A 52 year-old Caucasian male with a history of chronic obstructive airway disease (COPD) presented to the emergency department complaining of progressive shortness of breath. Two days prior, the patient had presented to the ED with similar complaints that resolved with aerosol treatments and the patient was discharged on a metered dose inhaler (MDI). The patient had been prescribed MDI’s (metered dose inhalers) previously for management of his COPD, but due to financial constraints he had been unable to fill his prescription for the past month. Emergency medical services (EMS) suspected COPD exacerbation and administered 40 mg prednisone IV and two albuterol-ipratropriumnebulisertreatments en route to the hospital, which improved the patient’s breathing symptoms.
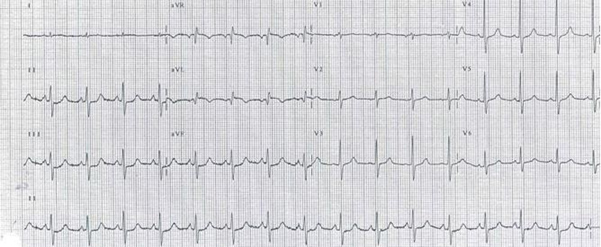
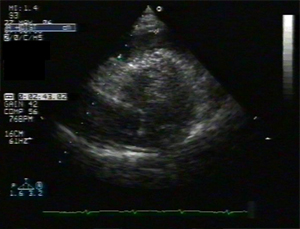
Upon arrival to the hospital, his blood pressure was 129/90, respirations 28, pulse 127, and he had an oxygen saturation of 100% on 7L/min. Physical examination revealed increased work of breathing, and wheezes in all lung fields with prolonged expiratory phase. The cardiovascular exam was normal except for tachycardia. A Routine electrocardiogram (ECG) revealed sinus tachycardia and T wave inversions in anterior leads. Chest x-ray showed old scarring in the left lower lobe. Routine cardiac enzymes showed mild elevation with a serum troponin level of 0.68ng/ml (normal range 0.0ng/ml-0.05ng/ml). The second set of troponin peaked at 1.66 ng/ml (normal 0.0ng/ml-0.05ng/ml). In view of the elevated cardiac enzymes atransthoracicechocardiogram was performed which demonstrated multiple wall motion abnormalities and reduced left ventricular ejection fraction of 25%. Coronary angiography demonstrated normal coronary arteries. Left ventriculography revealed hypokinetc mid-anterior and apical segment with a hypercontractile base with reduced ejection fraction (EF) of around 25% (normal range EF 55-65%) (Figure 1)
Figure 1. Left ventriculography demonstrating the classic appearance of Takotsubo cardiomyopathy
In light of the systolic dysfunction not in proportion with the degree of coronary artery stenosis and the multiple areas of wall motion abnormalities seen on echocardiogram, the diagnosis of Takotsubo cardiomyopathy (TCMP) was made. The diagnosis was further supported by the presence of ECG changes, troponin elevation, and the added social stresses of being unemployed. Over the course of his stay in hospital, the patient’s breathing improved with oral prednisone, inhaled tiotropium, and fluticasone/salmeterol. The patient was also treated with an angiotension converting enzyme inhibitor (ACE inhibitor), aspirin, statin, and beta-blockers. There were no adverse coronary events during the course of his hospital stay and the patient was discharged after four days. A Follow up echocardiogram after 4 weeks showed normal left ventricular systolic function.
DISCUSSION
Takotsubo cardiomyopathy (TCMP), also called stress-induced cardiomyopathy, apical ballooning syndrome, or broken heart syndrome, is a transient systolic dysfunction of the ventricles in the absence of significant coronary artery disease. Once thought to be a rare syndrome, TCMP is increasingly being identified in clinical practice, however, the prevalence and incidence are not known. It is estimated that 0.7-2.5% of patients who present with acute coronary syndrome are found to have TCMP1 .The majority of these patients are postmenopausal females, with a mean age of 62-75 years. They may present with chest pain and have a recent history of an emotional stress or severe medical illness. 1
The clinical manifestations of TCMP can mimic those of an acute myocardial infarction. Although, chest pain is a common presenting symptom, patients may also have complaints ofdyspnoeaand arrhythmias. In our casedyspnoeawas the predominant symptom and was easily confused with COPD exacerbation. Recently a few cases of concomitant stress cardiomyopathy with obstructive airway disease have been documented in literature. 2-4 While the pathophysiology of the coexistence of these two disorders is not fully understood, it is thought that both stress induced cardiac dysfunction due to exaggerated sympathetic activation and use of sympathomimetic bronchodilators instigates the myocardial stunning in such patients. Furthermore, an emotional stressor, such as death of a family member, or a physiological stressor, such as an acute medical illness, is thought to be a trigger for cardiomyopathy. 5 It is believed that the syndrome is not a result of anischemia, but there is some evidence to suggest thatoestrogenlevels may have a role in modulating the sympatho-adrenal outflow in TCMP. In mice models, chronic oestrogen supplementation seemed to have protective effects from exaggerated sympathetic outflow from the heart and brain6 . Postmenopausal women with low levels ofoestrogenmay be more vulnerable to the exaggerated catecholamine release in responses to stressors. 7
The characteristic finding in TCMP is a transient mid-ventricular or apical ballooning due to a hypokinetic portion seen on echocardiogram or on a left ventriculography. Systolic dysfunction is usually transient, inconsistent to the perfusion area of a single coronary artery, and usually resolves within 4-6 weeks. 8 Additional findings include ECG changes with ST segment deviations in precordial leads being the most common. Cardiac enzymes have been noted to have moderate elevations.9.
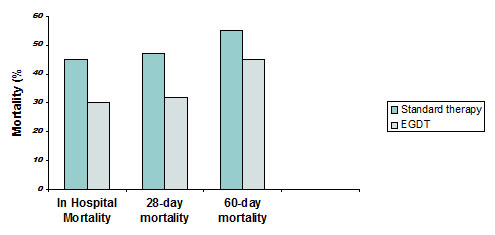
As data regarding the treatment of TCMP is limited, medical management mainly consists of symptomatic therapy with aspirin, ACE inhibitors, beta-blockers, and diuretics, also used in acute coronary syndrome.10 Patients who present acutely are treated as acute coronary syndrome and often receive emergency coronary angiography. However, less invasive imaging techniques, such as echocardiograms, should first be examined carefully. Due to the transient nature of the syndrome, the duration of treatment is unknown with some studies suggesting that there is no benefit with chronic treatment. 11 The prognosis is fairly good, with in hospital mortality rates being reported to range from 0-8%, and recovery of left ventricular function in the majority of patients. 9, 12
TCMP is difficult to distinguish from acute coronary syndrome on first presentation. Our patient had significant social stress. She presented with severedyspnoeaand was treated for COPD exacerbation. Elevation of cardiac enzymes and ECG changes lead to further evaluation and diagnosis of stress cardiomyopathy. This atypical presentation of TCMP showcases the importance ofutilisingthe routine noninvasive imaging and laboratory values to guide the diagnosis. Furthermore physicians need to maintain a high clinical suspicion for this syndrome.
Urinary tract infection (UTI) is the second most common infectious complaint in geriatric clinics overall, and the most common outpatient complaint caused by bacteria.1 The diagnosis and treatment of UTI in the elderly is not the same as treating UTI in adults. In frail elderly patients with age-associated multiple severe underlying disorders and cognitive impairment, early recognition of bacteraemic UTI and prompt, appropriate treatment are critical in reducing the mortality.2Also, the extensive and inappropriate use of antimicrobial agents has invariably resulted in the development of antibiotic resistance which, in recent years, has become a major problem worldwide.3 The diagnosis and empirical treatment of UTI in the elderly is challenging and a sound knowledge of the prevalent epidemiology of bacteria and their resistance pattern is necessary for the same. However, there is not much information on the aetiology and resistance pattern of UTI in the elderly in India. This study was done to find out the present uropathogen profile causing UTI in our centre and their antibiotic resistance patterns.
Subjects and methods
This prospective study was done at our tertiary care centre from January to December 2008. The study included all patients who were admitted or visited the outpatient departments in the hospital with symptoms of UTI during the study period and had UTI confirmed by positive urine culture reports. Only one sample from each subject was considered. Subjects with clinical symptoms of UTI but no growth on culture were excluded from final analysis. Subjects who were treated with another antimicrobial within the previous 48 hours, or within 24 hours if only a single dose and in the presence of an appropriate positive culture and ileal loops or vesicoureteral reflux were also excluded from the study. Complete data regarding demography, sex preponderance, associated symptoms, pathogenic organisms causing UTI and their antibiotic resistance were collected.
Overall, 194 subjects were included in the study (male: 116, female: 78). The mean age of the study population was 73.54±7.19 years, ranging between the ages of 65 and 96. The distribution of patients according to gender across various age groups is given in table 1. A general trend of more male subject enrolment was seen across all the age groups.
Table 1. Age and gender distribution of complicated and uncomplicated urinary tract infection.
Age group
Male
Percent
Female
Percent
Total
Percent
65-74
66
56.9
48
61.5
114
58.8
75-84
40
34.5
24
30.8
64
33.0
85-94
10
8.6
5
6.4
15
7.7
≥95
0
0
1
1.3
1
.5
Total
116
100.0
78
100.0
194
100.0
Isolation and identification of uropathogens
A clean catch midstream specimen, or suprapubic aspirate in subjects who were unable to give the former, was collected in a sterile, wide-mouth, leak-proof container to hold approximately 50ml from these subjects. Using a calibrated loop method of loop diameter 4 mm, 10 µL of the uncentrifuged specimen was transferred onto the agar plate and streak, using the modified Mayo’s technique without flaming the loop for isolation, and incubated at 35- 370C for 24 hours. A specimen was considered positive for UTI if a single organism was cultured at a concentration of >105 Colony Forming Units/ml. The Gram-positive and Gram-negative organisms culture isolates were further identified by using various biochemical reactions up to genus/species level wherever applicable.
Antibiotic sensitivity testing
In the presence of any potential growth, antibiotic sensitivity testing was done by the Modified Kirby-Bauer disc diffusion method according to the Clinical and Laboratory Standards Institute (CLSI) guidelines.4 The antibiotics tested were Imepenem, Meropenem, Ciprofloxacin, Ofloxacin, Norfloxacin, Amikacin, Gentamicin, Nitrofurantoin and Cotrimoxazole (Pathoteq Labs, India).
Extended Spectrum Beta-Lactamase (ESBL) detection
The screening for ESBL was done using Cefpodoxime (<17mm), Ceftazidime (<22mm), Aztreonam (<27mm), Cefotaxime (<27mm) and Ceftriaxone (<25mm). If the organisms showed the zone of inhibition lower than the minimum for any antibiotic disc, ESBL positivity was suspected. The phenotypic confirmation was done by testing the strain against Ceftazidime (Ca) and Ceftazidime/Clavulanic Acid. A > 5mm diameter of the zone of inhibition for Ceftazidime/Clavulanic Acid in comparison to Ceftazidime was considered indicative of ESBL production. Escherichia coli (E. coli) ATCC 25922 was used as ESBL negative and Klebsiella pneumoniae (K. pneumoniae) 700603 was used as ESBL positive reference strain.4
Statistical analysis
Descriptive statistics (totals, means, percentages, and standard deviations) were conducted using the statistical software package - SPSS Version 16.0 (SPSS Inc., Chicago, USA). Age, gender, organisms causing UTI, their antibiotic sensitivity and resistance, symptomatology of these subjects, and risk factors for UTI were included in the analysis and the results presented in tables and figures.
Results
Fever (57/194 - 29.4%) and dysuria (52/194 - 26.8%) were common symptoms of most UTI patients (Fig. 1). Diabetes mellitus (DM) and recent uro-genital instrumentation were the most common risk factors associated with UTI in the present study (Table 2). The organism profile and their antibiotic resistance profile were similar in patients with or without DM.
Figure 1. Various symptomatologies seen in patients with urinary tract infection during the initial presentation
Table 2. Frequency of various risk factors in subjects with urinary tract infection.
Risk Factor
Frequency
Percent
Catheterization
29
14.9
Diabetes Mellitus
97
50.0
Immunosuppression
2
1.0
Recent history of uro-genital Instrumentation
43
22.2
Recurrent urinary tract infection
14
7.2
Renal stones
5
2.6
E. coli (138/194 - 71.1%) was the most commonly isolated pathogen responsible for UTI in the present study (Figure 2). 56.2% of the total infection was caused by ESBL positive organisms. The antimicrobial potency and spectrum for nine selected antimicrobial agents (Imepenem, Meropenem, Ciprofloxacin, Norfloxacin, Ofloxacin, Gentamicin, Amikacin, Nitrofurantoin and Cotrimoxazole) against the uropathogens were studied. The highest and least antibiotic resistance was noted against fluoroquinolones (79.9%) and carbapenems (3.61%) respectively (Fig. 3).
Figure 2.Frequency and distribution pattern of urinary tract infection pathogens and percentage Extended Spectrum Beta-Lactamase (ESBL) production.
Figure 3. Resistance pattern to various antibiotics of the uropathogens
Discussion
While increased frequency and dysuria are usual symptoms of UTI, uncertainty looms around the same as these symptoms can be masked by catheterisation, or be common and chronic in the elderly even in the absence of UTI.5-10Fever was the most common symptom of UTI in the present study as with similar studies worldwide.11-13 Studies have found that the elderly do not lack a febrile response; that an elevated temperature was the most common initial symptom, a marker for a serious infection, and the most important clinical indicator for antibiotic treatment.14-16 Whitelaw et al17 reported that a delay in interpreting fever as a symptom of UTI led to a high mortality rate in the elderly within 24 hours of admission.
Diabetes isconsidered as an important risk factor for UTI with manyauthors having defined UTI in patients with DM as complicated when the UTI is symptomatic.18-19 However, the authors did not find that DM influenced the organism profile and their antibiotic resistance in the present study. Bonadio et al20 studied the influence of DM on the spectrum of uropathogens and antimicrobial resistance in elderly adult patients with asymptomatic UTI (mostly hospital-acquired). They found that DM per se did not seem to influence the isolation rate of different uropathogens and their susceptibility patterns to antimicrobials. These findings indicate that, although DM is a known immunomodulator, the role played by the same in altering the antibiotic resistance is minimal compared to recent invasive procedures.
Although the uropathogen profile of the present study resembles similar studies worldwide, the antibiotic resistance of these organisms was unusually high.2, 21 Cotrimoxazole is the recommended drug for treating UTI. However, more than one third of the study subjects were resistant to the first-line drug. 79.9% of the uropathogens were resistant to fluoroquinolones, which are considered as the second-line drug. As prior fluoroquinolone use is a known risk factor for fluoroquinolone-resistantE. coli infection, it is plausible that frequent fluoroquinolone prescriptions may be contributing to the observed resistance.22-23 Aypak et al 24 found that treatment durations were statistically longer than the recommended three-day course when patients were empirically treated with fluoroquinolones due to increased resistance rates, and suggested to discourage the empirical use of fluoroquinolones in UTI.
The most troublesome finding of the present study is that ESBL-positive organisms accounted for 56.2% of the total infection. Not much information on ESBL-producing organisms causing UTI is available from India and most of these reports are from the younger population. The prevalence of ESBL-positive UTI in these studies varied between 26.6% and 48.3%.25-26 To the best of our knowledge, this is the highest ever reported prevalence of ESBL-positive UTI in the elderly worldwide. ESBL-producing organisms are frequently resistant to many of the antimicrobial agents usually recommended for the treatment. As lesser new antibiotics are available for their management, we need to be concerned of this issue in years to come especially in tertiary care centres. A unified antibiotic protocol is necessary to limit the morbidity and mortality associated with inappropriate and under-treatment of UTI.
The limitations of the present study were that altered mental status was not considered as one of the clinical manifestations of UTI in the elderly, which could have mitigated the total number of study subjects included in the study. In addition, the phenotypic confirmation of ESBL-positive organisms was done using only Ceftazidime/Clavulanic Acid and not Cefotaxime/Clavulanic Acid as per the latest CLSI guidelines. As a result, there may be under-reporting of the incidence of ESBL organisms in the present study.
In conclusion, we report a significantly high resistance to common antibiotics among the uropathogens in the present study. Furthermore, the very high rate of ESBL-positive UTI is of concern, and monitoring for the same is necessary to prevent treatment failure and increased morbidity and mortality with UTI.
Diffuse Alveolar Haemorrhage (DAH) is a rare but serious and frequently life-threatening complication of a variety of conditions. DAH refers to a clinical syndrome resulting from injury to the alveolar capillaries, arterioles, and venules leading to red blood cell accumulation in the distal air spaces because of leakage of alveolar capillaries. Most cases of DAH are caused by capillaritis associated with systemic autoimmune diseases such as ANCA-associated vasculitis, anti-GBM disease, and systemic lupus erythematosus.1 Treatment is with immunosuppressants for patients with autoimmune causes and respiratory support if needed.
Diffuse alveolar haemorrhage syndrome is not a specific entity but is a syndrome that suggests a differential diagnosis and a specific sequence of testing.
Aetiology
Many disorders can cause alveolar haemorrhage; they include
Coagulation disorders caused by diseases or anticoagulant drugs
Isolated pauci-immune pulmonary capillaritis
Idiopathic pulmonary haemosiderosis
Bone marrow or solid organ transplantation.
Clinical Presentation
The clinical presentation of diffuse alveolar haemorrhage may reflect either alveolar bleeding alone or features of the underlying cause (e.g., haematuria in Wegener granulomatosis, arthritis in systemic lupus erythematosus). Hence, its recognition requires a high degree of suspicion. Some patients present with severe acute respiratory distress requiring mechanical ventilation. However, dyspnoea, cough, and fever are the common initial symptoms and are most often acute or subacute (i.e., present for less than a week). The fever is usually due to the underlying cause, such as lupus. Haemoptysis may be absent at the time of presentation in up to a third of patients because the total alveolar volume is large and can absorb large amounts of blood, without extending more proximally into the airways. Apparent haemoptysis, if present, must be differentiated from haematemesis or pseudohaemoptysis (alveolar flooding with fluid that resembles blood, as in Serratia marcescens pneumonia, in which the reddish hue of the infecting organism can create the impression of alveolar bleeding).
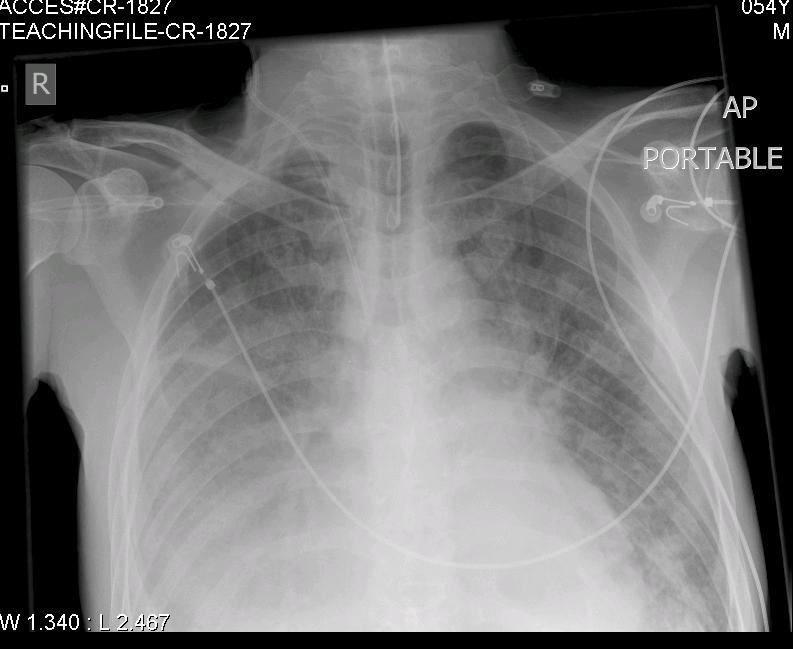
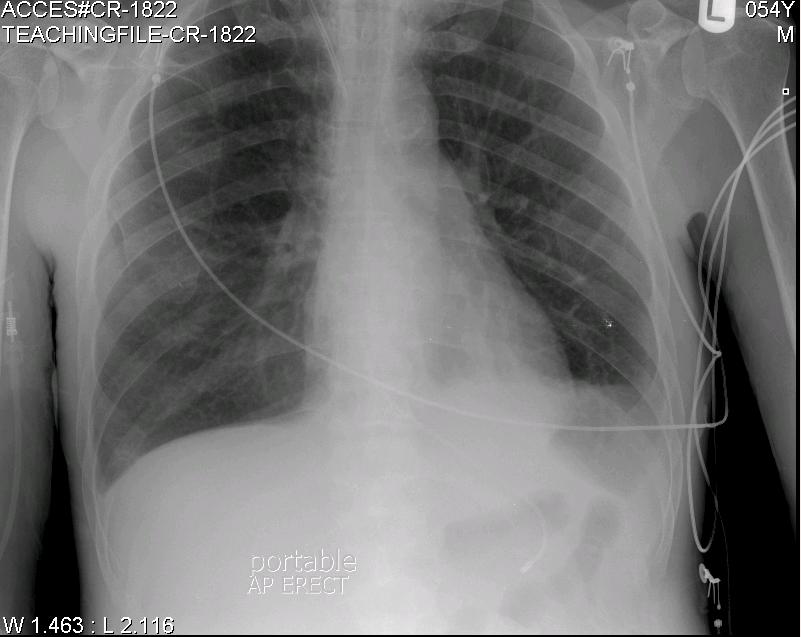
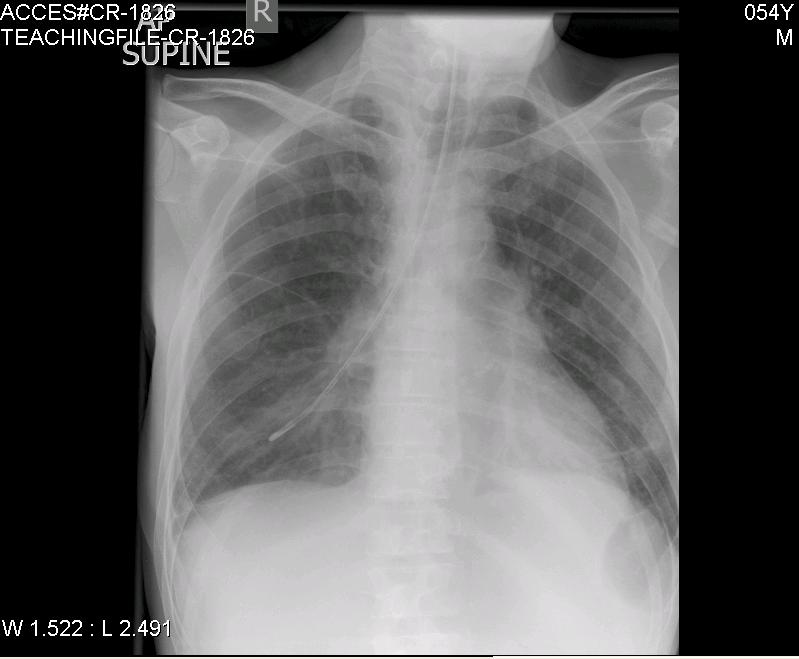
Chest X-ray and Chest CT scan typically shows bilateral infiltrates (figure 1 &2)
Figure 1
Figure 2
DAH & ANCA associated vasculitides
Wegener's Granulomatosis (WG) is an uncommon disease that affects about 1 in 20,000 to 1 in 30,000 people. WG is defined by the triad of granulomatous inflammation of the respiratory tract, vasculitis of small to medium-size vessels and necrotizing glomerulonephritis. The onset of WG may be indolent with few symptoms, or it may have a rapid and severe onset. About 90% of patients have symptoms of a cold or runny nose or sinusitis that fail to respond to the usual therapeutic measures and last considerably longer than the usual upper respiratory tract infection. Other symptoms include nasal membrane ulcerations and crusting, saddle-nose deformity, inflammation of the ear with hearing problems, inflammation of the eye with sight problems, cough (with or without the presence of blood), pleuritis, (inflammation of the lining of the lung), rash and/or skin sores, fever, lethargy weakness, loss of appetite, weight loss, arthritic joint pain, night sweats, and haematuria which may or may not be indicated by a change in urine colour.Thediagnosis of WG depends on the combination of clinical presentation, serological markers, and histopathological findings. ANCA is a sensitive and specific marker for ANCA-associated systemic vasculitis. In a study done by U. Schönermarck et al,9 624 ANCA- positive patients were included, (C-ANCA: 333, P-ANCA: 291). C-ANCA were highly sensitive (81%) and specific (99.5%) for WG, resulting in high positive predictive value (PPV) (94%). Many studies showed that combining proteinase 3 (PR3) and C-ANCA results(C-ANCA/PR3) increases specificity and Positive Predictive Value close to 100%, but reduces sensitivity close to 70%.10,11,13,14 In summary, the presence of C-ANCA & PR3 antibody is highly suggestive of WG. This led to reevaluation of the role of biopsy for diagnosis of WG in multiple studies.4, 14, 15
The site of biopsy is dependent upon the clinical status. A nasal or sinus biopsy may be the least invasive way to diagnose WG. Renal biopsy is helpful if there is evidence of renal insufficiency or glomerulonephritis. A lung biopsy should only be considered if potentially diagnostic tissue cannot be obtained from any other site.1 Hoffman et al performed a total of 82 open lung biopsies in patients with small vessel vasculitis of which 89% showed evidence of combined vasculitis and necrosis, granulomas and necrosis were found in 90%.16 59 transbronchial biopsies were performed in 48 patients and only four specimens had evidence of vasculitis and granulomas were identified in an additional three. Thus, the role of transbronchial biopsies in these patients is limited and open lung biopsies are more informative but carry a higher morbidity and mortality.
The incidence of DAH has beenreported as between 7-45% in Wegner’s Granulomatosis (WG), and 10-30% in Microscopic Polyangitis (MPA).3, 5, 6 The lungs are the most commonly affected organ in WG with evidence of involvement in over 90% of patients during the course of their disease; in 9% it is the only organ affected. 5,7 In MPA lung involvement is less common than inWG, and occurs in up to 50% of cases during the course of the disease.8 Pulmonary involvement ranges from subclinical changes on high resolution computed tomography to devastating haemoptysis. Approximately 5% of patients will have a fulminant presentation requiring assisted ventilation.
Treatment
Patients with DAH with or without glomerulonephritis, who are found to have ANCA positive can be generally assumed to have WG or MPA. The type of ANCA (PR3-ANCA or MPO-ANCA) found is irrelevant with respect to the initial management of this patients.1 The backbone of therapy is the early identification of disease followed by the rapid induction of disease control with immunosuppression. Early recognition is crucial, because the prompt institution of supportive measures and immunosuppressive therapy is required for survival. The intensity of the initial treatment depends on the severity of the disease. Based on the European Vasculitis Study Group (EUVAS), which categorized the patients in groups according to the severity of their disease, the presence of DAH put the patient in the severe disease group.17 The management of these patients is a combination of corticosteroid and cyclophospamide. S.L Hogan showed that cyclophosphamide reduces mortality and increase the likelihood of inducing remission in patients with ANCA-associated vasculitis. 18
DAH is animportant cause of morbidity and mortality in ANCA- associated vasculitis, the mortality rate may reach 66%, which is six times greater than vasculitis without alveolar hemorrhage.3,19,20,21 Based on the high mortality rate with DAH in ANCA-associated vasculitis, and reduction in mortality shown with cyclophosphamide, treatment with cyclophosphamide should be started as early as possible, based on the clinical presentation and the presence of ANCA, without waiting histological confirmation.
Conclusion
DAH leading to acute respiratory distress syndrome is a rare and life threatening condition in adults with ANCA positive vasculitis. Patients with DAH with or without glomerulonephritis, who are found to have ANCA positive can be generally assumed to have WG or MPA, and diagnostic lung biopsy may be deferred. Early institution of treatment with prednisone and cyclophosphamide can significantly reduce morbidity and mortality.
Key points
1.Patients with Wegner’s Granulomatosis often present with diffuse alveolar haemorrhage. These patients must be treated promptly as delay in treatment results in high morbidity and mortality.
2.Lung biopsy is very helpful if it shows granulomatous inflammation and vasculitis however it lacks sensitivity and specificity.
3.Detection of C-ANCA with Proteinase-3 can substitute for biopsy in the diagnosis of WG in patients who present with diffuse alveolar haemorrhage.
A 44 year old male presented to the emergency department complaining of shortness of breath. The symptoms had commenced suddenly four weeks ago. He had been breathless at rest, and subsequently developed a productive cough with white sputum. He denied chest pain. He was known to have the sickle cell trait but was otherwise in good health. He was a non-smoker.
Since the onset of symptoms, and prior to this admission, the patient presented to two different emergency departments. The working diagnosis was, and remained, community acquired pneumonia. On initial presentation empirical treatment for a community acquired pneumonia was commenced. Failure to improve resulted in additional cover for atypical organisms and the prescription of a short course of steroids on the subsequent admissions.
Initial observations revealed the patient was tachypnoeic and tachycardic, with a respiratory rate of 25 breaths per minute, heart rate of 114 beats per minute. He was apyrexial (temperature of 36.5°C ). Pulse oximetry showed an oxygen saturation of 94% on room air. His blood pressure was recorded as 183/99 millimetres of mercury.
On examination large volume peripheral pulses, raised jugular venous pressure (5 cm), bi-basal crepitations, and bilateral ankle oedema were elicited/identified. Auscultation of the heart revealed a loud diastolic murmur audible throughout the praecordium.
A 12 lead ECG showed normal sinus rhythm, normal axis and left ventricular hypertrophy. Arterial blood gas analysis on room air showed a pH of 7.46, pa02 9.6 kPa, pCO2 4.3 kPa, HCO3 23.8 mmol/L, BE + 0.8 and lactate of 0.7 mmol/L. Routine venous blood tests did not identify any elevated markers of infection or inflammation. A chest radiograph (Figure 1) showed cardiomegaly and pulmonary oedema.
Figure 1
The patient was administered oxygen and given a diuretic to improve his ventilation.
The working diagnosis was congestive cardiac failure in the presence of what was presumed to be a new murmur. Urgent echocardiography revealed an aortic root of 6.2cm diameter at sinus level, with an evident dissection flap. There was no obvious haematoma. Severe free flowing aortic regurgitation, a dilated hyperdynamic left ventricle and a 0.7 cm diameter pericardial effusion anteriorly were also noted. It was concluded that the patient had a sealed 7cm type A aortic dissection. This was confirmed by a CT scan (Figure 2).
Figure 2
Large bore venous access was obtained and an intravenous beta blocker (Labetalol) administered. Urgent transfer to a tertiary cardio-thoracic surgical centre was made. He underwent aortic root and valve replacement, along with coronary artery bypass grafting to the right coronary artery using a reversed long saphenous vein graft. Postoperatively, he was anticoagulated on Warfarin, and was also placed on beta blockade therapy (Bisoprolol), a diuretic (Frusemide), an ACE inhibitor (Ramipril), and a statin (Simvastatin).
Discussion
Aortic dissection is a medical emergency. If left unrecognised or untreated mortality can be as high as 80% in two weeks, or 90% within three months1,2. 96 % of patients with aortic dissection present primarily with chest pain. The remaining 10% present with symptoms secondary to impairment of blood supply to other organ systems3. Dissections involving the ascending aorta present with retrosternal chest pain, while interscapular pain suggests involvement of the descending aorta. Pleuritic pain may indicate haemorrhage in the pericardial sac, with the potential for acute cardiac tamponade.
Only 6% of aortic dissections present with acute congestive cardiac failure. Patients presenting with aortic dissection and congestive cardiac failure are more likely to present without chest pain and have a valvular abnormality. When chest pain is present, the pain is more often mild and less likely to be abrupt in onset. Patients are less likely to be hypertensive on presentation and more likely to present in shock. These patients are more likely to have Stanford type A dissection . Congestive cardiac failure does lead to a delay in surgical intervention4.
Congestive cardiac failure is usually due to aortic regurgitation from aortic valve disease, incomplete aortic leaflet closure, or aortic valve disruption. In the setting of unexplained cardiac failure aortic dissection should be considered, especially when an aortic regurgitant murmur has been detected clinically. Heart failure has been associated with supravalvular aortic stenosis in the presence of a painless type A dissection, in a patient presenting with persistent cough5. Rupture of aortic dissection into the right atrium, right ventricle, or main pulmonary artery may lead to a left to right shunt and congestive heart failure6.
Painless aortic dissection has been recorded in other contexts, particularly with chronic dissection and in patients with Marfan’s syndrome.The absence of chest pain should not exclude aortic dissection.
In anticipation of new recommendations from the Institute of Medicine and others, it behooves physicians and healthcare providers to review their knowledge base concerning adequate vitamin D intake for fall and fracture prevention in the elderly. There is enough new data for the Institute of Medicine to consider a new Dietary Reference Intake, or DRI, for vitamin D.1 A recent review by Bischoff-Ferrari et al, of numerous randomized controlled trials of vitamin D supplementation in older persons, concluded that both falls and fractures could be prevented. In addition, a dose-response relationship suggested that the optimal supplementation dose is 700 IU to 1000 IU per day.2 Epidemiologic associations between low vitamin D status and various cancers has led some to recommend balancing risk and benefit of moderate ultraviolet light (UV) exposure against complete UV protection for prevention of skin cancer.3 Others have reviewed the epidemiologic evidence for vitamin D supplementation in treatment of hypertension and prevention of cardiovascular disease.4 These epidemiologic studies are tantalizing, yet the evidence is not sufficient to support a causal relationship in making decisions about vitamin D supplementation for the prevention of cancer and cardiovascular disease. I will limit my editorial comments to preventing falls and fractures.
I would suggest looking at potential short- and long-term risks as well as the benefits of any intervention. What evidence do we have for the risks of vitamin D use for prevention? One recent study using a single dose of 500,000 IU of vitamin D daily showed an increased relative risk of fractures,5 but the dose of vitamin D in that study was far higher than other randomized controlled trials. Bischoff-Ferrari et al reviewed documented cases of hypercalcaemia in the randomized controlled trials;2 those authors add that only one trial reported nephrolithiasis, the Women’s Health Initiative.6 It is noteworthy that only the self-reported vitamin D and calcium dose was determined in that study, not the vitamin D status of the subjects. My opinion is that hypercalcaemia is uncommon and its complications are rare.
Many interventions that are routinely recommended for the older person probably have higher risks than the 700 IU to 1000 IU of vitamin D per day suggested by the evidence. Medications for hyperlipidaemia are one case in point; antihypertensives are another. Both are considered relatively safe and effective in primary and secondary prevention of cardiovascular disease. The long-term risks of the supplementation of 700 IU to 1000 IU of vitamin D are not well known compared to those long-term risks associated with lipid-lowering drugs or antihypertensives. On the other hand, some older persons at increased fall risk have more immediate threats to their health from a fall or fracture than any long-term risks of vitamin D supplementation. Given the detrimental consequences of falls and fractures in the elderly, the risks of vitamin D supplementation may be worth it.
Troponin T is a protein component of cardiac muscle. When death or damage of the myocardium occurs, it is released in to the circulation and can be detected by immunoassays 1. Troponin T is a sensitive and specific marker of myocardial damage when taken at least 12 hours after a suspected cardiac event and can be detected up to 7-10 days after myocardial damage 1,2. When used in conjunction with clinical history, electrocardiograms (ECGs) and cardiac imaging it is effective in excluding acute coronary syndrome (ACS) and myocardial infarction (MI). The cost of a Troponin T assay is £3.75 per sample inclusive of staff time.
Troponin concentrations have been incorporated in up to date definitions of acute MI. One of the criteria for diagnosis of acute MI is the detection of rise and/or fall of cardiac biomarkers (Troponin) with at least one value above the 99th percentile of the upper reference limit (URL) together with evidence of myocardial ischaemia with at least one of the following: ischaemic symptoms, new ischaemic ECG changes, pathological Q waves on ECG, or imaging suggesting loss of viable myocardium or new regional wall abnormality 3. Other criteria include unexpected cardiac death involving cardiac arrest, Troponin concentrations associated with percutaneous coronary intervention (PCI) and coronary bypass grafting (CABG) and pathological findings of acute MI 3. Troponin T is an important component of the risk stratification of patients with acute myocardial ischaemia and can be used to predict 30-day mortality 4,5.
Detection of a rise and/or fall in Troponin T concentration is important when diagnosing acute MI 3,6. It is the rise and fall that differentiates individuals who have sustained myocardial damage from other causes such as chronic kidney disease (CKD) 3, 7. In these other conditions the elevated Troponin T concentrations are sustained. To establish the diagnosis of MI, one elevated value above the decision level is required. The demonstration of a rise and/or fall in Troponin T levels assists clinicians in distinguishing elevated background Troponin T concentrations from elevations in the same patients suggestive of MI. Detection of rise and/or fall also identifies those patients with re-infarction within a short time period after an acute MI 8.
It is important to remember however that if the patient presents 24 hours after the onset of symptoms this rise and fall of Troponin T concentration is not necessary to make the diagnosis of MI. Troponin T levels must be interpreted in the light of the clinical presentation. An elevated concentration of Troponin T in the absence of clinical evidence of ischaemia should prompt a search for other aetiologies, such as CKD, congestive heart failure, myocarditis, aortic dissection, or pulmonary embolism 3, 6.
Risk stratification also includes the measurement of lipid profile in those presenting with suspected ACS or MI. To ensure that a cholesterol level representative of the patient’s normal baseline the blood sample must be organised within 24 hours of the event. In those with delayed presentation or where cholesterol is omitted on admission clinicians should wait until 3 months after the event to obtain a reliable cholesterol level, although most would be expected to have started lipid-lowering medications 9,10,11.
Method
We studied Troponin T requests made between 4pm and 7pm for a four-month period. Request cards were retrieved and the Troponin T result for each request was obtained. Any other Troponin T results obtained at any time relating to that event were noted as well as any rise and fall of the Troponin T concentrations. Review of the hospital notes for each patient established the working diagnosis, whether any other appropriate investigations had been carried out during admission, co-morbidities that were present and current relevant medications.
The final patient outcome was noted. The number of patients discharged on the same day, who would have otherwise been admitted overnight, based on Troponin T concentration was determined. Those patients with a Troponin T concentration above the 99th percentile of the upper reference limit (URL) used in the local laboratory (Troponin T <0.03ug/L) who were not discharged on the day of Troponin T measurement were identified and the reason for admission determined. The fiscal impact of the extended laboratory service was calculated.
Results
Of 162 Troponin T requests received during the four-month period, 140 (86%) were included in the study; 22 (14%) were excluded (12 haemolysed, 1 unlabelled, 2 not on computer system, 7 clinical notes unavailable).
The study population comprised of 74 (53%) male and 66 (47%) female patients. The age range was 21 – 101 years; mean (±SD) 67.6 (±16.8).
Half of Troponin T requests were received from the Acute Assessment Unit (AAU), 20% from the Emergency Department, 14% from inpatients, 8% from the Critical Care Complex (CCC) and 8% from the Coronary Care Unit (CCU).
Clinical notes indicated that 97 (69%) of Troponin T requests were taken appropriately at least 12 hours after the onset of the event, 19 (14%) were taken less than 12 hours after the event, in the remaining 24 (17%) the time of sample in relation to the event was not known. Interestingly only 30% of request cards had documented that sample was taken at least 12 hours after the event.
The indication documented on each request card is detailed in Figure 1. Indications detailed under other included: trauma, sepsis, collapse, cold & clammy, oesophageal cancer with hypercalcaemia, poor complex tachycardia, post-operative after abdominal aortic aneurysm repair, respiratory infection, sweating, palpitations, fall and repeat bleed because of previously unsuitable sample.
Figure 1: Indication noted on request card for Troponin T. ACS: acute coronary syndrome, MI: myocardial infarction, SOB: shortness of breath, LVF: left ventricular failure, CCF: congestive cardiac failure.
One hundred and two (73%) patients had a non-elevated Troponin T concentration of <0.030ug/L and 38 (27%) had an elevated Troponin T concentration >0.03ug/L. Only 5 (4%) patients had the rise and fall of Troponin T documented.
Eighty-three (59%) patients had no lipid profile measured during the attendance/admission. Of the remaining 57 patients, 31 (54%) had cholesterol assayed within 24 hours of the event, in 16 (28%) the cholesterol was taken between 2 and 17 days after the event and in 10 (18%) patients the time of cholesterol assay in relation to the event was not known. Overall only 1 in 5 patients had a lipid profile obtained within 24 hours of the event.
Interestingly of the 38 patients with raised Troponin T concentration of >0.03ug/L only 13 (34%) had a lipid profile organised. Only 7 of the 13 (54%) were obtained within 24 hours of the event, 4 were taken between 2 and 10 days after the event and in 2 patients it was not known when the lipid profile was obtained in relation to the event.
Overall no correlation was noted between cholesterol and Troponin T concentrations in all patients who had an elevated Troponin T concentration and cholesterol measured. Interestingly in those where cholesterol was measured within 24 hours of the suspected cardiac event there was some correlation, but the numbers involved were small.
The working diagnosis as stated in hospital notes is documented in Table 1.
Table 2: Reason why those patients with non-elevated Troponin T concentration of <0.03 (ug/L) were not discharged on the same day by the clinician.
Reason for admission
Number of patients
Trop T assayed <12hrs
5 (8%)
Ongoing chest pain
10 (15%)
ECG changes
3 (5%)
High CAD risk patient
2 (3%)
Monitoring and cardiology review
2 (3%)
Already inpatient
7 (10%)
Repeat attendance in 24hrs
1 (1%)
Other medical (non-cardiac) problem
28 (42%)
No reason documented
6 (9%)
Outcome not available
1 (1%)
Self discharge
2 (3%)
Total
67 (100%)
All of the 36 (26%) patients except one who were discharged on the day of Troponin T assay had a negative Troponin T concentration of <0.030ug/L. This patient had CABG one month previously and presented with chest pain and associated cough, although his Troponin T was 0.14ug/L, this was deemed not significant in view of a previous Troponin T concentration of 0.16ug/L assayed two days earlier.
Sixty three (45%) patients remained in the AAU or were admitted to a medical ward, 15 (11%) were admitted to CCU, 4 (3%) to CCC and 18 (13%) were already inpatients. Of the remaining 3 patients, 2 self-discharged and in 1 the final destination was not available.
Of those patients with a raised Troponin T concentration of >0.03ug/L 5 died during this attendance.
The majority (60/102) of patients in whom Troponin T was not raised (<0.030ug/L) still required hospital admission (Table 2). Another 6 patients with a non-elevated Troponin T concentration had no obvious reason for admission documented.
Based on an overnight stay cost of £657 we conclude that the laboratory’s extension of Troponin T service of 3 hours would save the hospital £70,956 annually. No additional manpower was required to provide the extended laboratory service as Biomedical Scientists are already providing urgent out of hour on-call service for other biochemical analysis. No additional laboratory costs were incurred, as the same number of samples would have been analysed during working hours the following day.
Discussion
There was sufficient demand for Troponin T assay to justify extension of the laboratory service for 3 hours each day. As expected most requests for Troponin T came from the AAU and the Emergency Department where the majority of patients with chest pain of potential cardiac origin would initially present. In those patients presenting with suspected myocardial damage 3 out of 4 had chest pain of non-cardiac origin.
In those patients where the time of event was known the majority had an appropriate Troponin T assay taken at least 12 hours after the event suggesting that most of the medical and nursing staff were well informed. In contrast it appears that only few of the medical profession were aware of the need to measure lipid profile soon after admission as only 1 in 5 patients had their lipid profile organised within 24 hours of the event.
The majority of requests had appropriate clinical details to justify Troponin T request. However one in four requests were deemed inappropriate (Fig. 1). Since Troponin T may be raised in other conditions the assay should be reserved for those patients where myocardial damage is suspected. Inappropriate testing is potentially hazardous and may expose patients to further unnecessary invasive investigations e.g. cardiac catheterisation with associated morbidity and mortality.
In patients presenting with chest pain, Troponin T assayed appropriately >12 hours after onset of the event can be used effectively to exclude myocardial damage and discharge can be made on the basis of this result without the need for admission. A small proportion (6%) of patients with non-elevated Troponin T concentrations who had no obvious reason for admission, were deemed unnecessary.
Dyslipidaemia plays an important role in the risk stratification of patients with suspected ACS or MI, yet only one in five patients with myocardial damage had a lipid profile organised within 24 hours of the event. Cholesterol measurements organised between 2 and 17 days after the event would not have been representative of the true concentration and were deemed inappropriate. Too few lipid profiles were assayed within 24 hours of the event in patients with an elevated Troponin T concentration to determine whether there is any correlation between cholesterol and Troponin T concentrations.
Similarly only a small number of patients had the rise and fall of Troponin T documented. The lack of serial measurements of Troponin T concentrations may have resulted in failure to recognise some patients with other conditions, which may cause elevated Troponin T concentrations and potentially subject them to unnecessary further invasive investigations.
The provision of the extended laboratory service had a positive impact; it enabled earlier discharge of patients with chest pain of non-cardiac origin, resulted in fewer unnecessary overnight hospital admissions and reduced the demand on hospital beds. Extending the service did not result in extra work for junior doctors, on the contrary by improving the efficiency of the process has not only speeded the patient journey but has improved junior doctors’ time-management.
We have shown that extending the provision of Troponin T assay for 3 hours daily has both fiscal and management benefits and reduces the number of unnecessary hospital admissions. Further extension to incorporate a 24-hour laboratory service for this assay would potentially reduce hospital admissions further with more potential savings.
Conclusion
Extending the provision of Troponin T assay for 3 hours daily has fiscal and management benefits and reduces the number of unnecessary hospital admissions of patients presenting with chest pain of non-cardiac origin.
Learning Points • Extending Troponin T service has a fiscal benefit. • Rise and fall of Troponin T values should be documented. • Lipid profile should be organised within 24 hours in all patients presenting with chest pain of potentially cardiac origin. • Measuring Troponin T where myocardial damage is not clinically suspected is potentially hazardous and may expose patients to further inappropriate and invasive investigations with associated morbidity and mortality. • In the current climate of litigation detailed documentation is necessary.
Irritable bowel syndrome (IBS) is a common disorder characterized by abdominal pain and altered bowel habit for at least three months.(1)
IBS is further defined depending on the predominant bowel symptom: IBS with constipation (IBS-C) or IBS with diarrhoea (IBS-D). Those not classified as either IBS-C or IBS-D are considered as mixed IBS (IBS-M). Alternating IBS (IBS-A) defines patients whose bowel habits oscillate from diarrhoea to constipation and vice versa.
IBS is a prevalent and expensive condition that is associated with a significantly impaired health-related quality of life (HRQOL) and reduced work productivity. IBS care consumes over $ 20 billion in both direct and indirect expenditures. Moreover, patients with IBS consume over 50% more health care resources than matched controls without IBS.(1)Based on strict criteria, 7 – 10 % of people have IBS worldwide. Community-based data indicate that diarrhoea-predominant IBS (IBS-D) and mixed IBS (IBS-M) subtypes are more prevalent than constipation-predominant IBS (IBS-C), and that switching among subtype groups may occur. IBS is 1.5 times more common in women than in men, is more common in lower socioeconomic groups, and is more commonly diagnosed
in patients younger than 50 years of age. Prevalence estimates of IBS range from 1 % to more than 20% in North America(7%).(1)In Asia the prevalence is about 5%.(3,4,5)Recently, a School-Based Study in chinareportedthe prevalence of IBS in adolescents and children was 13.25% and the ratio of boys to girls was 1:1.8.(6)Most patient with IBS in India are middle-aged men (mean age 39.4 years).(7)
Underlying pathophysiology:
Given the lack of definitive organic markers for IBS, the absence of aconsolidatedhypothesis regarding its underlying pathophysiology is not surprising. Nevertheless, important advances in research made during the past 50 years have brought us closer than ever to understanding the numerous existing aetiological factors involved in this multifaceted disorder, including environmental factors, genetic factors, previous infection, food intolerance, and abnormal serotonergic signaling in the GI tract.
Environmental factors:
The biopsychosocial model proposed by Engel(8)takes into account the interplay between biologic, psychological, and social factors. This model proposes that there is an underlying biologic predisposition for IBS that may be acted on by environmental factors and psychological stressors, which contribute to disease development, the patient's perception of illness, and impact on treatment outcomes. Different studies have shown that stress can result in release of stress-related hormones that affect colonic sensorimotor function (eg, corticotropin-releasing factor [CRF] and inflammatory mediators [eg, interleukin (IL)-1]), leading to inflammation and altering GI motility and sensation.
Genetics factors :
Twin studies have shown that IBS is twice as prevalent in monozygotic twins than in dizygotic twins.(9,10,11)IBS may be associated with selected gene polymorphisms, including those in IL-10, G-protein GNb3, alpha adrenoceptor, and serotonin reuptake transporter (SERT).
Post-infectious IBS (PI-IBS):
Culture positive gastroenteritis is a very strong risk factor for IBS. Different prospective studies show IBS symptoms developed in 7% to 32% of patients after they recovered from bacterial gastroenteritis.(12,13,14)Specific risk factors for the development of PI-IBS have been identified, including younger age, female sex, presence of severe infectious gastroenteritis for a prolonged period, use of antibiotics to treat this infection, and presence of concomitant psychological disorders (eg, anxiety).(12,13,15,16)
Small Intestinal bacterial overgrowth
Pimentel and colleagues(17,18)have shown that, when measured by the lactose hydrogen breath test (LHBT), small intestinal bacterial overgrowth (SIBO) has been detected in 78% to 84% of patients with IBS. Hence, a higher than usual population of bacteria in the small intestine has been proposed as a potential aetiological factor in IBS. While another study involving a review for the presence of gastrointestinal-related symptoms (including IBS) has shown that asensitivity of the LHBT for SIBO has been shown to be as low as 16.7%, and specificity approximately 70% and the test alone for small intestinal bacterial overgrowth were poor. Hence, combination with scintigraphy resulted in 100% specificity to assess the treatment responce, because double peaks in serial breath hydrogen concentrations may occur as a result of lactulose fermentation by cecal bacteria. (19,20)
Food intolerance :
Approximately 60% of IBS patients believe and different studies show that allergy to certain foods could trigger IBS symptoms. Recent research involving exclusion of foods patients had immunoglobulin (Ig) G antibodies, which are associated with a more delayed response after antigen exposure than IgE antibodies, resulted in significantly better symptom improvement than in patients in the non-exclusion group.(21)
Serotonin signaling in Gastrointestinal (GI) tract:
Normal gut physiology is predicated to be an interaction between the GI musculature and the autonomic nervous system (ANS), and central nervous system (CNS) by the neurotransmitter serotonin (5-hydroxytryptamine [5-HT]) . Impairment in this interaction affects GI motility, secretion, and visceral sensitivity leading to the symptoms associated with IBS .(22)
Preliminary steps toward making a positive diagnosis of IBS:
A careful history and physical examination are frequently helpful in establishing the diagnosis. A variety of criteria have been developed to identify a combination of symptoms to diagnose IBS. Different guidelines from different studies help in making a positive diagnosis of IBS based primarily on the pattern and nature of symptoms, without the need for excessive laboratory testing. In 1978, Manning and colleagues(23,24) proposed diagnostic criteria for IBS that were found to have a reasonable sensitivity of 78% and a specificity of 72%.(1)In 1984, Kruis and colleagues developed another diagnostic criteria with a high sensitivity of 77% and a specificity 89%. Likewise, in 1990 Rome I(25)criteria came with a sensitivity of 71% and specificity of 85%. RomeII(1999)(26)and Rome III(2006)(27)have not been evaluated yet. None of the symptom based diagnostic criteria have been evaluated and ideal reliability found.(1)
Summary of diagnostic criteria used to define IBS:(1)
In 1978, Manning defined IBS as a collection of symptoms, given below, but did not describe their duration. The number of symptoms that need to be present to diagnose IBS was also not reported in the paper, but a threshold of three positive is the most commonly used:
a) Abdominal pain relieved by defecation
b) More frequent stools with onset of pain
c) Looser stools with onset of pain
d) Mucus per rectum
e) Feeling of incomplete emptying
f) Patient-reported visible abdominal distension
Kruis in 1984, defined IBS by a logistic regression model that describes the probability of IBS. Symptoms need to be present for more than two years. Symptoms are as follows:
a) Abdominal pain, flatulence, or bowel irregularity
b) Description of character and severity of abdominal pain
c) Alternating constipation and diarrhea
Signs that exclude IBS (each determined by the physician) :
a) Abnormal physical findings and/or history pathognomonic for any diagnosis other than IBS
b) Erythrocyte sedimentation rate >20 mm/2 h
c) Leukocytosis >10,000/cc
d) Anaemia (Hemoglobin < 12 for women or < 14 for men)
e) Impression, the physician could perform a PR and see blood or the patient may report it.
Again in 1990, Rome I defined IBS as abdominal pain or discomfort relieved with defecation, or associated with a change in stool frequency or consistency, PLUS two or more of the following symptoms on at least 25% of occasions or days for three months:
a) Altered stool frequency
b) Altered stool form
c) Altered stool passage
d) Passage of mucus
e) Bloating or distension
Rome II, in 1999, redefined the criteria as abdominal discomfort or pain that has two of three features for 12 weeks (need not be consecutive) in the last one year.
a) Relieved with defecation
b) Onset associated with a change in frequency of stool
c) Onset associated with a change in form of stool
Recently , Rome III (2006) defined IBS as recurrent abdominal pain or discomfort three days per month in the last three months associated with two or more of:
a) Improvement with defecation
b) Onset associated with a change in frequency of stool
c) Onset associated with a change in form of stool
The role of routine diagnostic investigation in patients with IBS:
Routine diagnostic investigation is based on the age of the patient, family history of selected organic diseases including colorectal cancer, inflammatory bowel disease(IBD), coeliac sprue and the presence of ‘alarm’ features(table1), such as rectal bleeding, weight loss, iron deficiency anaemia and nocturnal symptoms.(1) In patient with typical IBS symptoms and no alarm features, routine diagnostic investigation (complete blood count, serum chemistry, thyroid function tests, stool for ova and parasites and abdominal imaging) is not recommended(1)because of a low likelihood of uncovering organic disease.
Table-1 Lists of alarm features:
Rectal bleeding
Weight loss
Iron deficiency anaemia
Nocturnal symptoms: abdominal pain
family history of of selected organic diseases: colorectalcancer, Inflammatory Bowel Disease(IBD), celiac sprue
Summary of diagnostic investigation in patient with IBS : (1,2)
Diagnostic Investigations:
Routine serologic screening for coeliac sprue for patients with IBS-D and IBS-M.
Lactose Breath test done in lactose maldigestion despite dietary modification.
Colonoscopic Imaging done in IBS patient (>50 yrs age) with alarm feature to rule out organic diseases and screening of colorectal cancer.
Colonoscopy with random biopsies taken in IBS-D to rule out microscopic colitis.
Management of IBS:
The goal of IBS management is to provide relief of symptoms and improve overall well-being.(28)Most studies use a combination therapy including patient education and psychological therapies, diet and fibre therapy along with different types of new emerging pharmacological therapies.
Patient education and psychological therapies:
The majority of patients with IBS have anxiety, depression and features of somatization. Psychological therapies, including cognitive behavioral therapy, dynamic psychotherapy, hypnotherapy(1)shed new light on the management of patients with IBS. The outcome of psychological therapies is improved when delivered by a trained professional (physician, occupational therapist, nurse).(29) A study by Guthrie(30)showed that psychological therapy is feasible and effective in two thirds of patients with IBS who do not respond to standard medical treatment.
Role of diet in IBS:
The concept of food intolerance and the consequent elimination of certain foods from the diet benefit symptoms of IBS. However, there is no sufficient evidence to support this.(1)
Therapeutic effectof dietary fibre, bulking agents and laxatives:The quality of evidence supporting the recommended use of dietary fibre or bulking agents to regularize bowel function is poor.(31)Ispaghula husk(Psyllium hydrophilic mucilloid ) and calcium polycarbophil are moderately effective and can be given a conditional recommendation because of the weakest type of evidence.(1) Polyethylene glycol(PEG) laxative has a role in improving stool frequency but no effect on abdominal pain. Different clinical studies and expert opinion suggest that increased fibre intake may cause bloating, abdominal distension and flatulence.(32)So gradual adjustment of dose is advised for the use of these agents.
Therapeutic effectof antispasmodic agents including peppermint oil:
Certain antispasmodics (hyoscine, cimetropium,and pinaverium and peppermint oil) may provide short-term relief of abdominal pain/discomfort in IBS.(33,34)Evidence for safety and tolerability
Agent
Mechanism of action
Targeted disorder
Clinical status
Crofelemer
CFTR
IBS-D
Phase2b complete
Linaclotide
Guanylate cyclase-c agonist
IBS-C
Phase 3
Arverapamil
Calcium channel blocker
IBS-D
Phase 3
Asimadoline
Kappa opioid agonist
IBS
Phase 2b complete
Mitemcinal
Motilin receptor agonist
IBS-C
Phase 2
Ramosetron
5-HT 3 antagonist
IBS-D
Phase 3
TD-5108
5-HT 4 agonist
IBS-C
Phase 2
DDP-773
5-HT 3 agonist
IBS-C
Phase 2
DDP-225
5-HT 3 antagonist and NE reuptake inhibition
IBS-D
Phase 2
BMS-562086
Corticotropin-releasing hormone antagonist
IBS-D
Phase 2
GW876008
Corticotropin-releasing hormone antagonist
IBS
Phase 2
GTP-010
Glucagon-like peptide
IBS pain
Phase 2
AGN-203818
Alpha receptor agonist
IBS pain
Phase 2
Solabegron
Beta-3 receptor agonist
IBS
Phase 2
Espindolol (AGI-011)
Beta receptor antagonist
IBS (all subtypes)
Phase 2
Dextofisopam
2,3 benzodiazepinereceptors
IBS-D and IBS-M
Phase 3
Table 1: Source: ACG Task Force on IBS(2009)
of these agents are very limited.The commonest adverse effects are dry mouth,dizziness and blurred vision.(34-36)
Therapeutic effectof anti-diarrhoeal medications:
The anti-diarrhoeal agent ‘Loperamide’ is effective at slowing down colonic transit and improving stool consistency for the treatment of IBS-D with no severe adverse effects.(37)But safety and tolerability datas are still lacking in many studies.
Therapeutic effect of antibiotics:
Many studies show well tolerance of a short term course of non-absorbable antibiotics (Rifaximin) is most effective for improvement of global symptoms in IBS-D and IBS patient with the predominant symptom of bloating and other associated symptoms, such as diarrhoea and abdominal pain.(38-40) While, the Unted States Food and Drug Administration (FDA or USFDA) approved Rifaximin for treatment of traveler’s diarrhoea. Other antibiotics, Neomycin(41), Clarithromycin and Metronidazole(42)have been well evaluated for the management of IBS.
Therapeutic effect of Probiotics:
Probiotics have a large number of properties that can benefit IBS. Bifidobacteria is the active agent in probiotic combination therapy.Whereas many studies show Lactobacilli to have no impact on symptoms.(43)But one Korean study concluded that thecomposite probiotics containing Bifidobacterium bifidum BGN4, Lactobacillus acidophilus AD031, and other species are safe and effective, especially in patients who excrete normal or loose stools.(44) Recently, P Moayyedi and colleague in their systematic review recommend that probiotics appear to be efficacious in IBS patients ,but the magnitude of benefit and the most effective species and strain are uncertain.(45)
Therapeutic effect of the 5HT3 receptor antagonists:
Alosetron (5-HT3 receptor antagonists), with dosage of 0.5 to 1 mg daily, is more effective and the commonest drug used for treatment of patients with IBS-D in spite of serious side effects including constipation and colon ischemia.The balance model of benefits and harms for ‘Alosetron’ is most encouraging in women who have not responded to conventional therapies.(46,47)
Therapeutic effect of 5-HT4 receptor agonists:
Tegaserod (5-HT4 receptor agonist) is more effective for the treatment of IBS-C mostly in female and IBS-M. The side effects reported among the patient receiving Tegaserod are diarrhoea (commonest), cardiovascular events i.e. myocardial infarction, unstable angina, or stroke.(48,49)Currently Tegaserod is available from FDA through an emergency investigational new drug protocol. Other 5-HT4 agonists (Cisapride,Renzapride) have not demonstrated improvement compared with placebo.(50,51)
Therapeutic effect of the selective C-2 chloride channel activators:
Lubiprostone (selective C-2 chloride channel activator) is effective for relieving symptoms of IBS-C, mostly in women, and has less frequent side-effects including nausea(8%), diarrhea(6%) and abdominal pain(5%).(52)
Therapeutic effect of antidepressants :
Patients with prominent symptom of abdominal pain in IBS that fails to respond to peripherally acting agents often are considered for treatment with antidepressants (TCAs and SSRIs), however, limited data on safety and tolerability of these agents is shown.(53)Antidepressants have the combined effect of both central and peripheral mechanism in IBS.(54)SSRIs are better tolerated than TCAs and have a prokinetic effect hence work better in IBS-C.(53,55)whereas TCAs are of greater benefit for IBS-D.
Therapeutic effect of herbal therapies and acupuncture:
Unique Chinese herbal mixtures show a benefit in IBS management.(56) Traditional Chinese herbal remedies are routinely used in China to treat the condition, but so far have not been generally accepted by conventional Western medicine.(56,57)Bensoussanand colleague in one randomized, double-blind, placebo-controlledtrial concluded that the Chinese herbal formulations appear to offerimprovement in symptoms for some patients with IBS.(57) A systematic review of different trials of acupuncture was inconclusive because of heterogenous outcomes.(58,59) Hence further work is needed before any recommendations on acupuncture or herbal mixtures therapy.
Emerging therapies :
The improved understanding of underlying mechanisms in IBS is beneficial for the development of new pharmacological treatment options.
A brief overview of emerging agents in IBS therapy summarized in Table 1(1)
Conclusion:
IBS is a true medical disorder that has significant impact on those in agony with regard to symptom severity, disability, and impaired quality of life, which exceeds that of most GI disorders. Advances in research over the past several decades have paved the way for anameliorableunderstanding of the underlying pathophysiology and standardized symptom-based approaches that can be implemented in making a positive diagnosis and development of innovative treatment options for multiple IBS symptoms. Although many unanswered questions remain, the progress is promising and it has equipped physicians better to efficiently diagnose IBS and choose from a growing armamentarium of treatment options.
Syncope is a common condition encountered in acute medical practice. Many patients with syncope are initially labelled as having “collapse query cause”. It is defined as transient loss of consciousness (T-LOC) due to transient global cerebral hypoperfusion characterized by rapid onset, short duration, and spontaneous complete recovery1. Incidence of syncope is difficult to determine accurately as many cases remain unreported. Some studies quote an overall incidence rate of a first report of syncope to be 6.2 per 100 person-years. Clearly this is age related and the incidence increases dramatically in patients over the age of 70 years2. Syncope accounts for 1-6% of hospital admissions and 1% of emergency department (ED) visits per year3-5. Hospital episode statistics from NHS hospitals in England reported a total of 119,781 episodes of collapse/syncope for the financial year 2008-09 which is about twice the number of episodes reported in the year 1999-2000. About 80% of patients were admitted and they have an average length of stay of 3 days accounting for over 269,245 bed days during that financial year6.
Syncope is also associated with significant mortality and morbidity if left untreated. Literature reports a 6-month mortality of 10%, which can go up to 30% if cardiac syncope is untreated7. Non-cardiac syncope is associated with a survival rate comparable to people with no syncope2. Syncope is also a risk factor for fractures related to falls especially in elderly and can cause significant morbidity in this group8. In addition, there are significant health care related costs associated with management of syncope. Cost per diagnosis can vary from over £611 in the UK to €1700 in Italy. Hospitalisation alone accounted for 75% of cost in some studies9,10. Diagnosis of this condition can be difficult especially if there is a lack of structured approach. Over the last few years this topic has attracted enormous interest and several studies have been published, aiming at improving the approach to this condition. Standardised syncope pathways improve diagnostic yield and reduced hospital admissions, resource consumption and over all costs10. Recently the task force for the diagnosis and management of syncope of the European Society of Cardiology published guidelines for the diagnosis and management of syncope1. However, in spite of the available evidence very few hospitals have standardised syncope pathways for the management of this complex condition. Only 18% of EDs have specific guidelines and access to a specialist syncope clinic11. This article focuses on evidence based structured evaluation of syncope. Current practice in the management of syncope Due to the difficulty in diagnosis and mortality associated with this condition, a cautious approach may be taken by physicians resulting in hospitalisation of majority of patients presenting with syncope. We recently audited the practice of syncope in our hospital, which is a tertiary centre in the north of Scotland. 58 patients admitted with this condition over a period of a month were included in the audit. It showed an average length of stay (LOS) of 4.76 days in these patients. Due to a lack of methodical approach and standardised pathway for management of this condition many patients were subjected to several inappropriate inpatient investigations significantly prolonging the LOS and increasing the cost. Only 7 (12%) cardiac events were observed in this group and in retrospect a good methodical approach would have predicted these events. It should be noted that even in the geriatric population, reflex syncope that carries a benign prognosis is more common than cardiac syncope2. A systematic approach to the management of syncope (Figures 1 and 2). The causes of syncope can be broadly divided in to cardiac causes and non-cardiac causes (Table 1). Initial evaluation leads to a diagnosis in less than 50% patients in most instances4,12-14. If there is uncertainty about diagnosis then the patient is risk stratified. High-risk patients are hospitalised, evaluated and treated whereas early discharge could be considered in low risk patients. Aetiology of Syncope41
Neurally-mediated (Reflex) Syncope
Cerebro vascular
Vasovagal syncope
Carotid sinus syncope
Situational syncope
e.g., Micturition, post prandial, defecation, cough
Relevant blood tests (e.g. to rule out metabolic abnormality)
Pacemaker check if appropriate
History Many patients with syncope are initially labelled as having “collapse query cause”. Loss of postural tone is termed “collapse”. Indeed, the term “collapse query cause” does not give any useful information regarding the underlying condition. A clear history from the patient and the bystander or witness (if available) is the key to the diagnosis. Firstly, determine if the collapse was associated with loss of consciousness (LOC). LOC can be transient (T-LOC) or prolonged. Categorising “collapse” is important at this stage as the aetiology and approach to each category is different (Figure 1). Secondly, establish if the collapse was syncopal. The LOC should be transient (e.g. did the patient regain consciousness in the ambulance, before or on arrival to hospital?), of rapid onset and associated with a spontaneous complete recovery. Also the mechanism should be due to transient global hypoperfusion. T-LOC secondary to other mechanisms such as trauma and brief seizures should be excluded. On occasions syncope could be associated with brief jerking movements mimicking seizures15. Also note that a transient ischemic attack (TIA), commonly listed as a differential diagnosis of syncope by physicians, is not a cause of syncope as this is not associated with global cerebral hypoperfusion. The absence of a coherent history because patient had no recollection of events and there was no witness account available can make this distinction difficult. This is also particularly difficult in the elderly with cognitive impairment. Other useful information includes whether the syncope was associated with postural change. Orthostatic hypotension occurs after standing. If present it will be useful to check drug history (new vasodepressive drugs). Features suggestive of Parkinson’s disease or amyloidosis may raise the possibility of autonomic neuropathy. A strong family history of sudden cardiac death may be of relevance. Table 3 summarises the features of neurally mediated and cardiac syncope. Table 3 Features suggesting neurally mediated and cardiac syncope42
Neurally mediated
Cardiac
Preceded by prodrome
Related to particular activity - e.g., Micturition, postprandial, prolonged standing, unpleasant situations
Associated with nausea and vomiting
After exertion
Absence of prodrome, no warning
Associated with chest pain, breathlessness, palpitation
During exertion or supine
History of cardiac disease
Family history of sudden cardiac death
Physical examination The next step is a thorough physical examination. This should include an ABC approach if the patient is very ill and particular attention should be given to exclude immediate life threatening conditions such as pulmonary embolism, acute myocardial infarction, life threatening arrhythmias, acute aortic dissection, seizures etc… Recording the vital signs is important as it may give a clue to diagnosis (e.g., acute hypoxia may indicate massive pulmonary embolism). Recording postural blood pressure when lying and during active standing for 3 minutes is useful to exclude orthostatic hypotension1. Recording a deficit in blood pressure in both arms may be a useful clinical finding especially if acute aortic dissection is suspected. Thorough cardio respiratory examination may reveal an obvious condition such as cardiac failure or aortic stenosis. Patients should also be examined for potential injuries as a result of syncope. Standard ECG A 12 lead ECG should be performed in all patients admitted with syncope. The abnormalities in table 4 would suggest a cardiac aetiology. The QT interval should always be measured, as it is a commonly overlooked abnormality. Blood tests Blood tests are usually unhelpful in establishing a diagnosis but can detect metabolic abnormalities such as hypoglycaemia, electrolyte abnormalities and other causes to explain LOC especially when witness account is not available. An acute drop in haemoglobin suggests blood loss. One recent study claims the usefulness of brain natriuretic peptide (BNP) for predicting adverse outcomes in syncope but it is not externally validated yet and it is too early to recommend for routine clinical practice16. Pacemaker check It is not uncommon to see a patient with a pacemaker implanted, admitted to hospital with syncope. In these circumstances, it is essential to rule out a device malfunction although this is not a common cause of syncope. A preliminary and easy test will be interrogating the pacemaker if available. This should pick up any problems with the pacemaker in most instances. With the above information establishing a diagnosis will be possible in a significant proportion of patients. Further investigations and management should be guided by the underlying diagnosis1. However in over half of patients the diagnosis may still be uncertain12,13,17. The following section explains the management of unexplained syncope. Risk stratification in patients with unexplained syncope (Tables 4 and 5)Table 4 ECG changes in ‘high-risk’ Syncope41
ECG changes favouring bradyarrhythmias
High degree AV blocks – Mobitz type 2 second degree AV block, complete heart block, trifascicular block (first degree heart block with left bundle branch block (LBBB) or right bundle branch block (RBBB) with axis deviation)
Bifascicular block (defined as either LBBB or RBBB combined with left anterior fascicular block or left posterior fascicular block) especially if new
Other intraventricular conduction abnormalities (QRS duration >0.12 s)
Asymptomatic sinus bradycardia (<50 bpm), sinoatrial block or sinus pause >3 s in the absence of negatively chronotropic medications
ECG changes favouring tachyarrhythmias
Pre-excited QRS complexes (e.g. WPW syndrome)
Prolonged QT interval
Right bundle branch block pattern with ST-elevation in leads V1–V3(Brugada syndrome)
Negative T waves in right precordial leads, epsilon waves and ventricular late potentials suggestive of arrhythmogenic RVD
Q waves suggesting myocardial infarction
Non sustained Ventricular Tachycardias
Table 5 – Clinical features of high-risk syncope1,18-23
History of severe structural heart disease or heart failure, presence of ventricular arrhythmia
Syncope during exertion or supine
Absence of prodrome or predisposing or precipitating factors
Preceded by palpitation or accompanied by chest pain or shortness of breath
Family history of sudden cardiac death
Examination suggestive of obstructive valvular heart disease
Syncope associated with trauma
Systolic blood pressure less than 90mm Hg
Hematocrit less than 30% (acute drop in hemoglobin)
When the cause of syncope is uncertain it is essential to risk stratify patients to enable appropriate treatment and further investigation. Risk stratification tools There are several scoring systems for risk stratification of syncope. Syncope Evaluation in the Emergency Department Study (SEEDS), Osservatorio Epidemiologico sulla Sincope nel Lazio (OESIL score), Evaluation of Guidelines in SYncope Study (EGSYS score), San Francisco Syncope Rule (SFSR), The Risk stratification Of Syncope in the Emergency department (ROSE) and American College of Emergency Physicians clinical policy are the popular ones and each has its own advantages and disadvantages1,16,18-23. Discussing each scoring system is beyond the scope of this article and we shall restrict the discussion to the summary of these risk stratification tools (Table 5). It will be too early to include all the factors mentioned in the ROSE study, as it is not externally validated yet. It could be argued that taking all the risk factors described may increase admission rates but this approach may at least not miss the high-risk patient. This is a developing field and more evidence is likely to be published soon. High-risk vs. low-risk syncope: A high-risk syncope patient is the one where a cardiac cause is likely and where the short-term mortality is high due to major cardiovascular events and sudden cardiac death. High-risk syncope is said to be present if any of the features in the table 4 or 5 are present. Management of low-risk syncope Patients with a single or very infrequent syncope are usually reassured and discharged, as the short-term mortality is low1,2. Tilt table test is not usually required where a single or rare episode of neurally mediated syncope is diagnosed clinically. One exceptional circumstance where single rare episodes are investigated further with a tilt table test is when there could be an occupational implication (e.g. aircraft pilot) or if there is a potential risk of physical injury. Patients with recurrent unexplained syncope need to be further investigated (see below). Management of high-risk syncope / suspected cardiac syncope High-risk patients usually require hospitalisation and inpatient evaluation. Other high-risk patients who may be considered for admission are vulnerable patients susceptible to serious injuries, for example, elderly patient or a patient with multiple co-morbidities. Further investigations (Table 6)
Non invasive
Invasive
Echocardiography
ECG monitoring
Telemetry
Holter monitoring
External loop recorder*
Carotid sinus massage
Cognitive testing (in elderly)
Ambulatory blood pressure monitoring
Tilt table test*
Exercise stress test
Implantable loop recorder*
Coronary angiography*
Electrophysiology*
* Specialist Investigation Echocardiography Echocardiography is a relatively inexpensive and non-invasive investigation. It should be performed if there is a clinical suspicion of a significant structural abnormality of heart such as ventricular dysfunction, outflow tract obstruction, obstructive cardiac tumours or thrombus, pericardial effusion etc… The yield of this test is low in the absence of clinical suspicion of structural heart disease. However in the presence of a positive cardiac history or an abnormal ECG, one study detected LV dysfunction in 27% of patients and half of these patients had syncope secondary to an arrhythmia. In patients with suspected obstructive valvular disease 40% had significant aortic stenosis as a cause of syncope24. ECG monitoring These tests have utility in identifying arrhythmogenic syncope. If a patient has syncope correlating with a significant rhythm abnormality during the monitoring period with the device, then the cause of syncope is due to the underlying rhythm abnormality. On the other hand, if no rhythm abnormality is recorded during a syncopal attack, then an underlying rhythm problem as a cause of syncope is excluded. Therefore, these tests are meaningful only if there is a symptom-rhythm correlation, which is the working principle of these devices. In the absence of syncope, during the monitoring period, these tests may pick up other abnormalities that may be relevant. For example, rapid prolonged supra-ventricular tachycardias, ventricular tachycardias, periods of high degree AV blocks (mobitz type 2 or complete heart block) or significant sinus pauses >3seconds (except during sleep, negatively chronotropic therapy and trained athletes), which will require further investigation or treatment. Telemetry Telemetry can be used in inpatients. Although the diagnostic yield of this investigation is only 16%, given the high short-term mortality, this test is indicated in the high-risk group 1. Usually patients are monitored for 24 to 48 hours although there is no agreed standard period for monitoring25. Holter monitoring This involves connecting the patient through cutaneous patch electrodes. It records the ECG activity conventionally over 24-48 hours or at times up to 7 days. It is particularly useful only in patients who have frequent regular symptoms (≥1 per week). For this reason, the yield of this test can be as low as 1-2% in unselected population1. Long inpatient waiting lists in some hospitals can significantly prolong the length of stay and cost. Selecting patients carefully for this test based on risk stratification will reduce costs and waiting lists. Carotid sinus massage This simple bedside test is indicated in patients over the age of 40 years with syncope of unexplained origin after initial evaluation. A ventricular pause lasting >3 s and/or a fall in systolic BP of >50mmHg defines carotid sinus hypersensitivity (CSH) syndrome. It is contraindicated in patients with recent cerebrovascular accidents (past 3 months) or with carotid bruit except when a Doppler study has excluded significant stenosis1. Cognition test If an elderly patient had forgotten about the events, in the absence of an obvious cause, it may be useful to test cognition. If cognitive impairment is present, common problems associated with cognitive dysfunction should be considered e.g. falls, orthostatic hypotension. Other investigations In spite of the above tests if a cause is not determined, early specialist input is recommended for further investigation and treatment. The following non-invasive and invasive investigations may be appropriate in these circumstances. An external loop recorder This is a non-invasive form of electrocardiographic monitoring. The principle is same as that of Holter monitoring. External loop recorders have a loop memory that continuously records and deletes ECG. When activated by the patient, typically after a symptom has occurred, 5 – 15 min of pre-activation ECG is stored and can be retrieved for analysis. Studies have shown that they have increased diagnostic yield compared to Holter1. They should be considered in patients who have symptoms on a monthly basis. A Tilt table test This is indicated in cases of recurrent unexplained syncope after relevant cardiac causes of syncope are excluded and a negative Carotid sinus massage performed in the absence of contraindications. It is also indicated when it is of clinical value to demonstrate patients susceptibility to reflex syncope and thereby to initiate treatment. Other less common indications are recurrent unexplained falls, differentiate jerking movements secondary to syncope and epilepsy, diagnose psychogenic pseudo syncope and differentiate orthostatic and reflex syncope. Indication of this test in the context of a single unexplained syncope is discussed above. Ambulatory blood pressure monitoring This may be useful in patients with unexplained syncope particularly in old age to check if there is an element of autonomic failure and if a single set of orthostatic blood pressure recording is not helpful. In one study, it has been shown that 25% of the elderly patients admitted with falls or syncope had postprandial hypotension especially after breakfast26. It may be more readily available than a tilt table test in some centres. Exercise stress test This may be useful in a rare entity called exercise induced syncope. Outflow tract obstruction should be excluded by echocardiography before subjecting a patient to this test especially in the presence of relevant signs. However there is no evidence for supporting this test in investigating syncope in general population. Implantable loop recorders These are implanted subcutaneously. It needs to be activated either by the patient or a bystander after a syncopal attack. It is indicated in high-risk patients where a comprehensive evaluation did not establish an underlying diagnosis. In the absence of high risk factors, it is also indicated in patients with recurrent unexplained syncope especially if infrequent. Conventionally it is used as a last resort in patients with recurrent unexplained syncope as the initial costs are high. It has been shown in one study to be more cost effective than the conventional strategy and was more likely to provide a diagnosis in patients with recurrent unexplained syncope27. However patients with poor LV function and those at high risk of life-threatening arrhythmias were excluded from this study. Coronary angiography or CT coronary angiography This may be helpful in suspected myocardial ischemia or ischemia related arrhythmias. Electrophysiological study may be considered in certain circumstances by cardiologists. When a standardised pathway is used, diagnosis is ascertained in 21% patients on initial evaluation and further 61% patients with early investigations. Only in 18% patients the diagnosis was still uncertain12. Other studies have shown similar results28. Although these results are from a dedicated syncope unit following a standardised pathway, these could be extrapolated to any unit following these standardised pathways. Further management is dictated by the underlying diagnosis with early specialist input for appropriate treatment. Treatments Single or rare episodes of reflex syncope do not require treatment. However, recurrent troublesome reflex syncope may warrant treatment. Treatment modalities are primarily non-pharmacological such as tilt training, physical counter pressure manoeuvres (leg crossing, hand gripping) and ensuring adequate hydration29. If refractory to non-pharmacologic measures midodrine (alpha agonist) may be considered in patients with frequent hypotensive symptoms30,31. Fludrocortisone may be used in elderly but there is no trial evidence to support this. Betablockers have been presumed to lessen symptoms but are shown to be ineffective in several studies 32. They may potentially exacerbate bradycardia in carotid sinus syncope and are not recommended in treatment of reflex syncope. Treatment with cardiac pacing in reflex syncope is controversial and may be considered in patients with predominant cardio inhibitory response on carotid sinus massage (in CSH syndrome) or on tilt test (in reflex syncope). It should be noted that cardiac pacing has no effect on the often-dominant vasodepressor component of reflex syncope. In patients with orthostatic hypotension, non-pharmacologic measures like increased salt and water intake, head up tilt sleeping, physical counter pressure manoeuvres, abdominal binders and compression stockings may help reducing symptoms. Midodrine is an efficient alternative in these circumstances and fludrocortisone also can be used.33,34Syncope secondary to cardiac arrhythmias needs treatment if a causal relationship is established. Potential reversible causes such as electrolyte abnormalities and drug induced causes should be excluded. Cardiac pacing is a modality of treatment in significant bradyarrhythmias secondary to sinus node or advanced AV nodal disease such as mobitz type 2 block, complete heart block or tri-fascicular block. Catheter ablation and anti-arrhythmic drug therapy are the main modalities of treatment for tachyarrhythmias. Implantable cardioverter defibrillator may be indicated in patients susceptible to malignant ventricular tachyarrhythmias. Treatment of syncope secondary to structural cardio pulmonary abnormality will need surgical intervention if possible. Driving and Syncope Doctors are poor at addressing and documenting this issue35. Table 7 gives some useful information from the DVLA website (http://www.dft.gov.uk/dvla/medical/ataglance)36. This information is country specific and subject to change. Table 7 – Driving and Syncope in the UK36
Type of Syncope
Group 1 entitlement (car, motorcycle etc.,)
Group 2 entitlement (Large goods vehicle, passenger carrying vehicle)
Simple faint
No restrictions
No restrictions
Unexplained syncope with low risk of recurrence*
Allowed to drive 1 month after the event
Allowed to drive 3 months after the event
Unexplained syncope with high risk of recurrence** and cause identified and treated
Allowed to drive 1 month after the event
Allowed to drive 3 months after the event
Unexplained syncope with high risk of recurrence** and cause not identified
Licence is refused or revoked for 6 months
Licence is refused or revoked for 12 months
*Absent clinical evidence of structural heart disease and normal ECG** Abnormal ECG, clinical evidence of structural heart disease, syncope causing injury, recurrent syncope Syncope unitsSyncope units aim to evaluate syncope (and related conditions) in dedicated units consisting of generalists and specialists with an interest in syncope. A sufficient number of patients are required to justify such a unit. They are well equipped with facilities for recording ECG, blood pressures, tilt table, autonomic function testing, ambulatory blood pressure monitoring, and invasive and non-invasive electrocardiographic monitoring. It has been shown to be cost effective and reduces health care delivery costs by reducing admission rates, readmission rates and event rates. Examples include the Newcastle model, Manchester model and the Italian model.12,18,37,38Conclusions The incidence of syncope is increasing in the UK with an aging population. There is significant cost incurred in the delivery of health care for this condition. The approach to syncope varies widely amongst practising physicians due to lack of a methodical approach. A thorough initial evaluation yields a diagnosis in less than half of the patients. When the cause of syncope remains unexplained after initial evaluation, the patients should be risk stratified. While a patient with a single episode of low risk syncope can be reassured and discharged, those with high-risk features should be hospitalised for further management. Outpatient evaluation could be offered for low risk patients if recurrent. Early specialist input should be sought in high-risk syncope and recurrent unexplained syncope. This standardised approach or pathway will reduce cost by reducing hospitalisation, inappropriate investigations and length of stay.
