



ISSN 1757-8515
“The Culture palette”- a randomized intervention study for women with burnout symptoms in Sweden.
Christina Grape Viding, Walter Osika, Töres Theorell, Jan Kowalski, Johan Hallqvist and Eva Bojner Horwitz
Cite this article as: BJMP 2015;8(2):a813
|
|
Abstract Burnout is common among women in Sweden. Cultural activities, i.e. arts, have benefitted different patient populations and may have potential for treating this group as well. |
Introduction
Population studies in Norway are showing that taking part of (creative) or receiving (receptive) cultural activities, i.e. arts, is associated with good health and good satisfaction with life among other things,1. Cultural activities have the potential to affect individuals beneficially: physiologically, biologically and emotionally, and several studies show that cultural activities can stimulate emotions and behaviors that make life easier, 2–5. Cultural activities can enrich and enhance our memory, stimulate connections among brain networks and enable us to accelerate learning and differentiate feelings of meaning and context,6,7 Cultural activities have also improved both physical health, social function and vitality among health care staff,8.
In an analysis of data from a large longitudinal cohort-study of a working population (called the SLOSH study = Swedish longitudinal occupational survey of health), some interesting associations were revealed between access to cultural activities in the workplace and health. Participants reporting many cultural activities at work had a more favorable improvement of emotional exhaustion during a follow-up period of two years than those whose workplaces did not offer these amenities,9. Other studies in which cultural activities have been offered to patients on long-term sick leave confirm that cultural activities have beneficial effects on both self-confidence and pain,10,11.
In a new approach, an artistic leadership program, called “Shibboleth”, affects not only managers included in the study, but also their employees (who did not participate in the artistic program). This one year art-based program showed statistically significantly more improvement of mental health, covert coping and performance-based self-esteem than the comparison group (who participated in an ordinary leadership program). They also experienced less winter/fall deterioration in the serum concentration of DHEA-S (dehydroepiandrostereone-sulfate), a regenerative/anabolic hormone,12.
Studies on singers, both amateur and professional singers and choir singers, show positive effects on different biological markers such as oxytocin and testosterone,13–15. On the basis of results from another Swedish project, ”Prescribed Culture”, which aimed to evaluate the effects of prescribed cultural experiences in the treatment of patients on long term sick leave, it was claimed that cultural experiences have their best effects when used in health promotion and prevention , rather than when the individual is already sick,16. Multimodal stimulation seems to have particularly strong effects. For instance, concomitant visual and auditory stimulation gives rise to stronger activation of “visual” and “auditory” parts of the brain than separate visual and auditory stimulation,17.
A mixture of different cultural activities seems to optimize influence on the limbic system since a broader emotional perception is activated,7. Cultural activities offered to participants that would not have chosen them spontaneously, could enhance already existing pathways in the brain enabling deeper cognitive behavioral change,17–20.
Despite this knowledge regarding the potential benefit of cultural activities in different contexts on both individuals and groups there is still a missing accessible practical functioning link between producers of culture and different groups of practitioners within health-care.
Burnout is characterized by emotional exhaustion, detachment from work and decreased effectiveness at work. This can develop in situations with excessive workload and insufficient resources as well as lack of control and support,21. If the process of burnout is a reaction to long-term stress, without enough recovery, this can lead to the more severe exhaustion syndrome,22. Symptoms include fatigue, impaired emotional regulation, cognitive problems and sleeping disorders. Most of these patients have an increased sensitivity for stress even after recovery,22. In recent years, Swedish rates of sick leave due to minor psychiatric morbidity , and burnout symptoms, have increased dramatically,23-24 . Complaints usually include physical, emotional and cognitive exhaustion, which in most cases appear to be related to chronic stress without restitution,25–28. Today many women in Sweden have stress related symptoms, and some are diagnosed with exhaustion syndrome. If these women are detected at an early stage, the prognosis is good,22.
Alexithymia, (the difficulty to differentiate your own and others feelings), can be a silent but severe problem for persons suffering from this personality trait. Grabe et al.,29 conducted a study in which the questionnaire TAS-20 was used for the assessment of alexithymia. Medical examination was also performed. In this study alexithymia was related to hypertension and arteriosclerotic plaques. Alexithymic personality traits may increase the risk for CVD (cardio vascular disease).
