



ISSN 1757-8515
Post MTAS: A Survey of the first MMC Surgical Trainees in the Oxford Deanery
Khurram K Khan, Karen A Eley, Bettina Lieske, and Mr Bob Soin
Cite this article as: BJMP 2010;3(3):a333
|
|
Abstract Introduction: The nationwide implementation of ‘run-through’ training in 2007, based upon the new system of postgraduate medical training known as Modernising Medical Careers (MMC), was the subject of much debate as to the suitability of the selection process, and the feasibility of the new system itself. One year after the start of the new Speciality Training (ST) grade this study obtains the views of core surgical trainees in the Oxford Deanery. Methods: Forty-six trainees in ST1, ST2, Fixed Term Specialty Training Appointment (FTSTA) 1 and FTSTA2 posts completed questionnaires at three and nine months from appointments in August 2007. Results: Fifty two percent (n=24) of respondents were appointed to their training posts from Round 1a, with 67% (n=16) to ST1 or ST2 level. Despite 61% (n=28) having initially selected Oxford as their first choice deanery, 93% (n=43) now wished to remain in the region for further training, with 57% (n=27) of all trainees satisfied with their current position. At three months, only 9% (n=4) felt well informed regarding their surgical training, and 28% (n=13) well supported by their seniors; however, six months later these figures had risen to 64% (n=29) and 60% (n=24) respectively. Nearly half (43%, n=20) of surgical trainees had looked into moving abroad to train, and two thirds had considered leaving surgery all together. From August 2008, 70% (n=9) of ST2 trainees and 57% (n=4) of FTSTA2 trainees had obtained ST3 positions, with all but one in their desired surgical specialty.
Conclusion: Despite MMC’s difficult introduction into higher specialist training, the majority of trainees surveyed expressed encouraging levels of job satisfaction, felt increasingly well informed and well supported, and had successfully negotiated the initial stages of the ‘run-through’ track. With continuing debate surrounding how MMC-based surgical training will work within the confines of National Health Service (NHS) provision and the European Working Time Directive, we present the opinions and outcomes of the first cohort of ‘run-through’ surgical trainees.
Keywords: Surgical training, MMC, ST trainee, FTSTA trainee |
Introduction
The Department of Health’s Modernising Medical Careers (MMC) has been uniformly implemented into specialty training across the United Kingdom (UK). This began with the controversial and subsequently redundant Medical Training Application System (MTAS) selection process in Spring 2007, and ended with the first MMC specialty training posts commencing in August 2007. During the application process itself one preliminary study reported that 85% of candidates demonstrated decreased levels of enjoyment in their work, and 43% caring less about patient care.1 The emergency introduction of the ‘golden ticket’ Round 1b guaranteed interview - though arguably justified in the face of a flawed application system - was a cause of further discontent and division amongst junior trainees and the consultants responsible for appointing them.
For surgical training in particular, the advent of the MMC initiative combined with the European Working Time Directive (EWTD) represents an estimated 50% reduction in the amount of specialist training hours when compared to the previous system.2 This has raised concerns not only from current consultants, but also from the already increased number of surgical trainees having to share the same caseload. A previous survey of Ear, Nose, and Throat senior house officers reported 71% were willing to opt out of the EWTD to safeguard their training and patient care.3
In the Oxford Deanery the selection process of shortlisted surgical trainees in Rounds 1a and 1b consisted of six stations assessing curriculum vitae, portfolio, clinical examination, data interpretation, and pre- and post-operative management (totalling one hour). Candidates were offered generic or specialty themed Core Training (CT) posts at Speciality Training (ST) 1 or 2, or Fixed Term Speciality Training Appointments (FTSTA) 1 or 2, depending upon the candidate’s ranking at interview (plus application form for Round 1a) irrespective of speciality preference. Following acceptance, individual appointments were made based on candidates ranking job preferences. Round 2 appointments were made at a local level via traditional selection methods. The most recent information from the deanery states that those trainees who received an offer of run-through training in the region will be guaranteed an interview for an ST3 post in surgery, however individual specialty preference and job allocation will be determined by re-ranking based on continuous appraisal during the core surgical training years, further Higher Specialist Training interviews, and training numbers available.
The media coverage that surrounded MTAS clearly highlighted the dissatisfaction amongst trainees and consultants leading up to and during the application process,4, 5 but no study has yet assessed the views of surgical trainees following the start of their new MMC-based training posts. This survey aimed to obtain the views and outcomes of core surgical trainees in the Oxford Deanery.