Key Facts
Collapse associated with transient loss of consciousness is called syncope if it is due to transient global cerebral hypoperfusion and characterized by rapid onset, short duration, and spontaneous complete recovery
Standardised syncope pathways improve diagnostic yield and reduce hospital admissions, resource consumption and over all costs
A thorough initial evaluation yields a diagnosis in less than half of patients. If the cause of syncope is undetermined after initial evaluation, patients should be risk stratified
Early discharge should be considered in low risk patients while high-risk patients need urgent evaluation.
Early specialist referral is recommended in patients with high risk syncope and recurrent unexplained syncope
Future Interests Syncope had been known for several decades and still remains a complex condition, as the exact mechanisms are poorly understood especially in non-cardiac syncope. Mechanism of syncope in the elderly patients may be different from those of young patients and studies should focus in understanding the mechanics. Further research is needed in risk stratifying syncope. It may enable us to develop more robust care pathways for management of syncope. The role of BNP in investigating and risk stratifying syncope need to be further clarified. In spite of sophisticated tests the cause of syncope in a proportion of patients remain uncertain. Studies should focus on the long-term outcome and management of syncope in this group. The role of implantable loop recorder in the investigation of syncope should be better defined and more studies should focus on when it should be offered in the pathway of management of syncope. Studies are also required to develop effective pharmacotherapies for this condition.
Cervicogenic headache (CH) refers to head pain originating from the pathology in the neck.1 However, the diagnosis of CH is still controversial 2,3 and it is often misdiagnosed. The author was called to consult a patient in a university hospital not so long ago. The patient was a 28-year-old female with a history of headache for six months. Her headache was described as continuous, dull and achy. It was mainly in the right side occipital and parietal areas. Sometimes she felt a headache behind the eyes. Her headache got worse periodically, several times a month, with nausea, photophobia, and phonophobia. She had no previous history of headache until a whiplash injury six months before. She had been diagnosed as having ‘migraine’ and ‘post-traumatic headache.’ She had used all anti-migraine medications. ‘Nothing was working.’ The patient was admitted into hospital because of ‘intractable headache.’
On the day when the author saw the patient, she was lying on the bed, with the room light turned off and a bed sheet covering her head and eyes. She was given Dilaudid, 2mg/h continuous intravenous (IV) drip, for the headache. The patient had normal results from magnetic resonance imaging (MRI) of the brain and lumbar puncture. According to the patient, no doctors had touched the back of her head and upper neck since admission. The author examined the patient and found a jumping tenderness over the right greater occipital nerve. The patient was given 2ml of 2% lidocaine with 40mg of Kenalog for the right greater occipital nerve (GON) block. Her headache was gone within five minutes and the Dilaudid drip was immediately discontinued. At follow-up four weeks later, the patient was headache-free. This was a typical missed case of CH (occipital neuralgia).
The concept of CH was first introduced by Sjaastad and colleagues in 1983.4 The International Headache Society published its first diagnostic criteria in 1998 which was revised in 2004.5 Patients with CH may have histories of head and neck trauma. Pain is often unilateral. Headache is frequently localized in the occipital area. However, pain may also be referred to the frontal, temporal or orbital regions. Headaches may be triggered by neck movement or sustained neck postures.6 Headache is constant with episodic throbbing attacks, like a migraine. Patients may have other symptoms mimicking a migraine such as nausea, vomiting, photophobia, phonophobia, and blurred vision. Due to the fact that there is a significant overlap of symptoms between CH and migraine without aura, CH is often misdiagnosed as migraine. CH is commonly found in patients after whiplash injuries, especially in the chronic phase.7
Anatomical studies have provided a basis for the pathogenesis of CH. The suboccipital nerve (dorsal ramus of C1) innervates the atlanto-occipital (AO)joint and dura matter over in the posterior fossa. Therefore, a pathologic condition of AO joint is a potential source for occipital headache. It has been reported that pain from the C2-3 and C3-4 cervical facet joints can radiate to the occipital area, frontotemporal and even periorbital regions. Even pathology in C5 or C6 nerve roots have been reported to cause headache.8 The trigeminocervical nucleus is a region of the upper cervical spinal cord where sensory nerve fibres in the descending tract of the trigeminal nerve (trigeminal nucleus caudalis) are believed to interact with sensory fibres from the upper cervical roots. This functional convergence of upper cervical and trigeminal sensory pathway sallows the bidirectional referral of painful sensations between the neck and trigeminal sensory receptive fields of the face and head.
Clinicians should always put CH in the list of differential diagnoses when they work up a headache patient. A history of head/neck injury, and detailed examination of the occipital and upper cervical area, should be part of the evaluation. Patients with CH may have tenderness over the greater or lesser occipital nerve, cervical facet joints and muscles in the upper or middle cervical region. Diagnostic imaging such as X-ray, computerized tomography (CT) and MRI cannot confirm CH, but can lend support to its diagnosis.
Treatment of CH is empirical. This headache does not respond well to migraine medications. Treatment should be focused on the removal of the pain source from the occipital-cervical junction. Initial therapy should be directed to non-steroidal anti-inflammatory drugs (NSAIDs) and physical therapy modalities.9 GON block is easy and safe to perform in office.10 It is effective for the treatment for occipital neuralgia and CH.11 The author followed a group of patients after GON block. The pain relief effects of GON block lasted an average of 31 days (unpublished data). If patients do not respond to GON block, diagnostic medial branch block and radiofrequency (RF) denervation of the upper cervical facet joints can be considered. Early studies have reported positive results.12 A subsequent randomized study found no benefit of RF. However, there were only six cases in each group,13 which significantly limited the power and validity of the conclusion from that study. Surgical treatment of cervical degenerative disc disease may offer effective pain relief for CH. Jansen14 reported 60 cases of CH patients treated mainly with C4/5, C5/6 and C6/7 nerve root decompression. More than 63% patients reported long lasting pain freedom or improvement (> 50%).
CH is common, with a prevalence of 0.4% and 2.5% in the general population. However, compared with other common pain conditions, CH is less studied. A Medline search found 6818 abstracts for migraine in 2009, whereas only 86 abstracts on CH were found. CH has not been well studied and it is often misdiagnosed. It is time to call for more attention.
Both Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) are diseases characterized by a high global prevalence, complex clinical course, and limited effectiveness of currently available antiviral therapy. Approximately 2 billion people worldwide have been infected with the HBV and about 350 million live with chronic infection. An estimated 600,000 persons die each year due to the acute or chronic consequences of HBV 1, 2. WHO also estimates that about 200 million people, or 3% of the world's population, are infected with HCV and 3 to 4 million persons are newly infected each year. This results in 170 million chronic carriers globally at risk of developing liver cirrhosis and/or liver cancer 3, 4. Hence, HBV and HCV infections account for a substantial proportion of liver diseases worldwide.
These viruses have some differences, like HBV belongs to the Hepadnaviridae family and HCV belongs to the Flaviviridae family. HBV has a circular, partially double-stranded DNA genome of approximately 3.2 kb, whereas HCV has a single RNA strand genome of approximately 9.6 kb. HBV and HCV show some common biological features. Both HBV and HCV show a large heterogenicity of their viral genomes producing various genotypes. Based on genomic nucleotide sequence divergence of greater than 8%, HBV has been classified into eight genotypes labeled A through H 5,6,7,8. Different isolates of HCV show substantial nucleotide sequence variation distributed throughout the genome. Regions encoding the envelope proteins are the most variable, whereas the 5’ non-coding region (NCR) is the most conserved 9. Because it is the most conserved with minor heterogeneity, several researchers have considered the 5’ NCR the region of choice for virus detection by reverse transcription (RT)-PCR. Sequence analysis performed on isolates from different geographical areas around the world has revealed the presence of different genotypes, genotypes 1 to 6 10. A typing scheme using restriction fragment length polymorphism analysis of the 5’ NCR was able to differentiate the six major genotypes 11. Hence both HBV and HCV genotypes display significant differences in their global distribution and prevalence, making genotyping a useful method for determining the source of HBV and HCV transmission in an infected localized population 12 - 27.
Many studies have been conducted to study the prevalence of HBV and HCV co-infection among HIV-infected individuals and intravenous drug users globally 28 -3 4.There are only a few studies relevant to the epidemiology of these types of infection in the normal healthy population 35,36,37. The objective in this study was to determine the seroprevalence of HBV and HCV, co-infection of both these viruses and their genotypes, among an apparently healthy female population as well as from known HBV patients in Karachi, a major city in the province of Sindh, Pakistan. This study is also aimed at providing the baseline data on HBV/HCV co-infection, in order to gain a better understanding of the public health issues in Pakistan. We evaluated the antigen, antibody and genotypes of both HBV and HCV in 144 otherwise healthy female individuals and 28 diagnosed HBV patients.
Materials and Methods:
Study duration:From March 2002 to October 2006 & April 2009
Study participants: Total 4000blood serum samples were collected from healthy female student volunteers and 28 serum samples (April 2009) from already diagnosed Hepatitis B positive patients, aged 16 to 65 years from two Karachi universities and one Karachi hospital. University samples were obtained through the Department of Microbiology, University of Karachi and the Department of Microbiology, Jinnah University for Women. Hospital samples were obtained through the Pathological Laboratory of Burgor Anklesaria Nursing Home and Hospital.
Ethical Consent: Signed informed consent forms were collected from all volunteers following Institutional Review Board policies of the respective institutes.
Pre study screening:All 4028 volunteers had health checkups by a medical doctor before collection of specimens, they were asked about their history of jaundice, blood transfusion, sexual contacts, and exposure to needles, and if they had undergone any surgical and dental procedures.
Biochemical & Hematological screening:On completion of the medical checkups, volunteers were asked to give 5mL of blood for different haematological [(complete blood picture (CP), haemoglobin percentage (Hb%) and erythrocyte sedimentation rate (ESR)] and 10mL for different biochemical tests [(direct bilirubin, indirect bilirubin, total bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP)]. Serological analysis:Samples were also subjected to serological analysis for hepatitis B surface Antigen (HBsAg), HBs antibodies and HCV antibodiesusing rapid immunochromatography kits (ICT, Australia and Abbott, USA). Confirmatory test for HBsAg was done by using ELISA (IMX, Abbott, USA).
All the above mentioned preliminary tests were conducted at the respective institutes in Karachi. Out of 4000 female volunteer from the two universities, 144 otherwise healthy females tested positive for HBsAg. 2 out of the 144 HBsAg positive females were also found to be positive for anti-HCV antibodies. The other 28 positive HBV patients from Anklesaria Hospital were only tested for HBsAg and all 28 were positive for HBsAg. Hence, a total of 172 HBV positive samples (144 + 28 = 172) including the 39 HCV positive serum samples obtained from Karachi were used for genotypic evaluation at Claflin University, South Carolina, USA. Specific ethnicity was not determined but we assume these study participants represent a collection of different ethnic groups in Pakistan.
DNA/RNA extraction and amplification of 172 HBV positive samples: DNA was extracted for HBV, and RNA was extracted for HCV analysis from 200μL of all 172 positive HBV serum samples using PureLink™ Viral RNA/DNA Mini Kit according to manufacturer’s instructions (Invitrogen, CA). Amplification was carried out using puReTaq Ready –To-Go PCR Beads (Amersham Biosciences, UK).
Determination of HBV and HCV genotypes by nested PCR: The primer sets for first-round PCR and second-round PCR, PCR amplification protocol, and primers for both HBV and HCV genomes and genotyping amplification for all 172 samples followed previously reported methods [45, 46]. First round amplification targeted 1063bp for the HBV genome and 470bp for the HCV genome. These respective PCR products for both HBV and HCV were used as a template for genotyping different HBV genotypes A to F and HCV genotypes from 1 to 6. HBV A through HBV F genotypes and HCV 1 through 6 genotypes for each sample were determined by separating the genotype-specific DNA bands on 2% agarose gels, stained with ethidium bromide. The sizes of PCR products were estimated according to the migration pattern of a 50bp DNA ladder (Promega, WI).
Results:
Before screening for HBV status, all 4000 healthy female volunteers from the Department of Microbiology, University of Karachi, and the Department of Microbiology, Jinnah University for Women were subjected to routine physical checkups for exclusion criteria i.e., either they were apparently unhealthy or malnourished (23 volunteers were excluded). All 4000 serum samples were screened by immunochromatography for the presence of HBsAg, anti HBs antibodies and anti-HCV antibodies. Positive results were confirmed by ELISA. Out of 4000 subjects 144 (3.6%) tested positive for HB surface antigen (HBsAg), 2 (0.05%) were positive for anti-HCV antibodies, and 3856 (96.4%) were negative for HBsAg and 3998 (99.95%) were negative for HCV antibodies by both immunochromatography and ELISA. Out of these 144 individuals who tested positive for HBsAg, 20 (13.8%) were positive for anti-HB surface antibodies and 2 (1.4%) tested positive for anti-HCV antibodies. The rest of the 28 serum samples obtained from already diagnosed HBV positive samples from Anklesaria Hospital were only tested for HBsAg and were all positive for HBsAg.
The haematological parameters: WBC count, RBC count, hematocrit and platelet count of the 172 HBsAg positive individuals were within the normal recommended range of values, while mean Hb% was 9.8±1.6 g/dL. Direct bilirubin (0 to 0.3 mg/dL), indirect bilirubin (0.1 - 1.0 mg/dL), total serum bilirubin (0.3 to 1.9 mg/dL), ALT (0 - 36 U/L), AST (0 - 31 U/L) and alkaline phosphatase (20 - 125 U/L) were also within the normal range for 129 HBsAg positive individuals, except for the raised ALT (>36 U/L) and AST (>31 U/L) levels in 38 participants with a previous history of jaundice who were also positive for HBsAg.
All 172 samples that were positive for HBsAg were confirmed for the presence of different HBV genotypes as well as for different HCV genotypes by PCR to see the co-infection of both these viruses. Genotyping was carried out at the South Carolina Center for Biotechology, Department of Biology, Claflin University, Orangeburg, SC, U.S.A. For HBV: Mix A primers were targeted to amplify genotypes A, B and C, and primers for Mix B were targeted to amplify genotypes D, E and F. For HCV: primers for Mix A were targeted to amplify genotypes 1a, 1b, 1c, 3a, 3c and 4. Primers of Mix B for HCV were targeted to amplify genotypes 2a, 2b, 2c, 3b, 5a, and 6a.
Table 1. Prevalence of both single and co-infection of HBV genotypes among the apparently healthy female student sample and known HBV positive patients from Anklesaria hospital in Karachi.
2 Universities
Samples
Percentage
Total HBV
144
Genotype D
70
48.6%
Genotype A
8
5.5%
Genotype F
7
4.9%
Genotype B
5
3.5%
Genotype E
3
2.1%
Genotype C
2
1.4%
Co-infections of HBV Genotypes
49/144
34%
Genotype B/D
30/144
20.8%
Genotype A/D
11/144
7.6%
Genotype A/D
4/144
2.8%
Genotype B/C
4/144
2.8%
Anklesaria Hospital
Samples
Percentage
Total HBV
28
Genotype D
19
67.9%
Genotype A
3
10.7%
Genotype B
1
3.6%
Genotype C
1
3.6%
Genotype F
1
3.6%
Co-infections of HBV Genotypes
Genotype B/A
3/28
10.7%
Figure 1: Electrophoresis patterns of PCR products from different HBV genotypes as determined by PCR genotyping system. Genotype A: 68bp, genotype B: 281bp, genotype C: 122bp, genotype D: 119bp, genotype E: 167bp and genotype F: 97bp.
Table 1 illustrates the prevalence of both single and co-infection of HBV genotypes from both the universities in Karachi and Anklesaria hospital. Representative 10 samples in Fig. 1 show single and co-infections for HBV.
Besides looking at the HBV genotypic status of these 172 patients by PCR, we also looked at the HCV genotypic status of the positive HBV patients by PCR so as to see if there was existence of co-infection of the two viruses i.e. HBV and HCV in the same individuals as only 2 samples tested positive for anti-HCV antibodies by rapid immunochromatography. Table 2 shows the prevalence of HCV genotypes among the apparently healthy female student population from the 2 universities in Karachi and known HBV individuals samples obtained from Anklesaria hospital. Fig. 2 shows different HCV genotype infection in the 10 representative samples shown in Fig. 1 showing HBV infection with different genotypes.
Table 2. Prevalence of HCV genotypes among the apparently healthy female student sample, and known HBV individuals from Anklesaria hospital in Karachi.
2 Universities
Samples
Percentage
Total HCV/Total HBV
39/144
27.1%
Genotype 3a
26/39
66.6%
Genotype 6a
5/39
12.8%
Genotype 3b
4/39
10.3%
Genotype 5a
4/39
10.3%
Anklesaria Hospital
Samples
Percentage
Total HCV/HBV
4/28
14.3%
Genotype 3a
2/28
7.14%
Genotype 2a
1/28
3.6%
Genotype 5a
1/28
3.6%
Figure 2: The sizes of the genotype-specific bands for HCV amplified by PCR genotyping method are as follows: genotype 2a, 190 bp; genotype 3a, 258 bp; genotype 3b, 232 bp; genotype 5a, 417 bp; and genotype 6a, 300 bp.
To summarize the results it was found that out of 172 HBsAg positive samples from the two universities (144 HBV samples) and Anklesaria Hospital (28 HBV samples), 89 (51.7%) were genotype D, 11 were genotype A (6.4%), 8 were genotype F (4.6%), 6 were genotype B (3.5%), 3 were genotype E (1.7%), and 3 were genotype C (1.7%). Out of 43 positive for HCV by PCR from the two universities (39/144 HBV samples) and Anklesaria Hospital (4/28 HBV samples), 65.1% (28/43) showed infection with 3a, followed by genotypes 5a (5/43 = 11.6%), 6a (5/43 = 11.6%), 3b (4/43 = 9.3%) and 2a (1/43 = 2.3%).
Discussion:
Viral hepatitis due to HBV and HCV has significant morbidity and mortality worldwide. The global prevalence of HCV is 3% 38 and the carrier rate of HBsAg varies from 0.1% to 0.2% in Britain and the USA, to 3% in Greece and southern Italy and up to 15% in Africa and the Asia 39. Pakistan is highly endemic with HBV. Studies are too limited to give a clear picture of the prevalence of HBV at the national level, especially among apparently healthy individuals. Most previous studies targeted different small groups of individuals with some clinical indications, so they do not accurately reflect the overall prevalence in Pakistan40. Our previous study was conducted on a first group of 4000 healthy female students from the two universities i.e., Department of Microbiology, University of Karachi and Department of Microbiology, Jinnah University for Women for the prevalence of HBV. We have reported earlier that genotype D appears to be the dominant genotype prevalent in Karachi, Pakistan’s apparently healthy female population, and genotype B appears to be the next most prevalent genotype 41, 42. In this study we checked the prevalence of both HBV and HCV in a second group of 4000 healthy female students from the same two universities in Karachi mentioned above, as well as the already 28 diagnosed HBV patients from Anklesaria Hospital in Karachi, Pakistan.
Both HBV and HCV are present in the Pakistani population and there are varying reports of disease prevalence. HCV is one of the silent killer infections spreading undetected in Pakistan because there are often no clinical symptoms and, when HCV is diagnosed, considerable damage has already been done to the patient. In Pakistan alone, the prevalence of HBsAg has been reported to be from 0.99% to 10% in different groups of individuals 43 - 52 and 2.2% to 14% for HCV antibodies 53 - 56. A recent study conducted in Pakistan showed that out of 5707 young men tested, 95 (1.70%) were positive for anti-HCV and 167 (2.93%) for HBsAg 57. Our previous study showed the prevalence of HBsAg among young otherwise healthy women to be 4.5% 41,42. Our present study shows that the prevalence of HBsAg in otherwise young healthy women to be 3.6%, with 0.98% testing positive for anti-HCV antibodies. On the basis of other studies conducted in different provinces of Pakistan, we can say that there is a variation in the prevalence of HBsAg and HCV antibodies in the Pakistani population as the population sample selected is limited to a particular area or segment of the provinces.
HBV and HCV genotyping is important to track the route and pathogenesis of the virus. In particular, the variants may differ in their patterns of serologic reactivity, pathogenecity, virulence, and response to therapy. Both HBV and HCV has genetic variations which correspond to the geographic distribution and has been classified into 8 genotypes (A to H) on the basis of whole genome sequence diversity of greater than 8% and 6 genotypes (1 to 6) using restriction fragment length polymorphism analysis of the 5’ non-coding region (NCR), respectively .
In this study genotyping was carried out for 6 HBV genotypes (A through F) and 6 HCV genotypes (1 through 6). This study suggests that the HBV D genotype is the most prevalent (114/144 = 79.2%) among otherwise healthy females alone or in co-infection with other HBV genotypes in Karachi, Sindh, Pakistan. In our previous study HBV D genotype was found to be ubiquitous (100%) among otherwise healthy females alone or in co-infection with other HBV genotypes in Karachi followed by genotype B 41,42. The earlier two studies conducted for prevalence of HBV genotypes in known hepatitis B positive patients in Pakistan report the prevalence of genotypes HBV A (68%) and HBV D (100%) in the province of Sindh 58,59. Interestingly, in this study we also found the HBV D genotype to be the prevalent genotype but it was followed by genotypes HBV A (5.5%) and HBV F (4.9%). The prevalence of genotype HBV B in this study was found to be 3.5% as our earlier study has shown the prevalence of genotype B in otherwise healthy females to be 16.1% 60. These findings respectively contradict and corroborate the previous studies for HBV genotype distributions reported here as the subjects in this study were also asymptomatic but comprised of second group of female volunteer students at the two universities. Out of 144 subjects positive for HBsAg, 10 reported a previous history of jaundice and the rest were not aware of their HBV status. In the nearby north Indian population, HBV D was reported as the predominant genotype (75%) in patients diagnosed with chronic liver disease (CLDB) 60. In this study we also found other HBV genotypes existed in the study population such as HBV genotype F (4.9%) followed by genotype E (2.1%), and genotype C (1.4%). We also saw mixed HBV infections of genotypes B and D, A and D, C and D as well as B and C (20.8%, 7.6%, 2.8% and 2.8%) among these otherwise healthy females.
Among the 28 diagnosed HBV patients from Anklesaria Hospital, 67.9% showed HBV genotype D infection followed by genotype A infection (10.7%). In this group of 28 HBV positive patients we also saw infections with genotypes B (3.6%), C (3.6%) and F (3.6%). This group exhibited 10.7% co-infection with genotypes B and A.
As far as the HCV status of these 144 otherwise healthy females who were HBV positive is concerned only 2 (1.4%) tested positive for HCV antibodies by rapid immunochromatography. But the PCR results showed 39 (27.15%) of these 144 otherwise healthy females that were HBV positive for different genotypes were also positive for HCV including the 2 otherwise healthy females that tested positive for HCV antibodies by rapid immunochromatography. Of the 39 HCV positive otherwise healthy females, we found the predominant HCV genotype to be 3a (66.6%) followed by genotypes 6a (12.8%), 3b (10.3%), and 5a (10.3%) infections. The earlier study conducted with samples from women at the two universities in Pakistan had shown that among the HCV positive apparently healthy females 51.44% were genotype 3a, 24.03% exhibited a mix of genotype 3a and 3b, 15.86% were genotype 3b, and 4.80% were genotype 1b 42. Interestingly, among the group of 28 diagnosed HBV patients, the prevalence of HCV 3a genotype infection was dominant but was 7.1% much lower than that found in the otherwise healthy females, followed by infections with genotypes 2a (3.6%) and 5a (3.6%). Hence we see there is 25% co-infection of both these viruses i.e., HBV and HCV among the HBsAg positive individuals. The sample of 28 HBV positive patients was from a hospital located in the center of the metropolis that represents an area of Karachi where sanitation, malnourishment, illiteracy, and lack of awareness is very common. Prostitution can also be considered as one factor in some of the localities of Karachi in the spread of both HBV and HCV.
Conclusion:
In conclusion, genotype D appears to be the dominant HBV genotype and genotype 3a for HCV appears to be prevalent in Sindh, Pakistan’s otherwise healthy young female population as well as in HBV diagnosed individuals. Co-infection of both the viruses i.e., HBV and HCV exists among HBsAg positive individuals. The young female participants were advised to seek appropriate medical care for both their own benefit and public health benefit.
Liver abscess accounts for 48% of visceral abscesses 1 and presents with significant morbidity and mortality. The overall incidence of pyogenic liver abscess is 3.6 per 100,000 populations, 2 however; elevated pancreatic enzymes within the content of a liver abscess have never been reported in the literature.
CASE REPORT:
A 36-year-old African American male with a history of chronic pancreatitis presented to the emergency department for abdominal pain in the epigastric area along with nausea, vomiting, diarrhoea, fever. His symptoms began 3-4 days before presentation. The abdominal pain was dull in nature and 6/10 in intensity, non-radiating. His past medical history was significant for HTN, diabetes mellitus and chronic diarrhoea secondary to chronic pancreatitis.
On admission the patient was alert and oriented, blood pressure was 97/44 mm Hg, heart rate 16 beats per minute, respiration 16 per minute, oxygen saturation 94% on room air and temperature 102*F. Abdominal examination revealed hyperactive bowel sounds and tenderness in the epigastrium & RUQ. Liver span was 14 cm. The rest of the examination was unremarkable.
Laboratory work revealed: Haemoglobin 9.8 g/dl, WBC 22.1 Thou/mm3 with segmented neutrophils of 81% and 9% bands, BUN 54 mg/dl, Cr 4.7 mg/dl, total protein 10.4 g/dl, albumin 1.8 g/dl, total bilirubin 1.1 mg/dl, direct bilirubin 0.3 mg/dl, AST 98 IU/L, ALT 38 IU/L, alkaline phosphatase 250 IU/L, amylase 81 units/L, lipase 10 units/L, lactate 2.3 mmol/L and INR 1.39.
The patient was started on fluids and meropenem for broad spectrum coverage. However his condition worsened and he developed acute respiratory distress syndrome secondary to sepsis necessitating intubation. Due to his abdominal pain he underwent a computer tomography (CT) scan of the abdomen, which revealed pancreatic calcifications and multiple liver abscesses; the largest measuring 7.5cm in the right lobe of the liver (Figure 1).
Figure 1
As the patient’s condition did not improve, he underwent liver abscess drainage. Fluid analysis showed ph 4.0, LDH 39 units/L, glucose 81 mg/dl, protein 1.6 g/dl, lipase of 16 units/L and amylase 68 units/L. The presence of amylase and lipase in the liver abscess without any evidence of a fistula between liver and pancreas on CT scan was unexpected, therefore it was decided to leave the catheter in situ for continuous drainage. 3 Even though his blood and fluid cultures remained negative during the hospital stay he was continued on antibiotics, which may have meant that the initial antibiotic therapy rendered the blood cultures negative. The success of management was assessed with a hepatic CT 10 days post drainage and was demonstrated by the observation of improvement in the patient’s general condition, as indicated by normal temperature, decreased draining catheter output and the resolution of deranged laboratory values. The catheter was then removed and the patient was discharged.
DISCUSSION:
Liver abscesses develop via seeding through portal circulation, directly via spread from biliary infections or from surgical or penetrating wounds and also from systemic organs via haematogenous spread. In our case the most reasonable explanation was through the involvement of portal circulation due to recurrent pancreatitis.
The morbidity and mortality rate for liver abscesses ranges from 2 – 12 % depending on the severity of underlying co-morbidities. 2 The clinical manifestations, as in our case, are characterized by abdominal pain (50-75%), 4, 5 fever (90%), nausea and vomiting. Other symptoms may include weight loss, malaise and diarrhoea. On physical exam RUQ tenderness, guarding, rebound tenderness, hepatomegaly and occasional jaundice can be appreciated. The diagnosis of a liver abscess can be made by radiographic imaging followed by aspiration and culture of the abscess material. Liver abscesses can be either polymicrobial or monomicrobial, unlike in the case with our patient, whose abscess was sterile. Depending on the microbial results additional sources of infection should be evaluated. Drainage of abscesses can be percutaneous 6 or open surgical. Percutaneous drainage with coverage of antibiotics was successful in our patient.
CONCLUSION:
In summary, we present a case of pancreato-liver abscess in a patient with a history of chronic calcified pancreatitis. It was treated with antibiotics and percutaneous drainage, with satisfactory resolution. To our knowledge this has never been reported in the literature and more work needs to be done to understand the pathophysiology of elevated pancreatic enzymes in the context of a liver abscess in a patient with a history of chronic pancreatitis.
Myocardial ischemia from coronary artery vasospasm can lead to variety of presentation including stable angina, unstable angina, myocardial infarction and sudden death 1. Although, pathognomic clinical scenario includes symptom of chest pain, transient ST-segment elevation on the electrocardiogram(ECG), and vasospasm on a coronary angiography, atypical presentations have also been reported 2. Various known physiological factors including stress, cold, hyperventilation and pharmacological agents including cocaine, ethanol, 5-Fluouracil, and triptans can precipitate a vasospastic attack. 3-7.We report a case of ST-segment elevation due to right coronary artery vasospasm, in patient with hypoxic respiratory failure, and successful treatment with calcium channel blockers.
Case description
A 56 year old man was admitted for the repair of a large ventral incisional hernia. The patient had a prior history of morbid obesity, chronic obstructive pulmonary disease (COPD), hypertension and cigarette smoking. The postoperative course was complicated by bilateral pneumonia leading to respiratory failure requiring mechanical ventilation. An electrocardiogram at the time of intubation was essentially normal. Aside from bilateral rhonchi and crackles on lung auscultation, the rest of the physical examination findings were unremarkable. Arterial blood gases at the time of intubation demonstrated PH 7.33, PO2 58 mmHg, PCO2 65 mmHg, HCO3ˉ 20 mmol/L, suggestive of hypoxia and concomitant respiratory acidosis. Baseline laboratory studies including cardiac enzymes were within normal limits. The patient was treated with intravenous vancomycin for methicillin-resistant staphylococcus pneumonia. On postoperative day 4, the patient had recurrent episodes of transient ST-elevation on a bedside monitor (Fig.1).
Figure 1
These episodes lasted for 3-5 minutes and were associated with significant bradycardia and hypotension. In view of recurrent episodes, haemodynamic instability, and underlying risk factors of coronary artery disease, cardiac catheterization was performed. Coronary angiography revealed a 90% stenosis with haziness of the mid-right coronary artery without any other significant epicardial disease. An intravascular ultrasound (IVUS) was performed and was followed by administration of 100 mcg of intracoronary nitroglycerin; the lesion was reduced to almost 20%. (Fig.2).
Figure 2
The diagnosis of prinzmetals angina was made, based on clinical course and angiographic results and prompt therapy with diltiazem (120 mg per day) was initiated. The patient had no further recurrences of similar episodes during the hospitalization and on follow up at 3 months.
Discussion
The prevalence of vasospasm has been reported to be higher in Japanese and Korean population as compared to the western population. A recent multi-institute survey in Japan documented spasm in 921 (40.9%) of the 2251 consecutive patients who underwent angiography for angina pectoris 8. In contrast to the traditional risk factors for atherosclerotic coronary artery disease, the incidence of smoking, age and dyslipdaemia has been reported higher in patients with coronary vasospasm 9. Endothelial dysfunction is now considered to the major inciting factor in the pathogenesis of the vasospasm 10. Vasospastic angina (VA) with normal coronary arteries on the angiography, impaired endothelial-dependent and endothelial-independent vasodilatation has been frequently observed in these patients. Vascular tone is normally regulated by production of vasodilator factors like nitrous oxide (NO), prostacyclin and vasoconstricting agents like endthelin-1. In the presence of dysfunctional endothelium the agents that normally cause vasodilatation lead to paradoxical vasoconstriction, due to direct muscle stimulation, like acetylcholine.
Stress, whether physical or mental stress has been shown to induce coronary vasospasm and myocardial ischemia. In a study by Kim et al, coronary spastic angina was diagnosed in 292 patients out of 672 coronary spasm provocation tests. Among 292 patients, 21 (7.2%) had myocardial infarction and 14 out of these 21 had experienced severe emotional stress before the event 11. Recently, animal studies have also shown that high circulatory level of stress hormones (cortisol) exaggerate coronary vasoconstriction through Rho-Kinase activation 12. Hypoxia has been seen in animal models to predispose to vasospasm through superoxide formation, which leads to loss of vasodilator function of NO.(13)
The ECG changes that occur during attack include ST-segment elevation, and or peaking of T wave from total or subtotal coronary occlusion 1. In some cases spasm can involve more than one artery leading to ST-segment elevation in multiple leads, which may predispose to ventricular tachycardia or fibrillation 14. Coronary spasm is diagnosed by angiography, and spasm can occur at the site of atherosclerotic plaque or in normal segment of the coronary artery. In patients with equivocal diagnosis, provocative tests including administration of acetylcholine, hyperventilation to induce spasm may be required for the diagnosis.
Current first line therapy involves used of calcium channel blockers (CCB) alone or in combination with long acting nitrates. In a study comparing the effect of long acting nitrates (Isosorbide dinitrate 40mg/day) versus calcium channel blockers (amlodipine 5mg/day or long acting nifedipine 20mg/day) on coronary endothelium and vasoconstriction between patients with normal or minimally diseased coronary artery, treatment with long acting nitrates was associated with less favourable effects on coronary endothelial functions 15. Sudden withdrawal of CCB in patients with known vasospasm can lead to rebound of symptoms and may prove dangerous. In patients with refractory symptoms alpha-blockers, nicorandil have been used. Although beta blockers are believed to enhance vasospasm, Betaxalol, a selective beta-1 blocker, has been found to be effective in the treatment of variant angina due to its vasorelaxing effects 16. In addition, elimination of or control of all other risk factors or precipitants is very important for successful treatment. In drug refractory cases the percutaneous coronary intervention or coronary artery bypass graft has been performed for the ischemia relief 17.
Our patient had multiple precipitating factors for vasospasm. Endothelial dysfunction from severe physical illness and sepsis could have precipitated the VA. Furthermore, hypoxia from respiratory failure could have also been an inciting agent and cannot be ruled out. It is worth mentioning that intensive care unit patients frequently have coexistence of both the underlying risk factors and the precipitating factors for vasospasm, yet VA as a clinical syndrome is uncommonly seen or reported.
Conclusion:
The clinician needs to be aware of coronary artery vasospasm as it can pose a serious medical threat. Early diagnosis and treatment may result in improved outcomes from vasospastic angina.
As highlighted in the World Health Report 2002, just a few Non Communicable Disease (NCD) risk factors, account for the majority of non communicable disease burden. These risk factors; tobacco use, alcohol consumption, raised blood pressure, raised lipid levels, increased BMI, low fruit/vegetable intake, physical inactivity, and diabetes, are the focus of the STEPs approach to NCD risk factor surveillance. 3
A tool for surveillance of risk factors, WHO STEPS, has been developed to help low and middle income countries get started. It is based on collection ofstandardised data from representative populations of specified sample size to ensure comparability over time and across locations. Step one gathers information on risk factors that can be obtained from the general population by questionnaire. This includes information on socio-demographic features, tobacco use, alcohol consumption, physical inactivity, and fruit/vegetable intake. Step two includes objective data by simple physical measurements needed to examine risk factors that are physiologic attributes of the human body. These are height, weight, and waist circumference (for obesity) and blood pressure. Step three carries the objective measurements of physiologic attributes one step further with the inclusion of blood samples for measuring lipid and glucose levels.4 The risk factors studied by MONICA project of the World Health Organization (WHO), included cigarette smoking, blood pressure, blood cholesterol and body weight.5In many resource-poor settings, laboratory access can be difficultand expensive. A screening algorithm that includesgender, age, cardiovascular disease history, blood pressure,weight and height, and a urine dipstick test for glucose andprotein is likely to be more practical and may well providemuch of the predictive value of more complex blood-based assessments.6In addition, such algorithms should, wherever possible, useregional data on morbidity and mortality, because backgroundrates vary considerably between regions.7 WHO/ISH (World Health Organization/International Society of hypertension) risk prediction charts provide approximate estimates of cardiovascular disease (CVD) risk in people who do not have established coronary heart disease, stroke or other atherosclerotic disease. They are useful as tools to help identify those at high cardio vascular risk, and to motivate patients, particularly to change behavior and, when appropriate, to take antihypertensive, lipid-lowering drugs and aspirin.8 After reviewing the above information about standardised methods available for identifying the risk factors for CAD, the present study was undertaken to assess the prevalence of risk factors in the community in Tripoli, the capital of Libya. The aim of this paper also includes suggesting priorities and strategy to deal with the risk factors that were found most important. Appropriate statistical tests were applied using the software SPSS 17 for determining the relative importance of different risk factors. The specific statistical tests have been stated below. Material and Methods 528 individuals were selected from general community for the study by random sampling from different geographical areas of Tripoli. They were interviewed about risk factors for CAD and where possible, facts stated by them were validated from medical records available with them. Their body weight, height and blood pressure were also recorded. The intern doctors posted with community medicine department were briefed and trained by faculty members for the above observations and recording the body measurement and blood pressure using the uniform technique. The WHO/ISH risk prediction colourcharts for Eastern Mediterranean Region B (which includes Libya) were used as questionnaire for the study. The option of charts available for settings where blood cholesterol can’t be measured was selected as it was found difficult to convince the individuals not suffering from disease to provide blood samples. The following criteria were used for defining Blood Pressure, BMI, Diabetes & MI : According to the WHO definition, individuals with systolic blood pressure ≥ 140 mmHg or those with diastolic blood pressure ≥ 90 mmHg were considered hypertensive. 21. Known cases of diabetes were termed as individuals for whom the diagnosis of diabetes had been established by a physician in the past, or those who were under treatment with anti diabetic drugs. 22 Body mass index (BMI) is calculated as weight divided by height squared (kg/m2). Overweight is defined as BMI 25–29.9 kg/m2, and obesity as BMI ≥ 30 kg/m2 for all subjects.19 Known cases of Myocardial Infarction (MI) were termed as individuals for whom the diagnosis of MI had been established by a physician in the past. ObservationsThe comparison of population characteristics of people with and without having a MI stated in the table below reveals that: distribution of males and females was similar in both the groups. 88% of individuals with a MI were from age group 35 and above. Whereas 11.43% of people with MI were from age group 15 to 34 years which shows the need of starting screening as well as control of risk factors from teenage. Using SPSS software, independent sample t test was applied on age distribution of individuals with and without history of MI. The result revealed that the mean age of individuals with a positive history of MI was 54. It was 43.74 for subjects with negative history of MI. The difference of age between the above 2 groups was found highly significant (P>0.001). In the same manner using SPSS software, Chi square test was applied on sex distribution of individuals with and without history of MI. The result revealed that the difference in sex distribution in the two groups was not significant (P = 0.522) Table 1 : Age & Sex wise distribution of persons with and without MI:
Characteristics
Individuals with MI in percentage, (N= 70)
Individuals without MI in percentage, (N = 458)
Sex; Male
68.57 (48)
68.78 (315)
Female
31.43 (22)
31.22 (143)
Age 15-34 years
11.43(8)
34.93 (160)
35-54 years
30.00 (21)
37.55 (172)
55 & above
58.57 (41)
27.51 (126)
Independent risk factorsAs presented in Fig.1, in males with MI in terms of percentage the most prevalent risk factor was found to be hypertension (11.05% higher than non MI group), followed by diabetes (higher by 10.78%), smoking (higher by 8.12%) and BMI 25 & above (higher by 5.13%). As presented in Fig.2, in females with MI in terms of percentage the most prevalent risk factor was found to be hypertension (20.55% higher than non MI group), followed by BMI 25 & above (higher by 8.77%) and diabetes (higher by 6.85%). There were no smokers in the female group with MI and only one smoker was found in the females without MI. Using SPSS software, under general linear model, multivariate analysis was performed after splitting the cases under male and female. History of MI was kept as fixed factor and age, history of hypertension, diabetes and stroke, smoking, systolic blood pressure and BMI were kept as dependent variables. The results reveal that in the males with positive history of MI, value of P was less than 0.001(highly significant) for age, History of hypertension & diabetes and systolic BP of140 and greater, followed by history of stroke (P>0.002) suggesting that prevalence of these variables were significantly higher in males with history of MI. The prevalence of BMI 25 & above (P>0.616) and smoking (P>0.882) in males with history of MI was found insignificant. In case of females with positive history of MI, the only variable having significant prevalence was f history of hypertension (P>0.008). An important reason for inability to assess significance for other variables in females may be the smaller number of females of only 22 with history of MI. Among the community members with MI, 94.38% males and 78.57% females had one or the other risk factor which have been stated above. Hence with focused attention to health education and screening for risk factors, identifying most of the individuals at risk of MI, should be possible. (Fig.1) Distribution of Risk Factors in Males with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) (Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factorsOut of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI. (Fig.3) Age wise distribution of blood pressure (both sexes)Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years. (Fig. 4) Age wise distribution of weight (both sexes) Discussion: Comparison with other relevant studies: In our study the most common risk factors observed in community members without MI were hypertension (total 24.35%, males 23.78 & females 25.88), followed by diabetes (total 21.13%, males 19.56 & females 25.29) and smoking (Total 27.26%, males 37.33 & females 0.59) as stated above in Fig.1 & 2. In similar studies performed in countries of Mediterranean region14-18 26% of study population were found to be suffering from hypertension, 40% males and 13% females were smokers and 14.5% were suffering from diabetes. 13 The percentage of diabetics was 10.6 in study population aged 30 years and above in Iran11. The percentage of diabetics were 11% in males and 7% in females in United Arab Emirates (UAE)10 and the figures were the similar in Saudi Arabia in subjects aged 30 years and above were 17.3% and 12.18% respectively.9. All the above studies were performed in the period from year 2000 to 2004 except the study in UAE which was performed in 1995. It can be seen from our study in Libya that in comparison to mean percentage for the same risk factors in other countries of Mediterranean Region, the percentage of hypertension was lower by about 2%. In Libya the percentage of total diabetics in the general community was greater by 6.6%, while the percentage of smokers were less by about 13% in males and 12.5% in females. The percentage of total overweight and obese individuals in all age groups and both sexes were 66.6 % in the general community without MI in our present study (Fig,4). The percentage for those overweight and obese in individuals above 19 years of age was 26.2% in study from Iran12 and 27 % in UAE10 in the age group of 30 to 64 years. The study of 12 countries of the Eastern Mediterranean Region(EMR) by the WHO conducted in 2004, reveals that regional adjusted mean for these countries was 43 % for overweight and obese individuals in all age groups and both sexes20. Hence in comparison to developing countries of the region having similar religious, social and dietary situation among the risk factors for CAD, diabetes and obesity can be seen as emerging major risk factors in Libya followed by hypertension and smoking. Smokers among females were found to be uncommon in Libya.Conclusion The findings of this study reveal that in comparison to those without MI the prevalence of following risk factors was higher in individuals with MI. In males aged 35 to 54, the percentage of those with a systolic BP of 140 and greater was more than double and in females 1.6 times greater. Those with diabetes were greater by 10.78% in males and 6.85% in females, while smokers were higher by 8.12% in males. The percentage of diabetes in individuals without MI was 21.13%. The prevalence of smokers was found to be 37.33% in males without MI which suggests urgent need for prevention and control measures. Considering multiple risk factors out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. In view of large number of individuals having risk factors of CAD in Tripoli, we would like to recommend that health education for preventing overweight and obesity, hypertension, smoking and diabetes may be started with school children and their parents as early as primary school. The screening for above risk factors needs to be implemented in the age group of 34 years and above for detecting individuals at risk as close to 34 years as possible. This step needs to be followed by relevant health education and treatment as soon as possible. More studies on a larger population sample are required from different geographical areas of Libya to refine our focus on the target population identified. At the same time waiting for action, till these additional studies are completed, is not recommended. To make the comparison of risk factors more fruitful among different countries and in the same country over time, we need to agree on uniform criteria such as using WHO/ISH risk prediction charts. Limitations of present studyIt is a cross sectional study based on the questions stated in WHO/ISH prediction charts for situations where collecting blood samples is not feasible. Due to the small sample size we can only say that the prevalence of MI is indicative of the pattern observed. These figures may get refined as we cover a larger number of the population over time. Due care has been taken in selecting sample size to represent different geographical divisions of Tripoli and to ensure that this is a random sample, but it is a systematic random sample and not the stratified random sample. Hence within each geographical division all the socio economic strata of community may not have been proportionately represented. AppendixThe questionnaire used for the study is stated below. It is based on the questionnaire recommended on page 21 of WHO/ ISH risk prediction charts for Eastern Mediterranean Region B of W.H.O. in which Libya is included.QuestionnairePrecautions: Do not interview persons below the age of 14 years. You should take height, weight and Blood Pressure of the person yourself, before recording it in the form below
S.N.
Question
Subject
1
2
3
4
5
1
Name of Person:
2
Address in Libya
4
Age
5
Sex: M / F
6
Do you smoke: Yes / No
8
Do you have History of suffering from Diabetes: Yes / No
9
Hist. of suffering from: Mayo cardial Infarction: Yes/ No
Initial reports of Obesity Hypoventilation Syndrome (OHS) date back as early as 18891, but it was not until 1955 that Auchincloss2 and colleagues described a case of obesity and hypersomnolence paired with alveolar hypoventilation. Burwell3 coined the term Pickwickian syndrome describing the constellation of morbid obesity, plethora, oedema and hypersomnolence. Hypercapnia, hypoxaemia and polycythemia were described on laboratory testing. Obstructive Sleep Apnea (OSA) had not been described at that time and came to be recognized for the first time in the mid 1970s. With attention shifting to upper airway obstruction, hypercapnia began to get lesser emphasis and confusion began to emerge in describing OSA and OHS. The term ‘Pickwickian’ began to be used for OSA-related hypersomnolence in the obese patient regardless of the presence of hypercapnia. This confusion was finally settled by the American Academy of Sleep Medicine (AASM) in its published guidelines in 1999.4 The AASM statement identified that awake hypercapnia may be due to a predominant upper airway obstruction (OSA) or predominant hypoventilation (Sleep Hypoventilation Syndrome) easily distinguished by nocturnal polysomnography (PSG) and response to treatment. Both disorders are invariably associated with obesity and share a common clinical presentation profile.
Salient features of OHS consist of obesity as defined by a BMI > 30kg/m2, sleep disordered breathing, and chronic daytime alveolar hypoventilation (PaCO2 ≥ 45 mmHg and PaO2 < 70 mmHg). 4 Sleep disordered breathing, as characterized by polysomnography in OHS, reveals OSA (Apnea-hypopnea index [AHI]>5) in up to 90% of patients and sleep hypoventilation (AHI<5) in up to 10%.5 Daytime hypercapnia and hypoxaemia are the hallmark signs of OHS and distinguish obesity hypoventilation from OSA. Severe obstructive or restrictive lung disease, chest wall deformities and hypoventilation from severe hypothyroidism, and neuromuscular disease need to be excluded before a diagnosis of OHS is established. As obesity is becoming more prevalent in western society, this disorder has gained more recognition in recent years. However, patients with this syndrome may still go undetected and untreated. No population-based prevalence studies of OHS exist till date but, at present, can be estimated from the relatively well known prevalence of OHS among patients with OSA. Recent meta-analysis with the largest cohort of patients (n=4250) reported a 19% prevalence of OHS among the OSA population, confirming an overall prevalence of about 3 per 1000.6
Whilst transient rectifiable nocturnal hypercapnia is common in patients with OSA, awake hypercapnia in OHS appears to be a final expression of multiple factors. There has been a debate about BMI and AHI not being the most important independent predictors of hypercapnia in obese patients with OSA. More definitive evidence for the role of OSA, however, is suggested by resolution of hypercapnia in the majority of patients with hypercapnic OSA or OHS with treatment, with either PAP or tracheostomy, without any significant changes in body weight or respiratory system mechanics. Yet some recent studies have shown that nocturnal hypoxaemia and diurnal hypercapnia, persist in about 50% of such individuals even after complete resolution of OSA with CPAP or tracheostomy. This raises questions such as how good is AHI as a measure of severity of OSA?
It is intuitive to argue that obesity may exert its effect through mass loading of CO2 due to (increased production via) higher basal metabolic rate or reduced functional residual capacity on lung function. But why do only some severely obese patients with OSA go onto develop OHS? Is the pathophysiology driven by the severity of BMI? Whilst weight loss, particularly surgically-induced, clearly shows resolution of both OSA and hypercapnia7, the role of BMI as an independent factor for hypercapnia has been challenged by the fact that only a small fraction of severely obese patients do in fact develop chronic diurnal hypercapnia. More importantly, not only can PaCO2 be normalized in a majority of patients without weight loss and with positive airway pressure therapy (PAP), but awake hypercapnia can develop even at lower BMIs among the Asian population. Some investigators have tried to explain the incremental role of BMI as follows. In situations where AHI is not a presumed independent predictor of nocturnal hypercapnia, potential pathophysiologic contributors can include pre-event (apnea or hypopnea) amplitude in relation to the post-event amplitude.8 Such inciting events for nocturnal hypercapnia may then be perpetuated in the daytime by factors such as AHI, functional vital capacity (FVC), FVC/FEV1, or BMI as shown in the largest pooled data to date.6 It has been shown that, for a given apnea/interapnea duration ratio, a greater degree of obesity is associated with higher values of PaCO2.9 However the same group of investigators, in another study, did not find any of these factors to be related to the post-event ventilatory response.8
Looking further at the breath by breath cycle, the post-event ventilatory response in chronic hypercapnia may relate to eventual adaptation of chemoreceptors perhaps in consequence to elevated serum bicarbonate known to blunt the ventilatory drive.10 Or it may relate to whole body CO2 storage capacity which is known to exceed the capacity for storing O2.11 With definite evolution in our understanding of hypercapnia among obese patients, these questions continue to dominate. Some of the more pressing ones include: are the predictors of daytime hypercapnia different from those of nocturnal hypercapnia in obese patients with OSA? An understanding of these facts can help us with the more important understanding of the associated morbidity and mortality from OHS and its correct management. In addition, what is the true effect of untreated OHS on mortality independent of the co-morbidities related to obesity and OSA? Can morbidities like cor pulmonale and pulmonary hypertension be reversed with treatment of OHS? How do we treat patients with OHS who fail CPAP/ BiPAP short of tracheostomy?
Forty one years after the last influenza pandemic, while everyone was worrying about the avian influenza A (H5N1) virus causing a pandemic, an apparent new chapter is opened with the emergence of new strain of influenza A virus. On 24th April, the World Health Organization (WHO) declared the first ever public health emergency of international concern indicating the occurrence of confirmed human cases of swine influenza in Mexico and United States.1 Subsequently the Centre for Disease Control and Prevention (CDC) confirmed that these human influenza cases were caused by a novel strain of influenza A virus to which there is little or no population immunity.2 On June 2009, the WHO rated the pandemic alert from phase 5 to 6, signalling that the first pandemic of the 21st century was underway. It was however stressed that the rise in the pandemic alert level was mainly attributed to the global spread of the virus rather than its severity. The pandemic potential of influenza A viruses has been ascribed to their genetic and antigenic instability and there ability to transform by constant genetic re-assortment or mutations, which can result in the emergence of novel progeny subtypes capable of both infecting and leading to sustained person to person transmission.3 The newly emerged strain contains a combination of gene segments that have not been previously identified in swine or human influenza viruses.4
Historical Perspectives
Influenza has been recognised for hundreds of years, but the cause was unknown for most of this time. Hippocrates had defined this disease about 2400 years ago, but lacked laboratory confirmation.5 The year 1580, marks the first instance of influenza recorded as an epidemic even though there is possibility that there were many prior influenza epidemics.6 The word influenza (meaning influence), first used in 1743 originated from the Latin word “Influenza”, named so because the disease was considered to be caused by unfavourable astrological conditions. Since 1700, there have been approximately a dozen influenza A virus pandemics and the lethal outbreak of 1918-1919 is dubbed as the greatest medical holocaust in recorded history, killing up to 50 million people worldwide.7
The earliest evidence of influenza A virus causing acute respiratory illness in pigs was traced to the 1930s. Swine influenza A viruses are antigenically very similar to the 1918 human influenza A virus and they may all have originated from common ancestor.8 From 1930 to 1990, classic swine influenza A was the commonest swine influenza virus circulating amongst the swine population during which the virus did not undergo much genetic change. Antigenic variants of these classical influenza viruses emerged in 1991 and the real antigenic shift occurred at the ends of last century when the classical swine influenza virus re-assorted with human influenza A virus and a North American lineage avian influenza virus. This resulted in the emergence of multiple subtypes including H1N2 and H3N2. In the past few years, sporadic cases of human infections caused by swine influenza A virus have occurred, mainly due to subtypes. Occupational exposure to swine was the most important risk factor for infection and fortunately all patients recovered without resulting in efficient, sustained human to human transmission.9
Origin of 2009 Strain
The pandemic that began in March 2009, was originally referred to as “swine flu” because laboratory testing showed that many of the genes in this new virus were very similar to influenza viruses that normally occur in pigs (swine) in North America. But further study has shown that this new strain of virus represents a quadruple re-assortment of two swine strains, one human strain and one avian strain of influenza. The largest proportion of genes come from swine influenza viruses (30.6% from North American swine influenza strains, and 17.5% from Eurasian swine influenza strains), followed by North American avian influenza strains (34.4%) and human influenza strains (17.5%).10 Analysis of the antigenic and genetic characteristics of the pandemic influenza A virus demonstrated that it’s gene segments have been circulating for many years, suggesting that lack of surveillance in swine is the reason that this strain had not been recognized previously.11 This novel strain is antigenically distinct from seasonal influenza A and possesses previously unrecognised molecular determinants that could be responsible for the rapid human to human transmission. Moreover, antigenic drift has occurred amongst different lineages of viruses, therefore, cross protection antibodies against avian, swine and human viruses are not expected to exist. Emerging scientific data support the hypothesis of a natural genesis, with domestic pigs a central role in the generation and maintenance of the virus. Protein homology analysis of more than 400 protein sequences from the new influenza virus as well as other homologous proteins from influenza viruses of the past few seasons also confirmed that this virus has a swine lineage.1 Phylogenetic analysis has suggested that initial transmission to humans occurred several months before the recognition of the outbreak and multiple genetic ancestry of this influenza A is not indicative of artificial origin.11
Situation Update
In March 2009, an outbreak of respiratory illness was first noted in Mexico, which was eventually identified as being related to influenza A.12 The outbreak spread rapidly to the United States, Canada and throughout the world as a result of airline travel.13 On 11th June 2009, the WHO raised its pandemic alert to the highest level i.e. phase 6, indicating widespread community transmission on at least two continents.14
Pandemic influenza was the predominant influenza virus circulating in the US, Europe, northern and eastern Africa and in Australia. Activity of the virus has initially peaked and then declined in North America and in parts of western, northern and Eastern Europe, but activity continued to increase in parts of central and southeastern Europe, as well as in central and south Asia. As of 28th February 2010, worldwide more than 213 countries and overseas territories or communities have reported laboratory confirmed cases of pandemic influenza 2009, including at least 16455 deaths; a number the WHO acknowledges significantly underreported the actual number.15 Most of the deaths have been related to respiratory failure resulting from severe pneumonia and acute respiratory distress syndrome.16
In India, the number of confirmed cases till March 2010 was 29,953 and a total of 1410 deaths were reported. The rate of infection has been highest among children and young individuals of <24 years of age. To date, pandemic influenza A infections are uncommon in persons older than 65 years, possibly as a result of pre-existing immunity against antigenically similar influenza viruses that circulated prior to 1957.17 High rates of morbidity and mortality has been noted among children and young adults with underlying health problems including chronic lung disease, immunosuppressive conditions, cardiac disease, pregnancy, diabetes mellitus and obesity.18
Transmission and Shedding
Novel virus is contagious and can transmit from human to human in ways similar to other influenza viruses. The main route of transmission between humans is via inhalation of infected respiratory droplets (range in size from 0.08 µm to 0.12 µm) produced after coughing and sneezing.19 Transmission via contact with surfaces that have been contaminated with respiratory droplets or by aerosolised small-particle droplets may also occur. In addition to respiratory secretions, all other body fluids (including diarrhoeal stool) should also be considered potentially infectious.
The estimated incubation period is unknown and could range from 1 to 7 days, although the median incubation period in most cases appears to be approximately 2 days.20 Shedding of the virus begins the day prior to the onset of symptoms and can persist for 5-7 days in immunocompetent individuals. The amount of virus shed is greatest during the first 2-3 days of illness. Persons who continue to be ill, for a period of longer than 7 days after illness onset, should be considered potentially contagious until symptoms have resolved. Longer periods of shedding may occur in children (especially young infants), elderly adults, and patients with chronic illnesses and immunocompromised hosts who might be contagious for longer periods.
Clinical Manifestations
According to the CDC, in humans the symptoms of the 2009 “flu” virus are similar to those of influenza and of influenza-like illness in general. The illness with the virus has ranged from mild to severe and symptoms include fever, cough, sore throat, body aches, headache, chills and fatigue, which are usual features of influenza virus. The 2009 outbreak has shown an increase percentage of patients reporting diarrhoea and vomiting.16 As these symptoms are not specific to swine flu hence a differential diagnosis of probable swine flu requires not only symptoms but also a high likelihood of swine flu due to person’s recent history. The CDC advised physicians to consider swine influenza infection in the differential diagnosis of patients with acute febrile respiratory illness who have either been in contact with persons with confirmed swine flu or who were in states that have reported swine flu cases during the 7 days preceding their illness onset.
The overall severity with this 2009 virus has been less than what was observed during the influenza pandemic of 1918-1919. Most patients appear to have uncomplicated, typical influenza-like illness and recovered without requiring any medical treatment. About 70% of people who have been hospitalised have had one or more medical conditions, which include pregnancy, diabetes, heart disease, asthma and kidney disease.21 The most common cause of death is acute respiratory distress syndrome. The other causes of death are severe pneumonia with multifocal infiltrates (leading to sepsis), high fever (leading to neurological problems), dehydration (from excessive vomiting and diarrhoea) and electrolyte imbalance. Fatalities are more likely in young children (<5 years), elderly (>65 years) and in people with underlying conditions, which include pregnancy, asthma, lung diseases, diabetes, morbid obesity, autoimmune disorders, immunosuppressive therapies, neurological disorders and cardiovascular disease.22
Laboratory Diagnosis
All diagnostic laboratory work on clinical samples from suspected cases of virus infection should be done in a Biosafety Level 2 (BSL-2) Laboratory. Suspected cases of novel infection should have respiratory specimens (nasopharyngeal, nasal or oropharyngeal swab, bronchoalveolar lavage and endotracheal aspirate) collected to test for the 2009 flu virus. Specimens should be placed into sterile viral transport media (VTM) and to be kept at 4°C. Real time reverse transcriptase polymerase chain reaction (RT-PCR) is the recommended sensitive method for the detection of virus, as well as to differentiate between pandemic 2009 and regular seasonal flu.23 The other rapid influenza diagnostic tests (RIDTs), although provide results within 30 minutes or even less, none of these tests can distinguish between influenza A virus subtypes. Moreover, RIDTs do not provide any information about antiviral drug susceptibility. Isolation of the virus in cell cultures or embryonated eggs is another method for diagnosis of infection, but may not yield timely results for clinical management and negative viral culture does not exclude the influenza A infection.
However, most people with flu symptoms do not need a test for pandemic 2009 flu, specifically because the test results usually do not affect the recommended course of treatment. The CDC recommends testing only for people who are hospitalised with suspected flu and persons having underlying medical conditions and those with weak immune systems.24 It is also expressed that treatment should not be delayed by waiting for laboratory confirmation of test results, but rather make diagnosis based on clinical and epidemiological backgrounds and start treatment early.
Treatment
The virus isolates in the 2009 outbreak are found to be resistant to amantidine and rimantidine. The CDC recommends the use of neuraminidase inhibitors as the drugs of choice for treatment and prevention of 2009 influenza in both children and adults.25 Tamiflu (oseltamivir phosphate) and Relenza (zanamivir) are the two FDA-approved influenza antiviral drugs and a third neuraminidase inhibitor peramivir is an experimental drug approved for hospitalised patients in cases where the other available methods of treatment are ineffective or unavailable. Antiviral drugs not only make the illness milder but also prevent serious flu complications. However, the majority of people infected with the virus make a full recovery without requiring medical attention or antiviral drugs. Treatment is recommended for patients with confirmed or suspected 2009 influenza who have severe, complicated or progressive illness or who are hospitalised. People who are not from the at-risk group and have persistent or rapidly worsening symptoms should also be treated with antivirals. Therapy should be started as soon as possible, since evidence of benefit is strongest when treatment is started within 48 hours of illness onset.26 Treatment should not be delayed while awaiting the results of diagnostic testing nor should it be withheld in patients with indications for therapy who present >48 hours after the onset of symptoms. Beside antivirals, supportive care at home or in hospital, focuses on controlling fevers, relieving pain and maintaining fluid balance as well as identifying and treating any secondary infections or other medical problems.
Major Concern
The neuraminidase inhibitors oseltamivir and zanamivir provide valuable defences and have been used widely for treatment and chemoprophylaxis of 2009 pandemic influenza A.But the recent emergence of resistance to these antiviral drugs is a matter of immediate concern. Influenza A strain resistant to oseltamivir has been reported from a variety of geographical locales and poses a challenge for the management of severely compromised patients.27 The CDC warned that the indiscriminate use of antiviral medications to prevent and treat influenza could ease the way for drug resistant strains to emerge, which would make the fight against the pandemic much harder. Most of the patients recover spontaneously without any medical attention and use of antiviral medications should be reserved primarily for people hospitalised with pandemic flu and persons, with pre-existing or underlying medical conditions who are at higher risk for influenza-related complications. It has also been emphasised that early treatment once a patient has developed symptoms, rather than chemoprophylaxis, should reduce opportunities for the development of oseltamivir resistance.26 The degree to which these drugs will remain effective for the treatment of the novel strain of influenza in the coming months is still a question.
What’s next?
The only possible way to combat the situation is large scale immunization. Antiviral drugs are not a substitute for vaccinination and are used only as an adjunct to vaccines in the control of influenza. Vaccines are one of the most effective ways to protect people from contracting illness during epidemics and pandemics of influenza. The seasonal vaccines do not confer any protection against 2009 H1N1; new vaccines have been licensed and are available.28 The vaccines are available in both live-attenuated and inactivated formulations. Two types of vaccines are approved by the FDA for use in the prevention of 2009 pandemic influenza virus. These are TIV (“flu shot” of trivalent inactivated vaccine) and LAIV (nasal spray of live attenuated vaccine). The inactivated vaccine is contraindicated in patients with severe allergic reaction to eggs or any other component of the vaccine. The live attenuated vaccine is licensed for persons aged 2 through 49 years who are not pregnant, are not immunocompromised and have no underlying medical conditions. Children less than 5 years who have asthma and are taking long term aspirin therapy should also not receive live vaccines. Otherwise, both vaccines are safe and highly immunogenic and a single administration leads to robust immune response in 80% to 90% of adults aged 18-64 years and in 56% to 80% of adults aged 65 years and older with in about 10 days.29 Children younger than 10 years will require two administrations of the vaccine separated by at least 21 days. Adverse effects following vaccination are minor, just like those of seasonal influenza vaccine and are self limiting. Concerns regarding the risk of Guillain-Barre syndrome (GBS) after vaccination have been raised. Various studies have suggested that the risk of GBS is higher from influenza itself rather than from the vaccine and the other adverse effects.30 The CDC is now encouraging everyone including people of 65 years and above to get vaccinated against the 2009 strain of influenza.
The Government of India has recently approved a split virus, inactivated, non-adjuvant monovalent vaccine (Panenza by Sanofi Pasteur) to inoculate frontline health workers and those who have a high risk of getting infected.31 Groups of health care workers has also been singled out by the European council for attention and immunization.32 Infection control practices in the health care settings should be followed along with as per the guidelines.33 Patients should also be educated regarding the other preventive measures, including using tissues to cover their mouth and nose when coughing and sneezing, developing good hand washing techniques, use of alcohol based hand-rubs, avoiding contact with ill persons if possible and staying home when ill unless medical attention has been given.
The flu season seems to be dying down in 2010 but the war is yet not over. Lessons must be learnt from the previous influenza pandemics and it is still important to get vaccinated against the flu and be prepared, as activity as well as virulence might increase again in the coming season. The words of Margaret Chan (Director General, WHO) to be remembered that “the virus writes the rule and this one like all influenza viruses can change the rules, without rhyme or reason, at any time”.
A 87-year old man was referred to hospital with a five day history of lethargy and increased urinary frequency. He denied symptoms of gastrointestinal bleeding or abdominal pain. His past medical history included diabetes mellitus, chronic kidney disease, peripheral vascular disease and surgery for repair of ruptured aortic aneurysm 6 weeks ago. Systemic examination, including per rectal examination, was normal. Haemoglobin was 83g/L and C-reactive protein was 148 (Normal <5). Twelve hours after admission he developed pyrexia (37.8 degree) accompanied with tachycardia (103 beats per minute) and hypotension (BP 87/43). Soon afterwards, he had a small amount (<50 mls) of fresh haemetemesis. He also complained of lower back pain and clinical examination revealed tenderness in the left iliac fossa. He was cross-matched for blood and initiated on intra-venous fluids. As his Rockall score was six an urgent oesophago-gastro-duodenoscopy (OGD) was planned. Over the next few hours he complained of increasing central abdominal pain and had several episodes of melaena. In view of the history of recent aortic surgery and current GI bleed the possibility of aorto-enteric fistula (AEF) was considered. An urgent contrast CT scan of the abdomen (Figure 1) was therefore arranged prior to OGD.
Figure 1: Contrast CT scan demonstrating the aorta (A) with extravasation of contrast (B) and a large collection (C) around it with trapped air suggestive of infection.
Contrast computed tomogram (CT) scan of the abdomen revealed an inflammatory soft tissue mass anterior to the infra-renal aortic graft with pockets of gas and leakage of contrast into it. These findings were suggestive of an AEF. The patient was informed of the diagnosis of AEF and the need for emergency surgical repair to which he consented. During the operation the vascular surgeons found that the duodenum was adherent to the aortic graft with evidence of fistulisation and infection, thus confirming the diagnosis. Although operative repair appeared to be successful, the patient continued to bleed on the table due to disseminated intravascular coagulation and died twenty fours after admission.
Discussion
AEF is defined as a communication between the aorta and the GI tract.1 The diagnosis of AEF should be considered in every patient with a GI bleed and a past history of aortic surgery.2 Our case patient had had emergency repair of a ruptured aortic aneurysm with a prosthetic graft 6 weeks prior to his current admission.
AEFs are a rare cause of gastro-intestinal (GI) hemorrhage. AEFs can be primary or secondary. Primary AEF (PAEF) is a communication between the native aorta and the GI tract.1 The incidence of PAEF ranges from 0.04 to 0.07%.3 PAEFs commonly arise from an abdominal aortic aneurysm of which 85% are atherosclerotic.1
Secondary AEFs (SAEF) are an uncommon complication of abdominal aortic reconstruction.4The incidence of SAEF ranges from 0.6% - 4%.5 Generally two types of SAEFs have been described. Type 1, termed as true AEF develops between the proximal aortic suture and the bowel wall. These usually present with massive upper GI hemorrhage.4 Type 2, or the paraprosthetic–enteric fistula does not develop a communication between the bowel and the graft and accounts for 15% to 20% of SAEFs.4 In this type of fistula, bleeding occurs from the edges of the eroded bowel by mechanical pulsations of the aortic graft. Sepsis is more frequently associated with this type of AEF (75% of cases).4 The mean time interval between surgery and presentation with SAEF is about 32 months6 but the time interval can vary from 2 days to 23 years.7 AEFs can involve any segment of the GI tract but, 75% involve the third part of the duodenum and the affected part is generally proximal to the aortic graft.8
The pathogenesis of AEF is not fully understood but two theories exist. One theory suggests repeated mechanical trauma between the pulsating aorta and duodenum causes fistula formation and the other suggests low-grade infection as the primary event with abscess formation and subsequent erosion through the bowel wall.9 The latter theory is felt to be most likely. The majority of grafts show signs of infection at the time of bleeding and up to 85% of cases have blood cultures positive for enteric organisms.10
The main symptom of AEF is GI bleeding. Secondary AEFs have been traditionally said to present with a symptom triad (as in our patient) of abdominal pain, GI bleeding and sepsis; however, only 30% of patients present in this manner.11 Patients often have a “herald bleed” which is defined as a brisk bleed associated with hypotension and hematemesis that stops spontaneously followed by massive gastro-intestinal haemorrhage in 20% – 100% of patients.8 Sometimes the GI bleeding can be intermittent.
The commonest investigations for diagnosis of AEFs are OGD, conventional contrast CT scan and angiography.12 OGD is often the initial investigation, as in any upper GI bleed mainly because of lack of clinical suspicion of the diagnosis. The endoscopic findings vary from those of a graft protruding through the bowel wall to fresh bleeding in distal duodenum to that of an adherent clot or extrinsic compression by a pulsating mass with a suture line protruding into the duodenum.13 Less than 40% of patients have signs of active bleeding at OGD.8 Conventional CT with contrast is widely available and most commonly performed to diagnose AEFs. Perigraft extravasation of contrast is a pathognomic sign of AEF and this may be associated with signs of graft infection i.e perigraft fluid and soft tissue thickening along with gas.12 Multi-detector CT and MRI are more sensitive diagnostic imaging tools with MRI now being used mainly in patients with renal failure to avoid the use of contrast.12
PAEFs can be treated with endovascular stent placement in selected cases especially in those who cannot tolerate emergency surgery.12 The treatment of choice in SAEFs is graft resection and establishment of an extra-anastomotic circulation with repair of the duodenal wall although overall survival rates vary from 30% to 70%.13
Conclusion
SAEFs are a catastrophic complication of aortic surgery. AEFs are relatively rare and need a high index of suspicion in the appropriate clinical situation in order to diagnose this condition. Left untreated they are universally fatal. Surgical repair carries a very high mortality.
A 55 year old white male with a history of hypertension, hyperlipidemia, smoking and transient ischaemic attacks was admitted to the hospital with worsening dyspneoa on exertion over a period of 6 weeks. He also reported significant weight loss, loss of appetite and fatigue over several weeks. Physical examination revealed tachycardia, and moderate respiratory distress with prominent jugular venous distention. Cardiac auscultation revealed normal S1 and loud P2. Also heard were an early diastolic heart sound ( tumour plop) and a mid-diastolic murmur at the apex. An ECG revealed evidence of left ventricular hypertrophy with repolarization abnormalities. A transthoracic echocardiogram (Figures 1 and 2) revealed a large, pedunculated, mobile left atrial mass measuring 3x4 cm, impinging on the mitral orifice with a mean gradient across the mitral valve of 15 mm Hg. Left ventricular systolic function was normal.
Figure 1: Parasternal long axis echocardiograph of the left atrial myxoma prolapsing into the mitral valve during diastole.
A diagnosis of probable left atrial myxoma was made. The patient had four episodes of syncope within 24 hrs, the first at 3: 53 am after returning from the bathroom, subsequently leading to cardiac arrest at 14:20 pm.
Figure 2: parasternal long axis echocardiograph showing the large left atrial myxoma during systole.
He was intubated and initiated on vasopressors. An emergent Left heart catheterization was performed prior to a referral for surgical excision, which revealed triple vessel coronary artery disease. During cardiac catheterization the patient became more hypotensive requiring an intra-aortic balloon pump. While arrangements were made for a referral for surgery, the patient’s clinical condition deteriorated rapidly and he went into pulseless electrical activity at 18:54 pm and could not be resuscitated. The patient’s death was presumably due to persistent intracardiac obstruction. On autopsy, the left atrial mass was identified as a haemorrhagic left atrial myxoma, 5x4x3.5cm in size attached by a stalk to an inter-atrial septum. Multiple organizsing thrombi were present in the 1tumour. Histology showed abundant ground substance with stellate myxoma cells and haemosiderin-laden macrophages (Figures 3 and 4). The cause of death was attributed to valvular “ball-valve” obstruction.
Figure 3: Histopathology of left atrial myxoma showing spindle shaped myxoma cells (white arrow) in a myxoid matrix (black arrow) and blood vessels (top arrow) (H & E 40X)
Figure 4: Histopathology of left atrial myxoma showing vascular spaces filled with relatively fresh blood and evidence of old bleeding (hemosiderin) suggesting repeated episodes of hemorrhage within the myxoma (H & E 4X)
Case 2
A 57 year old African American female presented with recurrent syncopal episodes and dyspnea on exertion, orthopnea, leg swelling, abdominal distention, loss of appetite and fatigue for the preceding nine months. Physical examination revealed jugular venous distention, a displaced apical cardiac impulse, a parasternal heave, and a loud S2. Also detected were a pan-systolic murmur at the lower left sternal border, an early diastolic heart sound with a mid diastolic murmur at the apex, bibasilar crackles, ascites, and oedema up to the thighs.
Significant laboratory values were a total bilirubin of 1.6 mg/dl, and B- Type Natriuretic Peptide of 1323 pg/ml. A chest x-ray revealed an enlarged cardiac silhouette, right lung atelectasis and effusion. An ECG revealed left atrial and right ventricular enlargement.
The patient was admitted with the diagnosis of new onset congestive heart failure and was treated with intravenous lasix, and fosinopril. A 2-D Echocardiogram revealed a large mass suggestive of myxoma in the left atrium measuring 4.5 x 7.5 cm, occupying the entire left atrium protruding through the mitral valve into the left ventricle (Figure 5) .
Figure 5: Apical four chamber echocardiograph of the left atrial myxoma prolapsing into the mitral valve during diastole.
This mass was obstructing flow with a mean trans mitral gradient of 17 mm Hg, with a reduced stroke volume and severe pulmonary hypertension with an estimated Right Ventricular systolic pressure of 120 mm hg. A presumptive diagnosis of left atrial myxoma was made and the patient was scheduled for its surgical removal the following morning. The patient was transferred to the intensive care unit for closer monitoring; and fosinopril and lasix were discontinued. At about 22:30 hours that night patient was noted to be hypotensive with systolic blood pressure of around 80mm Hg. The patient was treated with normal saline and concentrated albumin. She then developed acute respiratory distress at 23:00 hours requiring intubation and ventilator support. Intravenous dobutamine, dopamine and later norepinephrine were added for continued hypotension. The patient went into pulseless electrical activity, she was successfully coded with a return of her pulse but continued to be hypotensive. Cardiothoracic surgery decided not to take the patient for emergency surgery due to her unstable haemodynamic condition. The patient’s family was notified of the poor prognosis and the decision was made not to resuscitate her if her condition deteriorated further. The patient ultimately became bradycardic and went into asystole at 5: 30 am. An autopsy was not performed. The cause of death was attributed to large left atrial myxoma causing valvular obstruction and cardiovascular collapse.
Discussion
These two cases illustrate an uncommon, malignant course of a left atrial myxoma with rapid progression of symptoms which proved fatal. The most common primary tumour of the heart is myxoma accounting for 40-50% of primary cardiac tumours(2,3) .Nearly 90% of myxomas occur in the left atrium(3) .In over 50% of patients, left atrial myxoma causes symptoms of mitral stenosis or obstruction. Systemic embolic phenomena are known to occur in 30-40% of patients(3) .
Table 1. Summary of 17 published cases of sudden cardiac death associated with cardiac myxoma in adults (1950-2008)
Author/Reference
Year
No
Age
Gender
Symptoms
Interval Between Symptoms To Scd
Size Of Myxoma In Cm
Autopsy
Vassiliadis (8)
1997
1
17
M
Dizziness
3 months
6
yes
McAllister (10)
1978
5
40 to60
NA
NA
NA
5 to 6
yes
Cina (2)
1996
6
Below 40
NA
Embolic, syncope
16.6 months
5.7
yes
Puff (9)
1986
1
41
M
Syncope,
months
1.5
yes
Puff (9)
1986
1
19
F
Syncope
6 months
3
yes
Maruyama (7)
1999
1
20
M
Dizziness
1 day
8
None, Patient survived SCD; Myxoma resected
Turkman (6)
2007
1
73
M
DOE
months
8
yes
Ito (13)
1987
1
28
M
Syncope
7 days
NA
yes
NA: not available
Constitutional symptoms reported in approximately 20% of patients include myalgia, muscle weakness, athralgia, fever, fatigue, and weight loss. Around 20% of cardiac myxomas are asymptomatic (3) .Severe dizziness/syncope is experienced by approximately 20% of patients due to obstruction of the mitral valve. (4) Of all the symptoms associated with cardiac myxomas, syncope is one of the most ominous prognostic indicators.
Although sudden death is known to occur in patients with primary cardiac tumour it is rare and is estimated to constitute 0.01 to 0.005% of all sudden deaths (1). Association between sudden death and cardiac myxoma has been reported as early as 1953 by Madonia et al (5). A review of the literature on this subject between 1950 to2008 revealed 17 cases of sudden death attributed to cardiac myxoma in adults (1, 6, 7, 8, 9, 10, 13)(Table 1) .
In all patients with unexpected death syncope was a predominant presenting symptom and their age ranged from seventeen to seventy three. The majority of patients with sudden death were men even though the tumour is more common in women. The size of the tumour did not influence clinical presentation and in some reports of sudden cardiac death tumour was as small as 1.5 cm and without previous symptoms (3). Sudden death in myxoma is attributed to either severe acute disturbance in cardiac haemodynamics from cardiac obstruction (ball-valve syndrome) or to coronary embolization from the tumour. The latter is probably responsible for sudden death in patients with very small tumours. In the study of Alverez Sabin et al (11) the initial neurological manifestation was Transient Ischemic Attack (TIA), but in none of the patients’ was a diagnosis of myxoma made because of the initial neurological symptom. Even though cardiac myxomas are a rare cause of TIA and syncope, it is important to consider cardiac myxoma in the differential diagnosis of any patient with a TIA or syncope (11). The patients presented here had a TIA and recurrent syncope placing them at high risk for sudden death.
The timing of surgical excision of myxoma is not clear and it is not unusual for patients to die or experience a major complication while awaiting surgery (2, 12). Intraaortic balloon pump (IABP) use has been described in one case of left atrial myxoma and life-threatening cardiogenic shock with favorable outcome(14) .As illustrated by the cases presented here it is essential that surgery be performed urgently once it has been identified that a patient has a myxoma that is large enough to cause complete intracardiac obstruction.
Humans have always been interested in altering their body. Whether through piercings or tattoos, for aesthetics, religious reasons, or self-expression, the practice of body modification is a well known art.1 One not as familiar or easily observed body modification type is genital piercings. Genital piercings (GP) are defined as developing a tract under the skin with a large bore needle to create an opening into the anatomical region for decorative ornaments such as jewelry.2-3 Historically, GPs are not a new procedure.
Currently, this once taboo practice is on the rise and more men with GP are presenting with a variety of medical needs to clinics and hospitals.3 From the rare Pubic Piercing (a piercing through the dorsal base of the penis) to the Guiche (a piercing through the perineum), the male genitalia provides ample area to pierce. Men commonly choose from nine different types of GP and often use three major types of piercing jewellery (Figure 1).3-6
Figure 1 Common Types of Genital Piercings (GP) Worn by Men
Illustrations by Larry Starr, Senior Design Specialist Texas Tech University Health Sciences Center. Text modified with permission: Urologic Nursing 2006, 26(3), 175-176.