The rationale behind choosing symptoms of exhaustion, SOC and alexithymia as main outcome variables was the intention to examine whether cultural activities in this form can change pattern of thought, feelings and behavior in participants with burnout symptoms. If cultural activities prove effective for this participant group, they could have considerable benefits both financially in terms of reducing sick leave and health care consumption and of reduced individual suffering.
Aim
The aim of the study was to assess to what extent symptoms of exhaustion, sense of coherence, alexithymia and self-rated health among women with burnout symptoms can be beneficially influenced by cultural activities organized in health care centers.
Method
Participants
Four health care centers in Stockholm County hosted the cultural activities. Medical doctors and social workers distributed information about the study to women diagnosed with exhaustion disorder or exhaustion symptoms. Women, native and foreign born, with burnout/exhaustion symptoms (fatigue syndrome or stress-related fatigue) who were curious about new clinical approaches were asked by the doctor to participate in the study and screened for inclusion and exclusion criteria. Participants (women age > 18) with burnout/exhaustion symptoms such as strong fatigue, cognitive problems, and sleep disturbances were enrolled. There was an inclusion criterion with a score above 2 on the KEDS scale. The diagnosis was made by the doctor.
Exclusion criteria: Participants with difficulty in speaking and understanding Swedish, participants with alcohol or drug abuse problems, or/and participants with severe depression or psychiatric borderline. Also excluded were participants with severe somatic diseases (such as serious angina pectoris or participants who had had a stroke). Randomization was done using a 3:1 allocation to intervention or control groups.
The randomization was done using a stratified randomization by center. Randomization was done by the statistician. The group allocations were sent in individual envelopes which were distributed to centers and blinded to the site staff. Envelopes were further drawn in a consecutive order with regard to recruitment of subjects at each of the four health care centers. Thirty-six participants were allocated to the intervention group (nine patients in each group) and twelve participants to the control group. The standard care that each participant received included physiotherapy such as relaxation and physical light training.
All randomized participants gave their written consent to participation in the study. Data were collected over a period of 6 months. The project includes evaluation of six different culture activities. In the selection of the health care centers socio- economic diversity and employment status were considered. We used regularly occurring structured cultural activities in cooperation with culture producers, i.e. actors, musicians, dance teachers. The Regional Research Ethics Committee of Uppsala has approved the study (Dnr. 2012/359).
The culture palette: six different cultural packages
The following cultural activities were included in the study; five of them have previously been presented in the literature with good evidence on other groups of patients. One package (the musical show), which has not been presented previously on groups of patients, was chosen as it represents a combination of different modalities of activities at the same time. The active mechanism of all six cultural activities was to stimulate different modalities of the senses such as the visual, motor, verbal, auditory, emotional and sensational, according to Downing’s levels of perception, 30. All participants were offered six cultural packages:
1. Interactive theater: An experienced actor introduced poetical lyrics and poems and then initiated and participated in discussions with the participants regarding thoughts, emotions, and experiences evoked by the texts.
2. Movie: After showing a movie, a film expert initiated discussions among the participants about experiences and thoughts evoked by the movie.
3. Vocal improvisation and drawing: After participating in a vocal improvisation session with an experienced performance artist and pianist, the participants painted a picture representing emotions, thoughts and pictures evoked during the improvisation
4. Exploring Dance: The participants improvised dance movements under the guidance of a dance movement pedagogue/music teacher. The dance movements were staged according to the situation in the room and with focus on bodily awareness. Afterwards the group discussed their experiences during the dance session.
5. Mindfulness and contemplation: The participants contemplated and practiced mindfulness together with an experienced mindfulness instructor. Attention was on breathing and body awareness. Thoughts, feelings, images and sensations were in focus and experiences were reflected in the group after the contemplation.
6. Musical show: after a musical show including music, song and dance focusing on bodily awareness, the participants discussed thoughts regarding the body with the actor.
Every session in each one of the six different cultural packages lasted for 90 minutes.
Evaluations
Three different standardized scales, and also self-rated health and self-figure drawing, were used.
KEDS - Karolinska Exhaustion Disorder Scale,31. Questions about concentration, memory, physical fatigue, endurance, recovery, sleep, hypersensitivity to sensory input, experience requirements and irritation and anger. Higher scores indicate worse disease activity/performance.
