



ISSN 1757-8515
Daycase Anterior Cruciate Ligament Reconstruction: Success, Pitfalls and Patient Pain Scores
Al-Amin Kassam, Peter Schranz, Vipul Mandalia
Cite this article as: BJMP 2013;6(4):a632
|
|
Abstract Daycase Anterior Cruciate Ligament (ACL) reconstructions with hamstring autograft have been undertaken in this trust for the last 6 months. Performing the procedure as a daycase potentially reduces the risk of infection and cancellation as well as reaching government targets for the performance of at least 75% of all surgical procedures as a daycase. We analysed our attempted daycase ACL reconstructions between April 2009 and October 2009. We assessed success of the daycase discharge as well as reasons for failed discharge. Patients’ pain scores were assessed for the week post-surgery and patient satisfaction with the daycase procedure was also documented. Daycase ACL reconstructions were attempted in 50 patients. Average age was 31.0 years and there were 36 males and 14 females in the cohort. 29 patients were discharged as a daycase and 21 patients required inpatient stay (38% social reasons, 33% late back to ward, 10% due to pain, 10% dues to dizziness and 10% due to failed physiotherapist assessment) Patients having daycase ACL reconstructions have significantly less pain from days 1-3 post-operatively (p=0.05) compared to inpatients. There is no significant difference (p=0.05) between different nerve blocks used (Femoral vs Femoral and Sciatic). No correlation was noted between increased pain and additional procedures performed at the time of the ACL reconstruction. 100% of patients claiming they were happy with the daycase procedure and 96.6% would agree to have the procedure performed as a daycase again. New protocol has been devised to allow daycase ACL reconstructions to be performed only in the mornings. Anaesthetic has been standardised with General anaesthetic and only femoral nerve block. Re-audit has shown that the majority of patients are now discharged as a daycase and patient outcome is improved. We conclude that daycase ACL reconstruction does not cause significantly increased pain and grants excellent patient satisfaction. There is no apparent difference in pain scores between patients having femoral nerve blocks and those having sciatic blocks added in. The procedure is safe and efficient and will continue to be offered in the trust. Keywords: Daycase, Cruciate, Ligament, Reconstruction, Pain, Satisfaction, |
Introduction
Anterior Cruciate Ligament (ACL) reconstructions are increasingly being undertaken throughout the United Kingdom (UK). Advances in General and Local Anaesthetic as well as surgical technique allow reconstructions as a day case procedure.1,2,3 There are currently no studies showing post-operative pain suffered by ACL reconstruction patients, nor showing the comparison of day case and inpatient pain scores.
We document, prospectively, patients’ post-operative pain after ACL reconstructions. We aim to identify and assess factors that affect pain post-ACL reconstructions including additional procedures, type of nerve blocks and whether the procedure was performed as a day case or as an inpatient.
We propose that patients having ACL reconstruction have no difference in pain scores when having the procedure as a day case compared to performance with inpatient stay. We also propose that additional procedures do not cause an increase in pain. We hypothesise that patients having Femoral nerve block have no increase in pain compared to patients having combined Femoral and Sciatic nerve block.
Method
All patients having ACL reconstruction between April 2010 and September 2010 were evaluated prospectively. Four strand arthroscopic hamstring reconstructions were performed by two specialist knee surgeons using a similar technique. Anaesthetic was performed by varying anaesthetists with a General Anaesthetic and Regional Nerve Block with Bupivicaine (Femoral nerve block or Femoral plus Sciatic nerve block). This was performed in the anaesthetic room under ultrasound guidance. Intra-operatively, patients received standardised anaesthesia. All patients received one dose of intravenous Paracetamol and two intravenous doses of opiates (Morphine or Fentanyl, as tolerated) at the beginning and end of the procedure.
Inclusion criteria used were all ACL reconstructions performed on patients over 16 years of age. No exclusion criteria were used.
Arthroscopic hamstring reconstruction was undertaken using a four strand Semitendinosus and Gracilis graft. During the arthroscopy, any additional procedures necessary were performed (e.g. meniscal repair, menisectomy, etc.). No drains were used. The knee was placed into an immobilisation splint until the nerve blocks had worn off.
Patients were discharged once they were back on the ward and deemed safe for discharge by the physiotherapists, medical and nursing staff. They were discharged with Paracetamol, a non-steroidal anti-inflammatory (if tolerated) and a mild opiate (Tramadol or Codeine Phosphate).
