



ISSN 1757-8515
Giant Cerebral Hydatid Cyst in a Child- A Case Report and Review of Literature
Ali Nemati, Ahmad Kamgarpour, Murtaza Rashid and Sahar Sohrabi Nazari
Cite this article as: BJMP 2010;3(3):a338
|
|
Abstract Cystic hydatidosis is a rare disease which mainly involves the liver and lungs, and rarely the brain. Cysts may be single or multiple. A 6-year-old boy presented with the chief complaint of ataxia. Brain imaging revealed a huge cystic structure involving the right side of the brain. A diagnosis of brain hydatid cyst was made and the patient was operated on. A large cyst was successfully delivered without rupture. Antihelminthic medication was started and the patient was discharged with full recovery of neurological function. Hydatid cysts must be considered as a differential diagnosis in patients with cystic lesions of the brain, especially in children. Surgery remains the standard method of treatment, and care must be taken in order to recover the cyst without rupture to avoid severe complications and recurrence.
Keywords: Hydatid cyst; Brain; Imaging; Surgery |
Introduction A hydatid cyst is the larval stage of a small tapeworm, Echinococcus granulosus. This is an emerging zoonotic parasitic disease throughout the world, thought to cause an annual loss of US $193,529,740.1 Hydatid cysts are more prevalent in Australia, New Zealand, South America, Russia, France, China, India, the Middle East and Mediterranean countries.2,3,4 They are most commonly (about 50-75%) seen in children and young adults.4,5,6 The liver is the most common organ involved (77%), followed by the lungs (43%).7,8,9,10 However, some researchers report that the lung is the most common organ involved in children, possibly due to bypass of the liver by lymphatics, and higher incidental findings in the lungs when children are assessed for other respiratory infections.8,11,12,13 Hydatid cysts have been reported in the brain (2%),3,4,5,7,8,14,15 heart (2%),8,10,13,16 kidneys (2%),9,10,11 orbit (1%),17,18 spinal cord (1%),3,19 spleen,4 spine,3,8 spermatic cord20 and soft tissues.8 However, in the Mediterranean region, the incidence of brain hydatid cysts have been reported higher (7.4-8.8%).21 Surgery remains the treatment of choice, although recently some new modalities have been described.5,8,22 Careful removal of the lesion is of considerable importance, otherwise fatal complications are inevitable.23,24,25 We describe the case of a 6 year old boy who came to our department with various neurological manifestations. The main purpose of this study is to demonstrate the unusual symptoms of the patient and the enormity of the operated cyst, which was fully resected without rupture. Case Report A 6-year-old boy was referred to our Neurosurgery Department with a four week history of ataxia and left sided weakness. His vital signs were normal and his Glasgow Coma Scale (GCS) was 15. The symptoms had started about six months ago with numbness and parasthesia of the toes. Subsequently he developed intermittent nausea and vomiting. He then started to develop left sided weakness and finally ataxia. He also had a few focal convulsions but did not complain of headache. Fundoscopy revealed bilateral frank papilloedema. On examination, the patient had nystagmus and a positive Romberg’s test. Laboratory data showed mild leucocytosis without any significant rise in eosinophils, and liver enzymes were normal. The enzyme-linked immunosorbent assay (ELISA) for hydatid cysts was negative. Plain chest X-ray and ultrasound scan of the abdomen and pelvis were also normal. Brain computed tomography (CT scan) of the frontal and parietal lobes demonstrated a single large, spherical, well-defined, thin-walled homogenous cyst, with an inner density similar to that of cerebrospinal fluid (CSF), and a wall which did not show enhancement [fig 1(a)]. This cystic structure caused a mass effect and a midline shift towards the left, as well as hydrocephalus, possibly due to obstruction. Magnetic resonance imaging (MRI) of the brain showed cystic signal intensity similar to that of CSF, without ring enhancement or oedema [fig 2]. 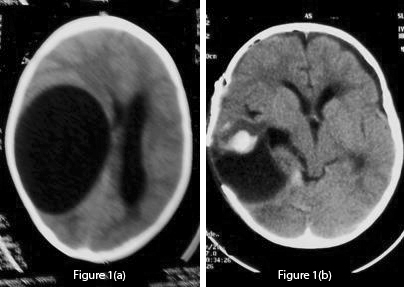 Fig 1 (a): Pre-operative unenhanced CT scan which shows a large CSF density cystic lesion on the right side causing mass effect and midline shift to the left. There is no peri-lesional oedema. Fig 1 (b): Post-operative CT scan of the lesion shows a large void which can lead to dangerous collapse. Mild haematoma is also seen.
