Sjögren’s syndrome (SS) is an autoimmune exocrinopathy characterised by a lymphoplasmacytic infiltration of the exocrine glands. Both xerophthalmia and xerostomia are the most common manifestations of the disease. However serious organ damage such as, pulmonary and neurological involvement, can occur. The prevalence of neurological manifestations of SS varies between 0% and 70% (average 20%), which is largely dominated by peripheral neuropathies¹. The cranial nerve involvement, especially when it is isolated, represents a rare facet of the peripheral neuropathy.
Observation
We report the case of a 62-year-old patient with no medical history, referred to the internal medicine department with a 6 years history of dry mouth and xerophthalmia. No other complaints were reported.
The mouth examination showed a fissured, smooth and left deviated tongue without evidence of atrophy or fasciculation (figure 1). The rest of the oropharyngeal examination was unremarkable with no angina or cervical lymphadenopathy. Neurological examination confirmed a deficit of the right XII cranial nerve and excluded other cranial nerve involvements, sensibility or motility deficit. A specialised ophthalmologic examination was performed and showed a bilateral superficial punctuate keratitis.
The search for antinuclear antibodies by indirect immunofluorescence was positive at the titre of 1/1280 (speckled) corresponding to Anti-SSA and Anti-SSB antibodies. Cryoglobulinemia search was negative.
The rest of the laboratory investigations (blood cell count, liver and renal function tests, thyroid balance and inflammation markers) were normal.
A labial salivary gland biopsy was performed and its histological examination showed a lymphoid cell cluster of more than 50 cells/ 4 mm² corresponding to a focus score 1.
Brain MRI was normal - no damage in the brain stem was seen. Electromyography was normal.
The diagnosis of SS was made according to the presence of five out of six criteria according to the European American study group. The diagnosis of primary SS was retained due to the lack of clinical or biological argues for an associated autoimmune disease. A symptomatic treatment of Sicca syndrome was prescribed but no specific therapy has been initiated for the hypoglossal nerve attempt because of its asymptomatic nature.
Discussion
In the case of our patient, the tongue deviation was discovered at physical examination and was totally asymptomatic. In other cases, the twelfth nerve palsy could be responsible for swallowing difficulties, and in advanced stages for a lingual or hemi lingual amyotrophy. The spectrum of its aetiologies is numerous. In a large case series of 100 patients, malignant tumors (about half of cases), neurological causes (16 %) and post-traumatic palsy (12% of cases) were the three most popular aetiologies². Other conditions could be associated with twelfth nerve palsy, such as, infections², vascular injury³ and non-invasive oxygen therapy⁴. Paroxysmal idiopathic hypoglossal nerve palsy has also been described⁵. Our patient had Sicca syndrome which was related to SS according to 5 criteria of the European American study group: it was a subjective sensation of dry mouth and dry eyes associated to a bilateral punctuated keratitis, a focus score > 1 at the histological examination of the salivary gland biopsy and positive anti-SSA and anti-SSB⁶.
SS is an autoimmune disease that often presents as dry eyes and dry mouth due to lacrimal and salivary gland involvement. It can be primitive or associated to other autoimmune diseases such as, Hashimoto’s Thyroiditis, Rheumatoid Arthritis or Systemic Lupus Erythematosus. Wide varieties of neurological complications are characteristic features of SS which occurs most frequently in the primary form. Peripheral neuropathy is the most frequent neurological manifestation. Its most common presentation is a symmetrical sensorimotor or pure sensory neuropathy of hands and feet. Sensitive neuropathy, small fiber neuropathy, multiple mononeuropathy and polyradiculoneuropathy have also been described¹. Cranial nerve involvement is rare. In a review of the literature, Colaci M found 267 patients suffering from SS with different types of cranial neuritis during their clinical history. The discovery of cranial neuritis was contemporary to SS diagnosis in 40% of the patients, as in the case of our patient.
Optic neuritis and trigeminal nerve injury were the most frequent attempts and represent respectively 46.4% and 38% of all cranial nerve palsies. All cranial nerves palsies have been described except the eleventh⁷. Involvement of the twelfth cranial nerve is very rare and only two cases have been described⁸′ ⁹. In these two cases, it was associated with an involvement of other cranial nerves (table 1). To the best of our knowledge, this is the first report of an isolated and permanent involvement of the twelfth cranial nerve in a patient with primary SS. Many mechanisms were proposed to explain the cranial nerve involvement in SS. Clinicopathological observations of Mori K⁸ suggest that an isolated trigeminal nerve attempt could be explained by an immune-mediated neuron death in the sensory gasser ganglion. Whereas, other cranial nerve involvements which are frequently associated together could be explained by a multiple mononeuropathy resulting from a vasculitis⁸.
Further clinical observations will be necessary to determine the exact mechanisms of such neurological involvement.
Table 1: Review of the literature regarding SS patients with hypoglossal nerve injury
Number of patients
Age
Nerves
involved
Treatment
Evolution
Mori/2005 [8]
1
No data
V, VII, IX, X, XII
No data
Paroxysmal
Ashraf/2009 [9]
1
47
V–IX–XII
No data
Paroxysmal
Our patient
1
62
XII
None
Permanent
Figure 1: Smooth and left deviated tongue
Conclusion
In front of cranial nerves neuritis, we should actively search for sicca syndrome, sometimes not spontaneously reported by patients. Examination of the mouth can be instructive and should not be omitted in the diagnosis and monitoring of Sjögren’s syndrome.
In the UK, all newly graduated doctors spend their first two years of work rotating between different specialities, usually spending four months in each placement, before applying for speciality training. This period is called the Foundation Programme.
In January 2016, the Royal College of Psychiatrists published its first ever strategy on Broadening the Foundation Programme to address the need to improve the psychiatric training experience for foundation doctors. The strategy’s aim is to “ensure the delivery of a high-quality training experience in all psychiatry foundation placements”.1
Over the last few years, the number of Foundation training posts in psychiatry in England and Wales has significantly increased. Health Education England aims that all Foundation doctors should rotate through a community or an integrated placement (psychiatry is considered as a community placement) from August 2017.2
As such, the College highlights the need to provide a supervised and well-structured psychiatric training experience for Foundation doctors. This aims not only to improve recruitment into psychiatry but also to ensure doctors have a good working knowledge and understanding of psychiatry and psychiatric services, no matter what career they pursue.
Mentoring provides an additional support and therefore can be helpful to improve the placement of Foundation doctors in psychiatry.
We implemented an ambitious mentoring scheme in Norfolk and Suffolk NHS Foundation Trust (the seventh largest mental health trust in the UK). The paper describes its essential component together with a brief review of the literature on mentoring in clinical settings, focusing on Foundation placements.
Why is mentoring is needed for Foundation doctors in psychiatry?
The literature on mentoring for medical professionals draws attention to the idea that it is beneficial to all doctors at all stages of their career to experience mentoring in some form or another. However, mentoring is of particular importance to doctors moving to a new job or organisation 3, thus making it highly relevant to Foundation trainees.
For newcomers, most of the mentoring support will focus on helping them settle into their new role, becoming familiar with, and developing an understanding of the expectations of their employers.4
Evidence shows that the quality of care in any organisation can be improved when clinical leaders support time for activities such as reflection, coaching and mentoring 5.
Most Foundation doctors will lack experience in psychiatry and will need a substantial amount of guidance from their supervisors and their teams.6 Research has shown that the transition from student to doctor is a difficult one and can be associated with significant levels of emotional stress.7
Foundation doctors find psychiatric assessments physically and emotionally challenging. They feel they lack the specialist knowledge and skills to deal with complex patients, especially concerning self-harm, personality and eating disorders. Dealing with such complex diagnostic categories requires knowledge, skill, understanding as well as physical and emotional robustness. Due to the relative lack of focus on such topics in most undergraduate medical training, a comprehensive support in psychiatric placements is essential.
Psychiatry is very different from other specialities in the way services are configured and delivered: junior doctors may face isolation as psychiatric units are typically spread across a wide geographical area and often lack a centralised meeting place for junior doctors (e.g. a doctors’ mess). In addition, they may find themselves the lone practitioner when on call, which can be daunting for many.
Clinical and Educational supervision is provided to Foundation doctors in similar ways to other rotations. However, the consultants delivering this essential support often focus only on clinical issues related to knowledge and skills. Furthermore, it is easy to see that the best guides to new trainees regarding the idiosyncrasies of the speciality and its services are likely to be trainees who have spent some time in those services and are more able to detect the specific stresses new doctors may experience and may find difficult to articulate.
Furthermore, mentoring fosters a productive peer-to-peer relationship. The learning needs of the Foundation doctor can be considered alongside their personal and professional interests and lifestyle. Questions can be posed in a non-judgmental forum, without fear of being ridiculed or condemned. The fundamentals of on-call systems, clinical cases and management options can all be considered at a level appropriate to their junior grade. Tips for examination success and information about essential courses and core texts can be shared. Job choices and research opportunities can be discussed. Day to day difficulties and mismatches between expectation and reality can be identified and possibly overcome. Where this is not possible next steps can be identified, and clinical and educational supervisors can be drawn in for higher level support. The benefits of the scheme are broad.
Finally, although mentoring is different from role-modelling (teaching by example and learning by imitation), it has been shown toserve some of the same aims of role-modelling, including enhancing problem-solving abilities of the mentee, improving professional attitudes, showing responsibility and integrity, and supporting career development. 8
What is mentoring?
Mentoring can mean different things to different people. There are various definitions which can create confusion between mentoring and other formal structures of support such as supervision, coaching, consultation, befriending or friend systems and even counselling. However, mentoring is none of the above but at the same time a combination of them.
The Standing Committee on Postgraduate Medical and Dental Education (UK) defined mentoring as ‘The process whereby an experienced, highly regarded, empathetic individual (the mentor) guides another individual (the mentee) in the development and re-examination of their ideas, learning, and personal and professional development”.9
The term “mentoring” takes us back to Greek mythology: Mentor was a person: he was the friend of Odysseus who was asked to look after Odysseus’ son Telemachus when Odysseus was fighting in the Trojan Wars. The name Mentor was later used to describe a trusted person, a supporter, or a counsellor.10
Mentoring as a professional developmental tool became popular in the private sector organisations in the USA during the 1970s and was introduced to the area of health during the 1990s 11. Since then, it has been widely used in various organisations.
Aims of mentoring
Mentoring has the advantage of being a flexible supporting tool, unlike other structured processes (e.g., clinical supervision or coaching) where the goals are set clearly from the start of the relationship between the supervisor and supervisee. The aims of mentorship are summarised in Table 1.
Table 1- Aims of mentorship
Help the mentees take the lead in managing their career and its development.
Provide support to discuss personal issues in a confidential and secure environment
Improve both the individual and the team performance
Types of mentoring
Buddeberg-Fischer and Herta 11 discussed various types of mentoring based on the numbers of mentors and mentees and their professional status or grade:
One to one mentoring (between a mentor and a mentee).
Group mentoring (one mentor and a small group of mentees)
Multiple-mentor experience model (more than one mentor assigned to a group of mentees).
Peer-mentoring (the mentor and mentee are equal in experience and grade): This mentoring is used mainly for personal development and improving interpersonal relationships. Mentor and mentee roles can be reversed. Also, called ‘co-mentoring’.
Distance or e-mentoring is becoming more popular, and it has the advantages of being “fast, focused, and typically centred on developmental needs”. 12
Structured vs. flexible mentoring
Evidence suggests that providing mentorship through a rigid and structured process can be counterproductive. 13 Mentors and mentees usually work in different locations, making it difficult for both to have a set of pre-planned meetings and topics for discussions.
Another advantage of the flexibility of mentoring is that it does not follow a “tick box” exercise but encourages informal discussions and exploration of whatever comes to mind during meetings. Doubtless, having some structure to the overall mentoring process is important as it ensures that the mentoring session doesn’t become an informal befriending or friend support system. Table 2 sets out the main benefits of mentoring.
Benefits to the organisations
Benefits to the mentee
Benefits to the mentor
Improve job satisfaction leading to improved performance, recruitment, and retention of employees
Enable early recognition and resolution of issues that face employees
Provide a valuable source of feedback that the organisations can use to improve working conditions
Ensure that the mentee has clear aims and objectives (development outcomes) at the start of their mentorship. These goals may include improving knowledge, performance and preparation for exams and interviews
Empowers the mentee to explore and pursue their career aims
Incorporates the mentee into a wider professional network and prevents isolation
Supports the mentee to use reflective practice and improve their self-awareness
Reducing stress and burnout
Formal recognition of informal practice within the profession
Structured program with support and supervision to the mentor
Development of knowledge and skills in management and supervision
Satisfaction of helping others and passing on their knowledge
Table 2-Benefits of mentoring. Developed from Mentoring – Chartered Institute of Personnel and Development (CIPD) Factsheet. Revised February 2009 14. Available from: https://www.shef.ac.uk/polopoly_fs/1.110468!/file/cipd_mentoring_factsheet.pdf
Are there any Disadvantages of mentoring?
There is extensive literature on the benefits of mentoring, but is there any harm associated with it?
As with any intervention, it does carry some potentially adverse effects. Mentoring can be perceived to “infantilise” junior employees rather than empowering them 10. This perception is probably more common among employees who see themselves as senior or very competent and think of themselves as able to adapt to change very quickly.
Mentoring might hinder creativity in new employees and inhibit them from thinking “outside the box” as it might re-enforce the message that ‘this is how we do things here’. 10
Clashes of personalities or other interpersonal factors could lead to a troubled mentor-mentee relationship and cause distress to both parties. Hence, plans must be put in place in any formal mentoring scheme to ensure an amicable ending to this relationship. Multiple mentor allocation mentioned earlier could also prevent such interpersonal problems and help to tackle them early on.
Furthermore, some mentees may feel uncomfortable with the influence or authority of the mentor, and this may hinder the progress of the mentoring relationship. 13 This is particularly relevant when the mentor is also involved in the formal assessment of the performance of the mentee (e.g. being the line manager or supervisor) or when a mentee who lacks self-confidence is paired with an overconfident mentor.
Good mentors avoid common pitfalls in the mentoring process, such as a patronising attitude, breaches of confidentiality and offering direct advice to the mentees. Instead, they encourage the mentee to reflect and come up with their answers. 15
Finally, mentoring can be perceived as an additional demand on doctors during their training, and some may feel that they are forced to provide it or receive it during placement. However, it must be remembered that mentoring should always be voluntary and flexible to meet the individual’s needs and not an additional ‘box to tick’ or a portfolio enrichment exercise.
The Mentoring Scheme for Foundation Doctors in Psychiatry Norfolk:
The scheme started in December 2015 and initially ran as a pilot in Norfolk with the support of all stakeholders. The mentoring scheme coordinator (YH) contacted twelve Foundation doctors by email, welcoming them to the Trust and inviting them to participate. The welcome email contained information about mentoring, including the benefits it may offer.
The voluntary nature of this scheme was highlighted so that the doctors didn’t feel they were being pressured to be enrolled.
Of the 12 doctors invited, five took up this opportunity. Uptake has remained constant over the consequent cohorts of Foundation doctors for many reasons. Those deciding not to enrol in this scheme explained that they felt happy with the support provided by their clinical supervisors. However, some doctors asked for a mentor halfway through their placement when they felt that they needed additional support. In these instances, a mentor was allocated to them as soon as possible.
Mentors were core and higher trainees already involved in supporting more junior psychiatric trainees through informal mentoring. Their experience meant there was no need for formal training. However, reading material was circulated to them to highlight the roles and responsibilities of mentors and what to do if any problem arose during mentoring. Monthly mentors’ meetings were very helpful to discuss issues arising in mentoring and offer peer to peer support.
Also, there were regular meetings and discussions between the mentoring coordinator, the Director of Medical Education, and Medical Director of the Trust to resolve any issues facing the Foundation doctors and provide feedback to improve the Psychiatric placement.
During the first meeting, the mentors and mentees agreed on the aims of mentoring drawing up a list of objectives that the Foundation doctor would like to achieve by the end of the placement. Following this initial meeting, there should have been once monthly face to face meetings throughout the placement. The mentor and mentee agreed on the most convenient means of communication (e.g. using text messages, emails, etc.) outside scheduled meetings.
All mentors kept a record of the mentoring meetings, with the mentoring coordinator informed about these meetings. Issues discussed were confidential and not shared with the coordinator or supervisors unless the mentee gave specific consent.
At the end of the mentoring scheme, the coordinator collected feedback from mentees and mentors using a structured questionnaire that was designed by the coordinator using SurveyMonkey® website. The feedback highlighted the positive aspects of mentoring as well as areas for improvement.
End of mentoring survey
Mentors reported that acting as a mentor without being involved in clinical supervision allowed them to offer objective advice and support in a way that would have been harder if they were directly involved in the workplace. One Foundation doctor experienced bullying from another member of the team who was a locum doctor. The mentor supported the Foundation doctor, and the issue was addressed and resolved promptly. There was a significant risk that they would have been left isolated and unsupported during this time if the mentor scheme had not been in place.
The topics discussed were varied, and this suggested that mentoring was not limited to a aspect of the job (see Table 3)
Table 3- Topics discussed in mentoring meetings
General guidance about the job
Assistance on completing competencies on e-portfolio
Advice regarding personal health, bullying, career choices
Leadership and research opportunities.
Mentees reported that they found mentoring useful and supportive of learning and development. This was especially important in a speciality that they had little experience of as an undergraduate. With a mentor in Psychiatry, the Foundation doctors reported that they could identify areas of development, including leadership and teaching opportunities for Foundation doctors.
Overall, mentoring was shown to be a useful tool to improving Foundation doctors’ experience in Psychiatry by offering extra support during placement in a challenging medical speciality.
Table 4 summarises the areas of development suggested by the mentors and mentees.
Table 4- Recommendations from the feedback of mentors and mentees
Early allocation of mentors at the start of the placement is vital.
The need to provide e-learning and classroom training on mentoring to develop the skills of mentors
Maintain the independence of the mentor from the clinical team of the mentee
Enhance the flexibility of the scheme to meet the demands of the training and the time constraints of the mentees and mentors
Limitations
Feedback from mentors and mentees showed an overall satisfaction with the scheme, but it was not possible to measure such satisfaction quantitatively, this was expected from an approach which is willfully kept outside the realm of performance management.
According to the literature on mentoring, most mentoring schemes lack a clear structure, as well as a clear evaluation process of its short and long terms, benefits 11.In our scheme, we addressed this by continually monitoring the mentoring process and collecting feedback from mentees and mentors. Another limitation involves training the mentor himself and finding the time in a highly pressurised and heavy workload environment.
There are many questions that the literature on mentoring is yet to answer. For example, what are the long-term benefits of mentoring? Would our Foundation doctors who received mentoring be more successful professionally and personally compared to their peers who decided not to participate? These questions remain unanswered as our pilot was not set up to address this general shortcoming of current knowledge and understanding.
Conclusions and recommendations
Mentoring provides a focused opportunity to target the wider needs of the trainee. Not only could this encourage Foundation doctors to pursue a career in Psychiatry, but it also provides the space for them to learn how to incorporate psychiatric skills into whatever speciality they choose to pursue.
As a new doctor in a novel environment, being expected, welcomed, and gently guided into the job is invaluable. With the hindsight of our training experiences (good and bad), junior doctors are ideally placed to support more junior colleagues at all levels.
There is a need to develop links with other mentoring schemes to exchange experiences and learn lessons from others. Research has shown the importance of supporting mentors in their roles through regular meetings where mentors learn from each other. 13
In our experience, the mentoring scheme worked both alongside and separately to clinical and educational supervision and the opportunity for reflective practice offered in Balint groups. Mentoring added another level of support for the Foundation doctors, which was deemed beneficial by those participating.
We recommend more research is required to determine whether mentoring will increase recruitment to psychiatry. Organisations responsible for the training of doctors should support formal mentoring schemes and supervisors should ensure that mentors and mentees have protected time in their timetable due to the benefits of the mentoring experience to the doctors and the employing organisations.
Finally, funding should be available to support training of mentors in their workplace and aim to develop their skills in helping their mentees. Many private organisations offer mentoring training packages (including classroom and online training) for competitive prices. These courses provide useful resources to mentors and may help to increase the motivation of mentors to continue their participations in mentoring.
Appendix:
How does mentoring work? A simple three stage model:
Figure 1- The three stage model of mentoring. Developed from Alred et al (1998). Alred, G., Gravey, B. and Smith, R, 1998, Mentoring pocketbook. Alresford: Management Pocketbooks.
One of the unique characteristics of mentoring is that it is a partnership between two individuals (mentor and mentee) where both contribute to its growth and sustainability. It is based on trust, eagerness to learn and mutual respect. 16
Alred et al (1998) 4 described a model of mentorship with three stages: exploration, developing new understanding and then action planning (Figure 1). Both the mentors and mentee have certain roles and responsibilities in each stage and it is only through their collaborative work that the benefits of mentoring can be obtained.
The stage of exploration is characterised by the building of a relationship between the mentor and the mentee. Trust, confidence and rapport start to develop and hopefully grow throughout the mentoring process. Methods such as active listening, asking open questions, and negotiating an agenda are essential to facilitate this growth.
The second stage is where new understanding develops, is characterised by showing support to the mentee, demonstrating skills in giving constructive feedback and challenging negative and unhelpful cognitions.
Key methods employed in this stage include recognition of the strengths and weaknesses of the mentee, giving them information, sharing experience and establishing priorities for the mentee to work on.
In the third and last stage of the mentoring, action planning, the mentee takes the lead in negotiating and agreeing on the action plan, examining their options and developing more independent thinking and decision-making abilities.
A good mentor should help the mentee to gain confidence and knowledge over time. In order to achieve this, the mentor helps the mentee to develop new ways of thinking and improve their problem-solving abilities.
Monitoring the progress and evaluating the outcomes of the mentoring process is essential to ensure that the mentoring relationship is going in the right direction.
Acknowledgement
We would like to thank Dr Stephen Jones (Consultant CAMHS and former Training Programme Director), Dr Trevor Broughton (Consultant Forensic Psychiatrist, Director of Medical Education), Dr Bohdan Solomka (Medical Director) from Norfolk and Suffolk NHS Foundation Trust for their unlimited support for the mentoring scheme.
We also would like to thank Dr Calum Ross (Foundation Training Programme Director-FY1) and Mr Am Rai (Foundation Training Programme Director -FY2), Norfolk and Norwich University Hospital for their support in implementing this scheme. Dr Srinaveen Abkari (Specialist Registrar, Norfolk, and Suffolk NHS Foundation Trust) is one of our mentors who also contributed useful ideas to the development of this paper.
Finally, we would like to thanks all our mentors who provided the support for the Foundation, without their efforts, this scheme would not have succeeded.
Oestrogen receptors (ERs) are expressed in a large proportion (approximately 70%1) of breast cancers (BCs). Oestrogen stimulates the growth of breast epithelial cells (both normal and cancerous) by binding to these receptors. Aromatase inhibitors (AIs) prevent the conversion of androstenedione to oestrogen by the enzyme aromatase in peripheral tissues, which is the predominant source of oestrogen in post-menopausal women. Consequently, they are routinely offered to post-menopausal women with ER-positive early invasive breast cancer as adjuvant therapy2. However, decreased residual oestrogen levels are associated with increased bone resorption by osteoclasts. The menopause initiates an accelerated phase of bone loss lasting 4 to 8 years, which is followed by a slower phase which continues indefinitely3. AI-induced bone loss (AIBL) occurs at a higher rate than natural menopausal bone loss4. Women are therefore at increased risk of fractures while they are on AI therapy5, with an associated higher rate of fractures as demonstrated in the ATAC trial6.
Recent data have supported more prolonged use of AIs (10 years instead of 5) to achieve lower BC recurrence rates7. This may lead to changes in future clinical practice in that ER-positive BC patients may be on an even longer course of AIs. This is likely to translate into a higher fracture risk in patients on long term treatment, and bone health in these patients should remain an important consideration.
Several guidelines have emerged over the years, as summarised by Hadji et al8, to aid the assessment of fracture risk in women receiving BC treatment, and management of AIBL. In the UK, the guidance in use and recommended by the National Institute of Health and Clinical Excellence (NICE) is a UK expert group consensus position statement issued in 2008 (Guidance for the Management of Breast Cancer Treatment-Induced Bone Loss)9. This includes two treatment algorithms for the assessment and management of bone loss in early BC: one for women with adjuvant treatment-induced premature menopause and the other for postmenopausal women starting adjuvant AI.
Despite the existence of various guidelines on the management of AIBL in BC patients, few articles have been published on the practical adherence to guidance. We carried out an audit of the management of AIBL in BC patients in a large general practice (with roughly 9000 registered patients) in Bradford (UK). Given the small number of eligible patients in our study, we undertook a review to identify all studies in the English literature assessing practical adherence to guidance on AIBL to establish whether gaps identified in our practice reflects a more widespread issue.
Our study
Methods
We carried out a retrospective study in a general practice in April 2015. Using the clinical electronic system used at the practice (SystemOne), we performed a search for all registered patients documented to currently be on AIs or to have previously been on them at any point, for the treatment of BC, using the search terms “anastrazole”, “Arimidex”, “exemestane”, “Aromasin”, “letrozole” and “Femara”. We excluded male patients (not addressed by current guidelines) and patients who started their treatment with AIs prior to the issuance of the UK guidance in 2008. For each patient we gathered data on the indication of treatment, menopause status, the date of initiation +/- completion of treatment, details of dual energy Xray absorptiometry (DEXA) scan and bone mass density (BMD), blood biochemistry results, documented risk factors for fractures and details of bone protection treatment. We audited our practice against the UK guidance.
Summary of the UK guidance
All post-menopausal patients starting AIs should have a baseline DEXA within 6 months of treatment initiation. Patients are stratified as low, medium and high risk for fractures based on the baseline T-scores. Medium and high risk patients should have vitamin D and calcium supplements, and high risk patients should be started bisphosphonates. A repeat DEXA scan should be performed 2 years later for medium and high risk patients to re-assess BMD and augment bone protection therapy as appropriate. Patients aged 75 years and above with at least one clinical risk factor for fractures should be started on a bisphosphonate regardless of their baseline BMD.
Results
There were 12 female patients who started AIs for BC treatment from 2008 onwards. Treatment was initiated between the years 2008 and 2014 (inclusive). The mean age was 67 years (range 57-81 years) and all 12 were post-menopausal at the time of adjuvant hormonal therapy initiation. Three were initially on tamoxifen and switched to an AI after 2 years of tamoxifen therapy.
Three patients (25%) did not receive an initial DEXA scan and had no subsequent risk fracture management. One of them was 75 years of age at the time of AI initiation and was on long term steroids (i.e. should have been on a bisphosphonate regardless of BMD), but she was not on a bisphosphonate.
Of the remaining 9 (75%) who did have a DEXA scan,
One was at high risk (T-score -2.7), and was appropriately started on a bisphosphonate and calcium and vitamin D supplements.
7 patients were at medium risk of osteoporotic fractures (T-score range -2.0 to -0.1). All were started on calcium and vitamin D supplements.
7 were eligible to have had a repeat DEXA scan at the time of the study but only 4 had a scan. Of these four, one was found to have incurred significant bone loss and was started on a bisphosphonate.
The mean interval between AI initiation and baseline DEXA was 1.9 months (range 0.2-4.4). The mean interval between the initial and repeat DEXA scans was 4.1 years (range 2.5-5.1).
Figure 1 illustrates the proportion of scans requested by different clinical teams involved in the patients’ care.
Figure 1: Who requests DEXA scans?
Literature review
Methods
We performed a search with the following terms on the Ovid Medline and Embase databases: “bone loss”, “osteoporosis”, “osteopenia”, “aromatase inhibitor”, “breast cancer”, “guidelines” and “guidance”. Of the 137 results returned after deduplication, we selected original and review articles assessing management of AIBL against established guidelines. We retrieved further papers by reviewing the references of these articles.
Results
The original articles generated are shown in Table 1. While conference abstracts have not been included here, they have been reviewed for the purpose of our discussion.
Table 1: Original articles publishing the results of audits of bone health management in BC patients on AIs against established guidelines
Authors
Place of study
Guidelines used to define audit standards
Sample size
Adjuvant therapy
Roberts R et al10
Australia
ASCO*, ESMO*, Hadji et al8, Belgian Bone Club
42
Both AI and tamoxifen
Spangler L et al11
Washington, USA
ASCO*
342
AI
Bosco D12
Italy
Results from the ARBI* trial13
39
AI
Gibson K et al14
Colorado, USA
ASCO*
54
AI
Ligibel et al15
USA
ASCO*, NCCN*, Hadji et al8
9138
AI
Dong et al16
UK
NICE guidelines based on UK expert group consensus9
100
AI
Zekri J et al17
Saudi Arabia
NICE guidelines based on UK expert group consensus9
367
AI
*ASCO: American Society of Clinical Oncology, ESMO: European Society for Medical Oncology, NCCN: National Comprehensive Cancer Network, ARBI: Arimidex Bone Mass Index and Oral Bisphosphonates
Discussion
The results of our audit show that we are failing to meet our current national standards pertaining to management of AIBL in BC patients. Our literature review confirms that this is a widespread issue and that results from larger studies are in agreement with ours.
25% of our patients never had a baseline BMD measurement. Similar findings have been reported in the literature11,12,14. However, Roberts et al report much higher rates of DEXA screening pre –AI10. Reasons for this were felt to be the presence of an institutional treatment algorithm as well as a survivorship programme.
We had a poor rate of repeat DEXA scans. Gibson et al and Spangler et al also noted that the highest rate of DEXA scanning was around the time of AI initiation compared to after initiation of therapy11,14. For the patients who had a repeat BMD measurement in our study, practice was not in line with recommendations as the interval between the initial and repeat DEXA scans (mean 4.1 years) was much longer than the recommended 2 years. This may be because recommendations made by the breast surgery team were different (intervals of 3 to 5 years being recommended in some cases in clinic letters written to the GP by the breast team).
Gibson et al found that 75% of their patients were on calcium and vitamin D, which deviates from the ASCO guidelines that they audited their results against14. The ASCO guidelines recommend that all BC patients should be on calcium and vitamin D therapy. In some studies10.12 not all women diagnosed with osteoporosis were started on bisphosphonates. Although women diagnosed with osteoporosis were started on bisphosphonates in our cohort, the suboptimal uptake of DEXA scans means that we may have missed the diagnosis in a number of patients.
From the articles included in our literature review, several reasons have been suggested as causes for deviation from guidelines when it comes to management of AIBL in BC patients. Lack of awareness of guidelines, especially amongst general practitioners (GPs), has been recognised as a barrier, as well as the expectation that other healthcare professionals should be addressing this aspect of care10. In our study, DEXA scans were mostly requested by the specialist breast team initiating AIs, or by the GP at the request of the breast team. Based on our experience, it is not clear who the responsibility of bone health management lies with – the breast surgery team, the oncologist or the GP. In a survey of 307 UK-based breast surgeons and oncologists 57% of responders felt that oncologists should be responsible for this18. In practice, patients may be discharged from specialist clinic follow-ups while they are still on hormonal therapy and GPs would be expected to continue their care. When this happened in our cohort of patients, there was no evidence of clear written communication from specialist teams to the GP regarding outstanding aspects of care that the GP would be expected to follow up.
An analysis of five different guidelines regarding antiresorptive treatment in postmenopausal women with hormone-receptor positive BC showed that little consistency exists among the five guidelines19. The variety of guidelines and recommendations regarding bone loss in BC patients probably leads to inconsistency in practice. In our study, specialist teams have sometimes recommended an interval of 3 to 5 years between BMD tests, deviating from the national recommendation of 2 years. This can translate into confusion when care is taken over by the community team after the patient is discharged from the specialist team.
Recommendations
We therefore suggest that institutional guidelines on bone health management in BC patients on AIs (as well as other hormonal therapies) should be created to improve awareness amongst clinicians as this has shown to improve rates of DEXA scanning10. Local guidelines should closely mirror national guidelines to allow delivery of standardised care across the country, but should include clear recommendations as to which local team should be responsible for bone health management, as well as recommendations regarding the creation of a care plan for general practitioners when the patient is discharged from specialist teams.
A UK-based study has shown that a “one stop” nurse-led bone health clinic within the breast care service can be a cost-effective way of ensuring adherence to guidelines20. Patients to be started on an AI are identified by the multidisciplinary team (MDT). They are referred to the clinic which arranges a baseline DEXA and other appropriate investigations. Such a clinic may be a consideration in institutions where resources allow. Studies have also shown that simple interventions such as presentations at MDT meetings and display of posters to increase awareness of guidelines amongst clinicians have led to significant improvement in compliance16,17.
Lack of patient awareness of the negative effects of AIs has also been highlighted in the literature21. Improving patient education can improve patients’ compliance with treatment and decrease the rates of unattended appointments for BMD screening. It can also give more control to patients over management of their bone health, as they may be able to discuss with their clinicians where they notice a gap (e.g. if they have failed to receive an appointment for a DEXA scan). Ligibel et al have noted that women from areas with lower levels of education are less likely to undergo BMD tests15.Patient education can also help reduce the impact that such health-seeking behaviours have on compliance to bone health management.
Current guidelines make no mention of bone health management in male BC patients on hormonal therapy. Although they constitute a small percentage of BC patients, it would be reasonable to include recommendations of their bone loss management in updated guidelines so that this aspect of their care is not neglected.
Strengths and limitations
Our audit is limited by its small sample size and its retrospective nature which meant that we relied on documentation of variable accuracy. We had no information regarding patients who failed to attend appointments despite their clinicians’ invitations for DEXA scans or biochemistry tests, and no information on compliance to medication. However, the results from recent conference abstracts on UK based studies22,23 generated from our literature review reflect our results, suggesting that this is indeed a national issue. The literature review presented is the most extensive currently available on the subject, gathering up-to-date evidence on worldwide compliance to guidelines on AIBL.
Conclusion
Although the sample size of our study does not allow us to draw conclusions purely based on our data, the literature review that it has prompted has shown that several years after issuance of various guidelines on the management of BC treatment-induced bone loss, in particular AIBL, important gaps still exist in practice. We have presented a summary of up-to-date evidence in the literature to identify potential reasons for this and possible solutions to the current problems, hoping that this will improve current practice.
However, the current guidelines are now several years old. In the last few years, there has been a lot of research on the role of bisphosphonates in BC. A consensus paper assessing recent evidence has suggested that bisphosphonates should be considered for the prevention of bone loss in patients with a T score of <-2.0 or with at least two clinical risk factors for fracture24. The paper also suggests considering the use of bisphosphonates as adjuvant BC treatment, based on a large meta-analysis including 18 766 patients which demonstrated significant benefits of bisphosphonates in terms of prevention of bone metastases and BC survival in postmenopausal women25. This may well change routine adjuvant treatment of BC in the next few years and must be taken into consideration if and when new guidelines on the management of AIBL are issued, or when writing local guidelines.
Metastatic bone disease is a relatively common event in the advanced stages of many malignancies.1 Bone-modifying agents decrease the incidence of skeletal-related events (SREs) such as spinal cord compression and bone fracture, as well as the need for skeletal radiotherapy or surgery.2
Bone modifying agents such as intravenous bisphosphonates (IV BPs) (e.g. pamidronate and zoledronic acid) and denosumab are approved for prevention of SREs. IV BPs are primarily used and effective in the treatment and management of cancer related conditions such as multiple myeloma (MM), and breast cancer with skeletal metastases, because they reduce bone pain, hypercalcemia, and the risk of pathologic fractures.3
Denosumab, a receptor activator of nuclear factor kappa-B ligand (RANKL) inhibitor, represents a breakthrough in the treatment of osteoporosis, MM, and bone metastases. The Food and Drug Administration (FDA) approved it in 2010 for the prevention of SREs in patients with bone metastases and in 2011 for the prevention of endocrine-therapy induced bone loss in patients taking aromatase inhibitors for breast cancer and in patients with non-metastatic prostate cancer.
Three international, randomised, double-blind, double-dummy phase III studies have evaluated denosumab versus zoledronic acid for the treatment of SREs in breast and prostate cancers, and in combined solid tumours and MM. Denosumab’s superior efficacy over zoledronic acid was demonstrated in the studies of patients with advanced breast or prostate cancer, as well as in a pre-specified integrated analysis of all patients enrolled across the three studies.4
In the 2014 position paper of the American Association of Oral and Maxillofacial Surgeons (AAOMS), the nomenclature “bisphosphonate-related osteonecrosis of the jaw” changed to “medication related osteonecrosis of the jaw” (MRONJ). MRONJ is defined as cases in which all of the following 3 characteristics are present5:
current or previous treatment with antiresorptive or antiangiogenic agents
exposed bone or bone that can be probed through an intraoral or extra-oral fistula in the maxillofacial region that has persisted for longer than 8 weeks
no history of radiation therapy to the jaws or obvious metastatic disease to the jaws
Other terminologies used previously include “denosumab related osteonecrosis of the jaw” (DRONJ), and “antiresorptive agent-induced ONJ” (ARONJ).
The aetiopathogenesis of MRONJ related to denosumab therapy remains enigmatic, and hypotheses have focused on reduced bony turnover, infection, toxicity of the soft tissue, and antiangiogenesis. The epidemiology also remains unclear, and reported incidence varies widely.6 Overall, it is estimated that bone necrosis can develop in about 0.7-1.9% of patients with malignancy who are given high-potency IV BPs (such as zoledronic acid), and in 0.01–0.1% of those with osteoporosis who take low-potency oral BPs (such as alendronate). Data relevant to denosumab given subcutaneously in patients with metastatic cancer and osteoporosis seem to replicate those when IV high-potency BPs are administered.7 The risk of osteonecrosis of the jaw (ONJ) is higher in patients exposed to concomitant antiagiogenic medication. The individuals’ risk of ONJ is further determined by factors such as the potency of agent, cumulative dosage or duration of antiresorptive treatment, route of administration, comorbidities and local factors such as periodontal disease.8,9 Oral hygiene plays a significant role with evidence supporting a strong correlation between bacteria associated with periodontal disease and MRONJ.10
MRONJ typically manifests as painful and often infected areas of necrotic bone, which subsequently may lead to severe chronic pain and facial disfigurement. This adversely affects the ability to eat, speak and lowers the quality of life. Adverse events related to RANKL inhibitors are usually considered to be infrequent and low in occurrence. Unfortunately from our recent clinical experience at Sheffield Teaching Hospitals' Trust, there have been several new cases presented in a very short period of time. In this paper we present a case series of MRONJ related to denosumab therapy since adverse events of denosumab in the mandible or maxilla have received relatively little attention.
The aim of this article is to highlight the elevated risk of MRONJ in patients receiving denosumab treatment and educate all health care providers involved in the management of such patients. Furthermore, the mechanisms of denosumab, comparison with bisphosphonates and the reported management strategies are reviewed.
Mechanism of Denosumab
Denosumab is an antiresorptive agent that exists as a human IgG2 monoclonal antibody and inhibits the binding of the receptor activator of nuclear factor kappa-B ligand (RANKL) to RANK (Receptor Activator of Nuclear Factor kappa-B). The binding normally signals the proliferation of osteoclasts, as RANK is expressed on the surface of osteoclasts and their precursors, whereas its ligand, RANKL, is a membrane bound protein expressed by bone marrow stromal cells, osteoblasts and T-lymphocytes. The activation of RANK is integral to the function of osteoclasts. Osteoprotegerin binds to membrane bound RANKL on osteoblast which in turns decreases the osteoclastic activity and in theory negatively effects bone turnover. Denosumab acts similarly to osteoprotegerin but has a higher affinity for RANKL.11-13
Denosumab follows nonlinear, dose-dependent pharmacokinetics. The bioavailability of one subcutaneous denosumab injection is 61% and serum concentrations are detected within 1 hour. Maximum serum concentrations occur in 5-21 days and cessation of osteoclast activity occurs within six hours of the subcutaneous injection. The normal function is restored approximately six to nine months later, whilst bone turnover returns to normal shortly after this.14 Based upon monoclonal antibody pharmacokinetics, denosumab is most likely cleared by the reticuloendothelial system with minimal renal filtration and excretion thus avoiding nephrotoxicity. Its elimination half-life is 32 days, and it does not incorporate into bone.15
It is currently marketed as Prolia® and Xgeva®, approved by FDA. Prolia® is administered subcutaneously every six months and has shown to reduce the incidence of new vertebral, non-vertebral, and hip fractures in osteoporotic patients.16,17 Xgeva® is also effective in reducing SRE related to metastatic bone disease from solid tumours when administered intravenously on a monthly basis.17,18
RANKL Inhibitors and BPs Pharmacokinetics
There are fundamental differences between denosumab and BPs with regard to their mode of action. Denosumab is an antibody and acts extracellularly whereas BPs act intracellularly. As such, BPs must be present in the circulation and available for reuptake into bone for prolonged periods to function.19 There is not any evidence of drug recycling with RANKL inhibitors, and therefore it is suggested that their adverse effects can be reversible with discontinuation, in fact leading to a transient rebound phenomenon, which can be restored, with subsequent treatment.14,20 On the other hand, recycling of BPs in the circulation system has been proposed as a reason for the long duration of action even after cessation which can be up to 12 years.
The US FDA-approved manufacturer’s package insert for both zolendronate and pamidronate states that “there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ in patients who require dental procedures during therapy and that clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/ risk assessment”. The package insert for denosumab does not address the issue of treatment continuation in patients who develop MRONJ to date.
Denosumab is a circulating protein capable of distributing throughout extravascular space. It is expected to reach all sites within bone including intracortical sites unlike with BPs. BPs have strong affinity for hydroxyapatite and bone mineral which limits their even distribution throughout the skeleton, particularly to sites deep within the bone.19,21 This can explain the more profound inhibition of bone remodelling with denosumab than that seen with BPs.
Case Series
Case 1
A 55 year-old lady referred to a dedicated Oral Surgery nerve injury clinic for an opinion and management of her left sided inferior alveolar nerve (IAN) paraesthesia. The patient presented with a history of numbness in the left sided inferior alveolar nerve distribution following removal of the left mandibular second premolar (LL5) in July 2014. She was asymptomatic until she had the LL5 removed and since had suffered with constant pain and numbness. A year later, she had removal of the left mandibular first molar (LL6) and gave a history of recurrent infections and excruciating pain in her mandible over the past two months. On presentation she had an obvious submental swelling and left sided IAN anaesthesia.
Medically she was diagnosed with breast cancer in 2011, for which she underwent wide local excision followed by chemotherapy. She then was placed on unknown clinical trial that we identified at the time to be denosumab trial, following liaison with the Oncology team. She is currently receiving intravenous denosumab every three months.
Clinical examination revealed a grossly mobile anterior mandible with widespread bony necrosis and associated osteomyelitis. Sensory testing revealed complete anaesthesia in the left sided IAN distribution secondary to MRONJ.
An OPG (Orthopantogram) and CBCT (Cone-Beam Computerised Tomography) revealed an extensive patchy area of ill-defined bone loss in the anterior mandible extending posteriorly to the premolar/molar areas bilaterally (Fig 1).
Figure 1 A) OPG showing non-healing sockets in the left mandible with extensive bony destruction together with periosteal reaction extending to the right mandible as shown by the arrows.
Rather interestingly, the bony destruction was evident bilaterally with the patient only having had extraction of teeth in the left mandible (Fig 1). This could be the case of spontaneous ONJ in the right mandible or an extensive ONJ arising from simple extractions on the left side.
Figure 2 3D reconstruction of the CBCT image demonstrating extensive bony destruction involving the lower border of anterior mandible in keeping with a spreading chronic bony infection and clinical presentation of submental swelling as showing by arrows.
Case 2
A 66-year-old female referred by her general medical practitioner (GMP) with a 3-month history of delayed healing following a tooth extraction in the left posterior mandible. She had moderate to severe discomfort and reported multiple previous infections and purulent discharge from the area, which treated with multiple courses of antibiotics. In addition, she reported discomfort from the root treated right mandibular first and second premolar teeth (LR4 and LR5).
Medically she was diagnosed with breast cancer over 10 years ago for which she underwent resection followed by chemotherapy. Three years ago, she diagnosed with metastatic deposits and therefore has been receiving intravenous denosumab every six weeks since then. Other medications include steroids, chemotherapy agents, antihypertensives and analgesics. She did not receive any radiotherapy or BPs treatment in the past.
Clinical presentation revealed a heavily restored dentition with chronic generalised periodontal disease. There was evidence of widespread bone loss clinically and radiographically. The slow healing socket in the left mandible was visible but did not have any exposed bone (Fig 3). The lower right first and second premolar teeth (LR4 and LR5) were clinically and radiographically sound.
Figure 3. Non-healing socket in the left posterior mandible with no evidence of exposed bone or suppuration as showing by white arrow. Gingiva recession (black arrows) is evident in the LL6 and LL5 teeth in keeping with chronic periodontal disease.
Figure 4 Coronal sections of CBCT A and B showing multiple lytic areas within the inferior cortex of the mandible and incomplete healing of the extraction sockets.
On follow-up appointments, the patient suffered multiple repeated infections in the right and left posterior mandible and due to deteriorating periodontal disease, the LR4, LR5, LR6 were extracted by her own general dental practitioner (GDP) due to severe mobility. All three extraction sockets failed to heal (Fig 5) leading to an extensive area of exposed bone in the right mandible, extending from the lower right first premolar (LR4) to lower left first molar (LL6) region. Conservative management was embarked which included antibiotics, chlorhexidine mouthwash and routine oral hygiene appointments. Selective sharp bone trimming and three sequestrectomies were undertaken. At the same time, liaison with the patient’s oncologist resulted in cessation of the denosumab therapy and complete resolution of her oral symptoms.
Figure 5 Clinical picture of exposed necrotic bone (white arrows) following simple extractions of periodontally involved teeth.
Case 3
A 76-year-old lady referred to the Oral Surgery department by her GDP with a 3-month history of a non-healing lower left first premolar (LL4) socket. The patient was treated with two courses of antibiotics prior to referral which provided only temporary relief to her symptoms.
Medically she was diagnosed with breast cancer 10 years ago and recently commenced intravenous denosumab for metastatic disease. She also receives hormone therapy and palliative radiotherapy to the spine.
On clinical examination, there was a partially healed LL4 socket with a rather granulomatous appearance. There was no clinical evidence of suppuration or bony exposure. Radiographs confirmed the absence of bony infill in the socket. Local debridement and biopsy of the granulomatous tissue was performed to exclude any metastatic disease. Biopsy report confirmed the presence of inflammation tissue.
Figure 6 CBCT scan; A and B sagittal views, C axial view and D 3D reconstruction. Extensive periosteal reaction extending from the midline of the mandible to the left molar region is evident in keeping with chronic osteomyelitis secondary to MRONJ.
Liaison with the microbiologist suggested a long-term antibiotic course to arrest osteomyelitis. Further liaison with the oncology team, resulted in denosumab being stopped for 4 months. On subsequent review appointments, patient’s symptoms improved however, there is now an area of exposed bone in the LL4 region as shown in Fig 7.
Figure 7 Clinical photo illustrating exposed bone (white arrow) in the LL4 region without evidence of local infection.
Case 4
A 65-year-old lady referred to the Oral Surgery department by her GDP with a history of a sore upper mouth and jaw underneath the dentures which is unable to wear.
Medically she was diagnosed with disseminated breast malignancy including bone metastases 3 years ago and for that, she is on exemestane and IV Denosumab monthly.
Clinical examination revealed multiple draining sinuses in the anterior maxilla. There was a partially healed LL4 socket with a rather granulomatous appearance and tenderness on palpation. There was neither discharge from the area nor any exposed bone. Radiographs confirmed the absence of bony infill in the LL4 socket. Local debridement and biopsy of the granulomatous tissue was performed to exclude any potential malignancy and it was confirmed as inflammation tissue.
Figure 8 CBCT scan; A axial view, B and C 3D reconstruction. A 25mm fragment of right anterior maxilla is beginning to sequestrate. This extends from the anterior margin of the right maxillary sinus approximately to the position of the upper left lateral incisor, crossing the midline. The sequestrated fragment involves the lateral margin of the nasal cavity. There is bilateral moderate mucosal thickening in the maxillary sinuses. Extensive periosteal reaction extending from the midline of the mandible to the left molar region is evident in keeping with chronic osteomyelitis secondary to MRONJ.
Table 1 Summary of cases
Cases
Indications
Duration (months)
Clinical Findings
Case 1
Metastatic deposits from primary breast malignancy
48
Anaesthesia in the distribution of the left inferior alveolar nerve Osteomyelitis Excruciating pain
Case 2
Metastatic deposits from primary breast malignancy
36
Chronic generalised adult periodontal disease Non-healing extraction sockets Exposed bone persisted for longer than 8 weeks Severe pain
Case 3
Metastatic deposits from primary breast malignancy and myeloma
24
Non-healing extraction socket with granulomatous tissue Severe pain
Case 4
Disseminated breast malignancy including bone metastases
30
Multiple draining sinuses in anterior maxilla Non-healing extraction socket with granulomatous tissue Severe pain
Discussion
ONJ associated with antiresorptive therapy deserves distinction from other causes and diseases/medications associated with the development of osteonecrosis of the jaw. AAOMS recently published stage specific treatment recommendation for MORNJ.22 The various stages and suggested stage-specific treatment strategies are not evidence-based, and in particular, stage 0 disease is not universally accepted. AAOMS recommendations echoed those stated in previous years for BRONJ, namely supporting conservative therapy, with aggressive surgery offered only to symptomatic patients. In contrast, the MRONJ guideline report from the German Dental and the German Oral and Maxillofacial Associations refrains from recommending therapy at least for certain stages of the disease. This might be attributed to the pitfalls of current MRONJ criteria. Furthermore, due to poor guidelines specifically related to RANKL inhibitors, no agreement exists on a universally acceptable therapy strategy of such cases.
Management strategies are largely based on expert opinion rather than experimental data. It includes prevention, conservative and surgical modalities. Prevention of the condition is the gold standard. It is highly recommended all patients have a comprehensive dental examination and preventive dentistry (pre-emptive extraction of unsalvageable teeth and optimised periodontal health) before commencing antiresorptive therapy.23,24 Oral hygiene should be kept meticulous during the course of therapy as periodontal disease and associated bacteria claim to be implicated in this condition and also observed in these cases.
The success rate of conservative treatment regimens range from less than 20% 25,26 to above 50%27,28 although some cases become chronic and develop complications.29
Microbial cultures from areas of exposed bone are not always helpful since normal oral microbes are isolated. However, when there is extensive soft tissue involvement, microbial cultures may help to define comorbid oral infections, which may guide the selection of an appropriate antibiotic regimen.30
Regardless of the stage of disease, areas of necrotic bone that are a source of chronic soft tissue irritation and loose bony sequestra should be removed or recontoured so that soft tissue healing can be optimised. This is in line with our clinical experience. The extraction of symptomatic teeth within exposed, necrotic bone should be considered as it appears unlikely that extraction will worsen the established necrotic process. Otherwise, surgical resection of necrotic bone should generally be reserved for refractory or advanced cases.31 Resection may occasionally result in even larger areas of exposed and painful infected bone.32
A recently published MISSION study7 reported that the AAOMS system misclassified/ underestimated the severity of the disease at a rate of about 1 in 3, in particular in patients suffering from MRONJ stage 1 and 2. The authors conclude that these findings may explain why the treatment of stage 3 ONJ, namely surgery with success rate over 85%33,34, has been deemed to be more predictable and therefore yields more favourable outcomes than the treatment of stages 1 and 2.35
Denosumab is characterised by reversibility of its effect after treatment discontinuation, in contrast with bisphosphonates. This is in line with our findings since cessation of denosumab in two cases helped to improve their symptoms significantly.
MRONJ has been reported to occur after a mean administration period of 39.3 months and 35 infusions in oncology patients.23 It is interesting that all published cases of denosumab-related ONJ occurred early after commencement of therapy, independent of the number of previous administrations.36,37 In our experience, all patients developed MRONJ within the first 3 months of teeth extractions; well ahead of the reported period and number of administrations of denosumab.
Furthermore, all four cases have had extensive lytic lesions developed following removal of a single tooth. The common radiographic findings in all cases include:
non-healing extraction socket
areas of focal and diffuse sclerosis
thickened lamina dura
early sequestrum formation
reactive periosteal bone
osteolysis of cortical and spongious bone
These findings, although common in MRONJ cases, have had extensive bony involvement and rapid progression of ONJ, demonstrating a far more aggressive nature of the disease compared to that seen with BPs.
In our experience, not all patients are adequately informed of the risks and adverse events of denosumab therapy. This highlights the importance of educating patients and inter-professional communication regarding the prevention and best management of MRONJ cases. In one of the cases, the lack of patient education concerning denosumab side effects and the failure of inter-professional communication had a detrimental effect on the patient’s overall management and subsequently patient’s oral health.
Table 2 Important Points
All patients prior to start of any antiresorptive medication should have a dental check-up and receive dental or surgical treatment beforehand to avoid the possibility of complications associated with antiresorptive medications
Strongly recommend regular dental check-ups to prevent
Patients should be advised to contact their Doctor/Dentist/Oral surgeon immediately if notice following symptoms:
Feeling of numbness, heaviness or other unusual sensation in the jaw
Pain in the jaw / toothache
Delayed healing to the gums, especially after dental work
Bad taste / infection
Swelling of the jaw
Loose teeth
Exposed bone
Pus like discharge from the affected area
Conclusion
We present our experience with denosumab-related ONJ from Sheffield Teaching Hospital’s NHS Trust. This case series should contribute to the existing sparse clinical literature on this topic. The pathogenesis, treatment and outcome of ONJ are complex and multifactorial. Patients treated with denosumab may be more prone to developing ONJ even without a precipitating dental event. ONJ may have a more aggressive profile and develop significantly earlier in patients receiving denosumab. Prevention of ONJ still remains the most important goal, and this is most directly accomplished by avoiding invasive dental procedures and establishing inter-professional communication.
Medicine is a dynamic science and discipline, which arise from the human need to face the suffering, pain and give hopes for better life. Since its inception, medicine has entered a career development that has brought great advances in science. Part of this momentum observed in medicine is defined as its reason for being, or rather, its primary goal, maintaining the health status in different populations1. This simple statement but becomes an object of great complexity which has received attention by many physicians and researchers from ancient times to the present, and in the tenth century, Ibn Hazm, a father of modern medicine enunciated the truth in this science was going to be impossible, since its dynamism is always present and the truth became a clear misrepresentation or significantly modified in the future2.
The goal of keeping adequate health status and prevent diseases has kept biomedical research in an alarming race in which the speedometer registering increases day by day. Today medical science is one of the most important sources of scientific innovation around the world; hundreds of manuscripts on health issues are published every day in multiple languages, in addition to numerous books and other non-official publications2-3. The increase in the medical literature during the last decade, led to think that the development of medicine has become a breakneck ratio, both the magnitude of the information obtained and its complexity.
However, the real reason for this phenomenon in biomedical sciences should be as a result of the new funding sources available for biomedical research either from the biomedical industry and government agencies. Each year new sources of money are offered to scientists to encourage innovation and the development of new ideas; and the resources existing to perform this goal increase. The OECD (Organization for Economic Co-operation and Development) suggests that countries spend about 500 billion dollars a year on research in biomedical sciences, including private laboratories and research institutes4. Medicine has become one of the most promising businesses in the economic field, and up today, and it is considered one of the greatest science future with wide range of prospects5.
Despite this encouraging situation, the concerning of development of modern medicine could be measured as a fundamental problem: the doctors and other scientists in charge of biomedical innovation are not trained in the administrative field. The above problem is clearly seen in different situation in the current medical and research practice, weak reflected on wasteful resource allocation processes6.
Each organization facilitating biomedical research resources requires that its resources are managed and used in an appropriate manner. Institutions demand to distribute funding for various interests not only in biomedical sciences. On the other hand, institutions have to verify the novelty and the ethical viability of the proposals, with the main idea of support ethical-approved studies, avoiding catastrophes in non-well-designed trials. Nowadays, as a result of better “quality control processes”, grant submissions involve a great number of administrative steps in order to be ready to submit any proposal. In this verification process, no only questions have to be addressed in term of sciences; a lot of administrative issues have to be explained in detail, including budget utilization and personnel management1, 4, 7.
Academics and scientists in universities are trained mostly in the technical aspects of their daily work, for this reason the horizon shows that the physician (M.D.) receives their training focus for the clinical management of patients, a doctor of science (Ph.D.) receive their training in the handling the samples to obtain the best results in the tests planned. In both cases, scientists are plainly educated out of the business and administrative field, leading important limitations with resources (personnel and funding) management3, 5.
