The British Journal of Medical Practitioners has adopted a “Continuous Publication” model from the beginning of year 2010 publishing articles online as soon as they are peer-reviewed and copy-edited. This provides faster publication of articles for the authors and a quicker access for readers.
The BJMP website will now be updated regularly with the latest articles and we will continue to collate published articles into archival "issues" (about 4 issues per year).
The United Kingdom kicked off its leading mass coronavirus disease-2019 (COVID-19) vaccination programme by vaccinating the first person, Margaret Keenan on 8th December 20201 which was followed by many other countries.2 COVID-19 vaccines were developed in less than 12 months after the pandemic began3, 4 and have offered hope of bringing normalcy back to many around the globe, but it is not without its challenges.5, 6 The infrastructure of coordinating frontline response and the development of confidence among various communities to accept vaccination posed significant challenges. This required input from governments, healthcare professionals, the media, and importantly the public who play a vital role in not only accepting the vaccines and busting the myths but also actively volunteering for this great cause.
After watching my father, a frontline COVID-19 healthcare worker, receive the vaccine and at the same time sensing the reluctance of some family and friends to take the vaccine, despite the pandemic hitting Black, Asian and minority ethnic (BAME) communities disproportionately, I felt energised to play my role. When I saw an exciting opportunity for volunteering for this noble cause coordinated by my school, Bolton School, I promptly put an application forward in February 2021. The whole process was streamlined, and soon afterwards I embarked on volunteering at the Bolton Wanderers Football Club vaccination centre.7 There was some initial anxiety about contracting COVID-19, but I discussed it with my mentor and was reassured about the safety standards of the vaccination centres.
I was pleasantly surprised to see a range of roles for a non-clinician volunteer including being the face of the vaccination programme by greeting patients, explaining the vaccination process and allying anxieties, handing out written information, managing patient flow, ensuring maintenance of social distancing, checking temperatures, and liaising with clinical staff. There was also an element of an administrative role and keeping the registers. However, what I found most fulfilling was to talk to some of the patients who said that they had been socially isolating for several months and were excited to talk to someone face to face. One could see a sense of liberation the vaccination was bringing to them. It was a truly humbling experience to go out of my way to support some of the BAME patients, and speaking to them in their native language to make the whole process a memorable experience. I remembered one elderly lady who seemed distressed as she could only communicate in Hindi and I was fortunate that she allowed me to take her through the whole process and later assist with arranging transport.
I am going to continue with my volunteering on weekly basis and I found that it revitalised me for the rest of the week to engage in my full-time academic studies at school. This being my first work experience, I must admit the shifts were well-paced, lasting 4-5 hours and not too demanding. I was made to feel safe, and the senior members of the team would regularly communicate and offer me guidance and support.
Working closely with clinicians helped me gain new insights into the importance of true multidisciplinary teamwork in healthcare. I appraised it as the epitome of how colleagues with a unique set of skills, and driven by a shared desire to bring about a real difference to people’s lives, strived together selflessly as a team. Furthermore, it was inspiring to observe the leadership of the senior volunteers acting as role models with their professionalism, unflinching dedication to their job and willingness to proactively offer support to others. However, the watershed moment that shaped my thinking to take on medicine as a career was the reward I got from the empathic interaction with patients and gratitude in their eyes. It was pleasing to see in practice the Good Medical Practice8 attributes of working collaboratively with colleagues, professionalism, communicating effectively, and treating patients with dignity.
I have been feeling proud to be at the frontline working shoulder to shoulder with my clinical colleagues in this battle to end the pandemic. I would highly recommend vaccination volunteering to others as it is truly a once in a lifetime opportunity to make a real difference in the lives of so many.
It is widely acknowledged that medicine can be a high-stress profession. The reasons behind this observation have been the focus of research over recent years, because concerns over the welfare of doctors have grown due to its relevance to burnout of individuals and safeguard of healthcare systems. However, a recent survey of hospital doctors still showed that 80% experienced workplace stress, and the junior doctors surveyed suffered significantly higher burnout rates than their consultants.1 Separate research has specifically found that junior doctors have a poor work-life balance, a composite measure of individual factors affecting wellbeing.2 There seem to be differences in the wellbeing of doctors in different specialities studied – a study in 2016 showed higher levels of leisure time enjoyed by general practitioners compared to doctors working in other specialities.3 Another survey showed that psychiatrists experienced lower levels of burnout than surgeons did.4 Furthermore, different burnout rates have been observed between consultants and junior doctors working in Psychaitry.5
We sought to build on existing research by studying the work-life balance of junior doctors and how some factors might affect that. We also decided to explore what factors might contribute to the differences in wellbeing between medical specialties and professional grades.
Method
Junior doctors working across an English county in general practice, medical and surgical specialities (the “non-psychiatric setting”), and in psychiatric specialities (the “psychiatric setting”), were recruited into a cross-sectional study between September and December 2019. To enable appropriate comparison between groups, junior doctors must have worked between the level of Foundation Year 2 (FY2) and consultant in their relevant speciality. This was necessary because the on-call responsibility of Foundation Year 1 (FY1) doctors in this locality varies significantly from that of more senior doctors.
All doctors were required to complete the SWING (Survey Work-home Interaction-NijmeGen), questionnaire6; a validated instrument measuring four aspects of work-home interaction. This questionnaire is split into negative (questions 1-12) and positive (questions 13-22) subscales, where lower and higher scores are better respectively. For each question four responses ranging from never to always could be returned. Demographic information was also collected to assess participant group similarity and identify any effect of these variables. These included age, gender, and whether they have children under the age of 18. No identifying information was requested to allow for staff anonymity, and no incentive was offered for participating.
Ethical approval for the study was granted by the local Medical Education Departments. Data from completed questionnaires was recorded in an Excel spreadsheet, which was used for collation and analysis. Significance of the between-group differences was calculated using the Chi-Squared test, with the threshold for statistical significance set at p<0.05. In order to allow comparison between the answers given for each questionnaire item, 1, 2, and 3 points were respectively allocated to each “sometimes”, “often”, or “always” response. The sum of these points for each question gave the “overall question score”, with lower and higher scores reflecting better work-life-balance on negative and positive subscales respectively. Overall question scores were also calculated as percentages of the maximum possible score for each question or subscale (i.e. if every respondent had answered “always”).
Results
Questionnaires were returned by 99 junior doctors (54 working in the non-psychiatric setting, and 45 working in the psychiatric setting). Demographic details are shown in Table 1. Not all respondents returned demographic details. There were no significant differences in the ages and genders of respondents between the two settings, but there were significantly more doctors with children <18 years in the psychiatric setting.
Table 1
Table 2
Questionnaire responses are shown in Table 2, along with calculated overall question scores and overall subscale scores for each subscale in both settings. Differences in overall question scores between settings are shown in Figure 1 and Figure 2.
Figure1
Figure 2
Overall question scores across the negative subscale were generally high, indicating a high incidence of negative work-home interaction among all respondents. Scores for questions 1-8, which ask about negative impact of work on home life, showed little/no difference between the two settings. Questions 9-12, which ask about negative impact of home life on work, recorded much lower scores in both settings, but there was separation between the settings, with scores in the psychiatric setting being higher than those in the non-psychiatric setting.
In the positive subscale, questions 13-17 ask about positive impact of work on home life, and questions 18-22 ask about positive impact of home life on work. Overall, there was a much more clear separation in scores between the two settings than that seen in the negative subscale. Aside from question 13, scores in the psychiatric setting being consistently higher than those in the non-psychiatric setting.
Main findings of this study can therefore be summarised as:
High negative impact of work on home life in both settings
Lower levels of negative impact of home life on work, but higher in the psychiatric setting
Higher positive impact of home life on work, and work on home life, in the psychiatric setting than in the non-psychiatric setting
Discussion
There has been a great interest in the wellbeing of junior doctors in recent years, resulting in a number of changes in working patterns, such as the move away from the old “firm” structure to medical training, and the introduction of the European Working Time Directive.7 However, the perceived wellbeing of junior doctors in the UK seems to still be poor, and has resulted in a so-called “Drexit” of junior doctors to other countries, such as Australia, providing a better quality of life or away from medicine altogether.7 One survey shockingly revealed that almost half of UK junior doctors have considered leaving the National Health Service, citing concerns over wellbeing.7 It is, therefore, unsurprising that in 2018, only 38% of FY2 doctors continued into speciality training.8
Various aspects of junior doctor wellbeing and contributory factors have been researched. For example, a large survey of Australian junior doctors published in 2020 showed that those working only a few more hours than the average were more than twice as likely to report common mental disorders.9 Many interacting themes have been qualitatively identified, such as those found in a recent Australian qualitative survey.10 These ranged from institutional issues such as discouragement to claim overtime, to cultural issues such as not wanting to ask for assistance, to personal issues such as time for personal care. Another study found multiple factors to be correlated with higher rates of burnout in hospital doctors, including male sex, younger age, and lower years of practice.1
It seems that wellbeing in junior doctors is a highly complex, multifactorial issue with many interacting contributory factors. In addition to considering the individual factors at work, it is also necessary to consider how these factors interact on a larger scale. One way which researchers have done this, and which we have replicated, is to consider the concept of “work-life balance”, which explores the interaction between work and home life, and vice-versa. Existing research in junior doctors has found work-life balance to be particularly poor in those with children and in women, who frequently cited that this had resulted in a change in career direction.2
Unsurprisingly, we have found high levels of work negatively impacting on home life in both psychiatric and non-psychiatric settings. Since work-life balance involves many interacting components, we speculated that it may differ between junior doctors working in different medical specialities. Indeed, we detected such differences, with the reported negative impact of home life on work being higher among those trainees in the psychiatric setting than those in the non-psychiatric setting. In a cross-sectional study like ours, it is not possible to comment on causality but we noted that there were significantly more trainees in the psychiatric setting who had children. This correlates with previous findings,2 and raises the possibility of a causative relationship between having children under 18 and negative impact on work. A study of stress in psychiatrists which gathered responses from 449 participants found that sickness of children and arranging childcare were among the top five stressors identified.11
Trainees in the psychiatric setting have consistently reported higher levels of positive impact of work on home life and vice-versa. One possible explanation is that the nature of psychiatry is inherently different to other areas of medicine, with a focus on promoting the quality of patient interaction, and training time dedicated to exploring this in detail. Supervision of patient contact is also conducted more thoroughly than in other specialities, which may lead to a greater sense of being supported in clinical decision making when trainees work in psychiatry.
Strengths and limitations
Regarding strengths of this study, we used an innovative method in seeking to compare trainees across two different settings. The questionnaire used was validated and holistic in examining bidirectional interaction between work and home life. Groups were well-matched in terms of the selection of trainees with broadly similar working rotas, and in their age and sex, which have been shown to be important variables which can affect work-life balance. We also used an innovative method in analysing the questionnaire responses which enabled us to compare directly between the two settings.
There are several limitations with this methodology which identify possible interesting and important areas for future research. For example, we did not investigate for differences in work-life balance between staff working in inpatient and community settings. Additionally, it was not possible to make conclusions about causality with this cross-sectional methodology, and the use of a longitudinal method with a more detailed exploration of demographic factors may provide interesting insights in the future. Due to local factors in the way psychiatric and general healthcare services are set up in our area, it was not practical to measure participant engagement with the study, and this would have presented a barrier making this study impossible. There were however 99 responses included in this study, with similar representation in both healthcare settings, which relative to the local population of doctors in the settings studied represents a good sample.
There will inherently be local differences in working patterns, and therefore the results of this study are not directly generalizable to a national or international population. The non-psychiatric setting is broad in its scope and includes trainees undertaking varied forms of medical and surgical training, and therefore there are likely to be more subtle variations which were missed in this approach.
Conclusion
This study adds to the literature on work-life balance in junior doctors, which is an important area of research in order to promote the wellbeing of the current and future medical workforce. It also explores how factors affecting wellbeing might interact on a higher level than when studied in isolation, and how these interactions may differ depending on the medical speciality in which the respective doctors work.
Because of the local variations in working patterns, we would suggest a replication of this research in other areas in the UK and abroad. We would also suggest that an interesting area for future research may be the exploration of differences in work-life balance between narrower groups of trainees, which may aid developmental policy generation in supporting doctors to maintain a healthy work-life balance across different specialities. The group we feel would benefit from further research in particular is the trainees with young children, as we found a possible negative association between this and impact of home life on work.
Processed sugar has a high glycaemic index (GI) as it is easily digested and absorbed triggering a prominent insulin response, which if repeated over time leads to insulin resistance and type two diabetes1, 2. The appealing nature of high calorific sugary food combined with their low satiating nature means they also tend to be eaten in excess which contributes to obesity and metabolic syndrome2, 3. Obesity and diabetes raises the long-term risk of poor gut health and chronic inflammation increasing the risk of chronic fatigue, low mood and degenerative disease conditions such as cancer, cardiovascular disease, dementia and stroke2, 3.
Despite these obvious risks, a recent survey of NHS health care professionals reported that over half are overweight and over a quarter are living with obesity4. Both obesity and high sugar content-foods are associated with musculoskeletal disorders, lower mood, unhappiness, fatigue and depression which significantly contribute to sickness absence from work4, 5, 6, 7.
Despite these risks, consumption growth continues to escalate especially in low and middle income countries. Since 2000 consumption has grown from 130 to 180 million tonnes in 20208, and its production is contributing to poor health as well as greenhouse gas emission and deforestation9, 10.
In an attempt to reduce sugar intake, NHS England introduced a voluntary reduction scheme in July 2017, recommending that NHS Trusts and retailers on NHS premises reduce the proportion of monthly sugar-sweetened beverages sales. They reported in March 2018, a reduction as a proportion of total drinks sales from 15.6% to 8.7%11. However, to date, there is no information as to whether this has had any impact on consumption of sugar, wellbeing or weight reduction. In our cancer unit there is a constant availability of sweet snacks, predominantly gifted by patients, and during busy clinics these often replace balanced meals. Some argue that this display of sugary foods, together with the high proportion of overweight staff undermines the NHS’ ability to give patients ‘credible and effective’ behavioural lifestyle advice.
The hypothesis for this intervention was that a removal of sugary foodstuffs from the field of vision on nurses’ stations and replacing with fruit, nuts and seeds enables healthy snacking, resulting in weight loss and increased mood.
Methodology
This pilot intervention used quantitative methods to observe the feasibility of delivery and outcome of a real-world intervention. This project was registered with and approved by Bedford Hospital NHS Trust Research and Development Department, but classed as a practical service evaluation, hence no Ethics approval or written consent was required.
Participants: Fifty eight members of staff at the Primrose unit, Bedford Hospital were invited to participate for this 3 month nutritional intervention; 44 (75%) volunteered. The cohort consisted of 36 nurses, 2 consultants, 2 secretaries and 4 administration staff. There were 41 females and 3 males, aged 28-72 years (average age 45 years). A further 100 consecutive patients attending for treatments were asked for their views on the intervention.
Measures and outcomes: The primary endpoints were Body Mass Index (BMI) (Kg/m2) and happiness measured with the previously validated Subjective Happiness Score (SHS)12. As a secondary end point, patients attending the Oncology unit during the intervention period were asked anonymously for their opinion and likely influence on their eating habits.
Procedure: At baseline the Primrose Unit research department recorded staff demographics, BMI and SHS questionnaire scores. From the date of entry of the first participant (June 2019) to completion of the last participant (September 2019), all sugary foodstuffs were removed and replaced with bowls of mixed whole and dried fruit, seeds and mixed nuts. Non-participating staff were asked to voluntarily keep sugary items out of general sight. At baseline, 3 months and 5 months, participants were weighed by one of the research team and completed a SHS questionnaire.
In the final month of the intervention, 100 consecutive patients attending for treatments at the unit were asked their opinion of this intervention, specifically if they felt that removing sugary items from public display was a welcome gesture and whether seeing staff making efforts to reduce sugar intake would encourage them to do the same.
Statistical methods and analysis
The completed dataset was compiled in an excel spreadsheet then transferred for independent statistical analysis. The pre- and post-intervention weight differences datasets were analysed by the T-test as were the difference in happiness scores. The differences in participants’ opinion were analysed by the chi squared test. There were no missing data and in view of the relatively small numbers in the cohort, sub-group analysis was not planned or performed. The study advisory committee predetermined that a change in weight of 1 kg was meaningful13.
Results
Average weight: At baseline the average was 72.12 kg, and 71.23 kg.at 3 months; an average loss of 0.89 kg (T-test p= 0.02). The average weight at 5 months was 71.09 kg; an average loss of 1.03 kg from baseline (T-test p= 0.01). Twenty participants (46%) lost >1kg in weight (average 3.01 kg) as opposed to 7 (16%) participants who gained >1kg (average 2.23 kg) T-test p< 0.03.
Happiness score: Average happiness score increased from 21.65 to 23.44 (+6.6%), T-test p< 0.04). Amongst those who lost >1kg weight, average happiness score increased from 21.54 to 23.75 (+9.3%), T-test p<0.03. In those who gained >1 kg weight, average happiness score decreased from 22.28 to 21.43 (-3.8% T-test p< 0.08. There was a 13.1% difference in the happiness score in those losing >1kg compared to those gaining >1kg in weight (p< 0.001).
Patient opinion: 94 (94%) of patients indicated that this initiative gave a good impression; 6 (6%) were not sure or felt it did not give a good impression (Chi2p<0.001). Ninety seven (97%) indicated that the initiative would encourage them to reduce sugar in their own diet versus 3 (13%) who were not sure or felt that it would not change their behaviour (Chi2 p<0.001).
Discussion
This small pilot evaluation has a number of methodological weaknesses but what it lacked in statistical strength it gained in novelty and potential importance. This was the first nutritional intervention involving hospital staff within a routine working practice. It addresses a health issue which affects hundreds of thousands of health workers every year, and demonstrated that a practical behavioural change initiative was welcomed by the majority of staff (75%), with no drop-outs or objections from non-participating staff. This implied a larger national study would be feasible.
These data clearly demonstrated a statistically significant reduction in meaningful weight similar to the best designed weight loss programmes14. A fundamental rule of behavioural change is not to dictate to people, but to encourage them to want to make the decision to change for themselves. This simple intervention did not stop staff eating what they wanted as there was no restriction to their overall food choices. The big difference was that, within their field of vision, there were healthier fruit and nuts instead of high-calorie, sugar-laden foods, which are usually readily available.
This intervention was overwhelmingly supported by patients. Surveys have repeatedly reported that patients look to health workers for guidance, and this study confirmed that this manoeuvre made patients think about their own eating habits. Although a further trial would have to establish whether this initiative objectively reduce processed sugar intake amongst patients, a reduction in intake would confer considerable benefits as several large cohort studies have linked high sugar intake with a higher risk of cancer, greater complications of treatments and worse outcomes, for several reasons3.
Sugary foods increase the risk of weight gain, already more common after cancer; increases levels of oestrogen in post-menopausal women; and increases insulin like growth factor (IGF) and other hormones such as leptin, all of which in laboratory experiments increase proliferation and markers of aggressiveness and spread of cancer cells 2, 15, 16, 17. Cohort studies have also reported that those who ate more than 10% of their daily calories as sugar had higher total LDL cholesterol levels further adding to the cardiac risks of herceptin and anthracycline chemotherapy drugs. Independent from obesity, high sugar intake directly increases the risk of type 2 diabetes (T2D) by overloading the insulin pathways1. Individuals with T2D have higher serum insulin levels (hyperinsulinemia) which triggers proliferation in cancer models18, is linked to higher oxidative stress and low-grade chronic inflammation, causing epigenetic genetic damage and ongoing malignant transformation19. These laboratory findings are supported by several cohort studies which have linked diabetes with a higher risk of cancer and a higher risk of relapse post-treatment20.
Patients on chemotherapy should be particularly discouraged from eating sweets and cakes as they are more prone to dental caries which contributes to the risk of osteonecrosis following consequent bisphosphonate therapy. Dental caries may also be an increased factor for bowel cancer itself as DNA codes from bacteria, commonly found in caries (Fusobacterium), have been detected in the genes of bowel cancer but not in normal guts21.
Patients receiving the new generation of targeted therapies should be particularly vigilant of their sugar intake. PD-1 inhibitors recruit the body's immunity to recognise and target cancer cells, the influence of diet and lifestyle is becoming even more important. Studies have demonstrated that better gut health is linked to significantly better response rates. Processed sugar is the preferred fuel for pro-inflammatory firmicutes bacteria whilst the healthy bacteroidetes utilise glycans from the breakdown of polyphenols, which explains why there is a reverse correlation between sugar intake and gut health22. However, whole fruit intake is associated with better gut and general health as it provides polyphenol which feed healthy bacteria3, 23. Despite having between 9-14% fructose, the fibre and pulp makes fruit satiating and slows gastric emptying, thus reducing the GI3. Additionally, the polyphenols in fruit, vegetables, nuts, legumes, herbs and spices slow transportation of sugar across the gut wall by inhibition of sodium-dependent glucose transporter 1. They enhance insulin-dependent glucose uptake, activate 5' adenosine monophosphate-activated protein kinase, which explain why their regular consumption is associated with a lower risk of T2D3, 23, 24. They also improve reduced gut and systemic inflammation; enhance anti-oxidant enzyme production so reduce intracellular oxidative stress; and reduce the risk of cancer and other chronic diseases including those associated with diabetes3, 25, 26.
The evaluation was not robust enough to measure whether this resulted in less sickness absence, but this endpoint should be included in a larger design. It also did not include data for those staff who did not actively participate, but who benefited from removal of sugary foods from their work areas; the evaluation committee did not receive any complaints or objections to their removal.
Government initiatives such as a sugar tax and public information campaigns may help but as individuals within the NHS, we have an opportunity to influence our staff, the patients whom we serve and the wider public. The evaluation reported in this paper is a small start, but demonstrates that a multicentre study would be feasible and if the results are confirmed, it could initiate a national cultural change attitude towards sugar in the NHS.
Health Education England (HEE) runs the Medical Training Initiative (MTI) scheme on behalf of the Department of Health (the Government Sponsor) and is influenced by the Home Office Tier 5 Government Authorised Exchange Visa Scheme1. The Academy of Medical Royal Colleges is the national sponsor for visa purposes. Major stakeholders involved in this scheme are the GMC and GMC Approved Sponsors (e.g. Medical Royal Colleges), Postgraduate Deaneries/Local Educational Training Boards (LETBs), and National Health Services (NHS) Trusts, with support from the Department of Health.
The Royal College of Psychiatrists (RCPsych) Medical Training Initiative (MTI) Scheme enables qualified overseas psychiatrists to undertake training posts in the National Health Service (NHS) for a maximum of two years (2). The purpose of the scheme is to provide training opportunities for international psychiatrists in the UK to improve capacity as a professional and return home with broad knowledge and experience. Vacant core training (CT3) posts approved by Deaneries/LETBs are offered to eligible international doctors. Thus, the MTI psychiatry scheme can benefit overseas doctors, the NHS and the countries that trained them.
Although the MTI scheme was first established in 2009, the RCPsych only formally adopted the program in 2014. Some lessons were learned from the experience of the scheme in other specialities and provided an opportunity for the RCPsych to develop its own scheme. It developed a selection process for successful candidates and matches them with relevant placements in NHS trusts across the UK. This process takes into consideration the training needs of the overseas doctor and vacancies available in NHS trusts. The MTI Psychiatry Scheme is now in its sixth year and has gradually grown over the years as evidenced by an increase in annual allocation of the training post to 40 placements, a rise in the number of applicants from different regions of the world and an increase interest from employing NHS trusts. However, there are areas for further development in this scheme and there is a need to ensure that it consistently provides a good training experience to international doctors.
Various researches suggest that there are diverse difficulties faced by overseas doctors during their transition into a new country 3,4. Lack of information about NHS; clinical, educational and work-culture challenges; language and communication challenges; and discrimination challenges were issues experienced by international doctors while initially working in the UK hospital settings 5. The College has recognised these difficulties and wanted to understand how these are impacting on the international doctors and what can be done to help them.
Aims
The aim of this survey was to evaluate the trainee’s experience of the MTI psychiatry training scheme and explore difficulties during the training and what can be done to help. The purpose of this survey was to gather feedback on the current implementation of the MTI scheme.
Methods
An anonymous online survey consisting of 28 questions was sent to doctors using SurveyMonkey as part of the RCPsych Annual MTI survey. All doctors enrolled in MTI Scheme were identified through the RCPsych MTI mailing list. The survey was open in November 2018 for one month.
Results
Out of seventy-six, a total of thirty-one trainees completed the survey with a response rate of 40.78%. Most of them (n= 13) were from the age group 31-35 years. The findings of the survey are summarised in Table 1-3.
