



ISSN 1757-8515
Coronary Artery Disease in Africa: Community based study of Risk Factors
R.K.Pal and Ali Grera
Cite this article as: BJMP 2010;3(2):326
|
|
Abstract According to estimates of the World Health Organization (WHO), in 2005, out of 58 million total deaths in the world due to different causes 30 percent (17.4 million) were due to cardio vascular diseases, mainly heart disease and stroke. 53 percent of global deaths due to coronary heart disease occurred in males and 47 percent in women. The common modifiable risk factors identified were unhealthy diet, physical inactivity and tobacco use, leading to raised blood pressure and blood glucose, abnormal blood lipids and becoming overweight.1 The WHO MONICA Project - an international collaboration of researchers from 21 countries, studied more than 30 populations, mainly from Europe, over a period of ten years, from the mid-1980s to the mid 1990s. More than seven million men and women aged between 35 and 64 years of age were monitored to examine if and how certain coronary risk factors and new treatments for heart disease contribute to the decline or increase of heart disease rates in these communities. 2 Hence it has been observed that there have been number of studies on risk factors in patients of Coronary Artery Disease (CAD) but comparatively few studies are available on risk factors in healthy community members in Africa and still fewer on comparison of risk factors for CAD in the patients and community members from the same population. The present study was conducted on 528 community members in Tripoli the capital of Libya including 70 individuals having a history of suffering from Myocardial infarction (MI). The comparison of both the groups of same community revealed that hypertension followed by smoking, diabetes and increased body mass index were more prevalent in the community members with history of MI. It was alarming to note that these risk factors earlier thought to be more frequent after the age of 50 years are now present in higher numbers in the younger age groups of 35 to 54 and 15 to 34 years as well. As most of the risk factors stated above are modifiable there seems to be urgent need of initiating a National Health Programme on prevention and control of these risk factors. The priorities and strategy of such a National Programme has also been suggested in brief for consideration of the national decision makers. Keywords: Coronary Artery Disease, Coronary Heart Disease, Risk factors |
Introduction
As highlighted in the World Health Report 2002, just a few Non Communicable Disease (NCD) risk factors, account for the majority of non communicable disease burden. These risk factors; tobacco use, alcohol consumption, raised blood pressure, raised lipid levels, increased BMI, low fruit/vegetable intake, physical inactivity, and diabetes, are the focus of the STEPs approach to NCD risk factor surveillance. 3
A tool for surveillance of risk factors, WHO STEPS, has been developed to help low and middle income countries get started. It is based on collection ofstandardised data from representative populations of specified sample size to ensure comparability over time and across locations. Step one gathers information on risk factors that can be obtained from the general population by questionnaire. This includes information on socio-demographic features, tobacco use, alcohol consumption, physical inactivity, and fruit/vegetable intake. Step two includes objective data by simple physical measurements needed to examine risk factors that are physiologic attributes of the human body. These are height, weight, and waist circumference (for obesity) and blood pressure. Step