



ISSN 1757-8515
SEPTIC SHOCK: A Review article
Khadija Qureshi and Abid Rajah
Cite this article as: BJMP 2008:1(2) 7-12
|
Abstract
Septic shock still remains one of the leading causes of death in hospital patients. Greater awareness, understanding of the condition .and the knowledge of most effective treatment measures available can decrease the rate of mortality. Making an early, accurate diagnosis of septic shock is the key to increasing survival rates. Excessive inflammation, excessive coagulation and suppression of fibrinolysis are the hallmarks of Sepsis. Infection control, haemodynamic stabilization, and modulation of the septic response are the cornerstones of treatment. The management is influenced more by appropriate treatment with antibiotics and fluids than by specific intensive care. Septic response can be modulated by the use of Steroids and Activated Protein C and with tight glucose control. Low Tidal Volume ventilation and high volume Haemofilteration are other beneficial strategies in Sepsis. As septic shock worsens and fails to respond to all therapy, one must be prepared to limit and withdraw treatment.
Septic shock still remains the one of the leading causes of death in hospital patients. Barely more than 50% of the patients with severe sepsis survive their hospital admission. This unacceptable high mortality can only be reduced if there is greater awareness and understanding of the condition .and the knowledge of most effective treatment measures available. Unplanned admissions to the Intensive Care Unit (ICU) and potentially preventable deaths on wards are associated with a failure to institute early preventive conditions. Greater than 40% of the intensive Care Unit admissions are potentially preventable with improved ward care.
Survival of patients with Septic shock appears to be better if shock develops while the patient is in Intensive Care Unit rather than on general ward despite greater severity of illness in the intensive care group [1].This suggests that the closer observation and earlier treatment can influence the outcome of sepsis.
INCIDENCE:
Septic shock is an increasingly common problem. The incidence of sepsis is increasing year by year. The reasons for this increase are that the people are living longer and this aged population are the most vulnerable to sepsis. We are using advanced technology to sustain life and there has been a rise in the number of immunocompromised patients due to aggressive cancer therapy and the increased prevalence of HIV. The widespread use of broad spectrum antibiotics has increased the rate of both antibiotic resistance and nosocomial infections.
A prospective, multicentre, observational study, recently conducted to evaluate the epidemiology of Sepsis and other characteristics of Intensive Care Unit patients in European countries (called the SOAP study) was endorsed by the European Society of Intensive Care Medicine [2]. This observational study showed a marked difference in the frequency of sepsis between countries, and higher frequencies of sepsis were mirrored by higher mortality rates. (Fig.1)
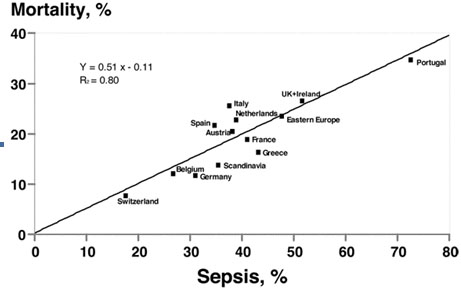
Fig 1: Incidence of Sepsis in European Countries
There was a direct relationship between the number of organs failing and the Intensive Care Unit mortality. Patients with no organ dysfunction on admission had mortality rates of 6% whereas those with four or more organ failures had mortality rates of 65 %. [2] (Fig. 2)
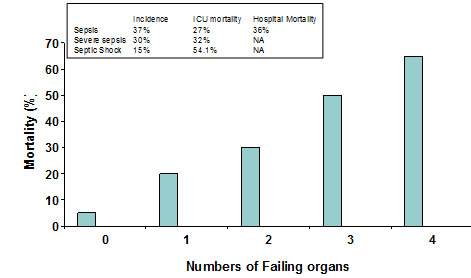
Fig 2: The SOAP study
As compared to the incidence of other pathologies in Europe the incidence of severe sepsis is higher (32%) [2] (Fig 3)
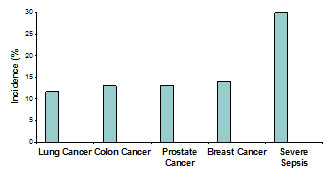
Fig 3: Incidence of different pathologies in Europe
In septic patients, older age, positive fluid balance, co morbid diseases on admission; cancer and cirrhosis are the most important variables of mortality.
