The concept of burnout has been used to describe emotional and psychological stress among healthcare workers in response to work-related stressors1. Maslach et al2 have defined burnout as a triad of characteristics: emotional exhaustion, depersonalisation (such as objectifying and treating patients indifferently) and lack of feelings of personal accomplishment. Since high time-pressure, high job- stress and excessive workload with poor support are among significant factors that contribute to burnout, physicians are at a greater risk of suffering from it as compared to the general population3.
Burnout affects approx. half of the doctors in the U.S. and in Western Europe working across multiple specialties including in family medicine and internal medicine4,5. Likewise, burnout is universally prevalent among healthcare workers from low and middle-income countries6.
Psychiatry presents specific range of stressors not encountered concurrently in other medical specialties, such as treating chronically ill patients, potentially difficult therapeutic relationships, threat of patient suicide/self-harm and stigma associated with this field of medicine7. Therefore, it is not surprising to discover that approx. 37% of psychiatric trainees working across 22 countries suffered from severe burnout8.
The COVID-19 pandemic resulted in a national lockdown in the U.K. with travel restrictions and unprecedented pressure on an already stretched healthcare system. Healthcare workers were, therefore, faced with extraordinary difficulties including increased working hours, heavy workload, staff shortages and lack of resources. A recent systematic review showed that a startling 40% of medical workers experienced acute stress disorder following COVID-19 pandemic, with burnout prevalent among 29% of them9.
During to the pandemic, there has been a huge increase in the pressure on mental health related admissions to hospitals10. A number of causative stressors may have instigated further strain on mental health workers, including bereavement, unemployment, and isolation, resulting in increased psychological morbidity11. Under such circumstances, ensuring the wellbeing of healthcare workers is of paramount importance to maintain a resilient healthcare system. However, limited research has been carried out so far on the effects of pandemics on psychiatrists and other frontline healthcare workers.
Following two surges of COVID-19 pandemic, we proposed to ascertain the frequency of burnout among doctors working in a large mental health trust in Southeast England, with a secondary aim of exploring possible contributory factors.
METHODOLOGY
We carried out a cross-sectional survey of all doctors working in a county-wide mental health Trust in England. Using the NHS Mail, a link to complete the online survey was sent to all doctors working at different experience levels and across a number of psychiatric specialties.
The survey was based on The Maslach Burnout Inventory12, which is considered to be a gold standard in assessing burnout among healthcare workforce. It consists of 22 questions, divided into domains that assess emotional exhaustion, depersonalisation and personal accomplishment based on a 7-point scale, ranging from “never” to “every day”. Scores for these domains range from 0 to 54, 0 to 30, and 0 to 48, respectively. High scores on the EE (≥ 30) and DP (≥ 12) subscales or a low score on the PA subscale (≤ 30) were considered highly suggestive of burnout symptoms.
The anonymised survey contained questions related to demographics, 22 questions as derived from the Maslach Burnout Inventory, and 14 other questions exploring specific work-related stressors regarding the COVID-19 pandemic. Responses to the questions were analysed and categorised into themes to allow further analysis and discussion.
RESULTS
Our response rate was 42% as 106 out of 254 doctors filled the questionnaire. Not all participants answered all questions, and response numbers for each question are indicated where applicable in the respective tables. There was an even distribution between trainees and consultants, but less representation from speciality doctors, which was expected due to their fewer numbers. Where gender was equally split, we found that age was relatively evenly distributed in our sample.
Figure 1: Participant demographics
Regarding the Maslach Burnout Inventory questions, higher aggregates in emotional exhaustion and depersonalisation subscales indicate higher chance of burnout. When comparing these two subscales, the levels of emotional exhaustion were higher than that of depersonalisation. Conversely, in the personal accomplishment subscale, more common occurrences indicate a lower chance of burnout.
Table 1: Maslach Burnout Inventory Results
Question
Possible responses
n
Never
A few times/ year
Once/ month
A few times/ month
Once/ week
A few times/ week
Every day
I feel emotionally drained by my work
7.6% (8)
23.8% (25)
10.5% (11)
27.6% (29)
6.7% (7)
20% (21)
3.8% (4)
105
Working with people all day long requires a great deal of effort
11.3% (12)
23.6% (25)
11.3% (12)
26.4% (28)
5.7% (6)
16.0% (17)
5.7% (6)
106
I feel like my work is breaking me down
20.0% (21)
39.0% (41)
9.6% (10)
18.1% (19)
1.9% (2)
9.6% (10)
1.9% (2)
105
I feel frustrated by my work
16.2% (17)
33.3% (35)
10.5% (11)
21.9% (23)
5.7% (6)
10.5% (11)
1.9% (2)
105
I feel I work too hard at my job
12.4% (13)
21.0% (22)
8.6% (9)
25.7% (27)
5.7% (6)
17.1% (18)
9.5% (10)
105
It stresses me too much to work in direct contact with people
46.2% (49)
28.3% (30)
9.4% (10)
7.5% (8)
0.9% (1)
4.7% (5)
2.8% (3)
106
I feel like I’m at the end of my tether
42.9% (45)
33.3% (35)
4.8% (5)
6.7% (7)
2.9% (3)
7.6% (8)
1.9% (2)
105
I feel I deal with my team/colleagues impersonally, as if they are objects
70.8% (75)
19.8% (21)
4.6% (5)
2.8% (3)
0.9% (1)
0.0% (0)
0.9% (1)
106
I feel tired when I get up in the morning and have to face another day at work
15.1% (16)
36.8% (39)
13.2% (14)
11.3% (12)
1.9% (2)
17.0% (18)
4.6% (5)
106
I have the impression that my team/colleagues make me responsible for some of their problems
41.0% (43)
21.9% (23)
10.5% (11)
20% (21)
0.0% (0)
4.8% (5)
1.9% (2)
105
I am at the end of my patience at the end of my work day
31.7% (33)
36.5% (38)
5.8% (6)
11.5% (12)
3.8% (4)
9.6% (10)
0.9% (1)
104
I really don’t care about what happens to some of my team/colleagues
85.7% (90)
6.7% (7)
1.9% (2)
1.9% (2)
1.9% (2)
0.9% (1)
0.9% (1)
105
I have become more insensitive to people in the workplace
67.0% (71)
22.4% (24)
2.8% (3)
3.8% (4)
0.9% (1)
2.8% (3)
0.0% (0)
106
I’m afraid that this job is making me uncaring
62.3% (66)
25.5% (27)
2.8% (3)
1.9% (2)
3.8% (4)
1.9% (2)
1.9% (2)
106
I accomplish many worthwhile things in this job
2.9% (3)
8.6% (9)
6.7% (7)
15.2% (16)
6.7% (7)
25.7% (27)
34.3% (36)
105
I feel full of energy
4.7% (5)
6.6% (7)
8.5% (9)
20.8% (22)
8.5% (9)
33.0% (35)
17.9% (19)
106
I am easily able to understand what my team/colleagues feel
0.9% (1)
2.8% (3)
3.8% (4)
13.2% (14)
8.5% (9)
34.0% (36)
36.8% (39)
106
I look after my team/colleagues problems very effectively
0.9% (1)
1.9% (2)
5.8% (6)
12.5% (13)
7.7% (8)
44.2% (46)
26.9% (28)
104
In my work, I handle emotional problems very calmly
0.9% (1)
4.8% (5)
1.9% (2)
2.9% (3)
13.3% (14)
31.4% (33)
44.8% (47)
105
Through my work, I feel that I have a positive influence on people
0.9% (1)
4.8% (5)
4.8% (5)
8.6% (9)
9.5% (10)
38.1% (40)
33.3% (35)
105
I am easily able to create a relaxed atmosphere with my team/colleagues
0.9% (1)
3.8% (4)
2.8% (3)
9.4% (10)
11.3% (12)
34.0% (36)
37.7% (40)
106
I feel refreshed when I have been close to my team/colleagues
1.9% (2)
8.5% (9)
3.8% (4)
17.0% (18)
11.3% (12)
34.9% (37)
22.6% (24)
106
In other quantitative questions, all respondents reported that their screen time had increased during the pandemic. A majority reported it to be by more than 2 hours/week, and 71% registered an increase of more than 4 hours/week. Despite this, there appears to be no increase in their home-working that could account for this difference.
The results of the remaining questions reflected a poorer work experience. The strongest evidence was for a feeling that mask wearing had affected rapport with patients. Other more common experiences included poor outcomes for patients during the pandemic, with decreased staffing levels, increased workload, and delayed treatments.
Table 2: Other Question Responses – Quantitative only
Question
Possible responses
n
0-1 hours
1-2 hours
2-3 hours
4-6 hours
6 hours +
During the pandemic, my screen time (e.g. due to meetings and teaching) increased by
4.0% (4)
5.0% (5)
20.0% (20)
37.3% (37)
33.3% (33)
99
Question
Possible responses
n
Yes
No
Were you working from home more often during the pandemic?
48%(48)
52%(52)
100
Question
Possible responses
n
Strongly disagree
Disagree
Neither agree nor disagree
Agree
Strongly agree
I felt that the increase in screen time negatively affected my mood
10.0% (10)
23.0% (23)
35.0% (35)
24.0% (24)
8.0% (8)
100
I felt that the increase in screen time increased my level of exhaustion
14.3% (14)
16.3% (16)
19.4% (19)
39.8% (39)
10.2% (10)
98
I felt that the increase in screen time resulted in depersonalisation of my patients
11.0% (11)
25.0% (25)
33.0% (33)
25.0% (25)
6.0% (6)
100
I felt that the increased screen time hindered the working relationship between colleagues
10.0% (10)
25.0% (25)
20.0% (20)
33.0% (33)
12.0% (12)
100
I felt that the increase in screen time resulted in feelings of burnout
17.0% (17)
26.0% (26)
27.0% (27)
23.0% (23)
7.0% (7)
100
I felt dissatisfied with my online/telephone consultations
8.2% (8)
31.6% (31)
41.8% (41)
13.3% (13)
5.1% (5)
98
I felt that wearing masks affected my rapport with patients
8.1% (8)
17.1% (17)
9.1% (9)
49.5% (49)
16.2% (16)
99
I felt dissatisfied with the patient care provided to patients during the pandemic
7.1% (7)
36.4% (36)
33.3% (33)
21.2% (21)
2.0% (2)
99
I felt that patients did have poorer outcomes during the pandemic
5.1% (5)
27.2% (27)
28.3% (28)
35.4% (35)
4.0% (4)
99
I felt that working from home affected my work-life balance
10.4% (10)
24.0% (23)
42.7% (41)
17.7% (17)
5.2% (5)
96
I felt that working from home resulted in increased work related stressors
12.5% (12)
30.2% (29)
37.5% (36)
18.8% (18)
1% (1)
96
I felt that working from home resulted in more difficulties in my job e.g. communicating with my team or patient
11.5% (11)
29.2% (28)
35.4% (34)
21.9% (21)
2.0% (2)
96
DISCUSSION
Our study provides a snapshot of difficulties encountered by different grades of psychiatrists, while working in a large English county, during the COVID-19 pandemic. We found a burnout rate of 44.2%, which is higher than 36.7% observed by Jovanović et al8 among those working in other countries before the pandemic. Since a higher prevalence is also documented in other recent studies13, it is reasonable to assume that the higher rate of burnout is due to increased work-related stressors during the COVID-19 pandemic. These stressors could be linked to the newly introduced guidelines, which involved social distancing, high staff sickness and redeployment.
In the personal accomplishment subset of our study, highest number of doctors experienced burnout, possibly suggesting a link to the COVID-19 pandemic. Unfortunately, we do not have a pre-COVID pandemic survey for the sake of comparison, which could have confirmed causality with greater certainty.
71% of our cohort reported an increase of more than 4 hours of computer screen time a week, which was not due to increased amount of working from home. Various factors could explain this finding including the introduction of remote medical consultations, online multidisciplinary team meetings and teaching/training. Virtual consultations may provide an alternative to face-to-face assessments, but complications such as difficulty in discussing sensitive topics and demonstrating empathy could influence therapeutic relationship, medical errors, and screen fatigue resulting in increased levels of burnout14, 15.
A compromised professional identity and reduced job satisfaction are considered among significant predictors of job burnout16, 17. It is, therefore, reasonable to question whether the increased screen time and reduced patient contact could have impacted the professional identity of our cohort and their job satisfaction. This could also provide possible explanation for our cohort scoring highly for low personal accomplishment. However, one study that examined burnout in medical residents, who had used virtual telemedicine to replace outpatient clinics, found that the burnout actually decreased with increased use of virtual consultations18. Therefore, more consideration and research needs to be conducted on telemedicine practices in different medical subspecialties and their impact on medical professionals’ working lives.
Burnout is associated with an increase in clinical errors and may manifest in irritability, fatigue, and reduced cognitive functioning that ultimately result in a reduction in quality of patient care12,19. Medical errors on the other hand cost the National Health Service (NHS) £3.3 billion in litigation costs and additional bed days due to both systemic and individual factors20. Overall, 41% of our cohort were dissatisfied with remote consultations and the care provided to their patients during the pandemic. The reported difficulties with providing good patient care primarily consisted of poorer quality of and reduced patient interaction, patients being unable to engage with services and delayed treatments.
Wearing face masks could affect both verbal and non-verbal communication that in turn hinder the therapeutic relationship, as previous research has shown that patient engagement, understanding and treatment success are influenced by a clinician’s facial expressions21. Poorer patient outcomes found in our study could partly be due to the difficulties experienced during the pandemic as approx. 62% of our cohort felt that face masks affected their rapport with patients. Other factors that could have contributed to these poorer outcomes include redeployment of staff due to NHS pressures and reduced services. Further work is, however, needed to ascertain the associated casual pathway.
During the height of pandemic, carrying out frenetic clinical work with limited resources and little respite, coupled with the loss of loved ones and colleagues, could have undoubtedly impacted the mental health of medical workforce including psychiatrists. On the other hand, the pandemic may have also heightened the sense of vocation for some doctors. It is, therefore, difficult to assess the lasting effects of burnout until the pandemic is finally over and we resume normal therapeutic practices, in both clinical and personal settings.
Lung carcinoma the most common malignancy worldwide, presents as a metastatic disease in majority of the cases. The most frequent sites of distant metastases are liver, adrenal glands, bones, and brain. Skeletal muscle metastasis is an unusual presentation of lung adenocarcinoma.
Case report
A fifty three year old male patient, labourer by occupation, beedi smoker for twenty five years, admitted to tertiary care hospital with pain and swelling over left arm, cough and expectoration for the past two months, accompanied with significant weight loss. There was no evidence of chest pain or haemoptysis. On local examination there was hard swelling over extensor compartment of left upper limb with mild tenderness, no loss of sensation and mild restriction of range of movements on flexion at elbow. Respiratory and other systemic examination was within normal results. Plain CT of thorax defined multilobulated lesion in right perihilar location in right middle lobe (Figure 1).
Figure 1: CT of Thorax: Well defined multi-lobulated lesion in right perihilar location in right middle lobe measuring 2.9 x 2.4 cm.
USG of left arm showed an irregular heterogenous soft tissue lesion noted within the triceps muscle with few areas of intra-lesional necrosis, MRI of left arm showed lobulated lesion in posteromedial aspect of mid and distal arm, involving triceps muscle, medial aspect of brachialis, encasing brachial artery, veins and median nerve (Figure 2).
Figure 2: MRI of Left arm: Well defined irregular lobulated enhancing T1 hypo intense, T2 and T2 flair hyperintense lesion in the posteromedial aspect of mid and distal arm.
PET scan showed enhancing nodular soft tissue lesion noted in middle lobe of right lung, 2.9 x 2.4 centimetres. Biopsy revealed metastatic adenocarcinoma. For further studies Immunophenotyping was done which showed negative for EGFR and ALK. Patient was treated with palliative RT, Pem-Carbo f/b Pemtrexed maintenance and recently 3# of Gemcitabine. The patient died of metastasis to brain within eight weeks of diagnosis.
Discussion
Lung carcinoma is a leading cause of cancer-related mortality. The most common sites of distant metastasis in lung carcinoma are brain, bones, the liver, and the adrenal gland1. The most common tumours that cause skeletal muscle metastasis are tumours originating from thyroid, oesophagus, stomach, pancreas, colon, rectum, bladder, breast, ovary, and prostateand skeletal muscle metastasis of lung carcinoma was first reported by Fisher ER2. Willis RA reported four skeletal muscle metastases in their autopsy series composed of 500 lung carcinoma patients3. Skeletal muscle metastasis is a rare occurrence for any tumour with a reported incidence lees than one percent4-5. The most common sites of muscle metastasis are thigh muscles, iliopsoas, and paraspinous muscles6.
The mechanism of skeletal muscle metastasis is unclear. Despite its rich vascular blood supply and a large mass in the body, it is resistant to haematogenous metastases. Organs that are frequently metastasized, including liver, lung, and bone have rich capillary networks and blood supply. As a result of the muscle metabolism, substances such as lactic acid, free oxygen radicals, and low pH in the environment constitute an infertile medium for proliferating tumour cells. In addition, mechanical insults due to contractions, high tissue pressure, and widely alternating blood flow are also against the survival of tumour cells7.
There are several hypotheses proposed for skeletal muscle metastasis in lung carcinoma. The most widely accepted hypothesis is the haematogenous route. In this hypothesis, it is believed that tumour cells are formed through tumour embolism. Some authors suggested that skeletal muscle metastases might originate from abnormal lymph nodes found in the muscle. In a study by Bocchino M et al. 1754 lung carcinoma patients treated between 2007 and 2012 were analyzed and forty six (2.6%) had skeletal muscle metastasis8. Despite the variations between different studies in terms of the association between histological subtypes and skeletal muscle metastasis, forty patients in that study (87%) had non small cell lung carcinoma and six had (13%) small cell lung carcinoma. Among non small cell lung carcinoma patients, twenty four (60%) had adenocarcinoma. The most common initial manifestation of skeletal muscle metastasis is a pain. Pain can be accompanied by extremity swelling. The case presented herein also applied with pain and swelling. Diagnostic methods for skeletal muscle metastasis are not specific. Direct films usually show only soft tissue shadows. MRI usually reveals hypointense signal in T1 and hyperintense signal in T2. MRI is preferred to distinguish soft tissue metastasis from an abscess, sarcoma, and other conditions9, similarly; our patient had hypointense signal on T1 and the hyperintense signal on T2 series. The optimum treatment and prognosis of skeletal muscle metastasis from lung cancer is unclear. Depending on the clinical characteristics, treatment options include observation, surgery, chemotherapy and radiotherapy.
Conclusion
Lung carcinoma with skeletal muscle metastasis should be considered as a potential differential diagnosis in patients presenting with an intramuscular mass.
Acknowledgements
Authors acknowledge the immense co-operation received by the patient and the help received from the scholars whose articles are cited and included in references of this case report. The authors also acknowledge the authors/editors/publishers of all those articles, journals and books from where the literature for this case report has been reviewed and discussed.
Clozapine is an atypical antipsychotic, it is the treatment of choice for treatment resistant schizophrenia and more effective than conventional neuroleptic medications. Clozapine is associated with potentially life-threatening side effects, some of which appear early in treatment.
Myocarditis is an uncommon but serious early adverse event of Clozapine, the majority of reported cases occurring in the first 4-8 weeks.1 Clozapine induced myocarditis (CIM) can present with mild symptoms, but can progress rapidly to fulminant symptoms and thereafter heart failure and death.1 These symptoms and signs typically include dyspnoea, palpitations, chest pain, fatigue, flu-like symptoms, pyrexia and tachycardia.
Case Report
A 21-year-old Caucasian male with a two year diagnosis of schizophrenia and previously inadequate responses to Risperidone and Olanzapine was commenced on Clozapine. The patient had previously tolerated Risperidone and Olanzapine and did not experience adverse events, but there was inadequate therapeutic response to both; hence it was decided to commence Clozapine.
On admission, his physical examination, baseline blood investigations (these did not include cardiac markers such as troponin or C-reactive protein (CRP)) and electrocardiogram (ECG) were normal. His medical history was unremarkable and he did not have a family history of cardiac disease. He smoked 15 cigarettes per day.
A rapid Clozapine titration compared with the standard UK titration[2] was commenced with a target dose of 200 mg/day on day 14. He was not on any other psychotropic medication.
The patient remained asymptomatic in the first 3 days. On day 4, he developed tachycardia (114 BPM). A repeat physical examination and ECG was normal, eventually his heart rate settled to 94 BPM. The tachycardia was deemed to be a benign side effect of Clozapine, and the rate of titration was slowed down as a precaution.
On day 12, the patient reported dizziness when standing and a ‘cold air’ sensation in his chest. Nurses reported that blood pressure was normal with a heart rate of 145 BPM but when reviewed clinically his heart rate was 89 BPM. His titration was continued.
On day 14, the patient complained that his ‘internal organs were hurting’. His Clozapine dose was 125 mg/day at the time. He reported chest tightness with central pain, pain in his legs and abdomen, intermittent breathlessness and palpitations. The duration of his symptoms was 24-36 hours. Examination was normal except for a heart rate of 110 BPM. His ECG showed sinus rhythm with no ST segment or T wave changes. Blood tests showed markedly elevated troponin I—1211.5 ng/L (normal range: <34.3 ng/L), CRP—176 mg/L (normal range: 0-10 mg/L) and eosinophil count —1.28 109/L (normal range: 0.02-0.5 109/L).
The patient was afebrile throughout the titration period.
He was admitted to an acute hospital and a provisional diagnosis of Clozapine induced myocarditis was made. The echocardiogram did not reveal structural abnormalities or damage. An EBV (Epstein Barr Virus) serology was negative. Clozapine was withheld and the patient improved along with the blood markers, after 4-5 days he was discharged back to the psychiatric hospital.
Discussion
CIM is an often overlooked adverse event associated with Clozapine titration. Currently there is no mandatory requirement of laboratory monitoring for detecting myocarditis during Clozapine titration unlike the mandatory requirement for detecting neutropenia, despite roughly similar estimated incidence of the two adverse events at 3%.[3,4]
This case was unusual because of the very early appearance of symptoms, the patient’s age and atypical symptom presentation. Although CIM is an early adverse event, the onset within 2 weeks of initiation was unusual. Literature suggests that myocarditis typically presents within 4-8 weeks.[1] The patient was also younger than the reported median age of patients (30).[1] The symptoms appeared at a low dose of 125mg/day which literature suggests is unusual, although CIM at doses of 50mg/day has been reported.[5]
Tachycardia and fever are common early side-effects of Clozapine. Tachycardia usually settles after 4-6 weeks of treatment[6] and fever typically for 2-3 days.[7] Both symptoms can be suggestive of myocarditis, especially when they co-occur. CIM often presents in a non-fulminant form.[8] As this case demonstrates many patients may not report symptoms when CIM is mild.
Increasing age, concomitant administration of sodium valproate and increased rate of dose titration are significant risk factors for CIM.[9] In this case, the patient was young and sodium valproate was not co-administered. The titration was originally intended to be rapid but slowed down soon after commencement.
Given the clinical difficulties in detecting mild CIM, we suggest that all patients have baseline troponin, CRP, heart rate, blood pressure, temperature, resipatory rate and ECG. If medical history reveals history of heart disease, a baseline echocardiogram can be obtained. If there is history of congestive cardiac failure, then baseline brain natriuretic peptide (BNP) or N-Terminal pro-B-type natriuretic peptide (NTproBNP) should be measured.[10]
In clinically asymptomatic patients, if there is elevated baseline CRP (>100 mg/L), troponin, BNP or NTproBNP then Clozapine titration should not commence and further advice from cardiology should be sought.
Weekly CRP and troponin should be done in the first month of titration and levels repeated once after stable dose of Clozapine is reached. The dose increase should not be rapid.
Tachycardia developed should be checked with reference to the baseline heart rate measured before commencing Clozapine. A heart rate of greater than 120 BPM or increase of more than 20 BPM over the baseline pulse rate should lead to the review of physical health, blood monitoring, ECG, and Clozapine titration rate.
An increase in troponin above upper limits or an increase in CRP should trigger consideration of CIM. Literature suggests that troponin levels greater than 2x the upper normal limit are indicative of acute myocarditis.[9] CRP is raised on average 3 days before any increase in troponin levels is detected.[9] If the troponin levels are within the normal range and the CRP levels are raised but less than 100 mg/L, clozapine titration can continue, but the pace must be slowed. Troponin levels and CRP levels should be monitored daily and the patient should be closely monitored for clinical signs of developing cardiotoxicity.
We do not recommend routine eaosinophil monitoring as the marker in 90% of cases does not exceed normal limits at the onset of CIM and typically peaks 7 days after cessation of Clozapine.[11]
Conclusion
Clozapine induced myocarditis often presents with low level cardiotoxicity. Mild symptoms may be missed; however, progression to fulminant myocarditis can be rapid, with high mortality rates.[1] Myocarditis, including clinically asymptomatic myocarditis remains a risk with Clozapine every time the patient is titrated onto this medication[12]. Close clinical monitoring, high index of suspicion and monitoring of cardiac parameters will help early detection of adverse cardiac events.
There have been continuing initiatives to transform and improve the National Health Service (NHS) in recent years. Mental health services in England have similarly shown evolution with regards to service provision. There has been a shift away from the perceived “medicalisation” of treatment, with traditional long-stay institutions replaced with more targeted and personalised care in the community.1 Furthermore, community services themselves have seen much remodelling over the years including decommissioning and integration, as well as increased involvement in outreach and early intervention teams.2
Mental health services are sometimes perceived as relatively well funded from outside but, as with most healthcare sectors, compared to the population requiring this service, these resources are inadequate to support the growing demand. This has been the case for some time, but it has become more evident with a significant reduction in funding observed since 2010/11.1 In addition, constant governmental pressures to meet key performance targets, as well as unachievable expectations from the public, have further stretched an already resource-depleted mental health service.
The implementation of new National policies3 was supposed to be a shift from large psychiatric hospitals to smaller specialist community centres with a promised reduction in the demand placed on inpatient services. In England, a peak number of 150,000 inpatient psychiatric beds was reported in 1955; this has since rapidly declined to 22,300 in 2012. Between 2010/11 and 2013/14, a further rapid reduction of 7% of all beds available was seen.4
Despite the promise of changes in service delivery within mental health to mitigate the continued reduction in the number of inpatient beds, demand for inpatient beds has not in fact reduced nationally.1 The recommended level of occupancy, for example, is 85% but 119 wards surveyed5 were operating at 91%, with some at 138% level of occupancy. The occupancy levels of over 100% usually occurred when long-stay inpatients were discharged home on short-term leave and their beds got filled during their absence.4 Where numbers of inpatient beds fail to meet the demands, or waiting list for their first assessment or review grows, the inadequacy lends these facilities to issues with regard to providing high quality and safe patient care. Examples of this may include inappropriate use of the Mental Health Act for detention of patients as a means of securing an inpatient bed,5 incomplete assessments of people detained in places of safety due to time or space constraints,6 and an increase in violent incidents on overcrowded inpatient wards.7
What is a Crisis Resolution and Home Treatment Team (CRHTT)?
In the late 1980s and 1990s, community mental health teams provided acute crisis support. This posed a number of issues including that these teams usually operated during normal working hours of 9am-5pm (Monday to Friday) and were not always available to provide support to patients in a crisis, and did not have the desired impact of reducing the number of acute admissions.8 This gap in service provision inspired the experimentation with and subsequent development of intensive home treatment services, some of which showed evidence of reduced hospital admissions, and holistic-working often preferred by families who were happy to have their loved ones receive the required support in the home environment.9 Over the last two decades, with remodelling of services, increased investment, NHS funding rising from £49 billion in 2000 to £122 billion in 2016, and a migration of mental health professionals, CRHTTs were established and are now available in every mental health trust across the United Kingdom (UK).10
CRHTT is a team of mental health professionals including psychiatrists, community psychiatric nurses, social workers and support workers, who provide rapid and intensive support at home during a mental health crisis.11 They are a 24-hour service operating seven days a week, and acting as the “gatekeeper” for acute services accepting referrals from various sources including inpatient, community, liaison and from outside the Trust for providing support to patients experiencing crises. These teams risk-assess patients and determine whether they require inpatient or home treatment. In the latter case, CRHTTs provide intensive home treatment by offering up to 2-3 visits a day as well as 24/7 phone support. These teams are also involved in facilitating early discharges from hospitals; in cases where patients are past the initial acute crisis, but may need further input prior to discharge to community mental health teams for longer term support.8
Definition of diagnosis and second opinion.
A second opinion is defined as “advice from a second expert (such as a doctor/psychiatrist) to make sure advice from the first such expert is correct” whilst diagnosis is defined as “the art or act of identifying a disease from its signs and symptoms”.12 Due to increased pressure on inpatient facilities and remodelling of community services, there has been a huge increase in the number of referrals made to CRHTTs. Between 2011/12 and 2013/14, it has been noted that referrals to CRHTTs increased by 16%.13 Reduction in inpatient beds and high workloads within community services often result in the formulation of arbitrary diagnoses and treatment plans. With increased pressures on other mental health services, the role of CRHTTs has begun to evolve. In addition to the previously discussed functions, CRHTTs appear to be becoming second opinion services by default enabled by the psychiatrists working in these teams.
We organised a project to establish whether a typical CRHTT is fulfilling the criteria of being a diagnostic or second opinion service provider.
Method
We examined 100 consecutively accepted referrals to a CRHTT from 1st December 2016. The patients were divided into three groups: those being discharged/referred from hospital (HR), those referred from the community (CR), and those who were not open to secondary mental health services at the time of referral (NR). The age range and gender of the groups were noted. Thereafter, the NR group was excluded from analysis for the obvious reason that the CRHTT was not providing a second opinion in their case. The HR and CR groups were further reduced by excluding patients who were not seen by a CRHTT psychiatrist. The remaining patients in both groups were scrutinised regarding a change in medication; this was also recorded for the previous and next care occasions. The likelihood of medication change at the next treatment event was analysed to establish whether it was affected by the previous event. The numbers of patients with CRHTT diagnosis change were also recorded for both groups.
Results
Figure 1: Project Flowchart
Figure 2: Group Demographics
n
Patient Gender
Patient Age
Time with CRHTT
Male
Female
Average
Range
1-7 days
> 7 days
No prior referral open (NR)
43
20 (47%)
23 (53%)
36.0
19-60
5 (12%)
38 (88%)
Community referral (CR)
36
13 (36%)
23(64%)
37.8
19-66
7 (19%)
29 (81%)
Hospital referral (HR)
21
10 (48%)
11 (52%)
39.0
19-63
6 (29%)
15 (71%)
There was little difference in age between the three groups (average ages were: CR=37.8, HR=39.0, NR=36.0). There was a lower proportion of men in the CR group than were present in the HR and NR groups (36% as against 48% and 47%). Whether a psychiatrist saw a patient appeared to be related to both the referral source and the length of CRHTT stay. Most (n=16, 76%) patients in the hospital-referred group (HR) were not seen by a psychiatrist while most (n=24, 67%) of those referred from the community (CR) did receive such an outcome. No community-referred patient was seen by a psychiatrist if they were with the CRHTT for less than a week. These short-stay patients accounted for 7 out of the 12 community-referred patients who were not seen. This suggests that a psychiatric assessment should be scheduled more quickly after community referrals so as to offer patients a more comprehensive service.
Psychiatric assessment led to changed diagnoses for 28% (8/29) of patients. This figure was 40% (2/5) for the HR group and 25% (6/24) for the CR group.
Medications were changed for 69% (20/29) of patients seen by a psychiatrist. In the subgroups; 60% (3/5) of HR psychiatric assessments resulted in a change of medication while 71% (17/24) of CR psychiatric assessments led to medication changes.
The chi-square statistic was used to evaluate whether a recent medication change, during the inpatient stay or at the most recent outpatient appointment, made the CRHTT less likely to adjust medication. This indicated that there was no relationship between the two events. A similar analysis indicated that the likelihood of a medication change at the patient’s next community appointment was increased by seeing a CRHTT psychiatrist but unrelated to whether that assessment had resulted in a change of medication.
Discussion
We have demonstrated in this study that a typical CRHTT is providing a diagnostic and second opinion service. Changes in medication were more than twice as frequent as changes in diagnosis – this is perhaps unsurprising as diagnostic changes would be likely to require a different prescription.
Most community referrals were actively evaluated in terms of both diagnosis and treatment. This is a significant change to the original function of the CRHTT where a psychiatric assessment was not a standard aspect of care when very few of the original CRHTTs included a psychiatrist. This may also reflect the current pressures on community teams, which are frequently short-staffed, leading to more competition for the available clinic appointments. Consequently, patients may not have seen a psychiatrist for some time and their requirements may have changed. It is, however, also known1 that community patients who have not been reviewed recently or who have a long wait before their first assessment are more likely to present in crisis.
The diagnostic and second opinion function of the CRHTT is more prevalent when patients have been referred by the community team (67% reviewed, 47% medication changed) rather than on discharge from hospital (24% reviewed, 14% medication changed). This appears to largely reflect the fact that relatively few discharges were seen by the CRHTT psychiatrist because these patients had just received a full consultant-led discharge treatment plan. This may be another example of community service pressures leading to patient crises and thus engagement with alternative services – in this case inpatient care may be offering a second opinion service. The current separation of community and inpatient services will augment this effect as previously the patient would have been more likely to receive continuous care from the same consultant. This is an interesting view of current service configuration. The reduced continuity of care is often seen as a disadvantage but it does present an opportunity for a fresh evaluation of a patient’s diagnosis and medication by a different psychiatrist.
Longer lengths of stay with the CRHTT made psychiatric assessments more likely. It was particularly clear that discharge within a week made a psychiatric review unlikely. The proportion of community-referrals seen by a CRHTT psychiatrist could be increased to 83% if patients were to be seen within 24 hours. This figure is derived from the assumption that psychiatrists would then see the same proportion of both long and short stay patients. The residue would include those patients who refuse to engage with such an appointment.
It is interesting that chi-square statistical analysis suggests that the only influence on prescription change at the next appointment is whether the patient was seen by a CRHTT psychiatrist. It is not related to whether or not the CRHTT psychiatrist changed the medication. It is difficult to see why this should be the case unless the community psychiatrists consider the patients’ needs in more detail or are tempted to regain control after the referral to another psychiatrist.
In conclusion, the addition of psychiatric care to CRHTTs may be a valuable adjunct to the current pressures on community teams. The current trend to separate community, inpatient and CRHTT care is often cited as a disadvantage due to reduced continuity of care for patients. This project has drawn attention to the fact that it also offers opportunities for new teams to re-evaluate both diagnosis and treatment which offers patients the advantage of an internal second-opinion service. This advantage could be offered to more community-referred patients, albeit with more resources, by ensuring that they are assessed by the CRHTT psychiatrist within 24 hours.
Limitations
This is a small study conducted in a single CRHTT. It does, however, offer an indication of the evolving role of the CRHTT and its relationship to other services.
Arrhythmogenic Right Ventricular Dysplasia (ARVD) was first described in a case series of 24 patients back in 1982 1, 2. Since then, our understanding of its pathophysiology has improved dramatically, with dedicated guidelines and literature being published to help with both diagnosis and management. Prompt diagnosis remains a struggle in majority of developing countries, including Malaysia, where resources and expertise are scarce, and obtaining both cardiac magnetic resonance imaging or endomyocardial biopsies remain a challenge. Furthermore, diagnosis is difficult in most cases as clinical presentation may vary and wide range of clinical mimics exist. We present a unique case of ARVD, diagnosed early through the knowledge of having a deceased sibling, whom had endomyocardial tissue characterization performed in the past confirming the presence of the disease in a first degree relative.
Case Report
A 21-year old gentleman presented to the emergency department following an episode of loss of consciousness, lasting approximately 30 minutes which recovered spontaneously. He denies having any similar episodes in the past. However, he had been suffering from reduced exercise tolerance, with a New York Heart Association (NYHA) Class II, over the past 1 year. He had no known medical illness at the time but smoked 6 cigarettes a day for the past 7 years.
His vital signs were stable on arrival, with a heart rate of 73 beats per minute, regular in rhythm, a blood pressure of 143/84 mmHg, respiratory rate of 19 breaths per minute, temperature of 37 degrees Celcius and oxygen saturation of 98% on room air. Cardio-respiratory examination revealed no murmurs, and normal heart and breath sounds. There were no carotid bruits audible. There was no evidence of any neurological deficits on neurological examination.
Figure 2 – Electrocardiogram revealing T-wave inversions in leads V2 to V4 with ventricular ectopic beats
Chest radiography revealed cardiomegaly (Figure 1). Electrocardiogram (ECG) revealed deep T-wave inversions in leads V2 to V4, with ventricular ectopic beats (Figure 2). Due to the suspicious-looking ECG, a serum Troponin-I test was performed, which was elevated at 480 pg/ml. The patient was treated for acute coronary syndrome complicated by cardiac syncope, and was later referred to the medical team for further inpatient management.
However, on further history, it was revealed that the patient had a sibling who had died from an unknown cause, 5 years prior. His younger brother, 14 years of age at the time, was brought in after collapsing whilst playing basketball in a school compound. Unfortunately, he was pronounced dead on arrival to the clinic. A post-mortem was performed due to the unexpected nature of the event. Fortunately, our patient was brought into the same hospital as his sibling, allowing us to trace previous autopsy reports and images, with consent.
Macroscopic examination of the right ventricular cavity revealed epicardial surfaces showing infiltration of excessive fat tissue with nodular fibrosis. The right ventricular cavity appeared dilated and cut sections showed diffuse transmural fibro-fatty replacement of the right ventricular free wall, extending into the endocardium and involving the right ventricular septum (Figure 3a).
Figure 3a – Macroscopic examination of right ventricular cavity, which was dilated and showing signs of transmural fibrofatty infiltration. Figure 3b – Histological evidence of focal lymphocytic infiltration, myocyte hypertrophy and degenerative cytoplasmic changes.
Histology revealed extensive fatty infiltration with interstitial fibrosis, primarily in the epicardium. There was associated myocyte loss with hypertrophy of cardiac muscle cells remaining (Figure 3b). Both macroscopic and microscopic findings were suggestive of ARVD.
After learning of the autopsy results, changes in clinical management took place, with priorities being shifted towards obtaining an echocardiogram, cardiac Magnetic Resonance Imaging (MRI) and Holter recording, as opposed to diagnostic angiography and coronary evaluation. Echocardiography revealed an ejection fraction of 25 to 30%, with evidence of left ventricular dyssynchrony, a tethered posterior mitral valve leaflet with mild eccentric regurgitation, consistent with dilated cardiomyopathy.
Cardiac MRI revealed both left and right ventricular dilatation, end diastolic dimensions being 5.8 cm and 4.4 cm and end-diastolic volume being 153 ml/m2 and 149 ml/m2 respectively, with evidence of bi-ventricular dyssynchrony. Left ventricular and right ventricular ejection fraction measured 31% and 8% respectively. There was also bilateral atrial dilatation. Gadolinium study revealed late enhancement in areas of the right ventricular wall (Figure 4).
Figure 4 – Four-chamber view of cardiac magnetic resonance imaging revealing evidence of right ventricular enhancement following gadolinium study.
A 24-hours Holter recording revealed up to significant ventricular ectopic burden, many of which were bigeminy and trigeminy in nature. In view of symptoms and the above investigative findings, the patient consented to insertion of an implantable cardiac defibrillator (ICD) 4 weeks later in our centre, and has since recovered well with regular monitoring.
Discussion
ARVD is rare, prevalence ranging between 1 in 2000 to 1 in 5000 (taking into consideration geographical variations) and accounts for 5% of deaths in young adults and 25% of deaths in athletes 3, 4. Typical histopathological feature of ARVD is the loss of right ventricular myocardium, replaced heavily by fibro-fatty tissue. Less commonly, left ventricle involvement have been reported 5, 6. Consequence from such pathological process leads to arrhythmias, heart failure and more importantly sudden cardiac death (SCD), with mortality rate ranging between 4 to 20% and peaking in the fourth decade, equally in both males and females 5.
Diagnosis is difficult in most cases as clinical presentation may vary and wide range of clinical mimic exist, including myocarditis, sarcoidosis, Brugada syndrome, idiopathic RV outflow tract VT and congenital heart diseases with right chambers overload amongst others 6. A Diagnostic Criteria was developed in 1994, with further modification in 2010 to assist in the diagnosis of ARVD and although the criterion has been shown to be specific, it lacks sensitivity 7. Nevertheless, it highlights several key areas, a mix of clinical, radiological, histological and electrophysiological features, that assist in diagnosis 4.
Despite not having any further evaluation or investigations performed at the time of presentation, in view of circumstances, our patient’s deceased sibling had supportive histological features. Therefore, our patient met the major criteria of having a first degree relative affected by the disease. More importantly, the suspicious family history had prompted further evaluation for the disease, allowing the medical team to prioritize investigations performed, specifically the Cardiac MRI and Holter evaluation. This led to early risk stratification and decision to implant an ICD for the patient, as he was deemed at high risk of SCD.
Conclusion
This case highlights the importance of good history taking, including a detailed family history of SCD or cardiac-related diseases, especially in young patients presenting with typical cardiac-related symptoms. Early identification and appreciation of risk will subsequently affect the outcomes of such patients affected by ARVD. Furthermore, important diagnosis like ARVD will have implications to relatives and future off-springs, further highlighting the need for detailed evaluation of patients similar to ours described in the above case report.
In a contemporary medical practice caring for complex patients with utmost efficiency, primary care physicians and specialists are expected to work together to organize a seamless transfer from acute to chronic care. The job of the generalist is to sort out and integrate different recommendations from numerous specialists and apply those strategies in the care of the patient long after the index admission. During such interactions with specialists, primary care physicians often realize the impact of differing viewpoints on the overall patient care well beyond the anticipated time frame, whether acute or chronic. To that end, and to better inform such recommendations, this paper proposes the top 10 things primary care physicians wish every specialist knew when addressing problems on the busy hospital ward.
1. Organ-systems work together, not independently
As we see in examples such as the cardio-renal syndrome, hepato-renal syndrome, or hepato-pulmonary syndrome, as the patient gets sicker, the interaction of organ-systems begins to dominate. Indeed, predicting the outcome in comorbid conditions depends not only on understanding the culprit organ, but rather quantifying a complicated interaction of multiple organ-systems. For example, the ADHERE registry algorithm shows the most important predictor for in-hospital death in heart failure patients is not the cardiac function per se, but rather creatinine clearance and BUN[1]. In other words, the commonly used comments from a specialist asked to evaluate their system of expertise, ‘such and such organ is fine’, might soon become irrelevant and obsolete in the context of multiple complex systems.
Moreover, recent research revealed that genotype, endotype and phenotype are quite different in COPD and asthma[2]. Therefore, even though a disease may manifest in a single system, the pathophysiological process from which it arose may have been triggered in different organs.
2. Mortality is not the only outcome measure
Specialists seem to treat all-cause mortality as the most important outcome measure in most cases. Or, they choose strategies based on organ specific survival as an alternative, such as MACE (major adverse cardiac events) or creatinine-doubling time[3]. Life is far more than just being alive. Subsequently, the quality of life (QOL) measures, which capture patient-centred outcomes, provide insight into the effectiveness of interventions but also their meaningfulness to patients, and such measures are gauging previously uncaptured positive aspects of interventions[4]. The difficulty of defining well-being remains a challenge for researchers and arises from the differences brought about by cultural and societal elements which are context-bound and unique to each community.
3. ADL is one of the most critical prognostic indicators
New biological markers are numerous around here - new renal injury markers, such as NGAL or KIM, to name a few. But a quick, old-fashioned, bedside assessment can easily reveal impairments in Activities of Daily Living (ADL) at each patient visit; and ADLs by Functional Assessment Measures have been consistently shown as strong outcome predictors in acute and chronic illnesses, especially within elderly populations[5]. In fact, functional measures were deemed to be as important as other objective measures in some prognoses[6]; for instance, in the BODE score for COPD survival prediction, the ADL measure carries the same weight as the PFT (Pulmonary Function Test). In the management of elderly patients, hospitalization[7] and initiation of haemodialysis[8] significantly influence the worsening of ADLs. In the development of a 1-year mortality index after hospital admissions among elderly patients, ADL was of pivotal importance[9].
Functional impairment is also a strong indicator for readmission: there is a dose-response correlation of severity of impairment and the risk of readmissions[10]. Intensifying the in-hospital post-ICU physical and nutritional therapy has been shown to improve many aspects of recovery[11]. In patients with numerous chronic illnesses, the number of comorbidities strongly correlates with the decline of ADL[12]. Interventions to maintain pre-hospitalization ADL is important in facilitating recovery from hospitalization, and in one study in-hospital mobility programs helped patients to maintain pre-hospitalization ADL while the usual care group experienced significant decline[13].
4. Effectiveness, not efficacy, matters most in the real-world
“Doctor, I cannot afford the medicine prescribed to me when I was discharged!” This is oft-repeated in offices of generalist physicians. If a patient cannot afford medication and therefore does not take it, the treatment lacks efficacy. In the inpatient setting, efficacy of intervention determines the outcome since patients are most likely to receive the prescribed intervention. This is not the case in the outpatient setting, and the effectiveness of an intervention depends on many other elements, such as the accuracy of diagnosis, patient compliance to the proven intervention, prescription drug coverage, access to care, and finally, efficacy of the intervention[14].
5. Mental wellness is essential to physical wellness
Health is not limited to the physical body; it also involves mental wellness. In fact, mental and physical health are inseparable. Naturally, serious illnesses affect mood and cognition: therefore, it is important to acknowledge that mental health issues lie squarely within the spectrum of physical disease management. Generalists can help patients with multiple comorbidities manage depressive symptoms through brief psychological interventions; such symptoms related to cognition and mood are expected consequences of any serious illnesses.
Studies have shown that among elderly patients without dementia at baseline, noncritical hospitalization is associated with the development of cognitive dysfunction[15]. Among elderly patients, the prevalence of cognitive dysfunction is significantly higher in ADHF (acute decompensated heart failure) admissions[16] or survivors of severe sepsis[17]. Depression and depressed mood are prevalent in patients suffering serious illnesses[18]. New models are emerging to integrate psychotherapy in multiple comorbid patients and have been proven to be effective[19].
6. Pay heed to illness trajectory
“My grandma has never been the same after her hip surgery. Please fix her!”
Primary care physicians often note a decline in the general function and cognition of their patients after index admissions to the hospital. As noted earlier, acute hospital admissions have a strong independent effect on the severity of disability amongst elderly persons[20]. The multidimensional frailty score, which incorporates ADL and cognitive function, predicts one-year mortality based on a simple scoring system[21]. Poor functional status attributes to frailty and has led to poor surgical outcomes in the elderly[22]. The prevalence of functional impairment steadily increases from 28% in the 2 years prior to death to 56% in the last month of life[23]. Studies demonstrate that gait speed is an important predictor for survival amongst the elderly[24][25] as well as grip strength[26][27].
Furthermore, elderly patients sustain significant impairments long after the index hospitalization[28]. Amongst elderly patients discharged from the ICU, more than 50% die within a month[29]. At one-year follow-up, critical ADL capacity, such as taking medications or shopping, was impaired in more than 70% of ICU survivors who remained ventilated for longer than 48 hours[30]. Delirium sustains a long-lasting effect even after patients are discharged from the hospital, the longer the duration of delirium, the more sustained is the cognitive impairment[31].
7. Care for the care-givers
There is increasing evidence that caregivers sustain long lasting effects from patient illnesses. Depressive symptoms increase overall for surviving spouses regardless of hospice use[32]. The RECOVER study[33] demonstrated that caregivers suffered from high levels of depressive symptoms up to 1 year after a loved one’s ICU admission. In the era of chronic illnesses, it is essential to be mindful of the contributions made by caregivers in disease management. Tools are widely available for the clinician to assess caregiver burden[34]. This is important because family-support interventions have been shown to improve the quality of communication and decrease the patient’s length of stay in ICU[35].
8. ‘Exercise and diet’ trumps ‘medicine and surgery’
The COURAGE trial demonstrated that after 7 years, there is no difference between medical management and percutaneous intervention (PCI) in managing coronary disease[36]. As time progresses after the initial event, the benefits of surgical intervention become less apparent. Similarly, in the long run, intensive statin therapy has not proven to be of greater clinical significance compared to those receiving moderate levels of statin[37]. As the saying goes, in the long run, “we are what we eat.” Innumerable studies have shown that diet and physical habits have a lasting effect on the health of individuals[38]. Bariatric surgery has been demonstrating dramatic and long-lasting effects on diabetes control, while the DiRECT study demonstrated that intensive exercise and diet successfully achieved remission in nearly half of the intervention group, compared to only 4% of controls[39]. Despite the substantial increase in chronic illnesses that are closely tied to our lifestyle and eating habits, physicians of all specialties are poorly trained to provide nutritional counselling to patients[40].
9. Whose definition of health matters?
If health is defined, as defined by the WHO, is not simply the lack of illness, but “a state of complete physical, mental and social well-being,” it must incorporate many other elements dictated by societal, cultural, moral and philosophical norms and values. Furthermore, the definition of health and the path to attain it should come from the society and community it reflects, since neither healthcare personnel nor the healthcare industry own health. Therefore, the definition should emerge from community interventions and multidisciplinary groups filled with varied stakeholders, rather than from the ivory tower of healthcare researchers. Therefore, medical decision-making processes are rapidly moving away from the paternalistic approach to consensus-based, collegial decisions. Shared decision-making, informed consent, discussions of different treatment options and acquiring second opinions have become standard practice and reflect the empowerment of patients, and communities, to define their own healthcare. Ultimately, as long as patients are competent, they decide their treatment after consulting with physicians, who advocate for the patients’ goals in care and advise them accordingly.
10. Empower healthcare recipients
In the long-term management of chronic illness, participation of the patient is essential. And transparent communication is pivotal for better participation and shared decision-making[41]. In the new model of health, healthcare providers must play an active role in advocating for patients and promoting well-being while acknowledging that health is a dynamic concept[42]; these physicians do not simply “coordinate care.” This shift from the physician-centred to the patient-centred approach, in and of itself, will be empowering for patients.
CONCLUSION
Transition of care is one of the most important steps connecting hospital care to primary care. Those problems currently labelled as miscommunication might be more than just a lack of handoff tools or timely messaging; they rather stem from a difference in priorities and varied interpretations of patients’ problems by these two groups of providers. Many questions remain unanswered when facing the future of collaborative healthcare: what kind of doctors are most suited to address the complex interaction of illnesses involving multiple organs? Who can develop a new framework to capture this dynamic and complex interaction of systems, covering many organs in a single patient? Moreover, the next generation of healthcare providers will need to be trained to bear in mind this fundamental concept of patient management. As the twenty-first century progresses, discoveries within medical science will continue to advance the field further away from the current organ-based specialization to pathophysiology-based specialization. This article advances the discussion on the altering role of generalist physicians and the advice of their specialist colleagues, as together they face more and more changes within the practice of medicine.
Sjögren’s syndrome (SS) is an autoimmune exocrinopathy characterised by a lymphoplasmacytic infiltration of the exocrine glands. Both xerophthalmia and xerostomia are the most common manifestations of the disease. However serious organ damage such as, pulmonary and neurological involvement, can occur. The prevalence of neurological manifestations of SS varies between 0% and 70% (average 20%), which is largely dominated by peripheral neuropathies¹. The cranial nerve involvement, especially when it is isolated, represents a rare facet of the peripheral neuropathy.
Observation
We report the case of a 62-year-old patient with no medical history, referred to the internal medicine department with a 6 years history of dry mouth and xerophthalmia. No other complaints were reported.
The mouth examination showed a fissured, smooth and left deviated tongue without evidence of atrophy or fasciculation (figure 1). The rest of the oropharyngeal examination was unremarkable with no angina or cervical lymphadenopathy. Neurological examination confirmed a deficit of the right XII cranial nerve and excluded other cranial nerve involvements, sensibility or motility deficit. A specialised ophthalmologic examination was performed and showed a bilateral superficial punctuate keratitis.
The search for antinuclear antibodies by indirect immunofluorescence was positive at the titre of 1/1280 (speckled) corresponding to Anti-SSA and Anti-SSB antibodies. Cryoglobulinemia search was negative.
The rest of the laboratory investigations (blood cell count, liver and renal function tests, thyroid balance and inflammation markers) were normal.
A labial salivary gland biopsy was performed and its histological examination showed a lymphoid cell cluster of more than 50 cells/ 4 mm² corresponding to a focus score 1.
Brain MRI was normal - no damage in the brain stem was seen. Electromyography was normal.
The diagnosis of SS was made according to the presence of five out of six criteria according to the European American study group. The diagnosis of primary SS was retained due to the lack of clinical or biological argues for an associated autoimmune disease. A symptomatic treatment of Sicca syndrome was prescribed but no specific therapy has been initiated for the hypoglossal nerve attempt because of its asymptomatic nature.
Discussion
In the case of our patient, the tongue deviation was discovered at physical examination and was totally asymptomatic. In other cases, the twelfth nerve palsy could be responsible for swallowing difficulties, and in advanced stages for a lingual or hemi lingual amyotrophy. The spectrum of its aetiologies is numerous. In a large case series of 100 patients, malignant tumors (about half of cases), neurological causes (16 %) and post-traumatic palsy (12% of cases) were the three most popular aetiologies². Other conditions could be associated with twelfth nerve palsy, such as, infections², vascular injury³ and non-invasive oxygen therapy⁴. Paroxysmal idiopathic hypoglossal nerve palsy has also been described⁵. Our patient had Sicca syndrome which was related to SS according to 5 criteria of the European American study group: it was a subjective sensation of dry mouth and dry eyes associated to a bilateral punctuated keratitis, a focus score > 1 at the histological examination of the salivary gland biopsy and positive anti-SSA and anti-SSB⁶.
SS is an autoimmune disease that often presents as dry eyes and dry mouth due to lacrimal and salivary gland involvement. It can be primitive or associated to other autoimmune diseases such as, Hashimoto’s Thyroiditis, Rheumatoid Arthritis or Systemic Lupus Erythematosus. Wide varieties of neurological complications are characteristic features of SS which occurs most frequently in the primary form. Peripheral neuropathy is the most frequent neurological manifestation. Its most common presentation is a symmetrical sensorimotor or pure sensory neuropathy of hands and feet. Sensitive neuropathy, small fiber neuropathy, multiple mononeuropathy and polyradiculoneuropathy have also been described¹. Cranial nerve involvement is rare. In a review of the literature, Colaci M found 267 patients suffering from SS with different types of cranial neuritis during their clinical history. The discovery of cranial neuritis was contemporary to SS diagnosis in 40% of the patients, as in the case of our patient.
Optic neuritis and trigeminal nerve injury were the most frequent attempts and represent respectively 46.4% and 38% of all cranial nerve palsies. All cranial nerves palsies have been described except the eleventh⁷. Involvement of the twelfth cranial nerve is very rare and only two cases have been described⁸′ ⁹. In these two cases, it was associated with an involvement of other cranial nerves (table 1). To the best of our knowledge, this is the first report of an isolated and permanent involvement of the twelfth cranial nerve in a patient with primary SS. Many mechanisms were proposed to explain the cranial nerve involvement in SS. Clinicopathological observations of Mori K⁸ suggest that an isolated trigeminal nerve attempt could be explained by an immune-mediated neuron death in the sensory gasser ganglion. Whereas, other cranial nerve involvements which are frequently associated together could be explained by a multiple mononeuropathy resulting from a vasculitis⁸.
Further clinical observations will be necessary to determine the exact mechanisms of such neurological involvement.
Table 1: Review of the literature regarding SS patients with hypoglossal nerve injury
Number of patients
Age
Nerves
involved
Treatment
Evolution
Mori/2005 [8]
1
No data
V, VII, IX, X, XII
No data
Paroxysmal
Ashraf/2009 [9]
1
47
V–IX–XII
No data
Paroxysmal
Our patient
1
62
XII
None
Permanent
Figure 1: Smooth and left deviated tongue
Conclusion
In front of cranial nerves neuritis, we should actively search for sicca syndrome, sometimes not spontaneously reported by patients. Examination of the mouth can be instructive and should not be omitted in the diagnosis and monitoring of Sjögren’s syndrome.
In the UK, all newly graduated doctors spend their first two years of work rotating between different specialities, usually spending four months in each placement, before applying for speciality training. This period is called the Foundation Programme.
In January 2016, the Royal College of Psychiatrists published its first ever strategy on Broadening the Foundation Programme to address the need to improve the psychiatric training experience for foundation doctors. The strategy’s aim is to “ensure the delivery of a high-quality training experience in all psychiatry foundation placements”.1
Over the last few years, the number of Foundation training posts in psychiatry in England and Wales has significantly increased. Health Education England aims that all Foundation doctors should rotate through a community or an integrated placement (psychiatry is considered as a community placement) from August 2017.2
As such, the College highlights the need to provide a supervised and well-structured psychiatric training experience for Foundation doctors. This aims not only to improve recruitment into psychiatry but also to ensure doctors have a good working knowledge and understanding of psychiatry and psychiatric services, no matter what career they pursue.
