World COVID-19 cases exceed 20 million as of today and the number of deaths surpass 733103. Behind these statistics is a great deal of pain and suffering. It is now increasingly getting recognized that COVID-19 is not just a respiratory disease at all. The face of COVID-19 is changing from a pulmonary disease to an inflammatory disease which particularly affects the blood vessels, the coronary vessels, the kidneys, the liver, brain and elsewhere. Its duration is also much longer with long term impact than initially speculated. Sufferers report a huge spectrum of problems beyond the three NHS-approved symptoms (persistent cough, fever and loss of taste or smell). These include fatigue, breathlessness, muscle aches, joint pain, 'brain fog,' memory loss, lack of concentration, and depression.
More morbidity is recognised in cases of infections among the aged populations and patients with suppressed immunity. The high incidence of complications among ethnic minority apparently points toward environmental factors of immunity rather than genetic factors. Underactive immune responses in cooler temperature and diminished synthesis of vit D and the genetic factors linked with these anomalies might explain only part of the higher incidence of COVID-19 among Black, Asian, and Minority Ethnic (BAME) communities.
Research on the first British patients to contract COVID-19 has shown that BAME people are more prone to critical impacts and care compared to white people. This research, conducted by the Intensive Care National Audit and Research Centre, observed that of nearly 2,000 COVID-19 patients, 35% were non-white, though people of BAME heritage only comprise 13% of the UK’s population.1 The study included data drawn from 286 critical care units across the UK and collected until 3 April 2020. According to another study from the UCL Institute for Global Health, Bangladeshi, Pakistani, Indian, Black African and Black Caribbean ethnic groups all had a substantially increased risk of death in comparison to white British and white Irish groups. Cook et al. pinpointed that of 119 NHS staff who died from COVID-19, 64 were from ethnic minority backgrounds.2 They also noted fewer deaths among critical care staff, highlighting PPE’s usefulness.
The UK BAME population’s mortality rate for the 2009 influenza A (H1N1) epidemic was nearly twice that of the white population.3 The Pakistani and Bangladeshi ethnic groups are now 1.8 times more likely to have a COVID-19-related morbidity than white males of a similar age, when other sociodemographic and health characteristics were compared.4Studies have also specified that Black men are 4.2 and Black women 4.3 times more likely to die from a COVID-19-related death than white people.5 Doherty et al. suggested that socioeconomic disadvantages and other circumstances only partially explicate this discrepancy, and that there are missing gaps that have not yet been expounded.6
There is some confusion regarding the cause of this higher incidence of morbidity and mortality among the BAME community, due to media propaganda failing to assess this relation’s intricacies. Higher morbidity and mortality have been observed among first-generation migrants to the UK, but not necessarily among the second generation, who were born and raised in the UK. Five months is a short period to develop any form of genetic immunity or susceptibility to a new viral infection. Each person’s genetic code differs only by 1% of 25,000 genes. The gene cluster largely responsible for our health is called the human leukocyte antigen (HLA), also known as the major histocompatibility complex (MHC). It also takes much longer for any sort of adaptation or mutation to occur. Suppressed general immunity due to various factors appears to be the main reason for the higher COVID-19 incidence among the BAME population. The following discussion examines the possible factors responsible for this anomaly.
a. Immunity and Temperature
Some data has suggested that immune cells are more active in higher temperatures, as supported by the fact that fevers are a bodily mechanism activated by the immune system to defend against pathogens. It has been established that if the body temperature is increased by 1°C, immunity instantly increases 5–6 times. Likewise, if the body temperature is reduced by 1°C, immunity decreases 5–6 times. This observation has some value in explaining the higher incidence of COVID-19 infection and mortality among BAME groups who were born and raised in warmer areas, then migrated to colder regions.
Temperature-dependent immune responses are linked to genetics. One probable explanation is that BAME individuals’ immune cells are genetically wired to function better in hot weather and are unable to optimally function in cold weather. Such a genetically determined immunological build-up means that their immune cells are slow to react to viral invaders. BAME individuals’ immune cells are well-adapted to warm weather but not so to cold weather, in comparison to white individuals who were born and raised in colder climates and adapted to lower temperatures. BAME individuals’ immune cells may even become underactive in cold weather. Though COVID-19 thrives equally well in hot and cold weather, the BAME population has immunity shortcomings in surviving colder months; this insight might prompt them to take special precautions in future cold seasons.
Low temperatures have been recognized as immunosuppressive. It has been observed that even coldblooded animals migrate to warmer places when they become ill. An increase in body temperature has long been a defence mechanism against infection and inflammation. The generation and differentiation of the lymphocytes CD8+ cytotoxic T-cells are enhanced by hyperthermia. Elevated body temperature changes T-cells’ membranes, which may help mediate micro-environmental temperature’s effects on cell function. Sub-thermoneutral laboratory housing temperature was shown to induce immunosuppression in mice experiments: when the mice were housed at a thermoneutral ambient temperature, striking reductions in tumour formation, growth rate and metastasis were observed.7
Mice experiments with antigens demonstrated that mice with antigen-induced raised temperatures showed a greater number of the CD8 T-cells capable of destroying infected cells.8,9 Parallels were observed in teleost fish.10 Higher temperatures also seem to interfere with microbe replication. This is particularly noticeable when a host has a high fever and their immune system temporarily enhances as their temperature rises. Hong Kong’s persistent cold weather was attributed to the rapid spread of SARS in 2003. BAME communities whose immune mechanisms are genetically evolved for survival in higher temperatures are compromised in Western countries’ lower temperatures. The cold weather puts additional stress on their immune cells, which give in to viral invaders.
This argument is further supported by the spread of the flu. During flu season, immune cells become less efficient and flu viruses, unaffected by low temperatures, are in an advantageous position to defeat these cells. Such a hypothesis explains the higher incidence of flu in the winter and challenges the misconception that the flu virus is killed by hot weather and thrives in cold weather. The 1918 Spanish flu that broke out in the United States in the winter seemed to ease off during the summer, but returned with a deadlier strain in the autumn, and a third wave followed the next year. The problem then seems to be in humans, as viruses are unaffected by seasonal temperature variations.
b. Diminished Vitamin D Synthesis
Other mitigating factors can explain the higher COVID-19 incidence among BAME people. Nearly all immune cells have vitamin D receptors that connect to vitamin D networks in the immune system. Vitamin D helps regulate both the innate and adaptive immune systems, and is critical for balancing immune function. Vitamin D has been demonstrated to reduce the production of pro-inflammatory cytokines associated with lung damage caused by acute viral respiratory infections, such as influenza and COVID-19.11 BAME communities are prone to vitamin D deficiency because higher melanin levels in their skin cause lower vitamin D absorption. Consequently, prolonged exposure to sunlight is required to accrue the equivalent vitamin D quantity produced in the white population. This is further exacerbated in colder countries like the UK, which see less sunlight, meaning BAME individuals spend more time indoors without much opportunity to absorb vitamin D. So, there may be a connection between lower vitamin D levels and more frequent COVID-19 cases in BAME communities, though there is no firm data defending this link.
Virtually all immune cells have vitamin D receptors, indicating vitamin D interacts with the immune system. Vitamin D is required to regulate both the innate and adaptive immune systems and its deficiency is associated with immune dysregulation. Many of the ways this vitamin affects the immune system are directly relevant to the body’s ability to defend against viruses. For example, vitamin D triggers the production of cathelicidin and other defensins, which are natural antivirals capable of preventing viruses from replicating and entering cells. Vitamin D also increases the number of CD8+ T-cells, which play a critical role in clearing acute viral infections in the lungs. Further, vitamin D suppresses pro-inflammatory cytokines and may also alleviate the cytokine storms occurring in the most severe COVID-19 cases. This vitamin plays an essential role as well in glucose homeostasis, insulin sensitivity and the regulation of adipokines, such as leptin and inflammatory cytokines.12
Evidence from randomized controlled trials suggested that regular vitamin D supplements may help protect against acute respiratory infections. Admittedly, the direct evidence of vitamin D’s role against COVID-19 is still scant. One study from the United States and another from Asia found a strong correlation between low vitamin D and severe COVID-19 infection. It is well-recognized that the elderly and people with pre-existing conditionsare more vulnerable to COVID-19. Notably, people with existing medical conditions are also often vitamin D–deficient. Studies assessing ICU patientshave reported these patients’ low vitamin D levels even before COVID-19. It appears logical to hypothesize a link between the high COVID-19 infection rates in UK and US BAME groups and their observed lower vitamin D levels. Moreover, it is not possible to gain a sufficient vitamin D supply through food alone, making exposure to sunlight indispensable.
c. Weakened Immunity
COVID-19’s spread in the UK is disproportionately high compared to its spread in the countries of origin of many BAME communities. BAME people should be mindful of their genetics in a new environment. These demographics also have higher rates of cardiovascular disease, type-2 diabetes and hypertension, conditions that have been linked to severe COVID-19 symptoms and complications. There may also be other genetic links that warrant further exploration.
Current evidence has illustrated that chronic stress can increase infection susceptibility by suppressing the T-helper 1 immune response in favour of the T-helper 2 immune response.40 Stress management, lifestyle changes and career management may reduce infection susceptibility in turn. When people are less mobile, food becomes a distraction and they can overindulge. Obesity is also an adaptation to cold weather, as fat protects against low temperatures. Black and South Asian populations in the UK have 3–5 times the prevalence of type-2 diabetes compared to the white population and are diagnosed 10–12 years sooner on average.13
Human immunity is generally fixed by age 5, as contributed to by bacterial flora, among other factors. Several trillion bacteria exist within our body, with the gut considered this bacterial colony’s front yard. We have 25,000 genes, but up to 3 million bacterial flora genes are the real immune cell trainers.14Bacterial worlds came into existence well before humans evolved. When people migrated to Western countries from tropical regions, their bacteria had to adjust to their host’s new lifestyle, with some even replaced. Others may not have survived at all; consequently, these individuals’ immunity may have weakened.
The high incidence of diabetes and coronary heart disease in the British Asian population has been well-recognized, along with many other risk factors and comorbidities, including obesity, chronic obstructive pulmonary disease, chronic kidney disease, hypertension, and age. These may partly account for this population’s increased COVID-19 mortality15,16, but warrant further exploration. Vitamin D level is also likely to drop with rising BMI and age.17Obesity is strongly associated with vitamin 19-22D deficiency.18 Admittedly, there are weaknesses in these data collections and interpretations, which are theoretical speculations yet to be confirmed, modified or falsified.
There are diverse genetically linked immune responses in a given population, and the spread and survival of complications in a pandemic like this are not well-defined. Research has suggested that people living in close communities, like certain regions of Lombardy, Italy, have a poor genetically linked immune response to COVID-19. Like our fingerprints, immunity genetics contribute to our physical identity, but our immunity is not permanently fixed by genetics. There thus remain many unknowns in immunity research.
It is now increasingly recognized that immune ageing and organismal ageing are intimately inter-related. Aging weakens the immune system and immunity decline further accelerates the aging process. Immune system protects the individuals against viruses and bacteria and it also helps identify and remove cancer cells and toxins. The potential for these elements to cause damage in the body increases as age advances. Critical cells in the immune system decrease in number and become less functional as people get older. COVID-19 affects seriously the aging people of the BAME community as in the case of general population, but they are more disadvantaged in terms of health care access.
d. Social Factors
Alongside these factors, many BAME individuals work in fields that carry a high risk of infection, such as healthcare, transport services and retail. In the UK, 40% of doctors, 20% of nurses and a large number of social care and unskilled migrant workers belong to BAME backgrounds. Another reason why these infections may become more prevalent among ethnic minorities is that BAME community members tend to spend more time indoors clustered together, often in cramped accommodations, which increases the likelihood of person-to-person transmission. A multigenerational family set-up is not helpful either to social distancing in a pandemic, so this lifestyle could contribute to higher infection rates. Some people living in this arrangement may also become stressed and obese due to unhealthy nourishment.
Migrant communities tend to visit and keep in contact with their country of origin, which involve international air travel and thus increased infection risk. Family studies demonstrate that BAME people living in the colder countries develop COVID-19 at a faster rate, but most of their family members living in the tropical climate in the countries of birth are spared from the infection. Such an observation point towards extrinsic factors like lifestyle and weather conditions rather than intrinsic genetic links-nurture than genetics. The second-generation immigrant population are less affected and the mixed-race individuals because of diversity of immune cells appear more resilient to the viral pandemic. There appears to exist an epidemiological trend of transmission concentrations within BAME communities living in colder countries, such a situation runs the risk of racial stigmatisation and discrimination and also risks to social cohesion.
BAME individuals should be cognizant of the additional risks and take preventive and precautionary measures. They should also adapt to balance their immunity. Enough sleep, healthy diet, moderate exercise, abstaining from excess alcohol and smoking and de-stressing are the cornerstones of enhancing immunity. Immunity is not absence of a specific disease or illness; rather, it is a balanced physiological and psychological state, the most sophisticated and elegant system of human physiology. Vaccines are pathogen-specific, and they do not bestow an overall balanced immunity.
Supporting Immunity
To defeat the tiger, one may need to become stronger than the tiger. To do this with COVID-19, we may need to foster our existing immune system, which can be done in many subtle ways. We all must grapple with the unprecedented threat posed by COVID-19, and frontline health workers must be mindful of their own immune systems when advising their patients to do the same. Unreasonable fear of COVID-19 only weakens the immune system, and fear attracts that which is feared. According to many COVID-19 survivors, remaining positive is a crucial factor in combatting this illness. Knowledge about the enemy and our potential resources lessens fears and helps us to plan strategies to defeat the adversary. With a quarter of the world’s population in the grip of COVID-19, it is a highly challenging period to learn to survive and strengthen our body and mind and enhance our immune system, even using the wisdom of unconventional medicines and faith traditions. We will have to battle with this invisible enemy until an effective vaccine is identified. Anything that fosters self-immunity should be encouraged in this time of a global medical emergency.
The two functions of immune system are defending the body’s health and maintaining health.The immune system is depicted as having two components: the innate and adaptive immune responses. The innate system is the more primitive and less specific. It is the body’s first line of defence against foreign substances that may lead to disease. The adaptive system, found only in vertebrates, is a much more specific, delayed response and requires sanction from the innate system to be instigated. Though considered separate, each interacts with the other in critical and complex manner. A basic understanding of both responses facilitates to clarify and further substantiate the significance of immune balance.
There are many myths surrounding immunity enhancement. Enrichment of the immune system is possible so that it becomes vigilant and active in the event of an invasion by pathogens and it may possibly prevent immunity anomalies. It is defending the defenders of the body. Immune system is our protective shield. Metaphorically, immune cells are the guardian angels of the body. Balancing of immunity can be achieved by focussing on ample sleep, healthy diet, moderate exercise, weight monitoring, restricting alcohol, free of smoking and destressing.In the nutshell, it warrants lifestyle changes- one size may not fit all and immune balancing has to be adjusted on an individual basis.
a. Restful Sleep
One healthy habit vital to preventing sickness is getting a full eight hours of sleep each night, which may help regulate immune function.19 Studies reveal that people who are deprived of quality sleep are more likely to get sick after being exposed to a virus. Respiratory infection has been linked to poor sleep.20 One study of over 22,000 people, for example, found that those who slept less than six hours per night or had a sleep disorder were more likely to suffer colds and other respiratory infections.21 Lack of sleep can affect immune system adversely.
During sleep, immune system releases cytokines, some of which even help promote sleep. Certain cytokines need to increase during an infection, or under stress. Sleep deprivation may decrease production of these protective cytokines. In addition, infection-fighting antibodies and cells are reduced during periods when person is deprived of ample sleep. Sleep and the circadian system are strong regulators of immunological processes.22 There is a bidirectional communication between CNS and immune system. This is mediated by shared signals though neurotransmitters, hormones and cytokines and direct innervations of the immune system by the autonomic nervous system. Differentiated immune cells with immediate effect or functions, like cytotoxic NK cells and terminally differentiated CTL, peak during the wake period. 23 These chemicals permit an efficient and fast combat of obtrusive antigens and reparation of tissue damage. The more slowly evolving adaptive immune response is initiated during nocturnal sleep and undifferentiated or less differentiated cells like naïve and central memory T cells peak during the night.
It is during sleep, the immune system heals, repairs, and prepares for the challenges of wakeful periods. During the deep stages of NREM sleep, the body repairs and recuperates, and this deep sleep also reinforces immunological memories of previous pathogens.23 The endocrine milieu during early sleep critically supports (a) the interaction between APC and T cells, as evidenced by an enhanced production of IL-12, (b) a shift of the Th1/Th2 cytokine balance towards Th1 cytokines and (c) an increase in Th cell proliferation and (d) probably also facilitates the migration of naïve T cells to lymph nodes.22 A feeling of lethargy when fighting an infection may be a signal from the body—which produces chemicals that act on the brain—to sleep, so that the body can recover. A single night of poor sleep can lead to a dramatic reduction in NK cells, the first line of defence against viruses and cancer cells, which negatively impacts other immune cells.
b. Nutrition
The size of the inoculum, the virulence of the exposure, the immune response of the host, and the health of the host are the four vulnerability factors of an infection. The former three ingredients are beyond the control of the host and the fourth one is within the control of the host and is very much based on the nutritional status. Food is generally viewed in terms of calories, but nutritionists have started appreciating the noncaloric micronutrients in the food, including those that are neither vitamins nor minerals, but phytochemicals (plant-chemicals) that strengthen and support normal immune function. The recent research discovery that food is not only a calorie supplier, but also adds to disease resistance and longevity benefits, has rekindled an interest in phytochemicals that support defensive and self-reparative functions. Modern diet consists of processed food mixed with additives, colouring agents, and preservatives; there is no room for unrefined vegetables in the dietary pie. Nutritional excellence can be achieved through green vegetations and friuts.
Antioxidants are vitamins, minerals and phytochemicals that support the clearance of free radicals and controlling its production in the body. Free radicals are molecules that contain an unpaired electron which causes them to be highly chemically reactive and these unstable molecules are destructive as they come in contact with structures and other molecules within the cells.24 Antioxidants are the natural enemy of free radicals which creates inflammation leading to dysfunctional immune system and to premature aging. Vitamin C, E, folate, selenium, and alpha and beta-carotene, as well as various other phytochemicals have antioxidant properties. They are available in plentiful amounts in vegetables and fruits and consumption of them enhances the immune functions. The Namboothiri caste of Kerala are famous for their strict vegetarian dietary habits and disease-free life, and longevity. The nutritional status of the host is critical in permitting or prophylaxis against viral and bacterial infections as well as the nutritional deficiencies in the host allow mutation of viruses into more lethal forms. 24 This is evident in the meat-eating food markets where the SARS-Cov-2 initially began to breed and mutate.
Pro-inflammatory foods can sabotage the immune system and should thus be checked in its quantity of consumption. Thirty minutes after they are consumed, carbohydrates may begin suppressing the immune system, and this effect may last for up to five hours. Foods with extreme diuretic properties also have detrimental effects on the immune system, which functions better when well hydrated. Drinking plenty of water facilitates efficient cell operation and allows the body to process food and eliminate waste. Following a diet rich in antioxidants is also essential to supporting the immune system, so eating fruits and vegetables is recommended. Fruits and vegetables are rich in antioxidants that combat free radicals—chemical by-products known to damage DNA and suppress the immune system.25 Choosing healthy fats—such as the omega-3 fatty acids found in oily fish, flaxseed and krill oil—over the saturated fats found in meat and dairy products is generally recommended by health authorities. These oils may help increase the body’s production of compounds involved in regulating immunity.26
Dietary supplements and medicines may be required for people who suffer from micronutrient deficiencies. Vitamin D is linked with a healthy immune system, and a large body of well-established data highlights its antiviral effects; it not only directly interferes with viral replication but also has immunomodulatory and anti-inflammatory effects.27-29 A research study in the U.S. suggests that having low levels of vitamin D doubles the risk of death due to heart attack compared to having higher levels.30 It is therefore recommended that all UK citizens take a vitamin D supplement between October and March to help maintain healthy levels during less sunny months. Such supplements are available in several forms, including capsules, sublingual sprays, and liquid drops, that are usually oil-based, as the vitamin is fat-soluble.
Nutritional excellence is in one’s own individual control. An over-boosted immune system, however, can lead to autoimmune reactions, so it is important to balance supplements and not over-boost. Moreover, vitamin D toxicity can cause hypercalcemia, which may lead to excess calcium deposits in the kidneys, lungs, or heart. A well-balanced diet is crucial in balancing immunity. An ideal immunity diet maintains caloric balance and consists of healthy fats, phytonutrients, fibre, quality carbs and diverse protein sources. Multiple micronutrients, including lutein, lycopene, folate, bioflavonoids, riboflavin, zinc, selenium, and many others have immune modulating functions.31 In general, the Mediterranean diet pattern has been praised as anti-inflammatory and good for fortifying immunity.32 The Mediterranean diet is associated with older age, as well as increased activity and reduced stress
c. Hygiene
Simply keeping the hands clean is one of the best ways to ward off illness, according to the Centres for Disease Control and Prevention (CDC). By washing the hands for 20 seconds using warm water and soap before preparing food or eating, as well as after coughing, sneezing, using the bathroom, or touching public surfaces can prevent the invasion of several pathogens. Hygiene hypothesis in medicine is quite often misinterpreted and misunderstood. It does not suggest that having more infections during childhood would be an overall benefit.
The hygiene hypothesis promulgates the view that early childhood exposure to particular microorganisms such as the gut flora and helminth parasites shields against allergic diseases by contributing to the maturation of the immune system. Lack of exposure is thought to lead to defects in the establishment of immune tolerance. The time period for exposure to microbes commences in utero and probably terminates at school age.
d. In Praise of Microbes and Nature
The preindustrial lifestyle that made available for the daily intake of trillions of friendly microbes is now replaced by a world of sanitisers and wet wipes. Alternative medicine takes into account the friendly bacterial flora inhabiting human body and we ought to be mindful of their role in balancing immunity. Even though humans are controlled by 25000 genes, the genes of the microbes cohabiting with ours are taken into account, it would be more than 3 million. In fact, these genes of the microbes are the immunity trainers and coaches of human immunological genes. Conventional medicine also takes into account the existence of intestinal microbes and their role in health and illness. Approximately, 95 percent of the total number of cells in the human body are constituted by these GI tract microflorae and play a prominent role in the health of our immune system. In fact, these guts bacterial flora is the meeting point of alternative medicine and modern medicine.33
The intestinal microflora serve several useful functions that may include the supplementation of the digestive process, produce vitamins, short-chain fatty acids, protect against the overgrowth of pathogenic bacteria and yeasts, strengthen immune abilities and generate beneficial nutrients that stop weight gain. 24 Pathogenic bacteria, on the other hand, produce toxic substances, become bacterial invaders, cause digestive disturbances, trigger immune system dysfunctions, and even stimulate weight gain.
Modern urban life is at a low level on microbial variety and has poor contact with helpful environmental microbes.34 Asthma and allergies are found to be much less among children brought up in farm and drunk farm milk.35 People living in urban areas are more susceptible to allergies and inflammatory diseases. Children exposed to outdoor microbes have more robust immunity. Obese people with 30% fewer intestinal microbes tend to gain more weight. 36
People should enjoy the smell of green grasses and appreciate the healing powers of mother nature. Ecopsychology, which is the study that explores the connection between the world of nature and the world of humans, is a new branch of psychology. Studies have revealed that spending some time outdoors, in the nature, can actually reduce stress, as well as improve our overall emotions and feelings of happiness and wellbeing, raise the levels of energy, and enhance immunity. It is healthier to do exercises outdoors than indoors. A lifestyle admirably adapted to mother nature alone can guarantee robust mental and physical health.
e. Antibiotic Overuse
Research findings suggest that antibiotic abuse can result in damage to the immune system, and memory problems caused by a lack of growth in new brain cells. Overusing antibiotics, which happens when antibiotics are overprescribed or prescribed inappropriately, has many negative outcomes. In the first place there is no relief of symptoms or rationale in prescribing antibiotics for a viral rather than bacterial infection. It results in disruption of the normal, healthy flora in the digestive system, which can take nearly two years to correct and lead to other infections. Antimicrobial resistance is another established complication of overprescribing antibiotics. Antibacterial adverse effects are attributed to 25% of all drug reactions in hospital patients.37
Even a single course of antibiotics has a detrimental effect on the gut flora and can result in harmful alterations in the composition and diversity of gut flora disrupting ecosystem. 38 Antibiotic exposure in children have long standing impact on the health and is linked with increased risk of immune system disorders. Antibiotic induced autoimmunity has been reported. Low levels of antibiotic administration lead to fatter mice by up to 40%.39
f. Physical Activity
To enjoy a good night sleep, one has to be pleasantly tired. Being active reduces stress and causes individuals to feel more energetic and alert, thereby helping the body prepare for better sleep. The main principle underlying exercise is keeping the body moving. Stress hormones are slowly released during exercise, which has a favourable effect on the immune system.40 Physical activity can also facilitate clearing of bacteria from the pulmonary system and can alter levels of white blood cells and antibodies. It is believed that during exercise, leucocytes and antibodies move faster in the circulatory system, allowing them to detect internal threats and diseases sooner; however, there is not yet proof that infections are prevented by these changes. Bacterial growth may also be blocked by the increased body temperature during and after exercise, which may help the body fight infection in a way similar to a fever.
Keeping muscles active releases high levels of interleukin 7 into the blood, which helps to stop the thymus from shrinking. This would help production of new T cells and balance our immunity. Maintaining a healthy basal metabolic rate is crucial. Walking is the simplest but highly effective exercise. Regular walks strengthen our immune system. It improves the mood and energizes the body. Walking in green spaces could give a big mood boost Walking has no set rules and can be carried out in the busiest cities and in the sprawling countryside. Too much of exercise can become a stressor for the body and turn out to be counterproductive.
g. Immunity and Obesity
Obesity is the result of a disruption of energy balance that leads to weight gain and metabolic disturbances that cause tissue stress and dysfunction. 41Metabolic syndrome is a cluster of metabolic disorders and is rampant in the 21st century. It results in conditions combining diabetes, hypertension, and obesity. Metabolic syndrome is also linked to several types of cancers and it has strong inflammatory underpinnings linked to dysregulated immunity.
Obesity and immunity are inversely related. It has been observed, for example, that the same amount of vaccine generates different immune responses from obese and lean people. Obesity has been identified as a modifiable risk factor of severe COVID-19, but weight loss also brings other health benefits. Having a healthy body weight is important in maintaining strong immunity because the presence of too many fat cells suppresses immunity. Obesity can depress the immune system by reducing the body’s ability to produce leucocytes, generate antibodies and locate infection sites. Persistently enlarged fat cells place a body in a constant state of inflammation, keeping the immune system permanently on the go. Maintaining the right amount of body fat is crucial to immunity and health.
h. Alcohol Impairs Immune Cells
Much remains unclear about the impact of alcohol consumption to immune system. Alcohol abuse result in diminished liver and pancreas functioning which can lead to immune system problems. Chronic alcohol abuse and pneumonia are linked. Alcohol has an immunosuppressant effect, and binge drinking is particularly detrimental. One study reports that after four shots of vodka within a 20-minute period, blood samples reveal initial ramping of the immune system followed by sluggish immune responses a few hours later. Acute and chronic alcohol use impedes cellular immune function, placing binge drinkers at greater risk for bacterial and viral infections. A multi-layered interaction between alcohol and immunity exists, and alcohol abuse has negative effects on both innate and adaptive immunity.42
Drinking alcohol immoderately can cause damage to the immune system in two ways. First, it reduces the availability of nutrients, thus depriving the body of resources that strengthen immunity. Second, it can hinder the ability of white blood cells to destroy microbes. It is well recognised that excessive alcohol consumption suppresses white blood cell replication, inhibits the action of killer white cells on cancer cells and hampers macrophages’ production of tumour necrosis factors. Immune system damage increases in proportion to the quantity of alcohol consumed. While wine promoters assert that one daily glass of red wine may be helpful to maintaining health, any amount of alcohol large enough to cause intoxication is also large enough to suppress immunity.
There is a perilous myth circulating among the inner quarters of the public that consuming high-strength alcohol can kill the COVID-19 virus and it has stemmed from fear and helplessness and is totally unfounded. Consuming any alcohol poses health risks, but consuming high-strength ethyl alcohol (ethanol), particularly if it has been adulterated with methanol, can result in severe health consequences, including death. Alcohol consumption is associated with a range of communicable and noncommunicable diseases and mental health disorders, which can make a person more vulnerable to COVID-19. In particular, alcohol compromises the body’s immune system as described above and increases the risk of harmful health effects. Though there is still limited data on the link between alcohol and COVID-19, past evidence shows alcohol consumption can worsen the outcomes from other respiratory illnesses by damaging the lungs and gut and impairing the cells responsible for immune function.
i. Avoiding Substance Use
Marijuana, cocaine, heroin, and other opiates are widely used illegal drugs. Drug abuse compromises immunity, so it is imperative to stay clear of illicit drugs during a pandemic. Numerous clinical reports indicate the association between infectious diseases and the use of illegal drugs. These drugs alter not only neurophysiological and pathophysiological responses but also immunity responses. Thus, it is vital to determine the mechanisms through which drugs compromise immune responses both independently and in concert with immunosuppressive viruses.43
Snorting cocaine harms mucous membranes in the nasopharynx and pulmonary areas. This increases the chance of upper respiratory infections.44Marijuana affects several kinds of cells in the body, which can ultimately harm the immune system. Smoking marijuana reduces the body’s ability to resist infections from viruses, bacteria, fungi, and protozoa. Because of the suppressed ability of the immune system, it may also reduce the ability of an immune system to be able to destroy cancer cells. Drugs of abuse include heroin, morphine, fentanyl, opium, and prescription painkillers. While all narcotics have some effect on the immune system, injecting drugs into the veins increases the risk of viral infections like HIV and hepatitis B or C (due to sharing needles) and bacterial or fungal infections. This is especially dangerous in people whose immune systems are already compromised. Crushing and snorting narcotic drugs can also increase the risk of upper respiratory infections due to damage to the mucous membranes in the nasopharyngeal regions. Morphine and related opioids have been found to directly impact white blood cells, which can reduce the ability of the immune system to react to diseases.45
j. Pulmonary Health
As with marijuana and crack cocaine, smoking cigarettes can lead to upper respiratory problems and a lowered immune system response to infections in the pulmonary system.46 Studies indicate that smoking increases the risk of more severe lung disease in cases of SARS-CoV-2 infection. It has been argued that exposure to cigarette smoke increased the number of infected and apoptotic cells in the airway and that SARS-CoV-2 prevented the usual repair response to airway injury.47 SARS-CoV-2, the causative agent of the COVID-19, infects cells by binding to the angiotensin-converting enzyme 2 (ACE2) receptor present on host cells. ACE2 is highly expressed in ciliated cells of the upper airways. Smoking is linked with both a negative progression and adverse outcomes of COVID-19.48
Smokers touch their lips frequently, which may accidentally pass the virus to their mouths, and they tend to have existing respiratory conditions consequent to their smoking habit. These factors make them more vulnerable to viral respiratory infections and more prone to COVID-19-related complications. Indeed, smoking has been linked to a plethora of respiratory diseases and poor disease prognosis.49 Smokers are more vulnerable to infectious diseases because smoking harms the immune system, adversely affecting how it responds to infections.50 During the previous MERS-CoV epidemic, for example, smokers were found to have high mortality rates.51 One retrospective analysis of 78 patients in China found that smoking was correlated with greater COVID-19 severity and poorer prognosis. Though analytical studies conflict,52 smoking continues to be linked with higher risk.53
k. Balancing Bodily Temperature
It has been recognised that an increase in body temperature by 1°C than normal would result in an instantaneous increase of immunity by 5 to 6 times. On the contrary, as soon as the body temperature drops, the activity of white blood cells will be retarded, resulting in a decrease in immunity. Low temperature is well recognised as immunosuppressive. It is an accepted fact that fever is the body’s defence mechanism that activates the immune system in response to inflammation. The immune system functions optimally at higher comfortable temperatures and becomes underactive in cold environments. This is why seasonal infectious diseases like influenza are more prevalent during lower temperatures. Warm temperature restricts viral replication through type I IFN-dependent and -independent mechanisms in vitro.54 In addition, both humidity and temperature affect the frequency of influenza virus transmission among guinea pigs.55 One way to warm the body is to be metabolically active while keeping a relatively high room temperature and/or wearing warm clothes. The significance of thermal balancing to maintain healthy immunity has been discussed in preceding paragraphs.
l. Destressing
Good relationships protect mental health and wellbeing. People who are more socially connected are happier, physically healthier and have longevity. One should put more time aside to connect with friends and family, learn to live in the present and switch out of work mode whenever possible. It is important to invest time on and value relationships and make them a priority, listen to others, and speak openly about feelings. People should be good listeners and concentrate on the needs of other people. Happiness is the reflection of what one does for others. People should make an effort to be surrounded by positive individuals and allow themselves to be listened and supported. The key to destressing and happiness is being honest and respecting others.
Severe anxiety suppresses the immune system and the coronavirus may thus literally feed on fear. Relaxing and focussing on the present, however, can improve mental health and counteract negative feelings. Various forms of meditation and progressive muscle relaxation techniques, for example, can help one unwind from the assault of daily stressors, and such post-work relaxation may enhance the immune system. Incorporating relaxing practices like meditation, yoga or deep breathing into a daily routine has been found to be helpful. Psychological health and immunity are causally related. The current pandemic is forcing us all to adjust to new and strange ways of life, which can adversely affect mental wellbeing.
While short-term exposure to stressors can accelerate immune defence, prolonged stress may wear down the immune system, increasing vulnerability to illness. 56 In this way, chronic stress can be a killer. Immuno-psychiatry is a fledgling sub-speciality which deals with the immunological components of psychosis and depression.57 The autoimmune aetiology of schizophrenia is gaining ground 58-60 and the neurotoxic effects of cytokine storm due to COVID-19 have recently caught high attention.
Extra-physiological Immunity?
The chemical effects of allopathic medicines are a scientific reality, but their therapeutic effects are also partially due to placebo effect. Placebos are aimed at the symptomatic relief of illnesses. Disease and illness have different connotations; disease is understood scientifically in terms of pathophysiology and illness is understood phenomenologically, as a lived experience. 61 It is increasingly being recognized that what we call the ‘placebo effect’ may involve changes in brain chemistry induced by quantum bioenergy fields. That implies the placebo effect may be a quantum reality that is created by the mobilisation of quantum bioenergy fields.62 The placebo effect is believed to be brought about when the subjective mind produces medicinal agents and accelerates the healing process. It is estimated that up to 40 per cent of the effects of medicinal drugs may be a placebo effect. The placebo effect often seems to be associated with measurable changes in brain chemistry and there have been observed quantifiable changes in neurotransmitters, hormones, and immune regulators. 63 Placebos also relate to the disposition to heal, no matter what treatment is offered, if those being treated believe the treatment is helpful. 64 Regarding the effects of drugs, expectations appear to have a significant influence. The very existence of placebos offers an indirect proof for the existence of extrasomatic energy system and we need to incorporate their effect in the immune balancing. A quantum conceptual model of placebo is essential to understand certain hidden channels of medical sciences. The placebo component of immunity is highly significant and needs further evaluation.
Immunity is not a single entity; it is a system, and for a system to function well, it requires balance and harmony. Not everything about the immune system is known to science, and according to integrated medicine, immunity may not be confined to physiology alone, but may have non-physiological aspects as well. Numerical age and physiological age are two different things. This is particularly so if extra-physiological energy system is brought into the equation of immunity. It is true that the existence of extra-physiological systems is not scientifically well established, but they are strong hypothetical possibilities.
Studies of quantum bioenergy fields should be an integral part of the science of human physiology and homeostasis should be redefined as the state of steady internal physical and chemical conditions maintained by different regulators, including extrasomatic energy fields.65 Humans are multidimensional or psycho-spiritual entities with several layers of energy bodies with increasing subtilty.66 Complementary medicines work on the assumption that humans are associated with a subtle energy system, in addition to their material body. Even though such extrasomatic energy systems are not recognised in the modern medical sciences, there are energy fields that cannot be explained by the classic Maxwell–Schrodinger equation.
The material body and energy bodies are in a complementary relationship: if the material body is the container, vital energy is the content.67 Beverly Rubik postulated that biological systems may be regarded as complex, non-linear, dynamic, self-organising systems of energy and field phenomena68,69 Many researchers have attempted to bring the existence of extrasomatic energy fields into the arena of mainstream sciences.70--73 If such quantum bioenergy fields really exist, they may play a major role in maintaining homeostasis in the human physiology, and it would be of great clinical interest to evaluate their role in immune system functionality, as long as they do not overrun the scientifically accepted views. To bring the concept of extra-physiological immunity into immunology, we may also have to accept the possibility of ‘nano immune cells’ and a ‘nano-level immune mechanism’.
Conclusion
The high incidence of complications among ethnic minority points toward the thermal conditioning and the role of immunogeneticsgenetics. Underactive immune responses in cooler temperature and diminished synthesis of vit D and the genetic factors linked with these anomalies might explain part of the higher incidence of COVID-19 among BAME. It is the physically and psychologically resilient people of a community who normally migrate to overseas countries. If migrants are to develop mental health problems, it would manifest within 6 months of migration, but physical health problems come about any time of their stay abroad as the weakening of immunity is a slow process. COVID-19 has a direct impact on co-existing disease processes worsening them because of the added immunity impairment. There are still missing gaps in the pervasive occurrence of this viral affliction among the BAME people. They should be mindful of the vulnerability factors and special precautionary measures should be adapted to prevent the infection.
COVID-19 appears to be a test of self-immunity. To combat COVID-19, efficient tests, novel treatments, and vaccines are the three means. An effective and safe vaccine would drastically change the pandemic situation for good. Vaccination and developing novel form of medication would take some time to become available. In such circumstances, one way of protecting from COVID-19 is by balancing one’s own immune mechanisms. It is a good thing that there is ample promotion of preventive measures of the contagion, there should be more awareness of improving personal immunity. More research works are warranted in immunology including extra-physiological immunity. Strengthening immunity is achievable for everybody if sufficient attention is paid. A safe and effective vaccine with long term immunological properties would drastically change the pandemic situation for good. Thus far, the research findings of the pandemic are inconsistent, and many dimensions of this pandemic warrant further clarification. COVID-19 will have a serious impact on virology and the neurotoxic effects of cytokine storm may be a stimulus for the growth of immuno-psychiatry.
Science is good enough to study the physical and visible, but it has obvious limitations when it comes to the unphysical and non-physical. Unphysical is undetectable only because they cannot be identified with the present-day instrumentation but can become detectable when our technology advances and their presence should not be stubbornly denied. The well-established placebo effects may point towards the existence of quantum bioenergy fields. Existence of extrasomatic energy system indirectly support the concept of extra-physiological immunity. Placebo effects are not psychological artefacts, but quantum manifestations. If extra-physiological immunity exists, it may be guarding and supervising the physiological immune system.
Processed sugar has a high glycaemic index (GI) as it is easily digested and absorbed triggering a prominent insulin response, which if repeated over time leads to insulin resistance and type two diabetes1, 2. The appealing nature of high calorific sugary food combined with their low satiating nature means they also tend to be eaten in excess which contributes to obesity and metabolic syndrome2, 3. Obesity and diabetes raises the long-term risk of poor gut health and chronic inflammation increasing the risk of chronic fatigue, low mood and degenerative disease conditions such as cancer, cardiovascular disease, dementia and stroke2, 3.
Despite these obvious risks, a recent survey of NHS health care professionals reported that over half are overweight and over a quarter are living with obesity4. Both obesity and high sugar content-foods are associated with musculoskeletal disorders, lower mood, unhappiness, fatigue and depression which significantly contribute to sickness absence from work4, 5, 6, 7.
Despite these risks, consumption growth continues to escalate especially in low and middle income countries. Since 2000 consumption has grown from 130 to 180 million tonnes in 20208, and its production is contributing to poor health as well as greenhouse gas emission and deforestation9, 10.
In an attempt to reduce sugar intake, NHS England introduced a voluntary reduction scheme in July 2017, recommending that NHS Trusts and retailers on NHS premises reduce the proportion of monthly sugar-sweetened beverages sales. They reported in March 2018, a reduction as a proportion of total drinks sales from 15.6% to 8.7%11. However, to date, there is no information as to whether this has had any impact on consumption of sugar, wellbeing or weight reduction. In our cancer unit there is a constant availability of sweet snacks, predominantly gifted by patients, and during busy clinics these often replace balanced meals. Some argue that this display of sugary foods, together with the high proportion of overweight staff undermines the NHS’ ability to give patients ‘credible and effective’ behavioural lifestyle advice.
The hypothesis for this intervention was that a removal of sugary foodstuffs from the field of vision on nurses’ stations and replacing with fruit, nuts and seeds enables healthy snacking, resulting in weight loss and increased mood.
Methodology
This pilot intervention used quantitative methods to observe the feasibility of delivery and outcome of a real-world intervention. This project was registered with and approved by Bedford Hospital NHS Trust Research and Development Department, but classed as a practical service evaluation, hence no Ethics approval or written consent was required.
Participants: Fifty eight members of staff at the Primrose unit, Bedford Hospital were invited to participate for this 3 month nutritional intervention; 44 (75%) volunteered. The cohort consisted of 36 nurses, 2 consultants, 2 secretaries and 4 administration staff. There were 41 females and 3 males, aged 28-72 years (average age 45 years). A further 100 consecutive patients attending for treatments were asked for their views on the intervention.
Measures and outcomes: The primary endpoints were Body Mass Index (BMI) (Kg/m2) and happiness measured with the previously validated Subjective Happiness Score (SHS)12. As a secondary end point, patients attending the Oncology unit during the intervention period were asked anonymously for their opinion and likely influence on their eating habits.
Procedure: At baseline the Primrose Unit research department recorded staff demographics, BMI and SHS questionnaire scores. From the date of entry of the first participant (June 2019) to completion of the last participant (September 2019), all sugary foodstuffs were removed and replaced with bowls of mixed whole and dried fruit, seeds and mixed nuts. Non-participating staff were asked to voluntarily keep sugary items out of general sight. At baseline, 3 months and 5 months, participants were weighed by one of the research team and completed a SHS questionnaire.
In the final month of the intervention, 100 consecutive patients attending for treatments at the unit were asked their opinion of this intervention, specifically if they felt that removing sugary items from public display was a welcome gesture and whether seeing staff making efforts to reduce sugar intake would encourage them to do the same.
Statistical methods and analysis
The completed dataset was compiled in an excel spreadsheet then transferred for independent statistical analysis. The pre- and post-intervention weight differences datasets were analysed by the T-test as were the difference in happiness scores. The differences in participants’ opinion were analysed by the chi squared test. There were no missing data and in view of the relatively small numbers in the cohort, sub-group analysis was not planned or performed. The study advisory committee predetermined that a change in weight of 1 kg was meaningful13.
Results
Average weight: At baseline the average was 72.12 kg, and 71.23 kg.at 3 months; an average loss of 0.89 kg (T-test p= 0.02). The average weight at 5 months was 71.09 kg; an average loss of 1.03 kg from baseline (T-test p= 0.01). Twenty participants (46%) lost >1kg in weight (average 3.01 kg) as opposed to 7 (16%) participants who gained >1kg (average 2.23 kg) T-test p< 0.03.
Happiness score: Average happiness score increased from 21.65 to 23.44 (+6.6%), T-test p< 0.04). Amongst those who lost >1kg weight, average happiness score increased from 21.54 to 23.75 (+9.3%), T-test p<0.03. In those who gained >1 kg weight, average happiness score decreased from 22.28 to 21.43 (-3.8% T-test p< 0.08. There was a 13.1% difference in the happiness score in those losing >1kg compared to those gaining >1kg in weight (p< 0.001).
Patient opinion: 94 (94%) of patients indicated that this initiative gave a good impression; 6 (6%) were not sure or felt it did not give a good impression (Chi2p<0.001). Ninety seven (97%) indicated that the initiative would encourage them to reduce sugar in their own diet versus 3 (13%) who were not sure or felt that it would not change their behaviour (Chi2 p<0.001).
Discussion
This small pilot evaluation has a number of methodological weaknesses but what it lacked in statistical strength it gained in novelty and potential importance. This was the first nutritional intervention involving hospital staff within a routine working practice. It addresses a health issue which affects hundreds of thousands of health workers every year, and demonstrated that a practical behavioural change initiative was welcomed by the majority of staff (75%), with no drop-outs or objections from non-participating staff. This implied a larger national study would be feasible.
These data clearly demonstrated a statistically significant reduction in meaningful weight similar to the best designed weight loss programmes14. A fundamental rule of behavioural change is not to dictate to people, but to encourage them to want to make the decision to change for themselves. This simple intervention did not stop staff eating what they wanted as there was no restriction to their overall food choices. The big difference was that, within their field of vision, there were healthier fruit and nuts instead of high-calorie, sugar-laden foods, which are usually readily available.
This intervention was overwhelmingly supported by patients. Surveys have repeatedly reported that patients look to health workers for guidance, and this study confirmed that this manoeuvre made patients think about their own eating habits. Although a further trial would have to establish whether this initiative objectively reduce processed sugar intake amongst patients, a reduction in intake would confer considerable benefits as several large cohort studies have linked high sugar intake with a higher risk of cancer, greater complications of treatments and worse outcomes, for several reasons3.
Sugary foods increase the risk of weight gain, already more common after cancer; increases levels of oestrogen in post-menopausal women; and increases insulin like growth factor (IGF) and other hormones such as leptin, all of which in laboratory experiments increase proliferation and markers of aggressiveness and spread of cancer cells 2, 15, 16, 17. Cohort studies have also reported that those who ate more than 10% of their daily calories as sugar had higher total LDL cholesterol levels further adding to the cardiac risks of herceptin and anthracycline chemotherapy drugs. Independent from obesity, high sugar intake directly increases the risk of type 2 diabetes (T2D) by overloading the insulin pathways1. Individuals with T2D have higher serum insulin levels (hyperinsulinemia) which triggers proliferation in cancer models18, is linked to higher oxidative stress and low-grade chronic inflammation, causing epigenetic genetic damage and ongoing malignant transformation19. These laboratory findings are supported by several cohort studies which have linked diabetes with a higher risk of cancer and a higher risk of relapse post-treatment20.
Patients on chemotherapy should be particularly discouraged from eating sweets and cakes as they are more prone to dental caries which contributes to the risk of osteonecrosis following consequent bisphosphonate therapy. Dental caries may also be an increased factor for bowel cancer itself as DNA codes from bacteria, commonly found in caries (Fusobacterium), have been detected in the genes of bowel cancer but not in normal guts21.
Patients receiving the new generation of targeted therapies should be particularly vigilant of their sugar intake. PD-1 inhibitors recruit the body's immunity to recognise and target cancer cells, the influence of diet and lifestyle is becoming even more important. Studies have demonstrated that better gut health is linked to significantly better response rates. Processed sugar is the preferred fuel for pro-inflammatory firmicutes bacteria whilst the healthy bacteroidetes utilise glycans from the breakdown of polyphenols, which explains why there is a reverse correlation between sugar intake and gut health22. However, whole fruit intake is associated with better gut and general health as it provides polyphenol which feed healthy bacteria3, 23. Despite having between 9-14% fructose, the fibre and pulp makes fruit satiating and slows gastric emptying, thus reducing the GI3. Additionally, the polyphenols in fruit, vegetables, nuts, legumes, herbs and spices slow transportation of sugar across the gut wall by inhibition of sodium-dependent glucose transporter 1. They enhance insulin-dependent glucose uptake, activate 5' adenosine monophosphate-activated protein kinase, which explain why their regular consumption is associated with a lower risk of T2D3, 23, 24. They also improve reduced gut and systemic inflammation; enhance anti-oxidant enzyme production so reduce intracellular oxidative stress; and reduce the risk of cancer and other chronic diseases including those associated with diabetes3, 25, 26.
The evaluation was not robust enough to measure whether this resulted in less sickness absence, but this endpoint should be included in a larger design. It also did not include data for those staff who did not actively participate, but who benefited from removal of sugary foods from their work areas; the evaluation committee did not receive any complaints or objections to their removal.
Government initiatives such as a sugar tax and public information campaigns may help but as individuals within the NHS, we have an opportunity to influence our staff, the patients whom we serve and the wider public. The evaluation reported in this paper is a small start, but demonstrates that a multicentre study would be feasible and if the results are confirmed, it could initiate a national cultural change attitude towards sugar in the NHS.
Across the UK there has been a reduction in the number of children and young people (CYP) presenting acutely to hospital during the COVID-19 pandemic. This was highlighted in a recent survey of consultant paediatricians in the UK and Ireland1. It showed that not only were fewer children being brought to emergency departments, but there were also delays in acute presentation of critical illness (such as sepsis and diabetic ketoacidosis) and reductions in referrals for cancer treatment and child protection assessments1.
The reasons for the reduced attendance are thought to be related to the initial government messaging of Stay Home, Protect the NHS, Save Lives2. However, as it became clear that not only parents, but other potential patients were not presenting even if warranted, the government adjusted the messaging to make it clear that the NHS was still open for urgent care that was not just COVID-19 related.
In CYP the cause of delayed presentations were likely to be manifold: parents following the initial governmental message; families concerned that hospitals were unsafe; the initial presumption that COVID-19 in CYP would present in the same manner as in adults potentially leading to primary care and NHS 111 pathways channelling them to domestic isolation. It may be that some delays in hospital presentations may be due to reduced referrals from primary care, and that in turn may be influenced by fewer CYP accessing their local General Practice facility. The ‘Take the Temperature’ survey which assessed the views of 1535 respondents (predominantly aged 16-25 years) found, “85% knew that they shouldn’t go to a doctor if they got the virus”3. However, it is possible that CYP and parents may not be able to make the often challenging differentiation between symptoms of COVID-19 and what may be another illness in need of medical attention.
There has been a significant increase in pressure on many aspects of the health service, including on primary care. Automated telephone messages have been used as a tool by General Practice to direct service users to the correct service or point of care for some time. As such, it is unsurprising that automated messages may be used to try to address some questions about the pandemic prior to speaking to a call handler at a practice. In addition to this, significantly limiting face to face contact with patients during the pandemic in Primary Care has been essential to prevent the potential spread of the virus and closure of services. We aimed to review the initial advice that parents and carers may be receiving from their first point of contact when telephoning their local General Practice and whether this considered CYP specifically.
Methods All General Practices within four Clinical Commissioning Groups (CCGs) in NHS Sheffield CCG, NHS Manchester CCG, NHS Leeds CCG and NHS Birmingham and Solihull CCG were identified using the NHS website. These were chosen as they are large cities, with diverse populations.
Practices were only contacted within their standard opening hours by three of the authors, within a four-day time period (7th July 2020 to 10th July 2020). The data collected is shown in table 1. All practices were telephoned and identified as to whether they had the following (see table 1):
Table 1: Questions asked during data collection
Was there an automated message?
Yes/No
Was COVID-19 was mentioned in the automated message?
Yes/No
Was there was advice to stay away from the practice if COVID-19 symptoms present?
Yes/No
Was there advice to self-isolate with COVID-19 symptoms
Yes/No
Was there any age segmentation or differing advice for children?
Yes/No
If worsening COVID-19 symptoms, was there advice to go to NHS website or telephone NHS 111 service?
Yes/No
What was the length of the automated message (In seconds)?
Percentages, means, standard deviation, and standard error of the mean were calculated. Proportions were compared using Fisher’s Exact test to calculate statistical significance of some data.
Table 2: Reasons for exclusion from analysis
Reason for exclusion from analysis
Number of practices
Private screening clinic
1
Duplication of practice already listed
5
Permanently closed
1
Call failed or no telephone number available
4
Line busy despite repeated attempts
1
Total
12
In total, 549 practices were listed under these four CCGs. 12 practices were excluded (see table 2), leaving 537 practices from which we could obtain results.
Table 3: Analysis of results from 537 GP practices
ALL GPS COMBINED
Automated message
Coronavirus mentioned in automated message
Advice to stay away from practice if coronavirus symptoms
Advice to self-isolate with coronavirus symptoms
Did have age segmentation
Advice if worsening COVID-19 symptoms to go to NHS Website or phone 111
Length of automated message (seconds)
TOTAL
440
290
153
120
5
169
23694
% of surgeries contacted
81.9%
54.0%
28.5%
22.3%
0.9%
31.5%
% of surgeries with automated message
100.0%
65.9%
34.8%
27.3%
1.1%
38.4%
Mean
54.1
Standard Deviation
26.9
Table 3 demonstrates that of the 537 practices, 81.9% (n=440) had an automated message. When an automated message was present, the mean length was 54.1 seconds (SD = 26.9). Of all of the practices with an automated message, 65.9% (n=290) mentioned ‘coronavirus’ or ‘COVID-19’ in their message, 34.8% (n=153) gave specific advice to stay away from the practice if the caller had symptoms of COVID-19, 27.3% (n=120) gave advice about self-isolating with COVID-19 symptoms, and 38.4% (n=169) re-directed callers to telephone NHS 111 or visit the NHS 111 website for advice on worsening symptoms. Only 1.1% (n=5) practices mentioned children specifically. Of these, two said that the advice about self-isolating also applied to children, and the other three said the following: “…anyone with a new continuous cough or fever of 37.8 degrees centigrade or higher must self-isolate for 7 days. This includes children. Travel history is now irrelevant. Anyone with these symptoms who are well are to stay at home and do not need to ring 111 or be tested. Anyone with these symptoms who are unwell should go to NHS 111 online for advice. You must not come to the surgery…” “…anyone with a new continuous cough and/or a high temperature should stay at home and self-isolate for the next 7 days. This includes children. All other members of your household will need to self-isolate for 14 days even if they remain asymptomatic. Do not attend the university health service, hospital, pharmacy or other NHS service in person. If you have these symptoms, use the NHS 111 online coronavirus service to find out what to do. Do not call NHS 111 unless you cannot get help online…”
“…anyone with a new continuous cough, a fever of 37.8 degrees or higher, or a loss or change to your sense of smell or taste must self-isolate for 7 days. This includes children. Anyone with these symptoms who are well must stay at home and order a COVID-19 test… Anyone with these symptoms who are unwell should go to 111 online for advice. You must not come to the surgery…”
Sheffield CCG had the fewest number of automated messages compared with all the other CCGs:
Sheffield CCG (n=75, 70.8%) vs Leeds CCG (n=119, 88.8%) p<0.0005;
Sheffield CCG (n=75, 70.8%) vs Manchester CCG (n=74, 81.3%) p=0.0974;
Sheffield CCG (n=75, 70.8%) vs Birmingham and Solihull CCG (n=172, 83.5%) p=0.012.
Sheffield CCG had the most automated messages with advice to stay away from the practice compared with the other CCGs:
Sheffield CCG (n=44, 58.7%) vs Leeds CCG (n=34, 28.6%) p<0.0001;
Sheffield CCG (n=44, 58.7%) vs Manchester CCG (n=26, 35.1%) p=0.0052;
Sheffield CCG (n=44, 58.7%) vs Birmingham and Solihull CCG (n=49, 28.5%) p<0.0001.
Manchester CCG had the fewest messages with advice to self-isolate compare with the other CCGs: Manchester CCG (n=9, 12.2%) vs Leeds CCG (n=30, 25.2%) p=0.0415;
Manchester CCG (n=9, 12.2%) vs Sheffield CCG (n=26, 34.7%) p=0.0018;
Manchester CCG (n=9, 12.2%) vs Birmingham and Solihull CCG (n=55, 32%) p=0.0009. See Table 4.
Table 4: Breakdown of results for individual CCGs
CCG
% of surgeries with automated message
% Coronavirus mentioned in automated message
% Advice to stay away from practice if coronavirus symptoms
% Advice to self-isolate with coronavirus symptoms
% Did have age segmentation
% Advice if worsening Covid-19 symptoms to go to NHS website or phone 111
Mean length of message in seconds (95%CIs)
Sheffield (n=106)
70.8 (n=75)
62.7 (n=47)
58.7 (n=44)
34.7 (n=26)
4.0 (n=3)
34.7 (n=26)
52 (46-57)
Leeds (n=134)
88.8 (n=119)
62.2 (n=74)
28.6 (n=34)
25.2 (n=30)
1.7 (n=2)
53.8 (n=64)
56 (51-60)
Manchester (n=91)
81.3 (n=74)
68.9 (n=51)
35.1(n=26)
12.2 (n=9)
0 (n=0)
56.8 (n=42)
58 (52-64)
Birmingham and Solihull (n=206)
83.5 (n=172)
68.6 (n=118)
28.5 (n=49)
32.0 (n=55)
0 (n=0)
21.5 (n=37)
52 (49-56)
Automated messages were all in English (although a small number of practices provided a translation in other languages after the message) and orated by a mixture of computerised voices, doctors or staff from the practice. Many automated messages indicated a range of options for the caller to be re-directed to a different line (such as to arrange an urgent appointment or to obtain a repeat prescription) but for the purposes of this study, the key data points listed in table 2 were the only parts of the message which were recorded.
There was no statistically significant difference in mean message length between the four CCGs. Sheffield CCG 51.7 seconds (95% confidence interval 46.5 to 56.8); Leeds CCG 55.7 seconds (95% confidence interval 51.2 to 60.1); Manchester CCG 58.0 seconds (95% confidence interval 52.2 to 63.7); Birmingham and Solihull CCG 52.4 seconds (95% confidence interval 48.7 to 56.0) (p<0.05).
Discussion
This study found that very few practices specifically mentioned children in their automated messaging in relation to the current pandemic. 81.9% of the practices contacted had automated telephone messaging. Of these, 65.9% mentioned COVID-19 in their message but only 1.1% (n=5) specifically mentioned children in their message.
38.4% of practices re-directed callers to either the NHS website or NHS 111 telephone advice line. The website advice states, "Call 111 if you're worried about a baby or child under 5. If your child seems very unwell, is getting worse or you think there's something seriously wrong, call 999”4. There is also further advice particularly focussed upon babies and very young children on the website. This is helpful advice for parents or carers of an unwell child and it is important that it is emphasised. However, it relies upon parents and carers to make an assessment as to when something may be getting worse or is ‘seriously wrong’. Whilst this would increase the workload for primary care, it perhaps would be more beneficial for CYP, particularly those under 5 years to be triaged by a call handler at the local practice and have a much lower threshold for a telephone consultation with a clinician at the surgery or advice to attend hospital.
This study provides a timely representation of first point of care health advice which is being provided in England during the current pandemic. It seeks to look specifically at automated advice given to CYP and whether this may contribute the delays in presentation to secondary care for acutely unwell CYP which have been seen.
It is difficult to know for certain how this may be directly attributable to the reported delays in presentation of serious illness.
Practices from within only four CCGs were contacted in this study. However, this covered a sizable number of different practices, 537 in total, all of which were in large cities and towns in England. It is notable that we did not assess any advice that may have been given by those answering the telephone call. Once the automated message had been completed there may have been opportunity to provide targeted advice. Also, for the 18.1% (n=97) practices where there was no automated message, we do not know if any further advice is relayed by those answering the call. It may have been at this point when age specific advice might have been received.
To our knowledge there have been no other studies looking at the spectrum of automated messages in General Practice during the COVID-19 pandemic.
This study highlights the need for tailored and consistent advice for CYP specifically during the COVID-19 pandemic.
There is significant variation in the advice being given by different General Practices. The Royal College of General Practitioners (RCGP) states that ‘as with all patients, children should be triaged prior to any face to face consultation’ and ‘every effort should be made to avoid face to face assessment’5. It is very important to note that the pandemic has been an extremely challenging time for General Practice with rapid adaptations to working being made in a very short time period. There have been repeated changes in guidance which highlight the challenges faced by General Practice in providing the most up to date information. Since 18th February 2020, patients with a travel history or suspected symptoms were advised to call NHS 111 and to not go to their local General Practice, pharmacy or hospital6. On 5th March 2020, General Practitioners (GPs) were advised by NHS England to switch to a telephone-only triage system, to reduce the change of potentially infected patients attending the practice7. The latest NHS England Standard operating procedure for General Practice (at the time of writing; 24 June 2020, Version 3.3)8 offersspecific advice for GPs regarding children; “Prolonged illness and/or severe symptoms should not be attributed to COVID-19 and should be evaluated as usual”. The rapidly changing advice, coupled with large amounts of uncertainty and anxiety among staff in Primary Care may have contributed to the challenges of providing consistent, standard information for service users such as through automated messaging. For some practices, a telephone triage service was a completely novel way of working, making this large process change over a very limited time frame must have been extremely challenging.
Logistically, the ability to alter automated telephone messaging is often not straightforward and, in many cases, requires outsourcing of this to external companies. This requires an already pressured service to keep up to date with rapidly altering advice whilst arranging for a staff member to formulate a new script and then arrange for this recording to be amended. A process which would have been required to be repeated multiple times over the preceding months, due to regularly changing government messaging.
Although evidence continues to emerge, we know that COVID-19 is less likely to develop into serious illness in healthy children and adolescents compared to adults9.
There have been concerns regarding a serious but rare complication of COVID-19 infection in children PIMS-TS (paediatric inflammatory multisystem syndrome temporarily associated with SARS-CoV-2). A recent paper in the Lancet10 reviewing children admitted to PICUs in the UK between 1st April 2020 and 10th May 2020 suggested that incidence of PIMS-TS requiring intensive care was around 1.5%. However, at the time only hospitalised patients were being tested for COVID-19 in the UK, so this does not take into account the number of children who may have had COVID-19 but were not tested. As a result, it is likely to be an overestimation. Whilst this condition can be serious, the likelihood of a child progressing to PIMS-TS after developing Covid-19 remains low. The greater concern is delayed presentation of other serious illness.
As other publications have suggested, there is a greater risk that children may delay in presenting to hospital or be delayed in being referred to secondary care for important investigations due to the widespread ‘stay away’ advice, seen in both the UK11 and in Europe12.
We suggest that adapting the messaging that parents or carers receive when they first contact their GP to include CYP would be possible and may reduce the number of unwell CYP who have delays in receiving medical care. It would also be important to aim to have consistent messaging across different practices, advice which perhaps should be standardised at a national level. This could greatly assist those working in Primary Care to be able to provide accurate and up to date messaging for their patients. Any adaptations required could be made by individual CCGs to take account of local differences.
Increased amounts of wider public health messaging directed towards encouraging parents and carers to seek medical advice if they are worried about their child, despite the pandemic, are paramount to aid in getting this vital message to those caring for CYP. It is important that additionally where appropriate, this advice is also available in languages other than English.
This study does not prove a direct link between the advice provided at the first point of contact in Primary Care and the delays in CYP presenting to hospital with serious illness. We do not know what influence the advice on automated messages has over CYP and their parents in their decision making about accessing care. Future research should seek to answer this question specifically, perhaps involving directly interviewing CYP and their parents or carers.
Depression and osteoporosis are two extremely common comorbidities in geriatric patients. Each have their associated mental and physical impacts on the patient, and economically on the wider healthcare system. Staggeringly, up to 39% of frail patients suffer with depression.1 Selective serotonin reuptake inhibitors (SSRIs) have long since been used in the management of depression and anxiety states and are one of the fastest-growing classes of drugs prescribed. Their use is not without the potential for negative effects; their side effect profile includes nausea, anxiety, insomnia, sexual dysfunction and gastro-intestinal upset, with the impact on bone mineral density (BMD) being controversial.
Statistics from the International Osteoporosis Foundation (IOF) reveal that in 2015, 6.8% of men and 21.8% of women over the age of 50 had osteoporosis. The estimated lifetime risk of hip fractures for women over 50 is 17.2%, with fracture-related costs at 5.3 billion pounds in 2017.2 Osteoporosis is a progressive, systemic skeletal disorder characterised by loss of bone tissue and disruption of bone microarchitecture, that leads to increased bone fragility and consequently an increased risk of fracture. As well as increasing age and female sex, other well documented risk factors for reduced BMD include early menopause, alcohol use, corticosteroid use, smoking, sedentary lifestyle, low body weight, impaired eyesight, and recurrent falls. What is more, depression itself cannot be overlooked as a risk factor for osteoporosis.
The mechanism by which depression leads to lower BMD is by that of alternation of the hypothalamic-pituitary-axis system, resulting in hypercortisolism. Cortisol is a well-known factor in bone loss. Proinflammatory cytokines have been implicated in depressive disorders, and they may directly stimulate osteoclastic activity.3 What must also be considered is the impact that depression has on certain lifestyle choices such as the potential for increased alcohol and nicotine consumption, inadequate nutrition and low physical activity.
The presence of serotonin receptors, neurotransmitters, and transporters have been found within osteoclasts and osteoblasts.4 95% of serotonin is synthesised in the gut and cannot cross the heteroencephalic barrier. Gut derived serotonin reduces osteoblast proliferation, thereby leading to bone loss. Brain derived serotonin signals to the ventromedial hypothalamic neurones leading to decreased sympathetic output and therefore favours bone formation by action on the beta-2 adrenergic receptors on the osteoblasts. It appears that with shorter duration of use, decreased bone resorption predominates, and with longer term use, bone loss outweighs.4
The impact of SSRIs on bone health has long since been the subject of research, with a possible link with both increased risk of fractures, and reduced bone mineral density being identified. In response to emerging evidence, the MHRA issued advise to healthcare practitioners, stating that we “should be aware of epidemiological data showing a small increased risk of fractures associated with the use of TCAs and SSRIs, and should take this risk into account in discussions with patients and in prescribing decisions”, yet this has not yet filtered down to prescribing guidelines.5 The National Institute for Health and Care Excellence (NICE) guidelines state that on choosing the antidepressant to prescribe, healthcare practitioners must consider that there is currently no evidence to support using specific antidepressants for specific physical health problems.6
We therefore present a case of recurrent depressive disorder in a patient with a background of osteoporosis. We also include a review of the most up-to-date literature, with the aim of increasing awareness of the impact of SSRIs on bone health for fellow prescribers. We aim to highlight the difficulties we face as clinicians whilst there are no formal recommendations regarding the use of SSRIs in high risk populations.
Case Description
This 78-year-old was referred to our services in late 2019 with low mood and loss of motivation. She lives alone following the death of her husband 3 years ago and sadly has no family. She has a past medical history of depression, hypertension, acute pericarditis, subclinical hypothyroidism, hiatus hernia, cataracts, previous cholecystectomy, and osteoporosis.