This rapid growth trend is creating its own set of complications and questions among clinicians. The medical literature suggests the most common risks are infection and bleeding, but there are other structural considerations as well.3-4, 6-8 An example of this is with the most widely known and commonly encountered male GP, the Prince Albert; the jewellery pierces the urethral meatus, exiting through the ventral surface of the penis. The piercing effectively creates a fistula for urine to drain, and many men report experiencing the need to sit down during urination due to the change in stream and difficulty in aiming.3,4 Other reported single case histories of more severe complications are Fournier’s gangrene, urethral tears, priapism, post-coital bleeding or lost jewellery in female partners, paraphimosis, and recurrent sexually transmitted diseases.8-20
Given the variety of negative issues that could arise from GP, any subject related to the health and well being of men having an intimate piercing should be directed to a well informed clinician. Currently, when questions or problems arise, men are more likely to seek assistance from the internet or a piercer rather than a health care provider.3,21-22 Considering the limited medical literature, as well as the minimal availability of clinicians knowledgeable about body piercings and modifications, men with GP are at high risk for delays in appropriate treatment of complications related to piercings as well as for overall preventive healthcare. Over concentration on the presence of GP by clinicians could delay important health care.23
Our purpose for this study was to elucidate information about men with GP in order to aid the clinician in providing relevant information for patients considering GP, as well as to provide further scientific evidence by examining their demographics, risk behaviours, procedural motives and post-piercing experiences. Additionally, several motives or characteristics of those with body art such as depression, abuse, self-esteem, and need for uniqueness were examined.24-29 Authors of this study have experience in urology, various aspects of piercing, and two decades of published body art research.
Problems in attempting any study about those with GP is reaching a sizeable sample for a study and an acceptable data collection methodology as those with GP have a hidden variable of study, making it difficult to make contact. Networking or “snowball” sampling for data collection, as well as anonymous questionnaires, becomes one approach,30 but this also makes it difficult to validate if respondents actually have GP. In an effort to address this issue, survey questions were specifically written for individuals with GP, making it extremely difficult and time-consuming to answer if the respondents did not have applicable experiences. Previous research experience also indicates that after about 10-15 questions, interest can wane and the questionnaire will not be completed.3,7,31
Only two published studies could be located to provide preliminary information about individuals with GP.21,22 In the first study21 data, collected in 2000 and actually published in 2005 had a national convenience sample of 63 women and 83 men with nipple and/or GP. Forty-eight men in the study had GP; the average man was 31 years of age, single, heterosexual, Caucasian, in good-excellent health, who sought out annual physicals, possessed some college education, and spoke of moderately strong religious faith. Almost all were employed, reporting an average annual salary of $36,000, or higher. Over half admitted and continued their belief they were risk takers; many of them also had 3 or more general body piercings. Most did not smoke or use drugs routinely and in this study, no questions about alcohol use were asked. Their average age at first sexual intercourse was 15.7 (the national male average is 16.9).32 Of those that participated (37%) in sport activities or exercise, they reported with no problems. They voiced minimal, if any, regrets to obtaining a genital piercing and would repeat the procedure. The Prince Albert was the most common male GP. Few (12%) voiced any problems with their GP, with urinary flow changes and site hypersensitivity being the most frequently mentioned. Six participants stated partners had refused sexual intercourse with them after their GP. One case of STD (Gonorrhoea) was reported post-procedurally.
As the internet survey demonstrated marked success in reaching those with GP, a similar study was undertaken to query a larger cohort of men with GP to increase clinician awareness in caring for men with GP. Thus, a cross-sectional descriptive study of men with GP was conducted so the collected information could be compared with the previously mentioned studies of those with GP.21,22 To ensure that the rights and dignity of all research participants were protected, exempt study status was obtained for this study from the university institutional review board. Notices of the study and a request for participation were posted on a number of popular body piercing sites with the assistance of an internationally-known Expert Piercer. The survey was available on the web for a total of 6 months during late 2008 and early 2009.
Questionnaire
Questionnaire items were based on a review of literature, the Armstrong Team Piercing Attitude Survey,31 previous work examining women with GP, 3,21-22, 33 and recent findings about those with body art. 24-29 The study purpose and benefits were presented on the front page of the survey. The subjects were informed that completion of the survey indicated their consent to participate in the study and that they could stop at any point during the survey if they were uncomfortable with a question (s). Ethnicity was included to note GP acquisition patterns; the ethnic categories were not defined and participants self-reported. Assurances were provided that the information would be analyzed as group data and no identifying information would be sought. Respondents were encouraged to answer questions honestly and not to be offended by any questions as some of them directly related to unsubstantiated assumptions written about GP in the medical literature. 21-22 There was no ability to tabulate how many individuals viewed the survey if they did not start the survey.
The survey had 4 sections: (a) Obtaining the GP (13 questions); (b) Personal experiences with the GP (32 questions); (c) General information including depression and abuse (26 questions), and (d) Sexual behaviour including forced sexual activity (12 questions). Four scales were also included: motives (14), outcomes (16), pre and post procedural self-esteem (16), and need for uniqueness (4). The previous reliabilities for the motive scale was 0.75,22 outcome scale 0.88,22 and need for uniqueness scale was 0.80;25 data was not available for the self-esteem scale.34 Various response formats were used throughout the survey such as a 5 point Likert scale (1 = strongly disagree or unlikely to 5 = strongly agree or likely), multiple choice, and short answers.
Data Analysis
The Statistical Package for the Social Sciences (16.0 Ed.) was used for data analysis to obtain frequencies, cross-tabulation, and chi-square analysis.30 Additionally, T-tests were used to compare means of similar questions from both the 2005 and 2008 studies with data from the current study. Significant differences were found in both study samples so they were judged as different groups from this current study.
RESULTS
Study Population
While 545 respondents started the survey, responses were analyzed from 445 men with GP (82%) residing in 42 states and 26 international countries; they declared a total of 656 piercings. Clusters of participants were evident from CA (22), NY (17), TX (16), FL (11), Europe (43), Canada (21), and Australia (20). Ages of the men with GP at survey time ranged from 15 to 72 (Table 1). The average participant in this study was 36 years of age, Caucasian, some college education, married, in excellent health, who sought out annual physicals, reported no/few friends with GPs, and declared a salary of $45,000 or higher. Religious beliefs were grouped into either non-existent or moderately to very strong faith. There was almost equal numbers of blue collar and white collar workers: others were from health care, arts, academia or military, while some were self-employed; very few mentioned unemployment, or retirement.
Table 1 Self-Reported Characteristics Of Men with Genital Piercings (GPs) continued
Demographics
Current Study* N = 445
Age at time of survey 20 or < 21-35 36-50 51+
61/29% 77/36% 41/19% 33/16%
Ethnicity Caucasian
319/89%
Martial Status Single Living/significant other Married with/out children
96/27% 69/20 143/41%
Education High school Diploma Some college Bachelor’s degree Graduate/Doctoral degree
34/10% 113/32% 77/22% 88/20%
Occupations Technical/vocational Professional Students Artists
90/28%
92/29%
44/14% 23/07%
Salary <45,000 $45,000+
135/44% 169/56%
Strength/Religious Faith Non-existent Mod Strong-Strong
135/39% 99/28%
State of Health Excellent
310/88%
Health care visits Annual physicals Only when problems
150/43% 142/40%
Close friends w/GPs None 1-3 4+
239/68% 100/28% 14/ 4%
Feel sad/depressed
Little/Some Pre-piercing Post-piercing
248/57% 210/59%
*Numbers will not always add up to 100 because of missing data or multiple answers.
Risk Behaviours
Those who reported pre-procedural risk taking tendencies continued to have significant tendencies for them post-procedurally (χ2 = 2.13) = 16; p = 0.000) (Table 2). Some risky behavior was observed; over half had body art, with an average of 2 piercings or more, as well as tattoos. Alcohol use was infrequent, but when they did, they had 5+ drinks. Other answers did not bear out the risk taker image with their monogamous, heterosexual relationships, limited tobacco, and drugs. Their average age at first intercourse was 17.05 (national male average 16.9).32 Most (391/88%) did not report STDs before their piercings, but of those that did itemize their STDs, Chlamydia was the most frequently mentioned (n =18).
Table 2 Self-Reported Risk Behavior From Men with Genital Piercings (GPs)
Risk Behaviour
Current Study* N = 445
Age at first intercourse Never had intercourse 12 or less 13-15 16-18 19+
12/03% 14/04% 80/25% 160/48% 74 /23%
Sexual Orientation Women
286/82%
Risk Taker Before Piercing
222/52%
Remains Risk Taker
198/52%
Cigarettes Smoked None ½-1 pack daily
252/75% 75/22%
Monthly Alcohol Consumption 1-3 times 5+ drinks @ one setting, 1-3x
118/33% 191/55%
Drugs Used monthly None 1-15 times
294/87% 27/08%
Sexual Partners in 6 months One Two or more
211/62% 98/32%
General body piercings None 1-4 piercings 5+ piercings
119/27% 259/59% 108/33%
Tattoos None 1-4 5+
115/35% 134/38% 76/21%
STDs before piercing
54/12%
*Numbers will not always add up to 100 because of missing data or multiple answers.
Genital Piercing Procedure
A deliberate time delay between their consideration to making the decision to have a GP was present as many had waited almost 5 years before procurement (Table 3). Over half reported the Prince Albert GP, with another third choosing a Frenum/Frenum Ladder (Figure 1). While a small-moderate amount of pain and bleeding was reported procedurally, virtually no drugs or alcohol were used before their GP.
Table 3 Self-Reported Procedural Information From Men with Genital Piercings (GPs)
Genital piercing procedure
Current Study* N = 445
Amt of decision time Waited long time, then a few minutes A long time (over a year)
49/24% 143/37%
Age of GP Decisions Consideration Procurement
29 years 34 years
Type of Genital Piercings Ampallang Apadavya Dydoe Foreskin Frenum/Frenum ladder Guiche Hafada Prince Albert Other
*Numbers will not always add up to 100 because of missing data or multiple answers.
Motives and Outcomes
Table 4 illustrates participant motives and outcomes for each group in the various GP studies.21,22 For the highest motive response of “just wanted one” there was consistency over the three studies; of the top five responses, they were similar but just ranked differently. Alpha measurements for the motive response scale ranged from 0.40 to 0. 75 except for our current study, where the covariance matrix was zero or approximately zero so the statistics based on its inverse matrix could not be computed. Motives centered around wanting a GP, trying something new, have more functional sexual control, and seeking uniqueness. Measureable outcomes (Alpha range 0.88-0.89) of their GP evolved around their sexual expression, uniqueness, and aesthetics, as well as the improvement of their personal and partner’s sexual pleasure. In review, their motives for the GP were met in their stated outcomes.
Table 4A Three Study Comparison Of Self-Reported Motives and Outcomes From Those Wearing Genital Piercings.
Variable
Caliendo et al, 2005 Study: Data Collected 2000 Men with GPs N = 48*
Young, et al, 2010 Study Data collected 2008 Women with GPs N = 240*
Current Study Data collected 2009 Men with GPs N = 445*
Motives for their genital piercing
34/71% “Just wanted one” 24/50% “Trying to feel sexier”
23/45% “For the heck of it”
18/38% “Wanted to be different” 18/38% “Make myself more attractive” (alpha 0.40)
163/70% “Just wanted one” 120/51% “Trying to feel sexier” 111/48% “More control over my body” 93/40% “Seeking uniqueness” 91/39% “Make myself more attractive” (alpha 0.75)
196/90% “Just wanted one”
73/60% “For the heck of it” 67/60% “Trying to feel sexier” 56/58% “More control over body” 51/56% “Seeking uniqueness” (alpha unobtainable)
Outcomes of their genital piercing
36/77% “Improved my sexual pleasure”
35/73% “Helped express myself sexually” 35/73% “Helped me feel unique”
176/76% “Helped express myself sexually 173/75% “Improved my sexual pleasure 157/68% “Helped me express myself 134/58% “Helped me feel feminine” 134/58% “Helped me feel unique” (alpha 0.88)
278/81% “Improved my sexual pleasure
234/71% “Helped express myself sexually”
218/67% “Helped me feel unique” 229/67% “Improved partners sexual pleasure 211/64% “Helped genital look better” (alpha 0.88)
*Numbers will not always add up to 100 because of missing data or multiple answers.
Post-piercing Experiences
The men reported continued satisfaction with their GP and would repeat the procedure. While not many were engaged in exercise/sport activities, those that did, were active (Table 5). A few reported partner refusal of sexual activities when their GP was in place. Almost half reported no piercing complications; of those that did, only 2 major problems were cited. First, with over half reporting Prince Albert piercings, it was not surprising that 25% discussed changes in their urinary flow. Site hypersensitivity was the second most reported problem (23%), otherwise there were no further trends of other severe complications. While 80 (18%) reported STDs after their GP, only 19 itemized the specific type: the most responses were Chlamydia (9). Those that had a history of STDs (Table 2 & 5) before their piercings were significantly more likely to have them post-procedurally (χ2 = 11.5) = 1; p = 0.001).
Table 5 Self-Reported Post Procedural Information From Men with Genital Piercings (GPs)
Complications from piercing No problems Change in urinary flow Site hypersensitivity Skin irritation Rips/tears at site Problems using condoms Keloids @ site Site infection Urinary tract infection Site hyposensitivity Sexual problems Jewellery embedded Erection problems Other, not named
*Numbers will not always add up to 100 because of missing data or multiple answers.
Depression, Abuse, Self-Esteem, and Need for Uniqueness
Four additional characteristics about individuals with GP were examined.24-29 Men with GP respondents reported a small amount of “sad or depressed feelings”; those that had these depressed feelings before their piercings were significantly more likely to continue these depressed feelings post-procedurally (χ2 = 4.1), = 16; p = 0.00). Only 5 (1%) reported being forced to participate in sexual activity against their will, while a few cited (56/12%) physical, emotional, or sexual abuse.
To extract a profile of self-esteem, 8 questions were asked in the pre and post piercing survey sections; internal consistency (Cronbach alpha) of both scales was 0.75. Their responses to both the pre procedure (M = 22.3, SD = 4.51) and the post piercing time (M = 23.1, SD = 3.97) was highly correlated at 0.79 (P<0.01). Two statements triggered split, negative and positive responses with “I make demands on myself that I would make on others” and “I blame myself when things do not work the way I expected.” Lastly, their Need for Uniqueness (NU) was asked using a four item scale24,25in the pre-piercing survey section. When all five responses of the scale were totaled (20), the mean was 11.3 documenting a more positive perspective about their GP, close to the moderate level (Cronbach alpha 0.86), for intentionally wanting to be different, distinctive, and unique. When asked if their overall feelings of NU had changed since obtaining their GPs, those that had NU before their piercings were significantly more likely to have them post-procedurally (χ2 = 11.5) = 16; p = 0.03).
DISCUSSION
When examining this data from men with GP alongside the 2005 published study,21 the cohort almost equalled 500 participants. To our knowledge this is the largest repository of data currently available to provide further evidence of the demographics and health issues regarding men with GP. The anonymous data, obtained by networking sampling and accessible, economical web-based survey, could be viewed as a study limitation. Yet, finding similarities between this data and data collected almost ten years ago suggests that our findings tapped into a core body of knowledge about men with GP. Similar data, obtained at different times, from different respondents increases the credibility and lends the information to further generalizability to influence use in practice.30
The “social reality” 2 of the GP phenomenon is here. All of the men had one type of GP, and some had multiple GP, and many had other general body piercings.35 Awareness of the current types of body modification including GP will help the clinician educate and inform adequately, to give professional advice, and also provide a realistic picture of structural considerations. Respondents stated their GP were an important and satisfying part of their life, they still liked them, and would repeat the procedure; the GP improved their sexual activities, few refused sexual intercourse, those that exercised were active, and they were not troubled by the GP complications. From a medical standpoint the insertion of a GP could be considered a minor surgical procedure, and yet the data suggests that when the GP is performed by experienced hands only minimal side effects are reported. Thus, finding a knowledgeable, expert piercer is an important educational theme. However, patients need to also be aware that certain types of piercing may require some behavioral changes such as toileting and consistent body cleaning. Unfortunately virtually no health care providers, including clinicians, were mentioned in the GP decision making process or care, they usually went to the internet or returned to a piercer for information.21,22 Hopefully, as more clinicians are made aware of GPs, those who are considering GP will find their physician to be a helpful and more informative resource.
These study participants with GP were older, well-educated men, often in a stable relationship, different than what is usually thought about people with body piercings.7, 22,26-27,29,31 This scientific evidence about their overall demographics pose challenges to the current medical literature. Sample demographics from this study and the other two cited GP studies 21,22 do not reflect individuals from stereotypical low performing social and economical backgrounds. Demographically, the people with GP were in their early thirties, Caucasian, heterosexual, well educated, employed, in good health, with some religious beliefs, but not ethnically diverse. In contrast to literature describing men with GP as antisocial miscreants or mostly homosexual, 2,4,18 our data support that these men are more part of the mainstream culture. The avoidance of “rushing to judgment”28 is an important aspect, especially in the way they are often perceived.
Men with GP did not deny their propensity to be risk takers, but being a risk taker was not synonymous with being deviant, but more with achieving individualization.21,28,31 Threads about stable relationships were provided throughout their information, including sexual orientation, marital status, GP complications, and even their lack of many risk behaviours. Their first time for sexual intercourse was close to the male national average. While procurement of any type of body art is thought to be impulsive 7,21-23, their time for GP decision-making was deliberate, as well as their practice of on-going, conscientious care of their piercings.21,22 Absence of alcohol and/or drug consumption before the GP procedure has been a frequent finding in other body art studies.7,21-22,31 Reputable piercing artists advocate for no use of alcohol and drugs as they want their customers to be making realistic procedural decisions about their GP and listening carefully to post GP care instructions.
The unsubstantiated assumptions in the literature about GP complications such as male infertility, scrotal infections, reduction of erotic stimulation, and frequent infections with bicycle rides were also challenged.6,21,36-40 Overall, only two problems of urinary flow changes and site hypersensitivity were reported with their GP. They took their sexual concerns seriously, as part of their internal influences of self esteem and their need for uniqueness. Their documented motives reflected sexual enhancement, aesthetics, as well as uniqueness. Their stated outcomes of the GPs reflected an ability to better express themselves sexually and create a sense of uniqueness; these elements obviously took precedence over the two problems of urinary flow changes and hypersensitivity. Both these motives and outcomes were similar when compared with the other two studies.21,22 Further procedural research is suggested to obtain more information about the reasons some with Prince Albert GP have urinary flow changes, while others do not, to eliminate this as a possible side-effect.
Negative bias continues with the assumption that individuals with GP frequently have STDs.18-20, 36-40 Historically, concern for those who have “exotic adornments” such as body piercings have led some health facilities to require STD screening, no matter what the nature of the presenting complaint.22,35 Yet, in this study and the other two related GP studies,21,22 respondents reported only a few STDs. Their reporting incidence of STD was low compared to the national Guttmacher Institute report of one in three sexually active people will have contracted a STD by age 24.32 As in this study, Chlamydia remains the most highly reported STD in the US.32 While it is important to always conduct a thorough sexual history, 20 perhaps the conscientious care related to the deliberate decision for the GP, and the mostly monogamous relationships reported may account for the limited reporting of STDs. One STD clinic study found that neither socioeconomic status, method of contraception, multiple partners, or the presence of genital infections correlated with GP.38 Further longitudinal research is suggested to examine the long-term effects of GPs, as well as further GP complications and STD prevalence.19
Men, like women, with GP21 reported depressed feelings26,27,29 both pre and post procedure, but gender differences were present with abuse and forced sexual activity. The men with GP reported few incidents of abuse (emotional, physical, or sexual) or forced sexual activity against their will whereas over a third of the women with GP22 reported this. Although women frequently spoke of their use of GPs to take more control in reclaiming their body to “free them from the bonds of molestation and give them strong feelings of empowerment,” 22 men verbalized their use of GPs to give them more sexual control.
STUDY LIMITATIONS
As with any study, several limitations to generalizability of data must be considered and one of methodology has been previously discussed. This was a non experimental, descriptive study design and the respondents self-selected to complete a web-based survey. Bias, inaccurate recall, and/or inflation can result from self-reporting.30 Respondents had to use their personal judgment to interpret questions with the use of an anonymous survey so socially desirable responses could have been entered. Participants with strong negative or positive feelings may have been more likely to complete the survey. Yet, as random sampling is almost impossible in a population with hidden variables, and in spite of these limitations, the respondents did contribute further quantitative data.21,22
CONCLUSIONS
The trend of those obtaining GP continues to increase and is not limited by age, gender, socio-economical backgrounds, or sexual preferences. Many in this study still reported seeking advice of a piercer or the internet. As an identified population at risk for quality health care, further evidence of demographics, piercings and jewellery, motivations, outcomes, and health issues were presented about men with GP so clinicians can provide clinically competent and applicable approaches for care. The collective data examined here, along with some collected almost ten years ago, begins to dispel some of the negative assumptions about this segment of the body modification population regarding their overall demographics, GP complications, and STD prevalence.
Oesophageal compression by a vascular structure resulting in dysphagia is uncommon. There have been multiple reports in the medical literature of almost every major vascular structure in the chest causing some degree of oesophageal compression and subsequent dysphagia(1, 2). In 1794, David Bayford, described a case of a 62 year-old lady having dysphagia due to an aberrant right subclavian artery. He coined the term “dysphagia lusus naturae”, which means “Freak of nature” (3).
Pill-induced esophagitis is associated with the ingestion of many pills and presents an uncommon cause of erosive oesophagitis (4). Multiple different classes of drugs have been described to be hazardous to the oesophageal mucosa and cause pill-induced oesophagitis (5, 6). Although uncommon in itself, dysphagia lusoria has not been described in literature to present as pill-induced oesophagitis. We present the first case of dysphagia lusoria causing pill-induced oesophagi's by testosterone pills in a young healthy man. Pubmed review of the English medical literature has been conducted to discuss the epidemiology, pathogenesis and management of this uncommon disorder.
Case Presentation:
A 26 year-old man with no significant past medical history presented with 5 days of dysphagia (for both solids and liquids), odynophagia and retrosternal chest discomfort. He admitted to having occasional difficulty swallowing for past 2-3 months for solids only. He denied any heartburn, cough, regurgitation, loss of appetite, weight loss, fever, chills, haematemesis or melaena. He denied tobacco or alcohol use. 2 weeks prior to presentation he had started taking testosterone pills for body-building. Physical examination was completely unremarkable.
A barium oesophagram showed extrinsic oblique compression of the oesophagus at the level of the carina as it passes through the aorta. CT scan and MRI of the chest revealed a right-sided aortic arch crossing posteriorly to the oesophagus with proximal oesophageal dilatation consistent with Dysphagia Lusoria. Endoscopy noted erosive oesophagitis/distinct ulceration extending from 18cm into a pulsatile area of narrowing at 20 cm with normal mucosa visualized distally.
Biopsies revealed oesophageal squamous mucosa with marked acute inflammation, reactive changes and no evidence of viral inclusions. Surgical management was discussed with the patient, but given the short duration of symptoms and the patient's stable weight, providing symptomatic relief with lifestyle changes, together with a trial of medications such as proton pump inhibitors were considered. At 2 weeks follow-up whilst taking proton pump inhibitors and having discontinued the testosterone pills, the patient experienced complete resolution of symptoms.
Epidemiology:
Dysphagia Lusoria: Moltz et al, found that lusorian artery has a prevalence of about 0.7% in the general population, based on the post-mortem findings(7). Also, out of 1629 patients who underwent endoscopy for various reasons, 0.4% had a finding of a lusorian artery in a report from Fockens et al(8). It has also been concluded based on the autopsy results and retrospective analysis of patients’ symptoms during life that about 60-70% of these patients remain asymptomatic (7). Coughing, dysphagia, thoracic pain, syncope and Horner's syndrome may develop, but usually present in old-age(9).
Pill-Induced Oesophagitis: The data on pill-induced oesophagitis is rather limited. A Swedish study found an incidence of 4 cases per 100,000 population/year(10). Wright found the incidence of drug-induced oesophageal injury to be 3.9/100,000(11). This may be underestimated and does not include subclinical or misdiagnosed cases. Also, cases are reported selectively, due to clustering of cases, newly implicated pills or rare complications. The incidence today is probably much higher due to increased use of prescription medications, widespread use of endoscopy and an ageing population. All these factors limit our ability to correctly assess the true epidemiology of this iatrogenic disorder.
Pathogenesis
Dysphagia Lusoria: During embryological development, the aortic sac gives rise to six aortic arches and with further development the arterial pattern is modified and the fourth arch persists on both sides and some vessels regress. In right arch anomaly, the left arch atrophies and disappears whereas the right arch persists. If both arches persist, they form a double arch or a vascular ring encircling the trachea and oesophagus (12).
Pill-induced oesophagitis: Several lines of evidence confirm that oesophageal mucosal injury is caused by prolonged contact with the drug contents(13, 14) .On clinical grounds, patients frequently report a sensation of a pill stuck in the oesophagus before the development of symptoms and the frequent occurrence of symptoms after improper pill ingestion. Endoscopically, the evidence includes occasional observation of pill fragments at the site of injury, sharp demarcation of the injury site from the normal tissue and the frequent localization of the injury to the areas of oesophageal hypomotility or anatomic narrowing(4, 15). Therefore factors predisposing to the drug-induced oesophageal injury can be divided into two main categories: patient or oesophageal factors (16, 17, 18,19,20,21) and drug or pharmaceutical factors as shown in tables 1 and 2 (13,14,22,23,24).
Table 1: Patient/Esophageal facors for pill-induced esophagitis
Old Age
Decreased Salivation
Pill intake in recumbent position
Lack of adequate fluid intake with the drug
Structural abnormalities of esophagus
Hypomobility of the esophagus
Table 2: Drug related factors for pill-induced esophagitis
Chemical structure(sustained release pills, gelatinous surface)
Formal structure (capsule increases risk over the tablet)
Solubility
Simultaneous administration of multiple medications
It is important to note that most patients who experience pill-induced damage have no antecedent oesophageal disorder, neither obstructive nor neuromuscular (25). It is the combination of anatomic narrowing coupled with the caustic effects of the implicated drug that caused the oesophageal injury in our case. Although testosterone pills have never been reported to cause pill-induced oesophagitis, 6 cases of corticosteroid-induced oesophagitis have been described in the literature(26) .
Clinical Presentation
Dysphagia Lusoria: As previously mentioned the disorder remains asymptomatic in majority of the patients. Symptomatic adults usually present with dysphagia for solids, (91%), chest pain (20% or less). Less commonly, patients may have cough, thoracic pain or Horner’s syndrome (27,28). In infants, respiratory symptoms are the most predominant mode of clinical presentation. This is believed to be due to absence of tracheal rigidity, allowing for its compression with resulting stridor, wheezing, cyanosis etc (9) . Richter et al. reported average age of presentation to be 48 years (27). Various mechanisms to explain this delayed presentation have been proposed such as increased rigidity of the oesophagus, rigidity of the vessel wall due to atherosclerosis, aneurysm formation (especially Kommerell’s diverticulum), elongation of the aorta etc (9, 29,30) .
Pill-induced oesophagitis: Patients with pill-induced injury usually present with odynophagia, dysphagia and/or retrosternal chest pain(4) . Symptoms can occur after several days after starting a drug, but frequently occur after the first dose. (13) .Fever and haematemesis signifying a possible mediastinal extension can occur without chest pain(32,33). Pharyngitis due to the pill lodged in the hypopharynx has been reported(34).
Our case presents a typical example of asymptomatic Dysphagia Lusoria, who developed acute dysphagia, odynophagia and retrosternal chest discomfort immediately after the initiation of the offending agent; which is very typical of pill-induced oesophageal injury.
Diagnostic approach
Dysphagia Lusoria: The best method to diagnose an aberrant right subclavian artery presenting with difficulty swallowing is initially with a barium oesophagram followed by a CT or MRI scan. (27) .Angiography although considered gold standard for the diagnosis of vascular abnormalities is now largely supplanted by newer less invasive techniques such as CT or MR angiography. Upper endoscopy may reveal a pulsating compression of the posterior wall of the oesophagus as in our case(9, 27). Endoscopic ultrasound, especially with Doppler technology may be helpful to confirm the vascular nature of the abnormality(27). Oesophageal manometry usually shows non-specific findings. High peristaltic pressures have been reported in the proximal oesophagus above the level of the compression (9, 35).
Pill-induced oesophagitis: Barium studies can be normal, and slowing of barium column may be the only abnormality seen(31). Double contrast studies may however, increase the yield of a positive result(36). Kikendall et al. reported that endoscopy revealed the evidence of injury in all the patients (5) . Endoscopy most commonly reveals one or more discrete well demarcated ulcers with normal surrounding mucosa. Ulcers may range from pin-point to several centimetres in diameter(5). Biopsies, if performed, help to distinguish the condition from infection and neoplasia.
Our case shows a distinct oblique compression in the posterior wall of oesophagus on the barium study (fig 1) and classic findings on MR/CT with contrast which also excluded any other thoracic vascular abnormalities (fig 2-5). Endoscopic images of a shallow ulcer are shown in fig 6,7.
Figure 1- Barium esophagram depicting the extrinsic indentation of the esophagus as it crosses the aorta.
Figure 2- CT scan of the thorax demonstrating esophageal compression from a posteriorly placed aorta.
Figure 3- Magnetic resonance image showing esophageal compression with proximally dilated esophagus.
Figure 4- CT image showing the right sided origin of the aortic arch.
Figure 5- Three Dimensional image of the heart and the right sided approach of the arch.
Figure 6- Endoscopic view of esophageal inflammation at the site of compression.
Figure 7- Endoscopic image of the esophageal injury using narrow band imaging.
Treatment
Dysphagia Lusoria: The treatment of patients with DL primarily depends upon the severity of symptoms. Mild to moderate cases are managed by lifestyle and dietary changes such as eating slower, chewing well, sipping liquids, weight reduction and reassurance as in our case.(9,27) Janssen et al also reported in a series of 6 patients that 3/6 improved with proton-pump inhibitor alone or in combination with the prokinetic drug cisapride (9) .Severe symptoms and failure of medical therapy may need surgical evaluation and treatment. Richter et al. reported 14/24 patients who underwent surgical repair of the aberrant vessel for DL(27) . Bogliolo et al proposed endoscopic dilation as a temporary alternative to relieve symptoms in patients who are poor surgical candidates (37) .
Pill-induced oesophagitis: Most uncomplicated cases of pill-induced oesophagitis may heal spontaneously, with resolution of symptoms in a few days to a few weeks. Withdrawal of the offending drug and avoidance of topically irritating foods such as citrus fruits, alcohol is imperative to aid healing (4, 13). Sucralfate, topical anaesthetics, and acid suppression are often used to aid in relief of pain(4, 15). Rarely, in severe cases, parenteral nutrition or endoscopic dilation of chronic strictures may be required. (15, 25)
Conclusion
Our case demonstrates a typical case of DL presenting with pill-induced oesophagitis who responded to conservative and acid suppressive therapy. Identifying the risk factors and adequate patient education is the key to prevention.
Bisphosphonates, which have been on the market for roughly a decade, have raised safety concerns in the past. Several case series and multiple individual case reports suggest that some subtrochanteric and femoral shaft fractures may occur in patients who have been treated with long-term bisphosphonates. Several unique clinical and radiographic features are emerging. Recent media spotlight in the United States (US), implying that long-term use of alendronate could cause spontaneous femur fractures in some women, has reignited the debate about the safety of bisphosphonates. The question posed: is the risk of bisphosphonate-associated fractures so great that treatment should be stopped?
Postmenopausal women with osteoporosis are commonly treated with the bisphosphonate class of medications, one of the most frequently prescribed medications in the US. While alendronate therapy has been shown to decrease the risk of vertebral and femoral neck fractures in postmenopausal osteoporotic patients, recent reports have associated long-term alendronate therapy with low-energy subtrochanteric and diaphyseal femoral fractures in a number of patients. In the past four years reports have been published implying that long-term bisphosphonate therapy could be linked to atraumatic femoral diaphyseal fractures.1, 2 According to two studies reported recently at the American Association of Orthopedic Surgeons 2010 Annual Meeting, an unusual type of bone fracture has been reported in women who have taken bisphosphonates for osteopenia and osteoporosis for more than four years.3, 4 The first report was published in 2005. Odvina et al5 reported on nine patients who sustained atypical fractures, including some with delayed healing, while receiving alendronate therapy. These authors raised the concern that long-term bisphosphonate therapy may lead to over-suppression of bone remodelling, an impaired ability to repair skeletal microfractures, and increased skeletal fragility. There have been other reports of "peculiar" fractures - i.e. low-energy femur fractures that are typically transverse or slightly oblique, diaphyseal, or subtrochanteric, with thickened cortices and a unicortical beak - in patients who have been on long-term bisphosphonate treatment.1-4, 6
In a small prospective study, Lane et al3 obtained bone biopsies from the lateral femurs of 21 postmenopausal women with femoral fractures. Twelve of the women had been on bisphosphonate therapy for an average duration of 8.5 years, and nine had no history of bisphosphonate use. They found that the heterogeneities of the mineral/matrix ratio were significantly reduced in the bisphosphonate group by 28%, and the crystallinity of the bone was significantly reduced by 33% (p < 0.05). The authors concluded that this suggested suppression of bone turnover, resulting in a loss of heterogeneity of the tissue properties, which may be a contributing factor to the risk of atypical fractures that we are starting to see. It is believed that long-term alendronate administration may inhibit normal repair of microdamage arising from severe suppression of bone turnover (SSBT), which, in turn, results in accumulation of microdamage. This process would lead to brittle bone and the occurrence of unexpected stress fractures, characteristically at the subtrochanter of femur. The typical presentation of these fractures consist of prodromal pain in the affected leg and/or a discrete cortical thickening on the lateral side of the femur in conventional radiological examination or the presentation with a spontaneous transverse subtrochanteric femur with typical features. The morbidity of atypical femoral fractures, particularly when bilateral, is high. Surgical intervention is generally required and healing may not be achieved for several years. Despite the lack of conclusive evidence of a causal relationship with bisphosphonate therapy, the current consensus is that treatment should be discontinued in patients who develop these fractures. In view of the high frequency of bilateral involvement, imaging of the contralateral femoral shaft with X-rays, MRI, or an isotope bone scan should be performed. MRI and bone scanning havegreater sensitivity than radiography for an incipient stressfracture. If lateral cortical thickening and/or an incipient stress fracture is seen, prophylactic surgical fixation should be considered. Suppressed bone formation in these patients provides a possible rationale for the use of anabolic skeletal agents, such as parathyroid hormone peptides, but at the present time the efficacy of this approach remains to be established. Parathyroid hormone not only has activated bone-formation markersin trials in humans but has also enhanced the healing of fracturesin studies in animals.
The question of whether these fractures are causally linked to bisphosphonate therapy is widely debated but as yet unresolved. Consequences of long-term suppression of bone turnover include increased mineralization of bone, alterations in the composition of its mineral/matrix composite and increased micro damage, all of which may reduce bone strength. Whilst these lend biological plausibility to a causal association, however, they do not constitute direct evidence. The bilateral fractures seen in many patients corroborate the suspicion that patients with bisphosphonate-associated stress fractures carry some other risk factor in addition to taking the drug. Microfractures,inadequate mineralization, and outdated collagen are some of the candidate causes. However, until further studies can provide definitive evidenceof bisphosphonate-associated fractures, it is premature to attributeatypical fractures to over-suppression of bone turnover alone,while disregarding secondary and patient-related factors. Many experts believe that prolonged suppression of bone remodelling with alendronate may be associated with a new form of insufficiency fracture of the femur. Studies have not shown if the entire class of medications produce a similar result, but patients who have been treated with any bisphosphonate for an extended period of time should be considered at risk.
A wealth of information from well-designed clinical trials clearly shows that, as a class, bisphosphonates are highly effective at limiting the loss of bone mass, deterioration of bone micro architecture, and increased fracture risk that occur with aging. The benefit/risk ratio of bisphosphonate therapy in patients at high risk of fracture remains overwhelmingly positive because of the very low incidence of atypical femoral fractures. Current estimates suggest that alendronate prevents 200 clinical fractures if 4000 women are treated over three years and will cause one femur fracture over the same course of time.7 A study by Schilcher et al8 found that the incidence density of a stress fracture for a patient on bisphosphonate was 1/1000 per year (95% CI: 0.3-2), which is acceptable considering that bisphosphonate treatment is likely to reduce the incidence density of any fracture by 15/1000.9 Nevertheless, limitation of treatment duration to five years in the first instance, with evaluation of the need to continue therapy thereafter, may be appropriate in clinical practice. The Fracture Intervention Trial Long-term Extension (FLEX), in which postmenopausal women who had received alendronate therapy for five years were randomised to continue receiving alendronate for five additional years or switched to placebo, provided clinical evidence that the effect of bisphosphonate therapy was maintained after discontinuation of therapy.7, 10 Women who are being treated with bisphosphonates should take a drug holiday if they have been on them for five years. Patients in whom bisphosphonate therapy is discontinued should typically follow up with bone mineral density measurements at 1- to 2-year intervals, with some experts advocating periodic measurement of biochemical markers of bone turnover to detect loss of the antiresorptive effect. Additional research is necessary to determine the exact correlation between the use of bisphosphonates and spontaneous or low-energy trauma fractures.
Headaches associated with or occurring around sexual activity have been recognized since the time of Hippocrates [1, 2]. Wolff [3] discussed headache during sexual activity in 1963. However, these headaches started to be formally reported in the 1970s, first by Kitz in 1970 [4] and then Paulson [5] and Martin [6] in 1974. The first published study was by Lance in 1976 [7].
Classification
This type of headache has been given many different names: benign sex headache (BSH), benign coital headache, coital cephalgia, orgasmic cephalgia, primary headache associated with sexual activity (PHSA), coital ‘thunderclap’ headache, primary thunderclap headache (PTH), orgasmic headache (OH) and preorgasmic headache.
In 2004the International Headache Society [8] classified HSA as a distinct form of primary headache.
These benign HSA are bilateral headaches, precipitated by sexual excitement (masturbation or coitus) occurring in the absence of any intracranial disorder and which can be prevented or eased by ceasing activity before orgasm. Type 1 consists of a bilateral, usually occipital, pressure-like headache that gradually increases with mounting sexual excitement. Type 2 headaches have an explosive, throbbing quality and appear just before or at the moment of orgasm. These often start occipitally but may generalize rapidly [9].
However, there are individuals who experience patterns of HSA that do not fall within the classifications and are included as a subgroup of HSA with unusual psychopathology [10]. For example, Paulson and Klawans [5] described a rare type postural sexual headache after coitus, which is present on standing, eased by lying, accompanied by a low CSF pressure, and persists for several weeks.
International Headache Society diagnostic criteria - ICHD-2(7) classification for HSA
4.4 Primary headache associated with sexual activity
4.4.1 Pre-orgasmic headache
A. Dull ache in the head and neck associated with awareness of neck and/or jaw muscle contraction
and fulfilling criterion B.
B. Occurs during sexual activity and increases with sexual excitement
C. Not attributed to another disorder
4.4.2 Orgasmic headache
A. Sudden severe (“explosive”) headache fulfilling criteria B
B. Occurs at orgasm
C. Not attributed to another disorder
7 Secondary headache disorder
7.2.3 Headache attributed to spontaneous (or idiopathic) low CSF pressure
Prevalence
HSA are not common but it is generally felt that they are under-reported due to patient embarrassment [1] at telling health professionals when their headaches occur. Prevalence in the general population is reported at around 1% [11, 12] and is greater in men than in women, by 3-4 times [11, 13-16]. There appear to be two peak times of onset: in the early 20s and then around age 40 [17]. About 22% of HSA are Type 1 and 78% are Type 2 [18]. The male:female ratio is the same for Type 1 and Type 2 headache.
Pathophysiology
HSA are not clearly understood but by definition lack serious underlying disease. They are however, unpleasant, frightening, repetitive and episodic. The clinical characteristics of Type 1 suggest a relationship with tension/muscular contraction headaches [2, 13, 15, 16]. There is a significant association between the risk of having more than one cluster of HSA and the presence of tension headaches or migraine [11, 14-17, 19-21]. Biehl [11] concluded that the association between migraine and HSA is bilateral. The prevalence of migraine in HSA patients is 25-47% [15, 16, 20]. Ostergaard [14] showed that the presence of concomitant migraine or tension headache was significantly associated with the recurrence of periods lasting weeks to months in which HSA occurred. Patients without another primary headache often have only one HSA period or episode and a more favourable prognosis . Migraine is co-morbid in 30% of Type 2 as opposed to 9% with Type 1. Co-morbidity is also seen in exertional headaches, 35% of Type 2 and 9% Type 1[17, 18]. There can be simultaneous onset of benign exertional headache (BEH) and HSA [22] as well as HSA after a history of BEH [16, 22].
Several drugs have been linked in case reports to sexual headaches associated with neurologic symptoms: Amiodarone [23], birth control pills [24], pseudoephedrine [7] and cannabis [25].An interesting more recent addition to HSA is that resulting from the use of PDE5 medication to assist in erectile difficulties [26, 27].
In type 2 headaches, increased intracranial pressure secondary to a Valsalva maneuver during orgasm has been proposed as a possible mechanism. Blood pressure may increase by 40-100mmHg systolic and 20-50mmHg diastolic during orgasm [7, 28-30]. A possible disruption of autoregulation of the cerebral vasculature has also been proposed [31-33].
Classic presentation
A male patient, middle-aged, in poor physical shape, mildly to moderately overweight, and mildly to moderately hypertensive [34]. In women muscle contraction and psychological factors are often involved [34].
The typical story is that the headache occurs during sexual activity, is bilateral and stops or is less severe if sexual activity stops prior to orgasm. The duration varies from 5 minutes to 2 hours if sexual activity stops and from 3 minutes to 4 hours, with the possibility of milder symptoms up to 48hours, if activity continues.
Differential diagnosis
With the first episode it is absolutely mandatory to exclude potentially life threatening and disabling causes. A thorough history and neurological examination with the option of imaging studies and CSF examination must be conducted.
Type 2 explosive “thunderclap” headaches can be secondary to subarachnoid haemorrhage, aneurysms without obvious rupture, intracerebral haemorrhage, pituitary apoplexy, venous sinus thrombosis, cervical artery dissection, subdural haematoma, haemorrhage into an intracranial neoplasm [35], cerebral tumour [36], intracranial hypotension and hypertension, significant cervical spine disease, and ischaemic stroke [37-43] and these serious conditions need to be excluded before an HSA diagnosis can be given. HSA may present similarly to paroxysmal headaches caused by phaeochromocytoma [44].
Sexual intercourse is reported as a precipitating cause of subarachnoid haemorrhage in 3.8% to 12% of patients with bleeding from a ruptured aneurysm [35].
Course of the disease
The unpredictable clinical course falls into 2 temporal patterns: an episodic course with remitting bouts, and a chronic course [20]. In most cases the headaches occur in bouts that recur over periods of weeks to months before resolving [16, 45].
The episodic type is defined as a bout of at least 2 attacks occurring in ≥ 50% of sexual activity followed by no attack for ≥ 4 weeks despite continuing sexual activity. The chronic course is defined as ongoing HSA attacks for ≥ 12 months without remission of ≥ 4 weeks [20].
Further uncertainty is experienced by the patient as HSA does not necessarily occur in every sexual encounter [7, 19]. A characteristic of HSA is the sporadic vulnerability of patients to the headache. Episodes can occur singly, in clusters or at irregular intervals. Recurrence can occur years later.
The acute HSA attacks are usually short lasting but the overall duration of pain can vary widely [17]. The mean duration of severe pain in HSA is similar (30 minutes) in type 1 and type 2 but the mean duration of milder pain is more prolonged with type 2 (4 hours vs 1 hour). About 15% of patients suffer from severe pain for >4hours needing acute treatment. Severe pain continuing for 2-24 hours occurs in up to 25% of patients with HSA [17]. Patients with episodic HSA compared to chronic HSA have an earlier age at onset and tend to suffer more often from concomitant BEH [20].
About 30% of patients report headaches with masturbation as well as intercourse. There are also reports of HSA occurring exclusively during masturbation [46, 47] and a case of this occurring with nocturnal emission [21].
Overall HSA occurs more commonly when the patient is tired, under stress or attempting intercourse for the second or third time in close succession [48]. HSA appears in bouts lasting weeks to months and can disappear without specific treatment [14, 16]. The number of attacks within one bout ranges from 2 to 50 [17]. About 25% of patients suffer attacks without longer remissions.
Prognosis
Prognosis is usually good for HSA as it is a benign self- limiting disorder and disappears without any specific treatment in the majority of patients [17]. It is usually better if there has been only one attack, especially if it was not associated with any other type of headache.
Frese [20] concluded that episodic HSA occurs in approximately 75% and chronic HSA in approximately 25% of patients. However even in chronic HSA, the prognosis is favourable, with remission rates of 69% in patients followed over 3 years.
Management
A thorough history and examination is mandatory in a first attack.
Referral is warranted if:
Atypical story and suspicious examination
First episode of severe headache where headache still present
A recurrent episode of severe headache with longer than average duration
Neck stiffness, photophobia or vomiting
Altered consciousness or confusion
Focal neurological signs
Previous history of AV malformation, neoplasms or neurosurgery
Investigations
Computed tomography
MRI
Lumbar puncture
Cerebral angiography
Urinary catecholamine
Medical treatment
Turner [49] has provided a good review.
Pre-emptive treatment
Propanolol hydrochloride ( Inderal) is effective in the prophylaxis of HSA[19]. Naratriptan 2.5mg has been reported as useful prior to sexual activity [50] but due to lower absorption rates needs to be taken more than 60 minutes before sexual activity [30]. Indomethacin 25-100mg can be taken 30-60 minutes prior to sexual activity [15, 16, 45, 51] and for acute severe pain management [20] but can cause serious gastrointestinal side-effects and is not tolerated by about 10% of headache patients [52].
Acute treatment
Triptans shorten the attack in about 50% of patients[30]. There is an 80% response rate [30]. Analgesics (ibuprofen, diclofenac, paracetamol, acetylsalicylic acid) given after onset of headache are of limited or no value in nearly all patients [45].
Other triptans, ergots and benzodiazepines have also been reported to have efficacy [5, 24, 53, 54] for acute and pre-emptive treatment for those patients not tolerating indomethacin. Taken 30 minutes before sexual activity they shorten orgasmic headache attacks in 66% of users [30].
Long term prophylaxis for longer lasting bouts or continued attacks
Options include indomethacin 25mg three times a day, propanolol 120-240mg per day, metoprolol 100-200 mg per day and diltiazem 180 mg per day [15, 19, 20, 22, 24, 45]. There is about an 80% response rate [30].
Sexual management
Trauma due to pain associated with sexual activity has the potential to affect immediate and long term satisfaction with sexual activity unless specifically addressed. HSA can be very distressing for both patient and partner with the development of fears around sexual activity and orgasm. Patients may develop patterns of impaired sexual arousal. If these fears are not exposed and dealt with, sexual problems may occur. Secondary avoidance behaviours may become established in the relationship leading to a decrease in couple’s physical affection, eroticism and sexual activity. Patients must be given the opportunity to talk about sexual fears in an ongoing way, especially if HSA is chronic.
The social and relationship history will disclose areas of stress which should be evaluated and managed as best possible. In type 1 HSA where neck and jaw tension may be a factor, conscious relaxation of these muscles during intercourse may help [7]. Relaxation exercises especially concentrating on neck and shoulder tension can be done regularly and particularly before anticipating sexual activity.
Individuals often sense early in the lovemaking process whether or not HSA will occur and encouragement not to pursue orgasm on that occasion can be helpful. Some patients can terminate the headache by stopping the sexual activity or suppressing orgasm and about 51% can lessen the intensity of pain by being more sexually passive [18].
Advice on continuing to engage with the partner despite ceasing or modifying one’s own sexual arousal needs to be given. Having a disappointed or resentful partner increases the distress of the condition so partner needs have to be discussed. Patients often have difficulty talking about sexual issues with both their partner and their doctor, therefore the doctor needs to be the one to raise the subject.
A brief sexual history will outline the love-making practice and modification to sexual positions, especially where neck tension is exaggerated, may help. In one report, the advice to engage in intercourse more frequently but less strenuously resulted in a reduction in headaches [5].
Avoiding sexual activity and strenuous activities until totally symptom free has been recommended by some [13, 22, 24, 55]. This may be difficult to follow as the capricious nature of HSA makes knowing when they have stopped difficult.
Conclusion
HSA are benign, but because they can mimic serious conditions, patients need to be properly assessed before reassurance is given and management of HSA started. Because pain can alter sexual experience and behaviour around sexuality for the patient and the couple, this aspect of patient wellbeing must be addressed by the treating physician for good holistic management. As not everyone is comfortable with addressing sexuality with patients, respectful acknowledgement of the situation and appropriate referral can be a useful approach.
Definition of restraint: a device or medication that is used to restrict a patient’s voluntary movement. Prevalence of physical restraints: up to 17% in acute care settings. Prevalence of chemical restraints: up to 34% psychotropic drug use in long term care facilities. Complications of restraints: include documented falls, decubitus ulcers, fractures, and death. Regulations: require documentation of indications plus failure of alternatives by a licensed professional. Prevention of removal of life sustaining treatment: is a relatively clear indication for restraints. Informed consent: including consideration of risks, benefits, and alternatives is necessary in all cases. Barrier to reducing restraints: a misguided belief that, by use, one is preventing patient injury. Steps can be taken to limit their use: including an analysis of behaviours precipitating their use.
Case study
A 79 year old female nursing home resident with frontotemporal dementia and spinal stenosis has a chronic indwelling catheter for cauda equina syndrome and neurogenic bladder. Attempts to remove the catheter and begin straight catheterization every shift were met by the patient becoming combative with the staff. Replacing the catheter led to repeated episodes of the patient pulling out the catheter. The patient lacks decision making capacity to weigh the risks, benefits, and alternatives; but she clearly doesn’t like having a catheter in. The attending physician instituted wrist restraints pending a team meeting. Unfortunately, attempts by the patient to get free led to dislocation of both shoulders and discharge to the hospital.
Introduction
A restraint is any device or medication used to restrict a patient’s movement. In the intensive care unit, for example, soft wrist restraints may be used to prevent a patient from removing a precisely placed endotracheal tube. A lap belt intended to prevent an individual from falling from a wheelchair in a nursing home is a restraint if the patient is unable to readily undo the latch.1 In the case study above of a catheterized, demented patient, if medication is used to prevent the patient from striking out at staff when performing or maintaining catheterization, then the medication is considered a restraint.
There is little data on efficacy and benefits of restraints1. Even when the indication to use a restraint is relatively clear, the outcome is often opposite of the intention. Consider that restraints used for keeping patients from pulling out their endotracheal tubes are themselves associated with unplanned self- extubation2. Complications of restraints can be serious including death resulting from medications or devices3,4.Use of restraints should be reserved for documented indications, should be time limited, and there should be frequent re-evaluation of their indications, effectiveness, and side effects in each patient. Lack of a Food and Drug Administration (FDA) approved indication for use of medications as restraints in agitated, aggressive, demented patients has led to recommendations that medications in these situations be used only after informed consent with proxy decision makers5. Medical, environmental, and patient specific factors can be root causes of potentially injurious behavior to self or others as in the case study above. To ensure consideration and possible amelioration of these underlying causes, the Center for Medicare and Medicaid Services (CMS ) in 2006 required face to face medical and behavioral evaluation of a patient within one hour after restraints are instituted by a physician (licensed independent practitioner). As a result of controversy surrounding this rule, clarification of that rule in 2007 allowed for a registered nurse or physician assistant to perform the evaluation provided that the physician is notified as soon as possible6 . In depth situational analysis of the circumstances surrounding the use of restraints in individual cases as well as education of the patient, family, and caregivers may lead to the use of less restrictive alternatives7.
Frequency of restraint use
Frequency of restraint use depends on the setting, the type of restraint, and the country where restraint use is being studied. In the acute care hospital setting, reported physical restraint use was 7.4% to 17%.a decade ago8.Two decades ago, in long term care facilities prevalence was reported as 28%-37%.9 . There has been a steady decline over the past several decades coincident with regulation such that, according to the Department of Health and Human Services, it is down to about 5% since newer CMS rules went into effect in 2007. In contrast, some European nursing homes still report physical restraint use from 26% to 56%10,11.
Chemical restraint is slightly more prevalent than physical restraint with a prevalence of up to 34% in long term care facilities in the US prior to regulations12.There is some indication that prevalence may be decreasing, some say markedly, perhaps as a result of government regulation13,12 .Interestingly, one case-control study of more than 71,000 nursing home patients in four states showed that patients in Alzheimer special care units were no less likely to be physically restrained compared to traditional units. Furthermore, they were more likely to receive psychotropic medication14.
Complications of restraint use
The use of chemical and physical restraints is associated with an increase in confusion, falls, decubitus ulcers, and length of stay15,16. Increase in ADL dependence, walking dependence, and reduced cognitive function from baseline has also been reported17. Use of restraints often has an effect opposite the intended purpose of protecting the patient, especially when the intent is prevention of falls18. Physical restraints have even caused patient deaths. These deaths are typically due to asphyxia when a patient, attempting to become free of the restraint, becomes caught in a position that restricts breathing4,19.
Antipsychotic medications may be used as restraints in elderly patients with delirium or dementia who become combative and endanger themselves and others; however, there is no FDA approval for these drugs for this use5. In a meta-analysis, an increased relative risk of mortality of 1.6 to 1.7 in the elderly prompted the FDA to mandate a “black box” label on atypical antipsychotic medications stating that they are not approved for use in the behavioral manifestations of dementia20. Other research suggests that conventional antipsychotics are just as likely to cause death, if not more so3. Forensic research also links antipsychotic medication and patient deaths21. The reported relative risk of falls from these drugs is 1.722. Given the risks, if antipsychotic medications are used at all, they need to be prescribed as part of a documented informed-consent process. Education of patients, families of patients, and facility staff about the harms of restraints is a good first step in a plan to avoid or eliminate their use. Over the past several decades, regulations have arisen in the United States because of complications of restraints and a lack of clear evidence supporting their use.
The regulatory environment in the United States
The Omnibus Budget Reconciliation Act of 1987 (OBRA 87) resulted in regulations that specify the resident’s right to be free of the use of restraints in nursing homes when used for the purpose of discipline or convenience and when not required to treat the resident’s medical symptoms23,24. OBRA87 related regulations also specified that uncooperativeness, restlessness, wandering, or unsociability were not sufficient reasons to justify the use of antipsychotic medications. If delirium or dementia with psychotic features were to be used as indications, then the nature and frequency of the behavior that endangered the resident themselves, endangered others, or interfered with the staff’s ability to provide care would need to be clearly documented24. Comprehensive nursing assessment of problem behaviors, a physician order before or immediately after instituting a restraint, and documentation of the failure of alternatives to restraint are required before the use of a restraint is permitted. The restraint must be used for a specific purpose and for a specified time, after which reevaluation is necessary.
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) instituted similar guidelines that apply to any hospital or rehabilitation facility location where a restraint is used for physical restriction for behavioral reasons25. In response to the 1999 Institute of Medicine report, To Err is Human, JCAHO focused on improving reporting of sentinel events to increase awareness of serious medical errors. Not all sentinel events are medical errors, but they imply risk for errors as noted in the revised 2007 JCAHO sentinel event definition: A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof6. The JCAHO recommends risk reduction strategies that include eliminating the use of inappropriate or unsafe restraints. The recommendations for restraint reduction are prioritized along with items like eliminating wrong site surgery, reducing post-operative complications, and reducing the risk of intravenous infusion pump errors6. It is clear that JCAHO considers placing restraints as a sentinel event to be monitored and reported. CMS and JCAHO have worked to align hospital and nursing home quality assurance efforts especially with respect to the standard concerning face to face evaluation of a patient within one hour of the institution of restraints. They held ongoing discussions that resulted in revised standards for the use of restraints in 200926. Among the agreed upon standards are: policies and procedures for safe techniques for restraint, face to face evaluation by a physician or other authorized licensed independent practitioner within one hour of the institution of the restraint, written modification of the patient’s care plan, no standing orders or prn use of restraints, use of restraints only when less restrictive interventions are ineffective, use of the least restrictive restraint that protects the safety of the patient, renewal of the order for a time period not to exceed four hours for an adult, restraint free periods, physician or licensed independent practitioner daily evaluation of the patient before re-ordering restraint, continuous monitoring, and documentation of strategies to identify environmental or patient specific triggers of the target behavior. The one hour face to face evaluation may be accomplished by a registered nurse provided that the attending physician is notified as soon as possible26.
Indications for use of restraints
The risk of using a restraint must be weighed against the risk of not using one when physical restriction of activity is necessary to continue life-sustaining treatments such as mechanical ventilation, artificial feeding, or fluid resuscitation. Every attempt should be made to allow earlier weaning from these treatments, thereby rendering the restraint unnecessary. Even in cases where the indication is relatively clear, the risks, benefits, and alternatives must be weighed (see Figure).
In an emergency, when it is necessary to get a licensed provider’s order for a restraint to prevent a patient from disrupting lifesaving therapy or to keep a patient from injuring others, an analysis of what may be precipitating the episode is essential. Are environmental factors such as noise or lighting triggering the behavio? Are patient factors such as pain, constipation, dysuria, or poor vision or hearing triggering the disruptive behavior? Is there an acute medical illness? Is polypharmacy contributing? Psychotropic drugs and drugs with anticholinergic activity are common culprits. Patient, staff, family, and other health care providers need to be queried.
One must guard against perceiving the continued need for life-sustaining treatment and the use of restraints as being independent factors, because that misconception can lead to a vicious cycle. For example, a patient who has persistent delirium from polypharmacy and needs artificial nutrition and hydration which perpetuates the need for continued chemical and physical restraints. Correcting the polypharmacy and the restraint as a potential cause of the delirium can break the cycle. When restraints are indicated, one must use the least-restrictive restraint to accomplish what is needed for the shortest period of time. Restraint-free periods and periodic reassessments are absolutely required.
A weaker indication is the use of restraints to prevent patient self-injury when the danger is not imminent. Such an indication exists when a patient repeatedly attempts unsafe ambulation without assistance or when he or she cannot safely ambulate early in the process of rehabilitation from deconditioning or after surgery. In these cases, weighing the risks and benefits of the restraint is more difficult than when considering restraints to maintain life-sustaining treatment.
Even more difficult to justify is the use of restraints to restrict movement to provide nonurgent care. An example might be a patient who repeatedly removes an occlusive dressing for an early decubitus ulcer. In these cases, it is more fruitful to use alternatives to restraints. For example, considering alternatives to a urinary catheter is more important than documenting that restraints are indicated to keep the patient from pulling it out.
If used, the specific indication, time limit, and plan for ongoing reevaluation of the restraint must be clearly documented. Effectiveness and adverse effects must be monitored. Restraint-free periods are also mandatory. The same is true for chemical restraints. Periodic trials of dosage reduction and outcome are mandatory.
Barriers to reducing the use of restraints
Perceived barriers to reducing restraints can be thought of as opportunities to build relationships between patients, physicians, staff, patients’ families, and facility leaders. A legitimate fear of patient injury, especially when the patient is unable to make his or her own decisions, is usually the root motivation to use restraints. Ignorance about the dangers of restraint use results in a sincere, but misguided, belief that one is acting in the patient’s best interest27. Attempts to educate physicians, patients, and staff may not have been made. These barriers are opportunities for the community to work together in creative partnerships to solve these problems. Even in communities where there are no educational institutions, there are opportunities for educational leadership among physician, nursing, and other staff. Conversely, lack of commitment to reducing restraints by institutional leaders will tend to reinforce the preexisting barriers. Regulatory intervention has been a key part of gaining the commitment of institutional leadership when other opportunities were not seized. On the other hand, competing regulatory priorities such as viewing a serious fall injury as a ‘never event’ and simultaneously viewing institution of a restraint as a sentinel event may lead to reduced mobility of the patient18. An example of this would be the use of a lap belt with a patient-triggered release. The patient may technically be able to release the belt, but the restricted mobility may lead to deconditioning and an even higher fall risk when the patient leaves the hospital. In the process of preventing the serious fall injury or ‘never event’ there is, even at the regulatory level, intervention that may not be in the patient’s best interest. These good intentions are, again, a barrier to the reduction of the use of restraints and an opportunity for physician leadership in systems based care collaboration. Physician leadership probably needs to extend beyond educational efforts. Evidence suggests education may be necessary but not sufficient to reduce the use of restraints10.
Reducing the use of restraints
Steps can be taken to reduce the use of restraints before the need for them arises, when the need for restraints finally does arise, and while their use is ongoing.
Programs to prevent delirium, falls in high-risk patients, and polypharmacy are all examples of interventions that may prevent the need for restraints in the first place. Attention to adequate pain control, bowel function, bladder function, sleep, noise reduction, and lighting may all contribute to a restraint-free facility.
When a restraint is deemed necessary, a sentinel event has occurred. Attempts to troubleshoot the precipitating factors must follow. Acute illness such as infection, cardiac, or respiratory illness must be considered when a patient begins to demonstrate falls or begins to remove life-sustaining equipment. Highly individualized assessment of the patient often requires input from physical therapy, occupational therapy, social work, nursing, pharmacy, and family. If root causes are determined and corrected, the need for restraints can be ameliorated and alternatives can be instituted.
The least restrictive alternative should be implemented when needed. For example, a lowered bed height with padding on the floor can be used for a patient who is at risk for falls out of bed in contrast to the use of bedrails for that purpose. Another example is the use of a lap belt with a Velcro release as opposed to a vest restraint without a release. A third example is the use of a deck of cards or a lump of modeling clay to keep the patient involved in an alternative activity to the target behavior that may be endangering the patient or staff. Alternatives to the use of restraints need to be considered both when restraint use is initiated and during their use. Judicious use of sitters has been shown to reduce falls and the use of restraints28. When danger to self or others from patient behaviors and restraints are deemed necessary, a tiered approach has been recommended by Antonelli29 beginning with markers and paper or a deck of cards for distraction and then proceeding up to hand mitts, lap belts, or chair alarms if needed. Vest or limb restraints are the default only when other methods have been ineffective29.
Literature from the mental health field provides some guidance to those attempting to use the least intrusive interventions for older patient behaviors that endanger themselves or others. A combination of system-wide intervention, plus targeted training in crisis management to reduce the use of restraints has been demonstrated to be effective in multiple studies30. In a recent randomized controlled study, one explanation the author gives for the ineffectiveness the educational intervention is that the intervention was “at the ward level unlike other restraint reduction programs involving entire organizations.”10. Research and clinical care in restraint reduction will likely need to be both patient-centered and systems-based in the future.
Case study revisited
Our 79 year old female with frontotemporal dementia and spinal stenosis noted in the above case pulls out her urinary catheter. The physician is called and determines that the patient’s urine has been clear prior to the episode, that she has no fever, nor does she have evidence of acute illness. The patient is likely pulling the catheter out simply because of the discomfort caused by the catheter itself since the patients behavior is at the same baseline as before the catheter was inserted as determined by discussion with the staff. The patient is unable to inhibit her behavior because of the frontotemporal dementia. The physician places a call to the medical power of attorney and explains the risks of bladder infection, bladder discomfort, renal insufficiency, and overflow incontinence from untreated neurogenic bladder. This is weighed against the risk of frequent infections and bladder discomfort from a chronic indwelling urinary catheter, or damage to the urethra from pulling the catheter out. The option of periodic straight catheterization is dismissed by the medical power of attorney as being too traumatic for this demented patient who becomes agitated during this procedure.
The medical power of attorney considers the options and agrees to observation by the staff without the catheter overnight with a team conference the next day. At the conference, it was noted that overnight the patient had several episodes of overflow incontinence in spite being toileted every few hours while awake. The patient had no signs of discomfort and was changed when found to be wet. A bladder scan done at the facility showed a few hundred cubic centimeters of residual urine after the patient was noted wet and changed. The team conference yielded the informed decision to continue checking the patient frequently and changing when wet as well as frequent toileting opportunities.
The patient continued at baseline for twelve weeks until she developed urinary sepsis and the patient’s medical power of attorney was contacted about additional care decisions.
Conclusion
A restraint is any device or medication used to restrict a patient’s movement. Complications of restraints can be serious including death resulting from both medications and devices. Use of restraints should be reserved for documented indications, should be time limited, and there should be frequent re-evaluation of their indications, effectiveness, and side effects in each patient. Analysis of environmental and patient specific root causes of potentially self-injurious behavior can lead to reduction in the use of restraints. Education of the patients, families, and the health care team can increase the use of less restrictive alternatives.
In the first part of this review we considered neurodegenerative and neurobehavioural diseases and the findings that these diseases commonly are associated with systemic and central nervous system bacterial and viral infections.1 In this second part we continue with psychiatric diseases, autoimmune diseases, fatiguing illnesses, and other chronic diseases where chronic infections play an important role.
Psychiatric diseases
Borrelia-associated psychiatric disorders
In addition to neurologic and rheumatologic symptoms Borrelia burgdorferi has been associated with several psychiatric manifestations2, 3 (see also below). Such infections can invade the central nervous system and may cause or mimic psychiatric disorders or cause a co-morbid condition. A broad range of psychiatric conditions have been associated with Lyme disease, including paranoia, dementia, schizophrenia, bipolar disorder, panic attacks, major depression, anorexia nervosa and obsessive-compulsive disorder.4-7 For example, depressive states among patients with late Lyme disease are fairly common, ranging from 26% to 66%.3 It is not known whether B. burgdorferi contributes to overall psychiatric morbidity, but undiagnosed chronic Lyme disease caused by this spirochete is considered a differential diagnosis in patients with certain psychiatric symptoms such as depressive symptoms, lack of concentration and fatigue.
The neuropsychiatric sequelae of chronic Lyme disease remains unclear. Studies were performed, some on large numbers of patients, to investigate whether a correlation exists between chronic Lyme disease (defined by seropositivity) and psychiatric disorders.8-11 Interestingly, different results were reported on the association between B. burgdorferi infection and psychiatric morbidity.8-11 For example, Hájek et al.8 compared the prevalence of antibodies to B. burgdorferi in groups of psychiatric patients and healthy subjects. Among the matched pairs, 33% of the psychiatric patients and 19% of the healthy comparison subjects were seropositive. In contrast, Grabe et al.11 did not find an association between Borrelia seropositivity and mental and physical complaints. In 926 consecutive psychiatric patients that were screened for antibodies and compared with 884 simultaneously recruited healthy subjects, seropositive psychiatric patients were found to be significantly younger than seronegative ones, and this was not found in the healthy controls.10 However, none of the psychiatric diagnostic categories used in this study exhibited a stronger association with seropositivity.10 These findings suggest a potential association between B. burgdorferi infection and psychiatric morbidity, but fail to identify any specific clinical 'signature' of the infection. This might be due to the very low incidence in an endemic region (0.2%, CI 95% 0.0% to 1.1%) as demonstrated in 517 patients hospitalized for psychiatric diseases.9
In addition to serological data, clinical evidence for the association of psychiatric symptoms and post-Lyme disease has also been investigated. If mental and physical complaints in patients were assessed with the von Zerssen's complaint scale using multivariate analyses, the data revealed that definitions of seropositivity were not associated with increased mental or physical complaints.11 In contrast, if the SF-36 was used to determine Quality of Life (QOL) in post-Lyme patients, the average SF-36 physical component summary (40±9, range 29-44) and mental component summary (39±14, range 23-46) of the QOL assessment were worse than the general USA population, and they could be significantly improved by anti-Lyme antibiotics (46% versus 18%, p=0.007).5 Barr et al.12 examined the relation between complaints of memory disturbance and measures of mood and memory functioning in 55 patients with serological evidence of late-stage Lyme borreliosis. There was a significant correlation between subjective memory ratings and self-reported depression (p<0.001) but not with objective memory performance, indicating memory disturbance in chronic Lyme patients. Using a structured psychiatric interview, the Positive and Negative Affect Schedule, the Lyme Symptom Checklist, and a battery of neuropsychological tests in 30 post-Lyme patients, participants did not appear to have an elevated incidence of psychiatric disorders or psychiatric history.13 Their mood, however, was characterized by lowered levels of positive affect and typical levels of negative affect that were similar to affect patterns in individuals with chronic fatigue syndrome (CFS). Similarly, Hasset et al.4, 7 reported on 240 consecutive post-Lyme patients who were screened for clinical psychiatric disorders, such as depression and anxiety. After adjusting for age and sex, these disorders were more common in symptomatic patients than in the comparison group (Odds Ratio=3.54, CI 95% 1.97-6.55, p<0.001), but personality disorders were comparable in both groups.
Although psychiatric co-morbidity and other psychological factors are prominent in post-Lyme patients, it remains uncertain whether these symptoms can be directly attributed to the chronic course of Borrelia infections or to other chronic illness-related factors.
Schizophrenia
Several microbes have been suspected as pathogenetic factors in schizophrenia, such as Chlamydia species, toxoplasma, and various viruses. For example, a number of studies have reported associations between Toxoplasma gondii infection and the risk of schizophrenia with an overall hazard ratio of 1.24.14 In addition, chlamydial infections have been found in 40% of schizophrenic patients compared to 7% in healthy controls.15 These infections represented the highest risk factor yet found to be associated with schizophrenia that was highly significant (Odds Ratio=9.43, p=1.39 x 10-10), especially with Chlamydophila psittaci (Odds Ratio=24.39, p=2.81 x 10-7). Interestingly, schizophrenic carriers of the HLA-A10 genotype were clearly the most often infected with Chlamydia, especially C. psittaci (Odds Ratio=50.00, p=8.03 x 10-5), pointing to a genetically related susceptibility.15 However, skepticism against the role of bacterial infection in schizophrenia was also fostered by the low impact of anti-infectious treatment on the course of disease progression in schizophrenia.16
Genetic backgrounds and viral infections and/or reactivations as well as cytokine-related pathomechanisms have also been proposed as causative for psychiatric disorders, such as schizophrenia. Specific genetic patterns of MICB polymorphism (MHC class I polypeptide-related sequence B, chromosome 6p21) were identified in patients seropositive for CMV and HSV-1.17 Similar polymorphisms were found for the COMT Val158Met related to serological evidence of HSV-1 infections in individuals with bipolar disorder.18 This serologic evidence of HSV-1 infection appeared to be associated with cognitive impairment in individuals with bipolar disorders19 and was found to be an independent predictor of cognitive dysfunction in individuals with schizophrenia.20 In addition, viral exposure during gestation has been described as a risk factor for schizophrenia. Offspring of mothers with serologic evidence of HSV-2 infection were at significantly increased risk for the development of psychoses (Odds Ratio=1.6; CI 95% 1.1-2.3). These results are consistent with a general model of risk resulting from enhanced maternal immune activation during pregnancy.21 However, this was not confirmed in another study.22 Similar contradictory results were observed in a small group of 8 patients with schizophrenia where reactivation of herpesviruses (HSV-1, CMV, EBV, varicella-zoster virus and human HHV-6) and other viruses (measles, rubella, mumps, influenzaA and B and Japanese encephalitis viruses) during acute onset or exacerbation of schizophrenia was investigated, but none of these viruses were detected in these patients.23 Also, a search for HSV-1 or varicella zoster virus infection in postmortem brain tissue from schizophrenic patients did not reveal evidence of persistent CNS infections with these viruses.24
Schizophrenic patients show a number of cytokine changes that may be important in their condition. For example, differences in interleukin-2, -4 and –6, among other cytokines, have been seen in schizophrenic patients.25-27 Often these changes in cytokines or cytokine receptors have been linked to associated genetic changes found in schizophrenia.28-30 Monji et al.31 recently reviewed the evidence for neuroinflammation, increases in pro-inflammatory cytokines and genetic changes in schizophrenia and concluded that these changes are closely linked to activation of microglia. Although the microglia comprise only about 10% of the total brain cells, they respond rapidly to even minor pathological changes in the brain and may contribute to neurodegeneration through the production of pro-inflammatory cytokines and free radicals. CNS infections could also activate microglia and cause similar events.
Neuropsychiatric Movement Disorders
Giles de la Tourette’s syndrome (TS) is a neurological condition that usually begins in childhood and results in involuntary sounds or words (vocal tics) and body movements (movement tics). An association between infection and TS has been repeatedly described.32 Abrupt onset of the disease, usually after infection, was noted in up to 11% of these patients.33-34 A role for streptococcal infections (PANDAS, see below) as causative or mediating agent in TS was established several years ago.35 Additionally, the involvement of other infectious agents, such as B. Burgdorferi or M. pneumoniae, has been described in case reports and small studies. For example, comparing 29 TS patients with 29 controls revealed significantly elevated serological titers in TS patients (59% versus 3%). This higher proportion of increased serum titers, especially IgA titers, suggested a putative role for M. pneumoniae in a subgroup of patients with TS.36 In predisposed persons, infection with various agents including M. pneumoniae should be considered as at least an aggravating factor, but an autoimmune reaction has to be taken into account in TS patients. In addition, co-infections with toxoplasmosis have been described in a few case reports of obsessive-compulsive disorder (OCD).37 As mentioned above, streptococcal infections are likely to play a pivotal role in these syndromes.35
The pathogenic mechanism may be secondary to an activation of the immune system, resulting in an autoimmune response. This will be discussed in the next section.
Autoimmune Diseases
Infections are associated with various autoimmune conditions.38-40 Autoimmunity can occur when infections like cell-wall-deficient bacteria are released from cells containing parts of cell membranes that are then seen as part of a bacterial antigen complex, or bacteria can synthesize mimicry antigens (glycolipids, glycoproteins or polysaccharides) that are similar enough in structure (molecular mimicry) to stimulate autoimmune responses against similar host antigens. Alternatively, viral infections can weaken or kill cells and thus release cellular antigens, which can stimulate autoimmune responses, or they can incorporate molecules like gangliosides into their structures.
In addition to molecular mimicry, autoimmunity involves several other complex relationships within the host, including inflammatory cytokines, Toll-like receptor signalling, stress or shock proteins, nitric oxide and other stress-related free radicals, among other changes that together result in autoimmune disease.38, 39
Guillain-Barré syndrome
Guillain-Barré syndrome (GB) is a demyelinating autoimmune neuropathy often associated with bacterial infections.40 Symptoms include pain, muscle weakness, numbness or tingling in the arms, legs and face, trouble speaking, chewing and swallowing. Of the types of infections found in GB, Campylobacter jejuni, Mycoplasma pneumoniae and Haemophilus influenzae are often found.39 For example, Taylor et al.41 found serological evidence of C. jejuni in 5 of 7 patients with GB and other motor neuropathies, and Gregson et al.42 found anti-ganglioside GM1 antibodies that cross-reacted with C. jejuni liposaccharide isolates. When infections were examined in GB cases in India, Gorthi et al.43 found that 35% and 50% of GB patients had serological evidence of C. jejuni and M. penumoniae infections, respectively, while one-third of cases showed evidence of both infections. In Japan Mori et al.44 found that 13% of GB patients had antibodies against Haemophilus influenzae . Autoantibodies stimulated by infections found in GB patients can cross-react with nerve cell gangliosides (anti-GM1, anti-GM1b, anti-GD1a, among others), and these are thought to be important in the pathogenesis of GB.45 Indeed, injection of C. jejuni lipo-oligosaccharide into rabbits induces anti-gangliosides and a neuropathy that resembles acute motor axonal neuropathy.46
Viruses have also been found to be associated with GB.40 Examples are: CMV,47 HIV,48 herpes simplex virus,49 West Nile virus,50 and HHV-6.51
Paediatric autoimmune neuropsychiatric disorders associated with Streptococci ('PANDAS')
Streptococcal infections in children are usually benign and self-limited. In a small percentage of children, however, prominent neurologic and/or psychiatric sequelae can occur. Post-streptococcal basal ganglia dysfunction has been reported with various manifestations, all of which fall into a relatively well-defined symptom complex or syndrome called paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS).52
Evidence from past studies indicates that adults and children with a symptom course consistent with PANDAS experience subtle neuropsychological deficits similar to those of primary psychiatric diagnosis of OCD and TS.53 PANDAS are now considered as a well-defined syndrome in which tics (motor and/or vocal) and/or OCD are consistently exacerbated in temporal correlation to a group A beta-hemolytic streptococcal infection. However, the pathological relationship between OCD or tics/TS in childhood to antecedent group A Streptococci is still not fully understood.52
In an epidemiological investigation Leslie et al.54 assessed whether antecedent streptococcal infection(s) increase the risk of subsequent diagnosis of OCD, TS, other tic disorders, attention-deficit hyperactivity disorder (ADHD) or major depressive disorder (MDD). Children with newly diagnosed OCD, TS, or tic disorder were more likely than controls to have had a diagnosis of streptococcal infection in the previous year (Odds Ratio=1.54, CI 95% 1.29-2.15). Previous streptococcal infection was also associated with incident diagnoses of ADHD (Odds Ratio=1.20, CI 95% 1.06-1.35) and MDD (Odds Ratio=1.63, CI 95% 1.12-2.30).54 Similar results were found in a retrospective, cross-sectional, observational study of 176 children and adolescents with tics, TS, and related problems.55 In a case-control study of children 4 to 13 years old patients with OCD, TS, or tic these disorders were more likely than controls to have had prior streptococcal infection (Odds Ratio=2.22; CI 95% 1.05-4.69) in the 3 months before onset date. The risk was higher among children with multiple streptococcal infections within 12 months (Odds Ratio=3.10; CI 95% 1.77-8.96).56 Having multiple infections with group A beta-hemolytic Streptococcus within a 12-month period was associated with an increased risk for TS (Odds Ratio=13.6; CI 95% 1.93-51.0). Similar results were found in patients with typical symptoms of Tourette's syndrome.57 The frequency of elevated anti-streptolysin O titers was also significantly higher (p=0.04) in patients with attention-deficit hyperactivity disorder (64%) than in a control group (34%).58
Sydenham's chorea is one manifestation of post-streptococcal neuropsychiatric movement disorders. A pathogenic similarity between Sydenham's chorea, TS and other PANDAS has been suggested since some patients can present with one diagnosis and then evolve with other neuropsychiatric conditions.59 These observations support a role of group A streptococcal infection and basal ganglia autoimmunity. Anti-basal ganglia antibodies that are associated with serologic evidence of recent streptococcal infection were found as potential diagnostic markers for this group of disorders, which includes Sydenham's chorea as the prototype.60
However, contradictory results were also reported.61 For example, an association between symptom exacerbations and new group A beta-hemolytic streptococcus infections among 47 paediatric patients with TS and/or OCD was not observed.59 In addition, the failure of immune markers for streptococcal infections to correlate with clinical exacerbations in a small study of children with paediatric autoimmune neuropsychiatric disorders raised concerns about the viability of autoimmunity as a pathophysiological mechanism in these syndromes.62 However, in a second study the same group reported that patients who fit published criteria for paediatric autoimmune neuropsychiatric disorders associated with streptococcal infections represented a subgroup of those with chronic tic disorders and OCD. These patients may be vulnerable to group A beta-hemolytic Streptococcus infection as a precipitant of neuropsychiatric symptom exacerbations. 63
Taken together, these findings provide epidemiologic evidence that some paediatric-onset neuropsychiatric disorders, including OCD, tic disorders, ADHD, and MDD, may be, at least partially, related to prior streptococcal infections. Group A beta-hemolytic Streptococcus infections are likely not the only event associated with symptom exacerbations for PANDAS patients, but they appear to play a role at least in a subgroup of these children. A potential genetic susceptibility for these post-infectious complexes has been recently proposed.64
The recent recognition that these paediatric neurobehavioural syndromes have infectious and/or immunologic triggers has pointed to important new avenues for their management.
Chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) is a fatiguing illness characterised by unexplained, persistent long-term disabling fatigue plus additional signs and symptoms, including neurophysiological symptoms.65 Brain imaging studies have shown that CFS/ME patients are dysfunctional in their ventral anterior cingulate cortex, and they also have other brain MRI abnormalities.66, 67 In addition, CFS/ME patients also have immunological and inflammation abnormalities, such as alternations in natural killer cell function68, 69 and cytokine profiles.70, 71 In addition, the hypothalamo-pituitary-adrenal axis, which plays a major role in stress responses, appears to be altered in CFS/ME.72
Most, if not all, CFS/ME patients have multiple chronic bacterial and viral infections.73-80 For example, when patients were examined for evidence of multiple, systemic bacterial and viral infections, the Odds Ratio for this was found to be 18 (CI 95% 8.5-37.9, p< 0.001).75 In this study CFS/ME patients had a high prevalence of one of four Mycoplasma species (Odds Ratio=13.8, CI 95% 5.8-32.9, p< 0.001) and often showed evidence of co-infections with different Mycoplasma species, C. pneumoniae (Odds Ratio=8.6, CI 95% 1.0-71.1, p< 0.01) and HHV-6 (Odds Ratio=4.5, CI 95% 2.0-10.2, p< 0.001).75 In a separate study the presence of these infections was also related to the number and severity of signs and symptoms in CFS/ME patients, including neurological symptoms.77 Similarly, Vojdani et al.76 found Mycoplasma species in a majority of CFS/ME patients, but this has not been seen in all studies.81 Interestingly, when European CFS/ME patients were examined for various Mycoplasma species, the most common species found was M. hominis,82 whereas in North America the most common species found was M. pneumoniae,75, 77 indicating possible regional differences in the types of infections in CFS/ME patients. In addition to Mycoplasma species, CFS/ME patients are also often infected with B. burgdorferi,80 and as mentioned above, C. pneumoniae.75, 77, 83
Other infections are also found in CFS/ME patients, such as viral infections: CMV,84 parvovirus B19,78 enterovirus79 and HHV-6.75, 77, 85-88 For example, Ablashi et al.88 found that 54% of CFS/ME patients had antibodies against HHV-6 early protein, compared to 8% of controls. Similarly, Patnaik et al.86 found that 77% of CFS/ME patients were positive for HHV-6 early antigen IgG or IgM antibodies, whereas only 12% of control subjects had IgG or IgM antibodies to HHV-6 early antigen. Recently a new retrovirus, XMRV, was found in mononuclear blood cells of 67% of 101 chronic fatigue syndrome patients compared to only 3.7% of healthy controls. Cell culture experiments determined that the patient-derived virus was infectious and could possibly be transmitted.89
Gulf War illnesses
GWI is a syndrome similar to CFS/ME.90 In most GWI patients the variable incubation time, ranging from months to years after presumed exposure, the cyclic nature of the relapsing fevers and the other chronic signs and symptoms, and their subsequent appearance in immediate family members, are consistent with an infectious process.90, 91 GWI patients were exposed to a variety of toxic materials including chemicals, radiochemicals and biologicals so not all patients are likely to have infections as their main clinical problem. Neurological symptoms are common in GWI cases.90 Baumzweiger and Grove92 have described GWI as neuro-immune disorder that involves the central, peripheral and autonomic nervous systems as well as the immune system. They attribute a major source of the illness to brainstem damage and central, peripheral and cranial nerve dysfunction from demyelination. They found GWI patients have muscle spasms, memory and attention deficits, ataxia and increased muscle tone.92
Bacterial infections were a common finding in many GWI patients.90 Mycoplasmal infections were found in about one-half of GWI patients, and more than 80% of these cases were PCR positive for M. fermentans.90, 91, 93-95 In studies of over 1,500 U.S. and British veterans with GWI, approximately 45% of GWI patients have PCR evidence of such infections, compared to 6% in the non-deployed, healthy population. Other infections found in GWI cases at much lower incidence were Y. pestis, Coxiella burnetii and Brucella species.90
When we examined the immediate family members of veterans with GWI who became sick only after the veteran returned to the home, we found that >53% had positive tests for mycoplasmal infections and showed symptoms of CFS/ME. Among the CFS/ME-symptomatic family members, most (>80%) had the same Mycoplasma fermentans infection as the GWI patients compared to the few non-symptomatic family members who had similar infections (Odds Ratio=16.9, CI 95% 6.0-47.6, p<0.001).91 In contrast, in the few non-symptomatic family members that tested Mycoplasma-positive, the Mycoplasma species were often different from the species found in the Gulf War Illness patients (M. fermentans).The most sensible conclusion is that veterans came home with M. fermentans infections and then transmitted these infections to immediate family members.91
Some other infectious diseases with neurological aspects
Lyme Disease
Lyme disease is caused by a tick bite and the entry of the spiral-shaped spirochete B. burgdorferi as well as other co-infections.96 Lyme disease is the most common tick-borne disease in North America. After incubation for a few days to a month, the Borrelia spirochete and co-infections migrate through the subcutaneous tissues into the lymph and blood where they can travel to near and distant host sites, including the central nervous system.3, 97-99 Transplacental transmission of B. burgdorferi and co-infections can occur in pregnant animals, including humans, and blood-borne transmission to humans by blood transfusion is likely but unproven. The tick-borne co-infections associated with Lyme disease can and usually do appear clinically at the same time, complicating clinical dignoses.100
Lyme disease signs and symptoms eventually overlap with the signs and symptoms of other chronic illnesses, and patients are often diagnosed with illnesses like CFS/ME, chronic arthritis or a neurological disease.80,97-100 About one-third of cases with Lyme disease start with the appearance of a round, red, bulls-eye skin rash (erythema migrans) at the site of the tick bite, usually within 3-30 days.100 Within days to weeks mild flu-like symptoms can occur that include shaking chills, intermittent fevers and local lymph node swelling. After this localised phase, which can last weeks to months, the infection can spread to other sites resulting in disseminated disease. In the disseminated (late) phase patients present with malaise, fatigue, fever and chills, headaches, stiff neck, facial nerve palsies (Bell’s palsy) and muscle and joint pain, and other signs and symptoms.100-104
The disseminated (late) phase of Lyme disease is a chronic, persistent disease with ophthalmic, cardiac, musculoskeletal, central nervous system and internal organ invasion. When it involves the central and peripheral nervous systems, it is often termed neuroborreliosis.100, 104 At this late stage, arthritis, neurological impairment with memory and cognitive loss, cardiac problems (such as myocarditis, endocarditis causing palpitations, pain, bradycardia, hypertension) and severe chronic fatigue are usually apparent.80, 100-102 The signs and symptoms of the chronic (late) phase of the disease usually overlap with other chronic conditions, such as CFS/ME, chronic arthritis, as well as neurodegenerative diseases, causing confusion in the diagnosis and treatment of the chronic phase in patients with Lyme Disease.80, 97, 100, 105 Patients with late stage neuroborreliosis exhibit neuropathologic and neuropsychiatric disease similar to some of the neurodegenerative diseases discussed in previous sections.1
Diagnostic laboratory testing for Lyme disease at various clinical stages is not fool-proof, and experts often use a checklist of signs and symptoms and potential exposures, along with multiple laboratory tests to diagnose Lyme disease.104 The laboratory tests include serology, Western blot analysis of B.burgdorferi associated bands, PCR analysis of blood and the nonspecific decrease in CD-57 natural killer cells. Unfortunately, similar to other intracellular bacteria, Borrelia spirochetes are not always released into the blood circulation or other body fluids, making the very sensitive PCR method less than reliable for diagnosing Lyme Borrelia with blood samples. Lebech and Hansen106 found that only 40% of cerebrospinal fluid samples from patients with Lyme neuroborreliosis were positive for B.burgdorferi by PCR.
Co-infections in Lyme disease are important but, in general, have not received the attention that B. burgdorferiattracts. Some of the Lyme Disease co-infections on their own, such as M. fermentans, have been shown to produce signs and symptoms comparable to B. burgdorferi infections.80, 102
The most common co-infections found in Lyme disease are species of Mycoplasma, mostly M. fermentans, present in a majority of cases.80, 103, 107 In some cases multiple mycoplasmal infections are present in patients with Lyme disease,80 while other common co-infections include Ehrlichia species, Bartonella species and Babesia species. Such co-infections are present in 10-40% of cases.103, 104, 108-112Ehrlichia and Bartonella species are usually found along with Mycoplasma species in Lyme disease.94, 98, 108-111 Bartonella species, such as B.henselae,111 which also causes cat-scratch disease,113 are often found in neurological cases of Lyme disease.100, 111
Protozoan co-infections have been found with B.burgdorferi, such as intracellular Babesia species.100, 108, 109, 112, 114 The combination of Borrelia, Mycoplasma and Babesia infections can be lethal in some patients, and ~7% of patients can have disseminated intravascular coagulation, acute respiratory distress syndrome and heart failure.109
Brucellosis
Brucellosis is a nonspecific clinical condition characterized by intracellular Brucella species infection.115 Approximately 40% of patients with Brucella spp. infections have a systemic, multi-organ chronic form of brucellosis that is similar to CFS/ME in its multi-organ signs and symptoms.115, 116Brucella infections can invade the central nervous system and cause neurological symptoms.117
Brucella species cause infections in animals, and often humans get the infections from prolonged contact with infected animals. Thus these bacteria are zoonotic, they are capable of being transmitted from animals to humans. Although there are at least eight species of Brucella that are pathogenic, only B. melitensis, B. abortus, B. suis and B. canis have been reported to be pathogenic in humans.116
When CFS/ME patients were examined for the presence of Brucella spp. infections, approximately 10% showed evidence by PCR of Brucella spp. infections (Odds Ratio=8.2, CI 95% 1-66, p<0.01).118 Interestingly, urban CFS/ME patients with Brucella infections were not as prevalent as rural patients with Brucella infections (Odds Ratio=5.5, CI 95% 3-23.5, p<0.02), while control subjects had very low (1.4%) rates of infection. Co-infections with Mycoplasma species were also found in Brucella-positive CFS/ME patients.118
Final comments to part 2
The progression, and in some cases, the inception of many chronic diseases are probably elicited by various bacterial and viral infections.1, 39, 40, 119 Even if infections are not directly involved in the pathogenesis of these diseases, patients with chronic conditions are at risk of a variety of opportunistic infections that could result in co-morbid conditions or promote disease progression. Infections can complicate diagnosis and treatment, and patients with late-stage disease with complex neurological manifestations, such as meningitis, encephalitis, peripheral neuropathy, psychiatric conditions, or with other signs and symptoms could have infections that are not recognized or treated.
Patients with chronic diseases are particularly difficult to treat using single modality approaches, and this is particularly true for patients who also have multiple chronic infections.103, 109 The multi-focal nature of chronic diseases and the fact that often treatments are given to suppress signs and symptoms, rather than treat causes of the disease or its progression, have resulted in incomplete or ineffective treatments. On the other hand, even if the causes of chronic diseases are known, by the time therapeutic intervention is undertaken, it may be entirely too late to use approaches that should work on the disease if chronic infections were not present. Moreover, if complex, chronic infections are ignored or left untreated, recovery may be difficult, if not impossible to achieve.
At the moment the evidence that particular or specific types of infections are responsible for the inception or pathogenesis of chronic diseases is inconclusive.119 One of the problems that arises in trying to prove this hypothesis is that not all patients appear to have similar chronic infections. Some individuals can harbour chronic infections without any observable signs or symptoms. Although the incidence of chronic infections of the types discussed in this review in symptom-free individuals is generally very low, usually only a few percent,74-76, 120 that does not prove that they are important in pathogenesis. Since patients with chronic diseases have been identified that do not have easily diagnosed chronic infections, most researchers have concluded that infections are not involved in the pathogenesis of chronic diseases. Unfortunately, the tools available to find chronic infections are not optimal, and many patients are likely go undiagnosed with chronic infections for purely technical reasons.1,119-121
In the history of medicine animal models of disease have provided useful information that could not be obtained through clinical studies alone. Indeed, the field of chronic diseases could benefit from the greater use of relevant animal models. We suggest that to be useful, the pathogenesis of the animal models of disease must be similar to the pathogenesis of human disease and the animal models must have a similar response to therapy as humans. Thus such models are only relevant if they closely mimic human disease and its response to treatment. For example, the infection of non-human primates with neuropathologic microorganisms, such as Mycoplasma fermentans, resulted in brain infections and fatal diseases with clinically typical neurological signs and symptoms.122 These primates also respond to therapies that have been used successfully to treat humans.93,123 Thus this particular model may be useful if it can be reproucibly infected with specific microorganisms and later develop neurological signs and symptoms that closely mimic chronic human neurological diseases. Future efforts to determine the relationship between specific infections and the pathogenesis of various chronic diseases may well depend on the further development of relevant animal models.
Malnutrition is defined as state of nutrition in which there is a deficiency or excess of energy, protein and other nutrients causing measurable adverse effects on tissue/body form, function and clinical outcome. (1) It is recognised that 30% of in-hospital patients are malnourished (undernourished) on admission and the majority of these will lose further weight while in hospital. (2) In this review article the term undernutrition will be used instead of the generalised term malnutrition. Undernutrition develops due to increased losses (vomiting, diarrhoea, malabsorption), decreased intake (anorexia, vomiting, nausea, dysphagia), increased requirements (catabolic state) or a combination of all these processes.
Is undernutrition important?
Consequences of undernutrition include reduced muscle mass, impaired immune function, poor tissue viability, poor clinical outcome and psychosocial effects. (3) Reduced muscle mass decreases cardio-pulmonary function, lean muscle mass and muscle weakness. Impaired immune function increases infection and sepsis risk. Poor tissue viability can cause pressure sores and poor wound healing. Undernutrition can amplify the length of hospital stay. Psychosocial effects include altered mood and poor quality of life. (4) It is therefore essential that undernutrition is properly treated to diminish patient morbidity and mortality.
How to recognise undernutrition:
1. Malnutrition screening tools
Screening tools should be performed easily with low-level staff training. Hospital patients at risk of undernutrition are identified by screening methods such as MUST (Malnutrition Universal Screening Tool) (5), SGA (Subjective Global Assessment) (6) or MNA (Mini Nutritional Assessment – validated for > 65 years) (7). These screening methods usually consider current body mass index (BMI), recent weight loss and possible future weight loss. MUST is currently well advertised as a nutritional screening tool within UK hospitals. The British Association of Parenteral and Enteral Nutrition have endorsed this 5 step-screening tool. The MUST score (low, moderate, high risk) has been shown to correlate with mortality (low risk group 8% vs. high risk group 32%, p 0.01) and length of hospital stay (low risk group 15 days vs. high risk group 28 days, p 0.02) (8). See Table 1.
Table 1
MUST Screening tool (5)
Step 1: BMI (can use alternatives such as ulna length for height or mid-upper arm circumference (MUAC) as approximation for BMI: MUAC <23 cm = BMI 20kg/m2, MUAC >32cm = BMI >30 kg/m2)
Step 2: Percentage weight loss
Step 3: Establish Acute Disease Effect and score
Step 4: Add scores step 1,2,3 together to obtain overall risk of malnutrition
Step 5: Develop care plan
2. Assessment of nutritional status:
If a patient is found to be at risk of undernutrition, following screening, then a formal nutritional assessment ensues. This assessment involves anthropometrics, biochemical testing, clinical methods and dietary history.
a) Anthropometrical data: appropriately trained staff can perform weight, height, waist circumference, mid-upper arm circumference and skinfold thickness measurements. Indices can subsequently be calculated. These include percentage weight loss, BMI and waist-hip ratio.
b) Biochemical data: information acquired from blood testing includes renal function as a marker of hydration. Also sepsis markers including CRP, ESR and WBC’s are valuable surrogate markers for stress response. Albumin is a poor marker of nutritional status. (9)
c) Clinical: medical history including past and present is valuable. It is essential to obtain plans regarding fasting for investigations. Knowledge of current treatment that may cause decreased intake or increased losses is essential.
d) Dietary History: there are assorted techniques of obtaining dietary history. Mostly recall, record diary and food frequency questionnaires methods are utilised.
The overall nutritional assessment entails considering all the information obtained from these different methods. Subsequently a clinical decision is reached regarding the overall nutritional status.
How to assess nutritional requirements:
In-patient energy requirements are calculated using a combination of:
a) basal metabolic rate equations such as Schofield, Harris Benedict and Ireton Jones
b) stress factors or weight gain/loss
c) combined factor for activity level and diet induced thermogenesis.
The basal metabolic rate is typically calculated using the Schofield equation (10). Schofield estimates basal metabolic rate of a healthy individual. An adjustment is then made for stress or weight gain/loss. Stress factors have been published for various clinical conditions including brain injury, infection, pancreatitis and surgery. Finally a combined factor (activity and diet-induced thermogenesis) is added to calculate total energy requirements. This combined factor is adjusted depending on patient mobility. Community patient’s energy requirements are calculated using a separate method. Occupational and non-occupational activity is estimated to determine a physical activity level which is multiplied by basal metabolic rate to achieve overall energy requirements.
Nitrogen/protein requirements are estimated using current patient clinical state i.e. hypermetabolic, depleted or normal state. Normal state nitrogen requirements are 0.14-0.20 g/kg/day. Depleted state patients nitrogen requirements are 0.20-0.40 g/kg/day. (1g nitrogen = 6.25g protein)
Methods of treating undernutrition
Following identification of undernutrition a patient’s treatment can be instituted. Undernutrition is typically treated using a graded stepwise approach and subsequently monitoring response. If however it appears clinically obvious that the first steps would not be advantageous then treatment can be commenced at a more aggressive phase. Improving energy intake using the following methods can treat undernutrition:
Step 1. Increase frequency and quantity of food intake. Consider nutrient dense foods. Encourage foods that are energy and nutrient dense such as meat, fish, cheese, eggs, dairy produce and snack foods.
Step 2. Increase nourishing drinks including milk based drinks, soups, fruit juices and sugary drinks. Nourishing drinks are simple to make and can provide high calories in a small quantity.
Step 3. Food fortification. This essentially increases the energy density of foods by adding high-energy components such as addition of cheese, milk powder, cream, jam and butter to other foods.
Step 4. Supplements. These can be milk, yoghurt or juice based. They contain varying calories (1-2kcal/ml) and protein (4-6g protein/100ml). Supplements are very useful at boosting energy intake. Most are nutritionally complete but others contain calories only. Examples include Ensure Plus, Fortisip, Calogen and Calshake.
Step 5. Enteral feeding. Enteral feeding is used to provide either supplementary or complete nutrition to patients that are unable to maintain adequate nutrition by oral route. It is only likely to benefit malnourished patients or those at risk of malnutrition. This includes patients that have had a failed trial of diet modification or supplementary feeds or patients at pulmonary aspiration risk from oral nutrition.
Step 6. Parenteral nutrition. The development of parenteral nutrition in the 1960’s meant that feeding was possible even in patients that did not have a functioning gastrointestinal tract. Although it is mentioned in this article as a final step in nutritional support it may also be appropriate to use early depending on clinical scenario.
Enteral versus Parenteral feeding
Enteral feeding produces gastro-intestinal luminal contents that can decrease the possibility of gut atrophy. Maintaining a normal intestinal mucosa reduces the hazard of bacteria and toxins crossing the gastro-intestinal wall and therefore can decrease proinflammatory mediator levels. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. (11) Hernandez et al have shown that enteral feeds decrease gut mucosal atrophy in critically ill patients. (12) A meta-analysis has shown that in acute pancreatitis use of EN was associated with a significant reduction in infectious morbidity, hospital length of stay, and a trend toward reduced organ failure when compared with use of parenteral nutrition. (13) However it is important to note that many of the studies involving parenteral nutrition had full dose daily calorie intake whereas enteral feeding studies were less likely to reach estimated energy requirements. This is significant since ill stressed patients should not be given full calorie energy requirements in the first 24-48 hours of commencing feeding. Therefore the parenteral feeding groups were disadvantaged in that the patients were overfed initially and received excess energy calorie intake. National Institute of Clinical Excellence states that parenteral nutrition is only to be used in patients with “inadequate or unsafe oral and/or enteral nutritional intake and a non-functional, inaccessible or perforated (leaking) gastrointestinal tract.” (14) Enteral nutrition can be provided by a number of methods including nasogastic tubes, nasojejunal tubes, gastrostomy tunes (including PEG tubes) and jejunostomy tubes (including PEG-J and D-PEJ). Parenteral nutrition can be given peripherally for approximately 14 days but central access should be used if greater than 14 days. Refeeding syndrome
Refeeding syndrome is a potentially lethal condition with severe electrolyte and fluid shifts with resulting metabolic disturbances in malnourished patients. (15) It is caused by refeeding in malnourished patients with resulting insulin release and intracellular movement of potassium, phosphate and magnesium and increased thiamine uptake. It is essential that patients are correctly identified (See Table 2) and electrolytes corrected and intravenous Vitamin B and C is given. Feeding should be initiated slowly. Fluid balance and electrolytes should be monitored closely.
Table 2
NICE guidelines: Risk of refeeding syndrome (14)
>1 of
BMI <16.5 kg/m2
Weight loss >15%
No food intake 10 days
Decreased magnesium/phosphate/potassium
>2 of
BMI <18.5 kg/m2
Weight loss <10%
No food intake 5 days
Alcohol abuse, Insulin, Chemotherapy
Cardiovascular disease and nutrition
Research has confirmed link between cardiovascular disease and serum cholesterol. The NHANES II data has shown that patients who died form myocardial infarction had increased cholesterol. (16) Hooper et al confirmed that dietary fat is linked to cardiovascular risk. (17) This group demonstrated that decreasing total dietary fat over 6 month period reduced cardiac events by 16%. The Seven Countries Study illustrated that cardiovascular mortality was linked to saturated fat intake. (18)
There has been recent interest in the role of the Mediterranean diet in the prevention of cardiovascular disease. (See Table 3)
Table 3
Mediterranean Diet Studies
Population Studies CARDIO2000. Panagiotakos et al 2002. (28) Greece. 2000-2002. CVD group versus control group. Intake of Mediterranean diet type foods significantly decreased risk of developing CVD. The daily use of olive oil and consumption of vegetables, legumes, cereals and fish was associated with 23% risk of developing acute coronary syndromes. Trichopoulou. 2005. (29) Studies relationship between Mediterranean diet and survival in 1302 Greek patients with CVD. Patients with higher compliance with Mediterranean diet had lower cardiac mortality. Martinez-Gonzalez. 2002. (30) Case-control study. Examined the relationship between a Mediterranean diet and risk of first MI. Better compliance with Mediterranean diet lowered risk of MI.
Intervention Studies Medi-RIVAGE. Dietary intervention Study. (31) 3 month diet. Compared Mediterranean diet and low fat diet. There was greater reduction in cardiovascular risk in Mediterranean diet group compared to low fat group (15% vs 9%). GISSI-Prevenzione. Barzi et al. (32) Supplement of Vit-E and omega-3 FA’s given to survivors of recent MI. Also informed to increase intake of Mediterranean diet foods. Outcomes showed that lower chance of premature death if higher intake of Mediterranean foods. Lyon Diet Heart Study. (33) Key study in relation to Mediterranean diet and CVD. Secondary prevention trial. Examined the effects of a Mediterranean diet in survivors of first MI. Experimental group supplied with margarine with high levels of alpha-linolenic acid (n-3 FA). Mediterranean diet group had lower total mortality (70%).
Patients were previously educated regarding low fat diet benefits but Mediterranean diet appears to have enhanced beneficial effects. There is however some complexity with definition of a Mediterranean diet. The diet is based on dietary patterns of Greece, Crete and Southern Italy in 1960’s. This diet was abundant in plant foods, fresh fruit, olive oil as principal fat source (monounsaturated fatty acid), low red meat intake, fish (polyunsaturated fatty acid) and red wine in low to moderate amounts. In respect to dietary fats the Mediterranean diet is low in saturated fat but high in monounsaturated fatty acid and polyunsaturated fatty acid.
Diabetes and nutrition
The diabetic diet is essentially a healthy diet. The total fat intake should be less than 35% with saturated fat less than 10%. Total monounsaturated fatty acid 10-20% and polyunsaturated fatty acid less than 10% which corresponds to oily fish 1-2 per week. Interestingly polyunsaturated fatty acid supplements should be avoided in this group as they have been shown to increase LDL-cholesterol. Diabetic patients should also be encouraged to eat regular starchy carbohydrate, avoid sugar, increase fibre, eat regular meals and snacks and avoid diabetic foods.
Cancer and nutrition
Is there a link between diet and cancer?
The World Cancer Research Fund states that 30% of all cancers could be prevented by a change in diet, increased physical activity and healthy weight. Animal studies and metabolic studies have been performed that reveal evidence linking diet and cancer. An ecological study linking diet and cancer compared risk of cancer against intakes of fat, cereals and vegetables in 39 countries (19). The ATBC was a clinical trial that related Vitamin A and E to increased lung cancer rates. (20) 2 large cohort studies have been performed in relation to colorectal cancer and dietary fibre. (21, 22). EPIC showed a significant benefit of dietary fibre against colorectal cancer. The EPIC data showed a 40% difference in colorectal cancer rates between the lowest and highest quintile dietary fibre groups. NIH-AARP however showed no benefit when adjusted for multivariate analysis. The American Gastroenterology Association suggest that available evidence form animal, epidemiological and interventional studies does not unequivocally support protective role of fibre against development of CRC. However the whole body of evidence is analysed overall the overall conclusion is that there is an inverse relationship between dietary fibre and CRC.
Cancer cachexia
Cancer cachexia is defined as anorexia, weight loss and muscle wasting, fatigue and weakness in a cancer patient. Cancer instigates an inflammatory response and production of tumour products. This triggers metabolic abnormalities that produce lipolysis, protein loss and anorexia. As with all disease processes the dietary management of cancer cachexia is initiated by a nutritional assessment. Any symptoms including vomiting and nausea should be treated. There has also been some research regarding fish oils and cancer cachexia. One available product contains docosahexaenoic acid, eicosapentaenoic acid and antioxidants. However a Cochrane review has shown no benefit in relation to beneficial effects of fish oils and cancer cachexia. (23)
Critical care
Injury and sepsis cause major disturbance to clinical state. There is rapid weight loss, increased metabolic rate, protein losses and sodium retention. There are also changes in hormone levels including increased insulin, catecholamines, growth hormone, glucagons and cortisol. The energy requirements in critical care can vary greatly. The Ireton-Jones equation is often used to calculate energy requirements in the critical care setting (See Table 4).
Table 4
Immunonutrition: ESPEN guidelines (34)
Surgical patients
Perioperatively for
Major Cancer Neck Surgery
Major Cancer Abdominal Surgery
Critical Care Patients
Elective Upper GIT surgery
Mild Sepsis
Trauma
ARDS (n-3 FA’s and antioxidants)
Glutamine (burns and trauma)
The specific immune modulating aspects of nutrients have been widely researched in the critical care setting. This field of immunonutrition has shown disparaging results.
Arginine has been investigated as an immune modulating nutrient. Arginine levels can increase or decrease in relation to clinical state. It produces nitric oxide that can lower blood pressure and has been revealed to have detrimental effects in critically ill patients. (24) Glutamine is another possible immune modulating nutrient. It has lots of metabolic functions. It enhances heat shock protein that protect against sepsis. It is thought to be useful in septic shock. Omega-3 fatty acids (alpha-linolenic acid, docosahexaenoic acid, eicosapentaenoic acid) have also been investigated as an immune modulating nutrient. Omega-3 fatty acids produce less proinflammatory eicosanoids than omega-6 fatty acids. There is some evidence that omega-3 fatty acids decrease duration of hospital stay (25) Antioxidants have also been researched as an immunomodulator. Antioxidant levels are lower in critically ill patients. Vitamins A,C,E and Selenium have been studied. A recent meta-analysis has suggested overall mortality benefit but no septic complications benefit in anti-oxidant trials. (26)
Gastrointestinal disease and nutrition
Liver disease
The energy requirements in chronic liver disease are dependent on clinical state i.e. compensated or decompensated. Nutritional requirements for compensated liver disease are 25-35 kcal per kg (dry body weight) day and protein 1.2g per day. Nutritional requirements for decompensated liver disease are energy 35-45 kcal per kg (dry body weight) day and protein 1.5grams per day.
Porto-systemic encephalopathy
This disease process is multifactorial and comprises increased ammonia levels, increased aromatic amino acids, decreased branched chain amino acids and alterations of brain neurotransmitters. There is a widely held belief among doctors that protein intake should be restricted but this is mistaken. Protein requirements are approximately 1g/kg/day and should be divided throughout day.
Ascites
Low salt intake (<6g per day) is an essential component of ascites treatment. Advice should include no salt in cooking, no added salt, avoid processed foods, and avoid foods rich in salt.
Inflammatory Bowel Disease
Inflammatory bowel disease patients are often undernourished due to meagre intake (anorexia, vomiting), amplified losses (diarrhoea and malabsorption) and increased demands (catabolic state). Protein requirements are also increased due to nitrogen losses and catabolic state. It is therefore important that nutritional measures are instituted to improve calorie and protein intake. Interestingly nutrition has been investigated as a treatment for active Crohn’s Disease. Elemental diet is used in active paediatric Crohn’s Disease more than adult Crohn’s Disease to achieve remission. (27). Often this has to be given via naso-gastric tube due to unpalatability. After 4-6 weeks if the patient is in remission foods are introduced slowly over a 3-week period.
Coeliac Disease
Coeliac disease is genetically determined chronic inflammatory disease secondary to gluten (glaidin is the alcohol-soluble fraction) that is a component of wheat. In addition the allergy involves similar proteins found in barley, rye and possibly oats. Coeliac patients consequently exclude these dietary sources. Oats can be reintroduced later depending on response. Dietary sources can be obvious or hidden as gluten can be found in numerous manufactured foods. Coeliac patients can however eat natural gluten-free foods or gluten-free proprietary foods (e.g. Schar, Juvela, Dietary Specials, Glutafin).
Irritable Bowel Syndrome
Simple healthy eating advice is suggested. Diet is tailored to either constipation or diarrhoea symptoms. Typically increasing dietary fibre gradually ameliorates constipation symptoms. Soluble fibre appears to offer benefit more than non-soluble fibre. Decreasing dietary fibre intake treats diarrhoea symptoms. There is not enough evidence regarding exclusion diets although some centres do offer exclusion diets.
Renal disease
Acute renal failure and nutrition is divided into non-catabolic and catabolic patients. Non-catabolic patients do not usually have increased energy requirements. Catabolic patients have high protein requirements but no benefit of >0.2 g nitrogen per kg per day. Their energy requirements should be no greater than >20% above resting energy expenditure.
Chronic kidney disease patients have estimated energy requirements of 35 kcal/kg/IBW/day. (IBW = Ideal Body Weight which in the UK this approximates to BMI 23kg/m2). There has been much research regarding protein restriction and possibility of slowing progression of chronic kidney disease. The Northern Italian Co-op study (protein <0.6grams/day) did show possible slower progression of CKD. However it is known that low protein diets have poor compliance and can increase risk of malnutrition. The Renal Association Standards suggest protein intake 0.75g/kg/IBW/day.
Discussing the dietary management of end-stage renal disease, nephrotic syndrome and renal stones is beyond the scope of this article.
Conclusion
This review article has highlighted the importance of undernutrition in patients under our care. There are numerous methods of screening and assessing patients for undernutrition. There is also a stepwise approach to improving calorie intake: improving oral intake by various methods to enteral and parenteral nutrition. Nutrition is an important aspect of treatment of different disease processes that include cardiovascular disease, diabetes, gastrointestinal disease, renal disease, critical care and cancer. This review article will hopefully provide the medical practitioner with improved knowledge that can be translated into improved awareness and treatment of undernutrition.
Chronic infections appear to be common features of various diseases, including neurodegenerative, psychiatric and neurobehavioral diseases, autoimmune diseases, fatiguing illnesses and other conditions.1-4 Neurodegenerative diseases, chronic degenerative diseases of the central nervous system (CNS) that cause dementia, are mainly diseases of the elderly. In contrast, neurobehavioral diseases are found mainly in younger patients and include autism spectrum disorders (ASD), such as autism, attention deficit disorder, Asperger’s syndrome and other disorders.5 For the most part, the causes of these neurological diseases remain largely unknown.2 Neurodegenerative diseases are characterized by molecular and genetic changes in nerve cells that result in nerve cell degeneration and ultimately nerve cell dysfunction and death, resulting in neurological signs and symptoms and dementia.2,3 On the other hand, neurobehavioral diseases are related to fetal brain development but are less well characterized at the cellular level and involve both genetic and environmental factors.6, 7 Even less well characterized at the cellular and genetic level are the psychiatric disorders, such as schizophrenia, paranoia, bipolar disorders, depression and obsessive-compulsive disorders.
Genetic linkages have been found in neurodegenerative and neurobehavioral diseases, but the genetic changes that occur and the changes in gene expression that have been found are complex and usually not directly related to simple genetic alterations.2, 6-8 In addition, it is thought that nutritional deficiencies, environmental toxins, heavy metals, chronic bacterial and viral infections, autoimmune immunological responses, vascular diseases, head trauma and accumulation of fluid in the brain, changes in neurotransmitter concentrations, among others, are involved in the pathogenesis of various neurodegenerative and neurobehavioral diseases.2, 3, 5-16 One of the biochemical changes found in essentially all neurological, neurodegenerative and neurobehavioral diseases is the over-expression of oxidative free radical compounds (oxidative stress) that cause lipid, protein and genetic structural changes.9-11 Such oxidative stress can be caused by a variety of environmental toxic insults, and when combined with genetic factors could result in pathogenic changes.14
Neurodegenerative diseases
Infectious agents are important factors in neurodegenerative and neurobehavioral diseases and may enter the brain within infected migratory macrophages. They may also gain access by transcytosis across the blood-brain-barrier or enter by intraneuronal transfer from peripheral nerves.15 Cell wall-deficient bacteria, such as species of Mycoplasma, Chlamydia (Chlamydophila), Borrelia and Brucella, among others, and various viruses are candidate brain infectious agents that may play important roles in neurodegenerative and neurobehavioral diseases.16-19 Such infections are systemic and can affect the immune system and essentially any organ system, resulting in a variety of systemic signs and symptoms.4, 15, 16, 19, 20
Amyotrophic lateral sclerosis
Amyotrophic lateral sclerosis (ALS) is an adult-onset, idiopathic, progressive neurodegenerative disease that affects both central and peripheral motor neurons.21 Patients show gradual progressive weakness and paralysis of muscles due to destruction of upper motor neurons in the motor cortex and lower motor neurons in the brain stem and spinal cord. This ultimately results in death, usually by respiratory failure.21, 22 The overall clinical picture of ALS can vary, depending on the location and progression of pathological changes.23
The role of chronic infections has attracted attention with the finding of enterovirus sequences in a majority of ALS spinal cord samples by polymerase chain reaction (PCR).24 However, others have failed to detect enterovirus sequences in spinal cord samples from patients with or without ALS.25-26 In spite of the mixed findings on enterovirus, infectious agents that penetrate the CNS could play a role in the aetiology of ALS. Evidence for transmission of an infectious agent or transfer of an ALS-like disease from man-to-man or man-to-animals has not been found.27
Using PCR methods systemic mycoplasmal infections have been found in a high percentage of ALS patients.28, 29 We found that 100% of Gulf War veterans from three nations diagnosed with ALS had systemic mycoplasmal infections.28 All but one patient had M. fermentans, and one veteran from Australia had a systemic M. genitalium infection. In nonmilitary ALS patients systemic mycoplasmal infections of various species were found in approximately 80% of cases.28 Of the mycoplasma-positive civilian patients who were further tested for various species of Mycoplasma, most were positive for M. fermentans (59%), but other Mycoplasma species, such as M. hominis (31%) and M. pneumoniae infections (9%) were also present. Some of the ALS patients had multiple infections; however, multiple mycoplasmal infections were not found in the military patients with ALS.28 In another study 50% of ALS patients showed evidence of systemic Mycoplasma species by PCR analysis.29
ALS patients who live in certain areas often have infections of Borrelia burgdorferi, the principal aetiological agent in Lyme disease. For example, ALS patients who live in a Lyme-prevalent area were examined for B. burgdorferi infections, and over one-half were found to be seropositive for Borrelia compared to 10% of matched controls.30 In addition, some patients diagnosed with ALS were subsequently diagnosed with neuroborreliosis.31 Spirochetal forms have been observed in the brain tissue of ALS patients and in patients with other neurodegenerative diseases.32 In general, however, the incidence of Lyme infections in ALS patients is probably much lower. In one recent study on 414 ALS patients only about 6% showed serological evidence of Borrelia infections.33 Some Lyme Disease patients may progress to ALS, but this is probably only possible in patients who have the genetic susceptibility genes for ALS as well as other environmental toxic exposures.34, 35
Additional chronic infections have been found in ALS patients, including human herpes virus-6 (HHV-6), Chlamydia pneumoniae andother infections.36, 37 There is also a suggestion that retroviruses might be involved in ALS and other motorneuron diseases.38 McCormick et al.39 looked for reverse transcriptase activity in serum and cerebrospinal fluid of ALS and non-ALS patients and found reverse transcriptase activity in one-half of ALS serum samples tested but in only 7% of controls. Interestingly, only 4% of ALS cerebrospinal fluid samples contained reverse transcriptase activity.39
Although the exact cause of ALS remains to be determined, there are several hypotheses on its pathogenesis: (1) accumulation of glutamate causing excitotoxicity; (2) autoimmune reactions against motor neurons; (3) deficiency of nerve growth factor; (4) dysfunction of superoxide dismutase due to mutations; and (5) chronic infection(s).24, 27-40 None of these hypotheses have been ruled out or are exclusive, and ALS may have a complex pathogenesis involving multiple factors. 28, 36
It is tempting to propose that infections play an important role in the pathogenesis or progression of ALS.28, 40 Infections could be cofactors in ALS pathogenesis, or they could simply be opportunistic, causing morbidity in ALS patients. For example, infections could cause the respiratory and rheumatic symptoms and other problems that are often found in ALS patients. Since the patients with multiple infections were usually those with more rapidly progressive disease,28 infections likely promote disease progression. Indeed, when Corcia et al.41 examined the cause of death in 100 ALS patients, the main causes were broncho-pneumonia and pneumonia. Finally, there are a number of patients who have ALS-like signs and symptoms but fall short of diagnostic criteria. Although a careful study has not been attempted on these patients, there is an indication that they have the same infections as those found in patients with a full diagnosis of ALS (personal communication). Thus ALS-like diseases may represent a less progressive state, in that they may lack additional changes or exposures necessary for full ALS.
Multiple sclerosis
Multiple sclerosis (MS) is the most common demyelinating neurological disease. It can occur in young or older people and is a cyclic (relapsing-remitting) or progressive disease that continues progressing without remitting.42 Inflammation and the presence of autoimmune antibodies against myelin and other nerve cell antigens are thought to cause the myelin sheath to break down, resulting in decrease or loss of electrical impulses along the nerve fibers.42, 43 In the progressive subset of MS neurological damage occurs additionally by the deposition of plaques on the nerve cells to the point where nerve cell death occurs. In addition, breakdown of the blood-brain barrier in MS is associated with local inflammation caused by glial cells.42, 43 The clinical manifestations of demyelinization, plaque damage and blood-brain barrier disruptions cause variable symptoms, but they usually include impaired vision, alterations in motor, sensory and coordination systems and cognitive dysfunction.43
There is strong evidence for a genetic component in MS.44, 45 Although it has been established that there is a genetic susceptibility component to MS, epidemiological and twin studies suggest that MS is an acquired, rather than an inherited, disease.46
MS has been linked to chronic infection(s).46, 47 For example, patients show immunological and cytokine elevations consistent with chronic infections.48-50 An infectious cause for MS has been under examination for some time, and patients have been tested for various viral and bacterial infections. 44, 45,47, 48, 51 One of the most common findings in MS patients is the presence of C. pneumoniae antibodies and DNAin their cerebrospinal fluid.51-53 By examining relapsing-remitting and progressive MS patients for the presence of C. pneumoniae in cerebrospinal fluid by culture, PCR and immunoglobulin reactivity Sriram et al.52 were able to identify C. pneumoniae in 64% of MS cerebrospinal fluid versus 11% of patients with other neurological diseases. They also found high rates (97% positive) of PCR-positive MOMP gene in MS- patients versus 18% in other neurological diseases, and this correlated with 86% of MS patients being serology-positive patients by ELISA and Western blot analysis.52 Examination of MS patients for oligoclonal antibodies against C. pneumoniae revealed that 82% of MS patients were positive, whereas none of the control non-MS neurological patients had antibodies that were absorbed by C. pneumoniae elemental body antigens.53 Similarly, Contini et al.54 found that the DNA and RNA transcript levels in mononuclear cells and cerebrospinal fluid of 64.2% of MS patients but in only 3 controls.
Using immunohistochemistry Sriram et al.55 later examined formalin-fixed brain tissue from MS and non-MS neurological disease controls and found that in a subset of MS patients (35%) chlamydial antigens were localized to ependymal surfaces and periventricular regions. Staining was not found in brain tissue samples from other neurological diseases. Frozen tissues were available in some of these MS cases, and PCR amplification of C. pneumoniae genes was accomplished in 63% of brain tissue samples from MS patients but none in frozen brain tissues from other neurological diseases. In addition, using immuno-gold-labeled staining and electron microscopy they examined cerebrospinal fluid sediment for chlamydial antigens and found that the electron dense bodies resembling bacterial structures correlated with PCR-positive results in 91% of MS cases.55 They also used different nested PCR methods to examine additional C. pneumoniae gene sequences in the cerebrospinal fluid of 72 MS patients and linked these results to MS-associated lesions seen by MRI.56
MRI was used by Grimaldi et al.57 to link the presence of C. pneumoniae infection with abnormal MRI results and found linkage in 21% of MS patients. These turned out to be MS patients with more progressive disease.58 In addition, higher rates of C. pneumoniae transcription were found by Dong-Si et al.58 in the cerebrospinal fluid of 84 MS patients. The data above and other studies strongly support the presence of C. pneumoniae in the brains of MS patients,59-61 at least in the more progressed subset of MS patients.
Other research groups have also found evidence for C. pneumoniae in MS patients but at lower incidence. Fainardi et al.62 used ELISA techniques and found that high-affinity antibodies against C. pneumoniae were present in the cerebrospinal fluid of 17% of MS cases compared to 2% of patients with non-inflammatory neurological disorders. They found that the majority of the progressive forms of MS were positive compared to patients with remitting-relapsing MS. The presence of C. pneumoniae antibodies was also found in other inflammatory neurological disorders; thus it was not found to be specific for MS.62
In contrast to the studies above, other researchers have not found the presence of C. pneumoniaeor other bacteriain the brains of MS patients.63-65 For example, Hammerschlag et al.66 used nested PCR and culture to examine frozen brain samples from MS patients but could not find any evidence for C. pneumoniae. However, in one study C. pneumoniae was found at similar incidence in MS and other neurological diseases, but only MS patients had C. pneumoniae in their cerebrospinal fluid.64 Swanborg et al.67 reviewed the evidence linking C. pneumoniae infection with MS and concluded that it is equivocal, and they also speculated that specific genetic changes may be necessary to fulfill the role of such infections in the aetiology of MS.
Another possible reason for the equivocal evidence linking MS with infections, such as C. pneumoniae, is that multiple co-infections could be involved rather than one specific infection. In addition to C. pneumoniae found in most studies, MS patients could also have Mycoplasma species, B. burgdorferi and other bacterial infections as well as viral infections.68 When multiple infections are considered, it is likely that >90% of MS patients have obligate intracellular bacterial infections caused by Chlamydia (Chlamydophila), Mycoplasma, Borrelia or other intracellular bacterial infections. These infections were found only singly and at very low incidence in age-matched subjects.68 In spite of these findings, others did not find evidence of Mycoplasma species in MS brain tissue, cerebrospinal fluid or peripheral blood.69
Viruses have also been found in MS. For example, HHV-6 has been found at higher frequencies in MS patients, but this virus has also been found at lower incidence in control samples.70 Using PCR Sanders et al.70 examined postmortem brain tissue and controls for the presence of various neurotrophic viruses. They found that 57% of MS cases and 43% of non-MS neurological disease controls were positive for HHV-6, whereas 37% and 28%, respectively, were positive for herpes simplex virus (HSV-1 and -2) and 43% and 32%, respectively, were positive for varicella zoster virus. However, these differences did not achieve statistical significance, and the authors concluded “an etiologic association to the MS disease process [is] uncertain.” They also found that 32% of the MS active plaques and 17% of the inactive plaque areas were positive for HHV-6.70 Using sequence difference analysis and PCR Challoner et al.71 searched for pathogens in MS brain specimens. They found that >70% of the MS specimens were positive for infection-associated sequences. They also used immunocytochemistry and found staining around MS plaques more frequently than around white matter. Nuclear staining of oligodendrocytes was also seen in MS samples but not in controls.71 Using immunofluorescent and PCR methods HHV-6 DNA has also been found in peripheral leukocytes in the systemic circulation of MS patients.72, 73 However, using PCR methods, others did not found herpes viruses in the peripheral blood or CSF of MS patients.74, 75 Evidence that prior infection with EBV could be related to the development of MS was proposed; however, EBV infects more than 90% of humans without evidence of health problems and 99% of MS patients.76 The difference in MS patients could be the presence of multiple infections, including EBV. Recently Willis et al.77 used multiple molecular techniques to examine MS tissue but failed to find EBV in any MS tissues but could find EBV in CNS lymphomas.
Current reviews and the information above points to an infectious process in MS.47, 48, 75, 76, 78-80 Although a few studies did not come to this conclusion,74, 75 most studies have found infections in MS patients. It is interesting that it is the progressive rather than relapsing-remitting forms of MS which have been associated with chronic infections; therefore, infections might be more important in MS progression than in its inception. Various infections may also nonspecifically stimulate the immune system.47, 48 Infections may also invade immune cells and alter immune cell function in a way that promotes inflammation and autoimmune activity.78 If infections like C. pneumoniae and Mycoplasma species are important in MS, then antibiotics effective against these infections should improve clinical status. Although preliminary, that is in fact what has been seen, but not in all patients.81 As in other neurodegenerative diseases, multiple factors appear to be involved in the pathogenesis of MS.
Alzheimer’s disease
Alzheimer’s Disease (AD) is a family of brain disorders usually found in elderly patients and is the most common cause of dementia. AD is characterized by slow, progressive loss of brain function, notable lapses in memory, disorientation, confusion, mood swings, changes in personality, language problems, such as difficulty in finding the right words for everyday objects, loss of behavioral inhibitions and motivation and paranoia. The course of AD varies widely, and the duration of illness can range from a few years to over 20 years. During this period the parts of the brain that control memory and thinking are among the first affected, followed by other brain changes that ultimately result in brain cell death.82
AD is characterized by distinct neuropathological changes in brain tissues and cells. Among the most notable are the appearance of plaques and tangles of neurofibrils within brain nerve cells that affect synapses and nerve-nerve cell communication. These structural alterations involve the deposition of altered amyloid proteins.83, 84 Although the cause of AD is not known, the formation of the amyloid plaques and neurofibrillary tangles may be due to genetic defects and resulting changes in the structure of beta amyloid proteins. This in turn may be caused by chemicals or other toxic events, inflammatory responses, excess oxidative stress and increases in reactive oxygen species, loss of nerve trophic factors and reductions in nerve cell transmission.83-87
Recently AD brain infections have become important.88-90 For example, one pathogen that has attracted considerable attention is C. pneumoniae.91, 92 As mentioned above, this intracellular bacterium has a tropism for neural tissue, and it has been found at high incidence in the brains of AD patients by PCR and immunohistochemistry.92C. pneumoniae has also been found in nerve cells in close proximity to neurofibrillary tangles.92, 93 Similarly to Mycoplasma species, C. pneumoniae can invade endothelial cells and promote the transmigration of monocytes through human brain endothelial cells into the brain parenchyma.94C. pneumoniae has been found in the brains of most AD patients,91 and it has been cultured from AD brain tissue.95 Injection of C. pneumoniae into mice stimulates beta amyloid plaque formation.96 Although the data are compelling, some investigators have not found C. pneumoniae infections in AD.97, 98
AD patients also have other bacterial infections, such as B. burgdorferi.99 Using serology, culture, Western blot and immunofluorenscence methods this Lyme Disease infection has been examined in AD.100, 101 Not all researchers, however, have found evidence of B. burgdorferi in AD patients.102, 103 The presence of intracellular infections like B. burgdorferi in AD patients has been proposed to be a primary event in the formation of AD beta amyloid plaques. This is thought to occur by the formation of “congophilic cores” that attract beta amyloid materials.104 Multiple reports indicate that AD nerve cells are often positive for B. burgdorferi, indicating that this intracellular bacteria could be important in the pathogenesis of AD.99, 100, 104, 105
The hypothesis in AD that intracellular microorganisms could provide “cores” for the attraction of beta amyloid materials is appealing, but other factors, including the induction of reactive oxygen species, lipid peroxidation and the breakdown of the lysosomal membranes releasing lysosomal hydrolases, are also thought to be important in beta amyloid deposition.105 That infections may be important in AD pathogenesis is attractive; however, some negative reports have not confirmed the presence of infections like B. burgdorferi in AD patients.99-101 This suggests that the infection theory, although compelling, remains controversial.102, 105
Herpes virus infections have also been found in AD,especially HSV-1.106, 107 Previously it was determined that HSV-1 but not a related neurotrophic virus (varicella zoster virus) is present more often in AD brains, and this could be linked to AD patients who have the risk factor ApoE e4 allele.108, 109 HSV-1 is thought to be involved in the abnormal aggregation of beta amyloid fragments within the AD brain by reducing the amount of full-length beta amyloid precursor protein and increasing the amounts of their fragments.110 HSV-1 infection of glial and neuronal cells results in a dramatic increase in the intracellular levels of beta amyloid forms, whereas the levels of native beta amyloid precursor protein are decreased.111 This is similar to what has been found in mice infected with HSV-1, indicating that HSV-1 is probably involved directly in the development of senile-associated plaques. Another herpes virus, HHV-6, has also been found in AD patients, but it is thought that this virus is not directly involved in AD pathogenesis. HHV-6 may exacerbate the effects of HSV-1 in AD ApoE e4 carriers.112
Other infections have been found in AD patients, for example, C. pneumoniae, Helicobacter pylori amongst others.113 It has been proposed that such infections may act as a trigger or co-factor in AD.114 Although experimental evidence that pathogens can elicit the neuropathological changes and cognitive deficits that characterize AD is lacking, this approach may yield interesting and important results. These authors also stressed that systemic infections must be considered as potential contributors to the pathogenesis of AD.114
Parkinson’s disease
Parkinson’s disease (PD) is characterized by akinesia, muscular rigidity and resting tremor.103 In addition, autonomic dysfunction, olfactory disturbances, depression, sensory and sleep disturbances and frequently dementia characterize this disease.115 The pathology of PD indicates a progressive loss of the dopamine neurons of the substantia nigra together with the presence of Lewy bodies and alpha-synuclein. More extensive brain degeneration also occurs, from the medulla oblongata to the cerebral cortex.116, 117
Age-related inclusion bodies and protein aggregations or defects in their degradation characteristically occur in PD, but their role in PD pathogenesis remains unclear.117, 118 Some evidence suggests a relationship between PD and specific genetic changes, such as changes in the genes affecting mitochondria, protein degradation, organelle trafficking and vesicular fusion, and in proteins involved in oxidative stress or antioxidant function.102 Inflammation has also been associated with PD pathology.119
The pathogenesis of PD has been proposed to be due to multiple genetic and neurotoxic events that produce oxidative damage and cell death. In the case of PD the relevant targets of toxic events are neuromelanin-containing dopaminergic neurons of the substantia nigra.118, 120 A case-control study indicated that multiple environmental factors and genetic background were statistically related risk factors for PD.121 Prominent among these were long-term toxic exposures and trauma early in life.122 For example,early life exposure to brain injury, chemicals and/or infections may initiate a cyclic inflammatory process involving oxidative damage, excitotoxicity, mitochondrial dysfunction and altered proteolysis that later in life results in substantia nigra neuron death.123, 124
A role for chronic infections in PD pathogenesis has been proposed.123, 124 One infection found in PD that has aroused considerable interest is the presence of chronic gastrointestinal Helicobacter pylori.125 Indeed, treatment of this infection offers relief to late stage cachexia in PD patients receiving L-dopa.126Helicobacter pylori-infected PD patients showed reduced L-dopa absorption and increased clinical disability,127 whereas treatment of this infection increased L-dopa absorption and decreased clinical disability.128H.pylori may not be directly involved in the pathogenesis of PD, but its systemic presence could affect the progression and treatment of PD, probably by stimulating inflammation and autoimmunity.128
Chronic infections in PD have been linked to inflammation and autoimmune responses.129-131 Experimental models of PD have been developed using neurological viral or bacterial infections to initiate the pathogenic process.132, 133 Spirochetes have also been found in Lewy bodies of PD patients.30 Other infections, such as viral encephalitis,134 AIDS-associated opportunistic infections of the basal ganglia,135 coronavirus,136 among other infections,68, 137, 138 have been found in PD and could be important in stimulating inflammation and autoimmune responses. It has been stressed that additional research will be necessary to establish whether a causal link exists between PD and chronic infections.139
Neurobehavioral diseases
Autism spectrum disorders
ASD, such as autism, Asperger’s syndrome, etc., are neurobehavioral diseases of primarily the young where patients generally suffer from an inability to communicate properly, form relationships with others and respond appropriately to their environment. Such patients do not all share the same signs and symptoms but tend to share certain social, communication, motor and sensory problems that affect their behavior in predictable ways. These patients often display repetitive actions and develop troublesome fixations with specific objects, and they are often painfully sensitive to certain sounds, tastes and smells.140, 141
ASD cases are likely to be caused by multiple factors, including genetic defects, heavy metal, chemical and biological exposures, among other important events, which are probably different in each patient. ASD patients appear to have similarities in genetic defects and environmental exposures that are important in patient morbidity or in illness progression.5-8, 140-142
Chronic infections appear to be an important element in the development of ASD.6, 16, 143, 144 In ASD patients more than 50 different bacterial, viral and fungal infections have been found,6 some apparently more important than others in causing symptoms. It has been known for some time that ASD patients have a number of nonspecific chronic signs and symptoms, such as fatigue, headaches, gastrointestinal, vision problems, occasional intermittent low-grade fevers and other signs and symptoms that are generally excluded in the diagnosis of ASD but are consistent with the presence of infections.143 Indeed, increased titres to various viruses as well as bacterial and fungal infections have been commonly seen in ASD patients.6, 16, 19, 143-145 Not withstanding these reports, epidemiological evidence for an association of childhood infections in the first two years of life and ASD has been mixed.146
Environmental exposures to chemicals and heavy metals also appear to be important in the development of ASD.140, 141, 147, 148 The relationship between ASD and heavy metals may involve the role of multiple vaccines in ASD pathogenesis.130, 141 ASD patients often show their first signs and symptoms after multiple childhood immunizations, and the sharp increase in Autism rates occurred only after the multiple MMR vaccine came into widespread use.141 In some states in the U.S. children receive as many as 33 vaccines before they can enroll in school.140 Such vaccines can contain mercury and other toxic preservatives, and some may also contain contaminating bacteria, as found in veterinary vaccines.149
There are very few studies that have followed the transmission of infections and subsequent autism. Previously we found that veterans of the Gulf War with chronic fatiguing illnesses (Gulf War illnesses, GWI) exhibited multiple nonspecific signs and symptoms similar to chronic fatigue syndrome/myalgic encephalomyopathy (CFS/ME).150, 151 After returning to the home with GWI, their children subsequently became symptomatic, and these children were often diagnosed with ASD.152, 153 Symptomatic children (mostly diagnosed with ASD) were infected with the same Mycoplasma species, M. fermentans, that was found in the veterans and their symptomatic family members, and this was not seen in aged-matched control subjects or in military families without GWI. In the GWI families some non-symptomatic family members did have mycoplasmal infections (~10%), but this was not significantly different from the incidence of mycoplasmal infections in healthy control subjects.152, 153
Subsequently ASD patients who were not in military families were examined for systemic mycoplasmal infections.153 The majority (~54%) were positive for mycoplasmal infections. However, in contrast to the children of GWI patients who for the most part had only M. fermentans, the civilian children tested positive for a variety of Mycoplasma species. We also tested a few siblings without apparent signs and symptoms, and for the most part few had these infections.153 In another study we examined the blood of ASD patients from Central and Southern California and found that a large subset (>58%) of patients showed evidence of Mycoplasma infections compared to age-matched control subjects (Odds Ratio=13.8, p<0.001).19 ASD patients were also examined for C. pneumoniae (8.3% positive, Odds Ratio=5.6, p<0.01) and HHV-6 (29.2% positive, Odds Ratio=4.5, p<0.01). The results indicated that a large subset of ASD patients display evidence of bacterial and/or viral infections (Odds Ratio=16.5, p<0.001).19
ASD patients have been examined for B. burgdorferi infections.154 Various studies revealed that 22-30% of ASD patients (N=76) have Borrelia infections.6, 154 The incidence of Borrelia infections in ASD patients may be related to Lyme disease distribution, with some Lyme-intense areas having high prevalence, and other areas having a low prevalence. Other infections, such as Lyme-associated Bartonella, Babesia, Ehrlichia and non-Lyme-associated CMV, Plasmodium species, Toxoplasma species and Treponema species may also be associated with ASD.6
Final comments to part 1
When neurological symptoms are present, infections of the CNS must be considered. Brain infections can stimulate glial responses, and the presence of viral and bacterial infections in nerve cells, can stimulate autoimmune responses against nerve cell antigens as well as the infections within them.155 For example, in MS some 20 different bacterial and viral infections have been found, but the link between these infections and the pathogenesis of MS is still being debated.16,47, 75 One or even a few types of infections cannot be causally linked to MS, and the reason for this is that there may be too many possibilities. No one infection or a group of infections needs to be the trigger in MS to be important in the pathogenesis of MS. In time combinations of certain infections may eventually be identified at least in a subset of MS patients, and this will allow the development of new therapeutic approaches for many MS patients that are not recognized today.
One problem that is rarely discussed is the apparent disparity between the laboratory results from different laboratories. Often different laboratories cannot agree on types of infections found in various chronic diseases.47 There are a number of reasons for this, including differences in the source of materials, qualities of reagents and techniques used.16 Some procedures, such as PCR, have specific challenges that must be overcome in the handling of specimens, their stability, presence of interfering substances, contamination, sensitivity and specificity of the tests and interpretation of the results. Variability in results from different laboratories will remain a problem unless research groups work closely together to solve these problems. One example of how this has been overcome is a multi-centre research study on the presence of C. pneumoniae in the cerebrospinal fluid of clinically defined, mono-symptomatic MS patients.156Sriram et al.156 conducted this diagnostic trial with good concordance of results between different laboratories. Cooperative studies such as this should eventually alleviate discrepancies in the types of infections found by different research groups.
This review continues in Part 2 with psychiatric diseases, autoimmune diseases, fatiguing illnesses, and other infectious diseases with neurological aspects and an overall discussion of the topic. 157
IntroductionHospital inpatient falls have remained the subject of extensive research and intervention over the past 55 years1. Despite risk factor identification, multiple prediction system developments and harm reducing technologies, the issue of falls remains. The incidence of falls varies between 2.2 and 14 per 1000 patient days 2,3 and increases with age 4. In the UK’s National Health Service, 32% of adverse incident reports are due to falls 2 . In 2007 it reported 200,000 inpatient falls to the National Patient Safety Association 5. Whilst most patients (96%) came to no harm or minor harm, they estimated that over 500 hip fractures and 26 deaths resulted from these falls.Inpatient falls lead to greater morbidity and mortality than equivalent fractures in the community, 6 and they significantly increase the length of stay in hospital7. Apart from physical harm, there are also psychological consequences for patients such as anxiety, loss of confidence, and fear of falling 4. The risk of falls leads to a conundrum in rehabilitative care. Ideally, patients’ mobility, autonomy and dignity must be encouraged and respected - yet slips, trips and falls must be pre-empted often with varying degrees of intrusion and even restraint. In order to selectively target individual patients who would benefit from closer attention, many risk stratification tools have been developed to predict potential fallers. They were developed on a background of over 400 independent risk factors identified with falls 8. The most prominent in the UK are STRATIFY (St Thomas's risk assessment tool in falling elderlyinpatients) and Downton with the recent addition of the Wandering Behaviour Assessment 8. STRATIFY 4 was designed to be used once per week and assesses 5 factors –falls history, patient agitation, visual impairment that limits daily function, frequent toileting, and a transfer or mobility score of 3 or 4 . Each factor scores 1 point and a score greater than 2 was found to have a 92% sensitivity and 68% specificity for a fall in the following week. In the Wandering Behaviour study the STRATIFY criteria results were not reproduced and were found to have only an 82% sensitivity and 34% specificity in their study population 8. Downton 9 also has 5 categories of assessment; falls history, medication subtypes, audio-visual-sensory deficits, mental state (using the Mini Mental State Score <24) and stability of gait. Each category scores 1 point and a score of greater than 3 is considered significant. In the Wandering Behaviour study, when applying the Downton criteria they only found an 82% sensitivity and 36% specificity 8. The Wandering Behaviour assessment looks for the presence of the following :checking, pottering, aimless walking, walking with inappropriate purpose, walking with appropriate purpose but inappropriate frequency, excessive activity, night-time walking, attempts to leave the hospital and being brought back to hospital. The presence of any one of these was found to have a sensitivity of 43% but specificity of 91% 8. Thus, both STRATIFY and Downton are limited by the multi-disciplinary assessments required, so that even when implemented, it is difficult to repeat them on a daily or weekly basis. The Wandering Score is easily repeatable on a daily basis, but lacks the sensitivity of STRATIFY and Downton 8. The aim of this study is to investigate whether changes in a patient’s physiology can be predictive of falls risk, and if so, can they become a useful tool for calculating risk? The reason why we have chosen to investigate this is that many of the commonly encountered risk factors can potentially be reflected in the patient’s routine observations 10. For example, fever could indicate infection and delirium. Hypotension could result from anti-hypertensives, sedatives, or dehydration. Hypertensive states could result from stroke, stress response to infection, or even be a surrogate marker of cardiovascular disease predisposing to arrhythmias. Blood pressure variation could also be predictive since dynamic orthostatic challenges such as lying and standing blood pressure measurements are known to predict falls 10. Thus, by measuring fluctuations in the observations we hypothesised that it may be possible to make an accurate short term prediction of falls riskMethodsSubjectsWe obtained consent for this retrospective study from the hospital’s ethics committee. We based this study in the Acute Medical Unit of our hospital, as it has the largest case mix of patients recently admitted and is therefore most likely to have the largest physiological instability. We aimed to detect a mean difference of 10% in the physiological variability prior to falling with 80% power, p-value < 0.05, and a common standard deviation of 5 %. Our power calculation indicated that we needed to study 12 patients. We identified all the falls in the calendar year of 2008 by examining the records of all the incident report forms submitted by the ward. A total of 33 incident reports related to falls were logged. Two reports related to staff slips and trips and were excluded, and a third incident report failed to adequately identify either the patient’s name, date of birth or hospital number and so had to be excluded. One of the 30 patients fell twice, and this was treated as its own incident as with the STRATIFY paper. The incident report forms were also used to identify the time, nature, and outcome of the fall. Of all the case notes related to the 30 falls requested from medical records, only 13 were available for detailed review. MeasurementsHeart rate (HR), Blood Pressure (BP), Temperature and Respiratory Rates were all recorded and analysed. The PAR (Patient at Risk) Score as calculated by the nursing staff was included too. PAR Scores are validated mechanisms of identifying sick patients who may go on to develop deterioration to the point of requiring Intensive Care. Scores of >3 are associated with a high risk of deteriorating health and are calculated using the routine nursing observations set. Oxygen saturations were not included in this study, as even small deviations tend to be rapidly corrected by staff with oxygen and therefore were not thought to be a useful marker. Recordings of blood pressure and heart rate were all done with ward based equipment. It is impossible to know which machines were used on individual patients as the equipment has varied, both over the course of time, and between multiple wards. However, because the subjects were their own controls, we are confident that the same machine and cuff were used for taking all the 12 hour recordings as each individual machine is allocated to a given bay. Blood pressures were obtained using semi-automatic Dynamap equipment, therefore the readings are in effect calculated from the Mean Arterial Pressure (MAP). We elected to study the systolic readings only, as this represents the maximum perfusion pressure to the brain and carotid sinus. Two of the thirteen patients were known to have undergone orthostatic challenges as part of their admission work up and these were included. Other parameters recorded included the time of the fall, number of medications on the drug chart, whether the fall was observed and any injuries sustained. ControlsWe had two sets of controls. The first set was used to compare the age and gender profile of the fallers to those of the general adult admissions. We had to do this because the official hospital statistics included obstetric and paediatric admissions and comparison would have been inaccurate. We therefore took 4 random days’ of acute adult medical admissions (i.e. over the age of 18) in order to compile an age and gender profile of patients admitted with a ratio of 4:1 (n=110). In order to compare the variability in physiological parameters between fallers and non fallers we generated a second set of controls matched for age (± 5 years) and gender in a ratio of 4 to 1 from a random week’s cohort of patients in February 2009 (for practical purposes). For each matched control, recordings were made at the equivalent length of stay and the controls were not known to have previously fallen. The patients were taken from across the hospital’s medical wards (not Intensive Care or Surgical) with their diagnosis blinded from the investigators. We were able to match 47 of the 52 controls that we were aiming for. Only BP and HR data were recorded in the controls, as we already established that temperature and respiratory rate were not sensitive markers from our faller data. StatisticsOur 13 patients allowed us to reach sufficient statistical power of 80%. Physiological parameters were tested within groups using the Students t-test (paired, two tailed) and when comparing to controls using the Students t-test (unpaired, two tailed). The null hypothesis were rejected when p<0.05. Variability in heart rate, temperature, respiratory rate and PAR (Patient At Risk Score) were calculated using the mean, range and standard deviation between maximum and minimum values. Blood pressure variability was measured by using the maximum and minimum systolic pressure and calculating the mean, range and standard deviation. We have chosen to primarily measure variability by the range as it is a simple calculation that can be done by anyone on a ward. It doesn’t require a calculator nor any detailed knowledge of mathematics. It is therefore an effective and repeatable measure which could be easily implemented as part of a scoring system. Data processing and Statistical Analyses was done in MS Excel 2002 and SPSS v.14. ResultsThe mean age of fallers was 79 years old (SD 16, n=30) and of the acute medical admission controls 67 years old (SD 20, n=110) with p=0.003. The gender distribution of males to females was 63% to 37% respectively for fallers (n=30), but 38% to 62% in general medical take controls (Fishers exact test p<0.001). 54% of fallers (n=13) were admitted from their own home with 31% from Residential Homes and 15% from Nursing Homes. 54% were known to have a preceding falls history (n=13). The timings of the falls showed that 60% of falls occurred between 08.00 and 20.00 (n=30). 77% of falls occurred within 48 hours of admission (n=13). The circumstances of the falls were consistent with the NPSA statistics with 20% falling out of bed, 17% from chair, 17% from commode / toilet, 20% when walking, 3% in the bath and 23% not documented. The significance of the falls as measured by the incident report forms (n=26, in 4 cases not recorded) was 70% under the level of 6 (i.e. low level and did not require further investigation), 13% were over the level of 6 (i.e. were serious and required further investigation) and 17% were unrecorded. Most of the injuries (n=30) were none or minor – 47%, 10% had a head injury and 43% were not recorded. 95% of the falls were not observed. 31% of the patients (n=13) were taking fewer than 4 medications, 38% were taking between 4 and 7 medications and 32% were taking over 8 medications. Comparing the demographic characteristics of our fallers to the age and gender matched controls; average age was 79 for both fallers and controls (p=0.94) and the gender distribution was 7 females : 6 males in the fallers, and 27 females: 21 males in the controls (Fisher’s Exact Test p=1.0). The overall PAR score (n=13) was not sufficiently sensitive to predict falls risk – 77% had no change in their PAR score, 8% had a 1 point change and 15% had a 2 point change ( Table 1). Temperature variation (n=13) was minimal with 69% having less than 1 degree Celsius change and 31% having change of 1 to 1.5 degrees Celsius . Recorded respiratory rate variation was also minor (n=13) with 85% having a maximum change of up to 4 breaths per minute. Table 1. Physiological Parameter Data * denotes p<0.05
Fallers N = 13Mean ± SDRange (x-x)
Controls N = 47Mean ± SDRange (x-x)
PAR Score
1.2 ± 0.6(1 – 3)
PAR Score Variability
0.4 ± 0.6(0 – 2)
Temperature (Celsius)
37.1 ± 0.5(36.4 - 38.1)
Temperature Variability (Celsius)
0.6 ± 0.5(0 – 1.3)
Respiratory Rate (Breaths/Minute)
18.5 ± 1.9(16 – 22)
Respiratory Rate Variability (Breaths/Minute)
1.1 ± 1.5(0 – 4)
Highest Heart Rate (Beats/Minute)
86 ± 13(70 - 110)
86 ± 14(60 -112)
Lowest Heart Rate(Beats/Minute)
71 ± 16(50 -101)
79 ± 14(55 – 110)
*Heart Rate Variability (Beats/Minute)
15 ± 10(0 – 39)
7 ± 7(0 – 27)
Highest Systolic BP (mmHg)
142 ± 22(102 – 180)
140 ± 24(99 – 218)
Lowest Systolic BP(mmHg)
116 ± 19(71 – 150)
129 ± 24(86 – 199)
*Systolic Variability (mmHg)
26 ± 12(2 – 40)
11 ± 7(0 – 26)
In fallers (n=13), the mean highest heart rate was 86 bpm (SD=13) and the mean lowest heart rate was 71 bpm (SD=16). The range was 15 bpm (SD=9.6) with p<0.001. In controls (n=47) the mean highest heart rate was 86 bpm (SD=14) and the mean lowest heart rate was 79 bpm (SD=14). The range was 7 bpm (SD=7) with p<0.001. The significance test when comparing the highest average heart rate between fallers and controls shows p=0.98 showing that they were well matched. The significance test for comparing the variation of the heart rate between fallers and controls is p<0.001. In fallers (n=13), the mean highest systolic BP was 142 mmHg (SD=22) and the mean lowest systolic BP was 116 mmHg (SD=19). The average variation was 26 mmHg (SD=12) with p<0.001. In controls (n=47) the mean highest systolic BP was 140 mmHg (SD=24) and the mean lowest systolic BP was129 mmHg (SD=24). The average variation was 11 mmHg (SD=6.5) with p<0.001. The significance test when comparing the highest average systolic BP between fallers and controls shows p=0.77 showing that they were well matched. The significance test for comparing the variation of the systolic BP between fallers and controls is p<0.001. Charts 1 and 2 show the spread of measurements in the cardiovascular parameters between fallers and controls.
Chart 1. Comparison of the heart rate variation between Fallers and Controls
Chart 2. Comparison of the systolic blood pressure variation between Fallers and Controls
DiscussionThe average age of the fallers was significantly greater than the average age of those admitted to the hospital in general. This is unsurprising considering both mechanical deterioration of the musculoskeletal system with advancing age and the accumulation of disease processes. It is noteworthy that despite making up the smaller percentage of admissions to the hospital, men made up the greater proportion of fallers. Other much larger studies show considerable variability in their gender proportions 11,12, therefore this finding is unlikely to be truly significant. Apart from age and gender, polypharmacy was also a feature of our fallers. This is consistent with other studies 13,14,15. Additionally, our data was consistent with the overall NPSA statistics in terms of the significance and circumstances of the falls 5. The main and novel finding of our study was that fallers were significantly more likely to display a larger range in their cardiovascular observations than the standard hospital population. Whilst it is generally expected that subjects undergoing any routine measurement of heart rate and blood pressure will have a variation in measurements of about 10% over the course of 12 hours 16,17, we found that our fallers had a variation in their heart rate and blood pressure of approximately 20%. This is similar to the dips experienced by the normal population over the course of the night and during orthostatic challenge. This was despite the fact that the baseline measurements of highest value were virtually the same for both populations. Furthermore, almost all the values recorded were within normal limits – and would not normally require specific remedial action to be taken. This could also explain why this risk factor has not previously been identified in other studies. Our study indicates that it is the cardiovascular lability rather than the cardiovascular measurements per se, which acts as an acute predictor of falls. In fact, the sensitivity for falls prediction with either a range of HR values > 15 beats per minute or range of BP systolic values >25 mmHg was 77%. We would therefore expect that when such patients mobilize, the superadded orthostatic challenge would be too great for cardiac output to be suitably matched and so patients are at greater risk of falling. In terms of the 12 hour prospective risk of falling this could certainly explain why a patient with known risk factors will fall during a given nursing shift. Indeed it may also explain why a patient may fall during a hospital admission when patients were, for example, already parkinsonian and arthritic and yet had not previously fallen. Interestingly, neither temperature, respiratory rate, nor PAR Score showed any significant lability in the lead up to the falls. This was surprising as we would have expected them to be predictive of other well known risk factors. The lack of fluctuation in temperature and respiratory rate could provide further evidence that the key short term factor responsible for falls is cardiovascular lability. More detailed analysis showed that it was more likely that these measurements were insufficiently sensitive. Only four of the fallers were admitted with infections, and those subjects showed some temperature fluctuations. However, only 2 had temperatures above 37.5 degrees Celsius, which is consistent with the blunted fever response that is well known to occur in 50% of the elderly population 19,20 (and most fallers were elderly). The lack of value in respiratory rate recordings probably reflects the lack of due care and attention paid to this, the only manually measured parameter. It has long been recognized that respiratory rate recordings tend to be inaccurate 21 . The highly limited range of measurements recorded (16-22 breaths per minute) amongst all the fallers, despite some patients having severe pneumonia, further supports this finding. Finally, the PAR score tended to be quite static. This was a result of its constituent parameters not being sensitive (temperature, respiratory rate) and the fact that most of the heart rate and blood pressure recordings were within normal limits. LimitationsDespite the fact that this study was well powered and statistically significant, ultimately it is quite limited in numbers with just 13 patients. It was disappointing that we were not able to obtain case-notes or the appropriate file in the other 17. We are also presenting calculated data from the MAP measurements, without knowing the exact algorithms being used. For this reason, we analysed the given systolic pressures as further data manipulation would have increased inaccuracies. Our data is taken from relatively acute admissions and as such may not necessarily be applicable to long stay patients, where cardiovascular lability may not play an important role.Furthermore, controls were not matched for diagnosis or for the number of medications taken. This could lead to criticism that the comparison was poor, though the baseline measurements for the two were remarkably consistent. One of our aims was to see if variability could be used to accurately model general falls risk. We therefore thought it would be more useful to study the hospital’s general physiology, in all its varying degrees of illness. ConclusionsThis study shows the value of looking closely at patients’ observations and that even ‘normal’ values have to be interpreted in context . The data supports the finding that the risk of falling at a given point in time relates not only to predisposing factors, but also to their current cardiovascular status. We therefore suggest that a one-off falls risk assessment is no longer appropriate, but should be continuously reviewed on a shift-by-shift basis by nursing staff. This has significant ramifications for modernizing current risk stratification tools so that they are able take this into account.
According to The National Kidney Foundation of The United States of America 1 CKD is defined as (1) evidence of kidney damage based on abnormal urinalysis results (e.g., proteinuria, hematuria) or structural abnormalities observed on ultrasound images or (2) an absolute GFR of less than 60 mL/min for 3 or more months. Based on this definition there are five stages. See Table 1. Anemia affects 60% to 80% of patients with chronic kidney disease (CKD) and reduces their quality of life. Treatment options are blood transfusion, epoietin alfa and darbepoetin alfa 2 . Anemia of CKD is, in most patients, normocytic and normochromic and primarily caused by depressed production of erythropoietin (EPO), oxidative stress and inflammation, erythropoiesis inhibition and reduction in red blood cell survival 3,4,5 . The other cause of anemia is deficiency of iron. The dialysis patient is in a state of continuous iron loss from gastrointestinal bleeding, blood drawing, and/or, most important with hemodialysis (HD), the dialysis treatment itself. HD patients lose an average of 2 g of iron per year. Thus, iron deficiency will develop in virtually all dialysis patients receiving EPO unless supplemental iron therapy is given orally or intravenously. DRIVE study, a randomized trial study, adds direct evidence that administration of intravenous iron to patients with functional iron deficiency who were on supplemental EPO therapy results in increase in the hemoglobin level 6. The aim of this review is to assess that whether Erythropoietin (EPO) treatment is beneficial or harmful in the management of anemia associated with CKD. To address these issues, we have analyzed randomized controlled trials, observational studies and meta-analyses.
Table 1: Stages of CKD according to NKF.
CKD Stage
Kidney damage
GFR
Stage 1
No kidney damage
>90 mL/min
Stage 2
mild kidney damage
60-90 mL/min
Stage 3
moderate kidney damage
30-59 mL/min
Stage 4
severe kidney damage
15-29 mL/min
Stage 5
Endstage kidney damage
<15 mL/mi
Methods:
Search strategy: The search strategy was designed to capture the patient population, suffering from CKD on supplemental erythropoietin (EPO) therapy. Literature search (1989 to 2008) was carried out using MEDLINE, PubMed as well as other electronic databases and in online journals using the keywords "Kidney failure, chronic and "erythropoietin" for studies up to 1996, and "epoetin alfa" for subsequent years.
Selection of studies: All papers identified were English-language, full text papers. In addition, the reference lists of identified relevant articles were also searched. The search was not limited to any specific study design, and we searched for randomized controlled trials (RCTs), observational studies, systemic review and meta-analysis. Citations identified in the literature search were independently screened by author to select potentially relevant articles. The full articles from this list were retrieved and subsequently reviewed by author for inclusion in the systematic review. During selection preference was given to articles published within last five years. Articles were included if they met the following inclusion criteria 1) published in a peer reviewed journal; 2) written in English; 3) reported randomized controlled trials of EPO; 4) observational studies regarding EPO and quality of life; 5) Review articles and meta-analyses about EPO therapy in CKD patients.
Results:
470 citations were identified in search from PubMed, Medline and from other online journals. Of these 470 citations, 444 did not meet the selection criteria and were excluded, leaving 26. Out of 26 citations 11 were RCTs, 10 were observational studies and 5 were reviews and meta-analysis.
Five studies (Parfrey et al7, Foley et al8, Furuland et al9, Drüeke et al10, and Canadian Erythropoietin Study Group11) showed that correction of anemia result in improvement of quality of life, although the singh et al12 showed such improvement with partial correction of anemia, and no detectable difference in the quality of life was evident in Roger et al13 study. Five studies Parfrey et al7, Foley et al8 and Levin et al14 and McMahon et al15 and Roger et al13 showed that normalization of hemoglobin does not lead to regression of established concentric LV hypertrophy or LV dilation. It may, however, prevent the development of LV dilation. In McMahon et al15 study the only factor that seemed to predict normalization of LV mass in patients who had LV hypertrophy at study entry was a lower pulse pressure. One study Sikole et al16 correction of renal anemia can normalize heart morphology and improve heart function. Three studies Besarab et al17, Drüeke et al10 and Singh et al12 demonstrated increased cardiovascular events whereas two studies Drüeke et al10 and Singh et al12 also showed progression to dialysis in patients assigned to the highest hemoglobin targets (>13.0 g/dL), compared with <12 g/dL, trial design of three studies was same in respect that both arms were on EPO. In comparison to Drüeke et al10 and Singh et al12 studies, in Roger et al13 study the renal function was not adversely affected in the group randomized to the higher Hb. (Table 2).
Table 2: Randomized controlled trials (RCTs)
Study
Study design
Patients enrolled
Parameters observed
Outcomes
Parfrey et al7
RCT double blind
596
QoL, LVVI
No change LVVI. QoL improved.
Foley et al8
RCT open label
146
QoL, LVH, LVD
QoL improved, No change LVMI
Furuland et al9
RCT open label
416
QoL, Safety.
QoL improved.
Drüeke et al10
RCT open label
603
CVE, QoL, LVMI, Renal function
QoL improved, No change LVMI.
Canadian Erythropoietin Study Group11
RCT double blind
118
QoL .
QoL improved.
Singh et al12
1432
CVE, QoL, Renal function
QoL not improved.
Roger et al et al13
RCT open label
155
LVMI. Renal function, QoL
No change.
Levin et al14
RCT open label
172
LVMI.
No change.
McMahon et al15
RCT open label
120
Change in LVMI.
Prevention&↓ in LVMI.
Sikole et al16
RCT open label
38
Heart morphology & functions.
Heart function
Improved.
Besarab et al17
RCT open label
1233
Effects of normal HCT.
↑CVE
Both Phrommintikul et al18andGiovanni et al19 addressed the similar issues, to evaluate the benefits and harms of different hemoglobin (Hb) targets in CKD in their meta-analyses. They reached to similar conclusion, increase in the risk of all-cause mortality in anemic patients with CKD in whom a higher Hb target (in the normal physiological range) is aimed for with treatment with EPO. Such patients are also at an increased risk of arteriovenous access thrombosis and poorly controlled hypertension, which could contribute to the increased risk of mortality. Furthermore, there seems to be no beneficial effect on left ventricular mass in such patients. There were similarities and differences in inclusion criteria. Both used the trials targeting different Hb concentrations in patients with anemia caused by CKD, majority of trials analyzed were different except 4 trials which were same in both. The difference in inclusion criteria was that Giovanni et. al analyzed two groups of studies: The first group contained studies in which the intervention was to achieve different Hb targets compared (higher versus lower Hb targets), both arms were on EPO and trials included individuals with clinical cardiovascular disease. The second group compared EPO treatment with no EPO treatment. The results of these two groups of studies were analyzed separately. In Phrommintikul only one group of studies “EPO treatment with no EPO treatment” was analyzed. Meta-analysis by Phrommintikul et alincludes nine RCTs, which enrolled 5143 patients.
In Jones et al20 meta-analysis both randomized controlled trials and uncontrolled trial were analyzed, all studies were of the “pre/post” design, in that measurements of anemia, quality of life, hospitalizations, and transfusions were taken before and after initiation of EPO therapy. They drew these conclusions from 16 published studies of which 5 were randomized clinical trials. He found that treatment with EPO raised hemoglobin levels, reduced transfusion requirements and improved quality of life. For quality of life outcome in these meta-analysis please review Table 3.
Table: 3 Meta-analysis.
Meta-analysis
Question addressed
No of studies included.
Assessed quality of life (QoL).
