



ISSN 1757-8515
Effects of Lornoxicam on the Haemodynamic and Catecholamine Response to Laryngoscopy and Tracheal Intubation
M. Daabiss, M. Hashish, R. AlOtaibi and R. AlDafterdar
Cite this article as: BJMP 2010;3(3):a328
|
|
Abstract Background and objectives: Laryngoscopy and tracheal intubation are associated with haemodynamic responses which might increase morbidity and mortality in some patients. Lornoxicam is a non-steroidal anti-inflammatory drug, which when added to fentanyl successfully attenuated the pressor response of intubation. The aim of this study was to evaluate the effect of lornoxicam individually on the haemodynamic response and serum catecholamine levels following laryngoscopy and tracheal intubation. Methods: Fifty adult patients scheduled for general anaesthesia with endotracheal intubation were enrolled in this randomised, double-blind placebo-controlled study. They were divided into two equal groups to receive intravenously either lornoxicam 16 mg or placebo, half an hour before surgery. Systolic, Diastolic and mean arterial pressure and heart rate were recorded before and after the induction of anaesthesia, and every minute after intubation for 10 minutes. Serum catecholamine levels were measured before induction and 1 minute after intubation. Results: After induction, there was a significant decrease in blood pressure in both groups.In the control group, a significant increase in serum catecholamine levels 1 minute after intubation as well as a significant increase in the haemodynamic parameters was observed in the first 3 minutes after tracheal intubation (P <0.05). Conclusion: Lornoxicam 16 mg attenuates the pressor response to laryngoscopy and intubation of the trachea. Keywords: Tracheal intubation, cardiovascular responses, Laryngoscopy, Lornoxicam, anaesthesia. |
Introduction
In 1940, Reid and Brace 1 first described the haemodynamic response to laryngoscopy and intubation due to noxious stimuli of the upper airway. Evidence from laboratory data demonstrates that epipharyngeal and laryngopharyngeal stimulation augments cervical sympathetic activity in the efferent fibres to the heart. This explains the increase in plasma levels of norepinephrine and, to a lesser extent, epinephrine, which occur during airway instrumentation 2. The rise in the pulse rate and blood pressure is usually transient occurring 30 seconds after intubation and lasting for less than 10 minutes 3. Usually these changes are well tolerated by healthy individuals. However, these changes may be fatal in patients with hypertension, coronary artery disease or intracranial hypertension 3. Numerous agents have therefore been utilised to blunt these stimulatory effects on the cardiovascular system induced by laryngoscopy and endotracheal intubation such as deepening of anaesthesia 3, pretreatment with vasodilators such as nitroglycerin 4, beta-blockers 5, and opioids 6 etc.
Lornoxicam is a nonsteroidal anti-inflammatory drug (NSAID) that belongs chemically to the oxicams and has been successfully used as a perioperative analgesic agent with a better safety profile regarding renal and hepatic function tests, in addition to better gastrointestinal tract tolerability compared to selective COX 2inhibitors 7. Riad and Moussa 8 reported that lornoxicam added to fentanyl attenuates the haemodynamic response to laryngoscopy and tracheal intubation in the elderly. Other than this, few data are available regarding the efficacy of lornoxicam in controlling the haemodynamic variations during the peri-intubation period. Therefore the present study was designed as a double-blind randomised placebo-controlled trial to investigate the effect of lornoxicam individually on the haemodynamic response and serum catecholamine levels following laryngoscopy and tracheal intubation.
Methods:
After obtaining the approval of the Hospital Research & Ethical Committee and patients' informed consent, fifty ASA I patients, aged 18-40 years, scheduled for elective surgical procedures under general anaesthesia requiring endotracheal intubation, were enrolled in this randomised, double-blinded placebo-controlled study. Those who had taken drugs that could influence haemodynamic and autonomic function, were excluded from the study. Further exclusion criteria consisted of patients with risk of pulmonary aspiration, predictably difficult airways or obesity (body mass index (BMI) > 30%) and patients with a known allergy to NSAIDs.
In a double-blind fashion and using a sealed envelope technique, patients were randomly allocated to one of two groups to receive intravenous injection (i.v.) of either Lornoxicam 16 mg diluted in 4 ml (Group L, n = 25) or placebo received saline 4 ml (Group S, n = 25) half an hour before induction of anaesthesia as the time taken by lornoxicam to reach peak plasma concentration (Tmax) was determined to be 0.5 h 9. Since lornoxicam is yellow while placebo is a clear fluid, syringes containing both solutions were prepared covered in a double blind fashion, by a collaborator not involved in data recording. The same collaborator administered drugs while a blind observer collected data.
