The pituitary gland is a tiny gland located at the base of the brain and is connected to the hypothalamus. Dubbed as the body’s “master gland”, it produces important hormones that control many bodily functions such as those involved in the control of haemodynamics, glucose, fight or flight response, body growth and many more. Any of the pituitary hormones may be affected in pituitary disease, with acute adrenocorticotropic hormone (ACTH) deficiency being the most catastrophic and life-threatening.
Pituitary apoplexy occurs following acute haemorrhage or infarction of the pituitary gland, causing patients to be acutely unwell due to hormonal as well as local compressive effects. These effects cause the usual presentation of pituitary apoplexy such as severe headache, diplopia, visual loss and hypopituitarism.
We report a case of pituitary apoplexy that presented with a 2-week history of loss of peripheral vision and lethargy with stable vital signs.
CASE PRESENTATION
A 49 years of age gentleman complained of loss of peripheral vision in the left eye and lethargy for 2 weeks. The loss of vision was sudden, painless and non-progressive and had caused him considerable difficulties with driving where he would shift into the wrong lane and was honked at. He had no known medical or surgical history of note. Prior to presentation, he had no history of eye pain, eye redness or a history of trauma to the left eye. There were no headaches, neurological deficits or constitutional symptoms.
Clinically, he had bitemporal hemianopia with no other cranial nerve deficits. His Glasgow Coma Scale was 15/15, vital signs were stable and there was no postural change in blood pressure. Examination of other systems was unremarkable. Blood investigations revealed a decreased morning cortisol of 46 nmol/L and a normal thyroid stimulating hormone (TSH) with borderline low free thyroxine. Serum electrolytes, plasma glucose and all other anterior pituitary hormones were within reference range.
A computed tomography (CT) of the brain showed an enlarged pituitary sella with a large well-circumscribed and heterogeneously enhancing mass within. This mass measured 3.5cm x2.7cm x3.5cm (AP xW xCC) and had no calcifications within. It was also compressing onto the optic chiasm.
Two days later, a brain pituitary Magnetic Resonance Imaging (MRI) was done which reported a heterogeneous mass occupying the sella with suprasellar extension measuring 2.7 x2.8 x2.9cm (AP xW xCC) (Figures 1.1 & 1.2). This mass returned mixed solid-cystic intensity with significant enhancement post-contrast administration. There was evidence of layering within the cystic component of this mass. Inferiorly, the right border ended lower than the left (Figures 2.1 & 2.2).
Following consultations with endocrinologists, neurosurgeons and radiologists, a clinical diagnosis of pituitary apoplexy with hypocortisolism and central hypothyroidism was reached. The patient was started on oral hydrocortisone 20mg in the morning and 10mg in the evening; and oral L-thyroxine 100mcg in the morning before he was referred to the neurosurgeon for trans-sphenoidal surgery. While awaiting surgery, no clinical deterioration was reported. An endoscopic trans-sphenoidal surgery successfully took place a week later which revealed an enlarged haemorrhagic pituitary gland (Figure 3.0). The patient was discharged well a week post-surgery.
His histopathology report later confirmed pituitary adenoma where monomorphic tumour cells arranged in nests and trabeculae and some pseudorosettes were seen. The tumour cells exhibited mild pleomorphism with moderate amount of cytoplasm. The stroma was highly vascularised. No necrosis, calcification or mitosis was seen. Immunohistochemistry studies were positive for follicle-stimulating hormone (FSH) and luteinising hormone (LH) and negative for ACTH, growth hormone, prolactin and TSH.
Figure 1.1 and 1.2: MRI brain on coronal view illustrating well-defined and heterogenous suprasellar mass
Figure 2.1 and 2.2: MRI brain on sagittal view illustrating mixed solid-cystic intensity pituitary mass
Figure 3.0: Intraoperative finding showing haemorrhage of the pituitary gland
DISCUSSION
Pituitary apoplexy is a potentially fatal condition caused by haemorrhage or infarction or both. Most cases occur during the fifth decade of life, predominantly in males.1 In the majority of cases, it is associated with a pre-existing non-functioning macro-adenoma which accounts for 14-54% of pituitary adenomas and has a prevalence of 7-41.3/100,000 population. The standardised incidence rate is 0.65-2.34/100,00.2
The many clinical presentations of pituitary apoplexy result from local compression of adjacent structures or deficiency of pituitary hormones – the former being more common where affected individuals present with headaches, visual disturbances and other symptoms of raised intracranial pressure.3
Subclinical haemorrhages refer to asymptomatic individuals with evidence of pituitary haemorrhage on MRI. In a 2018 retrospective transversal analysis involving 64 patients, 34.38% had subclinical haemorrhage within a non-functional adenoma.4 In another retrospective overview by Turgut et al, 186 cases of apoplectic pituitary adenoma presenting with monocular or binocular blindness were published in the last century.5 In a case report by Sasaki et al, a 65-year-old gentleman was only diagnosed with pituitary apoplexy following weeks of blood investigations for hyponatraemia and repeat imaging. His only presenting complaints were anorexia, low energy and fever for two weeks.6 These studies show that while an early correct diagnosis of pituitary apoplexy is important, it is not necessarily urgent.
On the other end of the spectrum, pituitary apoplexy may also present as a life-threatening situation where patients are unconscious and hemodynamically unstable due to hypopituitarism. In its acutely deficient state, ACTH causes acute adrenal insufficiency hence resulting in hypotension, hypoglycaemia, hyponatraemia and hyperkalaemia. Sometimes, non-specific symptoms precede the symptoms of hypocortisolism. A drop in consciousness level may be due to the tumour’s mass effect transmitting pressure to the brainstem or causing hypothalamic compression.7 Espinosa et al reported a 48-year-old gentleman with pituitary apoplexy who presented with the worst headache of his life, requiring urgent neurosurgical intervention which proved to be life-saving.8
Complex as it already is, diagnosing pituitary apoplexy may be further complicated when non-specific symptoms can be explained by other causes such as post-general anaesthesia drowsiness, hyponatraemia in a patient on diuretics and headaches in post-partum women receiving spinal anaesthesia.9, 10
While most patients consequently suffer from pituitary insufficiency, the extent, type and duration of therapy differs between patients. Cases of spontaneous recoveries whether a surgical or conservative approach was adopted have also been reported.11, 12 However, robust control studies comparing the outcome of surgical with conservative management in patients with pituitary apoplexy have yet to emerge. Nonetheless, studies have proven that visual outcomes significantly improve with surgery.13, 14
Having discussed the varied presentations of pituitary apoplexy, it can be agreed upon that the life-threatening endocrinal condition should be considered in any patient with abrupt neuro-ophthalmic deficits despite the state of clinical stability. This is imperative as prompt medical and surgical management may not only be life-saving, but also significantly improve visual and cranial nerve outcomes.15
CONCLUSION
Pituitary apoplexy is an endocrinal emergency which requires immediate investigation and treatment. Despite its disastrous pathology, there have been cases where affected patients present with isolated visual disturbances or with no symptoms at all. It is therefore important to have early suspicion of pituitary apoplexy in stable patients with eye complaints as early detection and management are life-saving and significantly improve neuro-ophthalmic outcome.
The Royal College of Psychiatrists and NICE Guidelines both stress the importance of carrying out physical examination on psychiatric in-patients due to their high level of physical health issues. Carrying out and carefully documenting these physical examinations at the time of admission allows physical health issues to be appropriately taken into account when creating management and medication plans and, in more severe cases, to allow diversion for medical treatment if that is required or the underlying cause of the presentation.
Monitoring physical health of patients in psychiatric settings is vital and is recommended by NICE in its guidelines; documentation of physical health assessment carried out at the right place is also imperative. According to Louth/Meath Mental Health Services Admission Policy, 2016, all psychiatric patients admitted should have their Physical Examination completed and recorded on Physical Examination Proforma.
Psychotropic medications can effect on physical health of psychiatric patients1. Patients with medical co-morbidities are more at risk from psychotropic medications compare to normal healthy population2. In addition, depression is considered as an independent risk factor for cardiac events in patients with coronary artery disease3. Adding that, depression may also possibly increase the risk of cardiovascular disease in population without medical co-morbidities. Hence, psychotropic medications are carefully chosen for treatment of individual patients to avoid any adverse events1. Depression is not the only risk factor for medical co-morbidities; other psychiatric problems also make patients vulnerable for physical health issues1. Moreover, prevalence of medical problems is relatively high in psychiatric patients compared to cohorts without mental health disorders4. The risk of medical co-morbidities do not always increase after prescribing psychotropic medications; the risk of cardiovascular disease also increases for patients suffering from anxiety and not necessarily using medications5.
Psychiatric patients receiving psychotropic medications should have their physical health monitored regularly as recommended by NICE6.
Methods
The audit cycle was completed in St Brigid’s Complex, Ardee. The audit cycle comprised initial audit (phase 1), implementing changes following recommendations and re-audit to compare results with initial audit. All patients in Unit 1, which is an acute admission ward, were included for the audit and re-audit. Patients admitted in another ward, which is a long stay ward, were excluded in the audit cycle. The rationale for not including patients admitted in long stay ward was that these cohorts of patients are already well established on psychotropic medications and their physical health is regularly monitored. Data collection was carried out from physical health proforma completed upon admission and filed in notes. No patient identifiable data was collected during the audit cycle.
During phase1, a review of the notes of all in-patients on a specific day in Unit 1, St Brigid’s Complex, Ardee was carried out. Data was collected from physical health proforma of each patient. This data was then entered in Xl-spread sheet for the analysis purpose. Results were analysed and feedback obtained from non-consultant hospital doctors. The findings were presented during local teaching to both the consultant and NCHD bodies and means of improving compliance were discussed openly. These discussions led to a redesign of the proforma to make it shorter and simpler to complete. This proforma was then attached to an assessment booklet, whereas physical health proforma was not part of an assessment booklet. A re-audit was carried out during a single day on all in-patients in Unit 1 several months after the first phase of the audit. In-patients who remained in Unit 1 since the initial phase of the audit were excluded from the re-audit.
Results
The results of initial audit demonstrated only 50% (10/20) compliance with physical health proforma. Furthermore, in phase 1 the proformas were only partially completed with elements of the physical exam documented on the proforma. In addition, other components were documented elsewhere in the admission notes and many elements omitted altogether. Only 15% (3/20) of the proformas contained a complete, documented physical examination.
One of the sections on proforma that lacked information significantly was information about patient’s current circumstances. On the other hand, demographic details were recorded for only 50% of patients. However, admitting doctor’s details were recorded on 35% (7/20) of proformas, the details of professional carrying out physical information was also not available on large number (19/20) of proformas.
Table 1:
Yes
No
Partial
Patient Demographics
10
10
0
Date & Time of Admission
6
11
3
Referral Agency
7
13
0
Admission Status
8
12
0
Drug Allergies
6
14
0
GP Details
7
13
0
NOK Details
3
17
0
Religion
1
19
0
Marital Status
2
18
0
No of Children
2
18
0
Occupation
2
18
0
Nationality
3
17
0
No of Previous Admissions
1
19
0
Medical Card No
0
20
0
V.H.I
0
20
0
Provisional Diagnosis
6
14
0
Admitting Doctor Name
7
13
0
Admitting Doctor Signature
7
13
0
General Examination
9
11
0
CVS
9
11
0
R.S
9
11
0
C.N.S
9
11
0
Alimentary System
6
14
0
G.U.S
3
17
0
L.M.P
1
19
0
Signature
1
19
0
Date
8
12
0
Data analysis of the re-audit shows that 80% (16/20) of the proformas were been completed. In overall, there was a huge improvement seen in the results of the re- audit and doctor’s details performing physical health was recorded on 75% of the proformas. Adding that, general examination section of the proforma demonstrated huge compliance of 80% along with Cardiovascular and Respiratory system.
Table 2:
Yes
% Yes
No
% No
Name
12
60%
8
40%
DOB
10
50%
10
50%
General Examination
16
80%
4
20%
CVS
15
75%
5
25%
R.S
15
75%
5
25%
C.N.S
14
70%
6
30%
Alimentary System
14
70%
6
30%
G.U.S
14
70%
6
30%
L.M.P
6
30%
14
70%
Signature
15
75%
5
25%
Date
15
75%
5
25%
Discussion
A total of 20 patients in each phase of the audit were included for data analysis. The number of patients included may seem small for a research study with a different design; however, quantitative number is not taken into account with this particular design used. On the other hand, number of patients admitted in any acute ward is similar.
During data collected, it was apparent that physical examination findings were recorded in the notes instead and proforma was not used for some of patients, which is evident through results. Even though physical examination may have been carried out, it was not possible to include in data analysis and results due to the study design.
The results of first phase demonstrated poor compliance with physical health proforma despite carrying out physical examinations and findings been recorded elsewhere in admission notes. It is an arguable fact that regardless of physical health proforma been filled, physical examination of patients are been carried out as per local and NICE guidelines. However, physical examinations documented elsewhere in the admission notes makes it difficult to locate; hence, a proforma is completed upon admission as a pre agreed standard procedure.
Once the results of initial audit were analysed, these results were presented in the local academic session to all the NCHDs and Consultant Psychiatrists. While all involved agreed the importance of carrying out physical examination on all patients upon admission; the design and complex nature of the initial proforma made very difficult for NCHDs to complete it. Adding that, some of the information, such as demographic details and personal information, was also repeated making it duplicate that had been recorded elsewhere in the notes. The physical health proforma was then redesigned and simplified to complete. Unnecessary and duplicate information was omitted in the new proforma and was attached with the initial psychiatric assessment booklet. The new physical health proforma was then implemented in the service after discussions with fellow NCHDs, Consultants and management.
Second phase of the audit cycle was conducted after number of months and redesigned physical health proforma been in circulation for some time. Data was again collected as per study design and methods and entered for analysis. These results demonstrated a huge improvement in compliance with physical health proforma after the change of practice. Although compliance with proforma has improved significantly, some gaps were noted to reach the desired outcome of 100% in practice. Case notes were studied to understand the reasons for not completing physical health proformas. Several themes emerged through case note reviews and one of the reasons was assumed that patient was transferred from medical ward of General Hospital after been medically cleared. Time and mode of admission also resulted in physical health proforma not been completed.
Conclusion
While all involved agreed that carrying out physical examination on all admissions was advisable; the length and complexity of the initial proforma contributed to poor completion rates by NCHDs. A combination of teaching to underline its importance and a redesign focused on usability and speed led to significantly increased completion of the proforma with attendant benefits for patient assessment and treatment.
Temporomandibular joint disorder (TMD) refers to a broad spectrum of disease states characterised mainly by pain and tenderness in the temporomandibular joint (TMJ) and adjacent soft tissues, TMJ clicking and limitation in jaw movements. TMD symptoms vary in severity and if left untreated, may lead to debilitating pain and limited function with a significant impact on quality of life. The estimated prevalence of TMD is 2-6 % 1 although up to 25 % has also been reported. The aetiology of TMD is not fully understood and it is multifactorial including organic disease of the TMJ, trauma, malocclusion and stress. Treatment options include reassurance and education, physical and splint therapy, simple analgesia and other drugs, surgical intervention or combined treatment. Most cases of TMD can be managed non-surgically. Most patients with TMD have traditionally been initially managed by a GDP and are often referred to a specialist for further non-surgical or surgical therapies if symptoms are not controlled.
Andersen et al (1999) reported approximately 3 out of every 100 attendances to GMP services in Wales, UK were due to oral and dental problems 2. The number of people attending their GMP for dental problems has been increasing 3, 4. GMPs have expressed concerns about their ability to treat dental diseases 5 as these conditions are beyond the scope of their expertise.
Consulting GMPs for TMD has been observed dating back to over nearly six centuries 6. Similar to the rising trend of attending GMP for oral problems in general, there has been an increasing tendency for patients with TMD symptoms to approach their GMP as the first point of contact due to comparatively easier availability and financial feasibility. Prompt referral to a GDP or relevant speciality is likely to improve management and reduce the adverse impact on quality of life. This could potentially reduce the burden on overstretched NHS hospitals in UK. There is paucity of data on the management of TMD among GMPs in UK. To the best of our knowledge, there has been no prior survey of their knowledge of and attitude towards assessment and management of TMD. The objectives of this study are to assess the current experience of UK GMPs with the care of TMD patients in primary care.
Method:
Design
A Single-Centre Cross-sectional survey
Study population and survey development
GMPs listed within the Leicester City Clinical commissioning groups 7 with access to refer to the regional NHS Oral and Maxillofacial Services Providers. GMPs were formally invited to complete a specifically prepared postal questionnaire (See Appendix) consisting of their knowledge and management of TMD. In order to ensure the reliability and validity of the results of survey, the questionnaire was pretested on the GMPs in five different Urban GP surgeries other than Leicester city. To maximise response rates, a follow-up questionnaire and telephone calls were arranged after four weeks if no reply had been received. Confidentiality was maintained by number-coding the questionnaires. Selection bias was avoided by sending the questionnaire to all the GMPs in the Leicester city area.
The questionnaire Survey was conducted in February 2018 and comprised of 16 questions on TMD and two demographic questions .The questionnaire assessed knowledge of TMD including clinical features, diagnostic criteria, prevalence and aetiology. Participants were asked about awareness of current guidelines and treatment options, and their management practice, whether they would refer to a GDP, or oral and maxillofacial surgeon or TMD specialist. They were asked whether they update or have updated their knowledge about TMD. They were also invited to propose which means of TMD knowledge provision they would prefer to receive demographic data included information on the gender and clinical experience. There were no open-ended questions and participants were asked to select the most correct statement from more than one option in some of the questions. Participant GMPs were informed in the invitation letter that participation was voluntary, all responses were anonymous and that the study would be published in a peer-reviewed journal. Participation in the survey implied consent.
Data analysis
Data was analysed descriptively using IBM SPSS Statistics for Windows version 21 (IBM Corp, Armonk, USA). We aimed to determine whether there is any relationship between GMPs knowledge of diagnostic features of TMD and their length of experience in practice. We stratified GMPs into two groups according to the seniority [certificate of completion of specialist training (CCST) obtained within 5 years or earlier]. Chi square test was used to compare the proportion between two groups and a p value < 0.05 was considered to be statistically significant.
Results:
Out of 259 GMPs who were contacted and invited to participate, a total of 126 practitioners returned the questionnaire by post {response rate (48.6%)}. Of the respondents, 2 did not correctly fill the survey questionnaire; the remaining 124 responses were analysed. There was a slight male preponderance (55%). Only 12% GMPs rated themselves above average (score >4) in terms of being familiar in general with TMD. Five percent of responders were aware of published guidelines of TMD management. None of them were familiar of Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD). Seventy-four percent of participants, including both GMPs with experience less than 5 years and more described the clinical features consistent with the diagnosis of TMD. 4% selected the correct option when asked about the possible causative factors. None of them knew about the actual prevalence of TMD symptoms in the community and majority of GMPs underestimated the proportion of population with TMD. Fourteen percent were correct in identifying the age group affected by TMD. While majority of them (56%) chose ‘ No’ and 12 % of them selected ‘Don’t know’ , thirty-two percent, participants believed that subjects with TMD symptoms require initial radiographic assessment before any treatment is commenced. 95% of respondents believed that they have seen on average 2 to 4 TMD patients per month. Eighty nine percent of respondents referred patients to GDPs whereas remaining 11 % of GMPs contacted Oral and maxillofacial surgery service providers for TMD management (see Figure). Only one of the participants was familiar of specialist-clinical services for TMD who, in addition to sending these patients to GDPs, also referred TMD patients directly to specialists. Majority of them (66%) were not comfortable in seeing and provide initial management of TMD and 34% of GMPs, in addition to referring TMD patients to other services, also provided initial treatment to these patients. All those who offered this initial non-surgical treatment to manage TMD, selected combined modalities i.e. patient education, pharmacological and physical therapy. In every 25 participants (6%) has updated their knowledge through internet resources in order to increase their awareness and knowledge about the TMD management in community. Almost all (97%) of the GMPs would welcome relevant continued education programmes and receiving leaflets / published literature. The summary of GMPs responses from survey is given in Table 1. Group analysis of participants (See Table 2) did not show any statistical association between the experience of GMPs and their knowledge of TMD clinical features (Chi-square statistics 3.78, p = 0.5).
Figure: GMPs Referral for TMD patients GMPs: General Medical practitioners, TMD: Temporomandibular joint disorders, GDPs: General Dental Practitioners
Table 1: Summary of the main responses from the GMPs survey about TMD knowledge
Familiarity of TMD rated as above average
12%
Awareness about TMD guidelines
5%
Familiarity with RDC Criteria of TMD
0%
Correctly identified the etiological factors of TMD
4%
Correctly identified TMD clinical features
74%
Correctly identified the TMD prevalence in General population
0%
Correctly identified the age group suffered most with TMD
14%
Selected ‘No’ about the need of radiograph before TMD management is initiated
56%
Not comfortable in seeing and provide initial management of TMD
66%
Selected combination of pharmacological and physiotherapy to treat TMD
34%
Have referred TMD patients to GDPs
89%
Have referred TMD patients to Oral and maxillofacial surgery
11%
Have updated the TMD knowledge through any resource
6%
Keen to receive further information about TMD
97%
GMPs: General Medical practitioners, TMD: Temporomandibular joint disorders
Table 2: Distribution of participant GMPs according to their seniority and familiarity with TMD clinical features
Experience as GMP
Correctly identified TMD features (n)
Incorrectly identified TMD features (n)
Greater than 5 years
50
11
Less than 5 years
42
21
Chi-square statistics 3.7894 p = 0.5 GMPs: General Medical Practitioners, TMD: Temporomandibular joint disorders
Discussion:
Main Findings
Our study is the first which has explored in-depth the experience of GMP with TMD management. Findings from the survey indicate that uncertainty exists among GMPs regarding their level of knowledge. Most GMPs had no awareness of TMD management guidelines. The RDC/TMD 8 is a valuable tool to assess signs and symptoms and to classify patients with TMDs. Participants were not aware of these guidelines. The response from GMPs indicated that the prevalence of TMD within the general population is not accurately recognised at all along. The majority of respondents do not appreciate that TMD patients require radiographic evaluation before treatment planning. None but one of the GMPs was aware of clinicians with a subspecialty in TMD. All patients with such condition were referred either to dentists or maxillofacial surgeons. This reflects an awareness of an appropriate chain of referral 9. There was a generalised consensus in considering the general medical practice environment as an unsuitable place to manage dental problems 5, including TMD. A positive finding of our study was that a significant proportion of GMPs in Leicester city are interested in learning about TMD. This indicates there is a need for designing formal training courses for GMPs. If appropriately trained, these practitioners will potentially have an enhanced capability of not only managing TMD at an initial level but also providing knowledge and guidance to other practices and community services
Comparison with existing literature
The knowledge, attitude and practices of GDPs regarding TMD management are widely reported 10-12 but there is hardly any study relating to General Medical Practice. Results of a questionnaire survey based on screening of TMD in 38 London teaching General Medical Practices were similar to our findings 13. .Thirty-six of 38 GMPs, who replied in that survey, routinely assess the TMJ as part of the physical examination for symptoms of TMD whereas TMJ assessment was not included in primary health care screening. Similarly to Cope et al 2015 5 another qualitative study in the North-west of England GMPs experiences of chronic orofacial pain, including TMD, revealed primary health care providers consider themselves unable to meet the diagnostic and management challenges of TMD 14 .GMPs in the face to face interviews explained that despite these limitations, they do offer TMD patients pharmacological and other complimentary approaches, particularly acupuncture. Similar experiences of GMPs are also reflected in our current findings.
Strength and limitations
The main strength of this survey is that, to the best of the authors' knowledge, it was the first study which determined Knowledge and experience of GMPs towards Management of TMD. In simple language but a comprehensive and pilot tested questionnaire was designed to assess GMPs knowledge of TMD which they were expected to have gained from available literature.
There were mainly two limitations in our survey. Firstly, the sample size was small as the study was confined only to the participant GMPs practising in Leicester City, hence it may not be representative of all GMPs across the country. Despite this weakness the results may serve as a scoping study to justify further research such as qualitative surveys. Secondly, there was a relatively low but acceptable response rate (48.6%). Although this raises concerns about the research validity, but studies have demonstrated that there is no direct correlation between response rate and validity 15. Also, Surveys with comparatively low response are only marginally less accurate than those with much higher reported response rates 16.
Implications for research and practice
In addition to other main areas of practice, the Royal College of General Practitioners (RCGP) curriculum also highlights the importance of Specialist GMP trainees attaining competency in learning about common oral and maxillofacial conditions 17. Considering the frequent attendance of patients with oral and facial diseases in primary care and the limited undergraduate Medical training, valuable suggestions have been made for GMPs to promote attendance at specialist oral medicine and oral surgery clinics to enhance exposure to common maxillofacial diseases. Despite these recommendations, surprisingly little no active interest has yet been shown by GMPs trainees. There is a need to integrate GMP training with some exposure to the specialty of Oral and Maxillofacial surgery to improve expertise in the management of TMD and other oral diseases, especially in view of the increasing trend for patients to initially present to their GMP for advice about TMD and other chronic orofacial pain conditions. .
Evidence based literature regarding dealing with TMD at a non-specialist level have been published in the medical literature 18-20. This provides clinicians including GMPs with sufficient knowledge to diagnose and refer TMD to the relevant clinician. The British association of Oral and Maxillofacial Surgeons (BAOMS) TMD commissioning guide 2014 8 suggests GMPs to refer TMD patients to a GDP in the first instance to start initial treatment. Early diagnosis, counselling and management of TMD tend to improve prognosis and reduces the severity of impact on the quality of life 21, 22. It is crucial that GMPs are have sufficient knowledge to make an early referral to an appropriate clinician in order to commence conservative measures including education and advice, use of a bite guard, medications and self-directed physical therapy. The limited access to dental care within the UK, despite a National Health Service (NHS), is a well-recognised challenge. There are multiple barriers to accessing dental care 23 including delays or failure in getting appointments which results in the patient turning to General Medical Practice for advice 4. GMPs have also expressed concerns regarding accessibility to and the collegiate relationship with GDPs in the management of chronic facial pain including TMD 14. Whether the aforementioned limitations are system related or simply patient factors, they are certainly hindrances to timely assessment and intervention. We suggest that suitably trained GMPs should be able to commence the initial conservative management of TMD patients whilst simultaneously referring patients to a GDP or appropriate specialist so as to optimize the management and possibly reduce subsequent referrals in the long term. There is an immense potential for primary care to be integral part of initial management of TMD. A large scale nationwide study could potentially help future planning for care within the community.
Conclusion:
Respondent GMPs in East midlands England, demonstrated limited knowledge and confidence related to the diagnosis and management of TMD. Appropriate post-graduate training and educational opportunities for ongoing continuing professional development related activities would improve the knowledge and awareness of TMD management, potentially leading to more effective care within the community.
The continuous growth in patient numbers and needs poses several challenges for medical professionals and support staff within the National Health Service (NHS).1 Health care services are under financial strain in the light of the changing demographic structure of the UK population that requires improved access to health services. Managing patient satisfaction represents another major challenge. Evidence from a recent national survey in the UK shoes that dissatisfaction with the NHS has increased by seven percentage points in 2017, reaching 29 percent, its highest level since 2007.2 Staff shortages, long waiting times for surgical operations and access to care, inadequate funding, and slow-paced government reforms are among the reasons for dissatisfaction. For hospitals, long waiting times at the A&E department, and delays for patients in need of critical care represent major concerns.3
Unsatisfactory health care service experiences generate negative outcomes for health service providers in terms of managing patients’ experience of care, and meeting performance targets. As patients are ultimately the receivers of health care provision, understanding their experiences of care is pivotal.4 The psychological processes underlying patients’ perceptions and evaluations of service provided by the health care professionals, play a crucial role in patient satisfaction. The cognitive processes of patients and their support network, such as friends and relatives, influence perceptions and attitudes towards health care treatment and service. Research underpinned by knowledge from social psychology can shed light on such cognitive processes and generate insights for effective management of patient satisfaction.
The concept of psychological threat in health care service experiences can be explained through the notion of ‘lock-in situations’5 perceived by the patients. For instance, when visiting a hospital or a GP surgery, patients often undertake externally-imposed activities, such as long waiting time for a doctor’s appointment, ease of self-service check-in, lack of acuity in self-care and monitoring, and/or unsatisfactory interactions with support staff – all parts of the service provision. Such situations can be perceived as a threat to the self-determination needs, such as the need for autonomy. Patients who regularly use health care services in the UK associate four main types of threat to health care service experiences, in response to which coping strategies are activated. We discuss these below.
Perceived threats associated with health care services
Patients who use health care services in the UK often report situations they find threatening or questioning their astuteness and sense of control. Interactions with health care staff can make patients feel unintelligent and/or incompetent and restricted in personal control. This is typical of encounters where healthcare support staff are unable to address patients’ queries accurately, and their attempt at resolving the issue is perceived subconsciously as unnecessary and inappropriate by the patients. The above seems to be due to a general lack of trust in the competence of health care personnel, and more conspicuously the perception that they were not willing to act in the interest of patients. Poor health status at the time of accessing health care services might also hinder patients’ willingness to accept advice from health care professionals. Such experiences of threat to self-competence are often associated with negative or even vengeful behavior towards the health service provider, which is the party perceived as threatening. The psychological mechanism behind such behavior is that retaliation alleviates the emotional discomfort caused by threat perceptions6.
Threats to personal control are often reported when processes in the health care service provision are perceived as inadequate and lead to, for instance, long waiting times for appointment booking and/or rescheduling. Our qualitative research show that patients perceive the process of booking a doctor’s appointment as ‘a nightmare’, ‘particularly time-consuming’ and ‘complicated’. They perceive a loss of control when seeking to book or reschedule an appointment. When appointments are not scheduled around their commitments, patients perceive that they are not being heard.
Furthermore, health care service experiences are perceived as threatening to the individual’s self-esteem; especially in situations where patients feel ignored by the health care personnel, and their own self-esteem and social identity are being undermined. A key reason is the perceived lack of empathy and concern of health care personnel during interactions with patients.
How patients activate coping strategies
The lock-in situations discussed above can affect satisfaction and well-being, despite patients’ general compliance with requests from health care personnel.5 Social psychology research shows that perceived threats, such as those reported in health care service experiences, increase feelings of anxiety, averseness, lack of control, and aggressiveness.6 Crucially, in response to threats and consequent negative feelings, patients activate coping strategyas a mechanism of self-defense. We postulate that coping strategies, in turn, influence their behavior, aimed at compensating for the unsatisfactory experience7. Such behaviour can be negative, and at times even vindictive towards the health care service provider.
Social psychology research distinguishes between individual’s coping strategies8 aimed at addressing the source of the threat (i.e. problem-focused coping), and those focused on re-establishing positive emotions, for instance through the act of venting dissatisfaction caused by the threat (i.e. emotion-focused coping). In health care services, patients often seek to proactively react to threats, thereby engaging in problem-solving. This is especially the case when unsatisfactory health care service experiences are aggravated by a serious illness. Severity of the illness markedly influences patients’ willingness to take actions in response to threats. Crucially, the decision to act seems to benefit patients, as they report feeling ‘back in control of the situation’ – a form of compensatory behaviour9. Cerebral activities, such as rational and positive thinking, influence the extent to which patients confront threats. Rational thinkingcan induce patients to take a step back from the experience, reconsider the factors at play, and plan their next actions.
Crucially, in the process of coping with threats imposed by health service experiences, patients often feel overwhelmed. Negative emotions in such threatening circumstances are heightened, and the support from their network of friends and family appears to be fundamental. Intriguingly, for some patients, social media is increasingly seen as a useful source of emotional support, which appears to be gradually replacing conventional forms of verbal, face-to-face support.
Final remarks
We offer an overview on how insights from social science research can be valuable for informing decision-making of health care service providers. This is especially the case in decisions related to staff hiring, training and development, service process improvement and supporting systems design. Lack of empathy and concern from frontline health care staff, outdated service processes and systems represent threats to patients. An implication is that innovative training of frontline staff is necessary for the development of soft skills, which are highly valued by patients. Developing caring and supportive relationships between health care personnel and patients is necessary, as these have considerable bearing on the outcome of healthcare service experiences. Similarly, introducing the practice of simulating patients’ care experience can help to identify threats whilst introducing service improvements and innovations. There is also need for health care service providers to be aware of the fact that patients’ health status at the time of seeking access to and experiencing health services influences their evaluations of the quality of care and of the service experience. It follows that the service provision needs to be adapted to account for patients’ health status and vary according to different patients’ groups. Insights from social science research can inform practice for enhanced provision of health care services. Further survey-based research focusing on the causal links between psychological threat, coping and patient well-being10 is on hand.
Colorectal cancer is the fourth most common cancer in the United Kingdom (UK), and accounts for 10% of all cancer deaths.1 The symptoms of colorectal cancer are often non-specific and in its early stages there may be no symptoms at all. Survival is directly linked to stage of disease at diagnosis – five-year survival falls from 98% for stage I disease down to 40% for stage IV disease.2
Thirty percent of all colorectal cancers are diagnosed via the ‘Two-Week Wait’ (2WW) referral route in the UK. The remainder are diagnosed following emergency presentation (24%), non-2WW GP referral (24%), bowel cancer screening (9%) or by other pathways (13%).3
The TWW referrals for patients with suspected cancer were introduced in 2000 by the NHS Cancer Plan,4 and built on the earlier recommendations of the Calman-Hine report into commissioning cancer services.5 These improvements sought to address the United Kingdom’s relatively low cancer survival rates compared to the rest of Europe, and to address the delays in diagnosis and treatment that some patients were encountering. In order to standardise cancer care nationally, 2WW referral guidelines were introduced by the Department of Health in 2000.6 These guidelines were reviewed and updated in 2005 by the National Institute for Clinical Health and Care Excellence (NICE).7
In November 2015, NICE updated all its 2WW referral guidelines, including those for suspected colorectal malignancy.8 The recommendations were developed following a systematic review of the literature which recommended referral for patients with symptoms deemed to have a positive predictive value for colorectal cancer of 3% or more. This was a reduction from the previous guidelines, which used a positive predictive value of greater than 5%.9 The original (2005) and updated (2015) NICE colorectal 2WW referral guidelines are outlined in Table 1.
This study measured the effect of the change in colorectal 2WW referral guidelines on the following outcomes:
Volume of referrals to the colorectal 2WW clinic
Rate of detection of colorectal cancer
Rate of detection of non-colorectal cancer
Adherence to the 2WW referral guidelines
Table 1. Summary of the 2005 and 2015 NICE Two-Week Wait referral guidelines for suspected colorectal cancer 7,8
2005 Criteria
2015 Criteria
Age >40 with rectal bleeding and a change in bowel habit for >6 weeks
Age >40 with unexplained weight loss and abdominal pain
Age >60 with rectal bleeding without a change in bowel habit for >6 weeks
Age >50 with unexplained rectal bleeding
Age >60 with change in bowel habit without rectal bleeding for >6 weeks
Age >60 with change in bowel habit or iron-deficiency anaemia
Right lower abdominal mass consistent with involvement of the large bowel
Positive faecal occult blood test
Palpable rectal mass (intra-luminal)
Palpable rectal or abdominal mass
Unexplained iron deficiency anaemia in: non-menstruating Women with an Hb <10g/100mL men with an Hb <11g/100mL
Age <50 with rectal bleeding and one of: abdominal pain change in bowel habit weight loss iron-deficiency anaemia
Methods and materials
We undertook a retrospective analysis of referrals to the colorectal 2WW service at a large inner city teaching hospital (Bristol Royal Infirmary, UK). All the patients referred in two-month periods before (July to August 2015) and after (July to August 2016) were included in the study. The referral guidelines changes were identified and their clinical notes were reviewed. The specific variables recorded for each referral included: age, gender, presenting symptoms and signs and subsequent diagnosis. All records were cross-referenced against the regional cancer registry.
Differences between the two groups were assessed for statistical significance using Chi-Squared and unpaired T-tests. Count data was assessed for significance using the Poisson Means test at a 95% confidence interval. Statistical tests were calculated using the MEDCALC statistical software.
Results
A total of 193 and 268 patients were referred in each of the two study periods. The data collection was complete for all patients. The demographics, referral data, and cancer detection rates are summarised in Table 2.
There was a significant increase in the volume of patients referred via the 2WW pathway following the change in the guidelines (193 vs. 268, p<0.01). There was no significant change in the rate of colorectal cancers detected (8.3% vs. 7.5%, p=0.75).
There was no significant difference in the rate of detection of any cancer (including colorectal cancer) following the 2WW referral (11.4% vs 10.8%, p=0.83). The non-colorectal cancers detected (15 in total) were predominantly metastatic cancers; from lung, ovarian, or prostatic primary malignancies. There was no significant difference in the detection rate of non-colorectal cancers (3.1% vs. 3.4%, p=0.85).
The rate of compliance to the referral guidelines was significantly higher following the update in referral guidelines (72% vs 89%, p<0.01).
In the second study period (July - August 2016), there was a sub-group of 31 patients whose referrals met the new (2015) referral guidelines, but who would not meet the previous (2005) referral guidelines. The mean age in this group was 58.5 and none of these patients had a cancer detected following the 2WW referral.
Table 2. Summary of the results
Jul-Aug 2015
Jul-Aug 2016
p value
Patients referred
193
268
<0.01 a
Cancers detected (% of total)
22 11.4%
29 10.8%
0.74 a 0.83 b
Colorectal cancers (% of total)
16 8.3%
20 7.5%
0.58 a 0.75 b
Non-Colorectal cancers (% of total)
6 3.1%
9 3.4%
0.61 a 0.85 b
% of referrals compliant with the guidelines (at that time)
72%
89%
<0.01 b
Mean age in years (Median age, range)
68.2 (69, 24-92)
67.9 (69, 22-93)
0.81 c
Sex ratio (M : F)
43 : 56
46 : 53
Frequency of referral signs/symptoms (%)
Change in bowel habit
60
63
0.51 b
Rectal bleeding
33
39
0.18 b
Abdominal pain
37
33
0.37 b
Unexplained weight loss
22
20
0.60 b
Iron deficiency anaemia
27
22
0.21 b
Statistical test used: a Poisson Means Test, b Chi squared test, c Unpaired t-test
Discussion
This study has shown that the volume of patients being referred to the colorectal 2WW service has significantly increased in a large inner city unit following the update to referral guidelines in 2015. A significantly greater proportion of referrals are compliant with the new guidelines compared with the previous guidelines. Despite this, we found no significant change in the rate of colorectal cancer detection. Our colorectal cancer detection rates following 2WW referral are similar to the published data series (6-14%).10,11,12
The factors contributing to the increased referral rate includes removal of time constraints and referral for symptoms not previously included within the guidelines (e.g. abdominal pain, unexplained weight loss). The updated guidelines are subsequently less specific and use signs and symptoms with a lower positive predictive value for colorectal cancer than previously.8
In their costing statement for the new guidelines, NICE acknowledge that the updated guidelines are likely to increase referral volumes. The justification given is that “benefits are anticipated from earlier diagnosis of cancer”.9 This study challenges that supposition – no cancers were detected in the latter group of 31 patients whose referrals met the new guidelines, but would not have met the old referral guidelines.
Studies prior to the update in guidelines have also challenged the view that 2WW referrals lead to earlier detection of cancer. When compared with ‘non-2WW’ outpatient referrals, patients referred via a 2WW pathway had no significant difference in the stage of disease at diagnosis,13,14 nor any significant difference in the related outcomes such as 2-year survival,15,16 5-year survival,15,17 or proportion undergoing curative surgery.14,15
Bowel cancer screening remains the only method with a strong evidence base for detecting colorectal cancers at an earlier stage.18 Cancers detected in this manner are disproportionately lower in stage,19 and are associated with a significant reduction in mortality.20 This study did not assess the impact of screening on cancer detection rates via the 2WW referral process, although the logical effect of increased detection of cancers via screening would be a proportional fall in cancers detected by other routes, including the 2WW pathway.
The findings of this study appear to challenge the anticipated benefits of the new 2WW referral guidelines. A group of patients were identified whose referrals only met the 2015 guidelines; these referrals would have been deemed inappropriate by the 2005 guidelines. This group of patients were generally younger and none went on to a cancer diagnosis. If other units (or multi-centre studies) corroborate these findings then this should prompt urgent review of the 2WW guidelines with regards to cancer stage at diagnosis and longer term outcomes.
Conclusion
The updated 2WW referral guidelines for suspected colorectal cancers have increased the volume of patients being seen via the 2WW service without increasing cancer detection rates. This is anticipated to have secondary effects on waiting times for routine and endoscopic services; this has not been evaluated in this study. Further research is needed to contextualise all of these findings with cancer detection rates via screening and other non-2WW routes to diagnosis.
According to DSM V, delirium is defined as disturbance in attention (i.e., reduced ability to direct, focus, sustain, and shift attention) and awareness (reduced orientation to the environment). This disturbance develops over a short period of time and it represents an acute change from baseline attention and awareness, and tends to fluctuate in severity during the course of a day.
The focus of the researchers has shifted from treatment to prevention of the syndrome. There is a need to study risk factors for prevention of delirium1. Data on delirium in the intensive care unit is scarce in the Indian subcontinent2.
A multicenter study indicated risk factors significantly contributing to delirium were related to patient characteristics (smoking, daily use of more than 3 units of alcohol, living alone at home), chronic pathology (pre-existing cognitive impairment), acute illness (use of drains, tubes, catheters, use of psychoactive medication, a preceding period of sedation, coma, mechanical ventilation) and the environment (isolation, absence of visit, absence of visible daylight, transfer from another ward, use of physical restraints)1. Psychoactive medications can provoke a delirious state. Lorazepam has an independent and dose related temporal association with delirium3.
Each additional day spent in delirium is associated with 20% increased risk of prolonged hospitalisation and 10% increased risk of death4.
Hence, the present study was done to assess risk factors and precipitating factors of delirium in a medical intensive care unit of a tertiary care hospital.
Materials and methods:
This is an observational study done over a period of 1 year in a tertiary care medical college hospital located in southern part of India. Ethical committee approval for the study was obtained from the institutional ethical committee.
All patients admitted to medical intensive care unit in our tertiary care hospital, were screened for presence of delirium during the first 72 hours of admission using Richmond Agitation Sedation Scale (RASS) and Confusion Assessment Method for ICU (CAM-ICU). Patients with delirium were classified as delirious and the remaining as non-delirious patients. Comatose patients (RASS score -4 or -5) were excluded from the study.
Patients were initially screened with Richmond Agitation Sedation Scale (RASS). It is a 10-point scale, with 4 levels of agitation (+1 to +4) and 5 levels of sedation (-1 to -5). Level zero indicates calm and alert patient. Patients with RASS score of -4 or -5 (deep sedation and unarousable patients) were excluded from the study. Patients with RASS score of +4 to -3 were then screened for presence of delirium using Confusion Assessment Method for ICU (CAM-ICU). CAM–ICU has 4 criteria:
1) Acute onset and fluctuating course of delirium
2) Inattention
3) Disorganized thinking
4) Altered level of consciousness
The diagnosis of delirium requires the presence of criteria 1 and 2 and of either criterion 3 or 4.
Risk factors for developing delirium were assessed in the study population. Risk factors are those proven factors which may also be present before patient’s admission to intensive care unit, and which predispose the patient to develop delirium. Risk factors were compared between delirious and non-delirious patients. Risk factors which were assessed were history of diabetes and hypertension, history of previous stroke, history of previous cognition impairment, history of previous psychiatric illness, history of previous trauma, history of previous episodes of delirium, history of bowel and bladder disturbances prior to admission (such as constipation and urinary retention respectively), history of alcohol abuse (consumption of more than 2 units of alcohol), history of smoking (more than 10 cigarettes per day), history of consumption of substances other than cigarettes and alcohol (such as cannabis, cocaine etc.), history of uncorrected visual or hearing disturbances before admission, history of usage of barbiturates (such as phenobarbital), benzodiazepines (such as alprazolam, chlordiazepoxide, clobazam, clonazepam) & opioids (such as morphine) before admission, history of usage of sedatives (such as haloperidol, midazolam, fentanyl) and pain killers (such as morphine, tramadol) at the time of admission. Metabolic risk factors which were compared between delirious and non-delirious subjects were uraemia, hyponatremia, hyperbilirubinemia, metabolic and respiratory acidosis.
Precipitating factors weredefined as factors that were the likely causes of delirium in delirious patients. Precipitating factors for delirium which were looked into were exposure to toxins (alcohol/drugs), deranged metabolic parameters, infections and central nervous system causes.
SPSS21 software was used to calculate statistics. Independent t-sample test and the Pearson Chi-square test were used to calculate differences between delirious and non-delirious subjects. Odds ratios (OR) was calculated for all factors using univariate binary logistic regression.
Results:
Total number of patients enrolled in the study was 1582, of which 406 were diagnosed with delirium. Percentage of patients developing delirium within first 72 hours of admission was 25.7%. Hypoactive delirium was present in 52% and hyperactive delirium in 48% of patients. Patients who experienced delirium (57.5 + 17 years) were older compared to their non-delirious (53.3 + 18.1 years) counterparts (p value <0.0001). Among delirious subjects, majority were in the age group of 61-70 years (Figure 1).
