The number of individuals surviving cancer is expected to rise by one-third according to estimates from the American Cancer Society and the National Cancer Institute1. This means that in the UK over 3 million individuals, and in the USA over 18 million individuals, will be living with the consequences of cancer by 2,022. The increase in the number of survivors is attributed to earlier diagnosis, an aging population, better cure rates and more effective systemic therapies to keep patients with metastatic disease alive for longer. To achieve these benefits, patients often have to endure more complex and arduous therapies, frequently leaving them beleaguered with acute and long-term adverse effects. In addition to being unpleasant, these adverse effects result in financial implications for patients and their families, as well as resulting in a greater usage of health resources.
Although the importance of exercise is beginning to be recognised by health professionals, advocacy groups and charities, it still remains an under-utilised resource. This article highlights the evidence that a physically active lifestyle and formal exercise programmes can help relieve many of the common concerns and adverse effects which plague individuals in the cancer survivorship period.
Physical activity improves well-being after cancer
Dozens of interventional studies have tested the feasibility and potential benefits of exercise in cancer survivors2,3,4. Recent meta-analyses of randomised trials involving exercise interventions after cancer, encouragingly demonstrate that the benefits of exercise spanned across several common cancer types and following a range of treatments including surgery, radiotherapy, chemotherapy, hormones and even the newer biological therapies. The most recent meta-analysis of 34 randomised trials published in the BMJ in 2012 involving patients exercising after cancer, demonstrated a benefit for a number of troublesome symptoms particularly fatigue, mood, anxiety and depression; muscle power, hand grip, exercise capacity and quality of life5.
The American College of Sports Medicine also published a comprehensive review of exercise intervention studies in cancer populations which included data from 85 RCT’s of exercise in cancer survivors. Evidence consistently demonstrated that exercise could be performed safely in adjuvant and post-treatment settings. Exercise led to significant improvements in aerobic fitness; increased flexibility and strength; quality of life; anxiety and depression; fatigue, body image, size and composition4.
The individual categories of symptoms which commonly afflict cancer survivors are now discussed in more detail:
Cancer related fatigue (CRF) is one of the most distressing symptoms experienced by patients during and after their anti-cancer therapies. It is reported by 60-96% of patients during chemotherapy, radiotherapy or after surgery, and by up to 40% of patients taking long-term therapies such as hormonal or biological therapies6. The first step to treating CRF is to correct, if possible, any medical conditions that may aggravate it, such as anaemia, electrolyte imbalance, liver failure and nocturia; or to eliminate drugs such as opiates, anti-histamines and anti-sickness medication7. The role of exercise was reviewed in 28 randomised, controlled trials (RCTs) involving 2083 participants in a variety of exercise programmes and showed that exercise improved CRF, although the benefit overall was small8. A second review of 18 RCTs involving 1,109 participants, sub-divided the data into types of exercise and demonstrated that supervised exercise programmes had the most impact on CRF9. Further meta-analyses and reviews have also showed that supervised exercise programmes had better results, with a greater reduction in CRF amongst breast cancer survivors assigned to exercise programmes compared to home-based programmes4,5,8,10.
Psychological distress, including anxiety and depression, is common after cancer with reported prevalence rates of 25-30%11. Patients with psychological distress have also been shown to have reduced survival compared to those who are psychologically healthy12. Exercise may help alleviate this symptom and improve mood, as a number of observational studies have shown that cancer patients who exercise have reduced levels of depression and anxiety, better self-esteem and are happier, especially if they involve group activities13. The recent meta-analyses of RCTs also demonstrated a reduction in anxiety and depression among individuals assigned to exercise programmes4,5.
Quality of life (QOL) is lower in many cancer sufferers and survivors, linked to other physical and psychological symptoms of cancer and its’ treatment. Meta-analyses of studies of exercise intervention programmes have demonstrated an improvement of QOL at all stages of the illness for the common cancer types and following several types of treatment4,5. For example, in a study involving 1,966 patients with colorectal cancer, patients achieving at least 150 minutes of physical activity per week had an 18% higher QOL score than those who reported no physical activity, as measured by the QOL FACT-C14. Another study showed similar benefits for breast cancer survivors who had completed surgery, radiotherapy or chemotherapy, and also demonstrated that change in peak oxygen consumption correlated with change in overall QOL15.
Weight gain:45% of women with breast cancer report significant weight gain16, and in a study of 440 prostate cancer survivors, 53% were overweight or obese17. For patients with bowel cancer, the CALBG 8980 trial showed that 35% of patients post-chemotherapy were overweight (BMI 25.0–29.9), and 34% were obese (BMI 30.0–34.9) or very obese (BMI >35)16. The reasons for this are multifactorial, but may include other symptoms of cancer treatment such as fatigue and nausea, causing patients to stop exercising. Regardless of the reasons for weight gain, numerous reviews and a comprehensive meta-analysis of the published literature have demonstrated that individuals who gain weight after cancer treatments have worse survival and more complications18. Fortunately, supervised exercise programmes have been shown to reduce weight and have significant other benefits on body constitution and fitness, such as improved lean mass indices, bone mineral density, cardiopulmonary function, muscle strength and walking distance18,19.
Bone mineral density (BMD): Pre-menopausal women who have had breast cancer treatment are at increased risk of osteoporosis, caused by reduced levels of oestrogen brought on by a premature menopause due to chemotherapy, surgery or hormones. Men who receive hormone deprivation therapy for prostate cancer are also at an increased risk of developing osteoporosis. Accelerated bone loss has also been reported for many other cancers, including testicular, thyroid, gastric and CNS cancers, as well as non-Hodgkin’s lymphoma and various haematological malignant diseases20,21. Lifestyle factors linked to an increase in the risk for developing osteoporosis include a low calcium and vitamin D intake, a diet low in plant-based protein, lack of physical activity, smoking and excessive alcohol intake22. A number of studies have linked regular physical activity with a reduction in the risk of bone mineral loss. Sixty six women with breast cancer were randomized to a control group or an exercise programme. The rate of decline of BMD was -6.23% in the control group, -4.92% in the resistance exercise group, and -0.76% in the aerobic exercise group. The statistically significant benefit was even greater in pre-menopausal women23. In another RCT of 223 women with breast cancer, it was found that exercise, over 30 minutes 4-7 times a week, helped preserve bone mineral density even when bisphosphonates (risedronate), calcium and vitamin D had already been prescribed24.
Thromboembolism: Those with pelvic involvement, recent surgery and immobility, previous history of varicose veins or thrombosis or receiving chemotherapy, are at higher risk25. Although strategies such as compression stockings, warfarin and low molecular weight heparin are essential, early mobilisation and exercise remains a practical additional aid in reducing this life-threatening complication18,26.
Constipation caused by immobility, opiate analgesics or anti-emetics during chemotherapy is a significant patient concern. Exercise reduces bowel transit time, and ameliorates constipation and its’ associated abdominal cramps26.
Physical activity improves survival and reduces relapse
In addition to improving the side effects of treatment for cancer, regular physical activity during and after cancer appears to improve overall survival and reduces the probability of relapse. One of the most convincing studies was an RCT in which 2,437 post-menopausal women with early breast cancer were randomised to nutritional and exercise counselling, or no counselling, as part of routine follow-ups19. In the group receiving counselling, fewer women relapsed and overall survival was greater in the oestrogen-negative subgroup. In another RCT, men with early prostate cancer were randomised to an exercise and lifestyle intervention or standard active surveillance. The average PSA in the intervention group went down, whilst in the control group it went up27. This supports a previous RCT of which the primary end point evaluated a salicylate-based food supplement, but it required men in both arms to receive exercise and lifestyle counselling. Although there was no difference in the primary end point, 34% of men, who’s prostate specific antigen (PSA) was climbing before trial entry, stabilized28.
The majority of the other published evidence for a reduced relapse rate and improved survival after cancer originates from retrospective analysis or prospective cohort studies. The National Cancer Institute, in a recent meta-analysis, reviewed 45 of these observational studies. The strongest evidence was demonstrated for breast cancer survivors; the next strongest evidence was for colorectal cancer survivors, followed by prostate cancer10. The most notable are summarised below:
Breast cancer: The five most prominent prospective cohort studies (in aggregate more than 15,000 women), have examined the relationship between physical activity cancer and prognosis:
Irwin et al. (2008)29 investigated a cohort of 933 breast cancer survivors and found that those who consistently exercised for >2.5 hours per week had a 67% lower risk of all deaths compared to sedentary women.
Holmes et al. (2005)30 performed a separate evaluation of 2,987 women in the Nurses’ Health Study and found that women walking >3 hours a week had lower recurrence rates, and better overall survival.
Holick et al. (2008)31 performed a prospective observational study of 4,482 breast cancer survivors, and found that women who were physically active for >2.8 hours per week had a 35-49% lower risk of dying from breast cancer.
Pierce et al. (2007)32 found that the benefits of 3 hours of exercise were even greater if combined with a healthy diet.
Sternfeld et al. (2009)33 in the LACE study, evaluated 1,870 women within 39 months of diagnosis. There was a significant difference in overall death rate between the highest and lowest quartile of exercise levels.
Colorectal cancer: The scientific community eagerly awaits the results of the CHALLENGE RCT mentioned above, but a number of retrospective analyses of randomised chemotherapy and cohort trials have been published:
Haydon et al. (2006)34retrospectively analysed a RCT involving patients with stage III bowel cancer and found a significant association between exercise and a 31% reduction in relapse rate.
Giles et al. (2002)35found that of 526 patients recruited into the Australian Cohort Study, those participating in recreational sport 1-2 days per week had a 5 year overall survival of 71%, as opposed to 57% in non exercisers.
Meyerhardt et al. (2006)16 found in an analysis of the Intergroup CALGB study, that physically active patients with bowel cancer had 35% reduction in relapse rate in after chemotherapy.
Meyerhardt et al. (2009)36 analysed 668 patients with colorectal cancer within the Health Professionals Study. Men who exercised >27 vs. < 3METS-hours / week had a lower cancer-specific mortality.
Prostate cancer: Three cohort studies have demonstrated a survival benefit for physically active men with prostate cancer:
Kenfield et al. (2011)37performed a subset analysis of 2,686 men with prostate cancer, within the Health Professional Study, who exercised >30minutes per week or >3 MET-hours of total activity, had a 35% lower risk of overall death, and men who walked at a brisk pace for >90 minutes had a 51% lower risk of overall death.
Richman et al. (2011)38 reported that 1,455 men with prostate cancer, walking more than 3 hours a week, correlated with an improved survival but only if >3miles/hour.
Giavannucci (2005)39, within a prospective analysis, reported that men who exercised vigorously had a lower risk for fatal prostate cancer, although this effect was only seen for men over the age of 65.
Quantity and type of exercise recommended for cancer patients
For reduced cancer relapse and improved well-being, most of the cohort studies summarized above suggest moderate exercise of around 2.5 to 3 hours a week for breast cancer survivors. However, for prostate cancer survivors, mortality continues to decrease if the patient walks 4 or more hours per week, and more vigorous activity is also associated with significant further reductions in risk for all-cause mortality37. When the mode of exercise is primarily walking, a pace of at least 3 miles/hour (for >3 hours/week) is recommended for a reduced risk of relapse 38. Therefore, both the pace and duration of exercise affect the survival benefit achievable from exercise, with more vigorous activity generally having a greater benefit (see Table 1). The best results appear to be with programmes including a combination of aerobic and resistance exercises, particularly within a social group.
Table 1: Summary of exercise guidelines for cancer survivors
· Exercising for >3 hours/week has proven benefits for cancer survival
· A pace of at least 3 miles/hour when walking provides greater benefit than a slower pace
· For optimal benefit, exercise should consist of a combination of resistance and aerobic exercises
· Supervised exercise programmes have shown greater benefits for cancer survivors than home-based programmes
The precise amount of exercise has to be determined on an individual basis and depends on pre-treatment ability, current disability caused by the cancer itself or the treatment, as well as time proximity to major treatments. An exercise programme supervised by a trained professional has major advantages, as they can design a regimen which starts slowly and gradually builds up to an acceptable and enjoyable pace. In addition, they can help motivate the individual to continue exercising for the short and the long-term, and they can judge the optimal exercise levels to improve fatigue, and not aggravate it.
The underlying mechanisms of the potential anti-cancer effects of exercise
The body’s chemical environment significantly changes after exercise, best demonstrated in the Ornish study, which found that serum from prostate cancer patients who exercised, had an almost eight times greater inhibitory effect on the growth of cultured androgen dependent prostate cancer cells compared to serum from patients in the control group27. The precise chemical mechanism, which the anti-cancer effect remains incompletely understood, but one of the most likely mechanisms involving growth factors such as insulin-like growth factor (IGF-1) and its’ binding proteins insulin-like growth factor binding proteins (IGFBPs), due to the central role of these proteins in the regulation of cell growth (see Table 2). After binding to its receptor tyrosine kinase, IGF-1 activates several signalling pathways including the AKT pathway, leading to the inhibition of apoptosis and the promotion of cell growth and angiogenesis34,40,41. An inverse relationship of cancer risk with IGFBP3 levels has also been shown, although this effect has not been confirmed in all studies42. Exercise has been shown to increase the levels of IGFBP3, and this was associated with a 48% reduction of cancer-specific deaths in a large prospective cohort study of 41,528 participants43. Decreased levels for IGF-1 in physically active patients have been reported with an associated survival benefit44.
Table 2: Summary of the potential biochemical pathways of the anticancer effects of exercise
Class of Effector Molecule
Effector Molecule
Effects of Exercise on Effector Molecule
Cell growth regulators
IGF1
Decreased levels
IGFBP3
Increased levels
Proteins involved in DNA damage repair
BRCA1
Increased expression
BRCA2
Increased expression
Regulator of apoptosis and cell cycle arrest
p53
Enhanced activity
Hormones
Oestrogen
Decreased levels
Vasoactive intestinal protein (VIP)
Decreased levels
Leptin
Decreased levels (indirect)
Immune system components
NK cells
Enhanced activity
Monocyte function
Enhanced activity
Circulating granulocytes
Increased proportion
Exercise has also been shown to have a large impact on gene expression, although the mechanisms through which the patterns of gene expression are affected remain to be determined. In a recent study of the mechanisms through which exercise impacts prostate cancer survival, it was found that 184 genes are differentially expressed between prostate cancer patients who engage in vigorous activity, and those who do not 37. Amongst the genes that were more highly expressed in men who exercise were BRCA1 and BRCA2, both of which are involved in DNA repair processes.
Another neuropeptide which changes after exercise is Vasoactive Intestinal Protein (VIP). Breast and prostate cancer patients have been found to have higher VIP titres compared to individuals who regularly exercise, and who have increased production of natural anti-VIP antibodies45. In hormone-related cancers such as cancers of the breast, ovaries, prostate and testes, the association between high levels of circulating sex hormones and cancer risk is well established46. Another mechanism through which exercise may affect cancer, is through decreasing the serum levels of these hormones. For breast cancer survivors, the link between exercise and lower levels of oestrogen has been shown13,34,47. An indirect, related mechanism is that exercise helps reduce adiposity, and adiposity in turn influences the production and availability of sex hormones48. In addition, greater adiposity leads to higher levels of Leptin, a neuropeptide cytokine with has cancer promoting properties49,50.
Other pathways include the modulation of immunity, such as improvements in NK cell cytolytic activity 11; the modulation of apoptotic pathways through impacting on a key regulator, p5351, and an exciting recent discovery, the messenger protein irisin, which is produced in muscle cells in response to exercise and is found is to be an important molecule in linking exercise to the health benefits52 , However, we are only beginning to scratch the surface with these and the other mechanisms discussed here, and much more research needs to be done to in this area.
Incorporating exercise into mainstream cancer management
The challenge for health professionals is how to encourage and motivate individuals with cancer to increase their exercise levels. Some, of course, are motivated to increase physical activity or remain active after cancer. However, a recent survey of 440 men with prostate cancer found that only 4% of patients exercised for more than the 3 hours a week recommended by the WCRF17. Macmillan Cancer Relief has produced a series of helpful booklets and web-based patient information materials designed to inform and motivate individuals to exercise as part of its ‘Move More’programme. The Cancernet website has a facility to search for local exercise facilities by postcode, which can be an aid for health professionals when counselling patients. It highlights activities that men will hopefully find feasible and enjoyable such as golf, exercise groups and walking groups, and are encouraged to attend in addition to work place activity and gardening.
Several pilot schemes have been started throughout the UK with the aim to incorporate exercise programmes into standard oncology practice. The difficulty with small schemes is that they tend to be poorly funded, often poorly attended and are unlikely to be sustainable in the longer term. Many agree that the gold standard model would be similar to the cardiac rehabilitation programme53. This would involve a hospital scheme run by a physiotherapist or an occupational therapist, supervising patients immediately after surgery, radiotherapy and even during chemotherapy. This is followed by refering the patient to a community-based scheme for the longer term. Unfortunately, this type of scheme is expensive and unlikely to be funded at present, despite the obvious savings by preventing patient relapsing and ultilising health care facilities to help late effects of cancer treatment54. However, expanding existing services, such as the National Exercise Referral Scheme, is a practical solution. The National Exercise Referral Scheme exists for other chronic conditions such as cardiac rehabilitation, obesity and lower back pain. The national standards for the scheme to be expanded to include cancer rehabilitation were written and accepted in 2010. Training providers have now developed training courses for exercise professionals set against these standards. Trainers completing the course gain a Register of Exercise Professionals (REPs) Level Four qualification, allowing them to receive referrals from GPs and other health professionals.
Conclusion
There are a wealth of well-conducted studies which have demonstrated an association between regular exercise and lower risk of side effects after cancer, as well as reasonable prospective data for a lower relapse rates and better overall survival. However, as there are several overlapping lifestyle factors, which are difficult to investigate on their own, there remain some concerns that exercisers may do better in these studies because they are less likely to be over-weight, more likely to have better diets and to be non-smokers. Although the existing RCTs provide encouraging evidence that exercise intervention programmes are beneficial, further large RCTs are needed, particularly in terms of cost-effectiveness, before commissioner’s start investing more in this area.
A 41 year old female patient (ASA II) underwent an incision and drainage of her perianal abscess under a general anaesthetic as an urgent procedure. She was known to have anorexia nervosa and was under medical management for it. She had a BMI of 18.5. She also suffered from eczema and mild asthma. She gave a history of irregular heart rhythm in the past. She had a normal ECG and echocardiogram. She was on fluoxetine, salbutamol inhaler, beclometasone inhaler and ricatriptan. She had normal blood investigations prior to induction.
Her anaesthetic was induced with propofol and fentanyl and was maintained on oxygen/ air/ sevoflurane. She was on spontaneous ventilation through a laryngeal mask. She also received paracetamol and ondansetron intraoperatively. She was haemodynamically stable during the twenty minute procedure, which was done in the lateral position.
The laryngeal mask came out ten minutes after her arrival in recovery. The patient asked for pain relief ten minutes after waking up. IV pethidine 25mg (diluted to 12.5 mg/ml) was given by the recovery nurse who, within five minutes, noted severe redness in the distribution of the vein into which it was injected (Figure 1). The anaesthetist was notified, who then flushed the IV line with normal saline. The redness settled down within 15-20 minutes of the start of the reaction ( Figure 2 to 4). The patient was haemodynamically stable and didn't complain of any local or systemic symptoms.
Discussion
Pethidine has been known to release histamine on systemic administration1. It can also have interactions with various drug groups like SSRIs and MAO inhibitors to cause serotonin syndrome2,3 and can present with tachycardia, hypertension, hyperthermia, agitation and even seizures, among other signs and symptoms. Pethidine is equipotent to morphine and codeine in terms of histamine release 4.
This case is most likely due to profound histamine release in a patient with atopic tendency. The factors thought to increase the incidence and severity of this reaction are 5:
Old age
Thin body structure
Poor peripheral circulation
Volar > dorsal veins
Repeated injection into the same superficial vein
High concentration of solution of injection (>10 mg/ml solution)
The factors that have no influence are:
Pretreatment with an antihistamine
History of previous pethidine use
Using pethidine as a premedication
In the past, diluting pethidine with 0.25% procaine also provided protection against the reaction.
There were no other signs of serotonin excess in this patient and she came to no harm. The presentation was dramatic enough to cause concern but was self-limiting.
The American Diabetic Association (ADA) and the American College of Endocrinology (ACE) recommend HbA1c levels as diagnostic criteria for diabetes mellitus. Physicians have adopted HbA1c levels as a convenient way to screen for diabetes, as well as to monitor therapy. There exists concern that because HbA1c is formed from the glycation of the terminal Valine unit of the β-chain of haemoglobin, it may not be an accurate surrogate to ascertain glycemic control in certain conditions that affect the concentration, structure and function of haemoglobin. It makes logical sense to infer that HbA1c levels should at least in part reflect the average haemoglobin concentration ([Hb]). Kim et al (2010) stated that iron deficiency is associated with shifts in HbA1c distribution from <5.0 to ≥5.5% 1 and significant increases was observed in the patients' absolute HbA1c levels 2 months after treatment of anaemia.2 There is a dearth of literature on HbA1c levels in the anaemia population, and a reference range for this unique population does not currently exist. There are a few documented studies on this matter, the findings of which are at best, inconsistent.
It is thought that the various types of haemoglobin found in the myriad of haemoglobinopathies may affect haemoglobin-glucose bonding and/or the lifespan of haemoglobin, and by extrapolation, HbA1c level. Hence, extending target HbA1c values to certain haemoglobinopathaties may be erroneous due to potential differences in glycation rates, analytical methods (HbF interfers with the immunoassay method) and some physiological challenges (markedly decreased red cell survival).3
There is a significant positive correlation between haemoglobin concentration and HbA1c in the patients with haemolytic anaemia.4,5 Cohen et al (2008) reported that observed variation in red blood cell survival was large enough to cause clinically important differences in HbA1c for a given mean blood glucose,6 and haemolytic disorders may cause falsely reassuring HbA1c values.7 Jandric et al (2012) inferred that in diabetic population with haemolytic anaemia, HbA1c is a very poor marker of both overall glycemia and haemolysis.8 Mongia et al (2008) report that immunoassay methods for measuring HbA1c may exhibit clinically significant differences owing to the presence of HbC and HbS traits.9 However, Bleyer et al report that sickle cell trait does not affect the relationship between HbA1c and serum glucose concentration and it does not appear to account for ethnic difference in this relationship in African Americans and Caucasians.10
Koga & Kasayama (2010) advise that caution should be entertained when diagnosing pre-diabetes and diabetes in people with low or high haemoglobin concentration when the HbA1c level is near 5.7% or 6.5% respectively, citing the implication of changes in erythrocyte turnover. They further assert that the trend for HbA1c to increase with iron deficiency does not appear to necessitate screening for iron deficiency to ascertain the reliability of HbA1c in this population.11
In the light of the uncertainty in the influence of anaemia and haemoglobinopathies on HbA1c, it is imperative that clinicians are aware of the caveats with HbA1c values when they make management decisions in the anaemic population.12 There is currently a call for the use of other surrogates for ascertaining average glycemic control in pregnancy, elderly, non-Hispanic blacks, alcoholism, in diseases associated with postprandial hyperglycemia, genetic states associated with hyperglycation, iron deficiency anaemia, haemolytic anaemias, variant haemoglobin states, chronic liver disease, and end-stage renal disease (ESRD).13,14
Study objectives and hypothesis
The study attempts to discern clinical differences in HbA1c levels in patients with anaemia compared to non-anaemic population, as well as to quantify and show the direction of such difference if they indeed exist. We hypothesize that as glucose is covalently bound to haemoglobin in glycosylated haemoglobin, HbA1c levels in non-diabetic anaemic population is significantly lower than in non-diabetic, non-anaemic population.2 However, this relationship may not hold true for certain anaemias, haemoglobinopathies and hyperglycation states in some genetic syndromes.
Study design and method
The study is a retrospective chart review of patients with and without anaemia who underwent haemoglobin concentration and HbA1c level testing at The Brooklyn Hospital Center (TBHC) from July, 2009 to June, 2013. Using Cohen (1987) power table, assuming a power of 0.8, alpha level of 0.05, and a small effect size of 0.2 standard deviations (SD), sample size estimation of 461 was computed. A convenient sampling method was used to select patients who meet inclusion criteria, absent exclusionary conditions. In using this sampling method, we queried the electronic medical record at the TBHC using the below-listed inclusion and exclusion criteria. The query generated a list of “potential subjects”. We then reviewed the electronic chart of each patient on this list to confirm that they indeed meet all study criteria (excluding further if any exclusion criteria was identified on “second look”. We continued the selection until the computed minimum sample size of 461 was significantly exceeded. During this process, we had to examine every patient on the “potential subject” list generated by the initial query to achieve this goal. For the purpose of the study, anaemia is defined as haemoglobin concentration <11g/dl.
Inclusion criteria:
iStudy participant must be at least 21 years of age. We adopted this age criteria because at TBHC, electronic medical records was only available for the non-pediatric population over the study period. Patients below 21 years were managed at the pediatrics department using paper charts until the recent adoption of the EMR system. It would have been difficult conducting the study using paper charts.
iStudy participant must have at least one documented HbA1c level obtained within a month of a haemoglobin concentration assay. This criterion was adopted to allow for more inclusiveness in the study. It is our experience that haemoglobin assays may not be available on the same day as HbA1C assays considering the retrospective nature of the study.
Exclusion criteria:
Confirmed cases of diabetes mellitus (using two or more of the following: presence of symptoms related to diabetes, fasting blood glucose, 2 hours post-prandial glucose, and oral glucose tolerance test).
Documented history of gestational diabetes (GDM)
Documented history of endocrinopathy with affect for glycemic control
Current or prior use of medication with potential to increase or decrease HbA1c (includes, but not limited to antidiabetics, corticosteroids, statins, and antipsychotics)
Pregnancy or pregnancy-related condition within three months of HbA1c assay
Haemoglobin concentration <6 g/dl or >16g/dl.
Blood loss or blood transfusion within two months of HbA1c assay
The study assumed a consistent HbA1c assay method at the study center over the study period. 482 (229 anaemic and 253 non-anaemic) were selected. The study reviewed electronic medical records of selected patients, extracting data on HbA1c, fasting blood glucose (FBG), 2-hour post-prandial serum glucose (2HPPG), 2-hour oral glucose tolerance test (OGTT), haemoglobin concentration and electrophoresis, and anaemia work-up results when available. Subsequent measures of HbA1c two months after correction of anaemia was also documented and compared to pre-treatment levels.
Results and Analysis
The mean age of the anaemic and non-anaemic was 51.8 and 64.6 years respectively. Using the student’s t-test and x2 analysis respectively, the difference in mean age of both groups (anaemia and non-anaemic) was significant at p0.05 while gender distribution was similar (p>0.05), see table 1. The mean HbA1c for anaemic and non-anaemic groups was 5.35% and 5.74% respectively, amounting to a 0.4 unit difference in (8%) in mean HbA1c. This difference was statistically significant (p0.02). A significantly higher variance was observed in the anaemia group (0.79 vs. 0.64).
Table 1: Gender and age distribution and statistics
Age in years Anaemia
#(%)
Gender (M/F)
Mean Age (in yrs)
21-44
20(8.7)
17/41
45-64
76(33.2)
43/86
≥65
133(58.1)
10/32
Total
229(100.0)
70/159
64.6
Non-anaemic
21-44
64(25.3)
23/42
45-64
134(53.0)
58/81
≥65
55(21.7)
18/31
Total
253(100)
99//154
51.8
p-Values: Age=0.023, Gender=0.061
Assuming that 95% of the population is normal, computation of HA1c reference range (mean ±1.96SD) for the anaemia and non-anaemic group yielded 3.8-6.9 and 4.5-7.0 respectively. There was a significantly positive spearman correlation between [Hb] and HbA1C (r=0.28, p0.00). The mean HbA1c level and proposed reference ranges for the five anaemia subgroups (anaemia of chronic disease [ACD], iron deficiency anaemia [IDA], mixed anaemia, macrocytic anaemia and sickle-cell disease) are shown in table 2. Using one-way ANOVA analysis, the difference in the mean [Hb] and HbA1c across anaemia subtypes was not statistically significant (p0.08 and p0.36 respectively), see table 2.
Table 2: Anaemia subtypes with HbA1c statistics
Anaemia Type
#
Mean[Hb]
MeanHbA1c
95% CI (HbA1c)
Ref. range (HbA1c)
ACD
92
9.23
5.41
5.24-5.59
3.5-7.1
IDA
78
9.41
5.38
5.22-5.54
3.9-6.8
Mixed
11
9.11
5.21
4.82-5.59
3.9-6.5
Macrocytic
43
8.83
5.14
4.92-5.37
3.7-6.6
SCD
5
9.12
5.55
4.84-6.26
3.8-7.3
Anaemia (all types)
229
9.21
5.35
5.24-5.44
3.8-6.9
Non-anaemic
253
12.87
5.735
5.66-5.81
4.5-7.0
p-values: [Hb] for anaemia subtypes=0.08, HbA1C for anaemia subtypes=0.36, HbA1C anaemia vs. non-anaemia=0.02. ACD: anaemia of chronic disease, IDA: iron deficiency anaemia, SCD: sickle cell disease.
The study also examined the anaemia group to document the effect of anaemia correction on HbA1c levels. Only 62 of the 229 anaemic participants had documented [Hb] and HbA1c after interventions to correct anaemia, see table 3 and 4.
Table 3: Trend in [Hb] and HbA1c
N
Mean
SD
SEM
Change
p-Value
[Hb]1
62
9.2
1.07
0.14
[Hb]2
62
10.1
1.98
0.25
[Hb]=0.9
0.00
HbA1c1
62
5.37
0.69
0.88
HbA1c2
62
5.35
0.66
0.83
HbA1c=0.02
0.78
[Hb]1 and [Hb]2: haemoglobin concentration pre- and post- treatment for anaemia. HbA1c1 and HbA1c2: HbA1c pre- and post-treatment for anaemia
Table 4: Trend in [Hb] and HbA1c for anaemia subtypes
N
Mean[Hb]1
Mean[Hb]2
Δ Hb
pValue
MeanHbA1c1
MeanHbA1c2
ΔA1c
pVal
ACD
33
9.1
9.7
0.6
0.0
5.44
5.35
0.09
0.3
IDA
21
9.4
10.7
1.3
0.0
5.30
5.33
0.03
0.8
Mixed
1
Macrocytic
6
SCD
1
Total
62
9.2
10.1
0.9
0.0
5.37
5.35
0.02
0.8
ΔHb: change in haemoglobin concentration ([Hb]), ΔA1c: change in HbA1c
Using the student’s t-test, analysis, a 0.9g/dl mean improvement in [Hb] in the anaemia group (significant at p0.00) did not result in a statistically significant change in HbA1c (-0.02 units, p0.78). Similar results were obtained with anaemia of chronic disease and iron deficiency anaemia (ICD: change [Hb] =+0.6g/dl, change HbA1c=0.09, p0.31; IDA: change [Hb]=+1.3g/dl, change HbA1c=0.03, p0.79).
Discussion
There was an over-representation of the elderly in the anaemia group (58.1% vs. 21.7%). This is not unexpected as nutritional anaemia and anaemia of chronic disease increase in prevalence with the increasing co-morbidities associated with increasing age. The linear relationship between [Hb] and HbA1c holds true for anaemic and non-anaemia populations. There is a statistically significant difference of 0.4units (8%) in the mean HbA1c between the anaemic and the non-anaemic population. This difference is even more marked when the lower limit of the range is compared (3.8 vs. 4.5, difference of 0.7unit, 18%), the significance of which is not as clinically impacting as the upper limit of the range (diabetes mellitus diagnostic criteria). However, the relatively lower limit of normal for HbA1c in anaemic subgroups (especially of anaemia of chronic disease) may make low values of HbA1c in these patients less indicative of over-enthusiastic glycemic control, as well as less predictive of the increase in mortality associated with such tight control.
The upper range of normal for HbA1c for the anaemia and the non-anaemic groups and by extrapolation the proposed diagnostic criteria for diabetes, is however more similar (6.9 vs. 7.0%). This result appear consistent with Koga and Kasavama (2010) assertion that the trend in HbA1c does not appear to necessitate screening for iron deficiency to ascertain the reliability of HbA1c in this population.11 Our observation is explained by the greater variance associated within the anaemia group. The significantly higher variance observed in the anaemia may be explained by the convenient homogenization of clinically heterogeneous anaemia entities in the anaemia group. Perhaps a prospective study that avoids this may report differently.
The significantly higher variance (23%) in the anaemia is explained by the heterogeneity of the subtypes within the anaemia group. The myriad of pathophysiologies (from variant haemoglobin affecting structure and function, and perhaps glycation rates of haemoglobin, to shortened erythrocyte lifespan due to intravascular and extravascular haemolysis) accounts for a less precise HbA1c reference range for the anaemia group. Separating the anaemia group into unique anaemia subtypes created less heterogeneity, reduced some within group variance and yielded a more precise references range for some anaemia subtypes.
The widened 95% CI of mean and reference ranges observed with mixed and sickle cell anaemia (95% CI of mean =4.82-5.59 and 4.84-6.26 respectively) may be attributable in part to the small number of participants in these subgroups (11 and 5 respectively, the normal curve is less robust in these circumstances [when n<30])). Furthermore, the marked variability in the type, severity, and the number of chronic morbidities and deficiencies causing mixed anaemia may be contributing. The imprecision of HbA1c observed with the sickle cell may be compounded by the unstable clinical course of sickle disease, marked by periodic crises with fluctuating [Hb] associated with intermittent or chronic haemolysis. These observations make the case for defining HbA1c reference ranges for each anaemia type.
A modest correction of anaemia (Δ [Hb] of +0.9g/dl, i.e <1g/dl) did not appear to cause a significant change in HbA1c levels. It is possible that higher increments in [Hb] may produce significant change in HbA1c (we predict in the direction of increment). A similar pattern was observed with anaemia of chronic disease and iron deficiency anaemia subtypes, where improvements in [Hb] of 0.6 and 1.3g/dl respectively did not cause a significant change in HbA1c. We propose that with anaemia of chronic disease, the change in [Hb] concentration was too modest to cause a significant change in HbA1c. The relative small size of participants (33) examined also makes type II statistical errors highly likely. We further propose that with anaemia of chronic disease, the myriad of functional cellular and system abnormalities (many, potentially affecting cellular homeostasis, especially acid-base balance and haemoglobin molecule covalent binding) associated with the primary disorder may impact on the potential for increase in HbA1c with increasing [Hb]. In view of the retrospective nature of the study, we could not ascertain the timelines of certain interventions and hence accurately determine the persistence of anaemia correction. Theoretically, a recent correction in [Hb] is less likely to impact on HbA1c. As alluded to above Kim et al (2010) evaluated for changes in HbA1c two months after correction of anaemia. Similar explanations are offered for the observation with iron deficiency anaemia. There were only 21 participants in the iron anaemia subgroup (i.e. <30, probable violation of a rule for use of parametric tests), making the parametric statistical tests less robust for the analysis. We did not study patterns with mixed, macrocytic and SCD, as each subtype had <7 (1,6,1) participants.
The study examined a large volume of data, eliminating as much as possible, potential extraneous factors in the relationship between [Hb] and HbA1c levels. However, the retrospective nature of the study made the control of other extraneous variables and certain patient attributes infeasible. It was also difficult to discern critical timelines and hence eliminate the potential impact of certain therapeutic interventions. Also, our exclusion of the younger population of patients (i.e. 16-20 years) does not necessarily indicate the result of the study may not be extended to this population of anaemia patients. In fact the similar human haemoglobin physiology in this group advises that the results may be extended to this younger population without concern. Due to the retrospective nature of the study, and in our attempt to increase inclusiveness, we allowed haemoglobin concentration and HbA1c assays done within a month of each other. In reality though, the majority (57%) had same day assays and even a greater majority (79%) had within same week assays. We recommend a larger scale prospective study with participants representative of all anaemia subtypes and ages so that the results can be extrapolated to the general population of anaemia patients.
Conclusion
The study emphasizes the need to exercise caution when applying HbA1c reference ranges to anaemic populations. It makes the case for defining HbA1c reference ranges and thus, therapeutic goals for each anaemia subtype. Redefining such reference ranges may increase the sensitivity of HbA1c in diagnosing diabetes in anaemic population if indeed the lower mean HbA1c (observed in this study) translates into significantly lower upper limits of references ranges (not observed in this study). Also, the realized reduced lower limits of reference range in this population will lead to appropriate clinical tolerance for lower HbA1c levels, with avoidance of inappropriate intervention for erroneous perception of over-enthusiastic control of diabetic hyperglycemia. We recommend that, absent risks factors for and symptoms relatable to diabetes, marginal elevations in HbA1c levels (i.e. HbA1c >6%) in anaemic patients should warrant confirmation of diagnosis using fasting blood glucose and 2HPPG or OGTT. The use of other surrogates of glycemic control, immune to the blur associated with haemoglobin type and concentration, may circumvent the problem associated with use of HbA1c in this special population. To this end, fructosamine and glycated albumin assays are currently being examined. 1,15
Metastatic carcinoma to the sinonasal tract is rare. We describe a patient with an aggressive follicular variant of papillary thyroid carcinoma who presented with an unusual metastasis to sphenoid sinus.
Case report
A 44 year old Hispanic woman presented at Queens Hospital Center in June 1988 with airway obstruction and was found to have a 10x12 cm firm mass in the left thyroid lobe, and palpable left supraclavicular node. She had no prior history of radiation, and no family of thyroid cancer. She underwent a total thyroidectomy with a modified radical neck dissection. Pathology revealed a follicular variant of papillary thyroid carcinoma: non-tall cell variant. Six of fifty (6/50) lymph nodes were positive. Post-surgery, patient received Iodine-131 ablation therapy (93 mCi) and was placed on thyroid hormone suppressive therapy. Non-stimulated thyrogen total body scan a week after therapy was negative. Thyrogen was not available at that time.
The patient was non-compliant with thyroxine and thyroid stimulating hormone (TSH) was often elevated (13-80 mlU/ml). However, the serum thyroglobulin remained less than 5.0 ng/ml and antithyroglobulin antibody was negative. A repeat total body scan (with 5 mCi I131) 6 months later and 4 years later with thyroxin withdrawal (TSH 36 mIU/ml and 48 mIU/ml respectively) was negative, and patient was continued on thyroxine suppression therapy.
Five years after initial presentation, the patient developed urinary retention and lower extremity weakness. A myelogram revealed block at T1-T2. Patient underwent laminectomy. Pathology revealed metastatic follicular variant of papillary thyroid carcinoma. Since iodine containing contrast was used during the myelogram, I131 iodine therapy was not given. External radiation of 2000 CGY to C7-T5 was administered.
A total body scan 8 weeks post laminectomy (when 24 hour urine iodine < 100 microgram/litre, and TSH was 38 mIU/ml after thyroid hormone withdrawal) was negative, the thyroglobulin level was 5 ng/ml and negative antithyroglobulin antibody (at that period of time, positron emission tomography (PET) scan was not an available option). For the next 2 years of follow up, the patient was maintained on thyroxin suppression therapy, this time with good compliance (TSH 0.1 mIU/ml, thyroglobulin less than 5 ng/ml and negative antithyroglobulin antibody). She did not show up for follow up lumbar computerised tomography (CT).
Seven years after the initial presentation, she complained of headache and double vision, and a three month history of amenorrhea. The thyroglobulin at this time was elevated (20 ng/ml). Chest X-ray was positive for two nodules in the right lung. Magnetic resonance imaging (MRI) revealed a soft tissue mass in the sphenoid sinus, eroding the basi-sphenoid and extending into the nasopharynx (Fig. 1 ABCD). The mass also eroded the sella floor displacing the pituitary gland upwards (arrows). Bone scan revealed focal abnormalities in the upper thoracic spine, ethmoid bones and base of the skull. At that period of time, PET scan was not an available option. Pituitary function testing revealed TSH 0.1 mIU/ml, free T4 level 1.2 mIU/ml. AM cortisol 5.3 mcg/dl, prolactin 182 ng/ml, ACTH 12 pg/ml, FSH 11.5 mIU/ml, LH 4.0 mIU/ml, and Estradiol 20 pg/ml.
Figure 1: A-T1 weighted midline sagittal MRI scan without contrast. B-T1 weighted midline sagittal MRI scan with contrast. C-T2 weighted axial MRI scan through the lesion. D-Axial CT scans without (on the left) and with (on the right) contrast. Note: The large destructive and enhancing lesion (*) in the sphenoid sinus associated with destruction of the basisphenoid, clivus and sellar floor. Note the normal pituitary gland (arrow) is displaced upwards out the sellaturcica.
Biopsy of the sphenoid sinus mass confirmed that it was metastatic papillary thyroid cancer, follicular variant. The tumour cell nuclear DNA was diploid and P53 and K167 were negative (Impat, NY). The patient was placed on hydrocortisone replacement and continued on thyroxine suppression therapy. Three months later the patient suffered a cardiorespiratory arrest and expired.
Discussion
Metastasis to the sphenoid sinus is rare from any tumour, and from papillary thyroid cancer it is extremely rare. An extensive world literature review revealed only 4 cases of spread to sphenoid sinus region from papillary thyroid cancer.1-4
Renal cell carcinoma is the most common tumour of paranasal sinus metastasis, 41.8%. The average age is 58 years, with slight predominance of males. The most common presentation was epistaxis, 31%. The most common causes of sphenoid metastasis are gastrointestinal and renal tumours5.
Von Eiselsberg et al. in 1893 described one case of metastasising thyroid carcinoma to sphenoid sinus.6 Harmer et al., 1899, reported a case of medullary thyroid carcinoma metastasis to sphenoid/ ethmoid sinus and nose. 7 Barrs et al. in 1979 reported a case of metastasis of follicular thyroid carcinoma to sphenoid sinus and sphenoid bone.8 Chang et al. in 1983 described a case of metastatic carcinoma of the thyroid to the sphenoid sinus.9 Renners et al. in 1992 reported one case of metastasis of follicular thyroid carcinoma to the paranasal sinuses, including the sphenoid sinus. 10Yamasoba et al. in 1994 reported a case with follicular thyroid carcinoma metastasising to sinonasal tract which also included sphenoid sinus.11 In the same year, Cumberworth et al. reported a case of metastasis of a thyroid follicular carcinoma to the sinonasal cavity which head CT showed sphenoid, ethmoid, frontal and maxillary sinuses. 12In 1997, Altman et al. described a case of follicular metastatic thyroid carcinoma to paranasal sinuses which included the sphenoid sinus. 13 The reported cases of thyroid cancer metastasis to sphenoid sinus are in table 1. Four cases were papillary thyroid carcinoma (included follicular variant of papillary thyroid carcinoma), six cases were follicular thyroid carcinoma, 1 case was medullary thyroid carcinoma and 1 case was unspecified thyroid carcinoma.
Table 1: Cases of thyroid metastases to the sphenoid sinus
Author
Age
Sex
Presenting symptoms
Histologic type
Present case
44
F
Headache, double vision and amenorrhea
Follicular variant papillary thyroid carcinoma
Mandronio (2011)
53
F
Blurring of vision of left eye
Papillary metastatic thyroid carcinoma
Nishijima (2010)
81
F
Epistaxis
Differentiated papillary thyroid carcinoma
Argibay Vasquez (2005)
53
F
Headache, paresthesia in the right eye region and left monocular diplopia
Differentiated carcinoma of thyroid, follicular variant of papillary cell
Altman (1997)
81
F
Progressive headache
Follicular thyroid carcinoma
Freeman (1996)
50
M
Facial pain, proptosis of the left globe and left horner’s syndrome
Metastatic papillary thyroid carcinoma
Yamatosoba (1994)
34
F
Hearing loss in right ear
Follicular thyroid carcinoma
Cumberworth (1994)
62
F
Right nasal blockage
Follicular carcinoma of the thyroid
Renner (1984)
61
F
Profuse right unilateral epistaxis
Follicular thyroid adenocarcinoma
Chang (1983)
50
F
Intermittent epistaxis, weight loss and pain in the right nasopharyngeal region
Follicular carcinoma with papillary foci
Barrs (1979)
54
F
Progressive loss of vision in the left eye
Follicular thyroid carcinoma
Harmer (1899)
44
F
Headache
Medullary thyroid carcinoma
von Eiselsberg (1893)
38
M
Chronic meningitis
Thyroid carcinoma
Pathologic lesions involving the sphenoid sinus include inflammatory disease, mucocele, chordoma, nasopharyngeal carcinoma, plasmacytoma, primary sphenoid sinus carcinoma, adenocystic carcinoma, pituitary adenoma, and giant cell granuloma. Benign disease often presents with a more gradual obstruction and disturbance of vision. This contrasts with the acute and progressive disturbances of vision in all cases reported with malignant lesions of the sphenoid sinus.14
Our patient presented with complaints of double vision for 6 months and headache. After imaging with MRI and given her previous history of metastatic thyroid cancer, the most likely diagnosis was metastases to the sphenoid sinus from the thyroid cancer, which was confirmed by tissue biopsy. Since this patient had evidence of bone metastasis, it is likely that the tumour first metastasised to the bone and then ruptured into the sphenoid sinus. The tumour appears to have eroded the sellar floor, extending into and displacing the pituitary gland, causing secondary hypoadrenalism.
In our patient, low thyroglobulin proved to be an unreliable marker because it was low when the patient had metastasis of the tumour in the spine. These tumours are more aggressive and today, PET scanning has proved more reliable in following them, a modality that was not available at the time for our patient. The possible explanations for negative total body scans in patients with metastatic differentiated thyroid cancer are a) technical limitations of the scan in detecting the tumour cells, and b) failure of the tumour tissue to trap iodine.
There are several unusual aspects in this patient’s presentation. Firstly, the initial presentation was unusual, since this tumour was very aggressive with rare sites of distant metastases. Perhaps the long periods of hypothyroidism when patient was noncompliant promoted the aggressive nature of this tumour. Secondly, the failure of known tumour markers, i.e. serum thyroglobulin and total body scan to identify these metastases. Thirdly, our patient’s tumour cell nuclear DNA was diploid. Investigations have shown that the DNA ploidy pattern as determined by flow cytometry is an important and independent prognostic variable.15-17 Fortunately, aggressive follicular variant papillary cancer of thyroid (non-tall cell type) is very uncommon.
Generally, total body scan negative with low stimulated thyroglobulin is an excellent prognostic sign. Our patient demonstrates that we need to remain vigilant for the unusual tumour especially when the initial presentation showed so much bulky disease. The need for additional tumour markers will help to identify aggressive well differentiated thyroid carcinoma cases.
Acknowledgement
Appreciation is extended to Ms. Deborah Goss and Mr. Timothy O’Mara, librarians, in helping with literature search and preparing the manuscript. No other financial sources or funding involved in the formation of manuscript. No potential financial conflicts of interest.
A 32-year old female with medical history of Diabetes Mellitus (type 2) presents to the outpatient clinic with a 2-day history of pain in the roof of her mouth. She described the pain as severe, throbbing, non-radiating, and unrelieved by analgesics. Fever was absent and there were no symptoms suggestive of an antecedent respiratory tract infection (RTI). She had no history of oral mucosa trauma or burns. She gave a remote history of herpes oralis and aphthous ulcers. Her diabetes is well controlled with Sitagliptan-Metformin and Lantus. An annual dental examination done in the past year was described as “normal” by the patient. She maintains oral hygiene with daily teeth brushing without flossing; she had never used dentures. Further review of systems was negative. On examination she was not in distress and vital signs were normal. No external orofacial or neck swelling was observed. Oral examination revealed dental plagues and periodontal lesions. A 2x2cm tender paramedian mass with a small central ulcer was seen and felt on the hard palate anteriorly (see Figure 1 and 2). There were no pharyngotonsillar lesions or regional lymphadenopathy. Tongue and deglutitive movements were normal. Systemic examination was normal. STD/HIV screening was negative. The clinical picture is most consistent with:
Torus palatinus with aphtous ulceration
Hyperplastic candidiasis
Palatal pleomorphic adenoma
Median palatine cyst
Palatal abscess
Answer
The clinical picture is most consistent with a palatal abscess. Palatal abscess is a pyogenic collection representing a palatally directed drainage of infective pulpal, pericoronal or periodontal process.1, 2The most common origin is from an infection of the palatal root of maxillary premolars or molars.3It presents as a very painful, fluctuant swelling, with lateral or paramedian localization. The surrounding edema may give an impression of midline involvement or contralateral extension.4The prevailing dental plagues and periodontitis present in this patient (her diabetic state abetting), creates a rich source of oral aerobes and anaerobes as well as the environment in which they thrive. An antecedent herpetic or aphthuos ulcer may also be portal of entry for causative microbes. The patient’s oral hygiene status, her diabetic state, the acuity of symptoms and markedly painful presentation are consistent with acute palatal abscess. The absence of fever in this patient does not preclude this diagnosis.
Hyperplastic candidiasis is the result of chronic colonization and superficial oral mucosa invasion by Candida sp, causing chronic inflammatory changes with edema and epithelial proliferation.2The result of these reactive responses is a raised pebbled-like –surfaced lesion. It is most commonly seen under denture sites in denture wearers.5,6The lesion depicted in the picture above is not typical for hyperplastic candidiasis, more so, though not an absolute discriminant, the patient had never used dentures.
Torus palatinus is a wide-based, smooth surfaced, bony protrusion in midline of the hard palate caused by cortical bone growth with a thin, poorly vascularized mucosa lining. The etiology is unclear, but is thought to be multifactorial; genetics (autosomal dominant trait) and recurrent superficial palatal injuries most often implicated.1Torus palatinus is often an incidental finding, though some affected persons may present out of concern for its increasing size or interval development of ulceration or pain in the area of the torus. Pleomorphic adenoma is the most common neoplasm of salivary glands. Though it may occur at any age, pleomorphic adenoma of salivary glands has peak incidence in the fourth to sixth decade of life. Palatal pleomorphic adenoma often presents as a painless, slow-growing tumor. Median palatine cyst is a rare, non-odontogenic lesion of the hard palate that usually presents as a painless, fluctuant swelling. They are composed histologically of a fibrous collagenous tissue wall, with infiltration of chronic inflammatory cells, and lined by stratified squamous and/or respiratory epithelium. Pain is unusual in the above three oral diagnostic entities, when present it arises from ulcerative, hemorrhagic or infective complications. A detailed history eliciting the chronicity of a preceding midline palatal swelling is often helpful. The patient reported normal palatal examination a year earlier, the relative short history, and the acuity of presentation (severity of pain) make torus palatinus, median palatine cyst or palatal pleomorphic adenoma unlikely. See Table 1 for discriminants and differential diagnoses.
Table 1: Differential Diagnoses of Palatal Swelling
Onset and course
Acute
Palatal abscess
Chronic
Torus palatinus, median palatal cyst, pleomorphic adenoma, hyperplastic candidiasis
Shape
Globular
Palatal abscess, torus palatinus, median palatal cyst, pleomorphic adenoma
Palatal abscess, hyperplastic candidiasis, infective or traumatic complications of: torus palatinus, median palatal cyst, pleomorphic adenoma
No
Uncomplicated: torus palatinus, median palatal cyst, pleomorphic adenoma
Associated fever
Yes
Palatal abscess (but may not be present)
No
Hyperplastic candidiasis, uncomplicated: torus palatinus, median palatal cyst, pleomorphic adenoma
Patient attributes
Poor oral hygiene/caries
Palatal abscess
Diabetes/HIV
Palatal abscess
Denture wearer
Hyperplastic candidiasis
The patient underwent definitive treatment with incision and drainage of abscess as well as extraction of her upper left second molar by a dental surgeon. She completed a course of Clindamycin as well as multiple scaling and polishing sessions by a dental hygienist. Maintaining oral hygiene by daily teeth brushing, and flossing, use of mouth antiseptic, as well as a biannual visit to her dentist was recommended.
Patella fractures account for 1% of all fractures but there is little in the contemporary literature regarding outcomes. It is accepted that where fixation is required it needs to be rigid and tension band wiring using cannulated screws or k-wires is the accepted standard.1 Recognised complications associated with this form of fixation occur in up to 15% of cases2 and include; infection, loss of fixation, knee stiffness, post-traumatic osteoarthritis, malunion, nonunion and irritation from hardware.3Thereis nothing in the literature regarding the natural history following fixation.
We report an unusual complication of an osteochondral defect being generated as a direct result of a malunion of a patella fracture previously fixed by a tension band wiring technique.
Case Report
A 35-year old lady presented to our unit after a direct fall on to her left knee with an associated dislocation of her patella that spontaneously reduced on extension, at the time of injury. Three years previously she had sustained a patella fracture that had been treated with tension band wiring. From the time of the original fixation she had experienced mild persistent anterior knee pain, with a reduced range of motion and grinding. She had been discharged from further follow up.
On this presentation, examination revealed that she had a marked knee effusion with a functional extensor mechanism and a range of motion from 0-60 degrees.
The initial radiographs demonstrated that she had broken hardware and an incongruency of the patella suggesting malunion on the articular surface with a residual step (figure 1). In addition, an osteochondral fragment was identified in the patellofemoral joint. Computer tomography was undertaken and confirmed the osteochondral fragment had come from the lateral femoral condyle and a spur like prominence on the articular surface of the patella (figure 2). The mechanism was that this bony spur had been driven into the articular surface of the lateral condyle on dislocation resulting in the osteochondral fragment being generated.
Intraoperative findings confirmed this and measured the osteochondral fragment as 40x15mm (figure 3). In addition it was found that the lateral longitudinal wire had protruded into the joint causing a vertical linear defect in the articular surface of the trochlea.
The osteochondral defect was reduced and stabilized with interrupted 3/0 PDS sutures achieving a smooth articular surface (figure 4). In addition a patelloplasty and a lateral release were performed to remove the bony prominence and restore patella tracking respectively. At 6-month follow up this patient was progressing well with rehabilitation and the majority of her chronic symptoms had resolved.
Figure 1. Lateral radiograph demonstrating an incongruency of the patella suggesting malunion on the articular surface with a residual step
Figure 2. Computerised Tomography confirming an osteochondral fragment that had come from the lateral femoral condyle.
Figure 3. Osteochondral fragment from the lateral femoral condyle measuring 40x15mm.
Figure 4. The osteochondral defect stabilized with interrupted 3/0 PDS sutures achieving a smooth articular surface
Discussion
Although patellae account for 1% of fractures their functional outcome remains largely ignored in the literature. This case presents an unreported complication and highlights that symptoms can remain following the initial fixation that are accepted either by the patient or the treating centre and not further investigated.
Osteoarthritis of the knee remains the most common musculoskeletal complaint in general practice but even then only a third of those with symptoms seek medical advice. Therefore the lack of re-referrals following fixation is not an accurate way to assess outcome following patella fractures treated with this mode of fixation.
Patella fractures represent only a small number of fractures and therefore assessment of treatment and outcomes is problematic, particularly as there is no standardised rehabilitation regimen.
We report on this case as it illustrates a complication of patella fracture fixation that has not been previously described or routinely recognised and, additionally, highlights the fundamental importance of a comprehensive standardised post-operative imaging follow-up regimen. It may be that patients are not currently being correctly counselled regarding the longer-term expectations following patella fracture. A study to define the natural history of patella fractures following contemporary management is needed.
Currently, depression is the leading cause of disability in the world and is predicted to become the second largest killer after heart disease by the year 20201. Eighty percent of individuals with depression report functional impairment while 27% report serious difficulties at work and home life2. According to a study conducted in 2011, India has the highest rate of depression (36%) in low income countries with women being affected twice more than men3. Cancer in children occurs randomly and spares no ethnic group, socio-economic class, or geographical region. An estimated 11,630 new cases are expected to occur among children aged 0-14 years in 2012 in the US, out of which 1,310 will die by end of 2013 due to it4. Based on Karachi Cancer Registry it is estimated that about 7500 children get cancer every year in Pakistan5. The mortality rates for childhood cancers have declined by 68% over the past four decades, from 6.5 per 100,000 in 1969 to 2.1 in 20094. However, the diagnosis of cancer in one’s child marks the beginning of social and psychological devastation for the whole family especially the mother. The length and intensity of treatment can be as distressing as the disease itself, negatively affecting their functionality as parents and in turn the child’s ability to handle the treatment6. As a primary care provider mother’s responsibility increases substantially starting a vicious cycle of anxiety and socio-economic uncertainty leading her to depression much more than the father7. The available data supports that mothers of children with cancer represent a group prone to high levels of emotional distress, and that the period following their child’s diagnosis and the initiation of treatment may be predominantly stressful and disturbing leading them to depression8. Such mothers have difficulty in taking care of themselves, their household and especially their sick children. Many parents continue to suffer from clinical levels of distress, even after five years off treatment of their child7. Many studies have shown that chronic depression and distress may lead to decrease in immune functioning and an increased risk of infectious disease in healthy individuals 9-11. Mothers are generally with the child mainly and hence are most affected from their child’s disease. In this study, we intended to estimate the frequency and severity of depression in mothers having children with cancer.
There is limited evidence from Pakistan regarding depression in mothers of children with cancer. The previous studies conducted had certain limitations such as small sample size, assessment of depression in both parents and that too of children with leukaemia only. This study intends to determine the frequency and severity of depression among mothers of children with cancer.
Methods
A cross sectional survey was conducted in the paediatric oncology clinics at The Aga Khan University Hospital, a teaching hospital in Karachi over a period of six months (September 2011- March 2012). Mothers of children with cancer were enrolled in the study, consecutively according to the inclusion and exclusion criteria. Mothers having children less than 15 years of age with any type of cancer, diagnosed by oncologist (2 months after diagnosis to rule out bias for normal grief period)12, mothers bringing their sick child for the first time to the teaching hospital or as follow up or for day care oncology procedures were included in the study. Mothers who had existing psychiatric illness (and or already diagnosed as having depression by a doctor) and/or taking medications for it, any recent deaths in family (within six months of interview) or having other co-morbidities (malignancy, myocardial infarction in previous year, neuromuscular disease limiting ambulation or blindness) were excluded.
A pre-coded validated and structured Urdu13, 14 and English15, 16 version of the questionnaire was used for data collection the questionnaire took about 20 minutes to complete and consisted of two sections. Section A, included mother’s and child’s demographic details and treatment status. Section B, consisted of Hamilton Depression Rating Scale (HAM-D 17) a validated scale (sensitivity 78.1% and specificity 74.6%) for assessing frequency and severity of depression in both hospitalised patients and the general population15. Scores of < 7 indicate no depression and scores > 7 are labelled as depressed. Mothers who were found to be depressed were further classified into mild (scores 8-13), moderate (scores 14-18), severe (scores 19-22) and very severe depression (scores > 23)16. Mothers with mild to moderate depression were referred to the family physicians; those with severe, very severe, or suicidal tendencies were urgently referred to a psychiatrist.
Institutional Ethical Committee of the Aga Khan University Hospital approved the study. Confidentiality of participants was maintained and informed written consent was obtained.
Sample sizecalculated by WHO software. The prevalence of maternal depression ranges from 56.5% to 61.5% 17, 18 as evident from different international studies. With 95%, confidence interval and bound on error of 10% the sample size came out to be 95. After an addition of 5% for non-responders, the total required sample size was 100 study participants. Data was double entered and analyzed in SPSS version19. The outcome variable was dichotomized as no depression and depression (cut off score7). Analysis was performed by calculating frequencies of categorical variables (maternal age, education, current marital status, employment, co- morbidities, diagnosed depression and treatment in mother, number of children, gender of sick child, cancer type, time since diagnosis of cancer in child, treatment given so far and current treatment status of child and family income). Means and Standard Deviation was reported for current age of the child.
Results
One hundred and sixty mothers were approached out of which 100 mothers consented to participate in the study yielding a response rate of 62.5% (100/160). With regards to the mothers the most common age group was the 30-39 year old category (43%). Fifty-five percent of mothers had a high level of education (those who had completed class 11-12 or engaged in professional education). Nearly all the mothers (98%) were married and were homemakers (95%). Only 5% of mothers were working outside the home. More than half of the participants (57%) had one to three children while 43% had more than three. Monthly financial income for 65% of the participants were more than fifty thousand Pakistani rupees (Table 1).
Table 1: Demographic Characteristics of Mothers (N=100)
Variables
N
%
Age of mother
20-29 years
39
39.00%
30-39 years
43
43.00%
40 years and above
18
18.00%
Education Level of mothers*
No education
13
13.00%
Primary/secondary/intermediate
32
32.00%
Higher
55
55.00%
Marital status of mothers
Currently Married
98
98.00%
Divorced
1
1.00%
Widow
1
1.00%
Maternal Employment Status
Housewife
95
95.00%
Working
5
5.00%
Number of children
1-3
57
57.00%
More than 3
43
43.00%
Family Income
< 20,000
4
4.00%
20,000-50,000
31
31.00%
>50,000
65
65.00%
* (Not Educated: Those who do not have primary education, Primary 1-5 years of schooling, Secondary: 6 to 10 years of schooling, Intermediate: Who have studied class 11 and 12, Higher: Who have completed or engaged in professional education)
The demographic characteristics of child are detailed in Table2. Seventy-five percent of sick children were male while 25% were females (n=100). Half the children were diagnosed with cancer between the age of three to nine. Fifty percent of children (n=50), had their diagnosis of cancer in the last one to five years. More than half of children (57%) were on treatment during study phase. Different types of cancers occurring in children are shown in Figure1.
Table 2: Demographics and social characteristics of sick child (N=100)
Variables
N
%
Current age of child *
6.90(±3.40)*
Gender of Sick Child
Male
75
75.0%
Female
25
25.00%
Age of child at cancer diagnosis
10months-3 years
40
40.0%
3 -9 years
50
50.00%
More than 9 years
10
10.00%
Time since diagnosis of child’s cancer
< 1 year
15
15.0%
1-5 years
50
50.00%
>5 years
35
35.00%
Current treatment status of child
On treatment
57
57.0%
Off treatment
43
43.00%
*Mean (SD) (t-test values)
Figure 1: Frequency of various types of cancer in children (N=100) *Others (BLL, Rhabdomyosarcoma, Glioblastoma, Nephroblastoma) Seventy eight percent of the mothers were depressed. Sixty-nine percent (n= 54) had mild depression, nearly 25% (n=19) had moderate, while 5% (n= 4) had severe and 1% (n=1) had very severe depression.(Table 3)
Table 3: Frequency and levels of severity of Depression in mothers
Variables
N
%
Frequency of Depression (n=100)
Depression present
78
78%
Depression absent
22
22%
Severity of Depression (n=78)
Mild
54
69%
Moderate
19
25%
Severe
4
5%
Very severe
1
1%
Discussion
Depressed patients are frequently encountered in nearly all specialty clinics. However, depression in caregivers accompanying patients is usually overlooked and hence missed, as doctors are mostly focused on the patient’s evaluation, condition, and treatment. When the patient is a child and the diagnosis is cancer, this difficult circumstance has a sudden and long term impact on both the child and the family. Many parents of a child with cancer will have very strong feelings of guilt. As such, parents of cancer survivors may be at risk for impaired physical and mental health. An increasing body of literature supports the conclusion that various levels of parental distress are ongoing, long after treatment is completed 19, 20.
The prevalence of depression in mothers in this study was as high as 78%. Mild depression was seen in 69% of mothers, moderate in 25%, severe in 5% while 1% had very severe depression. This high prevalence of depression in such mothers has not been reported from Pakistan before. The soaring levels of depression however have been consistent with the study conducted in Turkey in 2009 in mothers of children with leukaemia21 where 88% (n=65) mothers were depressed. Mild depression was reported in 22.7 % (n=18) and major depression in 61.5% (n=40). Similar results were reported from a study conducted on both parents of children with leukaemia in 2002 in Pakistan where 65% (n=60) of mothers were found to be depressed 17. Nevertheless, severity of depression in this study was not noted. A Sri Lankan study in 2008, showed moderate to severe depression to be 22.9% and 21.9% in mothers having children with mental and physical disorders respectively22. Another study conducted in Florida in 2008 suggests that an increased symptom of depression in mothers is related to significantly lower ratings in quality of life for their children18.
The existing data supports the argument that mothers of children with cancer represent a group prone to high levels of emotional distress. The time following their child’sdiagnosis and the commencement of treatment may be particularly stressful and traumatic 23 with an incidence as high as 40% 24-26. There could be multi-factorial reasons for this alarmingly high rate of depression seen in Pakistani mothers. One of the causes could be the political instability that Pakistan has been facing for past few years leading to economic volatility. The study conducted in 2002 in Karachi saw 65% of maternal depression17 which has now risen to 78% in this study. Due to political unrest, everyday strikes, bombasts, these mothers may also have difficulty in reaching hospital on scheduled visits leading to postponement of treatment. Other reason could be economic inflation. The cost of daily living has soared while allocated medical budget was 0.27% of its gross domestic product (GDP) on health in 2011-12, which is insufficient to cater the needs of the population (Economic Survey of Pakistan of 2011-2012).
Lately, there has been a recent trend towards nuclear families in Pakistan rather than living in extended families as before27. This in turn may lead to mother being the soul person in looking after the sick and her healthy children as well as managing house chores and doctor’s appointments leading to more frustration. This study also showed that 57% mothers had three children while 43% had more than three children. This could also be one of the factors for high rate of depression as looking after multiple children is demanding and may lead to decreased coping skills of mothers.
Other possible reason for this high rate of depression could be that mostly educated mothers were visiting the hospital that have access to internet and can search up all details, good or bad, on their child’s disease. This may start a vicious circle of worry for mothers. Other possible reasons for this growing depression could be gender of child (as in this society male child is thought to be the support and bread earner of the family), child’s current treatment status and time since diagnosis of cancer in child.
Strengths and Limitations
To the best of authors’ knowledge, this study has touched upon a topic that was not yet been attended to, in local context. Moreover, in this study adjustment phase of two months, for acute stress and posttraumatic stress disorder was given for diagnosis of depression in mothers. It was done to rule out bias in study. HAM-D also focuses on symptoms in the past 1 week, to minimize the recall bias. The findings in this study offer evidence and importance of the need for developing psychological support for families especially mothers who are caring for a child with cancer, in Pakistan.
This study has several limitations. The study was conducted in a tertiary care private hospital, which mostly caters a specific segment of population. Hence, the results may not be a true representation of the population. All data in this study was self-reported by the participants. Thus, it is anticipated that there may be some bias in their responses and recall. Lastly, since this was a cross-sectional study so temporality is difficult to establish.
Conclusion
In conclusion more than three-fourth of our study participants were depressed.
The outcome is expected to identify depressed mothers so that effective strategies can be developed to enhance their coping skills and medically treat them when required. This in the long term is expected to increase quality of life for both their sick and healthy children as well as mothers themselves.
