Organ transplantation is an effective therapy for end-stage organ failure and is widely practiced around the world. According to World Health Organization (WHO), kidney transplants are carried out in 91 countries. Around 66,000 kidney donations, 21,000 liver donations and 6000 heart transplants were performed globally in 2005. 1 In India the rate of organ donation is only 0.16 per million populations, compared to America's 26 and Spain's 35.2 The shortage of organ is virtually a universal problem. Though many efforts were undertaken by the government to motivate the public towards donation of organs, the rate of organ donors has not paralleled the growing waiting list3,4, 5 and inadequate organ donation in India remains a major limiting factor for transplantation. There are several factors which could facilitate and hinder the general public to donate a organ. Identifying these factors could help in planning effective strategies to combat the problem. Hence the present study was conducted with the aim to explore the general publics perceived barriers and facilitating factors of organ donation.
Materials and methods
The present study was a cross sectional, exploratory survey conducted among the general public of Puducherry U.T, India. 400 eligible subjects who fulfilled the following criteria were included a) Subjects aged 18 and above, and b) who understand either the local language Tamil or English. Subjects with intellectual, psychiatric and emotional disturbances that could affect the reliability of their responses were excluded from the study. The population registry in the primary health centers of the selected community area was used as a sample frame to select subjects randomly. Every eligible subject was explained about the purpose of the study and signed a written consent form. Formal ethical clearance was obtained from the institute ethics committee before actual data collection procedure.
Preparation of the questionnaire
An extensive literature review was carried out to understand the possible barriers and facilitators reported in the past. Reported barrier and facilitating factors in the literature were included in constructing the questionnaire, including specific cultural and religious oriented items specific to Indians. Subject’s intention to donate the organ was assessed using a single dichotomous question (yes or no). For assessing the barriers and facilitators related to organ donation a questionnaire with a total of 18 items (9 items each) was prepared in the form of closed ended question i.e. yes or no. Along with closed ended questions, an open ended question i.e. any other? was also included for obtaining an extended response apart from the framed questions. As knowledge is an important factor which could serve both as a barrier and facilitator for organ donation, 8 items related to knowledge were also included as a part of the questionnaire. Knowledge items of the questionnaire were evaluated by assigning a score of 1 for each correct response with a maximum possible score of 8. Interpretation of the knowledge component was also done by categorizing the knowledge as follows - Below 50% of the total score - Inadequate knowledge, 51 – 75% - Moderately adequate knowledge, above 75% - Adequate knowledge, for ease of understanding. The draft tool was validated for its content by 10 experts from the field of surgery, medicine, nursing, anthropology and psychology for its appropriateness. After appropriate modification the content validity index for the tool was calculated and it was found to be highly valid (0.98). The reliability of the tool was estimated by a test re-test reliability method among 10 subjects with an interval of 2 weeks from the first and second time of administration of the questionnaire. It was found to be highly reliable with reliability coefficient of 0.91. A face to face interview method was used to collect data from each subject. Collected data was analyzed using SPSS for windows version 14 (SPSS Inc., Chicago, Il, USA) with appropriate descriptive and inferential statistics. A probability value of < 0.05 was set as the level of significance
Results
Basic Demographic details
Of the total 400 subjects enrolled the majority were male (56%), between the age group of 31-40 years (48%), and followed Hinduism (68%) at the time of interview. Most of the subjects were literate (70%) with education up to high school and resided in a rural area (53%).
Knowledge regarding organ donation
The mean knowledge score of the subjects regarding organ donation was 4.74 1.45 score which ranged from a minimum score of 1 to a maximum score of 8. Most subjects responded correctly to questions related to organ matching (85.3%) and consent procedure (84.7%). Details of different aspects of knowledge regarding organ donation of the subjects can be found in Table 1. When subjects were asked about the source of information regarding organ donation, 51.3% of the subjects reported that they gained knowledge through television, 23% from health personnel, and 12% from friends and 7% through books and internet (Figure1). Whilecategorizing knowledge scores the majority of the subjects (38.6%) had inadequate knowledge, 50.6% had moderate knowledge and only 10.6% had adequate knowledge regarding organ donation.
Intention to donate organs: Barriers and Facilitators
Of the total 400 subjects interviewed 69.75% of the subjects reported that they wish to donate their organs, whereas the remaining 30.25% reported that they will not donate their organs either during their life or after their death. Subsequently the factors for barriers and facilitators were also analyzed using the pretested questionnaire. The most common barriers perceived by the subjects related to organ donation were as follows, ‘family opposition’ (82.8%), ‘complicated organ donation procedure’ (69%), ‘fear that donation affects their future’ (58.36%), and ‘misuse of organs’ (55.2%). More information about barriers is detailed in Table 2.The most important facilitating factors of organ donation as reported by the subjects were ‘thought of saving someone’s life’ (95.9%), ‘feeling of improved sense of humanity’ (95%), ‘to save the life of a close relative’, ‘thought that their organ live after their death (92.6%) and ‘being a role model for others’ (77.7%). More details of facilitating factor can be seen in Table 3
While associating the subject’s intention to donate organs with demographic variables like age, gender, residence, education, religion, marital status, type of family and knowledge; only educational level had a significant association with the subject’s intention to donate organ. Specifically graduate people are more likely to report intention to donate organ their organs than others (p<0.001).
Figure 1: Distribution of source of information regarding organ donation among the subjects.
Table 1: Item wise distribution of different aspects of knowledge regarding organ donation (n=400)
S. No
Aspects of Knowledge
Correct response
Incorrect response
1.
Definition of organ donation
24%
76%
2.
Knowledge regarding Commonly donated organ
71.3%
28.7%
3.
Knowledge regarding Consent procedure for living donor
76%
24%
4.
Knowledge regarding Consent procedure after death
84.7%
15.3%
5.
Knowledge regarding Consent for mentally retarded person
41.3%
58.7%
6.
Knowledge regarding Consent for unclaimed dead bodies
35.3%
64.7%
7.
Knowledge regarding Organ matching procedure
85.3%
14.7%
8.
Knowledge regarding legal consideration for organ donation
56%
44%
Table 2: Perceived Barriers towards organ donation (n=121)
S. No
Barrier factors
Percentage
1.
Oppose from the family
82.8%
2.
Fear
72.4%
3.
Procedures are complicated
69%
4.
Affects physical appearance
65.5%
5.
Affects the future
58.6%
6.
Create psychological problem
58.6%
7.
Organs could be misused
55.2%
8.
Against religious belief
48.3%
9.
Insults human rights and dignity
48.3%
Table 3: Perceived Facilitators towards organ donation (n=279)
S. No
Facilitating factors
Percentage
1.
Save someone’s life
95.9%
2.
Improve the sense of humanity
95%
3.
Save the life of a close relative
92.6%
4.
Wishes organ to be alive after death
92.6%
5.
To become a role model
77.7%
6.
Empathy for others
53.7%
7.
Rewarding experience
51.2%
8.
Due to family pressure
29.8%
9.
For economic benefit
27.3%
Discussion
The current study was conducted with the aim to explore the general publics intention towards organ donation and to identify the perceived barriers and facilitators. The present study revealed that 69.7% of the subjects have an intention to donate their organs either during their life or after their death, which is similar to the finding of Chung et al6 and Shahbazian H et al7. Similar to the previous studies8 the current study also confirmed a positive association between public intentions to donate their organ with their educational status. Though many studies in the past reported attitudes9,10 of public towards organ donation, the present study was the first of its kind to analyze specifically the barriers and facilitators of organ donation among the general public, this adds strength to this study. The most common barrier reported in the present study was ‘opposition form family in donating their organs’; these findings were similar to a previous study.6 Illegal organ donation and misuse of organ is a major problem in India for the low organ donation rate among public11, this fact was reflected even in the current study as 55.2% of the subjects reported misuse of an organ as barrier to organ donation. The most important facilitating factors of organ donation reported in the present study was ‘thought of saving someone’s life’ (95.9%), ‘feeling of improved sense of humanity’ (95%), ‘to save the life of a close relative’ (92.9%), these finding were similar to the findings of Neelam et al conducted in India12. The majority of the respondents in this study reported "lack of information" about organ donation and transplantation. These findings are comparable with those reported from previous studies, which all indicate the importance of public education about the importance of organ donation13,14,15,16. Our study identified that the principle respondents' source of information about organ donation was the television (TV). The contribution of other sources of information in providing respondents with knowledge about organ donation was minimal. Generally, studies had shown the importance of visual media in increasing the awareness of the public about organ donation. 17,18
Conclusion
Better knowledge may ultimately translate into the act of donation. Effective measures should be taken to educate people with relevant information with the involvement of media, doctors and religious scholars.
Isaac Asimov famously said: ‘The only constant is change.’ (Cited in Hartung, 2004).
So why is it so difficult for most of us to understand, manage, or embrace change?
Coping with change can be challenging for many and, depending on the change and what the impact or outcome of the change means to the individual, will depend upon how well they embrace and accept it. Should a person be fearful of change then it is natural that they will attempt to resist it which in turn can cause high levels of stress and anxiety.
Understanding how we typically react to change also helps us to cope better and manage change. The Kubler-Ross (2009) Model of Change is perhaps one of the best known and most applied models within clinical environments (her original work being around the five stages of grief) which is now also applied to businesses and organisations when looking at changes in the work place such as loss or change of job.
The five stages she refers to are:
Denial
Anger
Bargaining
Depression
Acceptance
A common example used to explain this model is to understand how we would typically respond to an unexpected change such as a dead car battery.
The dead car battery
Just imagine it is a cold winter day and you are dashing to get to work already running late…
You jump into the car, place the key in the ignition and turn it on.
Nothing happens, the battery is dead.
Applying the Kubler Ross Model to this situation, this is how a person may typically react:
Denial - This cannot be happening! Try again. And again! Check the other things in the car are working such as the lights and radio. Try again but still nothing.
Anger - Arrrrgh you stupid car!!! I’m sick of this car!! Why is this happening today of all days!! Slamming a hand against the steering wheel.
Bargaining - (realising that it really isn’t going to start and that you're going to be late for work)..., Oh please car, if you will just start one more time I promise I'll buy you a brand new battery and keep you clean and tidy. Please just start this one time.
Depression - Oh no! What am I going to do? I'm going to be late for work. I give up. I don't really care any more. What's the use?
Acceptance - Right I need to do something. It is not going to start. I need to call the breakdown service and ring into work.
The above example is a simple example yet I’m sure most of us have experienced it or something similar quite often. If you apply this to a situation where the stakes are far higher such as a sudden loss or change of a job, bereavement, house, relationship etc which may impact upon so many things including stability of finances, family, health and other forms of security, then you may be able to see the harsh effect this could have on an individual during this time.
Often individuals add to their stress by expecting themselves to be able to cope with such events. It is important to understand it is not about strength or weakness but about human nature to react by demonstrating the signs of loss and grief. Organisations, managers and individuals need to be understanding and supportive when situations like this happen.
Another way of understanding and coping with change is to consider what goes on in the mind of the individual at the time of the change and what it ‘means’ to them. Some people see risk and uncertainty as exciting and embrace change (depending on the change), whereas others can be fearful of any change, even those perceived to be minor changes, as for them any change is seen as a risk and takes them out of their comfort zone.
The comfort zone
Your comfort zone is where you are fully able, competent and comfortable. The job that you can do with your eyes shut or routines of life where you know exactly what you are doing. You may feel slightly challenged now and then, but there’s nothing you cannot easily handle.
When invited to step outside their comfort zone – or if they’re pushed outside of it - many people react with resistance. This is because of the human fear of failure which, when you look into it more deeply, comes from a desire to be accepted, liked and even loved. When most people ‘fail’ they feel embarrassed, ashamed, silly or stupid because they feel they can’t or couldn’t do whatever it was they tried.
So it’s understandable if at work, or any area of life where there is change, people react with resistance. Change is the unknown, and if you don’t know whether you can do something – especially if you have a ‘Be Perfect’ driver – you could have fears over whether you can do it, can be a success or even cope. Everyday changes such as new computers or telephone systems, new staff, new jobs, new routines and procedures, new management, merging of departments, sections or whole companies or, on a personal level, exams, weddings, divorce, births, deaths, moving house and so on, are all high on the list of stressors due to change.
How big is your zone?
Are you resistant to change? If you are, you’re causing yourself stress. Imagine what size a child’s comfort zone would be compared to an adult’s. Children do not have inhibitions and fears; it’s only as we grow older that we learn to feel fear, that we learn what embarrassment is and how to feel silly or stupid – that is, we learn to have an ego. This restricts our ability to have the freedom to learn, grow and be open to change, as we are nervous about asking questions for fear of looking silly, or trying new things for fear of failure, and we avoid doing anything that may cause us to feel embarrassed.
By being more fluid and open to change, accepting any fear and dealing with it effectively, you would not only grow your confidence and self-esteem, but you will be free to develop your life with more happiness and less stress.
By looking at change differently (for example, recognising that change can also be a good thing; focusing on the possible positives from a situation rather than being quick to look at the negatives from a point of fear and therefore resistance) stress can be greatly reduced.
Choose to flow with change rather than resist; choose to step out of your comfort zone and grow the size of your comfort zone daily. Aim to have a comfort zone the size of a child’s where nothing can faze or worry you, and you will notice a huge difference to the amount of stress you have in your life.
‘The greatest discovery of my generation is that a human being can change their life by altering their attitude of mind.’ William James (cited in Maxwell, 2007).
Remember – the only failure is not trying again. If we fail at something at least we know what NOT to do next time!
Identifying your zones and being rational
Following are three simple exercises you can complete to help you to gain a rational perspective on understanding how you cope with change and also being solution focused when embracing change.
The zones of change help us to understand the different levels of comfort or ‘risk’ and where changes may sit in terms of their percieved meanings to the individual.
Zones of change
Exercise 1
Think back to a significant change in your life or work (something from the past).
What were your perceived risks at the time?
…………………………………………………………………………………
…………………………………………………………………………………
What did you lose?
…………………………………………………………………………………
…………………………………………………………………………………
What did you gain?
…………………………………………………………………………………
…………………………………………………………………………………
This exercise demonstrates that our ‘perceived risks’ at the time of a change were often far different than the reality of how the change occurred. It is also common for an individual to notice that their ‘gains’ can be larger than their ‘losses’ (time can play a factor in this too, often a change can seem a disaster at the time but over time a person can look back and be glad it happened in comparison to how their life is now.)
Exercise 2
Think of a change that you are currently undergoing.
What aspects of the change are in your ‘comfort zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What aspects are in your ‘risk zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What aspects are in your ‘high risk zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What do you need to make the ‘high risk’ into ‘risk’ and the ‘risk’ into ‘comfort’?
…………………………………………………………………………………
…………………………………………………………………………………
This exercise is excellent for considering a current change and how it may affect a person.
Actually listing in categories the level of ‘risk,’ or even drawing the zones on a piece of paper and writing in each change in the place on the zone where the person believes it sits, will give a rational perspective.
Once all the ‘risks’ are highlighted then that is the time to minimize ‘risk’ and find solutions for the individual to cope or manage that change. This is good for action planning and allowing a person to take control to embrace a change rather than being reactive once the change has occurred.
Exercise 3
Think of a life or work change which is going to occur in the future.
Blockers
What I’d be sorry to lose.
…………………………………………………………………………………
…………………………………………………………………………………
My fears and concerns.
…………………………………………………………………………………
…………………………………………………………………………………
Drivers
Benefits of the change.
…………………………………………………………………………………
…………………………………………………………………………………
What I’d be glad to leave behind.
…………………………………………………………………………………
…………………………………………………………………………………
Answering these questions assists a person to determine how much resistance they may feel/have towards a change. Listing potential blockers will identify fears and concerns of the change as well as the levels of risk and loss. Listing drivers will encourage the individual to consider the benefits of the change, the gains, and that change can also be a good thing.
Typically, whichever list is the longest or has the most meaning/impact will be the strongest for that person. If this is the blockers they will resist the change and cause themselves pressure and stress. Therefore addressing the zones of change and looking for ways to reduce risk would be a good strategy in action planning to manage the change well. Should the drivers be the strongest for the person then they are likely to embrace the change more readily although they may still need to address their thoughts and rationale for any blockers listed.
Change tips:
Embrace change, as if you don’t accept it someone will push you into it.
Take every opportunity to grow your comfort zone.
Have the attitude that there is no failure and only learning and development – when we ‘fail’ we know what NOT to do next time.
The worst rarely happens, so why waste energy focusing on it and enforcing irrational fears?
Change CAN be a good thing.
There is always a solution, it may take time for you to see it, but if you look, you will find it.
The widespread use of office-software in general practice makes the idea of simple, automatic computerised support an attractive one. Different tools for different diseases have been tested with mixed results, and in 2009 a Cochrane review1 concluded that “Point of care computer reminders generally achieve small to modest improvements in provider behavior. A minority of interventions showed larger effects, but no specific reminder or contextual features were significantly associated with effect magnitude”. One year later another review2 reached similar conclusion: “Computer reminders produced much smaller improvements than those generally expected from the implementation of computerised order entry and electronic medical record systems”. Despite this, simple, non-expensive, automatic reminders are frequently part of GPs’ software, even if their real usefulness is seldom tested in real life.
Repeated hospitalisation for heart failure is an important problem for every National Health System; it is estimated that about half of all re-hospitalisation could be avoided3. Adherence to guidelines can reduce re-hospitalisation rate4, and pharmacotherapy according to treatment guidelines is associated with lower mortality in the community5. In 2004 a software commonly used in Italian primary care implemented a simple reminders’ system to help GPs to improve prescription of drugs recommended for heart failure. We evaluated if this could lead to a decrease in re-hospitalisation rate.
METHODS
In 2003, using Millewin ®, a software commonly used by Italian GPs, we showed that appropriate prescription could increase using a simple pop-up reminders6; a year later, using the Italian General Practitioners database ‘Health Search – CSD Patient database (HSD) (www.healthsearch.it), we observed a lower than expected prevalence of codified diagnosis of heart failure and of prescription of both beta-blockers and ACE-Inhibitors/ARBs (data on file). Therefore in 2004 Millewin® embedded a simple reminder system to help heart failure (HF) management. The first reminder aimed to identify patients with HF, but without codified diagnosis: in case of loop diuretic and/or digoxin prescription without codified HF diagnosis a pop-up told the GP that the patients could be affected by HF and invited the physician to verify this hypothesis and eventually to record the diagnosis. The second reminder appeared when a patient with codified HF diagnosis had no beta-blocker and/or ACE-inhibitor/ARB prescription: a pop-up invited the GP to prescribe the missing drug. This reminder system was already activated in the 2004 release of the software, but required voluntary activation in the successive releases. This is a common choice in real life, where positive choices in clinical practice by software-house neither are welcomed nor accepted by GPs. We had no possibility to know who decided to keep using the reminders.
We examined the 2004-2009 HF hospitalisations in Puglia, a Southern Italian Region with a population of over 4000000, and with high HF hospitalisation rate compared with the Italian mean7. We compared the hospitalisations for patients cared for by GPs who used Millewin® in 2004 to those of the patients cared for by GPs who never used Millewin®. Data were provided by the local Health Authority, and were extracted from the administrative database.
RESULTS
We identified 64591 patients (mean age 76 y, sd 12; 49.9% men) with one or more HF hospitalisation; 17810 had > 2 hospitalisations, and were analysed for the current study.
Figure 1 - Selection process leading to the identification of the patients with > 2 HF hospitalisations
The selection that led to this group is summarised in figure 1. There was no statistically significant difference between patients cared for GPs using or non using Millewin® software as far as age and gender are concerned. The re –hospitalisation rate according to the use or non-use of Millewin® of patients’ GPs is summarised in table 1.
Table 1: Re-hospitalisation rate of patients cared by Millewin® users and non-users
Patients with ≥ 2 hospitalisation (N, %)
Time
No MW users
MW users
Total
P
Within 1 year
11260 (23.1%)
1136 (22.9%)
12396 (23.1%)
=N.S.
Within 2 years
13851 (28.4%)
1410 (28.4%)
15261 (28.4%)
=N.S.
Within 3 years
15144 (31.0%)
1543 (31.1%)
16687 (31.0%)
=N.S.
Within 4 years
15803 (32.4%)
1612 (32.4%)
17415 (32.4%)
=N.S.
Within 5 years
16083 (33.0%)
1643 (33.1%)
17726 (33.0%)
=N.S.
Within 6 years
16156 (33.1%)
1654 (33.3%)
17810 (33.1%)
=N.S.
MW = Millewin®, N.S = Not significant
The mean time before the first re-hospitalisation was 108.5 day +/- 103.3 for Millewin® non-users and 116.4 +/- 107.5 for users (p < 0.05).
DISCUSSION
Even if reasonable and clinically sound, the availability of computerised reminders aimed to help GPs to identify HF patients and to prescribe them with recommended drugs didn’t reduce re-hospitalisation rate. The first possibility to explain this result is that, after the first year, GPs didn’t re-activate the reminders’ system. Unfortunately we couldn’t verify this hypothesis, but it is known that the level of use of such a system may be low in usual care8; furthermore providers may agree with less than half of computer generated care suggestions from evidence-based CHF guidelines, most often because the suggestions are felt to be inapplicable to their patients or unlikely to be tolerated9. Epidemiological studies have shown that heart failure with a normal ejection fraction is now a more common cause of hospital admission than systolic heart failure in many parts of the world10-11. Despite being common, this type of heart failure is often not recognised, and evidence based treatment—apart from diuretics for symptoms—islacking12. It is therefore possible that increasing ACE-I/ARBs and beta-blockers use in these patients doesn’t influence the prognosis and hospitalisation rate. Unfortunately administrative databases do not permit to distinguish the characteristic of HF. We must also consider that the use of appropriate drugs after HF hospitalisation could spontaneously increase in the last years; a survey in Italian primary care showed that 87% of HF patients used inhibitors of the renin-angiotensin system, and 33% beta-blockers13. A further relevant increase in ACE-I/ARBS is therefore unlikely, while a improvement is clearly needed for beta-blockers. Could more complex and information-providing reminders be more useful? This is unlikely since adding symptom information to computer-generated care suggestions for patients with heart failure did not affect physician treatment decisions or improve patient outcomes14. Furthermore, consultation with a cardiologist for starting beta-blocker treatment is judged mandatory by 57% of Italian GPs13, thus reducing the potential direct effect of reminders on prescription. Finally we must remember that part of the hospitalisation due to HF worsening can be due to non-cardiac disease, such as pneumonia, anemia, etc; all these cause cannot be affected by improved prescription of cardiovascular drugs.
Albeit simple and inexpensive, computerised reminders aren’t a neutral choice in professional software. Too many pop-ups may be disturbing and may lead to systematic skipping the reminders’ text. This can be a problem, since computerised reminders have proved to be useful for other important primary-care activity, such as preventive interventions15. In our opinion, at the moment, a computerised reminder-system should be proposed only as a part of a more complex strategy, such as long-term self or group audit and/or pay for performance initiative.
CONCLUSIONS
Availability of computerised automatic reminders aimed to improve detection of heart-failure patients and prescription of recommended drugs doesn’t decrease repeated hospitalisation; these tools should be probably tested in the context of a more complex strategy, such as a long-term audit.
The prevalence of current use of alcohol in India ranged from 7% in western states of Gujarat (officially under prohibition) to 75% in the North eastern state of Arunachal Pradesh 1.The prevalence of hazardous use of alcohol was 14.2% in rural south India2. Thus, alcohol abuse has a major public, family and health related problems withimpairment of social, legal, inter personal and occupational functioning in thoseindividuals who have been addicted to alcoholism.
A wide variety of biochemical and haematological parameters are affected by regular excessive alcohol consumption. The blood tests traditionally used most commonly as markers of recent drinking are the liver enzymes, gamma glutamyltranserase (GGT), aspartate aminotransferase (AST) and alanine aminotransferase (ALT), and the mean volume of the red blood cells (mean corpuscular volume (MCV). But they were not sensitive or specific enough for use as single tests3.
Elevated Gamma glutamyltransferase levels are an early indicator of liver disease; chronic heavy drinkers, especially those who also take certain other drugs, often have increased GGT levels. However, GGT is not a very sensitive marker, showing up in only 30–50 percent of excessive drinkers in the general population. It is not a specific marker of chronic heavy alcohol use, because other digestive diseases, such as pancreatitis and prostate disease, also can raise GGT levels 4.
AST and ALTare enzymes that help metabolize amino acids, the building blocks of proteins. They are an even less sensitive measure of alcoholism than GGT; indeed, they are more useful as an indication of liver disease than as a direct link to alcohol consumption. Nevertheless, research finds that when otherwise healthy people drink large amounts of alcohol, AST and ALT levels in the blood increase. Of the two enzymes, ALT is the more specific measure of alcohol-induced liver injury because it is found predominantly in the liver, whereas AST is found in several organs, including the liver, heart, muscle, kidney, and brain. Very high levels of these enzymes (e.g., 500 units per liter) may indicate alcoholic liver disease. Clinicians often use a patient’s ratio of AST to ALT to confirm an impression of heavy alcohol consumption. However, because these markers are not as accurate in patients who are under age 30 or over age 70, they are less useful than some of the other more comprehensive markers5.
AST /ALT ratio of more than1.5 strongly suggests and ratio >2.0 is almost indicative of alcohol induced damaged to liver 6.It has been suggested that an AST/ ALT ratio greater than 2 is highly suggestive or indicative of alcoholic etiology of liver disease. But extreme elevations of this ratio, with AST level greater than five times the normal should suggest non-alcoholic cause of hepatocellular necrosis 7.
Sialic acid, which is a derivative of acetyl neuraminic acid, attached to non-reducing residues of carbohydrate chain of glycoproteins and glycolipids is found to be elevated in alcohol abuse 8.
In this study we compared sensitivity, specificity and diagnostic efficiency of serum Sialic acid with other traditional markers like AST (Aspartate amino transaminase), ALT (Alanine amino transaminase), GGT (Gamma Glutamyl Transferase), as a marker of alcohol abuse.
MATERIALS AND METHODS:
This was a case-control study which was conducted on 100 male subjects aged 20-60 years, 50 cases and 50 controls. Cases comprised of patients diagnosed to have Alcohol Dependant Syndrome (ADS) who were admitted in Psychiatry-ADS ward, at Mahathma Gandhi Memorial Hospital,Warangal. Study was approved by the Institutional ethical committee. Amount, duration and the type of alcohol in the form of Rum, Whisky, Brandy, Vodka, Gin, Arrack, etc consumed was enquired, those subjects who consumed more than half bottles of these spirits daily (or intermittently with abstinence of 2-3 days), for more than 5 years were chosen for this study. Dependence of their alcoholism was enquired in the form of CAGE questionnaire 9.
