



ISSN 1757-8515
Paediatric fracture clinic referrals: what does it consist of?
Ravindra Thimmaiah and Alf Bass
Cite this article as: BJMP 2012;5(2):a521
|
|
Abstract Aim: To assess the pattern of new cases referred to fracture clinic at a large paediatric university teaching hospital. Materials and Methods: The study was carried out over a four-week period in May and June of 2010. A total of 864 patients were seen during this period, which included 310 new cases and 554 follow up cases. The radiographs and reports were analysed to collect the data. Results: Two hundred and ninety two new cases were analysed as 18 cases did not have radiographs available. One hundred and one (34%) cases did not have any fractures and 14 (5%) were suspected fractures. Fractures of the distal radius and ulna were the predominant cases (23%) followed by hand fractures (15%). Conclusion: Significant number of patients (34%) did not have fractures. Considerable amount of time can be saved especially in a busy fracture clinic if protocols are developed to manage new referrals. |
Introduction
Injuries in children are common.1 In the UK, incidence is found to be 20.2 fractures per 1000 per year. The peak age of incidence is on average of 9.7 years .2 Up to 42 per cent of boys and 27 per cent of girls will sustain at least one fracture during the paediatric age. 3
A study conducted in Northern Sweden in the age group of 0 - 19 years showed that there is a rise in injury related visits to emergency department over the years. Fractures and dislocations accounted for 21.4 per cent of the cases.1 Consequently, this will put a pressure on fracture clinics as new cases take a considerable in fracture clinic.
The purpose of this audit was to assess the pattern of new cases referred to fracture clinic at a large paediatric university teaching hospital
Materials and Methods
This prospective audit was carried out over a four-week period in May and June of 2010 and it was approved by the institutional clinical audit department. There were a total of 18 working days. A total of 864 patients were seen in the fracture clinic during this period, which included 310 new cases and 554 follow up cases. Data was collected from the fracture clinic patient list for the respective days and the new patient list was extracted from this. Using the picture archiving and communication system (PACS), the radiographs and reports were analysed to collect the data regarding the fracture sustained.
Results
Total number of cases seen during the 4 week period were 864, which included 310 new cases and 554 follow up cases. Two hundred and ninety two cases out of 310 were analysed, as 18 cases did not have radiographs available.
There were 170 males and 140 females. The average age was 9 years (range 1 month to 16 years).
One hundred and seventy seven (61%) showed fractures. One hundred and one (34%) cases did not have any fractures and 14 (5%) were suspected fractures.
The following figure 1 shows the pattern of cases on each working day. Those, which are left blank, are non working days or cancelled clinics. The average number of cases seen per day were 48 and of these, the average of new cases seen were 17.2 and the average number of follow up cases seen were 30.7.
As shown in figure 2, fractures of the distal radius and ulna were the predominant cases (23%) followed by hand fractures (15%). Other fractures included: lower limb excluding foot [23 (8%)], elbow and humerus [14 (5%)], clavicle [11 (4%)], foot [12 (4%)] and others [5 (2%)].
Further analysis of the fractures sustained showed that forearm injuries were the predominant cases and majority of them were buckle or greenstick fractures. The detailed distribution is shown in the figure 3 below.