Future Research and Policy Recommendations
Future studies are recommended in order to confirm our findings. Such studies need to be conducted on a larger scale, at national level, in various hospitals and settings to counteract limitations of our study with appropriate means of measuring depression in mothers. Factors, not explored in this study such as personality styles and coping skills of mothers can be explored as these may be significant aspects leading to depression. Further co-morbidities, such as anxiety and post traumatic stress disorder symptoms related to child’s cancer should also be investigated.
Other associated factors, such as the political and economic situation, which perhaps may also be a leading cause of depression in our part of the world, should also be assessed. Simultaneously, measures should be taken to root such factors out at national levels.
The results of current study show the need of incorporating mothers into a treatment process designed for psychological interventions, not only after the diagnosis of cancer in their child but also during their child’s treatment. Psychosocial services should be recognised as an important constituent of comprehensive cancer care for families of children with cancer.
It is highly advocated that the healthcare professionals who work with the families of children with cancer should evaluate the children and their families concerning the psychological and social aspects of their lives. Arrangements for family counselling for those needing help should be made. Mothers should also be referred to family physicians and social support if available. The mother’s crucial position in the family and the proximal and distal effects of her adaptation to the crisis of cancer in the family should lead to the design of interventions intended at decreasing her distress and at promoting her adaptive coping skills as improving mothers’ problem-solving skills has been associated with reductions depression and anxiety28. Thus, all hospitals, dealing with paediatric cancer cases should have a family counselling and support system.
Diabetic patients with peripheral neuropathy are predisposed to foot injury. In Asian countries, a common culture among patients with peripheral neuropathy is to immerse their feet in hot water baths, with a belief that it will “improve circulation” and hence “cure the numbness”. We hereby report three cases of severe burn injuries of the feet presented to our hospital over a span of six months due to the above belief.
Case Report
The first patient was a 53-year old Malay gentleman with poorly controlled diabetes mellitus for six years, complicated with peripheral neuropathy, diabetic nephropathy and right eye cataract (latest HbA1C 8.1%), treated with oral anti-diabetic agents. He had a habit of using hot footbaths for numbness of both feet. Two weeks prior to presentation, due to increased feeling of numbness, he immersed his right foot into a self-prepared tub of hot water with added salt, followed by application of traditional sea cucumber gel. That evening, he noticed blistering of his right foot. Despite advice for admission, he chose to do the dressing as an outpatient in a local clinic. He presented two weeks later due to a worsening wound. At presentation, 4% full thickness burn of his right foot was noted, complicated by secondary infection (Figure 1). He underwent wound debridement, and subsequent split skin grafting. He had a prolonged hospitalization of five weeks due to secondary pseudomonas wound infection requiring parenteral antibiotics.
Figure 1. Right lower limb upon presentation to our hospital
The second patient was a 26-year old Indian gentleman with type I diabetes mellitus for nine years, complicated with diabetic nephropathy and peripheral neuropathy. His wife usually prepared hot water footbaths for him to improve his feet circulation. He developed 5% full thickness burn when he immersed his right foot into a pail of boiling water, not knowing that his wife had not added cold water into the footbath. He presented himself after two days and was hospitalized for two weeks. He recovered after wound debridement and split skin grafting.
The third patient was a 17-year old Chinese lady with poorly controlled type I diabetes mellitus for eight years, complicated with diabetic nephropathy (latest HbA1C 10.0%). She used hot water steam therapy with an aim to cure her recent onset of left foot drop, but was unaware of the temperature of the water. She developed blisters on her left foot, but only presented herself two weeks later when she developed left foot gas gangrene. She had a prolonged hospital stay of eight weeks with recurrent hospital acquired infections, including Methicillin-resistant Staphylcoccus aureus (MRSA). Despite multiple wound debridement, she required amputation of her left fifth toe (Figure 2).
Figure 2. Left lower limb post Ray amputation
Discussion
Peripheral neuropathy is a known complication of diabetes mellitus. More than 50% of patients who are over 60 years old have this complication.1, 2 Thermal injury to the feet in patients with neuropathy has been reported after walking barefoot on hot surfaces3 and after application of hot water bottles or heating pads during winter months.4, 5 The use of thermal footbath as a cause of burn injury is mostly due to patient-misuse or ignorance of correct usage.6, 7 In contrast, in Asian countries, a common culture among patients with peripheral neuropathy is to immerse their feet in self-prepared hot water without checking the water temperature,8 with a belief that it will “improve circulation” and hence “cure the numbness”. This practice has led to accidental burn injuries as described in our case reports.
There are a few reasons why patients with diabetic peripheral neuropathy end up with such a severe complication after the use of thermal footbath. Firstly, the temperature of the thermal bath may be underestimated. The time to develop full thickness burn reduces exponentially with just minimal increments in water temperature.9 Secondly, lack of pain despite the burn can prolong exposure to the heat source. In addition, concomitant peripheral vascular disease and endothelial function can limit vasodilatation to conduct heat away hence further aggravate the thermal insult.
Another important contributing factor of complicated wounds are the delays in seeking treatment as the result of lack of pain despite the burn injury. In a study done by Memmel et al on 1794 patients (of which 130 were diabetics) who presented with burn injuries, the majority of non-diabetic burn patients (63%) presented within 48 hours of injury, but only 40% of diabetic patients sought treatment within that time frame. Significantly more patients with diabetes presented after two weeks compared to those without diabetes. As burn injuries are highly susceptible to secondary infection, any delay in presentation further complicates and prolongs hospital stay.10,11 Not surprisingly, our two patients who presented two weeks after their burn injury had a prolonged and complicated hospital course compared to our second patient who presented soon after the burn injury. Increased susceptibility to infection and delayed wound healing from poor circulation contribute to prolonged recovery and poorer clinical outcomes in patients with diabetes mellitus, with some needing amputation as noted in our third patient.
As a healthcare provider we play a role in preventing this misfortune. Routine screening for the presence of peripheral neuropathy and vascular disease should be done during clinic visits to identify high-risk patients. Specific education regarding avoidance of thermal footbath and consequences of this highly preventable injury should be incorporated into standard diabetic foot care education. If patients choose to immerse their feet in hot water, temperature of the water should always be measured with a thermometer and immersion time should be limited. If a wound develops, they should present early to hospital for immediate treatment.
Conclusion
Thermal footbath for therapeutic purposes is commonly practiced in Asian culture. Our case reports highlight the serious consequences of this practice in diabetic patients with peripheral neuropathy. More public awareness and patient education is needed to prevent these injuries and to avoid the high cost of prolonged hospital stay and losses to the patient.
Organ transplantation is an effective therapy for end-stage organ failure and is widely practiced around the world. According to World Health Organization (WHO), kidney transplants are carried out in 91 countries. Around 66,000 kidney donations, 21,000 liver donations and 6000 heart transplants were performed globally in 2005. 1 In India the rate of organ donation is only 0.16 per million populations, compared to America's 26 and Spain's 35.2 The shortage of organ is virtually a universal problem. Though many efforts were undertaken by the government to motivate the public towards donation of organs, the rate of organ donors has not paralleled the growing waiting list3,4, 5 and inadequate organ donation in India remains a major limiting factor for transplantation. There are several factors which could facilitate and hinder the general public to donate a organ. Identifying these factors could help in planning effective strategies to combat the problem. Hence the present study was conducted with the aim to explore the general publics perceived barriers and facilitating factors of organ donation.
Materials and methods
The present study was a cross sectional, exploratory survey conducted among the general public of Puducherry U.T, India. 400 eligible subjects who fulfilled the following criteria were included a) Subjects aged 18 and above, and b) who understand either the local language Tamil or English. Subjects with intellectual, psychiatric and emotional disturbances that could affect the reliability of their responses were excluded from the study. The population registry in the primary health centers of the selected community area was used as a sample frame to select subjects randomly. Every eligible subject was explained about the purpose of the study and signed a written consent form. Formal ethical clearance was obtained from the institute ethics committee before actual data collection procedure.
Preparation of the questionnaire
An extensive literature review was carried out to understand the possible barriers and facilitators reported in the past. Reported barrier and facilitating factors in the literature were included in constructing the questionnaire, including specific cultural and religious oriented items specific to Indians. Subject’s intention to donate the organ was assessed using a single dichotomous question (yes or no). For assessing the barriers and facilitators related to organ donation a questionnaire with a total of 18 items (9 items each) was prepared in the form of closed ended question i.e. yes or no. Along with closed ended questions, an open ended question i.e. any other? was also included for obtaining an extended response apart from the framed questions. As knowledge is an important factor which could serve both as a barrier and facilitator for organ donation, 8 items related to knowledge were also included as a part of the questionnaire. Knowledge items of the questionnaire were evaluated by assigning a score of 1 for each correct response with a maximum possible score of 8. Interpretation of the knowledge component was also done by categorizing the knowledge as follows - Below 50% of the total score - Inadequate knowledge, 51 – 75% - Moderately adequate knowledge, above 75% - Adequate knowledge, for ease of understanding. The draft tool was validated for its content by 10 experts from the field of surgery, medicine, nursing, anthropology and psychology for its appropriateness. After appropriate modification the content validity index for the tool was calculated and it was found to be highly valid (0.98). The reliability of the tool was estimated by a test re-test reliability method among 10 subjects with an interval of 2 weeks from the first and second time of administration of the questionnaire. It was found to be highly reliable with reliability coefficient of 0.91. A face to face interview method was used to collect data from each subject. Collected data was analyzed using SPSS for windows version 14 (SPSS Inc., Chicago, Il, USA) with appropriate descriptive and inferential statistics. A probability value of < 0.05 was set as the level of significance
Results
Basic Demographic details
Of the total 400 subjects enrolled the majority were male (56%), between the age group of 31-40 years (48%), and followed Hinduism (68%) at the time of interview. Most of the subjects were literate (70%) with education up to high school and resided in a rural area (53%).
Knowledge regarding organ donation
The mean knowledge score of the subjects regarding organ donation was 4.74 1.45 score which ranged from a minimum score of 1 to a maximum score of 8. Most subjects responded correctly to questions related to organ matching (85.3%) and consent procedure (84.7%). Details of different aspects of knowledge regarding organ donation of the subjects can be found in Table 1. When subjects were asked about the source of information regarding organ donation, 51.3% of the subjects reported that they gained knowledge through television, 23% from health personnel, and 12% from friends and 7% through books and internet (Figure1). Whilecategorizing knowledge scores the majority of the subjects (38.6%) had inadequate knowledge, 50.6% had moderate knowledge and only 10.6% had adequate knowledge regarding organ donation.
Intention to donate organs: Barriers and Facilitators
Of the total 400 subjects interviewed 69.75% of the subjects reported that they wish to donate their organs, whereas the remaining 30.25% reported that they will not donate their organs either during their life or after their death. Subsequently the factors for barriers and facilitators were also analyzed using the pretested questionnaire. The most common barriers perceived by the subjects related to organ donation were as follows, ‘family opposition’ (82.8%), ‘complicated organ donation procedure’ (69%), ‘fear that donation affects their future’ (58.36%), and ‘misuse of organs’ (55.2%). More information about barriers is detailed in Table 2.The most important facilitating factors of organ donation as reported by the subjects were ‘thought of saving someone’s life’ (95.9%), ‘feeling of improved sense of humanity’ (95%), ‘to save the life of a close relative’, ‘thought that their organ live after their death (92.6%) and ‘being a role model for others’ (77.7%). More details of facilitating factor can be seen in Table 3
While associating the subject’s intention to donate organs with demographic variables like age, gender, residence, education, religion, marital status, type of family and knowledge; only educational level had a significant association with the subject’s intention to donate organ. Specifically graduate people are more likely to report intention to donate organ their organs than others (p<0.001).
Figure 1: Distribution of source of information regarding organ donation among the subjects.
Table 1: Item wise distribution of different aspects of knowledge regarding organ donation (n=400)
S. No
Aspects of Knowledge
Correct response
Incorrect response
1.
Definition of organ donation
24%
76%
2.
Knowledge regarding Commonly donated organ
71.3%
28.7%
3.
Knowledge regarding Consent procedure for living donor
76%
24%
4.
Knowledge regarding Consent procedure after death
84.7%
15.3%
5.
Knowledge regarding Consent for mentally retarded person
41.3%
58.7%
6.
Knowledge regarding Consent for unclaimed dead bodies
35.3%
64.7%
7.
Knowledge regarding Organ matching procedure
85.3%
14.7%
8.
Knowledge regarding legal consideration for organ donation
56%
44%
Table 2: Perceived Barriers towards organ donation (n=121)
S. No
Barrier factors
Percentage
1.
Oppose from the family
82.8%
2.
Fear
72.4%
3.
Procedures are complicated
69%
4.
Affects physical appearance
65.5%
5.
Affects the future
58.6%
6.
Create psychological problem
58.6%
7.
Organs could be misused
55.2%
8.
Against religious belief
48.3%
9.
Insults human rights and dignity
48.3%
Table 3: Perceived Facilitators towards organ donation (n=279)
S. No
Facilitating factors
Percentage
1.
Save someone’s life
95.9%
2.
Improve the sense of humanity
95%
3.
Save the life of a close relative
92.6%
4.
Wishes organ to be alive after death
92.6%
5.
To become a role model
77.7%
6.
Empathy for others
53.7%
7.
Rewarding experience
51.2%
8.
Due to family pressure
29.8%
9.
For economic benefit
27.3%
Discussion
The current study was conducted with the aim to explore the general publics intention towards organ donation and to identify the perceived barriers and facilitators. The present study revealed that 69.7% of the subjects have an intention to donate their organs either during their life or after their death, which is similar to the finding of Chung et al6 and Shahbazian H et al7. Similar to the previous studies8 the current study also confirmed a positive association between public intentions to donate their organ with their educational status. Though many studies in the past reported attitudes9,10 of public towards organ donation, the present study was the first of its kind to analyze specifically the barriers and facilitators of organ donation among the general public, this adds strength to this study. The most common barrier reported in the present study was ‘opposition form family in donating their organs’; these findings were similar to a previous study.6 Illegal organ donation and misuse of organ is a major problem in India for the low organ donation rate among public11, this fact was reflected even in the current study as 55.2% of the subjects reported misuse of an organ as barrier to organ donation. The most important facilitating factors of organ donation reported in the present study was ‘thought of saving someone’s life’ (95.9%), ‘feeling of improved sense of humanity’ (95%), ‘to save the life of a close relative’ (92.9%), these finding were similar to the findings of Neelam et al conducted in India12. The majority of the respondents in this study reported "lack of information" about organ donation and transplantation. These findings are comparable with those reported from previous studies, which all indicate the importance of public education about the importance of organ donation13,14,15,16. Our study identified that the principle respondents' source of information about organ donation was the television (TV). The contribution of other sources of information in providing respondents with knowledge about organ donation was minimal. Generally, studies had shown the importance of visual media in increasing the awareness of the public about organ donation. 17,18
Conclusion
Better knowledge may ultimately translate into the act of donation. Effective measures should be taken to educate people with relevant information with the involvement of media, doctors and religious scholars.
Population-based studies indicated that diabetes remains as a nationwide epidemic that continues to grow tremendously affecting 25.8 million people or 8.3% of the US population.1 This number is expected to reach 68 million or 25% of the population by 20302 as incidence of obesity is rising.3
The American Diabetes Association (ADA) recognizes diabetes education (DE) as an essential part of comprehensive care for patients with diabetes mellitus and recommends assessing self-management skills and knowledge at least annually in addition to participation in DE.4 With the objective of improving the quality of life and reducing the disease burden, the ADA and the U.S. Department of Health and Human Services through its Healthy People 2020 program have emphasized three key components for effective disease management planning: regular medical care, self-management education and ongoing diabetes support.5,6
The hallmark of preventing the chronic complications of diabetes lies in optimizing metabolic parameters such as glycaemic control, blood pressure, weight and lipid profile. Pharmacologic intervention can only do so much in achieving treatment goals. It should be complemented with appropriate DE emphasizing dietary control, physical activity and strict medication adherence.7,8 Adequate glycaemic control is clinically important because a percentile reduction in mean HbA1C is associated with a 21% reduction in diabetes-related death risk, 14% reduction in heart attacks and 37% reduction in microvascular complications.9
Diabetes self-management (DSM) education programs are valuable strategy for improving health behaviours which have significant impact on metabolic parameters.10 This is supported by chronic care model that is based on the notion that improving the health of patients with chronic diseases depends on a number of factors that include patients’ knowledge about their disease, daily practice of self-management techniques and healthy behaviors.11,12,13
A systematic review by Norris et al. has shown that DSM training confers positive effect on patients’ knowledge about diabetes, blood glucose monitoring, and importance of dietary practices and glycaemic control.14 In another retrospective observational study, evidence has suggested that participation in a multifactorial diabetes health education significantly improved glycaemic and lipid levels in the short term.10
Diabetes education/support group provides a comprehensive patient education, fosters a sense of community, and engages the patients to become active part of a team managing their diabetes. The diabetes support group at Queens Hospital Centre provides services to a diverse population from different socioeconomic backgrounds and is offered to any patients with diabetes. It is facilitated by certified diabetes nurse educators in the hospital and in the clinic. Patients meet once a month per session and are provided education in self-management of diabetes, education in medication, diet, lifestyle modifications, regular exercise, weight management and translation in their respective languages, if needed.
Few researches have been conducted comparing the efficacy of DE and combination of diabetes education and peer support group (DE+PS) in improving the metabolic parameters of patients with DM. In patients with DM, the primary objective of this study was to assess the clinical impact of DE and combined DE+PS group on metabolic parameters such as lowering HbA1C, reducing weight or BMI, controlling blood pressure, and improving lipid profile.
Methods
The study subjects were identified through retrospective review of electronic medical records of adult patients aged more than 18 years old with diabetes and being treated at the Diabetes Centre and/or Primary Care Clinic of Queens Hospital Centre, Jamaica, New York from January 01, 2007 to June 01, 2011. A total of 188 study subjects were selected and assigned to three groups: (1) control group (n=62), who received primary care only, (2) DE group (n=63), who received diabetes teaching from DM nurse educator in addition to primary care, and (3) DE+PS group (n=63), who received both diabetes education and attended at least 2 or more sessions of peer support group in addition to primary care. The subjects in control group, education group, education plus peer support group were matched on age, sex, weight and BMI. Considering the data availability, the duration of follow up measured in each group varied; the control group was followed up for 8 months, the DE group for 13 months and the DE+PS group for 19 months. The changes from mean baseline to the third month, sixth month and final follow up period were calculated for the following metabolic parameters: HbA1C, weight, BMI, SBP, TC, HDL-C, LDL-C and TG-C. T sample T-test was used to compare statistical differences in the mean changes in the metabolic parameters in each group from baseline to follow up period. All data management and statistical analyses were conducted with MiniTab version 14. A p-value of less than 0.05 is considered statistically significant.
Results
Among the 188 study subjects included in our study between ages 20 to 88 years with mean age of 60, the predominant gender was female (n=132, 70%). African American makes up the majority (n=74, 39%), followed by Asian (n=40, 21%), Caucasian (n=34, 18%), Hispanic (n=22, 12%) and Indian (n=18, 10%). Majority of our patients with DM have concurrent hypertension (91%), hyperlipidemia (90%), and obesity (47%). See Table 1 for baseline demographics.
Table 1. Baseline demographic characteristics of the study population
Control [C] N=62
Diabetes Education [DE] N=63
Diabetes Education + Peer support [DE+PS] N=63
Baseline Characteristics
Age range (years) [median]
32-76 [61]
20-88 [58]
26-86 [62]
Sex-male [N (%)]
22 (35)
20 (32)
14 (22)
Race
African American
31 (50)
26 (41)
17 (27)
White
11 (17)
23 (37)
0 (0)
Indian
18 (29)
0 (0)
0 (0)
Asian
1 (2)
10 (16)
29 (46)
Hispanic
1 (2)
4 (6)
17 (27)
Comorbidities [N (%)]
Hypertension#
54 (87)
59 (94)
58 (92)
Hyperlipidemia¥
56 (90)
61 (97)
53 (84)
Obesity*
29 (47)
29 (46)
31 (49)
Active cigarette smoker
6 (10)
5 (8)
1 (2)
# Hypertension is defined as mean systolic blood pressure > 140 mmHg and/or diastolic > 90 mmHg measured on two separate occasions. These patients have either hypertension diagnosed prior to or after diagnosis of DM. ¥ Hyperlipidemia is defined as LDL > 100 mg/dl in patients with diabetes and diagnosis hyperlipidemia could be before or after diagnosis of DM. * Obesity is defined as body mass index (BMI) of at least 30 kg/m2 or greater.
The group analysis showed that the DE group had a statistically significant decrease in mean HbA1C (mean change: -0.78%, p=0.013), TC (mean change: -16.89 mg/dL, p=0.01) and LDL-C (mean change: -11.75 mg/dL, p=0.04) from baseline to final follow up (see Table 2). The DE group had non-significant mean weight gain of 2.17 pounds and BMI of 0.52 kg/m2.
* Final follow up varies for the three groups. 8 months for control (C), 13 months for education (DE) group and 19 months for education plus peer support (DE+PS) group
Although DE+PS group were observed to have decreased in mean HbA1C (-0.48%), weight (-0.38 pounds), SBP (-3.24 mmHg), TC (-4.43 mg/dL) and TG-C (-12.89 mg/dL) and increased in HDL-C (+095 mg/dL), they were not statistically significant from initial to final follow up period. There were greater improvements in HbA1C and SBP from baseline to final follow up in DE+PS group compared to the control group. Only the control and DE+PS groups showed a decrease in weight from initial to final follow up.
Between the two intervention arms, the DE group exhibited greater reduction compared to DE+PS group in mean HbA1C (-0.78 vs. -0.48%), SBP (-3.78 vs. -3.24 mmHg), TC (-16.89 vs. -4.43 mg/dL), LDL-C (-11.75 vs. +0.08 mg/dL) and TG-C (-14.75 vs. -12.89 mg/dL).
Discussion
Our results suggested that among patients with DM, the subjects who participated in DE exhibited significant reduction in baseline HbA1C, TC and LDL-C compared to control. Furthermore, the significant impact of DE alone on optimizing control of HbA1C and LDL-C appeared to persist through time. In addition patients who received DE+PS also demonstrated moderate improvement in HbA1C, SBP, TC and TG-C and HDL-C even though they were not statistically significant on final follow up. It must be noted that the baseline mean HbA1Cs were higher in both interventions DE and DE+PS groups compared to control group and this may be associated with greater reduction in HbA1C in the intervention groups and may skew the finding. Our study results showed that DE group had greater percentage reduction in HbA1C (9%) compared to DE+PS group (5%) from baseline to the first follow up. The average change in HbA1C and LDL-C levels recorded in our study is similar to what has been reported in a previous study which showed significantly greater improvement in mean glycaemic levels and LDL-C levels in patients who participated in DE.10
However our findings are in stark contrast to a previous study that showed that DE+PS intervention has led to substantially greater weight reduction and improvement in HbA1C at second month post-intervention compared to education and control group.15 This difference may be accounted for by the effect of sample size and the duration of follow up. The DE+PS group in our study included twice the number of patients being sampled compared to previous study (63 patients vs. 32 patients), and longer duration of follow up (19 months vs. 4 months)15. These differences are significant as they can influence the data trend.
In general, all groups had improvement in HbA1C, TC, TG-C levels, and SBP (though not significant). Only control and DE+PS groups had weight reduction and DE group had weight increase. Although the DE+PS group had improvement in most of the metabolic parameters they were not statistically significant throughout the entire follow up period compared to DE group. This scenario might be attributed to retrospective nature of the study, possible non-compliance of patients to medications, differences in duration of follow up between groups, and limited number of patients sampled thus hindering the appreciation of potential significant effect. The statistically significant differences in baseline HB A1C among the three groups could also explain the differing magnitude of change from baseline; DE group had higher baseline HbA1C compared to control group (9.3 vs. 7.5%; p=0.00) allowing for a greater change from baseline value. Similarly in DE+PS group, baseline HbA1C was considered statistically significant compared to control group (8.3 vs. 7.5%, p=0.018).
A previous randomized controlled trial assessing the effect of peer support on patients with type 2 diabetes with a 2-year follow up demonstrated no significant differences in HbA1C (-0.08%, 95% CI -0.35% to 0.18%), SBP (-3.9 mmHg, -8.9 to 1.1 mmHg) and TC (-0.03 mmol/l, -0.28 to 0.22 mmol/l).16 It was suggested that the effect of DSM education on glycaemic control is greatest in the short-term and progressively attenuated over time and this may suggest that learned behaviour changes with time.17,18 However, the result of the present study showed a persistently significant beneficial effect on HbA1C and LDL-C from the earliest follow up until the final month for patients receiving DE alone.
Previous meta-analysis of randomized trials of DSM education programs by Norris and colleagues (2002) demonstrated the beneficial effect of DE with estimated effect on glycaemic control (HbA1C) at -0.76% (95% CI: 0.34,1.18) compared to control immediately after the intervention.17 However, the findings of the present study on the effect of peer education are in direct contrast with the results of the randomized trial using the Project Dulce model of peer-led education showing significant improvement from baseline to the tenth month of follow-up in HB A1C (-1.5%, p=0.01), TC (-7.2 mg/dl, p=0.04), HDL-C (+1.6 mg/dl, p=0.01) and LDL-C (-8.1 mg/dl, p=0.02).19 This could be accounted for the different baseline values of the metabolic parameters in the present study, thus creating a bias in the magnitude of change.
It has been suggested that the most effective peer support model includes both peer support and a structured educational program. The emphasis on peer support is based on the recognition that people living with chronic illness can share their knowledge and experiences to one another.20 It has been observed that participants in peer support groups were not interested in the topic of diabetes itself but on the effect and meaning of the disease on the lives of the patients.21
There are a number of limitations to be taken into consideration when interpreting the results of our study. Since our study is a retrospective review of medical records, the data collection was limited to availability of the required clinical data. Some parameters were not possible to obtain on a consistently uniform time frame. This resulted in varying mean duration for the 3 study groups (8 months for control group, 13 months for DE and 19 months DE+PS group). Because of unavailability of some of the clinical parameters at a specific time frame, there were variables missing on the earlier follow-ups. Our study also examined the effect of the intervention over a relatively short time. A longer-term study is necessary to determine if the intervention has lasting impact on improving the metabolic parameters, uplifting the quality of life and preventing morbidity and mortality from diabetes. The limited sample size could also be important factor that may influence the generalizability of the data. The differing baseline values in the metabolic parameters could have blunted the appreciation of possible significant improvement in the metabolic parameters in the DE+PS group. Other confounding factors that were not analysed in the present study and could have affected the results include the use of insulin regimen among the different groups, initiation of additional oral hypoglycemic agents, medication adherence by the patients and adjustment by physicians, and whether the patients were seen by endocrinologists or not.
The present study suggested that participation in DE may assist with optimizing HbA1C, TC and LDL-C. The DE group had improvement in glycaemic control and other metabolic parameters. The significant metabolic improvement gained from DE appeared to be sustained over time. However, participation in both DE+PS showed relative improvement but not significant as it is likely due to confounding different baseline metabolic parameter and duration being compared. Our findings underscore the importance of DE as part of the treatment plan for patients with DM. The addition of peer support group may or may not contribute to significant improvement of metabolic parameters.
Electroconvulsive therapy (ECT) is an effective treatment for some individuals with severe neuropsychiatric illness. It is widely used to treat certain psychiatricdisorders, particularly major depression.1,2 ECT involves applying a brief electrical pulse to the scalp after the patients are administered muscle relaxants and general anaesthesia.3 This pulse excites the brain cells causing them to fire in unison and produce a seizure.
In 2003, the National Institute of Clinical Excellence (NICE) issued guidance on the use of ECT. Its use was recommended only to achieve rapid and short-term improvement of severe symptoms after an adequate trial of treatment options has proven ineffective and/or when the condition is considered to be potentially life-threatening in individuals with severe depressive illness, catatonia or a prolonged manic episode.4
The mechanism of action of ECT is not fully known. ECT affects multiple central nervous system components, including hormones, neuropeptides, neurotropic factors, and neurotransmitters. The induction of a bilateral generalized seizure is required for both the beneficial and adverse effects of ECT. Certain parameters like seizure duration, electric stimuli, seizure threshold, ECT practice factors and medication can influence its effectiveness. The degree to which electrical stimulation exceeds the seizure threshold, the positioning of electrodes on the head, pulse width, pulse frequency and seizure duration are all known to be important.5 This study aims to review the evidence base of these parameters in detail. The seizure duration and electric stimulus are the two critical parameters and are therefore the main focus of this review.
Literature Review
A review of literature regarding ECT was using search engines like MEDLINE, PsycInfo, and OVID using the key words “electroconvulsive therapy,” “seizure parameters,” “seizure duration,” “seizure threshold,” “stimulus dosing” and “effectiveness.”
Parameters Associated with Effectiveness of ECT
Seizure Duration Electrical Stimulus Seizure Threshold ECT Practice Factors Endocrine Factors Medication Other Parameters
Relationship between Seizure Duration and Effectiveness of ECT
Very little is documented on clinical studies that correlate ECT effectiveness and seizure duration. There is evidence that supports the direct relationship of seizure duration and the effectiveness of ECT. It was thought that measuring the seizure duration and the knowledge of measuring such parameters can help explain its therapeutic effect.6 There has been research which suggests that motor seizures of less than 15 seconds in duration do not exhibit tonic-clonic phases and are ineffective in treatment.7 Some of the studies in past years found a direct relationship between total seizure duration during a course of treatment and patient response to ECT.8
A retrospective study on ward patients found that a positive clinical outcome from depressive symptoms has a direct relationship with accumulative seizure time in the course of therapy.8 However, the study was neither randomized nor controlled. Stimulus intensity, diagnosis, and concurrent medication parameters were not properly considered. Another study that supports the correlation found that 88% of patients with cumulative seizure time of 300 seconds and over had a favourable response. The data was retrospectively and prospectively collected in a university hospital. It was mentioned that data gathering was very difficult specifically with regard to the variable number of patients’ ECT sessions; the confounding effect of medication and the treatment of different patients using unilateral or bilateral.9
However other studies challenge these statements. A prospective study of a sample of depressed patients undergoing ECT, the seizure duration did not correlate with Hamilton Depression Rating Scale (HAM-D) scores after treatment. However, it was found that significant nonverbal memory loss of patients was correlated with seizure duration.10 The seizure duration does not directly influence the frequency of ECT, longer seizures do not equate to fewer ECT treatments. Studies using HAM-D scores do not support the idea that seizure duration is a variable correlated to efficacy.11 Short seizures during ECT for few patients are the result of a medical condition or drug treatment interference. On the other hand, patients who have been subjected to ECT treatment encounter shortened seizures.12
There are studies which show that the length of the cerebral seizure activity or the tonic–clonic convulsion is not related to clinical effectiveness.6,13 However, the treating psychiatrist should question whether, or not, generalised cerebral seizure activity had occurred if, at the first treatment, the convulsion lasted less than 15 seconds or the EEG recording showed seizure activity lasting less than 25 seconds.14 Such brief seizure activity might be the result of a focal or partial seizure, and therefore be of questionable therapeutic efficacy. It has been noted that there are patients who recover with ECT and yet display only short tonic–clonic convulsions. This may be more likely in elderly patients.
Most recent evidence mentions that the quality of cerebral seizure activity and the quality of the desired activity cannot simply be related to its length in time alone. It is recommended that the convulsion be timed from the end of electrical stimulation to the end of generalised, that is, bilateral, clonic activity. EEG monitoring can also be done but one needs to have good experience using this technique and sometimes artefacts can cause misinterpretation of the results.15
Relationship between Electric Stimulus and Effectiveness of ECT
ECT is administered by a constant-current, brief-pulse ECT machine that is able to deliver a wide range of electrical dose, that is, 25–50 mC up to 750–800 mC. It is recommended that new machines deliver a range of dose from 25 to 1000 mC.15 One of the important parameters in predicting clinical response is the degree to which the electrical stimulus exceeds the seizure threshold.16 The maintenance of adequate seizure duration on patients is a complicated issue. Elderly patients are also more susceptible to cognitive side effects than younger patients.17 Patients regularly treated with ECT have records of shorten seizure duration over time, and clinicians need to increase stimulus to maintain duration, which in the long run can lead to complications.18
Electroencephalography (EEG) Findings
Voltage Suppression Studies. Postical voltage suppression refers to the decrease in resting EEG voltage after seizure activity as compared with baseline. Proper excitation of seizures invoke voltage-suppressing neural mechanisms intended to terminate and further seizure activity. This suppression is considered as a lower baseline on the EEG post ictus.19 According to studies, the degree of suppression correlates with seizure generalization, therapeutic adequacy, and bilateral stimulation.20
EEG Waveform Features. Greater ictal EEG amplitude, intensity, and symmetry obtained with bilateral ECT are not common with longer seizures, but they are related to antidepressant outcome.21 Studies found that the immediate post stimulus and mid ictal EEG amplitudes correlated with seizure therapeutic adequacy in depression. The symmetry of waveforms at the midpoint on the EEG tracing was also predictive.20 It was also proven that seizure duration had no impact as an EEG measure of treatment adequacy.21
Seizure Charge. The calculated product of EEG voltage, seizure uniformity throughout the brain, and seizure duration was hypothesized to be a measure of treatment intensity and efficacy.21 The variables included in total seizure charge are not physiologically independent of one another, which means longer seizure duration will not guarantee better results.
Low-dose bilateralelectroconvulsive therapy has a powerful antidepressant effectbut low-dose right unilateral therapy is ineffective.22 Evidence shows that the efficacy of rightunilateral electroconvulsive therapy depends on the electricaldose.23,24 There is some research showing that forboth unilateral and bilateral ECT, a higherelectrical dose leads to a more rapid clinical response.7,17,23
Seizure Threshold and Electroconvulsive Therapy
The knowledge of the seizure threshold is a guide to the selection of the electrical stimulus dose for ECT. In theory, the seizure threshold is the lowest dose of electrical charge for each particular patient that is required to induce seizure.25 In clinical applications the seizure threshold depends on individual patient’s characteristics, treatment history, and other stimulus factors.26
The therapeutic effectiveness of ECT is partly dependent on the degree that the stimulus intensity exceeds the seizure threshold.27,28 This statement is true on unilateral non-dominant electrode placement (UL) and on relative stimulus intensity. On bilateral (BL) ECT, the therapeutic response frequency is dependent on higher relative stimulus intensity,28 whereas barely suprathreshold UL ECT has significantly reduced antidepressant potency in contrast to moderately suprathreshold UL ECT (150% above threshold).6 The clinical use of this can be applied after determining the seizure threshold at the first treatment.22,29 The desired relative stimulus intensity to be maintained during treatments is confounded by variable increase in seizure thresholds during treatment.28 This rise in the seizure threshold lessens the degree to which a fixed stimulus dosage exceeds the seizure threshold which can result in possible diminished treatment therapeutic potency.
The seizure threshold can be higher in the elderly population and this may increase the difficulty of eliciting effective seizures.29,30,31 The choice of anaesthetic agent and other age related factors can also affect the seizure threshold. Propofol can reduce the seizure duration and has a possible effect on the seizure threshold.32 The seizure threshold may sometimes rise during the course of therapy. The dose would usually rise pari passu with a rise in the seizure threshold to maintain the dosing strategy. The seizure threshold can increase about 80% in bilateral ECT and 40% in unilateral ECT over a course of treatment.6 Some studies found increases of only 25–40% for bilateral ECT.33
ECT Practice Factors and Seizure Duration
As discussed earlier, the success of ECT treatment can be related to the degree to which the electrical stimulus exceeds seizure threshold and not the absolute dose that determines clinical outcome, especially in unilateral patients.6 Right unilateral (RUL) treatment at variable dosage can produce seizures of equal duration to bilateral treatment. With low levels electrical stimulation, RUL patients showed only 17% improvement inHAM-D scores compared to 70% in the BL group, despite the same mean seizure duration.22
Positioning electrodes over the non-dominant hemisphere causes lesssevere cognitive side effects than bilateral placement.11,24 In spite of extensive research however, the relative efficacy of right unilateraland bilateral electroconvulsive therapy is controversial.2,34,35 There are studies which have found superior efficacy with bilateral therapy,22,36,37 and then there are other studies which have reported equivalent efficacy.38,39 Because ofthis uncertainty, the American Psychiatric Association TaskForce on Electroconvulsive Therapy recommended thatelectrode placement be determined on a case-by-case basis.2
Multiple ECT stimuli (MECT) is given to patients to achieve longer cumulative seizure durations. The clinical improvement in depression correlates to patients’ total seizure time in MECT. But there is no proven study on the benefits of increased seizure time from the increased number of stimuli administered.40
Endocrine Measures
Oxytocin. According to studies, the measurement of oxytocin released from posteriorpituitary has a direct relationship with HAM-D measured improvement in depression.41 The concentration of oxytocin-associated neurophysin (AON) serum was calculated before and after the patient’s treatment of ECT. The increase in AON positively affects HAM-D. This neurophysin response was evident on ECT treatment but does not relate to EEG-measured seizure duration.
Prolactin. The surge of prolactin released during ECT treatment can be an indicator of clinical improvement. Seizure duration is associated with a rise in prolactin.42 However, the relationship between the magnitude of prolactin release and benefits of ECT is yet to be established.24
Cortisol. Although several variables have been studied as a possible predictor for the efficacy of ECT but results regarding hypercortisolism have been inconsistent. There has been a study to evaluate the relation between pre-treatment cortisol levels and the efficacy of ECT in a population of drug-free inpatients with severe major depression. This study suggests that higher levels of post-dexamethasone salivary cortisol at 9 AM are predictive of ECT efficacy.43
Elevated glucocorticoids may increase the vulnerability of the brain to the adverse effects of repeated seizures.This hypothesis was tested in a study and it was found that, ECT treatments delivered over 2 weeks resulted in a significant improvement in mood and a decline in most measures of cognitive performance. Elevated basal cortisol was associated with a greater decline in performance of executive function, visuospatial processing speed, and verbal memory. It was concluded that elevated cortisol predicts a greater degree of ECT-induced cognitive impairment. 44
Medication
Concurrent medication. Concurrent therapy can be considered under two headings: general medication and psychotropic medication. Both can affect seizure threshold. Anticonvulsants, hypnotics and membrane stabilisers tend to raise the seizure threshold, while preparations containing theophyllines can have the opposite effect. Concurrent psychotropic medication can have a significant effect upon ECT. Benzodiazepines are anticonvulsant and should be avoided if possible, but it is important to remember that there are risks associated with their sudden withdrawal. Some authorities have suggested short-term reversal with flumazenil if their presence is considered to be a limiting factor in the success of ECT, but experience is limited.45,46 Tricyclics tend to be proconvulsant, but there is little evidence of any detrimental effect on ECT. Selective serotonin reuptake inhibitors (SSRIs) tend to reduce seizure threshold and may be associated with prolonged seizures. Monoamine oxidase inhibitors increase seizure threshold and it is essential that the anaesthetist is aware that the patient is taking this class of medication or has done so within the previous 2 weeks. Lithium reduces seizure threshold and serum levels should be checked regularly and kept within a moderate range (0.4–1 mmol/l). Selective inhibitors of the reuptake of noradrenaline in common with SSRIs, can reduce seizure threshold and also cause hypertension. Neuroleptics tend to be proconvulsant at low dosage but increase seizure thresholds at higher dosage.
In a retrospective study of 455 patients involving 5482 treatments differences in tolerability and clinical effectiveness were found between combination therapy (ECT administered together with neuroleptic medication) and ECT monotherapy.47 Seizure duration which was assessed by EEG was significantly longer in patients treated with combination therapy using neuroleptics with lower antipsychotic potency; whereas seizure duration assessed by EEG-monitoring-electromyograph (EMG) was shorter in combination treatments done with atypical substances. In a parallel study, of ECT monotherapy or combination therapy with antidepressants using the same patient group, seizure duration was unaffected by most antidepressants but SSRIs lengthened seizure activity.48 In addition this study found that therapeutic effectiveness was significantly enhanced in the patients receiving tricyclic antidepressants, the tetracyclic antidepressant mirtazapine or SSRIs.
There may also be a role for antidepressants in the prevention of relapse following ECT. A small double-blind placebo controlled study of the tricyclic antidepressant imipramine involving 27 depressive inpatients who had failed on pharmacotherapy prior to ECT showed that imipramine, when compared to placebo, resulted in a significant decrease in the risk of relapse of patients receiving ECT.49 This study is in broad agreement with an earlier randomized, double-blind, placebo-controlled trial using another tricyclic antidepressant nortriptyline, or combination therapy of nortriptyline with lithium in the prevention of post-ECT relapse in patients with unipolar major depression.50 In 29 patients receiving placebo the relapse rate during the 24 week duration of the trial was 86%; whilst in 27 patients receiving nortriptyline 60% relapsed; and 39% of the 28 patients receiving nortriptyline and lithium combination therapy relapsed during the time of the study.
Other parameters
The effectiveness of the treatment is influenced by many other underlying factors, specifically the conditions and factors relating to individual patients. This would include age, sex, physical health status, co morbidities etc. Thus, one should always consider other factors that might affect the efficacy of ECT. Two recent small Japanese studies have suggested that some cardiovascular and EEG parameters may act as markers to predict the therapeutic response of ECT in depression. Postictal systolic heart rate and blood pressure were found to be significant predictors of the therapeutic efficacy of ECT in a study of 24 patients with depression;51 with higher systolic heart rate and blood pressure being associated with more effective ECT.
Discussion
ECT is widely used to treat certain psychiatricdisorders, particularly major depression. Although ECT has been extensively used there is little published information on the effect of seizure parameters and the effectiveness of ECT. There is evidence that supports the direct relationship of seizure duration and the effectiveness of ECT but the latest research suggests that the length in time of the cerebral seizure activity or the tonic–clonic convulsion is not related to clinical effectiveness.10,11 The effectiveness of ECT is related to the quality of cerebral seizure activity and cannot simply be related to its length in time alone. One of the important parameters in predicting clinical response is the degree to which electrical stimulus exceeds the seizure threshold.
Past research has shown that a generalized seizureof adequate duration is necessary and sufficient for antidepressanteffectsand that the intensity of the electrical stimuluscontributes to decreased cognitive function, the principal sideeffect, but not to effectiveness.7 Different types of anaesthetics, or concurrent medications can affect the seizure parameters and its efficacy.52,53 Research shows that a generalized seizureof adequate duration is necessary and sufficient for antidepressanteffects1,7 and that the seizures of less than 15 seconds duration are ineffective. There are other studies which mention that seizure duration does not influence the effectiveness of the ECT.10,11
The Future
Clinicians need to continue to research this difficult area within psychiatry to enhance the evidence base and fill such gaps in this evidence as highlighted by the ECT Handbook.54 On-going research is needed into what is a proven treatment of depressive illness and this should include more in depth research into the relationship of the above discussed parameters with its effectiveness.
“If ECT is ever legislated against or falls into disuse, it will not be because it is an ineffective or dangerous treatment, it will be because of a failure to supervise and monitor it correctly”55 and such supervision includes future quality research by concerned clinicians. Current NICE guidelines have limited the use of ECT to individuals with severe depressive illness, catatonia or a prolonged or severe manic episode who have been unresponsive to other treatment options.In addition, intervention of ECT should be considered to be short term and NICE does not recommend using it as maintenance therapy.56 As research into ECT develops, the consequences may be an even more targeted approach to the use of ECT as therapy.
Resource allocation in medicine applies to two complementary levels of care. One pertains to the organisation of public health and the provision of general rules informing the management of the system (macro-allocation). On the other hand, there is the need to specify decision criteria for the daily practice of health care providers who have to decide on the utilisation of their allocated resources, while dealing with a demand that often exceeds supply (micro-allocation).1
Beneficence, i.e. acting for the good of the patient, is one of the founding value of traditional ethics in medicine. However, the picture has changed when the core value of medicine shifted toward the centrality of the human person and the ideal of self-determination. The patient is now a 'health care user' who consults a professional whose knowledge and expertise is used in order to arrive at options. Good medical practice seems the result of a 'contract bargaining', which must take into account different criteria: clinical indication, patient preferences and subjective values, and appropriateness within the social context. Controlling how these three elements interact with each other requires a constant commitment and synchronised interventions.2
For cultural reasons, physicians consider, quite rightly, the costs of their interventions to be incommensurable with the life and the restoration to health of the diseased person. The most difficult problem in the distribution of resources remains the finding of convincing criteria to provide guidance, when often painful choices have to be made in the face of inadequacies in the availability of resources.3
Intensive care is one of the most expensive specialities of medicine and intensive care beds nowadays represent a limited resource.4, 5 The lack of beds is a daily problem in many ICU6, 7 and bed allocation has been considered one of the thorniest and stressful aspects of the intensivist's job.8 Studies have shown that resource use is often inefficient in European ICU. One of the main reasons for this inefficiency has been identified as nursing force “waste”.9
Monitoring and support of deficient vital functions are the main aims of intensive care. Usually, intensivists carry out the adequate diagnostic procedures and necessary medical and surgical treatments required to improve patient outcomes. There has been a considerable international effort to define the ethical, clinical and economical criteria for admission to ICU and to draft the relevant guidelines. The fundamental point is that resources should be utilised appropriately, i.e. that the patient be of the right category, in the right place and at the right time. Furthermore, ethics dictates that resources be allocated where they are more likely to make an impact.10-13
ICU admission and discharge can be ruled by means of a priority scale which classifies patients based on the expected benefit to result from intensive treatment.14 However, while it may be relatively easy to create “on-paper” scenarios affirming that patients who are too critical or not critical enough to benefit should not be admitted to intensive care, identifying these patients in everyday practice is far from simple.
As far as a reasonable doubt may be considered regarding the irreversibility of the clinical status, it is appropriate to initiate or continue intensive treatment. On the contrary, if the irreversibility of the clinical setting is deemed to be reasonably certain, it is appropriate not to initiate or to withdraw intensive measures to spare the patient the undue prolongation of the dying process. Excessive treatment is ethically unfair and should be strongly condemned, because it determines an inappropriate use of the means of treatment; it is likely to cause harm and pain to the patient and fails to respect the patient's dignity in death. Excessive treatment also increases the suffering of family members, is frustrating for care providers and generates an inequitable distribution of resources by curtailing them for other patients. The withdrawal of an intensive treatment, which was previously initiated because deemed to be indicated and accepted, or because the patient's clinical status and relevant prognosis were not clear enough at the time, should be considered whenever the clinical picture counter-indicates treatment continuation, the patient withdraws consent, or a previously defined therapeutic limit is reached.15
Immortality has always been an ambition for human beings. Today's medicine appears to be instrumental in dealing with this type of issues by making promises that will be hard not to break. The most urgent form of action to be undertaken regards these unwarranted expectations that society holds about the efficacy of medicine. The message to put across ought to be that death is inescapable and that the most severe diseases are incurable.
Once the inevitability of resorting to often dramatic measures in today's health care system is postulated, we are confronted with the problem of finding an ethical justification to subsequent decisions. On the basis of the choices made necessary by the paucity of available resources, medical treatment would be “apportioned”, i.e., distributed according to commitments and rules, with the inevitable exclusion of some from the utilization of the services themselves.
Rationalisation, intended as best utilisation and fair limitation, is an economic necessity, juridically and ethically legitimate. The ultimate objective must remain that of equitable apportionment.
Bortezomib is a reversible proteasome inhibitor, currently approved by US FDA for use in multiple myeloma and mantle cell lymphoma. It has been shown to cause new onset and exacerbation of underlying congestive cardiac failure (CHF) in some case reports. Although the exact mechanism of bortezomib induced congestive cardiac failure is unknown, studies have shown dysregulation of ubiquitin proteasome system (UPS) in human cardiac tissues in end stage heart failure1-3. Furthermore, a study in rats has shown reduced left ventricular contractility after bortezomib administration, which was attributed to reduced ATP synthesis in mitochondria of cardiac myocytes4. Our case demonstrates new onset severe reversible left ventricular systolic dysfunction after 4 cycles of bortezomib in a 58 year old female with multiple myeloma. It highlights the importance of monitoring cardiac function in patients receiving bortezomib.
Case Report
A 58 year old female with past medical history of well controlled hypertension presented with severe low back pain, anorexia and unintentional weight loss of around 20 pounds over a period of 3 months in medical clinic. On evaluation of her routine laboratory tests, she was found to have haemoglobin of 6.5 g/dl, haematocrit of 19.9%, white blood cell (WBC) count of 3.9 x 103/cc, red blood cell (RBC) count of 2.18 x 106/cc and platelet count of 1.52 x 105/cc. Her blood urea nitrogen and creatinine was 10 mg/dl and 0.7 mg/dl respectively and corrected calcium level was 10g/dl. On liver function test, her total protein was 12.4 g/dl and albumin level was 2.8 g/dl. X-ray of lumbosacral spine revealed a compression fracture at the level of T12and L2 vertebra. Bone survey confirmed diffuse osteopenia, severe collapse of the body of T12 and partial collapse of L2 and L3. Due to the presence of severe anaemia and compression fractures, multiple myeloma was suspected. Urine protein electrophoresis showed two monoclonal protein bands with concentration of 46.8% and 4.8% and urine immunofixation showed two intact monoclonal IgA-Kappa immunoglobulin bands. Beta-2 microglobulin level was 5.49. Bone marrow aspiration and biopsy confirmed the diagnosis of multiple myeloma. Patient was staged as IIIA according to Durie-Salmon staging system.
Subsequently, patient was planned to be treated with eight cycles of bortezomib and dexamethasone, with bortezomib being given on day 1, 4, 8 and 11 of each cycle at a dose of 1.3 mg/m2 body surface area. Prior to initiation of chemotherapy, she received radiotherapy to spine as well. However, after completing the fourth cycle of bortezomib/dexamethasone, she was admitted to the hospital with generalized weakness, nausea and vomiting. Chest X ray revealed possible right lower lobe infiltrate or effusion along with increased bronchovascular markings and she was treated with antibiotics for suspected community acquired pneumonia. However, an echocardiogram was obtained due to bilateral crackles on physical exam and increased bronchovascular markings on chest X ray, which revealed dilation of left ventricle with left ventricular ejection fraction of 30-35%, diffuse hypo kinesis of left ventricle, mild mitral and tricuspid regurgitation and diastolic dysfunction with abnormal relaxation(Tajik grade I). Left ventricular septal and posterior wall thickness was 0.8 cm. Infiltrative Cardiomyopathy in the setting of multiple myeloma was unlikely due to the absence of bi-atrial enlargement, pericardial effusion and thick bright myocardium on echocardiogram. Cardiology consultation was sought and their impression was new onset left ventricular dysfunction due to bortezomib therapy.
Patient did not receive any further cycles of chemotherapy due to cardiotoxicity and was on optimal medical management for heart failure with lisinopril, carvedilol and isosorbide dinitrate. An echocardiogram was repeated four months after discontinuation of bortezomib, which revealed normal left ventricular contractility with global left ventricular ejection fraction of 55% and trace mitral regurgitation.
Currently, at 2 year follow up, her echocardiogram shows global left ventricular ejection fraction of 65%, trace mitral and tricuspid regurgitation and diastolic dysfunction with abnormal relaxation(Tajik grade I).
Discussion and Review of Literature
Botezomib is a novel proteasome inhibitor which acts by inducing bcl-2 phosphorylation and cleavage, resulting in G2-M cell cycle phase arrest and apoptosis5. US Food and Drug Administration (FDA) have approved bortezomib for use in multiple myeloma and mantle cell lymphoma. The common adverse effects of bortezomib observed in clinical trials and post marketing surveillance include thrombocytopenia, neutropenia, hypotension, asthenia, peripheral neuropathy and nausea. US package insert for bortezomib states that acute development or exacerbation of congestive heart failure and new onset of decreased left ventricular ejection fraction have been reported, including reports in patients with no risk factors for decreased left ventricular ejection fraction and it is recommended to closely monitor patients with risk factor for, or existing heart disease.
The role of ubiquitin proteasome system (UPS) in heart failure has been studied extensively in recent years. Two studies by Hein et al and Weekes et al in 2003 have shown presence of increased amount of ubiquitinated proteins and substrates in cardiac tissues of heart failure patients, indicating reduced activity of UPS in end stage heart failure1-3. Another study has shown impaired proteasome activity in hypertrophic and dilated cardiomyopathy likely secondary to post translational modification of proteasome6.However, in early stage heart failure, there is increased activity of UPS, resulting in remodelling and high cardiac output2. Bortezomib, by inhibiting UPS, would lead to accumulation of ubiquitinated proteins in cardiac myocytes, similar to that seen in end stage heart failure. A study in rats exposed to bortezomib alone showed development of left ventricular systolic dysfunction by echocardiography and reduced synthesis of ATP was observed in the mitochondria of cardiac myocytes4. However, the exact mechanism of bortezomib induced systolic dysfunction in humans is not clear.
There have been a few reported cases of bortezomib induced congestive cardiac failure in literature (Table 1). The amount of bortezomib administered before development of symptoms of heart failure was 20.8 mg/m2 in four patients, 3 mg/m2 in one patient and 10.4mg/m2 in one patient. Three of them have received prior anthracycline based chemotherapy. Complete reversibility of heart failure after discontinuation of bortezomib was documented only in two cases by follow up echocardiograms and brain natriuretic peptide levels7, 8. The patient described in our index case had well controlled hypertension and no additional cardiac risk factors at baseline. She developed non-specific symptoms, including weakness, nausea and vomiting after the fourth cycle of chemotherapy and was admitted to the hospital for community acquired pneumonia. However, an echocardiogram was obtained due to pulmonary congestion, which uncovered the diagnosis of left ventricular systolic failure. The two echocardiograms obtained at a follow up of 4 months and 2 years showed gradual improvement in ejection fraction to 55% and 65% respectively from 15% after chemotherapy with bortezomib.
We did a review of major clinical trials of bortezomib in patients with multiple myeloma, Waldenstrom’s macroglobulinemia and plasma cell leukaemia (Table 2) to investigate the incidence of congestive cardiac failure reported after administration of bortezomib. In APEX trial, the incidence of congestive cardiac failure was 2% in both bortezomib and high dose dexamethasone group 11. In a study on melphalan refractory multiple myeloma by Hjorth et al, 3 cases of congestive cardiac failure was reported in bortezomib-dexamethasone group and 2 cases were reported in thalidomide-dexamethasone group12. Another study evaluating the safety of prolonged therapy with bortezomib by Berenson et al reported 1 case of cardiomegaly and 1 case of pulmonary edema13. However, further studies are needed to specifically evaluate the incidence of congestive cardiac failure with bortezomib therapy.
In summary, our case and review highlights the importance of maintaining a high level of suspicion for development of congestive cardiac failure after therapy with bortezomib. Given the widespread use of bortezomib and new generation proteasome inhibitors in multiple myeloma, there might be increased incidence of new onset and exacerbation of underlying congestive cardiac failure in future. Currently, there is no guideline for routine evaluation and monitoring of cardiac function in all patients during the course of bortezomib therapy. Furthermore, it is unclear whether the severity of congestive cardiac failure is proportional to the cumulative dosage of bortezomib administration and also, if there is any correlation between onsets of congestive cardiac failure with the timing of bortezomib therapy. Further studies are required in future to address these issues.
Table 1: Review of cases of bortezomib induced congestive cardiac failure reported so far.
Author
Age/sex
Prior cardiac history and risk factors
Baseline cardiac function
Number of Bortezomib containing cycles
Exposure to other cardiotoxic medications
Amount of Bortezomib received before onset of cardiac symptoms
Lowest EF** after Bortezomib administration
EF on follow up visits
Voortman et al7
53/M
36 pack years of smoking and COPD
Echo not available; NT-Pro BNP 1389 ng/l
4
Gemcitabine
3 mg/m2
10-15% on Echo after 4 cycles
45% on MUGA scan at 6 months
Orciuolo et al9
73/M
NK*
NK
6
1 Anthracycline containing regimen
20.8 mg/m2
EF 25%
NK
Orcioulo et al9
61/F
NK
NK
4
2 Anthracycline containing regimens
20.8 mg/m2
EF 20%
NK
Orciuolo et al9
80/F
NK
NK
4
1 prior non anthracycline chemotherapy regimen received
20.8 mg/m2
EF 35%
NK
Hasihanefioglu et al10
47/M
None
EF 70% and normal coronary angiogram
2
1 cycle of Vincristine, Doxorubicin and Dexamethasone
10.4 mg/m2
EF 10%
EF 20% at 6 month follow up
Bockorny et al8
56/F
Hypertension, well controlled
NK
4
None
20.8 mg/m2
EF 20-25%
EF 55-60%
INDEX CASE
58/F
Hypertension, well controlled
NK
4
None
20.8 mg/m2
EF 30-35%
EF 55% at 4 month and 65% at 2 year follow up.
*NK: Not Known; **EF: Ejection Fraction
Table 2: Review of cases of congestive cardiac failure reported in clinical trials with bortezomib in multiple myeloma, Waldenström’s Macroglobulinemia and plasma cell leukaemia.
Authors (ref)
Study
Study population
Significant Cardiac events (n)
Berenson, J.R. et al. 200513
Safety of prolonged therapy with bortezomib in relapsed or refractory multiple myeloma
Frontline chemotherapy with bortezomib-containing combinations improves response rate and survival in primary plasma cell leukaemia
29 patients with untreated PPCL
None reported
Hjorth, M. et al. 201212
Thal-Dex vs. Bort-Dex in refractory myeloma
131 patients with Melphalan refractory MM
2 cases of cardiac failure in Thal-Dex group and 3 in Bort-dex group
Jagannath, S. et al 200916
Bortezomib for Relapsed or Refractory Multiple Myeloma
54 patients with relapsed or refractory MM
None reported
Jagannath, S. et al 201017
Extended follow-up of Frontline Bortezomib ± Dexamethasone for MM
49 patients with untreated MM
None reported
Kobayashi, T. et al. 201018
Bortezomib plus dexamethasone for relapsed or treatment refractory multiple myeloma
88 patients with relapse/refractory MM
None reported
Mikhael, J.R. et al. 200919
High response rate to bortezomib with or without dexamethasone in patients with relapsed or refractory multiple myeloma
638 patients with refractory or relapsed MM
None reported
Richardson, P.G. et al. 200320
A Phase 2 Study of Bortezomib in Relapsed, Refractory Myeloma
202 patients with relapsed MM
None reported
Richardson, P.G. et al. 200511
Bortezomib or High-Dose Dexamethasone for Relapsed Multiple Myeloma(APEX trial)
669 patients with relapsed MM
Congestive cardiac failure in 2% of each arm.
Rosino, L. et al. 200721
Phase II PETHEMA Trial of Alternating Bortezomib and Dexamethasone As Induction Regimen Before Autologous Stem-Cell Transplantation in Younger Patients With Multiple Myeloma
40 patients with newly diagnosed MM
None reported
Sonneveld, P. et al. 201222
Bortezomib Induction and Maintenance Treatment in Patients With Newly Diagnosed Multiple Myeloma
827 patients with newly diagnosed MM
Cardiac Disorders in 5% of patient in VAD group vs. 8% of patients in PAD group.
Yuan, Z.G. et al. 201123
Different dose combinations of bortezomib and dexamethasone in the treatment of relapsed or refractory myeloma
168 patients with relapsed MM
None reported
Suvannasankha et al 200624
Weekly bortezomib/methylprednisolone in relapsed multiple myeloma
29 patients with relapsed multiple myeloma
1 case of congestive cardiac failure
Conclusion
CHF is an infrequent but serious adverse effect of bortezomib. Cardiac function should be closely monitored in patients receiving bortezomib, as case reports have shown that these patients might present with non-specific symptoms like weakness and fatigue. Further studies are required to establish the frequency and mode of monitoring of cardiac function during and after bortezomib therapy.
We report a case of worsening psychiatric symptoms in a patient who was serendipitously diagnosed with Primary Hyperparathyroidism.
Behavioural change in form of aggression sometimes occurs as a component of psychiatric disorders such as psychosis, attention deficit hyperactivity disorder, autistic spectrum condition, conduct disorder and various mood disorders. It may also present as a psychiatric manifestation of an endocrine disorder such as Primary Hyperparathyroidism (PHPT)1,2.
PHPT is rare in children and adolescents with an incidence of 2-5 in 100000 3. It is characterized by hypercalcaemia and elevation of parathyroid hormone. Children with PHPT may present with non-specific complaints such as behavioural change and deteriorating school performance.
Patients who present with non-renal symptoms have a longer duration of symptoms prior to diagnosis of PHPT4,6. It seems probable that it takes much longer for diagnosis to be made in those with pre-existing mental disorder. When left undiagnosed and untreated, PHPT can be a serious disease with significant morbidity.
The finding of elevated serum calcium levels in young people is often fortuitous as they often present with non-specific symptoms3,4. A significant number of hyperparathyroidism cases with neuropsychiatric manifestation have been reported in patients without recorded pre-existing psychiatric diagnosis 3-6.
This case report highlights the need for clinicians to always consider endocrine disorder as a differential diagnosis when treating patients with psychiatric symptoms which are poorly responsive to standard treatment. It also demonstrates the relevance of an integrated approach in healthcare delivery including the importance of good communication between primary and tertiary care clinicians.
Case Report:
A 15yr old Caucasian male known to Child & Adolescent Mental Health Service (CAMHS) for management of his behavioural problems presented in crisis as a consequence of physical aggression, suicidal ideation and homicidal thoughts.
His first contact with CAMHS had been at the age of 10 when he was referred for management of his frequent aggressive outbursts. He had always been boisterous but had no previous history of significant emotional or behavioural difficulties. His developmental history was unremarkable and there were no features indicative of any neurodevelopmental disorder. There was no family history of mental illness.
His biological parents were involved in an acrimonious divorce at the time of his first referral to CAMHS so it was felt that this conflict may have contributed to his presentation.
He was referred a Child Psychotherapist for weekly sessions as the initial assessment suggested significant weakness in his attachment and identification which manifested in the instability and immaturity of mood and behaviour.
The family described minimal improvements in his capacity for self-control having had three years of psychotherapy. His behaviour remained challenging but manageable within the community until six months prior to him being re-referred by his General Practitioner (GP) for urgent psychiatric assessment.
Following parental divorce, his mum remarried but her new marriage was also turbulent and the couple had to separate. During this period of increased psychosocial stresses within his family, the patient’s behaviour escalated to a point that he was regarded as a significant risk to himself and others. It was thought that the separation between his mother and step-father might have triggered this deterioration.
The night before his urgent referral to CAMHS, he set a trap for his mother; he had put a rope around some curtains on the floor and was planning to throw another curtain over her. He also had a knife and hockey stick with him at the time. As his mother stepped into the room, he put the curtain over her head and attempted to hit her with the hockey stick. He was promptly restrained by his father, who had come to visit, before he could do much damage.
He presented as unpredictable and aggressive but would often deny recollection of any reported outbursts. He was very upset when incidents were talked about as he believed he had no control whatsoever over this behaviour – it was clear how upsetting his behaviour was to him.
He displayed uncontrollable rage on many occasions. It was usually directed at his mother and home furniture, and might last up to two hours. He appeared to seek immediate gratification and was clearly hypersensitive to his setting with a significant degree of paranoia and irritability.
He repeatedly stated that he had thoughts of wanting to kill his mother and himself especially when angry. He did not appear able to accept any responsibility for his actions, blaming his temper outbursts on his older sibling. We heard she was extremely frightened of him; he had on two occasions broken down her door.
When he came out of these rages he would become very tearful and profoundly apologetic. These difficulties had been noticed at school where his grades had been falling. He told teachers he felt suicidal and would sometimes go into the school toilet to cry especially when he thought about his inability to control himself.
Physical examination at this point was unremarkable. The Community Psychiatrist commenced him on Fluoxetine and referred him to an in-patient psychiatric unit for further psychiatric evaluation including a forensic assessment.
He was diagnosed with Asperger’s Syndrome and Attention Deficit Hyperactivity Disorder in the inpatient unit and was prescribed risperidone and methylphenidate. His GP was asked to arrange a baseline blood test, consisting of full blood count (FBC), liver function test (LFT), urea & electrolytes (U&E) and thyroid function test (TFT). There was no request for blood glucose level or serum calcium.
The GP asked for a serum calcium level estimate purely out of ‘habit’. The laboratory result showed a high level of calcium 3.89mmol/L (normal range 2.2-2.6). Based on this significantly elevated serum calcium level, a referral was sent to the Paediatric Endocrinologist.
At the Endocrinology Clinic, he described a twelve month history of generalised aches and pains in association with emotional lability. A history of fracture of his right wrist and left hallux occurring within 18 months prior to presentation was also obtained. The X-ray report showed presence of a radiolucent area in his right femur. An assay of his parathyroid hormone, Sestamibi scan and ultrasound scan of his neck were done.
The elevated parathyroid hormone level, increased serum calcium, history of fractures and X-ray features indicated the diagnosis of Primary Hyperparathyroidism. The endocrinologist was of the opinion that his PHPT has been present for a number of years. He was referred for parathyroidectomy.
His serum calcium level dropped to 2.47mmol/L two days post surgery. As calcium level normalised, his symptoms improved remarkably and his psychotropic medications were discontinued. Since then, he has successfully commenced college full time and has succeeded in obtaining good grades in his chosen courses.
Discussion:
Psychiatric symptoms cause significant impairment in children and adolescents. Having additional symptoms of hyperparathyroidism would exacerbate the psychiatric symptoms and increase the degree of impairment. This patient presented with neuropsychiatric symptoms and evidence of end organ damage which is similar to those in published reports3,4.
Research shows that diagnosis of primary hyperparathyroidism is often delayed in young people but we suspect that it may even be more delayed in those with a pre-existing psychiatric disorder as the symptoms may be more likely to be attributable to the psychiatric condition.
It is possible that the behavioural problems in this patient may have co-existed independently of each other, but the rapid resolution of the psychiatric symptoms suggests that they may have been exacerbated by hyperparathyroidism.
Our findings in this case are similar to those reported by Spivak and colleagues’ which showed that early diagnosis of hypercalcaemia can prevent unnecessary and potentially harmful treatment with psychotropic medications7.
Psychiatric diagnoses are usually formed from identification of collective symptoms some of which may occur in other medical conditions. Adopting a multidisciplinary team approach is most helpful in the management of complex psychiatric cases. This approach may encourage clinicians to take a holistic view in management of children.
It is important for clinicians to be familiar with common psychiatric symptoms and medical conditions that may mimic or cause them because the presence of non-specific symptoms in PHPT poses a significant emotional burden for affected children and their families. It is a potentially treatable condition which if not diagnosed early could lead to impaired psychosocial well-being and damage of vital organs. Parathyroidectomy has been shown to improve general health, quality of life and cognitive functioning in patients with PHPT8.
The outcome for this particular young person could have included further episodes of in-patient hospitalisation or involvement with the juvenile justice system as a consequence of further violent episodes. The achievement of adolescent milestones and his education could have been severely disrupted and may have resulted in labelling detrimental to his future.