SOC - Sense of coherence,32. A key factor in being able to feel well-being and health. This factor has been shown to be crucial to helping individuals mobilize their self-healing systems. Higher scores indicate better performance.
TAS - Toronto Alexithymia Scale,33. Estimation of ability to recognize and interpret feelings in oneself and others. TAS contains three subscales; the inability to handle emotions due to emotions being poorly recognized (difficulty recognizing), the inability to describe feelings (difficulty describing), and mismatch between coping behavioral emotions (externally oriented thinking). This study used the full scale score, i.e. the summary of the three sub scores. Higher scores indicate worse performance.
Self-rated health (SRH) consists of a single item measure.
Procedures/implementation
The four different health care centers presented each activity on two consecutive occasions. After two weeks of one program, there was a new program on two consecutive occasions etc. Each participant has thus been offered 12 cultural packages during a three-month period, i.e. once a week. During the monitoring period between month 3 and month 6, there was no culture activity offered. The control group was monitored in parallel during the entire period monthly at 0, 3 and 6 months.
The participants evaluated the project individually with questionnaires prior to the sessions, after completion of the intervention at month 3, and at follow-up after 3 months i.e. month 6 (both intervention and control group). In-depth interviews with both participants and producers of culture, i.e. representatives for the various cultural activities and health care staff were conducted during the monitoring period (this data is not presented in this article).
Data analysis
The primary outcome efficacy end point/measure was mean change from baseline to three and six months in the KEDS summary score. The secondary outcome measures were mean change from baseline in the SOC summary score, the TAS summary score and the self-rated health, from baseline to three to six months.
All data were presented using descriptive statistics, i.e. mean and standard deviation for continuous variables and frequency and percentage for categorical variables. For all main outcome variables, data were further analyzed using the Linear Mixed Models, including group (intervention and control) and time (baseline, 3 month and 6 months) as fixed factors. Results were presented as marginal means, the estimated mean value adjusted for the factors included in the analyses model. The difference between intervention and control group with regard to the estimated and adjusted means are defined as the effect size, i.e. the mean difference between the intervention groups for each of the primary and secondary outcomes measures divided by the standard deviation. All tests were two-tailed and p<0.05 was regarded as statistically significant.
IBM SPSS version 22 was used for statistical calculations. In the presentation of the results from the statistical analyses, the measured effect size was used and derived as the absolute difference between active intervention and controls with regard to each of the outcome variables/endpoints used,34.
Results
There were 55 participants screened in this study, however seven participants who met the exclusion criteria of too serious/severe depression was not included into the study. In total, there were 48 participants randomized into the study, age between 41 and 70 years, mean 53.8 (SD= 8.15).
The results showed that for KEDS (exhaustion) there was a statistically significant two-way interaction (P<0.001) with a decreased mean from baseline to three and six month respectively in the intervention group whereas in the control group there was no change. The mean treatment effect size, i.e. the mean difference between groups, in favor of the intervention group was 9.9 (SE=3.0) at 6 months. See table 1 and figure 1a.
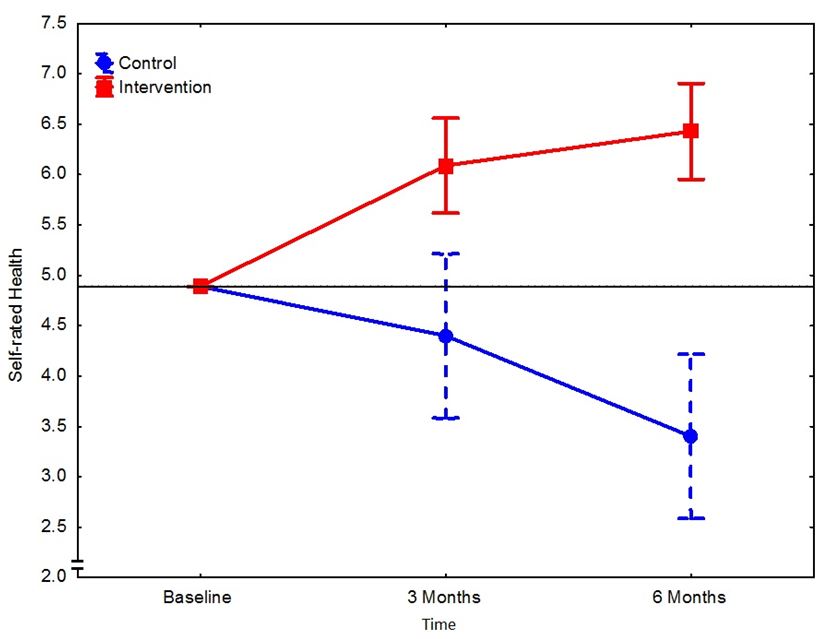
There was no difference in mean SOC - Sense of Coherence – scores between the groups. See figure 1b. Further, the results revealed a statistically significantly more pronounced decrease in the intervention group compared to the control group in the alexithymia items of total score, (P=0.007, mean treatment effect size=5.4 (SE=2.2) at 6 months in favor of the intervention group), difficulty describing (P=0.004, 2.4 (0.9)), difficulty identifying (P=0.051, 2.6 (1.3)) but not for external orientation (P=0.334 0.5 (0.8)). See table 1 and figure 1c. There was also a statistically significant difference between the groups with regard to self-rated health (P<0.001) where mean scores increased over time in the intervention group but decreased in the control group. See figure 1d.
