



ISSN 1757-8515
Ovarian masses in pregnancy: a single centre retrospective study
Tanja Eichenberger-Gautschi, Alison Smith & Ahmad Sayasneh
Cite this article as: BJMP 2018;11(1):a1109
|
|
Abstract Objectives: Ultrasound is proposed as being the first-choice modality to evaluate ovarian masses in pregnancy. The majority of cases are managed expectantly, unless suspicious features of malignancy or any complications, such as ovarian torsion, occur. The aim of this study was to evaluate the outcome of ovarian masses in pregnancy at a tertiary University Hospital in central London. Methods: In a retrospective cohort study in a tertiary referral centre in central London between 12/01/2014 and 14/11/2016 we have analysed the characteristics, size and subsequent management of cases of adnexal masses in early pregnancy. We included pregnant women who underwent a transvaginal ultrasound scan before 15 weeks of gestation and were found to have an adnexal mass. Exclusion criteria were women with corpus luteum or women who had recent induction of ovulation as part of their assisted conception. Results: 41 women were included in the study. Six cases were excluded. The mean diameter of ovarian cysts was 47.7mm (95%CI: 39.9-55.4). In 37/41 women, Ultrasound alone was performed to reach diagnosis with no other imaging or biomarker diagnostic modality. The most common diagnosis was mature teratoma in 20/41 women. One borderline tumour was found. 33/41 women (80.5%) did not require any surgical intervention. 8/41 women (19.5%) underwent surgical intervention in pregnancy. There was a significant difference in the mean diameter of ovarian cysts in the expectant management group (41.2mm; 95%CI: 34.7-47.7) and the mean diameter of cysts in the surgically managed group (74.5mm; 95%CI: 49.2-99.8). Conclusions: Invasive cancer in pregnancy is rare. The results show a significant relation between the size of adnexal mass and the probability of surgery. |
Introduction
With the increasing use of ultrasound as a standard examination in the first trimester, more incidental adnexal masses are detected. The reported incidence of adnexal masses in pregnancy varies, depending on the criteria used to define the mass. A literature review by Goh W. et al., found that 1% of all pregnancies are diagnosed with an adnexal mass 1. A more recent article has suggested adnexal masses are diagnosed in 5% of all pregnancies 2. Simple and functional cysts are very common, and they usually resolve after the first trimester 3. Mature teratomas are by far the most common persistent adnexal masses found in pregnancy 8. It has been estimated that up to 5% of adnexal masses in pregnancy are malignant 4.
Ovarian cysts are typically asymptomatic, but they can cause pain due to pressure on adjacent organs, rupture, bleeding or torsion. The latter case is a significant health condition which mainly requires emergency surgical intervention. During pregnancy, surgical management of ovarian cyst complications is more difficult and more challenging. This is mainly because of other differential diagnosis causing similar symptoms related to pregnancy such as ectopic pregnancy and miscarriage. In case of surgical intervention, the second trimester of pregnancy is supposed to be the safest window for surgery as the risk for drug-induced teratogenicity is smaller than in the first trimester, most functional cysts have disappeared by then and it is technically less difficult than operating during the third trimester 13.
Antenatally, ultrasound is considered to be the best first-line imaging to evaluate adnexal masses 5. Ovarian mass characterization into benign, malignant or borderline can be challenging in pregnancy. This is mainly due to the effect of high levels of gestational hormones which can cause decidualisation of the cystic or solid parts of the ovaries. Benign masses can mimic malignant masses due to this pregnancy related phenomena 12. One of the largest data in literature on ovarian mass characterization is published by the International Ovarian Tumor Analysis group (IOTA). All IOTA studies excluded pregnant women when they developed and validated the rules and models to characterize ovarian masses 14-17. This limits our knowledge and ability to use these models in pregnant women. It is known that tumour markers may be raised in pregnancy and should therefore not routinely been done 7. An alternative diagnostic tool is Magnetic Resonance Imaging (MRI) which is considered to be safe in pregnancy and can be helpful if the ultrasound imaging is inconclusive in evaluating whether a mass is benign or malignant 6; 10. The American College of Gynecology and Obstetrics recommends that pregnant patients should be reviewed on a case-to-case basis and stated that there are no known biological effects of MRI on fetuses. However, Gadolinium, which help in characterizing ovarian masses, should be avoided when examining a pregnant patient 11.