What measures of quality of life used in these trials.
Were the major gains in QoL seen with EPO.
Phrommintikul et.al18
Target Hb and cardiovascular events in CKD.
9
No
_____
_____
Giovanni et al19
Evaluate the benefits and harms of different Hb targets in CKD.
19
Yes
KDQ
QoL
Improved
↑KDQ
Jones et al20
Effects of
EPO on clinical efficacy, QoL hospitalizations,
and transfusions.
16
Yes
KPS
KDQ
SIP
QoL improved
↑KDQ
↑ KPS
↓SIP
Discussion:
Erythropoietin (EPO) has become an essential part of the management of anemic patients with CKD. It is also used to treat the anemia associated with chemotherapy and other diseases, and it improves quality of life 21,22 . The introduction of EPO in 1989 significantly improved the clinical management of anemia of CKD. By 2005, 99% of incenter hemodialysis patients received EPO treatment for their anemia. EPO dosing has changed dramatically in the past decade and a half; between 1991 and 2005, the mean dose of EPO increased about 4-fold in dialysis patients. Today, EPO therapy is the largest single Medicare drug expenditure totaling $1.8 billion in 2004 (an increase of 17% from 2003) and EPO comprised 11% of all Medicare ESRD costs 23
EPO and left ventricular hypertrophy. Randomized vs. Observational studies. Anemia is a contributing factor in many of the symptoms associated with reduced kidney function. These include fatigue, depression, reduced exercise tolerance, dyspnea.Data from observational studies shows that severe anemia may results in cardiovascular consequences, such as left ventricular hypertrophy (LVH) and left ventricular systolic dysfunction 24. Left ventricular hypertrophy (LVH) is present in nearly 80% of dialysis patients and is associated with higher rates of cardiovascular events 25. It is also associated with an increased risk of morbidity and mortality principally due to cardiac disease and stroke 26,27. As a result, patients with anemia due to CKD are at increased risk of hospitalization, hospital length of stay, reduced quality of life and mortality 28. Uncontrolled studies suggested that partial correction of anemia with EPO therapy may result in prevention or regression of CHF 29 and LVH 30,31. Several randomized controlled trials showed that left ventricular hypertrophy was not further improved by a complete correction of anemia compared to only partial correction 7,13,14,15,17. Robert N Foley et al. randomly assigned 146 patients with either concentric LV hypertrophy or LV dilation to receive EPO to achieve hemoglobin levels of 10 or 13.5 g/dL. He concluded that normalization of hemoglobin does not lead to regression of established concentric LV hypertrophy or LV dilation. It may, however, prevent the development of LV dilation, and it leads to improved quality of life 8. Partial correction of severe anemia <8 or 9g/dl to mild anemia (10-11 g/dL) likely reduces mortality, but further treatment to higher Hb levels has not been shown to further reduce mortality, and has actually increased mortality. Controlled studies with quality of life (QOL) and left ventricular mass as end points support partial correction of hemoglobin in dialysis patients 11,13,16,32, The fact that anemic renal failure patients have more LVH than non-anemic renal failure patients does not prove that anemia causes LVH. Vaziri et al in a review mentioned that the real culprits are oxidative stress, inflammation and diminished biological capacity that simultaneously cause treatment-resistant anemia and adverse cardiovascular and other outcomes 33.
EPO and quality of life:Numerous randomized, controlled trials have demonstrated that EPO significantly raises hemoglobin levels, reduces transfusion requirements, and improves quality of life in anemic patients with chronic renal failure. Lefebvre et al conducted an analysis on data from a multicenter, open-label, prospective study of EPO for anemia in patients with CKD not on dialysis to evaluate the relationship between Hb level and quality of life (QOL). The results showed that the maximal incremental gain in QOL occurred when Hb reached 11 to 12 g/dL. This suggests that treating anemic patients with non-dialysis CKD until their Hb level reaches 12 g/dL will result in the greatest QOL improvement per Hb unit increase 34.
Randomized vs. Observational studies. Many randomized controlled trials suggest an association between higher hemoglobin level and improved quality of life, physical function, and exercise capacity 7,8,9,35 but the association with survival is less clear. Whereas observational studies have generally shown increased survival with higher hemoglobin level 36,37,38,39,40 randomized trials have not shown such benefits. The extent anemia of inflammation varies between patients with renal failure. It is this factor that likely explains the following paradox: in observational studies, higher hemoglobin associates with better survival in CKD, while in controlled trials, higher hemoglobin achieved by escalated EPO dosing decreases survival. In the observational studies, those with the higher Hb levels were likely those patients who had the least component of anemia of inflammation, and therefore less resistant to EPO supplementation; they survived better not because they had better hemoglobin, but because they had less burden of inflammatory disease. Anemia of chronic disease is a highly conserved response that is mediated by multiple mechanisms acting in concert to lower the hemoglobin in the face of inflammation, and should be presumed until proven otherwise to be adaptive for most patients who exhibit it. That this is so is supported by the observation that the correction of anemia confers lower survival not only in renal failure, but also in cancer patients and in patients in the critical care unit.
Jones et al. in their very thorough meta-analysis 20 indeed found that treatment with EPO raised hemoglobin levels, reduced transfusion requirements and improved quality of life. Studies have demonstrated that morbidity and mortality rates are lower when hematocrit values are within the Disease Outcomes Quality Initiative (DOQI) target range (33 to 36%) 40. Ernesto Paoletti et alin their review of observational and randomized studies concluded from the results of observational studies that normalization of Hb in renal patients seems to be associated with further improvement in quality of life and physical activity but with no significant differences in mortality rate, hospitalization rate, and the extent of LVH regression, but the results of randomized trials show that achieving near-normal Hb did not reduce the risk for death from all causes or the risk for cardiac death. The latter risk actually increased slightly, in the group of dialysis patients with normalized Hb concentration 41. For CKD stage 3 and 4 patients, no improvement seen in CHOIR, but improvements reported in CREATE. There may be reporting bias in CREATE as it was an open label study, and the low target arm had to develop worsening anemia prior to initiating EPO therapy 10,12
EPO and Cardiovascular Events:Anemia is a common complication of chronic kidney disease. Determination of the appropriate target hematocrit level for patients undergoing hemodialysis continues to be a controversial area 40. The National Kidney Foundation Dialysis Outcomes Quality Initiative (K/DOQI) states when a decision to use EPO is made, some Hgb value in the range of 11 to 12, but no higher than 13 should generally be chosen. 42. The European Best Practice Guidelines (EBPGs) recommend that most patients with CKD achieve a target hemoglobin (Hb) 11 g/dl to reduce the risk of adverse outcomes 43.Randomized vs. Observational studies. Observational studies have shown a strong association between severity of anemia and risk of morbidity and mortality from cardiovascular disease and other causes in CKD patients 36,37,38,39,40. These findings have been interpreted as evidence for the causal role of anemia in the pathogenesis of adverse outcomes in these patients. On the hand, randomized clinical trials of anemia management revealed either no effect or increased morbidity and mortality in patients assigned to normal hemoglobin Hb targets 10,12,17. Meta- analyses of randomized clinical trials have shown a significant increase in cardiovascular and all-cause mortality and arteriovenous access thrombosis among patients assigned to the higher than those randomized to the lower Hb targets 18,19. Meta-analysis of Phrommintikul shows a significantly higher risk of all-cause mortality (targeting a Hb level higher than 12 g/dL results in a 17% increased risk of death compared with target hemoglobin levels less than 12 g/dL), arteriovenous access thrombosis and higher risk of poorly controlled blood pressure in the higher Hb target group than in the lower target Hb. The incidence of myocardial infarction was much the same in the two groups 18. Meta-analysis of Giovanni F.M et al shows that on the basis of available randomized, controlled trials, Hb targets of <12.0 g/dL are associated with a lower risk of death in the population with cardiovascular disease and CKD compared with Hb targets of >13.0 g/dL. For every 30 patients treated to an Hb target of <12.0 g/dL compared with an Hb target of >13.0 g/dL, approximately one death is avoided 19. Two large randomized controlled trials; CREATE [38] and CHOIR [39] demonstrated increased cardiovascular events and progression to dialysis in patients assigned to the highest hemoglobin targets (>13.0 g/dL), compared with <12 g/dL. US Food and Drug Administration (FDA) warned that use of erythropoiesis-stimulating agents (ESAs) increases mortality and morbidity risk. The warning follows publication of studies suggesting that correction of anemia in patients with CKD did not reduce the risk of cardiovascular events and that reaching a target Hb level of >13 g/dL, compared with a target level of 11.3 g/dL, was associated with increased risk of cardiovascular events. FDA said recent studies had found increased risk of death, blood clots, strokes, and myocardial infarctions in patients with chronic renal disease who received ESAs at higher-than-recommended doses that maintained their hemoglobin levels at more than 12 g/dL 44.
EPO and kidney:EPO has been found to interact with its receptor in a large variety of non-haematopoietic tissues, which result into cytoprotective cellular responses, like mitogenesis, angiogenesis, inhibition of apoptosis and promotion of vascular repair through mobilization of endothelial progenitor cells from the bone marrow. In experimental ischaemic and toxic acute renal failure administration of EPO, promotes renoprotection. Preliminary experimental and clinical evidence also indicates that EPO may be renoprotective in chronic kidney disease22 .EPO is used widely to treat anemia in patients with CKD, but the benefits of EPO use in patients with acute renal failure (ARF) are unclear. In vitro and animal studies suggest that EPO may promote renal recovery and decrease mortality in ARF 45. Partial amelioration of anemia with low doses of EPO was reported to slow the rate of progression to ESRD in a group of CKD patients 46. These cellular protection from EPO observed in animal models has not been confirmed in humans, and has been specifically addressed and disproven in large randomized trial. The CREATE study found as a secondary endpoint that early treatment with EPO increased the likelihood of starting dialysis. CHOIR found no reduction in the rate of progression of CKD in patients given more EPO (the higher target arm) compared to the lower target arm 10,12.
EPO for other Indications:In recent years, studies in animals and humans have focused on the use of EPO for other indications. It has been found to play a role in both cardioprotection and neuroprotection. It has effects on the immune system, and can cause regression in hematologic diseases such as multiple myeloma. It may also improve the response of solid tumors to chemotherapy and radiation therapy 21. Again the cellular protection from EPO observed in animal models has not been confirmed in humans.
EPO and Seizures:Seizures are reported to be a complication of EPO in the product information. However, in a meta-analysis conducted by Giovanni et alshowed that treating with EPO may be protective against seizures Lower Hb targets of <95 g/L in individuals who are not treated with EPO are associated with a significantly increased risk of seizures compared with treatment with EPO and Hb values of >100 g/L 19.
EPO and Hypertension:Administration of ESA may be associated with exacerbation of
hypertension in about 5% of patients. Robert N. Foley et alin his analysis of observational and randomized studies found that most of the trials that have been reported to date have shown that higher hemoglobin targets lead to higher BP levels and/or greater requirements for antihypertensive therapy, he drew this conclusion from nine randomized trials 47. The mechanism of ESA induced hypertension is thought to be related to stimulation of the vascular endothelium by ESA resulting in increased circulating levels of endothelin. Furthermore the increase in hemoglobin associated with ESA therapy may increase blood viscosity resulting in vasospasm. As such routine monitoring of blood pressure is essential in patients treated with ESA 48. Meta-analysis of Phrommintikul et al showed a significantly higher risk of poorly controlled blood pressure in the higher haemoglobin target group than in the lower target hemoglobin 18 . Giovanni et almeta-analysis showed lower Hb levels of <95 g/L with no EPO treatment are associated with a reduced risk of patients who present with hypertensive episodes. In absolute terms, the risk of developing hypertensive episodes is 16% lower with Hb values <95 g/L compared with Hb >100 g/L. For every seven patients treated to obtain an Hb >100 g/L, one patient will require additional antihypertensive medication 19
EPO and Access:Normalizing hemoglobin has been associated with a higher incidence of vascular access clotting 40. Randomized, prospective, open-label trial study of Besarab et al, showed a significantly higher risk of access thrombosis with the higher Hb targe17. Meta-analysis of Phrommintikul et alshowed a significantly higher arteriovenous access thrombosis in the higher Hb target group than in the lower target Hb 18.
EPO and Pure Red Cell Aplasia (PRCA):Although rare, administration of ESA may result in formation of anti-erythropoietin antibodies, thereby leading to pure red cell aplasia and erythropoietin resistance 49 In patients in whom ESA doses have been maximized without effect and no other causes can be identified, serum anti-erythropoietin levels and bone marrow biopsy should be performed. If confirmed, erythropoietin administration should be ceased and the patient treated with periodic blood transfusions.
Conclusion: Achieving hemoglobin control over time is a major challenge because of the various physiological factors that influence the response in individual patients and the potential risk for increased mortality, particularly for patients with co morbidities 50. The association data led to several hypotheses about what anemia was causing e.g. LVH, fatigue, and increased mortality. These hypotheses have been tested in RCT's and in most cases anemia is associated with but does not cause the outcome, such as LVH or mortality. Fatigue is improved somewhat by anemia treatment with EPO, and transfusion frequency is reduced, though the cost is high. In the case of EPO balance is critical. Too little treatment and patients with chronic kidney disease are subjected to a lifetime of exhaustion and blood transfusions. Too much and they could be threatened with an increased risk of death. The overall quality of life is improved when anemia is treated with EPO, but aiming for a target value of 13.5 g of hemoglobin per deciliter provided no additional quality-of-life benefit 12.
Key Points:
Anemia is associated with bad outcomes; Anemia is nearly universal in advanced renal disease. In these patients, anemia is associated with increased cardiovascular morbidity and mortality, reduced quality of life, and accelerated renal disease progression, though those associations do not necessarily establish causation.
Treatment of anemia reduces transfusion requirements and improves quality of life in anemic patients with CKD.
Mortality increases with treatment to higher targets; Recent studies have found an increased risk of death, blood clots, strokes, and myocardial infarctions in patients with chronic renal disease who received ESAs at doses that maintained their hemoglobin levels at more than 12g/dL, leading the Food and Drug Administration to apply a 'black box' warning to the product monographs of licensed ESAs.
Recent studies support partial correction, not normalization of hemoglobin.
Spasticity is a common symptom seen as a consequence of an injury to the brain (stroke, trauma, hypoxia, infection, cerebral palsy and post surgery), spinal cord injury or multiple sclerosis. It is a complex problem, which can cause profound disability alone or in combination with other features of upper motor neuron syndromes (figure 1). The word “spasticity” is derived from the Greek word “spasticus”, which means “To pull or To Tug”. Spasticity is defined1 as “Disordered sensori-motor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles”. Simply stated, spasticity is stiffness of muscles that occurs after injury to the spinal cord or brain. Awareness of the implications and associated symptoms can minimise development of long term secondary complications (table 1). The impact of spasticity can be devastating. If not managed early and appropriately it may result in progressive disability, resulting in secondary complications such as contractures and pressure sores. This significant impact has ensured that spasticity management is a prominent feature in the national management guidelines for long term neurological conditions, promoting coordination of care between primary, secondary and social care providers. Symptoms Spasticity can range from mild muscle stiffness to severe, painful and uncontrollable muscle spasms. It is associated with both positive and negative components of upper motor neuron syndromes. Positive components include muscle overactivity, flexor and extensor spasm, hyperreflexia, athetosis, spastic dystonia, clonus, and an extensor plantar response. Common negative symptoms comprise weakness/ paralysis, early hypotonia, fatigue and loss of dexterity. Spasticity can be distinguished from rigidity by its dependence on the speed of muscle stretch and characteristic distribution in antigravity muscle groups. Spasticity does not always cause harm and can occasionally assist in the rehabilitation process by enabling a patient to stand when their limb weakness would not otherwise allow it Table 1 Clinical and functional problems associated with severe Spasticity
Physical
Emotional / social
·Non- specific pain·Discomfort·Painful muscle spasm·Difficulties with activities of daily living. e.g. washing, dressing, eating, toileting, maintaining hygiene, sexual activity·Problems with posture and mobility·Physical deformity and longterm contracture·Pressure ulcers
·Emotional e.g. low mood, distorted self image, impaired motivation·Impact on fulfilment of life roles as a partner or a parent·Sleep disturbance – due to pain and discomfort·Vocational- impact on employment or education·Social isolation – due to restricted mobility
Figure 1 Vicious cycle of spasticity Assessment of spasticityBefore any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale
4 Rigid extremity 3 Loss of full joint movement, difficult movement, considerable tone2 Full joint/ limb movement, but more increase in tone, limb still easily moved.1+ Slight increase in tone, catch and resistance through out range of movement1 Slight increase in tone, catch or minimal resistance at end of range of movement0 no increase in tone
It is also important to remember that not every “tight” muscle is spastic. The clinically detectable increase in muscle tone may be due to spasticity, rigidity or a fixed muscle contracture.Management The key to successful spasticity management is education of the patient and carers with both verbal and written information. This allows them to understand, appreciate and be fully involved in the management plan. All patients with spasticity should be followed up by a coordinated multidisciplinary team, which allows more timely intervention and close monitor of the progress. Liaison between health and social services in both primary and secondary care is essential in long term management. This helps to deliver a more consistent approach to the individual over time (figure 2). Table 3 Aims of spasticity management.
1.Improve function- mobility , dexterity2.Symptom relief-· Ease pain- muscle shortening, tendon pain, postural effects· Decrease spasms· Orthotic wearing3. Postural- Body image4. Decrease carer burden- Care and hygiene, positioning, dressing5. Optimise service responses- to avoid unnecessary treatments, facilitate other therapy, delay/prevent surgery
The first step in the management of spasticity is to identify the key aims and realistic goals of therapy. Understanding the underlying pathology and possible prognosis is helpful in planning these goals (table 3). Other key points to consider are: · Identification and management of any trigger or aggravating factors-Initial assessment should exclude any co morbidity that may worsen spasticity such as pressure sores, chronic pain, infection (commonly urinary tract infection), constipation or in-growing toe nails.· Instigation of an effective and realistic physical programme including attention to posture and positioning Figure 2 Approach to spasticity assessmentComprehensive assessment of spasticityRecognition of underlying provocative factorsImpact on the individualMeasurement of spasticityPotential goals- individualised and person focussed Initial approachEducation to patient/ and their family /carersMultidisciplinary team assessmentIdentification of clear treatment goalsEstablish mechanism for monitoring and review Management Manage triggering factorsBalance between positioning and movementPosture and seatingPhysical therapy and active exercise programmeSplinting and use of orthoticsPharmacotherapy A) Physical modalities· Stretching- this intervention has the benefit of being benign and non-invasive. Maintaining muscle length through passive or active exerciseand stretching regimens including standing or splinting canbe key to managing spasticity both in the short and the longterm.· Cooling of muscles- this inhibits mono synaptic stretch reflex and lowers the receptor’s sensitivity, different techniques such as quick icing and evaporating spray like ethyl chloride are occasionally used.· Heat-heat may increase the elasticity of the muscles. Techniques used include ultrasound, fluidotherapy, paraffin, superficial heat and whirlpools. These techniques should be combined with stretching and exercise.· Orthosis/equipment/ aids – an orthosis or splint is an external device designed to apply, distribute or remove forces to or from the body in a controlled manner to control body motions and /or alter the shape of body tissues. E.g. ankle foot orthosis, insoles, ankle supports, wrist/ hand/ elbow splints, knee splints, spinal brace, hip brace, neck collar. Some equipment can also aid positioning e.g. T roles, wedges, cushions and foot straps.These are usually used in combination with other modalities like botox therapy. Attention to posture and positioning, whichmay include the provision and regular review of seating systems,is paramount in managing severe spasticity· Massage– althoughvarious techniques are in use there is no evidence to support this· Dynamic physiotherapy technique- many schools of physiotherapy claim that particular technique has antispastic and functional benefits, particularly for the more mobile person. E.g. Bobath technique, proprioceptive neuromuscular facilitation, Brunnstrom technique. B) Electrical therapy· Functional Electrical stimulation –Thisis an adjunct to physiotherapythat can be of benefit to selected individuals who are predominantlyaffected by upper motor neuron pathologies resulting in a foot drop. Randomised controlled trial by Burridge et al in patients following stroke found that the use of functional electrical stimulation in combination with physiotherapy was statistically superior to physiotherapy alone3· Transcutaneous electrical nerve stimulation – this has been found to reduce spasticitythrough its nociceptive action and reduction of pain.C) PharmacologicalMedicationshould always be used as adjunct to good general management and education. Identification of treatment goals will help optimise drug therapy not only in terms of choice of agent, but also in timing and dose. Aims of medication should be to improve function or relieve troublesome symptoms rather than to simply reduce the degree of spasticity. Table 4 Useful things to remember to optimise medication effects
1. Clear written/verbal information for patients about effects/adverse symptoms of drugs 2. Clear treatment goals3. Detailed drug history- Review of other medication and potential drug interaction4. Appropriate form of drug e.g. liquid preparation if swallowing difficulties5. Regular review of efficacy and side effects6. Aids to help administer drugs e.g. dossette box, timer to remind7. “Start low and go slow” to avoid deleterious effects on function or unwanted side effects8. Combination of drugs to obtain synergistic action
Table 5 Different methods of delivery of medication
·Enteral – orally or via PEG e.g. baclofen, benzodiazepins, dantrolene, clonidine, tizanidine, gabapentin·Transdermal system e.g. catapress TTS·Intrathecal e.g. baclofen pump (other drugs used alone or in combination intrathecally include clonidine, morphine, fentanyl, midazolam, lidocaine)·Intra muscular/ focal injection e.g. botulinum toxin·Nerve blocks e.g. Phenol, Ethanol
The oral agentsAlthough different categories of drugs are available, those most commonly used to treat spasticity are baclofen,tizanidine, benzodiazepines, dantrolene, and gabapentin4, 5, 6. Different agents act through different mechanisms (table 6 and 7) for e.g. GABA-like (baclofen, benzodiazepine), central alpha 2 agonists (tizanidine, clonidine) and peripheral anti-spastics (dantrolene). Antispastic drugs act in the CNS either by suppression of excitation (glutamate), enhancement of inhibition (GABA, glycine) or a combination of the two. Table 6 Mechanism of action of commonly used oral antispasticity medication
Drugs acting on
Drugs
GABA- ergic system
baclofen, benzodiazepines, piracetam, progabide
Ion flux
dantrolene sodium, lamotrigine, riluzole
Monoamines
tizanidine, clonidine, thymoxamine, beta blockers, and cyproheptadine
Excitatory amino acids
orphenadrine citrate, cannabinoids, inhibitory neuromediators and other miscellaneous agents.
Baclofen remains the most commonly used anti-spastic agent. The preferential indication is spasticity caused by spinal cord disease especially in multiple sclerosis. Many studies including the pilot study by Scheinberg et al 7 demonstrated that oral baclofen has an effect beyond placebo in improving goal-oriented tasks (such as transfers), in children with spastic quadriplegic cerebral palsy. In open-label studies of oral baclofen, the drug improved spasticity in 70-87 per cent of patients; additionally improvement in spasms was reported in 75-96 per cent of patients. In double-blind, crossover, placebo-controlled trials, baclofen was reported to be effective, producing statistically significant improvements in spasticity8.The main adverse effects of oral baclofen include sedation or somnolence, excessive weakness, vertigo and psychological disturbances. The incidence of adverse effects is reported to range from 10 to 75 per cent. The majority of adverse effects are not severe; most are dose related, transient and/or reversible. The main risks of oral baclofen administration are related to withdrawal; seizures, psychic symptoms and hyperthermia. These symptoms improve after the reintroduction of baclofen, usually without sequelae. When not related to withdrawal, these symptoms mainly present in patients with brain damage and in the elderly. The limited data on baclofen toxicity in patients with renal disease suggest that administration of the drug in these persons may carry an unnecessarily high risk. Tizanidine is an efficient and well tolerated antispastic. It is predominantlyan alpha 2 agonist and thus decreases presynaptic activity of theexcitatory interneurones. There is a large body of evidence for the effective use of tizanidine monotherapy in the management of spasticity 15. Tizanidine is the antispasticity drug that has been most widely compared with oral baclofen. Studies have generally found the two drugs to have equivalent efficacy, although tizanidine has better tolerability; in particular weakness was reported to occur less frequently with tizanidine than with baclofen.Dantrolene has a peripheral mechanism of action and acts primarily on muscle through inhibitingcalcium release from the sarcoplasmic reticulum. It decreasesthe excitation–coupling reaction involved in muscle contraction and can be prescribed in the different forms of spasticity. The efficacy of benzodiazepines (diazepam, tetrazepam, clonazepam) is comparable with baclofen. Although there is no evidence to suggest any difference in effectiveness between them, diazepam and dantrolene are associated with more side effects than baclofen and tizanidine. There are other compounds with anti-spastic properties (gabapentine, cyproheptadine, piracetam). Their advantage is
Table 7
Drug
Dosage
Doses per day
Mechanism of action
Common side effects
Initial dosage
Maximum dosage
Baclofen
5mg x3
90mg
4
GABA ergic
Seizure, Sedation, Dizziness, GI disturbances, psychosis, Muscle weakness
rather limited when used alone. Generally, they are administrated in combination with usual anti-spastic drugs. A few short term trials have trialed gabapentin with good results 19 .Pregabalin may be of value as a systemic agent in the treatment of spasticity, although properly controlled studies with clearly defined outcome measures are required to confirm this finding 22. The Sativex Spasticity in MS Study Group23 concluded that oromucosal whole plant cannabis-based medicine (CBM) containing delta-9 tetrahydrocannabinol (THC) and cannabidiol (CBD) may represent a useful new agent for treatment of the symptomatic relief of spasticity in MS. Intrathecal pump· Baclofen- If oral drug treatment is inadequate in controlling lower limb spasticity or is not tolerated, intrathecal delivery of baclofen should be considered. This has been found to be a cost-effective strategy when compared to conventional medical management alone by Bensmail et al 20 .The benefits of continuous intrathecal baclofen infusion have been demonstrated in more than 80 percent and over 65 percent of patients report an improvement in tone and spasms respectively. The main risks of intrathecal baclofen infusion are symptoms related to overdose or withdrawal. These are mostly related to catheter disruption, failure to refill the pump reservoir or failure of the pump's power source. Abrupt disruption of intrathecal baclofen can be a serious scenario with continuous spasms, tremors, temperature elevation, seizure and death having been reported.· Phenol- As phenol is a destructive agent which indiscriminately damagesmotor and sensory nerves, it is reserved for those individualswho do not have any functional movement in the legs, who havelost bladder and bowel function and who have impaired leg sensation. Intrathecal phenol can be an effective treatmentwhich, though it requires expert administration, does not havethe long term maintenance or cost issues that are associated with intrathecalbaclofen treatment. The effect of a single injection often lastsmany months and can be repeated if necessary 24. D) Nerve blockPeripheral nerve blockade/ Regional blocks/ Neurolytic blockade25 are another therapeutic possibility in the treatment of spasticity. This can be done with the help of fluoroscopy or nerve stimulation. Chemical neurolysis by phenol/ alcohol is irreversible and can be used at several sites. Blocks are applied most often to 4 peripheral sites: the pectoral nerve loop, median, obturator, and tibial nerves. The main indication is debilitating or painful spasticity. Peripheral blocks with local anaesthetics are used as tests to mimic the effects of motor blocks and determine their potential adverse effects. Peripheral neurolytic blocks are easy to perform, effective, and inexpensive30.E) Botulinum toxin injectionBotulinum toxin is the most widely used treatment for focal spasticity27,28,29. The effect of the toxin is to inhibit the release of acetylcholine at the neuromuscular junction. The clinical effect of injecting botulinum toxin is reversible due to nerve sprouting and muscle reinnervation, leading to functional recovery of the muscle in a few months. It is essential that botulinum toxin injections are given in conjunction with physiotherapy in order to obtain the maximum benefit. The toxin is injected directly into the targeted muscle and an effect can be noticed from as early as 2-3 days with a maximum effect seen by about 3 weeks, lasting at least 3 months. As it is not a permanent treatment it may have to be repeated after a few months.Many randomisedcontrolled trials show that botulinum toxin is effectivein reducing muscle tone in various conditions 28, 29. Brashear and colleaguesdemonstrated a reduction in spasticity in the wrist andfingers of patients following stroke with the use of botulinum toxin, together with an improvementin their disability assessment scale29.E) Surgical techniqueMost surgical procedures are irreversible. This means that realistic goal setting between the health care provider, family and patient is critical. Neurosurgical techniques have been proven useful in conditions like cerebral palsy 32, 33.· Neurosurgical techniques- Anterior and posterior rhizotomy, peripheral neurotomy 31, Drezotomy, percutaneous radiofrequency rhizotomy, spinal cord and deep cerebellar stimulation of the superior cerebellar peduncle 32, functional neurosurgery 33· Orthopaedic procedures- directly act on muscles and tendons e.g. lengthening operation, tenotomy, neurectomies, and transfer of tendons.
Key Points to remember1.Spasticity management is more effective in multidisciplinary settings2.Early multidisciplinary approach and goal setting is crucial3.Education and clear communication between patients, carers and health care providers is essential4.Early intervention and optimal therapy prevents long term complications.5.Focal spasticity responds well to botulinum toxin injection, while generalised spasticity needs oral/ intrathecal medications
The acquired immunodeficiency syndrome (AIDS) was first recognized among homosexual men in the United States in 19811,2. While initially limited, infection with the human immunodeficiency virus (HIV) has immensely increased over the past two decades to become the biggest epidemic of the twentieth century. However, we have witnessed dramatic improvement in prevention of disease progression and long-term survival in the era of Highly Active Anti Retroviral Therapy (HAART).
Apart from biological factors associated with the virus and host which play a role in the transmission and progression of HIV infection, several demographic and social variables have been studied and described in different studies worldwide. Understanding the variety of non-biological factors and behavioral patterns which can affect care and prognosis of HIV patients gives us the opportunity to design non-pharmacological interventions and where possible, to facilitate better care for our HIV positive population.
BACKGROUND:
J.E. Wood clinic of Pennsylvania Hospital in Philadelphia is a teaching outpatient care facility where Internal Medicine residents of Pennsylvania Hospital acquire their ambulatory care experience under supervision of teaching attendings. We have once a week clinic sessions dedicated to the care and follow-up of HIV/AIDS patients under close supervision of Infectious Disease specialists. Our patients have diverse socio-economic, educational and stages of HIV infection.
OBJECTIVE:
We aimed at finding out basic understanding of HIV infection, degree of awareness regarding the ongoing treatment and reasons behind irregular follow-up visits of our HIV patients who attend J.E. Wood outpatient clinic of Pennsylvania Hospital, Philadelphia for treatment of HIV/AIDS.
PARTICIPANTS AND METHODS:
In order to collect relevant information from our patients, a two paged, anonymous, study questionnaire was given to all patients who attended the clinic during January 2007 to December 2007. The questionnaire looked into three different areas of patient related factors which can influence the disease outcome: demographic and social information (Age, Sex, level of education), patients’ knowledge about their HIV disease (source of the infection, duration of HAART, individual recent CD4 count, names of current medications, duration of therapy, medication side-effects) and their behavior (sexual precautions, reasons for medication and follow-up non-compliance). Out of the 75 patients who were given the questionnaire, 7 questionnaires were rejected from the study because of the information received was incomplete, illegible or not related to the questions. 68 completed questionnaires were evaluated and comparative data was tallied using Microsoft excel sheet. We also reviewed relevant literature in pubmed to understand our findings in the light of previous studies related to demographic, socio-economic and psychological aspects of HIV treatment.
RESULTS:
We analyzed the information which was obtained from 68 patients by means of the questionnaire. Our patients consisted of 35 male, 33 female (Table 1). We had a wide range of patients regarding distribution of their age as shown in Table 2 below. Significant numbers of our patients (36%) were diagnosed with HIV for >10 years ago and more than 60% had the diagnosis at least for 5 years (Table 3)
Table 1: Socio-demographic characteristics of patients (n=68)
Variables
Percentage
Gender
Male
51.5%
Female
48.5%
Education
<High school
34%
High school graduate
50%
>High school
16%
Table 2: Age distribution of patients (n=68)
Age group
Percentage
Upto 30 years
19%
31 to 40 years
22%
41 to 50 years
37%
51 to 60 years
18%
61 years and above
4%
Table 3: Duration of diagnosis (in years)
Duration of
diagnosis (years)
Percentage of
total patients (n=68)
Unknown
3%
< 5
36%
>5 to 10
25%
>10
36%
Half of our patients (n= 68) completed high school education or equivalent. About 34% quit education before attaining high school diploma. Roughly, 10% of our patients went to college for further education and 6% acquired some vocational training after high school.
We tried to establish the level of our patients’ participation in their treatment by gathering information through the questionnaire whether they could recall the names of their HIV medicines and the last CD4 count. We found that 74% of our patients, who are on HIV medicines, could recall the names of their medicines but only about 45% of our patients remembered their last CD4 count. Our patients who had completed high school education or equivalent were 2.5 times more likely to remember the names of their HIV medications(95 % confidence interval CI=1.42 to 4.98) and 1.75 times more likely to remember their last CD4 count(95 % confidence interval CI=1.12 to 4.38).
We asked our patients whether they knew that HIV medications need to be taken life long and we also enquired about their knowledge about their safe sexual practices. Only 48% patients of our study group knew that HIV medicines are for life. About 50% of all our patients mentioned that they ensure use of condom during sexual activity and another 40% claimed they practice sexual abstinence. Women patients in our practice were 2.0 times more likely to practice use protective measures during sexual activity (95 % confidence interval CI=1.22 to 4.67).
In our study, only 32 patients (47%) attempted to answer the question where we asked about reason behind not turning up for their follow up appointments as scheduled. Eight patients could not specify a cause, 7 mentioned transport related problems and 2 had insurance issues. Five patients thought their appointments were too often whereas 3 just forget to keep the appointment. Although we did not specifically ask questions on psychological state of our patients, 7 out of the 32 patients mentioned significant psychological problems in their daily life as the reason for non-adherence to medication or follow-up appointments. The responses included responses like “still dealing with the diagnosis mentally”, “feel lack of energy in life”, “life seems to have too many problems”, “been drinking heavy lately” etc.
DISCUSSION:
Interestingly, our small patient cohort roughly reflects the sex ratio of HIV patients globally in 2007 as published by World Health Organization (WHO). In our study the ratio was Male : Female = 51.5% : 48.5% and in the WHO worldwide survey it was 50% : 50%; At the end of 2007, estimated total global HIV positive adults = 33 million (30million – 36 million) 3.
Rates of progression of HIV disease appear to be similar by sex and race category if adjusted for the quality of care 4, 5. Multiple studies on chronic disease management showed that patients’ level of education and health literacy has direct influence on the treatment compliance. Moreover, limited health literacy is thought to be a strong contributing factor to racial disparities in health care. A study was published in 2007 which examined the mediating effect of limited health literacy on the relationship between race and HIV-medication adherence. For the study, a total of 204 patients infected with HIV were recruited and structured in-person interviews were conducted to obtain information. In an adjusted analysis that excluded literacy, African Americans were 2.40 times more likely to be non-adherent to their HIV-medication regimen than whites (95% confidence interval [CI]=1.14-5.08). When literacy was included in the final model, the effect estimates of race diminished from 25% to insignificant level. Therefore, health care providers need to consider the potential utility of responding to literacy and communication barriers in health care as part of interventions to reduce racial disparities 6. In our study, we found that patients who had completed high school education or equivalent were more conscientious regarding their HIV care as demonstrated by the fact that they were more likely to remember their last CD4 count and current HIV medications.
Multiple studies have demonstrated that increasing age at the time of HIV infection is associated with more rapid progression to AIDS in the absence of antiretroviral therapy. In one series, for example, the median time from seroconversion to AIDS without therapy was 15 years for patients aged 16 to 24 years at seroconversion, compared to 6 years for those 35 years or older at seroconversion 7. In our study, it is notable that 36% of patients were diagnosed with HIV >10 years ago and more than 60% had the diagnosis at least for 5 years. The reason behind the high survival rate is clearly attributable to HAART. Fifty-four patients out of the 68 are currently on HAART and 25 of them are on it for more than last 5 years.
Patients' knowledge of their HIV condition and its treatment has been recognized as a factor that influences adherence to antiretroviral therapy. Patients’ knowledge & perception of the disease and participation in the treatment can be improved through targeted educational programs and support groups. One study done in Nigeria found that individuals living with HIV/AIDS who belonged to a support group and had availed themselves of relevant literature were more knowledgeable and positive about their illness than those who did not belong to support groups. The study concluded that HIV/AIDS support group membership is an important component of psycho-social care in HIV/AIDS patients 8. Another study done in France showed that an educational intervention improves adherence to antiretroviral regimens and health status and suggests that it should be initiated early in therapy 9. Communicating with patients about adherence issues is important issue, although this may not have an immediate impact on patients' behaviors. Health care professionals should play a pro-active role in this regard. The use of multi-disciplinary adherence teams to ensure that each HIV-positive patient receives the optimal amount of information and support for adherence is a practical approach. Health literacy should be provided in the context of different ethnicity, culturally sensitivity and individual needs associated with HIV, like any other chronic diseases. Epidemiological researches have shown that injection drug abusers and younger patients tend to have worse compliance, as well as subjects with depression and lack of self-perceived social support 10. Therefore, special care should be taken by health care providers to ensure treatment compliance and health literacy in these patients. In our J.E. Wood clinic, we have dedicated psychologist and social worker to for care of our HIV patients.
Psychological impact associated with treatment of any chronic illness is often neglected in clinical practice but indeed carries a huge significance in terms of long-term treatment compliance and outcome. We identified 7 of our patients who clearly expressed psychological issues related to their HIV infection and it was evident enough that those psychological problems were adversely affecting their treatment compliance. Formal and regular counseling sessions should be arranged for HIV/AIDS patients to promptly identify and manage any psychological or psychiatric disturbance that HIV patients might suffer from. We know that presence of a preexisting psychiatric disorder can increase the risk of HIV acquisition and can also complicate HIV treatment. Moreover, HIV infection can produce a number of psychiatric conditions and exacerbate many others; there is an intense co-morbidity and linkage between HIV and various types of psychiatric conditions. Personality disorders are more prevalent among HIV-infected (19 to 36 percent) and HIV at-risk (15 to 20 percent) individuals 11, 12 than the general population (10 percent). Antisocial personality disorder (ASPD) is the most common personality disorder among HIV infected individuals, and has been shown to significantly increase risk of HIV infection 13. Successful treatment can be achieved with even the most difficult patients by applying a comprehensive diagnostic formulation that includes psychiatric disease syndromes such as major depression, personality vulnerabilities, behavioral disorders such as addiction, and problems of life experiences such as trauma. With regards to anti-retroviral treatment of HIV positive or AIDS patients, nearly perfect compliance seems to be indispensable to obtain the maximum benefit from HAART. There is a clear relation between high adherence levels and virologic success. We reviewed relevant published literatures to understand the adverse effects and possible interventions of psychological problems in HIV patients. A prospective, randomized, two-arm controlled study was published in 2000 which included 116 patients starting their first-or second-line HAART who were randomized to receive psychoeducative intervention to implement adherence (experimental group [EG]) or a usual medical follow-up (control group [CG]). The study showed that specific and maintained psychoeducative interventions based on excellence on clinical practice are useful to keep high levels of adherence and therefore, high levels of viral suppression 14.
CONCLUSION:
Human Immunodeficiency Virus infection is one of the most serious disease entities in our modern time. We have witnessed dramatic improvement of long-term survival rate of HIV positive patients due to use of HAART in clinical practice. By identifying the demographic, socio-economic, behavioral and psychological variables which significantly influence patients’ adherence to treatment and understanding of the disease process, we can further improve treatment compliance and the long term prognosis of our HIV patients. These factors may not have very significant role individually, but collectively can dictate the course of success of HAART treatment in patients. Increasing awareness of these factors by practitioners caring for HIV-infected persons, recognizing and potentially treating some of them, should indirectly improve the effectiveness of antiretroviral therapy.
COMPETING INTERESTS None Declared AUTHOR DETAILS SUBHASISH BOSE, M.B.B.S., M.R.C.P, PGY1 in Internal Medicine, Pennsylvania Hospital, Philadelphia, USA. AJAY VARANASI, M.B.B.S.; PGY3 in Internal Medicine, Pennsylvania Hospital, Philadelphia, USA. GYI MO, M.B.B.S., M.P.H.; Director of J.E. Wood clinic, Pennsylvania Hospital, Philadelphia, USA. CORRESPONDENCE: DR SUBHASISH BOSE, Apartment 601, 269 South Ninth Street, Philadelphia, PA-19107, USA. Email: kumub@yahoo.com
Kaposi's sarcoma and Pneumocystis pneumonia among homosexual men--New York City and California. MMWR Morb Mortal Wkly Rep 1981; 30:305.
Status of the global HIV epidemic. http://data.unaids.org/pub/GlobalReport/2008/jc1510_2008_global_report_pp29_62_en.pdf. Accessed January 31, 2009.
Collaborative Group on AIDS Incubation and HIV Survival including the CASCADE EU Concerted Action. Time from HIV-1 seroconversion to AIDS and death before widespread use of highly-active antiretroviral therapy: a collaborative re-analysis. Lancet. 2000 Apr 1; 355(9210):1131-7.
Altisent, C, Montoro, JB, Ruiz, I, Lorenzo, JI. Long-term survivors and progression of human immunodeficiency virus infection. N Engl J Med 1996; 334:1065.
Osborn CY, Paasche-Orlow MK, Davis TC, Wolf MS. Health literacy: an overlooked factor in understanding HIV health disparities. Am J Prev Med. 2007 Nov; 33(5):374-8.
Mariotto, AB, Mariotti, S, Pezzotti, P, et al. Estimation of the acquired immunodeficiency syndrome incubation period in intravenous drug users. Am J Epidemiol 1992; 135():428.
Olley BO. The role of support group and duration of infection in HIV/AIDS patients' knowledge and attitudes to their illness. Afr J Med Med Sci. 2007 Mar; 36(1):11-6.
Goujard C, Bernard N, Sohier N, Peyramond D, Lançon F, Chwalow J, Arnould B, Delfraissy JF. Impact of a patient education program on adherence to HIV medication: a randomized clinical trial. J Acquir Immune Defic Syndr. 2003 Oct 1; 34(2):191-4.
Gordillo V, del Amo J, Soriano V, González-Lahoz J. Sociodemographic and psychological variables influencing adherence to antiretroviral therapy. AIDS. 1999 Sep 10; 13(13):1763-9.
Sher, KJ, Trull, TJ. Substance use disorder and personality disorder. Curr Psychiatry Rep 2002; 4:25.
Jacobsberg, L, Frances, A, Perry, S. Axis II diagnoses among volunteers for HIV testing and counseling. Am J Psychiatry. 1995; 152:1222.
Perkins, DO, Davidson, EJ, Leserman, J, et al. Personality disorder in patients infected with HIV: a controlled study with implications for clinical care. Am J Psychiatry. 1993; 150:309.
Tuldrà A, Fumaz CR, Ferrer MJ, Bayés R, Arnó A, Balagué M, Bonjoch A, Jou A, Negredo E, Paredes R, Ruiz L, Romeu J, Sirera G, Tural C, Burger D, Clotet B. Prospective randomized two-Arm controlled study to determine the efficacy of a specific intervention to improve long-term adherence to highly active antiretroviral therapy. J Acquired Immune Deficiency Syndrome. 2000; 25(3):221-8.
Hepatitis B is one of the world’s major health problems 1. By recent estimates, worldwide more than 2 billion people have been infected with hepatitis B virus (HBV) globally and more than 350 million have chronic (long term) liver infections2. The infection is supposed to be causally related to 1 to 2 million deaths per year worldwide 3. Hepatitis B is a blood borne infection that is transmitted 1) by an infected mother to the newborn, 2) by contact with infected blood through unsafe injection, transfusion, open wounds, and sharing toothbrush or razors, and 3) by unprotected sex. Approximately 90% of newborns infected with HBV develop chronic infection, whereas 30-50% of children under age 5 years, 10% of adolescents aged 15 years, and 2-5% of older individuals develop chronic infection 4,5.
In Pakistan, it is Hepatitis (B & C) not Human immuno deficiency virus (HIV) that is the most common serious viral infection. Number of hepatitis B carriers in Pakistan is estimated at around seven million4 that is about 5% of the world wide 350 million carriers of hepatitis B 5. Unlike HIV, there was no large-scale national awareness campaign to educate the public and healthcare professionals in Pakistan about these infections before 2006, but now a comprehensive national strategy that will lead to the elimination and control of hepatitis B is becoming a top public health priority in Pakistan after inclusion of HBV immunization in government’s expanded Program for Immunization (EPI). The World Health Organization (WHO) Assembly endorsed the recommendation of its Global Advisory Group that all countries should implement a hepatitis B immunization program6. The threat of HBV to the health of the nation is frequently under-recognized by epidemiologists, policy makers and the public because unlike the influenza virus, it is often not the acute infection that makes people sick, but the consequences of chronic HBV infection that occurs after 20-30 years. Fortunately, hepatitis B is a vaccine preventable disease, global eradication is therefore possible if everyone worldwide receives the HBV vaccine before they become infected. Despite advances in antiviral therapy, only a minority of patients with chronic hepatitis B will have a sustained response. Thus, primary prevention by vaccination to increase herd immunity remains the main thrust in the control of HBV infection.
The development of hepatitis B vaccine is considered to be one of the major achievements of modern medicine. Three different classes of hepatitis B vaccine are available based upon how they are derived (from plasma, yeast, or mammalian cells).The first generation HBV vaccine was prepared by concentrating and purifying plasma from Hepatitis B surface antigen (HbsAg) carriers to produce 22 nm sub viral particles, which contain HBsAg alone. Derivation from plasma has left lingering concerns regarding the potential to transmit blood-borne infections, although this vaccine has excellent efficacy and safety7. Yeast-derived recombinant HBV vaccines were first introduced in the mid 1980s. They are produced by cloning of the HBV-S gene in yeast cells. These vaccines contain non-glycosylated HBV small S protein as the envelope antigen which must be released from the yeast during the manufacturing process 8. These vaccines do not contain antigens of the pre-S regions. The third class of HBV vaccine is the mammalian cell-derived recombinant vaccine. Three vaccines of this class have been developed. In addition to the S antigen, one of these contain antigen from the pre-S2 region while the other two contain antigens from both the pre-S1 and pre-S2 regions 9
The efficacy of universal immunization has been shown in different countries, with striking reductions of the prevalence of HBV carriage in children, most importantly; the HBV vaccine can be considered the first successful anti-cancer vaccine, as 20 years of mass vaccination has clearly reduced the incidence of hepatocellular carcinoma in children, at least in Taiwan 10. Currently available hepatitis B vaccine in Pakistan’s market are genetically engineered DNA recombinant vaccines and the recommended series of three intramuscular doses of hepatitis B vaccines induces a protective antibody response (anti-HBs > =10 milli-international units {mIU/ml}) in > 90% of healthy adults and in >95% of infants, children and adolescents 7, 11.
A vaccine consists of many parts, only one of which is the antigen by which it is known. Other components of the presentation may include, for instance, an adjuvant, a preservative or other ingredient. There may be components not stated on the information sheet that are classified as proprietary and therefore the manufacturers are not obliged to declare them. Thus, the effect the vaccine has, on an individual may be influenced in various ways by each and all of these components. Preservatives are just one of a number of additives to vaccines that are carefully regulated and which come under special scrutiny from time to time 12. Several case reports raised concerns that hepatitis B (HB) immunization might be linked to new cases or reactivation of multiple sclerosis, could shift the immune system toward an auto-immune direction, or may cause central nervous system (CNS) demyelinating diseases etc 13, 14, 15, 16. The present study sought to compare the safety of four hepatitis B vaccine regimens available in Pakistan’s market, in apparently healthy young females, and to determine the sero-response (i.e. reactogenicity and immunogenicity) to these vaccine in the same group of volunteers.
MATERIALS AND METHODS: Study Duration: Jan 2003 to Jan 2006 Study Design: Prevention, Open Label, Dose Comparison, Parallel Assignment, Safety/Efficacy Study. Subject: A total of 243 apparently young healthy female students of two Universities of the city were included in this study. Informed Consent: Prior to immunization, all volunteers were requested to give written informed consent to participate in this study. The volunteers were also advised that they are free to withdraw from the study at any time without any obligation to disclose her reason (s) for so doing. Criteria For Inclusion In The Study: All volunteers after submitting their signed consents were subjected to selection criteria on the basis of health checkups by a medical doctor to record the various factors including: a) Age: 18 – 30 years, b) History of Jaundice, blood transfusion, exposure to syringe, surgical and dental, c) Weight: > 45 Kg, d) Body Temperature: 96 – 98°F, e) Hemoglobin: > 10 g/ dl, f) Blood Pressure: Systolic 100 – 180 mm of Hg, Diastolic: 60 – 100 mm of Hg, g) Pulse rate: > 65/min.
After qualifying for inclusion in this study, volunteers were asked to give 10 cc of blood sample for different hematological (CP i.e. complete blood picture and Hb% i.e. hemoglobin percentage by Sysmex blood analyzer & ESR i.e. erythrocyte sedimentation rate by Westergreen method ), and Biochemical analysis (Direct Bilirubin, Indirect Bilirubin, ALT, AST and, Alkaline phosphatase by MicroLab- Merck chemistry analyzer), this data was used to keep the record of health status of participants and its comparison with adverse effects if appeared. Screening for HBs antigen, anti HBs antibodies and HBc IgM antibodies by Immunochromatography (ICT, Australia and Abbott, USA) and confirmation by enzyme linked immunosorbent assay (IMX ELISA - Abbott, USA) was also done before first dose of immunization. Test Vaccines: Fourrecombinant yeast derived HB vaccine were used as test regimens i.e. Euvax-B (LG Chemicals Ltd., Korea), Heptis-B (Boryang, Korea), Amvax-B (Amson, Pakistan) and Engerix-B (GS & K, Belgium). To avoid complications related to multi dose vials, it was strictly followed that the vaccination dose for each subject should be company packed, individually in a sealed container and, formulated for intra muscular injection. The dosage vial should contain same amount i.e. 20 μgm/ ml of HBs Ag absorbed on to approximately 0.5 μgm / ml adjuvant (aluminum hydroxide) and 100 μgm / ml preservative (Thiomersal/ Thimerosol) in a final volume of 1.1 ml (1 dose/ vial). Storage temperature should maintain as 2ºC to 8ºC to ensure integrity. Participants were injected with the vaccine of their own choice. Information broachers of the four vaccines were distributed among participants to help them make a choice. Out of total 729 doses administered to 243 individuals during this study, 195 were of Engerix-B, 420 were Heptis-B, 75 were Amvax-B, and 39 doses were of Euvax-B. Categories for Determining Severity of an Adverse Effect:
Local Symptoms: Soreness, indurations, swelling and redness.
General Symptoms: Fever, headache and dizziness.
Mild: Adverse events easily tolerated
Moderate: Adverse event of sufficient discomfort to interfere with daily activity or requiring simple treatment (e.g. Paracetamol, Generic name: Paracip).
Severe: Adverse event incapacitating and preventing usual activity or which may be life threatening, requiring hospitalization or completed treatment.
The course of an adverse event was described as:
Spontaneous recovery without discontinuation of vaccination
Recovery after discontinuation of vaccination
Continuation of recovery after symptomatic treatment
Eight samples of Peripheral blood (2-3 ml) were taken from all vaccinees before administration of each dose, and at different intervals after completion of immunization as per schedule given below; the sera were collected and stored at - 20°C.
Table 1: Visits Were Scheduled As Follows:
Vaccination number & sample collection
1.
First sample Before 1st dose of Vaccine (Jan, 2003)
2.
Second sample Before 2nd dose of Vaccine (Feb, 2003)
3.
Third sample Before3rd dose of Vaccine (June, 2003)
4.
Fourth sample After 6 months of 3rd dose (Dec, 2003)
5.
Fifth sample After 15 months of 3rd dose (Sep, 2004)
6.
Sixth sample After 19 months of 3rd dose (Jan, 2005)
7.
Seventh sample After 22 months of 3rd dose (May, 2005)
8.
Eighth sample After 30 months of 3rd dose (Jan, 2006)
Antibody Estimation and Statistics:
Anti-HBs were detected by ELISA using IMX- Abbott and quantitated using appropriate dilution of a positive sample with a known concentration of anti-HBs expressed as IU/L, provided by the manufacturer. The assay determined IgG type of anti- HBs antibody and the protective level of antibody was considered >10 IU/L. P values of less than 0.05 were considered significant. On the whole Hepatitis B antibodies titer was determined in participants using five standards i.e. <10 IU/ml, Between 10 – 100IU/ml, Between 100 – 1000 IU/ml, >1000 IU/ml, and no response or no antibody titer for the period of 36 months starting Jan’2003 till Jan’ 2006.
RESULTS:
Percentage of Geometric mean titer (GMT) of antibodiesbelow 10 IU/ml was in between 0.0% to 0.22% in case of Engerix-B, 0.0% to 0.20% in case of Euvax B, 0.0% to 0.30% in case of Amvax-B and 0.0% to 0.25% in case of Heptis-B. Percentage of GMT of antibodies between 10 – 100 IU/ml was in between 0.0% to 10% in case of Engerix-B, 0.0% to 9% in case of Euvax B, 0.0% to 8.9% in case of Amvax-B and 0.0% to 9.3% in case of Heptis-B. Percentage of GMT of antibodies between 100 – 1000 IU/ml was in between 0.0% to 35% in case of Engerix-B, 0.0% to 30.1% in case of Euvax B, 0.0% to 39.3% in case of Amvax-B and 0.0% to 40% in case of Heptis-B. While, Percentage of GMT of antibodies above 1000 IU/ml was in between 0.0% to 23% in case of Engerix-B, 0.0% to 25% in case of Euvax B, 0.0% to 26% in case of Amvax-B and 0.0% to 23.7% in case of Heptis-B. When Percentage of GMT of negative response was calculated we found that on the whole Engerix-B showed no response after 6 months of 3rd dose in 0.9% recipients leading towards no response in 31.78% of recipients after 30 months of 3rd dose. Euvax-B showed no response after 6 months of 3rd dose in 7.9% recipients leading towards no response in 35.68% of recipients after 30 months of 3rd dose. Amvax-B showed no response after 6 months of 3rd dose in 11.6% recipients leading towards no response in 25.5% of recipients after 30 months of 3rd dose. While, Heptis-B showed no response after 6 months of 3rd dose in 9.88% recipients leading towards no response in 26.75% of recipients after 30 months of 3rd dose. Period after 6 months of 3rd dose and before 15th month of 3rd dose was the period when highest Percentage of GMT of anti- HBs was observed .
Local and generalized adverse effects observed during and after the immunization of volunteers were recorded separately for each vaccine (Table 2, 3, 4 & 5).
Table 2 Incidence of Local and/or Generalized Symptoms on Vaccination With Engerix-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
N
%
n
%
n
%
1
65
19
29
5
8
10
15
38
58
2
65
11
17
3
5
7
11
29
45
3
65
8
12
0
0
0
0
18
28
Total
195
38
19
8
4
17
9
85
44
Table 3 Incidence of Local and/or Generalized Symptoms on Vaccination With Euvax-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
13
4
31
2
15
3
23
8
62
2
13
2
15
1
0
2
15
6
46
3
13
2
15
0
0
0
0
0
0
Total
39
8
21
3
8
5
13
14
36
Table 4 Incidence of Local and/or Generalized Symptoms on Vaccination With Heptis-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
140
53
38
10
7
34
24
95
68
2
140
25
18
25
18
27
19
70
50
3
140
22
16
7
5
32
23
84
60
Total
420
100
24
42
10
93
22
249
59
Table 5 Incidence of Local and/or Generalized Symptoms on Vaccination With Amvax-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
25
13
52
8
32
3
56
23
92
2
25
2
8
6
24
4
16
9
36
3
25
14
56
3
12
25
100
12
48
Total
75
29
39
17
27
32
43
44
59
As Shown in Table 6 that one month after the first dose, 180/243 subjects (74.45%) had seroprotection with respect to anti-HBs. One month after the second dose, 189/243 subjects (77.92%) showed seroprotection, four months after second dose, at month 6, 224/243 subjects (92.43%) were seroprotective. After 15 months of 3rd dose 231/243 subjects (95.27%) showed maximum seroprotection level in the immunized women. Later on seroprotection level was determined after 19, 22 and 30 months of 3rd dose. 170/243 subjects (70.08%) subjects were seroprotected even after 30 months of 3rd dose without having any booster dose.
Table 6: Over All Seroprotection Levels and Geometric Mean Titers (GMT) of Anti- HBs Antibodies
Timing
N
S+
% of S+
GMT
Range of Anti HBs Titer
PRE
Before Vaccination (Jan, 03)
243
0
0
0
0
M1
Before 2nd dose (Feb, 03)
243
180
74.45
16
0-50
M2
Before 3rd dose (June, 03)
243
189
77.92
143
1-700
M3
After 6 months of 3rd dose(Dec, 03)
243
224
92.43
18500
45-50000
M4
After 15 months of 3rd dose(Sep, 04)
243
231
95.27
23000
40-50000
M5
After 19 months of 3rd dose(Jan, 05)
243
222
91.57
12100
39-33000
M6
After 22 months of 3rd dose(May, 05)
243
195
80.53
1875
5-17000
M7
After 30 months of 3rd dose(Jan, 06)
243
170
70.08
690
1-1500
Comparative results of serum protection analysis of 04 candidate vaccines determined after 15 months of third dose without giving any booster dose, were found effective in healthy young female volunteers, demonstrating induction of very good immunogenicity. No significant differences were observed in seroprotection level of test vaccines (Table7). Overall serum protection rate achieved in case of Engerix-B was 95.9%, in case of Euvax-B, it was 95.2%, in case of Heptis-B was 95.0% , and in case of Amvax-B it was 95.1%. Calculated P values for all four test vaccines were lesser than 0.05 indicating significance of the used vaccines.
Table 7: Comparative Serum Protection analysis of 04 different Hepatitis-B Vaccines(n= 243; mean age= 21.5+3.7 Years)
As yet no such immunogenicity trials have been conducted in Pakistan or risk factors indigenous to the region assessed for any of the vaccine being utilized at the population level for such long period. Our study, is one of the longest study, conducted between Jan’2003 and Jan’ 2006, which includes total 243 healthy women subjects of child bearing age group. In this study we have demonstrated that there is no significant difference in reactogenicity and serum protection level among all four candidate vaccines we tested here, excellent immunogenicity of vaccines in volunteers recommends their usage for immunization purpose among different communities without having any doubts related to reactogenicity and side effects.
Recombinant hepatitis B vaccines have long been used for protection in the serum of and three doses have been shown to produce Anti HBs in the serum of approximately 95% of people who have not encountered the virus. The antibody response declines with increasing age. Patientsolder than 30 years have an increased risk of no response toHBV vaccine, as compared with younger persons 17. Thus, immunizationduring childhood or adolescence offers the greatest potentialfor protection 17 and provides lifelong immunity. Ninety percent of healthy adults and 95 percent of infants, children, and adolescents have protective serum anti-HBs antibody concentrations after the vaccine series has been completed 18.
Two kinds of recombinant vaccine are used for active immunization against hepatitis B; one of them contains the PreS1 and PreS2 antigenic domains while the other kind contains S and PreS polypeptide. No important differences between the effectiveness of these two types of vaccine have been detected 19. In a series of studies it has been demonstrated that 90-99% of healthy neonates, children, adolescents and adults develop protective levels of anti-HBs antibody following a standard vaccination course with hepatitis B vaccine 20, 21, 22, 23, 24, 25.
Efficacy of vaccines in the field have been measured long after the vaccine have been introduced at large scale population levels and only selected countries have record keeping such as the Centers for Disease Control in USA and the National Health Services in UK. Most developing countries do not have infra structure to support these activities and therefore the efficacy and risk indigenous to the population remains unknown.
Procurement and delivery of high-quality vaccine has national and international public health and ‘public good’ implications far beyond the scope of most products. People immunized with vaccines of inadequate quality can become ill and die from the disease that the vaccine should have prevented. Even more lives are placed at risk if vaccination coverage declines as a result of reduced public confidence in immunization programs. If we look at the outcome of immunization programs in different countries then we will have a good idea that how mass vaccination helped in reduction of disease burden?26
Importance of dose size, number of doses and dose response is another important issue related to immunization programs. Published studies regarding the dose-response relationship in terms of immunogenicity and sero-protection are highly varied. Chiaramonte et al 27reported that the sero-protection reached a level of 99.6% within one month after primary immunisation with the recombinant hepatitis B vaccine. The findings of Assateerawatt et al28 and Just et al 29 also were the same. Baldy JLS et al carried out a comparative study with three recombinant hepatitis B vaccines, one Brazilian (Butang, Instituto Butantan) and two Korean vaccines (Euvax-B, LG Life Sciences Ltd. and Hepavax-Gene, Green cross Vaccine Corp.), administered intramuscularly to students aged 17to19 years in three doses (corresponding to half the amount of antigen routinely used for adult vaccination) at intervals of one month between the first and second dose, and of four months between the second and third dose. The GMT of anti-HBs induced by the Euvax-Band Engerix-B vaccines were higher than those obtained with the Butangvaccine (p < 0.05); this difference was not significant when comparing the other vaccines two-by-two. No spontaneous adverse effects attributable to the application of any dose of the three vaccines were reported 30.
Vaccine efficacy is defined as the reduction in the incidence of a disease among people who have received a vaccine compared to the incidence in unvaccinated people. The efficacy of a vaccine is measured in clinical trials by giving one group of people a vaccine and comparing the incidence of disease in that group to another group of people who do not receive the vaccine. In our study overall efficacy of the vaccines used was satisfactory, without producing sever adverse effects, also there is no report of incidence of disease till now, in those who were vaccinated during this study(Table 2, 3, 4, 5).
Maximum protection level in terms of immunogenicity was observed in Euvax-B, which showed GMAT of 35.68% in test population. Engerix-B showed GMAT of 31.78%, Heptis-B showed GMAT of 26.75% and, Amvax-B showed GMAT of 25.5% after 30 months of 3rd dose of immunization While highest serum protection level was achieved in case of Engerix -B i.e. 95.9%. On the whole, r-hepatitis B vaccines showed high immunogenicity and good safety profile in the test population.
The inclusion of Hepatitis B in the list of compulsory and Extended Program for Immunization (EPI) in Pakistan since 2005 will result in mass vaccination of pediatric population. However, a big chunk of the adult population, especially healthcare workers, also needs to be immunized against Hepatitis B infection. We believe that all of the above mentioned HB vaccines, which are easily available in Pakistan’s market can be used for these mass vaccination programs without having any doubts related to Reactogenecity and Immunogenicity.
CONCLUSION:
In conclusion, this prospective study reinforces that the four different recombinant hepatitis B vaccines licensed in Pakistan have a good tolerability and are highly immunogenic among young women. It is also recommended that government should ensure the serosurvey of HBsAg and vaccine coverage at country level in order to reduce the disease burden on country’s economy.
ACKNOWLEDGEMENTS We are thankful to the administration of Jinnah University for Women, Karachi-Pakistan, administration of University of Karachi, Karachi-Pakistan, and team of Volunteer students from Microbiology Department, JUW for their cooperation during vaccination camps and manufacturers of test vaccines for giving consents to include their vaccines in this study. COMPETING INTERESTS None Declared AUTHOR DETAILS SHAZIA TABASSUM HAKIM, Ph.D., Virology and Tissue Culture Lab, Jinnah University for Women and I.I.D.R.Lab., University of Karachi, Pakistan SAYYADA GHUFRANA NADEEM, Virology and Tissue Culture Lab, Jinnah University for Women and I.I.D.R.Lab., University of Karachi, Pakistan SHAHANA UROOJ KAZMI, I.I.D.R.Lab., University of Karachi, Pakistan CORRESPONDENCE: SHAZIA TABASSUM HAKIM, Associate Professor & Chairperson, Department of Microbiology, Jinnah University for Women, Nazimabad, Karachi-74600, Pakistan Email: Shaz2971@yahoo.com
References
1.Kane MA, and Clements J. Hepatitis B. D. T. Jamison, W. H. Mosley, A. R. Meashan, and J. Bobadilla , editors. Disease control priorities in developing countries. New York: Oxford University Press N.Y; 1993:321–330.
2.World Health Organization, Revised fact sheet, August 2008.
3.Park K. Textbook of prevention and social medicine, 15th edition, Jabalpur, India: Banarsidas Bhanot Publishers;1997:159
4.Wasim J, Nadim J, Yakoob K , Muhammad I, Tirmizi SFA, et al. Hepatitis B and C: prevalence and risk factors associated with seropositivity among children in Karachi, Pakistan. BMC Infectious Disease. 2006;6:101
5.Zaman AS. 2003. Daily Dawn Internet Edition. 23 January.
6.WHO, 45th World Health Assembly, expanded programme on immunization and vaccine quality—progress report by the Director General, A45/8. World Health Organization, Geneva, Switzerland. 1992.
7.Szmuness W, Stevens CE et al. Hepatitis B vaccine: demonstration of efficacy in a controlled clinical trial in a high-risk population in the United States. N Engl J Med. 1980; 9;303(15):833-41.
8.Stephenne J. Development and production aspects of a recombinant yeast-derived hepatitis B vaccine. Vaccine. 1990;8 Suppl:S69-73; discussion S79-80.
9.Young MD, Schneider DL et al. Adult hepatitis B vaccination using a novel triple antigen recombinant vaccine. Hepatology. 2001;34(2):372-6.
10.Kao JH, Chen DS. Global control of Hepatitis B infection. Lancet Infect Dis. 2002;2(7):395-403.
11. Zajac BA, West DJ, McAleer WJ, Scolnick E M. Overview of clinical studies with hepatitis B vaccine made by recombinant DNA. J. Inf. 1986; Suppl A0:39–45.
12.Clements CJ. Vaccine preservatives: what is the big deal?. Indian J Med Res. 2006;124:5–8.
13.Duclos P. Safety of immunisation and adverse events following vaccination against hepatitis B. Expert Opin Drug Saf. 2003;2:225-31.
14.Hall A, Kane M, Roure C, Meheus A. Multiple sclerosis and hepatitis B vaccine? Vaccine. 1999;17:2473-2475.
15.DeStefano F, Verstraeten T, Jackson LA et al. Vaccinations and risk of central nervous system demyelinating diseases in adults. Arch Neurol. 2003;60:504-509.
16.Ascherio A, Zhang SM, Hernán MA et al. Hepatitis B vaccination and the risk of multiple sclerosis. N Engl J Med. 2001;344:327-332.
17.Fisman DN, Agrawal D, Leder K. The effect of age on immunologic response to recombinant hepatitis B vaccine: a meta-analysis. Clin Infect Dis. 2002;35:1368-1375.
18.Mast E, Mahoney F, Kane M, Margolis H. Hepatitis B vaccine. Plotkin SA, Orenstein WA, editors. Vaccines. Philadelphia: Saunders. 2004:299-337.
19.Bertino JS Jr, Tirrell P, Greenberg RN et al. A comparative trial of standard or high-dose S subunit recombinant hepatitis B vaccine versus a vaccine containing S subunit, pre-S1, and pre-S2 particles for revaccination of healthy adult nonresponders. J Infect Dis. 1997;175:678-681.
20.Zannolli R, Morgese G. Hepatitis B vaccine: current issues. Ann Pharmacother. 1997;31(9):1059-1067.
21.West DJ, Calandra GB. Vaccine induced immunologic memory for hepatitis B surface antigen: implications for policy on booster vaccination. Vaccine. 1996;14(11):1019-1027.
22.Jafarzadeh A, Shokri F. The antibody response to HBs antigen is regulated by coordinated Th1 and Th2 cytokine production in healthy neonates. Clin Exp Immunol. 2003;131(3):451-456.
23.Shokri F, Jafarzadeh A. High seroprotection rate induced by low doses of a recombinant hepatitis B vaccine in healthy Iranian neonates. Vaccine. 2001;19(31):4544-4548.
24.Jafarzadeh A, Kardar GA, Khoshnoodi J, Shokri F. Downregulation of IL-12 production in healthy nonresponder neonates to recombinant hepatitis B vaccine. Iran Biomed J. 2004;8:41-45.
25.Jafarzadeh A, Shokrgozar MA, Khoshnoodi J, Shokri F. Unresponsiveness to recombinant hepatitis B vaccine in healthy Iranian neonates: association with HLA antigens. Irn J Med Sci. 2002;27:51-55.
26.Proceedings of Who’s third expert working group meeting on hepatitis B. Tokyo, Japan 6-7 March 2007.
27.Chiaramonte M, Majori S, Ngatchu T et al. Two different dosages of yeast derived recombinant hepatitis B vaccines: A comparison of immunogenicity. Vaccine. 1996;14:135-7.
28.Assateerawatt A, Tanphaichitr VS, Suvatte V, Yodthong S. Immunogenicity and efficacy of a recombinant DNA hepatitis B vaccine, Gen Hevac B Pasteur in high risk neonates, school children and healthy adults. Asian Pac J Allergy Immunol. 1993;11:85-91.
29.Just M, Berger R, Just V. Reactogenicity and immunogenicity of a recombinant hepatitis B vaccine compared with a plasma derived vaccine in young adults. Postgrad Med J. 1987;63 (Suppl 2):121-3.
30.Baldy JLS, Lima GZ, Morimoto HK et al. Immunogenicity of three recombinant hepatitis B vaccines administered to students in three doses containing half the antigen amount routinely used for adult vaccination. Rev Inst Med Trop S Paulo. 2004;46(2):103-7.
Ventilator Associated Pneumonia (VAP) is defined as pneumonia occurring in a patient within 48 hours or more after intubation with an endotracheal tube or tracheostomy tube and which was not present before1, 2. Early onset VAP occurs within 48 hours and late onset VAP beyond 48 hours of tracheal intubation.
Incidence
Between 5-15% of hospital in-patients develop infection during admission to ICU3. Patients are 5-10 times more likely to acquire nosocomial infections than patients in the wards4and approximately 86% of hospital associated pneumonia is linked with mechanical ventilation5.
Approximately 10-28% of critical care patients develop VAP6. VAP is also the most common and fatal infection of ICU7,8 and in the United States it affects 9-27% of intubated patients and doubles the risk of mortality as compared with similar patients without VAP9-13.
VAP may account for up to 60% of all Healthcare-Associated Infections14. VAP increases length of ICU stay by 28%16 and each incidence of VAP is estimated to generate an increased cost of £6000- £2200015.
Diagnosis
Despite the high incidence, diagnosis remains challenging because many conditions common to ICU patients like ARDS, sepsis, cardiac failure and lung atelectasis have similar clinical signs. More than 50% of patients diagnosed with VAP do not have the disease whereas upto one-third are not diagnosed17, 18. Unfortunately there is no clearly accepted gold standard for diagnosis of VAP19.
Centres for disease control and prevention (CDC) national healthcare safety network definition for VAP
Radiology signs (2 or more serial chest x-rays with at least one of the following)
New or progressive and persistent infiltrate
Consolidation
Cavitation
Clinical signs
At least one of the following
Fever (temperature > 38 deg C with no other recognised cause)
Leucocytosis > 12000WCC/uL or leucopenia (<4000 WCC /uL)
For adults 70 years or older, altered mental status with no other recognisable cause
and at least 2 of the following
New onset of purulent sputum, or change in character of sputum, or increased respiratory secretions, or increased suctioning requirements
New-onset or worsening cough, or dyspnoea or tachypnoea
Rales or bronchial breath sounds
Worsening gas exchange (eg. O2 desaturations [PaO2/FiO2 ≤ 240], increased O2 requirements, or increased ventilation demand)
Microbiological criteria (optional)
At least one of the following:
Positive growth in blood culture not related to another source of infection
Positive growth in culture of pleural fluid
Positive quantitative culture from bronchoalveolar lavage (≥104 colony forming units/ml) or protected specimen brushing (≥103colony forming units/ml)
5% or more of cells with intracellular bacteria on direct microscopic examination of Gram-stained bronchoalveolar lavage fluid
Histopathological evidence of pneumonia
Histological landmark of VAP is multifocal disease favouring dependant lung segments, often at different stages of development and severity with cultures growing heterogenous microbial flora.20,21
Risk Factors
Mechanical ventilation with Endotracheal intubation including Tracheostomy
Prolonged mechanical ventilation
Advanced age
Pre-existing sinusitis and lung disease
Micro or macroaspiration of oropharyngeal or gastric contents
Malnuitrition and immunosuppression
Obesity
Chronic lung disease
Several factors affect the aetiology of VAP
Time of onset of hospitalisation
Stress induced flora change
Antibiotic induced flora change
Exposure to contamination with nosocomial pathogens
Patient interventions
Pathogenesis:
VAP that occurs within 48 hours after tracheal intubation is usually termed as early onset often resulting from aspiration, which complicates intubation process22. VAP occurring after this period is late onset. Early onset VAP is often due to antibiotic sensitive bacteria (eg oxacillin-sensitive Staphylococcus aureus, Hemophilious influenza and Streptococcus pneumoniae), whereas late onset VAP is frequently caused by antibiotic resistant pathogens (eg.oxacillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa, acinetobacter species and enterobacter species) 23,24,25
The pathogenesis of VAP usually requires that two important processes take place:
Bacterial colonisation of the aero-digestive tract
Aspiration of contaminated secretions into the lower airway26.
Therefore, the strategies to prevent VAP usually focus on reducing the burden of bacterial colonisation in the aero-digestive tract, decreasing the incidence of aspiration or both.
The presence of invasive medical devices is an important contributor to the pathogenesis and development of VAP27. Many patients have nasogastric tubes that predispose them to gastric reflux and increase the potential for aspiration. Endotracheal tubes facilitate bacterial colonisation of the tracheo-bronchial tree and lower airway aspiration of contaminated secretions through mucosal injury, pooling of contaminated secretions above the endotracheal tube cuff and elimination of the cough reflex26. The ventilator circuit and the respiratory-therapy equipment may also contribute to the pathogenesis of VAP if they become contaminated with bacteria, which usually originate in the patient’s secretions26, 28.
Prevention:
The National Institute of Clinical Excellence (NICE) in collaboration with National Patient Safety Agency (NPSA) is examining four technical patient safety solutions for the prevention of VAP and in the process of publishing guidelines. The latest technical patient safety solutions for VAP was published in August 2008 which says
1. Body position-mechanically ventilated and intubated patients should be positioned with their upper body elevated for as long as possible. This may be inappropriate in some patients. eg. spinal injuries. 2. Oral antiseptics e.g. 2% chlorhexidine should be included as part of oral hygiene regimen for all patients who are intubated and ventilated. There is insufficient evidence to recommend any particular antibiotic regimen. 3. Use of kinetic beds - a lack of robust evidence meant the Committee was unable to make recommendations for action on the use of kinetic beds. 4. Care bundles - although the evidence supported the use of elements of care bundles; there was insufficient evidence to recommend a care bundle of any specific design.
The Department of Health published the following ‘High impact intervention’ for ventilated patients in June 2007
Elevation of the head of bed to 35-40 degrees
Sedation holding
Deep Vein Thrombosis prophylaxis
Gastric ulcer prophylaxis
Appropriate humidification of inspired gas
Appropriate tubing management
Suctioning of respiratory secretions (including use of gloves and decontaminating hands before and after the procedure)
Routine oral hygiene as per local policy
In addition the following also may contribute to the prevention of VAP
Prolonged nasal intubation (more than 48hrs) should be avoided because of the association between nosocomial sinusitis and ventilator-associated pneumonia29.
Several investigations have suggested that secretions that pool above the inflated endotracheal tube cuffs may be a source of aspirated material and thus VAP. Endotracheal tubes with separate dorsal lumen above the cuff to suction pooled secretions from the subglottic space are now available. The pressure of the endotracheal tube cuff should be adequate to prevent the leakage of colonised subglottic secretions into the lower airway26,30.
Antibiotic Administration:
Previous administration of antibiotics is an important risk factor for VAP because of the presence of antibiotic-resistant bacteria31. In an attempt to reverse the trend towards increasing rates of antimicrobial resistance among hospital acquired infections, more effective strategies for using antibiotics have been advocated that restrict antibiotic use or offer guidelines for their use 32, 33. Eliminating or reducing the unnecessary use of antibiotics should be the primary goal in reducing antibiotic-resistant nosocomial infections32.
The routine use of prolonged courses of empirical therapy i.e. therapy not supported by results of clinical cultures should be avoided to minimise the subsequent development of antibiotic-resistant infections.
The use of aerosolised antibiotics for the prevention of VAP has been abandoned because of its lack of efficacy and subsequent emergence of antibiotic-resistant infections28.
Similarly the routine use of selective digestive tract decontamination has not gained acceptance in the UK and USA because of its lack of demonstrated effect on mortality, emergence of antibiotic resistant infections and additional toxicity. NICE is currently in consultation for selective decontamination of digestive tract guidelines. The technical patient safety solutions for VAP in adults were published in August 2008.
The Committee examined evidence, which suggested that selective decontamination of the digestive tract (SDD) using topical antibiotics may reduce the incidence of VAP and that SDD regimes that include systemic antibiotics may also reduce mortality. However, Specialist Advisers stated that UK intensive care specialists had particular concerns about the risk of infection with Clostridium difficile and the induction and/or selection of resistant, including multiresistant, microorganisms as a result of SDD. Therefore the Committee recommended further research into SDD in a UK setting.
Use of broad-spectrum antibiotics is also not recommended for the prevention of VAP because of increasing antibiotic resistance among subsequent hospital acquired infections. Targeted antibiotic therapy with appropriate dose of appropriate antibiotic is the sensible thing to do.
Vaccines:
Various vaccination programmes in adults and children have reduced the incidence of pneumonia caused by specific pathogens including H.influenzae type B, Streptococcus Pneumoniae and Influenza virus 34, 35.Vaccinations against these may prevent some hospital acquired infections. Pneumococcal and influenza vaccination must be considered before hospital discharge or included in the discharge planning for all patients at increased risk for subsequent respiratory infections including VAP.
Newer Developments:
There have been new advances in equipment and techniques to help prevention of VAP
Endotracheal and tracheostomy tubes with an extra subglottic port to clear pooled secretions above the endotracheal and tracheostomy tube cuff.
Continuous suctioning of the subglottic secretions.
Endotracheal tubes with specially designed cuffs that do not allow pooled secretions above the cuff to trickle down causing micro-aspiration and ultimately leading to VAP. eg. Endotracheal tubes with microthin polyurethane cuff.
Specially designed closed Tracheal Suctioning Systems (TSS) as compared to open tracheal suctioning systems. However a meta analysis of randomised controlled trial showed that closed suctioning system is not associated with a lower incidence of VAP or mortality as compared to open suctioning36
ACKNOWLEDGEMENTS We thank Dr. S. Parida (Consultant Microbiologist) for her valuable contribution in helping us write this manuscript. COMPETING INTERESTS None Declared AUTHOR DETAILS HARSHAL WAGH, Registrar in Anaesthesia, St Albans City Hospital, United Kingdom DEVARAJA ACHARYA, Consultant in Anaesthesia and Critical Care, St Albans City Hospital, United Kingdom CORRESPONDENCE: DR HARSHAL WAGH, Registrar, Dept of Anaesthesia, Level I, St Julians Ward, St Albans City Hospital, St Albans, UK, AL3 5PN Email: drhdw@hotmail.com
References
Prevention of ventilator-associated pneumonia: consultation NICE, Sept 2007
Eggimann P, Pittet D. Infection control in the ICU. Chest 2001; 120: 2059-93
Weber DJ, Raasch R, Rutala WA. Nosocomial infections in the ICU: the growing importance of antibiotic-resistant pathogens. Chest 1999; 115: 34S-41S
Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in medical intensive care units in the United States. National Nosocomial infections Surveillance System.Crtic Care Med.1999 May; 27950: 887-92
The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee 1995.
Legras A, Malvy D, Quinioux AI, et al. Nosocomial Infections: prospective survey of incidence in five French intensive care units. Intensive Care Med.1998; 24: 1040-1046.
Urli T, Perone G, Acquarolo A, Zappa S, Antonini B, Ciani A. Surveillance of infections acquired in intensive care: usefulness in clinical practise. J Hosp Infect. 2002; 52: 130-135
Heyland DK, Cook DJ, Griffith L, keenan SP, Brun-Buisson C; Canadian Critical Trials Group. The attributable morbidity and mortality of ventilator-associated pneumonia. Am J Respir Crit Care Med. 1999; 159:1249-1256
Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gilbert C. Nosocomial pneumonia and mortality among patients in intensive care units. JAMA 1996; 275:866-869.
Rello J, Quintana E, Ausina V, et al. Incidence, etiology and outcome of nosocomial pneumonia in mechanically ventilated patients. Chest, 1991; 100:439-444.
Jiménez P, Torres A, Rodriguez-roisin R, et.al. Incidence and etiology of pneumonia acquired during mechanical ventilation. Crit care Med.1998; 17:882-885.