Table 1
KEDS (Karolinska Exhaustion Disorder Scale) and TAS (Toronto Alexithymia Scale) and SRH (self-rated health) at baseline, month 3 and month 6.
| Control Group (n=12) | Intervention Group (n=36) | |||||
| Count | Mean | Standard Deviation | Count | Mean | Standard Deviation | |
| KEDS | ||||||
| Baseline | 12 | 32.7 | 8.2 | 35 | 31.7 | 8.4 |
| Month 3 | 12 | 34.9 | 9.2 | 34 | 23.6 | 8.6 |
| Month 6 | 12 | 33.9 | 8.7 | 33 | 23.7 | 10.1 |
| Sense of Coherence | ||||||
| Baseline | 12 | 117.2 | 29.9 | 33 | 118.0 | 28.0 |
| Month 3 | 12 | 112.8 | 30.3 | 33 | 121.1 | 30.5 |
| Month 6 | 12 | 115.1 | 24.2 | 34 | 123.9 | 28.2 |
| Difficulty Describing | ||||||
| Baseline | 12 | 14.8 | 4.3 | 34 | 14.2 | 4.6 |
| Month 3 | 12 | 15.3 | 3.6 | 31 | 12.7 | 4.6 |
| Month 6 | 12 | 15.2 | 4.1 | 34 | 11.8 | 3.9 |
| Difficulty Identifying | ||||||
| Baseline | 12 | 20.0 | 6.0 | 34 | 20.3 | 6.3 |
| Month 3 | 12 | 20.6 | 6.5 | 31 | 19.0 | 6.9 |
| Month 6 | 12 | 20.0 | 6.1 | 34 | 17.4 | 5.0 |
| Externally Oriented | ||||||
| Baseline | 12 | 14.9 | 4.2 | 34 | 13.8 | 4.4 |
| Month 3 | 12 | 15.4 | 4.3 | 31 | 13.9 | 3.9 |
| Month 6 | 12 | 14.6 | 4.8 | 34 | 13.2 | 3.5 |
| TAS | ||||||
| Baseline | 12 | 49.7 | 13.1 | 34 | 48.3 | 13.4 |
| Month 3 | 12 | 51.3 | 13.3 | 31 | 45.6 | 13.9 |
| Month 6 | 12 | 49.8 | 13.9 | 34 | 42.4 | 10.8 |
| Self-rated Health | ||||||
| Baseline | 12 | 5.2 | 1.5 | 36 | 4.8 | 1.9 |
| Month 3 | 12 | 4.6 | 1.9 | 36 | 6.0 | 1.9 |
| Month 6 | 12 | 3.6 | 1.6 | 35 | 6.4 | 1.9 |
Figure 1a
Marginal means and 95 % confidence intervals for the KEDS (exhaustion) scale by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
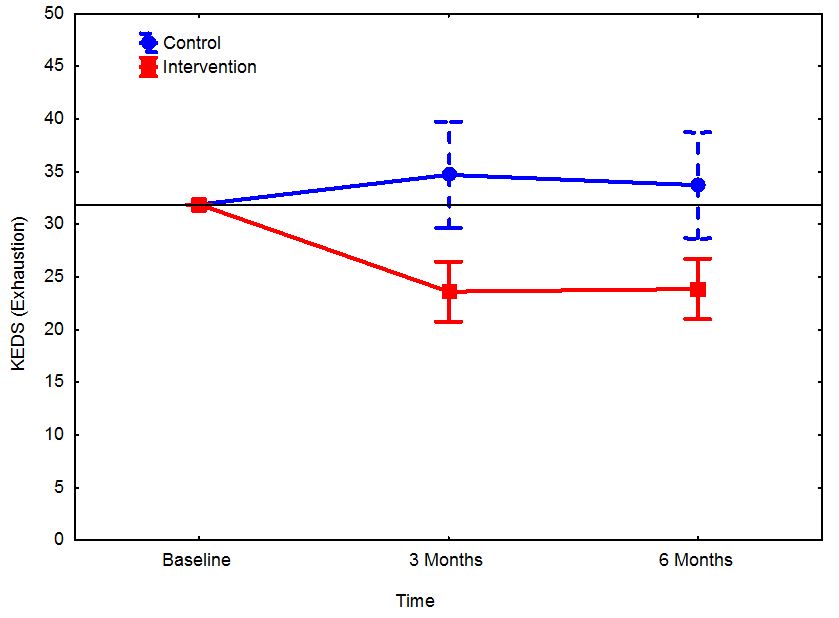
Figure 1b
Marginal means and 95 % confidence intervals for the sense of coherence (SOC) scale by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
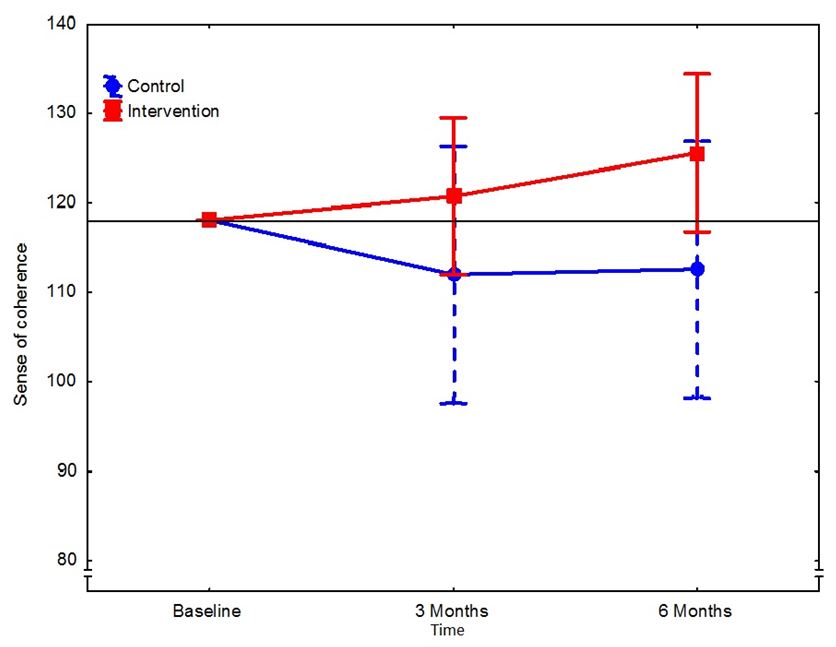
Figure 1c
Marginal means and 95 % confidence intervals for the Toronto Alexithymia Scale (TAS) by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
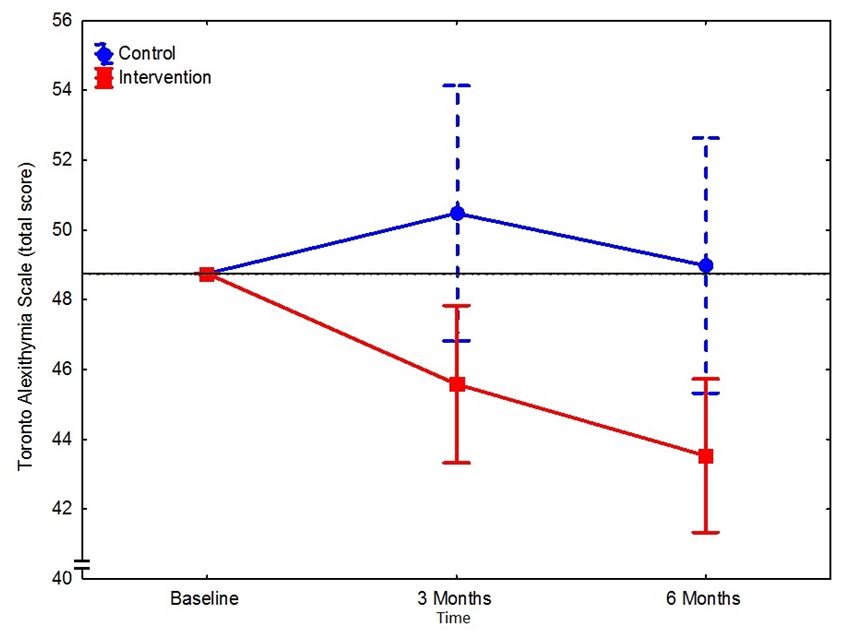
Figure 1d
Marginal means and 95 % confidence intervals for the self-rated health scale (SRH) by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Discussion