In the current economic climate and because of the rarity of Primary Hyperparathyroidism, we do not advocate routine serum calcium estimation in all behavioural problems but clinicians should have lower threshold for screening for this condition especially in patients with worsening symptoms despite conventional treatment.
In conclusion, Primary Hyperparathyroidism should be considered in the differential diagnosis in young people with worsening neuropsychiatric symptoms which are unresponsive to standard psychiatric treatment.
The US Food and Drug Administration (USFDA) considers the following as biologics: any therapeutic serum, toxin, antitoxin, vaccine, virus, blood, blood component or derivative, allergenic product, analogous product, or derivatives applicable to the prevention, treatment, or cure of injuries or disease of man1. However, generally, biologics refer to protein molecules therapeutically used in various diseases so as to target specific points in the inflammatory cascade of these disorders 2. Hope for an improved tolerability, convenience in usage and lasting remissions, combined with increased knowledge of immune-pathogenesis of various cutaneous diseases has lead to the introduction of biologics as alternative immune-modulating agents in the field of dermatology.
CLASSIFICATION
Biologics are generally divided into three major groups 3:
a) Monoclonal antibodies
b) Fusion antibody proteins
c) Recombinant human cytokines and growth factors
The main groups and the principal agents in each group are summarised in Box 1 and described below.
A) MONOCLONAL ANTIBODIES
Monoclonal antibodies target specific cell-surface receptors. In the early days of biologic therapy, purely murine monoclonal antibodies were used. However, due to the development of antimurine antibodies, which blocked their action, these could be given only for very short periods. The monoclonal antibodies used now have different amounts of murine sequences in the variable region. They may be categorised into three classes:
(a) chimeric antibodies comprising of 30% murine genes fused with human antibodies
(b) humanised antibodies, which have 10% murine sequences, and
(c) human antibodies, which are solely derived from human immunoglobulin genes 4.
Principal monoclonal antibodies with therapeutic relevance in Dermatology
The principal monoclonal antibodies known till date are enumerated in Box 1 and described briefly below.
· Anti-IL-12 and anti-IL-23 monoclonal antibody: Ustekinumab
· Anti-CD2 antibody: Siplizumab
· Anti-CD4 antibody: Orthoclone (OKTcdr4a)
· Anti-CD25 antibodies: Basiliximab, Daclizumab
· Anti-CD80r: Galiximab (IDEC 114)
· Anti-IgE: Omalizumab
Fusion antibody proteins
· Etanercept
· Alefacept
· Abatacept
· Onercept
· Denileukin Diftitox
Recombinant human cytokines and growth factors
a) Interferons
· Interferon α (IFNα)
· Interferon γ (IFNγ)
· Interleukin 1 Receptor antagonist (IL1Ra)
· Interleukin 2 (IL-2)
· Interleukin 4 (rhIL-4)
· Interleukin 10 (rhIL-10)
· Interleukin 11 (rhIL-11)
b) Granulocyte macrophage colony stimulating factor (GM-CSF)
c) Platelet derived growth factor (PDGF)
1. Infliximab
Infliximab (trade name Remicade) is a human-mouse monoclonal antibody that binds to and inhibits the activity of TNF-α, and also causes lysis of TNF-α producing cells5.
Important uses of Infliximab
Psoriasis: Infliximab is approved for the treatment of psoriatic arthritis and plaque psoriasis by FDA6, 7. Infliximab may also be of value in recalcitrant or unstable disease and in generalised pustular psoriasis. It is given as an IV (intravenous) infusion in doses of 5 or 10 mg/kg, over a period of 2 hours at weeks 0, 2, 6 and may be followed by repeat single infusions at 8-12 week intervals 8. In various controlled trials, improvement at 10 weeks has been noted in 87% of patients 7, 9.
Atopic dermatitis: Infliximab has also been evaluated in a study of atopic dermatitis 10. At 2 weeks, there was significant improvement in all patients. At 10, 14, and 30 weeks, variable response was seen.
Hidradenitis suppurativa: Long-term efficacy has also been evaluated in hidradenitis suppurativa. In one study, some patients had no evidence of recurrence after 2 years, while others relapsed within a mean of 8.5 months11.
2. Adalimumab
Adalimumab (Humira®) is a human IgG1 monoclonal antibody directed against TNF-α. Adalimumab is given in a dose of 40 mg subcutaneously (SC) every other week as self-injection 5, 12.
Important uses of Adalimumab
Psoriasis: Adalimumab rapidly reverses the decrease in epidermal Langerhans cell density in psoriatic plaques 13. In a trial, patients with psoriatic arthritis received adalimumab every other week for 24 week14. It was well-tolerated and helped improve joint and skin manifestations significantly.
Hidradenitis suppurativa: An increasing number of reports in refractory hidradenitis supprativa have shown successful control with adalimumab 15, 16, 17.
3. Basiliximab
Successful treatment for severe psoriasis and generalised pustular psoriasis has been reported with basiliximab, an interleukin-2 receptor (IL-2R; CD25) chimeric monoclonal antibody 18, 19.
4. Daclizumab
Daclizumab is a humanised monoclonal antibody thatbinds to the CD25 subunit of the IL-2 receptor onT-cells, thus blocking T-cell proliferation. It has been tried in recalcitrant psoriasis and HIV-associated psoriatic erythroderma with a mean reduction in PASI of 30% 20, 2122.
5. Siplizumab
Siplizumab (Medi-507) is a humanisedmonoclonal antibody directed against CD2. It is designed to block stimulationby inhibiting the CD2–LFA-3 interaction. In earlyphase studies in psoriasis, significant response to therapy has been noted23.
6. Efalizumab
Efalizumab is a recombinant humanised monoclonal IgG1 antibody that binds to CD11a, a subunit of leukocyte function-associated antigen 1 (LFA-1) 24. It destabilises and decreases the trafficking of T-cells into dermal and epidermal tissues.
Important uses of Efalizumab
Psoriasis: Efalizumab was approved by the US FDA in October 2003 for the treatment of psoriasis5. It is currently the only biologic agent approved for continuous administration to adult patients24. The licensed dose of efalizumab is 1 mg/kg weekly as a subcutaneous self- administered injection for 12 weeks, following a first conditioning dose of 0.7 mg/kg 24.
Lichen planus: There is one case report of 3 months duration of treatment with efalizumab for lichen planus with resolution of skin lesions and pruritis 25.
7. Rituximab
Rituximab is a monoclonal humanised antibody directed again in the B cell-specific antigen CD20.
Important uses of Rituximab
Lymphoma: It has been used in patients with CD20-positive non-Hodgkin's lymphoma in a dosage of 375 mg/m2 for four infusions26.
SLE: In systemic lupus, dose escalation studies revealed no differences with respect to clinical outcome in patients who received either a single infusion of 100 mg/m2, a single infusion of 375 mg/m2, or four weekly infusions of 375 mg/m227.
Blistering diseases: For patients with blistering diseases, most patients receive the lymphoma dosage schedule. However, serious side effects were considerably higher.
There are reports of refractory pemphigus patients who received infusions of rituximab and had rapid resolution of lesions and a long lasting clinical remission 28, 29, 30.
8. Galiximab
Galiximab a humanised monoclonal antibody directedagainst CD80 and blocks its interaction with CD28 on the T cell, for T-cell stimulation 31. Clinicaldata for this drug are just beginning to emerge with 40% of patients achieving at least 50% reduction in PASI after receiving4 biweekly doses in a trial32, 33.
9. Ustekinumab
It is a fully human monoclonal antibody targeting IL-12 and IL-23, presently undergoing clinical trials for psoriasis and psoriatic arthropathy2, 34. In placebo-controlled studies, (PHOENIX 1) and (PHOENIX 2) have shown that ustekinumab could control plaque psoriasis with only four injections a year resulting in greater ease of use and more sustained relief 35, 36.
10. Certolizumab pegol
Certolizumab is the recombinant antibody Fab' fragment of a humanised TNF inhibitor monoclonal antibody. A study in chronic plaque psoriasis showed that certolizumab pegol, given subcutaneously every two weeks, over a period of 12 weeks shows significant improvement 37.
11. Golimumab
Golimumab, a fully human monoclonal antibody is at present undergoing Phase III clinical trials in psoriatic arthropathy 38.
12. Orthoclone or OkT4a
It is a humanised antihuman CD4 IgG4 monoclonal antibody preventing the recognition of the MHC-bound antigen by an appropriate T-cell receptor, hence T cells do not get activated 39. Several studies have found orthoclone to be effective in moderate to severe psoriasis 40, 41.
13. ABX-IL8
ABX-IL8 is a fully human monoclonalantibody designed to bind free IL-8, a key chemokine in psoriasis and deactivate it in theskin42, 43. In early trials, the drug has demonstrated good clinical responsein psoriasis 44, 45.
14. Omalizumab
Omalizumab is a recombinant, humanised, monoclonal antibody against immunoglobulin IgE. This agent acts as a neutralising antibody by binding IgE at the same site on IgE as its high-affinity receptor, FcεR I, thus inhibiting the biological effects before the generation of allergic symptoms 46. There are reports of the efficacy of omalizumab in chronic urticaria 47, cold urticaria 48 and atopic dermatitis 49.
15. Mepolizumab
Mepolizumab is a humanised monoclonal IgG antibody to the IL-5 molecule, which is essential for eosinophil growth and differentiation. Two weekly infusions showed significant clinical improvement in atopic dermatitisand clinical trials are underway for hyper-eosinophillic disorders 50,51.
16. SMART Anti–IFN-γ
SMART anti–IFN- γ,a humanised monoclonal antibody, binds and inactivates IFN- γ, an important Th1 cytokinein psoriasis. Early phase studies are being performed at this time 52.
B) FUSION ANTIBODY PROTEINS
Fusion proteins, also known as chimeric proteins, are proteins which are created by the fusion of the receptor domain of a human protein with the constant region of human IgG. The resultant fusion protein binds specifically to a ligand or co-receptor 53. The most commonly used fusion proteins in dermatology are briefly described below and enumerated in Box 1.
1. Alefacept
Alefacept is a bivalent recombinant fusion protein composed of the first extracellular domain lymphocyte function antigen 3 (LFA-3), fused to the hinge domain of human IgG1. The LFA-3 portion of alefacept binds to CD2 receptors on T-cells, thereby blocking their natural interaction with LFA-3 on antigen presenting cells (APCs). The IgG1 portion of alefacept binds to FcγR receptor on natural killer cells to induce T-cell apoptosis 54.
Important uses of Alefacept
Psoriasis: The US FDA approved alefacept in January 2003 for treatment in adult patients with moderate to severe chronic plaque psoriasis. It is given by intramuscular or intravenous route with a dose of 10-15 mg IM weekly or 7.5 mg IV weekly and a 12 week course is recommended 5, 54. Two 12-week courses showed a75% or greater reduction in the PASI 55.
Alopecia areata: Case reports have shown that alefacept may be effective in the treatmentof AA56, 57.
Pyoderma gangrenosum: Alefacept has been used for pyoderma gangrenosum and improvement was shown in 25% of these patients 58.
Other Indications
Some of the off-label conditions where alefacept has been used with success are graft-versus-host disease (GVHD), lichen planus, alopecia areata, atopic dermatitis, mycosis fungoides,alopecia universalis, erosive lichen planus,Hailey-Hailey diseaseand hand dermatitis 58, 59, 60, 61, 62, 63.
2. Denileukin diftitox
Denileukin diftitox is a novel recombinant fusion protein consisting of fragments of diphtheria toxin linked to human interleukin-2 and works by targeting the high-affinity interleukin-2 receptors. It was tried in patients with recalcitrant psoriasis and the rate of improvement for treated patients was found to be significant 64.
3. Abatacept (Ctla4ig)
It is a fusion protein composed of the extracellular domain of CTLA4 and the Fc region of IgG4. It interferes with T-cell activation by competitively binding the B7.1 and B7.2 molecules on the surface of APC 65. In a study, patients with stable psoriasis vulgaris showed good improvement with IV infusion of abatacept 33. A second generation CTLA4Ig, Belatacept, is currently under Phase II clinical trial for allograft diseases 66.
4. Etanercept
Etanercept is a recombinant fully human dimeric fusion protein comprising of the human TNF-α p75 receptor and the Fc portion of human IgG1 molecule. It functions as a TNF inhibitor, thereby preventing interaction with its cell surface receptors on target cells and blocking its pro-inflammatory effects.
Important uses of Etanercept
Psoriasis: Etanercept (Enbrel®) is FDA approved for use as subcutaneous monotherapy in psoriasis. Several clinical trials have shown that it is effective67, 68, 69, 70. The adult dose is 50 mg/week, given subcutaneously for three months 5. The drug is also indicated for treatment of psoriatic arthritis 71, 72.
Hidradenitis supprivata:There is a study of etanercept in patients with severe hidradenitis with more than 50% score improvement12.
5. Onercept
Onercept is a recombinant human soluble p55 tumour necrosis factor binding protein under development for the potential treatment of psoriasis and psoriatic arthritis73. C) RECOMBINANT HUMAN CYTOKINES AND GROWTH FACTORS
Cytokines are non-immunoglobulin proteins and glycoproteins produced by a wide variety of cells in the human body and released in response to any immune stimulus 74, 75. Recombinant cytokines or cytokine antagonists have been used as immunomodulators 76. The principal recombinant cytokines used in dermatology, enumerated in Box 1, are described below.
1. Interferons (IFNs)
IFNs, a family of related proteins, are produced by virus-infected leucocytes. They exhibit anti-proliferative, immune-modulatory and anti-neoplastic functions 77.
· Interferon α
Recombinant IFNα is given as a subcutaneous or intramuscular injection to treat verruca vulgaris 78 , condyloma acuminatum 79, cutaneous T cell lymphoma 80, Kaposi's sarcoma (AIDS related) 81, melanoma 82, basal cell carcinoma 83, squamous cell carcinoma 84, actinic keratosis 85, Behçet's disease 86, hemangiomas 87 and keloids 88.
The injections are usually given thrice weekly and the dose (depending on the condition being treated) varies from low-dose therapy for condyloma acuminatum to high-dose therapy for melanoma 89, 90. Of late, pegylated IFNα is being used for convenience, because it has a longer half-life and hence can be given once weekly 80.
· Interferon-γ
It is FDA approved for the treatment of chronic granulomatous disease 91 and has also been used in atopic dermatitis 92 and cutaneous T cell lymphoma 90.
Anakinra is the non-glycosylated form of human IL-1Ra and acts by blocking the functions of the naturally occurring IL-193. Good results have also been reported in Schnitzler's syndrome94, familial cold auto-inflammatory syndrome 95 and psoriatic arthropathy96. It is given by subcutaneous injection 100 mg once a day.
3. Interleukin 2
Recombinant IL-2 is an antitumour cytokine that has been used in cutaneous T cell lymphoma (CTCL) and metastatic melanoma 97. When given intravenously in high doses of 600,000-720,000 IU/kg in melanoma, IL-2 has produced a 15-20% overall response, with complete cure in 4-6% 98.
4. Interleukin 4 (rhIL-4)
In a dose-escalation study (0.5 to 5mg/kg given by subcutaneous injection thrice a week), IL-4 has been shown to cause improvement in psoriasis by inducing Th2 differentiation in human CD4 + T cells 99.
5. Interleukin 11 (rhIL-11, Oprelvekin)
It has also shown reasonably good results in the treatment of psoriasis at doses of 2.5 or 5mg/ kg, by subcutaneous injection 100.
GM-CSF acts by stimulating stem cells to produce granulocytes, monocytes and macrophages 101. Recombinant human GM-CSF has been used to promote wound healing in ulcerated skin for example leg ulcers 102, 103, and for the treatment of melanoma 104 and Sezary syndrome 105.
7. Platelet derived growth factor (PDGF)
PDGF is a dimeric glycoprotein which regulates and promotes granulation tissue formation, re-epithelialisation and wound angiogenesis 106. Recombinant PDGF-BB topical gel (100ìg/g), applied once daily, has been approved by FDA for the treatment of diabetic foot ulcers 107, 108.
8. Recombinant Human IL-10
Recombinant Human IL-10 (Tenovil)can be given in subcutaneousinjections. Early phase clinical trials have shown thatrecombinant human IL-10 three times a week improved psoriasis 109, 110.
SIDE EFFECTS OF BIOLOGICS 5, 111, 112, 113
Some of the adverse effects of biologics are described below:
Allergic reaction and antibody formation: Mostly seen with TNF-α blockers.
Mild transient injection site reactions: Comprising of erythema, oedema and bruising, noted with etanercept in 10-20% of cases in the first month of therapy. Antibodies to etanercept may develop in 6% of patients.
Infusion reaction: Occurs during or within 1-2 hours of treatment and may affect up to 20% of all the patients treated with infliximab, rarely anaphylactic shock may occur.
Acute flu-like symptoms: Headache, chills, fever, nausea and myalgia may occur within 48 hours after administration of the first two doses of efalizumab and Interferon α.
Infections: Reactivation of tuberculosis may occur on treatment with anti-TNF-α agents and sepsis secondary to Listeria monocytogenes and Histoplasma capsulatum have been reported 113.
Malignancy: Patients previously treated with PUVA represent an at-risk group.
Demyelinating disease: Worsening of multiple sclerosis and demyelination reported with infliximab.
Thrombocytopenia: Occurs with efalizumab and warrants discontinuation of therapy.
Autoimmune haemolytic anemia: Occurs 4-6 months after the start of treatment with efalizumab.
Congestive cardiac failure: Worsening of congestive cardiac failure with TNF-α blockers is reported to occur.
Antinuclear antibodies and lupus-like syndrome: May develop during therapy with anti-TNF-α agents, but not associated with symptoms and signs of lupus in the majority.
Hepatitis: Reported following infliximab therapy, occurring from 2 weeks to more than a year after initiation of treatment. Treatment should be stopped in the event of jaundice and/ or marked elevations (>5 times the upper limit of normal) in liver enzymes.
PATIENT SCREENING FOR BIOLOGIC THERAPY 113, 114
All patients to be put on biologics should undergo a thorough evaluation including detailed clinical history, physical examination and relevant investigations with particular reference to known toxicity profile of the agent being considered. The investigations generally advised are113: full blood count, liver and renal function tests, screening for hepatitis and HIV infection, anti-nuclear antibodies, anti-ds DNA, urine analysis, chest X-ray and Tuberculin skin testing.
For efalizumab, haemogram (including platelet count) is recommended monthly for the first 3 months and then every 3 months. For TNF blockers, it is done at 3 months initially and repeated every 6 months.
Liver and renal function tests, serum electrolytes and urine analysis are done at 3 months initially and then every 6 months.
EXCLUSION CRITERIA/ CONTRAINDICATIONS
There are various contraindications for use of biologics, warranting their exclusion and precautions are to be exercised because of their immune-modulator properties. The main exclusion criteria are: active tuberculosis, severe congestive heart failure, patients having >200 treatments of PUVA (because of a risk of developing malignancies with anti- TNF agents), history of demyelinating disease or optic neuritis, hepatitis B and C positivity, HIV positivity, premalignant states, active infections and high risk states such as chronic leg ulcers, persistent or recurrent chest infections and indwelling urinary catheter infections, pregnancy and breast-feeding.
ASSESSMENT OF THE RESPONSE TO BIOLOGICS
Many scoring systems for assessing the severity of various dermatological diseases exist. These scoring systems and other indices can be used for assessment of response to the use of biologics. For example, for evaluation of improvement in psoriasis, PASI (psoriasis area and severity index) and DLQI (dermatology life quality index) are recommended at 3 months initially and then every 6 months 113. Reduction in baseline PASI score of >75% is the standard used by FDA to assess the efficacy of a new psoriasis agent 115. Similarly in atopic eczemas, improvement is monitored based on the Eczema Area and Severity Index, Pruritus Severity Assessment and DLQI. Reduction of the Eczema Area and Severity Index score by 50% is considered excellent, 30-49% moderate and <29% non-significant.
SUMMARY
To summarise, biologics represent the future of therapeutics, not only in dermatology but also in other fields of medicine. Among the various dermatological disorders where they are used, biologics have been most evaluated in psoriasis 116. However, the possibility of serious infections and the oncogenic potential combined with the high cost of the drugs limit their routine use at the present stage 117. Regular re-evaluation of efficacy and safety is essential if these agents are to be used to the maximum benefit of patients118.
Anterior Cruciate Ligament (ACL) reconstructions are increasingly being undertaken throughout the United Kingdom (UK). Advances in General and Local Anaesthetic as well as surgical technique allow reconstructions as a day case procedure.1,2,3 There are currently no studies showing post-operative pain suffered by ACL reconstruction patients, nor showing the comparison of day case and inpatient pain scores.
We document, prospectively, patients’ post-operative pain after ACL reconstructions. We aim to identify and assess factors that affect pain post-ACL reconstructions including additional procedures, type of nerve blocks and whether the procedure was performed as a day case or as an inpatient.
We propose that patients having ACL reconstruction have no difference in pain scores when having the procedure as a day case compared to performance with inpatient stay. We also propose that additional procedures do not cause an increase in pain. We hypothesise that patients having Femoral nerve block have no increase in pain compared to patients having combined Femoral and Sciatic nerve block.
Method
All patients having ACL reconstruction between April 2010 and September 2010 were evaluated prospectively. Four strand arthroscopic hamstring reconstructions were performed by two specialist knee surgeons using a similar technique. Anaesthetic was performed by varying anaesthetists with a General Anaesthetic and Regional Nerve Block with Bupivicaine (Femoral nerve block or Femoral plus Sciatic nerve block). This was performed in the anaesthetic room under ultrasound guidance. Intra-operatively, patients received standardised anaesthesia. All patients received one dose of intravenous Paracetamol and two intravenous doses of opiates (Morphine or Fentanyl, as tolerated) at the beginning and end of the procedure.
Inclusion criteria used were all ACL reconstructions performed on patients over 16 years of age. No exclusion criteria were used.
Arthroscopic hamstring reconstruction was undertaken using a four strand Semitendinosus and Gracilis graft. During the arthroscopy, any additional procedures necessary were performed (e.g. meniscal repair, menisectomy, etc.). No drains were used. The knee was placed into an immobilisation splint until the nerve blocks had worn off.
Patients were discharged once they were back on the ward and deemed safe for discharge by the physiotherapists, medical and nursing staff. They were discharged with Paracetamol, a non-steroidal anti-inflammatory (if tolerated) and a mild opiate (Tramadol or Codeine Phosphate).
After discharge from the ward, patients were brought back to an aftercare clinic, with a senior physiotherapist, any time up to 48 hours post-operatively, to assess whether the nerve block had worn off, perform a wound check and to reinforce physiotherapy advice.
Patients were given a discharge questionnaire asking them to record their pain scores daily, when the pain was at its worst, using the Numerical Rating Scale (NRS) from 0-10. Documentation commenced on the day of the procedure and was requested daily for one week. Complications were also documented by the patient. These questionnaires were handed in at the two week follow up appointment, at which point patients were also asked if they would have the surgery performed as a day case again.
Pain scores were analysed using a Box-whisker plot followed by a Shapiro-Wilk W test which showed a non-parametric data spread. Scores were subsequently analysed using a Mann-Whitney U test to assess significance (p=0.05).
Results
ACL Reconstruction was attempted in 50 patients from April 2009 up to and including September 2009. The average age of patients was 31.0 years (Range 16-55). Of the cohort, there were 36 male patients with 14 females. All of the ACL reconstructions had a General Anaesthetic and all had infiltration of their graft site and medial wound with Bupivicaine. 42 had a Femoral nerve block with Bupivicaine and eight had a Bupivicaine Femoral and Sciatic nerve block. Of the 50 patients, 13 patients had additional procedures formed.
29 patients from the group were discharged as a day case. 21 patients required inpatient stay for the reasons documented in Figure 1 below.
Figure 1. Reasons for inpatient stay after ACL reconstruction
Social reasons for inpatient stay included out-of-area patients and those who had no home support to care for them on the day of surgery. Patients who were unable to safely mobilise post-operatively were classified as having failed physiotherapist discharge assessment. Two patients were unable to be discharged due to excessive pain. Two patients had symptoms related to General Anaesthesia (e.g. nausea and dizziness) which prohibited discharge. Seven patients arrived back onto the ward with insufficient time for recovery and physiotherapy assessment, thus preventing day case discharge. In all seven cases, this was due to ACL reconstruction being performed late on the operating list.
On day one post-operatively the average NRS pain score for the day case group was 4.1, the average score for the inpatient group was 5.52. The pain score decreased steadily as the week went on. Pain scores on days one to four was statistically lower (p=0.05) in day case patients compared to inpatients (Table 1 and Figure 2). Figures 3 and 4 show the box whisker plots for inpatient vs day case pain scores on day 1 and 2.
Post-operative day
Daycase Pain Score (N1=29)
Inpatient Pain Score (N2=21)
P Value (*=significant)
1
4.1
5.52
0.03*
2
3.93
5.14
0.04*
3
3.62
4.81
0.03*
4
3.1
4.38
0.03*
5
3.1
4.29
0.09
6
2.69
4.00
0.03*
7
2.52
3.62
0.06
Table 1. Average NRS pain scores of patients undergoing ACL reconstruction
Figure 2. Comparison of NRS pain scores of day case and inpatient ACL reconstruction
Figure 3. Box Whisker plots for pain scores on day 1 for inpatients and day case patients
Figure 4. Box Whisker plots for pain scores on day 2 for inpatients and day case patients
Out of 50 patients, 42 patients had Femoral nerve blocks with the remaining eight patients having a combined Femoral and Sciatic nerve block. On average, patients receiving only a Femoral nerve block had lower pain scores compared to those receiving the combined block, although with the difference in cohort numbers, there was no statistical difference (p=0.09 on day 1 and p=0.5 on day 2) [Figure 5].
Figure 5. Comparison of daily pain scores with Femoral and Femoral/Sciatic nerve blocks
Of the 50 patients attempting the day case procedure, there were 17 additional procedures. Eight partial medial menisectomies, three partial lateral menisectomies, two lateral meniscal repairs, two medial meniscal repairs and two medial femoral condyle microfractures. There was no correlation identified between additional procedures and increased patient pain scores (Figure 6).
Figure 6. Comparison of pain scores of patients having additional procedures
When patient satisfaction among the 29 patients who had day case ACL reconstruction was asked, 100% were happy with the day case procedure. One patient felt that they would opt to have the operation done with an inpatient stay as they felt “groggy” overnight. They were otherwise happy with the day case procedure.
All patients had quadriceps function return at day 1 post-operatively and there were no re-admissions due to pain or being unable to cope at home. There were no infections amongst the groups.
Discussion
Day case ACL reconstructions are commonly undertaken in the UK. Literature from Sheffield, Glasgow and Romford1,2,3 shows that the rate of admission and complications is low and the procedure is safe and effective. It has been well tolerated by patients.
Day case surgery is encouraged by the government led Department of Health.3,4,5 It reduces the risk of cancellations and infections and can also have economic benefits for the National Health Service (NHS). In the United States (US), Bonsell has shown that a single day case ACL reconstruction saves the hospital $2234 compared to a procedure with an inpatient stay. Bonsell also proposed that day case ACL reconstructions are performed significantly quicker than inpatient reconstructions (approximately 23 minutes quicker) which could save the hospital $85000 per year.6
Day case patients were found to have statistically significant, lower pain scores compared to inpatients. Farrar et al have shown that, using the NRS pain scoring system, only a difference of greater than two points can be deemed clinically significant. However, the results of this study have shown that there is no clinical difference or worse pain when the procedure is performed as a day case.7 Krywulak et al noted that the average Visual Analogue Score (VAS) score for patients’ satisfaction post-day case ACL reconstructions was 85.1 compared to the inpatient average score of 78.2.8 This is validated in our study of which 100% of patients were happy with the day case procedure.
Patients were encouraged to take analgesia regularly for two weeks post-operatively but the amount of medication actually taken was not formally documented. This could potentially lead to some of the bias in this study. However, the significance of this bias is difficult to determine accurately as the NRS pain scores were recorded when the patients’ pain was at its worst. This would most likely be between analgesic doses so hopefully eliminating some of the bias.
Little is known about pain associated with the procedure of day case ACL reconstruction and also pain suffered compared to those undergoing inpatient stay. We have been able to compare pain scores of patients undergoing ACL reconstruction as a day case procedure with those undergoing the procedure as an inpatient. We found that patients having the procedure as a day case had significantly lower pain scores on days 1-4 post-ACL reconstruction compared to inpatients.
Day case ACL reconstructions are safe and not associated with any difference in pain compared to inpatient stays. This is important in pre-operative guidance given to patients and, in view of the risks of hospital inpatient stays and also additional costs to the Health Service and Primary Care Trust (PCT), ACL reconstruction as a day case procedure should be highly recommended to patients compared to an inpatient surgical procedure.9-11 Information can be given to patients advising them that pain will not be worse when the procedure is performed as a day case which will encourage more patients to accept same day discharge.
Further work needs to be done to assess the possible difference in pain scores associated with Femoral nerve blocks compared with combined Femoral and Sciatic nerve blocks but our results appear to show that significant difference is unlikely.
Patient satisfaction with the day case ACL procedure was excellent and subsequently day case ACL reconstruction is now routinely performed in this Trust.
Colorectal cancer (CRC) is the third most common cancer in men and women worldwide (1) and a leading cause of cancer related deaths (2). 5FU synthesized in 1957 by Heidelberger (3) is the mainstay in all current standard regimens for CRC (4). Chemotherapy induced hepatic toxicity in 5FU based regimens can be an acute or delayed outcome (5, 6); whereas steatosis is a hallmark of 5FU induced hepatic toxicity (7). Chemotherapy induced nephrotoxicity (8) is also an area of concern for oncologists. The antimetabolite 5FU is often linked with kidney damage (9). Therapeutic outcomes and toxicity of 5FU differs markedly in different doses, combinations, schedules of administration and routes of administration. Leucovorin (LV) incorporated in 5FU based regimen enhances the cytotoxicity of 5FU. In this study we opt to report abnormalities in hepatic enzymes and renal biomarkers biochemically assessed in the serum after alternate cycles of treatment in CRC patients subjected to 5FU/LV based chemotherapy.
Methods:
The study was designed in the Department of Pharmacology, University of Karachia and conducted in a leading cancer hospital in Pakistan. Following institutional authorisation, informed consent was obtained from patients being admitted during 2008-2011. The inclusion criteria was maintained on the following grounds:
1. Histologically confirmed advanced colorectal carcinoma 2. Adequate blood count before therapy 3. Age 20-80 years 4. ECOG score of < 3 5. Serum bilirubin < 5× normal 6. Serum creatinine < 135µmol/liter 7. Serum transaminases < ×2.5 normal
Twenty three patients (median age 59 years) who underwent surgery were included in the study. All the patients had measureable disease at CT scan, ultrasonography or clinical examination. Patient’s characteristics are shown in Table 1. Seventeen patients were treated with the adjuvant bimonthly regimen of 5FU/LV - high dose Folinic acid (de Gramont Regimen); whereas, six patients were treated with adjuvant monthly regimen of 5FU/LV –low dose Folinic acid(Mayo Clinic Regimen) as follows.
5Fluorouracil/ Leucovorin (de Gramont’s regimen)
5Fluorouracil: 400mg/m2 IV followed by 600mg/m2 CIV for 22 hours on day 1-2. Leucovorin: 600 mg/m2 IV as 2 hours infusion before 5FU on day 1-2. Cycle repeated after 2 weeks.
5Fluorouracil/ Leucovorin (Mayo clinic regimen)
5Fluorouracil: 425mg/m2 IV on day 1-5. Leucovorin: 20 mg/m2 IV before 5FU on day 1-5. Cycle repeated after 4-5 weeks.
Premedication with oral phenothiazines, 5HT3RA and 10-20 mg of dexamethasone was given.
The blood samples were collected before the initiation of the therapy and after each alternate cycle of treatment. The blood was drawn when the patient was rested and comfortable from the antecubital vein under minimal tourniquet pressure. The blood drawn was sampled and collected into vacutainers (BD). The biochemical profile of the pretreatment and subsequent treatment was comparatively assessed. SGOT, SGPT, bilirubin and alkaline phosphatase levels were measured after each cycle of treatment or on the clinical presentation of any hepatic adverse effect notified by the physician or oncologist and the levels were compared to the pretreatment values. The serum creatinine levels and BUN was measured before the start of chemotherapy and after each alternate cycle of treatment up to six times in each patient.
Table 1 Patient characteristics
Parameters
Arm A
Arm B
de Gramont
Mayo Clinic
No. of Patients
%
No. of Patients
%
Demographic Characteristics
Male
12
70.58
4
66.6
Female
5
29.41
2
33.3
Total Patients
17
6
Age: Years
Median
59
Range
56-65
ECOG Performance Status (21)
0
1
5.88
1
16.6
1
3
17.64
1
16.6
2
13
76.47
4
66.6
3
0
0
0
0
Primary Site
Colon
11
64.7
3
50
Rectum
5
29.4
2
32.3
Multiple
1
5.88
1
16.6
Metastases
Synchronous
11
64.7
4
66.6
Metachronous
6
35.2
2
32.3
Metastatic Site
Liver
8
47.0
1
16.6
Lymph nodes
4
23.5
2
32.3
Other*
5
29.4
3
50
No. of Sites
1
7
41.1
2
32.3
> 2
10
58.8
4
66.6
CEA
< 10ng/ml
2
11.7
1
16.6
>10ng/ml
8
47.0
1
16.6
Unknown
7
41.1
4
66.6
* = Peritoneal/ovary
Results:
Table 2shows that the SGOT levels are raised after each cycle of treatment and the difference between the SGOT levels of the patients before treatment and after subsequent cycle of treatment is significant in the patients treated with 5FU/LV (p value < 0.05). The difference in the SGPT levels of the patients from the pretreatment value is not highly significant (p value >0.05). The difference in the bilirubin levels of the patients after the sixth cycle of chemotherapy with 5FU/LV regimens is highly significant from the pretreatment level (p value < 0.05). The difference in the alkaline phosphatase levels of the patients after chemotherapy with the pretreatment value in the same patients is not significant (p value >0.05).The difference in the triglyceride levels is not significant before and after chemotherapy in the patients treated with 5FU/LV.
Table 2 Comparative changes in hepatic biomarkers in patients treated with 5FU/LV regimen
Paired Samples Test
Paired Differences
t
p-value
Mean
Std. Deviation
Hepatic
TGS
Control - Cycle 2
-1.200
1.643
-1.633
0.178
Control - Cycle 4
-3.200
3.033
-2.359
0.078
Control - Cycle 6
-3.400
2.966
-2.563
0.062
Control - Cycle 8
-10.000
10.198
-2.193
0.093
Control - Cycle 10
-3.600
8.414
-0.957
0.393
Control - Cycle 12
-8.800
12.872
-1.529
0.201
SGOT / AST
Control - Cycle 2
-12.667
5.033
-4.359
0.049
Control - Cycle 4
-22.000
3.464
-11.000
0.008
Control - Cycle 6
-22.667
3.055
-12.851
0.006
Control - Cycle 8
-25.333
3.055
-14.363
0.005
Control - Cycle 10
-27.000
7.810
-5.988
0.027
Control - Cycle 12
-28.667
7.024
-7.069
0.019
SGPT / ALT
Control - Cycle 2
-2.667
3.055
-1.512
0.270
Control - Cycle 4
-3.667
2.082
-3.051
0.093
Control - Cycle 6
-9.333
8.505
-1.901
0.198
Control - Cycle 8
-12.667
8.083
-2.714
0.113
Control - Cycle 10
-17.667
5.859
-5.222
0.035
Control - Cycle 12
-22.667
10.214
-3.844
0.062
Bilirubin
Control - Cycle 2
0.033
0.058
1.000
0.423
Control - Cycle 4
0.000
0.100
0.000
1.000
Control - Cycle 6
-0.267
0.058
-8.000
0.015
Control - Cycle 8
-0.267
0.058
-8.000
0.015
Control - Cycle 10
-0.267
0.058
-8.000
0.015
Control - Cycle 12
-0.367
0.115
-5.500
0.032
ALKPO4
Control - Cycle 2
-6.667
5.774
-2.000
0.184
Control - Cycle 4
-10.000
10.000
-1.732
0.225
Control - Cycle 6
-26.667
11.547
-4.000
0.057
Control - Cycle 8
-43.333
40.415
-1.857
0.204
Control - Cycle 10
-60.000
36.056
-2.882
0.102
Control - Cycle 12
-63.333
40.415
-2.714
0.113
Table 3 shows that the creatinine levels are raised in patients following each subsequent cycle of treatment with 5FU/LV regimens. The difference in the serum creatinine levels after the fourth and the tenth cycle of treatment with the pretreatment levels was significant (p<0.05). The difference in the BUN levels measures before and after chemotherapy with 5FU/LV was not significant following alternate cycles of treatment.
Table 3 Comparative changes in renal biomarkers in patients treated with 5FU/LV regimen
Paired Samples Test
Paired Differences
t
p-value
Mean
Std. Deviation
Renal
Creatinine
Control - Cycle 2
-0.120
0.130
-2.058
0.109
Control - Cycle 4
-0.160
0.114
-3.138
0.035
Control - Cycle 6
-0.242
0.204
-2.646
0.057
Control - Cycle 8
-0.264
0.225
-2.627
0.058
Control - Cycle 10
-0.546
0.422
-2.893
0.044
Control - Cycle 12
-0.566
0.463
-2.734
0.052
BUN
Control - Cycle 2
-1.800
1.924
-2.092
0.105
Control - Cycle 4
-1.800
1.924
-2.092
0.105
Control - Cycle 6
-2.000
2.449
-1.826
0.142
Control - Cycle 8
-3.000
2.550
-2.631
0.058
Control - Cycle 10
-4.400
4.037
-2.437
0.071
Control - Cycle 12
-6.400
8.204
-1.744
0.156
Discussion:
The hepatocellular enzyme findings are indicative of deteriorating liver function. The levels of SGOT and SGPT both differ from the control values and point toward 5FU induced hepatic toxicity. Increase in SGOT and SGPT up to grade 2 (CTC of NIC) is reported by Hotta and colleagues (10) in a study based on clinicopathological assessment of 36 patients treated with 5FU/LV. They did not report grade 3 or grade 4 elevations in SGOT and SGPT ratio. In our data there is considerable difference in SGOT levels (mean value) after the second cycle of treatment as compared to the pretreatment levels (mean value). Similarly SGPT levels are perturbed following treatment and the difference in the SGPT levels from the pretreatment control value is statistically significant after the tenth cycle of treatment. The pooled data of all the patients cannot be used for prognostic or diagnostic assessment; however, it shows a pattern of drug induced alterations in hepatic functions. An early effect on SGOT level show mild progressive damages correlated with a prominent rise in SGPT levels. SGOT is found in cytosol whereas SGPT is in mitochondria. Any mild to moderate damage to the hepatic cells will result in a rise in SGOT levels even though SGPT levels may remain normalised. Moderate to Severe hepatic damage will give a rise in both SGOT and SGPT elevation. SGOT is located in red blood cells, kidneys, brain, skeletal muscle and cardiac tissues; hence a prompt rise in SGOT level is indicative of associated damages. SGPT is present in skeletal muscles and cardiac tissues and the serum levels are affected with myocardial and skeletal muscle damages. Cytotoxic chemotherapy is frequently associated with fatty liver disease, chemical hepatitis and reactivation of hepatitis B (11). The elevation in triglyceride levels is indicative of drug induced steatosis (fat globule deposition in hepatocytes) leading to postoperative hepatic insufficiency(8). A significant change in bilirubin from the pretreatment level is observed after the 6th cycle of treatment. Biliary changes are detectable and persistent since the drug is excreted in the bile. Sclerosing cholangitis with elevation in alkaline phosphatase and bilirubin levels secondary to 5FU plus mitomycin therapy is reported by Fukuzumi et al (12). After intravenous administration, 5FU is converted into its active form ‘5-fluoro-deoxyuridine-monophosphate’ by anabolic reactions in the tissues. The drug undergoes catabolism primarily in the liver by reduction of the pyrimidine ring by enzymatic action of dihydrouracil dehydrogenase (13). The compound is then cleaved to urea, ammonia, carbondioxide and α-fluoro-β-alanine. The catabolic process in the liver amounts for 5FU induced hepatic toxicity. Hepatic and renal toxicity associated with 5FU is reported earlier with IV administration of 5FU (14). The risk of 5FU induced hepatic damages is increased in older patients (15). Older patients included in our study with increased post-treatment transaminase levels were more frequently presented with pruritus and hand and foot syndrome.This complexity of the situation is that altered hepatic function increases the risk of 5FU concentration (since it is catabolized in the liver cells), which in turn adds to the hepatic damage.
Creatinine clearance and blood urea nitrogen (BUN) are conventional biomarkers of renal function for convenient and cost-effective assessment (16). A detectable change in the creatinine levels of the patients ensue after the fourth cycle of treatment. Besides suggesting a decline in the renal function, it also indicates defect in hepatic functional status and progressive cachexia (muscle wasting), both of which are readily assessed in the patients during treatment. BUN levels are also affected by dexamethasone pretreatment, dehydration and azotemia besides renal function. Nephrotoxicity with 5FU chemotherapy is usually reported when it is combined with cisplatin with worsened creatinine levels (17, 18). Tubular damage induced by 5FU plus high dose leucovorin chemotherapy (similar to de Gramont’s regimen in our study) is reported by Kintzel, who also reported 50% decline in creatinine clearance in three patients (19). Chemotherapy induced renal damages are detected with abnormal creatinine and BUN levels, but in most cases the renal tubes remain intact and functional as the normal renal blood flow and GFR is reversibly attained (20). Adequate hydration and simultaneous treatment with mesna, which neutralises the toxic metabolites can effectively reduce chemotherapy induced renal damage (8).
Conclusion:
SGOT and bilirubin levels are raised after each cycle of treatment and the difference between the SGOT levels of the patients treated with 5FU/LV, before treatment and after subsequent cycle of treatment are highly significant indicative of mild to moderate progressive hepatic toxicity. Risk of clinical and subclinical renal damage is observed by a subsequent rise in serum creatinine and BUN levels. Renal toxicity marked by creatinine elevation is prominent after the fourth cycle of treatment.
Psoriasis is a common skin disorder characterized by erythematous papules and plaque formation with silver scaling. Guttate psoriasis is much less common and many studies cite a prevalence of less than 30% among patients who have psoriasis. It refers to the acute appearance of multiple skin eruptions mostly in a patient with no preexisting psoriasis and less commonly in a patient with psoriasis. We report here a case of guttate psoriasis associated with a flare of psoriatic arthritis.
Case report
A 53 year old man presented with a generalized body rash and multiple joint pains. His symptoms started a week prior to presentation. The skin rash initially appeared on his back and flanks but gradually progressed to involve the thighs and arms. He had ‘sausage fingers’, bilateral knee and ankle swelling associated with pain and sporadic metatarsophalyngeal joint pain as manifestations of his arthritis. His past medical history included hypertension, diabetes mellitus, hyperlipidemia and psoriasis with psoriatic arthritis. He did not report any recent changes in his medication. The patient denied any history of fever, sore throat, weight loss, visual problems, dyspnea, cough, gastrointestinal complaints or recent travel. Physical examination revealed a diffuse, non-blanching, pruritic, maculopapular and maculopustular rash over the trunk. He also had a scaly and diffuse erythematic rash over the lower abdomen which was non-blanching and pruritic. Auspitz’s sign was positive. He had multiple painful joints including both knees, right wrist, left proximal interphalangeal joint, and both his ankles. Left knee arthrocentesis was done which revealed joint fluid consistent with inflammatory joint disease without any evidence of crystals. Laboratory tests, including red and white blood cell count, haemoglobin, cyclic citrullinated peptide antibody, rapid plasma regain, hepatitis panel, antinuclear antibody, rheumatoid factor, lyme markers and serum uric acid revealed no abnormalities. ASO titer level was positive at 196. An x-ray of his left hand showed periarticular erosive changes along the distal aspect of the proximal phalanx. A skin biopsy was performed which revealed mild spongiosis and a perivascular lymphoplastic infiltrate. A diagnosis of guttate psoriasis was made. He was started on prednisone, methotrexate and folic acid and discharged from hospital. He was followed up in the rheumatology clinic 2 weeks after discharge and his rash had improved.
Discussion
Unlike psoriasis, guttate psoriasis is a much lesser known entity. It refers to the acute appearance of multiple skin eruptions, mostly in patients with no preexisting psoriasis and less commonly in chronic plaque psoriasis (guttate flare of chronic plaque psoriasis).
The characteristic skin lesions of guttate psoriasis are less than 1 cm in diameter, hence the name guttate (drop like). The lesions look like a shower of red, scaly tear drops that have fallen down on the body mainly involving the trunk, arms, thighs and face. Guttate psoriasis should be differentiated from diabetic dermopathy, also called shin spots, which typically begin as dull red, scaly papules or plaques and later develop into bilateral asymmetrical circumscribed shallow pigmented scars and/or brownish macular lesions with a fine scale. In diabetic dermopathy the lesions usually are greater than 4 cm in size.
Diagnosis is usually made on clinical examination; however skin biopsy is helpful in difficult cases. Histopathologic findings of guttate psoriasis vary with the age of the lesion. Findings in early lesions may be nonspecific and may include mild acanthosis, papillary dermal oedema and lymphocyte-predominant dermal infiltrate. Mature lesions exhibit parakeratosis alternating with hyperkeratosis, epidermal acanthosis, Munro microabscesses and dermal perivascular infiltrate containg neutrophils, lymphocytes and macrophages.
Streptococcal infections are well known to precipitate guttate psoriasis,1 however there have been no significant improvements in patients who were given penicillin or erythromycin when compared to those who were not treated.2 Other known precipitants are physical and psychological trauma.
The exact pathophysiologic mechanism is undetermined. The disease is believed to result from an immune reaction triggered by a previous streptococcal infection in a genetically susceptible host. Recent research points toward chromosome 6 as HLA-Cw*0602 allele positive patients are more prone to develop the guttate form.
Atopic dermatitis (AD), also known as atopic eczema is a chronic, relapsing, inflammatory skin disease that can cause significant physical, psychological and social stress for patients and their families.1 This article focuses primarily on AD in adults. It is the most frequent inflammatory skin disease in the western world and is often characterized by chronic inflammation and pruritus interrupted by acute flares and bacterial infection.2,3 The majority of the care of AD is provided in primary care, with a minority of patients being referred to secondary care. There are currently extensive cost implications to the National Health Service (NHS) for both treating patients and for lost working days.4 AD can be a therapeutic challenge, especially in primary care, and there appears to be a great potential for improving the outcome and cost effectiveness of treatment in the community setting.4
Epidemiology and pathogenesis
AD typically begins in young infants or early childhood and subsides spontaneously by adolescence in approximately 90% of patients although it can persist into adulthood in about 10% of patients.5 The incidence of AD is generally considered to be increasing worldwide.6 AD affects both sexes equally, and in the United kingdom (UK) approximately 15-20% of school-aged children and 2-10% of adults will be affected by the condition at some stage.7
AD appears to result from a complex interplay between defects in skin barrier function, environmental agents, modified immune responses of the immune system to exogenous and endogenous factors, IgE-mediated mechanisms and other factors. However, the pathogenesis leading to the precise manifestation of AD is not completely understood.3,8
Diagnosis
There are no laboratory or diagnostic tests for AD. The diagnosis is based on visual assessment and clinical history. The UK diagnostic criteria (Table1) has been shown to be the most extensively validated for AD in comparison to the Hanifin and Rajka criteria, Schulz-Larsen criteria, Diepgen criteria, and Kang and Tian diagnostic criteria. Although several different diagnostic criteria have been developed they should mainly be used for research purposes as opposed to daily clinical management.4
Skin tests and laboratory investigations (specific IgE) may be helpful in the investigation of provocative factors such as food or environmental allergens. It is important to note that laboratory investigations should be interpreted in the context of the patient’s history.9
It is often difficult to differentiate AD from other skin conditions (e.g. seborrhoeic dermatitis, contact dermatitis, psoriasis, scabies). However, a family history of atopy and the clinical distribution of the lesions are helpful in making the diagnosis. Other conditions that need to be considered in the differential diagnosis of AD are metabolic and nutritional deficiencies, malignancies and immunodeficiency syndromes that present with skin manifestations.8
Table 1 – UK Working Party Diagnostic Criteria4
The patient must report an itchy skin condition (or parental report of scratching or rubbing in a child) in the last 12 months, plus three or more of the following:
History of involvement of the skin creases (front of elbows, behind knees, fronts of ankles, around neck or around eyes)
Personal history of asthma or hay fever (or history of atopic disease in first degree relative if child aged under four years)
A history of generally dry skin in the last year
Onset under the age of two years (not used if child aged under 4 years)
Visible flexural dermatitis (including dermatitis affecting cheeks or forehead and outer aspects of limbs in children under four years)
Management
The management of AD should involve a combination that includes short-term treatment of flares and a long-term maintenance approach to prevent flares. For patients with mild to moderate AD, topical therapy may be sufficient to control the condition. Patients with more severe disease may require advanced therapy such phototherapy or systemic therapy.
Education
For optimal disease management, patients and/or their carers should be educated about the nature of AD, the need for continued adherence to prescribed treatment and about the appropriate use of topical therapies. Time spent educating patients and carers have been shown to have a positive effect on disease outcomes. Patients may also benefit from written information to reinforce learning.8
Emollients
Emollients soften the skin, aid in restoring the impaired barrier function, reduce itching, prevent moisture from leaving the skin and increase the efficacy of topical corticosteroids (TCS). They also replace the natural surface oils that are essential to preventing irritant materials, infection and allergy-inducing substances from entering the skin.4
Healthcare professionals should offer a range of emollients, and prescriptions should be reviewed frequently. To optimise adherence to emollient therapy, creams, lotions, and ointments, or a combination can be used depending on patient preference. Continued use of emollients during periods of disease quiescence can reduce the likelihood for exacerbations.10
When the treatment regimen involves both an emollient and TCS, there is no evidence on which to base the order of application. Patients should be advised to apply emollients liberally and frequently (at least 2-4 times a day). It is especially important to use emollients during or after bathing. The emollient should be applied in the general direction of growth of body hair in order to prevent accumulation at hair bases which might predispose to folliculitis. Emollients can become contaminated with bacteria and the use of pump dispensers minimises this risk. If the emollient is in a pot it should be removed with a clean spoon or spatula.4
Topical corticosteroid therapy (TCS)
TCS is considered first-line therapy for AD flares. Available preparations include ointments, creams, gels, lotions, liquids, and foams. Ointments and creams are generally the most effective in treating AD as they tend to be more moisturising.10 The least potent preparation required to control AD, particularly in sensitive areas, should be utilised. When possible the TCS should be stopped for short periods to reduce the risk of adverse events.8
TCS is categorised into four groups according to potency: mild, moderately potent, potent and very potent. The choice of TCS potency should be tailored to the age of the patient, the body region being treated, and the severity of inflammation. Patients should be advised to apply TCS once daily. If there is an inadequate response to once daily application, the frequency should be increased to twice daily.4 Once control has been achieved, twice weekly maintenance therapy with a TCS should be considered in patients with moderate to severe AD experiencing frequent relapses. The local adverse effects of TCS usage include skin thinning, bruising, perioral dermatitis, folliculitis, pruritus, allergic contact dermatitis and the spread of fungal infection. Patients being treated with intermittent courses of TCS should be reviewed regularly (depending on TCS potency and site of application) to determine response to therapy and assess skin for potentially reversible atrophic changes.4
Table 2 - The ‘fingertip unit’ (FTU) is a method of determining the amount of TCS to apply. It is described as “the amount of ointment expressed from a tube with a 5 mm diameter nozzle, applied from the distal skin crease to the tip of the palmar aspect of the index finger.” The following table is a guide to the use of FTU in adults.4
Skin area
FTU per dose
Face and neck
2.5
Torso and abdomen
7
Back and buttocks
7
Entire arm and hand
4
A hand and fingers (front and back)
1
Entire leg and foot
8
Topical calcineurin inhibitors (TCIs)
TCIs are non-steroidal immunomodulating agents licensed for the treatment of AD.4 TCIs work by inhibiting the phosphatase activity of calcineurin to block expression of cytokines and are thought to represent a more targeted way to limit inflammation and avoid many of the adverse effects of TCS. TCIs may be used either as monotherapy, as a combination or as sequential therapy. TCS are generally less expensive and more effective than TCIs although individual clinical situations will arise in which TCIs are preferred.10
Two TCIs are available: tacrolimus (0.03% and 0.1% ointments) and 1% pimecrolimus cream. The tacrolimus 0.03% and 0.1% ointments are both licensed for moderate to severe eczema and the 0.03% ointment is licensed for use in children aged two years and over. The 1% pimecrolimus cream is licensed for mild to moderate eczema in patients aged two years and over. The use of tacrolimus should be limited to doctors with a specialist interest and experience in treating AD.4
TCIs should not be used as first line treatment unless there is a specific reason to avoid the use of TCS.4 Given the high cost of TCIs, and the fact that their long-term safety is not fully known, they are generally reserved for patients with persistent disease or frequent flares that would require continuous TCS treatment. They are also of use in patients with severe disease in sensitive skin areas (e.g. around the eyes, face, neck and genitals) where systemic absorption and the risk of skin atrophy with TCS are of concern. Considering the possibility that the normal immunological response to infection may be suppressed, TCIs should not be applied to skin which appears actively infected.4, 8
Dressings and wet wrap treatment
Patients with non-infected moderate to severe AD can be advised to cover affected areas with dry wrap dressings to provide a physical barrier to scratching and improve the retention of emollients. Wet wrapping generally consists of two layers of bandage applied over topical preparations. The bottom layer is soaked in warm water, squeezed out and then put onto the skin over the topical preparation. The top layer is dry. Wet wraps can be worn under nightwear or ordinary clothes and used during the day or night. They are available in bandage form or as garments.4 Disadvantages include a high cost, inconvenience, a need for specialised training, and an increased potential for adverse effects from occluded corticosteroids (such as systemic absorption, atrophy, striae), and increased incidence of skin infection.10 There is currently insufficient consistent evidence on which to base a recommendation for wet wrap use in the primary care setting.4
Antimicrobial measures
Skin lesions of around 90% of patients with AD are colonised compared to less than 5% of individuals with healthy skin. Staphylococci are the main organisms isolated although other organisms such as streptococci may also cause infection. The routine swabbing of skin is not indicated although swabs of potential Staphylococcus aureus carriage sites should be considered in patients with recurrent infection. Oral antibiotics are not recommended in the routine treatment of non-infected AD but patients with clinically infected AD can be prescribed short term oral antibiotic treatment based on local/regional antibiotic sensitivities. However, first- or second-generation cephalosporins or penicillins for 7 to 10 days are usually effective in managing bacterial infection. Macrolides are less useful alternatives due to resistant patterns in patients with AD. Patients with AD are also prone to recurrent viral infections. Eczema herpeticum is a severe disseminated herpes infection that is a serious risk in patients with widespread AD and may be misdiagnosed as a bacterial infection. Patients with eczema herpeticum normally require systemic antiviral treatment4, 10.
Antihistamines
Although first-generation antihistamines do not directly affect the itching associated with AD, the sedative effects have been found to help improve sleep. Therefore, short-term bedtime use of sedating antihistamines should be considered in patients with AD where there is debilitating sleep disturbance. Daytime use of first generation antihistamines should be avoided given their sedative effects. Non-sedating antihistamines appear to have limited value in patients with AD but they may provide some benefit in patients with allergic triggers.4, 8
Dietary interventions
Although there is an association between IgE mediated food allergy and AD severity in infants, it is unclear whether hypersensitivity to food is a major factor in causing and maintaining AD. Dietary exclusion is not recommended for managing AD in patients without confirmed food allergy. The exclusion of foods during pregnancy and breast feeding to prevent the development of AD in infants is not recommended. Breast feeding for three months or more may help prevent the development of infant eczema where there is a family history of atopy. However, current UK guidelines state that weaning should start at six months.4
Table 3 - Guidance on when to refer to secondary care4
Poor control of the condition or failure to respond to appropriate topical treatments
Psychological upset or sleep problems
Recurrent secondary infection
Other therapies
Systemic corticosteroids are usually reserved for the acute treatment of severe AD exacerbations. Prolonged use of oral steroids is associated with potentially serious adverse effects and their long-term use should be avoided. Furthermore, relapses are common following discontinuation of oral corticosteroid therapy.8
Ultraviolet (UV) phototherapy may also be beneficial for the treatment of AD in adults. In addition, systemic therapies are available and may be broadly classified into traditional medications (e.g. cyclosporine, azathrioprine, methotrexate) and biologic agents (targeted monoclonal antibodies). These options are available for severe, refractory AD. These therapeutic options should generally be reserved for unique situations and require consultation with a dermatologist. These therapeutic options are beyond the scope of this article.8
A 26 year old male was brought to Emergency department with history of altered sensorium of 1 day duration. He had a 2 week history of fever prior to admission. On examination, meningeal signs were present. Fundus examination showed evidence of papilloedema and a round pale yellow spot near the optic disc (Figure 1). CT scan of head did not reveal any abnormality.
Mantoux test and HIV ELISA were negative. CSF analysis showed:
Glucose – 40mg/dl; Protein: 2gm/l;
Cell Count: 1200cells/µl;
Cell Type: 80% lymphocytes;
CSF VDRL- negative;
CSF Grams stain, India ink staining and Ziehl Neelsen staining were unremarkable.
What is the Fundus finding?
Roth Spot
Cotton Wool Spot
Choroidal tubercle
A-V malformation
Discussion:
Correct answer: 3) Choroidal Tubercle.
Intraocular tuberculosis is a rare event and occurs in 1% of all diagnosed cases of tuberculosis.1 It occurs by haematogenous spread of mycobacterial organism. Choroidal tuberculosis is the most common initial manifestation of intraocular tuberculosis. They may be seen in 1.4% to 60% of patients with different forms of tuberculosis and are highly specific for tuberculosis. 2, 3
Choroidal tubercles may be unilateral or bilateral and appear as polymorphic yellowish lesions with discrete borders. They are of 2 types, solitary tubercle or granuloma (seen in chronic tuberculosis) and choroidal miliary tubercles (seen in acute miliary tuberculosis). Their size varies from 0.4 to 5 mm and may be associated with retinal vasculitis, panuveitis, choroiditis and neuroretinitis.
When they involve macula they present with visual loss and any delay in appropriate treatment results in irreversible visual loss. Peripherally situated tubercles are asymptomatic. Definitive diagnosis can be daunting due to difficulty in getting ocular samples for histological evaluation, however when available reveal features of granulomatous inflammation. Fundus angiography exhibits hypofluorescence in early stages and hyperfluorescence in later stages.
On treatment they heal by varying degrees of scar formation and marginal pigmentation.4 Untreated tubercles grow into large tumour like mass called tuberculoma.
Roth spots are retinal haemorrhages with a pale centre and are associated with bacterial endocarditis. Cotton wool spots appear as fluffy white patches on the retina and are associated with diabetes. A-V malformations are developmental vascular anomalies and appear as marked arterial and venous dilation associated with a tortuous pattern of vessels. They may have an associated bruit or chemosis of the eye.
The presence of ocular tuberculosis may be subtle. A high index of suspicion is required for its diagnosis. Delay in treatment or misdiagnosis may lead to irreversible visual loss.
Clozapine has shown to have superior efficacy compared to other antipsychotics and is the drug of choice for treatment-resistant schizophrenia. 1 However there is evidence that this treatment is actually under-prescribed. 2 Clozapine requires careful monitoring during the initial titration period. In the UK, this has originally been done in hospital settings to follow the manufacturer’s recommendations because of the risks of hypotension, excessive sedation and fits. Starting clozapine in a hospital setting ceased to be a mandatory regulatory requirement in the UK when the Summary of Product Characteristics was harmonised across Europe following an opinion and recommendation issued on the 12th of November 2002 by the Committee for Proprietary Medical Products of the European Medicines Agency. 3 Despite this happening several years ago, there is little information published about the practicality of successfully commencing clozapine in the community, with previous studies ranging from a single case report 4 to a few small case series of patients 5-8. Our study aimed to examine this practice in a larger sample to highlight the advantages and difficulties of initiating clozapine in the community.
Method
The Central Manchester day hospital was established in 1985, with a focus on acute psychiatric treatment as an alternative to in-patient care. From March 1997, the acute day hospital in Central Manchester was extended to 24 hours, seven days a week, adopting the name of the Home Option Service, focussing on flexible individualised care delivered at patient’s home or team base according to patient choice. 9 In 2007 as part of implementation of new teams across the city to comply with NHS policy guidance 10 the Home Option service developed further to become the crisis resolution and home treatment team (CRHT) for central Manchester, whilst CRHTs were set up de novo in North, and South Manchester, thereby, providing acute community psychiatric care to a metropolitan area of about 500,000 people.
This study describes a large case series of patients referred for clozapine titration in the community to these teams during a three year period. We collected data retrospectively from April 2007 to April 2010 of all the referrals to the three crisis teams, which have assumed the responsibility of providing the service of initiating clozapine in the community. The teams followed the Trust protocol for non-inpatient clozapine titration, which includes recommended monitoring parameters, dosing schedule and algorithms for the management of complications. This protocol is in essence similar to established guidelines. 4,5, 11
Statistical analysis was done using SPSS version 15 for Windows. Comparisons were made using the Student t-test, non parametric tests or the Chi-Square test according to the type of data.
Results
There were 6542 referrals to the crisis teams and 66 of those were related to clozapine initiation. Out of these, 36 were for a first time titration and 30 were referred for re-titration. The latter group were patients previously taking clozapine but who had discontinued it abruptly for a period longer than 48 hours. The reasons for stopping clozapine in those cases were lack of adherence (n=21), a supplying difficulty (n=5) and medical complications (n=4), such as neutropenia, collapse secondary to dehydration, or undergoing surgery. Two of the patients in the re-titration group restarted clozapine in hospital but were discharged early to continue the titration in the community under the care of the crisis team. Six patients in the titration group were initially referred to the crisis team for stabilisation of their mental state following a crisis; however, during the course of this intervention it was decided to start them on clozapine as they showed poor response to other antipsychotic trials.
Fig. 1 - Referrals, number of patients starting clozapine and drop-outs
The characteristics of the sample are presented in Table 1. The majority of patients were single white males, with a diagnosis of schizophrenia and a mean age of 38.8 years (standard deviation = 9.2). The flowchart in Figure 1 outlines the number of referrals, titrations, and reasons for stopping. Clozapine titration commenced in 54 cases (81.8% of referrals), the other 12 patients refused this treatment. Out of the patients who refused treatment, 8 were severely mentally unwell and were admitted to hospital compulsorily under the Mental Health Act. There were 46 (85.2%) patients who successfully completed the community titration. The attrition rate of 14.8% (8 cases) was due to 7 patients withdrawing their consent and one patient who was unable to tolerate the titration. This person was admitted to hospital with hypotension and vomiting. The other 7 patients withdrew their consent for the following reasons: lack of adherence (n=2), deterioration in mental state (n=1), refusal to continue with the physical monitoring (n=1), lack of motivation (n=1), and reluctance to continue due to side-effects (n=2). The mean final dose of clozapine was 309.1 mg (s.d. - 75.1 mg). The mean duration of titration was 34.6 days (s.d. - 20.3) and the mean length of admission to the crisis team was 45.9 days (s.d. - 39.5). The median waiting time for crisis team intervention after the referral was 2 days (range 140 days). The median waiting time to start clozapine was 7 days (range 217 days) from the point of referral.
Table 1. Sample characteristics
Total
Age in years, mean (s.d.)
38.8
(9.2)
Gender, n (%)
Male
45
(68.2)
Female
21
(31.8)
Ethnicity, n (%)
White
45
(68.2)
Black
14
(21.2)
Asian
3
(4.5)
Other
4
(6.1)
Marital Status, n (%)
Single
54
(81.8)
Married or cohabiting
5
(7.6)
Separated or divorced
6
(9.1)
Widowed
1
(1.5)
Diagnosis, n (%)
Schizophrenia
54
(81.8)
Schizoaffective disorder
8
(12.1)
Bipolar affective disorder
1
(1.5)
Other
3
(4.5)
Crisis Team, n (%)
North
21
(31.8)
Central
31
(47.0)
South
14
(21.2)
Days waiting to crisis team intervention
Mean (standard deviation)
9.5
(25.6)
Median (range)
2
(140)
Days waiting to start clozapine
Mean (standard deviation)
23.1
(40.9)
Median (range)
7
(217)
Days taken to complete the titration
Mean (standard deviation)
34.6
(20.3)
Median (range)
28
(101)
Days under the care of the crisis team
Mean (standard deviation)
45.9
(39.5)
Median (range)
34
(235)
Final dose in mg
Mean (standard deviation)
309.1
(75.1)
There were few significant differences between the group of patients starting clozapine for the first time (titration) and those restarting it following a treatment break (re-titration). There was a shorter wait for patients in the re-titration group to recommence clozapine from the time of referral to the service (median=6 days, range = 41 days), compared to those starting clozapine for the first time (median=13 days, range= 217 days). This difference was statistically significant (Mann Whitney U= 201.5, z=-2.529, p=0.01). Patients with first titration on clozapine reached a lower final dose (mean=288 mg, s.d.=50 mg), compared to those having re-titration (mean dose =340 mg, s.d.=94 mg). The mean difference of 52.7 mg (95% C.I. 8.7 to 96.8) between these two groups was significant (t test=-2.178, d.f 42, p=0.02). In terms of ethnicity, patients in the initial titration group were more likely to be Caucasian (n=30, 83%), whereas only half of the patients in the re-titration group were Caucasian (n=15, 50%). This difference was statistically significant (Chi-square with continuity correction = 6.915, df = 1, p=0.009).
There were also significant differences in the distribution of titrations and re-titrations across the three crisis teams. The Central Team dealt with more re-titrations (n=23) than the North (n=4) and the South (n=3) teams. Conversely, the Central Team had fewer patients referred for initial titration (n=8), compared to the North (n=17) and the South (n=11) teams. These differences were significant (Chi-square=19.493, df=2, p<0.0001). Another difference between the teams was the duration of clozapine titration, with the South team taking shorter time (mean=24.15 days, s.d.=7.151), compared to the North (mean=29.5 days, s.d=16.342) and the Central team (mean =43.67 days, s.d.= 23.797). This difference was statistically significant (Kruskal-Wallis chi-square=8.823, d.f.=2, p=0.0121).
No significant differences were found between teams and titration or re-titration groups in terms of patient’s diagnosis, gender, marital status, age, rate of accepted referrals, proportion of successfully finished titrations or waiting time to crisis team intervention.