Table 1: Description of MTI doctors (n=31)
Gender
Male
17 (54.83%)
Female
13 (41.93%)
Prefer not to say
1 (3.22%)
Age (years)
<30
5 (16.12%)
31-35
13 (41.93%)
36-40
6 (19.35%)
41-45
5 (16.12%)
>45
2 (6.45%)
Year of MTI scheme
First
16 (51.61%)
Second
7 (22.58%)
Completed
8 (25.80%)
Country of Primary Medical Qualification
Egypt
3 (9.67%)
India
8 (25.80%)
Lebanon
2 (6.45%)
Nigeria
12 (38.70%)
Sri Lanka
3 (9.67%)
Trinidad & Tobago
1 (3.22%)
Skipped
1 (3.22%)
Previous psychiatric experience (Years)
3-5 years
17 (54.83%)
6-7 years
7 (22.58%)
8-10 years
5 (16.12%)
>10 years
2 (6.45%)
Worked in other countries besides the country of primary medical qualification prior to working in UK
Yes
2 (6.45%)
No
29 (93.54%)
Reason for choosing MTI Scheme
Recommendation from senior colleagues
15 (48.38%)
College reputation
16 (51.61%)
Training opportunities
24 (77.41%)
Research opportunities
6 (19.35%)
Job prospects
15 (48.38%)
Others
2 (6.45%)
Table 2: Induction, Supervision and Mentoring (n=31)
Initial induction at workplace prior to starting work
Yes
28 (90.32%)
No
3 (9.67%)
Allocation of educational supervisor
Yes
29 (93.54%)
No
2 (6.45%)
Frequency of educational supervision
Never
5 (16.12%)
1-2 times/year
14 (45.16%)
1-2 times/month
5 (16.12%)
Every week
5 (16.12%)
Other
2 (6.45%)
Able to attend course/study days
Yes
26 (83.87%)
Sometimes
4 (12.90%)
None
1 (3.22%)
Frequency of clinical supervision
Weekly
19 (61.29%)
Fortnightly
7 (22.58%)
Monthly
5 (16.12%)
Quality of clinical supervision
Excellent
7 (22.58%)
Good
16 (51.61%)
Fair
7 (22.58%)
Poor
1 (3.22%)
Access to out of hours support/advice
Always
18 (58.06%)
Sometimes
11 (35.48%)
Rarely
2 (6.45%)
Forced to cope with clinical problems
Weekly
2 (6.45%)
Monthly
3 (9.67%)
Rarely
17 (54.83%)
Never
9 (29.03%)
How often do you meet your MTI mentor?
I don’t have mentor
16 (51.61%)
1-2 times per year
5 (16.12%)
1-2 times per month
2 (6.45%)
Others
8 (25.80%)
Table 3: Work experience in MTI scheme (n=31)
Have you experienced any of the following?
Clinical training second to service
16 (51.61%)
Feeling unsafe
3 (9.67%)
Being punished for seeking help
4 (12.90%)
Being bullied
3 (9.67%)
Others
6 (19.35%)
Challenges encountered
Lack of relevant information about National Health Service (NHS)
14 (45.16%)
Lack of knowledge of regulatory framework
19 (61.29%)
Unfamiliarity with multidisciplinary teamwork approach
11 (35.48%)
Communication difficulties
8 (25.80%)
Cultural differences
15 (48.38%)
Varied level of training and support
11 (35.38%)
Others
7 (22.58%)
Reasons for choosing MTI Scheme
Training opportunities in the UK were considered by three quarters of the respondents for joining the MTI scheme. However, about half of the respondents reported job prospects, recommendation from senior colleagues and college reputation as pull factors.
Clinical and Educational Supervision
Three-fifths of trainees had weekly supervision with their designated clinical supervisor and three quarters (75%) of them rated the quality of supervision as either good or excellent. The majority (93.54%) of them had an educational supervisor and less than half met the supervisor 1-2 times per year. RCPsych has a mentoring scheme to support MTI doctors but half of the trainees (51%) did not have a mentor.
Out of hour support
Less than one-third of the trainees were never forced to cope with clinical problems beyond their competence. However, three-fifths of trainees reported that they always had access to out of hour support and advice.
Challenges encountered
Lack of knowledge of regulatory framework was reported by three-fifths of trainees while working in the UK settings. In addition to that, half of the trainees reported a lack of knowledge of NHS and cultural differences. One third had difficulty regarding multidisciplinary team settings and varied levels of support and training. About 51.61% felt that their clinical training was secondary to service and few reported feeling unsafe, being bullied and being punished.
Discussion
This is the first evaluation of the training experience of MTI psychiatric doctors. This study showed that most of the trainees had good work experience of psychiatry before coming to the UK. One of the undoubted strengths of the MTI psychiatry scheme is the recruitment of international psychiatrists with skills and experience of working in diverse cultural backgrounds and low resource settings. This is one of the potential benefits that the NHS can draw whilst delivering the health care smoothly. The majority of respondents in the present survey cited training opportunities as the main reason for choosing the MTI scheme. Child and Adolescent Psychiatry, Old Age Psychiatry, Addiction Psychiatry and Forensic Psychiatry were the subspecialties that received the highest interest in the MTI post in a 2017 survey 6. It is encouraging that most doctors were keen to gain further experience and training in subspecialties that were not readily available in their respective home countries.. A similar finding has been reported in the Royal College of Anaesthetists’ annual MTI survey where the majority chose subspecialties that were poorly developed in their respective countries, e.g. ICU and pain7.
Transition to the UK is not a smooth process for overseas doctors and must be supported during this transition phase (5). Lack of knowledge of the NHS, regulatory framework and cultural differences were the challenges faced by most MTI doctors in this study. The RCPsych International Medical Graduates (IMG) conference acknowledged that IMGs face more problems than British counterparts in succeeding in the system and recognised the importance of trainers, the role of employers in developing meaningful induction programmes and giving IMGs additional support and remediation if required8. This study showed that most of the trainees had attended local induction in the workplace before starting a job. Induction course content must be relevant and reflect issues concerning overseas doctors 9. It is particularly important to remember the specific needs of overseas doctors as they were trained in culturally diverse and low resource clinical settings. Several studies have shown that a structured induction program is a useful way to integrate doctors during the transition to the NHS10-12. Few trainees missed the local hospital induction as they arrived in the UK months later than expected and the trust could not arrange the training. With this hindsight, RCPsych organises the annual national MTI induction program to the new doctor in this scheme to complement and compensate for any shortcomings in the local hospital induction.
MTI posts should provide the trainee with an opportunity to train in a highly supported environment. Supervisors provide regular support and ongoing feedback during the training. Trainees value the support they receive through supervision, senior and peer support, and the opportunity to work in multidisciplinary team 13. It was reassuring to find that three-fifths of trainees had weekly clinical supervision as recommended by the Royal College of Psychiatrists.The quality of clinical supervision was rated as good by 51.61% of trainees and 22.58 % reported as excellent. Most of them had access to out-of-hour support/advice. Supervision is important for continued professional development as international doctors need more support than UK trained doctors 9. Unfortunately, few reported serious issues such as being bullied at the workplace and feeling unsafe. A survey of bullying of psychiatric trainees in the workplace reported that it was experienced equally by both IMGs and UK graduates, but IMGs were less likely to report the incident to the organisation14. It is important to educate IMGs about the mechanisms to escalate this concern for proper action. Besides that, it would also be prudent to include these pertinent issues during the annual MTI induction program to raise awareness among IMGs.
The MTI doctors had identified areas for additional support from the College, trusts, local deaneries, and senior colleagues in the 2017 annual survey6. The College took the following steps:
1. Annual MTI Induction Program: Full day induction program is held annually in the Royal College of Psychiatrists’ for new doctors in the scheme. The program is specifically tailored for doctors who are working in the UK for the first time. Highlights of the program include an introduction to the NHS, Good Medical Practice, Psychiatric training in the UK, ‘Person-Centred Care’, resources and support available for trainees and most importantly, communication skills workshop. It also provides an opportunity to meet with other MTI fellows and share experiences and set up informal support networks such as WhatsApp group. Twenty-three doctors attended the MTI induction program in 2019. Not all doctors recruited in the MTI scheme were able to attend the annual induction program because of the variable start date resulting from delay in visa processing. RCPsych could provide support to these IMGs by organizing the induction program two times a year.
2. MTI Mentoring Scheme: RCPsych runs a mentoring scheme and has been offering mentorship to MTI doctors for the past three years (15). Mentors are usually experienced RCPsych members who have volunteered in the mentoring scheme. RCPsych MTI team matches the mentor and mentee who will stay together for the duration of the placement. The current study shows that 50% do not have a mentor. We did not explore the reason for this, but we speculate that as doctors must actively express their interest in participating in this mentoring scheme and this might have shown less engagement.
3. Annual MTI Scheme Survey: Feedback is collected from MTI doctors each year as part of ongoing efforts to improve the RCPsych MTI scheme.
4. Sharing of experiences about the scheme between the trusts: Trust has varying levels of experience regarding the training scheme and the College has been facilitating the exchange of shared experience by the experienced trust to a new host trust.
This survey explored the experiences of doctors involved in the MTI scheme and it would be interesting to know findings from longer-term studies. Longer-term follow-up studies are needed to evaluate the positive impact of the scheme after the doctors return home on completion of the training. It is hoped that invaluable insight gained from the survey can be used to strengthen the scheme as well as provide learning points to other specialities with similar training scheme for international doctors.
Conclusions
This survey provides useful information regarding training experiences in the MTI psychiatry scheme. The first step in making the difference is getting feedback directly from those involved in the scheme. RCPsych MTI Scheme is an evolving program and measures were put in place to address the needs/concerns that emerged from the survey to enhance the training experience of the MTI doctors.
The way a doctor dresses is a fundamental part of establishing therapeutic alliance with patients.1,2 It has been shown that doctor’s dress can influence patient confidence, offer greater reassurance, higher levels of trust, better adherence to prescribed medication regimens, enhanced willingness to complete return visits, and discuss sensitive issues.3,4 The literature outcomes in this field are mixed; for example, some studies suggest a non-correlation with perceived courteousness or professionalism,5,6 but we believe there is enough evidence to suggest that the manner in which a doctor dresses forms an important part of non-verbal communication, which is important for their interaction with patients, carers and with other staff members.
Various studies have examined patient preferences towards doctors’ dress. Formal dress or a white coat have been cited as favoured due to their perceived association with empathy, competence and trust.2,4,7,8 This is in contrast to other studies which found semiformal dress as preferred.9
In psychiatry, studies of inpatients have indicated a preference for smart attire and white coats as part of their doctors' dress code.10,11 Mcguire et al also found that community patients preferred their psychiatrists to be dressed as “smart/formal”.12
In recent years, dress code policy for doctors in the UK has become more informal, and white coats have been abolished for a number of reasons.13 In this study, we sought to determine the attitudes of multiple stakeholders towards doctors’ dress in both general and psychiatric hospital settings.
Methods
We surveyed healthcare staff, patients, and carers in an emergency department at a district general hospital (“medical setting”), and in a psychiatric hospital (“psychiatric setting”) in the South East of England. The data was collected on a week day between 09.00 and 17.00 at both settings, using a questionnaire based on Rehman et al.14 There were no exclusion criteria.
The survey questionnaire sampled demographic details, and used nine questions and two sets of images (a male doctor & a female doctor) depicting three styles of dress; white coat, formal (tie & trousers for male; dark skirt and white shirt for female) and smart casual (“bare below the elbows”). The survey questionnaire was piloted amongst volunteer staff and assessed for their user-friendliness and ease of comprehension before use. It was amended in line with the feedback received.
Results
337 individuals responded to the questionnaire, giving a response rate of 94%. Our sample was predominantly white (72%), female (62%) and married (43%). Respondent age, ethnicity and employment status were broadly representative of the local population.
Overall (Table 1), we found that the majority of respondents felt that the way that doctors dress was important to them, and that the location of respondents significantly affected their preferences (p <0.001). Although in these overall results there was no majority preference for one dress code over another in either location, preferences within each varied significantly (medical: p<0.01 and psychiatric: p<0.001). This numerical preference appeared to be for formal dress in both settings, capturing 35% and 45% of respondent vote respectively.
Within the three stakeholder-specific breakdowns (Tables 2-4), differences in preference reached significance for medical staff (p<0.001), psychiatric staff (p<0.001), psychiatric patients (p<0.05), and psychiatric carers (p<0.01). Like the overall results, there was no majority preference in any of these groups, but formal dress captured the highest numerical vote in medical staff (41%), psychiatric staff (55%), and in psychiatric patients (41%). Psychiatric carers preferred formal and smart casual dress broadly equally, which captured 36% and 40% of the vote respectively. Carers were the only stakeholder whose preferences were significantly influenced by their location (p< 0.01).
Dress code statistically significantly influenced the attributes associated with the doctor wearing them (p< 0.0001), as shown in Table 5. Formal dress captured the greatest proportion of every attribute tested, and considering total responses, formally dressed doctors were almost twice as likely to be associated with these attributes as those dressed in smart causal or a white coat.
52% of respondents were not aware that a doctors’ dress code policy existed, and while 53% of respondents felt they should not be consulted when considering dress code, 41% believed they should. 59% of respondents believed doctors adhered to their sites’ dress code policies, while 27% did not think so.
Discussion
To our knowledge, this is the first study in the world to compare preferences in doctors’ dress code between a psychiatric hospital and a medical hospital. Also, no other study to our knowledge has simultaneously explored the attitudes of different key stakeholders in both medical and psychiatric settings regarding this important issue.
In this study, we have successfully captured the attitudes and perceptions of key stakeholders regarding doctors’ dress code. We found that overall, doctors’ dress code was felt to be important, and that in medical and psychiatric locations a formal dress code is preferred. Looking at staff, patients and carers specifically, we found a preference for formal dress among medical staff, psychiatric staff, and in psychiatric patients. Among psychiatric carers, formal dress was preferred equally to smart casual. There were no significant preferences among the other stakeholders surveyed.
This preference for formal dress is easily explained by the results shown in Table 5. Seeing a doctor in formal dress made it almost twice as likely that that doctor would be seen as possessing any of the eight positive attributes included. Clearly, in the eyes of the respondents to our survey, a formally dressed doctor was most likely to provide good care.
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
42
40
59
26
167
<0.01
-
Psychiatric
57
18
76
19
170
<0.001
-
Total
99
58
135
45
337
-
<0.001
Table 1. Dress code preferences among all stakeholders. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
22
10
27
7
66
<0.001
-
Psychiatric
22
4
35
3
64
<0.001
-
Total
44
14
62
10
130
-
NS
Table 2. Dress code preferences among staff. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
14
14
15
10
53
NS
-
Psychiatric
16
9
24
10
59
<0.05
-
Total
30
23
39
20
112
-
NS
Table 3. Dress code preferences among patients. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
6
16
17
9
48
NS
-
Psychiatric
19
5
17
6
47
<0.01
-
Total
25
21
34
15
95
-
<0.01
Table 4. Dress code preferences among carers. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Dress code
Associated doctor attribute
Total
Trust
Advice
Conf.
Return
Knowl.
Caring
Resp.
Auth.
Smart casual
77
57
59
74
49
109
51
38
514
White coat
74
91
89
77
107
65
87
103
693
Formal
142
138
142
134
132
110
143
145
1086
Table 5. Doctor attributes associated with different dress codes.Respondents were shown images of each dress code asked “Which doctor would you…”: Trust the most (trust), Follow the advice of (advice), Have confidence in their diagnosis and treatment (conf.), Return to for follow-up care (return), Regard as knowledgeable & competent (knowl.), Regard as caring & compassionate (caring), Regard as responsible (resp.), Regard as authoritative & in control (auth.). P <0.0001.(calculated using Chi-squared test). Results were excluded for where more than one dress code was selected for an attribute, or where no choice was made.
Discussion (continued)
Interestingly, we also found that the location of healthcare influenced the preferences of carers to such an extent that it offset the non-significant results among staff and patients; such that this significance was carried through to the overall results. Exploring this in more detail, we see a marked preference for smart casual in the psychiatric setting over the medical setting (40% vs. 13%), for a white coat in the medical setting over the psychiatric setting (33% vs. 11%), and an almost equal preference for formal dress in both. This starkness in difference in preference between care locations indicates differences in the cultural perceptions of doctors by carers, but not by staff or patients. Perhaps an explanation for this difference is that historically, carers have been more involved and influential in the psychiatric setting, being an essential component to care, whereas in the medical setting they have tended to be more passive partners in care. A negative perception of mental health care portrayed to the public through film and media may have driven preferences away from white coat in the psychiatric setting, whereas in the medical setting perhaps a positive association with the white coat and physical health may have done the opposite.
Conclusion
We have identified a clear preference for a formal dress code for doctors from all stakeholders at medical and psychiatric care locations studied. However, we identified several interesting variations in preferences among individual stakeholders, and found that the location of care significantly impacted the preferences of carers. We believe these findings could be harnessed in the future development of dress code policies for doctors in order to enhance the doctor-patient relationship, and to improve the quality of doctors’ relationships with both carers and with other staff members. Additionally, there may be merit in involving these stakeholders during the policy development process.
The continuous growth in patient numbers and needs poses several challenges for medical professionals and support staff within the National Health Service (NHS).1 Health care services are under financial strain in the light of the changing demographic structure of the UK population that requires improved access to health services. Managing patient satisfaction represents another major challenge. Evidence from a recent national survey in the UK shoes that dissatisfaction with the NHS has increased by seven percentage points in 2017, reaching 29 percent, its highest level since 2007.2 Staff shortages, long waiting times for surgical operations and access to care, inadequate funding, and slow-paced government reforms are among the reasons for dissatisfaction. For hospitals, long waiting times at the A&E department, and delays for patients in need of critical care represent major concerns.3
Unsatisfactory health care service experiences generate negative outcomes for health service providers in terms of managing patients’ experience of care, and meeting performance targets. As patients are ultimately the receivers of health care provision, understanding their experiences of care is pivotal.4 The psychological processes underlying patients’ perceptions and evaluations of service provided by the health care professionals, play a crucial role in patient satisfaction. The cognitive processes of patients and their support network, such as friends and relatives, influence perceptions and attitudes towards health care treatment and service. Research underpinned by knowledge from social psychology can shed light on such cognitive processes and generate insights for effective management of patient satisfaction.
The concept of psychological threat in health care service experiences can be explained through the notion of ‘lock-in situations’5 perceived by the patients. For instance, when visiting a hospital or a GP surgery, patients often undertake externally-imposed activities, such as long waiting time for a doctor’s appointment, ease of self-service check-in, lack of acuity in self-care and monitoring, and/or unsatisfactory interactions with support staff – all parts of the service provision. Such situations can be perceived as a threat to the self-determination needs, such as the need for autonomy. Patients who regularly use health care services in the UK associate four main types of threat to health care service experiences, in response to which coping strategies are activated. We discuss these below.
Perceived threats associated with health care services
Patients who use health care services in the UK often report situations they find threatening or questioning their astuteness and sense of control. Interactions with health care staff can make patients feel unintelligent and/or incompetent and restricted in personal control. This is typical of encounters where healthcare support staff are unable to address patients’ queries accurately, and their attempt at resolving the issue is perceived subconsciously as unnecessary and inappropriate by the patients. The above seems to be due to a general lack of trust in the competence of health care personnel, and more conspicuously the perception that they were not willing to act in the interest of patients. Poor health status at the time of accessing health care services might also hinder patients’ willingness to accept advice from health care professionals. Such experiences of threat to self-competence are often associated with negative or even vengeful behavior towards the health service provider, which is the party perceived as threatening. The psychological mechanism behind such behavior is that retaliation alleviates the emotional discomfort caused by threat perceptions6.
Threats to personal control are often reported when processes in the health care service provision are perceived as inadequate and lead to, for instance, long waiting times for appointment booking and/or rescheduling. Our qualitative research show that patients perceive the process of booking a doctor’s appointment as ‘a nightmare’, ‘particularly time-consuming’ and ‘complicated’. They perceive a loss of control when seeking to book or reschedule an appointment. When appointments are not scheduled around their commitments, patients perceive that they are not being heard.
Furthermore, health care service experiences are perceived as threatening to the individual’s self-esteem; especially in situations where patients feel ignored by the health care personnel, and their own self-esteem and social identity are being undermined. A key reason is the perceived lack of empathy and concern of health care personnel during interactions with patients.
How patients activate coping strategies
The lock-in situations discussed above can affect satisfaction and well-being, despite patients’ general compliance with requests from health care personnel.5 Social psychology research shows that perceived threats, such as those reported in health care service experiences, increase feelings of anxiety, averseness, lack of control, and aggressiveness.6 Crucially, in response to threats and consequent negative feelings, patients activate coping strategyas a mechanism of self-defense. We postulate that coping strategies, in turn, influence their behavior, aimed at compensating for the unsatisfactory experience7. Such behaviour can be negative, and at times even vindictive towards the health care service provider.
Social psychology research distinguishes between individual’s coping strategies8 aimed at addressing the source of the threat (i.e. problem-focused coping), and those focused on re-establishing positive emotions, for instance through the act of venting dissatisfaction caused by the threat (i.e. emotion-focused coping). In health care services, patients often seek to proactively react to threats, thereby engaging in problem-solving. This is especially the case when unsatisfactory health care service experiences are aggravated by a serious illness. Severity of the illness markedly influences patients’ willingness to take actions in response to threats. Crucially, the decision to act seems to benefit patients, as they report feeling ‘back in control of the situation’ – a form of compensatory behaviour9. Cerebral activities, such as rational and positive thinking, influence the extent to which patients confront threats. Rational thinkingcan induce patients to take a step back from the experience, reconsider the factors at play, and plan their next actions.
Crucially, in the process of coping with threats imposed by health service experiences, patients often feel overwhelmed. Negative emotions in such threatening circumstances are heightened, and the support from their network of friends and family appears to be fundamental. Intriguingly, for some patients, social media is increasingly seen as a useful source of emotional support, which appears to be gradually replacing conventional forms of verbal, face-to-face support.
Final remarks
We offer an overview on how insights from social science research can be valuable for informing decision-making of health care service providers. This is especially the case in decisions related to staff hiring, training and development, service process improvement and supporting systems design. Lack of empathy and concern from frontline health care staff, outdated service processes and systems represent threats to patients. An implication is that innovative training of frontline staff is necessary for the development of soft skills, which are highly valued by patients. Developing caring and supportive relationships between health care personnel and patients is necessary, as these have considerable bearing on the outcome of healthcare service experiences. Similarly, introducing the practice of simulating patients’ care experience can help to identify threats whilst introducing service improvements and innovations. There is also need for health care service providers to be aware of the fact that patients’ health status at the time of seeking access to and experiencing health services influences their evaluations of the quality of care and of the service experience. It follows that the service provision needs to be adapted to account for patients’ health status and vary according to different patients’ groups. Insights from social science research can inform practice for enhanced provision of health care services. Further survey-based research focusing on the causal links between psychological threat, coping and patient well-being10 is on hand.
Medical Student Syndrome (MSS) is a unique type of hypochondriasis which specifically causes health anxiety related to the diseases medical students study during their medical training.1 However, this phenomenon does not translate into an increased number of consultations differentiating it from hypochondriasis.2 Nevertheless, the common denominator in both conditions is that the affected person persistently experiences the belief or fear of having severe disease, due to the misinterpretation of physical symptoms.3 The medical examination on multiple occasions does not identify medical conditions that fully account for the physical symptoms or the person’s concerns about the disease, making it a diagnosis of exclusion. Unfortunately, the fears frequently persist among medical students despite medical reassurance, affecting their concentration during their training.4
Earlier studies have shown a higher prevalence of MSS in various medical schools, but recent studies show a declining trend. While Howes et al5 demonstrated that 70% of medical students have groundless medical fears during their studies, Weck et al,6 on the contrary, recorded the prevalence of health anxiety only among 5-30 % of study participants. One of the reasons ascribed to this could be that earlier studies, showing a high prevalence of MSS, were uncontrolled. Also, age-matched peers were not used as controls in some studies, and no direct interviews had been conducted.7,8 Methodological issues in previous data have led to inaccurate interpretations and over-generalization of findings. For example, the high emotional disturbance in medical students resulted from comparisons made with the general population, rather than with other students of their age. 9-11
We were prompted to conduct this study because the magnitude of MSS is variable from region to region, and in this study we compared medical students with their peers, studying in different colleges of Taif University to avoid observational bias.
Methods
This study was carried out from September 2017 to June 2018 at the female campus of Taif University, Kingdom of Saudi Arabia (KSA) in medical (pre-clinical and clinical years) and non-medical colleges in accordance with research guidelines of the College of Medicine, Taif University, KSA.
Inclusion criteria
Age and gender-matched students were selected for inclusion in the study. These included:
1. Female medical students from the second to the sixth grades enrolled in the College of Medicine, Taif University, KSA.
2. Female non-medical students from first to fourth grades enrolled in colleges of Arts, Admin and Financial Sciences, Computer and Information Technology, Science and Islamic Law.
Exclusion criteria
Biology students were excluded due to the medical content of their courses. At the time of enrolment, permission for participant recruitment was obtained from the concerned faculty administrators.
The participants were approached in the common/study rooms or lecture halls. The students were informed of the voluntary nature of the participation and were randomly selected. They were not required to provide their names during completion of the questionnaire and were assured of confidentiality. The Hypochondria/Health Anxiety Questionnaire (HAQ), developed by the Obsessive Compulsive Centre of Los Angeles (http://ocdla.com/hypochondria-test), was used to collect the data. The questionnaire was translated into Arabic and underwent a revision in order to ensure compatibility with the original one. The questionnaire was not designed to provide a formal diagnosis but provided an indication as to whether or not the persons were exhibiting significant signs of the disease.
Results of this questionnaire were analyzed as under:
A) 1 to 3 test items checked: there is a low probability that the student has health anxiety, and it is unlikely that her concerns significantly impact his life.