The results show that the different exhaustion factors measured by means of KEDS (Karolinska Exhaustion Disorder Scale) decreased in the intervention group compared to the control group. With regard to the total score of TAS (Toronto Alexithymic Scale) there was a statistically significant decrease in the intervention group compared to the controls, i.e. the participants started to improve their differentiation of feelings and emotions after three months with cultural activities. The same pattern was seen with regard to self-rated health, which improved in the intervention group. However, there was no significant difference between the groups with regard to the development of sense of coherence.
It seems that the different cultural activities have helped the participants become more aware of their feelings and sensations; to describe and to identify feelings. It is not easy to explain the positive results based on one clear paradigm. It is likely a mixture of psychological, neurological and social factors or changes that interact in a complex manner.
Previous studies have discussed the theory of the emotional brain - cultural modalities can “surprise” the cognitive brain unconsciously. LeDoux,20 discusses the upper/slower and the lower/faster pathway in the brain. Emotionally loaded visual and auditory stimuli are transmitted on both types of pathways. Music impulses are for example evoking activities in the emotional brain much more rapidly than in the cognitive brain. However, impulses spread secondarily from the emotional to the cognitive brain. This can trigger the participants awareness of different emotions and may start a process of differentiation, possibly initiating a change of life course. By using different cultural activities, that the participants normally would not try, the differentiation process may be amplified. This suggests that cultural activities can surpass automated thinking and create new "pathways '' with changes in behavior and increased well-being.
In other studies we have observed that a mixture of different cultural activities can increase the amount of stimuli affecting a broader network of emotional correlates, 14,16,18 . A very interesting long-term decrease in alexithymia, 35 was associated with lowered blood pressure and a decrease in sick leave. By allowing the participants to try new cultural stimuli we may have helped the participants change old habits. A hypothesis is that this may also have contributed to the observed decrease in exhaustion.