Nowadays, the easiest application to obtain resources requires the approval of at least 5 different offices responsible for reviewing ethical, financial, legal, logistical, and scientific issues. Now back to the main problem in this discussion, the fact that medical researchers are not trained as integrated researchers (sciences and business), we are in the position to deduct that this condition may generate a bottleneck, specifically in this time where biomedical research are gaining a lot of power and interest in the industry8.
A potential alternative for this dilemma is to offer manager and administration training to researchers in order to be able to efficiently manage the resources requested. Masters degree programs are now available in health sciences management and administration, gaining popularity in the last five years. Researchers are more committed to show better profiles in their grant applications. Modern scientists must be people with a proven knowledge on costs and productivity that allows performing biomedical research with scientific quality combined with attractive financial management in terms of production2, 5, 8.
Postgraduate medical training should equip trainees with the skills, knowledge and attributes for independent practice1. They need to be equipped with the skills to become lifelong learners and continually develop their abilities throughout their careers by learning from colleagues, mentors, patients and disease. The challenge for clinical teaching is how to provide an optimal learning environment in which trainees can achieve their competencies for practice within a defined training rotation; both the limitations in the number of hours within a working week and the balance between learning and service commitments all can negatively impact on the educational experience of trainees2. Moreover, trainees need to balance their own development of skills, knowledge and attributes for independent practice against the requirement to provide high quality and safe healthcare3. The appropriate level of supervision must be provided to trainees performing any patient interaction and this is gauged by the trainer-trainee relationship, regular assessment and feedback. The clinical workload of a trainee needs to be finely balanced between overstretching them with tasks outside their competencies and being left with all the routine and menial tasks4. Thus whilst trainees should work within their competencies, they must be given the opportunities to expand their repertoire of skills, which may result in errors (and potentially patient harm) – supervision should limit these errors, which should be reflected on to provide a learning opportunity within a ‘no-blame’ culture5. As a trainee gains competence of their necessary skills, the amount of supervision required can be stepped down, until distant supervision (i.e. advice via a telephone) may be all that is required.
An understanding of how each learning environment within the hospital setting can be maximized may enhance the learning opportunities conferred upon trainees. Both technical skills and the professional attributes of being a clinician can be learnt in clinical and non-clinical environments. These learning environments will be explored in the subsections below.
Bedside Teaching and Ward Rounds
Bedside teaching is a stalwart of medical education, allowing clinical history and examination to be performed under guidance, in an appropriate setting and with relevant clues (observation charts, oxygen, etc.) present. This patient-trainee interaction provides an opportunity to develop professionalism and communication, and can also be the source of training of diagnostic techniques ranging from venesection and cannulation to more invasive techniques (e.g., pleural aspiration, drainage of ascitic fluid)1.
Presentation of patients during ward rounds allows a professional conversation between trainees and trainers to occur, which justifies their role in management and provides an insight into understanding and thought processes6. The multidisciplinary nature of rounds creates a community of practice7, allowing social learning to occur, and an opportunity to voice differing perspectives on patient care3. In order to maximize these learning opportunities, learning objectives can be discussed prior to commencement and reflection undertaken once they it has been completed6. Teaching rounds should be carried out when the ward is quiet, at a suitable pace, with regular questioning and opportunities for trainees to ‘lead’ the process8. Factors that hinder this educational process include time pressures, patients not being available, and the availability of trainees8.
Outpatient Clinics
Outpatients provides a mixture of new and follow-up patients that enables a trainee to learn management of patients in an ambulatory setting. Trainees may be in the same room as their supervisor (learning the basics of the consultation), or can practice semi-autonomously as their experience increases (with discussion with their supervisor as required); they must select an appropriate investigation and treatment plan, with a time frame for review, once the investigation or intervention has been performed3. Outpatient teaching is more highly valued by trainees and students compared to ward based tuition9. Factors that hinder this educational opportunity include room availability, time constraints, staffing levels and attitudes to teaching9.
Operating Theatre and Interventional Suites
Invasive procedures should be performed by adequately trained (or supervised) personal in the relevant area of the hospital (e.g. endoscopy, interventional radiology suites, theatre), with the necessary equipment and monitoring for the technique to be performed. Even before patients enter these environments, trainees have an opportunity to review the patient and their relevant investigations, discuss the procedure with the patient and obtain consent for the intervention1. Trainees can learn a wide spectrum of skills within these environments including both technical (both procedural related and anesthetic related) and non-technical skills, including Human Factors, anatomy, identification of instruments, aseptic technique, effective hand-washing and donning of surgical gowns10. Teaching invasive procedures represents a dichotomy for clinicians, not only do trainees need to gain exposure and experience in the relevant technique, but patients need to be prevented from undue harm. Prior to undertaking an intervention, trainees should be familiar with the relevant anatomy and physiology of the system they are about to operate upon, will have watched the procedure being performed and may have learnt the basics of the procedure in a simulated setting.
Trainees must to be able to self-reflect on their own skills and record of the number of procedures they have performed (which can act as a proxy for ability) to ensure that the correct level of supervision is provided alongside an intervention of suitable difficulty. Trainers need to be sure that their trainees have the necessary skills and knowledge to perform a technique, with experience often being gained in a stepwise reflecting both the difficulty of intervention and the gaining of skills, competence and confidence by the trainee11. This skills acquisition should be accompanied by regular discussion and feedback to maximise learning opportunities; when no supervision is available, trainees should consider video-recording the procedure as this allows reflection and review at a later date. A video diary can also be used as a portfolio of a trainee’s repertoire from beginner to expert during their training rotation. The challenge for trainees is to achieve competence in the relevant invasive technique within their training rotation; the number of interventions required to gain competence will vary between each trainee and technique11.
Handover
Handover allows the care of patients to be transferred from one group of individuals to another on a temporary or permanent basis. Handover confers an opportunity to present a clinical synopsis of patients with key information to ensure continuity of care and patient safety is maintained3. Most handovers are trainee led which provides an opportunity for peer learning to occur, checking comprehension and sharing interesting cases or tips for practice12. Handovers should be considered to be a high risk procedure, as communication errors can result in vital information being omitted; as such the process should be undertaken in suitable environment away from distractions, in a structured written and oral manner supported by an electronic format12. A further review at the patient’s bedside can be performed if required, which can highlight high risk patients.
Multidisciplinary Team Meetings
Multidisciplinary team (MDT) meetings are small formal meetings focused on all aspects of a patient’s care that involve a wide range of medical personal, nursing staff and allied health care professionals1. Meetings ensure that evidence-based guidelines are followed, and help to streamline management, removing unnecessary delays in treatment and improving cost effectiveness. MDTs represent a Community of Practice7 allowing social learning to occur as each individual can share their relevant expertise; MDTs enable best practice to be shared and help break down barriers between different specialties. Trainees can learn from the didactic teaching that occurs within the MDT (in relation to clinical details, investigation and management), but can also contribute to the meetings and practice their presentation skills.
Morbidity and Mortality Meetings
Morbidity and Mortality (M&M) meetings can help ascribe accountability and be used to highlight improvements in patient safety. They provide an opportunity for professional education, especially if the discussion can be held within a no-blame culture, and the meeting can voice discrepancies in how to manage patients, especially in ambiguous situations13. Trainees may be tasked with presenting a case and the potential learning aspects associated with patient care.
Grand Rounds/Formal Teaching
Grand rounds are traditional formal teaching opportunities that typically revolve around a case, whereby salient findings are presented prior to a discussion of management. These meetings allow opportunities for trainees to present cases and learn management, but their educational benefit may be decreasing as they are being replaced with lectures with limited clinical relevance14. However “audience apathy, deteriorating decorum and shrinking attendance” have diminished these learning opportunities14. Targeted teaching and the establishment of learning objectives for trainees can improve the educational content and the provision of feedback to the speakers can also enhance these meetings.
Journal Club
Journal clubs confer an opportunity for current scientific research and developments to be presented, critiqued and discussed by trainees. These clubs confer an opportunity to appraise the current literature and how that can be translated into evidence based patient care15. Journal clubs tend to be both voluntary and occur outside of working hours, resulting in highly motivated groups of participants whom are protected from interruptions.
eLearning and mLearning
Electronic learning (eLearning) and multimedia learning (mLearning) enable trainees to work informally, away from desks and computers, and at their own pace through a series of educational modules. Any intervention that engages trainees and promotes learning should be encouraged and these online learning platforms can be combined traditional learning resources should be promoted to ensure that all aspects of the curriculum are covered. mLearning in particular can be ‘dipped into’ allowing the learner optimal flexibility of how and when they want to use it. elearning can be referred to during point-of-care patient interactions when a trainee is unsure of how to proceed with patient management1. These increasingly important and under-utilized resources should be supported by educational institutions that support both undergraduate and post graduate trainees. By developing a virtual learning environment, individual tailored learning programs can be created that allow a trainee to develop and control their own online learning16.
Simulation
Simulation is becoming increasingly important for medical training. , anything can be simulated from learning clinical skills to human factors training, for both individuals and teams, focused on patient care and current medical practice in both the undergraduate and postgraduate setting. The availability of simulators coupled with competency based training and a decreased amount of training within the workplace has led to an increase use of this teaching format1. In addition, trainees need to understand how to use certain pieces of equipment prior to employing them on patients and this familiarity can only be gained in a simulated setting. Simulation can either occur within the workplace (allowing point-of-care simulation to see how teams react in a situation) or on formal taught courses; it can be low-technology and cheap (e.g., tying surgical knots on the back of a chair), but can also be high-fidelity and expensive (e.g., a virtual reality training simulator for laparoscopic operations), or use animal or cadaveric tissue. Simulation that increases trainee’s familiarity with certain techniques is likely to improve their clinical performance, decreasing potential patient harm and shorten the time taken for trainees to achieve competence1. A simulation should be completed with feedback from the supervisor to ensure that trainees gain the most from the session and clarify any facts or concerns about the simulation; a video recording of the session can also enable participants to reflect on their performance in a manner that is almost impossible in everyday clinical practice.
The skeletal type of muscles are rarely affected by tuberculosis (TB) because they are not a preferred site for the survival and multiplication of Mycobacterium tuberculosis.1 Even in patients with widespread involvement of the disease, TB rarely involves muscles. Petter et al recorded only one case of primary skeletal muscles TB in over 8,000 cases of all types of TB, with an incidence of 0.015%.2 Few cases of tubercular myositis have been described in literature until now, mostly in adults. This, together with the decline in TB in general, makes it unlikely that one would immediately consider TB as the cause of a rectus sheath abscess.
There are only limited cases reports of isolated tubercular involvement of the anterior abdominal wall even though TB is rampant in developing countries, and with the rapid spread of acquired immune deficiency syndrome (AIDS) it has made inroads into the developed nations as well.3 We are presenting a case of primary tuberculous abdominal wall abscess, with no evidence of pulmonary, skeletal or gastrointestinal TB in an immunocompetent patient. This case report should serve as a reminder that TB, in all of its various manifestations, remains very much among us.
Case report
A 20-year-old female presented to the outpatient department of surgery, with a complaint of a progressive swelling in the left lower abdomen for the last three months. There was no history of preceding trauma, fever, cough, malaise or pain. There was no history of contact with any case of TB. On examination, there was a swelling in the left iliac fossa, measuring 8x8cm in size, non-tender with smooth and ill-defined margins, and normal overlying skin. The swelling was firm in consistency and moved with respiration. Examination of the cardiovascular and respiratory systems were within normal limits.
Laboratory investigation revealed: haemoglobin 11.5 g/dl; total leukocyte count 8510/cumm with a differential count of 54% neutrophils, 42% lymphocytes and 4% eosinophils; erythrocyte sedimentation ratio 70 mm; and enzyme-linked immunosorbent assay (ELISA) for human immunodeficiency virus (HIV) negative. The chest radiograph was unremarkable. Other biochemical blood investigations, including liver and kidney function tests, were within normal limits. Ultrasonography of the abdomen revealed a 6.5x8.5cm left iliac fossa cystic mass with a liquefied necrotic centre in the anterior abdominal wall (Fig. 1). Computerized Tomography (CT) scan of the abdomen showed an abscess in the left antero-lateral portion of the abdominal wall limited to the muscle layer (Fig. 2). Ultrasound-guided fine-needle aspiration and cytological examination revealed caseating granuloma with central necrosis, lymphocytes, and giant cells, consistent with TB (Fig. 3). The patient was diagnosed to have tuberculous abscess of the anterior abdominal wall and antituberculous treatment was started following internal medicine consultation. She improved rapidly over the next few days. After four weeks of antituberculous treatment, she responded well to the treatment and the abscess regressed considerably. The patient did not require any surgical intervention.
Figure 1. Ultrasonography of the abdomen revealed a left iliac fossa cystic mass.
Figure 2. Focal cystic collection seen in the anterior abdominal wall of the left iliac fossa with mild peripheral enhancement (white arrow)
Figure 3. Photomicrograph revealed caseating granuloma with central necrosis, lymphocytes, and giant cells, consistent with tuberculosis.
Discussion
TB of the anterior abdominal wall is a rare entity and only isolated cases are reported in the literature. Possible explanation for the rarity of muscle involvement in TB includes high lactic acid content, lack of reticulo-endothelial tissue in muscle, lack of lymphatic tissue, the abundant blood supply, and the highly-differentiated state of muscle tissue.4 Although none of them seems to be an adequate explanation, all theories (except the first one) have been criticized.2
Two forms of skeletal muscle involvement are recognized.5 In the first type the tuberculous process spreads into the muscle through direct extension from a neighbouring structure e.g. bone, joint, tendon, or lymph node. In the second type the spread is haematogenous. Our patient is of interest because she seems to have a primary tubercular anterior abdominal muscular lesion with no evidence of immunoincompetence.
A tuberculous focus in the muscle usually manifests as progressive swelling and pain. The infection is usually restricted to one muscle.6 There may be a frank tuberculous abscess (as seen in our case) or a nodular sclerosis followed by calcification. Ultrasonography usually shows a cystic mass of mixed echogenicity with irregular walls and a liquefied, necrotic centre. Computed scan of the abdomen usually shows a well-defined abscess in the abdominal wall.7, 8 Ultrasonography or CT-guided aspiration followed by cytological examination usually reveals tuberculous granulomas with areas of caseous necrosis.
Management of this entity is mainly in the form of antituberculous drugs. Surgical intervention in the form of sonography, CT-guided aspiration or open drainage is usually reserved to patients where medical treatment has failed.3 Our patient responded well to medical treatment.
Although localized swelling in the rectus abdominis muscle is commonly due to necrotizing fasciitis, rectus sheath haematoma or tumours (benign / desmoid / malignant), a rare possibility of TB should also be considered. The prognosis is good in tuberculous myositis with appropriate chemotherapy.
Conclusion
This case alerts clinicians and radiologists of the possibility of TB when considering the differential diagnosis of any lesion even in any unlikely anatomical area, especially in those regions where TB is endemic.
Endocrine disorders are frequently accompanied by psychological disturbances. Conversely, psychiatric disorders, to significant extent demonstrate consistent pattern of endocrine dysfunctions. [1] Endocrinopathies manifests as myriad of psychiatric symptoms, as hormones affect a variety of organ systems function. The presence of psychiatric symptoms in patients with primary endocrine disorders provides a new insight for exploring link between hormones and affective function.[2] Disturbance of hypothalamic-pituitary-thyroidal axis is of considerable interest in psychiatry and is known to be associated with a number of psychiatric abnormalities.[3]Thus, the main focus of psychoneuroendocrinology is on identifying changes in basal levels of pituitary and end-organ hormones in patients with psychiatric disorders. Psychiatric symptoms may be the first manifestations of endocrine disease, but often are not recognized as such. Patient may experience a worsening of the psychiatric condition and an emergence of physical symptoms with the progression of the disorder.[4] Psychiatric manifestations of endocrine dysfunction include mood disturbances, anxiety, cognitive dysfunction, dementia, delirium, and psychosis. While dealing with treatment-resistant psychiatric disorder, endocrinopathies should also be considered as a possible cause in management. Psychotropics medicine may worsen the psychiatric symptoms and improves only once the underlying endocrine disturbance is corrected. [5]The lifetime prevalence of depression and anxiety is 11.8% to 36.8% and 5.0% to 41.2% respectively in the group with previously known thyroid disorder. [6,7].The occurrence of major depression in DM is mostly estimated around 12% (ranging from 8-18%). 15-35 % of individuals with DM report milder types depression. [8]. Depressive symptom is seen in almost half of patients with Cushing's syndrome and these experience moderate to severe symptoms. Some patients with Cushing's syndrome also experience psychotic symptoms [9]. Patients suffering from Addison's disease may be misdiagnosed with major depressive disorder, personality disorder, dementia, or somatoform disorders [4, 10]. Women with hyperandrogenic syndromes are at an increased risk for mood disorders, and the rate of depression among women with PCOS has been reported to be as high as 50 percent. Central 5-HT, system dysregulation that causes depression might simultaneously affect peripheral insulin sensitivity, or vice versa, possibly via behavioral or neuroendocrinological pathways, or both. [10]
Hollinrake 2007 showed prevalence of depression has shown it to be four times that of women without PCOS. Hollinrake screened patients with PCOS for depression and found total prevalence of depressive disorders which included women diagnosed with depression before the study, was 35% in the PCOS group[11]. No specific psychiatric symptoms have been consistently associated with acromegaly or gigantism or with elevated GH levels. Adjustment disorder may occur from changes in physical appearance and from living with a chronic illness [11]. Sheehan’s syndrome (SS) refers to the occurrence of varying degree of hypopituitarism after parturition (1). It is a rare cause of hypopituitarism in developed countries owing to advances in obstetric care and its frequency is decreasing worldwide. Reports of psychoses in patients with Sheehan’s syndrome are rare. [13] Psychiatric disturbances are commonly observed during the course of endocrine disorders .The underlying cause can be hyper- or hyposecretion of hormones, secondary to the pathogenic mechanisms. medical or surgical treatment of endocrine diseases, or due to genetic aberrations[14]. Psychiatric disorders frequently mimic the symptoms of endocrinological disorders. In view of sizable number of patients seeking treatment from our department present with comorbid endocrinolgical disorders, we planned the present study to investigate psychiatric morbidity preferably anxiety and depression pattern among endocrinolgical disorders patients. With this background, we studied the depression and anxiety in different endocrinogical disorders.
Methods
The present study was conducted in the SMHS Hospital of Government medical college Srinagar and the study sample was drawn from patients attending the endocrinogical OPD in the Department of Medicine at Government Medical College Hospital Srinagar (SMHS).The study was conducted over a period of one and half year, from April 2011 to September 2012 in patients attending the Department of Medicine Government Medical College Hospital Srinagar enrolling 152 cases of Endocrinological disorders. All patients were first examined by Consultant endocrinologist. The patients were then selected using simple random sampling choosing every alternate patient. General information including age, sex, residence, economic status, past history of thyroid disorders, family history of psychiatric disorders was included. An endocrinology specialist first examined the patients, while a psychiatrist administers Hospital Anxiety and Depression scale (HADS). Hospital Anxiety and Depression scale (HADS) was used for purpose of screening anxiety and depressive disorders in patients suffering from different endocrinogical disorders. Hospital Anxiety and Depression scale (HADS) is used for purpose of screening anxiety and depressive disorders in patient suffering from chronic somatic disease. HADS contain 14 items and consist of two subscales: anxiety and depression with seven question each. Each question is rated on four point scale (0 to 3) giving maximum total score of 21 each for anxiety and depression. Score of 11 or more is considered a case of psychological morbidity, while as score of 8-10 represents borderline and 0-7 as normal. The forward backward procedure was applied to translate HADS from English to Urdu by a medical person and professional translator. [15]
The participating physicians subjected select patient of chronic Endocrinological disorders to HADS Questionnaire and recorded scores both for anxiety and for depression.
The patients were subjected to inclusion and exclusion criteria as given below:
Inclusion criteria
1. All endocrinological disorders.
2. Both sexes will be included.
3. Age > 15 yrs.
4. Those who will give consent.
Exclusion criteria
1. Those who don’t consent.
2. If diagnoses is not clear.
3. Age less than 15 years.
4. Presence of pregnancy or a history of pregnancy in the last six months.
5. Those who are on steroids or drugs known to interfere with thyroid function
General description, demographic data and psychiatric history was be recorded using the semi structured interview which was pretested
Statistical methods: Statistical analyses were performed using the SPSS, version 16.0 for Windows. A secure computerized database was established and maintained throughout the study. Patient names were replaced with unique identifying numbers. Descriptive statics were used to generate a profiles of each illness group based on presence of depression only, anxiety only and those with both anxiety and depression. To determine whether there were any significant differences between each illness group in the prevalence of depression and anxiety disorders , an unadjusted 3×2×2 test chi square was conducted. Data were analyzed by the Pearson chi-squared test and t test. P<0.05 was considered as the significance level in the evaluations.
Consent: Informed consent was obtained from each patient; those who were considered incapable of consenting were allowed to participate with consent of their closest family member or custodian. All patients were informed about the nature of the research within the hospital and willingly gave their consent to participate. Information sheets and preliminary interviews made it clear that the choice to consent or otherwise would have no bearing on the treatment offered. The project ensured the anonymity of the subjects by replacing patient names with unique identifying numbers before the statistical procedures began.
Results
A total of 152 patients from the endocrinological departments of Govt. Medical College, Srinagar hospitals were taken up for study. They were evaluated in detail with regard to socio-demographic profile regard to presence of psychiatric co-morbidity by HADS and the results have been presented below in the tabulated form .Only patients who consented for complete interview and respond to all HADS questions were considered in final analyses.
Out of total 152 subjects 71 were males (46.72%)), and 81 were females (53.28%) (Table 1). Most of cases belong to 35-45 year age group (26.3%) followed by age group 25- 35 years (24.3%) and 67.7% were married and 18.4% were unmarried. More than half (51.97 %) of the study subjects were from nuclear families and 82 (53.9%) were illiterate and majority 84(55.4 %) belonging to middle class family. The socio-demographic profile of the studied patients is shown in Table-2 .
Out of 152 patients with endocrine disorders, 56(37%) patients elicited HADS score of 10 or less indicating absent or doubtful association anxiety or depression. 96 (63.15%) patients were found positive to HADS Questionnaire with anxiety/depression score of 11 or more. The mean HADS score for anxiety alone, depression alone and anxiety/depression patients were 13.42, 15.7 and 25.62 respectively. On the basis of HADS screening, 96(63.157%) patients had varying degree of psychiatric co morbidity. 27 (28.12%) had anxiety alone, 30(43.47%) had depression alone where 39(40.62%) as patients had anxiety and depression both.(Table 3) The breakdown of total number of different Endocrinological disorders is given in table. Maximum psychiatric comorbidity is found in thyroid patients (69.35%) followed by diabetic patients (68.05). (Table 4).
Table 1: Age and sex distribution
Sex
Total
Male
Female
Age group
< 25
14
20%
7
9%
21
14%
25 – 35
20
28%
17
21%
37
24%
35 – 45
17
24%
23
28%
40
26%
45 – 55
11
16%
19
24%
30
20%
55 & above
9
13%
15
19%
24
16%
Total
71
100%
81
100%
152
100%
Mean ± SD
51.4± 13.7
56.4± 13.1
54.1± 13.6
Table 2: Demographic Characteristics of the Studied Patients
Characteristic
N
%
Dwelling
Rural
98
64.47
Urban
54
35.52
Marital status
Unmarried
28
18.4
Married
103
67.7
Widowed
21
13.8
Occupation
Household
61
40.1
Unskilled
29
19
Semiskilled
39
25.6
Skilled
23
15.1
Professional
8
5.26
Family type
Nuclear
79
51.97
Joint
28
18.4
Extended
45
29.6
Literacy status
Illiterate
82
53.9
Primary
22
14.4
Secondary
16
10.5
Matric
13
8.55
Graduate
11
7.23
Postgraduate/Professional
8
5.26
Family Income(Rs)
< 5000
45
29.6
5000 to 10000
85
55.92
≥ 10000
22
14.4
Socioeconomic status ( Kuppuswamy Scale )
Lower
32
21
Upper lower
11
7.23
Middle
84
55.2
Upper middle
19
12.5
Upper
6
3.94
Table 3: Result of HADS Scoring
Variable
Total (n=96)
Anxiety alone
Depression Alone
Anxiety depression both
p value
Male
37(38.54%)
8(29.6%)
18(60 %)
11(28.2%)
-
Female
59(61.4%)
19( 70.3%)
12( 40%)
28(71.7 %)
-
Age (Years)
54.1± 13.6
51.4± 13.7
56.4± 13.1
54.1± 13.1
< 0.005
Mean HADS Score
-
13.42±3.4
15.73±3.3
25.62±4.3
< 0.005
Table 4: Types of endocrinological disorders
Endocrinological disorders
Number of patients(N=152)
Psychiatric comorbidity
percentage
Thyroid disorders
62 (40.7%)
43
69.35
Diabetes mellitus
47(30.92%)
32
68.05
PCOD
28(18.4%)
16
57.1
Cushings syndrome
5(3.289%)
2
40
Acromegally
2(1.31%)
0
0
Addisions disease
1(0.65%)
0
0
Sheehan’s syndrome
3(1.97%)
2
66.6
Miscellaneous
4(2.63%)
1
25
Table-5 Psychiatric Co-morbidity across Socio-demography of the Patients
Present
Absent
p value
n
%
N
%
Dwelling
Rural
59
60.02
39
39.7
<0.005 (Sig)
Urban
37
68.5
17
31.4
Marital status
Unmarried
8
28.5
20
71.4
>0.005 (NS)
Married
72
69.9
31
30
Widowed
16
76.1
5
23.8
Occupation
Household
57
93.4
4
6.55
>0.005 (NS)
Unskilled
14
48.2
15
51.7
Semiskilled
9
39.1
30
76.9
Skilled
14
60.8
9
39.1
Professional
2
25
6
75
Family type
Nuclear
45
56.9
34
43.0
>0.005 (NS)
Joint
22
78.5
6
21.4
Extended
29
64.4
23
51.1
Literacy status
Illiterate
70
85.2
12
14.6
>0.005 (NS)
Literate
26
36.1
46
63.8
Family Income(Rs)
< 5000
17
37.7
28
62.2
>0.005 (NS)
5000 to 10000
65
76.4
20
23.5
≥ 10000
14
63.6
8
36.3
Socioeconomic status
Lower
18
50
18
50
>0.005 (NS)
Upper lower
7
63.6
4
36.3
Middle
59
70.2
25
29.7
Upper middle
10
52.6
9
47.3
Upper
2
33.3
4
66.6
Discussion
This study is the first to offer data on psychiatric morbidity among endocrine patients in the Kashmiri population. 63.15% (96) patients were found positive to HADS questionnaire with anxiety/depression score of 11 or more in our study. The results of this study suggest patient suffering from endocrinological disorders are likely to have a co-morbid psychiatric disorder. [5, 16].Depressive disorders and anxiety disorders are the commonest psychiatric disorders in endocrinogical patients. [3].Numerous studies have shown a high correlation between depression and endocrinological disorders and this study supports these findings, with 43.47 %( 30) of the participants having depressive symptoms on the HADS. [3, 16] 40.62% (39) respondents had both depressive symptoms and an anxiety disorder. 28.12% (27) participants were diagnosed with an anxiety disorder, which is slightly higher than the lifetime prevalence of anxiety disorder in men [16]. Our findings of a high proportion of respondents with endocrinological disorders (45.7%) Female were more in number than their male counterparts 59(61.4%) vs. 37(38.54%) and the majority of men presenting with endocrinological disorders were between the ages of 35 and 45 years has also been reported in a previous studies. [4, 8].The findings of our study suggest that psychiatric disorders are highly prevalent in endocrinological disorders and is largely unrecognized in the primary care setting. Endocrine disorders of different kinds, irrespective of treatment have been associated with Psychological distress. Psychological wellbeing of endocrine disorders may provide new insights in clinical endocrinology. Further psychological disorders comorbid with endocrinological disorders adds to their disability as well as cost to the individual and the society.[17] Most of the clinicians do not suspect this important association of endocrinological disorders in the beginning resulting in delayed diagnosis. Thus, the high prevalence of anxiety and depression in endocrinological disorders in our study supports a case for screening for these disorders in endocrinological clinics. Furthermore, recognition and treatment of these comorbidities could improve patient outcomes. Future studies should focus on replicating or refuting these findings in larger samples as well as in testing interventions aimed at targeting psychological morbidities in this patient group. Under-recognition of psychiatric morbidity is not an uncommon phenomenon, and has been found in similar local studies of psychiatric morbidity in other medical illnesses[8].Thus, more attention should be paid to recognizing psychiatric morbidities in this group of patients.. The reasons for increase in the frequency of psychiatric disorders are multi-factorial. Being chronic illness leads to psychological stress .The major limitation of our study was relatively small sample size. Another limitation of our study is its crossectional design, which does not allow us to determine direction of causality in the relationship between endocrinological disorders and depression/anxiety. More community based studies are required to assess the magnitude of the problem and to lay down principles to help such patients.In order to clarify the temporal relationship prospective studies with a bigger sample size are essential in the future. As far as we are aware, this is a first of its kind study in kashmir. Endocrinological disorders accounts for a huge proportion of referrals to psychiatric clinics and misery is added upon an already devastating metabolic disease. To add the cost associated with psychiatric morbidity accounts individual and to the society are substantial. Thus, the high prevalence of anxiety and depression in endocrinological disorders in our study supports a case for screening for these disorders in Endocrinological clinics. Furthermore, recognition and treatment of these comorbidities could improve patient outcomes.
Chest pain accounts for 1% of all GP consultations, but in only 8%-18% of cases is it an indicator of underlying ischemic heart disease.1 Given the potential diagnostic uncertainty associated with chest pain at initial presentation, specialist evaluation of patients in a Rapid Access Chest Pain Clinic (RACPC) is of value and represents an important process in the evaluation of symptoms. These clinics were established with the aim of providing rapid outpatient assessment of patients with suspected cardiac disease in order to permit earlier provision of appropriate treatment and investigations where required.
Stable chest pain typically presents as angina, a triad of dull central chest pain, brought on with exertion and relieved by rest or GTN spray. The aetiology is usually stable atherosclerotic plaque disease which is associated with low mortality and can be treated with oral anti-anginals, as demonstrated by meta-analyses and the landmark COURAGE study. 2, 3
NICE Clinical Guideline 95 (NICE CG95) suggests that choice of initial investigation for stable chest pain should be guided by a patient’s pre-test probability of having CAD. Calculations of the pre-test probability take into consideration a patient’s age, gender, cardiac risk factors and symptoms. Patients are defined as high risk of cardiac disease if they have diabetes, smoke or have hyperlipidaemia (total cholesterol >6.47mmol/litre). Patients with none of the above are considered low risk. Symptoms are defined as “typical angina” if the pain is: 1) constricting discomfort in the front of the chest or in the neck, shoulders, jaw or arms; 2) is precipitated by physical exertion and 3) is relieved by rest or GTN spray within approximately five minutes. Pain is defined as “atypical angina” if only two of the above criteria are met and defined as “non-anginal” if one or none of the above criteria are met.
NICE pre-test probabilities of CAD (Table 1), are based on a version of Diamond and Forrester’s pre-test probabilities published in 1979, modified using data from Duke’s cohort study, published in 1993.4, 5, 6 Recent studies suggest that these NICE pre-test probabilities may overestimate the prevalence of CAD in a primary care population and may risk over investigating patients.7, 8 In addition to having financial implications, this may cause patients undue anxiety and unnecessarily put them at risk of complications.
Table 1: NICE Clinical Guideline 95 pre-test probabilities table. Each cell represents the percentage risk of each group of patients having CAD, based on their typicality of symptoms, gender, age and cardiac risk factors (lo, low and hi, high)4
ESC guidelines utilise an updated, validated model of the Diamond-Forrester model by Genders et al. to create pre test probabilities of CAD (Table 2), based on patient’s age, gender and typicality of symptoms. 9, 10
Table 2: ESC guidelines clinical pre-test probabilities in patients with stable chest pain symptoms Each cell represents likelihood of each group of patients having CAD, based on typicality of symptoms, age and gender.9
We hypothesised that strict adherence to NICE guidelines results in over-estimation of the pre-test probability of CAD and therefore over-investigation of patients presenting with stable chest pain. ESC guidelines may offer more accurate pre-test probabilities of CAD and allow a more targeted and cost-effective use of investigations.
Methodology
Clinic records of all patients who attended the RACPC at Tunbridge Wells Hospital between July 2005 and December 2012 were reviewed. This service is run by a cardiology specialist. Patient demographics, cardiac risk factors and information regarding the nature of patient symptoms were collected prospectively and completed at the time of the patient’s RACPC appointment. Results of cardiac investigations were collected from paper and computerised records, and included diagnoses of significant CAD made following invasive coronary angiogram. These results were compared with patients’ pre-test probabilities of CAD calculated using both NICE and the ESC’s calculation methods. Outcome and readmissions were obtained from electronic records from the Maidstone and Tunbridge Wells NHS Trust computer records retrospectively.
Results
Study population
A total of 1968 records were reviewed. 59% (n = 1162) of patients were male and 41% (n = 806) were female. Their mean age was 60 years. At initial assessment, 69.8% patients (n=1373) had non-anginal chest pain, 19.5% (n=383) had atypical angina and 10.8% (n=212) had typical angina, based on the NICE guideline definitions of chest pain.
97.2% (n= 1912) patients underwent further investigation; 15% (n=256) of these were subsequently diagnosed as having significant CAD, accounting for their symptoms. The 2.8% (n=56) of patients who did not undergo investigation either chose not to, were unable to, were lost to follow up, or were diagnosed as having a non-cardiac cause of their symptoms at the initial RACPC appointment.
NICE CG95 pre test probabilities compared against cohort data
Table 3: NICE guidelines 95 pre test probabilities compared against cohort data Each cell represents the proportion (%) of cohort patients from each group who were diagnosed with CAD. We have colour-coded cells to represent the NICE estimated pre-test probability of CAD in each group. Red cells represent 61-90+% probability, pink cells represents 30-60% probability, blue cells represent 10-29% probability and white cells represents <10% probability of CAD according to NICE Guidelines. “ – “ marks a cell where pre-test probabilities of CAD could not be calculated for cohort patients.
Table 4: A comparison of NICE pre-test probabilities and cohort patient data. The risk of CAD as predicted by NICE guidelines 95 on the left compared with the actual number of cohort patients in each category and the proportion of those patients diagnosed with significant CAD.
The average discrepancy between the pre-test probability and actual incidence of CAD in cohort patients was 28% (range 20% - 88%). In 48% of cells in the NICE CG95 pre-test probability table (Table 1) the pre-test probability of CAD was overestimated by 30% or more (Table 3). A marked discrepancy between pre-test probability and actual incidence of CAD was found between “high risk” and “very low risk” patients. On average, high risk patients had an overestimated pre-test probability of 34.3 – 40.9% per cell compared with low risk patients whose pre-test probability was only overestimated by 6.5% (Table 3).
The cells highlighted in dark red in table 3 represent high risk patients whose pre-test probability was of 61-90+%, according to NICE CG95. In our cohort, only 31.2% (n=214, 95% CI 27.6-34.5) of high risk patients in this category were diagnosed with CAD. On average, actual incidence of CAD compared with pre-test probability was overestimated by 34.4% – 40.9% in each cell.
The pink cells in table 3 represent medium risk patients with a pre-test probability of CAD of 30-60%, according to NICE CG95. In our cohort, only 4.4% (n=24, 95% CI 3.0 – 6.5) of medium risk patients had a positive angiogram (Table 4). The average overestimate of actual incidence against pre-test probability was 35.9%.
The cells highlighted in blue in table 3 represent low risk patients with a pre-test probability of CAD of 10-29%, according to NICE CG95. In our cohort, only 2.5% (n=7, 95% CI 1.2 – 5.0) of low risk patients were diagnosed with CAD (Table 4). On average, the pre-test probability of CAD exceeded the found incidence of CAD by 18.6% (Table 3).
The white cells in table 3 represent very low risk patients with pre-test probability of CAD <10% according to NICE CG95. In our cohort, only 0.28% (n= 1, 95% CI 0.1 – 1.6) of patients were diagnosed with CAD. Average overestimation in this group was 6.5% in each cell.
ESC guidelines pre test probabilities compared against cohort data
Table 5: A comparison of ESC pre-test probabilities with cohort patient data. Each cell shows the proportion (%) of cohort patients from each group diagnosed with CAD. Each cell is colour coded to correspond with the ESC estimated pre-test probability. Dark red cells represent >85% probability, pale pink cells represent 66-85% probability, pale blue cells represent 15-65% probability and white cells represent <15% probability.
Table 6: A comparison of ESC pre-test probabilities and cohort patient data The risk of CAD as predicted by ESC guidelines on the left compared with the actual number of cohort patients in each category and the proportion of those patients diagnosed with significant CAD.
The average discrepancy between pre-test probability of CAD, according to the ESC’s risk stratification table, and actual incidence of CAD in cohort patients was 20.7%. In 28% of cells, the pre-test probability of CAD exceeded the found incidence of CAD by 30% or more (Table 5).
The cells highlighted in dark red in table 5 represent very high risk patients with a pre-test probability of CAD greater than 85%, according to ESC guidelines (Table 5). 73.4% (n= 58, 95% CI 63.7 – 82.7) of cohort patients in this high-risk category were diagnosed with CAD (Table 6). On average, incidence of CAD in each cell has been overestimated by 13% in this category.
The cells highlighted in pale pink in table 5 represent high risk patients, with a pre-test probability of CAD of 66-85%, according to ESC guidelines. 58.5% (n=103, 95% CI 51.1 – 65.5) of cohort patients in this high-medium risk category were diagnosed with CAD (Table 6). On average, the pre-test probability of CAD exceeded the found incidence of CAD in each cell by 17.7% (Table 5).
The cells highlighted in pale blue in table 5 represent medium risk patients with a pre-test probability of CAD of 15-65%, according to ESC guidelines. 6.4% (n=93, CI 5.3 –7.8) of cohort patients in this risk category were diagnosed with CAD (Table 6). On average, the pre-test probability of CAD exceeded the found incidence of CAD by 24.1%in each cell (Table 5).
The cells highlighted in white in table 5 represent patients whose pre-test probability of CAD was less than 15% according to ESC guidelines. Only 0.76% (n=2, 95% CI 0.2 –2.7) of cohort patients in this risk category were diagnosed with CAD (Table 6). On average, pre-test probability of CAD exceeded found incidence of CAD in each cell by 6.2% (Table 5).
Discussion
Only 15% of a total of 1968 patients referred to RACPC were diagnosed with significant CAD. The majority (70%) of referred patients had “non-anginal” chest pain and low pre-test probabilities of CAD, reflecting the importance ascribed by General Practitioners of ruling out ischemic heart disease as the underlying cause for chest pain, even in low risk patients. This may not be surprising given the large media attention to heart disease and sustained campaigns for early warning signs of heart attack in the British media. It is therefore of great public interest for cardiac disease to be identified.
NICE CG95 pre test probabilities compared against cohort data
Comparing cohort data to the pre-test probabilities of CAD outlined in NICE CG95, NICE have overestimated the number of patients likely to have CAD in the majority of groups. Strict adherence to NICE CG95 therefore carries the risk of over-investigating patients. NICE recommend CT calcium scoring as the first line investigation for patients with a low (10-29%) pre-test probability of CAD. 284 patients fall into this category and only 7 patients were shown to have CAD. This means that 40.5 patients need to be treated in order to identify 1 positive patient (NNT= 40.5).
In patients with a medium (30-60%) pre-test probability of CAD, NICE recommends functional imaging as the first line diagnostic investigation. In our cohort 544 patients would undergo functional imaging, but only 24 of these patients would be diagnosed with CAD, NNT=22.7.
Finally, in patient groups with a high (61-90%) pre-test probability of CAD, NICE recommends invasive coronary angiography as the first line diagnostic investigation. In our cohort of 1968 patients, 691 patients had a high pre-test probability of CAD, and 214 had significant coronary artery disease on angiography, NNT= 3.2.
Although invasive coronary angiography is considered the gold standard investigation for diagnosing CAD, and permits simultaneous therapeutic intervention, the procedure is not without risk, particularly in elderly patients and those with renal impairment.11 Furthermore, invasive angiography is expensive and is costed by the East Kent Hospitals University NHS Foundation Trust at £1166.02 per procedure (private correspondence).
NICE CG95 offers no guidance on managing patients who have a <10% pre-test probability of CAD. 347 of our cohort patients fell into this very low risk category and only 1 was diagnosed with CAD. Therefore, NICE CG95, if strictly adhered to, would have missed one diagnosis of CAD in our patient cohort.
ESC pre test probabilities compared against cohort data
ESC guidelines tend to offer more conservative estimates of pre-test probability of CAD compared with NICE guidelines. Using the ESC’s risk stratification table, almost all patients, except those with over 85% pre-test probability and those with less than 15% pre test probability, would be investigated for chest pain. This is due to their claim that non-invasive, image-based diagnostic methods for CAD have typical sensitivities and specificities of around 85%, so that roughly 15% of these investigations could be yielding false results. Hence, due to these inaccuracies, in patients with pre-test probabilities of CAD below 15% or above 85%, ESC state that performing no test at all could provide fewer incorrect diagnoses.9
In our patient cohort, 79 patients had very high (>85%) pre-test probability of CAD, but only 58 patients (73%) were diagnosed with CAD. For this patient risk group, ESC guidelines suggest that further investigation may not be necessary and that a diagnosis of CAD may be assumed. Thus, applying ESC guidelines to our cohort could result in 21 patients being incorrectly diagnosed with stable angina, and more serious causes of chest pain, for example pulmonary emboli or gastric ulceration, may be missed. However, in practice, it is likely that many patients in this very high pre-test probability category would have undergone angiography, because patients who have "severe symptoms" or who are clinically thought to have "high risk coronary anatomy" should be offered an invasive angiography with or without pressure wire studies. The vagueness of the guidelines allows interventionists to interpret this in the clinical context.
In ESC guidelines, invasive coronary angiography is not specifically recommended as a first line investigation for stable angina, regardless of the pre-test probability of CAD. In patients with a high (66-85%) pre-test probability of CAD, ESC guidelines recommend non-invasive functional imaging first line. Of the 176 patients who fell into this category, only 102 (58.0%) patients were ultimately diagnosed with CAD.
In patients with medium (15-65%) pre-test probability of CAD, ESC guidelines advise exercise ECG testing (or non-invasive imaging for ischemia if local expertise is available) as first line diagnostic investigations. Of the 1451 patients which fell into this category, only 93 were diagnosed with CAD, NNT= 15.6. Fortunately, exercise ECG testing would not expose the patient to potentially harmful radiation or medication, but their poor diagnostic power may result in the need for further investigations, despite a negative result.
In patients with low risk of CAD (<15%) ESC guidelines suggest making an assumption that the patient does not have CAD and advocates conducting no further investigations. In our cohort, 263 patients fell into this low risk category, two (0.8%) of which were diagnosed with CAD.
The ESC guidelines appear to have higher specificity than the NICE guidelines, and only two patients would have been missed had ESC guidelines been adhered to, compared to one patient missed if NICE guidance was used. Thus, although highly sensitive, ESC guidelines when applied to our cohort have lower sensitivity than NICE guidelines.
Comparison of number of investigations
Following ESC guidance for our cohort of patients would have resulted in fewer diagnostic invasive angiograms being performed than if NICE guidance had been followed. ESC guidance only recommends invasive angiography if first line, non-invasive investigations generate positive results. Overall, however, ESC guidance would result in a greater number of overall investigations being performed.
In total, NICE advises that all 691 of our high risk cohort patients should undergo invasive angiography as a first line investigation. 544 with medium risk should undergo functional testing first and 24 of these patients (assuming an angiogram would follow a positive result) would go on to have invasive angiography. 284 low risk patients should undergo CT calcium scoring first, of which 7 would go on to have functional imaging and angiography if the above logic is followed. This generates a total of 1557 investigations; 722 angiograms, 551 functional imaging investigations and 284 cardiac CT scans.
In comparison, using ESC guidance, 176 of our high risk patients would have functional imaging investigations, 103 patients with positive results would then undergo invasive angiography. 1451 patients would receive exercise ECGs, of which 93 with positive results would undergo functional imaging and invasive angiography. This generates a total of 1916 investigations; 196 angiograms, 269 functional imaging investigations and 1451 exercise ECGs.
If we assume that stress echocardiograms are used as “functional imaging” we can estimate costs for our cohort when applying each set of guidelines. Costs for each investigation are supplied by East Kent Hospitals University NHS Foundation Trust and are as follows: Outpatient elective coronary angiograms are costed at £1,166.02; stress echocardiograms are costed at £132.30; exercise ECGs at £40.26 and CTs of one area at £102.47 (private correspondence). If we were to apply NICE guidelines to our cohort, £841,866.44 would be spent on angiograms, £72,897.30 would be spent on stress echocardiograms and £29,101.48 on CT scans. This is a total of £943,865.22 on investigations.
If we were to apply ESC guidelines to our cohort, £228,539.92 would be spent on coronary angiograms, £35,588.7 would be spent on stress echocardiography and £58,417.26 would be spent on exercise ECGs. A total of £322,545.88 would be spent on investigations. Overall, this is £621,319.34 cheaper than applying NICE guidelines.
Limitations of study
This study is based on data from a single site and may not be nationally representative. The final diagnosis was made clinically by an experienced interventional cardiologist, which introduces subjectivity and the risk of interpreter bias. Not all patients underwent the gold standard of invasive coronary angiography to demonstrate the presence of CAD. However, all patients were seen and fully assessed by a cardiologist and 97% underwent investigations if deemed necessary.This study has all the limitations of a registry study. In addition, costs for investigations may vary throughout the country, and indeed the world, with varying expertise available.
Conclusion
In conclusion, strict adherence to NICE CG95 over-estimates the pre-test probability of CAD in our local population group. This is consistent with previous studies conducted in South London where there is a larger Afro-Caribbean population, as well as with studies conducted in the North of England.8,9 Adherence to ESC guidelines in place of NICE guidelines may enable a more targeted and cost-effective use of investigations. Strict application of the ESC guidelines to the study cohort would have resulted in investigations costing an estimated £322,545.88, compared to £943,865.22 if NICE guidelines were applied. However, conducting fewer investigations carries greater risk of misdiagnosis, and using ESC guidelines in isolation introduces the possibility of assuming CAD in patients without conducting investigations to confirm this.
It is advisable that local cardiology departments audit their stable chest pain guidelines to ensure that the interpretation of pre-test probabilities is in keeping with the local population. Unfortunately there is no ideal policy and local protocols should reflect the local population.
In the last few decades, the practice of medicine has seen swift changes, as well as its visualisation in the near future. It was designed and focused on serving the community and helping people in need. However, it is not a secret that there is a huge business around this labour and the economic interest of a diverse industry in the field. 1,2
Not intending to generalise, many have observed in daily practice a comparable trend with modern society. A phenomenon including both patients and health personnel, where there is a demand for health services, a growing supply, and a considerable revenue. Basic market economics, right? 3
Not that simple.
It would be the triumph of basic sciences to explain each disease under a biological substrate, minimising the involvement of other factors. A definitive targeting of biological research would be the key to unlocking knowledge. What is certain is that this approach has transformed pharmacotherapy, treatment alternatives and prognosis.2, 3, 4
Early physicians had little to nil information on what today we call aetiology, pathophysiology and therefore treatment. Patients were rarely relieved due to human intervention. Trepanations were frequently performed in the Classical and Renaissance periods and although having modern indications (decompressive craniotomy), its uses and technique were at best questionable. Belief and verbally transmitted understanding of a handful of medicinal plants whose effect were known empirically were standards of care.5
These times have changed, the pharmaceutical industry is a pillar of the economies in many countries, and the number of transactions and cash flow that they move are beyond the wildest dreams of the first physicians. Born each year, thousands of new pharmaceutical companies develop and market new drugs and medical supplies. 1, 6
As advocated by experts, pharmaceutical and medical supply companies are considered one the safest businesses nowadays, with everyone being a potential consumer/patient. It is the race for continuous development of new drugs to its current rate that guarantees soon we will have more drugs and procedures available. The drug industry may be easily overloaded by an oversupply of organic compounds and procedures to patients. 2, 4, 6
This pharmaceutical industry thriving is widening its horizon. Personalised medicine, the study of the influence of a patient’s genetic makeup on their disease susceptibility, prognosis, or treatment response (efficacy and safety), is actually in the spotlight. This can be assessed in different ways, being preventive and/or therapeutic. 7
In the preventive field, preconception screening studies have been unravelling genetic disorders, as recommended by different guidelines such as those of the American College of Medical Genetics, which are designed for individuals with known genetic conditions or high-risk patients who wish to become pregnant. 8
In the therapeutic filed, pharmacogenomics can aid in the identification of alterations of Single Nucleotide Polymorphism (SNPs) that affect the function or expression of proteins associated with pharmacokinetics or pharmacodynamics of different drugs. In recent years the research community has doubled efforts in personalising certain therapies. Hormonal therapy in breast cancer has been from the beginning a receptor-guided therapy, especially with ER (Oestrogen Receptor) therapy. Initial clinical results of trials conducted so far have allowed to establish single therapies regimens with Tamoxifen or combined with Arimidex. 9
Another model of the advances in this arena is reflected in the new alternatives for prostate cancer. This hormone-dependent tumour has demonstrated recurrent alterations in the androgen receptor and its pathway. In specific patients the disease can be found in Castration-Resistant Prostate Cancer (CRPC), a lethal clinical state in which the tumour has developed resistance to androgen deprivation therapy. This clinical scenario is commonly established in advanced or metastatic prostate cancer patients. The genomic landscape of localised prostate cancer has been well defined, describing putative pathogenic BRCA2 germ line mutations as well as somatic and germ line DNA repair alterations found such as BRCA1, CDK12, FANCA, and RAD51B. Furthermore, the research advances described above can allow clinicians to determine treatment, therefore achieving better outcomes. 10
It is unquestionable that personalising treatment will improve clinical outcomes for patients in the near future and help achieve a more effective use of available health care resources. The next challenge for scientists and researchers is to demonstrate with strong evidence the clinical and cost-effectiveness to support the use of personalised medicine and its implementation in different health care systems around the world. 2, 3, 5
In conclusion, individual patient variability currently studied in drug efficacy and drug safety has represented a major objective in current clinical practices. Years of research results have converged in progresses in pharmacogenetics and human genomics that have dramatically accelerated the discovery of genetic variations that potentially determine variability in drug response, providing better clinical outcomes for patients. The future in this field is expected to allow us to have effective and safe medications to targeted patients with appropriate genotypes.
Global recruitment in psychiatry has been falling for several decades because medical students and graduates have been finding it consistently unattractive 1,2. An analysis of the career choices of newly qualified doctors in the United Kingdom (U.K.) found the same trend from 1974 to 2009; psychiatry was the first career choice for only 3-5% of medical graduates annually3. In the U.K., lack of recruitment into psychiatry had reached a crisis point by 2003 when 15% of all unfilled consultants posts in England were in psychiatry and the Royal College of Psychiatrists was finding recruitment into specialist psychiatry posts increasingly difficult4,5. In 2012, only 78% of the Core Training year one (CT1) posts in psychiatry were filled; a serious shortfall which was overcome by overseas recruitment up until changes in immigration rules.
The factors that seem to dissuade medical students from taking up psychiatry as a future career may include: stigma, bad prognosis of psychiatric disorders, poor scientific base of psychiatry, ‘bad-mouthing’ from medical colleagues, lack of respect among peers & public, threats of violence from patients and lack of resources1-5. However, there is evidence to suggest that many students’ attitudes towards career choice changed in a positive direction after working in psychiatry due to the perceived ‘job satisfaction’, ‘life-style’, ‘training available’ and ‘multidisciplinary approach’3.
Psychiatry has previously been ranked higher in career choice at the end of students’ clinical year6. To ensure a stable psychiatric workforce for the future, there is an obvious need to motivate current and future cohorts of young doctors to take up psychiatry as a career. Das & Chandrasena (1988) found that attitudes changed positively towards mental health following clinical placement in this specialty7. It is also known that medical students’ attitudes to psychiatry and career intentions can be improved by their experiences of teaching8. Students were found to develop more positive attitudes when encouraged by senior psychiatrists, had direct involvement in patient care, or saw patients respond well to treatment. Improvement in attitudes during the placement was also related to an increased intention to pursue psychiatry as a career.
Previous research into attitude to psychiatry as a specialty and career choice seems to have produced conflicting results and most of it was carried out among medical students. Since career choices in the U.K. are actually made in the first clinical year following graduation, we carried out a survey among a recent cohort of foundation year one (FY1) doctors in the South East England before and after their first clinical year.
Method
Our study sample consisted of all FY1 doctors (n=101) in one region of South East England. They participated in the study at the beginning and then at the end of their first clinical year. We used a 20–item questionnaire devised by Das & Chandrasena(1988) to ascertain their perceptions and attitudes towards psychiatry before they commenced their first clinical placement. The questionnaire was sent to them via their Medical Education Managers (MEMS). It was handed out to the FY1 doctors as part of their induction pack for completion along with a study information sheet.
At the end of their first year of working, the participants were asked to complete an amended version of the questionnaire. This included two additional questions which ascertained whether the doctor had an opportunity to work in a psychiatric post, or had any experience of psychiatry in practice (such as taster days or cases in A&E). These amended questionnaires were sent to the foundation doctors electronically via their MEMS for completion.
The data was collected and entered into a spreadsheet to prepare descriptive statistics. Comparisons for before and after exposure to psychiatry, and between the psychiatry and non-psychiatry groups were made using the chi-square test. As the data was binary, a latent class model was developed using LatentGOLD software9 to explore the associations between different items in the questionnaire. Responses from the questionnaires were coded as: responses which agree with a positive attitude to psychiatry or disagree with a negative attitude were coded as +1; those not sure were coded as 0; and responses which agree with a negative attitude to psychiatry or disagree with a positive attitude were coded as -1.
Results
A 100% (n=101) response rate was obtained for the first set of questionnaires completed at the beginning of the year. However, there was a significant drop in the number of questionnaires completed at the end of the year - a 53.5% response rate (n=54) generally but 61.1% (22 out of 36) for those FY1 doctors who had the opportunity or access to a post in psychiatry within their clinical year.
Initial cohort at beginning of the clinical year vs. those with no exposure to psychiatry at the end
Table 1 shows the group means for each questionnaire item, for the whole cohort at the beginning of the year compared to those with no exposure to psychiatry by the end of the year.
Table 1: All FY1 doctors before training placements started (initial cohort) versus FY1 doctors without a psychiatric post after FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.591
0.095
-0.169
0.359
0.476
I may consider pursuing a career in psychiatry in the future
-0.539
-0.136
0.403
0.046
0.760
0.028
Psychiatry is attractive because it is intellectually comprehensive
-0.500
0.273
0.773
0.436
1.000
0.000
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
-0.500
-0.069
-0.442
0.305
0.717
Physicians do not have time to deal with patients emotional problems
-0.294
0.273
0.567
0.142
0.991
0.009
Psychiatrists understand and communicate better than other physicians
-0.127
0.364
0.491
0.090
0.892
0.017
Psychiatrists don't overanalyse human behaviour
0.147
0.364
0.217
-0.200
0.633
0.306
Expressing an interest in psychiatry is not seen as odd
0.157
-0.136
-0.293
-0.727
0.141
0.184
Hospitalised patients are not given too much medication
0.167
0.591
0.424
0.116
0.732
0.007
Psychiatrists don't make less money on average than other physicians
0.255
0.045
0.209
-0.537
0.118
0.208
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.727
0.365
0.033
0.696
0.032
Psychiatric curriculum and training are not too easy
0.520
0.682
0.162
-0.112
0.436
0.243
Psychiatrists are not fuzzy thinkers
0.578
0.818
0.240
-0.082
0.561
0.142
Psychiatrists should have the legal power to treat patients against their will
0.608
0.955
0.347
0.051
0.642
0.022
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.864
0.246
-0.066
0.558
0.121
Psychiatry is scientific and precise
0.627
0.818
0.191
-0.098
0.480
0.194
There is a place for ECT in modern medicine
0.755
0.727
-0.028
-0.239
0.184
0.797
Psychiatric consultations are often helpful
0.853
0.864
0.011
-0.210
0.231
0.924
Entering psychiatry is not a waste of a medical education
0.873
1.000
0.127
-0.048
0.303
0.153
Psychiatrists don't often abuse their legal powers
0.892
1.000
0.108
-0.049
0.264
0.175
Those FY1 trainees who had not worked in psychiatry during the year were significantly more positive (p = < 0.05) for psychiatry’s future, psychiatrist being better at patient communication and not over-medicating their patients. However, they remained significantly less convinced as compared to the whole cohort about psychiatry’s intellectual attraction or taking it up as a future career.
