



ISSN 1757-8515
Blue Macular Skin Lesions of Unknown Cause in a Tyre Factory Worker: A Case Report
Mohammed Al Abadie, Dilhara Karunaratne, Nabeel Salmons, Audrey Fong Juan Chin, Soha Ammar and Nisal Karunaratne
Cite this article as: BJMP 2015;8(2):a818
|
|
Abstract This report describes the case of a 61 year old gentleman who developed blue macular skin lesions of unknown cause. Biopsy of the lesion showed pigment deposition in the dermis that had the appearance of tattoo pigment, but oddly the patient had never been tattooed in the past. Carbon black is a chemical which can be used to give blue tattoos their colour. The patient was exposed to carbon black in his job as a tyre maker and it may have accumulated in the dermis by an unknown route. An occupational exposure may be the cause of the skin lesions and this case may play a part in the identification of more cases and a confirmation of the true diagnosis. Keywords: Macular lesion, dermis, carbon black, tattoo, tyre worker, occupational exposure |
Case Report
Blue discolouration of the skin can have a multitude of causes, including Mongolian spots, blue naevi, the naevi of Ito and Ota and metallic discolouration1 or the use of drugs such as minocycline. Here we report the case of a 61 year old gentleman who developed blue macular skin lesions that were not attributable to any obvious cause and may be the result of an unidentified occupational exposure.
A 61 year old Caucasian gentleman developed blue macular skin lesions over a 14 year period. The very first lesion appeared in the middle phalanx of the right middle finger (figure 1). It was light blue and pinpoint, eventually darkening and increasing in size to approximately 1mm x 1mm, at which point becoming permanent and non-evolving. The lesion had no notable associated features and the patient was in otherwise good health.

Figure 1: The first blue macular lesion on the middle phalanx of the right middle finger.

Figure 2: A blue macular lesion on the terminal phalanx of the left middle finger.

