



ISSN 1757-8515
COPD Exacerbation with Concurrent Stress Cardiomyopathy: A Case of Double Dyspnoea
Jennifer L. Pham, Steven R Bruhl and Mujeeb Sheikh
Cite this article as: BJMP 2011;4(1):a407
|
|
Abstract We present an interesting case of severe dyspnea due to chronic obstructive airway disease exacerbation and upon further evaluation a diagnosis of stress cardiomyopathy was entertained. We highlight a management of this particular case and provide a brief review of stress cardiomyopathy. |
Case presentation
A 52 year-old Caucasian male with a history of chronic obstructive airway disease (COPD) presented to the emergency department complaining of progressive shortness of breath. Two days prior, the patient had presented to the ED with similar complaints that resolved with aerosol treatments and the patient was discharged on a metered dose inhaler (MDI). The patient had been prescribed MDI’s (metered dose inhalers) previously for management of his COPD, but due to financial constraints he had been unable to fill his prescription for the past month. Emergency medical services (EMS) suspected COPD exacerbation and administered 40 mg prednisone IV and two albuterol-ipratropriumnebulisertreatments en route to the hospital, which improved the patient’s breathing symptoms.
Upon arrival to the hospital, his blood pressure was 129/90, respirations 28, pulse 127, and he had an oxygen saturation of 100% on 7L/min. Physical examination revealed increased work of breathing, and wheezes in all lung fields with prolonged expiratory phase. The cardiovascular exam was normal except for tachycardia. A Routine electrocardiogram (ECG) revealed sinus tachycardia and T wave inversions in anterior leads. Chest x-ray showed old scarring in the left lower lobe. Routine cardiac enzymes showed mild elevation with a serum troponin level of 0.68ng/ml (normal range 0.0ng/ml-0.05ng/ml). The second set of troponin peaked at 1.66 ng/ml (normal 0.0ng/ml-0.05ng/ml). In view of the elevated cardiac enzymes atransthoracicechocardiogram was performed which demonstrated multiple wall motion abnormalities and reduced left ventricular ejection fraction of 25%. Coronary angiography demonstrated normal coronary arteries. Left ventriculography revealed hypokinetc mid-anterior and apical segment with a hypercontractile base with reduced ejection fraction (EF) of around 25% (normal range EF 55-65%) (Figure 1)
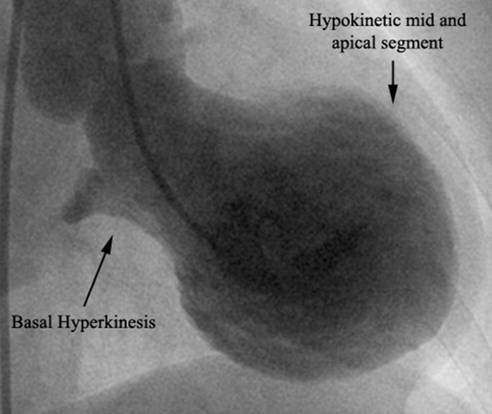
Figure 1. Left ventriculography demonstrating the classic appearance of Takotsubo cardiomyopathy
In light of the systolic dysfunction not in proportion with the degree of coronary artery stenosis and the multiple areas of wall motion abnormalities seen on echocardiogram, the diagnosis of Takotsubo cardiomyopathy (TCMP) was made. The diagnosis was further supported by the presence of ECG changes, troponin elevation, and the added social stresses of being unemployed. Over the course of his stay in hospital, the patient’s breathing improved with oral prednisone, inhaled tiotropium, and fluticasone/salmeterol. The patient was also treated with an angiotension converting enzyme inhibitor (ACE inhibitor), aspirin, statin, and beta-blockers. There were no adverse coronary events during the course of his hospital stay and the patient was discharged after four days. A Follow up echocardiogram after 4 weeks showed normal left ventricular systolic function.
DISCUSSION
Takotsubo cardiomyopathy (TCMP), also called stress-induced cardiomyopathy, apical ballooning syndrome, or broken heart syndrome, is a transient systolic dysfunction of the ventricles in the absence of significant coronary artery disease. Once thought to be a rare syndrome, TCMP is increasingly being identified in clinical practice, however, the prevalence and incidence are not known. It is estimated that 0.7-2.5% of patients who present with acute coronary syndrome are found to have TCMP1 .The majority of these patients are postmenopausal females, with a mean age of 62-75 years. They may present with chest pain and have a recent history of an emotional stress or severe medical illness. 1
The clinical manifestations of TCMP can mimic those of an acute myocardial infarction. Although, chest pain is a common presenting symptom, patients may also have complaints ofdyspnoeaand arrhythmias. In our casedyspnoeawas the predominant symptom and was easily confused with COPD exacerbation. Recently a few cases of concomitant stress cardiomyopathy with obstructive airway disease have been documented in literature. 2-4 While the pathophysiology of the coexistence of these two disorders is not fully understood, it is thought that both stress induced cardiac dysfunction due to exaggerated sympathetic activation and use of sympathomimetic bronchodilators instigates the myocardial stunning in such patients. Furthermore, an emotional stressor, such as death of a family member, or a physiological stressor, such as an acute medical illness, is thought to be a trigger for cardiomyopathy. 5 It is believed that the syndrome is not a result of anischemia, but there is some evidence to suggest thatoestrogenlevels may have a role in modulating the sympatho-adrenal outflow in TCMP. In mice models, chronic oestrogen supplementation seemed to have protective effects from exaggerated sympathetic outflow from the heart and brain6 . Postmenopausal women with low levels ofoestrogenmay be more vulnerable to the exaggerated catecholamine release in responses to stressors. 7
The characteristic finding in TCMP is a transient mid-ventricular or apical ballooning due to a hypokinetic portion seen on echocardiogram or on a left ventriculography. Systolic dysfunction is usually transient, inconsistent to the perfusion area of a single coronary artery, and usually resolves within 4-6 weeks. 8 Additional findings include ECG changes with ST segment deviations in precordial leads being the most common. Cardiac enzymes have been noted to have moderate elevations.9.