Initial cohort at beginning of the year vs. those with exposure to psychiatry at the end
Table 2 shows the group means for each questionnaire item, for the whole
cohort at the beginning of the year compared to those with exposure to psychiatry at the end of the year.
Table 2: All FY1 doctors before training placements started versus FY1 doctors with a psychiatric post during FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.745
-0.058
-0.242
0.125
0.531
I may consider pursuing a career in psychiatry in the future
-0.539
-0.617
-0.078
-0.332
0.177
0.547
Psychiatry is attractive because it is intellectually comprehensive
-0.500
-0.468
0.032
-0.214
0.278
0.798
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
0.106
0.538
0.248
0.827
0.000
Physicians do not have time to deal with patients emotional problems
-0.294
-0.383
-0.089
-0.401
0.224
0.575
Psychiatrists understand and communicate better than other physicians
-0.127
-0.085
0.042
-0.260
0.345
0.783
Psychiatrists don't overanalyse human behaviour
0.147
0.340
0.193
-0.123
0.510
0.229
Expressing an interest in psychiatry is not seen as odd
0.157
0.106
-0.050
-0.378
0.277
0.761
Hospitalised patients are not given too much medication
0.167
0.362
0.195
-0.044
0.434
0.109
Psychiatrists don't make less money on average than other physicians
0.255
0.404
0.149
-0.092
0.391
0.224
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.064
-0.299
-0.569
-0.029
0.030
Psychiatric curriculum and training are not too easy
0.520
0.596
0.076
-0.128
0.281
0.464
Psychiatrists are not fuzzy thinkers
0.578
0.596
0.017
-0.233
0.268
0.892
Psychiatrists should have the legal power to treat patients against their will
0.608
0.532
-0.076
-0.323
0.171
0.545
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.574
-0.043
-0.290
0.203
0.730
Psychiatry is scientific and precise
0.627
0.702
0.075
-0.155
0.304
0.521
There is a place for ECT in modern medicine
0.755
0.511
-0.244
-0.427
-0.061
0.009
Psychiatric consultations are often helpful
0.853
0.745
-0.108
-0.289
0.073
0.239
Entering psychiatry is not a waste of a medical education
0.873
0.808
-0.064
-0.218
0.090
0.412
Psychiatrists don't often abuse their legal powers
0.892
0.766
-0.126
-0.279
0.027
0.105
After a psychiatry placement, significant positive differences (p=<0.05) were observed in their responses to medical staff’s view of psychiatry, future of psychiatry and place of Electro Convulsive Therapy (ECT) in modern medicine. While there was a positive trend in most responses in favour of psychiatry, trainees remained negative about psychiatry’s status, its scientific base, curriculum & training and taking up psychiatry as a future career.
Those exposed to psychiatry vs. those not exposed to psychiatry
Table 3 compares responses between FY1 doctors exposed to psychiatry during the clinical year and those who were not.
Table 3: FY1 doctors who had a psychiatric post versus those who did not have one
Sorted by the size of the difference between the two groups.
t-test
ranksum
Psychiatry
No Psychiatry
Difference
L
U
p-value
p-value
Most non-psychiatric medical staff are not critical of psychiatry
0.106
-0.500
-0.606
-1.000
-0.144
0.011
0.011
Psychiatrists don't make less money on average than other physicians
0.404
0.045
-0.359
-0.694
-0.024
0.036
0.034
Expressing an interest in psychiatry is not seen as odd
0.106
-0.136
-0.243
-0.735
0.249
0.329
0.322
Psychiatrists don't overanalyse human behaviour
0.340
0.364
0.023
-0.421
0.467
0.917
0.907
Psychiatric curriculum and training are not too easy
0.596
0.682
0.086
-0.210
0.382
0.564
0.497
Psychiatry is scientific and precise
0.702
0.818
0.116
-0.187
0.419
0.447
0.777
Psychiatric consultations are often helpful
0.745
0.864
0.119
-0.173
0.411
0.419
0.388
Within medicine, psychiatry has a high status
-0.745
-0.591
0.154
-0.130
0.437
0.283
0.391
Entering psychiatry is not a waste of a medical education
0.808
1.000
0.191
-0.020
0.403
0.075
0.058
There is a place for ECT in modern medicine
0.511
0.727
0.217
-0.117
0.551
0.200
0.192
Psychiatrists are not fuzzy thinkers
0.596
0.818
0.222
-0.114
0.559
0.192
0.190
Hospitalised patients are not given too much medication
0.362
0.591
0.223
-0.139
0.597
0.218
0.192
Psychiatrists don't often abuse their legal powers
0.766
1.000
0.234
-0.005
0.473
0.055
0.040
A placement in psychiatry can change one's negative views of psychiatry
0.574
0.864
0.289
-0.045
0.623
0.088
0.064
Psychiatrists should have the legal power to treat patients against their will
0.532
0.955
0.423
0.097
0.748
0.012
0.011
Psychiatrists understand and communicate better than other physicians
-0.085
0.364
0.449
0.000
0.897
0.050
0.050
I may consider pursuing a career in psychiatry in the future
-0.617
-0.136
0.481
0.084
0.878
0.028
0.017
Physicians do not have time to deal with patients emotional problems
-0.383
0.273
0.656
0.195
1.000
0.006
0.007
Psychiatry is a rapidly expanding frontier of medicine
0.064
0.727
0.663
0.269
1.000
0.001
0.002
Psychiatry is attractive because it is intellectually comprehensive
-0.468
0.273
0.741
0.352
1.000
0.000
0.001
Those exposed to psychiatry agreed more often that non-psychiatric medical staffs were critical of psychiatry compared to the group not exposed to psychiatry. They also had comparatively negative responses for psychiatrists not abusing legal powers and to have the legal power to treat someone against their will. Trainees exposed to psychiatry also felt significantly (p=<0.05) positive towards psychiatry being intellectually comprehensive and adopting it as a career. However, they were less enthusiastic about psychiatrists treating patients against their will and psychiatry being the expanding frontier of medicine.
Discussion
In this study, we have ascertained attitudes of a regional cohort of FY1 doctors towards psychiatry as a specialty and as a career choice. Our findings are similar to previous research carried out among medical students, which found that there were generally negative attitudes towards psychiatry as a specialty and career choice but fairly positive attitudes towards the role of psychiatry in medicine and in society in general1-5,10. Like others, we also found that personal experience of psychiatry placement can improve trainees’ view of psychiatry as a specialty and as a future career 3,11.
It was interesting to find out that after a year in clinical practice but without any experience of psychiatry, trainees’ attitudes towards psychiatry as a specialty had been positive. It is difficult to know the exact reason but we can speculate that this respect for the specialty may have developed when they experienced limitations of the other specialties in medicine and/or perhaps due to the positive professional encounters with psychiatrists at the Accident & Emergency (A&E) or with psychiatric liaison teams during ward consultations. As opposed to previous research11, it was heartening to note that the group with no exposure to psychiatry agreed that non-psychiatric medical staff were not critical of psychiatry; a possible sign of reduced stigma for psychiatry within the medical profession.
Despite exposure to psychiatry, FY1 doctors’ attitudes to psychiatry’s status, scientific base, curriculum & training and career choice remained somewhat negative. Similar results were found by Lyons et al11 when they assessed students’ attitudes towards psychiatry after a clerkship in the specialty. There was a significant decrease in negative & stigmatising views towards mental illness after the clerkship, but no significant improvement in students' interest in psychiatry was detected1. Goldacre et al (2013) also acknowledged mixed outcomes of early experience of working in psychiatry as it might discourage some doctors. While highlighting positive effect of the doctors’ experience of the speciality, they also cited it as a negative factor that influenced some doctors who had previously considered psychiatry as a career3.
Our study has limitations because of having a small sample and being carried out in one small region of the country. It is also worth mentioning that the group exposed to psychiatry may not have had a psychiatry placement as it also included those who had had taster days or experience in A&E. The brevity of these latter exposures cannot give someone a real sense of the specialty. The nature of this and the overall experience needs to be differentiated and the exposure quantified in the future studies. Our study findings also need to be replicated with future cohorts and in other regions for confirmation because FY training programme in the U.K. is relatively recent and placements in psychiatry have evolved4 over the last few years through closer collaboration between different stakeholders in the Foundation Training Programmes.
Hypertension is the most common risk factor for perioperative cardiovascular emergencies. Acute episodes of hypertension may arise due to the aggravation of a pre-existing chronic hypertensive condition or as de novo phenomena1.
Emergency, anaesthesia, intensive care and surgery are among the clinical settings where proper recognition and management of acute hypertensive episodes is of great importance. Many surgical events may induce sympathetic activity, leading to sudden elevations in BP2.
The long term end-organ effects add to patient morbidity and mortality. Ensuring cardiovascular stability and pre-optimization of BP allows safe manipulation of physiology and pharmacology during anaesthesia2. Different medications are available for the management of hypertensive emergencies. The greatest challenge is the acute care setting where the need for proper and sustained control of BP exists.
Definition
Acute severe elevations in BP have several terms. The syndrome characterized by a sudden increase in systolic and diastolic BPs (equal to or greater than 180/120 mmHg) associated with acute end-organ damage that requires immediate management otherwise it might be life-threatening was defined as malignant hypertension3. The international blood pressure control guidelines removed this term and replaced it with hypertensive emergency or crisis4.
Criteria for hypertensive emergencies (crises) include: dissecting aortic aneurysm, acute left ventricular failure with pulmonary oedema, acute myocardial ischemia, eclampsia, acute renal failure, symptomatic microangiopathic haemolytic anemia and hypertensive encephalopathy5.
While they suggest 'hypertensive urgency' for patients with severe hypertension without acute end-organ damage3. The difference between hypertensive emergencies and urgencies depends on the existence of acute organ damage, rather than the absolute level of blood pressure5.
Causes of hypertensive crises
Cessation of antihypertensive medications is one of the main causes. Other common causes are autonomic hyperactivity, collagen-vascular diseases, drug use (stimulants, e.g. amphetamines and cocaine), glomerulonephritis, head trauma, pre-eclampsia and eclampsia, and renovascular hypertension6.
Signs and symptoms of hypertensive crisisinclude severe chest pain, severe headache accompanied by confusion and blurred vision, nausea and vomiting, severe anxiety, shortness of breath, seizures and unresponsiveness.
Pathogenesis
Humoral vasoconstrictors released in the hypertensive crises episodes result in a sudden increase in systemic vascular resistance. Endothelial injury accompanies severe elevations of BP resulting in fibrinoid necrosis of the arterioles with the deposition of platelets and fibrin, and a breakdown of the normal autoregulatory function. The resulting ischemia speeds the further release of vasoactive substances completing a vicious cycle7.
Perioperative hypertension
At least 25% of hypertensive patients who undergo noncardiac surgery develop myocardial ischemia associated with the induction of anaesthesia or during the intraoperative or early post-anaesthesia period8. Previous history of diastolic hypertension greater than 110 mmHg is a common predictor of perioperative hypertension. The level of risk depends on the severity of hypertension9.
Sympathetic activation during the induction of anaesthesia increases the BP by 20 to 30 mmHg and the heart rate by 15 to 20 beats per minute in normotensive individuals8. These responses may be more obvious in patients with untreated hypertension in whom the systolic BP can increase by 90 mmHg and heart rate by 40 beats per minute.
Intraoperative hypertension is associated with acute pain induced sympathetic stimulation besides certain types of surgical procedures like carotid surgery, intrathoracic surgery and abdominal aortic surgery. Paix et al, analysed 70 incidents of intraoperative hypertension and reported that drugs were the precipitating cause (inadvertent vasopressor administration by the anaesthetist or surgeon, intravenous adrenaline with local anaesthetic and failure to deliver a volatile agent or nitrous oxide) in 59% of the cases. Light anaesthesia and excessive surgical stimulation represented 21% of incidents, while equipment related causes (ventilation problems e.g. stuck valve, hypoventilation, soda lime exhaustion and endobronchial intubation) were 13% of incidents. Awareness under general anaesthesia, myocardial infarction and pulmonary oedema represented 7% of incidents10.
In the early postanaesthesia period, hypertension often starts within 10 to 20 minutes after surgery and may persist for 4 hours. Besides pain induced sympathetic stimulation, hypoxia, intravascular volume overload from excessive intraoperative fluid therapy and hypothermia can promote postoperative hypertension. If untreated, patients are at high risk for myocardial ischemia, cerebrovascular accidents and bleeding11. Hypertension might happen 24 to 48 hours postoperative due to fluid mobilisation from the extravascular space, besides cessation of antihypertensive medication in the early postoperative period12.
The absolute level of BP is as important as the rate of increase. For example, patients with chronic hypertension may tolerate systolic BPs (SBP) of 200 mm Hg without developing hypertensive encephalopathy, while pregnant women and children may develop encephalopathy with diastolic BPs of 100 mm Hg13.
Preoperative general considerations for hypertensive patients
During preoperative assessment we have to review associated medical problems such as ischaemic heart disease, cerebrovascular disease and renal failure. This can assess the risk for anaesthesia and so the hypertensive end-organ damage. Some patients with hypertension are asymptomatic and accidentally discovered during preoperative assessment. Incidental hypertension may suggest long standing hypertensive disease1. Idiopathic hypertension comprises about ninety percent of hypertensive patients6.
Management of perioperative hypertension crises
The treatment plan of perioperative hypertension differs from treatment of chronic hypertension. Hypertensive patients undergoing elective surgery are at risk for increased perioperative hypertensive attacks. Postponement of elective surgery is recommended in chronic hypertensive patients if the diastolic BP is ≥110 mm Hg until the BP is controlled14. We have to determine if it is a hypertensive emergency or urgency, besides the underlying causes of the patient’s BP elevation.
The most appropriate medication for management of hypertensive emergency should have a rapid onset of action, a short duration of action, be rapidly titratable, allow for dosage adjustment, have a low incidence of toxicity, be well tolerated and have few contraindications2,15. A parenteral antihypertensive agent is preferred due to rapid onset of action and ease of titration5.
The goal of therapy is to halt the vascular damage and reverse the pathological process, not to normalise the BP. Guidelines by the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High BP for treating hypertensive emergencies include starting intervention with reducing systolic BP by 10 to 15%, up to 25% within the first hour. Followed
by gradual reduction of the absolute BP to 160/110 mmHg over the following two to six hours5,16.
Hypertension that occurs with tracheal intubation, surgical incision and emergence from anaesthesia is best treated with short-acting β-blockers, calcium channel blockers, vasodilators, or angiotensin-converting enzyme inhibitors. Postoperative hypertension is best managed by correction of precipitating factors (pain, hypothermia, hypervolemia, hypoxia and hypercarbia)17.
Unintentional hypotension and associated organ hypoperfusion happens with aggressive attempts to lower BP since the homeostatic mechanisms depend on higher blood pressure for adequate organ perfusion. While inadequate lowering of BP may result in increased morbidity and mortality. However, the alteration between overshooting BP and severe hypotensive states and using vasopressors to get the normotensive levels may damage end-organs and the vasculature - precise control of BP in a hypertensive crisis is a challenge18.
Since chronic hypertension shifts cerebral and renal perfusion autoregulation to a higher level, the brain and kidneys are prone to hypoperfusion with rapid decrease in blood pressure. So control of blood pressure to baseline levels should take 24 to 48 hours5.
In cases of aortic dissection, the systolic BP should be reduced to less than 120 mmHg within twenty minutes. In ischemic stroke, BP must be lowered to less than 185/110 before administration of thrombolytic therapy19. Gentle volume expansion with intravenous saline solution will maintain organ perfusion and prevent sudden drop in BP with using antihypertensive medications5. Preoperative hypertension is a hypertensive urgency, not an emergency, as it rarely involves end-organ damage with adequate time to reduce the BP18. Longer acting oral medications such as Labetalol and Clonidine may be more suitable 20.
Common antihypertensive medications used in hypertensive crises
Sodium Nitroprusside is a combined venous and arterial vasodilator which decreases both afterload and preload. The onset of action is within seconds and duration of action lasts for one to two minutes, so continuous BP measurement is recommended. If the infusion is stopped, the BP rises immediately and returns to the pretreatment level within one to ten minutes. Prolonged intravenous administration with infusion rates more than 2 mcg/Kg/min may result in cyanide poisoning. Thus, infusion rates greater than 10 mcg/Kg/min should not be continued for prolonged periods21.
Labetalol, an alpha- and beta-blocking agent has proven to be beneficial to treat patients with hypertensive emergencies. Labetalol is preferred in patients with acute dissection and patients with end-stage renal disease. The onset of action is five minutes and lasts for four to six hours. The rapid fall in BP results from a decrease in peripheral vascular resistance and a slight fall in cardiac output22. A reasonable administration protocol is to give an initial intravenous bolus of Labetalol 0.25 mg/Kg, followed by boluses (0.5 mg/Kg) every 15 minutes until BP control or a total dose 3.25 mg/Kg. Once an adequate BP level is achieved, we can start oral therapy with gradual weaning from parenteral agents22.
Fenoldopam, a peripheral dopamine-1-receptor agonist, induces peripheral vasodilation; administered by intravenous infusion. Duration of action from 30 to 60 minutes. Gradual decrease in blood pressure to pretreatment values occurs without rebound once the infusion is stopped because of short elimination half-life. A starting dose of 0.1 μg/kg/min, titrated by 0.05 to 0.1 μg/kg/min up to 1.6 μg/kg/min. Fenoldopam provides rapid decline in blood pressure with reflex tachycardia so beware in patients at risk of myocardial ischemia23.
Clevidipine, a dihydropyridine calcium channel blocker, produces rapid and precise BP reduction. It has a short half-life of about one to two minutes with potent arterial vasodilation without affecting venous capacitance, myocardial contractility or causing reflex tachycardia24. Start intravenous infusion of Clevidipine at 1-2 mg/h; titrate the dose at short intervals (90s) initially by doubling the dose. Systolic pressure decreases by at least 15% from baseline within 6 minutes post-infusion24. A 1-2 mg/h increase in infusion rate produces an additional 2-4 mmHg reduction in SBP14. Clevidipine is an ideal agent to manage acute severe hypertension moreover safe for patients with hepatic and renal dysfunction2.
Rational approach to the management of hypertensive crises
Neurological emergencies
Subarachnoid haemorrhage, acute intracerebral haemorrhage, hypertensive encephalopathy, and acute ischemic stroke require rapid BP reduction. In hypertensive encephalopathy, reduce the mean arterial pressure (MAP) 25% over 8 hours. Labetalol, Nicardipine and Esmolol are the preferred medications; Nitroprusside and Hydralazine should be avoided25.
For acute ischemic stroke, the preferred medications are Labetalol and Nicardipine. The target BP is < 185/110 mm Hg especially if the patient is receiving fibrinolysis25.
In acute intracerebral haemorrhage, Labetalol, Nicardipine and Esmolol are preferred; avoid Nitroprusside and Hydralazine. If signs of increased intracranial pressure (ICP) exist, keep SBP < 180 mm Hg, while maintain SBP < 160 mm Hg in patients without increased ICP for the first 24 hours after onset of symptoms25. Early intensive BP control is recommended to reduce hematoma growth26,27.
In subarachnoid haemorrhage, Nicardipine, Labetalol and Esmolol are also the preferred agents; while Nitroprusside and Hydralazine should be avoided. Maintain the SBP < 160 mm Hg until the aneurysm is treated or cerebral vasospasm happens25.
Cardiovascular emergencies
Rapid BP reduction is also indicated in cardiovascular emergencies such as aortic dissection, acute heart failure, and acute coronary syndrome. Labetalol, Nicardipine, Nitroprusside (with beta-blocker), Esmolol, and Morphine are preferred in aortic dissection. Beta-blockers should be avoided if there is aortic valvular regurgitation or suspected cardiac tamponade. Keep the SBP < 110 mmHg unless signs of end-organ hypoperfusion exists28.
In acute coronary syndrome if the BP is >160/100 mm Hg, Nitroglycerin and beta blockers are used to lower the BP by 20-30% of baseline but, thrombolytics are avoided if the BP is >185/100 mm Hg28. In acute heart failure use intravenous Nitroglycerin and intravenous Enalaprilat. Give vasodilators (besides diuretics) when SBP is 140 mm Hg28.
Cocaine toxicity/Pheochromocytoma
Diazepam, Phentolamine and Nitroglycerin/Nitroprusside are the preferred drugs. In cocaine toxicity, tachycardia and hypertension rarely require specific treatment. Phentolamine is proper for cocaine-associated acute coronary syndromes.In pheochromocytoma, beta blockers can be added after alpha blockade for BP control29.
Pre-eclampsia/eclampsia
The proper medications are Hydralazine, Nifedipine and Labetalol however avoid Nitroprusside, Esmolol and angiotensin-converting enzyme inhibitors. The BP should be <160/110 mm Hg in the antepartum period and during delivery. The BP should be maintained below 150/100 mm Hg if the platelet count is less than 100,000 cells mm3. Intravenous Magnesium Sulphate should also be used to prevent seizures30.
Perioperative hypertension
Nitroprusside, Nitroglycerin and Esmolol are used. Target the perioperative BP to within 20% of the patient's baseline pressure. Perioperative beta blockers are best to use in patients undergoing vascular procedures or at risk of cardiac complications28.
CONCLUSION
Perioperative hypertension commonly occurs in patients undergoing surgery. The permitted value is based on the patient’s preoperative BP. It is approximately 10% above that baseline however more reduction in BP may be warranted for patients at high risk of bleeding or with severe cardiac problems. Accurate adjustment of treatment and monitoring of patient’s response to therapy are essential to safe and effective management of perioperative hypertension.
Bed bugs belong to the family Cimicidae and there are two species involved in the modern resurgence; the Common bed bug, Cimex lectularius and the Tropical bed bug, Cimex hemipterus. They are wingless insects with an oval-flat shape that allows them to hide in narrow cracks and crevices. The adults are dark brown, 4-5mm long, becoming to around 10mm when fully blood-engorged. There are five smaller juvenile stages (nymphs) that are similar in appearance, although lighter in colour. All nymphs require a blood meal to moult to the next stage, and both adults also bloodfeed for nutrition, and egg development in the case of the female. Bed bugs are solely haematophagous ectoparasites. After feeding they return to a harbourage and do not remain on the host. The main hosts are humans, but pets, bats, and birds may act as secondary hosts.
Epidemiology
In the past, bed bugs were particularly an affliction of the poor. However, in the early part of the modern resurgence it was the tourist areas and the hospitality sector that were initially impacted.1-3 Today, bed bugs have conquered quite diverse locations, ranging from hospitals, hotels and homes, to trains, cruise ships, and even airplanes. Most commonly, bed bugs travel in comfort as stowaways in luggage, although they can be transferred via furnishing and other belongings, as well by spreading to adjoining properties. Unfortunately, exact figures on the occurrence of bed bugs are unknown, as there are no mandatory reporting requirements. Additionally, due to the stigma associated with bed bugs, many infestations are simply not reported.
During the day, the largely nocturnal bed bugs will crawl deep into crevices of bed frames and mattresses (Fig.1), or behind wallpaper, and floor moldings. Here they tend to lay their eggs, often several hundred during the female lifetime. Live bed bugs, shed nymphal skins, and dark excrement spots indicate an active infestation. At night they are attracted by carbon dioxide, heat and other host odours to a victim, from which they may take a blood meal every 3-5 days. The adult bugs can survive long periods of starvation, up to five months at 22oC or even longer at cooler temperatures. When a host is found, they insert their mouthparts into the skin, blood feeding for 5-10 minutes. When bed bugs are in large numbers, often lines of bites occur on the unfortunate victim and this sign is almost a sure indication of the presence of the insect. The bites tend to occur along the arms and legs, down the back and across the shoulders.4,5
There has been long speculation whether bed bugs can transmit diseases, and in fact more than 40 different pathogens have been implicated. This has included Hepatitis B and C viruses, Human Immunodeficiency Virus (HIV), and Coxiella burnetii (Q fever). Recently, research has indicated that bed bugs are capable of transmitting the agent of Chagas Disease, Trypanosoma cruzi,in the laboratory. However, to date there is not one piece of evidence that bed bugs have transmitted any pathogen to humans.4,6
Clinical Features
During the act of feeding, saliva is injected which contains a variety of anticoagulants as well as other proteins whose function has yet to be determined. Contrary to popular belief, there is no evidence that bed bugs inject an anaesthetic. One protein, Nitrophorin, is involved in the transport of nitric oxide into the wound. This results in local vasodilation that increases blood supply to the feeding insect. The same protein can also induce a sensitivity to the bite.6
The diagnosis of Cimicosis is via the clinical appearance of the bite reaction and confirmation of an actual bed bug infestation (Table 1).3,5 The most commonly affected body parts are those that are left uncovered during sleep (Fig. 2,3,4), notably the arms, shoulders and legs. In young children, the face and even the eyelids can be bitten. Rarely, however, armpits are bitten, which are often preferred by other insects and ticks (Table 2).
Table 1. Bed bug infestation
Bites on the body
Wheals, 4-6cm in diameter, lines of bites
Any exposed body part
Often intense itching
Occasional central haemorrhage
Bed Sheet, mattress (clothing)
Small blood spots
Droppings (black dots)
Shed nymphal skins
Eggs, small (~1mm in length), white, oblong, glued to the substrate
Space
Pungent smell (mostly commonly noticed when an insect is squashed, or during the control program)
Table 2. Differential diagnosis of epidermatozoonoses
Bite preference
Pattern
Itching
Notes
Bed Bugs
Any exposed parts of the body, arms, legs, face, torso
In small infestations, bites will be random. In larger infestations, bite can occur in lines along the limbs and across the shoulder. Large wheals (up to 6cm across) may form, even some 14 days after the bite
Often intense, especially in the morning, but can be variable between individuals
Often associated with travel or used furniture
Fleas
Exposed parts of the body, especially the legs
Random, usually not grouped or in lines
During the day
Usually associated with pets
Mosquitoes
Exposed skin, particularly legs and arms
Random
Variable between individuals
Most commonly outdoors
Ticks
Potentially anywhere on the body
Erythema migrans with Lyme disease. Localised macules/papules at the bite site may occur
Low / no
Those who work or recreate in native forests are at greatest risk.
Itch Mites (Scabies, Sarcoptes scabiei)
Forearms, inter digital, genital area
Skin rashes, subcutaneous courses
At night
Most common in the elderly and infirmed
Harvest mites (Trombidiosis)
Skin surfaces under tight clothing
Red macules and wheals
Severe itching
Often occurs in gardens or meadows, most active during summer and autumn
Cheyletiellosis
Arms and trunk, contact points with pets
Polymorphic rash
Variable
Tends to be associated with pets
Bird mites
All over
Macular rash
Variable itching
Most commonly in homes as a result of birds roosting in roof cavities
Head Lice (Pediculosis)
In the hair of the head
Bar-shaped scratch effects with lichenification and hyper-pigmentation (Vagabond’s disease)
Night and day, generally mild itching
Most common in school aged children
Spiders, e.g. long-legged sac spiders
Arms, face
Necrotic lesion at bite site
Immediate severe pain, no itching
Uncommon
Figure 1: Typical appearance of bed bugs
Figure 2: Bites on the back, note the lines of bites common in moderate to large infestations
Figure 3: Bed bug bites on the arm, typical formation
Figure 4: Bed bug bites on the torso and arm
Figure 5: Bullae due to bed bug bites
Figure 6: Bed bugs, their droppings and eggs underneath a mattress
The degree of the bite reaction often depends on the level of prior exposure. With low level sensitization, individuals may develop a 1-2 cm wheal, with a small central haemorrhagic point. This haemorrhagic point can be recognized easily by diascopy. In contrast, a highly sensitized person will react immediately and may develop a wheal up to 15cm across (6 inches). If many bed bugs are present, an urticarial rash may develop as a result of the large number of bites and subsequent trauma to the area from scratching. On rare occasions, vesicles and bullae (Fig. 5) may form on the arms and legs. In the course of Cimicosis, papules that are extremely itchy may develop and can persist for several days to weeks. Due to the strong pruritus eczematous lesions, bacterial infections may occur, although this is extremely rare. There are case reports of systemic reactions such as anaphylaxis and asthma, although these are uncommon.
Through repeated exposure, some individuals may develop a tolerance to the bites. The clinical symptoms are then largely inapparent with small punctures at the bite site. Small blood spots are then the only clues that an infestation may be present.
Differential Diagnosis
Since reactions to stings and bites of various arthropods are non-specific, bed bug bites are commonly misdiagnosed. Single bites, notably that of other insects such as mosquitoes, fleas and biting midges may appear very similar morphologically (Table 2).
Consideration of where the bites are on the body can assist in the differential diagnosis. For bed bugs, lines of bites are very common in moderate to large infestations and this clinical picture is virtually unique amongst blood sucking arthropods. For the most part, the identification of the actual pest is required to confirm the diagnosis. Histologically, bed bug bites resemble perivascular eosinophilic infiltrates through the superficial and deep dermis, with minimal spongiosis.
Other possible diagnostic confounders can be various allergic reactions and other medical conditions such as urticaria, chickenpox, prurigo subacuta, and erythema multiforme.7,8 These do not show a central haemorrhagic point in the lesion which allows a correct diagnosis. However, in young children the diagnosis can sometimes be difficult.
Treatment
The treatment of Cimicosis is symptomatic. Local lesions can be treated with antipruritics e.g. Polidocanol 2-4% in Lotio alba (aqueous lotion) and topical antiseptic. Spirit of menthol may also be helpful. Local treatment with antihistamines is controversial. In severe reactions topical glucocorticoids such as Betamethasone may be required. In severe itching, the use of oral antihistamines is recommended. With infected bites, antibiotic therapy may be required. Uncomplicated bed bug bites tend to stop itching within 1-2 weeks, although temporary scarring from the bite may remain for several months.
Management
Treatment of patients with bed bug bites ultimately comes down to removing the source of the irritant, namely the eradication of the active infestation. Bed bugs have a typical pungent odor. This can be used to detect bed bugs through specially trained sniffer dogs that can rapidly locate the insects.9 Due to insecticide resistance, bed bugs are very difficult to control with traditional insecticides alone, and non-chemical means of eradication must be employed to reduce the overall insect biomass. Bed bug control should be undertaken by professionals trained in bed bug management, and the process may take some weeks to achieve.
Prevention
When travelling (1) always inspect the bed and surrounds for bed bugs hiding beneath the mattress and/or in seams of the bedding. Also, look for blood stains or small black dots (Figure 6, Table 1). (2) If present, request another room. (3) Always keep your luggage on the desktop or the luggage rack. A good preventative is to seal luggage in plastic or garbage bags during travelling, even when in transit. (4) When returning home, all clothing should be washed in at temperatures exceeding 60°C or frozen for one week with delicate fabrics. If there is no choice, then repellents containing N, N-Diethyl-meta-toluamide (DEET) should reduce the biting rate, but will not completely prevent all bed bug bites.10,11
Bed bugs can enter homes via an array of additional ways, particularly from objects bought second hand at flea markets or thrift stores, for example wooden frames, vintage clothes, furniture and the like. These should be heat-treated for a minimum of 10-20 minutes to kill bugs and their eggs.
Medical professional terminology is used to communicate with each other, allied professions and differentiates professionals from patients1. As a tradition, it has perhaps evolved into a language of its own with a vocabulary of terms used as expressions, designations or symbols such as ‘Patient’, ‘Ward Round’ and ‘Registrar’. This ‘language’ is not restricted to use by doctors or nurses - it is used among other professionals working in healthcare, e.g. medical coders and medico-legal assistants.
The National Health Service (NHS) in the U.K. has seen many changes in the last few decades. From within these changes, an interesting trend to change or alter the use of professional terminology, often without consultation with directly affected professionals or patients, has emerged. With new or changed roles, multidisciplinary teams have been observed to alter titles, even borrowing specific terms ascribed to doctors such as “consultant,” “practitioner” and “clinical lead”2,3. On the other hand, Modernising Medical Careers initiative4 has also led to changes in doctors’ titles reflecting their experience levels, which have been reported to be unclear to patients and fellow professionals5.
Medical professional terms can be traced back to Hippocratic writings and their development is a fascinating study for language scholars1. Psychiatric terminology is particularly interesting, as it has evolved through scientific convention while absorbing relevant legal, ethical and political trends along the way. Superficially, it may appear pedantic to quibble over terminology, but the power of language and its significance in clinical encounters is vital for high quality clinical care2,6. Since medical professional terminology is an established vehicle for meaningful communication, undue changes in its use can create inaccurate images and misunderstandings, leading to risks for professional identity. There is also evidence to suggest that such wholesale changes have been misleading7 and a source of inter-professional tension.
Understanding of a professional’s qualifications and experience is crucial for patient autonomy and for them to be able to give informed consent. We carried out a survey among foremost stakeholders of medical professional terminology, patients and doctors, within a psychiatric service to ascertain their attitudes to the changes they have experienced in recent years.
Method:
We gave out a self-report questionnaire to all adult psychiatric patients seen at a psychiatric service in the South East (U.K.) in a typical week and to all working psychiatrists/doctors. The questionnaire was developed after a review of the relevant literature and refined following feedback from a pilot project. The questionnaire contained demographic details and questions regarding attitudes towards medical professional terms for patient and professional identity, processes and working environments. The questions were mostly a “single best of four options” style, with one question involving a “yes” or “no” answer.
The datacollected was analysed by using SPSS statistical package8. Descriptive statistics were used to summarize the characteristics of the study population. The two sub-samples (patients & doctors) were compared with each other regarding different variables by using a t-test, which highlighted the absolute and relative differences among those.
Results:
196 subjects were approached to participate. 187 subjects (patients = 92, doctors = 95) participated, which represents a response rate of 95%.
Male to female ratio was roughly equal in the sample but there were more females in the medical group (56%) as compared to the patient (46%) group. Among responders, those over 40 years of age were more prevalent in the patient group (60% vs. 39%) compared to the medical group.
As shown in the Table 1, patients’ and doctors’ attitudes overwhelmingly leaned towards a patient being called a “patient” (as opposed to “client”, “service user” or “customer”); understanding “clinician” as a doctor (as compared to being a nurse, social worker or psychotherapist), and believing psychiatrist to be a “consultant” (preferred to nurse practitioner, psychologist or social worker).
Table1: Patients’ & doctors’ attitudes to medical professional terms = “patient”, “clinician” and “consultant”
What do you prefer to be called?
Doctors (%)
Patients (%)
Client
16 (17)
13 (14)
Patient
68 (72)
65 (71)
Service user
10 (11)
11 (12)
Customer
1 (1)
3 (3)
Don’t know
0
0
Total
95
92
Chi2 1.378, p = 0.710
Which of these is a clinician?
Doctors (%)
Patients (%)
Nurse
14 (15)
14 15)
Social worker
4 (4)
2 (2)
Doctor
56 (59)
70 (76)
Psychotherapist
7 (7)
6 (6)
Don’t know
14 (15)
0 (0)
Total
95
92
Chi2 16.3, p<0.05
Which of these is a consultant?
Doctors (%)
Patients (%)
Psychiatrist
71 (75)
68 (74)
Psychologist
3 (3)
6 (7)
Social worker
10 (11)
10 (11)
Nurse practitioner
3 (3)
8 (9)
Don’t know
8 (8)
0 (0)
Total
95
92
Chi2 11.3, p<0.05
Patients and doctors seemed to prefer (>70%) calling the person who provides the patient support in the community as “care-coordinator” or “key worker”.
It is worth noting that “key worker” is the main person looking after the patient admitted to hospital and “care-coordinator” has the same role when they are back in the community. Similarly, the majority of the patients deemed the terms “Acute ward” and “PICU” (psychiatric intensive care unit) appropriate for a psychiatric ward.
There was strong evidence to suggest that both patients and doctors were confused as to what a ‘medication review’ was; as approximately 35% of them thought it was a “nursing handover” and the rest were divided whether it was a “pharmacist meeting” or an “assessment”. See Table 2.
This is understandable because the patients are used to an “Out Patient Appointment/Review” where a psychiatrist reviews patients in a holistic manner, which includes prescribing and adjusting their medications. Similar confusion prevailed regarding what has replaced the term “ward round”, as both groups were universally divided among choices offered as “MDM” (multidisciplinary meeting), “Assessment”, “CPA” (Care Programme Approach) and “Review”.
Table 2: Patients’ & doctors’ attitudes to what a “ward round” and “medication review” means?
Which of these means a ward round?
Doctors (%)
Patients (%)
Assessment
26 (27)
34 (37)
MDM
18 (19)
15 (16)
Review
34 (36)
29 (32)
CPA
16 (17)
14 (15)
Don’t know
1 (1)
0 (0)
Total
95
92
Chi2 2.82, p = 0.588
Which of these is a medication review?
Doctors (%)
Patients (%)
OPD
19 (20)
11 (12)
Assessment
25 (26)
34 (37)
Pharmacist meeting
34 (36)
31 (34)
Nursing handover
14 (15)
12 (13)
Don’t know
3 (3)
4 (4)
Total
95
92
Chi2 3.89, p = 0.421
Both patients and doctors were clear (84% vs. 69%) that they expected to see a doctor when they attended a “clinic”. However, both groups were approximately equally divided between their preferences for what a psychiatry trainee should be called; “SHO” (37%) or “Psychiatric trainee” (36-40%). There was also a higher preference (approx. 50% vs. 30%) for the doctor a grade below consultant to be called a “Senior Registrar”.
Patients and doctors were equivocal in their response that they have never been consulted about medical professional terminology.
Fig. 1 Has anyone consulted you about these terms?
Discussion:
In a survey of attitudes to the use of medical professional terms among patients and doctors in a psychiatric service, we have found a significant preference for the older and established medical terms as compared to the newer terms such as MDM, CT trainee, Specialty Trainee, etc.
While replicating findings of other studies3,7, we also found that no single term was chosen by 100% of participants in either group, showing confusion surrounding most psychiatric terms. This lack of consensus and confusion can be explained by the fact that no participant had ever been consulted about the changes or new nomenclature.
Limitations to this study should be taken into account before generalising the results. The patients’ group is older than the doctors’ group, which could skew the results due to age related bias in favour of familiarity and against change9. In a questionnaire about preference and understanding, participants may intuitively prefer the easiest to understand terms and ignore the subtle difference between other styles. Possibility of bias may have been introduced by some of those giving out questionnaires being doctors
Our sample was drawn only from a psychiatric service, which may restrict the implications of our findings to mental health.
Furthermore, involvement of other professionals and carers working in the psychiatric service would have been useful to expand the scope of this study.
Inconsistency regarding doctors’ titles, unleashed by the Modernising Medical Careers (2008) initiative, has resulted in patients considering trainees as medical students5, not recognising ‘Foundation Year 1 Trainees’ as qualified doctors and being unable to rank doctors below consultant level3. Our findings have highlighted the uncertainty regarding qualifications and seniority of doctors – this can erode patients’ confidence in their doctors’ abilities, compromise therapeutic relationship10, especially in psychiatry, and result in poor treatment compliance. Medical students may also find themselves mistaken for doctors, and feel daunted by future job progression where training structures and status are unclear.
Title changes introduced by local management or Department of Health (DoH), without consultation with stakeholders, have the potential to create inter-professional tensions and devalue the myriad skills offered by healthcare workers other than doctors. This could also be damaging to their morale and the confidence instilled in patients. It is interesting to note, however, that titles that do not give the impression of status and experience, such as “trainee”, tend not to be adopted by non-doctor members of the multidisciplinary team3. On the other hand, in a profession steeped in tradition, there will be doctors who see other professionals’ adoption of their respect-garnering and previously uncontested titles as a threat to the status of the medical profession6. Previous studies have shown that terminology has a significant effect on the confidence and self-view of doctors5 and at a time where a multitude of issues has led to an efflux of U.K. junior doctors to other countries, and a vote for industrial action, re-examining a seemingly benign issue involving titles and terminology could have a positive impact.
Patients’ attitudes to development of surgical skills by surgical nurses show that they would like to be informed if the person doing a procedure is not a doctor7.
The roles of a number of professionals involved in an individual’s healthcare can be confusing and the possibility of mistaken identity could be considered misleading6, unethical, and even fraudulent. Introducing confusion by appropriating titles associated with doctors could be damaging to patients’ trust, and is inappropriate in a health service increasingly driven towards patient choice. The challenge lies in how to keep the terminology consistent and used in the best-understood contexts.
Commissioners and managers may instead evaluate the implications of changing professional terms by making sure that all stakeholders are consulted beforehand. Perhaps the pressing source of inconsistency in staff job titles could also be rectified by a broader scale study to find national, multidisciplinary and patient preferences, and taking simple measures such as standardising staff name badges.
Our study has highlighted once again how the landscape of nomenclature in psychiatry/medicine is pitted with inconsistency. While language naturally evolves with time and it may be understandable to see increasing application of business models & terminology in the NHS9, medical professional terms have been determined contextually over the years with significant implications for patient management and safety. Therefore, it is important to question how changes in terminology affect patients, whether it occurs by gradual culture change or due to new initiatives. It would benefit patient care if medical and psychiatric professional language could be standardised and protected from changes, which can lead to colleagues and patients being misled. DoH, Commissioners and Trust/Hospital management must recognise that changing terminology can have a significant impact and that serious discussion of such changes is important for reasons far beyond pedantry. For inter-professional communication a formalised consensus on titles would be beneficial for transparency, trust, patient safety and reducing staff stress levels.
Striae distensae, or stretch marks, are linear scars in the dermis which arise from rapid stretching of the skin over weakened connective tissue. It is a common skin condition that rarely causes any significant medical problems but is often a significant source of distress to those affected. Striae distensae were described as a clinical entity hundreds of years ago, and the first histological descriptions appeared in the medical literature in 1889.1 With a high incidence and unsatisfactory treatments, stretch marks remain an important target of research for an optimum consensus of treatment. These appear initially as red, and later, as white lines on the skin, representing scars of the dermis, and are characterized by linear bundles of collagen lying parallel to the surface of the skin, as well as eventual loss of collagen and elastin. The estimated prevalence of striae distensae range from 50 to 80%.2,3 The anatomical sites affected vary, with areas commonly affected including the abdomen, breasts, thighs and buttocks.4 The three maturation stages of striae include the acute stage (striae rubra) characterized by raised, erythematous striae, the sub-acute stage characterized by purpuric striae, and the chronic stage (striae alba), characterized by white or hypo-pigmented, atrophied striae.5 Although stretch marks are only harmful in extreme cases, even mild stretch marks can cause distress to the bearer6 (Table 1).
Table 1: Histological comparisons between striae rubrae and striae albae
Epidermis
Oedema Increased melanocytes
Epidermal atrophy Loss of rete ridges Decreased melanocytes
Papillary dermis
Dilatation of blood vessels
No vascular reaction
Reticular dermis
Structural alteration of collagen fibres Reduced and reorganized elastic fibres Fine elastic fibres in dermis
Densely packed collagen parallel to skin surface. Thick elastic fibres in dermis
Inflammatory cells
Lymphocytes and fibroblasts
Eosinophills
Aetiology
Striae may result from a number of causes, including, but not limited to, rapid changes in weight, adolescent growth spurts, corticosteroid use or Cushing Syndrome, and generally appear on the buttocks, thighs, knees, calves, or lumbosacral area.7 In addition, approximately 90% of all pregnant women develop stretch marks either on their breasts and/or abdomen by the third trimester.8 Genetic predisposition is also presumed, since striae distensae have been reported in monozygotic twins.9,10 There is decreased expression of collagen and fibronectin genes in affected tissue.11 The role of genetic factors is further emphasised by the fact that they are common in inherited defects of connective tissue, as in Marfan’s syndrome.12,13 Obesity and rapid increase or decrease in weight have been shown to be associated with the development of SD.14 Young male weight lifters develop striae on their shoulders.15 Striae distensae also occurs in cachetic states, such as tuberculosis, typhoid and after intense slimming diets.16 Rare etiologies include human immunodeficiency virus positive patients receiving the protease inhibitor indinavir and chronic liver disease.13,15 A case of idiopathic striae was also reported.17
Rosenthal18 proposed four aetiological mechanisms of striae formation: insufficient development of tegument, including elastic properties deficiency; rapid stretching of the skin; endocrinal changes; and other causes, possibly toxic.
Pathogenesis
The pathogenesis of striae is unknown but probably relates to changes in the components of extracellular matrix, including fibrillin, elastin and collagen.19 There has been emphasis on the effects of skin stretching in the pathogenesis of striae because the lesions are perpendicular to the direction of skin tension.20 A possible role of glucocorticoids in the pathogenesis of striae has been suggested because of an increase in the levels of steroid hormones and other metabolites found in patients exhibiting striae.21 There are studies suggesting the role of fibroblasts in the pathogenesis of striae. Compared to normal fibroblasts, expression of fibronectin and both type I and type III procollagen were found to be significantly reduced in fibroblasts from striae, suggesting that there exists a fundamental aberration of fibroblast metabolism in striae distensae.22
Pathological aspects
The earliest pathological changes are subclinical to be detected by electron microscopy only. These changes include mast cell degranulation and the presence of activated macrophages in association with mid-dermal elastolysis.23 When the lesions become become clinically visible, collagen bundles start showing structural alterations, fibroblasts become prominent, and mast cells are absent.23 On light microscopic examination, Inflammatory changes are conspicuous in the early stage, with dermal oedema and perivascular lymphocytic cuffing.24 In later stages, there is epidermal atrophy, loss of rete ridges and other appendages including hair follicles are absent.25
Evaluation of striae distensae
Approaches to evaluating SD severity visually include the Davey 26 and Atwal scores,27 although these have not been validated specifically for SD. An objective evaluation of SD may be carried out using skin topography, imaging devices including three-dimensional (3D) cameras, reflectance confocal microscopy and epiluminescence colorimetry.28,29,30
Table 2: Visual scoring systems for the assessment of striae distensae
Davey method
Used for evaluating striae rubrae and albae. Divide the abdomen into quadrants using midline vertical and horizontal lines. Each quadrant given a score (0 no SD; 1 moderate number of SD; 2 many SD). Score given out of 8.
Atwal score
Used for evaluating striae rubrae and albae. Six sites chosen (abdomen, hips, breasts, thigh/buttocks). Each site given a maximum score of six. Total score out of 24. Score 0–3 for the presence of striae (0 no SD; 1 < 5 SD; 2 5–10 SD; 3 > 10 SD). Score 0–3 for the presence of erythema (0 no erythema; 1 light red/pink; 2 dark red; 3 purple).
Management
Striae distensae (striae alba) is a very challenging cosmetic problem for dermatologists to treat. Various modalities of treatment have been tried. Although therapeutic strategies are numerous, there is no treatment which consistently improves the appearance of striae and is safe for all skin types.31 Weight loss by diet alone or a combination of diet and exercise do not change the degree of striae distensae.32
Topical treatments
Topical tretinoin (0.1%) ameliorates striae and the improvement may persist for almost a year after discontinuation of therapy.33 More recently, tretinoin has been shown to improve the clinical appearance of stretch marks during the active stage (striae rubra), although with not much effect during the mature stage (striae alba).34 Some of the studies have proven the inefficacy of the vitamin A derivative in the treatment of SD, but most of the patients included in these early studies presented with old lesions that had evolved into whitish atrophic scars.35 A study comparing topical 20% glycolic acid and 0.05% tretinoin versus 20% glycolic acid and 10% L-ascorbic acid, found that both regimens improved the appearance of striae alba.36
Hydrant Creams: 1) Trofolastin (a cream containing Centella asiatica extract, vitamin E, and collagen-elastin hydrolysates). The exact mechanism of action was identified as the stimulation of fibroblastic activity 37 and an antagonistic effect against glucocorticoids.38 2) Verum (a cream containing vitamin E, panthenol, hyaluronic acid, elastin and menthol). The results suggest that the product may show the benefit of massage alone.39 3) Alphastria (a cream composed of hyaluronic acid, allantoin, vitamin A, vitamin E, and dexpanthenol). Only one study was conducted, which concluded that the product markedly lowered the incidence of stretch mark development after pregnancy.40
Glycolic acid (GA): The exact mechanism of action of GA in the management of striae distensae is still unknown because, although GA is reported to stimulate collagen production by fibroblasts and to increase their proliferation in vivo and in vitro, which may be useful for the treatment of stretch marks.41,42 A study comparing topical 20% glycolic acid and 0.05% tretinoin versus 20% glycolic acid and 10% L-ascorbic acid, found that both regimens improved the appearance of striae alba.43
Trichloroacetic acid (TCA; 10–35%): It has been used for many years as a treatment option for striae distensae and is repeated at monthly intervals with reported improvement in texture and color of marks.44
Other topical products: Several oils have been used in the prevention of SD. A non-randomized, comparative study investigated the effect of almond oil in the prevention of SD in which they noted significant differences in the frequency of SD between the groups (almond oil and massage 20%, almond oil alone 38.8%, control 41.2%).45
Overall, there is limited evidence for the efficacy of topical therapy for the treatment of SD.
Microdermabrasion
Microdermabrasion may improve many skin problems including acne scars, skin texture irregularities, mottled pigmentation and fine wrinkles. Karimipour et al reported that microdermabrasion induces epidermal signal transduction pathways associated with remodelling of the dermal matrix.46 However, studies documenting the efficacy of rnicrodermabrasion in treatment of striae are lacking. Published in 1999, a book on microdermasion written by a French dermatologist, Francois Mahuzier, and translated to English, has a chapter "Microdermabrasion of stretch marks”.47 The author states that 10-20 sessions of microdermabrasion at an interval of not less than 1 month, each session resulting in bleeding points, provide satisfactory results. The author concludes that, "microdermabrasion is the only effective treatment of stretch marks today."
Lasers
Lasers have recently become a popular therapeutic alternative to ameliorate and improve the appearance of stretch marks. Most commonly used lasers used include pulsed-dye laser (PDL), short- pulse carbon dioxide and erbium-substituted yttrium aluminium garnet (YAG), neodymium- doped YAG (Nd:YAG), diode, and Fraxel.
Pulsed dye laser: The dilated blood vessels render the striae rubrae a good candidate for PDL.48 The 585- nm pulsed dye laser has a moderate beneficial effect in the treatment of striae rubra.49 To evaluate the effectiveness of the 585-nm flashlamp-pumped pulse dye laser in treating cutaneous striae, 39 striae were treated with four treatment protocols.50 Subjectively, striae appeared to return toward the appearance of normal skin with all protocols. Objectively, shadow profilometry revealed that all treatment protocols reduced skin shadowing in striae. Laser treatment of SD should be avoided or used with great caution in darker skin types (IV–VI), because of the possibility of pigmentary alterations after treatment.51
Excimer laser: Studies have shown temporary repigmentation and improvement of leukoderma in SD with excimer laser, although it failed to show any improvement in skin atrophy.52,53 To evaluate the true efficacy of the 308-nm excimer laser for darkening striae alba, 10 subjects were treated using the excimer laser on the white lines of striae, while the normal skin near to and between the lines was covered with zinc oxide cream. The results of this study showed the weakly positive effect of the 308-nm excimer laser in the repigmentation of striae alba.54
Copper Bromide laser: copper-bromide laser (577-511 nm) has been used for stretch marks. A clinical study was conducted in 15 Italian women with stretch marks, treated with the CuBr laser (577-511 nm) and followed-up for 2 years.55 The results of the study concluded that the copper-bromide laser was effective in decreasing the size of the SD and there were some pathogenic considerations that justified the use of this laser.
1,450-nm Diode Laser: The non-ablative 1,450-nm diode laser has been shown to improve atrophic scars and may be expected to improve striae. To evaluate the efficacy of the 1,450-nm diode laser in the treatment of striae rubra and striae alba in Asian patients with skin types 4-6, striae on one half of the body in 11 patients were treated with the 1,450-nm diode laser with cryogen cooling spray with the other half serving as a control.56 None of the patients showed any noticeable improvement in the striae on the treated side compared to baseline and to the control areas. The study concluded that the non-ablative 1,450-nm diode laser is not useful in the treatment of striae in patients with skin types 4, 5, and 6.
1,064-nm Nd:YAG Laser: A study was aimed to verify the efficacy of this laser in the treatment of immature striae in which 20 patients with striae rubra were treated using the 1,064-nm long-pulsed Nd:YAG laser.57 A higher number of patients (55%) considered the results excellent when compared to the same assessment made by the doctor (40%).
Intense Pulsed Light: In order to assess the efficacy of IPL in the treatment of striae distensae, a prospective study was carried out in 15 women, all of them having late stage striae distensae of the abdomen.58 All the study subjects showed clinical and microscopical improvement after IPL. It seems to be a promising method of treatment for this common problem with minimal side-effects, a wide safety margin and no downtime.
Fractional Photothermolysis: To determine the efficacy of fractional photothermolysis in striae distensae, 22 women with striae distensae were treated with two sessions each of fractional photothermolysis at a pulse energy of 30 mJ, a density level of 6, and eight passes at intervals of 4 weeks and response to treatment was assessed by comparing pre- and post-treatment clinical photography and skin biopsy samples.59 Six of the 22 patients (27%) showed good to excellent clinical improvement from baseline, whereas the other 16 (63%) showed various degrees of improvement. This study concluded that Fractional photothermolysis may be effective in treating striae distensae, without significant side effects.
Ablative 10,600-nm carbon dioxide fractitional laser: Ablative 10,600-nm carbon dioxide fractional laser systems (CO₂ FS) have been used successfully for the treatment of various types of scars. To assess the therapeutic efficacy of CO₂ FS for the treatment of striae distensae, 27 women with striae distensae were treated in a single session with a CO₂ FS and clinical improvement was assessed by comparing pre- and post-treatment clinical photographs and participant satisfaction rates.60 The evaluation of clinical results 3 months after treatment showed that two of the 27 participants (7.4%) had grade clinical 4 improvement, 14 (51.9%) had grade 3 improvement, nine (33.3%) had grade 2 improvement, and two (7.4%) had grade 1 improvement. None of the participants showed worsening of their striae distensae.To assess and compare the efficacy and safety of nonablative fractional photothermolysis and ablative CO(2) fractional laser resurfacing in the treatment of striae distensae, 24 ethnic South Korean patients with varying degrees of atrophic striae alba in the abdomen were enrolled in a randomized blind split study and were treated with 1,550 nm fractional Er:Glass laser and ablative fractional CO(2) laser resurfacing.61 These results of the study support the use of nonablative fractional laser and ablative CO(2) fractional laser as effective and safe treatment modalities for striae distensae of Asian skin with neither treatment showing any greater clinical improvement than the other treatment.
UVB/UVA1 Combined Therapy: Besides lasers, light sources emitting ultraviolet B (UVB) irradiation have been shown to repigment striae distensae. A study was conducted on 9 patients with mature striae alba who received 10 treatment sessions, and biopsies were taken at the baseline and end of the study.62 At the end of the study, all patients reported some form of hyperpigmentation that was transient and did not affect any surrounding tissues. No changes were seen on biopsy to indicate an effective remodelling collagen effect of the device, although it needs further assessment. Another study was conducted to analyse the histologic and ultrastuctural changes seen after UVB laser- or light source-induced repigmentation of striae distensae in which analyses of biopsied skin after treatment with both the UVB laser and light source showed increased melanin content, hypertrophy of melanocytes, and an increase in the number of melanocytes in all patients.63
Radiofrequency devices: RF devices are based on the principle of heat generation that occurs in response to poor electrical conductance according to Ohm’s law (heat generation is directly correlated with tissue resistance). The heat that is generated is sufficient to cause thermal damage to the surrounding connective tissue,64 which is responsible for the partial denaturation of pre-existing elastic fibers and collagen bundles.65 Initial collagen denaturation within thermally modified deep tissue is thought to represent the mechanism for immediate tissue contraction; subsequent neocollagenesis further tightens the dermal tissue and reduces striae.66 The efficacy and safety of combination therapy with fractionated microneedle radiofrequency (RF) and fractional carbon dioxide (CO2) laser in the treatment of striae distensae has been evaluated revealing that this combination therapy is a safe treatment protocol with a positive therapeutic effect on striae distensae.67 A recent study evaluating the effectiveness of a RF device in combination with PDL subjected 37 Asian patients with darker skin tone with SD to a baseline treatment with a RF device and PDL.68 All histological evaluations demonstrated an increase in the amount of collagen fibers, and six of the nine specimens showed an increase in the number of elastic fibers.TriPollar RF device appears to be a promising alternative for the treatment of striae distensae in skin phototypes IV-V.69
Needling therapy:
To evaluate the effectiveness and safety of a disk microneedle therapy system (DTS) in the treatment of striae distensae, 16 Korean volunteers with striae distensae alba or rubra were enrolled which received three treatments using a DTS at 4-week intervals.70 Marked to excellent improvement was noted in seven (43.8%) patients, with minimal to moderate improvement in the remaining nine. This study revealed that Disk microneedle therapy system (DTS) can be effectively and safely used in the treatment of striae distensae without any significant side effects. Another study assessed and compared the efficacy and safety of needling therapy versus CO2 fractional laser in treatment of striae and the results supported the use of microneedle therapy over CO2 lasers for striae treatment.71
Platelet-rich plasma:
Platelet-rich plasma has these wound-healing properties, affecting endothelial cells, erythrocytes, and collagen,72 which potentially aids in the healing of the localized chronic inflammation believed to be a factor in the aetiology of striae distensae. Platelet-rich plasma is well tolerated by the patients and is a safe and cost effective treatment option for striae distensae.