Mentoring provides an additional support and therefore can be helpful to improve the placement of Foundation doctors in psychiatry.
We implemented an ambitious mentoring scheme in Norfolk and Suffolk NHS Foundation Trust (the seventh largest mental health trust in the UK). The paper describes its essential component together with a brief review of the literature on mentoring in clinical settings, focusing on Foundation placements.
Why is mentoring is needed for Foundation doctors in psychiatry?
The literature on mentoring for medical professionals draws attention to the idea that it is beneficial to all doctors at all stages of their career to experience mentoring in some form or another. However, mentoring is of particular importance to doctors moving to a new job or organisation 3, thus making it highly relevant to Foundation trainees.
For newcomers, most of the mentoring support will focus on helping them settle into their new role, becoming familiar with, and developing an understanding of the expectations of their employers.4
Evidence shows that the quality of care in any organisation can be improved when clinical leaders support time for activities such as reflection, coaching and mentoring 5.
Most Foundation doctors will lack experience in psychiatry and will need a substantial amount of guidance from their supervisors and their teams.6 Research has shown that the transition from student to doctor is a difficult one and can be associated with significant levels of emotional stress.7
Foundation doctors find psychiatric assessments physically and emotionally challenging. They feel they lack the specialist knowledge and skills to deal with complex patients, especially concerning self-harm, personality and eating disorders. Dealing with such complex diagnostic categories requires knowledge, skill, understanding as well as physical and emotional robustness. Due to the relative lack of focus on such topics in most undergraduate medical training, a comprehensive support in psychiatric placements is essential.
Psychiatry is very different from other specialities in the way services are configured and delivered: junior doctors may face isolation as psychiatric units are typically spread across a wide geographical area and often lack a centralised meeting place for junior doctors (e.g. a doctors’ mess). In addition, they may find themselves the lone practitioner when on call, which can be daunting for many.
Clinical and Educational supervision is provided to Foundation doctors in similar ways to other rotations. However, the consultants delivering this essential support often focus only on clinical issues related to knowledge and skills. Furthermore, it is easy to see that the best guides to new trainees regarding the idiosyncrasies of the speciality and its services are likely to be trainees who have spent some time in those services and are more able to detect the specific stresses new doctors may experience and may find difficult to articulate.
Furthermore, mentoring fosters a productive peer-to-peer relationship. The learning needs of the Foundation doctor can be considered alongside their personal and professional interests and lifestyle. Questions can be posed in a non-judgmental forum, without fear of being ridiculed or condemned. The fundamentals of on-call systems, clinical cases and management options can all be considered at a level appropriate to their junior grade. Tips for examination success and information about essential courses and core texts can be shared. Job choices and research opportunities can be discussed. Day to day difficulties and mismatches between expectation and reality can be identified and possibly overcome. Where this is not possible next steps can be identified, and clinical and educational supervisors can be drawn in for higher level support. The benefits of the scheme are broad.
Finally, although mentoring is different from role-modelling (teaching by example and learning by imitation), it has been shown toserve some of the same aims of role-modelling, including enhancing problem-solving abilities of the mentee, improving professional attitudes, showing responsibility and integrity, and supporting career development. 8
What is mentoring?
Mentoring can mean different things to different people. There are various definitions which can create confusion between mentoring and other formal structures of support such as supervision, coaching, consultation, befriending or friend systems and even counselling. However, mentoring is none of the above but at the same time a combination of them.
The Standing Committee on Postgraduate Medical and Dental Education (UK) defined mentoring as ‘The process whereby an experienced, highly regarded, empathetic individual (the mentor) guides another individual (the mentee) in the development and re-examination of their ideas, learning, and personal and professional development”.9
The term “mentoring” takes us back to Greek mythology: Mentor was a person: he was the friend of Odysseus who was asked to look after Odysseus’ son Telemachus when Odysseus was fighting in the Trojan Wars. The name Mentor was later used to describe a trusted person, a supporter, or a counsellor.10
Mentoring as a professional developmental tool became popular in the private sector organisations in the USA during the 1970s and was introduced to the area of health during the 1990s 11. Since then, it has been widely used in various organisations.
Aims of mentoring
Mentoring has the advantage of being a flexible supporting tool, unlike other structured processes (e.g., clinical supervision or coaching) where the goals are set clearly from the start of the relationship between the supervisor and supervisee. The aims of mentorship are summarised in Table 1.
Table 1- Aims of mentorship
Help the mentees take the lead in managing their career and its development.
Provide support to discuss personal issues in a confidential and secure environment
Improve both the individual and the team performance
Types of mentoring
Buddeberg-Fischer and Herta 11 discussed various types of mentoring based on the numbers of mentors and mentees and their professional status or grade:
One to one mentoring (between a mentor and a mentee).
Group mentoring (one mentor and a small group of mentees)
Multiple-mentor experience model (more than one mentor assigned to a group of mentees).
Peer-mentoring (the mentor and mentee are equal in experience and grade): This mentoring is used mainly for personal development and improving interpersonal relationships. Mentor and mentee roles can be reversed. Also, called ‘co-mentoring’.
Distance or e-mentoring is becoming more popular, and it has the advantages of being “fast, focused, and typically centred on developmental needs”. 12
Structured vs. flexible mentoring
Evidence suggests that providing mentorship through a rigid and structured process can be counterproductive. 13 Mentors and mentees usually work in different locations, making it difficult for both to have a set of pre-planned meetings and topics for discussions.
Another advantage of the flexibility of mentoring is that it does not follow a “tick box” exercise but encourages informal discussions and exploration of whatever comes to mind during meetings. Doubtless, having some structure to the overall mentoring process is important as it ensures that the mentoring session doesn’t become an informal befriending or friend support system. Table 2 sets out the main benefits of mentoring.
Benefits to the organisations
Benefits to the mentee
Benefits to the mentor
Improve job satisfaction leading to improved performance, recruitment, and retention of employees
Enable early recognition and resolution of issues that face employees
Provide a valuable source of feedback that the organisations can use to improve working conditions
Ensure that the mentee has clear aims and objectives (development outcomes) at the start of their mentorship. These goals may include improving knowledge, performance and preparation for exams and interviews
Empowers the mentee to explore and pursue their career aims
Incorporates the mentee into a wider professional network and prevents isolation
Supports the mentee to use reflective practice and improve their self-awareness
Reducing stress and burnout
Formal recognition of informal practice within the profession
Structured program with support and supervision to the mentor
Development of knowledge and skills in management and supervision
Satisfaction of helping others and passing on their knowledge
Table 2-Benefits of mentoring. Developed from Mentoring – Chartered Institute of Personnel and Development (CIPD) Factsheet. Revised February 2009 14. Available from: https://www.shef.ac.uk/polopoly_fs/1.110468!/file/cipd_mentoring_factsheet.pdf
Are there any Disadvantages of mentoring?
There is extensive literature on the benefits of mentoring, but is there any harm associated with it?
As with any intervention, it does carry some potentially adverse effects. Mentoring can be perceived to “infantilise” junior employees rather than empowering them 10. This perception is probably more common among employees who see themselves as senior or very competent and think of themselves as able to adapt to change very quickly.
Mentoring might hinder creativity in new employees and inhibit them from thinking “outside the box” as it might re-enforce the message that ‘this is how we do things here’. 10
Clashes of personalities or other interpersonal factors could lead to a troubled mentor-mentee relationship and cause distress to both parties. Hence, plans must be put in place in any formal mentoring scheme to ensure an amicable ending to this relationship. Multiple mentor allocation mentioned earlier could also prevent such interpersonal problems and help to tackle them early on.
Furthermore, some mentees may feel uncomfortable with the influence or authority of the mentor, and this may hinder the progress of the mentoring relationship. 13 This is particularly relevant when the mentor is also involved in the formal assessment of the performance of the mentee (e.g. being the line manager or supervisor) or when a mentee who lacks self-confidence is paired with an overconfident mentor.
Good mentors avoid common pitfalls in the mentoring process, such as a patronising attitude, breaches of confidentiality and offering direct advice to the mentees. Instead, they encourage the mentee to reflect and come up with their answers. 15
Finally, mentoring can be perceived as an additional demand on doctors during their training, and some may feel that they are forced to provide it or receive it during placement. However, it must be remembered that mentoring should always be voluntary and flexible to meet the individual’s needs and not an additional ‘box to tick’ or a portfolio enrichment exercise.
The Mentoring Scheme for Foundation Doctors in Psychiatry Norfolk:
The scheme started in December 2015 and initially ran as a pilot in Norfolk with the support of all stakeholders. The mentoring scheme coordinator (YH) contacted twelve Foundation doctors by email, welcoming them to the Trust and inviting them to participate. The welcome email contained information about mentoring, including the benefits it may offer.
The voluntary nature of this scheme was highlighted so that the doctors didn’t feel they were being pressured to be enrolled.
Of the 12 doctors invited, five took up this opportunity. Uptake has remained constant over the consequent cohorts of Foundation doctors for many reasons. Those deciding not to enrol in this scheme explained that they felt happy with the support provided by their clinical supervisors. However, some doctors asked for a mentor halfway through their placement when they felt that they needed additional support. In these instances, a mentor was allocated to them as soon as possible.
Mentors were core and higher trainees already involved in supporting more junior psychiatric trainees through informal mentoring. Their experience meant there was no need for formal training. However, reading material was circulated to them to highlight the roles and responsibilities of mentors and what to do if any problem arose during mentoring. Monthly mentors’ meetings were very helpful to discuss issues arising in mentoring and offer peer to peer support.
Also, there were regular meetings and discussions between the mentoring coordinator, the Director of Medical Education, and Medical Director of the Trust to resolve any issues facing the Foundation doctors and provide feedback to improve the Psychiatric placement.
During the first meeting, the mentors and mentees agreed on the aims of mentoring drawing up a list of objectives that the Foundation doctor would like to achieve by the end of the placement. Following this initial meeting, there should have been once monthly face to face meetings throughout the placement. The mentor and mentee agreed on the most convenient means of communication (e.g. using text messages, emails, etc.) outside scheduled meetings.
All mentors kept a record of the mentoring meetings, with the mentoring coordinator informed about these meetings. Issues discussed were confidential and not shared with the coordinator or supervisors unless the mentee gave specific consent.
At the end of the mentoring scheme, the coordinator collected feedback from mentees and mentors using a structured questionnaire that was designed by the coordinator using SurveyMonkey® website. The feedback highlighted the positive aspects of mentoring as well as areas for improvement.
End of mentoring survey
Mentors reported that acting as a mentor without being involved in clinical supervision allowed them to offer objective advice and support in a way that would have been harder if they were directly involved in the workplace. One Foundation doctor experienced bullying from another member of the team who was a locum doctor. The mentor supported the Foundation doctor, and the issue was addressed and resolved promptly. There was a significant risk that they would have been left isolated and unsupported during this time if the mentor scheme had not been in place.
The topics discussed were varied, and this suggested that mentoring was not limited to a aspect of the job (see Table 3)
Table 3- Topics discussed in mentoring meetings
General guidance about the job
Assistance on completing competencies on e-portfolio
Advice regarding personal health, bullying, career choices
Leadership and research opportunities.
Mentees reported that they found mentoring useful and supportive of learning and development. This was especially important in a speciality that they had little experience of as an undergraduate. With a mentor in Psychiatry, the Foundation doctors reported that they could identify areas of development, including leadership and teaching opportunities for Foundation doctors.
Overall, mentoring was shown to be a useful tool to improving Foundation doctors’ experience in Psychiatry by offering extra support during placement in a challenging medical speciality.
Table 4 summarises the areas of development suggested by the mentors and mentees.
Table 4- Recommendations from the feedback of mentors and mentees
Early allocation of mentors at the start of the placement is vital.
The need to provide e-learning and classroom training on mentoring to develop the skills of mentors
Maintain the independence of the mentor from the clinical team of the mentee
Enhance the flexibility of the scheme to meet the demands of the training and the time constraints of the mentees and mentors
Limitations
Feedback from mentors and mentees showed an overall satisfaction with the scheme, but it was not possible to measure such satisfaction quantitatively, this was expected from an approach which is willfully kept outside the realm of performance management.
According to the literature on mentoring, most mentoring schemes lack a clear structure, as well as a clear evaluation process of its short and long terms, benefits 11.In our scheme, we addressed this by continually monitoring the mentoring process and collecting feedback from mentees and mentors. Another limitation involves training the mentor himself and finding the time in a highly pressurised and heavy workload environment.
There are many questions that the literature on mentoring is yet to answer. For example, what are the long-term benefits of mentoring? Would our Foundation doctors who received mentoring be more successful professionally and personally compared to their peers who decided not to participate? These questions remain unanswered as our pilot was not set up to address this general shortcoming of current knowledge and understanding.
Conclusions and recommendations
Mentoring provides a focused opportunity to target the wider needs of the trainee. Not only could this encourage Foundation doctors to pursue a career in Psychiatry, but it also provides the space for them to learn how to incorporate psychiatric skills into whatever speciality they choose to pursue.
As a new doctor in a novel environment, being expected, welcomed, and gently guided into the job is invaluable. With the hindsight of our training experiences (good and bad), junior doctors are ideally placed to support more junior colleagues at all levels.
There is a need to develop links with other mentoring schemes to exchange experiences and learn lessons from others. Research has shown the importance of supporting mentors in their roles through regular meetings where mentors learn from each other. 13
In our experience, the mentoring scheme worked both alongside and separately to clinical and educational supervision and the opportunity for reflective practice offered in Balint groups. Mentoring added another level of support for the Foundation doctors, which was deemed beneficial by those participating.
We recommend more research is required to determine whether mentoring will increase recruitment to psychiatry. Organisations responsible for the training of doctors should support formal mentoring schemes and supervisors should ensure that mentors and mentees have protected time in their timetable due to the benefits of the mentoring experience to the doctors and the employing organisations.
Finally, funding should be available to support training of mentors in their workplace and aim to develop their skills in helping their mentees. Many private organisations offer mentoring training packages (including classroom and online training) for competitive prices. These courses provide useful resources to mentors and may help to increase the motivation of mentors to continue their participations in mentoring.
Appendix:
How does mentoring work? A simple three stage model:
Figure 1- The three stage model of mentoring. Developed from Alred et al (1998). Alred, G., Gravey, B. and Smith, R, 1998, Mentoring pocketbook. Alresford: Management Pocketbooks.
One of the unique characteristics of mentoring is that it is a partnership between two individuals (mentor and mentee) where both contribute to its growth and sustainability. It is based on trust, eagerness to learn and mutual respect. 16
Alred et al (1998) 4 described a model of mentorship with three stages: exploration, developing new understanding and then action planning (Figure 1). Both the mentors and mentee have certain roles and responsibilities in each stage and it is only through their collaborative work that the benefits of mentoring can be obtained.
The stage of exploration is characterised by the building of a relationship between the mentor and the mentee. Trust, confidence and rapport start to develop and hopefully grow throughout the mentoring process. Methods such as active listening, asking open questions, and negotiating an agenda are essential to facilitate this growth.
The second stage is where new understanding develops, is characterised by showing support to the mentee, demonstrating skills in giving constructive feedback and challenging negative and unhelpful cognitions.
Key methods employed in this stage include recognition of the strengths and weaknesses of the mentee, giving them information, sharing experience and establishing priorities for the mentee to work on.
In the third and last stage of the mentoring, action planning, the mentee takes the lead in negotiating and agreeing on the action plan, examining their options and developing more independent thinking and decision-making abilities.
A good mentor should help the mentee to gain confidence and knowledge over time. In order to achieve this, the mentor helps the mentee to develop new ways of thinking and improve their problem-solving abilities.
Monitoring the progress and evaluating the outcomes of the mentoring process is essential to ensure that the mentoring relationship is going in the right direction.
Acknowledgement
We would like to thank Dr Stephen Jones (Consultant CAMHS and former Training Programme Director), Dr Trevor Broughton (Consultant Forensic Psychiatrist, Director of Medical Education), Dr Bohdan Solomka (Medical Director) from Norfolk and Suffolk NHS Foundation Trust for their unlimited support for the mentoring scheme.
We also would like to thank Dr Calum Ross (Foundation Training Programme Director-FY1) and Mr Am Rai (Foundation Training Programme Director -FY2), Norfolk and Norwich University Hospital for their support in implementing this scheme. Dr Srinaveen Abkari (Specialist Registrar, Norfolk, and Suffolk NHS Foundation Trust) is one of our mentors who also contributed useful ideas to the development of this paper.
Finally, we would like to thanks all our mentors who provided the support for the Foundation, without their efforts, this scheme would not have succeeded.
Oestrogen receptors (ERs) are expressed in a large proportion (approximately 70%1) of breast cancers (BCs). Oestrogen stimulates the growth of breast epithelial cells (both normal and cancerous) by binding to these receptors. Aromatase inhibitors (AIs) prevent the conversion of androstenedione to oestrogen by the enzyme aromatase in peripheral tissues, which is the predominant source of oestrogen in post-menopausal women. Consequently, they are routinely offered to post-menopausal women with ER-positive early invasive breast cancer as adjuvant therapy2. However, decreased residual oestrogen levels are associated with increased bone resorption by osteoclasts. The menopause initiates an accelerated phase of bone loss lasting 4 to 8 years, which is followed by a slower phase which continues indefinitely3. AI-induced bone loss (AIBL) occurs at a higher rate than natural menopausal bone loss4. Women are therefore at increased risk of fractures while they are on AI therapy5, with an associated higher rate of fractures as demonstrated in the ATAC trial6.
Recent data have supported more prolonged use of AIs (10 years instead of 5) to achieve lower BC recurrence rates7. This may lead to changes in future clinical practice in that ER-positive BC patients may be on an even longer course of AIs. This is likely to translate into a higher fracture risk in patients on long term treatment, and bone health in these patients should remain an important consideration.
Several guidelines have emerged over the years, as summarised by Hadji et al8, to aid the assessment of fracture risk in women receiving BC treatment, and management of AIBL. In the UK, the guidance in use and recommended by the National Institute of Health and Clinical Excellence (NICE) is a UK expert group consensus position statement issued in 2008 (Guidance for the Management of Breast Cancer Treatment-Induced Bone Loss)9. This includes two treatment algorithms for the assessment and management of bone loss in early BC: one for women with adjuvant treatment-induced premature menopause and the other for postmenopausal women starting adjuvant AI.
Despite the existence of various guidelines on the management of AIBL in BC patients, few articles have been published on the practical adherence to guidance. We carried out an audit of the management of AIBL in BC patients in a large general practice (with roughly 9000 registered patients) in Bradford (UK). Given the small number of eligible patients in our study, we undertook a review to identify all studies in the English literature assessing practical adherence to guidance on AIBL to establish whether gaps identified in our practice reflects a more widespread issue.
Our study
Methods
We carried out a retrospective study in a general practice in April 2015. Using the clinical electronic system used at the practice (SystemOne), we performed a search for all registered patients documented to currently be on AIs or to have previously been on them at any point, for the treatment of BC, using the search terms “anastrazole”, “Arimidex”, “exemestane”, “Aromasin”, “letrozole” and “Femara”. We excluded male patients (not addressed by current guidelines) and patients who started their treatment with AIs prior to the issuance of the UK guidance in 2008. For each patient we gathered data on the indication of treatment, menopause status, the date of initiation +/- completion of treatment, details of dual energy Xray absorptiometry (DEXA) scan and bone mass density (BMD), blood biochemistry results, documented risk factors for fractures and details of bone protection treatment. We audited our practice against the UK guidance.
Summary of the UK guidance
All post-menopausal patients starting AIs should have a baseline DEXA within 6 months of treatment initiation. Patients are stratified as low, medium and high risk for fractures based on the baseline T-scores. Medium and high risk patients should have vitamin D and calcium supplements, and high risk patients should be started bisphosphonates. A repeat DEXA scan should be performed 2 years later for medium and high risk patients to re-assess BMD and augment bone protection therapy as appropriate. Patients aged 75 years and above with at least one clinical risk factor for fractures should be started on a bisphosphonate regardless of their baseline BMD.
Results
There were 12 female patients who started AIs for BC treatment from 2008 onwards. Treatment was initiated between the years 2008 and 2014 (inclusive). The mean age was 67 years (range 57-81 years) and all 12 were post-menopausal at the time of adjuvant hormonal therapy initiation. Three were initially on tamoxifen and switched to an AI after 2 years of tamoxifen therapy.
Three patients (25%) did not receive an initial DEXA scan and had no subsequent risk fracture management. One of them was 75 years of age at the time of AI initiation and was on long term steroids (i.e. should have been on a bisphosphonate regardless of BMD), but she was not on a bisphosphonate.
Of the remaining 9 (75%) who did have a DEXA scan,
One was at high risk (T-score -2.7), and was appropriately started on a bisphosphonate and calcium and vitamin D supplements.
7 patients were at medium risk of osteoporotic fractures (T-score range -2.0 to -0.1). All were started on calcium and vitamin D supplements.
7 were eligible to have had a repeat DEXA scan at the time of the study but only 4 had a scan. Of these four, one was found to have incurred significant bone loss and was started on a bisphosphonate.
The mean interval between AI initiation and baseline DEXA was 1.9 months (range 0.2-4.4). The mean interval between the initial and repeat DEXA scans was 4.1 years (range 2.5-5.1).
Figure 1 illustrates the proportion of scans requested by different clinical teams involved in the patients’ care.
Figure 1: Who requests DEXA scans?
Literature review
Methods
We performed a search with the following terms on the Ovid Medline and Embase databases: “bone loss”, “osteoporosis”, “osteopenia”, “aromatase inhibitor”, “breast cancer”, “guidelines” and “guidance”. Of the 137 results returned after deduplication, we selected original and review articles assessing management of AIBL against established guidelines. We retrieved further papers by reviewing the references of these articles.
Results
The original articles generated are shown in Table 1. While conference abstracts have not been included here, they have been reviewed for the purpose of our discussion.
Table 1: Original articles publishing the results of audits of bone health management in BC patients on AIs against established guidelines
Authors
Place of study
Guidelines used to define audit standards
Sample size
Adjuvant therapy
Roberts R et al10
Australia
ASCO*, ESMO*, Hadji et al8, Belgian Bone Club
42
Both AI and tamoxifen
Spangler L et al11
Washington, USA
ASCO*
342
AI
Bosco D12
Italy
Results from the ARBI* trial13
39
AI
Gibson K et al14
Colorado, USA
ASCO*
54
AI
Ligibel et al15
USA
ASCO*, NCCN*, Hadji et al8
9138
AI
Dong et al16
UK
NICE guidelines based on UK expert group consensus9
100
AI
Zekri J et al17
Saudi Arabia
NICE guidelines based on UK expert group consensus9
367
AI
*ASCO: American Society of Clinical Oncology, ESMO: European Society for Medical Oncology, NCCN: National Comprehensive Cancer Network, ARBI: Arimidex Bone Mass Index and Oral Bisphosphonates
Discussion
The results of our audit show that we are failing to meet our current national standards pertaining to management of AIBL in BC patients. Our literature review confirms that this is a widespread issue and that results from larger studies are in agreement with ours.
25% of our patients never had a baseline BMD measurement. Similar findings have been reported in the literature11,12,14. However, Roberts et al report much higher rates of DEXA screening pre –AI10. Reasons for this were felt to be the presence of an institutional treatment algorithm as well as a survivorship programme.
We had a poor rate of repeat DEXA scans. Gibson et al and Spangler et al also noted that the highest rate of DEXA scanning was around the time of AI initiation compared to after initiation of therapy11,14. For the patients who had a repeat BMD measurement in our study, practice was not in line with recommendations as the interval between the initial and repeat DEXA scans (mean 4.1 years) was much longer than the recommended 2 years. This may be because recommendations made by the breast surgery team were different (intervals of 3 to 5 years being recommended in some cases in clinic letters written to the GP by the breast team).
Gibson et al found that 75% of their patients were on calcium and vitamin D, which deviates from the ASCO guidelines that they audited their results against14. The ASCO guidelines recommend that all BC patients should be on calcium and vitamin D therapy. In some studies10.12 not all women diagnosed with osteoporosis were started on bisphosphonates. Although women diagnosed with osteoporosis were started on bisphosphonates in our cohort, the suboptimal uptake of DEXA scans means that we may have missed the diagnosis in a number of patients.
From the articles included in our literature review, several reasons have been suggested as causes for deviation from guidelines when it comes to management of AIBL in BC patients. Lack of awareness of guidelines, especially amongst general practitioners (GPs), has been recognised as a barrier, as well as the expectation that other healthcare professionals should be addressing this aspect of care10. In our study, DEXA scans were mostly requested by the specialist breast team initiating AIs, or by the GP at the request of the breast team. Based on our experience, it is not clear who the responsibility of bone health management lies with – the breast surgery team, the oncologist or the GP. In a survey of 307 UK-based breast surgeons and oncologists 57% of responders felt that oncologists should be responsible for this18. In practice, patients may be discharged from specialist clinic follow-ups while they are still on hormonal therapy and GPs would be expected to continue their care. When this happened in our cohort of patients, there was no evidence of clear written communication from specialist teams to the GP regarding outstanding aspects of care that the GP would be expected to follow up.
An analysis of five different guidelines regarding antiresorptive treatment in postmenopausal women with hormone-receptor positive BC showed that little consistency exists among the five guidelines19. The variety of guidelines and recommendations regarding bone loss in BC patients probably leads to inconsistency in practice. In our study, specialist teams have sometimes recommended an interval of 3 to 5 years between BMD tests, deviating from the national recommendation of 2 years. This can translate into confusion when care is taken over by the community team after the patient is discharged from the specialist team.
Recommendations
We therefore suggest that institutional guidelines on bone health management in BC patients on AIs (as well as other hormonal therapies) should be created to improve awareness amongst clinicians as this has shown to improve rates of DEXA scanning10. Local guidelines should closely mirror national guidelines to allow delivery of standardised care across the country, but should include clear recommendations as to which local team should be responsible for bone health management, as well as recommendations regarding the creation of a care plan for general practitioners when the patient is discharged from specialist teams.
A UK-based study has shown that a “one stop” nurse-led bone health clinic within the breast care service can be a cost-effective way of ensuring adherence to guidelines20. Patients to be started on an AI are identified by the multidisciplinary team (MDT). They are referred to the clinic which arranges a baseline DEXA and other appropriate investigations. Such a clinic may be a consideration in institutions where resources allow. Studies have also shown that simple interventions such as presentations at MDT meetings and display of posters to increase awareness of guidelines amongst clinicians have led to significant improvement in compliance16,17.
Lack of patient awareness of the negative effects of AIs has also been highlighted in the literature21. Improving patient education can improve patients’ compliance with treatment and decrease the rates of unattended appointments for BMD screening. It can also give more control to patients over management of their bone health, as they may be able to discuss with their clinicians where they notice a gap (e.g. if they have failed to receive an appointment for a DEXA scan). Ligibel et al have noted that women from areas with lower levels of education are less likely to undergo BMD tests15.Patient education can also help reduce the impact that such health-seeking behaviours have on compliance to bone health management.
Current guidelines make no mention of bone health management in male BC patients on hormonal therapy. Although they constitute a small percentage of BC patients, it would be reasonable to include recommendations of their bone loss management in updated guidelines so that this aspect of their care is not neglected.
Strengths and limitations
Our audit is limited by its small sample size and its retrospective nature which meant that we relied on documentation of variable accuracy. We had no information regarding patients who failed to attend appointments despite their clinicians’ invitations for DEXA scans or biochemistry tests, and no information on compliance to medication. However, the results from recent conference abstracts on UK based studies22,23 generated from our literature review reflect our results, suggesting that this is indeed a national issue. The literature review presented is the most extensive currently available on the subject, gathering up-to-date evidence on worldwide compliance to guidelines on AIBL.
Conclusion
Although the sample size of our study does not allow us to draw conclusions purely based on our data, the literature review that it has prompted has shown that several years after issuance of various guidelines on the management of BC treatment-induced bone loss, in particular AIBL, important gaps still exist in practice. We have presented a summary of up-to-date evidence in the literature to identify potential reasons for this and possible solutions to the current problems, hoping that this will improve current practice.
However, the current guidelines are now several years old. In the last few years, there has been a lot of research on the role of bisphosphonates in BC. A consensus paper assessing recent evidence has suggested that bisphosphonates should be considered for the prevention of bone loss in patients with a T score of <-2.0 or with at least two clinical risk factors for fracture24. The paper also suggests considering the use of bisphosphonates as adjuvant BC treatment, based on a large meta-analysis including 18 766 patients which demonstrated significant benefits of bisphosphonates in terms of prevention of bone metastases and BC survival in postmenopausal women25. This may well change routine adjuvant treatment of BC in the next few years and must be taken into consideration if and when new guidelines on the management of AIBL are issued, or when writing local guidelines.
Metastatic bone disease is a relatively common event in the advanced stages of many malignancies.1 Bone-modifying agents decrease the incidence of skeletal-related events (SREs) such as spinal cord compression and bone fracture, as well as the need for skeletal radiotherapy or surgery.2
Bone modifying agents such as intravenous bisphosphonates (IV BPs) (e.g. pamidronate and zoledronic acid) and denosumab are approved for prevention of SREs. IV BPs are primarily used and effective in the treatment and management of cancer related conditions such as multiple myeloma (MM), and breast cancer with skeletal metastases, because they reduce bone pain, hypercalcemia, and the risk of pathologic fractures.3
Denosumab, a receptor activator of nuclear factor kappa-B ligand (RANKL) inhibitor, represents a breakthrough in the treatment of osteoporosis, MM, and bone metastases. The Food and Drug Administration (FDA) approved it in 2010 for the prevention of SREs in patients with bone metastases and in 2011 for the prevention of endocrine-therapy induced bone loss in patients taking aromatase inhibitors for breast cancer and in patients with non-metastatic prostate cancer.
Three international, randomised, double-blind, double-dummy phase III studies have evaluated denosumab versus zoledronic acid for the treatment of SREs in breast and prostate cancers, and in combined solid tumours and MM. Denosumab’s superior efficacy over zoledronic acid was demonstrated in the studies of patients with advanced breast or prostate cancer, as well as in a pre-specified integrated analysis of all patients enrolled across the three studies.4
In the 2014 position paper of the American Association of Oral and Maxillofacial Surgeons (AAOMS), the nomenclature “bisphosphonate-related osteonecrosis of the jaw” changed to “medication related osteonecrosis of the jaw” (MRONJ). MRONJ is defined as cases in which all of the following 3 characteristics are present5:
current or previous treatment with antiresorptive or antiangiogenic agents
exposed bone or bone that can be probed through an intraoral or extra-oral fistula in the maxillofacial region that has persisted for longer than 8 weeks
no history of radiation therapy to the jaws or obvious metastatic disease to the jaws
Other terminologies used previously include “denosumab related osteonecrosis of the jaw” (DRONJ), and “antiresorptive agent-induced ONJ” (ARONJ).
The aetiopathogenesis of MRONJ related to denosumab therapy remains enigmatic, and hypotheses have focused on reduced bony turnover, infection, toxicity of the soft tissue, and antiangiogenesis. The epidemiology also remains unclear, and reported incidence varies widely.6 Overall, it is estimated that bone necrosis can develop in about 0.7-1.9% of patients with malignancy who are given high-potency IV BPs (such as zoledronic acid), and in 0.01–0.1% of those with osteoporosis who take low-potency oral BPs (such as alendronate). Data relevant to denosumab given subcutaneously in patients with metastatic cancer and osteoporosis seem to replicate those when IV high-potency BPs are administered.7 The risk of osteonecrosis of the jaw (ONJ) is higher in patients exposed to concomitant antiagiogenic medication. The individuals’ risk of ONJ is further determined by factors such as the potency of agent, cumulative dosage or duration of antiresorptive treatment, route of administration, comorbidities and local factors such as periodontal disease.8,9 Oral hygiene plays a significant role with evidence supporting a strong correlation between bacteria associated with periodontal disease and MRONJ.10
MRONJ typically manifests as painful and often infected areas of necrotic bone, which subsequently may lead to severe chronic pain and facial disfigurement. This adversely affects the ability to eat, speak and lowers the quality of life. Adverse events related to RANKL inhibitors are usually considered to be infrequent and low in occurrence. Unfortunately from our recent clinical experience at Sheffield Teaching Hospitals' Trust, there have been several new cases presented in a very short period of time. In this paper we present a case series of MRONJ related to denosumab therapy since adverse events of denosumab in the mandible or maxilla have received relatively little attention.
The aim of this article is to highlight the elevated risk of MRONJ in patients receiving denosumab treatment and educate all health care providers involved in the management of such patients. Furthermore, the mechanisms of denosumab, comparison with bisphosphonates and the reported management strategies are reviewed.
Mechanism of Denosumab
Denosumab is an antiresorptive agent that exists as a human IgG2 monoclonal antibody and inhibits the binding of the receptor activator of nuclear factor kappa-B ligand (RANKL) to RANK (Receptor Activator of Nuclear Factor kappa-B). The binding normally signals the proliferation of osteoclasts, as RANK is expressed on the surface of osteoclasts and their precursors, whereas its ligand, RANKL, is a membrane bound protein expressed by bone marrow stromal cells, osteoblasts and T-lymphocytes. The activation of RANK is integral to the function of osteoclasts. Osteoprotegerin binds to membrane bound RANKL on osteoblast which in turns decreases the osteoclastic activity and in theory negatively effects bone turnover. Denosumab acts similarly to osteoprotegerin but has a higher affinity for RANKL.11-13
Denosumab follows nonlinear, dose-dependent pharmacokinetics. The bioavailability of one subcutaneous denosumab injection is 61% and serum concentrations are detected within 1 hour. Maximum serum concentrations occur in 5-21 days and cessation of osteoclast activity occurs within six hours of the subcutaneous injection. The normal function is restored approximately six to nine months later, whilst bone turnover returns to normal shortly after this.14 Based upon monoclonal antibody pharmacokinetics, denosumab is most likely cleared by the reticuloendothelial system with minimal renal filtration and excretion thus avoiding nephrotoxicity. Its elimination half-life is 32 days, and it does not incorporate into bone.15
It is currently marketed as Prolia® and Xgeva®, approved by FDA. Prolia® is administered subcutaneously every six months and has shown to reduce the incidence of new vertebral, non-vertebral, and hip fractures in osteoporotic patients.16,17 Xgeva® is also effective in reducing SRE related to metastatic bone disease from solid tumours when administered intravenously on a monthly basis.17,18
RANKL Inhibitors and BPs Pharmacokinetics
There are fundamental differences between denosumab and BPs with regard to their mode of action. Denosumab is an antibody and acts extracellularly whereas BPs act intracellularly. As such, BPs must be present in the circulation and available for reuptake into bone for prolonged periods to function.19 There is not any evidence of drug recycling with RANKL inhibitors, and therefore it is suggested that their adverse effects can be reversible with discontinuation, in fact leading to a transient rebound phenomenon, which can be restored, with subsequent treatment.14,20 On the other hand, recycling of BPs in the circulation system has been proposed as a reason for the long duration of action even after cessation which can be up to 12 years.
The US FDA-approved manufacturer’s package insert for both zolendronate and pamidronate states that “there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ in patients who require dental procedures during therapy and that clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/ risk assessment”. The package insert for denosumab does not address the issue of treatment continuation in patients who develop MRONJ to date.
Denosumab is a circulating protein capable of distributing throughout extravascular space. It is expected to reach all sites within bone including intracortical sites unlike with BPs. BPs have strong affinity for hydroxyapatite and bone mineral which limits their even distribution throughout the skeleton, particularly to sites deep within the bone.19,21 This can explain the more profound inhibition of bone remodelling with denosumab than that seen with BPs.
Case Series
Case 1
A 55 year-old lady referred to a dedicated Oral Surgery nerve injury clinic for an opinion and management of her left sided inferior alveolar nerve (IAN) paraesthesia. The patient presented with a history of numbness in the left sided inferior alveolar nerve distribution following removal of the left mandibular second premolar (LL5) in July 2014. She was asymptomatic until she had the LL5 removed and since had suffered with constant pain and numbness. A year later, she had removal of the left mandibular first molar (LL6) and gave a history of recurrent infections and excruciating pain in her mandible over the past two months. On presentation she had an obvious submental swelling and left sided IAN anaesthesia.
Medically she was diagnosed with breast cancer in 2011, for which she underwent wide local excision followed by chemotherapy. She then was placed on unknown clinical trial that we identified at the time to be denosumab trial, following liaison with the Oncology team. She is currently receiving intravenous denosumab every three months.
Clinical examination revealed a grossly mobile anterior mandible with widespread bony necrosis and associated osteomyelitis. Sensory testing revealed complete anaesthesia in the left sided IAN distribution secondary to MRONJ.
An OPG (Orthopantogram) and CBCT (Cone-Beam Computerised Tomography) revealed an extensive patchy area of ill-defined bone loss in the anterior mandible extending posteriorly to the premolar/molar areas bilaterally (Fig 1).
Figure 1 A) OPG showing non-healing sockets in the left mandible with extensive bony destruction together with periosteal reaction extending to the right mandible as shown by the arrows.
Rather interestingly, the bony destruction was evident bilaterally with the patient only having had extraction of teeth in the left mandible (Fig 1). This could be the case of spontaneous ONJ in the right mandible or an extensive ONJ arising from simple extractions on the left side.
Figure 2 3D reconstruction of the CBCT image demonstrating extensive bony destruction involving the lower border of anterior mandible in keeping with a spreading chronic bony infection and clinical presentation of submental swelling as showing by arrows.
Case 2
A 66-year-old female referred by her general medical practitioner (GMP) with a 3-month history of delayed healing following a tooth extraction in the left posterior mandible. She had moderate to severe discomfort and reported multiple previous infections and purulent discharge from the area, which treated with multiple courses of antibiotics. In addition, she reported discomfort from the root treated right mandibular first and second premolar teeth (LR4 and LR5).
Medically she was diagnosed with breast cancer over 10 years ago for which she underwent resection followed by chemotherapy. Three years ago, she diagnosed with metastatic deposits and therefore has been receiving intravenous denosumab every six weeks since then. Other medications include steroids, chemotherapy agents, antihypertensives and analgesics. She did not receive any radiotherapy or BPs treatment in the past.
Clinical presentation revealed a heavily restored dentition with chronic generalised periodontal disease. There was evidence of widespread bone loss clinically and radiographically. The slow healing socket in the left mandible was visible but did not have any exposed bone (Fig 3). The lower right first and second premolar teeth (LR4 and LR5) were clinically and radiographically sound.
Figure 3. Non-healing socket in the left posterior mandible with no evidence of exposed bone or suppuration as showing by white arrow. Gingiva recession (black arrows) is evident in the LL6 and LL5 teeth in keeping with chronic periodontal disease.
Figure 4 Coronal sections of CBCT A and B showing multiple lytic areas within the inferior cortex of the mandible and incomplete healing of the extraction sockets.
On follow-up appointments, the patient suffered multiple repeated infections in the right and left posterior mandible and due to deteriorating periodontal disease, the LR4, LR5, LR6 were extracted by her own general dental practitioner (GDP) due to severe mobility. All three extraction sockets failed to heal (Fig 5) leading to an extensive area of exposed bone in the right mandible, extending from the lower right first premolar (LR4) to lower left first molar (LL6) region. Conservative management was embarked which included antibiotics, chlorhexidine mouthwash and routine oral hygiene appointments. Selective sharp bone trimming and three sequestrectomies were undertaken. At the same time, liaison with the patient’s oncologist resulted in cessation of the denosumab therapy and complete resolution of her oral symptoms.
Figure 5 Clinical picture of exposed necrotic bone (white arrows) following simple extractions of periodontally involved teeth.
Case 3
A 76-year-old lady referred to the Oral Surgery department by her GDP with a 3-month history of a non-healing lower left first premolar (LL4) socket. The patient was treated with two courses of antibiotics prior to referral which provided only temporary relief to her symptoms.
Medically she was diagnosed with breast cancer 10 years ago and recently commenced intravenous denosumab for metastatic disease. She also receives hormone therapy and palliative radiotherapy to the spine.
On clinical examination, there was a partially healed LL4 socket with a rather granulomatous appearance. There was no clinical evidence of suppuration or bony exposure. Radiographs confirmed the absence of bony infill in the socket. Local debridement and biopsy of the granulomatous tissue was performed to exclude any metastatic disease. Biopsy report confirmed the presence of inflammation tissue.
Figure 6 CBCT scan; A and B sagittal views, C axial view and D 3D reconstruction. Extensive periosteal reaction extending from the midline of the mandible to the left molar region is evident in keeping with chronic osteomyelitis secondary to MRONJ.
Liaison with the microbiologist suggested a long-term antibiotic course to arrest osteomyelitis. Further liaison with the oncology team, resulted in denosumab being stopped for 4 months. On subsequent review appointments, patient’s symptoms improved however, there is now an area of exposed bone in the LL4 region as shown in Fig 7.
Figure 7 Clinical photo illustrating exposed bone (white arrow) in the LL4 region without evidence of local infection.
Case 4
A 65-year-old lady referred to the Oral Surgery department by her GDP with a history of a sore upper mouth and jaw underneath the dentures which is unable to wear.
Medically she was diagnosed with disseminated breast malignancy including bone metastases 3 years ago and for that, she is on exemestane and IV Denosumab monthly.
Clinical examination revealed multiple draining sinuses in the anterior maxilla. There was a partially healed LL4 socket with a rather granulomatous appearance and tenderness on palpation. There was neither discharge from the area nor any exposed bone. Radiographs confirmed the absence of bony infill in the LL4 socket. Local debridement and biopsy of the granulomatous tissue was performed to exclude any potential malignancy and it was confirmed as inflammation tissue.
Figure 8 CBCT scan; A axial view, B and C 3D reconstruction. A 25mm fragment of right anterior maxilla is beginning to sequestrate. This extends from the anterior margin of the right maxillary sinus approximately to the position of the upper left lateral incisor, crossing the midline. The sequestrated fragment involves the lateral margin of the nasal cavity. There is bilateral moderate mucosal thickening in the maxillary sinuses. Extensive periosteal reaction extending from the midline of the mandible to the left molar region is evident in keeping with chronic osteomyelitis secondary to MRONJ.
Table 1 Summary of cases
Cases
Indications
Duration (months)
Clinical Findings
Case 1
Metastatic deposits from primary breast malignancy
48
Anaesthesia in the distribution of the left inferior alveolar nerve Osteomyelitis Excruciating pain
Case 2
Metastatic deposits from primary breast malignancy
36
Chronic generalised adult periodontal disease Non-healing extraction sockets Exposed bone persisted for longer than 8 weeks Severe pain
Case 3
Metastatic deposits from primary breast malignancy and myeloma
24
Non-healing extraction socket with granulomatous tissue Severe pain
Case 4
Disseminated breast malignancy including bone metastases
30
Multiple draining sinuses in anterior maxilla Non-healing extraction socket with granulomatous tissue Severe pain
Discussion
ONJ associated with antiresorptive therapy deserves distinction from other causes and diseases/medications associated with the development of osteonecrosis of the jaw. AAOMS recently published stage specific treatment recommendation for MORNJ.22 The various stages and suggested stage-specific treatment strategies are not evidence-based, and in particular, stage 0 disease is not universally accepted. AAOMS recommendations echoed those stated in previous years for BRONJ, namely supporting conservative therapy, with aggressive surgery offered only to symptomatic patients. In contrast, the MRONJ guideline report from the German Dental and the German Oral and Maxillofacial Associations refrains from recommending therapy at least for certain stages of the disease. This might be attributed to the pitfalls of current MRONJ criteria. Furthermore, due to poor guidelines specifically related to RANKL inhibitors, no agreement exists on a universally acceptable therapy strategy of such cases.
Management strategies are largely based on expert opinion rather than experimental data. It includes prevention, conservative and surgical modalities. Prevention of the condition is the gold standard. It is highly recommended all patients have a comprehensive dental examination and preventive dentistry (pre-emptive extraction of unsalvageable teeth and optimised periodontal health) before commencing antiresorptive therapy.23,24 Oral hygiene should be kept meticulous during the course of therapy as periodontal disease and associated bacteria claim to be implicated in this condition and also observed in these cases.
The success rate of conservative treatment regimens range from less than 20% 25,26 to above 50%27,28 although some cases become chronic and develop complications.29
Microbial cultures from areas of exposed bone are not always helpful since normal oral microbes are isolated. However, when there is extensive soft tissue involvement, microbial cultures may help to define comorbid oral infections, which may guide the selection of an appropriate antibiotic regimen.30
Regardless of the stage of disease, areas of necrotic bone that are a source of chronic soft tissue irritation and loose bony sequestra should be removed or recontoured so that soft tissue healing can be optimised. This is in line with our clinical experience. The extraction of symptomatic teeth within exposed, necrotic bone should be considered as it appears unlikely that extraction will worsen the established necrotic process. Otherwise, surgical resection of necrotic bone should generally be reserved for refractory or advanced cases.31 Resection may occasionally result in even larger areas of exposed and painful infected bone.32
A recently published MISSION study7 reported that the AAOMS system misclassified/ underestimated the severity of the disease at a rate of about 1 in 3, in particular in patients suffering from MRONJ stage 1 and 2. The authors conclude that these findings may explain why the treatment of stage 3 ONJ, namely surgery with success rate over 85%33,34, has been deemed to be more predictable and therefore yields more favourable outcomes than the treatment of stages 1 and 2.35
Denosumab is characterised by reversibility of its effect after treatment discontinuation, in contrast with bisphosphonates. This is in line with our findings since cessation of denosumab in two cases helped to improve their symptoms significantly.
MRONJ has been reported to occur after a mean administration period of 39.3 months and 35 infusions in oncology patients.23 It is interesting that all published cases of denosumab-related ONJ occurred early after commencement of therapy, independent of the number of previous administrations.36,37 In our experience, all patients developed MRONJ within the first 3 months of teeth extractions; well ahead of the reported period and number of administrations of denosumab.
Furthermore, all four cases have had extensive lytic lesions developed following removal of a single tooth. The common radiographic findings in all cases include:
non-healing extraction socket
areas of focal and diffuse sclerosis
thickened lamina dura
early sequestrum formation
reactive periosteal bone
osteolysis of cortical and spongious bone
These findings, although common in MRONJ cases, have had extensive bony involvement and rapid progression of ONJ, demonstrating a far more aggressive nature of the disease compared to that seen with BPs.
In our experience, not all patients are adequately informed of the risks and adverse events of denosumab therapy. This highlights the importance of educating patients and inter-professional communication regarding the prevention and best management of MRONJ cases. In one of the cases, the lack of patient education concerning denosumab side effects and the failure of inter-professional communication had a detrimental effect on the patient’s overall management and subsequently patient’s oral health.
Table 2 Important Points
All patients prior to start of any antiresorptive medication should have a dental check-up and receive dental or surgical treatment beforehand to avoid the possibility of complications associated with antiresorptive medications
Strongly recommend regular dental check-ups to prevent
Patients should be advised to contact their Doctor/Dentist/Oral surgeon immediately if notice following symptoms:
Feeling of numbness, heaviness or other unusual sensation in the jaw
Pain in the jaw / toothache
Delayed healing to the gums, especially after dental work
Bad taste / infection
Swelling of the jaw
Loose teeth
Exposed bone
Pus like discharge from the affected area
Conclusion
We present our experience with denosumab-related ONJ from Sheffield Teaching Hospital’s NHS Trust. This case series should contribute to the existing sparse clinical literature on this topic. The pathogenesis, treatment and outcome of ONJ are complex and multifactorial. Patients treated with denosumab may be more prone to developing ONJ even without a precipitating dental event. ONJ may have a more aggressive profile and develop significantly earlier in patients receiving denosumab. Prevention of ONJ still remains the most important goal, and this is most directly accomplished by avoiding invasive dental procedures and establishing inter-professional communication.
Medicine is a dynamic science and discipline, which arise from the human need to face the suffering, pain and give hopes for better life. Since its inception, medicine has entered a career development that has brought great advances in science. Part of this momentum observed in medicine is defined as its reason for being, or rather, its primary goal, maintaining the health status in different populations1. This simple statement but becomes an object of great complexity which has received attention by many physicians and researchers from ancient times to the present, and in the tenth century, Ibn Hazm, a father of modern medicine enunciated the truth in this science was going to be impossible, since its dynamism is always present and the truth became a clear misrepresentation or significantly modified in the future2.
The goal of keeping adequate health status and prevent diseases has kept biomedical research in an alarming race in which the speedometer registering increases day by day. Today medical science is one of the most important sources of scientific innovation around the world; hundreds of manuscripts on health issues are published every day in multiple languages, in addition to numerous books and other non-official publications2-3. The increase in the medical literature during the last decade, led to think that the development of medicine has become a breakneck ratio, both the magnitude of the information obtained and its complexity.
However, the real reason for this phenomenon in biomedical sciences should be as a result of the new funding sources available for biomedical research either from the biomedical industry and government agencies. Each year new sources of money are offered to scientists to encourage innovation and the development of new ideas; and the resources existing to perform this goal increase. The OECD (Organization for Economic Co-operation and Development) suggests that countries spend about 500 billion dollars a year on research in biomedical sciences, including private laboratories and research institutes4. Medicine has become one of the most promising businesses in the economic field, and up today, and it is considered one of the greatest science future with wide range of prospects5.
Despite this encouraging situation, the concerning of development of modern medicine could be measured as a fundamental problem: the doctors and other scientists in charge of biomedical innovation are not trained in the administrative field. The above problem is clearly seen in different situation in the current medical and research practice, weak reflected on wasteful resource allocation processes6.
Each organization facilitating biomedical research resources requires that its resources are managed and used in an appropriate manner. Institutions demand to distribute funding for various interests not only in biomedical sciences. On the other hand, institutions have to verify the novelty and the ethical viability of the proposals, with the main idea of support ethical-approved studies, avoiding catastrophes in non-well-designed trials. Nowadays, as a result of better “quality control processes”, grant submissions involve a great number of administrative steps in order to be ready to submit any proposal. In this verification process, no only questions have to be addressed in term of sciences; a lot of administrative issues have to be explained in detail, including budget utilization and personnel management1, 4, 7.
Academics and scientists in universities are trained mostly in the technical aspects of their daily work, for this reason the horizon shows that the physician (M.D.) receives their training focus for the clinical management of patients, a doctor of science (Ph.D.) receive their training in the handling the samples to obtain the best results in the tests planned. In both cases, scientists are plainly educated out of the business and administrative field, leading important limitations with resources (personnel and funding) management3, 5.
Nowadays, the easiest application to obtain resources requires the approval of at least 5 different offices responsible for reviewing ethical, financial, legal, logistical, and scientific issues. Now back to the main problem in this discussion, the fact that medical researchers are not trained as integrated researchers (sciences and business), we are in the position to deduct that this condition may generate a bottleneck, specifically in this time where biomedical research are gaining a lot of power and interest in the industry8.
A potential alternative for this dilemma is to offer manager and administration training to researchers in order to be able to efficiently manage the resources requested. Masters degree programs are now available in health sciences management and administration, gaining popularity in the last five years. Researchers are more committed to show better profiles in their grant applications. Modern scientists must be people with a proven knowledge on costs and productivity that allows performing biomedical research with scientific quality combined with attractive financial management in terms of production2, 5, 8.
Postgraduate medical training should equip trainees with the skills, knowledge and attributes for independent practice1. They need to be equipped with the skills to become lifelong learners and continually develop their abilities throughout their careers by learning from colleagues, mentors, patients and disease. The challenge for clinical teaching is how to provide an optimal learning environment in which trainees can achieve their competencies for practice within a defined training rotation; both the limitations in the number of hours within a working week and the balance between learning and service commitments all can negatively impact on the educational experience of trainees2. Moreover, trainees need to balance their own development of skills, knowledge and attributes for independent practice against the requirement to provide high quality and safe healthcare3. The appropriate level of supervision must be provided to trainees performing any patient interaction and this is gauged by the trainer-trainee relationship, regular assessment and feedback. The clinical workload of a trainee needs to be finely balanced between overstretching them with tasks outside their competencies and being left with all the routine and menial tasks4. Thus whilst trainees should work within their competencies, they must be given the opportunities to expand their repertoire of skills, which may result in errors (and potentially patient harm) – supervision should limit these errors, which should be reflected on to provide a learning opportunity within a ‘no-blame’ culture5. As a trainee gains competence of their necessary skills, the amount of supervision required can be stepped down, until distant supervision (i.e. advice via a telephone) may be all that is required.
An understanding of how each learning environment within the hospital setting can be maximized may enhance the learning opportunities conferred upon trainees. Both technical skills and the professional attributes of being a clinician can be learnt in clinical and non-clinical environments. These learning environments will be explored in the subsections below.
Bedside Teaching and Ward Rounds
Bedside teaching is a stalwart of medical education, allowing clinical history and examination to be performed under guidance, in an appropriate setting and with relevant clues (observation charts, oxygen, etc.) present. This patient-trainee interaction provides an opportunity to develop professionalism and communication, and can also be the source of training of diagnostic techniques ranging from venesection and cannulation to more invasive techniques (e.g., pleural aspiration, drainage of ascitic fluid)1.
Presentation of patients during ward rounds allows a professional conversation between trainees and trainers to occur, which justifies their role in management and provides an insight into understanding and thought processes6. The multidisciplinary nature of rounds creates a community of practice7, allowing social learning to occur, and an opportunity to voice differing perspectives on patient care3. In order to maximize these learning opportunities, learning objectives can be discussed prior to commencement and reflection undertaken once they it has been completed6. Teaching rounds should be carried out when the ward is quiet, at a suitable pace, with regular questioning and opportunities for trainees to ‘lead’ the process8. Factors that hinder this educational process include time pressures, patients not being available, and the availability of trainees8.
Outpatient Clinics
Outpatients provides a mixture of new and follow-up patients that enables a trainee to learn management of patients in an ambulatory setting. Trainees may be in the same room as their supervisor (learning the basics of the consultation), or can practice semi-autonomously as their experience increases (with discussion with their supervisor as required); they must select an appropriate investigation and treatment plan, with a time frame for review, once the investigation or intervention has been performed3. Outpatient teaching is more highly valued by trainees and students compared to ward based tuition9. Factors that hinder this educational opportunity include room availability, time constraints, staffing levels and attitudes to teaching9.
Operating Theatre and Interventional Suites
Invasive procedures should be performed by adequately trained (or supervised) personal in the relevant area of the hospital (e.g. endoscopy, interventional radiology suites, theatre), with the necessary equipment and monitoring for the technique to be performed. Even before patients enter these environments, trainees have an opportunity to review the patient and their relevant investigations, discuss the procedure with the patient and obtain consent for the intervention1. Trainees can learn a wide spectrum of skills within these environments including both technical (both procedural related and anesthetic related) and non-technical skills, including Human Factors, anatomy, identification of instruments, aseptic technique, effective hand-washing and donning of surgical gowns10. Teaching invasive procedures represents a dichotomy for clinicians, not only do trainees need to gain exposure and experience in the relevant technique, but patients need to be prevented from undue harm. Prior to undertaking an intervention, trainees should be familiar with the relevant anatomy and physiology of the system they are about to operate upon, will have watched the procedure being performed and may have learnt the basics of the procedure in a simulated setting.
Trainees must to be able to self-reflect on their own skills and record of the number of procedures they have performed (which can act as a proxy for ability) to ensure that the correct level of supervision is provided alongside an intervention of suitable difficulty. Trainers need to be sure that their trainees have the necessary skills and knowledge to perform a technique, with experience often being gained in a stepwise reflecting both the difficulty of intervention and the gaining of skills, competence and confidence by the trainee11. This skills acquisition should be accompanied by regular discussion and feedback to maximise learning opportunities; when no supervision is available, trainees should consider video-recording the procedure as this allows reflection and review at a later date. A video diary can also be used as a portfolio of a trainee’s repertoire from beginner to expert during their training rotation. The challenge for trainees is to achieve competence in the relevant invasive technique within their training rotation; the number of interventions required to gain competence will vary between each trainee and technique11.
Handover
Handover allows the care of patients to be transferred from one group of individuals to another on a temporary or permanent basis. Handover confers an opportunity to present a clinical synopsis of patients with key information to ensure continuity of care and patient safety is maintained3. Most handovers are trainee led which provides an opportunity for peer learning to occur, checking comprehension and sharing interesting cases or tips for practice12. Handovers should be considered to be a high risk procedure, as communication errors can result in vital information being omitted; as such the process should be undertaken in suitable environment away from distractions, in a structured written and oral manner supported by an electronic format12. A further review at the patient’s bedside can be performed if required, which can highlight high risk patients.