She was diagnosed with osteoporosis in 2000. At that time, she had been seeing an osteopath due to back pain, who advised her to see her GP to investigate for arthritis or osteoporosis. She has a family history of osteoporosis on her mothers’ side. She was diagnosed by Dual-Energy X-ray Absorptiometry (DEXA) scan, with osteoporosis at the lumbar spine and pelvis, at which time she was started on calcium supplementation.
She was initially started on oral alendronic acid but developed reflux symptoms, so this was discontinued. Over the following years she was tried on various medications for bone protection but sadly developed side effects. Briefly, pamidronate infusion caused iritis, and nausea was reported whilst on sodium ranelate. Later she was to be commenced on sodium risedronate, however did not start this due to concerns she had following reading the information leaflet. Denosumab was discussed as the next suitable option, however she was undergoing dental work including tooth extraction and so this has been delayed due to the risk of avascular necrosis of the jaw.
DEXA scanning in March 2019 showed a T score of -0.8 at the neck of femur, -4.5 at the forearm, -1.3 at the total hip, and -4.2 at the spine. This had, unsurprisingly, worsened from her last DEXA in 2016 (-3.6 at the spine). Her risk of major osteoporotic fracture was last calculated at 21.6%, with the risk of hip fracture 11.5%. She has had no falls or fractures to date since her diagnosis.
Other than Adcal-D3 she is now no longer on bone protection. Her current medications also include levothyroxine, ramipril, bisoprolol, cetirizine, fluticasone nasal spray, and Hypromellose eye drops.
She had initially been started on citalopram by her GP which she had discontinued herself after a period of weeks as she felt it had no positive effect. In December 2019 she scored 92/100 on the Addenbrooke’s Cognitive Examination (ACE-III), with no significant deficits in any one category. As well as low mood and loss of motivation, she described frequent tearfulness, anhedonia, lack of energy, difficulty concentrating and poor sleep. There was no clear trigger for her current mental state, and her physical health was otherwise good. She had no suicidal ideation or thoughts of self-harm. There was some evidence of anxiety but no symptoms of psychosis. We could not identify any alcohol or substance use risks. Her mental state examination was unremarkable. She was given the diagnosis of moderate depressive episode, F32.1, and was started on sertraline. However, upon reading the patient information leaflet, she refused to start this medication due to it mentioning a link with bone disorders.
As a result of this discussion, we accessed the medicines.org patient information leaflet, where an increased risk of bone fractures is mentioned under the heading ‘symptoms that can occur when treatment is discontinued’. It also states that following clinical trials in adults, sertraline was found to cause ‘bone disorder’ in up to 1 in 1,000 people.7
Following in-depth discussions, our patient was very hesitant in agreeing to take any medication that may have an impact on her bone density. We were aware of the potential association between SSRIs and BMD but were unable to quantify this risk to our patient.
Discussion
Our case above represents a common situation; a patient that is worried about a side effect, concerning which there are no formal guidelines available to aid decision making. The link between depression, SSRIs and BMD is a complex one, with numerous confounders making analysis and application yet more difficult. We looked at the evidence surrounding SSRIs and their impact on bone health, in order to suitably advise our patient on the most appropriate treatment options.
Impact on BMD
We found several meta-analysis and systematic reviews concerning BMD. The majority showed no significant association between BMD and SSRI use.
Of note, a 2015 systematic review by Gebara et al, suggested that antidepressant use may well be associated with lower BMD. 4 of the included studies assessed the relationship with BMD, 3 of which highlighted an association with lower BMD. This association was reported with SSRIs but not TCAs. However, they concluded that there was insufficient evidence that SSRIs adversely affect bone health, and therefore a change in current recommendations for the use of antidepressants in older adults was not justified at the present time. They stated that the evidence did not satisfy the Bradford Hill criteria, it is inconsistent, and whilst there is biological plausibility, there are no experimental studies to support a causal relationship.8
Yet a 2012 literature review indicated effects on both BMD and fracture risk.9 Each and every study included, indicated a risk of reduced BMD, increased fracture risk, or both. Even when controlling for potential confounders this conclusion was drawn. Authors suggested on the basis of this evidence, that caution is advised when considering the use of SSRIs in those with osteoporosis or a history of osteoporotic fractures, despite there being no formal recommendations.
A 5-year longitudinal study involving 1988 women, 319 of which were using antidepressants, measured femoral neck BMD. A dose-response increase in bone mineral loss was evident.10 An older cohort study also showed that even after adjustment for potential confounders, mean total hip BMD decreased 0.47% per year in non-users, compared with 0.82% in SSRI users.11 A year later, and a community-based study revealed that after controlling for age, weight, height and smoking history, BMD among SSRI users was 5.6% lower at the femoral neck, 6.2% lower at the trochanter and 4.4% lower at the mid-forearm than nonusers.12
Fracture Risk
The evidence surrounding fracture risk is more unanimous. Of the systematic reviews and meta-analyses we found, all highlighted an increased risk of fracture in SSRI users.
Wu et al concluded that the significantly higher risks of fractures observed for patients who received SSRIs compared with patients with no exposure, remained statistically significant in studies that controlled for important risk factors and studies that scored highly in the quality assessment.13
Eom et al extrapolated their data, estimating that the increased risk of fractures translates to about one case of fracture for every 42 patients treated with SSRIs.14 The dose and duration of SSRIs also seems to contribute to fracture risk, with both an early increased risk (under 6 weeks), and a late risk associated with prolonged use.14,15
A notable literature review by Panday et al on medication-induced osteoporosis summarised that treatment decisions concerning SSRIs should be considered on an individual basis for patients with osteopenia, osteoporosis, or fracture risks greater than 3% and 20% for hip and major fractures respectively.16 Of particular note from this review, a 10-year cohort study revealed that 14.7% of SSRI users suffered at least one fragility fracture over the study period.17 Whilst those using SSRIs do tend to have more fracture risk factors than the general population; they are more likely to be women, have more comorbidities, use other antidepressants/ anxiolytics, and have a previous history of falls; the significant association remained even after these variables were controlled for. The risk of first fracture specifically was increased by more than 50%, and similar to other studies, a dose–response relationship was evident.17
Conclusion
The impact of SSRIs on bone health is clearly a topic of contention. Whilst the impact on BMD is unclear, the increased fracture risk is more unanimous. There are plausible biological mechanisms to explain these risks, yet there is also the fact that the risk of falls themselves are higher when taking SSRIs.
Yet why hasn’t this filtered down to making formal recommendations in prescribing guidelines? Questions remain as to whether we should be prescribing SSRIs in individual’s with osteoporosis at all. Regardless, the relatively high risk of fracture with SSRI use may have a significant clinical impact. These risks must be balanced against the benefits gained by the treatment for depression; both in terms of mental state and in osteoporosis risk factor modification. What would perhaps be more relevant would be to consider a patient’s falls risk independently to their bone health, when deciding whether to prescribe SSRIs. Consideration towards the use of concomitant medications, co-morbidities and other confounders is vital.
It is on this basis that we suggest discussing bone health with your patients (particularly those at high risk), prior to prescribing these medications, and being wary of prescribing SSRIs in those with osteoporosis or more importantly, those at high risk of falls.
Summary
Impact of SSRIs on bone health is complex with significant confounding factors
Whilst the impact on BMD is contentious, the increased fracture risk is more significant
Risk-benefit decision is needed
Consider the patients falls risk most importantly before prescribing an SSRI
General Practice is the first point of contact for most patients who ask for professional medical advice in the United Kingdom (UK) National Health Service (NHS)1. Primary care makes up around 90% of all NHS activity and, as a result of increasing populations overtaking the number of newly qualified General Practitioners (GPs), the burden of tasks from patients has increased exponentially. GPs characterise their workload as “unmanageable” or “unsustainable” and 93% have reported that patient care has been subsequently affected.1 Funding into General Practice from the NHS expenditure has fallen by almost 20% which has halted the expansion of new practices and recruitment of substantial GPs. The growth of new GPs increased by 0.2% only, between 2009-2014, and this has indirectly pressured existing doctors to care for more patients. This is reducing job morale as well as patients’ satisfaction with services. The main causes of increased workload are increased administrative load, high patient expectations and increased risk of litigation.2
Four years ago, there were four doctors at our practice. As time passed, one doctor emigrated, another doctor passed away and the third had retired. This has left two doctors at the practice at this current time. The practice currently employs locum GPs to cover the pressures of daily patient appointments as, according to new studies, there are now on average an astonishing 2,100 registered patients per GP.3 The loss of permanent doctors in this practice may be due to the location of the GP surgery. Barnsley, according to uSwitch in 2015, was ranked 122 out of 138 local areas across the UK based on 26 factors such as household income, life expectancy, hours of sunshine and the cost of essential goods including food bills, fuel costs and energy bills.4 Adding to the lack of permanent GPs, recruitment into General Practice as a specialty has been scarce. Studies have shown that medical graduates chose medical careers that they considered as more stimulating and interesting. One study mentions that medical students are attracted to technical or biomedical forms of medical practice, as opposed to a holistic view of medicine such as that of General Practice.5
Non-permanent GPs in the practice are keen on taking on flexible working hours, which meant the permanent doctors are left with a majority of the work including all of the on-call tasks. These tasks include dealing with patient requests that come through to the receptionist such as booking appointments, patient referrals, prescribing medication and issuing sick notes. We aim to identify the prevalence of specific tasks and evaluate ways to reduce the tasks performed by the doctor. We intend to analyse the number of prescribed acute medication that can be placed on a repeat or variable repeat prescription.
METHODS
Data was collected from a single NHS England GP Centre. This centre utilizes the Egton Medical Information Systems (EMIS) web platform for recording consultations, tracking investigation results, prescribing medications, and communicating within the practice.6 Using EMIS, we collected all the tasks of the on-call doctor for a single month. In this month, there were no school or public holidays. These tasks are sent to the on-call doctor from the receptionist who receives them directly from patients. At this centre, all tasks from 2pm on a particular day form part of the following days’ workload. Therefore, the tasks of each day were recorded from 2pm the previous day until 2pm that day.
We separated tasks by allocating them into 1 of 5 categories: medication request; request for appointment, advice, or test results; request for a referral; request for sick note; and other which included all miscellaneous tasks.
RESULTS
Total task distribution
A total of 969 tasks were performed in the month. The proportion of tasks over 4 weeks was as follows: week 1 had 26.7% (n=259) of the total tasks; week 2 had 25.6% (n=248); week 3 had 25.1% (n=243); and week 4 had 22.5% (n=218).
Figure 1: Total number (n) of tasks per day across each week for the four weeks of the month
Further to this, regarding the proportion of tasks over the days of the week: Monday had 23.1% (n=224) of the total tasks; Tuesday had 19.8% (n=192); Wednesday had 17.0% (n=165); Thursday had 18.0% (n=174); and Friday had 22.1% (n=214). Figures 1 and 2 show the number and percentage of task distribution respectively across the days and weeks for the month.
Figure 2: Percentage (%) of task distribution per day-of-the-week across each week for the four weeks of the month.
Type of task
The tasks for the month were separated unevenly across the five categories: medication tasks were 50.9% (n=493) of the total tasks; requests for appointments, results and advice were 35.9% (n=348) of the total tasks; referrals were 2.4% (n=24) of the total tasks; sick note were 4.6% (n=45) of the total tasks; and other tasks made up the remaining 6.1% (n=59) of the month. Figure 3 shows the distribution of tasks for the month.
Figure 3: Distribution of tasks/requests according to task-type for the month (total tasks n=969).
We recorded the type of tasks completed per week. Figure 4 shows the distribution of tasks according to task-type for weeks 1, 2, 3, and 4, respectively. Of the total 260 tasks recorded for week 1, 55.8% (n=145) were tasks involving medication; followed by 29.2% (n=76) request for appointments, results and advice; referrals made up 4.2% (n=11); sick notes were 7.3% (n=19); and miscellaneous tasks came to 3.5% (n=9).
The second week had a total of 248 tasks. Of these, 51.6% (n=128) were medication tasks; 34.7% (n=86) were requests for appointments, results and advice; referrals made up 2.4% (n=6); sick notes made up 2.8% (n=7); and miscellaneous tasks were 8.5% (n=21).
The third week had a total of 243 tasks. Of these, 44.4% (n=108) were medication tasks; 45.7% (n=111) were requests for appointments, results and advice; referrals made up 1.2% (n=3); sick notes made up 3.3% (n=8); and miscellaneous tasks were 5.3% (n=13).
The fourth week had a total of 218 tasks. Of these, 51.4% (n=112) were medication tasks; 34.4% (n=75) were requests for appointments, results and advice; referrals made up 2.8% (n=6); sick notes made up 5.0% (n=11); and miscellaneous tasks were 6.4% (n=14).
Figure 4: Comparison of distribution of tasks/requests according to task-type for week 1, 2, 3, and 4, respectively.
Medication tasks
Focusing on the medication category, we had a look at whether medication requests sent to the on-call doctor were drug prescriptions that should have been on a repeat/variable repeat prescription rather than on acute. Out of a total 493 medication tasks for the month, 49.1% (n=242) medication requests could have been on repeat prescription rather than being acutely prescribed. A further analysis of this data yielded comparable findings per week. In the first week, there were 145 total medication tasks, about 50.3% (n=73) of drug prescriptions could have been on repeat. In the second week, out of 128 medications, 46.1% (n=59) of medication could have been on a repeat or variable repeat prescription. In the third week, out of 108 medications, 39.8% (n=43) of drug prescriptions could have been on a repeat or variable repeat prescription. In the fourth week, out of 112 medications, 59.8% (n=67) could have been on a variable repeat or repeat prescription. Table 1 represents the total number of medication tasks that could have been on repeat or variable repeat prescription per day. Figure 5 represents the percentage of medication tasks that were on acute prescription but could have been on repeat or variable repeat prescription across each week.
Table 1: Total medication tasks that could have been on repeat or variable repeat prescription, per day across each week for the four weeks of the month.
Figure 5: Percentage (%) of medication tasks that could have been on repeat or variable repeat prescription, across each week for the four weeks of the month.
DISCUSSION
SUMMARY
The total number of tasks did not differ significantly day-to-day: each day per week (Monday-Friday) held about 15-25% of the total weeks’ tasks. The medication requests contributed to the majority of the total tasks (50.9%); followed by requests for appointments, results and advice (35.9%). Upon further analysis of the medication category, 10-25 medication tasks per day could have been avoided by having certain drugs on repeat prescription rather than being acutely prescribed. Taking into account that a GP would typically spend 2 minutes per task, this could save 20-50 minutes per day, which amount to 100-250 minutes per week, and 400-1000 minutes or 6.5-16 hours per month.
The drug prescriptions that we thought should have been on repeat or variable repeat prescription, rather than on acute prescription, included requests for drugs that patients typically take long-term. This included Proton Pump Inhibitors (PPIs) such as Omeprazole, statins such as Simvastatin, and Angiotensin Converting Enzyme Inhibitors (ACEIs) such as Ramipril. These are for chronic conditions such as gastric reflux, hypercholesterolemia, and hypertension, respectively. Other drugs that we considered would be more feasible if put on repeat or variable repeat prescription were those for palliative patients in care homes that require a constant need for laxatives such as Senna or Lactulose, or drugs such as Paracetamol. These are for constipation or pain management, respectively.
The medication requests that could not have been on repeat or variable repeat prior to the request being sent were drugs that were required acutely, such as for short-lived infection, transient pain relief, changing of drug doses, and prescribing of alternative drugs due to a possible manufacturing problem or unavailability from the pharmacy. These are tasks that we deem necessary to be sent to the GP so that drug doses are changed based on clinical judgement, and not merely on a request sent to the receptionist. This upholds a standard of drug-control and patient safety within the practice.
STRENGTHS & LIMITATIONS
This retrospective study provides an in-depth analysis of the on-call doctors’ day-to-day tasks in terms of the nature and number of tasks. This is a study involving a large number of tasks collected from a month in a single GP surgery which has produced significant results. As non-GPs collected all the data, including data in the medication category, this eliminated bias in reporting acute medication that could have been prescribed as repeat or variable repeat medication. Limitations include the sample size being considered as a relatively small number which cannot be representative of all on-call GPs’ tasks in the rest of England. In addition, this study took place in the month of September and the tasks can be distinctly different when looking into other months.
COMPARISON WITH EXISTING LITERATURE
To date, the existing literature that looks at GP tasks from this perspective is limited. Most studies look at the receptionists’ role in handling patient requests or focus on scrutinizing the technology that GPs rely on to issue repeat or variable repeat prescriptions.
Our study included the number of tasks completed in a single month as well the stratification of tasks done within the month. We separated our results week per week to see if there were any differences between them. In 2014, a quantitative analysis of incoming calls into three GP surgeries described basic numbers of calls and type of patient enquiries that came into the practice. They had received a total of 2,780 calls and found that the most dominant type of request was making a doctor’s appointment. The main finding in the study is that it identifies an aspect of non-effective communication in GP receptionists’ encounters with patients. It describes how some receptionists failed to meet the initial requests of the patient by directing the telephone call forward or even closing calls prematurely before understanding the problem. This increased ‘patient burden’ and lead to lower patient satisfaction score when recorded. Effective receptionists understood and summarized the patients’ requests as well as making alternative actions to help the patients enquiry.7
Repeat prescriptions are defined as those that are printed by a practice computer from its repeat prescribing program8. In the UK, repeat prescriptions account for up to three quarters of all drugs prescribed, and four fifths of drug costs in General Practice.9,10 Repeat prescriptions are mostly done as a technology-supported practice that requires collaboration between clinical and administrative staff to ensure patient safety.11 Two conflicting opinions exist around repeat prescribing: the first is that the increased automation aids in improving safety; the second is that the process as a whole may be weakened if assumptions built into the technology do not take full account of the nature of healthcare work such as real life demands like time, space, and resource constraints.11,12 It is important that the GPs at our practice are aware of the risks involved in potentially putting more drugs onto repeat prescription, and consequently monitor this closely.
IMPLICATIONS FOR RESEARCH AND/OR PRACTICE
The findings collected in our study demonstrate the increasingly demanding role of the on-call GP outside of consultation hours. According to recent surveys, the GP occupation has had its lowest job satisfaction since 2001 because of a higher workload which indirectly lowers quality of patient care and increases negative patient experiences.13,14 This should be taken with paramount importance, as this can cause harm to both patients and GPs. As results have described the huge number of tasks, it is important to find a way to avoid unnecessary tasks telephoned into the GP surgery. The results of our study were presented to all of the staff in the practice and the underlying message was well received. Medications that are prescribed by the doctors are double checked by the Clinical Commissioning Group pharmacist in the practice to ensure that drugs are safely given to patients.
CONCLUSION
As the funding formula has changed in the last decade, the government budget into the NHS primary care has decreased more than in secondary care even with the ever-growing pressures on primary care services.13 Some strategies, such as telephone triage, have been introduced at the practice to reduce workload crisis. However recent evidence has shown this is not effective.15 In 2015, the primary care workforce commission laid out recommendations to restructure primary care services as the current model for primary care was under doubt. The underlying message in the report was that continuity of care was important for the majority of GPs - the GPs understood patients better when they had been under their care for many years.16 With this, extra tasks can be avoided if GPs know their patients well. At a glance of primary care, from literature and our findings, it seems that General Practice may follow an unsustainable path. The pressures of workload include increasing patient lists, higher public expectations and growing bureaucracy.17 Our data collection has proven that there are a lot of tasks to be done in a month by an on-call doctor, however the amount of time that could be saved by prescribing repeat or variable repeat rather than acute medication can save significant time. From our positive results in the medication task section, we hope this can inspire further research into other areas of the GP surgery that can help optimize the time of the doctors. Furthermore, we would like to repeat our retrospective study in one year’s time with the suggestion implemented (appropriate acute medications changed to repeat or variable repeat prescriptions) over a longer period of time. With limitations corrected for, we want to re-analyse the number and type of tasks completed to determine whether this has truly optimized the time of the overworked on-call doctor.
Insomnia is a disturbance of normal sleep patterns. It is characterised by sleep onset latency and/or sleep maintenance. Short term insomnia is defined as having symptoms for less than four weeks, whilst long term insomnia is symptoms lasting more than four weeks1. Hypnotics can provide relief from the symptoms of insomnia; they do not treat any underlying cause.
Several hypnotic agents are licensed for the treatment of insomnia, including the benzodiazepines and Non-benzodiazepine hypnotics (Z-drugs)2.
NICE guidance for Insomnia management states “After consideration of the use of non-pharmacological measures, hypnotic drug therapy is considered appropriate for the management of severe insomnia interfering with normal daily life; it is recommended that hypnotics should be prescribed for short periods of time only, in strict accordance with their licensed indications” 1.
NICE guidance also advises to use the lowest effective dose of the hypnotic agent for the shortest time frame possible. The exact duration will depend on the underlying cause, but treatment should not continue for longer than two weeks. We should also inform the patient that further prescriptions for hypnotics will not usually be given, ensure that the reasons for this are understood, and document this information in the patient’s notes.
Side effects are common with hypnotic usage including, most importantly, the development of tolerance and rebound insomnia. Other side effects can occur such as daytime sedation, poor motor coordination, cognitive impairment, hallucinations, anxiety, delusions and sleep disorders2.
Aims
To reduce the amount of hypnotic medication being prescribed to patients on an Acute Inpatient psychiatric ward in the Northwest of UK. The ward is in a semirural psychiatric hospital and is a Male ward containing 17 inpatient beds. The patients are 18 years old onwards with varying diagnosis including Generalised Anxiety Disorder, Bipolar Affective Disorder, Schizophrenia, Depression, and patients with mental and behavioural disorders due to psychoactive substance use.
The reason for doing this project was most importantly for improving patient safety by reducing unnecessary prescriptions and therefore administration of hypnotic medications, but also to reduce NHS expenditure and carbon footprint.
Inclusion criteria
Patients who have been an inpatient on the selected ward between the 09/12/2020-20/01/202 and 28/01/2020-10/03/2020.
Intervention
We developed a prescription aid flow chart (Appendix 1) for all newly admitted patients to the ward. This will guide doctors when making the decision if a hypnotic prescription is warranted.
All patients on the ward during this intervention period, who are currently on a hypnotic agent and are not newly admitted, will have their hypnotic prescription reviewed using the flow chart (Appendix 1) at their weekly consultant ward round.
We then decided on some interventions to fulfil our aims. The interventions were as follows:
1) Development of an educational presentation about Insomnia and sleep management.
2) Development of an Insomnia management Flow chart (Appendix 1) to be used at admission point.
3) Training sessions for ward staff.
4) Shared teaching programme with patients at their sleep management sessions.
5) Face to face and E-mail correspondence to inform medical trainees about this project.
6) Gather feedback from ward patients and staff before and after this project.
The Hypnotic prescription flow chart aid (Appendix 1), has been put on the ward office notice board, the clinic room and the On Call Doctors Room. It was also e-mailed out to the regular ward doctors, as well as all on-call doctors working during the intervention period.
As discussed above, we created an educational PowerPoint presentation entitled “Insomnia and hypnotic agents”. This included insomnia definitions and types, NICE guidance on insomnia, sleep hygiene advice, the medications used for insomnia, their mode of actions, side effects, cautions and cost of these medications. We also included our new hypnotic prescription flow chart aid (Appendix 1).
From the 21/01/2020-27/01/2020 we had two of these educational training sessions. This was to ensure that all staff working on this ward attended at least one of these sessions. Staff in attendance included the ward managers, nursing staff, health care assistants, the pharmacist, a junior doctor, and the ward consultant. This was very important as all these health care professionals are involved with the management of patients on the ward, and those suffering from insomnia. We felt that this session was vital as we wanted to ensure that all the staff knew the importance of this project and could raise their own concerns and issues that they have with regards to managing patients with insomnia. This proved to be very useful as we all brainstormed and voiced some realistic ward changes that could happen on an inpatient psychiatric ward. We also acknowledged that sleeping on the ward as an inpatient can often be disturbed, due to regular nursing checks and noise from the staff and other patients. We did however discuss some feasible interventions which included:
1) The time at which all the automatic ward lights are turned on in the morning could be delayed.
2) Caffeine –free coffee/tea available only after a particular time in the evening.
3) Discourage daytime napping.
4) Have regular sleep-hygiene sessions on the ward.
Between 28/01/2020 to the 10/03/2020 we started these interventions, and this is the time period for collection of our next six weeks of data. We had multiple patient group sessions on sleep hygiene during this time led by the occupational therapist. Other health professionals assisted with this, including the ward pharmacist and the junior doctor. During these sessions we asked for patients to give their feedback on the current management of insomnia on the ward. Some responses included:
· One patient with Severe Generalised Anxiety Disorder stated that he feels that the sleep hygiene advice is helpful, as he doesn’t like to “jump straight into taking tablets” and likes to “fix the root” of his sleeping problem.
· A second patient with a diagnosis of Mental and Behavioural Disorder due to use of cannabinoids, stated that he needs both sleeping medications and sleep hygiene advice, as sometimes he still cannot get to sleep on the ward by solely using relaxation methods.
· A third patient with Generalised Anxiety Disorder stated that he found the sleep hygiene sessions useful. He is now using relaxation methods and is trying to avoid daytime naps which are both helping with his sleep. However, he still on occasions struggles with sleep. He said it is important to have a tidy, clean and relaxing sleeping environment, which is sometimes difficult to implement on the ward.
Appendix 1
Results:
Data was collected prior to any intervention on the ward between the dates 09/12/2020 and 20/01/2020.
The table below (Table No.1) includes the type and number of sleeping tablets prescribed on the ward between the dates 09/12/2020 and 20/01/2020. The total number of patients treated from 9 December 2019 to 20 January 2020 were 28 and the total number of patients were prescribed hypnotic medication during this time were 14.
Table No.1 - Hypnotic medication prescribed:
Name
dose
Number of tablets
Zopiclone
7.5mg
191
Zopiclone
3.75mg
12
Zolpidem
10mg
4
Nitrazepam
5mg
7
Temazepam
10mg
10
The table below (Table No.2) includes the number of hypnotics prescribed and administered after the interventions mentioned above. The total number of patients treated from 28 January 2020 to 10 March 2020 were 25 and the total number of patients who had prescribed hypnotic medication were 11.
Table No. 2- Hypnotic medication prescribed:
Name
dose
Number of tablets
Zopiclone
7.5mg
96
Zopiclone
3.75mg
6
Zolpidem
10mg
0
Nitrazepam
5mg
0
Temazepam
10mg
0
With our ward interventions we have significantly reduced the amount of hypnotic tablets being administered. The total number of tablets administered during this 6 week period was 102. The total number of patients who were prescribed hypnotics was 11. Prior to our interventions the total number of tablets administered between 9th December 2019 and 20th January 2020 was 224 and 14 patients in total were treated. This demonstrates a 44.5% reduction in tablets which is significant.
Discussion
The total reduction in tablet administration was very significant with a 44.5% reduction post-intervention. This demonstrates the positive change in our clinical practice that has resulted from using the flow chart aid (Appendix 1) as well as patient and staff educational and feedback sessions. This will improve patient safety by reducing the risk of side effects. The risk of patients developing tolerance to hypnotic medications has been reduced, as well as reducing those being discharged on a regular prescription which will further improve long term expenditure of hypnotic medications for the NHS. With the changes that have occurred in our clinical practice, we have reduced the number of hypnotics being unnecessarily prescribed and administered.
Over prescribing/unnecessary prescribing is an issue within the NHS and is impacting negatively on the environment. The NHS constitution states that the NHS is ‘committed to providing the most effective, fair and sustainable use of finite resources’3. By reducing the number of inpatients being unnecessarily started on hypnotic medications, another positive from this project will be the reduction in the negative pharmaceutical impact on the environment. The number patients being discharged with hypnotic medications, who may no longer need them, due to their insomnia improving when they are discharged from the inpatient setting will also improve. Furthermore, if they are unnecessarily started on a hypnotic prescription as an inpatient, they may continue this prescription regularly and become tolerant, which will inevitably have an undesirable effect on the environment.
The feedback that we received from the educational insomnia teaching sessions also proved to be very useful. As stated above the staff sessions allowed us to brainstorm simple ward-based interventions, as well as discussing possible drawbacks which may result. This allowed us to modify the flow chart so that it worked for all staff effectively.
The feedback given from patients was also very encouraging. As health professionals we sometimes overlook how some patients want and need more involvement in making decisions on aspects of their care. Ensuring patients are informed about medications prior to prescribing, especially about side effects is something that is very important and allows patients to make informed decisions which is a more holistic approach to clinical practice. This is vitally important prior to prescribing any medications but especially medications with more severe side effects which some hypnotics have.
The patient educational sessions were a key part of this project. We gathered feedback and established that the patients involved found these sessions informative. Some, but not all, of the sleep hygiene advice was feasible to implement into their daily routine on the ward. The ward can be disruptive at night, due to other patients, or due to regular staff checks in patient rooms, as well as rooms not being familiar surroundings, were two of the difficulties raised from the patients. This is something that we appreciate can’t be changed, however with the interventions that can be feasibly made on the inpatient psychiatric ward, we continue to strive to implement and improve for patients. For these reasons both the staff and the patient educational sessions should be continued and proved a vital part of this project
Following on from this initial intervention, we feel that we can continue to make further changes and expand the changes we made on this ward, to other similar wards in our hospital and to other inpatient psychiatric wards in the Trust.
Bed bugs belong to the family Cimicidae and there are two species involved in the modern resurgence; the Common bed bug, Cimex lectularius and the Tropical bed bug, Cimex hemipterus. They are wingless insects with an oval-flat shape that allows them to hide in narrow cracks and crevices. The adults are dark brown, 4-5mm long, becoming to around 10mm when fully blood-engorged. There are five smaller juvenile stages (nymphs) that are similar in appearance, although lighter in colour. All nymphs require a blood meal to moult to the next stage, and both adults also bloodfeed for nutrition, and egg development in the case of the female. Bed bugs are solely haematophagous ectoparasites. After feeding they return to a harbourage and do not remain on the host. The main hosts are humans, but pets, bats, and birds may act as secondary hosts.
Epidemiology
In the past, bed bugs were particularly an affliction of the poor. However, in the early part of the modern resurgence it was the tourist areas and the hospitality sector that were initially impacted.1-3 Today, bed bugs have conquered quite diverse locations, ranging from hospitals, hotels and homes, to trains, cruise ships, and even airplanes. Most commonly, bed bugs travel in comfort as stowaways in luggage, although they can be transferred via furnishing and other belongings, as well by spreading to adjoining properties. Unfortunately, exact figures on the occurrence of bed bugs are unknown, as there are no mandatory reporting requirements. Additionally, due to the stigma associated with bed bugs, many infestations are simply not reported.
During the day, the largely nocturnal bed bugs will crawl deep into crevices of bed frames and mattresses (Fig.1), or behind wallpaper, and floor moldings. Here they tend to lay their eggs, often several hundred during the female lifetime. Live bed bugs, shed nymphal skins, and dark excrement spots indicate an active infestation. At night they are attracted by carbon dioxide, heat and other host odours to a victim, from which they may take a blood meal every 3-5 days. The adult bugs can survive long periods of starvation, up to five months at 22oC or even longer at cooler temperatures. When a host is found, they insert their mouthparts into the skin, blood feeding for 5-10 minutes. When bed bugs are in large numbers, often lines of bites occur on the unfortunate victim and this sign is almost a sure indication of the presence of the insect. The bites tend to occur along the arms and legs, down the back and across the shoulders.4,5
There has been long speculation whether bed bugs can transmit diseases, and in fact more than 40 different pathogens have been implicated. This has included Hepatitis B and C viruses, Human Immunodeficiency Virus (HIV), and Coxiella burnetii (Q fever). Recently, research has indicated that bed bugs are capable of transmitting the agent of Chagas Disease, Trypanosoma cruzi,in the laboratory. However, to date there is not one piece of evidence that bed bugs have transmitted any pathogen to humans.4,6
Clinical Features
During the act of feeding, saliva is injected which contains a variety of anticoagulants as well as other proteins whose function has yet to be determined. Contrary to popular belief, there is no evidence that bed bugs inject an anaesthetic. One protein, Nitrophorin, is involved in the transport of nitric oxide into the wound. This results in local vasodilation that increases blood supply to the feeding insect. The same protein can also induce a sensitivity to the bite.6
The diagnosis of Cimicosis is via the clinical appearance of the bite reaction and confirmation of an actual bed bug infestation (Table 1).3,5 The most commonly affected body parts are those that are left uncovered during sleep (Fig. 2,3,4), notably the arms, shoulders and legs. In young children, the face and even the eyelids can be bitten. Rarely, however, armpits are bitten, which are often preferred by other insects and ticks (Table 2).
Table 1. Bed bug infestation
Bites on the body
Wheals, 4-6cm in diameter, lines of bites
Any exposed body part
Often intense itching
Occasional central haemorrhage
Bed Sheet, mattress (clothing)
Small blood spots
Droppings (black dots)
Shed nymphal skins
Eggs, small (~1mm in length), white, oblong, glued to the substrate
Space
Pungent smell (mostly commonly noticed when an insect is squashed, or during the control program)
Table 2. Differential diagnosis of epidermatozoonoses
Bite preference
Pattern
Itching
Notes
Bed Bugs
Any exposed parts of the body, arms, legs, face, torso
In small infestations, bites will be random. In larger infestations, bite can occur in lines along the limbs and across the shoulder. Large wheals (up to 6cm across) may form, even some 14 days after the bite
Often intense, especially in the morning, but can be variable between individuals
Often associated with travel or used furniture
Fleas
Exposed parts of the body, especially the legs
Random, usually not grouped or in lines
During the day
Usually associated with pets
Mosquitoes
Exposed skin, particularly legs and arms
Random
Variable between individuals
Most commonly outdoors
Ticks
Potentially anywhere on the body
Erythema migrans with Lyme disease. Localised macules/papules at the bite site may occur
Low / no
Those who work or recreate in native forests are at greatest risk.
Itch Mites (Scabies, Sarcoptes scabiei)
Forearms, inter digital, genital area
Skin rashes, subcutaneous courses
At night
Most common in the elderly and infirmed
Harvest mites (Trombidiosis)
Skin surfaces under tight clothing
Red macules and wheals
Severe itching
Often occurs in gardens or meadows, most active during summer and autumn
Cheyletiellosis
Arms and trunk, contact points with pets
Polymorphic rash
Variable
Tends to be associated with pets
Bird mites
All over
Macular rash
Variable itching
Most commonly in homes as a result of birds roosting in roof cavities
Head Lice (Pediculosis)
In the hair of the head
Bar-shaped scratch effects with lichenification and hyper-pigmentation (Vagabond’s disease)
Night and day, generally mild itching
Most common in school aged children
Spiders, e.g. long-legged sac spiders
Arms, face
Necrotic lesion at bite site
Immediate severe pain, no itching
Uncommon
Figure 1: Typical appearance of bed bugs
Figure 2: Bites on the back, note the lines of bites common in moderate to large infestations
Figure 3: Bed bug bites on the arm, typical formation
Figure 4: Bed bug bites on the torso and arm
Figure 5: Bullae due to bed bug bites
Figure 6: Bed bugs, their droppings and eggs underneath a mattress
The degree of the bite reaction often depends on the level of prior exposure. With low level sensitization, individuals may develop a 1-2 cm wheal, with a small central haemorrhagic point. This haemorrhagic point can be recognized easily by diascopy. In contrast, a highly sensitized person will react immediately and may develop a wheal up to 15cm across (6 inches). If many bed bugs are present, an urticarial rash may develop as a result of the large number of bites and subsequent trauma to the area from scratching. On rare occasions, vesicles and bullae (Fig. 5) may form on the arms and legs. In the course of Cimicosis, papules that are extremely itchy may develop and can persist for several days to weeks. Due to the strong pruritus eczematous lesions, bacterial infections may occur, although this is extremely rare. There are case reports of systemic reactions such as anaphylaxis and asthma, although these are uncommon.
Through repeated exposure, some individuals may develop a tolerance to the bites. The clinical symptoms are then largely inapparent with small punctures at the bite site. Small blood spots are then the only clues that an infestation may be present.
Differential Diagnosis
Since reactions to stings and bites of various arthropods are non-specific, bed bug bites are commonly misdiagnosed. Single bites, notably that of other insects such as mosquitoes, fleas and biting midges may appear very similar morphologically (Table 2).
Consideration of where the bites are on the body can assist in the differential diagnosis. For bed bugs, lines of bites are very common in moderate to large infestations and this clinical picture is virtually unique amongst blood sucking arthropods. For the most part, the identification of the actual pest is required to confirm the diagnosis. Histologically, bed bug bites resemble perivascular eosinophilic infiltrates through the superficial and deep dermis, with minimal spongiosis.
Other possible diagnostic confounders can be various allergic reactions and other medical conditions such as urticaria, chickenpox, prurigo subacuta, and erythema multiforme.7,8 These do not show a central haemorrhagic point in the lesion which allows a correct diagnosis. However, in young children the diagnosis can sometimes be difficult.
Treatment
The treatment of Cimicosis is symptomatic. Local lesions can be treated with antipruritics e.g. Polidocanol 2-4% in Lotio alba (aqueous lotion) and topical antiseptic. Spirit of menthol may also be helpful. Local treatment with antihistamines is controversial. In severe reactions topical glucocorticoids such as Betamethasone may be required. In severe itching, the use of oral antihistamines is recommended. With infected bites, antibiotic therapy may be required. Uncomplicated bed bug bites tend to stop itching within 1-2 weeks, although temporary scarring from the bite may remain for several months.
Management
Treatment of patients with bed bug bites ultimately comes down to removing the source of the irritant, namely the eradication of the active infestation. Bed bugs have a typical pungent odor. This can be used to detect bed bugs through specially trained sniffer dogs that can rapidly locate the insects.9 Due to insecticide resistance, bed bugs are very difficult to control with traditional insecticides alone, and non-chemical means of eradication must be employed to reduce the overall insect biomass. Bed bug control should be undertaken by professionals trained in bed bug management, and the process may take some weeks to achieve.
Prevention
When travelling (1) always inspect the bed and surrounds for bed bugs hiding beneath the mattress and/or in seams of the bedding. Also, look for blood stains or small black dots (Figure 6, Table 1). (2) If present, request another room. (3) Always keep your luggage on the desktop or the luggage rack. A good preventative is to seal luggage in plastic or garbage bags during travelling, even when in transit. (4) When returning home, all clothing should be washed in at temperatures exceeding 60°C or frozen for one week with delicate fabrics. If there is no choice, then repellents containing N, N-Diethyl-meta-toluamide (DEET) should reduce the biting rate, but will not completely prevent all bed bug bites.10,11
Bed bugs can enter homes via an array of additional ways, particularly from objects bought second hand at flea markets or thrift stores, for example wooden frames, vintage clothes, furniture and the like. These should be heat-treated for a minimum of 10-20 minutes to kill bugs and their eggs.
Medical professional terminology is used to communicate with each other, allied professions and differentiates professionals from patients1. As a tradition, it has perhaps evolved into a language of its own with a vocabulary of terms used as expressions, designations or symbols such as ‘Patient’, ‘Ward Round’ and ‘Registrar’. This ‘language’ is not restricted to use by doctors or nurses - it is used among other professionals working in healthcare, e.g. medical coders and medico-legal assistants.
The National Health Service (NHS) in the U.K. has seen many changes in the last few decades. From within these changes, an interesting trend to change or alter the use of professional terminology, often without consultation with directly affected professionals or patients, has emerged. With new or changed roles, multidisciplinary teams have been observed to alter titles, even borrowing specific terms ascribed to doctors such as “consultant,” “practitioner” and “clinical lead”2,3. On the other hand, Modernising Medical Careers initiative4 has also led to changes in doctors’ titles reflecting their experience levels, which have been reported to be unclear to patients and fellow professionals5.
Medical professional terms can be traced back to Hippocratic writings and their development is a fascinating study for language scholars1. Psychiatric terminology is particularly interesting, as it has evolved through scientific convention while absorbing relevant legal, ethical and political trends along the way. Superficially, it may appear pedantic to quibble over terminology, but the power of language and its significance in clinical encounters is vital for high quality clinical care2,6. Since medical professional terminology is an established vehicle for meaningful communication, undue changes in its use can create inaccurate images and misunderstandings, leading to risks for professional identity. There is also evidence to suggest that such wholesale changes have been misleading7 and a source of inter-professional tension.
Understanding of a professional’s qualifications and experience is crucial for patient autonomy and for them to be able to give informed consent. We carried out a survey among foremost stakeholders of medical professional terminology, patients and doctors, within a psychiatric service to ascertain their attitudes to the changes they have experienced in recent years.
Method:
We gave out a self-report questionnaire to all adult psychiatric patients seen at a psychiatric service in the South East (U.K.) in a typical week and to all working psychiatrists/doctors. The questionnaire was developed after a review of the relevant literature and refined following feedback from a pilot project. The questionnaire contained demographic details and questions regarding attitudes towards medical professional terms for patient and professional identity, processes and working environments. The questions were mostly a “single best of four options” style, with one question involving a “yes” or “no” answer.
The datacollected was analysed by using SPSS statistical package8. Descriptive statistics were used to summarize the characteristics of the study population. The two sub-samples (patients & doctors) were compared with each other regarding different variables by using a t-test, which highlighted the absolute and relative differences among those.
Results:
196 subjects were approached to participate. 187 subjects (patients = 92, doctors = 95) participated, which represents a response rate of 95%.
Male to female ratio was roughly equal in the sample but there were more females in the medical group (56%) as compared to the patient (46%) group. Among responders, those over 40 years of age were more prevalent in the patient group (60% vs. 39%) compared to the medical group.
As shown in the Table 1, patients’ and doctors’ attitudes overwhelmingly leaned towards a patient being called a “patient” (as opposed to “client”, “service user” or “customer”); understanding “clinician” as a doctor (as compared to being a nurse, social worker or psychotherapist), and believing psychiatrist to be a “consultant” (preferred to nurse practitioner, psychologist or social worker).
Table1: Patients’ & doctors’ attitudes to medical professional terms = “patient”, “clinician” and “consultant”
What do you prefer to be called?
Doctors (%)
Patients (%)
Client
16 (17)
13 (14)
Patient
68 (72)
65 (71)
Service user
10 (11)
11 (12)
Customer
1 (1)
3 (3)
Don’t know
0
0
Total
95
92
Chi2 1.378, p = 0.710
Which of these is a clinician?
Doctors (%)
Patients (%)
Nurse
14 (15)
14 15)
Social worker
4 (4)
2 (2)
Doctor
56 (59)
70 (76)
Psychotherapist
7 (7)
6 (6)
Don’t know
14 (15)
0 (0)
Total
95
92
Chi2 16.3, p<0.05
Which of these is a consultant?
Doctors (%)
Patients (%)
Psychiatrist
71 (75)
68 (74)
Psychologist
3 (3)
6 (7)
Social worker
10 (11)
10 (11)
Nurse practitioner
3 (3)
8 (9)
Don’t know
8 (8)
0 (0)
Total
95
92
Chi2 11.3, p<0.05
Patients and doctors seemed to prefer (>70%) calling the person who provides the patient support in the community as “care-coordinator” or “key worker”.
It is worth noting that “key worker” is the main person looking after the patient admitted to hospital and “care-coordinator” has the same role when they are back in the community. Similarly, the majority of the patients deemed the terms “Acute ward” and “PICU” (psychiatric intensive care unit) appropriate for a psychiatric ward.
There was strong evidence to suggest that both patients and doctors were confused as to what a ‘medication review’ was; as approximately 35% of them thought it was a “nursing handover” and the rest were divided whether it was a “pharmacist meeting” or an “assessment”. See Table 2.
This is understandable because the patients are used to an “Out Patient Appointment/Review” where a psychiatrist reviews patients in a holistic manner, which includes prescribing and adjusting their medications. Similar confusion prevailed regarding what has replaced the term “ward round”, as both groups were universally divided among choices offered as “MDM” (multidisciplinary meeting), “Assessment”, “CPA” (Care Programme Approach) and “Review”.
Table 2: Patients’ & doctors’ attitudes to what a “ward round” and “medication review” means?
Which of these means a ward round?
Doctors (%)
Patients (%)
Assessment
26 (27)
34 (37)
MDM
18 (19)
15 (16)
Review
34 (36)
29 (32)
CPA
16 (17)
14 (15)
Don’t know
1 (1)
0 (0)
Total
95
92
Chi2 2.82, p = 0.588
Which of these is a medication review?
Doctors (%)
Patients (%)
OPD
19 (20)
11 (12)
Assessment
25 (26)
34 (37)
Pharmacist meeting
34 (36)
31 (34)
Nursing handover
14 (15)
12 (13)
Don’t know
3 (3)
4 (4)
Total
95
92
Chi2 3.89, p = 0.421
Both patients and doctors were clear (84% vs. 69%) that they expected to see a doctor when they attended a “clinic”. However, both groups were approximately equally divided between their preferences for what a psychiatry trainee should be called; “SHO” (37%) or “Psychiatric trainee” (36-40%). There was also a higher preference (approx. 50% vs. 30%) for the doctor a grade below consultant to be called a “Senior Registrar”.
Patients and doctors were equivocal in their response that they have never been consulted about medical professional terminology.
Fig. 1 Has anyone consulted you about these terms?
Discussion:
In a survey of attitudes to the use of medical professional terms among patients and doctors in a psychiatric service, we have found a significant preference for the older and established medical terms as compared to the newer terms such as MDM, CT trainee, Specialty Trainee, etc.
While replicating findings of other studies3,7, we also found that no single term was chosen by 100% of participants in either group, showing confusion surrounding most psychiatric terms. This lack of consensus and confusion can be explained by the fact that no participant had ever been consulted about the changes or new nomenclature.
Limitations to this study should be taken into account before generalising the results. The patients’ group is older than the doctors’ group, which could skew the results due to age related bias in favour of familiarity and against change9. In a questionnaire about preference and understanding, participants may intuitively prefer the easiest to understand terms and ignore the subtle difference between other styles. Possibility of bias may have been introduced by some of those giving out questionnaires being doctors
Our sample was drawn only from a psychiatric service, which may restrict the implications of our findings to mental health.
Furthermore, involvement of other professionals and carers working in the psychiatric service would have been useful to expand the scope of this study.
Inconsistency regarding doctors’ titles, unleashed by the Modernising Medical Careers (2008) initiative, has resulted in patients considering trainees as medical students5, not recognising ‘Foundation Year 1 Trainees’ as qualified doctors and being unable to rank doctors below consultant level3. Our findings have highlighted the uncertainty regarding qualifications and seniority of doctors – this can erode patients’ confidence in their doctors’ abilities, compromise therapeutic relationship10, especially in psychiatry, and result in poor treatment compliance. Medical students may also find themselves mistaken for doctors, and feel daunted by future job progression where training structures and status are unclear.
Title changes introduced by local management or Department of Health (DoH), without consultation with stakeholders, have the potential to create inter-professional tensions and devalue the myriad skills offered by healthcare workers other than doctors. This could also be damaging to their morale and the confidence instilled in patients. It is interesting to note, however, that titles that do not give the impression of status and experience, such as “trainee”, tend not to be adopted by non-doctor members of the multidisciplinary team3. On the other hand, in a profession steeped in tradition, there will be doctors who see other professionals’ adoption of their respect-garnering and previously uncontested titles as a threat to the status of the medical profession6. Previous studies have shown that terminology has a significant effect on the confidence and self-view of doctors5 and at a time where a multitude of issues has led to an efflux of U.K. junior doctors to other countries, and a vote for industrial action, re-examining a seemingly benign issue involving titles and terminology could have a positive impact.
Patients’ attitudes to development of surgical skills by surgical nurses show that they would like to be informed if the person doing a procedure is not a doctor7.
The roles of a number of professionals involved in an individual’s healthcare can be confusing and the possibility of mistaken identity could be considered misleading6, unethical, and even fraudulent. Introducing confusion by appropriating titles associated with doctors could be damaging to patients’ trust, and is inappropriate in a health service increasingly driven towards patient choice. The challenge lies in how to keep the terminology consistent and used in the best-understood contexts.
Commissioners and managers may instead evaluate the implications of changing professional terms by making sure that all stakeholders are consulted beforehand. Perhaps the pressing source of inconsistency in staff job titles could also be rectified by a broader scale study to find national, multidisciplinary and patient preferences, and taking simple measures such as standardising staff name badges.
Our study has highlighted once again how the landscape of nomenclature in psychiatry/medicine is pitted with inconsistency. While language naturally evolves with time and it may be understandable to see increasing application of business models & terminology in the NHS9, medical professional terms have been determined contextually over the years with significant implications for patient management and safety. Therefore, it is important to question how changes in terminology affect patients, whether it occurs by gradual culture change or due to new initiatives. It would benefit patient care if medical and psychiatric professional language could be standardised and protected from changes, which can lead to colleagues and patients being misled. DoH, Commissioners and Trust/Hospital management must recognise that changing terminology can have a significant impact and that serious discussion of such changes is important for reasons far beyond pedantry. For inter-professional communication a formalised consensus on titles would be beneficial for transparency, trust, patient safety and reducing staff stress levels.
Hepatitis viruses are the most widespread cause of hepatitis and some cancer lymphomas in humans1.Hepatitis is a serious disease of the liver and described as a lifelong infection with swelling and inflammation (presence of inflammatory cells) in the liver, that if progresses, may lead to cirrhosis (scarring) of the liver, liver cancer, liver failure, and death. Hepatitis B (HBV) and Hepatitis C (HCV) are one of the viral types of hepatitis that leads to jaundice (a yellow discolouration of skin, mucous membrane and conjunctiva of the eye), anorexia (poor appetite), fatigue and diarrhoea and presumably it remains undiagnosed and leads to chronic carrier state but most infected individuals remain asymptomatic1-3. The hepatitis B virus is a DNA virus belonging to the Hepadnaviridae family of viruses and hepatitis C virus is a small, single stranded, RNA virus with a diameter of about 50 nm, belonging to Flaviviridae family of virus. Hepatitis B surface antigen (HBsAg) is present in the serum of those infected with hepatitis B, consisting of the surface coat lipoprotein of the hepatitis B virus. Anti-HCV antibody, a substance that the body makes to combat HCV 4. Hepatitis B virus is transmitted through blood and blood products, semen, vaginal fluids, and other body fluids. Hepatitis C virus is a blood borne or parenterally transmitted infection. Vehicles and routes of parenteral transmission include; contaminated blood and blood products, multi-transfusions (thalassemic and haemophilic patients), needle sharing, contaminated instruments (e.g. in haemodialysis, reuse of contaminated medical devices, tattooing devices, acupuncture needles, razors) and occupational and nosocomial exposure5-8. It stands to reason that an occupational risk for transmission of hepatitis virus in the health care setting, where unknown carriers of hepatitis infections are undergoing different procedures, in which there is a chance of contact of percutaneous blood, including transmission from infected patients to staff, from patient to patient, and from infected providers to patients9. There is a lack of routine serological screening prior to surgery, which is one of the factors responsible for increased disease transmission. The major risk factors include; re-use of contaminated syringes, surgical instruments and improperly screened blood products2. Without meticulous attention towards infection control and disinfection and sterilization procedures, the risk for transmission of blood borne pathogens in the health care setting is magnified.
The aim of our current study was to estimate the incidence of Hepatitis B and Hepatitis C among patients going through eye surgery at department of ophthalmology Liaquat University of Medical and Health Sciences Jamshoro at Hyderabad. This is one of the largest tertiary care centres in Sindh. This institution is a great referral centre for whole interior Sindh province.
MATERIAL AND METHODS
Study design and patients
This prospective observational study was carried out at Liaquat University Eye Hospital, Hyderabad, from June 2014 to February 2016. A total of 2200 patients undergoing eye surgery, who were unaware of hepatitis B & C infection were included in this study. No restriction was placed based on age and gender to ensure maximum participation.
Blood samples
The blood samples of all these patients were collected in the Hospital laboratory, Scientific Ophthalmic Diagnosis & Research Lab. Each patient was serologically screened, by using immuno-chromatography (ICT method) for qualitative detection of antigen for Hepatitis B and Hepatitis C virus antibodies, to find the carrier status of patients before surgery.
The blood was collected by a qualified technician / phlebotomist of our hospital laboratory under supervision of a consultant pathologist. Samples were allowed to coagulate at room temperature for 30 minutes, and then centrifuged at 3000 revolutions per minute (RPM) for 10 minutes. The serum samples were separated and kept frozen at -20°C for chemical and immunoassays. The HBV screening was based on the detection of antigen and detection of viral specific antibodies HCV in the sera using enzyme immunoassays. The test only shows whether a person has ever been infected by HBV or HCV, and not whether the virus is still present. According to the manufacturers’ literature, the relative sensitivity and specificity of HCV and HBV testing kits was 96.8% and 99% respectively.
Those patients with test results were found positive on screening test, were further confirmed by testing ELISA (Enzyme-Linked Immunosorbent Assay) method (4th generation ELISA) and were given advised for further testing on Polymerase Chain Reaction (PCR) for qualitative or quantitative detection of DNA/RNA (the viral gene).
All the data was entered in SPSS version 16 and the prevalence and percentage of all variables was measured.
RESULTS
A total number of 2200 patients were operated during the study, 1255 (57.04%) patients were male and 945 (42.95%) were female
Of these 2200 patients, 338 (15.36%) were serologically positive for hepatitis B virus & hepatitis C virus. Out of the 338 HBV or HCV positive patients, 56 patients (2.54%) were positive for hepatitis B surface antigen (HBsAg) and 282 patients (12.81%) were positive for hepatitis C antibody (HCVAb). (Figure 1&2). The majority of them were female, and 226 (66.86%) were in their 4th and 5th decade of life in both sexes (Figure 3).
Figure 1- A: Serologically positive for hepatitis C antibodies, B: Serologically negative for hepatitis C antibodies
Figure 2 - A: Serologically negative for hepatitis B antigen, B: Serologically positive for hepatitis B antigen
Figure 3: Incidence of Hepatitis B & C in different age group
DISCUSSION
Hepatitis B virus (HBV) and hepatitis C virus (HCV) are among the principal causes of liver diseases, with different frequency rates and various types all over the world. The World Health Organization (WHO) estimates that there are near 4 million people with chronic HBV infection and 170 million people with chronic HCV infection worldwide. Mortality rate of Hepatitis B is estimated to result in 563,000 deaths and hepatitis C in 366,000 deaths annually 1, 6, 10-12. The occurrence of hepatitis varies from country to country. The epidemiological estimates by WHO show that there is low prevalence of hepatitis C (<1%) in Australia, Canada and Northern Europe, and almost 1% in countries of medium endemism, such as the USA and most of Europe. The frequency is at its peak (>2%) in many countries of Africa, Latin America, Central and South-East Asia 5. As far as the Pakistani population is concerned, the incidence of hepatitis B and C is escalating. Previous studies reveal that the Pakistani population affected by HBV 10% and HCV is 5-10% 3. At times it will also vary among different regions of the same country, and is continuing to rising in certain parts, especially in the rural areas, the percentage of infected individuals is significantly higher 2. The total incidence of Hepatitis B and Hepatitis C in our study was found to be 15.36%. This was almost comparison to Naeem et al found to be 12.99% 2 and in our previous study reported incidence of anti HCV was 29.60% 7. W Ul Huda et al reported 17.33% incidence of HCV infection among their operated patients5, whereas a study conducted by Khurrum et al reported 6% incidence of anti HCV antibodies in health care workers in a local hospital13. The prevalence of Hepatitis B and Hepatitis C in preoperative cataract patients was found to be higher in males (59.18%) than females (40.82%), and Ahmed et al also showed that the total prevalence of Hepatitis B and Hepatitis C in males was very high compared to females among preoperative cataract patients14, which is controversial to our result. A study conducted in 2010 on different eye camps in Pakistan showed that 108 out of 437 patients were infected with Hepatitis B and Hepatitis C with a higher prevalence of the diseases in females with 60.18% (65/ 108) than in males with 39.81% (43/108) 15. Concerning demographic variables, the increase in the risk for HCV seropositive incidences increased with the age i.e. 7.1% at the age of 20 to 30 years whereas 21.4% at the age of 40 to 50 years. In our study, the higher prevalence of hepatitis B & C were in the age range of 30 – 60 years, which is comparable to the study of Talpur et al, in which 65% positive patients were above the age of 40 years16.
This study shows that the prevalence of these hepatitis causing viral pathogens are quite high. Doctors and paramedical staff in surgical and medical practice are at high risk of acquiring blood borne diseases from the patients on whom they operate.
CONCLUSION
The aim of the present study was to assess the prevalence of HBV and HCV infection among preoperative patients. The incidence of these hepatitis causing viruses are higher in our population. Therefore, it is a mandatory task to screen every patient for hepatitis B and C before any surgical procedure. The surgeons and health care professionals should protect themselves by using protective masks, eye protection glasses, and double gloves before handling infected cases. The used infected material, needles and other waste material should be destroyed properly using Biosafety protocols.
One in four adults are affected by musculoskeletal (MSK) problems, which account for up to 30% of General Practice (GP) consultations in the United Kingdom..1 Some GPs have direct access to community MSK services, but when not available, referrals are made to secondary care departments such as rheumatology. MSK training involves the skills that a rheumatologist needs to achieve competencies in the diagnosis and treatment of soft tissue rheumatism as opposed to inflammatory rheumatic joint disease.
It has been reported that junior doctors in the United Kingdom fail to routinely screen for MSK conditions on admission onto general medical or surgical wards2 which may be reflective of training issues. It was in our anecdotal opinion that MSK training at higher specialist training was being compromised as well. Within the United Kingdom doctors in training typically begin work as a first year rheumatology trainee four years after graduation from medical school following completion of both a two year foundation programme (encompassing a generic training programme which forms the bridge between medical school and specialist/general practice training) and a two year Core Medical Training programme, (involving 2 years of training, undertaking between four and six rotations in different medical specialties). At the time of writing, higher specialty training, such as in rheumatology, began at the level of Specialist Trainee 3 (ST3) and was either a four year training programme or a 5 year training programme if trainees were dually accrediting in general medicine.3 Higher specialist training involves rotating through different rheumatology departments within each Local Education Training Board (LETB).
In our opinion, the basic MSK skill set is essential to the training of a competent rheumatologist and trainees gain overall MSK competencies within routine clinical practice as they rotate through different hospitals during training. However, in some training programmes, there is very little MSK training opportunities, as MSK centres operating in the community in the United Kingdom, mean that these patient groups are not being treated in training hospitals. Faculty in these centres are competent to train, but training opportunities in MSK centres are reduced.
Rheumatology registrars in-training have expressed the anecdotal view that MSK training may be compromised, partly due to the reduction of referrals to secondary care and partly due to the inevitable focus on training in the more complex inflammatory conditions.
Rheumatology trainees in the UK were surveyed in 2015 on behalf of the Rheumatology Specialist Advisory Committee to assess confidence and ability in dealing with MSK conditions during and on recent completion of training. The survey was disseminated to rheumatology trainees via the trainee representative from each LETB.
77 responses were received across 15 LETBs from a total of an estimated 223 trainees. 20 of these surveys were incomplete, with not all questions being answered but those questions answered were considered in the results of this survey. Responses from trainees across all career grades from ST3 (1st year of specialist training) to 2 years post Certificate of Completion of Training were received.
58 out of 63 doctors (92%) thought MSK medicine to be an important part of rheumatology training. Free text comments recognised that MSK conditions were frequently referred to rheumatology and differentiating between inflammatory and non-inflammatory pain is important.
Only 41 out of 64 doctors (64%) felt they managed patients with soft tissue pathology on a daily basis and 20 out of 63 (32%), felt they were not yet confident in diagnosing and distinguishing between different types of soft tissue pathologies.
Exposure to, and experience with MSK medicine in current jobs and throughout training ranged from poor to excellent.
Only 9 out of 58 trainees (16%) felt they were lacking in competency for their level of training in managing the MSK pathologies outlined in the Joint Royal Colleges of Physicians Training Board (JRCPTB) 2010 rheumatology curriculum. The majority of trainees felt they were either partially competent in all, or some areas, satisfactory for their level of training.
Interestingly, only 39 out of 58 trainees (67%) felt their training in injection techniques had been at least ‘adequate’. Some trainees mentioned they had been self-taught in some injection procedures and training had been limited in certain soft tissue injections (most commonly plantar fasciitis, tendon sheath and elbow enthesis injections).
This survey has limitations in that the numbers of trainees surveyed were small. However, our total response number considering the usual poor response rate for online surveys is reasonable. Our survey was not validated and it is likely that there will be an element of selection bias in the responses received.
However, one of the strengths of our survey is the ability to review responses by seniority. We analysed further the confidence rating according to training level grade and we looked into two main subgroups, the more junior trainees (ST3 and ST4s) and the more senior trainees (ST6 and ST7). As expected the more junior cohort rated their confidence slightly lower compared to the more experienced group. Within the junior group (n=17) only 41% suggested they felt confident for their level of training when generically asked about their general diagnostic skills on MSK, which improved to 59% when this question was mapped to the curriculum. In the senior group of ST6 and ST7 (n=25), the confidence levels were significantly higher (80% felt confident appropriate to their level of training) and there was no change in confidence levels when skills were mapped to the curriculum. (Table 1). This may reflect the natural increase in experience and exposure to MSK medicine with progression in training, but also the better understanding of the curriculum requirements by the more senior trainees.Only one fully completed survey was received from a rheumatologist post Certificate of Completion of Training making this subgroup too small for further analysis.
Table 1:
(n)
Q6) Confidence in dealing with MSK
% Q6
Q9) Confidence mapped to curriculum
% Q9
ST3 and ST4- junior
17
7
0.41
10
0.59
ST6 and ST7- senior
25
20
0.8
20
0.8
Q6) How confident do you feel in diagnosing and distinguishing between different types of soft tissue pathologies/MSK in your daily practice? Q9) Do you feel competent in diagnosing and managing the above MSK pathologies outlined in the 2010 rheumatology curriculum?
Within this limited survey, the views of 77 trainees have shown that training in MSK could be improved for rheumatologists in training at all levels. Although trainees felt they were lacking confidence in dealing with certain areas of MSK medicine, when competencies were mapped out to the rheumatology curriculum, trainees felt they were achieving appropriate competency for their level of training although this was not assessed objectively.
The trainees’ perception of the level of competency needed in dealing with MSK conditions seemed to overestimate the requirement of the 2010 rheumatology curriculum. In clinical practice, trainees may feel they encounter different MSK pathologies, which they are being expected to manage which are not being given sufficient emphasis within their curriculum. Further questioning in this area may conceivably lead to adjustments within the curriculum and the training programmes.
In particular, to improve training in MSK medicine, rheumatology trainees valued teaching from physiotherapists and being able to attend specialist sports medicine clinics. Trainees who had ‘independently’ taken time to gain experience in this way felt that their training had benefitted. To support trainees in achieving these competencies it may be worthwhile adding a prerequisite in the Annual Review of Career Progression (ARCP) process (a formal method in UK medical training by which a trainee’s progression through their training programme is monitored and recorded) to ensure dedicated time is set aside for this aspect of MSK rheumatology training. Completion in a range of direct assessments such as Clinical Evaluation Exercises (miniCEX), and DOPs (Directly Observed Procedures) may ensure competency in this aspect of rheumatology training as well as secure confidence in dealing with MSK conditions and soft tissue pathology.
With changes in the nature and geography of rheumatology specialist services we feel these aspects of rheumatology training should not be overlooked so trainees are equipped to deal with MSK conditions independently by their completion of training.
Like doctors in other specialties, general medical practitioners (GPs) are exposed daily to human suffering which most of society try to avoid.1 The World Health Organisation (WHO) predicts that by 2030 depression will be ‘the leading cause of disease burden globally.’ And that 1 in 4 individuals seeking health care are ‘troubled by mental or behavioural disorders, not often correctly diagnosed and/or treated.’2, 3 Doctors suffer from stress, anxiety and depression (as well as vascular disease, cirrhosis of the liver and road traffic accidents) more than the general population.4-10 Help for doctors is inadequate and doctors are reluctant to seek help.1, 4, 11 Where improvement is suggested, it is usually as counselling and general support.11 Instead of ‘more of the same’, we suggest a radically different approach: Adaptation Practice, which Clive Sherlock pioneered and has taught since 1975. It is pragmatic and safe. This study tests its acceptability to a group of working doctors.
Doctors bear the responsibility for fellow human beings’ health, well-being and, often, for their very survival. Added to this, GPs are under increasing pressure from more patients who want more cures and from health service managers who demand clinical excellence and more administration and more managerial skills of them. GPs’ stress is related to increasing workloads, changes to meet requirements of external bodies, insufficient time to do the job justice, paperwork, long hours, dealing with problem patients, budget restraints, eroding of clinical autonomy, and interpersonal problems.6, 10, 12 The recent rise in the GMC’s Fitness to Practice complaints related to patients’ expectations of doctors is yet another stress making them feel threatened.13
Job satisfaction for GPs is at its lowest level since a major survey started ten years ago, while levels of stress are at their highest. In 2015 there had been a year on year increase in the number of GPs reporting a slight to strong likelihood of their leaving ‘direct patient care’ within five years, with 53% of those under 50 and 87% of those over 50.6
By nature and vocation, GPs want to help but too much pressure is unbearable and takes its toll. They work, not with numbers, data or profits, but with human suffering, which, inevitably, is an emotional burden because of compassion and because it makes them aware of their own vulnerabilities and mortality. 3, 14 When combined with heavy workloads and low morale, doctors themselves inevitably suffer emotionally and psychologically.7, 10, 14 At the same time they and others feel they should be invincible.1, 15-17 What professional help is available for them is inadequate.3, 4, 18, 19 Existing support services in the UK are underfunded and sporadic.4 Some are outsourced to counselling services, and some of these are by telephone. Doctors do not like to be counselled and are reluctant to use these services.4, 15, 17
Doctors themselves are the mainstay for diagnosis and treatment of mental illnesses but are not adequately trained.3, 20 Mental illness is not well understood and conventional treatments are insufficient and often harmful. 15, 20-23 Consequently, doctors do not have the wherewithal to deal with the emotional and psychological problems they face every day in their patients and often in themselves, their colleagues and their families.4, 12, 18
There is significant prejudice, stigmatisation and intolerance of mental ill health within the medical profession due to lack of understanding and fear.3, 4, 9, 15, 17, 20, 21, 22, 24 This not only affects how doctors treat their patients, it also exacerbates their own difficulties when they suffer with emotional and psychological problems themselves, and dissuades them from self-disclosure and from seeking professional help.3, 4, 8, 10, 18, 20, 25, 26 To succumb to stress, anxiety and depression is seen as being weak and inadequate as a person and in particular as a doctor. 3, 4, 15 Doctors think they should know the answers and should be able to cope.1, 4
However, doctors are willing to learn work-related skills as this present study set out to show.11 Adaptation Practice is training; not treatment or therapy. The course in this study was presented as a postgraduate programme for doctors to learn how to cope with stress, anxiety and depression.