Why did we not see any increase in the sense of coherence in the intervention group? It is very difficult to change patterns of thought and behavior although we can argue that the participants in the control group also found a new sense of coherence just by being invited to answer questions about themselves and being focused upon. Many of the participants did not go out spontaneously because of their fear of socializing. Some of them described their situation as black or white, not wanting to change routines that made them feel less safe,36.
Despite the fact that the health care staff did not participate in the culture palette, they were also affected by the cultural activities 36. This may be a mirroring effect, or emotional contagiousness on health care staff, which may also play a role between the participants and their staff. The passive cultural activation phenomenon has previously been presented in the literature,37 and there seem to be possible well-being effects of just watching dance or visiting a theatre, 6,10 which may explain the positive health care staff response to the culture palette. The results of this study underscore the importance of regarding the health care system as a whole, where patients, health care staff and visiting relatives affect each other. Empathic behaviors contaminate in all directions and we need to be aware of how we project ourselves when working in a caring context.
Modified “culture palettes” and “train the trainer” programs and workshops are now in use in Sweden, inspiring cultural producers to further develop the health care system and a cultural health box - a box with six different books about cultural activities and the research behind this - have been distributed to all health care centers in Sweden, 38.
Developing and adapting cultural programs to fit other kind of groups of participants could cross-fertilize health care thru culture production.
Limitations
This study was limited to women with exhaustion symptoms and therefore further research on implementation of cultural activities within different groups of participants and sexes is needed before we can generalize the results to other groups of participants. Another limitation is that we did not control for outside activities, such as doing walks in nature. In this study we only presented indoor cultural activities.
