



ISSN 1757-8515
Incidental adnexal mass at Caesarean section - the value of implementing a comprehensive consenting process
Ingrid Paredes, Marlon Pastrana, Alasdair Gordon and Toh Lick Tan
Cite this article as: BJMP 2011;4(1):a409
|
|
Abstract Informed consent is an important part of good medical practice. Potentially, added, but not essential procedures may only become obvious during surgery. Therefore comprehensive consent to cover such a situation is advisable. In this report, we illustrate the value of a standardised consent form which addresses the issue. |
Introduction
Examination of the ovaries at caesarean section is a normal practice as ovarian pathology may be found. The incidence of an adnexal mass found at caesarean section ranges from 1 in 123 1 to 329 2. Ovarian cysts rarely develop de novo in late pregnancy, but rather persist from early pregnancy. About 4 in 5 ovarian cysts detected in the first trimester scan resolve spontaneously. Also, 4 in 5 of ovarian cysts persisting into the second trimester will also be present in the post-natal period as complex cysts such as serous cystadenomas, mature cystic teratomas, endometriomas and mucinous cystadenomas 3. It therefore seems sensible to remove the ovarian cyst for histology at caesarean section rather than subject the woman to the anxiety of multiple investigations and/or another laparotomy, particularly when ovarian cystectomy during caesarean section does not appear to increase morbidity of the procedure 1.
We present a case of incidental ovarian cyst found at elective caesarean section to illustrate the value of a comprehensive consenting process.
Case Report
A 35 year-old para 1 + 0 healthy Polish woman was admitted for elective lower segment caesarean section (LSCS) at 39 + 4 weeks gestation in view of a previous caesarean section 2 years ago for failure to progress in the first stage of labour.She was booked in a neighbouring hospital for her antenatal care where she was counselled and consented for the procedure by her consultant. Her pregnancy was uncomplicated and routine pregnancy scans were unremarkable. Apart from drainage of a breast abscess 2 years ago, she had no medical history of note.
Written consent for elective LSCS was obtained by the junior doctor on duty before the consultant pre-operative ward round. However, the directorate’s standardised consent (figure 1) form was not used. The woman was therefore again counselled and written consent for elective LSCS obtained for the third time now including previously omitted additional procedures that might be performed during the course of the surgery.
At the uncomplicated LSCS under spinal anaesthetic, routine inspection of the uterus and adnexa revealed a 30 x 20 x 15 mm pedunculated firm pale mass attached to the left ovary suggestive of a fibroma. The findings were relayed to the woman, and confirmation of consent for the ovarian cystectomy was obtained. The abnormal ovarian mass was removed with conservation of the left ovary. Histology of the mass subsequently confirmed it to be an ovarian fibroma / fibrothecoma.
Discussion
The Royal College of Obstetricians and Gynaecologists (RCOG) recommend that clinicians should seek prior consent to treat any problem which might arise 4. Indeed, in its Consent Advice for caesarean section, it states that discussion of appropriate but not essential procedures, such as ovarian cystectomy at caesarean section, should take place before undertaking the procedure 5. This supports the position of the Department of Health which states that a procedure should not be performed merely because it is convenient, and that it is good practice where possible to seek the person’s consent to the proposed procedure well in advance, when there is time to respond to the person’s questions and provide adequate information 6.
In spite of the publication of the above guidelines well over a year ago, our case supports the belief that most obstetricians omit discussion and/or documentation of ovarian cystectomy at LSCS, and indeed other risks or additional procedures that may be relevant as showed in figure 1. This may be because the clinician is unaware of the recommendations, not familiar with the potential risks or findings at surgery, or that there is simply insufficient time to document comprehensively.
Our directorate has adopted the use of standardised consent forms for common procedures. These forms are available on our intranet which can be edited allowing clinicians to amend the risks and additional procedures as appropriate in each individual case. We believe the verified printed consent form offers legible and comprehensive documentation of the counselling process, as well as prompting clinicians to discuss key issues such as those recommended by the RCOG Consent Advice. We advocate the use of such standardised consent forms in improving the care of patients and supporting clinicians to deliver optimal services.
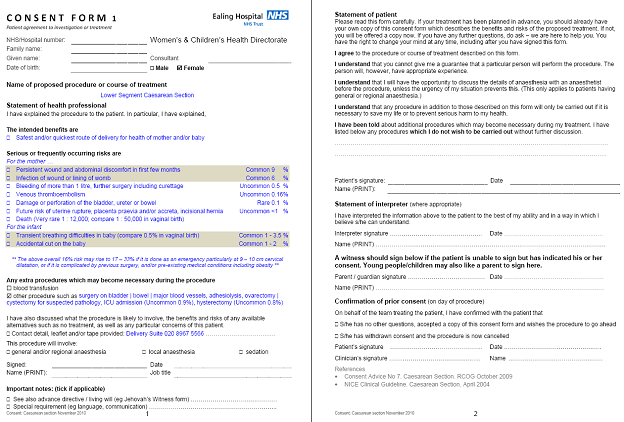
Figure 1. Standardised consent form for lower segment caesarean section
|
Competing Interests None declared Author Details INGRID PAREDES, BSc, Medical student, American University of the Caribbean School of Medicine, Florida, USA MARLON PASTRANA, BSc, Medical student, American University of the Caribbean School of Medicine, Florida, USA ALASDAIR GORDON, FRCS(Ed), MRCOG, Consultant obstetrician & gynaecologist, Department of Obstetrics and Gynaecology, Ealing Hospital, London, United Kingdom TOH LICK TAN, MRCOG, Consultant obstetrician & gynaecologist, Department of Obstetrics and Gynaecology, Ealing Hospital, London, United Kingdom CORRESPONDENCE: Mr TOH LICK TAN, Department of Obstetrics and Gynaecology,Ealing Hospital NHS Trust, Uxbridge Road, Southall UB1 3HW, United Kingdom Email: tohlick.tan@nhs.net |
References
- Dede M, Yenen MC, Yilmaz A, Goktolga U, Baser I. Treatment of incidental adnexal masses at caesarean section: a retrospective study. Int J Gynecol Cancer 2007; 17:3 39–341.
- Ulker V, Gedikbasi A, Numanoglu C, Saygı S, Aslan H, Gulkilik A. Incidental adnexal masses at caesarean section and review of the literature. J Obstet Gynaecol Research 2010; 36: 502-505.
- Condus A, Khalid A, Bourne T. Should we be examining the ovaries in pregnancy? Prevalence and natural history of adnexal pathology detected at first-trimester sonography. Ultrasound Obstet Gynecol 2004; 24: 62-66.
- RoyalCollegeof Obstetricians and Gynaecologists. Obtaining Valid Consent. Clinical Governance Advice No 6. December 2008
- RoyalCollegeof Obstetricians and Gynaecologists. Caesarean Section. Consent Advice No 7. October 2009
- Department of Health. Reference guide to consent for examination or treatment 2nd Edition. July 2009

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.