Fig 1 (a): Pre-operative unenhanced CT scan which shows a large CSF density cystic lesion on the right side causing mass effect and midline shift to the left. There is no peri-lesional oedema. Fig 1 (b): Post-operative CT scan of the lesion shows a large void which can lead to dangerous collapse. Mild haematoma is also seen. 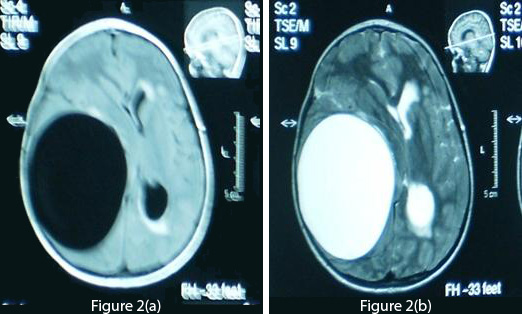 Fig 2 (a): T1-weighted axial MRI of the brain demonstrates a cyst density similar to CSF. Fig 2 (b): T2-weighted MRI shows no ring enhancement or oedema. The periventricular hyperintensity of the left side is probably due to obstructive hydrocephalus.
Fig 2 (a): T1-weighted axial MRI of the brain demonstrates a cyst density similar to CSF. Fig 2 (b): T2-weighted MRI shows no ring enhancement or oedema. The periventricular hyperintensity of the left side is probably due to obstructive hydrocephalus.  Fig 3: This shows the cyst removed in toto after operation. The cyst appears creamy and smooth. After summation of all the above data, the diagnosis of a hydatid cyst was made and a right frontotemporoparietal craniotomy was performed. A large cystic structure (14×14×12 cm) was delivered with utmost care to avoid rupture and spillage [fig 3]. A hydatid cyst was confirmed by pathology reports. A post-operative CT scan showed a large space without any residual matter [fig 1(b)]. Post-operatively, albendazole 15 mg/kg was started and continued for four weeks. The patient showed marked improvement in his neurological deficit and was discharged after one week with close follow-up. Discussion/Review Of Literature Life CycleHydatidosis is caused by Echinococcus granulosus, which occurs mainly in dogs. Humans who act as intermediate hosts get infected incidentally by ingesting eggs from the faeces of the infected animal. The eggs hatch inside the intestines and penetrate the walls, entering blood vessels and eventually reach the liver where they may form cysts or move on towards the lungs. Even after pulmonary filter, a few still make it to the systemic circulation and can lodge in almost any part of the body, including the brain, heart and bones.2,3,8,14,16,26 Brain hydatid cysts are relatively rare and only account for up to 2% of total cases.4,5,7 The actual percentage may be higher than what we have in literature, due to under-reporting. Brain hydatid cysts can be primary (single) or secondary (multiple).2,3,4,5,7 The latter are thought to arise from the multiple scolices released from the left side of the heart following cyst rupture in the heart2,3,5,27 or due to spontaneous, traumatic or surgical rupture of a solitary cranial cyst.3,5 Cysts mostly involve the territory of the middle cerebral artery4,7 but other regions like intraventricular, posterior fossa and the orbit have also been reported.15,17,18,28 The wall of the cyst consists of an inner endocyst (germinal layer) and outer ectocyst (laminated layer). The host reacts to the cyst forming a pericyst (fibrous capsule), which provides nutrients to the parasite. In the brain, due to minimal reaction, the pericyst is very thin. The endocyst produce scolices which bud into the cyst cavity and may sediment within the hydatid cavity, commonly known as hydatid sand.3,14,29,30 Presentation and DiagnosisMost hydatid cysts are acquired in childhood and are manifested during early adulthood.8,29 Cysts develop insidiously, usually being asymptomatic initially, and present with protean clinical and imaging features.3,5,6 In previous studies the most common presenting symptoms were headache and vomiting.4,5,7,14,15,28 Also in the literature, patients reported ataxia, diplopia, hemiparesis, abducens nerve palsy and even coma.5,7,15,28 Surprisingly, in the present study the patient did not have a headache and presented with parasthesia and numbness of the toes. Later he developed left sided weakness, convulsions and finally ataxia, which correlate with previous studies. Diagnosis of a hydatid cyst can sometimes be confused with other space occupying lesions of the brain, especially abscesses, neoplasms and arachnoid cysts.14,31 In this study the patient had bilateral frank papilloedema which is also mentioned in earlier reports.4,28 The Casoni and Weinberg tests, indirect haemagglutination, eosinophilia and ELISA are used