Multidisciplinary Team Meetings
Multidisciplinary team (MDT) meetings are small formal meetings focused on all aspects of a patient’s care that involve a wide range of medical personal, nursing staff and allied health care professionals1. Meetings ensure that evidence-based guidelines are followed, and help to streamline management, removing unnecessary delays in treatment and improving cost effectiveness. MDTs represent a Community of Practice7 allowing social learning to occur as each individual can share their relevant expertise; MDTs enable best practice to be shared and help break down barriers between different specialties. Trainees can learn from the didactic teaching that occurs within the MDT (in relation to clinical details, investigation and management), but can also contribute to the meetings and practice their presentation skills.
Morbidity and Mortality Meetings
Morbidity and Mortality (M&M) meetings can help ascribe accountability and be used to highlight improvements in patient safety. They provide an opportunity for professional education, especially if the discussion can be held within a no-blame culture, and the meeting can voice discrepancies in how to manage patients, especially in ambiguous situations13. Trainees may be tasked with presenting a case and the potential learning aspects associated with patient care.
Grand Rounds/Formal Teaching
Grand rounds are traditional formal teaching opportunities that typically revolve around a case, whereby salient findings are presented prior to a discussion of management. These meetings allow opportunities for trainees to present cases and learn management, but their educational benefit may be decreasing as they are being replaced with lectures with limited clinical relevance14. However “audience apathy, deteriorating decorum and shrinking attendance” have diminished these learning opportunities14. Targeted teaching and the establishment of learning objectives for trainees can improve the educational content and the provision of feedback to the speakers can also enhance these meetings.
Journal Club
Journal clubs confer an opportunity for current scientific research and developments to be presented, critiqued and discussed by trainees. These clubs confer an opportunity to appraise the current literature and how that can be translated into evidence based patient care15. Journal clubs tend to be both voluntary and occur outside of working hours, resulting in highly motivated groups of participants whom are protected from interruptions.
eLearning and mLearning
Electronic learning (eLearning) and multimedia learning (mLearning) enable trainees to work informally, away from desks and computers, and at their own pace through a series of educational modules. Any intervention that engages trainees and promotes learning should be encouraged and these online learning platforms can be combined traditional learning resources should be promoted to ensure that all aspects of the curriculum are covered. mLearning in particular can be ‘dipped into’ allowing the learner optimal flexibility of how and when they want to use it. elearning can be referred to during point-of-care patient interactions when a trainee is unsure of how to proceed with patient management1. These increasingly important and under-utilized resources should be supported by educational institutions that support both undergraduate and post graduate trainees. By developing a virtual learning environment, individual tailored learning programs can be created that allow a trainee to develop and control their own online learning16.
Simulation
Simulation is becoming increasingly important for medical training. , anything can be simulated from learning clinical skills to human factors training, for both individuals and teams, focused on patient care and current medical practice in both the undergraduate and postgraduate setting. The availability of simulators coupled with competency based training and a decreased amount of training within the workplace has led to an increase use of this teaching format1. In addition, trainees need to understand how to use certain pieces of equipment prior to employing them on patients and this familiarity can only be gained in a simulated setting. Simulation can either occur within the workplace (allowing point-of-care simulation to see how teams react in a situation) or on formal taught courses; it can be low-technology and cheap (e.g., tying surgical knots on the back of a chair), but can also be high-fidelity and expensive (e.g., a virtual reality training simulator for laparoscopic operations), or use animal or cadaveric tissue. Simulation that increases trainee’s familiarity with certain techniques is likely to improve their clinical performance, decreasing potential patient harm and shorten the time taken for trainees to achieve competence1. A simulation should be completed with feedback from the supervisor to ensure that trainees gain the most from the session and clarify any facts or concerns about the simulation; a video recording of the session can also enable participants to reflect on their performance in a manner that is almost impossible in everyday clinical practice.
The NHS is supplied with approximately 300 000 NG tubes per year1. There are approximately 800-1000 incidents reported to the NPSA every year related to the insertion and use of NG tubes. Difficulties are often encountered with their insertion, especially in the setting of general anaesthesia. Whilst stridor and injury related to the use of NG tubes has been previously reported2,3, it has been related to prolonged siting. We describe a case acute stridor occurring in the recovery room due to direct trauma of the airway upon NG tube insertion.
Case report
A 61-year-old male presented with clinical symptoms of bowel obstruction. His medical history included atrial fibrillation (AF) treated with flecainide, and a 30-pack year smoking history. He was previously independent with a World Health Organisation performance status of 0. After CT confirmation of bowel obstruction, he was scheduled for an emergency laparotomy. A predicted P-Possum 30 day mortality was calculated at over 10%. He required no organ support pre-operatively, although his AF was poorly controlled. He had a low thoracic epidural sited awake, followed by induction of general anaesthesia with a rapid sequence induction. An arterial line, a central venous line, and an NG tube were inserted once anaesthetised. The NG tube was documented as difficult to site, and there were several attempts at a blind insertion via the oral and nasal route, before successfully inserting under direct vision using a laryngoscope.
The operative finding was that of an unresectable caecal tumour, and a defunctioning loop colostomy was formed. The total duration was 150 minutes. Following peripheral nerve stimulation and administration of 2mg/kg Sugammadex, he was woken, extubated and escorted to recovery.
Within minutes of being in the recovery area, he was acutely stridulous. Emergency assistance was called, and after assessment he was given nebulized adrenaline (1mg diluted in 4mls 0.9% saline), and 200mg of intravenous hydrocortisone. The nasogastric tube was removed, and his breathing was then supported with CPAP via a Mapleson C circuit and 100% oxygen. Direct examination of his airway, and indirect nasendoscopy with a Storz fibre-optic scope were performed. Significant bruising of his soft palate was seen, in addition to bruising and oedema of the soft tissues around the arytenoid cartilages with a small haematoma within the valleculae [Figure 1]. After approximately twenty minutes his stridor settled.
He was transferred to a level 2 high dependency unit later that day. He did not suffer from any further airway compromise, and his symptoms completely resolved.
Discussion
The insertion of an NG tube, whilst often deemed low risk, may result in life threatening consequences4. There even exists a “NG tube syndrome” 5, the pathophysiological mechanism of which is thought to be paresis of the posterior cricoarytenoid muscles secondary to ulceration and infection over the posterior lamina of the cricoid. There is no doubt that insertion of an NG tube in the anaesthetised patient can prove to be difficult, with a failure rate of up to 50% on first pass6, with repeated attempts at insertion being required. However, this case highlights the need for a controlled and ordered approach to managing the difficulties that can be encountered. Medical training incorporates NG insertion as a basic skill within the curriculum, but this affords new anaesthetic trainees little help with the anaesthetised and intubated patient.
There are several techniques described to insert NG tubes in anaesthetised, intubated patients7. There is evidence to suggest that modified techniques such as a reverse Sellick’s manoeuvre or neck flexion with lateral pressure are better than blind insertion in the neutral position. In the right hands, insertion under direct vision can overcome most difficulties, but is again not without risk.
We feel it is important to remember that NG insertion can cause patient harm, and potentially lead to life threatening consequences. Whatever the approach or technique that is chosen, having a logical and ordered approach is paramount. Using suitable alternative methods for insertion, or abandoning the procedure, as opposed to blindly continuing to repeat the same unsuccessful method must be key for success, as would be the case for approaching any clinical encounter.
Published with the written consent of the patient.
The closure of asylums in the last century has resulted in an increased number of compulsory hospital admissions for psychiatric patients. Psycho-geriatric patients are highly vulnerable in this respect. Although the traditional buildings instituted for the care of the mentally afflicted have gone, misconceptions about provision and anecdotes about incarceration continue to haunt the community. Recent legislative changes have further extended the occurrence of involuntary hospital admission.1 Compulsory community care is under constant review. Concurrently the validity of the concept of mental illness, psychiatric classification and diagnostic dilemmas all continue to be debated. Confinement has regained respectability in the discourses of present-day British mental health system because of violent offences committed by psychiatric patients and the public media portraying them as a reflection of failure of community care.
Table 1, Advantages of Mental Health Acts
1. Mental health acts secure the safety of vulnerable people 2. Helps to regain control on their lives 3. Compulsory treatment helps to prevent further deterioration of mental health 4. Aimed to provide effective care and treatments 5. Ensure better after care 6. Protects the safety of other people 7. Prevents suicides 8. Provides opportunities for assessments and diagnosis 9. Can be therapeutic by unburdening personal responsibilities to an institution.
Numerical quantitative studies imply that generally involuntarily admitted patients show clinical improvement and retrospectively view their compulsory admission rather positively.2 It is an unquestionable fact that Mental Health Acts prevent suicides and homicides (table 1). Mental Health Acts have some unsatisfactory outcomes particularly on a subset of patients including senior citizens admitted formally. It is important to identify such patients and take additional precautions in their management as they run the risk of leaving hospital feeling inferior and inadequate. Patients’ specific characteristics, thought processes and past treatment experiences, colour their attitude towards coerced treatment and determine the gains and shortcomings of compulsory care.
Disadvantages
The Mental Health Acts are open to social abuse and elderly patients can be more defenceless in this respect. Specifically they may be: invoked to control behaviour; misused for material gain and implicated in subtle expressions of revenge. They are sometimes invoked to hasten divorce proceedings and to secure the custody of children by a specific parent. They are also used to control the behaviour of children by their parents. Mental Health Acts designed to control psychiatric patients are being enacted and enforced in some underdeveloped countries that lack an efficient tribunal system to monitor their effects.
A patient who has been detained is at risk of repeat detention and someone who has been inappropriately assessed becomes increasingly vulnerable to control on psychiatric grounds. The experience of being detained involuntarily has a reductive effect on behaviour after discharge – it may induce anxiety or post-psychiatric depression. The awareness of being deemed to require compulsory detention generates such negative attitudes as self-denigration, fear and unhealthy repression of anger. It may also impede self-direction and the normal sense of internal control and may encourage the view that in a world perceived as being divided into camps of mutually exclusive ‘normal’ and ‘abnormal’ people, the patient is in the latter category. Compulsory detention may lead to suicide because the patient loses their sense of integration within their own society. Furthermore, the fear and anxiety associated with involuntary admission delays the recovery process. There are other frequently occurring barriers to recovery for those affected such as, loss of capabilities, whether real or imagined, ineffectual medication due to poor elicitation of symptoms because of patient’s lack of cooperation and negative drug side effects.
Depressed patients have a higher suicide risk than the population at large and one of the reasons for detention is suicidality. Some of the subjective symptoms of depression can be ameliorated by denying them, while compulsory detention may reinforce depressive symptoms. Detention gives carers a false sense of security and this may lead them to relax their vigilance towards the patient. The Mental Health Acts increase the stigma associated with psychiatric illness and with the exuberant expression of emotions. Patients who are under section or are frightened of being placed under section may deliberately mask their symptoms in an attempt to have the section lifted or to avoid sectioning.
Trans-cultural studies
Trans-cultural studies show that members of migrated cultures, particularly the elderly, are more at risk of inappropriate sectioning than the rest of the population because of the lack of knowledge on part of professionals about the patient’s culture. For instance, the debate of over diagnosis of schizophrenia among Afro-Caribbean patients is still unsettled. A study conducted in South London has concluded that Black Africans and Black Afro-Caribbean patients with psychosis in that area are more likely than White patients to be detained under the Mental Health Act 1983.3 GreatBritain has become a multicultural society and a significant percentage of professionals working in psychiatric units have been trained overseas, in a wide range of countries. This creates further risk of inappropriate diagnosis. There needs to be more emphasis on the significance of trans-cultural psychiatry in the United Kingdom. In particular, psychiatrists should be aware that psychiatry is a medicine of language and culture as well as of the mind.
Medical Dilemmas
Countries in which Mental Health Acts are widely enforced have not achieved any reduction in suicide rates through their implementation. Sectioning is perceived by many patients affected as a psychological guillotine – a form of psychiatric terrorism. The medical profession is invested by the Acts with undue power over society. This is of particular concern because training in psychiatry does not include the study of free will and allied philosophical issues and also because there is no clear definition or description of mind and consciousness. In psychiatry there is a lack of clinical indicators and psycho-physiological parameters so the criteria for diagnosis are imprecise, with a concomitant risk of the Acts being erroneously implemented. It has been postulated that once a person has been classified as having deviant behaviour, that categorisation has a potent effect on the subsequent actions of the person concerned and those interacting with them.
Is it not justifiable to argue that even if a few mentally ill patients are underdiagnosed and not subjected to psychiatric admission, someone whom we would regard as normal should not be detained in a psychiatric hospital against their will? Such a view is analogous to the judicial view regarding capital punishment where even if ninety-nine murderers escape capital punishment because there is no death penalty, one innocent person should not be sentenced to death. Mental Health Acts may be a necessary evil but they present a dilemma for mental health professionals: the morality of helping patients and protecting the society from the consequences of their illness against the immorality of restricting their freedom. Clinicians become torn between the ideals of curing mental illness and defending the sanity of patients.
Patients’ Perception
A small survey conducted by the author revealed that no sectioned patient in the group studied sent a thank-you card after discharge to the ward in which they were confined. However, many voluntary patients expressed appreciation in that way. This is an indicator of the attitude of sectioned patients towards the Mental Health Acts. One reason must be that a record of being sectioned limits their freedom to travel and also affects their employment opportunities adversely. A patient has commented that it is easier for an ex-convict to gain employment than it is for a once-sectioned psychiatric patient.
There is anecdotal evidence illustrating the panic that may be generated with the word ‘section’ in psychiatric patients. A recovering elderly hypomanic patient explained that he misconstrued the word on hearing it when he was ill, taking it in relation to sectioning in Obstetrics and General Surgery. He remembered that as he resisted entering a taxi while being persuaded to agree to admission, the driver said that he was going to be sectioned if he refused hospital admission. The patient misunderstood this and interpreted it as he was going to be cut into pieces and tried to jump out of the vehicle.
Post-traumatic stress disorder
Any loss of intrinsic importance to an individual constitutes bereavement. Denial, anger and depression experienced in compulsory detention are comparable to bereavement.4 In the case of a detained patient, the loss of self-identity and of social functioning causes a grief reaction. It has been hypothesised that there are high levels of Post-traumatic Stress Disorder (PTSD) symptoms in detained patients.5 Very few repeat detainees become habituated to the implementation of the Mental Health Acts. The vast majority become increasingly frustrated and develop a pessimistic outlook towards their mental health. There is a high incidence of suicide among patients who have multiple detentions.
Post-hospitalisation Stress Disorder is much more common than generally recognised. Formal admission may lead to fear, anger, frustration, depression or loss of self-esteem, depending upon the individual’s psychological response.6 Involuntary admission may result in pervasive distress in any patient – this kind of hospital admission may be perceived as threatening and even as a catastrophe. Detained psychotic patients are less aware of their environment because of the preoccupation with their symptoms. Non-psychotic patients, when detained for instance because of a risk of suicide, are fully aware of their immediate environment and the chaos they have caused to themselves. They have a high risk of PTSD.
Preventive detention
Fear of liability may lead to compulsory hospitalisation solely to prevent violence on the part of patients who otherwise do not require in-patient care.6 Psychiatrists are not trained to police society and may lack sufficient knowledge and experience to participate in the social control responsibilities that are part of the remit of the criminal justice system - they are sometimes involved in that function. Psychiatry has to be safe and secure in the hands of individual psychiatrists and psychiatrists have to be protected when practising psychiatry. Mentally ill patients are sometimes mistakenly processed through the criminal justice system rather than the mental health system. When that happens, compulsory detention may be perceived as a form of criminalisation of mental illness. Unless there is scrupulous monitoring, mandatory treatment impinges on civil liberties. Preventive detention is legally ambiguous and clinically impractical.
Assessment
Amongst the government’s fundamental powers and responsibilities are, protecting people from injury by another and caring for less able people, whether physically or mentally incapacitated. These functions encompass the welfare and safety of both the individual concerned and the public.
A decision about compulsory detention is made on the basis of three considerations: loss of emotional control; psychotic disorder and impulsivity with serious thoughts, threats or plans to kill oneself or others. Any perceived risk must be imminent and provocative. The clinician is legally required to determine the least restrictive environment to which a patient may be safely assigned for continued care. To fulfil these requirements while implementing the Mental Health Acts, a psychiatrist needs the skills of a physician, lawyer, judge, detective, social worker and philosopher. The decision-making process is influenced by multiple factors such as: the clinician’s propensity to detain patients; the record of past untoward incidents involving the patient; attitude towards risk taking and availability of hospital beds and alternative safe treatment facilities. It is regrettable that in section 5(2) assessments, often it is a junior doctor, the least experienced person in the team, who is called upon to conduct the evaluation.4 A multitude of interviews with mental health staff, a social worker and solicitor will have to be endured by the patient - these are regarded as ordeals by most of them.
Non-detainable patients
Since the introduction of the Mental Capacity Act 2005, the number of assessments that are followed by a decision against compulsory detention is increasing. Patients who are assessed for formal admission but not found to be detainable may develop new risks subsequently as a result of the assessment procedure itself. Before assessment, mental health professionals may place themselves in covert locations around the patient’s house and neighbours may watch eagerly behind their curtains. Thereby the patient’s social image is damaged. After meticulous assessment, it may be a relief for the patient that they are not detained and that euphoria may continue for a short while but all too often damage has been done. The patient who is tormented by psycho-social stressors may find the assessment experience intensifies the injury. The decision about whether it is appropriate to assess someone is therefore an area in which more clarification and some management guidelines are much needed. In situations such as these, untoward incidents have been periodically reported. That may mean that the professionals involved and perhaps also family members who initiated the assessment, blame themselves and endure severe guilt feelings or blame each other. Furthermore, psychiatrists are not mind readers. It is possible that a patient will cleverly deny any suicidal intent during assessment, intending to fulfil a suicidal urge afterwards and that may falsely appear to be a reaction to the assessment. An interview for assessment may be the factor that takes them beyond their limit. Because of all these circumstances, the patient may need intensive home care and counselling after an assessment that does not lead to hospital care. In addition to treating mental illness, it is the duty of the psychiatrist to defend the sanity of patients. The difficulty of defining normalcy is notorious: it is easier to detect psychiatric symptoms than to describe normal behaviour.
Tribunals
Mental health tribunals are demanding and may be humiliating and intimidating. They are highly stressful for the patient and clinician and they involve the breach of patient confidentiality. Tribunals are often emotionally charged scenes for the patient and psychiatrist, they may result in traumatisation. The largely professional make-up of a tribunal is often perceived as intimidating by patients, who tend to be suspicious of collusion between professionals and above all of their reluctance to challenge the decision of a psychiatrist.7 Psychiatrists who are aware of legal profession’s ignorance on psychiatric issues dominate the tribunal scene by flamboyant linguistic expressions, while lawyers question the objectivity of psychiatry and the expertise of psychiatrists in legal matters. Tribunals are concerned with the legality of detention and not with the appropriateness of treatment. However, one study has shown that patients who appear before tribunals find it easy to accept they require compulsory admission. 8 Psycho-geriatric patients find it extremely distressing to attend tribunals. Hospital managers’ review hearings are often arranged and carried out promptly. Managerial hearings involve local people too which may make them less intimidating for detained patients.
Involuntary treatment
Although mental health staff usually have the best of intentions, when mandatory treatment is applied to patients it may prove traumatic and counter-therapeutic. The experience of undergoing forced treatment adds to the patient’s perception of stigma and discrimination. Involuntary psychiatric drug treatment is bound to be less effective than voluntary treatment. An outcome may be misdiagnosis, long-lasting and disabling side effects. Forced treatment potentially violates a person’s right to respect private life under Article 8 of the European Convention on Human Rights. Article 8 is violated only if patients can prove the treatment given is more harmful than the claimed therapeutic benefits, yet the clinician can administer the treatment if he thinks it is therapeutically necessary. Compulsory treatment makes patients feel infantilised, especially because forced psychiatric treatment often involves coercion, emotional intimidation, bullying and threats.
Community Treatment Order (CTO) is being constantly evaluated in terms of its merits and demerits. The results have been inconclusive and warrant more systematic studies. It was Section 41 of the Mental Health Act that inspired the introduction of CTO - the main purpose being to protect the community from the aggressive behaviour of some of the psychiatric patients as in the case of the successful Section 41. There are indications that CTO has fulfilled such a goal. It was also targeted to enhance compliance and concordance with the mental health services and to prevent suicides but studies indicate that those goals were not achieved.9,10 The Oxford Community Treatment Order Evaluation Trial (OCTET) substantiates a lack of any evident advantage in dropping relapse.
The “knee jerk” reaction from part of community service has apparently resulted in spontaneous readmissions of patients under CTO. It has also contributed to prolonged detention of patients awaiting community placement under CTO. This is because detained patients must stay on section 3 or 37 to allow the Mental Health Act to be converted to CTO upon discharge. Obviously, such a scenario curtails liberty. Patients always feel bitter about the “hanging feelings” of continued detention. Coercion runs the risk of weakening therapeutic alliance. It may be true that if fewer conditions are imposed, CTO could serve as a “memory knot” for patients with limited insight. Despite all the controversies surrounding the benefits of CTO, its use is increasing worldwide. 11
Assertive Human Rights
All human beings have individual rights and mental health professionals in particular must be mindful of those rights. Table 2 presents the list of assertive human rights, as modified from Gael Lindenfield (2001). 12
Table 2, Assertive Human Rights
1. The right to ask for what we want (realising that the other person has the right to say “No”). 2. The right to have an opinion, feelings and emotions and to express them appropriately. 3. The right to make statements which have no logical basis and which we do not have to justify (e.g. intuitive ideas and comments). 4. The right to make our own decisions and to cope with the consequences. 5. The right to choose whether or not to get involved in the problems of someone else. 6. The right to know about something and not to understand. 7. The right to be successful. 8. The right to make mistakes. 9. The right to change your mind. 10. The right to privacy. 11. The right to be alone and independent. 12. The right to change ourselves and be assertive people. 13. The right to be neutral. 14. The right to be empathetic and apathetic.
Discussion
Community care is more innovative than compulsory detention in hospital. For majority of patients, the best way forward is having high quality home treatment facilities as it is least restrictive and using compulsory detention should be the last resort. In some cases, forced psychiatric admission is indicative of failure in the supply of quality home treatment.One thing that sometimes leads to in-patient admission is lack of confidence in the service available. The perception of home treatment may be at fault here - it needs to be understood as more than merely staying outside hospital. Forensic patients and treatment resistant psychotic disorders lacking insight may be a different state of affairs. CTOs have serious impact on the autonomy and privacy interests of individuals and should not be applied to compensate for under-resourced community services.
Caring and supportive relationships between mental health staff and patients during involuntary in-patient care have considerable bearing on the outcome of compulsory detention. A recent study has revealed that among patients who have been detained involuntarily, perceptions of self are related to the relationships with mental health professionals during their inpatient stay. 13 Perceived coercion at admission predicts poor engagement with mental health staff in community follows up. When professionals demonstrate their genuineness and encourage patient participation in the treatment options, coercive treatment would be perceived as less of an infringement to the autonomy of patients and their sense of self-value. 14 If patients maintain both positive and negative views about detention, interventions should be designed to enhance positive experiences by focussing on respect and autonomy.Patients admit only compulsory detention gave them an opportunity to receive medication in a time of crisis and report it did not necessarily prevent thoughts relating to self-harm. It simply reduced the opportunities for impulsive acts.
‘Rooming-in’ is worth debating as an alternative to compulsory detention. This is the voluntary participation of so-called confidants, who may be chosen family members or trusted friends. They provide a 24-hour vigil for the patient in a safe hospital environment. An Australian study has suggested this system is highly valued by nursing staff, patients and their families.15 It is an initiative that needs further testing and evaluation. The resolution of angry feelings towards the mental health professionals has a significant bearing on their future compliance. The post-detention period tests the attention given to patients by mental health professionals. Here the staff members have to take the initial steps required to repair damaged relationships which may have developed in particular with angry patients. Detained patients should be offered counselling in post-discharge follow-ups and should be given satisfactory explanation of the circumstances for formal admission. Detained patients should be given the support to enable them to: rewrite their life story; reconstruct a sense of self; achieve healing of the assault of their illness and the treatment procedures inflicted on their personality. Specific interventions should be designed and evaluated in order to deal with any unresolved PTSD symptoms relating to formal psychiatric admission.
Bednar tumour, first described by Bednar in 1957, is a pigmented variant of dermatofibrosarcoma protuberans (DFSP).It is a rare entity, constituting1 to 5% of all DFSPs, which in turn, represent 0.1% of skin malignancies. It differs from DFSP by the presence of dendritic cells containing melanin, interspersed between the fusiform cells characteristic of DFSP. The most frequent location is in the trunk followed by upper and lower extremities and the head and neck region. We report a case of Bednar tumour occurring on the shoulder of a 29-year-old male.
Case report
A 29 year old male patient presented with a slow-growing swelling on his left shoulder for the past two years. Physical examination revealed a large, nodular, subcutaneous mass measuring 8x7 cm in left suprascapular region. Clinical impression was of soft tissue tumour and total resection with 3-cm margins was performed. Grossly, tumour measured 9x4.5 cm, with grey white to grey black cut surface (Figure 1a, 1b). Microscopy showed spindled cells arranged in a tight storiform pattern admixed with scattered heavily pigmented cells (Figure 2). On immunohistochemistry, tumour cells were positive for vimentin and CD34 (Figure 3a, 3b) and negative for S100, SMA and desmin. Pigmented cells were found positive for S100 and HMB 45 (Figure 4a, 4b) and negative for other markers. Thus, a final diagnosis of Bednar tumour was rendered.
Figure 1 - Gross appearance of the tumour with cut surface grey white to grey black
Figure 2 - Spindle cells in storiform pattern admixed with scattered heavily pigmented cells
Figure 3 - Tumour cells were positive for vimentin (3a) and CD34 (3b)
Figure 4 - Pigmented cells showed positivity for S100 (4a) and HMB 45 (4b)
Discussion
Dermatofibrosarcoma protuberans (DFSP) is a locally aggressive soft tissue neoplasm with intermediate malignant potential, regarded as a low grade sarcoma by the WHO classification of tumours of the skin.1,2,3
It was first described by Darier and Ferrand as a distinct cutaneous disease entity called progressive and recurring dermatofibroma in 1924. The term dermatofibrosarcoma protuberans was officially coined in 1925 by Hoffman.4
Histopathologically, DFSP is characterised by irregular, short, intersecting fascicles of tumour cells arranged in a characteristic storiform pattern. Cells have spindle-shaped nuclei which are embedded fairly uniformly in a collagenous stroma. There are several histological variants of DFSP. These include Bednar tumour, fibrosarcomatous, fibrosarcomatous with myoid/myofibroblastic change, myxoid, granular cell, palisaded, giant cell fibroblastoma, combined and indeterminate.5
Pigmented DFSP (Bednar tumour), first designated as storiform neurofibroma by Bednar, is a clinically and morphologicallydistinct variant of DFSP, constituting 5%-10% of all cases of DFSP.1,5 Clinical presentation is in the form of erythematous blue or brown coloured plaque lesions, with a smooth or irregular surface, often adhering to the deep tissue. The tumour may be exophytic, nodular or multilobulated and is generally firm in consistency.2 The lesions present as a slow growth, over a period of months or years. They have been described in all ethnic groups, with preponderance in blacks. They occur in third and fourth decades of life, however they may also occur in infancy and show a slight male predominance.1,5
The histogenesis of Bednar tumour is controversial. Some authors regard these tumours as being of neuroectodermal origin because of the presence of dendritic melanocytes and cells suggestive of Schwannian differentiation; while others believe attribute the origin to various kinds of local traumas, such as previous burns, vaccination scars, insect bites or vaccination such as BCG.3,6
Histopathologically, Bednar tumour is characterised by scattered melanosome-containing dendritic cells within an otherwise typical DFSP. The number of melanin-containing cells varies from case to case. Abundant pigmented dendritic cells can cause black discoloration of the tumor, whereas scant pigmented cells can be only identified microscopically.3,5 They grow invasively into the dermis and may reach the subcutaneous strata, fascia and musculature, in a manner similar to that of dermatofibrosarcoma protuberans. Occasionally, Bednar tumour may undergo fibrosarcomatous transformation with rare examples of pulmonary metastasis.5 Wang et al have reported a case of Bednar tumour with prominent meningothelial- like whorls.7
Immunohistochemically, most of the tumour cells stain positively with CD 34 and vimentin, and are negative for neuron-specific enolase, HMB-45 and protein S-100. However, cells containing melanin are positive for the usual melanocytic markers such as S-100 protein.5 On electron microscopy, three populations of cells have been identified, most of the cells being represented by fibroblasts. The second population exhibits fine elongations, enclosed in basal membrane while the third population consists of dendritic cells containing melanosomes and premelanosomes.3,5
The differential diagnoses include pigmented (melanotic) neurofibroma, psammomatous melanotic schwannoma, and desmoplastic (neurotrophic) melanoma. Pigmented neurofibroma can be differentiated from Bednar tumour by more extensive storiform growth and strong positivity for CD34 in latter. Psammamatous melanotic schwannoma is circumscribed, heavily pigmented with psammoma bodies, tumour cells being S- 100 positive and CD34 negative. Desmoplastic melanoma shows junctional activity and neurotropism.
Treatment consists of complete excision of the tumour with maximum preservation of normal tissue to maintain function and for optimal cosmesis. Moh’s Micrographic Surgery (MMS) or staged wide excision “Slow Moh’s “(with formal histopathological sectioning and delayed reconstruction for complete circumferential peripheral and deep margin assessment) has become the standard surgical treatment for DFSP.6,8
Bednar tumour presents a diagnostic challenge to the clinician because of resemblance to other commonly occurring pigmented lesions. Histopathological and immunohistochemical examination are necessary to arrive at the correct diagnosis.
A 74 year old female presented to the A&E department after waking with a swollen tongue. She called for an ambulance and the paramedic crew initially treated her for an allergic reaction with 200mg hydrocortisone IV, 20mg chlorphenamine IV and four doses of 0.5mg adrenaline 1 in 1,000 IM. She did not improve and was transferred to the local A&E.
In A&E, she was initially stable with no stridor or difficulty in breathing but noticeably swollen tongue. Saturations were 98% on 5L nasal O2. Blood pressure was stable at 135/75 mmHg. GCS was 15/15, but the patient was agitated from not being able to speak or retract the tongue. No further history was taken other than an allergy to shellfish, with no recent exposure. An obese habitus was noted.
A&E doctors called the anaesthetic on-call team, and on their request called the on-call ICU consultant and the on-call ENT consultant. Further adrenaline 100mcg IV, hydrocortisone 200mg IV and chlorphenamine 10mg IV were given. An attempt to look inside the mouth with a tongue depressor and torch was made by the anaesthetics/ICU team and it was quickly realised that the swelling continued into the mouth and larynx and was rapidly progressing. Given the lack of suitable equipment and the severity of the case, a decision was made to transfer to emergency theatres.
Once in emergency theatres, the on-call ENT consultant was scrubbed and ready. 100% oxygen via facemask and routine monitoring was instituted. At the request of the ENT consultant, a micro-tracheostomy was attempted with local anaesthesia but failed to pass into the trachea given the patient’s habitus. The ENT surgeons attempted an awake tracheostomy, but this was difficult due to her being agitated and unable to lie still, and a calcified trachea.
The rapidly progressing swelling compromised oxygen delivery to the lungs and the saturations began to drop quickly. The patient became bradycardic and lost consciousness. At this point, it became easier to attempt the tracheostomy. The ALS protocol was followed and CPR started. An attempt was made for direct laryngoscopy – a grade 3b view was obtained and a size four microlaryngeal tube was passed successfully. 100% O2, two doses of 1mg adrenaline IV, and 3mg atropine IV were given and the heart rate improved. Pulses were present and the defibrillator showed sinus rhythm; CPR was stopped and tracheostomy was continued. Due to abundant peri-tracheal fat, a number of tracheostomy tubes were tried before a secure tracheostomy was placed. However the microlaryngeal tube maintained airway patency.
An arterial line and larger cannula was secured. Propofol infusion and fentanyl IV were given to maintain anaesthesia and the patient was transferred to ICU.
On ICU, there was further difficulty in ventilation, with high airway pressures and saturations falling to the low 90s despite 100% O2. It was thought the tracheostomy tube was abutting the carina or posterior tracheal walls. The ENT surgeons were called urgently and in the interim the patient was re-intubated with a size 7 ETT to maintain the airway. The ENT team changed the size 8 cuffed non-fenestrated tracheostomy tube for a size 7 Shiley with a proximal extension. Despite the change, ventilation remained difficult. An urgent chest X-ray was performed which showed a right-sided pneumothorax. A chest drain was inserted and a ‘hiss’ was noted on insertion, indicating a possible tension pneumothorax. Ventilation then improved.
Further history was taken from previous notes and discharge letters. It was noted that the patient had allergies to shellfish, penicillin, erythromycin, and diclofenac, but no history of exposure. She had a background of hypertension, angina, chronic kidney disease and previous breast cancer. She was taking Lisinopril, Diltiazem, Nicorandil, Tamoxifen, Sertraline and Omeprazole. Her tongue swelling improved markedly over the next two days with antibiotic treatment and regular dexamethasone. She was awakened once appropriate and haemodynamically stable. A nasendoscopy was performed by the ENT team on day six and nothing remarkable was noted, with swelling having regressed totally. She was decannulated on day eight and transferred to the ward. Lisinopril was stopped.
Discussion
This case demonstrated a severe, acute presentation of tongue swelling (glossitis) leading to upper airway obstruction. Although a number of conditions may cause glossitis: infection, trauma, anaemia, liver disease, malnutrition. Acute glossitis is a hallmark of angio-oedema. This is a rare, but life threatening condition that requires prompt recognition and treatment.
Angio-oedema may result from anaphylactic, hereditary, acquired or idiopathic processes. Some 12-24% of anaphylaxis cases present with angio-oedema.1, 2 Hereditary and acquired cases usually result from a deficiency of C1 esterase inhibitor deficiency, which causes an accumulation of bradykinin, leading to soft tissue oedema. Such an increase in bradykinin may be caused by angiotensin converting enzyme inhibitors, leading to angio-oedema.3 If no cause can be found, it is termed idiopathic.
Management of angio-oedema requires rapid airway assessment and management; resuscitation; and treatment of the underlying cause. Anaphylaxis should respond to standard management as outlined by the AAGBI.4 Angio-oedema from other causes requires cessation of the suspected causative agent3, and in an emergency, nebulized adrenaline to reduce airway swelling. Infusion of plasma derived or recombinant C1 Esterase Inhibitor may also rapidly improve symptoms.1
Although airway support is the cornerstone of anaesthetic management, an acute, rapidly progressing case such as this requires a multi-disciplinary approach.5 Anaesthetists will require help from operating department practitioners and nurses to manage the initial airway compromise. A compromised airway presents a significant hazard to any form of anaesthesia, especially if it results in cardio-respiratory depression, which will expedite hypoxemia and impair tissue oxygenation. An awake, spontaneously ventilating approach to secure the airway needs to be undertaken. ENT staff should be scrubbed and ready to perform an emergency surgical tracheostomy if complete airway obstruction occurs or airway access cannot be secured.
An awake fibre-optic intubation can be attempted but this requires an experienced anaesthetist, timely access to equipment, preparation and a co-operative patient. These are unlikely to be provided in the resuscitation room. Fibre-optic manipulation causing bleeding or further swelling can lead to complete airway obstruction.
An inhalational induction to maintain spontaneous ventilation and then followed by direct laryngoscopy or fibre-optic intubation is another option and reduces the required co-operation of the patient. But this may cause haemodynamic instability in an already compromised patient and can lead to complete airway collapse.
An elective awake tracheostomy under local anaesthetic is the most likely route to ensure airway access without haemodynamic compromise.6 This will require a co-operative patient, senior help from trained operating department staff, and the ENT surgeons scrubbed and ready to perform a surgical tracheostomy if a percutaneous approach fails.
The Intensive Care Unit should be aware of the patient and ICU teams will be required to help with airway access as well as manage haemodynamic instability, secure arterial and central venous access. The patient will need further airway support and treatment in the Intensive Care Unit.
An acute upper airway obstruction therefore requires an emergent, yet controlled, approach to secure airway access and maintain oxygenation. Staff should have clear roles, ideally decided beforehand and practiced, with experience in the use of the equipment available. Senior ENT help should be available readily and again be versed in securing an emergency awake tracheostomy should other means fail or are not suitable.
As with any critical incident a debriefing should be undertaken to highlight points in the management of such patients that were handled well and those that were not, so that existing management plans can be improved and skills honed to improve management of future incidents.
A 46 year-old man presented to the Emergency department with chest pain and collapse, associated with loss of consciousness lasting several minutes. He had no significant past medical history and he had no risk factors for coronary artery disease. However, he did note a similar episode of collapse and loss of consciousness one year prior for which he did not seek medical attention. There was no known family history of heart disease or sudden death.
On examination he was haemodynamically stable with a blood pressure of 130/80 mmHg and heart rate of 85 beats per minute. Jugular venous pressure was measured at 2cm above the sternal angle and heart sounds were normal with no added sounds. His oxygen saturation was 98% on air and chest was clear to auscultation. Chest X-Ray demonstrated clear lung fields and laboratory investigations, including electrolytes and cardiac troponin T were within normal limits. Echocardiography showed a structurally normal heart. Figure 1 shows his 12-lead electrocardiogram (ECG) on admission.
Figure 1 – 12 lead ECG on admission
Questions
1. What is the likely diagnosis based on the clinical presentation and ECG findings?
2. What life-threatening arrhythmias can arise from this condition?
3. What is the pathophysiology of this condition?
4. How is the diagnosis of this condition made?
5. What treatment options are available for patients with this condition?
Answers
1. What is the likely diagnosis based on the clinical presentation and ECG findings?
Short answer
Brugada syndrome
Long answer
The ECG shows coved Type 1 ST segment elevation in keeping with a diagnosis of Brugada syndrome.
First described in 1992, Brugada syndrome is a primary cardiac electrical disease or channelopathy that is accompanied a structurally normal heart and carries an association with sudden cardiac death1.
Presentation often occurs in the third or fourth decades of life, with a male preponderance of 8:1, however sudden cardiac death due to Brugada syndrome has also been seen in patients at the extremes of age. It is estimated that it accounts for up to 20% of all sudden cardiac deaths in patients without structural heart disease, ischaemia or electrolyte abnormalities2. It is most commonly seen in south-east Asia, especially Thailand, where its incidence is around 1%, and is much less common in western countries1.
2. What life-threatening arrhythmias can arise from this condition?
Short answer
Brugada syndrome is associated with increased risk of ventricular tachycardia (VT), often polymorphic, and ventricular fibrillation (VF).
Long answer
Brugada syndrome often manifests clinically in the form of syncope or sudden cardiac death. It is most commonly associated with polymorphic VT and VF, which may or may not terminate spontaneously. There are a large proportion of patients with Brugada syndrome who never experience any symptoms and indeed, may not ever even be identified as having the condition, unless they are found to have incidental ECG abnormalities as part of routine medical testing or are under investigation for another problem3.
3. What is the pathophysiology of this condition?
Short answer
Brugada syndrome is understood as a genetic cardiac channelopathy, a disorder produced by the dysfunction of a cardiac ion channel participating in the action potential which can result in electrical change favouring the development of arrhythmias. Inheritance of the condition occurs via an autosomal dominant mode of transmission with incomplete penetrance4.
Long answer
Brugada syndrome is a genetic disorder, with a loss-of-function mutation of the SCN5A gene implicated in about 30% of sufferers. This gene codes for the α-subunit of the cardiac sodium channel. Other mutations of sodium and calcium channels have also been found. In inherited cases, the gene is passed in an autosomal dominant fashion, though sporadic mutations are also seen.
There is increased susceptibility to ventricular arrhythmias, because of altered depolarisation within the right ventricle. In SCN5A mutations, the defect in sodium channels leads to decrease in the sodium current and a shortening of the cardiac action potential by blunting phase 0 depolarisation. Potassium channels are also affected, with an increased number of transient outward potassium channel currents. This imbalance in the myocytes between sodium and potassium concentrations means the overall effect is to shorten the refractory period, making the myocytes more prone to re-entrant circuits, leading to the development of VT and degeneration to VF2,5.
4. How is the diagnosis of this condition made?
Short answer
Brugada syndrome is characterised by electrocardiographic changes demonstrating coved ST segment elevation in the right precordial leads.
Long answer
Electrocardiographic abnormalities constitute the hallmark of Brugada syndrome. There are three different ECG patterns and in all three types, the ECG shows ≥2mm J point (junction between the termination of QRS complex and beginning of ST segment) elevation and a characteristically shaped ST segment in the right precordial leads6.
Type I has a ‘coved’ pattern ST segment elevation ≥2mm, with a descending terminal portion in at least one right precordial lead.
Type II has a ‘saddle-back’ ST segment elevation ≥1mm and has a high elevation in its initial portion.
Type III has either coved or saddleback ST elevation but is less accentuated than types I or II (<1mm).
Although all the 3 patterns can be present in patients with Brugada syndrome, only the presence of a type-1 ECG pattern defines the diagnosis of the condition2,7. The patterns for type II or III are not diagnostic, and carrying out a Class I anti-arrythmic drug (AAD) test to confirm the diagnosis is recommended. This can be done with AADs such as ajmaline, flecainide or procainamide, though currently ajmaline is preferred due to its higher sensitivity in revealing Brugada type ECG changes1.
It is worth noting that the resting ECG changes associated with Brugada syndrome (in particular type I) are often transient, and therefore, in someone in whom the diagnosis is suspected, an AAD test may be indicated even if there are no resting spontaneous ECG abnormalities evident6.
Differential diagnoses of Brugada syndrome must be approached with care as ST segment elevation is associated with a wide variety of benign and malignant pathophysiologic conditions3.
5. What treatment options are available for patients with this condition?
Short answer
Currently, the implantable cardioverter defibrillator is the only proven effective treatment in the prevention of sudden cardiac death.
Long answer
Management of Brugada syndrome is focused on risk stratification of patients to prevent arrhythmic death in high risk individuals. ICD implantation can prevent sudden cardiac death in these groups1. Newer devices are now also being used, including the subcutaneous ICD which is implanted in a subcutaneous pocket and does not require any endovascular leads in the heart or access to the central venous circulation8.
Pharmacological options are focused on rebalancing the ion channel current active during the early phases of the epicardial action potential in the right ventricle3,9. Some studies have evaluated the role of quinidine in the treatment of Brugada syndrome and found it to be effective in preventing polymorphic VT and VF in this condition10. Quinidine has also been proposed as an alternative to ICD implantation in children and infants too young to receive an ICD11,12.
Data relative to the use of cryosurgical treatments or ablation therapy in Brugada syndrome are very limited at this point in time3.
Patient outcome
The patient underwent successful implantation of a subcutaneous cardioverter defibrillator. Figure 2 and Figure 3 show chest radiographs of the leadless device.
Polyarteritis nodosa (PAN) is a rare vasculitis in childhood. Since first described by Kussmaul and Maier in 1866 1, there have been approximately 140 pediatric case reports in the literature. Traditionally, children were classified as having one of three forms: infantile, cutaneous, and systemic. Infantile PAN is now recognized as a severe form of Kawasaki disease. Criteria for a diagnosis of systemic PAN in childhood have been proposed but not validated2.
Cutaneous PAN (cPAN) is recognized as a separate entity but there are no diagnostic criteria for cPAN2. cPAN is characterized by disease affecting the skin with no major organ system involvement. The cutaneous symptoms are similar to systemic PAN and mild fever, muscle, joint, and peripheral nervous system involvement may also occur. Fever, rash, and musculoskeletal symptoms are common in children and cPAN needs to be differentiated from other diagnostic entities. Definitive diagnosis is by histopathologic evidence of necrotizing inflammation of the medium and small-sized arteries. There is a paucity of knowledge of the spectrum of clinical presentation and management of children with cPAN. Here we describe a case of cPAN and summarize the clinical manifestations, laboratory data and treatment regimens of our patient.
Case report
This 10 year old female adolescent presented with pain in both the elbow joints followed by pain in the left knee joint and both the ankle joints in a course of 8 days and fever for the past 2 days .On admission her vitals were stable, both the elbow joints were tender and the knee and ankle joints were swollen and tender .She had multiple subcutaneous nodules over extensor aspect of both her forearms, both her tibial shins and few on her thighs. Systemic examination showed presence of a soft PSM of grade 2 intensity over left sternal edge. Blood investigations showed leucocytosis, elevated CRP, elevated ASLO titres and 2Decho revealed a mild tricuspid regurgitation. An initial diagnosis of acute rheumatic fever was made and child was started on penicillin and Aspirin. But child continued to have excruciating arthralgia and hence a rheumatologist opinion was taken. Child was advised a skin biopsy from the nodular lesions which showed small and medium vessel vasculitis suggestive of cutaneous polyarteritis nodosa. Hence she was stopped with aspirin therapy , given pulse therapy with methyl prednisolone and continued with penicillin therapy .Her arthralgia subsided within a day of pulse therapy and the subcutaneous nodules gradually disappeared .On discharge child was put on oral steroid therapy and penicillin prophylaxis and advised regular follow up.
Fig1 showing segmental fibrinoid necrosis with inflammatory infiltrates of small artery.
Fig2 showing leukocystoclastic vasculitis with fragmentation of neutrophils in and around blood vessels.
DISCUSSION:
cPAN is not common in the pediatric population with approximately 140 cases reported in the literature. Disease is limited to skin, joints, and muscles in the majority with a minority having nerve involvement. Constitutional symptoms are common. Most children have a chronic and relapsing benign course.
The precise etiology of cPAN remains to be unknown. However, an immune mediated mechanism has been postulated. Several infectious and noninfectious conditions have been associated both to initiation and relapse of the disease3,4,5. Among them, streptococcal infection has been commonly implicated6,7. Although some evidence of streptococcal infection as an initiating factor for cPAN is present, caution must be exercised when interpreting elevations in the serologic markers of streptococcal infection in the absence of an appropriate clinical presentation.
Cutaneous and systemic PAN share the same histopathologic features of necrotizing arteritis of small and medium sized vessels. Kussmaul and Meier described the first case of systemic PAN in 1866 1. Early reports 8,9 confirm that cPAN is a separate entity to systemic PAN. We have limited our definition of cPAN to disease affecting the skin, muscle, joints, and peripheral nervous system, with corresponding biopsy confirmation. Any evidence of visceral involvement, either clinically (central nervous system, pulmonary, cardiac, gastrointestinal, or renal), radiographically (abnormal angiography), or by histology (visceral biopsy) were classified as systemic PAN. Nakamura et al 10 proposed further restriction of the definition of cutaneous PAN in that any extracutaneous involvement such as peripheral neuropathy and myalgias must be limited to the same area as skin lesions. Systemic PAN and cPAN appear to be fairly distinct entities on a clinical continuum. There are only 5 reported cases of cPAN evolving into systemic PAN 11,12.
On review of treatment regimens reported in the literature, most children respond to corticosteroids. Penicillin should be considered in children with increased ASO titres 13,14. Recent case series report success with low-dose methotrexate, cyclophosphamide, intravenous immunoglobulin, and biologic therapies 15,16.
In summary, cPAN can be challenging to diagnose and manage. A diagnosis of cPAN should be considered in a child with fever, tender subcutaneous nodules, livido reticularis, and arthralgias/arthritis. Most children respond to corticosteroids and have a benign course, but some children may be corticosteroid dependent or corticosteroid resistant, necessitating other immunosuppressive agents including DMARDs and biologic therapy. Multicentre pediatric vasculitis disease registries are necessary to inform development and standardization of best clinical practice for childhood cPAN.
Surgery and anaesthesia have traditionally been viewed as expensive, resource-intensive and requiring highly specialized training.1 This misconception has led to surgery and anaesthesia taking a back seat to public health, maternal and child health, and infectious diseases in global health.2 Surgery has also been termed the “neglected stepchild of global health.3These concepts have changed rapidly since it has been found that surgical diseases contribute about 11% to Disability Adjusted Life Years4 and therefore would benefit from preventive and public health strategies necessary to achieve the Millennium Development Goals. The realization of the huge public health burden of surgical diseases in low and medium income countries (LMICs), and the fact that surgical services and treatment could be made cost effective, led World Health Organization (WHO) to launch the Global Initiative for Emergency and Essential Surgical Care (GIEESC) in 2005.5
The GIEESC is a global forum whose goal is to promote collaboration among diverse groups of stakeholders to strengthen the delivery of surgical services at the primary referral level in LMICs.5 Improvements in surgical services at the primary referral level in LMICs will equally require the provision of safe and effective anaesthesia. The provision of safe and effective anaesthesia will need adequately trained human resources and essential health technologies. The surgical and anaesthesia service capacity have generally been very low in sub-Saharan Africa (SSA) as evidenced through surveys conducted in Ethiopia,6 Gambia,7,8 Ghana,9,10 Liberia,8,11 Malawi,12 Nigeria,13 Sierra Leone,8,14 Rwanda,15,16 Tanzania,8,17 and Uganda.18 The survey from Nigeria was conducted among rural private hospitals and was administered to attending members in a conference of the Association of Rural Surgical Practitioners of Nigeria.13 This was done using the Personnel, Procedures, Equipment and Supplies (PIPES) survey tool developed by the non-governmental organization Surgeons Overseas (SOS).13 This is a tool developed to assess surgical capacity through the workforce, infrastructure, skill, equipment, and supplies of health facilities in LMICs.13 The other indicated surveys done in SSA used a comprehensive survey tool designed by the Harvard Humanitarian Initiative. This tool was adapted from the WHO Tool for Situational Analysis to Assess Emergency and Essential Surgical Care as part of an international initiative to assess surgical and anaesthesia capacity in LMICs.
The present survey used a rapid assessment tool known as the Lifebox Hospital Initial Needs Assessment questionnaire with another structured questionnaire to assess anaesthesia services in public hospitals in the Cross River State (CRS) of Nigeria. Lifebox (www.lifebox.org) is a non-profit organization saving lives by improving the safety and quality of surgical care in low-resource countries.19 Since 2001, Lifebox has trained more than 2000 anaesthesia providers, and more than 4200 pulse oximeters have been supplied to more than 70 low-resource countries thereby closing the operating room pulse oximetry gap in about 15 countries.19 This organization is supported by the World Federation of Societies of Anaesthesiologists (WFSA), Association of Anaesthetists of Great Britain and Ireland, Harvard School of Public Health and the Brigham and Women’s Hospital in Boston, United States of America.19 This survey was primarily aimed at the secondary health care facilities which are owned and managed by the CRS Ministry of Health (MOH). This survey audit will identify the anaesthesia providers in CRS, their level of training and retraining as well as equipment available for providing safe anaesthesia and monitoring patients in the peri-operative period. The data will also identify baseline information and gaps in anaesthesia and surgical capacity as a first step for the CRS MOH initiative to improve surgical and anaesthesia services. This information is a stepping-stone for national and international assistance since CRS is a relatively poor state in the Nigerian Federation.
Country and State overview
Nigeria is the most populous African country, located in the West African sub-region with a population of more than 160 million people.20 It is a Federal Republic with 36 states and a Federal Capital Territory. It is politically sub-divided into six geo-political zones: North-Central, North-Eastern, North-Western, South-Eastern, South-South and South-Western. There are 774 Local Government Areas (LGAs) where more than 60% of the population reside. The health care system is divided into three levels: primary, secondary and tertiary. There are public and private health facilities operating at all levels. The primary healthcare facilities (health centres) are managed by the Local Government, the secondary healthcare facilities (general hospitals) are managed by the State Government, while the tertiary facilities (University Teaching Hospitals and Federal Medical Centres) are managed by the Federal Government. Health indicators for Nigeria are among the worst in the world despite the fact that Nigeria is the sixth largest exporter of crude oil. The United Nations Human Development Index ranked Nigeria 156 out of 187 countries.21 In particular, Nigeria is one of the five countries contributing more than 50% to the global maternal mortality ratio22 and one of the countries with the highest physician’s and nurse’s emigration to developed countries.23 Physicians and nurses who remain in Nigeria predominantly practice in urban cities leaving the LGAs, most of them rural with severe shortages in health manpower.
CRS, with approximately 3.2 million population and 20156 square kilometres, is located in the South-South geo-political zone.24 The state has boundaries with the Republic of Cameroon in the East, Benue State in the North, Ebonyi State in the North West and Akwa-Ibom State in the South.24 It is divided into 18 LGAs with 18 general hospitals and 613 primary health centres. There is only one tertiary health facility, the University of Calabar Teaching Hospital (UCTH) located in Calabar, the capital city, which provides specialist care to the entire population. Being a tourism state, the importance of safe anaesthesia as a component of safe surgery cannot be overemphasized.
Physician-anaesthetist, nurse-anaesthetist and surgery training programs in Nigeria
Physicians are trained to be specialist anaesthetists or surgeons in a four-year training program leading to the Fellowship in Anaesthesia (FMCA) or Surgery (FMCS) of the National Postgraduate Medical College of Nigeria (NPMCN) or the Fellowship in Anaesthesia or Surgery (FWACS) of the West African College of Surgeons (WACS). This is after a six-year medical education program in the university leading to the Bachelor of Medicine and Bachelor of Surgery degree, one-year rotatory internship, and one-year of compulsory National Youth Service. Most Fellows, after completion (average time of completion is 7-8 years), work in University Teaching Hospitals and Federal Medical Centres, all located in urban cities. Another training program for doctors designed for primary and secondary healthcare is the Diploma in Anaesthesia (D.A) of the Universities or WACS, which is a 12-month training program. There is no short training program in Surgery.
Nurses are trained as nurse-anaesthetists after 18 months of training in a post-basic nursing program. The basic nursing training program is three-years of training in general nursing, after completing six years of secondary school education. There are now few university degree programs leading to the Bachelor’s degree in Nursing Science (BSN) from the universities. All these nursing training programs lead to certification by the Nursing and Midwifery Council of Nigeria.
Rural-urban practice
Physician-anaesthetists (Fellows and Diplomates), nurse-anaesthetists and consultant surgeons are all concentrated in urban hospitals leaving the rural areas and urban slums with a critical shortage of anaesthetic and surgical workforce. Therefore the majority of the surgical and anaesthetic procedures in rural areas in Nigeria are carried out by government-employed medical officers with almost all anaesthesia being provided by nurse-anaesthetists. In some very remote districts, Community Health Extension Workers (CHEWs) and Community Health Aids with little or no formal training in providing surgical care, are the only health workers available to provide some form of surgical care. The Association of Rural Surgical Practitioners of Nigeria (ARSPON) has been making some effort to address this workforce gap in rural areas by providing short on-the job training for medical officers to enable them to provide safe and affordable surgery to the rural population.13 The concept of surgical task-shifting to “non-physician clinicians” to address this rural-urban surgical workforce disparity, as is being officially done in other LMICs of SSA25 is not acceptable in Nigeria.
METHODOLOGY
A standardized questionnaire, the Lifebox Hospital Initial Needs Assessment Survey (Appendix 1) and another structured questionnaire (Appendix 2) was distributed to all 18 general hospitals (secondary health facilities) in CRS. All the general hospitals, which are the first referral hospitals in the districts, perform surgery. The site visit was conducted in April/May 2014. Permission to conduct the site visit was given by the CRS Honorable Commissioner for Health. The hospital surveys did not involve face-to-face interviews with the medical superintendents, hospital matrons or anaesthesia providers. The questionnaires were to be completed by the anaesthesia providers and medical superintendents in each of the hospitals visited. Each completed questionnaire was to be sent to the office of the Honorable Commissioner for Health at the MOH headquarters in Calabar, the capital city. The results are presented in frequency tables and charts.
RESULTS
A total of 16 well-completed questionnaires were received from 18 general hospitals/secondary healthcare facilities visited (88.9 % response rate). Averages of 3 - 53 surgeries are performed monthly in each of the hospitals (Table 1). The common procedures performed include: herniorrhaphy, appendicectomy, caesarean section, myomectomy, prostatectomy and exploratory laparotomy (Table 1). There are no practicing physician anaesthesiologists or surgeons employed by the State MOH except for one visiting consultant anaesthesiologist and five visiting consultant surgeons from the University of Calabar Teaching Hospital (UCTH), at the General Hospital, Calabar, which is located in the capital city of the State (Table 1). There are 13 nurse-anaesthetists distributed unevenly in the 16 hospitals (Table 1). There are no clinical officers cadres in the Nigerian healthcare system. Apart from the nurse-anaesthetists at the General Hospital in Calabar and Dr Lawrence Henshaw Memorial Hospital, also in Calabar, the other nurse-anaesthetists have had no refresher course or in-service training in the past two years. In the 16 general hospitals, the commonest anaesthetic technique used is Total Intravenous Anaesthesia (TIVA) with Ketamine (Table 1).