Figure 3: A lesion on the anterior abdomen from which a punch biopsy was taken.
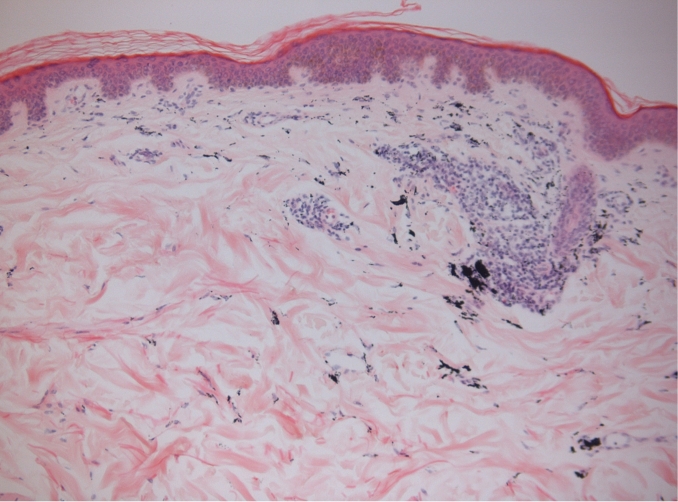
Figure 4: Haematoxylin and Eosin stained slide at 10x magnification. Abdominal skin biopsy showing dermal interstitial and perivascular distribution of black coloured pigment deposits
At present, he has approximately thirteen blue macular lesions in total, all of which have developed in the same manner. They are distributed predominantly on his hands with one on his left forearm and one on the right abdominal flank. New spots still continue to arise on his hands (figure 2).
A punch biopsy of the abdominal lesion (figure 3) was carried out. The histological findings were those of skin with normal intact epidermis and the presence of black coloured pigment granular deposits, located largely within the papillary dermis and occasional smaller deposits in the superficial reticular dermis (figure 4). The deep reticular dermis and subcutaneous fat were normal. The pigment had a perivascular distribution and in dendritic histiocytic cells, with close association to fibroblasts. Histiocytic cells form part of the mononuclear phagocyte system and these cells are abducted mainly for phagocytosis removal or storing material2. Apart from the pigment, the remaining skin was normal. The use of light microscopy alone does not identify all substances on examination of a Haematoxylin and Eosin (H&E) stained section of tissue. Applying polarisation light microscopy enables the identification of numerous structures, for example crystals, pigments, bone and amyloid3. However, the black coloured material here was non polarisable (no refractile foreign material could be identified). These appearances as seen on light microscopy alone are most frequently seen where there is a history of tattoo artistry, but tattoo pigment is typically identified as showing reflective properties using polarisation4. Interestingly, the patient had no clinical history of deliberate tattooing and other causes were considered.
Discussion
The discovery of black coloured deposits in the dermis excludes the diagnoses of Mongolian spots or blue naevi and the naevi of Ito and Ota, all of which are disorders of dermal melanocytes. Another important differential is malignant melanoma, but it is not the diagnosis as the histopathological findings did not find any evidence of dysplasia or malignancy.
In a disorder known as anthracosis, similar findings of black coloured deposits can be seen in other organs such as within the lung and draining lymph nodes. It is often found in smokers and urban populations and reflects the deposition of carbon which is the most commonly identified exogenous mineral substance within tissue sections. The skin is not a site where such carbon pigment is typically seen and therefore, this is not a credible diagnosis in this case.
Agyria is a condition that occurs as a result of silver particle impregnation of skin leading to blue-grey skin discolouration. Silver exposure may be due to occupational or surgical exposure (by use of silver sutures) or medication with silver salts. On interview, the patient denied any occupational exposure to silver and the use of silver salts. Although the patient had had previous shoulder surgery, silver sutures are no longer used in modern day surgical practice and therefore this cannot be the cause of his skin discolouration.
Unfortunately, histological examination of paraffin embedded tissue sections can only confirm the presence and distribution of an exogenous substance and it is not possible to precisely differentiate the exact type of material which is present. The use of an electron probe micro analyser may have been useful in identifying the substance, however, such equipment is not currently available and was not used in this case.
Interestingly, in tattoo artistry, carbon black may be used to give blue tattoos their colour5 and this is also a component of tyres and industrial rubber products6. This provided us with a link to occupational exposure, given that this gentleman is a tyre worker and has been involved in both the manufacture and assembly of tyres for 34 years. Carbon can cause discoloration of the skin, depending on the extent of deposition.
It is notable that in his 34 years of working with tyres, this gentleman did not routinely use gloves or protective uniform until only 10 years ago. This was as workplace safety precautions were not as strongly enforced in previous times. He admitted to have been in direct contact with the materials involved in tyre building and also suffered accidental superficial cuts on his hands whilst working, which may be a route by which carbon may have been introduced into the dermis. This is supported by the observation that the majority of the blue macular lesions were on the hands. Adding credibility to this theory is the identification of a colleague of this gentleman’s (who did not wish to be identified), whose job also involved the manufacture and assembly of tyres, who also has a similar single blue macular lesion on his hand.
In addition to this we have identified a forum on the internet7 that reports other similar cases of blue pin-point macular lesions appearing on the skin of tyre factory workers – some of whom worked for the same tyre company that this gentleman did. This may suggest that there is an association between exposure to a chemical, possibly carbon black, involved in the manufacture of tyres, and the appearance of these blue macular lesions.
In this case report, the identity of the material deposited and the route by which it accumulated in the dermis is unclear, but may have been related to an occupational exposure – this was in keeping with the general consensus upon presentation of this case at the West Midlands Dermatology Conference at New Cross Hospital Wolverhampton. We welcome any new case reports or literature that may be able to shed further light on this subject.
|
Competing Interests None declared Author Details MOHAMMED AL ABADIE, MBBS, DSBD, FAAD, PhD, FRCP, Consultant Dermatologist, The Royal Wolverhampton NHS Trust, New Cross Hospital, Wednesfield Road, Wolverhampton, WV10 0QP, United Kingdom. DILHARA KARUNARATNE, BSC FIRST CLASS HONOURS, Medical student at The University of Birmingham, Edgbaston, Birmingham, B15 2TT, United Kingdom. NABEEL SALMONS, MBChB, FRCPATH, Consultant Histopathologist, The Royal Wolverhampton NHS Trust, New Cross Hospital, Wednesfield Road, Wolverhampton, WV10 0QP, United Kingdom. AUDREY FONG JUAN CHIN, Medical student at The University of Birmingham, The University of Birmingham, Edgbaston, Birmingham, B15 2TT, United Kingdom. SOHA AMMAR, Medical student at The University of Birmingham, The University of Birmingham, Edgbaston, Birmingham, B15 2TT, United Kingdom. NISAL KARUNARATNE, Year 13 student at Brentwood School, Middleton Hall Lane, Brentwood, Essex, CM15 8EE, United Kingdom. CORRESPONDENCE: DILHARA KARUNARATNE, BSC FIRST CLASS HONOURS, Medical student at The University of Birmingham, Edgbaston, Birmingham, B15 2TT, United Kingdom. Email: diliekaru@yahoo.co.uk |
References
- Park JY, Shin DH, Choi JS, Kim KH. Metallic Discoloration on the Right Shin Caused by Titanium Alloy Prostheses in a Patient with Right Total Knee Replacement. Annals of Dermatology. 2013;25(3):356-9.
- Stevens A, Anderson PG. Immune System. In: Stevens A, Anderson PG (eds.) Stevens and Lowe's Human Histology. 4th edition. United Kingdom. Elsevier Mosby; 2015. p. 128-129.
- Bancroft JD, Floyd AD. Light Microscopy. In: Bancroft JD, Gamble M (eds.) Theory and Practice of Histological Techniques. 6th edition. United Kingdom. Churchill Livingstone; 2008. p. 45-48.
- Churukian CJ. Pigments and Minerals. In: Bancroft JD, Gamble M (eds.) Theory and Practice of Histological Techniques. 6th edition. United Kingdom. Churchill Livingstone; 2008. p. 252-257.
- Lehner K, Santarelli F, Vasold R, Koenig B, Landthaler M, Baeumler W. Black tattoo inks are a source of problematic substances such as dibutyl phthalate. Contact Dermatitis. 2011;65(4):231-8.
- International Carbon Black Association. Carbon Black Uses. [Online] Available from: http://www.carbon-black.org/index.php/carbon-black-uses [Accessed 19th December 2014]
- Topix LLC. Blue dots under skin. [Online] Available from: http://www.topix.com/forum/com/gt/TOIIO5NUTJE2050KS [Accessed 19th December 2014].

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.