METHOD
Recruitment
We asked by letter all 314 GPs registered in one UK urban and semi-rural Health Authority Area if they would be interested in a course of twelve fortnightly seminars to learn the basics of Adaptation Practice: a programme of self-discipline to cope with stress, anxiety and depression. Included, was the Hospital Anxiety and Depression Scale (HADS). Those who responded and whose HADS scores were ≥ 8 (the threshold for anxiety and depression) were invited to the course.
Stress, anxiety and depression
Anxiety and depression were assessed by the HADS and stress by a simple stress scale (SSS – see Table 1) one month before training started, immediately prior to training, at three months (mid-way through the training) and at six months (at the end of training).
Table 1: The Simple Stress Scaledeveloped by Clive Sherlock and used to assess the level of stress in a subject. A total score ≥ 8, out of a maximum of 24 is suggestive of a disturbing level of stress or burnout.
I feel I am under too much stress: 0 hardly ever 1 occasionally 2 most of the time 3 all the time
I feel exhausted: 0 seldom 1 some of the time 2 much of the time 3 most of the time
I care about other people: 0 as much as I ever did 1 rather less than I used to 2 definitely less than I used to 3 hardly at all
I have lost my appetite: 0 not at all 1 a little 2 moderately 3 significantly
I sleep well: 0 most of the time 1 quite often 2 occasionally 3 not at all
I am irritable: 0 not at all 1 occasionally 2 quite often 3 very often indeed
I feel dissatisfied: 0 never 1 occasionally 2 quite often 3 most of the time
I feel run down: 0 not at all 1 occasionally 2 quite often 3 most of the time
Evaluation of Adaptation Practice
Half of those GPs who applied for the course were unable to attend because of prior commitments on the days planned for the course. These acted as a control group. Those who attended the course were the study group. All those who attended were also assessed in private by the authors immediately before and throughout the course. At the end of the course the doctors wrote anonymous self-assessments.
Training in Adaptation Practice
Those attending the course were taught not to express and suppress upsetting and disturbing emotion, not to distract their attention from it (including not to think about it and not to analyse it) and not to numb themselves to it with chemicals (alcohol, recreational drugs or prescribed medication). Instead, they learned how to engage with their moods and feelings physically, not cognitively, and how not to engage with thoughts about them. They were instructed to practise this six days a week with whatever they were doing, wherever they were. They were all offered unrestricted confidential telephone and e-mail support from the authors between training sessions and after the course had finished.
Statistical Analyses
The results are reported as means ± standard errors of the means. The scores were normally distributed and the data were analysed by analysis of variance with additional paired comparisons within periods, using the LSD method. Correlations were determined using Pearson’s correlation. The analyses were carried out using the statistical software programme SPSS 17.0 for Windows.
RESULTS
Recruitment
Of 314 registered GPs, 225 (72%) responded to our initial contact, and of these 152 (68%) said they would be interested in participating in the training course. Recruitment was restricted to those with HADS scores ≥ 8. Of the 225 who responded there were 71 (32%) for anxiety, 35 (16%) for depression, and 79 (35%) for both. 29 (13%) applied to attend the course. All were experienced GPs. 15 of these attended and 14 were not able to attend because of pre-existing commitments on the course dates. They asked for alternative dates but these were not available.
At the initial assessment (one month before the course started) there were significant correlations between the scores for anxiety and depression (P < 0.001), anxiety and stress (P < 0.001) and depression and stress (P < 0.001). At the second assessment immediately before the course started these correlations remained highly significant.
Effects of Adaptation Practice
All those who attended the course reported a subjective improvement in their abilities to cope with their own stress, anxiety and depression, and in their sense of well-being.
Anxiety
There were no significant differences between the control and study groups either one month before the start (P=0.949) or immediately before the first session (P=0.914). The anxiety scores in both groups remained greater than 8 at both assessments (Figure 1). At the mid-point of the course the mean score had fallen slightly in the study group (Figure 1) but the difference was not significant (P=0.652) By the end of the course the mean anxiety score in the study group was significantly lower (P=0.008) than that of the control group (Figure 1). The mean scores for anxiety decreased over the 4 assessments. This tendency was significant in the study group (P=0.002) but not in the control group (P=0.567).
Figure 1: The mean anxiety scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of anxiety, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Depression
There were no significant differences between the control and the study groups either one month before the start (P=0.310) or immediately before the first session (P=0.880). The mean HADS scores for depression before training were all greater than 8 (Figure 2). At three months (the mid-point of the course) the difference between the mean scores in the two groups was not significant (P=0.631). At the end of the course the mean depression score in the study group was significantly lower (P=0.046) than the control group (Figure 2). The mean scores for depression decreased over the 4 assessments. This tendency was significant in the assessment group (P=0.003) but not in control group (P=0.689).
Figure 2: The mean depression scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of depression, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Stress
There were no significant differences between the control group and the study group either one month before the course started (P=0.234) or immediately before it started (P=0.505). The stress scores were all greater than 8 (Figure 3). At three months (the mid-point of the course) the difference between the mean scores between the two groups was not significant (P=0.621). At the end of the course the mean stress score in the study group was lower (P=0.077) than that of the control group (Figure 3). The mean assessment scores for stress decreased over the 4 assessments. This decrease was significant for the assessment group (P=0.001) but not for the control group (P=0.425).
Figure 3: The mean stress scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of stress, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Correlations
At all four assessments there were correlations among all three psychological parameters. At the initial assessment the correlation between anxiety and depression (r2= 0.405; P = 0.029) and between depression and stress (r2= 0.800; P < 0.0001) were significant but the correlation between anxiety and stress was not (r2= 0.253; P = 0.185). At the commencement of the course the correlation between anxiety and depression (r2= 0.479; P = 0.009), between depression and stress (r2= 0.765; P < 0.0001) and between anxiety and stress (r2= 0.486; P = 0.007) were all significant.
At three months (the mid-point) the correlation between anxiety and depression (r2= 0.526; P = 0.003), between depression and stress (r2= 0.622; P < 0.0001) and between anxiety and stress (r2= 0.790; P < 0.0001) were all significant and similarly at the and of the course: the correlation between anxiety and depression (r2= 0.604; P = 0.001), between depression and stress (r2= 0.577; P =0.001) and between anxiety and stress (r2= 0.740; P < 0.0001) were also all significant.
Assessments of the doctors’ psychological states and methods of coping
The doctors attending the course were assessed individually in private. They variously complained of stress, anxiety and depression. Notable findings included suicidal thoughts, plans for suicide, self-medication, excessive consumption of alcohol and an intention to leave the medical profession because of the unbearable pressures involved.
By the end of the course all these signs and symptoms had improved and the doctors felt confident in their ability to cope not only with pressures from outside but also with emotion, moods and feelings inside. One doctor still wanted to leave the profession but less adamantly than before, and stayed.
There was no qualitative assessment of the control group.
Qualitative Self-assessments
The anonymous self-assessment reports give meaningful, subjective accounts of what the doctors experienced individually. They fall into four main themes. There were no negative comments.
Connecting with emotion physically in the body
The following comments indicate contact with emotion:
‘I am more aware of my feelings.’
‘It is difficult to say “Yes” to unpleasant or upsetting feelings and situations. I have always preferred to avoid them and I have had a lifetime of suppressing emotions, so it is very difficult to say “Yes” to them, but this is what I am now doing.’
‘Since I’ve been more aware of my feelings there has been an enormous improvement in concentration.’
Developing inner emotional strength and coping.
A number of comments indicate the need to develop the strength to contain emotion physically in the body:
‘I am more accepting of daily stresses at work.’
‘I try to deal with problems instead of feeling so desperate and so wronged by them.’
‘I am calmer, and I lose my temper less often and less dramatically.’
‘The Practice was difficult initially because of my own resistances to it.’
‘I’ve always avoided seeking help for myself. I often feel worse than the patients I prescribe antidepressants for. I can now cope and I feel stronger but I don’t feel I’ve been treated and I now realise I didn’t need treatment: I needed to learn what to do and how to do it.’
Dealing with unpleasant, unwanted thoughts.
These comments illustrate the doctors’ new reactions to thoughts as they started to address the underlying emotion that normally drives worrying thoughts:
‘I now have less ruminations.’
‘As a long-standing ruminator I now realise these thoughts are the source of many anxieties. Thoughts were the main problem for me.’
‘I have learned to deal with obsessional thoughts by not giving time to them.’
General well-being.
The doctors commented on their sense of general well-being and ability to cope:
‘I am less tense and less anxious.’
‘I am now coping with episodes of work overload much better.’
‘I am feeling better generally.’
‘This has given me confidence to pursue the course of action I knew was correct.’
‘There are all-round improvements because of adapting myself to work and other people.’
‘I am happier and more content, optimistic and much less negative.’
DISCUSSION
Varying degrees of stress, anxiety or depression are universal.16, 26 Only about half of those thought to be clinically affected by these conditions seek help for them.26 If put into practice, sound medical knowledge and training can be beneficial to doctors’ own health.1, 11, 15 This does not seem to be true for stress, anxiety and depression.22 Too little is known about emotional and psychological problems, and treatment for them is inadequate.2, 9, 15, 17, 19, 21, 23, 28, 29
In this study, there was a high level of interest in how to deal with stress, anxiety and depression. Almost one third of respondents had scores on the HADS and SSS that suggested worrying levels of emotional and psychological problems amongst these working GPs. The fact that 152 doctors (68% of respondents) declared an interest in a six-month evening course (90 minute sessions after work on Thursday evenings) to learn how to deal with these conditions, suggests that:
stress, anxiety and depression are significant problems either amongst their patients or for the GPs themselves, or both
GPs are not confident in their ability to deal with them and want to learn more
although they have a strong tendency not to admit that they cannot cope and not to seek help, doctors are willing to attend a course to train and to learn.11
Most doctors tell their patients to seek professional help and to talk about their feelings but do not do so themselves.3, 5 They prescribe drugs for their patients that either the doctors will not take themselves or that they take but find ineffective. Of the 15 GPs on the course only one had mentioned psychological difficulties to a colleague and one to a partner and both only reticently. 16
ADAPTATION PRACTICE
Adaptation Practice strongly discourages self-disclosure, except in private to the Adaptation Practice teacher, which is necessary in order to assess the nature and severity of any problems and to lay the foundations for a rapport. Adaptation Practice sessions involve detailed discussion of moods and feelings as physical sensations and powerful forces that affect behaviour in all human beings. The ethos in Adaptation Practice is for participants to learn from their own experience how they are affected by emotion and how they can change this by containing themselves and not letting the emotion control them. It is not to criticise, judge, blame or condemn. Consequently, without the causes of stigmatisation, there is no prejudice and no stigma; instead there is respect and dignity and a pragmatic attitude to change.16
Adaptation Practice trains individuals to bear and endure upsetting, disturbing emotion by not expressing it, not suppressing it, not distracting themselves from it and not numbing themselves to it with drugs (alcohol, recreational drugs or prescribed medication). Bearing it this way develops emotional strength and resilience.
The high level of interest, the willingness to attend in groups and the positive results from this study indicate that Adaptation Practice is an acceptable way of teaching doctors how to cope with their own stress, anxiety and depression, that makes sense intellectually and emotionally. This, as well as the pragmatic approach mentioned above, makes Adaptation Practice radically different from other approaches.
GENERAL COMMENTS
Given that those who could not attend asked for an alternative day to attend, gave us reason to assume that the manner in which the study group and the control group were selected – individual availability on a given week night – would not have biased the sampling procedures and it seems reasonable to assume that the two groups did not differ in any meaningful way that would have biased the outcome.
Not surprisingly, there were strong positive correlations between anxiety and depression and between depression and stress on all assessments and between anxiety and stress on all but the first assessment, suggesting a strong association among these parameters of psychological states.
The mean scores for anxiety, depression and stress fell significantly in the participating GPs compared with the control group. The subjective reports from both the medical assessments and the self-assessments support these changes in the study group.
This study begs a number of important questions:
if doctors are prejudiced and stigmatise mental illness amongst themselves then what are their conscious, or unconscious, attitudes to mental illness in their patients? 3, 5, 9, 24
if doctors cannot cope with emotional problems themselves then whom are they and their patients to turn to for help? This is not the same as doctors suffering from physical conditions requiring surgery, or medications such as insulin or antibiotics.3, 5 Doctors expect, and are expected, to be able to cope with their emotions and, if necessary, that the treatment they give their patients will also work effectively for themselves
what are doctors to do and what are their patients to do, when doctors succumb to their own moods and feelings?
Adaptation Practice could be integrated in the medical curriculum at undergraduate and postgraduate levels, including Continuing Professional Development (CPD). Not only GPs but all doctors and other healthcare staff (nurses, physiotherapists, occupational therapists, social workers, etc.) could develop emotional resilience – which the GMC have proposed in recent years – and a better understanding of emotional and psychological problems and mental illnesses.
It is hoped that this preliminary study will stimulate and encourage a new way of looking at and investigating emotional and psychological problems and lead to further evaluation of Adaptation Practice.29, 30
With adequate training doctors and psychologists could teach Adaptation Practice.
The CASC (Clinical Assessment of Skills and Competencies) has been running since 2008 and is the final membership examination for the Royal College of Psychiatrists (MRCPsych).1 It is a clinical examination and follows an OSCE format (Objective Structured Clinical Examination), where candidates move through 16 short stations.2,3 We have been running a mock CASC in the West of Scotland for the last few years and have received consistently good feedback from candidates. This article describes our experience of organising the mock exam.
Step 1: Practicalities
The organising committee
Our mock CASC is arranged by the organising committee for the local core psychiatry education programme (MRCPsych course). This committee is comprised of a consultant chair, higher trainee chair and one or two trainee representatives from each higher subspecialty and each core training level. The higher trainee chair takes the lead with organising the mock, with the support of other committee members. This works well, as the trainees have recent experience of sitting or preparing for the exam and are enthusiastic about medical education.
Support from our postgraduate operations manager is invaluable. She works closely with the committee to book the venue and actors, and order equipment such as screens and a bell. She also has a key role in advertising the mock exam to trainees, booking places and being a point of contact for candidates. She assists with set up on the day of the exam and prints station instructions, marking schemes and labels for candidates.
Venue
Our mock exam is held in the same venue as our core trainee educational programme. We have 2 rooms to use for stations and a waiting area for candidates. Screens are borrowed from Glasgow University Medical School to create separate stations.
Timing
The mock exam takes place around 2 weeks before the CASC. This enables candidates to have prepared for the exam and leaves some time to work on any issues identified by the mock. Planning usually starts 4-5 months in advance of this, with increasing intensity and time commitment as the exam approaches.
Step 2: Mock Exam Format
CASC format and blueprint
The CASC itself includes morning and afternoon circuits, which all candidates will move through. There are 16 stations in total, with 90 seconds between each to read the task instructions. The morning session comprises 4 pairs of ‘linked’ stations, lasting 10 minutes each. In these paired stations, the second station is connected to the first in some way, such as taking a history in the first part then discussing with a family member in the second. Each station is marked independently. The afternoon consists of 8 single stations, lasting 7 minutes each. A passing list is posted online after a few weeks, with specific feedback made available to unsuccessful candidates.2
Mock CASC format
Our mock CASC is run in one afternoon session from 1.30-5pm. We have been able to include 16 stations by running the 2 circuits simultaneously. To make this possible, each station is 7 minutes in duration, with 90 seconds between stations. 4 candidates start after a delay, as it is not possible to start on part 2 of a linked station. Trainees are allocated candidate numbers and starting stations for both circuits to coordinate this effectively (figure 1). 16 candidates can take part in the mock exam.
Figure 1. Candidate numbers
Candidate Name
Number
1st loop starting station
2nd loop starting station
1
1a
5
2
2a
6
3
3a
7
4
4a
8
5
1a (8.5 min delay)
9
6
2a (8.5 min delay)
10
7
3a (8.5 min delay)
11
8
4a (8.5 min delay)
12
9
5
1a
10
6
2a
11
7
3a
12
8
4a
13
9
1a (8.5 min delay)
14
10
2a (8.5 min delay)
15
11
3a (8.5 min delay)
16
12
4a (8.5 min delay)
At least 3 other higher trainee helpers are recruited to assist the coordinator on the day of the exam. The same marking scheme is used for each station, covering domains common to all stations, such as building rapport and range and depth of questioning. There is also space for specific feedback, which examiners are encouraged to provide, though they do not interact with candidates directly during the exam. Forms are completed contemporaneously and distributed to candidates immediately after the mock exam.
Step 3: Writing the Stations
The content of the CASC follows a blueprint, which is available through the RCPsych website. A variety of skills are tested during the 16 stations of the exam, including history-taking, mental state examination, risk assessment, cognitive examination, physical examination, case discussion and difficult communication.3 We refer to the blueprint when selecting which stations to include in the mock. Each year, recent CASC candidates are asked to suggest stations and we combine these with previous stations to construct the mock exam. New stations are written by the trainee who suggested them, including candidate instructions and actor’s notes. The higher trainee organiser formats these to maintain consistency across the mock exam.
Role-play actors
For our most recent mock CASC, we employed paid actors for every station. These actors are part of a local agency which has experience in working as simulated patients for Glasgow University exams and communication skills sessions. In previous years, we have recruited a combination of core/higher trainees and actors. We have found pros and cons to each approach. The use of paid actors was more realistic for trainees but writing scripts proved more challenging as instructions required greater detailed in relation to specific psychiatric information, such as how a person with mania may present.
Step 4: Recruiting Examiners
There are a number of local consultant psychiatrists who are actively involved in teaching. They are supportive of the mock CASC and enthusiastic about examining stations. After the stations have been devised, consultants are invited to examine based on their areas of expertise. Higher trainees with particular interest in education are then asked to examine any remaining stations. Candidate instructions and actor’s notes are circulated to examiners in advance (figure 2). A simple guide to the mock exam is also sent to any new examiners. As we use the same marking scheme for each station, it is down to the experience of the examiner to consider whether the candidate has addressed the specific tasks appropriately.
Figure 2. Station template
Station
Title
Actor
Examiner
Written?
Sent?
1a
1b
2a
2b
3a
3b
4a
4b
5
6
7
8
9
10
11
12
Step 5: The Day of the Mock Exam
The higher trainee coordinators arrive at least 1.5 hours prior to the start time to set up the venue. Examiners, actors and candidates are asked to arrive 15-30 minutes before the scheduled start time. Each group is briefed on the exam format and given the opportunity to ask questions. Actors and examiners are shown to their stations and allowed time to discuss them. Candidates are provided with numbered labels to wear, for examiners to record on their marking sheets. The 4 candidates who will be starting later are asked to wait, while the others are shown to the examination rooms. They are shown which station they will be starting at, then queue in order at the door.
The mock exam coordinator stands where they can be heard by both rooms. There are 1 or 2 helpers in each room to guide the candidates around the circuit. The bell is rung to signify the start of the exam, the end of the 90 second preparation time (the start of each station), 1 minute warning and the end of each station. The candidates who were allocated to start later are brought into the circuit and shown to their station as the ‘end of station’ bell is rung, as this also signifies the start of the 90 second preparation time for the next station.
Marking schemes are collected and sorted during the break. Candidates are not kept separate from examiners, actors or each other. They are advised that they will get the most out of the afternoon if they don’t discuss the stations but this is ultimately their choice.
Examiners and actors return to their stations following the short break and candidates swap between circuits. Following the second round, there is another short break. Actors are excused at this point and most examiners remain for a feedback session. Marking schemes are collected, sorted and distributed to candidates. One room is re-set for group feedback. Examiners are thanked for their time and each is asked in turn for general feedback, hints and tips on their station (figure 3).
Figure 3. Mock CASC timing
11.30pm
Coordinators arrive & set up venue
12.30-12.45pm
Candidates, actors & examiners on site
1pm
Exam starts
2.15pm approx
Break
2.45pm
Exam re-starts - candidates switch circuits
4pm approx
Exam ends
4.30pm
Feedback forms distributed/ group feedback session
5pm
End
Overcoming Potential Problems
Examiners
Our examiners are all either higher trainee or consultant psychiatrists. It is therefore possible that unforeseen circumstances mean that they may have to cancel at very short notice, attend late or not at all, or be called away during the mock exam. Each of these has happened over the past few years but has been easily managed by the extra higher trainee helpers stepping in to examine a station.
Actors
All of our actors have attended as planned. If a paid actor has to cancel at short notice, the agency will find a replacement. If a trainee actor did not attend, one of the higher trainee helpers could step in. Another potential problem which we have encountered is actors not performing as intended. This can be minimised by preparing clear instructions for actors, with examiners providing some direction if needed.
Quality control of stations
It is difficult to know how a station will work until it is used in the mock exam. To minimise the risk of problems, stations are checked and formatted before the exam. They are circulated to actors and examiners in advance to allow time for them to raise any concerns and clarify any uncertainties. Despite following these processes, there are some stations which appear unclear or do not run smoothly on the day of the mock exam. It is helpful to receive feedback from examiners, so that stations can be amended or avoided in future.
Timing
Our mock exam follows a very tight schedule. If the mock exam itself overruns, then fewer examiners may be able to remain to provide feedback. The higher trainee coordinator should keep time carefully during the day of the mock exam, particularly during break times, which are very brief. Support from other higher trainee helpers is essential for this, in working together to collect and organise marking sheets and guiding examiners, actors and candidates to stations. Late arriving examiners remain a potential problem due to their other commitments. We provide a sandwich lunch to our examiners prior to the exam, which helps with prompt attendance.
Venue
The venue we use is quite cramped and can become noisy. We have access to only 14 screens to divide the 16 stations so they are close together and those at the ends of the room are not fully enclosed. The screens are thin so only muffle the noise from neighbouring stations. These issues of space and noise are difficult to overcome. Trainees are warned in advance and aim to focus on their own station as much as possible.
Recruiting actors, examiners and candidates
To date, we have not experienced any problems in recruiting actors, examiners or trainee helpers. We have been able to fill all candidate places and often have a waiting list. If necessary, the mock exam could be run with fewer stations and still provide helpful practice for trainees. If resources were tight, trainees could be role-play actors for some or all of the stations.
Conclusion
We run a local mock exam annually due to continued demand from trainees. It takes significant time and effort to arrange but is good experience for the organiser and local trainees and consultants remain enthusiastic. The mock CASC in the West of Scotland puts a strong emphasis on providing feedback for trainees to work on. The provision of completed marking sheets on the day of the exam and the group feedback session help with this ethos. Our experience has shown that a mock CASC can be delivered locally, at a low cost, while still providing trainees with a realistic exam experience.
Multiple Sclerosis (MS) is an inflammatory, demyelinating disease of the central nervous system (CNS) that affects approximately 400,000 people in the United States and 2.5 million worldwide.1 There are rare variants of this disease that can profoundly delay diagnosis and treatment. Examples of such variants include: Tumefactive MS, Acute Disseminated Encephalomyelitis, Neuromyelitis Optica, Marburg’s MS and Balo Concentric Sclerosis.2 These variants have a uniquely aggressive presentation and do not exhibit classic MS features.2 Classic MS features include relapsing and remitting sensory and motor impairments, optic neuritis and pain. These aggressive variants are more likely to present with symptoms similar to neoplasm such as motor impairments and seizures. When dealing with these aggressive MS variants diagnostic options include Magnetic Resonance Imaging (MRI), Single Photon Emission Computed Tomography (SPECT) scan, MR spectroscopy and Cerebrospinal Fluid (CSF) analysis.3
Invasive tests such as brain biopsy are not warranted unless absolutely necessary. In MS, a biopsy must not be completed in order to confirm a diagnosis. However, to confirm a diagnosis of cancer a biopsy is required.
We present a rare case of Tumefactive MS that exhibited a clinical picture identical to brain metastasis. This was diagnosed with surveillance MRI and CSF analysis in the absence of a brain biopsy.
Case presentation
A 48-year-old African American female was brought in by emergency medical services after falling with a brief loss of consciousness. Associated symptoms included dull chest pain, diaphoresis and shortness of breath. While in the emergency department she also developed nausea, vomiting and dizziness. The patient reported no similar previous episodes and denied precipitating events. There was nothing else to note on review of systems. The past medical history included hypertension with no previous surgeries and family history included breast cancer of the mother diagnosed at age 47. The patient denied tobacco, alcohol and intravenous drug use. She noted an allergy to iodine.
On physical examination the patient was afebrile, normotensive and tachycardic with an oxygen saturation of 89% on room air. She was alert and oriented but pale and diaphoretic with mild left sided chest pain. Cardiac examination revealed a normal rhythm tachycardia and no murmurs were heard. Her neurological examination showed a normal mental status, normal cognition/comprehension and that Cranial Nerves II-XII were intact.
Laboratory findings included haemoglobin of 9.8 g/dL, 30.8% haematocrit and potassium of 3.3 mmol/L. Electrolytes were otherwise normal. Cardiac workup showed a normal ECG and slightly elevated cardiac enzymes of 0.319 ng/mL.
Given the patients tachycardia and desaturation, a stat Ventilation-perfusion (V/Q) scan was completed (patient had an iodine allergy). The V/Q scan revealed a perfusion defect suggesting pulmonary embolism (PE) as the cause of symptoms. Subsequently the patient was placed on appropriate anticoagulation.
Head CT (computed tomography) showed a left centrum semiovale round hypodense lesion measuring 1.4 cm, a left basal ganglia round hypodense lesion measuring 1.0 cm and a left occipital lobe round hypodense lesion measuring approximately 1.0 cm (Figure 1). No midline shift was seen. MRI showed multiple hypointense T1/hyperintense T2 nonenhancing lesions, mainly within the left cerebrum (Figure 2 A-F). The three largest lesions within the left posterior centrum semiovale (2A), left globus pallidus (2B) and left posterior corona radiata adjacent to the occipital horn (2C) measured 1.5 cm, 1.0 cm and 1.0 cm respectively. Perilesional vasogenic oedema was seen in all except the basal ganglia lesion. There were bilateral cerebral scattered foci of hyperintense FLAIR/T2 signals (D-F). The imaging suggested a differential diagnosis which included metastasis, infection or primary CNS malignancy.
Further work up in search for possible malignancy was completed. Skin map revealed no concerning nevi. Mammogram showed no tumor. CT of the abdomen and pelvis revealed a 2.6 cm indeterminate hypodense lesion in the left lobe of the liver (Figure 3A) along with an enlarged fibroid uterus (17x 7 x 14 cm). Liver biopsy was considered but a repeat MRI and ultrasound showed the lesion to be cystic, so this was deferred following surgical oncology recommendations (Figure 3B). For the hypertrophic uterus found on imaging, gynecology felt no further workup was necessary as they attributed the findings to a fibroid uterus.
Tumor markers CA 27-29, CA 19-9, CA 125 and AFP were all sent and came back negative. Initial lumbar puncture with CSF analysis was not completed secondary to possible complications that could be incurred while on necessary PE anticoagulation.
Due to a non-focal neurological examination, she was discharged on Levetiracetam 500 mg for seizure prophylaxis and Dexamethasone 4 mg for perilesional oedema. Over subsequent months the patient did well without headaches, vision changes or seizure like activity. On subsequent visits to the clinic, she had no evidence of focal neurological deficits except for mild bilateral symmetric hyperreflexia. Given that the metastatic work up remained negative, we considered obtaining a baseline Positron emission tomography (PET) scan to ensure we were not missing any possible metastasis.
She subsequently went back to work full-time and reported no symptoms. Repeat MRI of the head (Figure 4 A-C) showed predominantly T1 hypointense and T2 hyperintense (A-B) lesions with significant decrease in size from MRI done three months ago. These lesions demonstrated no enhancement to incomplete ring enhancement, with diminished vasogenic oedema (A). These findings suggested an inflammatory demyelinating process so a lumbar puncture was obtained after anticoagulation was held. CSF analysis was done using Isoelectric Focusing (IEF) and immunoblotting methodology. This revealed a normal myelin basic protein but with eight oligoclonal bands restricted to the CSF. These findings solidified the suspicion of Tumefactive MS.
Figure 1. Head CT without contrast: left centrum semiovale round hypodense lesions measures 1.4 cm with perilesional vasogenic edema
Figure 2. MRI of brain showing axial T1-weighted (A-C) hypodense lesions of the left centrum semiovale(A), left basal ganglia(B) and left occipital lobe(C). Axial T2-weighted (D-F) views show multiple hyperdense lesions corresponding to the same locations. Perilesional vasogenic edema is seen.
Figure 3A. Thorax CT without contrast. 2.6 cm left lobe liver lesion.
Figure 3B. MRI of abdomen showing coronal T2-weighted half-Fourier acquisition single-shot turbo spin-echo (HASTE) hyperdense lesion. A mildly enlarged liver measuring 18.7 cm in craniocaudal span. Simple 2.8 x2.4 cm cyct in the medial segment of left lobe.
Figure 4. MRI of brain (3 month after initial scans) showing axial T-2 weighted (A-B) hyperdense lesions of the left centrum semiovale(A) and left basal ganglia(B). There is irregular peripheral enhancement. Considerable decrease in size is seen from previous MRI (Figure 2). Left posterior centrum semiovale, left globus pallidus and left occipital lobe lesion measure 1.3 cm, <1 cm and <1 cm respectively. Vasogenic edema is diminished in comparison to previous study.
Discussion
Tumefactive MS lesions are defined as solitary demyelinating plaques greater than 2 cm.5 Lesions are difficult to distinguish between primary or metastatic given similarity of imaging features.5 Imaging features suggestive of Tumefactive MS include incomplete ring enhancement, absence of mass effect and absence of cortical involvement.6 7 Kim describes that CT hypoattenuation of magnetic resonance enhancing lesions was found to be highly specific for distinguishing Tumefactive MS lesions from CNS cancer pathology.6 It has been shown that SPECT using I-IMP is useful for diagnosing CNS malignancy.3 This is because there would be increased uptake in comparison to the MS lesions - implying increased metabolic activity.3 However this study has its limitations in diagnosis. In a few isolated cases I-IMP was found in greater quantities in MS tumor-like lesions.3
The imaging studies for this patient established a concern for metastasis, infection or primary malignancy. Extensive cancer workup was completed as previously discussed. Since all tumor markers were negative a baseline PET scan was considered however, was not done secondary to insurance denial. Due to the asymptomatic presentation of her disease, a primary differential diagnosis of brain metastasis and anticoagulation therapy for PE, a CSF analysis was not considered until much later. We were able to use surveillance MRI and CSF analysis to see some resolution of these lesions and confirm the diagnosis. Brain biopsy was never warranted but in unique symptomatic cases it may have been.6
The cornerstone of diagnosing MS is the demonstration of lesions in both time and space - termed the McDonald Criteria.8 The revised criteria allow a diagnosis of MS, “possible MS” or “not MS”.8 This is what made the diagnosis of our patient difficult, as no clinical symptoms or attacks were evident. It was demonstrated that over the course of three months the lesions seen on MRI evolved. From the size of 1.5 cm, 1.0 cm and 1.0 cm they became 1.3 cm, <1.0 cm and <1.0 cm respectively (Figure 2, Figure 4). This was likely the effects of steroids that the patient was on due to her vasogenic oedema. Here an evolution in time and space is demonstrated which excluded brain metastasis and infection. This brings into discussion the diagnostic value of surveillance MRI, which in our case was helpful and appropriate as the patient did not have clinical symptoms.
Conclusion
The diagnosis of Tumefactive MS can be extremely difficult and time consuming. As seen in our case, it can mimic other conditions. Our patient was able to be diagnosed with MRI surveillance and CSF analysis. The definitive diagnostic test for MS is a brain biopsy but this is not preferred due to the invasiveness of the procedure. With the advent of newer diagnostic tests such as SPECT, MR Spectroscopy, surveillance MRI and CSF analysis, diagnosis can be attained and treated presumptively.
A 79 year old lady presented to the accident and emergency department with severe abdominal pain. On admission she was hypotensive and hypothermic. Blood tests demonstrated raised inflammatory markers and white count, but were otherwise unremarkable. A CT scan revealed no abnormalities. She was treated with intravenous fluids and empirical antibiotics.
She had multiple co-morbidities, including ischaemic heart disease, hypertension and chronic kidney disease.
Figure 1 – Upper Oesophagus
Figure 2 – Distal Oesophagus
Figure 3 - Gastro-eosophageal Junction
Figure 4 – Stomach (in retroflexion)
Figure 5 - Duodenum
Three days into her admission she had a single episode of hematemesis and a gastroscopy was arranged. Endoscopic features were as per figures 1- 5. Histology taken at the time showed necrotic tissue with evidence of candidiasis. Her treatment was optimised with a two-week course of fluconazole with the dose adjusted for her renal function and parenteral nutrition, with good clinical response. She was discharged after a two week hospital admission. A repeat gastroscopy 10 weeks later showed complete resolution of endoscopic features with no evidence of perforation or stricture formation.
DISCUSSION
The images seen at endoscopy demonstrate a region of oesophageal ulceration progressing to a diffuse, circumferential, black discoloration of the distal esophageal mucosa, with an abrupt transition to normal mucosa at the gastro-esophageal junction (Figs. 1-3). These endoscopic features, in the absence of a history of ingestion of caustic substances, are diagnostic of Acute Oesophageal Necrosis (AON), also known as ‘Black Oesophagus’. Whilst histology confirming necrosis is not necessary to make the diagnosis, it is confirmatory.
AON was first described in 1990 by Goldberg et al, since which over one hundred cases have been reported in the literature1. Population studies have suggested the incidence of this condition to be between 0.08% and 0.2%, although interestingly one post-mortem series of 1000 patients failed to reveal any cases2-4. There is a male preponderance, with an incidence four times greater than that for women and a peak incidence during the sixth decade of life5, 6.
The aetiology of this condition is not entirely clear; however case reports to date suggest that this is almost exclusively observed in those who are systemically unwell, usually in the context of multi-organ dysfunction5-7. It has been postulated that necrosis most commonly occurs as a consequence of hypo-perfusion caused by a low flow state in those with underlying vascular disease. This is likely to account for the predilection for the distal third of the esophagus, which is relatively less vascular5. Individual cases have occurred in association with bacterial, viral and fungal infections, whilst malnutrition, malignancy and immune-compromise appear to be important factors3, 5, 6.
The most common indication for the gastroscopy that makes the diagnosis of AON is hematemesis and melena, accounting for over 75% of cases6. It is therefore likely that AON is significantly under reported as endoscopy is often precluded in those who are clinically unstable. Further it is not clear whether hematemesis is a universal symptom of this condition; it is conceivable that AON may go undiagnosed in those in whom this is not a feature.
Whilst AON has no specific treatment, its presence is indicative of significant systemic compromise and predicts a poor prognosis. This diagnosis should alert physicians that close monitoring and aggressive treatment is required to optimise patient outcomes. There is no clear role for the use of anti-acid therapy, however this is commonly used in management due to patient symptoms, which usually includes hematemesis. Similarly, candidiasis may occur in conjunction with AON, whilst it is not thought to be causative, treatment is considered prudent given the poor prognosis associated with this condition.
For those that recover from their acute systemic insult the prognosis appears to be good. The long-term sequale of this condition includes oesophageal stenosis due to structuring. Evaluation with a repeat gastroscopy if therefore indicated if dysphagia develops.
CONCLUSION
The clinical course of AEN is variable, with an associated mortality of 32%5. The severity of the underlying clinical condition appears to be the most important factor in determining prognosis. There is no specific treatment for AON. The current body of experience suggests aggressive management of abnormal physiology optimises outcomes5, 6. Antibiotics, antifungals and nutritional support should be considered on an individual basis.
Angiogenesis is an integral process in biological programmes of embryonic development, tissue damage and regeneration, tumour growth and progression and pathogenesis of inflammatory and autoimmune diseases. MS (multiple sclerosis) is a demyelinating disease of the CNS (central nervous system). Angiogenesis has been a consistent feature of demyelinating plaques of MS1-3. Many inducers of angiogenesis are expressed in these plaques. They are also closely associated with the animal model of MS viz. EAE (experimental autoimmune encephalomyelitis)4 (Table 1). This has led to the suggestion that inhibition of angiogenesis by suppressing these effectors or inhibiting the elements of angiogenic signalling pathways might provide a viable way to target therapy to manage MS.
[Note: Inhibitory effects of thalidomides were described by Sherbet4; D’Amato et al.6; Kenyon et al.7; Lu et al.8]
Multiple sclerosis is an autoimmune inflammatory condition and so immunomodulators have been used in treatment. It is recognised that aberrant activation of the immune system and the associated network of its regulation are important events in the pathogenesis of the disease. This is the rationale for using immunomodulatory agents in disease control. Among immunomodulators of note are Fingolimod which prevents infiltration of auto-destructive lymphocytes into the CSF, Teriflunomide which reduces lymphocyte infiltration of the CNS, axonal loss and inflammatory demyelination, and dimethyl fumarate, which modulates the immune system by many mechanisms. Furthermore, much attention has been devoted to the immunomodulatory properties of MSCs (mesenchymal stem cells) 4,5. Thalidomides are also capable of modulating the function of key element of the immune system related to the pathogenesis of MS, but this brief article is intended to emphasise the potential of thalidomide and its analogues as potent inhibitors of angiogenesis and the latent possibility of their use as a therapeutic agent in the control of MS.
Thalidomide was introduced over four decades ago to treat respiratory infections and to combat morning sickness in pregnant women. It was withdrawn when it was found to be highly teratogenic. The teratogenic effects are a result of the binding of thalidomide to cereblon, a protein found in both embryonic and adult tissues. Cereblon is required for normal morphogenesis. It is inactivated by binding to thalidomide and this leads to teratogenesis9. Thalidomide possesses immunomodulatory, anti-inflammatory, anti-angiogenesis and cell proliferation inhibitory properties and this has suggested its use in the treatment of cancer5. Analogues of thalidomide, viz. lenalidomide and pomalidomide, have been synthesised and these possess reduced toxicity and greater efficacy10, 11. Recently, many studies have elucidated the signalling pathways which thalidomides inhibit and thereby suppress cell proliferation, promote apoptosis and inhibit angiogenesis. These have led to the suggestion of combining the modulators of these signalling pathways to synergise with thalidomides to deliver the suppressor effects with enhanced efficacy and at lower concentrations thus reducing the side effects5 (Figure 1).
Most of the work on the efficacy of thalidomide and the analogues has been carried out in preclinical models. Quite understandably, in the clinical setting very little effort is seen to check whether thalidomide or the analogues provide any beneficial effects in MS or neuro-inflammation. Clinically orientated investigations so far relate mainly to multiple myeloma and some other forms of haematological malignancies but not solid tumours5. Any perceived beneficial effects are probably outweighed by the side effects. We need to expend more effort and design and develop new analogues with reduced toxicity. In this context one should emphasise that pre-clinical exploration of the potential synergy between the thalidomides and the acknowledged modulators of the signalling pathways would be worthwhile. This might enable the delivery of benefits more effectively and at lower dosages. It is needless to say that safety of drug administration is of paramount importance.
Nearly 30% of seniors have chronic musculoskeletal pain. The most common cause of pain in seniors is related to the degenerative changes of the spine and joints9. Conventional treatments are often restricted to the management of symptoms. Use of chronic anti-inflammatory medications in seniors may bear serious risks in gastrointestinal and renal systems. Physical therapy has limited value. Epidural steroid injection(s) may provide up to three months of pain relief. However, there are some risks involved. Spine surgery for degenerative spine diseases has a limited success rate. Up to 30% or 40% of patients may continue to have pain after back surgery. Surgical repair of a knee injury and knee replacement surgeries are popular. However, the costs are relatively high. Many senior patients may not be ideal candidates for surgery due to cardiovascular conditions. Furthermore, all these treatments do not address the key cause of spine and joint pain due to degeneration of cells and subsequent tissue damage9. Recent development in stem cells therapy (SCT) has provided a new hope for seniors.
Back Pain
The major cause of back pain is the degeneration of the cells in the intervertebral discs. Over the last few years molecular, cell-based therapies and tissue-engineering strategies with SCT for disc regeneration have significantly increased. A recent report showed that injection of mesenchymal stem cells (MSC) into bovine intervertebral discs can increase the expression of extracellular type II collagen and maximize extracellular matrix production7. Chun et al 1injected human adipose-derived stem cells (ADSCs) into 20 mature male New Zealand white rabbits. The proliferation of ADSCs at the L4-5 disc was found at 10 weeks after cell injection. Histologically, the ADSC-injected discs exhibited elevated extracellular matrix secretion and little ossification of damaged cartilage in the nucleus pulposus compared with degenerative control discs.
In addition to the promising results from animal research, preliminary human studies showed mixed results. In 2006, Haufe et al3 reported 10 patients who underwent intradiscal injection of hematopoietic precursor stem cells (HSCs) obtained from their pelvic bone marrow. Of the 10 patients, none achieved any improvement of their discogenic low back pain after one year follow-up. More recently Orozco et al 8 reported a study of ten patients with chronic back pain treated with intradiscal injection of autologous expanded bone marrow MSC. Patients were followed for 1 year. Rapid improvements of pain and disability were reported (85% of maximum in 3 months). Although disc height was not recovered, water content was significantly elevated at 12 months. Advantages of intradiscal MSC therapy include simpler and preservation of normal biomechanics without surgery. However, long term survival of the transplanted MSCs in the harsh environment of the discs is still a major challenge. To the date, no double-blind, controlled studies have been published to confirm the clinical efficacy of SCT for the pain due to degenerative disc diseases.
Knee Pain
It is estimated there will be seven-fold increase in knee replacements in the United States between 2005 and 2030. However, SCT may reduce the future need for knee replacement5. Autologous MSC and ex vivo expanded skeletal SC all have shown promising results in the treatment of knee pain caused by osteoarthritis (OA).
In an experimental animal meniscus injury model, it has been reported 10 that transplantation of human meniscus stem/progenitor cells (hMeSPCs) effectively protected articular cartilage, promoted neo-tissue formation with better-defined shape and more matured extracellular matrix and smother surface cartilage, and maintained joint space at 12 weeks postsurgery11. MSC therapy may also reduce animal pain behavior14.
In human studies, Turajane et al13 conducted a case-series study with five patients that failed conservative treatment. It was reported that the combination of intra-articular autologous activated peripheral blood stem cells with growth factor addition/preservation along with hyaluronic acid in conjunction with arthroscopic microdrilling MCS resulted in Quality of Life improvements and succeeded in regenerating articular cartilage in early osteoarthritic knee disease. Skowronski12 reported 52 patients treated with autologous blood MSC for knee pain due to cartilage lesions. Scores improved across all scales with an average improvement of 23 points in the Knee Injury and Osteoarthritis Outcome Score scale and 35 points in the Lysholm knee scale at one year.
Koh et al4 treated eighteen patients with injection of autologous fat pad-derived MSC for knee pain due to OA. Patients were followed for 24 to 26 months after therapy. Western Ontario and McMaster Universities Osteoarthritis Index, Lyholm scores as well as VAS scores all significantly improved. Radiographic study showed the whole-organ MRI score had significantly improved from 60.0 points to 48.3 points at the final follow-up point. Particularly notable was the change in cartilage whole-organ MRI score, which improved from 28.3 points to 21.7 points. More recently, Vangsness et al reported15a randomized, double-blind, controlled study on adult human MSC delivered via intra-articular injection to the knee following partial medial meniscectomy. A single superolateral knee injection was given to 55 patients within seven to ten days after the meniscectomy. It was found that there was significantly increased meniscal volume determined by quantitative MRI in groups that received SCT. No patients in the control group had significant increase in meniscal volume. Patients with osteoarthritic changes who received MSC experienced a significant reduction in pain compared with those who received the control. This randomized, double-blind, controlled study confirmed that MSC could be a promising treatment for knee pain due to osteoarthritis and meniscus tear.
Challenges for SCT
The advantage of SCT is that stem cells can regenerate healthy and functionally specialized cells and tissues to replace the destroyed or degenerative tissues. Though it is promising, it is still facing a variety of challenges. Firstly, there are many studies reporting the clinical efficacy, most studies are open label. Only few, if any, double-blind, controlled studies have supported the efficacy of SCT for knee pain due to osteoarthritis. To the date, there are no controlled studies confirming the clinical efficacy of SCT for degenerative spine diseases. Thus more clinical studies are needed. Secondly, biological techniques for stem cell transplantation are waiting to be enhanced. For example, the stem cells transplanted into degenerated intervertebral discs will face a harsh environment, which has very high pressure, low nutrition and low oxygen. To enhance the cell survival rate and ensure the transplanted cells differentiating toward chondrocyte-like cells, which can produce proteoglycans and type II collagen, more basic science studies are needed2. The third challenge for SCT is iatrogenic cancerogenesis. Embryonic stem cells, including totipotent stem cells (produced from fusion of egg and sperm), and pluripotent stem cells (5-14 day old blastocytes) have a strong potency of cell reproducing and potentially highly teratogenic. Novel strategies such as using transgenic expression of the genetically engineered human recombinant DNases in proliferating and directed differentiation resisting stem cells are being developed to inhibit or prevent the iatrogenic cancerogenesis6. Adult SCs (Adipose, peripheral and bone marrow derived SCs) have the ability to differentiate and form a variety of tissues. These adult SCs have been used in researches to treat variety of human diseases. So far no iatrogenic carcinomas have been reported as the results of the treatment. The fourth major issue related to SCT is the legal challenge. Worldwide, different countries have different laws on SC research and use. Even President Barack Obama signed an executive order on March 9, 2009 to lift the restrictions on federally funded human embryonic stem cells (hESC) research, currently only adult stem cells (adipose, peripheral and bone marrow derived stem cells) are allowed to be used in most clinical settings. These cells should be minimally manipulated. Use of hESC from fetus, umbilical cord and amniotic fluid are all limited for research purposes. Researchers and clinicians must be familiar with the laws of their respective countries and states before becoming involved in SC therapy or research.
Conclusion
The treatment of chronic pain conditions is constantly evolving. Recent advancements in SCT for pain due to degenerative diseases in the spine and joints are promising and indicative that SCT will undoubtedly play a major role in the future. However, more studies are needed to enhance the biological techniques, confirm the clinical efficacy, reduce the risk of iatrogenic carcinoma and address the legal issues related to this exciting treatment. It is likely that SCT will be utilized more extensively in the future for replacing diseased tissues as an alternative to open back surgery or joint replacement.
Although it is well appreciated that pancreatitis is frequently secondary to biliary tract disease and alcohol abuse, it can also be caused by drugs, trauma and viral infections, or even be associated with metabolic and connective tissue disorders.1 Knowledge of the true incidence of drug-induced acute pancreatitis is dependent on the clinician’s ability to exclude other possible causes, and by promptly reporting the occurrence. Based on individual case reports and case control studies of drug-induced acute pancreatitis, the estimated overall incidence ranges from between 0.1 and 2% of pancreatitis cases.2,3 In particular, drug-induced acute pancreatitis is of mild severity and usually resolves without significant complications.4
Attempts have been made to categorize the risk of drugs causing acute pancreatitis. A previous classification system described by Mallory and Kern Jr. categorized drugs associated with acute pancreatitis as definite, probable, or possible.5 Trivedi et al. proposed a newer classification system for commonly used medications associated with drug-induced pancreatitis. Class I drugs are those medications with at least 20 reported cases of acute pancreatitis and at least one case with a positive rechallenge. Drugs with fewer than 20 but more than 10 reported cases of acute pancreatitis, with or without a positive rechallenge, are designated into Class II. While those medications with 10 or less reported cases, or unpublished reports in pharmaceutical or FDA files, are grouped into Class III.6
Acute pancreatitis as a result of either doxorubicin or cyclophosphamide, or a combination of both, or fluorouracil or epirubicin is a rare occurrence and has seldom been reported in the literature. Even the drug package labels registered with the FDA do not indicate the possible occurrence of pancreatitis. In this case report, we present a rare occurrence of drug-induced acute pancreatitis after the completion of the first cycle of the chemotherapy protocol involving cyclophosphamide and doxorubicin in a patient with stage 3 breast cancer, with recurrences of acute pancreatitis after re-challenging with cyclophosphamide and a derivative of doxorubicin, given individually on two separate occasions.
CASE PRESENTATION
A 58 year-old female presented to the emergency room with a one day history of severe, diffuse, deep-seated abdominal pain that radiated to her back, associated with nausea and vomiting, and was unrelieved despite the intake of NSAIDs. There was no reported fever, chills, diarrhea, dysuria, or antecedent trauma. Her medical history is notable for well-controlled hypertension, hyperlipidemia and hypothyroidism for which she takes amlodipine, atorvastatin and levothyroxine. She was recently diagnosed with left-sided breast cancer, Stage III, two months prior to admission and underwent a left modified radical mastectomy. Three days prior to the hospital visit, she was given her first cycle of chemotherapy with Doxorubicin 60 mg/m2 and Cyclophosphamide 600 mg/m2 along with Pegfilgrastim 6 mg and Fosaprepitant 150 mg. She is a former cigarette smoker, drinks alcohol infrequently, and denies illicit drug use. Her family history is unremarkable.
Physical examination revealed stable vital signs without a fever (36.6◦C). She had non-icteric sclerae and a dry oral mucosa. Chest exam revealed a well-healed left mastectomy scar and an infusaport located on the right anterior chest wall. Her breath sounds were clear bilaterally. Her heart sounds were normal. Her abdominal exam was significant for mild tenderness to palpation in the epigastric area without palpable masses, organomegaly or ascites. There was no evident ecchymosis observed. The extremities were warm to touch with intact and symmetrical pulses, and without bipedal edema.
Initial work-up revealed an elevated leukocyte count of 42,000 with 80% neutrophils and 17% band forms. Basic metabolic panel was normal except for mild hyponatremia of 129 mEq/L. Serum amylase and lipase were markedly elevated at 2802 units/L and >2000 units/L, respectively. Liver function panel was normal (Alk phos 63 U/L [ref range 30-115 U/L], GGT 21 U/L [ref range 3-40 U/L], total bilirubin 0.90 mg/dL [ref range 0-1.5 mg/dL]). The coagulation profile was within normal range. Imaging of the abdomen with a CAT scan with intravenous and oral contrast showed haziness in the pancreatic fat plane suggestive of pancreatic inflammation, with no gallstones, focal abscesses, hepatic masses, or biliary ductal dilatation (Figure 1). Right upper quadrant ultrasound was essentially normal (Figure 2).
Figure 1. Coronal view of CT scan of abdomen and pelvis with IV and oral contrast showing haziness in the peripancreatic fat plane.
Figure 2. Sonogram of the right upper quadrant of the abdomen showing gallbladder devoid of gallstones and non-dilated common bile duct.
She was admitted to the medicine unit with the assessment of acute pancreatitis likely secondary to doxorubicin and cyclophosphamide. Intravenous fluid hydration with normal saline was initiated. She was kept NPO (nothing per os) and was started on empiric Imipenem and IV Esomeprazole. Her abdominal pain was controlled with intravenous morphine and her nausea with Ondansetron as needed. The serial basic chemistry panel was monitored and electrolyte deficits were replaced accordingly. Further work-up was performed to identify other possible etiologies of pancreatitis. The lipid panel was within normal limits (cholesterol 169 mg/dL [0-200 mg/dL], HDL 74 mg/dL, LDL 71 mg/dL and triglycerides 54 mg/dL [0-150 mg/dL]). The serum calcium levels remained within the normal range throughout her hospital stay. An abdominal sonogram demonstrated absence of gallstones or dilatation of the common bile duct, with a normal appearing liver parenchyma and pancreas. During her stay in the medicine unit, the patient’s abdominal pain improved and she was gradually started on an oral diet, which she tolerated well. Her serum electrolytes remained stable, while her serial CBC revealed progressively decreasing trends in leukocytes, hemoglobin, hematocrit, and platelet count, findings which were attributed to her prior chemotherapy. Repeat serum amylase and lipase both trended downward. The patient was discharged with follow up in the Oncology clinic. A month later, she was started on another chemotherapy regimen that consisted of weekly administration of Paclitaxel 80 mg/m2 which, over the next two months, the patient completed without any complications. Then, after explaining the risks of recurrent pancreatitis, the patient consented to have a trial of cyclophosphamide 500 mg/m2 along with fluorouracil 500 mg/m2. Five days after receiving the chemotherapy, the patient developed acute pancreatitis which was attributed to cyclophosphamide. She again made a full recovery at that time. Three weeks later, her chemotherapy regimen was again changed, to epirubicin 90 mg/m2 and fluorouracil. Four days after receiving this regimen, she again, for the third time, had a recurrence of acute pancreatitis. At this time, a repeat abdominal sonogram revealed a 4mm echogenic focus adherent to the anterior gallbladder wall with a comet tail sign, suggestive of cholesterol crystals lodged within Rokitansky-Aschoff sinuses of the gallbladder wall. There were no visible gallstones. A subsequent MRI of the abdomen with contrast revealed a small rounded hypointensity in the dependent portion of the gallbladder wall that was suggestive of a gallstone, however, there was no biliary obstruction, choledocholithiasis or an obstructing pancreatic mass. At this point, chemotherapy was stopped and anastrozole along with radiation therapy was initiated. The patient continues to be followed regularly and has had no recurrence of pancreatitis since her last episode.
DISCUSSION
The case presented described the development of acute pancreatitis in a patient with breast cancer three days after receiving the chemotherapy regimen consisting of cyclophosphamide and doxorubicin. After re-challenging the patient with cyclophosphamide, and again a few weeks later with a derivative of doxorubicin, epirubicin, acute pancreatitis recurred on each occasion. Despite the presence of cholelithiasis detected on the abdominal MRI, the temporal presentation of acute pancreatitis after chemotherapy exposure is highly suggestive of the role these chemotherapeutic agents played in triggering these three acute attacks. Acute pancreatitis was diagnosed based on the clinical suspicion and symptoms suggestive of the acute pancreatitis and was supported by the marked elevation in serum amylase and lipase, as well as, the radiologic evidence of pancreatic inflammation, both of which are markers of acute pancreatitis.
Chemotherapy-induced acute pancreatitis involving cyclophosphamide and doxorubicin either alone or in combination, is quite rare that even the drug labels registered with the FDA do not indicate acute pancreatitis as one of the possible complications. This scenario highlights the importance of drug surveillance and prompt reporting in order to maintain a credible drug safety database.
Though the drug latency, which is the interval between the initial exposure to the drug and the development of acute pancreatitis, differs variably, the present case is considered to have an intermediate latency (1-30 days). Other drugs may have short (< 24 hours) or long (>30 days) latency periods. Examples of drugs with short latency are acetaminophen, codeine, erythromycin and propofol. Intermediate latency drugs include L-asparaginase, pentamidine and stibugluconate. Drugs with long latency are estrogen, tamoxifen, valproate and dideoxyinosine.7
Based on the revised classification of Badalov et al, the combination of cyclophosphamide and doxorubicin is classified as Class IV drugs, which have the weakest association with acute pancreatitis due to limited information and the lack of adequate detailed case reports. Fluorouracil, which has been known to cause a gastrointestinal ulcer, is also categorized as a Class IV drug, while epirubicin, which is derived from doxorubicin, has not been classified, as it has not been reported before to cause acute pancreatitis. In implicating drugs in the etiology of acute pancreatitis, two conditions must be considered to weigh the strength of the association between the causality and the disease process, namely: a positive rechallenge test resulting in the recurrence of pancreatitis and a similar latency period between the drug exposure and development of the disease.7
The combination of drugs rather than a single agent was implicated for drug-induced pancreatitis in a previous case report that described the development of acute pancreatitis shortly after the second cycle of the chemotherapy regimen composed of cyclophosphamide, doxorubicin, and vincristine in a patient with mediastinal immunoblastic lymphoma. The pancreatitis episode resolved over 48 hours without complications.8
Another case was described in a patient with breast cancer developing acute pancreatitis four days after the third cycle of chemotherapy, which involved docetaxel and carboplatin.9
Toprak et al. reported the occurrence of acute pancreatitis in a patient with multiple myeloma after the initial treatment with the triple regimen chemotherapy protocol consisting of vincristine, doxorubicin, and dexamethasone. In this case report, symptoms suggestive of acute pancreatitis started to manifest on the first day of the treatment, with resolution following discontinuation of the drugs.10
Other antineoplastic agents for breast cancer associated with drug-induced pancreatitis are alemtuzumab, trastuzumab and tamoxifen. Extended use of these medications may cause chronic pancreatitis as a result of their causing repeated clinical or subclinical episodes of acute pancreatitis.6 Most cases of drug-induced pancreatitis follow a mild clinical course.7
In a retrospective study involving 1613 patients diagnosed with acute pancreatitis in a gastroenterology center, the incidence of drug-induced pancreatitis had been reported in 1.4% of patients treated for acute pancreatitis. It has been observed that a higher incidence of drug-induced acute pancreatitis occurs in elderly or pediatric patients, and in those patients with inflammatory bowel disease or AIDS.11
The pathophysiology behind drug-induced pancreatic injury remains unclear. Potential mechanisms underlying such pancreatic injury might be related to drug hepatotoxicity which can be secondary to intrinsic toxicity of the drugs affecting the tissue, or due to an idiosyncratic reaction. In the vast majority of the cases, an idiosyncratic reaction could be the main pathway for tissue injury through a hypersensitivity reaction or production of toxic intermediate metabolites. Idiosyncratic reactions have a longer latency period of months to years before the onset of pancreatitis while the onset of hypersensitivity reactions is earlier (i.e. 1-6 weeks).7
CONCLUSION
Due to a variable latent period between the initial drug exposure and the onset of clinical symptoms, drug-induced pancreatitis must remain as a differential diagnosis in patients receiving chemotherapy regimens and presenting with the constellation of symptoms typical of acute pancreatitis. Due to the unclear pathogenesis of chemotherapy-induced pancreatitis, post-marketing surveillance and adverse drug reporting are paramount in elucidating the effect these drugs have on the pancreas.
The discharge summary is an integral part of continuing patient care. Apart from containing vital information regarding current admission, it also conveys key findings and plans to clinicians who will be taking over the care of the patient. This would mean communicating important information about patients to ensure appropriate and safe follow-up management. Studies involving discharge summaries have looked into role of communication from secondary to primary care and have highlighted the importance of accuracy and quality of information,1 errors2 and general practitioner (GP) preference.3 Systematic reviews have found low availability (12-34%) of discharge summary during first visit post-discharge as well as wide variations in content of discharge summaries thereby directly affecting patient management.4,5 The timing of discharge summary completion and reaching the follow-up physician is therefore of prime importance wherein this has been also found to influence and reduce the risk of rehospitalisation.6 The content necessary for a ‘good’ or ‘high-quality’ discharge summary has been studied via surveys. The inclusion of important data such as diagnosis, discharge drugs, complications, laboratory results and follow-up plans have been considered to be important clinical information by hospital physicians and GPs.7
Hospital discharge summaries can be hand-written, dictated or in electronic format. These formats have their benefits and downfalls. Hand-written summaries have been found to be well-accepted by primary care physicians although involve the factor of legibility.8 A randomised-controlled trial found no difference between electronic and dictated discharge summaries for primary care physician satisfaction.9 Although the use of electronic discharge summaries has significantly improved both the content and timing of discharge summaries reaching follow-up physician or healthcare staff,10 they have been found to contain higher number of errors in patient progress, additional diagnosis and free-text components.11
This audit examined the timing and content of discharge summaries at The Mount and whether they met local Trust standards. A follow-on audit was conducted to study the impact of recommendations that had been put forward at the end of Cycle 1 of the audit.
Aim and Objectives
Aim
Cycle 1: To study the content, accuracy and timing of discharge summaries at The Mount, Old Age Psychiatry hospital.
Cycle 2: To examine changes in clinical practice following recommendations from Cycle 1 of audit involving content and timing of discharge summaries from The Mount.
Objectives
Cycle 1: To ascertain whether Trust guidelines regarding content of discharge summaries are met and also whether the timeline guidance is being maintained.
Cycle 2: To examine adherence to the Trust guidelines as well as to study the changes brought about by recommendations at the end of Cycle 1.
Criteria/ Standards
Trust guidelines state:
Discharge summaries must be typed and sent in 5 working days post-discharge from hospital.
They must include the following information (Box 1):
Box 1 Trust guidelines for inclusion of information in discharge summaries
Patient ID
Date dictated
Patient Name
Date of Birth
Name of consultant
Admission address
Discharge address
Admission date
Discharge date
Reasons for admission
History of present illness
Past medical history
Past psychiatric history
Family history
Social history
Occupational history
Premorbid history
Mental health examination
Physical examination
Results of investigations
Progress & treatment during admission
Final diagnosis
Discharge medications
Follow-up arrangements
Name of key worker
Number of pages
Method
Audit Sample
Patients admitted and discharged from Ward 3 & 4 of The Mount, between 01.04.2011 to 31.10.2011. A total of 103 patient discharge summaries were therefore analysed in Cycle 1 of the study. For cycle 2, the audit sample comprised of patients admitted and discharged from Ward 3 & 4 of The Mount, between 01.04.2012 to 31.10.2012. A total of 97 patient discharge summaries were therefore analysed in this part of the study.
Data Collection
Data was collected using an anonymous data collection tool (Appendix 1) which was designed according to Trust guidelines. Administrative staff provided the clinical audit leads with list of patients discharged during the study dates. The electronic patient record system of the Trust (PARIS: Patient Record Information System) was used to study the discharge summary letters. Data collection was performed under the supervision of consultant responsible for the audit, between November 2011 and January 2012 for cycle 1 and for cycle 2 data collection was performed between October 2013 and November 2013. Patient confidentiality and anonymity was maintained.
Data Analysis
Qualitative data was gathered, coded and collated on to a Microsoft Excel spread sheet. The data collected was reviewed by the authors to ensure each aspect of data collection tool was filled. The data was analysed by the Clinical Audits Facilitator at the Trust Clinical Audit Support Team and placed into a report format for dissemination.
Results
The number of discharge summaries analysed in Cycle 1 and 2 of this study was 103 and 97 respectively.
Data were collected using the data collection tool (appendix 1). Dates of discharge, dictation and typing were recorded. Date of typing was used as a proxy of date sent to GP since there was no record of this. Seven days were permitted for discharges to be sent (equivalent to 5 working days). Discharge summaries were read and it was recorded if each stipulated heading from the Trust guidelines was present. No comment was made on quality of information; only consideration was whether information was present or absent.
Compliance with each point from the above categories is shown in the following series of tables and comparison is made between the studies in Cycles 1 and 2 (Table 1-4). The statistical significance of the differences found in the two audit cycles was evaluated using chi-square tests.
Table 1 Presence of information on discharge summary according to Trust guidelines
Criteria
Adherence % 2011 (n=103)
Adherence % 2013 (n=97)
Statistical significance
Patient code
100% (n=103)
97% (n=94)
p=0.721
Date dictated
72% (n=74)
98% (n=95)
p<0.001
Patient Name
100% (n=103)
100% (n=97)
No change
Date of birth
97% (n=100)
100% (n=97)
p=0.090
Name of consultant
98% (n=101)
99% (n=96)
p=0.596
Name of current GP
98% (n=101)
98% (n=95)
No change
Admission address
98% (n=101)
100% (n=97)
p=0.167
Discharge address
98% (n=101)
100% (n=97)
p=0.167
Admission date
97% (n=100)
100% (n=97)
p=0.090
Discharge date
97% (n=100)
99% (n=96)
p=0.342
Legal status
99% (n=102)
98% (n=95)
p=0.525
Reasons for admission
98% (n=101)
98% (n=95)
No change
History of present illness
100% (n=103)
99% (n=96)
p=0.301
Past medical history
89% (n=92)
95% (n=92)
p=0.150
Past psychiatric history
95% (n=98)
98% (n=95)
p=0.282
Family history
19% (n=20)
86% (n=83)
p<0.001
Social history
56% (n=58)
89% (n=86)
p<0.001
Occupational history
67% (n=69)
68% (n=66)
p=0.873
Premorbid history
37% (n=38)
52% (n=50)
p=0.036
Mental health examination
95% (n=98)
93% (n=90)
p=0.482
Physical examination
86% (n=89)
92% (n=89)
p=0.227
Results of investigations
84% (n=87)
78% (n=76)
p=0.265
Progress & treatment during admission
96% (n=99)
100% (n=97)
p=0.049
Final diagnosis
92% (n=95)
97% (n=94)
p=0.147
Discharge medications
98% (n=101)
97% (n=94)
p=0.602
Follow-up arrangements
86% (n=89)
79% (n=77)
p=0.007
Name of key worker
64% (n=66)
56% (n=54)
p=0.225
Number of pages
0% (n=0)
0% (n=0)
No change
Are there any spelling/typing errors in the list of medications?
90% (n=8)
98% (n=2)
p=0.064
Are there any spelling/typing errors in the diagnosis and medical terminology?
78% (n=21)
99% (n=1)
p<0.001
Table 1: The presence of information mentioned in the Trust guidelines is analysed. The percentage adherence in cycle 1 is compared with findings from cycle 2. Significant increase in inclusion of family history, social history, follow-up arrangements and date of dictation is observed. A healthy increase is also observed in inclusion of premorbid history and progression and treatment during admission. A significant reduction in spelling/typing errors is also seen. The decrease in inclusion of name of key worker, discharge medications, mental health examination and results of investigation amongst others is also noted. GP, general practitioner.
The comparison of findings from Cycle 1 and 2 establish a significant increase in adherence to family history (p<0.001), social history (p<0.001), premorbid history (p=0.036) as well as progress and treatment during hospital stay (p=0.049) components of the discharge summary. There was also a significant increase in inclusion of date of dictation of discharge summaries (p<0.001). Increase in adherence to most of the components of discharge summaries was observed. However, there was significant decrease in inclusion of follow-up arrangements (p=0.007) as well as a decrease in inclusion of name of key-worker assigned to patient (from 64% in cycle 1 to 56% in cycle 2; p=0.0225). A significant decrease in spelling/typing errors in diagnosis or medical jargon was observed (p<0.001).