Table 1 : Summary of audit of anaesthesia services in the 16 district hospitals in Cross River State, April/May2014
GA: General Anaesthesia. ETT: Endotracheal Intubation. C/S: Caesarean Section. CSE: Combined Spinal and Epidural anaesthesia.
Basic anaesthetic equipment such as anaesthetic machines, oxygen cylinders, suction machines, and pulse oximeters were lacking in most of the hospitals visited (Box 1).
Box 1. Summary of Equipment in the 16 General Hospitals, Cross River State, Nigeria: April-May 2014 · 10% of the hospitals had pulse oximeter · 20% of the hospitals had oxygen cylinders · 20% of the hospitals had suction machines · 30% of the hospitals had anaesthetic machines · 80% of the hospitals had recovery beds · 100% of the hospitals perform surgery
The WHO Surgical Safety Checklist Information was administered to the hospitals management team at the Districts Hospital (Box 2). This shows that all the surgical teams had never used the WHO checklist, never received training, and the checklist was not available in the operating rooms, although all surgical personnel would like to receive training on the WHO checklist and pulse oximetry
Box 2. World Health Organization (WHO) Surgical Safety Checklist Information · How often do the surgical teams at your hospital use the WHO Surgical Safety Checklist? NEVER · Has your hospital received training in the WHO Surgical Safety Checklist? NO · Is the WHO Surgical Safety Checklist available in your operating rooms? NO · Would you like to receive training in pulse oximetry and the WHO checklist? YES
DISCUSSION
This survey aimed to provide a quick assessment of anaesthesia and surgical services in public hospitals in CRS of Nigeria. The data shows gross and significant shortages in anaesthesia and surgical providers in all 16 general hospitals. There were no consultant anaesthetists, diplomate anaesthetists or consultant surgeons employed in the CRS MOH. There were only 13 nurse-anaesthetists working in the 16 general hospitals, and one visiting consultant anaesthetist and five visiting consultant surgeons at the General Hospital, Calabar, the capital city. In six of the hospitals, there were no nurse-anaesthetists providing care for the surgical procedures being conducted. As it has been reported from the many surveys in SSA.6, 18, 26 most of the procedures in all the hospitals are being done by generalist medical doctors and general nurses, many without any postgraduate training in surgery and anaesthesia.
The gross inadequacy of the anaesthetic workforce in this survey represents what is found in many of the 778 LGAs (Districts) in the Federal Republic of Nigeria. This is because many of the LGAs are rural and studies have indicated the general difficulties of most health workers seeking jobs in rural hospitals. The lack of specialist anaesthetists in peripheral hospitals in most of Nigerian Districts therefore requires a re-direction of the training programs for doctors in Nigeria with greater emphasis on the shorter training program design for primary and secondary healthcare levels. Inaddition, annual refresher courses should be made mandatory for nurse-anaesthetists especially for those practicing in rural areas.
A recent review of the met and unmet needs of surgical disease in rural SSA, where district and rural hospitals are the main providers of care, shows a very huge burden.27 An important finding is the discrepancy between surgical care needs and provision.27 Since the majority of the population in SSA reside in rural areas, there is the need to strengthen the surgical services at this level. This is the first of the four recommendations of the Bellagio Essential Surgery Group.28 Many of the surveys using the WHO Situational Analysis Tool have described the lack of capacity in many district hospitals to meet the local surgical and anaesthesia needs.6-18 One study, using pulse oximeter availability as a measure of operating room resources, showed that between 58.4% and 78.4% of operating rooms in West Africa, East Africa and Central SSA do not have pulse oximeters.29 This finding was also clearly shown by our own rapid survey and assessment. Three important factors have been responsible for these findings. These are lack of resources, lack of manpower and the need for training.27 The need for training to improve the quality of the surgical and anaesthesia providers at the district hospitals is the third recommendation of the Bellagio Essential Surgery Group.28
Training programs and improvement of the facilities at the District Hospital has been shown to increase the number of operations performed.27Also, the presence of a visiting consultant anaesthetist in the District Hospital has been shown to increase the scope of anaesthesia services during the visiting period.30 The visit left more knowledgeable local staff in the care of their patients especially in peri-operative care.30 The need for developing countries in SSA, particularly in Nigeria, to concentrate more on shorter training programs in surgery and anaesthesia at their current level of development has been advocated.31,32 This has been shown by Sani et al where a 12-month training program for General Practitioners in district hospitals in Niger significantly reduced the number of referrals to the regional and specialist hospital.33 In many other SSA countries, where gross shortages of medical manpower exist, surgical task shifting has been championed and research has shown that these are cost effective interventions.25, 34 This is, however, not acceptable in Nigeria which is Africa’s most populous country with very poor health indicators.
There are some limitations to this study. Firstly, it was a snapshot of anaesthesia and surgical services which did not highlight in detail the eight key areas of surgical and anaesthesia care, as in other surveys. These key areas include: access and availability of hospital services, human resources, physical infrastructures (including availability of water and electricity), surgical and anaesthetic procedures, surgical and anaesthesia outcome, essential equipment availability, NGO and international organizations providing care, and access to essential pharmaceuticals. Secondly, this assessment did not include the only public tertiary hospital in the State and private hospitals. Lastly, this was an initial assessment in preparation for a more detailed survey based on the WHO guidelines when research funds are received.
CONCLUSION AND RECOMMENDATIONS
Therehas been a paradigm shift in global public health and the concept of primary healthcare which has resulted in increased awareness of the importance and contributions of surgical disease to the overall burden of disease especially in LMICs. This rapid survey of anaesthesia services in CRS, one of the 36 states in Nigeria, will serve as a window to inform other Nigerian State governments of the need to increase surgical and anaesthesia capacity and funding in their development agenda. It is therefore recommended that visiting consultant’s services to all the general hospitals in an organized and planned fashion should be highly encouraged. All the anaesthesia caregivers should attend refresher courses at least once every two years. These courses can be arranged locally, or sponsorship provided for attendance of relevant courses by Anaesthesia Trainers within and outside the State. Basic anaesthesia equipment and guidelines as recommended by the Nigerian Society of Anaesthetists (Box 3) must be available and followed to enhance patient safety. It is also recommended that the government should give incentives to medical and nursing staff working in rural areas so that there will be a reversal of the rural- urban shift. The Lifebox global oximetry project is interested in making high quality, low-cost pulse oximeters available in every operating room. Therefore, every secondary care facility in the country should take advantage of this laudable program.
Box 3. Nigerian Society of Anaesthetists Standard Guidelines for the Practice of Anaesthesia Anaesthetic Personnel · Certified physician anaesthetist · Trained nurse-anaesthetist under supervision by physician-anaesthetists · Maximum number of nurses to physicians should be 4:1 · Where there is no physician-anaesthetist, nurses should adhere strictly to the guidelines and conditions of their certification · The surgeon should provide coverage especially in the area of patient resuscitation and fitness for surgery and take full responsibility for any decisions made against the guidelines.
Anaesthetic equipment for each theatre Standard Continuous Flow (Boyles) Anaesthetic Machine with: - Closed breathing system - Adult semi-closed breathing system - Paediatric breathing system Suction Machine - Electric - Manual Suction Catheters – disposable, various sizes Laryngoscope set with batteries and:- - 2 standard and 1 long curved blades - 2 standard and 1 long straight blades - Neonatal laryngoscope with 2 straight blades. Intubating Forceps (Magill) - Adult - Paediatric - Neonatal Self-inflating Resuscitation Bag - Adult - Paediatric - Infant Anaesthetic Face Masks : Size 0, 1, 2, 3, 4 Paediatric (Rendell-Baker) – Size 00,0,1 Naso-gastric tubes Head – Harness Oropharyngeal Airways 00 – 5 Endotracheal tubes (cuffed, noon-cuffed 2.5. – 9.0. mm) - Red rubber, latex reinforced, portex Plastic laryngeal Mask Airway (Sizes 1–5) Endobronchial tubes Bougies Fluid Warmer Warming Mattress (for paediatrics) Pressure Infusor Syringe Infusion Pump with lines
Maintaining its longstanding presence as one of the oldest forms of art, body tattooing has increased exponentially within mainstream society, as well as in social acceptance. Generally worn to display individuality and creativity, these distinctive forms of indelible markings are present in every culture, whether on tribal men, or people of status. Procedurally when inserting the decorative markings, the approach in studio tattooing has not changed significantly as artists are still using “an electrically powered, vertically vibrating instrument to inject tattoo pigment 50 to 3,000 times per minute up to or into the dermis at a depth of 1/64th to 1/16th of an inch”1
While no national registry provides prevalence, a 2012 Harris Poll cited one in five United States (U.S.) adults have at least one tattoo (21%), an increase of 16% and 14% from previous surveys taken in 2003 and 2008 respectively.2 Tattoo numbers were even higher in some variables including age between 30-39 years (38%), Hispanics (30%), females (23%), and those living in the Western part of the U.S. (26%). No questions were identified in the 2012 poll that queried tattooed body site locations. Other studies cite almost a 25% presence of tattoos.1,3-7 The amount of tattoo studios also echoes the growing body art phenomenon.
Given the societal blaze of tattooing, the medical literature on body art has also increased. Yet, most of the information still remains focused on small case reports6 about traditional locations (arms, legs, chest, back), their decision-making, various risk-taking behaviors,8 and the small amount of complications.7 Those with various adverse skin reactions or major complications seem to have had tattoos with colored pigment.6
While body art can be found virtually everywhere on the human anatomy, several articles have surfaced concerning genital body piecing.4-5, 9-11 Current studies validate the increasing rate of all types of tattooed 4,8 people, from a variety of occupations and social classes, with markings on visible and non-visible locations.7 This article reports on the limited medical literature found about men with genital tattoos (pubic and/or the glans penis). Also presented is a subsample data analysis of 14 men from a primary study examining male genital piercings,11-12 who responded affirmatively to one survey question about penile tattoos. This synopsis and subsample data analysis are provided for clinicians to have further, recent evidence about men with genital tattoos for decision making during patient encounters in health care settings. The terminology of penile and genital tattoos will be used interchangeably in this article.
METHODS
Literature Synopsis
Historically, the cross-cultural literature is rich in visual genital tattoo descriptions. In South America, the Moche on the North Coast of Peru (A.D. 150-800) produced ceramics illustrating vivid sexual imagery and highly decorated male genitals.13 Phallus decorations with dots, concentric lines, and other tattoo markings on the penile skin and mucosa during the Upper Paleolithic era in Europe 12,700 to 11,000 years ago have been reported.14-15 Likewise, the Samoan Island culture, where the word ”tattoo” is believed to have originated from “tatau,”, has maintained ritualistic16 traditions for over two thousand years; they are initiated at the time of puberty for future leadership roles. These 10+ days of ceremonies include very painful, repeated tattooing of the scrotum (tafumiti) and the penis (tafito). Other nearby primitive Polynesian tribes have believed this tattooing as highly erotic,16 whereas the indigenous Maori (New Zealand) trust that the pigment for these tattoos can trap cosmic energy.14 Circumcision and tattooing were thought to produce the same effect of magic protection and healing powers after scar healing.14 In the Japanese culture, an examination of Yakuza (racketeers or gangsters) also describes the genitalia as a site that is tattooed,17 fulfilling their principles of tattoos always being covered.
Searching for information about genital tattoos was more challenging within the medical literature. A comprehensive longitudinal 40 year search of the national and international electronic medical literature (1973-2013) published in English and their associated reference lists was conducted with MEDLINE, EMBASE, CINAHL, SCOPUS, and OVID. Only 20 articles were located that mentioned genital tattoos. Articles were from international authors (n = 11) and the U.S. (n = 9); they all produced interesting reading. One reference cited women with genital tattoos.7
Genital tattoos in the early literature were labeled as criminal, or personality disorders tattoos;18 one recent article discussed them under the header of genital self-mutilation.16 Others described them as a valuable clue for forensic pathology identification.19-20 World War II articles cited descriptive stories of soldiers with penile tattoos,21-22 with one reporting up to 10 sailors being seen.23 Besides reporting on how the fate of Bulgaria was determined by three tattooed men (Churchill with an anchor on his left arm, Roosevelt with a family coat of arms tattoo, and Stalin with a death’s head on his chest),24 Kazandjieva25 then provides vivid examples of auto-aggression markings that his countrymen self-inflicted after the Communist takeover. This included glans penis tattoos which are described as producing great pain.15,25 One political candidate, while campaigning, is reported as suggesting punitive action for those HIV+ by “putting indelible, glow-in-the-dark tattoos on [their] genitals.”26 Traumatic tattoos associated with gunpowder explosions and blast burns are also mentioned on the glans penis.27
Two studies also described inmates with genital tattoos and discussed how these markings demonstrated aggressive behavior within this type of environment. Here large, colorful tattoo designs and wording on the glans penis tattoos were described28-29 which seemed to satisfy the inmate’s flaunt of personal pain endurance. Additionally, Cuban refugees (Marielitos) fleeing to the U.S. were reported as having genital tattoos; they also were from prison subcultures and their markings had various sexual overtones.29
Four other reports described those with penile tattoos also routinely inserting foreign bodies12,30 and paraffinoma12,31,32 into the penis. In Pehlianov’s study (also in Bulgaria) they included a control group of another 25 men with genital tattoos. Recently, a unique case of non-ischemic priapism for 3 months was reported33 following prolonged bleeding from a manual penile tattoo procedure in Iran. The authors suggested the hand-held tattoo needle had penetrated too deeply producing an arteriovenous fistula and the subsequent persistent half-rigid priapism. The authors also noted that the 21 year old patient expressed no regret, depression, or other complications related to the genital tattoo.
Original Study
The initial study queried males with genital piercings using available internet survey software,12 as it was considered a hidden variable. Anonymity and access to people nationally and internationally were major advantages for using this nontraditional approach. The university institutional review board deemed the study status as Exempt. To obtain quantitative and qualitative data about those men with genital piercings, an 83 item web-based survey was used; overall results, and another subsample of this data, are published elsewhere.11-12
Subsample of those with Penile Tattoos
From the original 445 male genital pierced individuals that responded to the question regarding having tattoos on their penis, 14 replied affirmatively. This subsample had previously been determined not be an outlier of the larger group of genital pierced men.12 While a short general description (age span at the time of tattoo procurement, urethral “play,” design types, motives, and tattooists) about the 14 member genital tattoo subsample was published in 2010,12 further investigation leading to quantitative and qualitative (Figure 1) data is presented here.
Figure 1: Subsample Respondent Qualitative Quotes *Black tribal flames on the top of the shaft, done at [age] 38 * For erotic reasons, self done with no complications, done at [age] 54 *I got it because I wanted it. After it was finished I realized I needed it, done at [age] 30 * I self tattoo’d my penis on the glans and around the corona ridge in order to make up for its’ lack of size and to enhance its appearance. I used a sailmaker’s needle and Indian ink and there were no complications, done at [age] 43. *one small cross pigment tattoo! *I’m a little more than average in size, but I still have issues with my genitals. The way they look and their size. Piercings and tattoos have helped me quite a lot. *I sketched a rose one day, like[d] the design, decided to get it tattooed on my penis. The stem is green with some yellow highlights, the bud is red, all black outline. The tattoo was applied with a standard machine . . .healing was actually quicker and easier than any of my other tattoos. *It’s a little heart just next to ‘captain hemingway’ which I hand poked and used india ink for it when I was 17. . . thought our penis deserved a reminder of our affection . . .no complications experienced but since it was hand done with a [sterile] needle it’s kind of blurry
This subsample had significantly more foreskin genital piercings (chi-square = 11.5) = 1; P = .001), whereas the most common genital piercing of the larger group of those without genital tattoos11 had Prince Albert piercings (inserted through external urethra). No question inquired which came first, the genital piercing or genital tattoos.
Data Analysis
For this subsample analysis, (and original study11-12), IBM SPSS 21was used to obtain frequencies and chi-square analysis. Cross tabulations for the subsample were obtained by comparing those with and without penile tattoos.
RESULTS
Demographics
Almost all of the subsample respondents with penile tattoos were reportedly Caucasian (92%) and their ages ranged from 18 to 67 years (average 42.3). Of those that replied, six lived in the U.S. and five cited various international locations. Over half had vocational or college education (64%) and significantly more were likely to be single (25%) or divorced (25%), (chi-square 12.6) = 5; P = .027). Data regarding religious faith was weak to non-existent (75%). Respondents self-reported a good state of health (92%) (chi-square = 8.7) = 3; P = .034), yet 50% cited no annual health check-ups.
Risk Behaviors
Within this subsample, there was no consensus about being a “risk taker”. Recreational drugs were reportedly not used (91%), over half were non-smokers (55%), but monthly alcohol use with binge drinking (5+ or more drinks) was cited (78%). Their “motives for genital tattoos were for esthetics, sexual, and personal pleasure”12; a variety of penile tattoo designs were described (Figure 1), created either “by studio artists (n = 11) or self-inflicted (n = 3)”.12 All of them described having other body art, such as piercings and other general body tattoos. Some reported an average of 4 piercings (81%) and a significant amount of general body tattoos (average 3.5) (chi-square = 11.1) = 5; P = .049), that still interest them (85%) (chi-square = 8.9) = 3) P = .031).
Sexual Activity
This subsample’s average age of first intercourse was 17 years, with most citing women as their sexual partners (92%), most preferred penile/vaginal intercourse (79%), and only one respondent reported a sexually transmitted infection (gonorrhea). When asked about any forced sexual activity (rape), this subsample had a significant amount of those who answered affirmatively (23%) (chi-square = 7.7) = 1; P = .005). Virtually no sexual, physical, or mental abuse was reported.
Need for Uniqueness
A four-item scale called the Self-Attributed Need for Uniqueness (SANU)34 was present in the survey to determine the respondent’s self-view (Cronbach alpha = .86). Using a Likert scale, the subsample’s moderate, strong and very strong perspectives were collectively summarized. These respondents with penile tattoos preferred to be different (79%), distinctive (86%), intended to do things to make themselves different than those around them (72%), and reported a Need For Uniqueness (93%) (Cronbach alpha = .77). To validate this finding, when all 5 responses of SANU were totaled,12 the mean was 12.43 documenting a more positive perspective for intentionally wanting to be different, distinctive, and unique.
DISCUSSION
This article reviewed both the cross cultural and medical literature about those with genital tattoos, as well as included both a quantitative and qualitative subsample data analysis of a small group of men who specifically reported penile tattoos. Yet, with certainty this small sample size produced limitations and reporting/survey bias. Additionally, any generalizability with the findings of this subsample should be noted as the respondents could have self-selected their participation and used their personal judgment to interpret the survey questions in this non-experimental cross-sectional study using internet survey methodology.12
From this review and to our knowledge, few have studied groups of men with genital tattoos, a difficult group of subjects to find with this hidden variable.12,31 Cultural descriptions documented a long, rich history 12, 14-17, 29,31 of genital markings for esthetics, sexual enhancement, and tribal status, whereas the medical literature reflected limited observational type information, and few actual case histories or scientific studies. Although there were no mental health evaluations12 cited in this medical literature, more psychopathic, deviant behavior discussions were made about the individuals with genital tattoos.16-18,26,32,35 In contrast, two authors30,33 comment on the “normalcy” of their patients that presented with genital tattoos.
Genital tattoos may be more common than this very small subsample size suggested as great emphasis has been placed on male penile size in many cultures, for a long time.31,36 The augmentation of these genital markings and decorative designs seemed to have motivated their sexual health, self-enhancement9-10 and well-being.31 Thus, when further studies are considered for this population with a hidden variable, these findings should assist with further ideas of investigation.
Current society has a strong 25 year renaissance of procuring tattoos with at least one in five, and perhaps even four, individuals possessing a tattoo, on virtually every part of their body, without major complications. This small subsample of those who have genital tattoos validates some similarities to those who wear general body tattoos such as a single heterosexual orientation, possessing some college/vocational education, monthly binge drinking,1,3-5,10 and a strong propensity for a Need for Uniqueness.4-5,37 They were major body art wearers and continue to enjoy them, as others have also reported.4-5,10-12
Yet other demographic assumptions were challenged for this subsample of men with genital tattoos. These international respondents tended to be older Caucasians and not as ethnically diverse; there also was not a consensus as to them being risk takers, as has been repeatedly reported by many other body art respondents.1,3-5,11-12
Subsample respondents reported their average first occurance of sexual intercourse at age 17, similar to the national figures.38 Significant experiences of rape were also reported in this subsample, as in women with genital piercings.4-5,9-10 The national rate for forced sexual activity is 10.5%38 and those with genital tattoos reported over twice that amount (23%). No sexual abuse was reported in contrast to a recent German study39 examining general body tattooing.
As with any type of invasive procedure, there can be complications with certain types of body art. When these complications occur, body art wearers typically first seek the internet and/or their studio artist for health advice before presenting to clinicians.1,8,10-12 Yet, overall for the amount of general tattooing done, this type of body art produced limited documented complications and more potential concerns.7-8,11, 30,33 More complications were reported when the tattoos contained colored pigments.6
These tattoos are an integral part of their cultural and personal expression.12,31,33 From our experience many of these male patients with genital tattoos are not seen primarily because of their decorative markings,31 but during clinical evaluations for other issues presented with the normal range of urologic issues involving overall genitourinary and sexual function. Genital tattoos can be an ambivalent findings for many clinicians, but these indelible skin markings (tattoos) are only skin deep,40 and provide valuable cues such as a history of sexual trauma.39 Currently more genital tattoos are seen among our freedom-impaired patients, where the prevalence of general body tattoos among the inmates can be as high as 67%.41
Anecdotally, when healthcare staff discover a patient with genital body art, this discovery can be met with judgmental attitudes and behaviors which could impact care. To adequately assess, evaluate and treat the individuals that have chosen to have genital tattooing, clinicians should strive to provide a thoughtful, nonjudgmental patient-centered approach, along with a generous application of health education, for their present, or even future body art.11
Global Health can be defined as “an area for study, research, and practice that places a priority on improving health and achieving health equity for all people worldwide”. 1 Article 25 of the 1948 Universal Declaration of Human Rights declares that, “everyone has the right to a standard of living adequate for the health of himself and of his family”. 2 Unfortunately, the health disparity between high-income and low-income countries, as well as between individuals within a country, often makes this impossible, leaving many people living in unhealthy settings without sufficient access to care.
The field of global health is concerned with the health of populations worldwide, focusing on issues that typically have global, political, and economic significance. These health issues usually transcend national boundaries and are best solved through international collaboration. 3 Global health initiatives aim to improve the health and wellbeing of impoverished, vulnerable, and underserved people worldwide. 1 These initiatives include poverty reduction strategies, disease prevention measures (for HIV/AIDS, malaria, and tuberculosis, for instance), efforts to improve nutrition and food security, policy to raise environmental standards and living conditions, and the promotion of gender equality.
In 2001, the Commission of the World Health Organization (WHO) recommended to fund global health with 0.1% of GDP. 4
The average expenditure per capita for health in low-income countries is estimated at $ 20 per year while that of Western countries is estimated at $ 947. The target to be reached to help out the most disadvantaged countries is $ 44-60 per capita, which would ensure the populations of the poorest countries with the access to essential health services. Directing the 0.1% of the GDP of developed Western countries to the aids for global health would mean closing the gap to reach the target base of $ 44-60 that would allow the saving of 8 million lives a year. 4
Despite the good intentions, there is still a marked disparity between the current spending levels and the commitments made by developed countries in a context in which, among other things, the percentage of aid for global health has been in decline for almost all donor countries.
Activists claim that only 10 per cent of global health research is devoted to conditions that account for 90 per cent of the global disease burden – the so-called ‘10/90 Gap’. 5 They argue that virtually all diseases prevalent in low income countries are ‘neglected’ and that the pharmaceutical industry has invested almost nothing in research and development for these diseases.
In fact, the WHO acknowledges that there are only three diseases that are genuinely ‘neglected’: African trypanosomiasis, leishmaniosis and Chagas disease. 6
A large proportion of illnesses in low-income countries are entirely avoidable or treatable with existing medicines or interventions. Most of the disease burden in low-income countries finds its roots in the consequences of poverty, such as poor nutrition, indoor air pollution and lack of access to proper sanitation and health education. The WHO estimates that diseases associated with poverty account for 45 per cent of the disease burden in the poorest countries. 7 However, nearly all of these deaths are either treatable with existing medicines or preventable in the first place.
If treatments exist for the majority of poor countries’ health problems, why then do mortality rates remain so high? Any discussion of this question must address the problem of access to essential medicines, which remains an intractable political and economic problem. According to the WHO, an estimated 30 per cent of the world population lacks regular access to existing drugs, with this figure rising to over 50 per cent in the poorest parts of Africa and Asia. 8 And even if drugs are available, weak drug regulation may mean that they are substandard or counterfeit.
Within these populations, it is the poorest socioeconomic groups that disproportionately suffer from a lack of access to existing medicines. 9 The implications of this failure of public health policy on global mortality are profound – according to one study, over 10 million children die unnecessarily each year, almost all in low-income or poor areas of middle income countries, mostly from a short list of preventable diseases such as diarrhoea, measles, malaria and causes related to malnutrition. 10
Many governments fail their populations in this respect by imposing punitive tariffs and taxes on medicines, and by skewing their spending priorities in favour of defence over health. The governments of poor countries hinder the creation of wealth, imposing obstacles in the way of owning and transferring property, imposing unnecessary regulatory barriers on entrepreneurs and businesses, and restricting trade through extortionate tariffs. It is these and other political failures that have left poor populations without the necessary resources to access the medicines that could so easily transform their quality of life.
In conclusion, it appears more and more urgent and necessary to decide where to direct our efforts and investment in research, without prejudice, analyzing all the possible strategies for tackling global health issues, including those standing beyond the current economic paradigm based on the market.
Our patient is a 40-year-old lady who presented to our department feeling unwell with fever and numbness in both hands. Past medical history showed recurrent urinary tract infections, rheumatoid arthritis, chronic eczema and epilepsy .She was taking Levetiracetam 500mg twice daily and Clobazam 5 mg twice daily for the epilepsy. She is also known to have learning difficulties. Mild hypocalcaemia was documented few years back in a previous admission in other hospitals, but the cause was unclear. On admission, she was hemodynamically stable with mild facial dysmorphism, and positive Trousseau's and Chvostek's signs.
Blood tests showed a low corrected calcium 1.5 mmol/L (NR 2.25-2.5 mmol/L), high C-reactive protein, Leukocytosis, and 3.0 mmol/L serum potassium level (NR 3.5-5.0 mmol/L). Other routine blood tests were normal. Further investigations showed low Serum parathyroid hormone levels, normal magnesium levels and normal TSH level. A CT scan of the brain was unremarkable. Electrocardiogram showed QT prolongation (with QTc of 520 ms). The diagnosis of hypoparathyroidism and urinary tract infection was established and the patient was treated with antibiotics to cover urinary tract infection and calcium supplements for hypocalcaemia. The patient symptoms improved significantly and was discharged on calcium supplements and Calcitriol (Rocaltrol 0.25 mcg) with a calcium level of 2.1 mmol/L. The presence of hypoparathyroidism in association with learning difficulties, eczema and epilepsy prompted chromosomal analysis for DiGeorge syndrome. The microdeletion of chromosome 22q11.2 was confirmed by FISH (fluorescent in situ hybridization) analysis. Cardiac echo examination demonstrated no abnormalities and abdominal ultrasound examination showed no renal abnormalities. The patient was offered Genetic counselling together with her family.
Discussion:
DiGeorge syndrome is a well-known genetic disorder with a prevalence of 1:4000 live births1. It was initially described by Angelo DiGeorge a physician and paediatric endocrinologist in 1968 2. DiGeorge is a developmental defect caused by a microdeletion of chromosome 22q11.2; it is also known as velocardiofacial syndrome or CATCH 22 syndrome to describe the classical features of this syndrome (C-Congenital heart disease, A-Abnormal facies, T-Thymus hypoplasia, C-Cleft Palate and H- Hypocalcaemia due to Hypoparathyroidism. Autoimmune disorders, skeletal defects, renal abnormalities, psychiatric and behavioural disorders are also associated with this syndrome.
DiGeorge is an autosomal dominant syndrome but the majority of patients have de novo mutations caused mainly by the microdeletion of chromosome 22q11.2 which leads to developmental disorders such as the failure of development of pharyngeal pouch system 3, 4. These developmental disorders are the main cause of the classic features and presentation of DiGeorge syndrome such as congenital heart diseases, hypoplasia of the parathyroid glands and thymus, congenital immune deficiency and renal abnormalities5 .
Congenital Conotruncal cardiac defects that involve truncoaortic sac can present in 70% patients with DiGeorge Syndrome. The most common cardiac anomalies are interrupted aortic arch, Tetralogy of Fallot, Atrial septal defect and ventricular septal defects 4, 5, 6 .
Hypocalcaemia is due to hypoparathyroidism and is present in about 60 % of patients 5, 7 . Hypocalcaemia is a strong predictor of DiGeorge syndrome if it is associated with other clinical features such as cardiac defect and immunodeficiency. Hypocalcaemia commonly presents as muscle cramps, numbness, tetany, focal or generalized seizures, prolong QT and hypotension.
Immunodeficiency is rare in adults and but it may present in up to 70-80% of the children with DiGeorge syndrome. Immunodeficiency occurs because of the low T cell count due to thymus hypoplasia. The function of T cells is however, usually preserved. Patients with immunodeficiency may have recurrent viral chest infection, systemic fungal infections frequent bacterial infections 8 .
The characteristic facies of DiGeorge include long face, narrow palpebral fissures, broad nasal bridge, micrognathia and asymmetrical crying face.
Psychiatric disorders have been reported with 22q11.2 deletion syndromes such as schizophrenia, bipolar disorder, anxiety and affective disorders.
Other conditions that may be associated with DiGeorge are atopic disorders (asthma and eczema) rheumatoid arthritis, autoimmune thyroiditis, renal abnormalities (such as multicystic kidneys andVesicoureteral reflux).
Conclusion:
Due to the variety of symptoms and the de novo mutations, DiGeorge Syndrome should be considered in adults presenting with hypocalcaemia due to hypoparathyroidism even in the absence of the classical features. The syndrome has significant health implications, and confirming the diagnosis is important for future family planning.
Adiponectin, first reported in 1995 by Scherer et al, is a novel and important member of the adipokine family.1 It is a collagen-like protein that is exclusively synthesised in white adipose tissue and is the gene product of adipose most abundant gene transcript 1 (apM1).
Adiponectin has been postulated to play an important role in the modulation of glucose and lipid metabolism in insulin-sensitive tissues in both humans and animals. Various studies have reported a protective effect of plasma adiponectinagainst type 2 Diabetes Mellitus (T2DM) 2-6. Adiponectin is also inversely associated with traditional cardiovascular risk factors, such as total and low-density lipoprotein cholesterol (LDL-C) and triglyceride levels, and is positively related to high-density lipoprotein cholesterol (HDL-C).7 Recent studies suggest that it may have anti-atherogenic and anti-inflammatory properties .8-10 A few researchers who studied the combined effects of these findings reported inverse correlation between plasma adiponectin and risk of coronary heart disease.11-15
Recent epidemiological studies have shown that association of adiponectin with insulin resistance and cardiovascular risk factors vary with ethnicity. Mente et al studied the ethnic variations in adiponectin concentrations and insulin resistance and found that South Asians and aboriginal people display a greater increase in insulin resistance with decreasing levels of adiponectin compared to Chinese and Europeans .16 However, a similar study involving Asian Indian teenagers showed that adiponectin did not correlate directly with measures of insulin sensitivity, overweight, and other cardio-metabolic variables .17 Similar studies in adults are not available.
The present study was done to assess the association between plasma adiponectin levels and coronary event in patients with diabetes. Also the relation between plasma adiponectin level and various cardiovascular risk factors were studied in patients with diabetes with and without acute coronary event.
Subjects and Methods:
The prospective study was conducted at a tertiary care centre in Bangalore, India from January 2008 to December 2009. The study was approved by the institution ethics committee. Three groups of patients, age and sex matched, were included in the study. The first group included 30consecutive T2DM patients admitted with a diagnosis of myocardial infarction (MI) at the study centre. While the second consisted of patients with T2DM without MI, the third group were patients without diabetes without any history of acute coronary event. MI was diagnosed as per World Health Organization’s criteria.18 Patients aged less than 18 years were not included in the study. Patients with diabetes with chronic kidney disease or receiving Thiazolidinediones were also excluded from the study as it would alter plasma adiponectin levels.
Fasting Blood Glucose (FBG), Post-Prandial Blood Glucose (PPBG), Glycated Hemoglobin (HbA1C), Fasting Lipid Profile, Baseline Electrocardiogram and Plasma Adiponectin were done for all the study subjects. In addition, Coronary Angiogram was done for patients with diabetes with MI to confirm Coronary Artery Disease (CAD) and treadmill tests were done for patients with diabetes without MI to exclude underlying CAD.
FBG and PPBG, serum total cholesterol and serum triglycerides were estimated using enzymatic kit method (Vital Diagnostics, Mumbai, India); and serum HDL-C (Bayer Diagnostics, Baroda, India) using a semi-auto-analyser.
Plasma Adiponectin levels was estimated using Human Total Adiponectin/Acrp30 Quantikine ELISA Kit (R&D Systems Inc., India). This assay employs the quantitative sandwich enzyme immunoassay technique. A monoclonal antibody specific for the Adiponectin globular domain has been pre-coated onto a microplate. Standards and samples are pipetted into the wells and any Adiponectin present is bound by the immobilised antibody. After washing away any unbound substances, an enzyme-linked monoclonal antibody specific for the Adiponectin globular domain is added to the wells. Following a wash to remove any unbound antibody-enzyme reagent, a substrate solution is added to the wells and colour develops in proportion to the amount of Adiponectin bound in the initial step. The colour development is stopped and the intensity of the colour is measured.
Statistical Analysis
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) for Windows 16.0 (SPSS Inc., Chicago, USA). The results for each parameter (numbers and percentages) for discrete data and average (mean + standard deviation) for continuous data are presented in tables and figures using Microsoft office 2007 software package.
Two-way Analysis of Variance (ANOVA) was performed for plasma adiponectin in patients with diabetes with MI, patients with diabetes without MI and controls as the grouping factor. Two tailed ‘P’ values less than 0.05 were considered significant. Spearman correlation was performed to analyse the association between plasma adiponectin, BMI, FBG, PPBG, HbA1C, serum triglycerides, HDL-C and LDL-C.
Results
The following results are expressed as mean± standard deviation. The mean age of the study subjects in the three groups-patients with diabetes with MI, patients with diabetes without MI and Controls- was 58.00±8.77 years, 57.17±9.34 years and 54.20±7.28 years respectively. The descriptive statistics of the various parameters under study is given in table 1.
Patients with diabetes with MI had significantly lower plasma adiponectin levels (6.11±1.82) when compared to patients with diabetes without MI (9.47±1.55) which in turn was lower than normal subjects (17.82±1.30) (P<.001) . Plasma adiponectin was significantly correlated with BMI (r=-.31), FBG (r=-.61), HbA1C (r=-.63) and triglycerides (r=-.54) (all P<.001). We did not find any significant correlation between plasma adiponectin levels and HDL-C (Table 2).
Table 1: Descriptive statistics of various parameters under study
Variable
Controls Mean (±Std. Dev)
Patients with diabetes without MI Mean(±Std. Dev)
Patients with diabetes with MI Mean(±Std. Dev)
Plasma Adiponectin
6.11(±1.82)
9.47(±1.55)
17.82(±1.30)
Fasting Blood Glucose
123.50(±17.85)
133.23(±16.14)
88.80(±6.27)
Post-Prandial Blood Glucose
190.53(±19.27)
209.33(±28.72)
125.30(±6.200
Glycated Haemoglobin
7.81(±0.92)
8.04(±1.24)
4.06(±0.62)
Total Cholesterol
205.77(±19.92)
214.43(±21.54)
138.07(±10.38)
Serum Triglycerides
148.80(±11.32)
160.53(±14.61)
127.23(±6.11)
Serum HDL
45.13(±8.57)
37.43(±9.73)
44.87(±7.78)
Serum LDL
129.30(±22.55)
137.27(±18.83)
120.03(±8.27)
Body Mass Index
27.82(±2.39)
27.08(±2.20)
25.40(±2.63)
Table 1: Patients with diabetes with MI had significantly lower plasma adiponectin when compared to patients with diabetes without MI which in turn was lower than in normal subjects
Table 2: Spearman correlation between adiponectin and body mass index, blood lipids, HbA1C, fasting and post-prandial glucose levels
Adiponectin
BMI
FBG
HBA1C
TG
HDL
LDL
Adiponectin
1.00
-0.31**
-0.61**
-0.63**
-0.54**
0.02
-0.16
BMI
1.00
0.37**
0.29**
0.25*
-0.14
0.10
FBG
1.00
0.62**
0.61**
-0.17
0.21*
HBA1C
1.00
0.83**
-0.45**
0.35**
TG
1.00
-0.53**
0.33**
HDL
1.00
-0.07
LDL
1.00
** Correlation is significant at the 0.01 level (2-tailed); * Correlation is significant at the 0.05 level (2-tailed); (BMI- Body Mass Index, FBG- Fasting Blood Glucose, HDL- High Density Lipoprotein, LDL-Low Density Lipoprotein, HBA1C- Glycated Haemoglobin, TG- Serum Triglycerides); Plasma adiponectin was significantly correlated with BMI, FBG, HbA1C and triglycerides (all P<.001). The correlation between plasma adiponectin levels and HDL-C was not statistically significant.
Discussion
In the present study, we found decreased plasma adiponectin concentrationsin the patients with diabetes which was further lower in patients with an acute coronary event indicating that it may be a predictor of macroangiopathy. Hotta et al found similar results in their study and proposed that accumulation of adiponectinin atherosclerotic vascular walls may accelerate its half-lifein plasma, resulting in the reduction of the plasma concentrationof adiponectin in subjects with CAD .19 Ouchi et al studied the molecular basis of link between adiponectin and vascular disease and found that adiponectinmodulates endothelial inflammatory response and that the measurementof plasma adiponectin levels may be helpful in assessment ofCAD risk. 20 Large scale prospective experimental research is needed to clarify these theories.
The relation between plasma adiponectin and the various known metabolic risk factors were on par with the world literature, except for HDL-C. Koenig et al reported an additive effect of HDL-C and adiponectin on CAD risk prediction. 21 In their joint analyses, the highest risk for T2DM as well as acute coronary events was observed in men with low adiponectin in combination with low HDL-C levels. In the present study, the mean HDL-C levels were lower in patients with diabetes with MI compared to patients with diabetes without MI. However, we did not find any significant correlation between plasma adiponectin levels and HDL-C in the present study. Similar findings were obtained by Schulze et al indicating that although plasma adiponectin has been established to be correlated with insulin resistance, CAD and metabolic disease, the interrelation between these is far more complex.
The molecular mechanisms by which adiponectin exerts its multiple functions and whether its actions are receptor mediated still remain a mystery. Is the primary activity of adiponectin antiatherosclerotic, or is it principally a modulator of lipid metabolism and regulator of insulin sensitivity, or is it all of the above? The answers to these and other intriguing questions will undoubtedly provide additional insight into the metabolic roles of this new adipocyte hormone.
Conclusion
The present study and the recent evidence suggest that cross-talk between inflammatory signalling pathways and insulin signalling pathways may result in insulin resistance and endothelial dysfunction that synergise to predispose to cardiovascular disorders. Large scale prospective studies are needed to examine the ability of increase in adiponectin levels and insulin sensitivity to improve primary end points including incidence of diabetes and outcomes of cardiovascular events.
Organ transplantation is an effective therapy for end-stage organ failure and is widely practiced around the world. According to World Health Organization (WHO), kidney transplants are carried out in 91 countries. Around 66,000 kidney donations, 21,000 liver donations and 6000 heart transplants were performed globally in 2005. 1 In India the rate of organ donation is only 0.16 per million populations, compared to America's 26 and Spain's 35.2 The shortage of organ is virtually a universal problem. Though many efforts were undertaken by the government to motivate the public towards donation of organs, the rate of organ donors has not paralleled the growing waiting list3,4, 5 and inadequate organ donation in India remains a major limiting factor for transplantation. There are several factors which could facilitate and hinder the general public to donate a organ. Identifying these factors could help in planning effective strategies to combat the problem. Hence the present study was conducted with the aim to explore the general publics perceived barriers and facilitating factors of organ donation.
Materials and methods
The present study was a cross sectional, exploratory survey conducted among the general public of Puducherry U.T, India. 400 eligible subjects who fulfilled the following criteria were included a) Subjects aged 18 and above, and b) who understand either the local language Tamil or English. Subjects with intellectual, psychiatric and emotional disturbances that could affect the reliability of their responses were excluded from the study. The population registry in the primary health centers of the selected community area was used as a sample frame to select subjects randomly. Every eligible subject was explained about the purpose of the study and signed a written consent form. Formal ethical clearance was obtained from the institute ethics committee before actual data collection procedure.
Preparation of the questionnaire
An extensive literature review was carried out to understand the possible barriers and facilitators reported in the past. Reported barrier and facilitating factors in the literature were included in constructing the questionnaire, including specific cultural and religious oriented items specific to Indians. Subject’s intention to donate the organ was assessed using a single dichotomous question (yes or no). For assessing the barriers and facilitators related to organ donation a questionnaire with a total of 18 items (9 items each) was prepared in the form of closed ended question i.e. yes or no. Along with closed ended questions, an open ended question i.e. any other? was also included for obtaining an extended response apart from the framed questions. As knowledge is an important factor which could serve both as a barrier and facilitator for organ donation, 8 items related to knowledge were also included as a part of the questionnaire. Knowledge items of the questionnaire were evaluated by assigning a score of 1 for each correct response with a maximum possible score of 8. Interpretation of the knowledge component was also done by categorizing the knowledge as follows - Below 50% of the total score - Inadequate knowledge, 51 – 75% - Moderately adequate knowledge, above 75% - Adequate knowledge, for ease of understanding. The draft tool was validated for its content by 10 experts from the field of surgery, medicine, nursing, anthropology and psychology for its appropriateness. After appropriate modification the content validity index for the tool was calculated and it was found to be highly valid (0.98). The reliability of the tool was estimated by a test re-test reliability method among 10 subjects with an interval of 2 weeks from the first and second time of administration of the questionnaire. It was found to be highly reliable with reliability coefficient of 0.91. A face to face interview method was used to collect data from each subject. Collected data was analyzed using SPSS for windows version 14 (SPSS Inc., Chicago, Il, USA) with appropriate descriptive and inferential statistics. A probability value of < 0.05 was set as the level of significance
Results
Basic Demographic details
Of the total 400 subjects enrolled the majority were male (56%), between the age group of 31-40 years (48%), and followed Hinduism (68%) at the time of interview. Most of the subjects were literate (70%) with education up to high school and resided in a rural area (53%).
Knowledge regarding organ donation
The mean knowledge score of the subjects regarding organ donation was 4.74 1.45 score which ranged from a minimum score of 1 to a maximum score of 8. Most subjects responded correctly to questions related to organ matching (85.3%) and consent procedure (84.7%). Details of different aspects of knowledge regarding organ donation of the subjects can be found in Table 1. When subjects were asked about the source of information regarding organ donation, 51.3% of the subjects reported that they gained knowledge through television, 23% from health personnel, and 12% from friends and 7% through books and internet (Figure1). Whilecategorizing knowledge scores the majority of the subjects (38.6%) had inadequate knowledge, 50.6% had moderate knowledge and only 10.6% had adequate knowledge regarding organ donation.
Intention to donate organs: Barriers and Facilitators
Of the total 400 subjects interviewed 69.75% of the subjects reported that they wish to donate their organs, whereas the remaining 30.25% reported that they will not donate their organs either during their life or after their death. Subsequently the factors for barriers and facilitators were also analyzed using the pretested questionnaire. The most common barriers perceived by the subjects related to organ donation were as follows, ‘family opposition’ (82.8%), ‘complicated organ donation procedure’ (69%), ‘fear that donation affects their future’ (58.36%), and ‘misuse of organs’ (55.2%). More information about barriers is detailed in Table 2.The most important facilitating factors of organ donation as reported by the subjects were ‘thought of saving someone’s life’ (95.9%), ‘feeling of improved sense of humanity’ (95%), ‘to save the life of a close relative’, ‘thought that their organ live after their death (92.6%) and ‘being a role model for others’ (77.7%). More details of facilitating factor can be seen in Table 3
While associating the subject’s intention to donate organs with demographic variables like age, gender, residence, education, religion, marital status, type of family and knowledge; only educational level had a significant association with the subject’s intention to donate organ. Specifically graduate people are more likely to report intention to donate organ their organs than others (p<0.001).
Figure 1: Distribution of source of information regarding organ donation among the subjects.
Table 1: Item wise distribution of different aspects of knowledge regarding organ donation (n=400)
S. No
Aspects of Knowledge
Correct response
Incorrect response
1.
Definition of organ donation
24%
76%
2.
Knowledge regarding Commonly donated organ
71.3%
28.7%
3.
Knowledge regarding Consent procedure for living donor
76%
24%
4.
Knowledge regarding Consent procedure after death
84.7%
15.3%
5.
Knowledge regarding Consent for mentally retarded person
41.3%
58.7%
6.
Knowledge regarding Consent for unclaimed dead bodies
35.3%
64.7%
7.
Knowledge regarding Organ matching procedure
85.3%
14.7%
8.
Knowledge regarding legal consideration for organ donation
56%
44%
Table 2: Perceived Barriers towards organ donation (n=121)
S. No
Barrier factors
Percentage
1.
Oppose from the family
82.8%
2.
Fear
72.4%
3.
Procedures are complicated
69%
4.
Affects physical appearance
65.5%
5.
Affects the future
58.6%
6.
Create psychological problem
58.6%
7.
Organs could be misused
55.2%
8.
Against religious belief
48.3%
9.
Insults human rights and dignity
48.3%
Table 3: Perceived Facilitators towards organ donation (n=279)
S. No
Facilitating factors
Percentage
1.
Save someone’s life
95.9%
2.
Improve the sense of humanity
95%
3.
Save the life of a close relative
92.6%
4.
Wishes organ to be alive after death
92.6%
5.
To become a role model
77.7%
6.
Empathy for others
53.7%
7.
Rewarding experience
51.2%
8.
Due to family pressure
29.8%
9.
For economic benefit
27.3%
Discussion
The current study was conducted with the aim to explore the general publics intention towards organ donation and to identify the perceived barriers and facilitators. The present study revealed that 69.7% of the subjects have an intention to donate their organs either during their life or after their death, which is similar to the finding of Chung et al6 and Shahbazian H et al7. Similar to the previous studies8 the current study also confirmed a positive association between public intentions to donate their organ with their educational status. Though many studies in the past reported attitudes9,10 of public towards organ donation, the present study was the first of its kind to analyze specifically the barriers and facilitators of organ donation among the general public, this adds strength to this study. The most common barrier reported in the present study was ‘opposition form family in donating their organs’; these findings were similar to a previous study.6 Illegal organ donation and misuse of organ is a major problem in India for the low organ donation rate among public11, this fact was reflected even in the current study as 55.2% of the subjects reported misuse of an organ as barrier to organ donation. The most important facilitating factors of organ donation reported in the present study was ‘thought of saving someone’s life’ (95.9%), ‘feeling of improved sense of humanity’ (95%), ‘to save the life of a close relative’ (92.9%), these finding were similar to the findings of Neelam et al conducted in India12. The majority of the respondents in this study reported "lack of information" about organ donation and transplantation. These findings are comparable with those reported from previous studies, which all indicate the importance of public education about the importance of organ donation13,14,15,16. Our study identified that the principle respondents' source of information about organ donation was the television (TV). The contribution of other sources of information in providing respondents with knowledge about organ donation was minimal. Generally, studies had shown the importance of visual media in increasing the awareness of the public about organ donation. 17,18
Conclusion
Better knowledge may ultimately translate into the act of donation. Effective measures should be taken to educate people with relevant information with the involvement of media, doctors and religious scholars.
Population-based studies indicated that diabetes remains as a nationwide epidemic that continues to grow tremendously affecting 25.8 million people or 8.3% of the US population.1 This number is expected to reach 68 million or 25% of the population by 20302 as incidence of obesity is rising.3
The American Diabetes Association (ADA) recognizes diabetes education (DE) as an essential part of comprehensive care for patients with diabetes mellitus and recommends assessing self-management skills and knowledge at least annually in addition to participation in DE.4 With the objective of improving the quality of life and reducing the disease burden, the ADA and the U.S. Department of Health and Human Services through its Healthy People 2020 program have emphasized three key components for effective disease management planning: regular medical care, self-management education and ongoing diabetes support.5,6
The hallmark of preventing the chronic complications of diabetes lies in optimizing metabolic parameters such as glycaemic control, blood pressure, weight and lipid profile. Pharmacologic intervention can only do so much in achieving treatment goals. It should be complemented with appropriate DE emphasizing dietary control, physical activity and strict medication adherence.7,8 Adequate glycaemic control is clinically important because a percentile reduction in mean HbA1C is associated with a 21% reduction in diabetes-related death risk, 14% reduction in heart attacks and 37% reduction in microvascular complications.9
Diabetes self-management (DSM) education programs are valuable strategy for improving health behaviours which have significant impact on metabolic parameters.10 This is supported by chronic care model that is based on the notion that improving the health of patients with chronic diseases depends on a number of factors that include patients’ knowledge about their disease, daily practice of self-management techniques and healthy behaviors.11,12,13
A systematic review by Norris et al. has shown that DSM training confers positive effect on patients’ knowledge about diabetes, blood glucose monitoring, and importance of dietary practices and glycaemic control.14 In another retrospective observational study, evidence has suggested that participation in a multifactorial diabetes health education significantly improved glycaemic and lipid levels in the short term.10
Diabetes education/support group provides a comprehensive patient education, fosters a sense of community, and engages the patients to become active part of a team managing their diabetes. The diabetes support group at Queens Hospital Centre provides services to a diverse population from different socioeconomic backgrounds and is offered to any patients with diabetes. It is facilitated by certified diabetes nurse educators in the hospital and in the clinic. Patients meet once a month per session and are provided education in self-management of diabetes, education in medication, diet, lifestyle modifications, regular exercise, weight management and translation in their respective languages, if needed.
Few researches have been conducted comparing the efficacy of DE and combination of diabetes education and peer support group (DE+PS) in improving the metabolic parameters of patients with DM. In patients with DM, the primary objective of this study was to assess the clinical impact of DE and combined DE+PS group on metabolic parameters such as lowering HbA1C, reducing weight or BMI, controlling blood pressure, and improving lipid profile.
Methods
The study subjects were identified through retrospective review of electronic medical records of adult patients aged more than 18 years old with diabetes and being treated at the Diabetes Centre and/or Primary Care Clinic of Queens Hospital Centre, Jamaica, New York from January 01, 2007 to June 01, 2011. A total of 188 study subjects were selected and assigned to three groups: (1) control group (n=62), who received primary care only, (2) DE group (n=63), who received diabetes teaching from DM nurse educator in addition to primary care, and (3) DE+PS group (n=63), who received both diabetes education and attended at least 2 or more sessions of peer support group in addition to primary care. The subjects in control group, education group, education plus peer support group were matched on age, sex, weight and BMI. Considering the data availability, the duration of follow up measured in each group varied; the control group was followed up for 8 months, the DE group for 13 months and the DE+PS group for 19 months. The changes from mean baseline to the third month, sixth month and final follow up period were calculated for the following metabolic parameters: HbA1C, weight, BMI, SBP, TC, HDL-C, LDL-C and TG-C. T sample T-test was used to compare statistical differences in the mean changes in the metabolic parameters in each group from baseline to follow up period. All data management and statistical analyses were conducted with MiniTab version 14. A p-value of less than 0.05 is considered statistically significant.
Results
Among the 188 study subjects included in our study between ages 20 to 88 years with mean age of 60, the predominant gender was female (n=132, 70%). African American makes up the majority (n=74, 39%), followed by Asian (n=40, 21%), Caucasian (n=34, 18%), Hispanic (n=22, 12%) and Indian (n=18, 10%). Majority of our patients with DM have concurrent hypertension (91%), hyperlipidemia (90%), and obesity (47%). See Table 1 for baseline demographics.
Table 1. Baseline demographic characteristics of the study population
Control [C] N=62
Diabetes Education [DE] N=63
Diabetes Education + Peer support [DE+PS] N=63
Baseline Characteristics
Age range (years) [median]
32-76 [61]
20-88 [58]
26-86 [62]
Sex-male [N (%)]
22 (35)
20 (32)
14 (22)
Race
African American
31 (50)
26 (41)
17 (27)
White
11 (17)
23 (37)
0 (0)
Indian
18 (29)
0 (0)
0 (0)
Asian
1 (2)
10 (16)
29 (46)
Hispanic
1 (2)
4 (6)
17 (27)
Comorbidities [N (%)]
Hypertension#
54 (87)
59 (94)
58 (92)
Hyperlipidemia¥
56 (90)
61 (97)
53 (84)
Obesity*
29 (47)
29 (46)
31 (49)
Active cigarette smoker
6 (10)
5 (8)
1 (2)
# Hypertension is defined as mean systolic blood pressure > 140 mmHg and/or diastolic > 90 mmHg measured on two separate occasions. These patients have either hypertension diagnosed prior to or after diagnosis of DM. ¥ Hyperlipidemia is defined as LDL > 100 mg/dl in patients with diabetes and diagnosis hyperlipidemia could be before or after diagnosis of DM. * Obesity is defined as body mass index (BMI) of at least 30 kg/m2 or greater.
The group analysis showed that the DE group had a statistically significant decrease in mean HbA1C (mean change: -0.78%, p=0.013), TC (mean change: -16.89 mg/dL, p=0.01) and LDL-C (mean change: -11.75 mg/dL, p=0.04) from baseline to final follow up (see Table 2). The DE group had non-significant mean weight gain of 2.17 pounds and BMI of 0.52 kg/m2.
* Final follow up varies for the three groups. 8 months for control (C), 13 months for education (DE) group and 19 months for education plus peer support (DE+PS) group
Although DE+PS group were observed to have decreased in mean HbA1C (-0.48%), weight (-0.38 pounds), SBP (-3.24 mmHg), TC (-4.43 mg/dL) and TG-C (-12.89 mg/dL) and increased in HDL-C (+095 mg/dL), they were not statistically significant from initial to final follow up period. There were greater improvements in HbA1C and SBP from baseline to final follow up in DE+PS group compared to the control group. Only the control and DE+PS groups showed a decrease in weight from initial to final follow up.
Between the two intervention arms, the DE group exhibited greater reduction compared to DE+PS group in mean HbA1C (-0.78 vs. -0.48%), SBP (-3.78 vs. -3.24 mmHg), TC (-16.89 vs. -4.43 mg/dL), LDL-C (-11.75 vs. +0.08 mg/dL) and TG-C (-14.75 vs. -12.89 mg/dL).
Discussion
Our results suggested that among patients with DM, the subjects who participated in DE exhibited significant reduction in baseline HbA1C, TC and LDL-C compared to control. Furthermore, the significant impact of DE alone on optimizing control of HbA1C and LDL-C appeared to persist through time. In addition patients who received DE+PS also demonstrated moderate improvement in HbA1C, SBP, TC and TG-C and HDL-C even though they were not statistically significant on final follow up. It must be noted that the baseline mean HbA1Cs were higher in both interventions DE and DE+PS groups compared to control group and this may be associated with greater reduction in HbA1C in the intervention groups and may skew the finding. Our study results showed that DE group had greater percentage reduction in HbA1C (9%) compared to DE+PS group (5%) from baseline to the first follow up. The average change in HbA1C and LDL-C levels recorded in our study is similar to what has been reported in a previous study which showed significantly greater improvement in mean glycaemic levels and LDL-C levels in patients who participated in DE.10
However our findings are in stark contrast to a previous study that showed that DE+PS intervention has led to substantially greater weight reduction and improvement in HbA1C at second month post-intervention compared to education and control group.15 This difference may be accounted for by the effect of sample size and the duration of follow up. The DE+PS group in our study included twice the number of patients being sampled compared to previous study (63 patients vs. 32 patients), and longer duration of follow up (19 months vs. 4 months)15. These differences are significant as they can influence the data trend.
In general, all groups had improvement in HbA1C, TC, TG-C levels, and SBP (though not significant). Only control and DE+PS groups had weight reduction and DE group had weight increase. Although the DE+PS group had improvement in most of the metabolic parameters they were not statistically significant throughout the entire follow up period compared to DE group. This scenario might be attributed to retrospective nature of the study, possible non-compliance of patients to medications, differences in duration of follow up between groups, and limited number of patients sampled thus hindering the appreciation of potential significant effect. The statistically significant differences in baseline HB A1C among the three groups could also explain the differing magnitude of change from baseline; DE group had higher baseline HbA1C compared to control group (9.3 vs. 7.5%; p=0.00) allowing for a greater change from baseline value. Similarly in DE+PS group, baseline HbA1C was considered statistically significant compared to control group (8.3 vs. 7.5%, p=0.018).
