



ISSN 1757-8515
An aggressive follicular variant of papillary thyroid carcinoma with unusual metastases - A case report and review of literature
Isaac Sachmechi, Rachelle N Bitton, Susan Sanelli-Russo and Supat Thongpooswan
Cite this article as: BJMP 2014;7(1):a705
|
|
Abstract Metastatic carcinoma to the sinonasal tract is rare, by papillary thyroid cancer even rarer. We describe a 44-year old Hispanic woman with follicular variant papillary thyroid carcinoma treated with total thyroidectomy and post-surgery I 131 ablation. Post therapy, two consecutive body scans were negative and thyroglobulin level was less than 5 ng/ml. A year later, she presented with history of urinary retention and lower extremity weakness. A myelogram revealed block at T1-T2. Patient underwent laminectomy followed by external radiation. Pathology revealed metastatic follicular variant of papillary thyroid carcinoma. Total body scan post surgery was negative, and the thyroglobulin level was 5 ng/ml. Patient was maintained on thyroxine suppression therapy. Two years later, patient started complaining of headaches and double vision. Magnetic resonance imaging (MRI) was done and revealed a soft tissue mass in the sphenoid sinus, eroding the basi-sphenoid and extending into the nasopharynx. Biopsy was positive for metastatic papillary thyroid cancer, follicular variant. Pituitary function testing revealed TSH 0.1 mIU/ml, free T4 level 1.2 mIU/ml. AM cortisol 5.3 mcg/dl, prolactin 182 ng/ml, ACTH 12 pg/ml, FSH 11.5 mIU/ml, LH 4.0 mIU/ml, and Estradiol 20 pg/ml. Metastasis to the sphenoid sinus is rare from any tumour, and from papillary thyroid cancer is extremely rare. An extensive world literature review revealed only 4 cases of papillary thyroid carcinoma with spread to sphenoid sinus region. Of 12 case reports of thyroid carcinoma with spread to the sphenoid sinus, 6 were follicular thyroid carcinoma. Generally, total body scan negative with low stimulated thyroglobulin is an excellent prognostic sign. Our patient demonstrates that we need to remain vigilant for the unusual tumour especially when the initial presentation showed a large lesion. Keywords: papillary thyroid carcinoma, metastasis, sphenoid sinusAbbreviations: MRI- Magnetic resonance imaging TSH- Thyroid stimulating hormone PET- positron emission tomography CT- computerized tomography |
Introduction
Metastatic carcinoma to the sinonasal tract is rare. We describe a patient with an aggressive follicular variant of papillary thyroid carcinoma who presented with an unusual metastasis to sphenoid sinus.
Case report
A 44 year old Hispanic woman presented at Queens Hospital Center in June 1988 with airway obstruction and was found to have a 10x12 cm firm mass in the left thyroid lobe, and palpable left supraclavicular node. She had no prior history of radiation, and no family of thyroid cancer. She underwent a total thyroidectomy with a modified radical neck dissection. Pathology revealed a follicular variant of papillary thyroid carcinoma: non-tall cell variant. Six of fifty (6/50) lymph nodes were positive. Post-surgery, patient received Iodine-131 ablation therapy (93 mCi) and was placed on thyroid hormone suppressive therapy. Non-stimulated thyrogen total body scan a week after therapy was negative. Thyrogen was not available at that time.
The patient was non-compliant with thyroxine and thyroid stimulating hormone (TSH) was often elevated (13-80 mlU/ml). However, the serum thyroglobulin remained less than 5.0 ng/ml and antithyroglobulin antibody was negative. A repeat total body scan (with 5 mCi I131) 6 months later and 4 years later with thyroxin withdrawal (TSH 36 mIU/ml and 48 mIU/ml respectively) was negative, and patient was continued on thyroxine suppression therapy.