The aim of this retrospective study was to look into characteristics, size and subsequent management of cases of adnexal masses in early pregnancy.
Methods
This was a retrospective study of data collected between 12/01/2014 and 14/11/2016 in the Early Pregnancy and Gynaecology Unit (EPAGU) of a tertiary referral centre (Guy’s and St Thomas’ NHS Trust, GSTT) in central London. The Ultrasound reporting system (Astraia Software Gmbh, Version 1.24.10, Munich, Germany, 2016) was searched for data. Cases included were consecutive. The study was approved as a service evaluation audit by the Clinical Governance team at Guy’s and St Thomas’ NHS Trust. The study included women who were diagnosed with an adnexal mass while having a transvaginal ultrasound scan TVS at or before 15 weeks of gestation. Pregnancy was confirmed by a positive pregnancy test and an intrauterine gestation on transvaginal ultrasound scan. Women who had the first gestational TVS after 15 weeks of gestation, pregnancies of unknown location, ectopic or trophoblastic pregnancies and patients who had ovarian stimulation treatment were all excluded.
Repeat ultrasound scan reports were retrieved from the Astraia system. Further procedures, tests and imaging results were retrieved using the Electronic Patient Reporting system at GSTT (EPR application, iSOFT Group plc., USA, 2004), PACS (GE Medical Systems, Wisconsin, USA, 2006), Badgernet (Clevermed, Client version 2.9.1.0, Edinburgh, UK). We have used the subjective impression of the examiner as the index test. If surgery was performed the final outcome to identify benignity or malignancy was considered to be the histological diagnosis if any removed tissue. Cytology was used for a reference test in two cases when ovarian cysts were aspirated only. Borderline tumours were classified as malignant for statistical analysis. Tumours were classified using the criteria recommended by the World Health Organisation (WHO) 9; 10. All ultrasound scan images were available and reviewed by author TEG to confirm the US finding. For statistical analysis, the SPSS software package was used (version 24 for Windows, Chicago, IL, USA). A two tailed student’s t test was used to compare means in ovarian masses diameters and a p value of less than 0.05 was considered statistically significant.
Results
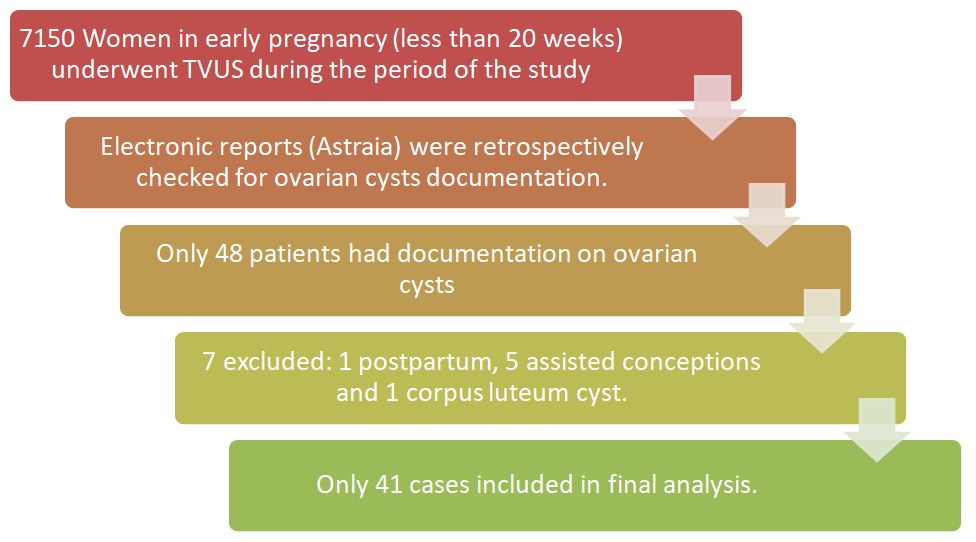
7150 patients underwent transvaginal scans for early pregnancy in that period. In total 48 cases of women with adnexal masses in pregnancy and completed data were analysed. Seven women have been excluded; one woman being postpartum at the time of the finding of a large endometrioma, five pregnancies due to assisted conception and one woman was found to have a corpus luteum cyst (Figure 1).
