



ISSN 1757-8515
Pictorial essay III: Permanent pacemakers and Oesophageal Doppler probe
Krishnan Melarkode and M Y Latoo
Cite this article as: BJMP 2009: 2(3) 66-68
|
INTRODUCTION
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the heart, lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In the previous two editions of pictorial essay, we have discussed the normal and abnormal positions of tracheal tube, nasogastric tube and central venous catheters on chest radiographs. In this edition, we shall look into permanent pacemakers and oesophageal Doppler probe on chest radiographs. PERMANENT PACEMAKERS A permanent pacemaker (artificial pacemaker) is a small battery powered medical device that is placed subcutaneously in the chest or abdomen to help control abnormal heart rhythms. They are inserted for different types of conduction problems (eg: sinus node disease, atrio-ventricular block, tachyarrhythmia etc). Permanent cardiac pacemakers consist of two parts:1. Pulse generator (power unit) – usually felt like a “bar of soap” beneath the skin and2. Pacing electrode leads The pulse generator consists of an energy source (battery) and all electrical circuits necessary for pacing and sensory function. The electrode is the exposed metal tip in contact with the myocardium. The electrode is connected to the pulse generator via an insulated wire (lead). Details regarding classification and functioning of a pacemaker is beyond the scope of this article and can be found in any standard cardiology text book. We shall now discuss what to look for in a chest radiograph in a patient with permanent cardiac pacemaker. Chest radiograph is one of the important diagnostic tools used in the evaluation of a patient with a pacemaker. However, it is not complete by itself and in addition to reviewing chest radiographs, it is important to take a detailed history from the patient, do a thorough examination of the patient, review all necessary case notes and analyse the ECG. If required, a cardiology opinion should be sought. Important points to note on a chest radiograph are: 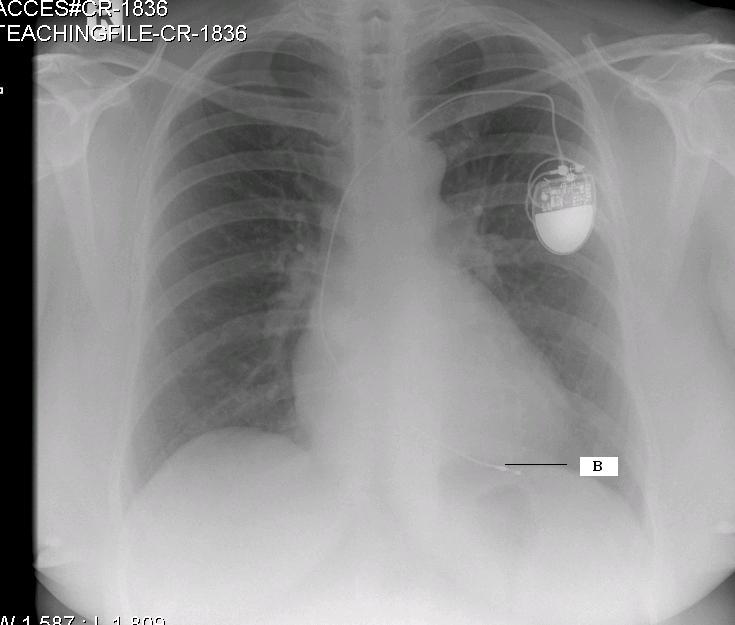 Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3.