DEFINITIONS
Sepsis is defined as an infection that triggers a particular Systemic Inflammatory Response Syndrome (SIRS). This is characterised by body temperature outside 36oC - 38oC, HR >90 beats/min, respiratory rate >20/min, WBC count >12,000/mm3 or < 4,000/mm3. (Fig 4)
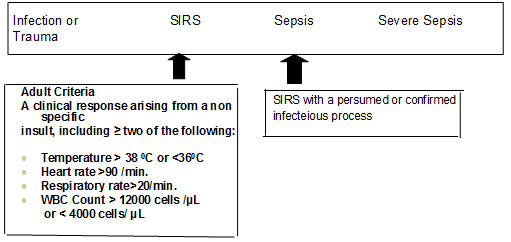
Fig 4: Definitions
There are three recognised stages in the hierarchy of the inflammatory response, with progressively increased risk of organ failure and death. Patients with infections plus two or more elements of the SIRS meet the criteria for sepsis. Those who have end organ failure are considered as having severe sepsis; and those who have refractory hypotension along with the above said criteria are consider to be in septic shock (Fig. 5)
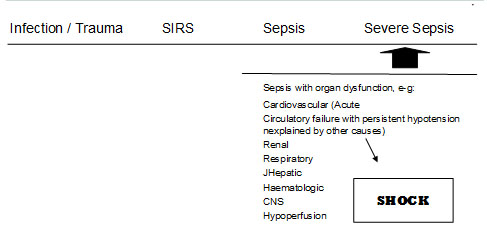
Fig 5: Definitions
PATHOPHYSIOLOGY:
Sepsis is a complex condition starting from an infective stimulus and resulting in an exaggerated immune response. The inflammatory response that was initiated to fight the infection ultimately leads to damage of various organs thorough out the body.
During the onset of sepsis, the inflammatory system becomes hyperactive, involving both cellular and humoral defence mechanisms Endothelial and epithelial cells, as well as neutrophils, macrophages and lymphocytes, produce powerful pro-inflammatory mediators, especially tumour necrosis factor-![]() (TNF-
(TNF-![]() ), interleukin (IL)-6, IL-1 and IL-8. Simultaneously, robust production of acute-phase proteins, such as C-reactive protein, occurs and humoral defence mechanisms such as the complement system are activated, resulting in production of pro-inflammatory mediators, including C5a, the complement split product. C5a ultimately enhances cytokine and chemokine production. Furthermore, the coagulation system becomes activated through various mechanisms, often resulting in disseminated intravascular coagulopathy.
), interleukin (IL)-6, IL-1 and IL-8. Simultaneously, robust production of acute-phase proteins, such as C-reactive protein, occurs and humoral defence mechanisms such as the complement system are activated, resulting in production of pro-inflammatory mediators, including C5a, the complement split product. C5a ultimately enhances cytokine and chemokine production. Furthermore, the coagulation system becomes activated through various mechanisms, often resulting in disseminated intravascular coagulopathy.
The hallmarks of the sepsis are excessive inflammation, excessive coagulation and suppression of fibrinolysis. In addition endogenous Activated Protein C which modulates coagulation, controls inflammation and supports fibrinolysis is also decreased. There is considerable variability in response which is almost certainly to a large degree genetically determined. Those with a tendency to produce excessive cytokines and TNF will have a greater inflammatory response. Simultaneously, the initial vascular damage results in neutrophil activation, neutrophil-endothelial cell adhesion, and further elaboration of inflammatory cytokines. In tissues already prone to dysfunctional oxygen uptake and metabolism, this vascular injury promotes further tissue hypoxia through regional hypo perfusion. This uncontrolled cascade of inflammation and coagulation fuels the progression of sepsis, resulting in tissue hypoxia and ischemia with resultant organ dysfunction and death.