After discharge from the ward, patients were brought back to an aftercare clinic, with a senior physiotherapist, any time up to 48 hours post-operatively, to assess whether the nerve block had worn off, perform a wound check and to reinforce physiotherapy advice.
Patients were given a discharge questionnaire asking them to record their pain scores daily, when the pain was at its worst, using the Numerical Rating Scale (NRS) from 0-10. Documentation commenced on the day of the procedure and was requested daily for one week. Complications were also documented by the patient. These questionnaires were handed in at the two week follow up appointment, at which point patients were also asked if they would have the surgery performed as a day case again.
Pain scores were analysed using a Box-whisker plot followed by a Shapiro-Wilk W test which showed a non-parametric data spread. Scores were subsequently analysed using a Mann-Whitney U test to assess significance (p=0.05).
Results
ACL Reconstruction was attempted in 50 patients from April 2009 up to and including September 2009. The average age of patients was 31.0 years (Range 16-55). Of the cohort, there were 36 male patients with 14 females. All of the ACL reconstructions had a General Anaesthetic and all had infiltration of their graft site and medial wound with Bupivicaine. 42 had a Femoral nerve block with Bupivicaine and eight had a Bupivicaine Femoral and Sciatic nerve block. Of the 50 patients, 13 patients had additional procedures formed.
29 patients from the group were discharged as a day case. 21 patients required inpatient stay for the reasons documented in Figure 1 below.
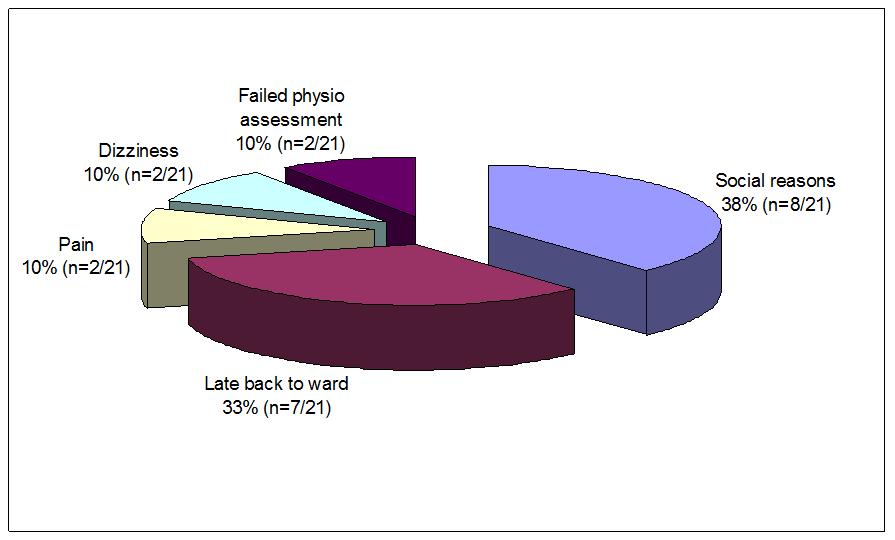
Figure 1. Reasons for inpatient stay after ACL reconstruction
Social reasons for inpatient stay included out-of-area patients and those who had no home support to care for them on the day of surgery. Patients who were unable to safely mobilise post-operatively were classified as having failed physiotherapist discharge assessment. Two patients were unable to be discharged due to excessive pain. Two patients had symptoms related to General Anaesthesia (e.g. nausea and dizziness) which prohibited discharge. Seven patients arrived back onto the ward with insufficient time for recovery and physiotherapy assessment, thus preventing day case discharge. In all seven cases, this was due to ACL reconstruction being performed late on the operating list.