Safdar N, Dezfulian C, Collard HR, Saint S. Clinical and economic consequences of ventilator-associated pneumonia; a systemic review.Crit Care Med.2005; 33:2184-2193
CDC. Guidelines for preventing Health -Care -Associated Pneumonia, 2003. Recommendation of the CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR 2004; 53(No.RR-3)
Nosocomial pneumonia: incidence, morbidity and mortality in the intubated-ventilated patient. Pittett 1994
Nosocomial viral ventilator-associated pneumonia in the intensive care unit: a prospective cohort study. Pfr Vincent 2005
Petersen IS, Aru A, SkØdt V, et al. Evaluation of pneumonia diagnosis in intensive care patients. Scand J infect Dis.1999; 31:299-303
Fagon JY, Chastre J, Hance AJ, Domart Y, Trouillet JL, Gilbert C. Evaluation of clinical judgement in the identification and treatment of nosocomial pneumonia in ventilated patients.Chest.1993; 103:547-553
American Thoracic Society; Infectious diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med.2005; 171:388-416.
Rouby JJ, Martin De Lassale E, Poete P, et al. Nosocomial bronchopneumonia in the critically ill: histologic and bacteriologic aspects. Am Rev Respir Dis.1992; 146:1059-1066.
Fabregas N, Torres A, El-Ebiary M, et al. Histopathologic and microbiologic aspects of ventilator-associated pneumonia. Anaesthesiology.1996; 84:760-761
Pingleton SK, Fagon JY, Leeper KV Jr. Patient selection for clinical investigation of ventilator-associated pneumonia: criteria for evaluating diagnostic techniques. Chest 1990; 97:170-81.
Niederman MS,Craven DE, Fein AM, Schultz DE. Pneumonia in the critically ill hospitalised patient. Chest 1990; 97:170-81.
Kollef MH, Silver P,Murphy DM, Trovillion E. The effect of late-onset ventilator-associated pneumonia in determining patient mortality. Chest 1995; 108:1655-62.
Rello J, ausina V, Ricart M, Castella J, Prats G. Impact of previous antimicrobial therapy on the therapy on the etiology and outcome of ventilator-associated pneumonia. Chest 1993; 104:1230-5.
Craven DE, Steger KA. Epidemiology of nosocomial pneumonia: new perspectives on an old disease. Chest 1995; 108: Suppl: 1S-16S.
Kollef M. Current concepts - the prevention of VAP. NEJM 340; 8:627-634.
Tablan OC, Anderson LJ, Arden NH, Breiman RF, Butler JC, Mcneil MM. Guideline for prevention of nosocomial pneumonia: The Hospital Infection Control Practices Advisory Committee, Centres For Disease Control And Prevention.Infect Control Hosp Epidemiol 1998; 19:304
Rouby JJ, Laurent P, Gosnach M et al. Risk factors and clinical relevance of nosocomial maxillary sinusitis in the critically ill. Am J Respir Crit Care Med 1994; 150: 776-83
Valles J, Artigas A, Rello J et al. Continuous aspiration of subglottic secretions in preventing ventilator associated pneumonia. Ann Intern Med 1995; 122:179-86.
Crouch Brewer S, Wuderink RG, Jones CB, Leeper KV Jr. Ventilator-associated pneumonia due to Pseudomonas aeruginosa. Chest 1996; 109:1019-29
Goldman DA, Weinstein RA, Wenzel RP, et al. Strategies to prevent and control the emergence and spread of antimicrobial-resistant microorganisms in hospitals: a challenge to hospital leadership. JAMA 1996; 275:234-40.
Evans RS, Pestotnik SL, Classen DC, et al. A computer-assisted management programme for antibiotics and other anti-infective agents. N Engl J Med 1998; 338:232-8.
Herceg A.The decline of Haemophilus influenza type b disease in Australia.Commun Dis Intell 1997; 21:173-6.
Gross PA, Hermogenes AW, Sacks HS, Lau J, Levandowski RA. The efficacy of influenza vaccine in elderly persons: a meta analysis and review of literature. Ann Intern Med 1995; 123:518-27.
I I Siempos, K Z Vardakas, M E Falagas. Br J Anaesth 2008; 100(3): 299-306.
Technical patient safety solutions for Ventilator-associated pneumonia in adults. NICE August 2008
Osteoporotic
fracture is common, expensive, and associated with increased morbidity
and mortality. The incidence of osteoporosis fracture annually is greater
than the risk of stroke, breast cancer, and heart attack combined. Bisphosphonates
(BPs) have recently been the subject of clinical controversies because
of the reported incidence of osteonecrosis of jaw (ONJ). Bisphosphonates
as a group of drugs were introduced for the management of various conditions
such as osteoporosis, Paget’s disease, multiple myeloma, and hypercalcemia
of malignancy. This group of drugs has improved the quality of life
in many patients with proven efficacy in limiting pain and skeletal-related
events. The efficacy of BPs as one method to prevent and treat osteoporosis
and avert future fractures, particularly vertebral fractures, is well
documented in large clinical trials. However, despite this evidence,
many patients at risk for osteoporosis are not screened or treated.
The controversy of osteonecrosis of the jaws and bisphosphonates is
a recent and growing problem.
Bisphosphonates:
Bisphosphonates
are fairly safe drugs to be used in the long term. There is a significant
amount of safety data for up to 10 years with alendronate or Fosamax
and up to 7 years with risedronate or Actonel. Every year, an estimated
30 million BP prescriptions are written in the U.S. alone.1
The bisphosphonates alendronate, risedronate, ibandronate, and zoledronic
acid are nitrogen containing compounds that increase bone mineral density
(BMD) by inhibiting osteoclast-mediated bone resorption.2
They have been shown to increase BMD approximately 2–8%, depending
upon the dose and site measured, and have demonstrated efficacy in primary
and secondary prevention of osteoporotic fractures.3–10
Nitrogen-containing
bisphosphonates are used widely for the management of metastatic cancer
in bone (intravenous zoledronic acid or Pamidronate), for the prevention
and treatment of osteoporosis (oral alendronate, risedronate, and ibandronate
and intravenous ibandronate), for the treatment of Paget’s disease
of bone (intravenous Pamidronate and oral alendronate and risedronate),
and for the short-term management of acute hypercalcemia (intravenous
zoledronic acid and Pamidronate).11 Bisphosphonates reduce
the survival and function of osteoclasts, the bone-resorbing cells.
The clinical pharmacology of intravenous (IV) BPs is characterized by
low intestinal absorption but highly selective localization and deposition
in bone. Oral BPs have a bioavailability of less than 5%.12
Once in the blood, BPs disappear very rapidly into the bone.13
After BPs are buried in the skeleton, they are released only when the
bone is destroyed in the course of turnover. In humans, the skeletal
half-lives of various BPs range from 3 months to as long as 10 years.
14
Osteoporosis:
Osteoporosis
is a devastating disease that may lead to significant morbidity and
mortality from resultant fractures. Approximately one in two women and
one in four men over age 50 will have an osteoporosis related fracture
in their remaining lifetime. 15 According to estimated
figures, osteoporosis was responsible for more than 2 million fractures
in US in 2005 15 (including approximately 297,000 hip fractures,
547,000 vertebral fractures, 397,000 wrist fractures , 135,000 pelvic
fractures , 675,000 fractures at other sites). The number of fractures
due to osteoporosis is expected to rise to more than 3 million by 2025.
15
Osteoporotic
fractures are associated with significant morbidity and mortality. Patients
who sustain a fracture are more likely to have lower health-related
quality of life, depression, pain, disability, physical deconditioning
due to inactivity, vertebral deformities with a resultant decrease in
pulmonary function and increase in gastrointestinal complications
(e.g., refractory reflux esophagitis), pressure ulcers, increased likelihood
of nursing home placement, and changes in self-image. 16-23
Hip fractures, which are the most serious complication of osteoporosis,
are associated with significant mortality. 24–27 Up to
38% of patients may die within one year after a hip fracture, and the
risk of death is approximately double that of patients who do not sustain
a hip fracture. 24, 25, 27
The economic
consequences of osteoporosis are enormous. In 1995 in USA, osteoporotic
fractures were responsible for approximately 432,000 hospital admissions,
2.5 million physician’s office visits, and 180,000 nursing home admissions.
15 Health care costs associated with osteoporotic fractures in
2005 were an estimated $19 billion. By 2025, experts predict that these
costs will rise to approximately $25.3 billion. 15 As the
population of the United States continues to age, these costs will likely
increase, with the number of hip fractures and associated costs possibly
tripling by 2040. 15
Oral
bisphosphonate associated osteonecrosis of the jaw:
Osteonecrosis
of the jaws (ONJ) is characterized by the death of bone as a natural
consequence of a wide variety of systemic and local factors compromising
the blood flow of the bone. Clinically it is diagnosed by an area of
exposed bone in the mandible, maxilla, or palate that typically heals
poorly or does not heal over a period of 6 to 8 weeks. The diagnosis
is primarily a clinical one, but imaging studies such as computed tomography
can be helpful. Approximately two thirds of cases involve the mandible
and the rest involve the maxilla. The lesion is painful in many, but
not all, patients, and infection is often present. In one unusual case,
osteonecrosis of the external auditory canal developed in a patient
with myeloma who had received intravenous zoledronic acid and amidronate.28
Predisposing factors for the development of osteonecrosis of the jaw
appear to be dental disease, dental surgery (e.g., tooth extraction),
oral trauma, periodontitis, and poor dental hygiene. The risk factors
for developing ONJ include trauma, female gender, advanced age, edentulous
regions, radiotherapy, chemotherapy, steroid therapy, blood dyscrasias/metastatic
disease, anemia, coagulopathy, surgical dental procedures, alcohol or
tobacco use, prior infection, and bisphosphonate therapy.29-32
Although there have been some reports in the literature about osteonecrosis
caused by steroids, this form is different from ONJ in the sense that
steroid-induced osteonecrosis does not cause bone exposure.
1,
33
ONJ in connection
with bisphosphonate use was first reported in 2003 34, or
5 to 10 years after these drugs were approved in the United States for
their current indications; it was rarely seen before then. Most of the
reported cases (95%) have been associated with zoledronic acid or Pamidronate
given intravenously to control metastatic bone disease. 35, 36,
11 Myeloma and breast cancer are by far the most common cancers
associated with intravenous bisphosphonate use and osteonecrosis of
the jaw.35
Osteonecrosis
of the jaw has developed far less often among patients who have received
oral bisphosphonates at the lower doses used for osteoporosis than among
patients who received the higher doses used for metastatic cancer. Among
several million patients who have received oral treatment for osteoporosis,
fewer than 50 cases of osteonecrosis of the jaw have been reported to
date.35 Moreover, with more than 60,000 patient- years of
exposure to nitrogen- containing bisphosphonates in clinical trials
of treatment for osteoporosis (involving follow-up for as long as 10
years in some patients), osteonecrosis of the jaw was not reported among
the adverse events. 11 The exact incidence of ONJ is unknown.
However, some reports have estimated it to be about 1 in 10,000 for
Intravenous use of BPs. 37 1 in 100,000 patient years
is a reasonable estimate of the incidence of osteonecrosis of the jaw
in patients receiving oral nitrogen-containing bisphosphonates for osteoporosis.
11 The risk of developing ONJ for patients taking alendronate,
the most commonly prescribed oral bisphosphonate, has been estimated
to occur in approximately 0.7 per 100,000 persons per years’ exposure
38; on the other hand, the incidence of ONJ for risedronate and
ibandronate cannot yet be quantified because too few cases have been
reported (12 cases for risedronate and one for ibandronate). 38
The Cartosos
medical claims database study also surveyed 260,000 subjects with osteoporosis,
and found an odds ratio for inflammatory necrosis of the jaw to be 0.65
in oral bisphosphonate users, and that for surgery for a necrotic process
to be 0.86. 39 Both these values are consistent with the
other data suggesting that oral bisphosphonate use does not increase
ONJ risk in osteoporosis patients. These findings are very similar to
those from a case-control study using a claims database, which found
that receiving at least
one oral bisphosphonate prescription was associated with an odds ratio for
jaw surgery of 0.91. 40 As per one consensus panel, there
have been 33 cases [reported] in the literature as of January 2007 --
out of the 33 million patients who have been treated worldwide with
an oral bisphosphonate -- which translates into approximately 200 million
prescriptions written. 41 In addition, there has been spontaneous
reporting in 1 of 100,000 patient-years for all of the approved bisphosphonates.
41 The fact that the majority of reported cases of osteonecrosis
of the jaw are associated with the use of high-dose intravenous bisphosphonates
for metastatic bone disease suggests that the dose, duration of treatment,
and route of administration, as well as coexisting conditions, concomitant
treatments (glucocorticoids or immunosuppressive agents), and dental
health, could all be related to the incidence of this complication.
11
Prevention
and management of bisphosphonate-associated osteonecrosis of the jaw:
Published
recommendations are based upon expert experience from a variety of sources.
35,36,1, 42-–45 As yet, there have been no randomized, controlled
trials that have evaluated strategies to prevent or manage ONJ in individuals
receiving long-term high-dose bisphosphonate therapy. Before initiating
BP therapy, all medical and dental practitioners are encouraged to follow
these guidelines:
All patients
should undergo a routine dental exam to rule out any dental source of
infection.
All medical practitioners
also should perform a baseline oral exam.
Invasive dental
or/and oral surgical procedures should be completed before initiating
therapy.
Practice preventive
dentistry, involving procedures such as oral prophylaxis, dental restorations,
and endodontic therapy, and check dentures for irritational foci.
Schedule routine
follow-up every 3 months to check for any signs of developing ONJ.
The risks associated
with oral surgical procedures such as dental implants, extractions,
and extensive periodontal surgeries must be discussed with the patient
and weighted against the benefits.
The following
recommendations are made by the American Association of Oral and Maxillofacial
Surgeons for management of patients on BP therapy and patients with
proven ONJ. 46
Management
of patients with proven ONJ based on staging of the condition:
Stage 1: Exposed/necrotic bone in patients who are asymptomatic and have no
evidence of infection
Stage 2: Exposed/necrotic bone in patients with pain and clinical evidence
of infection.
Stage 3: Exposed/necrotic bone in patients with pain, infection, and 1 or
more of the following: Pathologic fracture, extra oral fistula, or osteolysis
extending to the inferior border.
Treatment of patients with established ONJ:
Patients with stage 1 ONJ: Conservative management with oral rinse such as 0.12%
chlorhexidine.
Patients
with stage 2 ONJ: Manage with antibiotics and antimicrobial oral rinses.
Patients
with stage 3 ONJ: Surgical debridement/ resection in combination with
antibiotic therapy.
Extraction
of symptomatic teeth can be performed without any additional risks of
worsening the condition.
General
recommendations:
As with
all dental patients, routine dental examinations are recommended. A
comprehensive oral evaluation should be carried out of all patients
about to begin therapy with oral bisphosphonates (or as soon as possible
after beginning therapy). The dentist should inform the patient taking
oral bisphosphonates that there is a very low risk (estimated at 0.7
cases per 100,000 person-years’ exposure) of developing ONJ; there
are ways to minimize the risk, but not to eliminate the already low
risk; the consensus is that good oral hygiene along with regular dental
care is the best way to lower risk; there are no diagnostic techniques
to identify those at increased risk of developing ONJ.
Before undergoing
any invasive procedure that involves manipulation of the bone the patient
should understand that at this time, the risk of developing osteonecrosis
of the jaw is considered very small, and that the vast majority of patients
taking an oral bisphosphonate do not develop any oral complications.
(Dental management of patients receiving oral bisphosphonate therapy:
Expert panel recommendations)
Based on
the currently available information, National Osteoporosis Foundation
believes that in the vast majority of patient who are receiving them,
the benefits of oral bisphosphonate medications outweigh the potential
risk of ONJ. Patients for whom bisphosphonates are appropriate would
be at higher risk of fractures without treatment, and fractures are
the source of significant pain and disability that impact on function
and quality of life. If a patient receiving bisphosphonates has planned
dental surgery that involves the bone, a drug holiday beginning shortly
before the procedure and lasting until there is local healing could
be considered, although there is as yet no clinical evidence that this
will affect the incidence or severity of ONJ. (Osteonecrosis of the
Jaw (ONJ) June 14, 2006 / Reviewed and approved by the Science and Research
Committee of the NOF Board of Trustees March 3, 2007).
Conclusion:
There is
a need to clearly delineate the incidence of ONJ in osteoporosis patients
treated with oral bisphosphonates, and in appropriate control populations.
Based on current evidence, the risk of ONJ in osteoporosis patients
taking oral BPs appears to be comparable to that in the general population.
With the likely prevalence sitting at approximately 1 per 100,000 patient-years,
it is quite clear that this is no different from that in the general
population, since these problems can certainly occur in the absence
of bisphosphonate use. The documented benefits of using bisphosphonates
for established indications clearly outweigh whatever small risk of
osteonecrosis of the jaw might be incurred. 11, 47 Even if
the number of cases of ONJ in patients taking oral bisphosphonates are
still rare compared to the total exposure, primary care physicians treating
bone diseases with bisphosphonates need to be aware there is a small
risk their patients may develop this new complication, allowing for
prophylaxis, early diagnosis and prevention of potential consequences.
The benefits and risks of bisphosphonate therapy should be individually
discussed and, when necessary and possible, alternative therapy for
postmenopausal osteoporosis should be considered.
It is important
to understand that, based on the information currently available; the
risk for developing BON is much higher for cancer patients on intra
venous bisphosphonate therapy than the risk for patients on oral bisphosphonate
therapy. Therefore, there are different recommendations for dental management
of these patients.
In conclusion,
the risk of ONJ is extraordinarily low. The risk of being in a fatal
car accident is 10-15 times as high as the risk of ONJ from taking an
oral bisphosphonate. 41
Competeing Interests:
Serves as a speaker for Eisai Inc. and Pfizer Inc. for the 2008 ARICEPT LTC DELTA
2 (Dementia Education Leadership Training in Alzheimer's) Promotional
Education Program AUTHOR DETAILS
NASSEER A. MASOODI, MD,
FACP, CMD. Assistant Professor Clinical Sciences, Florida State University
College of Medicine, Tallahassee, FL-USA; Courtesy Assistant Professor
Geriatrics, University of Florida College of Medicine, Gainesville,
FL-USA; Medical Director Health Services, ACV Inc, Dowling Park, FL-USA
CORRESSPONDENCE: PO BOX: 4346, Dowling Park, FL-32064, USA.
Email: haadin@yahoo.com
References
Gutta R, Louis
P. Bisphosphonates and osteonecrosis of the jaws: Science and rationale.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:186-93
NIH Consensus
Conference. Optimal calcium intake. NIH Consensus Development Panel
on Optimal Calcium Intake. JAMA. 1994; 272:1942–8.
Cummings SR,
Black DM, Thompson DE et al. Effect of alendronate on risk of fracture
in women with low bone density but without vertebral fractures: results
from the Fracture Intervention Trial. JAMA. 1998; 280:2077–82.
Black DM, Cummings
SR, Karpf DB et al. Randomized trial of effect of alendronate on risk
of fracture in women with existing vertebral fractures. Lancet. 1996;
348:1535–41.
Harris ST, Watts
NB, Genant HK et al. Effects of risedronate treatment on vertebral and
nonvertebral fractures in women with postmenopausal osteoporosis: a
randomized controlled trial. JAMA. 1999; 282:1344–52.
Reginster J,
Minne HW, Sorensen OH et al. Randomized trial of the effects of risedronate
on vertebral fractures in women with established postmenopausal osteoporosis.
Osteoporos Int. 2000; 11:83–91.
McClung MR, Geusens
P, Miller PD et al. Effect of risedronate on the risk of hip fracture
in elderly women. N Engl J Med. 2001; 344:333–40.
Chesnut IC, Skag
A, Christiansen C et al. Effects of oral ibandronate administered daily
or intermittently on fracture risk in postmenopausal osteoporosis. J
Bone Miner Res. 2004; 19:1241–9.
Lyles KW, Colón-Emeric
CS, Magaziner JS et al. Zoledronic acid and clinical fractures and mortality
after hip fracture. N Engl J Med. 2007; 357:1799–809.
Black DM, Delmas
PD, Eastell R et al. Once-yearly zoledronic acid for treatment of postmenopausal
osteoporosis. N Engl J Med. 2007; 356:1809–22.
Bilezikian JP.
Osteonecrosis of the Jaw-Do Bisphosphonates pose a risk? N Engl J Med.
2006; 355:2278–81.
Conte P, Guarneri
V. Safety of intravenous and oral bisphosphonates and compliance with
dosing regimens. Oncologist 2004; 9(Suppl 4):28-37.
Bisaz S, Jung
A, Fleisch H. Uptake by bone of pyrophosphate, diphosphonates and their
technetium derivatives. Clin Sci Mol Med 1978; 54:265-72.
Kasting GB,
Francis MD. Retention of etidronate in human, dog, and rat. J Bone Miner
Res 1992; 7:513-22.
National Osteoporosis
Foundation. Physician’s guide to prevention and treatment of osteoporosis. www.nof.
org/physguide/index.htm (accessed Nov. 2008)
Lips P, Cooper
C, Agnusdei D et al. Quality of life in patients with vertebral fractures:
validation of the Quality of Life Questionnaire of the European Foundation
for Osteoporosis (QUALEFFO). Osteoporos Int. 1999; 10:150–60.
Gold DT, Shipp
KM, Lyles KW. Managing patients with complications of osteoporosis.
Endocrinol Metab Clin North Am. 1998; 27:485–96.
Hallberg I,
Rosenqvist AM, Kartous L et al. Health related quality of life after
osteoporotic fractures. Osteoporos Int. 2004; 15:834–41
Nevitt MC, Ettinger
B, Black DM et al. The association of radiographically detected vertebral
fractures with back pain and function: a prospective study. Ann Intern
Med. 1998; 128:793–800.
Fink HA, Ensrud
KE, Nelson DB et al. Disability after clinical fracture in postmenopausal
women with low bone density: the Fracture Intervention Trial (FIT).
Osteoporos Int. 2003; 14:69–76.
Ensrud KE, Thompson
DE, Cauley JA et al. Prevalent vertebral deformities predict mortality
and hospitalization in older women with low bone mass. J Am Geriatr
Soc. 2000; 48:241–9.
Margolis DJ,
Knauss J, Bilker W et al. Medical conditions as risk factors for pressure
ulcers in an outpatient setting. Age Ageing. 2003; 32:259–64.
Melton LJ 3rd.
Adverse outcomes of osteoporotic fractures in the general population.
J Bone Miner Res. 2003; 18:1139–41.
Empana JP, Dargent-Molina
P, Breart G. Effect of hip fracture on mortality in elderly women: the
EPIDOS prospective study. J Am Geriatr Soc. 2004; 52:685– 90.
Center JR, Nguyen
TV, Schneider D et al. Mortality after all major types of osteoporotic
fracture in men and women: an observational study. Lancet. 1999; 353:878–82.
Cauley JA, Thompson
DE, Ensrud KC et al. Risk of mortality following clinical fractures.
Osteoporos Int. 2000; 11:556–61.
Keene GS, Parker
MJ, Pryor GA. Mortality and morbidity after hip fractures. BMJ. 1993;
307:1248–50.
Hoff AO, Toth
B, Altundag K, et al. Osteonecrosis of the jaw in patients receiving
intravenous bisphosphonate therapy. J Bone Miner Res 2005; 20: Suppl
1:1218. Abstract
Bouquot JE,
McMahon RE. Neuropathic pain in maxillofacial osteonecrosis. J Oral
Maxillofac Surg 2000; 58:1003-20.
Assouline-Dayan
Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME. Pathogenesis and
natural history of osteonecrosis. Semin Arthritis Rheum 2002; 32:94-124.
Gruppo R, Glueck
CJ, McMahon RE, Bouquot J, Rabinovich BA, Becker A, et al. The pathophysiology
of alveolar osteonecrosis of the jaw: anticardiolipin antibodies, thrombophilia,
and hypofibrinolysis. J Lab Clan Med 1996;127:481-8.
Damato K, Gralow
J, Hoff A, Huryn J, Marx RE, Ruggiero S, et al. Available at: http://www.fda.gov/ohrms/dockets/ac/05/briefing/ 2005-4095B2_02_12-Novartis-Zometa-App-11.pdf.
(Accessed Oct, 2008).
Zigic TM, Marcous
C, Hungerford DS, Dansereau JV, Stevens MB. Corticosteroid therapy associated
with ischemic necrosis of bone in systemic lupus erythematosis. Am J
Med 1985;79:596.
Marx RE. Pamidronate
(Aredia) and zoledronate (Zometa) induced avascular necrosis of the
jaws: a growing epidemic. J Oral Maxillofac Surg 2003;61(9):1115–7.
Woo SB, Hellstein
JW, Kalmar JR. Bisphosphonates and osteonecrosis of the jaws. Ann Intern
Med 2006; 144:753-6. [Erratum, Ann Intern Med 2006; 145:235.]
Marx RE, Sawatari
Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis)
of the jaws: risk factors, recognition, prevention, and treatment. J
Oral Maxillofac Surg 2005; 63:1567-75.
Novartis Pharmaceuticals
Co. Updated safety: possible relationship of Aredia (Pamidronate disodium)
and/or Zometa (zoledronic acid) with osteonecrosis of the jaw [letter
to health care professionals]. Ottawa: Health Canada; Nov 2004. Available
at: www.hc-sc.gc.ca/ hpfb-dgpsa/tpd-dpt/aredia_zometa_hpc_e.html.
(Accessed Nov, 2008).
American Dental
Association Council on Scientific Affairs: Expert panel recommendations:
Dental management of patients receiving oral bisphosphonate therapy.
J Am Dental Assoc 2006, 137:1144-1150
Cartosos VM,
Zhu S, Zavras AI. Bisphosphonate use and the risk of adverse jaw outcomes.
JADA 2008; 139: 23-30.
Pazianas M,
Blumentals WA, Miller PD. Lack of association between oral bisphosphonates
and osteonecrosis using jaw surgery as a surrogate marker. Osteoporos
Int 2008;19: 773-779.
Postmenopausal
Osteoporosis: Putting the Risk for Osteonecrosis of the Jaw Into Perspective
Authors: Stuart L. Silverman, MD, FACR, FACP; Mone Zaidi, MD, PhD, FRCP;
E. Michael Lewiecki, MD, FACP; Regina Landesberg, DMD, PhD (Medscape
Online CME, accessed on April 23, 2007).
Migliorati CA,
Siegel MA, Elting LS. Bisphosphonate-associated osteonecrosis: a long-term
complication of bisphosphonate treatment. Lancet Oncol 2006;7(6):508–14
Expert panel
recommendations for the prevention, diagnosis, and treatment of osteonecrosis
of the jaws. LDA J 2005; 64(3):21–4.
Melo MD, Obeid
G. Osteonecrosis of the jaws in patients with a history of receiving
bisphosphonate therapy: strategies for prevention and early recognition.
J Am Dent Assoc 2005; 136(12):1675–81.
Hellstein JW,
Marek CL. Bisphosphonate induced osteochemonecrosis of the jaws: an
ounce of prevention may be worth a pound of cure. Spec Care Dentist
2006; 26(1):8–12.
AAOMS Position
Paper on Bisphosphonate-Related Osteonecrosisof the Jaws. Available
at: http://aaoms.org/docs/position_papers/osteonecrosis.pdf. (Accessed
October, 2008).
ASHP Therapeutic
Position Statement on the Prevention and Treatment of Osteoporosis in
Adults http://www.ashp.org/DocLibrary/BestPractices/TPS_Osteo.aspx (Accessed Nov 25, 2008)
Adjuvant
modes of breast cancer therapy following surgical intervention mainly
revolve round radiation therapy, chemotherapy, or hormone therapy designed
to eliminate residual cancer cells. The increase in the incidence of
breast cancer with age has sharply focused attention on the link between
incidence and progression. It follows from this that approaches to successful
treatment and patient management would converge on hormonal status as
a beneficial mode of targeted therapy. A number of growth factors, besides
the steroid hormones oestrogen and progesterone, are closely involved
in the growth and metastatic spread of breast cancer. Recent years have
seen intensive studies of the mechanisms of function of growth factors
and the pathways by which they stimulate the growth of cancer cells.
These studies have led the way to the targeting growth factor function
as a means of controlling breast cancer development and secondary spread.
The growth
factor receptors are transmembrane proteins. The binding of growth factors
to the external domain activates these receptors which have tyrosine
kinase activity. This activation therefore leads to the phosphorylation
of signalling proteins down stream in the signalling cascade. This in
turn leads to the expression of genes associated with cell proliferation
and often also to the inhibition of apoptotic loss of cells.
Growth
factors, growth factor receptors and tumour growth and progression
Growth factors
and their receptor play a major part in normal growth and differentiation
and also in tumour development and progression. Growth factors promote
proliferation and induce cancer invasion. Certain growth factors, e.g.
the insulin-like growth factor (IGF) might promote tumour growth by
inhibiting apoptotic loss of cells1. Mutations or over-expression
of growth factor receptors is associated with aggressive cancers and
poor prognosis for patients. Growth factor receptor genes are amplified
in a number of human cancers and this is reflected in the expression
of the respective receptor proteins in the cancers. Growth factor receptors
are transmembrane tyrosine kinase proteins and transduce the signals
imparted by the binding of the growth factors to their specific receptors;
this signal transmission ultimately results in the induction of cell
proliferation.
Among growth
factors of note in the context of this editorial are the epidermal growth
factor (EGF) and the Heregulins constituting a family of EGF related
growth factors. There are several isoforms of Heregulin generated by
alternative RNA splicing of the heregulin gene; these isoforms bind
to their receptors with different degree of affinity. The epidermal
growth factor receptor (EGFr) family (also often referred to as the
erb family) includes HER1 (human epidermal growth factor receptor 1
also called EGFr), HER2, HER3
and HER4. These receptor proteins significantly resemble one another
in aminoacid sequence2. Heregulin can bind HER3 and HER4
receptors but the ligand for HER2 has not been identified3
and so HER2 is often described as an orphan receptor. The receptor protein
consists of an external domain that binds growth factors, a transmembrane
domain and an intracellular domain which possesses tyrosine phosphorylation
sites4. Growth factors and their paralogues bind to these
receptors and induce receptor oligomerisation. This activates the cytoplasmic
kinase domains, which phosphorylate and activate target proteins that
induce the expression of genes responsive to the growth factors. The
binding and activation of the receptors is a highly specific process,
but often more than one receptor might be involved in the signalling
process. In this event heterodimerisation would occur between different
receptors; this seems to enhance the affinity of ligand binding5.
This process of engagement of co-receptors to enhance growth factor
signalling has been described as cross-talk between the receptors. HER2
is known to be involved in cross-talk with EGFr, HER3 as well as HER4.
So HER2 seems to occupy a pre-eminent position in the signalling cascade,
but recently it has been suggested that HER3 might also be a prominent
participant6.
The EGFr
family of receptors have been intensively investigated for their potential
relationship to cancer progression and prognosis and as a potential
route for treatment and patient management. Approximately 25% of breast
cancers show HER2 gene amplification and this correlates aggressive
behaviour and poor prognosis7-10. However, on the positive
side the presence of HER2 receptors has provided a new treatment modality
for many patients.
Monoclonal
antibodies (Herceptin) have been raised against the external domain
of HER2. Herceptin has provided a highly successful mode of treatment
for metastatic breast cancer showing high HER2 expression and HER2 gene
amplification11-13. Blocking receptor function with Herceptin
inhibits tumour growth and possibly also microvascular density associated
with tumours and vascular permeability. Furthermore, Herceptin treatment
appears to reduce VEGF (vascular endothelial growth factor) expression,
tumour associated microvascular density and cell proliferation in breast
cancers xenografted into mice14. Also in murine tumour models,
Herceptin reduces the number of circulating cancer cells even under
circumstances where the tumour is resistant to Herceptin treatment15,
which could be a manifestation of its effects on the vasculature independently
of its inhibition of HER2 signalling.
HER2
expression and tamoxifen resistance
Breast cancer
growth is influenced by the sex steroid hormones oestrogen and progesterone
and growth factors such as EGF and HER2 ligands. Patients with tumours
that are oestrogen receptor (ER) positive are treated with tamoxifen.
The latter binds ER and competitively blocks oestrogen signals. In the
context of the deployment of Herceptin to treat HER2+ patients, it has
emerged that tumours over-expressing HER2 are resistant to tamoxifen.
These patients could benefit from anti-oestrogen therapy combined with
blockade of HER2 signalling16. A randomized trial has indicated
that post-menopausal patients with advanced breast cancer can benefit
significantly from this combination therapy17.
Among other
factors that might confer tamoxifen resistance is AIB1, the steroid
receptor co-activator, which is often amplified in breast cancers. In
vitro studies with breast cancer cells and in vivo investigations of
murine tumours have suggested the involvement of AIB1 in tamoxifen resistance18
and in HER2 signalling19. In primary breast cancer also AIB1
has been linked with tamoxifen resistance20, 21. A second
factor deserving discussion in this context is the possibility that
EGFr and HER2 signalling systems might interact and contribute in this
way to resistance to hormonal therapy. As mentioned elsewhere in this
review, EGFr does recruit HER2 as a co-receptor in signal transduction.
This is of some significance for patients with ER-negative tumours.
For, we showed some years ago that a proportion of ER-ve tumours tended
to be EGFr+ve22-24. So this would suggest the possibility
that patients with ER-ve/EGFr+ tumours could conceivably benefit from
Herceptin treatment (see below).
Another
possible means by which tamoxifen resistance might arise has been suggested
by the finding that tamoxifen and Fulvestrant, also an anti-oestrogen,
appear to be able to induce breast cancer cell invasion in the absence
of E-cadherin25. Cadherins are transmembrane proteins, which
have considerable influence on cancer invasion because they alter intercellular
and cell-substratum adhesion. E-cadherin is regarded as a suppressor
of invasion and growth of carcinomas as the loss or mutation of E-cadherin
leads to the acquisition of invasiveness. Borley et al.25
showed that both tamoxifen and Fulvestrant induced invasion in E-cadherin
deficient MCF7 breast cancer cells, but this did not occur after oestrogen
depletion. These findings add a new dimension to tamoxifen resistance
as potentially being mediated by recurrence resulting from induced invasive
ability.
HER2
expression and adjuvant chemotherapy
It has been
recognised of late that combination of Herceptin with chemotherapy might
yield considerable benefits in terms of reduction of recurrence and
mortality. So HER2 expression has come into the reckoning when considering
the use of adjuvant chemotherapy. Combining Herceptin with either an
anthracycline plus cyclophosphamide or with Paclitaxel, as first-line
therapy for metastatic breast cancer over expressing the HER2 receptor,
has provided significant benefits in terms of objective response, duration
of response and survival as compared with chemotherapy alone. Furthermore,
the benefits were related to the degree of HER2 over-expression26.
A review of 35 clinical trials has indicated that patients with HER2+
cancers might benefit more from anthracycline-based and taxane-based
adjuvant chemotherapy than those with HER2-negative cancers27.
Indeed, anti-HER2 antibody combined with chemotherapy is superior to
HER2 anitibody and anti-oestrogen combination17. The benefits
of adjuvant chemotherapy with anthracyclines to patients with HER2 over-expressing
tumours seem to be beyond reasonable doubt. Gennari et al.28
have provided a combined analysis of eight studies. HER2+ patients on
anthracyclines had superior disease-free as well as overall survival
in comparison with patients on non-anthracycline regimen. No such benefits
emerged for HER2-ve patients, suggesting that one can exclude these
patients from anthracycline adjuvant therapy. Also being investigated
is potential synergy between antibodies against other growth factor
receptors and anti-HER2 antibodies.
Attempts
are also currently in progress to test the efficacy of conjugates of
anti-HER2 antibodies with cytotoxic drugs to achieve targeted delivery
of the cytotoxic agents. Laboratory studies are underway with Herceptin-platinum(II)
complexes29 and Herceptin-microtubule-depolymerising agents30.
Contraindications
of Herceptin regimen
The toxic
side-effects of the administration of monoclonal antibodies were recognised
some years ago. Cardiotoxicity, pulmonary toxicity and infusion-related
problems such as anaphylaxis occur, albeit infrequently with monoclonal
antibody therapies 31, 32. These toxicities have been described
with Herceptin treatment, more so in patients on anthracycline and cyclophosphamide
combined with Herceptin26. Cardiotoxicity could occur in
some patients when Herceptin is administered with anthracyclines33,
34. Herceptin itself can be cardiotoxic in patients receiving
concurrent or prior anthracyclines35, 36. Cardiotoxicity
is not due to structural abnormalities but Herceptin might cause myocardial
dysfunction. The toxicity of anthracyclines and Herceptin could be brought
about by different routes37. As Dinh et al.38
have emphasised, many questions relating to Herceptin treatment still
remain unanswered, e.g. optimising treatment, and combination with conventional
chemotherapeutic agents, among others. Even with these caveats Herceptin
may be regarded as a most efficacious agent in the treatment of HER2+
breast cancers.
EGFr
inhibitor Lapatinib (Tykerb) in breast cancer treatment
As stated
earlier, EGFr is over expressed in a proportion of breast cancers that
are ER-negative. EGFr expression also correlates with the expression
of metastasis promoting genes. Further, in the light of the function
of EGFr in conjunction with HER2, it would be of considerable clinical
benefit to test the effects of EGFr inhibitors in breast cancer treatment.
Lapatinib is a powerful dual inhibitor of EGFr and HER2 with marked
pharmacological potential.
Lapatinib
is a protein kinase inhibitor (a 4-anilinoquinazoline derivative), which
inhibits growth factor signalling by binding to the ATP-binding pocket
of both EGFr and HER2 receptor proteins and so prevents autophosphorylation
of the receptor and inhibits the signalling cascade leading to the suppression
of the growth of tumours, including advanced or metastatic breast cancers
resistant to Herceptin39. Objective responses have been achieved
in 28% of patients with untreated HER2-positive tumours40.
Clinical trials have provided promising results; Lapatinib is clinically
very effective especially in advanced or metastatic breast cancer and
patients with brain metastases. A phase III trial assessing the efficacy
of combination of Lapatinib with Capecitabine, which is converted to
5-Flurouracil and inhibits DNA synthesis, seems to suggest a significant
slowing down of disease progression by the combination as compared with
capecitabine alone41. The efficacy of combining Lapatinib
with other conventional chemotherapeutic agents is being evaluated.
First-line Paclitaxel-Lapatinib combination gave significant benefits
to HER-2-positive patients42.
Lapatinib
could be functioning synergistically with HER2 inhibitors, for its effect
on prominently EGFr over-expressing cancers, such as colorectal cancer
or squamous cell carcinoma of the head and neck, is said to be unexceptional
and moderate43. According to Press et al.44 the
benefits of Lapatinib appear to be restricted to patients with HER2
over-expressing cancers. Lapatinib has no cardiac toxicity but does
produce other toxic effects45. However, its toxicity whilst
administered in combination with other anticancer agents has not been
appraised.
Avastin
in breast cancer treatment
A different
route to control of tumour growth and metastatic spread has been afforded
by inhibitors that target the microvasculature associated with tumours.
Tumours induce the formation of neovascularisation so that tumour cells
can access the vascular system and become disseminated to form distant
metastases. The neovasculature is induced by VEGF, which transduces
its effects by binding specifically to its receptors VEGFr (see46).
A strategy similar to that adopted with EGF family growth factors has
been used to target VEGFr, inhibit its function and inhibit the signalling
by VEGF. Avastin (Bevacizumab), a humanised monoclonal anti-VEGFr antibody,
is such an inhibitor. Avastin with Paclitaxel chemotherapy has been
found to enhance progression-free survival and improve response rate
in patients with advanced breast cancer47. However, on account
of possible side effects, there is some reluctance to the use of Avastin.
It has been approved in Europe for first line treatment of women with
metastatic breast cancer, but has not been approved for use by the National
Institute for Health and Clinical Excellence UK48.
ACKNOWLEDGEMENTS
The author
thanks Professor Leif Bergkvist of the Department of Surgery and Centre
for Clinical Research of Uppsala University Central Hospital at Västerås,
and Dr M.S. Lakshmi for reading the manuscript and making helpful suggestions,
and Professor Bayan Sharif and Professor Satnam Dlay for research and
literary facilities
COMPETING
INTERESTS
None Declared AUTHOR
DETAILS
GAJANAN
V SHERBET, The Institute for Molecular Medicine, Huntington Beach CA,
USA and School of Electrical, Electronic and Computer Engineering, University
of Newcastle upon Tyne UK
CORRESPONDENCE:
GAJANAN V SHERBET, School of Electrical, Electronic and Computer Engineering,
University of Newcastle upon Tyne, Merz Court, Newcastle upon Tyne,
NE1 7RU, U.K.
Email:
gajanan.sherbet@ncl.ac.uk
References
Werner H, Le
Roith D. The insulin-like growth factor-I receptor signaling pathways
are important for tumorigenesis and inhibition of apoptosis., Critical
Reviews Oncol 1997; 8: 71-92.
Schlessinger
J, Ullrich A. Growth factor signalling by receptor tyrosine kinases.
Neuron 1992; 9: 383-391
Tzahar E, Levkowitz
G, Karunagaran D, et al. ErbB-3 and ErbB-4 function as respective low
and high affinity receptors of all Neu differentiation factor Heregulin
isoforms. J Biol Chem 1994; 269: 25226-25233.
Ullrich A, Schlessinger
J. Signal transduction by receptors with tyrosine kinase activity. Cell
1990; 61: 203-212.
Karunagaran D,
Tzahar E, Beerli RR, et al. ErbB-2 is a common auxiliary subunit of
NDF and EGF receptors: Implications for breast cancer. EMBO J 1996;
15: 254-264.
Lee-Hoeflich
ST, Crocker L, Yao E, et al. A central role for HER3 in HER2-amplified
breast cancer: implications for targeted therapy. Cancer Res 2008; 68:
5878-5887.
Slamon DJ, Clark
G, Wong S et al. Human breast cancer: correlation of relapse and survival
with amplification of the HER-2/neu oncogene. Science 1987; 235: 177-181.
Slamon DJ, Godolphin
W, Jones L, et al. Studies of the HER-2/neu proto-oncogene in human
breast and ovarian cancer. Science 1989; 244: 707-711.
Venter D, Kumar
S, Tuzi N, et al. Over expression of the c-erbB-2 oncoprotein in human
breast carcinomas: immunohistochemical assessment correlates with gene
amplification. Lancet 1987; 2: 69-72.
Natali P, Nicotra
M, Brigotti A, et al. Expression of the p185 encoded by HER2 oncogene
in normal and transformed human tissues. Int J Cancer 1990; 45: 457-461.
Cobleigh MA,
Vogel CL, Tripathy D, et al. Multinational study of the efficacy and
safety of humanized anti-HER2 monoclonal antibody in women who have
HER2-overexpressing metastatic breast cancer that has progressed after
chemotherapy for metastatic disease. J Clin Oncol 1999; 17: 2639-2648.
Vogel CL, Cobleigh
MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single
agent in first-line treatment of HER2-overexpressing metastatic breast
cancer. J Clin Oncol 2002; 20: 719-726.
Shepard HM,
Jin P, Slamon DJ, et al. Herceptin Handbook Exp Pharmacol 2008;
181: 183-219.
Le XF, Mao WQ,
Lu CH, et al. Specific blockade of VEGF and HER2 pathways results in
greater growth inhibition of breast cancer xenografts that over express
HER2. Cell Cycle 2008; 7: 3747-3758.
Barok M, Balazs
M, Nagy P, et al. Trastuzumab decreases the number of circulating and
disseminated tumor cells despite trastuzumab resistance of the primary
tumor. Can Lett 2008; 260: 198-208.
Rastelli F,
Crispino S. Factors predictive of response to hormone therapy in breast
cancer. Tumori 2008; 94: 370-383.
Prat A, Baselga
J. The role of hormonal therapy in the management of hormonal-receptor-positive
breast cancer with co-expression of HER2. Nature Clin Pratice Oncol
2008; 5: 531-542.
Su QB, Hu SY,
Gao HD, et al. Role of AIB1 for Tamoxifen resistance in estrogen receptor-positive
breast cancer cells. Oncology 2008; 75: 159-168.
Fereshteh MP,
Tilli MT, Kim SE, et al. The nuclear receptor coactivator amplified
in breast cancer-1 is required for neu (ErbB2/HER2) activation, signaling,
and mammary tumorigenesis in mice. Cancer Res 2008; 68: 3697-3706.
Kirkegaard T,
McGlynn LM, Campbell FM, et al. Amplified in breast cancer 1 in human
epidermal growth factor receptor-positive tumors of tamoxifen-treated
breast cancer patients. Clin Cancer Res 2007; 13: 1405-1411.
Dihge L, Bendahl
PO, Grabau D, et al. Epidermal growth factor receptor (EGFR) and the
estrogen receptor modulator amplified in breast cancer (AIB1) for predicting
clinical outcome after adjuvant tamoxifen in breast cancer. Breast Cancer
Res Treat 2008; 109: 255-262.
Sainsbury JRC,
Farndon JR, Harris AL, Sherbet GV. Epidermal growth factor receptors
are present in human breast cancers. Br J Surg. 1984; 71: 902.
Sainsbury JRC,
Farndon JR, Harris AL, Sherbet GV. Epidermal growth factor receptors
on human breast cancers. Br J Surg 1985; 72: 186-188.
Sainsbury JRC,
Farndon JR, Sherbet GV, et al. Epidermal growth factor receptors and
oestrogen receptors in human breast cancer. Lancet 1985; l: 364-366.
Borley AC, Hiscox
S, Gee J, et al. Anti-oestrogens but not oestrogen deprivation promote
cellular invasion in intercellular adhesion-deficient breast cancer
cells. Breast Cancer Res 2008; 10: R103.
McKeage K, Perry
CM. Trastuzumab - A review of its use in the treatment of metastatic
breast cancer over expressing HER2. Drugs 2002; 62: 209-243.
Dhesy-Thind
B, Pritchard KI, Messersmith H, et al. HER2/neu in systemic therapy
for women with breast cancer: a systematic review. Breast Cancer Res
Treat 2008; 109: 209-229.
Gennari A, Sormani
MP, Pronzato P, et al. HER2 status and efficacy of adjuvant anthracyclines
in early breast cancer: a pooled analysis of randomized trials. J Natl
Cancer Inst. 2008; 100: 14-20.
Gao J, Liu YG,
Liu R, et al. Herceptin-platinum(II) binding complexes: Novel cancer-cell-specific
agents. Chem Med Chem 2008; 3: 954-962.
Phillips GDL,
Li GM, Dugger DL, et al. Targeting HER2-positive breast cancer with
Trastuzumab-DM1, an antibody-cytotoxic drug conjugate. Cancer Res 2008;
68: 9280-9290.
Cersosimo RJ.
Monoclonal antibodies in the treatment of cancer, part 1. Amer J Hlth-System
Pharm 2003; 60: 1531-1548.
Klastersky J.
Adverse effects of the humanized antibodies used as cancer therapeutics.
Current Opinion Oncol 2006; 18: 316-320.
Perez EA. Cardiac
toxicity of ErbB2-targeted therapies: What do we know? Clin Breast Cancer
2008; 8: S114-S120
McKeage K, Lyseng-Williamson
KA. Trastuzumab - A pharmacoeconomic review of its use in early breast
cancer. Pharmacogenomics 2008; 26: 699-719.
Ewer SM, Ewer
MS. Cardiotoxicity profile of trastuzumab. Drug Safety 2008; 31: 459-467.
Popat S, Smith
IE. Therapy insight: anthracyclines and trastuzumab - the optimal management
of cardiotoxic side effects. Nature Clin Pract Oncol 2008; 5: 324-335.
Bria E, Cuppone
F, Milella M, et al. Trastuzumab cardiotoxicity: biological hypotheses
and clinical open issues. Expert Opinion Biol Therapy 2008; 8: 1963-1971.
Dinh P, de Azambuja
E, Cardoso F, et al. Facts and controversies in the use of trastuzumab
in the adjuvant setting Nature Clin Pract Oncol 2008; 5: 645-654.
Nelson MH, Dolder
CR. Lapatinib: A novel dual tyrosine kinase inhibitor with activity
in solid tumors. Ann Pharmacotherapy 2006; 40: 261-269.
Johnston SRD,
Leary A. Lapatinib: A novel EGFR/HER2 tyrosine kinase inhibitor for
cancer. Drugs Today 2006; 42: 441-453.
Bilancia D,
Rosati G, Dinota A, et al. Lapatinib in breast cancer. Ann Oncol 2007;
18 Suppl 6: 26-30.
Di Leo A, Gomez
HL, Aziz Z, et al. Phase III, Double-blind, randomized study comparing
Lapatinib plus Paclitaxel with placebo plus Paclitaxel as first-line
treatment for metastatic breast cancer J Clin Oncol 2008; 26: 5544-5552.
Montemurro F,
Valabrega G, Aglietta M. Lapatinib: a dual inhibitor of EGFR and HER2
tyrosine kinase activity. Expert Opinon Biol Therapy 2007; 7: 257-268.5
Press MF, Finn
RS, Cameron D, et al. HER-2 Gene amplification, HER-2 and epidermal
growth factor receptor mRNA and protein expression, and Lapatinib Efficacy
in women with metastatic breast cancer. Clin Cancer Res 2008; 14: 7861-7870.
Sherbet GV,
Lakshmi MS. The genetics of cancer: Genes associated with cancer invasion,
metastasis and cell proliferation. 1997; Academic Press, London.
National Cancer
Institute and Eastern Cooperative Oncology Group ECOG, 2005
The National
Institute for Clinical Excellence in June 2008 guidelines.
Severe pulmonary
hypertension (PH) is a rare disorder characterized by multifactorial
etiology and shared pathophysiology. The belief that primary pulmonary
hypertension (PPH) is an idiopathic variety mostly affecting younger
women may still be held by some. However, PH has often been reported
in overweight and obese individuals and postmenopausal women.1
Earlier studies have also suggested that combination of obesity and
higher altitude favors the development of pulmonary arterial hypertension.
Hypercapnic acidemia and increased total blood volume have been implicated
in this group of patients. Pulmonary artery systolic pressures (PASP)
greater than 40 mmHg is found in 6% of otherwise normal individuals
age 50 years or older and in 5% of individuals with a BMI greater than
30kg/m2 . 2
Overall,
the widely held view has been that alveolar hypoxia is the main pathophysiologic
cause of vasoconstriction in obese patients living at sea level or higher
altitudes. In 1947, Motley et al demonstrated that breathing a gas mixture
containing 10% oxygen induced a rise in pulmonary artery pressure (PAP).3Papers
dating back more than three decades have documented increases in PAP
associated with hypoxemia related to sleep disordered breathing (SDB).
It is well known that apneic episodes during sleep are associated with
transient elevations in PAP, which return to baseline when breathing
resumes after relief of obstruction. Earlier studies suggested
that daytime hypoxemia attributable to abnormal lung function was the
main cause of pulmonary hypertension in patients with sleep apnea. Whether
transient hypoxemias and associated elevations in PAP with obstructive
events during sleep are adequate to produce daytime resting “fixed”
pulmonary vascular disease, or whether daytime hypoxemia is required
remains unclear. It is also less certain whether daytime pulmonary
arterial hypertension also occurs in OSA patients without underlying
pulmonary or cardiac disease. Additionally, studies have shown
that the severity of SDB as measured by apnea-hypopnea index (AHI) and
the PAP elevations often fail to correlate.
Sajkov et
al 4 were amongst the first to demonstrate that hypoxemia
in PH patients with obstructive sleep apnea syndrome (OSAS) could not
be explained by impairment of lung or cardiac function, BMI and smoking
history. However, most of the studies that have tackled this question
(including the one done by Sajkov) have used echocardiography based
pulmonary artery pressures and the few that have used the gold standard
Right heart catheterization (RHC) used a definition of mean pulmonary
artery pressure (mPAP) >20 mmHg. At present, pulmonary arterial hypertension
is defined as a mean PAP greater than 25mmHg at rest or 30 mmHg with
exercise, as measured by RHC. The largest such study found PAH in 17%
patients but it also included some patients with chronic obstructive
pulmonary disease (COPD).5
Smaller series of patients with OSA but no clinical history of COPD
have reported daytime PAH as measured by RHC in 20-42% patients.
6, 7
Thus, despite
acute nocturnal increases in PAP associated with obstructive apneas,
proof that OSA causes PH has been limited by other co-morbidities related
to obesity. The three biggest confounders making this issue difficult
to be explored are associated COPD in OSAS patients (overlap syndrome),
Obesity Hypoventilation Syndrome (OHS) and underlying concomitant left
ventricular dysfunction in patients with OSA. OHS as defined at present
is characterized by combination of obesity (BMI ≥30kg/m2)
and chronic daytime hypercapnia (PaCo2 >45 mmHg); and sleep disordered
breathing in the absence of other known causes of hypercapnia.8
PH has been shown to be more frequent and mean PAP higher in patients
with OHS or the overlap syndrome when compared to patients with pure
OSAS only. 9 Elevated mPAP associated with higher pulmonary
capillary wedge pressure (PCWP) from underlying elevated left
ventricular end-diastolic pressure and in some studies apnea associated
have been other potential confounders.10 Other difficulties
related to exploring this issue are technical concerns regarding non-invasive
measurement of pulmonary artery pressure in obese OSA patients and difficulties
in identifying suitable controls i.e, obese patients with PH and without
OSA. Studies are also needed to investigate the role of humoral vasoactive
factors like natriuretic peptides, nitric oxide or norepinephrine and
individual genetic predisposition to account for different remodeling
responses to hypoxia in the pulmonary circulation. In OSAS patients
no neutrally mediated effect of apneas on PAP has been demonstrated.
PH seen
in association with OSA is generally regarded as mild and can be attributed
to elevated pulmonary vascular resistance (PVR) because cardiac output
and PCWP are normal atleast at rest. Although the association between
left sided-heart disease and OSA is widely accepted, most studies of
OSA patients with PH do not differentiate between pre-capillary (PAH)
and post-capillary pulmonary hypertension (PVH). Additionally a good
proportion of the studies do not even report PCWP.6, 9 while
some explain higher PAP on the basis of PCWP alone.
Elevations in both PCWP and PVR have been reported to contribute to
PH in patients with OHS. A recent study of referred patients who met
the WHO criteria for PAH from Duke University reported PCWP> 15 mmHg
in 25% of the patients. These patients were predominantly obese (58%)
and all had normal LVEF%. 11
In ourretrospective analysis of 8254 patients who underwent
RHC for suspected PH, mean Right atrial pressure, mean PA diastolic
pressure, mean PCWP and mean cardiac output increased proportionately
with increase in BMI regardless of the underlying contributory disease
process. 12
The debate
about whether OSA alone can be a cause of sustained pulmonary arterial
hypertension continues, but based on the above literature, the latest
revision of the Clinical Classification of Pulmonary Hypertension identifies
SDB as a part of the category of respiratory disorders associated with
PH.13 The most direct evidence comes from observations that
treatment of OSA with continious positive airway pressure (CPAP)
may lower daytime PAP. OSA patients with PH seem to have increased pulmonary
vascular reactivity to hypoxia compared to patients without PH and CPAP
has been reported to decrease pulmonary vascular reactivity to hypoxia.14
In studies from Stanford as early as 1978, 50% reduction in PAP
was noted in six selected patients with OSA after tracheostomy. In a
recent randomized placebo-controlled cross-over trial of effective versus
sham CPAP in 23 patients with OSA, effective CPAP was associated with
decreases in echocardiographic measurements of PASP especially in patients
with PH or left ventricular diastolic dysfunction at baseline.
15 This trial was limited by baseline differences in obesity and
lung function between the two groups. Larger randomized studies are
needed to identify more definitively any sustained effects of CPAP therapy
on PH and right heart function and to better establish any role for
CPAP as one of the rapidly evolving therapeutic options for PH.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
ROOP KAW, MD, Assistant Professor of Medicine, USA
CORRESPONDENCE: DR ROOP KAW,
Cleveland Clinic Main Campus, A12, 9500 Euclid Avenue, Cleveland, USA. OH44197
Email: KAWR@ccf.org
References
Taraseviciute
A, Voelkel NF et al. Severe pulmonary hypertension in postmenopausal
obese women. Eur J Med Res.2006 May 5; 11(5): 198-202.
McQuillan BM,
Picard MH, Leavitt et al. Clinical correlates and reference intervals
for pulmonary artery systolic pressure among echocardiographically normal
subjects. Circulation 2001; 104: 2797-2802.
Motley HL, Cournand
A, Werko et al. The influence of short periods of induced acute anoxia
upon pulmonary artery pressures in man. Am J Physiol 1947; 150: 315-320.
Sajkov D, Crowie
RJ, Thronton TH et al. Pulmonary hypertension and hypoxemia in obstructive
sleep apnea syndrome. Am J Respir. Crit. Care Med. 1994; 149: 416- 422.
Chaouat A, Weitzenblum
E, Krieger J et al. Pulmonary Hemodynamics in the Obstructive Sleep
Apnea Syndrome: Results in 220 Consecutive patients. Chest 1996; 109;380-386.
Laks L, Lehrhaft
B, Grunstein R et al. Pulmonary hypertension in obstructive sleep apnea.
Eur Respir J 1995 (8): 537-541.
Sanner BM, Doberauer
C, Konermann M et al. Pulmonary hypertension in patients with obstructive
sleep apnea syndrome. Arch Int Med 1997; 157: 2483-2487.
Olson AL, Zwillich
C. The Obesity hypoventilation syndrome. Am J Med 2005(118): 948-56.
Kessler R, Chaouat
A, Schinkewitch P et al. The Obesity-Hypoventilation Syndrome revisited.
A prospective Study of 34 cases. Chest 2001; 120(2): 369-376.
Buda AJ,
Schroeder JS, Guilleminault C et al. Abnormalities of pulmonary
artery wedge pressures in sleep-induced apneas. Int J Cardiol 1981;
I: 67-74.
Fortin TA, Krichman
A, Hargett CW et al. Characteristics of pulmonary arterial hypertension
associated with elevated pulmonary capillary wedge pressure. Chest 2005
Abstracts, Monday October 31.
Kaw R, Thota
A, Minai O. Pulmonary hypertension in Obese patients: An analysis of
hemodynamic data. Chest 2008; 134: p 134003.
Simmonneau G,
Galie N, Rubin LJ et al. Clinical classification of pulmonary hypertension.
J Am Coll of Cardiol. 2004; 43;5S-12S
Sajkov D, Wang
T, Saunders NA et al. Continous positive airway pressure treatment improves
pulmonary hemodynamics in patients with obstructive sleep apnea. Am
J Resp Crit Care Med. 2002; 165: 152-158.
Arias MA, Garcia-Rio
F, Alonso Fernandez A et al. Pulmonary hypertension in obstructive sleep
apnoea: effects of continous positive airway pressure: a randomized,
controlled cross-over study. Eur Heart J 2006; 27: 1106-1113.
Chest radiographs are one of the most common radiological procedures performed in medical practice. The chest radiograph should ideally include views of the heart, lungs, trachea, mediastinum, bones of the chest and upper part of the abdomen. Chest radiographs are normally taken in the posterior-anterior (PA) view with the patient in upright / standing position but for patients admitted in the intensive care unit (ICU) or other emergency situations, this is not possible and so they are taken in the supine (anterior-posterior views) or semi-erect position.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In this article, we aim to discuss and compare the normal and abnormal positions of both the endotracheal tube (ETT) and nasogastric tube (NG) on chest radiographs.
Endotracheal tube (ETT):
Endotracheal tubes are used to secure the patients airway. Modern ETTs have a radio-opaque line running along their length which enables us to determine their position on chest radiographs 1.
Clinical methods 2 that can be used to determine the appropriate position of the ETT include:
Symmetrical rise and fall of the chest wall with each breath (on inspection and palpation of the chest).
Auscultation of the lung fields
Use of capnography
However, clinical methods cannot confirm how high or low the ETT is situated in the trachea. This can be confirmed by chest radiography. Optimum position of the ETT is required to ensure ventilation of both lungs.
A correctly positioned ETT lies in the mid trachea and its tip is approximately 5-7 cm above the carina 3 as seen in Fig: 1 (CR-1827).
In Fig: 2 (CR-1820), the tip of the ETT is low lying and is at the origin of the right main bronchus. Further migration of the ETT will result in right sided endobronchial intubation and collapse of the left lung. This will result in decreased oxygen saturation values (SpO2) on a pulse oximeter and low arterial partial pressure of oxygen (PaO2) on analysis of an arterial blood gas specimen.
Nasogastric tube (NG):
Nasogastric tube (NG) or orogastric tube (OG) is inserted for providing enteral nutrition, administration of drugs or for gastric drainage. NG feeding is a common practice in all age groups. There is a risk that the NG feeding tube can be misplaced into the lungs during insertion or may move out of the stomach at a later stage.
In the past, various methods 4 have been used to determine the position of NG feeding tubes.
These included:
Auscultation of air insufflated through the feeding tube - whoosh test
Testing acidity/alkalinity of the aspirate using blue litmus paper
Interpreting absence of respiratory distress as an indicator of correct positioning
Monitoring bubbling at the end of the NG tube
Observing the appearance of the feeding tube aspirate
The National Patient Safety Agency (NPSA) have issued a patient safety alert and have recommended that the above methods are not reliable and therefore should not be used to detect the position of NG tubes.
The NPSA recommend 5:
Measuring the pH of the aspirate using pH indicator strips/paper
Use of radiography
The most accurate method for confirming the correct position of a NG feeding tube is radiography 5.
The pH of the gastric aspirate can be affected by ongoing enteral feeding and medications viz: antacids, H2 antagonists and proton pump inhibitors. In these cases, measuring the pH of the aspirate may not be useful and so use of radiography is recommended. The NPSA have issued guidance on how to confirm the position of nasogastric feeding tubes.
Fig: 3 (CR-1822) indicates the normal position of the NG tip below the diaphragm in the upper part of the stomach (fundus).
Fig: 4 (CR-1826) shows the abnormal position of the NG tube situated in the right lower lobe bronchus. If NG feeds are commenced, this will result in lung injury.
Conclusion
We have highlighted the optimum position of both the ETT and NG tube on chest radiographs. Optimum positioning is required not only for safety reasons to avoid complications but also for optimum monitoring and treatment of patients. This series of chest radiographs will benefit not only medical students and doctors from all specialties but also nurses, physiotherapists and paramedical teams who will be involved in the care of critically ill patients.
Self Assessment
MCQ 1:
On a chest radiograph, the tip of the ETT:
a. should lie very close to carina
b. should lie 5-7 cm above the carina
c. should lie 5-7 mm above the carina
d. The ETT cannot be visualised on a chest radiograph
MCQ 2:
Which one of the following tests is the most accurate method to determine the correct position of NG feeding tubes?
a. testing the aspirate from the NG tube using a blue litmus paper
b. whoosh test
c. measuring the pH using pH indicator strips/paper
d. radiography
Answers for MCQs:
MCQ 1: b
MCQ 2: d
ACKNOWLEDGEMENTS
We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Bedford Hospital NHS Trust, UK
DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK
CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Bedford Hospital, Bedford, UK
Email: drkrishnanmr@gmail.com
References
Tracheal and tracheostomy tubes and airways. In: Al-Shaikh B and Stacey S eds. Essentials of anaesthetic equipment. 2nd edition. Churchill Livingstone, 2002: 56-67.
Hutton P. Airway management II: assessment, control and problems. In: Hutton P, Cooper GM, James III FM and Butterworth J eds. Fundamental Principles and Practice of Anaesthesia. Martin Dunitz Ltd, 2002; 79.
Goodman LR. The postoperative and critically ill patient. In: Grainger RG and Allison DJ eds. Diagnostic Radiology. 2nd edition. Churchill Livingstone, 1992; 368.
Reducing the harm caused by misplaced nasogastric feeding tubes. Patient safety alert National Patient Safety Agency (NPSA)
How to confirm the correct position of nasogastric feeding tubes in infants, children and adults National Patient Safety Agency (NPSA), Interim advice for healthcare staff, February 2005.
For generations the mind has been mystifying physicians all around the world. It is the powerhouse behind everything we do, and everything that we are therefore there is no wonder that reams of time, research, money and effort has been poured into this1.
The Association of British Neurologist, through various publications in the last 10years, has stated that there are too few neurologist consultants, and that provisions need to be made to ensure that there is comprehensive care to patients in hospitals2. In light of this there has been a recent drive into increasing the number of clinical consultant posts in local hospitals. This drive has lead to more innovative measures being implemented in this field, including new research on pharmaceuticals as well as introduction of new technologies.
A general misconception of the field of Neurology by medical students is that it is too complicated3. However, I found my experience to be one of the most organised, patient orientated, enjoyable experiences I have encountered on a ward setting. The teaching sessions that accompanied the firm brought all of the previous years of knowledge together like a solved jigsaw puzzle linking the neuroanatomy with the pathophysiology of an illness and the role and impact pharmaceuticals have4. With everything falling into place and having a better understanding, it gave me more confidence to explore further into this field.
Having previously only had brief exposure to Neurology, to be in a committed arena focused on this speciality was a daunting experience. Opposed to other specialities, where history taking is the millstone to your diagnosis, management and follow-up care, there is a much bigger onus on clinical skills and interpreting findings. The obvious signs of loss of sensory or motor functions are evident, but more subtle focal lesions are sometimes harder to pick up, this is when drawing on your clinical knowledge and application is required. This remains one of the evident advantages to Neurology, compared to other disciplines - that it remains clinically orientated. There is only so much that could be galvanised from a case history. As medical students we had ample exposure to the ward, and were able to approach patients and hone in on our clinical skills. As our basic knowledge had been laid down, through teaching sessions and also clinical case studies, we had the theory behind many of the clinical assessments, but lacked confidence and appropriate patients to assess. This changed as we integrated ourselves with the close-knit multidisciplinary team and the patients. There seemed to be buoyancy in mood, as we became more proficient undertaking assessments, for instance a cranial nerve examination that once took 10minutes to carry out was halved, without feeling like we had missed anything vital out.
More so, it was an eye-opener to experience, (even for a brief period), the sub-specialities that Neurology caters for, an aspect that I particular enjoyed was neuropsychiatry. Essentially the brain is an intricate piece of machinery, as with all things in life, sometimes this goes awry. For me to observe from a clinicians point of view and come to the same conclusion as my peers, gave me a sense of pride, knowing that I was moving in the right direction in my medical career, and that all that pent up knowledge was at last being implemented on a practical level. Unlike other fields, for the most part we were left to our own devices we were not spoon fed. This was refreshing, although a little overwhelming at first. We were responsible to find, clerk, assess and present patients to our team-members. The feedback we received was invaluable; it illustrated the extent of our competency and also left you with a sense of achievement knowing that you are capable and apt.
For those that are looking for a speciality once they have started their medical career, Neurology is an exciting and innovative place to be at right now. With an aging population worldwide, more effort, resources and money is being spent on degenerative illnesses such as Alzheimers disease and Parkinsons disease.5
Although to some extent current treatments offer benefits to sufferers, there is hope that new pioneering forms of treatment will be developed to manage patients. Additionally this gives students and qualified peers alike a great opportunity to conduct research and audits and get the opportunity to be published. Neurology still remains a minefield of the unknown, and it seems to be constantly on a quest to better itself and find new measures and treatments to bring to the patients.
With its new advancements in the pipeline, Neurology seems to have a bright future. However, there is the obvious downside to being in a speciality of this nature. You will come into contact with a large number of patients with untreatable disorders. It needs someone with a strong constitution to see someone that has a poor prognosis and an almost certain decrease in quality of life. For some, there will be an obvious deterioration before your eyes, others may have already suffered severe neurological deficits that ethical questions on the continuation of the life may arise. These are tough decisions to make, and needs someone with conviction and strong-will to stand by their decision.
Overall Neurology is what you make it, as is every profession. What stands out with Neurology is the exposure you get to patients. For students this is a valuable and undoubtedly crucial time in their medical training to perfect skills that will be called on in the future. Where else would we find another welcoming and encouraging place to learn the tools of our future trade, that allows freedom to learn, exposure to patients, a myriad of different diagnosis, and most importantly a practical use of your knowledge and clinical skills?
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
MATHAVI UTHAYANAN and MASHUD SOUROYER, 4th Year Medical Students reading at the Barts and London School of Medicine and Dentistry
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) is a rare clinical syndrome, commonly seen in elderly patients who present with dorsal pitting edema of the hands and has a dramatic response to steroids, suggesting a benign nature. Sometimes it is associated with other rheumatologic conditions and potential underlying malignancy should be ruled out, especially when there is a poor response to steroids.
Elderly patients presenting with musculoskeletal symptoms such as painful, swollen or stiff jointsare challenging to physicians. The common conditions encountered are osteoarthritis, crystal arthropathies, spondyloarthropathies and rarely seropositive arthritis. RS3PE highlights a different inflammatory disease involving the tenosynovium of the tendons of the hands with a characteristic presentation. This case details such a presentation and aims to raise awareness amongst general physicians.
Case report:
An 83 year old man, with a history of chronic leg ulcers and poor mobility presented following a fall at home. On admission he also complained of a six to eight week history of bilateral hand swelling. This was of sudden onset, initially on the right hand and gradually progressed until the time of admission when it became prominent over the dorsum of both hands. Both hands were initially tender, but painfree at rest, and restricted in movement due to the swelling. Lately he had also noticed mild inactivity stiffness in his knees and shoulders, He had no previous musculoskeletal history, no skin rash or trauma to his hands.
Inspection of his hands revealed bilateral, symmetrical swelling, involving all the fingers and more pronounced on the dorsum. On palpation there was pitting oedema over the dorsum without signs of synovitis or joint deformity.(Figure 1 and 2).
On movement, finger flexion and opposition were limited, with reduced grip strength.
There was no girdle muscle weakness or pain. There was pitting oedema of both feet, with compression bandaging to the upper calf. This was chronic, and was likely to be secondary to peripheral vascular insufficiency.
Fig 1:Swollen hands
Fig 2: Dorsal pitting edema
Blood tests during this admission showed normocytic anaemia with low vitamin B12 levels but normal ferritin. Erythrocyte sedimentation rate (ESR) was raised at 100mm/hour and initial C-reactive protein (CRP) at 55 mg/l. Anti nuclear antibody (ANA) and rheumatoid factor were negative. X-rays of the hands revealed mild osteoarthrosis without any evidence of bony erosions. Computerised tomography (CT) of the chest and abdomen did not show any evidence of malignancy.
In view of the clinical presentation and seronegativity, a diagnosis of peritendinous rheumatoid arthritis was considered. He was commenced on low dose oral steroids following initial parenteral corticosteroid. Subsequent to the initiation of steroids, there was dramatic resolution of the swelling of the hands, within a week (Figure 3),
Fig 3: Response to steroids
Case discussion
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome was first described by McCarty et al in 1985 1 . It is also termed as peritendinous rheumatoid arthritis in Europe.
It predominantly affects elderly males and although not exceptionally rare, there is no clear documentation of the incidence of this condition (2).
The syndrome is a subset of symmetrical polyarthritis characterised by
Bilateral pitting oedema of both hands
Sudden onset of polyarthritis (A few cases report patients being able to state the time to the hour at which this occurred.1)
Age >50 years
Absence of rheumatoid factor (seronegativity).
Other features include symmetrical distal synovitis and tenosynovitis affecting the synovial sheaths of the flexor and extensor tendons of the hands and/or feet without evidence of joint erosions 2. It responds dramatically to corticosteroids with long term remission after withdrawal, suggesting a benign prognosis.
Although generally thought to be a characteristic benign syndrome with good outcomes, several studies have been published linking RS3PE to various rheumatic disorders such as spondyloathropathies, psoriasis (HLA associations), polymyalgia rheumatica, and temporal arteritis. 3 It may also be a paraneoplastic manifestation of haematological or solid malignancies 4 (eg. prostate, rectal, gastric and ovarian tumors) linked to the synthesis of interleukin, IL-6. Review of these cases suggested that RS3PE associated with neoplasia was associated with a poor response to steroid treatment. 4
Although MRI scanning offers the best imaging technique to diagnose the condition.,RS3PE is a clinical diagnosis. Scans typically demonstrate the tenosynovitis of the extensor tendons believed to cause the oedema which characterises the syndrome.3 MRIscans are valuable to exclude other bony pathologies like osteomyelitis.. An alternative imaging technique for identification of extensor tenosynovitis is ultrasonography. 5
Treatment generally involves steroids, but in some cases the patient may respond to NSAIDs or gold therapy
Learning points:
RS3PE should be considered as a diagnosis when a patient presents with bilateral symmetrical pitting oedema of the hands and or feet, and is found to be seronegative.
Patients are generally very responsive to corticosteroids.
A high index of suspicion is needed to search for underlying malignancy especially in the absence of associated rheumatic disorders and poor response to corticosteroid therapy.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. VIJAY JOSHI MD, Registrar, Internal Medicine, Chase Farm Hospital, UK
DR ANNA GREEN MBBS, FY1 Doctor, Chase Farm Hospital, UK
DR. JANE GRIFFIN FRCP, Consultant Rheumatologist, Chase Farm Hospital, UK
CORRESPONDENCE: DR. VIJAY JOSHI, Chase Farm Hospital, Enfield, UK
Mehmet Sayarlioglu Remitting Seronegative Symmetrical Synovitis with Pitting Edema (RS3PE) Syndrome and Malignancy. Eur J Gen Med 2004; 1(2): 3-5.
Oliveri I, Salvarani C,Cantini F. Remitting distal extremity swelling with pitting edema: a distinct syndrome or a clinical feature of different inflammatory rheumatic diseases.J.Rheumatol 1997;24:249-52
Sibilia J, Friess S, Schaeverbeke T et al. Remitting seronegative symmetrical synovitis with pitting edema (RS3PE): a form of paraneoplastic polyarthritis? J Rheumatol 1999;26:115-20
Agarwal et al . Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome: ultrasonography as a diagnostic tool. Clinical Rheumatology. Volume 25, Number 5/October 2005
Left ventricular free wall rupture is a serious complication of myocardial infarction (MI) with a mortality rate without intervention close to 100%. Its presentation is classically late following an MI but in some cases can present within 24 hours. There can be sudden overt clinical symptoms or it can present insidiously and therefore there must be a high index of suspicion. This report highlights the case of a gentleman with no prior history of ischaemic heart disease that presented with non-specific symptoms. A diagnosis of left ventricular (LV) free wall rupture near the atrial appendage, post MI was made and he was managed successfully.
Clinical Presentation
We present the case of a 75 year old gentleman who collapsed suddenly whilst riding his bicycle. According to an eye-witness he was unresponsive & confused for a few minutes after the episode. Paramedics attended and brought him to the Accident and Emergency department at a local hospital and he was subsequently transferred to the Admissions Unit. Initially he was confused with no recollection of the collapse however his confusion abated after a short period of time.
He was normally fit and well, his only past medical history of note being chronic neck pain requiring simple analgesia and mild asthma requiring when necessary salbutamol inhalers. He was however a life-long smoker with a minimal alcohol intake.
On arrival to the hospital, the patient was conscious, oriented, afebrile and not in any pain. His Glasgow Coma Scale (GCS) was 15/15, pulse was 92/min, regular but weak and the right radial and femoral pulses were absent. His systolic blood pressure was 55mmHg in the right arm and 105mmHg in the left arm. The only other positive finding on examination was muffled heart sounds. Bloods were taken and results are shown in Table 1 with normal ranges given for reference (results within normal limits are not shown).
Random Blood Glucose
16 mmol/l
<11.1 mmol/l
Troponin I (12 hour)
6.16 ng/ml
<0.04 ng/ml
WBC
14.0 x109/l
4-11 x109/l
CRP
179 mg/l
<10 mg/l
Hb
10.9 g/dl
13-18 g/dl (men)
Table 1. Blood results with normal ranges in italics.
In view of the high blood glucose and history of collapse, the patient was aggressively treated with insulin and intravenous fluids. However after receiving 2 litres of intravenous fluids, there was no haemodynamic response. An arterial blood gas on air was performed and the results are shown in Table 2 with normal ranges given for reference.
pH
7.40
(7.35-7.45))
pCO2
3.0 Kpa
(4.7-6.0 Kpa)
pO2
14.8 Kpa
(10.8-12.5 Kpa)
HCO3
13.6 mmol/l
(22-28 mmol/l)
Table 2. Arterial Blood Gas with normal ranges in italics.
A Chest X-ray was performed and showed nothing unusual. However an ECG demonstrated ST depression in the inferior leads & T- wave inversion with a Q wave in aVL (see figure 1). Differential diagnosis at this stage was therefore aortic dissection, carotid dissection and left ventricular wall rupture (post myocardial infarction).
A subsequent CT scan showed no aortic dissection, but probable haemopericardium together with an occluded right common iliac artery (see figure 2). Trans-thoracic echocardiogram confirmed haemopericardium with no suggestion of tamponade (see figure 3) and in addition demonstrated some mild LV diastolic dysfunction. CT scan of the brain and the carotids showed no evidence of carotid dissection but did indicate significant stenosis of the right subclavian artery. The diagnosis of left ventricular free wall rupture was made at this juncture. It was noted that the variability in blood pressure between both arms and between upper limbs and lower limbs was exacerbated by coincidental stenosis in the right common iliac and right subclavian arteries which possibly delayed diagnosis.
Subsequent coronary angiogram showed a blocked intermediate coronary artery (a branch of the left main coronary artery), 2 stenosed areas in the left anterior descending coronary artery (LAD) and a 50% occlusion of the right coronary artery (RCA). Later a trans-oesophageal echocardiogram (TOE) demonstrated separation of the ventricular free wall between the LAD artery and the left atrial appendage, high up in the heart a very unusual position indeed. The diagnosis of Left Ventricular Free Wall Rupture following a Silent Myocardial Infarction was therefore confirmed. The patient was transferred to a nearby cardiac surgery centre and an emergency patch repair of the ventricular free wall rupture was performed.
Figure 1. ECG demonstrating ST depression in II, III and aVL & T-wave inversion with a Q wave in aVL.
The patient had a prolonged recovery, spending 2 weeks on the Cardiac ICU and then subsequently developed hospital acquired pneumonia and remained an inpatient on a general medical ward for a further 4 weeks where he made slow progress. He later spent 4 weeks in a rehabilitation centre before finally returning home.
Figure 2. Thoracic CT with obvious haemopericardium.
Figure 3. Transthoracic echo with evidence of pericardial fluid.
Discussion
First described by William Harvey in 1647, left ventricular (LV) free wall rupture is a dramatic complication of myocardial infarction where there is a rupture of infarcted LV free wall tissue. The rupture is commonly insidious with bleeding into the pericardial sac and subsequent cardiac tamponade. It is hard to assess as clinical and autopsy results vary considerably. It contributes to nearly 15% of deaths due to acute MI1, with the average age of those affected being 69 years. It is third only to cardiogenic shock and arrhythmias as the leading cause of death following a myocardial infarction.2 Hutchins et al reviewed 153 post mortem results with gross and histological evidence of acute myocardial infarction and reported that 30.7% of patients in this group who had died from sudden death had a cardiac rupture.3 It is more common in females and classically occurs 3 to 6 days post MI, however in some studies, up to 50% of cases have been reported less than 24 hours post MI.4There is a history of previous MI in 25% cases but often LV free wall rupture can be the first presentation of ischaemic heart disease.5 Around 50% of the cases of LV free wall rupture are due to anterior MIs with LAD involvement.6There is a new murmur in 25% cases and echocardiography may often demonstrate a pericardial effusion. The prior use of NSAIDS and corticosteroids and a presentation which may mimic major artery dissection often delays thrombolytic therapy.
Unfortunately the current mortality rate in the UK is around 90%. Of note the incidence of LV free wall rupture post MI has increased since the more widespread availability of coronary care units and it is thought that this is because more people are now surviving the first few days post MI.7
The pathophysiological process involves thinning of the myocardial wall with the intensity of necrosis occurring at the terminal end of the vessel (watershed area) where there is often poor collateral flow. The shearing effect of myocardial contraction against a stiffened necrotic area causes rupture. The most common rupture location is on the anterior or lateral wall of the left ventricle.8 A midventricular position along the apex to base axis is most common. It can present either with sudden death or can present sub acutely e.g. with nausea, hypertension or pericardial type chest discomfort or pain. The gentleman discussed in this report collapsed with no preceding symptoms and as mentioned the location of his rupture was in a very unusual place, high up near the atrial appendage.
Transoesophageal echo (TOE) is diagnostic for this condition and is the gold standard.9 However it is found to have only a 70% sensitivity rate for LV free wall rupture10 and therefore some centres advocate the use of cardiac MRI when available.11 Initial management is haemodynamic stabilization and this is often followed by blood transfusion, pericardiocentesis12, inotropic support and the use of an intra-aortic balloon pump but ultimately prompt surgical repair is required.
Various surgical techniques have been applied including suturing of the infarcted ventricle but modern surgical repair involves the application of a Teflon felt patch over the ruptured area with a synthetic biocompatible glue (e.g. cyanoacrylate) as an adhesive to keep the patch attached to the epicardium.13,14 Crucially it can be performed without the use of cardiopulmonary bypass in most of cases. The current overall operative mortality for surgical intervention is reported to be around 24-35%15.
Ultimately survival depends on early recognition of the condition, prompt investigations & diagnosis and urgent surgical treatment. Unfortunately at the present time the condition is usually diagnosed at post-mortem.