in diagnosing hydatid cysts, but as brain tissue evokes minimal response many results tend to be false negatives.2,5,8,25 In our case also, serology for hydatid cyst was negative. CT scan and MRI are used frequently in diagnosing the cystic lesions.3,8,14,23,32,33 However, MRI is considered superior in demonstrating the cyst rim.5,8,11,21,32,34 On CT scan, a solitary cyst appears as well-defined, spherical, smooth, thin-walled and homogeneous, with an inner density similar to CSF, and non-enhancing walls.11,29,32The wall may appear iso-dense to hyper-dense on CT scan3,8, and rarely, may become calcified.11,29,32 There is usually no surrounding brain parenchymal oedema, which if exists along with ring enhancement, indicates inflammation and infection. 7,11,32,33,34,35 Ring enhancement and peri-lesional oedema differentiates brain abscesses and cystic neoplasms from uncomplicated hydatid cysts.3,8 These findings can in fact sometimes cause dilemma and misdiagnosis and lead to catastrophic events.14 The cyst shows low signal intensity on T1-weighted, and high signal intensity on T2-weighted MRI.2 MRI may also show peri-lesional oedema not seen on regular CT scan imaging.7 MRI may prove superior in determining exact cyst location, presence of super-added infections and cystic contents, and also in surgical planning and ruling out other diagnostic possibilities.14,33 We strongly recommend MRI for better evaluation of cystic brain lesions. Spontaneous cystic rupture can lead to different appearances depending on which layers have been obliterated, and produce some specific signs.3 When only the endocyst ruptures, cyst contents are held by the outer pericyst giving a peculiar water lily sign, which is pathognomic.3,8 TreatmentThough still in infancy, medical therapy for small or inoperable brain hydatid cysts has been promising. Albendazole alone or in combination with other compounds, such as praziquantel, has been reported with favourable results as an adjunct and, in certain circumstances, as the primary mode of treatment.2,36,37,38 It is reported that albendazole results in the disappearance of up to 48% of cysts and a substantial reduction in size of the cysts in another 28%.2 The duration of the treatment is four weeks or more, and recently many authors have favoured a prolonged therapy. The change in levels of cyst markers such as alanine, succinate, acetate and lactate, measured before and during treatment on Proton Magnetic Resonance Spectroscopy (MRS), correlate well with shrinkage and resolution of cyst findings on conventional MRI and help in evaluating the efficacy of chemotherapy.39 Cysts may drain into ventricles or rupture completely, causing spillage of contents into the subarachnoid space, leading to fatal anaphylactic shock, meningitis or local recurrence.3,5,22,25 Surgery is the mainstay for treating intracranial hydatid cysts and the aim is to excise the cysts entirely without rupture, which can otherwise lead to catastrophic events as described earlier 2,3,14,25. The Dowling-Orlando technique remains the preferred method, in which the cyst can be delivered by lowering the head of the operating table and instilling warm saline between the cyst and the surrounding brain.40 Even minimal spillage can cause deleterious effects (1 ml of hydatid sand contains 400,000 scolices).14 The thin cyst wall, periventricular location and micro-adhesions to the parenchyma are the main problems encountered during the surgical procedure.1,22 The large cavity remaining after the cystic removal can lead to many serious complications, such as cortical collapse, hyperpyrexia, brain oedema and cardio-respiratory failure.5 Recurrence remains a major concern, which is managed by both antihelminthic chemotherapy and surgery. In a study conducted by Ciurea et al, 25% of the patients had recurrence, which highlights the need for long term follow up.23 In the present study, due to the huge size of the cyst and progressive neurological deficit, it was not wise to completely rely on medical therapy. Surgery was performed and post-operatively albendazole was started as an adjunct. We recommend that for treating brain hydatid cyst, the size of the cyst, multiplicity, location and neurological deficit must all be taken into consideration.