Fig 1 (CR 1836): Single chamber pacemaker There is a single chamber permanent pacemaker. The pacing wire passes via the left subclavian vein and tricuspid valve. Its electrode is situated in the apex of the right ventricle (labelled B) and is anchored in the trabeculae by some sort of hook 2,3. 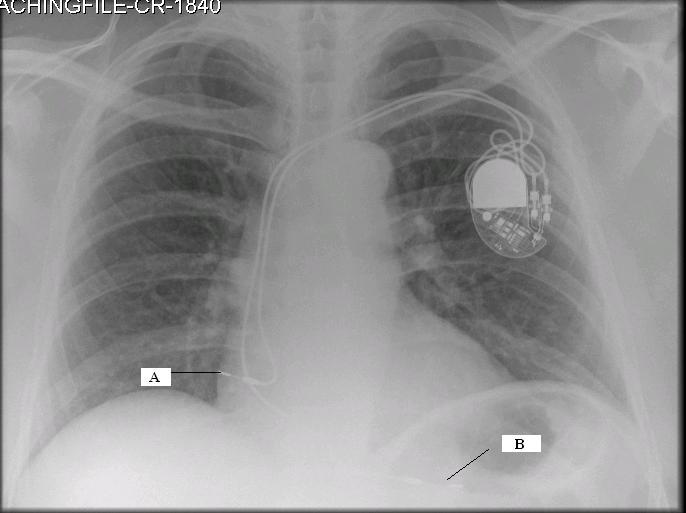 Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835).
Fig 2 (CR-1840): Dual chamber pacemaker with displaced right atrial lead This chest radiograph shows a dual chamber pacemaker. There are two pacing leads – one in the right atrium and another in the apex of the right ventricle (labelled B). The right atrial lead is displaced (labelled A). Note the normal position of the right atrial lead in Fig 3 (CR 1835). 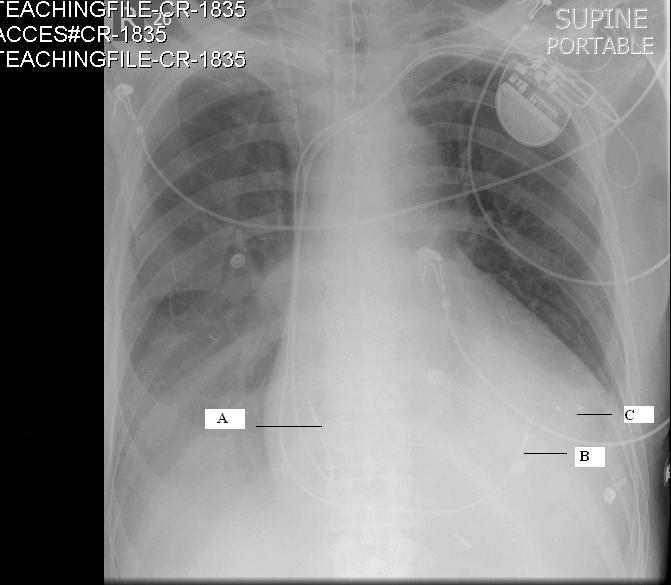 Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values.
Fig: 3 (CR-1835) Biventricular pacemaker This radiograph shows the presence of a permanent biventricular pacemaker and its pacing leads passing through the left subclavian vein. There are three pacemaker leads – the 1st lead is situated in the right atrium (J shaped wire- labelled A), the 2nd lead is in the apex of the right ventricle (labelled B) and the 3rd lead in the lateral wall of the left ventricle (labelled C). Pacing the apex of the right ventricle and the lateral wall of the left ventricle simultaneously improves the co-ordination of the left ventricular contraction 2. Biventricular pacemakers are used as cardiac synchronisation therapy in patients with cardiac failure. OESOPHAGEAL DOPPLER PROBE The oesophageal Doppler is a non-invasive cardiac monitoring device useful in critically ill patients in the Intensive care unit. The probe of the oesophageal Doppler monitor is inserted into the oesophagus and the ideal position for its tip is at the level between the 5th and 6th thoracic vertebra because at this level the descending aorta is adjacent and parallel to the oesophagus 4. The probe contains a crystal which produces continuous ultrasound wave of 4 MHz. The lubricated probe is inserted down till the 40 cm mark, rotated and slowly pulled back while listening to a good audible signal. It is essential that the probe is located in the correct position to record accurate values. 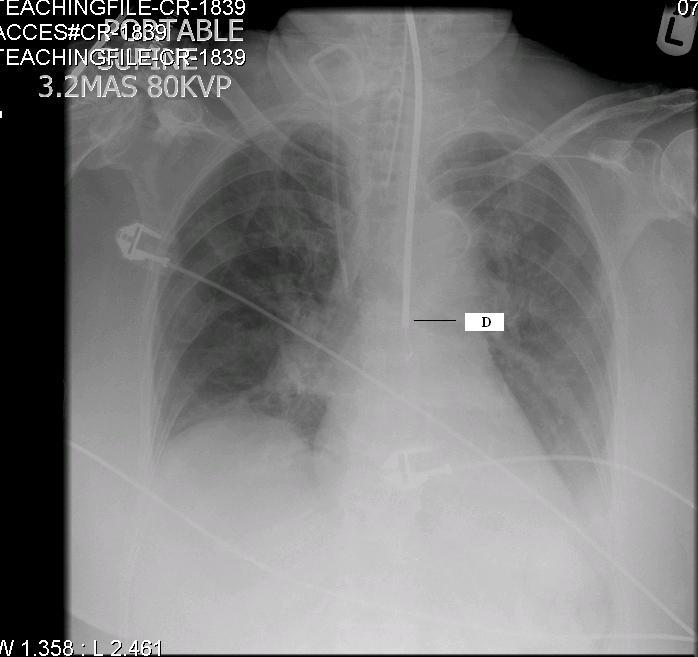 Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
Fig 4 (CR 1839) shows the normal position of the oesophageal Doppler probe (labelled D). Also, note the normal position of the tracheal tube and right Internal Jugular Vein catheter [discussed in detail in the previous two editions of pictorial essay 5,6].