Figure 1- Age distribution among delirious patients
38.2% of delirious patients and 39.3% of non-delirious patients were females. 61.8% of delirious patients and 60.7% of non-delirious patients were males.
Alcohol consumption [OR = 6.54 (95% CI 3.76-11.4, p = 0.0001)], previous psychiatric illness [OR = 3.73 (95% CI 1.712-8.159, p = 0.033)], previous cognition impairment [OR = 2.739 (95% CI 1.509-4.972, p = 0.001)], sedatives usage at the time of admission [OR = 2.488 (95% CI; 1.452-4.264), p = 0.001)], visual disturbances [OR = 2.227 (95% CI; 1.328-3.733, p = 0.002)], bowel and bladder disturbances [OR = 1.677 (95% CI 1.044-2.693, p = 0.032)] were significant risk factors contributing to delirium after univariate analysis (Table 1). Metabolic acidosis [OR = 1.996 (95% CI 1.469-2.711, p = 0.0001)] and hyperbilirubinemia [OR = 1.448 (95% CI 1.111-1.886, p = 0.006)] were significant metabolic parameters contributing to delirium after univariate analysis (Table 2).
Precipitating factors (Table 3) for delirium are those factors that were considered the most likely causes of delirium among the delirious patients. Precipitating factors for delirium were classified into toxins, deranged metabolic parameters, infections and central nervous system causes, of which metabolic parameters were most common. Among metabolic parameters, uraemia (25.1%), hepatic encephalopathy (22.7%) and hyponatremia (19.5%) contributed to the majority of cases with delirium.
Table 1 – Univariate analysis of risk factors of delirium
NO DELIRIUM
DELIRIUM
COUNT
%
COUNT
%
P
UNIVARIATE
Diabetes
No
729
62
226
55.7
.025
1.3(1.1-1.6)
Yes
447
38
180
44.3
Hypertension
No
684
58.2
239
58.9
.8
.97(0.8-1.2)
Yes
492
41.8
167
41.1
History of Stroke
No
1107
94.1
379
93.3
.6
1.14(0.7-1.8)
Yes
69
5.9
27
6.7
Previous memory disturbances
No
1149
97.7
264
89.7
<.0001
4.9(2.9-8)
Yes
27
2.3
42
10.3
Previous psychiatric illness
No
1161
98.7
386
95.1
<.0001
4(2-7.9)
Yes
15
1.3
20
4.9
Trauma
No
1137
96.7
396
97.8
.3
0.6(0.3-1.3)
Yes
39
3.3
9
2.2
Previous episodes of delirium
No
1155
98.2
402
99
.3
0.55(0.2-1.6)
Yes
21
1.8
4
1.0
Bowel & bladder disturbances
No
1107
94.1
350
86.2
<.0001
2.6(1.8-3.7)
Yes
69
5.9
56
13.8
Alcohol
No
1089
92.6
336
82.8
<.0001
2.6(1.8-3.7)
Yes
87
7.4
70
17.2
Smoking
No
981
83.4
354
87.2
.07
0.7(0.5-1.03)
Yes
195
16.6
52
12.8
Other substance abuse (apart from cigarettes and alcohol)
No
1071
91.1
391
96.3
.001
0.4(0.22-0.6)
Yes
105
8.9
15
3.7
Visual disturbances
No
1062
90.3
298
73.4
<.0001
3.4(2.5-4.5)
Yes
114
9.7
108
26.6
Hearing disturbances
No
1104
93.9
338
83.3
<.0001
3.1(2.2-4.4)
Yes
72
6.1
68
16.7
Barbiturates
No
1155
98.2
401
98.8
.5
0.7(0.3-1.8)
Yes
21
1.8
5
1.2
Benzodiazepines
No
1155
98.2
400
98.5
.7
0.8(0.3-2.1)
Yes
21
1.8
6
1.5
Opioids
No
1176
100
405
99.8
.9
4.7(0-IN)
Yes
0
.0
1
.2
Sedatives usage in present admission
No
1143
97.2
369
90.9
<.0001
3.5(2.1-5.6)
Yes
33
2.8
37
9.1
Pain killers usage in present admission
No
1080
91.8
400
98.5
<.0001
0.17(0.07-0.39)
Yes
96
8.2
6
1.5
Table 2- Univariate analysis of metabolic parameters
NO DELIRIUM
DELIRIUM
COUNT
%
COUNT
%
P
UNIVARIATE
Uraemia
NO
648
55.1
186
45.8
0.001
1.45(1.2-1.8)
YES
528
44.9
220
54.2
Hyponatremia
NO
645
54.8
202
49.8
0.08
1.2(0.98-1.5)
YES
531
45.2
204
50.2
Hyperbilirubinemia
NO
837
71.2
246
60.7
<0.0001
1.6(1.3-2)
YES
339
28.8
159
39.3
Metabolic acidosis
NO
990
84.2
286
70.4
<0.0001
2.2(1.7-2.9)
YES
186
15.8
120
29.6
Respiratory acidosis
NO
1092
92.9
377
92.9
1
1(0.6-1.5)
YES
84
7.1
29
7.1
Table 3- Precipitating factors of delirium in the present study
PRECIPITATING FACTORS
%
Toxins
Drug or Alcohol overdosage
1.5
Alcohol withdrawal
2.7
Metabolic conditions
Hyponatremia
19.5
Hyperglycaemia
6.2
Hypoglycaemia
2.5
Hypercarbia
5.7
Uraemia
25.1
Hepatic encephalopathy (hyperammonemia)
22.7
Infections
Systemic infective causes
16.5
Meningitis/ Encephalitis
8.9
Central Nervous System causes
Hypoperfusion states
14.5
Hypertensive encephalopathy
5.9
Cerebrovascular accident (CVA)
7.6
Intracranial space occupying lesion (ICSOL)
5.4
Seizures
10.3
Psychiatric illness
4.9
Discussion:
Delirium is classified into hyperactive, hypoactive and mixed type. Hyperactive subtype is present if there is definite evidence in the previous 24 hours of at least two out of the following factors - increased quantity of motor activity, loss of control activity, restlessness, wandering. Hypoactive subtype is present if there is definite evidence in the previous 24 hours of at least two of the following factors - decreased amount of activity, decreased speed of actions, reduced awareness of surroundings, decreased amount of speech, decreased speed of speech, listlessness, reduced alertness, withdrawal. Mixed subtype is present if there is evidence of both hyperactive and hypoactive subtypes in the previous 24 hours5. Percentage of patients with hypoactive delirium was high in this study (52%). Hypoactive delirium often carries relatively poor prognosis, occurs more commonly in elderly patients and is frequently overlooked or misdiagnosed as having depression or a form of dementia.
In the present study, delirium was more prevalent in the elderly population. Most of the elderly patients will have multiple risk factors making them more vulnerable to delirium. Delirium is often the only sign of an underlying serious medical illness in an elderly patient and particular attention should be given to identify and correct the underlying illness.
History of alcohol consumption of more than 2 units per day, prior to admission of the patient, was the major risk factor contributing to delirium in this study (OR = 6.54). This was similar to other studies done by Bart1 et al & Ouimet6 et al where consumption of more than 3 units of alcohol (OR 3.23) & 2 units of alcohol (OR 2.03) respectively, was a significant risk factor for delirium. Patients with a previous psychiatric illness were at increased risk for delirium in this study (OR – 3.73). However, other studies explaining its importance in contributing to delirium were not available. Previous cognition impairment was a significant risk factor contributing to delirium (OR = 2.73). The study by Bart1 et al found that previously diagnosed dementia was an important risk factor (OR = 2.41). Positive correlation with dementia was reported by McNicoll et al7 (RR 1.4) and Pisani et al8 (OR 6.3). Usage of sedatives (OR = 2.48) at the time of admission was a significant risk factor for developing delirium. Bart1 et al found that use of psychoactive medication may disturb the neurotransmission in the brain provoking a delirious state and use of benzodiazepines is a risk factor for delirium (OR – 3.34). Pandharipande3 et al found that Lorazepam was an independent risk factor for daily transition to delirium (OR – 1.2). Pisani8 et al found that use of benzodiazepines was a significant risk factor for developing delirium with odds ratio of 3.4. Uncorrected visual disturbances were a significant risk factor for developing delirium in this study (OR-2.22). Inouye9 et al found that vision impairment (adjusted relative risk – 3.5) was an independent baseline risk factor for delirium. Bowel and bladder disturbances were a significant risk factor contributing to delirium in this study (OR – 1.67). Morley10 opined that constipation is a frequent, often overlooked precipitating factor for delirium. Tony11 et al was of the opinion that a careful history and physical, including a rectal examination with consideration of disimpaction, may be helpful in assessing and managing delirious patients. Waardenburg12 concluded that significant urinary retention can precipitate or exacerbate delirium, a disorder referred to as cystocerebral syndrome. Liem and Carter13 suggested that increased sympathetic tone and catecholamine surge triggered by the tension on the bladder wall may contribute to delirium. Metabolic acidosis and hyperbilirubinemia were significant metabolic parameters contributing to delirium in this study.Similar findings were reported by Aldemir14 et al.
Among delirious patients, most common precipitating factors for delirium in this study were uraemia (25.1%), hepatic encephalopathy (22.7%) and hyponatremia (19.5%). Alterations of serum electrolytes, renal function predispose to delirium15. Hyponatremia causes delirium and the mechanism is not well understood16, 17. Blood urea nitrogen/creatinine ratio greater than 18 is an independent risk factor for delirium in general medical patients9.Hepatic failure leads to hyperammonemia, which leads to excessive NMDA (N-methyl-D-aspartate) receptor activation, resulting in dysfunction of glutamate-nitric oxide-cGMP pathway and causing impaired cognitive function in hepatic encephalopathy18.Excess activation of NMDA receptors results in neuronal degeneration and death19. In hepatic failure, there may be a shift in regional cerebral blood flow and cerebral metabolic rates from cortex to subcortex resulting in delirium20.
Patients who develop delirium during their stay in hospital have higher 6-month mortality rates, longer hospital stay, increased economic burden and a higher incidence of cognitive impairment at hospital discharge21. Limitation of this study was long term follow up of patients who developed delirium was not done.
Conclusion:
Delirium is common in intensive care unit patients and hypoactive delirium is more common. Major risk factor contributing to delirium was alcohol consumption before admission. Most common precipitating factors contributing to delirium were deranged metabolic parameters.
Delirium in ICU patients especially hypoactive delirium is easily missed. Hence, all ICUs should implement both RASS and CAM-ICU for early detection of delirium. Future research needs to be directed at development of scoring systems for detection of delirium, which are easy to use and are accurate.
Schizophrenia sufferers feel like abstract entities with non-animated bodies, often experiencing auditory verbal hallucinations (AVH) due to morbid “objectification” of inner dialogue.1 From the patient’s perspective, AVHs are a subjective–objective phenomenon. AVH is a non-consensual, dynamic and psychologically charged experience and the voices often echo significant emotions. Derogatory voices are common representations of unconscious self-hatred that cannot stand up to the external world’s logic. Thus, patients need help to incorporate it. Auditory hallucinations may be arising because of an interaction between biological predisposition, perceptual and cognitive factors. According to an integrated model of auditory hallucination (AHs) suggested by Waters et al,2 AHs arise from an interaction between abnormal neural activation patterns that generate salient auditory signals and top-down mechanisms that include signal detection errors, executive and inhibition deficits, a tapestry of expectations and memories. Recently, neuro-quantologists have proposed that AVHs may be an objectification of parallel thinking/quantum thinking.3 Parallel thinking is a source for thought insertion. There may be different variables of AVHs. Experiencing AVH has serious impact on the quality of life of the affected individual, and is a significant factor in prevalence of suicides among schizophrenic patients.4
Incidence
One in four schizophrenia sufferers experiences persistent AVH .5 AVHs are experienced by approximately 53% of schizophrenia sufferers 6 and are present in 28% of major affective disorders (Goodwin& Jamison, . 7 Evidence indicates that each patient responds differently to the voices, according to his/her evaluation of them (Table 1), which influences the degree of interventions. Specific dimensions of AVHs can give hints to the future likelihood of treatment resistance. Although the percentages differ in various studies, it is assumed that about 30% of patients have command hallucinations and they are seen as the ultimate betrayal of the mind. 8 Often, the content of such messages is negative; thus, commanding AVHs are more distressing than commenting ones. Schizophrenia predisposes them to a greater risk of suicides and homicides. Command hallucinations are more prevalent among forensic patients and contribute to their forensic status.
Table1. Patients’ Response to AVH
1.Anxiety and panic feelings 2.Fear 3.Feelings of humiliation 4.Entrapment 5.Self harm thoughts 6.Harm to others 7. Avoidant or withdrawn 8.Shouting and swearing 9.Ritualistic behaviour 10. Substance or alcohol abuse 11. Resistance. 12. Amusements 13. Engagement and courting the voices 14. Appeasement
The multi-factorial polygenic model of schizophrenic disorders has received great support and signifies that genetic factors play a bigger role than environmental factors in familial transmission of these disorders. Relevant studies provide little support for the mechanism of single major locus inheritance. A mechanism involving two, three, or four loci cannot be ruled out even though there is no compelling support for such models.9 It has also been proposed that a single gene may be even responsible for hallucinatory experiences 10 implying that those who have not inherited such a gene may not experience auditory hallucinations, but still could experience other characteristic symptoms of schizophrenia. One may also hypothesise that an individual who has inherited such a “hallucinatory gene” but not all the schizophrenia genes could hear non-clinical voices without having other schizophrenic symptoms. It is also arguable that those who carry such a specific gene are more vulnerable to experience hallucinations when they abuse psychoactive substances and could get misdiagnosed as having schizophrenia, but hallucinations may cease to occur once they abstain from illicit drug abuse.
Measurements for Assessment
AVH is a subjective experience and is hard to measure objectively. Several rating scales are now available for an efficient evaluation of different aspects of voice activities. Some are general and a number of them are specifically designed. Using rating scales facilitates better engagement with patients and helps in reinforcing the message that patients and the distress they experience are carefully considered.
Beliefs About Voice Questions (BAVQ) is an assessment scale useful in measuring the key beliefs about the voices.11 It is typically used in conjunction with the Cognitive Assessment Schedule (CAS).12 Voice Compliance Scale (VCS) is an observer rated scale aimed exclusively at measuring the frequency of command hallucinations and the level of obedience or confrontation with each recognized command.13 Voice Power Differential Scale (VPD) is another measure that can be applied to rate the perceived relative power differential between the voice and voice experience. 14 On the other hand, Omniscience Scale (OS) is intended to quantify the voice hearer’s beliefs about their voices’ knowledge regarding the bio data. 15 Another measure presently in use is Risk of Acting on Commands Scale (RACS), designed to assess the level of risk of acting on commands and the amount of associated distress. 16
The Bonn Scale (BSABS) is used for the assessment of basic symptoms, 17while the Schizophrenia Proneness Instrument (SPI-A) 18and the Examination of Anomalous Self Experience (EASE) 19 are useful aids in identifying minimal changes in subjective experience and for longitudinal monitoring (Table 2). In the extensively used Positive and Negative Syndrome Scale (PANSS), the hallucination item is one of seven in the positive subscale, which also includes delusions, conceptual disorganization, excitement, grandiosity, suspiciousness, and hostility. Given such a great number of scales in use, there is an obvious risk that differential anti-hallucinatory efficacy among antipsychotic drugs may be obscured by means of sum scores for the whole sample in clinical trials.
Table 2. Measurement scales
Beliefs About Voice Questions (BAVQ) Cognitive Assessment Schedule (CAS ). Voice co Voice Power Differential Scale (VPD) Voice Compliance scale (VCS) Voice Power Differential Scale (VPD) Omniscience Scale (OS) Risk of Acting on Commands Scale (RACS) Bonn Scale (BSABS) Schizophrenia Proneness Instrument (SPI-A) Examination of Anomalous Self Experience (EASE) Positive and Negative Syndrome Scale(PANSS)
Treatments
Although many forms of treatments aiming to eliminate AVH or improve quality of life are available, use of medication seems to be the most prevalent. Besides drug treatment, non-invasive physical treatments, such as TMS and different forms of psychological interventions, have recently evolved. Drug therapies are aimed at symptom eradication, whereas psychological therapies tend to foster healing, recovery and personal growth. Rather than being specifically anti-hallucinatory, typically, neuroleptics offer a generalised calming effect and patients are given some “breathing space” to work through their voices. Usage of non-pharmacological tools is needed in the long-term management of refractory cases. Presently, intervention strategies for AVH are based on different models of hallucinations, but regrettably no clear models have been established.
Pharmacotherapy
The current understanding of AVH and the neural mechanisms involved is limited, and knowledge on how CNS drugs, such as antipsychotics, influence the subjective experience and neurophysiology of hallucinations is inadequate. Consequently, using pharmacotherapy in the management of AVH remains very challenging. 20 Despite multiple trials of different combination and adjunctive therapies to an antipsychotic regime, AVH can remain drug resistant. It is also important to note that all antipsychotics are potentially anti-hallucinatory, even though these effects are usually modest. Moreover, given that, even when medications are effective, concordance can be an issue, antipsychotics should be used prudently and weighed up against effectiveness and side effects (Table 3). There are no clear guidelines for the drug treatment of AVH and comparisons of the efficacy of antipsychotics for AVHs are few. Clinical drug trials very rarely focus on single symptom scores, such as hallucinations, and tend to report group mean changes of overall psychopathology, or at best the positive subscale scores.
Evidences show that AVHs persist in spite of treatment in 32% of chronic patients 21 and 56% of acutely ill patients.22 Trifluperazine was popular as an anti-hallucinatory drug before the advent of atypical antipsychotic drugs. Clozapine is currently favoured for intractable AVHs and is beneficial in 30–60% of unresponsive patients.
Antipsychotic co-treatment is an option for clozapine augmentation. Olanzapine and risperidone may be alternative drugs in first episode psychosis. However, it is being debated whether clozapine should be used in such cases.
Table 3. Drug Treatment
Choice of antipsychotics Cautions and contraindications Titration of dose Switching antipsychotics Assessment of side effects, EPS, TD, Haematological effects etc. Measuring the beneficial effects Assess worsening of symptoms Compliance
Clozapine
Use of clozapine is suggested only after two other antipsychotics have been tried. It works better with continued usage and clinicians have to be patient in its upward titration. At six months, improvement in Global Assessment of Functioning score is significantly higher for clozapine in comparison to other antipsychotic drugs.23 However, when prescribing clozapine, cautions and contraindications must be noted (Table 4).
While higher doses of clozapine may not have more anti-hallucinatory effect, they still carry the risk of inducing the potential side-effects of this highly efficacious drug (Table 5). The most dreaded haematological side-effects are usually manifested within six months. For that reason, during clozapine therapy, patient has to be closely monitored, bearing in mind its limitations in achieving the anti-hallucinatory effects. If higher doses do not have the desired effect, clozapine dose should be titrated downwards to a point of its maximum anti-hallucinatory effect in a particular patient. Such an endeavour can prevent the emergence of serious side-effects, resulting in a complete failure of the therapy. The dose can also be adjusted to a safer level in cases where the psychological interventions are found to be successful. Clozapine can be effective even in lower doses, such as 200 mg/day. Only in the presence of command hallucinations, higher doses should be prescribed to patients whose other positive symptoms are well under control.
Prophylaxis with an antiepileptic drugs, such as lamotrigine or sodium valproate, or similar should be commenced before titrating the dose above 600 mg daily. Close monitoring and active treatment of metabolic dysregulation should be initiated concurrent with clozapine therapy. In clozapine therapy, weighing up safety and superior antipsychotic efficacy and educating the patients on “clozapine lifestyle” is immensely important, as it helps in treating refractory cases of AVH. Thirty percent of patients treated with clozapine may remain unresponsive and clinicians have to lower their expectations to the level of achievement without being cynical. Isolated cases of clozapine-induced joint visual and auditory hallucinations have been reported. 24 In spite of Clozaril treatment having the highest anti-hallucinatory effect, a good percentage of AVH sufferers remain symptomatic and are classed as super-refractory.8 According to Gonzales (2006), 25 50% of patients receiving antipsychotics achieve full remission, while 25% hear voices occasionally and 25% are unresponsive.
Table 4. Cautions & Contraindications of Clozapine
1.Patients with myeloproliferative disorders, a history of toxic or idiosyncratic agranulocytosis or severe granulocytopenia (with the exception of granulocytopenia / agranulocytosis from previous chemotherapy) 2.Bone marrow disorders 3-Patients with active liver disease, progressive liver disease and hepatic failure. 4-Severe CNS depression or comatose state, severe renal and cardiac disease, uncontrolled epilepsy, circulatory collapse, 5. Alcoholic/toxic psychosis and previous hypersensitivity to clozapine. 6.Pregnancy and breast feeding
Table 5. Benefits and risks of Clozapine
Benefits 1. Lower risk of suicide 2. Superior anti-delusional and anti-hallucinatory effects in refractory cases 3. Lower risk of tardive dyskinesia and suppression of TD. 4. Improvement in cognition 5.Higher quality of life and better adherence 6.Decreased relapse 7. Sexual functions unaffected Risks 1.Agranulocytosis 2.Metabolic syndrome 3.Myocardites 4.Chronic constipation and bowel complications 5.Incresed risk of seizure 6.Hypersalivation 7.Abrupt withdrawal cause marked discontinuation symptoms.
Benzodiazepines are often abused by voice hearers aiming to reduce their anxiety. Such patients might benefit by the addition of antidepressant, as this could enhance their mental resources to cope with the voices, even though they have no anti-hallucinatory effects per se. Mood stabilisers are sometimes used to augment the efficacy of antipsychotics without any clinical validation. Despite multiple trials of different adjuvant therapies to an antipsychotic regimen, there have been few promising results. Still, in practice, clinicians may get frustrated, as they struggle to provide symptomatic relief to the voice hearers at any cost. Recently allopurinol, an anti-gout agent has been used as an adjunctive therapy and based on three randomized controlled trials, the result has been encouraging. 26
Psychological Interventions
Persistent AVHs alone may not warrant pointless alteration of medication, as non-pharmacological interventions may achieve some control. When clinicians are not cognizant of non-pharmacological therapies, AVH patients that do not respond to antipsychotics alone may be mislabelled as having refractory AVH. In fact, they are only unresponsive to drug treatment, and could potentially respond to an integrated approach. Similarly, patients with treatment-refractory AVH are often over-diagnosed as suffering from hard to treat schizophrenia, even when other positive symptoms have been ameliorated.
There exists a false dichotomy between physical and psychological treatment approaches to AVH. In practice, both treatment modalities have to be modified in a personalised form. After all, psychiatry was originally known as psychological medicine. Presently, even though different forms of non-pharmacological interventions are available for drug-resistant AVH, some have questionable effects. 27,28,29 (Table 6).
Table 6. Psychological Interventions
1.Cognitive behavioural therapy (C.B.T.) 2. Acceptance and commitment therapy (ACT) 3. Competitive memory training (COMET) 4.Compassionate Mind Training therapy (CMT) 5.Hallucinations focussed integrative therapy (HIT) 6.Midfulness-based therapy 7.Normalizing techniques 8. Enhanced supportive psychotherapy 9. Attention training technique. 10. Distraction techniques 11. Self help approaches
CBT therapists predicate that AVHs are a manifestation of the morbid objectification of inner dialogue (thinking in words),and accordingly verbalised thoughts are the raw material for AVHs.Verbal thinking differs from external speech in many respects and has several distinct features. CBT therapists believe that cognitive dysfunctions underlie AVH and they target them with cognitive remediation strategies. Those experiencing voices commonly think that they are caused by a powerful external agency, and are controlling and potentially harmful. Psychological factors, such as meta-cognitive biases, beliefs, and attributions concerning the origins and intent of voices, also play critical modulatory role in shaping the experience of AVH. Teaching patients to recognize the source of the voices alone has yielded beneficial effects.
Specific techniques have been designed to modify the frequency of AVHs and restore a sense of control over them. Earlier methods involved behavioural approaches based upon addressing hypothesized antecedents and reinforcers of voices and explored a variety of specific interventions such as relaxation training, graded exposure to voice triggers, manipulation of environmental possibilities and even aversion therapy. 30 These behavioural techniques were eventually expanded on by the application of cognitive methods. The primary aim of psychological therapy is to change the belief that voices are omnipotent and uncontrollable and to suppress the associated attributes of false identity, wrong intentions, and urges to harm oneself and others. They encourage patients to challenge irrational interpretations and modify maladaptive behaviour, diverting attention from voices with distraction techniques (Table 7).
Reality testing and behavioural experiments are one form of CBT intervention, based on the view that behavioural changes can prompt cognitive changes. Attention switching can also be used to challenge the belief that hallucinations are uncontrollable. Command AVHs are more prevalent among the forensic population and are more distressing than the commenting ones. The risk of the sufferer acting on them is high when voices are perceived as omnipotent and uncontrollable. CBT has been proven beneficial in tackling command hallucinations. Lack of insight and formal thought disorder may not necessarily disqualify CBT for AVH; nonetheless, negative symptoms may pose a barrier to this form of psychological intervention. The current model of CBT for psychosis has been criticized, suggesting that it is simply an extension of general CBT concepts without taking into account the specificities of psychosis. 31 Patients with higher intelligence, who have the ability to grasp abstract concepts, might gain greater benefits from CBT. 32
Table 7. Goals of CBT
1. Change false beliefs about AVH . 2. Challenge irrational interpretations. 3. Modify maladaptive behaviour – e.g. fear of the voices or hiding from them. 4. Divert attention, using distraction techniques. 5. Build and maintain treatment strategies 6.Develop cognitive behavioural strategies 7.Develop newer understanding of hallucinatory experience 8. Address negative self-evaluation.
Combining psycho-education and supportive psychotherapy has been found to enhance the functioning and self-esteem of voice hearers, providing a therapeutic structure. In the increasingly popular self-help voice-hearing groups, the ethos of recovery is understanding, accepting and integrating the sufferer’s turmoil. Acceptance and non-judgemental support of people with similar experiences has helped many patients cope with the condition. In response, the number of books on AVH, aiming to educate the sufferers and carers, has grown considerably.
Newer Psychological Interventions
Attention Training Technique (ATT) focuses on negating psychological distress through cognitive and meta-cognitive modification. 33,34 Patients focus on up to five neutral sounds, such as a dripping tap, before switching their attention between different sounds. They then practise listening to all the sounds simultaneously. After a few weeks, they focus on neutral sounds and then on the AVH. Once this process is mastered, they switch attention between voices and other sounds, before being asked to divide their attention among them. This exercise continues for several weeks, whereby the aim is to replace the self-regulatory process with new processing configurations.
Acceptance and commitment therapy (ACT) is aimed at achieving psychological flexibility. It incorporates mindfulness and acceptance, considering AVH as a private experience and asserting that patients experience distress only when they try to deafen the voices. . By reducing struggle with voices and engagement with them, key responses such as arousal, attention and activation of brain areas are hypothesised to be reduced. 35 The ideas behind ACT are consistent with the emphasis on the recovery movement of finding a way to live a valued life despite the ongoing problems. To this effect, unique and effective coping strategies are offered, whereby patients are given the insights that parts of the self are behind the voices. Thus, accepting them means sending a loving message of compassion, acceptance and respect to oneself Two randomised control studies have yielded promising results. 36,37ACT follows a set manualised structure, rather than relying upon the complex and lengthy process of belief modification: therapy can be much briefer and potentially practiced by a wider range of clinicians and cost effective. 38
There are verbal and non-verbal routes to emotions. As CBT uses the former in voice therapy, it is less effective when patients are negatively involved with the voices. On the other hand, Competitive Memory Training (COMET) uses the non-verbal route. Generally COMET sessions involve four stages.39 A. identification of aspects of negative self-esteem reinforced by the voice; B. retrieval and re-living of memories associated with positive self-esteem; C. positive self-esteem is brought to compete with the content of the voices to weaken associations between voice content and negative self-valuation; and D. learning to disengage from the voices and to accept the voices as psychic phenomenon.
The significant past comes back to the conscious mind in AVH, as life experiences charged with emotion make a compelling impression on the brain. The observation that voices are knowledgeable about patients suggests that auditory hallucinations are linked to memory. In other words, negative experiences from memories evoke emotions, which should be deactivated. Distancing and decentring techniques could help patients to interpret voices as false mental events. As a result, incompatible memories could become tools to modify the power of voices—they are deactivated by new learning. Thus, when voices torment hearers, telling them that they are failures, a competing memory of such success as passing a significant examination is introduced. Posture, facial expression, imagination, self-verbalisation and music are all procedures included in the COMET protocol.40
Compassionate mind training (CMT) is used to encourage better resilience to unpleasant commenting voices.CMT involves practicing exercises which promote self-compassion and compassion towards others. It is targeted to activate brain systems involved in social and self-soothing that amend threat systems active when experiencing unfriendly voices. 41
Mindfulness is paying attention in a particular way – on purpose, in the present moment and non-judgementally. Clinical literature cautions against use of meditation in psychosis, but the effectiveness of mindfulness-based approaches for people with psychosis has been demonstrated in controlled clinical settings. 42and in the community. 43 Abba et al. 44 argue that effectiveness of mindfulness is a three-stage process: a. Becoming knowledgeable and developing more awareness of psychotic experiences and observing the thoughts and emotions that follow them. B. Permitting psychosis to come and go without reacting in order to cultivate understanding that distress is produced by the meanings one attaches to thoughts and sensations. C. Becoming autonomous by accepting psychosis and the self by acknowledging that the sensations only form part of the experience, and are not a definition of the self.
Neuroimaging studies are beginning to explain the neural mechanisms of how mindfulness might be working clinically. Structural changes have been observed in the anterior cingulate cortex, which is an area of the brain associated with emotional regulation. 45 . There is evidence to suggest that mindfulness practice is correlated to reduced brain activity in the default mode network. 46
Limited improvements with mono-therapy have prompted the development of multi-modular approaches. Hallucination-focused Integrative Therapy (HIT) is geared towards integrating CBT with neuroleptics, coping strategies, psycho-education, motivational intervention, rehabilitation and family treatment.47 Extant studies indicate that integrated treatment is more effective than TAU (treatment as usual).
The continuum model of psychosis and ordinary mental events has incited the development of normalisation of the voice hearing experience.48 Most psychiatric symptoms occur in normal people—just as breathlessness and palpitations occur while exercising—but are potential clinical symptoms. It is the frequency and duration that determine the borderline. According to the cognitive model, an internal mental event receives external attribution. Through normalisation, the external attribution can be reversed.
Although drug treatment may be the most practical way of managing AVH, refractory cases pose formidable challenges and it must be emphasized that psychological treatments are not counterproductive if applied skilfully. Clinicians who espouse the view that psychosis is a medical condition dismiss the usefulness of psychological interventions. The counter argument would be that a patient with a medical condition, such as stroke, benefits from physiotherapy, occupational therapy and psychological approaches.49
Repetitive Trans-cranial Magnetic Stimulation
There are several ongoing trials in which the aim is to treat refractory AVH (Table 4). Repetitive transcranial magnetic stimulation (rTMS) is thought to alter neural activity over language cortical areas. Several studies on rTMS have shown improvement in the frequency and severity of AVHs, albeit without offering any strong conclusive evidence for its efficacy .50 Moderate rates of AVH attenuation following rTMS have been noted in three meta analyses. Given that remarkable improvements in isolated cases have also been claimed, this suggests that rTMS may be appropriate mode of therapy for some patients.
Available data suggest that .rTMS selectively alters neurobiological factors that determine the frequency of AVH. However, a recent meta-analysis indicated that the effect of rTMS may be short-lived (less than one month).51 Studies seem to indicate that rTMS may be effective in reducing the frequency of AVHs, with little effect on their other topographical aspects.50,52 Sham stimulation has also led to improvements in a number of AVH parameters. Compared to bilateral stimulation, rTMS of left tempero-parietal region appears more effective in reducing the AVH frequency . 53 To reduce the distress associated with AVH and help patients to cope with hallucinatory predilection, rTMS could be combined with CBT. The side-effect profile is much cleaner for this biological approach when compared to medications. Still, like any other anti-hallucinatory treatments, neuro-stimulation technique does not guarantee long-term elimination of AVH. Electroconvulsive therapy (ECT) is considered a last resort for treatment resistant psychosis. Although several studies showed clinical improvement, a specific reduction in hallucinations severity has never been demonstrated.
Avatar Therapy
Computer-assisted voice therapy is a budding form of computerised psychological treatment that is currently undergoing trials.28 In this novel therapy, persecutory voices are directly depowered with the aid of a computerised dummy of the alleged persecutor through voice dialogue. Analytically-oriented therapists can even converse with “voices” and such committed clinicians will find computerised voice therapy as another helpful tool. It is hard to ascertain whether the benefits of the avatar therapy were due to the specific technique involved or simply the increased attention and care, and Leff’s team acknowledged the limitations of their work.54
Sound Therapy
Another important development in voice therapy is the use of tinnitus control instrument (TCI)—a form of sound therapy—in treating refractory AVH. Similar to AVH, subjective tinnitus is defined as the false perception of sound in the absence of acoustic stimuli. Even though their definitions are similar, the origin and underlying causes of these two conditions differ. Tinnitus is characterised by a simple sound—a monotone—and is non-verbal. In tinnitus, the brain is believed to interpret an internally generated electromagnetic signal as an acoustic sound or sounds.
Kaneko, Oda, and Goto29 reported successful intervention in two cases of refractory AVH with sound therapy, using tinnitus control instrument (TCI) alongside antipsychotic medications. They posited that, in sound therapy, the auditory system is directly helping the limbic nervous system and the neuro-mechanism for AVH is sensitive to sound therapy .55 They concluded that low-level auditory stimulation might be hindering the progression of voices and brain might be getting a breathing space to initiate self-healing process.
Future Directions
Hallucinogenic drugs, anti-hallucination medications and neuroimaging studies may lead to a better understanding of AVH. Animal models of hallucinations and pharmacogenetics might help to find more efficacious anti-hallucinatory drugs. AVHs themselves may have a genetic origin.10 Thus, not all patients that develop schizophrenia would experience AVHs. Such a finding might help shed more light on the genetics-linked mechanism and remedial measures of hallucinations in schizophrenia. Because the biological substrates facilitating drug effects on hallucinations remain largely unidentified, future studies with translational designs should address this important issue to find a more targeted drug treatment of psychosis.56
If a derivative of clozapine without the haematological side-effects is formulated in the future, it might be an important milestone in the treatment of refractory AVHs and schizophrenia because clozapine has the most potent anti-hallucinatory effect. Such a novel drug could become the first line of treatment for schizophrenia, as it would address many of schizophrenic symptoms at their onset. This is crucial, as symptoms and habits become stronger and more resistant the more frequently they occur. Fatty acid amide derivatives of clozapine, such as DHA-clozapine, are found to have better pharmacological properties and enhanced safety. However, such claims are awaiting substantiation in clinical trials.57 Thus, more attention needs to be directed into this potentially rewarding research arena. It is, however, very likely that, even after a better pharmacological cure is found for AVHs, a few symptoms might linger on for long periods. With this view, efficient non-pharmacological remedies have to be designed to deal with such residual symptoms.
Discussion
Medications help reduce the psychic pain, and protect the dignity of patients, as well as prevent suicides and homicides. From the patient’s perspective, the calming and relaxing effects of pharmacological therapies are a priority for relief from the distress due to AVH. Among the antipsychotics, clozapine has the maximum anti-hallucinatory effect and it is a shame that it cannot be used as a first line treatment choice. Treatment of AVH should be individualistic and clinicians should be prepared to apply several clinical and non-clinical approaches in concert to address them.
More research into the aetiology and mechanism of AVH is warranted in order to find effective treatment strategies. There is no shortage of theories about the mechanism of AVH, but there is no consensus among the investigators. It is unlikely that AVH is a pure neuro-chemical experience or a biological glitch, and this is where the currently available drug treatments fail. The distinction between primary and secondary symptoms was lost with the triumph of biological psychiatry in the last century. Thus, some authors presently claim that AVHs may even be a secondary symptom or a neuroquantological manifestation of an underlying biological disorder. We should not minimise the importance of eliminating symptoms when such symptoms are incapacitating, as in the case of hallucinatory experiences.
The present recovery model that emphasises and supports the patient’s potential for recovery involving hope, supportive relationship, empowerment, social inclusion, coping skills and meaning cannot be achieved without the help of psychological interventions. In this respect, CBT is a useful tool in the rehabilitation of psychotic patients with residual AVH. Jauhar et al.58 argued that the effectiveness of CBT in schizophrenia is influenced by failure to consider sources of bias. Consequently, the benefits are more apparent than real, prompting the question of whether CBT has been oversold.49 The verdict of Maudsley debate on the issue has been that CBT has not been oversold, but rather has a great impact on symptom reduction and enhancing concordance and insight. Perhaps the most informative trial so far accomplished has been the work on cognitive therapy for command hallucinations, which has proven the benefit of specific model development, and which productively, combined measurement of process and a targeted outcome.59
There is ample evidence suggesting that a combination of family and psychological interventions, alongside pharmacotherapy, can be the most effective way of dealing with refractory AVH.60 The inner dialogue hypothesis of AVH held by CBT therapists has its opponents.61 Patients respond to the voices they experience by utilising inner speech. Some observations with corresponding features weaken the inner-dialogue hypothesis. David and Lucas have demonstrated in a single case study that short-term maintenance of phonological representation (inner dialogue) may co-exist with AVHs – they are not synonymous experiences. The cost-effectiveness of psychological interventions is poorly studied, despite being highly relevant for policy decisions in healthcare.
Computerised voice therapy works better with technically minded, highly intelligent patients. In contrast, individuals of low to average intelligence may require a primarily behavioural approach, with limited efforts to understand concepts, such as automatic thinking and schema. Unlike sound therapy through music playing instruments (iPad, iPod, iPhone, etc.), TCI causes no disruption to daily functioning and can be used continuously. Computerised voice therapy and sound therapy warrant standardised case trials. When it comes to treating AVHs, optimizing compliance, reducing the burden of symptoms, and improving control, quality of life and social functioning should be the therapeutic goals.62 Neuroquantological views of AVHs63 explain the limitations of pharmacotherapy and the usefulness of psychological interventions.
Tuberculosis is an important and major infectious disease worldwide, especially in developing countries with an estimated global case fatality rate of 13% in 2007. The World Health Organization estimated that there were 13.7 million prevalent cases of TB infection worldwide, with each year bringing about 9.27 million new cases, 44% of which are new smear-positive cases1. Musculoskeletal tuberculosis is rare, chest wall tuberculosis is rarer and involvement of costochondral junction is among the rarest forms of tuberculosis. Tubercular costochondritis usually presents with insidious onset non-specific pain and swelling, resulting in delay in the diagnosis. Diagnosis is usually made by typical radiological findings and microbiological and histological evidence of tuberculosis. Treatment consists of antitubercular therapy with or without surgery.
Case report
30 year male, smoker, from low socio economic status presented with history of low grade fever, malaise and anorexia which began gradually two months back. For about one month he had pain in right side of chest just adjacent to lower part of sternum. The pain had started insidiously, gradually worsened with time, and was dull and aching in character. Pain was localized to the right lower parasternal area, occasionally radiating to the back. The pain was aggravated by physical activity and deep inspiration and was relieved to some extent by ordinary anti- inflammatory medications. There was significant history of pulmonary tuberculosis in the patient’s sister 1 year ago. There was no history of cough, haemoptysis, fever with chills or history of tuberculosis in the past.
On general physical examination, the patient was weak and febrile. On local examination, there was a bulge in the right lower parasternal area, corresponding to the right 9th costochondral junction. On palpation, there was severe tenderness in the same area. There was no peripheral lymphadenopathy and abdomen was soft and non-tender with no organomegaly. Chest examination was unremarkable. The rest of the examination was normal.
In terms of investigations, the chest radiograph, ECG, haemogram, kidney function tests and liver function tests were normal. ESR was high (34), Mantoux test was positive(15mm). Sputum for AFB was negative. Axial CT chest demonstrates expansion of the left 9th costal cartilage with soft tissue thickening on both the inner and outer aspect of the cartilage (Fig.1). FNAC (Fine Needle Aspiration Cytology) of the costochondral junction revealed Mycobacterium tuberculosis and on culture and histopathology of aspirated material revealed tubercular granuloma (Fig.2). A final diagnosis of tubercular costochondritis was made and the patient was treated with anti tubercular drugs for 9 months. Patient's symptoms improved after 2 weeks of treatment and swelling and tenderness subsided. Post treatment axial CT demonstrated complete resolution of soft tissue abnormality previously seen around the costal cartilage (Fig.3).
Figure 1: CT chest showing evidence of costochondritis.
Figure 2: Typical tubercular granuloma with central caseous necrosis on histopathology.
Figure 3: Post ATT CT showing complete resolution of costochondritis.
Discussion
Tuberculosis is very common infectious disease in developing countries like India, resulting in significant morbidity and mortality. Musculoskeletal tuberculosis is relatively uncommon and accounts for 1 to 2% of all the tuberculosis patients2,3 and accounts for about 10% of all extrapulmonary TB infections4. Tuberculosis of the chest wall constitutes 1 to 5% of all cases of musculoskeletal TB5,6. TB abscesses of the chest wall are usually seen at the margins of the sternum and along the rib shafts, and can also involve the costochondral junctions, costovertebral joints and the vertebrae7. In one study8, on the basis of the part of the rib involved, the roentgenographic findings for patients with rib tuberculosis was divided into four categories: Costovertebral (35%), Costochondral (13%),Shaft (61%), and Multiple cystic bone. TB of the thoracic wall is usually caused by reactivation of some latent foci of primary tuberculosis formed during hematogenous or lymphatic dissemination but direct extension from contiguous mediastinal lymph nodes can also occur9. In developing countries such as ours, tuberculosis is endemic and all the rare forms of the disease have been described, but in developed countries, resurgence of tuberculosis due to HIV may be responsible for atypical presentations .
Thoracic wall tuberculosis mostly presents insidiously with pain and swelling, but the diagnosis of chest wall TB is often delayed due to lack of specific symptoms and signs and gradual course10. Approximately less than 50% of chest wall TB patients may have active pulmonary TB11,12. Imaging techniques like X-Rays and CT scan play an important role in diagnosis and follow up of these patients. According to a study done by Vijay YB et al13, radiological signs may not be present initially at the time of presentation with symptoms, abscesses or sinuses may be present much before the imaging modalities detect them. Computed tomography (CT) scan is more valuable for localization and detection of bone destruction and soft tissue abnormalities. Atasoy et al demonstrated the role of Magnetic Resonance Imaging (MRI) for early detection of marrow and soft tissue involvement in sternal tuberculosis due to high contrast resolution of MRI14.Diagnosis is usually confirmed by finding acid fast bacilli (AFB) and positive AFB cultures of bone (positive in up to 75% of cases), and caseous necrosis and granuloma on histopathology11.
Complications of thoracic wall tuberculosis include secondary infection, fistula formation, spontaneous fractures of the sternum, compression or erosion of the large blood vessels, compression of the trachea and migration of tuberculosis abscess into the mediastinum, pleural cavity or subcutaneous tissues as discharging sinus. Chest wall TB needs to be differentiated from benign and malignant tumors [chondroma, osteochondroma, fibrous dysplasia, lipoid granuloma, chondrosarcoma, myeloma multiplex]11, metastatic carcinoma, lymphoma or other kinds of infection15,16.
The treatment of choice of chest wall TB is still not clear. Whether antitubercular therapy alone or surgical debridement (or excision based on lesion extension) combined with antitubercular therapy should be done needs further studies. But the general rule is if there are any complications, surgery is the treatment of choice followed by antitubercular therapy. We conclude that the diagnosis of thoracic wall tuberculosis is a challenge for physicians and is suspected by gradual onset clinical features and confirmed by microbiology, histopathology and radiography findings. Early diagnosis and treatment are important to prevent complications caused by bone and joint destruction.
Supporting Professional Activities (SPA) time is a part of each consultant’s new contract. When the new consultant contract evolved in 2003, a suggested breakdown of the week was 7.5 sessions (1 session equates to 4 hours) for direct clinical care (DCC) and 2.5 sessions for SPAs.1 This was driven by the need for consultants to continue their own professional development (CPD) as well as having the time for input into the development of trainees and medical students.
Examples of CPD work for consultants could include audit for improvement of service or patient care, teaching of patients, medical students or trainees, research, publications, aspects of hospital management and involvement in simulation courses e.g. Advanced Life Support (ALS)/Advanced Paediatric Life Support (APLS).