Platelet-rich plasma alone is more effective than microdermabrasion alone in the treatment of striae distensae, but it is better to use the combination of both for more and rapid efficacy.73
The plasma fractional radiofrequency and transepidermal delivery of platelet-rich plasma using ultrasound has also been found to be useful in the treatment of striae distensae.74
Since thermal damage from intradermal RF has characteristics similar to those of many wounds, combination treatment with intradermal RF and autologous PRP would eventuate in enhanced localized collagen neogenesis and redistribution. In one of the studies, three sessions of intradermal RF were used combined with autologous PRP administered once every four weeks.75 All of the participants showed satisfactory changes and no patient was reported to show no improvement.
Transepidermal retinoic acid:
Transepidermal retinoic acid delivery using ablative fractional radiofrequency associated with acoustic pressure ultrasound has also been used for the treatment of stretch marks.76
Conclusion
Striae distensae are an extremely common, therapeutically challenging form of dermal scarring. Adequate scientific knowledge and the evidence behind both preventative and therapeutic agents are vital in order to understand striae and to offer patients the best therapeutic options. The treatment of this cosmetically distressing condition has been disappointing and there is no widely accepted surgical procedure for improving the appearance of stretch marks. Laser therapy has been advocated as a treatment for striae distensae.
Hepatitis viruses are the most widespread cause of hepatitis and some cancer lymphomas in humans1.Hepatitis is a serious disease of the liver and described as a lifelong infection with swelling and inflammation (presence of inflammatory cells) in the liver, that if progresses, may lead to cirrhosis (scarring) of the liver, liver cancer, liver failure, and death. Hepatitis B (HBV) and Hepatitis C (HCV) are one of the viral types of hepatitis that leads to jaundice (a yellow discolouration of skin, mucous membrane and conjunctiva of the eye), anorexia (poor appetite), fatigue and diarrhoea and presumably it remains undiagnosed and leads to chronic carrier state but most infected individuals remain asymptomatic1-3. The hepatitis B virus is a DNA virus belonging to the Hepadnaviridae family of viruses and hepatitis C virus is a small, single stranded, RNA virus with a diameter of about 50 nm, belonging to Flaviviridae family of virus. Hepatitis B surface antigen (HBsAg) is present in the serum of those infected with hepatitis B, consisting of the surface coat lipoprotein of the hepatitis B virus. Anti-HCV antibody, a substance that the body makes to combat HCV 4. Hepatitis B virus is transmitted through blood and blood products, semen, vaginal fluids, and other body fluids. Hepatitis C virus is a blood borne or parenterally transmitted infection. Vehicles and routes of parenteral transmission include; contaminated blood and blood products, multi-transfusions (thalassemic and haemophilic patients), needle sharing, contaminated instruments (e.g. in haemodialysis, reuse of contaminated medical devices, tattooing devices, acupuncture needles, razors) and occupational and nosocomial exposure5-8. It stands to reason that an occupational risk for transmission of hepatitis virus in the health care setting, where unknown carriers of hepatitis infections are undergoing different procedures, in which there is a chance of contact of percutaneous blood, including transmission from infected patients to staff, from patient to patient, and from infected providers to patients9. There is a lack of routine serological screening prior to surgery, which is one of the factors responsible for increased disease transmission. The major risk factors include; re-use of contaminated syringes, surgical instruments and improperly screened blood products2. Without meticulous attention towards infection control and disinfection and sterilization procedures, the risk for transmission of blood borne pathogens in the health care setting is magnified.
The aim of our current study was to estimate the incidence of Hepatitis B and Hepatitis C among patients going through eye surgery at department of ophthalmology Liaquat University of Medical and Health Sciences Jamshoro at Hyderabad. This is one of the largest tertiary care centres in Sindh. This institution is a great referral centre for whole interior Sindh province.
MATERIAL AND METHODS
Study design and patients
This prospective observational study was carried out at Liaquat University Eye Hospital, Hyderabad, from June 2014 to February 2016. A total of 2200 patients undergoing eye surgery, who were unaware of hepatitis B & C infection were included in this study. No restriction was placed based on age and gender to ensure maximum participation.
Blood samples
The blood samples of all these patients were collected in the Hospital laboratory, Scientific Ophthalmic Diagnosis & Research Lab. Each patient was serologically screened, by using immuno-chromatography (ICT method) for qualitative detection of antigen for Hepatitis B and Hepatitis C virus antibodies, to find the carrier status of patients before surgery.
The blood was collected by a qualified technician / phlebotomist of our hospital laboratory under supervision of a consultant pathologist. Samples were allowed to coagulate at room temperature for 30 minutes, and then centrifuged at 3000 revolutions per minute (RPM) for 10 minutes. The serum samples were separated and kept frozen at -20°C for chemical and immunoassays. The HBV screening was based on the detection of antigen and detection of viral specific antibodies HCV in the sera using enzyme immunoassays. The test only shows whether a person has ever been infected by HBV or HCV, and not whether the virus is still present. According to the manufacturers’ literature, the relative sensitivity and specificity of HCV and HBV testing kits was 96.8% and 99% respectively.
Those patients with test results were found positive on screening test, were further confirmed by testing ELISA (Enzyme-Linked Immunosorbent Assay) method (4th generation ELISA) and were given advised for further testing on Polymerase Chain Reaction (PCR) for qualitative or quantitative detection of DNA/RNA (the viral gene).
All the data was entered in SPSS version 16 and the prevalence and percentage of all variables was measured.
RESULTS
A total number of 2200 patients were operated during the study, 1255 (57.04%) patients were male and 945 (42.95%) were female
Of these 2200 patients, 338 (15.36%) were serologically positive for hepatitis B virus & hepatitis C virus. Out of the 338 HBV or HCV positive patients, 56 patients (2.54%) were positive for hepatitis B surface antigen (HBsAg) and 282 patients (12.81%) were positive for hepatitis C antibody (HCVAb). (Figure 1&2). The majority of them were female, and 226 (66.86%) were in their 4th and 5th decade of life in both sexes (Figure 3).
Figure 1- A: Serologically positive for hepatitis C antibodies, B: Serologically negative for hepatitis C antibodies
Figure 2 - A: Serologically negative for hepatitis B antigen, B: Serologically positive for hepatitis B antigen
Figure 3: Incidence of Hepatitis B & C in different age group
DISCUSSION
Hepatitis B virus (HBV) and hepatitis C virus (HCV) are among the principal causes of liver diseases, with different frequency rates and various types all over the world. The World Health Organization (WHO) estimates that there are near 4 million people with chronic HBV infection and 170 million people with chronic HCV infection worldwide. Mortality rate of Hepatitis B is estimated to result in 563,000 deaths and hepatitis C in 366,000 deaths annually 1, 6, 10-12. The occurrence of hepatitis varies from country to country. The epidemiological estimates by WHO show that there is low prevalence of hepatitis C (<1%) in Australia, Canada and Northern Europe, and almost 1% in countries of medium endemism, such as the USA and most of Europe. The frequency is at its peak (>2%) in many countries of Africa, Latin America, Central and South-East Asia 5. As far as the Pakistani population is concerned, the incidence of hepatitis B and C is escalating. Previous studies reveal that the Pakistani population affected by HBV 10% and HCV is 5-10% 3. At times it will also vary among different regions of the same country, and is continuing to rising in certain parts, especially in the rural areas, the percentage of infected individuals is significantly higher 2. The total incidence of Hepatitis B and Hepatitis C in our study was found to be 15.36%. This was almost comparison to Naeem et al found to be 12.99% 2 and in our previous study reported incidence of anti HCV was 29.60% 7. W Ul Huda et al reported 17.33% incidence of HCV infection among their operated patients5, whereas a study conducted by Khurrum et al reported 6% incidence of anti HCV antibodies in health care workers in a local hospital13. The prevalence of Hepatitis B and Hepatitis C in preoperative cataract patients was found to be higher in males (59.18%) than females (40.82%), and Ahmed et al also showed that the total prevalence of Hepatitis B and Hepatitis C in males was very high compared to females among preoperative cataract patients14, which is controversial to our result. A study conducted in 2010 on different eye camps in Pakistan showed that 108 out of 437 patients were infected with Hepatitis B and Hepatitis C with a higher prevalence of the diseases in females with 60.18% (65/ 108) than in males with 39.81% (43/108) 15. Concerning demographic variables, the increase in the risk for HCV seropositive incidences increased with the age i.e. 7.1% at the age of 20 to 30 years whereas 21.4% at the age of 40 to 50 years. In our study, the higher prevalence of hepatitis B & C were in the age range of 30 – 60 years, which is comparable to the study of Talpur et al, in which 65% positive patients were above the age of 40 years16.
This study shows that the prevalence of these hepatitis causing viral pathogens are quite high. Doctors and paramedical staff in surgical and medical practice are at high risk of acquiring blood borne diseases from the patients on whom they operate.
CONCLUSION
The aim of the present study was to assess the prevalence of HBV and HCV infection among preoperative patients. The incidence of these hepatitis causing viruses are higher in our population. Therefore, it is a mandatory task to screen every patient for hepatitis B and C before any surgical procedure. The surgeons and health care professionals should protect themselves by using protective masks, eye protection glasses, and double gloves before handling infected cases. The used infected material, needles and other waste material should be destroyed properly using Biosafety protocols.
One in four adults are affected by musculoskeletal (MSK) problems, which account for up to 30% of General Practice (GP) consultations in the United Kingdom..1 Some GPs have direct access to community MSK services, but when not available, referrals are made to secondary care departments such as rheumatology. MSK training involves the skills that a rheumatologist needs to achieve competencies in the diagnosis and treatment of soft tissue rheumatism as opposed to inflammatory rheumatic joint disease.
It has been reported that junior doctors in the United Kingdom fail to routinely screen for MSK conditions on admission onto general medical or surgical wards2 which may be reflective of training issues. It was in our anecdotal opinion that MSK training at higher specialist training was being compromised as well. Within the United Kingdom doctors in training typically begin work as a first year rheumatology trainee four years after graduation from medical school following completion of both a two year foundation programme (encompassing a generic training programme which forms the bridge between medical school and specialist/general practice training) and a two year Core Medical Training programme, (involving 2 years of training, undertaking between four and six rotations in different medical specialties). At the time of writing, higher specialty training, such as in rheumatology, began at the level of Specialist Trainee 3 (ST3) and was either a four year training programme or a 5 year training programme if trainees were dually accrediting in general medicine.3 Higher specialist training involves rotating through different rheumatology departments within each Local Education Training Board (LETB).
In our opinion, the basic MSK skill set is essential to the training of a competent rheumatologist and trainees gain overall MSK competencies within routine clinical practice as they rotate through different hospitals during training. However, in some training programmes, there is very little MSK training opportunities, as MSK centres operating in the community in the United Kingdom, mean that these patient groups are not being treated in training hospitals. Faculty in these centres are competent to train, but training opportunities in MSK centres are reduced.
Rheumatology registrars in-training have expressed the anecdotal view that MSK training may be compromised, partly due to the reduction of referrals to secondary care and partly due to the inevitable focus on training in the more complex inflammatory conditions.
Rheumatology trainees in the UK were surveyed in 2015 on behalf of the Rheumatology Specialist Advisory Committee to assess confidence and ability in dealing with MSK conditions during and on recent completion of training. The survey was disseminated to rheumatology trainees via the trainee representative from each LETB.
77 responses were received across 15 LETBs from a total of an estimated 223 trainees. 20 of these surveys were incomplete, with not all questions being answered but those questions answered were considered in the results of this survey. Responses from trainees across all career grades from ST3 (1st year of specialist training) to 2 years post Certificate of Completion of Training were received.
58 out of 63 doctors (92%) thought MSK medicine to be an important part of rheumatology training. Free text comments recognised that MSK conditions were frequently referred to rheumatology and differentiating between inflammatory and non-inflammatory pain is important.
Only 41 out of 64 doctors (64%) felt they managed patients with soft tissue pathology on a daily basis and 20 out of 63 (32%), felt they were not yet confident in diagnosing and distinguishing between different types of soft tissue pathologies.
Exposure to, and experience with MSK medicine in current jobs and throughout training ranged from poor to excellent.
Only 9 out of 58 trainees (16%) felt they were lacking in competency for their level of training in managing the MSK pathologies outlined in the Joint Royal Colleges of Physicians Training Board (JRCPTB) 2010 rheumatology curriculum. The majority of trainees felt they were either partially competent in all, or some areas, satisfactory for their level of training.
Interestingly, only 39 out of 58 trainees (67%) felt their training in injection techniques had been at least ‘adequate’. Some trainees mentioned they had been self-taught in some injection procedures and training had been limited in certain soft tissue injections (most commonly plantar fasciitis, tendon sheath and elbow enthesis injections).
This survey has limitations in that the numbers of trainees surveyed were small. However, our total response number considering the usual poor response rate for online surveys is reasonable. Our survey was not validated and it is likely that there will be an element of selection bias in the responses received.
However, one of the strengths of our survey is the ability to review responses by seniority. We analysed further the confidence rating according to training level grade and we looked into two main subgroups, the more junior trainees (ST3 and ST4s) and the more senior trainees (ST6 and ST7). As expected the more junior cohort rated their confidence slightly lower compared to the more experienced group. Within the junior group (n=17) only 41% suggested they felt confident for their level of training when generically asked about their general diagnostic skills on MSK, which improved to 59% when this question was mapped to the curriculum. In the senior group of ST6 and ST7 (n=25), the confidence levels were significantly higher (80% felt confident appropriate to their level of training) and there was no change in confidence levels when skills were mapped to the curriculum. (Table 1). This may reflect the natural increase in experience and exposure to MSK medicine with progression in training, but also the better understanding of the curriculum requirements by the more senior trainees.Only one fully completed survey was received from a rheumatologist post Certificate of Completion of Training making this subgroup too small for further analysis.
Table 1:
(n)
Q6) Confidence in dealing with MSK
% Q6
Q9) Confidence mapped to curriculum
% Q9
ST3 and ST4- junior
17
7
0.41
10
0.59
ST6 and ST7- senior
25
20
0.8
20
0.8
Q6) How confident do you feel in diagnosing and distinguishing between different types of soft tissue pathologies/MSK in your daily practice? Q9) Do you feel competent in diagnosing and managing the above MSK pathologies outlined in the 2010 rheumatology curriculum?
Within this limited survey, the views of 77 trainees have shown that training in MSK could be improved for rheumatologists in training at all levels. Although trainees felt they were lacking confidence in dealing with certain areas of MSK medicine, when competencies were mapped out to the rheumatology curriculum, trainees felt they were achieving appropriate competency for their level of training although this was not assessed objectively.
The trainees’ perception of the level of competency needed in dealing with MSK conditions seemed to overestimate the requirement of the 2010 rheumatology curriculum. In clinical practice, trainees may feel they encounter different MSK pathologies, which they are being expected to manage which are not being given sufficient emphasis within their curriculum. Further questioning in this area may conceivably lead to adjustments within the curriculum and the training programmes.
In particular, to improve training in MSK medicine, rheumatology trainees valued teaching from physiotherapists and being able to attend specialist sports medicine clinics. Trainees who had ‘independently’ taken time to gain experience in this way felt that their training had benefitted. To support trainees in achieving these competencies it may be worthwhile adding a prerequisite in the Annual Review of Career Progression (ARCP) process (a formal method in UK medical training by which a trainee’s progression through their training programme is monitored and recorded) to ensure dedicated time is set aside for this aspect of MSK rheumatology training. Completion in a range of direct assessments such as Clinical Evaluation Exercises (miniCEX), and DOPs (Directly Observed Procedures) may ensure competency in this aspect of rheumatology training as well as secure confidence in dealing with MSK conditions and soft tissue pathology.
With changes in the nature and geography of rheumatology specialist services we feel these aspects of rheumatology training should not be overlooked so trainees are equipped to deal with MSK conditions independently by their completion of training.
Like doctors in other specialties, general medical practitioners (GPs) are exposed daily to human suffering which most of society try to avoid.1 The World Health Organisation (WHO) predicts that by 2030 depression will be ‘the leading cause of disease burden globally.’ And that 1 in 4 individuals seeking health care are ‘troubled by mental or behavioural disorders, not often correctly diagnosed and/or treated.’2, 3 Doctors suffer from stress, anxiety and depression (as well as vascular disease, cirrhosis of the liver and road traffic accidents) more than the general population.4-10 Help for doctors is inadequate and doctors are reluctant to seek help.1, 4, 11 Where improvement is suggested, it is usually as counselling and general support.11 Instead of ‘more of the same’, we suggest a radically different approach: Adaptation Practice, which Clive Sherlock pioneered and has taught since 1975. It is pragmatic and safe. This study tests its acceptability to a group of working doctors.
Doctors bear the responsibility for fellow human beings’ health, well-being and, often, for their very survival. Added to this, GPs are under increasing pressure from more patients who want more cures and from health service managers who demand clinical excellence and more administration and more managerial skills of them. GPs’ stress is related to increasing workloads, changes to meet requirements of external bodies, insufficient time to do the job justice, paperwork, long hours, dealing with problem patients, budget restraints, eroding of clinical autonomy, and interpersonal problems.6, 10, 12 The recent rise in the GMC’s Fitness to Practice complaints related to patients’ expectations of doctors is yet another stress making them feel threatened.13
Job satisfaction for GPs is at its lowest level since a major survey started ten years ago, while levels of stress are at their highest. In 2015 there had been a year on year increase in the number of GPs reporting a slight to strong likelihood of their leaving ‘direct patient care’ within five years, with 53% of those under 50 and 87% of those over 50.6
By nature and vocation, GPs want to help but too much pressure is unbearable and takes its toll. They work, not with numbers, data or profits, but with human suffering, which, inevitably, is an emotional burden because of compassion and because it makes them aware of their own vulnerabilities and mortality. 3, 14 When combined with heavy workloads and low morale, doctors themselves inevitably suffer emotionally and psychologically.7, 10, 14 At the same time they and others feel they should be invincible.1, 15-17 What professional help is available for them is inadequate.3, 4, 18, 19 Existing support services in the UK are underfunded and sporadic.4 Some are outsourced to counselling services, and some of these are by telephone. Doctors do not like to be counselled and are reluctant to use these services.4, 15, 17
Doctors themselves are the mainstay for diagnosis and treatment of mental illnesses but are not adequately trained.3, 20 Mental illness is not well understood and conventional treatments are insufficient and often harmful. 15, 20-23 Consequently, doctors do not have the wherewithal to deal with the emotional and psychological problems they face every day in their patients and often in themselves, their colleagues and their families.4, 12, 18
There is significant prejudice, stigmatisation and intolerance of mental ill health within the medical profession due to lack of understanding and fear.3, 4, 9, 15, 17, 20, 21, 22, 24 This not only affects how doctors treat their patients, it also exacerbates their own difficulties when they suffer with emotional and psychological problems themselves, and dissuades them from self-disclosure and from seeking professional help.3, 4, 8, 10, 18, 20, 25, 26 To succumb to stress, anxiety and depression is seen as being weak and inadequate as a person and in particular as a doctor. 3, 4, 15 Doctors think they should know the answers and should be able to cope.1, 4
However, doctors are willing to learn work-related skills as this present study set out to show.11 Adaptation Practice is training; not treatment or therapy. The course in this study was presented as a postgraduate programme for doctors to learn how to cope with stress, anxiety and depression.
METHOD
Recruitment
We asked by letter all 314 GPs registered in one UK urban and semi-rural Health Authority Area if they would be interested in a course of twelve fortnightly seminars to learn the basics of Adaptation Practice: a programme of self-discipline to cope with stress, anxiety and depression. Included, was the Hospital Anxiety and Depression Scale (HADS). Those who responded and whose HADS scores were ≥ 8 (the threshold for anxiety and depression) were invited to the course.
Stress, anxiety and depression
Anxiety and depression were assessed by the HADS and stress by a simple stress scale (SSS – see Table 1) one month before training started, immediately prior to training, at three months (mid-way through the training) and at six months (at the end of training).
Table 1: The Simple Stress Scaledeveloped by Clive Sherlock and used to assess the level of stress in a subject. A total score ≥ 8, out of a maximum of 24 is suggestive of a disturbing level of stress or burnout.
I feel I am under too much stress: 0 hardly ever 1 occasionally 2 most of the time 3 all the time
I feel exhausted: 0 seldom 1 some of the time 2 much of the time 3 most of the time
I care about other people: 0 as much as I ever did 1 rather less than I used to 2 definitely less than I used to 3 hardly at all
I have lost my appetite: 0 not at all 1 a little 2 moderately 3 significantly
I sleep well: 0 most of the time 1 quite often 2 occasionally 3 not at all
I am irritable: 0 not at all 1 occasionally 2 quite often 3 very often indeed
I feel dissatisfied: 0 never 1 occasionally 2 quite often 3 most of the time
I feel run down: 0 not at all 1 occasionally 2 quite often 3 most of the time
Evaluation of Adaptation Practice
Half of those GPs who applied for the course were unable to attend because of prior commitments on the days planned for the course. These acted as a control group. Those who attended the course were the study group. All those who attended were also assessed in private by the authors immediately before and throughout the course. At the end of the course the doctors wrote anonymous self-assessments.
Training in Adaptation Practice
Those attending the course were taught not to express and suppress upsetting and disturbing emotion, not to distract their attention from it (including not to think about it and not to analyse it) and not to numb themselves to it with chemicals (alcohol, recreational drugs or prescribed medication). Instead, they learned how to engage with their moods and feelings physically, not cognitively, and how not to engage with thoughts about them. They were instructed to practise this six days a week with whatever they were doing, wherever they were. They were all offered unrestricted confidential telephone and e-mail support from the authors between training sessions and after the course had finished.
Statistical Analyses
The results are reported as means ± standard errors of the means. The scores were normally distributed and the data were analysed by analysis of variance with additional paired comparisons within periods, using the LSD method. Correlations were determined using Pearson’s correlation. The analyses were carried out using the statistical software programme SPSS 17.0 for Windows.
RESULTS
Recruitment
Of 314 registered GPs, 225 (72%) responded to our initial contact, and of these 152 (68%) said they would be interested in participating in the training course. Recruitment was restricted to those with HADS scores ≥ 8. Of the 225 who responded there were 71 (32%) for anxiety, 35 (16%) for depression, and 79 (35%) for both. 29 (13%) applied to attend the course. All were experienced GPs. 15 of these attended and 14 were not able to attend because of pre-existing commitments on the course dates. They asked for alternative dates but these were not available.
At the initial assessment (one month before the course started) there were significant correlations between the scores for anxiety and depression (P < 0.001), anxiety and stress (P < 0.001) and depression and stress (P < 0.001). At the second assessment immediately before the course started these correlations remained highly significant.
Effects of Adaptation Practice
All those who attended the course reported a subjective improvement in their abilities to cope with their own stress, anxiety and depression, and in their sense of well-being.
Anxiety
There were no significant differences between the control and study groups either one month before the start (P=0.949) or immediately before the first session (P=0.914). The anxiety scores in both groups remained greater than 8 at both assessments (Figure 1). At the mid-point of the course the mean score had fallen slightly in the study group (Figure 1) but the difference was not significant (P=0.652) By the end of the course the mean anxiety score in the study group was significantly lower (P=0.008) than that of the control group (Figure 1). The mean scores for anxiety decreased over the 4 assessments. This tendency was significant in the study group (P=0.002) but not in the control group (P=0.567).
Figure 1: The mean anxiety scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of anxiety, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Depression
There were no significant differences between the control and the study groups either one month before the start (P=0.310) or immediately before the first session (P=0.880). The mean HADS scores for depression before training were all greater than 8 (Figure 2). At three months (the mid-point of the course) the difference between the mean scores in the two groups was not significant (P=0.631). At the end of the course the mean depression score in the study group was significantly lower (P=0.046) than the control group (Figure 2). The mean scores for depression decreased over the 4 assessments. This tendency was significant in the assessment group (P=0.003) but not in control group (P=0.689).
Figure 2: The mean depression scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of depression, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Stress
There were no significant differences between the control group and the study group either one month before the course started (P=0.234) or immediately before it started (P=0.505). The stress scores were all greater than 8 (Figure 3). At three months (the mid-point of the course) the difference between the mean scores between the two groups was not significant (P=0.621). At the end of the course the mean stress score in the study group was lower (P=0.077) than that of the control group (Figure 3). The mean assessment scores for stress decreased over the 4 assessments. This decrease was significant for the assessment group (P=0.001) but not for the control group (P=0.425).
Figure 3: The mean stress scores and standard errors of the means (SEM) for a control group and a study group of doctors with pre-existing signs of stress, assessed twice before, once during and once at the end of a six-month course in Adaptation Practice.
Correlations
At all four assessments there were correlations among all three psychological parameters. At the initial assessment the correlation between anxiety and depression (r2= 0.405; P = 0.029) and between depression and stress (r2= 0.800; P < 0.0001) were significant but the correlation between anxiety and stress was not (r2= 0.253; P = 0.185). At the commencement of the course the correlation between anxiety and depression (r2= 0.479; P = 0.009), between depression and stress (r2= 0.765; P < 0.0001) and between anxiety and stress (r2= 0.486; P = 0.007) were all significant.
At three months (the mid-point) the correlation between anxiety and depression (r2= 0.526; P = 0.003), between depression and stress (r2= 0.622; P < 0.0001) and between anxiety and stress (r2= 0.790; P < 0.0001) were all significant and similarly at the and of the course: the correlation between anxiety and depression (r2= 0.604; P = 0.001), between depression and stress (r2= 0.577; P =0.001) and between anxiety and stress (r2= 0.740; P < 0.0001) were also all significant.
Assessments of the doctors’ psychological states and methods of coping
The doctors attending the course were assessed individually in private. They variously complained of stress, anxiety and depression. Notable findings included suicidal thoughts, plans for suicide, self-medication, excessive consumption of alcohol and an intention to leave the medical profession because of the unbearable pressures involved.
By the end of the course all these signs and symptoms had improved and the doctors felt confident in their ability to cope not only with pressures from outside but also with emotion, moods and feelings inside. One doctor still wanted to leave the profession but less adamantly than before, and stayed.
There was no qualitative assessment of the control group.
Qualitative Self-assessments
The anonymous self-assessment reports give meaningful, subjective accounts of what the doctors experienced individually. They fall into four main themes. There were no negative comments.
Connecting with emotion physically in the body
The following comments indicate contact with emotion:
‘I am more aware of my feelings.’
‘It is difficult to say “Yes” to unpleasant or upsetting feelings and situations. I have always preferred to avoid them and I have had a lifetime of suppressing emotions, so it is very difficult to say “Yes” to them, but this is what I am now doing.’
‘Since I’ve been more aware of my feelings there has been an enormous improvement in concentration.’
Developing inner emotional strength and coping.
A number of comments indicate the need to develop the strength to contain emotion physically in the body:
‘I am more accepting of daily stresses at work.’
‘I try to deal with problems instead of feeling so desperate and so wronged by them.’
‘I am calmer, and I lose my temper less often and less dramatically.’
‘The Practice was difficult initially because of my own resistances to it.’
‘I’ve always avoided seeking help for myself. I often feel worse than the patients I prescribe antidepressants for. I can now cope and I feel stronger but I don’t feel I’ve been treated and I now realise I didn’t need treatment: I needed to learn what to do and how to do it.’
Dealing with unpleasant, unwanted thoughts.
These comments illustrate the doctors’ new reactions to thoughts as they started to address the underlying emotion that normally drives worrying thoughts:
‘I now have less ruminations.’
‘As a long-standing ruminator I now realise these thoughts are the source of many anxieties. Thoughts were the main problem for me.’
‘I have learned to deal with obsessional thoughts by not giving time to them.’
General well-being.
The doctors commented on their sense of general well-being and ability to cope:
‘I am less tense and less anxious.’
‘I am now coping with episodes of work overload much better.’
‘I am feeling better generally.’
‘This has given me confidence to pursue the course of action I knew was correct.’
‘There are all-round improvements because of adapting myself to work and other people.’
‘I am happier and more content, optimistic and much less negative.’
DISCUSSION
Varying degrees of stress, anxiety or depression are universal.16, 26 Only about half of those thought to be clinically affected by these conditions seek help for them.26 If put into practice, sound medical knowledge and training can be beneficial to doctors’ own health.1, 11, 15 This does not seem to be true for stress, anxiety and depression.22 Too little is known about emotional and psychological problems, and treatment for them is inadequate.2, 9, 15, 17, 19, 21, 23, 28, 29
In this study, there was a high level of interest in how to deal with stress, anxiety and depression. Almost one third of respondents had scores on the HADS and SSS that suggested worrying levels of emotional and psychological problems amongst these working GPs. The fact that 152 doctors (68% of respondents) declared an interest in a six-month evening course (90 minute sessions after work on Thursday evenings) to learn how to deal with these conditions, suggests that:
stress, anxiety and depression are significant problems either amongst their patients or for the GPs themselves, or both
GPs are not confident in their ability to deal with them and want to learn more
although they have a strong tendency not to admit that they cannot cope and not to seek help, doctors are willing to attend a course to train and to learn.11
Most doctors tell their patients to seek professional help and to talk about their feelings but do not do so themselves.3, 5 They prescribe drugs for their patients that either the doctors will not take themselves or that they take but find ineffective. Of the 15 GPs on the course only one had mentioned psychological difficulties to a colleague and one to a partner and both only reticently. 16
ADAPTATION PRACTICE
Adaptation Practice strongly discourages self-disclosure, except in private to the Adaptation Practice teacher, which is necessary in order to assess the nature and severity of any problems and to lay the foundations for a rapport. Adaptation Practice sessions involve detailed discussion of moods and feelings as physical sensations and powerful forces that affect behaviour in all human beings. The ethos in Adaptation Practice is for participants to learn from their own experience how they are affected by emotion and how they can change this by containing themselves and not letting the emotion control them. It is not to criticise, judge, blame or condemn. Consequently, without the causes of stigmatisation, there is no prejudice and no stigma; instead there is respect and dignity and a pragmatic attitude to change.16
Adaptation Practice trains individuals to bear and endure upsetting, disturbing emotion by not expressing it, not suppressing it, not distracting themselves from it and not numbing themselves to it with drugs (alcohol, recreational drugs or prescribed medication). Bearing it this way develops emotional strength and resilience.
The high level of interest, the willingness to attend in groups and the positive results from this study indicate that Adaptation Practice is an acceptable way of teaching doctors how to cope with their own stress, anxiety and depression, that makes sense intellectually and emotionally. This, as well as the pragmatic approach mentioned above, makes Adaptation Practice radically different from other approaches.
GENERAL COMMENTS
Given that those who could not attend asked for an alternative day to attend, gave us reason to assume that the manner in which the study group and the control group were selected – individual availability on a given week night – would not have biased the sampling procedures and it seems reasonable to assume that the two groups did not differ in any meaningful way that would have biased the outcome.
Not surprisingly, there were strong positive correlations between anxiety and depression and between depression and stress on all assessments and between anxiety and stress on all but the first assessment, suggesting a strong association among these parameters of psychological states.
The mean scores for anxiety, depression and stress fell significantly in the participating GPs compared with the control group. The subjective reports from both the medical assessments and the self-assessments support these changes in the study group.
This study begs a number of important questions:
if doctors are prejudiced and stigmatise mental illness amongst themselves then what are their conscious, or unconscious, attitudes to mental illness in their patients? 3, 5, 9, 24
if doctors cannot cope with emotional problems themselves then whom are they and their patients to turn to for help? This is not the same as doctors suffering from physical conditions requiring surgery, or medications such as insulin or antibiotics.3, 5 Doctors expect, and are expected, to be able to cope with their emotions and, if necessary, that the treatment they give their patients will also work effectively for themselves
what are doctors to do and what are their patients to do, when doctors succumb to their own moods and feelings?
Adaptation Practice could be integrated in the medical curriculum at undergraduate and postgraduate levels, including Continuing Professional Development (CPD). Not only GPs but all doctors and other healthcare staff (nurses, physiotherapists, occupational therapists, social workers, etc.) could develop emotional resilience – which the GMC have proposed in recent years – and a better understanding of emotional and psychological problems and mental illnesses.
It is hoped that this preliminary study will stimulate and encourage a new way of looking at and investigating emotional and psychological problems and lead to further evaluation of Adaptation Practice.29, 30
With adequate training doctors and psychologists could teach Adaptation Practice.
The CASC (Clinical Assessment of Skills and Competencies) has been running since 2008 and is the final membership examination for the Royal College of Psychiatrists (MRCPsych).1 It is a clinical examination and follows an OSCE format (Objective Structured Clinical Examination), where candidates move through 16 short stations.2,3 We have been running a mock CASC in the West of Scotland for the last few years and have received consistently good feedback from candidates. This article describes our experience of organising the mock exam.
Step 1: Practicalities
The organising committee
Our mock CASC is arranged by the organising committee for the local core psychiatry education programme (MRCPsych course). This committee is comprised of a consultant chair, higher trainee chair and one or two trainee representatives from each higher subspecialty and each core training level. The higher trainee chair takes the lead with organising the mock, with the support of other committee members. This works well, as the trainees have recent experience of sitting or preparing for the exam and are enthusiastic about medical education.
Support from our postgraduate operations manager is invaluable. She works closely with the committee to book the venue and actors, and order equipment such as screens and a bell. She also has a key role in advertising the mock exam to trainees, booking places and being a point of contact for candidates. She assists with set up on the day of the exam and prints station instructions, marking schemes and labels for candidates.
Venue
Our mock exam is held in the same venue as our core trainee educational programme. We have 2 rooms to use for stations and a waiting area for candidates. Screens are borrowed from Glasgow University Medical School to create separate stations.
Timing
The mock exam takes place around 2 weeks before the CASC. This enables candidates to have prepared for the exam and leaves some time to work on any issues identified by the mock. Planning usually starts 4-5 months in advance of this, with increasing intensity and time commitment as the exam approaches.
Step 2: Mock Exam Format
CASC format and blueprint
The CASC itself includes morning and afternoon circuits, which all candidates will move through. There are 16 stations in total, with 90 seconds between each to read the task instructions. The morning session comprises 4 pairs of ‘linked’ stations, lasting 10 minutes each. In these paired stations, the second station is connected to the first in some way, such as taking a history in the first part then discussing with a family member in the second. Each station is marked independently. The afternoon consists of 8 single stations, lasting 7 minutes each. A passing list is posted online after a few weeks, with specific feedback made available to unsuccessful candidates.2
Mock CASC format
Our mock CASC is run in one afternoon session from 1.30-5pm. We have been able to include 16 stations by running the 2 circuits simultaneously. To make this possible, each station is 7 minutes in duration, with 90 seconds between stations. 4 candidates start after a delay, as it is not possible to start on part 2 of a linked station. Trainees are allocated candidate numbers and starting stations for both circuits to coordinate this effectively (figure 1). 16 candidates can take part in the mock exam.
Figure 1. Candidate numbers
Candidate Name
Number
1st loop starting station
2nd loop starting station
1
1a
5
2
2a
6
3
3a
7
4
4a
8
5
1a (8.5 min delay)
9
6
2a (8.5 min delay)
10
7
3a (8.5 min delay)
11
8
4a (8.5 min delay)
12
9
5
1a
10
6
2a
11
7
3a
12
8
4a
13
9
1a (8.5 min delay)
14
10
2a (8.5 min delay)
15
11
3a (8.5 min delay)
16
12
4a (8.5 min delay)
At least 3 other higher trainee helpers are recruited to assist the coordinator on the day of the exam. The same marking scheme is used for each station, covering domains common to all stations, such as building rapport and range and depth of questioning. There is also space for specific feedback, which examiners are encouraged to provide, though they do not interact with candidates directly during the exam. Forms are completed contemporaneously and distributed to candidates immediately after the mock exam.
Step 3: Writing the Stations
The content of the CASC follows a blueprint, which is available through the RCPsych website. A variety of skills are tested during the 16 stations of the exam, including history-taking, mental state examination, risk assessment, cognitive examination, physical examination, case discussion and difficult communication.3 We refer to the blueprint when selecting which stations to include in the mock. Each year, recent CASC candidates are asked to suggest stations and we combine these with previous stations to construct the mock exam. New stations are written by the trainee who suggested them, including candidate instructions and actor’s notes. The higher trainee organiser formats these to maintain consistency across the mock exam.
Role-play actors
For our most recent mock CASC, we employed paid actors for every station. These actors are part of a local agency which has experience in working as simulated patients for Glasgow University exams and communication skills sessions. In previous years, we have recruited a combination of core/higher trainees and actors. We have found pros and cons to each approach. The use of paid actors was more realistic for trainees but writing scripts proved more challenging as instructions required greater detailed in relation to specific psychiatric information, such as how a person with mania may present.
Step 4: Recruiting Examiners
There are a number of local consultant psychiatrists who are actively involved in teaching. They are supportive of the mock CASC and enthusiastic about examining stations. After the stations have been devised, consultants are invited to examine based on their areas of expertise. Higher trainees with particular interest in education are then asked to examine any remaining stations. Candidate instructions and actor’s notes are circulated to examiners in advance (figure 2). A simple guide to the mock exam is also sent to any new examiners. As we use the same marking scheme for each station, it is down to the experience of the examiner to consider whether the candidate has addressed the specific tasks appropriately.
Figure 2. Station template
Station
Title
Actor
Examiner
Written?
Sent?
1a
1b
2a
2b
3a
3b
4a
4b
5
6
7
8
9
10
11
12
Step 5: The Day of the Mock Exam
The higher trainee coordinators arrive at least 1.5 hours prior to the start time to set up the venue. Examiners, actors and candidates are asked to arrive 15-30 minutes before the scheduled start time. Each group is briefed on the exam format and given the opportunity to ask questions. Actors and examiners are shown to their stations and allowed time to discuss them. Candidates are provided with numbered labels to wear, for examiners to record on their marking sheets. The 4 candidates who will be starting later are asked to wait, while the others are shown to the examination rooms. They are shown which station they will be starting at, then queue in order at the door.
The mock exam coordinator stands where they can be heard by both rooms. There are 1 or 2 helpers in each room to guide the candidates around the circuit. The bell is rung to signify the start of the exam, the end of the 90 second preparation time (the start of each station), 1 minute warning and the end of each station. The candidates who were allocated to start later are brought into the circuit and shown to their station as the ‘end of station’ bell is rung, as this also signifies the start of the 90 second preparation time for the next station.
Marking schemes are collected and sorted during the break. Candidates are not kept separate from examiners, actors or each other. They are advised that they will get the most out of the afternoon if they don’t discuss the stations but this is ultimately their choice.
Examiners and actors return to their stations following the short break and candidates swap between circuits. Following the second round, there is another short break. Actors are excused at this point and most examiners remain for a feedback session. Marking schemes are collected, sorted and distributed to candidates. One room is re-set for group feedback. Examiners are thanked for their time and each is asked in turn for general feedback, hints and tips on their station (figure 3).
Figure 3. Mock CASC timing
11.30pm
Coordinators arrive & set up venue
12.30-12.45pm
Candidates, actors & examiners on site
1pm
Exam starts
2.15pm approx
Break
2.45pm
Exam re-starts - candidates switch circuits
4pm approx
Exam ends
4.30pm
Feedback forms distributed/ group feedback session
5pm
End
Overcoming Potential Problems
Examiners
Our examiners are all either higher trainee or consultant psychiatrists. It is therefore possible that unforeseen circumstances mean that they may have to cancel at very short notice, attend late or not at all, or be called away during the mock exam. Each of these has happened over the past few years but has been easily managed by the extra higher trainee helpers stepping in to examine a station.
Actors
All of our actors have attended as planned. If a paid actor has to cancel at short notice, the agency will find a replacement. If a trainee actor did not attend, one of the higher trainee helpers could step in. Another potential problem which we have encountered is actors not performing as intended. This can be minimised by preparing clear instructions for actors, with examiners providing some direction if needed.
Quality control of stations
It is difficult to know how a station will work until it is used in the mock exam. To minimise the risk of problems, stations are checked and formatted before the exam. They are circulated to actors and examiners in advance to allow time for them to raise any concerns and clarify any uncertainties. Despite following these processes, there are some stations which appear unclear or do not run smoothly on the day of the mock exam. It is helpful to receive feedback from examiners, so that stations can be amended or avoided in future.
Timing
Our mock exam follows a very tight schedule. If the mock exam itself overruns, then fewer examiners may be able to remain to provide feedback. The higher trainee coordinator should keep time carefully during the day of the mock exam, particularly during break times, which are very brief. Support from other higher trainee helpers is essential for this, in working together to collect and organise marking sheets and guiding examiners, actors and candidates to stations. Late arriving examiners remain a potential problem due to their other commitments. We provide a sandwich lunch to our examiners prior to the exam, which helps with prompt attendance.
Venue
The venue we use is quite cramped and can become noisy. We have access to only 14 screens to divide the 16 stations so they are close together and those at the ends of the room are not fully enclosed. The screens are thin so only muffle the noise from neighbouring stations. These issues of space and noise are difficult to overcome. Trainees are warned in advance and aim to focus on their own station as much as possible.
Recruiting actors, examiners and candidates
To date, we have not experienced any problems in recruiting actors, examiners or trainee helpers. We have been able to fill all candidate places and often have a waiting list. If necessary, the mock exam could be run with fewer stations and still provide helpful practice for trainees. If resources were tight, trainees could be role-play actors for some or all of the stations.
Conclusion
We run a local mock exam annually due to continued demand from trainees. It takes significant time and effort to arrange but is good experience for the organiser and local trainees and consultants remain enthusiastic. The mock CASC in the West of Scotland puts a strong emphasis on providing feedback for trainees to work on. The provision of completed marking sheets on the day of the exam and the group feedback session help with this ethos. Our experience has shown that a mock CASC can be delivered locally, at a low cost, while still providing trainees with a realistic exam experience.
Schizophrenia sufferers feel like abstract entities with non-animated bodies, often experiencing auditory verbal hallucinations (AVH) due to morbid “objectification” of inner dialogue.1 From the patient’s perspective, AVHs are a subjective–objective phenomenon. AVH is a non-consensual, dynamic and psychologically charged experience and the voices often echo significant emotions. Derogatory voices are common representations of unconscious self-hatred that cannot stand up to the external world’s logic. Thus, patients need help to incorporate it. Auditory hallucinations may be arising because of an interaction between biological predisposition, perceptual and cognitive factors. According to an integrated model of auditory hallucination (AHs) suggested by Waters et al,2 AHs arise from an interaction between abnormal neural activation patterns that generate salient auditory signals and top-down mechanisms that include signal detection errors, executive and inhibition deficits, a tapestry of expectations and memories. Recently, neuro-quantologists have proposed that AVHs may be an objectification of parallel thinking/quantum thinking.3 Parallel thinking is a source for thought insertion. There may be different variables of AVHs. Experiencing AVH has serious impact on the quality of life of the affected individual, and is a significant factor in prevalence of suicides among schizophrenic patients.4
Incidence
One in four schizophrenia sufferers experiences persistent AVH .5 AVHs are experienced by approximately 53% of schizophrenia sufferers 6 and are present in 28% of major affective disorders (Goodwin& Jamison, . 7 Evidence indicates that each patient responds differently to the voices, according to his/her evaluation of them (Table 1), which influences the degree of interventions. Specific dimensions of AVHs can give hints to the future likelihood of treatment resistance. Although the percentages differ in various studies, it is assumed that about 30% of patients have command hallucinations and they are seen as the ultimate betrayal of the mind. 8 Often, the content of such messages is negative; thus, commanding AVHs are more distressing than commenting ones. Schizophrenia predisposes them to a greater risk of suicides and homicides. Command hallucinations are more prevalent among forensic patients and contribute to their forensic status.
Table1. Patients’ Response to AVH
1.Anxiety and panic feelings 2.Fear 3.Feelings of humiliation 4.Entrapment 5.Self harm thoughts 6.Harm to others 7. Avoidant or withdrawn 8.Shouting and swearing 9.Ritualistic behaviour 10. Substance or alcohol abuse 11. Resistance. 12. Amusements 13. Engagement and courting the voices 14. Appeasement
The multi-factorial polygenic model of schizophrenic disorders has received great support and signifies that genetic factors play a bigger role than environmental factors in familial transmission of these disorders. Relevant studies provide little support for the mechanism of single major locus inheritance. A mechanism involving two, three, or four loci cannot be ruled out even though there is no compelling support for such models.9 It has also been proposed that a single gene may be even responsible for hallucinatory experiences 10 implying that those who have not inherited such a gene may not experience auditory hallucinations, but still could experience other characteristic symptoms of schizophrenia. One may also hypothesise that an individual who has inherited such a “hallucinatory gene” but not all the schizophrenia genes could hear non-clinical voices without having other schizophrenic symptoms. It is also arguable that those who carry such a specific gene are more vulnerable to experience hallucinations when they abuse psychoactive substances and could get misdiagnosed as having schizophrenia, but hallucinations may cease to occur once they abstain from illicit drug abuse.
Measurements for Assessment
AVH is a subjective experience and is hard to measure objectively. Several rating scales are now available for an efficient evaluation of different aspects of voice activities. Some are general and a number of them are specifically designed. Using rating scales facilitates better engagement with patients and helps in reinforcing the message that patients and the distress they experience are carefully considered.
Beliefs About Voice Questions (BAVQ) is an assessment scale useful in measuring the key beliefs about the voices.11 It is typically used in conjunction with the Cognitive Assessment Schedule (CAS).12 Voice Compliance Scale (VCS) is an observer rated scale aimed exclusively at measuring the frequency of command hallucinations and the level of obedience or confrontation with each recognized command.13 Voice Power Differential Scale (VPD) is another measure that can be applied to rate the perceived relative power differential between the voice and voice experience. 14 On the other hand, Omniscience Scale (OS) is intended to quantify the voice hearer’s beliefs about their voices’ knowledge regarding the bio data. 15 Another measure presently in use is Risk of Acting on Commands Scale (RACS), designed to assess the level of risk of acting on commands and the amount of associated distress. 16
The Bonn Scale (BSABS) is used for the assessment of basic symptoms, 17while the Schizophrenia Proneness Instrument (SPI-A) 18and the Examination of Anomalous Self Experience (EASE) 19 are useful aids in identifying minimal changes in subjective experience and for longitudinal monitoring (Table 2). In the extensively used Positive and Negative Syndrome Scale (PANSS), the hallucination item is one of seven in the positive subscale, which also includes delusions, conceptual disorganization, excitement, grandiosity, suspiciousness, and hostility. Given such a great number of scales in use, there is an obvious risk that differential anti-hallucinatory efficacy among antipsychotic drugs may be obscured by means of sum scores for the whole sample in clinical trials.
Table 2. Measurement scales
Beliefs About Voice Questions (BAVQ) Cognitive Assessment Schedule (CAS ). Voice co Voice Power Differential Scale (VPD) Voice Compliance scale (VCS) Voice Power Differential Scale (VPD) Omniscience Scale (OS) Risk of Acting on Commands Scale (RACS) Bonn Scale (BSABS) Schizophrenia Proneness Instrument (SPI-A) Examination of Anomalous Self Experience (EASE) Positive and Negative Syndrome Scale(PANSS)
Treatments
Although many forms of treatments aiming to eliminate AVH or improve quality of life are available, use of medication seems to be the most prevalent. Besides drug treatment, non-invasive physical treatments, such as TMS and different forms of psychological interventions, have recently evolved. Drug therapies are aimed at symptom eradication, whereas psychological therapies tend to foster healing, recovery and personal growth. Rather than being specifically anti-hallucinatory, typically, neuroleptics offer a generalised calming effect and patients are given some “breathing space” to work through their voices. Usage of non-pharmacological tools is needed in the long-term management of refractory cases. Presently, intervention strategies for AVH are based on different models of hallucinations, but regrettably no clear models have been established.
Pharmacotherapy
The current understanding of AVH and the neural mechanisms involved is limited, and knowledge on how CNS drugs, such as antipsychotics, influence the subjective experience and neurophysiology of hallucinations is inadequate. Consequently, using pharmacotherapy in the management of AVH remains very challenging. 20 Despite multiple trials of different combination and adjunctive therapies to an antipsychotic regime, AVH can remain drug resistant. It is also important to note that all antipsychotics are potentially anti-hallucinatory, even though these effects are usually modest. Moreover, given that, even when medications are effective, concordance can be an issue, antipsychotics should be used prudently and weighed up against effectiveness and side effects (Table 3). There are no clear guidelines for the drug treatment of AVH and comparisons of the efficacy of antipsychotics for AVHs are few. Clinical drug trials very rarely focus on single symptom scores, such as hallucinations, and tend to report group mean changes of overall psychopathology, or at best the positive subscale scores.
Evidences show that AVHs persist in spite of treatment in 32% of chronic patients 21 and 56% of acutely ill patients.22 Trifluperazine was popular as an anti-hallucinatory drug before the advent of atypical antipsychotic drugs. Clozapine is currently favoured for intractable AVHs and is beneficial in 30–60% of unresponsive patients.
Antipsychotic co-treatment is an option for clozapine augmentation. Olanzapine and risperidone may be alternative drugs in first episode psychosis. However, it is being debated whether clozapine should be used in such cases.
Table 3. Drug Treatment
Choice of antipsychotics Cautions and contraindications Titration of dose Switching antipsychotics Assessment of side effects, EPS, TD, Haematological effects etc. Measuring the beneficial effects Assess worsening of symptoms Compliance
Clozapine
Use of clozapine is suggested only after two other antipsychotics have been tried. It works better with continued usage and clinicians have to be patient in its upward titration. At six months, improvement in Global Assessment of Functioning score is significantly higher for clozapine in comparison to other antipsychotic drugs.23 However, when prescribing clozapine, cautions and contraindications must be noted (Table 4).
While higher doses of clozapine may not have more anti-hallucinatory effect, they still carry the risk of inducing the potential side-effects of this highly efficacious drug (Table 5). The most dreaded haematological side-effects are usually manifested within six months. For that reason, during clozapine therapy, patient has to be closely monitored, bearing in mind its limitations in achieving the anti-hallucinatory effects. If higher doses do not have the desired effect, clozapine dose should be titrated downwards to a point of its maximum anti-hallucinatory effect in a particular patient. Such an endeavour can prevent the emergence of serious side-effects, resulting in a complete failure of the therapy. The dose can also be adjusted to a safer level in cases where the psychological interventions are found to be successful. Clozapine can be effective even in lower doses, such as 200 mg/day. Only in the presence of command hallucinations, higher doses should be prescribed to patients whose other positive symptoms are well under control.
Prophylaxis with an antiepileptic drugs, such as lamotrigine or sodium valproate, or similar should be commenced before titrating the dose above 600 mg daily. Close monitoring and active treatment of metabolic dysregulation should be initiated concurrent with clozapine therapy. In clozapine therapy, weighing up safety and superior antipsychotic efficacy and educating the patients on “clozapine lifestyle” is immensely important, as it helps in treating refractory cases of AVH. Thirty percent of patients treated with clozapine may remain unresponsive and clinicians have to lower their expectations to the level of achievement without being cynical. Isolated cases of clozapine-induced joint visual and auditory hallucinations have been reported. 24 In spite of Clozaril treatment having the highest anti-hallucinatory effect, a good percentage of AVH sufferers remain symptomatic and are classed as super-refractory.8 According to Gonzales (2006), 25 50% of patients receiving antipsychotics achieve full remission, while 25% hear voices occasionally and 25% are unresponsive.
Table 4. Cautions & Contraindications of Clozapine
1.Patients with myeloproliferative disorders, a history of toxic or idiosyncratic agranulocytosis or severe granulocytopenia (with the exception of granulocytopenia / agranulocytosis from previous chemotherapy) 2.Bone marrow disorders 3-Patients with active liver disease, progressive liver disease and hepatic failure. 4-Severe CNS depression or comatose state, severe renal and cardiac disease, uncontrolled epilepsy, circulatory collapse, 5. Alcoholic/toxic psychosis and previous hypersensitivity to clozapine. 6.Pregnancy and breast feeding
Table 5. Benefits and risks of Clozapine
Benefits 1. Lower risk of suicide 2. Superior anti-delusional and anti-hallucinatory effects in refractory cases 3. Lower risk of tardive dyskinesia and suppression of TD. 4. Improvement in cognition 5.Higher quality of life and better adherence 6.Decreased relapse 7. Sexual functions unaffected Risks 1.Agranulocytosis 2.Metabolic syndrome 3.Myocardites 4.Chronic constipation and bowel complications 5.Incresed risk of seizure 6.Hypersalivation 7.Abrupt withdrawal cause marked discontinuation symptoms.
Benzodiazepines are often abused by voice hearers aiming to reduce their anxiety. Such patients might benefit by the addition of antidepressant, as this could enhance their mental resources to cope with the voices, even though they have no anti-hallucinatory effects per se. Mood stabilisers are sometimes used to augment the efficacy of antipsychotics without any clinical validation. Despite multiple trials of different adjuvant therapies to an antipsychotic regimen, there have been few promising results. Still, in practice, clinicians may get frustrated, as they struggle to provide symptomatic relief to the voice hearers at any cost. Recently allopurinol, an anti-gout agent has been used as an adjunctive therapy and based on three randomized controlled trials, the result has been encouraging. 26
Psychological Interventions
Persistent AVHs alone may not warrant pointless alteration of medication, as non-pharmacological interventions may achieve some control. When clinicians are not cognizant of non-pharmacological therapies, AVH patients that do not respond to antipsychotics alone may be mislabelled as having refractory AVH. In fact, they are only unresponsive to drug treatment, and could potentially respond to an integrated approach. Similarly, patients with treatment-refractory AVH are often over-diagnosed as suffering from hard to treat schizophrenia, even when other positive symptoms have been ameliorated.
There exists a false dichotomy between physical and psychological treatment approaches to AVH. In practice, both treatment modalities have to be modified in a personalised form. After all, psychiatry was originally known as psychological medicine. Presently, even though different forms of non-pharmacological interventions are available for drug-resistant AVH, some have questionable effects. 27,28,29 (Table 6).
Table 6. Psychological Interventions
1.Cognitive behavioural therapy (C.B.T.) 2. Acceptance and commitment therapy (ACT) 3. Competitive memory training (COMET) 4.Compassionate Mind Training therapy (CMT) 5.Hallucinations focussed integrative therapy (HIT) 6.Midfulness-based therapy 7.Normalizing techniques 8. Enhanced supportive psychotherapy 9. Attention training technique. 10. Distraction techniques 11. Self help approaches
CBT therapists predicate that AVHs are a manifestation of the morbid objectification of inner dialogue (thinking in words),and accordingly verbalised thoughts are the raw material for AVHs.Verbal thinking differs from external speech in many respects and has several distinct features. CBT therapists believe that cognitive dysfunctions underlie AVH and they target them with cognitive remediation strategies. Those experiencing voices commonly think that they are caused by a powerful external agency, and are controlling and potentially harmful. Psychological factors, such as meta-cognitive biases, beliefs, and attributions concerning the origins and intent of voices, also play critical modulatory role in shaping the experience of AVH. Teaching patients to recognize the source of the voices alone has yielded beneficial effects.