41 women with 46 ovarian cysts could be included in the study. Two women had bilateral ovarian cysts, one had two ipsilateral cysts and one woman had three ipsilateral cysts. The mean age at the time of detection of the ovarian mass was 30 (95%CI:28-32) (Fig.2).
Figure 2: Age distribution in the study group. 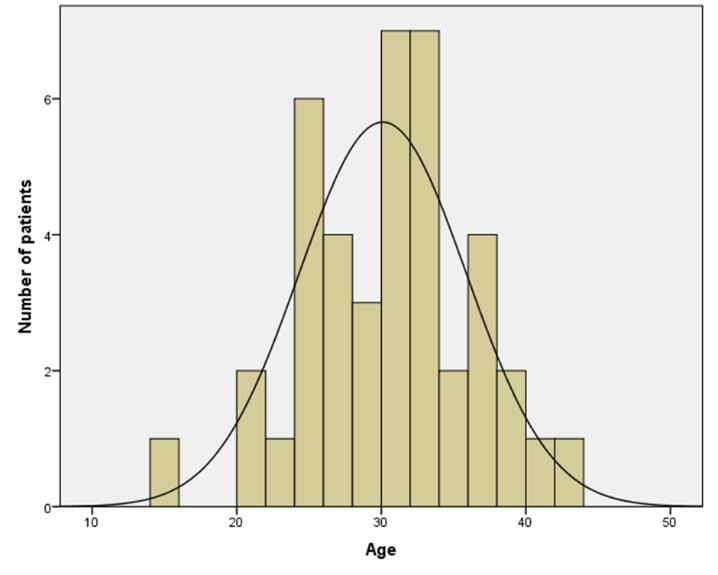
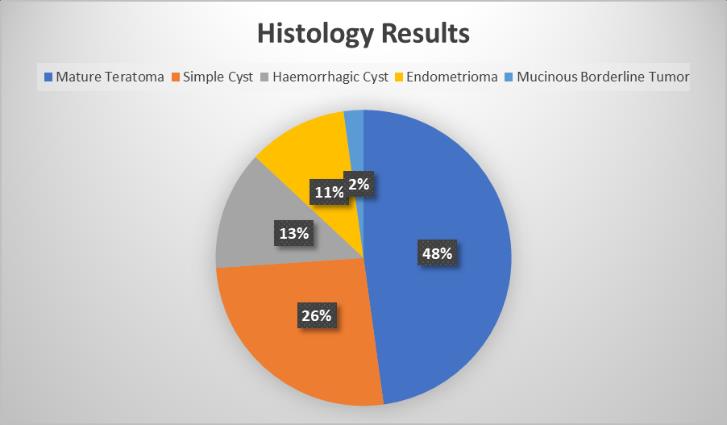
The mean gestation at the time of first ultrasound was 7.4 weeks (95%CI:6.6-8.3). The mean diameter of ovarian cysts measured 47.7mm (95%CI:39.9-55.4). In 36 women ultrasound alone was performed to reach diagnosis, one woman had an extra MRI scan, two women had tumour markers on top of the TVUS and in two women an MRI scan and tumour markers were performed after the TVUS. The ovarian cyst(s) was on the right ovary in 16/41 women, on the left in 22/41, bilateral in 2/41 and in one case the side of the cyst was not reported. The most common ultrasound subjective impression was mature teratoma (22/46 cysts), followed by simple cysts (12/46 cysts), haemorrhagic cysts (6/46 cysts), endometriomas (5/46 cysts) and one possible mucinous Borderline tumour. The latter was confirmed later on histology as the stage FIGO 1A intestinal type mucinous Borderline tumour (Fig.3).
