



ISSN 1757-8515
Coronary vasospasm in a patient with respiratory failure: A case report and a brief review.
Mujeeb Sheikh, Satjit Adlakha, Steven Bruhl and Shaffi Kanjwal
Cite this article as: BJMP 2010;3(3):a330
|
|
Abstract Coronary vasospasm is an episodic, augmented, contractile response of coronary smooth muscles to variety of stimuli in the setting of established endothelial dysfunction. Various physiological including cold, stress and pathological factors like smoking, and ethanol have been well known to precipitate vasospasm. Despite these omnipresent factors, coronary vasospasm has become infrequent, in particular due to judicious use of medication including calcium channel blockers, statins and aspirin. We present a case of severe coronary vasospasm resulting in haemodynamic instability, in a patient with hypoxic respiratory failure. Recurrent symptomatic episodes required coronary angiography for the diagnosis and patient was successfully treated with calcium channel blockers. Keywords: Myocardial infarction; respiratory failure; coronary vasospasm; Diltiazem |
Introduction
Myocardial ischemia from coronary artery vasospasm can lead to variety of presentation including stable angina, unstable angina, myocardial infarction and sudden death 1. Although, pathognomic clinical scenario includes symptom of chest pain, transient ST-segment elevation on the electrocardiogram(ECG), and vasospasm on a coronary angiography, atypical presentations have also been reported 2. Various known physiological factors including stress, cold, hyperventilation and pharmacological agents including cocaine, ethanol, 5-Fluouracil, and triptans can precipitate a vasospastic attack. 3-7.We report a case of ST-segment elevation due to right coronary artery vasospasm, in patient with hypoxic respiratory failure, and successful treatment with calcium channel blockers.
Case description
A 56 year old man was admitted for the repair of a large ventral incisional hernia. The patient had a prior history of morbid obesity, chronic obstructive pulmonary disease (COPD), hypertension and cigarette smoking. The postoperative course was complicated by bilateral pneumonia leading to respiratory failure requiring mechanical ventilation. An electrocardiogram at the time of intubation was essentially normal. Aside from bilateral rhonchi and crackles on lung auscultation, the rest of the physical examination findings were unremarkable. Arterial blood gases at the time of intubation demonstrated PH 7.33, PO2 58 mmHg, PCO2 65 mmHg, HCO3ˉ 20 mmol/L, suggestive of hypoxia and concomitant respiratory acidosis. Baseline laboratory studies including cardiac enzymes were within normal limits. The patient was treated with intravenous vancomycin for methicillin-resistant staphylococcus pneumonia. On postoperative day 4, the patient had recurrent episodes of transient ST-elevation on a bedside monitor (Fig.1).

Figure 1
These episodes lasted for 3-5 minutes and were associated with significant bradycardia and hypotension. In view of recurrent episodes, haemodynamic instability, and underlying risk factors of coronary artery disease, cardiac catheterization was performed. Coronary angiography revealed a 90% stenosis with haziness of the mid-right coronary artery without any other significant epicardial disease. An intravascular ultrasound (IVUS) was performed and was followed by administration of 100 mcg of intracoronary nitroglycerin; the lesion was reduced to almost 20%. (Fig.2).
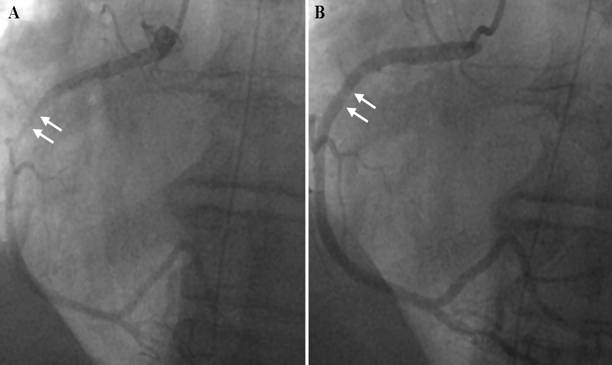
Figure 2
The diagnosis of prinzmetals angina was made, based on clinical course and angiographic results and prompt therapy with diltiazem (120 mg per day) was initiated. The patient had no further recurrences of similar episodes during the hospitalization and on follow up at 3 months.