On day one post-operatively the average NRS pain score for the day case group was 4.1, the average score for the inpatient group was 5.52. The pain score decreased steadily as the week went on. Pain scores on days one to four was statistically lower (p=0.05) in day case patients compared to inpatients (Table 1 and Figure 2). Figures 3 and 4 show the box whisker plots for inpatient vs day case pain scores on day 1 and 2.
| Post-operative day | Daycase Pain Score (N1=29) | Inpatient Pain Score (N2=21) | P Value (*=significant) |
| 1 | 4.1 | 5.52 | 0.03* |
| 2 | 3.93 | 5.14 | 0.04* |
| 3 | 3.62 | 4.81 | 0.03* |
| 4 | 3.1 | 4.38 | 0.03* |
| 5 | 3.1 | 4.29 | 0.09 |
| 6 | 2.69 | 4.00 | 0.03* |
| 7 | 2.52 | 3.62 | 0.06 |
Table 1. Average NRS pain scores of patients undergoing ACL reconstruction
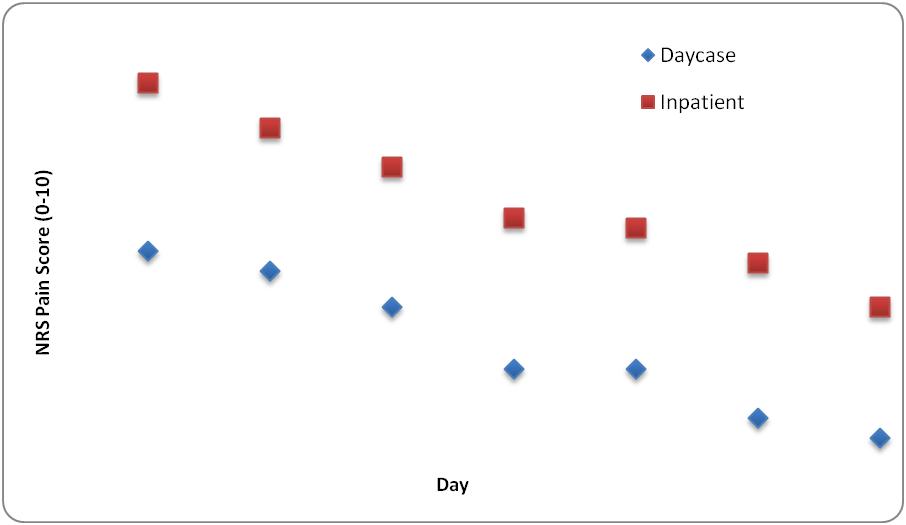
Figure 2. Comparison of NRS pain scores of day case and inpatient ACL reconstruction
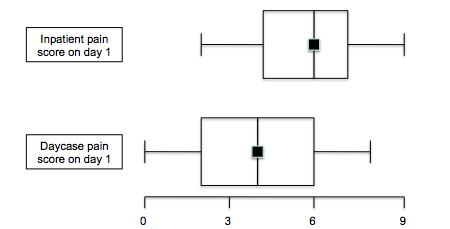
Figure 3. Box Whisker plots for pain scores on day 1 for inpatients and day case patients
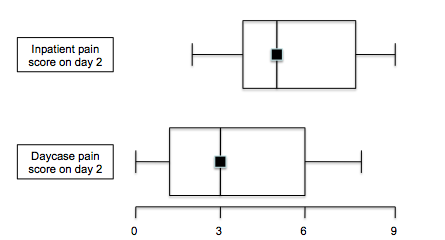
Figure 4. Box Whisker plots for pain scores on day 2 for inpatients and day case patients
Out of 50 patients, 42 patients had Femoral nerve blocks with the remaining eight patients having a combined Femoral and Sciatic nerve block. On average, patients receiving only a Femoral nerve block had lower pain scores compared to those receiving the combined block, although with the difference in cohort numbers, there was no statistical difference (p=0.09 on day 1 and p=0.5 on day 2) [Figure 5].
