



ISSN 1757-8515
Pictorial essay: endotracheal tube and nasogastric tube on chest radiographs
Krishnan Melarkode and M Y Latoo
Cite this article as: BJMP 2009:2(1) 54-56
|
Chest radiographs are one of the most common radiological procedures performed in medical practice. The chest radiograph should ideally include views of the heart, lungs, trachea, mediastinum, bones of the chest and upper part of the abdomen. Chest radiographs are normally taken in the posterior-anterior (PA) view with the patient in upright / standing position but for patients admitted in the intensive care unit (ICU) or other emergency situations, this is not possible and so they are taken in the supine (anterior-posterior views) or semi-erect position.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In this article, we aim to discuss and compare the normal and abnormal positions of both the endotracheal tube (ETT) and nasogastric tube (NG) on chest radiographs.
Endotracheal tube (ETT):
Endotracheal tubes are used to secure the patients airway. Modern ETTs have a radio-opaque line running along their length which enables us to determine their position on chest radiographs 1.
Clinical methods 2 that can be used to determine the appropriate position of the ETT include:
-
Symmetrical rise and fall of the chest wall with each breath (on inspection and palpation of the chest).
-
Auscultation of the lung fields
-
Use of capnography
However, clinical methods cannot confirm how high or low the ETT is situated in the trachea. This can be confirmed by chest radiography. Optimum position of the ETT is required to ensure ventilation of both lungs.
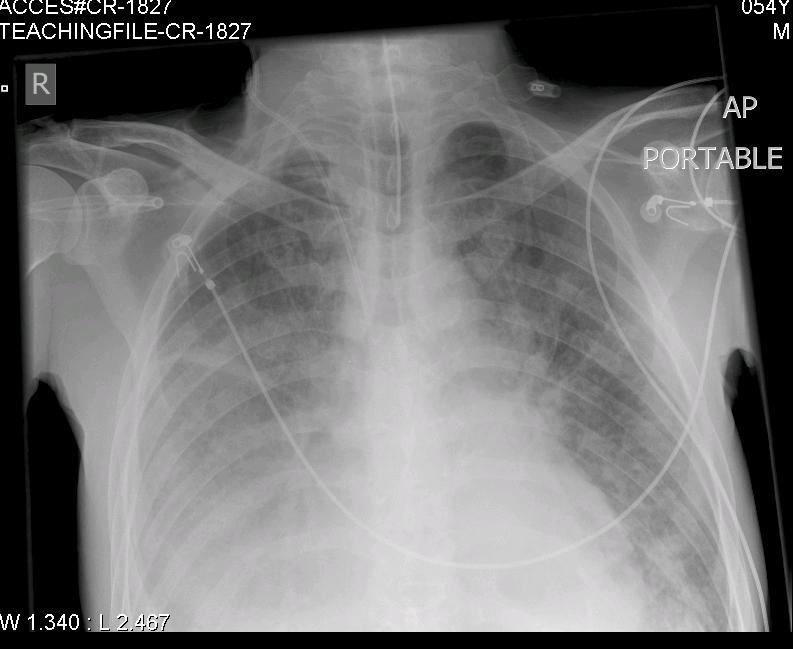
A correctly positioned ETT lies in the mid trachea and its tip is approximately 5-7 cm above the carina 3 as seen in Fig: 1 (CR-1827).

In Fig: 2 (CR-1820), the tip of the ETT is low lying and is at the origin of the right main bronchus. Further migration of the ETT will result in right sided endobronchial intubation and collapse of the left lung. This will result in decreased oxygen saturation values (SpO2) on a pulse oximeter and low arterial partial pressure of oxygen (PaO2) on analysis of an arterial blood gas specimen.
Nasogastric tube (NG):
Nasogastric tube (NG) or orogastric tube (OG) is inserted for providing enteral nutrition, administration of drugs or for gastric drainage. NG feeding is a common practice in all age groups. There is a risk that the NG feeding tube can be misplaced into the lungs during insertion or may move out of the stomach at a later stage.
In the past, various methods 4 have been used to determine the position of NG feeding tubes.
These included:
-
Auscultation of air insufflated through the feeding tube - whoosh test
-
Testing acidity/alkalinity of the aspirate using blue litmus paper
-
Interpreting absence of respiratory distress as an indicator of correct positioning
-
Monitoring bubbling at the end of the NG tube
-
Observing the appearance of the feeding tube aspirate
The National Patient Safety Agency (NPSA) have issued a patient safety alert and have recommended that the above methods are not reliable and therefore should not be used to detect the position of NG tubes.
The NPSA recommend 5:
-
Measuring the pH of the aspirate using pH indicator strips/paper
-
Use of radiography
The most accurate method for confirming the correct position of a NG feeding tube is radiography 5.
The pH of the gastric aspirate can be affected by ongoing enteral feeding and medications viz: antacids, H2 antagonists and proton pump inhibitors. In these cases, measuring the pH of the aspirate may not be useful and so use of radiography is recommended. The NPSA have issued guidance on how to confirm the position of nasogastric feeding tubes.