Methods
At three and nine months following the commencement of speciality training posts, questionnaires were distributed to junior surgeons (CT 1-2) in the Oxford Deanery School of Surgery. Questions were structured to obtain information about level of experience and qualification(s), current and desired surgical speciality, job satisfaction, attitudes towards ‘run-through’ training and levels of support. In the Oxford Deanery there were 40 appointments at CT1 (18 ST1 and 22 FTSTA), and 29 at CT2 (17 ST2 and 12 FTSTA) in August 2007. Data were expressed as the mean ± standard deviation (SD). Statistical comparison was performed using Mann-Whitney’s U test, with the significance level at p<0.05.
Results
The questionnaire was completed by a total of 46 and 45 surgical trainees at three and nine months respectively. At the three-month time point this represented 67% of all trainees in the Oxford Deanery School of Surgery (male: female, 33:13) and included 11 at ST1, 16 at ST2, 11 at FTSTA1, and 8 at FTSTA2. Of these 52% (n=24) had obtained their post via Round 1a, 41% (n=19) via Round 1b, and 7% (n=3) via Round 2. At both CT1 (ST1 & FTSTA1) and CT2 (ST2 & FTSTA2), trainees were on average 3.7 ± 1.9 years post graduation (from time surveyed; CT1 range 1-11 years, CT2 range 3-8 years); 16% (n=7) of all trainees had previously studied Medicine at Oxford University, and 93% had studied medicine in the UK. (Figures 1a, b). Most popular desired specialties at three and nine months are displayed in figure 2. Of the 46 respondents, all had worked in the speciality of their career choice during the course of the year.
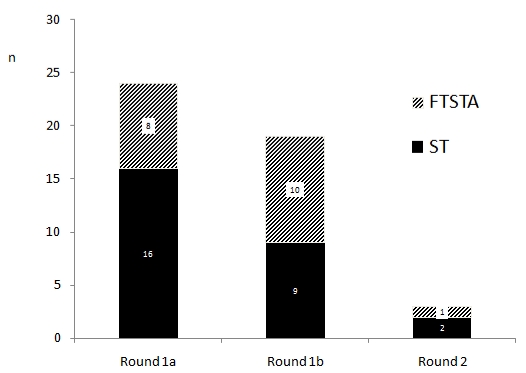
Figure 1a. Number of trainees selected in each MTAS round
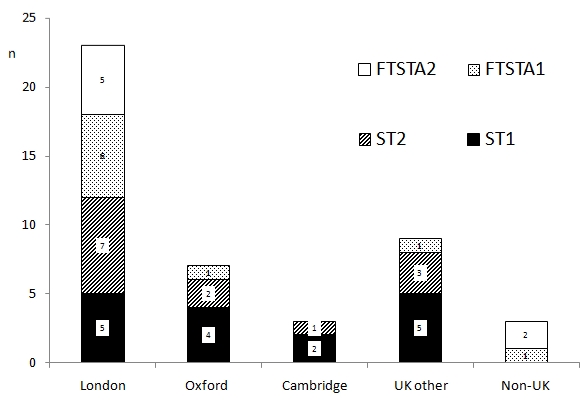
Figure 1b. Surgical trainee graduating medical school distribution
At time of appointment, 52% of trainees had completed the Membership to the Royal College of Surgeons (MRCS) exams, and 35% (n=16) of all trainees had completed a higher degree. (Figure 3). Furthermore, 22% (n=10) felt that there should be a further exam in addition to the MRCS to rank candidates for appointment to higher specialist training (ST3 onwards), with half of this number having already obtained their MRCS.