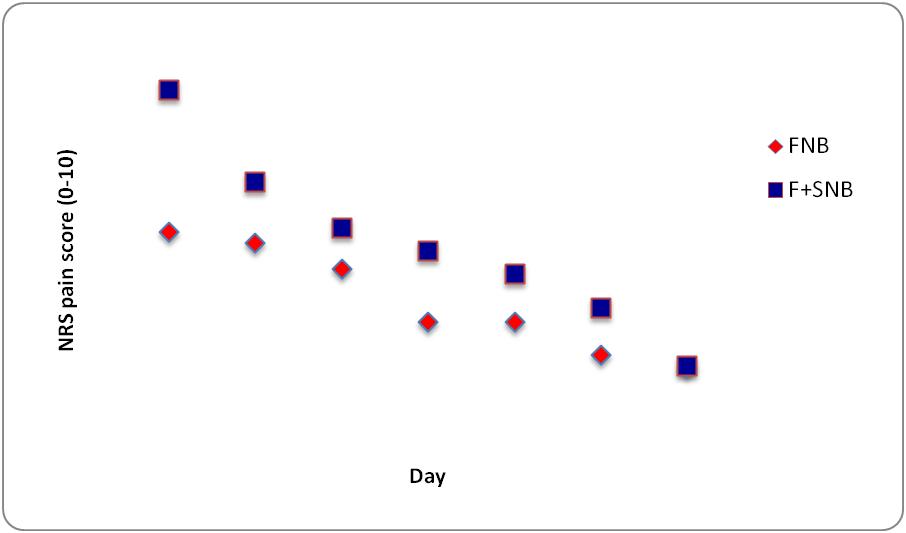
Figure 5. Comparison of daily pain scores with Femoral and Femoral/Sciatic nerve blocks
Of the 50 patients attempting the day case procedure, there were 17 additional procedures. Eight partial medial menisectomies, three partial lateral menisectomies, two lateral meniscal repairs, two medial meniscal repairs and two medial femoral condyle microfractures. There was no correlation identified between additional procedures and increased patient pain scores (Figure 6).
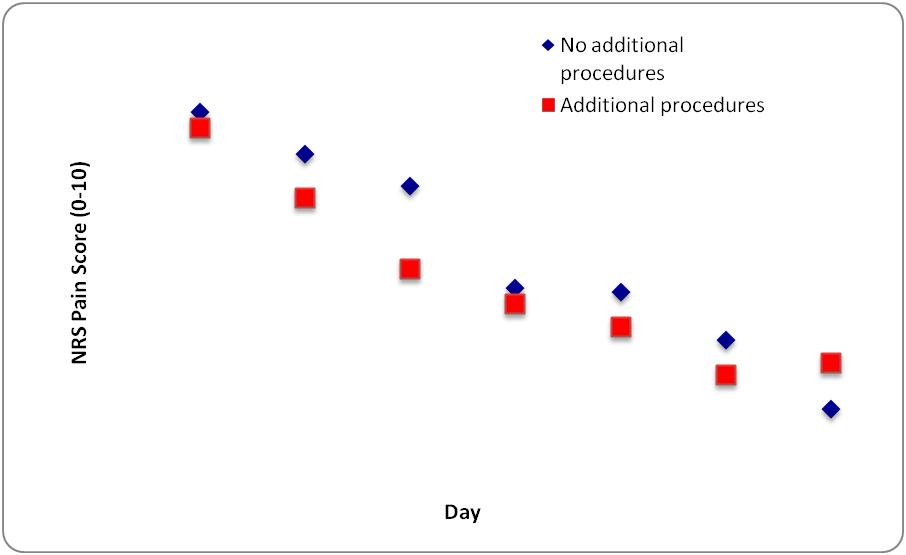
Figure 6. Comparison of pain scores of patients having additional procedures
When patient satisfaction among the 29 patients who had day case ACL reconstruction was asked, 100% were happy with the day case procedure. One patient felt that they would opt to have the operation done with an inpatient stay as they felt “groggy” overnight. They were otherwise happy with the day case procedure.
All patients had quadriceps function return at day 1 post-operatively and there were no re-admissions due to pain or being unable to cope at home. There were no infections amongst the groups.
Discussion
Day case ACL reconstructions are commonly undertaken in the UK. Literature from Sheffield, Glasgow and Romford1,2,3 shows that the rate of admission and complications is low and the procedure is safe and effective. It has been well tolerated by patients.
Day case surgery is encouraged by the government led Department of Health.3,4,5 It reduces the risk of cancellations and infections and can also have economic benefits for the National Health Service (NHS). In the United States (US), Bonsell has shown that a single day case ACL reconstruction saves the hospital $2234 compared to a procedure with an inpatient stay. Bonsell also proposed that day case ACL reconstructions are performed significantly quicker than inpatient reconstructions (approximately 23 minutes quicker) which could save the hospital $85000 per year.6
Day case patients were found to have statistically significant, lower pain scores compared to inpatients. Farrar et al have shown that, using the NRS pain scoring system, only a difference of greater than two points can be deemed clinically significant. However, the results of this study have shown that there is no clinical difference or worse pain when the procedure is performed as a day case.7 Krywulak et al noted that the average Visual Analogue Score (VAS) score for patients’ satisfaction post-day case ACL reconstructions was 85.1 compared to the inpatient average score of 78.2.8 This is validated in our study of which 100% of patients were happy with the day case procedure.