B) 4 to 7 test items checked: there is a medium probability that she has health anxiety, and a moderately high amount of distress related to specific health-related thoughts. She spends more time than most people doing unnecessary behaviours related to these thoughts.
C) More than 7 test items checked: there is a high probability that she has health anxiety. She most likely has a significant amount of distress related to certain health-related obsessions, and likely spends a significant amount of time doing unnecessary compulsive and avoidant behaviours directly related to these obsessions.
Statistical methods
Data were statistically described regarding frequencies (number of cases) and valid percentages for categorical variables. The response of the two groups was analyzed by student t-test. P values less than 0.05 were considered to be statistically significant. All statistical calculations were done using computer program IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 21 for Microsoft Windows.
Results
400 students were included in the study. There were 200 medical students, and the other 200 students were from various non-medical colleges of Taif University (Colleges of Arts, Admin and Financial Sciences, Computer and Information Technology, Science and Islamic Law).
All participating students were females (100%), and the mean age of the medical students was 21 years (ranged from 19-22years). The mean age in the non-medical group was 20.5 years (ranged from 19-23 years).
All students in the non-medical colleges completed the HAQ while five students in the medical college (clinical years) did not complete it, so the data on 395 participants were finally analyzed.
According to the scaling criteria, this study showed that the overall prevalence of MSS among the total sample (medical and non-medical female students) was 16.2% (64 out 395 students). However, it was higher in the medical students (34 out of 195 students; 17.4%) than in the non-medical students (30 students out of 200; 15%) – see Table 1.
Non-medical students n=200
Medical students
p value
Pre-clinical (95)
Clinical (100)
Age
19-23
19-20
21-22
Medical student syndrome (MSS)
30 (15%)
20 (21.1%)
14 (14%)
0.22
One visit to doctor
33.3 % (10 /30)
20 % (4/20)
14.3 % (2/14)
0.0043
More than one visit to doctor
40 % (4/10)
25 % (1/4)
0 %
0.001
Table 1. The frequency of Medical Student Syndrome (MSS) among medical and non-medical students.
Figure 1. The difference of Medical Student Syndrome (MSS) between pre-clinical and clinical years (p=0.028).
Figure 2. Fears related to diseases in the study cohort.
While comparing the response of the two groups by student t-test, there was no statistically significant difference between the responses obtained from medical and non-medical colleges (p=0.31). However, from the MSS diagnosed cases in the medical college, there was a significant difference between pre-clinical and clinical years – 21.1% vs 14% (p= 0.028) – see Figure 1.
Regarding the percentage of students who visited the doctors during the last year due to fears from disease, or medical condition, it was higher in the non-medical student's group than in the medical student's group with a significant difference observed (p=0.043).
The medical conditions that caused worry among medical and non-medical students were, diabetes mellitus followed by cancers especially breast cancer. The least worried diseases were headache and heart diseases – see Figure 2.
Regarding the percentage of students who consulted more than one doctor for the same medical concern, because of doubt about the previous doctor’s diagnosis and laboratory results, it was higher in the non-medical student's group compared to the medical student's group. The difference was significant (p=0.001).
The students with MSS in the total sample (of 395 students) were categorized according to the degree of probability into low, medium and high as shown in Figure 3.
Figure 3. The probability of Medical Student Syndrome (MSS) among all groups compared to their non-medical peers.
Discussion
The unrealistic fears about illnesses recorded in this study among medical students were higher than their peers studying various non-medical courses at Taif University; however, the difference was not significant. The subgroup analysis revealed a correspondingly higher prevalence of health anxiety during pre-clinical years than clinical years as shown in Figure 1. Possibly during the pre-clinical years, students have an increased sense of body awareness and stress as demonstrated by Moss-Morris et al.7 The authors in the above study described this syndrome as a normal perceptual process and differentiated it from common hypochondriasis. Other researchers 8,12 as well affirmed this. Our results are in parallel with the finding of Azuri et al13 who recorded that first-year students visited a general practitioner (GP) or specialist more often than in other years. The authors in the above study suggested that the pre-clinical students` visits may be due to registering with a new doctor closer to university or due to necessary health checks before the beginning of their medical school. The dream content of pre-clinical medical students frequently involved a preoccupation with a personal illness of the heart, the eyes and the bowels in the above study.
Additionally, the fear of acquiring a future disease is a core feature of health anxiety, while fear of already having a disease is considered more central to the MSS.14 There is a number of instances where this syndrome manifests among students from time to time during their training. The students are even known to change their diagnosis depending upon their clinical rotation. For example, in a psychiatry rotation the student conceptualizes having schizophrenia and later shifts his or her diagnosis to Meniere's disease during an ear, nose and throat (ENT) rotation. The symptoms are thought to occur due to intensive exposure to knowledge affecting symptom perception and interpretation.15 The fact remains that the affected student is devoid of either. At times, the simple knowledge of the location of the appendix transforms the most harmless sensations in that region into symptoms of a serious threat.16 The students who study "frightening diseases" for the first time routinely experience intense delusions of having the disease, reflecting a temporary kind of hypochondriasis.17
In a study by Waterman et al18 it was observed that 80% of medical students conceptualize diagnoses ranging from tuberculosis to cancer while studying these diseases during training. This caused emotional distress and conflict in them. It was suggested that this phenomenon was present in approximately 70-80% of students in the study mentioned above. There may be multiple reasons for precipitation of this condition among medical students. The vastness of medical studies are undebatable, and medical schools cause students to experience a large amount of psychological pressure due to work required to grasp the subject matter, the stress of examinations, and the competitive environment.19
In this study, we compared medical students with the students of the same age and gender with the same cultural background in order to avoid any bias. Our results are in parallel with a more recent study, which compared three groups, medical students, non-medical students, and their peers who were not undergoing any academic course. The authors in the study mentioned above observed no significant differences between the groups on total scores in the questionnaires. However, when considering the individual components of the questionnaires, it was found that medical students were less aware of bodily changes and sensations than the other groups; nevertheless, they did not avoid seeking medical advice for any health-related fears.20
Regarding the percentage of students who visited doctors in the past 12 months due to fear of disease, it was observed in this study that the non-medical group had significantly higher visits to doctors compared to their peers studying in the medical college of the university. It is entirely possible that they had increased access to personal advice from peers, relatives, and various mentors. Of the various diseases, fear of diabetes mellitus was the highest, possibly due to a high prevalence of the disease in Saudi Arabia.21 Further, it is entirely possible that medical students subconsciously conceive these metabolic disorders as these are discussed in greater details during their courses.
MSS may lead to cyberchondria, a phenomenon of the public, seeking to diagnose themselves via the internet,11 which in turn may lead to hypochondriasis in any given student. Thus, it becomes imperative that students suffering from this disorder must be dealt with an empathetic approach and counselled properly after ruling out an organic cause of their illness. A step to circumvent it further would be that MSS must be thoroughly discussed among medical students during their training.
Limitation of the study
The drawback of this study is that that the questionnaire was translated from English into Arabic, and although it underwent a revision, there were no other formal tests such as linguistic and cultural validation to validate the translated version. Further, we believe that our focus was only on female students, and it is well known that females have better ability to cope up with anxiety and depression compared to males22,23 so the figures of MSS among male medical students needs to be studied as it may be different from what we reported in this female cohort.
Conclusion
In conclusion, the students who are suffering from MSS often overuse medical resources and outpatient’s services compared to others. Therefore, clinicians should be aware of these students, to avoid unnecessary procedures and treatments. However, it is vital that a proper evaluation is done before labelling a given student with MSS.
Within the United Kingdom, all doctors are expected to teach.1 It is assessed throughout their professional career, during annual appraisals for doctors in training and during consultant revalidation. But how are those just embarking on their medical career expected to develop the necessary teaching skills? As three educators at various stages in our clinical careers, we developed and delivered a small course with the aim of addressing this issue.
The General Medical Council within the United Kingdom, suggest that a basic comprehension of teaching should be gained during the undergraduate and postgraduate training of doctors.2 Dandavino et al. further suggest that early development of these teaching skills may have additional benefits for the clinician; such as improving communication and assisting undergraduates to develop their own ability to learn.3 Our local training region, Yorkshire and the Humber Deanery (HEYH), have a mandatory post-graduate training day in teaching skills which focuses on generic and clinical teaching skills. This is delivered towards the end of the first foundation year. It is delivered by doctors who have various roles in medical education. Whilst useful in its content, for many it comes late. Doctors have often already been involved in providing teaching to medical students on placement at this time.
AMC recalls from her first postgraduate (foundation) year. One peer was thrilled to have ‘shaken-off’ a final year medical student who was supposed to accompany them on a shift as a learning experience; stating that they were now able to ‘do some work’. She couldn’t understand the desperation to escape one-to-one teaching. On reflection, it was probable that her colleague found it overwhelming to incorporate the additional responsibility of teaching alongside an already stressful clinical workload. Many share these feelings, with new doctors finding time pressures along with competing clinical demands a challenge to implementing clinical teaching.4
We thought that giving our graduates simple tools to understand and overcome these challenges may empower them as teachers. It may also improve their confidence in other areas, such as in their own learning and presentation skills.5-6 This paper proposes a solution; after creating a short course to be delivered immediately following graduation, to empower new doctors as teachers by providing some basic training in clinical teaching. These doctors are then able to use this training as soon as they begin their foundation training, which is ultimately the beginning of their teaching career.
Methods
Two versions of a half-day course, titled ‘Teach the Medic’ were developed in HEYH which ran in successive years. The original course was designed by a surgical trainee (AMC) and a general practitioner running the undergraduate education curriculum (MS). Initial topics were chosen based on experiences of the authors and colleagues. The optional course (see figure 1), was offered to the cohort of Leeds medical students who were in the transition period between finishing their final examinations and commencing their first post as a doctor.
Figure 1: A representation of the initial course structure. Stations were developed as interactive lectures and delivered to participants by doctors of various training levels.
The initial course received encouraging verbal and written feedback from the participants, which was collected on the day of the course. Further feedback was collected a few months into foundation training, allowing enough time to pass for delegates to use this knowledge. This feedback, whilst encouraging, included that delegates were keen for additional workshop style sessions. Subsequently, a modified half-day course ran the following year, with the recruitment of additional postgraduate teachers (including LES). A further 17 newly qualified doctors from various medical schools completed the course, prior to commencing their HEYH foundation post. This modified course (see figure 2) included scenario based sessions around potentially difficult situations for the clinical teacher, and also explored alternative styles of teaching that could be adopted successfully in the workplace.
Figure 2: A representation of the modified course structure. Building on feedback from the initial course, the three co-authors incorporated new small group scenario based discussions, alongside the interactive lectures.
Results
Initial feedback received from evaluation of the day was positive for both courses. For the second course, initial feedback found that all participants found every session very good (71%) or good (29%) overall. 12/17 (71%) thought that the course should be made compulsory to medical students. We also sent a follow-up survey, distributed six months after the course which generated 14 responses. All respondents felt that the course should be run again. All participants either strongly agreed (n=2, 14%) or agreed (n=12, 86%) that they felt more confident in teaching compared with their peers. Regarding individual sessions, 10 participants (71%) had directly incorporated learning from the ‘Teaching Theory’ session, 12 (86%) from the ‘Teaching for your Learning and Portfolio’ session, 11 (79%) from the ‘Teaching your Peers’ session, and 10 (71%) from the ‘Scenarios’ workshop. All participants stated they would still recommend this course to colleagues. They also reported directly incorporating their learning from the sessions into their teaching practice. The responses gathered from the second course implied that participants felt more confident in teaching when compared to their peers.
Discussion
We feel the course content in ‘Teach the Medic’ complements other courses available later in one’s career, such as the Royal College of Surgeons’ ‘Train the Trainer’ course. We propose this course could be run by a junior doctor who has a strong interest in clinical teaching with involvement of a senior colleague with extensive medical education experience. We felt the course was especially beneficial as participants had continued to find it useful long after its delivery.
To expand this project to include a whole year group as a compulsory course is ambitious. It would require development and the use of more resources, but initial feedback suggested participants will find it extremely useful. Bing-You et al.6 agree, having found that undergraduate students would be willing to undertake formal instruction in clinical teaching prior to graduation.
As our short course gains momentum within HEYH, this prospect becomes more achievable. When considering a wider delivered course, one must remember that attendance to ‘Teach the Medic’ was optional; suggesting that those who attended had already identified an interest in teaching. This has the potential to bias our data to some degree. However, we still believe that making the session compulsory would allow skill development and empowerment for those who may not consider themselves aspiring medical educators, but who are still in positions to deliver teaching.
Conclusion
Our evolving teaching skills course suggests that close work with both local medical schools and deaneries is important to allow this course to be incorporated into the training of newly qualified doctors. This may be included as a compulsory part of the final year medical school curriculum, an option for a SSC, or as an integrated part of the new starter induction programme delivered by individual hospitals.
Medical scientists who espouse a strict biological model of the mind tend to care less about the prolongation of life than do those who have faith in higher authority.1 The prevailing reductionist model of mind has recently been challenged effectively.2,3,4,5. That has led to a position in which there is some justification for claiming that there is scientific evidence to enable a suspension of disbelief in life after death. 6 Medical profession should respect the theology veiled in thanatology and should be careful not to become instrumental in creating a culture of death; alleviating suffering is not by eliminating the patient.
In the absence of spiritual conviction, human suffering lacks deep meaning and death is regarded as the ultimate tranquilliser. Prolonging life at any cost may be perceived as a worthless endeavour. To counter that, without suffering evolution would not take place and human consciousness would fail to expand. Without stress and struggle the spirit buds to which we may be likened would not mature and grow leaves and fruit, and our characters would not develop; we would lead the lives of lotus-eating sybarites. 7
Evidence for discarnate survival
According to those who are sceptical about after-death survival, there is only as much evidence to justify belief in life after death as there is for the historical existence of dinosaurs. Some scientific researchers however argue that there are compelling reasons to support those who are proponents of belief in life after death. Dr Vernon Neppe, a neuropsychiatrist turned parapsychologist, has declared that the combined body of evidence for discarnate survival is overwhelming – so great that it may be regarded as scientifically cogent.8 This emerging scientific view, coupled with the wisdom of the faith traditions, challenges the rationality of supporting assisted suicide. The following are examples of evidence for discarnate existence that are commonly cited:
clinical death experiences
pre-death visions
shared death experiences
collective apparitions
some forms of mediumistic incidents, particularly ones that involve cross-correspondence, drop-in communications and physical phenomena
children’s memories of previous lives
electronic voice phenomena
instrumental trans-communications
transplant cases
Scientifically studied Marian apparitions
The list is becoming longer as survival research progresses. Encouraged by the success of afterlife experiments with mediums,9 the multi-specialist professor Gary Schwartz of Arizona University claims to have invented a device to communicate with discarnate spirits; the holy grail of survival research that could possibly offer a fool proof scientific evidence of afterlife existence,10 but also takes account of all the potential negative consequences. He claims to have worked with black boxes in his laboratory, using a software programme that has generated proof that there is a spirit world by measuring light. 11It appears that he has developed a technique whereby faint light can be detected in a totally dark box. Measurements are taken at the beginning of an experimental session, and then a specific “hypothesized spirit collaborator” is asked to show a “spirit light” in the box and a second reading is taken. The finding is that instruction for specific spirits to enter a light sensing system was associated with reliable increase in the apparent measurement of photons. Such a curious result means that these communicating spirits are able to hear, respond and produce light in an otherwise dark enclosure. 12,13 The conclusion is that survival research opens up new vistas which seem much more important than cosmology or quantum electrodynamics.
Scientifically examined Marian apparitions are a recent addition to the evidences for discarnate existence. 14 Mainstream scientists seem never to have attempted to develop the conceptual tools and vocabulary needed to investigate the possibility of post-mortem existence. It may be that science will not accept the possibility of discarnate survival without a new theory of physical reality. In the early part of the twentieth century the prevailing view of scientists was that there was no possibility whatsoever of proving the existence of life after death. Over the years that have passed since then attitudes have evolved, and in the world, we are now in it is asserted by some researchers that there is scientific evidence for the existence of life after death. Some of the evidence relating to discarnate existence may not however satisfy the criteria of the physical sciences since the latter are based on speculative science and court room logic.
Paradigmatic shift
Demonstrating post-mortem existence as an irrefutable phenomenon is a route to establishing empirically that humans have a higher consciousness. Unfortunately, in survival research there are many phenomena that have multiple possible explanations, and these augments add to the complexity of this immensely significant area of scientific enquiry. All the types of evidence postulated as supporting discarnate survival are simultaneously a form of evidence of a non-biological component that operates in association with the brain. The existence of a non-biological component indirectly proves the possibility of survival after physical extinction. A huge paradigmatic shift towards non-reductionism is now taking place in the cognitive sciences – consciousness is no longer considered an epiphenomenon of brain activity, but asthe designer and prime mover of the material body. Nowadays, some mainstream scientists are themselves paradoxically trying to debunk mainstream science.
Suicide victims
Through suicide, a person is simply changing the location of their suffering. While wrapped in the physical planet by space and time, we are in an advantageous position for inducing personality changes swiftly, whereas in the timeless state of discarnate existence changes are sluggish and personality development is much slower. Contemporary data for survival research may be congruent with the wisdom of the faith tradition. 15 To use a simple analogy for this, carrying out assisted suicide is like destroying the shell of a pupa and forcefully freeing it in a premature state. Such a pupa will not be able to fly about like a butterfly. It is arguable that a person subjected to violent death – as in the case of suicide – may not be able to enjoy the beauty of God’s grand other-worldly dimensions until they have become spiritually compatible with them. They have to navigate through the physical plane like wingless birds. 10 To look at this way, if fruit that is unripe drops from a tree, it will be sour. Suicide breaks a solemn law because it deprives the conscious self of the natural growth that life in a physical body can best provide.7The Chinese saying “One day of earthly existence is not equivalent to a thousand days of ghostly existence” is a statement of the sanctity of terrestrial life.
Lord Alton has campaigned against the Assisted Suicide Bill of 2014 since its inception. Referring to his dying father’s account of how he had seen his own brother, a member of the Royal Air Force who had died in the Second World War, Lord Alton argued that a forced death, as opposed to a natural one, may deprive a person of their “healing moment.” 16 A graceful and natural death may be supposed to be accompanied by benign caretaker spirits with exuberant love who assist those who are dying by making them comfortable for the big transition.17,18 A person who terminates their own life prematurely may not be so fortunate as to get such benevolent assistance from the spiritual realm. Most hospice workers are very familiar with departing and death-bed visions such as that described by Lord Alton. Furthermore, it has been suggested that beings from the imperceptible spiritual sphere who assist in delivery from the terrestrial plane have a role in such matters as the timing of death, and it is arguable that their part in what happens should not be impeded by intervention.
It appears that human brain is designed to have some doubts about discarnate survival for some reason and a fool proof evidence of post-mortem existence may have its down side in that somebody who is fed up of life might use it to justify ending his earthly life voluntarily. 19An ultra-optimistic view of discarnate life is spiritually counterproductive and such an over optimism could be seen as a justification by the patient and carers in the decision making of assisted suicide. In a weak moment of extreme psychological or physical sufferings, such a belief can also become the final rationalization for ending one’s own life voluntarily. In my own clinical practice, I have come across suicidal patients telling me, “It will be always better on the other suicide.” A belief in discarnate existence based on parapsychological proof alone did not deter one such patient making a serious suicidal attempt
End-of-life concerns
The evening of life was considered as a great opportunity for spiritual, emotional and psychological growth and a celebration of one’s life journey. These are also times to harvest the wisdom of yesteryears and share them with the succeeding generation. Spiritually enlightened people consider this to be the time to conquer the fear of death. Fear of death is not the fear of the physical pain of death, but the fear of truthful self-judgement after death. Recent observations in thanatology favour a belief in post-mortem self-assessment and appraisal. For some, it would be voluntary or assisted, whereas for others it could turn out to be forced upon them. The final phase of life is the time to settle the errors committed against fellow beings that have not been remedied in life. Fortunately, modern medicine has prolonged this period, which grants an opportunity for most people to experience conscious ageing. Sadly, traditional attitudes towards the evening of life have changed in today’s youth-obsessed culture. For some, medical procedures have extended life and made dying a lingering process rather than a sudden event, and have contributed their own problems. For several reasons, terminally ill people who are in crisis may wish to die rather than being kept alive longer (Table 1).
From an evolutionary point of view, there can be only a survival instinct – no Freudian death instinct. Avoiding death rather than seeking it is a natural human urge and the fear of death may affect every individual action. The very concept of euthanasia is totally against the human make-up and is entirely artificial. Assisted dying and assisted suicide are the same thing when a member of the medical professional gives a lethal drug to a person so that they can take their own life. Euthanasia is different; it happens when, for example, someone injects a lethal substance into a patient. Involuntary euthanasia refers to a situation in which the patient has the capacity to give consent, but has not done so; and in non-involuntary euthanasia a person is unable to give consent, for example because of dementia or being in a coma. Mercy killing is claimed to be a compassionate act to end the life of a patient.
Table 1: End of Life Concerns
Losing autonomy
Less able to engage in activities making life enjoyable
Loss of dignity
Burden on family, friends/caregivers
Losing control of bodily functions
Inadequate pain control or concern about it
Financial implications of treatment
Moral and ethical issues
It has been observed that the risk of suicide is higher among people with a family history of suicide. Family culture and genetics may account for the increased incidence of suicide in such situations. Assisted suicide would create a trail in the culture of more families and more succeeding generations would perhaps be at increased risk of considering suicide as a serious option at a time of crisis. Kevil Yull (2013) comments that changes in the law of assisted suicide would have an additional impact on those left behind, because of their effect on the moral connections, assumptions and accepted responses to situations on which we base our relationships with fellow human beings and establish ourselves in the world. 20 He argues that the legalisation of assisted suicide would undermine freedom instead of promoting freedom of choice, and also that the proposed safeguards and regulations would breach the privacy of the death-bed.
Assisting someone to kill themselves is assisting them in murder. According to all the major faith traditions, life is a gift from God and ending it is like throwing a precious object back to the giver. All spiritual traditions teach and believe that bringing the human heart to a standstill is God's business (Table 2). There are patients who assert that even if all their limbs were amputated, they would still want to hold on to the treasured gift of life. It is very difficult to define what unbearable suffering is; extreme suffering is a subjective matter that it is not possible to separate from an individual’s outlook on life. A fundamental question is that of who would be the one to pronounce a verdict on when suffering is intolerable – the patient or medical personnel?
Laws are not precision-guided arrows and they may become perverted. In a world full of violence and crime, assisted suicide is unsafe and could be exploited. There would be many unintended consequences. For reasons of public safety alone, some people oppose assisted dying. Financial abuse by relatives of the elderly seems to be becoming more common; those with a vested interest could be tempted to put an inheritance before life.
The regulation of assisted dying has been modified in recent times in some countries, an example being the Netherlands in 2014. There it is now lawful to kill a patient without their consent, and euthanasia and assisted suicide may be offered to people with mental health problems (consensus with the family is required in all these situations). Inboth Belgium and the Netherlands the euthanasia of children is legal with family consent (in Belgium there is no age limit; in the Netherlands the child must be 12 or above and must give consent). In Belgium blind adults who were developing further problems were granted euthanasia at their own instigation a few years ago. There is public concern about collaboration between euthanasia teams and transplant surgeons in Belgium.
Table 2: Medical dilemmas
Assisted suicide promotes a human right to commit suicide and gives wrong messages to suicidal patients in psychiatry.
It undermines the Universal Declaration of Human rights and strikes at the foundations of all spiritual values.
It is hard to define unbearable sufferings.
Assisted suicide has many unintended consequences.
Death with dignity could deteriorate as death with indignity.
It might permit the unlawful killing of innocent people in certain circumstances.
It is founded on unethical principles-survival of the fittest.
In 2013, 1.7% of all deaths in Belgium were hastened without the explicit request of the patients. 21 Professor Cohen Almagor, the author of 2015 report on euthanasia in Belgium stated that the decision as to which is no longer worth-living is not in the hands of the patient but in the hands of the medical personal. 22 More than 500 people in the Netherlands are subjected to euthanasia without their consent.23 Data from Oregon where assisted suicide was legalised in 1977 shows that the top five reasons people choose assisted suicide are not because they are suffering from a terminal illness and 49% stated that feeling like a burden and a fear of loss of control are among the main reasons for choosing assisted suicide Oregon .24 In Washington state in 2013, 61% of people who were killed in assisted dying said that being a burden was a key factor for their choice of death. 25
Medical Dilemmas
Majority of British medical practitioners are against assisted suicide. 26 A 2013 survey showed that 77% hold the view that they would oppose a change in the current law to allow assisted dying, 18% favoured the RCGP moving to a neutral position, and only 5% favoured a change in the current law. They opined that a change in the law would make patients afraid of their doctor and would alter doctor –patient relationship, and would make vulnerable patients most at risk from assisted dying. According to Marris bill, some people should be given help to die meaning that some lives are worth less than others. Vulnerable people would feel pressurised to choose death and could be killed without their explicit consent. GPs feel that it is their privilege to protect the disadvantaged and vulnerable people of the society.