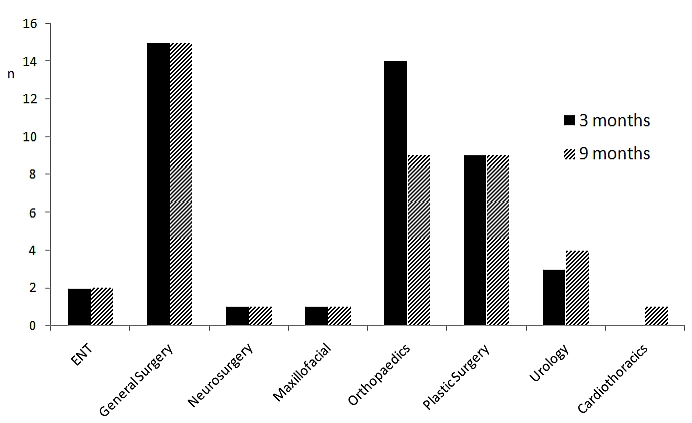
Figure 2. Desired surgical specialty at three and nine months
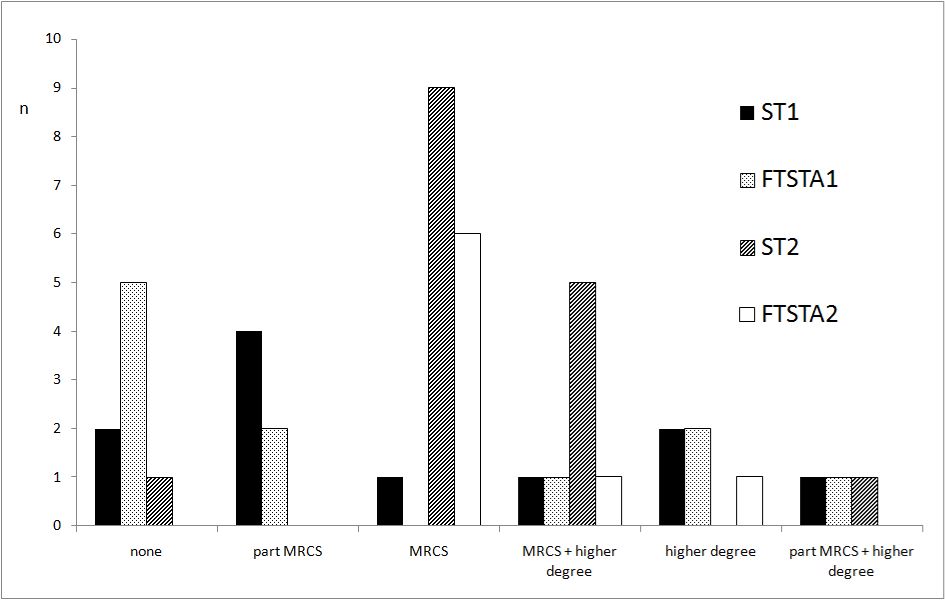
Figure 3. Trainee postgraduate qualifications at time of appointment
Those who had been allocated to ‘run-through’ ST posts were more satisfied with the concept of run-through training than those in FTSTA posts (where scores were assigned on a scale from 1 - very unsatisfied, to 5 - very satisfied), with the mean score at three months for ST trainees 4.1 ± 1.4, and FTSTA trainees 2.0 ± 1.4 (p<0.01), and at nine months 3.7 ± 1.1 for ST trainees versus 2.1 ± 1.1 for FTSTA trainees (p<0.01). Job satisfaction levels between these two groups of trainees were similar: at three months, mean score 3.5 ± 1.3 in ST posts versus 4.1 ± 0.8 in FTSTA posts (p>0.05), and at nine months, mean score 3.5 ± 1.0 in ST posts versus 3.2 ± 1.3 in FTSTA posts (p>0.05). In addition, a similar comparison between ST and FTSTA trainees was found when determining if trainees had thought about leaving surgery. On a scale where a score of 1 – never thought of leaving surgery to 5 – very frequently thought of leaving surgery, the mean score at three months was 2.3 ± 1.4 for ST trainees versus 3.0 ± 1.6 for FTSTA trainees (p>0.05), and at nine months 2.2 ± 1.4 for ST trainees versus 2.9 ± 1.5 for FTSTA trainees (p>0.05). (Figures 4a, b).
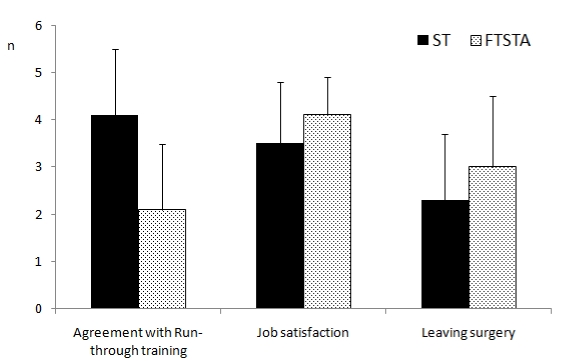
Figure 4a. Trainee attitudes at three months
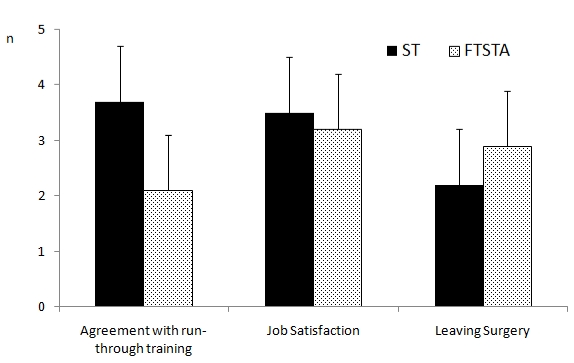
Figure 4b. Trainee attitudes at nine months
In fact, 43% (n=20) of all trainees surveyed reported having enquired about surgical training in another country, with 4% (n=2, both UK Medical School graduates) stating that if unsuccessful in securing a training post in their desired specialty for August 2008, they would move abroad to train.
