



ISSN 1757-8515
On the rise worlwide: Bed Bugs and Cimicosis
Sibylle Rahlenbeck, Jochen Utikal and Stephen Doggett
Cite this article as: BJMP 2016;9(3):a921
|
|
Abstract After they became rare in developed nations over some 30-50 years ago, bed bugs have dramatically increased in incidenceand rapidly spread worldwide over the last two decades. Insecticide resistance along with an increase in travel and trade are thought to be the main contributing factors for the resurgence of this public health pest. Bed bugs are not only a hoteliers’ nightmare, but they have also conquered many a private home. Keywords: bed bugs,inseciticides, bullae, hygiene, cimicosis |
Introduction
Bed bugs belong to the family Cimicidae and there are two species involved in the modern resurgence; the Common bed bug, Cimex lectularius and the Tropical bed bug, Cimex hemipterus. They are wingless insects with an oval-flat shape that allows them to hide in narrow cracks and crevices. The adults are dark brown, 4-5mm long, becoming to around 10mm when fully blood-engorged. There are five smaller juvenile stages (nymphs) that are similar in appearance, although lighter in colour. All nymphs require a blood meal to moult to the next stage, and both adults also bloodfeed for nutrition, and egg development in the case of the female. Bed bugs are solely haematophagous ectoparasites. After feeding they return to a harbourage and do not remain on the host. The main hosts are humans, but pets, bats, and birds may act as secondary hosts.
Epidemiology
In the past, bed bugs were particularly an affliction of the poor. However, in the early part of the modern resurgence it was the tourist areas and the hospitality sector that were initially impacted.1-3 Today, bed bugs have conquered quite diverse locations, ranging from hospitals, hotels and homes, to trains, cruise ships, and even airplanes. Most commonly, bed bugs travel in comfort as stowaways in luggage, although they can be transferred via furnishing and other belongings, as well by spreading to adjoining properties. Unfortunately, exact figures on the occurrence of bed bugs are unknown, as there are no mandatory reporting requirements. Additionally, due to the stigma associated with bed bugs, many infestations are simply not reported.
During the day, the largely nocturnal bed bugs will crawl deep into crevices of bed frames and mattresses (Fig.1), or behind wallpaper, and floor moldings. Here they tend to lay their eggs, often several hundred during the female lifetime. Live bed bugs, shed nymphal skins, and dark excrement spots indicate an active infestation. At night they are attracted by carbon dioxide, heat and other host odours to a victim, from which they may take a blood meal every 3-5 days. The adult bugs can survive long periods of starvation, up to five months at 22oC or even longer at cooler temperatures. When a host is found, they insert their mouthparts into the skin, blood feeding for 5-10 minutes. When bed bugs are in large numbers, often lines of bites occur on the unfortunate victim and this sign is almost a sure indication of the presence of the insect. The bites tend to occur along the arms and legs, down the back and across the shoulders.4,5
There has been long speculation whether bed bugs can transmit diseases, and in fact more than 40 different pathogens have been implicated. This has included Hepatitis B and C viruses, Human Immunodeficiency Virus (HIV), and Coxiella burnetii (Q fever). Recently, research has indicated that bed bugs are capable of transmitting the agent of Chagas Disease, Trypanosoma cruzi,in the laboratory. However, to date there is not one piece of evidence that bed bugs have transmitted any pathogen to humans.4,6
Clinical Features
During the act of feeding, saliva is injected which contains a variety of anticoagulants as well as other proteins whose function has yet to be determined. Contrary to popular belief, there is no evidence that bed bugs inject an anaesthetic. One protein, Nitrophorin, is involved in the transport of nitric oxide into the wound. This results in local vasodilation that increases blood supply to the feeding insect. The same protein can also induce a sensitivity to the bite.6
The diagnosis of Cimicosis is via the clinical appearance of the bite reaction and confirmation of an actual bed bug infestation (Table 1).3,5 The most commonly affected body parts are those that are left uncovered during sleep (Fig. 2,3,4), notably the arms, shoulders and legs. In young children, the face and even the eyelids can be bitten. Rarely, however, armpits are bitten, which are often preferred by other insects and ticks (Table 2).