Patients were encouraged to take analgesia regularly for two weeks post-operatively but the amount of medication actually taken was not formally documented. This could potentially lead to some of the bias in this study. However, the significance of this bias is difficult to determine accurately as the NRS pain scores were recorded when the patients’ pain was at its worst. This would most likely be between analgesic doses so hopefully eliminating some of the bias.
Little is known about pain associated with the procedure of day case ACL reconstruction and also pain suffered compared to those undergoing inpatient stay. We have been able to compare pain scores of patients undergoing ACL reconstruction as a day case procedure with those undergoing the procedure as an inpatient. We found that patients having the procedure as a day case had significantly lower pain scores on days 1-4 post-ACL reconstruction compared to inpatients.
Day case ACL reconstructions are safe and not associated with any difference in pain compared to inpatient stays. This is important in pre-operative guidance given to patients and, in view of the risks of hospital inpatient stays and also additional costs to the Health Service and Primary Care Trust (PCT), ACL reconstruction as a day case procedure should be highly recommended to patients compared to an inpatient surgical procedure.9-11 Information can be given to patients advising them that pain will not be worse when the procedure is performed as a day case which will encourage more patients to accept same day discharge.
Further work needs to be done to assess the possible difference in pain scores associated with Femoral nerve blocks compared with combined Femoral and Sciatic nerve blocks but our results appear to show that significant difference is unlikely.
Patient satisfaction with the day case ACL procedure was excellent and subsequently day case ACL reconstruction is now routinely performed in this Trust.
|
Competing Interests None declared Author Details AL-AMIN KASSAM, MRCS, BSc(Hons), MBBS. Exeter Knee Reconstruction Unit, Royal Devon and Exeter NHS Foundation Trust, Barrack Road, Exeter, UK. PETER SCHRANZ, FRCS (Trauma and Orth), Exeter Knee Reconstruction Unit, Royal Devon and Exeter NHS Foundation Trust, Barrack Road, Exeter, UK. VIPUL MANDALIA, FRCS (Trauma and Orth), Exeter Knee Reconstruction Unit, Royal Devon and Exeter NHS Foundation Trust, Barrack Road, Exeter, UK. CORRESPONDENCE: AL-AMIN KASSAM, Exeter Knee Reconstruction Unit, Royal Devon and Exeter NHS Foundation Trust, Barrack Road, Exeter, UK, EX2 5DW. Email: akassam@doctors.net.uk |
References
- Shaw AD, DiBartolo G, Clatworthy M. Daystay hamstring ACL reconstruction performed under regional anaesthesia. Knee. 2005; 12: 271-273
- Talwalker S, Kambhampati S, De Villiers S, booth R, Lang-Stevenson. Day case Anterior Cruciate Ligament Reconstruction: A study of 51 consecutive patients. Acta Orthopaedica Belgica. 2005; 71:309-314
- Kumar A, Bickerstaff DR, Johnson TR, Appleton DFJ. Day surgery anterior cruciate ligament reconstruction: Sheffield experiences. Knee. 2001; 8: 25-27
- Kao JT, Giangarra CE, Singer G, Martin S. A comparison of outpatient and inpatient anterior cruciate ligament reconstruction surgery. Arthroscopy 1995; 11: 151–6.
- Department of Health. Day Surgery: Operational Guide. August 2002 www.dh.gov.uk
- Bonsell SW. Financial analysis of anterior cruciate ligament reconstruction at Baylor University Medical Center. Proceedings (Baylor University Medical Center). 2000; 13(4):327-330
- Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2005; 94(2):149-158
- Krywulak Sa, Mohtadi NG, Russell ML, Sasyniuk TM. Patient satisfaction with inpatient versus outpatient reconstruction of the anterior cruciate ligament: a randomized clinical trial. Canadian Journal of Surgery. 2005; 48(3):201-206
- Acute hospital portfolio – review of national findings. Day Surgery Audit Commission 2001
- Day surgery – Report by the Day Surgery Task Force. NHS Management Executive (Department of Health) September 1993
- A short cut to better services – Day surgery in England and Wales Audit Commission 1990

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.