



ISSN 1757-8515
Retroperitoneal Teratoma in an adult presenting with painful abdominal mass: case history and literature review
Sadaqat Ali Khan, Tariq Mahmood, Muhammad Zeeshan Sarwar, Syed Hamad Rasool, Muhammad Danish Siddique and Zohaib Khan
Cite this article as: BJMP 2012;5(1):a509
|
|
Abstract Teratomas are congenital tumors that may contain derivatives of all three germ layers. They usually arise in the gonads and often occur in infancy and childhood. A primary retroperitoneal teratoma is a relatively rare disease in adults. Here we report a case of retroperitoneal teratoma in an adult female. It was benign but its wall was adherent to the aorta. It presented with right hypochondrial pain and examination revealed a mass in the abdomen. |
Introduction:
Although one cell type may predominate, teratomas usually comprise of tissue from all three embryonic germ layers1. Generally arising from the gonads, they may be found in extra-gonadal sites such as sacro-coccygeal region, mediastinum, neck and retroperitoneum.2 Here we report a case of retroperitoneal teratoma in an adult with successful surgical treatment. Its clinical presentation, diagnosis and treatment are reviewed.
Case Report:
A woman aged 28 years presented with pain in the right hypochondrium of one year duration. There was no associated bowel or urinary symptom. Examination showed minimal fullness in the right hypochondrium. Routine blood tests and urinalysis were within normal limits. A plain abdominal radiograph showed calcification in the right side of the abdomen (Fig. 1). Ultrasonography demonstrated 13.6 x 8.1 cm soft tissue mass in the retro-peritoneum between liver and the right kidney. It was heterogeneous, well circumscribed with sharply defined borders, and had some calcification and cystic areas. CT abdomen revealed a hypo-dense lesion between liver and the right kidney. It had fatty attenuation with internal hyper-dense areas representing calcification. (Fig. 2). Provisional diagnosis of a retroperitoneal teratoma was made and an open exploration was performed with a right sub-costal incision. There was a large cystic mass behind the ascending colon, duodenum and the pancreas. It was located in the retroperitoneal compartment. There were dense, fibrous adhesions of the mass with aorta but entire cystic mass was excised successfully.
Post operatively this tumor mass measuring 5 x 5 cm was excised in vitro and found to be filled with yellowish creamy material containing hair, sebum and bony tissue. Microscopically it was confirmed to be a cystic teratoma with no malignancy. Stratified squamous epithelium with sebaceous and sweat glands, hair shafts, calcification, few bony spicules and bone marrow elements were all demonstrated. (Fig. 3). The post operative course was uneventful and she was well at the 2 months follow up.
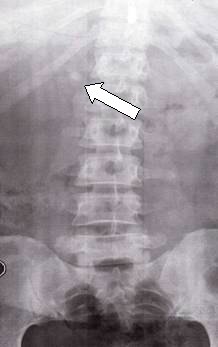
Figure 1. Plain abdominal radiograph showing radio-opaque shadow (arrow heads) in the right upper abdomen.