Five years after initial presentation, the patient developed urinary retention and lower extremity weakness. A myelogram revealed block at T1-T2. Patient underwent laminectomy. Pathology revealed metastatic follicular variant of papillary thyroid carcinoma. Since iodine containing contrast was used during the myelogram, I131 iodine therapy was not given. External radiation of 2000 CGY to C7-T5 was administered.
A total body scan 8 weeks post laminectomy (when 24 hour urine iodine < 100 microgram/litre, and TSH was 38 mIU/ml after thyroid hormone withdrawal) was negative, the thyroglobulin level was 5 ng/ml and negative antithyroglobulin antibody (at that period of time, positron emission tomography (PET) scan was not an available option). For the next 2 years of follow up, the patient was maintained on thyroxin suppression therapy, this time with good compliance (TSH 0.1 mIU/ml, thyroglobulin less than 5 ng/ml and negative antithyroglobulin antibody). She did not show up for follow up lumbar computerised tomography (CT).
Seven years after the initial presentation, she complained of headache and double vision, and a three month history of amenorrhea. The thyroglobulin at this time was elevated (20 ng/ml). Chest X-ray was positive for two nodules in the right lung. Magnetic resonance imaging (MRI) revealed a soft tissue mass in the sphenoid sinus, eroding the basi-sphenoid and extending into the nasopharynx (Fig. 1 ABCD). The mass also eroded the sella floor displacing the pituitary gland upwards (arrows). Bone scan revealed focal abnormalities in the upper thoracic spine, ethmoid bones and base of the skull. At that period of time, PET scan was not an available option. Pituitary function testing revealed TSH 0.1 mIU/ml, free T4 level 1.2 mIU/ml. AM cortisol 5.3 mcg/dl, prolactin 182 ng/ml, ACTH 12 pg/ml, FSH 11.5 mIU/ml, LH 4.0 mIU/ml, and Estradiol 20 pg/ml.
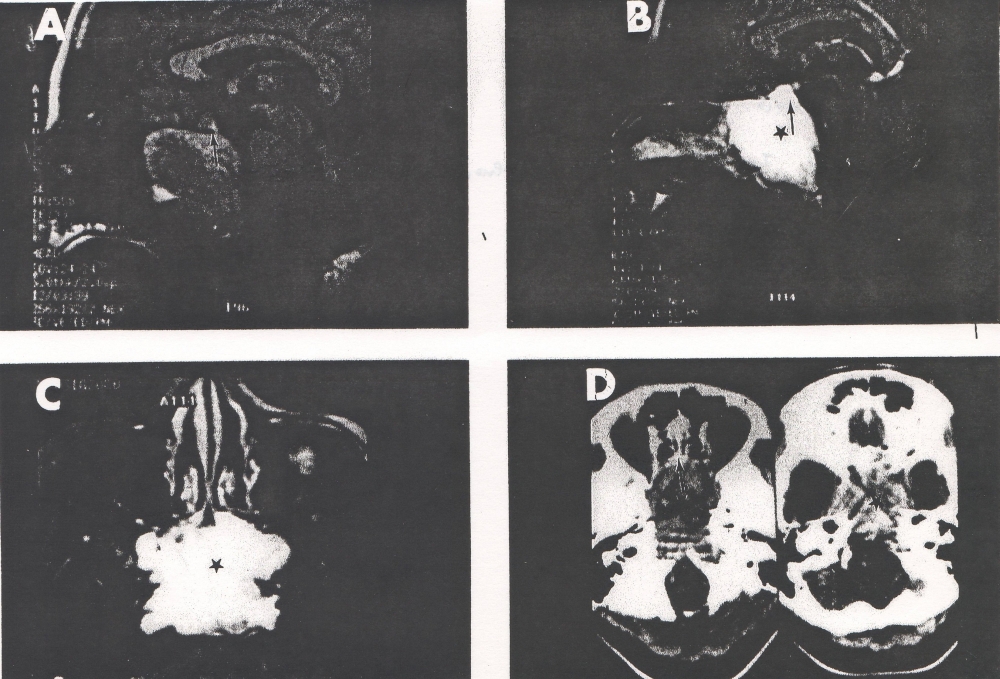
Figure 1: A-T1 weighted midline sagittal MRI scan without contrast. B-T1 weighted midline sagittal MRI scan with contrast. C-T2 weighted axial MRI scan through the lesion. D-Axial CT scans without (on the left) and with (on the right) contrast. Note: The large destructive and enhancing lesion (*) in the sphenoid sinus associated with destruction of the basisphenoid, clivus and sellar floor. Note the normal pituitary gland (arrow) is displaced upwards out the sellaturcica.