With regards to adverse events, most patients experienced transient tachycardia (n=30, 55.5%). Other side-effects were excessive salivation (n= 15), hypotension (n= 13), sedation (n=10), hyperthermia (n=8), dizziness (n=6), constipation (n=6), hypertension (n=5), headaches (n=4), nausea (n=2), and heartburn (n=2). Less common adverse events (n=1) were syncope, seizures, transient neutropenia, atrial fibrillation, blurred vision, swelling of the arms , acute dystonic reaction, nocturnal incontinence, exacerbation of asthma, diabetes, erectile dysfunction and delayed ejaculation. Only the patient who developed syncope, which was associated with vomiting and severe hypotension, had to be advised to stop the treatment in the community and was admitted to hospital. For the rest of the patients, the other reported adverse events did not impede the successful completion of clozapine titration in the community.
In terms of longer term outcomes, a total of 50 patients (75.8% of the total sample) were still taking clozapine at the time the data was collected. This is after a median 337 days (range 824 days) from being referred to the crisis team. The majority of patients (n=14, 21.2%) who were not on clozapine had chosen to discontinue the treatment. One patient had died, but the cause of death was not related to clozapine treatment. One patient had developed neutropenia and needed to discontinue clozapine for this reason. Out of the 46 patients who successfully completed the titration, 40 (86.96%) were still continuing clozapine at the time we collected the data. This is after a median 365.5 days (range 824 days) after they commenced clozapine in the community.
Discussion
The results of this study confirm that clozapine can be safely and successfully started in the community. Comparing this to published evidence, we found only one case report 4 and a small study 5,6 previously conducted in the UK. O’Brien et al. 5,6 initially considered 26 patients in their study; however, only 14 patients started clozapine in the community as the rest were considered too unwell and were admitted to hospital. One patient refused daily access and therefore only 13 patients completed the titration. The side effects reported in this study were minor, including sedation in 5 cases, dizziness in 4 patients, hypotension in two and nausea and vomiting once. Compared to our results, O’Brien et al. described a larger proportion of patients needing to be admitted to hospital for clozapine titration.
We found two published studies 7,8 regarding clozapine community titration that were conducted in the United States. The first study included 47 patients who started clozapine in a partial hospitalisation program. Adverse reactions here were common. Patients were titrated much more quickly than in our report, (i.e. to 350 mg over 2 weeks), which might explain the higher incidence of side effects reported, including drowsiness (93.6%), hypersalivation (93.6%), constipation (89.4%), weight gain (72.3%) and tachycardia (57.4%). However no patient discontinued clozapine, and the potentially serious complications were much less frequent, including 3 cases (6%) of seizures and 2 of leukopenia. The other study 8 conducted in the US demonstrated some evidence of cost savings associated with decreased hospitalisation in 28 patients who started clozapine on an outpatient basis.
Johnson et al. 7 discuss in their report that the reluctance to start clozapine outside inpatient settings may be due partly to the potential adverse reactions, but also to clinicians’ fears of making mistakes, avoidance of additional duties, and anticipation of difficulties in patients with a history of non-adherence to treatment. The results of our study support a careful approach to starting clozapine at home in this latter group of patients, as they represented the bulk of cases not achieving the intended outcome of a successful community clozapine titration. However, our study confirms that other reasons to deny a patient the opportunity to start clozapine at home, such as potential adverse events, are hardly justified.
The general advantages of community psychiatric care as opposed to inpatient treatment have been described elsewhere 9. These include accessibility, flexibility and user satisfaction. Treating patients in their own homes avoids the stigma of hospital admission, prevents the breakdown of important social networks and avoids disruption to patients' benefits. A recent Cochrane review 12 found that crisis/home care reduces the number of people disengaging early, reduces family burden, and is a more satisfactory form of care for both patients and families. Some patients who might have been reluctant to start clozapine if they had to be admitted to hospital can therefore benefit from starting this treatment at home supported by crisis teams.
Although a detailed cost-benefit evaluation of this service was not undertaken, it is fair to assume that the costs associated with titrating clozapine at home would be significantly lower than those associated with in-patient care, as demonstrated in previous studies. 8,12
In summary, clozapine can be safely started in the community, but has to be carefully monitored. Patients’ adherence to the treatment and to the physical monitoring requirements is the key element to a successful outcome. Crisis teams are in an ideal position to support patients undergoing initiation of clozapine at home, although this specific role was not originally identified in policy guidance.10 The results of this multi-site study are encouraging and can be applicable to other crisis or community teams nationally.
Insomnia is chronic inability to obtain the amount of sleep needed for optimal functioning and well-being. Insomnia has received much attention in last few decades, since it has become a growing and complex problem in our society.1 Insomnia is defined as the chronic complaint of difficulty initiating or maintaining sleep, early awakening, and interrupting or non-restorative sleep. Furthermore, it must be accompanied by clinically significant impairment in day time function, for which there is no identifiable cause such as another sleep, psychiatric or medical disorder.1
General Criteria for Insomnia:2
A complaint of difficulty initiating sleep, difficulty maintaining sleep, or waking up too early or sleep that is non-restorative or poor in quality. In children, the sleep difficulty is often reported by the caretaker and may consist of observed bedtime resistance or inability to sleep inadequately.
The above sleep difficulty occurs despite adequate opportunity and circumstances for sleep.
At least one of the following forms of daytime impairment related to the night-time sleep difficulty is reported by the patient:
Fatigue or malaise
Attention, concentration or memory impairment
Social or vocational dysfunction or poor school performance
Mood disturbance or irritability
Daytime sleepiness
Motivation, energy or initiative reduction
Proneness for errors, or accidents at work or while driving
Tension, headaches or GI symptoms in response to sleep loss
Concerns or worries about sleep
Insomnia is prevalent condition in both the general population and in clinical practice, and it is associated with significant morbidity and mortality. It may present as the primary complaint or in association with physical or mental health problem.
Classification:
Insomnia can be classified into two main etiologic groups:
Primary Insomnia: When identifiable etiologies for insomnia have been ruled out, a diagnosis of primary insomnia can be made.
Secondary Insomnia: Related to other medical disorders, mental disorders or related to known organic factors.
Insomnia can be divided in to three types based on duration:
Less than one month called Acute or Transient insomnia.
One to six months called Sub-acute or Short-term insomnia.
More than six months called Chronic insomnia.
Following types of Insomnia recognized in The International Classification of Sleep Disorders (ICSD) second edition, Diagnostic and Coding manual:2
Adjustment Insomnia (Acute Insomnia)
Psycho-physiological Insomnia
Paradoxical Insomnia
Idiopathic Insomnia
Insomnia Due to Mental Disorder
Inadequate Sleep Hygiene
Behavioural Insomnia of Childhood
Insomnia Due to Drug or Substance
Insomnia Due to Medical Condition
Insomnia Not Due to Substance or Known Physiological Condition, Unspecified (Nonorganic Insomnia, NOS)
Physiological (Organic) Insomnia, Unspecified
Prevalence:
One third of adult population reports insomnia, 9 to 12% experience day time consequences and approximately 6% meet formal criteria for an insomnia diagnosis.3 Insomnia is more common among women, middle-aged and increases with age, shift workers and with medical or psychiatric disorders.
Consequences:
Persistent insomnia can produce an important burden for individual and society, as evidenced by reduced quality of life, impaired daytime functioning and increased absenteeism at work, and higher health-care cost. Persistent insomnia is also associated with increased risks of depression and chronic use of hypnotics.
Diagnosis of insomnia is based on subjective complaint of difficulties falling or staying asleep or non-restorative sleep that is associated with marked distress or significant daytime impairments. Several indicators such as intensity, frequency and duration, needs to be evaluated to assess severity of insomnia.
Evaluation:
Insomnia is an important public-health problem that requires accurate diagnosis and effective treatment (Standard).4 Insomnia is a symptom of an underlying disorder or condition. The insomnia may be a problem directly related to the sleep-wake regulatory system and/or it might be associated with a comorbid psychiatric, behavioural, medical, or neurological condition.4 Insomnia is primarily diagnosed by clinical evaluation through a careful, detailed medical, psychiatric, and thorough sleep history (which includes assessment of sleep patterns and waking processes) (Standard).4
Treatment options:
Pharmacotherapy is currently the most common treatment modality for insomnia,5 but long-term use of hypnotics in chronic insomnia can become complicated by drug tolerance, dependence or rebound insomnia. Since insomnia is a chronic condition, long-term and safe treatments are warranted. Non-pharmacological options provide longer lasting benefits.
If a cause of insomnia is identified, initial treatment should be directed at the specific factor. If insomnia persists, non-pharmacologic and/or pharmacologic interventions should be instituted. Hypnotic agents are the treatment of choice for the management of acute or transient insomnia. The expected goal is to normalize the sleep pattern within a few days to weeks. Behavioural interventions are important aspect of the treatment of chronic primary insomnia.
Classification of evidence (Table 1) is used to determine different level of recommendations (Table 2), which is available for behavioural therapies in management of insomnia.
Table 1: AASM (American Academy of Sleep Medicine) Classification of Evidence (Based on Sackett system,6 the criteria for grading evidence level of each study)
Randomized well-designed trials with low alpha and beta error (Grade I) Randomized trials with high alpha and beta error (Grade II) Non-randomized concurrently controlled studies (Grade III) Non-randomized historically controlled studies (Grade IV) Case series (Grade V)
(Alpha (Type I error) refers to the probability that the null hypothesis is rejected when in fact it is true (generally acceptable at 5% or less, or p<0.05). Beta (Type II error) refers to the probability that the null hypothesis is mistakenly accepted when in fact it is false (generally trials accept a beta error of 0.20). The estimation of Type II error is generally the result of a power analysis. The power analysis takes into account the variability and the effect size to determine if sample size is adequate to find a difference in means when it is present (Power generally acceptable at 80-90%).
Table 2: AASM Levels of Recommendations (The following are recommendations of the SPC (Standards of Practice Committee) approved by the Board of Directors of the AASM).7
Term
Definition
Standard
This is a generally accepted patient-care strategy, which reflects a high degree of clinical certainty. The term standard enerally implies the use of Level I evidence, which directly addresses the clinical issue, or overwhelming Level II evidence.
Guideline
This is a patient-care strategy, which reflects a moderate degree of clinical certainty. The term guideline implies the use of Level II evidence or a consensus of Level III evidence.
Option
This is patient-care strategy, which reflects uncertain clinical use. The term option implies either inconclusive or conflicting evidence or conflicting expert opinion.
Recommendations according to type of Insomnia:10, 11, 12
For both, chronic primary insomnia and secondary insomnia, the standard psychological and behavioural interventions are effective and recommended.
Recommendations for specific therapies:
1. Stimulus control therapy
Effective and recommended therapy in treatment of chronic insomnia (Standard)
Objective is to train the insomnia patient by a set of instructions designed to re-associate the bed and bedroom with sleep and to re-establish a consistent sleep-wake schedule:
Go to bed only when sleepy;
Get out of bed when unable to sleep;
Use the bed/bedroom for sleep only (no reading, watching TV etc.);
Arise at the same time every morning;
No napping.
2. Relaxation training
Effective and recommended therapy in treatment of chronic insomnia (Standard)
Aimed at reducing somatic tension (e.g. progressive muscle relaxation, autogenic training) or intrusive thoughts at bed time (e.g. imagery training, meditation) that interfere with sleep.
3. Cognitive Behavioural Therapy (CBT) with or without relaxation therapy
Effective and recommended therapy in treatment of chronic insomnia (Standard)
CBT includes various combinations of both cognitive as well as behavioural interventions. The cognitive component is aimed at changing patient's beliefs and attitudes about insomnia. The behavioural component may include therapies such as stimulus control therapy, sleep restriction or relaxation training. Sleep hygiene education is often also included.
4. Sleep Restriction
Effective and recommended therapy in chronic insomnia (Guideline)
It involves curtailing the amount of time in bed to actual amount of time spent asleep. For example, if a patient reports sleeping an average of 6 hours per night, out of 8 hours spend in bed, the initial recommended sleep window (from lights out to final arising time) would restrict to 6 hours. Periodic adjustments to this sleep window are made contingent upon sleep efficiency, until optimal sleep duration is reached. Therapy creating mild sleep deprivation, and then lengthening sleep time as sleep efficiency improves.
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
Combining stimulus control therapy, relaxation training, sleep hygiene education
Combining stimulus control therapy, sleep restriction therapy, sleep hygiene education
Combining sleep restriction therapy, stimulus control therapy
6. Paradoxical intention
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
It involves instructing the patient to remain passively awake and avoid any effort (i.e. intention) to fall asleep. The goal is to eliminate performance anxiety, as it may inhibit sleep onset. This parameter is limited to sleep initiation insomnia.
7. Biofeedback
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
It provides visual or auditory feedback to patients to help them control some physiological parameters (e.g. muscle tension) in order to seek reduction in somatic arousal.
EEG Neurofeedback training: It is a self-regulation method that makes use of learning theory, more specifically, the paradigm of operant conditioning.8 While the EEG is measured; the patient receives instant feedback (visual and/or auditory) on the cortical activity of the brain. The goal of this treatment modality is to normalize the functioning of the brain by inhibiting and/or reinforcing specific frequency bands.
Recommendations relevant to specific patient groups:
Psychological and behavioural interventions are effective and recommended in treatment of insomnia in older adults (Standard) and among chronic hypnotic users (Standard)
Insufficient evidence is available for sleep hygiene education, imagery therapy, and cognitive therapy to be an option as a single therapy. (No recommendation level)
Sleep Hygiene Education: Please see table 3
Table 3: Sleep Hygiene Education:
1. Attempt to maintain a regular sleep-wake cycle 2. Obtain morning light exposure 3. Use the bedroom only for sleep and intimacy 4. Create a comfortable, quiet, dark and temperature-controlled bedroom environment 5. Develop a relaxing routine within an hour before bedtime 6. Exercise regularly, but not within a few hours of bed time 7. Avoid use of alcohol and other addicting substances 8. Avoid caffeine or nicotine, especially within a few hours of bedtime 9. Avoid empty stomach or heavy meals before bed time, a light snack may be of value 10. Avoid daytime napping, or if napping, be aware of the impact that napping has on nighttime sleep 11. Avoid disturbances at bedtime (e.g. disruptive noises, pets, family) 12. Avoid work, computers and emotional stress in the bedroom 13. Avoid keeping a clock close to the bed to prevent “clock watching” 14. Avoid excessive wakeful time in bed (>20 minutes)
Imagery therapy: It involves a visualization technique to focus on some pleasant or neutral images to block out unwanted thoughts before sleep.
Cognitive therapy: Psychological methods aimed at challenging and changing misconceptions about sleep and faulty beliefs and attitudes about insomnia and its perceived daytime consequences.
Limitations of non-pharmacological management:
Gains in sleep onset or total sleep time are not immediately attained.
Patient motivation and encouragement are required for success of management.
Non-pharmacological interventions are more expensive and time-consuming.
They require the availability of a skilled therapist.
Results:
Psychological and behavioural therapies produce reliable changes in several sleep parameters of individuals with either primary insomnia or insomnia associated with medical and psychiatric disorders.10 A Meta-analysis indicates that in patients with primary insomnia, behavioural interventions produce improvements in sleep parameters (sleep onset latency, time awake after sleep onset (WASO), number of awakenings and total sleep time) in about 70 to 80% of patients.9 Behavioural interventions are more expensive, time-consuming and require the availability of a skilled therapist, but the benefits are long lasting.13
Clinical Pearl:
Pharmacotherapy is currently the most common treatment modality for insomnia,5 but long-term use of hypnotics in chronic insomnia can become complicated by drug tolerance, dependence or rebound insomnia.
Psychological and behavioural therapies produce reliable changes in several sleep parameters of individuals with either primary insomnia or insomnia associated with medical and psychiatric disorders.
Behavioural interventions are important aspect of the treatment of chronic primary insomnia; they should be used in every patient of Insomnia.
Patients who present to physicians with altered mental health and behaviour may prematurely be diagnosed to have psychiatric illness. Psychiatric manifestations commonly accompany acute medical illnesses. As a rule of thumb, organic causes need to be ruled out before making a psychiatric diagnosis. A delay in arriving at a diagnosis could lead to prolonged psychiatric symptoms and unnecessary use of psychotropic medications. Prognosis and recovery will vary depending on the type of accompanying medical illness. Below, two cases are presented which varied significantly in terms of the sequelae.
Case 1
A female patient in her late 20’s was referred from primary care as she reported a sudden onset of “hearing voices”. The patient disclosed that she was bullied at work 6 months prior to this episode which resulted in change of job role and bullying has been dealt with. She described that the voices were talking about world politics and wanted her join MI5. She also believed that there were evil scientists who could read her mind through telepathy and felt that there were cameras and bugs planted in her house by a plumber. She became suspicious that her neighbours were spying on her. Her sleep was disturbed and she heard a ‘tick-tock ‘sound. This led to her checking pipes and walls to find the origin of the sounds. She believed that people were throwing things on to her bed and became very distressed - to the extent that the police were called on many occasions. She believed that people had been using telepathy on her and that aliens were invading the world. She was so distressed that she attempted to end her life by drinking bleach on one occasion and trying to cut her wrist on another.
There is no previous history of mental illness and no mental illness in the family.
Her medical history revealed that she had had mastoid surgery four years ago. Three weeks prior to the psychotic episode noted above, she had an ear infection with discharge from her ear. She presented to the general practitioner with psychotic symptoms at the same time. A CT scan of the brain was normal. A 2 week course of antibiotics in the form of Co-amoxiclav was given by the general practitioner. Her psychiatric manifestation resolved completely on follow up at two months without any psychotropics or Benzodiazepines, The patient was then kept under ‘wait and watch’ for six months in order to monitor any re-emergence of psychotic symptoms. She did not report any further episodes of ear infections during this period of follow up. Her diagnosis was Diseases of middle ear and mastoid (H65-H75).
Case 2
A 31 year old lady was referred to secondary mental health services from a Neurology team, presenting with psychotic symptoms following a viral encephalitis infection. A diagnosis of Herpes Simplex viral (HSV) encephalitis was confirmed by lumbar puncture and a CT scan by the Neurology team. She had made a gradual recovery from the encephalitis over a period of one month. She developed psychotic symptoms 2 weeks later, where she believed that doctors were trying to kill her and that she had been raped, with no evidence that this had occurred at any time. Her distress worsened which led to her informal admission to an inpatient mental health unit. A close assessment on the ward showed her to display an intermittent picture of worsening gait. A neuropsychiatry assessment confirmed that this lady had acquired brain injury following Herpes encephalitis. Single photon emission computed tomography (SPECT) showed extensive brain injury consistent with HSV. This lady presented with several acute episodes of psychosis where she complained of hearing voices and believed that people were trying to harm her. Her mood was labile and variably responsive to Olanzapine initially with a control of her psychotic symptoms as well as mood behaviour. She was diagnosed as suffering from Organic Delusional (Schizophrenia-like) Disorder (ICD 10 F06.2), with a picture of Paranoid Schizophrenia secondary to viral encephalitis. A maternal aunt was said to have suffered from Schizophrenia. Later on she had frequent relapses of psychosis and Quetiapine was initiated. As her symptoms did not respond to two different anti-psychotics, she was started on Clozapine which gave her reasonable stability. However, she still needs support while walking andhas been transferred to a suitable neuropsychiatric rehabilitation placement to maximise her independence and manage her ongoing needs.
Discussion
The two cases above display infective neurological diseases characterised by psychiatric presentations and greatly differing prognosis. The first case was an example of a chronic recurrent ear infection which was likely to have involved inner ear, mastoid or temporal lobe but has subsided without any long term sequelae. This was promptly treated with antibiotics at an early stage with complete recovery and there was no evidence of brain injury on imaging. The psychiatric manifestation was dramatically acute in this case and this could be partly attributable to stress at work. In particular there was neither previous history of mental illness nor a family history of psychiatric disorders.
In the second case, there was evidence of significant brain injury resulting in both physical and psychiatric sequelae following herpes encephalitis. Furthermore, this patient has a family history of schizophrenia which might have influenced the manifestation of the Mental Disorder.
There is significant evidence to suggest that childhood neurological viral infections increase the risk of psychotic illness 1. In both cases there was no suggestion of such illness in the childhood history. A recent study investigated whether HSV1 exposure was associated with structural brain abnormalities in individuals who, because of genetic or other factors, were deemed at high risk of developing psychosis. The results suggested that a history of HSV1 infection is associated with volumetric gray matter reductions in individuals at high risk for developing psychosis 2. In our second case, SPECT imaging confirmed grey matter loss and with the strong genetic risk would have led to the psychiatric illness.
The relationship between bacterial infections and psychotic illness in less well understood. Schizophrenic illnesses are often multifactorial in origin following a complex interplay between genetic and environmental factors such as infections. While there are various reports of Neurosyphilis, Mycoplasma Pneumoniae and Cryptococcal meningitis causing psychotic illness, specific bacteria could not be isolated in the first case presented 3-7. The improvement with antibiotics simply suggests that this could be a bacterial infection.
In summary, these cases clearly show the importance of identifying and treating medical illness presenting with psychiatric symptoms at the earliest to prevent long term complications.
Evidence has consistently shown that patients with mental illness have greater physical health morbidity and mortality compared to the general population.1 Many factors have been implicated and include a generally unhealthy lifestyle, side effects of medication, and inadequate physical healthcare.2, 3 Higher rates of suicide and accidents are other known risks. Psychiatric patients are more likely to smoke, have less inclination to exercise, and are prone to poor dietary habits and obesity, the latter through general inertia, the result of the adverse effects of neuroleptic medication, or increased alcohol use. Psychotropic medication is associated with impaired glucose tolerance and diabetes, metabolic syndrome, dyslipidemia, cardiovascular complications, extrapyramidal side effects and sexual dysfunction. A broad range of clinician and organisational factors prevent access to adequate physical healthcare that in turn compounds the above problems.
Scale of physical morbidity and mortality in mental illness
Patients suffering from depression are twice as likely to develop type 2 diabetes mellitus, and the prevalence of stroke and myocardial infarction is three- and five-fold respectively higher than people without depression.4 A mortality rate ratio (MRR) of 2 to 3 in patients with schizophrenia or bipolar disorder is a general finding.5 Schizophrenia is associated with higher rates of diabetes mellitus (side effects of medication partly to blame), osteoporosis (lifestyle risk factors play a role), obesity, and cardiovascular problems. 2, 6, 7, 8 It has been estimated that life expectancy is reduced by at least ten years. 9, 10 People with learning disabilities, particularly those with concurrent epilepsy, dementia and polypharmacy, are at greater risk of developing added complications.11 Eating disorders are associated with a high mortality because of physical disorders caused by anorexia/bulimia nervosa affecting other organ systems.12 Mental illness in general is associated with an increased risk of hepatitis, human immunodeficiency virus (HIV), tuberculosis, and poor dental health. 9, 10
Causes of raised physical health morbidity and mortality in psychiatric patients
Explanations for the higher morbidity and mortality in mental illness include cardiovascular and respiratory problems in addition to the increased suicide risk. Aetiological factors include adverse effects of medication (weight gain, diabetes, and dyslipidemia), lifestyle (smoking and the cost of smoking, poor diet and nutrition, lack of exercise, and obesity) and inability to access physical healthcare. Obesity, smoking and physical inactivity contribute to hypertension. Poor physical healthcare outcomes in mental illness are related to a combination of factors generally considered under the headings of patient/illness, psychiatrist/physician, and service provider/system issues.
De Hert and colleagues 9, 10 have outlined the factors that account for the raised physical health problems.For instance the patient/illness factors comprised difficulty in understanding health care advice combined with the motivation required to adopt new changes in lifestyle, poor compliance with treatment, cognitive deficits, reduced pain sensitivity (induced by antipsychotic medication), poor communication and deficient social skills (seen in many cases of schizophrenia, for example) which all accounted for the shortened life-span of patients with severe mental illness (SMI).
An additional patient/illness factor is that psychiatric symptoms may render patients less inclined to discuss physical problems. Some doctors are uncomfortable dealing with psychiatric patients because the latter may be cognitively compromised which may impair or impede a doctor’s clinical assessment. The stigma of mental illness, often the result of disparaging media coverage and negative stereotypes surrounding psychiatric patients, are other hurdles that prevent people from seeking treatment. Furthermore, psychiatric patients are less likely to see a primary care physician and therefore to receive other interventions such as screening for cancer.
Psychiatrist-related factors are characterised by an overemphasis on mental health to the exclusion of physical health, infrequent screening rates for metabolic abnormalities, omission of medical examination of patients because physical complaints frequently are part of the psychiatric presentation, poor communication with the patient and the primary care teams, a lack of awareness and perhaps adherence to treatment guidelines, insufficient medical knowledge, and erroneous, sometimes misguided beliefs about patients’ capability to change their lifestyle.9, 10 Even when risk factors are documented in the patient's clinical file, very little is done by way of further investigations or prevention.
Factors common to the psychiatrist and other physicians include a tendency to dismiss or interpret physical symptoms as psychosomatic, lack of good quality care, unequipped teams, insufficient assessment, and difficulties providing consistent monitoring and continuity of care. Other physician-related factors relate to problems coordinating psychiatric and medical care.9, 10
Service-provision factors included a lack of clarity and consensus as to where the responsibility of physical health lies.9, 10 Should general practitioners (GPs) supervise the majority of patients who do not suffer from severe, enduring mental illness? Should patients with acute alcohol withdrawal symptoms be managed at home by the GP, treated in a general hospital, or admitted to a psychiatric unit? The fragmentation of medical and mental health care systems, lack of integration of services (poor or absent liaison links) and insufficient funds to resource the mental health service, limit the ability of most psychiatrists to focus beyond their own speciality.
Service and system changes are prevalent in industrialised countries because reforms in mental health have led to reduced inpatient resources leading to shorter and infrequent hospital admissions with less time available to focus or investigate physical health problems. In the United Kingdom (UK) there is intense emphasis on community care and talking therapies, yet the management of physical health issues by community mental health teams may be poor because of inadequate training and learning.
Recommendations to improve physical health care in psychiatric patients
Health care professionals need to be more aware of these findings in order to improve medical screening and treatment of psychiatric patients. Currently there is no evidence this is happening, with increasing concerns regarding inequalities between those with and without mental illnesses.13
We propose the following recommendations to promote integration between mental and physical health care:
1.A greater effort to increase awareness of the problem among primary care and mental health care providers. The Royal College of Psychiatrists has launched a campaign called Fair Deal to highlight the importance of physical health of people with mental illness.1 Patients still feel stigmatised and therefore psychiatrists need to boost their efforts to reduce this discrimination. The excess mortality associated with this discrimination needs to be recognised as a human rights issue.13
2.Primary care providers need to change the culture of undertreating physical health in mental health patients. The National Institute for Health and Clinical Excellence (NICE) guidelines for schizophrenia and bipolar disorder highlight the importance of monitoring antipsychotics and mood stabilizers.14 The Royal College of Psychiatrists should lead by implementing the NICE guidelines for mental and behavioural conditions.
3.Education and training of doctors who pursue a career in psychiatry needs to be improved with mandatory trainee placements in acute medicine or neurology, regular personal development plan (PDP) courses, and training to update knowledge of recognising physical illness and the performance of basic medical tasks. The Royal College of Psychiatrists should develop a diploma in clinical psychiatry for GPs and clinicians with a specialist interest in psychiatry. The curriculum needs to be widened to include electrocardiogram (ECG) interpretation, basic endocrinology, and neurological investigations (magnetic resonance imaging and so forth). This would allow psychiatrists to develop better liaison with their fellow professionals and share responsibility with them, which undoubtedly would encourage good medical practice.
4.The Royal College Scoping Group’s report15 sets key standards for the physical healthcare of patients in a range of psychiatric services. It outlines the responsibilities of psychiatrists monitoring the physical health of patients, such as problems associated with adverse effects of medication. The report recommends that psychiatrists are trained and kept up to date in relevant physical health matters. These recommendationsneed to be followed.
5.Mental health professionals should encourage patients to monitor simple measures such as weight, dietary plans, and exercise programs, with the involvement of the voluntary sector (MIND, Mental Health Foundation) where possible. Patients and carers need to be educated about the health risks associated with unhealthy lifestyles: for example, smoking and alcohol misuse may interfere with the metabolism of neuroleptic medications. Smoking cessation clinics and alcohol treatment programmes may help. Advice from dieticians about patients' nutritional requirements to offset changes in metabolism caused by neuroleptics is important.
6.Because of the large-scale reduction of inpatient psychiatric beds and service redesign the majority of psychiatric care provision now exists in the community. Therefore community mental health teams and psychiatric outpatient clinics need to be appropriately designed and equipped to enable proper assessment of physical health monitoring. Annual health checks from the GP would benefit patients who require long-term monitoring in the community. Screening for deleterious effects of medication for example, hypothyroidism and renal dysfunction caused by lithium, at regular intervals would be appropriate.16 It should also be made clear to psychiatrists that they should resist working in clinical settings that compromise patient care and inhibit good medical practice.
7.Financial initiatives such as Commissioning for Quality and Innovation (CQUIN)17 may be used by commissioners to improve physical health monitoring.As part of this process, primary care commissioners could mutually agree with mental health providers to fulfil measured targets related to such monitoring.
8.In order to better understand the interplay between psychiatric conditions and medical complications contributing to the high physical morbidity and mortality, further studies are essential. To cite one example, we now know that psychotropic medications contribute to many physical problems (abnormal ECGs, weight gain, changes in plasma glucose) and lead to higher morbidity rates. The 'newer' generation of antidepressants and neuroleptics have not lived up to expectations and have as many untoward effects as the older drugs. Developments of newer drugs with different mechanisms of action are required, though this will take time.
9.The discrimination faced by people with mental illness and learning disabilities, with the accompanying excess mortality, represents a human rights issue13 that requires legislative changes. The Disability Right’s Commission18 has already recommended appropriate physical health care screening, for example, annual physical health checks. The government’s health inequality agenda should incorporate these conditions into its indicators of disadvantage and include mental illnesses and learning disability in the framework.
Conclusion
Traditionally the field of psychiatry involves a holistic approach in the management of patients. Unfortunately, over the decades psychiatry appears to have lost its way and therefore it is important to re-establish a more comprehensive system of treating mental illness that encompasses regular physical health monitoring. Physical morbidity and mortality in patients with mental illness is on the rise and is associated with a complex interplay of factors outlined above. The overall health care of psychiatric patients can be improved through the changes in education and training of clinicians, close liaison between primary and secondary care, implementation of recommendations by NICE and the Royal College of Psychiatrists, improved research through better funding, public health education of patients and carers, and legislative changes.
One in four people in general and one in five people in Canada suffer from a mental disorder and only half of these individuals will seek help for their mental health.1 Doctors have an increasingly demanding job with increasing expectations of excellence in clinical, academic and managerial roles. It seems surprising that with their rigorous training doctors have higher rates of suicide compared to the general population.2 Studies have revealed that two-thirds of Canada’s physicians consider their workload too heavy, and more than half say that personal and family life have suffered because of their career choice.3 One third of Canadian physicians disagreed with a statement that their work environment encourages them to be healthy .4
A systematic review of mental health studies of medical students in the US and Canada found consistently higher rates of psychological distress in medical students compared with both the general population and age-matched peers .5 Medical students were also less likely to seek help for psychological distress than their peers. 6
A survey of psychiatrists and physicians in the UK found that most would be reluctant to disclose personal mental illness to colleagues or professional institutions. Their choices regarding disclosure and treatment would be influenced by issues of confidentiality, stigma, and career implications rather than quality of care.7,8
To reduce stigma and ease physician access to mental healthcare it is important to understand and address the above issues. This will facilitate psychiatrists gaining optimized mental health as well as to improve recruitment and retention of these professionals.9 The objective of our study was to assess the understanding of Canadian psychiatrists to the incidence of mental illness amongst psychiatrists in comparison to the general population and also in comparison to their medical/surgical colleagues. The study also assessed the attitudes of psychiatrists towards preference for disclosure, and treatment should they develop a mental illness in addition to their own experience of mental illness.
Method
Ethics approval (Study code PSIY-336-11) from Queen’s University in Kingston, Ontario was granted. Funding was obtained from TH’s research initiation grant. A mailing list of all psychiatrists in the province of Ontario was provided by the College of Physicians and Surgeons of Ontario (CPSO) for specific use to this research project. The College of Physicians and Surgeons Ontario is a body similar to the General Medical Council (GMC) in the UK. Their role is to regulate the practice of medicine in the province of Ontario. Other provinces have their own respective College of Physicians and Surgeons. In the remainder of the text the term ‘psychiatrist’ refers to consultant psychiatrist.
The list obtained from the CPSO did not include approximately 10% of psychiatrists who opted out of having their postal details released for research purposes. In total 1231 psychiatrists were sent a survey package. This package included a covering letter, a 2-page questionnaire, and a stamped return addressed envelope. Consent was assumed based on taking part in the survey. The 10-item questionnaire was based on a review of the literature, previous research, and discussion with colleagues. It comprised broadly of three sections. The first collected information on the respondents’ perception of prevalence of mental illness in psychiatrists in comparison to the general population and then in comparison with other medical/surgical specialties. The second required psychiatrists to identify to whom they were most likely to disclose a mental illness and reasons for non-disclosure. The third asked psychiatrists their preference of treatment in both an outpatient and inpatient setting. The identifiable information requested was the amount of experience the respondent had as a psychiatrist and whether they had experienced mental illness in the past. A free-text box was included at the end for comments and complete anonymity was maintained. Psychiatrists were divided into 3 groups: Group 1 (less than 5 years of experience as a psychiatrist), Group 2 (5-10 years of experience) and Group 3 (greater than 10 years of experience).
Analysis
A series of two-sample chi-square tests (χ²) were conducted to examine associations between certain categorical variables. In cases where 20% of contingency cells were <5 or where any cell=0, Fisher’s Exact test was used. Phi (φ) or Cramer’s V (for associations >2x2) were used as measures of effect size, these provide an association coefficient between 0 and 1. All analyses were done using SPSS 19.
Results
Of the 1231 questionnaires sent to doctors 487 were returned, a response rate of 39.6%. The respondents were placed into three groups: those in attending for <5 years (55, 11.3%), 5-10 years (53, 10.9%) and >10 years (369, 75.8%). The frequency of responses to all questions, both overall and as a function of attending group are shown in Table 1.
Table 1. Responses to all questions and comparisons between attending groups. Discrepancies between the overall column and the sum of the attending group columns are due to missing cases in responses to the attending group question.
Attending Group
Overall
<5 years
5-10 years
>10 years
Incidence of psychiatric illness amongst doctors is higher than general population?
Yes
124 (25.5% )
15 (27.3%)
19 (35.8%)
89 (24.1%)
No
247 (50.7% )
30 (54.5%)
26 (49.1%)
184 (49.9%)
Don’t know
116 (23.8% )
10 (18.2%)
8 (15.1%)
96 (26.0%)
Incidence of psychiatric illness amongst medical/surgical professionals higher than that of psychiatrists?
Yes
37 (7.6% )
1 (1.8%)
8 (15.1%)
28 (7.6%)
No
285 (58.5% )
36 (65.5%)
29 (54.7%)
214 (58.0%)
Don’t know
165 (33.9% )
18 (32.7%)
16 (30.2%)
127 (34.4%)
Have you ever experienced a mental illness, which had affected your personal, social or occupational life?
Yes
151 (31.0%)
14 (25.5%)
18 (34.0%)
118 (32.0%)
No
336 (69.0%)
41 (74.5%)
35 (66.0%)
251 (68.0%)
If you were to develop a psychiatric illness affecting your personal, social or occupational life, to whom would you initially be most likely to disclose this?
Church/Clergy
3 (0.6% )
1 (2.0%)
0 (0.0%)
2 (0.6%)
GP/Family physician
153 (31.4%)
18 (35.3%)
16 (32.0%)
116 (32.3%)
Family/friends
204 (41.9% )
22 (43.1%)
27 (54.0%)
152 (42.3%)
Colleagues
54 (11.1% )
4 (7.8%)
1 (2.0%)
46 (12.8%)
Mental health profess.
32 (6.6%)
4 (7.8%)
5(10.0%)
22 (6.1%)
None
15 (3.1% )
1 (2.0%)
0 (0.0%)
14 (3.9%)
Other
9 (2.0% )
1 (2.0%)
1 (2.0%)
7 (1.9%)
What is the most important factor that would affect your decision not to disclose your mental illness?
Stigma
114 (23.4%)
12 (22.2%)
14 (26.4%)
86 (24.2%)
Career implications
168 (34.5%)
21 (38.9%)
22 (41.5%)
121 (34.1%)
Professional standing
80 (16.4%)
11 (20.4%)
6 (11.3%)
63 (17.7%)
Other
109 (22.4%)
10 (18.5%)
11 (20.8%)
85 (23.9%)
If you were to suffer from a mental illness affecting your personal, social or occupational life requiring out-patient treatment, what would be your first treatment preference?
Informal profess. advice
83 (17.0%)
6 (10.9%)
7 (13.5%)
70 (19.1%)
Formal profess. Advice
365 (74.9%)
42 (76.4%)
40 (76.9%)
275 (75.1%)
Self-medication
25 (5.1%)
7 (12.7%)
2 (3.8%)
15 (4.1%)
No treatment
9 (1.8%)
0 (0.0%)
3 (5.8%)
6 (1.6%)
If you were to develop a mental illness requiring in-patient treatment, where would be your first preference?
Local
109 (22.4%)
6 (10.9%)
5 (9.4%)
96 (26.5%)
Out of area
370 (76.0%)
49 (89.1%)
48 (90.6%)
266 (73.5%)
In choosing in-patient preference, which of the following influenced your decision most?
Quality of care
130 (26.7%)
7 (12.7%)
7 (13.2%)
112 (30.5%)
Convenience
44 (9.0%)
0 (0.0%)
5 (9.4%)
38 (10.4%)
Confidentiality
257 (52.8%)
39 (70.9%)
34 (64.2%)
180 (49.0%)
Stigma
32 (6.6%)
6 (10.9%)
4 (7.5%)
22 (6.0%)
Other
21 (4.3%)
3 (5.5%)
3 (5.7%)
15 (4.1%)
Perception of the incidence of mental illness
Just over half of respondents disagreed that the incidence of mental illness was higher in doctors than the general population (247, 50.7%). Just over a quarter (124, 25.5%) agreed and just under a quarter replied ‘don’t know’ (116, 23.8%). As can be seen in Table 1, the pattern of responding was similar across all attending groups on this question (χ²=5.92; df=4; p=.205; Cramer’s V=.08). Most disagreed that psychiatric illness was greater in medical/surgical professionals than in psychiatrists (285, 58.5%), a small minority agreed (37, 7.6%). Again the attending groups responded similarly on this question (χ²=7.06; df=4; p=.133; Cramer’s V=.09). Nearly a third of respondents (151, 31.0%) claimed to have experienced a mental illness, and once more the attending groups did not differ significantly in their responses to this (χ²=1.12; df=2; p=.57; Cramer’s V =.05).
Disclosure of mental illness
Respondents would be most likely to disclose their mental illness in the first instance to family and friends (204, 41.9%) although many would instead prefer to disclose to their family physician (153, 31.4%). Relatively few would disclose to a colleague (54, 11.1%) in the first instance or to a mental health professional (32, 6.6%), very few would choose no-one (15, 3.1%) and the clergy was the least endorsed option (3, 0.6%). When considering only the three most popular response options (family/friends, family physician, and colleague) the three attending groups responded similarly (χ²=6.63; df=4; p=.157; Cramer’s V=.09). When asked about the most important factor affecting the decision not to disclose, the most common response was career implications (168, 34.5%). However stigma (114, 23.4%) and professional standing (80, 16.4%) were also reasonably common responses.
Again, when including only the three most popular disclosure choices in the analysis, there emerged an association between choice of whom to disclose and factor affecting disclosure (χ²=12.52; df=6; p=.051; Cramer’s V=.13) (see Table 2). Those who would choose to disclose to their family physician or to family/friends were more likely to cite stigma as a factor influencing their choice than those who would choose to disclose to colleagues. Those who would disclose to colleagues would be more likely to cite professional standing as a factor influencing their choice compared to those who would disclose to their family physician or to their family/friends. There was no association between choice of whom to disclose and previous experience of mental illness (χ²=1.22; df=2; p=.545; Cramer’s V=.05).
Table 2. Preferences for disclosure and the factors influencing that preference.
Factors influencing disclosure
Stigma
Career implications
Professional standing
Other
Total
Preference for disclosure
Family Physician
33 (22.6%)
57 (39.0%)
29 (19.9%)
27 (18.5%)
146 (100.0%)
Family/friends
56 (28.1%)
71 (35.7%)
24 (12.1%)
48 (24.1%)
199 (100.0%)
Colleagues
7 (13.7%)
17 (33.3%)
14 (27.5%)
13 (25.5%)
51 (100.0%)
Treatment for mental illness
When considering out-patient treatment, the majority of respondents would opt for formal professional advice (365, 74.9%). A small proportion would choose informal professional advice (83, 17.0%) and very few would self-medicate (25, 5.1%) or have no treatment (9, 1.8%). With regard to in-patient treatment, the majority would opt for an out of area mental health facility (370, 76.0%). Only just over a quarter of respondents (130, 26.7%) claimed that quality of care would influence their choice of in-patient care, just over half would be most concerned about confidentiality (257, 52.8%) There was a strong association between in-patient preference and the factor influencing that preference (Fisher’s Exact=228.25; p<.001; Cramer’s V=.70). As shown in Table 3, those who would choose an out of area facility, were much more likely to cite confidentiality and stigma as factors influencing their choice, than those who would choose a local facility. Conversely, those choosing a local facility were more likely to cite quality of care and convenience as influencing factors.
Table 3. In-patient treatment choice and the factors influencing that choice.
Factors influencing in-patient choice
Quality of Care
Convenience
Confidentiality
Stigma
Total
In-patient treatment choice
Local MH Facility
57 (56.4%)
39 (38.6%)
4 (4.0%)
1 (1.0%)
101 (100.0%)
Out of area MH Facility
69 (19.4%)
4 (1.1%)
252 (70.8%)
31 (8.7%)
356 (100.0%)
There was an association between attending group and out-patient preference (Fisher’s Exact=12.00; p=.042; Cramer’s V=.13). As can be seen in Table 1, the >10 years group would be more likely to select informal advice than the <5 years group, but the >10 years group were less likely to self-medicate than the <5 years group. The >10 years group responded similarly to the 5-10 years group with regard to self-medication. There was also an association between attending group and in-patient preference (χ²=12.66; df=2; p=.002; Cramer’s V=.16). The >10 years group, although still largely in favor of out of area care, would be more likely than the other two groups to opt for local care. There was also a significant association between attending group and the factors influencing in-patient choice (Fisher’s Exact =25.335; p=.001; Cramer’s V=.16). As shown in Table 1, the >10 years group would be more influenced by quality of care and less influenced by confidentiality than the other two groups.
Finally, previous experience of mental illness was not associated with in-patient choice (χ²=0.542; df=1; p=.462; φ=-.04), but it was associated with out-patient choice (χ²=11.51; df=3; p=.009; Cramer’s V=.16). As Table 4 shows, although both groups are more likely to opt for formal over informal advice, this pattern is more pronounced in the group who have had mental illness, than in the group who have not previously had mental illness.
Table 4. Previous experience of mental illness and out-patient treatment preference.
Out-patient treatment preference
Informal prof. advice
Formal prof. advice
Self-medication
No treatment
Total
Previous experience of mental illness
No
69 (20.8%)
242 (72.9%)
17 (5.1%)
4 (1.2%)
332 (100.0%)
Yes
14 (9.3%)
123 (82.0%)
8 (5.3%)
5 (3.3%)
150 (100.0%)
Discussion
This is the first study to assess the attitudes of Canadian psychiatrists to becoming mentally ill themselves. As this study was carried out in one province of Canada and the results cannot be generalized across the country. There is a significantly large scope of research potential in this area especially among psychiatric residents and other healthcare professionals .10
Physician Impairment is any physical, mental or behavioral disorder that interferes with the ability to engage safely in professional activities.11 Impairment among medical practitioners and psychiatrists in particular is a significant problem characterized by chronicity, under reporting and in many cases, poor outcomes.12 However early detection, intervention and treatment programs that are more sensitive to the needs of impaired practitioners, that are more continuous, better structured, and rehabilitation and recovery focused may be more likely to produce a positive outcome. 13 It is extremely important to remember and advocate that although a physician may be mentally ill he/she is not necessarily impaired.
It is concerning that stigma continues to play a role in psychiatrists’ decision making process to obtain mental healthcare. This is consistent with the findings of a survey in the USA which showed that half of all psychiatrists with a depressive illness would self-medicate rather than risk having mental illness recorded in their medical notes.10 Both entertainment and news media provide a dramatic and distorted image of mental illness that emphasize dangerousness, criminality and unpredictability.14 With this increased stigma doctors subsequently are concerned whether to disclose a mental health problem to their Licensing Boards for fear of being discriminated.15 Studies of US medical licensing bodies have demonstrated a trend towards increasing stigmatizing approaches 16-19 and the concern is whether there is a similar trend in Canada.9 Most psychiatrists in Canada are not aware what to expect from provincial colleges once their mental illness is disclosed and as a result tend to expect the worst. More work is needed by psychiatrists to inform the Provincial Colleges on physician mental health. Only then can the Provincial Licensing Colleges do more to assure physicians that the recovery model of treatment applies to them as it does other psychiatric patients.
The gap however continues to lie between ‘I need help’ and active psychiatric management. Psychiatrists will be well aware of the profound impact that such illnesses can have on a person’s personal and professional competency. However to reflect it on oneself can at times be met with denial in the first instance. Dr. Mike Shooter (ex-President of the Royal College of Psychiatrists, UK) suffered from depression and he highlights the need to speak out and combat stigma. He points out the need to seek treatment early and how not doing so can adversely affect the doctor-patient relationship.20 For some however the fear of stigmatization by health professionals for health professionals can lead to very tragic consequences. Dr. Suzanne Killinger-Johnson was a family physician with a psychotherapy practice in Toronto. She suffered from postpartum depression and in November of 2000 she jumped in front of a subway train cradling her son. Her son died instantly and Dr. Killinger-Johnson died 9 days later.21
Over the past 15 years a greater understanding has developed on the incidence, stressors and complications of physician mental illness. 22 The CPA published its first position paper on the mentally ill physician as early as 1984 with the latest version in 1997 currently under review. 22 The Canadian Medical Association should be congratulated on the most comprehensive strategy document for mentally ill physicians. Physician Health Matters - A mental health strategy for physicians in Canada was published by the CMA in February 2010. In addition to outlining the mental health of medical students, residents and physicians it addresses the current gaps in services and strategic direction needed to achieve ‘optimal mental health for all physicians’. This sets out the necessary groundwork for institutions to implement based on current evidence. In Canada there was the inauguration of the position of ‘The Bell Mental Health and Anti-Stigma Research Chair’ with Queen’s University in February 2012. 23 This position was offered to Dr. Heather Stuart, Professor of Community Health and Epidemiology. Stigma is a social process characterized by exclusion, rejection, blame or devaluation resulting from an adverse social judgment about a person or group. 24 There is a cultural pressure amongst physicians not to be sick so that one can provide care resulting in physicians unfortunately trying to control their own illness and treatment. 25 This concept is exacerbated for mental health issues and the stigma is considerably attached to physicians acknowledging mental health issues or illness, as well as seeking help. 26
Over the past decade the physician health community has been working to destigmatise physician mental health and to provide support services in this regard. All Canadian provinces have Physician Health Programs (PHPs) to help physicians with mental health difficulties. Referrals can be from physicians, families, colleagues, and self. 9 Physicians with psychiatric or drug dependence problems are referred from outside the PHP though the PHP (depending on the province) may or will be involved in monitoring the physician.
One of the most important factors influencing where a doctor is treated is the issue of confidentiality. 8 At present in Canada many hospitals are either switching or have switched to electronic patient records. Patient data in an electronic environment will be accessed from multiple portals by different professionals. This potentially poses serious concerns for psychiatrists if they have significant concerns around confidentiality of their record. A mechanism by which patients can access a list of professionals who have accessed their information may alleviate some concern regarding confidentiality.
Conclusions
Education surrounding mental illness in physicians needs to begin in medical school. Medical students require more assurance that seeking help for psychological problems will not be penalized. Junior doctors are receptive to education on physician impairment and substance misuse and this should be a mandatory component of their training. 27 Education and training of medical students and psychiatric residents to assess doctors as patients would make this scenario less taboo than it is currently perceived.
CPSO in liaison with relevant partners must develop a clear and concise document outlining steps the CPSO will take in helping the mentally ill physician. This document must be clearly advertised on the CPSO website to ease access and would reduce the catastrophizing interpretation psychiatrists (and physicians) may make to the CPSO’s involvement with the mentally ill physician. By the CPSO taking a lead this will prove a stimulus for other provincial licensing colleges to follow suit.
The bridge from ‘I need help’ to ‘I am getting help’ is paved with multiple barriers. By addressing some of the concerns raised by psychiatrists will help the psychiatrist easily cross over.
Neuroleptic malignant syndrome (NMS) is a life-threatening neurologic disorder associated with the use of neuroleptic agents. NMS is typically characterized by a distinctive clinical syndrome of mental status change, muscle rigidity, fever, and autonomic instability. Atypical cases may present without muscle rigidity and/or hyperthermia. Association of infection in an atypical case can make the diagnosis challenging. We describe a case of NMS in a patient who presented with acute onset of altered mental status complicated with aspiration pneumonia.
Case Report
A 22-year-old female with a history of schizophrenia and seizure disorder presented with acute onset of altered mental status. Her home medications included haloperidol, clonazepam, olanzapine, trazodone, topiramate, benztropine, and trihexyphenadyl. The patient was found unarousable by her mother. She had multiple suicidal attempts in the past (overdosed on acetaminophen, drank cleaning detergent, and cut her wrist). She usually medicated herself without supervision. On examination, the patient was drowsy, afebrile (Temp 36.8oC/98.3oF), hypotensive (BP 85/64 mmHg), tachycardic (HR 105 bpm), and tachypnic (24/min). She was noted to be grunting with both inspiratory and expiratory stridor; therefore she was intubated for airway protection. Initial drug screen was negative for all substances of abuse. Acetaminophen and salicylate levels were undetectable. Head CT was unremarkable. Supportive care was provided as the patient was suspected to be overdosed with multiple medications. On the second day of admission the patient developed fever of 38.9oC/102oF. Chest xray and chest CT showed bilateral infiltrations (Fig.1), so empirical piperacillin/tazobactam and vancomycin were started for aspiration pneumonia. Sputum culture came back positive for Methicillin-resistant Staphylococcus aureus. However, the patient remained febrile with a temperature of 39.6 oC /103.2oF, despite appropriate antibiotic treatment. We suspected that there might be some other coexisting condition causing high fever. Serum creatine kinase (CK) was checked and found to be 8,105 U/L, up from 106 U/L on admission. We considered the diagnosis of NMS based on alteration of mental status, hyperthermia, autonomic instability, and elevated CK level, with the use of neuroleptic agents, although the patient did not have any muscle rigidity. The patient was started on dantrolene in addition to intravenous fluid and antibiotics. Shortly afterwards temperature and CK level started to trend down (Fig.2,3). Dantrolene was subsequently increased to maximum weight-based dose. Her mental status was gradually improved and returned to baseline. She became afebrile on day 10 of dantrolene treatment and serum CK went back to normal level after 2 weeks. Then bromocriptine was started orally and continued for 2 weeks.
Figure 1A: chest xray on admission
Figure 1B: chest xray on second day of admission
Figure 1C: chest CT on second day of admission
Figure 2. Temperature trend after starting treatment for NMS
Figure 3. CK trend after starting treatment for NMS
Atypical presentations of NMS can sometimes be difficult to diagnose, as in our patient who presented with altered mental status, fever, and coexisting infection, in the absence of muscle rigidity. We emphasize the importance of a high index of suspicion of NMS in patients using neuroleptic agents.
Discussion
NMS is an idiosyncratic drug reaction to antipsychotic medications and a potentially life threatening condition that occurs in an estimated 0.07% to 2.2% of patients treated with antipsychotics.1 Patients typically present with fever, rigidity, changes in mental status, and autonomic instability, often attributed to first generation antipsychotics, in particular after the start of medication or an increase in dosage.2 Atypical cases of NMS without muscle rigidity and/or hyperthermia have been reported, usually associated with atypical antipsychotic treatment. It has been hypothesized that atypical cases represent early or impending NMS; however pathogenesis remains unclear.3 Risk factors that have been established in case series and case-control studies include agitation, dehydration, acute medical illness, concomitant use of other psychotropic drugs, intramuscular injections and high doses of antipsychotic medications.4-6
Complications of NMS are often consequences of its symptoms. Pneumonia is the most common complication found in 13% of patient with NMS, likely due to altered mental status combined with difficulty swallowing that lead to aspiration.7 Renal failure is the second most common complication (8%), as a result of rhabdomyolysis and myoglobinuria. Other complications have been reported including myocardial infarction, disseminated intravascular coagulation, deep venous thrombosis, pulmonary embolism, hepatic failure, sepsis, and seizure.8 Mortality rate of NMS was around 20-30%.9-10 With early identification and treatment, mortality has significantly reduced to averages 10%.6
Withdrawal of the causative agent is the first step in the management of NMS. Supportive therapy, in particular, hydration, fever reduction, and careful monitoring, is the mainstay of management of NMS. In mild cases, supportive treatment alone may be sufficient.4 Adding specific therapies, such as dantrolene, bromocriptine, and benzodiazepine to supportive measures has been shown to reduce time to complete recovery, from a mean of 15 days with supportive care alone, to 9 days with dantrolene, and 10 days with bromocriptine.1 In severe cases, empirical trial of specific pharmacological agents should be started promptly. Electroconvulsive therapy is found to be effective when pharmacotherapy has failed.11
Sometimes NMS is difficult to identify in the presence of critical illnesses which can obscure the manifestation of NMS. As in our case, the patient presented with altered mental status, fever, and autonomic instability which could be simply explained by the presence of pneumonia and sepsis. However, due to lack of clinical response after appropriate antibiotic treatment, other coexisting condition was suspected. It is important to have a high index of suspicion for NMS in the setting of antipsychotic therapy. An absence of muscle rigidity should not exclude a diagnosis of NMS when the rest of the clinical picture points to this diagnosis. Elevated CK level helps support the diagnosis of NMS in patients with atypical presentation. Discontinuation of offending agent and supportive care should initiate promptly, and specific pharmacotherapy should be considered in severe cases. An early diagnosis is the key to successful treatment and patient outcome.
Conclusion
NMS is a rare but potentially life-threatening condition. Atypical presentation makes it more difficult to identify in patients with critical illnesses. Aspirated pneumonia is one of the common complications of NMS and sometimes can obscure signs and symptoms of NMS and delay diagnosis. High index of suspicion for NMS in patients taking antipsychotics is crucial. If not recognized or left untreated, NMD may be fatal.
Candida species is a leading cause of nosocomial infections and the most common fungal infection in intensive care units. Candida infection ranges from invasive candidal disease to blood stream infections (candidaemia). The incidence of Candida infection has been rising over the past two decades, particularly with the use of immunosuppressive drugs for cancer and HIV1,2,3 , and most of these infections occur in ICU settings.4 Candida infection is associated with high mortality and morbidity. Studies have shown that mortality attributable to candidaemia ranges from 5 to 71% depending on the study. 5.6.7Candidaemia is also associated with longer length of hospital stay and higher cost of care.
Early recognition of Candida BSI has been associated with improved outcome. Candida sepsis should be suspected in a patient who fails to improve and has multiple risk factors for invasive and bloodstream Candida infection. A variety of risk factors identified for candidaemia include previous use of antibiotics, sepsis, immunosupression, total parenteral nutrition, central venous line, surgery, malignancy and neutropaenia. Patients admitted to ICU are frequently colonised with Candida species. The role of colonisation in Candida blood stream infection and invasive candidal disease has always been debated. Few studies support the use of presumptive antifungal treatment in ICU based on colonisation and number of sites colonised by Candida. The NEMIS study has raised doubt about this approach of presumptive treatment. The Infectious Disease Society of America (IDSA) 2009 guidelines identify Candida colonisation as one of the risk factors for invasive candidiasis, but warn about the low positive predictive value of the level of Candida colonisation. 8 We conducted a retrospective cohort study in our medical ICU to identify risk factors for Candida blood stream infections including the role of Candida colonisation.
Hospital and Definitions:
This study was conducted at Interfaith Medical Center, Brooklyn, New York. It is a 280 bed community hospital with 13 medical ICU beds. A case of nosocomial Candida blood stream infection was defined as a growth of Candida Species in a blood culture drawn after 48 hours of admission. Cultures in our hospital are routinely done by the Bactec Method – aerobic and anaerobic cultures. Cultures are usually kept for 5 days at our facility and if yeast growth is identified, then species identification is done. In our ICU it is routine practice to do endotracheal culture and urine culture for all patients who are on mechanical ventilator supports and failing to improve. In patients who are not mechanically ventilated, it is routine practice to send sputum culture and nasal swabs to identify MRSA colonisation.
Study Design:
This study was a retrospective cohort study. We retrospectively reviewed all patients’ charts admitted to our medical ICU from 2000 to 2010 which stayed in the ICU for more than 7 days, irrespective of their diagnosis. Data were collected for demographics – age and sex. Data were also collected for risk factors for candidaemia – co-morbidities (HIV, cancer, COPD, diabetes mellitus, end-stage renal failure (ESRF)), presence or absence of sepsis, current or previous use of antibiotics, presence of central venous lines, steroid use during ICU stay, requirement of vasopressor support and use of total parenteral nutrition (TPN). Culture results for Candida including species identification were obtained for blood, urine and endotracheal aspirates.
Statistical Methods:
Patients were divided in two groups based on presence or absence of Candida BSI. Demographic data and risk factors were analysed using the chi square test to look at the difference between the two groups. Endotracheal aspirates and sputum cultures were combined to create a group with Candida respiratory tract colonisation. Binary logistic regression with forward likelihood ratio method was used to create models. Different models were generated for risk factors. Interactions between antibiotic use, steroid use, vasopressor support and sepsis were analysed in different models. Interactions between urine cultures and endotracheal aspirates/sputum cultures were also analysed by a different model. The model with the lowest Akaike information criterion (AIC) was chosen as the final model. The candidaemia risk score was calculated based on this final model to predict the risk of Candida BSI. Receiver operating curve (ROC) analysis was used to select the best cut-off value for the candidaemia risk score. Candida species in urine and endotracheal aspirates were compared with Candida species in blood culture using the kappa test. Data were analysed using SPSS statistical analysis software version 18.
Study Results:
A total of 1483 patients were included in the study. 56 patients (3.77%) had a blood culture positive for Candida species. Table 1 demonstrates demographic characteristics of the study population. There were no significant differences in the both groups for age, sex, diabetes mellitus, COPD, HIV, cancer and ESRF. As demonstrated in the table, 82.1% of patients in candidaemia groups recently used or were taking antibiotics as compared to 39.6% of patients in groups with no candidaemia. The P value was significant for this difference. Similarly, 71.4% of patients in the group with candidaemia had sepsis as compared to 30.6% in the other group with a P value of 0.000. Use of vasopressor (severe septic shock) was different between two groups – 23.2% and 10.1%, P value of 0.004. Steroid use, central lines and total parenteral nutrition use was higher in the candidaemia group as compared to the group without candidaemia. Similarly the rate of positive Candida cultures in urine and endotracheal aspirates was higher in the candidaemia group as compared to the group without.
Table 2 shows that 57.1% of Candida BSI were caused by C. Albicans, 30.4% by C. Glabrata and 12.5% by C. Parapsilosis. This incidence rate of species is similar to that found in other studies. Table 3 shows the two models with the lowest AIC value. The only difference between these two models was antibiotic use- previous or current use of antibiotics compared to current use of antibiotic in sepsis. Table 4 shows that when multifocal site positivity (urine and endotracheal culture) were used in the model, the AIC value increased significantly. This means that when multifocal sites were used in place of individual sites for the model, good amounts of information were lost and this model did not have good predictive value as compared to the model where individual sites are used for prediction of candidaemia. The model with lowest AIC was chosen as the final model. Binary logistic regression analysis with forward conditional analysis showed that only TPN, central venous line, previous or current antibiotic use, endotracheal aspirate culture positivity for Candida species and urine culture positive for Candida species were included in a statistical significant model. The final model had a P value of 0.000. Odds ratio with 95% confidence intervals and respective P values for all these risk factors are shown in Table 5. Age greater than 65 years, sex, sepsis or septic shock, co-morbidities and steroid use were not significant risk factors for candidaemia.
From this model, the candidaemia risk score calculated would be: Candidaemia risk score = 1.184 for previous or current antibiotic use + 0.639 for presence of central venous line + 1.186 for total parenteral nutrition + 0.760 for positive endotracheal culture for Candida + 1.255 for positive urine culture for Candida.
Table 6 shows the relationship between the Candida strain identified in endotracheal/sputum culture to that in blood culture. Similarly, Table 7 shows the relationship between the Candida strain identified in urine culture and that in blood culture. Strains identified in endotracheal aspirate culture had a very high value for the Kappa test and urine culture had a moderate value for agreement by the Kappa test. Thus, it can be inferred that Candida strain identified in blood culture was very similar to that identified in urine or endotracheal culture.
Table 1: Demographic characteristic of study population
Characteristic
Candidaemia (total 56) N (% of candidaemia)
No candidaemia (total 1427) N (% of no candidaemia)
Chi Square
Age >65 years
34 (60.7%)
676(47.40%)
0.06
Male sex
27 (48.2%)
694(48.6%)
0.530
Diabetes mellitus
22 (39.3%)
506(35.5%)
0.325
COPD
1(1.8%)
75(5.3%)
0.206
HIV
9 (16.1%)
253(17.7%)
0.458
Cancer
4(7.1%)
99(6.9%)
ESRF
11(19.6%)
251(17.6%)
0.401
Previous or current antibiotic use
46 (82.1%)
565(39.6%)
0.00
Sepsis
40(71.4%)
436(30.6%)
0.000
Vasopressor support (Septic shock)
13(23.2%)
144(10.1%)
0.004
Steroid use
27(48.2%)
431(30.2%)
0.004
Central line
30(53.6%)
267(18.7%)
0.000
Total parenteral nutrition
7(12.5%)
29(2.0%)
0.000
Candida in endotracheal aspirate/sputum culture
13(23.2%)
112(7.8%)
0.000
Candida in urine culture
34(60.7%)
262(18.4%)
0.000
Table 2: Candida strains responsible for Candida blood stream infection
Species in the blood culture
Number (%)
Candida Albicans
32(57.1%)
Candida Glabrata
17 (30.4%)
Candida Parapsilosis
7 (12.5%)
Table 3: Models with lowest two AIC
Variables
-2 log likelihood
AIC
Previous or current antibiotic use CVP line Total parenteral nutrition Endotracheal culture Urine culture
394.822
406.822
CVP line Total parenteral nutrition Endotracheal culture Urine culture Current antibiotic use in sepsis
395.730
407.73
Table 4: Model with 2 sites positive for Candida
Variables
-2 log likelihood
AIC
Sepsis CVP line Total parenteral nutrition Endotracheal and urine culture
407.920
417.92
Table 5: Odds ratio with 95% confidence interval for risk factors for candidaemia
Effect
Co efficient(β)
Odds ratio
95 % Confidence limit
P value
Lower
Upper
TPN
1.186
3.274
1.263
8.486
0.015
CVP line
0.639
1.895
1.032
3.478
0.039
Antibiotic Use
1.184
3.268
1.532
6.972
0.002
Endotracheal/ sputum culture
0.760
2.150
1.078
4.289
0.030
Urine
1.255
3.508
1.926
6.388
0.000
Table 6: Endotracheal aspirate culture in candidaemic patients
Endotracheal/Sputum Culture
Blood Culture
Kappa Test For Agreement
C. Albicans
C. Glabrata
C. Albicans
9
0
0.83
C.Glabrata
0
3
C. Tropicalis
0
1
Table 7: Urine cultures in candidaemic patients
Urine culture
Blood culture
Kappa Test for the agreement
C. Albicans
C. Glabrata
C. Tropicalis
C. Albicans
15
5
1
0.47
C. Glabrata
1
10
0
C. Krusei
1
1
0
Discussion
Candida is the most common nosocomial fungal infection in the ICU. Candidaemia accounts for approximately 5-8% of nosocomial BSI in the hospitals in the US.9,10,11 It accounts for approximately 50-75% of the cases of invasive fungal infection in the ICU12,13 and its rate varies from 0.2-1.73 per 1000 patient days.9,14,15 In a study done by Theoklis et al., candidaemia was associated with a mean 10.1 day increase in length of stay and a mean $39,331 increase in hospital charges.16 A study of 1,765 patients in Europe found that Candida colonisation was associated with increased hospital length of stay and increase in cost of care by 8000 EUR.17 ICU patients are at increased risk of infection because of their underlying illness requiring ICU care, immunosuppressant use, invasive or surgical procedures and nosocomial transfer of infections. A number of risk factors have been identified in different studies. In a matched case-control trial, previous use of antibiotic therapy, Candida isolated at other sites, haemodialysis and presence of a Hickman catheter were associated with increased risk of candidaemia.13 Similarly age of more than 65 years, steroid use, leucocytosis and prolonged ICU stays were risk factors for Candida BSI in 130 cases.18 Surgery, steroids, chemotherapy and neutropaenia with malignancy are the other identified risk factors.19
Candida BSI has a very high mortality rate. The attributable mortality varies from 5-71% in different studies.5,12,16,20 Even with treatment, there is high mortality as demonstrated in a study by Oude Lashof et al where out of 180 patients treated for candidaemia, 33% died during treatment and 55% completed treatment without complications.21 Risk factors for increased mortality in patients receiving antifungal treatment are delayed Candida antifungal treatment or inadequate dosing.22 Multivariate analysis of 157 patients with Candida BSI, APACHE II score, prior antibiotic treatment and delay in antifungal treatment were independent risk factors for mortality with odds ratio of 1.24, 4.05 and 2.09, respectively.23 Delayed treatment is also associated with increased fluconazole resistance as compared to early treatment and preventive treatment.24 Inadequate antifungal medication dose and retention of central venous catheters were also associated with increased mortality in a study of 245 Candida BSI, with adjusted odds ratios of 9.22 and 6.21, respectively.25,26
Candida albicans accounts for 38.8-79.4 % of the cases of Candida BSI. C. Glabrata is responsible for 20-25% of cases of candidaemia and C. tropicalis is responsible for less than 10% of cases of candidaemia in the US.9,20 ICU patients are frequently colonised with different Candida species. Candida colonisation can be from either endogenous or exogenous sources. Candida colonisation rates vary with the site- tracheal secretion (36%), throat swabs (27%), urine (25%) and stool (11%).27 Candida colonisation increases with the duration of the stay, use of urinary catheters and use of antibiotics. 28,29,30
The role of Candida colonisation in Candida BSI is frequently debated. Some studies have suggested that Candida colonisation of one or more anatomical sites are associated with increased risk of candidaemia.31,32,33,34 Typically, 84-94% of the patients developed candidaemia within a mean time of 5- 8 days after colonisation according to two studies.35,36 In another study, only 25.5% of colonised patients developed candidaemia.37 Similarity between strain identified in blood culture and that identified at various colonising sites was observed in one study.38 Candida colonisation by exogenously acquired species has also been implicated as a cause of candidaemia.39 In one study, 18-40% of cases of candidaemia were associated with clustering defined as “isolation of 2 or more strain with genotype that had more than 90% genetic relatedness in the same hospital within 90 days.” 40 Similar correlations for clusters are also noted for C. tropicalis candiduria41 and for C. Parapsilopsis.42 In a prospective study of 29 surgical ICU patients colonised with Candida, the APACHE II score, length of previous antibiotic therapy and intensity of Candida colonisation was associated with a significant risk of candidaemia. The Candida colonisation index calculated by non-blood body sites colonised by Candida over the total number of distinct sites tested for patients, was associated with a 100% positive and negative predictive value of candidaemia.29 Other studies do not support Candida colonisation as a risk factor for candidaemia. In a case-control study of trauma patients, only total parenteral nutrition was associated with an increased risk of candidaemia. Candida colonisation, steroid use, use of central venous catheters, APACHE II score, mechanical ventilation for more than 3 days, number and duration of antibiotics, haemodialysis, gastrointestinal perforation and number of units of blood transfused in first 24 hours of surgery. were not significant risk factors for candidaemia.43 NEMIS study found that in a surgical ICU, prior surgery, acute renal failure, total parenteral nutrition and triple lumen catheters were associated with increased risk of candidaemia; the relative risk for each risk factor being 7.3, 4.2, 3.6 and 5.4, respectively. Candida colonisation in urine, stool or both were not associated with increased risk of candidaemia.15
The effect of Candida colonisation of the respiratory tract on candidaemia and on mortality and morbidity is unclear. In a retrospective study of 639 patients, Candida respiratory tract colonisation was associated with increased hospital mortality (relative risk of 1.63) and increased length of stay (median increase of 21 days).30 In a study of 803 patients by Azoulay et al., respiratory tract colonisation was associated with prolonged ICU and hospital stays. These colonised patients were at increased risk of ventilator-associated Pseudomonas pneumonia, with an odds ratio of 2.22.44 However, in a postmortem study of 25 non-neutropaenic mechanically ventilated patients, 40% of the patients were colonised with Candida, but only 8% had Candida pneumonia.45,46 Jordi et al. found that out of 37 patients, definite or possible colonisation was found in 89% of patients and only 5% of cases were defined as Candida BSI.47.The effect of candiduria is also ill defined. Candida colonisation in urine has been implicated as a risk factor in certain studies. In a study done by Bross J et al., central lines, bladder catheters, 2 or more antibiotics, azotaemia, transfer from another hospital, diarrhoea and candiduria were significant risk factors for candidaemia. Candiduria had an odds ratio of 27 for development of candidaemia.48 Similar findings about candiduria were noted by Alvarez-Lerma et al.49
IDSA recommends starting empirical antifungal treatment for high risk neutropaenic patients who fail to improve on antibiotics after 4 days. Recommendation to start empirical antifungal therapy in low-risk neutropaenic patients and non-neutropaenic patients are not made by IDSA because of low risk of candidaemia.8 However, early detection of Candida BSI is vital because of increased mortality associated with delayed antifungal treatment and failure to remove central venous lines. Early detection of Candida BSI in a colonised patient can be facilitated by using a score based on the risk factors.50,51Similarly, b-D glucan assays can be used in patient colonised with Candida, to determine Candida BSI and need for antifungal treatment.52 Combined used of such risk factor identification systems and b-D glucan assays will help to detect candidaemia in earlier stages and will decrease mortality. Our study suggests that total parenteral nutrition, previous or current antibiotic use, central lines, candiduria and respiratory tract colonisation are risk factors for Candida BSI. With the help of our candidaemia risk score system, a score of more than 2 is associated with a higher risk of Candida BSI. This risk factor scoring system along with b-D glucan assays can be used to detect Candida BSI in earlier stages.