three carries the objective measurements of physiologic attributes one step further with the inclusion of blood samples for measuring lipid and glucose levels.4 The risk factors studied by MONICA project of the World Health Organization (WHO), included cigarette smoking, blood pressure, blood cholesterol and body weight.5In many resource-poor settings, laboratory access can be difficultand expensive. A screening algorithm that includesgender, age, cardiovascular disease history, blood pressure,weight and height, and a urine dipstick test for glucose andprotein is likely to be more practical and may well providemuch of the predictive value of more complex blood-based assessments.6In addition, such algorithms should, wherever possible, useregional data on morbidity and mortality, because backgroundrates vary considerably between regions.7 WHO/ISH (World Health Organization/International Society of hypertension) risk prediction charts provide approximate estimates of cardiovascular disease (CVD) risk in people who do not have established coronary heart disease, stroke or other atherosclerotic disease. They are useful as tools to help identify those at high cardio vascular risk, and to motivate patients, particularly to change behavior and, when appropriate, to take antihypertensive, lipid-lowering drugs and aspirin.8 After reviewing the above information about standardised methods available for identifying the risk factors for CAD, the present study was undertaken to assess the prevalence of risk factors in the community in Tripoli, the capital of Libya. The aim of this paper also includes suggesting priorities and strategy to deal with the risk factors that were found most important. Appropriate statistical tests were applied using the software SPSS 17 for determining the relative importance of different risk factors. The specific statistical tests have been stated below. Material and Methods
528 individuals were selected from general community for the study by random sampling from different geographical areas of Tripoli. They were interviewed about risk factors for CAD and where possible, facts stated by them were validated from medical records available with them. Their body weight, height and blood pressure were also recorded. The intern doctors posted with community medicine department were briefed and trained by faculty members for the above observations and recording the body measurement and blood pressure using the uniform technique. The WHO/ISH risk prediction colourcharts for Eastern Mediterranean Region B (which includes Libya) were used as questionnaire for the study. The option of charts available for settings where blood cholesterol can’t be measured was selected as it was found difficult to convince the individuals not suffering from disease to provide blood samples. The following criteria were used for defining Blood Pressure, BMI, Diabetes & MI : According to the WHO definition, individuals with systolic blood pressure ≥ 140 mmHg or those with diastolic blood pressure ≥ 90 mmHg were considered hypertensive. 21. Known cases of diabetes were termed as individuals for whom the diagnosis of diabetes had been established by a physician in the past, or those who were under treatment with anti diabetic drugs. 22 Body mass index (BMI) is calculated as weight divided by height squared (kg/m2). Overweight is defined as BMI 25–29.9 kg/m2, and obesity as BMI ≥ 30 kg/m2 for all subjects.19 Known cases of Myocardial Infarction (MI) were termed as individuals for whom the diagnosis of MI had been established by a physician in the past. Observations The comparison of population characteristics of people with and without having a MI stated in the table below reveals that: distribution of males and females was similar in both the groups. 