A previous randomized controlled trial assessing the effect of peer support on patients with type 2 diabetes with a 2-year follow up demonstrated no significant differences in HbA1C (-0.08%, 95% CI -0.35% to 0.18%), SBP (-3.9 mmHg, -8.9 to 1.1 mmHg) and TC (-0.03 mmol/l, -0.28 to 0.22 mmol/l).16 It was suggested that the effect of DSM education on glycaemic control is greatest in the short-term and progressively attenuated over time and this may suggest that learned behaviour changes with time.17,18 However, the result of the present study showed a persistently significant beneficial effect on HbA1C and LDL-C from the earliest follow up until the final month for patients receiving DE alone.
Previous meta-analysis of randomized trials of DSM education programs by Norris and colleagues (2002) demonstrated the beneficial effect of DE with estimated effect on glycaemic control (HbA1C) at -0.76% (95% CI: 0.34,1.18) compared to control immediately after the intervention.17 However, the findings of the present study on the effect of peer education are in direct contrast with the results of the randomized trial using the Project Dulce model of peer-led education showing significant improvement from baseline to the tenth month of follow-up in HB A1C (-1.5%, p=0.01), TC (-7.2 mg/dl, p=0.04), HDL-C (+1.6 mg/dl, p=0.01) and LDL-C (-8.1 mg/dl, p=0.02).19 This could be accounted for the different baseline values of the metabolic parameters in the present study, thus creating a bias in the magnitude of change.
It has been suggested that the most effective peer support model includes both peer support and a structured educational program. The emphasis on peer support is based on the recognition that people living with chronic illness can share their knowledge and experiences to one another.20 It has been observed that participants in peer support groups were not interested in the topic of diabetes itself but on the effect and meaning of the disease on the lives of the patients.21
There are a number of limitations to be taken into consideration when interpreting the results of our study. Since our study is a retrospective review of medical records, the data collection was limited to availability of the required clinical data. Some parameters were not possible to obtain on a consistently uniform time frame. This resulted in varying mean duration for the 3 study groups (8 months for control group, 13 months for DE and 19 months DE+PS group). Because of unavailability of some of the clinical parameters at a specific time frame, there were variables missing on the earlier follow-ups. Our study also examined the effect of the intervention over a relatively short time. A longer-term study is necessary to determine if the intervention has lasting impact on improving the metabolic parameters, uplifting the quality of life and preventing morbidity and mortality from diabetes. The limited sample size could also be important factor that may influence the generalizability of the data. The differing baseline values in the metabolic parameters could have blunted the appreciation of possible significant improvement in the metabolic parameters in the DE+PS group. Other confounding factors that were not analysed in the present study and could have affected the results include the use of insulin regimen among the different groups, initiation of additional oral hypoglycemic agents, medication adherence by the patients and adjustment by physicians, and whether the patients were seen by endocrinologists or not.
The present study suggested that participation in DE may assist with optimizing HbA1C, TC and LDL-C. The DE group had improvement in glycaemic control and other metabolic parameters. The significant metabolic improvement gained from DE appeared to be sustained over time. However, participation in both DE+PS showed relative improvement but not significant as it is likely due to confounding different baseline metabolic parameter and duration being compared. Our findings underscore the importance of DE as part of the treatment plan for patients with DM. The addition of peer support group may or may not contribute to significant improvement of metabolic parameters.
Electroconvulsive therapy (ECT) is an effective treatment for some individuals with severe neuropsychiatric illness. It is widely used to treat certain psychiatricdisorders, particularly major depression.1,2 ECT involves applying a brief electrical pulse to the scalp after the patients are administered muscle relaxants and general anaesthesia.3 This pulse excites the brain cells causing them to fire in unison and produce a seizure.
In 2003, the National Institute of Clinical Excellence (NICE) issued guidance on the use of ECT. Its use was recommended only to achieve rapid and short-term improvement of severe symptoms after an adequate trial of treatment options has proven ineffective and/or when the condition is considered to be potentially life-threatening in individuals with severe depressive illness, catatonia or a prolonged manic episode.4
The mechanism of action of ECT is not fully known. ECT affects multiple central nervous system components, including hormones, neuropeptides, neurotropic factors, and neurotransmitters. The induction of a bilateral generalized seizure is required for both the beneficial and adverse effects of ECT. Certain parameters like seizure duration, electric stimuli, seizure threshold, ECT practice factors and medication can influence its effectiveness. The degree to which electrical stimulation exceeds the seizure threshold, the positioning of electrodes on the head, pulse width, pulse frequency and seizure duration are all known to be important.5 This study aims to review the evidence base of these parameters in detail. The seizure duration and electric stimulus are the two critical parameters and are therefore the main focus of this review.
Literature Review
A review of literature regarding ECT was using search engines like MEDLINE, PsycInfo, and OVID using the key words “electroconvulsive therapy,” “seizure parameters,” “seizure duration,” “seizure threshold,” “stimulus dosing” and “effectiveness.”
Parameters Associated with Effectiveness of ECT
Seizure Duration Electrical Stimulus Seizure Threshold ECT Practice Factors Endocrine Factors Medication Other Parameters
Relationship between Seizure Duration and Effectiveness of ECT
Very little is documented on clinical studies that correlate ECT effectiveness and seizure duration. There is evidence that supports the direct relationship of seizure duration and the effectiveness of ECT. It was thought that measuring the seizure duration and the knowledge of measuring such parameters can help explain its therapeutic effect.6 There has been research which suggests that motor seizures of less than 15 seconds in duration do not exhibit tonic-clonic phases and are ineffective in treatment.7 Some of the studies in past years found a direct relationship between total seizure duration during a course of treatment and patient response to ECT.8
A retrospective study on ward patients found that a positive clinical outcome from depressive symptoms has a direct relationship with accumulative seizure time in the course of therapy.8 However, the study was neither randomized nor controlled. Stimulus intensity, diagnosis, and concurrent medication parameters were not properly considered. Another study that supports the correlation found that 88% of patients with cumulative seizure time of 300 seconds and over had a favourable response. The data was retrospectively and prospectively collected in a university hospital. It was mentioned that data gathering was very difficult specifically with regard to the variable number of patients’ ECT sessions; the confounding effect of medication and the treatment of different patients using unilateral or bilateral.9
However other studies challenge these statements. A prospective study of a sample of depressed patients undergoing ECT, the seizure duration did not correlate with Hamilton Depression Rating Scale (HAM-D) scores after treatment. However, it was found that significant nonverbal memory loss of patients was correlated with seizure duration.10 The seizure duration does not directly influence the frequency of ECT, longer seizures do not equate to fewer ECT treatments. Studies using HAM-D scores do not support the idea that seizure duration is a variable correlated to efficacy.11 Short seizures during ECT for few patients are the result of a medical condition or drug treatment interference. On the other hand, patients who have been subjected to ECT treatment encounter shortened seizures.12
There are studies which show that the length of the cerebral seizure activity or the tonic–clonic convulsion is not related to clinical effectiveness.6,13 However, the treating psychiatrist should question whether, or not, generalised cerebral seizure activity had occurred if, at the first treatment, the convulsion lasted less than 15 seconds or the EEG recording showed seizure activity lasting less than 25 seconds.14 Such brief seizure activity might be the result of a focal or partial seizure, and therefore be of questionable therapeutic efficacy. It has been noted that there are patients who recover with ECT and yet display only short tonic–clonic convulsions. This may be more likely in elderly patients.
Most recent evidence mentions that the quality of cerebral seizure activity and the quality of the desired activity cannot simply be related to its length in time alone. It is recommended that the convulsion be timed from the end of electrical stimulation to the end of generalised, that is, bilateral, clonic activity. EEG monitoring can also be done but one needs to have good experience using this technique and sometimes artefacts can cause misinterpretation of the results.15
Relationship between Electric Stimulus and Effectiveness of ECT
ECT is administered by a constant-current, brief-pulse ECT machine that is able to deliver a wide range of electrical dose, that is, 25–50 mC up to 750–800 mC. It is recommended that new machines deliver a range of dose from 25 to 1000 mC.15 One of the important parameters in predicting clinical response is the degree to which the electrical stimulus exceeds the seizure threshold.16 The maintenance of adequate seizure duration on patients is a complicated issue. Elderly patients are also more susceptible to cognitive side effects than younger patients.17 Patients regularly treated with ECT have records of shorten seizure duration over time, and clinicians need to increase stimulus to maintain duration, which in the long run can lead to complications.18
Electroencephalography (EEG) Findings
Voltage Suppression Studies. Postical voltage suppression refers to the decrease in resting EEG voltage after seizure activity as compared with baseline. Proper excitation of seizures invoke voltage-suppressing neural mechanisms intended to terminate and further seizure activity. This suppression is considered as a lower baseline on the EEG post ictus.19 According to studies, the degree of suppression correlates with seizure generalization, therapeutic adequacy, and bilateral stimulation.20
EEG Waveform Features. Greater ictal EEG amplitude, intensity, and symmetry obtained with bilateral ECT are not common with longer seizures, but they are related to antidepressant outcome.21 Studies found that the immediate post stimulus and mid ictal EEG amplitudes correlated with seizure therapeutic adequacy in depression. The symmetry of waveforms at the midpoint on the EEG tracing was also predictive.20 It was also proven that seizure duration had no impact as an EEG measure of treatment adequacy.21
Seizure Charge. The calculated product of EEG voltage, seizure uniformity throughout the brain, and seizure duration was hypothesized to be a measure of treatment intensity and efficacy.21 The variables included in total seizure charge are not physiologically independent of one another, which means longer seizure duration will not guarantee better results.
Low-dose bilateralelectroconvulsive therapy has a powerful antidepressant effectbut low-dose right unilateral therapy is ineffective.22 Evidence shows that the efficacy of rightunilateral electroconvulsive therapy depends on the electricaldose.23,24 There is some research showing that forboth unilateral and bilateral ECT, a higherelectrical dose leads to a more rapid clinical response.7,17,23
Seizure Threshold and Electroconvulsive Therapy
The knowledge of the seizure threshold is a guide to the selection of the electrical stimulus dose for ECT. In theory, the seizure threshold is the lowest dose of electrical charge for each particular patient that is required to induce seizure.25 In clinical applications the seizure threshold depends on individual patient’s characteristics, treatment history, and other stimulus factors.26
The therapeutic effectiveness of ECT is partly dependent on the degree that the stimulus intensity exceeds the seizure threshold.27,28 This statement is true on unilateral non-dominant electrode placement (UL) and on relative stimulus intensity. On bilateral (BL) ECT, the therapeutic response frequency is dependent on higher relative stimulus intensity,28 whereas barely suprathreshold UL ECT has significantly reduced antidepressant potency in contrast to moderately suprathreshold UL ECT (150% above threshold).6 The clinical use of this can be applied after determining the seizure threshold at the first treatment.22,29 The desired relative stimulus intensity to be maintained during treatments is confounded by variable increase in seizure thresholds during treatment.28 This rise in the seizure threshold lessens the degree to which a fixed stimulus dosage exceeds the seizure threshold which can result in possible diminished treatment therapeutic potency.
The seizure threshold can be higher in the elderly population and this may increase the difficulty of eliciting effective seizures.29,30,31 The choice of anaesthetic agent and other age related factors can also affect the seizure threshold. Propofol can reduce the seizure duration and has a possible effect on the seizure threshold.32 The seizure threshold may sometimes rise during the course of therapy. The dose would usually rise pari passu with a rise in the seizure threshold to maintain the dosing strategy. The seizure threshold can increase about 80% in bilateral ECT and 40% in unilateral ECT over a course of treatment.6 Some studies found increases of only 25–40% for bilateral ECT.33
ECT Practice Factors and Seizure Duration
As discussed earlier, the success of ECT treatment can be related to the degree to which the electrical stimulus exceeds seizure threshold and not the absolute dose that determines clinical outcome, especially in unilateral patients.6 Right unilateral (RUL) treatment at variable dosage can produce seizures of equal duration to bilateral treatment. With low levels electrical stimulation, RUL patients showed only 17% improvement inHAM-D scores compared to 70% in the BL group, despite the same mean seizure duration.22
Positioning electrodes over the non-dominant hemisphere causes lesssevere cognitive side effects than bilateral placement.11,24 In spite of extensive research however, the relative efficacy of right unilateraland bilateral electroconvulsive therapy is controversial.2,34,35 There are studies which have found superior efficacy with bilateral therapy,22,36,37 and then there are other studies which have reported equivalent efficacy.38,39 Because ofthis uncertainty, the American Psychiatric Association TaskForce on Electroconvulsive Therapy recommended thatelectrode placement be determined on a case-by-case basis.2
Multiple ECT stimuli (MECT) is given to patients to achieve longer cumulative seizure durations. The clinical improvement in depression correlates to patients’ total seizure time in MECT. But there is no proven study on the benefits of increased seizure time from the increased number of stimuli administered.40
Endocrine Measures
Oxytocin. According to studies, the measurement of oxytocin released from posteriorpituitary has a direct relationship with HAM-D measured improvement in depression.41 The concentration of oxytocin-associated neurophysin (AON) serum was calculated before and after the patient’s treatment of ECT. The increase in AON positively affects HAM-D. This neurophysin response was evident on ECT treatment but does not relate to EEG-measured seizure duration.
Prolactin. The surge of prolactin released during ECT treatment can be an indicator of clinical improvement. Seizure duration is associated with a rise in prolactin.42 However, the relationship between the magnitude of prolactin release and benefits of ECT is yet to be established.24
Cortisol. Although several variables have been studied as a possible predictor for the efficacy of ECT but results regarding hypercortisolism have been inconsistent. There has been a study to evaluate the relation between pre-treatment cortisol levels and the efficacy of ECT in a population of drug-free inpatients with severe major depression. This study suggests that higher levels of post-dexamethasone salivary cortisol at 9 AM are predictive of ECT efficacy.43
Elevated glucocorticoids may increase the vulnerability of the brain to the adverse effects of repeated seizures.This hypothesis was tested in a study and it was found that, ECT treatments delivered over 2 weeks resulted in a significant improvement in mood and a decline in most measures of cognitive performance. Elevated basal cortisol was associated with a greater decline in performance of executive function, visuospatial processing speed, and verbal memory. It was concluded that elevated cortisol predicts a greater degree of ECT-induced cognitive impairment. 44
Medication
Concurrent medication. Concurrent therapy can be considered under two headings: general medication and psychotropic medication. Both can affect seizure threshold. Anticonvulsants, hypnotics and membrane stabilisers tend to raise the seizure threshold, while preparations containing theophyllines can have the opposite effect. Concurrent psychotropic medication can have a significant effect upon ECT. Benzodiazepines are anticonvulsant and should be avoided if possible, but it is important to remember that there are risks associated with their sudden withdrawal. Some authorities have suggested short-term reversal with flumazenil if their presence is considered to be a limiting factor in the success of ECT, but experience is limited.45,46 Tricyclics tend to be proconvulsant, but there is little evidence of any detrimental effect on ECT. Selective serotonin reuptake inhibitors (SSRIs) tend to reduce seizure threshold and may be associated with prolonged seizures. Monoamine oxidase inhibitors increase seizure threshold and it is essential that the anaesthetist is aware that the patient is taking this class of medication or has done so within the previous 2 weeks. Lithium reduces seizure threshold and serum levels should be checked regularly and kept within a moderate range (0.4–1 mmol/l). Selective inhibitors of the reuptake of noradrenaline in common with SSRIs, can reduce seizure threshold and also cause hypertension. Neuroleptics tend to be proconvulsant at low dosage but increase seizure thresholds at higher dosage.
In a retrospective study of 455 patients involving 5482 treatments differences in tolerability and clinical effectiveness were found between combination therapy (ECT administered together with neuroleptic medication) and ECT monotherapy.47 Seizure duration which was assessed by EEG was significantly longer in patients treated with combination therapy using neuroleptics with lower antipsychotic potency; whereas seizure duration assessed by EEG-monitoring-electromyograph (EMG) was shorter in combination treatments done with atypical substances. In a parallel study, of ECT monotherapy or combination therapy with antidepressants using the same patient group, seizure duration was unaffected by most antidepressants but SSRIs lengthened seizure activity.48 In addition this study found that therapeutic effectiveness was significantly enhanced in the patients receiving tricyclic antidepressants, the tetracyclic antidepressant mirtazapine or SSRIs.
There may also be a role for antidepressants in the prevention of relapse following ECT. A small double-blind placebo controlled study of the tricyclic antidepressant imipramine involving 27 depressive inpatients who had failed on pharmacotherapy prior to ECT showed that imipramine, when compared to placebo, resulted in a significant decrease in the risk of relapse of patients receiving ECT.49 This study is in broad agreement with an earlier randomized, double-blind, placebo-controlled trial using another tricyclic antidepressant nortriptyline, or combination therapy of nortriptyline with lithium in the prevention of post-ECT relapse in patients with unipolar major depression.50 In 29 patients receiving placebo the relapse rate during the 24 week duration of the trial was 86%; whilst in 27 patients receiving nortriptyline 60% relapsed; and 39% of the 28 patients receiving nortriptyline and lithium combination therapy relapsed during the time of the study.
Other parameters
The effectiveness of the treatment is influenced by many other underlying factors, specifically the conditions and factors relating to individual patients. This would include age, sex, physical health status, co morbidities etc. Thus, one should always consider other factors that might affect the efficacy of ECT. Two recent small Japanese studies have suggested that some cardiovascular and EEG parameters may act as markers to predict the therapeutic response of ECT in depression. Postictal systolic heart rate and blood pressure were found to be significant predictors of the therapeutic efficacy of ECT in a study of 24 patients with depression;51 with higher systolic heart rate and blood pressure being associated with more effective ECT.
Discussion
ECT is widely used to treat certain psychiatricdisorders, particularly major depression. Although ECT has been extensively used there is little published information on the effect of seizure parameters and the effectiveness of ECT. There is evidence that supports the direct relationship of seizure duration and the effectiveness of ECT but the latest research suggests that the length in time of the cerebral seizure activity or the tonic–clonic convulsion is not related to clinical effectiveness.10,11 The effectiveness of ECT is related to the quality of cerebral seizure activity and cannot simply be related to its length in time alone. One of the important parameters in predicting clinical response is the degree to which electrical stimulus exceeds the seizure threshold.
Past research has shown that a generalized seizureof adequate duration is necessary and sufficient for antidepressanteffectsand that the intensity of the electrical stimuluscontributes to decreased cognitive function, the principal sideeffect, but not to effectiveness.7 Different types of anaesthetics, or concurrent medications can affect the seizure parameters and its efficacy.52,53 Research shows that a generalized seizureof adequate duration is necessary and sufficient for antidepressanteffects1,7 and that the seizures of less than 15 seconds duration are ineffective. There are other studies which mention that seizure duration does not influence the effectiveness of the ECT.10,11
The Future
Clinicians need to continue to research this difficult area within psychiatry to enhance the evidence base and fill such gaps in this evidence as highlighted by the ECT Handbook.54 On-going research is needed into what is a proven treatment of depressive illness and this should include more in depth research into the relationship of the above discussed parameters with its effectiveness.
“If ECT is ever legislated against or falls into disuse, it will not be because it is an ineffective or dangerous treatment, it will be because of a failure to supervise and monitor it correctly”55 and such supervision includes future quality research by concerned clinicians. Current NICE guidelines have limited the use of ECT to individuals with severe depressive illness, catatonia or a prolonged or severe manic episode who have been unresponsive to other treatment options.In addition, intervention of ECT should be considered to be short term and NICE does not recommend using it as maintenance therapy.56 As research into ECT develops, the consequences may be an even more targeted approach to the use of ECT as therapy.
Resource allocation in medicine applies to two complementary levels of care. One pertains to the organisation of public health and the provision of general rules informing the management of the system (macro-allocation). On the other hand, there is the need to specify decision criteria for the daily practice of health care providers who have to decide on the utilisation of their allocated resources, while dealing with a demand that often exceeds supply (micro-allocation).1
Beneficence, i.e. acting for the good of the patient, is one of the founding value of traditional ethics in medicine. However, the picture has changed when the core value of medicine shifted toward the centrality of the human person and the ideal of self-determination. The patient is now a 'health care user' who consults a professional whose knowledge and expertise is used in order to arrive at options. Good medical practice seems the result of a 'contract bargaining', which must take into account different criteria: clinical indication, patient preferences and subjective values, and appropriateness within the social context. Controlling how these three elements interact with each other requires a constant commitment and synchronised interventions.2
For cultural reasons, physicians consider, quite rightly, the costs of their interventions to be incommensurable with the life and the restoration to health of the diseased person. The most difficult problem in the distribution of resources remains the finding of convincing criteria to provide guidance, when often painful choices have to be made in the face of inadequacies in the availability of resources.3
Intensive care is one of the most expensive specialities of medicine and intensive care beds nowadays represent a limited resource.4, 5 The lack of beds is a daily problem in many ICU6, 7 and bed allocation has been considered one of the thorniest and stressful aspects of the intensivist's job.8 Studies have shown that resource use is often inefficient in European ICU. One of the main reasons for this inefficiency has been identified as nursing force “waste”.9
Monitoring and support of deficient vital functions are the main aims of intensive care. Usually, intensivists carry out the adequate diagnostic procedures and necessary medical and surgical treatments required to improve patient outcomes. There has been a considerable international effort to define the ethical, clinical and economical criteria for admission to ICU and to draft the relevant guidelines. The fundamental point is that resources should be utilised appropriately, i.e. that the patient be of the right category, in the right place and at the right time. Furthermore, ethics dictates that resources be allocated where they are more likely to make an impact.10-13
ICU admission and discharge can be ruled by means of a priority scale which classifies patients based on the expected benefit to result from intensive treatment.14 However, while it may be relatively easy to create “on-paper” scenarios affirming that patients who are too critical or not critical enough to benefit should not be admitted to intensive care, identifying these patients in everyday practice is far from simple.
As far as a reasonable doubt may be considered regarding the irreversibility of the clinical status, it is appropriate to initiate or continue intensive treatment. On the contrary, if the irreversibility of the clinical setting is deemed to be reasonably certain, it is appropriate not to initiate or to withdraw intensive measures to spare the patient the undue prolongation of the dying process. Excessive treatment is ethically unfair and should be strongly condemned, because it determines an inappropriate use of the means of treatment; it is likely to cause harm and pain to the patient and fails to respect the patient's dignity in death. Excessive treatment also increases the suffering of family members, is frustrating for care providers and generates an inequitable distribution of resources by curtailing them for other patients. The withdrawal of an intensive treatment, which was previously initiated because deemed to be indicated and accepted, or because the patient's clinical status and relevant prognosis were not clear enough at the time, should be considered whenever the clinical picture counter-indicates treatment continuation, the patient withdraws consent, or a previously defined therapeutic limit is reached.15
Immortality has always been an ambition for human beings. Today's medicine appears to be instrumental in dealing with this type of issues by making promises that will be hard not to break. The most urgent form of action to be undertaken regards these unwarranted expectations that society holds about the efficacy of medicine. The message to put across ought to be that death is inescapable and that the most severe diseases are incurable.
Once the inevitability of resorting to often dramatic measures in today's health care system is postulated, we are confronted with the problem of finding an ethical justification to subsequent decisions. On the basis of the choices made necessary by the paucity of available resources, medical treatment would be “apportioned”, i.e., distributed according to commitments and rules, with the inevitable exclusion of some from the utilization of the services themselves.
Rationalisation, intended as best utilisation and fair limitation, is an economic necessity, juridically and ethically legitimate. The ultimate objective must remain that of equitable apportionment.
Bortezomib is a reversible proteasome inhibitor, currently approved by US FDA for use in multiple myeloma and mantle cell lymphoma. It has been shown to cause new onset and exacerbation of underlying congestive cardiac failure (CHF) in some case reports. Although the exact mechanism of bortezomib induced congestive cardiac failure is unknown, studies have shown dysregulation of ubiquitin proteasome system (UPS) in human cardiac tissues in end stage heart failure1-3. Furthermore, a study in rats has shown reduced left ventricular contractility after bortezomib administration, which was attributed to reduced ATP synthesis in mitochondria of cardiac myocytes4. Our case demonstrates new onset severe reversible left ventricular systolic dysfunction after 4 cycles of bortezomib in a 58 year old female with multiple myeloma. It highlights the importance of monitoring cardiac function in patients receiving bortezomib.
Case Report
A 58 year old female with past medical history of well controlled hypertension presented with severe low back pain, anorexia and unintentional weight loss of around 20 pounds over a period of 3 months in medical clinic. On evaluation of her routine laboratory tests, she was found to have haemoglobin of 6.5 g/dl, haematocrit of 19.9%, white blood cell (WBC) count of 3.9 x 103/cc, red blood cell (RBC) count of 2.18 x 106/cc and platelet count of 1.52 x 105/cc. Her blood urea nitrogen and creatinine was 10 mg/dl and 0.7 mg/dl respectively and corrected calcium level was 10g/dl. On liver function test, her total protein was 12.4 g/dl and albumin level was 2.8 g/dl. X-ray of lumbosacral spine revealed a compression fracture at the level of T12and L2 vertebra. Bone survey confirmed diffuse osteopenia, severe collapse of the body of T12 and partial collapse of L2 and L3. Due to the presence of severe anaemia and compression fractures, multiple myeloma was suspected. Urine protein electrophoresis showed two monoclonal protein bands with concentration of 46.8% and 4.8% and urine immunofixation showed two intact monoclonal IgA-Kappa immunoglobulin bands. Beta-2 microglobulin level was 5.49. Bone marrow aspiration and biopsy confirmed the diagnosis of multiple myeloma. Patient was staged as IIIA according to Durie-Salmon staging system.
Subsequently, patient was planned to be treated with eight cycles of bortezomib and dexamethasone, with bortezomib being given on day 1, 4, 8 and 11 of each cycle at a dose of 1.3 mg/m2 body surface area. Prior to initiation of chemotherapy, she received radiotherapy to spine as well. However, after completing the fourth cycle of bortezomib/dexamethasone, she was admitted to the hospital with generalized weakness, nausea and vomiting. Chest X ray revealed possible right lower lobe infiltrate or effusion along with increased bronchovascular markings and she was treated with antibiotics for suspected community acquired pneumonia. However, an echocardiogram was obtained due to bilateral crackles on physical exam and increased bronchovascular markings on chest X ray, which revealed dilation of left ventricle with left ventricular ejection fraction of 30-35%, diffuse hypo kinesis of left ventricle, mild mitral and tricuspid regurgitation and diastolic dysfunction with abnormal relaxation(Tajik grade I). Left ventricular septal and posterior wall thickness was 0.8 cm. Infiltrative Cardiomyopathy in the setting of multiple myeloma was unlikely due to the absence of bi-atrial enlargement, pericardial effusion and thick bright myocardium on echocardiogram. Cardiology consultation was sought and their impression was new onset left ventricular dysfunction due to bortezomib therapy.
Patient did not receive any further cycles of chemotherapy due to cardiotoxicity and was on optimal medical management for heart failure with lisinopril, carvedilol and isosorbide dinitrate. An echocardiogram was repeated four months after discontinuation of bortezomib, which revealed normal left ventricular contractility with global left ventricular ejection fraction of 55% and trace mitral regurgitation.
Currently, at 2 year follow up, her echocardiogram shows global left ventricular ejection fraction of 65%, trace mitral and tricuspid regurgitation and diastolic dysfunction with abnormal relaxation(Tajik grade I).
Discussion and Review of Literature
Botezomib is a novel proteasome inhibitor which acts by inducing bcl-2 phosphorylation and cleavage, resulting in G2-M cell cycle phase arrest and apoptosis5. US Food and Drug Administration (FDA) have approved bortezomib for use in multiple myeloma and mantle cell lymphoma. The common adverse effects of bortezomib observed in clinical trials and post marketing surveillance include thrombocytopenia, neutropenia, hypotension, asthenia, peripheral neuropathy and nausea. US package insert for bortezomib states that acute development or exacerbation of congestive heart failure and new onset of decreased left ventricular ejection fraction have been reported, including reports in patients with no risk factors for decreased left ventricular ejection fraction and it is recommended to closely monitor patients with risk factor for, or existing heart disease.
The role of ubiquitin proteasome system (UPS) in heart failure has been studied extensively in recent years. Two studies by Hein et al and Weekes et al in 2003 have shown presence of increased amount of ubiquitinated proteins and substrates in cardiac tissues of heart failure patients, indicating reduced activity of UPS in end stage heart failure1-3. Another study has shown impaired proteasome activity in hypertrophic and dilated cardiomyopathy likely secondary to post translational modification of proteasome6.However, in early stage heart failure, there is increased activity of UPS, resulting in remodelling and high cardiac output2. Bortezomib, by inhibiting UPS, would lead to accumulation of ubiquitinated proteins in cardiac myocytes, similar to that seen in end stage heart failure. A study in rats exposed to bortezomib alone showed development of left ventricular systolic dysfunction by echocardiography and reduced synthesis of ATP was observed in the mitochondria of cardiac myocytes4. However, the exact mechanism of bortezomib induced systolic dysfunction in humans is not clear.
There have been a few reported cases of bortezomib induced congestive cardiac failure in literature (Table 1). The amount of bortezomib administered before development of symptoms of heart failure was 20.8 mg/m2 in four patients, 3 mg/m2 in one patient and 10.4mg/m2 in one patient. Three of them have received prior anthracycline based chemotherapy. Complete reversibility of heart failure after discontinuation of bortezomib was documented only in two cases by follow up echocardiograms and brain natriuretic peptide levels7, 8. The patient described in our index case had well controlled hypertension and no additional cardiac risk factors at baseline. She developed non-specific symptoms, including weakness, nausea and vomiting after the fourth cycle of chemotherapy and was admitted to the hospital for community acquired pneumonia. However, an echocardiogram was obtained due to pulmonary congestion, which uncovered the diagnosis of left ventricular systolic failure. The two echocardiograms obtained at a follow up of 4 months and 2 years showed gradual improvement in ejection fraction to 55% and 65% respectively from 15% after chemotherapy with bortezomib.
We did a review of major clinical trials of bortezomib in patients with multiple myeloma, Waldenstrom’s macroglobulinemia and plasma cell leukaemia (Table 2) to investigate the incidence of congestive cardiac failure reported after administration of bortezomib. In APEX trial, the incidence of congestive cardiac failure was 2% in both bortezomib and high dose dexamethasone group 11. In a study on melphalan refractory multiple myeloma by Hjorth et al, 3 cases of congestive cardiac failure was reported in bortezomib-dexamethasone group and 2 cases were reported in thalidomide-dexamethasone group12. Another study evaluating the safety of prolonged therapy with bortezomib by Berenson et al reported 1 case of cardiomegaly and 1 case of pulmonary edema13. However, further studies are needed to specifically evaluate the incidence of congestive cardiac failure with bortezomib therapy.
In summary, our case and review highlights the importance of maintaining a high level of suspicion for development of congestive cardiac failure after therapy with bortezomib. Given the widespread use of bortezomib and new generation proteasome inhibitors in multiple myeloma, there might be increased incidence of new onset and exacerbation of underlying congestive cardiac failure in future. Currently, there is no guideline for routine evaluation and monitoring of cardiac function in all patients during the course of bortezomib therapy. Furthermore, it is unclear whether the severity of congestive cardiac failure is proportional to the cumulative dosage of bortezomib administration and also, if there is any correlation between onsets of congestive cardiac failure with the timing of bortezomib therapy. Further studies are required in future to address these issues.
Table 1: Review of cases of bortezomib induced congestive cardiac failure reported so far.
Author
Age/sex
Prior cardiac history and risk factors
Baseline cardiac function
Number of Bortezomib containing cycles
Exposure to other cardiotoxic medications
Amount of Bortezomib received before onset of cardiac symptoms
Lowest EF** after Bortezomib administration
EF on follow up visits
Voortman et al7
53/M
36 pack years of smoking and COPD
Echo not available; NT-Pro BNP 1389 ng/l
4
Gemcitabine
3 mg/m2
10-15% on Echo after 4 cycles
45% on MUGA scan at 6 months
Orciuolo et al9
73/M
NK*
NK
6
1 Anthracycline containing regimen
20.8 mg/m2
EF 25%
NK
Orcioulo et al9
61/F
NK
NK
4
2 Anthracycline containing regimens
20.8 mg/m2
EF 20%
NK
Orciuolo et al9
80/F
NK
NK
4
1 prior non anthracycline chemotherapy regimen received
20.8 mg/m2
EF 35%
NK
Hasihanefioglu et al10
47/M
None
EF 70% and normal coronary angiogram
2
1 cycle of Vincristine, Doxorubicin and Dexamethasone
10.4 mg/m2
EF 10%
EF 20% at 6 month follow up
Bockorny et al8
56/F
Hypertension, well controlled
NK
4
None
20.8 mg/m2
EF 20-25%
EF 55-60%
INDEX CASE
58/F
Hypertension, well controlled
NK
4
None
20.8 mg/m2
EF 30-35%
EF 55% at 4 month and 65% at 2 year follow up.
*NK: Not Known; **EF: Ejection Fraction
Table 2: Review of cases of congestive cardiac failure reported in clinical trials with bortezomib in multiple myeloma, Waldenström’s Macroglobulinemia and plasma cell leukaemia.
Authors (ref)
Study
Study population
Significant Cardiac events (n)
Berenson, J.R. et al. 200513
Safety of prolonged therapy with bortezomib in relapsed or refractory multiple myeloma
Frontline chemotherapy with bortezomib-containing combinations improves response rate and survival in primary plasma cell leukaemia
29 patients with untreated PPCL
None reported
Hjorth, M. et al. 201212
Thal-Dex vs. Bort-Dex in refractory myeloma
131 patients with Melphalan refractory MM
2 cases of cardiac failure in Thal-Dex group and 3 in Bort-dex group
Jagannath, S. et al 200916
Bortezomib for Relapsed or Refractory Multiple Myeloma
54 patients with relapsed or refractory MM
None reported
Jagannath, S. et al 201017
Extended follow-up of Frontline Bortezomib ± Dexamethasone for MM
49 patients with untreated MM
None reported
Kobayashi, T. et al. 201018
Bortezomib plus dexamethasone for relapsed or treatment refractory multiple myeloma
88 patients with relapse/refractory MM
None reported
Mikhael, J.R. et al. 200919
High response rate to bortezomib with or without dexamethasone in patients with relapsed or refractory multiple myeloma
638 patients with refractory or relapsed MM
None reported
Richardson, P.G. et al. 200320
A Phase 2 Study of Bortezomib in Relapsed, Refractory Myeloma
202 patients with relapsed MM
None reported
Richardson, P.G. et al. 200511
Bortezomib or High-Dose Dexamethasone for Relapsed Multiple Myeloma(APEX trial)
669 patients with relapsed MM
Congestive cardiac failure in 2% of each arm.
Rosino, L. et al. 200721
Phase II PETHEMA Trial of Alternating Bortezomib and Dexamethasone As Induction Regimen Before Autologous Stem-Cell Transplantation in Younger Patients With Multiple Myeloma
40 patients with newly diagnosed MM
None reported
Sonneveld, P. et al. 201222
Bortezomib Induction and Maintenance Treatment in Patients With Newly Diagnosed Multiple Myeloma
827 patients with newly diagnosed MM
Cardiac Disorders in 5% of patient in VAD group vs. 8% of patients in PAD group.
Yuan, Z.G. et al. 201123
Different dose combinations of bortezomib and dexamethasone in the treatment of relapsed or refractory myeloma
168 patients with relapsed MM
None reported
Suvannasankha et al 200624
Weekly bortezomib/methylprednisolone in relapsed multiple myeloma
29 patients with relapsed multiple myeloma
1 case of congestive cardiac failure
Conclusion
CHF is an infrequent but serious adverse effect of bortezomib. Cardiac function should be closely monitored in patients receiving bortezomib, as case reports have shown that these patients might present with non-specific symptoms like weakness and fatigue. Further studies are required to establish the frequency and mode of monitoring of cardiac function during and after bortezomib therapy.
We report a case of worsening psychiatric symptoms in a patient who was serendipitously diagnosed with Primary Hyperparathyroidism.
Behavioural change in form of aggression sometimes occurs as a component of psychiatric disorders such as psychosis, attention deficit hyperactivity disorder, autistic spectrum condition, conduct disorder and various mood disorders. It may also present as a psychiatric manifestation of an endocrine disorder such as Primary Hyperparathyroidism (PHPT)1,2.
PHPT is rare in children and adolescents with an incidence of 2-5 in 100000 3. It is characterized by hypercalcaemia and elevation of parathyroid hormone. Children with PHPT may present with non-specific complaints such as behavioural change and deteriorating school performance.
Patients who present with non-renal symptoms have a longer duration of symptoms prior to diagnosis of PHPT4,6. It seems probable that it takes much longer for diagnosis to be made in those with pre-existing mental disorder. When left undiagnosed and untreated, PHPT can be a serious disease with significant morbidity.
The finding of elevated serum calcium levels in young people is often fortuitous as they often present with non-specific symptoms3,4. A significant number of hyperparathyroidism cases with neuropsychiatric manifestation have been reported in patients without recorded pre-existing psychiatric diagnosis 3-6.
This case report highlights the need for clinicians to always consider endocrine disorder as a differential diagnosis when treating patients with psychiatric symptoms which are poorly responsive to standard treatment. It also demonstrates the relevance of an integrated approach in healthcare delivery including the importance of good communication between primary and tertiary care clinicians.
Case Report:
A 15yr old Caucasian male known to Child & Adolescent Mental Health Service (CAMHS) for management of his behavioural problems presented in crisis as a consequence of physical aggression, suicidal ideation and homicidal thoughts.
His first contact with CAMHS had been at the age of 10 when he was referred for management of his frequent aggressive outbursts. He had always been boisterous but had no previous history of significant emotional or behavioural difficulties. His developmental history was unremarkable and there were no features indicative of any neurodevelopmental disorder. There was no family history of mental illness.
His biological parents were involved in an acrimonious divorce at the time of his first referral to CAMHS so it was felt that this conflict may have contributed to his presentation.
He was referred a Child Psychotherapist for weekly sessions as the initial assessment suggested significant weakness in his attachment and identification which manifested in the instability and immaturity of mood and behaviour.
The family described minimal improvements in his capacity for self-control having had three years of psychotherapy. His behaviour remained challenging but manageable within the community until six months prior to him being re-referred by his General Practitioner (GP) for urgent psychiatric assessment.
Following parental divorce, his mum remarried but her new marriage was also turbulent and the couple had to separate. During this period of increased psychosocial stresses within his family, the patient’s behaviour escalated to a point that he was regarded as a significant risk to himself and others. It was thought that the separation between his mother and step-father might have triggered this deterioration.
The night before his urgent referral to CAMHS, he set a trap for his mother; he had put a rope around some curtains on the floor and was planning to throw another curtain over her. He also had a knife and hockey stick with him at the time. As his mother stepped into the room, he put the curtain over her head and attempted to hit her with the hockey stick. He was promptly restrained by his father, who had come to visit, before he could do much damage.
He presented as unpredictable and aggressive but would often deny recollection of any reported outbursts. He was very upset when incidents were talked about as he believed he had no control whatsoever over this behaviour – it was clear how upsetting his behaviour was to him.
He displayed uncontrollable rage on many occasions. It was usually directed at his mother and home furniture, and might last up to two hours. He appeared to seek immediate gratification and was clearly hypersensitive to his setting with a significant degree of paranoia and irritability.
He repeatedly stated that he had thoughts of wanting to kill his mother and himself especially when angry. He did not appear able to accept any responsibility for his actions, blaming his temper outbursts on his older sibling. We heard she was extremely frightened of him; he had on two occasions broken down her door.
When he came out of these rages he would become very tearful and profoundly apologetic. These difficulties had been noticed at school where his grades had been falling. He told teachers he felt suicidal and would sometimes go into the school toilet to cry especially when he thought about his inability to control himself.
Physical examination at this point was unremarkable. The Community Psychiatrist commenced him on Fluoxetine and referred him to an in-patient psychiatric unit for further psychiatric evaluation including a forensic assessment.
He was diagnosed with Asperger’s Syndrome and Attention Deficit Hyperactivity Disorder in the inpatient unit and was prescribed risperidone and methylphenidate. His GP was asked to arrange a baseline blood test, consisting of full blood count (FBC), liver function test (LFT), urea & electrolytes (U&E) and thyroid function test (TFT). There was no request for blood glucose level or serum calcium.
The GP asked for a serum calcium level estimate purely out of ‘habit’. The laboratory result showed a high level of calcium 3.89mmol/L (normal range 2.2-2.6). Based on this significantly elevated serum calcium level, a referral was sent to the Paediatric Endocrinologist.
At the Endocrinology Clinic, he described a twelve month history of generalised aches and pains in association with emotional lability. A history of fracture of his right wrist and left hallux occurring within 18 months prior to presentation was also obtained. The X-ray report showed presence of a radiolucent area in his right femur. An assay of his parathyroid hormone, Sestamibi scan and ultrasound scan of his neck were done.
The elevated parathyroid hormone level, increased serum calcium, history of fractures and X-ray features indicated the diagnosis of Primary Hyperparathyroidism. The endocrinologist was of the opinion that his PHPT has been present for a number of years. He was referred for parathyroidectomy.
His serum calcium level dropped to 2.47mmol/L two days post surgery. As calcium level normalised, his symptoms improved remarkably and his psychotropic medications were discontinued. Since then, he has successfully commenced college full time and has succeeded in obtaining good grades in his chosen courses.
Discussion:
Psychiatric symptoms cause significant impairment in children and adolescents. Having additional symptoms of hyperparathyroidism would exacerbate the psychiatric symptoms and increase the degree of impairment. This patient presented with neuropsychiatric symptoms and evidence of end organ damage which is similar to those in published reports3,4.
Research shows that diagnosis of primary hyperparathyroidism is often delayed in young people but we suspect that it may even be more delayed in those with a pre-existing psychiatric disorder as the symptoms may be more likely to be attributable to the psychiatric condition.
It is possible that the behavioural problems in this patient may have co-existed independently of each other, but the rapid resolution of the psychiatric symptoms suggests that they may have been exacerbated by hyperparathyroidism.
Our findings in this case are similar to those reported by Spivak and colleagues’ which showed that early diagnosis of hypercalcaemia can prevent unnecessary and potentially harmful treatment with psychotropic medications7.
Psychiatric diagnoses are usually formed from identification of collective symptoms some of which may occur in other medical conditions. Adopting a multidisciplinary team approach is most helpful in the management of complex psychiatric cases. This approach may encourage clinicians to take a holistic view in management of children.
It is important for clinicians to be familiar with common psychiatric symptoms and medical conditions that may mimic or cause them because the presence of non-specific symptoms in PHPT poses a significant emotional burden for affected children and their families. It is a potentially treatable condition which if not diagnosed early could lead to impaired psychosocial well-being and damage of vital organs. Parathyroidectomy has been shown to improve general health, quality of life and cognitive functioning in patients with PHPT8.
The outcome for this particular young person could have included further episodes of in-patient hospitalisation or involvement with the juvenile justice system as a consequence of further violent episodes. The achievement of adolescent milestones and his education could have been severely disrupted and may have resulted in labelling detrimental to his future.
In the current economic climate and because of the rarity of Primary Hyperparathyroidism, we do not advocate routine serum calcium estimation in all behavioural problems but clinicians should have lower threshold for screening for this condition especially in patients with worsening symptoms despite conventional treatment.
In conclusion, Primary Hyperparathyroidism should be considered in the differential diagnosis in young people with worsening neuropsychiatric symptoms which are unresponsive to standard psychiatric treatment.
The US Food and Drug Administration (USFDA) considers the following as biologics: any therapeutic serum, toxin, antitoxin, vaccine, virus, blood, blood component or derivative, allergenic product, analogous product, or derivatives applicable to the prevention, treatment, or cure of injuries or disease of man1. However, generally, biologics refer to protein molecules therapeutically used in various diseases so as to target specific points in the inflammatory cascade of these disorders 2. Hope for an improved tolerability, convenience in usage and lasting remissions, combined with increased knowledge of immune-pathogenesis of various cutaneous diseases has lead to the introduction of biologics as alternative immune-modulating agents in the field of dermatology.
CLASSIFICATION
Biologics are generally divided into three major groups 3:
a) Monoclonal antibodies
b) Fusion antibody proteins
c) Recombinant human cytokines and growth factors
The main groups and the principal agents in each group are summarised in Box 1 and described below.
A) MONOCLONAL ANTIBODIES
Monoclonal antibodies target specific cell-surface receptors. In the early days of biologic therapy, purely murine monoclonal antibodies were used. However, due to the development of antimurine antibodies, which blocked their action, these could be given only for very short periods. The monoclonal antibodies used now have different amounts of murine sequences in the variable region. They may be categorised into three classes:
(a) chimeric antibodies comprising of 30% murine genes fused with human antibodies
(b) humanised antibodies, which have 10% murine sequences, and
(c) human antibodies, which are solely derived from human immunoglobulin genes 4.
Principal monoclonal antibodies with therapeutic relevance in Dermatology
The principal monoclonal antibodies known till date are enumerated in Box 1 and described briefly below.
· Anti-IL-12 and anti-IL-23 monoclonal antibody: Ustekinumab
· Anti-CD2 antibody: Siplizumab
· Anti-CD4 antibody: Orthoclone (OKTcdr4a)
· Anti-CD25 antibodies: Basiliximab, Daclizumab
· Anti-CD80r: Galiximab (IDEC 114)
· Anti-IgE: Omalizumab
Fusion antibody proteins
· Etanercept
· Alefacept
· Abatacept
· Onercept
· Denileukin Diftitox
Recombinant human cytokines and growth factors
a) Interferons
· Interferon α (IFNα)
· Interferon γ (IFNγ)
· Interleukin 1 Receptor antagonist (IL1Ra)
· Interleukin 2 (IL-2)
· Interleukin 4 (rhIL-4)
· Interleukin 10 (rhIL-10)
· Interleukin 11 (rhIL-11)
b) Granulocyte macrophage colony stimulating factor (GM-CSF)
c) Platelet derived growth factor (PDGF)
1. Infliximab
Infliximab (trade name Remicade) is a human-mouse monoclonal antibody that binds to and inhibits the activity of TNF-α, and also causes lysis of TNF-α producing cells5.
Important uses of Infliximab
Psoriasis: Infliximab is approved for the treatment of psoriatic arthritis and plaque psoriasis by FDA6, 7. Infliximab may also be of value in recalcitrant or unstable disease and in generalised pustular psoriasis. It is given as an IV (intravenous) infusion in doses of 5 or 10 mg/kg, over a period of 2 hours at weeks 0, 2, 6 and may be followed by repeat single infusions at 8-12 week intervals 8. In various controlled trials, improvement at 10 weeks has been noted in 87% of patients 7, 9.
Atopic dermatitis: Infliximab has also been evaluated in a study of atopic dermatitis 10. At 2 weeks, there was significant improvement in all patients. At 10, 14, and 30 weeks, variable response was seen.
Hidradenitis suppurativa: Long-term efficacy has also been evaluated in hidradenitis suppurativa. In one study, some patients had no evidence of recurrence after 2 years, while others relapsed within a mean of 8.5 months11.
2. Adalimumab
Adalimumab (Humira®) is a human IgG1 monoclonal antibody directed against TNF-α. Adalimumab is given in a dose of 40 mg subcutaneously (SC) every other week as self-injection 5, 12.
Important uses of Adalimumab
Psoriasis: Adalimumab rapidly reverses the decrease in epidermal Langerhans cell density in psoriatic plaques 13. In a trial, patients with psoriatic arthritis received adalimumab every other week for 24 week14. It was well-tolerated and helped improve joint and skin manifestations significantly.
Hidradenitis suppurativa: An increasing number of reports in refractory hidradenitis supprativa have shown successful control with adalimumab 15, 16, 17.
3. Basiliximab
Successful treatment for severe psoriasis and generalised pustular psoriasis has been reported with basiliximab, an interleukin-2 receptor (IL-2R; CD25) chimeric monoclonal antibody 18, 19.
4. Daclizumab
Daclizumab is a humanised monoclonal antibody thatbinds to the CD25 subunit of the IL-2 receptor onT-cells, thus blocking T-cell proliferation. It has been tried in recalcitrant psoriasis and HIV-associated psoriatic erythroderma with a mean reduction in PASI of 30% 20, 2122.
5. Siplizumab
Siplizumab (Medi-507) is a humanisedmonoclonal antibody directed against CD2. It is designed to block stimulationby inhibiting the CD2–LFA-3 interaction. In earlyphase studies in psoriasis, significant response to therapy has been noted23.
6. Efalizumab
Efalizumab is a recombinant humanised monoclonal IgG1 antibody that binds to CD11a, a subunit of leukocyte function-associated antigen 1 (LFA-1) 24. It destabilises and decreases the trafficking of T-cells into dermal and epidermal tissues.
Important uses of Efalizumab
Psoriasis: Efalizumab was approved by the US FDA in October 2003 for the treatment of psoriasis5. It is currently the only biologic agent approved for continuous administration to adult patients24. The licensed dose of efalizumab is 1 mg/kg weekly as a subcutaneous self- administered injection for 12 weeks, following a first conditioning dose of 0.7 mg/kg 24.
Lichen planus: There is one case report of 3 months duration of treatment with efalizumab for lichen planus with resolution of skin lesions and pruritis 25.
7. Rituximab
Rituximab is a monoclonal humanised antibody directed again in the B cell-specific antigen CD20.
Important uses of Rituximab
Lymphoma: It has been used in patients with CD20-positive non-Hodgkin's lymphoma in a dosage of 375 mg/m2 for four infusions26.
SLE: In systemic lupus, dose escalation studies revealed no differences with respect to clinical outcome in patients who received either a single infusion of 100 mg/m2, a single infusion of 375 mg/m2, or four weekly infusions of 375 mg/m227.
Blistering diseases: For patients with blistering diseases, most patients receive the lymphoma dosage schedule. However, serious side effects were considerably higher.
There are reports of refractory pemphigus patients who received infusions of rituximab and had rapid resolution of lesions and a long lasting clinical remission 28, 29, 30.
8. Galiximab
Galiximab a humanised monoclonal antibody directedagainst CD80 and blocks its interaction with CD28 on the T cell, for T-cell stimulation 31. Clinicaldata for this drug are just beginning to emerge with 40% of patients achieving at least 50% reduction in PASI after receiving4 biweekly doses in a trial32, 33.
9. Ustekinumab
It is a fully human monoclonal antibody targeting IL-12 and IL-23, presently undergoing clinical trials for psoriasis and psoriatic arthropathy2, 34. In placebo-controlled studies, (PHOENIX 1) and (PHOENIX 2) have shown that ustekinumab could control plaque psoriasis with only four injections a year resulting in greater ease of use and more sustained relief 35, 36.
10. Certolizumab pegol
Certolizumab is the recombinant antibody Fab' fragment of a humanised TNF inhibitor monoclonal antibody. A study in chronic plaque psoriasis showed that certolizumab pegol, given subcutaneously every two weeks, over a period of 12 weeks shows significant improvement 37.
11. Golimumab
Golimumab, a fully human monoclonal antibody is at present undergoing Phase III clinical trials in psoriatic arthropathy 38.
12. Orthoclone or OkT4a
It is a humanised antihuman CD4 IgG4 monoclonal antibody preventing the recognition of the MHC-bound antigen by an appropriate T-cell receptor, hence T cells do not get activated 39. Several studies have found orthoclone to be effective in moderate to severe psoriasis 40, 41.
13. ABX-IL8
ABX-IL8 is a fully human monoclonalantibody designed to bind free IL-8, a key chemokine in psoriasis and deactivate it in theskin42, 43. In early trials, the drug has demonstrated good clinical responsein psoriasis 44, 45.
14. Omalizumab
Omalizumab is a recombinant, humanised, monoclonal antibody against immunoglobulin IgE. This agent acts as a neutralising antibody by binding IgE at the same site on IgE as its high-affinity receptor, FcεR I, thus inhibiting the biological effects before the generation of allergic symptoms 46. There are reports of the efficacy of omalizumab in chronic urticaria 47, cold urticaria 48 and atopic dermatitis 49.
15. Mepolizumab
Mepolizumab is a humanised monoclonal IgG antibody to the IL-5 molecule, which is essential for eosinophil growth and differentiation. Two weekly infusions showed significant clinical improvement in atopic dermatitisand clinical trials are underway for hyper-eosinophillic disorders 50,51.
16. SMART Anti–IFN-γ
SMART anti–IFN- γ,a humanised monoclonal antibody, binds and inactivates IFN- γ, an important Th1 cytokinein psoriasis. Early phase studies are being performed at this time 52.
B) FUSION ANTIBODY PROTEINS
Fusion proteins, also known as chimeric proteins, are proteins which are created by the fusion of the receptor domain of a human protein with the constant region of human IgG. The resultant fusion protein binds specifically to a ligand or co-receptor 53. The most commonly used fusion proteins in dermatology are briefly described below and enumerated in Box 1.
1. Alefacept
Alefacept is a bivalent recombinant fusion protein composed of the first extracellular domain lymphocyte function antigen 3 (LFA-3), fused to the hinge domain of human IgG1. The LFA-3 portion of alefacept binds to CD2 receptors on T-cells, thereby blocking their natural interaction with LFA-3 on antigen presenting cells (APCs). The IgG1 portion of alefacept binds to FcγR receptor on natural killer cells to induce T-cell apoptosis 54.
Important uses of Alefacept
Psoriasis: The US FDA approved alefacept in January 2003 for treatment in adult patients with moderate to severe chronic plaque psoriasis. It is given by intramuscular or intravenous route with a dose of 10-15 mg IM weekly or 7.5 mg IV weekly and a 12 week course is recommended 5, 54. Two 12-week courses showed a75% or greater reduction in the PASI 55.
Alopecia areata: Case reports have shown that alefacept may be effective in the treatmentof AA56, 57.
Pyoderma gangrenosum: Alefacept has been used for pyoderma gangrenosum and improvement was shown in 25% of these patients 58.
Other Indications
Some of the off-label conditions where alefacept has been used with success are graft-versus-host disease (GVHD), lichen planus, alopecia areata, atopic dermatitis, mycosis fungoides,alopecia universalis, erosive lichen planus,Hailey-Hailey diseaseand hand dermatitis 58, 59, 60, 61, 62, 63.
2. Denileukin diftitox
Denileukin diftitox is a novel recombinant fusion protein consisting of fragments of diphtheria toxin linked to human interleukin-2 and works by targeting the high-affinity interleukin-2 receptors. It was tried in patients with recalcitrant psoriasis and the rate of improvement for treated patients was found to be significant 64.
3. Abatacept (Ctla4ig)
It is a fusion protein composed of the extracellular domain of CTLA4 and the Fc region of IgG4. It interferes with T-cell activation by competitively binding the B7.1 and B7.2 molecules on the surface of APC 65. In a study, patients with stable psoriasis vulgaris showed good improvement with IV infusion of abatacept 33. A second generation CTLA4Ig, Belatacept, is currently under Phase II clinical trial for allograft diseases 66.
4. Etanercept
Etanercept is a recombinant fully human dimeric fusion protein comprising of the human TNF-α p75 receptor and the Fc portion of human IgG1 molecule. It functions as a TNF inhibitor, thereby preventing interaction with its cell surface receptors on target cells and blocking its pro-inflammatory effects.
Important uses of Etanercept
Psoriasis: Etanercept (Enbrel®) is FDA approved for use as subcutaneous monotherapy in psoriasis. Several clinical trials have shown that it is effective67, 68, 69, 70. The adult dose is 50 mg/week, given subcutaneously for three months 5. The drug is also indicated for treatment of psoriatic arthritis 71, 72.
Hidradenitis supprivata:There is a study of etanercept in patients with severe hidradenitis with more than 50% score improvement12.
5. Onercept
Onercept is a recombinant human soluble p55 tumour necrosis factor binding protein under development for the potential treatment of psoriasis and psoriatic arthritis73. C) RECOMBINANT HUMAN CYTOKINES AND GROWTH FACTORS
Cytokines are non-immunoglobulin proteins and glycoproteins produced by a wide variety of cells in the human body and released in response to any immune stimulus 74, 75. Recombinant cytokines or cytokine antagonists have been used as immunomodulators 76. The principal recombinant cytokines used in dermatology, enumerated in Box 1, are described below.
1. Interferons (IFNs)
IFNs, a family of related proteins, are produced by virus-infected leucocytes. They exhibit anti-proliferative, immune-modulatory and anti-neoplastic functions 77.