Assisted dying would lead to less focus on investment in palliative care. The RCGPs also cautioned in the survey that a change in the position of the law makers would become like abortion legislation, which started as something for extreme circumstances and is now effectively on demand. They are also anxious for the fact that legalisation of assisted dying would make it impossible to tell the real reason why patients decided to die, because illness can cause people to become depressed and frightened. As debate on assisted suicide has become hotter, in clinical practice suicidal patients have already started enquiring about the prospects of assisted death.
Thanatology
Medical sciences have not advanced enough in matters of death to offer details to make informed choice for those who want to die voluntarily and thanatology is only a fledgling science. Thanatology is the scientific study of death and investigates the mechanisms and forensic aspects of death, such as bodily changes that accompany death and the post-mortem period, as well as wider psychological, parapsychological and social aspects related to death. They are not particularly interested in the meaning of life and related philosophical issues, but this is an area where science and philosophy not be separate. In recent years, studies of parting visions by Elizabeth Kubler Ross and Raymond Moody’s NDE studies. 27,28,29,30,31,32 have given a spiritual dimension to thanatology. Theology and Thanatology are two major corpuses of human wisdom that cannot but overlap. Assisted dying would probably become also an issue of forensic sciences.
It is the job of the doctor to keep the patient alive whereas it is the job of the psychotherapist to have a sense of a bigger picture. 33 People wanting to hasten death should also have the choice of receiving pastoral and psychotherapeutic assistances to distract themselves from their preoccupations of death and allow nature take its own natural course. New generation psychotherapists will have to be well versed in all aspects of death related sciences. Thanatology has a rightful place in medical studies, but I content that medical professionals need not to be unduly concerned about the different forms of afterlife existences, the borderland between religion and thanatology. Medical professionals are expected to be above religion and politics. Thanatologists now fear that if assisted suicide is legalised, they might be pressurised to slip from the original goal of acquiring more knowledge of human dying to serve the dying into the pursuit of death.
Concluding Remarks
Assisted suicide or euthanasia is incongruous with the theological view that it is the weakest and the vulnerable who can teach us the values of life and the concepts of euthanasia or assisted suicide have an indirect message of discarding them. The right to die would soon deteriorate as duty to die to prepare room for fittest ones. Instead of looking for reasons to live, people will be looking for reasons to die. What is need is better understanding of death process and advancements in the palliative care of the terminally ill, rather than doing away with them. Until we know more about the death process, assisted dying debate should be kept on hold. More research in palliative care and allowing people to die naturally with dignity should be the concern of medical profession.
Evolution may be taking place in biological and spiritual streams and they are interconnected: biological sufferings maybe aiding spiritual evolution. 34. From a philosophical perspective, the rationale of terminal sufferings is to help the individual to disengage from the “pleasant illusions” of earthly life. The debate of assisted suicide raises the question whether human beings are mere electrical animals, quantum beings or fundamentally spiritual personalities-humans maybe all the three.The sanctity of human sufferings need to be brought into the equation of assisted suicide discussion. Assisted suicide would only add to the growing violence in the present world that could do with reintroduction of principles of non-violence.
USA may have better legal infrastructure to negate the unwanted and unintended errors of assisted suicide, but in many third world countries, where there is no such legal infrastructure, the procedure would easily get dishonoured. Oriental religions as well as Abrahamic faith traditions are opposed to ending life voluntarily. In general, all faith traditions believe that life that is nearing the biological end need not be preserved at all costs and that one does not have to go to extraordinary lengths to preserve a terminally ill person’s life. This means, for instance, that while a terminally ill person should not be denied basic care, he or she could refuse treatment that might prove to be futile or unduly burdensome for the dying person - passive voluntary euthanasia.
A scientific belief in after death existence is not without its pitfalls unless it is accompanied by the spiritual corollary of sanctity of earthly life. Science alone cannot highlight the sanctity of life; Divine standards are helpful in comprehending the sacredness of life. In fact, science has taken us to a cross road with Professor Schwartz’s new instrumental communication and it is time mark the boundaries of healthy survival research and the unhealthy ones.
Medicine is a dynamic science and discipline, which arise from the human need to face the suffering, pain and give hopes for better life. Since its inception, medicine has entered a career development that has brought great advances in science. Part of this momentum observed in medicine is defined as its reason for being, or rather, its primary goal, maintaining the health status in different populations1. This simple statement but becomes an object of great complexity which has received attention by many physicians and researchers from ancient times to the present, and in the tenth century, Ibn Hazm, a father of modern medicine enunciated the truth in this science was going to be impossible, since its dynamism is always present and the truth became a clear misrepresentation or significantly modified in the future2.
The goal of keeping adequate health status and prevent diseases has kept biomedical research in an alarming race in which the speedometer registering increases day by day. Today medical science is one of the most important sources of scientific innovation around the world; hundreds of manuscripts on health issues are published every day in multiple languages, in addition to numerous books and other non-official publications2-3. The increase in the medical literature during the last decade, led to think that the development of medicine has become a breakneck ratio, both the magnitude of the information obtained and its complexity.
However, the real reason for this phenomenon in biomedical sciences should be as a result of the new funding sources available for biomedical research either from the biomedical industry and government agencies. Each year new sources of money are offered to scientists to encourage innovation and the development of new ideas; and the resources existing to perform this goal increase. The OECD (Organization for Economic Co-operation and Development) suggests that countries spend about 500 billion dollars a year on research in biomedical sciences, including private laboratories and research institutes4. Medicine has become one of the most promising businesses in the economic field, and up today, and it is considered one of the greatest science future with wide range of prospects5.
Despite this encouraging situation, the concerning of development of modern medicine could be measured as a fundamental problem: the doctors and other scientists in charge of biomedical innovation are not trained in the administrative field. The above problem is clearly seen in different situation in the current medical and research practice, weak reflected on wasteful resource allocation processes6.
Each organization facilitating biomedical research resources requires that its resources are managed and used in an appropriate manner. Institutions demand to distribute funding for various interests not only in biomedical sciences. On the other hand, institutions have to verify the novelty and the ethical viability of the proposals, with the main idea of support ethical-approved studies, avoiding catastrophes in non-well-designed trials. Nowadays, as a result of better “quality control processes”, grant submissions involve a great number of administrative steps in order to be ready to submit any proposal. In this verification process, no only questions have to be addressed in term of sciences; a lot of administrative issues have to be explained in detail, including budget utilization and personnel management1, 4, 7.
Academics and scientists in universities are trained mostly in the technical aspects of their daily work, for this reason the horizon shows that the physician (M.D.) receives their training focus for the clinical management of patients, a doctor of science (Ph.D.) receive their training in the handling the samples to obtain the best results in the tests planned. In both cases, scientists are plainly educated out of the business and administrative field, leading important limitations with resources (personnel and funding) management3, 5.
Nowadays, the easiest application to obtain resources requires the approval of at least 5 different offices responsible for reviewing ethical, financial, legal, logistical, and scientific issues. Now back to the main problem in this discussion, the fact that medical researchers are not trained as integrated researchers (sciences and business), we are in the position to deduct that this condition may generate a bottleneck, specifically in this time where biomedical research are gaining a lot of power and interest in the industry8.
A potential alternative for this dilemma is to offer manager and administration training to researchers in order to be able to efficiently manage the resources requested. Masters degree programs are now available in health sciences management and administration, gaining popularity in the last five years. Researchers are more committed to show better profiles in their grant applications. Modern scientists must be people with a proven knowledge on costs and productivity that allows performing biomedical research with scientific quality combined with attractive financial management in terms of production2, 5, 8.
Postgraduate medical training should equip trainees with the skills, knowledge and attributes for independent practice1. They need to be equipped with the skills to become lifelong learners and continually develop their abilities throughout their careers by learning from colleagues, mentors, patients and disease. The challenge for clinical teaching is how to provide an optimal learning environment in which trainees can achieve their competencies for practice within a defined training rotation; both the limitations in the number of hours within a working week and the balance between learning and service commitments all can negatively impact on the educational experience of trainees2. Moreover, trainees need to balance their own development of skills, knowledge and attributes for independent practice against the requirement to provide high quality and safe healthcare3. The appropriate level of supervision must be provided to trainees performing any patient interaction and this is gauged by the trainer-trainee relationship, regular assessment and feedback. The clinical workload of a trainee needs to be finely balanced between overstretching them with tasks outside their competencies and being left with all the routine and menial tasks4. Thus whilst trainees should work within their competencies, they must be given the opportunities to expand their repertoire of skills, which may result in errors (and potentially patient harm) – supervision should limit these errors, which should be reflected on to provide a learning opportunity within a ‘no-blame’ culture5. As a trainee gains competence of their necessary skills, the amount of supervision required can be stepped down, until distant supervision (i.e. advice via a telephone) may be all that is required.
An understanding of how each learning environment within the hospital setting can be maximized may enhance the learning opportunities conferred upon trainees. Both technical skills and the professional attributes of being a clinician can be learnt in clinical and non-clinical environments. These learning environments will be explored in the subsections below.
Bedside Teaching and Ward Rounds
Bedside teaching is a stalwart of medical education, allowing clinical history and examination to be performed under guidance, in an appropriate setting and with relevant clues (observation charts, oxygen, etc.) present. This patient-trainee interaction provides an opportunity to develop professionalism and communication, and can also be the source of training of diagnostic techniques ranging from venesection and cannulation to more invasive techniques (e.g., pleural aspiration, drainage of ascitic fluid)1.
Presentation of patients during ward rounds allows a professional conversation between trainees and trainers to occur, which justifies their role in management and provides an insight into understanding and thought processes6. The multidisciplinary nature of rounds creates a community of practice7, allowing social learning to occur, and an opportunity to voice differing perspectives on patient care3. In order to maximize these learning opportunities, learning objectives can be discussed prior to commencement and reflection undertaken once they it has been completed6. Teaching rounds should be carried out when the ward is quiet, at a suitable pace, with regular questioning and opportunities for trainees to ‘lead’ the process8. Factors that hinder this educational process include time pressures, patients not being available, and the availability of trainees8.
Outpatient Clinics
Outpatients provides a mixture of new and follow-up patients that enables a trainee to learn management of patients in an ambulatory setting. Trainees may be in the same room as their supervisor (learning the basics of the consultation), or can practice semi-autonomously as their experience increases (with discussion with their supervisor as required); they must select an appropriate investigation and treatment plan, with a time frame for review, once the investigation or intervention has been performed3. Outpatient teaching is more highly valued by trainees and students compared to ward based tuition9. Factors that hinder this educational opportunity include room availability, time constraints, staffing levels and attitudes to teaching9.
Operating Theatre and Interventional Suites
Invasive procedures should be performed by adequately trained (or supervised) personal in the relevant area of the hospital (e.g. endoscopy, interventional radiology suites, theatre), with the necessary equipment and monitoring for the technique to be performed. Even before patients enter these environments, trainees have an opportunity to review the patient and their relevant investigations, discuss the procedure with the patient and obtain consent for the intervention1. Trainees can learn a wide spectrum of skills within these environments including both technical (both procedural related and anesthetic related) and non-technical skills, including Human Factors, anatomy, identification of instruments, aseptic technique, effective hand-washing and donning of surgical gowns10. Teaching invasive procedures represents a dichotomy for clinicians, not only do trainees need to gain exposure and experience in the relevant technique, but patients need to be prevented from undue harm. Prior to undertaking an intervention, trainees should be familiar with the relevant anatomy and physiology of the system they are about to operate upon, will have watched the procedure being performed and may have learnt the basics of the procedure in a simulated setting.
Trainees must to be able to self-reflect on their own skills and record of the number of procedures they have performed (which can act as a proxy for ability) to ensure that the correct level of supervision is provided alongside an intervention of suitable difficulty. Trainers need to be sure that their trainees have the necessary skills and knowledge to perform a technique, with experience often being gained in a stepwise reflecting both the difficulty of intervention and the gaining of skills, competence and confidence by the trainee11. This skills acquisition should be accompanied by regular discussion and feedback to maximise learning opportunities; when no supervision is available, trainees should consider video-recording the procedure as this allows reflection and review at a later date. A video diary can also be used as a portfolio of a trainee’s repertoire from beginner to expert during their training rotation. The challenge for trainees is to achieve competence in the relevant invasive technique within their training rotation; the number of interventions required to gain competence will vary between each trainee and technique11.
Handover
Handover allows the care of patients to be transferred from one group of individuals to another on a temporary or permanent basis. Handover confers an opportunity to present a clinical synopsis of patients with key information to ensure continuity of care and patient safety is maintained3. Most handovers are trainee led which provides an opportunity for peer learning to occur, checking comprehension and sharing interesting cases or tips for practice12. Handovers should be considered to be a high risk procedure, as communication errors can result in vital information being omitted; as such the process should be undertaken in suitable environment away from distractions, in a structured written and oral manner supported by an electronic format12. A further review at the patient’s bedside can be performed if required, which can highlight high risk patients.
Multidisciplinary Team Meetings
Multidisciplinary team (MDT) meetings are small formal meetings focused on all aspects of a patient’s care that involve a wide range of medical personal, nursing staff and allied health care professionals1. Meetings ensure that evidence-based guidelines are followed, and help to streamline management, removing unnecessary delays in treatment and improving cost effectiveness. MDTs represent a Community of Practice7 allowing social learning to occur as each individual can share their relevant expertise; MDTs enable best practice to be shared and help break down barriers between different specialties. Trainees can learn from the didactic teaching that occurs within the MDT (in relation to clinical details, investigation and management), but can also contribute to the meetings and practice their presentation skills.
Morbidity and Mortality Meetings
Morbidity and Mortality (M&M) meetings can help ascribe accountability and be used to highlight improvements in patient safety. They provide an opportunity for professional education, especially if the discussion can be held within a no-blame culture, and the meeting can voice discrepancies in how to manage patients, especially in ambiguous situations13. Trainees may be tasked with presenting a case and the potential learning aspects associated with patient care.
Grand Rounds/Formal Teaching
Grand rounds are traditional formal teaching opportunities that typically revolve around a case, whereby salient findings are presented prior to a discussion of management. These meetings allow opportunities for trainees to present cases and learn management, but their educational benefit may be decreasing as they are being replaced with lectures with limited clinical relevance14. However “audience apathy, deteriorating decorum and shrinking attendance” have diminished these learning opportunities14. Targeted teaching and the establishment of learning objectives for trainees can improve the educational content and the provision of feedback to the speakers can also enhance these meetings.
Journal Club
Journal clubs confer an opportunity for current scientific research and developments to be presented, critiqued and discussed by trainees. These clubs confer an opportunity to appraise the current literature and how that can be translated into evidence based patient care15. Journal clubs tend to be both voluntary and occur outside of working hours, resulting in highly motivated groups of participants whom are protected from interruptions.
eLearning and mLearning
Electronic learning (eLearning) and multimedia learning (mLearning) enable trainees to work informally, away from desks and computers, and at their own pace through a series of educational modules. Any intervention that engages trainees and promotes learning should be encouraged and these online learning platforms can be combined traditional learning resources should be promoted to ensure that all aspects of the curriculum are covered. mLearning in particular can be ‘dipped into’ allowing the learner optimal flexibility of how and when they want to use it. elearning can be referred to during point-of-care patient interactions when a trainee is unsure of how to proceed with patient management1. These increasingly important and under-utilized resources should be supported by educational institutions that support both undergraduate and post graduate trainees. By developing a virtual learning environment, individual tailored learning programs can be created that allow a trainee to develop and control their own online learning16.
Simulation
Simulation is becoming increasingly important for medical training. , anything can be simulated from learning clinical skills to human factors training, for both individuals and teams, focused on patient care and current medical practice in both the undergraduate and postgraduate setting. The availability of simulators coupled with competency based training and a decreased amount of training within the workplace has led to an increase use of this teaching format1. In addition, trainees need to understand how to use certain pieces of equipment prior to employing them on patients and this familiarity can only be gained in a simulated setting. Simulation can either occur within the workplace (allowing point-of-care simulation to see how teams react in a situation) or on formal taught courses; it can be low-technology and cheap (e.g., tying surgical knots on the back of a chair), but can also be high-fidelity and expensive (e.g., a virtual reality training simulator for laparoscopic operations), or use animal or cadaveric tissue. Simulation that increases trainee’s familiarity with certain techniques is likely to improve their clinical performance, decreasing potential patient harm and shorten the time taken for trainees to achieve competence1. A simulation should be completed with feedback from the supervisor to ensure that trainees gain the most from the session and clarify any facts or concerns about the simulation; a video recording of the session can also enable participants to reflect on their performance in a manner that is almost impossible in everyday clinical practice.
Bed bugs belong to the family Cimicidae and there are two species involved in the modern resurgence; the Common bed bug, Cimex lectularius and the Tropical bed bug, Cimex hemipterus. They are wingless insects with an oval-flat shape that allows them to hide in narrow cracks and crevices. The adults are dark brown, 4-5mm long, becoming to around 10mm when fully blood-engorged. There are five smaller juvenile stages (nymphs) that are similar in appearance, although lighter in colour. All nymphs require a blood meal to moult to the next stage, and both adults also bloodfeed for nutrition, and egg development in the case of the female. Bed bugs are solely haematophagous ectoparasites. After feeding they return to a harbourage and do not remain on the host. The main hosts are humans, but pets, bats, and birds may act as secondary hosts.
Epidemiology
In the past, bed bugs were particularly an affliction of the poor. However, in the early part of the modern resurgence it was the tourist areas and the hospitality sector that were initially impacted.1-3 Today, bed bugs have conquered quite diverse locations, ranging from hospitals, hotels and homes, to trains, cruise ships, and even airplanes. Most commonly, bed bugs travel in comfort as stowaways in luggage, although they can be transferred via furnishing and other belongings, as well by spreading to adjoining properties. Unfortunately, exact figures on the occurrence of bed bugs are unknown, as there are no mandatory reporting requirements. Additionally, due to the stigma associated with bed bugs, many infestations are simply not reported.
During the day, the largely nocturnal bed bugs will crawl deep into crevices of bed frames and mattresses (Fig.1), or behind wallpaper, and floor moldings. Here they tend to lay their eggs, often several hundred during the female lifetime. Live bed bugs, shed nymphal skins, and dark excrement spots indicate an active infestation. At night they are attracted by carbon dioxide, heat and other host odours to a victim, from which they may take a blood meal every 3-5 days. The adult bugs can survive long periods of starvation, up to five months at 22oC or even longer at cooler temperatures. When a host is found, they insert their mouthparts into the skin, blood feeding for 5-10 minutes. When bed bugs are in large numbers, often lines of bites occur on the unfortunate victim and this sign is almost a sure indication of the presence of the insect. The bites tend to occur along the arms and legs, down the back and across the shoulders.4,5
There has been long speculation whether bed bugs can transmit diseases, and in fact more than 40 different pathogens have been implicated. This has included Hepatitis B and C viruses, Human Immunodeficiency Virus (HIV), and Coxiella burnetii (Q fever). Recently, research has indicated that bed bugs are capable of transmitting the agent of Chagas Disease, Trypanosoma cruzi,in the laboratory. However, to date there is not one piece of evidence that bed bugs have transmitted any pathogen to humans.4,6
Clinical Features
During the act of feeding, saliva is injected which contains a variety of anticoagulants as well as other proteins whose function has yet to be determined. Contrary to popular belief, there is no evidence that bed bugs inject an anaesthetic. One protein, Nitrophorin, is involved in the transport of nitric oxide into the wound. This results in local vasodilation that increases blood supply to the feeding insect. The same protein can also induce a sensitivity to the bite.6
The diagnosis of Cimicosis is via the clinical appearance of the bite reaction and confirmation of an actual bed bug infestation (Table 1).3,5 The most commonly affected body parts are those that are left uncovered during sleep (Fig. 2,3,4), notably the arms, shoulders and legs. In young children, the face and even the eyelids can be bitten. Rarely, however, armpits are bitten, which are often preferred by other insects and ticks (Table 2).
Table 1. Bed bug infestation
Bites on the body
Wheals, 4-6cm in diameter, lines of bites
Any exposed body part
Often intense itching
Occasional central haemorrhage
Bed Sheet, mattress (clothing)
Small blood spots
Droppings (black dots)
Shed nymphal skins
Eggs, small (~1mm in length), white, oblong, glued to the substrate
Space
Pungent smell (mostly commonly noticed when an insect is squashed, or during the control program)
Table 2. Differential diagnosis of epidermatozoonoses
Bite preference
Pattern
Itching
Notes
Bed Bugs
Any exposed parts of the body, arms, legs, face, torso
In small infestations, bites will be random. In larger infestations, bite can occur in lines along the limbs and across the shoulder. Large wheals (up to 6cm across) may form, even some 14 days after the bite
Often intense, especially in the morning, but can be variable between individuals
Often associated with travel or used furniture
Fleas
Exposed parts of the body, especially the legs
Random, usually not grouped or in lines
During the day
Usually associated with pets
Mosquitoes
Exposed skin, particularly legs and arms
Random
Variable between individuals
Most commonly outdoors
Ticks
Potentially anywhere on the body
Erythema migrans with Lyme disease. Localised macules/papules at the bite site may occur
Low / no
Those who work or recreate in native forests are at greatest risk.
Itch Mites (Scabies, Sarcoptes scabiei)
Forearms, inter digital, genital area
Skin rashes, subcutaneous courses
At night
Most common in the elderly and infirmed
Harvest mites (Trombidiosis)
Skin surfaces under tight clothing
Red macules and wheals
Severe itching
Often occurs in gardens or meadows, most active during summer and autumn
Cheyletiellosis
Arms and trunk, contact points with pets
Polymorphic rash
Variable
Tends to be associated with pets
Bird mites
All over
Macular rash
Variable itching
Most commonly in homes as a result of birds roosting in roof cavities
Head Lice (Pediculosis)
In the hair of the head
Bar-shaped scratch effects with lichenification and hyper-pigmentation (Vagabond’s disease)
Night and day, generally mild itching
Most common in school aged children
Spiders, e.g. long-legged sac spiders
Arms, face
Necrotic lesion at bite site
Immediate severe pain, no itching
Uncommon
Figure 1: Typical appearance of bed bugs
Figure 2: Bites on the back, note the lines of bites common in moderate to large infestations
Figure 3: Bed bug bites on the arm, typical formation
Figure 4: Bed bug bites on the torso and arm
Figure 5: Bullae due to bed bug bites
Figure 6: Bed bugs, their droppings and eggs underneath a mattress
The degree of the bite reaction often depends on the level of prior exposure. With low level sensitization, individuals may develop a 1-2 cm wheal, with a small central haemorrhagic point. This haemorrhagic point can be recognized easily by diascopy. In contrast, a highly sensitized person will react immediately and may develop a wheal up to 15cm across (6 inches). If many bed bugs are present, an urticarial rash may develop as a result of the large number of bites and subsequent trauma to the area from scratching. On rare occasions, vesicles and bullae (Fig. 5) may form on the arms and legs. In the course of Cimicosis, papules that are extremely itchy may develop and can persist for several days to weeks. Due to the strong pruritus eczematous lesions, bacterial infections may occur, although this is extremely rare. There are case reports of systemic reactions such as anaphylaxis and asthma, although these are uncommon.
Through repeated exposure, some individuals may develop a tolerance to the bites. The clinical symptoms are then largely inapparent with small punctures at the bite site. Small blood spots are then the only clues that an infestation may be present.
Differential Diagnosis
Since reactions to stings and bites of various arthropods are non-specific, bed bug bites are commonly misdiagnosed. Single bites, notably that of other insects such as mosquitoes, fleas and biting midges may appear very similar morphologically (Table 2).
Consideration of where the bites are on the body can assist in the differential diagnosis. For bed bugs, lines of bites are very common in moderate to large infestations and this clinical picture is virtually unique amongst blood sucking arthropods. For the most part, the identification of the actual pest is required to confirm the diagnosis. Histologically, bed bug bites resemble perivascular eosinophilic infiltrates through the superficial and deep dermis, with minimal spongiosis.
Other possible diagnostic confounders can be various allergic reactions and other medical conditions such as urticaria, chickenpox, prurigo subacuta, and erythema multiforme.7,8 These do not show a central haemorrhagic point in the lesion which allows a correct diagnosis. However, in young children the diagnosis can sometimes be difficult.
Treatment
The treatment of Cimicosis is symptomatic. Local lesions can be treated with antipruritics e.g. Polidocanol 2-4% in Lotio alba (aqueous lotion) and topical antiseptic. Spirit of menthol may also be helpful. Local treatment with antihistamines is controversial. In severe reactions topical glucocorticoids such as Betamethasone may be required. In severe itching, the use of oral antihistamines is recommended. With infected bites, antibiotic therapy may be required. Uncomplicated bed bug bites tend to stop itching within 1-2 weeks, although temporary scarring from the bite may remain for several months.
Management
Treatment of patients with bed bug bites ultimately comes down to removing the source of the irritant, namely the eradication of the active infestation. Bed bugs have a typical pungent odor. This can be used to detect bed bugs through specially trained sniffer dogs that can rapidly locate the insects.9 Due to insecticide resistance, bed bugs are very difficult to control with traditional insecticides alone, and non-chemical means of eradication must be employed to reduce the overall insect biomass. Bed bug control should be undertaken by professionals trained in bed bug management, and the process may take some weeks to achieve.