Biopsy of the sphenoid sinus mass confirmed that it was metastatic papillary thyroid cancer, follicular variant. The tumour cell nuclear DNA was diploid and P53 and K167 were negative (Impat, NY). The patient was placed on hydrocortisone replacement and continued on thyroxine suppression therapy. Three months later the patient suffered a cardiorespiratory arrest and expired.
Discussion
Metastasis to the sphenoid sinus is rare from any tumour, and from papillary thyroid cancer it is extremely rare. An extensive world literature review revealed only 4 cases of spread to sphenoid sinus region from papillary thyroid cancer.1-4
Renal cell carcinoma is the most common tumour of paranasal sinus metastasis, 41.8%. The average age is 58 years, with slight predominance of males. The most common presentation was epistaxis, 31%. The most common causes of sphenoid metastasis are gastrointestinal and renal tumours5.
Von Eiselsberg et al. in 1893 described one case of metastasising thyroid carcinoma to sphenoid sinus.6 Harmer et al., 1899, reported a case of medullary thyroid carcinoma metastasis to sphenoid/ ethmoid sinus and nose. 7 Barrs et al. in 1979 reported a case of metastasis of follicular thyroid carcinoma to sphenoid sinus and sphenoid bone.8 Chang et al. in 1983 described a case of metastatic carcinoma of the thyroid to the sphenoid sinus.9 Renners et al. in 1992 reported one case of metastasis of follicular thyroid carcinoma to the paranasal sinuses, including the sphenoid sinus. 10Yamasoba et al. in 1994 reported a case with follicular thyroid carcinoma metastasising to sinonasal tract which also included sphenoid sinus.11 In the same year, Cumberworth et al. reported a case of metastasis of a thyroid follicular carcinoma to the sinonasal cavity which head CT showed sphenoid, ethmoid, frontal and maxillary sinuses. 12In 1997, Altman et al. described a case of follicular metastatic thyroid carcinoma to paranasal sinuses which included the sphenoid sinus. 13 The reported cases of thyroid cancer metastasis to sphenoid sinus are in table 1. Four cases were papillary thyroid carcinoma (included follicular variant of papillary thyroid carcinoma), six cases were follicular thyroid carcinoma, 1 case was medullary thyroid carcinoma and 1 case was unspecified thyroid carcinoma.
