



ISSN 1757-8515
Frequency of Hepatitis B surface antigen (HBsAg) and Hepatitis C antibody (HCVAb) seropositivity among preoperative eye surgery patients
Mahesh Kumar Lohano, Li Su, Ashok Kumar Narsani, Muhammad Jawed & Hameem Naveed
Cite this article as: BJMP 2016;9(2):a918
|
|
Abstract The aim of this study was to analyse the prevalence of Hepatitis B & C Virus among the preoperative eye surgery patients at the Liaquat University Eye Hospital, Hyderabad, from June 2014 to February 2016. 2200 patients of various ages undergoing eye surgeries and being unaware of hepatitis B & C infection were included. The blood was collected by qualified technicians of our hospital laboratory under supervision of a consultant pathologist. Each patient was serologically screened by immuno-chromatography (ICT method) for qualitative detection of antigen for Hepatitis B and antibodies for Hepatitis C before surgery. 1255 (57.04%) patients were male and 945 (42.95%) were female. Large numbers of patients were in their 4th and 5th decade of life in both the sexes. Of these 2200 patients, 338 (15.36%) were serologically positive for Hepatitis B virus & Hepatitis C virus. The majority of them were female. The prevalence of Hepatitis B and Hepatitis C virus positive is higher in our population. Therefore, it is mandatory to screen every patient for Hepatitis B and C before any surgical procedure. The surgeon and health care professional should protect themselves by using protective masks, eye protection glasses, and double gloves before handling infected cases. Hence the used infected material, needles and other waste material should be destroyed properly using Biosafety protocols. Keywords: Hepatitis B virus, Hepatitis C virus, Cirrhosis |
INTRODUCTION
Hepatitis viruses are the most widespread cause of hepatitis and some cancer lymphomas in humans1.Hepatitis is a serious disease of the liver and described as a lifelong infection with swelling and inflammation (presence of inflammatory cells) in the liver, that if progresses, may lead to cirrhosis (scarring) of the liver, liver cancer, liver failure, and death. Hepatitis B (HBV) and Hepatitis C (HCV) are one of the viral types of hepatitis that leads to jaundice (a yellow discolouration of skin, mucous membrane and conjunctiva of the eye), anorexia (poor appetite), fatigue and diarrhoea and presumably it remains undiagnosed and leads to chronic carrier state but most infected individuals remain asymptomatic1-3. The hepatitis B virus is a DNA virus belonging to the Hepadnaviridae family of viruses and hepatitis C virus is a small, single stranded, RNA virus with a diameter of about 50 nm, belonging to Flaviviridae family of virus. Hepatitis B surface antigen (HBsAg) is present in the serum of those infected with hepatitis B, consisting of the surface coat lipoprotein of the hepatitis B virus. Anti-HCV antibody, a substance that the body makes to combat HCV 4. Hepatitis B virus is transmitted through blood and blood products, semen, vaginal fluids, and other body fluids. Hepatitis C virus is a blood borne or parenterally transmitted infection. Vehicles and routes of parenteral transmission include; contaminated blood and blood products, multi-transfusions (thalassemic and haemophilic patients), needle sharing, contaminated instruments (e.g. in haemodialysis, reuse of contaminated medical devices, tattooing devices, acupuncture needles, razors) and occupational and nosocomial exposure5-8. It stands to reason that an occupational risk for transmission of hepatitis virus in the health care setting, where unknown carriers of hepatitis infections are undergoing different procedures, in which there is a chance of contact of percutaneous blood, including transmission from infected patients to staff, from patient to patient, and from infected providers to patients9. There is a lack of routine serological screening prior to surgery, which is one of the factors responsible for increased disease transmission. The major risk factors include; re-use of contaminated syringes, surgical instruments and improperly screened blood products2. Without meticulous attention towards infection control and disinfection and sterilization procedures, the risk for transmission of blood borne pathogens in the health care setting is magnified.
The aim of our current study was to estimate the incidence of Hepatitis B and Hepatitis C among patients going through eye surgery at department of ophthalmology Liaquat University of Medical and Health Sciences Jamshoro at Hyderabad. This is one of the largest tertiary care centres in Sindh. This institution is a great referral centre for whole interior Sindh province.
MATERIAL AND METHODS
Study design and patients
This prospective observational study was carried out at Liaquat University Eye Hospital, Hyderabad, from June 2014 to February 2016. A total of 2200 patients undergoing eye surgery, who were unaware of hepatitis B & C infection were included in this study. No restriction was placed based on age and gender to ensure maximum participation.