C : Cut down drinking, A : Annoyed others by drinking, G : Guilty feeling of drinking. E : Eye-opener
Those who satisfied two or more questions were taken as cases 10 and their blood samples were collected for the study after their informed consent. Controls were selected from healthy subjects came for master health check up at MGMH health clinic, with no history ofalcoholism.
Exclusion criteria:
Patients with history of Diabetes mellitus, Cardiac disease, Viral/Bacterial Hepatitis, Alcoholic hepatitis, tumors, meningitis and history of current use of hepatotoxic and nephrotoxic drugs were excluded from the study.
4ml of blood was collected from each subject from median cubital vein by venipuncture, serum was separated and the different parameters were analyzed. Estimation of serum Sialic acid was done by modified thiobarbturic acid assay of warren11 (Lorentz and Krass) by colorimetric method. Estimations of Aspartate transaminase 12, 13, 14 Alanine transaminase 13, 15, 16 Gamma glutamyl transferase 17, 18 were done by IFCC recommended methods on Dimension Clinical chemistry system (auto analyzer).
Statistical analysis: Student t test (two tailed, independent) has been used to find the significance of study parameters between controls and cases. Receiving Operating Characteristics (ROC) tool (SPSS 17 version) has been used to find the diagnostic performance of study parameters.
RESULTS:
It was observed that all the study parameters were significantly increased (p value < 0.001) in subjects with alcohol abuse when compared to the controls as shown in the Table 1. The ROC analyses of the different parameters were shown in Fig 1 and Table 2. GGT was having highest Diagnostic efficacy followed by AST and SA as a marker of alcohol abuse.
Figure 1: ROC Curve analysis of different parameters
Table1: Comparison of study parameters between controls and cases
Parameters
controls
cases
P value
AST(U/L)
24.83±7.57
87.9 ±53.72
<0.001
ALT(U/L)
47.63 ±18.77
88.83± 46.53
<0.001
AST/ALT
0.58 ± 0.23
0.982 ± 0.29
<0.001
GGT(U/L)
39.36 ±v 20.23
264.13± 298.74
<0.001
SA(m mol/L)
1.81 ± 0.42
2.92±0.706
<0.001
Table 2: ROC Analysis of different study parameters
Parameters
Best-Cutoff value
Sensitivity
Specificity
Diagnosticefficacy
AUC
AST(U/L)
37.50
86.66 %
93.33%
90%
0.946
ALT(U/L)
71.00
63.33%
93.33%
78.33%
0.811
AST/ALT
0.732
83.33%
76.66%
80%
0.869
GGT(U/L)
55.50
96.66%
86.66%
91.66%
0.929
SA(m mol/L)
2.3
80%
93.33%
86.66%
0.939
DISSCUSSION:
Alcoholism is a serious health issue with major socio-economic consequences. Significant morbidity is related to chronic heavy alcohol use and alcoholics seek advice only when a complication of drinking sets in. The diagnosis is often based on patients self-reporting of alcohol consumption, which is unreliable and requires high degree of clinical suspicion.
Clinical histories and questionnaires are the commonest initial means of detection of alcohol abuse. They are cheap, easily administered but are subjective. If the history remains uncertain and there is suspicion of alcohol abuse, biological markers provide objectivity. A combination of markers remains essential in detection. Liver is the prime target organ for alcohol-induced disease. Liver enzymes are also important indicators of liver dysfunction, possibly as markers of alcohol dependence. Commonly used markers are GGT, AST and ALT. Laboratory markers help clinicians to raise the issue of excessive drinking as the possible cause of health problem, unfortunately because of lack of sensitive and specific methods, the detection of problem dinking in clinical settings has remained difficult. Therefore, findings of increased serum SA concentrations in alcoholics have raised the possibility of developing new tools for such purpose.
In the present study on analyzing the results it was found that an increased concentration of Serum Sialic acid and other traditional biochemical markers GGT, AST, ALT was observed in cases compared to that of controls. Over all GGT had a good sensitivity and specificity. The other traditional markers used in alcohol abuse varied considerably in their specificities and sensitivities. The increase in serum Sialic acid concentration in alcohol abusers in our present study is in accordance with the studies conducted by other investigators 8, 19, 20, 21.The diagnostic accuracy of SA was in accordance with the study by Antilla P et al 19 .The increase in serum GGT, ALT and AST concentration in alcohol abusers were in accordance with the studies conducted by other investigators 19, 22.
CONCLUSION:
In our study, Sialic Acid proved to be a good test with sensitivity of 80% and specificity of 93.33% with a diagnostic accuracy of 86.66% showing that SA can be used as a biochemical marker in alcohol abuse where secondary effects of liver disease hamper the use of traditional markers.
Limitations of the study are as follows: This study was done in small group of people only; a larger study consisting of alcohol abusers with and without specific liver disease should be conducted to confirm the role of SA as a new marker for alcohol abuse where the traditional markers will be altered by the different liver diseases.
Assessment and evaluation are the foundations of learning; the former is concerned with how students perform and the latter, how successful the teaching was in reaching its objectives. Case based discussions (CBDs) are structured, non-judgmental reviews of decision-making and clinical reasoning1. They are mapped directly to the surgical curriculum and “assess what doctors actually do in practice” 1. Patient involvement is thought to enhance the effectiveness of the assessment process, as it incorporates key adult learning principles: it is meaningful, relevant to work, allows active involvement and involves three domains of learning2:
Clinical (knowledge, decisions, skills)
Professionalism (ethics, teamwork)
Communication (with patients, families and staff)
The ability of work based assessments to test performance is not well established. The purpose of this critical review is to assess if CBDs are effective as an assessment tool.
Validity of Assessment
Validity concerns the accuracy of an assessment, what this means in practical terms, and how to avoid drawing unwarranted conclusions or decisions from the results. Validity can be explored in five ways: face, content, concurrent, construct and criterion-related/predicative.
CBDs have high face validity as they focus on the role doctors perform and are, in essence, an evolution of ‘bedside oral examinations’3. The key elements of this assessment are learnt in medical school; thus the purpose of a CBD is easy for both trainees and assessors to validate1. In terms of content validity, CBDs are unique in assessing a student’s decision-making and which, is key to how doctors perform in practice. However, as only six CBDs are required a year, they are unlikely to be representative of the whole curriculum. Thus CBDs may have a limited content validity overall, especially if students focus on one type of condition for all assessments.
Determining the concurrent validity of CBDs is difficult as they assess the pinnacle of Miller’s triangle – what a trainee ‘does’ in clinical practice (figure1)4. CBDs are unique in this aspect, but there may be some overlap with other work based assessments particularly in task specific skills and knowledge. Simulation may give some concurrent validity to the assessment of judgment. The professional aspect of assessment can be validated by a 360 degree appraisal, as this requests feedback about a doctor’s professionalism from other healthcare professionals1.
Figure 1: Miller’s triangle4
CBDs have high construct validity, as the assessment is consistent with practice and appropriate for the working environment. The clinical skills being assessed will improve with expertise and thus there should be ‘expert-novice’ differences on marking3. However the standard of assessment (i.e. the ‘pass mark’) increases with expertise – as students are always being assessed against a mark of competency for their level. A novice can therefore score the same ‘mark’ as an expert despite a difference in ability.
In terms of predictive validity performance-based assessments are simulations and examinees do not behave in the same way as they would in real life3. Thus, CBDs are an assessment of competence (‘shows how’) but not of true clinical performance and one perhaps could deduct that they don’t assess the attitude of the trainee which completes the cycle along with knowledge and skills (‘does’)4. CBDs permit inferences to be drawn concerning the skills of examinees that extend beyond the particular cases included in the assessment3. The quality of performance in one assessment can be a poor predictor of performance in another context. Both the limited number and lack of generalizability of these assessments have a negative influence on predictive validity3.
Reliability of Assessment
Reliability can be defined as “the degree to which test scores are free from errors of measurement”. Feldt and Brennan describe the ‘essence’ of reliability as the “quantification of the consistency and inconsistency in examinee performance” 5. Moss states that less standardized forms of assessment, such as CBDs, present serious problems for reliability6. These types of assessment permit both students and assessors substantial latitude in interpreting and responding to situations, and are heavily reliant on assessor’s ability. Reliability of CBDs is influenced by the quality of the rater’s training, the uniformity of assessment, and the degree of standardization in examinee.
Rating scales are also known to hugely affect reliability – understanding of how to use these scales must be achieved by all trainee assessors in order to achieve marking consistency. In CBD assessments, trainees should be rated against a level of completion at the end of the current stage of training (i.e. core or higher training) 1. While accurate ratings are critical to the success of any WBA, there may be latitude in the interpretation of these rating scales between different assessors. Assessors who have not received formal WBA training tend to score trainees more generously than trained assessors7-8. Improved assessor training in the use of CBDs and spreading assessments throughout the student’s placement (i.e. a CBD every two months) may improve the reliability and effectiveness of the tool1.
Practicality of Assessment
CBDs are a one-to-one assessment and are not efficient; they are labour intensive and only cover a limited amount of the curriculum per assessment. The time taken to complete CBDs has been thought to negatively impact on training opportunities7. Formalized assessment time could relieve the pressure of arranging ad hoc assessments and may improve the negative perceptions of students regarding CBDs.
The practical advantages of CBDs are that they allow assessments to occur within the workplace and they assess both judgment and professionalism – two subjects on the curriculum which are otherwise difficult to assess1. CBDs can be very successful in promoting autonomy and self-directed learning, which improves the efficiency of this teaching method9. Moreover, CBDs can be immensely successful in improving the abilities of trainees and can change clinical practice – a feature than is not repeated by other forms of assessment8.
One method for ensuring the equality of assessments across all trainees is by providing clear information about what CBDs are, the format they take and the relevance they have to the curriculum. The information and guidance provided for the assessment should be clear, accurate and accessible to all trainees, assessors, and external assessors. This minimizes the potential for inconsistency of marking practice and perceived lack of fairness7-10. However, the lack of standardization of this assessment mechanism combined with the variation in training and interpretation of the rating scales between assessors may result in inequality.
Formative Assessment
Formative assessments modify and enhance both learning and understanding by the provision of feedback11. The primary function of the rating scale of a CBD is to inform the trainee and trainer about what needs to be learnt1. Marks per see provide no learning improvement; students gain the most learning value from assessment that is provided without marks or grades12. CBDs have feedback is built into the process and therefore it can given immediately and orally. Verbal feedback has a significantly greater effect on future performance than grades or marks as the assessor can check comprehension and encourage the student to act upon the advice given1,11-12. It should be specific and related to need; detailed feedback should only occur to help the student work through misconceptions or other weaknesses in performance12. Veloski, et al, suggests that systemic feedback delivered from a credible source can change clinical performance8.
For trainees to be able to improve, they must have the capacity to monitor the quality of their own work during their learning by undertaking self-assessment12. Moreover, trainees must accept that their work can be improved and identify important aspects of their work that they wish to improve. Trainee’s learning can be improved by providing high quality feedback and the three main elements are crucial to this process are 12:
Helping students recognise their desired goal
Providing students with evidence about how well their work matches that goal
Explaining how to close the gap between current performance and desired goal
The challenge for an effective CBDis to have an open relationship between student and assessor where the trainee is able to give an honest account of their abilities and identify any areas of weakness. This relationship currently does not exists in most CBDs, as studies by Veloski, et al8and Norcini and Burch9 who revealed that only limited numbers of trainees anticipated changing their practice in response to feedback data. An unwillingness to engage in formal self-reflection by surgical trainees and reluctance to voice any weaknesses may impair their ability to develop and lead to resistance in the assessment process. Improved training of assessors and removing the scoring of the CBD form may allow more accurate and honest feedback to be given to improve the student’s future performance. An alternative method to improve performance is to ‘feed forward’ (as opposed to feedback) focusing on what students should concentrate on in future tasks10
Summative Assessment
Summative assessments are intended to identify how much the student has learnt. CBDs have a strong summative feel: a minimum number of assessments are required and a satisfactory standard must be reached to allow progression of a trainee to the next level of training1. Summative assessment affects students in a number of different ways; it guides their judgment of what is important to learn, affects their motivation and self-perceptions of competence, structures their approaches to and timing of personal study, consolidates learning, and affects the development of enduring learning strategies and skills12-13. Resnick and Resnick summarize this as “what is not assessed tends to disappear from the curriculum” 13. Accurate recording of CBDs is vital, as the assessment process is transient, and allows external validation and moderation.
Evaluation of any teaching is fundamental to ensure that the curriculum is reaching its objectives14. Student evaluation allows the curriculum to develop and can result in benefits to both students and patients. Kirkpatrick suggested four levels on which to focus evaluation14:
Level 1 – Learner’s reactions Level 2a – Modification of attitudes and perceptions Level 2b – Acquisition of knowledge and skills Level 3 – Change in behaviour Level 4a – Change in organizational practice Level 4b – Benefits to patients
At present there is little opportunity within the Intercollegiate Surgical Curriculum Project (ISCP) for students to provide feedback. Thus a typical ‘evaluation cycle’ for course development (figure 2) cannot take place15. Given the widespread nature of subjects covered by CBDs, the variations in marking standards by assessors, and concerns with validity and reliability, an overall evaluation of the curriculum may not be possible. However, regular evaluation of the learning process can improve the curriculum and may lead to better student engagement with the assessment process14. Ideally the evaluation process should be reliable, valid and inexpensive15. A number of evaluation methods exist, but all should allow for ongoing monitoring review and further enquiries to be undertaken.
Figure 2: Evaluation cycle used to improve a teaching course15
Conclusion
CBDs, like all assessments, do have limitations, but we feel that they play a vital role in development of trainees. Unfortunately, Pereira and Dean suggest that trainees view CBDs with suspicion7. As a result, students do not engage fully with the assessment and evaluation process and CBDs are not being used to their full potential. The main problems with CBDs relate to the lack of formal assessor training in the use of the WBA and the lack of evaluation of the assessment process Adequate training of assessors will improve feedback and standardize the assessment process nationally. Evaluation of CBDs should improve the validity of the learning tool, enhancing the training curriculum and encouraging engagement of trainees.
If used appropriately, CBDs are valid, reliable and provide excellent feedback which is effective and efficient in changing practice. However, a combination of assessment modalities should be utilized to ensure that surgical trainees are facilitated in their development across the whole spectrum of the curriculum.
Nosocomial pneumonia in patients receiving mechanical ventilation, also called ventilator-associated pneumonia (VAP), is an important nosocomial infection worldwide which leads to an increased length of hospital stay, healthcare costs, and mortality.(1,2,3,4,5) The incidence of VAP ranges from 9% to 27% with a crude mortality rate that can exceed up to 50%. (6,7,8,9) Aspiration of bacteria from the upper digestive tract is an important proposed mechanism in the pathogenesis of VAP.(9, 10) The normal flora of the oral cavity may include up to 350 different bacterial species, with tendencies for groups of bacteria to colonize different surfaces in the mouth. For example, Streptococcus mutans, Streptococcus sanguis, Actinomyces viscosus, and Bacteroides gingivalis mainly colonize the teeth; Streptococcus salivarius mainly colonizes the dorsal aspect of the tongue; and Streptococcus mitis is found on both buccal and tooth surfaces.(11) Because of a number of processes, however, critically ill patients lose a protective substance called fibronectin from the tooth surface. Loss of fibronectin reduces the host defence mechanism mediated by reticuloendothelial cells. This reduction in turn results in an environment conducive to attachment of microorganism to buccal and pharyngeal epithelial cells.(12) Addressing the formation of dental plaque and its continued existence by optimizing oral hygiene in critically ill patients is an important strategy for minimizing VAP.(13) Two different interventions aimed at decreasing the oral bacterial load are selective decontamination of the digestive tract involving administration of non absorbable antibiotics by mouth, through a naso-gastric tube, and oral decontamination, which is limited to topical oral application of antibiotics or antiseptics.(14) Though meta-analysis of antibiotics in decontamination of digestive tracts have found positive results(15) , the use of this intervention is, however, limited by concern about the emergence of antibiotic resistant bacteria.(16) One alternative to oral decontamination with antibiotics is to use antiseptics, such as chlorhexidine which act rapidly at multiple target sites and accordingly may be less prone to induce drug resistance.(17) Recently a meta-analysis of four trials on chlorhexidine failed to show a significant reduction in rates of ventilator associated pneumonia(18) but, subsequent randomised controlled trials, however, suggested benefit from this approach.(19) Current guidelines from the Centres for Disease Control and Prevention recommend topical oral chlorhexidine 0.12% during the perioperative period for adults undergoing cardiac surgery (grade II evidence). The routine use of antiseptic oral decontamination for the prevention of ventilator associated pneumonia, however, remains unresolved.(8) Despite the lack of firm evidence favouring this preventive intervention, a recent survey across 59 European intensive care units from five countries showed that 61% of the respondents used oral decontamination with chlorhexidine. As the emphasis on evidence based practice is increasing day by day, integrating recent evidence by meta-analysis could greatly benefit patient care and ensure safer practices. Hence we carried out this meta-analytic review to ascertain the effect of oral decontamination using chlorhexidine in the incidence of ventilator associated pneumonia and mortality in mechanically ventilated adults.(20)
Methods
Articles published from 1990 to May 2011 in English which were indexed in the following databases were searched: CINAHL, MEDLINE, Joanna Briggs Institute, Cochrane Library, EMBASE, CENTRAL, and Google search engine. We also screened previous meta-analyses and the references lists from all the retrieved articles for additional studies. Further searches were carried out in two trial registers (www.clinicaltrials.gov/ and www.controlled-trials.com/) and on web postings from conference proceedings, abstracts, and poster presentations.
Articles retrieved were assessed for inclusion criteria by three independent reviewers from the field of nursing with masters degrees. The inclusion criteria set for this meta-analysis were as follows: a) VAP definition meeting both clinical and radiological criteria b) Intubation for more than 48 hours in ICU.
We excluded the studies where clinical pulmonary infection score alone was considered for diagnosing VAP. Thereafter the articles were evaluated for randomisation, allocation concealment, blinding techniques, clarity of inclusion and exclusion criteria, outcome definitions, similarity of baseline characteristics, and completeness of follow-up. We considered randomisation to be true if the allocation sequence was generated using computer programs, random number tables, or random drawing from opaque envelopes. Finally, based on the above characteristics, only 9 trials which fulfilled the inclusion criteria was included for the pooled analysis. A brief summary of the 9 trials were listed in Table 1. The primary outcomes in this meta-analysis were incidence of VAP and mortality rate.
Table 1: Brief summary of trials
Source
Subjects
Intervention
ComparedWith
Outcome with respect to VAP
Outcome with respect to Mortality
C
E
C
E
DeRiso et al., 1996
353- Open Heart surgery patients
Chlorhexidine 0.12% 15 ml preoperatively and twice daily postoperatively until discharge from intensive care unit or death
Placebo
9/180
3/173
10/180
2/173
Fourrier et al., 2000
60- Medical and surgical patients
Chlorhexidine gel 0.2% dental plaque decontamination 3 times daily, compared with bicarbonate solution rinse 4 times daily followed by oropharyngeal suctioning until 28 days discharge form ICU or death
Standard treatment
15/30
5/30
7/30
3/30
Houston et al., 2002
561- cardiac surgery patients
Chlorhexidine 0.12% rinse compared with Listerine preoperatively and twice daily for 10 days postoperatively or until extubation, tracheostomy, death, or diagnosis of pneumonia.
Standard treatment
9/291
4/270
NA
NA
MacNaughton et al., 2004
194 – Medical and surgical patients
Chlorhexidine 0.2% oral rinse twice daily until extubation or death
Placebo
21/101
21/93
29/93
29/101
Fourrier et al., 2005
228 –ICU patients
Chlorhexidine 0.2% gel three times daily during stay in intensive care unit until 28 days
Placebo
12/114
13/114
24/114
31/114
Segers et al.,2005
954 – cardiac surgery patients
Chlorhexidine 0.12%, nasal ointment, and 10 ml oropharynx rinse four times daily on allocation and admission to hospital until extubation or removal of nasogastric tube
Placebo
67/469
35/485
6/469
8/485
Boop et al., 2006
5- cardiac surgery patients as pilot study
0.12% chlorhexidine gluconate oral care twice daily until discharge
Standard treatment
1/3
0/2
NA
NA
Koeman et al., 2006
385 –General ICU patients
2 treatment group: 2%Chlorhexidine, chlorhexidine and colistin, placebo four times daily until diagnosis of ventilator associated pneumonia, death, or extubation
Placebo
23/130
13/127
39/130
49/127
Tontipong et al., 2008
207 –General medical ICU or wards
2% chlorhexidine solution times per day until endotracheal tubes were removed.
Standard treatment
12/105
5/102
37/105
36/102
NA-Not available; C-Control group; E- Experimental group
Data analysis
Meta-analysis was performed in this study by using Review Manager 4.2 (Cochrane Collaboration, Oxford) with a random effect model. The pooled effects estimates for binary variables were expressed as a relative risk with 95% confidence interval. Differences in estimates of intervention between the treatment and control groups for each hypothesis were tested using a two sided z test. We calculated the number of patients needed to treat (NNT, with 95% confidence interval) to prevent one episode of ventilator associated pneumonia during the period of mechanical ventilation. A chi-squared test was used to assess the heterogeneity of the results. A Forest plot graph was drawn using Stats direct software version 2.72 (England: Stats Direct Ltd. 2008). We considered a two tailed P value of less than 0.05 as significant throughout the study.
Results
Effect of Chlorhexidine in reducing the Incidence of VAP
A total of nine trials were included in this meta-analysis(19,21,22,23,24,25,26,27,28). Pooled analysis of the nine trials with 2819 patients revealed a significant reduction in the incidence of VAP using chlorhexidine (Relative risk 0.60, 0.47 to 0.76; P< 0.01) (Figure 1). In relation to the Number Needed to Treat (NNT), 21 patients would need to receive oral decontamination with Chlorhexidine to prevent one episode of Ventilator associated pneumonia (NNT 21, 14 to 38).
Figure 1: Forest Plot showing the effect of Chlorhexidine oral decontamination in preventing the incidence of ventilator-associated pneumonia. Test for heterogeneity:χ2 =15.5, df =8, p < 0.01. Test for overall effect: z =4.33, p <0.05.
Effect of Chorhexidine in overall mortality rate
For assessing the outcomes in terms of mortality, only seven out of nine trials were included, since the other two(23,27) did not report the mortality rate. Pooled analysis of the seven trials with 2253 patients revealed no significant effect in reducing the overall mortality rate in patient who received chlorhexidine oral decontamination.(Relative risk 1.02, 0.83 to 1.26; P= 0.781 (Figure 2).
Figure 2: Forest plot showing the effect of Chlorhexidine oral decontamination in reducing overall mortality rate. Test for heterogeneity:χ2 =0.05, df =6, p = 0.81. Test for overall effect: z =0.27, p = 0.78
Discussion
The effectiveness of oral decontamination to prevent VAP in patients undergoing mechanical ventilation has remained controversial since its introduction, due to partly discordant results of individual trials. In the present meta-analysis nine trials were included to estimate the pooled effect size; the results revealed a significant reduction in the incidence of VAP among patients who were treated with oral chlorhexidine. But, it had no effect in reducing the overall mortality rate among these patients. There is a firm body of evidence that oropharyngeal colonization is pivotal in the pathogenesis of VAP. More than 25 years ago, Johanson et al described associations between increasing severity of illness, higher occurrence of oropharyngeal colonization, and an increased risk of developing VAP .(29,30)Subsequently, cohort and sequential colonization analyses identified oropharyngeal colonization as a important risk factor for VAP. (31,32,33) Our finding confirms the pivotal role of Oro- pharyngeal colonization in the pathogenesis of VAP , since this meta-analysis indicates that oral decontamination may reduce the incidence of VAP. Chlorhexidine was proven to have excellent antibacterial effects, with low antibiotic resistance rates seen in nosocomial pathogens, despite long-term use(34). Previous meta-analyses examining the effect of prophylaxis using selective decontamination of the digestive tract reported a significant reduction in the incidence of ventilator associated pneumonia(35,36,37). The most recent meta-analysis indicated that such an intervention combined with prophylactic intravenous antibiotics reduces overall mortality(38). In comparison our review suggests that oral antiseptic prophylaxis alone can significantly reduce the incidence of ventilator associated pneumonia, but not mortality. A similar result was documented by Ee Yuee Chan et al (2007)(14) who performed a meta-analysis with seven trials with a total of 2144 patients and found a significant result (Odds ratio 0.56, 0.39 to 0.81). Another comparable finding in the present study was, Mortality rate was not influenced by use of Chlorhexidine use, which was in line with the findings of Ee Yuee Chan et al (2007)(14) . Our meta-analysis on Chorhexidine differs from the findings of Pineda et al, who pooled four trials on chlorhexidine and did not report lower rates of ventilator associated pneumonia (odds ratio 0.42, 0.16-1.06; P=0.07)(18) . Our results also extend those of Chlebicki et al, who did not find a statistically significant benefit using the more conservative random effects model after pooling seven trials on chlorhexidine (relative risk 0.70, 0.47- 1.04; P=0.07), although their results were significant with the fixed effects model(39). Our meta-analysis included larger data set with a total of 9 trials including recent trials(28) which further adds strength to our analysis.
Limitations
Though our literature search was comprehensive, it is possible that we missed other relevant trials. Electronic and hand searches do not completely reflect the extent of research outcomes. For example, trials reported at conferences are more likely than trials published in journals to contain negative reports. In addition, more positive than negative results tend to be reported in the literature. This failure to publish more studies with negative outcomes is probably more due to authors’ lack of inclination to submit such manuscripts than to the unwillingness of editors to accept such manuscripts. Furthermore, many studies not published in English were not included e.g. a study by Zamora Zamora F (2011).(40) These limitations may lead to a risk for systematic reviews to yield a less balanced analysis and may therefore affect the recommendations resulting from the reviews. In addition, the heterogeneity which we found among the trials with respect to populations enrolled, regimens used, outcome definitions, and analysis strategies, may limit the ability to generalize results to specific populations.