DIAGNOSIS:
Diagnosis of sepsis is not easy. Making an early, accurate diagnosis of septic shock is a key to increasing survival rates. The signs and symptoms of severe sepsis may be subtle. Although the components of SIRS are non specific, the combination of suspected infection and the presence of SIRS may help alert the clinician to a possible diagnosis of sepsis. Although hypotension is another clinical sign that may signal the onset of septic shock, patient may present with sever sepsis and clinically significant global tissue hypoxia in its absence. Metabolic marker such as serum lactate, arterial base deficit may help to identify the severe cases. A single lactate measurement of 4mmol/l or more at initial presentation is associated with an increased rate of mortality [3]. There may well be signs of altered mentation and abnormalities of renal and liver function test, as well as coagulation abnormalities. At least two blood cultures and cultures of other sites as indicated before commencement of antibiotic therapy. Diagnostic studies such as Ultra sound and CT scan should be performed promptly.
D dimmers are grossly elevated in sepsis. Levels of Protein C are lowered which has therapeutic implications. The potential role of biomarkers for diagnosis of infection in patients presenting with severe sepsis remains undefined. Perhaps the most common considerations as diagnostic biomarkers for sepsis have been C-reactive protein and procalcitonin. Despite initial enthusiasm for their potential diagnostic strengths,[4] they have more recently been related to the growing heap of biomarkers that have failed to accurately differentiate sepsis from similar critical illnesses.
The most exciting development in the last 2 years is the recognition of "soluble triggering receptor expressed on myeloid cells-1" (sTREM-1) as a potential biomarker for sepsis. [5] For this marker, a level greater than 60 ng/mL was more accurate than any other clinical and laboratory findings indicating infection
TREATMENT:
The development of new treatment modalities has resulted in a spate of treatment algorithms, often promulgated by medical societies and healthcare improvement organizations. As these modalities have rolled out, increasing levels of evidence have emerged to support or refute their utility in treating patients with sepsis. One of the greatest endeavours to date is the Surviving Sepsis Campaign (SSC) [6] that was originally launched in 2002 with the stated goal to reduce mortality by 25%. The primary method to achieve this goal was the development of evidence-based sepsis care guidelines that were published in 2004. [6] and recently revised in 2008.
The Institute for Healthcare Improvement (IHI) has highlighted sepsis as an area of focus and has identified several deficiencies that may cause suboptimal care of patients with severe sepsis. These deficiencies include inconsistency in the early diagnosis of severe sepsis and septic shock, frequent inadequate volume resuscitation without defined endpoints, late or inadequate use of antibiotics, frequent failure to support the cardiac output when depressed, frequent failure to control hyperglycemias adequately, frequent failure to use low tidal volumes and pressures in acute lung injury, and frequent failure to treat adrenal inadequacy in refractory shock.
The management of patient with sepsis is influenced more by appropriate treatment with antibiotics and fluids than by specific intensive care. Therefore early intervention should never be delayed pending admission to the intensive care unit. The early and aggressive treatment of septic shock has been well documented in the survival sepsis campaign which is based on the best current practice.
The cornerstones of treatment are infection control, haemodynamic stabilization, and modulation of the septic response.
1. Infection Control:
Infection control is vital if the patient is to have any chance of survival. Appropriate broad-spectrum antibiotics must be given within the first hour of recognition of sepsis after obtaining various cultures. Evidence clearly shows that delay or inadequate antibiotic treatment results in poorer outcome. For every hour lost mortality climbs by 9%. [7]
Initial empirical anti-infective therapy should include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal) and that penetrate in adequate concentrations into the presumed source of sepsis[8] antimicrobial regimen be reassessed daily to optimize activity, to prevent the development of resistance, to reduce toxicity, and to reduce costs
A focus of infection must be sought for and if discovered dealt with immediately. The patient should be evaluated for a focused infection amenable to source control measures including abscess drainage or tissue debridement. One must weigh up the benefits and risks of the particular procedure chosen. If intravascular devices are a potential source, they must be promptly removed after establishing other vascular access. When source control is required, the effective intervention associated with the least physiologic insult be employed (e.g., percutaneous rather than surgical drainage of an abscess)
2. Haemodynamic Stabilization:
In septic shock there is extensive cardiovascular derangement. Hypotension is caused by myocardial depression, pathological vasodilatation and extravasation of circulating volume due to widespread capillary leak. The initial resuscitative effort is to attempt to correct the absolute and relative hypovolemia by refilling the vascular tree. There is no evidence to support one type of fluid crystalloid or colloid is superior to the other. There is good evidence that early gold directed aggressive volume resuscitation improves outcome of sepsis[9] During the first 6 hours of resuscitation the goals of initial resuscitation are a Central venous pressure of 8-12 mm Hg, Mean arterial pressure (MAP) ≥ 65 mmHg, Urine output ≥ 0.5 mL • kg-1 • hr and a central venous (superior vena cava) or mixed venous oxygen saturation ≥ 70% or ≥ 65%, respectively The Rivers study clearly shows a reduction in hospital mortality, 28 day mortality as well as 60 day mortality attributed to the Early Goal Directed Therapy (EGDT) [10]. Early goal-directed resuscitation has been shown to improve survival for emergency department patients presenting with septic shock in a randomized, controlled, single-centre study.[11] Resuscitation directed toward the previously mentioned goals for the initial 6-hr period of the resuscitation was able to reduce in hospital, 28-days as well as 60 days mortality rate (Fig. 6).