Timing of Discharge Summaries
Table 2 Time taken between discharge of patient and dictation of letter
Days
Adherence % 2011 (n=74)
Adherence % 2013 (n=94)
Statistical significance
0-7
30% (n=22)
73% (n=69)
p<0.001
8-15
24% (n=18)
22% (n=21)
p=0.762
16-22
18% (n=13)
4% (n=4)
p=0.004
23+
29% (n=21)
0% (n=0)
p<0.001
Table 2: The time taken between discharge of patient and dictation of letter is analysed. A significant increase is observed in the dictation of letter as per Trust guidelines (within 5 working days).
Table 3 Time taken between dictation and typing of discharge letter
Days
Adherence % 2011(n=75)
Adherence % 2013 (n=94)
Statistical significance
0-5
84% (n=63)
73% (n=69)
p<0.001
6-11
7% (n=5)
24% (n=23)
p=0.192
12+
9% (n=7)
2% (n=2)
p<0.001
Table 3: The time taken between dictation of letter and typing of discharge letter is analysed. A significant decrease is observed in the time taken for typing of letter within 5 days of dictation of letter.
Table 4 Time take between discharge and typing of discharge letter
Days
Adherence % 2011 (n=100)
Adherence % 2013 (n=96)
Statistical significance
0-7
18% (n=18)
52% (n=50)
p<0.001
8-15
32% (n=32)
34% (n=33)
p=0.724
16+
60% (n=60)
14% (n=13)
p<0.001
Table 4: The time taken between discharge of patient and typing of discharge letter is analysed. A significant increase is observed in the early typing of discharge letter from the date of discharge of patient.
The number of discharge summaries being dictated and typed within 7 days of discharge was significantly increased (p<0.001) and a significant decrease in discharge letters being dictated more than 2 weeks (p=0.004) or 3 weeks (p<0.001) of patient being discharged was observed. The time taken between dictation of letter and it being typed up was also found to have dropped, with 73% being done within 7 days, significant decrease (p<0.001) being observed since the first cycle. Furthermore, a significant increase is observed in early (less than 7 days) typing of discharge letter since patient being discharged (p<0.001).
Discussion:
The discharge summary is a very important means to communicate medical (both physical and psychiatric) and nursing interventions to the GP or community mental health team. This in turn helps in making invaluable decisions to patient care in the community. Hence, it is worth spending time on doing a good discharge letter which includes relevant information. A timely discharge letter can also be very useful in this regard.
At the end of Cycle 1 of the audit, recommendations that were made included (Appendix 2):
Disseminating information amongst all junior doctors, consultants and administrative staff on each ward to include the above mentioned headings in accordance with Trust guidelines.
Information was also provided regarding finding out Name of Keyworker in PARIS system.
A specific note was also placed regarding to spell out medical terminologies that would assist in the typing of discharge summaries by administrative staff.
From the results, it is evident that the content of the discharge summary has largely been maintained. In other words, good practice was maintained and recommendations from previous audit were implemented in most spheres of discharge letters. However, despite the recommendation of finding out name of key-worker from PARIS system, there was a decrease (from 64% in first cycle to 56% in second cycle) in its inclusion (p=0.225). Thus, training in usage of information technology system is essential. Providing appropriate instruction and training to junior doctors has been found to be useful in improving the quality of discharge summaries.12 Therefore, it might be beneficial to include instructions or guidelines for appropriate discharge summaries at local Trust or departmental inductions. This will help junior doctors in ensuring completion of accurate and succinct discharge summaries that will aid in patient management.
There was a reduction in documentation of discharge medication, follow up arrangement, mental state examination and physical health investigation carried out as an in-patient. This certainly needs improving as these are the relevant areas to facilitate smooth transition of care in the community and follow-up arrangement. With regard to the timing of the discharge summary, this was found to have significantly improved from the previous audit cycle. For example, the timing between discharge and dictation (within 7 days) has increased from 30% to 73% and almost all discharge summaries are dictated no later than 3 weeks. The possible reasons for delays in dictation could be ongoing workload, availability of medical staff and of the medical notes, as these are sometimes requested by the Intermediate Community Service (ICS) team. There was a slight drop in the time between dictation and typing (from 84% to 73%), which could possibly due to availability of administrative staff, dictation tapes or medical notes and proof reading by medical staff. Significant increase was observed in inclusion of date of dictation of discharge summaries which will be a useful component for future audits. A significant decrease in spelling/typing errors in diagnosis or medical terminologies was observed. Furthermore, there was significant increase in inclusion of family history, social history, premorbid history as well as information on progress and treatment during hospital in the discharge summary. Therefore, timely audit and feedback can be very useful in improvement of discharge summaries and patient care.
Recommendations & Actions:
Raise awareness amongst senior house officers (SHO’s) and other doctors in the Trust regarding recording of pre-morbid history, occupational history, name of keyworker as this was only done in 52%, 62%, 56% cases respectively. This could be done by disseminating findings from this audit amongst SHO’s and other doctors of Trust through hand-outs to wards as well as through local teaching session.
Remove number of pages from the list of sub-headings needed in discharge summary as this is dependent on typing and not necessarily possible to estimate while dictating discharge summary. However, it is an important part of discharge summary. Therefore, send information with audit findings to medical secretaries informing the need to keep number of pages in the discharge summary.
Consider adding a section on documentation of risk assessment should be included in the discharge summary as well as ‘early relapse signature’ which would enable early intervention in the community to avoid inpatient admission. This could be included in the discharge summary. This would involve liaising with consultants and the responsible person for making/printing discharge summaries for Trust.
Binge Eating Disorder (BED) was first defined by Stunkard in 19591; he identified peculiar food intake features characterized by a loss of control in a subgroup of obese patients. Various efforts have been made, ever since, to provide a non-sociological approach to individuals with such a behaviour disorder, which has long been considered a variant of Bulimia Nervosa.
Unlike patients affected by Bulimia Nervosa, patients with BED appear to be overweight and mainly obese. Thus, the treatment aims not only at reducing BED and its related psychopathology, but also at assessing the weight gain experienced by these patients to prevent a further worsening of physical health.
Walsh & Devlin2 evaluated the use of medication in the treatment of Bulimia Nervosa and BED, underlining the efficacy of antidepressant medication in the treatment of Bulimia Nervosa. The antidepressant efficacy led to consider its use in BED more accurately.
Williamson, Martin & Stewart3 stated that pharmacotherapy was not an effective treatment for Anorexia Nervosa. However, it did prove to be successful in Bulimia Nervosa and BED, although subjects affected with eating disorders apparently respond better to psychotherapy approaches.
Systematic investigations have been conducted on the aetiology of BED. Biological and genetic factors, neurotransmitters and hormones have been involved in the onset of binge eating and play an important role in the regulation of hunger and mood.4, 5 However, a definitive aetiological theory has not been developed and tested.3
BED is characterized by a relevant psychological component that in many cases is under-evaluated. Patients with BED have difficulty in interpreting the visceral sensations of hunger and satiety; they take large amounts of food even during regular meals and, moreover, their food contains more fat than protein.6, 7
In fact, Axis I and II disorders (DSM IV-TR) share common features with binge eating.8 Axis I psychiatric disorders (including depression, anxiety, body dysmorphic disorder, or chemical addiction) characterize many BED patients, and research has evidenced the presence of panic, loss of control, impulsivity, compulsive behavior, obsessive thoughts about food and social phobia.9 Axis II personality disorders (especially borderline personality disorder) are frequently related to patients suffering from eating disorder and comorbidity with Avoidant Personality Disorder and Obsessive-Compulsive Disorder was observed.10
BED is not associated with a restrained eating control, but probably with an increase of uncontrolled eating and emotional eating.11, 12
Pharmacological agents, compared to placebo, have been used in the treatment of BED. Appolinario, Bacaltuchuk, Sichieri et al13 evaluated the efficacy of Sibutramine to reduce the frequency of binge eating, while McElroy, Arnold, Shapira et al14 focused on Topiramate and evidenced a greater reduction in binge eating frequency but with side effects such as paraesthesia.
Other studies showed the efficacy of Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Noradrenaline Reuptake Inhibitors (SNRIs) in the treatment of obesity associated with BED15, 16, 17, 18 showing that SSRIs and Tricyclic Antidepressants (TCAs) reduced the frequency of BED compared to placebo.19 To determine which patients are most likely to benefit from medications, and how to sequence the various therapeutic interventions available better, are questions still open to debate.
Moreover, results in many cases appear to be divergent. Ciao, Latner and Durso20 underlined the influences of other factors that may influence treatment efficacy. They observed that many obese individuals who might benefit from weight loss treatment nevertheless do not plan or desire to seek treatment and perceive multiple barriers to treatments.
Pharmacotherapy may enhance weight loss,19 although other results suggest that pharmacotherapy may be associated with a reduction in binge frequency in obese patients with BED, but it does not lead necessarily to weight reduction.21 These medical treatments seem to be effective in reducing binge frequency over the short-term, and the subsequent discontinuation of the medication seems to be associated with a relapse of binge eating. Thus further studies of the role of pharmacotherapy in the treatment of BED need to be carried on.22
According to Williamson, Martin and Stewart3 the additive effects of psychotherapy, e.g. Cognitive Behavioural Therapy (CBT), and pharmacotherapy have to be investigated. At present it seems that adding pharmacotherapy to psychotherapy does not help to reduce binge frequency compared to psychotherapy alone.
The efficacy of CBT has been substantiated by scientific literature23, 24, 25, 26 and Vaidya27 stating that CBT helps patients reduce eating disorder habits by making them aware of the cause of their self-sabotage, while affecting weight indirectly.
Psychotherapy treatment over a one-year period deals with binge symptoms and aims at reducing the possibility of relapse by gathering different techniques for the maintenance of long-term results through the use of specific individual intervention protocols. The main target of the intervention is to facilitate the management of no-control food intake episodes and of impulsivity through the alteration of behaviour, and of cognitive and emotional factors related to eating disorders.
Thus, the main objective of this research was to verify the possible differences between those subjects with BED who underwent psychotherapy combined with pharmacotherapy and those who underwent psychotherapy only. In particular, it aimed at verifying possible differences between the various therapeutic strategies on eating behaviour (restrained eating, uncontrolled eating and emotional eating) and the behavioural and psychopathological features (psychopathic deviate, depression and hypomania).
The main hypothesis was to determine if patients who underwent CBT and pharmacotherapy with bio-equivalent doses of the SSRI Paroxetine or SNRI Venlafaxine obtained a considerable benefit from the pharmacotherapy on impulse regulation, on eating behavior and on personality features compared to those who underwent CBT alone.
The second hypothesis was to verify if Paroxetine and Venlafaxine treatments were equally effective on impulse regulation, eating behavior and on personality characteristics.
Methodology
Participants
A group of 30 subjects with BED were selected. All these subjects applied for support to the Inter-Service-Psychology Clinic for Eating Disorders and they were assisted by a Cognitive Behavioural Therapist. They were all of Italian nationality, aged 22 to 52, with a Body Mass Index (BMI) range of 26 to 35. All participants belonged to a middle class socio-cultural level. They were informed of the objectives of the research and signed a consent form. Those subjects who were diagnosed with binge eating less than two years ago, those aged over 65, or those who were suffering from other debilitating or chronic diseases were preliminarily excluded from this research.
Measures and procedure
Participants were recruited according to the nature of the assessments. More specifically, assessments had to address the effect of psychotherapy and pharmacotherapy in subjects with BED on their impulse regulation, their eating behavior (restrained eating, uncontrolled eating and emotional eating), and their personality features (Psychopathic Deviate, Depression and Hypomania). The 30 subjects selected were randomly assigned to three different treatments. Ten subjects had only CBT, ten subjects underwent psychotherapy with Paroxetine, and ten subjects underwent psychotherapy with Venlafaxine.
Each participant answered questionnaires during the assessment phase and in the post-training phase (after one year of psychotherapy). More specifically:
Binge Eating Scale (BES)28 is a 16-item questionnaire which assesses the presence of binge eating behaviour indicative of an eating disorder. The score ranges from 0 to 46 (non-binging <17; moderate binging = 18-26; severe binging = 27 and higher), which in this research had an adequate internal consistency (a = 0.84).
Eating Disorder Inventory-2(EDI-2)29 aims at quantifying some psychological and behavioural features. It consists of 64 questions grouped into 11 scales. For each item, the participants are asked to answer by using the following frequency adverbs: "always", "usually", "often", "sometimes", "rarely", and "never". The rating is measured with a score between 0 and 3: the maximum score of 3 corresponds to the intensity of the symptom ("always" or "never" depending on whether the direction of the item is positive or negative), score 2 corresponds to a degree intensity immediately below ("usually" or "rarely"), score 1 to an even lower level of intensity ("often" or "sometimes"), while a score of 0 is assigned to the three "asymptomatic" answers. So, those items with a positive direction are assigned the following scores: always = 3, usually = 2, often = 1, sometimes = 0, rarely = 0, never = 0; items with a negative direction are evaluated in the opposite way: never = 3, rarely = 2, occasionally = 1, and often, usually, always = 0. The sub-scale scores are calculated by simply adding all the scores of items of each specific sub-scale.
This research availed the Impulse Regulation Scale with an adequate internal consistency (a = 0.82). This scale shows the ability to regulate impulsive behaviour, especially binge behaviour.
Three Factor Eating Questionnaire (TFEQ)30 is a self-report questionnaire consisting of 51 items.The questionnaire refers to daily dietary practice and measures three different aspects of eating behaviour: (1) restrained eating (conscious restriction of food intake in order to control body weight or to promote weight loss – cut-off: ≤11; a = 0.79); (2) uncontrolled eating (tendency to eat more than usual due to a loss of control over intake accompanied by subjective feelings of hunger – cut-off: ≤8; a = 0.81): (3) emotional eating (inability to resist emotional cues – cut-off: ≤7; a = 0.83).
Minnesota Multiphasic Personality Inventory-2 (MMPI-2)31 consisting of 567 items with dichotomy answers (true/false) is most commonly used by mental health professionals to assess and diagnose mental illness. The MMPI is based on ten clinical scales that are used to indicate different psychotic conditions. In this research the scoring of the three following scales were taken into consideration: (1) Psychopathic Deviate Scale (Pd) (50 items) which measures social deviation, lack of acceptance of authority and amorality. This scale can be thought of as a measure of disobedience. High scorers tend to be more rebellious, while low scorers are more likely to accept authority. An adequate internal consistency was obtained in this research (a = 0.83); (2) Depression Scale (D) (57 items). The highest scores may indicate depression, while moderate scores tend to reveal a general dissatisfaction with one’s own life. A sound internal consistency was obtained through this research (a = 0.81); (3) Hypomania Scale (H), with 46 items, identifies such characteristics of hypomania as elevated mood, accelerated speech, locomotive activity, irritability, flight of ideas, and short periods of depression. In this research the internal consistency was a = 0.79.
Results
The Statistical Package for Social Science (SPSS 10.1) was implemented to verify the hypothesis. The limited number of subjects enabled analysis of data through non-parametric statistics. In order to verify statistical differences between simple comparisons on paired data the Mann-Whitney (U) test32 was applied. In order to verify statistical differences within phases (pre- Vspost-training), Wilcoxon Signed Ranks Tests33 were calculated separately on paired data.
Table 1 synthesizes the means and standard deviations of eating behaviour and of impulse regulation obtained by the three groups: CBT alone; psychotherapy with Paroxetine (CBT+P); and psychotherapy with Venlafaxine (CBT+V) in pre- and post-treatments.
Groups
Phases
Binge Eating Disorder
Impulse Regulation Scale
MIN
MAX
M
SD
MIN
MAX
M
SD
CBT (N=10)
Pre
28
35
31.43
2.41
74
94
85.93
6.84
Post
25
33
28.71
2.46
71
91
83.07
6.67
CBT+P (N=10)
Pre
26
35
30.90
3.54
77
94
86.80
5.29
Post
24
31
27.90
2.85
74
91
82.10
5.72
CBT+V (N=10)
Pre
27
35
30.80
2.78
83
94
87.80
3.91
Post
24
31
27.20
2.57
79
90
83.80
3.71
Table 1 – Minimum and maximum scores, Means and Standard Deviations of eating behaviour and of impulse regulation obtained by three differential groups.
By comparing the total scoring in BES during the pre-treatments phase, no statistical differences between groups were noticed. Subjects who only underwent CBT had the same result than those who had addition of Paroxetine (CBT+P) [U = 64; Z = 0.35; p = 0.75] and Venlafaxine (CBT+V) [U = 59; Z = 0.62; p = 0.55]. There were no initial statistical differences between the two groups that received pharmacotherapy [U = 50; Z = 0.1; p = 0.99].
In the post-treatment phases, the presence of binge eating behaviour appeared to be the same in all groups. Subjects belonging to the CBT group obtained the same results as those belonging to the CBT+P [U = 58; Z = 0.68; p = 0.5] and the CBT+V groups [U = 47; Z = 1.36; p = 0.19]. No statistical differences between medication use were noticed [U = 41; Z = 0.69; p = 0.53].
All groups in post-treatment phases seem to equally benefit from the treatment. Comparing scores obtained by participants in the pre- and post-treatments, statistically significant differences were found in subjects undergoing CBT [Z=3.38, p < 0.001] and those with the addition of Paroxetine [Z = 2.848; p < 0.004] and Venlafaxine [Z = 2.859, p < 0.004].
For this research, Impulse Regulation Scale scores were taken into consideration. In the pre-treatment phase relative to each group, all groups showed the same difficulties to regulate impulsive behaviour. The CBT group showed the same impulse regulation as those belonging to the CBT+P [U = 68; Z = 0.12; p = 0.93] and CBT+V group [U = 64; Z = 0.33; p = 0.75]. No initial statistical differences between pharmacotherapy groups were found [U = 45; Z = 0.39; p = 0.74].
In post-treatment, no statistical differences between groups were observed. The CBT group achieved the same results as the CBT+P [U = 60; Z = 0.56; p = 0.58] and CBT+V group [U = 64; Z = 0.32; p = 0.75]. No statistical differences between the use of Paroxetine and Venlafaxine were found either [U = 39; Z = 0.84; p = 0.44].
All groups seemed to benefit from the treatments. In fact, comparing the scores obtained by participants in the pre- and post-treatments, statistically significant differences were observed in subjects who underwent CBT [Z = 3.38, p < 0.001] as well as in subjects supported by Paroxetine [Z = 2.84; p < 0.005] and Venlafaxine [Z = 2.97, p < 0.003].
Table 2 synthesizes the means and standard deviations of different features of eating behavior (restrained eating,uncontrolled eating andemotional eating)showed by the three groups (CBT, CBT+P, and CBT+V) in pre- and post-treatment.
Groups
Scales
Pre-Treatment
Post-Treatment
MIN
MAX
M
SD
MIN
MAX
M
SD
CBT
restrained eating
5
9
6.64
1.28
5
8
5.86
.95
uncontrolled eating
13
16
14.71
1.07
11
15
12.93
1.21
emotional eating
8
13
9.93
1.21
7
11
8.57
1.22
CBT+P
restrained eating
5
9
6.50
1.43
5
7
6.00
.82
uncontrolled eating
13
16
14.10
1.11
10
13
11.60
1.07
emotional eating
8
13
10.70
1.64
8
11
9.80
1.03
CBT+V
restrained eating
5
8
6.10
1.11
4
7
5.50
.85
uncontrolled eating
12
16
13.90
1.37
10
13
11.40
1.17
emotional eating
9
13
10.60
1.43
7
11
9.10
1.19
Table 2 – Minimum and maximum scores, Means and Standard Deviations of different aspects of eating behavior (restrained eating, uncontrolled eating and emotional eating) obtained by three differential groups
In eating behaviour as well, all groups in pre-treatment phases appeared to be equivalent. The CBT group had the same mean result in restrained eating than those subjects who also underwent pharmacotherapy [CBT+P: U = 65; Z = 0.33; p = 0.74; and CBT+ V: U = 53; Z = 1.03; p = 0.55]. In the pre-training no statistical differences between groups with pharmacotherapy were noticed [U = 42; Z = 0.59; p = 0.58].
By analyzing the groups in pre-treatment phases no statistical differences in uncontrolled eating behaviour and emotional eating behaviour were found. In pre-treatment phase, the CBT subjects had the same statistical mean in uncontrolled eating [U = 48; Z = 1.33; p = 0.21] and in emotional eating [U = 48; Z = 1.32; p = 0.21] as those who took Paroxetine. No statistical differences were found when comparing CBT subjects with those that were taking Venlafaxine [uncontrolled eating: U = 48; Z = 1.33; p = 0.21; emotional eating: U = 48; Z = 1.32; p = 0.21]. In the pre-training phase there were no statistical differences between groups with pharmacotherapy [uncontrolled eating: U = 46; Z = 1.44; p = 0.17; emotional eating: U = 51; Z = 1.12; p = 0.28] were found.
All groups showed indistinctively less difficulty on restrained eating habits. In fact, by comparing post-training scores, the participants of CBT obtained the same results as those treated with Paroxetine [U = 61; Z = 0.56; p = 0.62] and Venlafaxine [U = 58; Z = 0.75; p = 0.51]. Therefore CBT alone appeared to be less effective on reducing uncontrolled eating than those with the addition of Paroxetine [U = 30; Z = 2.4; p < 0.02] and Venlafaxine [U = 26; Z = 2.6; p < 0.009]. Participants who underwent only CBT presented with less difficulties on emotional eating control than those with Paroxetine [U = 31; Z = 2.31; p < 0.02], but they achieved the same post-treatment score as those supported by Venlafaxine [U = 52; Z = 1.08; p = 0.31].
Comparing post-treatment outcomes, the effectiveness of Paroxetine and Venlafaxine appeared to be the same on restrained eating behaviour [U = 34; Z = 1.2; p = 0.25], on a better controlled eating behaviour [U = 45; Z = 0.39; p = 0.69] and on a higher emotional eating control behavior [U = 33; Z = 1.29; p = 0.2].
Comparing pre- and post-treatment results helped to observe a significant improvement in all groups. Participants who followed only CBT showed less difficulty to restrained eating behaviour [Z = 2.6; p < 0.009] in post-treatment. The same results were observed in those supported by Venlafaxine [Z = 2.12; p < 0.03], while no statistical differences were detected in a post-treatment phase in those groups supported by Paroxetine [Z = 1.89; p = 0.06].
Moreover it was possible to observe a considerable decrease in uncontrolled eating behaviour in all groups [CBT: Z = 3.49; p < 0.0001; CBT+P: Z = 2.84; p < 0.005; CBT+V: Z = 2.88; p < 0.004]. The same results were observed in the way emotional eating was handled. All groups benefited from treatments [CBT: Z = 3.27; p < 0.001; CBT+P: Z = 2.46; p < 0.01; CBT+V: Z = 2.87; p < 0.004].
Table 3 synthesizes means and standard deviations of Psychopathic Deviate (Pd), Depression (D) and Hypomania scales (H) obtained by the three groups (CBT, CBT+P, and CBT+V) in pre- and post-treatments.
Groups
Scale
Pre-Treatment
Post- Treatment
MIN
MAX
M
SD
MIN
MAX
M
SD
CBT
Psychopathic Deviate (Pd)
68
85
74.14
5.02
60
80
66
5.38
Depression (D)
63
81
72.50
5.58
61
78
69.86
5.39
Hypomania (H)
39
75
62
8.15
41
72
59.50
7.29
CBT+P
Psychopathic Deviate (Pd)
70
84
74.80
3.97
67
80
71.40
3.72
Depression (D)
66
76
70.80
3.91
64
74
67.80
3.58
Hypomania (H)
46
70
60.30
7.94
40
63
54.10
8.08
CBT+V
Psychopathic Deviate (Pd)
70
85
76.20
5.41
66
80
72.90
5.06
Depression (D)
65
80
70.80
4.76
61
75
66.60
4.69
Hypomania (H)
42
72
60.10
10.67
41
69
54
10.27
Table 3 – Minimum and maximum scores, Means and Standard Deviations of different aspects of Psychopathic Deviate obtained by three differential groups
As evidence of the homogeneity of the groups, the comparisons revealed no statistically significant differences in the pre-treatment phase. The CBT group subjects and those who received Paroxetine [Pd: U = 58; Z = 0.67; p = 0.51; D: U = 55; Z = 0.85; p = 0.39; H: U = 63; Z = 0.41; p = 0.71] showed similar scores. Likewise, the CBT group subjects and those treated with Venlafaxine [Pd: U = 53; Z = 0.99; p = 0.34; D: U = 58; Z = 0.71; p = 0.51; H: U = 65; Z = 0.26; p = 0.79] showed similar scores. The two groups treated subsequently with pharmacological support showed similar initial scores as well [Pd: U = 44; Z = 0.46; p = 0.68; D: U = 50; Z = 0.1; p = 0.99; H: U = 44; Z = 0.45; p = 0.68].
Comparing the results obtained in the post-treatment phase instead, those participants exposed to CBT alone showed a greater reduction of Pd compared to those who had taken Paroxetine [U = 23; Z = 2.76; p < 0.005] and Venlafaxine [U = 23; Z = 2.77; p < 0.005], whereas no differences were found comparing the scores obtained post-treatment in both groups of subjects with pharmacological treatments [U = 41; Z = 0.65; p = 0.53].
In post-treatment, the CBT group participants showed similar scores when compared to those taking Paroxetine [D: U = 54; Z = 0.91; p= 0.37; H: U = 41; Z = 1.67; p = 0.09] and Venlafaxine [D: U = 44; Z = 1.49; p = 0.14; H: U = 49; Z = 1.2; p = 0.23]. There have been no further significant differences in scores obtained post-treatment by the two pharmacotherapy groups [D: U = 39; Z= 0.84; p = 0.44; H: U = 0.47; Z = 0.23; p = 0.85].
All participants seem to have benefited from the proposed treatment. The CBT group had a significant reduction of Pd [Z = 3.3; p < 0.001], D [Z = 3.37; p < 0.001] and H [Z = 3.19; p < 0.001].
A similar result was found by comparing the pre- and post-treatment scores of the subjects supported by Paroxetine [Pd: Z = 2.7; p < 0.007; D: Z = 2.82; p < 0.005; H: Z = 2.82; p < 0.005].
Even in the group treated with Venlafaxine, a significant reduction of Pd [Z=2.87; p< 0.004], D [Z = 2.84; p < 0.004] and H [Z = 2.81; p < 0.005] was confirmed.
Discussion
The use of pharmacological therapy for overweight patients with BED has been less thoroughly studied. SSRIs (Citalopram, Sertraline, Fluoxetine, and Fluvoxamine) have mainly been used as the active compound in the pharmacological trials of patients with BED in order to improve mood symptoms and weight loss.34 Likewise, in many cases, promising results have been obtained with Venlafaxine in BED.35
Most of the research has focused on specific aspects of binge eating disorder, such as reduction in binge frequency and weight reduction. In general the results are associated with higher discontinuation rates.36
In this research, we did not only focus on the binge eating behaviour and impulse regulation in patients with BED. The main objective of this research was to analyze some aspects of eating behaviour (restrained eating, uncontrolled eating and emotional eating) and, more specifically, different psychotic conditions (psychopathic deviate, depression and hypomania).
The first hypothesis of this research was to verify differences between patients with binge eating disorder that followed CBT either with or without a pharmacotherapy support. The results confirmed that CBT and pharmacotherapy are equally effective in the treatment of BED and equally modified patients’ impulse regulation. Paroxetine and Venlafaxine medications did not enhance the control of binge eating or guarantee management of impulse regulation better than CBT alone.
This research also aimed at evaluating the efficacy of CBT with or without pharmacotherapy on some factors related to eating behaviour, such as the tendency to consciously monitor and reduce the caloric intake (restriction), the tendency to lose control on food intake (uncontrolled eating) and the conscious perception of the sensation of craving for food (emotional eating). The results suggest that CBT offers the same results regarding the reduction of caloric intake (restriction) as pharmacological treatment. It is less efficient in reducing the lack of control in food intake (uncontrolled eating), although it helps to reduce the sensation of craving for food (emotional eating) compared to pharmacotherapy.
In this research the effects of standardized treatments of CBT with or without the use of pharmacotherapy with bio-equivalent doses of Paroxetine and Venlafaxine were analyzed on psychopathic deviation, depression, and hypomania. The results confirmed that CBT showed a greater reduction of psychopathic deviation compared to those groups who underwent pharmacotherapy. Moreover, pharmacotherapy led to a higher reduction of depression and hypomania than CBT alone.
The second hypothesis was to verify if the SSRI Paroxetine and SNRI Venlafaxine were equally effective on impulse regulation, eating behaviour and personality features. The analysis showed that Paroxetine and Venlafaxine were equally effective on binge eating control and impulse regulation, but some differences in reducing dysfunctional eating behavior were found. Venlafaxine, compared to Paroxetine, seems to offer a greater improvement in emotional eating and restriction eating behavior. In fact CBT could be efficient to assess the tendency to reduce caloric intake (restriction) and to reduce the sensation of craving for food (emotional eating) more than Paroxetine alone. In order to reduce the tendency to lose control on food intake (uncontrolled eating) it could be helpful to administer Paroxetine or Venlafaxine.
Limitations
While the clinical groups were equivalent in all the parameters taken into consideration in the pre-treatment phase, the absence of a control group (no treatment) significantly reduced the possibility to accurately verify the conclusion. Due to ethical reasons we were not allowed to select a group of patients without any specific treatment. In order to correct this weakness in the research, it might be helpful to extend the sample and analyze the changes over a longer period of time.
It is relevant to analyze appropriately these aspects through controlled trials in order to test the efficacy and long-term outcome of psychotherapy, pharmacotherapy, and psychotherapy in combination with pharmacotherapy for treating BED.
Conclusion
In conclusion, patients with eating disorders usually suffer from other psychiatric disorders besides their eating disorder. Many results also confirm substantial comorbidity among obesity, BED, mood and anxiety disorders and metabolic syndrome in weight loss seeking populations.37
In such cases, it is important to understand the characteristics of the additional psychiatric disorders and the impact these ones have throughout the treatment.
As underlined by American Dietetic Association (ADA) Reports,38 understanding the complexities of eating disorders, such as influencing factors, comorbid illness, medical and psychological complications, is critical in the effectiveness of the treatment of eating disorders.
Eating disorders are complex medical illnesses since they have psychological, behavioural, and physiological components. Previous researchers underlined the importance to investigate gender differences in binge eating and associated behavioural correlates39 and, in order to prevent eating disorders, it is important to carry out individual treatment even on personality traits if the individual disorders have already occurred.40 Of course, a multidisciplinary approach involving a collaborative team of psychological, nutritional, and medical specialists as underlined in this research must be pursued in order to obtain important and at least short-term results.41
The results of this research confirm the need to analyze BED from an integrative perspective and to suggest treatments based on an interdisciplinary approach. The psychological (CBT) and pharmacological (Venlafaxine and Paroxetine) therapies were both efficient in different ways on the reduction of all the negative variables related to eating disorder. However any treatment could be inadequate in the absence of an accurate diagnosis that takes into consideration biological, genetic, psychological and nutritional components.
The assessment phase still plays an important role in determining which treatment is best for each patient. Accuracy in the medical examination when dealing with medical issues, as well as during the assessment examination and the psychological functioning evaluation is recommended.
Autism Spectrum Disorders (ASD) is the umbrella term increasingly used to describe the set of pervasive developmental disorders that included the diagnosis of Autism, Asperger’s Syndrome, and Pervasive Developmental Disorder Not Otherwise Specified under DSM IV. These are a group of disorders characterised by pervasive difficulties in a combination of the key areas of social communication interaction, and restrictive repetitive behaviours or activities 1, 2. The Diagnostic and Statistical Manual of Mental Disorders (the DSM-5), released by the American Psychiatric Association, officially eliminated many familiar autism spectrum diagnoses and now incorporated them into the single diagnosis of autism spectrum disorder. In DSM-IV, Asperger Syndrome was diagnostically differentiated from Autism by the lack of a significant language delay and intellectual functioning within the normal range.
The epidemiology of ASD is approximately estimated 30 in 10,000, although with increasing awareness of the disorder, this has led to greater rates of diagnosis, more recent estimates suggest the rate may be as high as 60 in 10,000 3. ASD may be as common as 1 in every 68 children according to the United States Centre for Disease Control 4.
Difficulties with an understanding of prevalence possibly related to early studies relying on clinically identified cases rather than community-based surveys, which may have resulted in cases not in treatment were being missed, and possibly only the most severe cases being recorded. Previous estimates may also have been incorrect due to previous narrower case definitions. As sampling methods have improved and better diagnostic instruments are used more cases have been identified and there has been a better delineation of ASD from other psychotic disorders. As more children with ASD are identified, there will be a likely rise in the number of families and children seeking treatment.
Comorbidities
There are very high levels of co-morbid psychiatric difficulties amongst this population with estimates ranging from 7-15%. Anxiety related concerns are among the most common presenting problems for school age children and adolescents with ASD 5. Several studies have examined the prevalence of anxiety within the ASD population. A review by white et al 6 of 11 such studies reported a prevalence to range from 11-84%. This large range in the prevalence may be accounted for by difference in methods used to measure anxiety, differences in definitions and in diagnostic subtypes.
Studies have also looked at prevalence rates of anxiety within the ASD population to other populations. Compared to groups of typically developing children, those with autism had a higher occurrence of anxiety 7, 8. Comparison with other groups considered to be at risk (children with conduct disorders and learning disabilities) children with ASD were more likely to be diagnosed with an anxiety disorder and/or have more intense anxiety symptoms 9,10.
A formal diagnosis of anxiety disorder in this group is hard for therapists due to overlap between comorbid anxiety and the core symptoms of ASD makes. Several anxiety disorders in DSM- IV and ICD 10 have autism as an exclusion criterion, implying that an anxious procession style is a feature of ASD.
The development of anxiety among children with ASD may relate to their cognitive impairment as they may lack the cognitive flexibility to generate strategies to adapt to varying circumstances and may experience distress over even trivial changes in the environment. The information processing style in children with ASD termed ‘weak central coherence’ is similar to non ASD anxious children whereby they selectively attend to threatening cues which results in the misinterpretation of ambiguous situations as threatening 11,12. As a consequence these cognitive deficits can result in a repertoire of social and communication difficulties resulting in children experiencing severe difficulties in social relationships which may in turn lead to the development of anxiety 13. If a child or adolescent has a co-occurring anxiety disorder, this could further negatively impact on the overall social impairment associated with ASD. This can impact on the child or adolescents ability to participate in activities at school, at home and within the community. Children with significant anxiety symptoms are at risk for serious educational difficulties, later unemployment, substance abuse and other psychiatric problems 14.
Some of the most frequently reported anxiety disorders and symptoms seen in children with Autistic Spectrum disorders are simple phobia, generalised anxiety disorder, separation anxiety disorder, obsessive-compulsive disorder and social phobia.
Treatment with Cognitive Behavioural Therapy
Pharmacological and psychosocial treatment have been the most common approaches to the treatment of anxiety in children with ASD but no single anxiety treatment has emerged to attain well established or probably efficacious empirically supported treatment status for children with an autistic spectrum disorder. Evidence for pharmacological intervention is limited. Also the effects of medication only appear to last as long as the medication is used, with relapse once regime is ceased.
The recommended treatment of choice by NICE guidelines for mood and anxiety disorders is cognitive behavioural therapy (CBT) and the primary psychosocial treatments have used CBT.
Despite the fact that CBT has been shown to be an effective empirically supported treatment for typical children, there continues to be differing views as to whether or not it can be used effectively with other populations. Some of the difficulties associated with treating children with ASD are due to suggestions from research that children with ASD have difficulty in identifying emotions and cognitions both in themselves and others. As CBT relies on the child’s ability to infer their own emotional states and thoughts in order to shift their cognitive style and in turn their anxious behaviour, standard CBT treatments need modification to address the difficulties associated with this.
Although there is recognition of the high comorbidity of anxiety with ASD, there have also been suggestions to the use of strict behavioural analysis 15 and an argument against using a cognitive component to treat this population. Lindsay 16 provides a different view, arguing children with ASD can benefit from the use of a cognitive component.
Various modifications have been proposed on the approach of CBT in this population. Some of the models have suggested adjustment of the developmental level to reflect the child’s ability, the use of coping model instead of curative model, the involvement of caretakers, and extending treatment both by the number of sessions and by overall session duration 17. Attwood 18 has recommended the use of role-plays and visuals, the involvement of special interests of the young person, the adjustment of material according to the developmental level and the incorporation of a social skills module due to the vast deficits associated with ASD. Anderson and Morris 19 recommend a more directive approach to treatment and the use of specifically in vivo practice to aid in the generalisation of skills. Each of these variations may contribute differently to the adaptation of CBT to meet the specific needs of the child being treated; however, the most appropriate pattern of practical and functional strategies is yet to be determined.
Chorpita and Daleiden 20 in their review of evidence based treatment for children and adolescents noted the most commonly used techniques to treat anxiety in typically developing children. These include exposure, relaxation, cognitive restructuring and modelling in that order. The most commonly used techniques to treat ASD include communication skills training, modelling, social skills training, goal setting and parent psycho-education.
CBT generally consists of six components which include assessment of the nature and degree of the disorder, affective education, cognitive restructuring, stress management, self-reflection and a schedule of activities to practice new cognitive skills. It is important to ensure that the young person has the same definition and interpretation of words, and affective education can help increase their vocabulary of emotional expression.
Attwood 21 has described several intervention components which can be added to CBT. Some of the suggestions include; a) Increasing the use of visual aids. b) Associating emotions with tangible objects. c) An emphasis on coping strategies that do not require the use of abstract language for instance the use of relaxation. d) Use of alternative communication modes. e) Embedding the use of preservative interests into CBT sessions. f) Increasing the focus on teaching social skills.
Attwood also developed the concept of an emotional toolbox and focused on working with the young person in identifying different tools to ‘fix’ problems that occur as a consequence of negative emotions including anger, anxiety and sadness. The ‘tools’ are further divided into those that constructively release or reduce energy and those that improve thinking. The therapist generally works together with the young person to draw a variety of tools and activities which encourage constructive emotions repair.
Cognitive restructuring aims to enable the young person to correct distorted conceptualisations and dysfunctional beliefs. It involves challenging the current thinking with logical evidence and ensuring rationalisation and cognitive control of their emotions. Young people with ASD can make false assumptions of their circumstances and intentions of others due to impaired or delayed theory of mind abilities. These young people also tend to make literal interpretations and are less able to seek alternative explanations or responses.
Summary of Case Reports, Case Series, and Randomised Control Trials
Method
Studies that used CBT with the aim of reducing anxiety symptoms in young people with an ASD diagnosis were looked at.
Search Procedures
A search was carried out in electronic bases: Psychinfo and Medline. The publication year was not restricted but the search was limited to English- language peer reviewed journals. Over the databases, the terms ‘Asperger’, ‘Autism’, or ‘developmental disability’, plus ‘anxiety’ or ‘CBT’ and the search was limited to children and adolescents.
Review of Case series and reports
There have been five case studies that used CBT in treatment of anxiety as well as one case report that used CBT in treatment of OCD in children with ASD.
The first case study by Reaven and Hepburn (2003)22 reported a 7 year old girl with Asperger syndrome who markedly responded to a 6 month modified CBT treatment which was primarily tailored for her OCD. Afterwards, Greig and MacKay (2005) 23, Sze and Wood (2007) 24 and (2008) 25, Reaven et al (2009) 26, and White et al (2009) 27 reported further successful outcomes of using modified CBT for treatment of Anxiety in children with ASD. See table 1 for a summary of published case reports and series of studies.
Table 1: A Summary of Published Case Reports and Series of studies using CBT for anxiety symptoms in young people with an ASD diagnosis
AUTHOR (year)
Sample
Anxiety Measure
Characteristics of intervention
Outcome
Reaven & Hepburn (2003)22
a 7 year old girl with Asperger syndrome
6 months modified CBT treatment based upon the work of March and Mulle
Obsessive-compulsive symptoms improved markedly
Greig and MacKay (2005) 23
12 year old male with ASD and unspecified anxiety disorder
TSCC, Teacher Report, SWQ
15 sessions
Anxiety score on TSCC reduced from 19 to 5. Teacher report suggested improvements at school.
Sze and Wood (2007) 24
11year old female SAD, OCD, GAD, HFA
ADIS
16 sessions 90 minutes each over 4 months family cognitive behavioural therapy (FCBT)
No longer met criteria for SAD, GAD or OCD on the ADIS by child or parent report
Sze and Wood (2008) 25
10 year old male with ASD,GAD, SAD
ADIS, CGI, MASC, CBCL, SSRS, VABS
Enhancing CBT
No longer met criteria for Social phobia or GAD, on the ADIS, improvement CGI , MASC
Reaven et al (2009) 26
7 male, 3 female mean age 11years, 12 weeks Active Treatment 10 parent-child dyads(n = 10) Wait List Control (n = 23)based on order of enrolment, not random assignment
SCARED
12 weekly sessions of 1.5 hours
Large group time, separate parent and child group meetings, and parent-child dyads
Parent report on SCARED showed significant decrease in severity of anxiety symptoms in treatment group
White et al (2009) 27
14 year old male with ASD, 14 yr old female with PDD-NOS,12 year old male with ASD, 12 year old female with ASD
ADIS
MCIT 12-13 individual therapy modules delivered over 11 weeks.
On the CASI-20 parent rated measure of anxiety, 3 out of 4 participants demonstrated significant improvement from baseline to endpoint.
There have been eight studies that have met criteria for a randomised controlled trial that identified CBT as a treatment for anxiety in children with ASD. See table 2 for published randomised controlled trials.
Table 2: Published randomised controlled trials of cbt
AUTHOR (year)
Age range/ Sample size
Anxiety Measure
Characteristics of intervention
Characteristics of Controlled
Outcome
Sofronoff, Atwood, Hinton (2005) 28
age 10-12
(n=71)
SCAS, SCAS-Parent,
child report measure
a 6 week CBT
child based (n=23) or combined child and parent (n=25) intervention
a waiting list group
Significant decreases Parent reports SWQ at follow-up and a significant increase in the child’s ability to generate positive strategies in an anxiety-provoking situation.
a 12 week group CBT based on ‘Cool Kids’ program(n=28)
Approx. 7 months waiting list (n=19)
71.4% of the treated children no longer met criteria for an anxiety disorder compared to 0% in the wait list condition (n=19)
Wood et al (2009) 30
ages 7-11 (n=40)
Anxiety symptom checklists at baseline and post treatment/ post waitlist
16 sessions of standard CBT augmented with multiple treatment components (n=17)
A 3 month wait list (n=23)
78.5% CGI improved compared to only 8.7% of the waitlist group, Remission of anxiety in CBT group, but child reported anxiety had no significant effect
Sung et al (2011) 31
age 9–16
(n=70)
SCAS-C,CGI-S
a 16-week CBT
program (n = 36)
a Social Recreational (SR) program on anxiety (n =34)
Children in both programs showed significantly lower levels of generalized
anxiety and total anxiety symptoms at 6-month follow-up on SCAS-C
Reaven et al (2012) 32
age 7-14
(n=50)
ADIS-P
modified CBT (n=24)
TAU (n=26)
50% in the CBT compared to 8.7% TAU group had a clinically meaningful positive treatment response, group CBT intervention specifically developed for children with ASD may be effective in decreasing anxiety
18 (75 %) of CBT arm, were treatment responders, versus only 3 of 21 (14%) in the TAU arm. CBT adapted for anxious youth with high-functioning ASD demonstrates large effects in reducing anxiety symptoms.
McNally et al (2013) 35
age 8-14
(n=22)
ADIS-P, SCAS-P, SCAS
a modified version of the Coping Cat program CBT package(n=12)
waiting-list
(n=10)
ADIS-P 58% of children with CBT had no anxiety / 36% after 2 month follow up. A modified version of the Coping Cat program may be a feasible and effective program for reducing clinically significant levels of anxiety in children with ASD.
Sofronoff, Atwood, and Hinton (2005) 28 evaluated the impact of a six week cognitive-behavioural intervention for anxiety in 71 school children aged between 10 to 12 with Asperger’s Syndrome. The authors also looked at the potential impact of parent involvement on outcome. The diagnosis of Asperger’s Syndrome was confirmed by semi-structured telephone interview and anxiety symptoms were based on parent report in the initial telephone interview. Children were randomly assigned to one of three groups: child based intervention, combined child and parent intervention or a waiting list group. The intervention focused on teaching the children strategies to manage feelings and expanding emotional knowledge and was delivered weekly in a group format. The focus was on teaching the children strategies to effectively manage feelings and expanding emotional knowledge. Parents served as co-therapists in the combined parent-child intervention as they were trained in all aspects of the intervention.
Using the Spence Child Anxiety Scale-Parent report, children in the combined parent-child intervention reported fewer symptoms of anxiety post–treatment and at a six week follow up than children in the child-only intervention. A child report measure (James and the Maths Test) was used to identify the number of strategies the child could identify for coping with anxiety. Compared to children on the waiting list, children who received either intervention were able to develop more coping strategies. Those in the combined intervention generated significantly more coping strategies at endpoint compared to those in the child only intervention.
Parental involvement is an important aspect of treatment of young people with ASD in ensuring better generalisation and therapy outcome. Authors of this study found that children whose parents were involved in treatment were significantly more improved at follow up than those whose parents were not involved. There are different models of parents involvement and include either only direct participation in each session or with a separate parent only component or both. It seems that regardless of which approach is used parent involvement increases the sustainability and success rate of CBT. Involvement of parents helps to improve their understanding of exposure and practice and helping the young person to learn how to master the skills on their own.
Limitations of this study include the reliance on the parent report of anxiety symptoms and both Asperger’s Syndrome and anxiety symptoms were not formally diagnosed. Parents who were involved in the delivery of treatment may have had a more vested interest in their children’s progress with higher expectations for improvement affecting outcome measure reports. However, no independent (blinded) ratings of anxiety were gathered.
Chalfant, Rapee, and Carroll (2006) 29 evaluated a 12 week group delivered cognitive –behavioural treatment for anxiety in 47 school children aged between 8 to 13 with ASD and no intellectual disability. The intervention was adapted from the ‘Cool Kids’ program (Lyneham et al, 2003), a 12 week group based activity for treatment of childhood anxiety. Cognitive strategies were simplified in the intervention, with a greater focus on visual aids, structured worksheets and homework and exposure and the programme was extended over a 6 month period of time.
The authors randomly assigned participants to either the CBT (n=28) or waiting list (n=19) before beginning of each treatment group. Those under waiting list condition were offered treatment after approximately 7 months, when the waiting list period ended. Multi-modal and Multi-person assessment of anxiety were used. At pre-treatment, over 75% of the sample met criteria for more than one anxiety disorder.
Structured diagnostic measures used in the study included the ADIS (Albano& Silverman, 1996), Spence Children’s Anxiety Scale (Spence, 1998), The Revised Children’s Manifest Anxiety Scale (Reynolds & Richmond, 1978), and Children’s Automatic Thoughts Scale (Schniering& Rapee, 2002). Parent report measures included the SDQ-Parent Report (Goodman, 1997), and SCAS-Parent Report (Spence, 1998).
At post treatment, 71.4% of the treated children (n=28) no longer met criteria for an anxiety disorder compared to 0% in the wait list condition (n=19). It was also found that children in the CBT condition were largely able to identify their automatic thoughts indicating some theory of mind ability and had a significant reduction in automatic thoughts, in comparison to the wait list condition.
Limitations of this study include the small sample size so the data may not be reflective of the wider population with high functioning autism and anxiety. Also the lack of confirmation of the diagnosis of ASD by the investigating clinicians reduced the validity of the participant’s diagnostic status. Participants were accepted based on previous evaluations completed within the community setting.
There was no time spent with the waiting list group to help ensure that the benefits of treatment could be attributed to the treatment alone and not to time spent with the therapist. Also the issue of the waiting list group being aware of the treatment programme and knowledge of future treatment may have attenuated the response of those on the waiting list. Clinicians who implemented the CBT groups and collected the relevant pre-and post-treatment data were not blind to the study’s aims.
Wood et al (2009) 30 used a standard CBT program augmented with multiple treatment components as a randomised controlled trial for 40 children aged between 7 to 11. It was designed to accommodate the social and adaptive skill deficit of children with ASD that could pose barriers to anxiety reduction. They also used a family based intervention program adapted for use with children with ASD. Enhancements included addressing of poor social skills, adaptive skill deficits, circumscribed interests and stereotypes, poor attention and motivation, common co-morbidities as well as school based problems. During modules, children were given social coaching by the therapist, parents and available school providers on appropriate ways to enter interactions and maintain conversation with peers.
Children were randomly assigned to 16 sessions of CBT (n=17) or a 3 month wait list (n=23). Independent evaluators blind to treatment condition, were involved in structured diagnostic interviews. Parents and children completed anxiety symptom checklists at baseline and post treatment/ post waitlist.
The Clinical Global Impressions Improvement Scale (CGI) criteria showed that 78.5% of the CBT group showed positive treatment response at post treatment as compared to only 8.7% of the waitlist group.
Children randomised to CBT had primary outcomes comparable to those of typically developing children receiving CBT for anxiety disorder, which were remission of all anxiety disorders for over half the children in immediate treatment at post treatment and follow up and a high rate of positive treatment response on the CGI. However child- reported anxiety did not yield a significant treatment effect.
Limitations of this study include the small sample size which precluded tests of moderation. The study was also undertaken by researchers who developed the intervention and would need independent replication to validate the intervention.
Also using measures not designed for children with ASD had major impact on the outcomes. The child report of Multidimensional Anxiety Scale for Children (MASC) scores did not yield a significant effect for treatment group largely due to a decrease in MASC scores from pre to post treatment for children in both groups. This may have been due to the MASC being not particularly effective in this population and children’s scores at baseline were relatively low on average. Parental scores showed less of a change from pre to post treatment in the waiting list group. The MASC does not specifically measure OCD and GAD symptoms and as there was a wide range of anxiety symptoms, the type of change that some children may have experienced may not have been properly assessed.
Sung et al (2011) 31 compared the effects of a 16-week cognitive-behavioural therapy program and a Social Recreational (SR) program for 70 children with ASD aged between 9 to16. 36 of them were randomised to CBT and 34 to Social Recreational program. Children in both programs showed significantly lower levels of generalized anxiety and total anxiety symptoms at 6-month follow-up on SCAS-C. They suggest factors such as regular sessions in a structured setting, consistent therapists, social exposure and the use of autism-friendly strategies are important components of an effective framework in the management of anxiety in children and adolescents with ASD.
Reaven et al (2012) 32 used a modified CBT intervention for anxiety in 50 children aged between 7 to 14 with high-functioning ASD and anxiety, who were randomized to group CBT (n=24) or treatment-as-usual (TAU) (n=26) for 12 weeks. Independent clinical evaluators blind to condition, completed structured ADIS-P pre- and post-intervention condition. They found a significant difference between CBT and TAU group.
47 children completed either the CBT or TAU condition. They also had 3 and 6 month follow-ups. Results indicated markedly better outcomes for the CBT group. Clinician Severity Ratings, diagnostic status, and clinician ratings of global improvement showed significant differences by group. In the intent-to-treat sample, the CBT group, 10 of 20 children (50%) had a clinically meaningful positive treatment response, compared to 2 of 23 children (8.7%) in the TAU group. Initial results from this randomized, designed treatment study suggest that a group CBT intervention specifically developed for children with ASD may be effective in decreasing anxiety.
Limitations of this study include small sample size, lack of an attention control group, use of outcome measures normed with typically developing children, and no use of teacher or child measures. TAU remained variable, and the study did not mention the situation of the children in TAU as were or weren’t receiving any treatment.
White et al (2012) 33 combined treatment approaches, and evaluated the feasibility and preliminary outcomes of the Multimodal Anxiety and Social Skills Intervention (MASSI) program in 30 adolescents aged between 12 to 17 with ASD and anxiety symptoms of moderate to greater severity who were randomised to CBT (n=15) or Wait list group (n=15). A 16 % improvement in ASD related social impairment (within-group effect size = 1.18) was observed on a parent-reported scale. Although anxiety symptoms declined by 26 %, the change was not statistically significant. These findings suggest MASSI as a feasible treatment program and further evaluation is warranted. High subject adherence and therapist fidelity demonstrate the treatment was acceptable to families.
Storch et al (2013) 34 examined the efficacy of the Behavioural Interventions for Anxiety in Children with Autism (BIACA), a modular cognitive behavioural therapy protocol, relative to treatment as usual (TAU) among 45 children with ASD aged between 7 to 11. Children with clinically significant anxiety (including OCD), and no intellectual disability, were randomised to receive 16 sessions of weekly CBT (n=22, 2 drop out) or TAU (n=21). After screening, assessments were conducted at baseline, post-treatment, and 3-month follow up for only CBT group which was not blind. The raters were blind to treatment condition. They did also use both child- and parent-report versions of ADIS. Children receiving CBT showed substantial improvement relative to TAU on primary anxiety outcomes. Of 24 children randomised to the CBT group, 18 (75 %) were treatment responders, versus only 3 of 21 children (14%) in the TAU group. Treatment gains were generally maintained at 3-month follow up for CBT responders. They concluded that relative to usual care, CBT adapted for anxious youth with high-functioning ASD demonstrates large effects in reducing anxiety symptoms.
The limitations of this study include that only about 75% of the TAU children were in fact getting treatment of any kind at all, as 25% of their TAU weren’t getting anything. Also TAU group was extremely variable, therefore the control group were getting a variety of treatments, or none, making comparisons with the children who received CBT difficult.
McNally et al (2013) 35 used a modified version of the Coping Cat Program in reducing anxiety in children with ASD. They randomly assigned 22 children with ASD aged between 8 to14, with clinically significant anxiety and no intellectual disability, to 16 sessions of the Coping Cat cognitive-behavioural therapy (CBT) program or a 16-week wait list group.
They used ADIS-parent at pre-treatment and post-treatment phases, and they also video-recorded therapy sessions to check for treatment fidelity. Children in the CBT condition evidenced significantly larger reductions in anxiety than those in the waitlist. Treatment gains were largely maintained at two-month follow-up. Results provide preliminary evidence that a modified version of the Coping Cat program may be a feasible and effective program for reducing clinically significant levels of anxiety in children with high-functioning ASD.
The limitations of this study include small sample size which recommended statistical and effect size to be interpreted with caution, and also the outcome measures were largely based on parent- ADIS reports by parents who were not blind to the treatment. Also, examining treatment response was limited to the primary author who delivered all of the treatment. Similarly, with waiting list as a comparison, there was a danger of getting placebo effects with the intervention arm, especially with parent-report measures, as most parents were very keen to get any help at all for their children.
Discussion and future perspective
It is clear from the 8 randomised controlled studies that young people on the autistic spectrum benefit from some form of CBT when modified as part of a therapeutic package. Unfortunately it is not clear what specific aspect of the therapy is making the difference. Cognitive Behavioural Therapy has many components to it as well as the actual cognitive, i.e. ‘thinking’ part and behavioural part. Which bit of the therapy is making a difference to the anxiety? Is it the cognitive reframing, the relaxation, the exposure, the parental involvement, or simply the therapeutic relationship with a therapist? As with CBT studies which are delivered as part of a package, positive results are often obtained when there is no control group or when compared to a waiting list.
Other limitation to research papers cited above include fairly small sample sizes, and outcome measures that are normed with a non ASD cohort.
Only 2 studies had non waiting list comparison 32, 34. These studies did show significant clinical improvement in anxiety levels. These studies have shown that CBT can be effective if modified for the ASD population. Many clinics often fail to pick up associated anxiety difficulties in the ASD cohort and if present, often are under the impression that CBT would not work in this population due to misunderstanding and ill informed prejudices about the ASD population. As there is such a high comorbidity with anxiety disorders, young people on the autistic spectrum should be offered effective interventions such as CBT. Research should focus on modifications of the CBT package to enable better engagement and better understanding of the CBT constructs.
Practice Points
Children with high-functioning Autism Spectrum Disorder (ASD) are at high risk for developing significant anxiety
Anxiety can adversely impact on functioning across school, home and community environments
Cognitive Behavioural Therapy (CBT) is frequently used with success for children with anxiety symptoms
Standard CBT treatments need modification to address the anxiety difficulties associated with ASD
Modified CBT interventions for anxiety in children with ASD have also yielded promising results
Brain injury is a major cause of mortality and morbidity all over the world and in Europe there is an estimated incidence of 235 brain injury inpatients per 100,000 population 1. Over the years, the medical care of brain injuries has developed with a resultant fall in mortality. However, with this fall in death rates the proportions of people with complications, especially the neuro-behavioural effects of brain injury, has risen 2. Of the complications, psychiatric disorders have a significant impact on the patient’s quality of life and rehabilitation prognosis3 and so are an important consideration from both a care delivery and public health perspective. This paper therefore aims to analyse the prevalence of psychiatric disorders following brain injury and highlight the practical and personal implications of these through an illustrative case series.
Depression Following Brain Injury
Jorge et al in 20044 conducted a prospective case controlled study on a sample of 91 patients with traumatic brain injury (TBI). Patients with penetrating head injury, spinal cord injury and severe deficits of comprehension was excluded and 27 patients without brain injury but with other trauma was included as controls. The sample was analysed at 3, 6 and 12 months with Present State Examination (PSE), structured clinical interview for DSM1V, and analysed with Mann Whitney and chi squared tests. The results showed that 33% of the TBI group had major depression compared to 22 % in the control group. Neuropsychological testing also demonstrated that depressed patients had a greater degree of impaired cognitive function. An earlier study with a larger sample was conducted by Kreutzer in 20015, studying 722 TBI patients (average time post injury for evaluation 2.5 years). Data was collected via survey, using the Neurobehavioral Functioning Inventory to identify depression; the response was studied by trained neuropsychologists and compared with DSM-IV Criterion for depression. A significant proportion (42%) of survey respondents met the DSM-IV criterion for depression. Fatigue, low concentration and frustration were most commonly reported symptoms. A similar study done by Seel et al in 20036, where 666 TBI outpatients from 17 centres was reviewed using DSM-IV Criterion, showed rates of major depression to be 27%.
Mania Following Brain Injury
Jorge in 19937 reviewed 66 patients with brain injury at 3, 6 and 12 month intervals to evaluate the prevalence of mania. The inclusion criteria was age above 18 years and absence of delirium, no previous history of mood disorder and absence of grave injuries to other areas of the body. Using the Present State Examination to gather data, 9% of the sample had symptoms in correlation with the DSM III criteria for mania.
Van Reekum in 19968 recruited 18 TBI patients attached to a rehabilitation unit for a study to evaluate mental illness in this population. 44% of patients had severe TBI while 56% had mild/moderate TBI; the average duration since TBI was 4.9 years. 27% met the DSM II criteria for bipolar affective disorder and 61% met criteria for depressive illness. The rate of anxiety disorder was 38% but psychosis was not reported.
Psychosis & Other Mental Illness Following Brain Injury
Fann et al in 20049 conducted a large prospective cohort study involving 1939 randomly selected TBI patients 1 year pre injury and 3 years post injury to study rates of psychiatric illness including psychosis. The sample was divided into the moderate/severe TBI and mild TBI compared to matched controls. The presence of psychiatric illness was detected by utilisation of mental health services by subjects, usage of psychotropic medication and presence of a psychiatric diagnosis in the records. Psychotic disorders were seen in 49% of the moderate to severe TBI patient group and for the mild TBI group psychosis was seen in 34% of the sample. This is significantly greater than the rate seen in the control group. However the lack of definitive diagnostic criteria and confounding factors such as social circumstances and other physical health issues which may have strong associations with mental illness were not accounted for.
Another observational prospective study done by Rao et al in 200910 looked into prevalence rates of aggression in the 3 months following brain injury. Overt Aggression Scale was used by trained examiners in the assessment of aggression in a sample of 107 TBI patients. Comorbidities were analysed using General Medical Health Rating scale; psychosocial functioning was analysed by Social Functioning Exam and the Social Ties Checklist. Results showed the prevalence of aggression in the sample to be 28.4% and this subgroup was also associated with new-onset major depression. Only 63% of the already small sample completed the study and the drop out group was unaccounted for; this may negatively impact the results.
Keenan et al in 200811 studied prevalence of attention-deficit hyperactivity disorder(ADHD) in 2782 post TBI children and demonstrated chance of a diagnosis of ADHD two folds higher amongst children with a head injury before age 2. Jellinger in 200412 studied links between brain injury and dementia, and found that although cognitive deficit was associated with brain injury, there was no established link between development of dementia and brain injury. Oquendo et al in 200413 studied 325 depressed patients to analyse the link with mild TBI and suicidal behaviour; 44% of the sample had mild TBI and suicidal behaviour was more common in this subgroup. Suicide Intent Scale and the Lethality Rating Scale was used to measure suicidal behaviour. However, exclusion of moderate to severe TBI and inclusion of only inpatients in this study would affect any generalisability of the results.
Case series: Psychiatric Disorders Following Brain Injury
Case 1- Patient A: Epilepsy, interictal psychosis and organic personality disorder following head injury
Patient A is a 37 year old female under mental health services with a diagnosis of organic personality disorder and interictal psychosis. She suffered from epilepsy from the age of 9 but coped well at school and went on to work successfully as a hairdresser. However, in 1998 at the age of 22 she was admitted to ITU with status epilepticus as a result of encephalitis of unknown cause, and remained severely unwell for several months. She recovered but was left with residual tonic clonic and complex partial seizures.
Since this episode, marked changes in her personality were noted. She developed mood swings with recurrent episodes of low mood, and expressed paranoid beliefs about people in the street talking about her. These beliefs resulted in her being agitated and physically aggressive, resulting in harm to both herself and others. She has required numerous admissions to acute wards and rehabilitation units because of her paranoid and suspicious behaviour and aggressive outbursts that her family were not able to manage in the community. She required restraint under Section 3 of the Mental Health Act in 2010, believing that care staff were poisoning her. Psychotic symptoms are most marked around seizures, with her displaying self harming behaviour such as cutting off hair or painting face with nail polish. She frequently accuses staff and family of acting against her in these periods and her behaviour is very difficult to manage.
Her case has been challenging to manage successfully in the community by family and community teams, and she has needed several short and long term stays in acute wards and residential units. Her care has been coordinated jointly between neurological and psychiatric services. She currently lives with her parents and has carers to support her. Her epilepsy is yet to be successfully controlled; antipsychotics can lower the seizure threshold and so a delicate balance between these and her antiepileptic medication is warranted. There is an on-going concern that further mental health problems may develop in light of this.
Case 2- Patient B: Schizophrenia following head injury
Patient B is a 43 year old female with a diagnosis of schizophrenia, learning difficulties and epilepsy. She suffers from epilepsy in the form of absence and tonic-clonic seizures from the age of 7 months, when there is high suspicion that she sustained a head injury whilst in the care of extended family. Patient B has difficulties with numeracy and literacy, identified through psychological assessment, and an IQ of around 70. She has required three admissions under Section 2 of the MHA due to her paranoid delusions and poor self care. Patient B frequently reports feeling monitored by cameras, suspicions that her food has been poisoned and that her personal belongings are being tampered with. She has attempted to take her own life due to feeling unable to cope with these delusions, laying in the road to be run over by a bus.
She is currently managed well in the community on oral risperidone for her psychosis and sodium valproate for her epilepsy; she resides in supported accommodation and has required stints in long term residential and rehabilitation beds due to her mental health problems and learning difficulties.
Case 3- Patient C:Depression and Personality disorder after head injury
Patient C first came in to contact with psychiatric services in 2007 and was diagnosed with depression and organic personality disorder. At the age of 16 this gentleman was knocked off his bicycle and sustained a severe head injury, from which he was left in a coma for over three weeks, but recovered well enough to go home. In 1994 he started having blackouts, was investigated extensively by neurology, and diagnosed with non-epileptic attack disorder. As part of these investigations, Patient C underwent an MRI which demonstrated significant brain damage including traumatic damage to the frontal lobes. This was likely due to his accident at age 16. From his first assessment by psychiatric services, he eluded to thoughts and behaviours that were of serious concern to his team. He reported feeling emotionally detached from his family, gaining little pleasure from life, getting in to fights frequently and allegedly having stabbed someone in an altercation several years ago. He described to practitioners only getting excitement out of reading and watching programmes about serial killers, and occasionally became sexually aroused by this. He had made extensive written plans on how he would capture, torture and kill the couple he believed were responsible for his accident at 16. He also struggles with auditory command hallucinations telling him to harm himself and others. He frequently self harms, often using a Stanley knife to cut his arms and legs. Patient C has been jointly managed by adult psychiatry and neuropsychiatry on an outpatient basis. His risks of aggression and violence have been carefully managed through regular assessment and involvement of forensic services.
Conclusion:
The literature search indicates that the prevalence of psychiatric disorders in patients with brain injury is much higher compared to general population. The significance of the results are however greatly affected by response bias, the impact of patients’ cognitive impairment on their study participation, observer biases and the small study population sizes; however, we believe that these short-fallings should be seen as a trigger to stimulate more comprehensive and wide-scale research in to this field. The methodologies used by authors described in the literature review demonstrate the wide variance in the tools used to assess psychiatric illness in patients following TBI; we therefore argue that universal case definitions need to be agreed on and implemented to standardise studies and reduce bias. The economic impacts and impacts on quality of life have often been neglected by researchers and warrant formal assessment. From a service delivery perspective, rehabilitation programs need to identify patients with signs of psychiatric illness post TBI earlier and involve psychiatric service in the development of integrated care plans to improve the total outcome and quality of life of the patient. The impact on the patient’s family and carers also need to be explored further to provide an evidence base for more effective and holistic interventions.
Various classes of medications have been known to cause drug induced liver injury (DILI), however not much literature has been published regarding angiotensin converting enzyme inhibitors (ACE-I) causing DILI. Recent years have seen tremendous increases in ACE-I prescriptions for coronary artery disease, diabetic nephropathy and hypertension. We report the first case of lisinopril induced hepatitis via a cholestatic mechanism.
Case:
A 47 year old female with history of diabetes mellitus type 2, hypertension, chronic kidney disease (CKD)stage III, non-obstructive coronary artery disease was admitted with complains of generalized weakness, lack of appetite, yellow discoloration of skin and eyes, dark urine and white stools for 1 week prior to admission. She denied history of alcohol abuse, past liver disease, illicit drug use, recent sick contacts, fever, chills, travel. Current patient medications included lisinopril, pioglitazone, furosemide, atenolol, metformin and detemir. Patient was started on these medications about 2 years prior to admission. Patient received enalapril for 5 months before switching to lisinopril about 2 years prior to presentation.
