



ISSN 1757-8515
Guttate psoriasis: A rare cause of diffuse rash.
Nauman Shahid, Muhammad Z Bawany, Ehsan Rafiq and Thomas Sodeman
Cite this article as: BJMP 2013;6(4):a627
|
|
Abstract Guttate psoriasis is a variant of psoriasis presenting as small, erythematous papules and plaques on the skin. Streptococcal infection is a common inciting factor. We are reporting a case of a 53 years old male, who presented with a generalized rash without any history of a recent infection and was diagnosed with guttate psoriasis on skin biopsy. |
Introduction
Psoriasis is a common skin disorder characterized by erythematous papules and plaque formation with silver scaling. Guttate psoriasis is much less common and many studies cite a prevalence of less than 30% among patients who have psoriasis. It refers to the acute appearance of multiple skin eruptions mostly in a patient with no preexisting psoriasis and less commonly in a patient with psoriasis. We report here a case of guttate psoriasis associated with a flare of psoriatic arthritis.



Case report
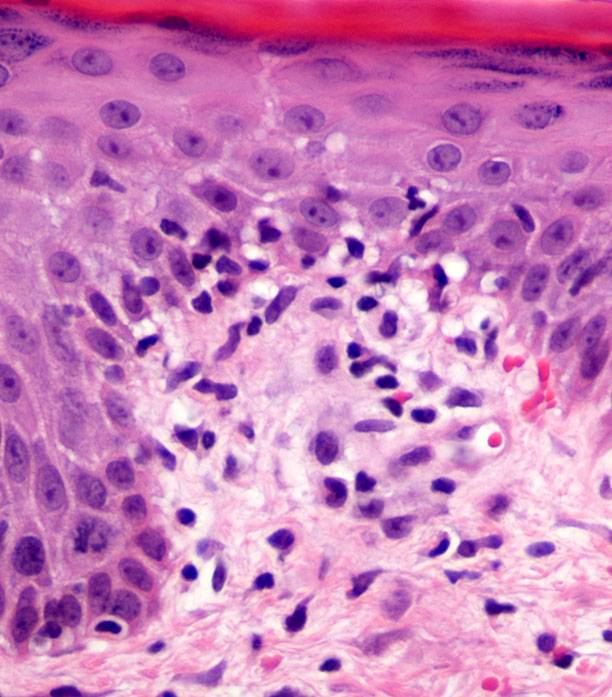
A 53 year old man presented with a generalized body rash and multiple joint pains. His symptoms started a week prior to presentation. The skin rash initially appeared on his back and flanks but gradually progressed to involve the thighs and arms. He had ‘sausage fingers’, bilateral knee and ankle swelling associated with pain and sporadic metatarsophalyngeal joint pain as manifestations of his arthritis. His past medical history included hypertension, diabetes mellitus, hyperlipidemia and psoriasis with psoriatic arthritis. He did not report any recent changes in his medication. The patient denied any history of fever, sore throat, weight loss, visual problems, dyspnea, cough, gastrointestinal complaints or recent travel. Physical examination revealed a diffuse, non-blanching, pruritic, maculopapular and maculopustular rash over the trunk. He also had a scaly and diffuse erythematic rash over the lower abdomen which was non-blanching and pruritic. Auspitz’s sign was positive. He had multiple painful joints including both knees, right wrist, left proximal interphalangeal joint, and both his ankles. Left knee arthrocentesis was done which revealed joint fluid consistent with inflammatory joint disease without any evidence of crystals. Laboratory tests, including red and white blood cell count, haemoglobin, cyclic citrullinated peptide antibody, rapid plasma regain, hepatitis panel, antinuclear antibody, rheumatoid factor, lyme markers and serum uric acid revealed no abnormalities. ASO titer level was positive at 196. An x-ray of his left hand showed periarticular erosive changes along the distal aspect of the proximal phalanx. A skin biopsy was performed which revealed mild spongiosis and a perivascular lymphoplastic infiltrate. A diagnosis of guttate psoriasis was made. He was started on prednisone, methotrexate and folic acid and discharged from hospital. He was followed up in the rheumatology clinic 2 weeks after discharge and his rash had improved.
Discussion
Unlike psoriasis, guttate psoriasis is a much lesser known entity. It refers to the acute appearance of multiple skin eruptions, mostly in patients with no preexisting psoriasis and less commonly in chronic plaque psoriasis (guttate flare of chronic plaque psoriasis).
The characteristic skin lesions of guttate psoriasis are less than 1 cm in diameter, hence the name guttate (drop like). The lesions look like a shower of red, scaly tear drops that have fallen down on the body mainly involving the trunk, arms, thighs and face. Guttate psoriasis should be differentiated from diabetic dermopathy, also called shin spots, which typically begin as dull red, scaly papules or plaques and later develop into bilateral asymmetrical circumscribed shallow pigmented scars and/or brownish macular lesions with a fine scale. In diabetic dermopathy the lesions usually are greater than 4 cm in size.
Diagnosis is usually made on clinical examination; however skin biopsy is helpful in difficult cases. Histopathologic findings of guttate psoriasis vary with the age of the lesion. Findings in early lesions may be nonspecific and may include mild acanthosis, papillary dermal oedema and lymphocyte-predominant dermal infiltrate. Mature lesions exhibit parakeratosis alternating with hyperkeratosis, epidermal acanthosis, Munro microabscesses and dermal perivascular infiltrate containg neutrophils, lymphocytes and macrophages.
Streptococcal infections are well known to precipitate guttate psoriasis,1 however there have been no significant improvements in patients who were given penicillin or erythromycin when compared to those who were not treated.2 Other known precipitants are physical and psychological trauma.
The exact pathophysiologic mechanism is undetermined. The disease is believed to result from an immune reaction triggered by a previous streptococcal infection in a genetically susceptible host. Recent research points toward chromosome 6 as HLA-Cw*0602 allele positive patients are more prone to develop the guttate form.
|
Competing Interests None declared Author Details NAUMAN SHAHID, MD; MUHAMMAD Z BAWANY, MD; EHSAN RAFIQ, MD; THOMAS SODEMAN, MD, FACP; Internal Medicine department, University of Toledo Medical Center, Toledo, Ohio. CORRESPONDENCE: Nauman Shahid, 200 High Park Avenue, Goshen, IN 46526. Email: nshahid1980@gmail.com |
References
- The role of streptococcal infection in initiation of Guttate Psoriasis ., Telfer ,Chalmer . Arch Dermatol 1992 Jan ;128 : 39-42 (Telfer NR, Chalmers RJG, Whale K, Colman G. The role of streptococcal infection in the initiation of guttate psoriasis. Arch Dermatol. 1992;128:39-42)
- Antistreptococcal treatment of guttate psoriasis: a controlled study.Dogan B, Karabudak O, Harmanyeri Y. Int J Dermatol. 2008 Sep;47(9):950-2.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.