Conclusion:
Our study suggests that urine or respiratory tract colonisation is associated with an increased risk of Candida BSI, along with total parenteral nutrition, central venous lines and previous or current antibiotic use. We identified a scoring system which can be used along with a b-D glucan assay to detect candidaemia earlier.
A 34 week preterm, small for gestational age, third born male neonate to a non consanguinous married couple with father having short extremities was admitted in our NICU prematurely with respiratory distress.
On examination the baby was tachypneic with grunt and lower chest indrawing. The baby was also found to have a narrow thorax, short fingers with postaxial polydactyly in both upper limbs and right lower limb, with syndactyly in right upper and lower limb (figures 1,2,3). The cardiovascular, respiratory, abdominal and neurological examination were unremarkable with no facial dysmorphism. The fundus examination was inconclusive.
The antenatal scan showed all long bones short in configuration. The liver function tests were normal except for mild elevation of alkaline phosphatase. The Ultrasound abdomen showed hepatomegaly and no evidence of any other mass lesions. The urine examination was negative for proteinuria and haematuria. The chest x ray showed short ribs, high position of clavicle and features of hyaline membrane disease (Figure 4).
The baby was put on continuous positive airway pressure and given surfactant through an endotracheal tube twice for two consecutive days, but as the condition deteriorated, with hypercarbia and hypoxia as evident on arterial blood gases, the baby was electively ventilated with minimal settings. The baby improved and hence was extubated. After a few hours of being extubation the baby gradually developed respiratory distress and started to deteriorate. Hence the baby was reintubated. The condition of baby was explained to attenders and as the attenders were not willing to continue the treatment, the baby was discharged from hospital against medical advice and later we were informed that the baby expired within few hours after discharge from the hospital.
Fig 1 : showing long narrow thorax and short upper extremities
Fig 2 : showing postaxial polydactyly with syndactyly in upper extremity
Fig 3 : showing polydactyly with syndactyly in lower extremity
Fig 4 : chest xray showing long narrow thorax and short and horizontally oriented ribs with irregular costochondral junctions and bulbous and irregular anterior ends
Discussion
Jeune syndrome or asphyxiating thoracic dystrophy is a rare autosomal recessive skeletal dysplasia characterised by a small chest and short ribs which restrict the growth and expansion of the lungs1. The inheritance is autosomal recessive and a locus has been identified on chromosome 15q13 2. Other symptoms may include shortened bones in the arms and legs, unusually shaped pelvic bones, and extra fingers and/or toes (polydactyly)3 . It is estimated to occur in 1 per 1,00,000 -1,30,000 (again is this 130,000?) live births4.. The diagnosis is based on clinical and radiological findings. Our patient fulfills the diagnostic criteria for Jeune syndrome. The most consistent and characteristic findings were the abnormalities of the thoraxand limbs. Jeune syndrome was first described in 1955 by Jeune in two siblings with severely narrow thorax5. It is known to be genetically heterogeneous.
Several complications of asphyxiating thoracic dystrophy have been described in the literature. The respiratory problems are the main concern. A large percentage of the children with asphyxiating thoracic dystrophy die as a result of these problems. Percentages up to 80% have been mentioned in literature6,7. In our case the baby experienced respiratory distress on day one of life needing ventilator support. The thoracic malformation tends to become less pronounced with age8. A possible explanation could be the improved mechanical properties of the chest wall with growth.
Clinically, Jeune syndrome is characterized by a small, narrow chest and variable limb shortness. Associated congenital abnormalities can be postaxial polydactyly of both hands and/or feet (20%). Typical radiographic findings include a narrow, bell-shaped thorax with short, horizontally oriented ribs and irregular costochondral junctions, elevated clavicles, short iliac bones with a typical trident appearance of the acetabula, relatively short and wide long bones of the extremities, and hypoplastic phalanges of both hands and feet with cone-shaped epiphyses9. The reported case has long narrow chest, short and horizontally oriented ribs with irregular costochondral junctions and bulbous and irregular anterior ends with post axial polydactyly in both upper extremities and right lower limb with left lower limb being normal.
Jeune syndrome is sometimes compatible with life, although respiratory failure and infections are often fatal during infancy. The severity of thoracic constriction widely varies. For those patients who survive infancy, the thorax tends to revert to normal with improving respiratory function. This suggests that the lungs have a normal growth potential and the respiratory problems are secondary to restricted rib cage deformity 10.
Routine pulse palpation is the recommended screening method to detect asymptomatic atrial fibrillation (AF) in clinical practice¹. Since this is part of the blood pressure (BP) measurement technique when using the Riva Rocci (mercury) device or the aneroid device, most patients are evaluated for rhythm irregularity while checking their BP, and, if pulse isn’t palpated, heart rhythm can be evaluated through auscultation of Koroktoff’ sounds. According to the European Community law (2007/51 CE; 2007 September 27th), the mercury sphygmomanometers should not be sold any more, therefore aneroid or automatic devices will replace them in a few years. Recently new devices with embedded algorithms to detect irregular heart beat and possible AF have been commercialised. Whether the switch from Riva-Rocci or aneroid sphygmomanometer to this device will affect detection of AF in usual care is unknown. We explored this issue using a retrospective, naturalistic observation of a group of GPs who abandoned the “old” Riva-Rocci or the aneroid sphygmomanometer and adopted this new device.
Methods
In September 2011 the members of the Italian College of General Practitioners based in Bologna (a medium size city in Central Italy) decided to standardize their office BP measurements. They received an unconditional grant for 30 automatic upper arm blood pressure monitors (Microlife- Afib ®) to be used in office by the GP him/herself. This device embeds an algorithm that calculates the irregularity index (standard deviation divided by mean) based on interval times between heartbeats; if the irregularity index is above a certain threshold value, atrial fibrillation is likely to be present and an atrial fibrillation icon is displayed on the screen. The 30 general practitioners who received the device agreed to a later proposal to examine their database to evaluate detection of new AF patients. They all had the same professional software (Millewin®), and used an automatic extraction. All the patients with recorded diagnosis of hypertension were identified, then BP recording and AF diagnosis were extracted before (365 days preceding the use of Microlife) and after (4 months since starting the use of Microlife) the adoption of the automatic devices. The proposal to examine AF detection was made after four months after they received the devices, therefore the GPs weren’t aware of this study during the usual professional activity. This study was also neither planned nor known by Microlife. Fourteen other GPs, who were using the traditional device, volunteered to provide the same data extraction from their personal database.
Results The 30 participants GPs cared for 48,184 individuals, 12,294 (25.5%) of whom had hypertension (mean age 69.9±13.4). The 16 control GPs cared for 23,218 patients, 5,757 (24.8%) with hypertension (mean age 69.7±13.6). The four-monthly AF detection rate for the original group and the control group is reported in table 1. All the new detected AF were then confirmed on ECG. Statistical analysis was made with the chi-square (χ²) test.
Table 1: Four-monthly AF detection rate in the original GP group and in the control group*
N° GPs and (n° hypertensive patients)
Detected AF % and (n° pts) October 2010- January 2011
Detected AF % and (n° pts) February 2011- May 2011
Detected AF % and (n° pts) June 2011- September 2011
Detected AF % and (n° pts) October 2011-January 2012
30 (12294) - original group
0.37% (46) *
0.3% (39) *
0.37% (45) *
0.63% (77) **
16 (5757) - controls
0.35% (20) ‡
0.45% (26) ‡
0.56% (32) ‡
0.33% (19) ‡‡
*‡ Use of the traditional device: original group vs controls: p NS ( χ² = 3.0421, df 1) ** use of the automatic device (other quarters use of traditional device) **‡‡ Original group: use of the automatic device vs traditional device in AF detection: p < 0.005 (χ ² = 9.487, df 1)
Discussion
Atrial fibrillation can be difficult to diagnose as it is often asymptomatic and intermittent (paroxysmal). The irregularity of heart rhythm can be detected by palpation of the pulse. It may therefore be detected in patients who present with symptoms such as palpitations, dizziness, blackouts and breathlessness, but may also be an incidental finding in asymptomatic patients during routine examination. The diagnosis must be confirmed with an ECG, which should be performed in all patients, whether symptomatic or not, in whom atrial fibrillation is suspected due to the detection of an irregular pulse. Heart rhythm should be evaluated while measuring BP with traditional sphygmomanometers, while this information may be lost with automatic devices, therefore the use of automatic devices with algorithms which can detect possible AF is an appealing choice. The hypothesis that these devices are equal or superior to systematic pulse palpation is currently under investigation by NICE². At the moment the consequences of switching from the classical Riva-Rocci devices to these new ones in usual care isn’t known. The AF opportunistic screening in people aged > 65 leads to a 1.63% detection rate while usual care has a detection rate of 1.04%, very similar to that observed in our hypertensive population (1.13%)³. Our data show that, at least in the short term, switching from the usual device to an automatic device with algorithm for irregular beat detection increases the identification rate of previously unknown AF in the hypertensive population. While waiting for a formal appraisal, GPs who wish or must renounce to their “old” Riva-Rocci can use this device implementing their “usual care” performances.
Mycobacterium tuberculosis was first isolated on 24th March 1882 by a German Physician Robert Koch, who received a Nobel Prize for this discovery in 1905 1. Tuberculosis is one of the oldest diseases in the history of mankind with evidence of tubercular decay found in some Egyptian mummies from 3000-2400 BC 2. The study of tuberculosis was also known as phthisiatry from phthisis, the Greek term for tuberculosis. Hippocrates identified phthisis as the most widespread disease of the time which involved the coughing up of blood, fever and was almost always fatal 3. Avicenna first identified that pulmonary TB was an infectious disease and developed the method of quarantine in order to limit the spread of disease 4 & 5. The disease was given the name of tuberculosis in 1839 by JL Schonlein 6.
Burden Of Disease
Tuberculosis (TB) is an infectious disease caused by various strains of mycobacteria; of which the commonest cause is Mycobacterium tuberculosis 7. The disease can affect any part of human body but commonly attacks the lungs. One third of the world’s current population has been infected by Mycobacterium tuberculosis and new infections occur at a rate of 1 per second 8. About 5-10% of these infections leads to active disease which, if left untreated, kills about 50% of its victims. TB affects approximately 8 million people worldwide and about 2 million people die of this disease annually. In the 19th century pandemic tuberculosis killed about 1/4th of the adult population of Europe 9. Nevertheless, these figures may be only the tip of the iceberg. Tuberculosis is again on the rise and main cause for the resurgence of TB is immunodeficiency as a result of HIV co-infection or, less commonly, immunosuppressive treatment such as chemotherapy or corticosteroids.
Introduction To Mycobacteria
Mycobacteria are aerobic and non-motile bacteria (with the exception of Mycobacterium marinum which is motile within macrophages) which are characteristically alcohol-acid fast 10. They are present in the environment widely in water and various food sources. They are usually considered to be Gram-positive bacteria, but they do not generally retain the crystal violet stain and are thus called Gram-positive acid-fast bacteria. These acid-fast bacilli (AFB) are straight or slightly curved rods 0.2-0.6 mm wide and 1-10 mm long. Mycobacteria are classified on the basis of growth & their ability to produce pigment.
On the basis of growth:
Rapid growing: Mycobacteria that forms colonies clearly visible to naked eye within 7 days on sub-cultures
Slowly growing: Mycobacteria that do not form colonies clearly visible to naked eye within 7 days on sub-culture
On the basis of pigmentation mycobacteria are divided into 3 groups:
Photochromogens (Group I): Produce non-pigmented colonies in dark and pigmented colonies when exposed to light and re-incubation e.g., M. kansasii, M. marinum etc
Scotochromogens (Group II): Produce deep yellow to orange colonies when grown in the presence of either light or darkness e.g., M. scrofulaceum, M. xenopi etc
Non-chromogens (Group III & IV): Non-pigmented in light and dark or only a pale yellow, buff or tan pigment that does not intensify after exposure to light e.g., M. tuberculosis, M. avium-intra-cellulare, M. ulcerans etc
For Clinical Purposes mycobacteria are divided into 3 main classes:
Mycobacterium tuberculosis complex: These are the mycobacteria which can cause TB and include M. tuberculosis, M. bovis, M. pinnipedii, M. africanum, M. microti and M. canetti.
Mycobacterium leprae causes leprosy, also known as Hansen’s disease.
Non-tuberculous mycobacteria (NTM) or environmental mycobacteria, atypical mycobacteria and mycobacteria other than tuberculosis (MOTT). These include all other mycobacteria which can cause pulmonary disease resembling tuberculosis, lymphadenitis, skin disease or disseminated disease. These include: Mycobacterium avium complex, Mycobacterium abscessus, Mycobacterium fortuitum and M. Kansasii which can cause both tuberculosis and leprosy in mammals.
Spread Of Tuberculosis
Today we know that TB is an airborne and highly infectious disease. A person becomes infected when he or she inhales Mycobacterium tuberculosis suspended in air as micro-droplets. Patients suffering from pulmonary TB who have detectable Mycobacterium tuberculosis in their sputum are known as smear positive cases of pulmonary TB. The bacterial load in sputum can be as high as 10,000,000 bacilli/mL. When such smear positive patients of pulmonary TB cough, sneeze or expectorate they produce micro-droplets of phlegm containing Mycobacterium tuberculosis (MTB). The size of these micro-droplets varies from 0.5 to 5mm in diameter. These micro-droplets can remain suspended in air up to 8 hours or even more (depending upon droplet size and environmental conditions including air flow). A single sneeze can produce up to 40,000 of these droplets 11. MTB cannot invade the mucous membranes of the respiratory tree and must reach the alveoli where it replicates. The size of the MTB-containing micro-droplet must be <1mm to be carried to the end of the bronchial tree otherwise it will be deposited on the walls of bronchial tree and cleared away by mucociliary action. Current knowledge asserts that even less than 10 bacteria may cause pulmonary infection 12 & 13. A sputum smear positive patient of TB, if left untreated, can cause infection in 10-15 new people each year.
Definition of TB contacts: People exposed to someone with infectious TB, generally including family members, roommates or housemates, close friends, coworkers, classmates, and others. They are a high priority group for latent-TB infection (LTBI) treatment as they are at high risk of being infected with TB.
Definition of close TB contacts:A person who had prolonged, frequent, or intense contact (i.e. >8 hours/day) with a person with sputum positive TB while he or she was infectious. They are more likely to become infected with TB than the contacts those who see the patient less often.
Pathogenesis
Once in the distal end of bronchial tree, MTB is engulfed by a macrophage in order to start replication within this host cell. Depending upon genetic factors, these macrophages can provide a variable environment for the replication of MTB. If this primary infection starts with a single mycobacteria and the initial host response is incapable of halting this process, within weeks or months there will be millions of tubercle bacilli within the body. MTB spreads in sequence from this primary site to the hilar-mediastinal lymph node initially. When seen on the X-ray, this primary focus of pulmonary infection is called a Gohn focus. It is generally located in the upper lobe or the apical segment of the lower lobe 7. The Gohn focus plus enlarged hilar-mediastinal node is called a Gohn complex. Tubercle bacilli enter the thoracic duct from the hilar-mediastinal lymph nodes, then by passing via the subclavian vein and right atrium, gain access to pulmonary and systemic circulation. As a result MTB can access, and subsequently infect, any organ of the body. Immunocompetent hosts can normally generate an effective immune response within 3-8 weeks, which tackles the primary Gohn focus and can cause involution of the lesions throughout the body. This immune response is a delayed type hypersensitivity reaction to the cell wall protein of bacilli and this is also responsible for positive tuberculin skin test, which appears 4-12 weeks after infection. The primary immune response is not however sufficient to sterilize the tissues and MTB can remain dormant in these foci. Latent foci may persist in the lungs or other organs of the body and are capable of producing disease reactivation which may be pulmonary or extra-pulmonary. In some cases where the initial host response is not capable of causing involution of the primary disease (such as infancy or an immunocompromised state) the infection proliferates and spreads, causing so-called “progressive primary disease”.
Mycobacterium bovis is a mycobacterium that causes tuberculosis in cattle but which can also infect humans. It can be transmitted from cattle to human by ingestion of infected milk and very rarely by inhalation of animal aerosol micro-droplets and by eating infected raw meat. The process of pasteurisation kills M. bovis and other bacteria in milk, meaning that infections in human are rare 14.
When To Suspect Tuberculosis
Primary Tuberculosis: Tuberculosis caused by infection with tubercle bacilli and characterized by the formation of a primary complex in the lungs consisting of a small peripheral pulmonary focus and hilar or para-tracheal lymph node involvement; it may cavitate and heal with scarring or progress. It is mainly seen in children but 10% cases of adults suffering from pulmonary TB have primary infection.
Reactivation Tuberculosis: Also known as chronic TB, post-primary disease, recrudescent TB, endogenous reinfection, and adult type progressive TB. It represents 90% of adult cases (in a non-HIV population), and is due to reactivation of dormant AFBs which are seeded at the time of the primary infection. The apical and posterior segments of the upper lobe and superior segment of the lower lobe of the lung are frequently involved.
Clinical Features:Symptoms and signs vary greatly as do radiological signs. A literature review showed that common signs and symptoms seen in TB infection were 15, 16, 17, 18:
Cough, which can be either productive or non-productive; it is often initially a dry cough which can later become productive.
Fever which seen in usually 70% of cases; generally it is low grade but could be as high as 390C, lasting for 14 to 21 days and in 98% cases is resolved completely by 10 weeks.
Night sweats which is usually seen in 50% of cases
Weight loss
Pleural effusion: 50% of the patients with pleuritic chest pain had pleural effusion
Chest pain: mainly pleuritic with some patients describing retrosternal and inter-scapular dull pain occasionally worsened by swallowing. This pain is believed to be due to enlarged bronchial/ mediastinal lymph nodes
Dyspnoea can be present in 33% of cases
Haemoptysis can be seen in 25%of cases
Fatigue
Arthralgia
Pharyngitis
Common radiological findings were as follows:
Hilar lymphadenopathy: can be seen as early as 1 week after the skin conversion and in almost all of cases within 2 months. It can be associated with right middle lobe collapse
Pleural effusion: typically within the first 3-4 months but can be seen as late as one year
Pulmonary infiltrates mainly in the upper zones and peri-hilar areas
How To Investigate19
HIV testing should be done in all patients presenting with clinical features of tuberculosis
Active Pulmonary TB
CXR: Perform an X-ray chest PA view. If the appearance is suggestive of active tuberculosis perform further investigations
Sputum smear & culture for AFB: send at least 3 sputums for AFB smear and culture including at least one early morning sample. This ideally should be before starting treatment or within 7 days of starting treatment.
If clinical features and CXR are suggestive of active TB, do not wait for culture and sensitivity results, start the patient on the 4 drug initial treatment. This can be modified according to culture results later on.
Active Non-Respiratory TB
A tissue sample should be taken from the suspected non-respiratory site and sent for histological analysis, AFB smear and culture analysis. Common examples of non-respiratory tuberculosis are tuberculous lymphadenopathy, tuberculous meningitis and disseminated tuberculosis.
Physicians should think about CNS tuberculosis such as TB meningitis if a patient with risk factors (i.e., immigrants from endemic areas, positive history of close contact etc) presents with signs and symptoms such as headache, low grade fever, photophobia and/ or focal neurological signs. Lumbar puncture (LP) after a CT brain to rule out any contra-indication for LP may yield the diagnosis in these scenarios. An MRI brain is also very sensitive for picking up tuberculomas in such cases.
Latent TB
Offer Mantoux testing to the household contacts and close contacts of the person with active TB (aged 5 and older). If the Mantoux is positive or if results are unreliable, as can be the case with BCG-vaccinated persons consider interferon gamma testing (T-spot TB Test). If Mantoux is inconclusive, the patient should be referred to a TB specialist. A similar approach should be used for new entrant TB screening.
QuantiFERON-TB Gold (QFT-G) Test & QuantiFERON-TB Gold in Tube (QFT-GIT) Test
Both of these tests have replaced the QuantiFERON-TB (QFT) Test. It is an interferon gamma release assay (IGRA) and measures a component of cell-mediated immune reactivity to mycobacterium tuberculosis. In QFT-G test a blood sample is mixed with antigens (2 Mycobacterium TB protein) and a control. Mixtures are incubated for 16 to 24 hours and then the amount of interferon gamma is measured. If the patient is infected with mycobacterium TB, white blood cells will release interferon gamma when they come in contact with TB antigens. Clinical features, chest X-ray and sputum/ tissue smear and culture for AFB are needed to differentiate between active and latent TB.
Its advantages over tuberculous skin testing are:
This test requires a single patient visit to draw a sample
Results are available within 24 hours
Results are not dependent on reader
It is not affected by prior BCG vaccination
Its limitations/ disadvantages include:
The blood sample must be processed within 12 hours of collection (while white cells are still viable)
There is limited data for use of QFT-G in immune-compromised patients, children under 17 years of age and persons recently exposed to MTB
False positive results may occur with Mycobacterium szulgai, kansasii and marinum infection
QFT-GIT is a modification of QFT-G test. It consists of 3 blood collection tubes containing: 1) no antigen, 2) TB antigen, 3) mitogen. These tubes must be transferred to an incubator within 16 hours of blood collection. Interferon gamma detection is then carried out via ELISA. Its specificity varies from 96-99% and sensitivity is as high as 92% in individuals with active disease.
T-Spot TB Test
It is a type of ELISPOT assay, developed by the researchers at the University of Oxford in England. It counts the number of effector T-cells in the blood that produce gamma interferon so gives an overall measurement of antigen load on immune system. As it does not depend upon production of antibody or recoverable pathogen, it can be used to detect latent TB and it is much faster. In one study it was found that its sensitivity is 97.2% 20.
Treatment Of Tuberculosis (Caused By Mycobacterium Tuberculosis)
Active TB will kill 2 of every 3 people affected, if left untreated. Disseminated TB is 100% fatal if untreated. For the treatment of TB, drugs are used in combination and never singly. Patients require regular supervision of their therapy during treatment to monitor compliance and side effects of medications. Treatment of atypical mycobacterial infections should be under the care of specialized units as this needs special care and drug regimens are complicated. Drugs for treatment of TB are divided into 3 categories:
1st Line Drugs: 1stline anti-TB drugs are very effective against TB. There are 5 first line drugs. All have 3 letter and 1 letter standard abbreviations.
Rifampicin is RMP or R
Isoniazid is INH or H
Ethambutol is EMB or E
Pyrazinamide is PZA or Z
Streptomycin is STM or S
Using a single drug usually results in treatment failure and drug resistant strains 21. The frequency of Mycobacterium tuberculosis developing spontaneous mutations conferring resistance to an individual drug is well known: 1 in 107for EMB, 1 in 108 for STM & INH, 1 in 1010 for RMP 22. A patient with extensive pulmonary TB usually has 1012bacteria in his body and hence will have about 105 EMB-resistant bacteria, 104 STM-resistant bacteria, 104 INH resistant bacteria and 102 RMP resistant bacteria. Drug-resistant tuberculosis occurs when drug-resistant bacilli outgrow drug-susceptible bacilli. Mutations can produce bacilli resistant to any of the anti-tuberculosis drugs, although they occur more frequently for some drugs than others. The average mutation rate in M. tuberculosis for resistance to isoniazid is 2.56 x 10-8mutations per bacterium per generation; for rifampicin, 2.25 x 10-10; for ethambutol, 1.0 x 10-7; and for streptomycin, 2.95 x 10-8. The mutation rate for resistance to more than one drug is calculated by multiplying the rates for the individual drugs. For example, the mutation rate for resistance to both isoniazid and rifampicin is approximately 2.56 x 10-8 times 2.25 x 10-10, or 5.76 x 10-18. The expected ratio of resistant bacilli to susceptible bacilli in an unselected population of M. tuberculosis is about 1:106 each for isoniazid and streptomycin and 1:108 for rifampicin. Mutants resistant to both isoniazid and rifampicin should occur less than once in a population of 1014 bacilli. Pulmonary cavities contain about 107 to 109 bacilli; thus, they are likely to contain a small number of bacilli resistant to each of the anti-tuberculosis drugs but unlikely to contain bacilli resistant to two drugs simultaneously 23.
There are different regimens available for the treatment of TB. The initial 2 months of treatment (usually rifampicin based) is called Initial Phase or Intensive Phase Treatment which later leads to Continuation Phase Treatment. Initial intensive phase treatment is designed to kill actively growing bacteria. Drugs are listed using their single letter abbreviation and a prefix denotes the number of months a treatment has to be given and a subscript denotes intermittent dosage. For example; 2RHEZ/4RH3 = 2 months of initial phase treatment with Rifampicin, Isoniazid, Ethambutol, Pyrazinamide and 4 months continuation phase treatment with Rifampicin and Isoniazid given 3 times per week. If there is no subscript, it means the drugs are given daily.
Usual anti-TB regimens are:
2RHEZ/4RH3 (in less endemic areas)
2RHEZ/4RH (mostly practised, especially in non-endemic areas including UK); standard recommended regimen 24
2RHEZ/7RH (in most endemic areas)
2RHEZ/10RHE (in cases of disseminated, bone and CNS tuberculosis)
2nd Line Drugs 25 & 26: These are less effective than 1st line drugs, have more toxic side effects and are usually not available in most of the developing countries of the world. There are 6 classes of 2ndline anti-TB drugs:
3rd Line Drugs: These are drugs which may be useful, but are not on the WHO list of second line drugs. These are not as effective. 3rdline drugs include:
Rifabutin (this is an effective drug but is very expensive for developing countries, so it not included in WHO list). Occasionally this can be used for patients who are intolerant to or have bacterial resistance to Rifampicin.
Macrolides: Clarithromycin (CLR), Azithromycin
Linezolid: (LZD) not of proven efficacy
Thioacetazone (T)
Thioridazine
Arginine
Vitamin D
R207910: efficacy not proven
Indications of Steroids in the treatment of TB
Steroids should be used along with anti-TB drugs in following situations:
CNS TB (proven benefit)
TB pericarditis (proven benefit)
TB involving eye (definitely beneficial)
TB pleuritis (beneficial – 20-40mg tapered over 4-8 weeks)
Extremely advanced TB (beneficial)
TB in children (may be beneficial)
Miliary TB (beneficial)
Genitourinary TB (beneficial)
Laryngeal TB (may be beneficial – scanty evidence)
TB peritonitis (may be beneficial – scanty evidence)
Important Definitions / Terms 25, 27, 28, 29
New Case: A patient diagnosed as having TB who has never had anti-TB treatment before or had taken anti-TB treatment for less than 4 weeks.
Sputum Smear Positive Case of Pulmonary TB: A patient who has 2 out of 3 consecutive sputum samples positive for AFB.
Sputum Smear Negative Case of Pulmonary TB: A patient clinically and radiologically suspected to have pulmonary TB but with 3 consecutive sputum samples which are negative for AFB and is also culture negative for AFB.
Culture Positive Case of Pulmonary TB: A patient with 3 consecutive sputum smear samples which are negative for AFB but with at least 1 specimen positive for AFB in culture.
Short Course Therapy for TB: The short course therapy for treatment of TB includes 2RHEZ/4RH and also known as standard regimen. If PZA is not included in the regimen for treating TB, the course should be extended from 6 months to 9 months. If rifampicin is not included in treatment regimen then the length of course should be 18 months in total.
Treatment Failure:A TB patient is said to have treatment failure if they remain smear or culture positive while on treatment at the 5th month or if they were initially smear positive, became negative but then reverted to positive at the end of 5months of treatment. Another scenario is that of a patient who was initially smear negative but then becomes smear positive after 2 months of treatment. Important things to note are:
Never add a single drug to a failing anti-TB regimen
Most cases are due to non-compliance
There is a high chance of Mycobacterium developing resistance to anti-TB drugs
Relapse of TB: A patient is said to have a relapse of TB if they were treated and declared cured but is again smear or culture positive; with the same organism. If the patient gets an infection with a new MTB then they are deemed to be a new case. Because genetic analysis of the infecting MTB is required to determine if re-infection is with the same organism or a new one, it is difficult to accurately diagnose TB relapse.
TB Default Case: A TB patient who completed 1 month of anti-TB treatment, stopped the treatment, and then returns for TB treatment over 2 months after treatment was first initiated. If the patient returns within 2 months of initial treatment, then his/ her initial regimen should be continued.
Re-treatment Regimen: A patient should be a given re-treatment regimen when they relapse or are a TB default case. In highly endemic areas for TB, most authorities prefer an initial intensive phase with 5 drugs for 3 months (2 months RHEZS and 1 month RHEZ).
Chronic Case of TB: A patient is said to be a chronic case of TB, who remains sputum smear positive after 1 re-treatment course. Such patients invariably have drug resistant TB.
Extra-pulmonary TB: TB involving organs other than lungs is called extra-pulmonary TB. For the purpose of treatment and understanding, TB of the central nervous system is excluded from this classification.
Pulmonary TB: Tuberculosis involving lungs is called pulmonary TB.
CNS Tuberculosis:TB can involve the meninges, brain & spinal cord. It is called TB-meningitis, cerebritis & myelitis respectively. Standard treatment is for 12 months and steroids are mandatory. INH & PZA have 100% penetration into CSF.
Miliary Tuberculosis: This a complication of 1–3% of all TB cases. Tuberculosis involving 2 or more organs/ systems of the body is called disseminated TB or miliary TB. It is also called tuberculosis cutis acuta generalisata and tuberculosis cutis disseminate. It is a form of tuberculosis that is characterized by the wide dissemination and by the tiny size of the TB lesions (1–5 mm). Its name comes from a distinctive pattern seen on a chest X-ray of many tiny spots distributed throughout the lung fields with the appearance similar to millet seeds—thus the term "miliary" tuberculosis. Miliary TB may infect any number of organs, including the lungs, liver, and spleen.
MDR-TB: Multi-drug Resistant TB (MDR-TB) is defined as TB caused by mycobacterium tuberculosis resistant to isoniazid and rifampicin. The diagnosis and appropriate treatment of MDR-TB is still a major challenge.
XDR-TB: Extensively-drug Resistant TB (XDR-TB) is defined as TB caused by mycobacterium tuberculosis resistant to isoniazid, rifampicin, quinolones and any 1 of 3 injectables: kanamycin, capreomycin or amikacin.
Treatment Categories of TB Patients:
There are four treatment categories of TB patients for details see table 1.
Table 1
Treatment Category
Type of TB Patient
Category I
New sputum smear +ve or Smear –ve pulmonary TB cases with extensive parenchymal involvement New severe extra-pulmonary TB cases
In this programme a trained person observes the patient swallowing tablets for preferably the whole course of treatment or at least the initial 2 months of treatment. Daily or thrice weekly dosages are recommended but twice weekly dosages are not recommended because of the risk of omitting (by mistake or by chance) one dose. This would result in once weekly dose and it is not acceptable. WHO recommends the DOTS strategy in an attempt to control tuberculosis. There are 5 main points of action:
Government commitment to control TB
Diagnosis based on sputum smear microscopy tests done on patients who actively report TB symptoms
Direct observation short course chemotherapy treatment
Definite supply of drugs
Standardized reporting and recording of cases and treatment outcomes
DOTS-Plus:
WHO extended the DOTS programme in 1998 to include treatment of MDR-TB and this is called DOTS-Plus. It requires the capacity for drug susceptibility testing and provision of 2nd line anti-TB drugs with facilities for identification and drug sensitivities.
Latent TB Infection (LTBI):
A patient is said to have LTBI when he is infected with MTB but does not have any symptoms and signs suggestive of active TB and has a normal chest X-ray. Such patients are non-infectious but 10% of these persons go on to develop active TB in their life at a later stage. They have positive tuberculin skin test and positive Interferon Gamma Release Assay (IGRA) tests (e.g. T-SPOT.TB test, QuantiFERON-TB Gold &QuantiFERON-TB Gold-in tube tests). There are different regimens for treatment of LTBI, commonly used are the following:
9H; 9 months INH (gold standard – only practised in USA)
6H; 6 months INH
3RH; 3 months INH + RMP (recommended in UK)
Common Causes Of Rising Burden Of Tuberculosis
The following are a few causes of rising burden of TB globally:
Non-compliance with medication
Presence of drug resistant strains of mycobacteria
Faulty regimens
Un-diagnosed cases
Under-diagnosed cases
Lack of newer, more effective anti TB medication.
Role Of Pcr In The Diagnosis Of Tuberculosis
There have been a number of studies regarding the role of PCR in the diagnosis of TB. They show that it has a high sensitivity and specificity but gold standard is still tissue smear and culture for AFB. In certain scenarios PCR of different tissue samples (pulmonary or extra-pulmonary) urine, CSF, sputum and blood can be useful and can also tell us about mycobacterial rifampicin resistance.
Role Of Physicians In Prevention & Control Of Tuberculosis In Relation To Airtravel30
Inform all patients with infectious TB that they must not travel by air on a flight exceeding 8 hours until they have completed at least 2 weeks of adequate therapy.
Inform all patients with MDR-TB and XDR-TB that they must not travel by air until they are culture-negative.
Advise patients with TB who undertake unavoidable air travel of less than 8 hours’ duration to wear a surgical mask or to otherwise keep the nose and mouth covered when speaking or coughing during the flight. This recommendation should be applied on a case-by-case basis and only with the agreement of the airline(s) involved and the public health authorities at departure and arrival.
Inform relevant health authorities of the intention of a patient with infectious TB to travel against medical advice.
Inform relevant health authorities when a patient with infectious TB has a recent history of air travel (travel within 3 months).
Side Effects Of Medications Used For Treatment Of Tuberculosis31, 32, 33, 34
Patients who are on treatment for TB should be monitored regularly for any signs of medication toxicity. This may include blood tests in addition to clinical examination. Common side effects of the routinely used 4 anti-TB medications (INH, rifampicin, Ethambutol & PZA) are as follows:
Hepatotoxicity: INH, PZA and rifampicin are known to cause liver toxicity. Ethambutol is a safer medication in patients with known liver problems. INH is contraindicated in patients with active hepatitis and end stage liver diseases. 20% patients can have an asymptomatic rise in AST concentration in the first 3 months of therapy. Symptoms of liver toxicity include anorexia, nausea, vomiting, dark urine, jaundice, fever, persistent fatigue, abdominal pain especially in the right upper quadrant. Routine base line LFTs are recommended prior to starting treatment. After that they should be repeated at least once a month and more frequently in those who are at risk of developing hepatotoxicity. Patients at increased risk of hepatotoxicity include:
HIV positive
Pregnant or post-partum (3 months after delivery)
History of or at risk of chronic liver disease (daily use of alcohol, IV drug users, hepatitis, liver cirrhosis)
Patients taking any other medication which have potential hepatotoxic side effects
The risk of hepatotoxicity increases with age (> 35 years old)
Suspect drug induced liver injury if there is AST/ ALT rise > 3 times base line with symptoms or > 5 times in the absence of symptoms, or disproportionate rise in ALP and total bilirubin. In such a situation:
Stop hepatotoxic anti-TB medications (INH, rifampicin and PZA) immediately
Admit the patient to hospital
Carry out serological tests for Hepatitis A, B, and C (particularly in those who are at risk for hepatitis)
Look for other causes (hepatotoxic medications, high alcohol consumption)
In acutely ill smear or culture positive patients start liver friendly medications i.e. Ethambutol Quinolones, and Streptomycin, until the cause for hepatotoxicity is identified.
Re-challenge: Once LFTs are normal (or < two times the upper normal limit) start with Ethambutol and add INH 1st. If LFTs do not rise after 1 week add Rifampicin. Next add PZA if there is no rise in LFTs after 1 week of adding Rifampicin. If at any point LFTs increase or symptoms recur, stop the last added drug – as this is the culprit drug.
Gastro-intestinal (GI) upset: GI upset is quiet common with anti-TB medications and usually occur in the first few weeks of therapy. Symptoms usually are nausea, vomiting, anorexia, abdominal pain. In such a case recommend good hydration, change the timing of medication (advise to take with a light snack and at bed time) and also check LFTs for possible hepatitis. Aluminium salt containing antacids can reduce bioavailability of INH, so avoid them 1 hour before and 2 hours after INH administration.
Rash: All anti-TB medications can cause a skin rash. Management is based on severity:
Mild rash or itching: administer anti-histamines 30 minutes prior to anti-TB medications and continue with the therapy. If no improvement, add prednisolone 40mg/day and gradually taper down when the rash clears.
Petechial rash: Red pinpoint sized dots under the skin due to leakage from capillaries – suspect rifampicin hypersensitivity. Monitor LFTs and full blood count. If platelet count is below normal (base line), stop rifampicin and do not restart it.
Erythematous rash with fever: and/ or mucous membrane involvement; stop all anti-TB medications immediately and hospitalize the patient. Rule out anaphylaxis (angio-oedema, swollen tongue, throat, stridor, wheezing, flushed face, hypotension) and Stevens-Johnson Syndrome (systemic shedding of mucous membranes and fever). If situation does not permit to stop TB medication then try 3 new drugs i.e. aminoglycoside and 2 oral agents from second line. Once the rash has settled, can re-introduce first line TB medications one by one every 2-3 days, 1st rifampicin, then INH, then PZA and then Ethambutol. While re-introduction, monitor the signs and symptoms of rash, if rash recurs at any point remove the last agent added.
Peripheral neuropathy: signs and symptoms include numbness and tingling in feet and hands, increased sensitivity to touch and stabbing pain. INH can cause peripheral neuropathy. It is more common in malnourished people, diabetes, HIV, renal failure, alcoholism, pregnancy and in breast feeding women. Prevention is the key; prophylaxis is with Pyridoxine (vitamin B6) 10mg/ 100mg INH (normally 25 – 50mg) per week is used in high risk patients.
Optic neuritis: the main agent responsible for this is Ethambutol. It is dose related and gets more intense if treatment is continued. Signs and symptoms are difficulty in reading road signs, decreased red-green colour discrimination, blurring or vision, and colour blindness. These can be unilateral or bilateral. Ethambutol is not recommended in children <5 years of age as visual changes are difficult to monitor. Visual acuity and colour blindness tests are recommended at baseline and also on a monthly basis. Fluctuations of 1 or 2 lines on the Snellen chart is considerable and Ethambutol must be stopped. More than 10% visual loss is considered significant.
Fatigue: INH can cause fatigue and in such situations patients should take the medication at bedtime. If it continues, check LFTs to look for hepatotoxicity.
Flu-like symptoms/joint aches and pains: These are usually seen with Rifampicin and treatment is symptomatic.
Drug-induced lupus: It is seen with INH and blood tests should be done to differentiate it from SLE. It can be managed with steroids while the patient is taking INH.
It seems that psychiatry is gradually losing its allure for future doctors. All around, one can detect an air of pessimism from colleagues about the creeping 'socialisation' of this important field of medicine. There is no longer the breadth of interest in the subject and each sub-branch, for want of a better expression, has its followers and adherents. Proponents of one particular facet of treatment are zealous in the pursuit of their own interests. Psychotherapy is pitched against the neurobiological, rehabilitation and social psychiatry against the pharmacologists, all trying to mark out their own piece of territory, with some yearning for a place in the history books, or at the very least, an acronym. Some psychiatrists do not believe in diagnoses; others ridicule the concept of personality disorder, autistic spectrum disorder, or drug treatment; some believe psychiatric illness is the fault of governments, and there are probably a few who do not believe in psychiatry at all! 'Research' studies are cherry-picked by all sides to illustrate the ineffectiveness of 'alternative' treatments. The full picture or perspective of ill health is blurred and narrowed by a minority who believe they alone know what is right for patients, and psychiatry is 'intellectualised' by others to give it an air of authority and profundity it does not possess. Morale and training are suffering and, if this state of chaos and insanity continues, the discipline itself will implode and cease to be of interest to anyone, save the warring factions in the profession itself.
Once upon a time it was considered that a reasonably broad mixture of community and hospital services would provide benefit for patients with mental illness. Staff involved in their care, who have the rather cumbersome and oxymoronic description of being called 'mental' health professionals, would also widen their experience because of the continuity of care provided. It was hoped patients who clearly did not need to be in hospital (for example, waiting for appropriate accommodation) could be discharged. Clinical need would determine those who required further rehabilitation/treatment in hospital, and would not be swayed by pressures, often financial, to discharge. Now, with the setting up of Home Treatment and other teams the situation has ironically worsened, because there is an implicit opinion in this arrangement that hospital admission, even for the seriously ill or indeed violent patients, is the least desirable option and something to avoid at all cost, even when care in the community is not immediately available or adequate. Care provision for the elderly is a separate concern and is not under discussion here.
In the domain of general adult psychiatry those patients who are in need of care, be it medical or social, are languishing at home, desperate for help, being offered assessment after assessment by disparate teams. There are not enough care professionals to cope with the demand. Home Treatment Teams in particular, are under considerable sustained pressure and stress to ensure further reduction in beds. Rehabilitation beds are being closed. 'It is cheaper to keep patients in the community', we are told. Or, if that does not suit, the liberal stance might be, 'What does hospital admission achieve'? That's fine if the problem is not on your doorstep. Psychiatrists who oversee inpatient care are also pressurised to discharge patients as soon as possible, so the very old notion of 'incarceration' (that worn-out cliché from the antipsychiatry lobby) seems facile, to say the least. On the contrary, doctors now have the added worry of prematurely discharging partially treated ('we need the beds') as well as more vulnerable patients who cannot cope. Most patients who take up psychiatric hospital beds do not want to be in hospital in the first place as they often, rightly or wrongly, do not see themselves as ill. Many hospital beds are now occupied by 'Section patients', and conversely, many very ill patients are left to go it alone because they refuse hospital admission and do not want community team involvement, yet are not 'sectionable'. The inference seems to be, 'If not sectionable or under CPA (Care Programme Approach) it is not our concern.'
Where there are sufficient provisions for outpatient care, some of the damage may be mitigated. Overworked staff including community psychiatric nurses (CPNs), support time recovery workers (STRs) and occupational therapists (OTs) often have the thankless task and enormous responsibility of seeing patients at home, some of whom are threatening and potentially dangerous, others erratic with their outpatient clinics attendance not always through deliberate evasion but often the result of the very condition causing the problem, for example, lack of insight. Other patients do not engage either through hostility or loss of motivation induced by the underlying problem, say, drug and alcohol misuse. Chronic patients are not ill enough to be on CPA and diagnostic 'conundrums' are left to others to sort out. With the introduction of the New Ways of Working,1 the traditional outpatient clinics are being abolished and replaced with community clinics ('short-term' outpatients really). Ideally a community clinic should be run by CPNs as they usually understand the medical, psychiatric, psychological, and social needs of patients. In the authors' opinion the clinics should be Consultant-led because despite the tendency to classify everyone as 'clinicians' many staff feel uncomfortable with this role as it implies or infers a degree of clinical responsibility for which they are not qualified. Psychiatric nurses (especially those with a general nursing background) are ideally placed to carry out this function by virtue of their wide experience; also they are aware when to seek medical help when needed. Often they are more informed about patients than the primary physician or indeed the psychiatrist because of more frequent contact, either via liaison with the hospital wards or through home visits in their role as CPNs. Nurses and other staff (for example, social workers) are involved in patients' discharge from hospital (usually determined at pre-discharge meetings) and are therefore an essential link in the continuity of patient care before patients are eventually seen in the 'community clinics'. Requests for domiciliary visits from general practitioners (GPs) to physicians themselves have become a thing of the past, with the exception of those psychiatrists working with Home Treatment Teams and Assertive Outreach Teams. Nowadays it is not uncommon for patients to be waiting months on end (more assessments) before being deemed 'appropriate' to see a Consultant Psychiatrist.
Certainly there are patients who do not need to continue seeing a Consultant Psychiatrist for years on end and should be discharged back to the GP to reduce unnecessary costs and to avoid a dependency culture, in the same way a patient with mild arthritis does not need to see a rheumatologist or a patient with anaemia does not always need the expertise of a haematologist, to use simple analogies. However, sometimes GPs are unwilling to reciprocate or feel out of depth with 'psychiatry' that this is not always possible. The chronicity of many psychiatric disorders perhaps harnesses the belief that new treatments may emerge which only a psychiatrist, with his/her specialized knowledge, can implement and deal with. This type of scenario is seen with many other illnesses in all fields of medicine (chronic psoriasis, rheumatoid arthritis, multiple sclerosis) yet no one is suggesting that GPs solely should be left to manage these conditions. It seems the clinical risk to patient care is not thought through and this no doubt will lead to serious repercussions later. In our estimation, physical and mental illnesses are so often intertwined that their management should be equally shared by physicians and psychiatrists.2
Swings and Roundabouts
Such is the pressure by management (under the thumb of civil servants) and 'those in the know', reverentially referred to as ‘Commissioners’, that health professionals in psychiatry have to defend their clinical judgment and carry out numerous risk assessments (defensive medicine) of patients who are to be discharged from the outpatient clinic back to the GP in any event. Patients may be fortunate enough to receive a few last appointments with the Community Clinic (when they are up and running: some are at the time of writing) before they are shown the door and sent back to the GP, all to save money. Packages of care will not disguise the fact that vulnerable patients are being left to fend for themselves, just as they were in the past when the large institutions closed down without any forward planning as to how and where patients would survive. Yet ‘management training’ and ‘mandatory courses’ continue inexorably, often provided by 'expert' outside speakers, costing Trusts considerable amounts of hours lost, let alone the expense, instead of employing more nursing staff to cope with the ever-increasing workload. We are led to believe that reducing 'outpatient numbers' will lead to less pressurised work on staff, which really does not fit. All that will be happening to the extent that 'outpatients' will now be filling to the brim with CPA patients (read 'psychoses') instead of a good case-mix of patients required for general experience and training. It seems to be forgotten that there are patients who feel very unwell and are unable to cope, yet are not suffering from major psychiatric disorders.
The next scenario will be the revolving door ‘GP - Access/Assessment Team - possible Consultant Psychiatrist advice and at most two follow-up appointments (if one is really ill) - Community Clinic - discharge to GP system’, to replace the premature hospital discharge-readmission system which failed miserably in the past. When the patient relapses (or rather, when the illness remains static) the GP refers back into the system and the whole process begins again. In this way the Trusts receive money by reaching their targets (discharging patients) and are paid a second time when GPs 'purchase' more care. Those patients with 'minor problems' (not in their GP's estimation) will whittle away and remain unhappy. 'They can always see a counsellor' is the unspoken passive riposte. Furthermore, there will be less clinical variety for doctors and students, as their work will amount to prescribing 'powerful drugs' (we are told by the antipsychiatrists), monitoring serum lithium (and other drug) levels or checking blood results and clozapine dosages, because the Talking Therapies will be curing all and sundry. If only. We are reverting to the bad old days of pseudomedicine and pseudoscience.
Academicians and those who sit on government advisory bodies with grandiose names would have us believe there are far more effective ways to support people at home, or if they have no home, a crisis house will do. Meaningless, empty statements such as 'randomised controlled trials' (given the complexity of the issues under study) often with some reference to National Institute for Health and Clinical Excellence (NICE) guidelines, are used to support questionable findings. Despite all the 'new ways of working' national stress levels are at their highest because of rising unemployment, unexpected redundancies, increasing debt through credit card borrowing, and suicide rates are going up. New ways of Working is not working and any 'ad hoc survey' (note we did not say 'research') will reveal the depth of disillusionment all professionals in the discipline of psychiatry are experiencing, and not just the hallowed psychiatrists. Rudderless multidisciplinary teams are not the answer: teams require management. The term 'leadership' is becoming redundant (one only has to look at successive governments) and is often merely a spur for making money out of meaningless and time-wasting leadership courses which seem to be sprouting everywhere. Among the many qualities 'leadership' embraces are a sense of humour, assertiveness, fairness, creativity, openness, integrity and dedication, all to be found in one individual; presumably! Hierarchical structures may work, contrary to the sweeping statements of some,3 because people who are experienced in medical, academic and management matters (with perhaps a sense of humour) tend to command respect from team members. It is not enough to be an expert in cognitive behavioural therapy (CBT).
No place like home
How does one establish trust and rapport with patients when there will be less opportunity to do so because their care and progress are determined by market forces? Instead of decreasing outpatient volume or confining this aspect of care to CPA patients only, outpatient departments should cater for the mounting levels of stress in the community (poverty, debts, redundancies, threatened job losses) through increased staffing levels and training/supervision of more social workers, CPNs and occupational health workers. Where possible such staff should attend as many clinics as possible (not just CPAs) to offer a more holistic approach to patient care. If anything, policy makers, clinicians, managers, carers and user groups need to collaborate and clamour for a more integrative mental health service, not fracture the already fragile set-up. Community clinics are seen as a stepping stone to discharging from the mental health services (those who set them up don't like this analogy), which in theory is a good idea. The problem lies in the precipitous nature of transfer from outpatient to community clinics. Some very ill patients with chronic conditions are ironically not a burden to the system, in that they do not need to be seen frequently nor do they not require repeated admissions to hospital, yet if left to their own devices and discharged back to Primary Care would soon find life unmanageable as they rely on the expertise of health professionals to remain reasonably stable. Many patients have physical problems, some partly the result of the very treatments given to alleviate their underlying condition (obesity, hypertension, ECG disturbances, Type 2 diabetes and so forth), and need careful monitoring and supervision which is best provided by CPNs and other staff, in the same way a Health Visitor, Practice Nurse, or Diabetes Nurse Specialist might offer his/her expertise to a GP practice.
There will always be patients who need to be seen in the outpatient department with the emotional security and staff support this provides. We are aware that some 20% of patients miss their mental health appointments but then people miss appointments for other interviews and not always because they are unwell.4 Some people miss appointments because they feel better. This is surely not a reason for abandoning the outpatient system, which serves the remainder of the patient population quite well. We have experienced an unprecedented expression of worry and disappointment by patients who have been told they are not ill enough to be followed up at the outpatient department. Now mental health professionals are also frustrated, because they perceive their remit is to refer back to the GP as swiftly as possible, without having thoroughly assessed a patient over a period of time. First on the target list will be those patients who have not been seen by a psychiatrist for several months (‘We don't see them very often, therefore what is the point?') yet many chronically unwell patients may not want to attend outpatients, or have sufficient insight to realize they need to attend, for reasons outlined above. Will Outreach Teams in every Trust be abandoned to save money? Was it not their role in the first place to help those reluctant to receive treatment? What messages are we giving to patients other than being 'just a number, a hospital statistic’'? Those who have had the ‘luxury’ of a hospital admission usually comprise the very psychotic, and the personality disordered, and of the latter some consider they should not be in hospital anyway. The gains that have been made over the past decade in early intervention and engagement with patients by Assertive Outreach Teams will be lost. Yet, there is a continuing demand from patients and their carers to be seen by doctors.5
Here is how the 'new' system works. New Ways of Working, set up some years ago 1 and imposed on us, was meant to be an innovative approach to consultants' contracts by encouraging multidisciplinary teamwork ('When did consultants ever not consult their fellow professionals'?), reviewing the continued necessity for outpatient clinics, advocating more scheduled time for carers (colleagues we have spoken to cannot ever recall not seeing relatives or carers!) and more prominent roles for all team members, encouraging further education and training. Unfortunately we have gone to the other extreme and are being bombarded by all sorts of courses to the extent that much time is lost not seeing patients. Team members may and should undertake postgraduate studies. For doctors, continued professional development is mandatory. We are the only profession that requires revalidation every five years. Nothing can substitute for the medical training doctors undergo and it is a shame that the expertise of psychiatrists is diluted and devalued by their current roles as medication gatekeepers. It is a curious state of affairs or perhaps conveniently forgotten that when Trusts or 'Health Care Reformers' talk nowadays about working in teams and 'shared responsibility', the Consultant-led team concept is dismissed. Where there are Consultants who do not feel up to the role of leading a team, or are uncomfortable making assertive decisions and would rather take a back-seat thus avoiding the responsibility of being in charge of a team, then a Specialist Registrar nearing the end of training could fill this position. Multidisciplinary means 'several' not 'equal' disciplines of learning, ideally each discipline contributing a part to the whole. The medical member of the team is nowadays confronted with the added indignity of having his/her patients described in management-speak as customers, consumers, clients, service users, in fact any title that does not describe the ill person as a patient. It also reflects a creeping normalisation of 'political correctness' thrust upon us by the social engineers and should be resisted. We want patients to be treated with respect not as 'service users’, waiting for the next bus or train. Trusts are now seen to promote a business approach to health care, thereby gaining the approval of their masters, the civil servants and politicians.6 Lots of tick boxes and targets, with subtle threats of redundancies or talks about 'natural wastage'. Meanwhile, the College sits idly by.
Another concern is the training of future psychiatrists which is slip-shod and bureaucratic (lots of forms and assessments). There is hardly any room to accommodate medical students. Junior doctors who practice psychiatry are not receiving the continuity of supervision which existed years ago. The 'junior doctor' is less visible because of European working time directives, on-call commitments with days off in lieu, study leave, annual leave, and the inevitable sick leave. Passing the Member of the Royal College of Psychiatrists (MRCPsych) exams nowadays does not necessarily equate with clinical experience anymore. Even the nomenclature is confusing - not just to doctors and management (‘CT1’, ‘ST1’ and so forth) but also to staff, and reduces the profession to an anomalous set of categories no outsider understands, not to mention the loss of identity it creates in the individual doctor. What was wrong with Senior House Officer (SHO), Registrar, Senior Registrar, and Consultant? Unfortunately, we believe it is now too late to revert this shambles born out of the chaotic modernisation of medical careers. 7
The future is bleak and many doctors (and indeed nurses) are becoming disenchanted by psychiatry, feeling let down by a Royal College which seems to accommodate every new social trend rather than concentrating on improving the status of a once fascinating field of medicine. Lots of wake-up calls, but no-one is getting out of bed.8 Strange having a 'trade union' that ignores its members! Could someone inform the College that nowadays most General Adult Psychiatrists are almost reduced to measuring lithium levels, advising on clozapine doses, and attending meetings. No wonder the numbers of potential psychiatrists are falling. How would this dilution of responsibility work in a surgical unit? Would the team members decide how an operation is to be carried out because one of them is trained in resuscitation? Contrary to reports3 consultants are not happy with the present set-up, though it is unlikely our Royal College hierarchy will do anything about it. Many psychiatrists nowadays have an extensive academic knowledge of medicine, psychology, sociology, and neuropsychiatry, and no longer want to be minor players in the game, or undermined by a system that encourages power without responsibility.
Fragmentation breeds disinterest
What is the answer? The previous system, though not perfect, worked well. This had its shortcomings too (oversized catchments areas, Consultants in charge of many wards, and so forth)7 but the continuity of care was there. Patients discharged from hospital were seen by the same team. GPs could refer directly to Consultants (as is the case in other medical specialties) and patients were then seen in the outpatient clinic. However, often the patient would attend such clinics for years because GPs were reluctant to resume care. Nowadays the training and education of GPs is exemplary and most are more than capable and indeed willing, to continue to provide support for their patients provided there is a back-up plan. The academic training of psychiatrists has never been better but their clinical skills are suspect. Therefore there needs to be an overhaul in the examination system as well. Actors are not patients. Simulated psychiatry is not the same as simulated surgery. Simulation is a technique not a technology, we are told. It is not a substitute for doctors examining real patients in real contexts. The same applies to nurses. All nurses (CPNs) could easily be trained to do ECGs, act as phlebotomists, and arrange routine tests. Many already do. Give back to nurses the skills they enjoy in other fields of medicine. For psychiatrists there are numerous courses one can attend to broaden their medical knowledge. Most GPs take an interest in a holistic approach to their patients (social, psychological, physical). As matters stand GPs now refer to a borough 'Access and Allocation Team' with no one held accountable, and even though requested by the GP, a Consultant Psychiatrist's opinion is not always provided. Responsibility is the province of senior doctors and management and should not be diluted by putting pressure on the Team as a whole whose individual experience varies considerably. Doctors (and nursing staff) should have mandatory training in psychological therapies (cognitive and behaviour therapies specifically). A fixed number of sessions in addition to their usual duties could be part of the job plan for those doctors interested in the psychotherapies per se, or put another way, a holistic approach to patient care, which is what most doctors do in any event. Patients would then have the benefit of medical and psychological input simultaneously (let's call it a cognitive-medical model). Waiting lists would be dramatically reduced at a stroke and Trusts would no longer have the responsibility of finding and employing unqualified (in medicine or psychology) 'talking therapists'. People who are generally physically well and who do not have serious psychosocial problems or psychiatric illnesses could receive treatment elsewhere through their GP, counsellors or other psychotherapists (those with no medical or psychology degrees) of their own volition. There is no need to clog up the system with 'customers'. We are not a supermarket!
Complaints will inevitably follow when patient dissatisfaction begins to emerge, which is only a matter of time. More serious incidents will be a consequence of too many bed closures and staff shortages. Dilution of responsibility means that no one person seems to be accountable when things go wrong and patients are left stranded (read the Francis Report 9). Already GPs are frustrated by the lack of informal contact with psychiatrists who are once again seen to be retreating to their ivory towers, having been overwhelmed by lots of courses, lots of training, lots of meetings, lots of empty rhetoric. Too much emphasis nowadays is placed on the sociological/psychological aspects of patients' illness and so serious conditions are missed. GPs should be able to refer directly to their colleagues where there are immediate concerns and not have to wait for triage meetings which delay this process. After all, GPs know their patients best. Community clinics could take the bulk of moderate conditions (which are causing undue stress) and see patients for as long as necessary (not a determined number of appointments) before deciding the GP can resume responsibility. 'Packages of Care' and other outdated expressions should be confined to the dustbin. Patients are not fooled by promises of cardboard boxes with little pink ribbons. Continuity of patient care requires a flexible approach which encompasses easy access to information and a direct pathway to services and medical care when needed.
Knowledge in the making
Psychiatrists should concentrate on more difficult and complicated cases (as was the case in the past) as well as routine moderate conditions, enabling them to use their broad skills more efficiently and effectively. Some psychiatrists see too few patients and this should be changed. Perhaps there is a case for psychiatrists rotating through some specialties say, every five years, for example, between Rehabilitation and General Adult Psychiatry. There are many patients who are not on mood stabilisers or clozapine who require intensive input and combined medical expertise and rotating between posts would offer valuable experience. A more varied approach is thus needed but do we really need all those subspecialties? What ever happened to the general psychiatrist with a special interest? In our view at least one year of neurology training should be mandatory for psychiatrists during their training. No formal examinations, just certificates to prove the courses have been completed; otherwise the system grinds to a halt. Under this system a doctor could still theoretically become a consultant after nine years postgraduate training (three years in foundation training and neurology), and six years Psychiatry (to include neurology, psychology and sociology) which is not unreasonable. Equal emphasis on neuromedical, sociological and psychological factors causing health problems would foster a healthier and friendlier relationship between disciplines which deal with mental illness and primary care providers. As it stands, with the fragmented role of general adult psychiatric services and the emphasis on e-learning and internet training for junior doctors (no hands-on clinical experience) we are facing yet another era of overemphasis on social psychiatry (or rather reverting to ancient belief systems) with its 'neutral' politically correct denigrating sound bites (customers, clients, service users). All will be well if we can just sort out the social problems! The simplistic notion that problems will disappear if we do not smoke, drink, take illicit drugs, keep our weight down, and have a home to go to, is the stuff of social engineering by the 'experts in living,' and alas by doctors who have lost touch with medicine.
Doctors need reminding that psychiatry is that branch of medicine that is concerned with the study, treatment, and prevention of mental illness using medical and psychological therapies as well as paying special attention to social hardship and isolation where present. It is not philosophy or social science. It is to medicine what metaphysics is to philosophy. Psychiatrists need to broaden their horizons and take their heads out of the therapy books to witness the advances in neuroscientific techniques and genetic advancements that have already transformed the nature of medicine. To develop their psychological skills they need to take on board that patients want more than drugs to alleviate distress. Therefore practical techniques such as CBT or DBT (dialectical behaviour therapy) will further heighten their expertise as physicians. Many doctors are already familiar with applying CBT and other therapies. However, doctors should also be aware of the limitations of psychotherapies in general, recognizing and acknowledging that such therapies do not always work either and indeed in some instances may be harmful. Psychiatrists should be part of separate Wellbeing Clinics (perhaps one session per week) to becoming better acquainted and proficient again with physical examinations, investigations, routine procedures (ECGs for example) and interpretation of results (not just screen, but to intervene). This overseeing of the physical health of patients is not always possible in a busy outpatient clinic. Many potentially serious conditions would be revealed and information to the GP or tertiary services made known immediately. Psychiatrists are not 'stuck in a medical model' no more than a physician believes all myocardial infarcts are caused by psychosocial factors or life style. But to ignore the medical advances in molecular biology and neuroscientific diagnostic techniques portrays a profound ignorance of biological psychiatry and is insulting to those scientists who work tirelessly, often without much recognition, to further our understanding of 'brain disorders'. It is all very well to talk about art, philosophy, social sciences and literature as having a great bearing on our interest in psychiatry and congratulate ourselves as 'lateral thinkers' but an understanding of the philosophy of say, Bertrand Russell or indeed the school of Zen Buddhism, will not eliminate mental disorder. Romantic as it might sound in retrospect, Vincent Van Gogh did not enjoy cutting his ear off, nor did Robert Schumann feel ecstatic when jumping into the Rhine before being carted off to the asylum.
If we do not embrace a holistic view of mental ill-health we risk not only throwing the baby out with the bath water but the bath itself, thereby causing further dissatisfaction and low morale among doctors with an inevitable negative impact on patient care. Psychiatrists are not bemoaning their loss of hegemony - a favourite word and another myth propagated by the antipsychiatry lobby; rather, it is only too obvious to them (as qualified medical doctors) that patients will suffer in the long term by not being referred appropriately to those who have the expertise to recognize and distinguish between human difficulties and illness. There is also a need to re-examine the impact of psychological therapies and not succumb to the popular and naive notion that they are all evidence-based in scientific terms. In the meantime the 'worried well' can indulge themselves with all the peripheral talking therapies and current fads they desire. Likewise, performance management, outcome measures and payment by results have become relentless tick-box exercises creating unnecessary stress among health care professionals (threats of job losses) who 'must meet targets at all costs', all for a slice of the Commissioners' cake. What a way to run a health service! Patients become meaningless statistics in the meantime. No! The wake-up call should be aimed at those who are intent on destroying the good will and values of the very same people they purport to support, through their social engineering and outdated attitudes.
Fifteen percent of elderly individuals report clinically significant depression due to variety of reasons. Osteoporosis is a disorder of bone metabolism which can be caused by multiple factors. The elder population has multiple risk factors for development of low Bone Mineral Density (BMD). Data supports that SSRI causes low BMD. There are numerous mediating processes, factors and causes that may contribute to relationship between depression and low BMD, therefore it has been suggested that depression may be an unrecognized risk factor for development of osteoporosis in this patient population.
Low BMD is a common condition among the elder population; prevalence of osteopenia and osteoporosis is expected to increase due to increasing elder population. Low BMD is associated with increased risk for debilitating fractures, particularly hip, vertebrae and distal forearm. There is a growing body of evidence that depression impact the risk for fractures in the older population.