Physical examination was positive for icteric sclera, icteric skin; negative for spider nevi, palmar erythema and asterixis. Exam did not reveal hepatomegaly or splenomegaly. Labs showed hemoglobin 8.7 gm/dl, normal white count and platelet, normal C-reactive protein, alkaline phosphatase (ALP) 750 U/L, aspartate transaminase (AST) 169 U/L, alanine transaminase (ALT) 210 U/L, gamma-glutamyl transferase (GGT) 813 U/L, total bilirubin 13.4mg/dl with conjugated fraction 7.7mg/dl, ammonia level 64. Prior to initiation of lisinopril ALP was 87 U/L, GGT 53 U/L, with AST18 U/L, ALT 11 U/L and normal bilirubin fractions. Hepatitis A, B, C and D serologies were negative. Serum acetaminophen level was normal. Anti nuclear antibody (ANA), anti- mitochondrial antibody (AMA), anti-endomysial antibody, c-anti-neutrophil cytoplasmic antibody (ANCA), p-ANCA was negative. Anti smooth muscle antibody was weakly positive in titre of 1: 40. Creatine kinase, ceruloplasmin and alpha -1 antitrypsin level were normal. Quantiferon gold was negative. Lipid panel was deranged with cholesterol level 1017 and low density lipoprotein 1006, triglycerides 255.
Ultrasonography and magnetic resonance imaging abdomen showed hepatomegaly 17.5cms but was negative for fatty infiltration of liver, stones, cirrhotic features or dilation of biliary tree. Liver biopsy was done which showed mild portal chronic hepatitis with lymphocytic infiltration (Fig: 1), cholestasis (Fig: 2), mild portal fibrosis (Fig: 3), negative for bile duct damage (Fig: 4), negative for cytoplasmic inclusion. Congo red stain was negative for amyloid.
Figure 1: Mild hepatitis with portal tract lymphocytic infiltration.
Patient was treated with fluids, anti-histaminic, ursodeoxycholic acid. Patient was unable to tolerate coleveselam. Impression was drug induced hepatitis, lisinopril was discontinued and patient improved clinically and biochemically. Discharge labs two weeks after discontinuation of lisinopril showed AST 80 U/L, ALT 70 U/L, ALP 1045 U/L and GGT 1212 U/L; total bilirubin of 3.93 mg/dl with conjugated fraction 2.43mg/dl. Patient was discharged uneventfully with follow up in Hepatology clinic. Six months after discontinuation of lisinopril ALP was 199 U/L, GGT 168 U/L with AST 19 U/L, ALT 17 U/L, total bilirubin 0.9mg/dl and conjugated bilirubin 0.21mg/dl. Patient is currently asymptomatic and icterus has resolved.
Discussion:
ACE-I has been used widely for coronary artery disease, hypertension and diabetic nephropathy and approximately 159 million prescriptions for ACE-I are written annually. Recent JNCC guidelines recommended ACE-I to be used as first line anti-hypertensives for patients with CKD and diabetes. The common side effects known about ACE-I use are cough and angioedema, hypersensitivity. However not much awareness exists regarding ACE-I induced hepatotoxicity. It is important to consider ACE-I as an etiology for drug-induced liver injury (DILI) since continuation of the ACE-I beyond onset of hepatitis is fatal1.
Literature review shows multiple reports of DILI with captopril2, 3, ramipril4, fosinopril5, 6 and enalapril.2,7 Most commonly implicated ACE-I are enalapril and captopril. The usual presentation for ACE-I induced hepatotoxicity is cholestasis mediated hepatitis. Till date there have been four case reports published reporting lisinopril as cause of hepatitis 1, 8, 9 All 4 cases of lisinopril induced hepatotoxicity have shown a hepatocellular pattern of liver injury and did not show any cholestatic features. We report the first case of lisinopril induced cholestasis mediated hepatotoxicity.
In our case, patient had received enalapril for 5 months before initiation of lisinopril; however patient developed symptoms 2 years after initiation of lisinopril. The patient had no past medical history of liver or biliary tract disease. A thorough investigative workup was negative for autoimmune and other viral causes of hepatitis. Older case reports of lisinopril induced toxicity have shown similar histopathological findings of portal inflammation by lymphocytes without centrilobular zonal necrosis.9 There are various theories regarding possible mechanisms for DILI with lisinopril, namely terminal proline ring mediated bile stasis8, 10 and hypersensitivity to the sulfhydryl group.2 Discontinuation of metformin, pioglitazone, furosemide, atenolol and detemir did not result in clinical or biochemical improvement. Patient was initially continued on lisinopril since suspicion was low and then later discontinued. Similarity in histopathological findings along with a strong temporal relationship between lisinopril withdrawal and improved biochemical and clinical scenario, with absence of other constitutional symptoms and eosinophilia strongly point toward lisinopril-induced hepatotoxicity.
Our case had a long period of latency between drug intake and onset of hepatic injury which is consistent with other published reports of lisinopril induced hepatocellular injury9, 10, 11; however the mechanism responsible for latency or hepatotoxicity remains unclear. Earlier report postulate metabolic idiosyncratic reaction as a possible molecular mechanism for hepatocellular injury9. However our case is unique as the primary mode of injury appears to be cholestatic. Since our patient received enalapril before initiation of lisinopril without any adverse events, this case adds further controversy as to whether this patient could have been safely continued on other ACE-I except lisinopril or whether she would have developed hepatotoxicity if enalapril was continued. This case highlights further need for research to evaluate ACE-I induced hepatotoxicity. Currently the awareness for ACE-I induced liver injury is low and there are no guidelines guiding physician to monitor for possible hepatic adverse events. Further research is needed to delineate the mechanism by which ACE-I cause hepatotoxicity and to define possible risk factors.
Conclusion:
Discontinuation of ACE-I beyond recognition of DILI hepatitis usually leads to normalization of liver enzymes, however continuing or reinitiating ACE-I can be severe and potentially fatal. Thus, it is important to be aware of ACE-I as a possible cause of DILI, which can present with either hepatocellular or cholestatic mechanism and to promptly discontinue ACE inhibitor use. Currently there are no guidelines in place for monitoring of liver enzymes following initiation of ACE-I and more research is required to delineate possible mechanisms and prevent further DILI in such patients.
Atopic dermatitis (AD), also known as atopic eczema is a chronic, relapsing, inflammatory skin disease that can cause significant physical, psychological and social stress for patients and their families.1 This article focuses primarily on AD in adults. It is the most frequent inflammatory skin disease in the western world and is often characterized by chronic inflammation and pruritus interrupted by acute flares and bacterial infection.2,3 The majority of the care of AD is provided in primary care, with a minority of patients being referred to secondary care. There are currently extensive cost implications to the National Health Service (NHS) for both treating patients and for lost working days.4 AD can be a therapeutic challenge, especially in primary care, and there appears to be a great potential for improving the outcome and cost effectiveness of treatment in the community setting.4
Epidemiology and pathogenesis
AD typically begins in young infants or early childhood and subsides spontaneously by adolescence in approximately 90% of patients although it can persist into adulthood in about 10% of patients.5 The incidence of AD is generally considered to be increasing worldwide.6 AD affects both sexes equally, and in the United kingdom (UK) approximately 15-20% of school-aged children and 2-10% of adults will be affected by the condition at some stage.7
AD appears to result from a complex interplay between defects in skin barrier function, environmental agents, modified immune responses of the immune system to exogenous and endogenous factors, IgE-mediated mechanisms and other factors. However, the pathogenesis leading to the precise manifestation of AD is not completely understood.3,8
Diagnosis
There are no laboratory or diagnostic tests for AD. The diagnosis is based on visual assessment and clinical history. The UK diagnostic criteria (Table1) has been shown to be the most extensively validated for AD in comparison to the Hanifin and Rajka criteria, Schulz-Larsen criteria, Diepgen criteria, and Kang and Tian diagnostic criteria. Although several different diagnostic criteria have been developed they should mainly be used for research purposes as opposed to daily clinical management.4
Skin tests and laboratory investigations (specific IgE) may be helpful in the investigation of provocative factors such as food or environmental allergens. It is important to note that laboratory investigations should be interpreted in the context of the patient’s history.9
It is often difficult to differentiate AD from other skin conditions (e.g. seborrhoeic dermatitis, contact dermatitis, psoriasis, scabies). However, a family history of atopy and the clinical distribution of the lesions are helpful in making the diagnosis. Other conditions that need to be considered in the differential diagnosis of AD are metabolic and nutritional deficiencies, malignancies and immunodeficiency syndromes that present with skin manifestations.8
Table 1 – UK Working Party Diagnostic Criteria4
The patient must report an itchy skin condition (or parental report of scratching or rubbing in a child) in the last 12 months, plus three or more of the following:
History of involvement of the skin creases (front of elbows, behind knees, fronts of ankles, around neck or around eyes)
Personal history of asthma or hay fever (or history of atopic disease in first degree relative if child aged under four years)
A history of generally dry skin in the last year
Onset under the age of two years (not used if child aged under 4 years)
Visible flexural dermatitis (including dermatitis affecting cheeks or forehead and outer aspects of limbs in children under four years)
Management
The management of AD should involve a combination that includes short-term treatment of flares and a long-term maintenance approach to prevent flares. For patients with mild to moderate AD, topical therapy may be sufficient to control the condition. Patients with more severe disease may require advanced therapy such phototherapy or systemic therapy.
Education
For optimal disease management, patients and/or their carers should be educated about the nature of AD, the need for continued adherence to prescribed treatment and about the appropriate use of topical therapies. Time spent educating patients and carers have been shown to have a positive effect on disease outcomes. Patients may also benefit from written information to reinforce learning.8
Emollients
Emollients soften the skin, aid in restoring the impaired barrier function, reduce itching, prevent moisture from leaving the skin and increase the efficacy of topical corticosteroids (TCS). They also replace the natural surface oils that are essential to preventing irritant materials, infection and allergy-inducing substances from entering the skin.4
Healthcare professionals should offer a range of emollients, and prescriptions should be reviewed frequently. To optimise adherence to emollient therapy, creams, lotions, and ointments, or a combination can be used depending on patient preference. Continued use of emollients during periods of disease quiescence can reduce the likelihood for exacerbations.10
When the treatment regimen involves both an emollient and TCS, there is no evidence on which to base the order of application. Patients should be advised to apply emollients liberally and frequently (at least 2-4 times a day). It is especially important to use emollients during or after bathing. The emollient should be applied in the general direction of growth of body hair in order to prevent accumulation at hair bases which might predispose to folliculitis. Emollients can become contaminated with bacteria and the use of pump dispensers minimises this risk. If the emollient is in a pot it should be removed with a clean spoon or spatula.4
Topical corticosteroid therapy (TCS)
TCS is considered first-line therapy for AD flares. Available preparations include ointments, creams, gels, lotions, liquids, and foams. Ointments and creams are generally the most effective in treating AD as they tend to be more moisturising.10 The least potent preparation required to control AD, particularly in sensitive areas, should be utilised. When possible the TCS should be stopped for short periods to reduce the risk of adverse events.8
TCS is categorised into four groups according to potency: mild, moderately potent, potent and very potent. The choice of TCS potency should be tailored to the age of the patient, the body region being treated, and the severity of inflammation. Patients should be advised to apply TCS once daily. If there is an inadequate response to once daily application, the frequency should be increased to twice daily.4 Once control has been achieved, twice weekly maintenance therapy with a TCS should be considered in patients with moderate to severe AD experiencing frequent relapses. The local adverse effects of TCS usage include skin thinning, bruising, perioral dermatitis, folliculitis, pruritus, allergic contact dermatitis and the spread of fungal infection. Patients being treated with intermittent courses of TCS should be reviewed regularly (depending on TCS potency and site of application) to determine response to therapy and assess skin for potentially reversible atrophic changes.4
Table 2 - The ‘fingertip unit’ (FTU) is a method of determining the amount of TCS to apply. It is described as “the amount of ointment expressed from a tube with a 5 mm diameter nozzle, applied from the distal skin crease to the tip of the palmar aspect of the index finger.” The following table is a guide to the use of FTU in adults.4
Skin area
FTU per dose
Face and neck
2.5
Torso and abdomen
7
Back and buttocks
7
Entire arm and hand
4
A hand and fingers (front and back)
1
Entire leg and foot
8
Topical calcineurin inhibitors (TCIs)
TCIs are non-steroidal immunomodulating agents licensed for the treatment of AD.4 TCIs work by inhibiting the phosphatase activity of calcineurin to block expression of cytokines and are thought to represent a more targeted way to limit inflammation and avoid many of the adverse effects of TCS. TCIs may be used either as monotherapy, as a combination or as sequential therapy. TCS are generally less expensive and more effective than TCIs although individual clinical situations will arise in which TCIs are preferred.10
Two TCIs are available: tacrolimus (0.03% and 0.1% ointments) and 1% pimecrolimus cream. The tacrolimus 0.03% and 0.1% ointments are both licensed for moderate to severe eczema and the 0.03% ointment is licensed for use in children aged two years and over. The 1% pimecrolimus cream is licensed for mild to moderate eczema in patients aged two years and over. The use of tacrolimus should be limited to doctors with a specialist interest and experience in treating AD.4
TCIs should not be used as first line treatment unless there is a specific reason to avoid the use of TCS.4 Given the high cost of TCIs, and the fact that their long-term safety is not fully known, they are generally reserved for patients with persistent disease or frequent flares that would require continuous TCS treatment. They are also of use in patients with severe disease in sensitive skin areas (e.g. around the eyes, face, neck and genitals) where systemic absorption and the risk of skin atrophy with TCS are of concern. Considering the possibility that the normal immunological response to infection may be suppressed, TCIs should not be applied to skin which appears actively infected.4, 8
Dressings and wet wrap treatment
Patients with non-infected moderate to severe AD can be advised to cover affected areas with dry wrap dressings to provide a physical barrier to scratching and improve the retention of emollients. Wet wrapping generally consists of two layers of bandage applied over topical preparations. The bottom layer is soaked in warm water, squeezed out and then put onto the skin over the topical preparation. The top layer is dry. Wet wraps can be worn under nightwear or ordinary clothes and used during the day or night. They are available in bandage form or as garments.4 Disadvantages include a high cost, inconvenience, a need for specialised training, and an increased potential for adverse effects from occluded corticosteroids (such as systemic absorption, atrophy, striae), and increased incidence of skin infection.10 There is currently insufficient consistent evidence on which to base a recommendation for wet wrap use in the primary care setting.4
Antimicrobial measures
Skin lesions of around 90% of patients with AD are colonised compared to less than 5% of individuals with healthy skin. Staphylococci are the main organisms isolated although other organisms such as streptococci may also cause infection. The routine swabbing of skin is not indicated although swabs of potential Staphylococcus aureus carriage sites should be considered in patients with recurrent infection. Oral antibiotics are not recommended in the routine treatment of non-infected AD but patients with clinically infected AD can be prescribed short term oral antibiotic treatment based on local/regional antibiotic sensitivities. However, first- or second-generation cephalosporins or penicillins for 7 to 10 days are usually effective in managing bacterial infection. Macrolides are less useful alternatives due to resistant patterns in patients with AD. Patients with AD are also prone to recurrent viral infections. Eczema herpeticum is a severe disseminated herpes infection that is a serious risk in patients with widespread AD and may be misdiagnosed as a bacterial infection. Patients with eczema herpeticum normally require systemic antiviral treatment4, 10.
Antihistamines
Although first-generation antihistamines do not directly affect the itching associated with AD, the sedative effects have been found to help improve sleep. Therefore, short-term bedtime use of sedating antihistamines should be considered in patients with AD where there is debilitating sleep disturbance. Daytime use of first generation antihistamines should be avoided given their sedative effects. Non-sedating antihistamines appear to have limited value in patients with AD but they may provide some benefit in patients with allergic triggers.4, 8
Dietary interventions
Although there is an association between IgE mediated food allergy and AD severity in infants, it is unclear whether hypersensitivity to food is a major factor in causing and maintaining AD. Dietary exclusion is not recommended for managing AD in patients without confirmed food allergy. The exclusion of foods during pregnancy and breast feeding to prevent the development of AD in infants is not recommended. Breast feeding for three months or more may help prevent the development of infant eczema where there is a family history of atopy. However, current UK guidelines state that weaning should start at six months.4
Table 3 - Guidance on when to refer to secondary care4
Poor control of the condition or failure to respond to appropriate topical treatments
Psychological upset or sleep problems
Recurrent secondary infection
Other therapies
Systemic corticosteroids are usually reserved for the acute treatment of severe AD exacerbations. Prolonged use of oral steroids is associated with potentially serious adverse effects and their long-term use should be avoided. Furthermore, relapses are common following discontinuation of oral corticosteroid therapy.8
Ultraviolet (UV) phototherapy may also be beneficial for the treatment of AD in adults. In addition, systemic therapies are available and may be broadly classified into traditional medications (e.g. cyclosporine, azathrioprine, methotrexate) and biologic agents (targeted monoclonal antibodies). These options are available for severe, refractory AD. These therapeutic options should generally be reserved for unique situations and require consultation with a dermatologist. These therapeutic options are beyond the scope of this article.8
A 26 year old male was brought to Emergency department with history of altered sensorium of 1 day duration. He had a 2 week history of fever prior to admission. On examination, meningeal signs were present. Fundus examination showed evidence of papilloedema and a round pale yellow spot near the optic disc (Figure 1). CT scan of head did not reveal any abnormality.
Mantoux test and HIV ELISA were negative. CSF analysis showed:
Glucose – 40mg/dl; Protein: 2gm/l;
Cell Count: 1200cells/µl;
Cell Type: 80% lymphocytes;
CSF VDRL- negative;
CSF Grams stain, India ink staining and Ziehl Neelsen staining were unremarkable.
What is the Fundus finding?
Roth Spot
Cotton Wool Spot
Choroidal tubercle
A-V malformation
Discussion:
Correct answer: 3) Choroidal Tubercle.
Intraocular tuberculosis is a rare event and occurs in 1% of all diagnosed cases of tuberculosis.1 It occurs by haematogenous spread of mycobacterial organism. Choroidal tuberculosis is the most common initial manifestation of intraocular tuberculosis. They may be seen in 1.4% to 60% of patients with different forms of tuberculosis and are highly specific for tuberculosis. 2, 3
Choroidal tubercles may be unilateral or bilateral and appear as polymorphic yellowish lesions with discrete borders. They are of 2 types, solitary tubercle or granuloma (seen in chronic tuberculosis) and choroidal miliary tubercles (seen in acute miliary tuberculosis). Their size varies from 0.4 to 5 mm and may be associated with retinal vasculitis, panuveitis, choroiditis and neuroretinitis.
When they involve macula they present with visual loss and any delay in appropriate treatment results in irreversible visual loss. Peripherally situated tubercles are asymptomatic. Definitive diagnosis can be daunting due to difficulty in getting ocular samples for histological evaluation, however when available reveal features of granulomatous inflammation. Fundus angiography exhibits hypofluorescence in early stages and hyperfluorescence in later stages.
On treatment they heal by varying degrees of scar formation and marginal pigmentation.4 Untreated tubercles grow into large tumour like mass called tuberculoma.
Roth spots are retinal haemorrhages with a pale centre and are associated with bacterial endocarditis. Cotton wool spots appear as fluffy white patches on the retina and are associated with diabetes. A-V malformations are developmental vascular anomalies and appear as marked arterial and venous dilation associated with a tortuous pattern of vessels. They may have an associated bruit or chemosis of the eye.
The presence of ocular tuberculosis may be subtle. A high index of suspicion is required for its diagnosis. Delay in treatment or misdiagnosis may lead to irreversible visual loss.
Clozapine has shown to have superior efficacy compared to other antipsychotics and is the drug of choice for treatment-resistant schizophrenia. 1 However there is evidence that this treatment is actually under-prescribed. 2 Clozapine requires careful monitoring during the initial titration period. In the UK, this has originally been done in hospital settings to follow the manufacturer’s recommendations because of the risks of hypotension, excessive sedation and fits. Starting clozapine in a hospital setting ceased to be a mandatory regulatory requirement in the UK when the Summary of Product Characteristics was harmonised across Europe following an opinion and recommendation issued on the 12th of November 2002 by the Committee for Proprietary Medical Products of the European Medicines Agency. 3 Despite this happening several years ago, there is little information published about the practicality of successfully commencing clozapine in the community, with previous studies ranging from a single case report 4 to a few small case series of patients 5-8. Our study aimed to examine this practice in a larger sample to highlight the advantages and difficulties of initiating clozapine in the community.
Method
The Central Manchester day hospital was established in 1985, with a focus on acute psychiatric treatment as an alternative to in-patient care. From March 1997, the acute day hospital in Central Manchester was extended to 24 hours, seven days a week, adopting the name of the Home Option Service, focussing on flexible individualised care delivered at patient’s home or team base according to patient choice. 9 In 2007 as part of implementation of new teams across the city to comply with NHS policy guidance 10 the Home Option service developed further to become the crisis resolution and home treatment team (CRHT) for central Manchester, whilst CRHTs were set up de novo in North, and South Manchester, thereby, providing acute community psychiatric care to a metropolitan area of about 500,000 people.
This study describes a large case series of patients referred for clozapine titration in the community to these teams during a three year period. We collected data retrospectively from April 2007 to April 2010 of all the referrals to the three crisis teams, which have assumed the responsibility of providing the service of initiating clozapine in the community. The teams followed the Trust protocol for non-inpatient clozapine titration, which includes recommended monitoring parameters, dosing schedule and algorithms for the management of complications. This protocol is in essence similar to established guidelines. 4,5, 11
Statistical analysis was done using SPSS version 15 for Windows. Comparisons were made using the Student t-test, non parametric tests or the Chi-Square test according to the type of data.
Results
There were 6542 referrals to the crisis teams and 66 of those were related to clozapine initiation. Out of these, 36 were for a first time titration and 30 were referred for re-titration. The latter group were patients previously taking clozapine but who had discontinued it abruptly for a period longer than 48 hours. The reasons for stopping clozapine in those cases were lack of adherence (n=21), a supplying difficulty (n=5) and medical complications (n=4), such as neutropenia, collapse secondary to dehydration, or undergoing surgery. Two of the patients in the re-titration group restarted clozapine in hospital but were discharged early to continue the titration in the community under the care of the crisis team. Six patients in the titration group were initially referred to the crisis team for stabilisation of their mental state following a crisis; however, during the course of this intervention it was decided to start them on clozapine as they showed poor response to other antipsychotic trials.
Fig. 1 - Referrals, number of patients starting clozapine and drop-outs
The characteristics of the sample are presented in Table 1. The majority of patients were single white males, with a diagnosis of schizophrenia and a mean age of 38.8 years (standard deviation = 9.2). The flowchart in Figure 1 outlines the number of referrals, titrations, and reasons for stopping. Clozapine titration commenced in 54 cases (81.8% of referrals), the other 12 patients refused this treatment. Out of the patients who refused treatment, 8 were severely mentally unwell and were admitted to hospital compulsorily under the Mental Health Act. There were 46 (85.2%) patients who successfully completed the community titration. The attrition rate of 14.8% (8 cases) was due to 7 patients withdrawing their consent and one patient who was unable to tolerate the titration. This person was admitted to hospital with hypotension and vomiting. The other 7 patients withdrew their consent for the following reasons: lack of adherence (n=2), deterioration in mental state (n=1), refusal to continue with the physical monitoring (n=1), lack of motivation (n=1), and reluctance to continue due to side-effects (n=2). The mean final dose of clozapine was 309.1 mg (s.d. - 75.1 mg). The mean duration of titration was 34.6 days (s.d. - 20.3) and the mean length of admission to the crisis team was 45.9 days (s.d. - 39.5). The median waiting time for crisis team intervention after the referral was 2 days (range 140 days). The median waiting time to start clozapine was 7 days (range 217 days) from the point of referral.
Table 1. Sample characteristics
Total
Age in years, mean (s.d.)
38.8
(9.2)
Gender, n (%)
Male
45
(68.2)
Female
21
(31.8)
Ethnicity, n (%)
White
45
(68.2)
Black
14
(21.2)
Asian
3
(4.5)
Other
4
(6.1)
Marital Status, n (%)
Single
54
(81.8)
Married or cohabiting
5
(7.6)
Separated or divorced
6
(9.1)
Widowed
1
(1.5)
Diagnosis, n (%)
Schizophrenia
54
(81.8)
Schizoaffective disorder
8
(12.1)
Bipolar affective disorder
1
(1.5)
Other
3
(4.5)
Crisis Team, n (%)
North
21
(31.8)
Central
31
(47.0)
South
14
(21.2)
Days waiting to crisis team intervention
Mean (standard deviation)
9.5
(25.6)
Median (range)
2
(140)
Days waiting to start clozapine
Mean (standard deviation)
23.1
(40.9)
Median (range)
7
(217)
Days taken to complete the titration
Mean (standard deviation)
34.6
(20.3)
Median (range)
28
(101)
Days under the care of the crisis team
Mean (standard deviation)
45.9
(39.5)
Median (range)
34
(235)
Final dose in mg
Mean (standard deviation)
309.1
(75.1)
There were few significant differences between the group of patients starting clozapine for the first time (titration) and those restarting it following a treatment break (re-titration). There was a shorter wait for patients in the re-titration group to recommence clozapine from the time of referral to the service (median=6 days, range = 41 days), compared to those starting clozapine for the first time (median=13 days, range= 217 days). This difference was statistically significant (Mann Whitney U= 201.5, z=-2.529, p=0.01). Patients with first titration on clozapine reached a lower final dose (mean=288 mg, s.d.=50 mg), compared to those having re-titration (mean dose =340 mg, s.d.=94 mg). The mean difference of 52.7 mg (95% C.I. 8.7 to 96.8) between these two groups was significant (t test=-2.178, d.f 42, p=0.02). In terms of ethnicity, patients in the initial titration group were more likely to be Caucasian (n=30, 83%), whereas only half of the patients in the re-titration group were Caucasian (n=15, 50%). This difference was statistically significant (Chi-square with continuity correction = 6.915, df = 1, p=0.009).
There were also significant differences in the distribution of titrations and re-titrations across the three crisis teams. The Central Team dealt with more re-titrations (n=23) than the North (n=4) and the South (n=3) teams. Conversely, the Central Team had fewer patients referred for initial titration (n=8), compared to the North (n=17) and the South (n=11) teams. These differences were significant (Chi-square=19.493, df=2, p<0.0001). Another difference between the teams was the duration of clozapine titration, with the South team taking shorter time (mean=24.15 days, s.d.=7.151), compared to the North (mean=29.5 days, s.d=16.342) and the Central team (mean =43.67 days, s.d.= 23.797). This difference was statistically significant (Kruskal-Wallis chi-square=8.823, d.f.=2, p=0.0121).
No significant differences were found between teams and titration or re-titration groups in terms of patient’s diagnosis, gender, marital status, age, rate of accepted referrals, proportion of successfully finished titrations or waiting time to crisis team intervention.
With regards to adverse events, most patients experienced transient tachycardia (n=30, 55.5%). Other side-effects were excessive salivation (n= 15), hypotension (n= 13), sedation (n=10), hyperthermia (n=8), dizziness (n=6), constipation (n=6), hypertension (n=5), headaches (n=4), nausea (n=2), and heartburn (n=2). Less common adverse events (n=1) were syncope, seizures, transient neutropenia, atrial fibrillation, blurred vision, swelling of the arms , acute dystonic reaction, nocturnal incontinence, exacerbation of asthma, diabetes, erectile dysfunction and delayed ejaculation. Only the patient who developed syncope, which was associated with vomiting and severe hypotension, had to be advised to stop the treatment in the community and was admitted to hospital. For the rest of the patients, the other reported adverse events did not impede the successful completion of clozapine titration in the community.
In terms of longer term outcomes, a total of 50 patients (75.8% of the total sample) were still taking clozapine at the time the data was collected. This is after a median 337 days (range 824 days) from being referred to the crisis team. The majority of patients (n=14, 21.2%) who were not on clozapine had chosen to discontinue the treatment. One patient had died, but the cause of death was not related to clozapine treatment. One patient had developed neutropenia and needed to discontinue clozapine for this reason. Out of the 46 patients who successfully completed the titration, 40 (86.96%) were still continuing clozapine at the time we collected the data. This is after a median 365.5 days (range 824 days) after they commenced clozapine in the community.
Discussion
The results of this study confirm that clozapine can be safely and successfully started in the community. Comparing this to published evidence, we found only one case report 4 and a small study 5,6 previously conducted in the UK. O’Brien et al. 5,6 initially considered 26 patients in their study; however, only 14 patients started clozapine in the community as the rest were considered too unwell and were admitted to hospital. One patient refused daily access and therefore only 13 patients completed the titration. The side effects reported in this study were minor, including sedation in 5 cases, dizziness in 4 patients, hypotension in two and nausea and vomiting once. Compared to our results, O’Brien et al. described a larger proportion of patients needing to be admitted to hospital for clozapine titration.
We found two published studies 7,8 regarding clozapine community titration that were conducted in the United States. The first study included 47 patients who started clozapine in a partial hospitalisation program. Adverse reactions here were common. Patients were titrated much more quickly than in our report, (i.e. to 350 mg over 2 weeks), which might explain the higher incidence of side effects reported, including drowsiness (93.6%), hypersalivation (93.6%), constipation (89.4%), weight gain (72.3%) and tachycardia (57.4%). However no patient discontinued clozapine, and the potentially serious complications were much less frequent, including 3 cases (6%) of seizures and 2 of leukopenia. The other study 8 conducted in the US demonstrated some evidence of cost savings associated with decreased hospitalisation in 28 patients who started clozapine on an outpatient basis.
Johnson et al. 7 discuss in their report that the reluctance to start clozapine outside inpatient settings may be due partly to the potential adverse reactions, but also to clinicians’ fears of making mistakes, avoidance of additional duties, and anticipation of difficulties in patients with a history of non-adherence to treatment. The results of our study support a careful approach to starting clozapine at home in this latter group of patients, as they represented the bulk of cases not achieving the intended outcome of a successful community clozapine titration. However, our study confirms that other reasons to deny a patient the opportunity to start clozapine at home, such as potential adverse events, are hardly justified.
The general advantages of community psychiatric care as opposed to inpatient treatment have been described elsewhere 9. These include accessibility, flexibility and user satisfaction. Treating patients in their own homes avoids the stigma of hospital admission, prevents the breakdown of important social networks and avoids disruption to patients' benefits. A recent Cochrane review 12 found that crisis/home care reduces the number of people disengaging early, reduces family burden, and is a more satisfactory form of care for both patients and families. Some patients who might have been reluctant to start clozapine if they had to be admitted to hospital can therefore benefit from starting this treatment at home supported by crisis teams.
Although a detailed cost-benefit evaluation of this service was not undertaken, it is fair to assume that the costs associated with titrating clozapine at home would be significantly lower than those associated with in-patient care, as demonstrated in previous studies. 8,12
In summary, clozapine can be safely started in the community, but has to be carefully monitored. Patients’ adherence to the treatment and to the physical monitoring requirements is the key element to a successful outcome. Crisis teams are in an ideal position to support patients undergoing initiation of clozapine at home, although this specific role was not originally identified in policy guidance.10 The results of this multi-site study are encouraging and can be applicable to other crisis or community teams nationally.
Evidence has consistently shown that patients with mental illness have greater physical health morbidity and mortality compared to the general population.1 Many factors have been implicated and include a generally unhealthy lifestyle, side effects of medication, and inadequate physical healthcare.2, 3 Higher rates of suicide and accidents are other known risks. Psychiatric patients are more likely to smoke, have less inclination to exercise, and are prone to poor dietary habits and obesity, the latter through general inertia, the result of the adverse effects of neuroleptic medication, or increased alcohol use. Psychotropic medication is associated with impaired glucose tolerance and diabetes, metabolic syndrome, dyslipidemia, cardiovascular complications, extrapyramidal side effects and sexual dysfunction. A broad range of clinician and organisational factors prevent access to adequate physical healthcare that in turn compounds the above problems.
Scale of physical morbidity and mortality in mental illness
Patients suffering from depression are twice as likely to develop type 2 diabetes mellitus, and the prevalence of stroke and myocardial infarction is three- and five-fold respectively higher than people without depression.4 A mortality rate ratio (MRR) of 2 to 3 in patients with schizophrenia or bipolar disorder is a general finding.5 Schizophrenia is associated with higher rates of diabetes mellitus (side effects of medication partly to blame), osteoporosis (lifestyle risk factors play a role), obesity, and cardiovascular problems. 2, 6, 7, 8 It has been estimated that life expectancy is reduced by at least ten years. 9, 10 People with learning disabilities, particularly those with concurrent epilepsy, dementia and polypharmacy, are at greater risk of developing added complications.11 Eating disorders are associated with a high mortality because of physical disorders caused by anorexia/bulimia nervosa affecting other organ systems.12 Mental illness in general is associated with an increased risk of hepatitis, human immunodeficiency virus (HIV), tuberculosis, and poor dental health. 9, 10
Causes of raised physical health morbidity and mortality in psychiatric patients
Explanations for the higher morbidity and mortality in mental illness include cardiovascular and respiratory problems in addition to the increased suicide risk. Aetiological factors include adverse effects of medication (weight gain, diabetes, and dyslipidemia), lifestyle (smoking and the cost of smoking, poor diet and nutrition, lack of exercise, and obesity) and inability to access physical healthcare. Obesity, smoking and physical inactivity contribute to hypertension. Poor physical healthcare outcomes in mental illness are related to a combination of factors generally considered under the headings of patient/illness, psychiatrist/physician, and service provider/system issues.
De Hert and colleagues 9, 10 have outlined the factors that account for the raised physical health problems.For instance the patient/illness factors comprised difficulty in understanding health care advice combined with the motivation required to adopt new changes in lifestyle, poor compliance with treatment, cognitive deficits, reduced pain sensitivity (induced by antipsychotic medication), poor communication and deficient social skills (seen in many cases of schizophrenia, for example) which all accounted for the shortened life-span of patients with severe mental illness (SMI).
An additional patient/illness factor is that psychiatric symptoms may render patients less inclined to discuss physical problems. Some doctors are uncomfortable dealing with psychiatric patients because the latter may be cognitively compromised which may impair or impede a doctor’s clinical assessment. The stigma of mental illness, often the result of disparaging media coverage and negative stereotypes surrounding psychiatric patients, are other hurdles that prevent people from seeking treatment. Furthermore, psychiatric patients are less likely to see a primary care physician and therefore to receive other interventions such as screening for cancer.
Psychiatrist-related factors are characterised by an overemphasis on mental health to the exclusion of physical health, infrequent screening rates for metabolic abnormalities, omission of medical examination of patients because physical complaints frequently are part of the psychiatric presentation, poor communication with the patient and the primary care teams, a lack of awareness and perhaps adherence to treatment guidelines, insufficient medical knowledge, and erroneous, sometimes misguided beliefs about patients’ capability to change their lifestyle.9, 10 Even when risk factors are documented in the patient's clinical file, very little is done by way of further investigations or prevention.
Factors common to the psychiatrist and other physicians include a tendency to dismiss or interpret physical symptoms as psychosomatic, lack of good quality care, unequipped teams, insufficient assessment, and difficulties providing consistent monitoring and continuity of care. Other physician-related factors relate to problems coordinating psychiatric and medical care.9, 10
Service-provision factors included a lack of clarity and consensus as to where the responsibility of physical health lies.9, 10 Should general practitioners (GPs) supervise the majority of patients who do not suffer from severe, enduring mental illness? Should patients with acute alcohol withdrawal symptoms be managed at home by the GP, treated in a general hospital, or admitted to a psychiatric unit? The fragmentation of medical and mental health care systems, lack of integration of services (poor or absent liaison links) and insufficient funds to resource the mental health service, limit the ability of most psychiatrists to focus beyond their own speciality.
Service and system changes are prevalent in industrialised countries because reforms in mental health have led to reduced inpatient resources leading to shorter and infrequent hospital admissions with less time available to focus or investigate physical health problems. In the United Kingdom (UK) there is intense emphasis on community care and talking therapies, yet the management of physical health issues by community mental health teams may be poor because of inadequate training and learning.
Recommendations to improve physical health care in psychiatric patients
Health care professionals need to be more aware of these findings in order to improve medical screening and treatment of psychiatric patients. Currently there is no evidence this is happening, with increasing concerns regarding inequalities between those with and without mental illnesses.13
We propose the following recommendations to promote integration between mental and physical health care:
1.A greater effort to increase awareness of the problem among primary care and mental health care providers. The Royal College of Psychiatrists has launched a campaign called Fair Deal to highlight the importance of physical health of people with mental illness.1 Patients still feel stigmatised and therefore psychiatrists need to boost their efforts to reduce this discrimination. The excess mortality associated with this discrimination needs to be recognised as a human rights issue.13
2.Primary care providers need to change the culture of undertreating physical health in mental health patients. The National Institute for Health and Clinical Excellence (NICE) guidelines for schizophrenia and bipolar disorder highlight the importance of monitoring antipsychotics and mood stabilizers.14 The Royal College of Psychiatrists should lead by implementing the NICE guidelines for mental and behavioural conditions.
3.Education and training of doctors who pursue a career in psychiatry needs to be improved with mandatory trainee placements in acute medicine or neurology, regular personal development plan (PDP) courses, and training to update knowledge of recognising physical illness and the performance of basic medical tasks. The Royal College of Psychiatrists should develop a diploma in clinical psychiatry for GPs and clinicians with a specialist interest in psychiatry. The curriculum needs to be widened to include electrocardiogram (ECG) interpretation, basic endocrinology, and neurological investigations (magnetic resonance imaging and so forth). This would allow psychiatrists to develop better liaison with their fellow professionals and share responsibility with them, which undoubtedly would encourage good medical practice.
4.The Royal College Scoping Group’s report15 sets key standards for the physical healthcare of patients in a range of psychiatric services. It outlines the responsibilities of psychiatrists monitoring the physical health of patients, such as problems associated with adverse effects of medication. The report recommends that psychiatrists are trained and kept up to date in relevant physical health matters. These recommendationsneed to be followed.
5.Mental health professionals should encourage patients to monitor simple measures such as weight, dietary plans, and exercise programs, with the involvement of the voluntary sector (MIND, Mental Health Foundation) where possible. Patients and carers need to be educated about the health risks associated with unhealthy lifestyles: for example, smoking and alcohol misuse may interfere with the metabolism of neuroleptic medications. Smoking cessation clinics and alcohol treatment programmes may help. Advice from dieticians about patients' nutritional requirements to offset changes in metabolism caused by neuroleptics is important.
6.Because of the large-scale reduction of inpatient psychiatric beds and service redesign the majority of psychiatric care provision now exists in the community. Therefore community mental health teams and psychiatric outpatient clinics need to be appropriately designed and equipped to enable proper assessment of physical health monitoring. Annual health checks from the GP would benefit patients who require long-term monitoring in the community. Screening for deleterious effects of medication for example, hypothyroidism and renal dysfunction caused by lithium, at regular intervals would be appropriate.16 It should also be made clear to psychiatrists that they should resist working in clinical settings that compromise patient care and inhibit good medical practice.
7.Financial initiatives such as Commissioning for Quality and Innovation (CQUIN)17 may be used by commissioners to improve physical health monitoring.As part of this process, primary care commissioners could mutually agree with mental health providers to fulfil measured targets related to such monitoring.
8.In order to better understand the interplay between psychiatric conditions and medical complications contributing to the high physical morbidity and mortality, further studies are essential. To cite one example, we now know that psychotropic medications contribute to many physical problems (abnormal ECGs, weight gain, changes in plasma glucose) and lead to higher morbidity rates. The 'newer' generation of antidepressants and neuroleptics have not lived up to expectations and have as many untoward effects as the older drugs. Developments of newer drugs with different mechanisms of action are required, though this will take time.
9.The discrimination faced by people with mental illness and learning disabilities, with the accompanying excess mortality, represents a human rights issue13 that requires legislative changes. The Disability Right’s Commission18 has already recommended appropriate physical health care screening, for example, annual physical health checks. The government’s health inequality agenda should incorporate these conditions into its indicators of disadvantage and include mental illnesses and learning disability in the framework.
Conclusion
Traditionally the field of psychiatry involves a holistic approach in the management of patients. Unfortunately, over the decades psychiatry appears to have lost its way and therefore it is important to re-establish a more comprehensive system of treating mental illness that encompasses regular physical health monitoring. Physical morbidity and mortality in patients with mental illness is on the rise and is associated with a complex interplay of factors outlined above. The overall health care of psychiatric patients can be improved through the changes in education and training of clinicians, close liaison between primary and secondary care, implementation of recommendations by NICE and the Royal College of Psychiatrists, improved research through better funding, public health education of patients and carers, and legislative changes.
Isaac Asimov famously said: ‘The only constant is change.’ (Cited in Hartung, 2004).
So why is it so difficult for most of us to understand, manage, or embrace change?
Coping with change can be challenging for many and, depending on the change and what the impact or outcome of the change means to the individual, will depend upon how well they embrace and accept it. Should a person be fearful of change then it is natural that they will attempt to resist it which in turn can cause high levels of stress and anxiety.
Understanding how we typically react to change also helps us to cope better and manage change. The Kubler-Ross (2009) Model of Change is perhaps one of the best known and most applied models within clinical environments (her original work being around the five stages of grief) which is now also applied to businesses and organisations when looking at changes in the work place such as loss or change of job.
The five stages she refers to are:
Denial
Anger
Bargaining
Depression
Acceptance
A common example used to explain this model is to understand how we would typically respond to an unexpected change such as a dead car battery.
The dead car battery
Just imagine it is a cold winter day and you are dashing to get to work already running late…
You jump into the car, place the key in the ignition and turn it on.
Nothing happens, the battery is dead.
Applying the Kubler Ross Model to this situation, this is how a person may typically react:
Denial - This cannot be happening! Try again. And again! Check the other things in the car are working such as the lights and radio. Try again but still nothing.
Anger - Arrrrgh you stupid car!!! I’m sick of this car!! Why is this happening today of all days!! Slamming a hand against the steering wheel.
Bargaining - (realising that it really isn’t going to start and that you're going to be late for work)..., Oh please car, if you will just start one more time I promise I'll buy you a brand new battery and keep you clean and tidy. Please just start this one time.
Depression - Oh no! What am I going to do? I'm going to be late for work. I give up. I don't really care any more. What's the use?
Acceptance - Right I need to do something. It is not going to start. I need to call the breakdown service and ring into work.
The above example is a simple example yet I’m sure most of us have experienced it or something similar quite often. If you apply this to a situation where the stakes are far higher such as a sudden loss or change of a job, bereavement, house, relationship etc which may impact upon so many things including stability of finances, family, health and other forms of security, then you may be able to see the harsh effect this could have on an individual during this time.
Often individuals add to their stress by expecting themselves to be able to cope with such events. It is important to understand it is not about strength or weakness but about human nature to react by demonstrating the signs of loss and grief. Organisations, managers and individuals need to be understanding and supportive when situations like this happen.
Another way of understanding and coping with change is to consider what goes on in the mind of the individual at the time of the change and what it ‘means’ to them. Some people see risk and uncertainty as exciting and embrace change (depending on the change), whereas others can be fearful of any change, even those perceived to be minor changes, as for them any change is seen as a risk and takes them out of their comfort zone.
The comfort zone
Your comfort zone is where you are fully able, competent and comfortable. The job that you can do with your eyes shut or routines of life where you know exactly what you are doing. You may feel slightly challenged now and then, but there’s nothing you cannot easily handle.
When invited to step outside their comfort zone – or if they’re pushed outside of it - many people react with resistance. This is because of the human fear of failure which, when you look into it more deeply, comes from a desire to be accepted, liked and even loved. When most people ‘fail’ they feel embarrassed, ashamed, silly or stupid because they feel they can’t or couldn’t do whatever it was they tried.
So it’s understandable if at work, or any area of life where there is change, people react with resistance. Change is the unknown, and if you don’t know whether you can do something – especially if you have a ‘Be Perfect’ driver – you could have fears over whether you can do it, can be a success or even cope. Everyday changes such as new computers or telephone systems, new staff, new jobs, new routines and procedures, new management, merging of departments, sections or whole companies or, on a personal level, exams, weddings, divorce, births, deaths, moving house and so on, are all high on the list of stressors due to change.
How big is your zone?
Are you resistant to change? If you are, you’re causing yourself stress. Imagine what size a child’s comfort zone would be compared to an adult’s. Children do not have inhibitions and fears; it’s only as we grow older that we learn to feel fear, that we learn what embarrassment is and how to feel silly or stupid – that is, we learn to have an ego. This restricts our ability to have the freedom to learn, grow and be open to change, as we are nervous about asking questions for fear of looking silly, or trying new things for fear of failure, and we avoid doing anything that may cause us to feel embarrassed.
By being more fluid and open to change, accepting any fear and dealing with it effectively, you would not only grow your confidence and self-esteem, but you will be free to develop your life with more happiness and less stress.
By looking at change differently (for example, recognising that change can also be a good thing; focusing on the possible positives from a situation rather than being quick to look at the negatives from a point of fear and therefore resistance) stress can be greatly reduced.
Choose to flow with change rather than resist; choose to step out of your comfort zone and grow the size of your comfort zone daily. Aim to have a comfort zone the size of a child’s where nothing can faze or worry you, and you will notice a huge difference to the amount of stress you have in your life.
‘The greatest discovery of my generation is that a human being can change their life by altering their attitude of mind.’ William James (cited in Maxwell, 2007).
Remember – the only failure is not trying again. If we fail at something at least we know what NOT to do next time!
Identifying your zones and being rational
Following are three simple exercises you can complete to help you to gain a rational perspective on understanding how you cope with change and also being solution focused when embracing change.
The zones of change help us to understand the different levels of comfort or ‘risk’ and where changes may sit in terms of their percieved meanings to the individual.
Zones of change
Exercise 1
Think back to a significant change in your life or work (something from the past).
What were your perceived risks at the time?
…………………………………………………………………………………
…………………………………………………………………………………
What did you lose?
…………………………………………………………………………………
…………………………………………………………………………………
What did you gain?
…………………………………………………………………………………
…………………………………………………………………………………
This exercise demonstrates that our ‘perceived risks’ at the time of a change were often far different than the reality of how the change occurred. It is also common for an individual to notice that their ‘gains’ can be larger than their ‘losses’ (time can play a factor in this too, often a change can seem a disaster at the time but over time a person can look back and be glad it happened in comparison to how their life is now.)
Exercise 2
Think of a change that you are currently undergoing.
What aspects of the change are in your ‘comfort zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What aspects are in your ‘risk zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What aspects are in your ‘high risk zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What do you need to make the ‘high risk’ into ‘risk’ and the ‘risk’ into ‘comfort’?
…………………………………………………………………………………
…………………………………………………………………………………
This exercise is excellent for considering a current change and how it may affect a person.
Actually listing in categories the level of ‘risk,’ or even drawing the zones on a piece of paper and writing in each change in the place on the zone where the person believes it sits, will give a rational perspective.
Once all the ‘risks’ are highlighted then that is the time to minimize ‘risk’ and find solutions for the individual to cope or manage that change. This is good for action planning and allowing a person to take control to embrace a change rather than being reactive once the change has occurred.
Exercise 3
Think of a life or work change which is going to occur in the future.
Blockers
What I’d be sorry to lose.
…………………………………………………………………………………
…………………………………………………………………………………
My fears and concerns.
…………………………………………………………………………………
…………………………………………………………………………………
Drivers
Benefits of the change.
…………………………………………………………………………………
…………………………………………………………………………………
What I’d be glad to leave behind.
…………………………………………………………………………………
…………………………………………………………………………………
Answering these questions assists a person to determine how much resistance they may feel/have towards a change. Listing potential blockers will identify fears and concerns of the change as well as the levels of risk and loss. Listing drivers will encourage the individual to consider the benefits of the change, the gains, and that change can also be a good thing.
Typically, whichever list is the longest or has the most meaning/impact will be the strongest for that person. If this is the blockers they will resist the change and cause themselves pressure and stress. Therefore addressing the zones of change and looking for ways to reduce risk would be a good strategy in action planning to manage the change well. Should the drivers be the strongest for the person then they are likely to embrace the change more readily although they may still need to address their thoughts and rationale for any blockers listed.
Change tips:
Embrace change, as if you don’t accept it someone will push you into it.
Take every opportunity to grow your comfort zone.
Have the attitude that there is no failure and only learning and development – when we ‘fail’ we know what NOT to do next time.
The worst rarely happens, so why waste energy focusing on it and enforcing irrational fears?
Change CAN be a good thing.
There is always a solution, it may take time for you to see it, but if you look, you will find it.
Case Presentation: Reflex Anoxic Seizures and Anaesthesia
Reflex anoxic seizures (‘RAS’) may present, as potentially life threatening events, but these are often preventable. They are most common in preschool children (but can occur in any age) and more so in females. As a cause of seizures they are not rare; one study estimated a frequency of 8 in 1000 preschool children1, but they are often misdiagnosed. The pathophysiology of RAS is vagally mediated – a noxious stimulus causes a supranormal vagal discharge resulting in bradycardia and then astystole2. This then results in cerebral under perfusion and hypoxia. During this time the patient is often noted to become very pale with dusky lips, initially flaccid and then tonic with rigid extension and clenched jaws. They may then have a generalised convulsion, often with rolling eyes and urinary incontinence. The patient spontaneously recovers (the whole episode lasting around 30 to 60 seconds) and will feel somnolent, often remaining pale for a while.
From this description it can be easily understood how such an event can be misdiagnosed as epilepsy; however it is not associated with the uncontrolled neuronal discharge of epilepsy and if monitored by EEG this is absent2. It may also be mistaken as breath-holding attacks (where intra-thoracic pressure restricts cerebral perfusion) or Stokes- Adams attacks (where there is abnormal electrical function of the heart).
The noxious stimuli responsible can be many different things. Ocular pressure2, venepuncture3, anaesthetics4, accidental trauma and fear have all been implicated. If these stimuli cannot be prevented, management is normally just supportive (positioning, protection from trauma, oxygen) and allowing the fit to self-resolve[U1] . Further management can involve atropine5 (either acutely of preventatively), maintenance anticonvulsants6 (though these often just stop the fitting but not the syncope) and even pacemaker [U2] insertion7.
The case we encountered was that of a 20 year old female student, presenting for a planned day case removal of a molar tooth. She was otherwise fit and well with no other past medical history, only taking the combined oral contraceptive pill. Her history with RAS started at age 1, when she was admitted to hospital following two seizures. The seizures occurred every few months and she was provisionally diagnosed as suffering from epilepsy, with prophylactic treatment started. However, as she grew older she was able to describe how the attacks were not associated with a preceding aura, but rather an unpleasant stimulus (such as accidental injury). A new diagnosis of RAS was made and the antiepileptics were stopped without the seizures becoming more frequent. As she entered late childhood and adolescence the frequency of the seizures became less, but (atypically) they did not stop entirely. On preassessment she reported being seizure free for just over a year and was anxious that today could precipitate another.
After consideration, we decided to proceed with anaesthesia with the following measures. The patient was kept calm by having a clear explanation of what to expect before coming to theatre, and then was reassured by an affable theatre team (who had been informed of her condition). Atropine was drawn up and available if vagal over stimulation occurred, as was suxamethonium in case of emergency airway intervention. For cannulation, cold spray was used along with distraction. Induction was with propofol (under full monitoring) and anaesthesia was maintained with sevoflurane/nitrous oxide via LMA. To prevent pain as a potential trigger, fentanyl (at induction) and paracetamol (after induction) were given and local anaesthetic (lidocaine) was administered before any surgery. Emergence was kept as smooth as possible by removing the LMA prior to any gagging and coughing and manually supporting the airway until she was awake.
With these measures the procedure was uneventful and the patient could be discharged home as planned. We hope this case report will help improve awareness and understanding of RAS, and the steps that can be taken peri-operatively to help ensure safe anaesthesia.
Foreign body ingestion is a common occurrence, especially in children, alcoholics, mentally handicapped and edentulous people wearing dentures. However, majority of the individuals pass these objects without any complications.1 Most foreign bodies pass readily into the stomach and travel the remainder of the gastrointestinal tract without difficulty; nevertheless, the experience is traumatic for the patient, the parents, and the physician, who must await the removal or the ultimate passage of the foreign body.2 The alimentary canal is remarkably resistant to perforation: 80% of ingested objects pass through the gastrointestinal tract without complications. 3 About 20% of ingested foreign bodies fail to pass through the entire gastrointestinal tract.4 Any foreign body that remains in the tract may cause obstruction, perforation or hemorrhage, and fistula formation. Less than 1% result in perforations from the mouth to the anus and those are mostly caused by sharp objects and erosions. 5, 18 Of these sharp objects, chicken bones and fish bones account for half of the reported perforations. The most common sites of perforation are the ileo-ceacal junction and sigmoid colon.3
Materials and Methods
This study, “Gastrointestinal tract perforations due to foreign bodies; a review of 21 casesover a ten year period” was carried out in the Department of General Surgery at the Sher-i-Kashmir Institute of Medical Sciences Srinagar (SKIMS), a tertiary care hospital in North India, from January 2002 to December 2011. A total of 21 consecutive patients who underwent surgery for an ingested foreign body perforation of the GI tract over a period of ten years were retrospectively reviewed. Computer database and extensive case note search of patient’s personal data including age, sex, residence, presenting complaints with special stress on clinical examination findings was done. The type and nature of the foreign objects, mode of entry into the gastrointestinal tract, preoperative diagnosis, perforation site, and treatment received were recorded. The complications arising due to perforation of GIT because of the foreign body ingestion and complications arising due to specific treatment received were noted. Important findings on various laboratory tests, including a complete blood count, erythrocyte sedimentation rate, [pre-op/post-op/follow up], blood cultures, and serum chemistry, chest and abdominal X-rays were penned down. Special efforts were made to identify the predisposing factors for ingestion of foreign bodies including edentulous patients with dentures, psychosis, extremes of age and hurried eating habits. Clinical, laboratory and radiological findings, treatment modalities, operative findings and therapeutic outcomes were summarized. Data collected as such was described as mean and percentage.
I/V Antibiotics ( Ceftriaxone + Metronidazole ) were given in the emergency room and changed to specific therapy as per the culture sensitivity postoperatively.
Results
The average follow up duration was 13 months (range 7 – 19 months). There were 14 male(66.66%) and 7 female (33.33%) patients ranging in age from 7 years to 82 years with a median age of 65 yrs at the time of diagnosis . The most frequently ingested objects were dietary foreign body (n = 17). Four patients had ingested objects like toothpicks (n =2) and metallic staples (n=2) {as shown in figure 1}. Among the dietary foreign bodies fish bone was found in 7(33.3%) and chicken bone in 10(47%) {as shown in figure 2} . All the patients described their ingestion as accidental and involuntary. A definitive preoperative history of foreign body ingestion was obtained in 4(19.04%) patients and an additional 9(42.8%) patients admitted ingestion of foreign body in the post operative period. Of these 13 patients the average duration between ingestion of foreign body and presentation was 9.3 days. Remaining 8 (38.09%) patients did not recall any history of foreign body ingestion; dietary or otherwise. In terms of impaction and perforation of ingested foreign body, ileum was the commonest site with 14(66.66%) patients showing perforation near the distal portions of the ileum followed by sigmoid colon in 5(23.8%). Jejunal perforation was seen in 2(9.5%) patients.
Fig 1: X ray abdomen AP view showing ingested metallic pin
Fig 2: Intra operative picture showing perforation of small gut due to chicken bone
All our patients presented with acute abdomen and were admitted first in emergency department. Since majority of patients did not give any specific history of foreign body ingestion, they were managed as cases of acute abdomen with urgency and level of care varying according to the condition of patients. Eight patients presented with free air in the peritoneum and air under the right side of diaphragm. The most common preoperative diagnoses were acute abdomen of uncertain origin: 12 (57.14%); acute diverticulitis:5 (23.8%) and acute appendicitis: 4 (19.04%).
Table 1: Showing demographic profile, site of perforation, etiology, presentation and management.
S No
Age
Sex
Site
Foreign Body
Presentation & Pre Op Diagnosis
Procedure Performed
1
78
Male
40 cm from ileo-caecal valve
Fish bone
Acute abdomen, peritonitis
Removal of foreign body and repair
2
65
Female
30 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Resection of the perforated distal ileum and ileum stoma
3
80
Male
30 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Resection of the perforated distal ileum and ileum stoma
4
43
Male
Jejunum
Tooth pick
Acute abdomen, peritonitis
Removal of foreign body and repair
5
10
Male
10 cm from ileo-caecal valve
Metallic staple
Acute abdomen, appendicitis
Removal of foreign body and repair
6
72
Female
Jejunum
Chicken bone
Acute abdomen, peritonitis
Resection of the perforated distal ileum and ileum stoma
7
65
Male
20 cm from ileo-caecal valve
Fish bone
Acute abdomen, peritonitis
Resection of the perforated distal ileum and ileum stoma
8
59
Male
Sigmoid colon
Chicken bone
Acute abdomen, diverticulitis
Removal of foreign body and repair
9
65
Female
30 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Removal of foreign body and repair
10
49
Female
40 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Removal of foreign body and repair
11
7
Male
Sigmoid colon
Metallic staple
Acute abdomen, diverticulitis
Removal of foreign body and repair
12
78
Female
15 cm from ileo-caecal valve
Fish bone
Acute abdomen, appendicitis
Resection of the perforated distal ileum and ileum stoma
13
72
Male
15 cm from ileo-caecal valve
Fish bone
Acute abdomen, appendicitis
Resection of the perforated distal ileum and ileum stoma
14
56
Male
20 cm from ileo-caecal valve
Tooth pick
Acute abdomen, appendicitis
Resection of the perforated distal ileum and ileum stoma
15
65
Male
Sigmoid colon
Fish bone
Acute abdomen, diverticulitis
Removal of foreign body and repair
16
63
Male
30 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Resection of the perforated distal ileum and ileum stoma
17
82
Female
30 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Removal of foreign body and repair
18
55
Female
Sigmoid colon
Fish bone
Hematochizia acute abdomen, diverticulitis
Removal of foreign body and repair
19
56
Male
20 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Resection of the perforated distal ileum and ileum stoma
20
69
Male
Sigmoid colon
Fish bone
Acute abdomen, diverticulitis
Removal of foreign body and repair
21
71
Male
40 cm from ileo-caecal valve
Chicken bone
Acute abdomen, peritonitis
Resection of the perforated distal ileum and ileum stoma
All the patients underwent an emergency celiotomy and confirmation of foreign body induced perforation was possible in all the 21 patients .Patients with a suspected appendicitis were explored via classical grid iron incision and rest via midline incision. Varying degrees of abdominal contamination was present in all the patients. Out of the 21 patients 11(52.38%) underwent removal of foreign body and primary repair of their perforations after minimal debridement. Intestinal resection with stoma formation (resection of the perforated ileum and ileum stoma) was done in 10 (47.6%) of the 21 patients as shown in Table 1. Take down of stoma was done at a later date. Three (14.28%) patients developed incisional superficial surgical site infection which responded to local treatment. Two (9.5%) patients died in the postoperative period due to sepsis. One patient (Patient no. 3 in table 1) who was a diabetic on Insulin, Chronic obstructive pulmonary disease and Hypertension died on 3rd postoperative day in surgical Intensive care unit due to severe sepsis. Another patient, (Patient no. 12 in table 1 ) an elderly female with no co-morbid illness developed severe sepsis due to Pseudomonas aeruginosa, died on 4th postoperative day. She was managed at a peripheral primary care center for first 3 days for her vague abdominal pain with minimal signs. All the other patients had an uneventful recovery and were discharged home between 6-14th postoperative day.
Discussion:
Foreign bodies such as dentures, fish bones, chicken bones, toothpicks and cocktail sticks have been known to cause bowel perforation6. Perforation commonly occurs at the point of acute angulation and narrowing. 7, 8 The risk of perforation is related to the length and the sharpness of the object.9 The length of the foreign body is also a risk factor for obstruction, particularly in children under 2 years of age because they have considerable difficulty in passing objects longer than 5 cm through the duodenal loop into the jejunum. In infants, foreign bodies 2 or 3 cm in length may also become impacted in the duodenum.10 The most common sites of perforation are the ileo-ceacal junction and sigmoid colon. Other potential sites are the duodeno-jejunal flexure, appendix, colonic flexure, diverticulae and the anal sphincter.3 Colonic diverticulitis or previously unsuspected colon carcinoma have been reported as secondary findings in cases of sigmoid perforation caused by chicken bones.11,12 Even colovesical or colorectal fistulas have been reported as being caused by ingested chicken bones. 13,14 .In our study ileum was the most common site with 14 patients showing perforation near the distal portions of the ileum followed by sigmoid colon. Jejunal perforation was seen in 2 patients.
The predisposing factors for ingestion and subsequent impaction are dentures causing defective tactile sensation of the palate, sensory defects due to cerebro-vascular accident, previous gastric surgery facilitating the passage of foreign bodies, achlorhydria where the foreign body passes unaltered from the stomach, previous bowel surgery causing stenosis and adhesions and diverticula predisposing to impaction.3 Overeating, rapid eating, or a voracious appetite may be contributing factors for ingesting chicken bones. The mean time from ingestion to perforation is 10.4 days.15 In cases when objects fail to pass the tract in 3 to 4 weeks, reactive fibrinous exudates due to the foreign body may cause adherence to the mucosa, and objects may migrate outside the intestinal lumen to unusual locations such as the hip joint, bladder, liver, and peritoneal cavity.16 The length of time between ingestion and presentation may vary from hours to months and in unusual cases to years, as in the case reported by Yamamoto of an 18 cm chopstick removed from the duodenum of a 71-year-old man, 60 years after ingestion.17 In our study the average duration between ingestion of foreign body and presentation was 9.3 days.
In a proportion of cases, definitive preoperative history of foreign body ingestion is uncertain.18 Small bowel perforations are rarely diagnosed preoperatively because clinical symptoms are usually non-specific and mimic other surgical conditions, such as appendicitis and caecal diverticulitis.19 In our study the most common preoperative diagnoses were acute abdomen of uncertain origin (n =12), acute diverticulitis (n = 5) and acute appendicitis (n = 4). Patients with foreign body perforations in the stomach, duodenum, and large intestine are significantly more likely to be febrile with chronic symptoms with a normal total white blood cell count compared to those with foreign body perforations in the jejunum and ileum.18 Plain radiographs of neck and chest in both anteroposterior and lateral views are required in all cases of suspect foreign body ingestion and perforations in addition to abdominal films. CT scans are more informative especially if radiographs are inconclusive.20 Computerised tomography (CT) scanning and ultrasonography can recognise radiolucent foreign bodies. An ultrasound scan can directly visualize foreign bodies and abscesses due to perforation. The ability to detect a foreign body depends on its constituent materials, dimensions, shape and position.21 Contrast studies with Gastrograffin may be required in excluding or locating the site of impaction of the foreign body as well as determining the level of a perforation. Using contrast is important in identifying and locating foreign bodies if intrinsically non-radiopaque substances, such as wooden checkers or fish and chicken bones are ingested.20 The high performance of computed tomography (CT) or multi-detector-row computed tomography (MDCT) scan of the abdomen in identifying intestinal perforation caused by foreign bodies has been well described by Coulier et al. 22 Although, in some cases imaging findings can be nonspecific, however, the identification of a foreign body with an associated mass or extraluminal collection of gas in patients with clinical signs of peritonitis, mechanical bowel obstruction, or pneumoperitoneum strongly suggests the diagnosis.8,20 Finally, endoscopic examination, especially in the upper gastrointestinal tract, can be useful in diagnosis and management of ingested foreign bodies.
Whenever a diagnosis of peritonitis subsequent to foreign body ingestion is made, an exploratory laparotomy is performed. However, laparoscopically assisted, or complete, laparoscopic approaches have been reported.17,23 The treatment usually involves resection of the bowel, although occasionally repair has been described.8 The most common treatment was simple suture of the defect. 24 Once the foreign body passes the esophagogastric junction into the stomach, it will usually pass through the pylorus25; however, surgical removal is indicated if the foreign body has sharp points or if it remains in one location for more than 4 to 5 days especially in the presence of symptoms. A decision should be based on the nature of the foreign body in those cases, as to whether a corrosive or toxic metal in ingested. 26 Occasionally, objects that reach the colon may be expelled after enema administration. However, stool softeners, cathartics and special diets are of no proven benefit in the management of foreign bodies.7
In traumatic brain injury (TBI) the primary insult to the brain and the secondary insults as a result of systemic complications may result in a multitude of sequelae ranging from subtle neurological deficits to significant morbidity and mortality. As the brain recovers by repair and adaptation, changes become apparent and may result in physical, cognitive and psychosocial dysfunction. Rehabilitation is usually structured to recover physical ability, cognitive and social retraining with the aim of gaining independence in activities of daily living.
Case Report:
A 76 year old male patient was admitted to an intermediate neurorehabilitation unit following a traumatic brain injury(TBI) .He had fallen from a height of 11 feet resulting in intracerebral haemorrhage in the left parietal lobe and a left parietotemopral subarachnoid hemorrhage which was managed conservatively in the neurosurgical unit. He developed recurrent post traumatic seizures in the form of myoclonic jerks for which he was started on antiepileptic drugs (AEDs) sodium valproate ,clobazam and levetiracetam .During his stay in the acute neurorehabilitation unit, he was noted to be confused and wandering with a disrupted sleep wake cycle. Cognitive assessment showed global impairment across all cognitive domains suggesting that cognitive impairment was secondary to TBI with the chaotic sleeping pattern and fatigue having a significant effect on his cognition. He was then transferred to an intermediate neurorehabilitation unit four months post head injury for rehabilitation prior to discharge.
On admission he was confused, and disorientated. His neurological examination was normal except for mild expressive dysphasia. On the first night of his stay in the unit, he did not sleep at all, was restless, agitated and aggressive towards the staff. His initial agitation was attributed to the change of surroundings and general disorientation. However during his first week at the rehabilitation unit it was noted that his sleep wake cycle was completely disrupted .He would have short fragmented naps through the day and would regularly get agitated at night with threatening behaviour towards staff. On admission the Rancho Los Amigos scale† was 4(confused-agitated) and he needed specialized supervision. Despite environmental modification and optimal pharmacotherapy to improve sleep and decrease agitation, the patient still continued to have aggressive outbursts and no identifiable sleep wake pattern. It was noted by the nursing staff that occasionally when very agitated, the patient refused to have his night time medications including all AEDs .On such occasions he was reported to have slept better at night and did not have any daytime naps. All blood investigations were within normal limits except for mild hyponatremia with a normal creatinine clearance and CT head showed changes consistent with previous TBI with no new pathology .A neurology opinion was sought and with a Naranjo adverse drug reaction probability score†† of 7/10, a decision was taken to slowly decrease levetiracetam and wean it to stop, while continuing all other regular AEDs. The levetiracetam was reduced from an original dose of 750mg twice daily by 500mg every week with an aim to stop. This resulted in a considerable improvement in the patient’s agitation with a complete halt in the nighttime aggressiveness. His sleep wake cycle normalized and he started sleeping longer at night. His Ranchos Los Amigos scale improved from 4(confused-agitated) to 6(confused-appropriate). The patient could now participate more with the team of trained therapists in memory and attention exercises as well as regaining independence in activities of daily living.