Conclusion
The finding that chlorhexidine oral decontamination can reduce the incidence of ventilator associated pneumonia could have important implications for lower healthcare costs and a reduced risk of antibiotic resistance compared with the use of antibiotics. These results should be interpreted in light of the moderate heterogeneity of individual trial results and possible publication bias. It may not be prudent to adopt this practice routinely for all critically ill patients until strong data on the long term risk of selecting antiseptic and antibiotic resistant organisms are available. Nevertheless, Chlorhexidine oral decontamination seems promising. Further studies are clearly needed in testing the effect of Chlorhexidine in specific populations with standard protocols (which includes specific concentration, frequency, and type of agents) to generalize the findings. Studies also may be done to test the effect of different oral antiseptics in reducing VAP, so as to enrich the body of knowledge within this area.
An 86-year-old lady was admitted from her residential home with acute on chronic confusion, new symptoms of expressive and receptive dysphasia, dysphagia, vacant episodes and urinary incontinence. She had a previous significant history of haemorrhagic stroke with residual right sided weakness, atrial fibrillation, hypertension, and moderate dementia. Following a CT head, this lady was started on acyclovir for encephalitis. She failed to respond to treatment, and developed constipation. With careful consideration of her poor prognosis and quality of life, this lady was placed on the End of Life Pathway. She was catheterised for comfort. Nine days after initial insertion of the urinary catheter, purple urine was noted in the catheter bag with yellow urine in the tubing leading to the bag. Urine dipstick showed Blood ++, Protein ++, Leuc +, Nit –ve, Glu -ve, Ketone +, pH 8.0. Urine microscopy showed: WCC 454, RBC 279, epithelial cells 52, no casts. Urine culture revealed heavy mixed growth with multiple organisms.
Question: What is the diagnosis?
Answers:
Porphyria
Propofol infusion syndrome
Purple urine bag syndrome
Blue diaper syndrome
Differential diagnoses: Discoloration of urine can be caused by trauma if blood stained, urinary tract infections, ingestion of dye (methylene blue), medications (amitriptyline, indomethacin, triamterene, flutamide, and phenol).
Explanation:
Porphyria usually presents with severe pain with neuropsychological symptoms or photosensitivity, and urine discoloration is likely to occur from initial onset of disease.
Propofol is an anaesthetic agent, excreted in the urine as phenol derivatives which can cause a green urine discolouration1. This medication is unlicensed for End of Life Pathway. Propofol infusion syndrome is associated with prolonged high dose infusion, but is not always accompanied by urine discoloration.
Blue diaper syndrome is an inherited metabolic disorder of tryptophan with presentation at infancy2-3.
Correct answer
Purple urine bag syndrome (PUBS)
Purple urine bag syndrome (PUBS)
PUBS is an uncommon condition with purple discoloration of the urine catheter system. This phenomenon is due to the presence of indigo and indirubin in the collected urine. PUBS was first published in 19784. Some academics would argue that PUBS was reported even earlier historically as an observation in Sir Henry Halford's bulletin in 18115-6. Two recent literature reviews suggested the prevalence of PUBS is as high as 9.8% in institutionalized patients with long-term urinary catheterisation8-9, 12.
A triad of key factors are suggested as cause of PUBS:
high level of tryptophan in the gut due to diet intake or bowel stasis
long term catheterisation8
urinary tract infection (UTI) with bacteria possessing indoxyl phosphatase and sulphatase enzymes, commonly Providencia stuarttiand rettgeri, Pseudomonas auruginosa, Proteus mirabilis, Escherichia coli,Klebsiella pneumoniae, Morganella, Citrobacter species, Group BStreptococci and Enterococci8, 13.
It is understood that bowel stasis causes accumulation of tryptophan, which leads to an increase in urinary indoxyl sulphate (UIS). In the presence of indoxyl phosphatase and sulphatase enzyme activities, whilst collected in the catheter system, UIS is degraded to form a mixture of indigo and dissolved indirubin in the plastic11, coating the catheter system with a purple appearance. Intensity of discoloration is deeper the longer the urine is in contact with the catheter plastic7, 10-12. The urine does not appear purple prior to entering the catheter.
Recent literature7-8 also suggested female gender, alkaline urine, bed bound debilitated patient population, PVC material7 and institutionalization are further predisposing factors of PUBS.
Management of PUBS requires catheter change and treatment of underlying UTI.
Good catheter hygiene and shorter duration of catheterisation can reduce PUBS1.
On discharge from hospital, secondary care providers have a duty and obligation to communicate with primary care provides – particularly the general practitioner – to give information regarding the reasons for admission, results of investigations, procedures performed, treatment instigated and importantly follow-up management. Therefore the transition of information between secondary and primary care is vital for care management and hence patients’ safety.
This information is shared in the form of a ‘discharge summary’. It is the responsibility of the secondary care team to provide this. The level of detail given has been found to vary not just between different NHS trusts or hospital but also between different wards and individual doctors completing the discharge summary – this can create many problems as communication plays a pivotal role in patient care.
The information given in the discharge summary is all that a patients’ GP knows in regards to their hospital admission and management. A discharge summary is effectively a form of ‘handover’. A hospital physician may instruct the GP to do certain things in regards to follow-up; for example check blood results, review results of investigations arranged as outpatients or simply review the patient clinically. The more information that is transferred across from secondary to primary care the more awareness the GP has to what has happened and what needs to happen, which leads to better patient care.
A discharge summary can also be a valuable document for when a patient is admitted to hospital; if their notes are not available a past discharge summary will provide useful information (re. past medical history and drug history in particular) to the medical team who may have no prior knowledge of the patient, this is invaluable if it not possible to take a history from a patient and is also useful in directing investigations if a patient has been admitted with the same complaint(s). Of course this depends on the patient having a copy of the discharge summary with them on admission or the ability to access previous discharge summaries electronically.
Good documentation is vital in the healthcare setting. All documentation, no matter in what form, must be clear, accurate and legible. Any type of document is useless if it cannot be read. The GMC and Royal College of Physicians stress the importance of documentation1, 2.
The importance of the discharge summary has been highlighted in the last few years. There has been a move from the traditional hand-written discharge summary – commonly referred to as the TTA (to take away) – to the use of computer software providing an electronic discharge summary (EDS). The latter not only provides more detail but also aims to deliver it to the primary care setting in a timelier manner; for example, in the future, once all EDSs are completed at Barking, Havering and Redbridge University Hospitals NHS Trust there are plans for them to be automatically emailed to a patients GP surgery – currently this scheme is being trailed at certain GP surgeries. This complies with the requirement and recommendations made to secondary care trusts to provide the GP with a discharge summary within 24hrs of a patients’ discharge from hospital – consequently reducing previous financial penalties when not achieved and thus being more cost efficient.
The advent of the EDS has impacted the daily working of the junior doctor, who is commonly, the individual on the secondary care team whose role it is produce the discharge summary. Previously with a TTA a patient could be discharged home without all the constituents on the form being completed and so a GP would be provided with an incomplete discharge summary. At BHR University Hospital NHS Trust in order to produce a finished EDS - and essentially discharge the patient - all constituent sections have to be completed before it can be electronically sent to pharmacy so that the patient sent home with their medications (the discharge summary acts as a prescription). Therefore producing an EDS is more time consuming in comparison to a TTA. However an EDS does have advantages (see Table 1).
Table 1: Comparison of EDS and TTA
Any form of discharge summary is user dependent; what is written is determined by the individual doctor producing the document therefore there is no guarantee that they have documented everything that occurred during admission. In the case of the TTA user dependence also refers to the legibility of the writing, the durability of the carbon copies produced, as well as the level of detail of the discharge summary produced.
In 2008 Newham University Hospital Trust introduced the EDS, the trust audited this process and found it to be successful3. 2010 saw the introduction of the EDS at BHR University Hospital NHS Trust. The EDS was piloted on Sunrise B ward of Queen’s Hospital, Romford. The purpose of this audit is to establish if the introduction of the EDS at BHR University Hospital NHS Trust has been successful. The audit aims to determine if the EDS method is superior to that of the traditional TTA – this will be achieved by comparing the completion rates for specific criteria of the discharge summary. This audit also aims to identify areas of improvement and recommendation for the EDS.
Design and Method:
An opportunistic sample of 50 TTAs and 50 EDSs were selected from the patients admitted to Sunrise B (‘Care of the elderly’) ward, Queen’s Hospital, Romford in a two-month period (January to February 2011). Thus this is a retrospective audit. No exclusion criteria for selection of discharge summaries was set. For each discharge summary completion rates for the different fields of the discharge summary were recorded. Table 2 shows the criteria fields included in each type of discharge summary.
Table 2: Comparison of EDS and TTA criteria
The Royal College of Physicians have published their recommendations for the structure and content of the discharge summary. Section headings include
GP details - name, address, practice code
Patient details – surname, forename, date of birth, gender, NHS number, address, telephone number
Admission details – method of admission, source of admission, hospital site, trust, date of, time of
Discharge details – date of, time of, discharge destination, discharging consultant, specialty
Clinical information – diagnosis at discharge, operations/procedures, reason for admission/presenting complaint, allergies, investigations and results, treatments, discharge medications, medication changes
Advice, recommendations and future plan – hospital/GP/community
Person completing summary – doctors name, grade, specialty, signature, date of completion4
This audit establishes which method of discharge summary is more compliant with these recommendations.
Data analysis was mainly descriptive. Data collected was tabulated and represented as percentages. Graphical representation of the data was performed using Microsoft Excel. Due to the nature of the study and data collected more sophisticated statistical analysis, such as that requiring the use of SPSS software, was not warranted.
Results:
Results demonstrate significant differences between the TTA and EDS completion rates for criteria of the discharge summary. Table 2 presents the data as percentages in a tabulated form. Compared to the TTA, the EDS had a higher rate of the following six criteria of the discharge summary documented; diagnosis, co-morbidities, investigations, drug history, discharge destination and instructions for GP.
Table 3: Summary table of data
Patient details and admission date.
The TTA had lower completion rates for these fields than the EDS. The EDS software automatically enters these fields therefore it is not possible for this criterion to be incomplete. The correct patient details ensure continuity of care and patient safety. If patient details – i.e. full name, date of birth, hospital number and address - are not present those with similar names could be mixed up.
Diagnosis.
The TTA performed poorly on documenting diagnosis. The EDS had a completion rate significantly higher than that of the TTA (EDS completion rate = 88%, TTA completion rate = 48%). Figure 1 represents these findings. The main objective of a discharge summary is to inform primary care of the diagnosis to enable healthcare management, therefore it is crucial and pivotal information, for it not to be included in the discharge summary is illogical.
Co-morbidities.
Neither TTAs nor EDSs documented co-morbidities well. However the EDS, yet again, outperformed the TTA. See Figure 1. Documenting co-morbidities has important repercussions for clinical coding and financial incentives (see below).
Investigations.
Coincidently, 62% of TTAs did not document investigations that the patient had had in contrast to 62% of EDSs that did. See Figure 1. There is no guarantee for either discharge method that all investigations are listed; it is dependent upon the doctor who is producing the discharge summary.
Figure 1: Graphical representation of data
Drug history.
As previously mentioned, EDS has to have a completed drug history before the patient can be discharged and hence they have to have a 100% completion rate for this criterion. TTAs only achieved a 64% completion rate as Table 3 demonstrates.
Review of case.
This is not a criteria field on the TTA document. Therefore 86% of TTAs provided no review. 88% of EDSs did provide a case review. Just fewer than 10% of EDSs were incomplete for this item.
Discharge date.
Like the admission date, a discharge date is automatically completed on an EDS thus the completion rate is 100%. However, this date is the date in which the EDS is completed and may not be the actual day the patient leaves hospital because sometimes the EDS is completed (and so the medications dispensed) the day prior to discharge or patient discharge may be delayed. The TTA achieved a 66% completion rate.
Discharge destination.
This is not a criterion present on the TTA and thus 100% of TTAs did not fulfil this requirement. EDSs had a 98% completion rate.
Follow-up arrangements.
The majority of EDSs documented the follow-up plans for a patient (88% in total, 70% specifically for GP follow-up). 46% of TTAs documented patient follow-up required, specifically 44% for hospital follow-up. 54% of TTAs documented no follow-up. In summary, 88% of EDSs documented follow-up in comparison to 46% of TTAs. These findings may be a limitation of the study i.e. patient selection rather than failings in documentation.
Instructions for GP and functional status.
Coincidently, 92% of TTAs did not document ‘instructions for GP’ in contrast to 92% of EDSs that did. ‘Instructions for GP’ is not a criterion on the TTA document.
Functional status.
‘Functional status’ is also not a criterion on the TTA document and so all TTAs were not complete for this. 64% of EDS had a completion rate for documenting ‘functional status’. Functional status indicates a patient’s mobility status, self-care abilities, hearing and sight impairment.
Discussion:
This audit has established that the EDS has a higher completion rate for criteria on the discharge summary, significantly so for documenting diagnosis, co-morbidities, investigations, drug history and instructions for the GP.
One major concern that has been highlighted in performing this audit is the documentation of co-morbidities. Due to variations in training many doctors are unaware of how and where to enter this information on the EDS – there is a specific window that opens on the software program to input this information. Junior doctors were documenting patients’ past medical history under the field of ‘diagnosis’. Co-morbidities should not be listed under ‘diagnosis’ - this infers a new diagnosis - as they are not the acute problem.
The coding of the diagnosis [the acute problem], in context of a patients co-morbidities, results in a condition specific ‘fee’ being paid to secondary care. For example the ‘fee’ received for a patient diagnosed with a respiratory tract infection is different for that when the patient is diagnosed with a respiratory tract infection on the background of dementia. Inaccuracies in diagnosis lead to incorrect coding and measures of incidence. Co-morbidity is ‘any condition which co-exists in conjunction with another disease’. It is a requirement of the discharge summary to document certain co-morbidities – as determined by the Clinical Coding Co-morbidity Working Group (CCCWG)5. Although the discharge summary is not the recommended source documents for use in clinical coding – patients medical notes are used instead – it can help direct and inform those responsible for clinical coding. In should be borne in mind that it is the treating clinicians’ responsibility to document co-morbidities relevant to the current admission. Accurate and correct clinical coding will result in financial gains. Clinical coding has more important purposes other than just financial; it allows the monitoring of health services, epidemiological research, NHS planning of provisions, as well as clinical audit and governance6.
The amount of information documented is user dependent; the level and amount of detail written is subjective. For example there is no guarantee that all the investigations that a patient had are documented. One doctor may provide a whole paragraph to summaries [‘review of case’] whereas another may just write one sentence. Educating those whose task it is to complete the discharge summary about how vital and important it is, along with the role it serves in healthcare management, may influence the effort and time dedicated to producing an EDS. The principles of clear, complete and concise documentation should be applied to both the patients’ discharge summary and their medical notes.
Other healthcare professionals should also contribute to producing the discharge summary, in particular occupational therapists and physiotherapists who are more aware of a patients ‘functional status’ than the doctors. More accurate completion of this item could be achieved with their input.
At the moment with the EDS software system used at BHR University Hospital Trust once an EDS has been printed there is no means of changing any of the information. It cannot be re-accessed to document new or change existing details. Often an EDS will be finalized and so printed for a patient to be discharged home on that day for the discharge then to be delayed. The discharge date document on the EDS should be the actual date the patient is discharged from hospital. Therefore it should be possible to be able to re-access and change details on the EDS.
The results of this audit show that the EDS system used at BHR University Hospital Trust is better then the EDS system audited at Newham in 2008. The Newham audit did not focus on all the criteria fields of the discharge summary or compare with a hand-written discharge summary method, however there is place for comparison with the results of this audit.
Table 4: Comparison of results with findings of Newham audit
This audit has established that the EDS method provides a discharge summary more compliant with the Royal College of Physician’s recommendations on the structure and content of discharge summary in comparison to the TTA.
The EDS will inevitably replace the TTA in time. However it should be remembered that there is still a place for the TTA in clinical practice e.g. locums do not have passwords to access the software programme, if computers are not working, fail or are unavailable. At the end of the day, a discharge summary is better than no discharge summary.
Conclusion:
The findings of this audit show that the EDS is a far superior method of producing a discharge summary than the TTA. The EDS provides a more informative and detailed discharge summary, which is always legible. The discharge summary is often the only source of information a GP is given in regards to a hospital admission and therefore secondary care providers have an obligation to provide clear, complete and concise information.
This audit does highlight that there are areas for improvement and recommendation:
The importance of a discharge summary should be highlighted to all individuals whose responsibility it is to complete them. This could promote better compliance at completing all items and completing them more thoroughly.
EDS training should make users aware of the ‘co-morbidity’ section. Past medical history should not be listed under new diagnosis. This should be a compulsory part that has to be completed before an EDS can be finished.
Occupational therapists and physiotherapists should be able to complete the ‘functional status’ criterion. This should be expanded to give more information and details to primary care providers.
The documentation of certain co-morbidities (those determined by the CCCWG) should be done by ‘tick list’ selection therefore it will not rely upon the individual doctor to remember to document such co-morbidities. All the co-morbidities that should be documented could be listed and the user selects those that the patient has. This will improve the trusts performance in regards to the financial rewards linked to discharge summaries.
The audit should be performed again in 12 months to access if EDS are maintaining high completion rates, to identify further improvement in completion rates and identify any further areas for improvement or recommendation.
Discussion of both TTA and EDS could be a part of the regular weekly supervision of junior medical staff by their prospective consultants.
A discharge summary should also be checked by nursing or clerical staff prior to letting the patient leave the ward to see if all components are completed.
Doris-Eva Bamiou is a Department of Health HEFCE funded Senior Lecturer at the UCL Ear Institute, and Consultant in Audiovestibular Medicine at the National Hospital for Neurology and Neurosurgery. She is also Honorary Consultant at the RNTNE Hospital and Great Ormond Street Hospital. She sees both adults, with vertigo, hearing problems or auditory processing disorders, and children with auditory processing disorders and complex communication needs in her clinics. She works in an academic, multidisciplinary environment.
After completing specialty training in ENT in Greece, Ms Bamiou trained in Audiological Medicine in the UK. During her training, she spent a three-month fellowship in Professor Musiek’s department in the States (on a stipendium from Professor Musiek and a grant from the TWJ foundation), where she trained in the diagnosis and management of patients with auditory processing disorders. Her PhD degree is onauditory processing in patients with structural brain lesions.
She is Director of the MSc in Audiovestibular Medicine at UCL. In addition, she has been Director and Organiser of the Current Trends in Auditory Processing Disorders instructional courses for the past several years. She is immediate past Secretaryof the British Society of Audiology (BSA), and Chair of the Auditory Processing Disorders Special Interest Group of the same Society. She is adviser in Audiology to the JLO, and in the Editorial Board of the Audiological Medicine journal.
She has a keen interest in research. Interests include the aetiology of hearing loss, auditory processing disorders in the presence of other neurological conditions as well as in the normal population, auditory neuropathy, vestibular rehabilitation and overlap between psychiatric and vestibular disorders.
How long have you been working in your speciality?
I first became interested as an ENT trainee in Greece, in 1993. At the time I was at a paediatric hospital, and we did a lot of paediatric testing (distraction and ABR). In 1994 I moved to an adult hospital, where I came across and learned to test and manage adult patients with vertigo and hearing loss.
Which aspect of your work do you find most satisfying?
Solving clinical problems, teaching postgraduate students, designing research projects and interpreting research results give me equal satisfaction – I enjoy equally the patient/doctor or student/teacher interaction and the intellectual challenges.
What achievements are you most proud of in your medical career?
I set up the first adult clinic for patients with auditory processing disorders at the National Hospital for Neurology, and the first multidisciplinary clinic in this field, again at the same hospital.
Which part of your job do you enjoy the least?
Administration and form filling exercises.
What are your views about the current status of medical training in your country and what do you think needs to change?
I wonder whether trainees get enough proper training in their very early days on and whether the length of the training is sufficient for them to be able to function independently by the end of their training.
How would you encourage more medical students into entering your speciality?
We do Audiovestibular Medicine Taster days, and we encourage them to come and “shadow” us to see what it is really like.
What qualities do you think a good trainee should possess?
He/she should be kind, hard working, highly motivated to learn and able to develop independent thinking.
What is the most important advice you could offer to a new trainee?
It may be hard work training as a Doctor, but it’s all worth it!
What qualities do you think a good trainer should possess?
Amongst many other things, empathy, and the ability to teach each trainee at their own level.
Do you think doctors are over-regulated compared with other professions?
Not more than is required.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what shouldbe done to counter this trend?
I think it is difficult to reconcile managerial activities with a doctor’s role.
Which scientific paper/publication has influenced you the most?
Several. I tend to read a lot of papers for lectures etc so this changes every few weeks!
What single area of medical research in your speciality should be given priority?
I could not separate one more than others.
What is the most challenging area in your speciality that needs further development?
Rehabilitation (auditory and vestibular) of the patient with complex needs.
Which changes would substantially improve the quality of healthcare in your country?
More funding and more rationalized use of free NHS services, depending on the patient’s income.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Yes, by working closely and by educating managers.
How has the political environment affected your work?
Not at all.
What are your interests outside of work?
I read a lot of books of every kind, I go to the theatre and to art exhibitions.
If you were not a doctor, what would you do?
This will sound very boring. I would still like to be a doctor!
Interest in cross-species transplantation has recently been rekindled1. This is due to many developments including the shortage of donor organs, advances in transplant medicine, investment in biotechnology research, and the non-availability of more ethically suitable alternatives to human organs. Increasing success rates in allotransplantations (organs from different member of the same species) has increased the demand on donor organs1, 2. Other types of transplantation include autotransplants (a person’s own organs or tissues are used for transplantation) and isotransplants (organs from one person are transplanted into another genetically identical person, like an identical twin). These options are limited in terms of body parts used and numbers.
Good facts inform good ethics. It is therefore obligatory to look into the current research knowledge about xenotransplants (organs from one species to another, for example animal to human) in more detail. The advocates of xenotransplantation argue that it could provide organs “relatively quickly” and hence save more lives. If animal organs were easily available for transplantation most eligible recipients would receive the transplantation much earlier on in their illness. It is argued that this may decrease distress and suffering. Whilst xenotransplantation may theoretically increase the survival time, it is unclear, however, whether the negative impact on recipients’ quality of life due to long-term immunosuppressant therapy and the risk of zoonotic infections would in fact worsen the overall long-term outcome3. Recent research suggests that xenotransplantation may be associated with the transmission of pig microorganisms including viruses, bacteria, fungi, and parasites. Because of the recipient’s likely immunosuppressed state, infection and pathologic consequences may be more pronounced. Transmission of most microorganisms with the exception of the porcine endogenous retroviruses may be prevented by screening the donor pig and qualified pathogen-free breeding. However, porcine endogenous retroviruses represent a special risk as they are present in the genome of all pigs and infect human cells in vitro. Until now, no porcine endogenous retrovirus transmission was observed in experimental and clinical xenotransplantations as well as in numerous infection experiments4. Nevertheless, strategies need to be developed to prevent their transmission to humans. It is equally possible that many eligible recipients may be denied having a trial of xenotransplantation by doctors who believe that there is an unfavourable risk-benefit ratio. The limited long-term data on outcomes of xenotransplants thus renders ethical analysis difficult.
There is some evidence to suggest that the recipients of animal organ donation may develop a different self image with possible consequences for their identity5,6. This happens with human organs at times, but may be a more significant problem with animal organs, as the recipient knows that they have been given a non-human organ. Loss of identity jeopardises the core principle of autonomy, which underpins all medical treatment.
The risk of zoonosis to the recipient and to the wider society cannot be accurately estimated7. Hence there is a requirement for vigilant post-operative monitoring5 with a possibility of engaging article5 and 8 of the European Convention of Human Rights (for England and Wales: Human Rights Act 1998)†. Article 12 may also be engaged as the recipients may be restricted from having physical relationships, carrying out their routine day to day activities and socialisation. This is because the prevention of possible risk to the wider public from zoonosis may require the recipient to be put under restrictions with regard to their engagement with others. This may include restrictions to go out, which can result into de facto temporary detentions at home. Hence consenting to xeno-transplantation would be “binding and contractual” over a long period of time. The subject may not have the right to withdraw. This is entering into a de facto contract with potential restrictions or even deprivation of human rights. This would restrict the ability to give informed consent even for a well informed patient, as it is difficult to be fully appreciative of future restrictions of one’s liberty.
Autonomous decision making and thus informed consent may also be put at risk by other factors surrounding xenotransplantation. The decision to embark on xenotransplantation may be primarily driven by an instinctual wish to survive due to a lack of other viable alternatives. Patients in these circumstances may have little or no consideration to medium and long-term effects on themselves and society. However, it is the consideration of such long-term consequences that make a truly autonomous decision, and differentiate it from a decision that is purely based on immediate instinct. Whilst the wish to survive is legitimate it is difficult to make decisions free of the pressure to survive when there is a lack of alternatives.
It also brings up an even more important question: Can any person everconsent to a future restriction or deprivation of their liberty or other human rights? Even if there were an option to define acceptable future restrictions it would be likely that patients could still challenge the legality of any such agreements. They could quite reasonably argue that they have agreed to the restrictions under duress because of a lack of viable alternatives to their xeno-transplants.
Xenotransplantation touches questions of utilitarianism (greatest good for the greatest numbers) and public protection2. Utilitarianism takes into account the reasonable interests of society in good outcomes, fairness in the distribution of resources, and the prevention of harm to others. The Nuffield council on bio-ethics embraces a utilitarian approach. However, there are limits to the utilitarian argument for xenotransplants. Even if they were widely available, the treatment would be immensely expensive. Production of a pathogen free donor organ would involve rearing animals in strictly controlled environments, subjecting them to rigorous standards of examination and surveillance. The additional costs of developing a sustainable work force to provide transplantation and post-transplant surveillance of the patient and the community would be high. The insurance providers may not cover expenses of a xenotransplant. Public health care providers may decline to provide this treatment as it may not be recommended by expert groups as cost effective. Xenotransplantation may commence in the developing world where the regulations are lax and the poor can be more easily exploited8. Patients who would potentially benefit from xenotransplantation may not be able to afford it due to its cost with serious implications for fairness.
Xenotransplantation also raises other ethical questions in relation to the wider community. We have seen that consent of an individual to a xenotransplant has significant bearing on the protection of society7. Should the members of a community therefore be consulted if there were any xeno-transplantation experiments in their region? The risk is primarily due to the risk of zoonotic infections, the need for surveillance, and possible quarantine of contacts7,9. In addition, if health authorities were to fund expensive experimental interventions like xenotransplantation, other routine treatments of greater potential benefits to society may be jeopardised. Society may also have views about particular animals being used as donor animals10. For example religions like Islam and Judaism may feel that pigs are ‘ritually unclean’. They may therefore not approve of certain animals to be used for donation, and more worryingly may fail to socially accept recipients with such ‘unclean’ transplants11.