· Interferon α
Recombinant IFNα is given as a subcutaneous or intramuscular injection to treat verruca vulgaris 78 , condyloma acuminatum 79, cutaneous T cell lymphoma 80, Kaposi's sarcoma (AIDS related) 81, melanoma 82, basal cell carcinoma 83, squamous cell carcinoma 84, actinic keratosis 85, Behçet's disease 86, hemangiomas 87 and keloids 88.
The injections are usually given thrice weekly and the dose (depending on the condition being treated) varies from low-dose therapy for condyloma acuminatum to high-dose therapy for melanoma 89, 90. Of late, pegylated IFNα is being used for convenience, because it has a longer half-life and hence can be given once weekly 80.
· Interferon-γ
It is FDA approved for the treatment of chronic granulomatous disease 91 and has also been used in atopic dermatitis 92 and cutaneous T cell lymphoma 90.
Anakinra is the non-glycosylated form of human IL-1Ra and acts by blocking the functions of the naturally occurring IL-193. Good results have also been reported in Schnitzler's syndrome94, familial cold auto-inflammatory syndrome 95 and psoriatic arthropathy96. It is given by subcutaneous injection 100 mg once a day.
3. Interleukin 2
Recombinant IL-2 is an antitumour cytokine that has been used in cutaneous T cell lymphoma (CTCL) and metastatic melanoma 97. When given intravenously in high doses of 600,000-720,000 IU/kg in melanoma, IL-2 has produced a 15-20% overall response, with complete cure in 4-6% 98.
4. Interleukin 4 (rhIL-4)
In a dose-escalation study (0.5 to 5mg/kg given by subcutaneous injection thrice a week), IL-4 has been shown to cause improvement in psoriasis by inducing Th2 differentiation in human CD4 + T cells 99.
5. Interleukin 11 (rhIL-11, Oprelvekin)
It has also shown reasonably good results in the treatment of psoriasis at doses of 2.5 or 5mg/ kg, by subcutaneous injection 100.
GM-CSF acts by stimulating stem cells to produce granulocytes, monocytes and macrophages 101. Recombinant human GM-CSF has been used to promote wound healing in ulcerated skin for example leg ulcers 102, 103, and for the treatment of melanoma 104 and Sezary syndrome 105.
7. Platelet derived growth factor (PDGF)
PDGF is a dimeric glycoprotein which regulates and promotes granulation tissue formation, re-epithelialisation and wound angiogenesis 106. Recombinant PDGF-BB topical gel (100ìg/g), applied once daily, has been approved by FDA for the treatment of diabetic foot ulcers 107, 108.
8. Recombinant Human IL-10
Recombinant Human IL-10 (Tenovil)can be given in subcutaneousinjections. Early phase clinical trials have shown thatrecombinant human IL-10 three times a week improved psoriasis 109, 110.
SIDE EFFECTS OF BIOLOGICS 5, 111, 112, 113
Some of the adverse effects of biologics are described below:
Allergic reaction and antibody formation: Mostly seen with TNF-α blockers.
Mild transient injection site reactions: Comprising of erythema, oedema and bruising, noted with etanercept in 10-20% of cases in the first month of therapy. Antibodies to etanercept may develop in 6% of patients.
Infusion reaction: Occurs during or within 1-2 hours of treatment and may affect up to 20% of all the patients treated with infliximab, rarely anaphylactic shock may occur.
Acute flu-like symptoms: Headache, chills, fever, nausea and myalgia may occur within 48 hours after administration of the first two doses of efalizumab and Interferon α.
Infections: Reactivation of tuberculosis may occur on treatment with anti-TNF-α agents and sepsis secondary to Listeria monocytogenes and Histoplasma capsulatum have been reported 113.
Malignancy: Patients previously treated with PUVA represent an at-risk group.
Demyelinating disease: Worsening of multiple sclerosis and demyelination reported with infliximab.
Thrombocytopenia: Occurs with efalizumab and warrants discontinuation of therapy.
Autoimmune haemolytic anemia: Occurs 4-6 months after the start of treatment with efalizumab.
Congestive cardiac failure: Worsening of congestive cardiac failure with TNF-α blockers is reported to occur.
Antinuclear antibodies and lupus-like syndrome: May develop during therapy with anti-TNF-α agents, but not associated with symptoms and signs of lupus in the majority.
Hepatitis: Reported following infliximab therapy, occurring from 2 weeks to more than a year after initiation of treatment. Treatment should be stopped in the event of jaundice and/ or marked elevations (>5 times the upper limit of normal) in liver enzymes.
PATIENT SCREENING FOR BIOLOGIC THERAPY 113, 114
All patients to be put on biologics should undergo a thorough evaluation including detailed clinical history, physical examination and relevant investigations with particular reference to known toxicity profile of the agent being considered. The investigations generally advised are113: full blood count, liver and renal function tests, screening for hepatitis and HIV infection, anti-nuclear antibodies, anti-ds DNA, urine analysis, chest X-ray and Tuberculin skin testing.
For efalizumab, haemogram (including platelet count) is recommended monthly for the first 3 months and then every 3 months. For TNF blockers, it is done at 3 months initially and repeated every 6 months.
Liver and renal function tests, serum electrolytes and urine analysis are done at 3 months initially and then every 6 months.
EXCLUSION CRITERIA/ CONTRAINDICATIONS
There are various contraindications for use of biologics, warranting their exclusion and precautions are to be exercised because of their immune-modulator properties. The main exclusion criteria are: active tuberculosis, severe congestive heart failure, patients having >200 treatments of PUVA (because of a risk of developing malignancies with anti- TNF agents), history of demyelinating disease or optic neuritis, hepatitis B and C positivity, HIV positivity, premalignant states, active infections and high risk states such as chronic leg ulcers, persistent or recurrent chest infections and indwelling urinary catheter infections, pregnancy and breast-feeding.
ASSESSMENT OF THE RESPONSE TO BIOLOGICS
Many scoring systems for assessing the severity of various dermatological diseases exist. These scoring systems and other indices can be used for assessment of response to the use of biologics. For example, for evaluation of improvement in psoriasis, PASI (psoriasis area and severity index) and DLQI (dermatology life quality index) are recommended at 3 months initially and then every 6 months 113. Reduction in baseline PASI score of >75% is the standard used by FDA to assess the efficacy of a new psoriasis agent 115. Similarly in atopic eczemas, improvement is monitored based on the Eczema Area and Severity Index, Pruritus Severity Assessment and DLQI. Reduction of the Eczema Area and Severity Index score by 50% is considered excellent, 30-49% moderate and <29% non-significant.
SUMMARY
To summarise, biologics represent the future of therapeutics, not only in dermatology but also in other fields of medicine. Among the various dermatological disorders where they are used, biologics have been most evaluated in psoriasis 116. However, the possibility of serious infections and the oncogenic potential combined with the high cost of the drugs limit their routine use at the present stage 117. Regular re-evaluation of efficacy and safety is essential if these agents are to be used to the maximum benefit of patients118.
Anterior Cruciate Ligament (ACL) reconstructions are increasingly being undertaken throughout the United Kingdom (UK). Advances in General and Local Anaesthetic as well as surgical technique allow reconstructions as a day case procedure.1,2,3 There are currently no studies showing post-operative pain suffered by ACL reconstruction patients, nor showing the comparison of day case and inpatient pain scores.
We document, prospectively, patients’ post-operative pain after ACL reconstructions. We aim to identify and assess factors that affect pain post-ACL reconstructions including additional procedures, type of nerve blocks and whether the procedure was performed as a day case or as an inpatient.
We propose that patients having ACL reconstruction have no difference in pain scores when having the procedure as a day case compared to performance with inpatient stay. We also propose that additional procedures do not cause an increase in pain. We hypothesise that patients having Femoral nerve block have no increase in pain compared to patients having combined Femoral and Sciatic nerve block.
Method
All patients having ACL reconstruction between April 2010 and September 2010 were evaluated prospectively. Four strand arthroscopic hamstring reconstructions were performed by two specialist knee surgeons using a similar technique. Anaesthetic was performed by varying anaesthetists with a General Anaesthetic and Regional Nerve Block with Bupivicaine (Femoral nerve block or Femoral plus Sciatic nerve block). This was performed in the anaesthetic room under ultrasound guidance. Intra-operatively, patients received standardised anaesthesia. All patients received one dose of intravenous Paracetamol and two intravenous doses of opiates (Morphine or Fentanyl, as tolerated) at the beginning and end of the procedure.
Inclusion criteria used were all ACL reconstructions performed on patients over 16 years of age. No exclusion criteria were used.
Arthroscopic hamstring reconstruction was undertaken using a four strand Semitendinosus and Gracilis graft. During the arthroscopy, any additional procedures necessary were performed (e.g. meniscal repair, menisectomy, etc.). No drains were used. The knee was placed into an immobilisation splint until the nerve blocks had worn off.
Patients were discharged once they were back on the ward and deemed safe for discharge by the physiotherapists, medical and nursing staff. They were discharged with Paracetamol, a non-steroidal anti-inflammatory (if tolerated) and a mild opiate (Tramadol or Codeine Phosphate).
After discharge from the ward, patients were brought back to an aftercare clinic, with a senior physiotherapist, any time up to 48 hours post-operatively, to assess whether the nerve block had worn off, perform a wound check and to reinforce physiotherapy advice.
Patients were given a discharge questionnaire asking them to record their pain scores daily, when the pain was at its worst, using the Numerical Rating Scale (NRS) from 0-10. Documentation commenced on the day of the procedure and was requested daily for one week. Complications were also documented by the patient. These questionnaires were handed in at the two week follow up appointment, at which point patients were also asked if they would have the surgery performed as a day case again.
Pain scores were analysed using a Box-whisker plot followed by a Shapiro-Wilk W test which showed a non-parametric data spread. Scores were subsequently analysed using a Mann-Whitney U test to assess significance (p=0.05).
Results
ACL Reconstruction was attempted in 50 patients from April 2009 up to and including September 2009. The average age of patients was 31.0 years (Range 16-55). Of the cohort, there were 36 male patients with 14 females. All of the ACL reconstructions had a General Anaesthetic and all had infiltration of their graft site and medial wound with Bupivicaine. 42 had a Femoral nerve block with Bupivicaine and eight had a Bupivicaine Femoral and Sciatic nerve block. Of the 50 patients, 13 patients had additional procedures formed.
29 patients from the group were discharged as a day case. 21 patients required inpatient stay for the reasons documented in Figure 1 below.
Figure 1. Reasons for inpatient stay after ACL reconstruction
Social reasons for inpatient stay included out-of-area patients and those who had no home support to care for them on the day of surgery. Patients who were unable to safely mobilise post-operatively were classified as having failed physiotherapist discharge assessment. Two patients were unable to be discharged due to excessive pain. Two patients had symptoms related to General Anaesthesia (e.g. nausea and dizziness) which prohibited discharge. Seven patients arrived back onto the ward with insufficient time for recovery and physiotherapy assessment, thus preventing day case discharge. In all seven cases, this was due to ACL reconstruction being performed late on the operating list.
On day one post-operatively the average NRS pain score for the day case group was 4.1, the average score for the inpatient group was 5.52. The pain score decreased steadily as the week went on. Pain scores on days one to four was statistically lower (p=0.05) in day case patients compared to inpatients (Table 1 and Figure 2). Figures 3 and 4 show the box whisker plots for inpatient vs day case pain scores on day 1 and 2.
Post-operative day
Daycase Pain Score (N1=29)
Inpatient Pain Score (N2=21)
P Value (*=significant)
1
4.1
5.52
0.03*
2
3.93
5.14
0.04*
3
3.62
4.81
0.03*
4
3.1
4.38
0.03*
5
3.1
4.29
0.09
6
2.69
4.00
0.03*
7
2.52
3.62
0.06
Table 1. Average NRS pain scores of patients undergoing ACL reconstruction
Figure 2. Comparison of NRS pain scores of day case and inpatient ACL reconstruction
Figure 3. Box Whisker plots for pain scores on day 1 for inpatients and day case patients
Figure 4. Box Whisker plots for pain scores on day 2 for inpatients and day case patients
Out of 50 patients, 42 patients had Femoral nerve blocks with the remaining eight patients having a combined Femoral and Sciatic nerve block. On average, patients receiving only a Femoral nerve block had lower pain scores compared to those receiving the combined block, although with the difference in cohort numbers, there was no statistical difference (p=0.09 on day 1 and p=0.5 on day 2) [Figure 5].
Figure 5. Comparison of daily pain scores with Femoral and Femoral/Sciatic nerve blocks
Of the 50 patients attempting the day case procedure, there were 17 additional procedures. Eight partial medial menisectomies, three partial lateral menisectomies, two lateral meniscal repairs, two medial meniscal repairs and two medial femoral condyle microfractures. There was no correlation identified between additional procedures and increased patient pain scores (Figure 6).
Figure 6. Comparison of pain scores of patients having additional procedures
When patient satisfaction among the 29 patients who had day case ACL reconstruction was asked, 100% were happy with the day case procedure. One patient felt that they would opt to have the operation done with an inpatient stay as they felt “groggy” overnight. They were otherwise happy with the day case procedure.
All patients had quadriceps function return at day 1 post-operatively and there were no re-admissions due to pain or being unable to cope at home. There were no infections amongst the groups.
Discussion
Day case ACL reconstructions are commonly undertaken in the UK. Literature from Sheffield, Glasgow and Romford1,2,3 shows that the rate of admission and complications is low and the procedure is safe and effective. It has been well tolerated by patients.
Day case surgery is encouraged by the government led Department of Health.3,4,5 It reduces the risk of cancellations and infections and can also have economic benefits for the National Health Service (NHS). In the United States (US), Bonsell has shown that a single day case ACL reconstruction saves the hospital $2234 compared to a procedure with an inpatient stay. Bonsell also proposed that day case ACL reconstructions are performed significantly quicker than inpatient reconstructions (approximately 23 minutes quicker) which could save the hospital $85000 per year.6
Day case patients were found to have statistically significant, lower pain scores compared to inpatients. Farrar et al have shown that, using the NRS pain scoring system, only a difference of greater than two points can be deemed clinically significant. However, the results of this study have shown that there is no clinical difference or worse pain when the procedure is performed as a day case.7 Krywulak et al noted that the average Visual Analogue Score (VAS) score for patients’ satisfaction post-day case ACL reconstructions was 85.1 compared to the inpatient average score of 78.2.8 This is validated in our study of which 100% of patients were happy with the day case procedure.
Patients were encouraged to take analgesia regularly for two weeks post-operatively but the amount of medication actually taken was not formally documented. This could potentially lead to some of the bias in this study. However, the significance of this bias is difficult to determine accurately as the NRS pain scores were recorded when the patients’ pain was at its worst. This would most likely be between analgesic doses so hopefully eliminating some of the bias.
Little is known about pain associated with the procedure of day case ACL reconstruction and also pain suffered compared to those undergoing inpatient stay. We have been able to compare pain scores of patients undergoing ACL reconstruction as a day case procedure with those undergoing the procedure as an inpatient. We found that patients having the procedure as a day case had significantly lower pain scores on days 1-4 post-ACL reconstruction compared to inpatients.
Day case ACL reconstructions are safe and not associated with any difference in pain compared to inpatient stays. This is important in pre-operative guidance given to patients and, in view of the risks of hospital inpatient stays and also additional costs to the Health Service and Primary Care Trust (PCT), ACL reconstruction as a day case procedure should be highly recommended to patients compared to an inpatient surgical procedure.9-11 Information can be given to patients advising them that pain will not be worse when the procedure is performed as a day case which will encourage more patients to accept same day discharge.
Further work needs to be done to assess the possible difference in pain scores associated with Femoral nerve blocks compared with combined Femoral and Sciatic nerve blocks but our results appear to show that significant difference is unlikely.
Patient satisfaction with the day case ACL procedure was excellent and subsequently day case ACL reconstruction is now routinely performed in this Trust.
Colorectal cancer (CRC) is the third most common cancer in men and women worldwide (1) and a leading cause of cancer related deaths (2). 5FU synthesized in 1957 by Heidelberger (3) is the mainstay in all current standard regimens for CRC (4). Chemotherapy induced hepatic toxicity in 5FU based regimens can be an acute or delayed outcome (5, 6); whereas steatosis is a hallmark of 5FU induced hepatic toxicity (7). Chemotherapy induced nephrotoxicity (8) is also an area of concern for oncologists. The antimetabolite 5FU is often linked with kidney damage (9). Therapeutic outcomes and toxicity of 5FU differs markedly in different doses, combinations, schedules of administration and routes of administration. Leucovorin (LV) incorporated in 5FU based regimen enhances the cytotoxicity of 5FU. In this study we opt to report abnormalities in hepatic enzymes and renal biomarkers biochemically assessed in the serum after alternate cycles of treatment in CRC patients subjected to 5FU/LV based chemotherapy.
Methods:
The study was designed in the Department of Pharmacology, University of Karachia and conducted in a leading cancer hospital in Pakistan. Following institutional authorisation, informed consent was obtained from patients being admitted during 2008-2011. The inclusion criteria was maintained on the following grounds:
1. Histologically confirmed advanced colorectal carcinoma 2. Adequate blood count before therapy 3. Age 20-80 years 4. ECOG score of < 3 5. Serum bilirubin < 5× normal 6. Serum creatinine < 135µmol/liter 7. Serum transaminases < ×2.5 normal
Twenty three patients (median age 59 years) who underwent surgery were included in the study. All the patients had measureable disease at CT scan, ultrasonography or clinical examination. Patient’s characteristics are shown in Table 1. Seventeen patients were treated with the adjuvant bimonthly regimen of 5FU/LV - high dose Folinic acid (de Gramont Regimen); whereas, six patients were treated with adjuvant monthly regimen of 5FU/LV –low dose Folinic acid(Mayo Clinic Regimen) as follows.
5Fluorouracil/ Leucovorin (de Gramont’s regimen)
5Fluorouracil: 400mg/m2 IV followed by 600mg/m2 CIV for 22 hours on day 1-2. Leucovorin: 600 mg/m2 IV as 2 hours infusion before 5FU on day 1-2. Cycle repeated after 2 weeks.
5Fluorouracil/ Leucovorin (Mayo clinic regimen)
5Fluorouracil: 425mg/m2 IV on day 1-5. Leucovorin: 20 mg/m2 IV before 5FU on day 1-5. Cycle repeated after 4-5 weeks.
Premedication with oral phenothiazines, 5HT3RA and 10-20 mg of dexamethasone was given.
The blood samples were collected before the initiation of the therapy and after each alternate cycle of treatment. The blood was drawn when the patient was rested and comfortable from the antecubital vein under minimal tourniquet pressure. The blood drawn was sampled and collected into vacutainers (BD). The biochemical profile of the pretreatment and subsequent treatment was comparatively assessed. SGOT, SGPT, bilirubin and alkaline phosphatase levels were measured after each cycle of treatment or on the clinical presentation of any hepatic adverse effect notified by the physician or oncologist and the levels were compared to the pretreatment values. The serum creatinine levels and BUN was measured before the start of chemotherapy and after each alternate cycle of treatment up to six times in each patient.
Table 1 Patient characteristics
Parameters
Arm A
Arm B
de Gramont
Mayo Clinic
No. of Patients
%
No. of Patients
%
Demographic Characteristics
Male
12
70.58
4
66.6
Female
5
29.41
2
33.3
Total Patients
17
6
Age: Years
Median
59
Range
56-65
ECOG Performance Status (21)
0
1
5.88
1
16.6
1
3
17.64
1
16.6
2
13
76.47
4
66.6
3
0
0
0
0
Primary Site
Colon
11
64.7
3
50
Rectum
5
29.4
2
32.3
Multiple
1
5.88
1
16.6
Metastases
Synchronous
11
64.7
4
66.6
Metachronous
6
35.2
2
32.3
Metastatic Site
Liver
8
47.0
1
16.6
Lymph nodes
4
23.5
2
32.3
Other*
5
29.4
3
50
No. of Sites
1
7
41.1
2
32.3
> 2
10
58.8
4
66.6
CEA
< 10ng/ml
2
11.7
1
16.6
>10ng/ml
8
47.0
1
16.6
Unknown
7
41.1
4
66.6
* = Peritoneal/ovary
Results:
Table 2shows that the SGOT levels are raised after each cycle of treatment and the difference between the SGOT levels of the patients before treatment and after subsequent cycle of treatment is significant in the patients treated with 5FU/LV (p value < 0.05). The difference in the SGPT levels of the patients from the pretreatment value is not highly significant (p value >0.05). The difference in the bilirubin levels of the patients after the sixth cycle of chemotherapy with 5FU/LV regimens is highly significant from the pretreatment level (p value < 0.05). The difference in the alkaline phosphatase levels of the patients after chemotherapy with the pretreatment value in the same patients is not significant (p value >0.05).The difference in the triglyceride levels is not significant before and after chemotherapy in the patients treated with 5FU/LV.
Table 2 Comparative changes in hepatic biomarkers in patients treated with 5FU/LV regimen
Paired Samples Test
Paired Differences
t
p-value
Mean
Std. Deviation
Hepatic
TGS
Control - Cycle 2
-1.200
1.643
-1.633
0.178
Control - Cycle 4
-3.200
3.033
-2.359
0.078
Control - Cycle 6
-3.400
2.966
-2.563
0.062
Control - Cycle 8
-10.000
10.198
-2.193
0.093
Control - Cycle 10
-3.600
8.414
-0.957
0.393
Control - Cycle 12
-8.800
12.872
-1.529
0.201
SGOT / AST
Control - Cycle 2
-12.667
5.033
-4.359
0.049
Control - Cycle 4
-22.000
3.464
-11.000
0.008
Control - Cycle 6
-22.667
3.055
-12.851
0.006
Control - Cycle 8
-25.333
3.055
-14.363
0.005
Control - Cycle 10
-27.000
7.810
-5.988
0.027
Control - Cycle 12
-28.667
7.024
-7.069
0.019
SGPT / ALT
Control - Cycle 2
-2.667
3.055
-1.512
0.270
Control - Cycle 4
-3.667
2.082
-3.051
0.093
Control - Cycle 6
-9.333
8.505
-1.901
0.198
Control - Cycle 8
-12.667
8.083
-2.714
0.113
Control - Cycle 10
-17.667
5.859
-5.222
0.035
Control - Cycle 12
-22.667
10.214
-3.844
0.062
Bilirubin
Control - Cycle 2
0.033
0.058
1.000
0.423
Control - Cycle 4
0.000
0.100
0.000
1.000
Control - Cycle 6
-0.267
0.058
-8.000
0.015
Control - Cycle 8
-0.267
0.058
-8.000
0.015
Control - Cycle 10
-0.267
0.058
-8.000
0.015
Control - Cycle 12
-0.367
0.115
-5.500
0.032
ALKPO4
Control - Cycle 2
-6.667
5.774
-2.000
0.184
Control - Cycle 4
-10.000
10.000
-1.732
0.225
Control - Cycle 6
-26.667
11.547
-4.000
0.057
Control - Cycle 8
-43.333
40.415
-1.857
0.204
Control - Cycle 10
-60.000
36.056
-2.882
0.102
Control - Cycle 12
-63.333
40.415
-2.714
0.113
Table 3 shows that the creatinine levels are raised in patients following each subsequent cycle of treatment with 5FU/LV regimens. The difference in the serum creatinine levels after the fourth and the tenth cycle of treatment with the pretreatment levels was significant (p<0.05). The difference in the BUN levels measures before and after chemotherapy with 5FU/LV was not significant following alternate cycles of treatment.
Table 3 Comparative changes in renal biomarkers in patients treated with 5FU/LV regimen
Paired Samples Test
Paired Differences
t
p-value
Mean
Std. Deviation
Renal
Creatinine
Control - Cycle 2
-0.120
0.130
-2.058
0.109
Control - Cycle 4
-0.160
0.114
-3.138
0.035
Control - Cycle 6
-0.242
0.204
-2.646
0.057
Control - Cycle 8
-0.264
0.225
-2.627
0.058
Control - Cycle 10
-0.546
0.422
-2.893
0.044
Control - Cycle 12
-0.566
0.463
-2.734
0.052
BUN
Control - Cycle 2
-1.800
1.924
-2.092
0.105
Control - Cycle 4
-1.800
1.924
-2.092
0.105
Control - Cycle 6
-2.000
2.449
-1.826
0.142
Control - Cycle 8
-3.000
2.550
-2.631
0.058
Control - Cycle 10
-4.400
4.037
-2.437
0.071
Control - Cycle 12
-6.400
8.204
-1.744
0.156
Discussion:
The hepatocellular enzyme findings are indicative of deteriorating liver function. The levels of SGOT and SGPT both differ from the control values and point toward 5FU induced hepatic toxicity. Increase in SGOT and SGPT up to grade 2 (CTC of NIC) is reported by Hotta and colleagues (10) in a study based on clinicopathological assessment of 36 patients treated with 5FU/LV. They did not report grade 3 or grade 4 elevations in SGOT and SGPT ratio. In our data there is considerable difference in SGOT levels (mean value) after the second cycle of treatment as compared to the pretreatment levels (mean value). Similarly SGPT levels are perturbed following treatment and the difference in the SGPT levels from the pretreatment control value is statistically significant after the tenth cycle of treatment. The pooled data of all the patients cannot be used for prognostic or diagnostic assessment; however, it shows a pattern of drug induced alterations in hepatic functions. An early effect on SGOT level show mild progressive damages correlated with a prominent rise in SGPT levels. SGOT is found in cytosol whereas SGPT is in mitochondria. Any mild to moderate damage to the hepatic cells will result in a rise in SGOT levels even though SGPT levels may remain normalised. Moderate to Severe hepatic damage will give a rise in both SGOT and SGPT elevation. SGOT is located in red blood cells, kidneys, brain, skeletal muscle and cardiac tissues; hence a prompt rise in SGOT level is indicative of associated damages. SGPT is present in skeletal muscles and cardiac tissues and the serum levels are affected with myocardial and skeletal muscle damages. Cytotoxic chemotherapy is frequently associated with fatty liver disease, chemical hepatitis and reactivation of hepatitis B (11). The elevation in triglyceride levels is indicative of drug induced steatosis (fat globule deposition in hepatocytes) leading to postoperative hepatic insufficiency(8). A significant change in bilirubin from the pretreatment level is observed after the 6th cycle of treatment. Biliary changes are detectable and persistent since the drug is excreted in the bile. Sclerosing cholangitis with elevation in alkaline phosphatase and bilirubin levels secondary to 5FU plus mitomycin therapy is reported by Fukuzumi et al (12). After intravenous administration, 5FU is converted into its active form ‘5-fluoro-deoxyuridine-monophosphate’ by anabolic reactions in the tissues. The drug undergoes catabolism primarily in the liver by reduction of the pyrimidine ring by enzymatic action of dihydrouracil dehydrogenase (13). The compound is then cleaved to urea, ammonia, carbondioxide and α-fluoro-β-alanine. The catabolic process in the liver amounts for 5FU induced hepatic toxicity. Hepatic and renal toxicity associated with 5FU is reported earlier with IV administration of 5FU (14). The risk of 5FU induced hepatic damages is increased in older patients (15). Older patients included in our study with increased post-treatment transaminase levels were more frequently presented with pruritus and hand and foot syndrome.This complexity of the situation is that altered hepatic function increases the risk of 5FU concentration (since it is catabolized in the liver cells), which in turn adds to the hepatic damage.
Creatinine clearance and blood urea nitrogen (BUN) are conventional biomarkers of renal function for convenient and cost-effective assessment (16). A detectable change in the creatinine levels of the patients ensue after the fourth cycle of treatment. Besides suggesting a decline in the renal function, it also indicates defect in hepatic functional status and progressive cachexia (muscle wasting), both of which are readily assessed in the patients during treatment. BUN levels are also affected by dexamethasone pretreatment, dehydration and azotemia besides renal function. Nephrotoxicity with 5FU chemotherapy is usually reported when it is combined with cisplatin with worsened creatinine levels (17, 18). Tubular damage induced by 5FU plus high dose leucovorin chemotherapy (similar to de Gramont’s regimen in our study) is reported by Kintzel, who also reported 50% decline in creatinine clearance in three patients (19). Chemotherapy induced renal damages are detected with abnormal creatinine and BUN levels, but in most cases the renal tubes remain intact and functional as the normal renal blood flow and GFR is reversibly attained (20). Adequate hydration and simultaneous treatment with mesna, which neutralises the toxic metabolites can effectively reduce chemotherapy induced renal damage (8).
Conclusion:
SGOT and bilirubin levels are raised after each cycle of treatment and the difference between the SGOT levels of the patients treated with 5FU/LV, before treatment and after subsequent cycle of treatment are highly significant indicative of mild to moderate progressive hepatic toxicity. Risk of clinical and subclinical renal damage is observed by a subsequent rise in serum creatinine and BUN levels. Renal toxicity marked by creatinine elevation is prominent after the fourth cycle of treatment.
Psoriasis is a common skin disorder characterized by erythematous papules and plaque formation with silver scaling. Guttate psoriasis is much less common and many studies cite a prevalence of less than 30% among patients who have psoriasis. It refers to the acute appearance of multiple skin eruptions mostly in a patient with no preexisting psoriasis and less commonly in a patient with psoriasis. We report here a case of guttate psoriasis associated with a flare of psoriatic arthritis.
Case report
A 53 year old man presented with a generalized body rash and multiple joint pains. His symptoms started a week prior to presentation. The skin rash initially appeared on his back and flanks but gradually progressed to involve the thighs and arms. He had ‘sausage fingers’, bilateral knee and ankle swelling associated with pain and sporadic metatarsophalyngeal joint pain as manifestations of his arthritis. His past medical history included hypertension, diabetes mellitus, hyperlipidemia and psoriasis with psoriatic arthritis. He did not report any recent changes in his medication. The patient denied any history of fever, sore throat, weight loss, visual problems, dyspnea, cough, gastrointestinal complaints or recent travel. Physical examination revealed a diffuse, non-blanching, pruritic, maculopapular and maculopustular rash over the trunk. He also had a scaly and diffuse erythematic rash over the lower abdomen which was non-blanching and pruritic. Auspitz’s sign was positive. He had multiple painful joints including both knees, right wrist, left proximal interphalangeal joint, and both his ankles. Left knee arthrocentesis was done which revealed joint fluid consistent with inflammatory joint disease without any evidence of crystals. Laboratory tests, including red and white blood cell count, haemoglobin, cyclic citrullinated peptide antibody, rapid plasma regain, hepatitis panel, antinuclear antibody, rheumatoid factor, lyme markers and serum uric acid revealed no abnormalities. ASO titer level was positive at 196. An x-ray of his left hand showed periarticular erosive changes along the distal aspect of the proximal phalanx. A skin biopsy was performed which revealed mild spongiosis and a perivascular lymphoplastic infiltrate. A diagnosis of guttate psoriasis was made. He was started on prednisone, methotrexate and folic acid and discharged from hospital. He was followed up in the rheumatology clinic 2 weeks after discharge and his rash had improved.
Discussion
Unlike psoriasis, guttate psoriasis is a much lesser known entity. It refers to the acute appearance of multiple skin eruptions, mostly in patients with no preexisting psoriasis and less commonly in chronic plaque psoriasis (guttate flare of chronic plaque psoriasis).
The characteristic skin lesions of guttate psoriasis are less than 1 cm in diameter, hence the name guttate (drop like). The lesions look like a shower of red, scaly tear drops that have fallen down on the body mainly involving the trunk, arms, thighs and face. Guttate psoriasis should be differentiated from diabetic dermopathy, also called shin spots, which typically begin as dull red, scaly papules or plaques and later develop into bilateral asymmetrical circumscribed shallow pigmented scars and/or brownish macular lesions with a fine scale. In diabetic dermopathy the lesions usually are greater than 4 cm in size.
Diagnosis is usually made on clinical examination; however skin biopsy is helpful in difficult cases. Histopathologic findings of guttate psoriasis vary with the age of the lesion. Findings in early lesions may be nonspecific and may include mild acanthosis, papillary dermal oedema and lymphocyte-predominant dermal infiltrate. Mature lesions exhibit parakeratosis alternating with hyperkeratosis, epidermal acanthosis, Munro microabscesses and dermal perivascular infiltrate containg neutrophils, lymphocytes and macrophages.
Streptococcal infections are well known to precipitate guttate psoriasis,1 however there have been no significant improvements in patients who were given penicillin or erythromycin when compared to those who were not treated.2 Other known precipitants are physical and psychological trauma.
The exact pathophysiologic mechanism is undetermined. The disease is believed to result from an immune reaction triggered by a previous streptococcal infection in a genetically susceptible host. Recent research points toward chromosome 6 as HLA-Cw*0602 allele positive patients are more prone to develop the guttate form.
A 29 year-old woman had been well until 7 months previously when, after a viral syndrome, she developed palpitations, fatigue, and frequent episodes of light headedness and near syncope. On further questioning she notes exercise intolerance and dyspnea on exertion. She has stopped working as cashier. Her mother thinks she is having panic attacks and needs “something to calm her nerves.” ECG, echocardiogram, and endocrine evaluation are all normal. On physical examination, she displayed a postural heart rate increase of 35 beats per minute on standing, along with a 15mmHg fall in diastolic blood pressure.
Introduction
Disorders of the autonomic nervous system present unique challenges to the practicing clinician. These syndromes have a significant impact on quality of life, offer subtle diagnostic clues, and have a propensity to mimic other disease processes. For these reasons clinicians should have basic familiarity with the differentiating features of autonomic disorders. While much investigation has focused on Neurocardiogenic syncope, a distinct subgroup has emerged characterized by postural tachycardia and exercise intolerance. Postural orthostatic tachycardia syndrome (POTS) is the final common pathway of a heterogeneous group of underlying disorders that display similar clinical characteristics .1
The constellation of symptoms associated with POTS reflects underlying dysautonomia including palpitations, exercise intolerance, fatigue, lightheadedness, tremor, headache, nausea, near syncope, and syncope. Foremost amongst these is orthostatic intolerance. Besides being limited in the functional activities of daily living, increased sleep disturbances including excess daytime sleepiness, fatigue are also common and have been associated poor health-related quality of life. 2 We aim to discuss the clinical presentation, classification, evaluation and management of POTS.
Diagnosis
The current diagnostic criteria for POTS is the presence of orthostatic intolerance symptoms associated with a sustained heart rate increase of 30 beat per minute (bpm) or absolute rate exceeding 120 bpm within the first 10 minutes of standing or upright tilt in the absence of other chronic debilitating disorders, prolonged bed rest, or medications that impair vascular or autonomic tone. 3 Most patients will have orthostatic symptoms in the absence of orthostatic hypotension (a fall in BP >20/10 mmHg). A grading system for POTS has been developed (Table 1). This system focuses on the functional severity of orthostatic intolerance in a way similar to the NYHA heart classification.
The physical exam should be methodical and directed. Supine, sitting, and immediate standing heart rate and blood pressure should be recorded. Orthostatic tachycardia and acrocyanosis of the lower extremities may be the only physical signs in these patients. Standing and supine blood pressure measurements and baseline electrocardiogram are generally recommended. In patients with physical examination or clinical history suggestive of cardiovascular abnormalities, other diagnostic test including echocardiogram , stress test or coronary angiography may be indicated before a tilt test. In addition, other possible clinical disorders with similar clinical manifestations must be kept in mind and ruled out. Upright tilt test remains the diagnostic test of choice for POTS and other autonomic disorders. Implantable loop recorders, electrophysiological tests and Holter monitoring are not helpful in the evaluation of these disorders. Supine and upright serum catecholamine levels should be obtained if hyperadrenergic type is suspected. In the presence of gastrointestinal symptoms bowel motility studies may reflect the degree of involvement and help to tailor therapy. 4
Table 1 : The Grading of Orthostatic Intolerance*
Grade 0 Normal orthostatic tolerance
Grade 1 Orthostatic symptoms are infrequent or occur only under conditions of increased orthostatic stress Subject is able to stand >15 minutes on most occasions Subject typically has unrestricted activities of daily living
Grade II Orthostatic symptoms are frequent, developing at least once a week Orthostatic symptoms commonly develop with orthostatic stress Subject is able to stand >5 minutes on most occasions Some limitation in activities of daily living is typical
Grade III Orthostatic symptoms develop on most occasions and are regularly unmasked by orthostatic stresses Subject is able to stand for >1 minute on most occasions Patient is seriously incapacitated, being bed or wheelchair bound because of orthostatic intolerance Syncope / presyncope is common if patient attempts to stand
*Symptoms may vary with time and state of hydration and circumstances. Orthostatic stresses include prolonged standing, a meal, exertion, and head stress.
Classification and Clinical Features
POTS is a heterogeneous group of disorders resulting in a common clinical scenario. This syndrome is classified as being either primary or secondary. Primary POTS is idiopathic and not associated with other disease processes. Secondary POTS occurs in association with a known disease or disorder. Subtype classification affects management and is therefore essential.1,4 (Figure 1)
Partial dysautonomic (PD) POTS (also referred to as Neuropathic POTS) is the predominant form.1, 2 This is a mild peripheral autonomic neuropathy, characterized by inadequate peripheral vasculature constriction in the face of orthostatic challenge. Female predominance is seen with 5:1 female to male ratio. Presentation is commonly abrupt onset of symptoms after a febrile viral illness, pregnancy, immunization, sepsis, surgery, or trauma. The etiology of PD type POTS is postulated to be an autoimmune molecular antigen mimicry type pathogenesis. Serum autoantibodies to peripheral autonomic ganglion alpha-3 acetylcholine receptors may be positive in 10-15% of the cases. Anhidrosis of lower extremities is seen in more than 50% of these patients at quantitative sudomotor axon reflex testingDependent blood pooling when upright is greater than normal and heart rate and contractility increase as normal compensatory physiologic mechanisms to maintain cerebral perfusion. This autoregulatory response may initially be fully compensatory; however, peripheral venous pooling may increase with time and exceed this compensatory effect. Patients with PD type POTS become dependent on the skeletal muscle pump to augment their autoregulatory physiology. Ultimately, venous blood pooling increases beyond the body’s total ability to compensate and adequate blood pressure maintenance fails.
“Developmental” partial dysautonomic POTS is an adolescent subtype.6 The mean age of onset is 14 years. The clinical scenario is that of orthostatic intolerance following a period of very rapid growth. Symptoms are progressive and peak at a mean age of 16 years. Orthostatic intolerance may be severe, including severe headaches, and can be functionally disabling. Following their peak symptoms will slowly improve and resolve into young adulthood (19-24 years). Roughly 80% of patients with developmental PD POTS will experience complete resolution of symptoms. The etiology of this subtype is unclear and appears to be a transient period of autonomic imbalance occurring in rapidly growing adolescents.
Hyperadrenergic POTS is less common than the PD type ,7This form is characterized by a gradual onset with slowly progressive symptoms. Patients report experiencing tremor, anxiety, and cold clammy extremities with upright posture. 7 Many patients note increased urine output when upright. True migraine headaches may be seen in over half of patients.7 Gastrointestinal symptoms in the form of recurrent diarrhea were seen in 30% of the patients. In contrast to PD type of POTS, the hyperadrenergic form demonstrates elevated serum catecholamine levels with serum norepinephrine levels >600ng/ml. This may be a familial syndrome in some instances determined by a careful history. The etiology of hyperadrenergic POTS is felt to be genetic with a single point mutation resulting in a dysfunctional norepinephrine reuptake transporter protein present in the intrasynaptic cleft. The result is excessive norepinephrine serum spillover with sympathetic stimulation resulting in a relative hyperadrenergic state appearing similar to pheochromocytoma. 8
A connective tissue disorder has been an increasingly recognized etiology of secondary POTS 9 . Joint hypermobility syndrome (JHS) is an inherited condition characterized by joint hypermobility, connective tissue fragility, and soft velvety skin with variable hyperextensibility. The condition is associated with ecchymotic predisposition, premature varicose veins, diffuse muscle and joint pain, and orthostatic acrocyanosis. The etiology of POTS in JHS patients is thought to be due to abnormal vascular (venous) elastic connective tissue. During orthostatic stress and increased hydrostatic pressure these patients exhibit increased vessel distensibility and orthostatic intolerance. Excessive peripheral venous pooling and compensatory tachycardia follows. Up to 70% of JHS patients suffer from some degree of orthostatic intolerance. It is observed that adolescent PD POTS patients have features similar to JHS patients and further studies may determine the significance of this potential relationship 10.
Secondary POTS refers to a group of conditions which result in peripheral autonomic denervation with sparing of cardiac innervation. Most commonly, secondary POTS is associated with diabetes mellitus. Less commonly, this form may occur with heavy metal intoxication, multiple sclerosis, parkinsonism and chemotherapy, especially vinca alkaloids.11,12
Severe autonomic nervous system disorders may present as POTS. These may include pure autonomic failure or multiple system atrophy. Paraneoplastic syndrome associated with adenocarcinoma of the lung, breast, ovary, or pancreas may also present as POTS. These tumors produce auto-antibodies targeting the acetylcholine receptors in the autonomic ganglia in a manner similar to post-viral syndromes.
Figure 1. Subtypes of postural orthostatic tachycardia syndrome
Evaluation and Management
Treatment is generally individualized to each patient. Confounding pharmacology should be identified and stopped if possible (Table 2). The presence of secondary POTS should be considered. Underlying diagnoses causing or augmenting POTS should be identified and treated appropriately. Deconditioning is frequent seen in POTS patient and a deliberate aerobic reconditioning program should be a component of the treatment plan. 13 This is encouraged to begin promptly working up to a goal of 20-30 minutes of activity at least 3 times a week. Resistance training of the lower extremities is helpful to increase the efficacy of the skeletal muscle pump. Salt and water ingestion are the most common employed non-pharmacolgical therapeutic intervention for POTS. Although, the intravenous saline infusion has been associated with reduction in standing tachycardia, the effect on this intervention on the symptom reduction remains unknown 14 . In general, since low blood volume may exacerbate symptoms patients are encouraged to have liberal salt and water intake. Excluding hyperadrenergic POTS, daily fluid and sodium intake should be greater than 2 liters and 3-5 grams.
Table 2: Pharmacologic Agents That May Cause or Worsen Orthostatic Intolerance
The goal of pharmacotherapy in the treatment of POTS is to ameliorate the symptoms of POTS and thus maintain the functional capacity. Currently no drug is US FDA approved for the treatment of POTS. All pharmacology is inherently off-label. (Table 3).
Majority of the evidence for the use of different pharmacological agents in the management of POTS is based on some small randomised , observational and retrospective single center studies. In clinical practice most patients are treated with a single agent and second medication from different class with a different mechanism of action is added in case of treatment failure. Resistant cases are often treated with polypharmacy.
Fludrocortisone, a potent mineralocorticoid resulting in sodium retention, augmented fluid volume, and sensitized peripheral alpha adrenergic receptors. The effects are more pronounced in the younger population. Starting dose is 0.1-0.2 mg daily with a maximum dose of 0.4 mg. Common side effects include electrolyte imbalance and hypertension. In a study of 11 female POTS patients, fludricortisone alone or in combination with bisoprolol was associated with improvement in symptoms 15. Midodrine is an alpha -1 adrenoreceptor agonist and causes both arterial and venous vasoconstriction. It is commonly used as add on therapy and with starting dose at 5 mg orally three times a day. In our clinical experience we advise patients to take their first dose of midodrine 15 minutes prior to getting out of bed. An additional 5mg dose can be used for breakthrough symptoms. Midodrine is usually well tolerated with the most common complaints being nausea, “goose bumps,” and scalp pruritus. In a small study of 6 patients with POTS acute combination therapy of midodrine (10mg) with octreotide (0.9mcg/kg) was significantly associated with reduction in upright tachycardia and improved standing time.In another study of 53 children with POTS, midodrine was significantly associated with both higher clinical cure rate and reduced recurrence rate as compared to children treated with metoprolol or conventional therapy.
Patients may continue to be symptomatic despite dual-therapy as outlined above. In this population we add a serotonin reuptake inhibitor (SSRI) or norepinephrine reuptake inhibitor (SNRI). SSRI therapy has been found to be helpful in the prevention of neurocardiogenic syncope. However, SNRI therapy is more useful in the treatment of POTS. Usually, we use bupropion XL beginning with 150 mg orally daily titratable to 300 mg daily if necessary.
The most effective SSRI therapies combine serotonin and norepinephrine reuptake inhibition (venlafaxine and duloxetine). The agents are usually well tolerated with the most common side effects being gastrointestinal upset, tremor, sleep disturbance, and less commonly agitation and sexual dysfunction. Bupropion and SSRI therapy can be combined to achieve a similar effect.
Pyridostigmine is an acetylcholinesterase inhibitor that facilitates sympathetic and parasympathetic ganglionic neural transmission. In our single center experience of 203 patients of POTS treated with pyridostigmine; improved symptoms of orthostatic intolerance were seen in 88 of 203 (43%) of total patients or 88 of 172 (51%) who were able to tolerate the drug. Fatigue (55%), palpitations (60%), presyncope (60%), and syncope (48%) were the most common symptoms that improved with pyridostigmine. Further, symptom reduction correlated with a statistically significant improvement in upright HR and diastolic blood pressure after treatment with pyridostigmine as compared to their baseline hemodynamic parameters (standing HR 94 ± 19 vs 82 ± 16, P < 0.003, standing diastolic blood pressure 71 ± 11 vs 74 ± 12, P < 0.02). Gastrointestinal problems were the most common adverse effects (n = 39, 19%) seen in our study. 18
Severely affected and refractory patients may benefit from erythropoietin (EPO) therapy. EPO increases red cell mass, central blood volume and augments response of blood vessels to the angiotensin-II and thus causes vasoconstriction. These effects are quite useful in the treatment of orthostatic disorders. Prior to initiation of EPO therapy obtain a complete blood count (CBC), total iron binding capacity, serum iron and ferritin levels. Hematocrit (HCT) levels must be monitored and should remain less than 50 on EPO. The starting dose is 10,000 units via subcutaneous injection once weekly. There is a 4-6 week delay between a given dose and the full clinical effect. The hematogenic and hemodynamic affects are independent but may occur simultaneously. A goal HCT of low to mid 40 will often result in optimum hemodynamic augmentation. Monitoring during EPO therapy should include monthly CBC to document HCT less than 50. EPO therapy may infrequently result in a “serum sickness” type reaction characterized by nausea, fever, chills, and general malaise. In another study of 39 patients (age 33 ± 12, 37 females) with resistant form of POTS, we reported sustained improvement in twenty-seven (71%) patients at mean follow-up of six month with EPO therapy. Eighty (21%) failed to respond to therapy while as 3 (8%) improved with therapy at 3months. Also, erythropoietin significantly improved sitting diastolic blood pressure but had no effect on other hemodynamic parameters.19 We reserve EPO therapy for patients that are refractory or intolerant of other forms of treatment because of its considerable expense and subcutaneous route of administration.
Beta blocker therapy such as metoprolol tartrate may be beneficial in adolescent type POTS patients. In a single center retrospective study of 121 patients with possible POTS, written survey at follow-up were used to evaluate response to therapy with beta-blockers and midodrine. 47 adolescents responded to survey (Walker Functional Disability Inventory Survey) and reported improvement with a β-blocker (100% vs 62%, P = 0.016) and more attributed their progress to medication (63.6% vs 36.4%, P = 0.011) than did those treated with midodrine 20.In addition, beta-blocker therapy was associated with improved quality of life. Great caution should be taken in using beta-blocker therapy in a rare form of hyperadrenergic POTS secondary to the mast cell activation disorders. Octreotide is a somatostatin analogue with potent vasoconstrictive effects and is useful in the treatment of orthostatic disorders. In patients with resistant POTS, octreotide may be a useful as add on therapy. It is administered by subcutaneous injection 2-3 times daily. The stating dose is 50 ug and may be titrated up to 100-200 ug three times daily.
Agents that block the release or effect of norepinephrine (noradrenaline) are very effective for hyperadrenergic type POTS patients. We use clonidine starting at 0.1 mg orally twice daily and titrating up as needed. The patch form may be preferable to some patients and has the added benefit of providing a steady state drug release for one week. Labetalol, an alpha and beta receptor blocker, is also useful in this group of patients. Dosages of 100-400 mg orally twice daily are used. Methyldopa may have a role in highly selected patients with POTS. Symptom control may be improved with both the SSRI and SNRI classes of medications.
Inappropriate sinus tachycardia (IST) is an important confounding finding in suspected POTS patients. This syndrome is similar to hyperadrenergic type POTS. The clinical presentation may be similar with IST being more common in females. These disease states display and exaggerated response to isoproterenol infusion. It has been postulated that they may represent different states of the same pathologic process. A greater degree of orthostatic change in heart rate is seen in POTS patients. The supine rate rarely exceeds 100 bmp (IST will often be >100). Postural changes in serum norepinephrine levels are much more pronounced in POTS patients. It is important to differentiate POTS and IST. Radiofrequency ablation of the sinus node will rarely benefit hyperadrenergic POTS patients and will make PD POTS patients markedly worse.
Treatment of secondary POTS should focus primarily on the underlying disorder to the greatest extent possible. Diabetes mellitus or JHS related POTS are treated as PD POTS. Secondary POTS due to sarcoidosis or amyloidosis may benefit from steroid therapy. Secondary POTS that is paraneoplastic may completely resolve with treatment of the underlying malignancy but may also respond to pyridostigmine.
Patients suffering from POTS have a disease that affects many aspects of their life. They are often unable to take advantage of meaningful employment or education opportunities. The pervasive life change experienced often results in significant psychosocial disruption as they may be excluded from social norms and certain environments. Frequently, patients require psychologists, social workers, and lawyers to address these aspects of living with POTS. The treating physician is a prominent and central figure who is a beacon of hope for this population. A positive, caring, and nurturing attitude may be the best medicine and lead to a rewarding rapport where an otherwise challenging disease exists.
Prognosis
There is limited data on the prognosis of POTS patients. Recent short term follow-up studies have shown better prognosis in patients with POTS. 21 Roughly 50% of post-viral POTS patients make a meaningful recovery over about 2-5 years. Meaningful recovery may be defined as the absence of orthostatic symptoms and the ability to perform the activities of daily living with little or no restriction. Some patients experience a partial recovery and still others may demonstrate a progressive functional decline with time. As a general principle, a younger age of onset portends a better prognosis. A majority of patients tend to adopt different lifestyle modifications including increased fluid and salt intake to improve and reduce exacerbation of the POTS symptoms. In secondary POTS syndromes have a prognosis consistent with the underlying causative disorder.
Conclusion
Disruption of normal autonomic function may manifest as one of a heterogeneous group of clinical disorders collectively referred to as postural orthostatic tachycardia syndrome. Treatment is most successful when diligence has been taken to investigate the underlying disorder or POTS subtype and a comprehensive targeted treatment program is instituted with frequent follow up. Goals of care should focus on functional milestones and maintenance of function.
The incidence and prevalence of hypertension is rife among first and second world countries and arguably, could be labelled the most common chronic disease in the UK1. It is estimated that a quarter of all adults in the UK have hypertension2. This is alarming in light of the incredible contribution of hypertension to mortality and morbidity. Evidence shows that for each 2mmHg rise of systolic blood pressure, mortality from ischaemic cardiac events rises by 7% and mortality from ischaemic intracranial events rises by 10%3-4. The key to reversing this lies in diagnosing hypertension accurately and quickly and knowing how to best treat each patient.
Understanding hypertension
It is still not entirely clear what mechanisms cause hypertension. Evidence has proven that systolic blood pressure increases in a linear fashion with age, which is due to the loss of elastic tissue in arteries with age1,5. This is known as ‘essential hypertension’. The majority of patients who are diagnosed with hypertension have ‘essential hypertension’, in other words, there is no clear cause found besides increasing age1-2. Research has shown that other factors can be associated with hypertension but alone may not necessarily cause it. Unalterable risk factors include genetic predisposition, age, sex and race. Other factors which have proven to raise blood pressure include environmental factors such as lifestyle and diet, obesity (randomised control trials have shown that a weight loss of one kilogram can be attributed to one mmHg fall in diastolic blood pressure5), excessive alcohol intake, smoking, stress at work or in the home, socio-economic status and recent major life events1-2,6.
How to take the perfect blood pressure
In the clinic setting, make sure the patient is relaxed, sit the patient comfortably with their arm outstretched, resting on the table and wait a few minutes. Make sure the sleeves are not too tight as this will alter the readings1,5. Be careful that the blood pressure cuff is the correct size for the patient as small cuffs can give a false high reading for larger patients and larger cuffs can give a false low reading for smaller patients3,5. Check the pulse is regular as irregular pulses can give incorrect readings from automated devices - if in doubt perform it manually5. Take the blood pressure in both arms and repeat several times, discard the first reading and always record the lowest reading in the patient’s file1.
The well recognised ‘white coat syndrome’ has a prevalence of about 10% in the UK and according to NICE data, the syndrome can cause a difference of 20/10mmHg between readings in a clinical setting and those at home1,3,5. In light of this, NICE altered the guidelines in 2011, stating that any patient with a reading close to 140/90mmHg is to be sent home with an Ambulatory Blood Pressure Monitor (ABPM)3. This is a device attached to the patient for a minimum of 24 hours and it records the patient’s blood pressure every 30 minutes of the patient’s waking day. The idea behind this is to rule out any ‘white coat syndrome’ and to get a range of readings as the patient goes about their usual day to day activities. In this way, when the readings are analysed (an average of at least 14 readings are taken by the clinician), it confirms diagnosis immediately and treatment can be initiated1,3.
The value of repeated measurements in different settings has been shown in evidence from as early as the 1970s2,5. Research has also shown that patients usually have a high blood pressure reading initially which drops after subsequent measurements, hence the new guidelines are in place to allow for a range of readings before diagnosing and treating hypertension1,3.
Investigations
While the patient is still in the clinic, assess the patient’s overall cardiovascular risk score using the cardiovascular risk assessment tool3. Perform a thorough physical examination, including looking for evidence of target organ damage, for example, left ventricular hypertrophy, renal disease, peripheral vascular disease and changes in the retina from raised blood pressure1,3,5. If there is suspicion of hypertension, send the patient home on an ABPM3. While waiting for the results of the ABPM, any patient under investigation for hypertension needs to have a baseline set of tests1,7-8. This includes a full blood count, renal function tests, liver function tests, a fasting glucose and cholesterol blood test, an ECG (electrocardiogram) and a urine dip. These tests are a basic screen for assessment of target organ damage6,9. If these investigations are not adequate, a patient can be referred for more extensive investigation for target organ damage, for example, an echocardiogram or a renal ultrasound/angiography1,3,5.
Any patient that is young or presenting with persistent hypertension, especially that which does not respond to treatment, needs further investigation for other causes, such as renal disease, adrenal disease, alcoholism or steroid use (not to forget the oral contraceptive pill can also cause hypertension1,7,9.
In general, a patient should be treated if their blood pressure readings are persistently 140/90mmHg or higher. For those that have borderline readings, for example, 135/85mmHg, clinicians must assess their cardiovascular risk score and look for target organ damage. If there is evidence for either of these, a patient should be started on treatment immediately1.
Treatment
Non-pharmacological
First line treatment of hypertension is always non-pharmaceutical; also known as ‘lifestyle changes’ 1,3,5,9. Attempt to find out the details of the patient’s diet, weight, employment, stress levels at work/home, exercise, alcohol intake and smoking habits. Once established, assist the patient in altering their lifestyle choices in order to lower their blood pressure. Patients often feel overwhelmed and many benefit from group activities, such as smoking cessation and weight loss groups3. Other ideas include a dietician referral, counsellors if they are struggling with motivation and low moods, gym sessions/personal trainers. Encourage the patient in that if they succeed in altering their lifestyle and therefore bringing down their blood pressure, they can avoid prescription medication.
Lifestyle changes can delay hypertension for many years but if the blood pressure continues to creep upwards in subsequent multiple visits and lifestyle options have been exhausted, it would then be appropriate to start pharmacological management1,3,5.
Pharmacological Treatment
In general terms, always start with monotherapy and increase the dose according to patient response. According to NICE guidelines from 2011, if a patient is over 55 years of age and/or Afro-Caribbean in origin, start with a calcium channel blocker, such as Amlodipine3. If these are contra-indicated, start with a thiazide diuretic3. In regards to thiazide diuretics, the new NICE guidelines state that Chlortalidone (12.5–25.0 mg once daily) or Indapamide (1.5 mg modified-release or 2.5 mg once daily) should be used in preference to what clinicians have been prescribing for years, namely Bendroflumethiazide and Hydrochlorothiazide3. For those who are already on these conventional thiazide diuretics, NICE state that if the patient’s blood pressure is stable, to continue with Bendroflumethiazide or Hydrochlorothiazide3.