Blood samples
The blood samples of all these patients were collected in the Hospital laboratory, Scientific Ophthalmic Diagnosis & Research Lab. Each patient was serologically screened, by using immuno-chromatography (ICT method) for qualitative detection of antigen for Hepatitis B and Hepatitis C virus antibodies, to find the carrier status of patients before surgery.
The blood was collected by a qualified technician / phlebotomist of our hospital laboratory under supervision of a consultant pathologist. Samples were allowed to coagulate at room temperature for 30 minutes, and then centrifuged at 3000 revolutions per minute (RPM) for 10 minutes. The serum samples were separated and kept frozen at -20°C for chemical and immunoassays. The HBV screening was based on the detection of antigen and detection of viral specific antibodies HCV in the sera using enzyme immunoassays. The test only shows whether a person has ever been infected by HBV or HCV, and not whether the virus is still present. According to the manufacturers’ literature, the relative sensitivity and specificity of HCV and HBV testing kits was 96.8% and 99% respectively.
Those patients with test results were found positive on screening test, were further confirmed by testing ELISA (Enzyme-Linked Immunosorbent Assay) method (4th generation ELISA) and were given advised for further testing on Polymerase Chain Reaction (PCR) for qualitative or quantitative detection of DNA/RNA (the viral gene).
All the data was entered in SPSS version 16 and the prevalence and percentage of all variables was measured.
RESULTS
A total number of 2200 patients were operated during the study, 1255 (57.04%) patients were male and 945 (42.95%) were female
Of these 2200 patients, 338 (15.36%) were serologically positive for hepatitis B virus & hepatitis C virus. Out of the 338 HBV or HCV positive patients, 56 patients (2.54%) were positive for hepatitis B surface antigen (HBsAg) and 282 patients (12.81%) were positive for hepatitis C antibody (HCVAb). (Figure 1&2). The majority of them were female, and 226 (66.86%) were in their 4th and 5th decade of life in both sexes (Figure 3).
Figure 1- A: Serologically positive for hepatitis C antibodies, B: Serologically negative for hepatitis C antibodies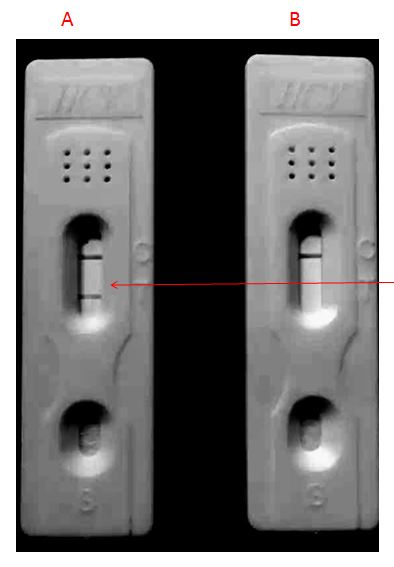
Figure 2 - A: Serologically negative for hepatitis B antigen, B: Serologically positive for hepatitis B antigen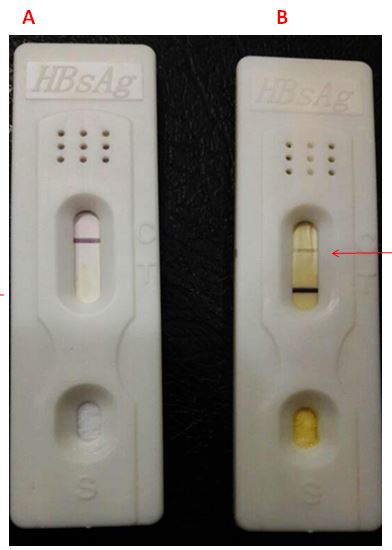
Figure 3: Incidence of Hepatitis B & C in different age group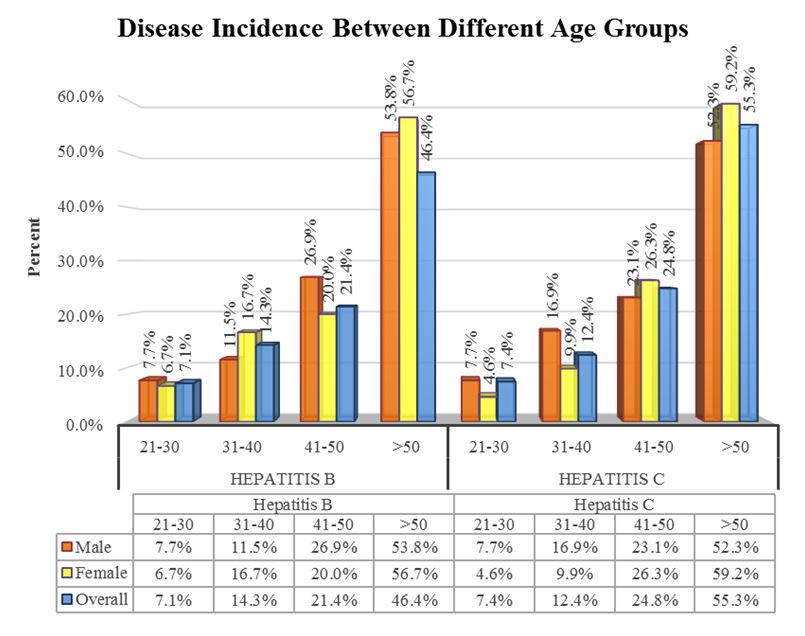
DISCUSSION
Hepatitis B virus (HBV) and hepatitis C virus (HCV) are among the principal causes of liver diseases, with different frequency rates and various types all over the world. The World Health Organization (WHO) estimates that there are near 4 million people with chronic HBV infection and 170 million people with chronic HCV infection worldwide. Mortality rate of Hepatitis B is estimated to result in 563,000 deaths and hepatitis C in 366,000 deaths annually 1, 6, 10-12. The occurrence of hepatitis