From a deontological perspective (this judges the morality of an action based on the action's adherence to a ruleor principle) some authors assert that animals have rights similar to those considered appropriate for humans12,13. The protection of animals has legal status in many countries. Consequentialists may view the suffering and death of an animal as acceptable for the betterment of a human patient, as they would judge the morality of an action primarily by its end result. They would argue that potential benefits and improvement in human welfare arising from xenotransplantation may justify the loss of animal life. However, this will never satisfy the animal rights lobby; especially as whilst minimising the risk of acquired infections, the animals have to forgo greater suffering in the form of isolation, monitoring and investigations. Furthermore, genetic modification can have both immediate and long-term negative effects on animals.
In summary, xenotransplantation has significant ethical consequences. On an individual level, there are the questions of pressure to consent that may negate autonomy and the validity of that consent as well as the difficulties that arise when patients are asked to consent to future restrictions of their human rights. On a societal level there are questions of cost and benefit analysis as well as risks from zoonotic infections. In addition, questions of animal rights need to be addressed before any programs are likely to go ahead.
†Appendix of articles of the Human Rights Act.
Article 8 of the Human Rights Act 1998 (The right to respect for private and family life, home and correspondence)
Article 5 (The right to liberty).
Article 12 (The right to marry and found a family)
“The more we care for the happiness of others, the greater our own sense of well being becomes.” The Medicine of Altruism: Dalai Lama
Introduction
The fundamental mission of any medical school is to select those individuals who possess the qualities and personality traits best suited to becoming a good doctor. The first part of this article takes a critical look at how United Kingdom (UK) medical schools select doctors, which can vary considerably, and asks whether it can be improved. The qualities needed to be a good doctor are discussed and asks whether work experience illustrates at least some of these personal qualities and should therefore be an essential prerequisite for applying to medical school. Such experience helps the student to make an informed career choice and exploring it at interview can reflect student motivation to study medicine. My experience in Ghana gave me the opportunity to find out at first hand if I had what it takes to become a doctor. The trip was totally inspirational. It made me realise that medicine is much more than being master of all sciences. In Ghana I saw many of the qualities one needs to be a doctor, how this contrasts with the current selection criteria in the UK, and made me wonder whether the UK system offers our society the best practice available.
Critique of UK medical school selection
Applying to medical school has become increasingly competitive. Selection into medical schools is not an exact science but one assumes that best available evidence is being used. The present system almost certainly turns away students who would make good doctors and accepts some who are mediocre or poor or even drop out of medicine altogether. The selection criteria for entry into medicine have to be accurate. However, no system is fool proof and the number of drop-outs in UK training stands at 6.8 – 12%.1,2,3 I believe that better selection criteria would reduce the drop-out rate and save personal distress among those who made an unwise choice. This makes economic sense. There is widespread agreement that we should select medical students on wider criteria than scores of academic success,4, 5 though in practice many medical schools have valued academic scores at the expense of other considerations.6, 7 A Levels alone should not be sufficient to gain a place at medical school. True communication calls for some shared life experiences and empathy with others. I believe that students who are totally absorbed in their studies to the exclusion of almost everything else are less likely to make good doctors. In one study, a ten-year follow-up after entry into medical school showed no correlation between academic score at entry and drop-out rate, but significant correlation between low interview scores and later drop-out.8 Reasons for drop-out were a variety of personal reasons including lack of motivation for study or for medicine. In a medical school that carefully evaluates applicants, empathy and motivation to be doctors were found to be particularly important in predicting both clinical and academic success.9
Another major study, looking at the dropping out from medical schools in the UK over a ten year period (1990-2000), 10 showed that drop-out rates increased during this period and concluded that the probability of dropping out of medical school is 20% lower for students with a parent who is a doctor. The authors comment that this may be the result of greater commitment or better preparation and insight before starting the course. Ethnic background of students was recorded only between 1998-2000. The study found that Indian females were around 1.9% less likely to drop out compared with white females, whereas Indian males were no different from white males. Other ethnic groups were less likely to drop-out by around 0.8%. A concerning fact in this paper was the degree to which drop-out rates varied between different medical schools. No study to date has been done to find the reasons for these differences. Surely potential applicants need to be aware of these results. The differences could be accounted for by variable selection processes among the medical schools.11 Some medical schools shortlist for interview only on predicted academic performance or the number of A* GCSEs or decide by the UK Clinical Aptitude Test (UKCAT) / BioMedical Admissions Test (BMAT) scores. Some use information presented in the candidate’s personal statement and referee’s report while others ignore this because of concern over bias. In some cases candidates fill in a supplementary questionnaire. Interviews vary in terms of length, panel composition, structure, content, and scoring methods. Some schools do not interview.
The commonest reasons cited in many papers for dropping out of medical school were because it is not for them, they found it boring, they did not like patients, the work environment was not what they want to spend their time on, or they did not like responsibility.12 Essentially they had realised too late that Medicine was not for them. They had failed to find out what they were letting themselves in for before applying and the medical school had failed to pick this up. There is a strong argument for pooling resources so that applicants get one good assessment instead of four poor ones.
A levels, used for medical selection, do not indicate any personality attributes of the candidate and are affected by socio-economic bias. The UKCAT was introduced to level the playing fields. This test doesn’t examine acquired knowledge and candidates can’t be coached to pass, so in theory it should provide a fairer assessment of aptitude than A level grades. It was also thought that the various components of the UKCAT, namely verbal reasoning, quantitative reasoning, abstract reasoning, and decision making, could help to pick the students who have the personality attributes to make good doctors. Unfortunately, a recent paper suggests that the UKCAT does not provide any more assessment of aptitude than A levels.13 However, an inherent favourable bias towards students from well-off backgrounds or from grammar and independent schools was also found. Moreover the test does not compensate for talented candidates whose education has been affected by attending a poor school. Another paper looked at the predictive validity of the UKCAT.14 This showed that UKCAT scores did not predict Year 1 performance at two medical schools. Although early prediction is not the primary aim of the UKCAT, there is some cause for concern that the test failed to show even the small-to-moderate predictive power demonstrated by similar admission tools.
There is no doubt that potential doctors must have enough intellectual capacity to do the job but they must also possess other important traits (Table 1):
Table 1: Personality traits potential doctors ought to possess
Concern for people
Committed to self-learning
Sense of responsibility
Emotionally stable
Professionalism
Good judgement and perception
Good communication skills
Good listener
Highly motivated
An enquiring mind
Honesty
Well organised
Integrity
Patience
Ability to handle pressure
Mental strength
Confident
Resilience
Determination
Respect for other people
Perseverance
Respect for confidentiality
Decisiveness
Tolerance
Conscientious
Hard working
Team player
An open mind
Leadership qualities
A rational approach to problems
Humility
Critical reasoning
Flexible and adaptable to change
Separate important points from detail
Logical thinking
Recognise limits of professional competence
What patients rate highly among the qualities of a good doctor are high levels of empathy and interpersonal skills.15 Personality traits such as conscientiousness have been positively associated with pre-clinical performance.16
The criteria being used more and more by admission tutors include the candidate’s insight into medicine including as evidenced from work experience.17Surprisingly, very little has been written on work experience and the value placed on it varies considerably between medical schools. Many would regard this experience as a prerequisite for entry into medical school. It enables a student to experience at first hand what he/she is letting him/herself in for. Some find the experience fascinating and challenging while others may find it is not for them. Work experience should not be seen as a hurdle to climb, but part of the decision-making process in determining whether medicine really is for you. I fear that another contributing factor to the increase in drop-out rates from medical schools is the increasing difficulty in obtaining work experience. Gone are the days when students could join theatre staff and watch an exciting operation or shadow doctors in Accident and Emergency (A&E). Useful work experience is so important and it is becoming harder and harder to get, but is still possible. Therefore considerable desire, commitment and motivation by the student are required to obtain it. The work does not need to be medically related, but work experience in any care setting is essential. These placements can be used to illustrate at least some of the personal qualities that are sought after in a good doctor including: appreciation of the communication skills required of a doctor; a thorough awareness of the realities of medicine and the National Health Service (NHS); an understanding of teamwork; an ability to balance commitments; and observation of the caring and compassionate nature of the doctors. Furthermore, as demonstrated in general practice,18 personal experiences can have a highly positive influence on an individual’s attitude to a particular speciality. Encouraging school students to experience general practice would therefore not only increase their awareness of the life to which they are about to commit, but could aid recruitment to general practice as a speciality.
My Ghana Experience
I decided that, as part of my work experience, I would go to Ghana with a charity organisation (Motec UK Life). The reason was not to impress medical admissions tutors, but to discover if I had what it takes to become a doctor. I realised how comfortably we live in our small bubble, with little appreciation of what goes on in the rest of the world. Ghana is a third world country, which not only has great poverty and malnutrition but also has many deadly diseases such as Acquired Immunodeficiency Syndrome (AIDS)/Human Immunodeficiency Virus (HIV), malaria, hepatitis, typhoid and sickle cell disease. My trip was demanding as I was stripped of my luxuries and removed from my comfort zone, but it helped me to understand the real values in life through helping the most needy and vulnerable people. I felt the suffering and the pain they went through, day in and day out, but knew that making even the slightest difference to their lives motivated me and enabled me to persevere through my time there.
One of the hospitals we stayedwas Nkawkaw, which was in the middle of a shantytown with houses made of metal sheets. Yet, despite the presence of great poverty and disease, I did not find a single person who was not extremely kind and welcoming and always smiling. It made me think of the contrasting situation back home in the UK where people were relatively well off, and yet so unhappy. I spoke to as many people as possible, not realising that I was developing my people- and communication-skills. I played football with the children and made them smile. I was able to visit the AIDS/HIV clinic and gained a first-hand account of how this devastating disease was controlled and dealt with in a third-world country. The pain, grief and suffering were immense and difficult to comprehend unless one was actually there witnessing it. AIDS here hurts everyone, but children are always the most vulnerable. The children were born with HIV from their mothers, or infected through breast milk, or in the past infected by unsafe medical treatments. They were often orphaned and destitute, having to build their own homes, grow their own food, and care for younger brothers and sisters. That is the cruel reality.
Equally heartbreaking was seeing so many people in the HIV clinic who could
not afford the anti-retroviral drug that would improve the quality and duration of life. This feeling of helplessness motivated me even further to pursue a career in medicine in order to help people at their most vulnerable. On this trip I was greatly impressed by the dedication, commitment and professionalism shown by the doctors in difficult situations. I saw doctors working with little supervision and little equipment, and yet they seemed confident, well organised, and adapted themselves well to the conditions. Their enthusiasm and compassion never waned despite working long hours.
I saw many types of operation being performed including joint replacements, hernia repairs and caesarean sections. On one particular day, I observed the team performing many knee and hip joint replacements. The deformities of the joints were much more severe than seen in the UK. I enjoyed and appreciated the skills of the orthopaedic surgeons in carrying out these operations, which were being done under spinal anaesthesia, and so I was able to talk to the patients and comfort them. Throughout the day, after seeing many operations, I did not flinch or feel queasy at the sight, and this further encouraged me to believe that I could handle a career in medicine. On watching the caesarean sections, the excitement of bringing new life into the world was overwhelming. Seeing another baby being born with severe hydrocephalus marred this. No treatment facilities for this condition were available for hundreds of miles and the baby was too ill to be transferred such a large distance. I witnessed the doctors conveying the heartbreaking news to the family with compassion. It became clear to me that there are negative aspects to this career. There is a great deal of emotion and stress to cope with in such circumstances but I believe that, given training, I would be mentally stronger to take control of these situations.
I was always allowed to follow the doctors on their ward rounds, and was encouraged to ask questions and make comments, so that I often felt that I was being treated as a medical student, which was strange in some ways but also very gratifying. On this trip I was involved in teaching and in helping to set up a workshop, which lasted for a whole day for doctors from all over Ghana. This involved lectures as well as demonstrating the latest surgical and theatre equipment. I was impressed by the teamwork and organisation shown by the group. The communication skills of the group had to be of the highest quality in order to get the message across. I found that teaching about the devastating effects of HIV, in a local school in Ghana, was particularly challenging as some of the students before me were sufferers and so I found it difficult to look them in the eye, knowing that although they were being taught the safety precautions, many did not have much of a future. This reinforced my feeling of helplessness but, although this situation was heartbreaking, I remained enthusiastic for the children, to keep their morale high in order to prepare them for their inevitable future.
Conclusion
My trip was totally inspirational. It made me realise that medicine is much more than being a master of all sciences. In Ghana I observed in doctors the real passion and drive needed for medicine as well as many other essential qualities I believed doctors needed. This contrasts with the current selection criteria in the UK; sadly we are missing out on too many good doctors because of our obsession with grades rather than looking for real qualities that are going to make a difference to our patients.I discovered that seeing the immense suffering, and the close bond of doctors and patients in an entirely different social and economic context, helped me to evaluate and shape my own emotions and personal values. My motivation in wanting to become a doctor has increased tremendously since this trip. My trip to Ghana also inspired me to create a medical journal in my school as a fund-raising initiative. I brought together a group of fellow students to write articles about common teenage problems (teenage drinking, anorexia, obsessive compulsive disorder (OCD), stress, smoking, sexually transmitted diseases (STDs)) as well as articles on euthanasia and assisted suicide, stem cell research and the NHS. I wrote about my personal experiences in Ghana in addition to editing and publishing the school journal. All the funds raised from the school medical journal will be going to the HIV victims in Ghana.
Malaria is a major worldwide scourge, infecting and killing several million individuals each year1. Malaria is common in mostly tropical and subtropical areas such as The Americas, Asia and Africa2, 3.
The NADPH oxidase complex is responsible for the reduction of oxygen in cells, yielding a superoxide anion (O2˚-) that is subsequently converted into other ROS; including hydrogen peroxide (H2O2) and the hydroxyl radical (OH˚)4.
The Sequence analysis showed that the NCF1 wild type gene is 15,236 bp long, contains 11 exons and has an intron/exon structure identical to the highly homologous pseudogene5. The pseudogene which is highly homologous to the wild type gene is located on the same region of the chromosome, which is 7q11.23 of chromosome 76. Comparative sequence analysis between the wild type gene and pseudogene demonstrates greater than 98% homology but the pseudogene has a GT deletion (ΔGT) at the start of exon 27. The genomic pattern of wild type NCF1 gene and its pseudogene may influence the production of reactive oxygen species (ROS) in parasitic and bacterial infections and also in autoimmune diseases.
During malarial infection, the ROS production can contribute to rapid parasite clearance in mild malaria8 but in severe malaria the high capacity production of ROS was associated with anaemia. This means that ROS has a possible role in both parasite clearance and anaemia during P.falciparum infection9. Genetic variation in components of the leukocyte NADPH oxidase may, therefore, influence disease susceptibility to, and disease duration of parasitic infection and autoimmune disease10.
Study Design
Inclusion and exclusion criteria
Patients who had fever with malarial parasites detected microscopically from blood smears and had no evidence of other illnesses were selected. Patients were excluded if they developed other illnesses within three days of admission or if there was any other present infection.
Relatives of patients in the hospital and in the laboratory and members of the community without malaria or any other febrile illness were included after clinical evaluation. These formed the control group of healthy individuals.
Patients and healthy individuals
To determine the association of NCF1 gene in malaria, the blood samples were collected from malarial patients and healthy individuals in storage tubes coated with EDTA. Malaria was diagnosed on the basis of clinical observation and positive smear test containing various types of plasmodium.
Materials and Methods
The restriction fragment length polymorphism (RFLP) method was performed to determine the prevalence of NCF1 gene GT deletion (ΔGT) among patients with malaria and among healthy individuals in a Pakistani population. In order to determine whether there was an association between NCF1 gene GT deletion (ΔGT) at the start of exon 2 with susceptibility to malaria, 88 malarial patients and 100 healthy individuals were genotyped for the GT deletion by restriction enzyme analysis.
Genetic Analysis
Genomic DNA of patients and of the healthy control subjects was extracted from venous blood samples using the nucleospin blood extraction kit (NucleoSpin® Blood, Germany) according to the manufacturer’s protocol. The NCF1 gene was analyzed by the restriction fragment length polymorphism (RFLP) method. The exon 2 was amplified using both forward and reverse primer as shown in Table 1. The reaction mixture (50 μl) for PCR was prepared in 0.2 ml tubes (Axygen®, California, USA) by adding the following: 1.2 μl of sample DNA (50 ng /μl), 5 μl (10X) from the PCR buffer (Fermentas, Burlington, Canada), 4 μl of 25mM magnesium chloride (MgCl2) (MBI Fermentas, Burlington, Canada), 3 μl of 2 mM deoxyribonucleotide triphosphates (dNTPs) mixture (MBI Fermentas, Burlington, Canada), 2.6μl of each forward primer (10 pm/μl), 2.6 μl of the reverse primers (10 pm/μl) and 1.2μl Taq DNA polymerase (MBI Fermentas, Burlington, Canada) in 30.40 μl nuclease free water with cycling conditions 95 °C for 5 min, followed by 35 cycles at 95 °C for 1 min, 60.6 °C for 1 min, 72 °C for 1 min and finally a 10 min extension at 72 °C.
The amplified products were then treated with the restriction enzyme BsrGI (Geobacillus stearothermophilus GR75) (Fermentas life science). For a 20 μl mixture we took 10 μl of PCR product, 2 μl 10X buffer tango, 1 μl BsrGI enzyme and 7 μl of nuclease free water to make the mixture volume up to 20 μl and checked the result on 2% agarose gel.
Table 1: sequence of primers and product size
Deletion Exon
primers
sequence
Product size
DNCF2F
5'-GCTTCCTCCAGTGGGTAGTG-3'
DNCF2R
5-GCAAGACCCTGGGTGACAGA-3'
GTGT
358 bp
GT
356 bp
Statistical Analysis
Statistical analysis was performed using the Study Result Software Version 1.0.4 (CreoStat HB Frolunda, Sweden). The association of both types of genes in malaria patients and healthy individuals were compared using the χ2 or Fischer’s exact test. Similarly to elucidate whether there was an association between the age and gender of both patients and healthy controls, analysis was done using the T-test and chi-square test by the online Graphpade software.
Results
Characteristics of patients
The characteristics of patients and healthy individuals are mentioned in Table 2 and table 3.
Table 2: Total number of patients and healthy individuals with their respective mean ages
Characteristic
Patients
Mean age
Control
Mean age
P value
± SD
Total number of subjects
88
22
100
26
0.43761
0.8627
Adults > 22 year
60
60
Children <22 year
28
40
Table 3: Total number of Patients and healthy individuals enlisted with respective mean age.
Characteristic
Patients
Mean age for patients
Control
Mean age for controls
No of males
75
24
80
26
No of females
13
20
20
27
Total
88
22
100
26
A chi-square test was performed to test the null hypothesis regarding whether there was an association between gender and the number of subjects in the control group and patient groups. No statistically significant association was found, c2 (1, N = 188) = 0.559, p = 0.4545”. Similarly, a chi-square test was performed to test whether there was any association between the gender and ages of subjects in the control group and in the patient group. Again no statistically significant association was found, c2 (1, N = 188) = 0.299, p = 0.5848”.
PCR amplification of exon 2 of NCF1 gene
The exon 2 was amplified by polymerase chain reaction to obtain 358 base pair long regions in the case of the wild type gene and 356 base pair long regions in the case of the pseudogene. The products were treated with a restriction enzyme, Geobacillus stearothermophilus, GR75 (BsrGI) which digests only the wild type gene (GTGT), which meant two bands of 265 bp and 93 bp were obtained respectively. Whereas with the pseudogene (ΔGT) there was no digestion and the original band of 356 bp was obtained. When the individuals had both the wild type gene (GTGT) and the pseudogene (ΔGT)three bands of 265 bp, 93 bp and 356 bp were obtained, two of the wild type gene and one of the pseudogene respectively, which is shown in figure 1.
Figure 1: Agarose gel (2%) showing genotypes of eight patients with malaria. The GT deletions (ΔGT) were checked using the RFLP method, using the restriction enzyme BsrGI. The lane L contains 50 base pair markers, while lane 1 contains a negative sample and 3 and 7 contain amplified wild type gene (GTGT) products. Lane 2, 5 and 6 contain amplified wild type gene and pseudogene (ΔGT) products and lane 4, 8 and 9 contain amplified pseudogene products respectively. The result shows that the 2nd, 5th and 6th patients have both the wild type gene and pseudogene (GT/GTGT). The 3rd and 7th patients have the wild type gene (GTGT) and THE 4th, 8th and 9th patients have the pseudogene (ΔGT).
Genotypic Frequencies of wild type gene and pseudogene in Malaria Patients
It was found that in the Pakistani population, the frequency of the wild type gene in malarial patients (37.5%) was no higher than in healthy individuals (45%) with P = 0.30427. The combination of wild type gene and pseudogene(GTGT/ ΔGT) was equally prevalent in malarial patients (39.8%) as it was in healthy individuals (40%) with P = 0.99999,while the pseudogene (ΔGT) was also slightly different among healthy individuals (15%) as compared to malarial patients (22.7%) with P = 0.19263 which is shown in table 4. There was no significant association found because the P values was greater than 0.05.
Table 4: Show the association of NCF1 gene with malaria
NCF1 gene
Control (n = 100)
Frequency (%)
Patients (n = 88)
Frequency (%)
P value
GTGT
45
45
33
37.5
0.30427
GT
15
15
20
22.7
0.19263
GTGT/GT
40
40
35
39.8
0.99999
Discussion
In this study the association of a wild type gene and a pseudogene with malarial infection, which affects the hepatic, haematological and respiratory systems was investigated.
There was no association found between the wild type gene and pseudogene and the severity of malaria. The innate immune mechanisms that have been proposed to kill malaria parasites are those mediated by ROS and RNS, especially NO and ONOO-, both generated early during infection prior to the activation of adaptive immune mechanisms and later as components of the effector arm of the adaptive immune response11, 12. The parasite-killing role for these molecules has often been conflicting, especially when looking at in vitro and in vivo studies13. It was confirmed that neither RNS nor ROS are essential for the elimination of blood stage malaria parasites14. It was also shown in other studies that on occasion the generation of ROS via NADPH oxidase does kill blood stage malaria parasites, which is a controversial finding. A possible explanation of the discrepancies between Brad et al. and those of Sanni et al. is that these Plasmodium parasites differ in their susceptibility to the action of ROS, with P. yoelii and P chabaudi being more resistant than P. berghei. ROS might be incapable of killing blood stage malarial parasites for several reasons:
(i) The in vivo ability to kill malaria parasites may be masked by the antibody response of the infected host, and (ii) the killing mechanisms mediated by these molecules may function in a redundant fashion15. The present data does not confer the association of the wild type gene and pseudogene with the severity of malaria but there is a need for further study involving a larger population. However within a group of children with severe malaria during the acute disease, a weak association of the wild type gene /pseudogene (ΔGT/GTGT) ratio with ROS production in whole blood was found. It has been suggested that the wild type gene/ pseudogene (ΔGT/GTGT) ratio influences the expression levels of ROS16. However, no influence of the wild type gene /pseudogene ( ΔGT/GTGT) ratio on Plasmodium falciparum malarial infection was detected, although it was previously shown that ROS production plays a role in parasite clearance as well as in the pathology of the disease17, 9. As for parasitic diseases, in humans there has been only one study conducted so far which examined the putative genetic associations of the wild type gene and pseudogene (ΔGT/GTGT) ratio with malaria18.
Chronic pain, arbitrarily defined as that lasting longer than six months, is a clinical, social, and economic problem. It is often accompanied by feelings of low mood and despondency.
Whether chronic pain induces clinical depression or depression initiates psychosomatic pain (through physiological mechanisms) is difficult to prove. The burden of illness increases when patients suffer from both. Financial hardship and medical costs affect the quality of life which leads to difficulties in coping and further decreased functioning, making the treatment of both conditions more complicated. Therefore, better recognition, assessment, and treatment of comorbid pain and depression should, at least in theory, lead to better outcomes.
Pain is broadly categorized into three groups: nociceptive (any painful stimulus), neuropathic (for example, diabetes), and psychogenic. Nociceptive pain occurs with direct noxious stimuli. Neuropathic pain is a result of disease or injury to the nervous system or spinal cord. Psychogenic pain has no discernible physical origin. Although the precise physiological mechanisms are not entirely understood, there are two basic categories of sensory neurones. The first type is myelinated and fast conducting; the second is unmyelinated and slow conducting.
Acute pain which follows damage to tissue (an ankle sprain, for example) is usually correlated with hyperalgesia (an increase in the pain elicited by a noxious stimulus and felt as a sharp, burning sensation) and allodynia (‘other’ pain evoked by a normally innocuous stimulus) and serves to protect the injury from further trauma while allowing the damage to be repaired.
Depression is often a chronic disorder and though its symptoms may be alleviated by appropriate medication and other therapies, physical complaints tend to be more intractable. For example, fibromyalgia (FM), a syndrome characterized by widespread muscle pain and generalized tender points, is often associated with major depressive disorder.1 However, although the vast majority of patients with fibromyalgia do not meet criteria for a psychiatric disorder, psychological symptoms are common. In a randomized controlled trial of primary care patients with musculoskeletal problems and depression, antidepressant medication followed by a self-management pain programme led to improvement in both.2 The tricyclic antidepressant amitriptyline was traditionally used usually in small doses, to treat pain, with moderate success. In addition to its own intrinsic analgesic effect amitriptyline appears to enhance the effects of opioid analgesia. Other antidepressants are now in vogue; for example, duloxetine, a serotonin (5-HT)/noradrenaline (NA) reuptake inhibitor, is sometimes used for diabetic neuropathic pain.
Of the numerous neurotransmitters at least two, namely 5-HT and NA, may prove to be one common link between depression and pain. Both serotoninergic and noradrenergic pathways ascend from subcortical areas (brainstem, hypothalamus and thalamus) to the whole neocortex and mediate emotional and physiological responses.3 Their pathways descend the spinal cord and suppress nociceptive inputs. Serotoninergic cell bodies located in the raphe nucleus in the brainstem, and noradrenergic neurones located in the locus coeruleus (also in the brainstem) send projections to various parts of the brain involved in the control of mood, appetite, sexual activity, attention and concentration. Theoretically at least, a dysfunction at the level of the serotoninergic and noradrenergic neurons could affect both ascending and descending pathways resulting in the psychological and physically painful symptoms of depression. Neurotransmitters may open or close the ‘gate’ on perception of painful stimuli. Therefore adrenergic and serotoninergic pathways from the brainstem to the spinal cord will inhibit incoming painful stimuli. This is perhaps an oversimplification as some sensory fibres enter via the ventral spinal roots.