The General Medical Council (GMC) requires that during annual appraisals, doctors should use supporting information to demonstrate they continue to follow “Good Medical Practice”. This mandates that doctors should ‘take part in educational activities that maintain and further develop’ their competence and performance.1 With regard to revalidation, the GMC states you will have to demonstrate that you regularly participate in these activities; at Annual Review of Competency Progression (ARCP) it is imperative that accurate records of these CPD activities are presented at the annual job plan review.2
It is clear, therefore, that the provision of allocated time during the working week to complete these aspects of work life are deemed necessary for consultants. The Royal College of Anaesthetists and Association of Anaesthetists of Great Britain and Ireland both support the original view that a consultant should “typically” have 2.5 SPAs in their contract (though this would have to be subject to individual workload). With the demands of service provision it is clear that consultant SPAs are under threat, with around 40% of new consultants offered jobs with fewer SPA sessions than are thought necessary to allow sufficient non-DCC work.3
Since trainees are subject to similar appraisal and development requirements, we wonder if trainees should be allocated SPA time? For progression through training years and to pass the ARCP, it is necessary to provide evidence of trainee development within clinical practice in a similar way to consultants. This can involve a great deal of extra time. Once (notoriously difficult) exams have been passed, each trainee must go through the application process and prove what skills they have assimilated during their training to date. In fact, the ST3 anaesthesia application criteria states that the following are some of the ‘desirable’ criteria that require evidence:
Relevant academic and research achievements
Involvement in an audit project, or quality improvement project
Interest and commitment to the specialty beyond the mandatory curriculum
Evidence of interest in, and experience of, teaching
Instructor status in an advanced life support course (ALS, APLS)
Involvement in management…and understanding of management
Effective multi-disciplinary team working and leadership
Effective leadership in and outside medicine
Achievement outside medicine
Altruistic behaviour, e.g. voluntary work
The list is extensive and clearly requires a lot of time and input outside of the normal working week. With the expectation that trainees should be prepared to move straight from CT2 to ST3 (assuming their exams are completed), these desirable criteria must be addressed alongside completing other mandatory aspects of training such as, for anaesthesia: an Initial Assessment of Competency (IAC), an Intensive Care Unit (ICU) module, an Initial Assessment of Obstetric Competency (IAOC) and 15 Units of Training. With all these challenges between a core anaesthetic trainee and potential specialist anaesthetic training, there seems little time to complete an adequate number of the desirable criteria; this is a compelling reason to facilitate some time into the trainee contract to help produce more well rounded trainees.
However, therein lies the challenge - anaesthetic training is such a busy programme. Trainees are involved with multiple areas within a hospital such as ICU, theatre work or Obstetric Delivery Suite that they must learn and practice a wide range of skills to demonstrate the proficiency expected of a consultant anaesthetist. With experience of clinical work already at a premium due to European Working Time Directive hours, creating a good teaching environment whilst providing service provision is a hard enough task. It might seem difficult, therefore, to justify taking away yet more clinical time for trainees.
The proposed “7 day National Health Service (NHS)” contract could also pose more difficulties. Current example rotas released by NHS Employers demonstrate an increased likelihood of shift-work for a typical ICU rota.4 This shows trainees will be working more weekends and nights than at present, which could reduce the time spent directly with consultants. This would make introducing more non-DCC work difficult to justify as it would likely occur during daylight hours – when training could occur.
How it could be introduced:
Assuming SPA sessions for trainees were implemented, there would also be practical aspects to address. For example, how many SPA sessions to allocate for each level of trainee and how to monitor that this time was spent effectively and efficiently.
Monitoring:
Trainees could propose which aspects to focus on during their SPA sessions, such as management, teaching, quality improvement projects or more time in their sub-specialty interest. The goals could then be set at the initial educational supervisor meeting, much like a Personal Development Plan (PDP), and monitored throughout the year. This would give focus to any SPA time and ensure it is effectively used. If a trainee abuses their time or is not using it appropriately then removal of SPA time could be enforced. This would give the trainees more ability to improve the skills so often considered additional to trainees.
Funding:
In times of NHS austerity, funding would also need addressing. Potentially neither Deanery nor Trust might be willing to pay a doctor for days spent working outside the hospital workload – such as in educational roles or as a college tutor.5 A trial in one single deanery could assess the efficacy of such a scheme.
A possible solution would be to remove a few days of study leave allowance, as many trainees do not use their whole entitlement, and re-assign these to SPA time, allowing a trainee more flexibility. Trainees could initially start with fewer SPA sessions when more junior, to allow more clinical time, increasing SPAs to one per week for intermediate or higher trainees who may well be approaching their Certificate of Completion of Training (CCT).
Conclusion:
There are some practical difficulties in establishing trainee SPA sessions and no doubt many feel all contracted time should be spent practicing anaesthesia. However, given the changing way trainees are recruited via a ‘tick-box’ national application system, together with the variety of non-clinical skills expected by consultancy such as an ability to teach, conduct audit work, engage in managerial roles etc., a small change in the training set-up could produce more rounded trainees, benefitting anaesthesia in general and training programmes in the future.
Communicating effectively with patients and families is a vital component of high quality care. Studies have shown that patients feel excellent communication in consultations is vital for instilling confidence in the medical practitioner.1,2 There is evidence that doctors are not meeting this fundamental need.3
Some consider it an ethical obligation of doctors to balance their training needs against providing optimal care for patients. It is well known that junior trainees have significant level of performance anxiety that translates through to their consultations.4
Simulation based training is now an integral part of postgraduate curriculum in training a variety of medical specialties in managing acute scenarios. As an education method it provides a controlled environment in which it is safe to learn from errors,5 and improves learner outcomes.6 Simulation has been shown to be a valid approximation of true clinical practice.7 It therefore allows trainees to reach higher levels of proficiency prior to embarking on real patient encounters.
Current Core Medical Trainees (i.e. junior doctors who have embarked on the first stage of physician training within England) in the London deanery are expected to be able to manage complex communication scenarios effectively prior to entering specialty training. This is demonstrated by requirements set out in the Core Medical Curriculum, as detailed in Box 1. Whilst significant emphasis is placed on communication skills training in basic scenarios at a medical student level, there is very little formal postgraduate communication skills training within this deanery and others.
Box 1: Excerpts from Core Medical Trainee curriculum
Counsel patients, family, carers and advocates tactfully and effectively when making decisions about resuscitation status, and withholding or withdrawing treatment
Able to explain complex treatments meaningfully in layman's terms and thereby to obtain appropriate consent even when there are problems of communication and capacity
Skillfully delivers bad news in any circumstance including adverse events
This deficit in training led us to conduct a survey exploring Core Trainees’ views regarding communication skills training in the London deanery. Findings from the survey are detailed in Box 2.
Box 2: Results from Core Trainee Survey
83% received less than 2 hours of post-graduate training in communication skills since the start of Core Medical Training
Only 50% felt somewhat competent in engaging in difficult communication scenarios
88% reported significant challenges when conducting these discussions. They have had difficult on-calls experiences relating to communication difficulties
100% displayed interest in attending further Simulation Training in advanced communication skills
Method
We devised a pilot project using simulation to develop trainees’ competencies in advanced communication skills. After application to our local training board, we secured funding to run a number of sessions for core medical trainees within the London area.
The objectives of our pilot project were to provide experience of realistic communication based scenarios in a structured and safe environment to core trainees; provide feedback on trainees’ communication styles and offer suggestions for improvement; improve confidence of trainees in difficult communication situations.
Each session was conducted in an afternoon session and candidates were divided into three groups of three trainees who would remain together for the entire session. We ran four sessions, with a total of 36 trainees. Each group was facilitated by a consultant or a higher trainee in either elderly or palliative care medicine, given our focus on resuscitation/end of life discussions and assessment of capacity. We employed three actors to rotate around each group performing a variety of roles including patients and relatives. With a total of six scenarios, each trainee had the opportunity to participate in at least two scenarios lasting approximately 15 minutes, with feedback thereafter for approximately 10 minutes.
The scenarios employed were based on personal experience of regularly occurring, challenging communication situations encountered in our own clinical practice. We created detailed scripts for the actors as well as corresponding clinical vignettes for the candidates.
The scenarios were:
End-of-life discussion with a challenging family regarding a patient with end-stage dementia.
Discussing resuscitation with a family opposed to do not attempt resuscitation (DNAR) regarding an acutely unwell patient with poor functional baseline.
Discussing resuscitation with a young patient with metastatic cancer undergoing palliative chemotherapy who has little understanding of the terminal nature of the disease.
Assessing mental capacity regarding discharge planning in a patient with mild to moderate dementia.
Assessing mental capacity regarding treatment in a patient with moderate learning difficulties.
Assessing mental capacity in a medically unwell patient with mental health issues who wishes to self discharge from the ward.
Box 3 outlines the session structure.
Box 3: Timetable for the session
12.30-12.45:
Actors briefing
12.45- 13.00:
Facilitators briefing
13.00-13.30:
Core trainee briefing
13.30-14.45:
Scenarios 1-3 in small groups
14.45-15.00:
Tea/Coffee break
15.00-16.15:
Scenarios 4-6 in small groups
16.15-16.45:
Feedback and closing
Results
Written feedback was obtained from all participants by distributing a post-course evaluation form, with a 100% response rate. A number of areas were assessed via a Likert scale of 1 – 5, with 1 being ‘not at all’ and 5 being ‘very much’. 100% of trainees felt the content was useful and their knowledge/skills had increased. 100% felt more confident after the session and all trainees and facilitators felt this would be beneficial for medical trainees. A full breakdown of results is detailed in Table 1.
Table 1: Results from post-course feedback
The post-course feedback form allowed for free text feedback from participants, with some individual examples given below:
“Realistic scenarios - good opportunity to experience them and get feedback in a safe environment, good practice of common communication problems”
“It builds confidence in dealing with these situations and provides basis for building up ”
“This work dealt with complicated cases and actors were not too easy which I liked. Good and unforgettable”
Discussion
With the European Working Timing Directive and resulting shorter working hours, gaining proficiency in a number of key skill areas is limited due to reduced patient encounters. A recurrent complaint among core medical trainees is the lack of observed clinical encounters that leads to individualised feedback.
Feedback from more experienced speciality practitioners was only one component of our attendees learning experience. They also benefited from personal practise in a non-threatening environment, observation of their colleagues communication styles and finally learning through reflection with their colleagues
This innovation has shown a clear benefit in amplifying the confidence and preparedness of our core medical trainees in approaching these higher level communication scenarios. Future directions include introducing quantitative assessments pre- and post- course to objectively demonstrate improved confidence and performance. Providing the course to trainees in other specialties as well as across the multidisciplinary team would also be beneficial given the universal requirement of healthcare professionals to communicate skilfully.
A 41-year-old woman with a 6-year history of mild psoriasis presented with a rash under her breasts. The differential diagnosis included flexural psoriasis, an allergy to the nickel in her under wired bra, and intertriginous dermatitis (moisture-associated skin damage). She was prescribed Trimovate cream (GlaxoSmith Kline) and developed a florid weeping eczema within 48 hours of application (Figure 1). The eczema settled with the withdrawal of Trimovate and application of Betnovate RD cream (GlaxoSmith Kline). The history was very suggestive of a contact dermatitis to Trimovate cream.
Figure 1 showing eczema
She was referred to the Dermatology department and was patch tested to the European standard, medicament and steroid batteries. She had a number of positives including cetearyl alcohol, sodium metabisulphite, and clobetasone butyrate. These are all components of Trimovate. She was given advice sheets on all her allergens and on avoiding them she has had no recurrence of eczema.
Discussion
Contact dermatitis is a type IV allergy and usually appears within 2 to 3 days after contact with an external allergen. This case is likely to be an example of concomitant sensitisation, where one sensitivity facilitates the acquisition of another sensitivity to a chemically unrelated ingredient within a product.Whilst there has been a previous case report of concomitant sensitivity to sodium metabisulphite and clobetasone butyrate in a patient using Trimovate cream,1 this is the first report of a patient reacting to three of the ingredients found in Trimovate - sodium metabisulphite, clobetasone butyrate, and cetearyl alcohol. Allergy to clobetasone butyrate is rare, with only 5 previously reported cases.1, 2, 3 Allergy to sodium metabisulphite is not uncommon, producing a positive reaction in approximately 4% of patients who are patch tested.4, 5 Allergy to cetearyl alcohol is also rare, with one study estimating the incidence of positive reactions to be 0.8% among 3062 patients that were patch tested.6
Detection of the allergen, or allergens, is important, as avoidance results in resolution of the eczema. Our patient highlights the fact that it is insufficient to simply advise a patient to avoid the topical medicament that has caused a reaction. Ideally, patients with a topical medicament allergy should be patch tested to identify which components the patient is allergic to, so that they can be avoided in all products. In this case, in addition to Trimovate, there are a number of other products that our patient will now avoid. This is of particular significance in view of her history of psoriasis, for which she has used moisturizers and topical steroid preparations in the past, and will likely need again in the future. Clobetasone butyrate is often used in facial and flexural psoriasis. Cetearyl alcohol is a particularly important allergen to identify, as it is found in many products including a number of commonly used moisturizers such as Diprobase (MSD), Cetraben (Genus) and Epaderm (Mölnlycke) cream, and most steroid creams although not steroid ointments. Our patient was therefore advised to use only steroid ointments and has had no recurrence of the contact dermatitis. To conclude, GPs should consider sending their patients with contact dermatitis for patch testing, as the identification of all allergens is valuable to management.
A 38 year male presented to our centre with a two-month history of jaundice. Past medical & family history was insignificant. Clinical examination revealed a icterus and greenish brown ring in both eyes (Figure 1). Laboratory investigations revealed a mild thrombocytopenia (platelet count-1.2 lakh/mm3) and a prolonged prothrombin time. Liver function tests showed elevated serum levels of alanine aminotransferase & aspartate aminotransferase. Serology for hepatotropic viruses was negative. Serum ceruloplasmin was 9.8 mg/dl (reference range 20-60mg/dl) and 24 hour urinary copper was elevated.
Figure 1
What is the eye finding?
Arcus Senilis
Pterygium
Kayser Fleischer ring
Phlycten
Correct Answer:
3. Kayser Fleischer ring
Discussion:
Wilson’s disease is a consequence of defective biliary excretion of copper. This leads to its accumulation in the liver and brain 1. It is due to mutations of the ATP7B gene on chromosome 13, which codes for a membrane-bound copper transporting ATPase 2.
Kayser-Fleischer ring is an outcome of abnormal copper deposition in the membrane in the limbus of cornea. Slit-lamp examination by an experienced observer is required to identify a K-F ring. The colour may range from greenish gold to brown. When well developed, a K-F ring may be readily visible to the naked eye. K-F ring is observed in most individuals with symptomatic Wilson disease and are almost invariably present in those with neurologic manifestations. They are not entirely specific for Wilson’s disease, since they may also be found in patients with chronic cholestatic diseases.
Clinical presentation is variable and patients presenting with chronic hepatitis, cirrhosis & at times acute liver cell failure. The most common presenting neurologic feature is asymmetric tremor. The characteristic tremor is coarse, irregular proximal tremulousness with a “wing beating” appearance.
Typically, the combination of K-F rings and a low serum ceruloplasmin (<0.1 g/L) level is sufficient to establish a diagnosis of Wilson’s disease 3.However delayed diagnosis in patients with neuropsychiatric presentations is frequent and was in one case as long as 12 years 4.Our patient was treated with a none copper diet, oral zinc and d pencillamine. His liver functions became normal over 6 months of treatment and without progression of liver disease.
Arcus Senilis is a grey band of apacity near the sclero-corneal margin, commonly found in the elderly and associated with hypercholesterolemia. Pterygium is a benign wedge shaped fibrovascular growth of conjunctiva that extends onto the cornea. Phylecten is consequence of allergic response of the conjunctive & corneal epithelium usually associated with tuberculosis, staphylococcus protein and moraxella.
The rate of primary and secondary syphilis reported in the United States is gradually increasing. Reported cases of syphilis decreased during the 1990s, were lowest in 2000, after which it gradually increased annually during 2001-20091. In a recent report published by CDC, primary and secondary syphilis rates have increased among men of all ages, races and ethnicities, largely among MSM, from 5.1 cases per 100,000 population in 2005 to 9.8 in 2013. Rates of 50%–70% HIV coinfection among MSM infected with primary and secondary syphilis have been reported2. Syphilis and the behaviours associated with acquiring it, increase the likelihood of acquiring and transmitting HIV. Although the incidence of HIV has remained stable, the incidence of syphilis has been increasing disproportionately possibly due to adaptive behaviour like serosorting among HIV concordant couples and oral sex that decrease transmission of HIV but not syphilis3.
Syphilis may manifest differently in patients with HIV. HIV positive patients present more often with secondary syphilis and the disease course is more aggressive4. Malignant syphilis also known as lues maligna or ulceronodular syphilis is a severe form of secondary syphilis and is more common among HIV infected persons5. Although HIV patients present with varied clinical symptoms, it is uncommon to present with florid secondary syphilitic skin lesions. Here we present a case report of a patient, who presented with diffuse ulceronodular skin lesions, whose serology and skin biopsy confirmed syphilis and was subsequently found to have HIV.
Case report
A 20-year-old African American man was admitted to Interfaith Medical Center with a generalised body rash for a month. He noticed a rash on his chest, which in few days spread centrifugally to his whole body, face and arms, including palms and soles. The rash was non-pruritic, painless, progressive in size and gradually oozed and crusted (Figure 1a). Besides significant unintentional weight loss of 26 pounds in the last two months, he did not report any other systemic complaints. He denied any travel or unwell contacts. He is a homosexual man and has had two male sexual partners in the last two years; one of them was treated for syphilis two years ago. He denied smoking, alcohol or drug use.
Figure 1a - Skin lesions reveal papulosquamous nodular and ulcerative changes in upper limbs
On admission, he was afebrile with normal vital signs. His physical examination revealed widespread papulonodular and ulcerated lesions on his whole body including the scalp and oral mucosa, and measured up to 2-3 cm. Skin lesions were prominent on his face, some with sero-purulent discharge and some covered with crusts and scabs, which would bleed on removal of crusts and scabs. No skin lesions were noted in genital area. Besides bilateral enlarged axillary lymph nodes, nosignificant lymphadenopathy was noted. Other systemic examinations were within normal limits.
His full blood count showed microcytic hypochromic anaemia with a mean corpuscular volume of 77.2 fL (normal reference range, 80-100 fL) and thrombocytosis with platelets of 546 per microliter (reference range, 130-400 per microliter). Renal and hepatic function tests were normal. He tested positive for HIV using serum enzyme linked immunosorbent assay (ELISA), rapid plasma reagin was 1:128 (reference range, nonreactive), fluorescent treponemal antibody absorption test was reactive (reference range, nonreactive) and neurosyphilis was ruled out with negative spinal fluid studies. Hepatitis B and Cserologieswere negative. Nucleic acid amplification test of the urine sample was negative for Neisseria gonorrhea and Chlamydia trachomatis. The patient was treated with doxycycline100 mg every 12 hours for secondary syphilis as he was allergic to penicillin.
The patient developed chills, fever, sweating, tachycardia and hypotension 18 hours after treatment with doxycycline. A Jarisch-Herxheimer reaction was suspected, which was managed with observation, intravenous hydration and a single dose of methylprednisone. Despite being on antibiotics, he had intermittent fever for two weeks, possibly related to the syphilis and its treatment. Further investigations included blood and urine culture, chest x-ray, CT scan of the head, chest, abdomen and pelvis and a gallium scan, which were unremarkable. Brucella IgM antibody, Q fever phase I and II antibodies, coccidioides antibody, histoplasma urine antigen, cryptococcal antigen and blood culture for acid fast bacilliwere all negative. His EBVserologies suggested past infection and CMV serologies for IgG and IgM were positive. Wound culture taken from the purulent skin lesions grew methicillin sensitive Staphylococcus aureus (MSSA)which was treated with antibiotics. His HIV-1 RNA was 1050118 (reference range, <20) and CD4 was 276 cells per microlitre (reference range, 317-1868 cells per microlitre), CD4 was 17.4% (reference range, 25.7-62.8%) and CD4:CD8 ratio was 0.32 (reference range, 0.20-3.50). Skin biopsy from the left forearm lesion showed lichenoid lymphohistiocytic infiltrate with plasma cells (Figure 1b). Immunochemical stain was positive for spirochetes, which confirmed secondary syphilitic skin lesions (Figure 1c). After three weeks of doxycycline therapy, significant clinical improvement in the skin lesions were noted. The skin lesions healed well with hyperpigmentation. Combination anti-retroviral therapy was initiated upon discharge and on follow-up a month later, the skin lesions had resolved and the RPR titre was 1:32; showing a four-fold reduction.
Figure 1b - A lymphocyhistiocytic infiltrate was present in the dermis and extended around blood vessels.
Figure 1c - Immunohistochemical stain showing delicate and spiral shaped spirochaetes, highly specific and sensitive of Treponema pallidum
Discussion
Skin lesions of secondary syphilis in patients with HIV may have varied appearance that mimic other diseases like cutaneous lymphomas, mycobacterial infections, bacillary angiomatosis, fungal infections or Kaposi’s sarcoma6. Detail workup was done in our patient and systemic fungal and bacterial infections were ruled out. He had secondary infection of the skin lesions due to MSSA and was treated with doxycycline. Skin biopsy confirmed secondary syphilitic skin lesions. Histology showed abundant plasma cells and lymphocytesandtreponomes were demonstrated in the special immuno-histochemical stains. Fisher’s diagnostic criteria for lues maligna include strongly positive RPR titre, a severe Jarisch-Herxheimer reaction, characteristic gross and microscopic morphology and rapid resolution of the lesions with antibiotics7. Our patient had all of these features. Because of variable presentation of skin lesions and increased rate of false negative serological tests due to prozone phenomenon in patients with HIV, alternative diagnostic techniques like biopsy of skin lesions and special stains should be performed8,9. The relative paucity of spirochetes in the biopsy of skin lesions makes the demonstration of microorganisms difficult. Yanagishawa et al were able to find 6 published cases of pathologically confirmed malignant syphilis with the demonstration of spirochetes10. Treatment of secondary syphilis in HIV infected patient is the same as that of HIV non infected patients. Benzathine penicillin is first line therapy and doxycycline is an alternative drug for penicillin allergic patients11. A severe Jarish-Herxheimer reaction occurred in our patient, which might not be observed in some cases with HIV and syphilis due to concurrent immunosuppression10. Experience from case reports have shown that malignant syphilitic skin lesions respond very well to antibiotics regardless of CD4 count12. With the increasing incidence of syphilis in HIV infected patients, it is important to recognise and diagnose malignant syphilis early and institute appropriate treatment as complete cure can be achieved.
Phytochemicals, are not regarded as essential nutrients in humans although an increasing number of well-conducted studies are linking higher intake with a lower risk of developing cancer, as well as lower relapse after initial treatment completion 1,2,3. There is a wide range of dietary phytochemicals, but one of the largest and well-known groups being the polyphenols [Table.1]. The average total dietary intake of polyphenols is reported to be over 1g per day, which is up to ten times higher than that of all other classes of phytochemicals and known dietary antioxidants4. The health benefits of phytochemical rich foods or concentrated nutritional supplements are often being highlighted in the medical and popular media and hence they are an increasing topic of conversation between medical practitioners and their patients especially those with cancer who have a particular interest in over the counter self help strategies 5,6. This article provides an overview of the major classes of phytochemicals with examples of their common food sources. It highlights the international evidence for their anti-cancer mechanisms of action, their clinical benefits, as well as discuss the pros and cons of concentrating them and, into nutritional supplements in an attempt to harness and boost their health benefits. Hopefully this review will provide some useful learning points to aid communication between patients and clinicians [Table. 2].
Classification
There are three major groups of phytochemicals: the polyphenols which can be subcategorized as the flavonoids, phenolic acids and other non-flavonoid polyphenols; the terpenoids, which can be subcategorized as the carotenoids and non-carotenoid terpenoids; and the thiols, which includes the glucosinolates, allylic sulfides and non-sulphur containing indoles (Table. 1). There are other phytochemical group, which although have some properties within these groups, have been classified within a miscellaneous category and examples of these include the betaines, chlorophylls and capsaicin.
Table.1 Classification of phytochemicals with notable food rich sources
Polyphenols
1. Flavonoids
o Flavonols:quercetin, kaempferol (onions, kale, leeks, broccoli, buckwheat, red grapes, tea, apples)
o Glucosinolates: isothiocyanates (sulforaphane) and dithiolthiones (cruciferous vegetables such as broccoli, asparagus, brussel sprouts, cauliflower, horseradish, radish and mustard)
o Allylic sulfides: allicin and S-allyl cysteine (garlic, leeks, onions)
o Indoles: Indole-3-carbinol (broccoli, Brussel sprouts)
Other phytochemicals
o Betaines found in beetroot
o Chlorophylls found in green leafy vegetables
o Capsaicin found in chilli
o Peperine in black peppers
Table. 2 learning points
Higher intake of phytochemical-rich foods such as colourful fruit, vegetables, herbs, pulses, spices and teas is associated with a lower risk of cancer and relapse after treatments.
Their anti-oxidant properties help to protect our DNA from ingested or environmental carcinogens.
Phytochemicals, particularly polyphenols have direct anti-cancer mechanism of action via inflammation, modulation of cellular and signalling events involved in growth, invasion and metastasis.
Concentrating element of foods such as minerals, vitamins and phytoestrogenic polyphenols to potentially boost their health effects have largely been unsuccessful in preventing cancer in clinical trials.
Whole food phytochemical-rich supplements have demonstrated significant benefits in phase II and well conducted RCT and their true potential is been evaluated in ongoing studies.
Clinical evidence for cancer prevention.
Although not all, many studies have linked a higher intake of phytochemical-rich foods, such as vegetables, fruit, legumes, nuts, herbs and spices, with a lower incidence of cancer as highlighted in the latest comprehensive review from the World Cancer Research Fund and other systemic reviews2,3.
More specifically, certain elements of food have been addressed within a number of cohort studies. Carotenoids found in leafy green vegetables and carrots have been linked with a lower risk of breast cancer in a recent meta-analysis demonstrated7 and a lower risk of ovarian and pancreatic cancers, especially among smokers in either questionnaire or serum-based studies8, 9, 10. Higher intake of cruciferous vegetables such as cabbage, cauliflower, Brussel sprouts, radishes and broccoli have been associated with a lower prostate cancer risk11, as have foods rich in isoflavones such as pulses and soy products12, lycopene rich colourful fruits and tomatoes13. Foods with abundant levels of flavonoids such as onions, rich in quercetin, have been shown to reduce the incidence of numerous cancers particularly those arising from the lung, especially amoung smokers14, 15. The anthoxanthins, in dark chocolate, have been reported to lower the risk of colon cancer16 and higher green tea intake lowers the risk of breast, prostate, ovarian and oesophageal cancer, again particularly among smokers and alcoholics17, 18. Finally, coffee consumption has been shown to reduce the risk of non-melanomatous skin cancers and melanoma, even after removing other factors such as ultraviolet radiation exposure, body mass index, age, sex, physical activity, alcohol intake and smoking history19,20.
Clinical evidence for a benefit after cancer
The benefits of healthy foods do not stop after a diagnosis, especially if combined with other healthy lifestyle habits. For example, breast cancer survivors who regularly consumed more than the government recommended five portions of fruit and vegetables a day, had a third lower breast cancer recurrence risk if combined with regular physical activity21. In another study, women with breast cancer who had the highest serum lignan levels, reflecting good intake of legumes, cereals, cruciferous vegetables and soya, were reported to have the lowest risk of death22. Likewise, a lignan and polyphenol rich diet was associated with a lower colorectal cancer relapse rate23.
The large Shanghai Breast Cancer Survival Study demonstrated that women with the highest intake of the phytoestrogenic polyphenols isoflavones and flavanone found in soya and other beans, had a 29% lower risk of relapse and death24. Similar findings were seen for green tea after breast25 and colorectal cancer23. Green tea also decreased the abnormal white cell count in 30% of patients with chronic leukaemia and reduced the levels of several markers of proliferation, as well as serum Prostate Specific Antigen (PSA) among men with prostate cancer26. A slowing of PSA progression has similarly been observed in other dietary studies, most notably the randomised trial involving a plant-based diet together with other lifestyle changes27 and a phase II study of pomegranate juice28.
Another cancer influenced by nutrition is skin cancer, as highlighted by a study of individuals who have been treated for basal cell carcinoma or squamous cell carcinoma, and who have a high risk of further lesions due to their on-going solar damage. Those who consumed the highest levels of lutein and zeaxanthin-rich foods, such as leafy green vegetables, had the lowest levels of new cancer formation29.
A number of other studies evaluating the impact of phytochemicals are underway, the largest and probably most comprehensive is the UK’s DietCompLyf prospective trial involving 3159 women treated for breast cancer30.
What are the likely anti-cancer mechanisms of phytochemicals?
The precise biochemical mechanisms through which phytochemicals exert their anti-cancer effects are still being explored, as their actions are wide-ranging and complex but significant advances have been made of late in the understanding the mode of action. The most quoted cancer prevention mechanism is via their antioxidant activity, elicited either through direct free radical absorption or through induction of antioxidant enzymes such as superoxide dismutase (SOD), catalase and glutathione via a variety of molecular mechanisms31, 32. One of these mechanisms is activation of Nrf2, which switches on genes that code for antioxidant as well as detoxification enzymes31, 32. Phytochemicals, particularly the thiol class such as sulforaphane,have also been shown to inhibit the conversion of procarcinogens to their electrophilic, DNA damaging, chemicals32,33.
A number studies involving known, common carcinogens have highlighted the antioxidant properties of phytochemicals. A good example of their protective effect was an experiment involving the known house-hold carcinogen triclocarban, commonly found in detergents and cleaning agents. Healthy cells exposed to triclocarban tend to mutate into pre-malignant cells, however, the amount and rate of carcinogenesiswas significantly reduced byadding curcumin to the petri dish culture feeds34. In another study, volunteers who ate a diet rich in kaempferol were found, on serum and urine analysis, to have improved SOD activity and higher urinary concentration of these polyphenols35. Rats exposed to cigarette smoke given indole-3-carbinol, a phytochemical rich in cruciferous vegetables, had a lower lung cancer rate than those not given idole-3-carbinol36. Subjects eating a meal of onions, which increased their serum levels of quercetin, demonstrated decreased levels of oxidative metabolites including 8-hydroxydeoxyguanosine (8-OHdG) a marker of DNA damage and repair1618, 37. Quercetin supplementation has also been shown to improving mitochondrial dysfunctions induced by the toxin 3-nitropropionic acid38. A clinical study in Singapore gave Chinese smokers 170g of watercress a day, rich in the indole-3-carbinol, and found a similar effect on urinary markers of DNA damage39. Finally, marinating meat in rosemary and thyme, has been reported to reduced the serum levels of carcinogenic heterocyclic amines (HCA) by 87% compared to subjects who eat the meat unseasoned40.
Another key anti-cancer mechanism of phytochemicals appears to be their ability to reduce inflammation. It is now well established that inappropriate inflammation is intimately involved in the cancer process, particularly in the promotion and progression stages of cancer. Inflammation is closely associated with oxidative stress and activation of NF-kappa B family of transcription factors. These factors regulate more than 150 genes involved in mechanisms of cell survival and these target genes are not just pro-inflammatory but also oncogenic. Numerous phytochemicals have been shown to inhibit NF-kappa B signalling, particularly the green tea polyphenol epigallocatechin-3-gallate (EGCG), quercetin, curcumin, caffeic acid and caffeic acid phenethyl ester and the phytochemicals within bilberries31,41.
More recently, it has been reported mainly from laboratory studies that phytochemicals have an affect on several cancer process through modulation of cellular and signalling events involved in growth, invasion and metastasis32. Pomegranate, for example, rich in the polyphenol ellagic acid, has been shown to directly inhibit cell growth and induce apoptosis in androgen sensitive and aggressive human prostate cancer cells42. Pomegranate extract has also been reported to inhibit processes involved in cancer metastasis in a study involving oestrogen sensitive and resistant breast cancer cell lines, showing increased markers of cell adhesion and migration in cancer but not normal cells43. In another study it inhibited a chemokine that attracts breast cancer cells to the bone44. Curcumin slows cancer cell growth by blocking the cell cycle, increasing the rate of apoptosis and preventing the invasion and migration of cells45, 46, 47, 48. It has also been found to halt the growth of stem cells that give rise to breast cancer without harming normal breast stem cells49. Curcumin has been shown to modulate miRNA expression in breast cancer cells leading to a reduced expression of Bcl-250 and stabilisation of tumour suppressor gene in colorectal cancer cell lines52. Green tea, rich in epigallocatechin gallate (EGCG), has demonstrated significant reduction of several factors that promote cancer cell proliferation by inhibiting DNA synthesis, de-differentiation and angiogenesis26, 52, 53. It has also been shown to block ornithine decarboxylase, an enzyme which signals cells to proliferate faster and bypass apoptosis50, 54. Resveratrol has demonstrated epigenetic regulatory properties which influence regulate proliferation, cell survival and apoptosis in prostate cancer by global modulation of gene expression through deacetylation of FOXO transcription factor46. Caffeic acid and phenethyl ester, as well as inhibiting NF-κB signaling, also have been shown to inhibit cell motility in vitro and inhibit metastasis of tumour models in vivo47. Luteolin, as well as inhibiting tumour growth and metastasis, inhibits epithelial mesenchymal transition which is a basic biological process related to cancer initiation and development47.
Finally some polyphenols and other phytochemicals are also able to influence cancer via a hormonal mechanism. Phytoestrogenic compounds, most notably isoflavones and lignans found in soy products, legumes and some cruciferous vegetables, weakly bind to the oestrogen receptor without stimulating proliferation of the cells, yet at the same time blocking the binding of more harmful oestrogens, including those produced endogenously39. This explains why in the previously mentioned Shanghai Breast Cancer Survival Study, women with the highest intake of isoflavones and flavanones-rich foods had a lower risk of death24. In men, phytoestrogenic compounds have been shown to affect 5 alpha reductase lowering endogenous testosterone levels. This may partly explain why men who eat phytoestrogenic foods such as beans and pulses have a lower risk of prostate cancer.
Can concentrating foods into supplements enhance their anti-cancer effect?
If certain foods have anti-cancer effects, then it is not unreasonable to hypothesise that concentrating them into a pill may be a good way to supplement individuals with poor diets or further enhance the benefits in those whoes diets are already adequate. People living with and beyond cancer (PLWBC) are certainly attracted to the potential health benefits of food supplements, as over 65% report regular intake5,6. There are two main categories of supplements commercially available: the first involves chemicals extracted from food, or made synthetically, such as minerals and vitamins; the second involves purifying and concentrating whole foods:
Vitamins and mineral supplements: The majority of studies, to date, have evaluated extracted chemicals such as vitamins and minerals. Some have shown a benefit. For example, a recent meta-analysis of studies reported that women who took supplements providing an average daily intake of vitamin C over 100mg had a reduced risk of breast cancer relapse57. The SU.VI.MAX study randomised French adults to a single daily capsule of ascorbic acid, vitamin E, beta carotene, selenium and zinc, or a placebo, and found no reduction in mortality or cancer-specific mortality overall58, although a further analysis in men found a reduction in the risk of prostate cancer. The authors postulated that this difference between the sexes was related to French men having a lower baseline micro-nutrient status59. A major trial of selenium and vitamin supplements in a poor region of China, demonstrated reduced risks of oesophageal cancer; at the time this population was known to have widespread micro-nutrient deficiencies60.
Unfortunately, most other studies of vitamin, minerals and other extracted nutrients have shown no benefit, or have actually shown an increased risk of cancer. For example, the CARET study found that beta carotene and retinol increased the risk of lung cancer61. The Health Professionals Follow-up study (HPFS) which followed the lifestyle habits of 51,529 male professionals for over 15 years found that men who took very high doses of zinc (>100mg/day), or took it for long durations were more than twice as likely to develop advanced prostate cancer compared with controls62. The randomised SELECT study demonstrated an increased prostate cancer incidence with vitamin E and selenium supplementation63. A further analysis of the HPFS found that of the 4,459 men who had developed prostate cancer, those who took selenium supplementation of ≥ 140 μg/d after diagnosis were associated with a 2.60-fold greater risk of prostate cancer mortality64.
The negative effects of vitamin E and beta carotene were once again demonstrated in the ATBC study which found them to increase lung cancer risk, although subsequent analysis showed that men with pre-intervention low plasma levels of beta-carotene had a lower prostate cancer risk following supplementation, and that those with high levels had a higher risk, particularly in smokers65. This u-shaped distribution of risk was also observed in the EPIC study where those with folate-deficient diets and those with the highest intake both had a higher risk of cancer66. These data have prompted organisation such as the National Cancer Institute to issue statements stating that long term vitamin and mineral supplements should ideally be given to correct a known deficiency67, which is rarely routinely detected unless individuals have self funded micro-nutrient analysis (cancernet.co.uk).
Whole food supplements: More recently academic attention has turned towards the evaluation of concentrated whole food supplements, particularly foods rich in polyphenols and other phytochemicals such as herbs, spices, green vegetables, teas and colourful fruits which have appeared to be beneficial in environmental cohort studies. Despite some initial encouragement from smaller evaluations, studies of extracted lycopene or genistein given on their own in more scientifically robust analyses have not demonstrate a benefit for either prostate cancer or benign prostatic hypertophy68, 69, 70 neither were there links with the reduction in the risks of breast cancer with regular intake5. Of more concern, a randomised study from Memorial Sloan Kettering reported that serum taken from women who had take very high dose soy supplementation (25.8 g twice a day) added to laboratory tumour cells caused them to proliferate faster (Increased K67 expression) and overexpress the tumorigenic growth factor receptor FGFR271. This supports the notion that phytoestrogen foods are healthy, but concentrating them into strong supplements is not recommended.
On the other hand, no study of non-phytoestrogenic foods supplements has shown any detrimental effects on cancer outcomes and some have beneficially influenced progression rates. For example, a study carried out at John Hopkins involving pomegranate seed extract, found that men taking the supplements had a reduction in PSA progression rate72. A study conducted at the Mayo Clinic found that green tea concentrate decreased the abnormal white cell count in 30% of patients with chronic leukaemia, and a small study from Louisiana University reported that green tea concentrate significantly reduced levels of several cancer-promoting growth factors as well as PSA levels in participants26. In the Vitamins and Lifestyle (VITAL) cohort study, a regular intake of grapeseed extract was shown to be linked with a lower risk of prostate cancer70, and another small RCT found that a dietary supplement containing isoflavones, plus other phytochemicals and anti-oxidants delayed PSA progression73. Interestingly one of the most popular supplements, Saw Palmetto, despite an effect in early small studies, showed no benefit for prostate cancer or benign prostatic hypertrophy in the largest randomised evaluation74. Likewise, another popular supplement, lycopene, despite similar suggestions from smaller non-randomised trials68, 69, demonstrated no benefits in a more robust evaluation.
So far, the largest trial analysing phytochemical-rich food extracts was the National Cancer Research Network adopted Pomi-T study75. This study combined four different food types (pomegranate, green tea, broccoli and turmeric) in order to provide a wide spectrum of synergistically acting nutrients, whilst at the same time avoiding over-consumption of one particular phytochemical. It involved two hundred men, with localised prostate cancer managed with active surveillance or watchful waiting experiencing a PSA relapse, following initial radical interventions.
The results, presented as an oral presentation at the American Society of Clinical Oncology Conference (ASCO), Chicago, showed a statistically significant, 63% reduction in the median PSA progression rate compared to placebo in both men on active surveillance and experiencing a PSA relapse post-treatment. A further analysis of MRI images, demonstrated the cancers size and growth patterns correlated with PSA changes, excluding the possibility that this was just a PSA rather than tumour effect75. It was well tolerated, apart from some mild loosening of the bowels in 10% of men, and there was no effect on testosterone levels. At 6 months, significantly more men opted to remain on surveillance rather than proceeding to expensive radiotherapy, surgery or medical castration which can cause unpleasant effects such as depression, hot flushes, weight gain, osteoporosis and erectile dysfunction75.
A number of other RCT’s involving whole food phytochemical-rich supplement have demonstrated benefits for some of the distressing symptoms common after cancer treatments, such as fatigue76 and urinary infections77. There are currently over ten, on-going studies registered with the National Institute of Health. In the UK, the Institute of Preventative Medicine has plans to include the Pomi-T supplement into the next national prostate cancer prevention study. This study will be recruiting men with a higher genetic risk of prostate cancer identified in the national RAPPER study, co-ordinated by the Institute of Cancer Research. Further trials are being designed involving men with prostate cancer already on androgen deprivation therapy and individuals with skin, colorectal and bladder cancer. In the meantime, a trial is passing through the regulatory process to investigate whether the natural anti-inflammatory properties of these ingredients could help joint pains after breast cancer.
Conclusion
There is increasingly convincing evidence to show that plant phytochemicals, particularly polyphenols have significant benefits for humans. Not only do they improve our daily lives by helping our food taste, smell and look appetising, they also reduce our risk of cancer and help people living with and beyond treatments. Living well programmes, slowly being introduced in the UK, are beginning to highlight the importance of phytochemical-rich diets, along side other lifestyle factors, largely being driving by the National Survivorship Initiative and guidelines from influential organisations such as ASCO. Going a step further and concentrating these foods, or extracted elements of these foods, into nutritional supplements gives an opportunity to boost their beneficial anti-cancer effects, but have their pitfalls. Studies of concentrated minerals, vitamins and phytoestrogenic supplements have reported detrimental effects. No study has reported detrimental effects of whole, non-phytoestrogenic food supplements and some have reported significant advantages. Despite these potential benefits and reports that over 60% of patients living with and beyond cancer take nutritional supplements, oncologists have been reluctant to discuss their pros and cons due to a lack of RCTs from academic institutions55, 56. Hopefully this trend will change, particularly following the success of the Pomi-T study75 and ongoing studies registered with the National Cancer Institute.
Pellagra is a nutritional disorder due to an insufficiency in vitamin B3 also called vitamin PP (‘Pellagra preventing’). The disease was characterized by the following ‘3 D’s’: ‘Dermatitis’, ‘Dementia’ and ‘Diarrhoea’. When it is misdiagnosed, it can lead to the fourth ‘D’ which is ‘Death’.1 It was very common in past centuries, particularly in populations that had an exclusively maize diet. Nowadays, this diet problem is rare in developed countries, so the disease is less frequent. However, many recent studies suggest that the disease has not been eradicated and can be under-diagnosed. Alcohol, drugs and malabsorption seem to be the new aetiologies of the disease. So, it is important to recognize the ‘3 D’s’ triad in such situations to avoid fatalities.
Observation
A 61-year-old patient presented to the Internal Medicine Department with an 8-month history of deterioration in her general state. She had a medical history of Epilepsy treated by Phenobarbital since she was 16.
Review of systems revealed gastrointestinal symptomatology consisting of intermittent diarrhoea (6-7 watery stools a day without blood), dysphagia and diffuse abdominal pain. The patient also reported a skin photosensitive eruption affecting her hands and feet.
Physical examination showed a listless patient with a low Body Mass Index (17 kg/m²).
On dermatological examination, symmetric, well-defined, brown-coloured and scaly eruption was observed on the dorsa of her feet (Picture 1) and hands (Picture 2). The mucous examination showed a commissural Cheilitis and Glossitis.
Picture 1: Brown well-defined patches on feet.
Picture 2: Brown pigmentation and scales of hands.
Picture 3: Hands aspect after treatment.
The nervous system examination revealed a pyramidal and cerebellar syndrome. The response to neurocognitive tests was altered suggesting Dementia.
The rest of physical examination was normal. In particular, there were neither peripheral lymph nodes, nor spleen or liver enlargements, nor abdominal mass.
The laboratory tests (glucose, calcaemia, creatinine, liver function tests, urine analysis, haemoglobin, hematocrit, sedimentation rate, C-reactive protein and protein electrophoresis) were within normal limits.
Oesogastroduodenal endoscopy was normal. The cranial, thoracic and abdominal CT scans were normal.
The diagnosis of Pellagra was made on dermatological, abdominal and neurological signs. The patient was treated by Niacin (1000 mg/day) and multivitamin complex. Phenobarbital was discontinued and switched to Clobazam. The patient’s symptoms started to improve quickly. Ten days after the treatment began the skin lesions (Picture 3) and gastrointestinal signs completely disappeared.
Discussion
Pellagra was diagnosed clinically in our patient based on the skin aspects. The skin lesions have been described since 1771 by Frapolli whose name was given to the disease: Pellagra which means rough skin in Italian.1 The typical lesions consist of a brown pigmentation and scales with a photosensitive distribution and well-defined borders as seen in our patient. The face, the neck and the dorsa of the hands are the preferential locations.2 The skin lesions are not always found, and cases of Pellagra Sine Pellagra have been described.3 The extra-cutaneous manifestations are less specific, but their association with pellagrous skin lesions are sufficient to reach a diagnosis. The neurological involvement is classically a Dementia syndrome, but ‘Pellagrous Encephalopathy’ can also consist of delirium, insomnia, depression, cerebellar and extrapyramidal syndrome.4 The gastrointestinal signs are non-specific; they can be Glossitis, dysphagia, nausea, vomiting and abdominal pain. An intractable diarrhoea may occur in advanced stages of disease and can quickly lead to death.5
In 1929, Goldberger attributed such clinical manifestations to a Niacin (vitamin B3 or PP) deficiency. Niacin is a precursor for two important coenzymes namely ‘Nicotinamide Adenine Dinucleotide (NAD)’ and ‘NAD-Phosphate’ which are essential for many oxidative reactions. This probably explains why Pellagra affects tissues with a high rate of cell turnover such as the skin and digestive tract.4
Niacin can be directly absorbed by the gastrointestinal tract or synthesized from Tryptophan.