Patients were not premedicated. In the holding area, an i.v. cannula was inserted and an i.v. infusion of Lactated Ringer’s 10 ml Kg-1 was started half an hour before induction of anaesthesia. Additionally, a 16-gauge i.v. catheter, attached to a stopcock and flushing device, was inserted into an antecubital vein of the contralateral arm to collect blood samples. Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP) and arterial oxygen saturation (SpO2) were recorded before induction (baseline value).
After 3 min of pre-oxygenation, anaesthesia was induced with propofol 2.5mg kg-1 and cisatracurium 0.15 mg kg-1 to facilitate tracheal intubation which was performed using direct laryngoscopy when neuromuscular block was achieved by train of four-Guard monitor. SBP, DBP, MAP and HR were recorded before and after administration of the i.v. anaesthetic, immediately after intubation and cuff inflation, and every minute (min) for 10 mins. after intubation. All intubations were performed by a single anaesthetist, the duration of laryngoscopy and intubation were limited to the minimum possible time and were recorded. Data from patients in whom intubationrequired longer than 20 seconds (sec) were excluded.
Blood samples were drawn before (baseline) and 1 min. after intubation and cuff inflation for measurement of serum catecholamine concentrations. The samples were collected into pre-chilled tubes containing EDTA/Na and immediately centrifuged. Plasma concentrations of epinephrine and norepinephrine were measured in duplicate by using high-pressure liquid chromatography 10.
After tracheal intubation, patients were ventilated to normocapnia with sevoflurane (2-3% end tidal) in 50% oxygen in air. Two mins. after intubation (after collecting the blood sample), all patients received fentanyl i.v. 1.5 µg kg-1 and were monitored with ECG, SBP, DBP, MAP, SpO2 and end tidal carbon dioxide (EtCO2). All measurements were completed before skin incision. At the end of surgery, muscle relaxation was reversed and patients were extubated.
Statistical analysis was performed using SPSS version 17. Numerical data are presented as mean ± SD. Statistical comparisons among the groups were performed using unpaired t-test. Haemodynamic responses to induction and intubation in a given group were analysed using a paired t-test. The number of subjects enrolled was based on a power calculation of finding a 20% difference between the two groups in MAP and HR from the baseline values at alpha error of 0.05 and beta of 0.2. Categorical data were expressed as numbers and wereanalysed by using the 2 test where appropriate. A P value <0.05was considered statistically significant.
Results:
The two groups were comparable in demographic profile, duration of laryngoscopy and intubation as well as baseline haemodynamic parameters (table 1).
Table 1: Demographic, baseline haemodynamic characteristics and duration of laryngoscopy
|
|
Group S (Saline)
|
Group L (Lornoxicam)
|
|
No. of patients
|
25
|
25
|
|
Sex (female/male)
|
10/15
|
12/13
|
|
Age (yrs)
|
31.5 ± 5.6
|
33.1 ± 4.4
|
|
ASA (I/II)
|
19/6
|
20/5
|
|
Weight (Kg)
|
69.7 ± 4.2
|
66.9 ± 6.7
|
|
Height (cm)
|
167.9 ± 8.6
|
170.2 ± 4.5
|
|
Duration of laryngoscopy and intubation (sec)
|
14.9 (1.7)
|
16.2 (1.2)
|
|
HR/ minute
|
80.13±8.69
|
81.87±11.62
|
|
MAP mmHg
|
89.97±10.1
|
85.83±9.23
|
|
Systolic BP mmHg
|
120.2±11.2
|
117.44±17.1
|
|
Diastolic BP mmHg
|
78.7±9.91
|
73.13±12.42
|
(mean ± SD or number). No significant difference among groups
Table 2: Changes in Heart rate/minute
|
|
Group S
(Saline)
|
Group L
(Lornoxicam)
|
P
|
|
After induction
|
85.15±10.76
|
83.32±8.44
|
.062
|
|
0 minute after intubation
|
106±14.3
|
88.17±8.89
|
.000*
|
|
1 minute
|
101.71±11.15
|
86.92±9.11
|
.000*
|
|
2 minute
|
97.39±12.07
|
84.88±10.36
|
.019*
|
|
3 minute
|
95.48±12.95
|
81±9.91
|
.036*
|
Table 3: Changes in mean arterial pressure mmHg
|
|
Group S
(Saline)
|
Group L
(Lornoxicam)
|
P
|
|
After induction
|
84.65±8.3
|
79.77±9.92
|
.055
|
|
0 minute after intubation
|
129±16.54
|
91.73±10.7
|
.000*
|
|
1 minute
|
119.95±18.2
|
86.01±8.99
|
.000*
|
|
2 minute
|
105.33±13.15
|
83.62±10.63
|
.008*
|
|
3 minute
|
96.1±10.11
|
83.47±8.8
|
.024*
|
(mean ± SD). *P ≤ 0.05 is statistically significant change.