Fig 3: This shows the cyst removed in toto after operation. The cyst appears creamy and smooth. After summation of all the above data, the diagnosis of a hydatid cyst was made and a right frontotemporoparietal craniotomy was performed. A large cystic structure (14×14×12 cm) was delivered with utmost care to avoid rupture and spillage [fig 3]. A hydatid cyst was confirmed by pathology reports. A post-operative CT scan showed a large space without any residual matter [fig 1(b)]. Post-operatively, albendazole 15 mg/kg was started and continued for four weeks. The patient showed marked improvement in his neurological deficit and was discharged after one week with close follow-up. Discussion/Review Of Literature Life CycleHydatidosis is caused by Echinococcus granulosus, which occurs mainly in dogs. Humans who act as intermediate hosts get infected incidentally by ingesting eggs from the faeces of the infected animal. The eggs hatch inside the intestines and penetrate the walls, entering blood vessels and eventually reach the liver where they may form cysts or move on towards the lungs. Even after pulmonary filter, a few still make it to the systemic circulation and can lodge in almost any part of the body, including the brain, heart and bones.2,3,8,14,16,26 Brain hydatid cysts are relatively rare and only account for up to 2% of total cases.4,5,7 The actual percentage may be higher than what we have in literature, due to under-reporting. Brain hydatid cysts can be primary (single) or secondary (multiple).2,3,4,5,7 The latter are thought to arise from the multiple scolices released from the left side of the heart following cyst rupture in the heart2,3,5,27 or due to spontaneous, traumatic or surgical rupture of a solitary cranial cyst.3,5 Cysts mostly involve the territory of the middle cerebral artery4,7 but other regions like intraventricular, posterior fossa and the orbit have also been reported.15,17,18,28 The wall of the cyst consists of an inner endocyst (germinal layer) and outer ectocyst (laminated layer). The host reacts to the cyst forming a pericyst (fibrous capsule), which provides nutrients to the parasite. In the brain, due to minimal reaction, the pericyst is very thin. The endocyst produce scolices which bud into the cyst cavity and may sediment within the hydatid cavity, commonly known as hydatid sand.3,14,29,30 Presentation and DiagnosisMost hydatid cysts are acquired in childhood and are manifested during early adulthood.8,29 Cysts develop insidiously, usually being asymptomatic initially, and present with protean clinical and imaging features.3,5,6 In previous studies the most common presenting symptoms were headache and vomiting.4,5,7,14,15,28 Also in the literature, patients reported ataxia, diplopia, hemiparesis, abducens nerve palsy and even coma.5,7,15,28 Surprisingly, in the present study the patient did not have a headache and presented with parasthesia and numbness of the toes. Later he developed left sided weakness, convulsions and finally ataxia, which correlate with previous studies. Diagnosis of a hydatid cyst can sometimes be confused with other space occupying lesions of the brain, especially abscesses, neoplasms and arachnoid cysts.14,31 In this study the patient had bilateral frank papilloedema which is also mentioned in earlier reports.4,28 The Casoni and Weinberg tests, indirect haemagglutination, eosinophilia and ELISA are used in diagnosing hydatid cysts, but as brain tissue evokes minimal response many results tend to be false negatives.2,5,8,25 In our case also, serology for hydatid cyst was negative. CT scan and MRI are used frequently in diagnosing the cystic lesions.3,8,14,23,32,33 However, MRI is considered superior in demonstrating the cyst rim.5,8,11,21,32,34 On CT scan, a solitary cyst appears as well-defined, spherical, smooth, thin-walled and homogeneous, with an inner density similar to CSF, and non-enhancing walls.11,29,32The wall may appear iso-dense to hyper-dense on CT scan3,8, and rarely, may become calcified.11,29,32 There is usually no surrounding brain parenchymal oedema, which if exists along with ring enhancement, indicates inflammation and infection. 