



ISSN 1757-8515
Correspondence - Another case report of a unusual reaction to IV Pethidine
Premila Hirubalan and Pierre Christian Ip-Yam
Cite this article as: BJMP 2016;9(1):a903
|
A 38 year old BMI 20.2 ASA 2 female underwent an elective robotic-assisted laparoscopic extirpation of endometriosis and dissection of endometriomas. Her medical history included hypertension, migraine, atopic dermatitis, sciatica, cervical spine spondylosis and dysplastic spondylolisthesis of L4/5. Of note, the patient had allergies to Aspirin (causing angioedema), Morphine and Tramadol (both causing generalized rash).
An 18gauge IV cannula was inserted into the cephalic vein at the left wrist, and connected to a bag of Hartmann’s solution. The patient was induced with Propofol 100mg, Rocuronium 30mg and a Remifentanyl infusion running at Ce 1ng/mL. Cefazolin 2g and Dexamethasone 4mg were also administered post-intubation. No rashes were noted on the patient’s skin, and her arms were subsequently enclosed with green towels by her sides for the duration of the surgery. During the procedure, the patient was sustained in a steep trendelenberg position, with her face and eyes checked periodically. No rashes were noted on any exposed skin. Peri-operatively, she was maintained with O2/air/Desfluorane, top-up doses of Rocuronium, and titration of the Remifentanyl infusion. At the end of the surgery, the patient was administered Ondansetron 4mg and Pethidine 50mg (in 2mL), and reversed with Neostigmine 2.5mg and Glycopyrrolate 0.4mg. The patient’s arms were subsequently exposed in preparation for transfer, and it was noted that she had developed severe erythema and inflammation in specific tributaries of the cannulated vein (Figure 1). The patient was extubated uneventfully five minutes later, and did not complain of any symptoms systemically or pertaining to the cord inflammation. She was monitored in recovery for three hours post-op, and the inflammation subsided significantly 90 minutes post-op (Figure 2) and completely 150 minutes post-op (Figure 3).
There have not been many reports of such a reaction in published materials, and we take this opportunity to provide further pictorial evidence of the possible sequelae of IV administration of a high concentration Pethidine solution. The variances in analgesia effectiveness and potential side effects between Morphine and Pethidine are negligible2. As such, and given that Pethidine is commonly used as a mode of analgesia on our wards and in the peri- and immediate post-operative periods when other classes of drugs are contraindicated, we hope to provide further pictorial support of such an extraordinary reaction for other interested clinicians. It is also interesting to note that in both cases the patient was female, around 40 years old, had a thin body structure, had an atopic tendency, and the concentration of injected solution was higher than 10mg/mL. Additionally, these are known factors believed to increase reaction severity3 4. We acknowledge that 3 other drugs were administered at the same approximate time as Pethidine, and as such any of the 4 medications could be culprit to the reaction, although this is unlikely as our patient had been given those medications in previous procedures with no issues or complications.
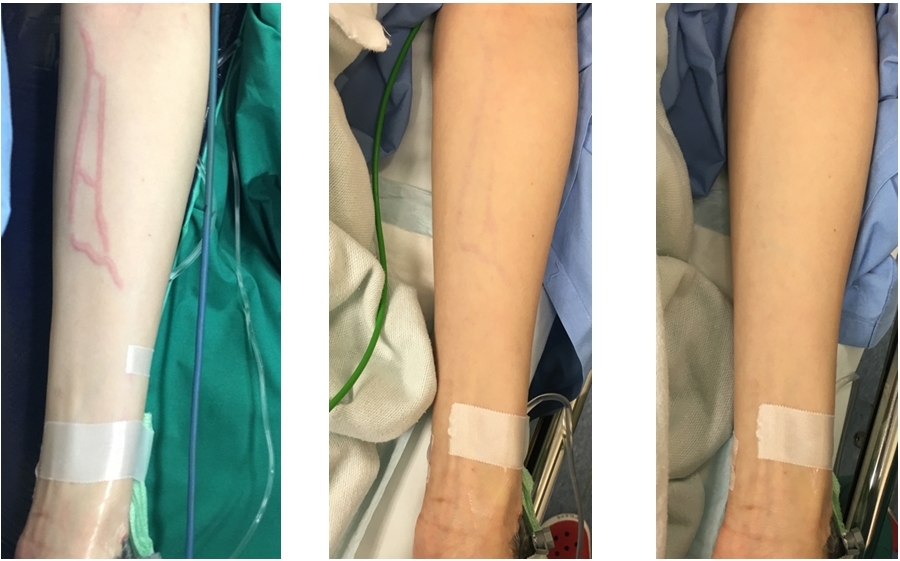
Figure 1: Post-op, Figure 2: 90 mins post-op, Figure 3: 150 mins post-op
|
Competing Interests None declared Author Details PREMILA HIRUBALAN, MBBS, BBiomedSc (Hons), Department of Anaesthesiology, Singapore General Hospital, Duke-NUS Medical School, Singapore. PIERRE CHRISTIAN IP-YAM, MBChB, DA, FRCA, FFARCSI, FAMS, Department of Anaesthesiology, Singapore General Hospital, Duke-NUS Medical School, Singapore. CORRESPONDENCE: PREMILA HIRUBALAN, Department of Anaesthesiology, Singapore General Hospital, Outram Road, Singapore 169608, Singapore. Email: premila.hirubalan@gmail.com |
References
- Krishnan, P. & Sultan, A. An unusual reaction to IV pethidine – A Case Report. BJMP 2014;7(1):a707
- O’Connor A., Schug, S.A. & Cardwell, H. A comparison of the efficacy and safety of morphine and pethidine as analgesia for suspected renal colic in the emergency setting. J Accid Emerg Med 2000;17:261-264
- Evans S.R. Risk factors for adverse drug events: a 10-year analysis. Ann. Pharmacother. 2005; 42(1): 53-61
- Argent D.E., Dinnick O.P. Pethidine phlebitis. Br Journal of Anaesthesia 1954; 26: 260

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.