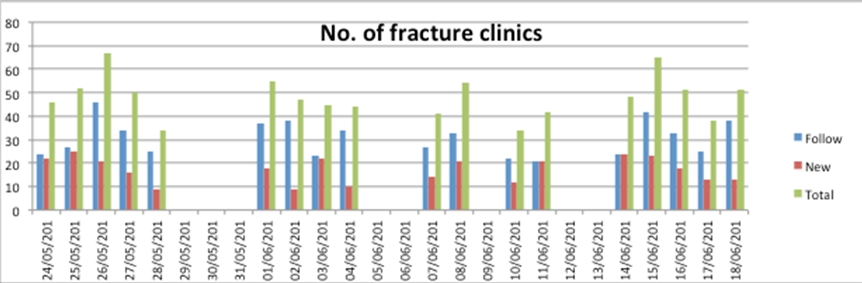
Figure 1 showing the daily pattern of cases
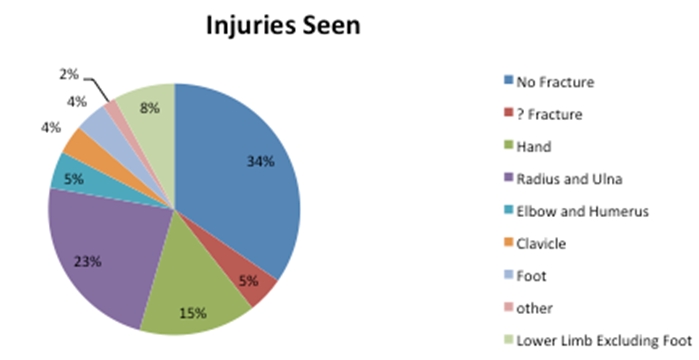
Figure 2 showing the area involved
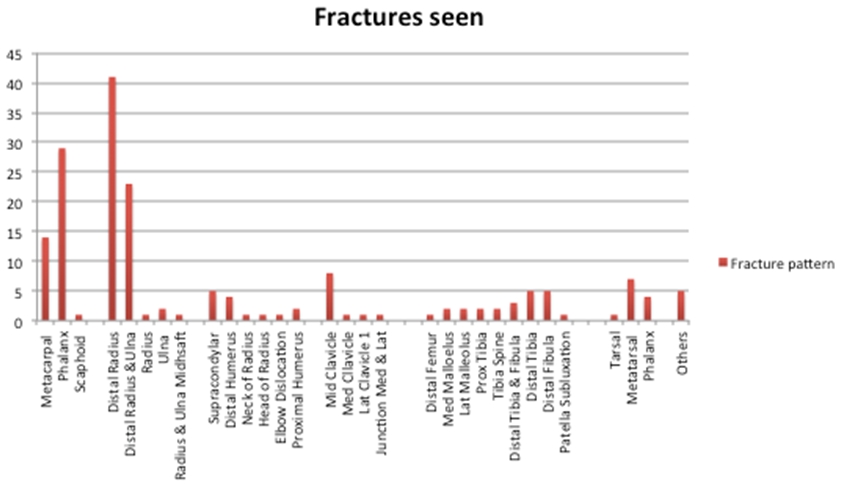
Figure 3 showing the pattern of fracture
Discussion
Fracture clinics are a part of any trauma and orthopaedic department. One must consider the benefits of providing such a service and routine audits are necessary to improve the efficiency, accuracy and above all, best possible patient care.
Although there is evidence that simple fracture like buckle fractures of the distal radius do not need orthopaedic input and can be safely treated in emergency department using a splint, and can be discharged without follow up 4, concerns have been raised against the possibility of a misdiagnosis and providing patient information 5.
Radiographic interpretation is often done by junior doctors in the emergency department. Guly6 demonstrated that there is significant issue in misreading radiographs and missing the injuries. The second problem was noted to be not requesting a radiograph. It has been suggested that better training in interpreting radiographs and rapid reporting by radiologist could solve this problem.
Others have adapted local departmental audits and guidelines and have shown to reduce the risk.7
Another possibility is a rapid review of radiographs by orthopaedic consultants on the same day as suggested by Beiri et al.8 But if the hospital is covering a large population area including peripheral walk in centres, this becomes difficult due to accessibility and logistic reasons.
Toeh and collegues9 investigating attitudes of parents towards paediatric fracture clinic found that mothers were the one who predominantly accompanied their children and most children had to take time off school to attend the clinic. It was also interesting to note that parents perception of severity of injury prompted attendance at follow up clinics.
In another study, ninety nine per cent of the parents thought attendance at the fracture clinic was important. However, when evaluating the socio economic costs, they found that this led to loss of 0.25 working days of parents, 0.18 daily wages and 0.54 schooling days per visit.1
A combination of factors may lead to fracture clinic appointments especially in paediatric population. Departmental protocols and guidelines may help in reducing the fracture clinic visits, however careful consideration must be given while drawing up these for a successful outcome.