varies from country to country. The epidemiological estimates by WHO show that there is low prevalence of hepatitis C (<1%) in Australia, Canada and Northern Europe, and almost 1% in countries of medium endemism, such as the USA and most of Europe. The frequency is at its peak (>2%) in many countries of Africa, Latin America, Central and South-East Asia 5. As far as the Pakistani population is concerned, the incidence of hepatitis B and C is escalating. Previous studies reveal that the Pakistani population affected by HBV 10% and HCV is 5-10% 3. At times it will also vary among different regions of the same country, and is continuing to rising in certain parts, especially in the rural areas, the percentage of infected individuals is significantly higher 2. The total incidence of Hepatitis B and Hepatitis C in our study was found to be 15.36%. This was almost comparison to Naeem et al found to be 12.99% 2 and in our previous study reported incidence of anti HCV was 29.60% 7. W Ul Huda et al reported 17.33% incidence of HCV infection among their operated patients5, whereas a study conducted by Khurrum et al reported 6% incidence of anti HCV antibodies in health care workers in a local hospital13. The prevalence of Hepatitis B and Hepatitis C in preoperative cataract patients was found to be higher in males (59.18%) than females (40.82%), and Ahmed et al also showed that the total prevalence of Hepatitis B and Hepatitis C in males was very high compared to females among preoperative cataract patients14, which is controversial to our result. A study conducted in 2010 on different eye camps in Pakistan showed that 108 out of 437 patients were infected with Hepatitis B and Hepatitis C with a higher prevalence of the diseases in females with 60.18% (65/ 108) than in males with 39.81% (43/108) 15. Concerning demographic variables, the increase in the risk for HCV seropositive incidences increased with the age i.e. 7.1% at the age of 20 to 30 years whereas 21.4% at the age of 40 to 50 years. In our study, the higher prevalence of hepatitis B & C were in the age range of 30 – 60 years, which is comparable to the study of Talpur et al, in which 65% positive patients were above the age of 40 years16.
This study shows that the prevalence of these hepatitis causing viral pathogens are quite high. Doctors and paramedical staff in surgical and medical practice are at high risk of acquiring blood borne diseases from the patients on whom they operate.
CONCLUSION
The aim of the present study was to assess the prevalence of HBV and HCV infection among preoperative patients. The incidence of these hepatitis causing viruses are higher in our population. Therefore, it is a mandatory task to screen every patient for hepatitis B and C before any surgical procedure. The surgeons and health care professionals should protect themselves by using protective masks, eye protection glasses, and double gloves before handling infected cases. The used infected material, needles and other waste material should be destroyed properly using Biosafety protocols.