Primary Pellagra occurs when the diet is deficient in Niacin or Tryptophan as in poor populations with an exclusive maize diet (which contain Niacin but in an indigestible form).
Despite sufficient dietary Niacin, Secondary Pellagra may be caused by a problem in Niacin absorption or metabolism. Many causes of Secondary Pellagra were identified as alcohol, intestinal malabsorption, carcinoid tumours, Hartnup’s Syndrome, Anorexia Nervosa and drugs (Table 1).5 Our patient did not consume alcohol and had no biological signs of malabsorption, but she was taking Phenobarbital for about 45 years. In the English literature, we found only two cases of Phenobarbital-induced Pellagra, and with a fatality in one case.6, 7 The underlying mechanism of Pellagra caused by Phenobarbital, or other antiepileptic drugs, is an alteration in Niacinamide synthesis due to an enzymatic induction.5
Chemotherapy and immunosuppressive drugs 6-Mercaptopurine 5-Fluorouracil Chlorambucil Azathioprine Chloramphenicol
The treatment is first based on correction of predisposing factors. In our patient, it consisted of using another antiepileptic drug instead of Phenobarbital. Second-line treatment is a vitamin therapy based on Niacin. There is no consensus on the doses, form and duration of the treatment, but the minimal dose is 300 mg of Niacin/day. A multivitamin complex containing other B-vitamins is often necessary because of the frequency of other deficits in such patients.2 With treatment, the skin lesions and gastrointestinal symptoms generally disappear within a few hours or days, as in the case of our patient, and it is a good argument for a retrospective diagnosis of pellagra.1 Testing for Niacin levels or urinary metabolites is not frequently available and it’s not necessary for the diagnosis.
Conclusion
We described a typical case of Pellagra in which the ‘3 D’s’ were present. In such a case, we should begin the treatment before the results of the laboratory investigations are known. The improvement of all symptoms within a few days is sufficient to confirm the diagnosis. However, the ‘3 D’s’ triad is not always present, and the clinician should consider the diagnosis in face of unexplained abdominal or neurological signs in certain patient groups.
Population studies in Norway are showing that taking part of (creative) or receiving (receptive) cultural activities, i.e. arts, is associated with good health and good satisfaction with life among other things,1. Cultural activities have the potential to affect individuals beneficially: physiologically, biologically and emotionally, and several studies show that cultural activities can stimulate emotions and behaviors that make life easier, 2–5. Cultural activities can enrich and enhance our memory, stimulate connections among brain networks and enable us to accelerate learning and differentiate feelings of meaning and context,6,7 Cultural activities have also improved both physical health, social function and vitality among health care staff,8.
In an analysis of data from a large longitudinal cohort-study of a working population (called the SLOSH study = Swedish longitudinal occupational survey of health), some interesting associations were revealed between access to cultural activities in the workplace and health. Participants reporting many cultural activities at work had a more favorable improvement of emotional exhaustion during a follow-up period of two years than those whose workplaces did not offer these amenities,9. Other studies in which cultural activities have been offered to patients on long-term sick leave confirm that cultural activities have beneficial effects on both self-confidence and pain,10,11.
In a new approach, an artistic leadership program, called “Shibboleth”, affects not only managers included in the study, but also their employees (who did not participate in the artistic program). This one year art-based program showed statistically significantly more improvement of mental health, covert coping and performance-based self-esteem than the comparison group (who participated in an ordinary leadership program). They also experienced less winter/fall deterioration in the serum concentration of DHEA-S (dehydroepiandrostereone-sulfate), a regenerative/anabolic hormone,12.
Studies on singers, both amateur and professional singers and choir singers, show positive effects on different biological markers such as oxytocin and testosterone,13–15. On the basis of results from another Swedish project, ”Prescribed Culture”, which aimed to evaluate the effects of prescribed cultural experiences in the treatment of patients on long term sick leave, it was claimed that cultural experiences have their best effects when used in health promotion and prevention , rather than when the individual is already sick,16. Multimodal stimulation seems to have particularly strong effects. For instance, concomitant visual and auditory stimulation gives rise to stronger activation of “visual” and “auditory” parts of the brain than separate visual and auditory stimulation,17.
A mixture of different cultural activities seems to optimize influence on the limbic system since a broader emotional perception is activated,7. Cultural activities offered to participants that would not have chosen them spontaneously, could enhance already existing pathways in the brain enabling deeper cognitive behavioral change,17–20.
Despite this knowledge regarding the potential benefit of cultural activities in different contexts on both individuals and groups there is still a missing accessible practical functioning link between producers of culture and different groups of practitioners within health-care.
Burnout is characterized by emotional exhaustion, detachment from work and decreased effectiveness at work. This can develop in situations with excessive workload and insufficient resources as well as lack of control and support,21. If the process of burnout is a reaction to long-term stress, without enough recovery, this can lead to the more severe exhaustion syndrome,22. Symptoms include fatigue, impaired emotional regulation, cognitive problems and sleeping disorders. Most of these patients have an increased sensitivity for stress even after recovery,22. In recent years, Swedish rates of sick leave due to minor psychiatric morbidity , and burnout symptoms, have increased dramatically,23-24 . Complaints usually include physical, emotional and cognitive exhaustion, which in most cases appear to be related to chronic stress without restitution,25–28. Today many women in Sweden have stress related symptoms, and some are diagnosed with exhaustion syndrome. If these women are detected at an early stage, the prognosis is good,22.
Alexithymia, (the difficulty to differentiate your own and others feelings), can be a silent but severe problem for persons suffering from this personality trait. Grabe et al.,29 conducted a study in which the questionnaire TAS-20 was used for the assessment of alexithymia. Medical examination was also performed. In this study alexithymia was related to hypertension and arteriosclerotic plaques. Alexithymic personality traits may increase the risk for CVD (cardio vascular disease).
The rationale behind choosing symptoms of exhaustion, SOC and alexithymia as main outcome variables was the intention to examine whether cultural activities in this form can change pattern of thought, feelings and behavior in participants with burnout symptoms. If cultural activities prove effective for this participant group, they could have considerable benefits both financially in terms of reducing sick leave and health care consumption and of reduced individual suffering.
Aim
The aim of the study was to assess to what extent symptoms of exhaustion, sense of coherence, alexithymia and self-rated health among women with burnout symptoms can be beneficially influenced by cultural activities organized in health care centers.
Method
Participants
Four health care centers in Stockholm County hosted the cultural activities. Medical doctors and social workers distributed information about the study to women diagnosed with exhaustion disorder or exhaustion symptoms. Women, native and foreign born, with burnout/exhaustion symptoms (fatigue syndrome or stress-related fatigue) who were curious about new clinical approaches were asked by the doctor to participate in the study and screened for inclusion and exclusion criteria. Participants (women age > 18) with burnout/exhaustion symptoms such as strong fatigue, cognitive problems, and sleep disturbances were enrolled. There was an inclusion criterion with a score above 2 on the KEDS scale. The diagnosis was made by the doctor.
Exclusion criteria: Participants with difficulty in speaking and understanding Swedish, participants with alcohol or drug abuse problems, or/and participants with severe depression or psychiatric borderline. Also excluded were participants with severe somatic diseases (such as serious angina pectoris or participants who had had a stroke). Randomization was done using a 3:1 allocation to intervention or control groups.
The randomization was done using a stratified randomization by center. Randomization was done by the statistician. The group allocations were sent in individual envelopes which were distributed to centers and blinded to the site staff. Envelopes were further drawn in a consecutive order with regard to recruitment of subjects at each of the four health care centers. Thirty-six participants were allocated to the intervention group (nine patients in each group) and twelve participants to the control group. The standard care that each participant received included physiotherapy such as relaxation and physical light training.
All randomized participants gave their written consent to participation in the study. Data were collected over a period of 6 months. The project includes evaluation of six different culture activities. In the selection of the health care centers socio- economic diversity and employment status were considered. We used regularly occurring structured cultural activities in cooperation with culture producers, i.e. actors, musicians, dance teachers. The Regional Research Ethics Committee of Uppsala has approved the study (Dnr. 2012/359).
The culture palette: six different cultural packages
The following cultural activities were included in the study; five of them have previously been presented in the literature with good evidence on other groups of patients. One package (the musical show), which has not been presented previously on groups of patients, was chosen as it represents a combination of different modalities of activities at the same time. The active mechanism of all six cultural activities was to stimulate different modalities of the senses such as the visual, motor, verbal, auditory, emotional and sensational, according to Downing’s levels of perception, 30. All participants were offered six cultural packages:
1. Interactive theater: An experienced actor introduced poetical lyrics and poems and then initiated and participated in discussions with the participants regarding thoughts, emotions, and experiences evoked by the texts.
2. Movie: After showing a movie, a film expert initiated discussions among the participants about experiences and thoughts evoked by the movie.
3. Vocal improvisation and drawing: After participating in a vocal improvisation session with an experienced performance artist and pianist, the participants painted a picture representing emotions, thoughts and pictures evoked during the improvisation
4. Exploring Dance: The participants improvised dance movements under the guidance of a dance movement pedagogue/music teacher. The dance movements were staged according to the situation in the room and with focus on bodily awareness. Afterwards the group discussed their experiences during the dance session.
5. Mindfulness and contemplation: The participants contemplated and practiced mindfulness together with an experienced mindfulness instructor. Attention was on breathing and body awareness. Thoughts, feelings, images and sensations were in focus and experiences were reflected in the group after the contemplation.
6. Musical show: after a musical show including music, song and dance focusing on bodily awareness, the participants discussed thoughts regarding the body with the actor.
Every session in each one of the six different cultural packages lasted for 90 minutes. Evaluations
Three different standardized scales, and also self-rated health and self-figure drawing, were used.
KEDS - Karolinska Exhaustion Disorder Scale,31. Questions about concentration, memory, physical fatigue, endurance, recovery, sleep, hypersensitivity to sensory input, experience requirements and irritation and anger. Higher scores indicate worse disease activity/performance.
SOC - Sense of coherence,32. A key factor in being able to feel well-being and health. This factor has been shown to be crucial to helping individuals mobilize their self-healing systems. Higher scores indicate better performance.
TAS - Toronto Alexithymia Scale,33. Estimation of ability to recognize and interpret feelings in oneself and others. TAS contains three subscales; the inability to handle emotions due to emotions being poorly recognized (difficulty recognizing), the inability to describe feelings (difficulty describing), and mismatch between coping behavioral emotions (externally oriented thinking). This study used the full scale score, i.e. the summary of the three sub scores. Higher scores indicate worse performance.
Self-rated health (SRH) consists of a single item measure.
Procedures/implementation
The four different health care centers presented each activity on two consecutive occasions. After two weeks of one program, there was a new program on two consecutive occasions etc. Each participant has thus been offered 12 cultural packages during a three-month period, i.e. once a week. During the monitoring period between month 3 and month 6, there was no culture activity offered. The control group was monitored in parallel during the entire period monthly at 0, 3 and 6 months.
The participants evaluated the project individually with questionnaires prior to the sessions, after completion of the intervention at month 3, and at follow-up after 3 months i.e. month 6 (both intervention and control group). In-depth interviews with both participants and producers of culture, i.e. representatives for the various cultural activities and health care staff were conducted during the monitoring period (this data is not presented in this article).
Data analysis
The primary outcome efficacy end point/measure was mean change from baseline to three and six months in the KEDS summary score. The secondary outcome measures were mean change from baseline in the SOC summary score, the TAS summary score and the self-rated health, from baseline to three to six months.
All data were presented using descriptive statistics, i.e. mean and standard deviation for continuous variables and frequency and percentage for categorical variables. For all main outcome variables, data were further analyzed using the Linear Mixed Models, including group (intervention and control) and time (baseline, 3 month and 6 months) as fixed factors. Results were presented as marginal means, the estimated mean value adjusted for the factors included in the analyses model. The difference between intervention and control group with regard to the estimated and adjusted means are defined as the effect size, i.e. the mean difference between the intervention groups for each of the primary and secondary outcomes measures divided by the standard deviation. All tests were two-tailed and p<0.05 was regarded as statistically significant.
IBM SPSS version 22 was used for statistical calculations. In the presentation of the results from the statistical analyses, the measured effect size was used and derived as the absolute difference between active intervention and controls with regard to each of the outcome variables/endpoints used,34.
Results
There were 55 participants screened in this study, however seven participants who met the exclusion criteria of too serious/severe depression was not included into the study. In total, there were 48 participants randomized into the study, age between 41 and 70 years, mean 53.8 (SD= 8.15).
The results showed that for KEDS (exhaustion) there was a statistically significant two-way interaction (P<0.001) with a decreased mean from baseline to three and six month respectively in the intervention group whereas in the control group there was no change. The mean treatment effect size, i.e. the mean difference between groups, in favor of the intervention group was 9.9 (SE=3.0) at 6 months. See table 1 and figure 1a.
There was no difference in mean SOC - Sense of Coherence – scores between the groups. See figure 1b. Further, the results revealed a statistically significantly more pronounced decrease in the intervention group compared to the control group in the alexithymia items of total score, (P=0.007, mean treatment effect size=5.4 (SE=2.2) at 6 months in favor of the intervention group), difficulty describing (P=0.004, 2.4 (0.9)), difficulty identifying (P=0.051, 2.6 (1.3)) but not for external orientation (P=0.334 0.5 (0.8)). See table 1 and figure 1c. There was also a statistically significant difference between the groups with regard to self-rated health (P<0.001) where mean scores increased over time in the intervention group but decreased in the control group. See figure 1d.
Table 1
KEDS (Karolinska Exhaustion Disorder Scale) and TAS (Toronto Alexithymia Scale) and SRH (self-rated health) at baseline, month 3 and month 6.
Control Group (n=12)
Intervention Group (n=36)
Count
Mean
Standard Deviation
Count
Mean
Standard Deviation
KEDS
Baseline
12
32.7
8.2
35
31.7
8.4
Month 3
12
34.9
9.2
34
23.6
8.6
Month 6
12
33.9
8.7
33
23.7
10.1
Sense of Coherence
Baseline
12
117.2
29.9
33
118.0
28.0
Month 3
12
112.8
30.3
33
121.1
30.5
Month 6
12
115.1
24.2
34
123.9
28.2
Difficulty Describing
Baseline
12
14.8
4.3
34
14.2
4.6
Month 3
12
15.3
3.6
31
12.7
4.6
Month 6
12
15.2
4.1
34
11.8
3.9
Difficulty Identifying
Baseline
12
20.0
6.0
34
20.3
6.3
Month 3
12
20.6
6.5
31
19.0
6.9
Month 6
12
20.0
6.1
34
17.4
5.0
Externally Oriented
Baseline
12
14.9
4.2
34
13.8
4.4
Month 3
12
15.4
4.3
31
13.9
3.9
Month 6
12
14.6
4.8
34
13.2
3.5
TAS
Baseline
12
49.7
13.1
34
48.3
13.4
Month 3
12
51.3
13.3
31
45.6
13.9
Month 6
12
49.8
13.9
34
42.4
10.8
Self-rated Health
Baseline
12
5.2
1.5
36
4.8
1.9
Month 3
12
4.6
1.9
36
6.0
1.9
Month 6
12
3.6
1.6
35
6.4
1.9
Figure 1a
Marginal means and 95 % confidence intervals for the KEDS (exhaustion) scale by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Figure 1b
Marginal means and 95 % confidence intervals for the sense of coherence (SOC) scale by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Figure 1c
Marginal means and 95 % confidence intervals for the Toronto Alexithymia Scale (TAS) by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Figure 1d
Marginal means and 95 % confidence intervals for the self-rated health scale (SRH) by group and time. Results were based on the linear mixed models analysis adjusted for baseline.
Discussion
The results show that the different exhaustion factors measured by means of KEDS (Karolinska Exhaustion Disorder Scale) decreased in the intervention group compared to the control group. With regard to the total score of TAS (Toronto Alexithymic Scale) there was a statistically significant decrease in the intervention group compared to the controls, i.e. the participants started to improve their differentiation of feelings and emotions after three months with cultural activities. The same pattern was seen with regard to self-rated health, which improved in the intervention group. However, there was no significant difference between the groups with regard to the development of sense of coherence.
It seems that the different cultural activities have helped the participants become more aware of their feelings and sensations; to describe and to identify feelings. It is not easy to explain the positive results based on one clear paradigm. It is likely a mixture of psychological, neurological and social factors or changes that interact in a complex manner.
Previous studies have discussed the theory of the emotional brain - cultural modalities can “surprise” the cognitive brain unconsciously. LeDoux,20 discusses the upper/slower and the lower/faster pathway in the brain. Emotionally loaded visual and auditory stimuli are transmitted on both types of pathways. Music impulses are for example evoking activities in the emotional brain much more rapidly than in the cognitive brain. However, impulses spread secondarily from the emotional to the cognitive brain. This can trigger the participants awareness of different emotions and may start a process of differentiation, possibly initiating a change of life course. By using different cultural activities, that the participants normally would not try, the differentiation process may be amplified. This suggests that cultural activities can surpass automated thinking and create new "pathways '' with changes in behavior and increased well-being.
In other studies we have observed that a mixture of different cultural activities can increase the amount of stimuli affecting a broader network of emotional correlates, 14,16,18 . A very interesting long-term decrease in alexithymia, 35 was associated with lowered blood pressure and a decrease in sick leave. By allowing the participants to try new cultural stimuli we may have helped the participants change old habits. A hypothesis is that this may also have contributed to the observed decrease in exhaustion.
Why did we not see any increase in the sense of coherence in the intervention group? It is very difficult to change patterns of thought and behavior although we can argue that the participants in the control group also found a new sense of coherence just by being invited to answer questions about themselves and being focused upon. Many of the participants did not go out spontaneously because of their fear of socializing. Some of them described their situation as black or white, not wanting to change routines that made them feel less safe,36.
Despite the fact that the health care staff did not participate in the culture palette, they were also affected by the cultural activities 36. This may be a mirroring effect, or emotional contagiousness on health care staff, which may also play a role between the participants and their staff. The passive cultural activation phenomenon has previously been presented in the literature,37 and there seem to be possible well-being effects of just watching dance or visiting a theatre, 6,10 which may explain the positive health care staff response to the culture palette. The results of this study underscore the importance of regarding the health care system as a whole, where patients, health care staff and visiting relatives affect each other. Empathic behaviors contaminate in all directions and we need to be aware of how we project ourselves when working in a caring context.
Modified “culture palettes” and “train the trainer” programs and workshops are now in use in Sweden, inspiring cultural producers to further develop the health care system and a cultural health box - a box with six different books about cultural activities and the research behind this - have been distributed to all health care centers in Sweden, 38.
Developing and adapting cultural programs to fit other kind of groups of participants could cross-fertilize health care thru culture production.
Limitations
This study was limited to women with exhaustion symptoms and therefore further research on implementation of cultural activities within different groups of participants and sexes is needed before we can generalize the results to other groups of participants. Another limitation is that we did not control for outside activities, such as doing walks in nature. In this study we only presented indoor cultural activities.
Conclusion
The cultural activities in this study made exhausted women understand what makes them vital, confirmed, curious, healthy and creative. The study also illustrated that there could be synergistic effects when bringing cultural activities into the health care system36.
Once upon a time there lived a quite wealthy young man - in the sense that he was quite smug and comfortable, never really wanting for anything. ‘Wealthy people don’t have to concern themselves about others or indeed material matters, he used to say to himself, blissfully unaware of the dramatic irony in his statement. He had tons of clothes (which made it difficult to decide what to wear each day), lived on his own in a big house almost the size of a mansion, went on lots of holidays to exotic places, ate in the best restaurants, and by all accounts had no worries whatsoever. He was a man of modest intelligence, quite tall and stout with an arrogant (or should I say confident) manner. He could quite easily win an argument because he would literally wear his opponent down with the ferocity of his delivery, even though it bore little substance. 'I could be a politician because I am so good at debating sensitive issues which affect ordinary people, he would reflect when on his own, which was frequent.
His parents had so much money (from their banking business) to fritter away and therefore had no trouble finding him a suitably big house (almost as large as a mansion as stated) in a fashionable area of London. He also owned a house in Richleymanor, a wealthy, prosperous suburb of Richleyshire. ‘Because I have no worries and am in perfect health', he said when he was only 16, 'I am going to become a doctor and heal people who are not rich enough to see me privately and who are a million times less fortunate than me.' Such was his altruistic spirit. And so he studied as hard as he could because he had to (he was not the brightest card in the pack). With the help of his parents' influential circle of friends in the whole of Richleyshire who knew people in high places, he managed to secure a place in an elite medical school where only top doctors were trained - even though he did not possess any outstanding qualifications on leaving school. But that sort of thing doesn’t really matter if you possess an altruistic spirit. 'I mean', he reasoned, – 'Lots of famous people (including entrepreneurs) did not pass their final school year exams with Honours and I am just like them in that respect - really down-to-earth, a man of the people.'
On the first day of entry to the Royal Breedington University Medical School he was already planning his future career. Not for him the humdrum life of a family doctor. No - he was aiming for prestige and acclaim. He did not need the money though extra money would help 'because you can never have enough, especially if you want to help others less fortunate than yourself', he would say to himself. Such was his determination. 'Should I become a great brain surgeon', he pondered one evening. Should I become an eminent cardiologist or a revered obstetrician? You see, for him it was not enough to be an ordinary doctor - one had to be special in some way. These careers and others (the field of Medicine is huge) he considered. Then one day he decided: 'I know now what to do'; I will get my basic qualifications out of the way and then embark on a career in Mentalology - a subject which was gaining great interest in the popular press. Even students at the University were talking about it. It was a higher degree than Neurodevelopmental Psychobabble (another much sought-after career, normally the reserve of doctors studying cerebrotherapy). So after lots and lots of postgraduate courses in Mentalology he finally passed the higher degree, becoming a member of the Royal College of Mentalologists (MRCM), spent 5 more years in training and became a Consultant Mentalologist at a very prestigious hospital, one which had links to a university, as it happened. His ultimate ambition was to become a Doctor in Medical Politics because he wanted to be in charge of doctors and patients but without the encumbrance of having to care for patients per se or to actually meet doctors. Not for him the drudgery of life in a hospital or general practice – no - one needs to earn as much as possible by doing the least work, rather like Business Executives, he would ruminate.
Initially he enjoyed seeing a few patients here and there as par for the course, but because he felt he was a very important doctor, he needed to move up the ladder to the higher echelons, managing other doctors who might in turn benefit from his great wisdom and enormous insight, accrued in just 8 years training! He decided that he was too important to be seen hanging around hospital wards or in the outpatient department and so spent nearly all his time in the library and at meetings, apart from breakfast and lunch. He always had breakfast in the hospital canteen to show he had the common touch, and sometimes he would make a point of staying on longer after lunch in order to mix with other not-so-important doctors, who would laugh and grovel obsequiously at his every spoken word. Then suddenly he was off, and would be seen bustling and rushing through the canteen doors on his way to a very important event at the prestigious headquarters of the Organization, where he would sit three seats away from the Lord High Superexecutive Chief of the Organization (LHSCO), a very long title indeed but when one is important one usually has imposing if not long titles. Such was the circle the very important doctor was mixing, it explained why he was hardly ever seen in the hospital outside lunch hours or breakfast. Because, you see, in his estimation or rather esteemed opinion, if one is not around much then one must be a very important person indeed.
Sometimes he was seen rushing off to other very important meetings at a top-class hotel where there would be a special Conference Room; sometimes he was at meetings all day. However, often it was difficult to find out exactly what he was doing or where he was because many of the meetings were high level top-secret meetings; for example, a Superexecutive meeting lasting a whole hour might have on the agenda a motion to close down the hospital outpatient department because patients were costing the Organisation too much money. That superfluous-to-requirements money could be better spent on holidays and pay rises for other but not-so-important medical chums as well as serious-minded managers who in turn might do him a favour later on. 'You never know what's around the corner', he always used to say in one of his contemplative moments. The Organization often talked about very big issues such as Doctor Management Downcasting (how to keep those grasping medics in line) and Patient Empowerment, even though patients were never included in any discussions about where they would go when their hospital closed down. Sometimes meetings would extend until the early hours of the morning, which suited the very important doctor because he had no family to worry about or other personal commitments and could come and go as he pleased. Others had to stay on at the very important meetings regardless of their personal circumstances. Sometimes he was so exhausted attending meetings he would spend the following afternoon on the golf course relaxing before attending another evening conference. 'I don't know how he does it', his reverential colleagues would mutter, in hushed tones. 'He deserves another award for taking time off to recharge his batteries for the next meeting'. 'It is quite astonishing how much energy some people have', he would say contentedly to himself.' 'What would the Organisation do without someone of my great leadership skills’?, he asked himself many times in a semi-congratulatory tone.
Nothing would deter the very important doctor from achieving his goals and pleasing the Organisation. After all, this was the way to the top of the medical hierarchy – Doctor of Medical Politics (DMP) and Chief Scientist and Supervisor of the Faculty of Mentalology (CSSFM for short) was his goal. First he set out some decrees or edicts. These would all come under the rubric 'Management Directives', or put in another way, informing his colleagues in a polite but firm manner how he would delegate them to do ‘this and that', and therefore no one would blame the very important doctor for say, dismantling any part of the service; besides, his sheer tenacity and doggedness (character traits which he had cultivated from his seniors) gained him further admiration from the legions of subdoctors (doctors who were under his control) who had to yield to his commands. He would sometimes act very humble when questioned about his ruthless tactics and would feign innocence (or was it impotence) in the face of criticism. No, it was the Organization 'calling the shots', as he used to describe it, callously ignoring the plight of his colleagues and patients.
It was strange that he could never recall or at least did not seem to know any of the names of people in the Organization who were responsible for the targets to be achieved. 'Anyway, most patients are not really ill, they just complain and they can jolly well go back to their own general practitioner if they want to bother someone', he would argue in one of his rare insights into the human condition, particularly when colleagues challenged him. His doctor 'associates' (he could never really truthfully call them friends) were stupefied by his perspicacity and visionary zeal and were in no doubt that in order to achieve a change in their practice it was better they were paid less and worked more intensely between 9am and 5pm. They could come in earlier or stay later if they wanted to of course, but no extra money was available for overtime because it was costing the Organization thousands of pounds annually. Best to give the bonuses to those who really deserved them - those Manager Doctors who were extremely busy writing protocols about Best Practice and Risk Assessments - real life-and - death issues, and spending at least 4 hours every six months at very special high-powered meetings drafting 'outcome protocols'. So many emails to send out. This agenda was 'all in a day's work' for the very important doctor who needed to supervise this superhuman task in between meals.
But even the very important doctor himself needed resources and time to carry out all this work. 'I know what', he said to himself one bright sunny Sunday morning on the golf course, - 'I will reduce the amount of time doctors spend seeing patients and cut costs further in this way for all those dedicated doctors because dedication is costing too much'. One hospital in-patient could cost the Organization £1000 a week, even more. 'The doctors can still attend meetings in the hospital (no costs incurred) and do extra administrative work.' 'The bonuses will only go to those who have achieved a special distinction in doing the work of Managers and follow the party line'. 'Yes, that's the way forward', he thought to himself, in one of his rare flashes of brilliance. 'From now on doctors will only have to work 9-5pm'. 'The on-call commitments can be covered by NHS Indirect', the latter being a new company set up to replace doctors and nurses at night-time and weekends, usually manned by staff from one of the local supermarkets. Surgeons would be then free to down tools at 5pm instead of wasting time (and the Organization's money) battling through endless hours of unnecessary exhaustive operations such as cardiac bypasses or hip replacements, which could easily be carried out in the patients' homes anyway. Psychobabble experts could use tick-box rating scales or instruments to assess new referrals (no need to see patients, too costly).
There is no way to describe the tumultuous reception these ideas received at the Managers Annual Conference in Bristol, and the very important doctor received even more accolades. In fact, he was considered for a Rhodium Medal, the highest award in the land given to any doctor. Before being conferred with this precious and prestigious medal (because it can only be worn around your neck, or else it lies on the mantelpiece where nobody really notices it) he was given two lots of pay rises - one for services to the Organisation, the other for keeping the common grasping subdoctors in line by forcing them to sign in and out of work every day and by reducing their salaries. After all, there were rumours that the grasping, greedy subdoctors were beginning to think that perhaps the very important doctor was becoming too very very important. But they kept quiet in any event.
His great achievement was the setting up of SCRAP (Strategic Commission for Rapid Abolition Programme) which set out a one-year plan of how to prevent any patient being seen by a doctor. The patient could be seen by any number of people, from the tea lady to the hospital porter, who were already working flat out on the minimum wage. At least they were not so expensive to keep on the pay roll. The next brilliant idea he concocted was to replace the word 'patient' with 'customer'. 'Patient', he did not like. It gave the impression that someone was ill and needed to see a doctor. But with the New Opinion About Hospital Patients (NOAHPS in short) charter, the word 'patient' did not fit the profile of an enterprising Organisation and so NOAHCS (New Opinion About Hospital Customers) sounded much better. All staff were thence ordered to use this terminology or face the consequences. It was rumoured that it was a sacking offence to use the word patient. He even sent an email to the same effect around the whole Organisation. No one spoke out for fear of reprisal and possible instant dismissal. He was applauded at every Organization meeting from that time on and was rewarded by being given Freedom of the Hospital. This meant he did not have to do anything really - just walk around shaking hands with everybody, telling them what a great job they were doing, and so forth. He used the phrase 'Congratulations on a job well done' as many as four times a day to different staff in the hospital. In private he would be irritated because he had to praise other people for what he truly believed were his achievements.
By the end of each week he was so exhausted from sitting on comfortable chairs (some were so comfortable it was a real effort to get out of them) at the many meetings he attended that he would fly off to some far away country for a rest, though of course would endeavour to find out how that country dismantled its health service. Because of his enterprising attitude on behalf of the Organization these trips would be paid for and the very important doctor would not have to spend a penny. 'I deserve it because of all the hard work I am putting in', he used to say, to justify his huge salary and the enormous expenses paid for by the Organization. 'They obviously think very highly of me.' Besides, they know I would get a better salary elsewhere if they did not pay me such gigantic sums of money here', he would rationalise. But this suits me for the time. I have a big house in London near the University and an even bigger house in Richleyshire where I can play golf on the weekends and charge all my expenses to the Organization, even the Golf Club fees. 'Why not? Politicians were doing it', he would argue, in a rare utterance of cognitive dissonance (or pangs of conscience others might think) a term he had picked at one of the many important half-hour psychology conferences he attended (he was much too busy to stay to the end of any conference.
As time passed he was beginning to think he needed a higher salary because time off and holidays were costing him money (domestic shopping, clothes, food, heating bills) despite the freebies. During his days off he would spend lots of time going to museums, visiting the theatre, eating in expensive restaurants and staying in luxury hotels not too far from home, say 10 miles or less. However, for him a real holiday was travelling abroad in a first class seat on a prestigious airline to faraway places. This gave him an edge over his less wealthy colleagues and he would often spend hours on his return recounting his great adventures and experiences abroad in exotic lands. 'He is so broadminded and well-travelled', his managerial associates would say with a feeling of unrequited envy. It is quite remarkable how he manages to be in so many places at the same time - if only he could do the same at this hospital, we would be top of the League Tables for Hospital Risk (LTHR) and gain the recognition we deserve'. 'For all his hard work spent travelling abroad researching better ways of closing down wards and hospitals he now deserves a huge rise in salary'.
And so it came to be. The very important doctor was given an extra allowance (EA for short) worth half his salary and a Credit for Working Hard Allowance (CWHA), both linked to his pension. He was also given a bonus allowance (BA) for sitting twice yearly on a Doctors Work Review Panel (DWRP) set up to deal with those doctors who were not pulling their weight or taking more than one day sick leave or 2 days annual leave at a time. Study leave had already been dropped because the very important doctor argued that if he did not need study leave then no one else did. Besides, ‘Who needs study leave when you can look things up on the internet – even how to carry out open heart surgery’. He would argue. Commitment to the Organization was his raison d'être.
And so it continued. After 10 years nearly all the patients had been discharged from the hospital and family doctors were sending them elsewhere into more luxurious, expensive, private hospitals for 'reviews, assessments, and second, third, even fourth opinions'. The Organization would pay for all this from the money it saved closing down the local hospital. This was the very important doctor's finest hour and for his services to the Organization he was awarded the Rhodium Medal at the Annual Convention of Supermanagers Conference. This award was inevitable, given all the time both home and abroad he had invested in this venture. Now the entire hospital could be closed down thereby saving the Organization millions of pounds.
However, there was a problem with this way of operating, he began to think: ‘If the hospital were to close down there would be no need for an Organization to run it. There would be no management posts and my post as MDP and CSSFM might be superfluous to requirements. 'I know what I will do' - he decided - 'When that happens I will apply for another post in a different Organisation and I am sure I will be successful given all the accolades I have received, and when that Organisation closes down with my help I will get an even bigger salary and move on to the next post' - maybe Minister for Health?
A 40 year old patient presented to the hospital outpatient department with one year history of cough, choking sensation following swallowing, hoarseness of voice and loss of weight. History revealed his previous hospital admission 1 year back for management of organophosphorus poisoning during which he was intubated and put on mechanical ventilator for 10 days. Patient developed the symptoms a month after his discharge from the hospital. Cranial nerve examination was within normal limits. What is the possible diagnosis?
Gastro-oesophageal reflux disease
Tracheo-oesophageal fistula
Oesophageal diverticula
Oesophageal rupture
Fig 1: Barium swallow illustrating a dilated oesophagus and the TOF with resultant contamination of the trachea and bronchial tree
Fig 2: Oesophagoscopy showing TOF
Correct answer:
2. Tracheo-oesophageal fistula
Discussion:
A tracheo-oesophageal fistula (TOF) is a communication between the trachea and oesophagus which can be congenital or acquired. Congenital and acquired TOFs are associated with multiple complications, including poor nutrition, recurrent pneumonia, acute lung injury, acute respiratory distress syndrome, lung abscess, bronchiectasis from recurrent aspiration, respiratory failure, and death. Acquired TOFs occur secondary to malignant disease, infection, ruptured diverticula, and trauma.1, 2 Acquired TOFs are quite rare, and incidence rates have not been well documented. Post intubation TOFs uncommonly occur following prolonged mechanical ventilation with an endotracheal or tracheostomy tube. TOFs caused by endotracheal tube intubation depend on several factors, including prolonged intubation, an irritating or abrasive tube, and pressure exerted by the cuff. Pressures exceeding 30 mm Hg can significantly reduce mucosal capillary circulation and result in tracheal necrosis. Cuff pressure is particularly risky when exerted posteriorly against a rigid nasogastric tube in the oesophagus. Poor nutrition, infection, and steroid use cause tissue alteration, which predisposes patients for the development of TOFs. As a result of laryngeal bypass, spillage of oesophageal contents occurs into the trachea. Saliva, food and gastric juice contaminate the airways. This leads to congestion, infection, pneumonia, bronchial obstruction, atelectasis and respiratory distress. The severity of contamination depends on the width and length of the fistula as well as the posture of the patient. Spontaneous closure of non-malignant TOFs is exceptional.
Patients with acquired TOFs have high mortality and morbidity rates because of critical illnesses and co-morbidities. Acquired TOFs may occur in individuals of any age, and elderly individuals are at increased risk if they become ventilator dependent because of respiratory failure. Acquired TOFs can be diagnosed by instillation of contrast media into the oesophagus (Fig.1) or during direct visualization by flexible oesophagoscopy (Fig.2) or bronchoscopy. A high index of suspicion is needed to diagnose tracheo-oesophageal fistula in a post intubated patient presenting with symptom of cough following deglutition. Since acquired TOFs do not close spontaneously, surgical repair is needed if the patient is stable enough.3, 4 Critically ill patients are managed conservatively until stable enough for a major surgical procedure.
Typical oesophageal symptoms of gastro-oesophageal reflux disease include heartburn, regurgitation and dysphagia. The classic presentation of spontaneous oesophageal rupture is chest pain and subcutaneous emphysema after recent vomiting or retching (Mackler’s triad) in a middle-aged man with a history of dietary over-indulgence and over consumption of alcohol. Oesophageal diverticula presents with oropharyngeal dysphagia, usually to both solids and liquids, which is the most common symptom. Retention of food material and secretions in the diverticulum, particularly when it is large, can result in regurgitation of undigested food, halitosis, cough, and even aspiration pneumonia. The patient may note food on the pillow upon waking up in the morning.
An 87-year-old gentleman was admitted after sudden dysarthria and left facial palsy due to a right internal carotid artery occlusion. On examination, incidental spontaneous movements were seen at rest in the left leg (video), with bilaterally diminished Achilles reflexes. Patient was unaware of this finding. Muscle atrophy and hypoesthesia were not present. When walking on heels, left foot dorsiflexion was impaired.
What kind of physical finding is shown in this video?
A. Myoclonus B. Dystonia C. Tremor D. Chorea E. Fasciculation F. Myokymia
Answer / Discussion
Focal fasciculations in the tibialis anterior muscle are shown. When walking on heels, left foot dorsiflexion was slightly impaired.
Fasciculation is a brief, twitching, spontaneous involuntary contraction affecting muscle fibres served by one motor unit, which may be visible under skin. When present, they reflect denervation.
A complete history intake and neurological examination will lead to a sensible diagnostic work-up and to set a prognosis. Clinical differential diagnosis is presented in table 1.
Table 1: Key points for clinical diagnosis
Myoclonus
Brief, shocklike involuntary contraction of a muscle or group of muscles
Dystonia
Involuntary muscle contraction that can cause slow repetitive movements or abnormal postures
Tremor
Involuntary rhytmic contraction of antagonistic muscles
Chorea
Involuntary irregular movement that starts in one part of the body and moves unpredictably and continously to another part, like “dancing”
Myokymia
Involuntary spontaneous quivering, writhing movements within a single muscle not extensive enough to cause a movement of a joint
Localization helps in diagnosis: fasciculations can be generalised, in metabolic-toxic conditions, the benign fasciculation syndrome and degenerative disorders of anterior horn of spinal cord, as amyotrophic lateral sclerosis; segmental, as in syringomyelia; or focal, affecting the muscles controlled by a nerve or spinal root. When fasciculations are in a distribution that cannot be explained by plexus, root or nerve lesion amyotrophic lateral sclerosis (ALS) must be ruled out as soon as possible.
Evolution findings are also pivotal. The absence of muscle atrophy suggests that an acute or subacute nerve lesion is present, although a limited chronic nerve lesion cannot be excluded based on that observation alone. A clinical examination should be repeated at least every six months to assess progression, muscle weakness, upper motor neuron signs and other findings, such as bilateral wasting of the tongue, the “split hand”, head drop, emotionality and cognitive or behavioral impairment1
It is also very important to rule out any possible metabolic disorder, as toxic conditions. Earl Grey tea intoxication has been reported as a cause of widespread fasciculations and cramps2
Electromyography (EMG) is the recording of the electrical activity of the muscles. It supports the clinical suspicion and helps in the topographic diagnosis. If ALS is suspected, a systematic examination of clinically uninvolved muscles has to be done for 2 minutes as fasciculations are the hallmark of this condition. As fasciculation potentials in ALS and benign fasciculation syndrome are indistinguishable on grounds of waveform parameters3 and there is not a reliable biological marker of the disease, a minimum follow-up of 6 months is required before setting a prognosis. When non-progressive isolated fasciculations of the tibialis anterior muscle, it has to been examined the 5th lumbar root and the deep peroneal nerve, as localizer sensory symptoms may be absent4, and to rule out any more diffuse neurogenic processes.
Magnetic resonance imaging (MRI) is supportive to EMG findings as it is very sensitive in detecting anatomic changes that could be responsible for the radiculopathy, but there are other causes of radiculopathy besides nerve root compression. Moreover, lumbar disk protrusions can be found in asymptomatic patients independent of age5. Therefore, MRI is not appropriate if pain or foot drop are not present.
Finally, an isolated chronic left L5 radiculopathy was diagnosed related to lumbar spondyloarthrosis.
A 26-year-old previously healthy male presented with a two day history of pain in his left wrist following trauma inflicted while playing volleyball. It was aggravated by movements around the affected joint. Clinical examination revealed mild tenderness over the left wrist with full range of movements and absence of any swelling. Distal neurovascular status was intact. X-ray of the left hand and wrist was done to rule out an injury to the bones (Fig. 1). Fig. 1: X-Rays of left hand and wrist
What diagnosis does the X-ray findings indicate?
Fracture of left scaphoid bone
Osteoblastic metastases
Osteopathia striata
Tuberous sclerosis
Osteopoikilosis
Answer / Discussion
The X-ray in Fig. 1 shows multiple small hyperdense oval and circular lesions scattered in all small bones of the left hand, with preservation of cortical thickness. These findings are suggestive of osteopoikilosis. Similar lesions were also present in the contralateral hand and wrist, as well as the pelvis (Fig. 2), on X-rays done subsequently.
Fig. 2: X-Ray Pelvis showing bone islands
Patient was counselled and reassured about the radiological findings. He was prescribed oral Paracetamol and topical Piroxicam for three days and asked to rest the affected joint. Osteopoikilosis (also called spotted bone) is a benign, possibly autosomal dominant dysplasia of bones, occurring in 1 per 50,000 people.1 Small bones of hand and feet, long tubular bones and pelvis are most frequently affected. The condition is asymptomatic and is diagnosed incidentally on radiographs taken for other problems. The diagnosis is straightforward, based on the typical radiological appearances of small (up to 10mm) hyperdense opacities distributed symmetrically. No further investigations or any specific treatment are indicated. Patients need to be reassured about the benign nature of radiological findings.
Osteoblastic metastases occur in the older age group, are generally larger in size and do not have such a uniformly symmetric distribution. Osteopathia striata is another rare bone dysplasia, characterized by long hyperdense striations mainly in the metaphyses of long bones and pelvis.2 Sclerotic bone lesions in tuberous sclerosis are frequently seen in the axial skeleton especially calvarias and spine, are at times distributed focally and have irregular borders and variable size.3 Subperiosteal new bone formation may be present and other clinical features like epilepsy may also provide a clue. As seen in Fig. 1, there is no break in the continuity of scaphoid bone, thus ruling out a fracture.
Hyperthyroidism is a common endocrine disorder and is mainly treated with anti-thyroid medications like propylthiouracil (PTU) and carbimazole. These medications have a large number of adverse effects, the commonest being skin rashes, and some are rare like agranulocytosis. Vasculitis is uncommon, but ANCA positivity is reported more in propylthiouracil and rarely with carbimazole or methimazole (1).We report a female patient with Graves’ disease who developed ANCA associated vasculitis while on carbimazole treatment.
Case report
A 29 year old female Filipino patient came to us with history of palpitations, tremors and weight loss for the last one month. Her thyroid profile showed severe hyperthyroidism (TSH <0.005, FT3-11.5, FT4-45.6) She was diagnosed with Graves’ disease as her anti-TSH receptor positive and was started on carbimazole 10mg tds. After three weeks of treatment, she developed macular rash over arms and legs and swelling of small joints of both hands. She noticed pain and colour change of both the hands and experienced typical Raynaud’s phenomenon. She had no renal or lung involvement.
On examination her blood pressure was 120/84mmHG, pulse 104 beats per min, temperature -37.1̊C. She had a mild diffuse goiter. Her X-ray chest, ECG and urine dipstick routine were all normal. Her CRP and ESR were raised. X-rays of the hands were normal. P-ANCA was positive. Antimyeloperoxidase antibody was positive. Anti-TPO and TSH receptor antibodies were positive.
Diagnosis of carbimazole induced vasculitis was made. The patient was treated with prednisolone 40mg daily once daily which was tapered over three weeks. She improved within 48hours and was asymptomatic after three weeks. She was treated successfully with radioiodine ablation. Her MPO-ANCA after 6 months was negative.
Figure 1. Pictures of the hands showing Raynaud’s phenomenon
Figure 2. Pictures of the hands showing Raynaud’s phenomenon
Discussion
ANCA positive vasculitis in association with antithyroid drugs was first reported in 1992 (2).There has been 32 cases of ANCA positive vasculitis associated with antithyroid medications reported up until now (3). The presenting symptoms are variable and may include renal involvement (67%), arthralgias (48%), fever (37%), skin involvement (30%), respiratory tract involvement (27%), myalgias (22%), scleritis (15%) and other manifestations (18%) (3).
In these patients the underlying thyroid disease is most commonly Graves’ disease but ANCA positive vasculitis has also been seen with association with toxic multinodular goitre (4). Recent studies have shown high frequency of ANCA positivity in patients with Graves’ disease treated with antithyroid medications, especially with PTU. Most cases of ANCA positivity are seen in patients on long term therapy (greater than 18 months) or in those with recent commencement of therapy as seen in our patient. However, a small percentage of these go on to develop features of vasculitis (3).