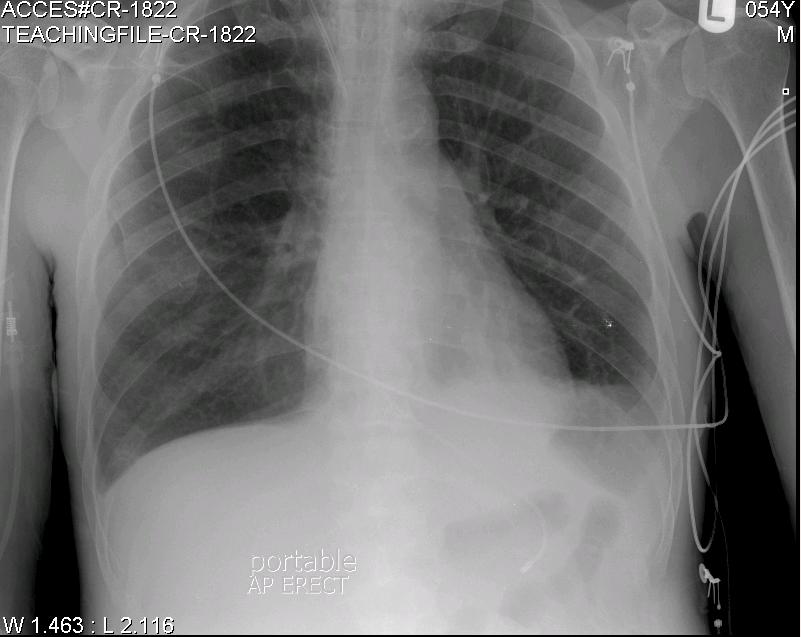
Fig: 3 (CR-1822) indicates the normal position of the NG tip below the diaphragm in the upper part of the stomach (fundus).
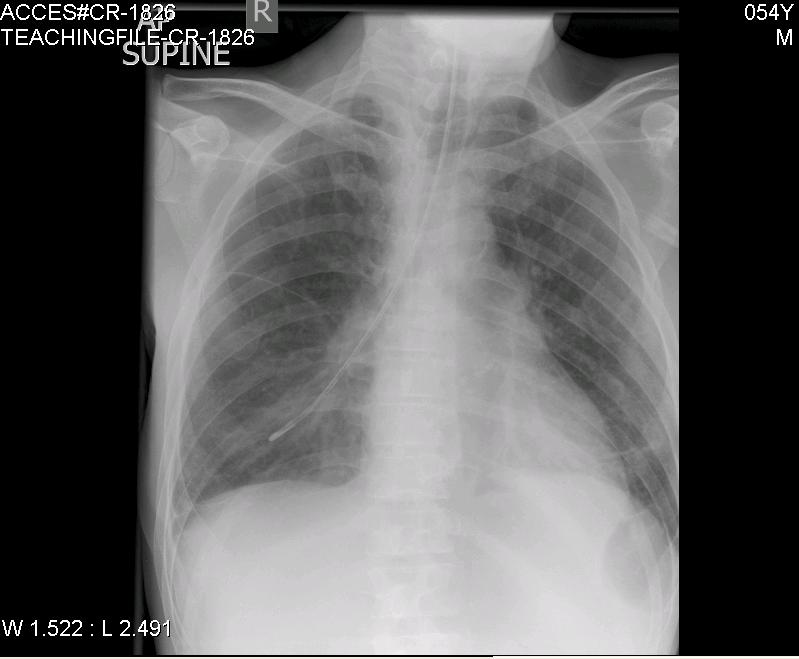
Fig: 4 (CR-1826) shows the abnormal position of the NG tube situated in the right lower lobe bronchus. If NG feeds are commenced, this will result in lung injury.
Conclusion
We have highlighted the optimum position of both the ETT and NG tube on chest radiographs. Optimum positioning is required not only for safety reasons to avoid complications but also for optimum monitoring and treatment of patients. This series of chest radiographs will benefit not only medical students and doctors from all specialties but also nurses, physiotherapists and paramedical teams who will be involved in the care of critically ill patients.
Self Assessment
MCQ 1:
On a chest radiograph, the tip of the ETT:
a. should lie very close to carina
b. should lie 5-7 cm above the carina
c. should lie 5-7 mm above the carina
d. The ETT cannot be visualised on a chest radiograph
MCQ 2:
Which one of the following tests is the most accurate method to determine the correct position of NG feeding tubes?
a. testing the aspirate from the NG tube using a blue litmus paper
b. whoosh test
c. measuring the pH using pH indicator strips/paper
d. radiography
Answers for MCQs:
MCQ 1: b
MCQ 2: d
ACKNOWLEDGEMENTS
We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Bedford Hospital NHS Trust, UK
DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK
CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Bedford Hospital, Bedford, UK
Email: drkrishnanmr@gmail.com
References
-
Tracheal and tracheostomy tubes and airways. In: Al-Shaikh B and Stacey S eds. Essentials of anaesthetic equipment. 2nd edition. Churchill Livingstone, 2002: 56-67.
-
Hutton P. Airway management II: assessment, control and problems. In: Hutton P, Cooper GM, James III FM and Butterworth J eds. Fundamental Principles and Practice of Anaesthesia. Martin Dunitz Ltd, 2002; 79.
-
Goodman LR. The postoperative and critically ill patient. In: Grainger RG and Allison DJ eds. Diagnostic Radiology. 2nd edition. Churchill Livingstone, 1992; 368.
-
Reducing the harm caused by misplaced nasogastric feeding tubes. Patient safety alert National Patient Safety Agency (NPSA)
-
How to confirm the correct position of nasogastric feeding tubes in infants, children and adults National Patient Safety Agency (NPSA), Interim advice for healthcare staff, February 2005.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.