Discussion:
TBI particularly in elderly aged over 64 years has a worse functional outcome as compared to non elderly.1Closed head injury in older adults produces considerable cognitive deficits in the early stages of recovery2 and there have been studies suggesting TBI to be a risk factor for developing Alzheimer’s disease.3Memory deficits, attention problems, loss of executive function and confusion are common after TBI.4This impaired cognitive function reduces the patient’s ability to recognize environmental stimuli often resulting in agitation and aggression towards perceived threats.TBI by itself may result in a variety of sleep disorders ranging from hypersomnia, narcolepsy, alteration of sleep wake cycle, insomnia to movement disorders. 5Sleep wake schedule disorders following TBI are relatively rare and may clinically present as insomnia.6Often these sleep disorders result in additional neurocognitive deficits and functional impairment, which might often be attributed to the original brain injury itself and thus be left without specific treatment.
While dealing with disrupted sleep pattern and agitation in the elderly following TBI, treatable causes such as neurological, infectious, metabolic, and medications should be ruled out. This is imperative as they disrupt rehabilitation and achievement of functional goals. Long duration of agitation post TBI has been associated with longer duration of rehabilitation stay and persisting limitations in functional independence.7After ruling out all the treatable causes the first focus is on environmental management with provision of a safe, quiet, familiar, structured environment while reducing stimulation and providing emotional support. The next step is introduction of pharmacotherapy to reduce agitation. Though a variety of pharmacological agents are available, there is no firm evidence of efficacy of any one class and often the choice of drug is decided by monitoring its effectiveness in practice and watching for side-effects.8In pharmacotherapy, the general principle followed is start low and go slow while developing clear goals to help decide when to wean and stop medications. Atypical antipsychotics are often used for the agitation while benzodiazepines and non benzodiazepine hypnotics such as zopiclone are recommended for treatment of insomnia.9 However atypical antipsychotics carry a FDA black box warning being associated with increased risk of stroke and death among elderly.
But what does one do when all optimal non pharmacologic and pharmacologic measures fail? That brings us back to the drawing board which in this case led the team to rethink Levetiracetam, a novel new antiepileptic that has been used as monotherapy for partial seizures and adjunctive therapy for generalized tonic clonic and myoclonic seizures. Levetiracetam treated patients have been reported to have psychiatric adverse effects10 including agitation, hostility, anxiety, apathy, emotional lability, depersonalization, and depressionwith few case reports of frank psychosis 11.While in healthy volunteers levetiracetam is noted to consolidate sleep12,in patients with complex partial seizures, levetiracetam has been noted to cause drowsiness decreasing day time motor activity and increasing naps without any major effects on total sleep time and sleep efficiency during night.13There has been an isolated report of psychic disturbances following administration of levetiracetam and valproate in a patient with epilepsy which resolved following withdrawal of valproate. 14However in practice it is used for recurrent post TBI seizures as it is a potent AED with a relatively mild adverse effect profile and no clinically significant interactions with commonly prescribed AEDs.15
Any adverse drug reaction (ADR) should be evaluated while keeping the patients clinical state in mind. This was, indeed, difficult in our case. With a history of TBI and cognitive decline, it became difficult to ascertain whether the neurocognitive issues were purely due to the nature of TBI or due to an ADR. Assigning causality to a single agent is difficult and fraught with errors. Using the Naranjo algorithm 16, with a score of 7/10(probable ADR) and a notable response on withdrawal of the offending drug as in this case helps establish possible causality.
This is a rare instance where sleep wake cycle disorder and agitation resolved following withdrawal of Levetiracetam in an elderly patient with TBI. This in turn led to the patient having a stable mood so that therapists could communicate and interact with him in order to improve basic cognitive functions such as attention, memory, thinking and executive control. This case illustrates the constant need to systematically and frequently reassess patients as they recover from TBI.
†Appendix: Ranchos Los Amigos Levels of cognitive functioning.
Total knee replacement (TKR) is an effective and cost-effective intervention for advanced osteoarthritis (OA). Pain is the main indication for the procedure, and the majority of patients undergoing a TKR gain significant pain relief 1-3.
However, an important minority of those who undergo a TKR have persistent pain in the operated knee 4. Baker showed that 19.8% of patients with data in the National Joint Registry had persistent knee pain, and 18.2% were dissatisfied with the procedure 5. Anderson, in a study of 98 patients, found that 8.1% claimed that the operated knee was worse at follow-up (2-3 years after surgery) than prior to surgery and 9.2% were dissatisfied Wylde et al reviewed the available literature in 2009, and found that 10-20% of patients report significant pain in the operated knee, and that the patient centred outcomes of TKR appear to be considerably worse than those of total hip replacement, where as implant survivorship figures are fairly similar 7.
There are numerous possible causes of pain after a TKR, including anterior knee pain arising from the patello-femoral joint and extensor apparatus, prosthesis loosening, or infection. Other likely causes include soft-tissue periarticular problems, referred pain, pain sensitisation, or neuropathic painBecause of the risk of infection, and the possible need for further surgery, orthopaedic surgeons are generally keen to investigate these patients thoroughly and exclude surgical causes of the problem. However, there seems to be background pain vulnerability in the knee causing this high incidence of post-operative pain. The pain itself clearly needs appropriate management but patients also need surgical evaluation to exclude important reversible causes.9
In spite of this being a sizeable and worrying problem in orthopaedics, very little has been written about the assessment or management of these patients. No protocols or guidelines are available and the costs of management have not been explored.
In this paper we describe the first case series of patients with chronic knee pain after a TKR, and document the investigations and treatment undertaken, and the direct financial costs of their care to the NHS Trust in which they were seen.
RD&E provides an Arthroplasty tertiary referral service for a large area but is a large District General Hospital and as such the costs and results we report should be representative of most trusts within the UK
Methods:
A specialist service for revision knee surgery is available at the Royal Devon and Exeter Hospital, resulting in the referral of patients with problems in a knee after a TKR. A registry of such patients has been established at the hospital. The data presented here is based on examination of the records of 41 of these patients. These were patients with a painful TKR who had been referred to one of the authors from Orthopaedic specialists in various institutions including the resident hospital.
The notes of these patients were analysed to ascertain the number of appointments patients’ had attended to address the TKR problem, and what investigations and treatments had been undertaken for that problem both by the originating surgeon and by the revision knee specialist.
In addition data was obtained from the Trust on the current costs of the clinic appointments, investigations and any treatment or interventions undertaken.
Results:
The 41 patients studied included 27 women and 14 men, with a mean age of 63.9 years (range 49-81) at time of initial TKR. In the year 2009, 536 TKR’s were performed in the trust with an average age of 70.5 years (range 37-94) with 298 females and 238 males.
Investigations were commenced for abnormal pain post total knee replacement on average 15 months (range 1-84) after their knee replacement. Appointments and investigations were undertaken over a mean time of 20 months from initial investigation (range 7-45).
Neuropathic pain was diagnosed in 6 patients and instability was identified as a cause in 5 patients. 4 patients suffered aseptic loosening and no diagnosis was made in 26 patients (63%).
Table 1 shows the average number of appointments attended and investigations undertaken on these 41 patients.
Data on the costs of these appointments, investigations and treatments to the local NHS Trust are presented in Table 2.
Table 1- Number of appointments and investigations per patient with a painful TKR
Ave appt/pt
Range
Orthopaedic appointment
4.37
2 – 11
Pain team appointment
2.05
0 – 6
Physiotherapy appointment
3.05
0 – 12
Hydrotherapy appointment
0.8
0 – 8
ESR/CRP/WCC/PV
7.75
2 – 38
X-rays
7.92
2 – 35
MRI/CT/Bone scan
0.41
0 – 2
Aspiration/Arthroscopies
0.51
0 – 3
Table 2 – Costs of appointments, investigations and treatments per patient
Ave cost/pt (£)
Orthopaedic appointment
370
Pain team appointment
235
Physiotherapy appointment
45
Hydrotherapy appointment
68
ESR/CRP/WCC/PV
21
X-rays
*
MRI/CT/Bone scan
70
Aspiration/Arthroscopies
1529
Operative Costs
2624
Drug Costs
174
Average cost/patient
5136
*= X-ray radiographs costs were insignificant and not charged to the NHS Trust
The outcomes of these 41 patients included medical management alone in 19 (14 of whom reported significant improvement) and further surgical interventions in 22 (14 of whom reported improvement). The calculated direct costs of investigation and management of those treated solely medically (i.e. non-surgically) was £190/patient, while the cost of those treated surgically was £5,051/patient. This is shown in table 3.
Table 3 – Comparison of operative versus non-operative costs
Average Surgical intervention cost/pt
Average drug therapy cost/pt
Total cost/pt
Operative patients (22)
4891.09
160.22
5051.31
Non-operative patients (19)
N/A
190.63
190.63
Discussion:
We have analysed the management of a case series of patients with persistent pain in the knee after TKR. The results show that most of the 41 people studied attended numerous appointments with different specialists, and had the same investigations (serology and x-rays) repeated on many occasions over a relatively short period of time (less than 2 years), often before referral to a surgeon with a specific revision knee interest. We have also shown that the investigations and treatment undertaken were costly to the NHS, particularly if specialist imaging investigations (CT or MRI) or further surgical procedures (including aspiration or arthroscopy) were undertaken. The costs to the patients of the numerous appointments and repeated investigations have not been included, but are likely to have been considerable.
The fact that many different appointments were offered, and many investigations repeated, along with the wide range of different approaches to the different patients, are indicative of the absence of clear patient pathways or of a co-ordinated clinical service for these patients. Patients were seen by orthopaedic surgeons, pain specialists and physiotherapists, but definitive diagnoses or management plans did not often result from these appointments, and investigations were often repeated unnecessarily. We do not believe that this situation is unique to our area, as there are no clear guidelines or protocols to help us know how best to investigate or manage these patients before referral and the natural history of the condition is unknown.
The investigations carried out most frequently were serological tests (ESR and CRP) to try to exclude infection, and x-rays to look for prosthesis loosening or other bony problems. Previous work has shown that a single test of ESR greater than 22.5 or CRP greater than 13.5, in this situation, has a sensitivity of 0.77 and a specificity of 0.93 for the diagnosis of infection Repeating these tests offers little help, and if these were positive it would seem more appropriate to proceed to joint aspiration 11, 12-15.
Similarly, there is little point in doing more than one x-ray study a year, as the rate of change in radiographic findings is slow. If a bone problem is suspected, other more sophisticated imaging modalities can be used 16-18.
The cost data obtained from our Trust show that high costs are incurred from new clinic referrals and visits, sophisticated imaging procedures (CT, MRI and bone scans), and surgical procedures – in particular revision surgery. These high costs of investigations would indicate that patients with a painful TKR would be more appropriately investigated and managed by specialist centres with early and meticulous evaluation by surgeons with a special interest in revision knee surgery.
The surgical costs of management of painful TKR’s dwarf the amount of money spent on medical (i.e. non-surgical) approaches. This considerable difference suggests that it is of paramount importance to manage the pain early, irrespective of whether surgery is required. Good pain management will allow the surgeon, and particularly the patient, to evaluate the problem in a clearer manner, weighing up the treatment options and making a decision from a more balanced position.
According to data from the National Joint Registry, over 53,000 TKRs were performed in NHS hospitals in England and Wales in 2009 19. Using the estimates of Baker, and Wylde and others on the numbers of these patients who are in pain or dissatisfied, we calculate that over 10,000 patients each year, in this country alone, are acquiring the problem of persistent pain in a TKR ,7This represents a huge public health problem, and one that, if our Trust’s cost figures are representative, is probably costing the NHS over £10 Million/annum. In view of that, we believe that this issue needs urgent attention from the research community and health care providers.
Figure 1 – Algorithm for assessment of a patient with a painful TKR
Our recommendation is that research is undertaken to document the natural history of pain in a TKR knee, differentiate the main causes of this pain, and develop simple algorithms to help clinicians make the correct diagnosis. We suggest a protocol that can be utilised by healthcare professionals to investigate painful TKR’s to allow correct assessment and diagnosis (Figure 1). We believe that health care providers in major orthopaedic centres should set up interdisciplinary clinics in which surgeons, pain specialists and physiotherapists can work together to help investigate and manage these patients.
Pre-eclampsia is a multisystem disorder of pregnancy that forms an integral part of the spectrum known as hypertensive diseases of pregnancy. The National High Blood Pressure Education Program (NHBPEP) Working Group1classifies hypertensive diseases in pregnancy into 4 groups:
1) Gestational hypertension
· New onset hypertension in pregnancy presenting after 20 weeks
· No proteinuria
· BP returns to normal less than 12 weeks postpartum
· Final diagnosis made only postpartum
2) Chronic hypertension
· BP >140/90 mm Hg before pregnancy or diagnosed before 20 weeks gestation not attributable to gestational trophoblastic disease or
· Hypertension first diagnosed after 20 weeks gestation but persistent after 12 weeks postpartum.
3) Pre-eclampsia/eclampsia
· BP > 140/90 mm Hg after 20 weeks gestation in a women with previously normal blood pressure
· Proteinuria (>0.3 gm urine protein in 24 hr).
· Eclampsia is defined as seizures that cannot be attributed to other causes in a woman with pre-eclampsia
4) Superimposed pre-eclampsia (on chronic hypertension)
· New onset proteinuria (>300 mg/24 hr) in a woman with hypertension but no proteinuria before 20 weeks gestation
· A sudden increase in proteinuria or blood pressure, or platelet count less than 100,000 in women with hypertension and proteinuria before 20 weeks gestation
Epidemiology
Pregnancy induced hypertension complicates about 10% of pregnancies, but there is a widespread geographic variation in its incidence.The incidence is higher in developing countries. The highest reported rate of pre-eclampsia is 7.1% (deliveries) from Zimbabwe2, while the incidence is as low as 0.81% (deliveries) in Colombia3. In UK, the incidence of severe pre-eclampsia is 5/1000 maternities4, while the incidence of eclampsia is 4.9/10,000 maternities5. The incidence of severe pre-eclampsia in European countries ranges from 2/1000 (deliveries) in Norway to 6.4/1000 (deliveries) in Belgium and Hungary6.
The 8th Confidential Enquiry into maternal and child heath7 revealed pre-eclampsia and eclampsia as the second leading cause of direct maternal death, thereby contributing to a maternal death rate of 0.83 / 100,000 maternities.
Worldwide studies show that mortality from pre-eclampsia can be as high as 0.4%, while that in eclampsia varies from 6.1% in developing countries to 1.8% in UK 5, 8-9.
Estimates of maternal mortality from the developing countries (in Asia, Africa, Latin America and the Caribbean) suggest that 10-15% of maternal deaths are associated with hypertension in pregnancy, while eclampsia is associated with 10% maternal mortality10.
Severe pre-eclampsia is also associated with significant maternal morbidity, including eclamptic seizures, intracerebral haemorrhage, pulmonary oedema due to capillary leak or heart failure, acute renal failure, liver dysfunction, and coagulation abnormalities.
Fetal complications include abruptio placentae, intrauterine growth restriction, premature delivery, and intrauterine fetal death. The incidence of stillbirths and neonatal deaths in mothers who suffered eclampsia was 22.2/1000 and 34.1/1000, respectively, in the UK with a higher incidence in developing countries5.
More than half a million women die each year from pregnancy related causes across the globe. The Millennium Development Goals have placed maternal health as a basic human right, one that is integral to the core of the fight against poverty and inequality. The high incidence of pre-eclampsia and its complications makes its prevention and effective management important. The following article attempts to outline the pathophysiology and management of pre-eclampsia.
Aetiology & Risk factors
Pre-eclampsia is commonly referred as the “disease of theories” making its prevention and management an ongoing challenge worldwide. Although the aetiology is still largely unknown, there are a few hypotheses regarding the pathophysiology and prediction of pre-eclampsia.
It has been postulated that pre-eclampsia may be autoimmune in nature. Seminal-vesicle-derived transforming growth factor 1 (TGF-1) initiates a post mating inflammatory reaction, which is a type 2 immune response towards paternal antigens resulting in maternal-fetal (paternal) immune maladaptation11. This idea originates from epidemiological studies demonstrating the protective effect of long-term sperm exposure and is supported by the fact that frequency of pre-eclampsia is higher in nulliparous women or multiparous women with a new partner, teenagers, women who conceive after donor insemination or oocyte donation, and women with autoimmune conditions.
Another potential mechanism responsible for pathogenesis of pre-eclampsia is placental hypoperfusion which in turn releases various factors that trigger endothelial activation / dysfunction. Nitric oxide, disordered endothelin metabolism, thromboxane/prostaglandin imbalance, cellular fibronectin, inflammatory cytokines (TNF-α, IL-6, IL-1α, and IL-1β) and otherfactors such as lipid peroxides and reactive oxygen intermediateshave all been implicated in mediating the endothelial cell injury12. This is well-supported by the fact that pre-eclampsia commonly occurs in pre-existing metabolic (diabetes, hypercholesterolemia), renal, vascular disorders (hypertension) and connective tissue disorders that result in poor placental circulation. In cases of multiple gestation or increased placental mass, it is not surprising for the placenta to become underperfused.
However, majority of the pre-eclamptic women do not suffer from any underlying medical conditions. In these women, lack of placental cytotrophoblastic invasion of uterine spiral arterioles and arrest of arteriolar remodelling results from failure of pseudo-vascularisation of the invasive cytotrophoblasts13. Deregulation of angiogenesis-related gene products such as vascular endothelial growth factor (VEGF), angiopoietin and ephrin family proteins, placental growth factor (PlGF) and their receptors have been implicated in this process14.Shallow placentation leads to reduced placental perfusion and subsequent ischaemia.
Obese (BMI ≥30 Kg/m2) women are at higher risk for pre-eclampsia compared to lean women (odds ratio = 3.3). The exact mechanism is not completely understood but possible explanations are: increased stress due to the hyperdynamic circulation associated with obesity; dyslipidaemia or increased cytokine-mediated oxidative stress; and direct haemodynamic effects of hyperinsulinaemia15 (increased sympathetic activity and increased tubular sodium resorption).
On the other hand, smoking actually decreases a woman’s risk of pre-eclampsia. Inhibition of thromboxane A2production by nicotine might explain the decreased risk. However, the adverse effects of smoking on pregnancy significantly outweigh any beneficial effects16.
Epidemiological and clinical risk factors for pre-eclampsia are classified as maternal, paternal, and/or pregnancy-specific2, 17 (Table 1, below).
Table 1: Pre-eclampsia Risk Factors
Maternal Considerations
Inherent
Ø Age < 20 or 35–40 years
Ø Nulliparity
Ø Afro-Caribbean origin
Ø Prior or family history of PE or cardiovascular disease
Ø Woman born small for gestational age
Medical conditions
Ø Obesity
Ø Chronic hypertension
Ø Chronic renal disease
Ø Diabetes mellitus (insulin resistance, type 1, and gestational)
Ø Antiphospholipid antibody syndrome
Ø Connective tissue diseases
Ø Thrombophilia
Ø Stress
Pregnancy specific
Ø Multiple gestation
Ø Oocyte donation
Ø New partner
Ø Urinary tract infection
Ø Congenital conditions affecting the fetus
Ø Hydatidiform mole
Ø Hydrops fetalis
Ø Structural anomalies
Paternal Considerations
Ø Limited sperm exposure
Ø Barrier contraception
Ø First-time father
Ø Donor insemination
Ø Partner who fathered a pre-eclamptic pregnancy in another woman
What exactly happens in Pre-eclampsia?
The triad of physiological derangements in pre-eclampsia include 1. Vasospasm 2. Plasma volume contraction 3. Local or disseminated intravascular coagulation.
Although the cause of pre-eclampsia is unknown, we have already discussed that the placenta is largely implicated. The sequence of events starts with vasospasm caused by increased production or sensitivity to vasoconstrictors (angiotensin II, serotonin and endothelin) and/or decreased production or sensitivity to vasodilators (prostacyclin and nitric oxide). This is followed by plasma volume contraction, increased capillary permeability and, in severe cases, low plasma oncotic pressures. Redistribution of fluid occurs from the intravascular to interstitial fluid spaces causing peripheral tissue oedema. Along with this, intravascular coagulation may occur due to platelet activation, thrombocytopenia and, often, reduced production of anti-thrombin III.
The net effect is organ hypoperfusion. Commonly affected systems are kidney (manifested by reduced GFR, proteinuria, hyperuricaemia and occasionally oliguria), liver (manifested by elevated transaminases with or without epigastric and right upper quadrant pain), and the brain (manifested by headaches, transient visual disturbances due to occipital lobe ischaemia and rarely convulsions, i.e. eclampsia). This leads to increased maternal morbidity.
Placental insufficiency resulting from uterine hypoperfusion is characterised by intrauterine fetal growth retardation and less commonly placental abruption or fetal death. Preterm delivery, low birth weight, respiratory distress syndrome, and admission to the neonatal intensive care lead to increased perinatal morbidity.
In spite of major advances in understanding the pathophysiology of the disease in recent years, interventions to prevent hypertensive disorders in pregnancy have had disappointing results, hence early detection, continued surveillance and timely intervention still remains the key towards decreasing the inherent maternal and fetal morbidity and mortality associated with severe pre-eclampsia and eclampsia.
Prevention of pre-eclampsia
Till date there is no well-established measure for prevention of pre-eclampsia in the general population. Calcium is clearly of benefit amongst high risk women in communities where low dietary calcium intake is prevalent. A Cochrane systematic review in 2010 concludes that calcium supplementation approximately halves the risk of pre-eclampsia, reduces the risk of preterm birth and the rare occurrence of the composite outcome 'death or serious morbidity18.
Low dose aspirin (antiplatelet agent) therapyefficiently reduces the development of pre-eclampsia in women with abnormal uterine artery Doppler studies. If started in early gestation (< 16 weeks), it also causes a significant reduction in the incidence of severe pre-eclampsia, gestational hypertension and IUGR19.
Some studies have suggested that prophylactic use of antioxidants (vitamin C, E) may be beneficial as well but this is not routinely recommended20 in practice.
Evidence is also lacking to support lifestyle preventative interventions for pre-eclampsia, such as rest, exercise and reduced dietary salt intake.
The pre-eclampsia community guideline (PRECOG)
This has been developed for screening and detection of onset of pre-eclampsia in the community21. It includes:
Initial risk assessment at community booking using pre-determined criteria, to identify factors that predispose women to pre-eclampsia in a given pregnancy. Following this, women are offered referral before 20 weeks gestation for specialist input to their antenatal care plan if they have been identified as high risk: this may be for clarification of risk, necessary investigations, advice on early intervention or pharmacological treatment.
Systematic community assessment for onset of pre-eclampsia from 20 weeks gestation. The frequency of assessment is determined by the likelihood of developing pre-eclampsia. Women with no risk factors for pre-eclampsia are offered assessments at weeks 16, 28, 34, 36, 38, 40, and 41 weeks.Women with one risk factor for developing pre-eclampsia (excluding previous pre-eclampsia, multiple pregnancy and underlying medical conditions like hypertension, renal disease, diabetes, antiphospholipid syndrome) are reviewed in the community at least once every three weeks before 32 weeks, and then at least once every two weeks, until delivery. At every visit, recommendation is to look for presence of any signs or symptoms like new hypertension, new proteinuria, headache/visual disturbance, or both, epigastric pain/vomiting, or both, reduced fetal movements, small for gestational age infant. In the presence of two such, they are referred for early specialist input, individual assessment, and discussion of obstetric risk.
Recommendations have been made within the scope of this guideline for improving accuracy inblood pressure measurement, increasing reliability of proteinuria test with dipstick and community assessment of fetal growth and well being which provide the parameters for referral. Referral is made forstep-up assessment in hospital day unit within 24/48 hoursor admission in accordance with set criteria. All pregnant women are also made aware that pre-eclampsia may develop between antenatal assessments, and they could self-refer at any time.
It is recognised that all women benefit from a continuity of care in the community and need midwifery or GP care as part of their individual antenatal care plan, whatever be their obstetric risk.
Management of Pre-eclampsia
Antenatal Care
These patients should be under consultant led care with multidisciplinary input from the anaesthetic and neonatal teams as necessary.
Women with risk factors for developing pre-eclampsia may be considered for uterine artery doppler velocimetry at 20-24 weeks to look for increased impedance to flow (resistance index >95th centile or early diastolic notch), which is predictive of developing pre-eclampsia or IUGR in late gestation, however the specificity and sensitivity varies widely between different studies22-25.
At diagnosis of pre-eclampsia, the best practice is to offer initial hospital admission for assessment and formulation of follow-up care. Assessment of proteinuria should be done by automated reagent strip reading device. Visual assessment of the dipstick is not recommended nowadays because of high error rates26-28. If the automated reagent strip reading of urine yields a result of 1+ or more, this should be followed up with a spot urinary protein:creatinine ratio or a 24 hour urine collection to quantify the proteinuria. Significant proteinuria is diagnosed if the urinary protein:creatinine ratio is more than 30mg/mmol or the validated 24 hr urine sample has more than 300 mg of protein. Baseline blood investigations should include full blood count, liver function (bilirubin and transaminases), electrolytes and kidney function tests. Antihypertensive medications may need to be commenced with the aim of maintaining the systolic blood pressure below 150 mm Hg, and the diastolic pressure between 80 - 100 mm Hg. Labetalol is the first line treatment. However, in patients in whom labetalol cannot be used (e.g. in patients with bronchial asthma), alternatives include nifedipine (contraindicated before 20 weeks of gestation), methyldopa, atenolol and metoprolol. 4-6 hourly blood pressure, daily assessment of proteinuria, along with haematological and biochemical monitoring are also carried out. Inpatient management is required till the blood pressure stabilises.
Following discharge blood pressure can be checked in the community or in antenatal day assessment 2-3 times a week depending on clinical circumstances. Quantification of urinary protein is not necessary after the initial assessment, however, blood tests for full blood count, liver and kidney functions need to be repeated at least twice weekly (thrice weekly if the hypertension is moderate or severe). There is often a rise in serum uric acid level, which has been associated with poor maternal and fetal outcome29, 30. However, there is no evidence to use serum uric acid levels for clinical management.
Fetal monitoring:
Ultrasound assessment of fetal growth and amniotic fluid volume along with umbilical artery doppler velocimetry needs to be done at initial diagnosis of pre-eclampsia to exclude IUGR and then every 2 weeks if the pregnancy is managed conservatively and the results remain normal CTG monitoring is commonly done at diagnosis, along with the ultrasound assessment. If normal, further CTG should be performed weekly unless otherwise clinically indicated.
Delivery
In pre-eclampsia with mild or moderate hypertension, women may be delivered between 34 and 37 weeks of gestation, depending on maternal and fetal condition, presence of risk factors and availability of neonatal intensive care facilities. If severe pre-eclampsia develops, refractory to treatment or fetal wellbeing delivery may need to be done earlier.
Pre-eclampsia is considered to be severe in case of
1) Severe hypertension with proteinuria or
2) Mild / moderate hypertension and proteinuria with one or more of the following signs / symptoms:
Ø Severe headache , not responding to medications
Ø Visual disturbance (blurring or flashing of light)
Ø Severe pain in upper abdomen or vomiting
Ø Papillo-oedema
Ø Signs of clonus (³ 3 beats)
Ø Liver tenderness
Ø HELLP syndrome
Ø Decrease in platelet count to less than 100 x 109 per litre
Ø Abnormal liver enzymes (ALT or ASTrising to above 70 iu/litre).
HELLP syndrome
HELLP Syndrome (haemolysis, elevated liver enzyme, low platelets) is a form of severe pre-eclampsia that is associated with high maternal and perinatal morbidity and mortality and may be present without hypertension or, in some occasions, without proteinuria.
A diagnosis of HELLP syndrome is made after confirmation of haemolysis, either by blood film microscopy showing fragmented red cells or increased serum LDH level. An AST or ALT level of above 70 iu/l is significant while a level more than 150 iu/l is associated with increased morbidity to the mother, though neither of them are independent risk factors for increased maternal morbidity 31. A low platelet count (less than 100 x 10 6 /ml) supports the diagnosis.
There is some evidence to suggest that the severity of pre-eclampsia differs according to the time of onset. More severe form occurs with the onset of pre-eclampsia prior to 34 weeks of gestation. This form is associated with abnormal uterine artery blood flow, IUGR and adverse maternal and fetal outcomes32-33.
There may be some difference in the pathophysiology of these two disease types. The early onset disease may be associated with placental abnormalities, while the late onset one is more linked to maternal constitutional factors such as increased BMI34.
In severe pre-eclampsia, delivery is appropriate anytime beyond 34 weeks of gestation following corticosteroid administration to achieve fetal lung maturity. Delivery before 34 weeks is only indicated in maternal/fetal compromise or hypertension refractory to treatment35-37. Prolonging pregnancy at early gestation may improve the perinatal outcome but has to be carefully balanced against maternal wellbeing. If conservative management is planned, ultrasound assessment of fetal growth, amniotic fluid volume and umbilical artery doppler flow should be done at admission, and thereafter, every two weeks. In case of normal ultrasound findings, weekly CTG monitoring should suffice, unless clinically indicated otherwise (for e.g. reduced fetal movement, vaginal loss, abdominal pain or deterioration of maternal condition).
Eclampsia
Generalised tonic-clonic seizures, with or without raised blood pressure and proteinuria, occurring during or after pregnancy with no other identifiable cause is classified as eclampsia. The cause is usually multi-factorial including cerebral vasoconstriction, ischaemia, vasogenic oedema, or other pathology. Although it is more likely to occur in women with severe rather than mild pre-eclampsia, there is no convincing test for predicting the onset of eclampsia. Convulsions may occur antepartum (38-53%), intrapartum (18-36%), or postpartum (11-44%)38. Women with a history of previous eclampsia are at increased risk of eclampsia (1-2%) and pre-eclampsia (22-35%) in subsequent pregnancies39.
Intrapartum Care
During labour, hourly blood pressure monitoring in women with mild or moderate hypertension, and continuously in severe hypertension is ideal. Antenatal hypertensive treatment should be continued, with the aim of maintaining the systolic blood pressure below 150 mm Hg, and the diastolic pressure between 80-100 mmHg. If oral medications fail to control the blood pressure, then intravenous anti-hypertensives are indicated to prevent the known risk of vascular damage due to uncontrolled hypertension.
Hydralazine, a peripheral arteriolar vasodilator, has been widely used as the first-line treatment for acute hypertension in pregnancy, in the past.It is administered as bolus doses (5-10 mg) intravenously, every 20 minutes to a maximum dose of 30 mg, with careful monitoring of blood pressure. The side effects include headache, nausea, and vomiting. Importantly, hydralazine may result in maternal hypotension, which may subsequently cause fetal distress. Preloading with 500 ml of crystalloid fluid before or with the first dose of intravenous hydralazine may avoid this40. Labetalol is another antihypertensive that can be given intravenously, either as bolus doses or as an infusion to manage severe hypertension. It is commonly used as the first line drug in many centers in UK. However, it is not suitable for patients with bronchial asthma. Nifedipine may also be used orally to control blood pressure (sublingual administration is not recommended).However, it can interact with magnesium sulphate to produce profound muscle weakness, maternal hypotension and fetal distress41-43. Recent evidence suggests labetalol and nifedipine as better alternatives than hydralazine40. In all cases, the blood pressure should be monitored closely, along with fetal monitoring, as sudden decrease in maternal blood pressure will reduce the utero-placental blood flow, resulting in fetal distress.
Magnesium sulphate isthe agent of choice for treatment of eclampsia. It is also used in women with severe pre-eclampsia for prophylaxis of eclampsia andis usually commenced once delivery decision is made or in immediate postpartum period. In women with less severe disease the decision will depend on individual case assessment. Evidence shows that magnesium sulphate more than halves the risk of eclamptic seizures44.It has also been shown to reduce maternal morbidity related to pneumonia, mechanical ventilation and intensive care45.However, there is little evidence to suggest that it decreases the risk of stillbirth or neonatal death.Magnesium sulphate is usually continued for 24 hours following delivery or 24 hours after the last seizure, whichever is the later, unless there is a clinical reason to do otherwise. This is based on the findings of the Collaborative Eclampsia Trial, 1995. However, recent evidence suggests that magnesium infusion may be stopped earlier (12 hours postpartum), especially when used in conjunction with other clinical parameters46, 47. Regular assessment of the urine output, deep tendon reflexes, respiratory rate, oxygen saturation and serum concentration is done as long as magnesium sulphate is continued to avoid toxicity. Features of magnesium toxicity include suppression/loss of patellar reflexes, drowsiness and respiratory depression. Intravenous calcium gluconate is used for reversal of magnesium toxicity.
Fluid restriction is the usual practice, unless there is associated maternal haemorrhage, to reduce the chance of fluid overload and pulmonary oedema. As per NICE guidelines, total fluids should be limited to 80 ml/hour in women with severe pre-eclampsia. Strict intake-output chart should be maintained. The regime of fluid restriction should continue until postpartum diuresis commences.
The mode of delivery should be individualised taking into account the gestation, presentation, cervical favourability for induction of labour and well-being of the fetus. Vaginal delivery is generally preferable but in case of extreme prematurity or fetal compromise, caesarean section is more likely.
Haematological and biochemical monitoring needs to be continued in labour and is dictated by the patient condition and need for analgesia/anaesthesia. For those on magnesium sulphate, bloods must be repeated every 6 hours.
Anaesthetic management
The anaesthetic management in pre-eclamptic patients is important, and should start with a detailed pre-anaesthetic assessment. Appropriate history and physical examination are important. Pre-eclamptic patients are at increased risk of oedema of the pharyngolarynx and assessment of airway is vital48-49. Clinical assessment of the cardiopulmonary and fluid status is required, along with laboratory investigations including renal biochemistry and coagulation status.An appropriate understanding of the obstetric interventions such as antihypertensive medications, and magnesium sulphate infusion is required.
Anaesthetic management should include appropriate monitoring, and should include NIBP, pulse oximetry and urine output. Invasive blood pressure monitoring (arterial line) is indicated in patients with poorly controlled blood pressure, or when NIBP is difficult to obtain (e.g. in the obese patients).
Pulmonary oedema is a rare but serious complication of severe pre-eclampsia, which can lead to increased maternal mortality (10%) and perinatal mortality as high as 50%50. Central venous pressure monitoring is indicated in patients with pulmonary oedema, poor urine output or when difficulty in fluid management is anticipated in the peripartum period. Pulmonary arterial catheters are rarely needed. Non-invasive monitoring of cardiac output may be required in patients with difficult fluid management or coexisting cardiac problems.
The safety of regional anaesthesia in pre-eclamptic patients is now well established51. Lumbar epidural may be used for labour analgesia in women with pre-eclampsia if the mothers opt for it. Early epidural should be considered as it helps to diminish the hypertensive responses to pain. Platelet count >75x109/L in the absence of other coagulation abnormalities is not associated with increased likelihood of regional anaesthetic complications in the setting of pre-eclampsia52. The presence of a functioning epidural catheter allows the epidural block to be titrated for LSCS if indicated. If central neuraxial block is contraindicated, then intravenous opioids may be used for labour analgesia53-54. Few studies have mentioned the successful use of remifentanil PCA in these patients55.Regional blockade is currently the preferred mode of anaesthesia for caesarean section. It has long been argued that while titrated epidural blocks are safe, single shot spinal or CSE techniques may produce profound hypotension. However, multiple studies have demonstrated the safety of spinal and CSE in pre-eclamptic patients for LSCS with no adverse effects on mother or fetus56-58. In fact the incidence of hypotension in pre-eclamptic patients following regional anaesthesia is less than that in healthy patients, and is successfully managed by intravenous boluses of ephedrine or phenylephrine59-60.Doses of local anaesthetics in regional anaesthesia remain the same in pre-eclamptic patients as in normal healthy parturients.
Though regional anaesthesia is preferred for LSCS, a general anaesthesia may still be needed if regional anaesthesia is contraindicated (e.g. coagulopathy as in HELLP syndrome), and in emergency situations where the baby has to be delivered as early as possible. General anaesthesia increases the risk of hypertension during induction and emergence, loss of airway due to pharyngolaryngeal oedema, aspiration and transient neonatal depression. Extreme care is to be undertaken to obtund the hypertensive response during induction-intubation, as this has been a significant past cause of maternal mortality61. Several agents (alfentanil, fentanyl, remifentanil, magnesium sulphate, intravenous lignocaine and esmolol) have been suggested for induction, and clinicians should use familiar ones. All opioids rapidly cross the placenta and increase the risk of neonatal depression, and appropriate facilities for neonatal resuscitation must be available. Remifentanil has the advantage as it is rapidly metabolised by the neonate, and any respiratory depression is usually brief62- 63.Maintenance of anaesthesia is done by inhalational anaesthetic agents. Isoflurane is considered to be a good choice, because of its vasodilating properties. Vigilance is also required during emergence from anaesthesia, to prevent hypertension, as well as aspiration.
Anaesthetists must also be aware of the potential drug interactions of agents commonly used in pre-eclampsia. Magnesium sulphate and calcium channel blockers may potentiate the action of muscle relaxants and appropriate monitoring is vital.
Post delivery analgesia
This is maintained by simple analgesics like paracetamol. Non-steroidal anti-inflammatory agents have been used; however, caution must be exercised due to their effect on cyclo-oxygenase pathway, especially those with renal insufficiency and coagulopathy. A few case reports of significant increase in blood pressure in postpartum women have been reported following their use64. Patient controlled analgesia with opioids has been used widely, and is considered to be a safe option.
Use of oxytocic agents
Syntocinon is the drug of choice. Ergometrine should be avoided because of its propensity to cause hypertension. Synthetic prostaglandins such as Carboprost (15 methyl PGF 2 alpha) may be given with caution after considering the risk-benefit ratio, especially because it can aggravate hypertension.
Use of thromboprophylaxis
This should be considered in all patients with pre-eclampsia.
Table 2: Management strategies for chronic hypertension and gestational hypertension
Preconception
Antenatal
Delivery
Postpartum
Further follow-up
Chronic Hypertension
Optimise antihypertensives, change ACE inhibitors, diet and lifestyle modification
Continue treatment to maintain BP <150/100. Offer uterine artery dopplers to detect risk of developing pre-eclampsia/IUGR
At 37 weeks, if BP is controlled.
Aim to maintain BP <140/90 with antihypertensives
Medical review at 6-8 weeks
Gestational Hypertension
Assessment of risk factors
Hospital admission if severe hypertension. Antihypertensive if BP > 150/100. Test for proteinuria at each visit, blood tests as indicated
At 37 weeks, if BP <160/110, with/without antihypertensives
Titrate antihypertensives to keep BP <140/90
Medical review at 6-8 weeks, or earlier if need to continue antihypertensives
Pre-eclampsia
Assessment of risk factors.
Hospital admission at diagnosis. Antihypertensives to be started if BP>150/100. Regular blood investigations (2-3/week)
Delivery between 34-37 weeks, depending on maternal/ foetal condition
Initial monitoring as inpatient, to be discharged to the community when BP <149/99 with/without treatment and blood results are stable
Medical review at 2 weeks, if continuing antihypertensives. Otherwise at 6-8 weeks
Postpartum Care
Following childbirth, mobilisation of the extravascular fluid occurs increasing the intravascular volume, and consequently increasing the blood pressure. This fluid shift also increases the risk of pulmonary oedema, cerebral oedema and eclampsia.
Most of the existing guidance focuses on management of blood pressure and its associated problems in the antenatal and intrapartum period but the postpartum phase can often be poorly looked after 65. Regular blood pressure monitoring at an interval of 4-6 hours should be done as an inpatient initially and blood platelet count, transaminases and creatinine should be measured to note any changing trends. The aim is to maintain blood pressure <160/110mmHg, thereby preventing cerebral injury from occurring. In order to achieve this, beta-blockers, calcium-channel blockers and ACE inhibitors can be used in a stepwise manner. Use of methyldopa is usually avoided as it has the potential to cause depression and psychosis in postpartum period. Women are discharged to the community care if they are asymptomatic, blood pressure, with or without treatment, is 149/99 mmHg or lower and blood test results are stable or improving. Blood pressure isthen checked daily/alternate days in the community till 2 weeks postpartum. Antihypertensives should continue till blood pressure falls below 130/80 mm of Hg and the dose adjustments need to be made by the GP. If blood pressure becomes uncontrolled, then women would require urgent referral to the hospital.
In most cases, the hypertension and/or proteinuria resolve within six weeks postpartum. Any women whohad pre-eclampsia complicating their pregnancy, needs to have blood pressure and urine protein checked at 6-8 week postnatal visit at the GP surgery. If still requiring antihypertensive treatment at that stage or persistent proteinuria further assessment is warranted to find out cause for raised blood pressure if any and also identify and advise on risk factors for cardiovascular disease and lifestyle changes.
For all these women preconception counselling should be offered for subsequent pregnancies especially if risk factors are identified so that potentially preventative strategies can be initiated.
Table 2 outlines briefly the management strategies for mothers with chronic hypertension and gestational hypertension. However, a detailed discussion is outside the scope of this article.
On discharge from hospital, secondary care providers have a duty and obligation to communicate with primary care provides – particularly the general practitioner – to give information regarding the reasons for admission, results of investigations, procedures performed, treatment instigated and importantly follow-up management. Therefore the transition of information between secondary and primary care is vital for care management and hence patients’ safety.
This information is shared in the form of a ‘discharge summary’. It is the responsibility of the secondary care team to provide this. The level of detail given has been found to vary not just between different NHS trusts or hospital but also between different wards and individual doctors completing the discharge summary – this can create many problems as communication plays a pivotal role in patient care.
The information given in the discharge summary is all that a patients’ GP knows in regards to their hospital admission and management. A discharge summary is effectively a form of ‘handover’. A hospital physician may instruct the GP to do certain things in regards to follow-up; for example check blood results, review results of investigations arranged as outpatients or simply review the patient clinically. The more information that is transferred across from secondary to primary care the more awareness the GP has to what has happened and what needs to happen, which leads to better patient care.
A discharge summary can also be a valuable document for when a patient is admitted to hospital; if their notes are not available a past discharge summary will provide useful information (re. past medical history and drug history in particular) to the medical team who may have no prior knowledge of the patient, this is invaluable if it not possible to take a history from a patient and is also useful in directing investigations if a patient has been admitted with the same complaint(s). Of course this depends on the patient having a copy of the discharge summary with them on admission or the ability to access previous discharge summaries electronically.
Good documentation is vital in the healthcare setting. All documentation, no matter in what form, must be clear, accurate and legible. Any type of document is useless if it cannot be read. The GMC and Royal College of Physicians stress the importance of documentation1, 2.
The importance of the discharge summary has been highlighted in the last few years. There has been a move from the traditional hand-written discharge summary – commonly referred to as the TTA (to take away) – to the use of computer software providing an electronic discharge summary (EDS). The latter not only provides more detail but also aims to deliver it to the primary care setting in a timelier manner; for example, in the future, once all EDSs are completed at Barking, Havering and Redbridge University Hospitals NHS Trust there are plans for them to be automatically emailed to a patients GP surgery – currently this scheme is being trailed at certain GP surgeries. This complies with the requirement and recommendations made to secondary care trusts to provide the GP with a discharge summary within 24hrs of a patients’ discharge from hospital – consequently reducing previous financial penalties when not achieved and thus being more cost efficient.
The advent of the EDS has impacted the daily working of the junior doctor, who is commonly, the individual on the secondary care team whose role it is produce the discharge summary. Previously with a TTA a patient could be discharged home without all the constituents on the form being completed and so a GP would be provided with an incomplete discharge summary. At BHR University Hospital NHS Trust in order to produce a finished EDS - and essentially discharge the patient - all constituent sections have to be completed before it can be electronically sent to pharmacy so that the patient sent home with their medications (the discharge summary acts as a prescription). Therefore producing an EDS is more time consuming in comparison to a TTA. However an EDS does have advantages (see Table 1).
Table 1: Comparison of EDS and TTA
Any form of discharge summary is user dependent; what is written is determined by the individual doctor producing the document therefore there is no guarantee that they have documented everything that occurred during admission. In the case of the TTA user dependence also refers to the legibility of the writing, the durability of the carbon copies produced, as well as the level of detail of the discharge summary produced.
In 2008 Newham University Hospital Trust introduced the EDS, the trust audited this process and found it to be successful3. 2010 saw the introduction of the EDS at BHR University Hospital NHS Trust. The EDS was piloted on Sunrise B ward of Queen’s Hospital, Romford. The purpose of this audit is to establish if the introduction of the EDS at BHR University Hospital NHS Trust has been successful. The audit aims to determine if the EDS method is superior to that of the traditional TTA – this will be achieved by comparing the completion rates for specific criteria of the discharge summary. This audit also aims to identify areas of improvement and recommendation for the EDS.
Design and Method:
An opportunistic sample of 50 TTAs and 50 EDSs were selected from the patients admitted to Sunrise B (‘Care of the elderly’) ward, Queen’s Hospital, Romford in a two-month period (January to February 2011). Thus this is a retrospective audit. No exclusion criteria for selection of discharge summaries was set. For each discharge summary completion rates for the different fields of the discharge summary were recorded. Table 2 shows the criteria fields included in each type of discharge summary.
Table 2: Comparison of EDS and TTA criteria
The Royal College of Physicians have published their recommendations for the structure and content of the discharge summary. Section headings include
GP details - name, address, practice code
Patient details – surname, forename, date of birth, gender, NHS number, address, telephone number
Admission details – method of admission, source of admission, hospital site, trust, date of, time of
Discharge details – date of, time of, discharge destination, discharging consultant, specialty
Clinical information – diagnosis at discharge, operations/procedures, reason for admission/presenting complaint, allergies, investigations and results, treatments, discharge medications, medication changes
Advice, recommendations and future plan – hospital/GP/community
Person completing summary – doctors name, grade, specialty, signature, date of completion4
This audit establishes which method of discharge summary is more compliant with these recommendations.
Data analysis was mainly descriptive. Data collected was tabulated and represented as percentages. Graphical representation of the data was performed using Microsoft Excel. Due to the nature of the study and data collected more sophisticated statistical analysis, such as that requiring the use of SPSS software, was not warranted.
Results:
Results demonstrate significant differences between the TTA and EDS completion rates for criteria of the discharge summary. Table 2 presents the data as percentages in a tabulated form. Compared to the TTA, the EDS had a higher rate of the following six criteria of the discharge summary documented; diagnosis, co-morbidities, investigations, drug history, discharge destination and instructions for GP.
Table 3: Summary table of data
Patient details and admission date.
The TTA had lower completion rates for these fields than the EDS. The EDS software automatically enters these fields therefore it is not possible for this criterion to be incomplete. The correct patient details ensure continuity of care and patient safety. If patient details – i.e. full name, date of birth, hospital number and address - are not present those with similar names could be mixed up.
Diagnosis.
The TTA performed poorly on documenting diagnosis. The EDS had a completion rate significantly higher than that of the TTA (EDS completion rate = 88%, TTA completion rate = 48%). Figure 1 represents these findings. The main objective of a discharge summary is to inform primary care of the diagnosis to enable healthcare management, therefore it is crucial and pivotal information, for it not to be included in the discharge summary is illogical.
Co-morbidities.
Neither TTAs nor EDSs documented co-morbidities well. However the EDS, yet again, outperformed the TTA. See Figure 1. Documenting co-morbidities has important repercussions for clinical coding and financial incentives (see below).
Investigations.
Coincidently, 62% of TTAs did not document investigations that the patient had had in contrast to 62% of EDSs that did. See Figure 1. There is no guarantee for either discharge method that all investigations are listed; it is dependent upon the doctor who is producing the discharge summary.
Figure 1: Graphical representation of data
Drug history.
As previously mentioned, EDS has to have a completed drug history before the patient can be discharged and hence they have to have a 100% completion rate for this criterion. TTAs only achieved a 64% completion rate as Table 3 demonstrates.
Review of case.
This is not a criteria field on the TTA document. Therefore 86% of TTAs provided no review. 88% of EDSs did provide a case review. Just fewer than 10% of EDSs were incomplete for this item.
Discharge date.
Like the admission date, a discharge date is automatically completed on an EDS thus the completion rate is 100%. However, this date is the date in which the EDS is completed and may not be the actual day the patient leaves hospital because sometimes the EDS is completed (and so the medications dispensed) the day prior to discharge or patient discharge may be delayed. The TTA achieved a 66% completion rate.
Discharge destination.
This is not a criterion present on the TTA and thus 100% of TTAs did not fulfil this requirement. EDSs had a 98% completion rate.
Follow-up arrangements.
The majority of EDSs documented the follow-up plans for a patient (88% in total, 70% specifically for GP follow-up). 46% of TTAs documented patient follow-up required, specifically 44% for hospital follow-up. 54% of TTAs documented no follow-up. In summary, 88% of EDSs documented follow-up in comparison to 46% of TTAs. These findings may be a limitation of the study i.e. patient selection rather than failings in documentation.
Instructions for GP and functional status.
Coincidently, 92% of TTAs did not document ‘instructions for GP’ in contrast to 92% of EDSs that did. ‘Instructions for GP’ is not a criterion on the TTA document.
Functional status.
‘Functional status’ is also not a criterion on the TTA document and so all TTAs were not complete for this. 64% of EDS had a completion rate for documenting ‘functional status’. Functional status indicates a patient’s mobility status, self-care abilities, hearing and sight impairment.
Discussion:
This audit has established that the EDS has a higher completion rate for criteria on the discharge summary, significantly so for documenting diagnosis, co-morbidities, investigations, drug history and instructions for the GP.
One major concern that has been highlighted in performing this audit is the documentation of co-morbidities. Due to variations in training many doctors are unaware of how and where to enter this information on the EDS – there is a specific window that opens on the software program to input this information. Junior doctors were documenting patients’ past medical history under the field of ‘diagnosis’. Co-morbidities should not be listed under ‘diagnosis’ - this infers a new diagnosis - as they are not the acute problem.
The coding of the diagnosis [the acute problem], in context of a patients co-morbidities, results in a condition specific ‘fee’ being paid to secondary care. For example the ‘fee’ received for a patient diagnosed with a respiratory tract infection is different for that when the patient is diagnosed with a respiratory tract infection on the background of dementia. Inaccuracies in diagnosis lead to incorrect coding and measures of incidence. Co-morbidity is ‘any condition which co-exists in conjunction with another disease’. It is a requirement of the discharge summary to document certain co-morbidities – as determined by the Clinical Coding Co-morbidity Working Group (CCCWG)5. Although the discharge summary is not the recommended source documents for use in clinical coding – patients medical notes are used instead – it can help direct and inform those responsible for clinical coding. In should be borne in mind that it is the treating clinicians’ responsibility to document co-morbidities relevant to the current admission. Accurate and correct clinical coding will result in financial gains. Clinical coding has more important purposes other than just financial; it allows the monitoring of health services, epidemiological research, NHS planning of provisions, as well as clinical audit and governance6.
The amount of information documented is user dependent; the level and amount of detail written is subjective. For example there is no guarantee that all the investigations that a patient had are documented. One doctor may provide a whole paragraph to summaries [‘review of case’] whereas another may just write one sentence. Educating those whose task it is to complete the discharge summary about how vital and important it is, along with the role it serves in healthcare management, may influence the effort and time dedicated to producing an EDS. The principles of clear, complete and concise documentation should be applied to both the patients’ discharge summary and their medical notes.
Other healthcare professionals should also contribute to producing the discharge summary, in particular occupational therapists and physiotherapists who are more aware of a patients ‘functional status’ than the doctors. More accurate completion of this item could be achieved with their input.
At the moment with the EDS software system used at BHR University Hospital Trust once an EDS has been printed there is no means of changing any of the information. It cannot be re-accessed to document new or change existing details. Often an EDS will be finalized and so printed for a patient to be discharged home on that day for the discharge then to be delayed. The discharge date document on the EDS should be the actual date the patient is discharged from hospital. Therefore it should be possible to be able to re-access and change details on the EDS.
The results of this audit show that the EDS system used at BHR University Hospital Trust is better then the EDS system audited at Newham in 2008. The Newham audit did not focus on all the criteria fields of the discharge summary or compare with a hand-written discharge summary method, however there is place for comparison with the results of this audit.
Table 4: Comparison of results with findings of Newham audit
This audit has established that the EDS method provides a discharge summary more compliant with the Royal College of Physician’s recommendations on the structure and content of discharge summary in comparison to the TTA.
The EDS will inevitably replace the TTA in time. However it should be remembered that there is still a place for the TTA in clinical practice e.g. locums do not have passwords to access the software programme, if computers are not working, fail or are unavailable. At the end of the day, a discharge summary is better than no discharge summary.
Conclusion:
The findings of this audit show that the EDS is a far superior method of producing a discharge summary than the TTA. The EDS provides a more informative and detailed discharge summary, which is always legible. The discharge summary is often the only source of information a GP is given in regards to a hospital admission and therefore secondary care providers have an obligation to provide clear, complete and concise information.
This audit does highlight that there are areas for improvement and recommendation:
The importance of a discharge summary should be highlighted to all individuals whose responsibility it is to complete them. This could promote better compliance at completing all items and completing them more thoroughly.
EDS training should make users aware of the ‘co-morbidity’ section. Past medical history should not be listed under new diagnosis. This should be a compulsory part that has to be completed before an EDS can be finished.
Occupational therapists and physiotherapists should be able to complete the ‘functional status’ criterion. This should be expanded to give more information and details to primary care providers.
The documentation of certain co-morbidities (those determined by the CCCWG) should be done by ‘tick list’ selection therefore it will not rely upon the individual doctor to remember to document such co-morbidities. All the co-morbidities that should be documented could be listed and the user selects those that the patient has. This will improve the trusts performance in regards to the financial rewards linked to discharge summaries.
The audit should be performed again in 12 months to access if EDS are maintaining high completion rates, to identify further improvement in completion rates and identify any further areas for improvement or recommendation.
Discussion of both TTA and EDS could be a part of the regular weekly supervision of junior medical staff by their prospective consultants.
A discharge summary should also be checked by nursing or clerical staff prior to letting the patient leave the ward to see if all components are completed.
First described in 1971 by Spillane et al.1, painful legs and moving toes (PLMT) is a syndrome consisting of pain in lower legs with involuntary movements of the toes or feet. Pain varies from moderate discomfort to diffuse and deep and usually precedes movements by days to years. The movements themselves are often irregular and range from flexion/extension, abduction/adduction to clawing/straightening and fanning/ circular movements of the toes.1,2 This syndrome may affect one leg or spread to involve both legs.3
PMLT incidence and prevalence remain largely unknown since it is still a relatively rare disorder worldwide. Age of onset is between the second and seventh decades of life. It has been postulated that lesions of the peripheral or central nervous system after nerve or tissue damage might lead to impulse generation that subsequently causes the symptoms seen in PLMT.4 We report a case of PMLT that presented to our Neurology Movement Disorder Clinic along with a discussion on the pathophysiology, differential diagnosis and clinical management of this rare debilitating condition.
Case report
63 year old, morbidly obese (BMI 41.7) Caucasian male patient with past medical history of stroke 10 years ago, on long term anticoagulation, hypertension, type II controlled diabetes mellitus, asbestos exposure, bilateral hip and knee osteoarthritis, left total knee replacement 2 years ago, and non-traumatic ruptured Achilles tendon; presented with complaints of involuntary movements in both legs over the last 8-10 years. He had unprovoked flexion and extension of the toes along with feet movement at all times with no diurnal variation. He admitted to having a constant severe pain described as 'twisting a rubber band' with 10/10 intensity that radiated up to his calf accompanied by numbness and dorsal swelling of both feet for many months. He claimed to have partial relief whilst walking but had difficulty walking without a cane as he ‘“could not balance with constantly moving [his] feet”’. Tylenol 500mg as required and amitriptyline 20mg at night prescribed by his primary care physician provided no relief.
He also has a history of snoring, daytime fatigue, and non-restorative sleep with frequent nocturnal awakenings due to bilateral feet pain. He recalled having a stroke with transient confusion and focal hand weakness along with visual problems about 10 years previously. All laboratory and radiological investigations were negative and he recovered fully. He had previously served with the US armed forces and had been exposed to ‘Agent Orange’ in Vietnam.
He had no medical allergies and his current medications include amitriptyline 25mg at night, hydrochlorothiazide 25mg once daily, lisinopril 10mg once daily, loradatine 10mg once daily, metoprolol tartrate 20mg twice daily, simvastatin 20mg once daily, vitamin B complex one tablet once daily and warfarin once daily. He denied any history of alcohol, tobacco, or recreational drug abuse in the past. His mother had a history of hypertension and chronic low back pain; no members of his family had any neurological or movement disorders.
Physical examination revealed an alert, awake, and well oriented male with bilateral lower extremity varicose veins. He was observed to have semi-rhythmic flexion-extension and occasionally abduction movements of the phalanges, especially in the great toes. There was a profound decrease in vibration sense below both knees and it was almost absent on both feet, decreased reflexes in both feet, and absent proprioception in the phalangeal joints. He was also observed to have decreased pinprick and monofilament sensation in both legs below the knee. Bilateral ankle reflexes were diminished with negative Babinski sign. Both lower extremity dorsalis pedis and posterior tibial pulsations were palpable. He did not have any cerebellar signs. He did have pitting oedema up to his shins in both lower extremities, extending from his feet to upper one third of the legs. There were no abnormalities noted on the bilateral lower extremity EMG and there was no electrodiagnostic evidence of large-fiber neuropathy.
He was diagnosed with painful legs and moving toes syndrome and started on a trial of gabapentin 300mg at night. He was advised to increase it to 1200mg and to continue taking his amitriptyline 25mg at night. Scheduled MRI of the brain could not be done due to his morbid obesity. He was arranged follow up in three months in the clinic.
Methods
A review of published literature on PLMT was done using MEDLINE and PubMed databases. Searches were conducted to find articles from 1971 – 2010. Medical subject headings used to search the databases included PLMT with subheadings of Movement disorder, Electromyography, and Polysomnography as well as keyword search using ‘PLMT’. Single author reviewed titles and abstracts of potentially relevant articles.
Review of current literature
We reviewed approximately 19 PLMT articles that have been published to date with a total of 72 patients: 30.5% males, 69.5% females (median age 55 & 64 years,
respectively). Clinical presentations in the majority of the cases were burning pain in lower extremities and involuntary movements of the toes. The most common predisposing conditions were neuropathy and radiculopathy (see Table 1).
Table 1 - Painful Legs & Moving Toes Syndrome ~ Review of Literature (1971- 2010)
Author
Year
Sex/ Subjects
Subject age
# of cases
Clinical presentation
Spillane et al
1971
M (4) F (2)
51, 52, 52, 53 66, 68
6
Burning/throbbing LE pain followed by writhing/clawing and flexion/extension movements of the toes
Dressler et al
1994
M (4) F (16)
28, 36, 54, 73 28-76
20
Pain in LE followed by involuntary flexion/extension and abducion/adduction of the toes
Shime et al
1998
F (1)
63
1
Involuntary flexion/extension of the toes bilaterally and aching/crampy pain in both feet
Schott et al
1981
M (1) F (4)
66 56, 57, 69, 77
5
Crushing pain in both feet followed by involuntary writhing and flexion/extension of the toes; burning pain in foot followed by writhing toe movements
Montagna et al
1983
M (1) F (2)
57 74, 76
3
Burning pain in one or both LE followed by involuntary flexion/extension, abduction/adduction, and fanning/clawing of the toes
Shime et al
1998
F (1)
63
1
Involuntary flexion/extension of the toes bilaterally and aching/crampy pain in both feet
Villarejo et al
2004
M (1)
66
1
Paresthesias/burning pain in both feet followed by involuntary flexion/extension and abduction/adduction of the toes
Aizawa et al
2007
F (1)
73
1
Tingling pain in both feet followed by involuntary abduction/adduction of the toes
Guimaraes et al
2007
M (1)
60
1
Wringing-like pain in in L foot and R leg followed by flexion/extension and abduction/adduction of the toes
Eisa et al
2008
M (1) F (1)
62 76
2
Burning pain in bilateral LE followed by semirhythmic flexsion/extension of the toes
Alvarez et al
2008
M (6) F (8)
25-84 (mean 69)
14
Burning pain of LE followed by involuntary flexion/extension, abduction/adduction, fanning, or clawing of the toes
Tan et al
1996
F (1)
57
1
Severe burning pain in both LE followed by involuntary flexion/extension and abduction of the toes
Dressler et al
1994
M (4) F (16)
28, 36, 54, 73 28-76
20
Pain in LE followed by involuntary flexion/extension and abducion/adduction of the toes
Yoon et al
2001
F (1)
56
1
Burning pain in R foot with flexion and lateral deviation of the toes
Miyakawa et al
2010
M (1) F (1)
36 26
2
Burning pain in R arm followed by involuntary flexion/extension of R thumb; pain in L leg accompanied by flexion/extension and abduction/adduction of L toes
Schoenen et al
1984
M (2) F (4)
49, 74 68, 69, 71, 80
6
Burning/aching pain in LE followed by involuntary flexion/extension and writhing of the toes
Sanders et al
1999
F (1)
76
1
Deep/throbbing pain in L leg followed by invloluntary flexion/extension and abduction/adduction of L toes
Ikeda et al
2004
F (1)
75
1
Involuntary flexion/extension of the toes bilaterally followed by pain in both legs
Kwon et al
2008
F (1)
75
1
Painless wriggling movements of the toes in both feet
Total Number of articles reviewed = 19 Total Number of Cases: Male = 22 (Median Age = 55 years); Female = 50 (Median Age = 64 years) Author/Article References in chronological order (Top to below): 1, 2, 3, 4, 5, 6, 7, 8, 9, 11, 16, 17, 23, 24, 25, 29, 31, 32, 33
In 1981 Schott GD et al reported that in 3 PLMT patients the EMG revealed evidence of denervation in the affected muscles. Montagna et al of the University of Bologna, Italy reported 3 cases of PLMT that exhibited evidence of peripheral neuropathy on EMG. Polysomnography (PSG) studies on these patients showed reduced movements during sleep with increase in slow wave or rapid eye movement sleep.5 This suggested the movements could have arisen centrally.
Guimaraes et al of the Universidade Nova Lisboa, Portugal reported one patient with a history of Hashimoto’s disease whose lower extremity EMG showed spontaneous arrhythmic bursts of the affected muscles during wakefulness which disappeared during sleep6. Both suggested the movements could have arisen centrally.
Alvarez et al of the Mayo Clinic described 14 cases of PLMT in 2008 in which burning pain often preceded the movements. PSG studies confirmed these movements would also persist in light stages of sleep which pointed to a central origin.7 Eisa et al of Yale University School of Medicine, Connecticut described 2 cases of PLMT in which one patient had a past history of lumbosacral root injury and the other systemic lupus erythematosus with peripheral neuropathy on EMG.8 Interestingly, in the latter patient her pain occurred years after the onset of involuntary toe movements.8
Discussion
Spinal cord and cauda equina diseases, neuropathies, radiculopathies, drugs and other systemic diseases are the main cause of this syndrome although many cases are still idiopathic. The most common predisposing conditions were neuropathy (i.e. polyneuropathy from alcoholism, hypertrophic mononeuritis, or tarsal tunnel syndrome) and radiculopathy.7 Other etiologies include nerve root lesions, peripheral nerve trauma, spinal ganglia lesions, cauda equina lesion, Wilson’s disease, herpes zoster myelitis, HIV, neuroleptics, and chemotherapeutic agents.9-19
The involuntary movements appeared bilaterally in the toes in our patient, which suggests that central reorganization (especially in the spinal level) is the cause of PLMT. EMG and nerve conduction studies have proven helpful in demonstrating spontaneous arrhythmic bursts of affected muscles and underlying neuropathy in some patients. Although the exact mechanism remains elusive, it has been proposed that impulses generated in lesioned peripheral nerve, posterior nerve root/ganglion, or afferent fibers pass into the spinal cord - some to higher areas to cause pain, while others into the local interneuron and motor neurons to generate involuntary movements of the toes.5
In patients with clinical or electrophysiological evidence of peripheral nerve or root problem, these lesions can initiate or even alter afferent input to the spinal cord and cause subsequent central and efferent motor reorganization, which may explain the limited
success these patients had with nerve blocks or lumbar sympathetic blockade.2 Similarly, some have suggested that even though the radiation of pain following local trauma seemed to resemble causalgia,20 there was a lack of hyperpathia and changes in the soft tissue, bones, and blood vessels as well as a poor response to sympathetic blockade, thus making clinical features of PLMT inconsistent with known radicular disorders.3
Interestingly, some believed that the central nervous system played an essential role in PLMT via a central oscillator.21 It has also been proposed that hyper-excitability of the damaged peripheral nerves could cause symptoms of PLMT by way of the sympathetic nervous system. More specifically, the sympathetic nervous system could potentially serve as a bridge between injured afferent fibers and sympathetic nerve fibers,22 allowing abnormal afferent impulse to travel to efferent fibers and ultimately leading to continuous pain with involuntary movements. This was evident in the fact that lumbar sympathetic ganglion blockade provided moderate symptomatic relief for some patients even though it was short-lived.4 Interestingly, one of the explanations put forth was the possibility of spinal/supraspinal reorganization,23 which coincided with the hypothesis of central reorganization mentioned above.