88% of individuals with a MI were from age group 35 and above. Whereas 11.43% of people with MI were from age group 15 to 34 years which shows the need of starting screening as well as control of risk factors from teenage. Using SPSS software, independent sample t test was applied on age distribution of individuals with and without history of MI. The result revealed that the mean age of individuals with a positive history of MI was 54. It was 43.74 for subjects with negative history of MI. The difference of age between the above 2 groups was found highly significant (P>0.001). In the same manner using SPSS software, Chi square test was applied on sex distribution of individuals with and without history of MI. The result revealed that the difference in sex distribution in the two groups was not significant (P = 0.522) Table 1 : Age & Sex wise distribution of persons with and without MI:
| Characteristics | Individuals with MI in percentage, (N= 70) | Individuals without MI in percentage, (N = 458) |
| Sex; Male | 68.57 (48) | 68.78 (315) |
| Female | 31.43 (22) | 31.22 (143) |
| Age 15-34 years | 11.43(8) | 34.93 (160) |
| 35-54 years | 30.00 (21) | 37.55 (172) |
| 55 & above | 58.57 (41) | 27.51 (126) |
Independent risk factors As presented in Fig.1, in males with MI in terms of percentage the most prevalent risk factor was found to be hypertension (11.05% higher than non MI group), followed by diabetes (higher by 10.78%), smoking (higher by 8.12%) and BMI 25 & above (higher by 5.13%). As presented in Fig.2, in females with MI in terms of percentage the most prevalent risk factor was found to be hypertension (20.55% higher than non MI group), followed by BMI 25 & above (higher by 8.77%) and diabetes (higher by 6.85%). There were no smokers in the female group with MI and only one smoker was found in the females without MI. Using SPSS software, under general linear model, multivariate analysis was performed after splitting the cases under male and female. History of MI was kept as fixed factor and age, history of hypertension, diabetes and stroke, smoking, systolic blood pressure and BMI were kept as dependent variables. The results reveal that in the males with positive history of MI, value of P was less than 0.001(highly significant) for age, History of hypertension & diabetes and systolic BP of140 and greater, followed by history of stroke (P>0.002) suggesting that prevalence of these variables were significantly higher in males with history of MI. The prevalence of BMI 25 & above (P>0.616) and smoking (P>0.882) in males with history of MI was found insignificant. In case of females with positive history of MI, the only variable having significant prevalence was f history of hypertension (P>0.008). An important reason for inability to assess significance for other variables in females may be the smaller number of females of only 22 with history of MI. Among the community members with MI, 94.38% males and 78.57% females had one or the other risk factor which have been stated above. Hence with focused attention to health education and screening for risk factors, identifying most of the individuals at risk of MI, should be possible. 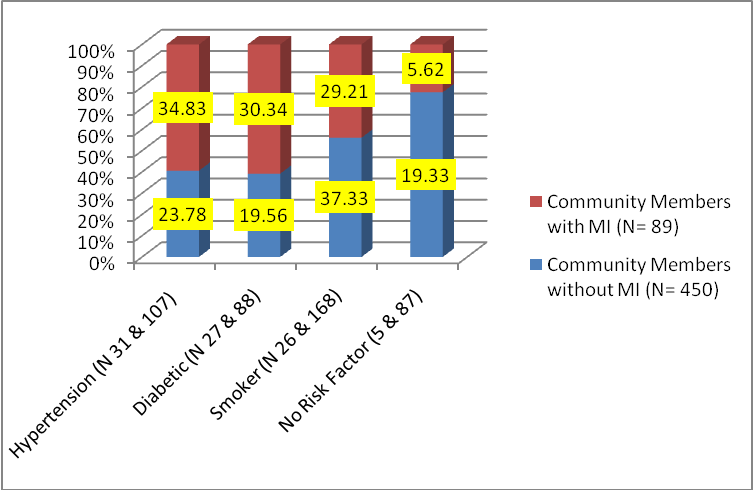
(Fig.1) Distribution of Risk Factors in Males with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) 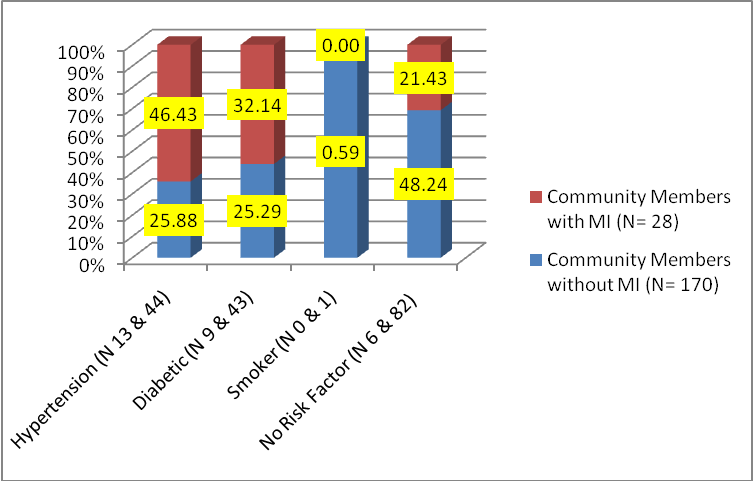 (Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI.
(Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI. 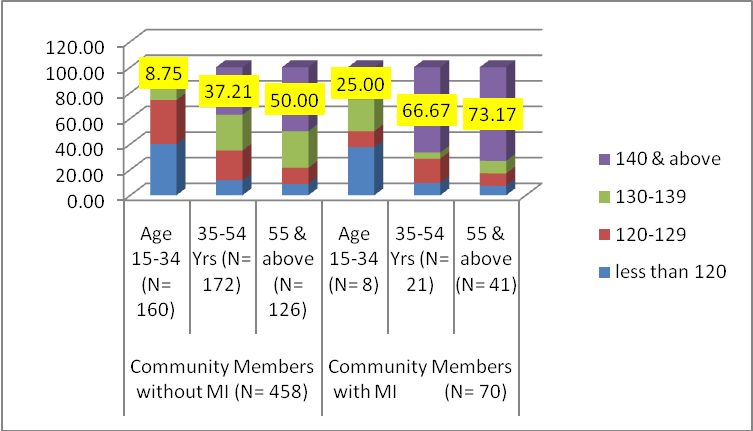 (Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years.
(Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years. 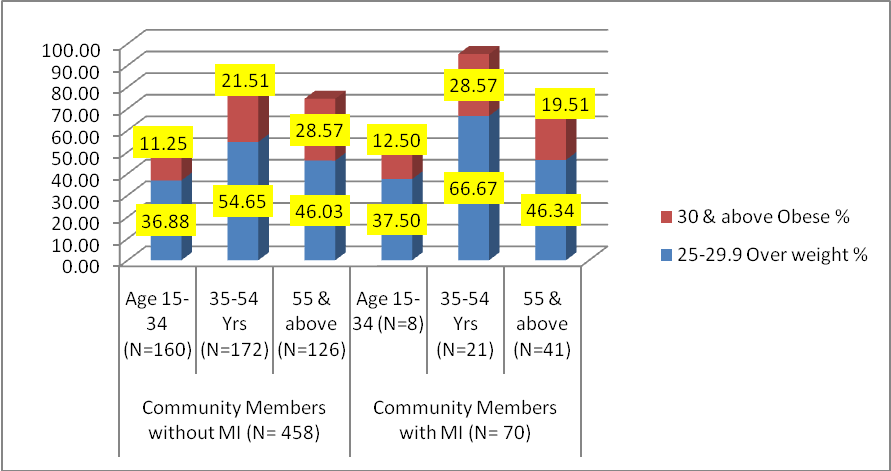 (Fig. 4) Age wise distribution of weight (both sexes)
(Fig. 4) Age wise distribution of weight (both sexes)
Discussion: Comparison with other relevant studies: In our study the most common risk factors observed in community members without MI were hypertension (total 24.35%, males 23.78 & females 25.88), followed by diabetes (total 21.13%, males 19.56 & females 25.29) and smoking (Total 27.26%, males 37.33 & females 0.59) as stated above in Fig.1 & 2. In similar studies performed in countries of Mediterranean region14-18 26% of study population were found to be suffering from hypertension, 40% males and 13% females were smokers and 14.5% were suffering from diabetes. 13 The percentage of diabetics was 10.6 in study population aged 30 years and above in Iran11. The percentage of diabetics were 11% in males and 7% in females in United Arab Emirates (UAE)10 and the figures were the similar in Saudi Arabia in subjects aged 30 years and above were 17.3% and 12.18% respectively.9. All the above studies were performed in the period from year 2000 to 2004 except the study in UAE which was performed in 1995. It can be seen from our study in Libya that in comparison to mean percentage for the same risk factors in other countries of Mediterranean Region, the percentage of hypertension was lower by about 2%. In Libya the percentage of total diabetics in the general community was greater by 6.6%, while the percentage of smokers were less by about 13% in males and 12.5% in females. The percentage of total overweight and obese individuals in all age groups and both sexes were 66.6 % in the general community without MI in our present study (Fig,4). The percentage for those overweight and obese in individuals above 19 years of age was 26.2% in study from Iran12 and 27 % in UAE10 in the age group of 30 to 64 years. The study of 12 countries of the Eastern Mediterranean Region(EMR) by the WHO conducted in 2004, reveals that regional adjusted mean for these countries was 43 % for overweight and obese individuals in all age groups and both sexes20. Hence in comparison to developing countries of the region having similar religious, social and dietary situation among the risk factors for CAD, diabetes and obesity can be seen as emerging major risk factors in Libya followed by hypertension and smoking. Smokers among females were found to be uncommon in Libya. Conclusion The findings of this study reveal that in comparison to those without MI the prevalence of following risk factors was higher in individuals with MI. In males aged 35 to 54, the percentage of those with a systolic BP of 140 and greater was more than double and in females 1.6 times greater. Those with diabetes were greater by 10.78% in males and 6.85% in females, while smokers were higher by 8.12% in males. The percentage of diabetes in individuals without MI was 21.13%. The prevalence of smokers was found to be 37.33% in males without MI which suggests urgent need for prevention and control measures. Considering multiple risk factors out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. In view of large number of individuals having risk factors of CAD in Tripoli, we would like to recommend that health education for preventing overweight and obesity, hypertension, smoking and diabetes may be started with school children and their parents as early as primary school. The screening for above risk factors needs to be implemented in the age group of 34 years and above for detecting individuals at risk as close to 34 years as possible. This step needs to be followed by relevant health education and treatment as soon as possible. More studies on a larger population sample are required from different geographical areas of Libya to refine our focus on the target population identified. At the same time waiting for action, till these additional studies are completed, is not recommended. To make the comparison of risk factors more fruitful among different countries and in the same country over time, we need to agree on uniform criteria such as using WHO/ISH risk prediction charts. Limitations of present study It is a cross sectional study based on the questions stated in WHO/ISH prediction charts for situations where collecting blood samples is not feasible. Due to the small sample size we can only say that the prevalence of MI is indicative of the pattern observed. These figures may get refined as we cover a larger number of the population over time. Due care has been taken in selecting sample size to represent different geographical divisions of Tripoli and to ensure that this is a random sample, but it is a systematic random sample and not the stratified random sample. Hence within each geographical division all the socio economic strata of community may not have been proportionately represented. AppendixThe questionnaire used for the study is stated below. It is based on the questionnaire recommended on page 21 of WHO/ ISH risk prediction charts for Eastern Mediterranean Region B of W.H.O. in which Libya is included.QuestionnairePrecautions: Do not interview persons below the age of 14 years. You should take height, weight and Blood Pressure of the person yourself, before recording it in the form below
| S.N. | Question | Subject | ||||
| 1 | 2 | 3 | 4 | 5 | ||
| 1 | Name of Person: | |||||
| 2 | Address in Libya | |||||
| 4 | Age | |||||
| 5 | Sex: M / F | |||||
| 6 | Do you smoke: Yes / No | |||||
| 8 | Do you have History of suffering from Diabetes: Yes / No | |||||
| 9 | Hist. of suffering from: Mayo cardial Infarction: Yes/ No | |||||
| 10 | History of suffering from Stroke: Yes / No | |||||
| 12 | History of suffering from Hypertension: Yes / No | |||||
| 13 | Height in Cms: | |||||
| 14 | Weight in Kg: | |||||
| 15 | Systolic Blood Pressure ( in mm of Hg): | |||||
|
Competing Interests None Declared Author Details R.K.PAL, Department of Community Medicine, Al Fateh University of Medical Sciences, Tripoli, Libya. ALI GRERA, Department of Community Medicine, Al Fateh University of Medical Sciences, Tripoli, Libya. CORRESPONDENCE: R.K.PAL, Department of Community Medicine, Al Fateh University of Medical Sciences, Tripoli, Libya. Email: palrk2002@gmail.com |