The hypothalamic pituitary axis (HPA) is probably also involved. The hypothalamus, which synthesises and secretes neurohormones, has a wide range of physiological functions including regulation of thirst and hunger, sexual behaviour, defence reactions such as fear and rage, and circadian rhythm: disturbances of all these functions are frequently seen in depressed or anxious patients. The HPA is also affected in patients with physical stress as well as major depression, as shown by increased levels of adrenocorticotropic hormone and cortisol in the plasma. Stimulation of the lateral areas of the hypothalamus produces a diffuse sympathetic discharge possibly because some areas of the hypothalamus control adrenaline and NA secretion. Prolonged stress associated with pain leads to depletion of central 5-HT and malfunction of other associated receptors.4
The hypothalamus and limbic system (whose boundaries are difficult to define) with its associated structures – the amygdala, hippocampus and septal nuclei, are involved in the mental and affective aspects of emotions. The amygdala, a cluster of nuclei in the medial temporal lobe, may have a role in the reciprocal relationship between pain and depression. The amygdala controls not only emotional behaviour but also memory. However, mixed results have been reported regarding the level of activity of the amygdala in response to pain.
Nociceptor afferents terminate within distinct regions of the dorsal horn and within the spinal cord, synapses are sites of considerable modification, hence the term ‘gate’ for the dorsal horn cells. The neurotransmitter for slow pain is believed to be substance P, and glutamate is the putative transmitter secreted by primary afferent fibres subserving fast pain.5
5-HT and NA neurotransmitter systems influence neuroplasticity in the brain. Most currently available antidepressants act through reuptake inhibition of either or both. Therefore, it would seem feasible to prescribe dual-action antidepressants when pain symptoms are associated with depression. However depressed patients with pain comorbidity are less likely to take antidepressant medications compared to those with depression alone. Also, individuals who develop pain or depression are at risk for developing the other, thus escalating the clinical management. Furthermore, when pain is refractory to treatment, it is associated with more depressive symptoms and worse depression outcomes, and vice versa. Depressive symptoms are very common in physically ill patients. Unfortunately, depression is often overlooked in pain patients because pain symptoms take priority or worse still, comorbid depression is not considered.
It is difficult to state with certainty whether or not unexplained pain is ‘psychological’. Such an assumption might be perceived as demeaning and patronizing to patients and the suggestion of providing cognitive therapy misinterpreted as him/her overplaying their reaction to pain or that the pain is ‘psychological’. Others do not like being labelled ‘psychiatric’, and are therefore reluctant to take antidepressants even when a physiological explanation is given. Pain perception involves physical and emotional factors and its primary function is to protect the organism from harm. It follows therefore, that pain thresholds and pain tolerance vary from individual to individual, and especially among patients with depression.
Antidepressants are frequently used in the treatment of depression and generalized anxiety disorders. Their use extends beyond these areas, however, and it is now accepted that antidepressants are efficacious in treating chronic pain syndromes in addition to their effects on psychological features such as low mood, inordinate guilt, or feelings of worthlessness. Because physical symptoms are often the main complaint in many depressed patients and pain is common as a presenting symptom, clinicians need to know about the dual use of antidepressants for both. Future antidepressants may involve neurotransmitters, other than 5-HT and NA, which could include dopaminergic pathways, opioid (antagonists of morphine-type drugs) receptors and the pentapeptides (enkephalins) which bind to these receptors.
Controlled teaching environment can be provided to undergraduate medical students for learning certain basic clinical skills through using manikins or models before they have to perform them on real patients. Many medical schools in the United Kingdom now have clinical skills laboratories which are equipped with a large host of such learning resources. Many medical schools promote their clinical laboratories and have dedicated lead consultants to teach, monitor and develop clinical skills. Furthermore, a wide variety of skills can be taught in these laboratories. For example, the University of Leeds Medical school offers teaching to second year undergraduate medical students in basic life support, vital signs, injections, blood glucose monitoring, cannulation and venepuncture while third year medical students are taught fundoscopy, rectal examination, urinary bladder catheterisation, doing an ECG and examination of the breast. Similarly, simulators have also been used in postgraduate medical teaching, for example, Colonoscopy simulators have been used to calculate efficiency ratio of learners. 1
However not all places in the world have clinical skills laboratories. Alternatively, some institutions teach the undergraduate medical students various basic skills in clinical supervised settings before they take up their first job as physicians. Some have assessed the level of training that their institutions have thus offered and tried to improve upon deficits. Mario Sicaja et al 2 from Zagreb University evaluated 252 students using a questionnaire asking the students to self assess their abilities on nine groups of skills and asked 129 faculty teachers to simultaneously assess the minimum necessary level of skills they expected from the graduating students. They concluded that the teachers expected higher level of clinical skills from students than that assessed by the students. Similarly, in postgraduate teaching, the students’ learning needs have been assessed by determining the difference in expectation of trainers and the trainees. 3
Effectiveness of basic clinical skills training programmes has been documented and it has been suggested that longitudinal skills training offers superior preparation for abilities during the clerkship 4. It has also been suggested that whereas students from medical schools using traditional curriculum may not differ in their knowledge based performance, (demonstrated by Multiple Clinical Questions i.e. MCQ scores) from students at medical schools with clinical skills training, the later perform better on clinical examination (measured by Objective Structured Clinical Examination i.e. OSCE). 5
However, in many other medical schools worldwide, which implement the traditional undergraduate medical curriculum, there are no clinical skills teaching sessions for undergraduate medical students. The students get to learn this first time when they are doing internship and are in direct contact with the patients. It was the same situation in Liaquat University of Medical and Health Sciences (LUMHS) in Hyderabad, Pakistan. This is a large medical school which is based in the second largest city of Sindh province of Pakistan. The first author was invited from United Kingdom to review and advise on the undergraduate medical curriculum at LUMHS. The professor of plastic surgery (second author) had started to run a voluntary clinical skills course in his department covering some general basic clinical skills and provided his data to the first author for analysis and review.
This study was devised to analyse the views of participating students regarding the course and determine their learning needs. Based on the learning needs, one could identify which resources are needed and what the University should aim to provide. Furthermore, there are no such published studies from Pakistan. This study was aimed at providing scientific information on the learning needs of undergraduate medical students from the developing world, which may be deemed to be different from the medical students in the western world.
Methods:
All medical students from fourth and final year at LUMHS were invited to attend four weeks of clinical skills course at the plastic surgery department voluntarily. The students had to attend the department after their normal working hours. There were dedicated junior doctors in the department who were given the responsibility to teach the attendees hands on clinical skills in a structured manner. The skills included history taking, organising blood tests, vene-puncture, giving intravenous and intra-muscular injections, intravenous cannulation, urinary bladder catheterisation, passing naso-gastric tube, dressing of surgical wounds, basic pre-operative assessment, basic post-operative assessment including haemo-dynamic stability, surgical theatre mannerism, principles of sterilization, identification of common surgical instruments and equipment and identification of types of drugs used in anaesthesia. The students were provided a questionnaire asking for feedback on the course which they had to fill at the end. The study was approved by the University Research and Ethics Committee. The data was computerised and statistically analysed using a statistical package. It involved all students who went through the course during consecutive sixteen months commencing from October 2008 and ending in January 2010.
Results:
90 students were recruited to the study. Students were from both sexes and both fourth year and final year. There were 32 male (35.6%) and 58 female (64.4%) students. Of the total 90 students, 62 (68.9%) were from 4th year while 28 (31.1%) students were from final year. They were all volunteers who were willing to attend the course after their normal working hours and were allocated seats on a first come first serve basis. No student was refused entry to the course and all participants were provided questionnaire on feedback at the time of completion of the course. The response rate was 100% although this may be because students were actively encouraged by the teaching staff to ensure that feedback questionnaires were filled in.
History taking and laboratory investigations were deemed least important by students, perhaps because these are taught to them during normal attachments in all wards for clinical teaching.
The Friedman mean rank was highest for catheterisation of urinary bladder (11.66) and passing of a naso-gastric tube (12.44). The students felt the greatest need to learn these two basic clinical skills perhaps because they are not taught elsewhere. This was followed by anaesthesia, sterilisation and passing an intravenous cannulation. The students ranked learning of the learning of the following skills in the middle: giving injections, taking blood, providing pre or post-operative care and being able to identify surgical instruments. Taking history and arranging laboratory investigations were both ranked the lowest at 6.22. The Friedman asymptotic significance was high (p<0.000). Despite being a good sample size, Monte Carlo significance at confidence interval of 99% was very high (p<000.0). Table below summarises the statistics
Ranks
Mean Rank
History taking
6.22
Lab investigations
6.22
Venesection
6.29
Giving injection
6.68
I/v cannulation
7.46
Catheterisation
11.66
Naso-gastric intubation
12.24
Dressing wound
6.29
Pre-operative assessment
6.71
Theatre environment
6.53
Post-operative assessment
6.62
Principles of sterilisation
7.73
Types of anaesthesia
7.81
Surgical instruments
6.54
Test Statistics a
N
90
Chi-Square
615.431
Df
13
Asymp. Sig.
0.000
Monte Carlo Sig.
0.000
99% Confidence Interval Lower Bound
0.000
99% Confidence Interval Upper Bound
0.000
a : Friedman Test
Discussion:
Our study has shown that undergraduate medical students from the developing world greatly value a basic clinical skills course, and are particularly keen on being taught naso-gastric intubation and urinary bladder catheterisation. They seem to get enough exposure in the wards on history taking and arranging laboratory tests, but identify learning needs in other clinical skills.
This study is limited to data collection from one large medical university, but the sample size has been large, observation has been over a period of one year, statistical significance has been very high and response rate has been extremely good. The teaching staff actively encouraged the students to fill the feedback questionnaires, and this could arguably lead to some response bias.
There are no such previous studies from Pakistan to compare our findings with. This study therefore can make a good baseline for local institutions to further develop and build upon. Roy Remmen’s group compared four medical schools on clinical skills of students, and demonstrated positive effect of both longitudinal skill training as well as utilisation of problem based approach in these skill courses. Our study did not provide any longitudinal data and problem based learning approach was not utilised either. Our data is a cross sectional study.
There seem to be three levels of engagement in learning basic clinical skills. One side of the spectrum has structured teaching in clinical skills laboratories with simulation, models and manikins, while the other has no teaching of clinical skills at all, until the physician starts to work with real patients. In the middle is the model of teaching clinical skills on the wards, before graduating as doctors. The former model with clinical skills laboratories requires the most resource. Which model of teaching is adopted by any individual medical university may be dependant upon the local resources, as well as the demands of the local regulatory bodies. During this study, we were able to realise the pattern of clinical skills teaching at some other medical universities in Pakistan, India and Bangladesh as random examples of southeast Asia. We learned that most institutions in this part of the world do not undertake any formal clinical skills teaching, and certainly there are hardly any clinical skills laboratories. This voluntary attempt by the professor of plastic surgery at LUMHS is therefore commendable.
This study has also identified the keenness of students to learn some specific skills through such courses prior to graduation. With a move to more globalisation of medical protocols and guidelines, a greater uniformity should also emerge in the ways in which doctors in the east or the west hemisphere of the world learn medical knowledge, attitudes and skills. There may thus be need for researchers in medical education to encourage and push for adoption of clinical skills teaching courses prior to medical graduation in the developing world.
Furthermore this study has yet again reiterated that student’s views should form a key part in the curriculum design when considering development of a clinical skills course, and resources should be geared to meet these learning needs of students.
Dr James Moon is a Senior Lecturer and Consultant Cardiologist at UCL and the Heart Hospital. He set up and runs the cardiac MRI department dividing his time between clinical practice and research.
He is part of a team of 5 research fellows in the new Heart Hospital Imaging department. He is interested in understanding the structure and function of the heart, particularly the heart muscle, and in detecting abnormalities of the heart to better target treatment.
How long have you been working in your speciality?
12 years (3 as consultant)
Which aspect of your work do you find most satisfying?
The creative aspects of research - joining the dots on information that does not fit and constructing a coherent body of work.
What achievements are you most proud of in your medical career?
Changing statin prescribing in England – as a registrar, I did not having access to cardiac MRI for 2 years and I worked relentlessly at all levels of the healthcare system –including up to Commons Health Select Committee - on this with the result that £1billion was saved or diverted to treat more individuals with statins – the UK now has the highest uptake of statins for primary prevention in the world.
Developing new ways of detecting different types of disease with MRI or CT scanners – in its latest iteration, we may be onto a technique that can measure a fundamental process common to most diseases and organs – not just the heart, and with CT as well as MRI: the volume of cells, fibrosis and their ratio.
Which part of your job do you enjoy the least?
New bureaucracy which we did without just a few years ago..
What are your views about the current status of medical training in your country and what do you think needs to change?
I worry about a tickbox ‘learning portfolio’ culture which dumbs down initiative and personal responsibility leaving a misplaced sense of entitlement.
How would you encourage more medical students into entering your speciality?
I’ve not seen the need to – cardiology is a fantastic, over-subscribed specialty with something for everyone so its pretty competitive.
What qualities do you think a good trainee should possess?
The same as those of a doctor. I have never seen this trainee:consultant divide; there is a continuum of learning and responsibility development.
What is the most important advice you could offer to a new trainee?
My advice is about learning rather than being a trainee. Medicine does not have that many raw facts to learn. What it does have is interconnected systems. Rarely consciously try and learn information – rather, try and link everything you have ever learned together, preventing isolated islands of knowledge. It takes longer to create the story, but you will never forget it and it’s far more rewarding. If you encounter something new - a tricky JVP waveform, an ECG repolarisation abnormality or some esoteric MRCP clinical sign, invoke your know of the physical world and apply it to explain the new phenomena – write the essay, deconvolute the phenomena and build it back up, perhaps with subtle changes to see where that gets you. You have spent decades learning about the Krebb’s cycle, anatomy, electron transport, fractals, Newtonian dynamics, Brownian motion, fluid dynamics, conservation of energy, entropy, cell structure, evolutionary biology, statistics etc etc – use them.
What qualities do you think a good trainer should possess?
I am not sure I know, but generating enthusiasm in people, and then rewarding and promoting it - that’s a good starting point.
Do you think doctors are over-regulated compared with other professions?
No.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what shouldbe done to counter this trend?
It’s the effects on individuals that concern me. I fully understand the need for process, protocol teamwork and hierarchy, but these remove individual responsibility
Which scientific paper/publication has influenced you the most?
The non-medical maths/science/philosophy books and magazines I read at school and university. I particularly remember Martin Gardner recreational maths books. Recently I have used fractals and the concepts behind trapdoor ciphers in my understanding of cardiology.
What single area of medical research in your speciality should be given priority?
Prioritize individual researchers/teams rather than topics to create progress through their enthusiasm and own perceptions of priorities.
What is the most challenging area in your speciality that needs further development?
Managing our increasing technical capability which comes with ever reducing incremental benefit.
Which changes would substantially improve the quality of healthcare in your country?
I would overhaul the way society pays for and develops drugs. I would focus on increasing drug company reward for the risk associated with genuine innovation whilst reducing reward for expensive ‘me too’ drugs with no added value. My group estimated that about 10% of the NHS drug budget could immediately be reallocated improving societal value for money in prescribing, paying for all those much needed NICE decision cancer type drugs and concurrently turbocharging rather empty pharmaceutical drug development pipelines.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Absolutely. If you have transparently good and altruistic ideas, are selfless about who gets he credit for them, and sufficiently driven to achieve results, the NHS is a wonderful place - its like a demagnetized iron – apply a sufficiently persuasive external field, and the domains line up, generating far more force and direction than expected.
How has the political environment affected your work?
The UK has been great for my field –new techniques are adopted early and the international bane of my field - cardiology-radiology turf wars are less acrimonious here as socialized medicine does not reimburse on a pay per procedure basis..
What are your interests outside of work?
My young family, recreational science, cooking.
If you were not a doctor, what would you do?
Who knows. Perhaps an economist or maybe evolutionary biologist.
Prof Griffiths is a Professor of Medicine (Intensive Care), Dept of Musculoskeletal Biology, Institute of Ageing & Chronic Disease, Faculty of Health & Life Sciences University of Liverpool, and Honorary Consultant Physician in Intensive Care Medicine, Whiston Hospital, UK.
He obtained a BSc in Physiology during undergraduate training in medicine (MBBS) at University College London during the ‘70s. During the early ‘80s in London obtained a research MD studying muscle energetics in the early days of human Magnetic Resonance Spectroscopy. Became a consultant in adult Intensive Care Medicine in 1985 following a move to Liverpool in 1984 and continued research interests in muscle and expanded these into nutrition (glutamine) and the critically ill. Since then has been a pioneer of the rehabilitation of the post-ICU patient. He extensively involved over the last two decades in undergraduate curriculum reform and as the Director of the Final Year has pioneered a fully portfolio based professional learning programme.
How long have you been working in your speciality?
I have been a consultant intensive care physician for more than 25 years.
Which aspect of your work do you find most satisfying?
To be able to improve patient care through clinical research and the training of medical students.
What achievements are you most proud of in your medical career?
Raising the awareness of the physical, psychological and cognitive challenges ICU patients and relatives face during recovery and contributing to the evidence base guiding rehabilitation.Clinical nutrition research on glutamine and identifying the need to use six month mortality outcomes in the critically ill. Creating a final year of undergraduate medical training that fosters professionalism and critical self awareness based upon a clinical portfolio and appraisal process that produces graduates fit for practice.
Which part of your job do you enjoy the least?
Very little, but perhaps the ever increasing bureaucracy of regulation in practice and research.
What are your views about the current status of medical training in your country and what do you think needs to change?
In the UK most medical schools have radically reformed their curriculum to meet the needs of modern medicine and life- long learning. In Liverpool our students are recognized to be well prepared with the skills to ensure patient safety and start foundation training following a course commended by clinicians, hospitals, examiners and GMC alike. Post-graduate changes have paralleled these developments and while the training structures and closer observations are to be commended the restrictions on working time remains a concern for the acquisition of real “shop floor” experience. Our trainees simply don’t get enough “flying hours” as in the past.
How would you encourage more medical students into entering your speciality?
Intensive care medicine is popular. The problem for students is to understand how to get there. The new Faculty of Intensive Care medicine, that has just starte, brings an independent speciality out from under the umbrella of its various parent specialities and hopefully will provide the focus to make the career pathway clearer in the future.
What qualities do you think a good trainee should possess?
All those attributes that the GMC expect of a practitioner! In particular I like to see enthusiasm, self awareness and measured confidence, an enquiring and questioning mind and a degree of professional flexibility mixed with the ability to ask for help and advice. I need to trust them just as their patients need to as well.
What is the most important advice you could offer to a new trainee?
Stay calm, be professional and follow the basic principles of good medical practice doing the simple things well, and don’t be afraid to ask for help.
What qualities do you think a good trainer should possess?
Maintain professionalism and be a role model at all times with the ability to listen, support and recognize the strengths as well as being firm with those things that need developing.
Do you think doctors are over-regulated compared with other professions?
No, while regulation does not itself prevent bad medicine it does prevent it being ignored.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what should be done to counter this trend?
De-professionalising only occurs when doctors avoid taking leadership roles. I think this was a fear in the recent past but in the last 10 years in the UK there has been a strong drive to redefine professionalism and the role of the doctor for the 21st century and it is central now to modern undergraduate and post graduate training with the importance of Consultants and GPs taking leadership roles in planning health care delivery.
Which scientific paper/publication has influenced you the most?
Huxley AF 1957 A theory of muscular contraction” Prog. In Biophys. And Biophys. Chem; 7:255.
Professor Sir Andrew Huxley was awarded the Nobel prize in medicine in 1963 with AL Hodgkin for nerve conduction but my personal memory is in muscle physiology (as one of my tutors) for his work on the theory of muscle contraction and the role of cross bridges. His clarity of thought was demonstrated in his ability to always ask the question everyone else wished they had asked! He was a kind and gentle teacher that gave time even for a simple medical student.
What single area of medical research in your speciality should be given priority?
The brain is the forgotten organ in multiple organ failure. We now recognize that acute brain dysfunction is a serious problem but we know little about its pathology, how to prevent it or recover from it.
What is the most challenging area in your speciality that needs further development?
There has been a rush towards ill conceived large scale pragmatic clinical effectiveness studies of various therapies few of which have shown much to change practice. Rather there is a need for more detailed scientific research to better define efficacy of therapies by exploring the pathological processes and the genetic and environmental influences of common disorders that result in multiple organ failure.
Which changes would substantially improve the quality of healthcare in your country?
Addressing the challenge of an ageing population and in particular the community medical and non-medical support of the aged infirm so that modern medicine does not grind to a halt.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
By showing leadership and making the changes happen and not leaving it to others perhaps less informed to direct change.
How has the political environment affected your work?
I have tried to ignore it as much as possible. Politics is a business best left to politicians while the rest of the world gets on with life.
What are your interests outside of work?
I treasure my family, a marriage of 28 years, with two undergraduates in medicine and one in architecture and doing all the jobs they ask of a father. When not escaping to the south of France or walking I become a generalist handyman so it can be a gardener, electrician, plumber, decorator, carpenter, car mechanic………and the Sunday Roast!
If you were not a doctor, what would you do?
With the exception of playing a musical instrument anything that combines academia, teaching and its practical application, but with preference in the natural world.
The Department of Health’s Modernising Medical Careers (MMC) has been uniformly implemented into specialty training across the United Kingdom (UK). This began with the controversial and subsequently redundant Medical Training Application System (MTAS) selection process in Spring 2007, and ended with the first MMC specialty training posts commencing in August 2007. During the application process itself one preliminary study reported that 85% of candidates demonstrated decreased levels of enjoyment in their work, and 43% caring less about patient care.1 The emergency introduction of the ‘golden ticket’ Round 1b guaranteed interview - though arguably justified in the face of a flawed application system - was a cause of further discontent and division amongst junior trainees and the consultants responsible for appointing them.
For surgical training in particular, the advent of the MMC initiative combined with the European Working Time Directive (EWTD) represents an estimated 50% reduction in the amount of specialist training hours when compared to the previous system.2 This has raised concerns not only from current consultants, but also from the already increased number of surgical trainees having to share the same caseload. A previous survey of Ear, Nose, and Throat senior house officers reported 71% were willing to opt out of the EWTD to safeguard their training and patient care.3
In the Oxford Deanery the selection process of shortlisted surgical trainees in Rounds 1a and 1b consisted of six stations assessing curriculum vitae, portfolio, clinical examination, data interpretation, and pre- and post-operative management (totalling one hour). Candidates were offered generic or specialty themed Core Training (CT) posts at Speciality Training (ST) 1 or 2, or Fixed Term Speciality Training Appointments (FTSTA) 1 or 2, depending upon the candidate’s ranking at interview (plus application form for Round 1a) irrespective of speciality preference. Following acceptance, individual appointments were made based on candidates ranking job preferences. Round 2 appointments were made at a local level via traditional selection methods. The most recent information from the deanery states that those trainees who received an offer of run-through training in the region will be guaranteed an interview for an ST3 post in surgery, however individual specialty preference and job allocation will be determined by re-ranking based on continuous appraisal during the core surgical training years, further Higher Specialist Training interviews, and training numbers available.
The media coverage that surrounded MTAS clearly highlighted the dissatisfaction amongst trainees and consultants leading up to and during the application process,4, 5 but no study has yet assessed the views of surgical trainees following the start of their new MMC-based training posts. This survey aimed to obtain the views and outcomes of core surgical trainees in the Oxford Deanery.
Methods
At three and nine months following the commencement of speciality training posts, questionnaires were distributed to junior surgeons (CT 1-2) in the Oxford Deanery School of Surgery. Questions were structured to obtain information about level of experience and qualification(s), current and desired surgical speciality, job satisfaction, attitudes towards ‘run-through’ training and levels of support. In the Oxford Deanery there were 40 appointments at CT1 (18 ST1 and 22 FTSTA), and 29 at CT2 (17 ST2 and 12 FTSTA) in August 2007. Data were expressed as the mean ± standard deviation (SD). Statistical comparison was performed using Mann-Whitney’s U test, with the significance level at p<0.05.
Results
The questionnaire was completed by a total of 46 and 45 surgical trainees at three and nine months respectively. At the three-month time point this represented 67% of all trainees in the Oxford Deanery School of Surgery (male: female, 33:13) and included 11 at ST1, 16 at ST2, 11 at FTSTA1, and 8 at FTSTA2. Of these 52% (n=24) had obtained their post via Round 1a, 41% (n=19) via Round 1b, and 7% (n=3) via Round 2. At both CT1 (ST1 & FTSTA1) and CT2 (ST2 & FTSTA2), trainees were on average 3.7 ± 1.9 years post graduation (from time surveyed; CT1 range 1-11 years, CT2 range 3-8 years); 16% (n=7) of all trainees had previously studied Medicine at Oxford University, and 93% had studied medicine in the UK. (Figures 1a, b). Most popular desired specialties at three and nine months are displayed in figure 2. Of the 46 respondents, all had worked in the speciality of their career choice during the course of the year.
Figure 1a. Number of trainees selected in each MTAS round
Figure 1b. Surgical trainee graduating medical school distribution
At time of appointment, 52% of trainees had completed the Membership to the Royal College of Surgeons (MRCS) exams, and 35% (n=16) of all trainees had completed a higher degree. (Figure 3). Furthermore, 22% (n=10) felt that there should be a further exam in addition to the MRCS to rank candidates for appointment to higher specialist training (ST3 onwards), with half of this number having already obtained their MRCS.
Figure 2. Desired surgical specialty at three and nine months
Figure 3. Trainee postgraduate qualifications at time of appointment
Those who had been allocated to ‘run-through’ ST posts were more satisfied with the concept of run-through training than those in FTSTA posts (where scores were assigned on a scale from 1 - very unsatisfied, to 5 - very satisfied), with the mean score at three months for ST trainees 4.1 ± 1.4, and FTSTA trainees 2.0 ± 1.4 (p<0.01), and at nine months 3.7 ± 1.1 for ST trainees versus 2.1 ± 1.1 for FTSTA trainees (p<0.01). Job satisfaction levels between these two groups of trainees were similar: at three months, mean score 3.5 ± 1.3 in ST posts versus 4.1 ± 0.8 in FTSTA posts (p>0.05), and at nine months, mean score 3.5 ± 1.0 in ST posts versus 3.2 ± 1.3 in FTSTA posts (p>0.05). In addition, a similar comparison between ST and FTSTA trainees was found when determining if trainees had thought about leaving surgery. On a scale where a score of 1 – never thought of leaving surgery to 5 – very frequently thought of leaving surgery, the mean score at three months was 2.3 ± 1.4 for ST trainees versus 3.0 ± 1.6 for FTSTA trainees (p>0.05), and at nine months 2.2 ± 1.4 for ST trainees versus 2.9 ± 1.5 for FTSTA trainees (p>0.05). (Figures 4a, b).