All tracheal intubations were performed successfully by the same anaesthetist at the first attempt. Following the induction of anaesthesia; SBP, DBP and MAP decreased in both groups (fig. 1 and 2).
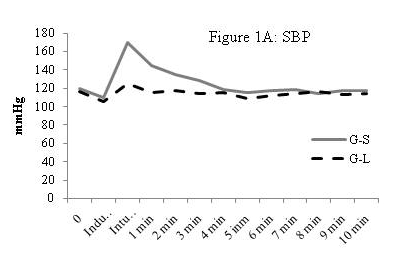
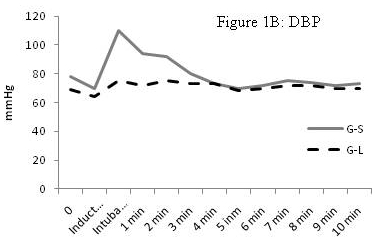
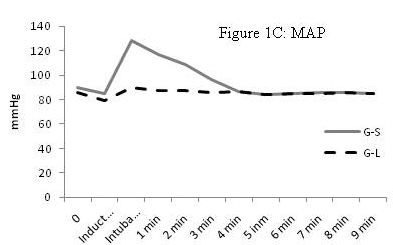
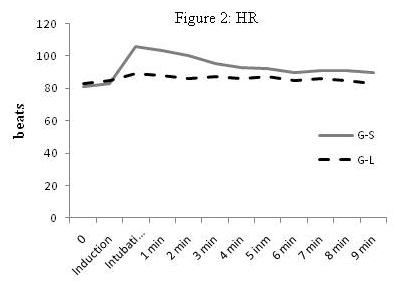
After intubation the attenuation of the increase in SAP, DBP, MAP and HR in group L was statistically significant compared to group S, and then remained significant until 3 mins. after intubation. Haemodynamic variables are summarised in tables 2,3,4,5. The maximum rise in MAP and HR in group S at intubation was 30.5% and 42% respectively. While in group L the maximum rise in MAP and HR was 7.1% and 6.2% respectively over the entire observation period. After that, SBP, DBP, MAP and HR decreased gradually in both groups to values similar to those noted before induction. Furthermore, blood samples collected one minute following intubation showed a significant increase in serum epinephrine and norepinephrine concentrations in group S compared to group L in the same observation period (fig. 3) (table 6).
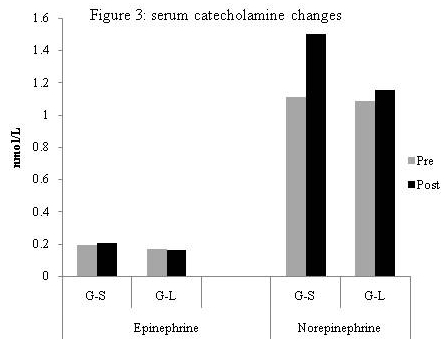
Table 4: Changes in systolic blood pressure mmHg
|
|
Group S
(Saline)
|
Group L
(Lornoxicam)
|
P
|
|
After induction
|
107.38±11.71
|
102.25±12.89
|
.069
|
|
0 minute after intubation
|
169.27±18.29
|
117.35±13.5
|
.0001*
|
|
1 minute
|
141.53±15.51
|
113.68±12.91
|
.005*
|
|
2 minute
|
128 ±11.2
|
115.39±14.17
|
.014*
|
|
3 minute
|
122.99±12.56
|
111.67±14.8
|
.037*
|
(mean ± SD). *P ≤ 0.05 is statistically significant change
Table 5: Changes in diastolic blood pressure mmHg
|
|
Group S
(Saline)
|
Group L
(Lornoxicam)
|
P
|
|
After induction
|
72.49±8.79
|
68.99±8.1
|
.085
|
|
0 minute after intubation
|
109.53±14.22
|
78.48±8.51
|
.000*
|
|
1 minute
|
92.18±10.63
|
74 ±7.75
|
.007*
|
|
2 minute
|
89.77 ±11.34
|
78.12±7.98
|
.02*
|
|
3 minute
|
81.45±8.8
|
73.6±8.21
|
.043*
|
(mean ± SD). *P ≤ 0.05 is statistically significant change
Table 6: Changes in serum catecholamine level nmol/L
|
|
|
Group S
(Saline)
|
Group L
(Lornoxicam)
|
P
|
|
Epinephrine
|
Pre intubation
|
.195±.119
|
.179±.104
|
.085
|
|
|
1 min postintubation
|
.206±.112
|
.181±.087
|
.038*
|
|
Norepinephrine
|
Pre intubation
|
1.11±.633
|
1.098±.51
|
.059
|
|
|
1 min postintubation
|
1.499±.903
|
1.107±.524
|
.000*
|
(mean ± SD). *P ≤ 0.05 is statistically significant change
Discussion:
Lornoxicam has been successfully used in prevention and treatment of postoperative pain 11. It was reported that i.v. 8 mg of lornoxicam was equianalgesic with 20 mg of morphine 12, 50 mg of pethidine 13, while 16 mg of lornoxicam had a superior analgesic effect compared with 100 mg of tramadol 14 and was comparable to 100 µg of fentanyl as intraoperative analgesia in mild to moderate day case ENT surgical procedures 15.