7,11,32,33,34,35 Ring enhancement and peri-lesional oedema differentiates brain abscesses and cystic neoplasms from uncomplicated hydatid cysts.3,8 These findings can in fact sometimes cause dilemma and misdiagnosis and lead to catastrophic events.14 The cyst shows low signal intensity on T1-weighted, and high signal intensity on T2-weighted MRI.2 MRI may also show peri-lesional oedema not seen on regular CT scan imaging.7 MRI may prove superior in determining exact cyst location, presence of super-added infections and cystic contents, and also in surgical planning and ruling out other diagnostic possibilities.14,33 We strongly recommend MRI for better evaluation of cystic brain lesions. Spontaneous cystic rupture can lead to different appearances depending on which layers have been obliterated, and produce some specific signs.3 When only the endocyst ruptures, cyst contents are held by the outer pericyst giving a peculiar water lily sign, which is pathognomic.3,8 TreatmentThough still in infancy, medical therapy for small or inoperable brain hydatid cysts has been promising. Albendazole alone or in combination with other compounds, such as praziquantel, has been reported with favourable results as an adjunct and, in certain circumstances, as the primary mode of treatment.2,36,37,38 It is reported that albendazole results in the disappearance of up to 48% of cysts and a substantial reduction in size of the cysts in another 28%.2 The duration of the treatment is four weeks or more, and recently many authors have favoured a prolonged therapy. The change in levels of cyst markers such as alanine, succinate, acetate and lactate, measured before and during treatment on Proton Magnetic Resonance Spectroscopy (MRS), correlate well with shrinkage and resolution of cyst findings on conventional MRI and help in evaluating the efficacy of chemotherapy.39 Cysts may drain into ventricles or rupture completely, causing spillage of contents into the subarachnoid space, leading to fatal anaphylactic shock, meningitis or local recurrence.3,5,22,25 Surgery is the mainstay for treating intracranial hydatid cysts and the aim is to excise the cysts entirely without rupture, which can otherwise lead to catastrophic events as described earlier 2,3,14,25. The Dowling-Orlando technique remains the preferred method, in which the cyst can be delivered by lowering the head of the operating table and instilling warm saline between the cyst and the surrounding brain.40 Even minimal spillage can cause deleterious effects (1 ml of hydatid sand contains 400,000 scolices).14 The thin cyst wall, periventricular location and micro-adhesions to the parenchyma are the main problems encountered during the surgical procedure.1,22 The large cavity remaining after the cystic removal can lead to many serious complications, such as cortical collapse, hyperpyrexia, brain oedema and cardio-respiratory failure.5 Recurrence remains a major concern, which is managed by both antihelminthic chemotherapy and surgery. In a study conducted by Ciurea et al, 25% of the patients had recurrence, which highlights the need for long term follow up.23 In the present study, due to the huge size of the cyst and progressive neurological deficit, it was not wise to completely rely on medical therapy. Surgery was performed and post-operatively albendazole was started as an adjunct. We recommend that for treating brain hydatid cyst, the size of the cyst, multiplicity, location and neurological deficit must all be taken into consideration.