| Table 1. Bed bug infestation | |
| Bites on the body | Wheals, 4-6cm in diameter, lines of bites |
| Any exposed body part | |
| Often intense itching | |
| Occasional central haemorrhage | |
| Bed Sheet, mattress (clothing) |
Small blood spots |
| Droppings (black dots) | |
| Shed nymphal skins | |
| Eggs, small (~1mm in length), white, oblong, glued to the substrate |
|
| Space | Pungent smell (mostly commonly noticed when an insect is squashed, or during the control program) |
| Table 2. Differential diagnosis of epidermatozoonoses | ||||
| Bite preference | Pattern | Itching | Notes | |
| Bed Bugs | Any exposed parts of the body, arms, legs, face, torso | In small infestations, bites will be random. In larger infestations, bite can occur in lines along the limbs and across the shoulder. Large wheals (up to 6cm across) may form, even some 14 days after the bite | Often intense, especially in the morning, but can be variable between individuals | Often associated with travel or used furniture |
| Fleas | Exposed parts of the body, especially the legs | Random, usually not grouped or in lines | During the day | Usually associated with pets |
| Mosquitoes | Exposed skin, particularly legs and arms | Random | Variable between individuals | Most commonly outdoors |
| Ticks | Potentially anywhere on the body | Erythema migrans with Lyme disease. Localised macules/papules at the bite site may occur | Low / no | Those who work or recreate in native forests are at greatest risk. |
| Itch Mites (Scabies, Sarcoptes scabiei) | Forearms, inter digital, genital area | Skin rashes, subcutaneous courses | At night | Most common in the elderly and infirmed |
| Harvest mites (Trombidiosis) | Skin surfaces under tight clothing | Red macules and wheals | Severe itching | Often occurs in gardens or meadows, most active during summer and autumn |
| Cheyletiellosis | Arms and trunk, contact points with pets | Polymorphic rash | Variable | Tends to be associated with pets |
| Bird mites | All over | Macular rash | Variable itching | Most commonly in homes as a result of birds roosting in roof cavities |
| Head Lice (Pediculosis) | In the hair of the head | Bar-shaped scratch effects with lichenification and hyper-pigmentation (Vagabond’s disease) | Night and day, generally mild itching | Most common in school aged children |
| Spiders, e.g. long-legged sac spiders | Arms, face | Necrotic lesion at bite site | Immediate severe pain, no itching | Uncommon |
Figure 1: Typical appearance of bed bugs
Figure 2: Bites on the back, note the lines of bites common in moderate to large infestations
Figure 3: Bed bug bites on the arm, typical formation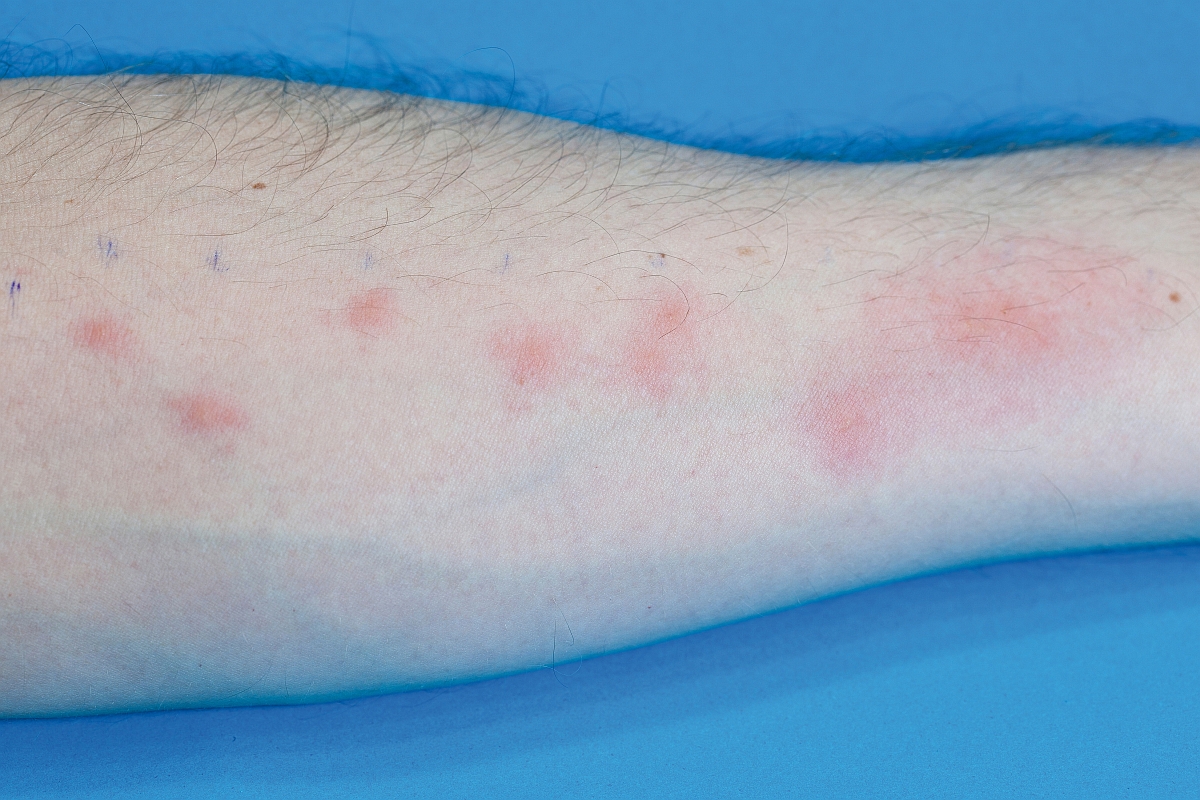
Figure 4: Bed bug bites on the torso and arm
Figure 5: Bullae due to bed bug bites
Figure 6: Bed bugs, their droppings and eggs underneath a mattress