Figure 3: Distribution of origin of cysts by histology.
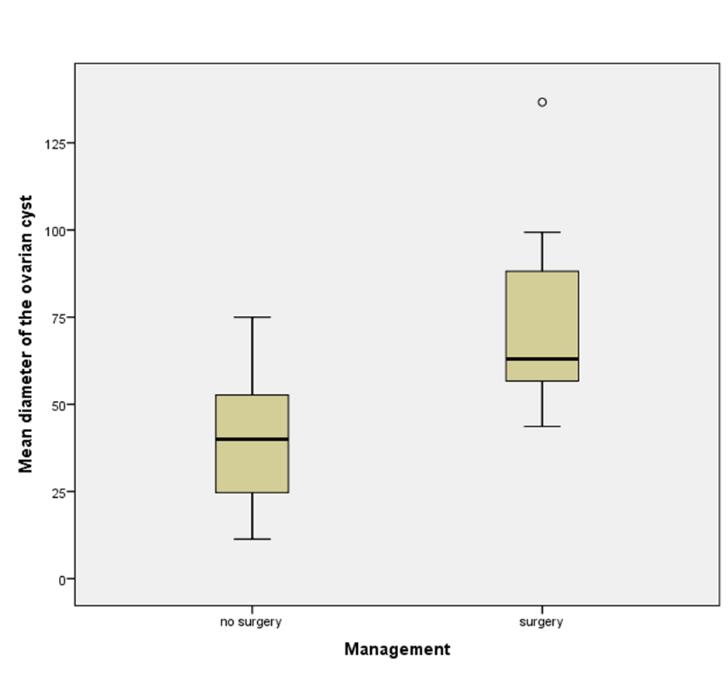
In total 8/41 women (19.5%) underwent surgical intervention; of these eight cases six underwent major surgery under GA and two had a cyst aspiration under local anaesthesia. Seven out of these eight masses were classified as benign on USS and were subsequently confirmed to be benign by histology or cytology. In only one case a complex adnexal mass was found on USS examination at 9 weeks of gestation and the MRI scan reported possible malignancy. Tumour markers in this 23-year-old woman were normal and a laparotomy was performed at 17 weeks of gestation to remove the mass. Histology showed the mass to be a mucinous borderline tumour, FIGO stage IA. In another patient, an oophorectomy had to be performed at the time of the Caesarean section at term for fetal distress as the ovary was found to be necrotic. In this patient an ultrasound at 10 weeks of pregnancy had demonstrated a 6cm diameter haemorrhagic cyst, which had presumably torted during the pregnancy without any symptoms to prompt the patient to refer herself. Histology in this case had shown an infarcted cyst with fibrosis and calcification. In four of the major surgery cases performed under GA uncomplicated laparoscopies were performed to remove the adnexal mass; in one case a laparoscopic salpingoophorectomy was performed as an emergency for a suspected ovarian torsion at 16/40 weeks. In three cases a laparoscopic procedure for cystectomy was performed electively for ongoing pain. In the first case a cyst was diagnosed in early pregnancy subsequently there was a miscarriage and the cyst was removed 4 months after the diagnosis. In the second case a cyst was found in early pregnancy the woman had a termination at 11 weeks of pregnancy and a cystectomy 5 months later. In the third case a laparoscopic cystectomy was performed 8 weeks after the diagnosis, however the woman suffered a miscarriage at 12 weeks of gestation. Histology confirmed dermoid cysts in all four of these cases. The two cyst aspirations performed under local anaesthesia and ultrasound guidance were both symptomatic for torsion, one at nine weeks and one at ten weeks of pregnancy. In both patients the procedure has been successful. 33/41 (80.5%) with no indication for surgical intervention. There was a significant difference in the mean diameter of ovarian cysts in the expectant management group (41.2mm; 95%CI:34.7-47.7) compared with the mean diameter of cysts in the surgically managed group (74.5mm; 95%CI: 49.2-99.8) (Fig.4).