Patients diagnosed with hypertension who are under 55 years of age, should be started on an ACE inhibitor (Angiotensin Converting Enzyme inhibitor), for example, Ramipril3, but if this is not tolerated, replace it with an ARB (Angiotensin II Receptor Blocker) such as Losartan3.
Review the patient every few weeks initially and extend the reviews to 6 months once the blood pressure is within therapeutic range6.Do not forget to check the patient’s renal function in the first few months of starting a new drug and always be aware that if a patient’s blood pressure drops drastically after starting an ACE inhibitor this suggests underlying renal disease and must be investigated1,3,5,9.
Continue to titrate the dose of the drug until the patient’s blood pressure is satisfactory. Consider adding in a second agent when the patient is nearing maximum dose of the first agent and the blood pressure is rising again3,5. Depending on what the patient is on, add in either an ACE inhibitor, ARB or a calcium channel blocker, for example, if patient is on Ramipril, add in Amlodipine and vice versa3. If a calcium channel blocker is not tolerated as second line, consider using thiazide diuretics. Afro-Caribbean patients who are already on calcium channel blockers, add in an ARB, rather than an ACE inhibitor3.
Following that, if the blood pressure is still not within therapeutic range, consider adding in a third agent or alternatively, discontinue the first agent and continue with the second and add a third from among an ACE inhibitor, ARB or calcium channel blocker. Consider a thiazide diuretic if patients are intolerable to any of the above3.
Beta-blockers should not be considered in treating hypertension, according to NICE, unless the patients are very young or intolerant to ACE inhibitors, ARBs or calcium channel blockers3.
Beware and monitor closely any elderly patients who are on antihypertensives as the physiology of ageing interferes with the drugs, for example, decreased clearance of drugs from the kidney or liver, decreased sensitivity to baroreceptors (postural hypotension), chronic sodium retention and reduced cardiac reserve. Do not forget communication and compliance issues with the elderly also1,7.
Make sure there is an annual review for each patient that has been diagnosed with hypertension in order to get blood pressure readings, medication review and how the patient is coping with lifestyle changes or side effects of the antihypertensives.
When to Refer
Resistant hypertension is defined as a patient remaining hypertensive despite being on triple or quadruple drug therapy3,7. Consider starting a low dose of Spironolactone (if the serum potassium is less than 4.5mmol/l) and refer to a specialist for advice3-4.
If subsequent readings are 180/110mmHg or more, start antihypertensives immediately and refer the patient to hospital. Also refer immediately if retinal haemorrhages or papilloedema are seen1,3.
Summary
If a patient is suspected to have hypertension, send them home with an ABPM and perform baseline tests1,3.
Start treatment if blood pressure is 140/90mmHg and ABPM average is 135/85mmHg and/or patient has one of the following:
target organ damage
established cardiovascular disease
renal disease
diabetes
10-year cardiovascular risk equivalent to 20% or greater (NICE guidelines, 2011)3
Start on monotherapy and review every few months, until blood pressure is stable3.
Review yearly after stability has been reached and consider adding in further antihypertensives if the blood pressure rises again.
Book patients in for annual reviews of end organ damage as this is an excellent overview of disease progression.
Hypertension is to be respected in light of its incredible contributor to morbidity and mortality. Never underestimate the importance of keeping a patient’s blood pressure within the desired range4.
An unquestioning belief in the power and efficacy of nature's healing remedies and processes, the placebo effect, disappointment and dissatisfaction with conventional medicines, outright rejection of orthodox treatments, convincing and persuasive advertising, reinforcement from others with similar views, endorsement by influential celebrities, perceived hand-me-down wisdom, bogus pseudoscientific claims, uncritical journalism, scare-mongering, feelings of desperation for a 'cure', and anecdotal case studies or surveys masquerading as research, are among the many reasons why patients and the public choose to alternative medicines either bought through local stores, pharmacies or on the internet. Over-the-counter drugs (OTCs) or over-the internet remedies are taken either with or without conventional medicines by millions of people every year and while most are harmless and safe to use there are inherent dangers of additive effects and interference with prescribed medications.
Benefits for patients who use OTCs include the convenience and sometimes less costly outlay on prescription drugs (analgesics, for example). Preparations may vary in price, according to the pharmaceutical provider. Self-treatment of minor ailments should theoretically lead to less pressure on GPs. Unfortunately, some patients tend to self-medicate for long periods (for example, analgesics) without visiting their GP for a health check to monitor the condition(s) for which they are using the OTC remedy to begin with. There is also the incorrect but widespread belief that because a prescription is not necessary to obtain these drugs they must be much less harmful than prescription-only preparations. Medicines may be used inappropriately, such as paracetamol for insomnia, or aspirin for stomach aches. Very often no record of OTCs is documented in the patient's notes. The list of OTCs is too numerous to cover in any detail here and for practical reasons the authors will concentrate on common legal products which most people are familiar with.
What causes the adverse effects?
An understanding of drug interactions gained momentum through the study of metabolizing enzymes. Cytochrome P450 inhibition or induction is probably the main mechanism for the pharmacokinetic interactions of drugs. CYP450 enzymes are haemoproteins (like haemoglobin) which comprise many related though distinct enzymes referred to as CYP. Over 70 CYP gene families have been described so far and are further divided into families and subfamilies of which CYP1, CPY2 and CYP3, are involved in hepatic drug metabolism.1 Thus, CYP3A denotes a cytochrome P450 enzyme that is a member of family 3 and subfamily A. It is abundant in liver and intestine. In the liver CYP450s are found mainly in the smooth endoplasmic reticulum. Any inhibition of CYP enzymes may result in enhanced plasma and tissue concentration of drugs, leading to toxicity. Likewise, induction may result in reduced drug concentration leading to decreased drug efficacy and treatment failure. Tricyclic antidepressants are substrates of 2D6 (CYP450 2D6 in full), which inactivates them by hydroxylation. For example, if a tricyclic antidepressant is given concomitantly with the serotonin/ noradrenaline reuptake inhibitor venlafaxine, the levels of the tricyclic antidepressant will rise because venlafaxine inhibits CYP450 2D6 and therefore prevents the breakdown of the tricyclic compound. Similar effects can occur with paroxetine, duloxetine, fluoxetine and atomoxetine. However, in clinical practice only atomoxetine requires dosage reduction when given with a 2D6 inhibitor. 2
Diphenhydramine (a common ingredient in sleeping tablets) in therapeutic doses inhibits CYP45 2D6-mediated metabolism of venlafaxine in humans. Venlafaxine has a low potential to inhibit the metabolism of substrates for CYP2D6 such as imipramine and desipramine compared with several of the most widely used SSRIs, as well as the metabolism of substrates for several of the other major human hepatic P450s 3 Of all the marketed drugs, about 60% are metabolized by the CYP450 system. The presence of the latter in red blood cells and hepatocytes contributes to the first-pass metabolism of drugs. This will have add-on effects when CYP450 inhibitors are simultaneously ingested. For example, grapefruit juice inhibits this enzyme system and therefore the bioavailability of drugs taken by mouth will increase causing a reduction in first-pass effect (presystemic metabolism).4
Common varieties of OTCs
Many commonly used OTC preparations (other than food supplements and analgesics) contain the ingredient dextromethorphan (related to codeine), used to treat coughs, colds and flu symptoms. Up to 125 different types of cold medicines contain dextromethorphan. It is an effective cough suppressant (antitussive) that works by raising the coughing threshold. It is not an analgesic. Cough syrups and tablet or capsule forms of medicine that contain dextromethorphan may lead to loss of coordination, dizziness and, nausea when used in high doses. Dextromethorphan is the d-isomer of the codeine analogue of levorphanol which mimics morphine. It is relatively nontoxic and its antitussive effects last for about 6 hours. It should be avoided when an MAO inhibitor is concomitantly given.
The generic term antihistamine refers in general to the H1 receptor antagonists used for inflammatory and allergic conditions. Sedation is a prominent feature of the H1 antagonist, diphenhydramine, used for allergies such as hay fever (short-term beneficial effect) and for symptomatic relief of the common cold. Guaifenesin, derived from the guaic tree, is a common ingredient found in cough expectorants. It is usually harmless though may cause problems in patients with compromised renal function. The mechanism of action, if any, is not known, save that it 'reduces viscosity’ of respiratory secretions.
OTCs believed to help weight loss, such as laxatives, diuretics and diet pills, are often purchased either for genuine health concerns or for misuse. All have serious and potentially fatal side effects if taken for a long time, particularly electrolyte disturbances.5Where diet pills are concerned problems may emerge insidiously with a few pills, quickly escalating to addiction. The alkaloid eephedrine is the principal active ingredient in the herb ephedra or ma huang. It is a potentially dangerous stimulant (sympathomimetic amine) contained in diet pills. Among the many possible side effects of diet pills are of course excessive weight loss with its attendant problems, alopecia, insomnia, and anxiety.
Used daily by millions of people worldwide, coffee and tea contain the methylxanthines caffeine and theophylline which act mainly by antagonism at purine receptors and by inhibiting phosphodiesterase. The effect is akin to a beta-adrenoreceptor agonist action. Caffeine is naturally found in certain leaves, beans, and fruits of over 60 plants worldwide. Its bitterness acts as a deterrent to pests. It can also be produced synthetically. Other than coffee and tea, the most common sources in the diet are cocoa beans, cola, and energy drinks. Product labels are required to list caffeine in the ingredients. Caffeine consumption in excess of 250mg daily produces symptoms indistinguishable from anxiety, including nervousness, irritability, tremulousness, muscle twitching, sleep disturbance, tachycardia, tachypnoea, palpitations, ectopic beats, and diuresis. A withdrawal syndrome can also occur and is associated with headache and a general muzziness. Caffeine may interfere with the effectiveness of drug treatment. For example, clozapine plasma levels can be raised, presumably through competitive inhibition of CYP1A2.6 In general terms, an average cup of brewed coffee contains 100mg caffeine per cup, Red Bull 80 mg/ 250ml per can, tea 45mg/ cup, instant coffee 60mg/ cup and filter coffee 120mg of caffeine per cup. Excess consumption of Red Bull may cause myopathy due to caffeine-mediated hypokalemia and rhabdomyolysis.7
Paracetamol (acetaminophen in the USA) is metabolized in the liver. It is probably the most common household analgesic and is present in a variety of preparations and is usually well tolerated. Drugs that increase the action of liver enzymes which metabolize it for example, carbamazepine, isoniazid, and rifampin, reduce the levels of paracetamol and decrease its action. Doses greater than recommended may result in liver damage and in overdose a potentially fatal hepatic necrosis can occur.
Not much is known about the contents of home medication cabinets (HMCs), the management of leftover medications, and the inclination of patients toward self-initiated treatment using non-prescription drugs. One cross-sectional study conducted in 72 Belgian community pharmacies revealed that the most frequently encountered categories of registered medicines were NAIDs, nasal decongestants, and drugs used for nausea. Despite their high prevalence, NSAIDs and non-opioid analgesics did not predominate (14%) among the most frequently used drugs: food supplements were used daily in 23.3% of households. Twenty-one per cent of the drugs were expired, 9% were not stored in the original container, and the package insert was missing for 18%. Self-medication, although generally acceptable in terms of indication and dosage, was commonly practiced, also with prescription drugs. Taking into account that younger people showed a significantly higher rate of self-medication, awareness of the risks of self-medication is warranted. 8
Relevance to Psychiatrists
Many psychiatric conditions are associated with excess alcohol use which complicates the picture when OTCs are used concurrently. Mixing alcohol with medication has the potential to cause nausea and vomiting, headaches, drowsiness, fainting, and loss of coordination. Because so many drugs can be bought without a prescription potential interactions with alcohol are often forgotten. Teenagers see OTCs as safer than illegal drugs and OTCs are sometimes taken to get a buzz or to help stay awake while studying. The home medicine cabinet allows quick access. Besides, parents will most likely have given an OTC preparation to their children for colds or other minor everyday ailments. Most drug education programmes however, focus primarily on illegal drugs, not OTC drugs and their potential for abuse.
Of some interest and importance to psychiatrists is the interaction when warfarin is combined with ginkgo (Ginkgo biloba) causing bleeding, a mild serotonin syndrome in patients who mix St John's wort (Hypericum perforatum) with serotonin-reuptake inhibitors. decreased bioavailability of digoxin when combined with St John's wort, induction of mania in depressed patients who mix antidepressants and ginseng, exacerbation of extrapyramidal effects with neuroleptic drugs and betel nut (Areca catechu); increased risk of hypertension when tricyclic antidepressants are combined with yohimbine. Disulfiram which inhibits aldehyde dehydrogenase inhibits the metabolism of warfarin. Metronidazole causes an unpleasant disulfiram-like reaction when mixed with alcohol. Consumption of 6-8 glasses of grapefruit per day may raise levels of carbamazepine and pimozide. Grapefruit juice is thought to the metabolism of many drugs and inhibition can last a number of hours. 9 The St John's wort component, hyperforin, contributes to the induction of CYP3A4. St John's wort also enhances the metabolism of other CYP3A4 substrates including the protease inhibitors indinavir and nevirapine, oral contraceptives, and tricyclic antidepressants such as amitriptyline. Other herbal remedies with the potential to modulate cytochrome P450 activity include ginseng, garlic preparations, and liquorice. 10Intake of St John's wort increases the expression of intestinal P-glycoprotein and the expression of CYP3A4 in the liver and intestine. The combined up-regulation in intestinal P-glycoprotein and hepatic and intestinal CYP3A4 impairs the absorption and stimulates the metabolism of cyclosporine, leading to subtherapeutic plasma levels.
The hormone melatonin plays a role in regulating the sleep-wake cycle but does not induce sleep per se. It is easily available through the internet and over-the-counter in the USA and many people use it for jet lag. Melatonin has side effects including diarrhoea, abdominal pain, headaches, nightmares, morning hangover, nausea, mild depression and loss of libido. Melatonin is used for many other complaints including tinnitus, depression, chronic fatigue syndrome (CFS), fibromyalgia, migraine and other headaches. Valerian root, a medicinal herb has been known to cause liver damage and should be used with caution. It too is most commonly used for insomnia and frequently combined with hops, lemon balm, or other herbs.
Many complementary medicines prescribed for anxiolysis/sedation (e.g. kava kava, valerian, passion flower and chamomile) are GABAergic, GABA (formed from glutamate) being the major inhibitory mediator in the brain, though for some, such as hops, the mechanism of action remains unknown. As expected, all remedies can lead to drowsiness when taken in high doses and can potentiate the effect of synthetic sedatives.11 Kava has been taken off the market because of its hepatoxicity.
Although sufficient dietary fibre and water are effective for the treatment of constipation some patients fear they are building up 'toxins' if they do not have 'regular' bowel habits. Often constipation is caused by opiate analgesics which are widely available, and in many cases patients are using antidepressant/psychotropic medication concurrently. The tendency to misuse laxatives is commonly seen in anorexia nervosa though is not confine to that disorder. The osmotic laxative lactulose is a disaccharide of galactose and fructose and therefore care is needed where diabetic patients are concerned particularly if they are taking neuroleptic medications such as clozapine or olanzapine. Abdominal cramps and diarrhoea can occur with high doses. Laxatives have the potential to interfere with potassium levels, usually causing hypokalemia. 5
Ordinary foods and drinks may interfere with prescribed medications.12 Grapefruit juice reduces the metabolism of calcium channel antagonists. Vegetables such as broccoli, cabbage, and Brussels sprouts are putative cytochrome P450 inducers and are known sources of vitamin K. Red wine, ethanol and cigarette smoke are also believed to induce the cytochrome P450 system and have the potential to interfere with the metabolism and catabolism of many drugs. Smoking interferes with clozapine metabolism. When smokers are prescribed clozapine abrupt smoking cessation may lead to high plasma concentrations with potentially serious consequences. Clozapine plasma concentrations can rise 1.5 times in the 2–4 weeks following smoking cessation.13 and in some instances by 50–70% within 2–4 days. Where baseline plasma concentrations are higher, particularly over 1 mg/litre, the plasma concentration may rise dramatically owing to non-linear kinetics. If patients smoking more than 7–12 cigarettes per day while taking clozapine decide to quit, the dose may need to be reduced by 50%.14 Smoking also interferes with duloxetine levels due to an induction of CYP1A2 by hydrocarbons contained in tobacco smoke. It cannot be expected that patients would be aware of these facts, let alone understand the pharmacology of the multitude of chemicals contained in OTCs. 15
Availability does not mean harmless
Most people using OTCs are unaware of the potential for harm. Herbal remedies, for instance, with their attractive packaging, convey the impression of being beneficial merely because they contain 'earth minerals' and other 'natural ingredients:' therefore they must be beneficial for health, rather like eating vegetables or taking vitamins.10 There are numerous instances of drug interactions and many preparations may contain contaminants such as mercury, lead, and arsenic. One of the commonest ingredients in many lotions and potions is hydrocortisone, which if used liberally may cause skin atrophy. The most worrying aspect of OTCs is that they give hope to people with serious conditions which might be better treated with conventional medicines - multivitamins for cancer, mineral supplements for constipation, and so forth. With buzz words such as 'healing, energy, vitality, harmony, body balance, healthy living, total well-being, holistic', and 'traditional', targeting the sometimes gullible consumer, OTCs become very appealing. Others are taken in by the pseudoscientific jargon, 'healing powers, purifying the blood, eliminating toxins from the bowel', boosting one's immune system, and so forth. The outcome can be serious: for example, Chinese herbal medicines containing extracts from Aristolochia plants have been implicated in the high incidence of urinary tract cancer in Taiwan, a study has suggested 16 because aristolochic acid has a consistent pattern of inducing DNA damage.
Some patients may be coincidentally taking conventional, proven medicines yet attribute their improved health to the alternative remedy. Other beneficial factors which are often conveniently ignored include a change in diet, increased wellbeing through physical exercise, or going on holiday! There is of course, the natural remission of the illness, particularly with transient viral infections, or unexplained lower back pain, to cite two instances. 17
Some common problems
Although the dangers of the common analgesics are relatively well-known (paracetamol causing liver damage, gastrointestinal upset with ibuprofen), patients are often unaware of the potential for adverse effects with other preparations. Nor are they always aware that many compounds combine two analgesics, for example, paracetamol and aspirin, or paracetamol and ibuprofen. Nonsteroidal anti-inflammatory drugs (NSAIDs) interfere with renal clearance and may result in elevated lithium levels with resultant toxicity.18 Combined use of an antidepressant or sodium valproate with an OTC could lead to abnormal liver function tests attributed solely to the former agents and not the OTC. Even reading the label does not guarantee insight and understanding of what is on offer. Labels are carefully and handsomely packaged by advertisers to persuade people their product is better than conventional medicines. Most consumers spend little time reading the labels about ordinary foodstuffs, never mind the chemical constituents of OTCs. In transplant patients, self-medication with St John's wort (hypericum perforatum) may lead to a drop in plasma levels of the immunosuppressant drug cyclosporine, causing tissue rejection. In the US, the Food and Drug Administration (FDA) with branches in other cities, including London (European Medicines Agency) approved a regulation in 1999 requiring that all OTC drug labels contain certain information such as ingredients, doses and warnings in a standardized format. This covers thousands of non-prescription products, including sunscreens. In the same way that people understand the nutritional value of foods, it is hoped that its efforts will help people use OTCs safely.
Sexual side effects are a frequent accompaniment of psychotropic drugs and patients are often bothered by impotence to such a degree they resort to surfing the internet to acquire sildenafil (Viagra) and the like. Such over-the-internet medicines are easy to acquire. Carbamazepine and St John's will decrease the level of sildenafil by competition with CYP3A4. Ketoconazole, the antifungal agent, works in a similar mechanism and may in increase the levels of citalopram. Metronidazole has a disulfiram-like reaction with alcohol.
There is also the problem of addiction with OTCs because of ease of access to opioid compounds. Patients often do not perceive them as having addictive potential. Preparations containing ephedrine or dextromethorphan can be abused. Ephedrine is still used as a nasal decongestant. As an indirectly-acting sympathomimetic amine it can react dangerously with monoamine oxidase inhibitors because of the increased amount of noradrenaline stored in noradrenergic neurones. Opioids may be crushed and the powder snorted or injected leading to euphoria or elation, followed by addiction when compulsive use takes over. Patients may be subject to mood swings making underlying psychiatric disorders and drug treatment difficult to manage. Opioids produce drowsiness, and depress respiration in high doses. The combination with sedative psychotropic medication such as mirtazapine, olanzapine or quetiapine could be deleterious especially where there is concomitant weight gain. Buspirone (a 5-HT1A receptor agonist used for anxiety) may interact with monoamine oxidase inhibitors (MAOIs), such as isocarboxazid, phenelzine, and tranylcypromine. Use of buspirone with these drugs can increase blood pressure. The combination of buspirone and trazodone may raise LFTs. The combination of buspirone and warfarin may accentuate the effects of warfarin and increase the risk of bleeding. Patients taking buspirone should not drink grapefruit juice, since even some time after a dose is taken, the amount of buspirone in the blood may be increased. Carbamazepine increases the metabolism of the pill reducing its effectiveness. The pill is more easy to acquire now (clinics and/or the Internet) and therefore unexpected pregnancies may occur in patients taking both. Cimetidine may increase the blood levels of sertraline by reducing its elimination by the liver. St John's wort interacts with the metabolism of the pill and this can result in unwanted pregnancies.
Overall OTCs are generally safe, though not where young children and pregnant women are concerned. Vitamins are safe unless taken in very high doses. Deficiency is rare in developed countries (apart from vitamin D) and therefore they are often taken unnecessarily 'to achieve balance' or for 'vitality and energy', and other eye-catching spurious claims. Glucosamine, an amino sugar, seems to be the most popular OTC dietary supplement for the treatment of osteoarthritis. It is naturally present in shellfish and in some fungi. Apart from occasional allergic reactions and mild gastrointestinal symptoms, it is generally innocuous, though conclusive evidence for its efficacy in osteoarthritis is lacking. Fish oil supplements usually come from mackerel, herring, tuna, halibut, salmon and cod. There is some evidence that omega-3-fatty acids contained in fish oils are beneficial for cardiovascular problems but more trials are needed. Side effects are minimal and include mild gastrointestinal upset. 19
Doctors' dilemma
Is there a solution? Probably not, though one way to increase consumers’ awareness of the dangers associated with OTCs could be to change their status to match that of drugs such as simvastatin—they would still be sold over the counter, but with a pharmacist’s supervision. The list of OTCs is rising leading to increased intake of phytochemicals in addition to the usual gamut of medicines used to treat upper respiratory infections. Potentially fatal interactions can occur with OTCs and traditional drugs. Providing better training for pharmacy staff, and restriction of the quantity sold per costumer, should also be considered, though with so many retail outfits selling these products this is probably unrealistic. Besides, many of these products are available on the shelves, not necessarily at the pharmacy counter.
The most common addictions are combinations of opioids with standard analgesics. The Internet is an easy source for prescription drugs, increasing their availability and eliminating the need to see a doctor. Is there an epidemic of prescription opiate use? It is difficult to tell. Effective prevention, public information, and treatment policies require sound epidemiological data about drug use to ensure policy-making is not distorted by stories of celebrity arrests and media-generated hysteria which tend to give that impression that use of illegal drugs is rife. The lack of knowledge about the ubiquitous presence of unknown ingredients in OTCs may be a source of concern in the future when even more become easily available.
It is difficult for doctors and other health care professionals to advise patients on the effectiveness and safety of OTCs. The numbers of well-designed studies available for review are limited, often conducted in a small number of healthy participants, and for short time periods only.20 A survey conducted by questionnaire in 238 follow-up UK rheumatology outpatients in three centers found nearly half (44%) had taken various herbal remedies or over-the-counter (OTC) preparations over the past 6 months. The most commonly used were: cod-liver oil, glucosamine, and/or chondroitin, and evening-primrose oil. Rheumatology outpatients have a particularly high risk of interactions with conventional medication because of polypharmacy and comorbidity. Gingko biloba, devil's claw, ginger, and garlic may have antiplatelet or anticoagulant effects and may exacerbate the gastrointestinal bleeding risk of nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids. Echinacea (taken by 4%) may be hepatotoxic and could exacerbate the adverse effect of disease-modifying antirheumatic drugs (DMARDs). Most patients are unaware of the potentially harmful interactions.21
The authors carried out a small audit of consecutive outpatients and staff on a random basis seen in our unit. Of the 45 people who completed the questionnaire 70% affirmed use of OTCs, either presently or in the past. A high percentage (73%) had never been asked by their GP about these 'alternate medicines' and among health professionals 25% never enquired from patients about the use of OTCs. More than half (63%) were unaware of possible side effects before taking them and nearly 50% had not considered that the OTCs might interact with prescribed medication. As would be expected, the majority of users (84%) did not experience any side effects. Nonetheless 16% experienced unpleasant adverse effects such as tachycardia, nightmares, drowsiness, cough, constipation, and exacerbation of asthma. When asked who had recommended the preparation/s the response was generally, 'friends' or 'I knew about it myself'. When asked why they bought it over-the-counter, the response was 'just in case I need it', 'cheaper than prescription' 'it is a natural remedy' 'it's only Nurofen'. As with most surveys, the commonest preparations were analgesics, laxatives, glucosamine for arthritis, and decongestants. Others bought OTCs to promote good health because they are herbal and natural', for example, ginkgo biloba. In a separate random survey of 50 consecutive outpatients carried out by FJD and N El-H, some 40% were taking herbal remedies.
Conclusion
Medical care has become fragmented in recent years. The family doctor of old no longer acts as a gatekeeper to coordinate medications patients are prescribed. A gynaecologist may prescribe the pill to a patient and a walk-in clinic may prescribe an antibiotic to the same patient. How does a doctor inform the patient that antibiotics decrease the effectiveness of the pill if the doctor is unaware of the myriad of other supplements including OTC medications, a patient is taking? Although a patient should bear some responsibility, in reality he/she may not have the expertise to discern the complications and interactions of medications. Besides multiple use of preparations is more often a problem of older age groups who frequently have many health problems. The family pharmacist has also been lost to mail-order pharmacies and sometimes suspect internet web sites. Because of the increase in numbers of prescriptions and OTCs, doctors and pharmacists are using computer programs to establish what is safe and what is not.
Strategies to mitigate these problems could include more general enquiries about prescriptions, OTC, and herbal drug use at the initial examination. 22 Even though some patients may be aware of the potential for drug misuse, others are naive and do not realize the harm involved. Providing containers to enable patients to dispose of unused or unneeded prescriptions or OTC medications is another tactic. Treating the underlying causes (of pain, for example) more aggressively may obviate the need for patients adding OTCs to their drug list. Practicing careful record keeping of prescription refills and tightening controls over prescription blanks are other practical measures. Where patients have become addicted to medications, programmes such as Narcotics Anonymous may help.
Prolactin is a polypeptide hormone that is secreted by lactotrophs of the anterior pituitary gland. Prolactin secretion shows a circadian rhythm1, with highest levels occurring during the night and the nadir occurring during the afternoon and eveningThe best known function of prolactin is the stimulation and maintenance of lactation.
Normal basal levels of serum prolactin are approximately 20 to 40 ng/ml in women (depending on the phase of their menstrual cycle), and 15 ng/ml in men. However, these concentrations can also vary with ageHyperprolactinemia is diagnosed when serum prolactin concentrations are >20-25 ng/ml (400-500 mU/l) on two separate occasions3.
Hyperprolactinemia is the most common disorder of the hypothalamic-pituitary-gonadal (HPG) axis4 and can have physiological causes - pregnancy, nursing, sleep, stress, sexual intercourse or pathological causes - tumor called prolactinomaMultiple factors are involved in prolactin secretion (Figure 1). However, hyperprolactinemia is also a common side-effect of traditional antipsychotics (e.g. haloperidol) and is associated with the use of some newer second generation agents2, 6.
Figure 1: Factors involved in Prolactin secretion
The prevalence of hyperprolactinemia is low in the general population (0.4%), but it can be as high as 9 to 17 % in women with reproductive disordersThe disease occurs more frequently in women than in men, multiple signs and symptoms associated with hyperprolactinemia (Table 1).
Multiple variables affect probability of development of breast cancer (Table 2) and a number of important factors determine the risk for breast cancer, and the most important of these seem to be related to estrogen and possibly prolactin (Table 3).
Sexual dysfunction: decreased libido, impaired arousal, impaired orgasm
Acne and hirsutism in women (due to relative androgen excess compared with low estrogen levels)
Behavioural effects
Decreased bone mineral density (BMD) which may lead to increased risk of osteoporosis.
Table 2: Probability of Developing Breast Cancer32 Risk of Breast cancer
Variables
Increased
Decreased
Age
Older
Younger
Socioeconomic status
Higher
Lower
Family history of breast cancer
Present
Absent
Racial
Caucasian
Oriental
Geographic
America
Asia
Marital status
Single
Married
Age at first pregnancy
Older
Younger
History of multiple pregnancies
Present
Absent
Age at menarche
Younger
Older
Age at natural menopause
Older
Younger
Artificial menopause
Absent
Present
Table 3: Epidemiology of breast cancer7
Age of menarche
Late pregnancy
Obesity
Caucasian females have slightly higher incidence
The highest incidence of breast cancer occurs after age 35, with 83% of the cases occurring after age 50 and only 1.5% under age 30
1 in 11 women will develop breast cancer sometime during their lifetime
The highest incidence of breast cancer in the US is found in the northeastern part of the country
The women with previous cancer of one breast are at risk for cancer in the opposite breast
A woman whose natural menopause occurs before age 45 has only half the breast cancer risk of those whose menopause occurs after the age of 557.
Methods
Pubmed.gov searched by using keywords
Antipsychotics and Hyperprolactinemia
Hyperprolactinemia is caused by these agents by blocking D2 receptors on lactotrophs and thus preventing inhibition of prolactin secretion. Furthermore, it has been suggested that the degree of elevation of prolactin correlates with the degree of occupation of D2 receptors in excess of 50%8.
Most studies have shown that conventional antipsychotics are associated with a two to tenfold increase in prolactin levels9, 10. In general, second generation antipsychotics produce a lower increase in prolactin than conventional agentsAmong second generation antipsychotics associated with increased prolactin are amisulpride, zotepine and risperidone11, 12, 13.
Antipsychotic induced Hyperprolactinemiaand Breast cancer
Prolactin is known to increase the incidence of spontaneously occurring mammary tumors in mice14 and increase the growth of established carcinogen-induced mammary tumors in rats15.
Prolactin and other sex hormones such as, estradiol and progesteroneare important in normal mammary gland growth and developmentas well as lactation. Both animal and in vitro data suggestthat prolactin is involved in tumorigenesis by promotingcell proliferation, increasing cell motility,and improving tumor vascularization. Whereas prolactinand its receptor are found in normal and malignant tissues,concentrations of both are generally higher in malignant tissue16.
Several studies have linked hyperprolactinemia to an increased risk of breast cancer in women17, 18. Mechanisms that have been suggested to explain this possible action of prolactin include the increased synthesis and expression of prolactin receptors in malignant breast tissue and a prolactin-induced increase in DNA synthesis in breast cancer cells in vivo18.
One of the hypothesized roles of prolactin in the development of mammary tumors is to create mammary gland conditions favorable for the action of carcinogens through its stimulation of the rate of mammary gland DNA synthesis, a measure of the frequency of mammary gland cell division19.
Several epidemiological studies have investigated whether female psychiatric patients receiving treatment with antipsychotics have a higher incidence of breast cancer but results have been conflicting. However, the most recent and methodologically strong study, found that antipsychotic dopamine receptor antagonists conferred a small but significant risk of breast cancer. This study had a retrospective cohort design and compared women who were exposed to prolactin-raising antipsychotics with age-matched women who were not20.
Conversely, other studies have shown no correlation between hyperprolactinemia and breast cancer21, 22. Furthermore, as most breast cancers are thought to be fueled by estrogen23, and hyperprolactinemia causes estrogen deficiency24, it is perhaps surprising that hyperprolactinemia has been linked with an increased risk of breast cancer. Indeed, post-operative hyperprolactinemia in breast cancer patients has been shown to improve disease free and overall survivalObviously, more studies are necessary to define any possible links between hyperprolactinemia and breast cancer.
In view of these problems it would be of interest to go around the contentious issue of possible carcinogenic effects of dopamine antagonists using a classical condition of dopamine loss or attenuation as in Parkinson's disease (PD). Using computerized registers of death data of the National Center of Health Statistics for years 1991 through 1996, estimated 12,430,473 deaths of persons over forty, and extracted 144,364 cases with PDTellingly, PD patients showed a highly significant reduction of overall cancer incidence. PD resistance to breast cancer might conceivably be attributed to dopaminergic treatment antagonizing hyperprolactinemia26, 27, 28.
Another recent study showed that dopaminergic therapy inhibits angiogenesis thereby acting as an anti-tumor agent29.
Epidemiological studies of women who have received prolactin-releasing drugs such as reserpine and perphenazine have not disclosed increased risk30.
Antipsychotic induced Hyperprolactinemia and Other cancers
Antipsychotics have been hypothesized to account for the reduced cancer occurrence observed in patients with schizophrenia in a number of studies. This reduction has been found primarily in men in smoking-related cancers, and in prostate and rectal cancer.
In addition, a study found a reduced risk of rectal cancer in both men and women as well as indications of a reduced risk of colon and prostate cancer in this population-based cohort of neuroleptic users. Reassuringly, they observed no increased risk of breast cancer in female users31.
Comments and recommendations
Hyperprolactinemia results from treatment with any drug that disrupts dopaminergic function on the HPG axis and is not limited to the use of antipsychotics.
Management of supposed anti-psychotic associated hyperprolactinemia should exclude all other causes, involve regular monitoring of adverse effects and include a regular risk-benefit discussion with patient.
Switching the patient to prolactin-sparing antipsychotic (i.e. Aripiprazole, Olanzapine, Quetiapine or Clozapine) usually proves effective, though there is also a risk of relapse.
It seems prudent to avoid prescribing prolactin-raising antipsychotics in patients with past history or family history of breast cancer.
It is premature to mandate warning patients of an unknown and undemonstrated increase in the risk of developing breast cancer associated with neuroleptic treatment.
Before initiating antipsychotic treatment a careful examination of patient is necessary.
One should examine the patient for evidence of sexual adverse events, including menorrhagia, amenorrhoea, galactorrhoea and erectile/ejaculatory dysfunction. If evidence of any such effects is found, then the patient's prolactin level should be measured.
Patient history, physical examination, pregnancy test, thyroid function test, blood urea and creatinine level can help determine if other etiologies are responsible.
Presence of headache and visual field defects is suggestive of a sellar space-occupying lesion (MRI indicated), but the absence of these features does not exclude such pathology.
History of menstrual cycling (duration, amount and intervals of menstruation) as well as lactation and sexual functioning should be taken before antipsychotic medication is initiated.
Obtain a pretreatment prolactin level, which one can compare with subsequent samples if the patient develops symptoms associated with relatively modest hyperprolactinemia.
The risk-benefit ratio for treatment of antipsychotic-induced hyperprolactinemia needs to be assessed on an individual basis.
If there is doubt about the cause of the hyperprolactinemia, patient should be referred to an endocrinologist.
Current recommendation
A rise in prolactin concentration should not be of concern unless complications develop, and until such time no change in treatment is required.20
Conclusions
There is no definitive data suggesting increased risk of breast cancer available at this time, thus author concludes:
Further prospective studies are needed in this area, with large number of patients, before a more definitive answer can be provided.
Detection of existing mammary tumor by breast examination or studies (mammogram) is recommended prior to administration of neuroleptics.
Development of newer antipsychotic drugs that do not increase serum prolactin level may be indicated.
Strengths
Each article found by search term was reviewed
Data were extracted from each article to find answer of research question
Pubmed.gov is a huge database for search.
Limitations
This literature review has been conducted by a single author, thus bias on part of author cannot be ruled out
Author was limited by time to review articles available in other databases.
Key Points
Most studies report no increased risk of breast cancer associated with use of these medications.
Only one study reported a positive correlation between neuroleptic induced hyperprolactinemia and increased risk of breast cancer.
Other studies report inconclusive data.
At this time we do not have definitive data suggesting increased risk of breast cancer secondary to hyperprolactinemia caused by antipsychotics.
Further prospective studies are desirable.
Author concludes that thorough screening of patient should be best desirable before starting of antipsychotics to avoid any add-on risk.
A 73 year old male retired civil servant with a background of spinal bulbar atrophy and hypertension presented to his General Practitioner (GP) for a routine health check. He was taking bendroflumethiazide, propranolol, atorvastatin and aspirin. His brother also has spinal bulbar atrophy.
The GP sent routine blood tests, which came back as follows: Haemoglobin 8.5 (13-17g/dL), Mean Cell Volume 84.9 (80-100fl), White Cell Count 3.4 (4-11 x10^9/L), Neutrophil Count 0.68 (2-8 x10^9/L), Platelets 19 (150-400 x10^9/L). A random blood sugar reading was 18 (3.9-7.8mmol/L). Renal function, bone profile and hepatic function tests were normal. The General Practitioner referred the patient urgently to the local Haematology unit for further assessment.
On further review the patient complained of tiredness but had had no infections or bleeding. There were no night sweats or recent foreign travel. Physical examination was unremarkable, with no lymphadenopathy or organomegaly.
A blood film showed marked anaemia with red cell anisopoikilocytosis, prominent tear drop cells and neutropenia with normal white cell morphology. There were no platelet clumps. A diagnostic investigation followed.
QUESTIONS
What are the differential diagnoses of pancytopenia and which causes are likely here given the findings on examination of the peripheral blood film?
Infections - Viral infections including cytomegalovirus, hepatitis A-E, Epstein-Barr virus, Parvovirus B19 and non A-E hepatitis viruses can cause aplastic anaemia1. The classical picture would be pancytopenia in a young patient who has recently had ‘slapped cheek syndrome’ from parvovirus B19 who has transient bone marrow aplasia. Tropical infections such as visceral leishmania may cause pancytopenia, splenomegaly and a polyclonal rise in immunoglobulins2. Overwhelming sepsis may also cause pancytopenia with a leucoerythroblastic blood film (myeloid precursors, nucleated red blood cells and tear drop red cells). HIV is also an important cause of cytopenias.
Medications - common medications may cause aplastic anaemia, such as chloramphenicol, azathioprine and sodium valproate. The history in this case did not have any recent medications introduced. The other very common cause of pancytopenia in modern practice would be in the context of chemotherapy.
Bone marrow disorders - tear drop cells are a key finding and clue in this case. They suggest an underlying bone marrow disorder and stress. In the context of a known active malignancy they are nearly indicative of bony metastases. Our patient did not have a known malignancy and there was nothing to suggest this on the history or physical examination, although in a man of this age metastatic prostate cancer should be considered. Other bone marrow disorders that would need to be considered are acute leukaemia (which was the diagnosis here), myelodysplasia and myelofibrosis. Splenomegaly would be especially significant in this case as it would be highly suggestive of myelofibrosis in combination with tear drop cells wit pancytopenia in an elderly patient3.
B12 and folate deficiency – this may cause pancytopenia, tear drop cells and leucoerythroblastic blood findings4&5. The mean corpuscular volume in this case however is normal which would somewhat argue against B12 and folate deficiency, as well as the fact that there were no hypersegmented neutrophils seen on the blood film. This cause is however very important given how it is easily reversible and treatable.
Haemophagocytosis – this is a bone marrow manifestation of severe inflammation and is a manifestation of systemic disease6. It has various causes including viruses (e.g. Epstein Barr virus), malignancy and autoimmune disease. It should be considered in patients with prolonged fever, splenomegaly and cytopenias. It is diagnosed by characteristic findings on bone marrow biopsy.
Paroxysmal nocturnal haemoglobinuria – this is a triad of pancytopenia, thrombosis and haemolysis caused by a clonal stem cell disorder with loss of membrane proteins (e.g. CD55 and CD59) that prevent complement activation7.
Genetic disease – Fanconi anaemia is a rare autosomal recessive disease with progressive pancytopenia, malignancy and developmental delay. It is caused be defects in DNA repair genes.
The key finding in this case was tear drop cells on the blood film. These are part of a leucoerythroblastic blood picture seen in bone marrow disease, malignant marrow infiltration, systemic illness and occasionally haematinic deficiency. See above for why this is unlikely to be haematinic deficiency. Although tear drop cells can occur in systemic illness such as severe infection, the history here was not in keeping with this. The diagnoses remaining therefore are malignant bone marrow infiltration or a primary bone marrow disorder (myelodysplasia, acute leukaemia or myelofibrosis). There were no features in the history pointing towards a metastatic malignancy and therefore primary bone marrow disorder is the most likely diagnosis. The diagnosis was later established as acute myeloid leukaemia on bone marrow examination.
What investigations would help to confirm or eliminate the possible diagnoses?
Blood tests including a clotting screen, liver function tests, inflammatory markers and renal function shall help to exclude other systemic disease such as disseminated intravascular coagulation, sepsis, liver disease and thrombotic thrombocytopenic purpura which may all give rise to cytopenias. Autoimmune screening may also suggest vasculitis which can cause cytopenias.
Microbiology studies including virology tests (e.g. human immunodeficiency virus, Epstein Barr virus and hepatitis viruses) may also be requested as appropriate given the clinical scenario and findings. Visceral leishmania should be tested for according to travel history and clinical likelihood. Leishmania may be identified through serology and light microscopy (for amastigotes) or polymerase chain reaction of the bone marrow aspirate. Tuberculosis could be cultured from the bone marrow is suspected.
Haematinics are a crucial test and the aim should be to try and withhold transfusion until these results are known in case they can easily be replaced thereby negating the need for blood products. Remember that if haematinics are not tested before transfusion then the blood products will confound the tests results.
Bone marrow biopsy, including aspirate and trephine are a crucial investigation for morphological examination and microbiological testing if indicated. This will distinguish the bone marrow disorders including acute leukaemia, myelofibrosis, bone marrow metastatic infiltration and myelodysplasia. Haemophagocytic syndrome may also be suggested by bone marrow examination findings.
Imaging if there is suspicion of an underlying malignancy (e.g. CT chest, abdomen and pelvis) and then further blood tests such as the prostate specific antigen. Ultrasound could also be used to check for splenomegaly where clinical examination has not been conclusive.
Medication review is vital as this may reveal the diagnosis (e.g. use of chloramphenicol)
Flow cytometry may be considered to investigate for an abnormal clone in the case of paroxysmal nocturnal haemoglobinuria and may be used on bone marrow samples to further evaluate the cells.
Unless a very clear cause for the pancytopenia is obvious (e.g. haematinic deficiency or malignant infiltration) then bone marrow examination is crucial for establishing a diagnosis. This will also prevent inappropriate treatments being initiated.
What immediate management steps and advice would be given to this patient?
General measures for pancytopenia include blood product support. Red cells and platelets can be given for symptomatic anaemia and bleeding. There is no need to transfuse platelets in the patient if there are no signs of bleeding. Alternatively he could also be treated with tranexamic acid as an alternative to avoiding risks associated with platelet transfusion. Infection should be treated urgently. Due to the neutropenia he should be advised to seek medical help if he develops a fever or sore throat. He should urgently be followed up in clinic with the results and given the contact details for the haematology department in the interim period in case he develops any problems.
The specific treatments for pancytopenia rests on the exact cause found after investigation. In this case the diagnosis was acute myeloid leukaemia arising from a background of myelodysplasia. The treatment for acute myeloid leukaemia in general, with curative intent, would consist of induction chemotherapy with DA (daunorubicin and cytosine arabinoside) followed by consolidation with further chemotherapy, the type of which (e.g. high dose cytosine arabinoside or FLAG-Ida) would depend on the risk assessment of the disease and possible consideration of an allograft bone marrow transplant after consolidation. Currently different approaches to consolidation chemotherapy, transplantation and small molecule inhibitors are being evaluated in clinical trial (e.g. AML 17 clinical trial).
The other options, in older more frail patients where high dose chemotherapy will be very toxic, are low dose palliative chemotherapy and support with transfusion.
PATIENT OUTCOME
He has been supported with blood products (platelets and packed red cells for bleeding and anaemia respectively). After discussion with him and his wife he has elected to have palliative chemotherapy with low dose cytosine arabinoside. He will be seen regularly in the haematology clinic and day unit for review. We do not suspect a link between the leukaemia and spinal bulbar atrophy.
Claiming historic triumph, that has defined his presidency ever since, President Barak Obama signed the $ 1 trillion Patient Protection and Affordable Care Act (in short called as ACA) in a highly visible white house ceremony on Tuesday March 23, 2010 (using 20 different pens) thereby establishing health care as a ‘right’ of every American for the first time. It took all the legislative and political skills from him to get the bill passed through both houses of Congress as was suggested on these pages previously.1
Soon after President Obama signed the landmark legislation, 26 States filed law suit contesting that the health care legislation, which earned the nickname of “Obamacare” from its opponents, was unconstitutional for several reasons. The legal challenge created significant uncertainty about the viability and future implementation of the legislation. There was also growing concern about the law’s impact on the national debt that became, and continues to be, an extremely divisive issue between the Democrats and the Republicans in the US Congress.
The law suit finally, as expected, made its way to the Supreme Court of the United States. The Court was looking at the legislation from three angles. First, at the core of the legislation, was the requirement that nearly all Americans obtain health insurance by 2014 or face a financial penalty- a provision that came to be known as the ‘individual mandate’ . The penalty would be recycled into “health exchanges” providing alternate options to low income Americans and small businesses for purchase of health care. The ‘individual mandate’ was the backbone of the legislation that wouldcover millions of uninsured Americans, majority of whom would be healthy young individuals. And, if this ‘individual mandate’ were to be struck down by the Court (as was expected by many), then the second question would be what happens to the rest of the ACA as insurance industry was supporting the legislation since it would provide them with tens of millions of new healthy ‘customers’. If such healthy individuals were left out, the pool would have mostly sicker individuals compromising the profitability, and perhaps the very viability, of the insurance industry. The third issue related to the mandate for the states to accept a large number of individuals into Medicaid program that provides health care for the poor and those with income of up to 133 % of the federal poverty level.2
The Supreme Court, mercifully for President Obama, upheld virtually the entire legislation in its historic decision on June 28, 2012. The four ‘liberal justices’ ( Justices Stephen Breyer, Ruth Ginsburg, Elena Kagan and Sonia Sotomayor) were joined by the conservative Chief Justice John Roberts in upholding the ‘individual mandate’. In what many observers of the court called a surprising twist, the justices held that the mandate was not constitutional under the ‘interstate commerce clause’, as argued by the administration, but was constitutional under Congress’ power of taxation. The other four dissenting conservative justices (Justices Samuel Alito, Anthony Kennedy, Antonin Scalia and Clarence Thomas) held that the Congress had exceeded its authority on several levels.
The reaction to the ruling was prompt and mixed. Dr. Jeremy A. Lazarus, President American Medical Association said “The AMA has long supported health insurance coverage for all, and we are pleased that this decision means millions of Americans can look forward to the coverage they need to get healthy and stay healthy”. The President and CEO of American Hospital Association, Mr Rich Umbdenstock, said “The decision means that hospitals now have much-needed clarity to continue on their path toward transformation”Perhaps the President of the American College of Physicians stated it best “We hope that a day will come when the debate will no longer be polarized between repeal on one hand, or keeping the law exactly as it is on the other, but on preserving all of the good things that it does while making needed improvements.”
The President of the U.S. Chamber of Commerce, Thomas J. Donohue, lamented that “While we respect the court’s decision, today’s Supreme Court ruling does not change the reality that the health care law is fundamentally flawed. It will cost many Americans their employer-based health insurance, undermine job creation and raise health care costs for all.” And in a scathing statement, the President of National Federation of Independent Business, Dan Danner, echoing the sentiments of a growing number of small businesses said “Under [the ACA], small-business owners are going to face an onslaught of taxes and mandates, resulting in job loss and closed businesses. We will continue to fight for the repeal of [the ACA] in the halls of Congress; only with [the ACA’s] full repeal will Congress have the ability to go back to the drawing board to craft real reform that makes reducing costs a No. 1 priority.” 3
This line of argument, apart from bringing some uncertainly, provided politicians fodder as they move closer to the Presidential elections. And as expected, the Republicans (who control the House of Representatives) passed legislation repealing the law but the bill died in the US Senate (controlled by Democrats). And the Republican Presidential candidate, Gov. Mitt Romney, framed the decision as a political call to arms. “What the Court did not do on its last day in session, I will do on my first day if elected President of the United States. And that is I will act to repeal Obamacare.” While both President Obama and Gov. Romney agree that Medicare costs have to be reined in but there is fundamental difference in their approach to cost cutting. President Obama’s plan relies on a powerful board to reduce payments to service providers and gradually changing how hospital and doctors are paid in order to eliminate fee for service and establish pay for performance (pay for the quality, not quantity). Gov. Romney would limit the amount future retirees would receive from the federal government to approximately $ 7000 (also called as Voucher System) and relying on the private industry to find an efficient solution.
It is clear that Gov. Romney, who previously implemented ‘Obamacare’ type of legislation as the governor of Massachusetts, flipped his position to appease extreme right wing of the Republican Party. As usual politics trumps policy. This drama continues to play out as we get closer to the election on November 6, 2012.
As identified by an independent nonpartisan educational institute based in Washington, The Centre for American Progress (CAP), some of the popular provisions of the law are 4:
The law provides for young adults to stay on their parents’ insurance to age 26 enabling 2.5 millionyoung Americans toenrol on their parents policies (73 % of young adults now have coverage as a result of this provision);
For seniors living on fixed income (Medicare patient population), one of the immediate benefits of the ACA was the closure of prescription drug coverage gap (known as the ‘donut hole’) saving 4 million seniors about$ 2 billion on prescription drugs or approximately $604 per person, in 2011 alone;
The law provides $11 billion to support and expand community health centres nationwide. More than 350 new community health centres were established in 2011 serving 50 million Americans in medically underserved areas;
Starting in 2014, the law prohibits health insurance carriers from excluding and/or denying coverage or charging higher premiums and limiting benefits to those with pre-existing medical conditions (as happens currently in too many cases);
50,000 Americans have already enrolled in the Pre-existing Condition Insurance Plan (PCIP) that ensures medical services including prescription drugs for those with pre-existing conditions as soon as possible ;
Provision of $200 million to expand school-based health centres for primary care, dental care, behavioural health services and substance abuse counselling;
In 2011 alone, 85 million Americans benefitted from preventive services included in the legislation. Many more will benefit since a major provision of the preventive services for women took effect in August 2012;
However, several components of the legislation remain unclear and their impact rather unknown. As an example the Obama administration fought hard for formation of the Independent Payment Advisory Board (IPAB) to address the inordinate influence of stakeholders in Congressional decisions over Medicare. This group of 15 nonpartisan experts is responsible for developing payment and related Medicare policy changes to assure that Medicare spending does not exceed budget targets tied to economic growth. Although now the law, the IPAB may never be formed because the Senate is unlikely to find 60 votes required to confirm IPAB members (unless the election brings unforeseen changes in the makeup of the Senate). Politics may again triumph policy. The payment approaches that need to evolve from “volume” to “value,” remain vexing. The Centre for Medicare & Medicaid Innovation charged with developing the pilot programs that may result in a reformed delivery system, have no pilots that focus on developing alternative models to reimburse physicianservices.5, 6
And the “invisible problem” of physician shortage! While there is growing bipartisan appreciation that the primary care workforce is insufficient to handle increasing demand for primary care services, the problem has not been fully addressed. The Association of American Medical Colleges estimates that in 2015 the country will have 62,900 fewer doctors than needed and those numbers will more than double by 2025. 7, 8
In coming months the States may become the battleground for implementing the “health exchanges”. By 2014 States are required to establish American Health Benefits exchanges and small business health operations program (SHOP) exchanges. These exchanges called in short, “health exchanges”, are basically subsidized market places with tax credits for consumers to shop for their health insurance at very competitive rates. Individuals who will not be eligible for Medicaid and with income of up to 400% of the Federal poverty level will have access to these health exchanges to purchase insurance. Such subsidies and tax credits will also be available to businesses with less than 100 employees. 9
It is also becoming apparent that the financial burden of the legislation will be significantly higher than initially estimated.For example the non-partisan Congressional Budget Office (CBO) estimates that 80 % of Americans who will face penalty for lack of health insurance under the ‘individual mandate’ would be those with yearly income of $ 55, 250 (for individuals) and $ 115, 250 (for couples). This is in contrast to the statements of President Obama who continues to pledge that he will not raise taxes on individuals making less than $ 200,000 and couples making less than $ 250, 000. And the Republican side of the Senate Budget Committee estimates that Obamacare will cost $2.6 trillion dollars in its first real decade since the bill does not fully go into effect until 2014. 10
Fortunately for President Obama, the prestigious Institute of Medicine released a report,last month on September 6, confirming what has been suggested by him and others, that the US health care system wastes almost 30 % ($750 Billion) each year on unnecessary procedures, fraud and waste. Therefore, the administration has redoubled its efforts to check the waste and fraud in order to pay for the cost of ACA. However, the real battle will begin as soon as the Congress reconvenes in January 2013. They are immediately faced with dealing with “Sequestration”. Originally a legal term referring to the act of valuable property being locked away for safe keeping by an agent of the court, the term has been adapted by Congress in 1985 for fiscal discipline. Under this rule, an amount of money equal to the difference between the cap set in the Budget Resolution and the amount actually appropriated is "sequestered" by the department of Treasury and not handed over to the departments it may have been appropriated originally by the Congress. The balanced budget act of 2011established a Congressional task force (called ‘Super Committee’) that was charged to make recommendations to cut the US Budget deficit by $ 1.5 trillion by November 23, 2011. Failure to do so would automatically trigger “Sequestration”. On November 21, 2011, the committee issued a statement that it had failed to reach agreement. This failure is viewed by most as a triumph of political ideology over genuine leadership. But the prospect of ‘sequestration’ has come to be seen so catastrophic that key members of Congress and the Presidentare expected to abandon brinkmanship and come to an agreement in early 2012.
So, as the drama and the debate continue vigorously in the days leading up to the November 6 elections, it is clear that “Obamacare” will continue to divide the US congress and the country. Irrespective of the party that will control the Congress and who becomes the next President of the US, “Obamacare” is here to stay. And, no matter how hard the Republican Party may try, they will face a monumental task in reversing the course of the history. There will be bickering, name calling, finger pointing and horse trading. But, the warring factions will realize that the escalating costs and complexities of the health care system demand that the legislators and the President come together to find real solutions to keep the American health care system as the best in the world. The real challenges will remain the same no matter who is elected as President: to stem the unsustainable tide of national health expenditure as percentage of the gross national product (rising from 7.2 % in 1970 to over 17 % in 2010), rapidly increasing number of Americans without health insurance (approaching almost 50 million), exploding national debt and, more immediately, the looming threats from sequestration.