The degree of the bite reaction often depends on the level of prior exposure. With low level sensitization, individuals may develop a 1-2 cm wheal, with a small central haemorrhagic point. This haemorrhagic point can be recognized easily by diascopy. In contrast, a highly sensitized person will react immediately and may develop a wheal up to 15cm across (6 inches). If many bed bugs are present, an urticarial rash may develop as a result of the large number of bites and subsequent trauma to the area from scratching. On rare occasions, vesicles and bullae (Fig. 5) may form on the arms and legs. In the course of Cimicosis, papules that are extremely itchy may develop and can persist for several days to weeks. Due to the strong pruritus eczematous lesions, bacterial infections may occur, although this is extremely rare. There are case reports of systemic reactions such as anaphylaxis and asthma, although these are uncommon.
Through repeated exposure, some individuals may develop a tolerance to the bites. The clinical symptoms are then largely inapparent with small punctures at the bite site. Small blood spots are then the only clues that an infestation may be present.
Differential Diagnosis
Since reactions to stings and bites of various arthropods are non-specific, bed bug bites are commonly misdiagnosed. Single bites, notably that of other insects such as mosquitoes, fleas and biting midges may appear very similar morphologically (Table 2).
Consideration of where the bites are on the body can assist in the differential diagnosis. For bed bugs, lines of bites are very common in moderate to large infestations and this clinical picture is virtually unique amongst blood sucking arthropods. For the most part, the identification of the actual pest is required to confirm the diagnosis. Histologically, bed bug bites resemble perivascular eosinophilic infiltrates through the superficial and deep dermis, with minimal spongiosis.
Other possible diagnostic confounders can be various allergic reactions and other medical conditions such as urticaria, chickenpox, prurigo subacuta, and erythema multiforme.7,8 These do not show a central haemorrhagic point in the lesion which allows a correct diagnosis. However, in young children the diagnosis can sometimes be difficult.
Treatment
The treatment of Cimicosis is symptomatic. Local lesions can be treated with antipruritics e.g. Polidocanol 2-4% in Lotio alba (aqueous lotion) and topical antiseptic. Spirit of menthol may also be helpful. Local treatment with antihistamines is controversial. In severe reactions topical glucocorticoids such as Betamethasone may be required. In severe itching, the use of oral antihistamines is recommended. With infected bites, antibiotic therapy may be required. Uncomplicated bed bug bites tend to stop itching within 1-2 weeks, although temporary scarring from the bite may remain for several months.
