



ISSN 1757-8515
Oral oxygenating airway
Mohamed Daabiss and Nashat ElSaid
Cite this article as: BJMP 2010;3(2):322
|
Immediate postoperative care of patients undergoing nasal surgery, e.g. septoplasty or rhinoplasty, could be hazardous as desaturation happens frequently especially if the patient is not fully recovered struggling for nasal breathing while the nose is packed with gauze.1,2 Moreover, ice may be applied to the nose in the operating room to decrease swelling, and an external splint could be taped by the surgeon onto the patient’s face.3 All make it difficult to apply and fit a Hudson recovery face mask in the post-anaesthesia care unit (PACU) to maintain adequate oxygenation.
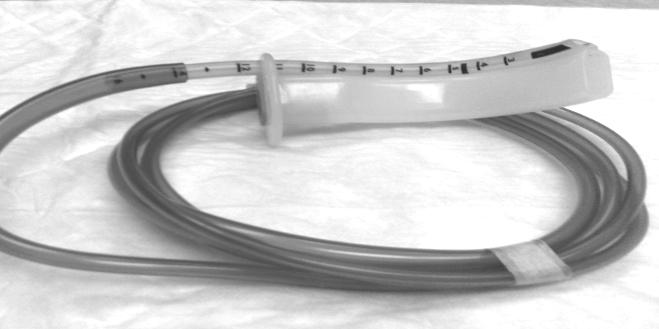
Figure 1
Facing this problem, we prepared an oral oxygenating airway device, to maintain an open unblocked airway in addition to adequate oxygenation, in the early recovery period for patients undergoing nasal surgery. Our device (Fig 1,2) is an oral airway size 4 or 5 with a siliconised soft endotracheal tube (ETT) size 5.5 mm fixed alongside the airway with its bevel directed laterally to provide easy insertion of the airway. The distal end of the ETT is cut 4-5 cm from the airway to be connected to a breathing circuit through a 15 mm connector or connected directly to tubing of oxygen flow-meter supplying humidified oxygen at a low flow rate of 1-2 L/minute to provide FIO2 35-40%. This device was tried successfully in 54 patients scheduled to septoplasty and rhinoplasty.

Figure 2
In conclusion, this device is simple, cheap, easily inserted, efficiently maintains adequate arterial oxygen saturation as long as the oral airway is tolerated in the early recovery period, reduces the oxygen flow rate and, in addition, an oxygen analyzer can be connected to the 15 mm connector to provide monitoring of the delivered FIO2.
|
Competing Interests None declared Author Details Mohamed Daabiss MD; Nashat ElSaid MSc. Department of Anesthesia Riyadh Military Hospital, Saudi Arabia. P.O.Box 7897 – D186, Riyadh 11159, Saudi Arabia. CORRESPONDENCE: Mohamed Daabiss MD Department of Anesthesia Riyadh Military Hospital, Saudi Arabia. P.O.Box 7897 – D186, Riyadh 11159, Saudi Arabia Email: madaabiss@yahoo.com |
References
1.Kimmelman CP. The problem of nasal obstruction. Otolaryngol Clin North Am 1989;22:253-64.
2.Serpell MG, Padgham N, McQueen F, et al. The influence of nasal obstruction and its relief on oxygen saturation during sleep and the early postoperative period. Anaesthesia 1994;49:538-40.
3.Buckley JG, Hickey SA, Fitzgerald O'Connor AF. Does post-operative nasal packing cause nocturnal oxygen desaturation? J Laryngol Otol 1991;105:109-11.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.