Figure 4a. Trainee attitudes at three months
Figure 4b. Trainee attitudes at nine months
In fact, 43% (n=20) of all trainees surveyed reported having enquired about surgical training in another country, with 4% (n=2, both UK Medical School graduates) stating that if unsuccessful in securing a training post in their desired specialty for August 2008, they would move abroad to train.
At three months, 9% (n=4) of all trainees felt well-informed about what will happen in the future regarding their training, with 20% (n=9, ST to FTSTA ratio 2:7) responding that had they been better informed prior to August 2007, then they would not have accepted their current post, and 28% (n=13) felt well-supported by their senior colleagues with regard to their future training. However at nine months from appointment, 69% (n=29) of all trainees felt well informed, and nearly two thirds well supported by their seniors (n=27). (Figure 5). Ninety three percent (n=43) of applicants wished to remain in the region for their future training, with 61% (n=28) having initially selected Oxford as their first choice deanery.
Figure 5. How well informed and supported trainees felt at three and nine months
The majority of both ST2 (85%, n=11) and FTSTA2 (71%, n=5) trainees secured ST3 posts from August 2008, mainly within the Oxford Deanery, and all within their desired surgical specialty. All ST1 (n=16) trainees successfully moved into ST2 posts, and the majority of FTSTA1 (78%, n=7) trainees secured CT positions. (Table 1).
Grade (n)
August 2008 Post (n)
ST1 (16)
ST2 (16)
FTSTA1 (9)
CT1 (3) CT2 (4) FTSTA (2)
ST2 (13)
ST3 (11) Research Fellow (1) GP Trainee (1)
FTSTA2 (7)
ST3 (5) ST1 Radiology (1) CT2 (1)
Table 1. ST2 and FTSTA2 trainee outcomes from August 2008
Discussion
MMC has and will have profound implications on the way junior doctors will henceforth be trained in the National Health Service (NHS). Last year’s difficult introduction into specialist training, has for obvious reasons, directly affected the perceptions of trainees having to negotiate their careers through the ‘transition’ period.1, 6 This survey provides an interesting insight into the demographics, current viewpoints, and outcomes of the first cohort of MMC surgical trainees in the Oxford Deanery.
Just over half of all trainees in the survey were appointed after Round 1a (52%, n=24) of which two thirds (n=16) were to ST posts: a further 41% (n=19) were appointed after Round 1b, of which roughly half (n=9) were to ST posts. This highlights the large number of very good surgical trainees that may have been left unemployed had MTAS interim measures not been introduced to permit all candidates the opportunity of at least one interview, and that in the Oxford Deanery at least, candidates were given an equal chance of obtaining a ‘run-through’ post between the two rounds. Despite MMC person specifications at the time of application stating that MRCS was not an absolute requirement for entry at ST1-2, 52% (n=24) had completed their MRCS, with a further 20% (n=9) having completed at least Part I or more.
Overall job satisfaction levels were good amongst all trainees (mean score 3.7 ± 1.1), with 57% (n=26) still agreeing with the concept of ‘run-through’ training, and hence MMC. This view is maintained despite the problems associated with last years application process, and in the face of an uncertain future. However, nearly half (43%, n=20) of trainees had enquired about training abroad, with several committed to leaving the UK next year if unable to obtain their desired surgical specialty. With the average cost to train a UK medical graduate being at least £150,000,7 and the amount of dedication and effort needed to embark on a surgical career thereafter, care must be taken to improve morale amongst junior surgeons, and to provide adequate and timely information. Encouragingly, between the two time points surveyed, levels of senior support and how well informed surgical trainees felt with regards to their training, increased from 28% to 60% and from 9% to 69% respectively; this may be secondary to a combination of extensive effort from the Deanery and the Royal College of Surgery to address trainee concerns.
The realistic future of those in FTSTA posts is cause for concern. This is highlighted in the recently released Tooke Report, in which it is stated they are “in danger of becoming the next ‘lost tribe’, the very category of doctor MMC sought to avoid”, but at the same time that “core [training] should not repeat the errors of previous SHO arrangements and must be time limited”.6 Those in FTSTA posts face higher levels of future uncertainty than their ST colleagues, and this was reflected in reporting a higher likelihood of consideration of alternative careers outside of surgery. However, both groups of trainees demonstrated statistically similar scores when questioned about how frequently they had thought of leaving surgery (2.3 ± 1.4 for ST trainees versus 3.0 ± 1.6 for FTSTA trainees, p>0.05), and 71% of FTSTA2 trainees surveyed within the Oxford Deanery went on to secure ST3 level posts in their desired specialty.
The authors note the limitations inherent to surveys in general namely the validity and reliability of responses obtained to questions asked due to the self-report method of data collection, the questionnaire entirely constructing the information obtained, and that the data does not capture the decision process that produced the observed outcomes and is therefore descriptive rather than explanatory. More specifically, the authors note that candidates who were successful in obtaining an ST3 post may have been more likely to complete the questionnaire, leading to further potential bias.
Conclusion
MMC has crossed the threshold into higher specialist training, and the first cohorts of MMC surgeons are being trained. The majority of trainees we surveyed expressed good levels of job satisfaction, had successfully negotiated their first year of the new system, and encouragingly felt better informed and supported over the course of their first year. However, this study encompassed a proportion of surgical trainees in one Deanery in the UK, and further study on a larger scale at regular time intervals is certainly warranted. Consequent to the problems of MMC’s difficult introduction, positive steps included travelling tours by the Royal College of Surgeons (England), and in the Oxford Deanery at least, regional meetings to address concerns and expectations, and outline the realistic future for surgical trainees. Perhaps a key determinant of sustainability for MMC in surgery in 2008 and beyond will be the relative success of the Intercollegiate Surgical Curriculum Programme (ISCP), and this represents a significant area for further study.
Problem based learning (PBL) has been an important development in health professions education in the latter part of the twentieth century. Since its inception at McMaster University1 (Canada), it has gradually evolved into an educational methodology being employed by many medical schools across the globe2,3. PBL presents a paradigm shift in medical education, with a move away from ‘teacher centered’ to ‘student centered’ educational focus. The assumptive difference between a pedagogy learner and an androgogy learner (Table 1) was summarised by Knowles4, and the androgogy approach underpins PBL. This shift has redefined the role of a teacher in the PBL era, from being a teacher to a facilitator.
Table 1: Differences between Androgogy and Pedogogy learner (Knowles)
Characteristics
Pedagogy
Androgogy
Concept of the learner
Dependent personality
Self-directed
Readiness to learn
Uniform by age-level & curriculum
Develops from life tasks & problems
Orientation to learning
Subject-centered
Task- or problem-centered
Motivation
By external rewards and punishment
By internal incentives curiosity
It is well known that implementing PBL as an educational methodology required additional resources compared to a traditional lecture based curricula5. In addition, there was a need to recruit and train a large number of tutors to facilitate the PBL process6.Training PBL tutors is an important component of a successful curriculum change, and is a continuous process. Training workshops and role plays were employed to train conventional teachers, but challenges were faced in developing them into effective PBL tutors5.
The aim of this paper is to evaluate the literature for any evidence supporting the theory that a PBL background student may develop into an effective PBL tutor. The Medline, EMBASE and CINHAL databases were searched to look for any pre-existing literature or research supporting this theory.
Results:
To the best of my knowledge, there has been no reported evidence supporting this theory. With limited literature evidence, this paper aims to identify common grounds between a PBL student and a PBL tutor, and whether being a PBL student may contribute to the overall development as a PBL tutor. The discussion evolves around the following domains:
1. Teaching Styles:
The ideal teaching style of a PBL tutor is a facilitative-collaborative style, which augments and supplements the PBL process. The teaching style inventory developed by Leung et al7 hypothesised four domains of teaching styles: the assertive, suggestive, collaborative and facilitative styles. Though a PBL tutor assumes himself in possessing this style (facilitative), it does not necessarily match with the students perceptions, as reported by Kassab et al8.
Some of the characteristics of being a PBL student may foster the development of a collaborative teaching style. Being a student, you are expected to be a collaborative learner which is critical for achieving and improving group performance9. Initial years as a student in PBL may contribute to developing attributes required to develop a preferential teaching style.
2. Facilitating critical thinking:
PBL is grounded in cognitive psychology and is set out to stimulate curiosity and build durable understanding. One of the roles of the tutor is to foster critical thinking and enhance the group’s ability to analyse and synthesise the given information. This attribute stems from the tutors ability to facilitate, rather than teach. Irby10 opined that clinical teachers tended to teach as they themselves were taught using traditional approaches, which may affect the process of stimulating critical thinking among the students.
A tutor from a PBL background would have the ability to think critically, through a process of developing thoughtful and well-structured approach to guide their choices11. Tiwari et al12 showed in their study that PBL students showed significantly greater improvement in critical thinking compared to traditionalist courses. Hence, prior exposure to a certain learning style can create a cognitive psychology that can contribute to tutor development.
3. Group dynamics:
One of the prime roles of a PBL tutor is to facilitate the PBL process by keeping the group focused on tasks, and guiding them to achieve their goals. Tutors who are skilled in group dynamics are evaluated more highly than those who are not so skilled11,13 . Tutors need to develop sound appreciation of the group dynamics, failing which may lead to fostering uncertainty with in the group. Bowman et al13 commented about the lack of consideration on the emotional implications placed on prospective PBL tutors when tutoring small groups, especially the skills required to balance between short term anxieties and potential serious problems. This imbalance which usually serves as unconscious incompetence may affect group dynamics.
PBL students would have experience of group dynamics and the pressures of working within it. They would have developed a model of working with members with varying attributes. Blighet al14 showed in their study that students from a PBL curriculum rated themselves better in team working and motivation compared to conventional course peers. This highlights the fact that an apprenticeship model may be necessary in developing the right skills to be an effective tutor.
The characteristics of a student that may foster ideal attributes in a PBL tutor are briefly summarised in Table 2, and has evolved from the work of Samy Azer9,11 .
Table 2: Common ground
Ideal PBL student
Ideals of a PBL tutor
Knows his role within a group
Would help in identifying different roles students may play
Knows to ask empowering questions
Would help in guiding groups in achieving learning objectives
Monitors his own progress by self evaluation and motivation
Would help in monitoring individual progress and motivate group
Bonds with other members to achieve goals
Would help in building trust and encourage bonding of group members
Develops thoughtful and well structured approach to guide choices
Would help in facilitating critical thinking
Fosters collaboration with other group members to create a climate of trust
Would facilitate collaborative teaching style
4. Tutor training
Considerable resources are exhausted in teaching new tutors the art of facilitating a PBL group6, and the usual cohort is teachers from a conventional taught background. The shift from didactic expertise to facilitated learning is difficult for those tutors who feel more secure in their expert role. Finucane et al5 published their study which showed that only a minority of staff had volunteered to be PBL tutors, possibly reflecting the fact that absence of prior exposure to PBL style of learning may have contributed to this. In spite of tutor training workshops, they could only retain 73% at the end of two years.
Prior exposure as a student may help negate much of the stigma associated with PBL. They would have observed and learnt from their PBL tutors, and would have analysed their contribution to the PBL process. They could reflect on their experience and evolve into an ideal PBL tutor. This would help in minimising resource expenditure and contribute towards retention of staff.
5. Tutor comfort zones:
PBL contextualises learning to practical situations, with integration across disciplinary boundaries. Dornan et al15 reported on how some teachers felt PBL to be a frustrating drain on time as it did not fit their educational style, and was a distraction from clinical teaching, demonstrating the ‘conditioning effect’ of prior experiences. This further fuels the debate between content vs. process expertise, but prior knowledge of the process would benefit the students and the PBL process.
6. Role modeling:
Role models have long been regarded as important for inculcating the correct attitudes and behaviors in medical students. Being an ideal role model is considered as one of the prime requisites of a teacher. In a recent study, Mclean et al16 showed that PBL students tended to have a higher percentage of role models compared to students from a traditional programme (73% vs. 64%). In an ideal setting, a “content and process expert” would be the perfect role model for the PBL students, but this may not be realised in all settings.
Paice et al17 commented on the resistance to change within the medical profession, and highlighted the need for training to emphasise the values and attitudes required. This puts an added emphasis on the tutor to demonstrate tenacity and virtues to be an effective role model, avoiding ‘cognitive clouding’ from previous experiences.
As a PBL student, they would be exposed to variety of PBL tutors. They would have incorporated the good points of an effective PBL tutor, and would have reflected on the negative aspects. Reflective practice enables them to develop the right attributes. Though these attributes may be difficult to develop through training workshops, having a background of PBL education may help mould the tutor characteristics.
Conclusion:
As PBL continues to be employed across different specialties, there would be increased emphasis on the medical schools to match the resources needed to implement it. There is an argument for developing an apprenticeship model or recruiting tutors from PBL background, which would help in reducing the cost in training new tutors, along with nullifying the negative influences a new tutor may bring. The biggest limitation in the present setting is finding a cohort of PBL background tutors, but an apprenticeship model may benefit teachers from conventional background. A prospective research study exploring the attributes of tutors, successful and less successful, from traditional, PBL and hybrid curricula and those who have crossed the Rubicon from traditional to PBL can effectively answer this question.
Professor Elisabeth Paice is currently on secondment to NHS London having been appointed to the new post of Acting Director of Medical and Dental Education from her role as Dean Director at London Deanery. The new role will ensure that the right number of doctors and dentists have the right training to deliver the service ambitions outlined in Healthcare for London. Elisabeth will be leading on the Medical and Dental Education Commissioning System (MDECS). This is the name of the programme of work that will manage the changes to postgraduate medical and dental training.
She was born in Washington DC, brought up in Canada, and studied medicine first at Trinity College Dublin and later at Westminster Medical School. She was the originator of the 'Hospital at Night' concept; developed the 'Point of View Surveys'; chaired PMETB working parties on Generic Standards and the National Trainee Survey and has published variously including on doctors in difficulty; workplace bullying; women in medicine. She was Chair of COPMeD, Conference of Postgraduate Medical Deans, from July 2006 to July 2008.
How long have you been working in your speciality?
I have been a full-time postgraduate dean since 1995. Before that I was a consultant rheumatologist for 13 years.
Which aspect of your work do you find most satisfying?
I get great satisfaction out of developing and implementing new ideas, especially when they work well enough to be taken up by others. I think most doctors have a creative streak and sometimes bureaucracy can damp this down. One of the reasons why medical education and training is so enjoyable is that it has to keep changing because of changes in the way the service is developing. There are standards to be met, of course, and regulators to satisfy, but within those constraints there is plenty of room for innovation. The better the quality of education and training, the better and safer the care of patients.
What achievements are you most proud of in your medical career?
As Dean Director of London, I have been very proud to lead postgraduate medical and dental education in one of the world’s great cities, with its five world-renowned medical schools, numerous centres of clinical excellence, and over 10,000 trainees. In order to understand trainees’ views, I introduced a regular survey through which they could voice their views about the quality of training they were receiving. I was very pleased when this formed the basis of the very successful National Trainee Doctor Survey, now embarking on its fourth iteration. This survey has enabled postgraduate deans across the UK to identify departments where training is not meeting the minimum standards for training and to take appropriate action.
Other achievements of which I am proud include the development of a multiprofessional team-based approach to out of hours services, known as the Hospital at Night initiative, which has improved patient safety while providing a solution for reducing the hours of junior doctors. Most recently I am delighted with the success of London’s Simulation and Technology-enhanced Learning Initiative (STeLI) which recently won the prestigious Health Service Journal Award for Patient Safety.
Which part of your job do you enjoy the least?
I least enjoy dealing with performance issues, whether internal to my staff or among trainees or their trainers.
What are your views about the current status of medical training in your country and what do you think needs to change?
Medical education is recognized in the UK as being a vital factor in providing the high quality doctors necessary for a high quality health service. It needs to be better resourced, and in particular every doctor with responsibility for educational supervision needs to have the training, the time, and the tools to do a good job. The way in which training has traditionally taken place, known as the ‘apprenticeship model’, is no longer suitable because of restrictions on the hours of work. I am all in favour of these restrictions, because long hours have a negative impact on learning and pose a risk to the health and safety of both doctors and patients. But we need radical change in the way we depend on doctors in training to provide out of hours cover and we need to find robust ways to ensure they gain the practical experience they need.
How would you encourage more medical students into entering your speciality?
I would strongly encourage any medical student to consider taking an interest in medical education from the start. Whatever the field of medicine that they enter, there will inevitably be an expectation that they will teach the next generation of doctors and of other healthcare professionals. Teaching is increasingly being recognized as one of the duties of a doctor, and like anything else, the more effort you put in, the more rewarding the outcomes.
What qualities do you think a good trainee should possess?
Trainees need to have a solid grounding in the basic sciences, because it is the foundation on which their postgraduate training will build. They need to be both conscientious and curious, doing what is required of them, but also going the extra mile in the search for knowledge. They should be motivated by the desire to make a positive difference to the lives of others, because I believe that is the only motivation that stands the test of time.
What is the most important advice you could offer to a new trainee?
Read the curriculum, establish what is expected of you and what you can expect from your seniors and your team, and engage with the educational programme.
What qualities do you think a good trainer should possess?
Kindness, honesty, expertise - and a passion for developing these qualities in their juniors.
Do you think doctors are over-regulated compared with other professions?
No, it is a profession in which we can potentially harm others, regulation is a necessity.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what should be done to counter this trend? The responsibility for the professionalism of a doctor lies with the doctor. There are no policies in the UK that de-professionalise doctors.
Which scientific paper/publication has influenced you the most? I have been heavily influenced by the body of work by Charles Czeisler in the USA and Philippa Gander in New Zealand about the impact of long hours and sleep deprivation on health, safety, errors and retention of learning of doctors in training.
What single area of medical research in your speciality should be given priority? Simulation technology.
What is the most challenging area in your speciality that needs further development? Fitting adequate training into a 48 hour week without lengthening the duration of training
Which changes would substantially improve the quality of healthcare in your country?
Improving the training of general practitioners
Do you think doctors can make a valuable contribution to healthcare management? If so how?
All doctors need to learn to look after the system of care as well as the patient in front of them. Medical leadership is crucial to modernizing services. During training all doctors should be involved in quality improvement initiatives and all should learn how to champion change effectively.
How has the political environment affected your work?
The most recent impact has come from the national policy to introduce a separation between the commissioning of education and its provision. This has meant a reorganization of the way we work, with much of the work we did being commissioned from lead providers. While change is always disconcerting, there are real benefits to be realized from this one, in particular a better alignment between service and education planning.
What are your interests outside of work?
Looking after our four delightful grandchildren
If you were not a doctor, what would you do?
When I was at school I planned to write plays, but a medical career has sated my appetite for drama.
He'd try to sit, couldn't hold on for long,
Fidgety, restless, frustration would only prolong
Tried hard to listen to parents and teacher,
Distracted, voices sounding like a background clutter
Kept working on sitting listening and learning
Realized wasn't at par with kids and his sibling
This sentence would redundantly echo in his head
"Sit, listen, learn" you dumb head!!!
"How come life can't be better than what I feel?"
Why is it so hard for me to deal
My head hurts after constant listening,
Nothing I do is gratifying
They say, am not in same learning standard curve as other kids
My parents are worried for me, not understanding my needs
Have tried all avenues, anger, love , comfort, compassion,
Yet everyday is a challenge for them to find a solution
They interpreted his "not sitting still as restlessness",
Not listening and disruptive behaviour as impulsiveness
His attention level considered as poor learning skills
parents embarrassed, trying to overcome his hills
"Trust me”, He'd say, “you don’t understand, I'm trying my best"
Parents instead kept echoing sit, listen and learn, and accept it as a test
All this felt repetitive and redundant in his head,
Until someone said "maybe something is wrong with his brain instead"
Suggested see a doctor who might help clear the clutter away
Who observed his behaviour without decision to change him right away,
That's when he told the parents "Your child has had attention deficit disorder"
They felt was a mental taboo, and asked not to speak about it louder
The doctor insisted on strict compliance and periodic follow-up
Meds, mental stimulation exercises worked, felt no more like empty cup
Before he knew, he was sitting longer, nothing felt like clutter
Realized the deficit had prevented him from thinking better
Parents and doctors worked together, we salute them for the joint effort,
helped him evolve into the person altogether different
He listens to his inner and external suggestions alone and in group discussions,
Has learned realities of life, applying them in every day decisions
Sits down for hours working on his research projects
Sit, listen, learn, now all sound real, not mystical acts
The implementation of Modernising Medical Careers (MMC) significantly altered the structure of postgraduate medical education in the UK. MMC oversees the training of all UK doctors from the outset of their career, the first two years of which comprise the Foundation Programme. Successful completion of the Foundation Programme is based upon doctors’ Foundation Portfolios in which they must demonstrate achievement of essential competences and work-based assessments. Doctors are also encouraged to attain additional competencies and to develop their portfolio further. Voluntary educational activities undertaken outside the workplace form the basis of this.
Application into Specialist Training following the Foundation Programme is highly competitive, with an average of three applicants for each post in 20081. Points-based shortlisting criteria are used to select candidates, and are based upon the contents of the Foundation Portfolio and application form. This means that points can be scored for activities not required for completion of the Foundation Programme, such as Royal College membership examinations and course attendance. Foundation Programme doctors undertake voluntary activities to improve their portfolios however no quantifiable evidence currently exists as to what doctors undertake in this respect.
We aimed, therefore, to determine firstly what voluntary educational activities Foundation doctors are undertaking. We also aimed to establish their underlying motivating and deterring factors, financial costs incurred, and use of annual and study leave and ‘specialty taster days’, to assess the overall extent and impact of portfolio activities. The authors hope the results are useful in informing medical students and Foundation trainees of the scope of activities of their peers, and in advising supervisors of the activities of their trainees.
Methods
A two page anonymous questionnaire was posted at random to 100 Foundation doctors across five hospitals in East Midlands Deanery (50 Foundation Year 1, 50 Foundation Year 2). See Appendix 1
Demographics
The first section of the questionnaire asked for the sex and grade of respondents (Foundation Year 1 (FY1), or Foundation Year 2 (FY2))
Activities
Respondents were directly asked whether they were attending courses or conferences, using on-line e-learning packages, joining professional bodies/societies or sitting higher professional examinations such as royal college membership examinations/higher degrees.
Cost
Doctors were asked how much money (excluding that of teaching allowances) and days of annual leave they used on the above activities. They were also asked how many of their allowed ‘specialty taster days’ they had taken during each year.
Motivating and deterring factors
Doctors were asked to rank from a list the motivating and deterring factors determining what activities they were undertaking.
Professional development
Doctors were finally asked to rank which educational activities they thought would make them a better overall Foundation doctor.
Results
Response rate was 49% with 49 doctors returning the questionnaire. Of these 69.4% (n=34) were Foundation Year 1 (FY1) and 30.6% (n=15) were Foundation Year 2 (FY2), with 53.1% female and 46.9% male.
Activities
Overall 89.8% (n=44) of respondents were engaged in voluntary educational activity (FY1 85.3%, FY2 100%). The most common mode (89.8%, n=44) was e-learning packages (FY1 85.3% (n=29), FY2 100% (n=15)) followed by joining/ becoming a member of professional bodies or societies ie BMA etc (73.5%, n=36) (FY1 64.7% (n=22), FY2 93.3% (n=14)), followed by courses (69.4%, n=34) (FY1 55.9% (n=19), FY2 100% (n=15)), undertaking higher qualifications (36.7%) (FY1 14.7% (n=5), FY2 86.7% (n=13)) and attending conferences (14.3%) (FY1 14.7% (n=5), FY2 13.3% (n=2))– See figure 1.
Fig 1 – A graph to show the percentage of Foundation year 1 and 2 doctors involved in each mode of voluntary educational activity.
Of the courses attended, 25.5% pertained to teaching, 25.5% to advanced life support and 18.0% to surgical skills. The remaining 31% of courses related to a variety of other interests such as anaesthetic skill days, expedition medicine courses, and sub speciality specific courses such as movement disorder workshops and laparoscopic surgery.
Cost
The mean amount spent by Foundation Year 1 Doctors on these activities was £581 (range £0 - £3100) Foundation Year 2 Doctors spent significantly more at £1842 (range £0 - £3500). The mean cost per activity is shown in figure 2.
Fig 2 – A graph to show the mean amount of money spent by foundation year 1 and 2 doctors on each mode of
educational activity.
The mean number of days of annual leave used by doctors for these activities was 2.8 in FY1 and 5.3 in FY2, therefore combining to average 8.1 days in total that would be used over the whole foundation programme. Of their five allowed ‘taster – days’ the mean number attended was 1.3 and 2.9 by FY1 and FY2 doctors respectively. Only 20.4% of doctors took their full entitled allowance.
Motivating and deterring factors
The most common factor motivating Foundation doctors to undertake portfolio educational activities was the belief they would help candidates achieve a specialist training post (67.3%). Only 12.2% engaged primarily out of personal interest with 8.2% to improve their medical competence (See Table 1).
Primary Motivating Factor
FY1 Doctors
FY2 Doctors
Overall
Percentage (%)
Number
Percentage (%)
Number
Percentage (%)
Number
Improve chance of specialist training post
58.8
20
86.7
13
67.3
33
Personal interest
14.7
5
6.7
1
12.2
6
To improve medical competencies
11.8
4
0
0
8.2
4
On advice of seniors
11.8
4
6.7
1
10.2
5
Other
2.9
1
0
0
2
1
TOTAL
100
34
100
15
100
49
Table 1 – A table to show the primary motivating factors of foundation doctors to undertake voluntary portfolio educational activities.
The most common deterrents were a lack of study leave (42.9%), lack of annual leave (22.4%) and expense (20.4%) (See Table 2).