The majority of cases of vasculitis (88%) have been reported in association with PTU, vasculitis associated with carbimazole is very rare (5, 6, and 7). The pathogenesis of ATD associated vasculitis is not clearly understood. PTU has been shown to accumulate within neutrophils (8) and bind myeloperoxidase (9). The binding alters the configuration of myeloperoxidase (9) and may promote formation of autoantibodies in susceptible people. There has been no data with regards to whether carbimazole can alter the configuration of myeloperoxidase. ANCA positive vasculitis may be more common in patients of Asian ethnic origin, with half of cases reported from Japan (3). Our patient was from Philippines.
Wadw et al have reported 25% of patients were positive for MPO-ANCA in PTU group whereas in methimazole group 3.4% were positive (10).
This case highlights the awareness of this relatively rare adverse effect of a thyroid medication which may lead to fatal renal and pulmonary complications. Early diagnosis and withdrawal of the offending medication is important. In asymptomatic patients the significance of ANCA positivity is not clear but early definitive therapy in the form of radioiodine ablation or surgery should be considered.
A 44-yr-old patient with history of ileal Crohn’s disease was admitted to our Department because of asthenia, subclinical jaundice, painful hepatomegaly, fluid retention and ascites. In 2008 the patient was diagnosed with bladder cancer and was treated by surgical resection of the cancer and intravesical chemotherapy with mitomicyn C. In 2010 he was given azathioprine (AZA) at 2 mg/kg for Crohn’s disease and 3 months later he developed an increase in serum alkaline phosphatase, gamma-glutamyl transpeptidase and transaminases. He was then started on 1.5 mg/kg 6-mercaptopurine (6-MP) once daily. After 9 months he stopped 6-MP because of nausea, vomiting and abnormal liver function tests; 6-MP was therefore discontinued until the normalisation of markers of liver function. Two months later, when the transaminases were within the normal range, he received 6-thioguanine (6-TG) 25 mg a day, that was progressively increased to 80 mg a day. Three months later, the patient was referred to our Department with painful hepatomegaly, ascites and asthenia. Laboratory tests on admission revealed an elevation in AST 198 U/l and ALT 209 U/l. Total bilirubin was 3 mg/dl (direct bilirubin 1.5 mg/dl), LDH 784 U/l, alkaline phosphatase 191 U/l and ammonia 112 umol/l. Virological markers (HBsAg, HBcAb, anti HCV, HBV DNA) were negative. Patient was apyrexial, showed normal blood pressure (130/80 mmHg), tachycardia (110 bpm) and 97% SaO2 on room air. Physical examination revealed right hypochondrial tenderness, abdominal distension and shifting dullness, suggesting the presence of ascites. The rest of the physical examination was unremarkable. An echo-Doppler evaluation revealed thin linear suprahepatic veins and confirmed the presence of ascites. A CT scan of the abdomen showed hepatomegaly with dishomogeneous enhancement after dye injection (mosaic pattern). There was no evidence of any venous thrombosis or splenomegaly (Figure 1A); 6-TG was withdrawn empirically and the patient was started on therapy with albumin 25 g/day and spironolactone 200 mg/day. The average serum Na+ level during diuretic treatment was 134 mEq/l. An abdominal paracentesis of two litres was necessary, due to the progressive increase of ascites.
FIGURE 1A. CT scan of the abdomen on admission: Dishomogeneous enhancement of the liver after dye injection (mosaic pattern) (arrow). Suprahepatic veins are not detectable.
FIGURE 1B. Histological pattern of the liver biopsy specimen: marked centrilobular congestion (arrows) with hepatocyte dropout. There is no evidence of centrolobular veins thrombosis.
A routine laboratory investigation of ascitic fluid showed < 500 leukocytes/µL and < 250 polymorphonuclear leukocytes (PMNs)/µL. The ascitic fluid total protein level was 2.1 g/dl and serum-ascites albumin gradient (SAAG) was > 1.1 g/dL. No neoplastic cells were found. A transjugular liver biopsy was then performed, showing marked centrilobular hemorrhage with hepatocyte necrosis. There was mild ductular reaction, with no evidence of centrilobular vein thrombosis. The histologic diagnosis confirmed veno-occlusive disease (VOD) (Figure 1B). Screening for thrombophilia was also done, showing low levels of serum protein C and protein S. There was no mutation of JAK-2 V617F. The patient was then treated with a hyposodic diet, mild hydric restriction, enoxaparin,spironolactone, lactulose and omeprazole. He was discharged two weeks later, and after 3 months a complete regression of ascites and hepatomegaly occurred, and echography of the liver was unremarkable (Figure 2A and 2B).
FIGURE 2A. Echography of the liver at follow up. No evidence of ascites.
FIGURE 2B. Echography of the liver at follow up. No evidence of ascites. Suprahepatic veins are detectable (arrow)
Discussion
Although VOD was known among complications of 6-TG in childhood, this case-report emphasises the occurrence of VOD in adults with Crohn’s disease, as first described by Kane et al. in 20041. The thiopurine drugs were developed more than 50 years ago, and 6-MP was first used as a drug in 19522. Since then, 6-MP and 6-TG have been widely used to treat acute lymphoblastic leukemia in children. VOD mimicking Budd-Chiari like disease was then described as a frequent complication of 6-TG in pediatric patients given the drug for lymphoblastic leukaemia. Later on, in 1976, Griner et al. described the cases of two adult male patients with acute leukaemia developing a fatal Budd-Chiari-like disease while receiving 6-TG3. Since patients were given 6-TG plus cytosine arabinoside, authors were unable to ascribe this complication solely to 6-TG3. VOD exclusively related to 6-TG was first described by Gill et al., who observed a clinically reversible liver VOD developing in a young man with acute lymphocytic leukemia after 10 month administration of 6-TG4. Furthermore, sinusoidal obstruction was also reported in a patient with psoriasis treated with 6-TG and other cytotoxic therapy5. In 2006, a European 6-TG Working Party established that 6-TG should be considered a rescue drug in stringently defined indications in inflammatory bowel diseases (IBD). The indication for administration of 6-TG should only include its use for maintenance therapy as well as intolerance and/or resistance to aminosalicylates, azathioprine, 6-mercaptopurine, methotrexate and infliximab. Moreover, 6-TG must be withdrawn in case of overt or histologically proven hepatotoxicity6. Although Ansari et al 7 found no nodular regenerative hyperplasia (NRH) in the liver of patients given 6-TG, Dubinsky et al.8 described NHR as a common finding in 6-TG-treated patients with inflammatory bowel disease in the absence of VOD. By contrast, in our case report we showed histological pattern of VOD and, in accord with Gisbert et al.9, would suggest that 6-TG should not be administered out of a clinical trial setting. Given that the proportion of patients with Crohn’s disease achieving an improvement of symptoms during 6-TG treatment is similar to that after methotrexate10 or infliximab6, these drugs should therefore be considered as second line therapy in patients intolerant or resistant to azathioprine and 6-mercaptopurine.
Patients who present to physicians with altered mental health and behaviour may prematurely be diagnosed to have psychiatric illness. Psychiatric manifestations commonly accompany acute medical illnesses. As a rule of thumb, organic causes need to be ruled out before making a psychiatric diagnosis. A delay in arriving at a diagnosis could lead to prolonged psychiatric symptoms and unnecessary use of psychotropic medications. Prognosis and recovery will vary depending on the type of accompanying medical illness. Below, two cases are presented which varied significantly in terms of the sequelae.
Case 1
A female patient in her late 20’s was referred from primary care as she reported a sudden onset of “hearing voices”. The patient disclosed that she was bullied at work 6 months prior to this episode which resulted in change of job role and bullying has been dealt with. She described that the voices were talking about world politics and wanted her join MI5. She also believed that there were evil scientists who could read her mind through telepathy and felt that there were cameras and bugs planted in her house by a plumber. She became suspicious that her neighbours were spying on her. Her sleep was disturbed and she heard a ‘tick-tock ‘sound. This led to her checking pipes and walls to find the origin of the sounds. She believed that people were throwing things on to her bed and became very distressed - to the extent that the police were called on many occasions. She believed that people had been using telepathy on her and that aliens were invading the world. She was so distressed that she attempted to end her life by drinking bleach on one occasion and trying to cut her wrist on another.
There is no previous history of mental illness and no mental illness in the family.
Her medical history revealed that she had had mastoid surgery four years ago. Three weeks prior to the psychotic episode noted above, she had an ear infection with discharge from her ear. She presented to the general practitioner with psychotic symptoms at the same time. A CT scan of the brain was normal. A 2 week course of antibiotics in the form of Co-amoxiclav was given by the general practitioner. Her psychiatric manifestation resolved completely on follow up at two months without any psychotropics or Benzodiazepines, The patient was then kept under ‘wait and watch’ for six months in order to monitor any re-emergence of psychotic symptoms. She did not report any further episodes of ear infections during this period of follow up. Her diagnosis was Diseases of middle ear and mastoid (H65-H75).
Case 2
A 31 year old lady was referred to secondary mental health services from a Neurology team, presenting with psychotic symptoms following a viral encephalitis infection. A diagnosis of Herpes Simplex viral (HSV) encephalitis was confirmed by lumbar puncture and a CT scan by the Neurology team. She had made a gradual recovery from the encephalitis over a period of one month. She developed psychotic symptoms 2 weeks later, where she believed that doctors were trying to kill her and that she had been raped, with no evidence that this had occurred at any time. Her distress worsened which led to her informal admission to an inpatient mental health unit. A close assessment on the ward showed her to display an intermittent picture of worsening gait. A neuropsychiatry assessment confirmed that this lady had acquired brain injury following Herpes encephalitis. Single photon emission computed tomography (SPECT) showed extensive brain injury consistent with HSV. This lady presented with several acute episodes of psychosis where she complained of hearing voices and believed that people were trying to harm her. Her mood was labile and variably responsive to Olanzapine initially with a control of her psychotic symptoms as well as mood behaviour. She was diagnosed as suffering from Organic Delusional (Schizophrenia-like) Disorder (ICD 10 F06.2), with a picture of Paranoid Schizophrenia secondary to viral encephalitis. A maternal aunt was said to have suffered from Schizophrenia. Later on she had frequent relapses of psychosis and Quetiapine was initiated. As her symptoms did not respond to two different anti-psychotics, she was started on Clozapine which gave her reasonable stability. However, she still needs support while walking andhas been transferred to a suitable neuropsychiatric rehabilitation placement to maximise her independence and manage her ongoing needs.
Discussion
The two cases above display infective neurological diseases characterised by psychiatric presentations and greatly differing prognosis. The first case was an example of a chronic recurrent ear infection which was likely to have involved inner ear, mastoid or temporal lobe but has subsided without any long term sequelae. This was promptly treated with antibiotics at an early stage with complete recovery and there was no evidence of brain injury on imaging. The psychiatric manifestation was dramatically acute in this case and this could be partly attributable to stress at work. In particular there was neither previous history of mental illness nor a family history of psychiatric disorders.
In the second case, there was evidence of significant brain injury resulting in both physical and psychiatric sequelae following herpes encephalitis. Furthermore, this patient has a family history of schizophrenia which might have influenced the manifestation of the Mental Disorder.
There is significant evidence to suggest that childhood neurological viral infections increase the risk of psychotic illness 1. In both cases there was no suggestion of such illness in the childhood history. A recent study investigated whether HSV1 exposure was associated with structural brain abnormalities in individuals who, because of genetic or other factors, were deemed at high risk of developing psychosis. The results suggested that a history of HSV1 infection is associated with volumetric gray matter reductions in individuals at high risk for developing psychosis 2. In our second case, SPECT imaging confirmed grey matter loss and with the strong genetic risk would have led to the psychiatric illness.
The relationship between bacterial infections and psychotic illness in less well understood. Schizophrenic illnesses are often multifactorial in origin following a complex interplay between genetic and environmental factors such as infections. While there are various reports of Neurosyphilis, Mycoplasma Pneumoniae and Cryptococcal meningitis causing psychotic illness, specific bacteria could not be isolated in the first case presented 3-7. The improvement with antibiotics simply suggests that this could be a bacterial infection.
In summary, these cases clearly show the importance of identifying and treating medical illness presenting with psychiatric symptoms at the earliest to prevent long term complications.
One in four people in general and one in five people in Canada suffer from a mental disorder and only half of these individuals will seek help for their mental health.1 Doctors have an increasingly demanding job with increasing expectations of excellence in clinical, academic and managerial roles. It seems surprising that with their rigorous training doctors have higher rates of suicide compared to the general population.2 Studies have revealed that two-thirds of Canada’s physicians consider their workload too heavy, and more than half say that personal and family life have suffered because of their career choice.3 One third of Canadian physicians disagreed with a statement that their work environment encourages them to be healthy .4
A systematic review of mental health studies of medical students in the US and Canada found consistently higher rates of psychological distress in medical students compared with both the general population and age-matched peers .5 Medical students were also less likely to seek help for psychological distress than their peers. 6
A survey of psychiatrists and physicians in the UK found that most would be reluctant to disclose personal mental illness to colleagues or professional institutions. Their choices regarding disclosure and treatment would be influenced by issues of confidentiality, stigma, and career implications rather than quality of care.7,8
To reduce stigma and ease physician access to mental healthcare it is important to understand and address the above issues. This will facilitate psychiatrists gaining optimized mental health as well as to improve recruitment and retention of these professionals.9 The objective of our study was to assess the understanding of Canadian psychiatrists to the incidence of mental illness amongst psychiatrists in comparison to the general population and also in comparison to their medical/surgical colleagues. The study also assessed the attitudes of psychiatrists towards preference for disclosure, and treatment should they develop a mental illness in addition to their own experience of mental illness.
Method
Ethics approval (Study code PSIY-336-11) from Queen’s University in Kingston, Ontario was granted. Funding was obtained from TH’s research initiation grant. A mailing list of all psychiatrists in the province of Ontario was provided by the College of Physicians and Surgeons of Ontario (CPSO) for specific use to this research project. The College of Physicians and Surgeons Ontario is a body similar to the General Medical Council (GMC) in the UK. Their role is to regulate the practice of medicine in the province of Ontario. Other provinces have their own respective College of Physicians and Surgeons. In the remainder of the text the term ‘psychiatrist’ refers to consultant psychiatrist.
The list obtained from the CPSO did not include approximately 10% of psychiatrists who opted out of having their postal details released for research purposes. In total 1231 psychiatrists were sent a survey package. This package included a covering letter, a 2-page questionnaire, and a stamped return addressed envelope. Consent was assumed based on taking part in the survey. The 10-item questionnaire was based on a review of the literature, previous research, and discussion with colleagues. It comprised broadly of three sections. The first collected information on the respondents’ perception of prevalence of mental illness in psychiatrists in comparison to the general population and then in comparison with other medical/surgical specialties. The second required psychiatrists to identify to whom they were most likely to disclose a mental illness and reasons for non-disclosure. The third asked psychiatrists their preference of treatment in both an outpatient and inpatient setting. The identifiable information requested was the amount of experience the respondent had as a psychiatrist and whether they had experienced mental illness in the past. A free-text box was included at the end for comments and complete anonymity was maintained. Psychiatrists were divided into 3 groups: Group 1 (less than 5 years of experience as a psychiatrist), Group 2 (5-10 years of experience) and Group 3 (greater than 10 years of experience).
Analysis
A series of two-sample chi-square tests (χ²) were conducted to examine associations between certain categorical variables. In cases where 20% of contingency cells were <5 or where any cell=0, Fisher’s Exact test was used. Phi (φ) or Cramer’s V (for associations >2x2) were used as measures of effect size, these provide an association coefficient between 0 and 1. All analyses were done using SPSS 19.
Results
Of the 1231 questionnaires sent to doctors 487 were returned, a response rate of 39.6%. The respondents were placed into three groups: those in attending for <5 years (55, 11.3%), 5-10 years (53, 10.9%) and >10 years (369, 75.8%). The frequency of responses to all questions, both overall and as a function of attending group are shown in Table 1.
Table 1. Responses to all questions and comparisons between attending groups. Discrepancies between the overall column and the sum of the attending group columns are due to missing cases in responses to the attending group question.
Attending Group
Overall
<5 years
5-10 years
>10 years
Incidence of psychiatric illness amongst doctors is higher than general population?
Yes
124 (25.5% )
15 (27.3%)
19 (35.8%)
89 (24.1%)
No
247 (50.7% )
30 (54.5%)
26 (49.1%)
184 (49.9%)
Don’t know
116 (23.8% )
10 (18.2%)
8 (15.1%)
96 (26.0%)
Incidence of psychiatric illness amongst medical/surgical professionals higher than that of psychiatrists?
Yes
37 (7.6% )
1 (1.8%)
8 (15.1%)
28 (7.6%)
No
285 (58.5% )
36 (65.5%)
29 (54.7%)
214 (58.0%)
Don’t know
165 (33.9% )
18 (32.7%)
16 (30.2%)
127 (34.4%)
Have you ever experienced a mental illness, which had affected your personal, social or occupational life?
Yes
151 (31.0%)
14 (25.5%)
18 (34.0%)
118 (32.0%)
No
336 (69.0%)
41 (74.5%)
35 (66.0%)
251 (68.0%)
If you were to develop a psychiatric illness affecting your personal, social or occupational life, to whom would you initially be most likely to disclose this?
Church/Clergy
3 (0.6% )
1 (2.0%)
0 (0.0%)
2 (0.6%)
GP/Family physician
153 (31.4%)
18 (35.3%)
16 (32.0%)
116 (32.3%)
Family/friends
204 (41.9% )
22 (43.1%)
27 (54.0%)
152 (42.3%)
Colleagues
54 (11.1% )
4 (7.8%)
1 (2.0%)
46 (12.8%)
Mental health profess.
32 (6.6%)
4 (7.8%)
5(10.0%)
22 (6.1%)
None
15 (3.1% )
1 (2.0%)
0 (0.0%)
14 (3.9%)
Other
9 (2.0% )
1 (2.0%)
1 (2.0%)
7 (1.9%)
What is the most important factor that would affect your decision not to disclose your mental illness?
Stigma
114 (23.4%)
12 (22.2%)
14 (26.4%)
86 (24.2%)
Career implications
168 (34.5%)
21 (38.9%)
22 (41.5%)
121 (34.1%)
Professional standing
80 (16.4%)
11 (20.4%)
6 (11.3%)
63 (17.7%)
Other
109 (22.4%)
10 (18.5%)
11 (20.8%)
85 (23.9%)
If you were to suffer from a mental illness affecting your personal, social or occupational life requiring out-patient treatment, what would be your first treatment preference?
Informal profess. advice
83 (17.0%)
6 (10.9%)
7 (13.5%)
70 (19.1%)
Formal profess. Advice
365 (74.9%)
42 (76.4%)
40 (76.9%)
275 (75.1%)
Self-medication
25 (5.1%)
7 (12.7%)
2 (3.8%)
15 (4.1%)
No treatment
9 (1.8%)
0 (0.0%)
3 (5.8%)
6 (1.6%)
If you were to develop a mental illness requiring in-patient treatment, where would be your first preference?
Local
109 (22.4%)
6 (10.9%)
5 (9.4%)
96 (26.5%)
Out of area
370 (76.0%)
49 (89.1%)
48 (90.6%)
266 (73.5%)
In choosing in-patient preference, which of the following influenced your decision most?
Quality of care
130 (26.7%)
7 (12.7%)
7 (13.2%)
112 (30.5%)
Convenience
44 (9.0%)
0 (0.0%)
5 (9.4%)
38 (10.4%)
Confidentiality
257 (52.8%)
39 (70.9%)
34 (64.2%)
180 (49.0%)
Stigma
32 (6.6%)
6 (10.9%)
4 (7.5%)
22 (6.0%)
Other
21 (4.3%)
3 (5.5%)
3 (5.7%)
15 (4.1%)
Perception of the incidence of mental illness
Just over half of respondents disagreed that the incidence of mental illness was higher in doctors than the general population (247, 50.7%). Just over a quarter (124, 25.5%) agreed and just under a quarter replied ‘don’t know’ (116, 23.8%). As can be seen in Table 1, the pattern of responding was similar across all attending groups on this question (χ²=5.92; df=4; p=.205; Cramer’s V=.08). Most disagreed that psychiatric illness was greater in medical/surgical professionals than in psychiatrists (285, 58.5%), a small minority agreed (37, 7.6%). Again the attending groups responded similarly on this question (χ²=7.06; df=4; p=.133; Cramer’s V=.09). Nearly a third of respondents (151, 31.0%) claimed to have experienced a mental illness, and once more the attending groups did not differ significantly in their responses to this (χ²=1.12; df=2; p=.57; Cramer’s V =.05).
Disclosure of mental illness
Respondents would be most likely to disclose their mental illness in the first instance to family and friends (204, 41.9%) although many would instead prefer to disclose to their family physician (153, 31.4%). Relatively few would disclose to a colleague (54, 11.1%) in the first instance or to a mental health professional (32, 6.6%), very few would choose no-one (15, 3.1%) and the clergy was the least endorsed option (3, 0.6%). When considering only the three most popular response options (family/friends, family physician, and colleague) the three attending groups responded similarly (χ²=6.63; df=4; p=.157; Cramer’s V=.09). When asked about the most important factor affecting the decision not to disclose, the most common response was career implications (168, 34.5%). However stigma (114, 23.4%) and professional standing (80, 16.4%) were also reasonably common responses.
Again, when including only the three most popular disclosure choices in the analysis, there emerged an association between choice of whom to disclose and factor affecting disclosure (χ²=12.52; df=6; p=.051; Cramer’s V=.13) (see Table 2). Those who would choose to disclose to their family physician or to family/friends were more likely to cite stigma as a factor influencing their choice than those who would choose to disclose to colleagues. Those who would disclose to colleagues would be more likely to cite professional standing as a factor influencing their choice compared to those who would disclose to their family physician or to their family/friends. There was no association between choice of whom to disclose and previous experience of mental illness (χ²=1.22; df=2; p=.545; Cramer’s V=.05).
Table 2. Preferences for disclosure and the factors influencing that preference.
Factors influencing disclosure
Stigma
Career implications
Professional standing
Other
Total
Preference for disclosure
Family Physician
33 (22.6%)
57 (39.0%)
29 (19.9%)
27 (18.5%)
146 (100.0%)
Family/friends
56 (28.1%)
71 (35.7%)
24 (12.1%)
48 (24.1%)
199 (100.0%)
Colleagues
7 (13.7%)
17 (33.3%)
14 (27.5%)
13 (25.5%)
51 (100.0%)
Treatment for mental illness
When considering out-patient treatment, the majority of respondents would opt for formal professional advice (365, 74.9%). A small proportion would choose informal professional advice (83, 17.0%) and very few would self-medicate (25, 5.1%) or have no treatment (9, 1.8%). With regard to in-patient treatment, the majority would opt for an out of area mental health facility (370, 76.0%). Only just over a quarter of respondents (130, 26.7%) claimed that quality of care would influence their choice of in-patient care, just over half would be most concerned about confidentiality (257, 52.8%) There was a strong association between in-patient preference and the factor influencing that preference (Fisher’s Exact=228.25; p<.001; Cramer’s V=.70). As shown in Table 3, those who would choose an out of area facility, were much more likely to cite confidentiality and stigma as factors influencing their choice, than those who would choose a local facility. Conversely, those choosing a local facility were more likely to cite quality of care and convenience as influencing factors.
Table 3. In-patient treatment choice and the factors influencing that choice.
Factors influencing in-patient choice
Quality of Care
Convenience
Confidentiality
Stigma
Total
In-patient treatment choice
Local MH Facility
57 (56.4%)
39 (38.6%)
4 (4.0%)
1 (1.0%)
101 (100.0%)
Out of area MH Facility
69 (19.4%)
4 (1.1%)
252 (70.8%)
31 (8.7%)
356 (100.0%)
There was an association between attending group and out-patient preference (Fisher’s Exact=12.00; p=.042; Cramer’s V=.13). As can be seen in Table 1, the >10 years group would be more likely to select informal advice than the <5 years group, but the >10 years group were less likely to self-medicate than the <5 years group. The >10 years group responded similarly to the 5-10 years group with regard to self-medication. There was also an association between attending group and in-patient preference (χ²=12.66; df=2; p=.002; Cramer’s V=.16). The >10 years group, although still largely in favor of out of area care, would be more likely than the other two groups to opt for local care. There was also a significant association between attending group and the factors influencing in-patient choice (Fisher’s Exact =25.335; p=.001; Cramer’s V=.16). As shown in Table 1, the >10 years group would be more influenced by quality of care and less influenced by confidentiality than the other two groups.
Finally, previous experience of mental illness was not associated with in-patient choice (χ²=0.542; df=1; p=.462; φ=-.04), but it was associated with out-patient choice (χ²=11.51; df=3; p=.009; Cramer’s V=.16). As Table 4 shows, although both groups are more likely to opt for formal over informal advice, this pattern is more pronounced in the group who have had mental illness, than in the group who have not previously had mental illness.
Table 4. Previous experience of mental illness and out-patient treatment preference.
Out-patient treatment preference
Informal prof. advice
Formal prof. advice
Self-medication
No treatment
Total
Previous experience of mental illness
No
69 (20.8%)
242 (72.9%)
17 (5.1%)
4 (1.2%)
332 (100.0%)
Yes
14 (9.3%)
123 (82.0%)
8 (5.3%)
5 (3.3%)
150 (100.0%)
Discussion
This is the first study to assess the attitudes of Canadian psychiatrists to becoming mentally ill themselves. As this study was carried out in one province of Canada and the results cannot be generalized across the country. There is a significantly large scope of research potential in this area especially among psychiatric residents and other healthcare professionals .10
Physician Impairment is any physical, mental or behavioral disorder that interferes with the ability to engage safely in professional activities.11 Impairment among medical practitioners and psychiatrists in particular is a significant problem characterized by chronicity, under reporting and in many cases, poor outcomes.12 However early detection, intervention and treatment programs that are more sensitive to the needs of impaired practitioners, that are more continuous, better structured, and rehabilitation and recovery focused may be more likely to produce a positive outcome. 13 It is extremely important to remember and advocate that although a physician may be mentally ill he/she is not necessarily impaired.
It is concerning that stigma continues to play a role in psychiatrists’ decision making process to obtain mental healthcare. This is consistent with the findings of a survey in the USA which showed that half of all psychiatrists with a depressive illness would self-medicate rather than risk having mental illness recorded in their medical notes.10 Both entertainment and news media provide a dramatic and distorted image of mental illness that emphasize dangerousness, criminality and unpredictability.14 With this increased stigma doctors subsequently are concerned whether to disclose a mental health problem to their Licensing Boards for fear of being discriminated.15 Studies of US medical licensing bodies have demonstrated a trend towards increasing stigmatizing approaches 16-19 and the concern is whether there is a similar trend in Canada.9 Most psychiatrists in Canada are not aware what to expect from provincial colleges once their mental illness is disclosed and as a result tend to expect the worst. More work is needed by psychiatrists to inform the Provincial Colleges on physician mental health. Only then can the Provincial Licensing Colleges do more to assure physicians that the recovery model of treatment applies to them as it does other psychiatric patients.
The gap however continues to lie between ‘I need help’ and active psychiatric management. Psychiatrists will be well aware of the profound impact that such illnesses can have on a person’s personal and professional competency. However to reflect it on oneself can at times be met with denial in the first instance. Dr. Mike Shooter (ex-President of the Royal College of Psychiatrists, UK) suffered from depression and he highlights the need to speak out and combat stigma. He points out the need to seek treatment early and how not doing so can adversely affect the doctor-patient relationship.20 For some however the fear of stigmatization by health professionals for health professionals can lead to very tragic consequences. Dr. Suzanne Killinger-Johnson was a family physician with a psychotherapy practice in Toronto. She suffered from postpartum depression and in November of 2000 she jumped in front of a subway train cradling her son. Her son died instantly and Dr. Killinger-Johnson died 9 days later.21
Over the past 15 years a greater understanding has developed on the incidence, stressors and complications of physician mental illness. 22 The CPA published its first position paper on the mentally ill physician as early as 1984 with the latest version in 1997 currently under review. 22 The Canadian Medical Association should be congratulated on the most comprehensive strategy document for mentally ill physicians. Physician Health Matters - A mental health strategy for physicians in Canada was published by the CMA in February 2010. In addition to outlining the mental health of medical students, residents and physicians it addresses the current gaps in services and strategic direction needed to achieve ‘optimal mental health for all physicians’. This sets out the necessary groundwork for institutions to implement based on current evidence. In Canada there was the inauguration of the position of ‘The Bell Mental Health and Anti-Stigma Research Chair’ with Queen’s University in February 2012. 23 This position was offered to Dr. Heather Stuart, Professor of Community Health and Epidemiology. Stigma is a social process characterized by exclusion, rejection, blame or devaluation resulting from an adverse social judgment about a person or group. 24 There is a cultural pressure amongst physicians not to be sick so that one can provide care resulting in physicians unfortunately trying to control their own illness and treatment. 25 This concept is exacerbated for mental health issues and the stigma is considerably attached to physicians acknowledging mental health issues or illness, as well as seeking help. 26
Over the past decade the physician health community has been working to destigmatise physician mental health and to provide support services in this regard. All Canadian provinces have Physician Health Programs (PHPs) to help physicians with mental health difficulties. Referrals can be from physicians, families, colleagues, and self. 9 Physicians with psychiatric or drug dependence problems are referred from outside the PHP though the PHP (depending on the province) may or will be involved in monitoring the physician.
One of the most important factors influencing where a doctor is treated is the issue of confidentiality. 8 At present in Canada many hospitals are either switching or have switched to electronic patient records. Patient data in an electronic environment will be accessed from multiple portals by different professionals. This potentially poses serious concerns for psychiatrists if they have significant concerns around confidentiality of their record. A mechanism by which patients can access a list of professionals who have accessed their information may alleviate some concern regarding confidentiality.
Conclusions
Education surrounding mental illness in physicians needs to begin in medical school. Medical students require more assurance that seeking help for psychological problems will not be penalized. Junior doctors are receptive to education on physician impairment and substance misuse and this should be a mandatory component of their training. 27 Education and training of medical students and psychiatric residents to assess doctors as patients would make this scenario less taboo than it is currently perceived.
CPSO in liaison with relevant partners must develop a clear and concise document outlining steps the CPSO will take in helping the mentally ill physician. This document must be clearly advertised on the CPSO website to ease access and would reduce the catastrophizing interpretation psychiatrists (and physicians) may make to the CPSO’s involvement with the mentally ill physician. By the CPSO taking a lead this will prove a stimulus for other provincial licensing colleges to follow suit.
The bridge from ‘I need help’ to ‘I am getting help’ is paved with multiple barriers. By addressing some of the concerns raised by psychiatrists will help the psychiatrist easily cross over.
Neuroleptic malignant syndrome (NMS) is a life-threatening neurologic disorder associated with the use of neuroleptic agents. NMS is typically characterized by a distinctive clinical syndrome of mental status change, muscle rigidity, fever, and autonomic instability. Atypical cases may present without muscle rigidity and/or hyperthermia. Association of infection in an atypical case can make the diagnosis challenging. We describe a case of NMS in a patient who presented with acute onset of altered mental status complicated with aspiration pneumonia.
Case Report
A 22-year-old female with a history of schizophrenia and seizure disorder presented with acute onset of altered mental status. Her home medications included haloperidol, clonazepam, olanzapine, trazodone, topiramate, benztropine, and trihexyphenadyl. The patient was found unarousable by her mother. She had multiple suicidal attempts in the past (overdosed on acetaminophen, drank cleaning detergent, and cut her wrist). She usually medicated herself without supervision. On examination, the patient was drowsy, afebrile (Temp 36.8oC/98.3oF), hypotensive (BP 85/64 mmHg), tachycardic (HR 105 bpm), and tachypnic (24/min). She was noted to be grunting with both inspiratory and expiratory stridor; therefore she was intubated for airway protection. Initial drug screen was negative for all substances of abuse. Acetaminophen and salicylate levels were undetectable. Head CT was unremarkable. Supportive care was provided as the patient was suspected to be overdosed with multiple medications. On the second day of admission the patient developed fever of 38.9oC/102oF. Chest xray and chest CT showed bilateral infiltrations (Fig.1), so empirical piperacillin/tazobactam and vancomycin were started for aspiration pneumonia. Sputum culture came back positive for Methicillin-resistant Staphylococcus aureus. However, the patient remained febrile with a temperature of 39.6 oC /103.2oF, despite appropriate antibiotic treatment. We suspected that there might be some other coexisting condition causing high fever. Serum creatine kinase (CK) was checked and found to be 8,105 U/L, up from 106 U/L on admission. We considered the diagnosis of NMS based on alteration of mental status, hyperthermia, autonomic instability, and elevated CK level, with the use of neuroleptic agents, although the patient did not have any muscle rigidity. The patient was started on dantrolene in addition to intravenous fluid and antibiotics. Shortly afterwards temperature and CK level started to trend down (Fig.2,3). Dantrolene was subsequently increased to maximum weight-based dose. Her mental status was gradually improved and returned to baseline. She became afebrile on day 10 of dantrolene treatment and serum CK went back to normal level after 2 weeks. Then bromocriptine was started orally and continued for 2 weeks.
Figure 1A: chest xray on admission
Figure 1B: chest xray on second day of admission
Figure 1C: chest CT on second day of admission
Figure 2. Temperature trend after starting treatment for NMS
Figure 3. CK trend after starting treatment for NMS
Atypical presentations of NMS can sometimes be difficult to diagnose, as in our patient who presented with altered mental status, fever, and coexisting infection, in the absence of muscle rigidity. We emphasize the importance of a high index of suspicion of NMS in patients using neuroleptic agents.
Discussion
NMS is an idiosyncratic drug reaction to antipsychotic medications and a potentially life threatening condition that occurs in an estimated 0.07% to 2.2% of patients treated with antipsychotics.1 Patients typically present with fever, rigidity, changes in mental status, and autonomic instability, often attributed to first generation antipsychotics, in particular after the start of medication or an increase in dosage.2 Atypical cases of NMS without muscle rigidity and/or hyperthermia have been reported, usually associated with atypical antipsychotic treatment. It has been hypothesized that atypical cases represent early or impending NMS; however pathogenesis remains unclear.3 Risk factors that have been established in case series and case-control studies include agitation, dehydration, acute medical illness, concomitant use of other psychotropic drugs, intramuscular injections and high doses of antipsychotic medications.4-6
Complications of NMS are often consequences of its symptoms. Pneumonia is the most common complication found in 13% of patient with NMS, likely due to altered mental status combined with difficulty swallowing that lead to aspiration.7 Renal failure is the second most common complication (8%), as a result of rhabdomyolysis and myoglobinuria. Other complications have been reported including myocardial infarction, disseminated intravascular coagulation, deep venous thrombosis, pulmonary embolism, hepatic failure, sepsis, and seizure.8 Mortality rate of NMS was around 20-30%.9-10 With early identification and treatment, mortality has significantly reduced to averages 10%.6
Withdrawal of the causative agent is the first step in the management of NMS. Supportive therapy, in particular, hydration, fever reduction, and careful monitoring, is the mainstay of management of NMS. In mild cases, supportive treatment alone may be sufficient.4 Adding specific therapies, such as dantrolene, bromocriptine, and benzodiazepine to supportive measures has been shown to reduce time to complete recovery, from a mean of 15 days with supportive care alone, to 9 days with dantrolene, and 10 days with bromocriptine.1 In severe cases, empirical trial of specific pharmacological agents should be started promptly. Electroconvulsive therapy is found to be effective when pharmacotherapy has failed.11
Sometimes NMS is difficult to identify in the presence of critical illnesses which can obscure the manifestation of NMS. As in our case, the patient presented with altered mental status, fever, and autonomic instability which could be simply explained by the presence of pneumonia and sepsis. However, due to lack of clinical response after appropriate antibiotic treatment, other coexisting condition was suspected. It is important to have a high index of suspicion for NMS in the setting of antipsychotic therapy. An absence of muscle rigidity should not exclude a diagnosis of NMS when the rest of the clinical picture points to this diagnosis. Elevated CK level helps support the diagnosis of NMS in patients with atypical presentation. Discontinuation of offending agent and supportive care should initiate promptly, and specific pharmacotherapy should be considered in severe cases. An early diagnosis is the key to successful treatment and patient outcome.
Conclusion
NMS is a rare but potentially life-threatening condition. Atypical presentation makes it more difficult to identify in patients with critical illnesses. Aspirated pneumonia is one of the common complications of NMS and sometimes can obscure signs and symptoms of NMS and delay diagnosis. High index of suspicion for NMS in patients taking antipsychotics is crucial. If not recognized or left untreated, NMD may be fatal.
In rheumatology clinics chronic painful conditions are the norm. Although many pain syndromes are associated with low mood and sometimes clinical depression, the mood disorder often goes unrecognised. Fibromyalgia is one such chronic pain syndrome, 'chronic' arbitrarily defined as lasting longer than six months. It is a common, poorly understood, musculoskeletal disorder which more often affects women between the ages of 25-50 years generally.
In nearly all patients three symptoms predominate, namely, neuropathic pain (nerve injury pain), fatigue and non-restorative sleep disturbance. The chronic neuropathic diffuse pain, described as whole body pain, is felt particularly in deep tissues such as ligaments, joints, and muscles of the axial skeleton in mainly the lower cervical and lumbar spine. The pain is often characterised by an exaggerated and prolonged response to a noxious stimulus (hyperalgesia). Patients may be considered to be malingering because there is no obvious explanation for the symptoms. Anxiety, stress and depression caused by fibromyalgia add insult to injury, with personality and cognitive factors coming into play in addition.1 Paraesthesiae (abnormal sensory sensations) or dysaesthesiae (painful sensations) of the extremities may also occur. There is no objective muscular weakness or neurological disorder to account for the symptoms, which adds to the diagnostic dilemma. For example, fibromyalgia affecting the supraspinatus muscle of the shoulder would limit initial abduction of the arm because of pain, not because of any muscle weakness. Cognitive function is sometimes described as 'fibrofog' or 'conscious confusion' and may be a primary symptom of fibromyalgia, reflecting impairments in working memory (a form of short-term memory), episodic (memory for events), and semantic memory (memory for words, rules, language).
Nociception refers to the process of information about harmful stimuli conveyed by neuronal activity up to the point of perception in the dorsal horn of the spinal cord where primary afferents synapse.2 Evidence is accumulating which shows that atypical sensory processing in the central nervous system (CNS) and dysfunction of skeletal muscle nociception are important in the understanding of fibromyalgia and other chronic pain syndromes.3The concept of 'central pain sensitization' or 'central sensitivity syndrome' considers fibromyalgia to be a disturbance of nociceptive processing which causes a heightened experience of pain or pain amplification.4 Because pain signals are subject to variation in amplitude, the modulation of sensory processing may be the key to understanding the pain response not only in fibromyalgia but also in other conditions, such as irritable bowel syndrome. Descending spinal noradrenergic and serotonergic neurons inhibit the neurotransmitters noradrenaline and serotonin, released from primary afferent neurons and dorsal horn neurons. Therefore, when descending inhibition is decreased, irrelevant nociceptive stimuli are more readily felt. Put another way, in patients with chronic pain syndromes descending inhibition may not be functioning adequately to prevent or mask irrelevant pain stimuli. When appropriate medication is used this normal descending inhibition is enhanced and pain is no longer troublesome.
The release of neurotransmitters (ligands) also requires a mechanism that involves voltage-sensitive calcium and sodium channels. Repetitive action potentials cause the calcium channels to open with the ensuing release of neurotransmitters into the synaptic cleft. The postsynaptic neurons are thus stimulated leading to molecular and structural changes (sprouting) which cause neuropathic pain. Drugs such as Pregabalin and Gabapentin bind to voltage-sensitive calcium channels and reduce calcium influx, which in turn diminishes pain. The concept of central pain sensitization now incorporates affective spectrum disorders and functional somatic syndromes. It seems that the more painful symptoms one has which are difficult to explain, the more likely the patient is suffering from a mood disorder. Dopamine may be involved in the regulation of cognition in the dorsolateral prefrontal cortex and could account for the cognitive deficits.5Because cingulate and prefrontal cortices are particularly implicated in pain modulation (inhibition and facilitation of pain), structural changes in these systems could contribute to the chronic pain associated with fibromyalgia.6
Many patients with fibromyalgia have an increased sensitivity to sensory stimuli that are not normally or previously painful (allodynia). In other words, minor sensory stimuli that ordinarily would not cause pain in most individuals induce disabling, sometimes severe pain in patients with fibromyalgia.7 In normal individuals 4 kg/square cm2pressure (approximately the pressure needed to blanch the skin at the top of one’s thumb) causes patients with fibromyalgia to wince with pain or suddenly withdraw when the tender point is palpated. This indicates that pain occurs at a lower pain threshold in fibromyalgia sufferers when this pressure is applied.
The pain of fibromyalgia may be aggravated by emotional stress though the latter is difficult to quantify and evaluate. For instance, corticosteroid hormones are released in high amounts after stress yet fibromyalgia is associated in some patients with a decreased cortisol response to stress. Stress may therefore initiate, inhibit or perpetuate alterations in the corticotrophin-releasing hormone (CRH) neuron, with associated effects on the hypothalamic pituitary axis (HPA) and other neuroendocrine axes.8
There are many other possible explanations for fibromyalgia pain. One of the major neurotransmitters involved in nociception is substance P, found in high concentrations in the spinal cord, limbic system, hypothalamus, and nigrostriatal system. It is involved in the transmission of pain impulses from peripheral afferent receptors to the central nervous system. Nerve growth factor (NGF), a cytokine-like mediator may indirectly exert its effect through enhancing glutaminergic transmission and could account for sustained central sensitization in fibromyalgia. 9, 10 Another neuropeptide, calcitonin gene-related peptide, a potent vasodilator, present in non-myelinated afferent neurons, may also play a role in pain pathology.5
Levels of the neurotransmitter serotonin have been found to be low in some studies in fibromyalgia patients. Although serum levels of serotonin are lower than in some patients with rheumatoid arthritis and healthy controls, the variation is too broad and therefore measurement of serotonin has not proved useful tool in determining a diagnosis of fibromyalgia. 11
Logically, pharmacologic agents used to treat pain in fibromyalgia would act by either increasing levels of inhibitory neurotransmitters or decreasing levels of excitatory neurotransmitter. In the United States of America (USA), Pregabalin was the first drug to be approved by the Food and Drug Administration (FDA) for the treatment of fibromyalgia and has been shown to improve pain, sleep and quality of life. It is ineffective against depression. The main inhibitory mediator in the brain, gamma amino butyric Acid (GABA), is formed from glutamate (excitatory) by the enzyme glutamate decarboxylase (GAD). It is particularly plentiful in the nigrostriatal pathways. About 20% of CNS neurons are GABAergic and it serves as a neurotransmitter at some 30% of all CNS synapses.12 Pregabalin increases neuronal GABA levels by producing a dose-dependent increase in glutamate decarboxylase activity. In a meta-analysis of 21 clinical trials to estimate treatment differences vs. placebo, statistically significant improvement was observed with Duloxetine, Milnacipran 200 mg/day, Pregabalin 300 or 450 mg/day, and Tramadol plus Paracetamol. The meta-analysis showed a statistically increased risk of discontinuation because of adverse events related to Milnacipran and Pregabalin.13
Antidepressants may improve fibromyalgia symptoms by reducing pain, stabilizing mood and improving sleep, though the effect seems to be modest. If abnormal sleep, and hence subsequent tiredness, precedes the development of fibromyalgia the effect of antidepressants may be primarily associated with improved sleep. However, the efficacy of tricyclic antidepressants is difficult to quantify and their limited superiority over placebo lasts no more than a few months. A meta-analysis of ten randomized double-blinded, placebo-controlled studies revealed only poor to moderate evidence for a beneficial effect at low doses of Amitriptyline (25mg daily) over 6-8 weeks. Even when given in higher doses or prescribed for a longer duration, Amitriptyline did not make a great deal of difference. 14
The efficacy of Selective Serotonin Reuptake Inhibitors (SSRIs) is also inconclusive. More promising results have been demonstrated with Serotonin and Noradrenaline Reuptake Inhibitors (SNRIs) such as Duloxetine. Both serotonin (5-HT) and noradrenaline (NA) exert analgesic effects via descending pain pathways. Pain is a prominent feature of depression and vice versa and the alleviation of one modifies the other. 15, 16 The reduction in pain reduces fatigue and Duloxetine improves mood.
Other drugs used in this condition include Milnacipran and Cyclobenzaprine (a muscle relaxant structurally related to tricyclic antidepressants). Milnacipran and Cyclobenzaprine are not available in the United Kingdom (UK). Tramadol (a serotonin and noradrenaline reuptake inhibitor) is a weak mu-receptor opioid agonist used to control pain but its adverse effects are those of opiates in general, mainly nausea and dependence.