Prevention
When travelling (1) always inspect the bed and surrounds for bed bugs hiding beneath the mattress and/or in seams of the bedding. Also, look for blood stains or small black dots (Figure 6, Table 1). (2) If present, request another room. (3) Always keep your luggage on the desktop or the luggage rack. A good preventative is to seal luggage in plastic or garbage bags during travelling, even when in transit. (4) When returning home, all clothing should be washed in at temperatures exceeding 60°C or frozen for one week with delicate fabrics. If there is no choice, then repellents containing N, N-Diethyl-meta-toluamide (DEET) should reduce the biting rate, but will not completely prevent all bed bug bites.10,11
Bed bugs can enter homes via an array of additional ways, particularly from objects bought second hand at flea markets or thrift stores, for example wooden frames, vintage clothes, furniture and the like. These should be heat-treated for a minimum of 10-20 minutes to kill bugs and their eggs.
Like doctors in other specialties, general medical practitioners (GPs) are exposed daily to human suffering which most of society try to avoid.1 The World Health Organisation (WHO) predicts that by 2030 depression will be ‘the leading cause of disease burden globally.’ And that 1 in 4 individuals seeking health care are ‘troubled by mental or behavioural disorders, not often correctly diagnosed and/or treated.’2, 3 Doctors suffer from stress, anxiety and depression (as well as vascular disease, cirrhosis of the liver and road traffic accidents) more than the general population.4-10 Help for doctors is inadequate and doctors are reluctant to seek help.1, 4, 11 Where improvement is suggested, it is usually as counselling and general support.11 Instead of ‘more of the same’, we suggest a radically different approach: Adaptation Practice, which Clive Sherlock pioneered and has taught since 1975. It is pragmatic and safe. This study tests its acceptability to a group of working doctors.
Doctors bear the responsibility for fellow human beings’ health, well-being and, often, for their very survival. Added to this, GPs are under increasing pressure from more patients who want more cures and from health service managers who demand clinical excellence and more administration and more managerial skills of them. GPs’ stress is related to increasing workloads, changes to meet requirements of external bodies, insufficient time to do the job justice, paperwork, long hours, dealing with problem patients, budget restraints, eroding of clinical autonomy, and interpersonal problems.6, 10, 12 The recent rise in the GMC’s Fitness to Practice complaints related to patients’ expectations of doctors is yet another stress making them feel threatened.13
Job satisfaction for GPs is at its lowest level since a major survey started ten years ago, while levels of stress are at their highest. In 2015 there had been a year on year increase in the number of GPs reporting a slight to strong likelihood of their leaving ‘direct patient care’ within five years, with 53% of those under 50 and 87% of those over 50.6
By nature and vocation, GPs want to help but too much pressure is unbearable and takes its toll. They work, not with numbers, data or profits, but with human suffering, which, inevitably, is an emotional burden because of compassion and because it makes them aware of their own vulnerabilities and mortality. 3, 14 When combined with heavy workloads and low morale, doctors themselves inevitably suffer emotionally and psychologically.7, 10, 14 At the same time they and others feel they should be invincible.1, 15-17 What professional help is available for them is inadequate.3, 4, 18, 19 Existing support services in the UK are underfunded and sporadic.4 Some are outsourced to counselling services, and some of these are by telephone. Doctors do not like to be counselled and are reluctant to use these services.4, 15, 17
Doctors themselves are the mainstay for diagnosis and treatment of mental illnesses but are not adequately trained.3, 20 Mental illness is not well understood and conventional treatments are insufficient and often harmful. 15, 20-23 Consequently, doctors do not have the wherewithal to deal with the emotional and psychological problems they face every day in their patients and often in themselves, their colleagues and their families.4, 12, 18
There is significant prejudice, stigmatisation and intolerance of mental ill health within the medical profession due to lack of understanding and fear.3, 4, 9, 15, 17, 20, 21, 22, 24 This not only affects how doctors treat their patients, it also exacerbates their own difficulties when they suffer with emotional and psychological problems themselves, and dissuades them from self-disclosure and from seeking professional help.3, 4, 8, 10, 18, 20, 25, 26 To succumb to stress, anxiety and depression is seen as being weak and inadequate as a person and in particular as a doctor. 3, 4, 15 Doctors think they should know the answers and should be able to cope.1, 4
However, doctors are willing to learn work-related skills as this present study set out to show.11 Adaptation Practice is training; not treatment or therapy. The course in this study was presented as a postgraduate programme for doctors to learn how to cope with stress, anxiety and depression.
METHOD
Recruitment
We asked by letter all 314 GPs registered in one UK urban and semi-rural Health Authority Area if they would be interested in a course of twelve fortnightly seminars to learn the basics of Adaptation Practice: a programme of self-discipline to cope with stress, anxiety and depression. Included, was the Hospital Anxiety and Depression Scale (HADS). Those who responded and whose HADS scores were ≥ 8 (the threshold for anxiety and depression) were invited to the course.
Stress, anxiety and depression
Anxiety and depression were assessed by the HADS and stress by a simple stress scale (SSS – see Table 1) one month before training started, immediately prior to training, at three months (mid-way through the training) and at six months (at the end of training).
Table 1: The Simple Stress Scaledeveloped by Clive Sherlock and used to assess the level of stress in a subject. A total score ≥ 8, out of a maximum of 24 is suggestive of a disturbing level of stress or burnout.
I feel I am under too much stress: 0 hardly ever 1 occasionally 2 most of the time 3 all the time
I feel exhausted: 0 seldom 1 some of the time 2 much of the time 3 most of the time
I care about other people: 0 as much as I ever did 1 rather less than I used to 2 definitely less than I used to 3 hardly at all
I have lost my appetite: 0 not at all 1 a little 2 moderately 3 significantly
I sleep well: 0 most of the time 1 quite often 2 occasionally 3 not at all
I am irritable: 0 not at all 1 occasionally 2 quite often 3 very often indeed
I feel dissatisfied: 0 never 1 occasionally 2 quite often 3 most of the time
I feel run down: 0 not at all 1 occasionally 2 quite often 3 most of the time
Evaluation of Adaptation Practice
Half of those GPs who applied for the course were unable to attend because of prior commitments on the days planned for the course. These acted as a control group. Those who attended the course were the study group. All those who attended were also assessed in private by the authors immediately before and throughout the course. At the end of the course the doctors wrote anonymous self-assessments.
Training in Adaptation Practice
Those attending the course were taught not to express and suppress upsetting and disturbing emotion, not to distract their attention from it (including not to think about it and not to analyse it) and not to numb themselves to it with chemicals (alcohol, recreational drugs or prescribed medication). Instead, they learned how to engage with their moods and feelings physically, not cognitively, and how not to engage with thoughts about them. They were instructed to practise this six days a week with whatever they were doing, wherever they were. They were all offered unrestricted confidential telephone and e-mail support from the authors between training sessions and after the course had finished.
Statistical Analyses
The results are reported as means ± standard errors of the means. The scores were normally distributed and the data were analysed by analysis of variance with additional paired comparisons within periods, using the LSD method. Correlations were determined using Pearson’s correlation. The analyses were carried out using the statistical software programme SPSS 17.0 for Windows.
RESULTS
Recruitment
Of 314 registered GPs, 225 (72%) responded to our initial contact, and of these 152 (68%) said they would be interested in participating in the training course. Recruitment was restricted to those with HADS scores ≥ 8. Of the 225 who responded there were 71 (32%) for anxiety, 35 (16%) for depression, and 79 (35%) for both. 29 (13%) applied to attend the course. All were experienced GPs. 15 of these attended and 14 were not able to attend because of pre-existing commitments on the course dates. They asked for alternative dates but these were not available.
At the initial assessment (one month before the course started) there were significant correlations between the scores for anxiety and depression (P < 0.001), anxiety and stress (P < 0.001) and depression and stress (P < 0.001). At the second assessment immediately before the course started these correlations remained highly significant.
Effects of Adaptation Practice
All those who attended the course reported a subjective improvement in their abilities to cope with their own stress, anxiety and depression, and in their sense of well-being.
Anxiety
There were no significant differences between the control and study groups either one month before the start (P=0.949) or immediately before the first session (P=0.914). The anxiety scores in both groups remained greater than 8 at both assessments (Figure 1). At the mid-point of the course the mean score had fallen slightly in the study group (Figure 1) but the difference was not significant (P=0.652) By the end of the course the mean anxiety score in the study group was significantly lower (P=0.008) than that of the control group (Figure 1). The mean scores for anxiety decreased over the 4 assessments. This tendency was significant in the study group (P=0.002) but not in the control group (P=0.567).
Figure 1: The mean anxiety scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of anxiety, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Depression
There were no significant differences between the control and the study groups either one month before the start (P=0.310) or immediately before the first session (P=0.880). The mean HADS scores for depression before training were all greater than 8 (Figure 2). At three months (the mid-point of the course) the difference between the mean scores in the two groups was not significant (P=0.631). At the end of the course the mean depression score in the study group was significantly lower (P=0.046) than the control group (Figure 2). The mean scores for depression decreased over the 4 assessments. This tendency was significant in the assessment group (P=0.003) but not in control group (P=0.689).
Figure 2: The mean depression scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of depression, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Stress
There were no significant differences between the control group and the study group either one month before the course started (P=0.234) or immediately before it started (P=0.505). The stress scores were all greater than 8 (Figure 3). At three months (the mid-point of the course) the difference between the mean scores between the two groups was not significant (P=0.621). At the end of the course the mean stress score in the study group was lower (P=0.077) than that of the control group (Figure 3). The mean assessment scores for stress decreased over the 4 assessments. This decrease was significant for the assessment group (P=0.001) but not for the control group (P=0.425).
Figure 3: The mean stress scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of stress, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Correlations
At all four assessments there were correlations among all three psychological parameters. At the initial assessment the correlation between anxiety and depression (r2= 0.405; P = 0.029) and between depression and stress (r2= 0.800; P < 0.0001) were significant but the correlation between anxiety and stress was not (r2= 0.253; P = 0.185). At the commencement of the course the correlation between anxiety and depression (r2= 0.479; P = 0.009), between depression and stress (r2= 0.765; P < 0.0001) and between anxiety and stress (r2= 0.486; P = 0.007) were all significant.
At three months (the mid-point) the correlation between anxiety and depression (r2= 0.526; P = 0.003), between depression and stress (r2= 0.622; P < 0.0001) and between anxiety and stress (r2= 0.790; P < 0.0001) were all significant and similarly at the and of the course: the correlation between anxiety and depression (r2= 0.604; P = 0.001), between depression and stress (r2= 0.577; P =0.001) and between anxiety and stress (r2= 0.740; P < 0.0001) were also all significant.
Assessments of the doctors’ psychological states and methods of coping
The doctors attending the course were assessed individually in private. They variously complained of stress, anxiety and depression. Notable findings included suicidal thoughts, plans for suicide, self-medication, excessive consumption of alcohol and an intention to leave the medical profession because of the unbearable pressures involved.
By the end of the course all these signs and symptoms had improved and the doctors felt confident in their ability to cope not only with pressures from outside but also with emotion, moods and feelings inside. One doctor still wanted to leave the profession but less adamantly than before, and stayed.
There was no qualitative assessment of the control group.
Qualitative Self-assessments
The anonymous self-assessment reports give meaningful, subjective accounts of what the doctors experienced individually. They fall into four main themes. There were no negative comments.
Connecting with emotion physically in the body
The following comments indicate contact with emotion:
‘I am more aware of my feelings.’
‘It is difficult to say “Yes” to unpleasant or upsetting feelings and situations. I have always preferred to avoid them and I have had a lifetime of suppressing emotions, so it is very difficult to say “Yes” to them, but this is what I am now doing.’
‘Since I’ve been more aware of my feelings there has been an enormous improvement in concentration.’
Developing inner emotional strength and coping.
A number of comments indicate the need to develop the strength to contain emotion physically in the body:
‘I am more accepting of daily stresses at work.’
‘I try to deal with problems instead of feeling so desperate and so wronged by them.’
‘I am calmer, and I lose my temper less often and less dramatically.’
‘The Practice was difficult initially because of my own resistances to it.’
‘I’ve always avoided seeking help for myself. I often feel worse than the patients I prescribe antidepressants for. I can now cope and I feel stronger but I don’t feel I’ve been treated and I now realise I didn’t need treatment: I needed to learn what to do and how to do it.’
Dealing with unpleasant, unwanted thoughts.
These comments illustrate the doctors’ new reactions to thoughts as they started to address the underlying emotion that normally drives worrying thoughts:
‘I now have less ruminations.’
‘As a long-standing ruminator I now realise these thoughts are the source of many anxieties. Thoughts were the main problem for me.’
‘I have learned to deal with obsessional thoughts by not giving time to them.’
General well-being.
The doctors commented on their sense of general well-being and ability to cope:
‘I am less tense and less anxious.’
‘I am now coping with episodes of work overload much better.’
‘I am feeling better generally.’
‘This has given me confidence to pursue the course of action I knew was correct.’
‘There are all-round improvements because of adapting myself to work and other people.’
‘I am happier and more content, optimistic and much less negative.’
DISCUSSION
Varying degrees of stress, anxiety or depression are universal.16, 26 Only about half of those thought to be clinically affected by these conditions seek help for them.26 If put into practice, sound medical knowledge and training can be beneficial to doctors’ own health.1, 11, 15 This does not seem to be true for stress, anxiety and depression.22 Too little is known about emotional and psychological problems, and treatment for them is inadequate.2, 9, 15, 17, 19, 21, 23, 28, 29
In this study, there was a high level of interest in how to deal with stress, anxiety and depression. Almost one third of respondents had scores on the HADS and SSS that suggested worrying levels of emotional and psychological problems amongst these working GPs. The fact that 152 doctors (68% of respondents) declared an interest in a six-month evening course (90 minute sessions after work on Thursday evenings) to learn how to deal with these conditions, suggests that:
stress, anxiety and depression are significant problems either amongst their patients or for the GPs themselves, or both
GPs are not confident in their ability to deal with them and want to learn more
although they have a strong tendency not to admit that they cannot cope and not to seek help, doctors are willing to attend a course to train and to learn.11
Most doctors tell their patients to seek professional help and to talk about their feelings but do not do so themselves.3, 5 They prescribe drugs for their patients that either the doctors will not take themselves or that they take but find ineffective. Of the 15 GPs on the course only one had mentioned psychological difficulties to a colleague and one to a partner and both only reticently. 16
ADAPTATION PRACTICE
Adaptation Practice strongly discourages self-disclosure, except in private to the Adaptation Practice teacher, which is necessary in order to assess the nature and severity of any problems and to lay the foundations for a rapport. Adaptation Practice sessions involve detailed discussion of moods and feelings as physical sensations and powerful forces that affect behaviour in all human beings. The ethos in Adaptation Practice is for participants to learn from their own experience how they are affected by emotion and how they can change this by containing themselves and not letting the emotion control them. It is not to criticise, judge, blame or condemn. Consequently, without the causes of stigmatisation, there is no prejudice and no stigma; instead there is respect and dignity and a pragmatic attitude to change.16
Adaptation Practice trains individuals to bear and endure upsetting, disturbing emotion by not expressing it, not suppressing it, not distracting themselves from it and not numbing themselves to it with drugs (alcohol, recreational drugs or prescribed medication). Bearing it this way develops emotional strength and resilience.
The high level of interest, the willingness to attend in groups and the positive results from this study indicate that Adaptation Practice is an acceptable way of teaching doctors how to cope with their own stress, anxiety and depression, that makes sense intellectually and emotionally. This, as well as the pragmatic approach mentioned above, makes Adaptation Practice radically different from other approaches.
GENERAL COMMENTS
Given that those who could not attend asked for an alternative day to attend, gave us reason to assume that the manner in which the study group and the control group were selected – individual availability on a given week night – would not have biased the sampling procedures and it seems reasonable to assume that the two groups did not differ in any meaningful way that would have biased the outcome.
Not surprisingly, there were strong positive correlations between anxiety and depression and between depression and stress on all assessments and between anxiety and stress on all but the first assessment, suggesting a strong association among these parameters of psychological states.
The mean scores for anxiety, depression and stress fell significantly in the participating GPs compared with the control group. The subjective reports from both the medical assessments and the self-assessments support these changes in the study group.
This study begs a number of important questions:
if doctors are prejudiced and stigmatise mental illness amongst themselves then what are their conscious, or unconscious, attitudes to mental illness in their patients? 3, 5, 9, 24
if doctors cannot cope with emotional problems themselves then whom are they and their patients to turn to for help? This is not the same as doctors suffering from physical conditions requiring surgery, or medications such as insulin or antibiotics.3, 5 Doctors expect, and are expected, to be able to cope with their emotions and, if necessary, that the treatment they give their patients will also work effectively for themselves
what are doctors to do and what are their patients to do, when doctors succumb to their own moods and feelings?
Adaptation Practice could be integrated in the medical curriculum at undergraduate and postgraduate levels, including Continuing Professional Development (CPD). Not only GPs but all doctors and other healthcare staff (nurses, physiotherapists, occupational therapists, social workers, etc.) could develop emotional resilience – which the GMC have proposed in recent years – and a better understanding of emotional and psychological problems and mental illnesses.
It is hoped that this preliminary study will stimulate and encourage a new way of looking at and investigating emotional and psychological problems and lead to further evaluation of Adaptation Practice.29, 30
With adequate training doctors and psychologists could teach Adaptation Practice.
Supporting Professional Activities (SPA) time is a part of each consultant’s new contract. When the new consultant contract evolved in 2003, a suggested breakdown of the week was 7.5 sessions (1 session equates to 4 hours) for direct clinical care (DCC) and 2.5 sessions for SPAs.1 This was driven by the need for consultants to continue their own professional development (CPD) as well as having the time for input into the development of trainees and medical students.
Examples of CPD work for consultants could include audit for improvement of service or patient care, teaching of patients, medical students or trainees, research, publications, aspects of hospital management and involvement in simulation courses e.g. Advanced Life Support (ALS)/Advanced Paediatric Life Support (APLS).
The General Medical Council (GMC) requires that during annual appraisals, doctors should use supporting information to demonstrate they continue to follow “Good Medical Practice”. This mandates that doctors should ‘take part in educational activities that maintain and further develop’ their competence and performance.1 With regard to revalidation, the GMC states you will have to demonstrate that you regularly participate in these activities; at Annual Review of Competency Progression (ARCP) it is imperative that accurate records of these CPD activities are presented at the annual job plan review.2
It is clear, therefore, that the provision of allocated time during the working week to complete these aspects of work life are deemed necessary for consultants. The Royal College of Anaesthetists and Association of Anaesthetists of Great Britain and Ireland both support the original view that a consultant should “typically” have 2.5 SPAs in their contract (though this would have to be subject to individual workload). With the demands of service provision it is clear that consultant SPAs are under threat, with around 40% of new consultants offered jobs with fewer SPA sessions than are thought necessary to allow sufficient non-DCC work.3
Since trainees are subject to similar appraisal and development requirements, we wonder if trainees should be allocated SPA time? For progression through training years and to pass the ARCP, it is necessary to provide evidence of trainee development within clinical practice in a similar way to consultants. This can involve a great deal of extra time. Once (notoriously difficult) exams have been passed, each trainee must go through the application process and prove what skills they have assimilated during their training to date. In fact, the ST3 anaesthesia application criteria states that the following are some of the ‘desirable’ criteria that require evidence:
Relevant academic and research achievements
Involvement in an audit project, or quality improvement project
Interest and commitment to the specialty beyond the mandatory curriculum
Evidence of interest in, and experience of, teaching
Instructor status in an advanced life support course (ALS, APLS)
Involvement in management…and understanding of management
Effective multi-disciplinary team working and leadership
Effective leadership in and outside medicine
Achievement outside medicine
Altruistic behaviour, e.g. voluntary work
The list is extensive and clearly requires a lot of time and input outside of the normal working week. With the expectation that trainees should be prepared to move straight from CT2 to ST3 (assuming their exams are completed), these desirable criteria must be addressed alongside completing other mandatory aspects of training such as, for anaesthesia: an Initial Assessment of Competency (IAC), an Intensive Care Unit (ICU) module, an Initial Assessment of Obstetric Competency (IAOC) and 15 Units of Training. With all these challenges between a core anaesthetic trainee and potential specialist anaesthetic training, there seems little time to complete an adequate number of the desirable criteria; this is a compelling reason to facilitate some time into the trainee contract to help produce more well rounded trainees.
However, therein lies the challenge - anaesthetic training is such a busy programme. Trainees are involved with multiple areas within a hospital such as ICU, theatre work or Obstetric Delivery Suite that they must learn and practice a wide range of skills to demonstrate the proficiency expected of a consultant anaesthetist. With experience of clinical work already at a premium due to European Working Time Directive hours, creating a good teaching environment whilst providing service provision is a hard enough task. It might seem difficult, therefore, to justify taking away yet more clinical time for trainees.
The proposed “7 day National Health Service (NHS)” contract could also pose more difficulties. Current example rotas released by NHS Employers demonstrate an increased likelihood of shift-work for a typical ICU rota.4 This shows trainees will be working more weekends and nights than at present, which could reduce the time spent directly with consultants. This would make introducing more non-DCC work difficult to justify as it would likely occur during daylight hours – when training could occur.
How it could be introduced:
Assuming SPA sessions for trainees were implemented, there would also be practical aspects to address. For example, how many SPA sessions to allocate for each level of trainee and how to monitor that this time was spent effectively and efficiently.
Monitoring:
Trainees could propose which aspects to focus on during their SPA sessions, such as management, teaching, quality improvement projects or more time in their sub-specialty interest. The goals could then be set at the initial educational supervisor meeting, much like a Personal Development Plan (PDP), and monitored throughout the year. This would give focus to any SPA time and ensure it is effectively used. If a trainee abuses their time or is not using it appropriately then removal of SPA time could be enforced. This would give the trainees more ability to improve the skills so often considered additional to trainees.
Funding:
In times of NHS austerity, funding would also need addressing. Potentially neither Deanery nor Trust might be willing to pay a doctor for days spent working outside the hospital workload – such as in educational roles or as a college tutor.5 A trial in one single deanery could assess the efficacy of such a scheme.
A possible solution would be to remove a few days of study leave allowance, as many trainees do not use their whole entitlement, and re-assign these to SPA time, allowing a trainee more flexibility. Trainees could initially start with fewer SPA sessions when more junior, to allow more clinical time, increasing SPAs to one per week for intermediate or higher trainees who may well be approaching their Certificate of Completion of Training (CCT).
Conclusion:
There are some practical difficulties in establishing trainee SPA sessions and no doubt many feel all contracted time should be spent practicing anaesthesia. However, given the changing way trainees are recruited via a ‘tick-box’ national application system, together with the variety of non-clinical skills expected by consultancy such as an ability to teach, conduct audit work, engage in managerial roles etc., a small change in the training set-up could produce more rounded trainees, benefitting anaesthesia in general and training programmes in the future.
Communicating effectively with patients and families is a vital component of high quality care. Studies have shown that patients feel excellent communication in consultations is vital for instilling confidence in the medical practitioner.1,2 There is evidence that doctors are not meeting this fundamental need.3
Some consider it an ethical obligation of doctors to balance their training needs against providing optimal care for patients. It is well known that junior trainees have significant level of performance anxiety that translates through to their consultations.4
Simulation based training is now an integral part of postgraduate curriculum in training a variety of medical specialties in managing acute scenarios. As an education method it provides a controlled environment in which it is safe to learn from errors,5 and improves learner outcomes.6 Simulation has been shown to be a valid approximation of true clinical practice.7 It therefore allows trainees to reach higher levels of proficiency prior to embarking on real patient encounters.
Current Core Medical Trainees (i.e. junior doctors who have embarked on the first stage of physician training within England) in the London deanery are expected to be able to manage complex communication scenarios effectively prior to entering specialty training. This is demonstrated by requirements set out in the Core Medical Curriculum, as detailed in Box 1. Whilst significant emphasis is placed on communication skills training in basic scenarios at a medical student level, there is very little formal postgraduate communication skills training within this deanery and others.
Box 1: Excerpts from Core Medical Trainee curriculum
Counsel patients, family, carers and advocates tactfully and effectively when making decisions about resuscitation status, and withholding or withdrawing treatment
Able to explain complex treatments meaningfully in layman's terms and thereby to obtain appropriate consent even when there are problems of communication and capacity
Skillfully delivers bad news in any circumstance including adverse events
This deficit in training led us to conduct a survey exploring Core Trainees’ views regarding communication skills training in the London deanery. Findings from the survey are detailed in Box 2.
Box 2: Results from Core Trainee Survey
83% received less than 2 hours of post-graduate training in communication skills since the start of Core Medical Training
Only 50% felt somewhat competent in engaging in difficult communication scenarios
88% reported significant challenges when conducting these discussions. They have had difficult on-calls experiences relating to communication difficulties
100% displayed interest in attending further Simulation Training in advanced communication skills
Method
We devised a pilot project using simulation to develop trainees’ competencies in advanced communication skills. After application to our local training board, we secured funding to run a number of sessions for core medical trainees within the London area.
The objectives of our pilot project were to provide experience of realistic communication based scenarios in a structured and safe environment to core trainees; provide feedback on trainees’ communication styles and offer suggestions for improvement; improve confidence of trainees in difficult communication situations.