Specific techniques have been designed to modify the frequency of AVHs and restore a sense of control over them. Earlier methods involved behavioural approaches based upon addressing hypothesized antecedents and reinforcers of voices and explored a variety of specific interventions such as relaxation training, graded exposure to voice triggers, manipulation of environmental possibilities and even aversion therapy. 30 These behavioural techniques were eventually expanded on by the application of cognitive methods. The primary aim of psychological therapy is to change the belief that voices are omnipotent and uncontrollable and to suppress the associated attributes of false identity, wrong intentions, and urges to harm oneself and others. They encourage patients to challenge irrational interpretations and modify maladaptive behaviour, diverting attention from voices with distraction techniques (Table 7).
Reality testing and behavioural experiments are one form of CBT intervention, based on the view that behavioural changes can prompt cognitive changes. Attention switching can also be used to challenge the belief that hallucinations are uncontrollable. Command AVHs are more prevalent among the forensic population and are more distressing than the commenting ones. The risk of the sufferer acting on them is high when voices are perceived as omnipotent and uncontrollable. CBT has been proven beneficial in tackling command hallucinations. Lack of insight and formal thought disorder may not necessarily disqualify CBT for AVH; nonetheless, negative symptoms may pose a barrier to this form of psychological intervention. The current model of CBT for psychosis has been criticized, suggesting that it is simply an extension of general CBT concepts without taking into account the specificities of psychosis. 31 Patients with higher intelligence, who have the ability to grasp abstract concepts, might gain greater benefits from CBT. 32
Table 7. Goals of CBT
1. Change false beliefs about AVH . 2. Challenge irrational interpretations. 3. Modify maladaptive behaviour – e.g. fear of the voices or hiding from them. 4. Divert attention, using distraction techniques. 5. Build and maintain treatment strategies 6.Develop cognitive behavioural strategies 7.Develop newer understanding of hallucinatory experience 8. Address negative self-evaluation.
Combining psycho-education and supportive psychotherapy has been found to enhance the functioning and self-esteem of voice hearers, providing a therapeutic structure. In the increasingly popular self-help voice-hearing groups, the ethos of recovery is understanding, accepting and integrating the sufferer’s turmoil. Acceptance and non-judgemental support of people with similar experiences has helped many patients cope with the condition. In response, the number of books on AVH, aiming to educate the sufferers and carers, has grown considerably.
Newer Psychological Interventions
Attention Training Technique (ATT) focuses on negating psychological distress through cognitive and meta-cognitive modification. 33,34 Patients focus on up to five neutral sounds, such as a dripping tap, before switching their attention between different sounds. They then practise listening to all the sounds simultaneously. After a few weeks, they focus on neutral sounds and then on the AVH. Once this process is mastered, they switch attention between voices and other sounds, before being asked to divide their attention among them. This exercise continues for several weeks, whereby the aim is to replace the self-regulatory process with new processing configurations.
Acceptance and commitment therapy (ACT) is aimed at achieving psychological flexibility. It incorporates mindfulness and acceptance, considering AVH as a private experience and asserting that patients experience distress only when they try to deafen the voices. . By reducing struggle with voices and engagement with them, key responses such as arousal, attention and activation of brain areas are hypothesised to be reduced. 35 The ideas behind ACT are consistent with the emphasis on the recovery movement of finding a way to live a valued life despite the ongoing problems. To this effect, unique and effective coping strategies are offered, whereby patients are given the insights that parts of the self are behind the voices. Thus, accepting them means sending a loving message of compassion, acceptance and respect to oneself Two randomised control studies have yielded promising results. 36,37ACT follows a set manualised structure, rather than relying upon the complex and lengthy process of belief modification: therapy can be much briefer and potentially practiced by a wider range of clinicians and cost effective. 38
There are verbal and non-verbal routes to emotions. As CBT uses the former in voice therapy, it is less effective when patients are negatively involved with the voices. On the other hand, Competitive Memory Training (COMET) uses the non-verbal route. Generally COMET sessions involve four stages.39 A. identification of aspects of negative self-esteem reinforced by the voice; B. retrieval and re-living of memories associated with positive self-esteem; C. positive self-esteem is brought to compete with the content of the voices to weaken associations between voice content and negative self-valuation; and D. learning to disengage from the voices and to accept the voices as psychic phenomenon.
The significant past comes back to the conscious mind in AVH, as life experiences charged with emotion make a compelling impression on the brain. The observation that voices are knowledgeable about patients suggests that auditory hallucinations are linked to memory. In other words, negative experiences from memories evoke emotions, which should be deactivated. Distancing and decentring techniques could help patients to interpret voices as false mental events. As a result, incompatible memories could become tools to modify the power of voices—they are deactivated by new learning. Thus, when voices torment hearers, telling them that they are failures, a competing memory of such success as passing a significant examination is introduced. Posture, facial expression, imagination, self-verbalisation and music are all procedures included in the COMET protocol.40
Compassionate mind training (CMT) is used to encourage better resilience to unpleasant commenting voices.CMT involves practicing exercises which promote self-compassion and compassion towards others. It is targeted to activate brain systems involved in social and self-soothing that amend threat systems active when experiencing unfriendly voices. 41
Mindfulness is paying attention in a particular way – on purpose, in the present moment and non-judgementally. Clinical literature cautions against use of meditation in psychosis, but the effectiveness of mindfulness-based approaches for people with psychosis has been demonstrated in controlled clinical settings. 42and in the community. 43 Abba et al. 44 argue that effectiveness of mindfulness is a three-stage process: a. Becoming knowledgeable and developing more awareness of psychotic experiences and observing the thoughts and emotions that follow them. B. Permitting psychosis to come and go without reacting in order to cultivate understanding that distress is produced by the meanings one attaches to thoughts and sensations. C. Becoming autonomous by accepting psychosis and the self by acknowledging that the sensations only form part of the experience, and are not a definition of the self.
Neuroimaging studies are beginning to explain the neural mechanisms of how mindfulness might be working clinically. Structural changes have been observed in the anterior cingulate cortex, which is an area of the brain associated with emotional regulation. 45 . There is evidence to suggest that mindfulness practice is correlated to reduced brain activity in the default mode network. 46
Limited improvements with mono-therapy have prompted the development of multi-modular approaches. Hallucination-focused Integrative Therapy (HIT) is geared towards integrating CBT with neuroleptics, coping strategies, psycho-education, motivational intervention, rehabilitation and family treatment.47 Extant studies indicate that integrated treatment is more effective than TAU (treatment as usual).
The continuum model of psychosis and ordinary mental events has incited the development of normalisation of the voice hearing experience.48 Most psychiatric symptoms occur in normal people—just as breathlessness and palpitations occur while exercising—but are potential clinical symptoms. It is the frequency and duration that determine the borderline. According to the cognitive model, an internal mental event receives external attribution. Through normalisation, the external attribution can be reversed.
Although drug treatment may be the most practical way of managing AVH, refractory cases pose formidable challenges and it must be emphasized that psychological treatments are not counterproductive if applied skilfully. Clinicians who espouse the view that psychosis is a medical condition dismiss the usefulness of psychological interventions. The counter argument would be that a patient with a medical condition, such as stroke, benefits from physiotherapy, occupational therapy and psychological approaches.49
Repetitive Trans-cranial Magnetic Stimulation
There are several ongoing trials in which the aim is to treat refractory AVH (Table 4). Repetitive transcranial magnetic stimulation (rTMS) is thought to alter neural activity over language cortical areas. Several studies on rTMS have shown improvement in the frequency and severity of AVHs, albeit without offering any strong conclusive evidence for its efficacy .50 Moderate rates of AVH attenuation following rTMS have been noted in three meta analyses. Given that remarkable improvements in isolated cases have also been claimed, this suggests that rTMS may be appropriate mode of therapy for some patients.
Available data suggest that .rTMS selectively alters neurobiological factors that determine the frequency of AVH. However, a recent meta-analysis indicated that the effect of rTMS may be short-lived (less than one month).51 Studies seem to indicate that rTMS may be effective in reducing the frequency of AVHs, with little effect on their other topographical aspects.50,52 Sham stimulation has also led to improvements in a number of AVH parameters. Compared to bilateral stimulation, rTMS of left tempero-parietal region appears more effective in reducing the AVH frequency . 53 To reduce the distress associated with AVH and help patients to cope with hallucinatory predilection, rTMS could be combined with CBT. The side-effect profile is much cleaner for this biological approach when compared to medications. Still, like any other anti-hallucinatory treatments, neuro-stimulation technique does not guarantee long-term elimination of AVH. Electroconvulsive therapy (ECT) is considered a last resort for treatment resistant psychosis. Although several studies showed clinical improvement, a specific reduction in hallucinations severity has never been demonstrated.
Avatar Therapy
Computer-assisted voice therapy is a budding form of computerised psychological treatment that is currently undergoing trials.28 In this novel therapy, persecutory voices are directly depowered with the aid of a computerised dummy of the alleged persecutor through voice dialogue. Analytically-oriented therapists can even converse with “voices” and such committed clinicians will find computerised voice therapy as another helpful tool. It is hard to ascertain whether the benefits of the avatar therapy were due to the specific technique involved or simply the increased attention and care, and Leff’s team acknowledged the limitations of their work.54
Sound Therapy
Another important development in voice therapy is the use of tinnitus control instrument (TCI)—a form of sound therapy—in treating refractory AVH. Similar to AVH, subjective tinnitus is defined as the false perception of sound in the absence of acoustic stimuli. Even though their definitions are similar, the origin and underlying causes of these two conditions differ. Tinnitus is characterised by a simple sound—a monotone—and is non-verbal. In tinnitus, the brain is believed to interpret an internally generated electromagnetic signal as an acoustic sound or sounds.
Kaneko, Oda, and Goto29 reported successful intervention in two cases of refractory AVH with sound therapy, using tinnitus control instrument (TCI) alongside antipsychotic medications. They posited that, in sound therapy, the auditory system is directly helping the limbic nervous system and the neuro-mechanism for AVH is sensitive to sound therapy .55 They concluded that low-level auditory stimulation might be hindering the progression of voices and brain might be getting a breathing space to initiate self-healing process.
Future Directions
Hallucinogenic drugs, anti-hallucination medications and neuroimaging studies may lead to a better understanding of AVH. Animal models of hallucinations and pharmacogenetics might help to find more efficacious anti-hallucinatory drugs. AVHs themselves may have a genetic origin.10 Thus, not all patients that develop schizophrenia would experience AVHs. Such a finding might help shed more light on the genetics-linked mechanism and remedial measures of hallucinations in schizophrenia. Because the biological substrates facilitating drug effects on hallucinations remain largely unidentified, future studies with translational designs should address this important issue to find a more targeted drug treatment of psychosis.56
If a derivative of clozapine without the haematological side-effects is formulated in the future, it might be an important milestone in the treatment of refractory AVHs and schizophrenia because clozapine has the most potent anti-hallucinatory effect. Such a novel drug could become the first line of treatment for schizophrenia, as it would address many of schizophrenic symptoms at their onset. This is crucial, as symptoms and habits become stronger and more resistant the more frequently they occur. Fatty acid amide derivatives of clozapine, such as DHA-clozapine, are found to have better pharmacological properties and enhanced safety. However, such claims are awaiting substantiation in clinical trials.57 Thus, more attention needs to be directed into this potentially rewarding research arena. It is, however, very likely that, even after a better pharmacological cure is found for AVHs, a few symptoms might linger on for long periods. With this view, efficient non-pharmacological remedies have to be designed to deal with such residual symptoms.
Discussion
Medications help reduce the psychic pain, and protect the dignity of patients, as well as prevent suicides and homicides. From the patient’s perspective, the calming and relaxing effects of pharmacological therapies are a priority for relief from the distress due to AVH. Among the antipsychotics, clozapine has the maximum anti-hallucinatory effect and it is a shame that it cannot be used as a first line treatment choice. Treatment of AVH should be individualistic and clinicians should be prepared to apply several clinical and non-clinical approaches in concert to address them.
More research into the aetiology and mechanism of AVH is warranted in order to find effective treatment strategies. There is no shortage of theories about the mechanism of AVH, but there is no consensus among the investigators. It is unlikely that AVH is a pure neuro-chemical experience or a biological glitch, and this is where the currently available drug treatments fail. The distinction between primary and secondary symptoms was lost with the triumph of biological psychiatry in the last century. Thus, some authors presently claim that AVHs may even be a secondary symptom or a neuroquantological manifestation of an underlying biological disorder. We should not minimise the importance of eliminating symptoms when such symptoms are incapacitating, as in the case of hallucinatory experiences.
The present recovery model that emphasises and supports the patient’s potential for recovery involving hope, supportive relationship, empowerment, social inclusion, coping skills and meaning cannot be achieved without the help of psychological interventions. In this respect, CBT is a useful tool in the rehabilitation of psychotic patients with residual AVH. Jauhar et al.58 argued that the effectiveness of CBT in schizophrenia is influenced by failure to consider sources of bias. Consequently, the benefits are more apparent than real, prompting the question of whether CBT has been oversold.49 The verdict of Maudsley debate on the issue has been that CBT has not been oversold, but rather has a great impact on symptom reduction and enhancing concordance and insight. Perhaps the most informative trial so far accomplished has been the work on cognitive therapy for command hallucinations, which has proven the benefit of specific model development, and which productively, combined measurement of process and a targeted outcome.59
There is ample evidence suggesting that a combination of family and psychological interventions, alongside pharmacotherapy, can be the most effective way of dealing with refractory AVH.60 The inner dialogue hypothesis of AVH held by CBT therapists has its opponents.61 Patients respond to the voices they experience by utilising inner speech. Some observations with corresponding features weaken the inner-dialogue hypothesis. David and Lucas have demonstrated in a single case study that short-term maintenance of phonological representation (inner dialogue) may co-exist with AVHs – they are not synonymous experiences. The cost-effectiveness of psychological interventions is poorly studied, despite being highly relevant for policy decisions in healthcare.
Computerised voice therapy works better with technically minded, highly intelligent patients. In contrast, individuals of low to average intelligence may require a primarily behavioural approach, with limited efforts to understand concepts, such as automatic thinking and schema. Unlike sound therapy through music playing instruments (iPad, iPod, iPhone, etc.), TCI causes no disruption to daily functioning and can be used continuously. Computerised voice therapy and sound therapy warrant standardised case trials. When it comes to treating AVHs, optimizing compliance, reducing the burden of symptoms, and improving control, quality of life and social functioning should be the therapeutic goals.62 Neuroquantological views of AVHs63 explain the limitations of pharmacotherapy and the usefulness of psychological interventions.
Tuberculosis is an important and major infectious disease worldwide, especially in developing countries with an estimated global case fatality rate of 13% in 2007. The World Health Organization estimated that there were 13.7 million prevalent cases of TB infection worldwide, with each year bringing about 9.27 million new cases, 44% of which are new smear-positive cases1. Musculoskeletal tuberculosis is rare, chest wall tuberculosis is rarer and involvement of costochondral junction is among the rarest forms of tuberculosis. Tubercular costochondritis usually presents with insidious onset non-specific pain and swelling, resulting in delay in the diagnosis. Diagnosis is usually made by typical radiological findings and microbiological and histological evidence of tuberculosis. Treatment consists of antitubercular therapy with or without surgery.
Case report
30 year male, smoker, from low socio economic status presented with history of low grade fever, malaise and anorexia which began gradually two months back. For about one month he had pain in right side of chest just adjacent to lower part of sternum. The pain had started insidiously, gradually worsened with time, and was dull and aching in character. Pain was localized to the right lower parasternal area, occasionally radiating to the back. The pain was aggravated by physical activity and deep inspiration and was relieved to some extent by ordinary anti- inflammatory medications. There was significant history of pulmonary tuberculosis in the patient’s sister 1 year ago. There was no history of cough, haemoptysis, fever with chills or history of tuberculosis in the past.
On general physical examination, the patient was weak and febrile. On local examination, there was a bulge in the right lower parasternal area, corresponding to the right 9th costochondral junction. On palpation, there was severe tenderness in the same area. There was no peripheral lymphadenopathy and abdomen was soft and non-tender with no organomegaly. Chest examination was unremarkable. The rest of the examination was normal.
In terms of investigations, the chest radiograph, ECG, haemogram, kidney function tests and liver function tests were normal. ESR was high (34), Mantoux test was positive(15mm). Sputum for AFB was negative. Axial CT chest demonstrates expansion of the left 9th costal cartilage with soft tissue thickening on both the inner and outer aspect of the cartilage (Fig.1). FNAC (Fine Needle Aspiration Cytology) of the costochondral junction revealed Mycobacterium tuberculosis and on culture and histopathology of aspirated material revealed tubercular granuloma (Fig.2). A final diagnosis of tubercular costochondritis was made and the patient was treated with anti tubercular drugs for 9 months. Patient's symptoms improved after 2 weeks of treatment and swelling and tenderness subsided. Post treatment axial CT demonstrated complete resolution of soft tissue abnormality previously seen around the costal cartilage (Fig.3).
Figure 1: CT chest showing evidence of costochondritis.
Figure 2: Typical tubercular granuloma with central caseous necrosis on histopathology.
Figure 3: Post ATT CT showing complete resolution of costochondritis.
Discussion
Tuberculosis is very common infectious disease in developing countries like India, resulting in significant morbidity and mortality. Musculoskeletal tuberculosis is relatively uncommon and accounts for 1 to 2% of all the tuberculosis patients2,3 and accounts for about 10% of all extrapulmonary TB infections4. Tuberculosis of the chest wall constitutes 1 to 5% of all cases of musculoskeletal TB5,6. TB abscesses of the chest wall are usually seen at the margins of the sternum and along the rib shafts, and can also involve the costochondral junctions, costovertebral joints and the vertebrae7. In one study8, on the basis of the part of the rib involved, the roentgenographic findings for patients with rib tuberculosis was divided into four categories: Costovertebral (35%), Costochondral (13%),Shaft (61%), and Multiple cystic bone. TB of the thoracic wall is usually caused by reactivation of some latent foci of primary tuberculosis formed during hematogenous or lymphatic dissemination but direct extension from contiguous mediastinal lymph nodes can also occur9. In developing countries such as ours, tuberculosis is endemic and all the rare forms of the disease have been described, but in developed countries, resurgence of tuberculosis due to HIV may be responsible for atypical presentations .
Thoracic wall tuberculosis mostly presents insidiously with pain and swelling, but the diagnosis of chest wall TB is often delayed due to lack of specific symptoms and signs and gradual course10. Approximately less than 50% of chest wall TB patients may have active pulmonary TB11,12. Imaging techniques like X-Rays and CT scan play an important role in diagnosis and follow up of these patients. According to a study done by Vijay YB et al13, radiological signs may not be present initially at the time of presentation with symptoms, abscesses or sinuses may be present much before the imaging modalities detect them. Computed tomography (CT) scan is more valuable for localization and detection of bone destruction and soft tissue abnormalities. Atasoy et al demonstrated the role of Magnetic Resonance Imaging (MRI) for early detection of marrow and soft tissue involvement in sternal tuberculosis due to high contrast resolution of MRI14.Diagnosis is usually confirmed by finding acid fast bacilli (AFB) and positive AFB cultures of bone (positive in up to 75% of cases), and caseous necrosis and granuloma on histopathology11.
Complications of thoracic wall tuberculosis include secondary infection, fistula formation, spontaneous fractures of the sternum, compression or erosion of the large blood vessels, compression of the trachea and migration of tuberculosis abscess into the mediastinum, pleural cavity or subcutaneous tissues as discharging sinus. Chest wall TB needs to be differentiated from benign and malignant tumors [chondroma, osteochondroma, fibrous dysplasia, lipoid granuloma, chondrosarcoma, myeloma multiplex]11, metastatic carcinoma, lymphoma or other kinds of infection15,16.
The treatment of choice of chest wall TB is still not clear. Whether antitubercular therapy alone or surgical debridement (or excision based on lesion extension) combined with antitubercular therapy should be done needs further studies. But the general rule is if there are any complications, surgery is the treatment of choice followed by antitubercular therapy. We conclude that the diagnosis of thoracic wall tuberculosis is a challenge for physicians and is suspected by gradual onset clinical features and confirmed by microbiology, histopathology and radiography findings. Early diagnosis and treatment are important to prevent complications caused by bone and joint destruction.
Supporting Professional Activities (SPA) time is a part of each consultant’s new contract. When the new consultant contract evolved in 2003, a suggested breakdown of the week was 7.5 sessions (1 session equates to 4 hours) for direct clinical care (DCC) and 2.5 sessions for SPAs.1 This was driven by the need for consultants to continue their own professional development (CPD) as well as having the time for input into the development of trainees and medical students.
Examples of CPD work for consultants could include audit for improvement of service or patient care, teaching of patients, medical students or trainees, research, publications, aspects of hospital management and involvement in simulation courses e.g. Advanced Life Support (ALS)/Advanced Paediatric Life Support (APLS).
The General Medical Council (GMC) requires that during annual appraisals, doctors should use supporting information to demonstrate they continue to follow “Good Medical Practice”. This mandates that doctors should ‘take part in educational activities that maintain and further develop’ their competence and performance.1 With regard to revalidation, the GMC states you will have to demonstrate that you regularly participate in these activities; at Annual Review of Competency Progression (ARCP) it is imperative that accurate records of these CPD activities are presented at the annual job plan review.2
It is clear, therefore, that the provision of allocated time during the working week to complete these aspects of work life are deemed necessary for consultants. The Royal College of Anaesthetists and Association of Anaesthetists of Great Britain and Ireland both support the original view that a consultant should “typically” have 2.5 SPAs in their contract (though this would have to be subject to individual workload). With the demands of service provision it is clear that consultant SPAs are under threat, with around 40% of new consultants offered jobs with fewer SPA sessions than are thought necessary to allow sufficient non-DCC work.3
Since trainees are subject to similar appraisal and development requirements, we wonder if trainees should be allocated SPA time? For progression through training years and to pass the ARCP, it is necessary to provide evidence of trainee development within clinical practice in a similar way to consultants. This can involve a great deal of extra time. Once (notoriously difficult) exams have been passed, each trainee must go through the application process and prove what skills they have assimilated during their training to date. In fact, the ST3 anaesthesia application criteria states that the following are some of the ‘desirable’ criteria that require evidence:
Relevant academic and research achievements
Involvement in an audit project, or quality improvement project
Interest and commitment to the specialty beyond the mandatory curriculum
Evidence of interest in, and experience of, teaching
Instructor status in an advanced life support course (ALS, APLS)
Involvement in management…and understanding of management
Effective multi-disciplinary team working and leadership
Effective leadership in and outside medicine
Achievement outside medicine
Altruistic behaviour, e.g. voluntary work
The list is extensive and clearly requires a lot of time and input outside of the normal working week. With the expectation that trainees should be prepared to move straight from CT2 to ST3 (assuming their exams are completed), these desirable criteria must be addressed alongside completing other mandatory aspects of training such as, for anaesthesia: an Initial Assessment of Competency (IAC), an Intensive Care Unit (ICU) module, an Initial Assessment of Obstetric Competency (IAOC) and 15 Units of Training. With all these challenges between a core anaesthetic trainee and potential specialist anaesthetic training, there seems little time to complete an adequate number of the desirable criteria; this is a compelling reason to facilitate some time into the trainee contract to help produce more well rounded trainees.
However, therein lies the challenge - anaesthetic training is such a busy programme. Trainees are involved with multiple areas within a hospital such as ICU, theatre work or Obstetric Delivery Suite that they must learn and practice a wide range of skills to demonstrate the proficiency expected of a consultant anaesthetist. With experience of clinical work already at a premium due to European Working Time Directive hours, creating a good teaching environment whilst providing service provision is a hard enough task. It might seem difficult, therefore, to justify taking away yet more clinical time for trainees.
The proposed “7 day National Health Service (NHS)” contract could also pose more difficulties. Current example rotas released by NHS Employers demonstrate an increased likelihood of shift-work for a typical ICU rota.4 This shows trainees will be working more weekends and nights than at present, which could reduce the time spent directly with consultants. This would make introducing more non-DCC work difficult to justify as it would likely occur during daylight hours – when training could occur.
How it could be introduced:
Assuming SPA sessions for trainees were implemented, there would also be practical aspects to address. For example, how many SPA sessions to allocate for each level of trainee and how to monitor that this time was spent effectively and efficiently.
Monitoring:
Trainees could propose which aspects to focus on during their SPA sessions, such as management, teaching, quality improvement projects or more time in their sub-specialty interest. The goals could then be set at the initial educational supervisor meeting, much like a Personal Development Plan (PDP), and monitored throughout the year. This would give focus to any SPA time and ensure it is effectively used. If a trainee abuses their time or is not using it appropriately then removal of SPA time could be enforced. This would give the trainees more ability to improve the skills so often considered additional to trainees.
Funding:
In times of NHS austerity, funding would also need addressing. Potentially neither Deanery nor Trust might be willing to pay a doctor for days spent working outside the hospital workload – such as in educational roles or as a college tutor.5 A trial in one single deanery could assess the efficacy of such a scheme.
A possible solution would be to remove a few days of study leave allowance, as many trainees do not use their whole entitlement, and re-assign these to SPA time, allowing a trainee more flexibility. Trainees could initially start with fewer SPA sessions when more junior, to allow more clinical time, increasing SPAs to one per week for intermediate or higher trainees who may well be approaching their Certificate of Completion of Training (CCT).
Conclusion:
There are some practical difficulties in establishing trainee SPA sessions and no doubt many feel all contracted time should be spent practicing anaesthesia. However, given the changing way trainees are recruited via a ‘tick-box’ national application system, together with the variety of non-clinical skills expected by consultancy such as an ability to teach, conduct audit work, engage in managerial roles etc., a small change in the training set-up could produce more rounded trainees, benefitting anaesthesia in general and training programmes in the future.
Communicating effectively with patients and families is a vital component of high quality care. Studies have shown that patients feel excellent communication in consultations is vital for instilling confidence in the medical practitioner.1,2 There is evidence that doctors are not meeting this fundamental need.3
Some consider it an ethical obligation of doctors to balance their training needs against providing optimal care for patients. It is well known that junior trainees have significant level of performance anxiety that translates through to their consultations.4
Simulation based training is now an integral part of postgraduate curriculum in training a variety of medical specialties in managing acute scenarios. As an education method it provides a controlled environment in which it is safe to learn from errors,5 and improves learner outcomes.6 Simulation has been shown to be a valid approximation of true clinical practice.7 It therefore allows trainees to reach higher levels of proficiency prior to embarking on real patient encounters.
Current Core Medical Trainees (i.e. junior doctors who have embarked on the first stage of physician training within England) in the London deanery are expected to be able to manage complex communication scenarios effectively prior to entering specialty training. This is demonstrated by requirements set out in the Core Medical Curriculum, as detailed in Box 1. Whilst significant emphasis is placed on communication skills training in basic scenarios at a medical student level, there is very little formal postgraduate communication skills training within this deanery and others.
Box 1: Excerpts from Core Medical Trainee curriculum
Counsel patients, family, carers and advocates tactfully and effectively when making decisions about resuscitation status, and withholding or withdrawing treatment
Able to explain complex treatments meaningfully in layman's terms and thereby to obtain appropriate consent even when there are problems of communication and capacity
Skillfully delivers bad news in any circumstance including adverse events
This deficit in training led us to conduct a survey exploring Core Trainees’ views regarding communication skills training in the London deanery. Findings from the survey are detailed in Box 2.
Box 2: Results from Core Trainee Survey
83% received less than 2 hours of post-graduate training in communication skills since the start of Core Medical Training
Only 50% felt somewhat competent in engaging in difficult communication scenarios
88% reported significant challenges when conducting these discussions. They have had difficult on-calls experiences relating to communication difficulties
100% displayed interest in attending further Simulation Training in advanced communication skills
Method
We devised a pilot project using simulation to develop trainees’ competencies in advanced communication skills. After application to our local training board, we secured funding to run a number of sessions for core medical trainees within the London area.
The objectives of our pilot project were to provide experience of realistic communication based scenarios in a structured and safe environment to core trainees; provide feedback on trainees’ communication styles and offer suggestions for improvement; improve confidence of trainees in difficult communication situations.
Each session was conducted in an afternoon session and candidates were divided into three groups of three trainees who would remain together for the entire session. We ran four sessions, with a total of 36 trainees. Each group was facilitated by a consultant or a higher trainee in either elderly or palliative care medicine, given our focus on resuscitation/end of life discussions and assessment of capacity. We employed three actors to rotate around each group performing a variety of roles including patients and relatives. With a total of six scenarios, each trainee had the opportunity to participate in at least two scenarios lasting approximately 15 minutes, with feedback thereafter for approximately 10 minutes.
The scenarios employed were based on personal experience of regularly occurring, challenging communication situations encountered in our own clinical practice. We created detailed scripts for the actors as well as corresponding clinical vignettes for the candidates.
The scenarios were:
End-of-life discussion with a challenging family regarding a patient with end-stage dementia.
Discussing resuscitation with a family opposed to do not attempt resuscitation (DNAR) regarding an acutely unwell patient with poor functional baseline.
Discussing resuscitation with a young patient with metastatic cancer undergoing palliative chemotherapy who has little understanding of the terminal nature of the disease.
Assessing mental capacity regarding discharge planning in a patient with mild to moderate dementia.
Assessing mental capacity regarding treatment in a patient with moderate learning difficulties.
Assessing mental capacity in a medically unwell patient with mental health issues who wishes to self discharge from the ward.
Box 3 outlines the session structure.
Box 3: Timetable for the session
12.30-12.45:
Actors briefing
12.45- 13.00:
Facilitators briefing
13.00-13.30:
Core trainee briefing
13.30-14.45:
Scenarios 1-3 in small groups
14.45-15.00:
Tea/Coffee break
15.00-16.15:
Scenarios 4-6 in small groups
16.15-16.45:
Feedback and closing
Results
Written feedback was obtained from all participants by distributing a post-course evaluation form, with a 100% response rate. A number of areas were assessed via a Likert scale of 1 – 5, with 1 being ‘not at all’ and 5 being ‘very much’. 100% of trainees felt the content was useful and their knowledge/skills had increased. 100% felt more confident after the session and all trainees and facilitators felt this would be beneficial for medical trainees. A full breakdown of results is detailed in Table 1.
Table 1: Results from post-course feedback
The post-course feedback form allowed for free text feedback from participants, with some individual examples given below:
“Realistic scenarios - good opportunity to experience them and get feedback in a safe environment, good practice of common communication problems”
“It builds confidence in dealing with these situations and provides basis for building up ”
“This work dealt with complicated cases and actors were not too easy which I liked. Good and unforgettable”
Discussion
With the European Working Timing Directive and resulting shorter working hours, gaining proficiency in a number of key skill areas is limited due to reduced patient encounters. A recurrent complaint among core medical trainees is the lack of observed clinical encounters that leads to individualised feedback.
Feedback from more experienced speciality practitioners was only one component of our attendees learning experience. They also benefited from personal practise in a non-threatening environment, observation of their colleagues communication styles and finally learning through reflection with their colleagues
This innovation has shown a clear benefit in amplifying the confidence and preparedness of our core medical trainees in approaching these higher level communication scenarios. Future directions include introducing quantitative assessments pre- and post- course to objectively demonstrate improved confidence and performance. Providing the course to trainees in other specialties as well as across the multidisciplinary team would also be beneficial given the universal requirement of healthcare professionals to communicate skilfully.
Ventilator-associated pneumonia (VAP) is a type of nosocomial pneumonia that occurs in patients who receive mechanical ventilation and is usually acquired in the hospital setting approximately 48–72 hours after mechanical ventilation.1 VAP is one of the most frequent hospital-acquired infections occurring in mechanically ventilated patients and is associated with increased mortality, morbidity, and health-related costs. Several risk factors have been reported to be associated with VAP, including the duration of mechanical ventilation, and the presence of chronic pulmonary disease, sepsis, acute respiratory distress syndrome (ARDS), neurological disease, trauma, prior use of antibiotics, and red cell transfusions.2 VAP occurrence is closely related to intubation and the presence of the endotracheal tube (ETT) itself.
Since there are inadequate objective tools that are utilized to make an assessment of bacterial-induced lung injury in a heterogeneous group of hosts, the diagnosis of VAP is challenging. Around 90% of ICU-acquired pneumonias occur during mechanical ventilation, and 50 % of these ventilator-associated pneumonias begin in the first 4 days after intubation.3 VAP has a cumulative incidence of 10-25% and accounts for approximately 25% of all ICU infections and 50% of its antibiotic prescription, making it the primary focus for risk-reduction strategies.1,4 For all these reasons, early diagnosis and prevention of VAP has held a prominent position on the research agenda of intensive care medicine in the past 25 years, with an ultimate goal of improving patient outcome, preferably by reducing mortality.
The keywords, ‘ventilator-associated pneumonia,’ in PUBMED revealed a total of 3612 titles and 625 review articles within the search limit of 10 years, between 2005 and 2014. Only articles in English were chosen.
PATHOGENESIS
Understanding the pathogenesis of VAP is the first step in the formulation of its appropriate preventive and therapeutic strategies. The initial step in the pathogenesis of VAP is bacterial colonization of the oropharynx and gastric mucosa, followed by translocation of the pathogens to lower respiratory tract. The most common means of acquiring pneumonia is via aspiration which is promoted by supine position and upper airway and nasogastric tube placement.2,5 In a mechanically ventilated patients, aspiration occurs around the outside of the endotracheal tube rather than through the lumen. Secondly, aerobic Gram-negative bacteria presumably reach the lower airway via aspiration of gastric contents or of upper airway secretions. Other means by which VAP can be acquired include aspiration from the stomach or nose and paranasal sinuses. Figure 1 depicts the essential elements favoring colonization of lower respiratory tract with the bacterial pathogens with subsequent development of pneumonia.2,5,6
Figure 1: Pathogenesis of Ventilator-associated pneumonia5 *Gastric alkalinization; prior antimicrobials; ICU stay; intubation; supine position; circuit/airway manipulation and mishandling; device cross-contamination; sedation; diminished cough reflex; and malnutrition predispose to colonization and aspiration. As the duration of ICU stay increases, colonization with MDR Gram-negative pathogens like Pseudomonas and Acinetobacter increases. †Via contaminated nebulizers/aerosols Reproduced with permission from the publisher.
COMMON CAUSES
The specific microbial causes of VAP vary widely depending in epidemiological and clinical factors. Common pathogens include aerobic gram negative bacteria such as Pseudomonas aeruginosa and members of family Enterobacteriaceae, staphylococci, streptococci, and Haemophilus species. Microorganisms like Pseudomonas spp., Acinetobacter spp. and Methicillin-Resistant Staphylococcus aureus occur commonly after prior antibiotic treatment, prolonged hospitalization, mechanical ventilation or when other risk factors are present.6,7
Moreover, deliberated ill patients may have defect in phagocytosis and behave as functionally immunosuppressed even prior to emergence of nosocomial infection as seen by many recent studies.8,9
DIAGNOSIS
Clinical Diagnosis
No gold standard of diagnosis for identifying VAP is there inspite of variety of proposed definitions. VAP has traditionally been diagnosed by clinical criteria of Johanson and colleagues (appearance of new or progressive pulmonary infiltrates, fever, leucocytosis and purulent tracheobronchial secretions), which are non-specific. When findings on histologic analysis and cultures of lung samples obtained immediately after death were used as references, a new and persistent (>48-h) infiltrate on chest radiograph plus two or more of the three criteria (i) fever of >38.3°C, (ii) leukocytosis of >12 × 109/ml, and/or (iii) purulent tracheobronchial secretions had a sensitivity of 69% and a specificity of 75% for establishing the diagnosis of VAP.10
Because of the poor specificity of the clinical diagnosis of VAP and of qualitative evaluation of ETAs, Pugin et al. developed a composite clinical score, called the clinical pulmonary infection score (CPIS), based on six variables: temperature, blood leukocyte count, volume and purulence of tracheal secretions, oxygenation, pulmonary radiography, and semi-quantitative culture of tracheal aspirate. The score varied from 0 to 12. A CPIS of >6 had a sensitivity of 93% and a specificity of 100%.11 Accuracy of CPIS in diagnosis of VAP is debated, despite of its clinical popularity. In one meta-analysis study evaluating the accuracy of CPIS in diagnosing VAP reported pooled estimates for sensitivity and specificity for CPIS as 65 % (95 % CI 61-69 %) and 64 % (95 % CI 60-67 %), respectively.12 The poor accuracy of clinical criteria for diagnosing VAP is due to purulent tracheobronchial secretions in patients receiving prolonged mechanical ventilation which are rarely caused by pneumonia. Moreover, in pneumonia systemic signs such as fever, tachycardia, and leukocytosis are nonspecific; they can be caused by any state that releases the cytokines interleukin-1, interleukin-6, interleukin-8, tumor necrosis factor alpha (TNFα), and gamma interferon.13,14 The weak point of CPIS is probably the inter-individual variability (kappa= 0.16), since a subjective evaluation is required when we are judging the quality of tracheal secretion (purulent/not purulent) and the presence of infiltrate at chest ray.15
Radiologic Diagnosis
Radiographical evidence of pneumonia in ventilated patients is also notoriously inaccurate. In a study of autopsy proven VAP, of the total population, only air bronchograms correlated with pneumonia and no specific roentgenographic sign correlated with pneumonia in patients with adult respiratory distress syndrome. The differential diagnoses of VAP based on radiographical appearance, include adult respiratory distress syndrome, congestive heart failure, atelectasis, pulmonary embolism and neoplastic infiltration.16
Microbiologic Diagnosis
The type of specimen that should be obtained for microbiologic processing as soon as VAP is suspected is another area of importance. The use of quantitative cultures is one of the main issues for any diagnostic laboratory because there is oropharyngeal bacterial contamination of all respiratory secretion samples, despite this is not always undertaken in many hospitals today.16,17
Blood cultures
Blood cultures have limited value because organisms isolated from blood in suspected VAP cases are often from extrapulmonary sites of origin.18 Blood cultures in patients with VAP are clearly useful if there is suspicion of another probable infectious condition, but the isolation of a microorganism in the blood does not confirm that microorganism as the pathogen causing VAP.
Quantitative cultures of airway specimens
Simple qualitative culture of endotracheal aspirates has high percentage of false-positive results due to bacterial colonization of the proximal airways observed in most patients in the ICU.20 Quantitative culture techniques suggest that endotracheal aspirate cultures (QEA) may have an acceptable overall diagnostic accuracy, similar to that with several other, more invasive techniques including BAL, protected BAL (pBAL) ,protected specimen brush (PSB) or tracheobronchial aspirate(TBA).7,19,20 Threshold values often employed for diagnosing pneumonia by quantitative cultures are ≥105 to 106, ≥104, and ≥103 CFU/ml for QEA, bronchoscopic BAL, and PSB, respectively, with ≥105 CFU/ml being the most widely accepted value for QEA.21,22,23 Also, blind aspiration sampling can lead to errors but bronchoscope also carries risks, such as inducing cardiac arrhythmia, hypoxemia, bleeding, pneumothorax, along with greater costs both in terms of time and resources. It is accepted that before administering the first dose of antibiotic or before any change in treatment patient specimens for culture should be taken, so that the results interpreted are valid.24 Lalwani et al., in their study, observed that culture results of a properly collected tracheal aspirate should be taken into consideration along with Centre for Disease Control and Prevention (CDC's) diagnostic criteria to maximize the diagnosis of VAP.25
The recent guidelines of Society for Healthcare Epidemiology of America/ Infectious Diseases Society of America (SHEA/IDSA) recommend Gram staining of endotracheal aspirates. However, the sensitivity (57-95%) and specificity (48-87%) of this technique are highly variable. The role of procalcitonin and other biomarkers for the diagnosis of VAP is yet unsubstantiated.5,26
Since VAP diagnosis founded on radiographic findings of pneumonia, which have intrinsic variability in technique, interpretation, and reporting, and on clinical signs and symptoms- that are subjective- in 2011 a Working Group of the CDC proposed a new approach to surveillance for Ventilator-Associated Events (VAE). Table 1 According to the new CDC definition algorithm, VAP is an Infection-related Ventilator-Associated Complication (IVAC) occurring after 3 days of mechanical ventilation and 2 days before or after the onset of worsening oxygenation, if purulent respiratory secretions with positive cultures or objective signs of respiratory infection have been found.27
Table 1: CDC Algorithm for VAP diagnosis30
1= Purulent respiratory secretions AND one of the following:
2= One of the following (without requirement for purulent respiratory secretions):
Positive culture of endotracheal aspirate, ≥ 105 CFU/ml *
Positive pleural fluid culture
Positive culture of bronchoalveolar lavage, ≥ 104 CFU/ml*
Positive lung histopathology
Positive culture of lung tissue, ≥ 104 CFU/ml*
Positive diagnostic test for Legionella spp.
Positive culture of protected specimen brush, ≥ 103 CFU/ml*
Positive diagnostic test on respiratory secretions for influenza virus, respiratory syncytial virus, adenovirus, parainfluenza virus
On or after calendar day 3 of mechanical ventilation and within 2 calendar days before or after the onset of worsening oxygenation, criteria 1 or 2 is met (*or equivalent semi-quantitative result).
Table 2: Practices for which insufficient evidence or no consensus exists about Efficacy8,57
Rotational or turning therapy
Routine use of turning or rotational therapy, either by ‘kinetic’ therapy or by continuous lateral rotational therapy
Systemic antimicrobial agent prophylaxis
Routine administration of systemic antimicrobial agent(s) to prevent pneumonia in those receiving mechanically-assisted ventilation. Changes in the antimicrobial agents class used for empiric therapy
Oral chlorhexidine
rinse for oropharyngeal colonization
Routine use of an oral chlorhexidine rinse for the prevention of healthcare-associated pneumonia in all postoperative or critically ill patients and/or other patients at high risk for pneumonia.
Ventilator breathing circuits with HMEs
No recommendation can be made for the preferential use of HMEs to prevent pneumonia in patients receiving mechanically assisted ventilation No recommendation can be made for placing a filter or trap at the distal end of the expiratory-phase tubing of the breathing circuit to collect condensate
Suctioning of respiratory tract secretions
No recommendation can be made for the preferential use of either the multiuse closed-system suction catheter or the single-use open-system suction catheter
Prevention of aspiration associated with enteral feeding
Small-bore tubes for enteral feeding Enteral feedings continuously or intermittently should be given
Patient care with tracheostomy
Daily application of topical antimicrobial agent at the tracheostoma
Gloving
Wearing sterile rather than clean gloves when performing endotracheal suctioning
STRATEGIES FOR VAP PREVENTION
There are multiple recommended measures for prevention of VAP. Practices for which insufficient evidence or no consensus exists about efficacy are summarized in Table2. Preventive VAP strategies can be grouped into two classes: non-pharmacologic strategies, which are focused on preventing aspiration, and pharmacologic strategies, which are aimed at preventing colonization.
Non-Pharmacologic Strategies
Staff Education in the Intensive Care Unit
Various barriers to adhering to VAP prevention recommendations include disagreement with the reported results of source studies, resource paucity, elevated costs, inconvenience for nurses, fear of potential adverse effects and patient discomfort. There is considerable variability in practice between countries regarding humidification systems, intubation route, endotracheal suction system, kinetic therapy beds, subglottic secretion drainage and body position. For efficient patient care staffing must be sufficient while ensuring that staff is able to comply with essential infection control practices and other prevention strategies.17,28
Hand Hygiene
Microorganisms can be spread easily from patient to patient on the hands of healthcare workers. Moreover, wrist watches, rings, bangles and other jewelry commonly act as reservoirs for organisms, and impede effective hand cleaning. Moreover, healthcare workers compliance to hand hygiene is low, and high workload decreases their compliance.29
Impact of patient position
Patients positioned semi-recumbently 45 degrees have significantly lower incidence of clinically diagnosed VAP compared to patients positioned supinely.30 Moreover, the incidence of clinically diagnosed VAP among patients positioned prone, does not differ significantly from the incidence of clinically diagnosed VAP among patients positioned supine.31,32
Kinetic Beds
Critical patients often for a long time remain immobile in the supine position so the functional residual capacity is decreased because of alveolar closure in dependent lung zones and impaired mucociliary clearance. This leads to the accumulation of mucus, atelectasis onset and ensuing infection.33 Rotational therapy uses a special bed designed to turn continuously, or nearly continuously, the patient from side to side; specific designs include kinetic therapy and continuous lateral rotation therapy (CLRT).34,35
Artificial Airway Management
Oral vs Nasal Intubation: Both nasogastric and nasotracheal tubes can cause oropharyngeal colonization and nosocomial sinusitis. Thus, use of the oral route for both endotracheal and gastric intubation should be considered to decrease the risk of VAP.36
Endotracheal tube cuff pressure: The secretions that pool above inflated endotracheal tube cuffs may be a source of aspirated material and ensuing VAP. The pressure of the endotracheal tube cuff should be optimized in order to prevent the leakage of colonized subglottic secretions into the lower airways. Persistent pressures into the tube cuff below 20 cm H2O have been associated with the development of VAP.37
Silver-Coated Endotracheal Tubes: Silver-coated endotracheal tubes appear to be safe, reduces bacterial biofilm formation, has bactericidal activity, reduces bacterial burden and can delay airway colonization. However, further studies are needed to for determing its efficacy.38,39
Mechanical Ventilation Management
Ventilator Circuit Change: The CDCs recommendation was ‘do not change routinely, on basis of duration of use, the breathing circuit that is in use on an individual patient. Change the circuit when it is visibly soiled or mechanically malfunctioning.40
Humidification With Heat and Moisture Exchangers: The effect of HME in preventing VAP is still controversial and recent studies have failed to show a significant difference in rates of infection.41
Subglottic secretion drainage: Intermittent subglottic secretions drainage using inspiratory pause during mechanical ventilation results in a significant reduction in VAP.42 SSD reduces VAP in patients ventilated for >72 hours and should be considered with other recommended strategies such as semi-recumbent positioning.43
Pharmacologic Strategies
Modulation of Oropharyngeal Colonization
Policies encouraging routine tropical oral decontamination with chlorhexidine for patients merit reevaluation. It is a cheap measure, but whether is it a safe one − it does not select resistant microorganisms − remains to be investigated.8,44
Selective Decontamination of the Digestive Tract
Selective decontamination of the digestive tract (SDD) is the decontamination ofpotentially pathogenic microorganisms living in the mouth and stomach, whilst preserving the indigenous anaerobic flora. SDD is an effective and safe preventive measure in ICUs where incidence rates of MRSA and VRE are low, but in ICUs with high rates of multi-resistant microorganisms it is a measure that is effective but not safe.45,46
Stress Ulcer Prophylaxis
Patients at risk from important gastrointestinal bleeding (shock, respiratory failure requiring mechanical ventilation or coagulopathy) should receive H2 antagonists such as ranitidine rather than sucralfate.47
Ventilator sedation protocol
In patients receiving mechanical ventilation and requiring sedative infusions with midazolam or propofol, the use of a nurse-implemented sedation protocol decreases the rate of VAP and the duration of mechanical ventilation.48 An objective assessment-based Analgesia-Delirium-Sedation (ADS) protocol without daily interruption of medication infusion decreases ventilator days and hospital length of stay in critically ill trauma patients.49
Antibiotic Policy and Infection Control
Rational antibiotic policy is a key issue for better patient care and preventing antimicrobial resistance.50,51 Infection control programs like using a scheduled switch of antibiotic class have demonstrated efficacy in reducing nosocomial infection rates and restraining multidrug resistant (MDR) microorganism emergence.52
VAP prevention in low resource/developing countries
Though the incidence of VAP has declined in the developed countries, it continues to be unacceptably high in the developing world. Its incidence in these countries is 20 times that in the developed nations with significant morbidity, mortality, and increase in ICU length of stay, which may represent an additional burden on the scarce resources in developing countries.53 Insufficient preventive strategies and probably inappropriate antibiotics administration may have lead to this scenario. Since microbiology and resistance pattern in India is different from other countries, there is need for data from our country to choose appropriate antimicrobials for management.54 Simple and effective preventive measures can be instituted easily and at minimal costs. Such measures might include hand hygiene, diligent respiratory care, elevation of head, oral and not nasal cannulation, minimization of sedation, institution of weaning protocols, judicious antibiotics use, de-escalation, and leveraging PK/PD characteristics for antibiotics administered. More costly interventions should be reserved for appropriate situations. Strategies to prevent VAP, probably by emphasis on practical, low-cost, low technology, easily implemented measures is need of the hour.
Ventilator-associated events (VAE) surveillance: an objective patient safety opportunity
Surveillance for ventilator-associated pneumonia is challenging and contains many subjective elements, including the use of chest x-ray evidence of pneumonia. In January 2013, CDC convened a VAP Surveillance Definition Working Group which transitioned VAP surveillance to ventilator-associated event (VAE) surveillance in adult inpatient settings.55 The VAE algorithm—which is a surveillance algorithm and not intended for use in the clinical management of patients—consists of 3 tiers of definitions: Tier 1, Ventilator-Associated Conditions (VAC); Tier 2, Infection -related Ventilator-Associated Complications (IVAC); and Tier 3, Possible and Probable VAP.27 The tier 1, VAC attempts to identify sustained respiratory deterioration episodes, and capture both infectious and noninfectious conditions and complications occurring in patients receiving mechanical ventilation. The tier 2, IVAC, is intended to identify the subset of VACs that are potentially related to pulmonary and extra pulmonary infections of sufficient severity to trigger respiratory deterioration. The tier 3, possible and probable VAP, attempts to identify IVAC patient subsets with respiratory infections as manifested by objective evidence of purulent respiratory secretions (where purulence is defined by using quantitative or semi-quantitative criteria for the number of neutrophils on Gram stain) and/or positive results of microbiological tests done on respiratory specimens. Because of the wide range of the lower respiratory tract specimens, their collection procedure as well as in laboratory processing and reporting of results, the Working Group of CDC determined that it was not appropriate to include these data elements in the VAC and IVAC definitions.56
This 3 tier approach is ineffective to accurately identify VAP for surveillance purposes and focuses on more mechanical ventilation complications. This approach may also reduce the likelihood of manipulation that could artificially lower event rates. Most VAEs are caused by pneumonia, pulmonary edema, atelectasis, or acute respiratory distress syndrome. In few recent studies concordance between the VAE algorithm and VAP was found to be poor.57 Thus, more studies are needed to further validate VAE surveillance compared with conventional VAP by using strong microbiologic criteria, particularly bronchoalveolar lavage with a protected specimen brush for diagnosing VAP and to better characterize the clinical entities underlying VAE.
Bundle approach to prevention of VAP
One of the five goals of the ‘Saving 100,000 Lives’ campaign, launched by the Institute for Healthcare Improvement is to prevent VAP and deaths associated with it by implementing a set of interventions for better patient care known as the ‘ventilator bundle’. The interventions should have scientific support of effectiveness, based on randomized controlled trials. All the elements of the bundles must be executed at the same time. The bundles for VAP includes four components: (a) elevation of the head end of the bed to 30-45º, (b) daily interruption of sedation, (c) daily assessment of readiness to extubate and (d) prophylaxis for deep venous thrombosis and peptic ulcer disease. The bundle approach to prevention of VAP has been found to be highly effective in reducing the incidence, mortality and ICU stay.5,58,59 The ventilator bundle should be modified and expanded to include specific processes of care that have been definitively demonstrated to be effective in VAP reduction. A multidimensional framework with a long-lasting program can successfully increase compliance with preventive measures directly dependent on healthcare workers bedside performance.
CONCLUSION
Ventilator Associated Pneumonia is one of the most common nosocomial infections in ICU presenting with non specific symptoms and clinical signs. Quantitative culture obtained by different methods, including EA, BAL, pBAL, PSB or TBA seem to be rather equivalent in diagnosing VAP. Clinical criteria used in combination, may be useful in VAP diagnosis; however, inter-observer variability and the moderate performance are to be considered.
Preventive strategies should focus on better secretion management and on reduction in bacterial colonization. Further research on targeted interventions is needed to effectively reduce VAP incidence. For VAP an approach based on multidisciplinary group is required including setting preventive benchmarks, establishing goals and time lines and providing appropriate education and training, audits and feedback to the staff, while continually updating themselves based on relevant clinical and preventive strategies.
During my placement in Psychiatry at the Brooker Centre, Runcorn, UK, I have come into contact with a wide array of psychiatric disorders, none more so than borderline personality disorder (BPD). It is undoubtedly one of the most prevalent problems in the area which the Brooker Centre serves. I can recall an example of a patient with BPD who had been quite unwell for a prolonged period of time and had struggled with affective instability. This patient had been quite successfully treated with Lithium therapy, has exhibited stability and is happy on the current treatment. There is a pattern of pharmacological treatment in BPD patients despite the fact that guidelines suggest otherwise…
Personality disorders are defined as ‘an enduring pattern of inner experience and behaviour that deviates markedly from the expectations of the individual’s culture, is pervasive and inflexible, has an onset in adulthood, is stable over time, and leads to distress or impairment’ . Personality disorders are representative of long-term functioning and are not considered in terms of episodes of illness 1.
The Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), groups the various personality disorders into three clusters based on their descriptive similarities.
Cluster A includes the Paranoid, Schizoid, and Schizotypal personality disorders which are categorised as ‘odd/eccentric’;
Cluster B includes the Antisocial, Borderline, Histrionic, and Narcissistic personality disorders which are categorised as ‘dramatic/emotional/erratic’;
Cluster Cincludes the Avoidant, Dependent, and Obsessive-compulsive personality disorders which are categorised as ‘anxious/fearful’ 2.
The International Classification of Diseases, 10th edition (ICD-10), specifies the condition of emotionally unstable personality disorder which has two subtypes: The impulsive type and the borderline type. The borderline type in essence overlaps with the DSM-5 definition 3.
It has proven difficult to provide robust clinical recommendations with regards to the treatment of personality disorder. This is, in part, due to the fact that study populations are diverse but also compounded by the use of different assessment criteria. Furthermore, it is important to consider that personality disorders often present with a great deal of psychiatric comorbidity. Of the personality disorders, particular attention has been paid to borderline personality disorder (BPD) as the symptom clusters which it involves have been shown to improve considerably with treatment 4.
Figure 1: Diagnostic Criteria for Borderline Personality Disorder according to DSM-5 2:
A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following: 1. Frantic efforts to avoid real or imagined abandonment. (Note: Do not include suicidal or self-mutilating behaviour covered in Criterion 5.) 2. A pattern of unstable and intense interpersonal relationships characterised by alternating between extremes of idealization and devaluation. 3. Identity disturbance: markedly and persistently unstable self-image or sense of self. 4. Impulsivity in at least two areas that are potentially self-damaging (e.g. spending, sex, substance abuse, reckless driving, binge eating). (Note: Do not include suicidal or self-mutilating behaviour covered in Criterion 5.) 5. Recurrent suicidal behaviour, gestures, or threats, or self-mutilating behaviour. 6. Affective instability due to a marked reactivity of mood (e.g. intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days). 7. Chronic feelings of emptiness. 8. Inappropriate, intense anger or difficulty controlling anger (e.g. frequent displays of temper, constant anger, recurrent physical fights). 9. Transient, stress-related paranoid ideation or severe dissociative symptoms.
Borderline personality disorder is characterised by a pervasive instability in mood, interpersonal relationships, self-image and behaviour. The condition was first recognised in the United States by Adolf Stern in 1938. He described that these are a group of patients who neither fit into psychotic or psychoneurotic group, which gave rise to the term ‘borderline’. BPD is often diagnostically comorbid with depression and anxiety, eating disorders (notably bulimia), post-traumatic stress disorder, substance misuse and bipolar affective disorder. Furthermore, psychotic disorders have also been found to overlap. Due to this extent of comorbidity it is rare to see a patient who has a pure BPD 5.
The pharmacological treatments of BPD are tailored according to the symptom clusters that present. These include impulsivity, affective instability, transient stress-related psychotic symptoms and suicidal & self-injurious behaviours 5,6.
Recommended Psychological and Pharmacological treatment, 2009 National Institute for Health and Clinical Excellence (NICE) guidelines on Borderline Personality Disorder5, 7:
Psychological
NICE guidelines state that when offering psychology for BPD or for the individual symptoms of the disorder, brief psychological interventions (i.e. less than a 3 month period) should not be used. It states that the frequency of psychotherapy sessions should be adapted to the patient’s needs and ‘context of living’ and suggests that twice-weekly session may be considered. The guidelines also specify that for women with BPD for whom recurrent self-harm is a priority, a comprehensive dialectical behaviour therapy programme should be considered. NICE recommends that when psychological treatment is provided in BPD, the effects should be monitored using a broad range of outcomes. These should include personal functioning, drug and alcohol use, self-harm, depression and the symptoms of BPD.