Our results showed a significant fall in SBP, DBP and MAP in both groups after induction. This might be due to the vasodilatation associated with the administration of propofol. Patients in both groups exhibited an increase in heart rate since no medicine other than Lornoxicam was added to propofol to decrease pain on injection. Propofol can cause significant tachycardia from pain in addition to reflex tachycardia due to a decrease in SVR. As the SBP, DBP and MAP rose significantly for the first 3 minutes after intubation in the control group, a further reduction in SVR due to the vasodilator effect of sevoflurane is the probable reason for the return of the MAP to nearly baseline values over the entire observation period. The fall in HR over the same period might be partly due to the bradycardia associated with fentanyl administered 2 minutes after intubation in both groups.
In our study, lornoxicam attenuated the pressor response to laryngoscopy and tracheal intubation; SBP, DBP, MAP and HR were significantly lower in L group compared to S group in the first 3 min after intubation. This may be attributable to the analgesic action of lornoxicam mediated through the antiprostaglandin effect of COX inhibition, the release of endogenous dynorphin and β-endorphin 14, a decrease in peripheral and central prostaglandin production, 16 as well as it exerting some of its analgesic activity via the central nervous system 17.
In agreement with our results, Bruder and colleagues 18 reported that laryngoscopy and intubation violate the patient's protective airway reflexes with marked reflex changes in the cardiovascular system and lead to an average increase in blood pressure by 40-50% and a 20% increase in heart rate. Kihara and colleagues 19, when comparing the haemodynamic response to direct laryngoscopy with the intubating laryngeal mask and the Trachlight device, reported that the HR increased compared with preoperative baseline values in all groups. Moreover, both systolic and diastolic pressure increased after tracheal intubation for 2 mins. with the highest values in the hypertensive group receiving direct laryngoscopy.
In a previous study done by Riad and Moussa 7, i.v. administration of 8 mg lornoxicam half an hour before surgery added to fentanyl 1 µg Kg-1 during induction of anaesthesia was found to attenuate the haemodynamic response to laryngoscopy and tracheal intubation in the elderly. However, it was unclear whether this was attributed to the drug's narcotic effect. Therefore, our study was designed to evaluate the use of lornoxicam individually, in a single i.v. administration of 16 mg lornoxicam half an hour before surgery. Lornoxicam 8 mg was not used as it was proven to have an inadequate analgesic effect 15.
There have been a few studies which have measured catecholamine levels after intubation. Our results are consistent with those of Russell et al 2 and Shribman et al 20 who reported significant elevations in serum levels of norepinephrine and epinephrine following laryngoscopy and tracheal intubation. Hassan and colleagues 21 concluded that during laryngoscopy and endotracheal intubation, placing the tube through the cords and inflating the cuff in the infraglottic region contributes significantly to sympathoadrenal response caused by supraglottic stimulation.
When assessing techniques to ameliorate the cardiovascular responses to intubation; the drugs used to induce anaesthesia may influence the results. We induced anaesthesia with propofol which produces hypotension. This may compensate in part for the cardiovascular changes attributable to laryngoscopy and tracheal intubation. This could be considered a limitation of the present study. The omission of opioids during the induction of anaesthesia in healthy young patients should not be a concern.