Each session was conducted in an afternoon session and candidates were divided into three groups of three trainees who would remain together for the entire session. We ran four sessions, with a total of 36 trainees. Each group was facilitated by a consultant or a higher trainee in either elderly or palliative care medicine, given our focus on resuscitation/end of life discussions and assessment of capacity. We employed three actors to rotate around each group performing a variety of roles including patients and relatives. With a total of six scenarios, each trainee had the opportunity to participate in at least two scenarios lasting approximately 15 minutes, with feedback thereafter for approximately 10 minutes.
The scenarios employed were based on personal experience of regularly occurring, challenging communication situations encountered in our own clinical practice. We created detailed scripts for the actors as well as corresponding clinical vignettes for the candidates.
The scenarios were:
End-of-life discussion with a challenging family regarding a patient with end-stage dementia.
Discussing resuscitation with a family opposed to do not attempt resuscitation (DNAR) regarding an acutely unwell patient with poor functional baseline.
Discussing resuscitation with a young patient with metastatic cancer undergoing palliative chemotherapy who has little understanding of the terminal nature of the disease.
Assessing mental capacity regarding discharge planning in a patient with mild to moderate dementia.
Assessing mental capacity regarding treatment in a patient with moderate learning difficulties.
Assessing mental capacity in a medically unwell patient with mental health issues who wishes to self discharge from the ward.
Box 3 outlines the session structure.
Box 3: Timetable for the session
12.30-12.45:
Actors briefing
12.45- 13.00:
Facilitators briefing
13.00-13.30:
Core trainee briefing
13.30-14.45:
Scenarios 1-3 in small groups
14.45-15.00:
Tea/Coffee break
15.00-16.15:
Scenarios 4-6 in small groups
16.15-16.45:
Feedback and closing
Results
Written feedback was obtained from all participants by distributing a post-course evaluation form, with a 100% response rate. A number of areas were assessed via a Likert scale of 1 – 5, with 1 being ‘not at all’ and 5 being ‘very much’. 100% of trainees felt the content was useful and their knowledge/skills had increased. 100% felt more confident after the session and all trainees and facilitators felt this would be beneficial for medical trainees. A full breakdown of results is detailed in Table 1.
Table 1: Results from post-course feedback
The post-course feedback form allowed for free text feedback from participants, with some individual examples given below:
“Realistic scenarios - good opportunity to experience them and get feedback in a safe environment, good practice of common communication problems”
“It builds confidence in dealing with these situations and provides basis for building up ”
“This work dealt with complicated cases and actors were not too easy which I liked. Good and unforgettable”
Discussion
With the European Working Timing Directive and resulting shorter working hours, gaining proficiency in a number of key skill areas is limited due to reduced patient encounters. A recurrent complaint among core medical trainees is the lack of observed clinical encounters that leads to individualised feedback.
Feedback from more experienced speciality practitioners was only one component of our attendees learning experience. They also benefited from personal practise in a non-threatening environment, observation of their colleagues communication styles and finally learning through reflection with their colleagues
This innovation has shown a clear benefit in amplifying the confidence and preparedness of our core medical trainees in approaching these higher level communication scenarios. Future directions include introducing quantitative assessments pre- and post- course to objectively demonstrate improved confidence and performance. Providing the course to trainees in other specialties as well as across the multidisciplinary team would also be beneficial given the universal requirement of healthcare professionals to communicate skilfully.
Poetry is a way of expressing the subjective experiences that spill over the rational mind and it permits spontaneous overflow of subjective feelings. The ability to express oneself through poetry, and share that experience, is one of the unique human experiences that distinguish us from lower biological forms. The strife and struggle of modern men have made them miserable wretches on the face of this beautiful cosmos, and the technological revolution has taken the poetic sense from them; a time old coping mechanism. Those not capable of expressing their own sorrows and joys of everyday life in poetic words could find a surrogate writer in The Gushing Fountain.
In his collection of poetry, Dr Latoo (who is currently working as a Consultant Psychiatrist in United Kingdom) has catered poems for every mood and occasion: love, parting and sorrow, inspiration, rapture, memory, nature, solitude, and contemplation. Some of them are deeply personal and the author is trying to unearth a time capsule he had left in his native country of Kashmir. Dr Latoo appears to be searching for inner truths and making a self exploratory pilgrimage in his collection of poetry. Poetry has the power to describe and dramatize one’s own life, and Dr Latoo has done it well. The themes generally move from childhood to old age, love to grief, sorrow to joyfulness, aggressive nationalism to corrupted politicians, and depression to psychosis. There are pearls of mystical wisdom embedded in the poetry:
“Be choreographed by a great master for our sustenance Rather than just be a part of random unplanned accident?”
There are wise statements in “Divine Justice”:
“Anything like fatalism shall be a contradiction Of the Divine justice, free will and Lord’s will.”
All poetries have some hidden messages, and the book as a whole stands for immense moral values. “Woman” stands for women’s rights and dignity. The thoughts about the forgotten orphans are heart touching. “Behold a Man - Judging others” points towards the fallacy of judging other people without correcting oneself. Mental health professionals are particularly prone to this error because they are often professionally bound to assess their clients; we are only supposed to assess others and not judge others. We should not even judge ourselves, but only do self-assessment - God is the only Judge. The author writes about very ordinary humble human beings like the barber, Rupa, Ayesha, Ahmed, Puja etc. “Marriage” highlights the sanctity of wedlock. These poetries reflect the world view of the author. “Hold fast to thy dreams” may be inspired by Langston Hughes (1902 - 1967) and reminded me of my father who liked the verses of Hughes on dreams. “A raven who wants to be a dove” refers to people who pretend to be what they are not - wearing borrowed garments.
There are also poems about the author’s travelling experiences. A century ago, if a poet wrote about airport, he would have been frowned upon by the peer group, but in the 21st century it is appropriate to write such poetry. “Noisy airport and my mind” illustrates the hustle and bustle of contemporary life and gives the book a modern flavour. “By the Dal Lake” is nostalgic and the author is trying to recapture and share his lost Kashmiri literary Empire with the readers. Born in Kashmir, there is no surprise that the author renders beautiful nature in his poems. One wonders, if William Wordsworth were born in Kashmir, what would have been the content of his writings. Dr Latoo’s dual identity is evident when he writes about Kashmir and London.
In these days of global union through mere technology, poetry may have a serious role in the “international soul-union.” The days of regional poetry are over. Poets like Dr Latoo may be able to contribute to the formation of a healthier global village; poetry penetrates beyond the psychic realm into the spiritual dimension. There is a mission of peace and love in the Gushing Fountain, and the author is not enforcing any strong convictions on the readers. There is a poet-philosopher in the author of the Gushing Fountain.
The author has used rhyming and free verse styles of poetry. Metaphors and similes are appropriately embedded in various situations:
“A smile on our face blooms the gardens of her innocent soul A tear in our eyes arises from the blood of her bruised heart.” (From the poem, “Mother”)
Lyrical poetries are ravishingly harmonious and there are no repetitions. The thoughts are clear and there is an exotic element in all the poetry. On the whole, all the poems are cerebral and riveting. The works are relevant to the present century and can be appreciated by scholar and casual readers alike. Every poem is an experience to be savoured and memorised. Let these pieces of poetry echo and reverberate not only in the conflict-ridden valleys of Kashmir, but all around the world until they find rest in the minds of the waiting millions.
Psychiatry is going through an identity crisis because the newer medications are not as effective as expected to be and clinicians are turning to different forms of psychotherapy. Poetry/lyric therapy could be another form of psychotherapy that needs attention in the field of soft psychiatry. Dr Latoo’s book could be an inspiration and encouragement in this line of treatment. Hypnotherapists readily recognize that words are like loaded bullets and are highly potent. To an extent, poetry therapy involves the principles of both hetero- and self- hypnotherapy. Primitive and modern religions take advantage of the potentials of different forms of poetry in religious rituals for healing and promoting health.
A study of the mechanism of poetry writing is helpful in developing better conceptual models of creativity and deeper understanding of mental process. Sudden flashes of creative insight and other intuitive leaps, which arise from states of mind through intermediate steps that remain hidden beneath consciousness, and such ultrafast processing involving a concealed intermediate step, is consistent with quantum computations. A poet who enjoys superior mental health is capable of swinging from the unconscious quantum logic to the classical logic of consensus consciousness with an ultrafast speed. In psychotic states, “the quantum gates” do not shut swiftly as in normal mental states and the sufferers get trapped in the quantum logic. The usefulness of poetry therapy in psychotic patients, who get stuck in the quantum logic of the unconscious mind back to the classical logic of ordinary consciousness, needs further analytical studies. The primary aetiology of psychotic disorders may be biological, but secondary symptoms are quantum-linked and the new generation of psychotherapists have to learn the quantum meta-languages to communicate with psychotic and depressed patients. Poetry is such a source of quantum meta-language.
Poetry therapy promotes abstract thinking and develops imaginative powers. It is also a means of relieving and revealing innermost sentiments; it helps to ventilate overpowering emotions and hidden tensions. It is a form of self-expression and aids to build greater self-esteem; useful in strengthening interpersonal skills and communication skills. It would be valuable in repairing the assault of psychosis on the personalities of the sufferers. Quoting from my own memory lane, I became interested in poetry therapy when I comprehended the core problem of a patient who wrote:
“Moon, you shine at the centre of the sky, Catching attention from all over the world, Don’t you know that I am lonely?”
Poetry is of the heart and imagination whereas science is about reason and logic and may be grounded on contradictory principles. If science is about objectivity, poetry is essentially about subjectivity and to blend those human experiences harmoniously is a hard task; Dr Latoo has successfully achieved this goal. A man of science, when he writes poetry, has to liberate himself from the shackles of rationalism so that he can be a wholly free human: to be a poet one has to be a natural human being. To quote from Jean-Jacques Rousseau: “Man is born free and everywhere he is in chains.” Let us hope that the Gushing Fountain will have a part two and even more!
Population studies in Norway are showing that taking part of (creative) or receiving (receptive) cultural activities, i.e. arts, is associated with good health and good satisfaction with life among other things,1. Cultural activities have the potential to affect individuals beneficially: physiologically, biologically and emotionally, and several studies show that cultural activities can stimulate emotions and behaviors that make life easier, 2–5. Cultural activities can enrich and enhance our memory, stimulate connections among brain networks and enable us to accelerate learning and differentiate feelings of meaning and context,6,7 Cultural activities have also improved both physical health, social function and vitality among health care staff,8.
In an analysis of data from a large longitudinal cohort-study of a working population (called the SLOSH study = Swedish longitudinal occupational survey of health), some interesting associations were revealed between access to cultural activities in the workplace and health. Participants reporting many cultural activities at work had a more favorable improvement of emotional exhaustion during a follow-up period of two years than those whose workplaces did not offer these amenities,9. Other studies in which cultural activities have been offered to patients on long-term sick leave confirm that cultural activities have beneficial effects on both self-confidence and pain,10,11.
In a new approach, an artistic leadership program, called “Shibboleth”, affects not only managers included in the study, but also their employees (who did not participate in the artistic program). This one year art-based program showed statistically significantly more improvement of mental health, covert coping and performance-based self-esteem than the comparison group (who participated in an ordinary leadership program). They also experienced less winter/fall deterioration in the serum concentration of DHEA-S (dehydroepiandrostereone-sulfate), a regenerative/anabolic hormone,12.
Studies on singers, both amateur and professional singers and choir singers, show positive effects on different biological markers such as oxytocin and testosterone,13–15. On the basis of results from another Swedish project, ”Prescribed Culture”, which aimed to evaluate the effects of prescribed cultural experiences in the treatment of patients on long term sick leave, it was claimed that cultural experiences have their best effects when used in health promotion and prevention , rather than when the individual is already sick,16. Multimodal stimulation seems to have particularly strong effects. For instance, concomitant visual and auditory stimulation gives rise to stronger activation of “visual” and “auditory” parts of the brain than separate visual and auditory stimulation,17.
A mixture of different cultural activities seems to optimize influence on the limbic system since a broader emotional perception is activated,7. Cultural activities offered to participants that would not have chosen them spontaneously, could enhance already existing pathways in the brain enabling deeper cognitive behavioral change,17–20.
Despite this knowledge regarding the potential benefit of cultural activities in different contexts on both individuals and groups there is still a missing accessible practical functioning link between producers of culture and different groups of practitioners within health-care.
Burnout is characterized by emotional exhaustion, detachment from work and decreased effectiveness at work. This can develop in situations with excessive workload and insufficient resources as well as lack of control and support,21. If the process of burnout is a reaction to long-term stress, without enough recovery, this can lead to the more severe exhaustion syndrome,22. Symptoms include fatigue, impaired emotional regulation, cognitive problems and sleeping disorders. Most of these patients have an increased sensitivity for stress even after recovery,22. In recent years, Swedish rates of sick leave due to minor psychiatric morbidity , and burnout symptoms, have increased dramatically,23-24 . Complaints usually include physical, emotional and cognitive exhaustion, which in most cases appear to be related to chronic stress without restitution,25–28. Today many women in Sweden have stress related symptoms, and some are diagnosed with exhaustion syndrome. If these women are detected at an early stage, the prognosis is good,22.
Alexithymia, (the difficulty to differentiate your own and others feelings), can be a silent but severe problem for persons suffering from this personality trait. Grabe et al.,29 conducted a study in which the questionnaire TAS-20 was used for the assessment of alexithymia. Medical examination was also performed. In this study alexithymia was related to hypertension and arteriosclerotic plaques. Alexithymic personality traits may increase the risk for CVD (cardio vascular disease).
The rationale behind choosing symptoms of exhaustion, SOC and alexithymia as main outcome variables was the intention to examine whether cultural activities in this form can change pattern of thought, feelings and behavior in participants with burnout symptoms. If cultural activities prove effective for this participant group, they could have considerable benefits both financially in terms of reducing sick leave and health care consumption and of reduced individual suffering.
Aim
The aim of the study was to assess to what extent symptoms of exhaustion, sense of coherence, alexithymia and self-rated health among women with burnout symptoms can be beneficially influenced by cultural activities organized in health care centers.
Method
Participants
Four health care centers in Stockholm County hosted the cultural activities. Medical doctors and social workers distributed information about the study to women diagnosed with exhaustion disorder or exhaustion symptoms. Women, native and foreign born, with burnout/exhaustion symptoms (fatigue syndrome or stress-related fatigue) who were curious about new clinical approaches were asked by the doctor to participate in the study and screened for inclusion and exclusion criteria. Participants (women age > 18) with burnout/exhaustion symptoms such as strong fatigue, cognitive problems, and sleep disturbances were enrolled. There was an inclusion criterion with a score above 2 on the KEDS scale. The diagnosis was made by the doctor.
Exclusion criteria: Participants with difficulty in speaking and understanding Swedish, participants with alcohol or drug abuse problems, or/and participants with severe depression or psychiatric borderline. Also excluded were participants with severe somatic diseases (such as serious angina pectoris or participants who had had a stroke). Randomization was done using a 3:1 allocation to intervention or control groups.
The randomization was done using a stratified randomization by center. Randomization was done by the statistician. The group allocations were sent in individual envelopes which were distributed to centers and blinded to the site staff. Envelopes were further drawn in a consecutive order with regard to recruitment of subjects at each of the four health care centers. Thirty-six participants were allocated to the intervention group (nine patients in each group) and twelve participants to the control group. The standard care that each participant received included physiotherapy such as relaxation and physical light training.
All randomized participants gave their written consent to participation in the study. Data were collected over a period of 6 months. The project includes evaluation of six different culture activities. In the selection of the health care centers socio- economic diversity and employment status were considered. We used regularly occurring structured cultural activities in cooperation with culture producers, i.e. actors, musicians, dance teachers. The Regional Research Ethics Committee of Uppsala has approved the study (Dnr. 2012/359).
The culture palette: six different cultural packages
The following cultural activities were included in the study; five of them have previously been presented in the literature with good evidence on other groups of patients. One package (the musical show), which has not been presented previously on groups of patients, was chosen as it represents a combination of different modalities of activities at the same time. The active mechanism of all six cultural activities was to stimulate different modalities of the senses such as the visual, motor, verbal, auditory, emotional and sensational, according to Downing’s levels of perception, 30. All participants were offered six cultural packages:
1. Interactive theater: An experienced actor introduced poetical lyrics and poems and then initiated and participated in discussions with the participants regarding thoughts, emotions, and experiences evoked by the texts.
2. Movie: After showing a movie, a film expert initiated discussions among the participants about experiences and thoughts evoked by the movie.
3. Vocal improvisation and drawing: After participating in a vocal improvisation session with an experienced performance artist and pianist, the participants painted a picture representing emotions, thoughts and pictures evoked during the improvisation
4. Exploring Dance: The participants improvised dance movements under the guidance of a dance movement pedagogue/music teacher. The dance movements were staged according to the situation in the room and with focus on bodily awareness. Afterwards the group discussed their experiences during the dance session.
5. Mindfulness and contemplation: The participants contemplated and practiced mindfulness together with an experienced mindfulness instructor. Attention was on breathing and body awareness. Thoughts, feelings, images and sensations were in focus and experiences were reflected in the group after the contemplation.
6. Musical show: after a musical show including music, song and dance focusing on bodily awareness, the participants discussed thoughts regarding the body with the actor.
Every session in each one of the six different cultural packages lasted for 90 minutes. Evaluations
Three different standardized scales, and also self-rated health and self-figure drawing, were used.
KEDS - Karolinska Exhaustion Disorder Scale,31. Questions about concentration, memory, physical fatigue, endurance, recovery, sleep, hypersensitivity to sensory input, experience requirements and irritation and anger. Higher scores indicate worse disease activity/performance.
SOC - Sense of coherence,32. A key factor in being able to feel well-being and health. This factor has been shown to be crucial to helping individuals mobilize their self-healing systems. Higher scores indicate better performance.
TAS - Toronto Alexithymia Scale,33. Estimation of ability to recognize and interpret feelings in oneself and others. TAS contains three subscales; the inability to handle emotions due to emotions being poorly recognized (difficulty recognizing), the inability to describe feelings (difficulty describing), and mismatch between coping behavioral emotions (externally oriented thinking). This study used the full scale score, i.e. the summary of the three sub scores. Higher scores indicate worse performance.
Self-rated health (SRH) consists of a single item measure.
Procedures/implementation
The four different health care centers presented each activity on two consecutive occasions. After two weeks of one program, there was a new program on two consecutive occasions etc. Each participant has thus been offered 12 cultural packages during a three-month period, i.e. once a week. During the monitoring period between month 3 and month 6, there was no culture activity offered. The control group was monitored in parallel during the entire period monthly at 0, 3 and 6 months.
The participants evaluated the project individually with questionnaires prior to the sessions, after completion of the intervention at month 3, and at follow-up after 3 months i.e. month 6 (both intervention and control group). In-depth interviews with both participants and producers of culture, i.e. representatives for the various cultural activities and health care staff were conducted during the monitoring period (this data is not presented in this article).
Data analysis
The primary outcome efficacy end point/measure was mean change from baseline to three and six months in the KEDS summary score. The secondary outcome measures were mean change from baseline in the SOC summary score, the TAS summary score and the self-rated health, from baseline to three to six months.
All data were presented using descriptive statistics, i.e. mean and standard deviation for continuous variables and frequency and percentage for categorical variables. For all main outcome variables, data were further analyzed using the Linear Mixed Models, including group (intervention and control) and time (baseline, 3 month and 6 months) as fixed factors. Results were presented as marginal means, the estimated mean value adjusted for the factors included in the analyses model. The difference between intervention and control group with regard to the estimated and adjusted means are defined as the effect size, i.e. the mean difference between the intervention groups for each of the primary and secondary outcomes measures divided by the standard deviation. All tests were two-tailed and p<0.05 was regarded as statistically significant.
IBM SPSS version 22 was used for statistical calculations. In the presentation of the results from the statistical analyses, the measured effect size was used and derived as the absolute difference between active intervention and controls with regard to each of the outcome variables/endpoints used,34.
Results
There were 55 participants screened in this study, however seven participants who met the exclusion criteria of too serious/severe depression was not included into the study. In total, there were 48 participants randomized into the study, age between 41 and 70 years, mean 53.8 (SD= 8.15).
The results showed that for KEDS (exhaustion) there was a statistically significant two-way interaction (P<0.001) with a decreased mean from baseline to three and six month respectively in the intervention group whereas in the control group there was no change. The mean treatment effect size, i.e. the mean difference between groups, in favor of the intervention group was 9.9 (SE=3.0) at 6 months. See table 1 and figure 1a.
There was no difference in mean SOC - Sense of Coherence – scores between the groups. See figure 1b. Further, the results revealed a statistically significantly more pronounced decrease in the intervention group compared to the control group in the alexithymia items of total score, (P=0.007, mean treatment effect size=5.4 (SE=2.2) at 6 months in favor of the intervention group), difficulty describing (P=0.004, 2.4 (0.9)), difficulty identifying (P=0.051, 2.6 (1.3)) but not for external orientation (P=0.334 0.5 (0.8)). See table 1 and figure 1c. There was also a statistically significant difference between the groups with regard to self-rated health (P<0.001) where mean scores increased over time in the intervention group but decreased in the control group. See figure 1d.
Table 1
KEDS (Karolinska Exhaustion Disorder Scale) and TAS (Toronto Alexithymia Scale) and SRH (self-rated health) at baseline, month 3 and month 6.
Control Group (n=12)
Intervention Group (n=36)
Count
Mean
Standard Deviation
Count
Mean
Standard Deviation
KEDS
Baseline
12
32.7
8.2
35
31.7
8.4
Month 3
12
34.9
9.2
34
23.6
8.6
Month 6
12
33.9
8.7
33
23.7
10.1
Sense of Coherence
Baseline
12
117.2
29.9
33
118.0
28.0
Month 3
12
112.8
30.3
33
121.1
30.5
Month 6
12
115.1
24.2
34
123.9
28.2
Difficulty Describing
Baseline
12
14.8
4.3
34
14.2
4.6
Month 3
12
15.3
3.6
31
12.7
4.6
Month 6
12
15.2
4.1
34
11.8
3.9
Difficulty Identifying
Baseline
12
20.0
6.0
34
20.3
6.3
Month 3
12
20.6
6.5
31
19.0
6.9
Month 6
12
20.0
6.1
34
17.4
5.0
Externally Oriented
Baseline
12
14.9
4.2
34
13.8
4.4
Month 3
12
15.4
4.3
31
13.9
3.9
Month 6
12
14.6
4.8
34
13.2
3.5
TAS
Baseline
12
49.7
13.1
34
48.3
13.4
Month 3
12
51.3
13.3
31
45.6
13.9
Month 6
12
49.8
13.9
34
42.4
10.8
Self-rated Health
Baseline
12
5.2
1.5
36
4.8
1.9
Month 3
12
4.6
1.9
36
6.0
1.9
Month 6
12
3.6
1.6
35
6.4
1.9
Figure 1a
Marginal means and 95 % confidence intervals for the KEDS (exhaustion) scale by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Figure 1b
Marginal means and 95 % confidence intervals for the sense of coherence (SOC) scale by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Figure 1c
Marginal means and 95 % confidence intervals for the Toronto Alexithymia Scale (TAS) by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Figure 1d
Marginal means and 95 % confidence intervals for the self-rated health scale (SRH) by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Discussion
The results show that the different exhaustion factors measured by means of KEDS (Karolinska Exhaustion Disorder Scale) decreased in the intervention group compared to the control group. With regard to the total score of TAS (Toronto Alexithymic Scale) there was a statistically significant decrease in the intervention group compared to the controls, i.e. the participants started to improve their differentiation of feelings and emotions after three months with cultural activities. The same pattern was seen with regard to self-rated health, which improved in the intervention group. However, there was no significant difference between the groups with regard to the development of sense of coherence.
It seems that the different cultural activities have helped the participants become more aware of their feelings and sensations; to describe and to identify feelings. It is not easy to explain the positive results based on one clear paradigm. It is likely a mixture of psychological, neurological and social factors or changes that interact in a complex manner.
Previous studies have discussed the theory of the emotional brain - cultural modalities can “surprise” the cognitive brain unconsciously. LeDoux,20 discusses the upper/slower and the lower/faster pathway in the brain. Emotionally loaded visual and auditory stimuli are transmitted on both types of pathways. Music impulses are for example evoking activities in the emotional brain much more rapidly than in the cognitive brain. However, impulses spread secondarily from the emotional to the cognitive brain. This can trigger the participants awareness of different emotions and may start a process of differentiation, possibly initiating a change of life course. By using different cultural activities, that the participants normally would not try, the differentiation process may be amplified. This suggests that cultural activities can surpass automated thinking and create new "pathways '' with changes in behavior and increased well-being.
In other studies we have observed that a mixture of different cultural activities can increase the amount of stimuli affecting a broader network of emotional correlates, 14,16,18 . A very interesting long-term decrease in alexithymia, 35 was associated with lowered blood pressure and a decrease in sick leave. By allowing the participants to try new cultural stimuli we may have helped the participants change old habits. A hypothesis is that this may also have contributed to the observed decrease in exhaustion.
Why did we not see any increase in the sense of coherence in the intervention group? It is very difficult to change patterns of thought and behavior although we can argue that the participants in the control group also found a new sense of coherence just by being invited to answer questions about themselves and being focused upon. Many of the participants did not go out spontaneously because of their fear of socializing. Some of them described their situation as black or white, not wanting to change routines that made them feel less safe,36.