Pharmacological
The NICE guidance states that drug treatment should not be used specifically for BPD or for the individual symptoms or behaviour associated with the disorder (e.g. repeated self-harm, marked emotional instability, risk taking behaviour and transient psychotic symptoms). It goes on to suggest that antipsychotics should not be used for the medium- and long term treatment of BPD. However, with regards to the management of comorbidities, it specifies that drug treatment may be considered and that in each case, the NICE guidelines for each comorbid condition must be referred to. Antidepressants, mood stabilisers and antipsychotics are commonly used in clinical practice. The guidelines mention that short-term use of sedative medication may be considered in a crisis. ‘Short-term’ denotes treatment lasting no longer than one week.
With regards to drug treatment during a period of crisis, NICE recommends that there should be a consensus among prescribers and other involved professionals about the proposed drug treatment and also that a primary prescriber should be identified. There should be an appreciation of the likely risks of prescribing, including alcohol and illicit drug use. NICE emphasises that the psychological role of prescribing (both from the patient’s and prescriber’s perspective) should be taken into account, and the impact that such prescribing decisions may have on the therapeutic relationship and overall care plan. NICE recommends that a single drug be used and that polypharmacy is to be avoided as much as possible.
In a crisis NICE recommends prescribing ‘a drug that has a low side-effect profile, low addictive properties, minimum potential for misuse and relative safety in overdose.’ The minimum effective dose is favourable, prescribing fewer tablets more frequently if there is a significant risk of overdose and also agreeing with patient on the symptoms that are being targeted. NICE suggests that following a crisis, a plan should be made to stop drug treatment that was started during a crisis. If this is not possible, a regular review of the effectiveness, side effects, misuse and dependency of the drug is advised. BPD patients can often have concomitant insomnia and for this, NICE details basic advice regarding sleep hygiene and forwards on to the guidance on the use of zaleplon, zolpidem and zopiclone for the short-term pharmacological management of insomnia.
AIMS AND OBJECTIVES
This report will review the current guidelines specifically regarding the management of borderline personality disorder and explore the literature according to the research recommendations that are set by NICE. The report is to focus on the two aspects of the management of BPD – The psychological/psychosocial aspect and the pharmacological aspect.
CURRENT NICE GUIDELINES ON PSYCHOLOGICAL AND PHARMACOLOGICAL TREATMENT OF BPD 7:
Psychology
Mentalisation-based therapy and dialectical behavioural therapy are proposed in the setting of a ‘well structured, high quality community based service’ e.g. a day hospital setting or a community mental health team. NICE suggests that these techniques should be compared with ‘high-quality community care delivered by general mental health service without the psychological intervention for people with BPD’ in order to measure efficacy. For outpatients, cognitive analytic therapy, cognitive behavioural therapy, schema-focussed therapy and transference focussed therapy are suggested and are catered to those with less severe BPD (i.e. fewer comorbidities, higher level of social functioning, greater ability to depend on self-management methods). Randomised controlled trials reporting medium term outcomes (e.g. quality of life, psychosocial functioning, employment outcomes and BPD symptomatology) of a minimum of 18 months are recommended
Pharmacology
Mood stabilisers are proposed as it is detailed that emotional instability is a key feature in BPD. In particular, topiramate and lamotrigine are mentioned as they have been shown to produce encouraging results in small-scale studies. A randomised placebo-controlled trial with medium to long-term follow up is recommended.
ANALYSIS
Psychology: Dialectical Behaviour Therapy (DBT)
Dialectics can be defined as the art of investigating the relative truth of opinions, principles, and guidelines 8. Dialectical in DBT refers to a means of arriving at the truth by examination of the argument i.e. the ‘thesis’ and ‘antithesis’ and resolving the two into a rational synthesis. DBT was introduced in 1991 by Marsha Linehan (a psychology researcher) and colleagues tailored as a treatment for BPD. In this, patients are supported in understanding their own emotional experiences and are taught new skills for dealing with their stresses. A combination of individual and group sessions are used. More adaptive responses and effective problem-solving techniques are integrated to improve functioning and quality of life as well as improving morbidity and mortality 9, 10.
A study published in 2015 by M. Linehan et al detailed a randomized clinical trial that set out to compare
1) Standard DBT (DBT group skills training + DBT individual therapy) with
2) A treatment that evaluated DBT group skills training with manual case management (i.e. with the removal of DBT individual therapy) and
3) A treatment that removed DBT skills training by providing only DBT individual therapy with an activities group and prohibited individual therapists from teaching DBT skills.
All 3 versions of the treatment were found to be comparably effective at reducing suicide attempts, suicidal ideation, medical severity of intentional self-harm, use of crisis services owing to suicidality and improving reasons for living 11.
Psychology: Mentalization based therapy
Mentalization is ‘the process by which we make sense of each other and ourselves, implicitly and explicitly, in terms of subjective states and mental processes.’ It is a social construct suggesting that we are attentive to the mental states of those we are with, physically or psychologically 12. Mentalization based treatment is a psychosocial treatment for BPD in which therapists monitor attachment and mentalizing capacity, and use interventions that aim to reinstate or maintain the capacity of patients to mentalize 13.
A longitudinal study, published in 2008, involving an eight-year follow-up of patients treated for BPD evaluated the effect of mentalization-based treatment (MBT) with partial hospitalization compared with treatment as usual. Five years after discharge from MBT, the MBT group exhibited clinical and statistical superiority to treatment as usual measured on suicidality, diagnostic status, service use, medication use, global function and vocational status 14. A more recent review article, published in 2015, emphasises the consideration of disruptions in three closely related domains in individuals with BPD. These are ‘in attachment relationships, in different polarities of mentalizing, and in the quality of epistemic vigilance and trust’. It is suggested that this approach allows seemingly paradoxical features of BPD patients appear more coherent. It is supposed that this approach provides a clear focus for the therapist enabling them to monitor the therapeutic process in terms of imminent mentalizing impairments and epistemic mistrust due to activation of the attachment system.
The article goes on to assert that the effectiveness of MBT in BPD may be elucidated due to the fact that it ‘enables the therapist to maintain and foster a mentalizing stance, even–and perhaps particularly–under high arousal conditions that are so characteristic of work with these patients’ 15.
Psychology: Cognitive analytic therapy (CAT)
CAT is a brief focal therapy that is informed by cognitive therapy, psychodynamic psychotherapy and elements of cognitive psychology. It was originally developed by Anthony Ryle tailored towards the needs of the NHS 16. It is based on a collaborative therapeutic position which sets out to create narrative and diagrammatic reformulations with patients concerning their difficulties. The theory centres on descriptions of sequences of linked external, mental and behavioural events. At first, the emphasis was on how such procedural sequences prevented revision of dysfunctional ways of living. More recently, this has been extended to understanding the origins of reciprocal role procedures in early life and their repetition in current relationships and self-management 17.
One study detailed a randomised controlled trial which aimed to investigate the effectiveness of time-limited CAT for participants with personality disorder. The study found that participants receiving CAT exhibited reduced symptoms and showed considerable improvement compared with the control group who showed signs of deterioration during the treatment period. They concluded that CAT is superior to treatment as usual in improving outcomes associated with personality disorder 18.
Psychology: Cognitive behavioural therapy (CBT) and Schema-focussed therapy
CBT is a time-limited, problem focussed psychotherapy that has been applied to a wide range of psychiatric disorders. The development of this technique was born out of the observation that patients referred for psychotherapy often would hold ingrained, negatively skewed assumptions of themselves, their future and their environment. The therapy is based on the notion that disorder is caused not by life events, but by the view the patient adopts of events. The therapy focusses on current problems and helps to develop new skills to provide symptom relief and sustain recovery 9, 19.
Initially CBT was predominantly insight-orientated, using introspection to bring about change. Beck et al began to integrate a range of behavioural techniques to improve the impact on dysfunctional controlling belief systems (schemas). The goal of treatment is not to replace the dysfunctional schemas; it aims to modify beliefs and develop new ones allowing the patient to cope more effectively in challenging situations 20, 21.
A 2013 review article that set to explore schema-focussed therapy concluded that schema-therapy is based on a ‘cohesive theoretical model’ and that there seems to be sufficient evidence supporting its validity. Regarding effectiveness, it goes on to indicate that one should be encouraged by the results of studies, however it points out that due to the small number of ‘methodologically-good efficacy studies’ it is difficult to be certain. The article claims that when evaluated against other psychotherapeutic treatments, specifically DBT and MBT, schema-therapy requires more investigation 22. A pilot study (2013) set out to monitor the effects of group schema-based CBT on global symptomatic distress in young adults with personality disorders or features of personality disorder. Their findings provide preliminary evidence that schema-based CBT might be an effective treatment 23.
Furthermore, there is a multicentre randomized controlled trial being conducted with the aim of investigating schema-focussed therapy versus treatment as usual in BPD, which has a closing date of 1st February 2016 24.
Psychology: Transference focussed therapy (TFT)
The classic use of the term transference originates in psychoanalysis and comprises “the redirection of feelings and desires and especially of those unconsciously retained from childhood toward a new object” 25. Transference-focussed psychotherapy is an evidence-based manualised treatment using a psychodynamic approach with a focus on object relations theory 26. TFT aims to ‘facilitate the reactivation, under controlled circumstances, of the dissociated internalised object relations in the transference relationship to observe the nature of the patient’s split polarised internal representations, and then, through a multistep interpretive process, work to integrate them into a fuller, richer, and more nuanced identity 27.
Yeomans et al produced an article in 2013 consisting of vignettes to illustrate the techniques used in TFT with the view to evaluate its use in treating BPD. Their findings supported the validity of TFT in treating BPD patients who specifically had difficulty with relationships.
They distilled TFT down to three important components 28:
1) The treatment contracting/setting the frame
2) Managing one’s affective response
3) The interpretative process
Pharmacology
A Cochrane intervention review assessing the effects of drug treatments in BPD, included twenty-eight randomised control trials, published in the period 1979-2009 (20 of 28 trials dating from 2000 or later), involving a total of 1742 participants 29.
Figure 2: The pharmacological agents that were tested included the following:
The authors arrived at the conclusion that pharmacotherapy in BPD ‘is not based on good evidence from trials’. The review found that there is support for the use of Second-generation antipsychotics (in improving cognitive-perceptual symptoms and affective dysregulation); Mood stabilisers (in diminishing affective-dysregulation and impulsive-aggressive symptoms); and Omega-3 fatty acids.
However, these claims were made based on single study effects and therefore require replication. No drug was found to significantly affect the symptom clusters, specific to BPD, including avoidance of abandonment, chronic feelings of emptiness, identity disturbance, and dissociation.
One noteworthy finding was that Olanzapine was associated with an increase in self-harming behaviour. Furthermore, the review states that ‘special attention’ is needed in BPD when prescribing tricyclic antidepressants (due to toxic effects in overdose) and hypnotics & sedatives (due to there being potential for misuse or dependence). Another problem that was highlighted was that in comorbid eating disorders the use of Olanzapine can contribute to weight gain and Topiramate can produce weight loss.
The review goes on to elucidate that there is not any evidence from randomised controlled trials that any drug reduces the severity of BPD and that it consists of ‘distinct pathology facets’. They recommend that the pharmacotherapy of BPD should be targeted at ‘defined symptoms’ and that polypharmacy is not supported by the latest evidence and should be avoided as much as possible.
The authors end by reaffirming that the evidence is not robust and that the studies may not satisfactorily reflect certain characteristics of the clinical environment. They propose that further research is needed in order to produce reliable recommendations. They detail the complications that arise from the ‘polythetic nature’ of BPD i.e. each patient is likely to experience different aspects of the disorder. There lacks a consensus among researchers about a common battery of outcome variables and measures. They comment that there is a fragmentary view on drug effects and that it is unknown as to how the alteration of one symptom affects another.
Comorbidity
Comorbidity is a foremost concern in the interpretation of data concerning personality disorders 30. A majority of individuals diagnosed with one personality disorder often meet criteria for at least one other personality disorder 30. A large proportion of patients with personality disorder have one axis I 31 disorder comorbidly, mostly depression, anxiety and alcohol and substance use disorders 32. [Axis I is a reference to the multi-axial classification system used in the Diagnostic and Statistical Manual of Mental Disorders that was removed in the latest version, DSM-5 2
It is important to consider therefore that, an improvement in the symptom clusters in personality disorders might be an improvement in comorbid axis I disorder symptoms. It is reported that the rates of depression are very high in BPD 33 and that the response to antidepressants in depressed individuals with comorbid personality disorders appears lower than in those without comorbid personality disorder 32.
The most recent guidance on the treatment of BPD from the National Health and Medical Research Council of Australia (NHMRC), which reviewed the literature and integrated a series of meta-analyses, details that pharmacotherapy does appear to be effective in altering the nature and course of BPD and that evidence does not warrant the use of pharmacotherapy as a sole or first-line treatment for BPD 34.
DISCUSSION
All of the aforementioned psychotherapy techniques are shown to produce promising results when applied to the treatment of BPD, with some standing out, such as DBT and MBT, due to the presence of a relatively robust evidence base. With such a wide variety of different approaches that all show some propensity for successful treatment of BPD it is clear that these approaches must be taken more seriously in clinical practice. These treatments have been shown to considerably improve symptomatic outcomes however there is a shortcoming in that they have failed to significantly improve social functioning. Each of the therapies follow distinct theories, however, when each treatment modality is applied to BPD, similar effects are seen. This is intriguing and should be explored further.
An analysis of these therapies revealed some common features which are now suggested as core requirements for all effective psychotherapeutic treatments:
Figure 3: Five common characteristics of evidence-based treatments for BPD 35, 36.
1. Structured (manual directed) approaches to prototypic BPD problems 2. Patients are encouraged to assume control of themselves (i.e. sense of self-agency) 3. Therapists help connections of feelings to events and actions 4. Therapists are active, responsive, and validating 5. Therapists discuss cases with others, (including personal reactions)
An update to the aforementioned Cochrane review 29 was published in 2013. The update focussed on the psychotherapies that are available for the treatment of BPD and included a total of 1804 participants spread over 28 studies. The psychotherapies discussed were divided into ‘comprehensive’ if they substantially involved an individual psychotherapy element or as ‘non-comprehensive’ if they did not. The comprehensive therapies included dialectical behaviour therapy, mentalization-based therapy (delivered in either a partial hospitalisation or outpatient setting), transference-focussed therapy, cognitive behavioural therapy, dynamic deconstructive psychotherapy, interpersonal psychotherapy and interpersonal therapy for BPD. These were assessed against a control condition and also with some direct comparisons against each other. Non-comprehensive psychotherapies included DBT-group skills training, emotion regulation group therapy, schema-focussed group therapy, systems training for emotional predictability and problem solving for borderline personality disorder (STEPPS), STEPPS plus individual therapy, manual assisted cognitive treatment, and psychoeducation 37.
The authors concluded that both comprehensive and non-comprehensive therapies indicated beneficial effects for the core pathology of BPD and associated general psychopathology. The authors identified that dialectical behaviour therapy had been studied the most comprehensively followed by mentalization-based therapy, transference-focussed therapy, schema-focussed therapy and STEPPS. However, the authors do state that none of the treatments presented a very robust evidence base and that there are concerns over the quality of individual studies 37.
In terms of pharmacotherapy, the NICE and NHMRC guidelines agree with the 2006 Cochrane interventional review among others 38, 39 that there is some evidence that some second-generation antipsychotics (aripriprazole and olanzapine) and some mood stabilisers (topiramate, lamotrigine and valproate) could improve BPD symptoms in the short term. However, for some of these agents, it is necessary to balance risks against benefits as they have considerable long-term risks (e.g. with antipsychotics, extrapyramidal side effects such as tardive dyskinesia can persist even after withdrawal of the drug 40). Such risks are not a problem in psychological treatments and it is probable that this influences guidelines. In practice, off-label use of psychotropics is widespread, despite the fact that the NICE guidance negates their use. It is arguable that clinicians should preferentially use pharmacological treatments that have the strongest evidence base (i.e. antipsychotics and mood stabilisers) and refrain from using agents with the least evidence (i.e. antidepressants and benzodiazepines).
CONCLUSION
Specialist treatments, in particular DBT and MBT substantiate the use of psychotherapy in BPD and these findings support the validity of the NICE guidance. However, the array of such treatments must be amalgamated with the view to provide a comprehensive, multi-faceted treatment approach. Each treatment must be broken down in order to outline the components that are particularly useful in BPD with the view to understand the condition in greater depth and to provide more focussed therapies.
The 2013 Cochrane review 37 highlights that further psychotherapies are available and have been shown to successfully treat BPD core pathology, however, as it is clearly stated the evidence base lacks robustness and there is a need for further studies that can replicate results. The therapies that have been included in this Cochrane review that have not been covered in the guidelines (e.g. STEPPS) may prove to be superior to those put forward by NICE, and I recommend that these be explored thoroughly when the guidelines are due for update.
While the NICE guidance emphasises that the use of psychotropics is reasonable in the management of comorbidities, it worth noting that to understand BPD, it is necessary to explore both the underlying aberrant psychological processes and biological processes that manifest in the disorder. This will enable the use of more specific pharmacological therapies in targeting the symptoms of BPD in the future.
Anterior knee pain or patellofemoral pain is a common clinical presentation especially in females. It is a challenging clinical problem. The specific cause can be difficult to diagnose as the aetiology remains poorly understood and there are various pathologic entities that can result in pain in the anterior aspect of knee.
Multiple surgical options have been used to treat the condition. Lateral retinacular release is one of these options and has been used to treat anterior knee pain with variable results1-5. The aim of this study was to assess isolated patella lateral retinaculum release as a treatment for anterior knee pain.
Materials and Methods
We performed a retrospective review of all the patients who underwent isolated arthroscopic lateral patella retinacular release under a single surgeon between July 2007 and July 2010. Exclusion criteria included significant patellar instability and severe mal-alignment on both radiological and clinical assessment and additional procedures including cartilage debridement, meniscal tear repair/excision or patella stabilization.
Data was collected from case notes (demographics, pre-operative and intra-operative findings and any post-operative complications), archived radiographs and postal questionnaires including pre and post procedure Oxford Knee Score (OKS), as well as patient satisfaction. Patient satisfaction questions included a grading of satisfaction of 1(completely dissatisfied) - 10 (completely satisfied) and whether patient would reconsider the procedure if given the choice again.
Independent factors assessed were age, sex, tight lateral retinaculum, osteoarthritic x-ray changes of all compartments, intraoperative findings of grade of arthritis and lateral subluxation and postoperative physiotherapy. The primary outcome assessed was patient reported outcome measures, including the improvement in post procedure OKS and patient satisfaction scores. SPSS Version 20 was used for analysis.
Preoperative and Postoperative OKS – total and components - were compared using Wilcoxon Signed Rank Test. The Mann Whitney U test was used for nominal data and Kruskal-Wallis test was used for continuous data for total OKS. Individual OKS components compared were ability to kneel and ability to climb stairs - more representative of patellofemoral joint.
Results
59 patients were identified with male to female ratio of 1:1.5. The mean age was 58.7 (range 25 to 77). 40 patients (67%) returned completed forms. Four patients had further surgery; three total knee replacement and one subsequent arthroscopic procedure for meniscal tears. These patients were excluded from the study. Four patients had bilateral procedures. Therefore after the exclusions for further surgery and those who failed to return completed forms 36 patients were included, on whom 40 procedures had been performed. Changes of osteoarthritis - graded according to Kellgren and Lawrence system - on the medial and lateral facets of the patella were noted on preoperative Merchant views (Table 1) and the tibiofemoral compartment as well.
Table 1 – Pre-Operative Radiographic grades of Patellofemoral change
Medial Facet
Lateral Facet
Grade
Frequency
%
Frequency
%
0
2
5
1
2.5
1
6
15
4
10
2
15
37.5
13
32.5
3
16
40
15
37.5
4
1
2.5
7
17.5
Total
40
100
40
100
All patients had undergone standardized preoperative physiotherapy regimen with no significant benefit. Two had, had intra-articular hyaluronic acid injection with no benefit.
All procedures were performed by a single surgeon (PE) and intraoperative findings of cartilage Outerbridge grade were noted in all compartments. Closed lateral retinacular release was performed with Smiley’s knife from just below lower end up to the upper border of patella.
Mean follow up duration was 20.43 months +/- 10.64. Patients were divided into three groups of follow up durations. 6-12 months had 6, 12-18months had 18 and >18months had 16 cases. The best results were in 12-18 month follow up but no statistically significant difference was found between different groups. There was no significant difference in age and gender distribution amongst different durations of follow up. Also there was no significant difference in age, gender and different durations of follow up between responders and non-responders of the questionnaire. There were no reported postoperative complications.
24(60%) underwent post-operative physiotherapy. The mean OKS improved from 23.05 (range11-40) to 35.30 (range14-48) [p value <0.0001]. Individual components of OKS, particularly ability to climb stairs and ability to kneel, also showed statistically significant improvements (Figure 1, Figure 2).
Fig 1 – OKS – ability to climb stairs
Fig 2 – OKS – ability to kneel
Univariate analysis showed improvement of total OKS and OKS for ability to kneel were significantly associated with higher grade of radiographic lateral patellofemoral joint wear (p value 0.025 and 0.042 respectively) and postoperative physiotherapy (p value 0.018 and 0.003) and improvement in OKS for ability to climb stairs was significantly associated with higher grade cartilage wear, noted intraoperatively, for trochlea (p value 0.042) and patella (p value 0.022).
However the OKS components lost this significance if there was Outerbridge Grade 3 or more wear in tibiofemoral articulation.
The procedure had a high mean satisfaction score of 8.2 (range 4 to 10), and 32 of 36 patients would have the procedure again if needed.
Discussion
Anterior Knee pain or patella pain syndrome is a very common clinical problem faced by orthopaedic surgeons. However the aetiology remains poorly understood. Mori et al6identified evidence of degenerative neuropathy in 29 out of 35 histologically examined specimens of resected lateral retinaculum; thus suggesting it may originate in the lateral retinaculum. Lateral Retinacular release would denervate this tissue producing symptomatic relief. Osterneier et al7 measured patellofemoral contact pressures and kinematics using fresh-frozen cadaver specimens both before and after lateral release. They concluded that release could decrease pressure on the lateral patella facet in flexion but did not stabilize the patella or medialise patella tracking. This possibly explains our finding of improvement with lateral patellofemoral joint wear.
Arthroscopic lateral release remains a controversial topic because of lack of well-designed randomised studies. Fulkerson and Shea8 suggested that knees showing lateral patellar tilt without subluxation were more likely to benefit from a lateral release in the absence of grade III or grade IV changes in the articular cartilage. Korkala et al9 showed that a lateral release tended to improve symptoms in patients with grade II to grade IV chondromalacia. Our findings concur that greater the patellofemoral articulation cartilage wear the more significant the improvement.
Lodhi et al10 performed a prospective study of elderly patients with patellofemoral osteoarthritis and pain which conservative management had failed to improve and concluded that the procedure improves function and provides significant pain relief successfully deferring need for arthroplasty; therefore they recommended the procedure in middle aged to elderly patients with symptomatic patellofemoral osteoarthritis.
Twaddle and Parkinson11 suggested lateral release to be an effective, reliable and durable procedure in ‘carefully selected patients’ through their retrospective study.
Our study has deficiencies regarding single surgeon series and retrospective review. However it reflects some of the findings from previous studies suggesting that it is an effective procedure to improve symptoms associated with cartilage changes in patellofemoral articulation without significant tibiofemoral joint osteoarthritis. Further well designed randomized controlled trials are needed to give a more definitive answer.
Conclusion
Isolated lateral patella retinacular release can be effective for anterior knee pain in carefully selected patients, (without significant instability or mal-alignment, with high patellofemoral but low tibiofemoral wear), who have failed conservative management. It particularly improves patients’ ability to kneel and climb stairs, giving a high satisfaction score. The grade of wear of patellofemoral cartilage is the most significant factor in determining this, with post-operative physiotherapy further augmenting the good results.
Three and half year old male child presented to PICU, Narayana health BANGALORE, with a short history of fever of 8 days with headache and cough for 2 days. At admission the child was febrile, dull looking, haemodynamically stable with no meningeal signs or focal neurological deficit. He was admitted and evaluated for the cause of fever. Same day child developed generalized seizures along with fever, hence a possibility of meningitis or electrolyte imbalance (hyponatremia) kept as child had initial serum sodium of 128meq/l. The cause of hyponatremia was looked into and child managed with antiepileptic drugs and 3% normal saline infusion. The initial sepsis screen was in-conclusive and CSF analysis showed 3 lymphocytes with low glucose and elevated protein levels, hence partially treated meningitis was considered (as h/o admission to a hospital for 3 days prior to admission in our hospital). The antimeningitic dose of IV antibiotics were given. On day 3 of admission child developed meningeal signs with worsening sensorium, hence neuro imaging was done (MRI brain) which showed multiple well defined ring enhancing lesion at bilateral central and cerebrallar hemisphere, thalamus, pons with mild perilesional edema. This radiological picture suggested a possibility of nerucysticercosis, however the clinical picture did not match with the same, hence pediatric neurology opinion was taken and simultaneous workup for tuberculosis were started. Child was also started on IV steroid. A strong possibility of CNS toxoplasmosis was kept by neurologist based on radiological picture. The workup for TB was inconclusive (negative mantoux, normal ESR, negative gastric aspirate for AFB) however child was empirically started on category II ATT in view of deteriorating clinical state. Repeat CSF evaluation showed increasing cell counts and similar biochemical picture as before, the sample was also send for Gene-Xpert (DNA amplification study). On day 6 of admission child developed lethargy and drowsiness hence antiedema measures were initiated. Same day he developed tonic posturing with unequal pupil, hypertension and bradycardia indicating raised Intracranial pressure (ICP), for which he was intubated and ventilated and urgent repeat CT head was done which showed increase in ventricular size and hydrocephalus. Immediately EVD was put by neurosurgeons after which there was gradual improvement in child’s condition and he was extubated within 48 hours. The reports showed negative HIV and toxoplasma serology and positive CSF gene study for AFB confirming the diagnosis of CNS tuberculosis, hence ATT and antiedema measures were continued and the EVD was later converted into VP shunt. Child by 2nd week of illness became afebrile with improved sensorium and function.
Fig 1 & 2: MRI showing multiple ring enhancing lesions
Discussion
Tuberculosis remains a leading cause of morbidity and mortality in the developing world. CNS involvement is thought to occur in 2-5% of patients with tuberculosis and up to 15% of those with AIDS related tuberculosis 1,2. Although CNS involvement by tuberculosis is seen in all age groups, there is a predilection for younger patients, with 60-70% of cases occurring in patients younger than 20 years of age 2. Haematogeneous spread from the lungs or gastrointestinal tract is most common, leading to small subpial or subependymal infective foci. These are termed Rich foci and form a reservoir from which intracranial manifestations may arise 3,4. Tuberculomas often present with symptoms and signs of focal neurological deficit without evidence of systemic disease. The radiologic features are also nonspecific and differential diagnosis includes malignant lesions, sarcoidosis, pyogenic abscess, toxoplasmosis and cysticercosis.5,6
Regarding treatment, the Center for Disease Control and Prevention recommends 12 months of treatment for CNS TB when the MT strain is sensitive to all drugs.7 However numerous variables can affect the response of the disease to therapy and it has been suggested that treatment duration should be tailored to the radiological response.8 After 12 months of treatment more than two-thirds of the patients still have contrast enhancing lesions. Although it is not clear if this represents an active lesion or just inflammation, continuing treatment is probably prudent. Total resolution of the tuberculoma is observed when scans demonstrate no enhancing lesions or only an area of calcification.8
In the case described above child had tubercular mengitis, multiple tuberculous, hydrocephalus and raised ICP. Although clinical presentations were suggestive of same, however the radiological picture and initial CSF finding raised suspicion is diagnosis. As tuberculoma and NCC shows many common clinical features, there are few distinguishing features such as the cysticercosis is smaller, less perilesional edema, multiple numbers and less of midline shift as compared to tuberculoma. However in our patient the multiple tuberculi gave a suspicion of NCC. It was only gene expert which confirmed our diagnosis.
Hence clinical cases like Tuberculoma, the radiological findings of which can usually be distinguished from other common illness like Neurocysticercosis or Toxoplasmosis, sometimes pose challenge in terms of radiological diagnosis suggesting the need for detailed evaluation to reach the diagnosis and guide treatment.
The state of pregnancy results in a multitude of cutaneous changes in the female. These are a reflection of the profound alterations in the endocrine, metabolic and immunological profiles that occur during this period.1 Skin manifestations occur due to the production of a number of proteins and steroid hormones by the fetoplacental unit and also by the maternal pituitary, thyroid and adrenals.2 The placenta, a new endocrine organ in the woman, produces progesterone. Dehydroepiandrosterone is produced by the fetal adrenals from pregnenolone and this is aromatized to estriol. At term, the level of progesterone is 7 times, estradiol is 130 times and prolactin level is 19 times of that present at 8 weeks of gestation.3 There occurs an overall preference for the Th2 cytokine profile, which helps in fetal protection from the immune system.4 This is due to the high levels of progesterone, which promotes Th2 cytokines like IL-4, IL-5 and IL-10 and has inhibitory effects on TNF alpha production. Oestrogen suppresses IL-2 production. The postpartum period is marked by withdrawal of hormones and consequent elevation of Th1 cytokine levels.4
Cutaneous changes develop in more than 90% of all pregnant females.5 These include common cutaneous changes that occur in most cases to severe diseases, some of which are seen exclusively in the pregnant and postpartum state. Cutaneous manifestations can be grouped into three broad categories: physiological cutaneous changes related to pregnancy; diseases modified by pregnancy and specific dermatoses of pregnancy.6
PHYSIOLOGICAL CHANGES IN PREGNANCY
These changes are so common that they are not considered abnormal. Rather, they provide contributory evidence of a pregnant state. This however, does not mean they are cosmetically acceptable to all patients. The various physiological changes during pregnancy have been summarized in Table 1.
Table 1: Physiological changes in pregnancy
Pigmentation Generalized hyperpigmentation Pigmentation of inner thigh, genitalia, axilla Secondary areola Linea nigra Chloasma Prominence/ appearance of pigmentary demarcation lines Enlargement and darkening of freckles, naevi and scars
Vascular changes Oedema of distal extremities and hands Spider angiomas Palmar erythema Leg varicosities Rectal haemorrhoids Cutis marmorata Capillary haemangioma
Glandular changes Miliaria Dyshidrotic eczema Montgomery’s tubercles Aggravation of acne
Oral mucosal changes Oedema and hyperaemia of gingivae Pregnancy epulis
Hair changes Hirsuitism Hypertrichosis Delayed anagen release after delivery
Nail changes Brittle nail plate Onycholysis Beau’s lines after delivery
Pigmentation:
Hyperpigmentation is one of the most common and early signs of pregnancy, seen in more than 90% of patients.7 High levels of Melanocyte Stimulating Hormone (MSH), oestrogen and progesterone are believed to be responsible for hyperpigmentation. Progesterone augments the oestrogen mediated melanin output, the levels of which correlate with pigmentary changes.8
Generalized hyperpigmentation is seen which is more marked in the dark haired skin.6 Pigmented areas of the body, namely the genitalia, perineum, areolae and upper medial thighs, demonstrate more pronounced pigmentation. Linea nigra, a hyperpigmented line extending from the pubic symphysis to umbilicus and further up to the xiphisternum, replaces the linea alba.9 Chloasma, also termed as mask of pregnancy, is the well marginated brownish pigmentation of the face like melasma. It is seen in 45-75% of pregnant women in western literature but in less than 10% cases in women with pigmented skin.5,10,11 Pigmentary demarcation lines appear on the limbs with borders of abrupt transition; freckles, naevi and scars tend to darken and enlarge.12
The pigmentation gradually fades after delivery, though the resolution of skin colour is usually incomplete. Chloasma tends to persist in 30% cases postpartum.13 Sun protection and reassurance is all that is needed. Topical formulations containing hydroquinone and tretinoin are avoided in pregnancy and can be added after delivery.
Physiological connective tissue changes:
Gross distension of abdomen with adrenocortical activities are responsible for the red-blue depressed streaks seen on abdomen and breasts in 70-90% pregnancies, called striae distensae.5,14 These usually develop in the second trimester. Females with pre-existing striae on breasts and thighs are more likely to develop striae gravidarum15, seen in White women more than Asian and African-American.14 Preventive therapies are controversial and postpartum treatment options include topical tretinoin, excimer laser or surgery.10
Soft tissue fibromas of pregnancy are called molluscum fibrosum gravidarum. They appear in the second trimester on the neck, face and beneath the breasts. These disappear after delivery.16
Physiological vascular changes:
Vascular growth factors released during pregnancy by the pituitary, adrenals and placenta are believed to be causative and this has been demonstrated in vitro as well.17 Non-pitting oedema of the face, hands and feet is present in around half of all females in the later part of pregnancy.13 This is probably due to sodium and fluid retention and pressure of the gravid uterus on the inferior vena cava. Spider naevi or spider angiomas are small raised lesions with a central pulsatile punctum and radiating telangiectatic vessels frequently present over the area drained by the superior vena cava. They are present in 67% of White women and 11% Black women during the second trimester.5 Palmar erythema is seen in two-thirds of White and one-third of Black women.8 Other vascular changes include varicosities of legs and anus (40%)13, cutis marmorata (0.7%)18 and capillary haemangioma (5%)9. These changes revert after the postpartum period.
Physiological glandular changes:
Eccrine gland activity is usually increased but the palms show decreased sweating. Thus, the incidence of miliaria and dishidrotic eczema is increased. There is inconclusive evidence to suggest that apocrine gland activity is decreased during pregnancy.19 Sebaceous activity increases in the third trimester leading to acne and enlargement of Montgomery’s tubercles.14 One-third to half of all pregnant women develop these tubercles, which are modified sebaceous glands.5,8 However, sebum excretion has not been found to decrease in lactating females post-delivery.20
Oral mucosal changes:
Oedema and hyperaemia of the gingivae in pregnancy is attributable to local irritation and nutritional deficiencies and is seen in around 80% women.5 Gingivitis not related to poor oral hygiene may occur. Granuloma gravidarum or pregnancy epulis might occur that regresses postpartum.
Hair changes:
Hair changes are seen in 3-12% of pregnant females.21 Hirsuitism and hypertrichosis occurs due to oestrogen. This leads to an increase in the percentage of hair in anagen.2 Approximately 2-3 months after delivery, loss of telogen hair occurs.22 This is termed as late anagen release as the hair follicles are no longer stimulated to stay in anagen phase by the maternal hormones. The hair recovery occurs in 3-12 months. A small number of females may experience episodic shedding of hair for long periods. This has been proposed to be due to the inability of some hair follicles to revert to asynchronous shedding.23 Rarely, male pattern baldness may occur in women.2
Nail changes:
Nail growth increases during pregnancy.6 Brittleness of the nail plate and distal onycholysis may be seen.19 Beau’s lines may develop after delivery.12 Reassurance is all that is needed for these benign nail problems.
DISEASES MODIFIED BY PREGNANCY
Many pre-existing dermatoses may be exacerbated or ameliorated by pregnancy. Certain tumours may also show remission or exacerbation. This is due to the shift in pregnancy to the Th2 state and a return to Th1 state in the postpartum period and also the discontinuation of some drugs due to their teratogenic potential.
Infections:
Depressed cell-mediated immunity makes the pregnant woman susceptible to more severe and frequent infections.24
Candidiasis is quite common and was found to be the commonest cause of white discharge per vagina, being present in 22% pregnant females.5 Half of all neonates born to infected mothers are positive for Candida and some may show signs of infection.25 Pityrosporum folliculitis, caused by Pityrosporum ovale, is more common in pregnancy.25
Genital warts are the commonest sexually transmitted disease seen in 4.7% subjects, these increase in size during pregnancy.9,25 Prophylactic caesarian section to prevent laryngeal papillomas in the neonate is not recommended now.26 Herpes simplex virus infection carries 50% risk of transmission to neonate in the primary episode and 5% risk in recurrent episode, caesarean section might be warranted to prevent such transmission.26 Varicella zoster virus infection has been reported to cause pneumonia in 14% of mothers and death in 3%.27 Bowenoid papulosis, caused by human papilloma virus appears first during pregnancy or may get aggravated.6
Pregnancy prepones the clinical manifestations in HIV infected females, possibly due to additive immune suppression. Pneumocystis pneumonia or listeriosis may prove to be fatal.27 Kaposi’s sarcoma may occur in these females.27 20-30% women present with leprosy for the first time in pregnancy and the postpartum period.28 The disease tends to downgrade towards the lepromatous pole in pregnancy and upgrades during lactation.29 Type 1 lepra reactions are more frequent in the first trimester and after delivery, whereas type 2 lepra reactions peak in third trimester.29 Trichomoniasis is diagnosed in 60% of pregnant women.25
Autoimmune diseases:
Systemic Lupus Erythematosus (SLE) is associated with a better prognosis than previously thought, if the disease is in remission and nephropathy and cardiomyopathy are not present.10 If the disease is active, half of the patients’ disease will get worse and there might be fatalities.14 SLE tends to be more severe if it first presents in pregnancy.14 Babies of such mothers are likely to develop neonatal lupus.
Patients with scleroderma are usually unaffected and some are improved in pregnancy. However, occasional reports of renal crisis, hypertension and pre-eclampsia are reported.30 Course of dermatomyositis is usually unaltered but the disease may worsen in some patients.31
Pemphigus tends to be exacerbated or present for the first time in pregnancy.32 The clinical presentation in pregnancy is similar to that of the regular presentation. Differentiation from herpes gestationis is important.
Metabolic diseases:
Effect of pregnancy on porphyria cutanea tarda is not clear, though some females show biochemical and clinical deterioration.33 Acrodermatitis enteropathica shows clinical worsening.34
Connective tissue diseases:
Pregnancy can lead to bleeding, uterine lacerations and wound dehiscence in patients of Ehlers-Danlos syndrome. Pseudoxanthoma elasticum patients may suffer massive gastrointestinal bleeds.35 Lichen sclerosis et atrophicus of the vulva usually improves in pregnancy and a normal delivery is mostly possible.
Disorders of glands:
Acne can aggravate during pregnancy. Hidradenitis suppurativa and Fox-Fordyce disease become better as a result of decreased apocrine gland activity.27
Keratinization diseases:
The course of psoriasis remains unaltered in 40% females during pregnancy while it improves in a similar percentage of females and worsens in the remaining.36 It is more likely to deteriorate in the postpartum period.37 Psoriatic arthritis has been found to worsen or present for the first time in pregnancy.2
Generalized pustular psoriasis of Von Zambusch may rarely occur. Though most patients have a preceding or family history of psoriasis, some may develop the disease without ever having a preceding episode.38 Peak incidence is seen in the last trimester and the disease tends to recur.38 Multiple, discrete, sterile pustules at the margins of erythematous macules on the umbilicus, medial thigh, axillae, inframammary folds, gluteal creases and sides of neck are seen. These break to form erosions and crusts. Painful, circinate mucosal erosions may form. Prednisolone is used for management.12 Von Zambusch pustular psoriasis of pregnancy was earlier termed ‘Impetigo Herpetiformis’ but the term is best avoided as it is impossible to differentiate it from the former, both clinically and histologically.6 Erythrokeratoderma variabilis is reported to worsen during pregnancy.27
Tumours:
A melanoma that develops during pregnancy carries worse prognosis but if pregnancy occurs after the tumour is resected, the prognosis is unaltered.39 Metastasis in the fetus has been seen and a minimum period of two years following tumour resection is recommended.32 A female with neurofibromatosis may develop neurofibroma for the first time in pregnancy or older neurofibromas may grow in size. Rupture of major vessels may occur.6 Pregnancy may worsen mycosis fungoides and eosinophilic granuloma.6
Miscellaneous diseases:
Prognosis of atopic dermatitis is unpredictable in pregnancy, with reports of both improvement and worsening.27 Predisposed patients may first develop atopic dermatitis during pregnancy.40 Allergic contact dermatitis may improve in pregnancy.12 Hand eczema may worsen in the puerperal period.6 Erythema multiforme may be precipitated by pregnancy.6 Autoimmune progesterone dermatitis has been described in pregnancy.12 This disease is characterized by hypersensitivity to progesterone demonstrated by a positive intradermal skin test and cutaneous lesions resembling urticaria, eczema, erythema multiforme and dermatitis herpetiformis.41 The disease is associated with fetal mortality and recurs in subsequent pregnancies.12
PREGNANCY SPECIFIC DERMATOSES
These are a heterogeneous group of inflammatory skin diseases specific for pregnancy.42 Most of these conditions are benign and resolve spontaneously in the postpartum period but a few of these are associated with fetal complications.42 Almost all of them present with pruritus and a cutaneous eruption of varying severity.5
Classification:
The first attempt to classify these conditions was made by Holmes and Black in 1982-83 who classified them into: a) Pemphigoid Gestationis (PG) or Herpes Gestationis(HG), b) Polymorphic Eruption of Pregnancy (PEP) or Pruritic Urticarial Papules and Plaques of Pregnancy (PUPPP), c) Prurigo of Pregnancy (PP) and d) Pruritic Folliculitis of Pregnancy (PF).43,44 Shornick was of the view that all patients with PF also had papular dermatitis, so he included PF in the PP group. He included Intrahepatic Cholestasis of Pregnancy (ICP) in his classification for dermatoses where secondary skin lesions due to scratching are produced. He proposed that failure to consider ICP in the classification has led to confusion in terminology of pregnancy specific diseases. Thus, his classification included PG, PEP, PP and ICP.45 Ambros-Rudolph et al carried out a retrospective review of 505 pregnant patients over a 10 year period and gave a more rationalised classification system in 2006. They clubbed PP, PF and eczema of pregnancy in one group called Atopic Eruption of Pregnancy (AEP) due to their overlapping features and found this group to be the most common pruritic condition in pregnancy. Thus, they proposed four conditions: a) AEP, b) PEP, c) PG and d) ICP.46 The various specific pregnancy dermatoses have been elaborated in Table 2.
Table 2: Comparison of different pregnancy specific dermatoses in relation to clinical characteristics, prognosis, investigations and treatment.
AEP
PEP
PG
ICP
Pruritus
+
+
+
+
Primary cutaneous involvement
+
+
+
-
Skin lesions
Eczematous or papular
Papules, vesicles and urticarial lesions
Vesiculo bullous lesion on urticarial base
Excoriations, papules secondary to scratching
Site of lesions
Trunk, extensors of limbs, rest of the body also involved
Abdominal involvement, in striae distensae, periumbilical sparing
Abdominal, particularly periumbilical involvement
Palms and soles followed by rest of the body
Time
First trimester
Third trimester, Post partum
Second and third trimester, post partum
Second and third trimester
Risk with primigravidae
-
+
-
-
Association with multiparity
-
+
-
+
Flare at delivery
-
-
+
-
Recurrence
+
-
+
+
Family history
+
+
-
+
Histopathology
Non-specific
Non-specific
Specific, sub epidermal vesicle
Non-specific
Immunofluorescence
-
-
Linear deposition of C3
-
Other lab findings
Ig E elevated
-
Indirect IMF +
Increased serum bile acids
Maternal risk
-
-
Progression to pemphigoid, thyroid dysfunction
Gallstones, Jaundice
Fetal risk
-
-
Prematurity, Small for age baby, neonatal blistering
Premature births, fetal distress, stillbirth
Treatment
Steroids, antihistaminics
Steroids, antihistaminics
Oral steroids, antihistaminics
Ursodeoxycholic acid
Atopic eruption of Pregnancy (AEP): (Syn: Besnier’s prurigo, prurigo gestationis, Nurse’s early onset prurigo of pregnancy)
It is the most common pregnancy specific dermatoses that includes eczematous or papular lesions in females with personal or family history of atopy and elevated IgE - accounting for nearly half of all patients.46 The disease tends to recur in subsequent pregnancies with 75% of all cases occurring before the start of the third trimester.47 It carries no risk for the mother or baby however, infant may develop atopy later in life.48 Treatment is symptomatic with antihistamines and corticosteroids.
E-type AEP: This group comprises of 67% of AEP patients and includes patients with eczematous features; previously referred to as Eczema of Pregnancy (EP). It was not until 1999 that a high prevalence of atopic eczema was noted in pregnancy.49 80% of pregnant women develop the first episode of atopic dermatitis during pregnancy.46 This is attributed to the Th2 cytokine profile in pregnancy and a dominant humoral immunity.4 It is more common in primigravida, in single gestation, begins in early pregnancy and affects whole body including face, palms and soles.46
P-type AEP: This group includes what was referred to previously as Prurigo of Pregnancy and Pruritic Folliculitis of Pregnancy. Prurigo of Pregnancy (PP) is seen in one out of 300 to 450 pregnancies and occurs predominantly in the second to third trimester.50 Excoriated or crusted papules are seen over the extensors of extremities and abdomen and are associated with some eczematization. The eruption lasts up to 3 months after delivery and recurrences in subsequent pregnancies are common.51 PP is associated with ICP with the differentiating feature being the absence of a primary lesion in the latter.50 Personal and family history of atopic dermatitis or raised IgE may be seen in PP.52 Serology is normal. There are no specific changes on histopathology and immunofluorescence results are found to be negative.50 There appears to be no maternal or fetal risk.45
Pruritic Folliculitis of Pregnancy (PF), first described by Zoberman and Farmer, is now believed to be as common as PG or PP, though only a few cases have been reported.50 It begins in the latter two trimesters and affects roughly one in 3000 pregnancies.51 Pruritus is not a defining feature, despite what the name suggests.2 Multiple, follicular papules and pustules occur on the shoulders, arms, chest, upper back and abdomen and are acneiform in nature.42 The lesions tend to resolve in a couple of months following delivery. Histopathological examination reveals non-specific features with sterile folliculitis and immunofluorescence studies are negative.50 No maternal or fetal risk is described except for low birth weight neonates in a single study.52 Pathogenesis of PF is unknown with no definite role of androgens or immunologic abnormalities.53 There is no evidence to suggest that it is a hormonally aggravated acne as proposed by some workers.54
Polymorphic Eruption of Pregnancy (PEP): (Syn: Pruritic Urticarial Papules and Plaques of Pregnancy or PUPPP, Bourne’s Toxaemic Rash of Pregnancy, Toxic Erythema of Pregnancy, Nurse’s Late Prurigo of Pregnancy)
With a prevalence of a case in every 130-300 pregnancies, this disease is the second most common pregnancy specific dermatoses and was seen in 21.6% pregnancies reviewed by Ambros-Rudolph et al.46 They found it began in late pregnancy in 83% cases and 15% in the postpartum period.46 The disease occurs predominantly in primigravida and a familial predisposition is present.55 Lesions are pleomorphic, usually urticarial but purpuric, vesicular, polycyclic and targetoid lesions may be present. The striae on the abdomen are the first to be involved and there is a characteristic periumbilical sparing.56 The lesions seldom occur on the body above the breast and on hands and feet.12 The lesions resolve with scaling and crusting in six weeks. The disease is more common in excessive weight gain during pregnancy and in multiple gestation.57,58 Histopathology is non-specific and shows spongiosis, occasional subepidermal split and eosinophilic infiltration. Serology and immunofluorescence is negative.50 Treatment is symptomatic, oral steroids are needed in severe cases. There are no associated maternal or fetal complictions,59 although infants may later develop atopic dermatitis.2
The pathogenesis is unknown however, the abdominal distension leading to collagen and elastic fibre damage in striae is hypothesized, leading to formation of antigens and triggering inflammatory cascade.60 The role of progesterone has been suggested by the increased progesterone receptor immunoreactivity in skin lesions of PEP.61 The discovery of fetal DNA in skin lesions of women with PEP has furthered the hypothesis that abdominal distension leads to increased permeability of vessels and permit chimeric cell migration in the maternal skin.62 Linear IgM dermatosis of pregnancy is an entity characterized by pruritic, red, follicular papules and pustules on the abdomen and proximal extremities seen after 36 weeks gestation and a linear band of IgM deposition on basement membrane zone. It has been characterized as a variant of PEP or PP by different authors.12
Pemphigoid Gestationis (PG): (Syn: Herpes Gestationis or HG, Gestational Pemphogoid, Dermatitis Herpetiformis of Pregnancy)
PG is the most clearly characterized pregnancy dermatosis and the one which also affects the fetal skin.63 It is a rare, self-limiting, autoimmune bullous disease with an incidence of 1:1700 to 1:50000 pregnancies.63 Mean onset occurs at 21 weeks gestation, though it occurs in the postpartum period in a fifth of all cases.64 Constitutional symptoms, burning and itching herald the onset of the disease. Half of patients develop urticarial lesions on the abdomen, particularly in the periumbilical region, that change rapidly to a generalized bullous eruption usually sparing the face, palms, soles and mucosae. Vesicles may arise in herpetiform or circinate distribution. Face is involved in 10% cases and oral mucosa in 20%.12 The disease shows spontaneous improvement in late gestation but flares may occur at the time of delivery in 75% of the cases.63 Though the disease may remit after a few weeks after delivery, a protracted course, conversion to bullous pemphigoid or recurrence with menstrual cycle and use of oral contraceptive pills has been reported.50 PG tends to recur in subsequent pregnancies in a more severe form and at an early stage with longer stay in postpartum.50 Skipped pregnancies have been described.63,65 The disease is also linked with hydatiform mole and choriocarcinoma.66
The classical histopathological finding is the presence of a subepidermal vesicle, spongiosis and an infiltrate consisting of lymphocytes, histiocytes and eosinophils.64 An inverted tear drop appearance due to oedema in the dermal papilla is seen in early urticarial lesions.15 Direct immunofluorescence reveals a linear deposition of C3 along the dermo-epidermal junction in 100% cases and is diagnostic of the disease, while a salt split skin shows an epidermal staining.67 Antithyroid antibodies may be present but thyroid dysfunction is not common.63 Systemic corticosteroids are the mainstay of management. About one in ten children born to women with PG develop blisters due to passive transfer of antibodies, this resolves on its own. Severity of the disease has been correlated with the risk of prematurity and small for gestational age babies.68
Pathogenesis of PG involves the production of IgG1 antibodies against NC16A domain of carboxyl terminus of Bullous Pemphigoid Antigen 2 (BPAg2), leading to activation of complement, recruitment of eosinophils to the local site and damage of the basement membrane and consequent blistering.2 The aberrant expression of MHC class II antigens of paternal haplotype is believed to stimulate an allogenic response to placental basement membrane and this is believed to cross react with the skin in PG.63,69
Intrahepatic Cholestasis of pregnancy (ICP): (Syn: Obstetric Cholestasis, Pruritus Gravidarum, Icterus Gravidarum, Recurrent Jaundice of Pregnancy, Idiopathic Jaundice of Pregnancy)
Pruritus in pregnancy is fairly common and can be due to various reasons like pregnancy specific dermatoses and other co-existing dermatoses such as scabies, urticaria, atopic dermatitis, drug reactions etc. It was found to be present in more than half of 170 pregnant women in an Indian study.70 This must be differentiated from ICP where the skin lesions arise secondary to itching.
ICP was first described by Kehr in 1907.63 ICP being referred to Pruritus Gravidarum (for pruritus without skin changes occurring early in pregnancy and related to atopic diathesis and no cholestasis) and Prurigo Gravidarum (for pruritus associated with PP like skin lesions and associated with cholestasis) lead to much confusion regarding nomenclature.63 The disease has an incidence of 10-150 cases per 10,000 pregnancies71, being more common in South America and Scandinavia, probably due to dietary factors.50 Patients complain of sudden onset pruritus beginning from the palms and soles and later generalizing to the whole body. Skin lesions are secondary to itching and range from excoriations to prurigo nodularis, extensors are more severely involved. Jaundice is seen in 20% cases only.72 Clay coloured stools, dark urine and haemorrhage secondary to vitamin K malabsorption can occur. Family history can be elicited in half of the cases and an association with multiple gestation is described.73 Resolution of ICP occurs soon after delivery. Recurrence in subsequent pregnancies is seen in 45-70% cases and routinely with the use of oral contraceptive pills, though no detectable abnormalities are seen in the duration between two pregnancies.63 Histopathology is non-specific and immunofluorescence is negative. Diagnosis is made by increased serum bile acid levels, transaminases are elevated. Prothrombin time may be prolonged. A 2.7 times increased risk of gallstones is reported in primigravida with ICP compared to non-pregnant women.74 ICP is associated with significant fetal morbidity including premature births in 20-60% cases, intrapartum fetal distress including meconium aspiration in 20-30% and fetal mortality in 1-2%.71 Risk is particularly more if serum bile acid levels exceed 40 micromoles per litre.75 Meconium may cause umbilical vein compression and induction of labour at 36 weeks gestation has been recommended in severe cases.50 The goal of treatment is reduction of serum bile acids. Ursodeoxycholic acid, given in the dose of 15mg/kg orally daily is the only proven therapeutic agent that decreases fetal mortality.63,76 Cholestyramine reduces vitamin K absorption and increases the risk of haemorrhage. Other agents like S-adenosylmethionine, dexamethasone, silymarin, phenobarbitone, epomediol and activated charcoal are not that effective and do not affect fetal risk.63 Topical emollients and antipruritic agents offer symptomatic relief but antihistamines are not that effective.50
The key event in the pathogenesis of ICP is elevation of bile acids. Oestrogens are said to have cholestatic properties by reducing hepatocyte bile acid uptake and also by inhibiting basolateral transport proteins.50 Progesterone may additionally saturate the transport capacity of these transport proteins in hepatocyte.71 Genetic predisposition occurs due to mutation in genes encoding bile transport proteins, with cholestasis developing in pregnancy as their capacity to secrete substance is exceeded.63 Bile acids passing through the placenta produce vasoconstriction of placental veins, fetal cardiomyocyte dysfunction and also abnormal uterine contractility, all leading to fetal hypoxia.71
CONCLUSION
Pregnancy is associated with a wide variety of cutaneous changes. These may range from common, benign changes termed physiological or more severe, posing significant risk to the mother as well as the baby. Physiological pregnancy changes may be of cosmetic concern to the patient and seldom need anything more than counselling. Pre-existing dermatoses may aggravate during this period, posing a challenge to the treating physician. Women suffering from such diseases need to be warned of complications and risks before trying to conceive. A strict watch for possible complications and appropriate management at an early stage is warranted. Women should also be looked for pregnancy specific dermatoses and their complaints should not be lightly overlooked as non-specific or physiological. Careful history and examination with a judicious use of investigations will help to arrive at a diagnosis and in prompt institution of treatment.
Meningiomas are common intracranial neoplasms with a wide range of histopathological appearances. The WHO classification of tumours of the central nervous system recognises 15 subtypes of meningiomas, of which meningothelial, fibrous and transitional subtypes are most common. Lymphoplasmacyte-rich meningiomas (LPM) are rare WHO subtype that belong to Grade I meningiomas.1 The estimated incidence is less than 1% of all meningiomas.2 LPM usually occurs in young and middle age patients, with most common locations being cerebral convexities, skull base, parasagittal area within the superior sagittal sinus, cervical canal, optic nerve and tentorium.3 Histopathological examination shows extensive infiltrates of lymphocytes and plasma cells often obscuring the meningothelial component.
Case report
A 21-year-old man presented with a history of headache since 4 months. It was a dull pain not associated with vomiting, seizures or visual symptoms. The patient did not have any features suggestive of cranial nerve involvement. Physical examination was unremarkable except for the presence of papilloedema. Non-contrast CT scan showed a large isodense lesion with peri- lesional oedema and eccentric enhancing nodular component in the right fronto-parietal region (Figure 1). A radiological diagnosis of glioma with mass effect and shift to left was rendered. A right frontoparietal free bone flap craniotomy was performed. Operatively, a well encapsulated tumour probably arising from the dura mater was found. Gross total removal of the tumour was done and the excised tumour was sent for histopathological examination with a provisional clinical diagnosis of meningioma.
Histopathological examination revealed a tumour arranged as sheets and whorls of meningothelial cells without any mitoses or atypia. A dense infiltrate of lymphocytes and plasma cells was seen in large areas of the tumour (Figure 2).
On immunohistochemistry, tumour cells were positive for epithelial membrane antigen (EMA) (Figure 3) and vimentin. The lymphoplasmacytic infiltrate contained mixture of CD3 and CD20 positive lymphocytes. A diagnosis of lymphoplasmacyte- rich meningioma was given.