Conclusion
The cultural activities in this study made exhausted women understand what makes them vital, confirmed, curious, healthy and creative. The study also illustrated that there could be synergistic effects when bringing cultural activities into the health care system36.
|
Acknowledgements The authors thank all participants, health care staff and cultural producers who made this study possible. The authors also thank the Postal Code lottery, Sweden, for sponsoring this project. Competing Interests None declared Author Details CHRISTINA GRAPE VIDING, RN, PHD stud., Dept. of Public Health and Caring Sciences, Uppsala University, Uppsala, Sweden. WALTER OSIKA, MD, PHD, Center for Social Sustainability, Dept. of Neurobiology, Care Sciences and Society, Karolinska Institutet and Dept. of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden. TÖRES THEORELL, MD, PHD,PROF., Stress Research Institute, Stockholm University, Stockholm, Sweden. JAN KOWALSKI, Biostatistician, Dept. of Science, Intervention and Technology, Pediatric Unit, Karolinska Institutet, Stockholm, Sweden. JOHAN HALLQVIST, MD, PHD, PROF. Dept. of Public Health and Caring Sciences, Uppsala University, Uppsala, Sweden. EVA BOJNER HORWITZ, PHD, PHT, Dept. of Public Health and Caring Sciences, Uppsala University, Uppsala and Center for Social Sustainability, Dept. of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden. CORRESPONDENCE: CHRISTINA GRAPE VIDING, BMC, Husargatan 3, Box 564, SE-751 22 Uppsala, Sweden. Email: tina.grape.viding@pubcare.uu.se |
References
- Cuypers, K., Krokstad, S., Holmen, TL. et al. Patterns of receptive and creative cultural activities and their association with perceived health, anxiety, depression and satisfaction with life among adults: the HUNT study, Norway. Journal of Epidemiology & Community Health. 66(8):698–703 (2012).
- Theorell, T., Konarski, k., Engström, R. et al. Behandling av långvariga psykosomatiska sjukdomstillstånd med konstpsykoterapi[Treatment of longterm psychosomatic states with creative art psychotherapy]. Vård [Care] 94–97 (1993).
- Theorell, T. Psychological health effects of musical experiences -theories, studies and reflections in music health science. (Springer, 2014).
- Clift, S. M. & Hancox, G. The perceived benefits of singing: findings from preliminary surveys of a university college choral society. J. R. Soc. Promot. Health 121(4):248–256 (2001).
- Cohen, G. D., Perlstein, S., Chapline, J. et al. The impact of professionally conducted cultural programs on the physical health, mental health, and social functioning of older adults. Gerontologist 46(6):726–734 (2006).
- Bojner Horwitz, E. Kultur för hälsans skull[Culture for the sake of health]. (Gothia, 2011).
- Immordino-Yang, M. H., McColl, A., Damasio, H. et al. Neural correlates of admiration and compassion. Proc. Natl. Acad. Sci. U. S. A. 106(19):8021–8026 (2009).
- Bygren, L. O., Weissglas, G., Wikstrom, BM. et al. Cultural participation and health: a randomized controlled trial among medical care staff. Psychosom. Med. 71(4):469–473 (2009).
- Theorell, T., Osika, W., Leineweber, C. et al. Is cultural activity at work related to mental health in employees? Int. Arch. Occup. Environ. Health. 86(3): 281–288 (2013).
- Bojner Horwitz, E., Kowalski, J. & Anderberg, U. M. Theater for, by and with fibromyalgia patients – Evaluation of emotional expression using video interpretation. Arts Psychother. 37(1):13–19 (2010).
- Ikonomidou, E., Rehnstrom, A. & Naesh, O. Effect of music on vital signs and postoperative pain. AORN J 80(2):269–274,277–278 (2004).
- Romanowska, J. Larsson, G., Eriksson, M. et al. Health effects on leaders and co-workers of an art-based leadership development program. Psychother. Psychosom. 80(2):78–87 (2011).
- Grape, C., Sandgren, M., Hansson, L.-O. et al. Does singing promote well-being?: An empirical study of professional and amateur singers during a singing lesson. Integr. Physiol. Behav. Sci. 38(1):65–74 (2003).