Despite the fact that the health care staff did not participate in the culture palette, they were also affected by the cultural activities 36. This may be a mirroring effect, or emotional contagiousness on health care staff, which may also play a role between the participants and their staff. The passive cultural activation phenomenon has previously been presented in the literature,37 and there seem to be possible well-being effects of just watching dance or visiting a theatre, 6,10 which may explain the positive health care staff response to the culture palette. The results of this study underscore the importance of regarding the health care system as a whole, where patients, health care staff and visiting relatives affect each other. Empathic behaviors contaminate in all directions and we need to be aware of how we project ourselves when working in a caring context.
Modified “culture palettes” and “train the trainer” programs and workshops are now in use in Sweden, inspiring cultural producers to further develop the health care system and a cultural health box - a box with six different books about cultural activities and the research behind this - have been distributed to all health care centers in Sweden, 38.
Developing and adapting cultural programs to fit other kind of groups of participants could cross-fertilize health care thru culture production.
Limitations
This study was limited to women with exhaustion symptoms and therefore further research on implementation of cultural activities within different groups of participants and sexes is needed before we can generalize the results to other groups of participants. Another limitation is that we did not control for outside activities, such as doing walks in nature. In this study we only presented indoor cultural activities.
Conclusion
The cultural activities in this study made exhausted women understand what makes them vital, confirmed, curious, healthy and creative. The study also illustrated that there could be synergistic effects when bringing cultural activities into the health care system36.
Once upon a time there lived a quite wealthy young man - in the sense that he was quite smug and comfortable, never really wanting for anything. ‘Wealthy people don’t have to concern themselves about others or indeed material matters, he used to say to himself, blissfully unaware of the dramatic irony in his statement. He had tons of clothes (which made it difficult to decide what to wear each day), lived on his own in a big house almost the size of a mansion, went on lots of holidays to exotic places, ate in the best restaurants, and by all accounts had no worries whatsoever. He was a man of modest intelligence, quite tall and stout with an arrogant (or should I say confident) manner. He could quite easily win an argument because he would literally wear his opponent down with the ferocity of his delivery, even though it bore little substance. 'I could be a politician because I am so good at debating sensitive issues which affect ordinary people, he would reflect when on his own, which was frequent.
His parents had so much money (from their banking business) to fritter away and therefore had no trouble finding him a suitably big house (almost as large as a mansion as stated) in a fashionable area of London. He also owned a house in Richleymanor, a wealthy, prosperous suburb of Richleyshire. ‘Because I have no worries and am in perfect health', he said when he was only 16, 'I am going to become a doctor and heal people who are not rich enough to see me privately and who are a million times less fortunate than me.' Such was his altruistic spirit. And so he studied as hard as he could because he had to (he was not the brightest card in the pack). With the help of his parents' influential circle of friends in the whole of Richleyshire who knew people in high places, he managed to secure a place in an elite medical school where only top doctors were trained - even though he did not possess any outstanding qualifications on leaving school. But that sort of thing doesn’t really matter if you possess an altruistic spirit. 'I mean', he reasoned, – 'Lots of famous people (including entrepreneurs) did not pass their final school year exams with Honours and I am just like them in that respect - really down-to-earth, a man of the people.'
On the first day of entry to the Royal Breedington University Medical School he was already planning his future career. Not for him the humdrum life of a family doctor. No - he was aiming for prestige and acclaim. He did not need the money though extra money would help 'because you can never have enough, especially if you want to help others less fortunate than yourself', he would say to himself. Such was his determination. 'Should I become a great brain surgeon', he pondered one evening. Should I become an eminent cardiologist or a revered obstetrician? You see, for him it was not enough to be an ordinary doctor - one had to be special in some way. These careers and others (the field of Medicine is huge) he considered. Then one day he decided: 'I know now what to do'; I will get my basic qualifications out of the way and then embark on a career in Mentalology - a subject which was gaining great interest in the popular press. Even students at the University were talking about it. It was a higher degree than Neurodevelopmental Psychobabble (another much sought-after career, normally the reserve of doctors studying cerebrotherapy). So after lots and lots of postgraduate courses in Mentalology he finally passed the higher degree, becoming a member of the Royal College of Mentalologists (MRCM), spent 5 more years in training and became a Consultant Mentalologist at a very prestigious hospital, one which had links to a university, as it happened. His ultimate ambition was to become a Doctor in Medical Politics because he wanted to be in charge of doctors and patients but without the encumbrance of having to care for patients per se or to actually meet doctors. Not for him the drudgery of life in a hospital or general practice – no - one needs to earn as much as possible by doing the least work, rather like Business Executives, he would ruminate.
Initially he enjoyed seeing a few patients here and there as par for the course, but because he felt he was a very important doctor, he needed to move up the ladder to the higher echelons, managing other doctors who might in turn benefit from his great wisdom and enormous insight, accrued in just 8 years training! He decided that he was too important to be seen hanging around hospital wards or in the outpatient department and so spent nearly all his time in the library and at meetings, apart from breakfast and lunch. He always had breakfast in the hospital canteen to show he had the common touch, and sometimes he would make a point of staying on longer after lunch in order to mix with other not-so-important doctors, who would laugh and grovel obsequiously at his every spoken word. Then suddenly he was off, and would be seen bustling and rushing through the canteen doors on his way to a very important event at the prestigious headquarters of the Organization, where he would sit three seats away from the Lord High Superexecutive Chief of the Organization (LHSCO), a very long title indeed but when one is important one usually has imposing if not long titles. Such was the circle the very important doctor was mixing, it explained why he was hardly ever seen in the hospital outside lunch hours or breakfast. Because, you see, in his estimation or rather esteemed opinion, if one is not around much then one must be a very important person indeed.
Sometimes he was seen rushing off to other very important meetings at a top-class hotel where there would be a special Conference Room; sometimes he was at meetings all day. However, often it was difficult to find out exactly what he was doing or where he was because many of the meetings were high level top-secret meetings; for example, a Superexecutive meeting lasting a whole hour might have on the agenda a motion to close down the hospital outpatient department because patients were costing the Organisation too much money. That superfluous-to-requirements money could be better spent on holidays and pay rises for other but not-so-important medical chums as well as serious-minded managers who in turn might do him a favour later on. 'You never know what's around the corner', he always used to say in one of his contemplative moments. The Organization often talked about very big issues such as Doctor Management Downcasting (how to keep those grasping medics in line) and Patient Empowerment, even though patients were never included in any discussions about where they would go when their hospital closed down. Sometimes meetings would extend until the early hours of the morning, which suited the very important doctor because he had no family to worry about or other personal commitments and could come and go as he pleased. Others had to stay on at the very important meetings regardless of their personal circumstances. Sometimes he was so exhausted attending meetings he would spend the following afternoon on the golf course relaxing before attending another evening conference. 'I don't know how he does it', his reverential colleagues would mutter, in hushed tones. 'He deserves another award for taking time off to recharge his batteries for the next meeting'. 'It is quite astonishing how much energy some people have', he would say contentedly to himself.' 'What would the Organisation do without someone of my great leadership skills’?, he asked himself many times in a semi-congratulatory tone.
Nothing would deter the very important doctor from achieving his goals and pleasing the Organisation. After all, this was the way to the top of the medical hierarchy – Doctor of Medical Politics (DMP) and Chief Scientist and Supervisor of the Faculty of Mentalology (CSSFM for short) was his goal. First he set out some decrees or edicts. These would all come under the rubric 'Management Directives', or put in another way, informing his colleagues in a polite but firm manner how he would delegate them to do ‘this and that', and therefore no one would blame the very important doctor for say, dismantling any part of the service; besides, his sheer tenacity and doggedness (character traits which he had cultivated from his seniors) gained him further admiration from the legions of subdoctors (doctors who were under his control) who had to yield to his commands. He would sometimes act very humble when questioned about his ruthless tactics and would feign innocence (or was it impotence) in the face of criticism. No, it was the Organization 'calling the shots', as he used to describe it, callously ignoring the plight of his colleagues and patients.