Primary Deterring Factor
FY1 Doctors
FY2 Doctors
Overall
Percentage (%)
Number
Percentage (%)
Number
Percentage (%)
Number
Lack of study leave
38.2
13
53.3
8
42.9
21
Lack of annual leave
23.5
8
20
3
22.4
11
Financial expense
17.6
6
26.7
4
20.4
10
Lack of career choice
11.8
4
0
0
8.2
4
Not relevant to Foundation doctors
8.8
3
0
0
6.1
3
Other
0
0
0
0
0
0
TOTAL
100
34
100
15
100
49
Table 2 – A table to show the primary deterring factors listed by foundation doctors that deter them from undertaking voluntary educational portfolio activities.
Professional development
The final section of the questionnaire asked respondents which educational activity they felt was most influential in making them a better Foundation doctor. Interestingly 83.7% (n=41)(FY1 88.2% (n=30), FY2 73.3%( n=11)) felt on-call experience was most influential, with only 6.1% (FY1 2.9% (n=1), FY2 13.3% (n=2)) citing courses, 6.1 % (FY1 2.9% (n=1), FY2 13.3% (n=2)) e-learning packages and 4.1% (FY1 2.9% (n=1), FY2 6.7% (n=1)) qualifications (Fig 3).
The academic conference was ranked least influential by 89.8% (n=44) (FY1 85.3% (n=29), FY2 100% (n=15)) of respondents, followed by 6.1% (n=3) (FY1 8.8% (n=3), FY2 0.0% (n=0)) citing courses, and 4.8% (FY1 5.8% (n=2), FY2 0.0% (n=0)) e-learning packages (Fig 3).
Fig 3 – The above graph was the response of Foundation doctors when asked which activities they thought were most and least influential in making them a better foundation doctor.
Discussion
This survey suggests that Foundation doctors undertake numerous activities at significant personal expense to expand their portfolios, and are primarily motivated by a belief that this will increase their chance of obtaining higher specialist training posts.
Educational activities and opportunities
The advent of the European Working Time Directive and New Deal document2 have resulted in junior doctors working considerably fewer hours than in previous years. This has led some authors to conclude that the quality of learning opportunities in the working environment has reduced 3 .With 89.8% of Foundation doctors in this survey actively undertaking some form of educational activity outside of work, this suggests that Foundation doctors may be going some way to re-dressing this balance. It may also come as a surprising yet reassuring figure to Foundation Programme educational supervisors who may be unaware of the education of their trainees outside of work.
We found the most popular mode of educational activity to be the e-learning package. E-learning is an effective and extensively employed method for both distance learning4 , and as an adjunct to “traditional” lecture-based techniques across several disciplines. It has also been shown to be a well received and practical method of supplementary education for doctors5 and our study suggests this is particularly true for the Foundation years. The reasons why e-learning is popular in this group was not explored, but its low cost, easily accessible and modular nature may have some part to play. As medical schools continue to utilise this modality to a greater extent, its follow-through into the Foundation years and postgraduate medical education in general is inevitable. With such high uptake, e-learning packages are a promising format for delivering education to this group.
Popular courses undertaken by Foundation doctors related to obtaining teaching skills, or advanced life support. This suggests that Foundation doctors place a high emphasis on teaching and training, and on recognising and managing acutely ill patients. These are two core objectives of the Foundation Programme. However, one could also argue that doctors undertaking courses outside work to achieve essential competencies casts doubt on the ability of the Foundation Programme to deliver them. We submit that educational supervisors are in a prime position to appraise this issue.
The least popular mode of activity in our survey was the attendance of a medical conference. It was also regarded as least influential by 89.7% of respondents. There is a global shortage of medical academics6, and as conferences serve to introduce junior doctors to academic medicine and research, perhaps academic doctors should take a more prominent role in promoting conferences as an educational activity.
Time and money
Doctors incur the majority of their costs attending courses with Foundation Year 1 and 2 doctors spending £365 and £1120 respectively on this area (fig 2). This highlights the possibility that Foundation doctors may be prone to financial exploitation by a growing number of courses which are often unvalidated. As senior advice was the primary motivating factor for only 10.2% of activities, this suggests that educational supervisors could play a greater role in assessing, appraising and advising their trainees on the courses best suited for them and their professional development.
The overall financial cost incurred for all portfolio educational activities was £581 for FY1 and £1842 for FY2. Whilst previous estimates have been made in this area, this is the first specific to the Foundation Programme and to include non-mandatory outlay, and represents 3 % and 7% of the basic salary for FY1 and FY2 doctors before tax. As our survey found financial expense to be a significant deterrent to portfolio activity (20.4% of respondents), a potentially serious implication is that expense will limit the uptake of postgraduate education in the future. From the authors’ own experience such professional costs are not explained to medical students and that this issue merits more attention in undergraduate education.
A lack of study leave was highlighted as the main deterring factors to educational portfolio activities (42.9%). This is of particular interest as only 20.4% of Foundation doctors use their full ‘taster-day’ entitlement. These ‘taster days’ are a fundamental aspect of the Foundation Programme, offering doctors the opportunity to explore a specialty for up to five days per year. However, whilst doctors fail to utilise them, they take an average of 8.1 days’ annual leave over the two year programme for educational purposes.
The reasons behind this are unclear, but may be due to a lack of awareness of these ‘taster days’. With a lack of study leave hindering educational activities, a potential solution might be for doctors to have the option to utilise ‘taster days’ as a form of study leave.
Professional education and motivation
Between 1998 and 2005, the number of medical students in the UK has risen by 57%7. Increasing numbers of doctors and decreasing working hours may reduce the amount of on-call experience for those in the Foundation Programme. However, it is this on-call experience that is regarded by the vast majority (83.7% in this study) as the most important educational modality in making them a better foundation doctor. Although time and money are perceived as barriers to portfolio educational activities it appears that doctors value this on-call experience above all. With key aims of the Foundation Programme being training and emergency competence, efforts must be made to preserve this experience.
Whilst Foundation doctors are engaging in numerous portfolio activities, their underlying motivations are interesting. It appears this group are primarily motivated not by the educational benefits of these activities, but rather by their perceived ability to help attain a specialist training post. This could suggest that the educational portfolio is at risk of becoming a ‘tick-box’ means for career progression, rather than addressing limitations, exploring interests and aspiring to clinical excellence. This contrasts with the conclusions of the most recent assessment of postgraduate medical education in the UK8.
As competition for jobs appears to be driving Foundation doctors to undertake educational activities it remains unclear whether engaging in these activities to obtain jobs, rather than competencies, reduces their validity and educational outcomes. Furthermore it is unclear whether trainees will be more likely to achieve their overriding aim of obtaining a specialist training post through these activities. Determining the career outcomes of doctors undertaking these activities will provide an evidence base, allowing educational supervisors to optimally advise their trainee in portfolio educational activities.
Conclusions
This is a baseline survey quantifying portfolio educational activities in the Foundation Programme, applicable to trainees and supervisors alike. Whilst the latter are well aware of assessments such as DOPS (Direct Observation of Procedural Skills) and CbD’s (Case-based Discussions), they are often less aware of the voluntary educational activities of their trainees.
Our study would suggest that Foundation Programme doctors are a cohort driven to undertake numerous voluntary educational activities, albeit largely to achieve career progression rather than accrue educational benefit. To this end they undertake activities such as e-learning, courses and higher qualifications at the expense of conferences. For this they spend significant amounts of money and leave, yet continue to site a lack of traditional study leave as a barrier to further educational development. The authors would suggest that further work is needed to develop the role of educational supervisors in the Foundation Programme in harnessing the motivation of their trainees, and guiding them appropriately.
Key Points
·Foundation Doctors spend significant amounts of time and money on voluntary educational activities.
·Foundation Doctors are primarily driven to undertake these activities due to the belief that it will help them obtain specialist training posts.
·A lack of study leave is the primary barrier to voluntary education.
·The academic medical conference is viewed as the activity least likely to improve medical competence, whereas on-call experience is regarded as the most likely.
·Foundation Programme educational supervisors are best placed to guide their trainees towards the most appropriate educational modalities
BJMP 2009: 2(3) 57-58
A case of accidental carotid artery cannulation in a patient for Hemofilter: complication and management
Sanil Nair , Harshal Wagh , Kavita Mordani and Salim Bhuiyan
In the 'Author Details' block of the left column on page 58, the correct details of SALIM BHUIYAN should be
Kenneth Brummel-Smith, MD is the Charlotte Edwards Maguire Professor of Geriatrics and the chair of the Department of Geriatrics at the FSU College of Medicine. He is editor of five textbooks, Geriatric Rehabilitation, Practical Ambulatory Geriatrics, Interviewing and Patient Care, Geriatric Assessment, and Reichel’s Care of the Elderly. His research has addressed the effect of a support group on caregivers of patients with Alzheimer’s disease, methods of assessing pain in persons with Alzheimer’s disease, and advance care planning. He serves on the National Advisory Council on Aging for the National Institute on Aging.
How long have you been working in your speciality?
I started in geriatrics in 1983. I completed a residency in family medicine, then a fellowship in faculty development. While teaching in a family medicine residency 3 years after that, I was sent to a Society of Teachers in Family Medicine conference on integrating geriatrics into family practice teaching. I feel in love with the concept of the “functional approach” and dedicated myself to learning more geriatrics. After taking a 1-year certificate course in geriatrics at UCLA I was offered the position of Co-Chief of the Clinical Gerontology service at Rancho Los Amigos Hospital, the largest rehabilitation hospital in the US. And that was the start of it all!
Which aspect of your work do you find most satisfying?
Although my work now is primarily academic, I still get the most satisfaction is working closely with a elder in guiding them through difficult medical decision-making situations. I never cease to be amazed how well people can think through difficult medical decisions, if they are fully engaged in the process and educated about their options. We rarely give patients enough credit to do this.
What achievements are you most proud of in your medical career?
Being selected by the American Geriatrics Society for the Dennis W Jahnigen Memorial Award for outstanding contributions to geriatric education in 2006, and by the students of the Florida State University College of Medicine (FSUCOM) for the Hippocratic Award in 2008 for best representing professionalism, compassionate care, and inspirational teaching.
Which part of your job do you enjoy the least?
Dealing with personnel issues in my department
What are your views about the current status of medical training in your country and what do you think needs to change?
I think we need to make some fundamental changes. The future of medicine is in managing chronic conditions in a team environment. Much of the ways we teach medicine today is just like we did 30 years ago when I was in school. First, I would rethink the role of basic science teaching. Not every student needs the same thing. I see the best value of basic science is to teach critical thinking, but most of it today focuses on memorizing and regurgitating minute details. Second, I would provide most clinical teaching in teams of providers – especially medicine, social work, nursing and pharmacy. Third, I would equip students with real skills for helping patients to manage chronic conditions – patient-centered compassionate care, using motivational interviewing. Finally, I would adopt what most other advanced countries do – require a service commitment after graduation in rural and underserved areas, in exchange for more subsidies of educational costs.
How would you encourage more medical students into entering your speciality?
Start with positive role models – we use a senior mentor program where each student is assigned a mentor in the community in the 1st year of med school. The senior mentors are relatively healthy, very active and engaged in their communities and a real hoot to be around! We train every student in geriatric issues as a normal part of clinical care, not something special or different. And we have required integration of geriatrics into all other classes and a required 4th year rotation. Perhaps that’s why we have the highest rating by our graduates of their geriatric skills in the country.
What qualities do you think a good trainee should possess?
Compassion for others, an inquisitive mind, the recognition that authority is often wrong, and a commitment to evidence.
What is the most important advice you could offer to a new trainee?
Relax and remember you (and all of us) are not that important in the large scheme of things
What qualities do you think a good trainer should possess?
Relax and remember you (and all of us) are not that important in the large scheme of things
Do you think doctors are over-regulated compared with other professions?
No – we under-regulated. Nobody should let us do all the things we get away with. What other business can kill tens of thousands clients a year and get away with it? If you doubt this, you have not read the Institute of Medicine’s report “To Err is Human.” But you should!
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what should be done to counter this trend?
Yes. Calling patients “consumers.” Allowing doctors to advertise – especially plastic surgeons. And the growing influence of money on medicine – unnecessary surgeries and diagnostic tests, and unthinking acceptance of pharmaceutical companies information.
Which scientific paper/publication has influenced you the most?
Donald Berwick, “What patient-centered should mean: Confessions of an extremist,” Health Affairs 28, no. 4 (2009): w555–w565 (published online 19 May 2009; 10.1377/hlthaff.28.4.w555)
What single area of medical research in your speciality should be given priority?
Non-pharmaceutical management of behavioral disturbance in dementia
What is the most challenging area in your speciality that needs further development?
Developing a reasonable reimbursement system that recognizes the role of cognitive work and support of families in the patient’s care
Which changes would substantially improve the quality of healthcare in your country?
A single-payer national health insurance program, dissolution of the fee-for-service model of reimbursement, cost-effectiveness research, regulation of pharmaceutical costs
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Absolutely – if they put the patient first in all considerations.
How has the political environment affected your work?
Mostly through frustration. Washington seems to be in the lobbyist’s pocket and while I had great hopes of health care reform, I think we will be worse off if the present plans go through.
Contrary to the period in 1993, when the United States (US) President Bill Clinton failed to gain any traction on his healthcare reform, the current President, Barack H Obama, has been able to embark on historic healthcare reform. This is because major stakeholders agree that US healthcare is in crisis and requires major reform. Businesses and consumer groups have joined the insurance industry, pharmaceutical industry, and physician groups in asking for this healthcare reform that would blunt the rapidly escalating costs and provide healthcare for all Americans. While the number of uninsured Americans increased from 39.8 million in 2001 to 46.3 million in 2008, the National Health Expenditure (NHE) grew from 7.2% of the gross domestic product (GDP) in 1970 to 16% in 2005 1. This growth is projected to climb further to 19.5% in 2016. To put these figures into perspective, the US is projected to spend almost $13 trillion on healthcare over the ten years from 2010 to 2019 if the current trend continues2. Add to that the number of bankruptcies filed in the US due to healthcare expenses. Himmelstein and colleagues have recently demonstrated that of all the bankruptcies filed in the US in 2007, 62.1% were due to medical reasons as opposed to 46.2% in 2001 and only 8% in 19813 .
Hence, there is no longer any debate about ‘whether there is a problem’ but rather ‘what can be done to fix this problem’. How to fix it has been, and will continue to be, a highly contentious issue that will pitch Democrats against Republicans even after the passage of the pending legislation. Some of the key elements President Obama had identified as his basic objectives in healthcare legislation, that he is expected to sign into law by the end of 2009, include:
Providing universal coverage to all Americans and requiring employers to provide health insurance to their employees.
Barring insurance companies from providing policies that would exclude patients with ‘pre-existing conditions’ thereby ensuring uniform health insurance premiums for all Americans irrespective of their health status.
Providing a one-stop marketplace for national health insurance exchange to allow consumers to compare and shop for different insurance plans.
Promoting the use of electronic medical records and the practice of evidence-based medicine.
Introducing a government-run health insurance option providing low cost, affordable health insurance that would directly compete with the private insurance industry.
This last provision, often called the ‘Public Option’, has been regarded by its opponents as an indication of how the federal government would grab political power and control the lives of all Americans. Some have gone as far as to say that the Administration is trying to introduce a ‘socialist system’ and set up ‘death panels’ to decide the fate of terminally ill Americans.
The raging debate in both Houses of Congress (House of Representatives and US Senate), since the introduction of the legislation early this year, has been highly partisan and, at times, acrimonious. The primary debate will continue to target accessibility and the ‘Public Option’ on one hand and affordability and deficit reduction on the other. Additionally, fundamental ideological issues of the rights of women to their health (read right for abortion) and accusations of ‘socialist medicine’ (read demand for free market healthcare with little or no government oversight) will continue to fuel this debate well after the legislation has been enacted into law. At the time of writing it is clear that President Obama’s deadline of this year will not be met.
On 7th November 2009, President Obama won a major battle in this war when the House of Representatives passed the ‘Affordable Healthcare for America Act’. The vote was 220-215 and essentially along party lines with the Democrats and only one Republican voting for this legislation. According to Representative John Dingle, the 83-year-old Michigan lawmaker who had introduced national health insurance in every congress since 1955, this 1990-page bill provides coverage for ‘96% of Americans and offers everyone, regardless of health or income, the peace of mind that comes from knowing that they will have access to affordable healthcare when they need it’. However, in the run-up to the final vote, conservatives from both political parties joined hands to impose tough restrictions on abortion coverage that will continue to be a divisive issue throughout the legislative process 4 .
President Obama won the second major victory on 21st November 2009 when the Democrats (with the help of two independents) in the US Senate pushed the legislation past a key hurdle, despite vocal Republican opposition, with 60-39 votes. Sixty votes are needed in the US Senate to prevent ‘filibuster’ or an indefinite discussion on any bill 5 . With this vote the bill will now be debated in the Senate. Table 1 highlights some of the important features of the two bills:
Table 1: Important features of the Senate Bill and House Bill.
Senate Bill
House Bill
Cost*
$848 billion
$1.02 trillion
Projected deficit savings*
$127 billion
$104 billion
New patients*
31 million
36 million
Protection against generic drugs**
12 years
12 years
Government sponsored program
New plan to compete with private plans; government to negotiate payment rates.
New public plan through insurance exchanges; government to negotiate payment rates.
Projected reduction in Medicare growth***
$400 billion
$400 billion
How is it paid for?
Fees on insurance companies, pharmaceutical and medical devices industries. A new payroll tax and 5% tax on elective cosmetic surgery.
$460 billion over the next decade from income tax on individuals making over $500,000 and couples making over $1 million per year.
* These are the estimates for the 10-year-period (2009-2019) from the Congressional Budget Office 6 .
** Both bills would protect biological drugs (made from living organisms rather than chemical
compounds) from competition from generic drugs.
*** The reduction in Medicare spending is non-binding and future Congress can restore these cuts.
In this national debate, two well-known medical centres in the US, the Mayo Clinic of Minnesota and the Cleveland Clinic in Ohio, have frequently been cited as examples that could perhaps be emulated to deliver quality care in an efficient and cost-effective fashion. Both centres practise a ‘medical home’ concept based on a coordinated team approach that was introduced by the American Academy of Paediatrics in 1967. This has been further refined into the ‘patient-centred medical home’ by the American College of Physicians (ACP), American Academy of Family Physicians, and the American Academy of Paediatrics in 2007. This concept is exceedingly important for the management of chronic illnesses because the cost associated with unmanaged chronic conditions is astronomically high. It is estimated that 45% of the US population has a chronic medical condition. Amongst Medicare recipients aged 65 and above, 83% have at least one chronic health problem and almost 25% have at least five co-morbidities. Whereas the current system rewards acute care, it generally does not reimburse preventative care, chronic care management or active integrated inter-specialty management 7. A medical home provides expanded primary care that is personalized, focuses on prevention, actively involves patients in making decisions about their care and helps coordinates all of their care.
One of the deficiencies of the proposed reform is the absence of any tort reform. For physicians in the US the threat of a malpractice lawsuit is real. Without legislative relief, ‘defensive medicine’ will take a significant chunk out of healthcare dollars. Estimates suggest that savings accrued from such legislation could account for 20-25% of the NHE and may be prudently used to reduce the healthcare costs. President Obama’s outright rejection to consider tort reform in his address to the American Medical Association in June is very unfortunate and runs counter to his passionate plea to help reduce medical waste. Some of the important discussions that will take place relate to the need to revamp the physician reimbursement schedules and empower the Medicare Payment Advisory Commission to enhance primary care reimbursement, establish incentives to implement health information technology (including electronic medical records), and mandate the use of evidence based medicine and established protocols to stem the tide of escalating costs with ‘pay for performance’ and other quality measurements 8.
Healthcare reform must also address the physician shortage issue. Several studies, including those from the Institute of Medicine and the American Association of Medical Colleges (AAMC), have indicated a growing physician shortage particularly in Primary Care. In order to address this rising tide of physician shortages the Balanced Budget Act of 1996, that froze the number of reimbursable training positions at the 1996 level, needs to be revisited. As a preliminary target ACP and AAMC have recommended that the availability of Medicare-funded training positions in adult primary care specialties be increased by 3000 each year for the next 15 years 9-11.
From here on I suspect a bruising legislative debate (and drama) will continue with passion and, undoubtedly, some acrimony. Since mid-term elections are coming up in 2010, both the parties are jockeying their position as best as they can. To end the ‘filibuster’ the Democrats will need, yet again, 60 votes to pass the bill in the Senate. However that is not guaranteed at this time since many Democratic senators continue to have concerns and Republicans have made it clear that they will do whatever they can to derail this initiative. Hence further deliberation, particularly in the Senate, will entail significant manoeuvring and arm-twisting, passionate appealing, horse-trading, and perhaps additional funding for select senators to achieve 60 votes. However, in the end there will be a bill from the Senate, perhaps in mid to late January 2010. Subsequently, a conference committee will hammer out the differences in the two bills that can be presented to both houses for final passage and submitted to the President for signature. I believe the President will have the bill on his desk for signature at the end of January or early February 2010.
BJMP 2009:2(2) 4-5
Obesity and Pulmonary Hypertension. What’s the Link?
Roop Kaw.