Most studies support that depression is associated with increased risk for both low BMD and fractures. There are many risk factors for low BMD, but some are unalterable. Therefore it is crucial to identify modifiable risk factors to reduce the public health burden of osteopenia, osteoporosis and fractures, and complications associated with them.
Objective:
A literature review was performed to extract evidence and to evaluate risk of Osteoporosis in depression.
Educational Objectives:
At the conclusion of this article, the reviewer will be able to understand,
The risk of development of osteoporosis,
Need for close monitoring and early assessment of risk,
Need for prophylactic treatment to avoid complications due to development of osteoporosis.
Method:
Pubmed.gov was searched by using pre-determined key word.
Key words:
“Depression AND Osteoporosis"
Background:
Osteoporosis was first recognized as a disorder of bone metabolism in 1947 by Albright. It is the most common degenerative disease in developed countries; it is characterized by low bone mineral density (BMD), causing bone fragility and increased fracture incidence. Over past quarter century, it has emerged as a major public health problem in the Western world, prevalence of osteopenia and osteoporosis is expected to increase dramatically in the next 50 years as the population pyramid shift toward old age. In United States alone, app 10 million individuals over age of 50 have osteoporosis. In addition, 33.6 million Americans in this age group have osteopenia (i.e. a decrease in bone mineral density [BMD] that precedes osteoporosis and its potential complications later in life). The estimated annual fracture rate due to an underlying bone disease is 1.5 million. These fractures lead to pain, skeletal mutilation, disability, loss of independence and increased mortality.1
Low BMD has been shown to be major risk factor for debilitating bone fractures, particularly of the hip, vertebrae and distal forearm.2 The established risk factors for osteoporosis include increasing age, female sex, oestrogen deficiency, glucocorticoid therapy and other medications, smoking, alcohol use, inactivity, and low calcium intake.3 Many prominent risk factors are unalterable, it is therefore crucial to identify modifiable risk factors in order to reduce the public health burden of osteopenia, osteoporosis and the fractures associated with them. In the USA, depression is a common disorder that affects 5 to 9% of women and 1 to 2% men.4 It ranks second only to hypertension as the most common chronic illness encountered in general medical practice.5 This disorder carries a considerable risk of death and is associated with a two to three fold increase in all-cause of non-suicide-related death.6 Fifteen percent of elderly individuals report clinically significant depression.
Definition of Osteopenia and Osteoporosis:
Osteopenia is a condition where bone mineral density is lower than normal, more specifically; it is defined as BMD T-Score between -1.0 and -2.5. It is considered to be precursor to osteoporosis. However, not every person diagnosed with osteopenia will develop osteoporosis. Osteoporosis causes bones to become weak and brittle – so brittle that a fall or even mild stresses like bending over or coughing can cause a fracture.
Osteoporosis-related fractures most commonly occur in the hip, wrist or spine. Bone is a living tissue, which is constantly being absorbed and replaced. Osteoporosis occurs when the creation of new bone does not keep up with the removal of old bone. Osteoporosis affects men and women of all races, but White and Asian women especially those who are past menopause are at highest risk. Medications, dietary supplements and weight-bearing exercise can help strengthen bones.
Literature evidence:
Current evidence supports a bidirectional link between major depressive disorders (MDD), several other mood disorders, and various medical conditions such as osteoporosis and cardiovascular disease.7 A significant association was found between BMD and depressive symptoms after adjustment for osteoporosis risk factors. In Caucasians, depressive symptoms were associated with both osteoporotic and osteopenic levels of BMD.8 A meta-analysis reported BMD is lower in depressed than non-depressed subjects. The association between depression and BMD is stronger in women than men, and in premenopausal than postmenopausal women. Only women psychiatrically diagnosed for MDD display significantly low BMD; women diagnosed by self-rating questionnaires do not.9 Depression is a significant risk factor for fracture in older women.14 Numerous studies have examined association between antidepressant use (both SSRI and TCA) and fracture risk. The majority have found that use of these medications, regardless of class is associated with increased risk of fracture.10 Animal studies have also indicated that serotonin may influence bone mass, particularly during stages of bone growth.11, 12
Daily SSRI (Table 1) use in adults 50 years and older remained associated with a 2-fold increased risk of clinical fragility after adjustment for potential covariates. Depression and fragility fractures are common in this age group, and the elevated risk attributed to daily SSRI use may have important public health consequences.15 (Figure 1). SSRI may increase fracture risk because of their effect on bone physiology and on the risk of falling. Functional serotonin receptors and transporters have been localized to bone, while the administration of SSRI decreases bone mass and strength in growing mice. SSRI function by inhibiting the serotonin transporter. Functional serotonin transporters in osteoblasts, osteoclasts and osteocytes raises the possibility that serotonin transporters may play a role in bone metabolism and those medications that affect this transporter system may also affect bone metabolism. Use of SSRI is associated with an increased rate of bone loss at the hip in this cohort of older women; use of a TCA was not similarly associated with increased rates of hip bone loss in our cohort.16 In men, BMD was lower among those reporting current SSRI use, but not among user of other antidepressants.17 Meta-analysis proved that MDD is associated with low BMD and should therefore be considered a risk factor for osteoporosis. BMD in subjects with MDD was 4.7% lower at the AP spine, 3.5% lower at the total femur, and 7.3% lower at the femur neck as compared to healthy controls.18 NIH meta-analysis concluded MDD was associated with lower BMD at the AP spine, femoral neck and total femur. The deficits in BMD in subjects with depression are of clinical significance and likely to increase fracture risk over the lifetime of these subjects.18
Table 1: List of SSRI (Selective Serotonin Reuptake Inhibitor) and dosages range:
Generic Name
Brand Name
Dose range
Citalopram
Celexa
10 to 40 mg
Escitalopram
Lexapro
10 to 20 mg
Fluoxetine
Prozac
20 to 80 mg
Fluvoxamine
Luvox
50 to 300 mg
Paroxetine
Paxil
10 to 40 mg
Sertraline
Zoloft
50 to 200 mg
Figure 1: Fracture-free survival by Selective Serotonin Reuptake Inhibitors (SSRI) use
Potential mechanisms of bone loss in depression:
Depression is associated with alterations of the hypothalamic-pituitary-adrenal (HPA) axis at multiple levels, including altered secretion of hypothalamic corticotrophin-releasing hormone (CRH), as indicated by CRH levels in the cerebrospinal fluid, and change in the set point threshold for negative feedback; these changes generally result into hyper-cortisolism.
Pro-inflammatory cytokines are increased in depression and IL-6 is a potent activator of the osteoclast. Oestrogen deficiency in women and androgen deficiency in men may affect bone mass and there is at least theoretical evidence for decreased sexual hormones in both genders during the acute phases of depression. Serotonin transporter receptors are present on the osteoblast and use of antidepressants has been associated with more fractures. Commonly accepted life style risk factors for osteoporosis include smoking, inadequate calcium intake, excessive alcohol intake and physical inactivity.
There are three pathophysiologic pathways leading to low BMD.13 (Figure 2):
Inadequate acquisition of bone mass early in life
Elevated resorption of bone mass later in life, and
Inefficient bone formation during continuous bone remodelling
These pathways are interdependent and the relative importance of each mechanism changes over development and varies by sex.
Figure 2: Pathways linking depression, low bone mneral density and fracture. 13
Bottom line:
Current available evidence supports that there is increase of development of osteoporosis due to various factors, pathways and medications used in treatment of depression.
Conclusion:
Major depressive disorder is an important but still unrecognized risk factor for osteoporosis. Depression should be considered as an important risk factor for osteoporosis. Depression is associated with low BMD, with a substantially greater BMD decrease in depressed women and in cases of clinical depression. These patients need close monitoring, early assessment of risk and preventive measures to avoid complications. Premenopausal women with major depression should undergo DXA screening. Similar recommendation may be made for postmenopausal women with depression especially in the presence of one or more known risk factors for development of osteoporosis.
Once a diagnosis of osteoporosis is made in subjects with major depression, DXA measurements should be performed with a frequency based on the current WHO algorithm; this model takes into account the presence of other risk factors and age of the subjects.
Clinical Point:
Periodic BMD measurements and anti-osteoporotic prophylactic and curative measures are strongly advocated for these patients.
People with intellectual disabilities are a heterogeneous group, who can pose a challenge to services in terms of meeting a wide range of needs. Following the closure of large institutions, the optimum means of service provision for people with intellectual disabilities with additional mental illness and challenging behaviour has been a matter of debate.
Challenging behaviour can be defined as a ‘culturally abnormal behaviour of such an intensity, frequency or duration that the physical safety of the person or others is likely to be placed in serious jeopardy, or behaviour which is likely to seriously limit use of, or result in the person being denied access to, ordinary community facilities’ – Emerson, 19951. Examples of challenging behaviours include self-injury, aggressive outbursts, destruction of property and socially inappropriate behaviour.
The credit-crunch of recent years has led to an increased use of private sector services delivering care to NHS funded patients. The Winterbourne Scandal unearthed by BBC Panorama in June 2011 (an investigation into the physical abuse and psychological abuse suffered by people with learning disabilities and challenging behaviour at this private hospital in South Gloucestershire), highlighted that whist this maybe an economically viable option, fundamental questions were raised about whether private sector services’ safeguards and monitoring protocols were as robust as the NHS in protecting vulnerable patients. It also reawakened longstanding disputes around the way people with complex needs are cared for in residential settings. The discussions centred around ‘institutional’ versus ‘community’ care styles; specialist intellectual disabilities services versus generic adult psychiatric services; local versus specialist expertise congregated around a single unit; and also financial questions regarding how best to meet the needs of this population at a time of austerity. Opinions vary widely, and at times are even polarised, as a result of several factors including position within this competitive and complex system, personal and cultural politics and also personal experience. As a result of the government review, subsequent to the Winterbourne investigation, a number of recommendations have been made which will affect the future of care of this vulnerable group of patients. These include, “by June 2013, all current placements will be reviewed, everyone in hospital inappropriately will move to community-based support as quickly as possible, and no later than June 2014… as a consequence, there will be a dramatic reduction in hospital placements for this group of people”2
The Department of Health Policy, Valuing People3, set out ‘ambitious and challenging programme of action for improving services’, based on four important key principles – civil rights, independence, choice and inclusion. Government Policy as detailed in both Valuing People and the Mansell Report3, 4 recognises that NHS specialist inpatient services are indeed necessary on a short-term basis for some people with intellectual disabilities and complex mental health needs. Inpatient facilities for people with Intellectual Disability have been described as highly specialised services that are a valuable, but also expensive, component of mental health services5. The Enfield Specialist Inpatient unit - the Seacole Centre - is one such service.
The Seacole Centre consists of two inpatient units, with a total of 12 inpatient beds, for people with intellectual disabilities with acute mental illness and/or challenging behaviour. It is located within Chase Farm Hospital in Enfield, Greater London. The Seacole Centre has a multidisciplinary team consisting of nurses, psychologists, psychiatrists, a resident GP, occupational therapists, intensive support team staff, physiotherapists, speech and language therapists, a physical exercise coach and administrative staff. Patients are admitted from a variety of sources, including general psychiatric wards, general medical wards and community intellectual disability teams. Since patients are often referred from other boroughs, in addition to this multidisciplinary team, each patient has their own community and social care team based within their own borough. The use of out-of-area units faces similar challenges to out-of-area placements, use of which has been increasing in the UK, and it is important to explore ways in which service users, out-of-area, can be supported effectively6.
In 2002, a review of admissions to the unit was completed to describe the management of mental illness and challenging behaviour. Since then there have been several service reconfigurations within the trust, in order to accommodate national, political and financial recommendations. However, despite these changes, it was observed clinically that certain clinical problems including delayed discharges continue to occur. We decided to complete a similar review, to describe current admission trends in further detail, in order to enable us to identify areas of improvement, and also to ascertain the nature and severity of ongoing problems to focus future recommendations.
METHOD:
A retrospective review of the case records of all inpatient admissions to the Seacole Centre was completed over a three-year period – from 1st January 1999 to 31st December 2001.
Data collected included age on admission, gender, borough, diagnosis, psychotropic medication on discharge, date of admission and discharge, length of stay, legal status on admission, delays on discharge, and reason for delay, and living arrangements prior to and after discharge
A successful outcome of admission was discharge from hospital to community care. We used the following definition of the delayed discharge:
"A delayed transfer occurs when a patient is ready for transfer from a general and acute hospital bed but is still occupying such a bed. A patient is ready for transfer when:
a clinical decision has been made that the patient is ready for transfer
a multi-disciplinary team decision has been made that the patient is ready for transfer
the patient is safe to discharge/transfer.7
The review was repeated during a further three-year period between 1st January to 2009 and 31st December 2011.
RESULTS:
Characteristics of 1999-2001 cohort, and comparison with 2009-2011
The basic demographic details can be seen in Table 1.
Table 1 - Demographic details
1999-2001
2009-2011
Number of admissions
60
41
Number of patients
46
40
Average (mean) age/years
29.58
36.16
Age Range / years
14-63
19-72
M:F ratio
1.4:1
3.1:1
Total number of boroughs from which patients admitted
10
7
Trends in Admission Rates
As seen in Tables 1 and 2, there has been a reduction in the total number of admissions between the studies. There has also been a marked reduction in re-admissions. The average length of stay has increased, and although the number of delayed discharges has slightly decreased, it can be seen that this is still a factor in a significant proportion of the admissions.
Table 2 - Trends in admission
1999-2001
2009-2011
Total Number of admissions
60
41
Average (mean) length of stay / days
198.6
244.6
Number of readmissions
16
1
Number of delayed discharges
40 (67%)
24 (59%)
Reason for admission
The trends in reason for admission are shown in Figure 1.
Figure 1 – Trends in Reason for Admission, 1999-2001 compared to 2009-2011
In both time periods, the most frequent reason for admission is challenging behaviour (62%, n=37 between 1999-2001; 63%, n=29, between 2009-2011), followed by psychosis (22%, n=13 between 1999-2001; 11%, n=5, between 2009-2011. Social admissions were the third most common reason for admission in the recent study (0% between 1999-2001; 4%, n=2 between 2009-2011). The range of psychiatric presentations was widest during the original time period.
Patterns on discharge
As shown in Figure 2, most patients in the original study were discharged to either the same residential home or back to the family home, where as in the latter time period patients were most frequently discharged to either a different residential home or to supported living. Figure 3 summarises this effect, demonstrating the change in discharging the majority of patients to a different place of residence.
Figure 2 – A graph to show the place of discharge, 1999-2001 compared to 2009-2011
Figure 3 – A Graph to Demonstrate Trends in Place of Discharge – comparing 1999-2001 and 2009-2011
Delayed discharges
The primary cause for delay in both studies was finding appropriate placement, although this was more marked in the recent cohort.
One of the major factors contributing to delayed discharges was lack of identification of suitable placement, which was identified as a major contributing factor to delayed discharges in 69% of cases in 2009-2011 and in 44% in 1999-2001, and apparent delays in the role played by social services (table 2).
DISCUSSION:
Throughout this study spanning 10 years, challenging behaviour followed by psychotic disorder remained the most common cause for admission. Interestingly, by 2008-2011, the third most common cause for admission was related to social reasons (4%). There were no admissions in the original study for this reason. Between 1999 and 2001, there were a wider range of reasons for admission across the mental illness spectrum compared to 10 years on. In previous studies, the largest diagnostic group for all admissions was schizophrenia spectrum disorders7,8. However, between 2009-2011, more than a quarter of patients admitted to the Seacole Centre did not have any psychiatric diagnosis on admission. It is important to keep in mind that individuals with intellectual disabilities accessing specialist inpatient services are more likely to present with complex clusters of symptoms and behavioural problems that may span several diagnostic categories.
The most significant improvement from the original review and the re-review is that the number of re-admissions significantly reduced from 24% (14 patients) to 2% (1 patient). Of interest to note is that during 1999-2001 a large proportion of patients were discharged to their original place of accommodation (often the family home) whereas in 2009-2011, it was more common for patients to be discharged to a new place of living, more suited to managing increasing complex needs and behaviours. This may account for some of the reduction in re-admission rates.
The length of stay over the 10-year period has slightly increased from an average of 198.6 days up to 244.6 days, which demonstrate that admissions are considerably longer than in more generic medical settings. The findings are in keeping with a number of other studies regarding patients with intellectual disability who are admitted to a specialist unit and continue as inpatients for significantly longer periods. One study showed a mean length of stay 23.2 weeks for a specialist unit versus 11.1 weeks in generic settings 8. Another study in South London revealed similar finds of 19.3 weeks compared with generic unit stays of 5.5. weeks9. An exploratory national survey of intellectual disability inpatient services in England has shown that 25% of residents had been in the units for more than two years. Only 40% of residents had a discharge plan, and only 20% had both this and the type of placement considered ideal for them in their home area10. Reasons for length of stay are not fully understood in any of these studies. They may include fear of taking risks, lack of local safe or competent amenities, lack of experience or authority amongst those charged with sourcing bespoke services for complex people with challenging needs, and also a potential lack of such resource in terms of time available to see people, read reports, meet with stake holders and find the right services. The results of another retrospective study comparing the generic and specialist models in two districts in the UK by Alexander et al11 suggested that, within the same district, patients do stay longer in the specialist unit, but they are less likely to be discharged to an out of area placement.
There is no evidence to suggest that comprehensive care for people with intellectual disabilities can be provided by community services alone. Likewise, there is also no clear evidence to suggest that a balanced system of mental health care can be provided without acute beds12. There is, however, clear evidence that services created by the private sector are used very widely and seen as at time as an economically viable option in the current climate of credit crunches.
The different models of inpatient service provision that have been suggested range from mainstream adult mental health services; alternatively an integrated inpatient scheme whereby people with Intellectual disabilities with additional mental illness or severe challenging behaviour are admitted to adult mental health beds, with provision for extra support from a multidisciplinary learning disabilities team; ranging across to specialist assessment and treatment units13,14.
Inpatient care is known to consume most of the mental health budget15 and specialist inpatient units are an expensive component of these services. Cost containment and cost minimisation of inpatient beds within the current economic recession presents a real challenge for those charged with responsibility to provide high-quality, effective, specialist care for adults with intellectual disability. Such cost reduction could be approached in a number of ways, through the reduction of length of stay, optimising drug budgets, reducing rates of re-admissions, and establishment of projects in association with the voluntary and statutory sector to facilitate prompt and safe discharge.
Reducing the average length of stay where possible can reduce the cost, and the resources and budget freed up in this way could be used for other service components15. However, this single agenda can lead to problems of pressured early discharge to unsuitable placements. It is known that resource consumption is most intense during the early stages of admission. As such, we observe a position whereby reducing length of stay requires proactive planning throughout the whole process of care, as well as active discharge planning, with a need for clearly defined pathways of care.
A crucial aspect of the patient's transition through inpatient placement to life in the community is efficient and regular communication between the relevant professionals and teams who form part of continuity of on-going care back in the community. This can at times be particularly challenging owing to differences in values and perceptions about patient need and problem, and also varying pressures. Understanding and resolving problems for individuals with complex and severe challenging behaviour or mental illness that requires a period of containment in a specialist service also requires specialist on-going work and risk management to ensure that when the problems are contained and understood, they remain contained and understood on discharge and thereafter so long as the individual remains vulnerable to the point of requiring any care giving. Many people from the general population who develop a serious mental illness requiring hospitalisation, have capacity once well, to make decisions for themselves and articulate a need or otherwise for specific care or intervention. This is rarely completely the case for people with Intellectual disabilities. Collaborative approaches together with those involved in community care is crucial to getting the right care at the right financial cost for this relatively small but very complex and vulnerable group of individuals.
The effective relief of pain is of paramount importance to anyone treating patients undergoing surgery. Not only does effective pain relief mean a smoother postoperative course with earlier discharge from hospital, but it may also reduce the onset of chronic pain syndromes1. Regional anaesthesia is a safe, inexpensive technique, with the advantage of prolonged postoperative pain relief. Research continues concerning different techniques and drugs that could prolong the duration of regional anaesthesia and postoperative pain relief with minimal side effects1. Magnesium is the fourth most plentiful cation in the body. It has antinociceptive effects in animal and human models of pain 2,3. Previous studies had proved the efficacy of intrathecally administered magnesium in prolonging intrathecal opioid analgesia without increase in its side effectsThese effects have prompted the investigation of epidural magnesium as an adjuvant for postoperative analgesia4.
Midazolam, a water-soluble benzodiazepine, has proved epidural analgesic effect in patients with postoperative wound painSerum concentrations of midazolam after an epidural administration were smaller than those producing sedative effects in humans5.
The purpose of this study is to compare the analgesic efficacy of epidural magnesium to that of midazolam when administered with bupavacaine in patients undergoing total knee replacement.
Methods:
After obtaining the approval of the Hospital Research & Ethical Committee and patient’s informed consent, 120 ASA I and II patients of both sexes, aged 50-70 years undergoing total knee replacement surgery were enrolled in this randomised, double blinded placebo-controlled study. Those who had renal, hepatic impairment, cardiac disease, spine deformity, neuropathy, coagulopathy or receiving anticoagulants for any cause were excluded from the study.
Prior to surgery, the epidural technique as well as the visual analogue scale (VAS; 0: no pain; 10: worst pain) and the patient-controlled epidural analgesia device (PCEA) were explained to the patients.
The protocol was similar for all patients. Patients received no premedication. Heart rate (HR), mean arterial pressure (MAP) and oxygen saturation (SpO2) were measured. Intravenous access had been established and an infusion of crystalloid commenced.
Before the induction of anaesthesia, an epidural catheter was placed at the L3-L4 or L4-L5 intervertebral space under local anaesthesia with the use of loss of resistance technique, and correct position was confirmed by injection of lidocaine 2% (3ml) with epinephrine in concentration 1: 200 000. An epidural catheter was then inserted into the epidural space. The level to be blocked was up to TIn a double blind fashion and using a sealed envelope technique, patients were randomly allocated to one of three equal groups to receive via epidural catheter either 50 mg magnesium sulphate (MgSO4) in 10 ml as an initial bolus dose followed by infusion of 10 mg/h (diluted in 10 ml saline) during the surgery (Mg group) or 10 ml saline followed by infusion of saline 10 ml/h during the surgery (control group) or 0.05 mg/kg of midazolam in 10 ml saline (Midazolam group) followed by infusion of saline 10 ml/h during the surgery. All patients received epidural bupivacaine 0.5 % in a dose of 1ml/segment .
Sensory block was assessed bilaterally by using loss of temperature sensation with an ice cube. Motor block was evaluated using a modified Bromage scale 6 (0: no motor block, 1: inability to raise extended legs, 2: inability to flex knees, 3: inability to flex ankle joints). During the course of operation, epidural bupivacaine 0.5% was given, if required, to achieve a block above T10MAP, HR, SpO2 and respiratory rate (RR) were recorded before and after administration of the epidural medications and every 5 minutes till end of the surgery.
When surgery was complete, all patients received PCEA using a PCEA device (Infusomat® Space, B.Braun Space, Germany) containing fentanyl 2 µg/ml and bupivacaine 0.08% (0.8 mg/ml). The PCEA was programmed to administer a demand bolus dose of fentanyl 5 ml with no background infusion and lockout interval 20 min. The PCEA bolus volume was titrated according to analgesic effect or occurrence of side-effects. Patients’ first analgesic requirement times were recorded. The time from the completion of the surgery until the time to first use of rescue medication by PCEA was defined as the time to first requirement for postoperative epidural analgesia. A resting pain score of ≤ 3 was considered as a satisfactory pain relief. If patients had inadequate analgesia, supplementary rescue analgesia with intramuscular pethidine 50 mg was available. MAP, HR, SpO2, RR and pain assessment using VAS were recorded at 30 minutes, and then at 1, 2, 4, 8, 12, and 24 h in the postoperative period. Epidural fentanyl consumption was also recorded at the same time points. Patients were discharged to the ward when all hemodynamic variables were stable with completely resolved motor block, satisfactory pain relief, and absence of nausea and vomiting. Adverse events related with the epidural drugs (sedation, respiratory depression, nausea, vomiting, prolonged motor block) and epidural catheter were recorded throughout the 24 h study period. Sedation was assessed with a five-point Scale: 1: Alert/active, 2: Upset/wary, 3: Relaxed, 4: Drowsy, 5: Asleep. A blinded anaesthesiologist who was unaware of the drug given, performed all assessments.
The results were analyzed using SPSS version 17. The number of subjects enrolled was based on a power calculation of finding a 20% change in HR and MAP. The α-error was assumed to be 0.05 and the type II error was set at 0.20. Numerical data are presented as median and 95% CI. The groups were compared with analysis of variances (ANOVA). The VAS pain scores were analyzed by Mann-Whitney U test. Categorical data were compared using the Chi square test. P value of 0.05 was used as the level of significance.
Results:
The three groups were comparable in respect of age, weight, height, sex, ASA status and duration of surgery (Table 1). Patients in all groups were comparable regarding intra or postoperative MAP, HR (Figure 1,2), RR and SpO2 during the observation period with no case of hemodynamic or respiratory instability. No difference in the quality of sensory and motor block before and during the surgery was noted between groups, and none of the patients required supplemental analgesia during surgery.
Control
Mg
Midazolam
of patients
40
40
40
Sex (female/male)
17/23
20/20
19/21
Age (yrs)
59.5 ± 6.1
61.1 ± 4.9
61.9 ± 3
ASA (I/II)
12/28
14/26
11/29
Weight (Kg)
69.7 ± 4.2
66.9 ± 6.7
70.1 ± 5.5
Height (cm)
165.9 ± 8.6
170.2 ± 4.5
167.2 ± 6.9
Duration of surgery (min)
144 ± 21
129 ± 30
130 ± 27
( median and 95% CI or number). No significant difference among groups
Table 1: Demographic data and duration of surgery.
Figure 1: Heart rate changes (HR) of study groups. Data are mean±SD.
Figure 2: Mean Arterial pressure changes (MAP) of study groups. Data are mean±SD.
The intraoperative VAS was significantly less in magnesium and midazolam groups compared to control group after 15 and 30 minutes (Figure 3). Whereas the postoperative VAS was significantly less in the magnesium group in the first postoperative hour compared to other groups (Figure 4).
Figure 3: The intra-operative Visual analogue score of study groups. Data are mean±SD.
Figure 4: The post-operative Visual analogue score of study groups. Data are mean±SD.
The time of request for postoperative analgesia was significantly delayed and the number of patients requesting postoperative analgesia was significantly reduced in magnesium group (Figure 5). Moreover, the pethidine rescue analgesia consumption and the total amount of postoperative fentanyl infusion were significantly reduced in magnesium group compared to other groups (Table 2) (Figure 5).
Control
Mg
Midazolam
P
Pethidine (mg)
92.38±10.91
52.56±9.67
70±9.23
0.014*
Total Fentanyl infusion (mcg)/24H
320.67±112.19
219.9±56.86
256.2±53.49
0.00*
Data are expressed as median and 95% CI. * Significant difference (P < 0.05).
Table 2: Pethidine rescue analgesia and total fentanyl infusion over 24 hours of study groups
Figure 5: The number of patients and time of requesting analgesia in the first 3 postoperative hours in the study groups. Data are numbers.
No significant differences were recorded regarding the incidence of sedation or any adverse effects between groups (Table 3).
Control
Mg
Midazolam
P
Sedation
0
0
2
0.068
Bradycardia
1
0
0
0.103
Nausea & Vomiting
3
1
2
0.571
Data are expressed as numbers. Significant difference (P < 0.05).
Table 3: Incidence of sedation, bradycardia and nausea & vomiting in the study groups
Discussion:
The efficacy of postoperative pain therapy is a major issue in the functional outcome of the surgery7. It was evident that epidural analgesia regardless the agent used provides better postoperative analgesia compared with parental analgesiaThe addition of adjuvants to local anaesthetics in epidural analgesia gained widespread popularity as it provides a significant analgesia which allows the reduction of the amount of local anaesthetic and opioid administration for postoperative pain and thus the incidence of side effects9.
Our study demonstrates a significant intraoperative improvement in VAS in magnesium and midazolam groups, while in the postoperative period magnesium group showed a significant reduction in the number of patients requesting early postoperative analgesia as well as total fentanyl consumption.
The antinociceptive effects of magnesium are primarily based on the regulation of calcium influx into the cell, as a calcium antagonism and antagonism of N-methyl-D-aspartate (NMDA) receptorTanmoy and colleagues10 evaluated the effect of adding MgSO4 as adjuvants to epidural Bupivacaine in lower abdominal surgery and reported reduction in time of onset and establishment of epidural block. Whereas, Arcioni and colleagues 11 proved that combined intrathecal and epidural MgSO4 supplementation reduce the postoperative analgesic requirements. Farouk et al12 found that the continuous epidural magnesium started before anesthesia provided preemptive analgesia, and analgesic sparing effect that improved postoperative analgesia. Also, Bilir and colleagues 4 showed that the time to first analgesia requirement was slightly longer with significant reduction in fentanyl consumption after starting epidural MgSO4 infusion postoperatively. Asokumar and colleagues13 found that addition of MgSO4 prolonged the median duration of analgesia after intrathecal drug administration.
On the other hand, Ko and colleagues14 found that peri-operative intravenous administration of magnesium sulfate 50 mg/kg does not reduce postoperative analgesic requirements which could be attributed to the finding that the perioperative intravenous administration of MgSO4 did not increase CSF magnesium concentration due to inability to cross blood brain barrier.
Nishiyama et al17,18,19 reported that epidural midazolam was useful for postoperative pain relief. It was suggested that epidurally administered midazolam exerts its analgesic effects through the ᵞ-aminobutyric acid receptors in the spinal cord, particularly in lamina II of the dorsal horn15 as well as through the opioid receptorsNishiyama et al20 showed that intrathecally administered midazolam and bupivacaine had synergistic analgesic effects on acute thermal- or inflammatory-induced pain, with decreased behavioral side effects. While, Kumar et al21 reported that single-shot caudal coadminstration of bupivacaine with midazolam 50 µg/kg was associated with extended duration of postoperative pain relief in lower abdominal surgery. Whereas, Jaiswal et al22 concluded that epidural midazolam can be useful and safe adjunct to bupivacaine used for epidural analgesia during labor.
In the present study, there were no significant hemodynamic changes between groups. This is in agreement with many authors who used epidural MgSO44,12,23 and midazolam 24 and did not report any hemodynamic or respiratory instability during the observation period.
This study did not record any neurological or epidural drugs related complications postoperatively. Our results are in accord with some of the trials that have previously examined the neurological complications of using epidural MgSO4,11,12,23.Moreover, Goodman and colleagues 25, found that inadvertent administration of larger doses MgSO4 (8.7 g and 9.6 g) through epidural catheter did not reveal any neurological side effects.
Regarding epidural midazolam, Nishiyama19 said that epidural administration of midazolam has a wide safety margin for neurotoxicity of the spinal cord due to the small dose used.
Our results did not reveal any significant difference regarding the sedation score. This is in agreement with Bilir et al4 and El-Kerdawy23 who did not report any case with drowsiness or respiratory depression when using epidural magnesium.
Whereas, De Beer et al26 and Nishiyama et al27 reported that a dose of 50 µg/kg midazolam appears to be the optimum dose for epidural administration, while many patients fell into complete sleep with no response to verbal command and respiratory depression when they used epidural midazolam 0.075 mg/Kg or 0.01 mg/KgMoreover, Nishiyama et al17,28 reported that when 50 µg/kg epidural midazolam was used, serum midazolam concentration was less than 200 ng/ml which was considered as the lower limit for sedation by intravenous administration.
In conclusion, co-administration of epidural magnesium provides better intraoperative analgesia as well as analgesic-sparing effect on PCEA consumption without increasing the incidence of side-effects compared to bupivacaine alone or with co-administration of epidural midazolam in patients undergoing total knee replacement. The results of the present investigation suggest that magnesium may be one of the useful adjuvants to epidural analgesia.
It is well documented that many HBsAg-positive / HBeAg-negative patients show normal alanine aminotransferase (ALT) levels. However, two different scenarios have been proven to exist: inactive Hepatitis B Virus (HBV) carriers (previously defined as “healthy” HBV carriers) and patients with chronic hepatitis B (CHB) with transient virological and biochemical remission. These subsets of patients share HBsAg positivity and normal ALT levels; however, progression of disease, outcome, HBV DNA levels, severity of liver damage, requirement for liver biopsy and antiviral treatment significantly differ between the two patient populations.
Thus, among HBsAg-positive / HBeAg-negative subjects with normal liver biochemistry, it is important and sometimes difficult to distinguish the ‘true inactiveHBV carriers’ from patients with ‘activeCHB’ in whom phases of spontaneous remission have occurred. The former have a good prognosis with a low risk of complications, while the latter patient population have active liver disease with a high risk of progression to liver cirrhosis and/or hepatocellular carcinoma (HCC). Therefore, prolonged biochemical and virological follow-up are mandatory for diagnosis and decision to treat.
The term ‘chronic hepatitis B’ refers to a chronic necroinflammatory disease of the liver caused by persistent HBV infection 1. The term ‘necroinflammatory’ describes the presence of death of periportal hepatocytes (periportal necrosis) with or without disruption of the limiting plate by inflammatory cells, intralobular necrosis, portal or intralobular inflammation, and formation of bridges between vascular structures (the so-called bridging necrosis). Chronic hepatitis B can be subdivided into HbeAg positive and HBeAg-negative chronic hepatitis B 1,2. These two forms may have different natural histories and different response rates to antiviral treatment, although both may progress to more severe liver damage 3, such as, liver cirrhosis 4 or HCC 5.
The second subset is called the ‘inactive HBsAg carrier state’. It means a persistent HBV infection of the liver but without continual significant necroinflammatory disease. It is characterized by very low or undetectable serum HBV DNA levels and normal serum aminotransferases 1. It has been shown that histologically significant liver damage is rare in these patients, particularly when HBV DNA is lower than 2000 IU/ml, and thus a liver biopsy is not indicated in these subjects 4. Even among HBeAg-negative carriers with serum HBV DNA between 2000 and 20,000 IU/ml, histologically significant liver disease is also rare 6. Thus, these subjects should be followed up closely, but biopsy and treatment are not currently indicated.
As mentioned above, it is sometimes difficult to distinguish true inactive HBV carriers from patients with active HBeAg-negative CHB in whom phases of spontaneous remission may have occurred 1. The former patients have a good prognosis with a very low risk of complications, while the latter have active liver disease with a high risk of progression to advanced hepatic fibrosis, cirrhosis and subsequent complications such as decompensated cirrhosis and HCC 3-6. Thus, a minimum follow-up of 1 year with ALT levels every 3–4 months and periodical measurements of serum HBV DNA levels are required before classifying a patient as an inactive HBV carrier 1. ALT levels should remain consistently within the normal range, and HBV DNA should be below 2000 IU/ml 7. Thereafter, the inactive HBV carrier with undetectable or very low HBV DNA levels should be followed up with ALT determinations every 6 months after the first year and periodical measurement of HBV DNA levels 6 for the rest of their lifetime. This follow-up policy usually allows detection of fluctuations of activity in patients with true HBeAg-negative CHB 8.
It is important to underline that some inactive carriers may have HBV DNA levels greater than 2000 IU/ml (usually below 20,000 IU/ml), despite their persistently normal ALT levels 1,6,9. In these carriers the follow-up should be much more condensed, with ALT determinations every 3 months and HBV DNA measurements every 6–12 months for at least 3 years 1. After these 3 years, these patients should be followed up for life like all inactive chronic HBV carriers 6. After all, the inactive HBV carrier state confers a favourable long-term outcome with a very low risk of cirrhosis or HCC in the majority of patients 1,10,11. Patients with high baseline viremia levels have higher risk of subsequent reactivation. A liver biopsy should be recommended if ALT levels become abnormal and HBV DNA increases above 20,000 IU/ml. Non-invasive evaluation of liver fibrosis 12 may be useful, although these non-invasive tools, such as transient elastography, need further evaluation 6.
HBsAg clearance and seroconversion to anti-HBs antibody may occur spontaneously only in 1–3% of cases per year, usually after several years with persistently undetectable HBV DNA 7. On the other hand, progression to HBeAg-negative CHB may also occur 10.
Although the optimal definition of persistently normal ALT (PNALT) levels has not been established, the fluctuating nature of chronic HBV infection reasonably justifies serial ALT determinations. These should be done with a minimum of four to five tests 3–4 months apart within the first year of presentation, before determining whether an HBeAg-negative patient truly has PNALT. An initial follow-up of at least 1 year is supported by the finding of mild histological lesions in HBeAg-negative patients with true PNALT during the first year 6. The risk of developing abnormal ALT levels in HBeAg-negative patients with a normal baseline ALT have been reported to be higher during the first year (15–20%) and decline after 3 years of follow-up, therefore frequent monitoring during the first 1–3 years is critical 6,10.
Antiviral treatment of inactive HBsAg subjects is not indicated 1. Patients should be considered for treatment only when they have HBV DNA levels above 2000 IU/ml, serum ALT levels above the upper limit of normal and severity of liver damage assessed by liver biopsy showing moderate to severe active necroinflammation and/or at least moderate fibrosis 1,2.
Irritable bowel syndrome (IBS) is a chronic and often debilitating condition with a complex aetiology1. It is the most common diagnosis made by gastroenterologists worldwide2. The incidence and prevalence of IBS vary depending on the diagnostic criteria used but it is estimated that the prevalence in the UK is 17% overall, with a prevalence of 11% among men and 23% among women3-4. IBS can have a significant negative impact on quality of life and social functioning, although it is not known to be associated with the development of serious disease or excess mortality. However, patients with IBS are more likely to undergo specific surgical operations such as hysterectomy and cholecystectomy. IBS further represents an economic burden on society due to the high consumption of healthcare resources and the non-productivity of IBS patients5. It appears that 33–90% of patients do not consult a physician, and that a proportion of patients who meet the IBS criteria are not diagnosed with IBS. The frequency of IBS symptoms peaks in the third and fourth decades, and there is a female predominance of about 2:1 in the 20s and 30s, although this discrepancy is less apparent in older patients6. The female predominance is less apparent in the general population, which suggests that women with IBS are more likely to seek healthcare for their symptoms7. IBS symptoms which persist beyond middle life continue to be reported by a substantial proportion of individuals in their seventh and eighth decades.
Pathogenesis
The pathogenesis of IBS appears to be multifactorial. The following factors play a central role in the pathogenesis: heritability and genetics, dietary and intestinal microbiota, low-grade inflammation and disturbances in the neuroendocrine system of the gut2.
IBS is known to aggregate in families and to affect multiple generations but not in a manner consistent with a major Mendelian effect. Relatives of an individual with IBS are two to three times as likely to have IBS8.
Psychological distress is not only a common co-morbidity in IBS patients, but also a factor which is likely to play a direct role in the pathogenesis4. Interestingly, parental modelling and the reinforcement of illness behaviour can also contribute to IBS. Having a mother with IBS has been shown to account for as much variance as having an identical set of genes as a co-twin who has IBS. This insinuates that the contribution of social learning to IBS is at least as great as the contribution of heredityFurthermore, the role of childhood events such as nasogastric tube placement, poor nutrition, abuse, and other stressors have been clearly associated with IBS8.
A substantial proportion of patients with IBS report onset of their symptoms after acute gastroenteritis9. Post-infectious (PI)-IBS has been reported after viral, bacterial, protozoa and nematode infections, with the incidence of PI-IBS varying between 7% and 31%. In this subset of IBS patients GI symptoms appear following gastroenteritis, with approximately 10% developing persistent symptomsRecent studies suggest that some individuals are genetically predisposed to developing PI-IBS, with some people demonstrating a specific cytokine response to infection4.
It is important to note that women appear to have more frequent and severe IBS symptoms during menses compared to other phases of the menstrual cycle and that female gender is a significant independent risk factor for the development of IBS7.
Diagnosis and Investigations
Adult patients who present to their general practitioner (GP) with lower gastrointestinal tract disorders account for one in 20 of all general practice consultations. The possibility of sinister conditions such as colorectal cancer or inflammatory bowel disease may create diagnostic uncertainty and reluctance for the doctor to attribute the symptoms to IBS. In the United Kingdom up to 29% of patients with IBS are referred to a specialist but the majority of these will return to their GP for long term management6.
Primary care differs from specialist care because the GP’s greater familiarity with the patient, and their previous consultations, enable presenting problems to be seen in context rather than in isolation. Furthermore, it involves the first contact for care of problems at a stage when they are likely to be poorly defined. Lastly, primary care is characterised by a biopsychosocial model of care that takes into account the context of the person’s problem. These characteristics are especially important when managing chronic disorders, such as IBS, where there is a high priority on continuity of care6.
There is currently no biochemical, histopathological or radiological diagnostic test for IBS. The diagnosis is based principally on symptom assessment. The Rome III criteria (Figure 1) is the most recent, updated and universal diagnostic criteria for IBS. However, although the Rome III criteria are widely used in clinical studies, it is not used by most cliniciansIn fact, most primary care physicians are not aware of diagnostic criteria for IBS and about one third of secondary care doctors do not use them in practice6.
IBS patients are grouped on the basis of the most predominant bowel symptom as diarrhoea- predominant, constipation-predominant, a mixture of both diarrhoea and constipation, and un-subtyped IBS in patients with an insufficient abnormality of stool consistency to meet the criteria for the other sub-groups. Approximately one third of patients have diarrhoea- predominant, one third have constipation-predominant, and the remainder have a mixture of both diarrhoea and constipation. The classification of IBS patients into sub-groups is useful for clinical practice, but it is common for IBS patients to switch from one subtype to another over time. More than 75% of IBS patients change to either of the other 2 subtypes at least once over a 1-year period2,10.
Figure 1 - Rome III diagnostic criteria* for IBS 6
Recurrent abdominal pain or discomfort** at least 3 days a month in the past 3 months, associated with two or more of the following:
Improvement with defecation
Onset associated with a change in frequency of stool
Onset associated with a change in form (appearance) of stool
* Criteria fulfilled for the past 3 months with symptom onset at least 6 months before diagnosis
** “discomfort” means an uncomfortable sensation not described as pain
According to the National Institute for Health and Clinical Excellence (NICE), healthcare professionals should consider assessment for IBS if a patient presents with any of the following symptoms for at least six months11:
abdominal pain/discomfort
bloating
or a change in bowel habit
NICE has also given the following guideline pertaining to “red flag” indicators. All people presenting with possible IBS symptoms should be asked if they have any of the following indicators. Referral to secondary care should be made if any are present11:
unintentional and unexplained weight loss
rectal bleeding
family history of bowel or ovarian cancer
change in bowel habit to looser and/or more frequent stools persisting for more than 6 weeks in a person aged over 60 years.
Furthermore, all patients presenting with IBS symptoms should be appropriately assessed and clinically examined for the following 'red flag' indicators. A referral should be made to secondary care if any are present11:
Anaemia
Abdominal masses
Rectal masses
Inflammatory markers for inflammatory bowel disease
Serum CA125 should be measured in women with symptoms that suggest ovarian cancer
In addition, NICE have stated that IBS should be considered only if the person has abdominal pain or discomfort that is either relieved by defecation or associated with altered bowel frequency or stool form. This should be accompanied by at least two of the following four symptoms11:
abdominal bloating (more common in women), distension, tension or hardness
symptoms made worse by eating
passage of mucus
Other features such as lethargy, nausea, backache and bladder symptoms are common in people with IBS, and may be used to support the diagnosis.
According to NICE, patients who meet the IBS diagnostic criteria should have the following tests to exclude other diagnoses (Figure 2):
Figure 2 11 - Tests to exclude other diagnoses
Full blood count (FBC)
Erythrocyte sedimentation rate (ESR) or plasma viscosity
C-reactive protein (CRP)
Antibody testing for coeliac disease (endomysial antibodies [EMA] or tissue transglutaminase [TTG])
The value of serological tests for coeliac disease (EMA or TTG antibodies) in patients with IBS diarrhoea-predominant depends on the population and is generally considered cost-effective if the incidence of coeliac disease is above 1%. It is therefore likely to be beneficial in the United Kingdom, where up to 3% of cases of IBS diarrhoea-predominant in primary care have coeliac disease6.
The following tests are not necessary to confirm diagnosis in people who meet the IBS diagnostic criteria11:
Ultrasound
Rigid/flexible sigmoidoscopy
Colonoscopy/barium enema
Thyroid function test
Faecal ova and parasite test
Faecal occult blood
Hydrogen breath test (for lactose intolerance and bacterial overgrowth)
It is important to note that IBS is associated with several other conditions. At least half of IBS patients can be described as depressed, anxious, or hypochondriacal. In addition, between 20% and 50% of IBS patients have fibromyalgia. Furthermore, IBS is common in several chronic pain disorders, being present in 51% of patients with chronic fatigue syndrome, in 64% with temporomandibular joint disorder, and in 50% with chronic pelvic pain. The lifetime rates of IBS in patients with these syndromes are even higher. Patients with such co-morbidities generally have more severe IBS. A careful history to identify such associated disorders is helpful in identifying patients who are likely to have severe IBS and associated psychiatric disorder6.
Management
The treatment of IBS is determined by the patient’s most troublesome symptoms. Although there is overlap in the therapies offered to the different IBS sub-groups, treatment decisions are primarily based on the frequency and severity of symptomsThe management discussed in this section is largely based on the NICE guidelines11.
Dietary and lifestyle advice
People with IBS should be given information about the importance of self-help in effectively managing their IBS. This should include information on general lifestyle, physical activity, diet and symptom-targeted medication. Healthcare professionals should assess the physical activity levels of people with IBS (ideally using the General Practice Physical Activity Questionnaire). People with low activity levels should be given advice to encourage them to increase their activity levels. Healthcare professionals should also encourage people with IBS to make the most of their available leisure time and to create time for relaxation11.
Figure 3 summarises the general advice that should be given to patients regarding their diet and nutrition. If diet continues to be considered a major factor in a person's symptoms and they are following general lifestyle/dietary advice, they should be referred to a dietician for further advice and treatment, including single food avoidance and exclusion diets. Such advice should only be given by a dietician11.
Probiotics are live microorganisms which when taken in sufficient quantities, confer a health benefitPeople with IBS who try probiotics should be advised to take the product for at least 4 weeks while monitoring the effect. Probiotics should be taken at the dose recommended by the manufacturer11.
Figure 3 - Diet and nutrition should be assessed and the following general advice given 11
Have regular meals and take time to eat
Avoid missing meals or leaving long gaps between eating
Drink at least eight cups of fluid per day, especially water or other non-caffeinated drinks, for example herbal teas
Restrict tea and coffee to three cups per day
Reduce intake of alcohol and fizzy drinks
It may be helpful to limit intake of high-fibre food (such as wholemeal or high-fibre flour and breads, cereals high in bran, and whole grains such as brown rice)
Reduce intake of 'resistant starch' (starch that resists digestion in the small intestine and reaches the colon intact), which is often found in processed or re-cooked foods
Limit fresh fruit to three portions per day (a portion should be approximately 80 g)
People with diarrhoea should avoid sorbitol, an artificial sweetener found in sugar-free sweets (including chewing gum) and drinks, and in some diabetic and slimming products.
People with wind and bloating may find it helpful to eat oats (such as oat-based breakfast cereal or porridge) and linseeds (up to one tablespoon per day).
Healthcare professionals should review the fibre intake of patients, adjusting (usually reducing) it while monitoring the effect on symptoms. People with IBS should be discouraged from eating insoluble fibre (for example, bran). If an increase in dietary fibre is advised, it should be soluble fibre such as ispaghula powder or foods high in soluble fibre (for example, oats)
Pharmacological therapy
Healthcare professionals should consider prescribing antispasmodics for patients. These should be taken as required, alongside dietary and lifestyle advice. Laxatives should be considered for the treatment of constipation, but patients should avoid taking lactulose. Patients should be advised how to adjust their doses of laxative or antimotility agent according to the clinical response. The dose should be titrated according to stool consistency, with the aim of achieving a soft, well-formed stool (corresponding to Bristol Stool Form Scale type 4). Loperamide should be the first choice of antimotility agent for diarrhoeaOne advantage of loperamide is its peripheral site of action with little penetration of the blood brain barrier and thus, little potential for CNS side effects or habituation4.
Psychotropics possess a variety of peripheral and central effects which make them attractive treatments for IBS. These effects include modulation of pain perception, mood stabilisation, treatment of associated psychiatric conditions, and possible direct effects on GI motility and secretionHealthcare professionals should consider tricyclic antidepressants (TCAs) as second-line treatment for patients if laxatives, loperamide or antispasmodics have not helped. Treatment should be started at a low dose (5–10 mg equivalent of amitriptyline), which should be taken once at night and reviewed regularly. The dose may be increased, but does not usually need to exceed 30 mg11.
Selective serotonin reuptake inhibitors (SSRIs) should be considered only if TCAs have been ineffective. The anticholinergic effects of TCAs and their ability to prolong intestinal transit times are the reasons they are particularly preferred over SSRIs in IBS diarrhoea-predominant. Furthermore, given the propensity of SSRIs to commonly cause GI adverse events of nausea, vomiting, and diarrhoea, indicate that TCAs may have more utility in IBS diarrhoea-predominant than SSRIs12. Healthcare professionals should take into account the possible side effects when prescribing TCAs or SSRIs. After prescribing either of these drugs for the first time at low doses, the patient should be followed up after 4 weeks and then at 6–12 monthly intervals11.
Psychological interventions
Anxiety and depression are common in IBS and patients report a correlation between stress and their symptoms, providing a rationale for psychological therapyReferral for psychological interventions (cognitive behavioural therapy, hypnotherapy and/or psychological therapy) should be considered for people with IBS who do not respond to pharmacological treatments after 12 months and who develop a continuing symptom profile (refractory IBS).11 Hypnotherapy reduces patient anxiety and improves symptom control in the majority of patients with refractory IBS. The benefits extend well beyond symptom control and include improvements in quality of life and reduction in emotional distress13. Data from general practice shows that hypnotherapy is effective during the first three months, although the effect is less marked after that6.
Prognosis of IBS depends on the length of the history, those with a long history being less likely to improveFollow-up should be agreed between the healthcare professional and the patient based on the response of the person's symptoms to interventions. The emergence of any 'red flag' symptoms during management and follow-up should prompt further investigation and/or referral to secondary care11.
Acute gastrointestinal ulcerations and erosions (stress ulcers) are common in major trauma victims and in intensive care units. In fact, 75% of all critically ill admissions may have endoscopic evidence of gastroduodenal or upper gastrointestinal bleeding1. The bleeding could be in mutiple forms such as haematemesis,coffee ground aspirates, melaena, or haematochezia. Clinically significant haemorrhage causes hypotension and tachycardia and requires blood transfusion. Aggressive management is required in order to improve the outcomes of this potentially fatal complication. Prevention of stress ulcers helps reduce the morbidity and mortality of major bleeding2. Multiple causes may be responsible for gastrointestinal ulceration in patients with spinal cord injury1. Furthermore, steroids, thrombophylactic agents, anticoagulants and heavy cigarette smoking may act as predisposing factors to gastrointestinal bleed.
The aim of this study was to review our practice of stress ulcer prophylaxis after spinal cord injury and analyse morbidity and mortality associated with stress ulcer bleeding.
Patients and Methods
The Queen Elizabeth National Spinal Injuries Unit is the sole spinal cord injury centre in Scotland. It serves a population of 5.1 million and admits approximately 175 acute spinal injuries patients per year.
This study is retrospective. Only cases of life threatening or massive gastrointestinal haemorrhage were included. The period studied is between January 2006 and May 2008.
The department policy is to start all patients on Ranitidine 150 mg twice daily provided they are not on alternative medications before their admission, in which case the policy is to continue with the original pre admission medication.
Clinical notes of included patients were reviewed and information on patient’s demographics, cause and level of injury, past medical history, preadmission medications, clotting profile, prophylaxis, and management of bleeding were collected.
Results
A total of 360 patients were admitted. Out of them 19 (2 Female:17 Male) met the inclusion criteria as they suffered a life threatening GI bleed or major haemorrhage. The age range was 19 to 78 years with a mean age of 51.2 years. The majority of patients had a cervical spine injury (63%) followed by lumbar (21%) and thoracic (16%) spine injuries . Fall down stairs was the most common cause of injury occurring in 6 (31.5%) patients followed by road traffic accidents (26.3%) and fall from a height (21%). One patient suffered spinal injury whilst playing rugby and 1 patient suffered a cycling accident. The majority of cases (17 out 19) were admitted with acute injuries. However, 2 patients were admitted for complications of chronic injuries (one with a post surgical abscess and one with pressure sores). The various causes of spinal injuries are shown in table 1.
The American Spinal Injury Association (ASIA) impairment scales of all 19 patients are shown in Table 2. Associated injuries were encountered in 4 (21%) of patients. These associated injuries include sternum fracture, rib fractures, clavicle fracture, tendon injury and a calcaneum fracture. Significant past medical history was found in 14 (73.6%) patients whereas 5 (26.4%) did not have any previous medical illness. The list of all the significant past medical problems is shown in Table 3.
4 (21%) patients were already taking Omeprazole before admission, whereas 2 (10.5%) were taking Ranitidine and 1 (5.2%) patient was taking Lansoprazole.
7 out of 19 patients (36.8%) had either one or two episodes of significant coffee ground vomiting, 6 (31.5%) patients had an episode of haematemesis and 4 (21%) patients had combined coffee ground vomiting and haematemesis. Two (10.5%) patients had positive nasogastric aspirate for bleeding.
All 19 patients were started on intravenous Omeprazole and Sucralfate was added in 13 patients. Low molecular weight heparin, Ibuprofen and Aspirin was discontinued in all patients. Six (31.5%) patients were transfused 40 units of fresh frozen plasma and packed red cells (Figure 1). Eight patients (42.1%) underwent endoscopic treatment (Table 4) and 3 (15.7%) patients underwent laparotomy. There was one (5.2%) fatality reported.
Table 1:Causes of Spinal Cord Injury
Cause of Injury
Number of Patients
Percentage
Fall from stairs
6
31.5%
Road traffic accidents
5
26.3%
Fall from height
4
21%
Rugby injury
1
5.2%
Cycling accident
1
5.2%
Old injury admitted with skin problem
1
5.2%
Post surgical abscess
1
5.2%
Table 2:American Spinal Injury Association Impairment Scale
ASIA Impairment Scale
Number of Patients
Percentage
A= Complete: No motor or sensory function is preserved in the sacral segments S4-S5.
3
15.7%
B=Incomplete: Sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-S5
1
5.2%
C=Incomplete: Motor function is preserved below the neurological level, and more than half of key muscles below the neurological level have a muscle grade less than 3
10
52.6%
D=Incomplete: Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more
2
10.5%
E=Normal: motor and sensory function are normal
3
15.7%
Table 3: Previous Risk Factors in Spinal Cord Injured Patients with Stress Ulcers
Adverse Factor
Number of Patients with the Problem
Smoking
13 (68.4%)
Alcohol
5 (26.3%)
Reflux Oesophagitis
4 (21%)
Hypertension
3 (15.8%)
Diabetes Mellitus
3 (15.8%)
Hiatus Hernia
2 (10.5%)
Ischemic Heart Disease
2 (10.5%)
Asthma
1 (5.3%)
Duodenal Ulcers
1 (5.3%)
Anaemia
1 (5.3%)
Pyloric Stenosis
1 (5.3%)
Table 4:Endoscopic Findings, Procedures and Outcome
Number of Patients
Endoscopic findings, Procedures and Outcome
2
Bleeding Duodenal Ulcer injected with adrenaline Bleeding stopped
1
Had Endoscopy twice and bleeding Duodenal Ulcer injected with adrenaline on both occasions Continuous bleeding Underwent Laparotomy and over Sewing of the ulcer
1
Endoscopic findings were Oesophagitis, Hiatus Hernia and superficial ulcerations No procedure performed Treated Conservatively
1
Bleeding Duodenal Ulcer injected with adrenaline Continuous bleeding Prepared for Laparotomy but could not survive
1
Bleeding Duodenal Ulcer injected with adrenaline Bleeding stopped Barrett’s oesophagus was found and biopsied but biopsy results were negative
2
Bleeding Duodenal Ulcer injected with adrenaline Continuous bleeding Laparotomy and over sewing
Figure 1: Packed Red Cells and Fresh frozen Plasma Transfusion Units Patients
Discussion
The development of “stress” ulceration in the upper GI tract has been part of critical care folklore for a long time. In 1823 Curling described a series of severe duodenal ulceration associated with burns3; in 1832 Cushing reported ulcer disease associated with surgery and trauma4In the early years of intensive care, a strong association between severity of illness and the incidence of GI bleeds was established. Patients who had major bleeds had a high mortality rate and, consequently, prophylaxis against this complication has become a central issue in ICU care.
Gastrointestinal haemorrhage in patients with spinal cord disease was not reported until 1933 when Polstorff described gastric ulceration in an epileptic patient with spontaneous hematomyelia5. El Marsi and colleagues in 1982 reported 5.5% incidence of gastrointestinal bleeding in acute spinal cord injury patients6. Lesions of the spinal cord including traumatic, viral and infectious have been described with gastrointestinal bleeding7. It has been found mainly associated with injury to the cervical spinal cord8.
Controversy still exists regarding the appropriate prophylaxis of stress ulcers in trauma patients. There have been numerous randomized, controlled trials and several meta-analyses evaluating the use of drug therapy for stress ulcer prophylaxis in trauma patients9. One meta-analysis concluded that Sucralfate is as effective as pH-altering medications in preventing stress ulcer bleeding10. There is currently no large study that proves the superiority of proton pump inhibitors over H2- receptor antagonists for stress ulcer prophylaxis 11, 12. A survey of all the Level I trauma centers in the United States by Barletta et al9 revealed that H2-receptor blockers were the preferred agents. It is important to mention that some studies have questioned the need for prophylaxis altogehter but these were mainly retrospective studies that primarily evaluated medical patients as compared to trauma patients13, 14, 15, 16. The reported incidence of gastrointestinal haemorrhage in the medical literature in acute spinal cord injuries is between 5 and 22% 6, 17,18. In our study 19 out of 360 patients (5.2%) suffered a major bleed from the gastrointestinal tract. This incidence is similar to lower percentage reported in the medical literature17, 18. The strict adherence to the department policy of early prophylaxis for all admitted patients could be the reason for this low percentage of significant bleeding.
It is interesting to note that despite the increasing use of steroids and anticoagulants in the last decade, the incidence of gastrointestinal bleeding in acute spinal cord injuries have remained the same. The possible reason for this could be the increased awareness of this condition by spinal cord injury specialists and the regular prophylaxis initiated in the early phases of the injury. Our unit aims to admit patients as soon as they are fit for transfer and approximately 50% of our patients are transferred within the 48 hours of their injury from the peripheral hospitals. The referring hospitals are advised to commence H2 receptor antagonist at the time of referral.
Increasing use of antacids, H2 receptor antagonists and proton pump inhibitors in primary care19 may also contribute to the reduction of the incidence of gastrointestinal bleeding in patients with spinal cord injuries. This assumption is supported by our study as 7 (36.8%) patients in our study were already on these medications prior to their spinal cord injury.
The aetiology of gastroduodenal bleeding in spinal cord injury is multifactorial including, synergetic effects of the stress of the accident along with added effects of concomitant surgery, sepsis, unopposed reduced vagal tone and mucosal ischemia20. Also prolonged mechanical ventilation and coagulopathy has been shown to be associated with increased risk of stress ulcers in spinal injuries21.Other identified risk factors include multiple injuries, acute renal failure and use of high dose steroids22. Croft23 in 1977 first described the dynamics of the surface epithelium in the stomach. He reported that various agents were responsible for the damage of the gastric mucosa; stress, steroids and uraemia were causing decrease in the production of the mucosal cells; and alcohol and aspirin were causing increase in the shed of the gastric mucosal cells. This serious complication usually develops during the first four weeks after the spinal cord injury20,24. However, the period of greatest risk for gastrointestinal haemorrhage is reported to be between the fourth and tenth day after the injury8Nuseilben also reported focal ischemia of the gastric mucosa as early as 24 hours following the acute spinal cord injuries25.
Spinal injuries seldom occur in isolation; in a study by Silver26 in 1985 a 15% incidence of associated injuries was reported. The incidence of associated injuries in our study was 21%.
In a study by Walters and Silver1 all patients that bled had a combination of at least 3 risk factors. In our study 73.6% of patients who developed gastroduodenal bleeding had significant history of risk factors with smoking (68.4%) and alcohol (26.3%) being the major contributors. The other risk factors in our study were reflux oesophagitis (21%), hypertension (15.8%), diabetes mellitus (15.8%), hiatus hernia (10.5%) and ischemic heart disease (10.5%). However, only 7 (36.8%) patients had a combination of three or more risk factors at the time of admission. The reason for this decreased incidence as compared to Walter and Silver1 is difficult to explain.
In this study the majority of patients with gastrointestinal bleeding had cervical cord injuries (63.1%) as compared to thoracic and lumbar spine injuries. Kewalramani20 also showed predominance of gastrointestinal bleeding in patients with cervical cord injuries. This favours the neurogenic hypothesis as a major cause of gastrointestinal bleeding following the spinal injury 20.
Finally, there is no consensus, in literature, over the discontinuation of stress ulcer prophylaxis. Some studies suggest the continuation of prophylaxis throughout the duration of the critical illness or intensive care unit stay27, 28, 29.
Conclusion:
Gastrointestinal haemorrhage is a serious complication in spinal cord injured patients. Appropriate prophylaxis, early diagnosis and prompt management may help to avoid a possible fatality. Patients with spinal cord injury especially with cervical cord injury are at a high risk of gastrointestinal bleeding at all times even during period of rehabilitation30, 31. All acute spinal cord injured patients and patients who are undergoing rehabilitation who become critically ill may benefit from receiving chemical prophylaxis for stress ulceration. The duration of treatment is ill defined but is maybe better to continue while risk factors are present. Prevention could be the cornerstone in the overall management of this problem.
The WHO estimated that 171 million people had diabetes in the year 2000 and predicted this number to increase to 366 million in the year 2030. Given the increasing prevalence of obesity it is likely that these figures provide an underestimate of future diabetes prevalence1. Peripheral diabetic neuropathy (PDN) may be present in 60 to 65% diabetic patients, with 11% patients of diabetic neuropathy complaining of pain. The management of this condition can be particularly challenging as these patients may not get good response to the medications used for the treatment and the medications used are associated with side effects which the patients may find difficult to tolerate.
Pathophysiology:
Pathophysiology of PDN is complex and incompletely understood. Both peripheral and central processes contribute to the chronic neuropathic pain in diabetes. Peripherally at the molecular level due to hyperglycaemia, glycosylated end products are generated, which deposit around the nerve fibres causing demyelination, axonal degeneration and reduction in nerve conduction velocity. Deposition of glycosylated end products around the capillary basement membrane causes basement membrane thickening and capillary endothelial damage, which in association with a hypercoaguable state causes peripheral arterial disease. The peripheral arterial disease leads to neuronal ischemia which worsens nerve damage. There also occurs depletion of NADPH by activation of NADPH oxidase causing increased oxidative stress and generation of oxidative free radicals which aggravate the nerve damage. Calcium and sodium channel dysfunction, changes in receptor expression are the other peripheral processes which cause further neuronal tissue injury. The nerve damage can cause neuronal hyperexcitability. Neurotropic factors are required for nerve regeneration. In diabetes there occurs a low level of both nerve growth factors and insulin-like growth factors resulting in impaired neuronal regeneration. This can lead to peripheral hyperexcitability. Central sensitization is cause by increased excitability at the synapse, which recruits several sub-threshold inputs and amplifies noxious and non-noxious stimuli. Loss of inhibitory interneurons, growth of non-damaged touch fibres into the territory of damaged pain pathways, increased concentration of neurotransmitters and wind up caused by NMDA receptors are responsible for central sensitization at the level of dorsal horn in the spinal cord2.
Clinical Presentation:
Chronic sensorimotor distal polyneuropathy is the most common type of diabetic neuropathy. Acute sensorimotor neuropathy is rare and is usually associated with diabetic ketoacidosis and acute neuritis caused by hyperglycaemia. Autonomic neuropathy is common and often under reported. It can affect cardiovascular, gastrointestinal and genitourinary system. The other presentations can be cranial neuropathies, thoraco-abdominal neuropathies or peripheral mononeuropathies involving median, ulnar, radial, femoral, lateral cutaneous nerve of the thigh or common peritoneal nerve.
The patients usually complain of one or more of the following symptoms. They can have a chronic continuous or intermittent pain described as burning, aching, crushing, cramping or gnawing pain. The pain can be associated with numbness. They can have brief abnormal stimulus evoked pain like allodynia or hyperalgesia. Some patients also complain of brief lancinating pains described as electrical or lightening pains which can be spontaneous or evoked. The symptoms typically start in the toes and feet and ascend in the lower limb over years and are worse at night. Diabetic distal polyneuropathy is typically described in glove and stocking distribution but the upper limb involvement is rare. On examination there can be paradoxically reduced sensation to light touch and pin prick in the area of pain. Examination can also show features of allodynia (pain caused by a stimulus that does not normally cause pain), hyperalgesia (pain of abnormal severity in response to a stimulus that normally produces pain), hyperpathia (painful reaction to a repetitive stimulus associated with increased threshold to pain), dysaesthesia (unpleasant abnormal sensation as numbness, pins and needles or burning), paraesthesia (abnormal sensation which is not unpleasant) or evoke electric shock like pains. There can be features of peripheral autonomic neuropathy including vasomotor changes like colour changes of feet which can be red, pale or cyanotic and temperature changes like warm or cold feet. With autonomic neuropathy there can also occur trophic changes which includes dry skin, callouses in pressure areas and abnormal hair and nail growth and sudomotor changes involving swollen feet with increased or decreased sweating. Mechanical allodynia is the most common type of allodynia, but there can be thermal allodynia described as cold or warmth allodynia. Patient often describes cold allodynia as the pain getting worse in cold weather and warmth allodynia can make the patient keep the effected limb cool by using fan or ice bags. There can be reduced joint position sense, reduced vibration sense, reduced temperature sensation and reduced ankle jerks.
Diagnosis:
The diagnosis of PDN can be made by clinical tests using pinprick, temperature and vibration perception (using a 128-Hz tuning fork). The feet should be examined for ulcers, calluses and deformities. Combinations of more than one test have >87% sensitivity in detecting PDN. Other forms of neuropathy, including chronic inflammatory demyelinating polyneuropathy, B12 deficiency, hypothyroidism and uraemia, occur more frequently in diabetes and should be ruled out. If required these patients should be referred to a neurologist for specialized examination and testing3.
Treatment Options:
US Food and Drug Administration has approved duloxetine in 2004 and pregabalin in 2005 for the treatment of painful DPN. Amitriptyline, nortriptyline and imipramine are not licenced for the treatment of neuropathic pain.