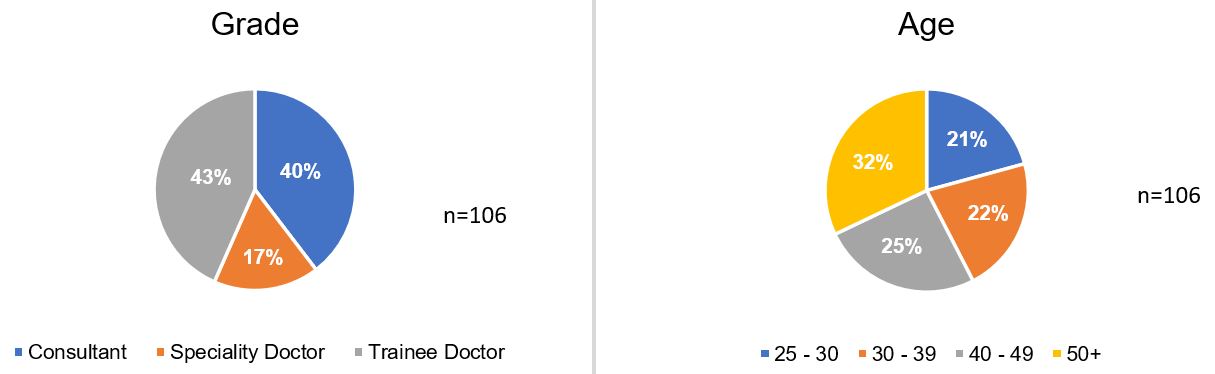
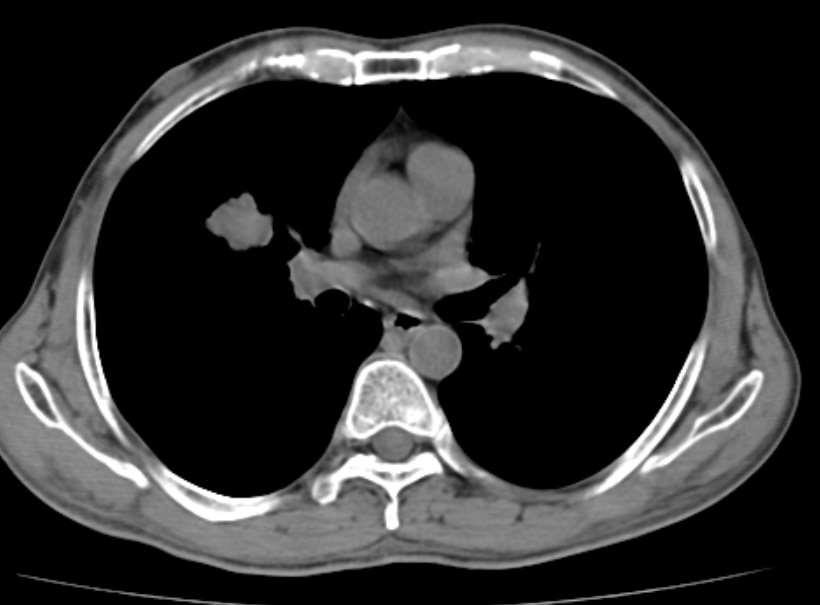
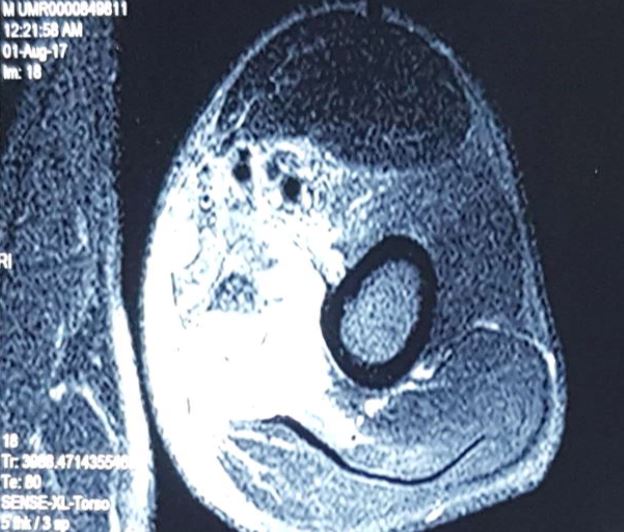
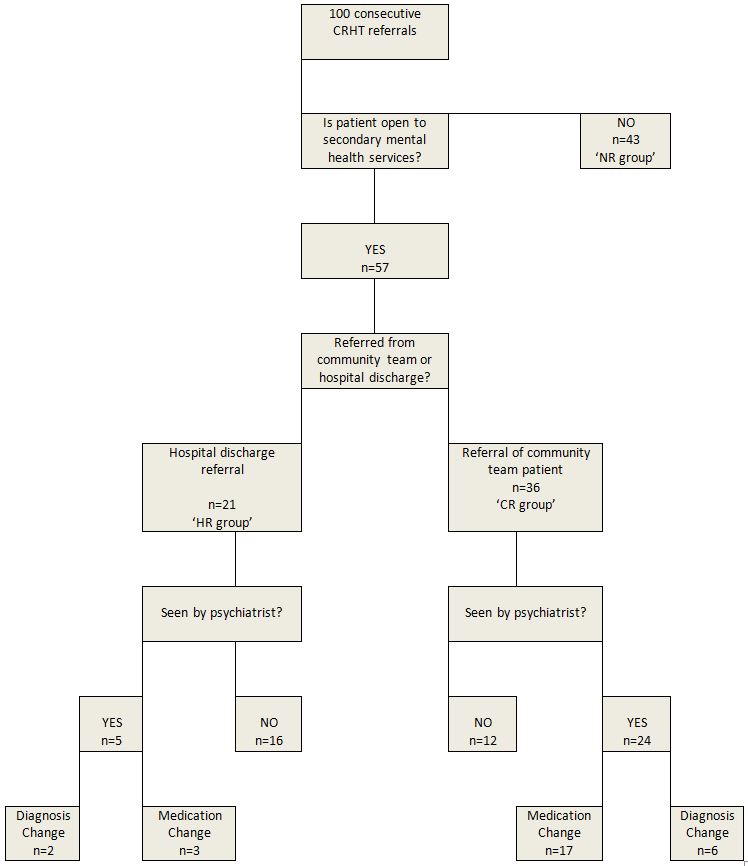
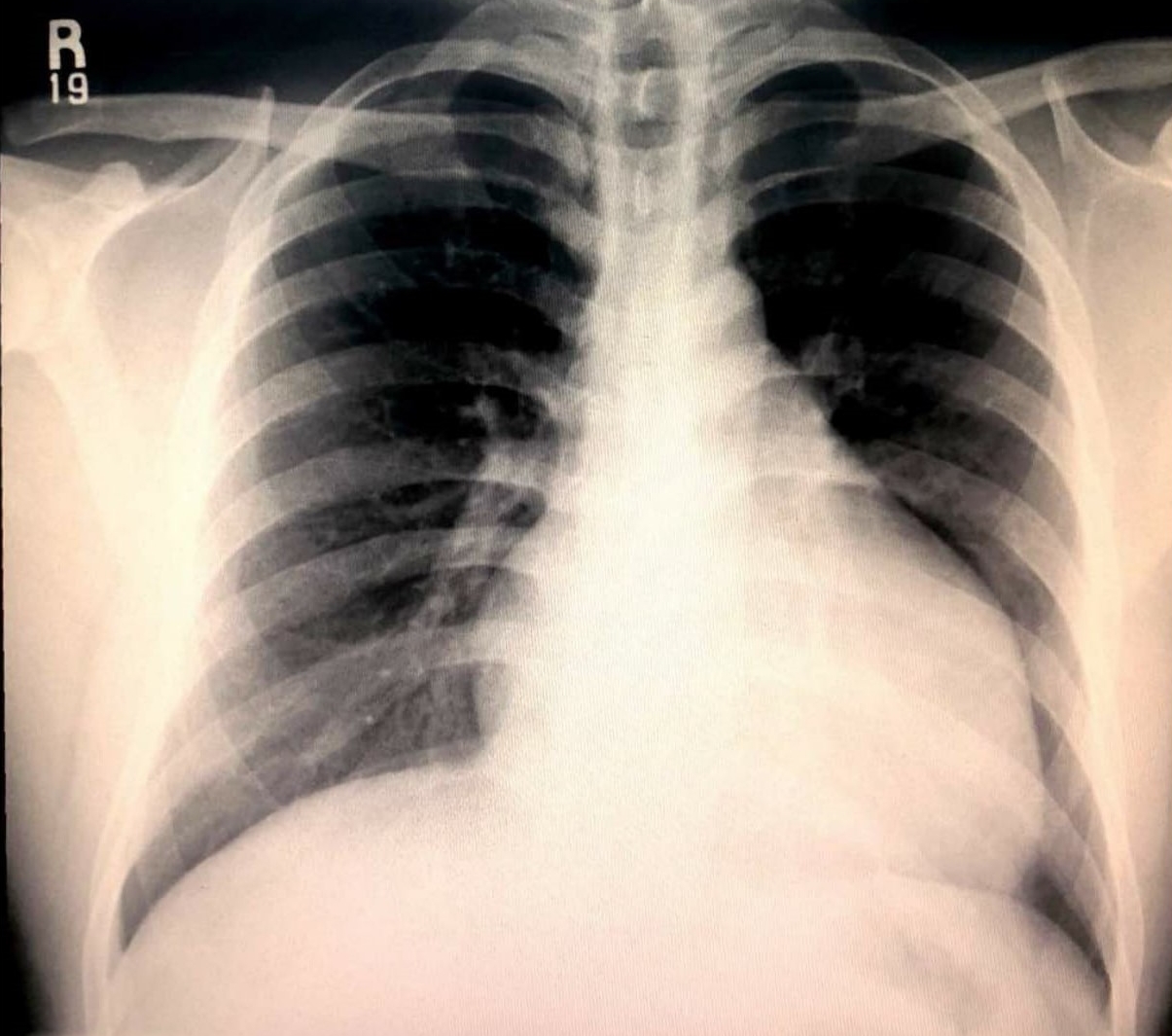
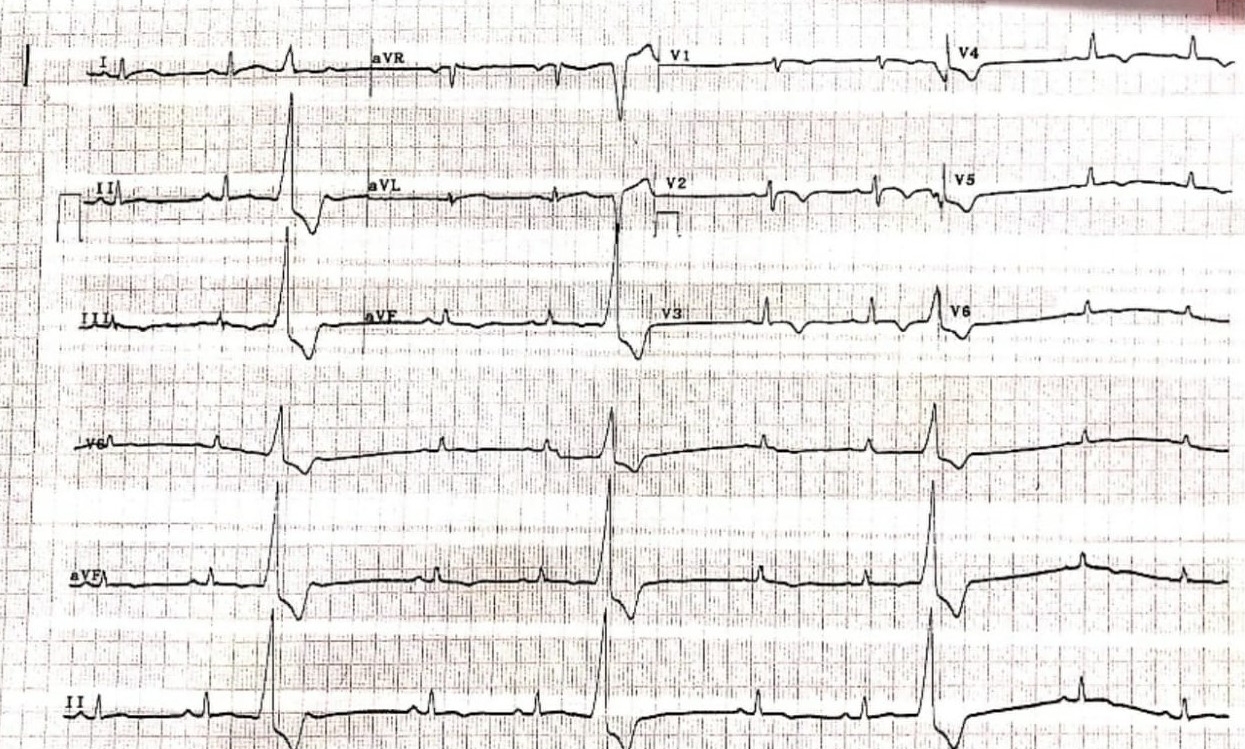
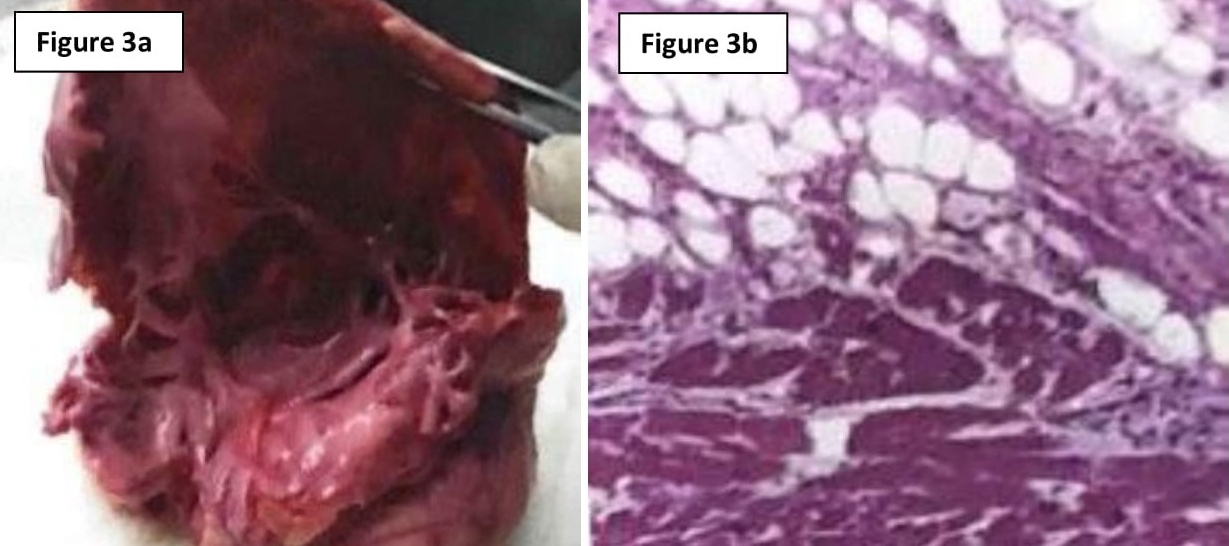
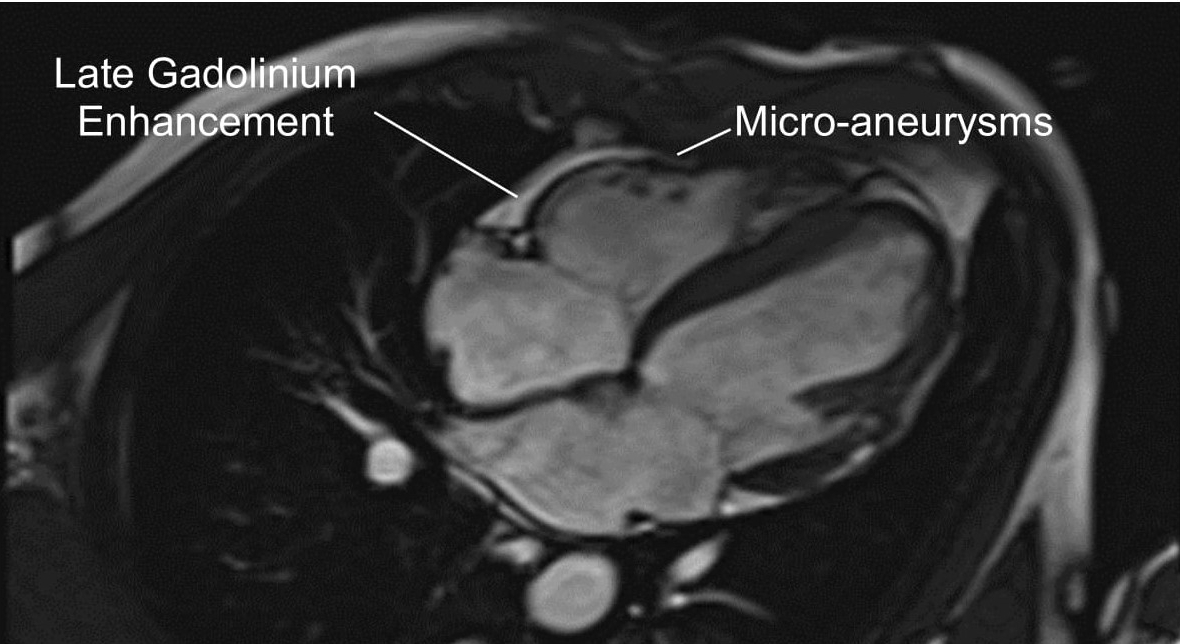

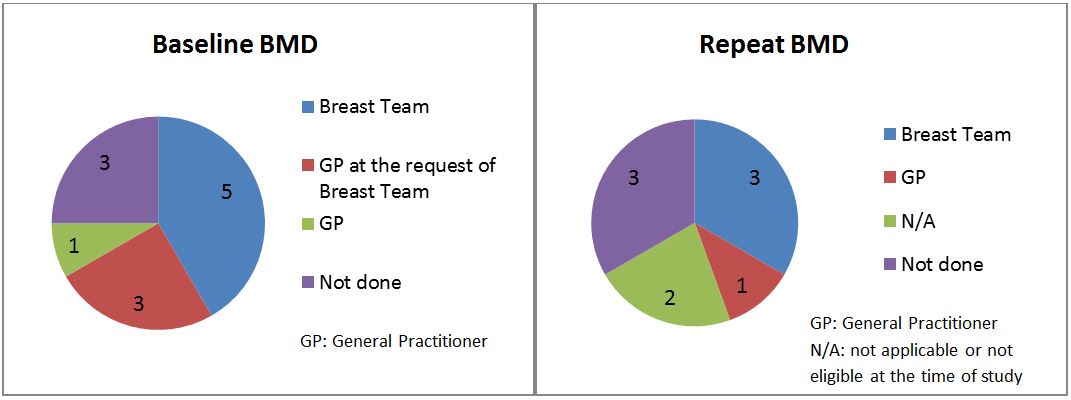





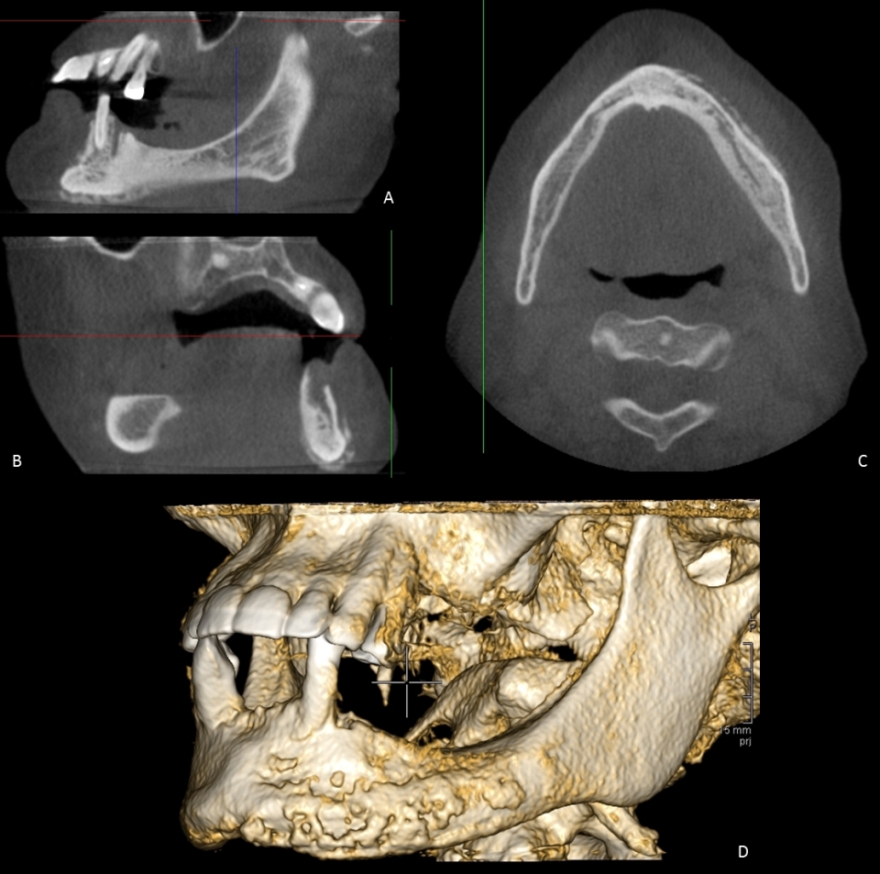

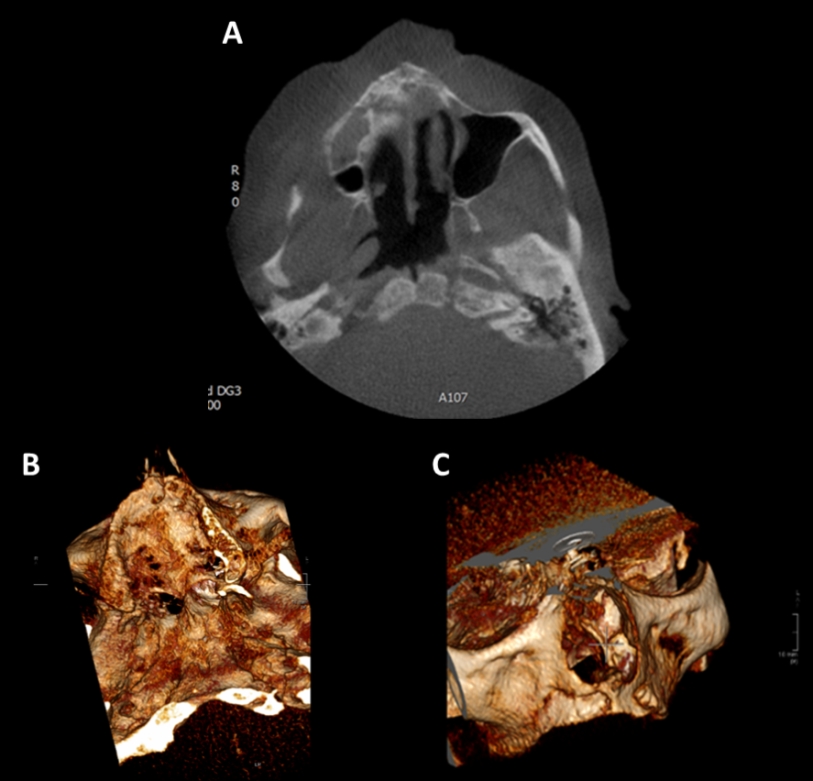

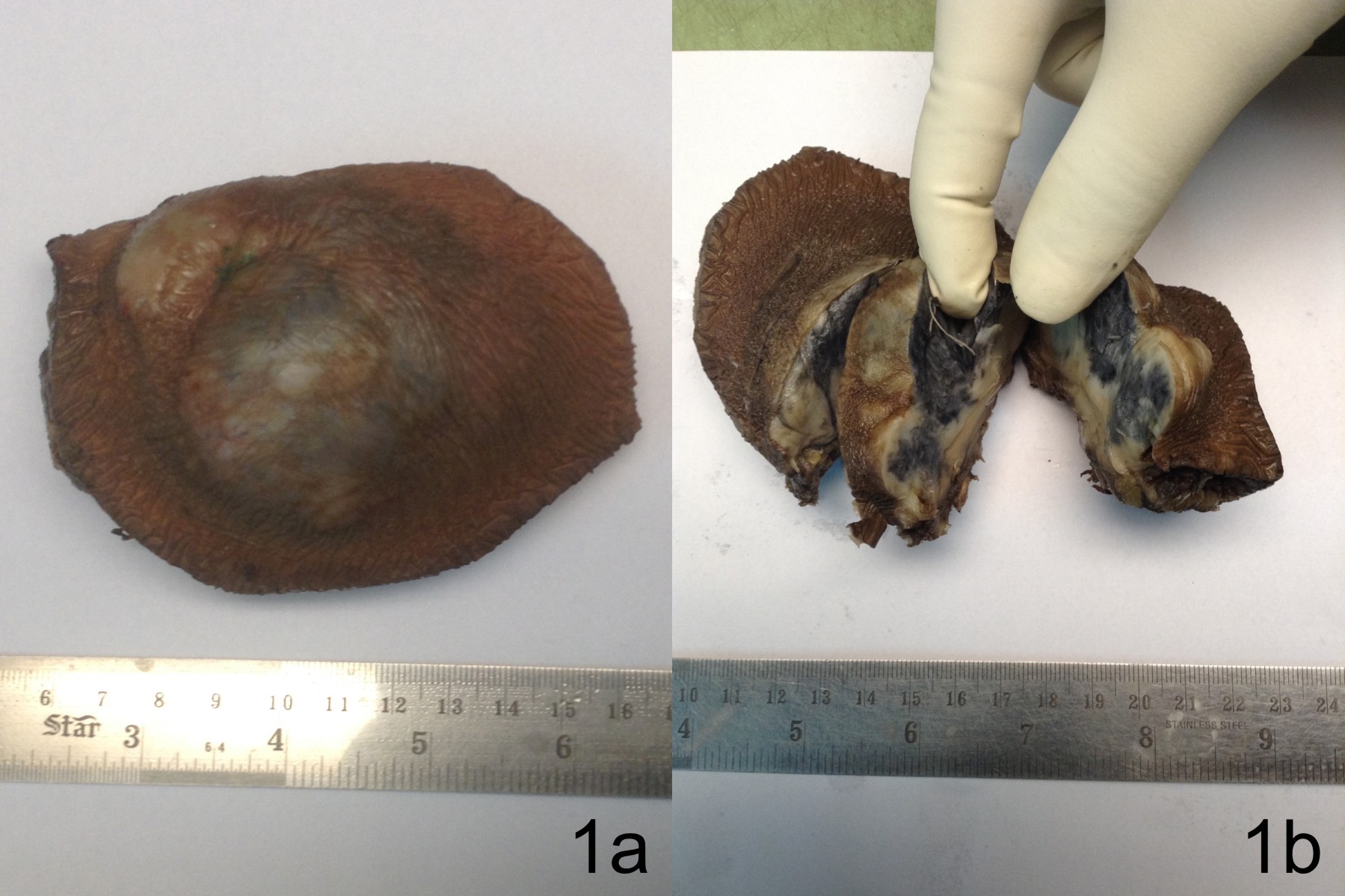
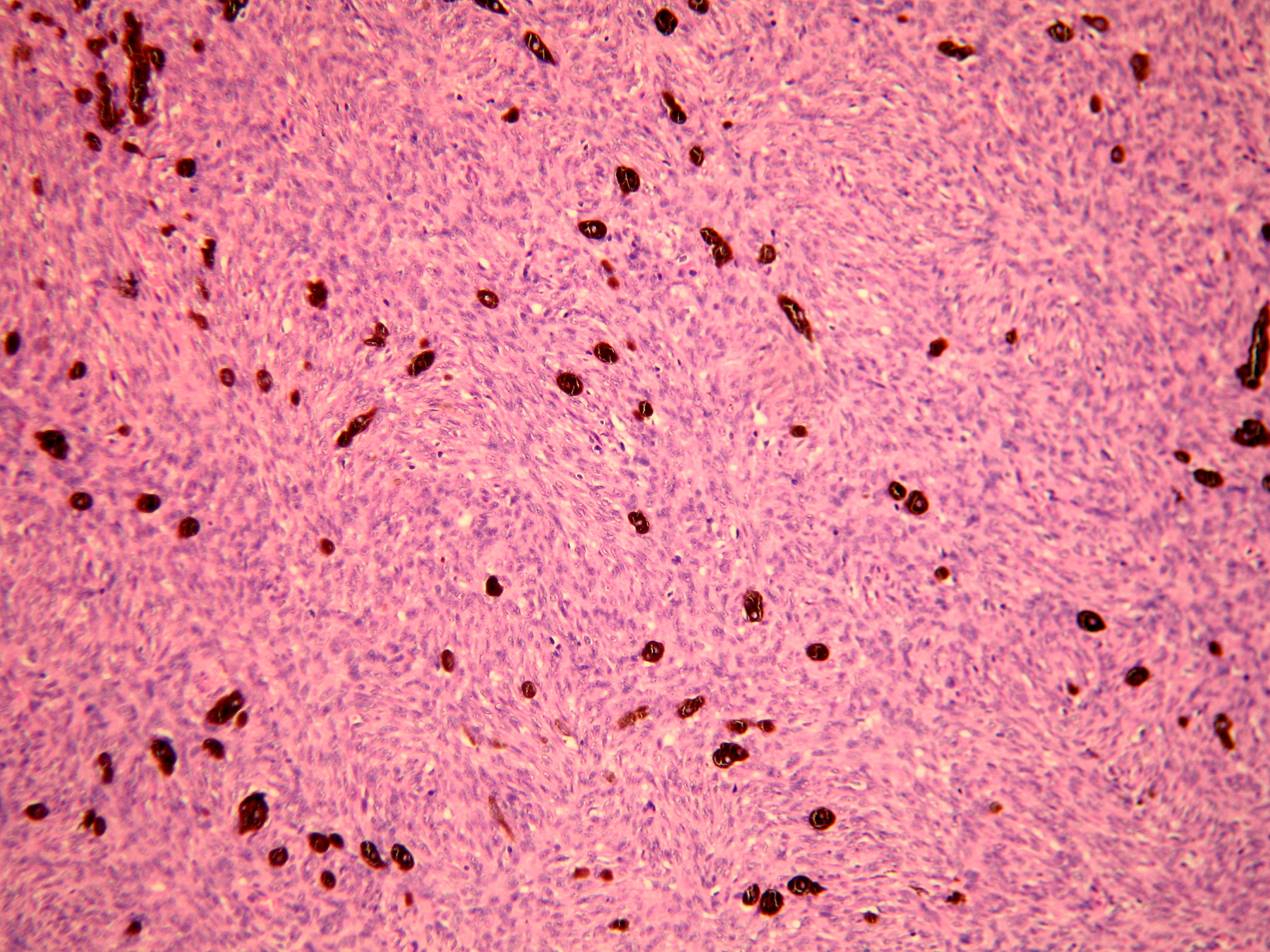
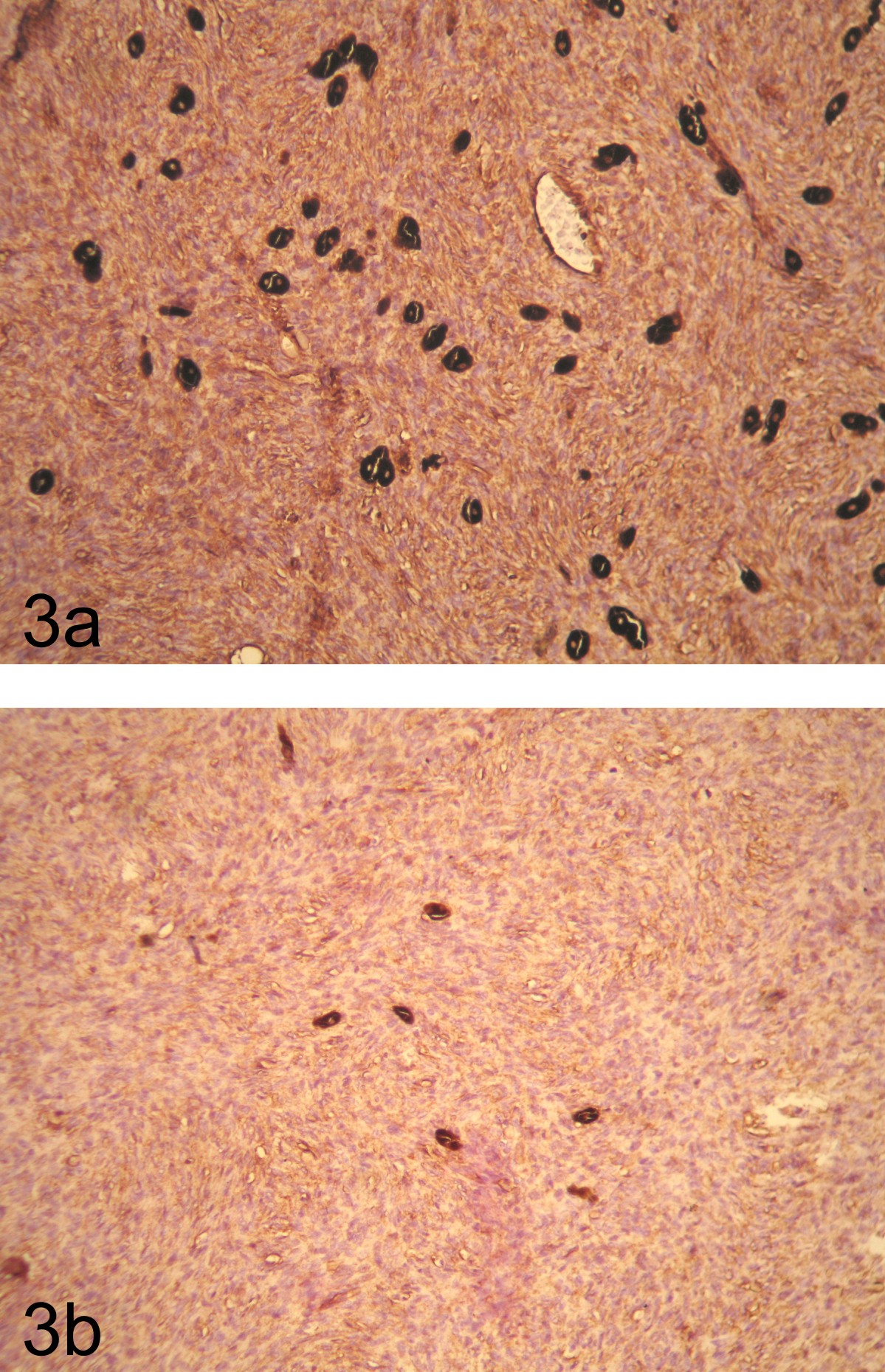
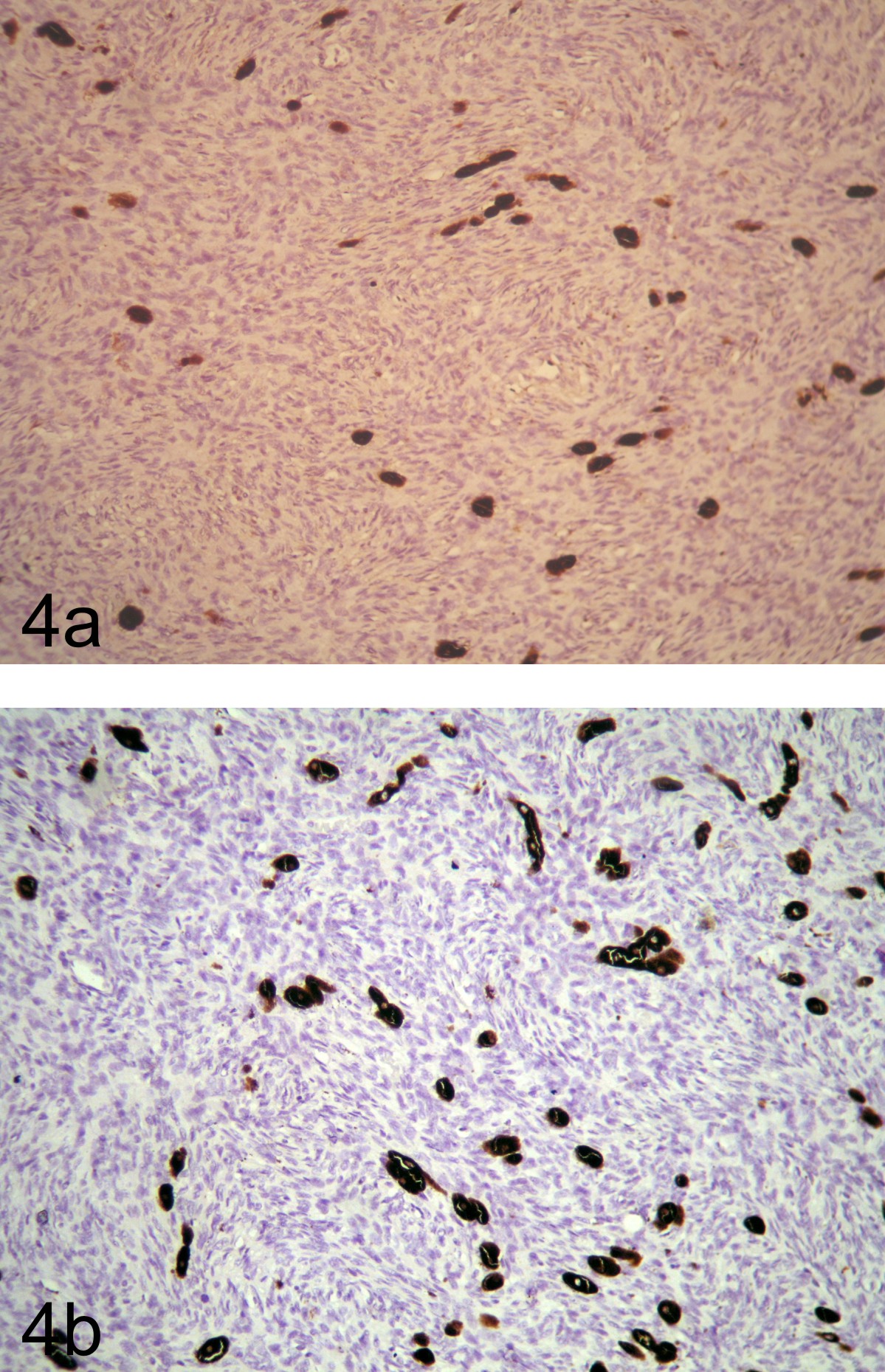
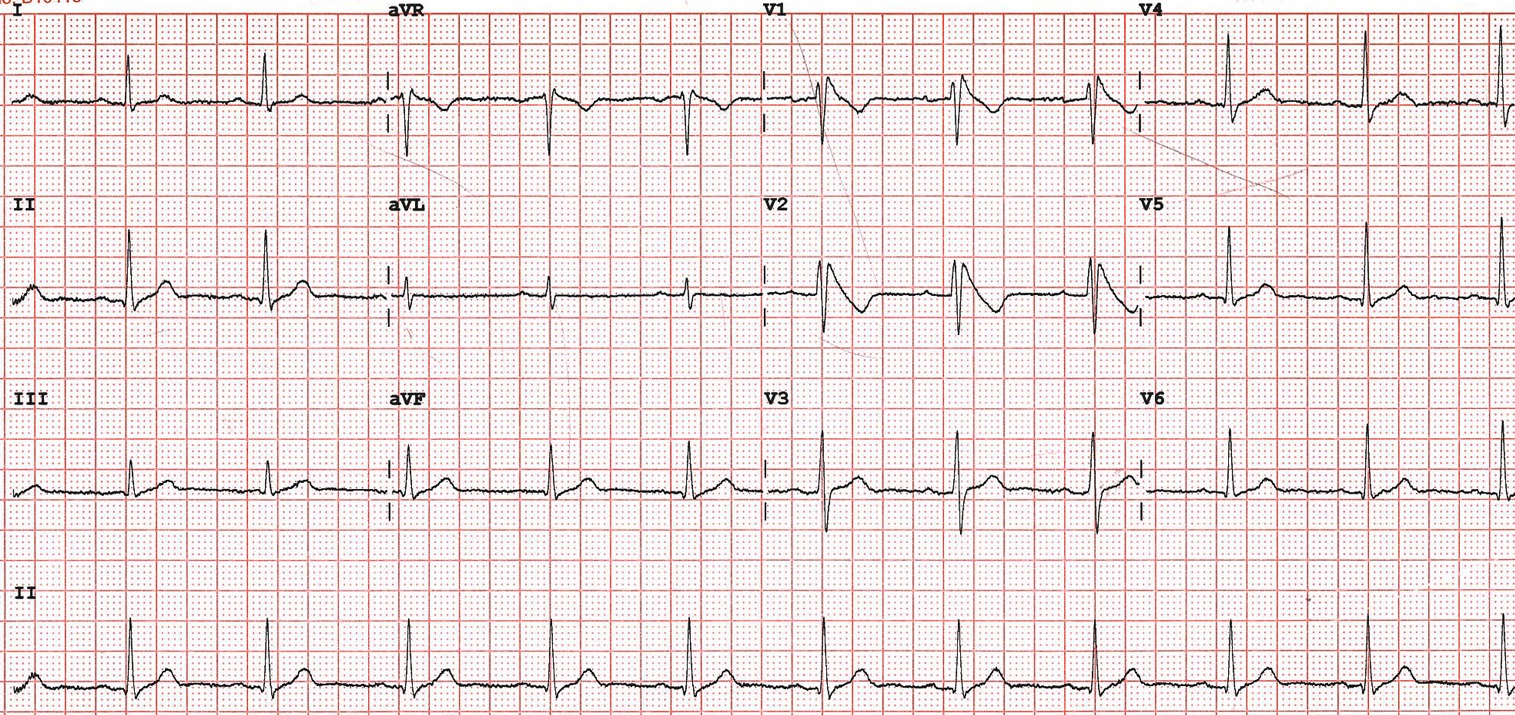
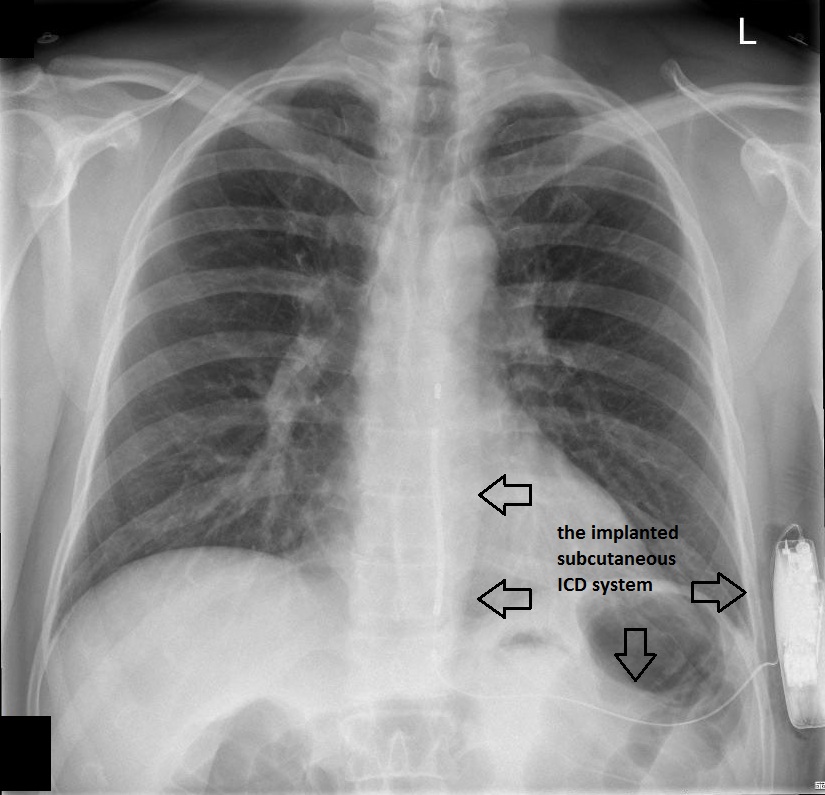
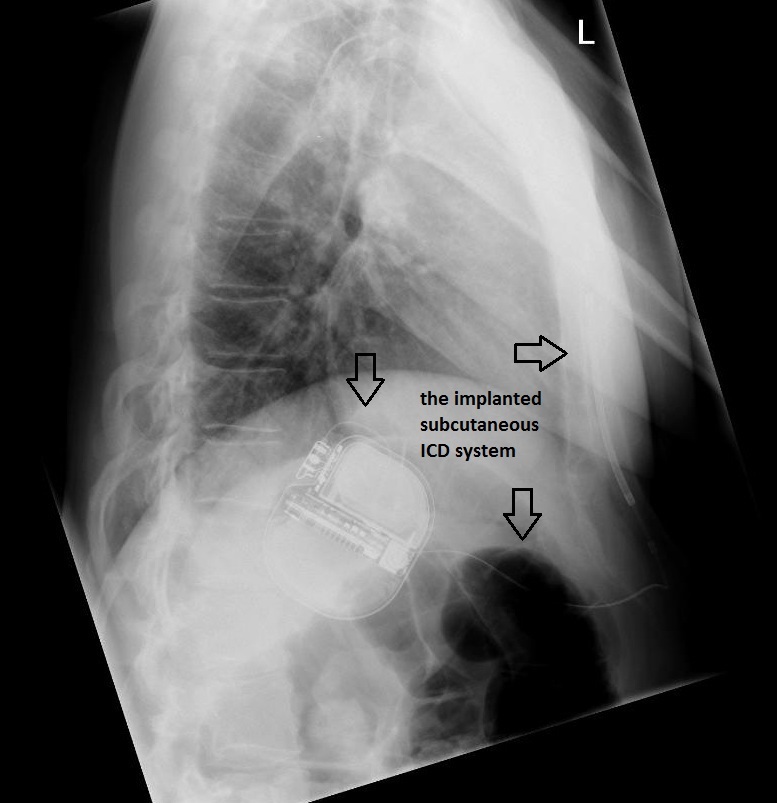
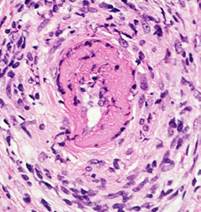
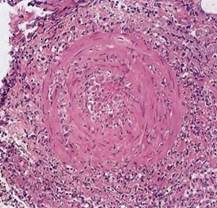

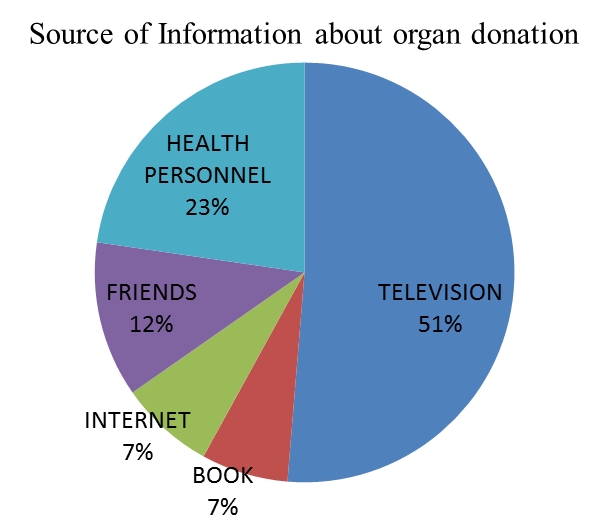
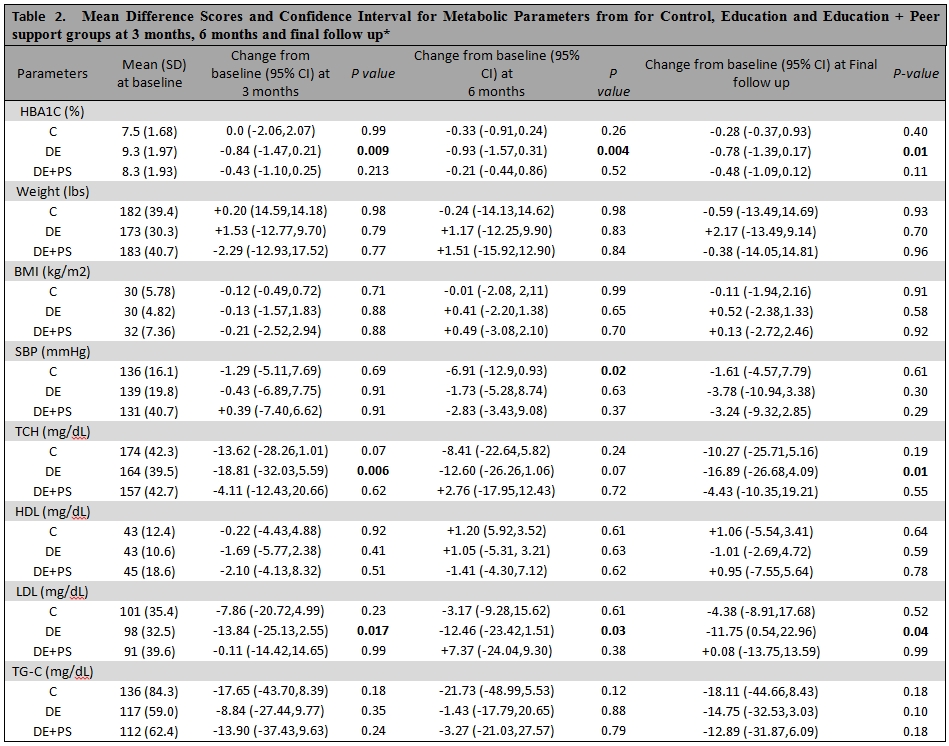
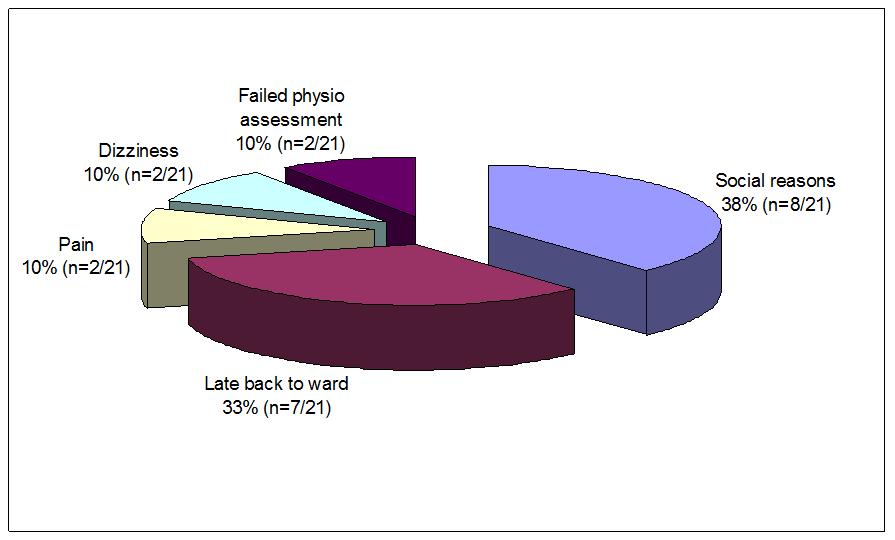
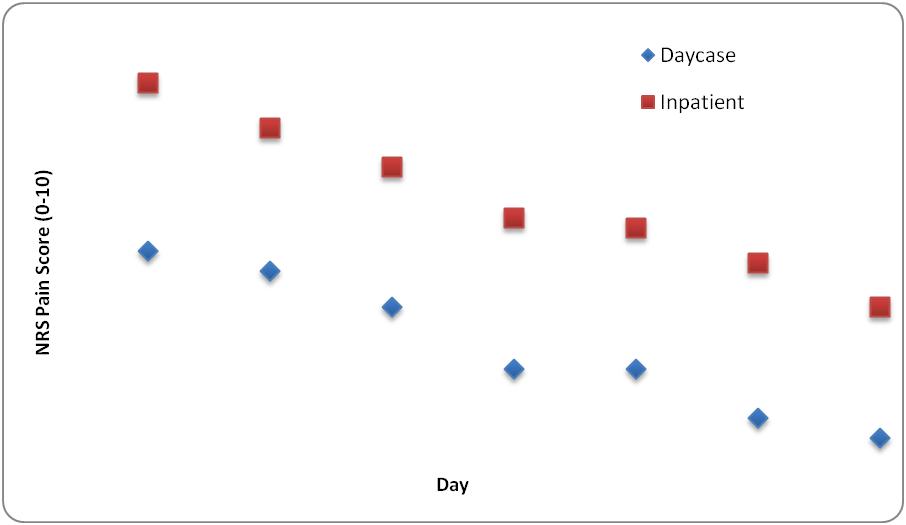
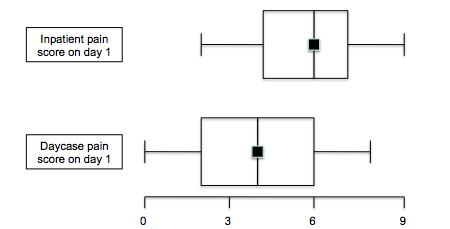
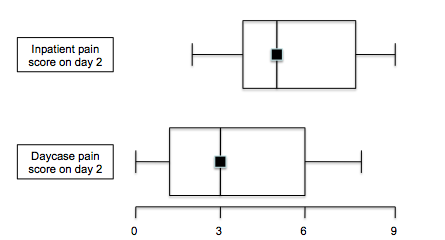
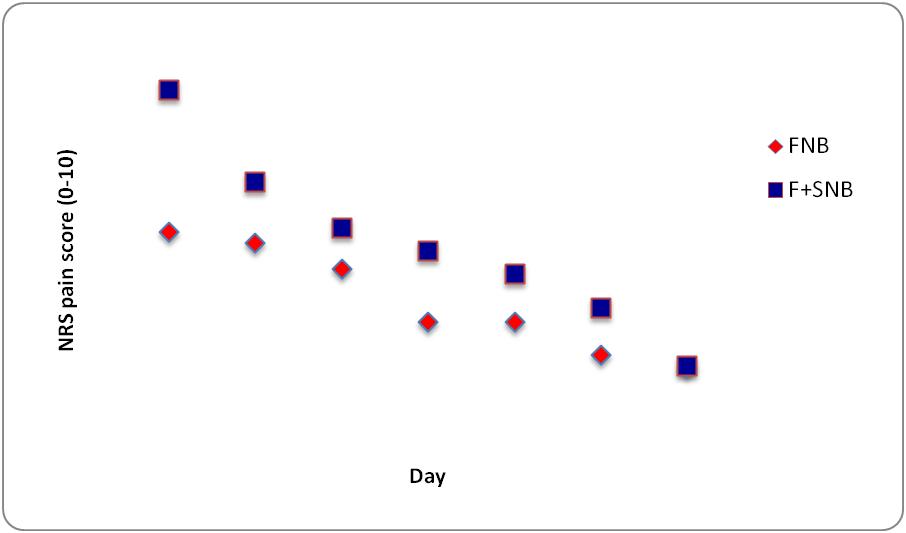
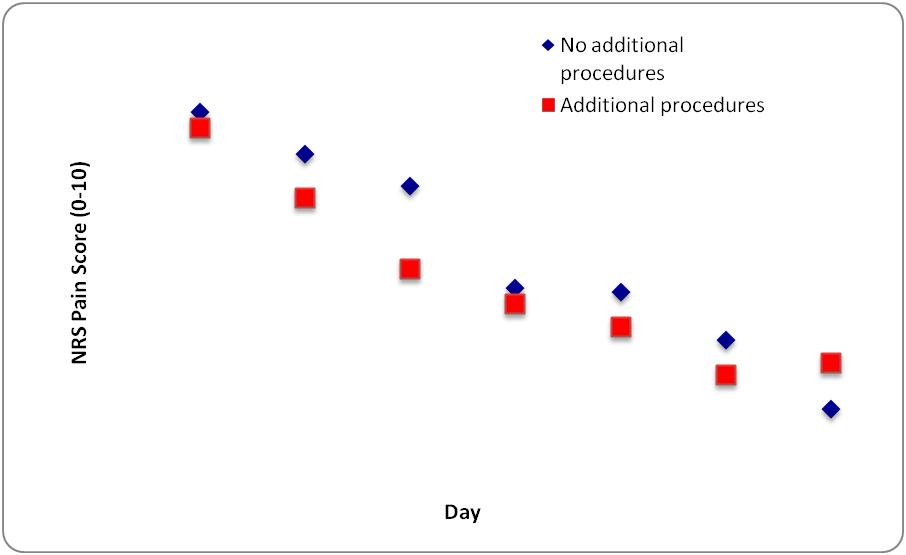


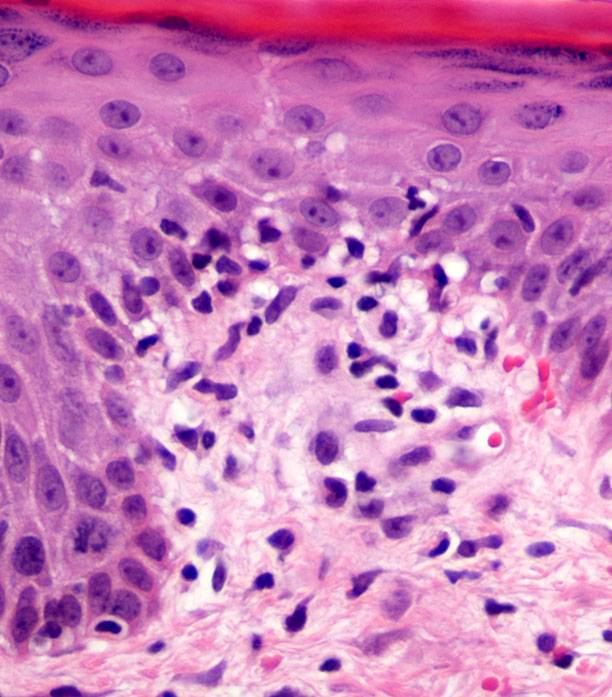

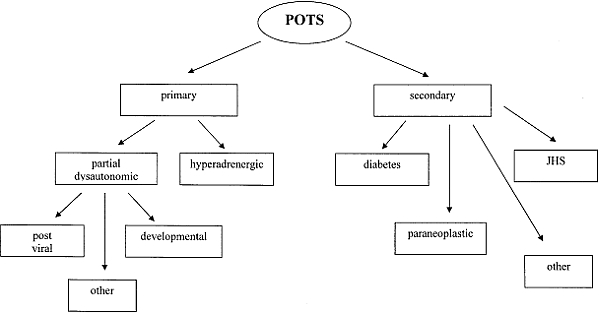

Browse the December 2010 PDF Booklet (Volume 3 Number 4)