Table 1: Cases of thyroid metastases to the sphenoid sinus
| Author | Age | Sex | Presenting symptoms | Histologic type |
| Present case | 44 | F | Headache, double vision and amenorrhea | Follicular variant papillary thyroid carcinoma |
| Mandronio (2011) | 53 | F | Blurring of vision of left eye | Papillary metastatic thyroid carcinoma |
| Nishijima (2010) | 81 | F | Epistaxis | Differentiated papillary thyroid carcinoma |
| Argibay Vasquez (2005) | 53 | F | Headache, paresthesia in the right eye region and left monocular diplopia | Differentiated carcinoma of thyroid, follicular variant of papillary cell |
| Altman (1997) | 81 | F | Progressive headache | Follicular thyroid carcinoma |
| Freeman (1996) | 50 | M | Facial pain, proptosis of the left globe and left horner’s syndrome | Metastatic papillary thyroid carcinoma |
| Yamatosoba (1994) | 34 | F | Hearing loss in right ear | Follicular thyroid carcinoma |
| Cumberworth (1994) | 62 | F | Right nasal blockage | Follicular carcinoma of the thyroid |
| Renner (1984) | 61 | F | Profuse right unilateral epistaxis | Follicular thyroid adenocarcinoma |
| Chang (1983) | 50 | F | Intermittent epistaxis, weight loss and pain in the right nasopharyngeal region | Follicular carcinoma with papillary foci |
| Barrs (1979) | 54 | F | Progressive loss of vision in the left eye | Follicular thyroid carcinoma |
| Harmer (1899) | 44 | F | Headache | Medullary thyroid carcinoma |
| von Eiselsberg (1893) | 38 | M | Chronic meningitis | Thyroid carcinoma |
Pathologic lesions involving the sphenoid sinus include inflammatory disease, mucocele, chordoma, nasopharyngeal carcinoma, plasmacytoma, primary sphenoid sinus carcinoma, adenocystic carcinoma, pituitary adenoma, and giant cell granuloma. Benign disease often presents with a more gradual obstruction and disturbance of vision. This contrasts with the acute and progressive disturbances of vision in all cases reported with malignant lesions of the sphenoid sinus.14
Our patient presented with complaints of double vision for 6 months and headache. After imaging with MRI and given her previous history of metastatic thyroid cancer, the most likely diagnosis was metastases to the sphenoid sinus from the thyroid cancer, which was confirmed by tissue biopsy. Since this patient had evidence of bone metastasis, it is likely that the tumour first metastasised to the bone and then ruptured into the sphenoid sinus. The tumour appears to have eroded the sellar floor, extending into and displacing the pituitary gland, causing secondary hypoadrenalism.
In our patient, low thyroglobulin proved to be an unreliable marker because it was low when the patient had metastasis of the tumour in the spine. These tumours are more aggressive and today, PET scanning has proved more reliable in following them, a modality that was not available at the time for our patient. The possible explanations for negative total body scans in patients with metastatic differentiated thyroid cancer are a) technical limitations of the scan in detecting the tumour cells, and b) failure of the tumour tissue to trap iodine.
There are several unusual aspects in this patient’s presentation. Firstly, the initial presentation was unusual, since this tumour was very aggressive with rare sites of distant metastases. Perhaps the long periods of hypothyroidism when patient was noncompliant promoted the aggressive nature of this tumour. Secondly, the failure of known tumour markers, i.e. serum thyroglobulin and total body scan to identify these metastases. Thirdly, our patient’s tumour cell nuclear DNA was diploid. Investigations have shown that the DNA ploidy pattern as determined by flow cytometry is an important and independent prognostic variable.15-17 Fortunately, aggressive follicular variant papillary cancer of thyroid (non-tall cell type) is very uncommon.
Generally, total body scan negative with low stimulated thyroglobulin is an excellent prognostic sign. Our patient demonstrates that we need to remain vigilant for the unusual tumour especially when the initial presentation showed so much bulky disease. The need for additional tumour markers will help to identify aggressive well differentiated thyroid carcinoma cases.
Acknowledgement
Appreciation is extended to Ms. Deborah Goss and Mr. Timothy O’Mara, librarians, in helping with literature search and preparing the manuscript. No other financial sources or funding involved in the formation of manuscript. No potential financial conflicts of interest.