In conclusion, pretreatment with lornoxicam in the doses given in this study, attenuates the pressor response to laryngoscopy and the intubation of the trachea.
|
Competing Interests None declared Author Details M. Daabiss, Riyadh Armed Forces Hospital, Department of Anesthesia, KSA M. Hashish, Armed Forces Hospital King Abdulaziz Airbase Hospital Dhahran, Department of Anesthesia, KSA R. AlOtaibi, Riyadh Armed Forces Hospital, Department of Anesthesia R. AlDafterdar, Riyadh Armed Forces Hospital, Department of Laboratory, Riyadh, KSA CORRESPONDENCE: Mohamed Daabiss Department of Anesthesia, Riyadh Armed Forces Hospital Mail box: 7897-D186 Riyadh 11159 Saudi Arabia Email: madaabiss@yahoo.com |
References
1.Reid LC, Brace DE. Irritation of the respiratory tract and its reflex effect upon heart. Surg Gynaec & Obst; 1940; 70: 157-62. (s)
2.Russell WJ, MorrIs RG, FrewIn DB, Drew SE. Changes in plasma catecholamine concentration during endotracheal intubation. Br J Anaesth; 1981, 53:837-9.3.Kovac AL. Controlling the hemodynamic response to laryngoscopy and endotracheal intubation. J Clin Anesth 1996; 8: 63–79.4.Fassoulaki A and Kaniaris P. Intranasal administration of nitroglycerin attenuates the pressor response to laryngoscopy and intubation of the trachea. Br J Anaesth 1983; 55:49–525.Vucevic M, Purdy GM, Ellis FR. Esmolol hydrochloride for management of the cardiovascular stress responses to laryngoscopy and tracheal intubation. Br J Anaesth 1992; 68:529–306.Anila D. Malde, Vineet Sarode, Attenuation of the Hemodynamic Response to Endotracheal Intubation: Fentanyl versus Lignocaine. The Internet J Anesthesiol 2007; 12 (1).7.McCormack K. The evolving NSAID: focus on Lornoxicam. Pain Rev 1999; 6 (4), 262-78.8.Riad W, Moussa A. Lornoxicam attenuates the hemodynamic responses to laryngoscopy and tracheal intubation in the elderly. Eur J Anaesthiol 2008; 25: 732–6.9.Ankier SI, Brimelow AE, Crome P, Johnston A, Warrington SJ, Turner P, Ferber HP. Chlortenoxicam pharmacokinetics in young and elderly human volunteers. Postgrad Med J 1988; 64: 752–754.10. Holly JMP, Makin HLJ. The estimation of catecholamines in human plasma: a review. Anal Biochem 1983; 128: 257–74.11. Zhao H, Ye TH, Gong ZY, Xue Y, Xue ZG, Huang WQ. Application of lornoxicam to patient-controlled analgesia in patients undergoing abdominal surgeries. Chin Med Sci J 2005; 20: 59-62.12. Norholt ES., Pedersen S, Larsen U. Pain control after dental surgery: a double blind, randomized trial of lornoxicam versus morphine. Pain 1996; 67: 335-43.13. Balanika M., Tsitsika M., Wilczynski W. The use of lornoxicam-mepridine combination for postoperative analgesia. Eur J Anaesthiol 2000;17, 771-8.14. Staunstrup H, Ovesen J, Larsen T. Efficacy and tolerability of lornoxicam versus tramadol in postoperative pain. J Clin Pharmacol 1999; 39: 834-41.15. Daabiss M, Al-Sherbiny M, Al-Otaibi R, El-Nimar R. Analgesia in day-case ENT surgery: The efficacy of lornoxicam. Br J Med Practitioner 2009; 2(3); 46-50.16. Hitzenberger G, Radhofer-Welte S, Takacs F, Rosenow D. pharmacokinetics of lornoxicam in man. Postgrad Med J. 1990; 66(Suppl 4): S22-7.17. Buritova J, Besson JM. Dose-related anti-inflammatory analgesic effects of lornoxicam: a spinal c-Fos protein study in the rat. Inflamm Res 1998;47 (1), 18-25.18. Bruder N, Granthil C, Ortega D. Consequences and prevention methods of hemodynamic changes during laryngoscopy and intubation. Ann Fr Anaesth Reanim 1992; 11(1):57-71.19. Kihara S, Brimacombe J, Yaguchi Y, Watanabe S, Taguchi N, Komatsuzaki T. Hemodynamic responses among three tracheal intubation devices in normotensive and hypertensive patients. Anesth Analg 2003; 96: 890–895.20. Shribman AJ, Smith G, Achola kJ. Cardiovascular and catecholamine response to laryngoscopy with and without endotracheal intubation. Br J Anaesth; 1987, 59:295-9.21. Hassan, HG, El-Sharkawy, Renk H, Mansour G, Fouda A. Haemodynamic and catecholamine responses to laryngoscopy with Vs without endotracheal intubation. Acta Anaesthesiol Scand 1991; 35: 442.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.