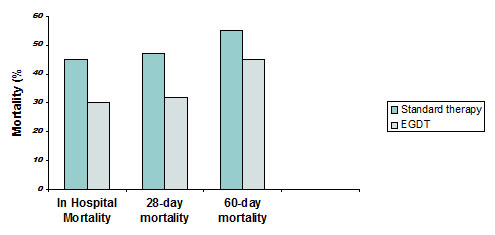
Fig 6: Results of Early Goal Directed Therapy (EGDT)
If Scvo2 or SVo2 of 70% or 65%, respectively, is not achieved with fluid resuscitation to the central venous pressure target, then transfusion of packed red blood cells to achieve a hematocrit of ≥ 30% and/or administration of a dobutamine infusion (up to a maximum of 20 µg • kg-1 • min-1) be used to achieve this goal.
It is important to remember that vasopressors should be utilized not only when fluids fail to reverse hypotension, but also during resuscitation to maintain minimally adequate blood pressure. Traditionally, the use of noradrenalin in patients with shock has been restricted by the fear of excessive vasoconstriction that may result in end-organ hypo perfusion. In the past it was usually given only when other vasopressin agents failed, and thus such patients would be predicted to have a poor outcome. Recent studies indicate that the fear of deleterious effect was unwarranted and that noradrenalin may have a role as a first-line vasopressor agent in patients with septic shock.
Vasopressin should be considered in refractory shock despite high dose conventional vasopressors. Vasopressin is an endogenously produced hormone that is deficient in many patients with septic shock. Exogenously administered vasopressin in physiologic replacement doses may act synergistically with other vasopressor agents, and has been associated with early withdrawal of catecholamine. Most studies have evaluated short-term infusions of vasopressin at 0.08 U/minute or less as add-on therapy in patients requiring adrenergic agents. The results show that starting vasopressin in patients with septic shock increases systemic vascular resistance and arterial blood pressure, thus reducing the dosage requirements of adrenergic agents [12]. These effects are rapid and sustained. Substantial enhancement of urine production, likely due to increased glomerular filtration rate, was shown in several studies. A few studies demonstrated clinically significant reduced cardiac output or cardiac index after vasopressin was begun, necessitating cautious use in patients with cardiac dysfunction.
3. Modulation of Septic Response:
There are a number of ways to modulate the septic response. These includes use of steroids, tight glucose control and the use of Activated Protein C. Septic shock causes adrenal suppression and this can be confirmed by measuring cortisol levels or by using the synacthan test. Compare to placebo, the administration of low dose of hydrocortisone (200-300 mg/day in divided doses) to patients with septic shock decrease there requirements for vasopressors [13] and lowered their mortality rate [14]. Low dose hydrocortisone should only be given to non responders of the synacthan test but in practice all patient receive this treatment until the result of the test are received. Following the Corticosteroid Therapy of Septic Shock (CORTICUS) study there is now an increasing trend towards restricting the use of low dose hydrocortisone only to patients with refractory hypotension who are already on high doses on vasopressors [15]. The trial did show a faster resolution of septic shock in patients who received steroids but failed to show a mortality benefit with steroids therapy. Close control of blood glucose has been shown to increase survival in critically ill septic patient. When conservative (10 – 11.1 mol/L) glycemic control was compared with tight control (4.4-6.1mmol/L) in a multi centre, randomized controlled trial, tight control lead to a significant reduction in mortality (8% versus 4-6%), p < 0-04 and improved morbidity at 12 months [16].