|
Competing Interests None Declared Author Details ALI NEMATI MD; Chief Resident, Department Of Neurosurgery, Shiraz Medical School AHMAD KAMGARPOUR MD; Associate Professor, Department Of Neurosurgery, Shiraz Medical School MURTAZA RASHID MD; House Officer, Department Of Neurosurgery, Shiraz Medical School SAHAR SOHRABI NAZARI MD; House Officer, Department Of Neurosurgery, Shiraz Medical School CORRESPONDENCE: MURTAZA RASHID MD,Department of Neurosurgery, Shiraz University of Medical Sciences, Iran. P.O. Box: 71455-166 Tel: +98 917 910 5372 Email: dr.murtazarashid@gmail.com |
References
1. Budke CM. Global socioeconomic impact of Cystic echinococcosis. Emerg Infec Dis 2006;12(2):296-303.
2. Reddy DR. Managing cerebral and cranial hydatid disease. Neurol India 2009;57:116-118.
3. Kovoor JME, Thomas RD, Chandrashekhar HS, Jayakumar PN, Pillai S, Shankar SK. Neurohydatidosis. Australas Radiol 2007;51:406-411.
4. Ersahin Y, Mutluer S, Güzelbag E. Intracranial hydatid cysts in children. Neurosurgery 1993;33(2): 219-224.
5. Cavusoglu H, Tuncer C, Ozdilmaç A, Aydin Y. Multiple Intracranial Hydatid cysts in a boy. Turk Neurosurg 2009; 19(2):203-207.
6. Sierra J, Oviedo J, Berthier M, Leiguardo R. Growth rate of secondary hydatid cysts of the brain. Case report. J Neurosurg 1985;62:781-782.
7. Gana R, Skhissi M, Maaqili R, Bellakhdar F. Multiple infected cerebral hydatid cysts. J Clin Neurosci 2008;15(5):591-593.
8. Andronikou S, Welman C, Kader E. Classic and unusual appearances of hydatid disease in children. Pediatr Radiol 2002;32: 817-828
9. Afsar H, Yagci N, Aybasti N, et al. Hydatid disease of the kidney. Br J Urol 1994;73:17-22
10. Dahniya MH, Hanna RM, Ashebu S, et al. The imaging appearances of hydatid disease at some unusual sites. Br J Radiol 2001;74:283–289.
11. Pedrosa I, Saiz A, Arrazola J, et al. Hydatid disease: radiologic and pathologic features and complications. Radiographics 2001;20:795–817.
12. Rebhandl W, Turnbull J, Felberbauer F. Pulmonary echinococcosis (hydatidosis) in children: results of surgical treatment. Pediatr Pulmonol 1999;27:336–340.
13. Macedo AJ, Magalhaes MP, Jalles Tavares N, et al. Cardiac hydatid cyst in a child. Pediatr Cardiol 1997; 18:226–228.
14. Anvari M, Amirjamshidi A, Abbassioun K. Gradual and complete delivery of a hydatid cyst of the brain through a single burr hole, a wrong happening! Childs Nerv Syst 2009:25(12):1639-1642.
15. Kayaoglu CR. Giant hydatid cyst in the posterior fossa of a child: a case report. J Int Med Res 2008; 36(1)198-202.
16. Salehi M, Soleimani A. Cardiac echinococcosis with negative serologies: a report of two cases. Heart lung circ 2009;18(1):59-61.
17. Ergun R, Okten AI, Yuksel M, et al: Orbital hydatid cysts. report of four cases. Neurosurg Rev 1997;20:33–37
18. Karakaþ HM, Tokoðlu F, Kacar M, et al: Retrobulbar hydatid cyst:assessment of two cases. Australas Radiol 1997;41:179–180.
19. Mazyad MA, Mostafa MM, Morsy TA. Spinal cord hydatid cysts in Egypt. J Egypt Soc Parasitol 1998; 28:655–658.
20. Yurtçu M, Gündüz M, Toy H, Günel E. Spermatic cord hydatid cyst: an unusual localization. J Pediatr Surg 2007;42(12):e15-6.