|
Acknowledgements Appreciation is extended to Ms. Deborah Goss and Mr. Timothy O’mara, Librarians, in helping with literature search. No other financial sources or funding involved in the formation of manuscript. No potential financial conflicts of interest. Competing Interests None declared Author Details ISAAC SACHMECHI, MD, FACE, FACP, Queens Hospital Center, Department of Medicine, 82-68 164th street, Jamaica, New York 11432, USA. RACHELLE N. BITTON, MD, FACE, Pro Health, New Hyde Park, New York 11040, USA SUSAN SANELLI-RUSSO, MD, Queens Hospital Center, Department of Medicine, 82-68 164th street, Jamaica, New York 11432, USA. SUPAT THONGPOOSWAN, MD, Queens Hospital Center, Department of Medicine, 82-68 164th street, Jamaica, New York 11432, USA. CORRESPONDENCE: SUPAT THONGPOOSWAN, MD, Queens Hospital Center, Department of Medicine, 82-68 164th street, Jamaica, New York 11432. Email: th.supat@gmail.com |
References
- Mandronio EB, Lantion-Ang FL. The tale of two tumours: an undiagnosed case of papillary thyroid carcinoma. BMJ Case Reports. 20 Dec 2011.
- Nishijima H, Kitahara N, Murata M, Egami N. A case of papillary thyroid carcinoma metastatic to the sphenoid sinus presenting with epistaxis. Nihon Jibiinkoka Gakkai Kaiho. 2010; 113(2):62-66.
- Argibay Vázquez S, Lancha Hernández C, Martínez Muñiz A. Metastasis in the sphenoidal sinus in a patient with papillary thyroid cancer. Clin Transl Oncol. 2005; 7(7):324-327.
- Freeman JL, Gershon A, Liavaag PG, Walfish PG. Papillary thyroid carcinoma metastasizing to the sphenoid-ethmoid sinuses and skull base. Thyroid. 1996; 6: 59-61.
- Bernstein JM, Montgomery WW, Baloh K Jr. Metastatic tumours to the maxilla, nose and paranasal sinuses. The Laryngoscope. 1966; 76:621-650.
- Von Eiselsberg, A. Uber Knochen-metastasen des schilddrusenkrebses. Verhandlungen der Deutschen Gesellschaft für Chirurgie. 1893; 22:225-268.
- Harmer, L. Schilddrusenmetastase in der Nasenhohle. Weiner Klinische Wochenschrift. 1899; 23: 628-631.
- Barrs DM, McDonald TJ, Whisnant JP. Metastatic tumours to the sphenoid sinus. The Laryngoscope. 1979; 89:1239-1242.
- Chang G, Weber A, Pappanikov A. X-ray study of the month-Metastatic carcinoma of the thyroid to the sphenoid sinus. Ann Otol Rhinol Laryngol. 1983; 92:309-310.
- Renner GJ, Davis WE, Templer JW. Metastasis of thyroid carcinoma to the paranasal sinuses. Otolaryngology-Head and Neck Surgery. 1984; 92:233-237.
- Yamasoba T, Kikuchi S, Sugasawa M, Higo R, Sasaki T. Occult follicular carcinoma metastasizing to the sinonasal tract.ORL J Otorhinolaryngol Relat Spec. 1994 Jul-Aug; 56(4):239-43.
- Cumberworth VL, Ohri A, Morrissey G, Stirling R. Late sino-nasal metastasis from follicular thyroid carcinoma. J Laryngol Otol. 1994; 108:110-111.
- Altman KW, Mirza N, Philippe L. Metastatic follicular thyroid carcinoma to the paranasal sinuses: a case report and review. J Laryngol Otol 1997;111: 647-651.
- Wyllie JW III, Kern EB and Djalilian M. Isolated sphenoid sinus lesions. The Laryngoscope. 1973; 83:1252-1265.
- Hay ID. Papillary thyroid carcinoma. Endocrinol Metab Clin North Am. 1990; 19:545-576.
- Backdahl M, Carstensen J, Auer G, Tallroth E. Statistical evaluation of the prognostic value of nuclear DNA content in papillary, follicular, and medullary thyroid tumours. World J Surg 1986; 10:974-980.
- Ozata M, Suzuki S, Miyamoto T, Liu RT, Fierro-Renoy F, DeGroot LJ. Serum thyroglobulin in the follow-up of patients with treated differentiated thyroid cancer. J Clin Endocrinol Metab. 1944; 79:98-105.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.