Figure 4: Mean diameter of the ovarian cysts.
In 33/41 patients no surgical intervention was needed during pregnancy. 13/33 patients had no follow up of their ovarian cyst arranged and no further mentioning of the cysts on routine growth and anomaly scans during pregnancy was found. In 20/33 patients at least one routine follow-up scan was performed 1-2 weeks after the diagnosis and in 12 of these 20 patients a second follow-up had taken place at least 1 month after the diagnosis. In one of the 20 patients with recorded follow-up’s an MRI scan had been arranged 2 months after the initial USS finding of a dermoid cyst.
Discussion
The results of our study confirm findings from previous studies: The vast majority of ovarian masses in pregnancy are benign and invasive cancer in pregnancy is rare; The results show a significant relation between size of adnexal mass and probability for surgery; Ultrasound examination of adnexal masses has been proven to be accurate and safe in pregnancy; Managing ovarian cysts in pregnancy can be challenging. Goh et al. have reported similar outcomes, namely that ovarian torsion is still reported as a rare event in pregnancy and that the management of most adnexal masses in pregnancy can be conservatively managed if asymptomatic and if there are no ultrasound findings suspicious for malignancy 8. If a surgical intervention is needed for persistent masses with complications such as torsion Goh et al. have found that laparoscopy during 1st and 2nd trimester can be safely performed 1. In our cohort two out of six women underwent successful major surgery during the 2nd trimester of pregnancy. One had an emergency laparoscopy for a torsion at 16 weeks of pregnancy and the other had a laparotomy at 17 weeks of pregnancy for a mucinous borderline tumour.
However, to our knowledge currently no evident guidelines exist on how to manage and follow-up ovarian masses during pregnancy. The characteristics and presentation of ovarian mass complications in pregnancy can be mimicked by similar symptoms related to pregnancy, such as ectopic pregnancy. In one of our cases a woman with a known ovarian cyst was found to have a necrotic ovary at the time of Caesarean section, despite no signs of torsion at any time during pregnancy. This only highlights how challenging and difficult the assessment of ovarian masses during pregnancy can be. Additional diagnostic examinations such as tumour markers in suspicious ovarian masses have been found difficult to interpret in pregnancy. However, there has been literature suggesting that if a mass is strongly suspicious for malignancy, it is likely that CA-125 will be severely elevated (1000-10 000) 7.
The strength of this study is that the data has been collected using the expertise and facilities of a tertiary referral centre in London (GSTT). The limitations of this study include retrospective data collection, small numbers of cases and loss of follow-up. Although, our study shows the benign nature of most ovarian masses in pregnancy and the ability of ultrasound to safely characterize ovarian masses, a prospective study is required to validate our results. As it is difficult to interpret ovarian cancer tumour markers in pregnancy 7, other models, such as the IOTA Simple Rules14,16 or the ADNEX model17 may play a role for further characterisation of ovarian masses. A prospective trial is required to validate these models in pregnancy.