At three months, 9% (n=4) of all trainees felt well-informed about what will happen in the future regarding their training, with 20% (n=9, ST to FTSTA ratio 2:7) responding that had they been better informed prior to August 2007, then they would not have accepted their current post, and 28% (n=13) felt well-supported by their senior colleagues with regard to their future training. However at nine months from appointment, 69% (n=29) of all trainees felt well informed, and nearly two thirds well supported by their seniors (n=27). (Figure 5). Ninety three percent (n=43) of applicants wished to remain in the region for their future training, with 61% (n=28) having initially selected Oxford as their first choice deanery.
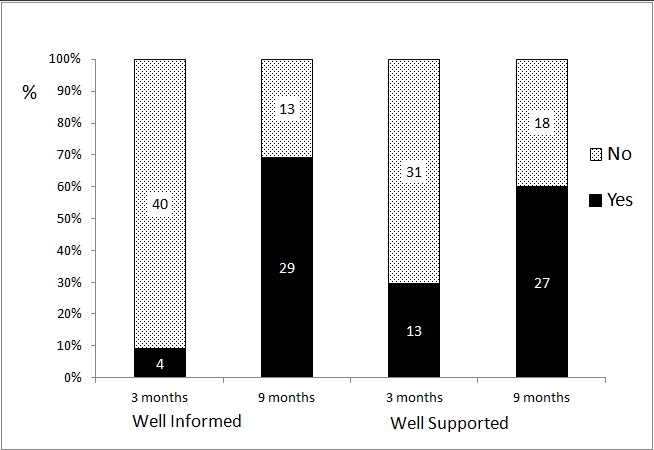
Figure 5. How well informed and supported trainees felt at three and nine months
The majority of both ST2 (85%, n=11) and FTSTA2 (71%, n=5) trainees secured ST3 posts from August 2008, mainly within the Oxford Deanery, and all within their desired surgical specialty. All ST1 (n=16) trainees successfully moved into ST2 posts, and the majority of FTSTA1 (78%, n=7) trainees secured CT positions. (Table 1).
| Grade (n) | August 2008 Post (n) |
| ST1 (16) | ST2 (16) |
| FTSTA1 (9) | CT1 (3) CT2 (4) FTSTA (2) |
| ST2 (13) | ST3 (11) Research Fellow (1) GP Trainee (1) |
| FTSTA2 (7) | ST3 (5) ST1 Radiology (1) CT2 (1) |
Table 1. ST2 and FTSTA2 trainee outcomes from August 2008
Discussion
MMC has and will have profound implications on the way junior doctors will henceforth be trained in the National Health Service (NHS). Last year’s difficult introduction into specialist training, has for obvious reasons, directly affected the perceptions of trainees having to negotiate their careers through the ‘transition’ period.1, 6 This survey provides an interesting insight into the demographics, current viewpoints, and outcomes of the first cohort of MMC surgical trainees in the Oxford Deanery.
Just over half of all trainees in the survey were appointed after Round 1a (52%, n=24) of which two thirds (n=16) were to ST posts: a further 41% (n=19) were appointed after Round 1b, of which roughly half (n=9) were to ST posts. This highlights the large number of very good surgical trainees that may have been left unemployed had MTAS interim measures not been introduced to permit all candidates the opportunity of at least one interview, and that in the Oxford Deanery at least, candidates were given an equal chance of obtaining a ‘run-through’ post between the two rounds. Despite MMC person specifications at the time of application stating that MRCS was not an absolute requirement for entry at ST1-2, 52% (n=24) had completed their MRCS, with a further 20% (n=9) having completed at least Part I or more.