Figure 1. Non-contrast CT scan showing a large isodense cystic lesion with perilesional oedema and eccentric enhancing nodular component in the right frontoparietal region
Figure 2: Tumour arranged as sheets and whorls of meningothelial cells without any mitoses or atypia. A dense infiltrate of lymphocytes and plasma cells seen in large areas of the tumour (H & E x 100)
Meningiomas are common neoplasms accounting for 24-30% of all primary intracranial tumours. They arise from the arachnoidal cells, and are typically attached to the inner surface of the duramater.1 Most of the meningiomas are benign, corresponding to WHO grade I and associated with a favourable clinical outcome. LPM is a rare low grade histopathological subtype of meningioma, usually seen in younger patients, with the mean age of onset being 34 years.4,5 The patients with LPM have variable clinical manifestations according to the location of the tumour. The common presentations include headache, hemiparesis, seizure, vomiting, dizziness, visual disturbance, dyscalculia, dysgraphia and slurred speech.3 Although the natural history of LPM is often over one year, few cases might occur in short duration due to inflammatory cell infiltration and oedema.6 Systemic haematological abnormalities such as hyperglobulinemia and iron refractory anaemia have been documented in some patients with LPM, believed by some to be due to the plasma cell infiltrate.3,6,7
Radiologically, LPMs are usually globular, highly vascular, contrast- enhancing, and dural based tumours. The typical characters of LPM on MRI are isointense lesions on T1-weighted images and hyperintense lesions on T2-weighted images, with a strong homogenous enhancement after the administration of gadolinium; obvious peritumoural brain oedema and dural tail signs.3 Sometimes, cystic component and heterogeneous enhancement may also be encountered, making pre-operative diagnosis difficult, as in our case.8
On microscopic examination, this tumour is characterised by a conspicuous infiltrate of lymphocytes and plasma cells, sometimes completely obscuring the tumour cells. The massive infiltration of lymphocytes and plasma cells has been postulated to play a central role in the development of brain oedema associated with LPM. The origin of this tumour (neoplastic or inflammatory) is unclear, so it is considered closer to intracranial inflammatory masses rather than typical meningiomas.7
The differential diagnoses include collision tumour of meningioma and plasmacytoma, inflammatory pseudotumour, idiopathic hypertrophic pachymeningitis (IHP), and intracranial plasma cell granuloma.3,7 The use of staining for EMA and vimentin is useful in indicating the meningothelial origin of the tumour, and differentiates LPM from other intracranial lesions.9
The pathological findings of IHP usually include thickened fibrotic dura mater with marked infiltration of lymphocytes and plasma cells, occasionally accompanied with small islands of meningothelial proliferation mimicking those of LPM. Localised nodular lesion can sometimes rule out this diagnosis in that IHP usually shows diffused lamellar thickenings or plaque-like features.4
Chordoid meningiomas often contain regions that are histologically similar to chordoma, with cords or trabeculae of eosinophilic, vacuolated cells in a background of abundant mucoid matrix background.3 Detailed histological studies can aid the differential diagnosis. The plasma cell component is not neoplastic and thus plasmacytoma with reactive meningothelial hyperplasia or a collision tumour involving meningioma and plasmacytoma can both be excluded.10
The knowledge of this rare entity is important to avoid its underdiagnosis as an inflammatory pseudotumour or plasma cell granuloma and overdiagnosis as a plasmacytoma.
The non-vitamin K antagonist oral anticoagulants have demonstrated favourable benefit–risk profiles in large phase III trials, and these findings have been supported by real-world studies involving unselected patients representative of those encountered in routine clinical practice and including those deemed ‘challenging-to-treat’
Accurate detection of atrial fibrillation and assessment of stroke and bleeding risk is crucial in identifying patients who should receive anticoagulation
Elderly populations represent a significant proportion of patients seen in general practice, and advanced age should not be regarded as a contraindication to treatment; acetylsalicylic acid is not considered an effective treatment option to reduce the risk of stroke in patients with non-valvular atrial fibrillation (except for those declining oral anticoagulation), particularly in fragile elderly patients, for whom this drug was historically prescribed
The frequency of follow-up visits, in particular to check compliance, should be tailored according to patients’ clinical characteristics and needs, but there is no requirement for routine coagulation monitoring, unlike vitamin K antagonists
Atrial fibrillation: a clinical and economic burden to society
Atrial fibrillation (AF) is the most frequently encountered sustained cardiac arrhythmia, with a prevalence of about 1.5–2% in the general population1,2. Its incidence is predicted to rise sharply over the coming years as a consequence of the ageing population and increased life expectancy in those with ischaemic and other structural heart disease2. In addition to being associated with significantly increased rates of mortality3, AF is also associated with significantly increased rates of heart failure, which is both a common cause and consequence of AF and greatly worsens the prognosis4. However, it is stroke that is the most devastating consequence of AF, with an average fivefold increased risk5.
AF-related strokes are often more severe than other strokes6,7because the clots that embolise from the left atrium or left atrial appendage are often much larger8than from other sources of emboli. These clots usually lodge in large cerebral vessels, commonly the middle cerebral artery, resulting in huge neurological and functional deficits and increased mortality compared with other stroke types. Moreover, the strokes suffered by patients with AF are more likely to lead to extended hospital care than strokes in patients without AF, thus impacting on patients’ quality of life7.
Current evidence suggests that, in the UK, AF has a causative role in almost 20% of all strokes9. This is likely to represent a significant underestimate given that long term electrocardiogram (ECG) monitoring in patients who would previously have been diagnosed as having cryptogenic stroke has demonstrated a significant AF burden in these patients10.
With improved AF detection and stroke prevention, it is estimated that approximately 8000 strokes could be avoided and 2100 lives saved every year in the UK, resulting in substantial healthcare savings of £96 million11,12.
A key objective of this short review is to provide primary care clinicians with the confidence to manage patients with AF in need of anticoagulation, including the safe and appropriate use of the non-vitamin K antagonist oral anticoagulants (NOACs) apixaban, dabigatran, rivaroxaban (approved in the EU, US and several other countries worldwide) and edoxaban (approved in the EU, US and Japan).13-20The focus will be on how to accurately identify, risk-stratify and counsel patients on the risks and benefits associated with the different treatment options.
Who to treat. Accurate detection and assessment of stroke and bleeding risk
Many patients with AF are asymptomatic, particularly the elderly, less active patients who may not notice the reduction in cardiac performance associated with AF. Unfortunately, it remains the case that AF is undetected in up to 45% of patients21, and stroke is very often the first presentation of AF.
Both the National Institute for Health and Care Excellence (NICE) and the European Society of Cardiology (ESC) guidelines recommend opportunistic screening in patients aged ≥65 years by manual pulse palpation followed by ECG in patients found to have an irregular pulse1,22. Opportunistic screening (manual pulse palpation) was shown to be as effective as systematic screening (ECG) in detecting new cases23, and this simple strategy should be used to screen at-risk patient groups as often as possible. Hypertension and increasing age are the two leading risk factors for developing AF, but other high-risk groups include patients with obstructive sleep apnoea, morbid obesity or a history of ischaemic heart disease24-26. In the context of proactive AF detection, many initiatives have been launched worldwide to encourage primary care clinicians to integrate manual pulse checks into their routine practice. The Know Your Pulse campaign was launched by the AF Association and Arrhythmia Alliance during Heart Rhythm Week in 2009 and was quickly endorsed by the Department of Health in the UK and by many other countries. This initiative has assisted in diminishing some of the gaps in AF detection21.
The most frequently used tools to evaluate stroke risk in patients with non-valvular AF (AF that is not associated with rheumatic valvular disease or prosthetic heart valves) are the CHADS227 and CHA2DS2-VASc28scores, with recent guidelines favouring the use of the latter and emphasising the need to effectively identify ‘truly low-risk’ patients1. The CHA2DS2-VASc score is superior to CHADS2 in identifying these truly low-risk patients, who should not be routinely offered anticoagulation1. Patients with any form of AF (i.e. paroxysmal, persistent or permanent), and regardless of whether they are symptomatic, should be risk stratified in this way. The risk of stroke should also be assessed using CHA2DS2-VASc in patients with atrial flutter and probably for the majority of patients who have been successfully cardioverted in the past22. Unless the initial underlying cause has been removed (e.g. corrected hyperthyroidism) and there is no significant underlying structural heart disease, the risk of patients suffering from a recurrence of AF following ‘successful’ cardioversion remains high29. The ESC guidelines recommend that anticoagulation should be offered to patients with a CHA2DS2-VASc score ≥1 based on assessment of risk of bleeding complications and the patient’s clinical features and preferences1.
The new Quality and Outcomes Framework (QOF) for 2015–2016 now recommends the use of CHA2DS2-VASc for risk stratification and no longer recommends antiplatelet agents as a therapeutic option for stroke prevention in patients with non-valvular AF30; this should result in significantly more patients receiving anticoagulation for this indication. The changes to QOF 2015–2016 compared with 2014–2015 are summarised in Table 130.
Table 1. Summary of changes to UK the Quality and Outcomes Framework (QOF) 2015–201630
NICE indicator ID
Changes
2014–2015 points
2015–2016 points
NM45: Patients with AF and CHADS2=1 currently treated with anticoagulant therapy or antiplatelet therapy
Retired
6
–
NM46: Patients with AF and a latest record of a CHADS2 ≥1 currently treated with anticoagulant therapy
Replaced by NM82
6
–
NM82: Patients with AF and CHA2DS2-VASc ≥2 currently treated with anticoagulant therapy
Replacement
–
12
NM81: Patients with AF in whom stroke risk has been assessed using the CHA2DS2-VASc risk-stratification scoring system in the preceding 12 months (excluding those with a previous CHADS2 or CHA2DS2-VASc ≥2)
New indicator
–
12
Key: AF = atrial fibrillation; CHADS2 = Congestive heart failure, Hypertension, Age ≥75 years, Diabetes, Stroke (doubled); CHA2DS2-VASc = Congestive heart failure or left ventricular dysfunction Hypertension, Age ≥75 years (doubled), Diabetes, Stroke (doubled)-Vascular disease, Age 65–74 years, Sex category (female); NICE = National Institute for Health and Care Excellence
The Guidance on Risk Assessment and Stroke Prevention in Atrial Fibrillation (GRASP-AF) clinical audit software detection tool is now very widely used in primary care to improve clinical outcomes in the AF population by identifying patients likely to benefit from anticoagulation. GRASP-AF systematically scans general practice software systems and calculates CHADS2 and CHA2DS2-VASc scores in patients who are coded as having AF, thus enabling physicians to identify high-risk patients who are not adequately treated for stroke prevention31. Identification of AF patients who are poorly controlled on warfarin (defined as having a time in therapeutic range <65% or a labile international normalised ratio [INR], e.g. one INR value >8 or two INR values <1.5 or >5 within the past 6 months)22 is crucial because these patients are more likely to experience major bleeding or stroke. These patients should be reviewed and, if possible, the cause for the poor warfarin control should be identified. The Warfarin Patient Safety Audit tool is another software tool that has been developed to help identify patients with poor warfarin control32.
Primary care clinicians are being urged to objectively assess the bleeding risk of AF patients who are receiving, or about to receive, anticoagulation1,22,32. HAS-BLED is the bleeding assessment scheme advocated by both NICE and the ESC1,22, this has been validated in several independent cohorts and was shown to correlate well with the risk of major bleeding, in particular intracranial bleeding1. The key aspect of HAS-BLED is that, unlike CHADS2 and CHA2DS2-VASc, it consists of risk factors that are modifiable. It should, therefore, not be a tool to influence the decision of whether to anticoagulate, but instead to identify ways to reduce the risk of bleeding in patients receiving an anticoagulant; for example, optimising blood pressure control, stopping unnecessary antiplatelet or anti-inflammatory agents and reducing alcohol consumption can all significantly reduce HAS-BLED scores and bleeding risk1. In addition, it needs to be emphasised that the absolute number of patients with AF experiencing a serious bleeding event while receiving anticoagulant therapy is low (~2–3%/year in the XANTUS, PMSS and Dresden NOAC Registry real-world studies) , with prospective real-world studies indicating that most bleeding events can be managed conservatively33-35. Whilst concerns have been raised about not having a reversal agent to counter the anticoagulant action of NOACs in patients who experience serious bleeding, the low incidence of major bleeding in real-world and phase III studies and its conservative management in most cases demonstrate that such agents would not be required routinely. Despite these low rates of major bleeding, reversal agents have been developed and successfully completed phase III studies and undergone approval in some markets, including idarucizumab in the UK36,37. Notably, high-risk patients with AF were shown to be more willing to endure bleeding events in order to avoid a stroke and its consequences38, thus reinforcing the message that “we can replace blood but we cannot replace brain tissue”.
Adequate anticoagulation therapy should follow appropriate patient identification
Identifying the right treatment option for patients with AF is likely to improve clinical outcomes. Involving patients in the decision-making process and rationale, and ensuring they understand the net benefit–risk of treatment options, is likely to lead to better compliance and improved clinical outcomes. The ESC guidelines consider patients with valvular AF (patients with AF in the presence of either rheumatic mitral stenosis [very rare now in the UK] or prosthetic heart valves) to be at high risk, and these patients should be anticoagulated with a VKA regardless of the presence of any other risk factors1. Warfarin is very effective at reducing the risk of stroke compared with acetylsalicylic acid (ASA)39,40, but an unpredictable dose–response relationship and multiple drug and food interactions can be problematic for some patients, and many patients remain sub-optimally treated41. ASA is also not considered an effective treatment option to reduce the risk of stroke in patients with non-valvular AF especially in frail, elderly patients in whom ASA was historically prescribed. The GARFIELD-AF registry (10,614 patients enrolled in the first cohort) revealed that real-world anticoagulant prescribing in AF populations deviates substantially from guideline recommendations: 40.7% of patients with a CHA2DS2-VASc score ≥2 did not receive anticoagulant therapy, and a further 38.7% with a score of 0 received anticoagulant therapy. At diagnosis, 55.8% of patients overall were given a VKA, just over one quarter (25.3%) received an antiplatelet drug alone, and ~4.5% received a NOAC24. Inappropriate prescribing was further confirmed by data from UK general practices (n=1857, representing a practice population of 13.1 million registered patients) using the GRASP-AF tool. Only 55% of patients with high-risk AF (CHADS2 ≥2) were receiving oral anticoagulation (OAC) therapy, whereas a further 34% of patients with no known contraindication did not receive OAC therapy42.
The NOACs have altered the landscape in terms of stroke prevention management by increasing the available options for patients. These agents exhibit some important practical advantages over traditional therapy (e.g. no requirement for routine anticoagulation monitoring, simple fixed dosing oral regimens, fast onset of action, fewer drug reactions and no food interactions), leading to their increased uptake in primary care.
Key patient groups who are likely to benefit from the NOACs include patients poorly controlled on VKAs, those predicted to require medications that interact with VKAs (e.g. patients who require frequent antibiotics), those without severe renal impairment or those with a prior ischaemic stroke while receiving a VKA with an adequate INR. These agents could also be a good choice for patients living a considerable distance from their local hospital or surgery and commuters. The NICE guidelines state that primary care clinicians should consider clinical features and patient preference before deciding on the most appropriate option for patients22. In addition, cost may be important in some settings. All of the NOACs have demonstrated cost-effectiveness versus warfarin, and although cost models vary by country, there is little doubt that these agents provide cost-effectiveness largely through the number of adverse events avoided and their associated costs43.
Choice of anticoagulant: which to choose?
The demonstration of a favourable benefit–risk profile (stroke prevention vs bleeding events) in large phase III studies involving over 70,000 patients has resulted in the regulatory approval of apixaban, dabigatran, edoxaban and rivaroxaban44-47for the prevention of stroke and systemic embolism in patients with non-valvular AF and one or more risk factors.
Overall, NOACs have demonstrated an improved benefit compared with warfarin, with lower rates of intracranial haemorrhage (for all NOACs) and similar or superior efficacy for stroke prevention44-48. Statistically significant relative risk reductions (RRRs) in the incidence of fatal bleeding events were seen with low-dose dabigatran (110 mg twice daily [bd]; RRR=42%), both tested doses of edoxaban (30 mg once daily [od] and 60 mg od; RRR=65% and 45%, respectively) and rivaroxaban (20 mg od; RRR=50%)46,47,49; rates of fatal bleeding were also lower in patients treated with apixaban compared with warfarin (34 patients vs 55 patients, respectively)44. These data are promising, especially considering the current lack of a specific antidote for any of the NOACs, and it is likely that the very short half-life of these drugs play an important role in mitigating the bleeding risk.
Owing to a lack of head-to-head comparisons between the NOACs in phase III clinical trials, patient characteristics, drug compliance, tolerability issues and cost may be important considerations1. In addition, subanalyses of phase III trial data for rivaroxaban, apixaban and dabigatran indicate that the challenging-to-treat patient groups often encountered by primary care clinicians can be treated effectively and safely with the NOACs (Table 2). A recent meta-analysis showed a similar treatment effect for almost all subgroups encountered in clinical practice; NOACs appeared to be at least as effective as VKAs in reducing the risk of stroke and systemic embolism and no more hazardous in relation to the risk of major bleeding events, irrespective of patient co-morbidities50.
Table 2.Novel oral anticoagulants studied in key patient subgroups*
Subgroup analysis
Rivaroxaban
Dabigatran
Apixaban
Factors related to disease
ROCKET AF
RE-LY
ARISTOTLE
Heart failure
ü59
ü60
ü61
Renal impairment
ü62
ü63
ü64
Prior stroke
ü65
ü66
ü67
VKA-naïve
ü68
ü69
ü70
Prior MI or CAD
ü(prior MI)71
ü(CAD or prior MI)72
üCAD73
PAD
ü74
–
–
PK/PD
ü75
ü76
–
East Asian patients
ü77
ü78
79
Elderly
ü80
ü49
ü81
Major bleeding predictors
ü82
–
–
Obesity
–
–
–
Diabetes
ü83
ü84
ü85
Valvular heart disease
ü86
–
ü87
Paroxysmal versus persistent AF
ü88
ü89
ü90
*No subgroup analyses have been presented for edoxaban Key: AF = atrial fibrillation; ARISTOTLE = Apixaban for Reduction In STroke and Other ThromboemboLic Events in atrial fibrillation; CAD = coronary artery disease; CHADS2= Congestive heart failure, Hypertension, Age ≥75 years, Diabetes, Stroke (doubled); MI = myocardial infarction; PAD = peripheral artery disease; PK/PD = pharmacodynamics/pharmacokinetics; RE-LY = Randomized Evaluation of Long-term anticoagulation therapy; ROCKET AF = Rivaroxaban Once daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation; VKA = vitamin K antagonist
Because patient selection in clinical trials is based on strict inclusion/exclusion criteria, patient populations in such studies are not always representative of patients routinely seen in real-world practice. In addition, bleeding events may be managed differently in clinical trials versus routine clinical practice. Real-world data are, therefore, needed to help validate drug safety and effectiveness in unselected patient populations. Following phase III clinical trials and the widespread approval of the NOACs in stroke prevention in patients with non-valvular AF, real-world experience has been steadily accumulating. The current real-world data for rivaroxaban, apixaban and dabigatran have been very reassuring and bridge the evidence gap between clinical studies and real-world experience33-35,51-57.
The lack of routine coagulation monitoring with NOACs does not remove the necessity for regular follow-up. Instead, the frequency of visits can be tailored according to patients’ clinical characteristics and needs. NOACs are all partially eliminated by the kidneys; therefore, regular monitoring of renal function is important either to use a lower recommended dose of these drugs or to avoid them. For example, renal function should be monitored every 6 months in patients who have stage III chronic kidney disease (creatinine clearance [CrCl] 30–60 ml/min)58. Apixaban, rivaroxaban and edoxaban are not recommended in patients with CrCl <15 ml/min, and dabigatran is contraindicated in patients with CrCl <30 ml/min13,15,17,19. Reduced-dose regimens of NOACs are recommended for patients at higher risk of bleeding events, including those with reduced renal function. For example, a reduced apixaban dose of 2.5 mg bd is indicated in patients with at least two of the following characteristics: age ≥80 years, body weight ≤60 kg or serum creatinine ≥1.5 mg/dl (133 μmol/l); a reduced rivaroxaban dose of 15 mg od is indicated in patients with CrCl 15‒49 ml/min58; edoxaban is recommended at a reduced dose of 30 mg od in patients with CrCl 15‒50 ml/min and contraindicated in patients with CrCl >95 ml/min58; and a reduced dose of 110 mg bd dabigatran should be considered in patients with CrCl 30‒50 ml/min who are at a high risk of bleeding58. Follow-up visits should also systematically document patient compliance, thromboembolic and bleeding events, side-effects, co-medications and blood test results58.
Conclusions
The NOACs have demonstrated favourable benefit–risk profiles in large phase III trials, and these findings have been supported by real-world studies involving unselected patients, including those deemed challenging to treat. The NOACs also address many of the limitations associated with VKA use, thus assisting with their integration into clinical practice for stroke prevention in patients with non-valvular AF. In addition, the results from subgroup analyses should provide primary care clinicians with the confidence to manage stroke-prevention strategies in a wide variety of patients with AF.
A 38 year old BMI 20.2 ASA 2 female underwent an elective robotic-assisted laparoscopic extirpation of endometriosis and dissection of endometriomas. Her medical history included hypertension, migraine, atopic dermatitis, sciatica, cervical spine spondylosis and dysplastic spondylolisthesis of L4/5. Of note, the patient had allergies to Aspirin (causing angioedema), Morphine and Tramadol (both causing generalized rash).
An 18gauge IV cannula was inserted into the cephalic vein at the left wrist, and connected to a bag of Hartmann’s solution. The patient was induced with Propofol 100mg, Rocuronium 30mg and a Remifentanyl infusion running at Ce 1ng/mL. Cefazolin 2g and Dexamethasone 4mg were also administered post-intubation. No rashes were noted on the patient’s skin, and her arms were subsequently enclosed with green towels by her sides for the duration of the surgery. During the procedure, the patient was sustained in a steep trendelenberg position, with her face and eyes checked periodically. No rashes were noted on any exposed skin. Peri-operatively, she was maintained with O2/air/Desfluorane, top-up doses of Rocuronium, and titration of the Remifentanyl infusion. At the end of the surgery, the patient was administered Ondansetron 4mg and Pethidine 50mg (in 2mL), and reversed with Neostigmine 2.5mg and Glycopyrrolate 0.4mg. The patient’s arms were subsequently exposed in preparation for transfer, and it was noted that she had developed severe erythema and inflammation in specific tributaries of the cannulated vein (Figure 1). The patient was extubated uneventfully five minutes later, and did not complain of any symptoms systemically or pertaining to the cord inflammation. She was monitored in recovery for three hours post-op, and the inflammation subsided significantly 90 minutes post-op (Figure 2) and completely 150 minutes post-op (Figure 3).
There have not been many reports of such a reaction in published materials, and we take this opportunity to provide further pictorial evidence of the possible sequelae of IV administration of a high concentration Pethidine solution. The variances in analgesia effectiveness and potential side effects between Morphine and Pethidine are negligible2. As such, and given that Pethidine is commonly used as a mode of analgesia on our wards and in the peri- and immediate post-operative periods when other classes of drugs are contraindicated, we hope to provide further pictorial support of such an extraordinary reaction for other interested clinicians. It is also interesting to note that in both cases the patient was female, around 40 years old, had a thin body structure, had an atopic tendency, and the concentration of injected solution was higher than 10mg/mL. Additionally, these are known factors believed to increase reaction severity3 4. We acknowledge that 3 other drugs were administered at the same approximate time as Pethidine, and as such any of the 4 medications could be culprit to the reaction, although this is unlikely as our patient had been given those medications in previous procedures with no issues or complications.
Figure 1: Post-op, Figure 2: 90 mins post-op, Figure 3: 150 mins post-op
India ranks second in world not only in terms of its population but also in disaster proneness.1 Disasters, whether they are natural or man-made, result in a wide range of mental and physical health consequences.2 International public agenda has taken notice of protection and care of children in natural and man-made disasters. This, in large part, is due to observations that those affected and overlooked often include children and adolescents.3 There is continuous controversy about the impact of disasters on victims including children4, 5and some investigations deny that serious psychological effects occur.6, 7, 8However further researchhas found that the criterion used in these studies were extremely narrow and inadequate and hence more systematic, clinically relevant investigations are required.9 For children and adolescents, response to disaster and terrorism involve a complex interplay of pre-existing psychological vulnerabilities, stressors and nature of support in the aftermath. Previous research has shown that direct exposure to differenttypes of mass traumatic events is associated with an increasein post-traumatic stress symptoms, 10, 11, 12, 13 anxiety, and depression, 11, 14 which are frequently comorbid withpost-traumatic stress reactions among youth.15 To the best of our knowledge, studies on long term psychological effects of disasters on younger age groups from South Asian countries are only a handful even though the frequency and the extent of natural disasters in this part of the world are considerable. As trauma during childhood and adolescents can etch an indelible signature in the individual's development and may lead to future disorder,16 it underscores the need for such studies.
A snowstorm followed by an avalanche took over a small mountainous village “Waltengu Nard” in South Kashmir, India on 19th Feb. 2005, about a month after the devastating Indian Ocean Tsunami. Of the total population, 24.77% (n=164) had perished. 17 As reported, the total population of children and adolescents prior to disaster was 242, of whom 52 died (21.49%).17 The present study is a discreet one which aims to determine long term psychiatric morbidity among the surviving children and adolescents of this disaster affected region five years after the snowstorm disaster. This is based on the notion that psychiatric disturbances can be present in children and adolescents years after a disaster has occurred.18, 19, 20 The socio-demographic variables of the patients are also studied. The results may support the need to apply wide area epidemiological approaches to mental health assessment after any large scale disaster.
Material and Methods
The study was designed as a survey of children attending school. Children from ages 6 years to 17 years from the high school near Waltengu Nard were taken up for the study. Only those children who were present in the area during the disaster were included in the study. Those with presence of any psychiatric disorder prior to the time of disaster, mental retardation, organic brain disorder, serious physical disability prior to disease (e.g. blindness, polio, amputated limbs etc.) or severe medical condition (e.g. congenital or rheumatic heart disease, tuberculosis, malignancy etc.) were excluded from the study. Within the school, an alphabetically ordered list was prepared including all classes of school with children aged 6-17 years 11 months. Every 3rd student on this list was chosen and subjected to inclusion and exclusion criteria until a sample size of 100 children was complete. Informed consent was obtained both from the child and one of his/her caregivers or parents.
Selected children were subjected to the Mini International Neuropsychiatric interview for children and adolescents (MINI-KID) for evaluation of symptoms and diagnosis which is a DSM-IV based diagnostic interview with high reliability and validity. 21, 22 A semi structured proforma was prepared for socio-demographic profile. Kuppuswamy's Socioeconomic Status Scale, 2007 was used for determining socio-economic status. 23 Oslo-3 Social Support Scale (OSS-3) was used to calculate social support. 24
Interviews were conducted following formal training in instituting MINI-KID by trained psychiatrists of the Department of Psychiatry GMC Srinagar. The data was then subjected to appropriate statistical methods. A p-value less than 0.05 was taken as significant.
Results
Of the 100 children and adolescents studied (41.32% of the affected population of children and adolescents) 41 were noted to have at least one psychiatric diagnosis (patients). The socio-demographic profile of these patients is represented in Table 1. Age and sex distribution of diagnoses is presented in Table 2 and Table 3 respectively.
A total of 54 diagnoses were observed in these 41 patients (Figure 1), with comorbidities present in 12 patients (29.27%). 11 of these 12 patients were experiencing two psychiatric disorders present concurrently and 1 was enduring three concurrent psychiatric diagnoses. Post-Traumatic Stress Disorder (PTSD) was the commonest comorbidity seen in 6 patients. This comes to 42.86% of total PTSD cases. This was followed by Major Depressive Disorder (MDD), Generalized Anxiety Disorder (GAD), Suicidality, Social Phobia, Panic Disorder, Agoraphobia and Separation Anxiety Disorder (SAD) in 2 each. Attention Deficit/Hyperactivity Disorder (ADHD), Conduct Disorder (CD), Specific Phobia (dark), Substance Abuse and Dysthymia were comorbid in one patient each. Studies have consistently shown presence of psychiatric comorbidities post-disaster.48, 49 Of the total 54 diagnoses, the commonest were Anxiety disorders (except PTSD), PTSD and affective disorders (includes MDD, dysthymia and mania) comprising 37.04% (N=20), 25.93% (N=14) and 14.81% (N=8) of total diagnosis respectively.
Figure 1: Diagnostic profile of the patients
Discussion
When children and their families are involved in natural or man-made disasters they may be exposed to diverse stressors which may impact mental health of the survivors, including children.25 Studies have suggested that reliance on parental reports of children’s distress may not be valid as parents typically under-report symptoms compared with child and adolescent self-report in mental health surveys.26 Thus in our study the psychiatric interview of each child was done individually without getting leads from their parents. In the early "heroic" and "honeymoon" phases of disaster relief there is much energy, optimism, and altruism. As fatigue sets in over the time and frustrations and disillusionment accumulate, more stress symptoms may appear.27 Accordingly, the study was carried out five years after disaster to catch this delayed response to disaster in the form of psychiatric morbidity.
Consequences of the extensive amount of stress on our sample population due to the snowstorm resulted in a high prevalence of psychiatric disorders in our sample which was apparently not due to any other psychological stress during this period. Despite the fact that the study was done five years after the disaster, the research generated high psychiatric morbidity. Many young survivors reported restlessness and fear with the return of the season in which snowstorm occurred. All these kept the memories of the disaster and the losses fresh in their mind thus not allowing the wounds to heal. Some said that they couldn't keep their minds off the snowstorm during the weeks approaching the anniversary. This was much like the so called anniversary reactions.28 Even children and adolescents, who have rebuilt their homes or found new dwellings to rent, frequently feel a sense of loss at the anniversary. Though the area was provided with adequate relief in terms of better infrastructure, education, employment and financial help in years post disaster to make their life without psychological distress, but, perhaps four such anniversary reactions and the fact that they are still living in the same geographical area and climate conditions have not allowed them to settle down in a routine since the psychological distress. Of the total sample of 100 patients, 41 % (N=41) reported at least one diagnosis. This is almost similar to a study by Kar and Bastia after a natural disaster in Orissa (cyclone) who found 37.9 % of adolescents with any diagnosis.29 Similarly Margoob et al found that 34.39 % had a psychiatric disorder at the end of one year, after disaster.17 Other studies yielded results in the range of 12% to 70% in terms of total psychiatric morbidity.26, 30-33
PTSD was the commonest individual diagnosis in our study with 14% (N=14) of the total population. Studies have shown PTSD prevalence after disaster from as high as 72 %34 to as low as 8 %.35 However, these were done immediately or within a few months after the disaster and the longitudinal pattern was not studied. A study conducted by Margoob et al reported a prevalence of 18.51 % in a sample of survivors one year after the same snowstorm on which this present study is based.17 Similarly, Bockszczanin et al 2.5 years after a flood in Poland reported 18 % of children to be suffering from PTSD.36 Thus our results of 14 % patients suffering from PTSD are also similar to the trend as we are studying them after a period of five years following the disaster. Diagnosis of PTSD in our study was more common among the pre-adolescent age group, 22.58 % (N=7) and adolescents 33.33% (N=2). Similar findings were reported by Hoven et al who found a prevalence of 20.1 % in this age group.30 Also PTSD was more frequent in females in our study. It was observed in 16.98 % females (N=9) as compared to 10.64 % for males. Hoven et al also found high prevalence in girls (13.3 % vs. 7.4 %).30
Anxiety Disorders (excluding PTSD) formed the most common collective diagnostic category in our sample. Anxiety disorders were present in 20 % (N=20) of our sample population which formed about 37.04 % of total diagnosis. These included cases of GAD 5% (N=5), SAD 4% (N=4), Social Phobia 3% (N=3), Agoraphobia 3% (N=3), Panic Disorder 2% (N=2), OCD 2% (N=2) and Specific Phobia 1% (N=1). Similarly Norris et al found anxiety in various forms in 32% of their sample of disaster victims.25 Similar findings were also reported by Reijneveld et al.37 Hoven et al in an important study after 9/11 found prevalence of various anxiety disorders to the magnitude of 28.6%.30 Our study correlated very closely to the above mentioned study. GAD was the commonest anxiety disorder among the above group. A prevalence of 5% (N=5) was found in the study sample. This prevalence was almost half of the earlier studies in children and adolescents after a disaster by Kar and Bastia29 where it was 12% and by Hoven et al 30 where it came out to be 10.3 %. However these studies were conducted within a few months after the disaster and hence came out with a higher prevalence of GAD than ours. It was more common in girls in contrast to boys (7.55 % vs. 2.12%) similar to study by Hoven et al.30 SAD was also seen to predominate in anxiety disorders with 4 % (N=4) of the sample receiving the diagnosis. Some studies like one by Hoven et al found it to be prevalent in 12.3 % of their sample 6 months after 9/11.30 However other studies have found SAD to be comparatively less frequent post disaster in children and adolescents.34 Thus our findings are modest and lie somewhere between the above two studies. Also ours was a long term study hence SAD figures are a bit low. SAD in our study was more prevalent in girls than boys (5.66% vs. 2.12%). Moreover, it was exclusively seen in ages below 10 years. The above findings are in tune with the study by Hoven et al.30 Panic disorder showed a low prevalence in our study and was found in only 2 % (N=2) patients. In both of these patients it was found to be comorbid, with MDD in one and with Agoraphobia in another. Studies immediately post disaster found the prevalence to be around 10.8 % (Math et al)32 and 8.7% (Hoven et al).30 However in the survivors of the same area, in which our study is based, an earlier study one year after the disaster found 3.08 % prevalence of panic disorder which is very similar to our study.17 It was more prevalent in females and is well correlated to a study by Hoven et al.30 Agoraphobia was present in 3 % (N=3) patients. It was comorbid in two patients with panic disorder and with PTSD, and an individual diagnosis in one. Hoven et al have found high rates of Agoraphobia post disaster i.e., about 14.8%.30 But again this study was done only 6 months after 9/11 hence more morbidity. Female preponderance of the diagnosis was established (3.77 % vs. 2.12 %) as with earlier studies.30 Obsessive traits are known to increase subsequent to disaster in the surviving population.38 Similarly 2 % of cases satisfying the criteria for OCD were seen in our study. The commonest obsessions were recurrent intrusive and annoying themes related to the disaster and ruminations about whether it could have been prevented, followed by worries related to harm befalling themselves, family members, or fear of harming others due to losing control over aggressive impulses. Other obsessive themes were related to scenes of trauma and commonly blood. Obsessions regarding extreme fears of contamination were also present.
The affective disorders have been studied less often than PTSD after disaster. Depression is known to occur with increased frequency subsequent to disaster.25 MDD was present in 4 % (N=4) of the total sample population. Studies conducted immediately after disasters have found higher prevalence. Math et al,32 Kar & Bastia29 and Catani et al33 found the prevalence of 13.5 %, 17.6 % and 19.6 % in their studies respectively. A study at three months and at one year after disaster on the adults in the same population as our study found the prevalence of MDD as 29.6 % and 14.28 % respectively.17 This decreasing trend is substantiated by the findings of our study and is in line with it. MDD was more common in females (5.66 % vs. 2.12%) which is similar to the study of Hoven et al.30 Our findings of increased prevalence of MDD in middle adolescents (7.69 %) as compared to other age groups is also comparable to Hoven et al.30 Of the Dysthymia cases, 3 % (N=3) were observed in our studies. Increased prevalence of dysthymia has not been reported post disaster in earlier studies. Our findings could be a part of large affective diaspora with dysthymia resulting from diminished self-esteem and a sense of helplessness subsequent to disaster. In addition to the time period for depression these patients were given the diagnosis of dysthymia because the depressed mood in them was more apparent subjectively than objectively. Finally these patients could have been on a natural course of dysthymia which usually begins in childhood. Combined dysthymia and MDD accounted for 7 % (N=7) of patients which if taken as a collective depression category, the results are slightly more comparable with the above studies. One patient had Mania (past). This patient had a positive family history of Bipolar Affective Disorder. This could be an incidental finding even though psychological stress is known to precipitate mania.39 Also the prevalence is 1 % in our study which is even less than the prevalence in general population thus it could be an artifact.40Studies have consistently found increased prevalence of adjustment disorder after disaster.41 In our study prevalence of adjustment disorder was 3% (N=3, anxiety 2, depression 1). In a study by Math et al 3 months after tsunami it was 13.5%.32 A lower prevalence in our study was again due to the long term nature of study. The role of trauma, stress, and negative life events as risk factors for suicidal ideation and behavior has long been recognized.42 A longitudinal investigation looking at the trends in suicidality and mental illness in the aftermath of Hurricane Katrina found significant increases in suicidal ideation and plans in the year after the disaster as a result of unresolved hurricane related stresses.43 The suicidality in our population sample was found to be 2% (N=2) of sample. These results were in tune with that of Kessler et al, although it was immediately after hurricane Katrina and hence a higher prevalence of 6.4%.43
Many symptoms of PTSD overlap with the symptoms of ADHD and CD.44 In our study, each of the disorders were present in 2 % of the sample. In one patient, they were comorbid with each other (ADHD with CD). In a study by Hoven et al 6 months after 9/11, the prevalence of CD was found to be as high as 12.8 %.30 This could be because of immediate post disaster nature of the study. Also because of the symptom overlap more weight was given to the PTSD diagnosis.
Three patients had a diagnosis of Substance Abuse, Tic Disorder and PDD, 1 % each. Though substance abuse is known to increase subsequent to disaster in adolescents,30 no evidence was found for relation of tic disorder or PDD to the post-disaster psychiatric stress. The cause of a low prevalence of substance abuse in our sample was because of the fact that the area is inhabited by Muslim population and hence alcohol is not religiously sanctioned, and, harder substances are either not available or they can’t be afforded. The only substance which is available is marijuana or cannabis. However, most used it only recreationally and the criterion for abuse was not met. Even the sole patient of substance abuse was also taking cannabis. Also, it is a well known phenomenon that drug dependent subjects do not reveal the true information and deny any history of abuse at first contact with the investigating team.45 Tic disorder and PDD are regarded as biological disorders and their relation to trauma is only incidental.46, 47
Studies have consistently shown presence of psychiatric comorbidities post disaster.48, 49 The same was observed in our study where 29.27 % of total patients had comorbid psychiatric diagnosis. Similar results were found by Kar and Bastia who found comorbidities in 39% of adolescents.29 PTSD is the most common comorbid disorder observed during the period post disaster48, 49 and the same was observed in our study with PTSD comorbid in 14.63 % (N=6) of cases. However when all the anxiety disorders were combined except PTSD, they were found to exceed the comorbidity of PTSD and they were comorbid in 21.95 % (N=9) patients. There is expanding literature regarding comorbidity of anxiety and depression in children and adolescents.50, 51, 52Similar comorbidity of an anxiety disorder (including PTSD) and depressive disorder (including Dysthymia) were seen in 7.32 % (N=3) of patients in our study. These results show that psychiatric diagnoses are frequently comorbid after the disaster and there is a need to be vigilant about them for a holistic psychiatric assessment, treatment and rehabilitation of the survivors.
Sociodemographic Profile: In our sample the prevalence of psychiatric morbidity was at maximum in pre-adolescents (6-10 years age group) and it was 61.29 % of the sample of pre-adolescents.This is consistent with the research that has suggested that younger children possess fewer strategies for coping with both the immediate disaster impact and its aftermath, and thus may suffer more severe emotional and psychological problems.53 Second commonest group was of 11-13 years with 40 % morbidity in them which was consistent with an earlier study which also found significant morbidity in this age group.54 The age characteristics of the total population also closely matched the above findings. More females than males were found to exhibit psychiatric morbidity in our study (47.17 % vs. 34.04 %). Though these findings were in tune with those of Hoven et al,their findings were a little lower than ours (34.7 % vs. 21.8 %).30 Some studies have found that girls express more anxiety-depressive disorders30 and PTSD symptoms55, 56 and boys seen to exhibit more behavioral problems.57 Similarly in our study rates of anxiety disorders, depressive disorders and PTSD were higher in girls and conduct disorder was exclusively found in boys.
Our study suggested that children up to 5th standard were (51.02 %) more susceptible than those in higher classes. This was in accordance with an earlier study by Kar et al.54 These findings are also in accordance with the findings of a study by Hoven et al. which found maximum morbidity (34.1 %) in preschoolers.30 Thus it could be said that higher educational status was protective, in addition to increasing age. Psychiatric morbidity was highest in children who were from joint family systems (48.15%). This was followed by children from extended nuclear (37.5%) and nuclear (27.27%) families. This pattern is consistent with an earlier study by Margoob et al.58 This could be because of the fact that in the sample of joint families there was loss of more family members in the tragedy. There were no cases of upper and upper-middle socio-economic class and lower-middle class was significantly less in our sample. This was because of the demographics per se and was not a sampling error. Consequently, higher morbidity was seen in the upper-lower socio-economic class (49.09%) followed by the lower class (31.71%). All the above findings are in accordance with an earlier study by Margoob et al.58
Psychiatric morbidity was not found to be influenced by the source of family income. Same was observed by Kar and Bastia in their study.29 The majority of the patients had poor social support (52.17%, p=0.03). These findings are substantiated by earlier studies.59 Loss of a parent was strongly associated with lower social support and high psychiatric morbidity. This was also reported by earlier studies.31, 60 Our study reported higher psychiatric morbidity in first-born children (71.43%). This could be due to increased burden of family matters on an eldest child subsequent to a disaster especially when head of family or mother has perished in such a catastrophe. This was in accordance with earlier studies on birth order and psychiatric morbidity.61 However in our study only childs also documented significant morbidity which is in contrast to earlier studies.61 This could be due to the fact that an only child had significantly less social support due to fewer siblings and death in the family due to disaster considerably compounding the problem. Also, often the youngest born is more pampered and hence more likely to feel emotionally insecure when attention is shifted from him in the aftermath of a disaster.
There was an unavoidable limitation in the study; the disaster-affected population was not compared with a normal or control population. The difficulty we faced was finding a control population as the area has a racially, geographically and culturally distinct population of Gujjars and all of them were affected. So no appropriate control group could be found. However if we compare it with most of the studies done in populations from the north India, the prevalence in our study is largely greater than those found In those studies.62
Conclusion
This research portrays and scrutinizes the experience of children and adolescents in the aftermath of a snowstorm disaster and supports the idea that children are susceptible to morbid psychological experiences long after the traumatic event has occurred. With that said, we want to stress the decisive role of support agents for children. These agents include the adults and peers who help children and youth recuperate in the long term. Provision of an outreach psychosocial and clinical service long after the disaster when no one is around to help after the initial knee jerk response of relief agencies is also stressed.
A 61-year-old lady underwent a modified radical mastectomy and axillary clearance in 2008 for a carcinoma of the left breast. Histopathology examination revealed two tumours within the left breast; a 16mm Grade 2 lobular carcinoma with probable vascular invasion and a 9mm Grade 1 infiltrating ductal carcinoma with no vascular invasion. She had clear resection margins. 21 out of 34 removed lymph nodes were positive for metastatic deposits. The tumour was oestrogen receptor positive and HER2 negative. She was staged as T1 N3a Mx and the tumour had a Nottingham Prognostic Index of 5.32. Metastatic workup revealed no distant metastasis.
Postoperatively, she required aspiration of a seroma but her recovery was otherwise satisfactory. She received adjuvant chemotherapy in the form of three cycles of Fluorouracil, Epirubicin and Cyclophosphamide and 3 cycles of Docetaxel. In addition, she had postoperative radiotherapy to the chest wall and supraclavicular fossa (40 Gy in 15 Fractions over 3 weeks) and hormonal therapy with Letrozole 2.5mg once daily.
The patient opted to undergo a prophylactic right mastectomy in 2010. She was regular in follow up and appeared to be free of disease recurrence for 6 years.
Her past surgical history included abdominal hysterectomy and bilateral salpingo-ophorectomy for fibroid disease as well as varicose vein stripping. She is a non-smoker and doesn’t consume alcohol. She had a family history of colon and cervical cancer in her uncle and sister respectively.
The patient visited the surgical outpatient clinic complaining of abdominal cramps, altered bowel habits and fatigue of a few months duration. There was no associated rectal bleeding, haematemesis, melaena, weight loss or urinary symptoms. Physical examination was unremarkable but she was noted to have gradually worsening renal function. Her symptoms were at first attributed to side effects of intravenous antibiotic treatment, which she received during an admission for cellulitis. She had already undergone an upper GI endoscopy which showed oesophagitis and ulceration; biopsies were within normal limits. She received treatment with proton pump inhibitors but her symptoms persisted.
A non-contrast abdominal CT scan was done, on account of her poor renal function, which showed bilateral hydronephrosis and thickening of the postero-superior aspect of the bladder wall. Considering the limitations of the non-contrast study, there were no other abnormalities. A colonoscopy was also done to investigate her altered bowel habit and it revealed a benign-looking stricture in the sigmoid about 25cm from the anal verge which was easily bypassed by the scope.
Figure 1. Benign stricture on flexible sigmoidoscopy
Biopsies of the sigmoid stricture showed an infiltrate of small to medium sized tumour cells in the submucosa, which had an Indian file pattern. They were positive for AE1/AE3 (pancytokeratins) and negative for CD68. They were positive for CK7 and negative for CK20, strongly positive for oestrogen receptors and HER2 negative. Taken in conjunction with the patient’s past history of an invasive lobular carcinoma of the breast, the appearance was consistent with a metastatic lobular carcinoma.
Figure 2. Clusters and cords of cells with positive cytoplasm for the cytokeratin immunostain CK7. Although the classical ‘Indian filing’ of lobular carcinoma is not well seen, the image clearly demonstrates that the large bowel glands are negative (normally CK20+, CK7-) and that the infiltrate is beneath the glandular mucosa (i.e. not originating from dysplastic glands within the mucosa and raising the possibility of infiltration from outside the bowel wall). The magnification is x200. Lobular carcinoma is usually CK7 +, CK20 -, ER +.
Figure 3. The same cells with their nuclei staining positively with an immunostain to oestrogen receptors. There are a few short chains of ‘Indian filing’ with the cells appearing rather rectangular in shape with straight margins. You can make out slight ‘moulding’ of the nuclei as they press against one another. The magnification is x 400.
Figure 4. Haematoxylin and Eosin section at 400 magnification. This shows a diffuse infiltrate of single cells with eccentric nuclei.
The patient required a right nephrostomy and a cystoscopy with left double J ureteric stent insertion to address her hydronephrosis and deteriorating renal function before undergoing restaging of her disease.
DISCUSSION
In patients with history of breast cancer, isolated GI metastases are less common than benign disease processes or second primaries of the GI tract.1.2 In a retrospective review, 73 out of 12001 cases of breast cancer had gastrointestinal metastases, out of which 24 were to the colorectum3 and invasive lobular carcinoma was the commonest histological subtype. 3.4 However, sixteen percent of patients with breast cancer have GI metastases at postmortem examination1.
There might be a long interval of time between the diagnosis of breast cancer and development of gastrointestinal metastasis which together with their rare occurrence and nonspecific clinical and radiological manifestations adds to the diagnostic challenge. The median interval between the diagnosis and the development of GI metastasis was reported to be 6 years (range 0.25 to 12.5 years) by Schwarz et al 5with 25 years being the longest reported in the literature.6 Because of this long interval the history of a primary breast cancer can be missed. This also highlights the importance of long term follow up and maintaining an index of suspicion when these patients develop GI symptoms.
In our case, the interval between the diagnosis of breast cancer and colonic metastasis was 81 months. Her GI symptoms were initially attributed to side effects of antibiotic treatment for cellulitis and dyspepsia before investigating her with a colonoscopy. Even at colonoscopy the appearance was that of a smooth benign-looking stricture which did not seem to harbour any sinister pathology
Histological examination is probably the most reliable tool to make a diagnosis and it is prudent in such cases to compare the specimen with the original breast tumour. In this case, there were two primary tumours; an invasive ductal carcinoma as well as a lobular carcinoma but the metastatic disease favoured the lobular component, which is consistent with other published reports in the literature. The reasons why metastases favour lobular carcinoma are poorly understood. One explanation is the loss of E-cadherin expression, a molecule involved in cellular adhesion, in invasive lobular carcinoma7. A similar case in which the primary was a mixed ductal and lobular type with lobular subtype colonic metastasis was reported by Uygun et al.8 Immunohistochemistry can also help in establishing a diagnosis. Metastatic breast cancers tend to be positive for Oestrogen or Progesterone receptors as well as Gross Cystic Disease Fluid Protein-15.9, 10 It is, however, worth noting that primary colonic cancers can be oestrogen receptor positive in 30 to 70% of cases.11
Accurate histopathological diagnosis probably saved our patient an unnecessary surgical treatment for a primary colonic neoplasm as the main focus of her treatment should be systemic therapy for metastatic breast cancer.
CONCLUSION
GI tract metastases from breast cancer are a rare occurrence. The patients may present after a long interval from the original diagnosis and the clinical and radiological features are nonspecific with the diagnosis often established on histological examination. Moreover, the history of breast cancer may not be elicited in all cases and these patients may present to a gastroenterologist or colorectal surgeon rather than a breast surgeon or oncologist. Therefore, remaining vigilant to this possibility is advised in any patient with a history of breast cancer who presents with unexplained GI symptoms.