|
Acknowledgements We would like to extend special thanks to Adnan Nazir, College of Economics and Management, Huazhong Agriculture University, Wuhan, China, for their invaluable help and assistance in technical assistance and improving image quality. Competing Interests None declared Author Details MAHESH KUMAR LOHANO, PhD Scholar, College Of Life Science And Technology, Hust, Wuhan, China. PROF DR SU LI, Dean, College Of Life Science And Technology, Hust, Wuhan, China. PROF DR ASHOK KUMAR NARSANI, Chairman Dept Ophthalmology, Liaquat Medical University, Hyderabad, Sindh, Pakistan. MUHAMMAD JAWED, College of Life Science and Technology, Hust, Wuhan, China. HAMEEM NAVEED, College of Life Science and Technology, Hust, Wuhan, China. CORRESPONDENCE: MAHESH KUMAR LOHANO, PhD Scholar, College of Life Science and Technology Huazhong University of Science and Technology,Wuhan, China; and Consultant Pathologist, Liaquat Medical University, Hyderabad, Sindh, Pakistan. Email: mklohana@yahoo.com |
References
- Chaudhary M, Sharma M. Management of Psychological Effects through Counselling During HCV (Hepatitis) Treatment. The International Journal of Indian Psychology, Volume 3, Issue 2, No 3. 2016:106.
- Naeem SS, Siddiqui EU, Kazi AN, Khan S, Abdullah FE, Adhi I. Prevalence of Hepatitis ‘B’and Hepatitis ‘C’among preoperative cataract patients in Karachi. BMC research notes. 2012;5(1):492.
- Tahir MA, Cheema A, Tareen S. Frequency of Hepatitis-B and C in patients undergoing cataract surgery in a tertiary care Centre. Pakistan journal of medical sciences. 2015;31(4):895.
- Spradling PR, Tong X, Rupp LB, Moorman AC, Lu M, Teshale EH, et al. Trends in HCV RNA Testing Among HCV Antibody–Positive Persons in Care, 2003–2010. Clinical infectious diseases. 2014;59(7):976-81.
- ul Huda W, Jameel N, Fasih U, Rehman A, Shaikh A. Prevalence of Hepatitis B and C in Urban Patients Undergoing Cataract Surgery. Pakistan Journal of Ophthalmology. 2013;29(3):147.
- KHAN M, HUSSAIN U, AHMAD I, KHAN A. PREVALENCE OF HEPATITIS B AND C SEROPOSITIVITY IN PATIENTS PRESENTING FOR DENTAL TREATMENT. Pakistan Oral & Dental Journal. 2015;35(2).
- Jatoi SM, Narsani AK, Kumar M. Frequency of Anti Hepatitis C Virus in Eye Surgery Patients at Tertiary Referral Center LUMHS. Pak J Ophthalmol. 2009;25(2).
- Nadol P, O'Connor S, Duong H, Mixson-Hayden T, Tram TH, Xia G-L, et al. High hepatitis C virus (HCV) prevalence among men who have sex with men (MSM) in Vietnam and associated risk factors: 2010 Vietnam Integrated Behavioural and Biologic Cross-Sectional Survey. Sexually Transmitted Infections. 2016:sextrans-2015-052518.
- Mahmood T, Iqbal M. Prevalence of anti Hepatitis C virus (HCV) antibodies in cataract surgery patients. Pak J Ophthalmol. 2008;24(1):16-9.
- Ali SA, Donahue RM, Qureshi H, Vermund SH. Hepatitis B and hepatitis C in Pakistan: prevalence and risk factors. Int J Infect Dis. 2009;13(1):9-19.
- Lavanchy D. Global surveillance and control of hepatitis C. Report of a WHO Consultation organized in collaboration with the Viral Hepatitis Prevention Board, Antwerp, Belgium. Journal of viral hepatitis. 1999;6(1):35-47.
- Papatheodoridis G, Thomas H, Golna C, Bernardi M, Carballo M, Cornberg M, et al. Addressing barriers to the prevention, diagnosis and treatment of hepatitis B and C in the face of persisting fiscal constraints in Europe: report from a high level conference. Journal of viral hepatitis. 2016;23(S1):1-12.
- Khurum M. Prevalence of anti-HCV antibodies among health care workers of Rawalpindi and Islamabad. Rawal Med J. 2003;28(1):7-11.
- Ahmad I, Khan SB, ur Rehman H, Khan MH, Anwar S. Frequency of Hepatitis B and Hepatitis C among cataract patients. Gomal Journal of Medical Sciences. 2004;4(2).
- Nangrejo KM, Qureshi MA, Sahto AA, Siddiqui SJ. Prevalence of Hepatitis B and C in the patients undergoing cataract surgery at eye camps. Pak J Ophthalmol. 2011;27(1):27-9.
- Talpur A, Ansari A, Awan M, Ghumro A. Prevalence of hepatitis B and C in surgical patients. Pak J Surg. 2006;22(3):150-3.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.