As data regarding the treatment of TCMP is limited, medical management mainly consists of symptomatic therapy with aspirin, ACE inhibitors, beta-blockers, and diuretics, also used in acute coronary syndrome.10 Patients who present acutely are treated as acute coronary syndrome and often receive emergency coronary angiography. However, less invasive imaging techniques, such as echocardiograms, should first be examined carefully. Due to the transient nature of the syndrome, the duration of treatment is unknown with some studies suggesting that there is no benefit with chronic treatment. 11 The prognosis is fairly good, with in hospital mortality rates being reported to range from 0-8%, and recovery of left ventricular function in the majority of patients. 9, 12
TCMP is difficult to distinguish from acute coronary syndrome on first presentation. Our patient had significant social stress. She presented with severedyspnoeaand was treated for COPD exacerbation. Elevation of cardiac enzymes and ECG changes lead to further evaluation and diagnosis of stress cardiomyopathy. This atypical presentation of TCMP showcases the importance ofutilisingthe routine noninvasive imaging and laboratory values to guide the diagnosis. Furthermore physicians need to maintain a high clinical suspicion for this syndrome.
|
Competing Interests None Declared Author Details Mujeeb Sheikh, M.D Cardiovascular Fellow, University of Toledo Medical Center, Toledo, OH, 43614 Steven Bruhl, M.D Cardiovascular Fellow, University of Toledo Medical Center, Toledo, OH, 43614 Jennifer L. Pham, B.S ,Fourth year medical student, Medical College of Ohio, Toledo, 43614 CORRESPONDENCE: Mujeeb Sheikh, M.D Cardiovascular Fellow, University of Toledo Medical Center, Toledo, OH, 43614 Email: skmujiba@yahoo.co.in |
References
1. Bybee, K.A., et al., Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med, 2004. 141(11): p. 858-65.
2. Bilan, A., et al., Dyspnea as a dominant clinical manifestation in a patient with takotsubo cardiomyopathy treated for chronic obstructive pulmonary disease and hyperthyroidism. Pol Arch Med Wewn, 2009. 119(4): p. 265-8.
3. Hernandez Lanchas, C., et al., [Tako-Tsubo syndrome in a patient with exacerbated bronchial asthma]. Rev Clin Esp, 2007. 207(6): p. 291-4.
4. Saeki, S., et al., [Case of bronchial asthma complicated with Takotsubo cardiomyopathy after frequent epinephrine medication]. Nihon Kokyuki Gakkai Zasshi, 2006. 44(10): p. 701-5.
5. Tsuchihashi, K., et al., Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol, 2001. 38(1): p. 11-8.
6. Ueyama, T., Emotional stress-induced Tako-tsubo cardiomyopathy: animal model and molecular mechanism. Ann N Y Acad Sci, 2004. 1018: p. 437-44.
7. Ueyama, T., et al., Catecholamines and estrogen are involved in the pathogenesis of emotional stress-induced acute heart attack. Ann N Y Acad Sci, 2008. 1148: p. 479-85.
8. Nef, H.M., et al., Mechanisms of stress (Takotsubo) cardiomyopathy. Nat Rev Cardiol. 7(4): p. 187-93.
9. Banihashemi, M.R. and I.A. Khan, Acute stress-induced cardiomyopathy: a brief observation. Int J Cardiol, 2009. 134(2): p. 273-7.
10. Cocco, G. and D. Chu, Stress-induced cardiomyopathy: A review. Eur J Intern Med, 2007. 18(5): p. 369-79.
11. Fazio, G., et al., Chronic pharmacological treatment in takotsubo cardiomyopathy. Int J Cardiol, 2008. 127(1): p. 121-3.
12. Regnante, R.A., et al., Clinical characteristics and four-year outcomes of patients in the Rhode Island Takotsubo Cardiomyopathy Registry. Am J Cardiol, 2009. 103(7): p. 1015-9.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.