NICE clinical guidance on pharmacological management of neuropathic pain in adults in non-specialist settings as shown in Figure 1, recommends duloxetine as the first line treatment, which if contraindicated amitriptyline is suggested to be the first line. Second line treatment is amitriptyline or pregabalin. Pregabalin can be used alone or in combination with either amitriptyline or duloxetine, which if ineffective the patient should be referred to specialist pain services. While awaiting the referral tramadol can be started as the third line treatment. NICE also recommends that these patients should be reviewed to titrate the doses of the medication started, to assess the tolerability, adverse effects, pain reduction, improvement in daily activities, mood, quality of sleep and the overall improvement caused by the medication as reported by the patient4.
The Mayo clinic recommends5 the first tier of drugs for peripheral diabetic neuropathy are duloxetine, oxycodone CR, pregabalin and tricyclic antidepressants. The second tier of drugs iscarbamazepine, gabapentin, lamotrigine, tramadol and venlafaxine extended release. The topical agents suggested are capsaicin and lidocaine.
“Evidence Based guideline on treatment of Painful Diabetic Neuropathy”, was formulated by American Academy of Neurology; American Association of Neuromuscular and Electrodiagnostic Medicine; American Academy of Physical Medicine and Rehabilitation. A systematic review of the literature between time period 1960 to 2008 was carried out. The review included the articles which looked at the efficacy of a given treatment either pharmacological or non-pharmacological to reduce pain and improve physical function and quality of life (QOL) in patients with PDN. They subsequently recommended that Pregabalin is established as effective and should be offered for relief of PDN (Level A). Venlafaxine, duloxetine, amitriptyline, gabapentin, valproate, opioids (morphine sulfate, tramadol, and oxycodone controlled-release), and capsaicin are probably effective and should be considered for treatment of PDN (Level B). Other treatments have less robust evidence or the evidence is negative. Effective treatments for PDN are available, but many have side effects that limit their usefulness, and few studies have sufficient information on treatment effects on function and quality of life6.
Non-pharmacological techniques:
Letícia et al. following their literature review on therapies used for PDN concluded that for non-pharmacological techniques like acupuncture, reiki, photic stimulation, electromagnetic stimulation of neural electrical stimulation, laser therapy, there is a lack of consensus about their effectiveness and there is scarce knowledge about them. They suggested new researches, including treatments for a longer period of time, with dosimetry control, and representative samples are necessary to discover the actual importance of these therapies for pain relief7.Spinal Cord Stimulators have however been shown to be effective and safe in severe resistant cases8,9.
Pharmacological Therapies:
Pregabalin: Pregabalin is a gamma aminobutyric acid analogue which binds to α2δ subunit of calcium channels and modulates them. Its starting dose is 150 mg/day with a maximum dose of 600 mg/day. As 98% of the drug is excreted unchanged in the urine, its dose is reduced in patients with renal impairment (creatinine clearance below 60 ml/min)10. A Cochrane Database Systematic Review in 2009 showed that Pregabalin was effective at daily doses of 300 mg, 450 mg and 600 mg, but a daily dose of 150 mg was generally ineffective. The NNT for at least 50% pain relief for 600 mg daily pregabalin dose compared with placebo was 5.0 (4.0 to 6.6) for PDN11.
Duloxetine: Duloxetine reduces the reuptake of serotonin and noradrenaline at the level of spinal cord, thereby potentiating the descending inhibitory pain pathways to reduce pain. It is started at a dose of 30 mg/day and its dose can be increased to 120mg/day10. Sultan et al. in their systematic review found that pain relief achieved with daily dose of 60 mg Duloxetine was comparable with daily dose of 120 mg of Duloxetine. The number needed to treat (NNT) for at least 50% pain relief at 12 to 13 weeks with duloxetine 60 mg versus placebo was 5.8 as compared to NNT of 5.7 for daily dose of 120 mg of duloxetine. The side effects reported with Duloxetine were reduction in appetite, nausea, constipation and somnolence12. Systematic Reviews and cohort studies have shown that duloxetine provides overall savings in terms of better health outcomes and reduction in opioid use, in comparison to gabapentin and pregabalin, tricyclic antidepressants and venlafaxine, in pain caused by PDN13, 14.
Gabapetin: Gabapentin is structurally related to gamma-aminobutyric acid (GABA) but acts by binding to the alpha2-delta subunit of voltage-gated calcium channels and thereby reducing the transmission of neuronal signals. Gabapentin bioavailability is non-linear and it tends to decrease with increasing dose. Gabapentin is not bound to plasma proteins and has a high volume of distribution. It is eliminated unchanged by the kidneys so in elderly patients and in patients with impaired renal function, its dose must be reduced. Gabapentin can be started froma daily dose of 300 to 900 mg and the dose can be increased to a maximum daily dose of 3600 mg over 3 weeks period10. Gabapentin provides good pain relief in about one third of patients when taken for neuropathic pain. Adverse events are frequent, but most of them are tolerable15.
Tricyclic Antidepressants (TCA): Amitriptyline and nortriptyline are the commonly used TCA for PDN. They may be used if there is no benefit from pregabalin or gabapentin and duloxetine. They may be used alone or in combination with pregabalin or gabapentin. In small RCTs, amitriptyline has been found to relieve pain better than placebo in patients with diabetic neuropathy10. Amitriptyline is a tricyclic antidepressant with marked anticholinergic and sedative properties. It increases the synaptic concentration of noradrenaline and serotonin in the CNS by inhibiting their re-uptake by the pre-synaptic neuronal membrane. For neuropathic pain it is started at 10-25 mg orally once daily at bed time initially and increased according to response to a maximum of 150 mg/day.
TCA should be used with caution in patients with a history of epilepsy, cardiovascular disorders, deranged liver function, prostatic hypertrophy, history of urinary retention, blood dyscrasias, narrow-angle glaucoma or increased intra-ocular pressure. It’s other side-effects are agitation, confusion and postural hypotension in elderly patients10. Amitriptyline is the most studied TCA for DPN and has been compared with placebo, imipramine, and desipramine. Amitriptyline, when compared with placebo, reduced pain to a significant degree. Pain relief was evident as early as the second week of therapy, with greater pain relief noted at higher doses (at a mean dose of 90 mg). A decrease in pain was not associated with improvement in mood. A systematic review of the TCAs, including fewer than 200 patients, found no difference in efficacy between the agents16. Nortriptyline is associated with fewer adverse events than amitriptyline and therefore it should be preferred in elderly patients.
Opioids: The use of opioids in chronic neuropathic pain has been a topic of debate because of uncertainty about their effectiveness, the concerns about addiction problems, the loss of efficacy with their long term use due to development of tolerance with their long term use and the development of hyperalgesia associated with their use. Cochrane review of twenty-three trials of opiates was carried out. The short-term studies showed equivocal evidence, while the intermediate-term studies showed significant efficacy of opioids over placebo, in reducing the intensity of neuropathic pain. Adverse events of opioids were reported to be common but were not life threatening. The authors recommended the need for further randomized controlled trials to establish long-term efficacy, safety (including addiction potential) and effects on quality of life17. In RCT Tramadol/Acetaminophen combination was shown to be associated with significantly greater improvement than placebo (p < or = 0.05) in reducing pain intensity, sleep interference and several measures of quality of life and mood18. In another RCT, controlled release (CR) oxycodone was compared with placebo, CR oxycodone resulted in significantly lower mean daily pain, steady pain, brief pain, skin pain, total pain and disability. In this study the number needed to treat to obtain one patient with at least 50% pain relief is 2.619. Gabapentin and morphine combination in randomised controlled trial showed that the combination of the two drugs provided better analgesia at lower doses of each drug than either of the drugs used as a single agent20.
Capsaicin: Capsaicin is the active component of chilli peppers. Capsaicin works by releasing the pro-inflammatory mediators like substance P from the peripheral sensory nerve endings and thereby causes its depletion from the peripheral nerve. Pharmacological preparations of Capsaicin are available as 0.025% cream, 0.075% cream and 8% capsaicin patches10. Repeated application of a low dose (0.075%) cream, or a single application of a high dose (8%) patch has been shown to provide a degree of pain relief in some patients with painful neuropathy. Common side effect includes local skin irritation which causes burning and stinging. It is often mild and transient but sometimes severe and not tolerated by the patients leading to withdrawal from treatment. Capsaicin rarely causes systemic adverse effects. Capsaicin can be used either alone or in combination with other treatment to provide useful pain relief in individuals with neuropathic pain21.
5% Lidocaine medicated plasters: A recent systematic review showed that 5% Lidocaine medicated plaster causes pain relief comparable to pain relief caused by amitriptyline, capsaicin, gabapentin and pregabalin in treatment of painful diabetic peripheral neuropathy. Lidocaine plaster being a topical agent may be associated with lesser clinically significant adverse events than the side effects of systemic agents. The need for further studies has been recommended by the reviewer as limited number and size of studies were included in the systematic review 22.
Conclusion:
The American Academy of Neurology, Mayo Clinic and NICE have both developed guidelines for treatment of peripheral diabetic neuropathic pain. There are several peripheral and central pathological mechanisms leading to the development of this condition and no single drug is available to target all these pathological mechanisms. Therefore often a combination of drugs is required for their management. Despite using a combination of medicines, managing these cases can be challenging. At the same time there is limited evidence on combination therapy in diabetic neuropathy and much work is required in this area. While using opioids for this condition the controversies over the use of opioids in non-malignant pain should be kept in mind and the advantages and disadvantages of using them should be discussed with the patients. Opioids should only be started with patient’s consensus. The treatment should be modified from the guidelines on an individual basis to achieve the optimal pain relief.
A 54-year-old male presented to the psychosexual clinic with symptoms suggestive of persistent genital arousal disorder of 2years duration. Physical examination and investigations ruled out any underlying urological or neurological causes. He was treated with Diazepam and Pregabalin and his symptoms reduced in intensity.
Introduction:
Persistent genital arousal disorder (PGAD), also known as persistent sexual arousal syndrome (PSAS) or restless genital syndrome (ReGS), is recently recognised as a sexual health problem in western countries although it is not been considered as a physical or psychiatric disorder by DSM IV or ICD 10. PGAD is associated with constant, spontaneous and intrusive feelings of genital arousal in the absence of conscious sexual thoughts or stimuli.
The working definition of PGAD1,2 is as follows:
1) Persistent physical arousal in the genital area
2) in the absence of conscious thoughts of sexual desire or interests
3) associated with spontaneous orgasm or feelings that orgasm is imminent and
4) the symptoms not diminished by orgasm.
It may be present throughout the person’s life (primary PGAD) or develop at any age (secondary PGAD). It is associated with varying degrees of distress in the patients. This new disorder has been reported in women by numerous clinicians in the last decade. However, so far, there is only one report of two males suffering with ReGS in the literature.3 We report a case of PGAD in a male and aim to analyse the cause.
Case Report
A 54-year-old male was referred to the psychosexual clinic by an urologist with 2 years history of constant feelings of physical arousal in the genital area as if he was about to ejaculate. These feelings were associated with pain which was relieved to an extent after ejaculation. These symptoms started suddenly for the first time when he was browsing the internet and accidentally ended up in pornographic websites. But later on, the symptoms were constant without any sexual stimuli and he got some relief from attaining climax.
He described that the physical arousal in the genital area increased in intensity to a point he had to ejaculate to have some relief. He felt this “as if wanting to have climax all the time”. Post- ejaculation, he felt anxious, tired and nauseated for sometime, during which the symptoms intensified again that he needed climax. Initially this cycle repeated every 2-3 days but later on the frequency increased to 2-3 times a day. He achieved climax both by masturbation and sexual intercourse. He felt these ejaculations were unpleasant and not enjoyable. He felt frenzied if he couldn’t ejaculate and the post orgasmic feelings were severe if he avoided orgasm for a day or two. He described regular ejaculations led to less severe “come downs” but left him constantly drained.
His medical history included vasectomy four years ago with minor complication of painful scrotum which subsided fully with pain killers. He also had few urinary tract infections (UTI) in the past which were treated with antibiotics. He was initially seen by urologist who carried out physical examination which was noted to be normal. Then investigations including CT- KUB, CT- Abdomen, Urogram, Transrectal Ultrasound of prostate and seminal vesicles, Flexible Cystoscopy were done and no abnormalities noted. He also had MRI- Brain which was normal. He had no symptoms of hyperactive bladder and no varicocele was noted.
When he was seen in the psychosexual clinic, he was noted to be very anxious and expressed guilty feelings around the incident of watching pornography which initiated the onset of symptoms. There were no depressive or psychotic symptoms. Prior to attending this clinic he was prescribed duloxetine 30mgs by the urologist, which he took only for few weeks. He stopped it as there was no symptom relief. He was started on diazepam and pregabalin. The dose was increased to 2mgs qds of diazepam and 50mgs qds of pregabalin. His symptoms diminished gradually and now he remains mildly symptomatic although feeling “more in control”. He was also referred to psychologist and had an assessment. As he was not psychologically minded and unable to engage in sessions, he stopped attending.
Discussion
The clinical features in this man were consistent with the definition of PGAD. He had physical arousal symptoms, which were not related to sexual desire or thoughts and was causing severe distress to him. The symptoms were relieved by ejaculation to a certain extent. He was treated with diazepam and pregabalin which reduced the intensity of the symptoms.
There is an emerging literature on the pathophysiology, possible aetiological factors and the management options of PGAD. There are various associations reported including psychological4,5 and organic6-9 pathologies with some convincing evidence.
In this case, he suffered few UTI and a minor complication of painful scrotum following vasectomy, few years before the onset of PGAD. However he had a full urological and neurological work-up recently which didn’t show any underlying organic cause for his current symptoms. He suffered no previous depressive or anxiety disorder. Hence his current symptoms may be induced by anxiety which is further worsened by the fact that he became focussed on the genital arousal and attaining climax to relieve the pain. When he was prescribed diazepam and pregabalin, his anxiety eased and his physical symptoms diminished in intensity. However the possibility of an organic cause cannot be ruled out completely as he previously suffered sensory neuropathic pain following vasectomy. Further pregabalin is useful for both generalised anxiety and neuropathic pain. Therefore we conclude that his symptoms may be a result of interaction between physical and psychological factors. This suggests that PGAD could be a psychosomatic condition, which was already proposed as a cause for PGAD in women by Goldmeier and Leiblum.4
Similar to the causes for PGAD, there is few treatment modalities reported in the literature. These include treatment of the underlying organic causes if any found, electro-convulsive therapy (ECT) if co-morbid with mood symptoms,10 transcutaneous electrical nerve stimulation (TENS),3 cognitive behavioural therapy11 and medications like varenicline.2 We used anti-anxiety medications (diazepam and pregabalin) and achieved adequate symptom relief. This also supports the idea that PGAD could be a psychosomatic condition related to the peripheral nerves of the genito-urinary system.
This case is reported to confirm that PGAD also occurs in males, which is quite different from priapism and it could be a psychosomatic condition. More research is needed into the pathophysiology of PGAD and its management.
Major Obstetric haemorrhage (MOH) remains one of the leading causes of maternal mortality & morbidity worldwide. In the 2003-2005 report of the UK Confidential Enquiries into Maternal Deaths, haemorrhage was the third highest direct cause of maternal death (6.6 deaths/million maternities) with the rate similar to the previous triennium 1, 2. Postpartum haemorrhage (PPH) accounts for the majority of these deaths. This triennium, 2006-2008, unlike in previous reports there has been a change in the rankings of direct deaths by cause. Deaths from haemorrhage have dropped, to sixth place, following genital tract sepsis, preeclampsia, thromboembolism, amniotic fluid embolism and early pregnancy deaths 3. A well-defined multidisciplinary approach that aims to act quickly has probably been the key to successful management of MOH. In the developing world, several countries have maternal mortality rates in excess of 1000 women per 100,000 live births, and WHO statistics suggests that 25 % of maternal deaths are due to PPH, accounting for more than 100,000 maternal deaths per year 4.The blood loss may be notoriously difficult to assess in obstetric bleeds 5, 6. Bleeding may sometimes be concealed & presence of amniotic fluid makes accurate estimation challenging.
Definition
MOH is variably defined as blood loss from uterus or genital tract >1500 mls or a decrease in haemoglobin of >4 gm/dl or acute loss requiring transfusion of >4 units of blood. Blood loss may be:
1. Antepartum: Haemorrhage after 24th week gestation & before delivery; for example: placenta praevia, placental abruption, bleeding from vaginal or cervical lesions.
2. Postpartum: Haemorrhage after delivery
Primary PPH: Within 24 hours of delivery, which is >500 mls following vaginal delivery & > 1000mls following a caesarean section 7.
Secondary PPH: 24 hours to 6 weeks post-delivery; for example: Uterine atony, retained products of conception, genital tract trauma, uterine inversion, puerperal sepsis, uterine pathology such as fibroids 8.
PPH can be minor (500-1000 mls) or major (> 1000 mls). Major PPH could be divided to moderate (1000-2000 mls) or severe (>2000 mls).
Causes
Causes of PPH may be conveniently remembered using 4 T’s as a mnemonic:
Tone(Uterine atony)
Tissue (retained products)
Trauma( cervical & genital tract trauma during delivery)
Thrombosis (coagulation disorder)
Other Risk factors include:-Prolonged labour, multiple pregnancy, polyhydramnios, large baby, obesity, previous uterine atony & coagulopathy.
Prevention
The most significant intervention shown to reduce the incidence of PPH is the active management of the third stage of labour (see below).Other measures to prevent or reduce the impact of MOH include
Avoidance of prolonged labour
Minimal trauma during assisted vaginal delivery
Detection & treatment of anaemia during pregnancy
Identification of placenta praevia by antenatal ultrasound examination.
Where facilities exist, magnetic resonance imaging (MRI) may be a useful tool and assist in determining whether the placenta is accreta or percreta. Women with placenta accreta/percreta are at very high risk of major PPH. If placenta accreta or percreta is diagnosed antenatally, there should be consultant-led multidisciplinary planning for delivery 9.
Active management of the third stage
This represents a group of interventions including early clamping of the umbilical cord, controlled cord traction for placental delivery & prophylactic administration of uterotonic at delivery (e.g. oxytocin) 10. Active management of the third stage is associated with a lower incidence of PPH and need for blood transfusion 11. A longer acting oxytocin derivative, carbetocin, is licensed in the UK specifically for the indication of prevention of PPH in context of caesarean delivery. Randomised trials suggest that a single dose (100 mcg) of carbetocin is at least as effective as oxytocin by infusion 12, 13.
Management of MOH
Pregnant women are often young, healthy & have an increased blood volume of up to 20 % at term and therefore likely to compensate well to haemorrhage until the circulating blood volume is very low 14. MEOWS are a useful bedside tool for predicting morbidity. A validation study of the CEMACH recommended modified early obstetric warning system (MEOWS) in all obstetric inpatients to track maternal physiological parameters, and to aid early recognition and treatment of the acutely unwell parturient. In addition, blood loss may sometimes be concealed and difficult to calculate. More commonly massive haemorrhage may be obvious; signs other than revealed haemorrhage include:
Tachycardia
Hypotension( BP may not drop until significant blood is lost)
Pallor
Oliguria
Cool peripheries
Lower abdominal pain
Management of anticipated MOH
On some occasions, cases at high risk of MOH can be predicted; e.g. caesarean section in a lady with a low lying placenta and previous uterine scar. These cases may be at a risk of placenta accreta and massive blood loss.
2 large bore IV cannulae
Rapid infusion device or pressure bags in theatre
Blood warmer & warming blanket
Blood cross-matched & available
Consider preoperative invasive monitoring
Consider cell salvage if available (see below)
Consider interventional radiological procedures if available ( see below)
Management of unanticipated MOH
Management involves four components, all of which must be undertaken SIMULTANEOUSLY: communication, resuscitation, monitoring and investigation, arresting the bleeding 9, 15. Most maternity units in UK have CODE RED bleep system for alerting MOH.
Communication & teamwork:
Communication and teamwork are essential in cases of both anticipated & unanticipated maternal haemorrhage. This includes:
Call for help. Alert the midwife-in-charge, senior obstetrician & anaesthetist.
Alert Blood transfusion service & haematologist.
Alert portering service for transport of blood samples & collection of blood products
Check blood is available. In the UK 2-4 units of O-neg blood is kept on labour ward for emergency use.
Allocate roles to team members.
Ensure departmental guidelines exist for the management of MOH & regularly practice ‘fire drills’.
Alert one member of the team to record events, fluids, drugs and vital signs 9.
The use of standard form of words (such as ‘on going major obstetric haemorrhage’, ‘we need compatible blood now or group specific blood’) 9.
Goals of management:
Early identification of maternal bleed and institution of major haemorrhage drill
Rapid access to infusion of fluid in first instance with rapid availability & administration of blood.
Avoidance/limitation of complications of massive blood transfusion namely: acid/base disturbance, transfusion related acute lung injury (TRALI), hypocalcaemia, hyperkalaemia, hypothermia & thrombocytopenia.
Efficient team working & management decision making.
Resuscitation & immediate management:
ABC, 100% oxygen
2 large bore cannulae & bloods for X-match
Fluid resuscitation; crystalloid/colloid 2000mls via rapid infuser or pressure bags e.g. Level 1 Rapid infuser ( can achieve >500mls/min warmed fluid flow)
Fluid therapy and blood product transfusion 9
Crystalloid Up to 2 litres Hartmann’s solution
Colloid up to 1–2 litres colloid until blood arrives
Blood Crossmatched
If crossmatched blood is still unavailable, give uncrossmatched group-specific blood OR give ‘O RhD negative’ blood
Fresh frozen plasma 4 units for every 6 units of red cells or prothrombin time/activated partial thromboplastin time > 1.5 x normal (12–15 ml/kg or total 1litres)
Platelets concentrates if platelet count < 50 x 109
Cryoprecipitate If fibrinogen < 1 g/l
Thromboelastography and rotational thromboelastometry coagulation tests: In most cases, medical and transfusion therapy is not based on the actual coagulation state because conventional laboratory test results are usually not available for 45 to 60 minutes. Thromboelastography and rotational thromboelastometry are point-of-care coagulation tests. A good correlation has been shown between thromboelastometric and conventional coagulation tests, and the use of these in massive bleeding in non-obstetric patients is widely practiced and it has been proven to be cost-effective.
A 2006 guideline from the British Committee for Standards in Haematology 1, 4summarizes the main therapeutic goals of management of massive blood loss is to maintain:
Haemoglobin > 8g/dl
Platelet count > 75 x 109/l
Prothrombin < 1.5 x mean control
activated prothrombin times < 1.5 x mean control
Fibrinogen > 1.0 g/l.
In addition, the Confidential Enquiry into Maternal and Child Health recommends that women with known risk factors for PPH should not be delivered in a hospital without a blood bank on site 1.
Transfer to theatre.
Non-surgical intervention for uterine atony.
Bimanual uterine compression (rubbing up the fundus) to stimulate contractions.
Ensure bladder is empty (Foley catheter, leave in place). ‘Rub up ‘the uterus
Syntocinon 5 units by slow intravenous injection (may have repeat dose).
Ergometrine 0.5 mg by slow iv/im injection (contraindicated in women with hypertension) 16.
Syntocinon infusion (40 units over 4 hours).
Carboprost 0.25 mg by intramuscular injection repeated at intervals of not less than 15 minutes to a maximum of 8 doses (contraindicated in women with asthma).
Direct intramyometrial injection of carboprost 0.5 mg im (Haemobate or Prostaglandin F2a) with responsibility of the administering clinician as it is not recommended for intramyometrial use. Can be repeated up to 5 doses (contraindicated in women with asthma, may cause bronchospasm, flushing & hypertension 17).
Misoprostol 1000 micrograms rectally.
If pharmacological measures fail to control the haemorrhage, initiate surgical haemostasis sooner than later.
Surgical treatment and other interventions
The most common cause of primary PPH is uterine atony. However, clinical examination must be undertaken to exclude other or additional causes:
Retained products (placenta, membranes, clots)
Vaginal/cervical lacerations or hematoma
Ruptured uterus
Broad ligament hematoma
Extra genital bleeding (for example, subcapsular liver rupture)
Uterine inversion.
Intrauterine balloon tamponade is an appropriate first line ‘surgical’ intervention for most women where uterine atony is the only or main cause of haemorrhage. If this fails to stop the bleeding, the following conservative surgical interventions may be attempted, depending on clinical circumstances and available expertise:
Haemostatic brace suturing (such as B-Lynch or modified compression sutures).
Bilateral ligation of uterine arteries.
Bilateral ligation of internal iliac (hypogastric) arteries.
Selective arterial embolisation or balloon occlusion radiologically.
Compression/ clamping aorta to buy time.
Uterine replacement if uterine inversion
It is recommended that a laminated diagram of the brace technique be kept in theatre. Resort to hysterectomy sooner rather than later (especially in cases of placenta accreta or uterine rupture). A second consultant clinician should be involved in the decision for hysterectomy.
Interventional Radiological techniques
Interventional techniques are gaining popularity if the facilities & expertise exist and are especially useful for the anticipated massive bleeds e.g. planned LSCS in a woman with anticipated placenta accrete. Though evidence of effectiveness is still limited, there are increasing case reports of its successful use. This suggests that prophylactic arterial catherisation (with a view to embolisation) could be considered where facilities permit until such time as further evidence becomes available 22-28.
Bilateral internal iliac artery balloons may be placed electively & inflated at C. section/ should bleed occur.
Selective pelvic artery (internal iliac arteries, anterior division of internal iliac or uterine artery) embolisation can be performed.
Interventional radiology may be considered in cases of placenta praevia with accreta if intra-arterial balloons can be placed in the radiology department before the woman goes to theatre for caesarean section. Follow up studies of women who had undergone arterial embolisation for control of PPH suggest that the intervention does not impair subsequent menstruation and fertility 29, 30.
Intraoperative cell salvage in obstetrics (ICSO)
Cell salvage has now been used in numerous cases of obstetric bleeds and appear safe. Concerns relate to re-infusion of foetal cells which could theoretically cause haemolytic disease in future pregnancies and also the potential for amniotic fluid embolus. If cell salvage techniques are utilised, separate suction of amniotic fluid is recommended and a leukocyte depletion filter used during re-infusion of salvaged blood. Setting up cell salvage measures should not divert staff an attention from initial resuscitation.
Intraoperative cell salvage (the process whereby bloodshed during an operation is collected, filtered and washed to produce autologous red blood cells for transfusion to the patient) is commonly being used in cardiac, orthopaedic and vascular surgery with relative reduction of blood transfusion by 39% and absolute risk reduction by 23%, with cell salvage not appearing to impact adversely on clinical outcomes 31, 32. Although large prospective trials of cell salvage with auto transfusion in obstetrics are lacking, to date, no single serious complication leading to poor maternal outcome has been directly attributed to its use. Several bodies based on current evidence have endorsed cell salvage in obstetrics. Current evidence supports the use of cell salvage in obstetrics, which is likely to become increasingly commonplace, but more data are required concerning its clinical use 33. A National UK survey in 2007 showed that, in 2005–2006, 38% of all UK maternity units were using cell salvage and that 28% incorporated cell salvage into their massive haemorrhage guidelines 34. In particular, this survey showed that a lack of training was the main perceived barrier to its use: 48% of units specifically stated that their reason for not using cell salvage was lack of training and equipment, with fears about safety being expressed by only 10%. However, the potential difficulty is the effective removal of amniotic fluid and the degree of contamination with fetal red cells with potential maternal sensitization, intraoperative cell salvage may be a useful technique in women who refuse blood or blood products (Jehovah’s Witnesses guideline) 9 or those where massive blood loss is anticipated (placenta percreta or accreta). For women who are Rh-negative, to prevent sensitization, the standard dose of anti-D should be given and a Kleihauer test taken 1 hour after cell salvage has finished, to determine whether further anti-D is required 35.
Recombinant activated factor VII (rFVIIa)
Recombinant activated factor VII (rFVIIa) was developed for the treatment of haemophilia. Over the past decade, it has also been used to control bleeding in other circumstances. A 2007 review identified case reports of 65 women treated with rFVIIa for PPH 36.Although the case reports suggested that rFVIIa reduced bleeding, 30 of the 65 women underwent peripartum hysterectomy and particular caution is required in interpreting data from uncontrolled case reports. In the face of life-threatening PPH, and in consultation with a haematologist, rFVIIa may be used as an adjuvant to standard pharmacological and surgical treatments. A suggested dose is 90 micrograms/kg, which may be repeated in the absence of clinical response within 15–30 minutes 37. Although there is no clear evidence of thrombosis with the use of rFVIIa in obstetric practice, there have been case reports of thrombosis with the use in cardiac surgery 38-40. Women with PPH are particularly susceptible to defibrination (severe hypofibrinogenaemia) and this is particularly relevant to the most severe cases that will be considered for rFVIIa; rFVIIa will not work if there is no fibrinogen and effectiveness may also be suboptimal with severe thrombocytopenia (less than 20 x 109/l).Therefore, fibrinogen should be above 1g/l and platelets greater than 20 x 109/l before rFVIIa is given. If there is a suboptimal clinical response to rFVIIa, these should be checked and acted on (with cryoprecipitate, fibrinogen concentrate or platelet transfusion as appropriate) before a second dose is given 36-40.
Anaesthetic management15:
GA with RSI is generally advocated if actively bleeding or coagulopathy.
Reduce dose of induction agent if severe on going bleeding.
Regional anaesthesia is relative contraindication but may be maintained if the patient has an epidural insitu & bleeding is controlled.
Alert Blood bank & haematologist.
Consider arterial line, central line and urinary catheter but only after definitive treatment has commenced. Their insertion must not delay resuscitation & fluid management.
Use fluid warmer & aim to keep the patient normothermic.
Regular monitoring of haemoglobin level and coagulation using near patient devices if available (e.g. Haemacue). FFP, platelets transfusion & cryoprecipitate may be necessary if coagulopathy develops. Liaise early with haematology department for optimal & timely product replacement.
Perioperative monitoring as per AAGBI guidelines.
Recording of parameters on a flow chart such as the modified obstetric early warning system charts.
Consider systemic haemostatic agents such as Aprotonin, Vit K, Tranexemic acid, Recombinant factor VII a (Novo seven R). Although evidence is conflicting, there is a consensus view that fibrinolytic inhibitors seldom, if ever, have a place in the management of obstetric haemorrhage 41, 42.
Postoperative management includes transfer to ITU/HDU.
Anticipate coagulopathy & treat clinically until coagulation results available.
It is also important that, once the bleeding is arrested and any coagulopathy is corrected, thromboprophylaxis is administered, as there is a high risk of thrombosis. Alternatively, pneumatic compression devices can be used, if thromboprophylaxis is contraindicated in cases of thrombocytopenia.
Conclusion
Globally, postpartum haemorrhage (PPH) is the leading cause of maternal morbidity and mortality. Major obstetric haemorrhage is managed by multidisciplinary approach. In the current treatment of severe PPH, first-line therapy includes transfusion of packed cells and fresh-frozen plasma in addition to uterotonic medical management and surgical interventions. In persistent PPH, tranexamic acid, fibrinogen, and coagulation factors are often administered. Secondary coagulopathy due to PPH or its treatment is often underestimated and therefore remains untreated, potentially causing progression to even more severe PPH. The most postnatal haemorrhage is due to uterine atony and can be temporarily controlled with firm bimanual pressure while waiting for definitive treatment.
The global epidemiology of PD varies widely which could be partly accounted for by differences in survival rates.1 One review paper examined the epidemiology of PD in Austria, the Czech Republic, France, Germany, Italy, The Netherlands, Portugal, Spain, Sweden and United Kingdom. It revealed that the prevalence rates range from 65.6 per 100,000 to 12,500 per 100,000 and annual incidence estimates ranged from 5 per 100,000 to 346 per 100,000.2 The wide variation in incidence and prevalence rates of PD across Europe could be due to environmental and genetic factors. Differences in methodologies for case ascertainment, diagnostic criteria, or age distributions of the study populations, could also account for the wide variations.2
Described by James Parkinson in 1817, PD is the second most common neurodegenerative disorder next to Alzheimer’s dementia. Depletion of dopaminergic neurones in the substantia nigra is the main pathology found in PD. Symptoms usually appear when dopamine levels are reduced by 50-80%.3 Noradrenergic, cholinergic and serotonergic pathways are also affected. Clinically PD is characterised by rigidity, tremor (cogwheel, lead pipe, and resting), akinesia, bradykinesia (poverty and slowness of movement), and postural instability (leading to frequent falls).4 These symptoms may also be accompanied by a range of non-motor symptoms other than well-known neuropsychiatric syndromes of depression, psychosis, and cognitive impairment.
In essence, a syndrome is a combination of signs and symptoms related to an underlying pathological process. PD may present with neuropsychiatric syndromes of depression, psychosis (usually affective in origin) and cognitive impairment.5 These syndromes are not under discussion here as readers are likely to be familiar with them. However, PD may also present with other neuropsychiatric syndromes and for the purpose of this article we have classified them into: 1) Anxiety disorders, 2) Apathy, 3) Involuntary emotional expression disorder, 4) Sleep disorders, and 5) Impulse control disorders.
Drugs used to treat PD themselves are associated with neuropsychiatric side effects. For example, dopamine agonists are well-known to cause sleep disturbance, dizziness (usually due to postural hypotension), hallucinations, hypersexuality, and compulsive gambling. Anticholinergics may cause confusion, hallucinations and impaired memory. Surgery also may cause adverse effects including depression, confusion and cognitive impairment.6 Table 1 illustrates the groups of drugs used in PD.
Overlooked neuropsychiatric syndromes in Parkinson’s disease
The prevalence of overlooked neuropsychiatric syndromes found in PD, summarised in Table 2, is generally less common than PD syndromes of depression (up to 50%),psychosis (up to 60%) and dementia (ultimately develops in 80%).7, 8, 9
Table 2. Overlooked neuropsychiatric syndromes found in Parkinson’s Disease.
Neuropsychiatric syndrome
Prevalence
Anxiety disorders
Up to 40%
Apathy
16-42%
Involuntary emotional expression disorder
Up to 16.8%
Sleep disorders
60-98%
Impulse control disorders
Up to 13.6%
Anxiety Disorders
Epidemiology
There is a wide range in the reporting of the prevalence of anxiety in patients with PD. Anxiety is significantly more prevalent in PD sufferers compared with age and sex matched non-sufferers. Prevalence is quite high with estimates indicating that up to 40% of PD patients suffer significant anxiety.10 However, clinicians’ recognition and awareness of anxiety in PD need to be raised because it is likely to be under-diagnosed and untreated.11, 12 Consequently the prevalence of anxiety may be even higher. Severity of anxiety is not correlated with severity of parkinsonian symptoms, duration of levodopa use, or current dose of levodopa.
Aetiology and risk factors
Anxiety is an understandable psychological response to the physical symptoms, to the neurochemical changes of the disease itself, or as a side effect of the various medications used to treat the condition.10 Sleep disturbances and cognitive impairment have been proposed as possible aetiological factors for anxiety in PD.11, 12 Depression in PD may manifest in two clinical phenotypes, one ‘anxious-depressed’ and the other ‘depressed’. However, a further large proportion of patients can have relatively isolated anxiety.13
Anxiety frequently precedes the development of motor symptoms, suggesting specific neurobiological processes are involved, not merely social and psychological reactions in learning to adapt to PD.14
Patients with postural instability and gait dysfunction have a higher incidence of anxiety compared with tremor-dominant patients. Younger-onset PD patients are also more likely to experience anxiety. The pathogenesis of anxiety involves noradrenergic, serotonin and dopamine neurotransmitters. GABAergic pathways may also be involved.14 Right hemisphere disturbances have also been implicated, particularly with panic disorder.Symptom variation in PD may be due to medication, as well as motor fluctuations.11 One study revealed that although the dose of levodopa was not associated with anxiety, the experience of dyskinesia or on-off fluctuations increased the risk of anxiety.12, 14, 15
Presentation and diagnosis
The commonest disorders found in PD are generalised anxiety, panic disorder, and social phobia. Anxiety contributes to the complexity of PD and lowers quality of life. 14, 15 The degree of comorbidity between anxiety and depression in PD patients is in excess of that found in patients without PD. While anxiety is significantly associated with depression, some patients show anxiety without depression.10
The main features of anxiety are inappropriate feelings of apprehension as well as mood, cognitive, and somatic changes. Some symptoms may be common to PD, such as autonomic symptoms, fatigue, muscle tension, insomnia and attention problems. Psychologically, anxiety in PD is understandable because being diagnosed with a chronic disease with no known cure and an inexorable course, would be difficult for anyone to contemplate. Motor signs and changes in appearance could explain social anxiety. However, the frequency of anxiety in PD seems to be higher than in other chronic diseases and unrelated to the severity of motor signs. Even in social phobia the phobic symptoms do not correlate with disease severity and are not restricted to performance situations. Furthermore, anxiety can precede motor signs by several years, suggesting that the neurobiological substrate of PD is responsible for anxiety at least in part.
Treatment
Treatment comprises the use of selective serotonin reuptake inhibitors (SSRIs) such as sertraline, fluoxetine and citalopram as well as other newer antidepressants - serotonin and noradrenaline reuptake inhibitor (SNRIs) for example, venlafaxine, cognitive behavioural therapy (CBT), exercise, the occasional use of atypical neuroleptics, and benzodiazepines.14 However, benzodiazepines have a tendency to cause sedation, unsteadiness of gait, and even confusion. Antidepressants are useful because they treat both anxiety and depression that often overlap: depression coexists with anxiety in 14% of cases.15 Low dose tricyclic antidepressants with minimal anticholinergic effects may be useful in those patients who do not respond to benzodiazepines.
Apathy
Epidemiology
Apathy, a state of lethargic indifference and loss of motivation, and fatigue are prominent non-motor symptom in PD with a prevalence of between 16-42%.16, 17 Fatigue is a sense of tiredness or exhaustion, due to mental or physical causes. Apathy and fatigue are important because they have significant repercussions for the quality of life in PD.18, 19 Apathy can exist without depression but, by definition, patients themselves do not complain of apathy, though are found to be unmotivated to engage in activities. Apathy and fatigue are often difficult to distinguish from low mood and daytime sleepiness, both of which are common to depression.
A four-year prospective longitudinal study of 79 patients found that 13.9% of those with PD had persistent apathy and 49.4% had developed apathy at follow up. The study showed apathy to be a frequent and persistent behavioural feature in PD with a high incidence and prevalence over time, and associated with neurotransmitter deficits.20
Aetiology and risk factors
The dorsolateral, medial and orbital frontal cortices, as well as subcortical structures such as the basal ganglia, thalamus and internal capsule are implicated in the pathogenesis of apathy.The independent risk factors for apathy are dementia at baseline, a more rapid decline in speech, and axial impairment (e.g. poor ability to turn in bed) during follow up.20, 21 A more recent study showed that male gender, higher depressive scores, and severe motor symptoms, were significantly associated with apathy, but not with greater cognitive impairment.22 It has been observed that deep brain stimulation (DBS) may contribute to the development of apathy23 but other studies show conflicting results.24
Presentation and diagnosis
There is a higher incidence of depression and dementia in PD patients with apathy.Therefore differential diagnosis between apathy and cognitive deficits and depression is essential because the therapeutic approaches are different.19, 20 It is equally important to differentiate between apathy and depression that are different clinical entitiesalthough both may coexist.The crucial difference is that people with apathy lack serious self-reproach or feelings of guilt. 21, 25 The Lille Apathy Rating Scale (LARS), administered as a structured interview, can be a useful tool to distinguish them both26 though further research is needed to differentiate the neurological and neurochemical basis for depression and apathy.
Treatment
Treatment options for apathy are limited. The use of methylphenidate, a stimulant drug related to amphetamine, has been suggested but evidence is scarce and side effects may outweigh its clinical benefit.27 Methylphenidate has been described as effective for both apathy and fatigue28 but more studies are necessary. Antidepressants are not effective, can cause unnecessary side effects and can even aggravate apathy, demonstrating that these syndromes are really independent.29 The association between cognition and apathy, along with the potential benefit of cholinesterase inhibitors on both cognition and apathy, suggests that cholinergic mechanisms take part in the pathophysiology of apathy.30, 31 ’Off-time’ refers to periods of the day when the medication is not working well, causing worsening symptoms of fatigue and apathy. ‘Wearing-off’ episodes may occur predictably and gradually, or they may emerge suddenly and unexpectedly. Wearing-off periods may be improved with appropriate changes in the medication regimen. This would mean optimizing dopaminergic agents or using a long-acting levodopa or a catechol-O-methyltransferase (COMT) inhibitor. Wearing off may be also better controlled by shortening the time between medication doses. In a study of 23 PD patients in both the 'on' and 'off' states compared to 28 controls, L-dopa had a positive effect on motivation suggesting striatofrontal loops are involved.32
Involuntary emotional expression disorder
Epidemiology
Involuntary emotional expression disorder (IEED) has been found to occur in 16.8% of PD patients, and in 15.3% if comorbid depressive disorder was excluded.33 However, other studies suggest that the symptoms of IEED are present in up 15% of PD patients but the actual IEED disorder occurs in half of these cases.34 This implies that IEED symptoms occur in PD but the condition of IEED is not present although this may depend on the criteria used for the diagnosis. If IEED does develop in PD it is particularly common in the later stages of PD and is likely to be distinct from depressive disorderwhich remains an important differential diagnosis.33, 35
Aetiology and risk factors
IEED can occur in neurological conditions such as stroke, traumatic brain injury, amyotrophic lateral sclerosis, multiple sclerosis, seizure disorders, multiple system atrophy, corticobasal degeneration, and Alzheimer’s disease.35 Injury to the neurological pathways that control the expression of emotion have been implicated in its pathogenesis. Emotional expression involves various pathways within the frontal lobe, limbic system, brainstem and cerebellum, with disruption of regulatory and inhibitory mechanisms in this network implicated.36, 37
Presentation and diagnosis
IEED is described as sudden episodes of laughing or crying that may be spontaneous or disproportionate to the triggering stimuli.The emotional outbursts of IEED may involve laughter, crying or anger. The episodes all share common features in that they are involuntary, uncontrollable, and excessive, not sustained, and usually last from seconds to minutes. Outbursts are often stereotyped though single individuals may have episodes of both laughing and crying.IEED is also known as pseudobulbar affect, pathological laughter and crying, emotional lability, emotionalism, and emotional dysregulation.Despite the various terms used to describe the disorder, IEED is often missed and even sometimes mistaken for depression.33, 35 Symptoms of IEED are important because they are associated with an impairment of social and occupational functioning.38 It is hypothesized that neurological disease and injuries affect the excitatory action of glutamate, leading to excessive glutaminergic signalling and increased electrical activity in neurons. As glutamate is the primary excitatory neurotransmitter of the central nervous system, stabilizing or reducing glutaminergic activity could prove useful in the treatment of IEED.39
Treatment
Medication options include the use of SSRIs, tricyclic antidepressants (TCAs) for example, amitriptyline, and less frequently dopaminergic agents.A combination of dextromethorphan and quinidine has also been suggested. 35 38
Sleep disorders
Epidemiology
Sleep disorders have been known to affect 60-98% of patients with PD.40
Aetiology and risk factors
The aetiology of sleep disorders includes PD itself or other comorbid conditions such as depression, and cognitive impairment.41 Nocturnal pain from rigidity or dystonia, restless legs syndrome, and autonomic disturbance leading to nocturnal frequency and urgency, also contribute to insomnia. Degeneration of sleep regulatory centres in the brainstem and thalamocortical pathways, side effects of drugs, motor impairment, and incontinence may affect sleep. Sleep disorders may precede the onset of motor symptoms. Rapid Eye Movement (REM) sleep behaviour disorder (RBD), which occurs in almost a third of PD patients,is often associated with cognitive impairment and hallucinations. This disorder is directly related to the degenerative process of the pedunculopontine nucleus, the locus subceruleus and the retrorubral nucleus. A sudden onset of the disorder is almost always due to the introduction or the withdrawal of drugs, especially antidepressants. Curiously, parkinsonism can disappear during the RBD.42
Sleep fragmentation is the earliest and most common sleep disorder in PD, and gradually worsens as the disease progresses. Vivid dreaming, nightmares and night terrors are common and occur in up to 30% of patients using levodopa for long periods. Dream content is probably altered in PD and many patients vocalize during sleep. Vocalization may vary from incomprehensible sounds to detailed conversations, laughing, cursing or screaming. Excessive daytime sleepiness and 'sleep attacks' affect half of patients with PD and may precede disease onset. The causes are a combination of the disease process, the consequence of other sleep disorders and medication. A sudden onset of sleep during the day is a phenomenon in PD which resembles narcolepsy, and it is commonly associated with dopaminergic drugs. PD patients may be more prone to restless legs syndrome, periodic limb movements and obstructive sleep apnoea.
Sleep disorders in PD are seldom diagnosed and treated. Although an accurate diagnosis of a particular sleep disorder depends on polysomnography, sometimes the diagnosis can be based on clinical observation. Treatment is based on the correct diagnosis and underlying cause of the sleep disorder. Often it is difficult to decide whether excessive daytime sleepiness is cause or consequence of insomnia.43
Presentation and diagnosis
Sleep disorders may manifest as insomnia, excessive daytime sleepiness and sleepwalking.44, 45 Sudden attacks of sleepiness are known to occur during stimulating activities such as walking, eating, and even driving a car. These sudden sleep episodes can be associated with medication such as dopamine agonists and levodopa.46
RBD is characterised by the loss of the normal atonia during dreaming. In other words, patients act out their dreams as manifested by crying out, kicking or thrashing about during their sleep. RBD can predate the development of motor symptoms by several years and a longitudinal study of a cohort of 26 patients found an association between RBD and the later development of PD. 47
Treatment
Management involves the review of medication that may be contributing to the sleep disorder. Treatment of comorbid conditions such as depression and cognitive impairment is essential.
Sleep hygiene is the initial and basic measure applied to all patients. For instance, stimulating patients during the day can decrease the excessive naps and improve sleep at night, thus improving daytime sleepiness. Additional techniques include going to bed only when sleepy, exposure to natural and bright light during day, reduction of light and noise exposure at night as much as possible, and maintenance of a regular schedule.
Long-acting dopaminergic drugs might improve insomnia caused by worsening of motor symptoms at night. Clonazepam, a benzodiazepine, is efficacious and well tolerated by the majority of patients afflicted by RBD and should be considered as initial treatment.48 Antidepressants with a sedative effect might be helpful in cases of insomnia with comorbid depression or anxiety. Quetiapine, an antipsychotic which has sedative properties as a side effect, may be a safe and effective treatment for insomnia in PD because it has no untoward effects on motor function.49 Small clinical trials with Modafinil for excessive daytime sleepiness had controversial results. An additional remark concerning treatment of sleep disorder in PD is that sleep may provide a short-term benefit on motor symptoms.28, 43
Impulse control disorders
Epidemiology
A large multi-centre investigation (the DOMINION study) of 3,090 patients with PD revealed that impulse control disorder (ICD) was identified in 13.6% of PD patients; specifically, pathological gambling in 5%, compulsive sexual behaviour in 3.5%, compulsive buying in 5.7% and binge-eating disorder in 4.3%.50 The prevalence of ICD rises to 14% for patients taking dopamine agonists, compared with 0.7% for patients taking levodopa alone.51 It is not clear whether these ICD symptoms reflect a primary pathology of PD or whether dopaminergic medication is interacting with an underlying predisposition or vulnerability.52 Possible neurobiological explanation centres around dopamine-receptor binding profiles. Dopamine D2 and D1 receptors, abundant in the dorsal striatum, may mediate the motor effects of dopamine replacement therapies, whereas D3 receptors are abundant in the ventral striatum, a brain region associated with addictive behaviour and substance misuse disorders. Second generation non-ergot dopamine agonists (e.g. pramipexole and ropinirole) demonstrate relative selectivity for D3 receptors compared with D2 and D1 receptors.50
Aetiology and risk factors
Addiction to dopaminergic medication used in the treatment of PD may explain behaviours such as drug-seeking, gambling, and hypersexuality. The risk of pathological gambling increases if dopamine agonists are used in those with younger age of onset, higher novelty seeking traits, and a personal and family history of alcohol misuse.53
Presentation and diagnosis
In addition to the above PD patients with ICD may present with compulsive shopping, compulsive eating, and compulsive medication use, all of which can have potentially devastating psychosocial consequences because they are often hidden. Complex stereotyped repetitive behaviours (punding) may also be present.54Punding behaviour is stereotyped and purposeless and includes hoarding, shuffling papers, sorting labels, assembling and disassembling objects, to name a few.
Treatment
Stopping dopaminergic medication should be considered in the first instance. Further treatment options are limited but one double-blind crossover study demonstrated the use of amantadine in abolishing or reducing pathological gambling.55 In addition, one case report suggested the antipsychotic quetiapine to be effective in treating pathological gambling.56 Whether other treatments, such as DBS, are effective for these compulsive repetitive behaviours, remains to be seen.
Management of overlooked neuropsychiatric syndromes in PD
Because of the significant disability and impact on quality of life caused by overlooked neuropsychiatric symptoms in PD, it is important for neurologists and psychiatrists to recognise them and develop their clinical skills in order to be aware of their significance. Early detection is crucial. We have shown there is a limited range of treatment strategies available to guide the clinician in treatment choices. Because neuropsychiatric diagnoses in PD are different in phenomenology it is important to remember that treatment with 'psychiatric' drugs will often be insufficient and therefore more consideration should be given to 'antiparkinsonian' medications because the underlying pathology of PD is causing the various syndromes mentioned.
Table 3 provides an overview of the medical treatment of overlooked neuropsychiatric syndromes in PD, although it should be noted that overall very few studies document the effectiveness of the solutions proposed and more controlled studies are needed. Nonetheless, the reader should find the following useful.
Table 3. Summary of the medical treatment of overlooked neuropsychiatric syndromes in Parkinson’s Disease.
- Possible use of amantadine or quetiapine in pathological gambling - Further research required
Conclusion and implications
The management of PD is often complicated because of the diverse factors underlying its aetiology. Dopaminergic, serotonergic, noradrenergic and cholinergic pathways are involved.57 Clinicians are generally competent in recognising the more common disorders such as depression, psychosis and cognitive impairment associated with PD though there is a tendency to focus too much on these at the expense of other nonmotor symptoms. Anxiety, apathy, involuntary emotional expression disorder, sleep disorders, and impulse control disorders cause significant disability and impact heavily on patients and carers.
Before introducing treatment for psychiatric complications it is essential to exclude causes such as antiparkinson’s medication, DBS (implicated in apathy), and underlying medical conditions. Once excluded or treated, subsequent management includes psychotropic pharmacotherapy but there are limited options. With no specific drug designed to treat the overlooked conditions, a wide range of medications (e.g. antidepressants, antipsychotics, benzodiazepines, dopaminergic agents, and psychostimulants) are available to manage the symptoms.
Neurologists and psychiatrists need to work together to manage these syndromes and they must be innovative in setting up joint research ventures into developing treatment options. Simple questionnaires may alert physicians when presenting symptoms are abstruse because many of the nonmotor symptoms predate the motor symptoms58 (the presymptomatic phase of stages 1-2 of Braak's classification system).59 60 For example, anosmia, constipation and other autonomic symptoms are not considered neuropsychiatric syndromes per se, but are some of the nonmotor problems associated with PD and may give clues that PD is developing.
Despite research highlighting the presence of these disorders in PD, they generally go unrecognised by clinicians, being less common, and therefore psychiatrists in old age and adult psychiatry as well as general neurologists may lack skills to recognise them. Besides, there are no clear treatment guidelines on how to manage the conditions.
Trigeminal Neuralgia (TN) is relatively rare in Multiple Sclerosis (MS) affecting approximately 2% of patients1. The severity of the pain is indistinguishable whether TN is an isolated impairment or is associated with MS. However, when associated with MS, TN is often bilateral, affecting younger patients and is more refractory to medical treatment 2.
Several pharmacological agents are reported to be effective in TN associated with MS. Topiramate3,4, gabapentin5 and lamotrigine6 were all reported to benefit patients with TN associated with MS in small uncontrolled trials. Several other drugs such as phenytoin, misoprostol and amitriptyline are routinely tried in patients with TN despite the lack of convincing evidence of their efficacy7.
In 2008, Both the American Academy of Neurology and the European Federation of Neurological Societies launched joint Task Force general guidelines for the management of TN. After systematic review of the literature the Task Force came to a series of evidence-based recommendations 8. Carbamazepine and oxcarbazepine had the strongest evidence of efficacy and were recommended as the first line treatment. An earlier Cochrane systematic review reached the same conclusion. 9.
Case report
A 62 year old female patient had been suffering from MS for about 20 years. The MS presented with trigeminal neuralgia from the outset and this was then followed by pyramidal lower limbs’ weakness and sphincteric dysfunction. The patient started to use a wheelchair 10 years ago but she became totally wheelchair dependent about 6 years later.
Trigeminal neuralgia remained active throughout the 20 years. Carbamazepine (300 mg daily) provided the patient with a satisfactory control of TN. Despite having occasional break through TN pain; the patient declined having higher doses of carbamazepine as excessive sedation was an unacceptable side effect.
Recently; the patient was admitted to hospital in two separate occasions complaining of increasing malaise and confusion. Plasma sodium levels were found to be low in both occasions (first presentation 118 mmol/l and second admission 114 mmol/l). Clinical evaluation confirmed Syndrome of Anti Diuretic Hormone Secretion (SIADH) as the cause of the hyponatremia and in the absence of any other explanation for the SIADH; carbamazepine was thought to be the main reason and was duly discontinued.
Unfortunately, TN attacks came back with vengeance. During the following 6 months, therapeutic trials using gabapentine, topiramate and amitriptyline failed to show any beneficial effect on either the severity or the frequency of the TN attacks. All three drugs were duly discontinued.
The patient was started on eslicrbazepine 400 mg on a single daily dose. This dose lead to almost complete eradication of the TN attacks. The control of TN and the plasma sodium levels remained stable a year following the initiation of the therapy.
Comments
Hyponatremia, defined as a sodium level < 135 mmol/l is a common side effect of carbamazepine and oxcarbazepine therapy. The incidence of hyponatremia secondary to carbamazepine therapy ranges between 4.8 and 40 % depending on the population studied10,11. In most cases, hyponatremia is asymptomatic and continuation of the carbamazepine use is possible whilst a close eye is kept on the plasma sodium level10. In rare occasions hyponatremia is symptomatic and discontinuation of carbamazepine is warranted. Administration of demeclocycline to normalise the sodium level was suggested by some authors12 However, the long term use of demeclocycline is associated with several complications and this approach is hardly a standard practice.
Clinicians often face a dilemma when carbamazepine is the only agent able to control a specific clinical problem. With many antiepileptics available, it is unusual to face such a problem in epileptic patients. Trigeminal neuralgia on the other hand can be extremely difficult to control and carbamazepine was found to have a unique ability to manage such unpleasant condition even before its antiepileptic effects were noticed on 196213.
Eslicarbazepine is promoted as an alternative to carbamazepine when side effects occurs on otherwise responsive patients to its favourable antiepileptic effects14. Hyponatremia is rare in eslacarbazepine users with only an incidence of less than 1% in the small populations studied15,16. Frequency of hyponatraemia increased with increasing eslicarbazepine dose. In patients with pre-existing renal disease leading to hyponatraemia, or in patients concomitantly treated with medicinal products which may themselves lead to hyponatraemia17.
Our patient showed the same favourable response to eslicarbazepine as she experienced with carbamazepine. However, hyponatremia did not occur with eslicarbazepine therapy. This enabled our patient to continue with pharmacological management and avoid surgical interventions.
With the exception of epilepsy, no reports are available commenting on the use of eslicarbazepine on the wide range of conditions that carbamazepine is traditionally used for such as mental health problems and neuropathic pain. When patients are well controlled on carbamazepine whatever the indication is, the occurrence of side effects such as hyponatremia is often managed by an automatic replacement with another agent. We feel that in such patients a therapeutic trial of eslicarbazepine might be appropriate especially if the control on carbamazepine was robust or if the benefits of carbamazepine therapy were clearly superior to other pharmacological agents potentially useful for the targeted clinical condition.
Driven by a global rise in opioid dependence, Opioid Substitution Treatment (OST), the prescribing of opioids (usually methadone or buprenorphine) as maintenance treatment, has expanded worldwide over the last two decades3. Participation in OST reduces the risk of death by overdose4, reduces the risk of HIV transmission5 and reduces participants’ involvement in property crime6. For these reasons, maintenance with methadone remains the major public health response to reduce the harms caused by heroin addiction.
In the United Kingdom (UK) in the late 1990s, government funding to expand access to OST was provided, with the explicit objective of reducing crime7. The expansion of treatment was supported with clinical guidelines2, and targets were set to try to ensure good outcomes. Given the research evidence on the importance of retention in producing better outcomes, service providers were set a target of retaining at least 75% of people in treatment for 3 months. A tool to monitor outcomes, the Treatment Outcomes Profile (TOP)8, was developed and service providers nationally were set a target of 80% of people in OST completing TOP at entry and after 6 months9. This 20-item self-report questionnaire records a set of core data for the previous 28 days, including the number of days on which heroin and cocaine have been used.
The amount of methadone prescribed in England and Scotland increased fourfold over the decade 1998 – 20083. However, in 2010, Britain’s newly-elected government signalled a change in the direction of drug policy1. The paradigm on which the new policy is based is “recovery”, a concept embracing self-help, mutual support, and optimism about the possibility of positive change. The policy is in part driven by the perception that treatment services have a defeatist attitude, expecting little positive change – hence the claim that there are too many patients “parked on methadone”. To counteract this perceived pessimism, the “recovery agenda” includes incentives to services to promote abstinence from all drugs including prescribed OST medication. This policy has been criticized as being inconsistent with the available evidence10, but has been defended on the grounds that many patients on methadone were doing poorly, and needed encouragement to make positive changes in their lives.
In 2010, we decided to investigate to what extent people were responding poorly to treatment, and whether this could be improved by implementation of evidence-based treatment.
Methods
This quality improvement project was undertaken in two OST clinics in Merseyside, managing in total over 1000 patients. The services had the same senior leadership and medical staff, but separate teams of nurses and key workers. Supervised administration was provided by local retail pharmacies.
In October 2010 key workers were provided with list of patients currently under their care and asked to identify patients they thought were using heroin regularly. A research assistant then checked case notes of identified patients, looking at self-reported heroin use as recorded in TOP monitoring forms, and at the results of previous urine toxicology tests. Those whose most recent TOP was performed at entry to treatment were excluded (since their self-reported heroin use covered a time when they were not in treatment). Among the remainder patients reporting use of heroin on at least 8 days in the 4 weeks preceding their last TOP interview were classified as “non-responding” patients. The case notes of all identified “non-responders” were reviewed using an audit tool covering age, sex, postcode, date of entry into treatment, duration of treatment, dose of medications, extent of supervised administration, dates and results of recent urine toxicology, and date and self-reported drug use from previous TOP questionnaires. This data was collected at baseline and again at re-audit (follow-up) 9 months later.
Postcodes were used to derive Index of Multiple Deprivation (IMD) scores11. The English index of multiple deprivation (IMD) is a measure of multiple deprivations, with domains including employment deprivation, health deprivation and disability, education skills and training deprivation, barriers to housing and services, living environment deprivation, and crime.
In one clinic, the “implementation clinic”, beginning January 2011, key workers were asked to refer all non-responders for a medical review. Patients were also screened for comorbidity, taking advantage of a separate project running concurrently which was designed to test the psychometric properties of a new questionnaire on mental health and well-being. All service users at the implementation clinic were invited to take part. The study had National Research Ethics approval and approval from the Merseycare NHS Trust R&D Office. Quality of life was assessed with the EQD12 which comprises 5 domains measuring health-related quality of life: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Depression was screened for with the Beck Depression Inventory13.
UK guidelines recommend for patients doing poorly “..ensuring medication is provided within evidence-based optimal levels, changing to another substitute medication, increasing key working or psychosocial interventions and increasing supervised consumption” 3. The recommended dosage for effective treatment is listed as in the range 60-120mg/day of methadone. At medical review, the plan was for the doctor to assess the non-responding patients, and propose raising methadone dose progressively until heroin use ceased, or a maximum dose of 120mg/day was reached; and requiring supervised consumption of methadone for patients persisting in heroin use.
Establishing the medical reviews in one of the two clinics was necessary for logistic reasons, but it also allowed an opportunity to assess the impact of the reviews, by comparing the outcomes of non-responders in the two clinics. If effective, it was proposed to extend this approach to the second ‘treatment as usual’ service. Referrals for medical review ceased in June 2011, and over the next three months staff feedback about the process was sought. In October 2011 a repeat audit of case notes including TOP results of all previously identified non-responders at both services was undertaken.
At follow-up data on the frequency of medical appointments in the preceding 6 months were also collected. In cases where people had left treatment, the TOP performed on exit from treatment was used. Those non-responders who had left treatment were identified and tabulated according to the reason for leaving treatment.
Flowchart 1: The audit and re-audit process
Ethics
The audit was approved by the local NHS Trust R&D Office. Funding was obtained to undertake the work by Mersey Care NHS Trust.
Analysis
Data was entered into SPSS version 18 (for windows). Summary statistics and standard hypothesis tests compared non responders in the intervention service to non responders in treatment as usual to ensure there were no statistically significant differences between the two groups at baseline. Chi-square and t-tests compared age, sex distribution, IMD scores, methadone dose and months in treatment this episode. Mann-Whitney U tests compared the number of TOP forms completed in each group during the previous 6 and 12 months. Regression analysis explored whether there was a relationship between attendance for supervised administration, self-reported quality of life and depression for non responders in the implementation group. Differences in baseline and at 9 month re audit methadone dose and heroin use were tabulated for each group. Mann-Whitney U-tests compared any differences between the two groups. Differences within each group were also compared using the Wilcoxon signed ranks test.
Results
The implementation service managed 534 patients, of whom 130 (24%) were initially identified as non-responders, reporting heroin use on 8 or more days in the previous month at their last TOP interview. At the TAU service there were 485 patients, of whom 112 (23%) were identified as non-responders. Of the 242 non-responders in total, 67 (28%) were new to treatment, and were excluded. This is illustrated in the flowchart 2.
Flowchart 2: Sample Algorithm
Approximately 50% of the non-responders in each group reported daily heroin use at baseline. The two groups of non-responders did not differ significantly in terms of age, sex distribution, nor on the Index of Multiple deprivation scores (mean of 62 reflecting very severe social exclusion across both groups). Non responders in the implementation service had been in treatment a median of 18 months compared to 17 months for those in treatment as usual. Urine testing was performed infrequently in both services, but a result was available from the six months prior to baseline for 133 of the remaining 175 subjects. The urine tests results were broadly consistent with the patients self-report. Aspects of treatment at the two services differed, as shown in Table 1. At baseline, doses did not differ significantly, but the treatment as usual group was significantly less likely to have their methadone administration supervised, and had less frequent TOP monitoring.
Table 1 Profile of non-responders and their treatment at baseline
Implementation
TAU
Total
N
104
71
175
Mean age in years (min, max)
42 (25,66)
43 (23,63)
42 (23,66)
Male (%)
65 (63%)
48 (68%)
113 (65%)
Mean IMD Score (SD)
62 (14.6)
62 (14.7)
62 (14.7)
Mean methadone dose in mg (SD)
60 (17.8)
60 (21.3)
60 (20.3)
Median Months in this Rx episode (IQR)
18 (20)
17 (10)
18 (14)
Any supervised doses
56 (54%)
22 (31%)*
78 (45%)
Last TOPS > 6/12 ago
15 (15%)
29 (42%)**
44 (25%)
*Pearson Chi square 9.995, df=2, p=0.007 **Mann-Whitney U =2654, p=0.002
Despite almost all non-responders being booked in for an appointment and given reminders at the implementation service, only 47 (45%) of the 104 identified attended at least one medical review. Keyworkers commented that the main reason for non-attendance was that clients were quite happy continuing heroin use and did not see stopping as something they wanted to do. When patients were told they would only receive their prescription renewal after attending, some patients chose to go without methadone and make contact a few days later, rather than attend an appointment. Among those who did attend, there was frequently resistance to increasing their methadone dose, and anger at the suggestion that medication administration should be supervised. Word of mouth spread through the service that doctors were proposing dose increases and more supervision. This increased resistance among patients, and appears to have generated some resistance among keyworkers, some of whom saw their role as advocates for the patients.
The attempt to implement change in one clinic appears to have had small effects in increasing average doses there, and having more patients seen by a doctor. Between baseline and 9 month re-audit (follow-up), mean methadone doses increased in the implementation group and fell in the TAU group, as shown in Table 2. There was a small and statistically significant increase in methadone dose in the implementation group compared to the TAU group. The difference in change in methadone dose between the two groups was statistically significant (Mann-Whitney U= 2745, p=0.002), but the mean dose increase (3mg) in the implementation group was small. In the 6 months prior to the collection of follow-up data, medical reviews in both services were infrequent; 36% of patients in the implementation group and 66% of patients in the TAU group had not seen a doctor in their OST service (Chi square =13.38, df=1, p=0.001).
In both groups, the reductions in heroin use over time were statistically significant (Wilcoxon signed ranks test p = <0.05), but the change in heroin use over time did not differ significantly between the two services (Mann-Whitney U 2832.5, p=0.7). The changes from baseline audit to 9 month re audit are shown in Table 2. Among the 47 patients who attended a medical review, the mean prescribed methadone dose rose from 58 to 66mg/day, but the number receiving supervised doses actually fell, from 23 at baseline to 20 at follow-up. Mean days of reported heroin use fell from 20 to 12 (6 patients reported abstinence) – changes almost identical to what was observed in the TAU group.
Table 2 Changes in dose and heroin use between baseline (T1) and follow-up/re audit (T2)
Implementation
TAU
Time 1
Time 2
Time 1
Time 2
N
104
103
71
68
Mean Self-report heroin days/28 (SD)
19.9 (8.6)
13.4 (10.8)
19.6 (8.3)
11.7 (10.8)
Reported daily heroin use
52 (50%)
33 (32%)
25 (42%)
17 (25%)
Heroin abstinence
-
14 (14%)
-
15 (22%)
Urine test positive morphine %
88%
76%
85%
70%
Mean daily methadone dose
59.5
62.9
60.1
57
Proportion self-report cocaine
67%
54%
53%
44%
Urine test cocaine positive
66%
57%
58%
45%
29 non responders (28%) from the implementation service, and 27 (38%) from the TAU service had left the service between baseline and 9 month re audit. Most discharges (31/56) were transfers to another service as part of a local policy to move more people into treatment in primary care. Eight patients from the Implementation service dropped out of treatment, and 4 patients from the TAU service did so. Differences in the pattern of leaving the two services did not approach significance.