It was strange that he could never recall or at least did not seem to know any of the names of people in the Organization who were responsible for the targets to be achieved. 'Anyway, most patients are not really ill, they just complain and they can jolly well go back to their own general practitioner if they want to bother someone', he would argue in one of his rare insights into the human condition, particularly when colleagues challenged him. His doctor 'associates' (he could never really truthfully call them friends) were stupefied by his perspicacity and visionary zeal and were in no doubt that in order to achieve a change in their practice it was better they were paid less and worked more intensely between 9am and 5pm. They could come in earlier or stay later if they wanted to of course, but no extra money was available for overtime because it was costing the Organization thousands of pounds annually. Best to give the bonuses to those who really deserved them - those Manager Doctors who were extremely busy writing protocols about Best Practice and Risk Assessments - real life-and - death issues, and spending at least 4 hours every six months at very special high-powered meetings drafting 'outcome protocols'. So many emails to send out. This agenda was 'all in a day's work' for the very important doctor who needed to supervise this superhuman task in between meals.
But even the very important doctor himself needed resources and time to carry out all this work. 'I know what', he said to himself one bright sunny Sunday morning on the golf course, - 'I will reduce the amount of time doctors spend seeing patients and cut costs further in this way for all those dedicated doctors because dedication is costing too much'. One hospital in-patient could cost the Organization £1000 a week, even more. 'The doctors can still attend meetings in the hospital (no costs incurred) and do extra administrative work.' 'The bonuses will only go to those who have achieved a special distinction in doing the work of Managers and follow the party line'. 'Yes, that's the way forward', he thought to himself, in one of his rare flashes of brilliance. 'From now on doctors will only have to work 9-5pm'. 'The on-call commitments can be covered by NHS Indirect', the latter being a new company set up to replace doctors and nurses at night-time and weekends, usually manned by staff from one of the local supermarkets. Surgeons would be then free to down tools at 5pm instead of wasting time (and the Organization's money) battling through endless hours of unnecessary exhaustive operations such as cardiac bypasses or hip replacements, which could easily be carried out in the patients' homes anyway. Psychobabble experts could use tick-box rating scales or instruments to assess new referrals (no need to see patients, too costly).
There is no way to describe the tumultuous reception these ideas received at the Managers Annual Conference in Bristol, and the very important doctor received even more accolades. In fact, he was considered for a Rhodium Medal, the highest award in the land given to any doctor. Before being conferred with this precious and prestigious medal (because it can only be worn around your neck, or else it lies on the mantelpiece where nobody really notices it) he was given two lots of pay rises - one for services to the Organisation, the other for keeping the common grasping subdoctors in line by forcing them to sign in and out of work every day and by reducing their salaries. After all, there were rumours that the grasping, greedy subdoctors were beginning to think that perhaps the very important doctor was becoming too very very important. But they kept quiet in any event.
His great achievement was the setting up of SCRAP (Strategic Commission for Rapid Abolition Programme) which set out a one-year plan of how to prevent any patient being seen by a doctor. The patient could be seen by any number of people, from the tea lady to the hospital porter, who were already working flat out on the minimum wage. At least they were not so expensive to keep on the pay roll. The next brilliant idea he concocted was to replace the word 'patient' with 'customer'. 'Patient', he did not like. It gave the impression that someone was ill and needed to see a doctor. But with the New Opinion About Hospital Patients (NOAHPS in short) charter, the word 'patient' did not fit the profile of an enterprising Organisation and so NOAHCS (New Opinion About Hospital Customers) sounded much better. All staff were thence ordered to use this terminology or face the consequences. It was rumoured that it was a sacking offence to use the word patient. He even sent an email to the same effect around the whole Organisation. No one spoke out for fear of reprisal and possible instant dismissal. He was applauded at every Organization meeting from that time on and was rewarded by being given Freedom of the Hospital. This meant he did not have to do anything really - just walk around shaking hands with everybody, telling them what a great job they were doing, and so forth. He used the phrase 'Congratulations on a job well done' as many as four times a day to different staff in the hospital. In private he would be irritated because he had to praise other people for what he truly believed were his achievements.
By the end of each week he was so exhausted from sitting on comfortable chairs (some were so comfortable it was a real effort to get out of them) at the many meetings he attended that he would fly off to some far away country for a rest, though of course would endeavour to find out how that country dismantled its health service. Because of his enterprising attitude on behalf of the Organization these trips would be paid for and the very important doctor would not have to spend a penny. 'I deserve it because of all the hard work I am putting in', he used to say, to justify his huge salary and the enormous expenses paid for by the Organization. 'They obviously think very highly of me.' Besides, they know I would get a better salary elsewhere if they did not pay me such gigantic sums of money here', he would rationalise. But this suits me for the time. I have a big house in London near the University and an even bigger house in Richleyshire where I can play golf on the weekends and charge all my expenses to the Organization, even the Golf Club fees. 'Why not? Politicians were doing it', he would argue, in a rare utterance of cognitive dissonance (or pangs of conscience others might think) a term he had picked at one of the many important half-hour psychology conferences he attended (he was much too busy to stay to the end of any conference.
As time passed he was beginning to think he needed a higher salary because time off and holidays were costing him money (domestic shopping, clothes, food, heating bills) despite the freebies. During his days off he would spend lots of time going to museums, visiting the theatre, eating in expensive restaurants and staying in luxury hotels not too far from home, say 10 miles or less. However, for him a real holiday was travelling abroad in a first class seat on a prestigious airline to faraway places. This gave him an edge over his less wealthy colleagues and he would often spend hours on his return recounting his great adventures and experiences abroad in exotic lands. 'He is so broadminded and well-travelled', his managerial associates would say with a feeling of unrequited envy. It is quite remarkable how he manages to be in so many places at the same time - if only he could do the same at this hospital, we would be top of the League Tables for Hospital Risk (LTHR) and gain the recognition we deserve'. 'For all his hard work spent travelling abroad researching better ways of closing down wards and hospitals he now deserves a huge rise in salary'.
And so it came to be. The very important doctor was given an extra allowance (EA for short) worth half his salary and a Credit for Working Hard Allowance (CWHA), both linked to his pension. He was also given a bonus allowance (BA) for sitting twice yearly on a Doctors Work Review Panel (DWRP) set up to deal with those doctors who were not pulling their weight or taking more than one day sick leave or 2 days annual leave at a time. Study leave had already been dropped because the very important doctor argued that if he did not need study leave then no one else did. Besides, ‘Who needs study leave when you can look things up on the internet – even how to carry out open heart surgery’. He would argue. Commitment to the Organization was his raison d'être.
And so it continued. After 10 years nearly all the patients had been discharged from the hospital and family doctors were sending them elsewhere into more luxurious, expensive, private hospitals for 'reviews, assessments, and second, third, even fourth opinions'. The Organization would pay for all this from the money it saved closing down the local hospital. This was the very important doctor's finest hour and for his services to the Organization he was awarded the Rhodium Medal at the Annual Convention of Supermanagers Conference. This award was inevitable, given all the time both home and abroad he had invested in this venture. Now the entire hospital could be closed down thereby saving the Organization millions of pounds.
However, there was a problem with this way of operating, he began to think: ‘If the hospital were to close down there would be no need for an Organization to run it. There would be no management posts and my post as MDP and CSSFM might be superfluous to requirements. 'I know what I will do' - he decided - 'When that happens I will apply for another post in a different Organisation and I am sure I will be successful given all the accolades I have received, and when that Organisation closes down with my help I will get an even bigger salary and move on to the next post' - maybe Minister for Health?




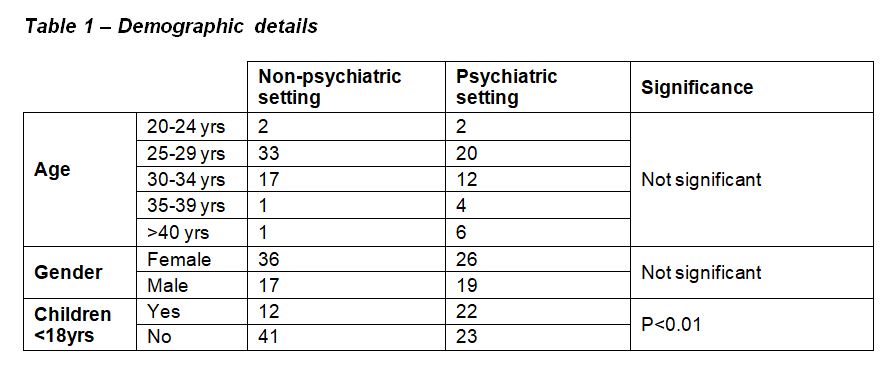
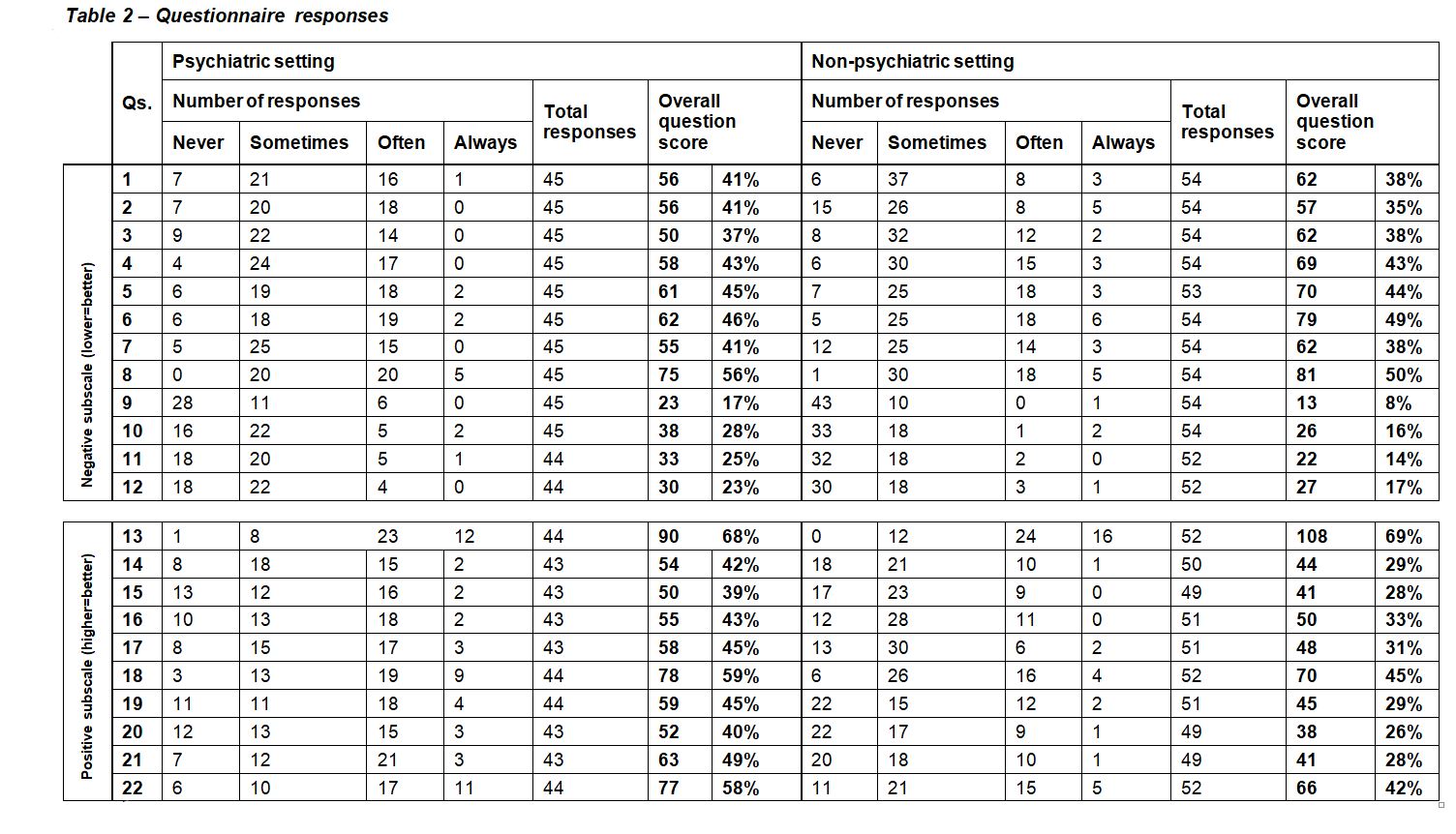
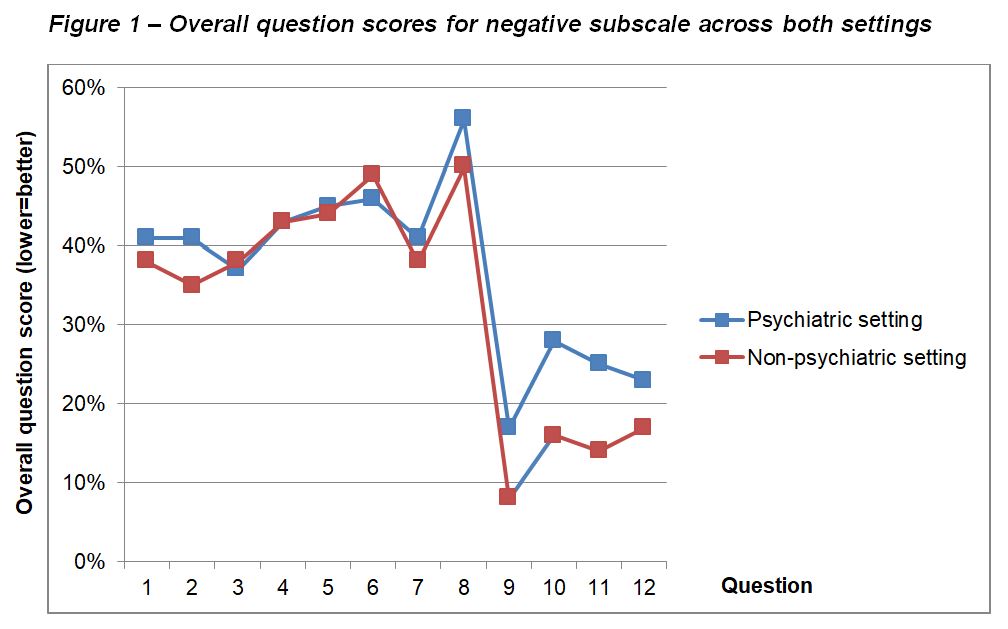
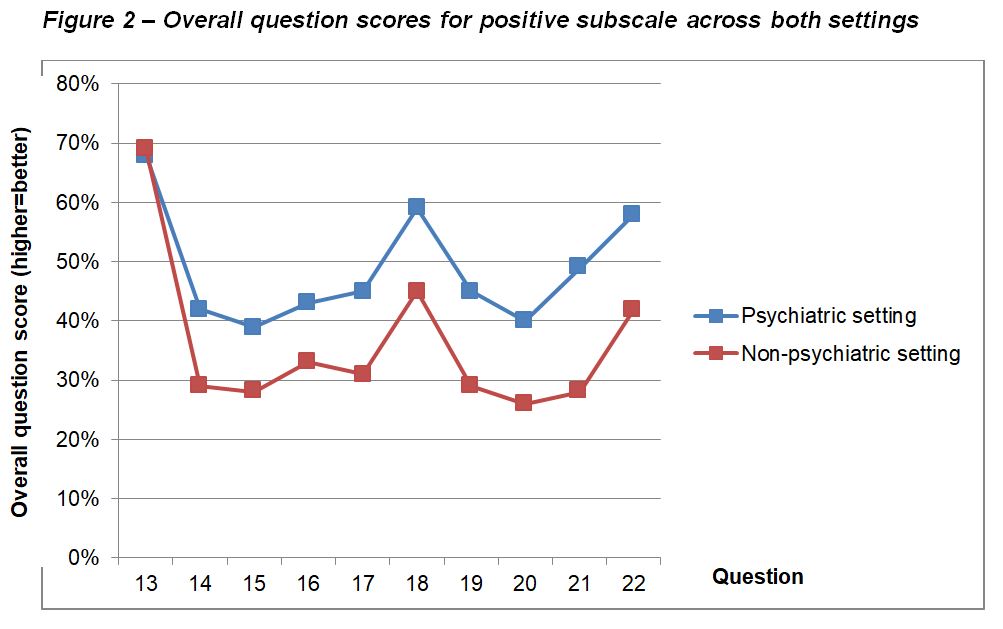
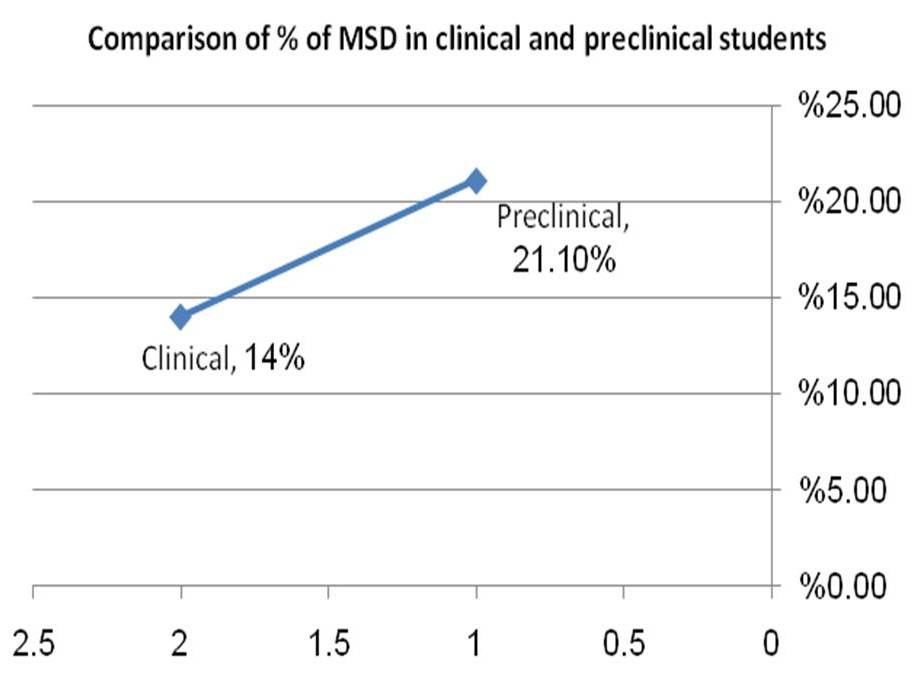
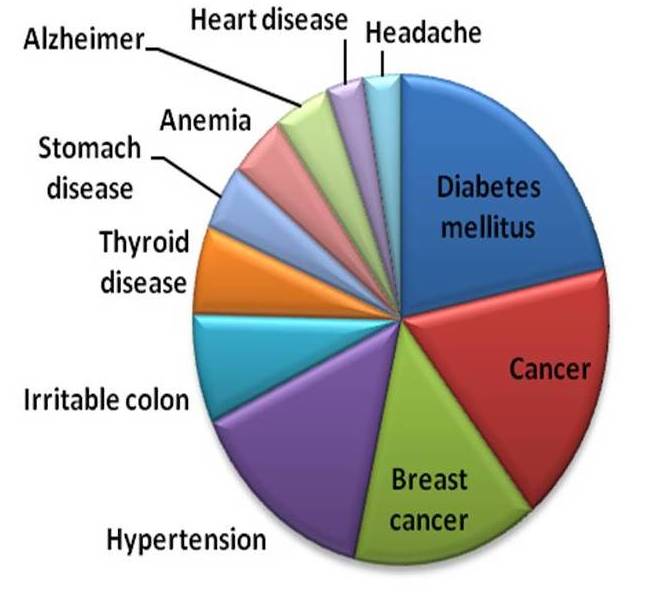
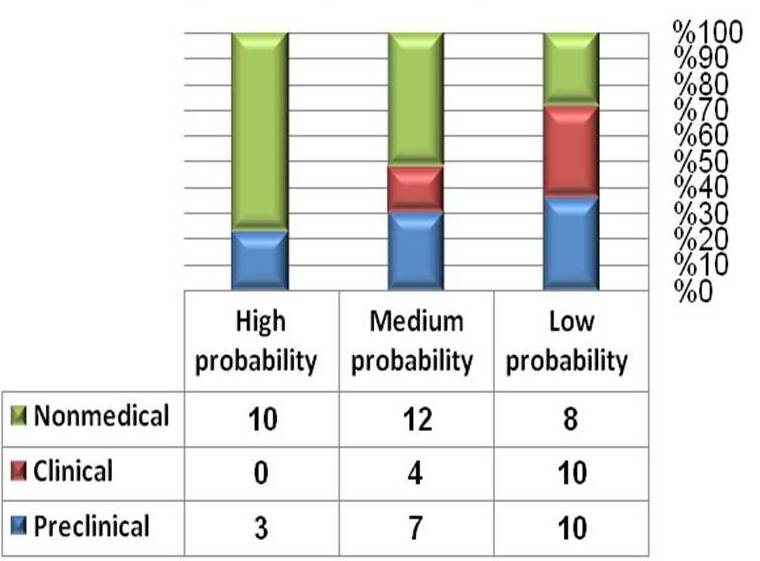
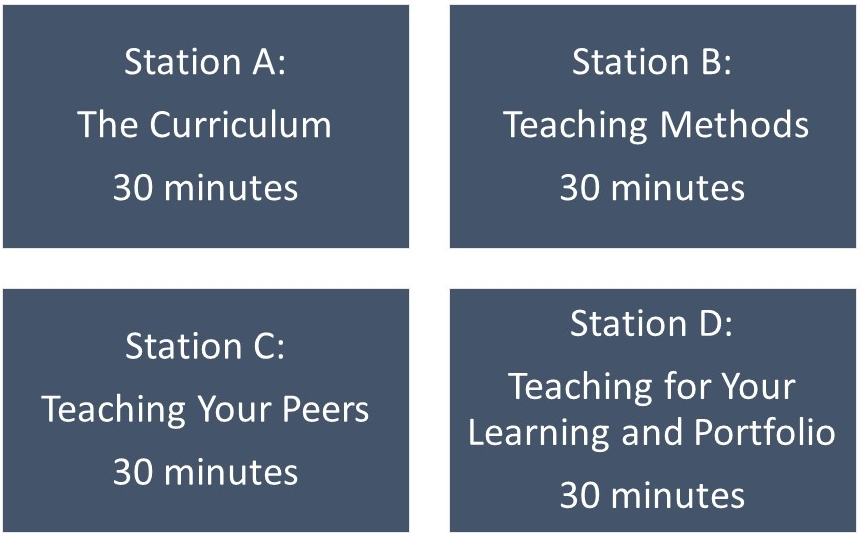


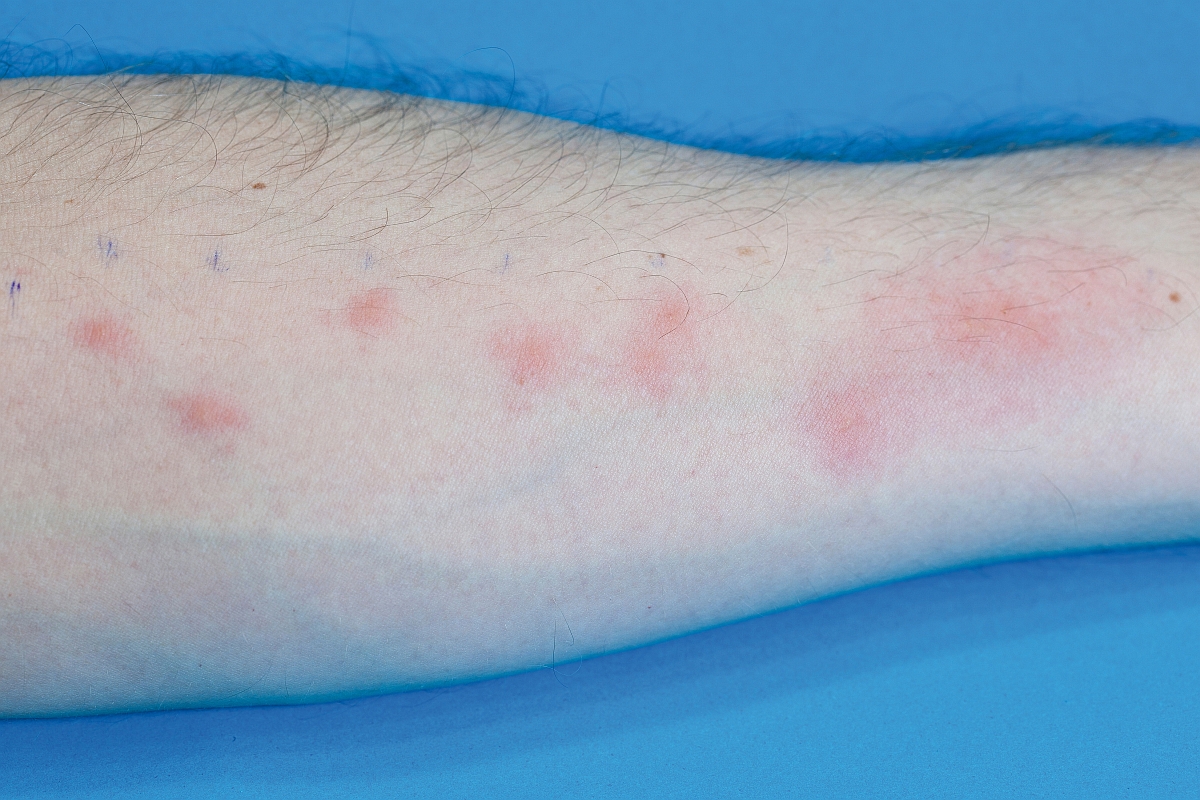



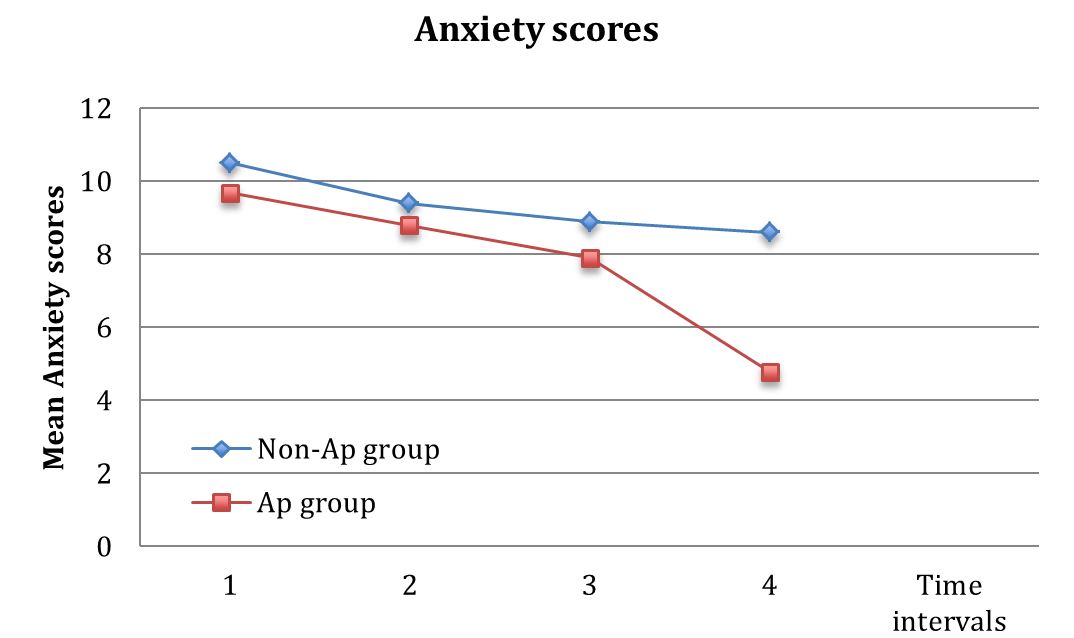
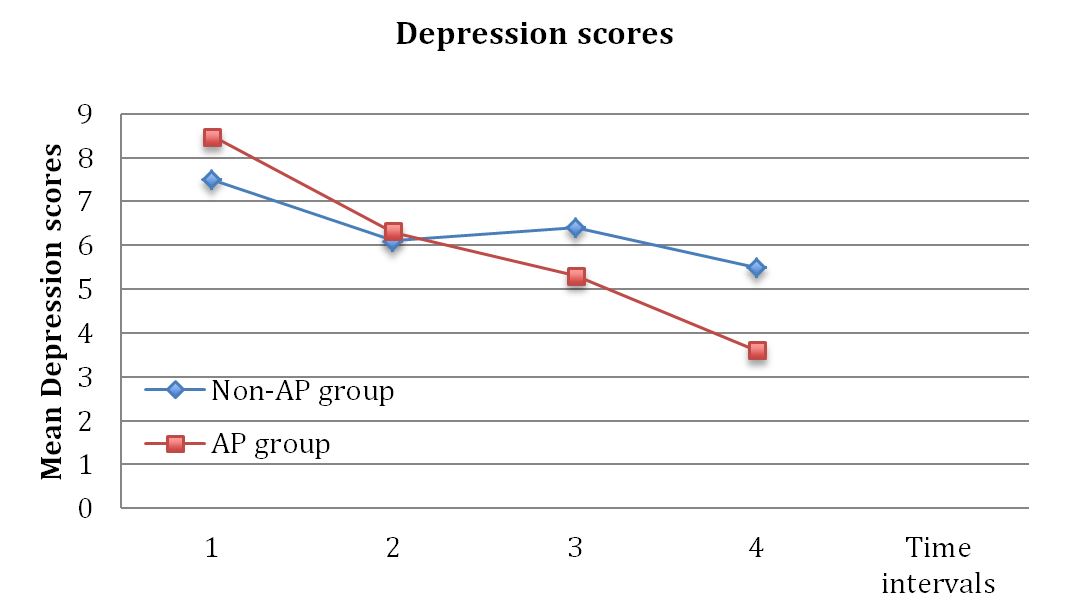
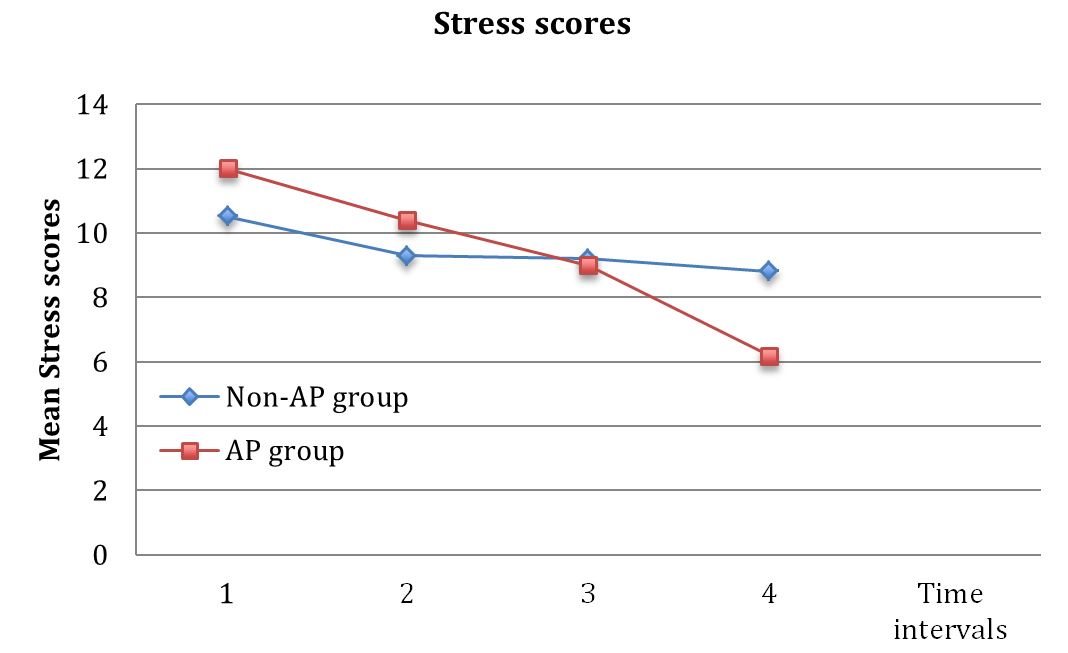
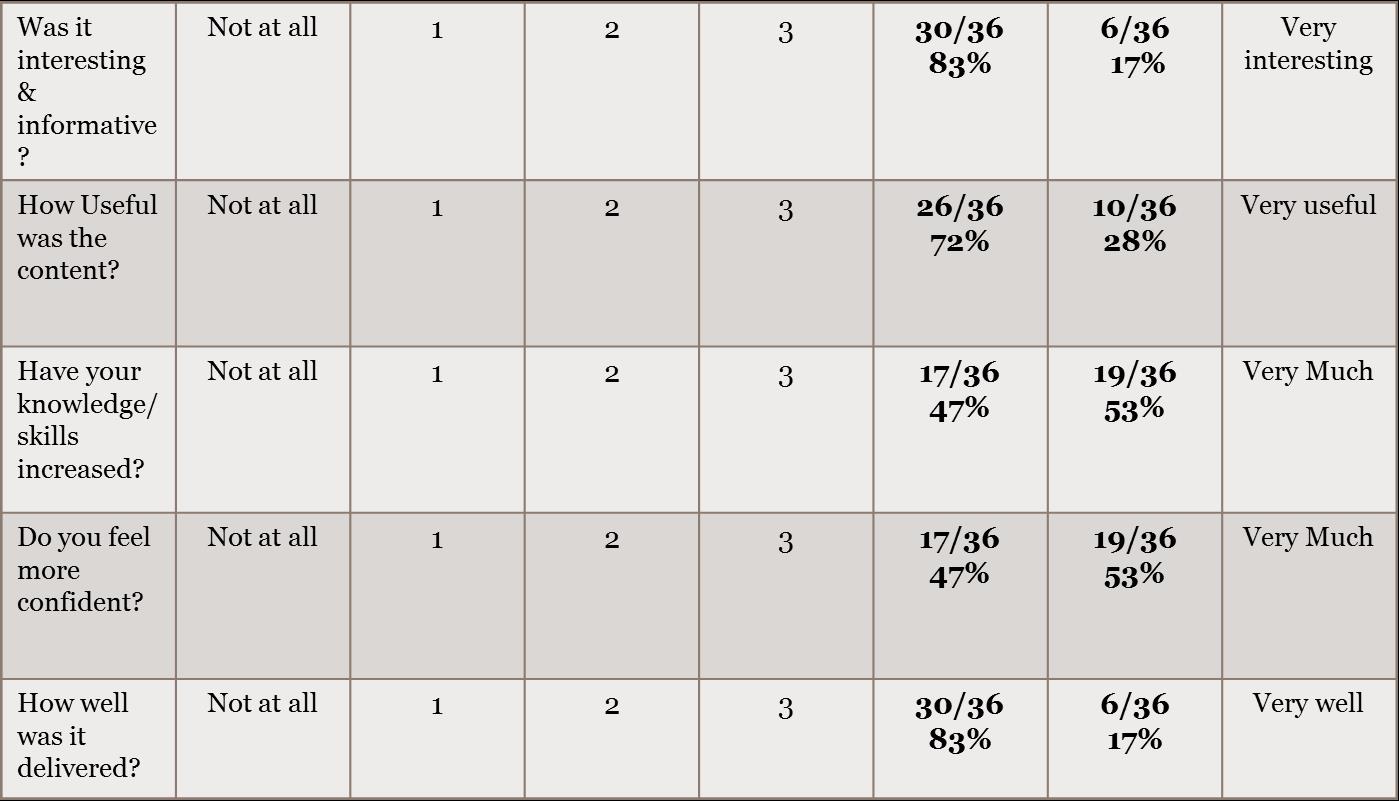
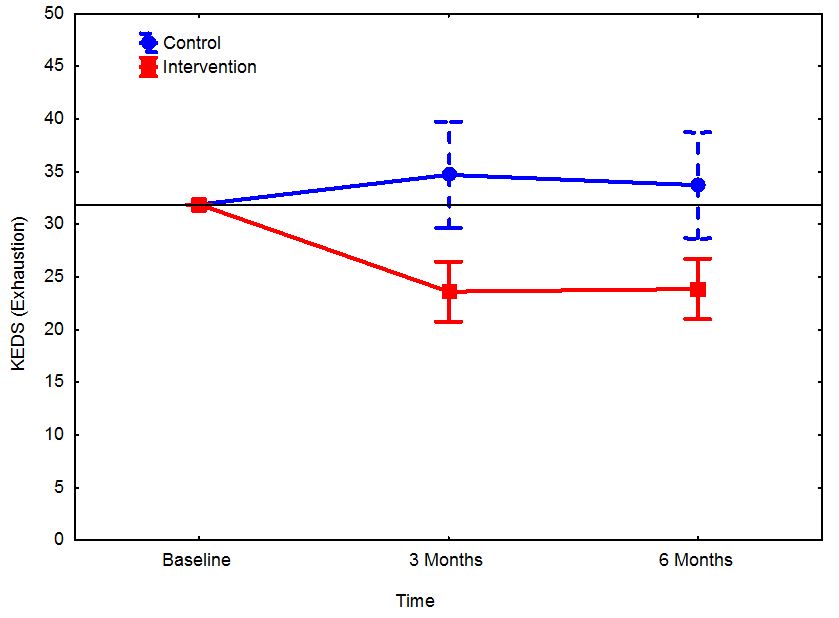
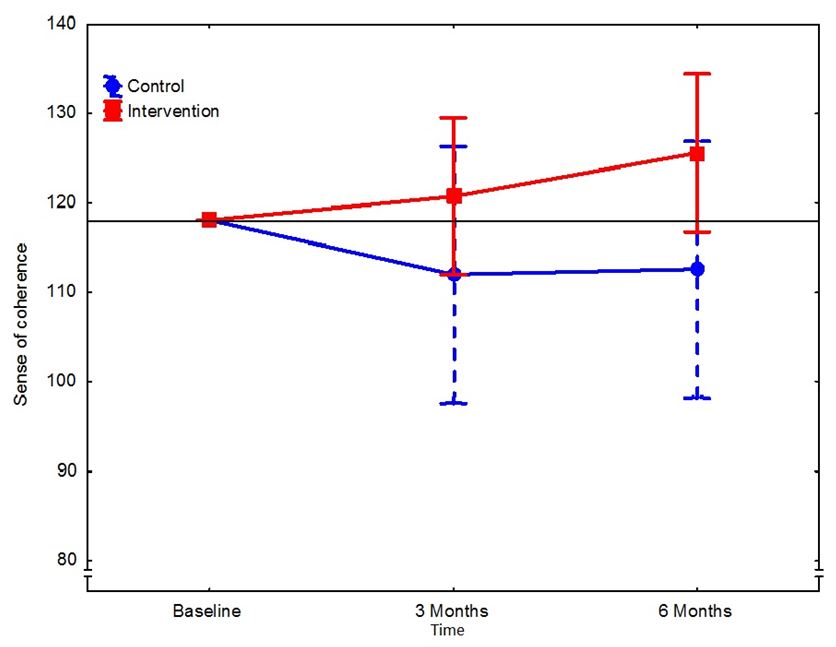
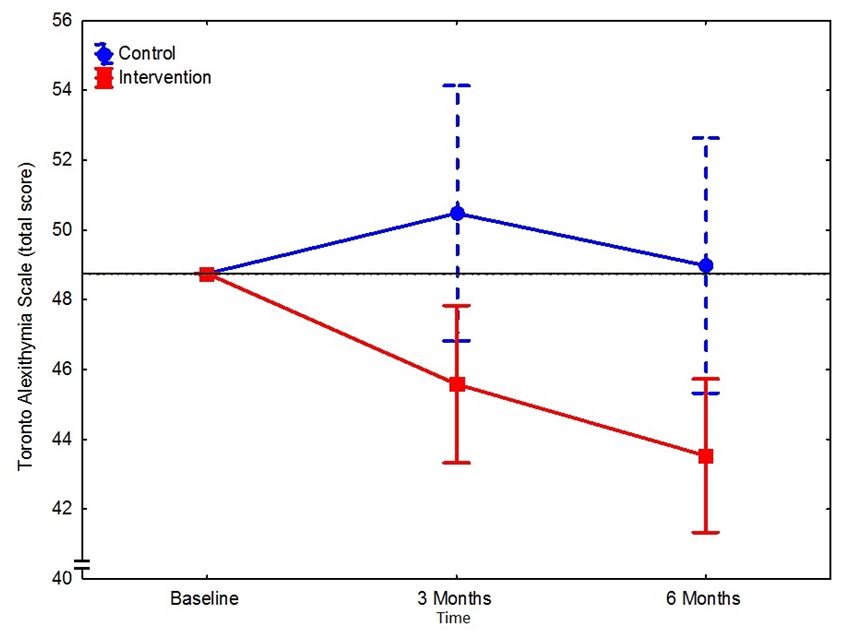
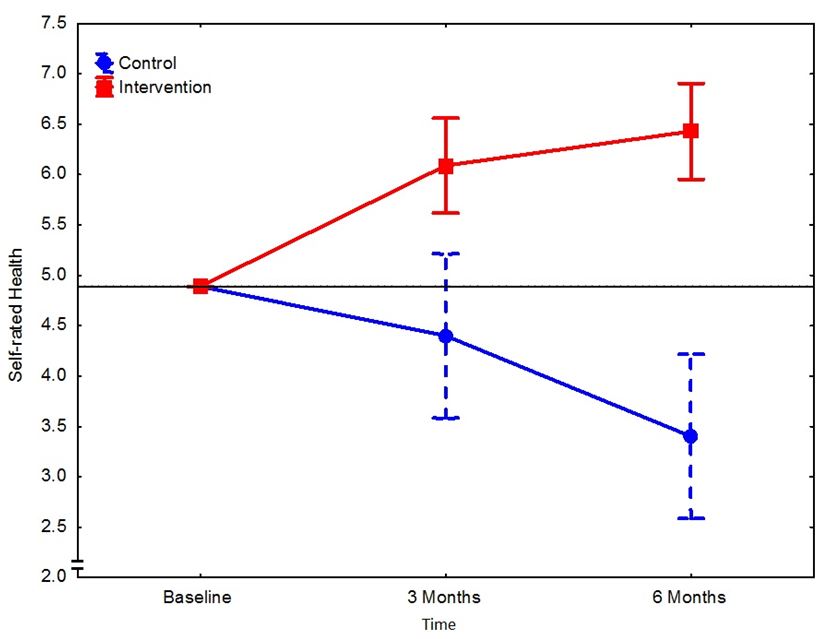
Browse the December 2010 PDF Booklet (Volume 3 Number 4)