|
Competing Interests None declared Author Details TANIA EICHENBERGER-GAUTSCHI Dr Med, Specialist Registrar in Obstetrics and Gynaecology, Guy's and St Thomas' NHS Foundation Trust, London UK. ALISON SMITH MSc, DMU Tutor Sonographer, Guy's and St Thomas' NHS Foundation Trust, London, UK. AHMAD SAYASNEH MBChB MD(Res) MRCOG, Consultant Gynaecological Oncology Surgeon, Honorary Senior Clinical Lecturer, Guy's and St Thomas' NHS Foundation Trust, London UK. CORRESPONDENCE: Dr Tania Eichenberger-Gautschi Dr Med, Specialist Registrar in Obstetrics and Gynaecology, Guy's and St Thomas' NHS Foundation Trust, London UK email: eichenberger.tt@gmail.com Email: eichenberger.tt@gmail.com |
References
- Goh W., Bohrer J., Zalud I. Management oft the adnexal mass in pregnancy. Curr Opin Obstet Gynecol 2014; 26:49-53.
- Mukhopadhyay A, Shinde A, Naik R. Ovarian cysts and cancer in pregnancy. Best Pract Res Clin Obstet Gynaecol 2016; 33:58-72.
- Giuntoli R, Vang R, Bristow R. Evaluation and management of adnexal masses during pregnancy. Clin Obstet Gynecol 2006; 49:492-505
- Smith L, Dalrymple J, Leiserowitz G, et al. Obstetrical deliveries associated with maternal malignancy in California, 1992 through 1997. Am J Obstet Gynecol 2001; 184 :1504-1512.
- Yakasai I, Bappa L. Diagnosis and management of adnexal masses in pregnancy. J Surg Tech Case Rep 2012 ; 4 :79-85.
- Adusumilli S, Hussain H, Caoili E, et al. MRI of sonographically indeterminate adnexal masses. AJR Am J Roentgenol 2006; 187:732-740.
- Spitzer M, Kaushal N, Benjamin F. Maternal CA-125 levels in pregnancy and the puerperium. J Reprod Med 1998; 43:387-392.
- Goh W, Rincon M, Bohrer J, et al. Persistent ovarian masses and pregnancy outcomes. J Matern Fetal Neonatal Med 2013 ; 26 :1090-1093.
- Tavassoli FA, Devilee P International Agency for Research on Cancer (2003) Pathology and Genetics of Tumours of the Breast and Female Genital Organs. International Agency for Research on Cancer: Lyon.Tavassoli FA, Devilee P. Pathology and genetics of tumours of the breast and female genital organs.
- Ray JG et al. Association Between MRI Exposure During Pregnancy and Fetal and Childhood Outcomes. JAMA. 2016;316(9):952-961
- Guidelines for diagnostic imaging during pregnancy and lactation. Committee Opinion No. 723. American College of Obstetricians and Gynecologists. Obstet Gynecol 2017;130:e210–6.
- Sayasneh A, Naji O, Adallah Y et al. Changes seen in the ultrasound features of a presumed decidualised ovarian endometrioma mimicking malignancy. J Obstet Gynaecol. 2012 Nov;32(8):807-11.
- Cavaco-Gomes J, Jorge Moreira C, Rocha A et al. Investigation and Management of Adnexal Masses in Pregnancy. Scientifica (Cairo). 2016;2016:3012802.
- Sayasneh A, Kaijser J, Preisler J et al. A multicenter prospective external validation of the diagnostic performance of IOTA simple descriptors and rules to characterize ovarian masses. Gynecol Oncol. 2013 Jul;130(1):140-6.
- Timmerman D, Testa AC, Bourne T et al. Logistic regression model to distinguish between the benign and malignant adnexal mass before surgery: a multicenter study by the International Ovarian Tumor Analysis Group. J Clin Oncol. 2005 Dec 1;23(34):8794-801.
- Timmerman D, Ameye L, Fischerova D et al. Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: prospective validation by IOTA group. BMJ. 2010 Dec 14;341:c6839.
- Sayasneh A, Ferrara L. De Cock B et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model: a multicentre external validation study. Br J Cancer 2016; 115, 542-548.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.