| First of all, check whether you are looking at the correct chest radiograph (not another patient’s chest radiograph)Identify the pulse generatorIdentify whether it is a single chamber, dual chamber or biventricular pacemaker. This can be done by counting the number and tracing the pacing leads to the cardiac chamber it is implantedCheck that the pacing leads are not dislodgedCheck that the pacemaker leads are intact and not brokenFinally, look for any abnormal shadowing behind the pacemaker as these can be easily missed1 |
CONCLUSION Valuable information can thus be obtained on reviewing chest radiographs. Our aim is to provide a quick overview on what to look for in pacemakers and oesophageal Doppler probe on chest radiographs. It is by no means an exhaustive description. This article is for the benefit of medical students, junior doctors in training, nurses and paramedical teams who would be involved in the care of critically ill patients. Self Assessment Multiple Choice questions (only one option is correct):1. The wires of permanent pacemakers are usually inserted viaA. Femoral veinB. Basilic veinC. Subclavian veinD. Subclavian artery 2. A chest radiograph is not useful in one of the followingA. To detect intact pacemaker wiresB. To indicate whether a pacemaker is working optimallyC. To detect whether pacemaker wires are dislodgedD. To identify a single chamber or dual chamber pacemaker Answers:1. C2. B
|
Acknowledgements We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs Competing Interests None Declared Author Details <p>DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Great Ormond Street Hospital for Children, London, UK<br /> DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK</p> CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Great Ormond Street Hospital for Children, London, UK Email: drkrishnanmr@gmail.com |
References
1. Mylotte DM, O’Regan A. What lies beneath? The New England Journal of Medicine 2008; 359: 1822.
2. Cardiac pacing. Advanced Life Support. 5th edition, revised June 2008: 103-108.
3. Hutton P. The patient with an abnormal ECG. In: Hutton P, Cooper GM, Jmmes III FM and Butterworth JF eds. Fundamental Principles and Practice of Anaesthesia. Martin Dunitz Ltd. 2002; 820-824.4. Anaesthesia UK. Positioning the probe. ttp://www.frca.co.uk/article.aspx?articleid=1005565. Krishnan Melarkode, Yaqub Latoo. Pictorial essay: endotracheal tube and nasogastric tube on chest radiographs. British Journal of Medical Practitioners2009; 2: 54-56.6. Krishnan Melarkode, MY Latoo. Pictorial essay: central venous catheters on chest radiographs. British Journal of Medical Practitioners 2009; 2: 55-56.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.