Discussion
The prevalence of vasospasm has been reported to be higher in Japanese and Korean population as compared to the western population. A recent multi-institute survey in Japan documented spasm in 921 (40.9%) of the 2251 consecutive patients who underwent angiography for angina pectoris 8. In contrast to the traditional risk factors for atherosclerotic coronary artery disease, the incidence of smoking, age and dyslipdaemia has been reported higher in patients with coronary vasospasm 9. Endothelial dysfunction is now considered to the major inciting factor in the pathogenesis of the vasospasm 10. Vasospastic angina (VA) with normal coronary arteries on the angiography, impaired endothelial-dependent and endothelial-independent vasodilatation has been frequently observed in these patients. Vascular tone is normally regulated by production of vasodilator factors like nitrous oxide (NO), prostacyclin and vasoconstricting agents like endthelin-1. In the presence of dysfunctional endothelium the agents that normally cause vasodilatation lead to paradoxical vasoconstriction, due to direct muscle stimulation, like acetylcholine.
Stress, whether physical or mental stress has been shown to induce coronary vasospasm and myocardial ischemia. In a study by Kim et al, coronary spastic angina was diagnosed in 292 patients out of 672 coronary spasm provocation tests. Among 292 patients, 21 (7.2%) had myocardial infarction and 14 out of these 21 had experienced severe emotional stress before the event 11. Recently, animal studies have also shown that high circulatory level of stress hormones (cortisol) exaggerate coronary vasoconstriction through Rho-Kinase activation 12. Hypoxia has been seen in animal models to predispose to vasospasm through superoxide formation, which leads to loss of vasodilator function of NO.(13)
The ECG changes that occur during attack include ST-segment elevation, and or peaking of T wave from total or subtotal coronary occlusion 1. In some cases spasm can involve more than one artery leading to ST-segment elevation in multiple leads, which may predispose to ventricular tachycardia or fibrillation 14. Coronary spasm is diagnosed by angiography, and spasm can occur at the site of atherosclerotic plaque or in normal segment of the coronary artery. In patients with equivocal diagnosis, provocative tests including administration of acetylcholine, hyperventilation to induce spasm may be required for the diagnosis.
Current first line therapy involves used of calcium channel blockers (CCB) alone or in combination with long acting nitrates. In a study comparing the effect of long acting nitrates (Isosorbide dinitrate 40mg/day) versus calcium channel blockers (amlodipine 5mg/day or long acting nifedipine 20mg/day) on coronary endothelium and vasoconstriction between patients with normal or minimally diseased coronary artery, treatment with long acting nitrates was associated with less favourable effects on coronary endothelial functions 15. Sudden withdrawal of CCB in patients with known vasospasm can lead to rebound of symptoms and may prove dangerous. In patients with refractory symptoms alpha-blockers, nicorandil have been used. Although beta blockers are believed to enhance vasospasm, Betaxalol, a selective beta-1 blocker, has been found to be effective in the treatment of variant angina due to its vasorelaxing effects 16. In addition, elimination of or control of all other risk factors or precipitants is very important for successful treatment. In drug refractory cases the percutaneous coronary intervention or coronary artery bypass graft has been performed for the ischemia relief 17.
Our patient had multiple precipitating factors for vasospasm. Endothelial dysfunction from severe physical illness and sepsis could have precipitated the VA. Furthermore, hypoxia from respiratory failure could have also been an inciting agent and cannot be ruled out. It is worth mentioning that intensive care unit patients frequently have coexistence of both the underlying risk factors and the precipitating factors for vasospasm, yet VA as a clinical syndrome is uncommonly seen or reported.
Conclusion:
The clinician needs to be aware of coronary artery vasospasm as it can pose a serious medical threat. Early diagnosis and treatment may result in improved outcomes from vasospastic angina.
|
Competing Interests None Declared Author Details MUJEEB SHEIKH MD Assistant Professor, Department of Internal Medicine, 3000, Arlington Avenue, University of Toledo Medical Center, Toledo, Ohio SATJIT ADLAKHA, D.O Cardiology fellow 3000, Arlington Avenue, University of Toledo Medical Center, Ohio, USA STEVEN BRUHL M.D Cardiology fellow 3000, Arlington Avenue, University of Toledo Medical Center, Ohio, USA SHAFFI KANJWAL M.D, 3000, Arlington Avenue Department of Pulmonary and Critical Care, University of Toledo Medical Center, Toledo, Ohio, USA CORRESPONDENCE: Mujeeb Sheikh, Assistant Professor, Department of Internal Medicine 3000, Arlington Avenue, University of Toledo Medical Center, Toledo, Ohio. Email: skmujiba@yahoo.co.in |
References
1. Nakamura M, Takeshita A, Nose Y. Clinical characteristics associated with myocardial infarction, arrhythmias, and sudden death in patients with vasospastic angina. Circulation. 1987 Jun;75(6):1110-6.