Clinical Management
Numerous treatments including antiepileptics, benzodiazepines, antispasmodic agents, and antidepressants have been tried with little success.1,2,24,25 However, temporary success was observed with local anesthetic nerve blocks, epidural blocks, sympathectomy/sympathetic blockade, neurectomies, botulinum toxin type A injection, transcutaneous electrical nerve stimulation, vibratory stimulation, and epidural spinal cord stimulation.1,2,15,26,27 Analgesics, steroids, anti-inflammatory agents, vitamin B12 injections, propranolol, quinine sulphate, and local anesthetics only offered temporary relief as well.3 GABAergic agents such as gabapentin and pregabalin were the most effective in attenuating the pain and the movements, possibly via both central and peripheral mechanisms.7,24,25 It has been reported that gabapentin as high as 600mg three times daily could control symptoms of PLMT long-term.25
Treatment of PLMT has also been attempted with botulinum toxin A at the level of lumbosacral roots and peripheral nerves with moderate relief of symptoms, although toe movements did return after a few months.8 It was suggested that botulinum toxin A might have acted via reduction of muscle spindle discharge leading to decreased central sensitization, as well as antisympathetic, antiglutamergic, or anti-inflammatory effects.28
Differential Diagnosis
The syndrome of PLMT exhibits certain features similar to the restless leg syndrome (RLS). In RLS the sensation in the legs could be burning, creeping, or tingling coupled with an urge to move them, especially early in the night. Movements such as walking or stretching relieve the symptoms whereas rest makes them worse. However, in PLMT pain is severe, constant, unrelated to the sleep-wake cycle, and is not relieved by
movements or walking.23 In addition, its involuntary movements of the toes or feet also differ from the myoclonic jerks of RLS.
In conditions such as thalamic syndrome and limb pain with myoclonus, patients may experience pain and involuntary movements as well but they often occur simultaneously as opposed to in PLMT where pain often precedes the movements.17 In disorders such as Parkinson’s disease and dystonia, sustained involuntary movements in the feet can be present and pain can be an associated feature. But the movements are typically sustained muscle contractions, which are different from the typical movements associated with PLMT.
Prognosis
PLMT is a newly discovered syndrome and since there has not been a systematic study following these patients long-term, it is currently quite difficult to predict the outcome of this syndrome and its effect on lifespan, though there has yet been a report of a patient actually dying from this syndrome. However, it is known that PLMT is a debilitating condition that greatly reduces patients’ quality of life.
Conclusion
Since Spillane et al first described it in 1971, there have been more reported cases of PLMT and its variants over the years. Though much progress has been made in elucidating its etiology, its exact mechanism still remains a mystery. Similarly, even though EMG and nerve conduction studies have proven helpful in demonstrating spontaneous arrhythmic bursts of affected muscles and underlying neuropathy in some patients, diagnosis of PLMT remains largely on history and clinical presentation.
Physicians should be aware of this rare debilitating condition. It is important to consider PLMT in a patient with painful legs and/or restless leg syndrome without any significant history of neurological disease or trauma. Treatments such as different combinations of medications and invasive techniques are complex and generally lead to a poor outcome.
Thyrotoxic periodic paralysis (TPP) is an uncommon disorder characterised by simultaneous thyrotoxicosis, hypokalaemia, and paralysis that occurs primarily in males of South Asian descent.1 Many affected patients do not have obvious symptoms and signs of hyperthyroidism and hence may be misdiagnosed or overlooked on presentation.2 We hereby report a male patient who presented to us with weakness of all four limbs. The patient was evaluated and diagnosed to be having TPP.
Case History
A 30-year-old male patient, who was an agriculturist by profession, presented with weakness of all four limbs of one-day duration. The weakness first appeared in his lower limbs and then in the upper limbs. There were no sensory symptoms or bladder involvement. He was not a known hypertensive, diabetic or thyrotoxic patient. He was not on any medication for any significant illness.
On general physical examination, there was no pallor, icterus, cyanosis, clubbing, lymphadenopathy or pedal oedema. Multinodular goitre was noted on thyroid examination. There was no exopthalmos, lid lag, pretibial myxoedema or other signs of thyrotoxicosis. Thyroid bruit was absent. Pulse rate was 96/minute, blood pressure of 140/80mmHg, and respiratory rate 18/minute. On central nervous system examination, the higher mental functions and cranial nerve examination were within normal limits. Motor system examination showed the presence of flaccid quadriparesis with areflexia. Sensory system examination was within normal limits. Cardiovascular and respiratory system examination were normal.
Investigations revealed: haemoglobin (Hb) -13.1 gm%, total count (TC) - 11,400/cmm, platelet count - 49,000/cmm, random blood sugar (RBS) - 110mg/dl, blood urea - 29 mg/dl, serum creatinine - 0.8 mg/dl. Serum electrolyte profile showed sodium - 143 mEq/L, potassium - 2.2mEq/L, chloride - 112mEq/L. Serum calcium and magnesium levels were within normal limits. Electrocardiogram (ECG) was normal. Human Immunodeficiency Virus (HIV) ELISA was non reactive. Bone marrow biopsy and ultrasonography of abdomen were normal. Fine Needle Aspiration Cytology (FNAC) of thyroid showed features of hyperplastic colloid goitre. Ultrasonography of thyroid showed hyperechoic small nodules in both lobes as well as isthmus suggestive of multinodular goitre. Thyroid profile was: total T3 - 2.34 (normal: 0.60 - 1.81ng/ml), total T4 - 13.9 (normal: 4.5 - 10.9 mcg/dl), thyroid-stimulating hormone (TSH) - 0.01 (normal: 0.35 - 5.5IU/ml). Antithyroid antibodies and antiplatelet antibodies were negative. Nerve conduction study was normal. A final diagnosis of TPP with idiopathic thrombocytopenia was made.
The patient was administered 40mmol potassium chloride intravenously. He was treated with tablet carbimazole 10mg three times a day and tablet propanolol 10mg twice a day. The patient’s weakness in all four limbs improved dramatically within an hour after potassium chloride administration. As he had persistent thrombocytopenia during his stay in hospital, he was commenced on tablet prednisolone (1mg/kg body weight). His platelet count normalized in one month after which the steroid dose was tapered and stopped.
Discussion
TPP is an uncommon disorder characterised by simultaneous thyrotoxicosis, hypokalaemia and paralysis that occurs primarily in males of South Asian descent. The overall incidence of TPP in Chinese and Japanese thyrotoxic patients is 1.8% and 1.9% respectively.3, 4 Sporadic cases have been reported in non-Asian populations such as Caucasians, Afro-Americans, American Indians and Hispanics. With population mobility and admixture, TPP is becoming more common in Western countries. Many affected patients are in the age group of 20 - 40 years and do not have obvious symptoms and signs of hyperthyroidism.5 The attack is characterised by recurrent, transient episodes of muscle weakness that range from mild weakness to complete flaccid paralysis. The proximal muscles are affected more severely than distal muscles. Attacks usually first involve the lower limbs, and progress to the girdle muscles and subsequently the upper limbs. Sensory function is not affected. Although patients can present with quadriparesis that resembles Guillain-Barre Syndrome or transverse myelitis, the bladder and bowel functions are never affected. Patient may experience recurrent episodes of weakness that last from a few hours up to 72 hours with complete recovery between the attacks. In the majority of patients, deep tendon jerks are markedly diminished or absent although some patients may have normal jerks.
Patients with TPP usually experience the attacks a few hours after a heavy meal or in the early morning hours upon waking. More than two-thirds present to the emergency department between 2100 and 0900 hours; hence it was initially described as nocturnal palsy or night palsy.6 It has been shown that plasma glucose and insulin responses to meals are markedly higher in the evening than in the morning in control subjects. Such a phenomenon suggests a possible mechanism for the nocturnal preponderance of TPP. Another explanation could be the circadian rhythmicity of many hormones reaching their peak levels during sleep. Hypokalaemia is considered to be the most consistent electrolyte abnormality in TPP and a hallmark of the syndrome along with hyperthyroidism. It has been demonstrated that hypokalaemia is a result of potassium shift into cells and that it is not caused by total body potassium depletion.7 Patients with thyrotoxic periodic paralysis have an underlying predisposition for activation of Na+/K+-ATPase activity either directly by thyroid hormones or indirectly via adrenergic stimulation, insulin or exercise. Increased Na+-K+ ATPase activity is postulated to contribute to hypokalaemia.8
The majority of cases of hyperthyroidism associated with thyrotoxic periodic paralysis are due to Graves disease although other conditions including thyroiditis, toxic multinodular goitre, toxic adenoma, TSH secreting pituitary tumour, ingestion of T4 and inadvertent iodine excess have also been implicated.9 Assaying of thyroid function in patients with hypokalaemic paralysis distinguishes thyrotoxic periodic paralysis from other forms of hypokalaemic periodic paralysis. Thyrotoxic periodic paralysis occurs only in the presence of hyperthyroidism and is abolished when thyroid hormones are normalised.
Immediate therapy with potassium supplementation and beta-adrenergic blockers can prevent serious cardiopulmonary complications and may hasten recovery of periodic paralysis.10 Potassium chloride is given intravenously and/or orally. Regular potassium supplementation as prophylaxis against further paralysis when the patient has normal serum potassium level is ineffective. Effective control of hyperthyroidism is indicated to prevent recurrence of paralysis.
Conclusion
To conclude, although the association of thyrotoxicosis and periodic paralysis has been well known, TPP is often not recognised when first seen because of lack of familiarity with the disorder and partly because of the subtleness of thyrotoxicosis. When a young male of South Asian descent is initially seen with severe lower limb weakness or paralysis, TPP should be considered in the differential diagnosis and investigated for its presence since it is a curable disorder that resolves when euthyroid state is achieved.
Chronic obstructive pulmonary disease (COPD) is a debilitating condition resulting in significant morbidity and mortality. It is the fifth leading cause of death in the UK 1, estimated to be the third by 2020 2.
Definition:
COPD is a preventable and treatable disease with some extra-pulmonary effects that may contribute to the severity in individual patients Its pulmonary component is characterised by airflow limitation that is progressive and not fully reversible. There is an abnormal inflammatory response of the lung to noxious gases and particles, most commonly cigarette smoke 3.
Airflow obstruction is defined as post-bronchodilator FEV1/FVC ratio (where FEV1 is the forced expiratory volume in one second and FVC is the forced vital capacity) of less than 0.7 If FEV1 is ≥ 80% predicted, a diagnosis of COPD should only be made in the presence of respiratory symptoms 4.
Incidence/ Prevalence:
Within the UK it is estimated that 3 million people are affected with COPD 4. However, only 900,000 are diagnosed -4An estimated two million people who have COPD remain undiagnosed 4.
Causes:
90% of cases are smoking related 4, particularly those with >20 pack year smoking histories 5. Environmental and occupational factors can also play a role, including exposure to biomass fuels such as: coal, straw, animal dung, wood and crop residue which are used to cook in some countries and heat poorly ventilated homes COPD occurs in 10-20% of smokers, suggesting there is an element of genetic susceptibility 2-3, 5.
Diagnosis:
To make a diagnosis of COPD an obstructive deficit must be demonstrated on spirometry in patients over the age of 35 years with risk factors (mainly smoking) and signs and symptoms of the disease 4.
Signs and Symptoms:
Progressive dyspnoea on exertion
Chronic cough
Chronic sputum production
Wheeze
Frequency of exacerbations – particularly during winter months 4
Functional status – bearing in mind gradual progression of disability, effort intolerance and fatigue.
Features suggestive of Cor pulmonale 5:
Peripheral oedema
Elevated jugular venous pressure
Hepatomegaly
Right ventricular heave
Tricuspid regurgitation
Investigations/ Tests to consider:
Post-bronchodilator Spirometry – essential in confirming the diagnosis of COPD.
Demonstrating an obstructive picture.
FEV1 is used to assess the progression and severity of COPD, but correlates poorly with the degree of dyspnoea 3-6. (Table 1)
Pulmonary functions tests – Markers suggesting the presence of emphysema include:
Reduced TLCO and KCO due to a reduced surface area for gaseous exchange 5.
Raised Total lung capacity, residual volume and functional residual capacity due to air trapping 5.
Chest radiograph – Is not required for the diagnosis, but is recommended to exclude other conditions such as interstitial lung disease, pleural effusions or pneumothorax. It may demonstrate features of the condition, such as 3, 5:
Hyperinflated lung fields
Flattened diaphragms
Bullous changes, particularly at the apices
BODE index prognostic indicator – This is grading system shown to be better than FEV1 at predicting the risk of hospitalisation and death in patients with COPD. Patients are scored between 0 and 10, with higher scores having an increased risk of death. It encompasses 3, 5-7: (Table 2)
BMI
Airflow Obstruction – taking into account the FEV1
Dyspnoea – in accordance with the Medical Research Council (MRC) scale 5.
Exercise capacity – measured by the distance walked in 6 minutes. (Table 3)
Table 1. Severity of airflow obstruction 4
Stage
Severity post-bronchodilator
FEV1 (%) Predicted
Comments
1
Mild
≥ 80%
Only diagnosed in the presence of symptoms
2
Moderate
50- 79%
Managed within the community
3
Severe
30-49%
TLCO usually Low
Hospitalization may be needed only with exacerbations
4
Very Severe
<30%
Or FEV1 <50% with respiratory failure
Table 2. BODE Index 3, 5-8
1
2
3
FEV1 Predicted (%)
≥ 65
50- 64
36- 49
≤ 35
Distance walked in 6 minutes (meters)
≥ 350
250- 349
150- 249
≤ 149
MRC dyspnoea scale
0-1
2
3
4
BMI
≥ 21
≤ 21
Table 3. Medical research council (MRC) Dyspnoea scale 5, 8
1
Dyspnoeic only on strenuous activity
2
Dyspnoeic on walking up a slight incline or when hurrying
3
Walks slower than contemporaries on the flat, or has to stop for breath, or has to stop for breath when walking at own pace
4
Stops for breath on walking 100m or after a few minutes on walking on the flat
5
Breathless on minimal exertion e.g. dressing/ undressing. To breathless to leave the house
Differential Diagnosis:
Asthma – the most important differential diagnosis to consider.
This is steroid and bronchodilator responsive
Indicative of reversible airway obstruction.
It is not associated with smoking.
Patients with asthma may exhibit 3, 9: chronic non-productive cough, variability in breathlessness, diurnal /day-to-day variation, nocturnal wheeze and dyspnoea
However both conditions may coexist creating diagnostic uncertainty.
Alpha1 antitrypsin deficiency is an autosomal dominant condition associated with an increased risk of developing emphysema at an early age 3, 5, 9.
It can occur in non-smokers
Can be asymptomatic and thus under-diagnosed with an estimated 1 in 2000-5000 individuals being affected 5.
The disease is worse in smokers
COPD can develop in patients < 35years of age
It is associated with liver cirrhosis.
All patients with COPD should be screened.
Emphasis should be made to avoid smoking, including passive smoking.
Other conditions to consider include:
Bronchiectasis
Interstitial lung disease
Cardiac failure.
Treatment:
Goals of management include:
Early and accurate diagnosis
Improve symptoms and quality of life
Reduce the number of exacerbations
Improve mortality
Non-pharmacological management:
Smoking cessation – an accurate smoking history should be obtained, including the number of pack years smoked. All current smokers with COPD should be encouraged to stop at every opportunity, and offered smoking cessation advice. Advising the patient alone will help a certain proportion to stop, whilst referral to smoking cessation services has been shown to further increase in quit rates. There are a range of nicotine and other pharmacological therapies available such as Bupropion (Zyban®) and Varenicline (Champix®) 3-4, 7, 8.
Vaccinations – A once off Pneumococcal and annual Influenza vaccine should be offered.
Pulmonary rehabilitation – Should be offered to patients who have had a recent exacerbation requiring hospitalisation and those that have an MRC score of ≥ 3, but are still able to mobilise and thus have the potential for further rehabilitation. It is not suitable for those patients that are immobile or limited in their mobility due to symptoms of unstable angina or a recent cardiac event. Benefits are seen in terms of reduced hospital admission, improved quality of life and exercise tolerance Commitment to the programme should be relayed to the patient, and each programme should be tailored to their individual needs. This usually includes 3-5:
Disease education – which can improve the ability to manage their illness.
Exercise – tailored programmes to prevent de-conditioning and improve functional exercise capacity, dyspnoea and quality of life 4. This includes strength and endurance training of upper limbs and respiratory muscles Benefits may be seen even after 6 months.
Physiotherapy – to teach active cycle breathing techniques or to use positive expiratory pressure masks in patients with excessive sputum production.
Nutritional support – in the form of supplementation or dietician advice in patients with a suboptimal BMI. A low BMI is associated with increased mortality as it is associated with poor exercise capacity, reduced diaphragmatic mass and impaired pulmonary status. Alternatively, weight loss is recommended in patients who are in the obese range.
Psychological – Assessment for support at home, introduction of patients to day centres, assessing for features of depression and anxiety, and aiding in the obtainment of a car disability badges may require referral to occupational therapy and social services.
Travel advice – Patients who are planning air travel and have FEV1 <50%, Sa02 < 93%, or are on long term oxygen therapy (LTOT) should undergo formal assessment -4Patients with bullous disease should be informed that they are at increased risk of pneumothorax during high altitude flights 4.
Pharmacological management:
Bronchodilators – Provide long term benefit in reducing dyspnoea. This is not reflected in improvements in FEV1 as it may not show reversibility 4.
Start with an inhaled SABA (short-acting beta2-agonist) or a SAMA (short-acting muscarinic antagonist) on an as required basis for symptomatic relief. If symptoms remain despite regular SABA therapy (i.e. four times a day), then treatment will need to be stepped up.
If symptoms persist or if the patient is having recurrent exacerbations add in a LABA (long-acting beta2 agonist) or a LAMA (long acting muscarinic antagonist).
If symptoms continue, add in a LAMA if already on a LABA (or vice versa).
If FEV1 <50% add in an inhaled corticosteroid (ICS). This can be offered as a combination inhaler.
Inhaled therapy should offer sufficient bronchodilator response. A spacer can be used for those with poor technique. Nebulisers are reserved for patients who demonstrate respiratory distress despite maximal inhaled therapy, and for those that show an improvement in symptoms or exertional capacity 4.
Diagram 1: Summary of step-by-step management 4
Corticosteroids – A short course of oral steroids may be used during exacerbations. A maintenance course however is not recommended Any patients on long term steroids should be weaned off.
Mucolytic agents – May be considered in patients with a chronic cough who have difficulty expectorating. They should only be continued if symptomatic benefit is evident, otherwise they can be stopped. There is no evidence to show that they reduce the exacerbation frequency.
Theophylline – Should only be offered in people that are unable to use inhaled therapy or after trials of SA and LA bronchodilators 4. The same generic brand should be prescribed as individual brands will have different efficacy. It is usually used as an adjunct to beta2-agonists and muscarinic antagonists. Interactions with macrolides and fluroquinolones and other drugs are also common, and as such the theophylline dose should be reduced if interactions are known. Caution should be taken in prescribing theophylline in the polypharmacy patient 3, 5. Little evidence has been shown to support theophylline usage in COPD (compared to asthma), however it is used for its anti-inflammatory effects As such levels are only performed if toxicity is suspected and should not be adjusted if in the sub-therapeutic range.
Oxygen therapy – Patients should be assessed for long-term oxygen therapy(LTOT) if they exhibit 4:
Severe airflow obstruction
Features of Cor pulmonale
Hypoxaemia (Sa02 ≤ 90%)
Cyanosis
Polycythaemia
Patients with stable COPD who are receiving maximum medical therapy are assessed by measuring arterial blood gases taken on two separate occasions at least 3 weeks apart. To meet the criteria patients must have 4:
A Pa02 < 7.3 kPa when stable, or
A Pa02 >7.3 but < 8.0 kPa when stable and:
Pulmonary hypertension or
Peripheral oedema or
Secondary polycythaemia or
Nocturnal hypoxaemia
LTOT should be used for a minimum of 15L per day, including during sleep 3-4.
Patients who continue to smoke should be made aware of the serious risk of facial injuries due to the highly flammable nature of oxygen.
When to refer:
Referrals for specialist advice or specialist investigations may be appropriate at any stage of the disease.
Other possible reasons for referral 4
§ Diagnostic uncertainty
§ Suspected severe COPD
§ Onset of Cor pulmonale
§ Rapid decline in FEV1
§ Assessment for LTOT, home nebulisers or oral corticosteroid therapy
§ Symptoms that do not correlate to lung function deficit
§ Pulmonary rehabilitation assessment
§ Frequent infective exacerbations
§ Family history of alpha-1-antitrypsin deficiency
§ Haemoptysis
§ Onset of symptoms < 40 years
§ Bullous lung disease
§ Assessment for lung volume reduction surgery/ lung transplantation
§ Dysfunctional breathing
Follow-up:
Patients with stable mild-moderate COPD should be reviewed by their general practitioner at least once a year and those with severe COPD twice yearly.
At each visit 4:
An opportunity should be taken to ask about their current smoking status and the desire to stop.
Assessment of adequate control of symptom: dyspnoea, exercise tolerance and the estimated number of exacerbations per year.
Assessment of inhaler technique.
To assess the effects/side effects of each drug treatment.
The need for pulmonary rehabilitation.
For those patients with very severe airflow obstruction (FEV1 < 30%), the above still remains, in addition to the assessment of 4:
Features of Cor pulmonale
Nutritional status
The need for LTOT
Signs of depression
The need for occupational therapy and social services input
Referral to specialist and their services
Measurements of:
FEV1 and FVC
BMI
MRC dyspnoea scale
Sa02 via pulse oximetry
Those patients requiring long term non-invasive ventilation will be reviewed by a specialist on a regular basis.
Interest in cross-species transplantation has recently been rekindled1. This is due to many developments including the shortage of donor organs, advances in transplant medicine, investment in biotechnology research, and the non-availability of more ethically suitable alternatives to human organs. Increasing success rates in allotransplantations (organs from different member of the same species) has increased the demand on donor organs1, 2. Other types of transplantation include autotransplants (a person’s own organs or tissues are used for transplantation) and isotransplants (organs from one person are transplanted into another genetically identical person, like an identical twin). These options are limited in terms of body parts used and numbers.
Good facts inform good ethics. It is therefore obligatory to look into the current research knowledge about xenotransplants (organs from one species to another, for example animal to human) in more detail. The advocates of xenotransplantation argue that it could provide organs “relatively quickly” and hence save more lives. If animal organs were easily available for transplantation most eligible recipients would receive the transplantation much earlier on in their illness. It is argued that this may decrease distress and suffering. Whilst xenotransplantation may theoretically increase the survival time, it is unclear, however, whether the negative impact on recipients’ quality of life due to long-term immunosuppressant therapy and the risk of zoonotic infections would in fact worsen the overall long-term outcome3. Recent research suggests that xenotransplantation may be associated with the transmission of pig microorganisms including viruses, bacteria, fungi, and parasites. Because of the recipient’s likely immunosuppressed state, infection and pathologic consequences may be more pronounced. Transmission of most microorganisms with the exception of the porcine endogenous retroviruses may be prevented by screening the donor pig and qualified pathogen-free breeding. However, porcine endogenous retroviruses represent a special risk as they are present in the genome of all pigs and infect human cells in vitro. Until now, no porcine endogenous retrovirus transmission was observed in experimental and clinical xenotransplantations as well as in numerous infection experiments4. Nevertheless, strategies need to be developed to prevent their transmission to humans. It is equally possible that many eligible recipients may be denied having a trial of xenotransplantation by doctors who believe that there is an unfavourable risk-benefit ratio. The limited long-term data on outcomes of xenotransplants thus renders ethical analysis difficult.
There is some evidence to suggest that the recipients of animal organ donation may develop a different self image with possible consequences for their identity5,6. This happens with human organs at times, but may be a more significant problem with animal organs, as the recipient knows that they have been given a non-human organ. Loss of identity jeopardises the core principle of autonomy, which underpins all medical treatment.
The risk of zoonosis to the recipient and to the wider society cannot be accurately estimated7. Hence there is a requirement for vigilant post-operative monitoring5 with a possibility of engaging article5 and 8 of the European Convention of Human Rights (for England and Wales: Human Rights Act 1998)†. Article 12 may also be engaged as the recipients may be restricted from having physical relationships, carrying out their routine day to day activities and socialisation. This is because the prevention of possible risk to the wider public from zoonosis may require the recipient to be put under restrictions with regard to their engagement with others. This may include restrictions to go out, which can result into de facto temporary detentions at home. Hence consenting to xeno-transplantation would be “binding and contractual” over a long period of time. The subject may not have the right to withdraw. This is entering into a de facto contract with potential restrictions or even deprivation of human rights. This would restrict the ability to give informed consent even for a well informed patient, as it is difficult to be fully appreciative of future restrictions of one’s liberty.
Autonomous decision making and thus informed consent may also be put at risk by other factors surrounding xenotransplantation. The decision to embark on xenotransplantation may be primarily driven by an instinctual wish to survive due to a lack of other viable alternatives. Patients in these circumstances may have little or no consideration to medium and long-term effects on themselves and society. However, it is the consideration of such long-term consequences that make a truly autonomous decision, and differentiate it from a decision that is purely based on immediate instinct. Whilst the wish to survive is legitimate it is difficult to make decisions free of the pressure to survive when there is a lack of alternatives.
It also brings up an even more important question: Can any person everconsent to a future restriction or deprivation of their liberty or other human rights? Even if there were an option to define acceptable future restrictions it would be likely that patients could still challenge the legality of any such agreements. They could quite reasonably argue that they have agreed to the restrictions under duress because of a lack of viable alternatives to their xeno-transplants.
Xenotransplantation touches questions of utilitarianism (greatest good for the greatest numbers) and public protection2. Utilitarianism takes into account the reasonable interests of society in good outcomes, fairness in the distribution of resources, and the prevention of harm to others. The Nuffield council on bio-ethics embraces a utilitarian approach. However, there are limits to the utilitarian argument for xenotransplants. Even if they were widely available, the treatment would be immensely expensive. Production of a pathogen free donor organ would involve rearing animals in strictly controlled environments, subjecting them to rigorous standards of examination and surveillance. The additional costs of developing a sustainable work force to provide transplantation and post-transplant surveillance of the patient and the community would be high. The insurance providers may not cover expenses of a xenotransplant. Public health care providers may decline to provide this treatment as it may not be recommended by expert groups as cost effective. Xenotransplantation may commence in the developing world where the regulations are lax and the poor can be more easily exploited8. Patients who would potentially benefit from xenotransplantation may not be able to afford it due to its cost with serious implications for fairness.
Xenotransplantation also raises other ethical questions in relation to the wider community. We have seen that consent of an individual to a xenotransplant has significant bearing on the protection of society7. Should the members of a community therefore be consulted if there were any xeno-transplantation experiments in their region? The risk is primarily due to the risk of zoonotic infections, the need for surveillance, and possible quarantine of contacts7,9. In addition, if health authorities were to fund expensive experimental interventions like xenotransplantation, other routine treatments of greater potential benefits to society may be jeopardised. Society may also have views about particular animals being used as donor animals10. For example religions like Islam and Judaism may feel that pigs are ‘ritually unclean’. They may therefore not approve of certain animals to be used for donation, and more worryingly may fail to socially accept recipients with such ‘unclean’ transplants11.
From a deontological perspective (this judges the morality of an action based on the action's adherence to a ruleor principle) some authors assert that animals have rights similar to those considered appropriate for humans12,13. The protection of animals has legal status in many countries. Consequentialists may view the suffering and death of an animal as acceptable for the betterment of a human patient, as they would judge the morality of an action primarily by its end result. They would argue that potential benefits and improvement in human welfare arising from xenotransplantation may justify the loss of animal life. However, this will never satisfy the animal rights lobby; especially as whilst minimising the risk of acquired infections, the animals have to forgo greater suffering in the form of isolation, monitoring and investigations. Furthermore, genetic modification can have both immediate and long-term negative effects on animals.
In summary, xenotransplantation has significant ethical consequences. On an individual level, there are the questions of pressure to consent that may negate autonomy and the validity of that consent as well as the difficulties that arise when patients are asked to consent to future restrictions of their human rights. On a societal level there are questions of cost and benefit analysis as well as risks from zoonotic infections. In addition, questions of animal rights need to be addressed before any programs are likely to go ahead.
†Appendix of articles of the Human Rights Act.
Article 8 of the Human Rights Act 1998 (The right to respect for private and family life, home and correspondence)
Article 5 (The right to liberty).
Article 12 (The right to marry and found a family)
Introduction A hydatid cyst is the larval stage of a small tapeworm, Echinococcus granulosus. This is an emerging zoonotic parasitic disease throughout the world, thought to cause an annual loss of US $193,529,740.1 Hydatid cysts are more prevalent in Australia, New Zealand, South America, Russia, France, China, India, the Middle East and Mediterranean countries.2,3,4 They are most commonly (about 50-75%) seen in children and young adults.4,5,6 The liver is the most common organ involved (77%), followed by the lungs (43%).7,8,9,10 However, some researchers report that the lung is the most common organ involved in children, possibly due to bypass of the liver by lymphatics, and higher incidental findings in the lungs when children are assessed for other respiratory infections.8,11,12,13 Hydatid cysts have been reported in the brain (2%),3,4,5,7,8,14,15 heart (2%),8,10,13,16 kidneys (2%),9,10,11 orbit (1%),17,18 spinal cord (1%),3,19 spleen,4 spine,3,8 spermatic cord20 and soft tissues.8 However, in the Mediterranean region, the incidence of brain hydatid cysts have been reported higher (7.4-8.8%).21 Surgery remains the treatment of choice, although recently some new modalities have been described.5,8,22 Careful removal of the lesion is of considerable importance, otherwise fatal complications are inevitable.23,24,25 We describe the case of a 6 year old boy who came to our department with various neurological manifestations. The main purpose of this study is to demonstrate the unusual symptoms of the patient and the enormity of the operated cyst, which was fully resected without rupture. Case Report A 6-year-old boy was referred to our Neurosurgery Department with a four week history of ataxia and left sided weakness. His vital signs were normal and his Glasgow Coma Scale (GCS) was 15. The symptoms had started about six months ago with numbness and parasthesia of the toes. Subsequently he developed intermittent nausea and vomiting. He then started to develop left sided weakness and finally ataxia. He also had a few focal convulsions but did not complain of headache. Fundoscopy revealed bilateral frank papilloedema. On examination, the patient had nystagmus and a positive Romberg’s test. Laboratory data showed mild leucocytosis without any significant rise in eosinophils, and liver enzymes were normal. The enzyme-linked immunosorbent assay (ELISA) for hydatid cysts was negative. Plain chest X-ray and ultrasound scan of the abdomen and pelvis were also normal. Brain computed tomography (CT scan) of the frontal and parietal lobes demonstrated a single large, spherical, well-defined, thin-walled homogenous cyst, with an inner density similar to that of cerebrospinal fluid (CSF), and a wall which did not show enhancement [fig 1(a)]. This cystic structure caused a mass effect and a midline shift towards the left, as well as hydrocephalus, possibly due to obstruction. Magnetic resonance imaging (MRI) of the brain showed cystic signal intensity similar to that of CSF, without ring enhancement or oedema [fig 2]. Fig 1 (a): Pre-operative unenhanced CT scan which shows a large CSF density cystic lesion on the right side causing mass effect and midline shift to the left. There is no peri-lesional oedema. Fig 1 (b): Post-operative CT scan of the lesion shows a large void which can lead to dangerous collapse. Mild haematoma is also seen. Fig 2 (a): T1-weighted axial MRI of the brain demonstrates a cyst density similar to CSF. Fig 2 (b): T2-weighted MRI shows no ring enhancement or oedema. The periventricular hyperintensity of the left side is probably due to obstructive hydrocephalus. Fig 3: This shows the cyst removed in toto after operation. The cyst appears creamy and smooth. After summation of all the above data, the diagnosis of a hydatid cyst was made and a right frontotemporoparietal craniotomy was performed. A large cystic structure (14×14×12 cm) was delivered with utmost care to avoid rupture and spillage [fig 3]. A hydatid cyst was confirmed by pathology reports. A post-operative CT scan showed a large space without any residual matter [fig 1(b)]. Post-operatively, albendazole 15 mg/kg was started and continued for four weeks. The patient showed marked improvement in his neurological deficit and was discharged after one week with close follow-up.Discussion/Review Of LiteratureLife CycleHydatidosis is caused by Echinococcus granulosus, which occurs mainly in dogs. Humans who act as intermediate hosts get infected incidentally by ingesting eggs from the faeces of the infected animal. The eggs hatch inside the intestines and penetrate the walls, entering blood vessels and eventually reach the liver where they may form cysts or move on towards the lungs. Even after pulmonary filter, a few still make it to the systemic circulation and can lodge in almost any part of the body, including the brain, heart and bones.2,3,8,14,16,26 Brain hydatid cysts are relatively rare and only account for up to 2% of total cases.4,5,7 The actual percentage may be higher than what we have in literature, due to under-reporting. Brain hydatid cysts can be primary (single) or secondary (multiple).2,3,4,5,7 The latter are thought to arise from the multiple scolices released from the left side of the heart following cyst rupture in the heart2,3,5,27 or due to spontaneous, traumatic or surgical rupture of a solitary cranial cyst.3,5 Cysts mostly involve the territory of the middle cerebral artery4,7 but other regions like intraventricular, posterior fossa and the orbit have also been reported.15,17,18,28 The wall of the cyst consists of an inner endocyst (germinal layer) and outer ectocyst (laminated layer). The host reacts to the cyst forming a pericyst (fibrous capsule), which provides nutrients to the parasite. In the brain, due to minimal reaction, the pericyst is very thin. The endocyst produce scolices which bud into the cyst cavity and may sediment within the hydatid cavity, commonly known as hydatid sand.3,14,29,30Presentation and DiagnosisMost hydatid cysts are acquired in childhood and are manifested during early adulthood.8,29 Cysts develop insidiously, usually being asymptomatic initially, and present with protean clinical and imaging features.3,5,6 In previous studies the most common presenting symptoms were headache and vomiting.4,5,7,14,15,28 Also in the literature, patients reported ataxia, diplopia, hemiparesis, abducens nerve palsy and even coma.5,7,15,28 Surprisingly, in the present study the patient did not have a headache and presented with parasthesia and numbness of the toes. Later he developed left sided weakness, convulsions and finally ataxia, which correlate with previous studies. Diagnosis of a hydatid cyst can sometimes be confused with other space occupying lesions of the brain, especially abscesses, neoplasms and arachnoid cysts.14,31 In this study the patient had bilateral frank papilloedema which is also mentioned in earlier reports.4,28 The Casoni and Weinberg tests, indirect haemagglutination, eosinophilia and ELISA are used in diagnosing hydatid cysts, but as brain tissue evokes minimal response many results tend to be false negatives.2,5,8,25 In our case also, serology for hydatid cyst was negative. CT scan and MRI are used frequently in diagnosing the cystic lesions.3,8,14,23,32,33 However, MRI is considered superior in demonstrating the cyst rim.5,8,11,21,32,34 On CT scan, a solitary cyst appears as well-defined, spherical, smooth, thin-walled and homogeneous, with an inner density similar to CSF, and non-enhancing walls.11,29,32The wall may appear iso-dense to hyper-dense on CT scan3,8, and rarely, may become calcified.11,29,32 There is usually no surrounding brain parenchymal oedema, which if exists along with ring enhancement, indicates inflammation and infection. 7,11,32,33,34,35 Ring enhancement and peri-lesional oedema differentiates brain abscesses and cystic neoplasms from uncomplicated hydatid cysts.3,8 These findings can in fact sometimes cause dilemma and misdiagnosis and lead to catastrophic events.14 The cyst shows low signal intensity on T1-weighted, and high signal intensity on T2-weighted MRI.2 MRI may also show peri-lesional oedema not seen on regular CT scan imaging.7 MRI may prove superior in determining exact cyst location, presence of super-added infections and cystic contents, and also in surgical planning and ruling out other diagnostic possibilities.14,33 We strongly recommend MRI for better evaluation of cystic brain lesions. Spontaneous cystic rupture can lead to different appearances depending on which layers have been obliterated, and produce some specific signs.3 When only the endocyst ruptures, cyst contents are held by the outer pericyst giving a peculiar water lily sign, which is pathognomic.3,8TreatmentThough still in infancy, medical therapy for small or inoperable brain hydatid cysts has been promising. Albendazole alone or in combination with other compounds, such as praziquantel, has been reported with favourable results as an adjunct and, in certain circumstances, as the primary mode of treatment.2,36,37,38 It is reported that albendazole results in the disappearance of up to 48% of cysts and a substantial reduction in size of the cysts in another 28%.2 The duration of the treatment is four weeks or more, and recently many authors have favoured a prolonged therapy. The change in levels of cyst markers such as alanine, succinate, acetate and lactate, measured before and during treatment on Proton Magnetic Resonance Spectroscopy (MRS), correlate well with shrinkage and resolution of cyst findings on conventional MRI and help in evaluating the efficacy of chemotherapy.39 Cysts may drain into ventricles or rupture completely, causing spillage of contents into the subarachnoid space, leading to fatal anaphylactic shock, meningitis or local recurrence.3,5,22,25 Surgery is the mainstay for treating intracranial hydatid cysts and the aim is to excise the cysts entirely without rupture, which can otherwise lead to catastrophic events as described earlier 2,3,14,25. The Dowling-Orlando technique remains the preferred method, in which the cyst can be delivered by lowering the head of the operating table and instilling warm saline between the cyst and the surrounding brain.40 Even minimal spillage can cause deleterious effects (1 ml of hydatid sand contains 400,000 scolices).14 The thin cyst wall, periventricular location and micro-adhesions to the parenchyma are the main problems encountered during the surgical procedure.1,22 The large cavity remaining after the cystic removal can lead to many serious complications, such as cortical collapse, hyperpyrexia, brain oedema and cardio-respiratory failure.5 Recurrence remains a major concern, which is managed by both antihelminthic chemotherapy and surgery. In a study conducted by Ciurea et al, 25% of the patients had recurrence, which highlights the need for long term follow up.23 In the present study, due to the huge size of the cyst and progressive neurological deficit, it was not wise to completely rely on medical therapy. Surgery was performed and post-operatively albendazole was started as an adjunct. We recommend that for treating brain hydatid cyst, the size of the cyst, multiplicity, location and neurological deficit must all be taken into consideration.
Cervicogenic headache (CH) refers to head pain originating from the pathology in the neck.1 However, the diagnosis of CH is still controversial 2,3 and it is often misdiagnosed. The author was called to consult a patient in a university hospital not so long ago. The patient was a 28-year-old female with a history of headache for six months. Her headache was described as continuous, dull and achy. It was mainly in the right side occipital and parietal areas. Sometimes she felt a headache behind the eyes. Her headache got worse periodically, several times a month, with nausea, photophobia, and phonophobia. She had no previous history of headache until a whiplash injury six months before. She had been diagnosed as having ‘migraine’ and ‘post-traumatic headache.’ She had used all anti-migraine medications. ‘Nothing was working.’ The patient was admitted into hospital because of ‘intractable headache.’
On the day when the author saw the patient, she was lying on the bed, with the room light turned off and a bed sheet covering her head and eyes. She was given Dilaudid, 2mg/h continuous intravenous (IV) drip, for the headache. The patient had normal results from magnetic resonance imaging (MRI) of the brain and lumbar puncture. According to the patient, no doctors had touched the back of her head and upper neck since admission. The author examined the patient and found a jumping tenderness over the right greater occipital nerve. The patient was given 2ml of 2% lidocaine with 40mg of Kenalog for the right greater occipital nerve (GON) block. Her headache was gone within five minutes and the Dilaudid drip was immediately discontinued. At follow-up four weeks later, the patient was headache-free. This was a typical missed case of CH (occipital neuralgia).
The concept of CH was first introduced by Sjaastad and colleagues in 1983.4 The International Headache Society published its first diagnostic criteria in 1998 which was revised in 2004.5 Patients with CH may have histories of head and neck trauma. Pain is often unilateral. Headache is frequently localized in the occipital area. However, pain may also be referred to the frontal, temporal or orbital regions. Headaches may be triggered by neck movement or sustained neck postures.6 Headache is constant with episodic throbbing attacks, like a migraine. Patients may have other symptoms mimicking a migraine such as nausea, vomiting, photophobia, phonophobia, and blurred vision. Due to the fact that there is a significant overlap of symptoms between CH and migraine without aura, CH is often misdiagnosed as migraine. CH is commonly found in patients after whiplash injuries, especially in the chronic phase.7
Anatomical studies have provided a basis for the pathogenesis of CH. The suboccipital nerve (dorsal ramus of C1) innervates the atlanto-occipital (AO)joint and dura matter over in the posterior fossa. Therefore, a pathologic condition of AO joint is a potential source for occipital headache. It has been reported that pain from the C2-3 and C3-4 cervical facet joints can radiate to the occipital area, frontotemporal and even periorbital regions. Even pathology in C5 or C6 nerve roots have been reported to cause headache.8 The trigeminocervical nucleus is a region of the upper cervical spinal cord where sensory nerve fibres in the descending tract of the trigeminal nerve (trigeminal nucleus caudalis) are believed to interact with sensory fibres from the upper cervical roots. This functional convergence of upper cervical and trigeminal sensory pathway sallows the bidirectional referral of painful sensations between the neck and trigeminal sensory receptive fields of the face and head.
Clinicians should always put CH in the list of differential diagnoses when they work up a headache patient. A history of head/neck injury, and detailed examination of the occipital and upper cervical area, should be part of the evaluation. Patients with CH may have tenderness over the greater or lesser occipital nerve, cervical facet joints and muscles in the upper or middle cervical region. Diagnostic imaging such as X-ray, computerized tomography (CT) and MRI cannot confirm CH, but can lend support to its diagnosis.
Treatment of CH is empirical. This headache does not respond well to migraine medications. Treatment should be focused on the removal of the pain source from the occipital-cervical junction. Initial therapy should be directed to non-steroidal anti-inflammatory drugs (NSAIDs) and physical therapy modalities.9 GON block is easy and safe to perform in office.10 It is effective for the treatment for occipital neuralgia and CH.11 The author followed a group of patients after GON block. The pain relief effects of GON block lasted an average of 31 days (unpublished data). If patients do not respond to GON block, diagnostic medial branch block and radiofrequency (RF) denervation of the upper cervical facet joints can be considered. Early studies have reported positive results.12 A subsequent randomized study found no benefit of RF. However, there were only six cases in each group,13 which significantly limited the power and validity of the conclusion from that study. Surgical treatment of cervical degenerative disc disease may offer effective pain relief for CH. Jansen14 reported 60 cases of CH patients treated mainly with C4/5, C5/6 and C6/7 nerve root decompression. More than 63% patients reported long lasting pain freedom or improvement (> 50%).
CH is common, with a prevalence of 0.4% and 2.5% in the general population. However, compared with other common pain conditions, CH is less studied. A Medline search found 6818 abstracts for migraine in 2009, whereas only 86 abstracts on CH were found. CH has not been well studied and it is often misdiagnosed. It is time to call for more attention.
Introduction: Most experts define infertility as not being able to get pregnant after at least one year of trying. Women who are able to get pregnant but then have recurrent miscarriages are also said to be infertile. The infertility definition made a difference. The World Health Organization definition based on 24 months of trying to get pregnant is recommended as the definition that is useful in clinical practice and research among different disciplines.1Magnitude of the Problem: It is a growing problem and across virtually all cultures and societies almost all over the World and affects an estimated 10%-15% of couples of reproductive age. In recent years, the number of couples seeking treatment for infertility has dramatically increased due to factors such as postponement of childbearing in women, development of newer and more successful techniques for infertility treatment, and increasing awareness of available services. This increasing participation in fertility treatment has raised awareness and inspired investigation into the psychological ramifications of infertility. Consideration has been given to the association between psychiatric illness and infertility. Researchers have also looked into the psychological impact of infertility per se and of the prolonged exposure to intrusive infertility treatments on mood and well-being. There is less information about effective psychiatric treatments for this population; however, there is some data to support the use of psychotherapeutic interventions2. Why infertility has a psychological effect on the couple? Parenthood is one of the major transitions in adult life for both men and women. The stress of the non-fulfilment of a wish for a child has been associated with emotional squeal such as anger, depression, anxiety, marital problems and feelings of worthlessness. Partners may become more anxious to conceive, ironically increasing sexual dysfunction and social isolation. Marital discord often develops in infertile couples, especially when they are under pressure to make medical decisions. Couples experience stigma, sense of loss, and diminished self-esteem in the setting of their infertility3. Male and female partner respond differently: In general, in infertile couples women show higher levels of distress than their male partners4; however, men’s responses to infertility closely approximate the intensity of women’s responses when infertility is attributed to a male factor3. Both men and women experience a sense of loss of identity and have pronounced feelings of defectiveness and incompetence. Women trying to conceive often have clinical depression rates similar to women who have heart disease or cancer. Even couples undertaking IVF face considerable stress. Emotional stress and marital difficulties are greater in couples where the infertility lies with the man. Therefore the psychological impact of infertility can be devastating to the infertile person and to their partner. Factors influencing psychological stress: According to one study done in Sweden, three separate factors seem to contribute to the psychological stress men and women experience as a result of their infertility. The three factors, in order of importance for the women were,1. "Having Children is a Major Focus of Life"2. "The Female Role and Social Pressure"3. "Effect on Sexual Life"The men in the study reversed the order of importance of factors 1 and 2. The third factor was equally significant to both the men and women. It was also shown that women experienced their infertility more strongly than the men. Women also showed a more intense desire to have a baby than men.5.Behaviour of the couple as a result of infertility: Stress, depression and anxiety are described as common consequences of infertility. A number of studies have found that the incidence of depression in infertile couples presenting for infertility treatment is significantly higher than in fertile controls, with prevalence estimates of major depression in the range of 15%-54%6,7,8,9. Anxiety has also been shown to be significantly higher in infertile couples when compared to the general population, with 8%-28% of infertile couples reporting clinically significant anxiety9,10. The causal role of psychological disturbances in the development of infertility is still a matter of debate. A study of 58 women from Lapane and colleagues reported a 2-fold increase in risk of infertility among women with a history of depressive symptoms; however, they were unable to control for other factors that may also influence fertility, including cigarette smoking, alcohol use, decreased libido and body mass index11. Psychological factors may also affect the reproductive capacity: Although infertility has an effect on a couple’s mental health, different psychological factors have been shown to affect the reproductive ability of both partners. Proposed mechanisms through which depression could directly affect infertility involve the physiology of the depressed state such as elevated prolactin levels, disruption of the hypothalamic-pituitary-adrenal axis, and thyroid dysfunction. One study of 10 depressed and 13 normal women suggests that depression is associated with abnormal regulation of luteinizing hormone, a hormone that regulates ovulation12. Changes in immune function associated with stress and depression may also adversely affect reproductive function13. Further studies are needed to distinguish the direct effects of depression or anxiety from associated behaviours (e.g., low libido, smoking, alcohol use) that may interfere with reproductive success. Since stress is also associated with similar physiological changes, this raises the possibility that a history of high levels of cumulative stress associated with recurrent depression or anxiety may also be a causative factor. Result of treatment: While many couples presenting for infertility treatment have high levels of psychological distress associated with infertility, the process of assisted reproduction itself is also associated with increased levels of anxiety, depression and stress14. A growing number of research studies have examined the impact of infertility treatment at different stages, with most focusing on the impact of failed IVF trials15. Comparisons between women undergoing repeated IVF cycles and first-time participants have also suggested that ongoing treatment may lead to an increase in depressive symptoms16. The data, however, is still controversial since other studies have found minimal psychological disturbance induced by the infertility treatment process or IVF failure17,18. In light of the discrepancy in results, there has been increasing interest in the factors that contribute to drop out from infertility treatment since this population is often not included or decline to participate in studies. Whereas cost or refusal of physicians to continue treatment have been cited as reasons for discontinuing treatment, recent research suggests that a significant number of drop outs are due to psychological factors19,20,21. The outcome of infertility treatment may also be influenced by psychological factors. A number of studies have examined stress and mood state as predictors of outcome in assisted reproduction. The majority of these studies support the theory that distress is associated with lower pregnancy rates among women pursuing infertility treatment7,16,22,23,24,25. Conclusion: In light of all the data suggesting that psychological symptoms may interfere with fertility, success of infertility treatment and the ability to tolerate ongoing treatment; interest in addressing these issues during infertility treatment has grown. Since psychological factors play an important role in the pathogenesis of infertility, exploration of this is also an important task to manage this devastating problem, which has cultural and social impact.
Both Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) are diseases characterized by a high global prevalence, complex clinical course, and limited effectiveness of currently available antiviral therapy. Approximately 2 billion people worldwide have been infected with the HBV and about 350 million live with chronic infection. An estimated 600,000 persons die each year due to the acute or chronic consequences of HBV 1, 2. WHO also estimates that about 200 million people, or 3% of the world's population, are infected with HCV and 3 to 4 million persons are newly infected each year. This results in 170 million chronic carriers globally at risk of developing liver cirrhosis and/or liver cancer 3, 4. Hence, HBV and HCV infections account for a substantial proportion of liver diseases worldwide.
These viruses have some differences, like HBV belongs to the Hepadnaviridae family and HCV belongs to the Flaviviridae family. HBV has a circular, partially double-stranded DNA genome of approximately 3.2 kb, whereas HCV has a single RNA strand genome of approximately 9.6 kb. HBV and HCV show some common biological features. Both HBV and HCV show a large heterogenicity of their viral genomes producing various genotypes. Based on genomic nucleotide sequence divergence of greater than 8%, HBV has been classified into eight genotypes labeled A through H 5,6,7,8. Different isolates of HCV show substantial nucleotide sequence variation distributed throughout the genome. Regions encoding the envelope proteins are the most variable, whereas the 5’ non-coding region (NCR) is the most conserved 9. Because it is the most conserved with minor heterogeneity, several researchers have considered the 5’ NCR the region of choice for virus detection by reverse transcription (RT)-PCR. Sequence analysis performed on isolates from different geographical areas around the world has revealed the presence of different genotypes, genotypes 1 to 6 10. A typing scheme using restriction fragment length polymorphism analysis of the 5’ NCR was able to differentiate the six major genotypes 11. Hence both HBV and HCV genotypes display significant differences in their global distribution and prevalence, making genotyping a useful method for determining the source of HBV and HCV transmission in an infected localized population 12 - 27.
Many studies have been conducted to study the prevalence of HBV and HCV co-infection among HIV-infected individuals and intravenous drug users globally 28 -3 4.There are only a few studies relevant to the epidemiology of these types of infection in the normal healthy population 35,36,37. The objective in this study was to determine the seroprevalence of HBV and HCV, co-infection of both these viruses and their genotypes, among an apparently healthy female population as well as from known HBV patients in Karachi, a major city in the province of Sindh, Pakistan. This study is also aimed at providing the baseline data on HBV/HCV co-infection, in order to gain a better understanding of the public health issues in Pakistan. We evaluated the antigen, antibody and genotypes of both HBV and HCV in 144 otherwise healthy female individuals and 28 diagnosed HBV patients.
Materials and Methods:
Study duration:From March 2002 to October 2006 & April 2009
Study participants: Total 4000blood serum samples were collected from healthy female student volunteers and 28 serum samples (April 2009) from already diagnosed Hepatitis B positive patients, aged 16 to 65 years from two Karachi universities and one Karachi hospital. University samples were obtained through the Department of Microbiology, University of Karachi and the Department of Microbiology, Jinnah University for Women. Hospital samples were obtained through the Pathological Laboratory of Burgor Anklesaria Nursing Home and Hospital.
Ethical Consent: Signed informed consent forms were collected from all volunteers following Institutional Review Board policies of the respective institutes.
Pre study screening:All 4028 volunteers had health checkups by a medical doctor before collection of specimens, they were asked about their history of jaundice, blood transfusion, sexual contacts, and exposure to needles, and if they had undergone any surgical and dental procedures.
Biochemical & Hematological screening:On completion of the medical checkups, volunteers were asked to give 5mL of blood for different haematological [(complete blood picture (CP), haemoglobin percentage (Hb%) and erythrocyte sedimentation rate (ESR)] and 10mL for different biochemical tests [(direct bilirubin, indirect bilirubin, total bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP)]. Serological analysis:Samples were also subjected to serological analysis for hepatitis B surface Antigen (HBsAg), HBs antibodies and HCV antibodiesusing rapid immunochromatography kits (ICT, Australia and Abbott, USA). Confirmatory test for HBsAg was done by using ELISA (IMX, Abbott, USA).
All the above mentioned preliminary tests were conducted at the respective institutes in Karachi. Out of 4000 female volunteer from the two universities, 144 otherwise healthy females tested positive for HBsAg. 2 out of the 144 HBsAg positive females were also found to be positive for anti-HCV antibodies. The other 28 positive HBV patients from Anklesaria Hospital were only tested for HBsAg and all 28 were positive for HBsAg. Hence, a total of 172 HBV positive samples (144 + 28 = 172) including the 39 HCV positive serum samples obtained from Karachi were used for genotypic evaluation at Claflin University, South Carolina, USA. Specific ethnicity was not determined but we assume these study participants represent a collection of different ethnic groups in Pakistan.
DNA/RNA extraction and amplification of 172 HBV positive samples: DNA was extracted for HBV, and RNA was extracted for HCV analysis from 200μL of all 172 positive HBV serum samples using PureLink™ Viral RNA/DNA Mini Kit according to manufacturer’s instructions (Invitrogen, CA). Amplification was carried out using puReTaq Ready –To-Go PCR Beads (Amersham Biosciences, UK).
Determination of HBV and HCV genotypes by nested PCR: The primer sets for first-round PCR and second-round PCR, PCR amplification protocol, and primers for both HBV and HCV genomes and genotyping amplification for all 172 samples followed previously reported methods [45, 46]. First round amplification targeted 1063bp for the HBV genome and 470bp for the HCV genome. These respective PCR products for both HBV and HCV were used as a template for genotyping different HBV genotypes A to F and HCV genotypes from 1 to 6. HBV A through HBV F genotypes and HCV 1 through 6 genotypes for each sample were determined by separating the genotype-specific DNA bands on 2% agarose gels, stained with ethidium bromide. The sizes of PCR products were estimated according to the migration pattern of a 50bp DNA ladder (Promega, WI).
Results:
Before screening for HBV status, all 4000 healthy female volunteers from the Department of Microbiology, University of Karachi, and the Department of Microbiology, Jinnah University for Women were subjected to routine physical checkups for exclusion criteria i.e., either they were apparently unhealthy or malnourished (23 volunteers were excluded). All 4000 serum samples were screened by immunochromatography for the presence of HBsAg, anti HBs antibodies and anti-HCV antibodies. Positive results were confirmed by ELISA. Out of 4000 subjects 144 (3.6%) tested positive for HB surface antigen (HBsAg), 2 (0.05%) were positive for anti-HCV antibodies, and 3856 (96.4%) were negative for HBsAg and 3998 (99.95%) were negative for HCV antibodies by both immunochromatography and ELISA. Out of these 144 individuals who tested positive for HBsAg, 20 (13.8%) were positive for anti-HB surface antibodies and 2 (1.4%) tested positive for anti-HCV antibodies. The rest of the 28 serum samples obtained from already diagnosed HBV positive samples from Anklesaria Hospital were only tested for HBsAg and were all positive for HBsAg.
The haematological parameters: WBC count, RBC count, hematocrit and platelet count of the 172 HBsAg positive individuals were within the normal recommended range of values, while mean Hb% was 9.8±1.6 g/dL. Direct bilirubin (0 to 0.3 mg/dL), indirect bilirubin (0.1 - 1.0 mg/dL), total serum bilirubin (0.3 to 1.9 mg/dL), ALT (0 - 36 U/L), AST (0 - 31 U/L) and alkaline phosphatase (20 - 125 U/L) were also within the normal range for 129 HBsAg positive individuals, except for the raised ALT (>36 U/L) and AST (>31 U/L) levels in 38 participants with a previous history of jaundice who were also positive for HBsAg.
All 172 samples that were positive for HBsAg were confirmed for the presence of different HBV genotypes as well as for different HCV genotypes by PCR to see the co-infection of both these viruses. Genotyping was carried out at the South Carolina Center for Biotechology, Department of Biology, Claflin University, Orangeburg, SC, U.S.A. For HBV: Mix A primers were targeted to amplify genotypes A, B and C, and primers for Mix B were targeted to amplify genotypes D, E and F. For HCV: primers for Mix A were targeted to amplify genotypes 1a, 1b, 1c, 3a, 3c and 4. Primers of Mix B for HCV were targeted to amplify genotypes 2a, 2b, 2c, 3b, 5a, and 6a.
Table 1. Prevalence of both single and co-infection of HBV genotypes among the apparently healthy female student sample and known HBV positive patients from Anklesaria hospital in Karachi.
2 Universities
Samples
Percentage
Total HBV
144
Genotype D
70
48.6%
Genotype A
8
5.5%
Genotype F
7
4.9%
Genotype B
5
3.5%
Genotype E
3
2.1%
Genotype C
2
1.4%
Co-infections of HBV Genotypes
49/144
34%
Genotype B/D
30/144
20.8%
Genotype A/D
11/144
7.6%
Genotype A/D
4/144
2.8%
Genotype B/C
4/144
2.8%
Anklesaria Hospital
Samples
Percentage
Total HBV
28
Genotype D
19
67.9%
Genotype A
3
10.7%
Genotype B
1
3.6%
Genotype C
1
3.6%
Genotype F
1
3.6%
Co-infections of HBV Genotypes
Genotype B/A
3/28
10.7%
Figure 1: Electrophoresis patterns of PCR products from different HBV genotypes as determined by PCR genotyping system. Genotype A: 68bp, genotype B: 281bp, genotype C: 122bp, genotype D: 119bp, genotype E: 167bp and genotype F: 97bp.
Table 1 illustrates the prevalence of both single and co-infection of HBV genotypes from both the universities in Karachi and Anklesaria hospital. Representative 10 samples in Fig. 1 show single and co-infections for HBV.
Besides looking at the HBV genotypic status of these 172 patients by PCR, we also looked at the HCV genotypic status of the positive HBV patients by PCR so as to see if there was existence of co-infection of the two viruses i.e. HBV and HCV in the same individuals as only 2 samples tested positive for anti-HCV antibodies by rapid immunochromatography. Table 2 shows the prevalence of HCV genotypes among the apparently healthy female student population from the 2 universities in Karachi and known HBV individuals samples obtained from Anklesaria hospital. Fig. 2 shows different HCV genotype infection in the 10 representative samples shown in Fig. 1 showing HBV infection with different genotypes.
Table 2. Prevalence of HCV genotypes among the apparently healthy female student sample, and known HBV individuals from Anklesaria hospital in Karachi.
2 Universities
Samples
Percentage
Total HCV/Total HBV
39/144
27.1%
Genotype 3a
26/39
66.6%
Genotype 6a
5/39
12.8%
Genotype 3b
4/39
10.3%
Genotype 5a
4/39
10.3%
Anklesaria Hospital
Samples
Percentage
Total HCV/HBV
4/28
14.3%
Genotype 3a
2/28
7.14%
Genotype 2a
1/28
3.6%
Genotype 5a
1/28
3.6%
Figure 2: The sizes of the genotype-specific bands for HCV amplified by PCR genotyping method are as follows: genotype 2a, 190 bp; genotype 3a, 258 bp; genotype 3b, 232 bp; genotype 5a, 417 bp; and genotype 6a, 300 bp.
To summarize the results it was found that out of 172 HBsAg positive samples from the two universities (144 HBV samples) and Anklesaria Hospital (28 HBV samples), 89 (51.7%) were genotype D, 11 were genotype A (6.4%), 8 were genotype F (4.6%), 6 were genotype B (3.5%), 3 were genotype E (1.7%), and 3 were genotype C (1.7%). Out of 43 positive for HCV by PCR from the two universities (39/144 HBV samples) and Anklesaria Hospital (4/28 HBV samples), 65.1% (28/43) showed infection with 3a, followed by genotypes 5a (5/43 = 11.6%), 6a (5/43 = 11.6%), 3b (4/43 = 9.3%) and 2a (1/43 = 2.3%).
Discussion:
Viral hepatitis due to HBV and HCV has significant morbidity and mortality worldwide. The global prevalence of HCV is 3% 38 and the carrier rate of HBsAg varies from 0.1% to 0.2% in Britain and the USA, to 3% in Greece and southern Italy and up to 15% in Africa and the Asia 39. Pakistan is highly endemic with HBV. Studies are too limited to give a clear picture of the prevalence of HBV at the national level, especially among apparently healthy individuals. Most previous studies targeted different small groups of individuals with some clinical indications, so they do not accurately reflect the overall prevalence in Pakistan40. Our previous study was conducted on a first group of 4000 healthy female students from the two universities i.e., Department of Microbiology, University of Karachi and Department of Microbiology, Jinnah University for Women for the prevalence of HBV. We have reported earlier that genotype D appears to be the dominant genotype prevalent in Karachi, Pakistan’s apparently healthy female population, and genotype B appears to be the next most prevalent genotype 41, 42. In this study we checked the prevalence of both HBV and HCV in a second group of 4000 healthy female students from the same two universities in Karachi mentioned above, as well as the already 28 diagnosed HBV patients from Anklesaria Hospital in Karachi, Pakistan.
Both HBV and HCV are present in the Pakistani population and there are varying reports of disease prevalence. HCV is one of the silent killer infections spreading undetected in Pakistan because there are often no clinical symptoms and, when HCV is diagnosed, considerable damage has already been done to the patient. In Pakistan alone, the prevalence of HBsAg has been reported to be from 0.99% to 10% in different groups of individuals 43 - 52 and 2.2% to 14% for HCV antibodies 53 - 56. A recent study conducted in Pakistan showed that out of 5707 young men tested, 95 (1.70%) were positive for anti-HCV and 167 (2.93%) for HBsAg 57. Our previous study showed the prevalence of HBsAg among young otherwise healthy women to be 4.5% 41,42. Our present study shows that the prevalence of HBsAg in otherwise young healthy women to be 3.6%, with 0.98% testing positive for anti-HCV antibodies. On the basis of other studies conducted in different provinces of Pakistan, we can say that there is a variation in the prevalence of HBsAg and HCV antibodies in the Pakistani population as the population sample selected is limited to a particular area or segment of the provinces.
HBV and HCV genotyping is important to track the route and pathogenesis of the virus. In particular, the variants may differ in their patterns of serologic reactivity, pathogenecity, virulence, and response to therapy. Both HBV and HCV has genetic variations which correspond to the geographic distribution and has been classified into 8 genotypes (A to H) on the basis of whole genome sequence diversity of greater than 8% and 6 genotypes (1 to 6) using restriction fragment length polymorphism analysis of the 5’ non-coding region (NCR), respectively .
In this study genotyping was carried out for 6 HBV genotypes (A through F) and 6 HCV genotypes (1 through 6). This study suggests that the HBV D genotype is the most prevalent (114/144 = 79.2%) among otherwise healthy females alone or in co-infection with other HBV genotypes in Karachi, Sindh, Pakistan. In our previous study HBV D genotype was found to be ubiquitous (100%) among otherwise healthy females alone or in co-infection with other HBV genotypes in Karachi followed by genotype B 41,42. The earlier two studies conducted for prevalence of HBV genotypes in known hepatitis B positive patients in Pakistan report the prevalence of genotypes HBV A (68%) and HBV D (100%) in the province of Sindh 58,59. Interestingly, in this study we also found the HBV D genotype to be the prevalent genotype but it was followed by genotypes HBV A (5.5%) and HBV F (4.9%). The prevalence of genotype HBV B in this study was found to be 3.5% as our earlier study has shown the prevalence of genotype B in otherwise healthy females to be 16.1% 60. These findings respectively contradict and corroborate the previous studies for HBV genotype distributions reported here as the subjects in this study were also asymptomatic but comprised of second group of female volunteer students at the two universities. Out of 144 subjects positive for HBsAg, 10 reported a previous history of jaundice and the rest were not aware of their HBV status. In the nearby north Indian population, HBV D was reported as the predominant genotype (75%) in patients diagnosed with chronic liver disease (CLDB) 60. In this study we also found other HBV genotypes existed in the study population such as HBV genotype F (4.9%) followed by genotype E (2.1%), and genotype C (1.4%). We also saw mixed HBV infections of genotypes B and D, A and D, C and D as well as B and C (20.8%, 7.6%, 2.8% and 2.8%) among these otherwise healthy females.
Among the 28 diagnosed HBV patients from Anklesaria Hospital, 67.9% showed HBV genotype D infection followed by genotype A infection (10.7%). In this group of 28 HBV positive patients we also saw infections with genotypes B (3.6%), C (3.6%) and F (3.6%). This group exhibited 10.7% co-infection with genotypes B and A.
As far as the HCV status of these 144 otherwise healthy females who were HBV positive is concerned only 2 (1.4%) tested positive for HCV antibodies by rapid immunochromatography. But the PCR results showed 39 (27.15%) of these 144 otherwise healthy females that were HBV positive for different genotypes were also positive for HCV including the 2 otherwise healthy females that tested positive for HCV antibodies by rapid immunochromatography. Of the 39 HCV positive otherwise healthy females, we found the predominant HCV genotype to be 3a (66.6%) followed by genotypes 6a (12.8%), 3b (10.3%), and 5a (10.3%) infections. The earlier study conducted with samples from women at the two universities in Pakistan had shown that among the HCV positive apparently healthy females 51.44% were genotype 3a, 24.03% exhibited a mix of genotype 3a and 3b, 15.86% were genotype 3b, and 4.80% were genotype 1b 42. Interestingly, among the group of 28 diagnosed HBV patients, the prevalence of HCV 3a genotype infection was dominant but was 7.1% much lower than that found in the otherwise healthy females, followed by infections with genotypes 2a (3.6%) and 5a (3.6%). Hence we see there is 25% co-infection of both these viruses i.e., HBV and HCV among the HBsAg positive individuals. The sample of 28 HBV positive patients was from a hospital located in the center of the metropolis that represents an area of Karachi where sanitation, malnourishment, illiteracy, and lack of awareness is very common. Prostitution can also be considered as one factor in some of the localities of Karachi in the spread of both HBV and HCV.
Conclusion:
In conclusion, genotype D appears to be the dominant HBV genotype and genotype 3a for HCV appears to be prevalent in Sindh, Pakistan’s otherwise healthy young female population as well as in HBV diagnosed individuals. Co-infection of both the viruses i.e., HBV and HCV exists among HBsAg positive individuals. The young female participants were advised to seek appropriate medical care for both their own benefit and public health benefit.