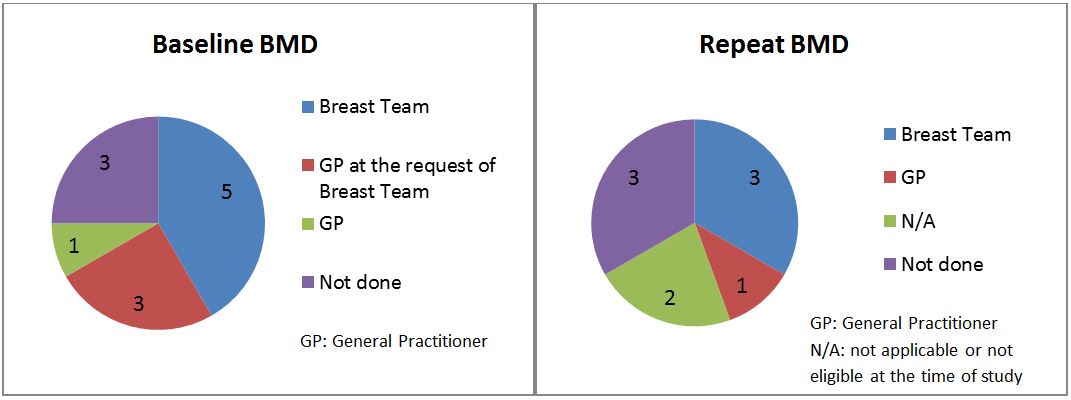





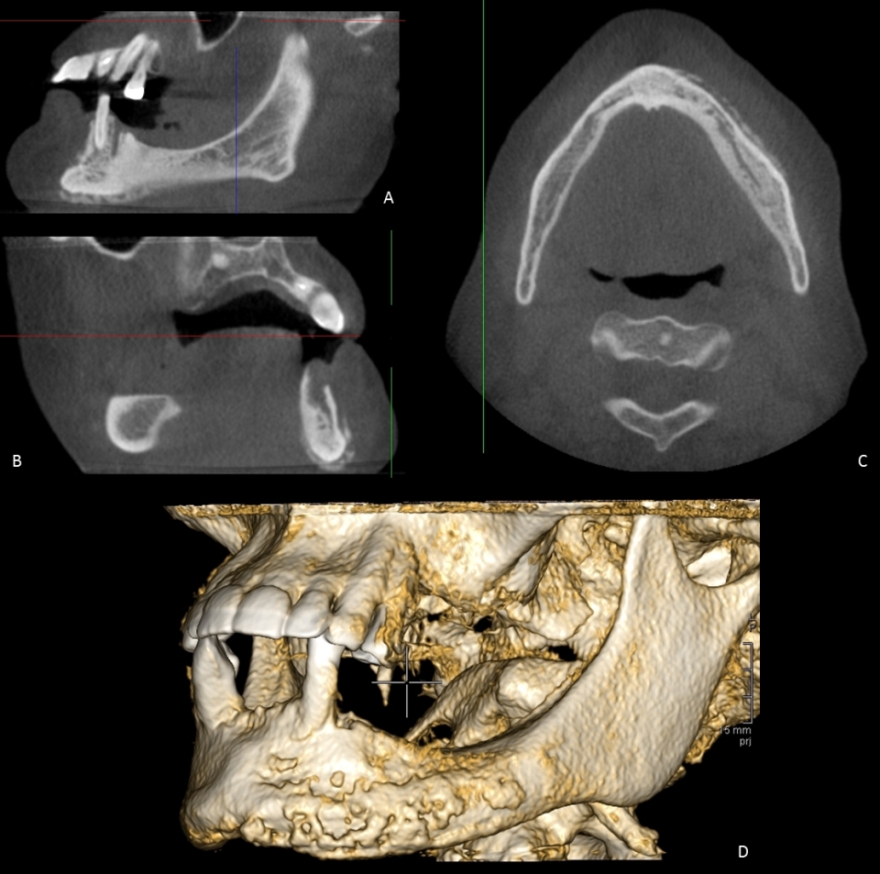

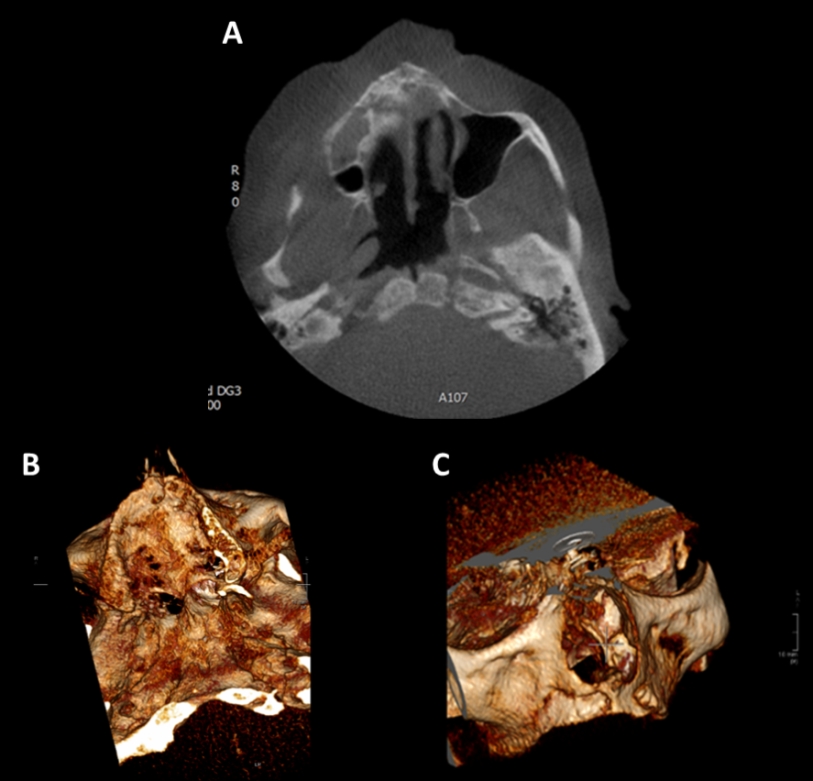
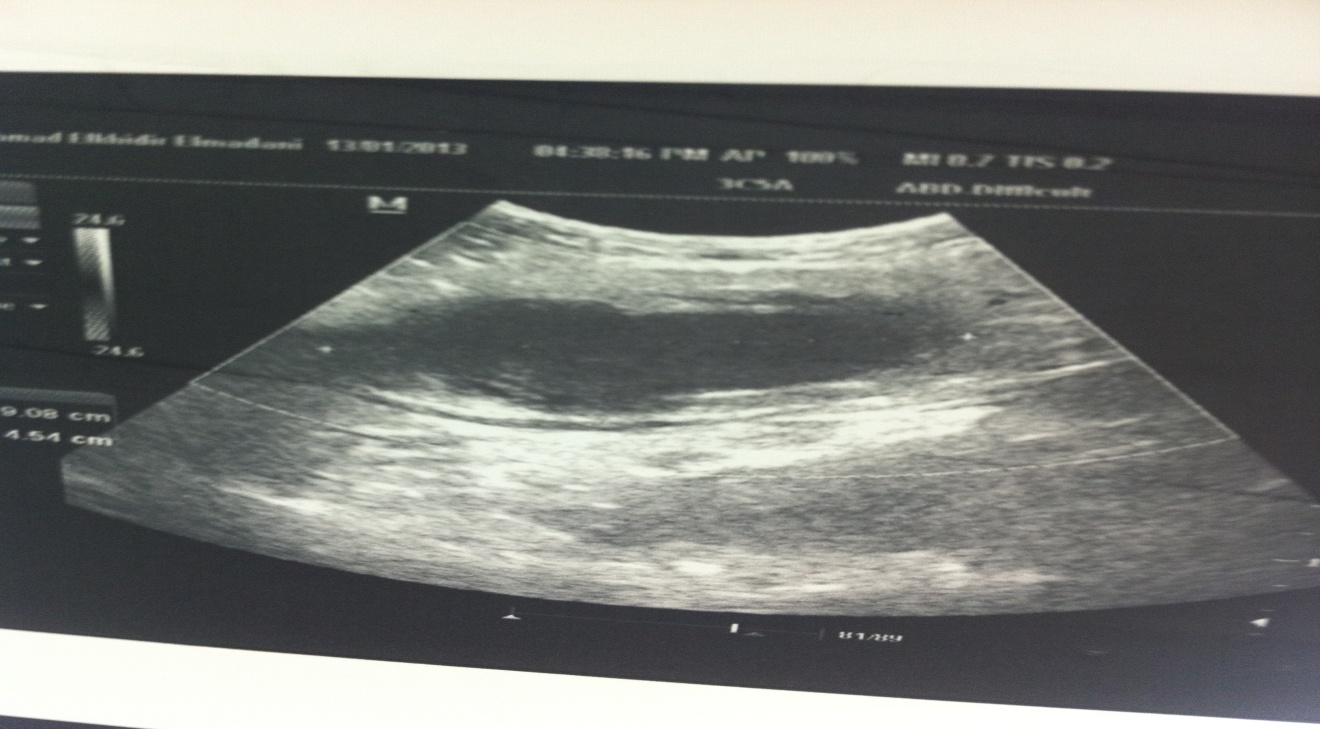
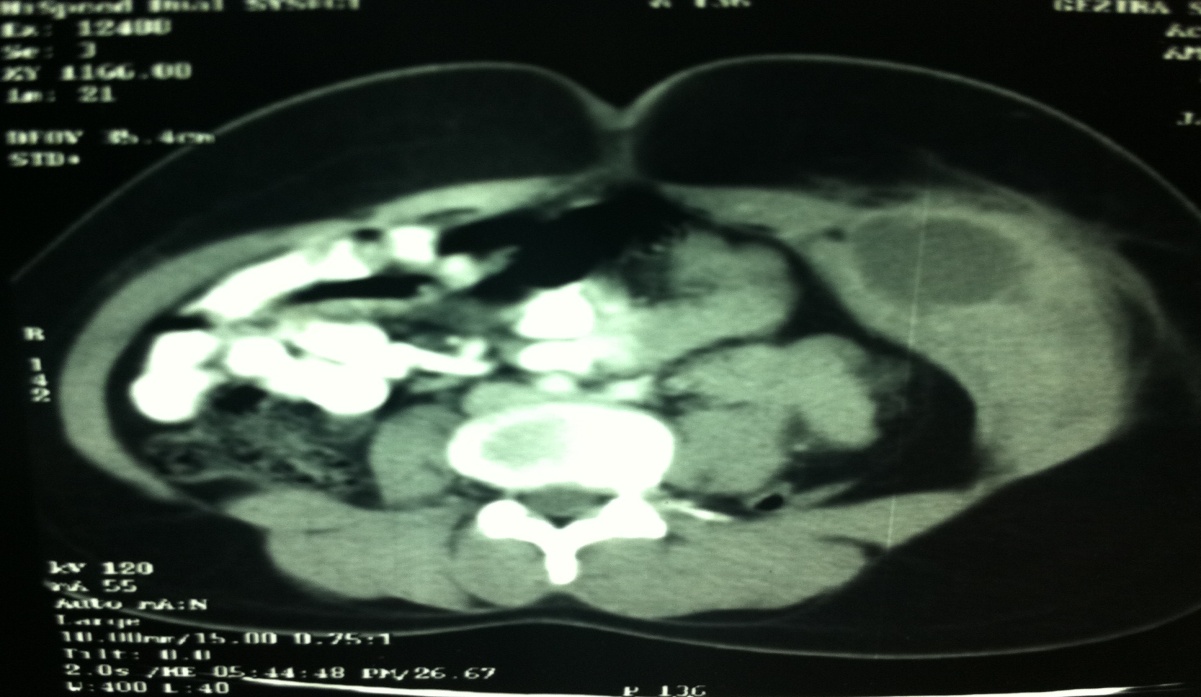
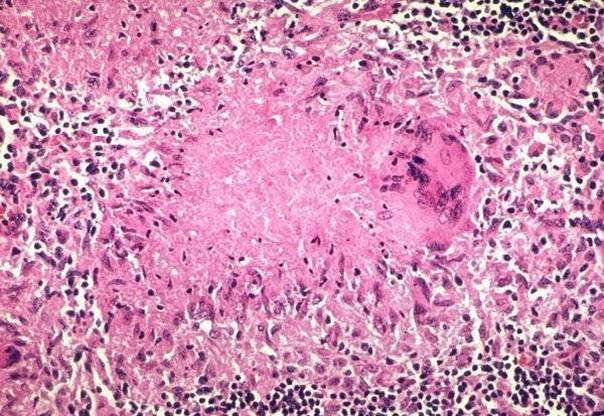
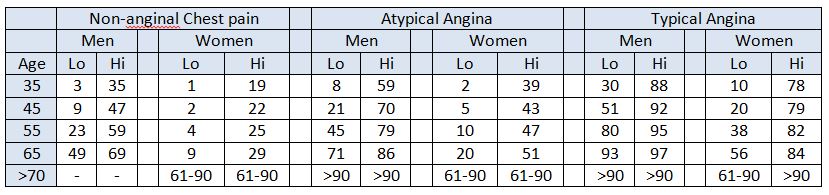
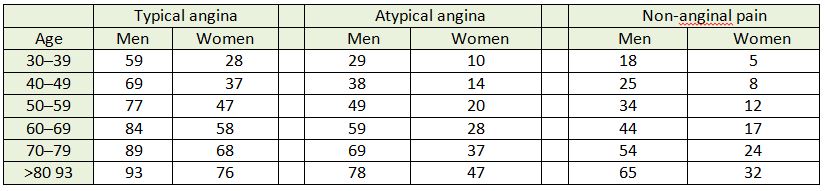
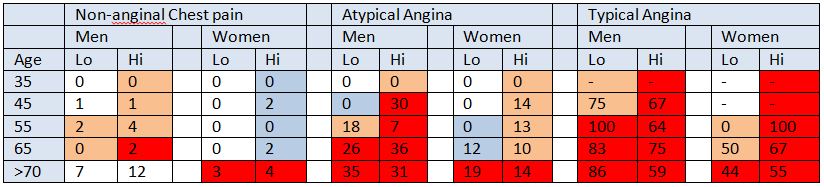

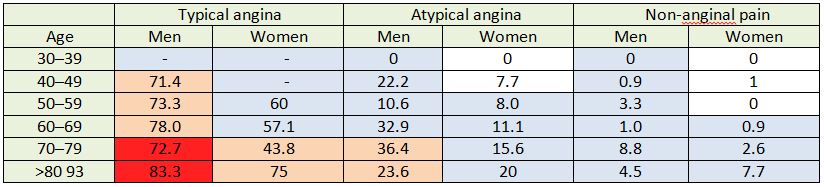



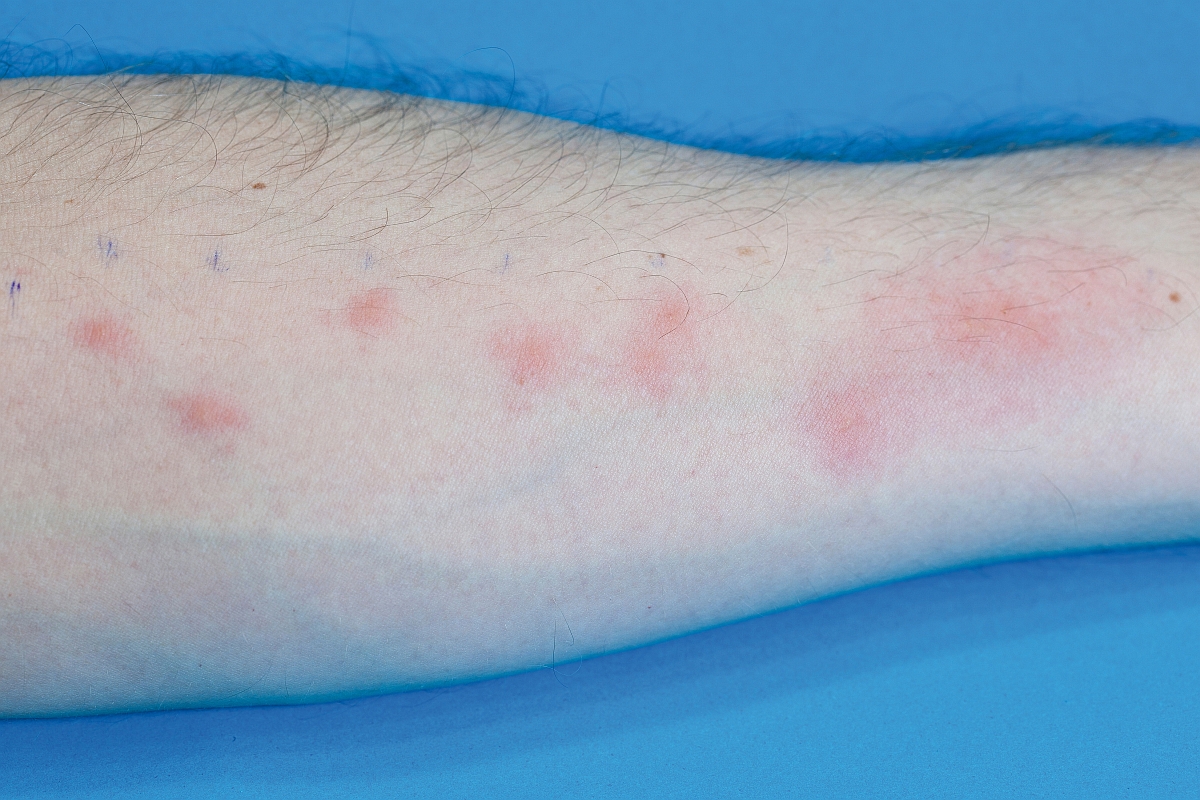



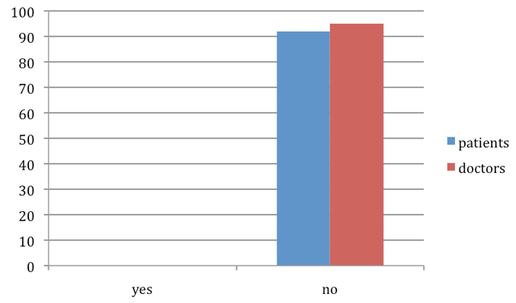
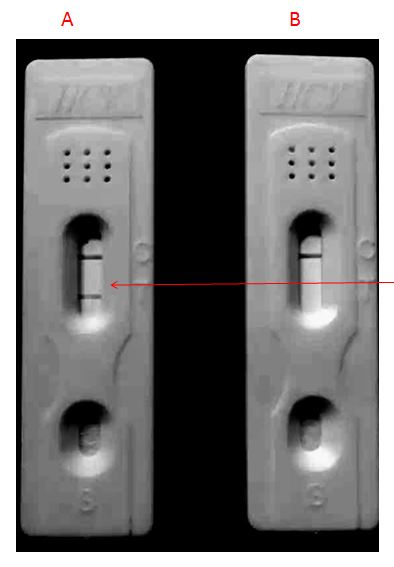
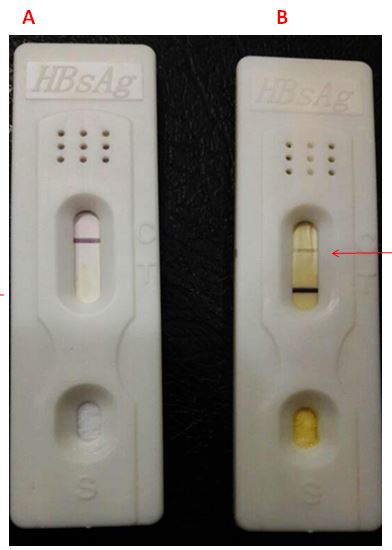
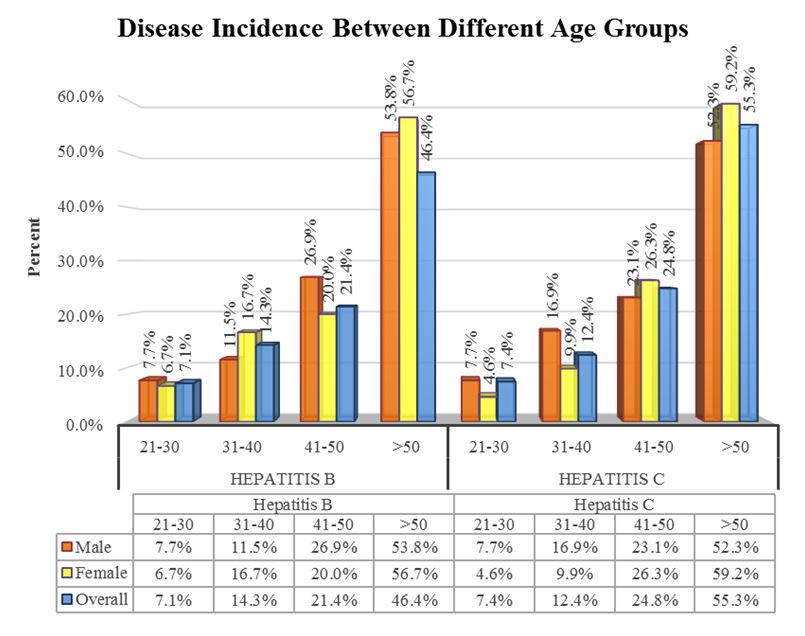
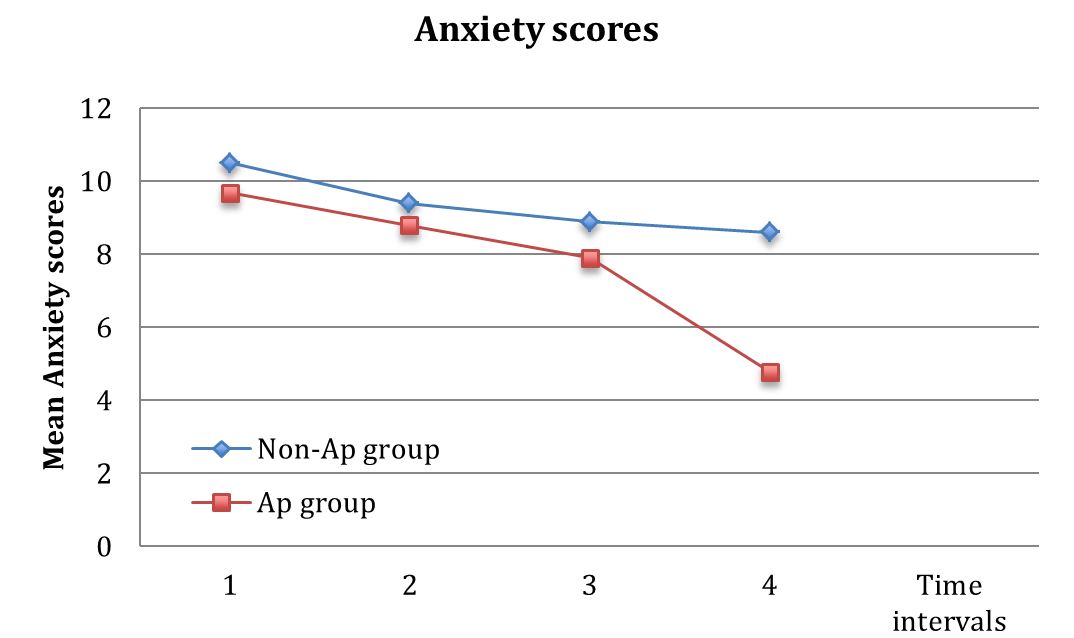
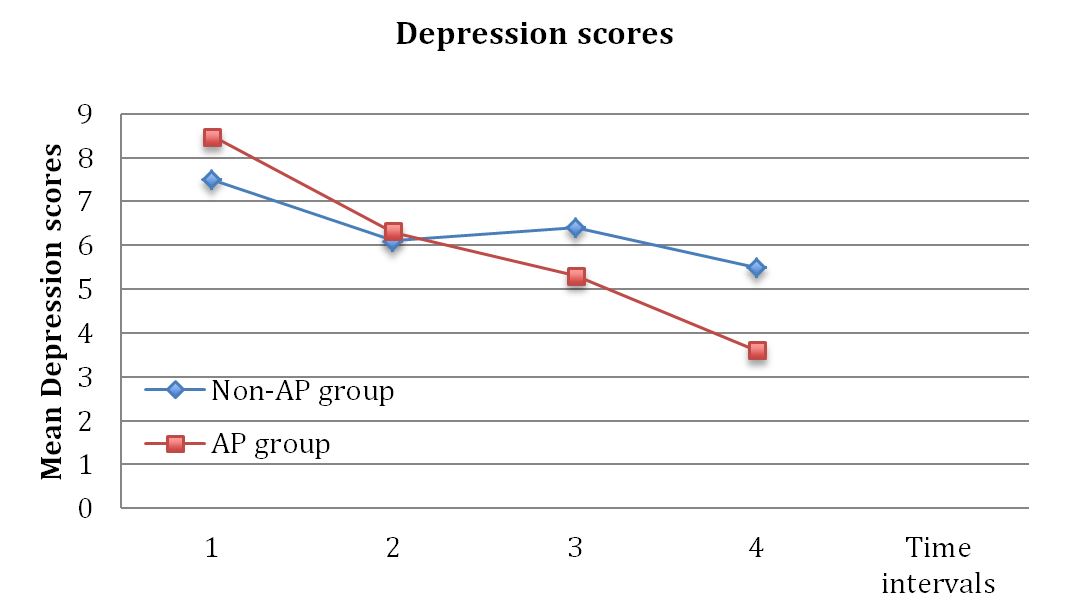
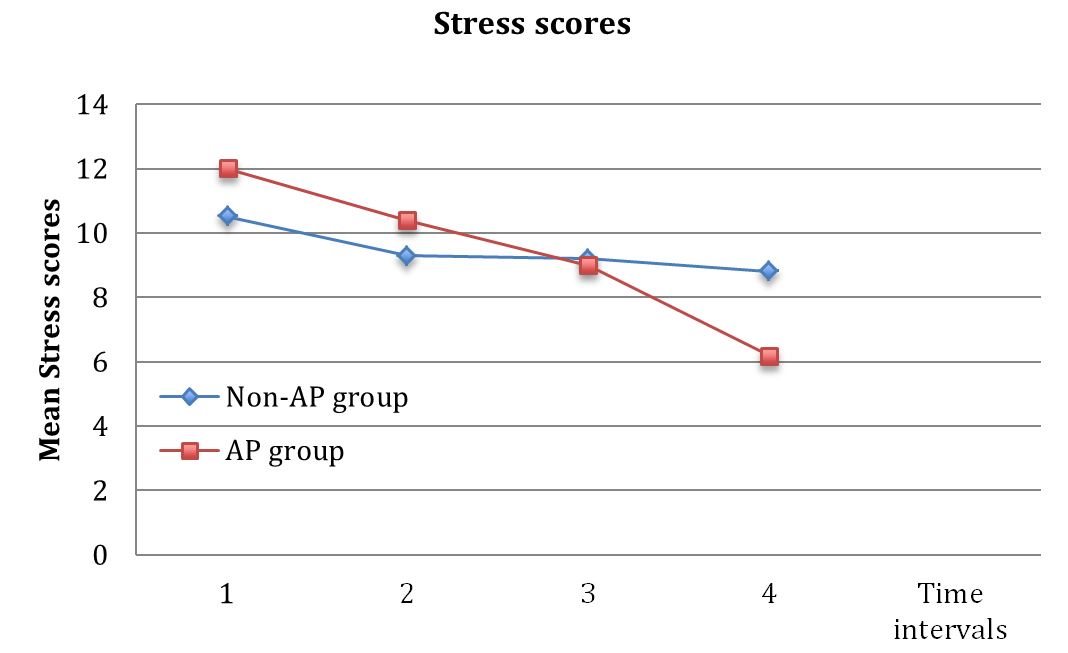
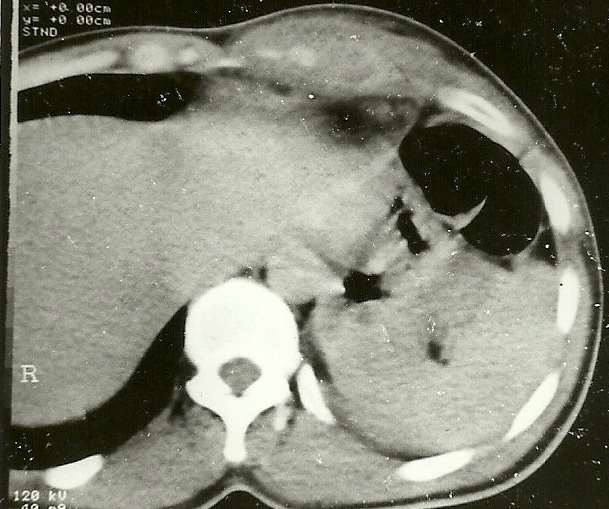
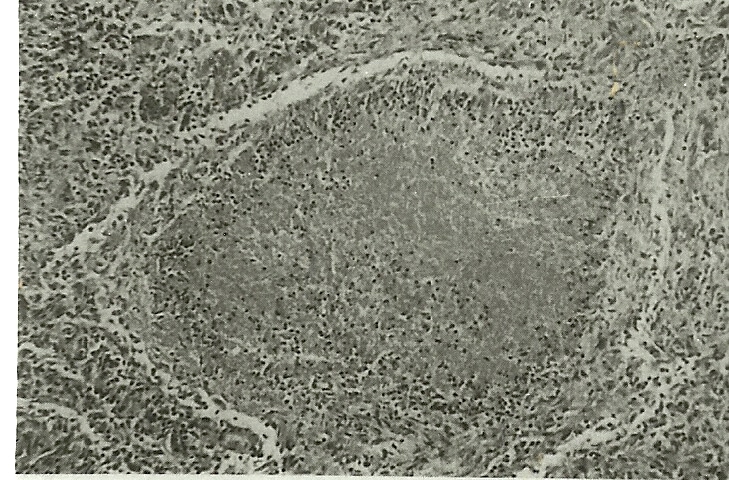
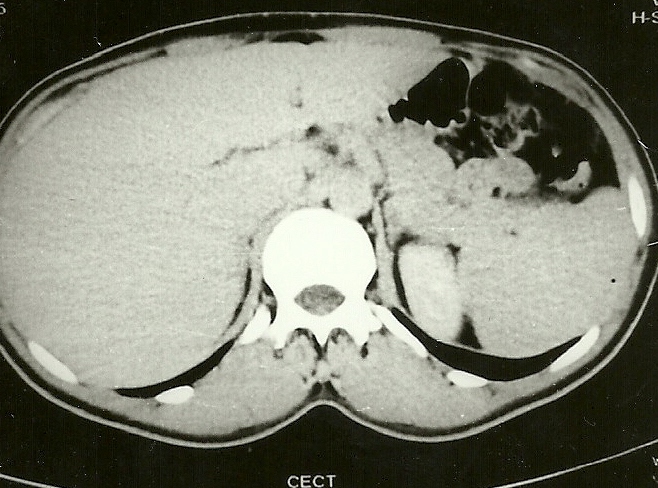
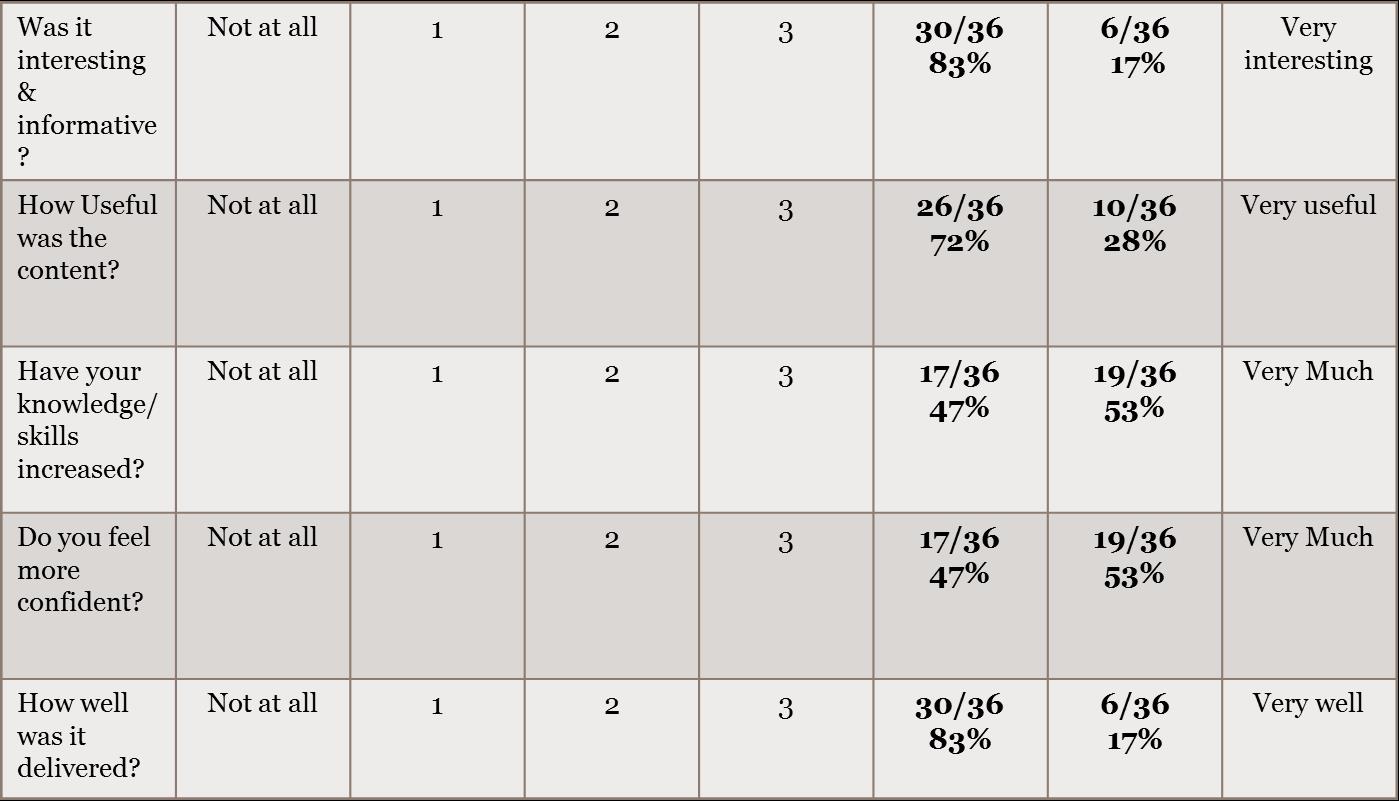
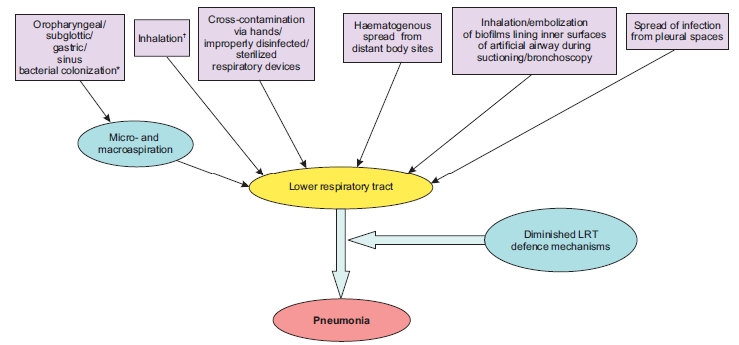
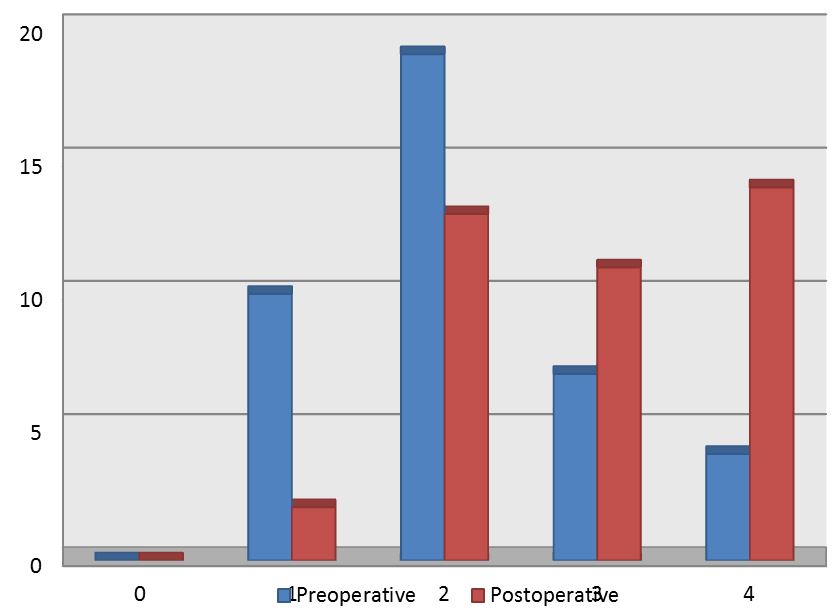
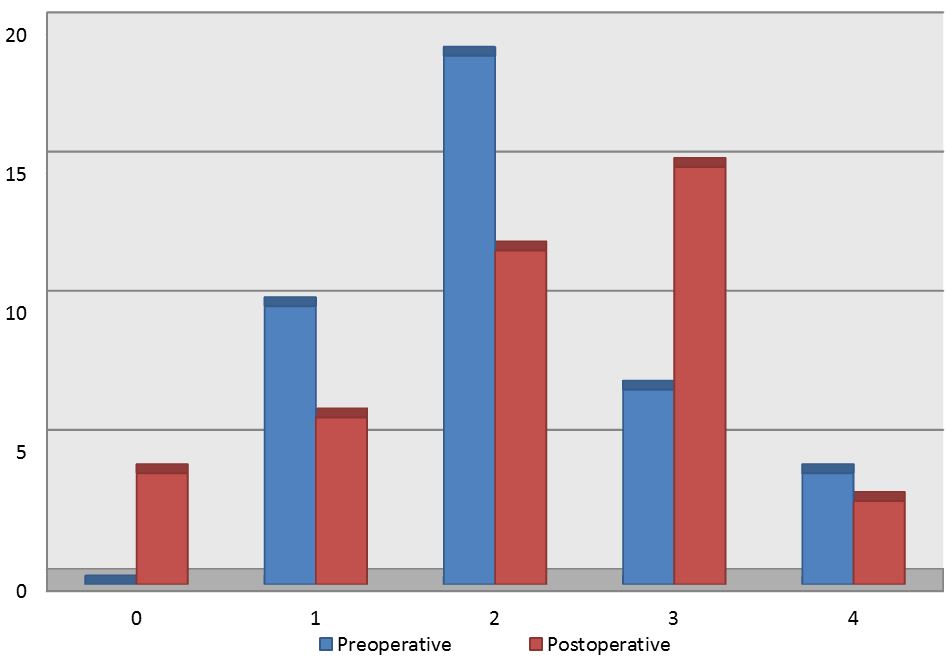

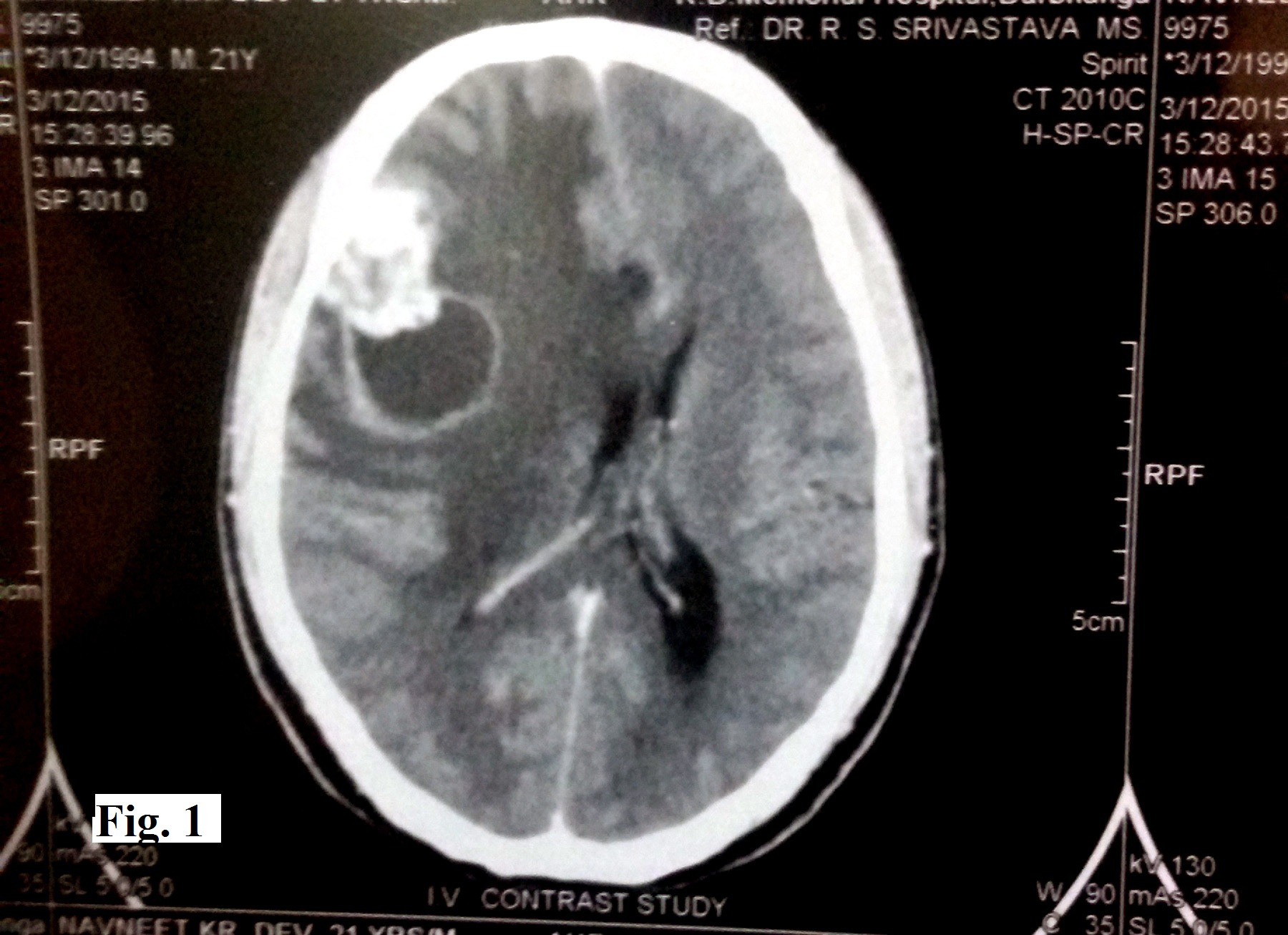
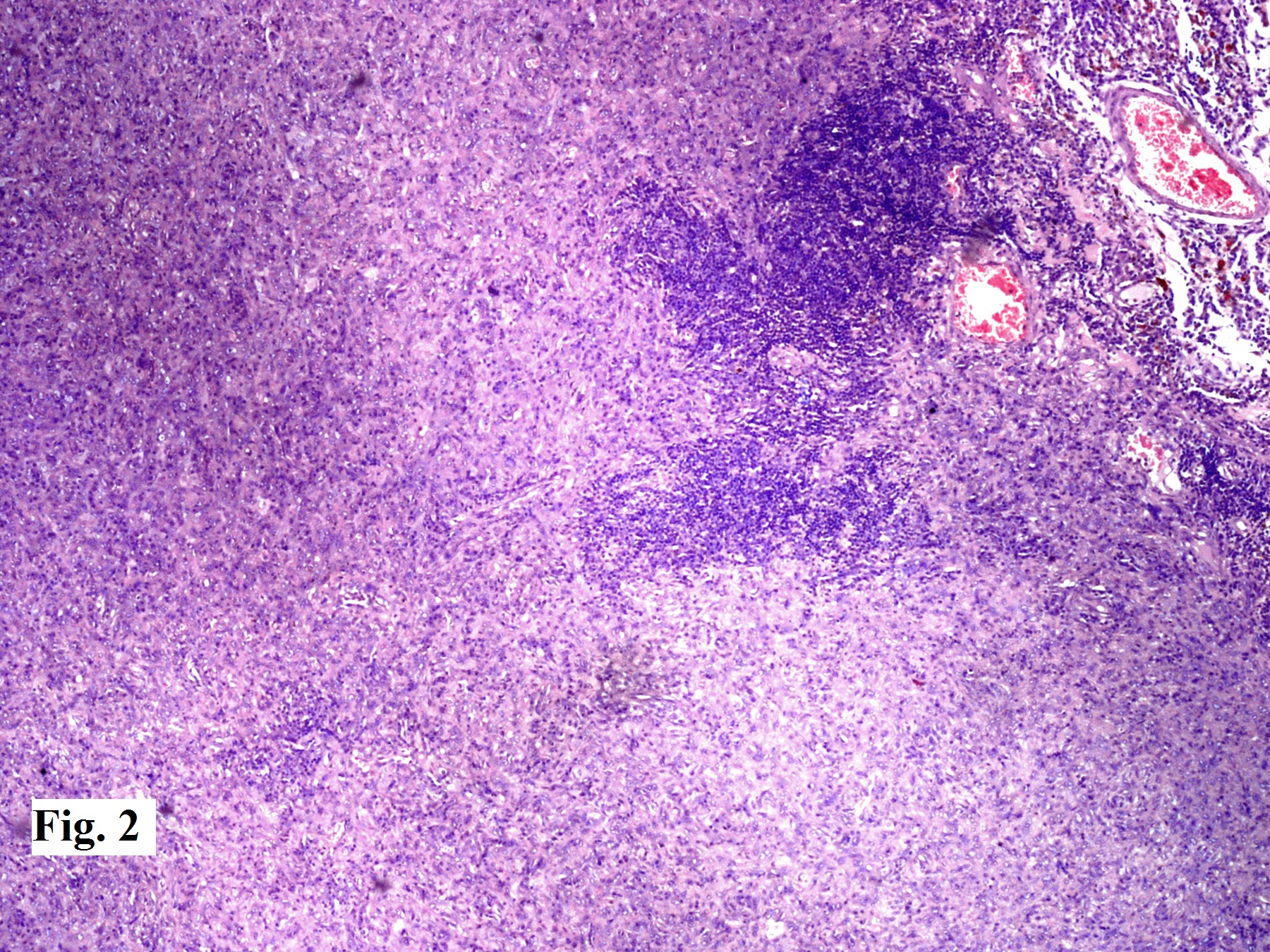
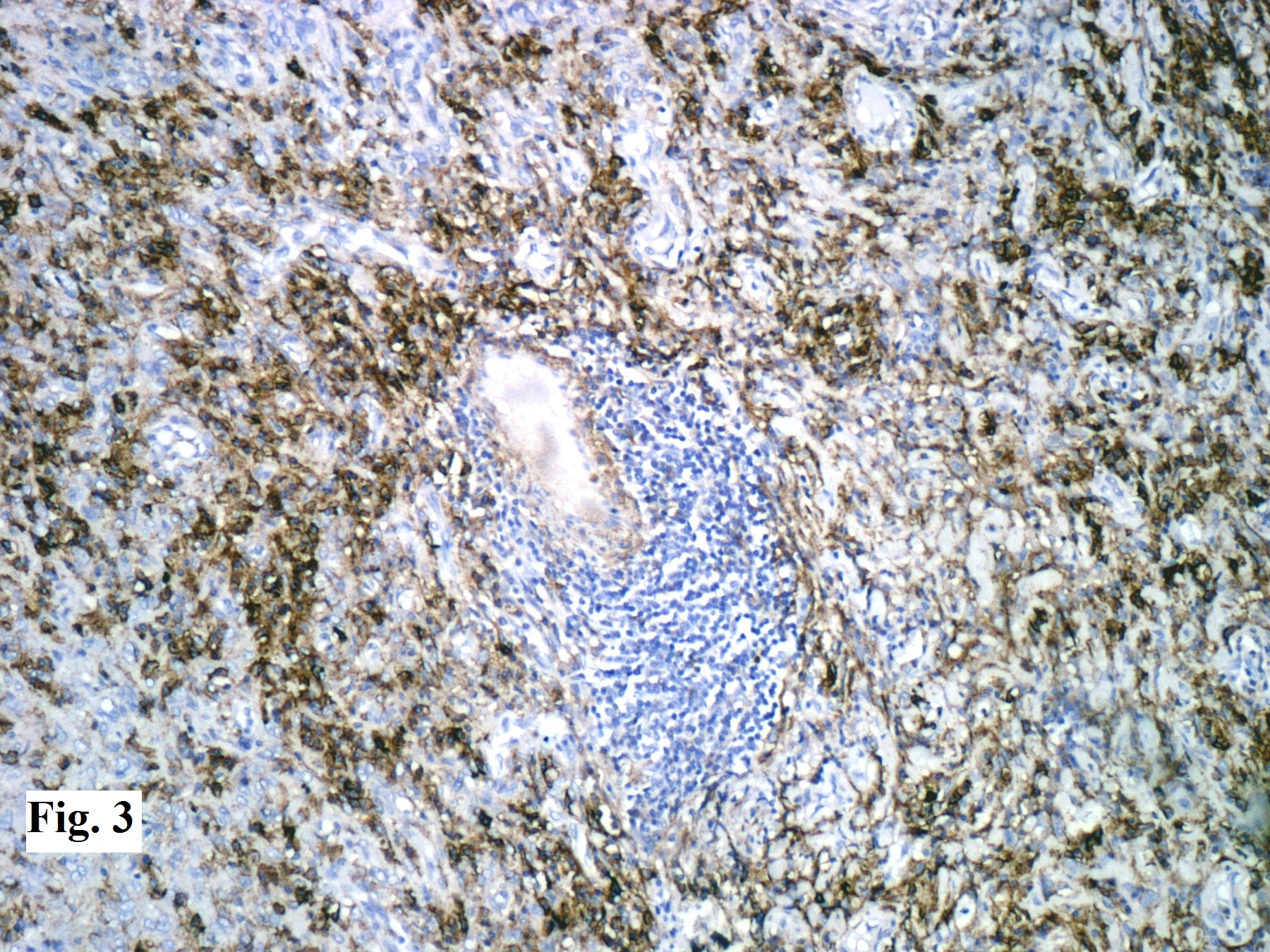
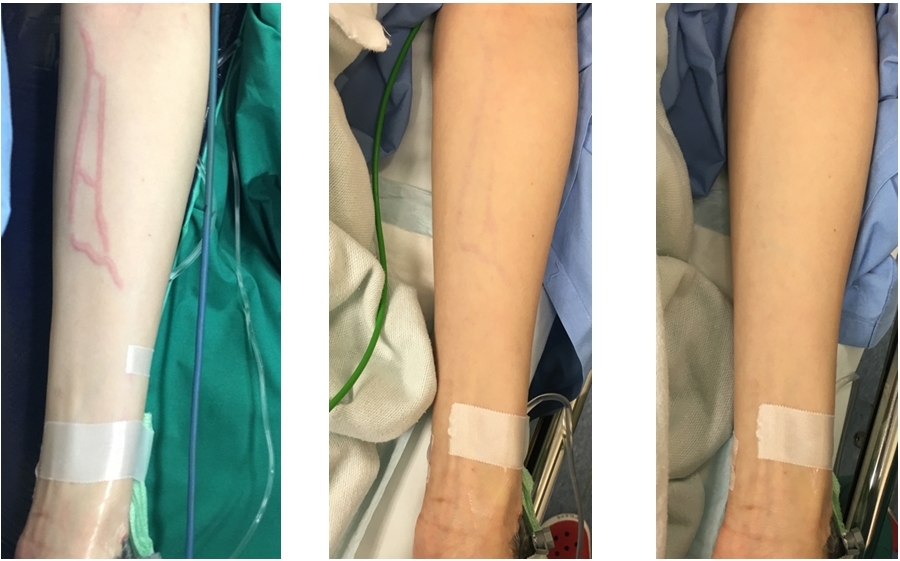


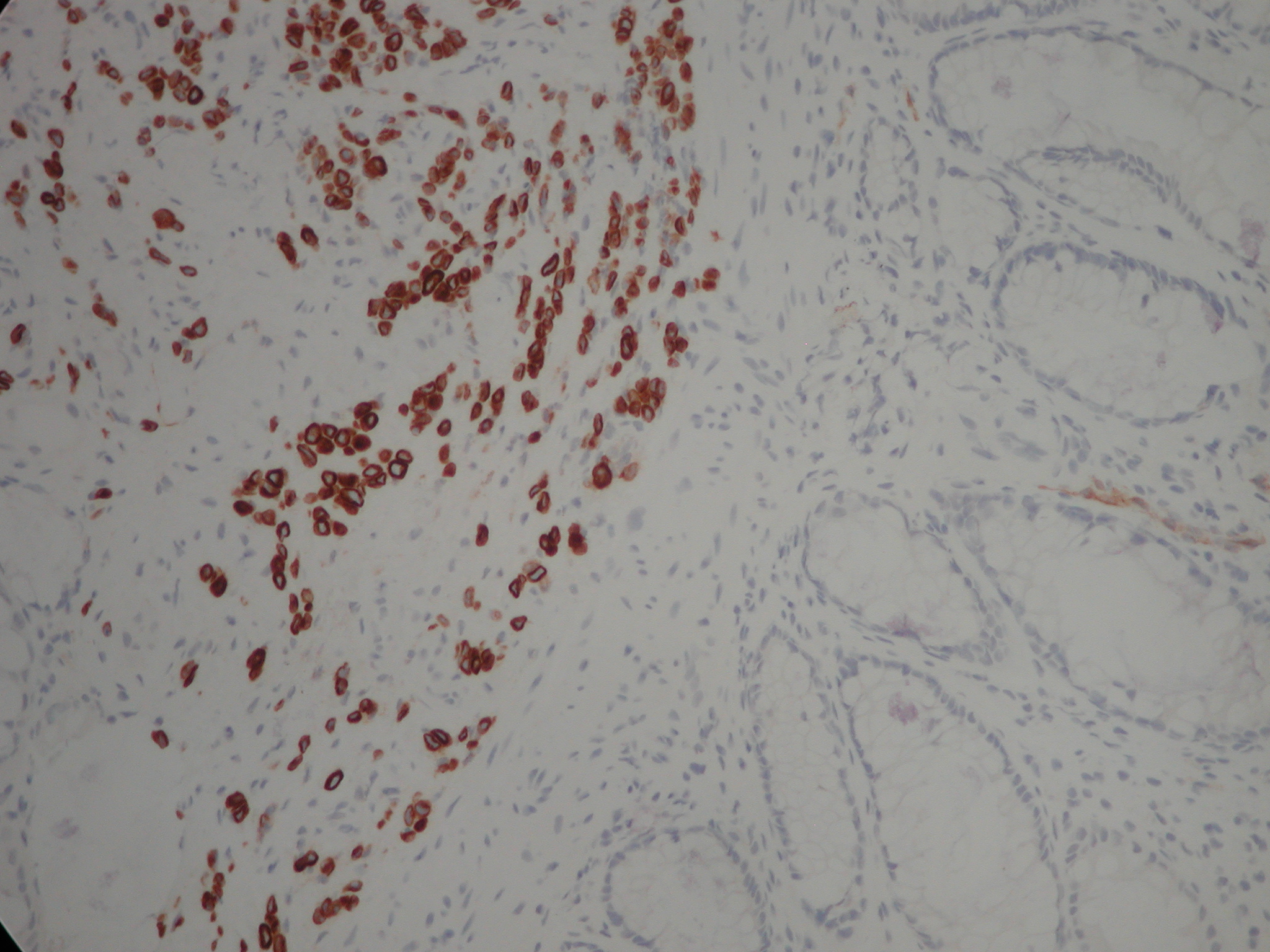
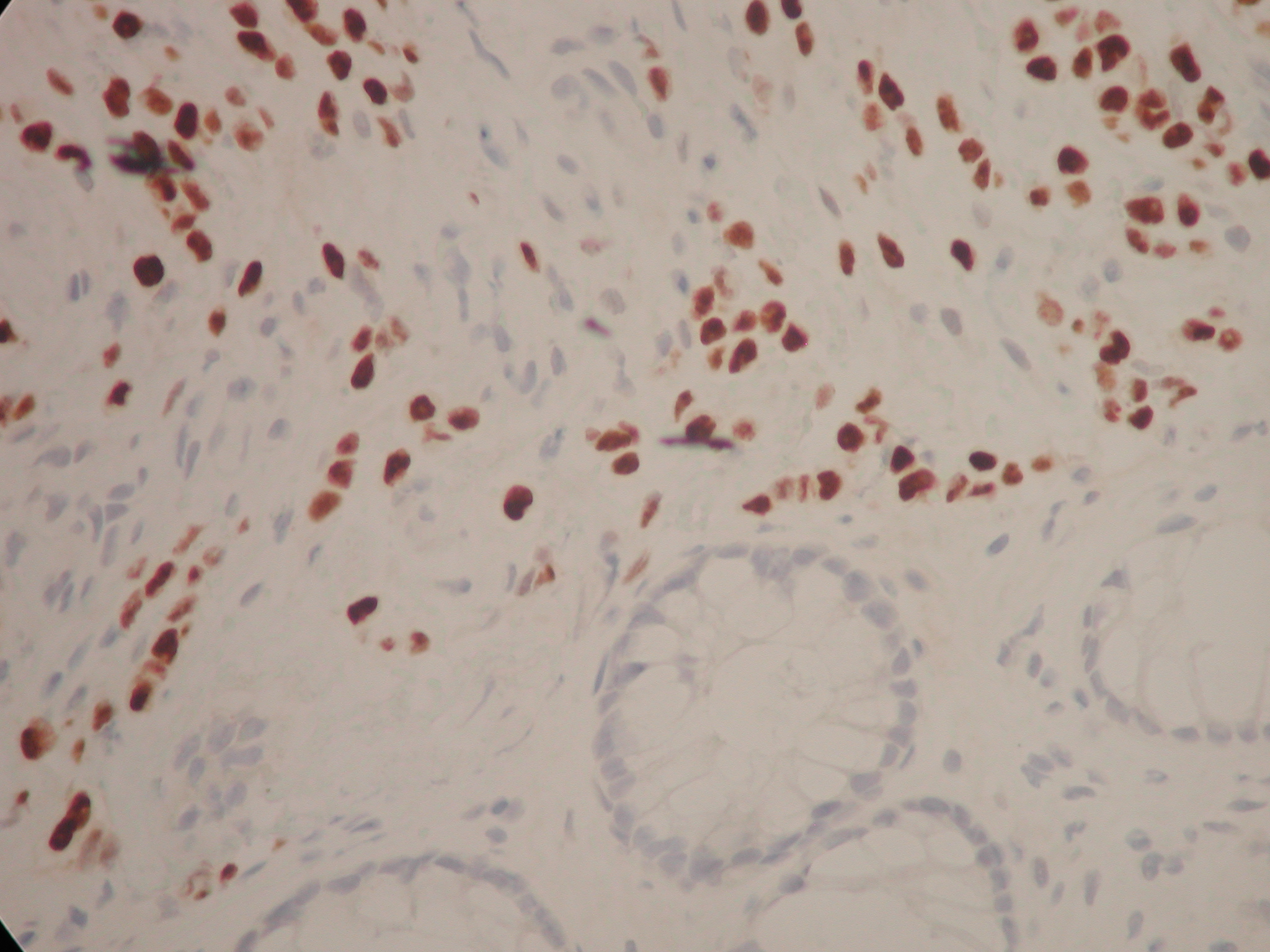
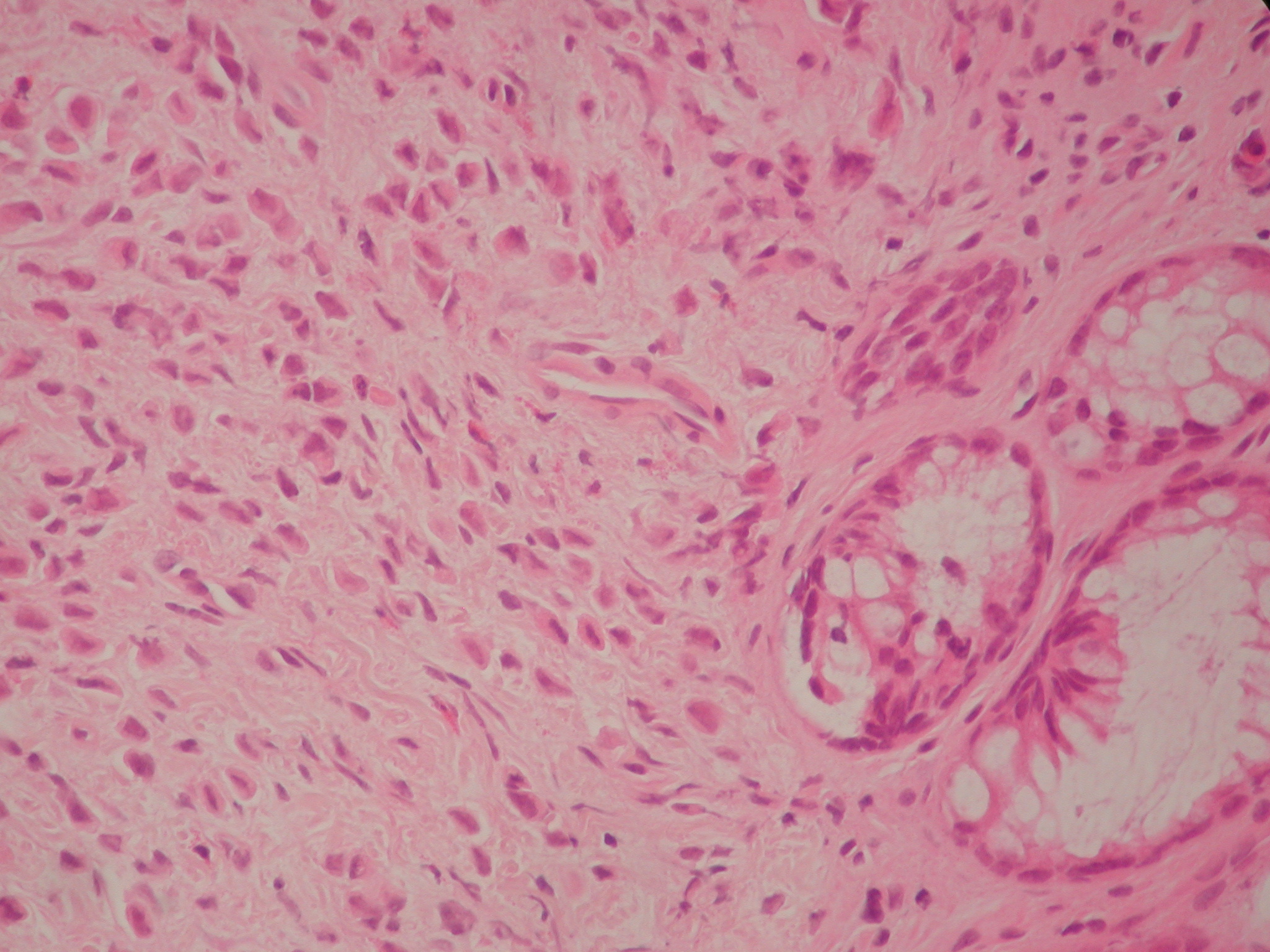
BJMP December 2016 Volume 9 Issue 4
Editorial
Clinical Practice
Education and Training