In the second paragraph of the left column on page 5, the second sentence must have read
"The most direct evidence comes from observations that treatment of OSA with continious positive airway pressure (CPAP) may lower daytime PAP"
BJMP 2009:2(1) 38 - 40
The ‘Lost’ Mirena: What Investigations Are Required ? An Intraperitoneal Levonorgestrel-Releasing Intrauterine System Following Uterine Perforation: Case Report
Shambhu S and Pappas M
The correct name of the author must have read Pappas A on pages 4,39, 41
REFRESHER DAY ON OBSTETRIC ANAESTHESIA AND ANALGESIA
Contact: Obstetric Anaesthetists' Association Secretariat Tel: 011-44-20-8741-1311 Fax: 011-44-20-8741-0611 Email: available through webpage Website: www.oaa-anaes.ac.uk
Anesthesiology
October 07, 2009 United Kingdom / London
UPPER & LOWER LIMB PERIPHERAL NERVE BLOCK WORKSHOP
Contact: Aynsley Pix, B. Braun Medical Limited Email: aynsley.pix@bbraun.com Website: www.aesculap-academy.com
Anesthesiology / Pain Management
October 08, 2009 United Kingdom / Sheffield
2009 DIFFICULT AIRWAY SOCIETY ANNUAL MEETING
Contact: Anne Griffin, Abbey Conference & Corporate Tel: 011-353-1-648-6130 Fax: 011-353-1-648-6197 Email: das2009@abbey.ie Website: www.das2009.co.uk/cms/
Anesthesiology
November 04-06, 2009 United Kingdom / Perth
ASSOCIATION OF CARDIOTHORACIC ANAESTHETISTS AUTUMN MEETING 2009
Contact: Mrs. Andrea Reid, Secretary to Cardiac Anaesthetists Tel: 011-44-125-365-7789 Fax: 011-44-125-365-7134 Email: andrea.reid@bfwhospitals.nhs.uk Website: www.actablackpool2009.nhs.uk
Anesthesiology
November 05-06, 2009 United Kingdom / Blackpool
2009 THREE-DAY COURSE ON OBSTETRIC ANAESTHESIA AND ANALGESIA
Contact: Obstetric Anaesthetists' Association Secretariat Tel: 011-44-20-8741-1311 Fax: 011-44-20-8741-0611 Email: available through webpage Website: www.oaa-anaes.ac.uk
Anesthesiology
November 09-11, 2009 United Kingdom / London
GENERAL MEDICINE
DIABETES & ENDOCRINOLOGY: CLINICAL CHALLENGES & EXPERT ADVICE
Contact: Christine Berwick Tel: 011-44-131-247-3634 Fax: 011-44-131-220-4393 Email: c.berwick@rcpe.ac.uk Website: www.rcpe.ac.uk
Endocrinology / Family Medicine / General Medicine / Geriatrics / Internal Medicine
October 01, 2009 United Kingdom / Edinburgh
2ND NATIONAL CONFERENCE: ANXIETY & DEPRESSION
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Family Medicine / General Medicine / Psychiatry
October 01-02, 2009 United Kingdom / London
3RD ROYAL COLLEGE OF GENERAL PRACTITIONERS (RCGP) ANNUAL NATIONAL PRIMARY CARE CONFERENCE
Contact: Terri Myers, RCGP Tel: 011-44-20-7581-3232 Fax: 011-44-20-7225-3047 Email: courses@rcgp.org.uk Website: www.rcgpannualconference.org.uk
Family Medicine / General Medicine
November 05-07, 2009 United Kingdom / Glasgow
NEW CLINICAL SOLUTIONS IN DIABETES CARE CONFERENCE: OPPORTUNITIES & CHALLENGES
Contact: Alison Bone, Diabetes UK Tel: 011-44-1325-488-606 Email: alison.bone@diabetes.org.uk Website: www.diabetes.org.uk
Family Medicine / General Medicine
November 05, 2009 United Kingdom / York
INNOVATIONS AND PROGRESS IN HEALTHCARE FOR WOMEN
Contact: Confab Consulting, Conference Organisers Tel: 011-44-20-8906-7778 Fax: 011-44-20-8906-7790 Email: IPHW09@confab-consulting.co.uk Website: www.womenshealth.uk.com
Family Medicine / General Medicine / Obstetrics/Gynecology / Oncology
November 09-11, 2009 United Kingdom / London
GYNAE & OBSTETRICS
TRAINING THE TRAINERS
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
October 01-02, 2009 United Kingdom / London
POSTMENOPAUSAL HEALTH
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
October 12-13, 2009 United Kingdom / London
ADVANCED TECHNIQUES IN VAGINAL HYSTERECTOMY
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
October 15, 2009 United Kingdom / London
BASIC PRACTICAL SKILLS IN OBSTETRICS AND GYNAECOLOGY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
October 26-28, 2009 United Kingdom / London
ADVANCE LABOUR WARD PRACTICE
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
November 02-04, 2009 United Kingdom / London
BRITISH SOCIETY OF UROGYNAECOLOGY / ROYAL COLLEGE OF OBSTETRICIANS & GYNAECOLOGISTS JOINT MEETING
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
November 05-06, 2009 United Kingdom / London
MEDICAL COMPLICATIONS IN PREGNANCY
Contact: Symposium Office, Imperial College London Tel: 011-44-20-7594-2150 Fax: 011-44-20-7594-2155 Email: sympreg@imperial.ac.uk Website: www.prossl.com/symposiassl/events.asp
Obstetrics/Gynecology
November 11-13, 2009 United Kingdom / London
PROMPT (PRACTICAL OBSTETRICS MULTI-PROFESSIONAL TRAINING) COURSE: TRAINING THE TRAINERS
Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings
Obstetrics/Gynecology
November 12, 2009 United Kingdom / London
PROMPT (PRACTICAL OBSTETRICS MULTI-PROFESSIONAL TRAINING) COURSE: TRAINING THE TRAINERS
Contact: Conference Office, Royal College of Obstetricians and Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings
Obstetrics/Gynecology
November 13, 2009 United Kingdom / London
NEONATAL UPDATE 2009
Contact: Symposium Office, Imperial College London Tel: 011-44-20-7594-2150 Fax: 011-44-20-7594-2155 Email: sympreg@imperial.ac.uk Website: www.prossl.com/symposiassl/events.asp
Obstetrics/Gynecology
November 16-20, 2009 United Kingdom / London
QUALITY MANAGEMENT OF A FERTILITY SERVICE STUDY DAY 2009
Contact: British Fertility Society Tel: 011-44-14-5464-2217 Fax: 011-44-14-5464-2222 Email: bfs@bioscientifica.com Website: www.britishfertilitysociety.org.uk
Obstetrics/Gynecology / Other Specialties / Urology
November 17, 2009 United Kingdom / London
REPRODUCTIVE GENETICS
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
November 19, 2009 United Kingdom / London
LAPAROSCOPIC SURGERY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk/events Website: www.rcog.org.uk/events
Obstetrics/Gynecology / Surgery
December 02, 2009 United Kingdom / London
RECENT ADVANCES IN GYNAECOLOGICAL SURGERY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology / Surgery
December 03-04, 2009 United Kingdom / London
HANDS ON LAPAROSCOPIC HYSTERECTOMY WORKSHOP
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
December 03, 2009 United Kingdom / London
BASIC PRACTICAL SKILLS IN OBSTETRICS & GYNAECOLOGY
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
December 07-09, 2009 United Kingdom / London
PAEDIATRICS
EUROPEAN SYMPOSIUM ON LATE COMPLICATIONS AFTER CHILDHOOD CANCER
Contact: Margaret Falconer, Event Co-ordinator Tel: 011-44-131-226-0821 Fax: 011-44-131-226-0801 Email: eslccc2009@colpitts.co.uk Website: www.eslccc2009.com
Oncology / Pediatrics
October 29-30, 2009 United Kingdom / Edinburgh
3RD NATIONAL CONFERENCE: PAEDIATRICS ASTHMA & ALLERGY
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Immunology/Allergy / Pediatrics
November 09-10, 2009 United Kingdom / London
PSYCHIATRY
2ND NATIONAL CONFERENCE: ANXIETY & DEPRESSION
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Family Medicine / General Medicine / Psychiatry
October 01-02, 2009 United Kingdom / London
DRUG TREATMENTS IN AFFECTIVE DISORDERS
Contact: Mrs. Susan Chandler, British Association for Psychopharmacology Tel: 011-44-1223-358-428 Email: susan@bap.org.uk Website: www.bap.org.uk
Psychiatry
October 08-09, 2009 United Kingdom / Manchester
DRUG TREATMENTS IN OLD AGE PSYCHIATRY
Contact: Mrs. Susan Chandler, British Association for Psychopharmacology Tel: 011-44-1223-358-428 Email: susan@bap.org.uk Website: www.bap.org.uk
Psychiatry
November 11-13, 2009 United Kingdom / London
BRITISH ASSOCIATION FOR PSYCHOPHARMACOLOGY (BAP) MASTERCLASSES IN CLINICAL PSYCHOPHARMACOLOGY
Contact: Lynne Harmer, BAP Tel: 011-44-1223-358-421 Email: lynne@bap.org.uk Website: www.bap.org.uk
Clinical Pharmacology / Psychiatry
November 11, 2009 United Kingdom / London
CAREIF 2009 INTERNATIONAL CONFERENCE*
Contact: Hampton Medical Conferences Tel: 011-44-20-8979-8300 Fax: 011-44-20-8979-6700 Email: careif@hmconline.co.uk Website: www.careif.ukevents.org
Other Specialties / Psychiatry
December 04, 2009 United Kingdom / London
7TH NATIONAL CONFERENCE: BIPOLAR DISORDERS
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Psychiatry
December 10, 2009 United Kingdom / London
SLEEP DISORDERS
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Psychiatry / Respirology
RADIOLOGY
ECHOCARDIOGRAPHY
Contact: Robina, Intensive Care Society Tel: 011-44-20-7280-4350 Email: events@ics.ac.uk Website: www.ics.ac.uk
Internal Medicine / Radiology/Imaging
September 04, 2009 United Kingdom / London
PET / CT COURSE
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
October 01, 2009 United Kingdom / Glasgow
WELSH BRANCH, BRITISH INSTITUTE OF RADIOLOGY, AUTUMN MEETING
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
October 16-17, 2009 United Kingdom / Llantrisant
OBESITY: THE CHALLENGES & SOLUTIONS IN IMAGING
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
October 19, 2009 United Kingdom / London
ROYAL COLLEGE OF RADIOLOGISTS BREAST GROUP MEETING*
Contact: Hampton Medical Conferences, Conference Manager Tel: 011-44-20-8979-8300 Fax: 011-44-20-8979-6700 Email: hmc@hamptonmedical.com Website: www.hamptonmedical.com
Radiology/Imaging
November 02, 2009 United Kingdom / Belfast
CONTROLLING RADIATION RISKS IN DIAGNOSTIC RADIOLOGY
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
November 24, 2009 United Kingdom / London
RPS UPDATE TRAINING SESSION
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
November 25, 2009 United Kingdom / London
BRITISH SOCIETY OF THORACIC IMAGING AUTUMN MEETING
Contact: British Institute of Radiology Tel: 011-44-20-7307-1400 Email: available through website Website: www.bir.org.uk
Radiology/Imaging
November 27, 2009 United Kingdom / London
7TH ANNUAL CONFERENCE OF UK & IRELAND NEUROENDOCRINE TUMOUR SOCIETY (UKI NETS)
Contact: UKI NETS Secretariat Tel: 011-44-145-464-2277 Fax: 011-44-145-464-2222 Email: enquiries@ukinets.org Website: www.ukinets.org
Endocrinology / Gastroenterology / Oncology / Other Specialties / Pathology / Radiology/Imaging / Surgery
November 30, 2009 United Kingdom / London
SURGERY
2ND ANNUAL ROYAL MARSDEN BREAST CANCER MEETING: HOT TOPICS IN BREAST CANCER
Contact: The Royal Marsden Tel: 011-44-20-7808-2921 Fax: 011-44-20-7808-2334 Email: conferencecentre@rmh.nhs.uk Website: www.royalmarsden.nhs.uk
Oncology / Pathology / Radiology/Imaging / Surgery
October 02, 2009 United Kingdom / London
CURRENT CONCEPTS IN EXTERNAL FIXATION IN TRAUMA
Contact: Jean Fretwell Tel: 011-44-113-392-3819 Email: jean.fretwell@leedsth.nhs.uk Website: www.rcseng.ac.uk
Orthopedics / Surgery
October 05, 2009 United Kingdom / Leeds
ADVANCED TECHNIQUES IN VAGINAL HYSTERECTOMY
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
October 15, 2009 United Kingdom / London
CARE OF THE CRITICALLY ILL SURGICAL PATIENT INSTRUCTOR COURSE
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6311 Email: ccrisp@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Other Specialties / Surgery
October 26-27, 2009 United Kingdom / London
21ST CENTURY DECONTAMINATION: SHARING EXPERTISE
Contact: Aynsley Pix, B. Braun Medical Limited Email: aynsley.pix@bbraun.com Website: www.aesculap-academy.com
Surgery
November 03-04, 2009 United Kingdom / Sheffield
CORE SKILLS IN OPERATIVE ORTHOPAEDIC SURGERY
Contact: Mrs. Kelly Westlake Tel: 011-44-29-2068-2129 Email: westlakekm@cardiff.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
November 04-06, 2009 United Kingdom / Cardiff
CORE SKILLS IN OPERATIVE ORTHOPAEDIC SURGERY
Contact: Lesley Izzard Tel: 011-44-114-271-4027 Email: Lesley.izzrd@sth.nhs.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
November 04-06, 2009 United Kingdom / Sheffield
HANDS ON GYNAECOLOGICAL ENDOSCOPY SKILLS WORKSHOP
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
November 11-13, 2009 United Kingdom / London
ONEHEALTH STUDY DAY
Contact: Aynsley Pix, B. Braun Medical Limited Email: aynsley.pix@bbraun.com Website: www.aesculap-academy.com
Surgery
November 11, 2009 United Kingdom / Tankersley




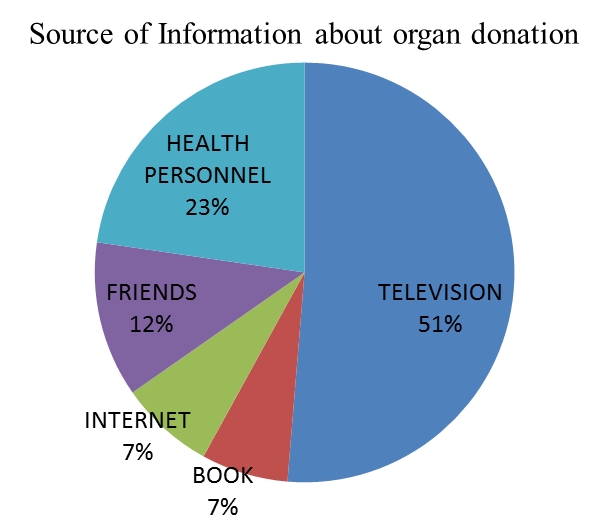
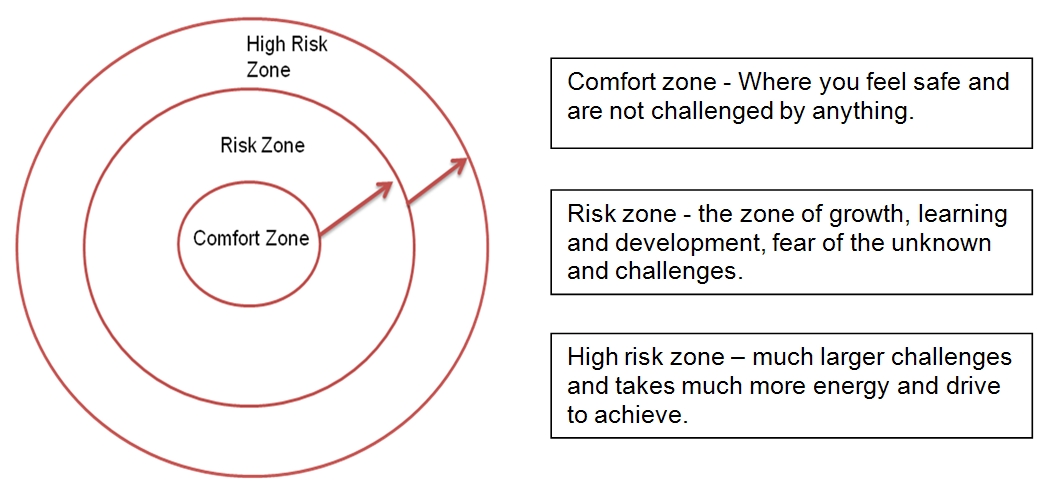
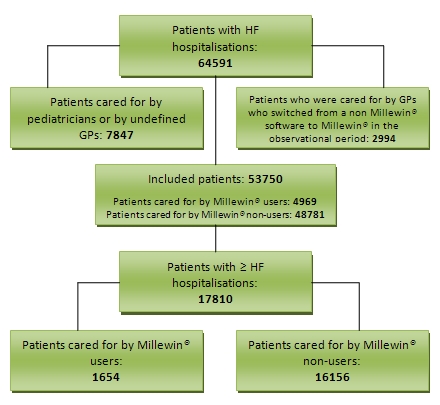
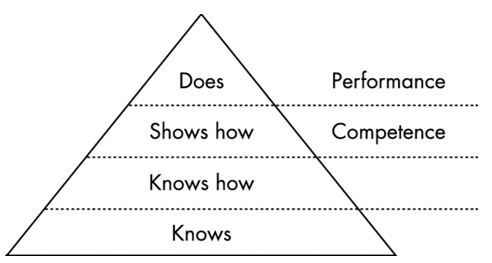
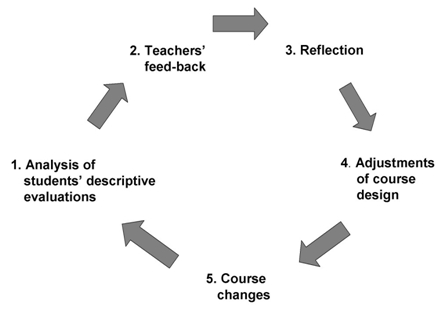
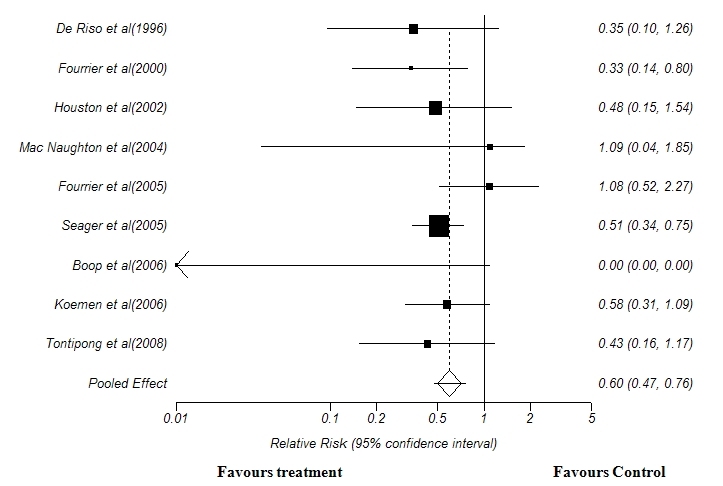
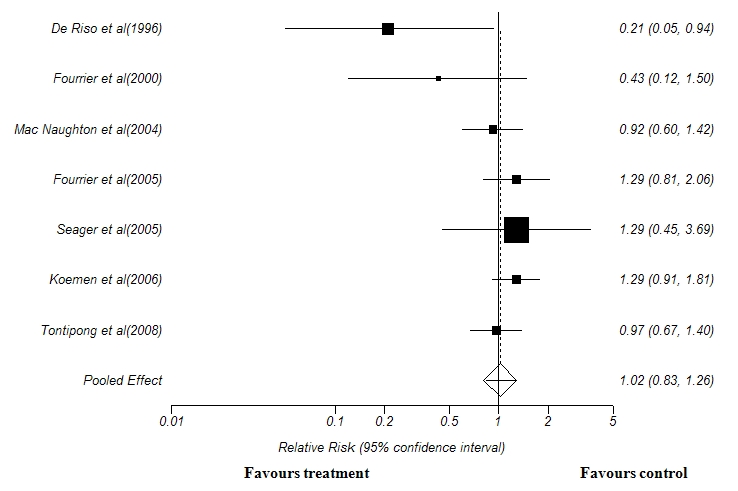

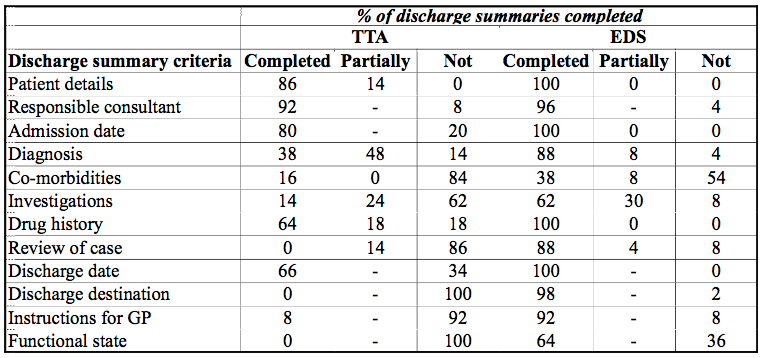
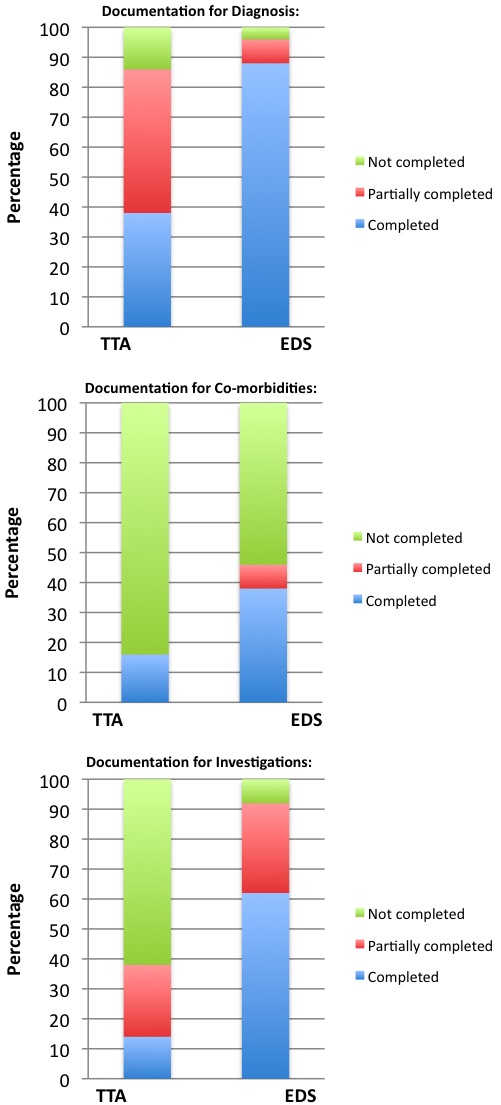
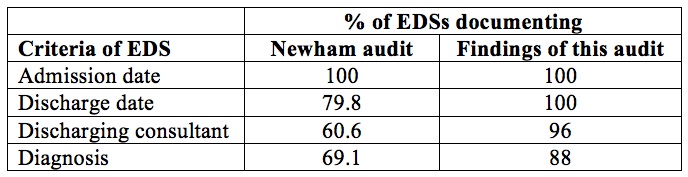



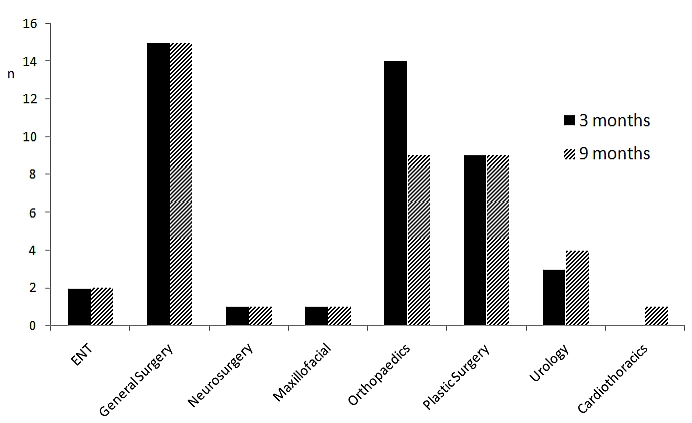
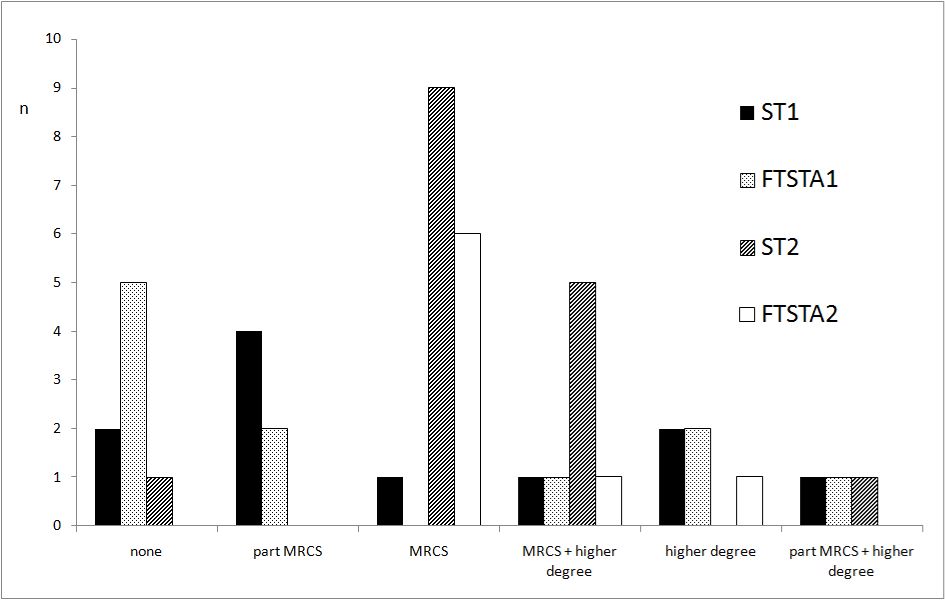
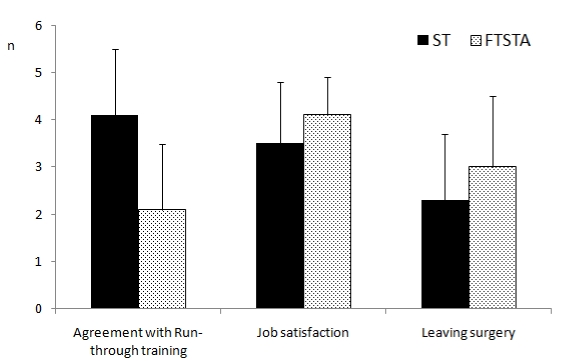
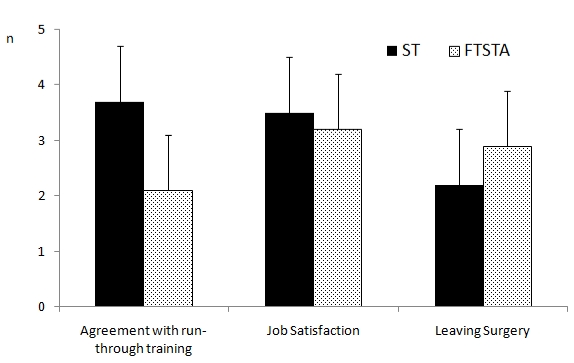
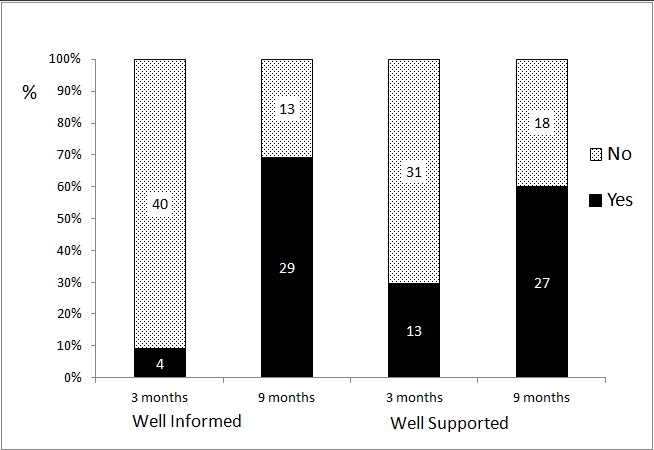

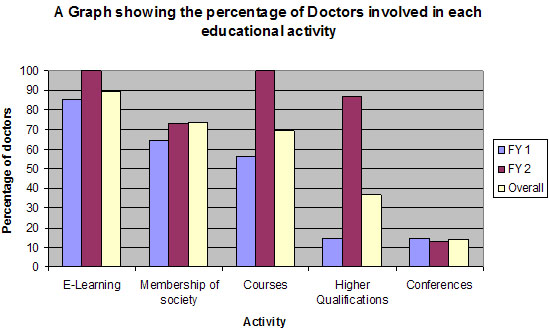
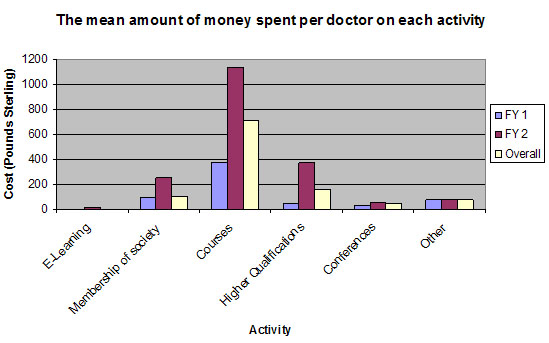
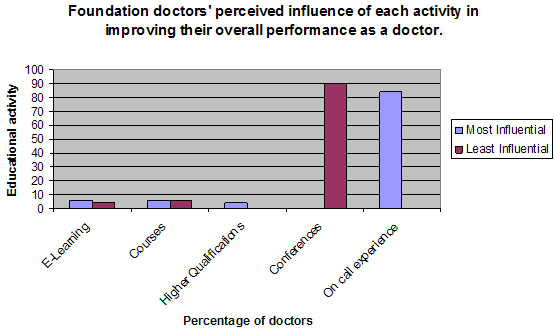
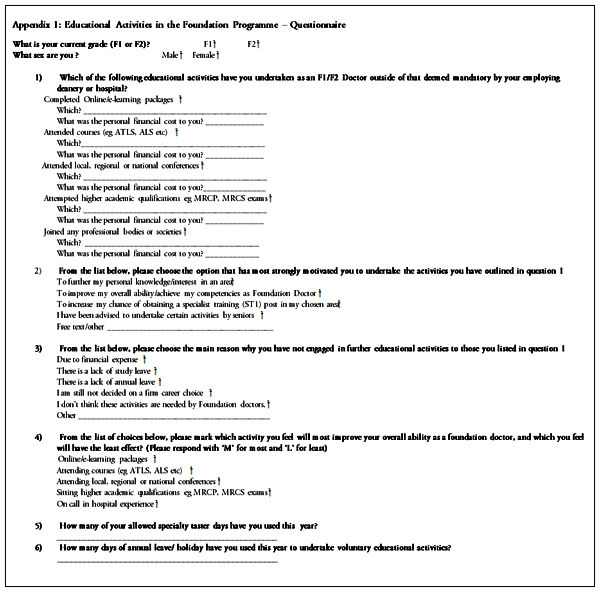

BJMP December 2013 Volume 6 Number 4
BJMP December 2013 Volume 6 Number 4
Editorial
Research Articles
Review Articles
Case Reports/Series