Although other adjunctive non-pharmacological treatments have been advocated the results are disappointing. Assessments of non-drug treatments are generally mediocre. Aerobic exercises benefit some patients, especially when combined with biofeedback, patient education and cognitive therapy. A whole gamut of treatments such as graded exercises, yoga, dietary advice, balneotherapy (heated pool bathing), homeopathy, massage, acupuncture, patient education, group therapy and cognitive behaviour therapy, have been suggested and tried, but few of them demonstrated clear-cut benefits in randomized controlled trials.Support groups may help some patients. 17, 18, 19
Fibromyalgia is now considered to be, in part, a disorder of central pain processing. Central sensitization manifests as pain hypersensitivity, particularly allodynia, and hyperalgesia. It is believed that central sensitization occurs in part through the action of glutamate on the N-methyl-D-aspartate (NMDA) receptor, resulting in an increase in intracellular calcium and kinase activation, leading to hyperalgesia and allodynia.20
Response to standard analgesics is erratic and more promising results have emerged with drugs such as the SNRIs Duloxetine and Milnacipran, the anticonvulsants Gabapentin and Pregabalin, either used alone or in combination, or with other agents such as Amitriptyline. There is only modest evidence to support SSRIs and Tramadol. Treatment needs to be holistic and multidisciplinary, focussing on both physical pain management and psychological dysfunction. The multidisciplinary approach, though difficult to measure, may help by imparting a sense of empathy and support for patients. Overall, most patients with fibromyalgia continue to have chronic pain and fatigue with symptoms persisting for many years, but it is not necessarily a progressive disorder and some patients may show moderate improvement.
Ganglioneuroma is a rare, benign, neuroblastic tumour that originates from the neural crest cells. Ganglioneuroma, ganglioneuroblastoma and neuroblastoma are three maturational manifestations of a common neoplasm in the progressive order of loss of differentiation. Ganglioneuromas may be found anywhere along the line of the embryonic neural crest, from clivus to sacrum and are very rare in the pelvis. Less than twenty cases have been described in the literature with various presentations based upon location including extradural, retroperitoneal, spinal, thoracic and one solely intradural medullary location. Ganglioneuromas may stay asymptomatic for a long period and give rise to no pressure symptoms either due to slow growth leading to progressive increase in size accompanied by adaptive changes. Ganglioneuromas demonstrate long-term disease-free survival even with an incomplete surgical removal. Here we present a case of a girl aged 11 years with pelvic ganglioneuroma.
Case Report:
A girl aged eleven years was brought from a remote hilly area in Pakistan by her mother to the city hospital many miles away. She had noticed that her daughter’s lower abdomen had progressively enlarged over last few months. Her menstrual cycle was normal so the mother was concerned that despite not being pregnant, her daughter had a distended abdomen as if she was pregnant She had a good appetite and unaltered bowel and bladder function. She had no heartburn, regurgitation, nausea, vomiting, heamatemesis or melaena. She denied any bleeding par rectum, shortness of breath, cough, loss of consciousness or convulsions. Her past medical history was mundane. She had not had any surgery in the past and was not taking any medication. Examination revealed a smooth, large, fixed hard mass in the right lower abdomen and pelvis. It was palpable in the pelvis on rectal examination which was otherwise normal. Liver or spleen was not palpable and she had no ascites. Her chest was clear, heart sounds were normal and there were no neurological abnormalities. Laboratory tests including FBC, LFT, U&E and Creatinine were normal. Her MRI scan was not of a good quality due to limitation of resources and technology at place of her diagnosis, but it showed an 11.4 x 11.8cm solid, well-defined mass arising from pelvis and extending up to the umbilicus. The mass showed intermediate low signals on T1 and hyper intense signals on T2 images (Fig. 1). Mid line surgical exploration was undertaken which showed a large, solid, retroperitoneal mass arising from sacral nerves within the pelvis. Mass was lying in front of great vessels, overlapping the confluence of common iliac vessels. The left ureter was displaced laterally while the right ureter was lying over the mass. The mass was excised completely. Post operative course was uneventful and patient was discharged home on the fifth post operative day.
Figure1: MRI showing showing a large soft tissue mass.
Macroscopically, the specimen was a 13x13x5cm rounded well-encapsulated mass (Fig. 2). Upon sectioning in vitro, mass was seen to be solid, whorled and grey white. Microscopically, groups and singly scattered ganglion cells were seen with surrounding neural tissue. There was no evidence of atypia, mitosis or necrosis. Features were suggestive of a ganglioneuroma. (Figure 3) The patient was well at two months follow up and required no further treatment.
Figure2: Photograph of the resected specimen shows a well-encapsulated ovoid mass.
Neuroblastoma, ganglioneuroblastoma and ganglioneuromas are tumours of sympathetic nervous system that arise from the neural crest cells.1 These tumours differ only in their progressive degree of cellular and extracellular maturity, with ganglioneuroma being the most mature hence well differentiated and neuroblastoma being the least.2 Ganglioneuroma are rare, benign and slow growing. They may occur spontaneously or as a down grading from therapy for Neuroblastoma with either chemotherapy or radiation.3 International Neuroblastoma Pathology Classification (INPC) has been devised after studying 552 such tumours. Out of 300 with favourable prognosis three groups were identified as; ganglioneuroma maturing (GN-M), ganglioneuroblastoma intermixed (GNB-I) and ganglioneuroblastoma nodular with favourable subset (GNB-N-FS). These are resectable in 91% cases in one or more surgical sessions. In contrast, the remaining 252 tumours had unfavourable prognosis and were called ganglioneuroblastoma nodular unfavourable subset (GNB-N-US). This group was not amenable to surgical resection and usually already had metastasis at the time of presentation.4
Ganglioneuromas although are mostly sporadic, may be associated with Neurofibromatosis (Von Recklinghausens Disease) and Multiple Endocrine Neoplasia type II (MEN).1 Ganglioneuroma usually presents before the second decade and rarely after the sixth.2 The median age at diagnosis has been reported to be approximately 7 years. There is a slight female preponderance.5 The common locations are the posterior mediastinum, and the retroperitoneal space. Retroperitoneal pelvic location is very rare and only few case histories have been reported.1
Although retroperitoneal ganglioneuromas are usually asymptomatic, some patients may get compression symptoms, diarrhea, hypertension, virilization and myasthenia gravis owing to release of certain peptides.1 Radiological examination may localize the lesion. MRI may show low intensity on T1-weighted images and heterogenous hyper intensity on T2-weighted images with gradual increasing enhancement on dynamic images.6
Surgical excision is sufficient for treatment of ganglioneuromas. Chemotherapy or radiotherapy has no role in the treatment. Even with an incomplete excision, close follow up alone may be adequate. If any progression of the tumour is seen then repeat laparotomy may be indicated.2
Conclusion:
Although pelvic ganglioneuroma is a very rare lesion, it should be considered in the differential diagnosis of any abdomeno-pelvic mass. As it is a slow growing tumour, gross total surgical removal with preservation of organ function is a feasible surgical option.
The widespread use of office-software in general practice makes the idea of simple, automatic computerised support an attractive one. Different tools for different diseases have been tested with mixed results, and in 2009 a Cochrane review1 concluded that “Point of care computer reminders generally achieve small to modest improvements in provider behavior. A minority of interventions showed larger effects, but no specific reminder or contextual features were significantly associated with effect magnitude”. One year later another review2 reached similar conclusion: “Computer reminders produced much smaller improvements than those generally expected from the implementation of computerised order entry and electronic medical record systems”. Despite this, simple, non-expensive, automatic reminders are frequently part of GPs’ software, even if their real usefulness is seldom tested in real life.
Repeated hospitalisation for heart failure is an important problem for every National Health System; it is estimated that about half of all re-hospitalisation could be avoided3. Adherence to guidelines can reduce re-hospitalisation rate4, and pharmacotherapy according to treatment guidelines is associated with lower mortality in the community5. In 2004 a software commonly used in Italian primary care implemented a simple reminders’ system to help GPs to improve prescription of drugs recommended for heart failure. We evaluated if this could lead to a decrease in re-hospitalisation rate.
METHODS
In 2003, using Millewin ®, a software commonly used by Italian GPs, we showed that appropriate prescription could increase using a simple pop-up reminders6; a year later, using the Italian General Practitioners database ‘Health Search – CSD Patient database (HSD) (www.healthsearch.it), we observed a lower than expected prevalence of codified diagnosis of heart failure and of prescription of both beta-blockers and ACE-Inhibitors/ARBs (data on file). Therefore in 2004 Millewin® embedded a simple reminder system to help heart failure (HF) management. The first reminder aimed to identify patients with HF, but without codified diagnosis: in case of loop diuretic and/or digoxin prescription without codified HF diagnosis a pop-up told the GP that the patients could be affected by HF and invited the physician to verify this hypothesis and eventually to record the diagnosis. The second reminder appeared when a patient with codified HF diagnosis had no beta-blocker and/or ACE-inhibitor/ARB prescription: a pop-up invited the GP to prescribe the missing drug. This reminder system was already activated in the 2004 release of the software, but required voluntary activation in the successive releases. This is a common choice in real life, where positive choices in clinical practice by software-house neither are welcomed nor accepted by GPs. We had no possibility to know who decided to keep using the reminders.
We examined the 2004-2009 HF hospitalisations in Puglia, a Southern Italian Region with a population of over 4000000, and with high HF hospitalisation rate compared with the Italian mean7. We compared the hospitalisations for patients cared for by GPs who used Millewin® in 2004 to those of the patients cared for by GPs who never used Millewin®. Data were provided by the local Health Authority, and were extracted from the administrative database.
RESULTS
We identified 64591 patients (mean age 76 y, sd 12; 49.9% men) with one or more HF hospitalisation; 17810 had > 2 hospitalisations, and were analysed for the current study.
Figure 1 - Selection process leading to the identification of the patients with > 2 HF hospitalisations
The selection that led to this group is summarised in figure 1. There was no statistically significant difference between patients cared for GPs using or non using Millewin® software as far as age and gender are concerned. The re –hospitalisation rate according to the use or non-use of Millewin® of patients’ GPs is summarised in table 1.
Table 1: Re-hospitalisation rate of patients cared by Millewin® users and non-users
Patients with ≥ 2 hospitalisation (N, %)
Time
No MW users
MW users
Total
P
Within 1 year
11260 (23.1%)
1136 (22.9%)
12396 (23.1%)
=N.S.
Within 2 years
13851 (28.4%)
1410 (28.4%)
15261 (28.4%)
=N.S.
Within 3 years
15144 (31.0%)
1543 (31.1%)
16687 (31.0%)
=N.S.
Within 4 years
15803 (32.4%)
1612 (32.4%)
17415 (32.4%)
=N.S.
Within 5 years
16083 (33.0%)
1643 (33.1%)
17726 (33.0%)
=N.S.
Within 6 years
16156 (33.1%)
1654 (33.3%)
17810 (33.1%)
=N.S.
MW = Millewin®, N.S = Not significant
The mean time before the first re-hospitalisation was 108.5 day +/- 103.3 for Millewin® non-users and 116.4 +/- 107.5 for users (p < 0.05).
DISCUSSION
Even if reasonable and clinically sound, the availability of computerised reminders aimed to help GPs to identify HF patients and to prescribe them with recommended drugs didn’t reduce re-hospitalisation rate. The first possibility to explain this result is that, after the first year, GPs didn’t re-activate the reminders’ system. Unfortunately we couldn’t verify this hypothesis, but it is known that the level of use of such a system may be low in usual care8; furthermore providers may agree with less than half of computer generated care suggestions from evidence-based CHF guidelines, most often because the suggestions are felt to be inapplicable to their patients or unlikely to be tolerated9. Epidemiological studies have shown that heart failure with a normal ejection fraction is now a more common cause of hospital admission than systolic heart failure in many parts of the world10-11. Despite being common, this type of heart failure is often not recognised, and evidence based treatment—apart from diuretics for symptoms—islacking12. It is therefore possible that increasing ACE-I/ARBs and beta-blockers use in these patients doesn’t influence the prognosis and hospitalisation rate. Unfortunately administrative databases do not permit to distinguish the characteristic of HF. We must also consider that the use of appropriate drugs after HF hospitalisation could spontaneously increase in the last years; a survey in Italian primary care showed that 87% of HF patients used inhibitors of the renin-angiotensin system, and 33% beta-blockers13. A further relevant increase in ACE-I/ARBS is therefore unlikely, while a improvement is clearly needed for beta-blockers. Could more complex and information-providing reminders be more useful? This is unlikely since adding symptom information to computer-generated care suggestions for patients with heart failure did not affect physician treatment decisions or improve patient outcomes14. Furthermore, consultation with a cardiologist for starting beta-blocker treatment is judged mandatory by 57% of Italian GPs13, thus reducing the potential direct effect of reminders on prescription. Finally we must remember that part of the hospitalisation due to HF worsening can be due to non-cardiac disease, such as pneumonia, anemia, etc; all these cause cannot be affected by improved prescription of cardiovascular drugs.
Albeit simple and inexpensive, computerised reminders aren’t a neutral choice in professional software. Too many pop-ups may be disturbing and may lead to systematic skipping the reminders’ text. This can be a problem, since computerised reminders have proved to be useful for other important primary-care activity, such as preventive interventions15. In our opinion, at the moment, a computerised reminder-system should be proposed only as a part of a more complex strategy, such as long-term self or group audit and/or pay for performance initiative.
CONCLUSIONS
Availability of computerised automatic reminders aimed to improve detection of heart-failure patients and prescription of recommended drugs doesn’t decrease repeated hospitalisation; these tools should be probably tested in the context of a more complex strategy, such as a long-term audit.
The use of convulsive therapy for psychiatric conditions evolved after its first use by Meduna using camphor in 1934, and by 1938, Cerletti and Bini had documented the use of electricity to induce convulsions and therapeutic benefit. The technique has been extensively modified by the addition of muscle relaxants and general anaesthesia. Electroconvulsive Therapy is now an important and effective treatment option for certain severe neuropsychiatric disorders.
Most developments and changes in the practice of ECT have been driven to reduce the adverse effects and not by the need to make it more efficacious. The aim is to induce a generalised tonic-clonic seizure with a sufficient dose to maximise efficacy but not too high to reduce cognitive side effects. The newer brief-pulse, constant-current, square-wave machines are more efficient in inducing seizure than the older sine-wave, constant-voltage machines.
Between January and March 2002, there were nearly 12800 ECT administrations in England to 2300 individuals 1. The National Institute of Clinical Excellence currently recommends that ECT is only used to achieve rapid and short term improvement of severe symptoms after an adequate trial of other treatment options have proved inefficient and/or when the condition is life threatening as in people with severe depression, catatonia or prolonged/severe manic episode2. The newer guidelines on depression suggest that ECT be considered as a treatment option in moderate depression when it has failed to respond to multiple treatments15. It has been noted from the observation of the users experiences that the cognitive impairment often outweighed their perception of any benefit after ECT treatment.
It has been recognised that the induction of a generalised tonic-clonic seizure is necessary to achieve a therapeutic response and a number of studies demonstrate superiority of ECT over Sham ECT. It is also noted that administration of an electrical stimulus that fails to induce a seizure and immediate termination of a seizure after induction does not result in clinical improvement. Stimulus which just about produces a generalised tonic-clonic seizure may not ensure therapeutic potency, but the degree to which the stimulus intensity exceeds the Seizure Threshold is an important determinant of the therapeutic effectiveness. Unfortunately, this also corresponds to the cognitive side effects3.
Seizure Threshold
Seizure Threshold is empherically defined as the minimal electrical dose that induces generalised tonic clonic seizure activity. Boylan et alfound that greater that 40% of individuals had an initial seizure threshold of less than 50mC with unilateral electrode placement4 and Scott and Dykes and Sakheim concluded that for bilateral ECT, this was around 7%5,9.
Standard fixed doses continue to be used in UK, and this can result in a dose which is several times the seizure threshold, contributing to acute and long term cognitive side effects without any additional benefits of clinical efficacy. It is also associated with a greater risk of missed or partial seizures that have no therapeutic effect.
There is a great deal of variability between seizure thresholds in different individuals. Many factors influence it and Box 1 summarises them. Seizure threshold is generally higher in older men than younger women. Electrolyte imbalances, particularly, hyponatremia and hypocalcaemia can lower the seizure threshold. It is important for the clinician to consider these before starting the course of ECT.
Initiation of a course of Electroconvulsive Therapy treatment should routinely involve the estimation of the seizure threshold by gradual dose titration (Stimulus dosing) and then treatment by using the supra threshold doses. Once seizure threshold is determined a dose of 1.5 to 2 times the seizure threshold for bilateral ECT and at least 2.5 to 3 times the seizure threshold for unilateral ECT may provide the best balance of clinical efficacy and cognitive side effects3. This is supposed to be a better practice compared to the fixed dose method used to initiate the ECT treatment.6
Missed Seizure
An adequate electrical dose will manifest as generalised tonic, followed by clonic activity of skeletal muscle, accompanied by a typical seizure pattern on EEG. The absence of both is deemed a missed seizure7.Pippard’s audit of ECT practice showed that in nearly 22% of ECT treatments, there was either no seizure or a brief seizure.
Box 2: Causes for Missed Seizure
Low stimulus intensity
Excess impedance
Premature stimulus termination
Excess Anaesthetic Agent
Increase of seizure threshold by ECT
Other factors increasing seizure threshold
The causes of Missed Seizures are summarised in Box 2. Missed seizures may be due to faulty technique leading to insufficient stimulus intensity, excess impedance or premature stimulus termination. Individual patient factors such as electrolyte imbalances, particularly dehydration and hypercarbia can lead to missed seizures. A common reason for raised seizure threshold is the administration of high dose of anaesthetic induction agent 5. Propofol, the most commonly used agent for ECT increases seizure threshold and also decreases the seizure duration. Use of alternatives like Methohexital, Etomidate or Ketamine may be successful as they either have minimal or no effect on seizure threshold and may increase the seizure duration.
During the course of treatment seizure threshold usually rises and this may lead to missed seizures. In addition to delaying the improvement, missed seizures cause more irritability and restlessness10. By measuring the seizure duration during the course of ECT missed seizure could be anticipated and appropriate steps can be taken. Some of the effects of a missed seizure are listed in Box 3.
Box 3: Consequences of Missed Seizure
Anxiety
Headache
Confusion
Lethargy
Tiredness
A missed seizure should prompt monitoring and correction of electrolyte imbalance if any. Seizure activity during the ECT procedure is affected by medication as well. Administration of seizure threshold increasing drugs should be reviewed and where possible stopped or reduced. If the treatment is for depression, consider using tricyclic drugs which lower the seizure threshold and augment ECT.
The maximum dose deliverable by the ECT machines is restricted in some countries and this may be inadequate due to very high seizure threshold in a few individuals. The US Food and Drug Administration restrict the maximum output of ECT machines to 576 millicoulombs compared to the Royal College of Psychiatrists which has recommendeda maximum output charge of 1200millicoulombs8. While higher electric doses may be able to induce generalised seizure activity, the cognitive side effects are also increased11. Therefore attempts must be made to decrease the seizure threshold to minimise these side effects.
Seizure Threshold Lowering Techniques
The aim of ECT treatment is to induce a generalised seizure activity; failure to do so makes the treatment session ineffective and of no therapeutic benefit. If a patient does not have generalised tonic-clonic seizure after a stimulus it is important to wait for at least 20 seconds after a non-seizure and at least 45 seconds after a partial/focal seizure prior to restimulating. Using appropriate techniques to avoid like low stimulus intensity, inappropriate application of electrodes, premature stimulus termination, etc are important6.
Charter and Simpson established the use of hyperventilation immediately before the application of the electrical stimulus and it has been shown to enhance seizure duration12. Sleep deprivation safely reduces the seizure threshold and also increases the seizure duration13. Caffeine prolongs the seizure duration, but has no effect on the seizure threshold14.
Conclusions
ECT remains the most maligned and misunderstood of psychiatric treatments. Whilst it has no doubt, successfully saved many lives and provided relief from the abyss of depression, proving its efficacy, the thrust of recent developments have been towards minimising the side effects. Adequate training and supervision of trainee psychiatrists will be essential to raise the standards of ECT administration techniques and skills.
Being aware of the significance of seizure threshold and ways to lower it, as an alternative to electric dose increase may address to some extent, the concerns about cognitive difficulties.
Warfarin is the most commonly used oral anticoagulant and has established efficacy for more than 50 years for the prevention of thromboembolic events, but its use is limited by fear of bleeding, drug-drug and drug-food interactions, and routine monitoring of international normalized ratio (INR). In patients with atrial fibrillation (AF), warfarin prevents 64% of strokes in research studies but the real-world effectiveness drops to 35% because of various factors leading to its suboptimal use.1 In October 2010 the United States (US) Food and Drug Administration (FDA) approved Pradaxa capsules (dabigatran etexilate) as the first new agent to prevent stroke and systemic emboli in patients with non-valvular AF. In this article we will discuss some of the evidence for and against the use of dabigatran.
In the RE-LY study2 (Randomized Evaluation of Long-term Anticoagulant Therapy), high-dose dabigatran (150mg twice a day) was found to be superior to warfarin for the prevention of stroke and systemic emboli, required no routine INR monitoring, and had few food and drug interactions. James Freeman and colleagues,3 using data from the RE-LY trial, found that high-dose dabigatran (150mg twice a day) was the most efficacious and cost-effective strategy compared with adjusted-dose warfarin among adults older than 65 with AF.
Dabigatran has been shown to specifically and reversibly inhibit thrombin, the key enzyme in the coagulation cascade. Studies in healthy volunteers4 and in patients undergoing orthopaedic surgery have indicated that dabigatran has a predictable pharmacokinetic/pharmacodynamic profile, allowing for a fixed-dose regimen. Peak plasma concentrations of dabigatran are reached approximately two hours after oral administration in healthy volunteers, with no unexpected accumulation of drug concentrations upon multiple dosing. Excretion is predominantly via the renal route as unchanged drug. Dabigatran is not metabolized by cytochrome P450 isoenzymes. Though use of dabigatran for non-valvular AF and venous thromboembolism (VTE) is gaining practice,5 it remains far from being the standard of care.
What are the concerns with use of dabigatran? In the RE-LY study the INR control was relatively poor (64% TTR (time in the therapeutic range)) but, probably more importantly, the relationship between events and individual’s INR control was not reported. The use of centre’s time in therapeutic range (cTTR) in the RE-LY study as a surrogate for INR control may not truly reflect TTRs for individual patients. Also in RE-LY study, randomization was stratified for centre and by the centre-based analyses, and the quality of oral anticoagulant services was the basis for the comparisons in this report. A subgroup analysis6 concluded that relative effectiveness of dabigatran versus warfarin was mainly seen at centres with poorer INR control. For example, Swedish centres had good TTR and the relative effectiveness and safety of dabigatran was virtually the same as with warfarin; thus, it is only the price difference that counts. It also highlights how local standards of care affect the benefits of use of new treatment alternatives and hence further limits the generalizability of any ‘overall average’ cost-effectiveness of dabigatran, raising the question that if an intervention does not do more, why should a payer pay more for it? There are several other factors that could impact on the cost-effectiveness7 of dabigatran such as patient medication adherence, dosing frequency, and the potential effect of new efficient methods of warfarin management improving INR control by patient self-testing.
The other shortcomings of dabigatran include lack of antidotes when patients do bleed and lack of any alert to physicians that patients are not compliant with dabigatran (INR serves this purpose for warfarin). Additionally, in the RE-LY trial, dabigatran was used twice daily thus raising compliance issues compared to once daily warfarin (the rates of discontinuation of dabigatran were higher at 15% and 21% at one and two years, respectively); 11.3% reported dyspepsia (twice the rate of warfarin group); high rate of gastrointestinal bleed compared with warfarin; patients in the dabigatran cohort were at slightly higher risk of myocardial infarction (not sure how it will translate in real world practice); and contraindication of dabigatran in severe renal dysfunction raises some more questions about its use and cost effectiveness. In addition, the RE-LY trial excluded patients who had: contraindications to anticoagulation, severe heart-valve disorder, stroke within 14 days or severe stroke within six months before screening, a condition that increased risk of haemorrhage, creatinine clearance of less than 30ml per minute, active liver disease, and pregnancy. Clinicians will need to use their judgement to weigh and balance the risk for bleeding with this new agent in a setting of an acute stroke versus the risk of having another ischaemic stroke in someone with AF if not given anti-coagulation therapy immediately. Safety and efficacy at extremes of body weight is not well established with current FDA approved doses of dabigatran either.
In summary dabigatran is a very exciting new agent with significant advantages over warfarin. However, in view of dabigatran’s higher non-adherence rate and greater risk of non-haemorrhagic side effects, patients already taking warfarin with excellent INR control have little to gain by switching to dabigatran.1 Until more studies and post-marketing data become widely available, we should advocate tight INR control for which there is a wealth of evidence for benefits, and promote strategies to improve the management of therapy with warfarin.
Sedation is frequently administered outside of the operating theatre by non-anaesthetic doctors to facilitate minor procedures. This can be in both primary care including dental surgeries as well as in hospital departments such as radiology, endoscopy and the emergency department. Clinical practice including medication and monitoring equipment available and the personnel involved, varies not only between hospitals and regions but also between departments.
In the emergency department sedation is often performed in a busy clinical setting by junior doctors. This enables minor procedures to be carried out with subsequent discharge home reducing admission rates and the requirement for general anaesthesia. Other advantages include less workload pressure on the anaesthetic team and a significant improvement in the patient experience. Sedation is not without risk and significant morbidity and mortality is still associated with its use, particularly in the elderly and in combination with other medication1,2. Guidelines and protocols do exist to ensure safe practice but often it is only anaesthetic doctors who are aware of them3-7. A recent study by Fanning highlighted discrepancies in practice, skills and knowledge of doctors of various specialities and grades who administered sedation8. Anecdotal reports from orthopaedic colleagues suggested the variability in competence of doctors with clear implications for patient safety. We therefore sought to ascertain the current clinical practice, knowledge and prior training in sedation techniques of specialist registrars in orthopaedic and trauma surgery in our region.
Materials and Methods
A questionnaire based survey of 53 specialist registrars in orthopaedic and trauma surgery in the neighbouring Severn and South Wales regions was carried out. The questionnaire was modified from that developed by Fanning8 and circulated for completion at regional teaching sessions in Swansea and Bristol (Appendix 1). Each respondent had 15 minutes to complete the questionnaire based on their own experience, practice and knowledge. Respondents were not allowed to confer and full confidentiality was assured. The questionnaire was split into several sections that ascertained the respondents’ clinical practice including the procedures that sedation was used for, prior training, awareness of protocols and safety issues. Knowledge of the basic pharmacology of commonly used sedative agents was also tested. The final section asked respondents whether they had ever encountered any adverse events, the nature of the adverse event and whether assistance was required from the anaesthetic department.
Results
Orthopaedic specialist registrars (post basic surgical training) who were in higher surgical training completed 53 questionnaires. Sedation was performed in the emergency department by all respondents for manipulating fractures, reducing dislocated joints and for applying traction. Twenty-four respondents (45%) had read the sedation protocol for their hospital/emergency department. Thirteen respondents (25%) completed pre-sedation assessment forms, whilst only eleven (21%) completed the during-procedure monitoring data forms and twelve (23%) filled the after-procedure forms (Figure 1). Twenty-eight (53%) respondents ensured that either they or an assistant provided the patient with discharge advice.
Figure 1The percentage of respondents who had read the departmental protocol, completed monitoring forms and given advice prior to discharge.
Table 1: Sedative agents used.
Medication/Sedative Agent
No of Respondents
Diazepam
31
Pethidine
1
Midazolam
35
Propofol
15
Fentanyl
3
Morphine
44
Opiates with BDZs
12
Local anaesthesia with sedation
17
Almost all (98%) respondents administered sedation in the presence of an assistant. Forty-seven (89%) checked their medication with another healthcare professional. All fifty-three respondents supplied patients with concurrent oxygen whilst fifty-two ensured that resuscitation equipment was available nearby. In terms of specific training, forty-seven (89%) registrars had undergone Advanced Life Support training (ALS) but this qualification was only valid (within three years) for thirty-six (68%). Sixteen registrars (30%) stated they had undergone formal training or teaching regarding sedation (Figure 2). With regards to monitoring of patients, thirty-six (68%) respondents used pulse oximetry, fourteen (26%) used electrocardiogram (ECG) monitoring and twenty-eight (53%) measured blood pressure.
Figure 2The proportion of respondents who had received training in administering sedation
Morphine and other opioids were the most commonly used sedative medication (44 responses), followed by midazolam (35 responses), diazepam (31 responses) and propofol (15 responses). Twelve respondents combined opiates and benzodiazepines, whilst seventeen combined local anaesthesia with sedation (Table 1). Two-thirds of respondents (35 out of 53, 66%) administered sedation in boluses rather than calculating the correct dose per kilogram. The pharmacology questions devised by Fanning8 tested knowledge of metabolic pathways, duration of action and side effects. Overall, each question was answered correctly by over 50% of respondents (Figure 3). The mean score was 4.29 out of 7.
Figure 3The percentage of correct answers for each of the seven pharmacology questions.
Eighty percent of surveyed orthopaedic doctors (43 respondents) reported an adverse event after administering sedation. Twenty-nine respondents had at some stage contacted the anaesthetic department for assistance in managing a patient following sedation (Table 2).
Table 2: Adverse Events reported.
Adverse Effects
No of Respondents
Hypoxia
20
Respiratory Depression
13
Loss of consciousness
7
Hypotension
14
Prolonged Sedation
13
Nausea and Vomiting
14
Discussion
Non-anaesthetic doctors are permitted and often required to administer sedation to perform procedures in settings outside of the operating theatre. There are various published guidelines that detail the level of care and monitoring that should be provided when sedation is given3-7. It has been recommended that the same standards of monitoring apply to procedures under sedation or local anaesthesia as to procedures under general anaesthesia, and are irrespective of the location of the procedure3.
The report by an intercollegiate working party led by the Royal College of Anaesthetists summarised the key aspects of administering sedation based on existing guidelines6. Patients should be first assessed before the procedure by attendant staff, risk factors noted and further examination or investigations performed as necessary. Drug administration technique should be “one defined by a relevant specialty organisation”6 and doses adjusted to individual patient requirements. Combinations of drugs should be “employed with particular caution” especially sedatives and opioids. The opioids should be administered first and given time to be maximally effective before any sedative is given. The patient should be monitored during the procedure by a suitably trained individual recording pulse oximetry, blood pressure and electrocardiography. High flow oxygen should also be available. Doctors administering sedation should be able to control an airway using basic manoeuvres or airway adjuncts.
There is significant morbidity and mortality associated with sedation1,2. It is difficult to know the true incidence of cardio-respiratory complications after sedation, as this is often related to the procedure and patient factors. An audit of 14,000 endoscopic procedures reported a 30-day mortality of 1 in 20009 and there are several anecdotal reports of death following sedation10,11.
It is apparent that not all doctors are aware of or follow sedation guidelines. In the study by Fanning8, 42% of respondents completed a pre-procedure assessment form and 70% completed monitoring data sheets. In this study, whilst 45% of respondents had read departmental protocols, only 25% completed a dedicated pre-assessment of the patient and an equally low number recorded monitoring data forms during (21%) and after the procedure (25%). These low numbers are of potential concern. Time and resource constraints may play a part, particularly in a busy emergency department. Also, as junior doctors frequently rotate between hospitals, they may not be aware of departmental policies in each unit. It is understandably impractical to perform a procedure and concurrently complete a data monitoring form. This role should be delegated to an assistant.
Knowledge of basic pharmacology amongst respondents seemed reasonable and indeed better scores were achieved than in Fanning’s original paper. It would appear that a large number of respondents (n=29) have contacted anaesthetic colleagues for help following adverse events. This may simply reflect an acknowledgement of limited anaesthetic capabilities amongst respondents and a pre-emptive call for assistance rather than an anaesthetic “bail out” after cardio-respiratory compromise.
Whilst the questionnaire used is neither a formal assessment tool of clinical competence nor an accurate log of experience, it serves to highlight the potential limitations of current training. A clear issue is the low number of respondents who claim to have received formal teaching or training with regards to sedation. This may be due to the fact that little or no postgraduate training is provided in hospital specialities that require sedation. This is an area that needs to be addressed. The issues raised by this study are not new. In fact, a similar survey by Hewitt and Hartley in 1994 had similar findings and suggested that “sedation techniques should be included in induction teaching for A&E and orthopaedic juniors” and that all doctors administering sedation should have the “opportunity of resuscitation refresher courses”12.
Conclusion
Sedation is widely administered by non-anaesthetic doctors including orthopaedic surgeons in order to perform basic procedures outside of the operating theatres, mainly in the Accident and Emergency department. Whilst this study only involves 53 doctors in one speciality across two regions, it does give an insight into the self-reported clinical practice, knowledge and experience of a group of surgical doctors who are often required to administer sedation. Significantly, the majority of doctors surveyed reported they had not received any formal training. It is also apparent that departmental guidelines are not always known or followed. Due to the inherent risks of sedation, it is important that doctors are aware of and follow available guidelines. It is crucial that adequate training should be given to non-anaesthetic doctors to ensure they have the knowledge and skills to safely administer sedation. Otherwise a medical doctor, perhaps a registrar level from the Accident and Emergency department, should be present for patient assessment and management of airway compromise or any arising complication.
Lactic acidosis is an important cause of metabolic acidosis in hospitalised patients. This usually occurs either due to over production or under utilisation of lactate1 . Most cases of lactic acidosis are due to marked tissue hypoperfusion or hypoxia in systemic shock.
Asymptomatic lactic acidosis has been reported previously during acute severe asthma and attributed to fatiguing respiratory muscles, hypoxaemia and liver ischaemia. It has also been linked to β2 agonist therapy in asthma, although lactic acidosis causing increasing dyspnoea in the asthmatic patient has only been recorded rarely.
Case presentation
We present a case of lactic acidosis in a patient with acute severe asthma who did not have any overt signs of sepsis or tissue hypoperfusion.
Mr IL was a 49 years old male who was known to have moderate asthma. He had multiple previous admissions to hospital with exacerbation of asthma but had never required an intensive care admission and had never been intubated. His other comorbidities included atrial fibrillation, ischaemic heart disease and depression.
His usual medications included salbutamol, budesonide and salmeterol inhalers, aspirin, atorvastatin and digoxin. He was a mechanic by trade with no obvious occupational sensitisation. He had no pets at home. He was a smoker with a 20 pack year history. Recent lung function tests showed an FEV1/FVC of 0.68 with a post bronchodilator FEV1 of 4.17 L (95% predicted).
He was admitted with a 1 week history of worsening shortness of breath, dry cough and wheeze. His baseline blood tests including full blood count, C reactive protein, liver and renal function were normal. Chest radiograph was unremarkable. Arterial blood gas showed no evidence of hypoxia or acidosis.He was treated as acute severe asthma with back to back nebulisers, intravenous hydrocortisone and magnesium sulphate resulting in gradual improvement in bronchospasm and peak expiratory flow rate.
Despite optimal treatment, his breathing started to deteriorate. Arterial blood gas at this time showed lactic acidosis with normal oxygenation (Table 1). There was no clinical or biochemical evidence of haemodynamic compromise or sepsis. A presumptive diagnosis of lactic acidosis secondary to salbutamol was made. The nebulisers were withheld and he has transferred to high dependency unit for closer monitoring. The acidosis completely resolved in the following 12 hours on stopping salbutamol and the patient made an uneventful recovery.
Table 1: Serial Arterial Blood Gases (On admission, 4 hours later and on stopping salbutamol)
00:22
04:06
07:42 *
10:50
11:35
12:24
14:29
17:33
23:32
FiO2
100%
60%
60%
60%
60%
40%
40%
35%
28%
pH (7.35-7.45)
7.36
7.28
7.26
7.32
7.34
7.37
7.37
7.39
7.41
pCO2 (4.5-6.0 kPa)
4.87
4.74
4.15
3.31
3.98
3.9
4.7
5.08
5.49
pO2 (11-14 kPa)
27
19.2
16.5
19
18
14.1
12.5
13
11.8
HCO3 (22-28 mmol/L)
22
16.3
13.6
12.4
15.6
16.6
19.9
22
25.6
BE (2- -2)
-2
-9.1
-12
-12
-9
-7.6
-4.4
-1.5
1.4
Lactate (0.5-2 mEq/L)
1.8
7.6
9.7
9.3
7.6
6.8
3.6
1.4
1.1
* Salbutamol witheld
Discussion
Lactate is a product of anaerobic glucose metabolism and is generated from pyruvate. Normal plasma lactate concentration is 0.5-2 meq/L. Most cases of lactic acidosis are due to marked tissue hypoperfusion or hypoxia in systemic shock2 .
Lactic acidosis can occur in acute severe asthma due to inadequate oxygen delivery to the respiratory muscles to meet an elevated oxygen demand3 or due to fatiguing respiratory muscles4 . A less recognised cause of lactic acidosis is treatment with salbutamol. The mechanism of this complication is poorly understood.
Salbutamol is the most commonly used short acting βagonist. Stimulation of β adrenergic receptors leads to a variety of metabolic effects including increase in glycogenolysis, gluconeogenesis and lipolysis5 thus contributing to lactic acidosis.
Table 2 shows an assortment of previously published case reports and case series of lactic acidosis in the context of acute asthma.
Table 2: Details of etiology and consequences of lactic acidosis in previously published case reports
Reference
n
Suggested etiology of lactic acidosis
Effect of lactic acidosis
Roncoroni et al, 1976 [6]
25
Uncertain: increased respiratory muscle production, decreased muscle or liver metabolism
None observed
Appel et al, 1983 [7]
12
Increased respiratory muscle production, decreased muscle or liver metabolism
8 out of 12 developed respiratory acidosis, 6 required invasive ventilation
Braden et al, 1985 [8]
1
β2 agonist, steroid and theophylline therapy
None
O’Connell & Iber, 1990 [9]
3
Uncertain: intravenous β2 agonist versus severe asthma
None
Mountain et al, 1990 [10]
27
Hypoxia and increased respiratory muscle production
None
Maury et al, 1997 [11]
1
β2 agonist therapy
Inappropriate intensification of β2 agonist therapy
Prakash and Mehta, 2001 [2]
2
β2 agonist therapy
Contributed to hypercapneic respiratory failure
Manthous, 2001 [12]
3
β2 agonist therapy
None
Stratakos et al, 2002 [3]
5
β2 agonist therapy
None
Creagh-Brown and Ball, 2008 [13]
1
β2 agonist therapy
Patient required invasive ventilation
Veenith and Pearce, 2008 [14]
1
β2 agonist therapy
None
Saxena and Marais, 2010 [15]
1
β2 agonist therapy
None
Conclusion
In this case, the patient developed lactic acidosis secondary to treatment with salbutamol nebulisers. The acidosis resolved spontaneously without any specific treatment.
Lactic acidosis secondary to β agonist administration may be a common scenario which can be easily misinterpreted and confuse the clinical picture. Acidosis itself results in hyperventilation which could be mistaken for failure to treat the response. This may in turn lead to inappropriate intensification of treatment.
Tumefactive multiple sclerosis (MS) is a rare variant of MS. This form of MS can masquerade as neoplasm or infectious etiology. Understanding of the disease is limited to case report but it is associated with high morbidity and mortality.
Case report
A 44 year old man presented with a 2-month history of progressive right upper extremity weakness, confusion and visual change. Physical exam revealed weakness, hyperreflexia on the right side and right homonymous hemianopia. MRI of the brain showed multiple ring-enhancing lesions located in both cerebral hemispheres. CSF analysis disclosed elevated protein with positive oligoclonal bands and myelin basic protein. Stains and cultures for bacteria and mycobacteria were negative. Serologies including HIV, Toxoplasmosis, and Lyme were all negative. Patient was treated with high-dose IV corticosteroid and clinically improved. One month later, he presented with increasing confusion, aphasia and progressive weakness. Repeat MRI of the brain revealed worsening multiple ring-enhancing lesions with surrounding vasogenic edema in most lesions. High-dose corticosteroid was promptly started. There was also concern about infection, especially brain abscess; hence, intravenous ceftriaxone, vancomycin, and metronidazole were empirically given. Due to uncertainty of diagnosis, first brain biopsy at right frontal lobe lesion yielded non-specific gliosis. Repeat MRI brain showed increasing number of ring-enhancing lesions in both cerebral hemispheres. As a result, a second brain biopsy was performed, which showed an active demyelinating process consistent with multiple sclerosis. Patient experienced severe disability and was discharged to long-term facility with slowly tapered schedule of corticosteroid. He was readmitted several times and eventually family decided hospice care.
Discussion
Multiple sclerosis is diagnosed by demonstrating clinical and/or radiographic evidence of dissemination of disease in time and space1. Tumefactive MS is a term used when the clinical presentation and/or MRI findings are indistinguishable from a brain tumor2. Not all case of tumefactive MS are fulminant. Marburg variant MS is an acute rare variant of MS which has a rapidly progressive course with frequent, severe relapses leading to death or severe disability within weeks to months3. The tumefactive demyelinating lesions are defined as large (>2 cm.) white matter lesions with little mass-like effect or vasogenic edema, and post-gadolinium magnetic resonance imaging (MRI) typically showing an incomplete ring enhancement2,4. The clinical and imaging characteristics of these demyelinating lesions may mimic primary and secondary brain tumors, brain abscess, tuberculoma, and other inflammatory disorders e.g. sarcoidosis, primary sjogren’s syndrome5. As a result, tumefactive MS is frequently misdiagnosed. There are some MRI characteristics that are more suggestive of tumefactive demyelinating lesions than of other etiologies. These include incomplete ring enhancement, mixed T2-weighted iso-and hyperintensity of enhanced regions, absence of a mass effect and absence of cortical involvement2,6. Differential diagnosis of rapidly progressive neurological deficit with ring-enhancing lesions include brain abscess, primary brain neoplasm or brain metastasis, acute disseminated encephalomyelitis (ADEM) and tumefactive multiple sclerosis. Careful clinical history, CSF study, serial MRI evaluation and follow-up are usually sufficient to make a diagnosis. Some cases pose considerable diagnostic difficulty owing to clinical and radiographical resemblance to brain tumor, for which biopsy may be warranted. Pathologically, the lesions are characterized by massive macrophage infiltration, acute axonal injury, and necrosis. No specific histological features distinguished specimens derived from patients developing classic multiple sclerosis from those who had tumefactive form7. A limited number of cases of Marburg’s variant MS have been reported in the literature whereby most patients died within a period of weeks to months. Only two cases survived after one year7,8. There is no current standard treatment for this condition. Plasma exchange and Mitoxantrone are reportedly showed some promising options9,10.
Figure A: FLAIR imaging at first presentation showed lesion in both hemisphere. Figure B: FLAIR imaging at one month later showed progression of multiple lesion in both hemisphere. Figure C: T1 Post contrast imaging showed intense ring enhancement pattern in almost all lesions with mild edema and minimal mass effect. Figure D: Showed lesion view as sagittal section.
Our patient presented somewhat like a stroke with visual field defect and right hemiparesis which is unusual in MS, but MRI and CSF exam yielded a diagnosis of probable MS. Because of his abrupt clinical deterioration and impressive worsening of his MRI, concern was raised about possibility of infection or neoplasm. Hence, he received two brain biopsies, the second of which showed active demyelination, confirming the diagnosis of severe tumefactive multiple sclerosis and can be consider as a Marburg variant multiple sclerosis.
Conclusion
Marburg variant multiple sclerosis carries a high morbidity and mortality. This disease notoriously mimics other conditions leading to delay diagnosis and treatment. Absence of definitive diagnosis test apart from brain biopsy makes diagnosis, prognosis and treatment decisions difficult.
Robert Moots is Professor of Rheumatology at the University of Liverpool and Director for Research and Development at the University Hospital, Aintree. He is also a Consultant Rheumatologist at the hospital.
He graduated from St Mary’s Hospital, London University in 1985 and also worked at Harvard Medical School. He became a Consultant Rheumatologist at University Hospital Aintree in 1997 and the youngest full-time professor of Rheumatology and Head of Department in 2003.
Professor Moots has published extensively in rheumatology, winning the prestigious Michael Mason prize for rheumatology research. He advises the UK Department of Health and NICE. His research interests are inflammatory rheumatic diseases, in particular innate cellular immunity in rheumatoid arthritis, immunotherapy, new therapeutic targets and clinical trials.
How long have you been working in your speciality?
I’ve been working as a consultant in rheumatology since1997, when I returned to the UK from the USA. Of course I was a trainee in rheumatology for a few years before then.
Which aspect of your work do you find most satisfying?
Its hard to single out any one thing. The great fun of being Professor is that no two days are the same. My job varies so much from looking after patients, to teaching, running research and also communicating and sharing research findings with other clinicians and scientists throughout the world – giving me the opportunity to visit countries, where I would not normally have visited.
What achievements are you most proud of in your medical career?
Clinically, I often deal with rare rheumatic diseases, or situations where normal treatments have failed and other doctors have said there is “no more that can be done”. Each patient that I see in this situation, who then goes on to recover and have a normal happy life, gives me a great satisfaction. Academically, building up a successful research team of talented individuals in Liverpool, the first academic rheumatology unit in that city, has been a great privilege.
Which part of your job do you enjoy the least?
Trying to balance the demands of patient care with the many other calls on my time can be rather wearing. But nothing is worse than the ever expanding administration tasks and bureaucracy!
What are your views about the current status of medical training in your country and what do you think needs to change?