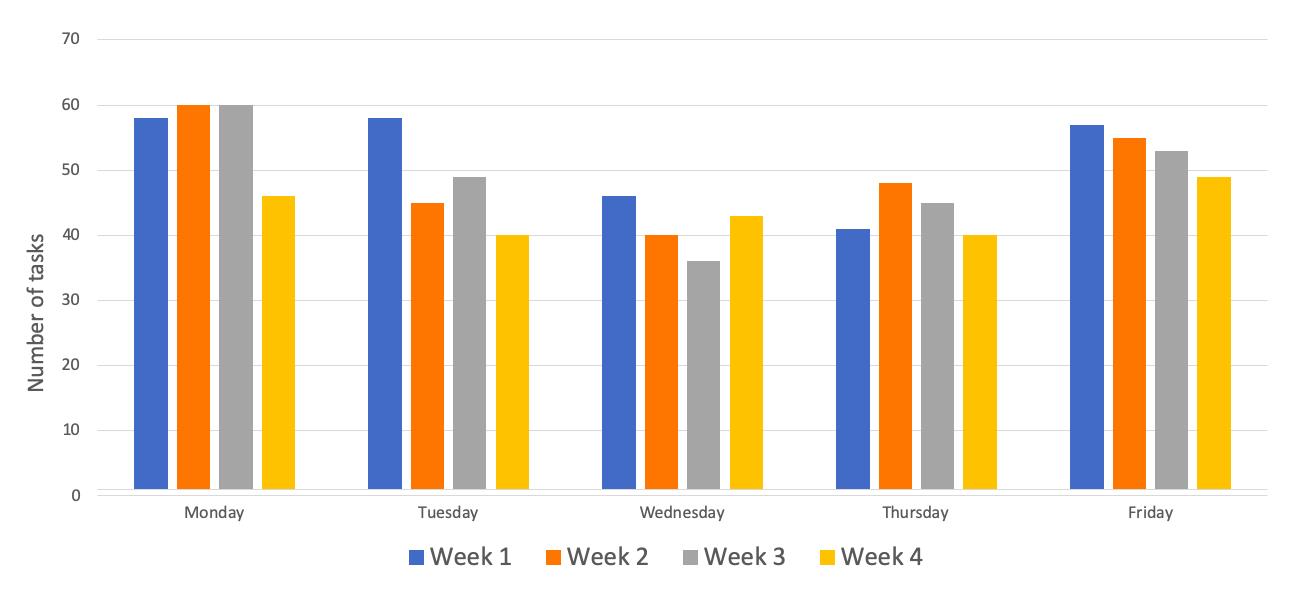
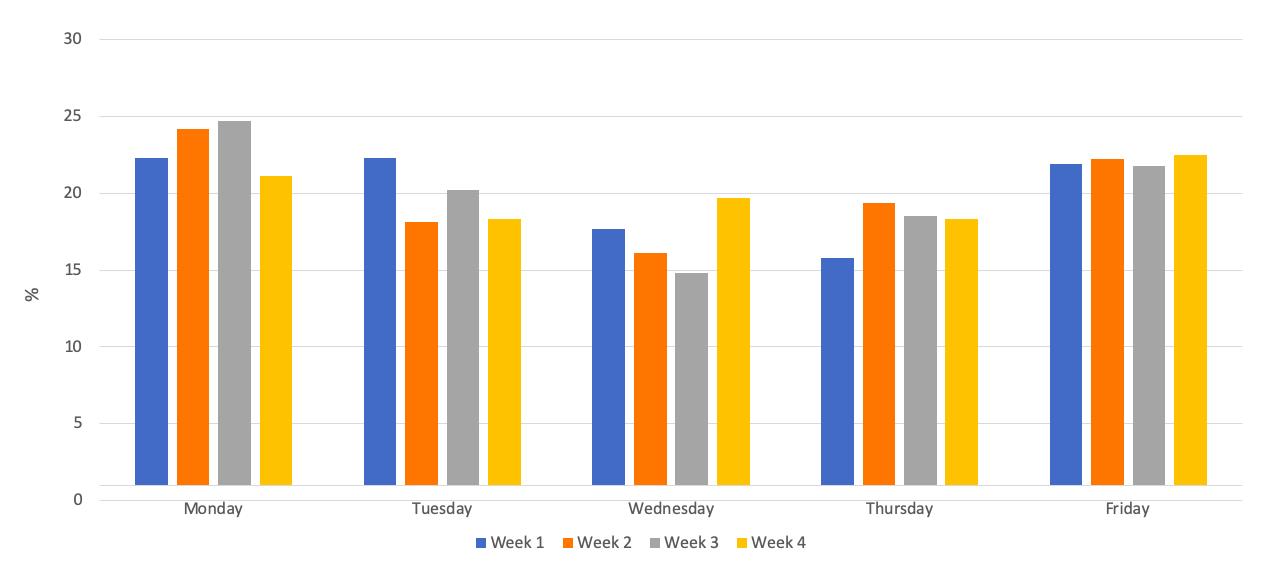
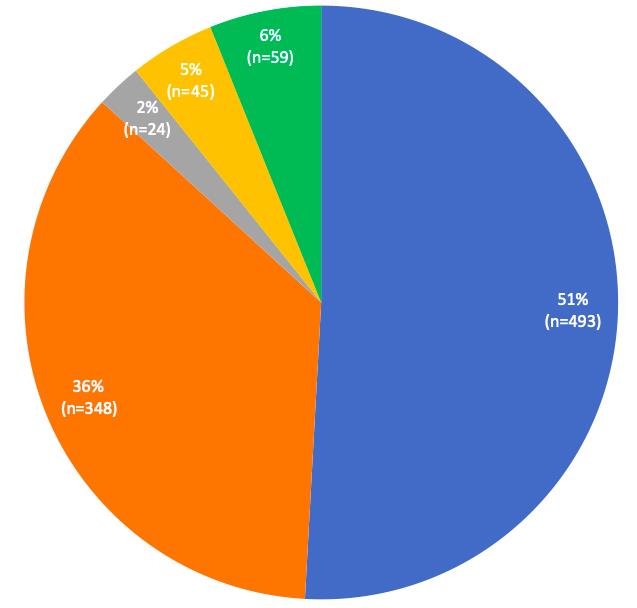
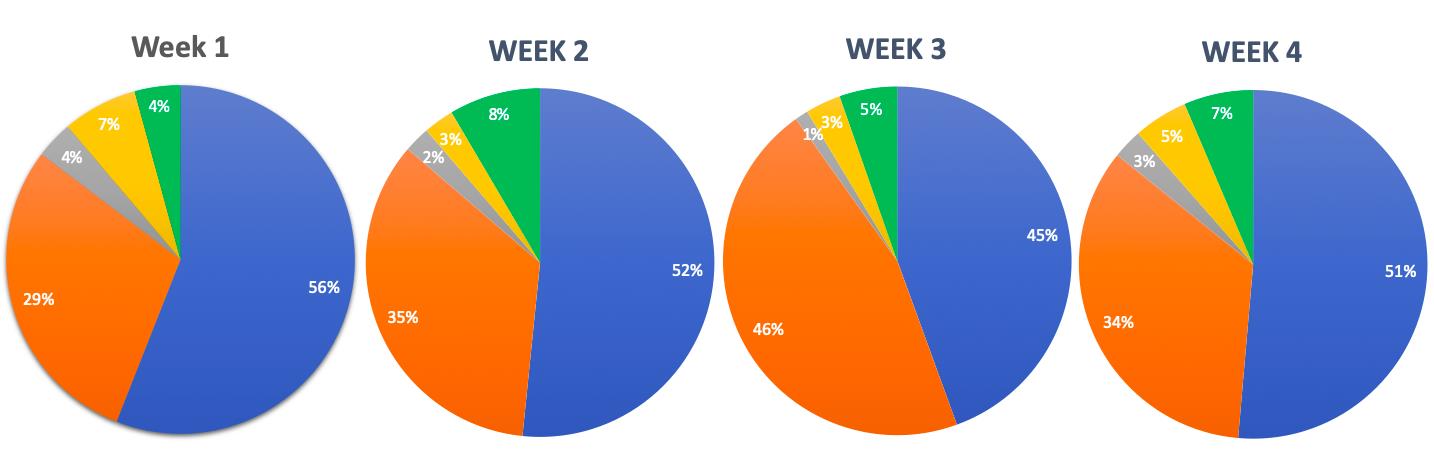
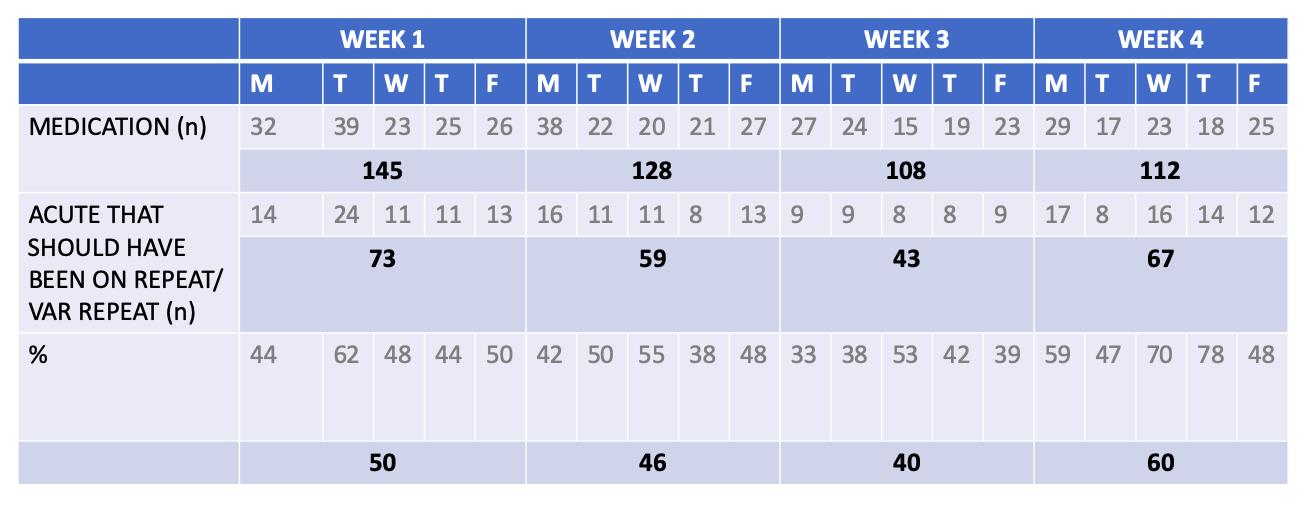
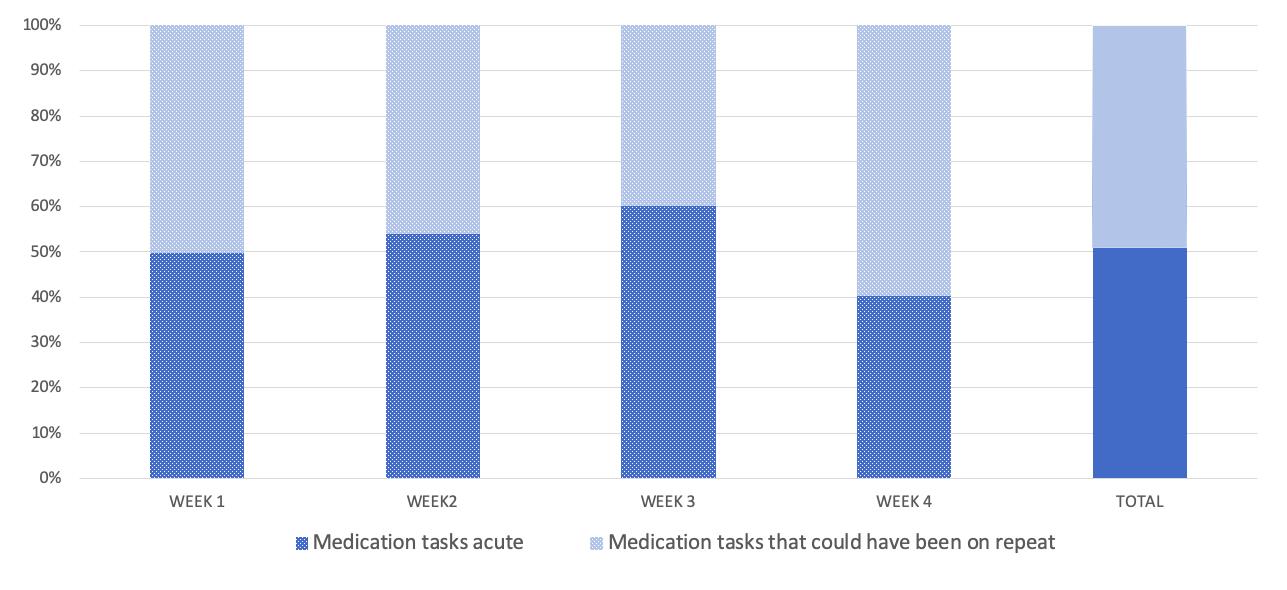
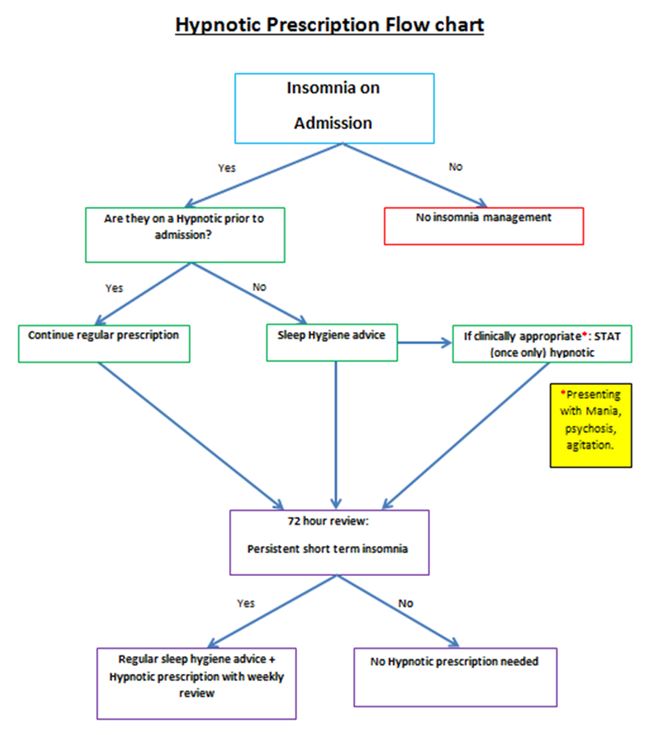


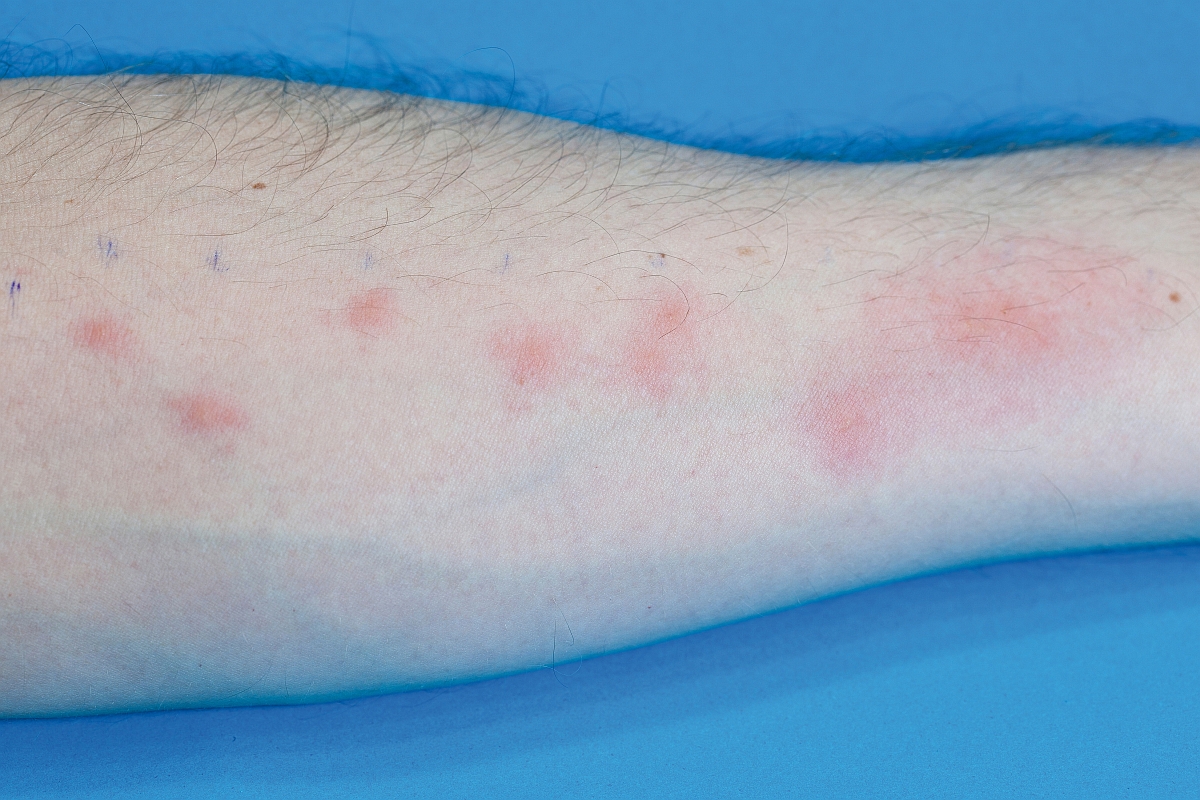



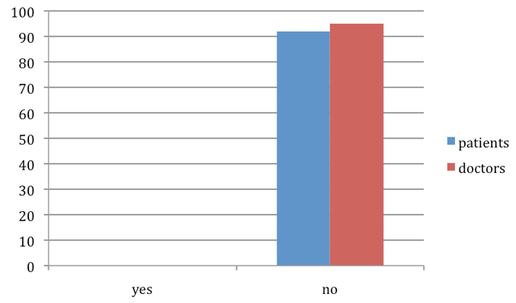
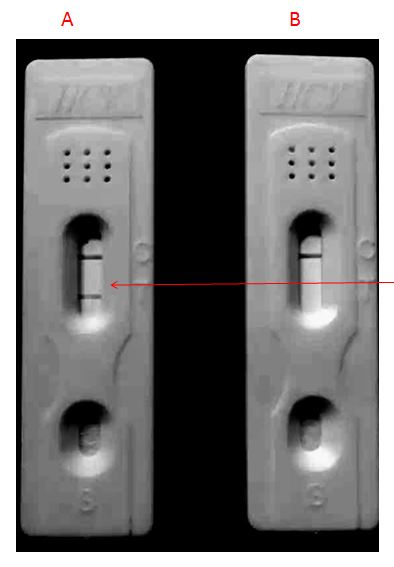
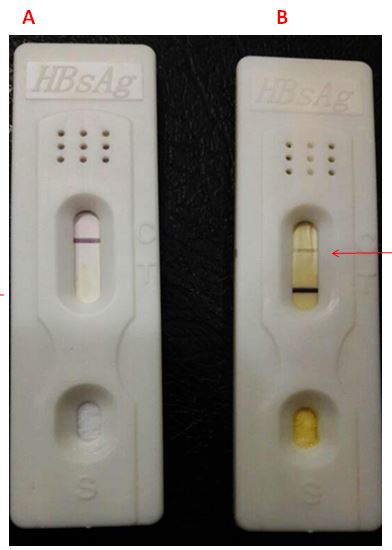
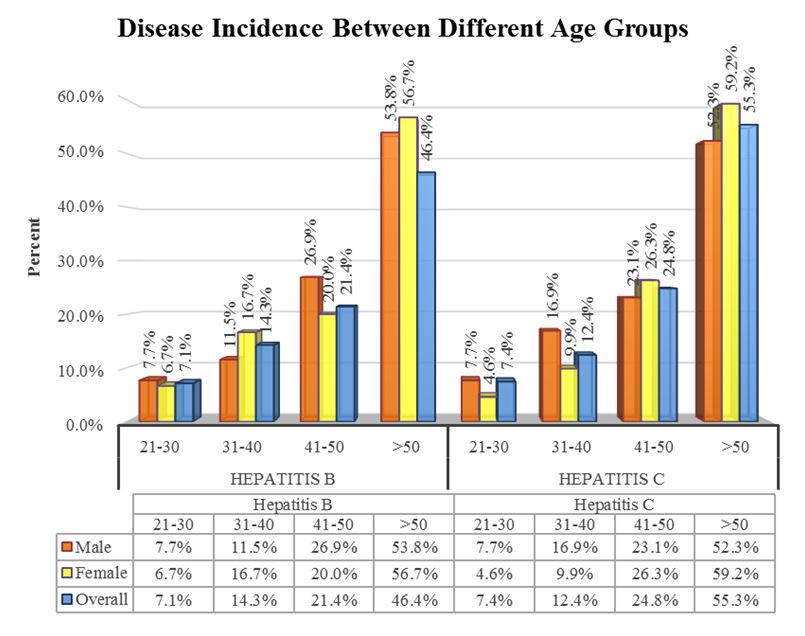
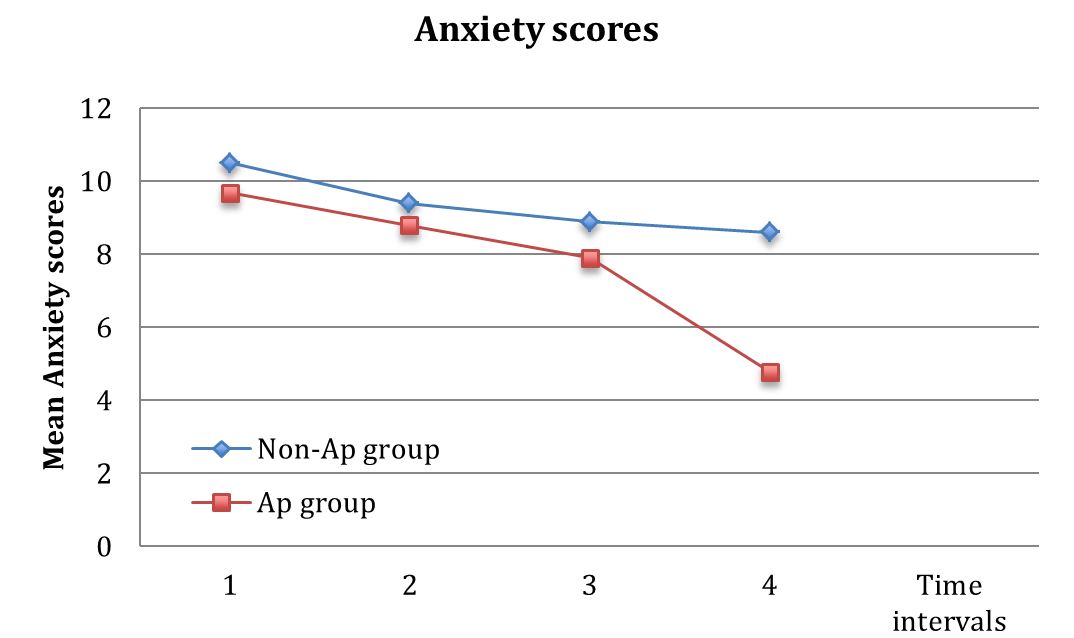
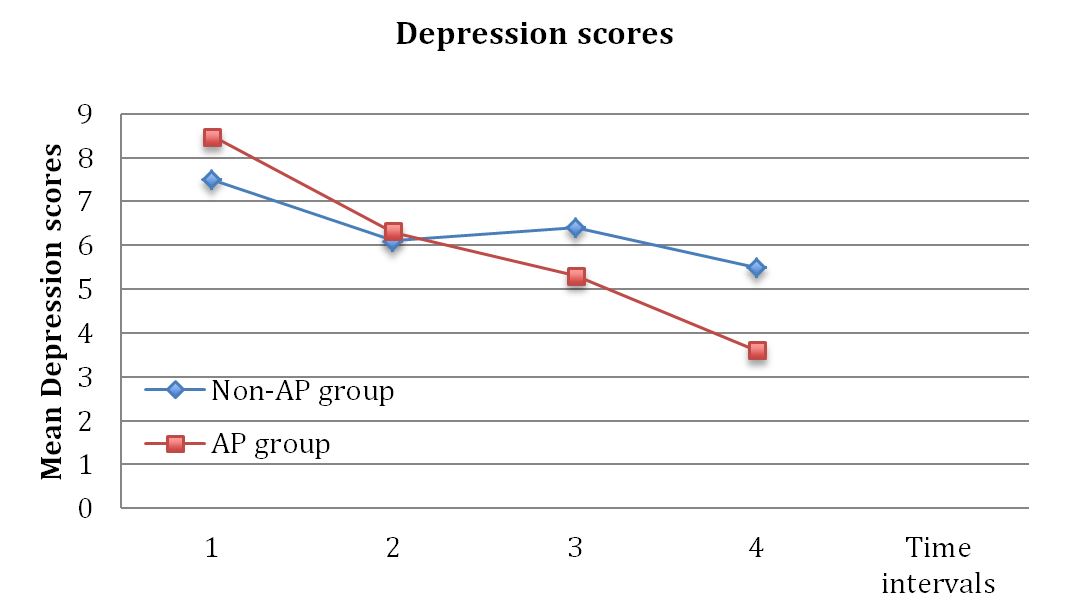
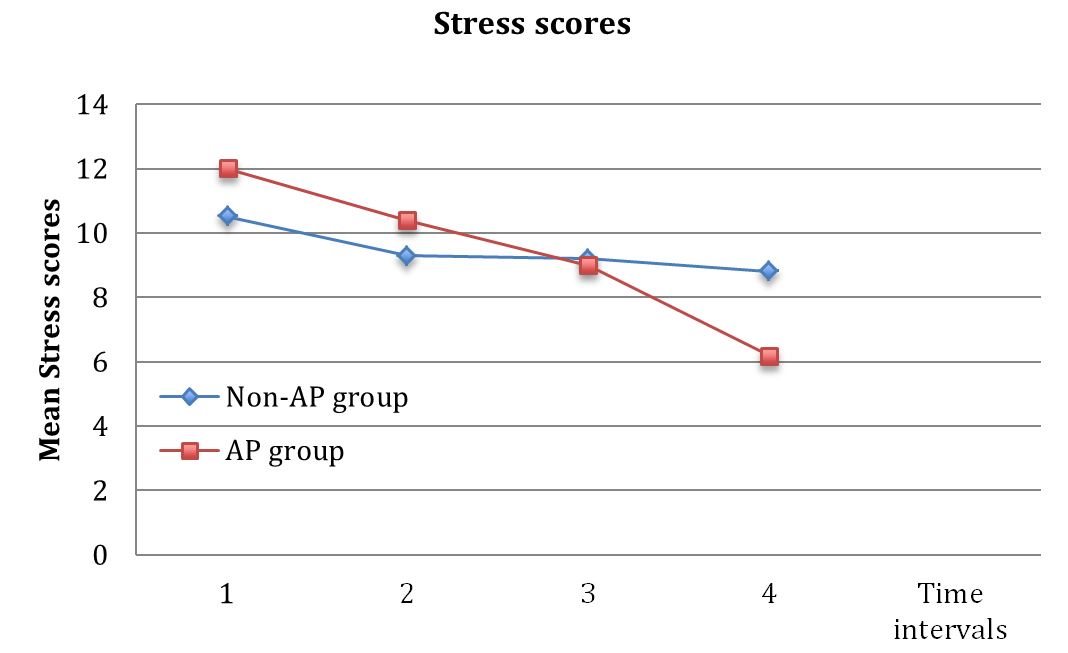
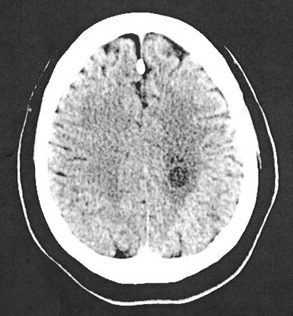
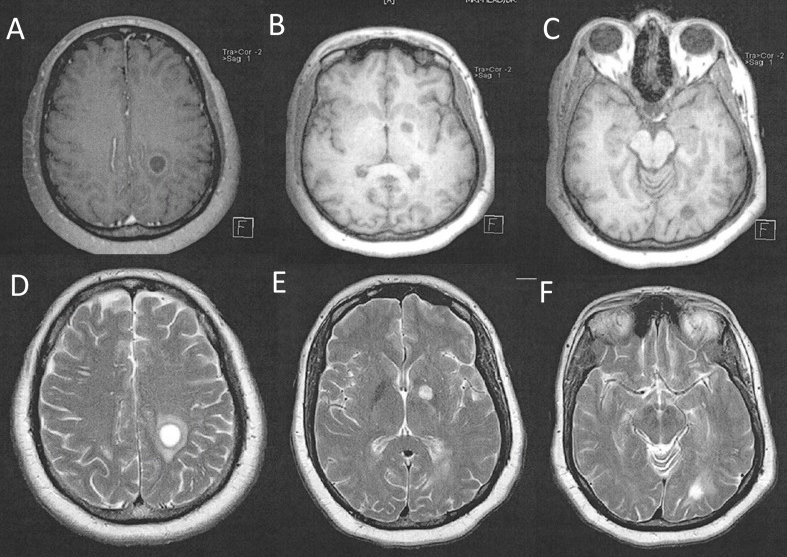
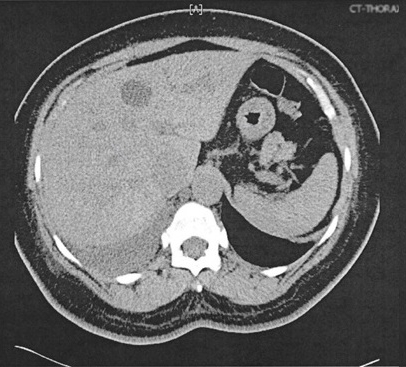
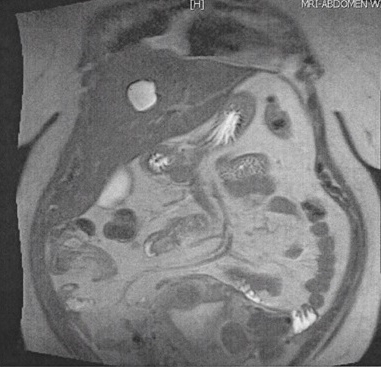
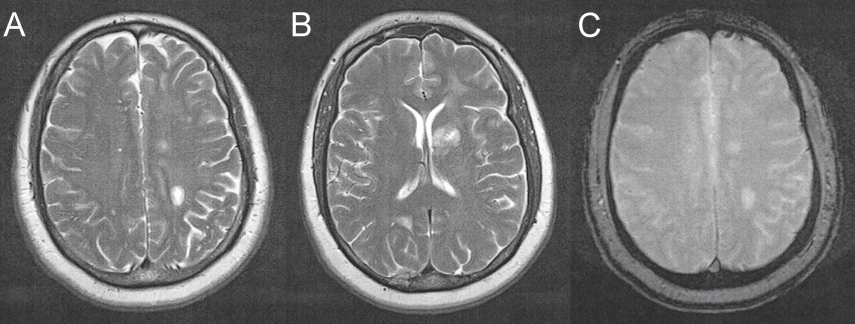

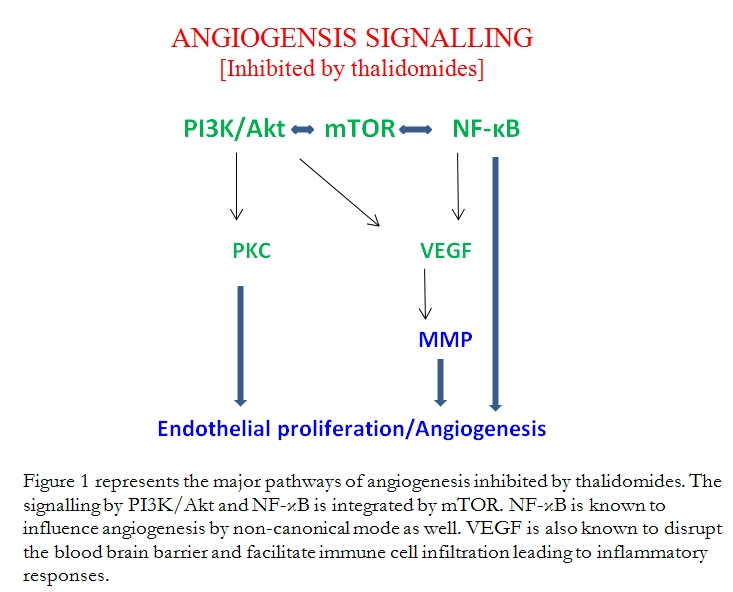

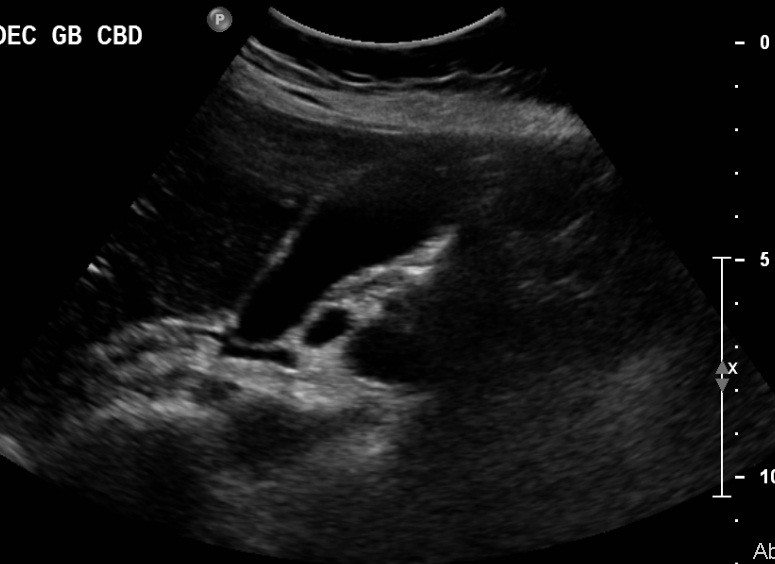
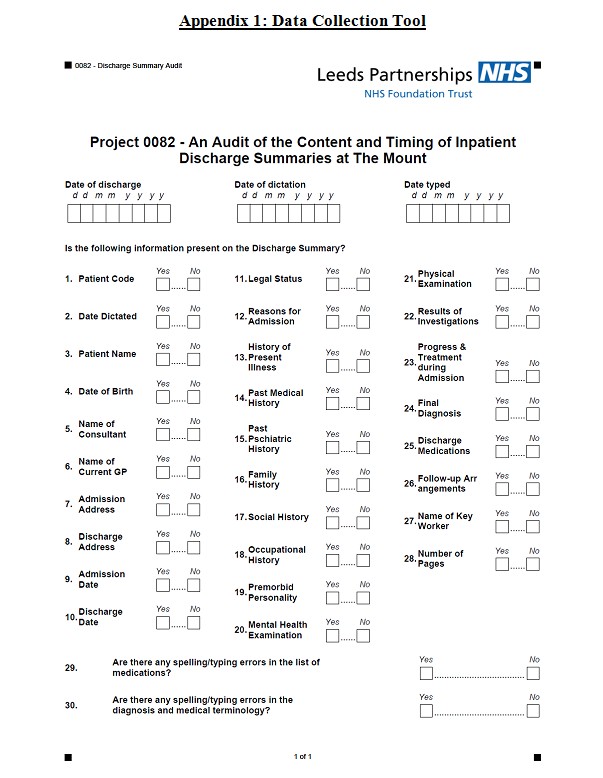
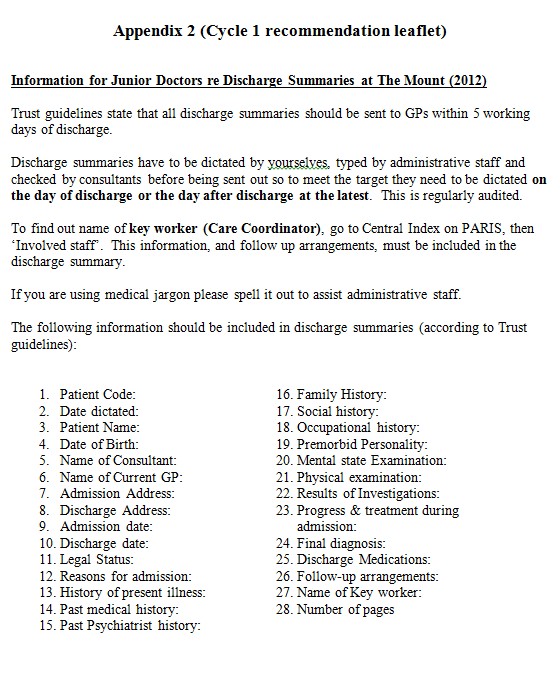
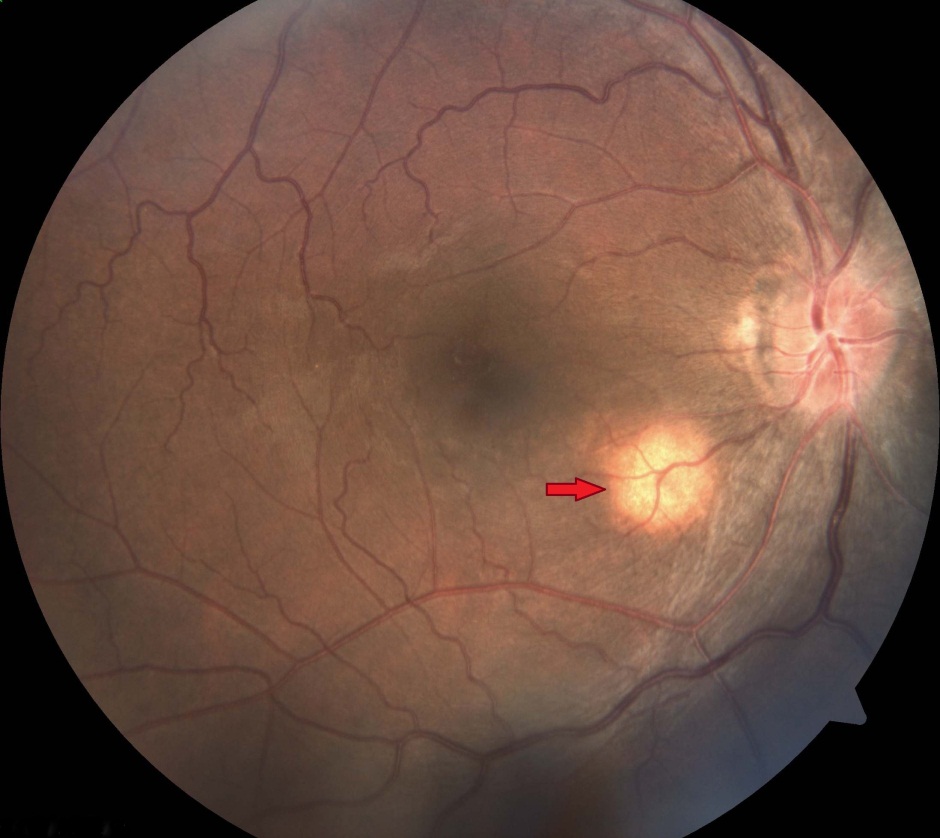
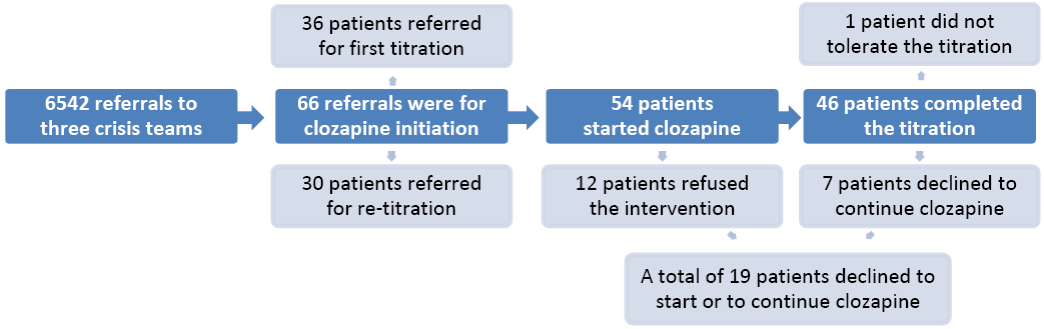
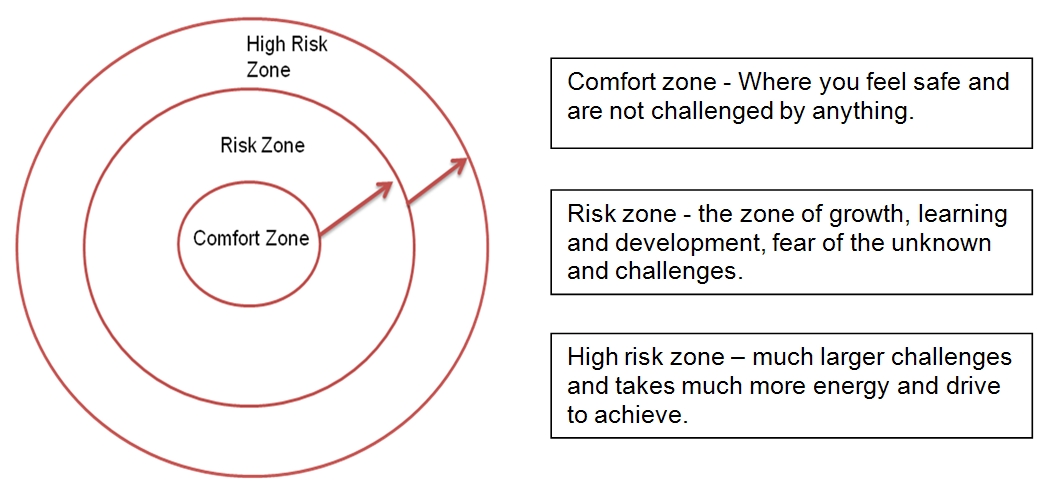


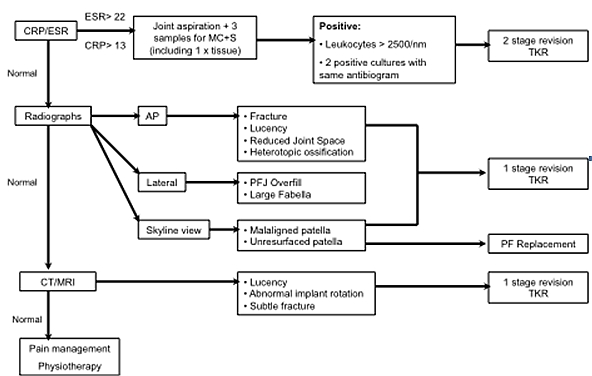
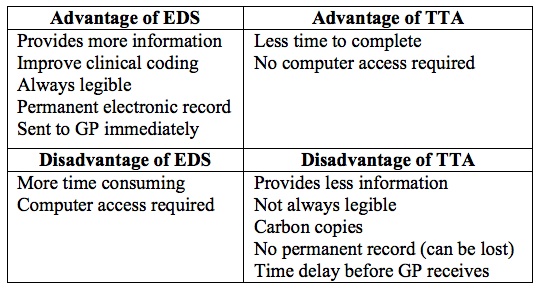
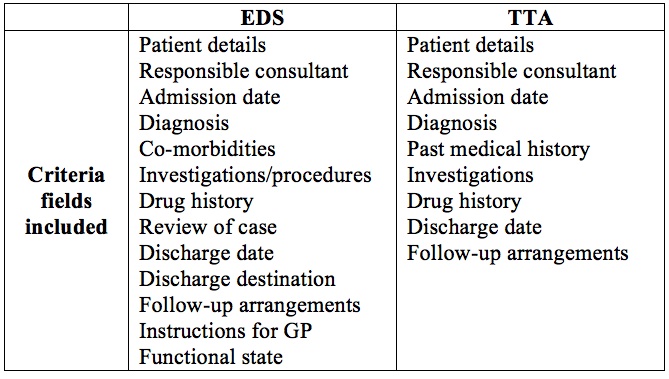
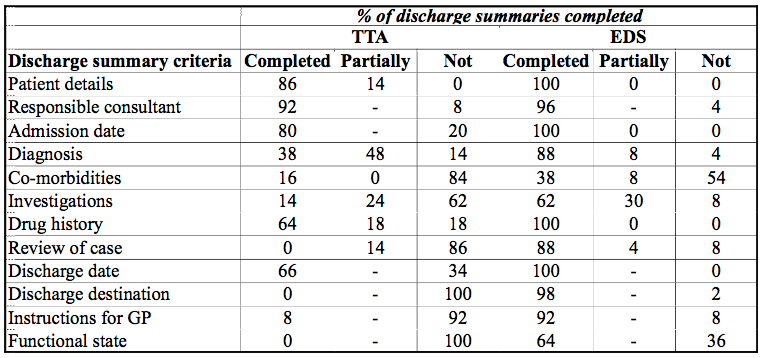
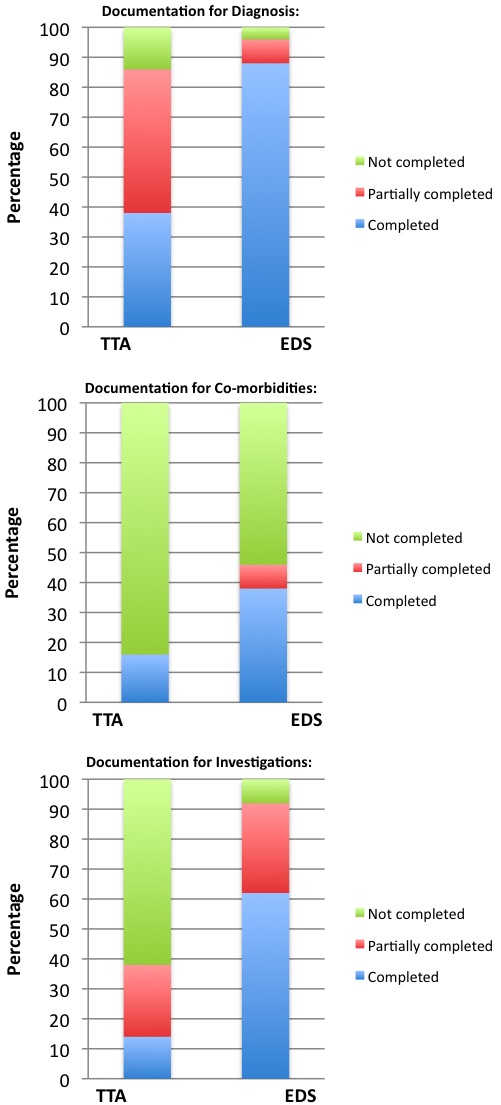
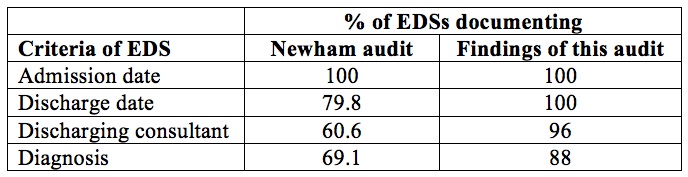
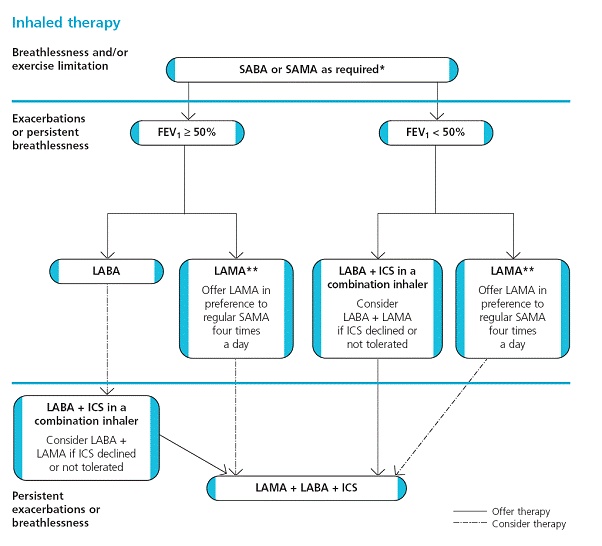
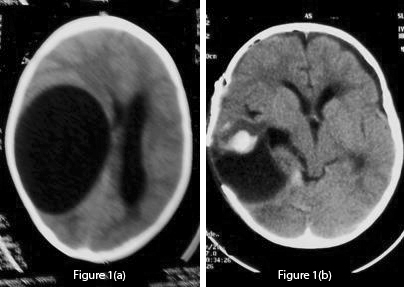 Fig 1 (a): Pre-operative unenhanced CT scan which shows a large CSF density cystic lesion on the right side causing mass effect and midline shift to the left. There is no peri-lesional oedema. Fig 1 (b): Post-operative CT scan of the lesion shows a large void which can lead to dangerous collapse. Mild haematoma is also seen.
Fig 1 (a): Pre-operative unenhanced CT scan which shows a large CSF density cystic lesion on the right side causing mass effect and midline shift to the left. There is no peri-lesional oedema. Fig 1 (b): Post-operative CT scan of the lesion shows a large void which can lead to dangerous collapse. Mild haematoma is also seen. 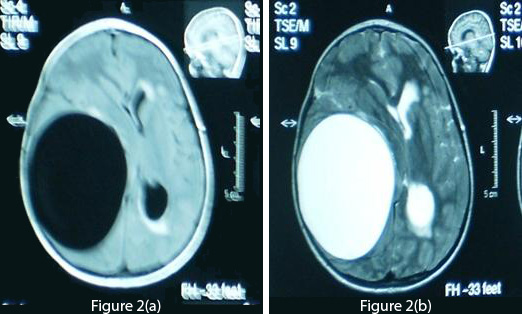 Fig 2 (a): T1-weighted axial MRI of the brain demonstrates a cyst density similar to CSF. Fig 2 (b): T2-weighted MRI shows no ring enhancement or oedema. The periventricular hyperintensity of the left side is probably due to obstructive hydrocephalus.
Fig 2 (a): T1-weighted axial MRI of the brain demonstrates a cyst density similar to CSF. Fig 2 (b): T2-weighted MRI shows no ring enhancement or oedema. The periventricular hyperintensity of the left side is probably due to obstructive hydrocephalus.  Fig 3: This shows the cyst removed in toto after operation. The cyst appears creamy and smooth. After summation of all the above data, the diagnosis of a hydatid cyst was made and a right frontotemporoparietal craniotomy was performed. A large cystic structure (14×14×12 cm) was delivered with utmost care to avoid rupture and spillage [fig 3]. A hydatid cyst was confirmed by pathology reports. A post-operative CT scan showed a large space without any residual matter [fig 1(b)]. Post-operatively, albendazole 15 mg/kg was started and continued for four weeks. The patient showed marked improvement in his neurological deficit and was discharged after one week with close follow-up. Discussion/Review Of Literature Life CycleHydatidosis is caused by Echinococcus granulosus, which occurs mainly in dogs. Humans who act as intermediate hosts get infected incidentally by ingesting eggs from the faeces of the infected animal. The eggs hatch inside the intestines and penetrate the walls, entering blood vessels and eventually reach the liver where they may form cysts or move on towards the lungs. Even after pulmonary filter, a few still make it to the systemic circulation and can lodge in almost any part of the body, including the brain, heart and bones.2,3,8,14,16,26 Brain hydatid cysts are relatively rare and only account for up to 2% of total cases.4,5,7 The actual percentage may be higher than what we have in literature, due to under-reporting. Brain hydatid cysts can be primary (single) or secondary (multiple).2,3,4,5,7 The latter are thought to arise from the multiple scolices released from the left side of the heart following cyst rupture in the heart2,3,5,27 or due to spontaneous, traumatic or surgical rupture of a solitary cranial cyst.3,5 Cysts mostly involve the territory of the middle cerebral artery4,7 but other regions like intraventricular, posterior fossa and the orbit have also been reported.15,17,18,28 The wall of the cyst consists of an inner endocyst (germinal layer) and outer ectocyst (laminated layer). The host reacts to the cyst forming a pericyst (fibrous capsule), which provides nutrients to the parasite. In the brain, due to minimal reaction, the pericyst is very thin. The endocyst produce scolices which bud into the cyst cavity and may sediment within the hydatid cavity, commonly known as hydatid sand.3,14,29,30 Presentation and DiagnosisMost hydatid cysts are acquired in childhood and are manifested during early adulthood.8,29 Cysts develop insidiously, usually being asymptomatic initially, and present with protean clinical and imaging features.3,5,6 In previous studies the most common presenting symptoms were headache and vomiting.4,5,7,14,15,28 Also in the literature, patients reported ataxia, diplopia, hemiparesis, abducens nerve palsy and even coma.5,7,15,28 Surprisingly, in the present study the patient did not have a headache and presented with parasthesia and numbness of the toes. Later he developed left sided weakness, convulsions and finally ataxia, which correlate with previous studies. Diagnosis of a hydatid cyst can sometimes be confused with other space occupying lesions of the brain, especially abscesses, neoplasms and arachnoid cysts.14,31 In this study the patient had bilateral frank papilloedema which is also mentioned in earlier reports.4,28 The Casoni and Weinberg tests, indirect haemagglutination, eosinophilia and ELISA are used in diagnosing hydatid cysts, but as brain tissue evokes minimal response many results tend to be false negatives.2,5,8,25 In our case also, serology for hydatid cyst was negative. CT scan and MRI are used frequently in diagnosing the cystic lesions.3,8,14,23,32,33 However, MRI is considered superior in demonstrating the cyst rim.5,8,11,21,32,34 On CT scan, a solitary cyst appears as well-defined, spherical, smooth, thin-walled and homogeneous, with an inner density similar to CSF, and non-enhancing walls.11,29,32The wall may appear iso-dense to hyper-dense on CT scan3,8, and rarely, may become calcified.11,29,32 There is usually no surrounding brain parenchymal oedema, which if exists along with ring enhancement, indicates inflammation and infection. 7,11,32,33,34,35 Ring enhancement and peri-lesional oedema differentiates brain abscesses and cystic neoplasms from uncomplicated hydatid cysts.3,8 These findings can in fact sometimes cause dilemma and misdiagnosis and lead to catastrophic events.14 The cyst shows low signal intensity on T1-weighted, and high signal intensity on T2-weighted MRI.2 MRI may also show peri-lesional oedema not seen on regular CT scan imaging.7 MRI may prove superior in determining exact cyst location, presence of super-added infections and cystic contents, and also in surgical planning and ruling out other diagnostic possibilities.14,33 We strongly recommend MRI for better evaluation of cystic brain lesions. Spontaneous cystic rupture can lead to different appearances depending on which layers have been obliterated, and produce some specific signs.3 When only the endocyst ruptures, cyst contents are held by the outer pericyst giving a peculiar water lily sign, which is pathognomic.3,8 TreatmentThough still in infancy, medical therapy for small or inoperable brain hydatid cysts has been promising. Albendazole alone or in combination with other compounds, such as praziquantel, has been reported with favourable results as an adjunct and, in certain circumstances, as the primary mode of treatment.2,36,37,38 It is reported that albendazole results in the disappearance of up to 48% of cysts and a substantial reduction in size of the cysts in another 28%.2 The duration of the treatment is four weeks or more, and recently many authors have favoured a prolonged therapy. The change in levels of cyst markers such as alanine, succinate, acetate and lactate, measured before and during treatment on Proton Magnetic Resonance Spectroscopy (MRS), correlate well with shrinkage and resolution of cyst findings on conventional MRI and help in evaluating the efficacy of chemotherapy.39 Cysts may drain into ventricles or rupture completely, causing spillage of contents into the subarachnoid space, leading to fatal anaphylactic shock, meningitis or local recurrence.3,5,22,25 Surgery is the mainstay for treating intracranial hydatid cysts and the aim is to excise the cysts entirely without rupture, which can otherwise lead to catastrophic events as described earlier 2,3,14,25. The Dowling-Orlando technique remains the preferred method, in which the cyst can be delivered by lowering the head of the operating table and instilling warm saline between the cyst and the surrounding brain.40 Even minimal spillage can cause deleterious effects (1 ml of hydatid sand contains 400,000 scolices).14 The thin cyst wall, periventricular location and micro-adhesions to the parenchyma are the main problems encountered during the surgical procedure.1,22 The large cavity remaining after the cystic removal can lead to many serious complications, such as cortical collapse, hyperpyrexia, brain oedema and cardio-respiratory failure.5 Recurrence remains a major concern, which is managed by both antihelminthic chemotherapy and surgery. In a study conducted by Ciurea et al, 25% of the patients had recurrence, which highlights the need for long term follow up.23 In the present study, due to the huge size of the cyst and progressive neurological deficit, it was not wise to completely rely on medical therapy. Surgery was performed and post-operatively albendazole was started as an adjunct. We recommend that for treating brain hydatid cyst, the size of the cyst, multiplicity, location and neurological deficit must all be taken into consideration.
Fig 3: This shows the cyst removed in toto after operation. The cyst appears creamy and smooth. After summation of all the above data, the diagnosis of a hydatid cyst was made and a right frontotemporoparietal craniotomy was performed. A large cystic structure (14×14×12 cm) was delivered with utmost care to avoid rupture and spillage [fig 3]. A hydatid cyst was confirmed by pathology reports. A post-operative CT scan showed a large space without any residual matter [fig 1(b)]. Post-operatively, albendazole 15 mg/kg was started and continued for four weeks. The patient showed marked improvement in his neurological deficit and was discharged after one week with close follow-up. Discussion/Review Of Literature Life CycleHydatidosis is caused by Echinococcus granulosus, which occurs mainly in dogs. Humans who act as intermediate hosts get infected incidentally by ingesting eggs from the faeces of the infected animal. The eggs hatch inside the intestines and penetrate the walls, entering blood vessels and eventually reach the liver where they may form cysts or move on towards the lungs. Even after pulmonary filter, a few still make it to the systemic circulation and can lodge in almost any part of the body, including the brain, heart and bones.2,3,8,14,16,26 Brain hydatid cysts are relatively rare and only account for up to 2% of total cases.4,5,7 The actual percentage may be higher than what we have in literature, due to under-reporting. Brain hydatid cysts can be primary (single) or secondary (multiple).2,3,4,5,7 The latter are thought to arise from the multiple scolices released from the left side of the heart following cyst rupture in the heart2,3,5,27 or due to spontaneous, traumatic or surgical rupture of a solitary cranial cyst.3,5 Cysts mostly involve the territory of the middle cerebral artery4,7 but other regions like intraventricular, posterior fossa and the orbit have also been reported.15,17,18,28 The wall of the cyst consists of an inner endocyst (germinal layer) and outer ectocyst (laminated layer). The host reacts to the cyst forming a pericyst (fibrous capsule), which provides nutrients to the parasite. In the brain, due to minimal reaction, the pericyst is very thin. The endocyst produce scolices which bud into the cyst cavity and may sediment within the hydatid cavity, commonly known as hydatid sand.3,14,29,30 Presentation and DiagnosisMost hydatid cysts are acquired in childhood and are manifested during early adulthood.8,29 Cysts develop insidiously, usually being asymptomatic initially, and present with protean clinical and imaging features.3,5,6 In previous studies the most common presenting symptoms were headache and vomiting.4,5,7,14,15,28 Also in the literature, patients reported ataxia, diplopia, hemiparesis, abducens nerve palsy and even coma.5,7,15,28 Surprisingly, in the present study the patient did not have a headache and presented with parasthesia and numbness of the toes. Later he developed left sided weakness, convulsions and finally ataxia, which correlate with previous studies. Diagnosis of a hydatid cyst can sometimes be confused with other space occupying lesions of the brain, especially abscesses, neoplasms and arachnoid cysts.14,31 In this study the patient had bilateral frank papilloedema which is also mentioned in earlier reports.4,28 The Casoni and Weinberg tests, indirect haemagglutination, eosinophilia and ELISA are used in diagnosing hydatid cysts, but as brain tissue evokes minimal response many results tend to be false negatives.2,5,8,25 In our case also, serology for hydatid cyst was negative. CT scan and MRI are used frequently in diagnosing the cystic lesions.3,8,14,23,32,33 However, MRI is considered superior in demonstrating the cyst rim.5,8,11,21,32,34 On CT scan, a solitary cyst appears as well-defined, spherical, smooth, thin-walled and homogeneous, with an inner density similar to CSF, and non-enhancing walls.11,29,32The wall may appear iso-dense to hyper-dense on CT scan3,8, and rarely, may become calcified.11,29,32 There is usually no surrounding brain parenchymal oedema, which if exists along with ring enhancement, indicates inflammation and infection. 7,11,32,33,34,35 Ring enhancement and peri-lesional oedema differentiates brain abscesses and cystic neoplasms from uncomplicated hydatid cysts.3,8 These findings can in fact sometimes cause dilemma and misdiagnosis and lead to catastrophic events.14 The cyst shows low signal intensity on T1-weighted, and high signal intensity on T2-weighted MRI.2 MRI may also show peri-lesional oedema not seen on regular CT scan imaging.7 MRI may prove superior in determining exact cyst location, presence of super-added infections and cystic contents, and also in surgical planning and ruling out other diagnostic possibilities.14,33 We strongly recommend MRI for better evaluation of cystic brain lesions. Spontaneous cystic rupture can lead to different appearances depending on which layers have been obliterated, and produce some specific signs.3 When only the endocyst ruptures, cyst contents are held by the outer pericyst giving a peculiar water lily sign, which is pathognomic.3,8 TreatmentThough still in infancy, medical therapy for small or inoperable brain hydatid cysts has been promising. Albendazole alone or in combination with other compounds, such as praziquantel, has been reported with favourable results as an adjunct and, in certain circumstances, as the primary mode of treatment.2,36,37,38 It is reported that albendazole results in the disappearance of up to 48% of cysts and a substantial reduction in size of the cysts in another 28%.2 The duration of the treatment is four weeks or more, and recently many authors have favoured a prolonged therapy. The change in levels of cyst markers such as alanine, succinate, acetate and lactate, measured before and during treatment on Proton Magnetic Resonance Spectroscopy (MRS), correlate well with shrinkage and resolution of cyst findings on conventional MRI and help in evaluating the efficacy of chemotherapy.39 Cysts may drain into ventricles or rupture completely, causing spillage of contents into the subarachnoid space, leading to fatal anaphylactic shock, meningitis or local recurrence.3,5,22,25 Surgery is the mainstay for treating intracranial hydatid cysts and the aim is to excise the cysts entirely without rupture, which can otherwise lead to catastrophic events as described earlier 2,3,14,25. The Dowling-Orlando technique remains the preferred method, in which the cyst can be delivered by lowering the head of the operating table and instilling warm saline between the cyst and the surrounding brain.40 Even minimal spillage can cause deleterious effects (1 ml of hydatid sand contains 400,000 scolices).14 The thin cyst wall, periventricular location and micro-adhesions to the parenchyma are the main problems encountered during the surgical procedure.1,22 The large cavity remaining after the cystic removal can lead to many serious complications, such as cortical collapse, hyperpyrexia, brain oedema and cardio-respiratory failure.5 Recurrence remains a major concern, which is managed by both antihelminthic chemotherapy and surgery. In a study conducted by Ciurea et al, 25% of the patients had recurrence, which highlights the need for long term follow up.23 In the present study, due to the huge size of the cyst and progressive neurological deficit, it was not wise to completely rely on medical therapy. Surgery was performed and post-operatively albendazole was started as an adjunct. We recommend that for treating brain hydatid cyst, the size of the cyst, multiplicity, location and neurological deficit must all be taken into consideration. 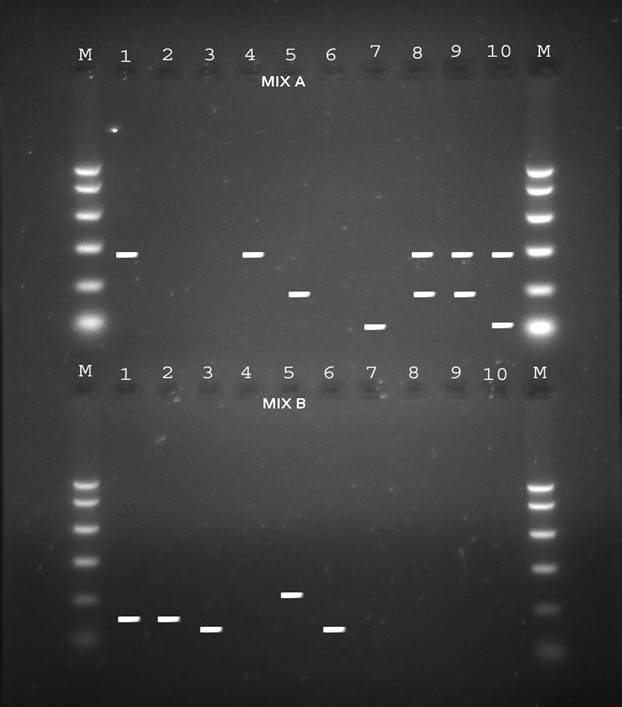
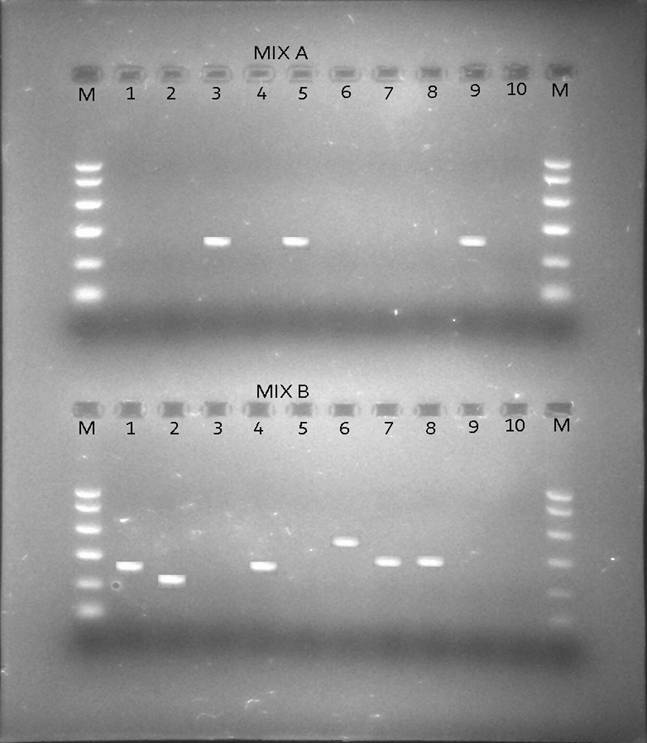
BJMP September 2016 Volume 9 Number 3
BJMP September 2016 Volume 9 Number 3
Editorial
Research Articles
Review Articles
Clinical Practice
Education and Training