



ISSN 1757-8515
Painless aortic dissection presenting with congestive heart failure
Usman Ali, Wai Hang Cheung and Ashis Banerjee
Cite this article as: BJMP 2011;4(1):a401
|
|
Abstract A 44 year old man, previously in good health, presented with congestive heart failure, the onset of which was probably four weeks previously. A diagnostic label of community acquired pneumonia led to delay in the diagnosis of type A aortic dissection. This required surgical management which resulted in a good outcome. The absence of chest pain may have contributed to the delay in diagnosis. Aortic dissection should form part of the differential diagnosis of unexplained acute congestive heart failure. |
Case History
A 44 year old male presented to the emergency department complaining of shortness of breath. The symptoms had commenced suddenly four weeks ago. He had been breathless at rest, and subsequently developed a productive cough with white sputum. He denied chest pain. He was known to have the sickle cell trait but was otherwise in good health. He was a non-smoker.
Since the onset of symptoms, and prior to this admission, the patient presented to two different emergency departments. The working diagnosis was, and remained, community acquired pneumonia. On initial presentation empirical treatment for a community acquired pneumonia was commenced. Failure to improve resulted in additional cover for atypical organisms and the prescription of a short course of steroids on the subsequent admissions.
Initial observations revealed the patient was tachypnoeic and tachycardic, with a respiratory rate of 25 breaths per minute, heart rate of 114 beats per minute. He was apyrexial (temperature of 36.5°C ). Pulse oximetry showed an oxygen saturation of 94% on room air. His blood pressure was recorded as 183/99 millimetres of mercury.
On examination large volume peripheral pulses, raised jugular venous pressure (5 cm), bi-basal crepitations, and bilateral ankle oedema were elicited/identified. Auscultation of the heart revealed a loud diastolic murmur audible throughout the praecordium.
A 12 lead ECG showed normal sinus rhythm, normal axis and left ventricular hypertrophy. Arterial blood gas analysis on room air showed a pH of 7.46, pa02 9.6 kPa, pCO2 4.3 kPa, HCO3 23.8 mmol/L, BE + 0.8 and lactate of 0.7 mmol/L. Routine venous blood tests did not identify any elevated markers of infection or inflammation. A chest radiograph (Figure 1) showed cardiomegaly and pulmonary oedema.
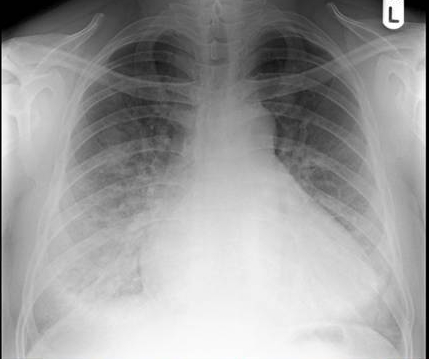
Figure 1
The patient was administered oxygen and given a diuretic to improve his ventilation.
The working diagnosis was congestive cardiac failure in the presence of what was presumed to be a new murmur. Urgent echocardiography revealed an aortic root of 6.2cm diameter at sinus level, with an evident dissection flap. There was no obvious haematoma. Severe free flowing aortic regurgitation, a dilated hyperdynamic left ventricle and a 0.7 cm diameter pericardial effusion anteriorly were also noted. It was concluded that the patient had a sealed 7cm type A aortic dissection. This was confirmed by a CT scan (Figure 2).
Figure 2
Large bore venous access was obtained and an intravenous beta blocker (Labetalol) administered. Urgent transfer to a tertiary cardio-thoracic surgical centre was made. He underwent aortic root and valve replacement, along with coronary artery bypass grafting to the right coronary artery using a reversed long saphenous vein graft. Postoperatively, he was anticoagulated on Warfarin, and was also placed on beta blockade therapy (Bisoprolol), a diuretic (Frusemide), an ACE inhibitor (Ramipril), and a statin (Simvastatin).
Discussion
Aortic dissection is a medical emergency. If left unrecognised or untreated mortality can be as high as 80% in two weeks, or 90% within three months1,2. 96 % of patients with aortic dissection present primarily with chest pain. The remaining 10% present with symptoms secondary to impairment of blood supply to other organ systems3. Dissections involving the ascending aorta present with retrosternal chest pain, while interscapular pain suggests involvement of the descending aorta. Pleuritic pain may indicate haemorrhage in the pericardial sac, with the potential for acute cardiac tamponade.
Only 6% of aortic dissections present with acute congestive cardiac failure. Patients presenting with aortic dissection and congestive cardiac failure are more likely to present without chest pain and have a valvular abnormality. When chest pain is present, the pain is more often mild and less likely to be abrupt in onset. Patients are less likely to be hypertensive on presentation and more likely to present in shock. These patients are more likely to have Stanford type A dissection . Congestive cardiac failure does lead to a delay in surgical intervention4.
Congestive cardiac failure is usually due to aortic regurgitation from aortic valve disease, incomplete aortic leaflet closure, or aortic valve disruption. In the setting of unexplained cardiac failure aortic dissection should be considered, especially when an aortic regurgitant murmur has been detected clinically. Heart failure has been associated with supravalvular aortic stenosis in the presence of a painless type A dissection, in a patient presenting with persistent cough5. Rupture of aortic dissection into the right atrium, right ventricle, or main pulmonary artery may lead to a left to right shunt and congestive heart failure6.
Painless aortic dissection has been recorded in other contexts, particularly with chronic dissection and in patients with Marfan’s syndrome.The absence of chest pain should not exclude aortic dissection.
|
Competing Interests <p> None declared</p> Author Details <p> Usman Ali, MB,BS FY2 doctor, Wai Hang Cheung, MB,BS ST3 in Medicine, Ashis Banerjee, MS, FRCS, FCEM Consultant, Emergency Department Chase Farm Hospital, Enfield</p> CORRESPONDENCE: <p> Ashis Banerjee, Consultant/ lead clinician in emergency medicine Chase Farm Hospital, The Ridgeway, Enfield EN2 8JL, Middlesex</p> Email: libra19542003@yahoo.co.uk |
References
1. Hirst AE, Johns VJ, Kime SW, Dissecting aneurysm of the aorta. A review of 505 cases. Medicine 1958; 37:217-279
2. Harris PD, Malm JR, The management of acute dissection of the thoracic aorta. Am Heart J 1969; 78: 419-422
3. Link MS, Pletrzak MP, Aortic dissection presenting as superior vena cava syndrome. Am J Emerg Med 1994; 12:326-328
4. Januzzi, JL, Eagle KA, Cooper JV, Fang J, Sechtem U, Mymel T, Evangelista A, Oh JK, Llovet A, O’Gara PT, Nienaber CA, Isselbacher EM: Acute aortic dissection presenting with congestive heart failure: results from the International Registry of Acute Aortic Dissection. J AM Coll Cardiol. 2005,46:733-735
5. Sakamoto, H, Watanabe, Y, Sugimori, H, Heart failure due to severe supravalvular aortic stenosis in painless type A aortic dissection. Ann Thorac Surg, 2008, 85: 1441-1443
6. Spier, LN, Hall, MH, Nelson, RL, et al. Aortic dissection: rupture into right ventricle and right pulmonary artery. Ann Thorac Surg,1995, 59: 1017-1019

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.