21. Krajewski R, Stelmasiak Z. Cerebral hydatid cysts in children. Childs Nerv Syst 1991;7:154-155.
22. Izci Y, Tüzün Y, Seçer HI, Gönül E. Cerebral hydatid cysts: technique and pitfalls of surgical managemen.Neurosurg Focus 2008;24(6):E15.
23. Ciurea AV, Fountas KN, Coman TC, Machinis TG, Kapsalaki EZ, Fezoulidis NI, Robinson JS. Long-term Surgical outcome in patients with intracranial hydatid cyst. Acta Neurochir (wien) 2006:148(4):421-426.
24. Pearl M, Kosilimbos DG, Lehrer HZ, Rao AH, Fink H, Zaiman H. Cerebral echinococcosis, a pediatric disease. Report of 2 cases with one successful five year survival. Pediatrics 1987;61:915–920 .
25. Khaldi M, Mohamed S, Kallel J, Khouja N. Brain hydatidosis: report on 117 cases. Childs Nerv Syst 2000; 16:765-769.
26. Guillot J, Bouree P. Zoonotic worms from carnivorous pets: risk assessment and prevention. Bull Acad Natl Med 2007;191(1):67-78.
27. Turgut M, Benli K, Eryilmaz M. Secondary multiple intracranial hydatid cysts caused by intracerebral embolism of cardiac echinococcosis: an exceptional case of hydatidosis. J Neurosurg 1997;86:714–718.
28. Guzel A, Tatli M, Maciaczyk J, Altinors N; Primary Cerebral Intraventricular Hydatid Cyst. A Case Report and Review of the Literature. J Child Neurol 2008;23(5):585-588.
29. Haliloglu M, Saatcsi I, Akhan O, Ozmen MN, Besin A. Spectrum of imaging finding in pediatric hydatid disease. AJR 1997;169: 1627–1631.
30. Iyigun O, Uysal S, Sancak R, Hokelek M, Uyar Y, Bernay F, Ariturk E. Multiple organ involvement hydatid cysts in a 2-year-old boy . J Trop Pediatr 2004;50(6):374-376.
31. Bahloul K, Ouerchefani N, Kammoun B, Boudouara MZ . Unusual brain edema caused by an intracranial hydatid cyst: case report and literature review. Neurochirurgie 2009;55(1):53-56.
32. Tuzun M, Hekimoðlu B: Hydatid disease of the CNS. imaging features. AJR 1998;171:1497-1500.
33. El-Shamam O, Amer T, El-Atta MA. Magnetic resonance imaging of simple and infected hydatid cysts of the brain. Magn Reson Imaging 2004;22(9):1339-1340.
34. Altinörs N, Bavbek M, Caner HH, Erdogan B. Central nervous system hydatidosis in Turkey: A cooperative study and literature survey analysis of 458 cases. J Neurosurg 2000;93:1–8.
35. Behari S, Banerji D, Phadke RV, Shukla S, Krishnani N, Kumar D. Multiple infected extradural parasellar hydatid cysts. Surg Neurol 1997;48: 53–57.
36. Davis A, Dixon H, Pawloski ZS. Multicentre clinical trials of benzimidazole-carbamates in human cystic echinococcosis (phase 2), Bull World Health Organ 1989;67:503–508.
37. Singounas EG, Leventis AS, Sakas DE, Hadley DM, Lampadarios DA, Karvounis PC. Successful treatment of intracerebral hydatid cyst with albendazole: case report and review of the literature. Neurosurgery 1992;31:571–574.
38. Todorov T, Vutova K, Mechkov G, Tonchev Z, Georgiev P, Lazarova I. Experience in the chemotherapy of severe, inoperable echinococcosis in man. Infection 1992;20:19–24.
39. Seckin H, Yagmurlu B, Yigitkanli K, Kars HZ. Metabolic changes during successful medical therapy for brain hydatid cyst: case report. Surg Neurol 2008;70(2):186-189.
40. Carrea R, Dowling E Jr, Guevara JA. Surgical treatment of hydatid cysts of the central nervous system in the pediatric age (Dowling's technique). Childs Brain 1975;1(1):4-21.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.