2. Xiang DC, He JX, Hong CJ, Qiu J, Ma J, Gong ZH, et al. [Clinical features of patients with atypical coronary artery spasm]. Zhonghua Xin Xue Guan Bing Za Zhi. 2006 Mar;34(3):227-30.
3. Keller KB, Lemberg L. The cocaine-abused heart. Am J Crit Care. 2003 Nov;12(6):562-6.
4. Ando H, Abe H, Hisanou R. Ethanol-induced myocardial ischemia: close relation between blood acetaldehyde level and myocardial ischemia. Clin Cardiol. 1993 May;16(5):443-6.
5. Bathina JD, Yusuf SW. 5-Fluorouracil-induced coronary vasospasm. J Cardiovasc Med (Hagerstown). 2009 Jun 25.
6. Shimizu M, Hata K, Takaoka H, Kanazawa K, Shinke T, Matsumoto H, et al. Sumatriptan provokes coronary artery spasm in patients with variant angina: possible involvement of serotonin 1B receptor. Int J Cardiol. 2007 Jan 8;114(2):188-94.
7. Teragawa H, Kato M, Yamagata T, Matsuura H, Kajiyama G. The preventive effect of magnesium on coronary spasm in patients with vasospastic angina. Chest. 2000 Dec;118(6):1690-5.
8. Yasue H, Sasayama S, kikuchi K, Okumura K, Matsubara T, Miwa K. The study on the role of coronary spasm in ischemic heart disease. Osaka:National Cardiovascular Center; 2000; Osaka:National Cardiovascular Center. Osaka: Annual report of the research on cardiovascular diseases; 2000. p. 96-7.
9. Sugiishi M, Takatsu F. Cigarette smoking is a major risk factor for coronary spasm. Circulation. 1993 Jan;87(1):76-9.
10. Yasue H, Nakagawa H, Itoh T, Harada E, Mizuno Y. Coronary artery spasm--clinical features, diagnosis, pathogenesis, and treatment. J Cardiol. 2008 Feb;51(1):2-17.
11. Kim PJ, Seung KB, Kim DB, Her SH, Shin DI, Jang SW, et al. Clinical and angiographic characteristics of acute myocardial infarction caused by vasospastic angina without organic coronary heart disease. Circ J. 2007 Sep;71(9):1383-6.
12. Hizume T, Morikawa K, Takaki A, Abe K, Sunagawa K, Amano M, et al. Sustained elevation of serum cortisol level causes sensitization of coronary vasoconstricting responses in pigs in vivo: a possible link between stress and coronary vasospasm. Circ Res. 2006 Sep 29;99(7):767-75.
13. Zou MH, Bachschmid M. Hypoxia-reoxygenation triggers coronary vasospasm in isolated bovine coronary arteries via tyrosine nitration of prostacyclin synthase. J Exp Med. 1999 Jul 5;190(1):135-9.
14. Nishizaki M, Arita M, Sakurada H, Suzuki M, Ashikaga T, Yamawake N, et al. Polymorphic ventricular tachycardia in patients with vasospastic angina--clinical and electrocardiographic characteristics and long-term outcome. Jpn Circ J. 2001 Jun;65(6):519-25.
15. Ninomiya Y, Hamasaki S, Saihara K, Ishida S, Kataoka T, Ogawa M, et al. Comparison of effect between nitrates and calcium channel antagonist on vascular function in patients with normal or mildly diseased coronary arteries. Heart Vessels. 2008 Mar;23(2):83-90.
16. Suzuki J, Watanabe K, Tsuruoka T, Sueda S, Funada J, Kitakaze M, et al. Beneficial effects of betaxolol, a selective antagonist of beta-1 adrenoceptors, on exercise-induced myocardial ischemia in patients with coronary vasospasm. Int J Cardiol. 2003 Oct;91(2-3):227-32.
17. Sugimoto A, Morino Y, Ikari Y. Stent implantation for diffuse and multiple coronary spasm in a patient with variant angina refractory to optimal medical therapy. J Invasive Cardiol. 2007 Nov;19(11):E320-3.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.