Management
Treatment of patients with bed bug bites ultimately comes down to removing the source of the irritant, namely the eradication of the active infestation. Bed bugs have a typical pungent odor. This can be used to detect bed bugs through specially trained sniffer dogs that can rapidly locate the insects.9 Due to insecticide resistance, bed bugs are very difficult to control with traditional insecticides alone, and non-chemical means of eradication must be employed to reduce the overall insect biomass. Bed bug control should be undertaken by professionals trained in bed bug management, and the process may take some weeks to achieve.
Prevention
When travelling (1) always inspect the bed and surrounds for bed bugs hiding beneath the mattress and/or in seams of the bedding. Also, look for blood stains or small black dots (Figure 6, Table 1). (2) If present, request another room. (3) Always keep your luggage on the desktop or the luggage rack. A good preventative is to seal luggage in plastic or garbage bags during travelling, even when in transit. (4) When returning home, all clothing should be washed in at temperatures exceeding 60°C or frozen for one week with delicate fabrics. If there is no choice, then repellents containing N, N-Diethyl-meta-toluamide (DEET) should reduce the biting rate, but will not completely prevent all bed bug bites.10,11
Bed bugs can enter homes via an array of additional ways, particularly from objects bought second hand at flea markets or thrift stores, for example wooden frames, vintage clothes, furniture and the like. These should be heat-treated for a minimum of 10-20 minutes to kill bugs and their eggs.
|
Competing Interests None declared Author Details SIBYLLE RAHLENBECK, MD, MPH, Consultant in Public Health, Berlin, Germany. JOCHEN UTIKAL, MD, Dermatologist, Dep. of Dermatology, Venereology and Allergology, University Medical Center Mannheim and German Cancer Research Center Heidelberg Germany. STEPHEN DOGGETT, Dr. Sc, Dep. Medical Entomology, Westmead Hospital, Locked Bag 9001, Sydney, NSW 2145, Australia. CORRESPONDENCE: Sibylle Rahlenbeck, MD, MPH, Consultant in Public Health, Berlin, Germany. Email: rahlenbeck@hotmail.com |
References
- Cooper R, Wang C, Singh N. Mark-release-recapture reveals extensive movement of bed bugs (Cimex lectularius L.) within and between apartments. PLoS One 10(9), e0136462.doin:10.1371/journal.pone.0136462
- Bernadeschi C, Le Cleach L, Delaunay P, Chosidow O. Bed bug infestation. BMJ 2013;346:f138doi: http://dx.doi.org/10.1136/bmj
- Kolb A, Needham GR, Neyman KM, High WA. Bedbugs. Dermatol 2009;22:347-52. doi: 10.1111/j.1529-8019.2009.01246.x.
- Doggett SL, Dwyer De, Penas P, Russell R. Bed bugs: clinical relevance and control options. Clin Microbiol Rev 2012; 25:164-92 doi: 10.1128/CMR.05015-11
- Goddard J & deShazo R. Bed bugs (Cimex lectularius) and clinical consequences of their bites. JAMA 2009;301:1358-66
- Salazar R, Castillo-Neyra R, Tustin AW, Borrini-Mayorí K, Náquira C, Levy MZ. Bed bugs (Cimex lectularius) as vectors of Trypanosoma cruzi.Am J Trop Med Hyg 2015 Feb;92(2):331-5. doi: 10.4269/ajtmh.14-0483
- Scarupa MD, Economides A. Bedbug bites masquerading as urticaria. J Allergy Clin Immunol 2006;117(6):1508-9
- Braun-Falco’ s Dermatology, 6th edition; Burgdorf W.H.C., Plewig G., Wolff H.H., Landthaler M. (Eds.). Springer Berlin Heidelberg, 2012; ISBN 978-3-642-24162-8
- Vaidyanathan R & Feldlaufer MF. Bed bug detection, current technologies and future directions. Am J Trop Hyg 2013;88:619-25. doi: 10.4269/ajtmh.12-0493
- Todd RG, 2011. Repellents for Protection from Bed Bugs: The Need, the Candidates, Safety Challenges, Test Methods, and the Chance of Success. IN: G. Paluch & J.Coats (eds): Recent Developments in Invertebrate Repellents. Merican Cehmical Soc., Washington, DC, 2011
- Wang C, Lü L, Zhang A, Liu C. Repellency of selected chemicals against the bed bug (Hemiptera: Cimicidae). J Econ Entomol 2013;106:2522-9

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.