References
1. Preventing chronic diseases – a vital investment, World Health Organization, www.who.int/chp.
2. WHO Study on Heart Disease, Press Release WHO/10, 28 February 2000. (http://www.who.int/inf-pr-2000/en/pr2000-10.html).
3. The World Health Report 2002: reducing risks, promoting healthy life. Geneva, World Health Organization, 2002:57– 61, 162.
4. Summary, Surveillance of risk factors for non communicable diseases, The WHO STEP wise approach, WHO/NMH/CCS/01.01 Rev.1, 2003.
5. Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998; 97: 1837–1847.
6. Mendis S, Lindholm LH, Mancia G, Whitworth J, Alderman M, Lim S, Heagerty T. World Health Organization (WHO) and International Society of Hypertension (ISH) risk prediction charts: assessment of cardiovascular risk for prevention and control of cardiovascular disease in low and middle-income countries. J Hypertens. 2007; 25: 1578–1582.
7. Barzi F, Patel A, Gu D, Sritara P, Lam TH, Rodgers A, Woodward M. Cardiovascular risk prediction tools for populations in Asia. J Epidemiol Community Health. 2007; 61: 115–121.
8. CVD Risk reduction guide, questions and answers, page 9, W.H.O.,September 2007.
9. Risk factors of coronary artery disease in different regions of Saudi Arabia, A.K. Osman and M.M. Al-Nozha, Vol. 6, Issue 2/3, 2000, page 465-474.
10. El-Mugamer IT et al. Diabetes, obesity and hypertension in urban and rural people of Bedouin origin in United Arab Emirates. Journal of tropical medicine and hygiene, 1995, 98(6):407-15.
11. Azizi F., Modifying life style for the prevention of non-communicable disease, Iranian journal of endocrinology and metabolism, 2002, 4(2):81–4.
12. Clustering of coronary artery disease risk factors in patients with type 2 diabetes and impaired glucose tolerance, F. Sajjadi, N. Mohammadifard, R. Kelishadi, N. Ghaderian, H. Alikhasi and M. Maghrun, 1088 La Revue de Santé de la Méditerranée orientale, Vol. 14, No 5, 2008.
13. Al-Nozha MM et al. Coronary artery disease, in Saudi Arabia, Saudi medical journal, 2004, 25(9):1165–71.
14. National survey on the major non communicable diseases, Lebanon. Final Report,2003. Cairo, WHO Regional Office for the Eastern Mediterranean.
15. Diabetes atlas, 2nd ed. Brussels, International Diabetes Federation, 2003.
16. Mokhtar N et al. Diet, culture and obesity in northern Africa. Journal of nutrition, 2001, 131(3):887–92s.
17. Mokdad AH et al. Prevalence of obesity, diabetes, and obesity-related health factors.Journal of the American MedicalAssociation, 2003, 289(1):76–9.
18. National Health Survey of Pakistan1990–1994. Islamabad, Pakistan Medical Research Council, 1998.
19. North American Association for the Study of Obesity,The practical guide. Identification,evaluation and treatment of overweight and obesity in adults. Bethesda, Maryland, National Institutes of Health, 2000 (NIH Publication No. 00–4084).
20. O. Khatib, Noncommunicable diseases, risk factors and regional strategies for prevention and care, Eastern Mediterranean Health Journal, Vol. 10, No. 6, 2004.
21. Azizi F et al. Determinates of serum HDLC level in a Tehran urban population: the Tehran Lipid and Glucose study. Nutrition, metabolism and cardiovascular diseases, 2002, 12:80–9.
22. The Expert Committee of the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes, 2000, 25:S5–20.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.