Activated Protein C
Human activated Protein C (APC) is an endogenous regulator of coagulation. In order for protein C in the plasma to become activated, it must combine with thrombin and thrombomodulin along with the endothelial protein C receptor. With endothelial damage this activation does not take place resulting in its deficiency. Therefore APC supplementation is a rational therapeutic option. APC has an important role in the management of severe sepsis. It protects against the disruption of the endothelial cell membrane, improves micro circulatory perfusion, and has anti inflammatory, procoagulant, fibrinolytic and anti apoptotic activity. APC must ideally be started with in the first 24 hours of the onset of septic shock. The Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) trial found activated protein C to reduce the risk of death among all severe sepsis patients by 20% [17] This study has also recognized the risk of complications specially haemorrhages.
Subsequent studies have shown similar results. “Administration of Drotrecogin Alfa (Activated) in Early Stage Severe Sepsis” (ADDRESS trial) also provides the evidence concerning use of rhAPC in adults [18]. Additional safety information comes from an open-label observational study, “Extended Evaluation of Recombinant Activated Protein C” (ENHANCE trail). [19] The ENHANCE trial also suggested that early administration of rhAPC was associated with better outcomes.
Other beneficial Strategies in Sepsis
Low Tidal Volume Ventilation: using normal or high tidal volume (10-12mls/Kg) ventilation will cause over expansion of the normal lung segments. This will in turn result in inflammatory mediators being released in the lung tissue. The consequences of this are the development of Acute Lung Injury (ALI) or Acute Respiratory Distress Syndrome (ARDS). Therefore it is crucial to use low tidal volume Ventilation (6ml/kg) to keep plateau airway pressure less than 30 cm of water [20, 21]
High volume Haemofilteration: In the past five years, many studies have been conducted to evaluate and demonstrate benefits of increasing the volume of ultra filtration and replacement fluid during Continuous Renal replacement therapy [22, 23] particularly in complex and very severe syndromes such as Severe Sepsis and Septic Shock, associated with or without acute renal failure.
In general, the high-volume approach provides higher clearances for middle/high molecular weight solutes than a simple diffusive transport, Continuous veno venous haemodialysis (CVVHD) or a convection-based transport at lower volumes, Continuous veno venous haemofiltration (CVVH). These solutes seem to be primarily involved in the Systemic Inflammatory Response Syndrome, which characterizes the Sepsis syndrome, and their efficient removal may thus be beneficial. [24]
Alternative approaches have been based on more efficient removal of inflammatory mediators by high cut-off hemofilters, which are characterized by an increased effective pore size. Most commercially available hemofilters do not permit a substantial elimination of cytokines because of the low cut-off point of their membranes. The use of high cut-off hemofilters is a new and effective approach to cytokine removal, but it has potentially harmful side effects, such as the loss of essential proteins like albumin [25].
Because the reversibility of this disease and the resultant mortality may be greatest during the earliest stages of presentation, proper sepsis management should not be confined within the walls of an Intensive Care Unit. Specific emphasis on appropriate triage to ensure prompt diagnosis of the high-risk patient is vital to the launch of a coordinated and cooperative effort by the primary treating clinician and the intensivist
Ethical Dilemmas in Septic Shock
Patient with septic shock have a high mortality and as yet there is no predictive scoring system which gives accurate predictions of outcome for individual patient. Survival from an episode and septic shock is dependent on patient’s age, number of failed organs, previous health and the time delay before the onset of medial intervention, as well as the appropriateness and quality of medical care. The resources available to us are not limitless and so difficult decisions have to be made deciding between the potential benefits for one critically ill patient and need for several less critically ill patients. As an intensivist one must set realistic expectations which must be clearly communicated to the families concerned. As septic shock worsens and fails to respond to all therapy, one must be prepared to limit and withdraw treatment.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
KHADIJA E QURESHI, BSC, MBBS, DA, FCPS, ST2- Anaesthetics, Hemel Hempstead General Hospital, United Kingdom
ABID RAJAH, MB ChB, FRCA, FFARCSI, Lead Clinician & Consultant in Intensive Care, Hemel Hempstead General Hospital, United kingdom
CORRESPONDENCE: Dr Abid Rajah, Lead Clinician & Consultant in Intensive Care, Hemel Hempstead General Hospital, Hill field Road, Hemel Hempstead, HP2 4AD
Email: ARajah@aol.com
REFERENCES
- Lundberg J, Perl TM. Septic shock: an analysis of outcomes for patients with onset on hospital wards vs. Intensive care units. Crit care Med 1998; 26: 1020-24
- Vincent JL, Sakr Y, and Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006; 34:344-353.