Conclusion
The patients presentation i.e. collapse with no proceeding symptoms coupled with the fact that he was suffering a silent MI with no prior indications of ischaemic heart disease e.g. angina, shortness of breath etc and the rapid subsequent development of left ventricular free wall rupture in such an high position made this quite an unusual case. Stenosis in the right common iliac and subclavian arteries did delay diagnosis slightly, as aortic and carotid dissection had yet to be ruled out but ultimately this patient survived probably because of early diagnosis despite these obstacles and subsequent prompt treatment.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
ANDREW PETER VANEZIS MBChB BSc, FY2 Doctor, Barts and The London NHS Trust, UK.
REHAN QUADERY MBBS, ST3 Medicine, Bedford Hospital NHS Trust, UK
MOHAMMAD WASIL PhD, Assistant Director of Research & Development, Bedford Hospital NHS Trust, UK
MOHAMMED AZHER FCCP FRCP, Consultant Chest Physician, Bedford Hospital NHS Trust, UK
CORRESPONDENCE: REHAN QUADERY, Bedford Hospital NHS Trust, UK
Pohjola-Sintonen S, Muller JE, Stone PH, Willich SN, Antman EM, Davis VG, Parker CB, Braunwald E. Ventricular septal and free wall rupture complicating acute myocardial infarction: experience in the Multicenter Investigation of Limitation of Infarct Size. Am Heart J. 1989;117:809818
Hutchins, Kenneth D, Skurnick, Joan, Lavenhar, Marvin, Natarajan, Geetha A. Cardiac Rupture in Acute Myocardial Infarction: A Reassessment. American Journal of Forensic Medicine & Pathology. 23(1):78-82, March 2002.
Becker AE, Anderson RH. Cardiac pathology. An integrated text and colour atlas. London: Gower Medical Publishing; 1983.
Shirani J, Berezowski K, Roberts WC. Out-of-hospital sudden death from left ventricular free wall rupture during acute myocardial infarction as the first and only manifestation of atherosclerotic coronary artery disease. Am J Cardiol 1994 Jan; 73(1): 88-92
Slater J, Brown RJ, Antonelli TA, et al. Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction:A report from the SHOCK trial registry. J Am Coll Cardiology. 2000;36:1117-1122
Reddy SG, Roberts WC. Frequency of rupture of the left ventricular free wall or ventricular septum among necropsy cases of fatal acute myocardial infarction since introduction of coronary care units. Am J Cardiol 1989;63:90611
David, TE. Surgery for post infarction rupture of the free wall of the ventricle. In: David TE. , editor. Mechanical Complications of Myocardial Infarction. Austin, R.G. Landes Company; 1993. p. 142.
Cheitlin, MD et al. ACC/AHA/ASE 2003 Guideline update for the clinical application of echocardiography. J Am Coll Cardiol. 2003;42:95470
Lopez-Sendon J, Gonzalez A, Lopez de Sa E, Coma-Canella I, Roldan I, Dominguez F, et al. Diagnosis of subacute ventricular wall rupture after acute myocardial infarction: sensitivity and specificity of clinical, hemodynamic and echocardiographic criteria. J Am Coll Cardiol 1992;19: 114553.
Rajiv Agarwal, Pedro Diaz-Ortiz, Ravinder Reddy, Veronica Lenge, R. David Fish, David A. Ott, John Connelly, and Scott D. Flamm. Asymptomatic Incomplete Left Ventricular Apical Rupture Diagnosed by Cardiac Magnetic Resonance Imaging. Tex Heart Inst J. 2006; 33(1): 9395
Rolf Svedjeholma, Erik Hkansonb, Mrten Lindstrmc and Per Hjort. Case report - Cardiac general. Post-infarct left ventricular free wall rupture and ventricular septal defect managed by pericardial aspiration during transport to referral hospital. Interactive Cardiovascular and Thoracic Surgery. 2003; 2:193-195
Padro JM, Mesa JM, Silvestre J, Larrea JL, Caralps JM, Cerron F, Aris A. Subacute cardiac rupture: repair with a sutureless technique. Ann Thorac Surg. 1993;55:2023
Alejandro Aris. Surgical repair of left ventricular free wall rupture. Multimedia Manual of Cardiothoracics. 2004. doi:10.1510/mmcts.2004.
Malek G, Massas MD, Alexander SG. Surgical Repair of Mechanical Complications of Myocardial Infarction. World J Surg. 2004;28:847-856
BACKGROUND : The present study was designed to measure changes in markers of antioxidant capacity (measured individually and total) following acute ischemic stroke.
METHODS : The study included 135 subjects. 62 were controls and 73 were ischemic stroke patients diagnosed clinically and by CT scan of the brain. The cases were divided into two groups, The ischemic stroke patients with large vessel / cortical, subcortical infarcts (Group. I) and small vessel / lacunar infarcts (Group. II) based on CT scan of the brain. Serum vitamin E, vitamin C, superoxide dismutase, uric acid and total antioxidant capacity were estimated in all the subjects.
RESULTS : Group I and Group II ischemic stroke cases had significantly lower levels of vitamin E, vitamin C and superoxide dismutase and significantly higher levels of uric acid compared to controls. The group I ischemic stroke cases had significantly lower levels of vitamin E, vitamin C, and superoxide dismutase and significantly higher levels of uric acid than group II ischemic stroke cases. Total antioxidant capacity strongly correlated with serum uric acid in cases
CONCLUSION: The present study suggests that estimation of vitamin E, vitamin C, SOD, uric acid and total antioxidant capacity may be used as an indirect evidence of oxidative stress induced neuronal damage in acute ischemic stroke which may be useful for monitoring and optimizing antioxidant therapy.
KEY WORDS: Stroke, oxidative stress, SOD, vitamin C, vitamin E. Total antioxidant capacity.
Several studies provide evidence of an association between ischemic stroke and oxidative stress. Increased free radical formation together with a reduced antioxidant defense causes oxidative stress, that may play an important role in the pathogenesis of stroke associated neuronal injury. Several studies demonstrate increased oxidative damage to neuronal cells during cerebral ischemia and reperfusion. Antioxidant activity is known to reflect the altered redox balance of affected fluids, tissues or organs in acute ischemic stroke patients. Therefore antioxidant concentrations or measures of their activity have been used to estimate the amount of oxidative stress 1. No single component of serum antioxidant complex could fully reflect the protective efficiency of blood, probably because of interactions that occur in vivo among different antioxidant compounds. Total antioxidant capacity considers the cumulative effect of all antioxidants present in blood and body fluids 2. The aim of this study was therefore to measure changes in markers of antioxidant capacity (measured individually and total) following acute ischemic stroke.
Materials and methods:
This study was conducted at Bapuji Hospital and Chigateri General Hospital, Davangere (Both Hospitals attached to J.J.M. Medical College, Davangere, karnataka), by including 62 healthy controls (of which 34 were men and 28 were women aged between 36 and 73 years) and 73 cases clinically diagnosed
as acute ischemic stroke patients of less than 48 hrs duration after the onset of symptoms) and confirmed by computerized tomography of the brain (of which 41 were men and 32 were women aged between 36 and 73 years). The cases were divided into two groups, The ischemic stroke patients with large vessel / cortical, subcortical infarcts (Group. I) and small vessel/lacunar infarcts (Group. II) based on CT scan of the brain. The stroke patients due to cerebral hemorrhage, malignancy, sepsis, severe medical or psychiatric illness, language disorders, swallowing difficulties, cognitive impairment, gout, renal failure and patients who were taking antioxidant vitamins were excluded from the study. The study was conducted after informed consent was obtained from them and the study has been approved by the ethical committee of the institution.
Under aseptic precautions about 6 ml of a non-fasting venous blood sample was collected from cases within 24 h following stroke onset and from healthy controls. Blood was collected in appropriate tubes and centrifuged at 3000 g for 15 min to separate plasma from red blood cells. The supernatant was stored at 40 C until analysis was carried out.
Serum vitamin E was estimated by Baker and Frank method 3, Vitamin C by 2, 4 DNPH method 4, SOD by Marklund and Marklund method 5, and uric acid by Henry Caraway method 6 and total antioxidant capacity (TAC) by FRAP assay method 2 in both the controls and cases. All the chemicals used were of highest analytical grade available in India.
TABLE I. Comparison of Serum Vitamin E, Vitamin C, SOD, Uric Acid and Total Antioxidant Capacity (Mean SD)
Vit. E mg/L
Vit. C mg/dl
SOD units/ml
Uric acid mg/dl
TAC (mol/l)
Controls (n = 62)
11.04 0.97
1.16 0.13
9.01 1.03
4.66 0.47
1079.7 197.9
Cases (n = 73)
7.22 0.81
0.52 0.16
4.35 0.70
6.56 0.73
1043.4 140.7
Comparison
p < 0.05
p < 0.05
p < 0.05
p < 0.05
p > 0.05
TABLE II. Comparison of Serum Vitamin E, Vitamin C, SOD, Uric Acid and Total Antioxidant Capacity (Mean SD) between Group I and Group II Cases.
Vit. E mg/L
Vit. C mg/dl
SOD units/ml
Uric acid mg/dl
TAC (mol/l)
Cases Group. I (n = 56)
6.93 0.67
0.45 0.08
4.14 0.61
6.78 0.62
1048.9 140.3
Cases Group. II (n = 15)
8.24 0.17
0.80 0.10
5.12 0.49
5.73 0.55
1038.1 142.9
Comparison (one way ANOVA and student t test)
p < 0.05
p < 0.05
p < 0.05
p < 0.05
p > 0.05
Statistical analysis :
Statistical analysis was performed with one way ANOVA test, student t test and Pearsons correlation coefficient using SPSS version 16.0. A value of p < 0.05 was taken to indicate statistical significance.
Results:
It was observed that the serum levels of Vitamin E, Vitamin C, TAC and SOD were significantly lower in ischemic stroke cases than those of controls and serum uric acid levels were significantly higher in ischemic stroke cases table I . Further it was observed that the group I ischemic stroke cases had significantly lower levels of serum Vitamin E, Vitamin C and SOD than group II ischemic stroke cases and significantly higher serum levels of uric acid in group I cases than group II ischemic stroke cases table II . Significant negative correlations were observed between vitamin C, vitamin E, SOD and TAC and significant positive correlation was observed between uric acid and TAC among cases table III.
TABLE III. Correlations of Vitamin E, Vitamin C, SOD, Uric Acid with Total Antioxidant Capacity in cases.
Vitamin C and TAC
Vitamin E and TAC
SOD and TAC
Uric acid and TAC
R value
-0.24
-0.1
-0.19
0.16
p value
< 0.05
< 0.05
< 0.05
< 0.05
Discussion:
In this study, there were reduced concentrations of vitamin E, vitamin C, SOD and TAC and increased concentrations of uric acid in stroke patients compared with controls. FRAP assay is presented as a novel method of assessing total antioxidant capacity 2 which is believed to be a useful measure of the ability of antioxidant present in the fluids to protect against oxidative damage to membranes and other cellular components..
Vitamin E, a potent chain breaking lipid soluble antioxidant, reacts with lipid peroxyl radicals eventually terminating the peroxidation chain reaction and thereby reducing oxidative damage. Some studies have shown reduced serum vitamin E levels in stroke patients and this may be due to high lesion volume resulting in production of more number of free radicals from a large ischemic injury. It is also shown that reduced vitamin E levels resulted in poor clinical outcome in stroke patients 7,8. In the present study serum vitamin E levels were significantly decreased in ischemic stroke cases (significantly decreased in large vessel infarcts than in small vessel infarcts) when compared to controls.
Vitamin C represents the major water-soluble antioxidant in the human body. Many studies show that reduced vitamin C levels are associated with increased risk of both ischemic and hemorrhagic strokes 9. In our present study the serum vitamin C levels were decreased significantly in ischemic stroke cases (decreased significantly in large vessel infarcts than in small vessel infarcts) compared to controls. It may be due to the exhaustion of this antioxidant in the neutralization of free radicals which are formed in excess during ischemia and reperfusion 10,11.
SOD is an endogenous antioxidant that catalyses the dismutation of the superoxide anion radical. SOD plays an important role in the defense against free radical damage in reperfusion injury and helps in reducing the infarct size during ischemia and reperfusion 12,13. In the present study the serum SOD levels were decreased significantly in ischemic stroke cases decreased in large vessel infarcts than in small vessel infarcts) compared to controls.
Uric acid, most abundant endogenous aqueous antioxidant in humans, may protect against oxidative modification of endothelial enzymes and preserves the ability of endothelium to mediate vascular dilatation during oxidative stress 14. Several studies have shown that increased oxidative stress is associated with high circulating uric acid levels due to elevation of xanthine oxidase in stroke induced brain damage 15,16. In this study, there was a significant increase in the serum levels of uric acid in ischemic stroke cases (increased significantly in large vessel infarcts than in small vessel infarcts) than in controls. Serum TAC strongly correlated with serum uric acid. Under multivariate analysis, serum uric acid explained most of the variance in TAC during the study period.
This study suggests that estimation of serum vitamin E, vitamin C, SOD, uric acid and total antioxidant capacity may be used as an indirect evidence of oxidative stress induced neuronal damage in ischemic stroke.
The limitations of our study are as follows: We have not estimated any markers of lipid peroxidation such as malondialdehyde which along with antioxidant levels would better explain oxidative stress. Antioxidant levels were measured only once, but prospective serial estimations would better predict the antioxidant status with prognosis of stroke. This study was conducted on a small group of stroke patients. Larger clinical studies in this area are needed to establish the relationships between antioxidant capacity and oxidative damage following ischemia and reperfusion in man, and to form the basis of appropriate antioxidant intervention strategies to minimize long-term brain injury following cerebral ischemia.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. SRIKRISHNA R, M.D., Assistant Professor, Department of Biochemistry, JJM Medical college, Davangere, India
DR. SURESH D R, M.D., Assistant Professor, Sri Siddhartha Medical College, Sri Siddhartha Academy of Higher Education (SSAHE), Tumkur, India
CORRESPONDENCE: DR. SURESH D R, 3/1, Seethappa layout, 5th Block, Doddabommasandra, Vidyaranyapura.P.O, Bangalore, Karnataka, INDIA- 560097.
Email: drsuri77@gmail.com
References
Leinonen JS, Ahonen JP, Lonnrot K, Jehkonen M, Dastidar P,Molnar G. Low plasma antioxidant activity is associated with high lesion volume and neurological impairment in stroke (2000). Stroke 31(9), 33-39.
Benzie FF, Strain JJ. The ferric reducing ability of plasma (FRAP) as a measure of antioxidant power: the FRAP assay (1996). Analytical Biochem 239, 7076.
Baker H, Frank O (1969). Clinical vitaminology. Academic Press. New York, pp169173.
Omage ST (1979). Ascorbic acid analysis II. Determination after derivatization with 2, 4, - Dinitrophenylhydrazine, Methods in Enzymology, 62, 7-8.
Nandi A, Chatterjee IB (1988). Assay of superoxide dismutase activity in animal tissues. J Biosci, 13 (3), 305-315.
Price CP, James DR (1988). Analytical reviews in clinical biochemistry: the measurement of urate. Ann Clin Biochem, 25 (5), 484-498.
Cherubini A, Ruggiero C, Polidori MC, Mecocci P. Potential markers of oxidative stress in stroke. Free Radical Biology and Medicine (2005), 39 (7), 841-852.
Tornwall ME, Virtamo J, Korhonen PA, Virtanen MJ, Albanes D, Huttunen JK (2004). Postintervention effect of alpha tocopherol and beta carotene on different strokes. A 6 year follow-up of the alpha tocopherol, beta carotene cancer prevention study. Stroke, 35(8), 1908-1913.
Yokoyama T, Date C, Kokubo Y, Yoshiike N, Matsumura Y, Tanaka H (2000). Serum vitamin C concentration was inversely associated with subsequent 20 year incidence of stroke in a Japanese Rural Community. Stroke, 31(10), 2287-2294.
Kurl S, Tuomainen TP, Laukkanen JA, Nyyssonen K, Lakka T, Sivenius J, Salonen JT (2002). Plasma vitamin C modifies the association between hypertension and risk of stroke. Stroke, 33(6), 1568-1573.
Kim GW, Kondo T, Noshita N, Chan PH (2002). Manganese superoxide dismutase deficiency exacerbates cerebral infarction after focal cerebral ischemia / reperfusion in mice. Stroke, 33(3), 809-815.
Zimmermann C, Winnefeld K, Streck S, Roskos M, Haberl RL (2004). Antioxidant Status in Acute Stroke Patients and Patients at Stroke Risk. Eur Neurol, 51(3), 157-161.
Weir CJ, Muir SW, Walters MR, Lees KR (2003). Serum urate as an independent predictor of poor outcome and future vascular events after acute stroke. Stroke, 34 (8), 1951-1957.
Hariklia VD, Apostolos IA, Haralambos IK (2008). The Role of Uric Acid in Stroke: The Issue Remains Unresolved. Neurologist, 14(4), 238-242.
Hozawa A, Folsom AR, Ibrahim H, Nieto JF, Rosamond WD, Shahar E (2006). Serum uric acid and risk of ischemic stroke : the ARIC study. Atherosclerosis, 187(2), 401-407.
Society of Hospital Medicine (SHM) defines 'Hospitalists' as physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital medicine.
The term "hospitalist"1was first introduced in 1996 by Robert M. Wachter and L Goldman to describe physicians who devote much of their professional time and focus to the care of hospitalized patients. In the most prevalent American model of hospitalist care, several doctors practice together as a group and work full-time caring for inpatients. Most of the (80%) of practicing hospitalists are board certified or eligible in internal medicine, and some (5%) have completed subspecialty fellowships. Although hospitalists first emerged in the care of adult inpatients, the field has grown rapidly in pediatrics, now accounting for nearly 10% of U.S. hospitalists2. Hospitalists typically provide 24/7 inpatient coverage and thus are more readily available to a patient than a doctor who spends much of the day outside the hospital in an office or clinic setting.
Over the past decade, the United States has undergone a remarkable evolution in the way it delivers inpatient medical care. In the mid-1990s, much of American health care was dominated by a managed care paradigm, which gave incentives to control health care inflation3. Hospitalist model was uniquely well versed in evidence based practice and systems improvement. Their focus on providing clinically appropriate care, improving efficiency, reduce length of inpatient stay and helping to make the hospital system work better, without compromising patient satisfaction & outcome was big boon for its growth. Hospitalist field has now become the fastest growing specialty in the history of American medicine, approximately today close to 15,000 hospitalists practice in America, and the field is likely to grow to about 30,000 making it a larger specialty than cardiology4.
Hospitalist Program, St Joseph's Hospital/Marshfield Clinic
In keeping pace with nation wide trend, St. Joseph's Hospital (SJH) Marshfield Clinic, Marshfield was developed in 2000 by the General Internal Medicine Department at the request of clinic leadership. Hospitalst Program was formally launched in October 2001. SJH was pioneer and leader during the time in the Midwest. Dr Qasim Raza & Dr Mark Schwartz were instrumental in establishing a full fledged hospitalist program that has grown tremendously over the years. Dr Bill Yanke, then Chairman of Internal Medicine made into a full subdivision in October 2005 under the leadership of Dr Qasim Raza as Medical Director and Dr Mark Schwartz as Associate Program Director. Today there are 24 full-time hospitalists providing 24/7 hours inpatient medical services, including consultative services to all sub-specialists at Marshfield Center. Their job also includes surgical co-management of all orthopedic patients admitted to St. Josephs hospital.
Hospitalists typically work in shift system, and on any given day we have about 7 day time non-teaching, 2-3 academic teaching, 1 back-up, 2 evening and 1 night time hospitalist covering all medical inpatient services. St. Joseph's Hospital/Marshfield has always been able to recruit the top graduating residents from Internal Medicine Residency/Med-Peds Programs across United States as we believe this is the first step towards success of our program. Many of our hospitalists are actively involved in academic research & teaching and hold Clinical Assistant Professor rank with School of Medicine & Public Health, University of Wisconsin, Madison.
Andy Weir, Director Quality & Strategic Analysis, St. Joseph's hospital (SJH), Ministry Health places our program among the top 15 in the State of Wisconsin. SJH continues to have a lower Length of Stay (LOS) for the top 25 DRG (Diagnosis Related Group) that usually makes typical hospitalist patients. In FY 2007 we still held a 0.16 LOS advantage compared to other 14 hospitals that round up the top 15 hospitals of Wisconsin. This literally means thousands of dollars saved for the patients in todays world of skyrocketing health care costs. This was achieved without significant compromise on quality of care or patient satisfaction. We have far few readmits when compared to our peers in other hospitals of the state. This was only achieved with hard work and dedication of our hospitalist team under the able leadership of Dr Roderick Koehler, Chairman of Internal Medicine Department and full support of Marshfield Clinic Board of Directors.
Marshfield Clinic physicians work in four other hospitalist programs besides St Joseph's Hospital/Marshfield Center. Marshfield Clinic Euclaire, Minocqua & Wausau Centers have 4 full time hospitalists each. Marshfield Clinic Lake View Medical Center; Rice Lake has one full time hospitalist. This makes Marshfield Clinic almost the largest employer of Hospitalists (total of 37 today) in Wisconsin.
The Future : Hospitalists are here to stay
Proponents say Hospitalists fill a growing gap in continuity of patient care. Typically Physicians spend more time today in treating patients in their offices than at hospitals. Hospitals are traditionally getting sicker patients than ever before, and no primary are physicians are willing to take care of unassigned patients (patients with no primary care provider privileged to work in their hospital). Hospitalists are easily available 24 hours daily to take are of these acutely ill patients. Primary care physicians and sub-specialists are happy in that they can spend more time in their practices. There is no competition as Hospitalists have no out-patient practice and their patients return back for follow-up appointments. Its a win-win situation for patients and physicians. Medicare and more insurance companies have now tagged reimbursement with quality of care provided to patients. Research has proven that in-house physicians are good for hospitals goal to achieve these targets5.
Table 1 Potential roles for hospitalists. ( Swiss Med Wkly 2006; 136:591-596 )
Clinical
Inpatient Wards
Intensive Care Unit
Medicine Consultation Services
Palliative Care Services
Post-discharge Clinic Services
Pre-operative Clinic Services
Non-teaching services (in Teaching Hospitals)
Skilled Nursing Facilities
Educational
Residency Program Directorship
Student Clerkship Directorship
Curriculum Development and Leadership
Operational
Emergency Department Triage Officers
Bed Flow Coordination
Discharge Planning Coordination
Transfer Center Coordination
Quality & Safety
Patient Safety Officer
Director of Quality (Compliance)
Quality Improvement Officer
Other
Clinical Information Technology Implementation
Hospital Leadership Positions
Dr Robert Watcher in his landmark article in JAMA concluded that implementation of Hospitalist programs was associated significant reductions in resource use, usually measured as hospital costs (average decrease , 13.4%) or average LOS (average, 16.6%). All research till date has empirically proven that hospitalists improve in-patient efficiency without harmful effects on quality or patient satisfaction6.
Hospitalists come from diverse training backgrounds and hence SHM has started implementing a process to start early training programs for hospitalists, including residency track and fellowship programs. Current educational deficits include training in communication skills, end-of-life care, quality improvement and patient safety, medical economics, follow-up of acute post-op surgical patients. Hospitalists are slowly expanding into other roles beyond the traditional role of medical consultant Table 1.
Hospital Medicine : New Specialty
Specialists in medicine are traditionally defined by organ disease, example Cardiology; Gastroenterology, Nephrology, Radiology, Oncology, General Surgery etc. The hospitalist, on the other hand is a site defined generalist specialist similar to ER physicians. They care for acutely ill patients with wide array of organ derangements and ages in a given specific location7. Hospitalist co-ordinate and integrate patient care within the health delivery system and reduce the distance between office and hospital with their round of clock availability. Hospitalists already have their own Clinical Textbook8 and SHM is the fastest growing medical society in United States and soon plan to get credentials from ABME (American Board of Medical Specialties) to start an accredited fellowship program in Hospital Medicine.
Critical Issues Facing Hospitalists today
There is significant variation in hospitalists training level, and in the way hospitalists groups are managed. Starting a Hospitalist core curriculum in Residency Training program is the key step towards this goal. Marshfield Clinic Internal Medicine Residents already do Hospitalist Service elective rotation for one month during their post-graduate training period at SJH. Funding of hospitalist programs remains a challenge for hospital administrators. Stagnant Medicare reimbursement, rise in uninsured patients, more acutely ill patients are increasing costs, while their ability to support these costs from hospital budgets is decreasing. There is increasing diversity of hospitalists clinical and non-clinical duties, burn out myth due to ever increasing work-loads, rise in demand for hospitalists (1 available for 10 jobs!), perceived shortage may potentially compromising the efficiency and advantages of hospitalists9. Division between out-patient and inpatient practices continues to widen, hence it is vital to maintain connections between referring and primary care physicians. All of these may in-turn negatively impact hospiltalist and patient satisfaction10.
Respondents (patients and allied health care providers) have overwhelming positive impressions of hospitalist movement. In one survey over 76% believed that they improve Emergency Room efficiency, and 66% felt hospitalists lower costs. Interestingly majority 69% would prefer hospitalists have additional certification or training. In 2007 at least 59% and probably closer to 2/3 of California Hospitals have hospitalists. I believe its true for Wisconsin as well. Quality improvement, keeping patients satisfaction (health care customer), challenging all the above critical issues discussed will be the key to success of this hospitalist program at St. Josephs Hospital/Marshfield Clinic in future.
The impact of this revolution in Inpatient care is just beginning to be felt, and history will tell us if this is the best thing that has happened to medicine this decade. Nevertheless, hospital care will likely remain a highly pluralistic system in which organization of care is determined by efforts to improve the value of care in context to local demands and needs11. I am sure everybody will agree that, method of care chosen should always be the one that promotes the best clinical outcomes and highest patient satisfaction at lowest costs. With these goals hospitalists will definitely have increasingly visible role in many institutions across the country in near future.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
MOHAMMED MOIZUDDIN MD, Clinical Assistant Professor of Medicine, School of Medicine & Public Health, University of Wisconsin, Madison. Hospitalist, St. Josephs Hospital/Marshfield Clinic, Marshfield, USA
QASIM RAJA, MD, Director, Hospitalist Division, Department of Internal Medicine, Marshfield Clinic, Marshfield, USA
QURETUL QURESH, MD, Deccan College of Medical Sciences, India
CORRESPONDENCE: MOHAMMED MOIZUDDIN, MD, Department of Internal Medicine, Hospitalist office 3J3, Marshfield Clinic, 1000 North Oak Avenue, Marshfield, USA, WI 54449
Email: moizuddin.mohammed@marshfieldclinic.org
References
1. Watcher RM, Goldman L. The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996; 335:514-7.
2. Bellet PS and Watcher RM. The hospitalist movement and its implications for care of hospitalized children. Pediatrics 1999; 103:47377
3. Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington DC: National Academy Press, 2001.
4. Niraj L Sehgal, RM Watcher The emerging role of "hospitalists" in the American health care system. Swiss Med Wkly 2006; 136:591-596
5. Hospitals & Health Network; June 2006, Vol. 80 Issue 6, p56-60, 3p
Bacterial infections are associated with many autoimmune diseases involving chronic inflammation and demyelination. The possible mechanisms of bacterial involvement as aetiological agents or in the exacerbation of these diseases have been investigated intensively. This review focuses the role of bacterial infections in the pathogenesis of autoimmune, inflammatory and demyelinating diseases. Possible modes of pathogenic action of bacteria are discussed, viz. the role of cytokines, Toll-like receptor signalling, the interaction of heat shock proteins with the immune system, and the role of nitric oxide. An auto-regulatory loop might exist in the interaction of bacteria with the host and in pathogenic signal processing. These studies reveal potential therapeutic targets.
Abbreviations: AQP4 Aquaporin-4; AS ankylosing spondylitis; CSF cerebrospinal fluid; EAE autoimmune encephalomyelitis; GB Guillain-Barre syndrome; HLA human leukocyte antigens; HSP heat shock protein; IL interleukin; LPS lipopolysaccharides; MAM Mycoplasma arthritidis antigen; MHC [proteins encoded by] major histocompatibility gene complex; MS multiple sclerosis; NK natural killer cells; NMO neuromyelitis optica; NO nitric oxide; NOS nitirc oxide synthase; PCR polymerase chain reaction; RA rheumatoid arthritis; SLE systemic lupus erythematosus; TLR Toll-like receptors; TNF tumour necrosis factor
Introduction
Bacterial and viral infections are commonplace in a variety of autoimmune and chronic illnesses such as the chronic fatigue syndrome (myalgic encephalomyelitis), fibromyalgia syndrome, Gulf War illnesses and rheumatoid conditions1-3. Much attention is focused at present on the role of bacteria and the possible mechanisms of their involvement in the pathogenesis of several diseases. The route of infection and penetration and the immune responses of the host can not only make any bacterial infection pathogenic but probably can also determine the aggressiveness of the disease and the chance for full recovery. Therefore the two basic elements addressed here are the association between bacterial infection and autoimmune disease and the involvement of the immune system in the disease process.
Bacterial infections in rheumatoid conditions
A wide variety of bacterial infections have been associated with rheumatoid conditions. Rheumatic diseases might have a manifold aetiology with varying genetic susceptibility, but bacteria-related autoimmunity might be an important factor4.
Mycoplasma infection, e.g. by M. pneumoniae, M. salivarum, and M. fermentans, has been strongly associated with RA (rheumatoid arthritis)5-8. There is often systemic infection of more than one species8. Mycoplasma antigens induce both cell-mediated and humoral immune responses. Enhanced levels of antibodies against MAM (Mycoplasma arthritidis antigen) have been found in sera from RA patients in comparison with antibodies against Staphylococcal enterotoxins A and B. Also antibody titers were higher in RA serum than in systemic lupus erythematosus, ankylosing spondylitis, psoriatic arthritis, Reiter's syndrome, or healthy controls.
The mycoplasma antigen MAM can activate T cells. MAM contains two domains, one of which can inhibit lymphocyte proliferation; the second domain, which contains concanavalin A motif-, is required for T cell activation9. It can also up regulate natural killer cell activity10. Furthermore, synovial tissues of RA patients contain T-cells, which bear the same T-cell receptors as used by MAM. The mitogen seems to be capable of initiating and exacerbating arthritic changes11, 12. MAM is a zinc-dependent antigen that binds to MHC class II molecules. Zinc induces MHC protein dimerisation required for MAM binding, MHC-induced cell-cell adhesion, and efficient T cell activation13, 14. As discussed in later sections, MAM can alter cytokine expression profiles and activate and modulate nitric oxide synthase (NOS) signalling pathways.
Bacterial DNA isolated from rheumatoid arthritis (RA) and juvenile arthritis has included Haemophilus influenzae, Bordatella and Yersinia as possible infecting organisms15. Lyme arthritis, which resembles rheumatoid synovial infiltration by Borrelia burgdorferi, has often been suggested to be an autoimmune condition. The B. burgdorferi surface protein A (OspA161-175) is recognised by T-cells and HLA (human leukocyte antigen)-DR molecules that bind this T-cell epitope and to these events is attributed the development of autoimmunity following B. burgdorferi infection. However, these decline with antibiotic therapy16. Therefore, in spite of the perceived association, Drouin et al.17 diligently searched for peptides with sequence homology with OspA (165-173) and have concluded from their study that molecular mimicry might not be significant to pathogenesis. The epitope OspA (163-175) is the predominant epitope associated with Lyme disease. Serum reactivity against OspA is also found in RA patients18. Our knowledge concerning the interaction of B. burgdorferi with host tissues and cells is rather scant. Ghosh et al.19 have suggested cytokeratin 10 as a potential autoantigen. Gavanescu et al.20 reported that mycoplasma infections can result in the production of autoantibodies against centrosomes. It is not known if this cellular organelle is involved with autoimmunity in RA.
B. burgdorferi seems to be able to induce inflammatory responses including secretion of cytokines and cellular responses of the T-helper cell-1 (Th-1) type21. Beermann et al.22 generated lipoprotein vesicles (LV) from this bacterium and incorporated them into peripheral blood mononuclear cells. The resultant LV-T cells were predominantly the immune effector CD8+. Furthermore, these cells destroyed autologous T-cells carrying LV. These data do indeed support the existence of an autoimmune condition. Overall, a conservative conclusion would be that the molecular mimicry and autoimmunity thesis is yet to be fully tested.
Proteus mirabilis has been implicated in the pathogenesis of RA23-26 and in osteoarthritis (OA)27, 28. Again, the HLA DRB1 alleles appear to be the major genetic susceptibility factors as postulated some years ago29.
Bacterial infection associated with other autoimmune conditions
Bacterial infections have been identified in association with other autoimmune conditions besides RA. Members of the Enterobacteriaceae family are associated with autoimmune conditions such as Kawasaki syndrome and Graves disease. Demyelinating diseases have been a focus of active investigation in the past few years. Kollef et al.30 suggested that central and peripheral nerve demyelination might occur following M. pneumoniae infection. Since then patients with the autoimmune condition SLE (systemic lupus erythematosus) have been investigated for mycoplasma infections. Early studies revealed differences between SLE patients and control subjects in respect of genitourinary mycoplasma infections31. However, the deployment of more sensitive methods of detection has not supported these early claims. Runge et al.32, for instance, found no difference in the incidence of Ureaplasma urealyticum in SLE patients, and they discount the notion that this mycoplasma species has any role to play in the pathogenesis of SLE. Nonetheless, there should be no serious doubts that mycoplasma infection can lead to demyelination.
The demyelinating neuropathy known as Guillain-Barre (GB) syndrome often has pathogenic association with bacterial infections. Campylobacter jejuni, Haemophilus influenzae and M pneumoniae have been implicated as possible causative agents of GB. C. jejuni is the major infecting organism here together with M. pneumoniae infection in some cases33, 34. GB is associated with the presence of antibodies against galactocerebroside, which is a major component of myelin35, 36. Some bacterial LPS (lipopolysaccharides) apparently bear molecular similarity to the human gangliosides GM1, GM1b, GD1a, and GalNAc-GD1a of the motor axolemma and are said to be the target epitopes for antibodies occurring in the GB subtype acute motor axonal neuropathy. The antiganglioside antibodies cause axonal neuropathy37. The host immune response to LPS moieties of the HB93-13 strains of C. jejuni cross-reacts with human nerve gangliosides and induce GBS38. .
Multiple sclerosis (MS) is a chronic inflammatory and demyelinating disease of the central nervous system. The pathogenesis of MS is possibly a consequence of autoimmune condition or infection by viral or bacterial agents. Both infections lead to the development of demyelinating plaques. Bacterial infections can evoke immune responses and induce demyelination. Infections of the brain parenchyma are sequestered from the immune system. Matyszak39 has postulated a loss of the integrity of the blood-brain barrier at the foci of infection by a delayed-type hypersensitivity response leading to demyelination. Nitric oxide (NO), which enhances the permeability of the blood brain barrier, is found in greater quantities in the CSF (cerebrospinal fluid) of MS patients than of control subjects4. Also NO metabolite levels reportedly correlate with disease activity41. Other explanations have also been advanced. Gay42 has drawn attention to the putative link of bacterial nasopharyngeal infections with optic neuritis, optochiasmatic arachnoiditis and MS. The possibility is aired that the blood barrier may be by-passed. Gay42 points out the physical connection between CSF and the lymphatic drainage channels of the nasopharyngeal mucosa. So in the event, the CNS could be exposed to bacterial toxins and generate an immunological response. Many autoimmune diseases involve HLAs. The latter play a key role in antigen presentation to CD4+ Th cells. Specific regions of HLA e.g. HLA-C have robust association with MS and Graves' disease43.
More recently serology and PCR (polymerase chain reaction) have provided ample evidence of Chlamydia pneumoniae, Borrelia burgdorferi, Mycoplasma species, human herpesvirus-1 and -6, among others in MS, amyotrophic lateral sclerosis Alzheimer's and Parkinson's disease3. Parratt et al.44 looked at Chlamydia pneumoniae-specific immune complexes and have reported that C. pneumoniae infection is more frequent in MS patients and detected early in the course of the disease, presumably indicating an aetiological link. A tentative relationship between MS and streptococcal infection has been suggested45. But Budak et al.46 have found no evidence of C. pneumoniae DNA in CSF samples. Similarly no Mycoplasma-specific nucleic acid sequences were detected47 (Casserly et al. 2007). Lindsey and Patel48 found no trace of bacterial 16S DNA in the CSF of MS patients with progressive diseases or patients in remission. They tested for Campylobacter, Mycoplasma, Chlamydia, Bartonella, Mycobacteria and Streptococcus.
The aetiology and pathogenesis of MS and neuromyelitis optica (NMO) have been studied intensively from another angle in recent years. MS and NMO are related conditions; NMO could be a variant of greater severity than MS. Specific autoantibody responses have been identified in NMO patients. These are AQP4 (Aquaporin-4) antibodies generated against the water channel protein AQP449. 50 and they selectively target astrocytic end feet at the glia limitans (the external glial limiting membrane).
AQP4 antibodies are regarded as autoantibodies and so associated with the pathogenesis of NMO. The occurrence of lesions in the brain and spinal cord of NMO patients are consistent with the degree of AQP-4 expression51. The damage of astrocytes encountered in NMO is attributed to these antibodies. Serum IgG from patients with NMO binds to the extracellular domain of aquaporin-4; it is predominantly IgG1. Antibody binding to membranes expressing aquaporin-4 probably initiates demyelination52. HSP (heat shock protein) 70 has also been implicated in the autoimmune response leading to demyelination53.
Possible modes of pathogenic action of bacteria
Molecular mimicry in pathogenesis
Most autoimmune diseases are associated with HLA types. RA and AS (ankylosing spondylitis) are classical examples of the association of HLA with rheumatoid conditions. More than 90% of RA patients possess HLA-DR1 or other sub-type and >96% of AS patients reportedly possess HLA-B2754. HLA-B27 antigen is also involved in reactive arthritis55. Spondyloarthropathies (SAP) are a group of HLA-B27-linked diseases, characterised by inflammatory pain in the spine and asymmetrical arthritis in the lower limbs. HLA-B27 transgenic mice spontaneously develop arthritis and they are susceptible to collagen-induced arthritis56. The involvement of HLA antigens in the pathogenesis of autoimmune diseases has been suggested to be due to the molecular similarities between certain bacterial antigens and HLA antigens. But there are no cross-reactive antibodies against bacteria and HLA-B27 in significant titres57.
The autoimmune conditions of Graves disease and Kawasaki syndrome are a result of the hyperactivation of the immune system. Bacterial infections have been implicated in both disease states. Yersinia enterocolitica, a member of the Enterobacteriaceae family, produces lipoproteins that are well known for their mimicry of the extracellular domain of the human thyrotropin receptor protein58, 59. This lipoprotein is mitogenic to B-cells60 and induces the production of autoantibodies against the thyrotropin receptor. This could be the cause of hyperthyroidism associated with Graves disease.
Chlamydial infection occurs commonly in chronic and acute diseases of the upper and lower respiratory tract and. also with atherosclerosis and asthma. Rheumatic autoimmune conditions also often show antibodies against the ribosomal protein L7. The L7 protein has been reported to contain epitopes bearing homology with a specific aminoacid sequence of the C. trachomatis RNA polymerase61. This has led to the suggestion that certain rheumatoid conditions could be due to the molecular similarity between L7 and the homologous sequence of the polymerase and generation of autoantibodies.
The autoimmune condition of SLE causes glomerulonephritis, arthritic changes and neurological alterations. SLE is another example of pathogenesis attributable to molecular mimicry between antigens of infecting agents and autologous proteins. As stated earlier, Campylobacter jejuni is the major infecting agent in patients with this disease. Hughes et al.62 demonstrated the presence of antibodies against the ganglioside GM1 in SLE patients. Campylobacter infection has been linked with the perceived molecular mimicry of bacterial LPS with the human gangliosides of the motor axolemma and these are the target epitopes for antibodies that are believed cause axonal neuropathy37.
The role of cytokines in the pathogenesis of autoimmune conditions
Another line of evidence that links bacterial infections with RA and other inflammatory autoimmune conditions is the demonstration that bacterial antigens, such as MAM, induce the synthesis of pro-inflammatory cytokines, interleukin (IL)-1, IL-6, and IL-863, 64. Furthermore, the modulation of the synthesis of cytokines by MAM corresponds with the induction of arthritic changes in mice65. The induction of IL-13 expression appears to be up regulated in human fibroblast cell lines when the cell cultures are contaminated by mycoplasmas66. IL-6 and IL-8 are induced in human gingival fibroblasts by a host of mycoplasma species, e.g. M. hominis, M. arthritidis, M. arginini, M. fermentans, M. penetrans, M. pirum and M. pneumoniae64. Glycolipid antigens of M. fermentans have been identified as important mediators of pathogenicity. The induction of TNF (tumour necrosis factor) together with cytokines and prostaglandins was reported some years ago67, 68. TNF is produced in response to M. fermentans antigens69. TNF- induced by M. fermentans appears to enhance cytokines that can modulate the immune system. Exposure of human lung fibroblasts to M. fermentans induces IL-6, IL-10 and IL-12, IL-1b, IL-8 (now designated as CXCL8), the monocyte chemoattractant protein-1 (MCP-1) also known as CCL2 (CC chemokine ligand 2), and the chemokine (C-X-C motif) ligand 1 (CXCL1) production69, 70. Kawahito et al.71 used monoclonal antibody against the M. fermentans glycolipid antigen GGPL-III and detected it in synovial tissues from RA patients. The antigen was not detectable in OA or normal synovial tissues. Furthermore, GGPL-III induced TNF-a and IL-6 production by peripheral blood mononuclear cells, and also induced proliferation of synovial fibroblasts. However, anti-phospholipid antibodies are generated in response to a number of bacterial infections72. So their presence alone might not be clearly linked with pathogenesis.
Toll-like receptor signalling in immune responses to infection
The generation of immune responses to lipopolysaccharides (LPS) is mediated by a class of receptors called Toll-like receptors (TLRs). These are transmembrane receptors that activate immune cell responses. TLR can recognise molecular patterns associated with pathogenic infectious agents; among them of note are LPS, viral RNA, and unmethylated CpG-oligonucleotides.
The TLR signalling mechanism has been the focus of much attention. Exposure of cells to LPS or other toxins induces the expression of different forms of TLR and different pro-inflammatory interleukins and interferons73. Inflammatory responses to M. arthritidis lipoproteins require TLRs74. MAM of M. arthritidis has been shown to interact with TLRs75. MAM generates a differential immune reactivity mediated by different TLR types. The co-stimulatory molecules associated with the immune stimulation determine the outcome in terms of IL isoform produced and this depends upon which co-stimulatory factor interacts with MAM. Thus inhibition of co-stimulatory factor B7-1 leads to a shift from IL-2 to IL-176. TLR signalling also involves caspases required for processing the precursors of IL-1 and IL-18. The TLRs use the adapter protein MyD88 and the so-called adapter-like MyD88 to activate signaling pathways, but only the latter interacts with caspase77. So here we have another potential means of regulating the expression pattern of pro-inflammatory cytokines. In other words, IL production pattern is determined by the co-operation TLRs. TLRs can synergistically or competitively modulate IL expression in immune response to infectious agents78. Equally, one can attribute specific TLRs of T-cells with the ability to directly stimulate Th1 and Th2 effector function and modulate the synthesis of cytokines and interferons, and influence cell proliferation and survival79. TLR function is closely related to Fc? receptor (Fc?R) expression. The cells of the immune system express receptors for the Fc region of Ig isotypes. Fc?R for IgG links IgG mediated responses of the immune system80. TLR4 up regulates the expression of Fc?R. IL10 is said to be involved in and mediate this up regulation81. Probably, as Loof et al.82 have implied, TLRs might be functioning as a cohort of signalling channels interacting with one another rather than acting individually to generate an immune outcome. TLR signalling might be autoregulated; a concept that is worthy of investigation.
LPS seems to induce the production of interleukins via a TLR-mediated pathway. Exposure of the macrophage RAW264.7 cell line to LPS leads to Janus kinase (JAK)2 tyrosine phosphorylation with TLR4 mediation, then down stream to the phosphorylation of JNK {c-jun N terminal kinase) resulting in IL production83.
Finally, TLR signalling is involved in the activation of innate immunity in defence from infections not only bacterial, but also viral and parasitic. NK cells, macrophages, dendritic cells are all capable of enlisting TLRs signalling in their function. The recognition of bacterial infection by NK cells seems to be mediated by TLR84, 85. Other infections e. g. by the parasitic protozoan Leishmania major, result in the induction of IL-12 in bone marrow-derived dendritic cells, IFN-? expression and activation of NK cells. These events are mediated by TLR986.
The interaction of heat shock proteins with the immune system
Heat shock proteins (HSP) are a highly conserved family of stress-related proteins with diverse function such as protein folding and chaperoning, and novel and differential modes of function have now been ascribed to their functional repertoire. HSPs might chaperone antigenic peptides.
Antibodies against a number of HSPs have been detected in autoimmune diseases. Marked increases in antibodies against HSP70 and HSP90 occur in patients with RA87, Klebsiella pneumoniae HSP60 in ankylosing spondylitis patients88, HSP27 and HSP90 antibodies in patients with arthritis accompanying cystic fibrosis89 and so on. T lymphocytes react to heat shock proteins and this probably plays an important regulatory role in the progression of autoimmune diseases. HLA-DR-T cell epitopes have been identified in HSP60 and HSP7090-92. In experimental systems HSP60 induces the production of IL-8 and TNF (tumor necrosis factor)-a and this is enhanced by HSP auto-antibodies. Sera from RA patients with higher anti-HSP60 auto-antibody titers also markedly increased the IL-8 production induced by HSP60 in a human monocytic cell line93. As yet, it is unclear what role HSP auto-antibodies might play in pathogenesis.
HSP are known to be able to influence both innate and adaptive immune response and induce the expression of interleukins under a variety of experimental conditions. Some HSPs induce and other can inhibit the production of interleukins. Bacterial HSPs bear sequence homology to human HSPs, and immunisation with bacterial HSPs has often inhibited disease progression94. Several HSP receptors have been identified to-date on antigen presenting cells. Among them are the Toll-like receptors TLR2 and TLR4. HSPs are recognised by appropriate receptors to initiate their participation in the signalling cascade95, 96. Singh et al.97 showed that heat shock activated transcription factor HSF-1 (heat shock factor-1) binds to heat shock responsive elements in the promoter of genes coding for certain interleukins.
The TLR signalling pathway has been robustly implicated in HSP function. HSPs recognise and bind to pathogen-associated molecules and activate TLR mediated signalling. It appears possible that different HSPs might differentially activate TLRs thus determining the functional pathway. Thus HSP60 is said to bind to TLR1 but not to TLR298; this could have differing consequences in terms of induction of cytokines. HSP70 bound to the cell membrane is said to specifically activate NK cells, whilst intracellular HSP70 exerts immunomodulatory effects by binding specifically to TLR2 and TLR4. In vitro studies have suggested that HSP70 is actively released in response to heat shock and induces the production of IL-10 in fibroblast-like synoviocytes by TLR4 signalling99. HSP72 induces IL-8 expression by activating TLR4 and NF-kappa B100.
The role of nitric oxide in the pathogenesis of autoimmune, inflammatory and demyelinating diseases
Nitric oxide (NO) is synthesised by NO synthase (NOS) which occurs as neuronal, endothelial and inducible isoforms. NO subserves many functions. Most prominently, it is a vasoactive agent regarded as contributing significantly to the pathogenesis of inflammatory immune and neurodegenerative diseases. RA, SLE, MS, and experimental autoimmune encephalomyelitis (EAE), an experimental model of MS, all show associated synthesis of NO, superoxide and their toxic products. Upon infection bacterial components bind to macrophages using TLRs and this leads to the production of TNF-a, which in turn induces to the synthesis of NO. NO is also expressed by cells when exposed to IFN-?. NOS is required for bacterial clearance during infection101. The general and overall effects would be bactericidal in nature.
Arthritic changes occurring in an animal model called adjuvant-induced arthritis, which exhibits features similar to those of RA, accompany the induction of NOS. Furthermore, NOS inhibitors suppress the arthritic changes102. Mouse peritoneal macrophages and a macrophage cell line have been reported to synthesise NO in response to MAM. This is enhanced by LPS possibly via TLR2 but not TLR4 signalling103, 104. M. hominis lipophilic component also interacts with TLR2 not TLR4105. M. synoviae lipoprotein lipid moiety induces NO secretion by chicken macrophages106.
Nitric oxide (NO) enhances the permeability of the blood brain barrier. The invasion of the CNS by inflammatory cells and the development of EAE are prevented if the toxic product peroxynitrite of NO and superoxide are scavenged107. Both constitutive isoforms of NOS, neuronal and endothelial, and inducible NOS are active in the demyelination process108. NOS has also been implicated in the pathogenesis of Parkinsons disease109.
Demyelination can be induced by mycoplasmas. NO, inflammatory cytokines, and prostaglandins are induced when glial cells are exposed to M. fermentans antigens68. Heat shock inhibits both NO and iNOS (inducible NOS)110, 111. Bacterial LPS-induced expression of NOS can be inhibited by exposure of cells to hyperthermia at 43C. Transfection of HSP70 reduces iNOS expression111, 112. From the foregoing discussions one can visualize a complete regulatory picture of the involvement of HLAs, HSPs, cytokines and nitric oxide in the pathogenesis of inflammatory immune diseases.
Although NO is harmful to bacteria, it can induce apoptosis in some cell systems113 and cause necrosis (see Naito et al.114). The toxicity of NO can result in immune suppression and in turn lead to enhanced infection115. Bacteria also seem to have evolved protective mechanisms against these deleterious effects. So host resistance to bacterial infections and the ability of bacteria to initiate inflammatory and demyelinating conditions leading to pathogenesis are finely tuned. The understanding of the control mechanisms has not only expanded our knowledge of the possible modes of bacterial involvement in pathogenesis, but it has also led to the identification of potential targets for therapy. The activation of signalling pathways mediated by TLRs has afforded an avenue of therapeutic approaches to autoimmune conditions. TLR signalling together with its cognate receptors and adapter molecules can conceivably be employed as specific targets for therapeutic intervention. The TLR agonists have been found to enhance immune responses, especially against tumours116. Some agonists have been approved for the treatment of certain human disease conditions117, 118. There is also much scope for the detection of bacterial infections via TLRs. As discussed earlier the TLR signalling pathway might be implicated in potential crosstalk with other interacting signalling systems. In other words, a composite regulatory operation of many pathways involving TLRs can be delineated in the pathogenesis of autoimmune diseases.
It would not be out of place to inquire here into the potential clinical benefits of studying the role of bacterial infections and the mode of their participation in the disease process. The prevention of disease progression is one of the benefits, in which not only the identification of the infecting agent but also the mode by which the infectious agents might trigger initiation and progression would make a valuable contribution. Specifically targeted intervention modalities using antibacterial therapy can evolve and develop from such basic research. Also these would find much application in the development of healthcare facilities such as antimicrobial stewardship programmes and infection control programmes to monitor effects of treatment and treatment costs119. Unavoidably the cost effectiveness of treatment regimes comes into reckoning. This makes it imperative that factors which determine antibiotic-resistance of bacteria are identified and adequately addressed.
ACKNOWLEDGEMENTS
I thank Professor Jrg Haier of the Cancer Centre of the University Hospital at Mnster and Dr M.S. Lakshmi for reading the manuscript and making valuable suggestions, and Professor Bayan Sharif and Professor Satnam Dlay for supporting my research and literary efforts.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
GAJANAN V SHERBET, The Institute for Molecular Medicine, Huntington Beach CA, USA
CORRESPONDENCE: GAJANAN V SHERBET, School of Electrical, Electronic and Computer Engineering, University of Newcastle upon Tyne, Merz Court, Newcastle upon Tyne, NE1 7RU, U.K.
Email: gajanan.sherbet@ncl.ac.uk
References:
1. Nicolson GL, Nasralla M, Haier J, et al. Diagnosis and treatment of mycoplasmal infections in fibromyalgia and chronic fatigue syndromes. Relationship to Gulf war illness. Biomed Therapy 1998; 16: 266-271.
2. Nicolson GL, Nasralla MY, Franco AR, et al. Role of mycoplasmal infections in fatigue illnesses. Chronic fatigue and fibromyalgia syndromes, Gulf War illness and rheumatoid arthritis. J Chronic Fatigue Syndrome (Microbiol) 2000; 6: 23-29.
3. Nicolson, GL. Chronic bacterial and viral infections in neurodegenerative and neurobehavioral diseases. Labmed 2008; 39: 291-299.
5. Furr PM, Taylor-Robinson D, Webster ADR. Mycoplasmas and ureaplasmas in patients with hypogammaglobulinemia and their role in arthritis: Microbiological observations over twenty years. Ann Rheum disease 1994; 53: 183-187.
6. Simecka JW, Rosss SE, Cassell GH, et al. Interactions of mycoplasmas with B cells. Production of antibodies and nonspecific effects. Clin Infectious Dis 1993; 17: S176-S182.
7. Hoffman RW, OSullivan FX, Schafermeyer KR, et al. Mycoplasma infection and rheumatoid arthritis. Analysis of their relationship using immunoblotting and an ultrasensitive polymerase chain reaction detection method. Arthritis Rheum 1997: 40: 1219-1228.
8. Haier J, Nasralla M, Franco AR, et al. Detection of mycoplasmal infections in blood of patients with rheumatoid arthritis. Rheumatol 1999; 38: 504-509.
9. Cole BC, Knudtson KL, Oliphant A, et al. The sequence of the Mycoplasma arthritidis superantigen, MAM. Identification of functional domains and comparison with microbial superantigens and plant lectin mitogens. J Exp Med 1996; 183: 1105-1110.
10. DOrazio JA, Cole BC, Stein-Streilein J. Mycoplasma arthritidis mitogen up regulates human NK cell activity. Infection Immunity 1996; 64: 441-447.
11. Cole BC, Griffiths MM. Triggering and exacerbation of autoimmune arthritis by the mycoplasma arthritidis superantigen MAM. Arthritis Rheum 1993; 36: 994-1002.
12. Cole BC, Sawitzke AD, Mu HH. Mycoplasma arthritidis and its superantigen M-arthritidis mitogen as a model for inflammatory and autoimmune disease. EFFECTS Mcrobes Immune Sys 2000; 93-107.
13. Langlois MA, El Fakhry Y, Mourad W. Zinc-binding sites in the N terminus of Mycoplasma arthritidis-derived mitogen permit the dimer formation required for high affinity binding to HLA-DR and for T cell activation. J Biol Chem 2003; 278: 22309-22315.
14. Li HM, Zhao YW, Guo Y, et al. Zinc induces dimerization of the class II major histocompatibility complex molecule that leads to cooperative binding to a superantigen. J Biol Chem 2007; 282: 5991-6000.
15. Wilkinson NZ, Kindsley GH, Jones HW, et al. The detection of DNA from a range of bacterial species in the joints of patients with a variety of arthritides using a nested, broad-range polymerase chain reaction. Rheumatology 1999; 38: 260-266.
16. Kannian P, Drouin EE, Glickstein L, et al. Decline in the frequencies of Borrelia burgdorferi OspA(161-175)-Specific T cells after antibiotic therapy inHLA-DRB1*0401-positive patients with antibiotic-responsive or antibiotic-refractory Lyme arthritis. J Immunol 2007; 179: 6336-6342.
17. Drouin EE, Glickstein L, Kwok WW, et al. Human homologues of a Borrelia T- cell epitope associated with antibiotic-refractory Lyme arthritis. Mol Immunol 2008; 45: 180-189.
18. Hsieh YF, Liu HW, Hsu TC, et al. Serum reactivity against Borrelia burgdorferi OspA in patients with rheumatoid arthritis. Clin Vaccine Immunol 2007; 14: 1437-1441.
19. Ghosh S, Seward R, Costello CE, et al. Autoantibodies from synovial lesions in chronic, antibiotic treatment-resistant Lyme arthritis bind cytokeratin-10. J Immunol 2006; 177: 2486-2494.
20. Gavanescu I; Pihan G, Halilovic E, et al. Mycoplasma infection induces a scleroderma-like centrosome autoantibody response in mice. Clin Exptl Immunol 2004; 137:288-297.
21. Franz JK, Priem S, Rittig MG, et al. Studies on the pathogenesis and treatment of Lyme arthritis. Wiener Klini Wochenschrift 1999; 111, 981-984.
22. Beermann C, Wunderli-Allenspach H, Groscurth P, et al. Lipoproteins from Borrelia burgdorferi applied in liposomes and presented to dendritic cells induce CD8+ T-lymphocytes in vitro. Cell Immunol 2000; 201: 124-131.
23. Subair H, Tiwana H, Fielder M, et al. Elevation of anti-Proteus antibodies in patients with rheumatoid arthritis from Bermuda and England. J Rheumatol 1995; 22: 1825-1828.
24. Blankenberg-Sprenkels SHD, Fielder M, Feltkamp TEW et al. Antibodies to Klebsiella pneumoniae in Dutch patients with ankylosing spondylitis and acute anterior uveitis and to Proteus mirabilis in rheumatoid arthritis. J Rheumatol 1998; 25: 743-747.
25. Tiwana H, Wilson C, Walmsley RS, et al. Antibody responses to gut bacteria in ankylosing spondylitis, rheumatoid arthritis, Crohns disease and ulcerative colitis. Rheumatol Int 1997; 17: 11-16.
26. Tani Y, Tiwana H, Kukuda S, et al. Antibodies to Klebsiella, Proteus, and HLA-B27 peptides in Japanese patients with ankylosing spondylitis and rheumatoid arthritis. J Rheumatol 1997; 24: 109-114.
27. Wanchu A, Deodhar SD, Sharma M, et al. Elevated levels of anti-Proteus antibodies in patients with active rheumatoid arthritis. Indian J Med Res 1997; 105: 39-42.
28. Van der Heijden IM, Wilbrink B, Tchetverikov I, et al. Presence of bacterial DNA and bacterial peptidoglycans in joints of patients with rheumatoid arthritis and other arthritides. Arthritis Rheum 2000; 43: 593-598.
29. Silman AJ, Pearson JE. Epidemiology and genetics of rheumatoid arthritis. Arthritis Res 2002; 4: Suppl 3S265-72.
30. Kollef MH, West S, Davis DR, et al. Central and peripheral nervous system demyelination after infection with Mycoplasma pneumoniae. Evidence of an autoimmune process. Southern Med J 1991; 84, 1255-1258.
31. Ginsburg KS, Kundsin RB, Walter CW, et al. Ureaplasma urealyticum and Mycoplasma hominis in women with systemic lupus erythematosus. Arthritis Rheum 1992; 35: 429-433.
32. Runge M, Rykena S, Wildhagen K, et al. Detection of Ureaplasma urealyticum in urine of patients with systemic lupus erythematosus and healthy individuals by culture and polymerase chain reaction. J Med Microbiol 1997; 46: 413-418.
33. Komatsu H, Kuroki S, Shimizu Y, et al. Mycoplasma pneumoniae meningo-encephalitis and cerebellitis with antiganglioside antibodies. Pediatric Neurol 1998; 18: 160-164.
34. Yuki, N. Ganglioside mimicry and peripheral nerve disease. Muscle Nerve 2007; 35: 691-711.
35. Kusunoki S, Chiba A, Hitoshi S, et al. Anti-GAL-c antibody in autoimmune neuropathies subsequent to mycoplasma infection. Muscle Nerve 1995; 18: 409-413.
36. Nishimura M, Saida T, Kuroki S, et al. Post-infectious encephalitis with anti-galactocerebroside antibody subsequent to Mycoplasma pneumoniae infection. J Neurol Sci 1996; 140: 91-95.
37. Kuwabara, S. Guillain-Barre syndrome. Current Neurol Neurosci Rep 2007; 7: 57-62.
38. Perera VN, Nachamkin I, Ung H, et al. Molecular mimicry in Campylobacter jejuni: role of the lipo-oligosaccharide core oligosaccharide in inducing anti-ganglioside antibodies. FEMS Immunol Med Microbiol 2007; 50: 27-36.
39. Matyszak MK. Inflammation in the CNS. Balance between immunological privilege and immune response. Progress Neurobiol 1998; 56: 19-35.
40. Speciale L, Sarasella M, Ruzzante S, et al. Endothelin and nitric oxide levels in cerebrospinal fluid of patients with multiple sclerosis. J Neurovirol 2000; 6: S62-S66.
41. Svenningsson A, Petersson AS, Andersen O, et al. Nitric oxide metabolites in CSF of patients with MS are related to clinical course of the disease. Neurology 1999; 53: 1880-1882.
42. Gay, F. Bacterial toxins and multiple sclerosis. J Neurol Sci 2007; 262 :105-112.
43. Gough SCL, Simmonds MJ. The HLA region and autoimmune disease: Associations and mechanisms of action. Current Genomics 2007; 8: 453-465.
44. Parratt J, Tavendale R, O'Riordan, J, et al. Chlamydia pneumoniae-specific serum immune complexes in patients with multiple sclerosis. Multiple Sclerosis 2008; 14: 292-299.
45. Topkaya AE, Sahin S, Aksungar FB, et al. Is there any relationship between streptococcal infection and multiple sclerosis?. Med Sci Monitor 2007; 13: CR567-CR569.
46. Budak F, Keceli S, Efendi H, et al. The investigation of Chlamydophila pneumoniae in patients with multiple sclerosis. Int J Neurosci 2007; 117: 409-415.
47. Casserly G, Barry T, Tourtellotte WW, et al. Absence of Mycoplasma-specific DNA sequence in brain, blood and CSF of patients with multiple sclerosis (MS): A study by PCR and real-time PCR. J Neurol Sci 2007; 253: 48-52.
48. Lindsey JW, Patel S. PCR for bacterial 16S ribosomal DNA in multiple sclerosis cerebrospinal fluid. Multiple Sclerosis 2008; 14: 147-152.
49. Lennon VA, Kryzer TJ, Pittock SJ, et al. IgG marker of optic-spinal multiple sclerosis binds to the aquaporin-4 water channel. J Exp Med 2005; 202: 473-477.
50. Weinshenker BG, Wingerchuk DM, Pittock SJ, et al. NMO-IgG: A specific biomarker for neuromyelitis optica. Dis Markers 2006; 22: 197-206.
51. Bradl M, Lassmann H. Anti-Aquaporin-4 Antibodies in Neuromyelitis Optica: How to Prove their Pathogenetic Relevance? Int MS J 2008; 15:75-78.
52. Hinson SR, Pittock SJ, Lucchinetti CF, et al. Pathogenic potential of IgG binding to water channel extracellular domain in neuromyelitis optica. Neurology 2007; 69: 2221-2231.
53. Mycko MA, Cwiklinska H, Walczak A, et al. A heat shock protein gene (Hsp70.1) is critically involved in the generation of the immune response to myelin antigen. Eur J Immunol 2008; 38: 1999-2013.
54. Ebringer A, Wilson C. HLA molecules, bacteria and autoimmunity. J Med Microbiol 2000; 49: 305-311.
55. Beutler AM, Schumacher HR. Reactive arthritis. Is it a useful concept? Br J Clin Practice 1997; 51: 169-172.
56. Lee S, Khare SD, Griffiths MM, et al. HLA-B27 transgenic mice are susceptible to collagen-induced arthritis. Type II collagen as a potential target in human disease. Human Immunol 2000; 61: 140-147.
57. Ringrose JH. HLA-B27 associated spondyloarthropathy, an autoimmune disease based on cross-reactivity between bacterial and HLA-B27? Ann Rheum Dis 1999; 58: 598-610.
58. Zhang HW, Kaur I, Niesel DW, et al. Lipoprotein from Yersinia enterocolitica contains epitopes that cross react with the human thyrotropin receptor. J Immunol 1997; 158: 1976-1983.
59.Luo CY, Seetharamaiah GS, Niesel DW, et al. Purification and characterization of Yersinia enterocolitica envelope protein which induce antibodies that react with human thyrotropin receptor. J Immunol 1994; 152: 2555-2561.
60. Zhang HW, Kaur I, Niesel DW, et al. Yersinia enterocolitica envelope proteins that are corss reactive with thyrotrpin receptor (TSHR) also have B-cell mitogenic activity. J Autoimmunity 1996; 9: 509-516.
61. Hemmerich P, Neu E, Macht M, et al. Correlation between chlamydial infection and autoimmune response. Molecular mimicry between RNA polymerase major sigma subunit from Chlamydia trachomatis and human L7. Eur J Immunol 1998; 28: 3857-3866.
62. Hughes RAC, Hadden RDM, Gregson NA, Pathogenesis of Guillain-Barre syndrome. J Neuroimmunol 1999; 100: 74-97.
63. Rink L, Nicklas W, Luhm J, et al. Induction of a pro-inflammatory cytokine network by Mycoplasma arthritidis-derived superantigen (MAS). J Interferon Cytokine Res 1996; 16: 861-868.
64. Shibata K, Hasebe A, Sasaki T, et al. Mycoplasma salivarum induces interleukin-6 and interleukin-8 in human gingival fibroblasts. FEMS Immunol Med Microbiol 1997; 19: 275-283.
65. Mu HH, Sawitzke AD, Cole BC. Modulation of cytokine profiles by the mycoplasma superantigen Mycoplasma arthritidis mitogen parallels susceptibility to arthritis induced by M. arthritidis. Infection Immunity 2000; 68: 1142-1149.
66. Zurita-Salinas CS, Palacios-Boix A, Yaanez A, et al. Contamination with mycoplasma species induces interleukin-13 expression by human skin fibroblasts in culture. FEMS Immunol Med Microbiol 1996; 15: 123-128.
67. Brenner T, Yamin A, Abramsky O, R. et al. Stimulation of tumour necrosis factor alpha production by mycoplasmas and inhibition by dexamethasone in cultured astrocytes. Brain Res 1993; 608: 273-279.
68. Brenner T, Yamin A, Gallily R. Mycoplasma triggering of nitric oxide production by central nervous system glial cells and its inhibition by glucocorticoids. Brain Res 1994; 641; 51-56.
69. Kikkawa S, Matsumoto M, Sasaki T, et al. Complement activation in Mycoplasma fermentans-induced clearance from infected cells. Probing of the organism with monoclonal antibody against M161Ag. Infection Immunity 2000; 68: 1672-1680.
70. Fabisiak JP, Gao F, Thomson RG, et al. Mycoplasma fermentans and TNF-beta interact to amplify immune-modulating cytokines in human lung fibroblasts. Amer J Physiol-Lung Cell Mol Physiol 2006; 291: L781-L793.
71. Kawahito, Y; Ichinose, S; Sano, H; Tsubouchi, Y; Kohno, M; Yoshikawa, T; Tokunaga D, Hojo T, Harasawa R, et al. Mycoplasma fermentans glycolipid-antigen as a pathogen of rheumatoid arthritis. Bichem Biophys Res Commun 2008; 369: 561-566.
72. Avcin T, Toplak, N. Antiphospholipid antibodies in response to infection. Current Rheumatol Rep 2007; 9:212-218.
73. Moue M, Tohno M, Shimazu T, et al. Toll-like receptor 4 and cytokine expression involved in functional immune response in an originally established porcine intestinal epitheliocyte cell line. Bichem Biochem Acta Gen Subjects 2008; 1780: 134-144.
74. Hasebe A, Mu HH, Washburn LR, et al. et al. Inflammatory lipoproteins purified from a toxigenic and arthritogenic strain of Mycoplasma arthritidis are dependent on Toll-like receptor 2 and CD14. Infection Immunity 2007; 75: 1820-1826.
75. Mu HH, Pennock ND, Humphreys J, et al. Engagement of Toll-like receptors by mycoplasmal superantigen: downregulation of TLR2 by MAM/TLR4 interaction. Cell Microbiol 2005; 7: 789-797.
76. Mu HH, Humphreys J, Chan FV, et al. TLR2 and TLR4 differentially regulate B7-1 resulting in distinct cytokine responses to the mycoplasma superantigen MAM as well as to disease induced by Mycoplasma arthritidis. Cell Microbiol 2006; 8: 414-426.
77. Miggin SM, Palsson-McDermott E, Dunne A, et al. NF-kappa B activation by the Toll-IL-1 receptor domain protein MyD88 adapter-like is regulated by caspase-1. Proc Natl Acad Sci USA. 2007; 104: 3372-3377.
78 Vanhoutte F, Paget C, Breuilh L, et al. Toll-like receptor (TLR)2 and TLR3 synergy and cross-inhibition in murine myeloid dendritic cells. Immunol Lett 2008; 116: 86-94.
80. Ravetch JV, Bolland S. IgG Fc receptors. Annu Rev Immunol 2001: 19: 275-90.
81. van Lent PLEM, Blom AB, Grevers L, et al. Toll-like receptor 4 induced Fc gamma R expression potentiates early onset of joint inflammation and cartilage destruction during immune complex arthritis: Toll-like receptor 4 largely regulates Fc gamma R expression by interleukin 10. Ann Rheum Dis 2007; 66: 334-340.
82. Loof TG, Goldmann O, Medina E. Immune recognition of Streptococcus pyogenes by dendritic cells. Infection Immunity 2008; 76: 2785-2792.
83. Okugawa S, Ota, Y, Kitazawa, T, et al. Janus kinase 2 is involved in lipopolysaccharide-induced activation of macrophages. Am. J. Physiol.-Cell Physiol 2003; 285: C399-C408.
84. Marcenaro E, Ferranti B, Falco M, et al. Human NK cells directly recognize Mycobacterium bovis via TLR2 and acquire the ability to kill monocyte-derived DC. Int Immunol 2008; 20: 1155-1167.
85. Tu Z, Bozorgzadeh A, Pierce RH, et al. TLR-dependent cross talk between human Kupffer cells and NK cells. J Exp Med 2008; 205: 233-244.
86. Liese J, Schleicher U, Bogdan C. TLR9 signaling is essential for the innate NK cell response in murine cutaneous leishmaniasis. Eur J Immunol 2007; 37: 3424-3434.
87. Hayem G, De Bandt M, Palazzo E, et al. Anti-heat shock protein 70 kDa and 90 kDa antibodies in serum of patients with rheumatoid arthritis. Ann Rheum Dis 1999; 58: 291-296.
88. Cancino-Diaz ME, Perez-Salazar JE, Dominguez-Lopez L, et al. Antibody response to Klebsiella pneumoniae 60 -kDa protein in familial and sporadic ankylosing spondylitis. Role of HLA-B27 and characterisation as a GroEL-like protein. J Rheumatol 1998; 25: 1756-1764.
89. Al Shamma MRR, McSharry C, McLeod K, et al. Role of heat shock proteins in the pathogenesis of cystic fibrosis arthritis. Thorax 1997; 52: 1056-1059.
90. Musfata AS, Lundin KEA, Meloen RH, et al. HLA-DR4-restricted T cell epitopes from the mycobacterial 60,000 MW heat shock protein (hsp60) do not map to the sequence homology regions with the human hsp60. Immunology 1996; 87: 421-427.
91. Auger I, Escola JM, Gorvel JP, et al. HLA-DR4 and HLA-DR10 motifs that carry susceptibility to rheumatoid arthritis bind to 70-kD heat shock proteins. Nature Med 1996; 2: 306-310.
92. Vinasco J, Beraun Y, Nieto A, et al. Heat shock protein 70 gene polymorphism in rheumatoid arthritis. Tissue Antigens 1997; 50: 71-73.
93. Yokota S, Minota S, Fujii N. Anti-HSP auto-antibodies enhance HSP-induced pro-inflammatory cytokine production in human monocytic cells via Toll-like receptors. Int Immunol 2006; 18: 573-580.
94. Hauet-Broere F, Wieten L, Guichelaar T, et al. Heat shock proteins induce T cell regulation of chronic inflammation. Ann Rheum Dis 2006; 65: 65-68.
95. Binder, RJ, Vatner R.The heat-shock protein receptors: some answers and more questions. Tissue Antigens 2004; 64: 442-451.
96. Calderwood SK, Mambula SS, Gray PJ, et al.. Extracellular heat shock proteins in cell signaling. FEBS Lett 2007: 581: 3689-3694.
97. Singh IS, Gupta A, Nagarsekar A, et al. Heat shock co-activates interleukin-8 transcription. Amer J Resp Cell Mol Biol 2008; 39: 235-242.
98. Brown V, Brown RA, Ozinsky A, et al. Binding specificity of Toll-like receptor cytoplasmic domains. Eur J Immunol 2006; 36:742-753.
99. Luo XJ, Zuo XX, Zhang B, et al. Release of heat shock protein 70 and the effects of extracellular heat shock protein 70 on the production of IL-10 in fibroblast-like synoviocytes. Cell Stress Chaperones 2008; 13: 365-373.
100. Chase MA; Wheeler DS, Lierl KM, et al. Hsp72 induces inflammation and regulates cytokine production in airway epithelium through a TLR4- and NF-kappa B-Dependent mechanism. J Immunol 2007; 179: 6318-6324.
101. Cui XZ, Besch V, Khaibullina A, et al. Neuronal nitric oxide synthase deficiency decreases survival in bacterial peritonitis and sepsis. Intensive Care Med 2007; 33: 1993-2003.
102. Connor JR, Manning PT, Settle SL, et al. Suppression of adjuvant-induced arthritis by selective inhibition of inducible nitric oxide synthase. Eur J Pharmacol 1995; 273: 15-24.
103. Ribeiro-Dias F, Shio MT, Timenetsky J, et al. Mycoplasma arthritidis superantigen (MAM)-induced macrophage nitric oxide release is MHC class II restricted, interferon gamma dependent, and toll-like receptor 4 independent. Exp Cell Res 2003; 286:345-354.
104. Cole BC, Mu HH, Pennock ND, et al. Isolation and partial purification of macrophage- and dendritic cell-activating components from Mycoplasma arthritidis: Association with organism virulence and involvement with toll-like receptor 2. Infection Immunity 2005; 73: 6039-6047.
105. Peltier MR, Freeman AJ, Mu HH, et al. Characterization and partial purification of a macrophage-stimulating factor from Mycoplasma hominis. Amer J Reprod Immunol 2005; 54: 342-351.
106. Lavric M, Bencina D, Kothlow S, et al. Mycoplasma synoviae lipoprotein MSPB, the N-terminal part of V1hA haemagglutinin, induces secretion of nitric oxide, IL-6 and IL-1 beta in chicken macrophages. Vet Mircobiol 2007; 121: 278-287.
107 Hooper DC, Scott GS, Zborek A, et al. Uric acid, a peroxynitrite scavenger, inhibits CNS inflammation, blood-CNS barrier permeability changes, and tissue damage in a mouse model of multiple sclerosis. FESEB J 2000; 14: 691-698.
108. Linares D, Taconis M, Mana P, et al. Neuronal nitric oxide synthase plays a key role in CNS demyelination. J Neurosci 2006; 26: 12672-12681.
109. Kavya R, Saluja R, Singh S, et al. Nitric oxide synthase regulation and diversity: Implications in Parkinson's disease. Nitric Oxide Biol Chem 2006; 15: 280-294.
110. Scarim AL, Heitmeier MR, Corbett JA. Heat shock inhibits cytokine-induced nitric oxide synthase expression by rat and human islets. Endocrinology 1998; 139: 5050-5057.
111. Feinstein DL, Galea E, Aquino DA, et al. (). Heat shock protein 70 suppresses astroglial-inducible nitric oxide synthase expression by decreasing NF kappa B activation. J Biol Chem 1996; 271: 17724-17732.
112. Song MC, Pinsky MR, Kellum JA. Heat shock factor 1 inhibits nuclear factor-kappa B nuclear binding activity during endotoxin tolerance and heat shock. J Crit Care 2008; 23: 406-415.
113. Mangipudy RS, Vishwanatha JK. Role of nitric oxide in the induction of apoptosis by smokeless tobacco extract. Mol Cell Biochem 2000; 200, 51-57.
114. Naito Y, Yoshikawa T, Boku Y, et al. Protective role of intracellular glutathione against nitric oxide-induced necrosis in rat gastric mucosal cells. Alimentary Pharmacol Therapeutics 2000; 14:145-152.
115. Cassidy RA, Burleson DG, Delgado AV, et al... Effects of heme proteins on nitric oxide levels and cell viability in isolated PMNs. A mechanism of toxicity. J Leukocyte Biol 2000; 67, 357-368.
116. Zheng RX, Cohen PA, Paustian CA, et al. Paired toll-like receptor agonists enhance vaccine therapy through induction of interleukin-12. Cancer Res 2008; 68: 4045-4049.
117. Meyer T, Stockfleth E. Clinical investigations of Toll-like receptor agonists. Expert Opinion Invest Drugs 2008; 17: 1051-1065.
118. Himmel ME, Hardenberg G, Piccirillo CA, et al. The role of T-regulatory cells and Toll-like receptors in the pathogenesis of human inflammatory bowel disease. Immunology 2008; 125: 145-153.
119. Owens, RC. Antimicrobial stewardship: concepts and strategies in the 21st century. Diag Microbiol Infectioius Dis 2008; 61: 110-128.
Post-operative urinary retention affects up to 38% of the 200,000 patients undergoing elective TKRs or THRs in the UK every year, according to literature.
Objectives:
This study aims to identify both patient and anaesthetic factors that predispose to urinary retention, and in doing so develop a protocol of pre-operative urinary catheterisations that will minimize its incidence and subsequent complications, as well as hasten patient recovery and discharge.
Methods:
Analysis of prospectively collected data of 54 patients over a three-month period at a British district general hospital.
Results:
10% of patients in the study developed urinary retention, and 60% of these developed renal failure complicating recovery and lengthening stay. All were male, and a history of renal disease and a current elevated serum creatinine were identified as common factors in these patients.
Conclusions:
A protocol of pre-operatively catheterizing males with either a history of renal disease or a current elevated creatinine is suggested – this would potentially reduce incidence rates of urinary retention by 80% whilst only increasing the rate of unnecessary catheterizations by 2%.
Introduction:
Every year, approximately 200,000 people undergo elective total hip and knee replacement surgery in the UK 1. There is limited available literature on the incidence of post-operative urinary retention and even less regarding the onset of subsequent renal failure which, besides posing immediate medical problems, necessitates treatment and can significantly prolong recovery – all of which have personal and financial implications for both patient and healthcare trust.
Summary of Current Literature:
Surprisingly little research is available which offers data on the association on the incidence of, risk factors for, and associations with urinary retention for patients undergoing elective total hip or knee replacement surgery. The following table summarises seven studies conducted between 1980 and 2007:
Study
Year
n
Males
Females
Retention
Sepsis
TKR
THR
Overall
Wroblewski & Del Sel 2
1980
195
195
6.20%
Waterhouse et al. 3
1987
103
103
0
10.70%
O' Riordan et al. 4
2000
116
47
69
18.10%
Kumar et al. 5
2004
19%
22%
0.93%
Cronin et al. 6
2005
118
118
0
38.10%
Kumar et al. 7
2006
142
19.70%
2.10%
Lingaraj et al. 8
2007
119
10
109
10%
Analysing the available literature, the following conclusions can be made.
Males are more likely than females to develop urinary retention.
Risk factors include a history of urinary retention, the use of epidural analgesia and patient-controlled analgesia (PCA).
Retention rates varied between 10% and 38.1% (mean 19.6%).
Deep sepsis rates varied between 0.93% and 2.1% in the total post-operative group, rising to 6.2% in those developing urinary retention.
Objectives:
This study aims to develop a policy of pre-operative catheterisation, anaesthetic technique and post-operative analgesia in patients undergoing elective total hip and knee replacement surgery that will:
Minimize the incidence of urinary retention.
Minimize the incidence of subsequent complications.
Hasten patient recovery and discharge.
Methods:
A prospective study was conducted between February and April 2008 in the operating theatres and on the Orthopaedic wards at Bedford Hospital, a district general hospital in Bedfordshire, UK. Data was collected that would enable the following questions to be addressed:
Are these patients catheterised pre-operatively?
Of those who are not, how many develop urinary retention?
Is any particular anaesthetic technique associated with an increased incidence of retention?
Is antibiotic prophylaxis administered for catheterisation?
How frequently does renal failure arise in those patients who develop urinary retention?
Can a protocol be created which might reduce the incidence of retention?
How effective and efficient would this be?
54 patients undergoing elective total hip and knee replacements were recruited into the study. Of these, 4 were catheterised pre-operatively and hence were excluded (n = 50).
Data Collection:
The primary source of data collection was from patients’ notes and anaesthetic charts, assessed pre- and post-operatively. Data was gathered in the following areas:
Demographics – Name, Age, Sex
ASA Classification – 1 to 4
History of Renal disease
History of Urological disease
Pre-operative Creatinine
Nature & Date of Operation
Type of Anaesthetic Technique employed
Onset of post-operative Urinary Retention necessitating catheterization
Duration of Epidural Analgesia (if applicable)
Administration of Antibiotic Prophylaxis for catheterization
Progress from urinary retention to Renal Failure
Results:
As mentioned, 4 of the original 54 patients were excluded from the study as they had already been catheterised pre-operatively. All were female, 75% of whom were over the age of 80; it appears that the main indication for pre-operatively catheterisation was existing urinary incontinence.