Overall job satisfaction levels were good amongst all trainees (mean score 3.7 ± 1.1), with 57% (n=26) still agreeing with the concept of ‘run-through’ training, and hence MMC. This view is maintained despite the problems associated with last years application process, and in the face of an uncertain future. However, nearly half (43%, n=20) of trainees had enquired about training abroad, with several committed to leaving the UK next year if unable to obtain their desired surgical specialty. With the average cost to train a UK medical graduate being at least £150,000,7 and the amount of dedication and effort needed to embark on a surgical career thereafter, care must be taken to improve morale amongst junior surgeons, and to provide adequate and timely information. Encouragingly, between the two time points surveyed, levels of senior support and how well informed surgical trainees felt with regards to their training, increased from 28% to 60% and from 9% to 69% respectively; this may be secondary to a combination of extensive effort from the Deanery and the Royal College of Surgery to address trainee concerns.
The realistic future of those in FTSTA posts is cause for concern. This is highlighted in the recently released Tooke Report, in which it is stated they are “in danger of becoming the next ‘lost tribe’, the very category of doctor MMC sought to avoid”, but at the same time that “core [training] should not repeat the errors of previous SHO arrangements and must be time limited”.6 Those in FTSTA posts face higher levels of future uncertainty than their ST colleagues, and this was reflected in reporting a higher likelihood of consideration of alternative careers outside of surgery. However, both groups of trainees demonstrated statistically similar scores when questioned about how frequently they had thought of leaving surgery (2.3 ± 1.4 for ST trainees versus 3.0 ± 1.6 for FTSTA trainees, p>0.05), and 71% of FTSTA2 trainees surveyed within the Oxford Deanery went on to secure ST3 level posts in their desired specialty.
The authors note the limitations inherent to surveys in general namely the validity and reliability of responses obtained to questions asked due to the self-report method of data collection, the questionnaire entirely constructing the information obtained, and that the data does not capture the decision process that produced the observed outcomes and is therefore descriptive rather than explanatory. More specifically, the authors note that candidates who were successful in obtaining an ST3 post may have been more likely to complete the questionnaire, leading to further potential bias.
Conclusion
MMC has crossed the threshold into higher specialist training, and the first cohorts of MMC surgeons are being trained. The majority of trainees we surveyed expressed good levels of job satisfaction, had successfully negotiated their first year of the new system, and encouragingly felt better informed and supported over the course of their first year. However, this study encompassed a proportion of surgical trainees in one Deanery in the UK, and further study on a larger scale at regular time intervals is certainly warranted. Consequent to the problems of MMC’s difficult introduction, positive steps included travelling tours by the Royal College of Surgeons (England), and in the Oxford Deanery at least, regional meetings to address concerns and expectations, and outline the realistic future for surgical trainees. Perhaps a key determinant of sustainability for MMC in surgery in 2008 and beyond will be the relative success of the Intercollegiate Surgical Curriculum Programme (ISCP), and this represents a significant area for further study.
|
Competing Interests None declared Author Details KHURRAM K KHAN, MRCS, BSc. ST3 trainee, Department of Plastic Surgery, Salisbury District Hospital. KAREN A ELEY, MBChB, MRCS(Ed), PGCTLCP, FHEA, MSc. Research Fellow & Doctoral Candidate, Oxford Radcliffe Hospitals & University of Oxford. BETTINA LIESKE, MRCS. Specialist Registrar, Department of General Surgery, Royal Berkshire Hospital. BOB SOIN, MA, MBBChir(Hons), FRCS(Gen Surg), MD. Consultant General Surgeon, Department of General Surgery, Heatherwood & Wexham Park Hospitals. CORRESPONDENCE: KHURRAM K KHAN, MRCS, BSc. ST3 trainee, Department of Plastic Surgery, Salisbury District Hospital Email: drkkhan@gmail.com |
References
1. Lydall GJ, Malik A, Bhugra D. MTAS: Mental health of applicants seems to be deteriorating. Br Med J 2007; 334(7608):1335.
2. Devey L. Will modernised medical careers produce a better surgeon? Br Med J 2005; 331:1346.
3. Anwar M, Irfan S, Daly N, Amen F. EWTD has negative impact on training for surgeons. Br Med J 2005; 331(7530):1476.
4. Brown MJ. Raging against MTAS (UK Medical Training Application Service). Br Med J 2007; 334(7593):549.
5. Coombes R. How specialist training reform sparked crisis of confidence. Br Med J 2007; 334(7592):508-9.
6. Tooke J. Aspiring to Excellence. Final Report of the Independant Inquiry into Modernising Medical Careers. In Inquiry M, ed. London: Aldridge Press, 2008.
7. Jefferis T. Selection for specialist training: what can we learn from other countries? Br Med J 2007; 334:1302-1304.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.