- Grape, C., Theorell, T., Wikström, B. M. et al. Choir singing and fibrinogen. VEGF, cholecystokinin and motilin in IBS patients. Medical Hypotheses. 72(2):223–225 (2009).
- Grape, C., Wikström, B.-M. M., Ekman, R., et al. Comparison between choir singing and group discussion in irritable bowel syndrome patients over one year: saliva testosterone increases in new choir singers. Psychother. Psychosom. 79, 196–198 (2010).
- Augustinsson, S. Kultur på recept/Prescribed Culture. (2011). at <http://www.skane.se/kulturparecept>
- Baumgartner, T., Lutz, K., Schmidt, C. F. et al. The emotional power of music: How music enhances the feeling of affective pictures. Brain Res. 1075(1):151–164 (2006).
- Pennebaker, J. W. Writing About Emotional Experiences as a Therapeutic Process. Psychological Science. 8(3):162–166 (1997).
- Lumley, M. A. Alexithymia, emotional disclosure, and health: A program of research. Journal of Personality. 72(6):1271–1300 (2004).
- LeDoux, J. E. The Emotional Brain: The Mysterious Underpinnings of Emotional Life. (Weidenfeld & Nicolson, 1998).
- SBU. Swedish Counsil on Health Technology Assessment. Role of the work environment in the development of symtoms of depression and burnout. (2014). doi:SBU-report nr 223. ISBN 978-91-85413-64-5.
- Åsberg, M., Grape, T.,Krakau, I., et al. Stress som orsak till psykisk ohälsa/Stress as the cause of mental illness. Lakartidningen. 107(19-20):1307–1310 (2010).
- Swedish Social Insurance Agency. Follow-up of the development of sickness insurance. (2013). doi:Dnr. 3023-2013
- Norlund, S., Reuterwall,C., Höög, J., et al. Burnout,working conditions and gender - results from the northern Sweden MONICA Study. BMC Public Health. 10:326 (2010).
- Åsberg, M., Sköld, C., Wahlberg, K., et al. Mindfulness-meditation/ An old fashion method for stress relief. Lakartidningen. 103(42):3174–3177 (2006).
- NBHW. National Board of Health and Welfare. Exhaustion syndrome. Stress related psychological ill health. (2003).
- NBHW. National Board of Health and Welfare. Changes and additions to classifikation of diseases and health problems, ksh97-systematic list. (NBHW, 2005).
- Golkar, A., Johansson, E., Kasahara, M., et al. The influence of work-related chronic stress on the regulation of emotion and on functional connectivity in the brain. PLoS One. 9(9):e104550 (2014).
- Grabe, H. J., Schwahn, C., Barnow, S., et al. Alexithymia, hypertension, and subclinical atherosclerosis in the general population. J. Psychosom. Res. 68(2):139–147 (2010).
- Downing, G. Kroppen och Ordet [The Body and the Word]. (Natur & Kultur, 1997).
- Besèr, A., Sorjonen, K., Wahlberg, K. et al. Construction and evaluation of a self rating scale for stress-induced Exhaustion Disorder, the Karolinska Exhaustion Disorder Scale. Scand. J. Psychol. 55(1):72–82 (2014).
- Langius, A. & Lind, M. G. Well-being and coping in oral and pharyngeal cancer patients. Eur. J. Cancer. B. Oral Oncol. 31B(4):242–249 (1995).
- Bagby, R. M., Ayearst, L. E., Morariu, R. et al. The Internet administration version of the 20-item Toronto Alexithymia Scale. Psychol. Assess. 26(1):16–22 (2014).
- Moher, D., Schulz, K. F. & Altman, D. G. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. Lancet. 357 (9263):1191-4 (2001).
- Jorgensen, R. S. & Houston, B. K. Cardiovascular reactivity, hostility, and family history of hypertension. Psychother Psychosom. 50(4):216–222 (1988).
- Grape Viding,C., Osika,W., Theorell,T. et al. “Culture palette” in Swedish Health Care centres - a qualitative interview with health care staff, culture producers and patients. Work in progress (2015).
- Rizzolatti, G., Fadiga, L., Gallese, V. et al. Premotor cortex and the recognition of motor actions. Cogn. Brain Res. 3(2):131–141 (1996).
- Red. Eva Bojner Horwitz. The Culture health box of books. Six books referring different cultural activities within health care. (Gothia, 2014).

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.