When I visit other countries to lecture, I always try to see how medicine runs there. I attend clinics and hospitals, see patients and learn how practice compares to the UK. I am pleased to note that the standard in the UK remains amongst the highest of all countries.
How would you encourage more medical students into entering your speciality?
Its hard to image why students and doctors could consider any specialty other than Rheumatology! Rheumatology provides the opportunity to see patients of all ages, develop a close rapport with patients as the diseases tend to be chronic and prevalent, perform cutting edge research to understand pathophysiological process underlying the diseases and access drugs that can make a revolution to lives with great outcomes.
What qualities do you think a good trainee should possess?
Be keen to learn, open, honest and bright. I also like trainees to challenge accepted wisdom – a considered critical approach is needed to move things forward and to keep us on our toes.
What is the most important advice you could offer to a new trainee?
Don’t accept non-evidence based dogma. Don’t learn bad habits. Be critical and try to improve things. Try to spend some time away from your unit and ideally out of your country – seeing how medicine works in other environments to get life and work in a better perspective.
What qualities do you think a good trainer should possess?
Good trainers should be excellent clinicians, inspirational leaders and listeners with patience. If you know someone like this, you should really treasure them!
Do you think doctors are over-regulated compared with other professions?
No – but I fear that we are getting there in the UK.
Is there any aspect of current health policies in your country that are de-professionalising doctors? If yes what shouldbe done to counter this trend?
With a recent change in government in the UK and major changes to the Health Service planned, it’s a little too early to tell. We have to be vigilant though.
Which scientific paper/publication has influenced you the most?
For much of my working life, I was focused on the T cell as the major driver for diseases such as rheumatoid arthritis. The paper that changed that was: Edwards SW, Hallett MB. Seeing the wood for the trees: the forgotten role of neutrophils in rheumatoid arthritis. Immunol Today.1997 Jul;18(7):320-4. This crucial paper from Steve Edwards, the world leader in neutrophil biology opened my eyes to a whole new field of work. I didn’t know at the time that I would eventually have the privilege of working with Steve.
What single area of medical research in your specialty should be given priority?
That’s an easy one – it should be whatever my group are working on at the time.(I just wish that were the case!)
What is the most challenging area in your specialty that needs further development?
Many rheumatic diseases such as rheumatoid arthritis can be treated extremely successfully (with patients enjoying a full remission) if they can access the right drugs at the right time. There is still much variability in time to diagnosis and in provision of appropriate medications – the challenge is to ensure that best practice can be rolled out more effectively.
Which changes would substantially improve the quality of healthcare in your country?
There needs to be a greater understanding of the importance of rheumatic diseases in the UK. These conditions are prevalent, may cause significant morbidity (and indeed mortality), cost the nation considerably in reduced productivity and in disability payments – yet many of these conditions can be treated most effectively.
Do you think doctors can make a valuable contribution to healthcare management? If so how?
Its crucial that doctors are fully engaged in management. We are in the best position to be advocates for our patients but cannot do this effectively without understanding the health care system and take the lead in ensuring this works for the best.
How has the political environment affected your work?
The consequences of the recent change in Government in the UK are likely to be considerable for the National Health Service. This will involve major changes to the work of staff at all levels. It is too early to know the full extent of this – but we all wait with trepidation
What are your interests outside of work?
With so much to do, its hard to find the time for much else apart from relaxing with my family. I travel a lot and especially enjoy taking my children with me. My 10 year old has heard me lecture so much that I suspect she can give my talk for me (and do it better). She has also taken to asking questions at the end of my lecture, which always scares the chairperson of the meeting!
If you were not a doctor, what would you do?
I’m not sure that I would be fit for anything else!
As highlighted in the World Health Report 2002, just a few Non Communicable Disease (NCD) risk factors, account for the majority of non communicable disease burden. These risk factors; tobacco use, alcohol consumption, raised blood pressure, raised lipid levels, increased BMI, low fruit/vegetable intake, physical inactivity, and diabetes, are the focus of the STEPs approach to NCD risk factor surveillance. 3
A tool for surveillance of risk factors, WHO STEPS, has been developed to help low and middle income countries get started. It is based on collection ofstandardised data from representative populations of specified sample size to ensure comparability over time and across locations. Step one gathers information on risk factors that can be obtained from the general population by questionnaire. This includes information on socio-demographic features, tobacco use, alcohol consumption, physical inactivity, and fruit/vegetable intake. Step two includes objective data by simple physical measurements needed to examine risk factors that are physiologic attributes of the human body. These are height, weight, and waist circumference (for obesity) and blood pressure. Step three carries the objective measurements of physiologic attributes one step further with the inclusion of blood samples for measuring lipid and glucose levels.4 The risk factors studied by MONICA project of the World Health Organization (WHO), included cigarette smoking, blood pressure, blood cholesterol and body weight.5In many resource-poor settings, laboratory access can be difficultand expensive. A screening algorithm that includesgender, age, cardiovascular disease history, blood pressure,weight and height, and a urine dipstick test for glucose andprotein is likely to be more practical and may well providemuch of the predictive value of more complex blood-based assessments.6In addition, such algorithms should, wherever possible, useregional data on morbidity and mortality, because backgroundrates vary considerably between regions.7 WHO/ISH (World Health Organization/International Society of hypertension) risk prediction charts provide approximate estimates of cardiovascular disease (CVD) risk in people who do not have established coronary heart disease, stroke or other atherosclerotic disease. They are useful as tools to help identify those at high cardio vascular risk, and to motivate patients, particularly to change behavior and, when appropriate, to take antihypertensive, lipid-lowering drugs and aspirin.8 After reviewing the above information about standardised methods available for identifying the risk factors for CAD, the present study was undertaken to assess the prevalence of risk factors in the community in Tripoli, the capital of Libya. The aim of this paper also includes suggesting priorities and strategy to deal with the risk factors that were found most important. Appropriate statistical tests were applied using the software SPSS 17 for determining the relative importance of different risk factors. The specific statistical tests have been stated below. Material and Methods 528 individuals were selected from general community for the study by random sampling from different geographical areas of Tripoli. They were interviewed about risk factors for CAD and where possible, facts stated by them were validated from medical records available with them. Their body weight, height and blood pressure were also recorded. The intern doctors posted with community medicine department were briefed and trained by faculty members for the above observations and recording the body measurement and blood pressure using the uniform technique. The WHO/ISH risk prediction colourcharts for Eastern Mediterranean Region B (which includes Libya) were used as questionnaire for the study. The option of charts available for settings where blood cholesterol can’t be measured was selected as it was found difficult to convince the individuals not suffering from disease to provide blood samples. The following criteria were used for defining Blood Pressure, BMI, Diabetes & MI : According to the WHO definition, individuals with systolic blood pressure ≥ 140 mmHg or those with diastolic blood pressure ≥ 90 mmHg were considered hypertensive. 21. Known cases of diabetes were termed as individuals for whom the diagnosis of diabetes had been established by a physician in the past, or those who were under treatment with anti diabetic drugs. 22 Body mass index (BMI) is calculated as weight divided by height squared (kg/m2). Overweight is defined as BMI 25–29.9 kg/m2, and obesity as BMI ≥ 30 kg/m2 for all subjects.19 Known cases of Myocardial Infarction (MI) were termed as individuals for whom the diagnosis of MI had been established by a physician in the past. ObservationsThe comparison of population characteristics of people with and without having a MI stated in the table below reveals that: distribution of males and females was similar in both the groups. 88% of individuals with a MI were from age group 35 and above. Whereas 11.43% of people with MI were from age group 15 to 34 years which shows the need of starting screening as well as control of risk factors from teenage. Using SPSS software, independent sample t test was applied on age distribution of individuals with and without history of MI. The result revealed that the mean age of individuals with a positive history of MI was 54. It was 43.74 for subjects with negative history of MI. The difference of age between the above 2 groups was found highly significant (P>0.001). In the same manner using SPSS software, Chi square test was applied on sex distribution of individuals with and without history of MI. The result revealed that the difference in sex distribution in the two groups was not significant (P = 0.522) Table 1 : Age & Sex wise distribution of persons with and without MI:
Characteristics
Individuals with MI in percentage, (N= 70)
Individuals without MI in percentage, (N = 458)
Sex; Male
68.57 (48)
68.78 (315)
Female
31.43 (22)
31.22 (143)
Age 15-34 years
11.43(8)
34.93 (160)
35-54 years
30.00 (21)
37.55 (172)
55 & above
58.57 (41)
27.51 (126)
Independent risk factorsAs presented in Fig.1, in males with MI in terms of percentage the most prevalent risk factor was found to be hypertension (11.05% higher than non MI group), followed by diabetes (higher by 10.78%), smoking (higher by 8.12%) and BMI 25 & above (higher by 5.13%). As presented in Fig.2, in females with MI in terms of percentage the most prevalent risk factor was found to be hypertension (20.55% higher than non MI group), followed by BMI 25 & above (higher by 8.77%) and diabetes (higher by 6.85%). There were no smokers in the female group with MI and only one smoker was found in the females without MI. Using SPSS software, under general linear model, multivariate analysis was performed after splitting the cases under male and female. History of MI was kept as fixed factor and age, history of hypertension, diabetes and stroke, smoking, systolic blood pressure and BMI were kept as dependent variables. The results reveal that in the males with positive history of MI, value of P was less than 0.001(highly significant) for age, History of hypertension & diabetes and systolic BP of140 and greater, followed by history of stroke (P>0.002) suggesting that prevalence of these variables were significantly higher in males with history of MI. The prevalence of BMI 25 & above (P>0.616) and smoking (P>0.882) in males with history of MI was found insignificant. In case of females with positive history of MI, the only variable having significant prevalence was f history of hypertension (P>0.008). An important reason for inability to assess significance for other variables in females may be the smaller number of females of only 22 with history of MI. Among the community members with MI, 94.38% males and 78.57% females had one or the other risk factor which have been stated above. Hence with focused attention to health education and screening for risk factors, identifying most of the individuals at risk of MI, should be possible. (Fig.1) Distribution of Risk Factors in Males with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) (Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factorsOut of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI. (Fig.3) Age wise distribution of blood pressure (both sexes)Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years. (Fig. 4) Age wise distribution of weight (both sexes) Discussion: Comparison with other relevant studies: In our study the most common risk factors observed in community members without MI were hypertension (total 24.35%, males 23.78 & females 25.88), followed by diabetes (total 21.13%, males 19.56 & females 25.29) and smoking (Total 27.26%, males 37.33 & females 0.59) as stated above in Fig.1 & 2. In similar studies performed in countries of Mediterranean region14-18 26% of study population were found to be suffering from hypertension, 40% males and 13% females were smokers and 14.5% were suffering from diabetes. 13 The percentage of diabetics was 10.6 in study population aged 30 years and above in Iran11. The percentage of diabetics were 11% in males and 7% in females in United Arab Emirates (UAE)10 and the figures were the similar in Saudi Arabia in subjects aged 30 years and above were 17.3% and 12.18% respectively.9. All the above studies were performed in the period from year 2000 to 2004 except the study in UAE which was performed in 1995. It can be seen from our study in Libya that in comparison to mean percentage for the same risk factors in other countries of Mediterranean Region, the percentage of hypertension was lower by about 2%. In Libya the percentage of total diabetics in the general community was greater by 6.6%, while the percentage of smokers were less by about 13% in males and 12.5% in females. The percentage of total overweight and obese individuals in all age groups and both sexes were 66.6 % in the general community without MI in our present study (Fig,4). The percentage for those overweight and obese in individuals above 19 years of age was 26.2% in study from Iran12 and 27 % in UAE10 in the age group of 30 to 64 years. The study of 12 countries of the Eastern Mediterranean Region(EMR) by the WHO conducted in 2004, reveals that regional adjusted mean for these countries was 43 % for overweight and obese individuals in all age groups and both sexes20. Hence in comparison to developing countries of the region having similar religious, social and dietary situation among the risk factors for CAD, diabetes and obesity can be seen as emerging major risk factors in Libya followed by hypertension and smoking. Smokers among females were found to be uncommon in Libya.Conclusion The findings of this study reveal that in comparison to those without MI the prevalence of following risk factors was higher in individuals with MI. In males aged 35 to 54, the percentage of those with a systolic BP of 140 and greater was more than double and in females 1.6 times greater. Those with diabetes were greater by 10.78% in males and 6.85% in females, while smokers were higher by 8.12% in males. The percentage of diabetes in individuals without MI was 21.13%. The prevalence of smokers was found to be 37.33% in males without MI which suggests urgent need for prevention and control measures. Considering multiple risk factors out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. In view of large number of individuals having risk factors of CAD in Tripoli, we would like to recommend that health education for preventing overweight and obesity, hypertension, smoking and diabetes may be started with school children and their parents as early as primary school. The screening for above risk factors needs to be implemented in the age group of 34 years and above for detecting individuals at risk as close to 34 years as possible. This step needs to be followed by relevant health education and treatment as soon as possible. More studies on a larger population sample are required from different geographical areas of Libya to refine our focus on the target population identified. At the same time waiting for action, till these additional studies are completed, is not recommended. To make the comparison of risk factors more fruitful among different countries and in the same country over time, we need to agree on uniform criteria such as using WHO/ISH risk prediction charts. Limitations of present studyIt is a cross sectional study based on the questions stated in WHO/ISH prediction charts for situations where collecting blood samples is not feasible. Due to the small sample size we can only say that the prevalence of MI is indicative of the pattern observed. These figures may get refined as we cover a larger number of the population over time. Due care has been taken in selecting sample size to represent different geographical divisions of Tripoli and to ensure that this is a random sample, but it is a systematic random sample and not the stratified random sample. Hence within each geographical division all the socio economic strata of community may not have been proportionately represented. AppendixThe questionnaire used for the study is stated below. It is based on the questionnaire recommended on page 21 of WHO/ ISH risk prediction charts for Eastern Mediterranean Region B of W.H.O. in which Libya is included.QuestionnairePrecautions: Do not interview persons below the age of 14 years. You should take height, weight and Blood Pressure of the person yourself, before recording it in the form below
S.N.
Question
Subject
1
2
3
4
5
1
Name of Person:
2
Address in Libya
4
Age
5
Sex: M / F
6
Do you smoke: Yes / No
8
Do you have History of suffering from Diabetes: Yes / No
9
Hist. of suffering from: Mayo cardial Infarction: Yes/ No
Antibiotics serve a very useful therapeutic purpose in eradicating pathogens1,2. Unfortunately excessive and inappropriate use of antibiotics results in antibiotic resistance which is a rapidly increasing global problem with a strong impact on morbidity and mortality 3-5. It is now evident that self-medication is widely practiced in both developing 6-11, as well as developed countries 12-18. India is also experiencing this problem of inappropriate use of self-medications in significant numbers 19,20.
Unlike the rest of the population, when physicians become ill,they can prescribe medicines for themselves very easily. Medical knowledgeand access to prescription of medications increase the potentialfor self-treatment. Although many warn of the loss of objectivitythat can accompany self-prescription, previous studies suggest that self-prescription is common among practicing physicians 21-24. The purpose of the present studyis to evaluate self-prescription and self-care practices amonggovernment doctors in the Hassan District of Karnataka. Materials and methods
A cross section of doctors attending the CME programme at Hassan Institute of Medical Sciences, Hassan, was selected for the project during August 2009. A self –assessment questionnaire was distributed amongst the participants after explaining the purpose of the study and after taking informed oral consent. The study was given prior approval from the institutional ethics committee. A total of 160 doctors (all participants were male) were chosen randomly for participation in the study.
The questionnaire consisted of both closed and open-ended questions. A total of 21 questions were stated concerning the following: Socio-demographic characteristics (like age, sex and personal habits), patterns of self – medication with antibiotics (e.g. type of antibiotics used, frequency, whether the course of antibiotic was completed, and the health condition that lead to self-medication).
After completion of data collection, it was reviewed, organized and evaluated using the Chi-square test and analysis of variance (One-way ANOVA) using the Statistical Package of Social Science (SPSS Inc., Chicago, IL) for windows version 14 and p-value of <0.05 was considered statistically significant. Results
A total of 160 male doctors agreed to participate in the study. Twenty eight percent of them were postgraduate qualified (e.g. MD, MS in different specialities) and 72% were only MBBS qualified. Eighty six percent of them were aged between 36-45 years.
Fifty three percent of doctors had used self-prescribed antibiotics with self-diagnosis within the last 6 months before the study.
Table – 1
Characteristics of the Respondents
Variables
Doctors %
Used self-medication with antibiotics
53.0
How many times
Once / day
55.8
Twice / day
10.4
> 3 times
16.1
Completed the course
26.8
Table – 2
Factors that lead to Self-medication
Conditions
Doctors %
Respiratory Infections
66.7
GI problems
23.4
Systemic Problems
7.7
Skin Problems
2.6
Urinary tract conditions
0
Table – 3
Antibiotics used for self-medication
Name of the antibiotic
Doctors %
Penicillines
68.0
Amoxicillin
40.0
Flouroquinolones
13.3
Co-amoxiclav
6.8
Macrolides
8.0
Tetracyclines
2.7
Cephalosporins
4.0
Sulphonamides
2.2
Metronidazole
1.2
Tinidazole
2.0
The frequency of antibiotic use was once in 55.8%, twice in 10.4% and thrice or more in 16.1% in the study period (p < 0.05). Only 26.8% of all doctors attended in this study completed the course of antibiotic therapy (p < 0.05) (Table 1).
The factors that lead to self-medication among respondents were perceived respiratory infections in 66.7%, gastrointestinal diseases in 23.4%, systemic diseases in 7.7% and skin diseases in 2.6% (Table 2).
Table 3 shows the antibiotics that were most frequently used for self-medication. Penicillins were ranked highest (68%) and in this group Amoxicillin was most frequently used (40%). Next were the flouroquinolones with 13.3% followed by Macrolides 8%. Other relatively lesser used drugs were co-amoxiclav, cephalosporins, tetracyclines, sulphonamides, Tinidazole and Metronidazole. Discussion
The current study examined antibiotic self-medication among government medical doctors in Hassan district. They were attending a CME programme at HIMS, Hassan. Studies on factors associated with antibiotic use are important to prevent the occurrence of antibiotic resistance 9, which is a well known problem in many countries 7-18. Antibiotic use in different diseases was always empirical without proper opinion and laboratory investigation in self- medication.
The source of the antibiotics was from medical representatives (47.8%), from drug stores (44.8%) without prescription, even though antibiotics are prescription only medicines. The fact that the violation of this law is subject to financial penalty and is not strictly implemented in case of doctors, has resulted in the continuation of this practice. Self-medication with antibiotics may increase the risk of inappropriate use and the selection of resistant bacterial strains 25,26. There have been several reports addressing the extent of self-medication practices with antibiotics among university students in other countries 27,28, but few about doctors. This should be further analyzed.
In this study, more than 53% of the respondents practiced self-medication with antibiotics within the last 6 months before the study. This rate is similar to the findings of a study in Turkey with 45.8% of self-medication with antibiotics 29 and also a recent study in Jordan (40.7%) 9 and other studies in Sudan (48%) 7, Lithuania (39.9% ) 30 and also in USA ( 43% ) 17.
Higher rates of self-medication are reported from China(59.4%) and Greece (74.6%) 14. Lower rates are reported from Palestinian students (19.9) 27, Mexico (5%) 31, Malta (19.2%) 18 and Finland (28%) 12. It seems that the lower rates of self-medication in these cases were due to respiratory diseases being treated symptomatically rather that with antibiotics.
Only 26.8% of respondents completed the course of antibiotic therapy. This is similar to the result of study in Jordan (37.6%) 9.
The most common disease treated by antibiotics was respiratory tract infections (common cold, sore throat, and sinusitis). Such diseases were also reported to be the common cause for self-medicated in Jordan 9, Palestine 27, Turkey 28 and European countries 16. The above conditions are known to be of viral origin 32, requiring no antibiotic treatment.
The main antibiotics used in self-medication were penicillins in general, and particularly Amoxicillin. Similar results are reported by other studies from different parts of the world 8,33. This may be due to the low cost of broad spectrum penicillin throughout the world 8.
It is agreed by some researchers that adverse effects due to inadequate and inappropriate use of antibiotics without prescription can be minimized by proper education 34. This can be effectively done through national awareness programmes, educational programmes (Rational Drug Use, Intensive Medical Monitoring of Prescription, evidence based practice, and essential drug use) and CME programmes.
We also suggest specific education about antibiotics in all educational and research institutions.
There are a few limitations in this study for all doctors irrespective of gender. First, is its reliance on self-reported dataabout self-medication with antibiotics. Secondly, it refers to any previous use of self-medication with antibiotics (retrospective study). Another limitation is that our population samplemay not be representative of the doctors’ population in the entire district. National education programmes about the dangers of irrational antibiotic use and restriction of antibiotics without prescriptions should be the priority. This study indicated that with reference to doctors, knowledge regarding antibiotics cannot be evaluated alone since it did not always correlate with behaviour. Conclusion
Almost all medical doctors practice self-treatment when they are ill. Although they prefer to be treated by a physician, due to complex reasons including ego and a busy professional work pattern, there is a certain amount of hesitation in consulting professional colleagues when they need medical help.
The prevalence of self medication practices is alarmingly high in the medical profession, despite the majority knowing that it is incorrect. We recommend that a holistic approach must be taken to prevent this problem from escalating, which would involve: (i) awareness and education regarding the implications of self medication (ii) strategies to prevent the supply of medicines without prescription by pharmacies (iii) strict rules regarding pharmaceutical advertising; and (iv) strategies to make receiving health care much less difficult.
Our study has also opened gateways for further research on this issue, besides showing that it is a real problem and should not be ignored in and around Karnataka, India and all over the world.
Acute Lung Injury (ALI) is a continuum of clinical and radiographic changes affecting the lungs, characterised by acute onset severe hypoxaemia, not related to left atrial hypertension, occurring at any age. At the severe end of this spectrum lies Acute Respiratory Distress Syndrome (ARDS) and therefore unless specifically mentioned this review will address ARDS within the syndrome of ALI.
It was first described by Ashbaugh in the Lancet in 1967. This landmark paper described a group of 12 patients with “Respiratory Distress Syndrome” who had refractory hypoxaemia, decreased lung compliance, diffuse infiltrates on chest radiography and required positive end expiratory pressure (PEEP) for ventilation.1
Key Points on Acute Lung Injury
Common, life threatening condition which is a continuum of respiratory dysfunction with ALI and ARDS being at either end of the spectrum
Risk factors include conditions causing direct and indirect lung injury, leading to an inflammatory response which can cause multiple organ failure
Damage to alveolar epithelial cells and capillary vasculature impair gas exchange and can lead to fibrosis
Management aims include supportive care, maintaining oxygenation and diagnosing and treating the underlying cause
Evidence supports low tidal volume ventilation and conservative fluid management
Long term outcomes relate to neuromuscular, neurocognitive and psychological problems rather than pulmonary dysfunction
This initial description gave only vague criteria for diagnosis, focused on the most severe end of the continuum and was not specific enough to exclude other conditions. A more precise definition was described by Murray et al. in 1988 using a 4 point lung injury scoring system including the level of PEEP used in ventilation, ratio of arterial oxygen tension to fraction of inspired oxygen (PaO₂/FiO₂), static lung compliance and chest radiography changes2. Despite being more specific and assessing severity it was too large and complex for practical purposes in the ICU setting.
It was not until 1994 that The American –European Consensus Conference on ARDS set the criteria used today to define both ALI and ARDS in research and clinical medicine. It recommended ALI be defined as “a syndrome of inflammation and increased permeability that is associated with a constellation of clinical, radiological and physiological abnormalities that cannot be explained by, but may coexist with, left atrial or pulmonary capillary hypertension” .3 They distinguished between ALI and ARDS based upon the degree of hypoxaemia present, as determined by the ratio of partial pressure of arterial oxygen to fractional inspired oxygen concentration (PaO₂/FiO₂), with ALI patients demonstrating a milder level of hypoxaemia. Additionally ARDS changed from Adult Respiratory Distress Syndrome to Acute Respiratory Distress Syndrome to account for its occurrence at all ages.
DIAGNOSIS AND PROBLEMS RELATED TO THIS
There are no gold standard radiological, laboratory or pathological tests to diagnosis ALI and ARDS and patients are given the diagnosis based on meeting the criteria agreed in 1994. (See Table 1)
ALI is diagnosed clinically and radiologically by the presence of non-cardiogenic pulmonary oedema and respiratory failure in the critically ill.
Table 1 – Diagnostic Criteria for ALI and ARDS
ALI
ARDS
Onset
Acute
Acute
Oxygenation (PaO₂/FiO₂) ratio in mmHg, regardless of ventilatory settings
<300
<200
Chest Radiological Appearance
Bilateral Pulmonary Infiltrations which may or may not be symmetrical
Bilateral Pulmonary Infiltrations which may or may not be symmetrical
Pulmonary Wedge Pressure
(in mmHg)
<18 or no clinical evidence of left atrial hypertension
<18 or no clinical evidence of left atrial hypertension
Meeting criteria, in itself, is not a problem when diagnosing conditions in the ICU setting, as sepsis and multi-organ failure are defined using consensus based syndrome definitions, however there are problems specifically related to ALI’s diagnosis.
In practice ALI and ARDS are clinically under-diagnosed, with reported rates ranging between 20 to 48% of actual cases.4 This is due to poor reliability of the criteria related to;
Non-specific radiological findings which are subject to inter-observer variability
Oxygenation criteria is independent of inspired oxygen concentration or ventilator settings including lung volumes and PEEP
Excluding cardiac causes of pulmonary oedema including left ventricular failure, mitral regurgitation and cardiogenic shock, in the ICU setting is difficult even when pulmonary artery catheters are used
The definition includes a heterogeneous population who behave very differently in response to treatment, duration of mechanical ventilation and severity of pulmonary dysfunction.
However this is the definition used by the ARDS network (a clinical network set up in 1994 by The National Heart, Lung and Blood Institute and the National Institutes of Health in the USA) for its clinical trials and on this basis it is validated.
EPIDEMIOLOGY
Incidence
Incidence of ALI is reported as 17-34 per 100,000 person years.5 Unfortunately despite population studies demonstrating fairly consistent trends regarding age (mean approximately 60years), mortality (35-40%) and ratio of ARDS to ALI (around 70%), incidence figures are less consistent internationally. A recent prospective population-based cohort study in a single US county demonstrated a higher incidence around 78.9 per 100,000 person years and inferred from this that 190,600 cases could occur in the USA alone each year.6 This variation is likely due to problems with reliability of diagnosis as illustrated above and also related to ALI generally presenting as a critical care illness making its epidemiology directly linked to availability of ICU resources.
Cases are only “captured” in the ICU setting and it potentially exists outside this environment in unknown quantities.7 Taking this into account means ALI and ARDS are probably far commoner in clinical practice than reported and many patients may meet the diagnosis yet be managed outside the ICU environment.8
Risk Factors
ALI is a multi-factorial process which occurs due to environmental triggers occurring in genetically predisposed individuals, as ALI-inducing events are common, yet only a fraction of those exposed develop the syndrome.
Environmental triggers for developing ALI can be divided into those causing direct and those causing indirect lung injury, with sepsis, either intrapulmonary or extrapulmonary being the commonest cause. (See table 2)
Table 2 Direct and Indirect triggers for ALI
Direct Lung Injury
Indirect Lung Injury
Common
Pneumonia
Aspiration of gastric contents
Less Common
Pulmonary contusion
Fat / Amniotic fluid embolism
High Altitude
Near Drowning
Inhalation Injury
Reperfusion Injury
Common
Sepsis
Severe trauma with shock and multiple transfusions
Less Common
Burns
Disseminated intravascular coagulation
Cardiopulmonary bypass
Drug overdose (heroin, barbiturates)
Acute pancreatitis
Transfusion of blood products
Hypoproteinaemia
At present there is research into the role of genetic factors and how they contribute to susceptibility and prognosis.9 It is difficult to assess the molecular basis of ALI due to the range of ALI inducing events which can cause the lung injury, the heterogeneous nature of the syndrome itself, presence of additional comorbidities, potentially incomplete gene penetrance and complex gene-environment interactions. However possible candidate genes which predispose patients to ALI have been identified and other genes exist which may influence its severity, thus providing targets for research in treatment development.
Secondary factors including chronic alcohol abuse, chronic lung disease and low serum pH may increase risk of developing ALI.⁷ There may be factors which are protective against its development, such as diabetes in septic shock patients,10 but further research is required.
PATHOPHYSIOLOGY
It is thought ALI patients follow a similar pathophysiological process independent of the aetiology. This occurs in two phases; acute and resolution, with a possible third fibrotic phase occurring in a proportion of patients.
Acute Phase
This is characterised by alveolar flooding with protein rich fluid secondary to a loss of integrity of the normal alveolar capillary base, with a heterogeneous pattern of alveolar involvement.
There are two types of alveolar epithelial cells (Table 3), both of which are damaged in ALI, likely via neutrophil mediation, with macrophages secreting pro-inflammatory cytokines, oxidants, proteases, leucotrienes and platelet activating factor.
Table 3 Characteristics of Type I and Type II Alveolar Epithelial Cells
Type I
Type II
Percentage of cells
90%
10%
Shape
Flat
Cuboidal
Function
Provide lining for alveoli
Replace damaged type I cells by differentiation
Produce surfactant
Transport ions and fluids
Damage to type I alveolar epithelial cells causes disruption to alveolar-capillary barrier integrity and allows lung interstitial fluid, proteins, neutrophils, red blood cells and fibroblasts to leak into the alveoli.
Damage to type II cells decreases surfactant production and that produced is of low quality, likely to be inactivated by fluid now in alveoli, which leads to atelectasis. Additionally there is impaired replacement of type I alveolar epithelial cells and an inability to transport ions and therefore remove fluid from the alveoli.
Coagulation abnormalities occur including abnormal fibrinolysis and formation of platelet and fibrin rich thrombi which result in microvascular occlusion, causing intrapulmonary shunting leading to hypoxaemia.
Ventilation-perfusion mismatch, secondary to alveolar collapse and flooding, decreases the number of individual alveoli ventilated, which in turn increases alveolar dead space, leading to hypercapnia and respiratory acidosis. Additionally pulmonary compliance decreases and patients start to hyperventilate in an attempt to compensate the above changes.
The release of inflammatory mediators from damaged lung tissue triggers systemic inflammation and systemic inflammatory response syndrome (SIRS) which may progress to multiple organ failure, a leading cause of death in ARDS patients.
Resolution Phase
This phase is dependent on repair of alveolar epithelium and clearance of pulmonary oedema and removal of proteins from alveolar space.
The type II alveolar epithelial cells proliferate across the alveolar basement membrane and then differentiate into type I cells. Fluid is removed by initial movement of sodium ions out of the alveoli via active transport in type II alveolar epithelial cells, with water then following, down a concentration gradient through channels in the type I alveolar epithelial cells.
Soluble proteins are removed by diffusion and non soluble proteins by endocytosis and transcytosis of type I alveolar epithelial cells and phagocytosis by macrophages.
Fibrotic Phase
Some patients do not undergo the resolution phase but progress to fibrosing alveolitis, with fibrosis being present at autopsy in 55% non-survivors of ARDS.11 This occurs by the alveolar spaces filling with inflammatory cells, blood vessels and abnormal and excessive deposition of extracellular matrix proteins especially collagen fibres.12 Interstitial and alveolar fibrosis develops, with an associated decrease in pulmonary compliance and only partial resolution of pulmonary oedema with continued hypoxaemia.
CLINICAL FEATURES
Acute Phase
The diagnosis should be considered in all patients with risk factors who present with respiratory failure, as the onset though usually over 12 to 72 hours, can be as rapid as 6 hours in presence of sepsis.
Patients present with acute respiratory failure where hypoxaemia is resistant to oxygen therapy and chest auscultation reveals diffuse, fine crepitations, indistinguishable from pulmonary oedema.
Resolution Phase
This phase usually occurs after around 7 days after onset of ALI, where a resolution of hypoxaemia and improvement in lung compliance is seen.
Fibrotic Phase
There is persistent impairment of gas exchange and decreased compliance. In severe cases it can progress to pulmonary hypertension through damage to pulmonary capillaries and even severe right heart failure, with the signs and symptoms of this developing over time.
INVESTIGATIONS
Diagnostic criteria require arterial blood gas analysis to demonstrate the required ratio between the partial pressure of arterial oxygen and fractional inspired oxygen concentration.
Radiological Findings
Although there are no pathognomonic radiographic findings for ALI, features on plain chest radiography include;
Bilateral patchy consolidation, which may or may not be symmetrical
Normal vascular pedical width
Air bronchograms
Pleural effusion may be present
10-15% patients have pneumothoraces independent of ventilator settings
Computer tomography of the chest can show the heterogeneous nature of ALI, with dependent areas of the lung showing patchy consolidation with air bronchograms, atelectasis and fibrosis. As with plain radiography there may be pneumothoraces present.
Computer tomography and Chest radiograph of ARDS
MANAGEMENT
The aims of management are to provide good supportive care, maintain oxygenation and to diagnose and treat the underlying cause.
General
Good supportive care, as for all ICU patients, should include nutritional support with an aim for early enteral feeding, good glycaemic control and deep venous thrombosis and stress ulceration prophylaxis. It is important to identify and treat any underlying infections with antibiotics targeted at culture sensitivities and if unavailable, towards common organisms specific to infection site.
It is not uncommon for ALI patients to die from uncontrolled infection rather than primary respiratory failure.
Ventilator associated pneumonia is common in patients with ALI and can be difficult to diagnoses, as ALI radiological findings can mask new consolidation and raised white cell count and pyrexia may already be present. If suspected this should be treated with appropriate antibiotics, although long term ventilation can cause colonisation which leads to endotracheal aspirate culture results being difficult to interpret.
Although the role of physiotherapy in ALI is unclear, aims of treatment should be similar to those in all ICU patients, including removal of retained secretions and encouragement of active and passive movements, as patients are often bed bound for prolonged periods of time.
Ventilation
MODE OF VENTILATION
Ventilation is usually via endotracheal intubation using intermittent positive pressure ventilation with PEEP. There may be a role for non invasive ventilation in early stages of ALI, but it is poorly tolerated at higher PEEP settings which may be required to maintain oxygenation, and no evidence supports its use at present. Additionally there is no evidence to suggest an advantage of either volume or pressure controlled ventilation.
Principles of ventilation in ALI are to maintain adequate gas exchange until cell damage resolves whilst avoiding ventilator associated injury from;
Barotrauma – alveolar overdistension associated with ventilation at high volumes
Volutrauma – alveolar overdistension associated with ventilator high pressures
Biotrauma – repeated opening and closing of collapsed alveoli causing shearing stress which can initiate a proinflammatory process
Lungs in patients with ALI are heterogeneous and therefore can react variably to changes in ventilator settings. Therefore settings which provide adequate oxygenation, may damage more “healthy” areas of lung.13
Table 4 Lung ventilation in different parts of lung with acute lung injury
Area
Characteristics
Behaviour when ventilated
1
Normal compliance and gas exchange
Easily over ventilated
Exposed to potential damage
2
Alveolar flooding and atelectasis
Alveoli can still be recruited for gas exchange by safely raising airway pressures
3
Severe alveolar flooding and inflammation
Alveoli cannot be recruited without using unsafe airway pressures
TIDAL VOLUMES
Old strategies of high volume ventilation are likely to over inflate healthy lung portions leading to barotrauma and ventilator management in ALI has moved towards lower tidal volumes. This is a consequence of the ARDSnet tidal volume study, which demonstrated significant reduction in mortality (40 to 31%) when using a low volume ventilator strategy based on predicted body weight (6mls/kg and peak pressures <30cmH₂O vs. 12mls/kg and peak pressures <50cmH₂O).14 Furthermore they showed a decrease in systemic inflammatory markers, lower incidence of multiple organ failure and an increase in ventilator free days in the lower tidal volume group.
PEEP
It was postulated that PEEP may be beneficial in ARDS as it reduces biotrauma, maintains the patency of injured alveoli, reduces intrapulmonary shunting and improves ventilation-perfusion mismatch. However evidence regarding its use is inconclusive. Numerous large centre trials have demonstrated no difference in outcome or mortality between patients ventilated with lower PEEP vs. higher PEEP (8 vs. 14 cm H₂O).151617 Yet a recent JAMA systematic review and meta-analysis showed that although higher PEEP ventilation was not associated with improved hospital survival, it was associated with improved survival among the ARDS subgroup of ALI and suggested that an optimal level of PEEP remains unestablished but may be beneficial.18
ECMO (Extracorporeal membrane oxygenation)
This is a modified longer term form of cardiopulmonary bypass which aims to provide gas exchange across an artificial membrane external to the body, allowing the lungs time to recover. It is confined to a few specialist centres in the UK and the first results from the CESAR multicentre randomised controlled trial were published in the Lancet in 2009. It showed improved survival in adult patients with severe but potentially reversible respiratory failure on ECMO, as compared to conventional ventilation and demonstrated cost effectiveness in settings like the UK healthcare system.19 This therefore may be a treatment strategy to consider in extreme cases resistant to conventional therapy.
OTHER STRATEGIES
A current meta-analysis looking at prone positioning concluded that randomised controlled trials failed to demonstrate improved outcomes in ARDS patients overall. There is a decrease in absolute mortality in severely hypoxaemic patients with ARDS but as long term proning can expose ALI patients to unnecessary complications, it should only be used as rescue therapy for individuals resistant to conventional treatment.20
No evidence supporting specific weaning programmes exists and a recent Cochrane review showed no evidence to support recruitment manoeuvres in ALI. 21
Therefore the aim of ventilation is low volumes with permissive hypercapnia, providing adequate oxygenation (regarded as a partial pressure of arterial oxygen >8kPa) whilst trying to avoid oxygen toxicity lung injury.
Fluid Management
Fluid management has to balance the need for enough fluid to maintain an adequate cardiac output and end organ perfusion, with a low enough intravascular pressure to prevent high capillary hydrostatic pressures, which could cause pulmonary oedema, worsen oxygen uptake and carbon dioxide excretion. Evidence supports a negative fluid balance in patients not requiring fluid for shock.
Studies as early as 1990 showed a reduction in pulmonary wedge pressure was associated with increased survival22 and extravascular lung water was associated with poor outcomes23 in ARDS patients.
The ARDSnet FACTT study looked at two fluid regimens comparing liberal fluid management (a net gain of approximately 1 litre per day) with a conservative fluid management (zero net gain over first seven days).24 Although there was no significant difference in (the) primary outcome of 60 day mortality, the conservative management group had improved lung function, shortened duration of mechanical ventilation and intensive care and had no increased incidence of shock or use of renal replacement. This is supported by a recent retrospective review, which concluded negative cumulative fluid balance at day 4 of acute lung injury is associated with significantly lower mortality, independent of other measures of severity of illness.25
Pharmacotherapy
To date no pharmacological agent has been demonstrated to reduce mortality among patients with ALI.26 However ALI encompasses a wide range of patients with varying aetiology and comorbidities. It may be that on subdividing ALI patients, some therapies may be suitable for specific circumstances but at present there is little literature to support this.
EXOGENOUS SURFACTANT
Since the 1980’s numerous randomised controlled trials have demonstrated no benefit from synthetic, natural or recombinant surfactant use in adults with ALI.
INHALED NITRIC OXIDE
Despite providing selective vasodilatation and improving ventilation perfusion mismatch, trials have only showed short lived improvement in oxygenation and no change in mortality with nitric oxide use. At present it plays no role in standard ALI treatment and should be reserved for rescue therapy in patients difficult to oxygenate.27
STEROIDS
Despite the potential for steroids to benefit ALI patients due to anti-inflammatory properties, clinical trials demonstrate no improved mortality when given early or late in disease progression and given concerns regarding their role in development of neuromuscular disorders associated with critical illness, a recent large randomised controlled trial argued against steroid use in ALI.28
INTRAVENOUS SALBUTAMOL
Beta 2 agonists were shown to be experimentally beneficial in ALI due to increasing fluid clearance from alveolar space, anti-inflammatory properties and bronchodilation.29 The BALTI trial published in 2006, investigated the effects of intravenous salbutamol in patients with ARDS. It showed decreased lung water at day 7, lowered Murray lung injury scores and lower end expiratory plateau pressures but an increase in incidence of supraventricular tachycardias and therefore further investigation is needed before it can be recommended as treatment for ALI.30 The BALTI-2 trial is currently underway in the UK, to further assess possible benefits and complications.
Other new and promising treatments which are currently being evaluated in trials are activated protein C and granulocyte-macrophage colony-stimulating factor (GM-CSF).
MORTALITY
Mortality rates of patients with ALI and ARDS are similar, with both being around 35-40%.³ Controversy exists regarding whether mortality rates in ALI are decreasing,31 or have stayed static.32 Nonetheless death in patients with ALI is rarely from unsupportable hypoxaemic respiratory failure but from complications of the underlying predisposing conditions or multiple organ failure.33
There is some evidence related to racial and gender differences in mortality (worse in African Americans and males)34 and that thin patients have increased mortality and obese patients have somewhat lower mortality than normal weight individuals35 but the main independent risk factors for increased mortality are shown in Table 5.
Table 5 Independent risk factors for increased mortality in ALI as identified in multicentre epidemiological cohorts
·Old age
·Worse physiological severity of illness
·Shock, on admission to hospital
·Shorter stay in the ICU after ALI onset
·Longer hospital stay before ALI onset
·Increased opacity on chest radiography
·Immunosupression
OUTCOMES
Long term problems are related to neuromuscular, neurocognitive and psychological dysfunction rather than pulmonary dysfunction. (Table 6) There is poor understanding of the mechanisms which cause these sequelae and therefore prevention of these outcomes and planning rehabilitation can be difficult.
Table 6 Long Term Outcomes in ARDS survivors and caregivers
Neuromuscular dysfunction
·critical illness polyneuropathy
·critical illness myopathy
·entrapment neuropathy
Neurocognitive dysfunction involving
·memory
·executive function
·attention
·concentration
Psychological dysfunction
·Post traumatic stress disorder
·Depression
·Anxiety
Other
·Pulmonary dysfunction
·Tracheostomy site complications
·Striae
·Frozen joints
Caregiver and financial burden
A recent study into patients who survived ALI showed they require support during discharge from ICU to other hospital settings and again once in the community regarding guidance on home care, secondary prevention and support groups.36
CONCLUSION
The syndrome which encompasses ALI and ARDS is common and under-recognised, with many clinicians encountering it outside the ICU setting. Despite advances in identification and management, morbidity and mortality is still high. Care should focus on supportive treatment and managing the underlying cause, whilst specifically aiming for low volume ventilation and conservative fluid balance. Ongoing research is still needed to hone the diagnostic criteria, define genetic risk factors and develop new treatment strategies to improve outcome. The new challenge for clinicians is how to address the long term outcomes of survivors and their relatives which will be an increasingly important problem in the future.²⁶
Initial reports of Obesity Hypoventilation Syndrome (OHS) date back as early as 18891, but it was not until 1955 that Auchincloss2 and colleagues described a case of obesity and hypersomnolence paired with alveolar hypoventilation. Burwell3 coined the term Pickwickian syndrome describing the constellation of morbid obesity, plethora, oedema and hypersomnolence. Hypercapnia, hypoxaemia and polycythemia were described on laboratory testing. Obstructive Sleep Apnea (OSA) had not been described at that time and came to be recognized for the first time in the mid 1970s. With attention shifting to upper airway obstruction, hypercapnia began to get lesser emphasis and confusion began to emerge in describing OSA and OHS. The term ‘Pickwickian’ began to be used for OSA-related hypersomnolence in the obese patient regardless of the presence of hypercapnia. This confusion was finally settled by the American Academy of Sleep Medicine (AASM) in its published guidelines in 1999.4 The AASM statement identified that awake hypercapnia may be due to a predominant upper airway obstruction (OSA) or predominant hypoventilation (Sleep Hypoventilation Syndrome) easily distinguished by nocturnal polysomnography (PSG) and response to treatment. Both disorders are invariably associated with obesity and share a common clinical presentation profile.
Salient features of OHS consist of obesity as defined by a BMI > 30kg/m2, sleep disordered breathing, and chronic daytime alveolar hypoventilation (PaCO2 ≥ 45 mmHg and PaO2 < 70 mmHg). 4 Sleep disordered breathing, as characterized by polysomnography in OHS, reveals OSA (Apnea-hypopnea index [AHI]>5) in up to 90% of patients and sleep hypoventilation (AHI<5) in up to 10%.5 Daytime hypercapnia and hypoxaemia are the hallmark signs of OHS and distinguish obesity hypoventilation from OSA. Severe obstructive or restrictive lung disease, chest wall deformities and hypoventilation from severe hypothyroidism, and neuromuscular disease need to be excluded before a diagnosis of OHS is established. As obesity is becoming more prevalent in western society, this disorder has gained more recognition in recent years. However, patients with this syndrome may still go undetected and untreated. No population-based prevalence studies of OHS exist till date but, at present, can be estimated from the relatively well known prevalence of OHS among patients with OSA. Recent meta-analysis with the largest cohort of patients (n=4250) reported a 19% prevalence of OHS among the OSA population, confirming an overall prevalence of about 3 per 1000.6
Whilst transient rectifiable nocturnal hypercapnia is common in patients with OSA, awake hypercapnia in OHS appears to be a final expression of multiple factors. There has been a debate about BMI and AHI not being the most important independent predictors of hypercapnia in obese patients with OSA. More definitive evidence for the role of OSA, however, is suggested by resolution of hypercapnia in the majority of patients with hypercapnic OSA or OHS with treatment, with either PAP or tracheostomy, without any significant changes in body weight or respiratory system mechanics. Yet some recent studies have shown that nocturnal hypoxaemia and diurnal hypercapnia, persist in about 50% of such individuals even after complete resolution of OSA with CPAP or tracheostomy. This raises questions such as how good is AHI as a measure of severity of OSA?