Inappropriate referrals lead to usage of time and resources, which can lead to delay of service meant for those in need of specialist opinion. In our audit, 34% of the cases seen did not have any fractures and 5% were suspected fractures.
One of the drawbacks of this audit includes lack of case note review of those cases where fractures were not present. It would have been ideal to investigate the nature of cases seen, and whether this was treated as soft tissue injuries, or seen just for reassurance or used as a safety net.
The following recommendations could be used as possible solutions to decrease inappropriate referrals to fracture clinic.
If the patient is seen in Accident and Emergency (A&E), where appropriate and when diagnosis is in doubt, there should be an opportunity for the patient to be seen or discussed with a more senior doctor in A&E.
With regards to Peripheral Walk In Centres, there should be an opportunity to discuss it with the on call Orthopaedic team with the integration of PACS, so that images are readily available for viewing, and to consider rapid reporting of images.
The use of Specialist Physiotherapists for soft tissue injuries in A&E with follow up in physiotherapy clinics were shown to have high patient satisfaction rates and reduce fracture clinic follow up. Similar strategy could be considered.11, 12
Conclusion
This study has shown that although the majority of patients needed treatment, a significant number (34%) did not have fractures. Considerable amounts of time can be saved, especially in a busy fracture clinic if unnecessary appointments could be avoided. It would also benefit patients by avoiding unnecessary visits to the fracture clinic. A repeat study following the consideration of recommendations would reveal any benefit of such a strategy.
|
Competing Interests None declared Author Details Ravindra Thimmaiah, MRCS, MSc. Orthopaedic Registrar, Southport Hospital, Town Lane, Kew, Southport PR8 6PN, United Kingdom Mr Alf Bass, FRCS Address: Consultant, Department of Trauma & Orthopaedics, Alder Hey Children’s Hospital, Liverpool L12 2AP, United Kingdom CORRESPONDENCE: Ravindra Thimmaiah, MRCS, MSc. Orthopaedic Registrar, Southport Hospital, Town Lane, Kew, Southport PR8 6PN, United Kingdom Email: Email: travi@hotmail.co.uk |
References
- Hedstrom E M, Bergstrom U, Michno P. Injuries in children and adolescents-Analysis of 41,330 injury related visits to an emergency department in northern Sweden. Injury 2011. Article in Press.
- Rennie L, Court-Brown C M, Mok J Y, et al. The epidemiology of fractures in children. Injury 2007;38(8):913-922.
- Landin LA. Epidemiology of children's fractures. J Pediatr Orthop B 1997;6:79-83.
- May G, Grayson A. Bet 3: Do buckle fractures of the paediatric wrist require follow up? Emerg Med J 2009;26:819-822.
- Hamilton T W, Alsousou J, Willett K M. PostScript: Do buckle fractures of the paediatric wrist require follow up? Emerg Med J 2010;27:413.
- Guly HR. Diagnostic errors in an accident and emergency department. Emerg Med J 2001;18:263–269.
- Jenkins D P, Cooke M W, Glucksman EE. Audit of upper limb fracture management in an accident and emergency department. Journal of Accident and Emergency Medicine 1994;11:105-108.
- Beiri A, Alani A, Ibrahim T, et al. Trauma rapid review process: efficient out patient fracture management. Ann R Coll Surg Engl 2006;88:408–411.
- Teoh K H, Chee Y H, Simpson P M, et al. Attitudes of parents towards an urban paediatric fracture clinic. International Journal of Orthopaedic and Trauma Nursing 2010;14(2):82-87.
- Morris M W J, Bell M J. The socio-economical impact of paediatric fracture clinic appointments. Injury, Int. J. Care Injured 2006;37:395-397.
- Jibuike O O, Paul-Taylor G, Maulvi S, Richmond P, Fairclough J. Management of soft tissue knee injuries in an accident and emergency department: the effect of the introduction of a physiotherapy practitioner. Emerg Med J 2003;20:37–39.
- McClellan C M, Greenwood R, Benger J R. Effect of an extended scope physiotherapy service on patient satisfaction and the outcome of soft tissue injuries in an adult emergency department. Emerg Med J 2006;23:384–387.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.