Figure 2: Computed Tomography showing an encapsulated mass that contains multiple tissue elements including fat and areas of calcification.
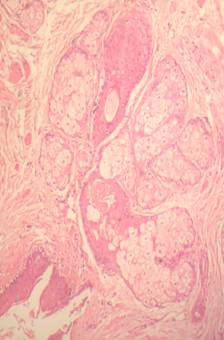
Figure 3: Microscopic examination of the tumor showing squamous epithelium (SE), hair shaft (HS), sebaceous glands (SBG)
Discussion:
Teratomas are congenital tumours arising from pluri-potential embryonic cells and therefore have several recognizable somatic tissues3, Teratomas are usually localized to the ovaries, testis, anterior mediastinum or the retro-peritoneal area in descending order of frequency.4 Teratomas constitute less than 10% of all primary retroperitoneal tumours and hence are relatively uncommon5. Furthermore, retroperitoneal teratomas occur mainly in children and have been very rarely described in the adults. Half of these cases present in children less than 10 years of age and only a fifth of them present after 30 years of age. Retroperitoneal teratomas are often located near the upper pole of the kidney with preponderance on the left. The case described here is therefore unusual in that it was a primary retroperitoneal teratoma in an adult, on the right side and with adhesions to the aorta.
Retroperitoneal teratomas are seen in females twice as commonly than males. Teratomas are usually benign if they are cystic and contain sebum or mature tissue. They are more likely to be malignant if they are solid and have immature embryonic tissue like fat, cartilage, fibrous and bony elements.6 In these regards our case is similar to other described cases as our patient is also female and as her teratoma was cystic, it showed lack of malignancy.
Teratomas are usually asymptomatic as the retroperitoneal space is extensive enough to allow for their free growth. When compression of the surrounding structure occurs, patients may get compression symptoms.The diagnosis of a retroperitoneal teratoma cannot be made on clinical grounds alone. Ultrasound and computed tomography are important in its diagnosis and may show the presence of calcification, teeth or fat. Calcification on the rim of tumour or inside the tumour is seen in 53-62% of teratomas and although radiologically three quarters of patients with a benign teratoma may have calcification within it, a quarter of malignant cases may also demonstrate calcification. Computed tomography is better than Ultrasonography in defining the extent and spread of teratoma to the surrounding organs.7
The prognosis is excellent for benign retroperitoneal teratoma if complete resection can be accomplished.
|
Competing Interests Dr Tariq Mahmood helped only in the scientific writing up of this case based upon material provided by the co-authors. He was not involved in clinical management and therefore cannot verify clinical details of the case. Author Details Sadaqat Ali Khan MBBS, MCPS, FRCSEd, FICS, Professor and Head of Department, Surgical unit III, Services Institute of Medical Sciences, Lahore, Pakistan. Tariq Mahmood Consultant Physician and Gastroenterologist Ickenham, United Kingdom. (Involved only in helping to write up the case in scientific manner. Not involved in management of the case) Muhammad Zeeshan Sarwar MBBS, FCPS, Senior Registrar, Surgical Unit III, Services Institute of Medical Sciences, Lahore. Syed Hamad Rasool MBBS, FCPS, Senior Registrar, Surgical Unit III, Services Institute of Medical Sciences, Lahore. Muhammad Danish Siddique MBBS, House Officer, Surgical Unit III, Services Institute of Medical Sciences, Lahore. Zohaib Khan MBBS, Medical Officer, Surgical Unit III, Services Institute of Medical Sciences, Lahore CORRESPONDENCE: Tariq Mahmood, Consultant Physician and Gastroenterologist Ickenham, United Kingdom. Email: Tm123@btinternet.com |
References
- Muguti GI and Kanakambaran B. Retroperitoneal mature cystic teratoma in an infant. Cen Afr J Med 1997; 43: 274-6
- Engel RM, Elkins RC, and Fletcher BD. Retroperitoneal teratoma. Review of the literature and presentation of an unusual case. Cancer 1968; 22: 1068-73
- Barbara W, Joseph LL and Scott W. Ultrasound and CT demonstration of a benign cystic teratoma arising from the retroperitoneum. AJR 1979; 133: 936-38
- Jean NB, Francois D, Jacques PD, Jean CS and Jean FT. Primary retroperitoneal teratomas in adults. Radiology 1980; 134: 613-16
- Taori K, Rathod J, Deshmukh A, Sheorain VS, Jawale R, Sanyal R, et al. Primary extragonadal retroperitoneal teratoma in an adult. Br J Radiol 2006; 79: 120-22
- Pantoja E, Llobet R and Gonzalez-Flores B. Retroperitoneal teratoma: a historical review. J Urol 1976; 115: 520-23
- Davidson AJ, Hartman DS and Goldman SM. Mature teratoma of the retroperitoneum: radiologic, pathologic and clinical correlation. Radiology 1989; 172: 421-5

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.