- Shapiro NI, Homel MD, Talmor D, Nathanson LA, Lisbon A, Wolfe RE, et al. Serum lactates as a predictor of mortality in emergency department patient with infection. Ann Emerg Med. 2005; 45: 524-8.
- Harbarth S, Garbino J, Pugin J, et al. Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med. 2003; 115:529-535.
- Gibot S, Kolopp-Sarda MN, Bene MC, et al. Plasma level of a triggering receptor expressed on myeloid cells-1: its diagnostic accuracy in patients with suspected sepsis. Ann Intern Med. 2004; 141:9-15.
- Surviving Sepsis Campaign. Available at: http:// www.surviving sepsis.org/ Accessed March 6, 2007.
- Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis C guidelines for management of severe sepsis and septic shock. Crit Care med. 2004;32: 858-873
- Battleman DS, Callahan M, Thaler HT. Rapid antibiotic delivery and appropriate antibiotic selection reduce length of hospital stay of patients with community acquired pneumonia: link between quality of care and resource utilization. Arch Intern Medicine 2002; 162(6):682-8.
- Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003; 31:1250-1256.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377
- Emanuel Rivers. The outcome of patients presenting to the emergency department with severe sepsis or septic shock. Crit Care. 2006; 10(4): 154.
- Obritsch MD; Bestul DJ; Jung R; Fish DN; MacLaren R. The role of vasopressin in vasodilatory septic shock. Pharmacotherapy. 2004; 24(8):1050-63 (ISSN: 0277-0008)
- Briegel J, Frost H, Haller M, Shelling G, Kilger E, Kuprat G et. Stress doses of hydrocortisone reverse hyper dynamic septic shock: a prospective randomised double blind single centre study. Crit care Med 1999; 27:723-32.
- Annane D, Sebille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002; 288:862-871.
- Sprung CL. Update on clinical trials in severe sepsis. CORTICUS trial. Program and abstracts of the Society of Critical Care department patient with infection. Ann Emerg Med 2005: 45 (524-8).
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354:449-461
- Bernard GR, Vincent JL, Laterre PF, et al. Recombinant human protein C Worldwide Evaluation in Severe Sepsis (PROWESS) study group. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001; 344:699-709.
- Abraham E, Laterre PF, Garg R, et al: Drotrecogin alfa (activated) for adults with severe sepsis and a low risk of death. N Engl J Med 2005; 353:1332-1341.
- Vincent JL, Bernard GR, Beale R, et al: Drotrecogin alfa (activated) treatment in severe sepsis from the global open-label trial ENHANCE: Further evidence for survival and safety and implications for early treatment. Crit Care Med 2005; 33:2266-2277.
- ARDS Network Investigators. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000; 342:1301-1308.
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wiedemann HP, Wheeler AP, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006; 354:2564-2575.
- Piccinni P, Dan M, Barbacini S, Carraro R, Lieta E, Marafon S, Zamperetti N, Brendolan A, D'Intini V, Tetta C, et al.: Early iso-volaemic haemofiltration in oliguric patients with septic shock. Intensive Care Med 2006, 32:80-86.
- Reiter K, D'Intini V, Bordoni V, Baldwin I, Bellomo R, Tetta C, Brendolan A, Ronco C: High-volume hemofiltration in sepsis. Nephron 2002, 92:251-258.
- Ronco C, Tetta C, Mariano F, Wratten ML, Bonello M, Bordoni V, Cardona X, Inguaggiato P, Pilotto L, d'Intini V, Bellomo R: Interpreting the mechanisms of continuous renal replacement therapy in sepsis: the peak concentration hypothesis. Artif Organs 2003, 27:792-801.
- Mariano F, Fonsato V, Lanfranco G, Pohlmeier R, Ronco C, Triolo G, Camussi G, Tetta C, Passlick-Deetjen J: Tailoring high-cutoff membranes and feasible application in sepsis-associated acute renal failure: in vitro studies.Nephrol Dial Transplant 2005, 20:1116-1126.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.