There was a female preponderance amongst the sample population, with females outnumbering males by a ratio of 3 to 2. In terms of the sample population’s co-morbidities and anaesthetic risk, the majority of patients were classified as ASA 2 (60%) by the assessing anaesthetist, with ASA 3 patients (26%) outnumbering ASA 1 patients (14%) by a ratio of approximately 2 to 1 in the remainder. Over the period covered, knee replacements (70%) outnumbered hip replacements (30%) by a ratio of 7 to 3.
A range of anaesthetic techniques were employed, including:
Combined Spinal Epidural (CSE)
Spinal Anaesthetic (Spinal)
General Anaesthetic + Epidural (GA + Epidural)
General + Spinal Anaesthetic (GA + Spinal)
General Anaesthetic + Lumbar Plexus Block (GA + LPB)
General Anaesthetic + Femoral Nerve Block (GA + FNB)
General Anaesthetic +/- Patient Controlled Analgesia (GA + PCA)
Spinal anaesthetics appeared to be most commonly employed, either alone or in conjunction with a general anaesthetic. GAs in combination with a nerve block was also often used, followed by CSEs.
In total, there were a total of 5 cases of post-operative urinary retention, all of which necessitated catheterisation. This results in an incidence rate of 10% across elective total hip and knee replacements. Of these anaesthetic techniques, spinal anaesthesia was associated with the highest risk of post-operative urinary retention (22.2%), followed by GAs (20%), CSEs (14.3%) and GA + FNBs (14.3%). No cases were reported for patients who underwent GA + Spinals (n = 13), GA + LPBs (n = 8) or GA + Epidurals (n = 1).
Of those patients who had undergone epidural anaesthesia, whether in combination either with a GA or a spinal, no documentation was found regarding the duration for which they had been active in 25% of cases. In the remainder, the epidural had been functional for less than 24 hours in 50% of cases.
All five patients who developed post-operative urinary retention were male; three of whom were below the age of 80. Only three of these patients received the recommended antibiotic prophylaxis on catheterisation (60%), and on following up their subsequent inpatient progress and serum creatinine, it appeared the same number progressed to renal failure (60%).
Analysis:
Two factors were identified in this study which may have predisposed these five patients into developing post-operative urinary retention. The first is a history of renal disease – 4% of the total sample had such a history (n = 2) and both went on to develop retention. The second is a currently elevated serum creatinine – 6% of the total sample had this at the time of surgery (n = 3), and of these, two went on the develop retention. The remaining patient who developed retention had neither of these risk factors.
The table below compares the results found in this study with those described in existing literature, namely the aforementioned publications. As can be seen, the post-operative urinary retention rate was on the lower extreme of that noted in the literature; only the studies by Waterhouse et al.3 and Lingaraj et al.7 demonstrated similar rates.
Factor
Study
Literature
Pre-op Cath Rate
7.4%
Unknown
Post-op Retention Rate
10%
10 - 38.1%
Hx of Renal Disease
Increased
Unknown
Elevated Creatinine
Increased
Unknown
Male Incidence
Increased
Increased
Epidural Incidence
Average
Increased
This study concurred with the existing opinion that males have a higher incidence of retention, but the study population was insufficient to draw any specific conclusions regarding the influence of epidural anaesthesia on post-operative urinary retention. It was noted however, that in half of the cases for which data was available, the epidural was functional for less than 24 hours – one might argue that the risk/benefit ratio of epidural anaesthesia would cause it to be a relative contraindication if only employed for relatively short durations, particularly if the patient is admitted to a ward on which nursing staff are unfamiliar with its care.
Conclusions:
Existing literature fails to comment upon the impact of the aforementioned risk factors for retention highlighted in this study, namely a history of renal disease and a current elevated serum creatinine. However, these two factors in conjunction with the increased incidence in males allows for the creation of a system by which patients who are at high risk of developing post-operative urinary retention may be successfully identified and catheterised pre-operatively, hence preventing the problem from arising.
If a protocol had been established in which males with either of these two factors were catheterised pre-operatively, 5 patients from the sample population of 50 would have qualified; this includes 4 of the 5 patients who developed urinary retention post-operatively. In addition, only 1 patient who did not develop urinary retention post-operatively would have met these criteria and been unnecessarily catheterised pre-operatively. These figures are demonstrated in the graph below.
On the basis of these findings, one can deduce that a protocol indicating pre-operative catheterisation in males with either a history of renal disease and a current elevated serum creatinine undergoing total hip and knee replacement surgery would have a profound impact on the incidence of post-operative urinary retention, essentially reducing it by 80%. Unnecessary catheterisations as a result of this protocol would be minimal, affecting only 2% of patients.
Although this study has obvious limitations in terms of its size and its single-centred nature, findings were comparable to existing literature and are likely to be representative of incidence rates on a national, if not international basis. Further research, ideally with a larger population spread across multiple centres would allow for more accurate data to be collected, which in turn would allow for a more effective and efficient protocol to be developed.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
SUMIT DUTTA, MBBS, Speciality Trainee Registrar in Emergency Medicine, Bedford Hospital, United Kingdom
CORRESPONDENCE: Sumit Dutta, Specialty Trainee Registrar in Emergency Medicine, Bedford Hospital, Kempston Road, Bedford, MK429DJ, United Kingdom.
Waterhouse N, Beaumont AR, Murray K, Staniforth P, Stone MH. Urinary Retention after Total Hip Replacement. A Prospective Study. Journal of Bone and Joint Surgery, British Volume. 1987 Jan; 69 (1): 64-6
O’Riordan JA, Hopkins PM, Ravenscroft A, Stevens JD. Patient controlled analgesia and urinary retention following lower limb joint replacement: prospective audit and logistic regression analysis. European Journal of Anaesthesiology. 2000 Jul; 17 (7): 431-5
Kumar P, Mannan K, Chowdhury AM, Kong KC, Pati J. Urinary retention following arthroplasty. Urology, 2005 Sep; 66(3); Supp I: 22
Cronin JJ, Shannon FJ, Bale E, Quinlan W. Prediction of post-operative urinary retention following hip and knee arthroplasty in a male population. European Journal of Orthopaedic Surgery and Traumatology. 2007 Jan; (17): 47-50
Kumar P, Mannan K, Chowdhury AM, Kong KC, Pati J. Urinary retention and the role of indwelling catheterization following total knee arthroplasty. International Brazilian Journal of Urology 2006 Jan-Feb; (32): 1
Lingaraj K, Ruben M, Chan YH, De Das S. Identification of risk factors for urinary retention following total knee arthroplasty: a Singapore hospital experience. Singapore Medical Journal. 2007 Mar; 48 (3): 213-6
Septic shock still remains one of the leading causes of death in hospital patients. Greater awareness, understanding of the condition .and the knowledge of most effective treatment measures available can decrease the rate of mortality. Making an early, accurate diagnosis of septic shock is the key to increasing survival rates. Excessive inflammation, excessive coagulation and suppression of fibrinolysis are the hallmarks of Sepsis. Infection control, haemodynamic stabilization, and modulation of the septic response are the cornerstones of treatment. The management is influenced more by appropriate treatment with antibiotics and fluids than by specific intensive care. Septic response can be modulated by the use of Steroids and Activated Protein C and with tight glucose control. Low Tidal Volume ventilation and high volume Haemofilteration are other beneficial strategies in Sepsis. As septic shock worsens and fails to respond to all therapy, one must be prepared to limit and withdraw treatment.
Septic shock still remains the one of the leading causes of death in hospital patients. Barely more than 50% of the patients with severe sepsis survive their hospital admission. This unacceptable high mortality can only be reduced if there is greater awareness and understanding of the condition .and the knowledge of most effective treatment measures available. Unplanned admissions to the Intensive Care Unit (ICU) and potentially preventable deaths on wards are associated with a failure to institute early preventive conditions. Greater than 40% of the intensive Care Unit admissions are potentially preventable with improved ward care.
Survival of patients with Septic shock appears to be better if shock develops while the patient is in Intensive Care Unit rather than on general ward despite greater severity of illness in the intensive care group [1].This suggests that the closer observation and earlier treatment can influence the outcome of sepsis.
INCIDENCE:
Septic shock is an increasingly common problem. The incidence of sepsis is increasing year by year. The reasons for this increase are that the people are living longer and this aged population are the most vulnerable to sepsis. We are using advanced technology to sustain life and there has been a rise in the number of immunocompromised patients due to aggressive cancer therapy and the increased prevalence of HIV. The widespread use of broad spectrum antibiotics has increased the rate of both antibiotic resistance and nosocomial infections.
A prospective, multicentre, observational study, recently conducted to evaluate the epidemiology of Sepsis and other characteristics of Intensive Care Unit patients in European countries (called the SOAP study) was endorsed by the European Society of Intensive Care Medicine [2]. This observational study showed a marked difference in the frequency of sepsis between countries, and higher frequencies of sepsis were mirrored by higher mortality rates. (Fig.1)
Fig 1: Incidence of Sepsis in European Countries
There was a direct relationship between the number of organs failing and the Intensive Care Unit mortality. Patients with no organ dysfunction on admission had mortality rates of 6% whereas those with four or more organ failures had mortality rates of 65 %. [2] (Fig. 2)
Fig 2: The SOAP study
As compared to the incidence of other pathologies in Europe the incidence of severe sepsis is higher (32%) [2] (Fig 3)
Fig 3: Incidence of different pathologies in Europe
In septic patients, older age, positive fluid balance, co morbid diseases on admission; cancer and cirrhosis are the most important variables of mortality.
DEFINITIONS
Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response Syndrome (SIRS). This is characterised by body temperature outside 36oC - 38oC, HR >90 beats/min, respiratory rate >20/min, WBC count >12,000/mm3 or < 4,000/mm3. (Fig 4)
Fig 4: Definitions
There are three recognised stages in the hierarchy of the inflammatory response, with progressively increased risk of organ failure and death. Patients with infections plus two or more elements of the SIRS meet the criteria for sepsis. Those who have end organ failure are considered as having severe sepsis; and those who have refractory hypotension along with the above said criteria are consider to be in septic shock (Fig. 5)
Fig 5: Definitions
PATHOPHYSIOLOGY:
Sepsis is a complex condition starting from an infective stimulus and resulting in an exaggerated immune response. The inflammatory response that was initiated to fight the infection ultimately leads to damage of various organs thorough out the body.
During the onset of sepsis, the inflammatory system becomes hyperactive, involving both cellular and humoral defence mechanisms Endothelial and epithelial cells, as well as neutrophils, macrophages and lymphocytes, produce powerful pro-inflammatory mediators, especially tumour necrosis factor- (TNF-), interleukin (IL)-6, IL-1 and IL-8. Simultaneously, robust production of acute-phase proteins, such as C-reactive protein, occurs and humoral defence mechanisms such as the complement system are activated, resulting in production of pro-inflammatory mediators, including C5a, the complement split product. C5a ultimately enhances cytokine and chemokine production. Furthermore, the coagulation system becomes activated through various mechanisms, often resulting in disseminated intravascular coagulopathy.
The hallmarks of the sepsis are excessive inflammation, excessive coagulation and suppression of fibrinolysis. In addition endogenous Activated Protein C which modulates coagulation, controls inflammation and supports fibrinolysis is also decreased. There is considerable variability in response which is almost certainly to a large degree genetically determined. Those with a tendency to produce excessive cytokines and TNF will have a greater inflammatory response. Simultaneously, the initial vascular damage results in neutrophil activation, neutrophil-endothelial cell adhesion, and further elaboration of inflammatory cytokines. In tissues already prone to dysfunctional oxygen uptake and metabolism, this vascular injury promotes further tissue hypoxia through regional hypo perfusion. This uncontrolled cascade of inflammation and coagulation fuels the progression of sepsis, resulting in tissue hypoxia and ischemia with resultant organ dysfunction and death.
DIAGNOSIS:
Diagnosis of sepsis is not easy. Making an early, accurate diagnosis of septic shock is a key to increasing survival rates. The signs and symptoms of severe sepsis may be subtle. Although the components of SIRS are non specific, the combination of suspected infection and the presence of SIRS may help alert the clinician to a possible diagnosis of sepsis. Although hypotension is another clinical sign that may signal the onset of septic shock, patient may present with sever sepsis and clinically significant global tissue hypoxia in its absence. Metabolic marker such as serum lactate, arterial base deficit may help to identify the severe cases. A single lactate measurement of 4mmol/l or more at initial presentation is associated with an increased rate of mortality [3]. There may well be signs of altered mentation and abnormalities of renal and liver function test, as well as coagulation abnormalities. At least two blood cultures and cultures of other sites as indicated before commencement of antibiotic therapy. Diagnostic studies such as Ultra sound and CT scan should be performed promptly.
D dimmers are grossly elevated in sepsis. Levels of Protein C are lowered which has therapeutic implications. The potential role of biomarkers for diagnosis of infection in patients presenting with severe sepsis remains undefined. Perhaps the most common considerations as diagnostic biomarkers for sepsis have been C-reactive protein and procalcitonin. Despite initial enthusiasm for their potential diagnostic strengths,[4] they have more recently been related to the growing heap of biomarkers that have failed to accurately differentiate sepsis from similar critical illnesses.
The most exciting development in the last 2 years is the recognition of "soluble triggering receptor expressed on myeloid cells-1" (sTREM-1) as a potential biomarker for sepsis. [5] For this marker, a level greater than 60 ng/mL was more accurate than any other clinical and laboratory findings indicating infection
TREATMENT:
The development of new treatment modalities has resulted in a spate of treatment algorithms, often promulgated by medical societies and healthcare improvement organizations. As these modalities have rolled out, increasing levels of evidence have emerged to support or refute their utility in treating patients with sepsis. One of the greatest endeavours to date is the Surviving Sepsis Campaign (SSC) [6] that was originally launched in 2002 with the stated goal to reduce mortality by 25%. The primary method to achieve this goal was the development of evidence-based sepsis care guidelines that were published in 2004. [6] and recently revised in 2008.
The Institute for Healthcare Improvement (IHI) has highlighted sepsis as an area of focus and has identified several deficiencies that may cause suboptimal care of patients with severe sepsis. These deficiencies include inconsistency in the early diagnosis of severe sepsis and septic shock, frequent inadequate volume resuscitation without defined endpoints, late or inadequate use of antibiotics, frequent failure to support the cardiac output when depressed, frequent failure to control hyperglycemias adequately, frequent failure to use low tidal volumes and pressures in acute lung injury, and frequent failure to treat adrenal inadequacy in refractory shock.
The management of patient with sepsis is influenced more by appropriate treatment with antibiotics and fluids than by specific intensive care. Therefore early intervention should never be delayed pending admission to the intensive care unit. The early and aggressive treatment of septic shock has been well documented in the survival sepsis campaign which is based on the best current practice.
The cornerstones of treatment are infection control, haemodynamic stabilization, and modulation of the septic response.
1. Infection Control:
Infection control is vital if the patient is to have any chance of survival. Appropriate broad-spectrum antibiotics must be given within the first hour of recognition of sepsis after obtaining various cultures. Evidence clearly shows that delay or inadequate antibiotic treatment results in poorer outcome. For every hour lost mortality climbs by 9%. [7]
Initial empirical anti-infective therapy should include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal) and that penetrate in adequate concentrations into the presumed source of sepsis[8] antimicrobial regimen be reassessed daily to optimize activity, to prevent the development of resistance, to reduce toxicity, and to reduce costs
A focus of infection must be sought for and if discovered dealt with immediately. The patient should be evaluated for a focused infection amenable to source control measures including abscess drainage or tissue debridement. One must weigh up the benefits and risks of the particular procedure chosen. If intravascular devices are a potential source, they must be promptly removed after establishing other vascular access. When source control is required, the effective intervention associated with the least physiologic insult be employed (e.g., percutaneous rather than surgical drainage of an abscess)
2. Haemodynamic Stabilization:
In septic shock there is extensive cardiovascular derangement. Hypotension is caused by myocardial depression, pathological vasodilatation and extravasation of circulating volume due to widespread capillary leak. The initial resuscitative effort is to attempt to correct the absolute and relative hypovolemia by refilling the vascular tree. There is no evidence to support one type of fluid crystalloid or colloid is superior to the other. There is good evidence that early gold directed aggressive volume resuscitation improves outcome of sepsis[9] During the first 6 hours of resuscitation the goals of initial resuscitation are a Central venous pressure of 8-12 mm Hg, Mean arterial pressure (MAP) ≥ 65 mmHg, Urine output ≥ 0.5 mL • kg-1 • hr and a central venous (superior vena cava) or mixed venous oxygen saturation ≥ 70% or ≥ 65%, respectively The Rivers study clearly shows a reduction in hospital mortality, 28 day mortality as well as 60 day mortality attributed to the Early Goal Directed Therapy (EGDT) [10]. Early goal-directed resuscitation has been shown to improve survival for emergency department patients presenting with septic shock in a randomized, controlled, single-centre study.[11] Resuscitation directed toward the previously mentioned goals for the initial 6-hr period of the resuscitation was able to reduce in hospital, 28-days as well as 60 days mortality rate (Fig. 6).
Fig 6: Results of Early Goal Directed Therapy (EGDT)
If Scvo2 or SVo2 of 70% or 65%, respectively, is not achieved with fluid resuscitation to the central venous pressure target, then transfusion of packed red blood cells to achieve a hematocrit of ≥ 30% and/or administration of a dobutamine infusion (up to a maximum of 20 µg • kg-1 • min-1) be used to achieve this goal.
It is important to remember that vasopressors should be utilized not only when fluids fail to reverse hypotension, but also during resuscitation to maintain minimally adequate blood pressure. Traditionally, the use of noradrenalin in patients with shock has been restricted by the fear of excessive vasoconstriction that may result in end-organ hypo perfusion. In the past it was usually given only when other vasopressin agents failed, and thus such patients would be predicted to have a poor outcome. Recent studies indicate that the fear of deleterious effect was unwarranted and that noradrenalin may have a role as a first-line vasopressor agent in patients with septic shock.
Vasopressin should be considered in refractory shock despite high dose conventional vasopressors. Vasopressin is an endogenously produced hormone that is deficient in many patients with septic shock. Exogenously administered vasopressin in physiologic replacement doses may act synergistically with other vasopressor agents, and has been associated with early withdrawal of catecholamine. Most studies have evaluated short-term infusions of vasopressin at 0.08 U/minute or less as add-on therapy in patients requiring adrenergic agents. The results show that starting vasopressin in patients with septic shock increases systemic vascular resistance and arterial blood pressure, thus reducing the dosage requirements of adrenergic agents [12]. These effects are rapid and sustained. Substantial enhancement of urine production, likely due to increased glomerular filtration rate, was shown in several studies. A few studies demonstrated clinically significant reduced cardiac output or cardiac index after vasopressin was begun, necessitating cautious use in patients with cardiac dysfunction.
3. Modulation of Septic Response:
There are a number of ways to modulate the septic response. These includes use of steroids, tight glucose control and the use of Activated Protein C. Septic shock causes adrenal suppression and this can be confirmed by measuring cortisol levels or by using the synacthan test. Compare to placebo, the administration of low dose of hydrocortisone (200-300 mg/day in divided doses) to patients with septic shock decrease there requirements for vasopressors [13] and lowered their mortality rate [14]. Low dose hydrocortisone should only be given to non responders of the synacthan test but in practice all patient receive this treatment until the result of the test are received. Following the Corticosteroid Therapy of Septic Shock (CORTICUS) study there is now an increasing trend towards restricting the use of low dose hydrocortisone only to patients with refractory hypotension who are already on high doses on vasopressors [15]. The trial did show a faster resolution of septic shock in patients who received steroids but failed to show a mortality benefit with steroids therapy. Close control of blood glucose has been shown to increase survival in critically ill septic patient. When conservative (10 – 11.1 mol/L) glycemic control was compared with tight control (4.4-6.1mmol/L) in a multi centre, randomized controlled trial, tight control lead to a significant reduction in mortality (8% versus 4-6%), p < 0-04 and improved morbidity at 12 months [16].
Activated Protein C
Human activated Protein C (APC) is an endogenous regulator of coagulation. In order for protein C in the plasma to become activated, it must combine with thrombin and thrombomodulin along with the endothelial protein C receptor. With endothelial damage this activation does not take place resulting in its deficiency. Therefore APC supplementation is a rational therapeutic option. APC has an important role in the management of severe sepsis. It protects against the disruption of the endothelial cell membrane, improves micro circulatory perfusion, and has anti inflammatory, procoagulant, fibrinolytic and anti apoptotic activity. APC must ideally be started with in the first 24 hours of the onset of septic shock. The Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) trial found activated protein C to reduce the risk of death among all severe sepsis patients by 20% [17] This study has also recognized the risk of complications specially haemorrhages.
Subsequent studies have shown similar results. “Administration of Drotrecogin Alfa (Activated) in Early Stage Severe Sepsis” (ADDRESS trial) also provides the evidence concerning use of rhAPC in adults [18]. Additional safety information comes from an open-label observational study, “Extended Evaluation of Recombinant Activated Protein C” (ENHANCE trail). [19] The ENHANCE trial also suggested that early administration of rhAPC was associated with better outcomes.
Other beneficial Strategies in Sepsis
Low Tidal Volume Ventilation: using normal or high tidal volume (10-12mls/Kg) ventilation will cause over expansion of the normal lung segments. This will in turn result in inflammatory mediators being released in the lung tissue. The consequences of this are the development of Acute Lung Injury (ALI) or Acute Respiratory Distress Syndrome (ARDS). Therefore it is crucial to use low tidal volume Ventilation (6ml/kg) to keep plateau airway pressure less than 30 cm of water [20, 21]
High volume Haemofilteration: In the past five years, many studies have been conducted to evaluate and demonstrate benefits of increasing the volume of ultra filtration and replacement fluid during Continuous Renal replacement therapy [22, 23] particularly in complex and very severe syndromes such as Severe Sepsis and Septic Shock, associated with or without acute renal failure.
In general, the high-volume approach provides higher clearances for middle/high molecular weight solutes than a simple diffusive transport, Continuous veno venous haemodialysis (CVVHD) or a convection-based transport at lower volumes, Continuous veno venous haemofiltration (CVVH). These solutes seem to be primarily involved in the Systemic Inflammatory Response Syndrome, which characterizes the Sepsis syndrome, and their efficient removal may thus be beneficial. [24]
Alternative approaches have been based on more efficient removal of inflammatory mediators by high cut-off hemofilters, which are characterized by an increased effective pore size. Most commercially available hemofilters do not permit a substantial elimination of cytokines because of the low cut-off point of their membranes. The use of high cut-off hemofilters is a new and effective approach to cytokine removal, but it has potentially harmful side effects, such as the loss of essential proteins like albumin [25].
Because the reversibility of this disease and the resultant mortality may be greatest during the earliest stages of presentation, proper sepsis management should not be confined within the walls of an Intensive Care Unit. Specific emphasis on appropriate triage to ensure prompt diagnosis of the high-risk patient is vital to the launch of a coordinated and cooperative effort by the primary treating clinician and the intensivist
Ethical Dilemmas in Septic Shock
Patient with septic shock have a high mortality and as yet there is no predictive scoring system which gives accurate predictions of outcome for individual patient. Survival from an episode and septic shock is dependent on patient’s age, number of failed organs, previous health and the time delay before the onset of medial intervention, as well as the appropriateness and quality of medical care. The resources available to us are not limitless and so difficult decisions have to be made deciding between the potential benefits for one critically ill patient and need for several less critically ill patients. As an intensivist one must set realistic expectations which must be clearly communicated to the families concerned. As septic shock worsens and fails to respond to all therapy, one must be prepared to limit and withdraw treatment.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
KHADIJA E QURESHI, BSC, MBBS, DA, FCPS, ST2- Anaesthetics, Hemel Hempstead General Hospital, United Kingdom
ABID RAJAH, MB ChB, FRCA, FFARCSI, Lead Clinician & Consultant in Intensive Care, Hemel Hempstead General Hospital, United kingdom
CORRESPONDENCE: Dr Abid Rajah, Lead Clinician & Consultant in Intensive Care, Hemel Hempstead General Hospital, Hill field Road, Hemel Hempstead, HP2 4AD
Email: ARajah@aol.com
REFERENCES
Lundberg J, Perl TM. Septic shock: an analysis of outcomes for patients with onset on hospital wards vs. Intensive care units. Crit care Med 1998; 26: 1020-24
Vincent JL, Sakr Y, and Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006; 34:344-353.
Shapiro NI, Homel MD, Talmor D, Nathanson LA, Lisbon A, Wolfe RE, et al. Serum lactates as a predictor of mortality in emergency department patient with infection. Ann Emerg Med. 2005; 45: 524-8.
Harbarth S, Garbino J, Pugin J, et al. Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med. 2003; 115:529-535.
Gibot S, Kolopp-Sarda MN, Bene MC, et al. Plasma level of a triggering receptor expressed on myeloid cells-1: its diagnostic accuracy in patients with suspected sepsis. Ann Intern Med. 2004; 141:9-15.
Surviving Sepsis Campaign. Available at: http:// www.surviving sepsis.org/ Accessed March 6, 2007.
Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis C guidelines for management of severe sepsis and septic shock. Crit Care med. 2004;32: 858-873
Battleman DS, Callahan M, Thaler HT. Rapid antibiotic delivery and appropriate antibiotic selection reduce length of hospital stay of patients with community acquired pneumonia: link between quality of care and resource utilization. Arch Intern Medicine 2002; 162(6):682-8.
Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003; 31:1250-1256.
Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377
Emanuel Rivers. The outcome of patients presenting to the emergency department with severe sepsis or septic shock. Crit Care. 2006; 10(4): 154.
Obritsch MD; Bestul DJ; Jung R; Fish DN; MacLaren R. The role of vasopressin in vasodilatory septic shock. Pharmacotherapy. 2004; 24(8):1050-63 (ISSN: 0277-0008)
Briegel J, Frost H, Haller M, Shelling G, Kilger E, Kuprat G et. Stress doses of hydrocortisone reverse hyper dynamic septic shock: a prospective randomised double blind single centre study. Crit care Med 1999; 27:723-32.
Annane D, Sebille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002; 288:862-871.
Sprung CL. Update on clinical trials in severe sepsis. CORTICUS trial. Program and abstracts of the Society of Critical Care department patient with infection. Ann Emerg Med 2005: 45 (524-8).
Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354:449-461
Bernard GR, Vincent JL, Laterre PF, et al. Recombinant human protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study group. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001; 344:699-709.
Abraham E, Laterre PF, Garg R, et al: Drotrecogin alfa (activated) for adults with severe sepsis and a low risk of death. N Engl J Med 2005; 353:1332-1341.
Vincent JL, Bernard GR, Beale R, et al: Drotrecogin alfa (activated) treatment in severe sepsis from the global open-label trial ENHANCE: Further evidence for survival and safety and implications for early treatment. Crit Care Med 2005; 33:2266-2277.
ARDS Network Investigators. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000; 342:1301-1308.
National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wiedemann HP, Wheeler AP, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006; 354:2564-2575.
Piccinni P, Dan M, Barbacini S, Carraro R, Lieta E, Marafon S, Zamperetti N, Brendolan A, D'Intini V, Tetta C, et al.: Early iso-volaemic haemofiltration in oliguric patients with septic shock. Intensive Care Med 2006, 32:80-86.
Reiter K, D'Intini V, Bordoni V, Baldwin I, Bellomo R, Tetta C, Brendolan A, Ronco C: High-volume hemofiltration in sepsis. Nephron 2002, 92:251-258.
Ronco C, Tetta C, Mariano F, Wratten ML, Bonello M, Bordoni V, Cardona X, Inguaggiato P, Pilotto L, d'Intini V, Bellomo R: Interpreting the mechanisms of continuous renal replacement therapy in sepsis: the peak concentration hypothesis. Artif Organs 2003, 27:792-801.
The effectiveness and quality of care for patients is largely dependent on communication between physicians both in secondary care and in primary care. Written communication between secondary and primary care in the form of a discharge summary is vitally important for informing General Practitioners (GPs) and other healthcare professionals of the details regarding patients’ admission into hospital, as well as ensuring there is continuity of care in the community. Discharge summaries are often the only form of communication that occurs at the transition between secondary and primary care.
Prior to discharging patients from hospital, a discharge summary (whether this be hand written or typed) is required to be completed. Ideally copies are kept in patient files and given to the patient, as well as forwarding a copy to the GP. Correctly completing all relevant sections on a discharge summary is part of good medical practice, Clinical Governance and hospital/patient documentation.
Historically, discharge summaries have been found to be poorly written, contain inaccurate and ineffective information. Several studies have identified areas which are lacking in discharge summaries when looking at the quality of the discharge summary. These include: inadequacies of medical evaluation, level of experience of the discharge author and accuracy. Subsequently, there has been a general move towards electronic discharge summaries with a standard format.
In April 2005, Newham University Hospital Trust (NUHT) began using the Cerner Millennium Electronic Patient Record (EPR) system. This electronically stores information about a patient, for example discharge summaries, previous blood results, imaging results etc. It is intended that all discharge summaries are typed directly onto this computerized system. The summaries are then available to view by all authorized parties anywhere in the hospital. This system has the advantage of enabling access to portions of a patient’s medical record whilst waiting for patients’ old notes. Furthermore, more information can be added to the discharge summaries contemporaneously or even after the point of discharge. Table 1. Shows some advantages and disadvantages of EPR vs paper discharge summaries.
Advantages of EPR over a paper-bases system
More information included
Do not need to later type or dictate a formal letter
Permanent electronic record
Available immediately
Always legible
Full details with GP at time of discharge
Allows more accurate clinical coding
Disadvantages of EPR
Takes longer to complete than a paper summary
AIMS AND OBJECTIVES
This study assessed the quality of discharge summaries completed by medical specialties at Newham University Hospital Trust using the EPR system. The aim was to identify any problems and where they are occurring. The information gained would help in addressing any problems identified, to improve the quality of discharge summaries.
METHODS
I had an in-depth discussion with my supervisor about the feasibility, methodology, data collection, patient confidentiality, ethics and relevance of this audit to the Hospital.
I undertook a thorough literature search in Medline and other internet searches, reviewed the Journals in NUHT Library for similar audits which looked at the quality of discharge summaries.
A sample of 100 Medical (respiratory, endocrine and gastroenterology) and Care of the Elderly (CoE) discharge summaries of patients from NUHT were retrospectively audited. The hospital Audit Department provided me with the names of the last 100 patients who had been discharged from Medicine and CoE during October 2007. These were sequential discharges, not selected at random. We did not analyze any patients from the specialties of Surgery, Gynaecology, Paediatrics, Cardiology or Emergency Medicine.
After obtaining the names, the discharge summaries were analysed and information was collected on the following fields:
Name of Consultant on the discharge summary sheet
Which team the consultant belonged to: Medical, CoE or A&E
If the discharge consultant was correct
If date of admission had been completed
If date of discharge had been completed
If the patient was given a diagnosis
If a follow up appointment was suggested and what type of follow up this was (GP or NUHT or another hospital)
If a follow up appointment had been made
If the discharge summaries had been signed and bleep number provided
This data was then tabulated using simple statistical analysis (mainly descriptive) and the results calculated into a percentage.
The names of the consultants on the discharge summaries were divided into Medical, Care of the Elderly and Accident & Emergency. The medical team was further divided into team A, B and C, according to the specialty they worked under, for example Team A: endocrine, team B: gastroenterology, and team C: respiratory medicine. By dividing the consultants under different teams allowed me to confirm if they were the right consultant. A&E was included into this field as many discharges still have A&E consultants on them despite the patients being admitted to hospital.
This audit did not address the following issues:
1. If the GP is correct
2. If the GP received the summary
3. If the GP made follow up arrangements post discharge
4. The accuracy of the diagnosis
5. If the patient has more than one electronic medical records
RESULTS
The examination of 100 medical records yielded 94 discharge summaries available for audit, leaving 6 medical records with no evidence of a discharge summary.
As mentioned above, the consultants on the discharge summary were divided into the following categories. The number beside them represents how many discharge summaries belonged to each respective team.
Care of the elderly team: 46
Adult medicine: 36
A&E: 9
Other: 3
It was found that 57(60.6%) of the discharge summaries contained the correct consultant name. However, on 22(23.4%) of the discharge summaries it was unclear if the discharge consultant was correct.
From the 96 discharge summaries completed, every single summary had an admission date on it, however, only 75(79.8%) of discharge summaries had a discharge date.
Seventy five (79.8%) of discharge summaries had been signed by the author (with their name), but only 71(75.5%) had wrote their bleep number.
Sixty five (69.1%) summaries were identified to have a diagnoses under the heading of acute problems, whereas only 22(23.4%) had only symptoms. The remaining 13 (13.8%) summaries had no diagnosis or symptoms completed.
Finally, when analyzing the discharge summaries regarding follow up arrangements, 91(96.8%) discharge summaries had a follow up suggested, of which 27(29.7%) were to be followed up by GP, 59(64.8%) were to be followed in NUHT and 5 patients were to be followed up at another hospital.
Of the discharge summaries which had follow up arranged in NUHT, only 40(67.8%) patients had a follow up appointment made.
DISCUSSION
This study supports previous studies, confirming that a new approach to discharge summary completion is required. One of the main problems identified in this summary, was the use of incorrect consultants on the discharge summary. The current method used is clearly not effective; therefore it is important that the author completing the discharge summary ensures that the correct consultant is on the summary.
Changing the Consultant name on the discharge summaries is of great importance because this means that GPs are able to refer patients back to the correct consultants when seeking advice or trying to arrange further follow up with that consultant. Furthermore, it allows the appropriate National Health Service (NHS) funding to be given to the relevant department.
It was unclear in 22 discharge summaries if the discharge Consultant was correct. This was partly due to the fact that several discharge summaries had no author name or bleep number. By documenting your name and bleep number on a discharge summary, is not only accessible to physicians in primary and secondary care, but also to hospital pharmacist, in case they need to contact you when medication needs to be amended.
The second important problem identified in this study, was the lack of follow up appointments made, despite having it requested on the discharge summary. Of the patients that had follow up appointments suggested at NUHT, only 40(67.8%) patients had follow appointments made, which meant that 19(32.2%) patients had no appointment made. The only possible explanations for this may be that I started analyzing the patient summaries and follow up appointments too early post discharged, therefore not allowing enough time for the appointments to be made, or perhaps the appointments are simply not being made.
As this study did not look to see whether follow appointments with GPs had been made, we are unable to comment on this. However, previous studies have shown that follow up appointments are not always made with the GPs post discharge. As a result, the percentage of patients actually receiving a follow up post discharge from hospital may be lower than anticipated.
The third problem this study identified was the lack of discharge dates on the summaries. Having the discharge date on discharge summaries is not only important for hospital doctors but its of vital importance for GPs, as it provides them with information about how long a patient remained in hospital, and the severity of their illness. For example, if a patient was discharged from hospital after 2 days with an Asthma Exacerbation, we can assume that the severity of their exacerbation was not too severe. However, if the same pt remains in hospital for 15 days, this gives us more information about the severity of their exacerbation.
The fourth problem demonstrated in this study, was the infrequent number of diagnoses entered under the acute problems section in the discharge summaries. Only 65 (69.1%) summaries were identified to have a diagnoses, 22(23.4%) summaries had symptoms only. The remaining 13 (13.8%) summaries had no diagnosis or symptoms completed. It is important to document diagnosis or symptoms as it allows accurate medical coding. It is also often difficult to fathom why a patient was admitted to hospital even after reading the entire discharge summary. Furthermore, the benefit of accurate clinical coding is accurate payment for the services provided by the hospital.
The final problem which needs to be addressed is the completion of a discharge summary for all patients that have been admitted to hospital. This study found that 6 medical records showed no evidence of a discharge summary. One possible explanation for this would be if a patient had self discharged from the hospital, and not been formally discharged by a team or if a patient had died. However, in this case it is still important that a discharge summary is completed. A GP will still need to know why a patient was admitted and why they self discharged
CONCLUSION
It is clear from this study that there needs to be more robust processes put in place to ensure accurate recording of data on the information sent out to General Practitioners. Medical Practitioners completing the summaries should be encouraged to ensure that all fields on the discharge summary are adequately completed in order for us to reap the benefits.
Poor communication in the discharge summaries impacts poorly on patient care and increases the costs to the NHS due to increased rates of readmission into hospital. We can recognize this as a major problem confronting the NHS and so completing discharge summaries in full can help reduce his burden.
RECOMMENDATIONS
A number of recommendations have been identified and include:
The need to raise the awareness of this problem amongst hospital colleagues including Clinical Governance and Audit department with the objective to improve the quality of the summary. The preferred format may be a presentation or advisory email.
For consultants to communicate with junior doctors on a regular basis and go through their discharge summaries, highlighting areas of improvement. This is currently done by some medical teams at NUHT.
For the author of the discharge summary to ensure the correct consultant name is on the discharge summary.
All medical teams should complete a discharge summary regardless if a patient has self discharged or died.
To relay this information back to the ward clerks and ensure that they understand the importance of making follow up appointments as soon as they have been given a discharge summary.
A repeat audit should be performed in 12 months to look for improvements in the data completion.
CONFLICT OF INTERESTS None declared
ACKNOWLEDGMENTS The author would like to thank Dr T. O’Shaughnessy, Medical Student Umair Mohammed, Dr David Ward, and the Audit Department for all their help and support
AUTHOR DETAILS SYEDA M. B. KAZMI, Foundation Year 2 Trainee, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, London, United Kingdom
CORRESPONDENCE: DR S M B Kazmi, 15 Kevelioc Road, Tottenham, London, N17 7PR
Email: mar1amkazmi@hotmail.com
REFERENCES
Mann R and Williams J. Standards in medical record keeping. Clinical medicine. 2003 jul-Aug; 3 (4): 329-32
Paterson JM, Allega RL. Improving communication between hospital and community physicians. Feasibility study of a handwritten, faxed hospital discharge summary. Discharge Summary Study Group. Can Fam Physicians. 1999 Dec; 45: 2893-9
Wilson S, Ruscoe W, Chapman M, Miller R. General practitioner –hospital communications: a review of discharge summaries. Journal of Quality in Clinical Practice. 2001 Dec; 21(4): 104-8
Foster DS, Paterson C, Fairfield G. Evaluation of immediate discharge documents–room for improvement? Scott Med J. 2002 Aug; 47(4): 77-9
Garasen H and Johnsen R. The quality of communication about older patients between hospital physicians and general practitioners: a panel study assessment. BMC Health Services Research. 2007 Aug24; 7: 133
Population demographics are changing worldwide, with life expectancy and the proportions of older persons increasing. Older people are the greatest consumers of medications and healthcare resources in developed countries. It is assumed that as more drugs become available and life expectancy continues to increase, the consumption of prescription drugs by older people will increase further and the incidence of potentially inappropriate prescribing will grow. A survey of non-institutionalized older adults in the United States showed an increased usage of all medications with advancing age, the highest prevalence of drug use being in women 65 years of age and older with 12% taking 10 or more medications and 23% taking at least five prescribed drug therapies 1. In most industrialized nations older people consume three times as many prescription medications as younger people and purchase 70% of non-prescription medications 2. In the United States, 12•5% of the population is over 65 years of age but consume 32% of all prescription medications and account for 25% of drug expenditure and 30% of total national healthcare expenditure 3-5. In Ireland, 11•13% of population is over the age of 65 years but consume 47% of all prescription medications 6. In Europe, people over 65 years of age consume on average 2•3 times the amount of health care than do those <65 years of age 7.
POLYPHARMACY:
Polypharmacy has been defined in many different ways and the appropriate definition may differ according to patient population and study setting 9. Fulton and Allen 10 define polypharmacy as: 'the use of medications that are not clinically indicated'. In practice, polypharmacy is defined as using more than a certain number of drugs, irrespective of the appropriateness of drug use 8, 11, 12. Inappropriate prescribing includes the use of medicines that introduce a significant risk of an adverse drug-related event where there is evidence for an equally or more effective but lower-risk alternative therapy available for treating the same condition. Inappropriate prescribing also includes the use of medicines at a higher frequency and for longer than clinically indicated, use of multiple medicines that have recognized drug–drug interactions and drug–disease interactions, and importantly, the under-use of beneficial medicines that are clinically indicated but not prescribed for some reasons. As older patients seek treatment for various ailments from a variety of physicians, they are at increasing risk of accumulating layers of drug therapy. Individuals aged 65 and older use a disproportionate number of prescriptions and over-the-counter medications; 31% use more than one pharmacy and 50% receive prescriptions from more than one prescriber 13. A higher number of primary care physicians and multiple dispensing pharmacies increase the risk of drug–drug interactions 14. The number of medications prescribed to elderly patients, and the complexity of their drug regimens increase over time 15. The potential for an increased risk of drug–drug interactions and adverse drug reactions, and factors such as age-related changes in pharmacodynamics (PD) and pharmacokinetics (PK) must be considered. Diabetes and chronic lung disease predict a greater complexity and cost of drugs regimen in elderly patients with heart failure 16. Besides the increase in diseases and worsening of diseases, the literature also mentions other factors as being responsible for the increase in polypharmacy, i.e. ageing, moving to a residential or nursing home and hospitalization 17, 18. The patient's expectations, the General Practitioner's attitude and consultations with several doctors have been associated with an increase in multiple drug use 19, 20.
EFFECTS OF AGING ON DRUG METABOLISM:
Drug absorption, distribution, metabolism and elimination change as a natural consequence of the ageing process. Changes in drug absorption in older patients may result from decreases in splanchnic blood flow and gastric motility, and increases in gastric pH, and other physiological changes that are associated with ageing. Blood flow and gastric motility may be further diminished by cardiovascular and gastrointestinal drugs used to treat co-morbid conditions. Ageing influences drug excretion. Age-related decreases in glomerular filtration rate are well known. These physiological declines coupled with co-morbid conditions and the use of multiple drugs means that medications eliminated by the renal route requires dose adjustment. Drugs that influence renal function and thus elimination/excretion have the potential to pose serious clinical problems if used concomitantly. With ageing, there is a decrease in lean body mass and total body water with a relative increase in total body fat 21. These changes lead to a decreased volume of distribution for hydrophilic drugs such as lithium, and digoxin where unadjusted dosing can result in higher plasma concentrations, thus increasing the potential for adverse effects. Conversely, lipid soluble drugs such as long-acting benzodiazepines have an increased volume of distribution, thereby delaying their maximal effects and resulting in accumulation with continued use. There is a reduction in hepatic mass and blood flow with ageing 22.
Drugs such as beta-blockers, nitrates and tricyclic anti-depressants that have a first pass effect in the liver may have a higher bioavailability in older people and thus be effective at lower doses. Cytochrome P450 oxidation declines with ageing 24 and drug–drug interactions involving these enzymes are important to recognize. Larger drug storage reservoirs and decreased clearance prolong drug half-lives and lead to increased plasma drug concentrations in older people. If serum albumin is decreased there will be an increase in the active unbound drug concentration for highly protein-bound drugs such as phenytoin, theophylline, warfarin and digoxin. Ageing is also associated with changes in the end-organ responsiveness to drugs at receptor or post-receptor level 25. There is decreased sensitivity to beta-receptors along with a possible decreased clinical response to beta-blockers and beta-agonists 26. Increased sensitivity to drugs such as opiates and warfarin is common 27, 28.
ADVERSE DRUG REACTIONS (ADRs):
The number of elderly is increasing dramatically. In United States, in the next 25 years, as the baby boomer generation begins to turn 65 years old, the number of elderly is expected to double to approximately 70 million. Those older than 85, is now the fastest growing segment of our population. Thus, we can expect the number of adverse drug reactions to increase proportionately. Polypathology, the age-related increase of concurrent diseases, is likely to be the main determinant of drug consumption. However, both over-prescribing and improper prescribing has been reported and seems to contribute to the age-related increase in the prevalence of adverse drug reactions (ADRs) 29, 30. A hospital-based study from Norway showed that the risk of experiencing a drug-related problem increased linearly with the number of drugs on admission 31. A study carried out in the USA found that nursing home patients receiving nine or more drugs were more than twice as likely as patients receiving a lower number of drugs, of experiencing an adverse effect 32. On average, ADRs account for 3%–13% of all the admissions 33-35 and complicate 5%–20% of the stays of patients over 65 years 36-38. More than 40% of persons aged 65 and older use five or more different medications per week, and 12% use 10 or more different medications 39. If an elderly patient takes five or more drugs, he or she has a 35% chance of experiencing an adverse drug event 40. Drug interactions are significant contributors to morbidity 35. Office visits for an adverse drug event increase from 9% of the population per year at age 25–44 years to as high as 56•8% between age 65 and 74 years 41. Inappropriate drug use is one of the risk factors for adverse drug reactions in the elderly. The risk for an adverse drug event is 13% with the use of two medications, but the risk increases to 58% for five medications 42. If seven or more medications are used, the incidence of adverse drug events increases to 82% 42.
INTERVENTIONS:
Older people are a heterogenous group, often with multiple concomitant illnesses and multiple prescriptions. There is a thin line between a healthy old person and an ill old person. Prescribing for older people is challenging as any new medication must be considered in the context of altered pharmacokinetics, altered pharmacodynamics and age-related changes in body composition and physiology. Both over prescription and undue prescription seem to characterize the overall pharmacological therapy of the elderly. Polypharmacy is the main risk factors for ADRs 43. Thus, attempts should be made to curtail inappropriate drug prescription by utilizing different available tools 44. An interdisciplinary medication review of older individuals in the community helps to reduce the cost and number of medications. Polypathology seems the most obvious explanation of the high number of drugs taken by older people, but additional factors deserve consideration. Changes in patient’s medical status over time can cause medications that have been used chronically to become unsafe or ineffective. Particular care must be taken in determining drug dosages and treatment options when prescribing for older adults. “Pill for an ill” approach should be discouraged as many a time pharmacological treatment may carry more adverse effects then the illness itself. Use of electronic medical records and other hand held devices to prescribe appropriate medication doses and check drug to drug interactions has been found useful in reducing the medication related errors and hence adopted by various medical groups and hospital practices. Reviewing medications at every visit is a simple and very helpful tool too especially if patients are encouraged to bring with them a printed list of their current medications (including over the counter drugs). Printing an updated list of the medication changes in bold and large font after a visit with their physician helps patients to follow the recommendations especially in case of geriatric patients who may not remember all the new changes made at an office visit.
CONCLUSIONS:
Polypharmacy is an important issue in the elderly. The problem involves many issues, a number of which have been explored in this article. One of the most important issues involves adverse drug reactions. All pharmaceutical agents have the potential for side effects; therefore, it is obvious that the more drugs one takes the more side effects one will experience. The aging process results in altered metabolism and excretion of medications, and deficits in cognition and senses. Incidence of adverse drug reaction and interactions is increased with polypharmacy. Since adverse drug reactions are a significant cause of morbidity and mortality, as well as an important cause for hospital admissions, minimizing polypharmacy is an important consideration. The general principle of “Start Low and Go Slow” holds true in most scenarios but should be modified to “Start Low, Go Slow but Use Enough” to achieve desired therapeutic effect.




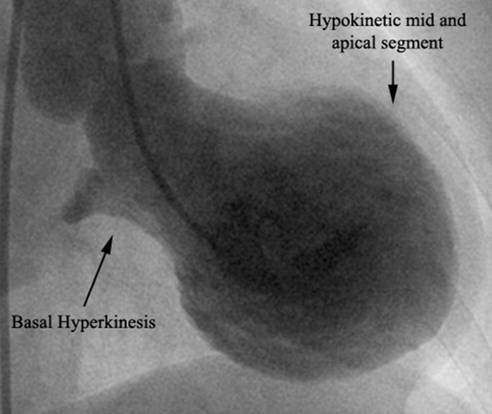
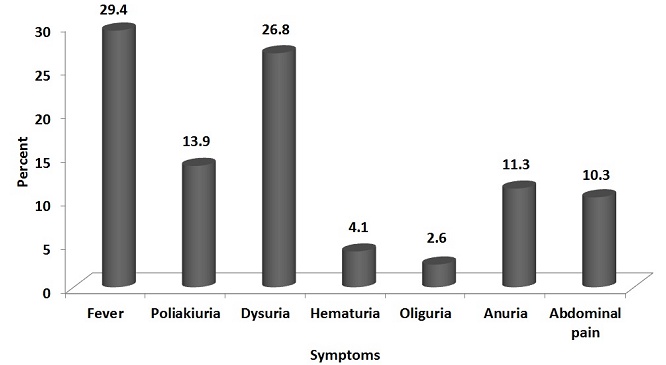
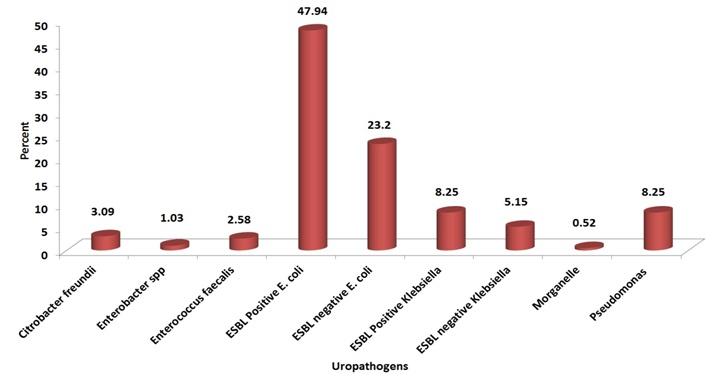
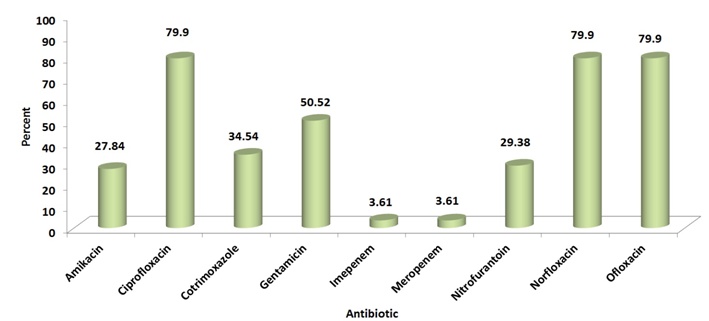
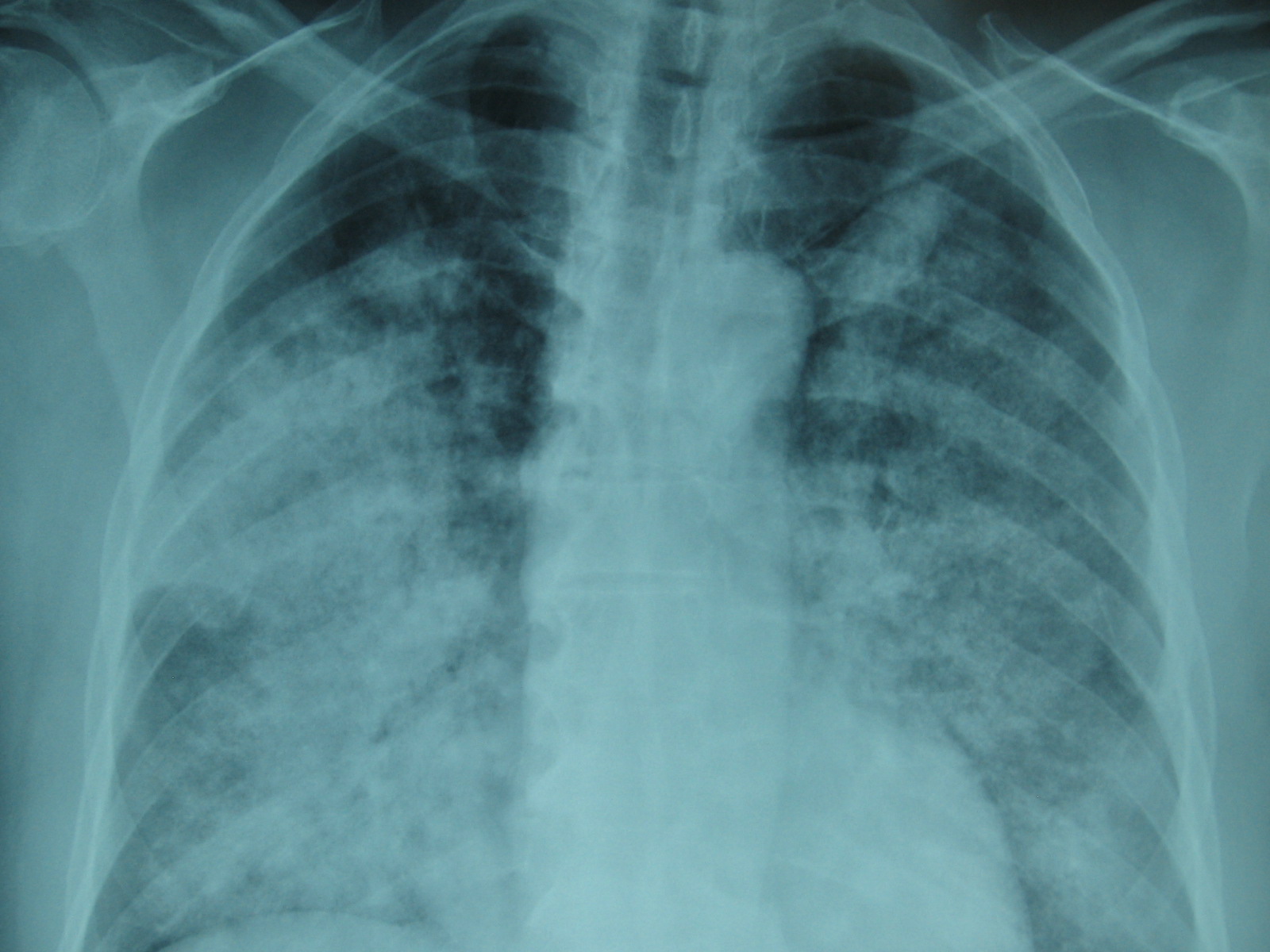
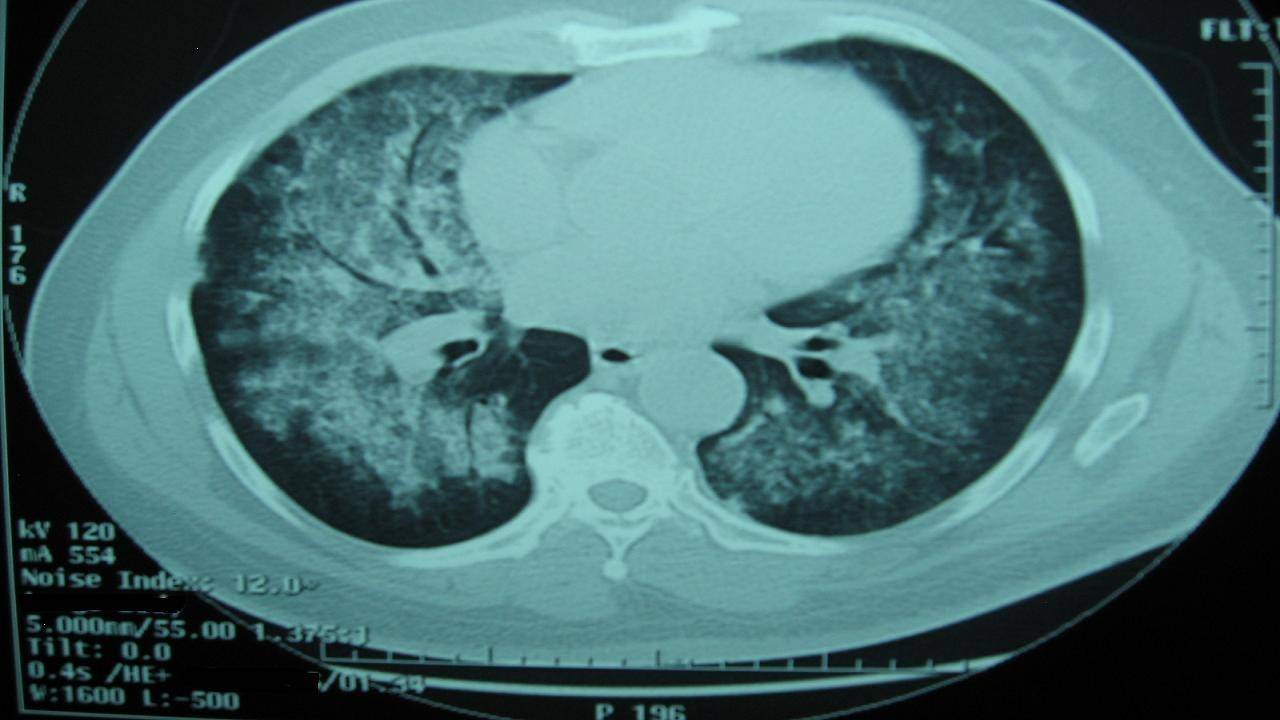
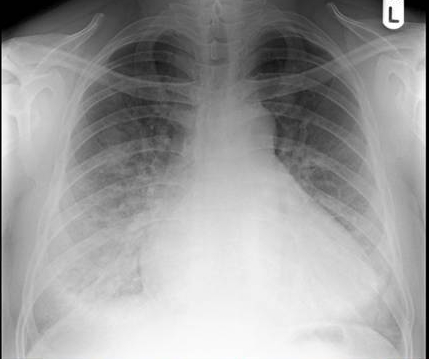
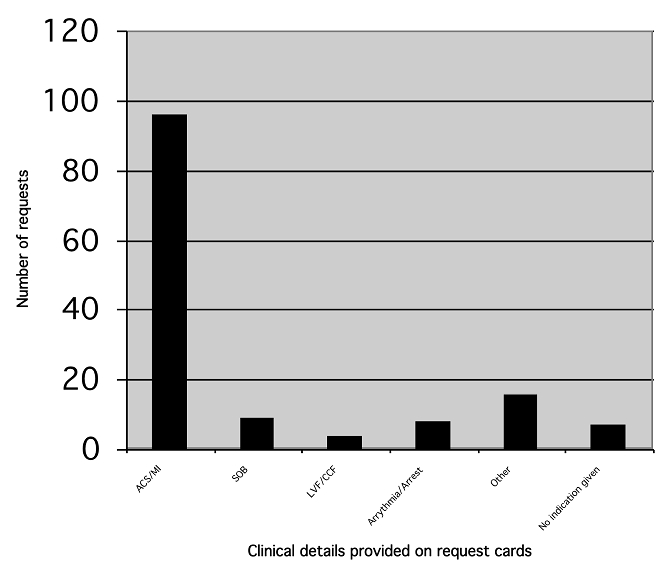

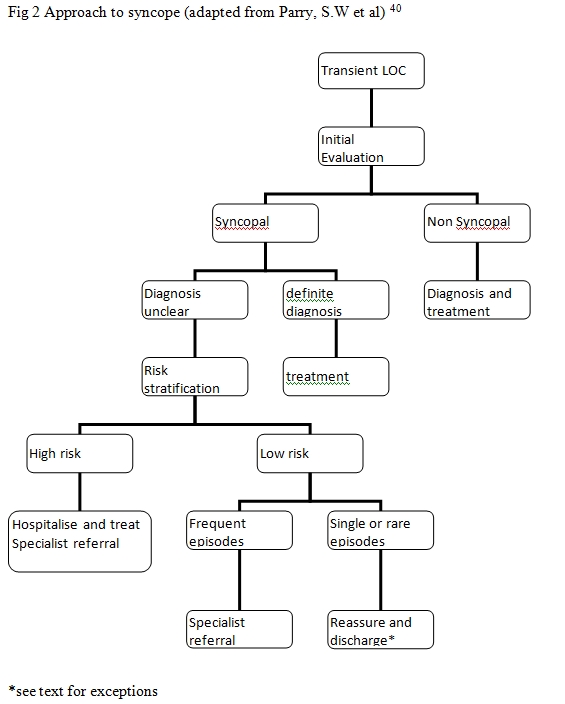 The causes of syncope can be broadly divided in to cardiac causes and non-cardiac causes (Table 1). Initial evaluation leads to a diagnosis in less than 50% patients in most instances4,12-14. If there is uncertainty about diagnosis then the patient is risk stratified. High-risk patients are hospitalised, evaluated and treated whereas early discharge could be considered in low risk patients. Aetiology of Syncope41
The causes of syncope can be broadly divided in to cardiac causes and non-cardiac causes (Table 1). Initial evaluation leads to a diagnosis in less than 50% patients in most instances4,12-14. If there is uncertainty about diagnosis then the patient is risk stratified. High-risk patients are hospitalised, evaluated and treated whereas early discharge could be considered in low risk patients. Aetiology of Syncope41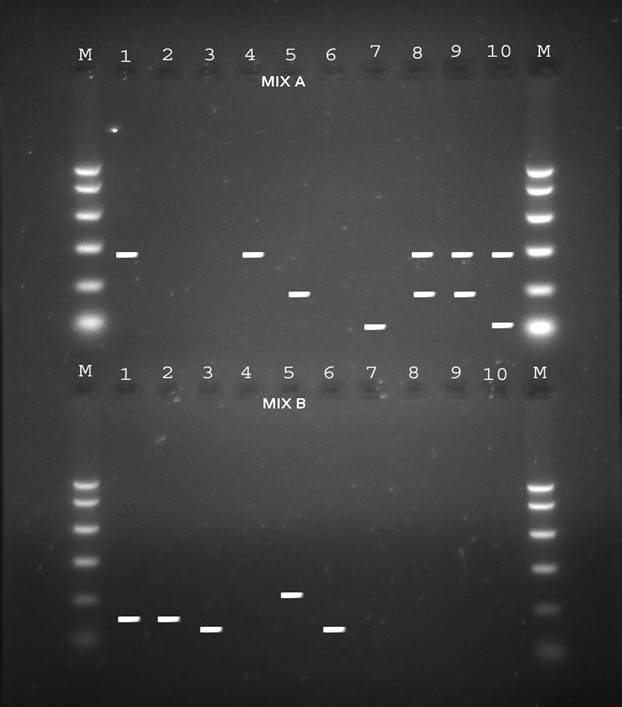
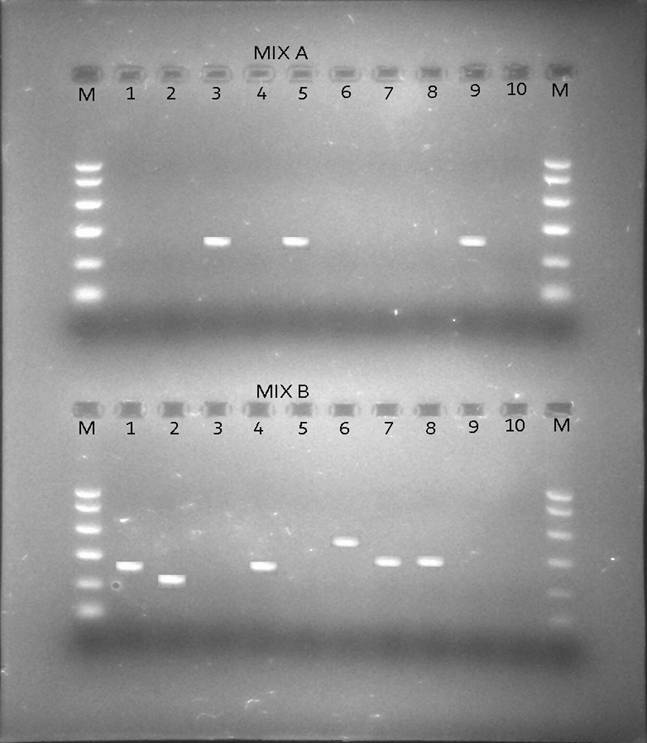
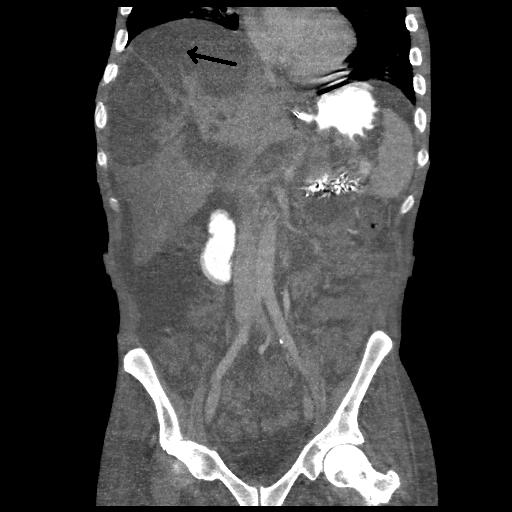

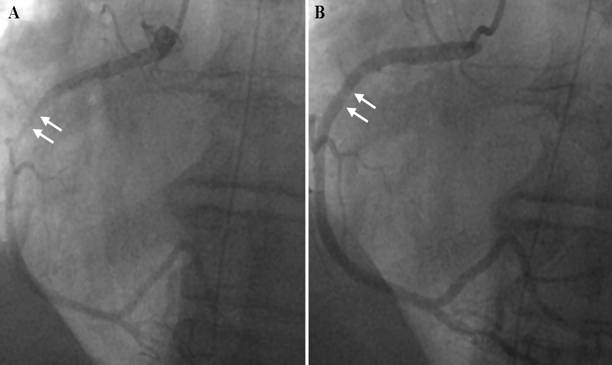
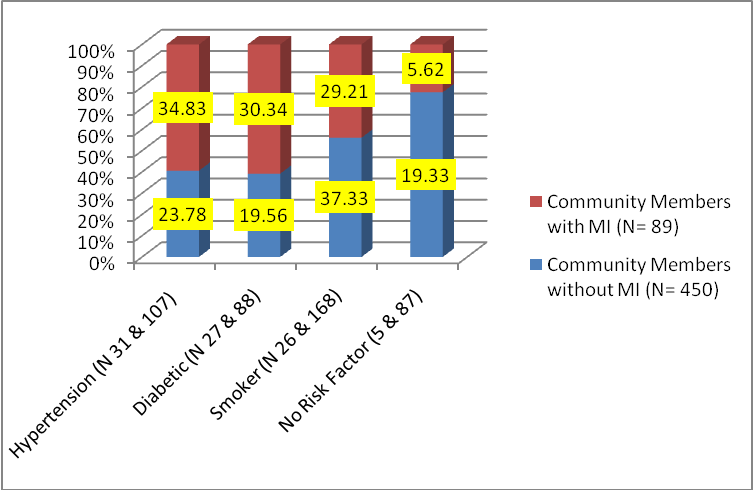
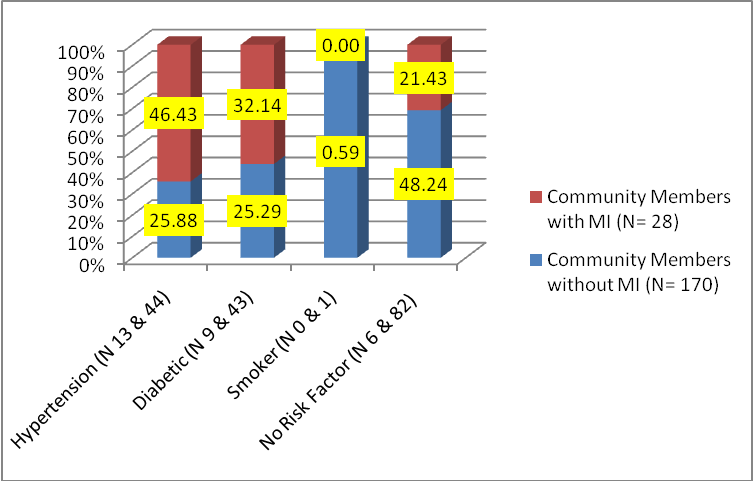 (Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI.
(Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI. 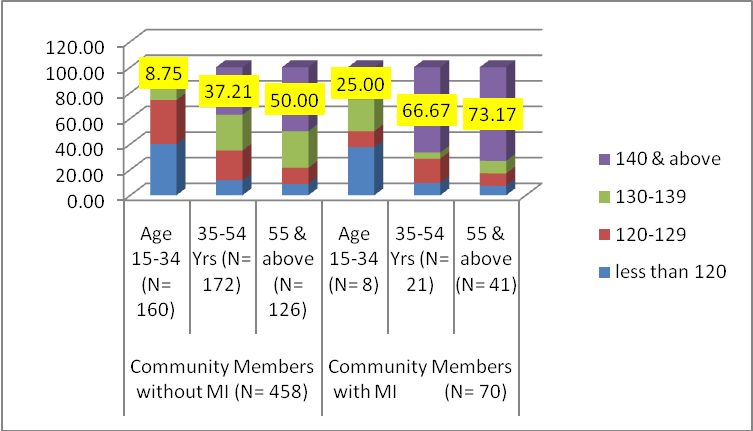 (Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years.
(Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years. 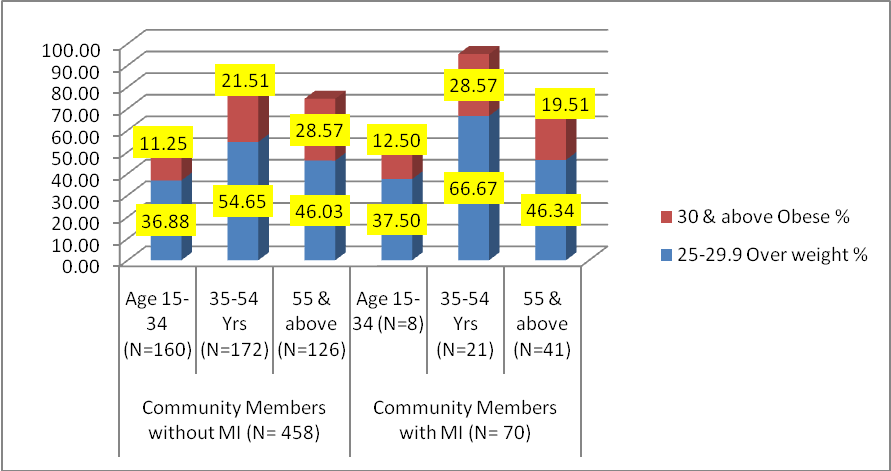
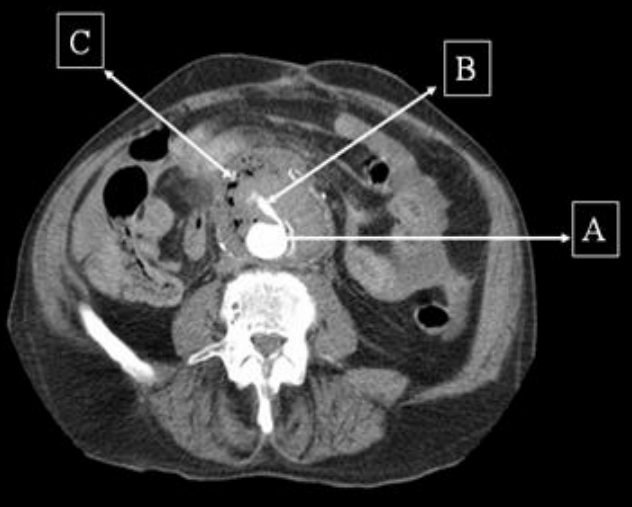

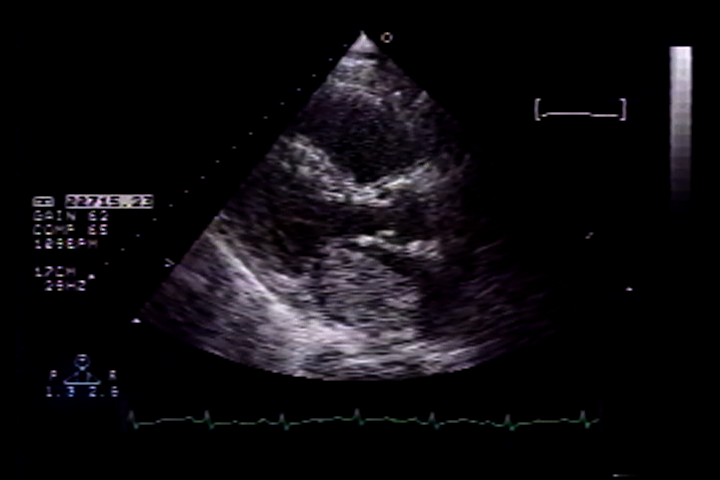



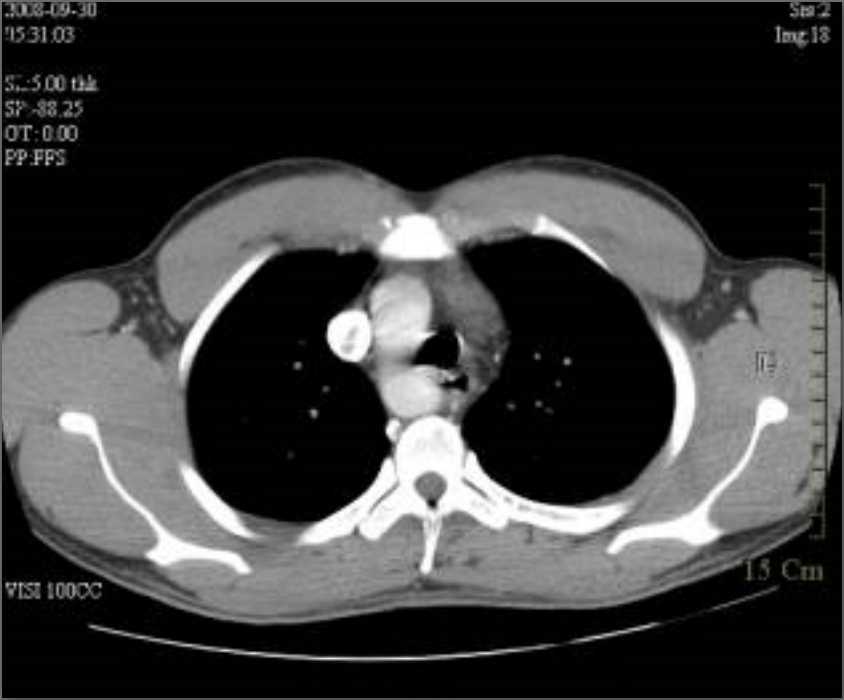

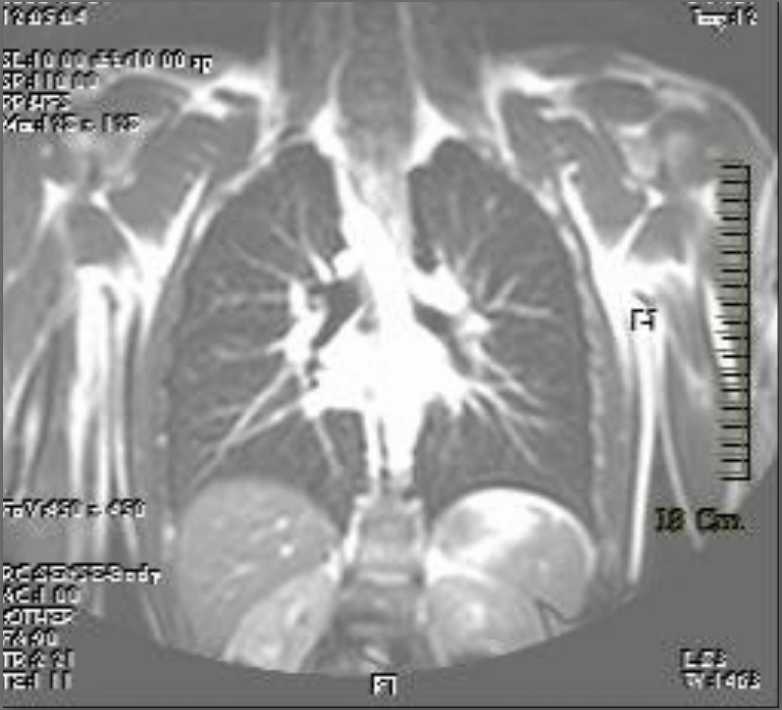
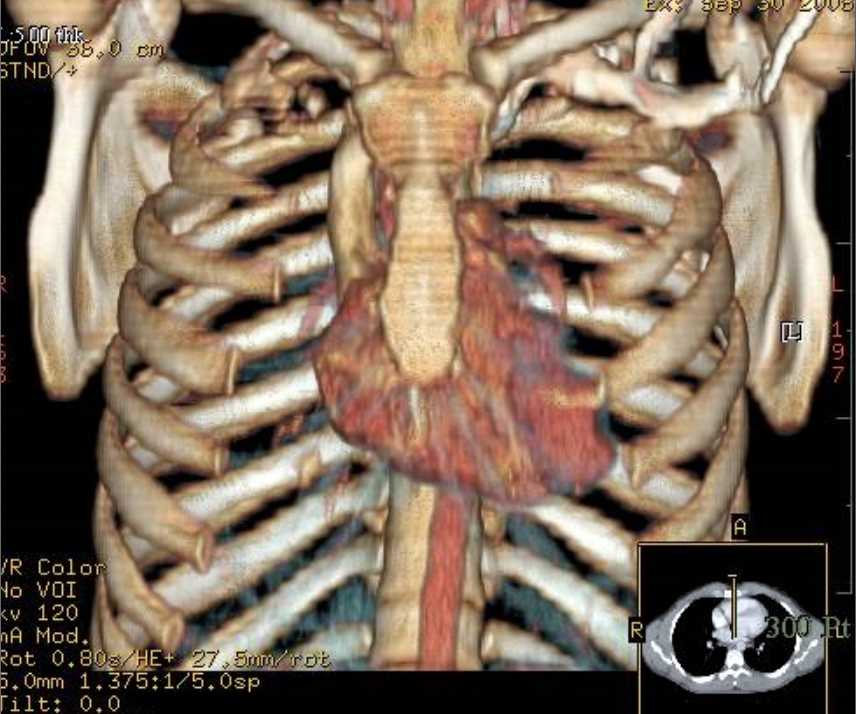

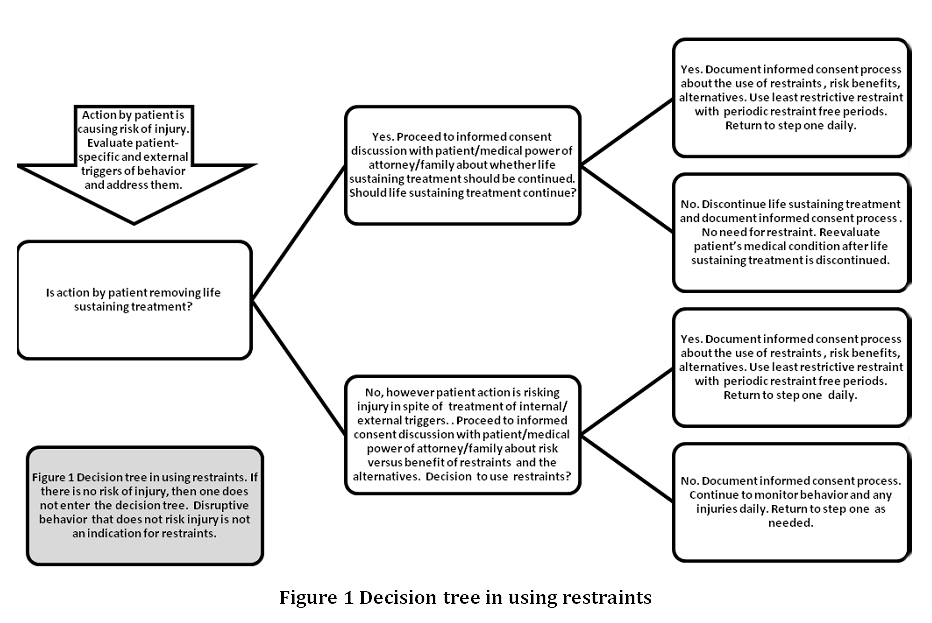
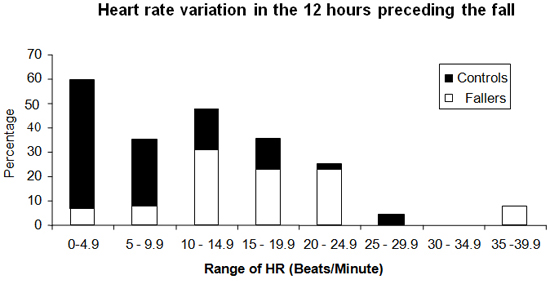
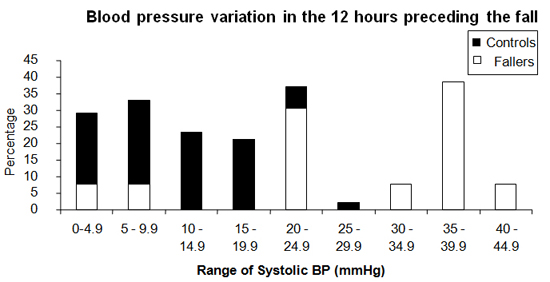
 Assessment of spasticity Before any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale
Assessment of spasticity Before any intervention is undertaken to modulate hypertonicity, it is important to attempt to assess the severity of spasticity. Many grading scales are used to quantify spasticity. These address the degree of muscle tone, the frequency of spontaneous spasms and the extent of hyperreflexia. Goniometry, Ashworth scale, Tardieu Scales, Goal attainment scale are only a few of these scales. One of the most widely used scales is the modified Ashworth scale2. Table 2 Modified Ashworth scale