It is intuitive to argue that obesity may exert its effect through mass loading of CO2 due to (increased production via) higher basal metabolic rate or reduced functional residual capacity on lung function. But why do only some severely obese patients with OSA go onto develop OHS? Is the pathophysiology driven by the severity of BMI? Whilst weight loss, particularly surgically-induced, clearly shows resolution of both OSA and hypercapnia7, the role of BMI as an independent factor for hypercapnia has been challenged by the fact that only a small fraction of severely obese patients do in fact develop chronic diurnal hypercapnia. More importantly, not only can PaCO2 be normalized in a majority of patients without weight loss and with positive airway pressure therapy (PAP), but awake hypercapnia can develop even at lower BMIs among the Asian population. Some investigators have tried to explain the incremental role of BMI as follows. In situations where AHI is not a presumed independent predictor of nocturnal hypercapnia, potential pathophysiologic contributors can include pre-event (apnea or hypopnea) amplitude in relation to the post-event amplitude.8 Such inciting events for nocturnal hypercapnia may then be perpetuated in the daytime by factors such as AHI, functional vital capacity (FVC), FVC/FEV1, or BMI as shown in the largest pooled data to date.6 It has been shown that, for a given apnea/interapnea duration ratio, a greater degree of obesity is associated with higher values of PaCO2.9 However the same group of investigators, in another study, did not find any of these factors to be related to the post-event ventilatory response.8
Looking further at the breath by breath cycle, the post-event ventilatory response in chronic hypercapnia may relate to eventual adaptation of chemoreceptors perhaps in consequence to elevated serum bicarbonate known to blunt the ventilatory drive.10 Or it may relate to whole body CO2 storage capacity which is known to exceed the capacity for storing O2.11 With definite evolution in our understanding of hypercapnia among obese patients, these questions continue to dominate. Some of the more pressing ones include: are the predictors of daytime hypercapnia different from those of nocturnal hypercapnia in obese patients with OSA? An understanding of these facts can help us with the more important understanding of the associated morbidity and mortality from OHS and its correct management. In addition, what is the true effect of untreated OHS on mortality independent of the co-morbidities related to obesity and OSA? Can morbidities like cor pulmonale and pulmonary hypertension be reversed with treatment of OHS? How do we treat patients with OHS who fail CPAP/ BiPAP short of tracheostomy?




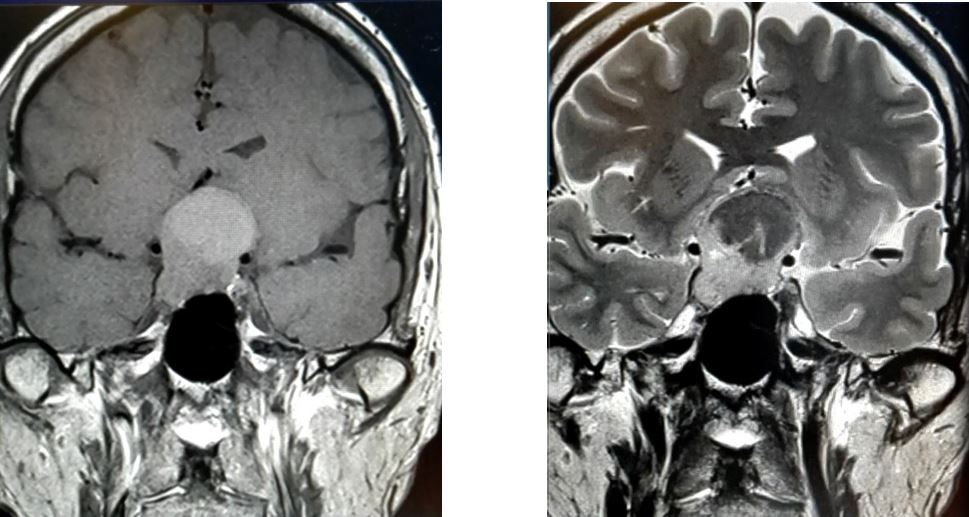
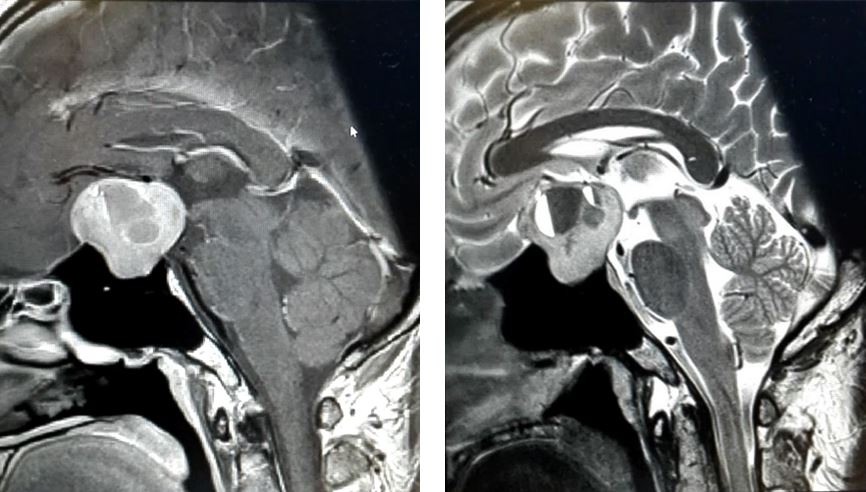
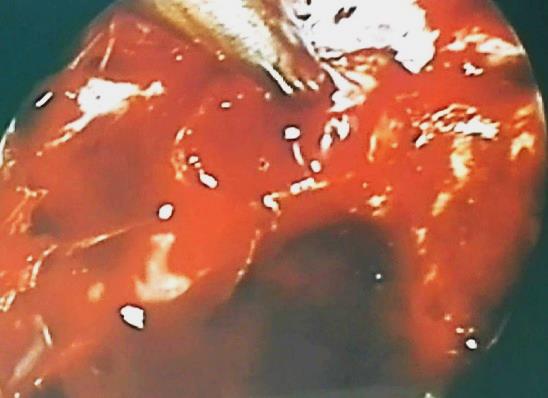
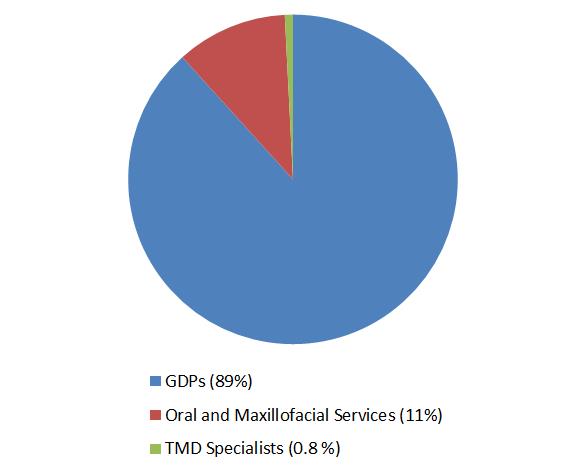
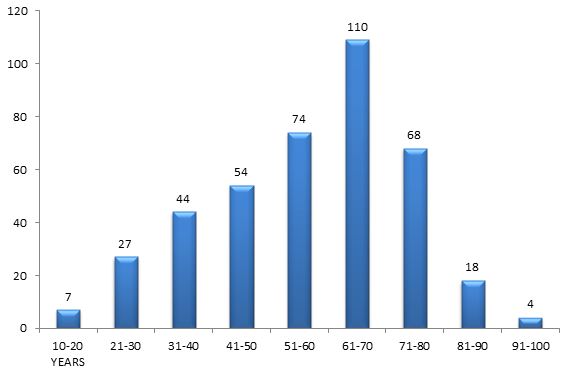
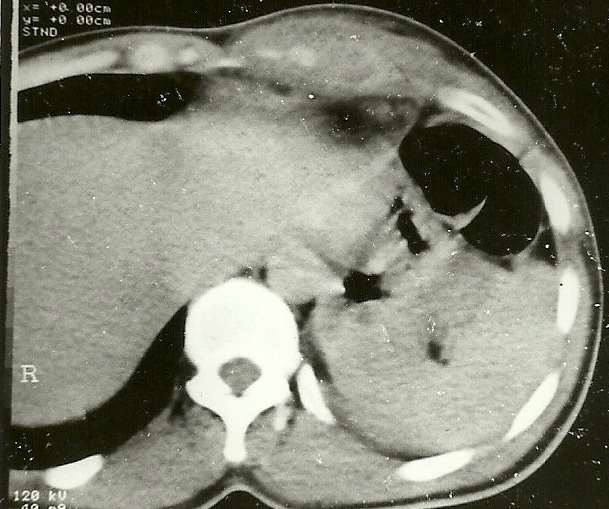
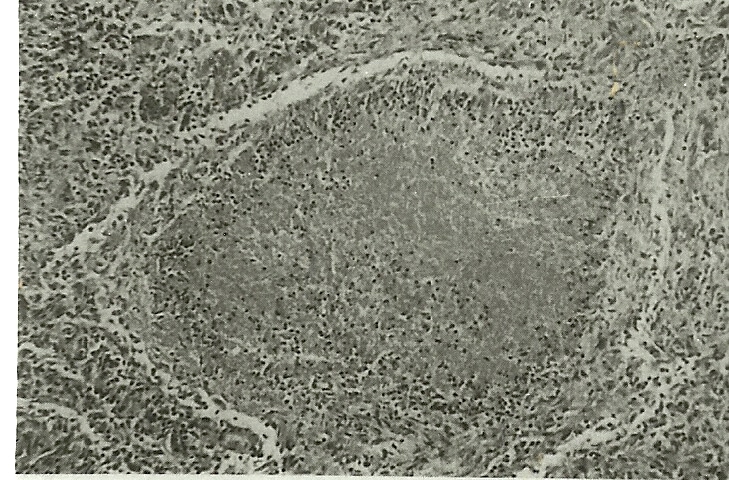
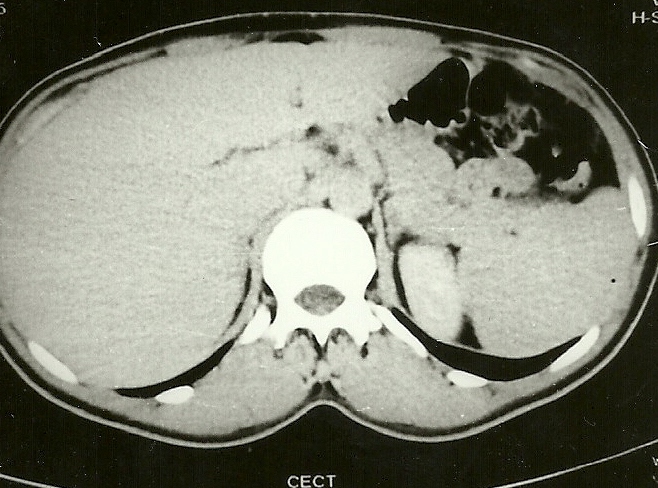
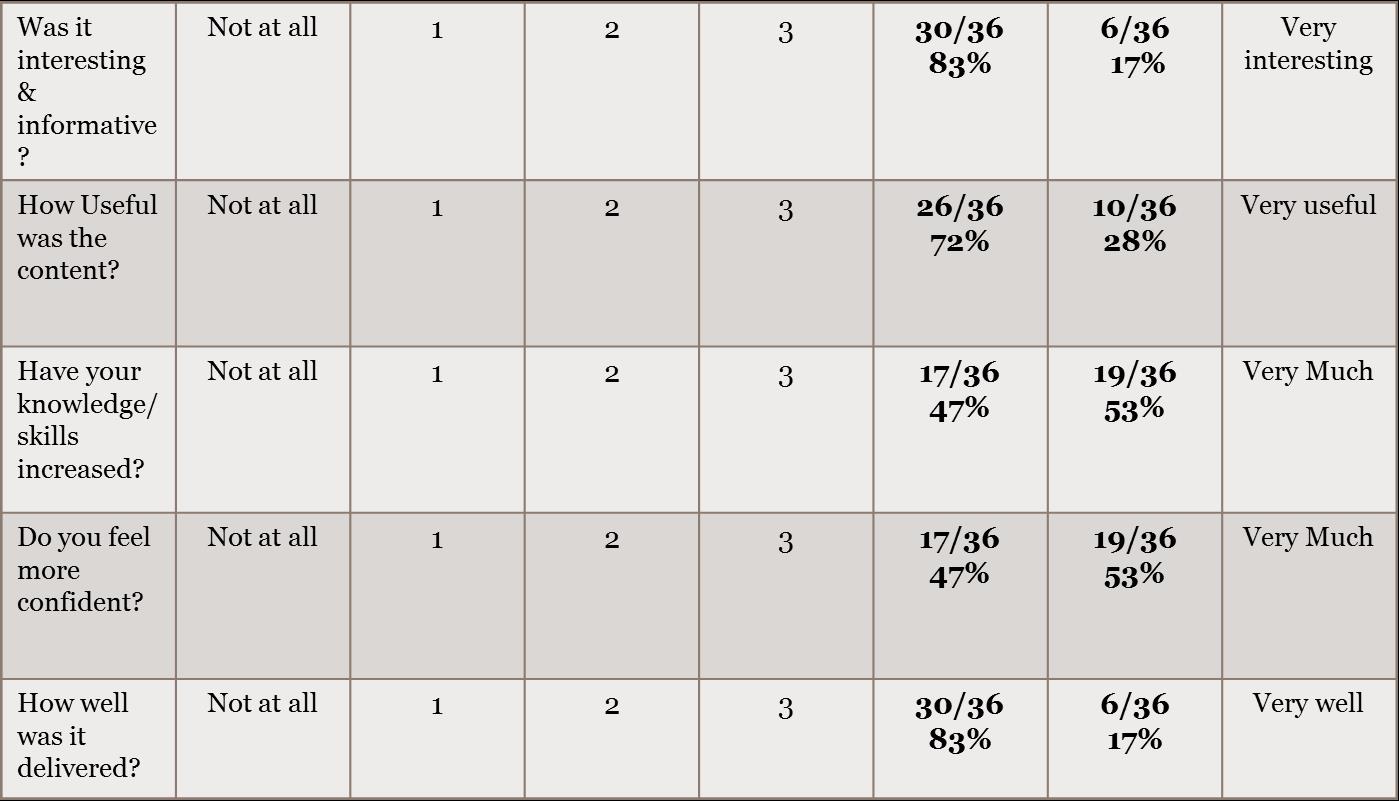

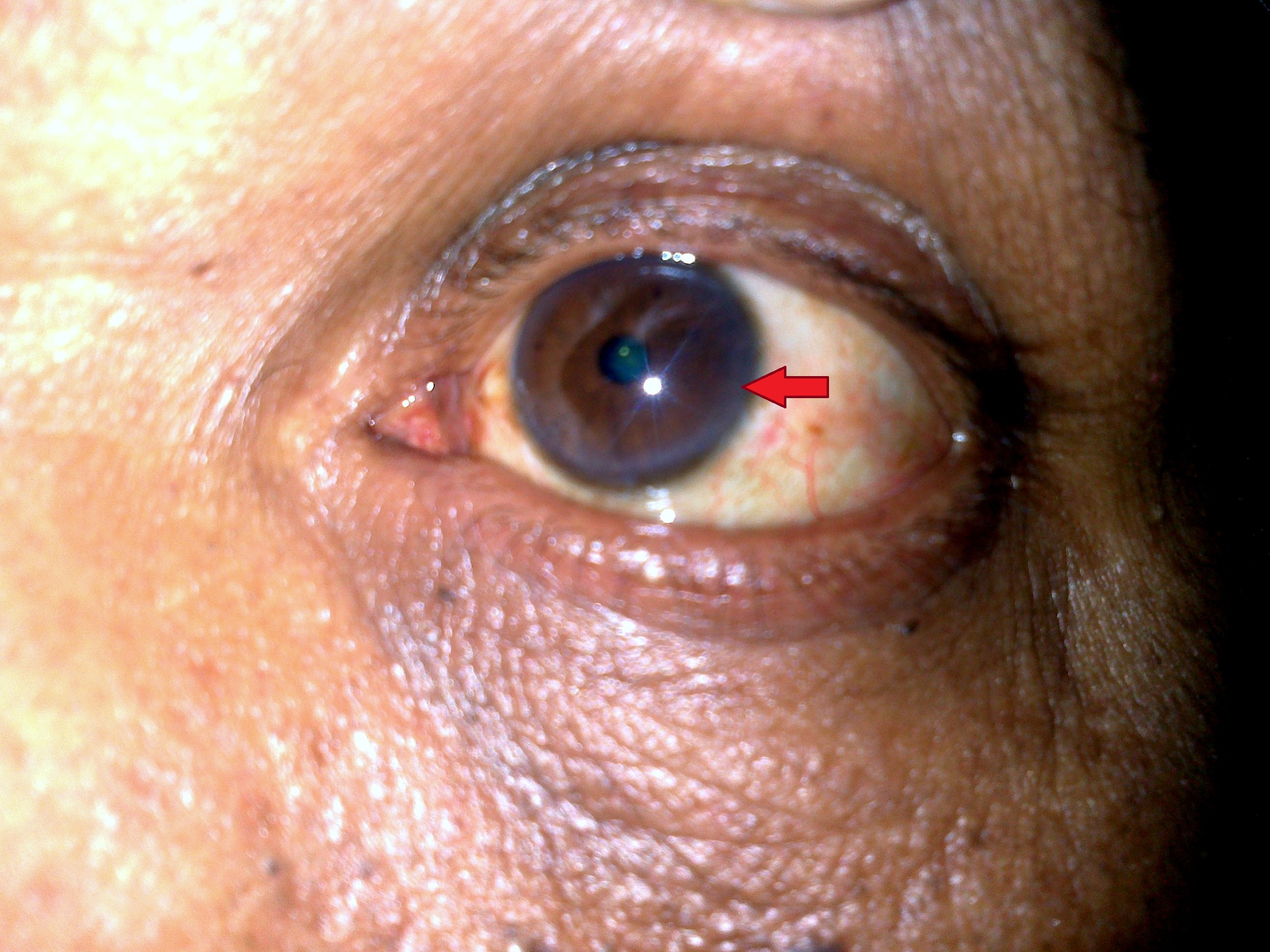

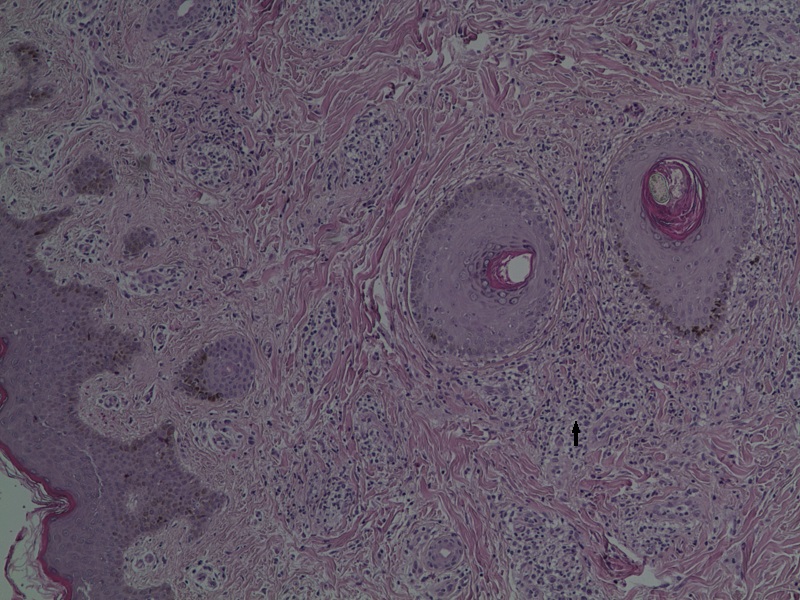
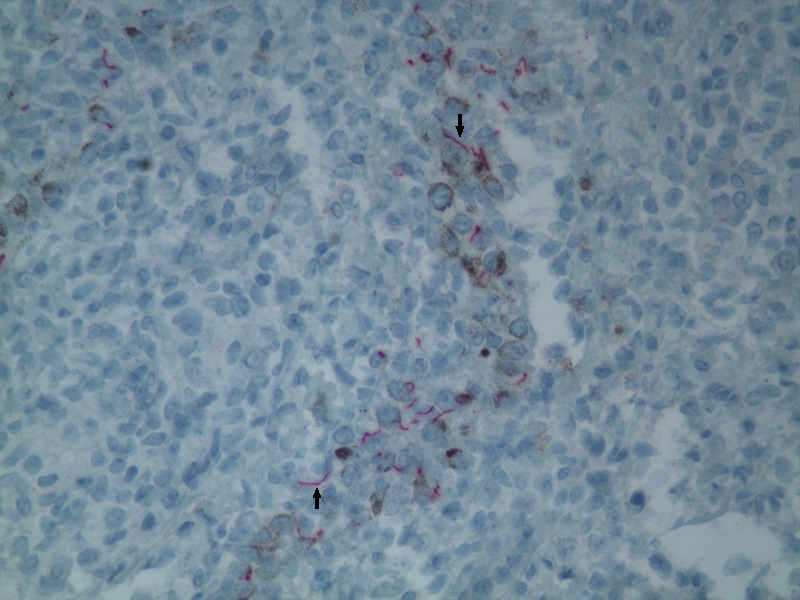



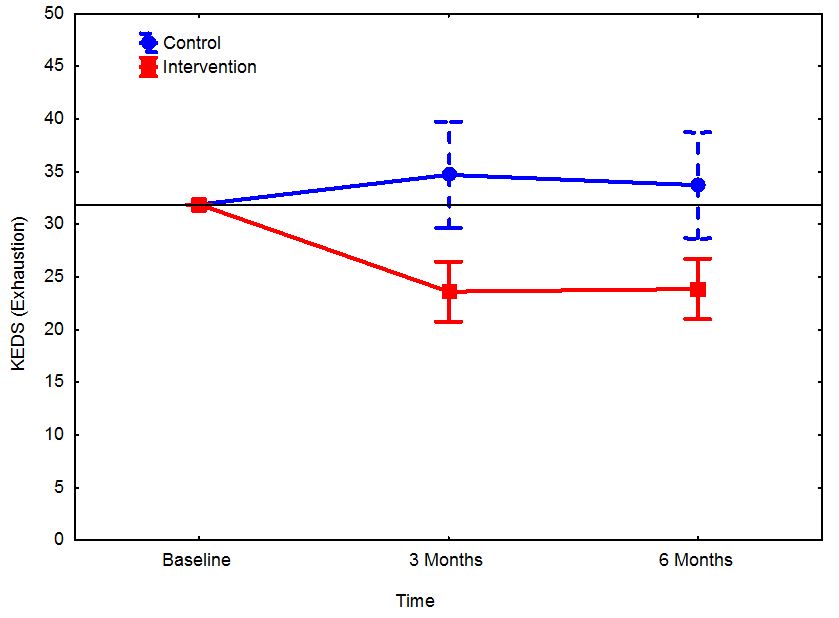
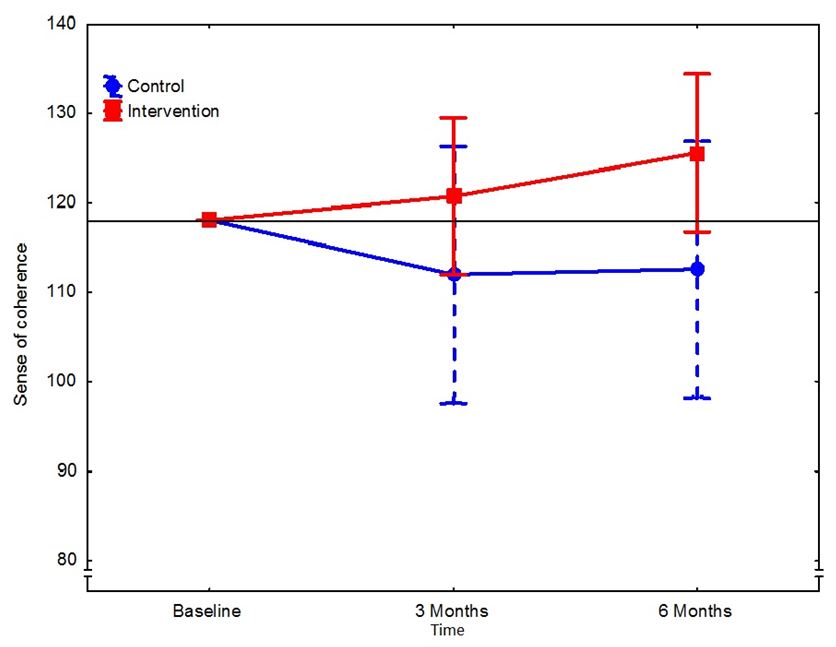
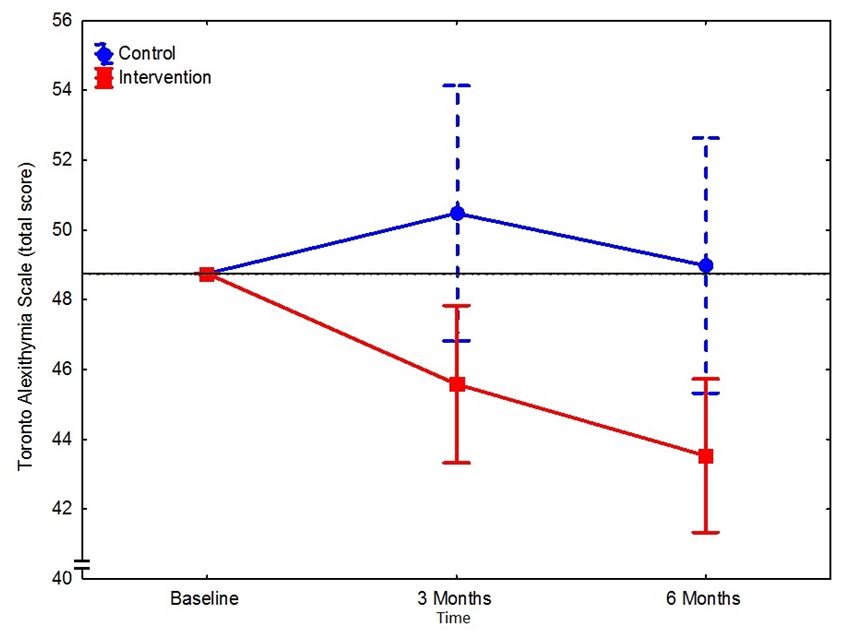
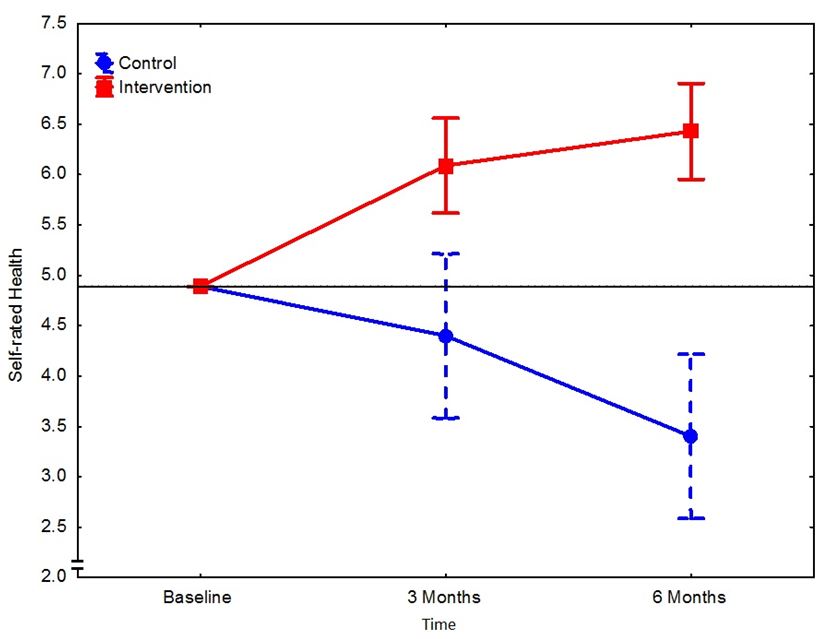
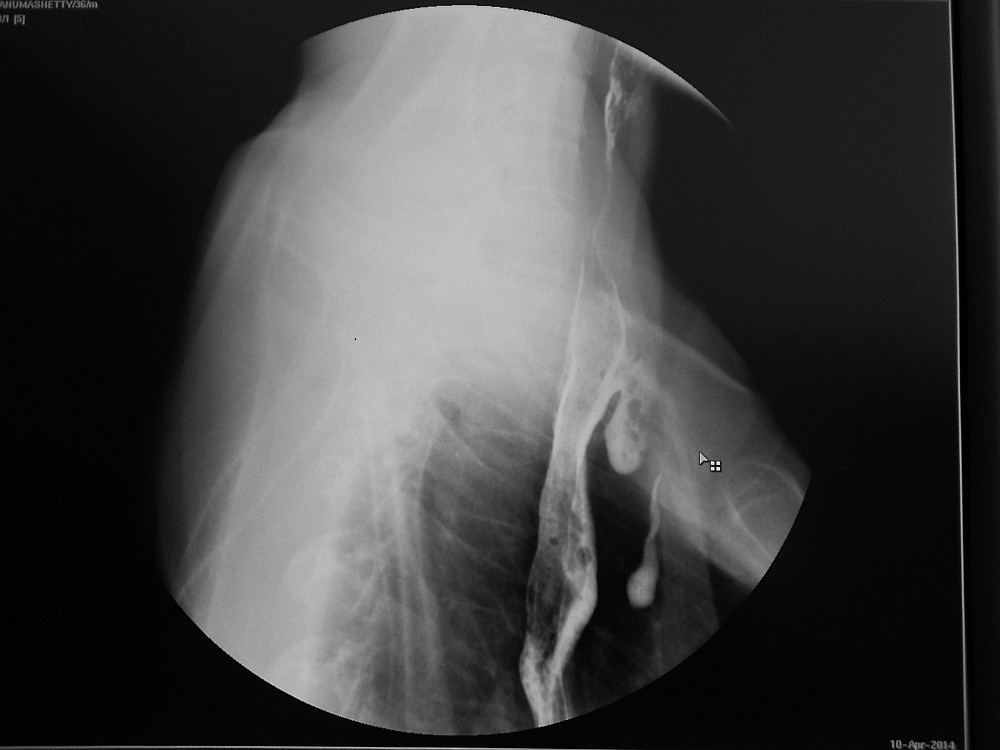
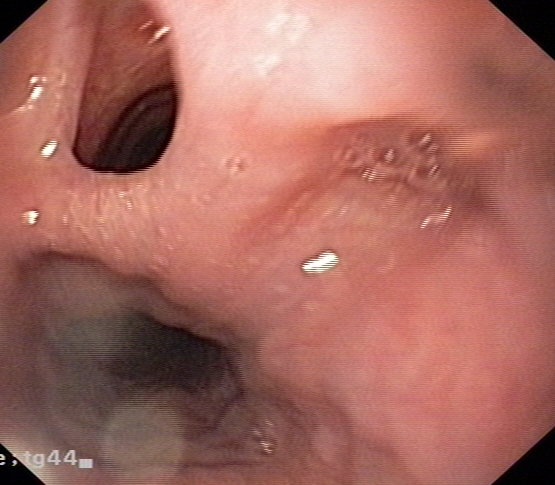




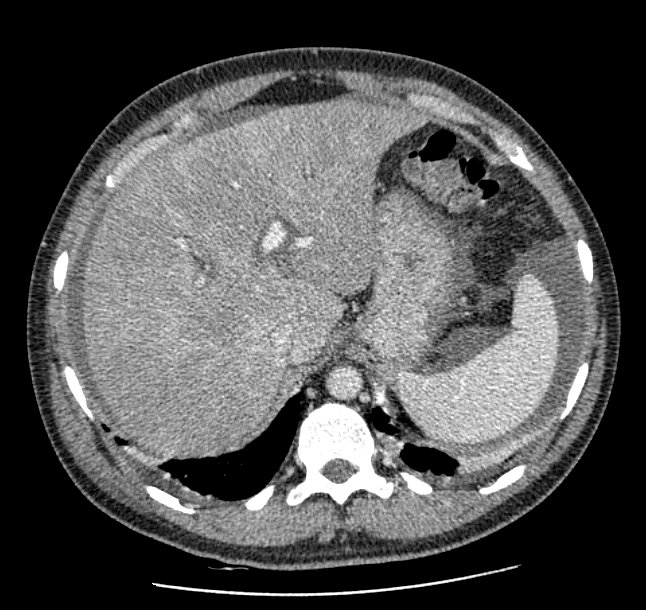
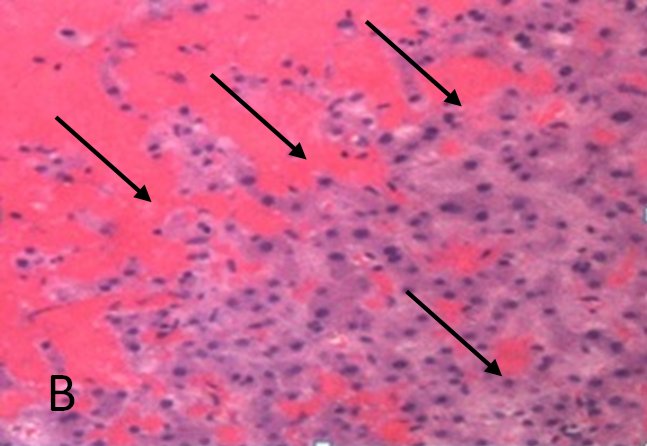
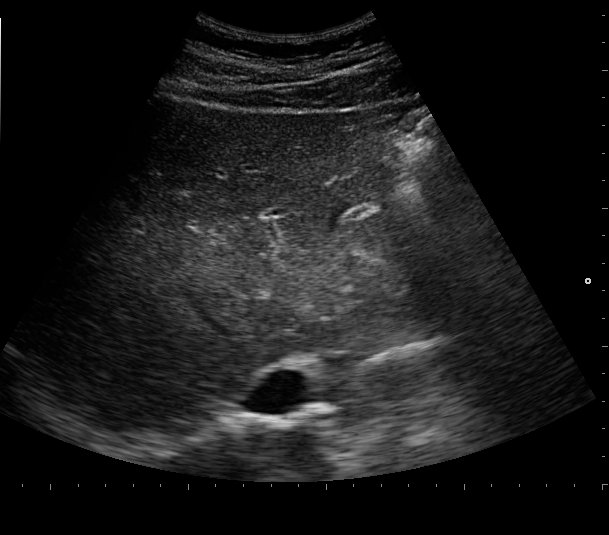
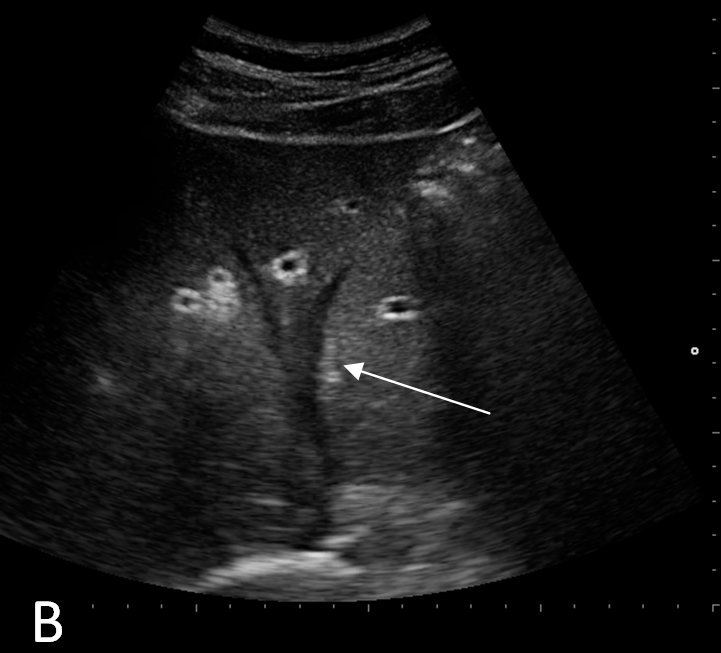



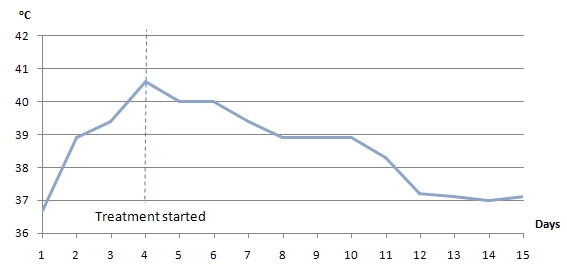
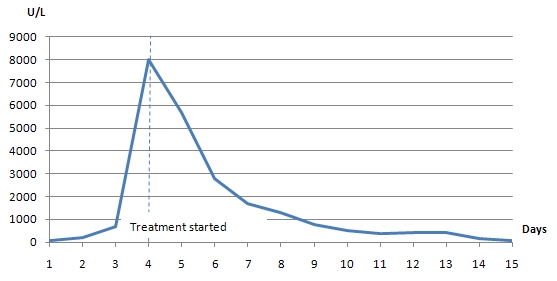

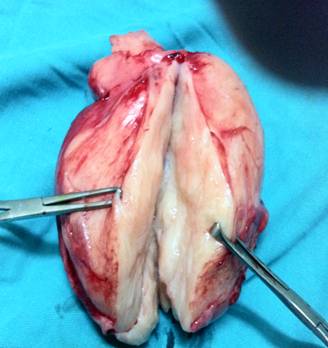
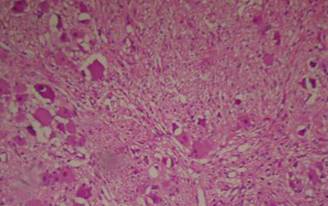
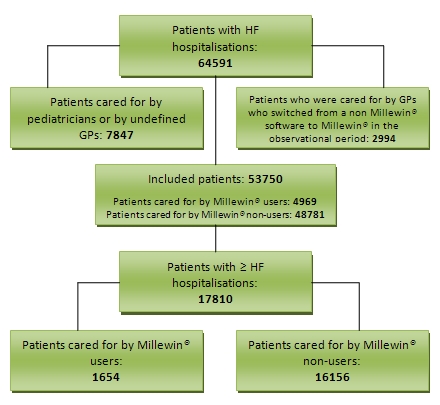

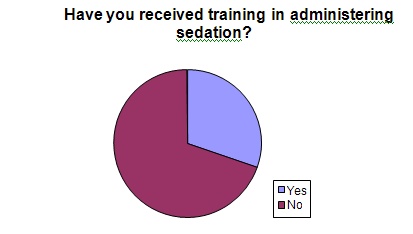
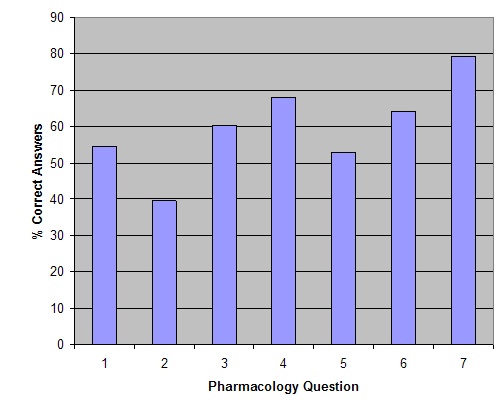


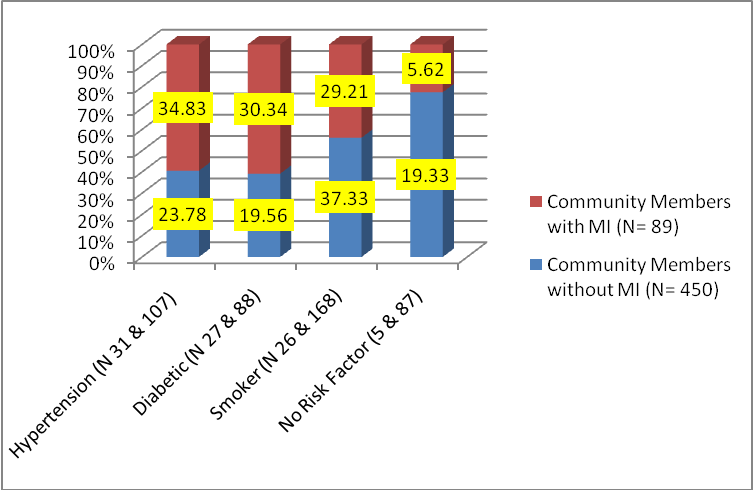
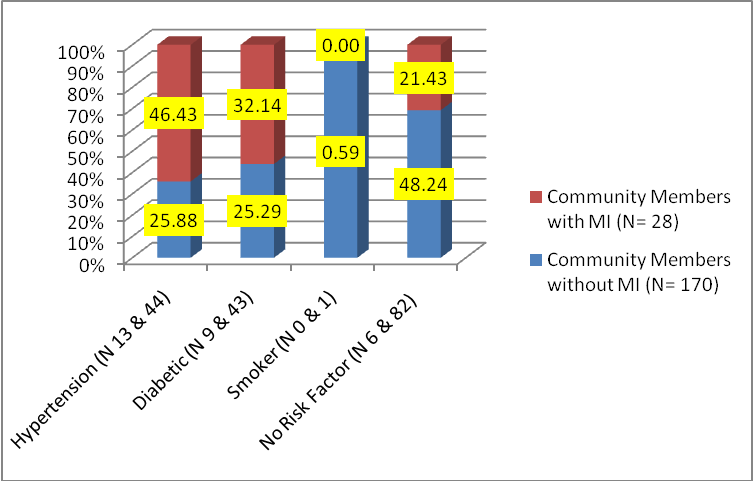 (Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI.
(Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI. 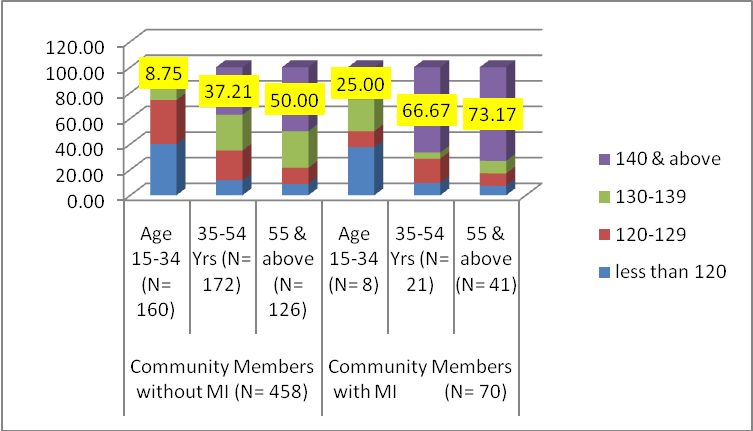 (Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years.
(Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years. 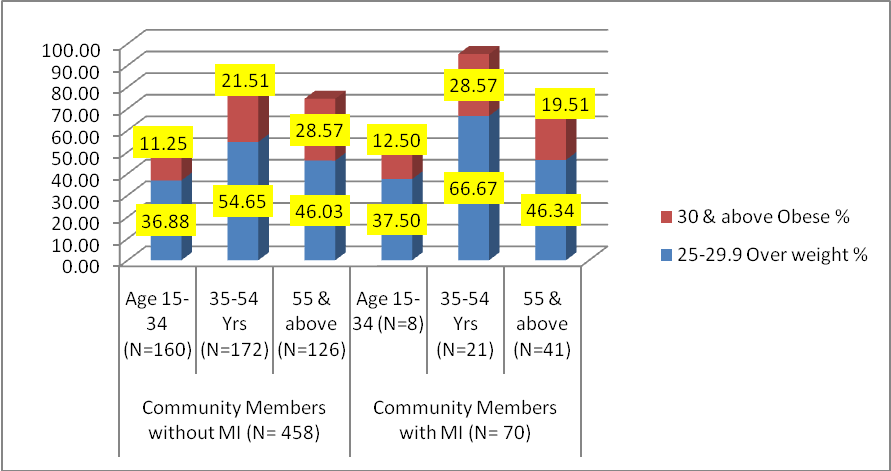


BJMP June 2019 Volume 12 Issue 2
Editorial
Review Articles
Audits
Case Reports/Series
Clinical Practice
Education and Training