Table 3 Reason for discharge
Reason
Implementation
TAU
Total
Transfer of Rx
13
17
30
Did not attend (DNA)
8 (28%)
4 (15%)
12
Elective Withdrawal
3
3
6
Deceased
2
0
2
Prison/drug diversion program
3
3
6
Total
29
27
56
44 non responders who attended a medical review at the implementaion service completed questionnaires on health, quality of life, and depression. Ninety-six percent were not in education, employment or training (NEET). On the Beck Depression Inventory, 50% of respondents reported depression in the moderate to severe range. Regression analysis indicated that having to attend for supervised doses was associated with less depression measured on the BDI (r=-.332, p=0.039), and with better quality of life in terms of EDQ scale of self-care (r=-.598, p<0.001) and being able to undertake usual activities (r=-.605, p<0.001).
Discussion
Many people persisting in heroin use were receiving care that was out of line with guidelines – doses below 60mg, often with no supervised doses, and seldom attending for medical reviews. However, the attempt to systematically implement guidelines was not effective. Most patients did not attend, and many of those who did attend resisted changes. Although patients who attended received slightly higher doses, changes in heroin use in the subset who actually attended for review were no different to the changes observed in the TAU group.
Higher methadone doses, and patients having control over their doses, have been shown in a meta-analysis to be independently predictive of better outcomes14. One possible explanation for the failure to implement guidelines is that it may have been perceived as challenging clients’ control over their treatment. If so, it was a challenge easily defeated. Patients clearly had substantial control over their treatment, choosing whether to attend appointments, whether to accept higher doses, and whether to accept supervised doses. However, this degree of control over their treatment did not appear to be beneficial. “Non-responders” reported depression, disability and a poor quality of life.
Guidelines need to move beyond systematic reviews of effectiveness, to include evidence about implementing evidence in a real world setting15. Our conclusion is that the failure to implement guidelines was that the approach adopted was not congruent with clinic culture, which emphasised “support” rather than “structure”. “Structure” refers to both cognitive and behavioural elements of treatment. The cognitive elements are defined and agreed objectives, a sense of the direction and purpose of treatment. In all areas of mental health, clinical interactions are most useful if focused on specific performance goals related to the patient’s circumstances16. In the OST services studied, there appeared to be a focus on process and on supporting patients, rather than achieving outcomes.
Structure also includes behavioural elements - expectations and rules regarding attendance, and daily attendance for supervised administration. Interviews with UK patients in OST have indicated that they understand and value the role of supervision, not only in minimizing diversion and misuse, but in providing an activity for many people without social roles17. Consistent with the benefits of supervision, in the current audit more supervision was associated with less depression and less-poor quality of life.
This audit had several limitations. It did not attempt to measure the proportion of patients responding poorly to long-term methadone treatment, and it is possible that the true proportion may be higher than the 17% identified by key workers. Documentation of treatment outcomes, using TOP reports and UDS results, was unsystematic, limiting the number of patients in whom complete data was available. “Non-responders” self-reported heroin use to keyworkers, who administered the TOP questionnaire, and there may have been under-reporting. However, while this study may not have identified all non-responding patients, this does not invalidate the observation that attempting to implement guidelines was not successful.
Most importantly, the observations from these clinics may not be generalisable to other treatment settings. However, certain key data are available suggesting the treatment and outcomes observed in this study were not atypical. A report on national TOP monitoring noted patchy availability of follow-up data, and confirmed a high rate of persisting heroin use in treatment, with 38% of participants reporting abstinence from heroin18. Despite this high rate of heroin use, a recent survey reported a mean dose of 56mg of methadone in a national survey19. In this regard, the clinics in this report thus seem representative.
Medical staff appeared to have a peripheral role in delivery of OST in these clinics. Most non-responders did not have a medical review in 6 months – despite persisting heroin use, and self-reported depression. In the 1980s in the US, methadone treatment underwent a process labelled “demedicalisation”, marginalisation of the role of medical practitioners, and a loss of the sense that methadone was a medical treatment with clearly defined objectives and guidelines20. This contributed to a situation in which much methadone treatment in the US was out of line with research evidence21. The current audit suggests that a similar process of demedicalisation and deviation from evidence-based treatment has been occurring in some NHS services in the UK.
If these observations are representative of at least some treatment culture in the UK, they lend support to the criticisms made of methadone treatment in the new UK drug strategy1. To the extent that the recovery agenda challenges clinic culture and shifts the focus of treatment onto outcomes, it is a positive development.
However, many well-intentioned policies have unintended consequences, and there are well-based fears that the new policy promoting abstinence from OST as an objective of recovery will lead to an increase in overdose deaths3. This is specifically because of the risk of overdose deaths after leaving treatment. The reason for the increased risk of overdose after leaving treatment is that newly abstinent addicts who have reduced opioid tolerance, and a dose of heroin they previously used during periods of addiction becomes a potentially fatal dose once they are abstinent. This risk attaches to all forms of drug free treatment, as well as to patients who have left methadone. The critical issue is that lapses to heroin use, and relapses to dependent heroin use, are very common among newly-abstinent addicts. It is the high probability of relapse to heroin use which is the basis of long-term maintenance treatment – better to keep people safe and functioning normally, albeit while still taking a medication, than the risk of relapse and re-addiction, or relapse and fatal overdose. In the UK, implementation of the recovery agenda has included incentives to abstinence, and this is not consistent with evidence about the risk of relapse. If the recovery agenda can accommodate the evidence that indefinite maintenance as a valid option for many, perhaps most heroin users, then the evidence of this study is that far from being in contradiction, the recovery agenda may facilitate the implementation of evidence-based practice.
A 29 year-old woman had been well until 7 months previously when, after a viral syndrome, she developed palpitations, fatigue, and frequent episodes of light headedness and near syncope. On further questioning she notes exercise intolerance and dyspnea on exertion. She has stopped working as cashier. Her mother thinks she is having panic attacks and needs “something to calm her nerves.” ECG, echocardiogram, and endocrine evaluation are all normal. On physical examination, she displayed a postural heart rate increase of 35 beats per minute on standing, along with a 15mmHg fall in diastolic blood pressure.
Introduction
Disorders of the autonomic nervous system present unique challenges to the practicing clinician. These syndromes have a significant impact on quality of life, offer subtle diagnostic clues, and have a propensity to mimic other disease processes. For these reasons clinicians should have basic familiarity with the differentiating features of autonomic disorders. While much investigation has focused on Neurocardiogenic syncope, a distinct subgroup has emerged characterized by postural tachycardia and exercise intolerance. Postural orthostatic tachycardia syndrome (POTS) is the final common pathway of a heterogeneous group of underlying disorders that display similar clinical characteristics .1
The constellation of symptoms associated with POTS reflects underlying dysautonomia including palpitations, exercise intolerance, fatigue, lightheadedness, tremor, headache, nausea, near syncope, and syncope. Foremost amongst these is orthostatic intolerance. Besides being limited in the functional activities of daily living, increased sleep disturbances including excess daytime sleepiness, fatigue are also common and have been associated poor health-related quality of life. 2 We aim to discuss the clinical presentation, classification, evaluation and management of POTS.
Diagnosis
The current diagnostic criteria for POTS is the presence of orthostatic intolerance symptoms associated with a sustained heart rate increase of 30 beat per minute (bpm) or absolute rate exceeding 120 bpm within the first 10 minutes of standing or upright tilt in the absence of other chronic debilitating disorders, prolonged bed rest, or medications that impair vascular or autonomic tone. 3 Most patients will have orthostatic symptoms in the absence of orthostatic hypotension (a fall in BP >20/10 mmHg). A grading system for POTS has been developed (Table 1). This system focuses on the functional severity of orthostatic intolerance in a way similar to the NYHA heart classification.
The physical exam should be methodical and directed. Supine, sitting, and immediate standing heart rate and blood pressure should be recorded. Orthostatic tachycardia and acrocyanosis of the lower extremities may be the only physical signs in these patients. Standing and supine blood pressure measurements and baseline electrocardiogram are generally recommended. In patients with physical examination or clinical history suggestive of cardiovascular abnormalities, other diagnostic test including echocardiogram , stress test or coronary angiography may be indicated before a tilt test. In addition, other possible clinical disorders with similar clinical manifestations must be kept in mind and ruled out. Upright tilt test remains the diagnostic test of choice for POTS and other autonomic disorders. Implantable loop recorders, electrophysiological tests and Holter monitoring are not helpful in the evaluation of these disorders. Supine and upright serum catecholamine levels should be obtained if hyperadrenergic type is suspected. In the presence of gastrointestinal symptoms bowel motility studies may reflect the degree of involvement and help to tailor therapy. 4
Table 1 : The Grading of Orthostatic Intolerance*
Grade 0 Normal orthostatic tolerance
Grade 1 Orthostatic symptoms are infrequent or occur only under conditions of increased orthostatic stress Subject is able to stand >15 minutes on most occasions Subject typically has unrestricted activities of daily living
Grade II Orthostatic symptoms are frequent, developing at least once a week Orthostatic symptoms commonly develop with orthostatic stress Subject is able to stand >5 minutes on most occasions Some limitation in activities of daily living is typical
Grade III Orthostatic symptoms develop on most occasions and are regularly unmasked by orthostatic stresses Subject is able to stand for >1 minute on most occasions Patient is seriously incapacitated, being bed or wheelchair bound because of orthostatic intolerance Syncope / presyncope is common if patient attempts to stand
*Symptoms may vary with time and state of hydration and circumstances. Orthostatic stresses include prolonged standing, a meal, exertion, and head stress.
Classification and Clinical Features
POTS is a heterogeneous group of disorders resulting in a common clinical scenario. This syndrome is classified as being either primary or secondary. Primary POTS is idiopathic and not associated with other disease processes. Secondary POTS occurs in association with a known disease or disorder. Subtype classification affects management and is therefore essential.1,4 (Figure 1)
Partial dysautonomic (PD) POTS (also referred to as Neuropathic POTS) is the predominant form.1, 2 This is a mild peripheral autonomic neuropathy, characterized by inadequate peripheral vasculature constriction in the face of orthostatic challenge. Female predominance is seen with 5:1 female to male ratio. Presentation is commonly abrupt onset of symptoms after a febrile viral illness, pregnancy, immunization, sepsis, surgery, or trauma. The etiology of PD type POTS is postulated to be an autoimmune molecular antigen mimicry type pathogenesis. Serum autoantibodies to peripheral autonomic ganglion alpha-3 acetylcholine receptors may be positive in 10-15% of the cases. Anhidrosis of lower extremities is seen in more than 50% of these patients at quantitative sudomotor axon reflex testingDependent blood pooling when upright is greater than normal and heart rate and contractility increase as normal compensatory physiologic mechanisms to maintain cerebral perfusion. This autoregulatory response may initially be fully compensatory; however, peripheral venous pooling may increase with time and exceed this compensatory effect. Patients with PD type POTS become dependent on the skeletal muscle pump to augment their autoregulatory physiology. Ultimately, venous blood pooling increases beyond the body’s total ability to compensate and adequate blood pressure maintenance fails.
“Developmental” partial dysautonomic POTS is an adolescent subtype.6 The mean age of onset is 14 years. The clinical scenario is that of orthostatic intolerance following a period of very rapid growth. Symptoms are progressive and peak at a mean age of 16 years. Orthostatic intolerance may be severe, including severe headaches, and can be functionally disabling. Following their peak symptoms will slowly improve and resolve into young adulthood (19-24 years). Roughly 80% of patients with developmental PD POTS will experience complete resolution of symptoms. The etiology of this subtype is unclear and appears to be a transient period of autonomic imbalance occurring in rapidly growing adolescents.
Hyperadrenergic POTS is less common than the PD type ,7This form is characterized by a gradual onset with slowly progressive symptoms. Patients report experiencing tremor, anxiety, and cold clammy extremities with upright posture. 7 Many patients note increased urine output when upright. True migraine headaches may be seen in over half of patients.7 Gastrointestinal symptoms in the form of recurrent diarrhea were seen in 30% of the patients. In contrast to PD type of POTS, the hyperadrenergic form demonstrates elevated serum catecholamine levels with serum norepinephrine levels >600ng/ml. This may be a familial syndrome in some instances determined by a careful history. The etiology of hyperadrenergic POTS is felt to be genetic with a single point mutation resulting in a dysfunctional norepinephrine reuptake transporter protein present in the intrasynaptic cleft. The result is excessive norepinephrine serum spillover with sympathetic stimulation resulting in a relative hyperadrenergic state appearing similar to pheochromocytoma. 8
A connective tissue disorder has been an increasingly recognized etiology of secondary POTS 9 . Joint hypermobility syndrome (JHS) is an inherited condition characterized by joint hypermobility, connective tissue fragility, and soft velvety skin with variable hyperextensibility. The condition is associated with ecchymotic predisposition, premature varicose veins, diffuse muscle and joint pain, and orthostatic acrocyanosis. The etiology of POTS in JHS patients is thought to be due to abnormal vascular (venous) elastic connective tissue. During orthostatic stress and increased hydrostatic pressure these patients exhibit increased vessel distensibility and orthostatic intolerance. Excessive peripheral venous pooling and compensatory tachycardia follows. Up to 70% of JHS patients suffer from some degree of orthostatic intolerance. It is observed that adolescent PD POTS patients have features similar to JHS patients and further studies may determine the significance of this potential relationship 10.
Secondary POTS refers to a group of conditions which result in peripheral autonomic denervation with sparing of cardiac innervation. Most commonly, secondary POTS is associated with diabetes mellitus. Less commonly, this form may occur with heavy metal intoxication, multiple sclerosis, parkinsonism and chemotherapy, especially vinca alkaloids.11,12
Severe autonomic nervous system disorders may present as POTS. These may include pure autonomic failure or multiple system atrophy. Paraneoplastic syndrome associated with adenocarcinoma of the lung, breast, ovary, or pancreas may also present as POTS. These tumors produce auto-antibodies targeting the acetylcholine receptors in the autonomic ganglia in a manner similar to post-viral syndromes.
Figure 1. Subtypes of postural orthostatic tachycardia syndrome
Evaluation and Management
Treatment is generally individualized to each patient. Confounding pharmacology should be identified and stopped if possible (Table 2). The presence of secondary POTS should be considered. Underlying diagnoses causing or augmenting POTS should be identified and treated appropriately. Deconditioning is frequent seen in POTS patient and a deliberate aerobic reconditioning program should be a component of the treatment plan. 13 This is encouraged to begin promptly working up to a goal of 20-30 minutes of activity at least 3 times a week. Resistance training of the lower extremities is helpful to increase the efficacy of the skeletal muscle pump. Salt and water ingestion are the most common employed non-pharmacolgical therapeutic intervention for POTS. Although, the intravenous saline infusion has been associated with reduction in standing tachycardia, the effect on this intervention on the symptom reduction remains unknown 14 . In general, since low blood volume may exacerbate symptoms patients are encouraged to have liberal salt and water intake. Excluding hyperadrenergic POTS, daily fluid and sodium intake should be greater than 2 liters and 3-5 grams.
Table 2: Pharmacologic Agents That May Cause or Worsen Orthostatic Intolerance
The goal of pharmacotherapy in the treatment of POTS is to ameliorate the symptoms of POTS and thus maintain the functional capacity. Currently no drug is US FDA approved for the treatment of POTS. All pharmacology is inherently off-label. (Table 3).
Majority of the evidence for the use of different pharmacological agents in the management of POTS is based on some small randomised , observational and retrospective single center studies. In clinical practice most patients are treated with a single agent and second medication from different class with a different mechanism of action is added in case of treatment failure. Resistant cases are often treated with polypharmacy.
Fludrocortisone, a potent mineralocorticoid resulting in sodium retention, augmented fluid volume, and sensitized peripheral alpha adrenergic receptors. The effects are more pronounced in the younger population. Starting dose is 0.1-0.2 mg daily with a maximum dose of 0.4 mg. Common side effects include electrolyte imbalance and hypertension. In a study of 11 female POTS patients, fludricortisone alone or in combination with bisoprolol was associated with improvement in symptoms 15. Midodrine is an alpha -1 adrenoreceptor agonist and causes both arterial and venous vasoconstriction. It is commonly used as add on therapy and with starting dose at 5 mg orally three times a day. In our clinical experience we advise patients to take their first dose of midodrine 15 minutes prior to getting out of bed. An additional 5mg dose can be used for breakthrough symptoms. Midodrine is usually well tolerated with the most common complaints being nausea, “goose bumps,” and scalp pruritus. In a small study of 6 patients with POTS acute combination therapy of midodrine (10mg) with octreotide (0.9mcg/kg) was significantly associated with reduction in upright tachycardia and improved standing time.In another study of 53 children with POTS, midodrine was significantly associated with both higher clinical cure rate and reduced recurrence rate as compared to children treated with metoprolol or conventional therapy.
Patients may continue to be symptomatic despite dual-therapy as outlined above. In this population we add a serotonin reuptake inhibitor (SSRI) or norepinephrine reuptake inhibitor (SNRI). SSRI therapy has been found to be helpful in the prevention of neurocardiogenic syncope. However, SNRI therapy is more useful in the treatment of POTS. Usually, we use bupropion XL beginning with 150 mg orally daily titratable to 300 mg daily if necessary.
The most effective SSRI therapies combine serotonin and norepinephrine reuptake inhibition (venlafaxine and duloxetine). The agents are usually well tolerated with the most common side effects being gastrointestinal upset, tremor, sleep disturbance, and less commonly agitation and sexual dysfunction. Bupropion and SSRI therapy can be combined to achieve a similar effect.
Pyridostigmine is an acetylcholinesterase inhibitor that facilitates sympathetic and parasympathetic ganglionic neural transmission. In our single center experience of 203 patients of POTS treated with pyridostigmine; improved symptoms of orthostatic intolerance were seen in 88 of 203 (43%) of total patients or 88 of 172 (51%) who were able to tolerate the drug. Fatigue (55%), palpitations (60%), presyncope (60%), and syncope (48%) were the most common symptoms that improved with pyridostigmine. Further, symptom reduction correlated with a statistically significant improvement in upright HR and diastolic blood pressure after treatment with pyridostigmine as compared to their baseline hemodynamic parameters (standing HR 94 ± 19 vs 82 ± 16, P < 0.003, standing diastolic blood pressure 71 ± 11 vs 74 ± 12, P < 0.02). Gastrointestinal problems were the most common adverse effects (n = 39, 19%) seen in our study. 18
Severely affected and refractory patients may benefit from erythropoietin (EPO) therapy. EPO increases red cell mass, central blood volume and augments response of blood vessels to the angiotensin-II and thus causes vasoconstriction. These effects are quite useful in the treatment of orthostatic disorders. Prior to initiation of EPO therapy obtain a complete blood count (CBC), total iron binding capacity, serum iron and ferritin levels. Hematocrit (HCT) levels must be monitored and should remain less than 50 on EPO. The starting dose is 10,000 units via subcutaneous injection once weekly. There is a 4-6 week delay between a given dose and the full clinical effect. The hematogenic and hemodynamic affects are independent but may occur simultaneously. A goal HCT of low to mid 40 will often result in optimum hemodynamic augmentation. Monitoring during EPO therapy should include monthly CBC to document HCT less than 50. EPO therapy may infrequently result in a “serum sickness” type reaction characterized by nausea, fever, chills, and general malaise. In another study of 39 patients (age 33 ± 12, 37 females) with resistant form of POTS, we reported sustained improvement in twenty-seven (71%) patients at mean follow-up of six month with EPO therapy. Eighty (21%) failed to respond to therapy while as 3 (8%) improved with therapy at 3months. Also, erythropoietin significantly improved sitting diastolic blood pressure but had no effect on other hemodynamic parameters.19 We reserve EPO therapy for patients that are refractory or intolerant of other forms of treatment because of its considerable expense and subcutaneous route of administration.
Beta blocker therapy such as metoprolol tartrate may be beneficial in adolescent type POTS patients. In a single center retrospective study of 121 patients with possible POTS, written survey at follow-up were used to evaluate response to therapy with beta-blockers and midodrine. 47 adolescents responded to survey (Walker Functional Disability Inventory Survey) and reported improvement with a β-blocker (100% vs 62%, P = 0.016) and more attributed their progress to medication (63.6% vs 36.4%, P = 0.011) than did those treated with midodrine 20.In addition, beta-blocker therapy was associated with improved quality of life. Great caution should be taken in using beta-blocker therapy in a rare form of hyperadrenergic POTS secondary to the mast cell activation disorders. Octreotide is a somatostatin analogue with potent vasoconstrictive effects and is useful in the treatment of orthostatic disorders. In patients with resistant POTS, octreotide may be a useful as add on therapy. It is administered by subcutaneous injection 2-3 times daily. The stating dose is 50 ug and may be titrated up to 100-200 ug three times daily.
Agents that block the release or effect of norepinephrine (noradrenaline) are very effective for hyperadrenergic type POTS patients. We use clonidine starting at 0.1 mg orally twice daily and titrating up as needed. The patch form may be preferable to some patients and has the added benefit of providing a steady state drug release for one week. Labetalol, an alpha and beta receptor blocker, is also useful in this group of patients. Dosages of 100-400 mg orally twice daily are used. Methyldopa may have a role in highly selected patients with POTS. Symptom control may be improved with both the SSRI and SNRI classes of medications.
Inappropriate sinus tachycardia (IST) is an important confounding finding in suspected POTS patients. This syndrome is similar to hyperadrenergic type POTS. The clinical presentation may be similar with IST being more common in females. These disease states display and exaggerated response to isoproterenol infusion. It has been postulated that they may represent different states of the same pathologic process. A greater degree of orthostatic change in heart rate is seen in POTS patients. The supine rate rarely exceeds 100 bmp (IST will often be >100). Postural changes in serum norepinephrine levels are much more pronounced in POTS patients. It is important to differentiate POTS and IST. Radiofrequency ablation of the sinus node will rarely benefit hyperadrenergic POTS patients and will make PD POTS patients markedly worse.
Treatment of secondary POTS should focus primarily on the underlying disorder to the greatest extent possible. Diabetes mellitus or JHS related POTS are treated as PD POTS. Secondary POTS due to sarcoidosis or amyloidosis may benefit from steroid therapy. Secondary POTS that is paraneoplastic may completely resolve with treatment of the underlying malignancy but may also respond to pyridostigmine.
Patients suffering from POTS have a disease that affects many aspects of their life. They are often unable to take advantage of meaningful employment or education opportunities. The pervasive life change experienced often results in significant psychosocial disruption as they may be excluded from social norms and certain environments. Frequently, patients require psychologists, social workers, and lawyers to address these aspects of living with POTS. The treating physician is a prominent and central figure who is a beacon of hope for this population. A positive, caring, and nurturing attitude may be the best medicine and lead to a rewarding rapport where an otherwise challenging disease exists.
Prognosis
There is limited data on the prognosis of POTS patients. Recent short term follow-up studies have shown better prognosis in patients with POTS. 21 Roughly 50% of post-viral POTS patients make a meaningful recovery over about 2-5 years. Meaningful recovery may be defined as the absence of orthostatic symptoms and the ability to perform the activities of daily living with little or no restriction. Some patients experience a partial recovery and still others may demonstrate a progressive functional decline with time. As a general principle, a younger age of onset portends a better prognosis. A majority of patients tend to adopt different lifestyle modifications including increased fluid and salt intake to improve and reduce exacerbation of the POTS symptoms. In secondary POTS syndromes have a prognosis consistent with the underlying causative disorder.
Conclusion
Disruption of normal autonomic function may manifest as one of a heterogeneous group of clinical disorders collectively referred to as postural orthostatic tachycardia syndrome. Treatment is most successful when diligence has been taken to investigate the underlying disorder or POTS subtype and a comprehensive targeted treatment program is instituted with frequent follow up. Goals of care should focus on functional milestones and maintenance of function.
Hydatid disease is due to Echinococcus species commonly granulosus sometimes multilocularis. The common locations of hydatid cyst are the liver (65% to 75%) and lungs (25%-30%) 1,2,3. Hydatid disease rarely develops in some locations such as the spleen, kidney, bones, heart, brain, peritoneum, myocardium and muscles (1-4%)1. In our review of literature, concomitant paraspinal and intrahepatic hydatid is reported rarely.
Case Report
A 25 year old male presented with backache on the right for 1 month and fullness in the right paraspinal region. No history of trauma, fever, burning micturition, pain in abdomen, weight loss or hematuria.
On clinical examination he had non ballotable lump in the right paraspinal region, measuring 15x5x5cm with ill defined margins intra muscular plane extending from the posterior subcostal margin to the iliac region with no overlying skin changes and no organomegaly.
Blood investigations including liver function tests and kidney function tests were normal. Ultrasound examination revealed hepatomegaly with thick walled cystic lesion in the right lobe of the liver and the in muscle plane in the right renal angle region.
CT abdomen (P+C) revealed a well defined hypodence non-enhancing cystic lesion measuring 45x40 cm seen in the right lobe of the liver with peripheral calcification with another lesion of similar morphology of size 14x5x3.6cm in the right paraspinal muscles with no intercommunication between them and no bone, spinal canal alteration or compression of the right kidney.
Figure 1: Right paraspinal hydatid
Figure 2: Intrahepatic hydatid
Figure 3: Coronal view of CT image
The diagnosis of paraspinal hydatid cyst was confirmed. As the patient was symptomatic for paraspinal hydatid cyst only and the size of the hepatic cyst was small, exploration of the right paraspinal region was done after 21 days of antiscolicidal treatment. There was a cyst measuring 15x5x5 cm beneath the oblique and lattisimus dorsi ,superficial to the psoas muscle without invasion into it .The cyst opened multiple daughter cysts along with pus evacuated. The cyst excised in totto without rupture & spillage. Negative suction drain was kept. Post operatively on day 3 the drain was removed, stitches removed on day 10 and discharged. Histopathology confirmed diagnosis.
Figure 4: Intraoperrative photograph
Figure 5: Photograph of multiple daughter cysts
Discussion
Hydatid disease is most prevalent in sheep and cattle-breeding areas, which is where the first step in the chain of transmission occurs. The causative agent is introduced to the dog (the primary host) through the faeces of livestock. The minute larval form of E. granulosus lives in the small intestine of the dog species. The eggs are passed in the faecesof an infected dog and can be transferred to mammal (man – intermediate host) that ingests them. After ingestion, the embryos are released from the eggs, traverse the intestinal mucosa and disseminate systemically via venous and lymphatic channels and develop into hydatid cysts in various body parts.
The cysts cannot easily grow in muscles due to their contractility and lactic acid content. The wall of a cyst in the muscle is formed by three layers: the inner germina, intermediate and outer granulomatous adventitial layer. The most common skeletal sites include hip, thigh, shoulder and humerus regions. Hydatid cysts are frequently asymptomatic1. The latent period of cyst development varies between 5 and 20 years4,5.
Serological tests are widely used to diagnose hydatid cysts. However, positive serological results do not confirm, nor negative results exclude the disease1,6. The imaging features of hydatid cysts are well described in the literature. Ultrasound scans are a sensitive, safe, non-invasive method. It is the procedure of choice for the diagnosis of cysts with a “honeycomb” pattern (type 3), as observed in our patient. Gharbi’s classification provides morphological description on ultrasound. Type 1-pure fluid collection, type 2-fluid collection with split wall (floating membrane), type 3-fluid collection with septa, type 4-heterogenous echographic pattern, type 5-reflecting thick walls.
As seen in our case the cyst fluid appears anechoic at USS, yields an attenuation value of 3-30HU at CT. Calcifications in the cyst wall as in our case are best detected on CT scans. CT has the advantage of detecting smaller cysts when located outside the liver and sometimes differentiating parasitic from non-parasitic cysts, for follow-up studies during chemotherapy. Other diagnostic means such as fine needle aspiration should be avoided because of dangerous anaphylactic reactions7.
Surgery is the optimal treatment for hydatid cyst. Open cyst evacuation is indicated for gharbi types 4 & 5, posterior cysts, central cysts, more than 3 cysts, large cysts, heavy calcification, infected cysts with above criteria, biliary communication, pulmonary communication and peritoneal rupture. Laparoscopic evacuation is indicated in Gharbi type 1 or 2, anterior cysts, peripheral cysts,1-3 cysts, small cysts, no or minimal calcification. Pericystectomy is complete resection of cyst wall without entering the cyst cavity.
Alternative therapy with non-toxic scolocidal agents or combination chemotherapy using imidazole derivatives, particularly albendazol, has been advocated in the management of patients with recurrence and high risk of contamination8.








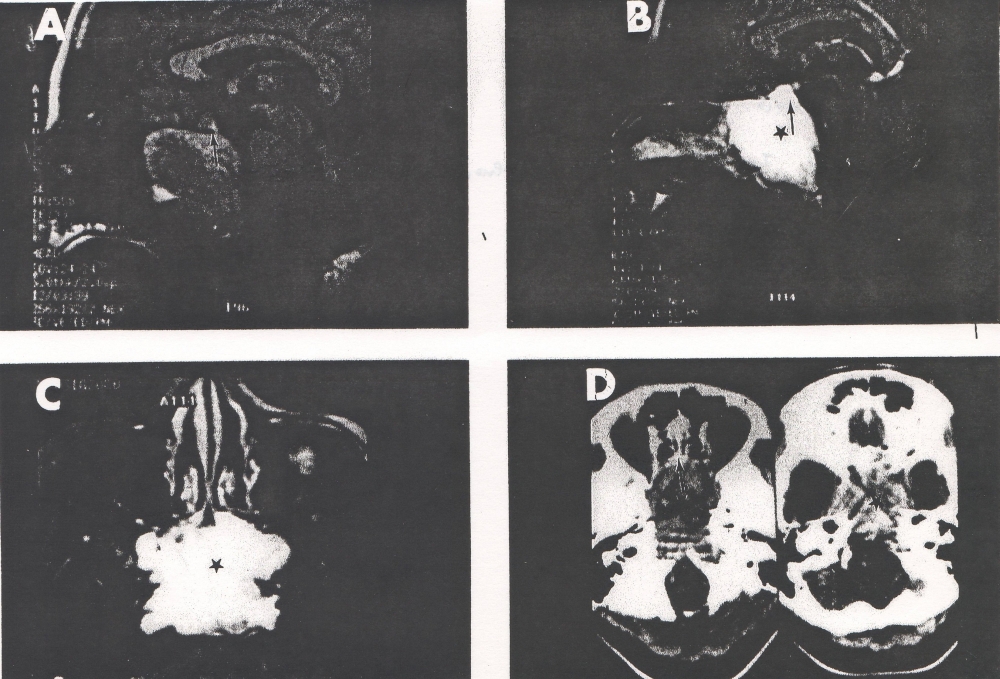




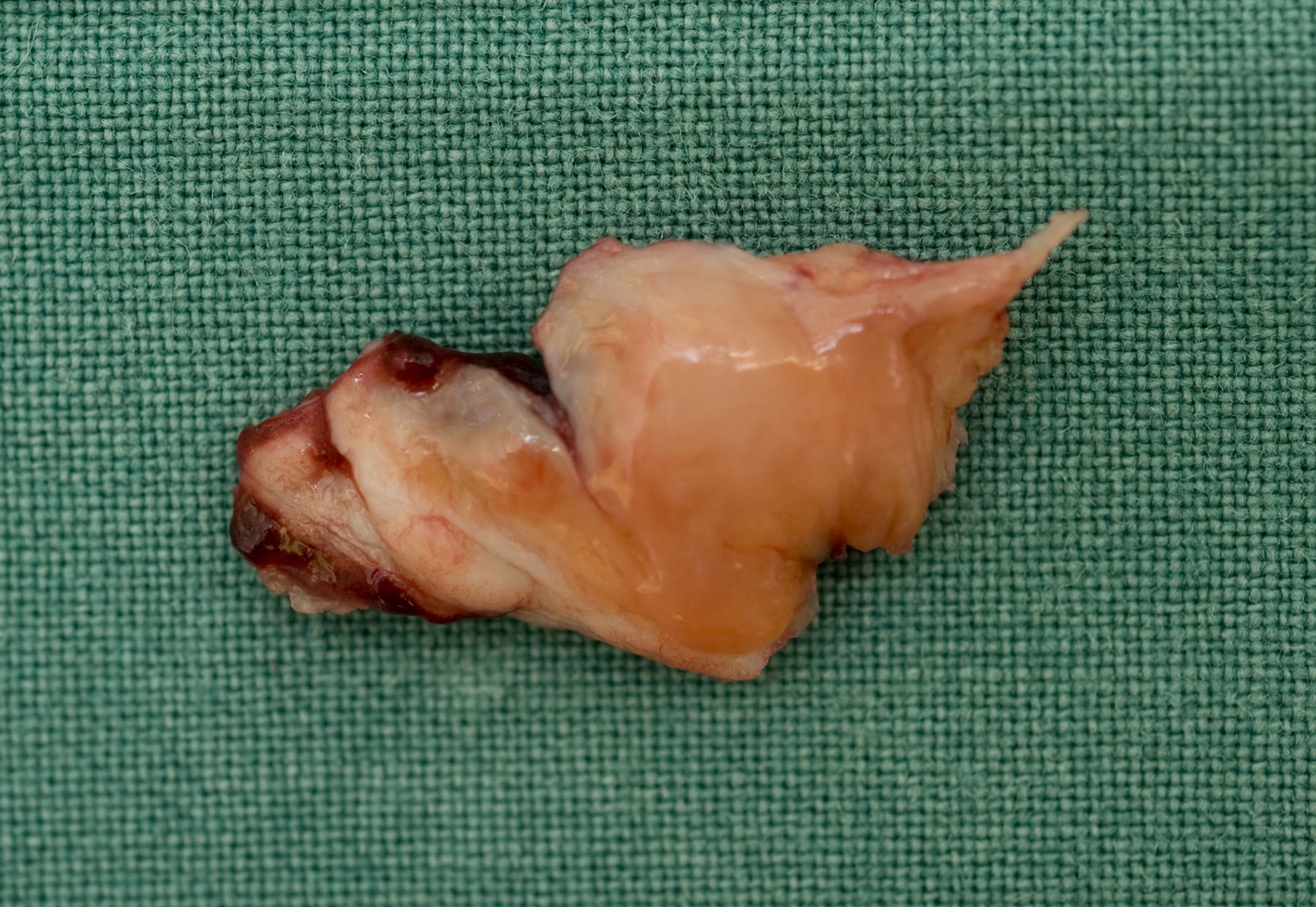
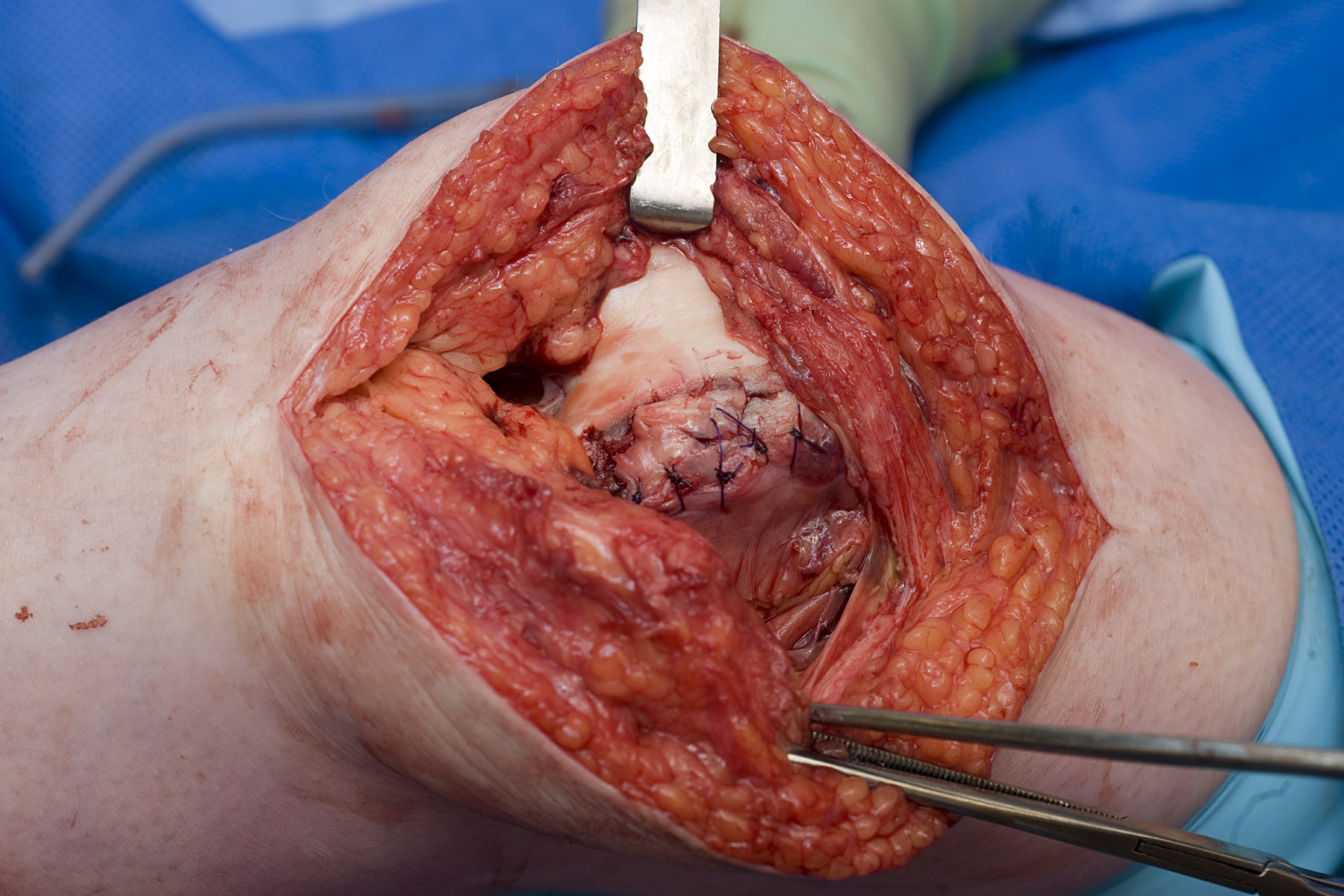
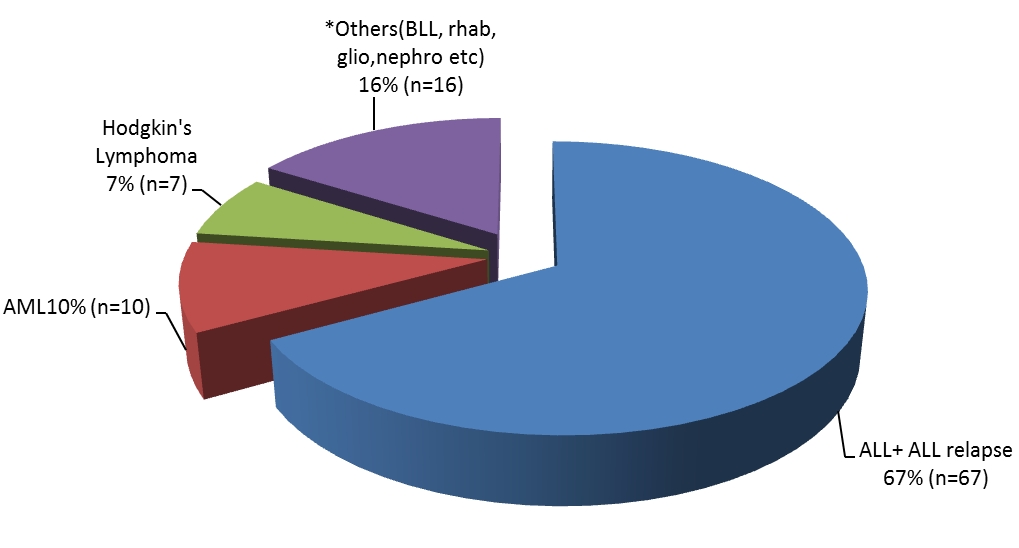


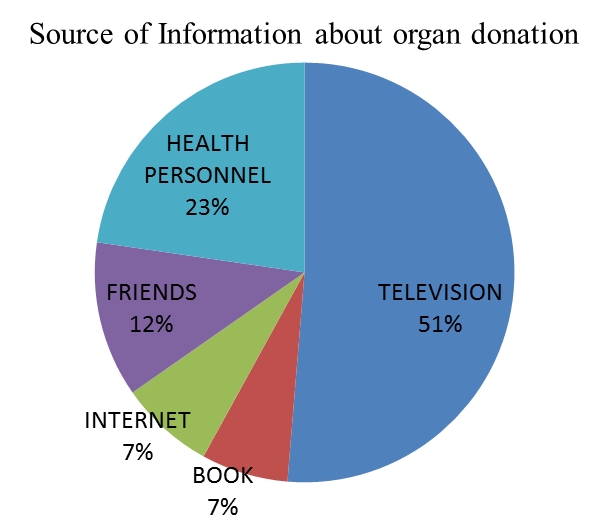
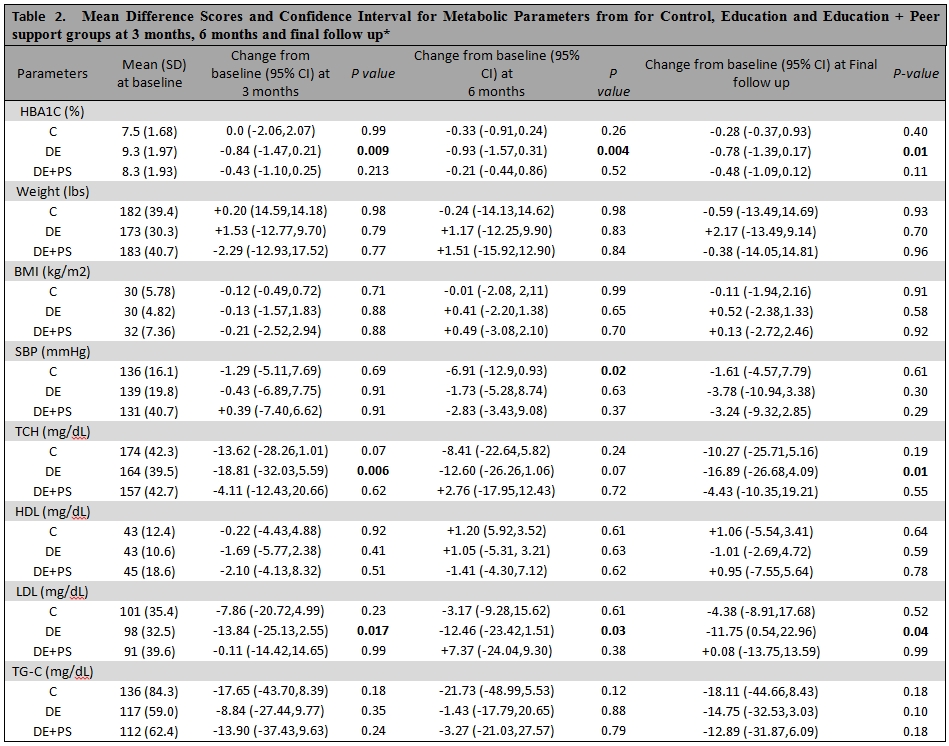
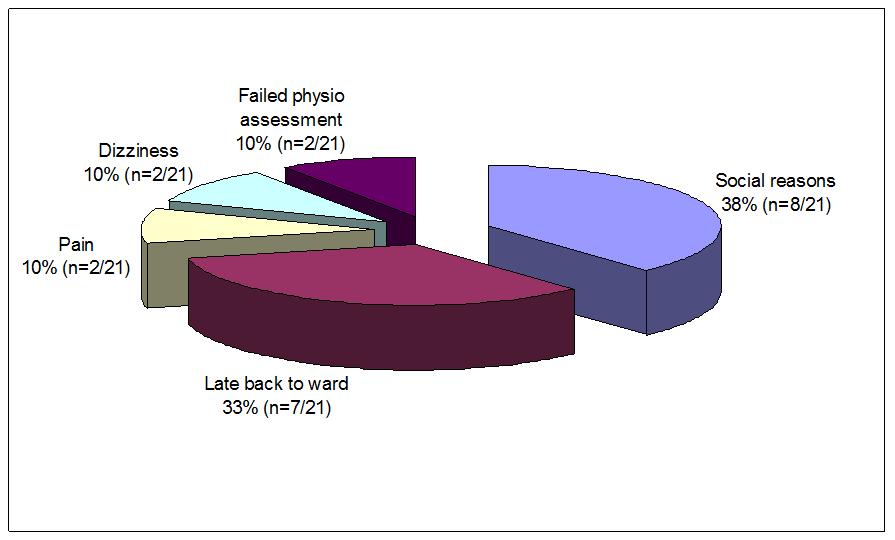
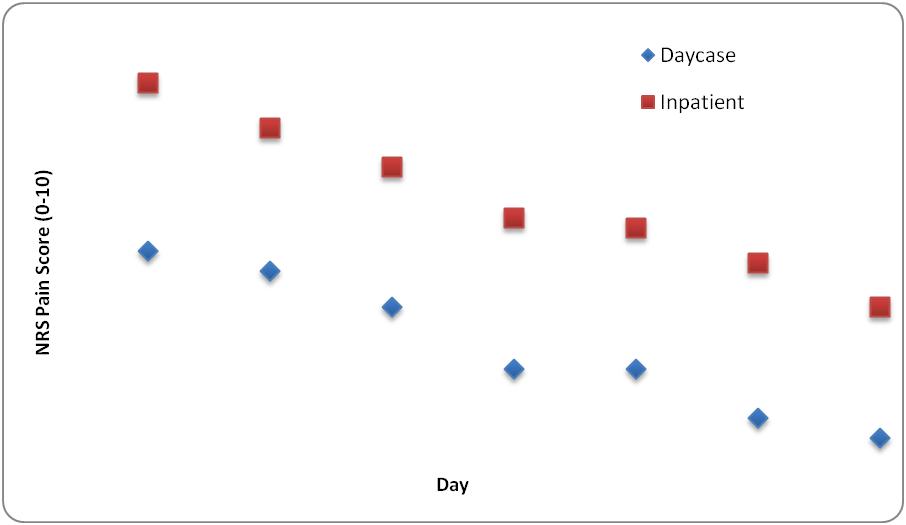
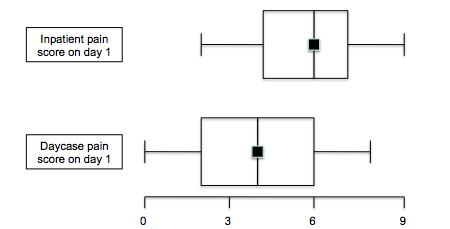
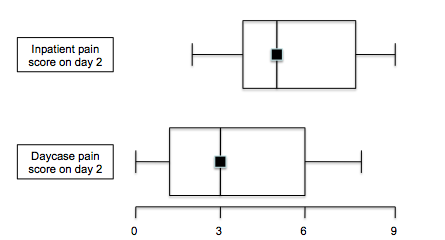
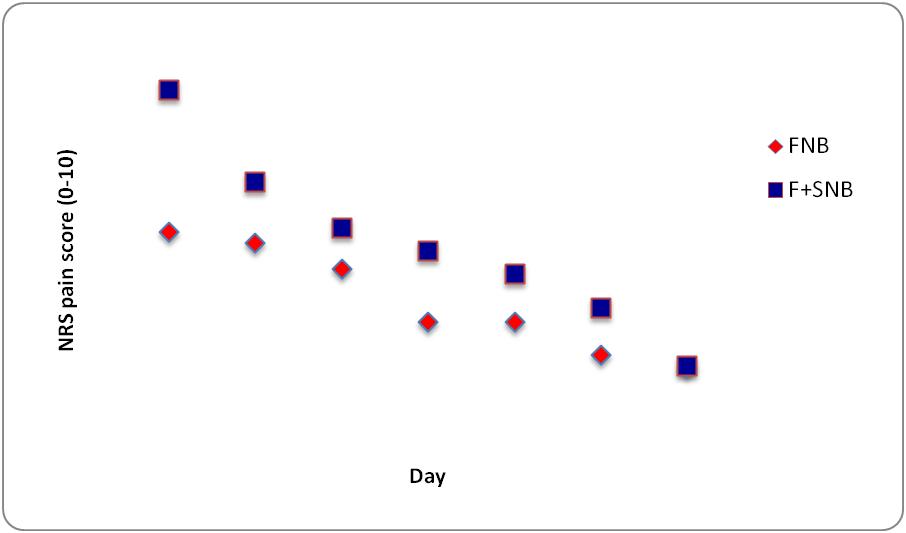
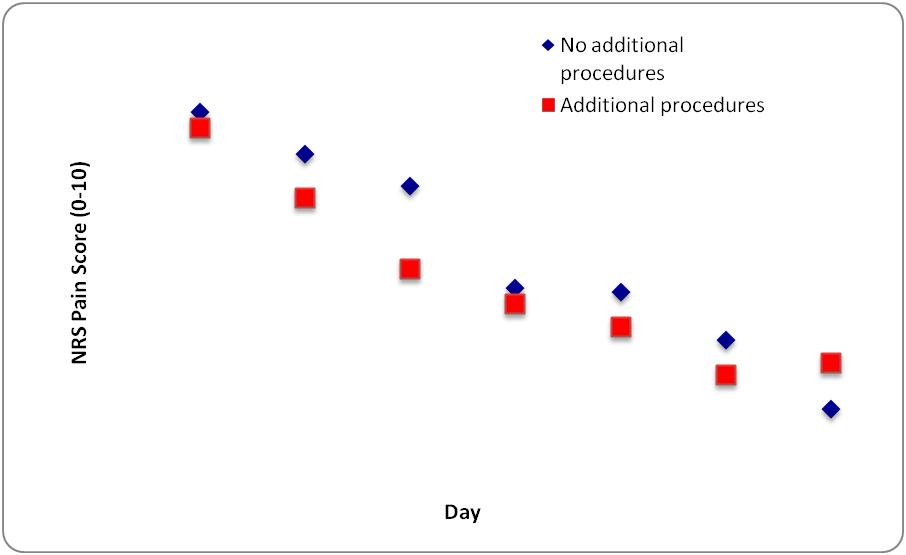


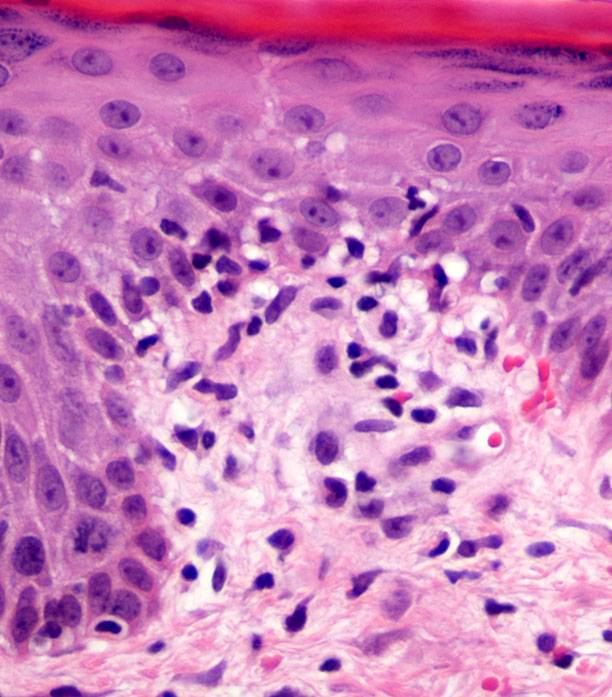

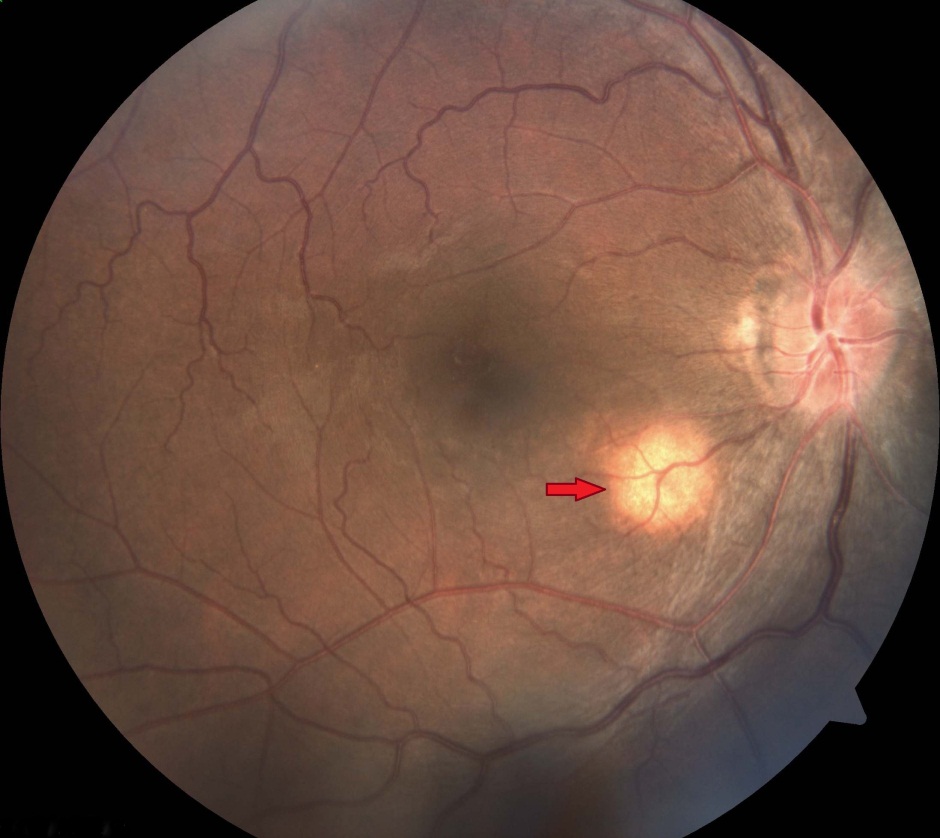
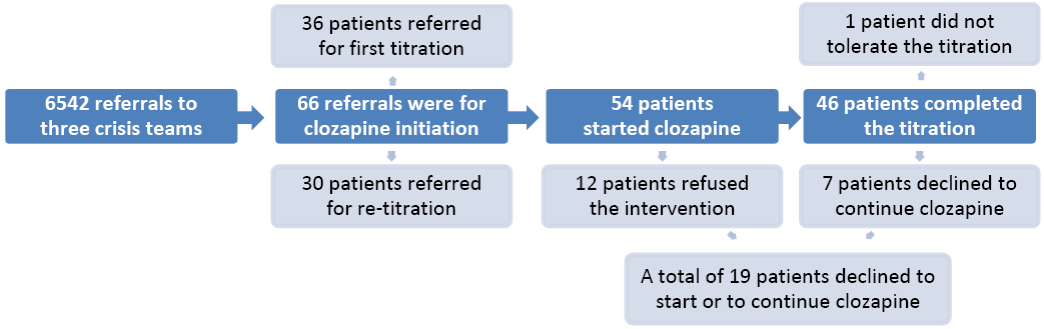



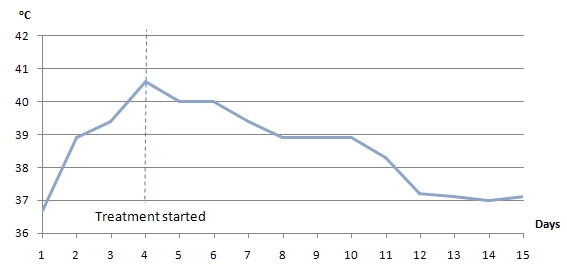
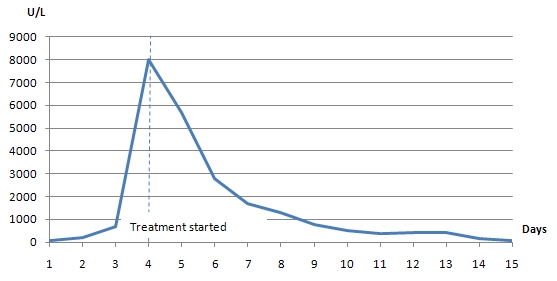



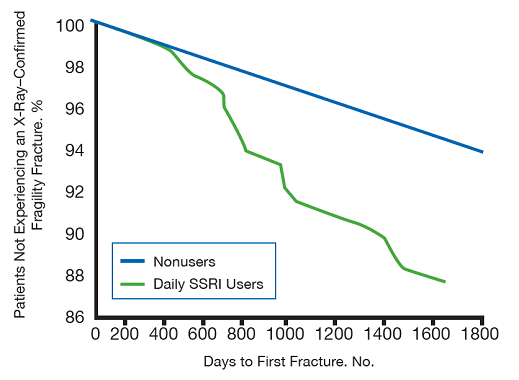
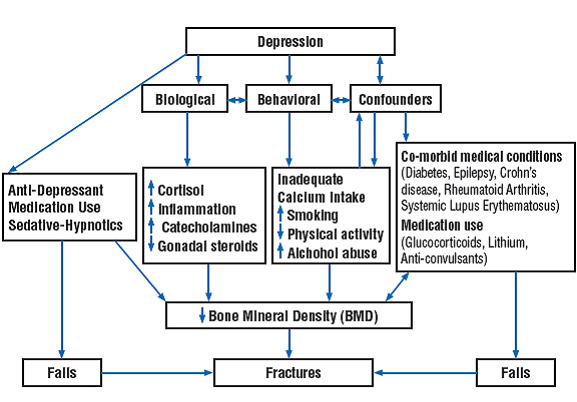
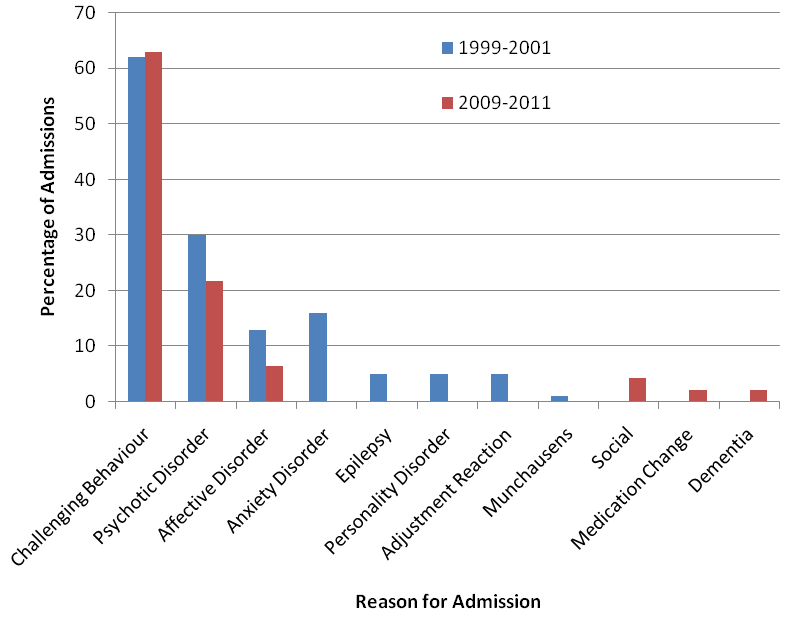

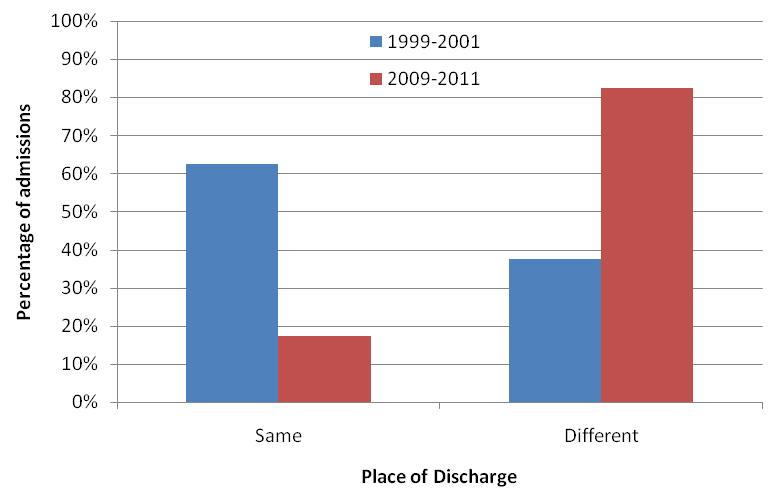
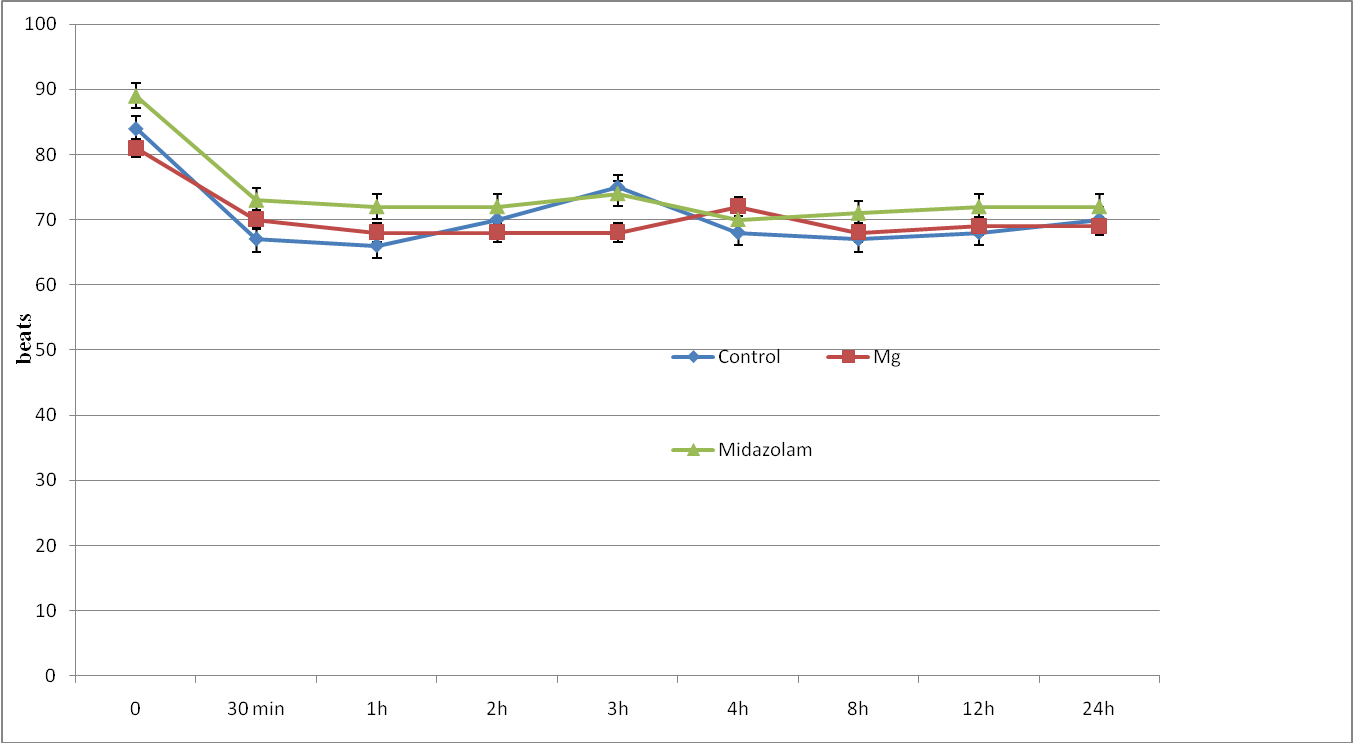
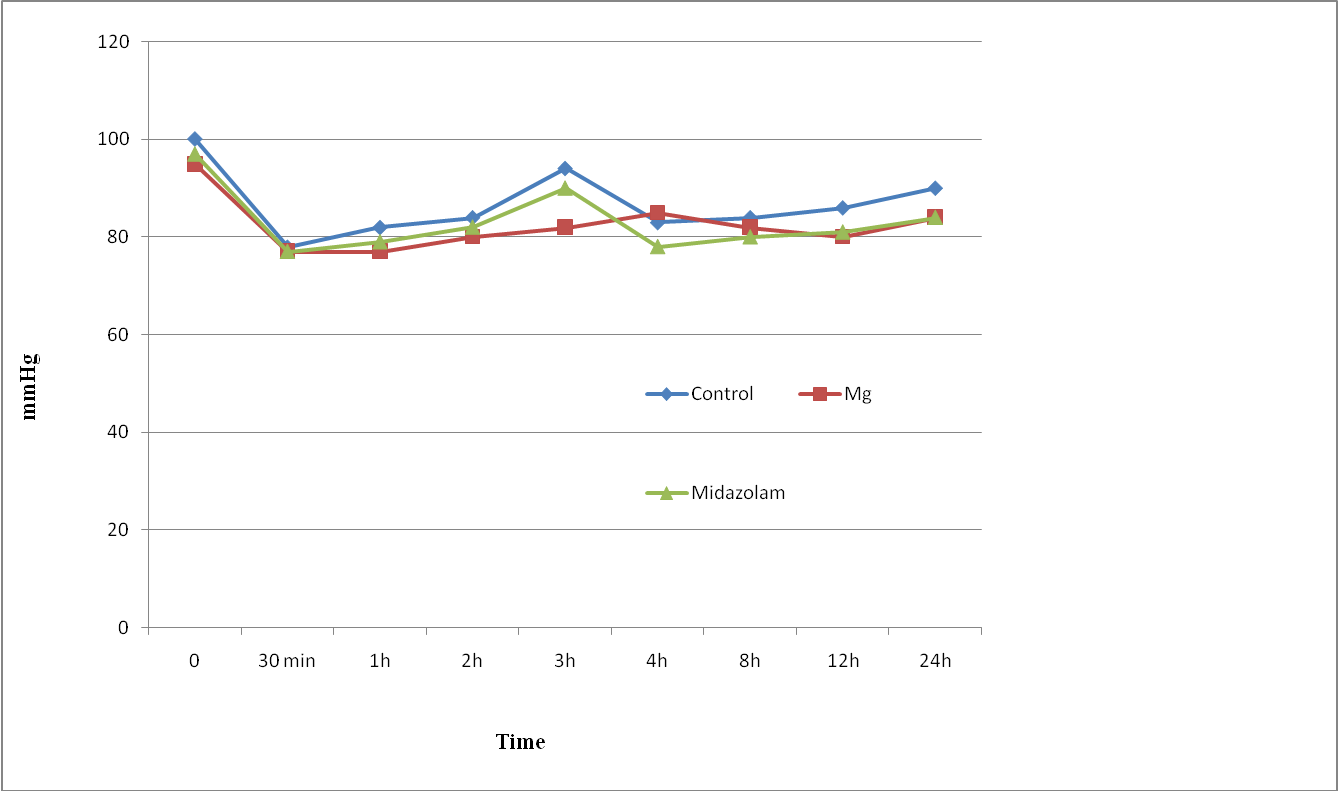
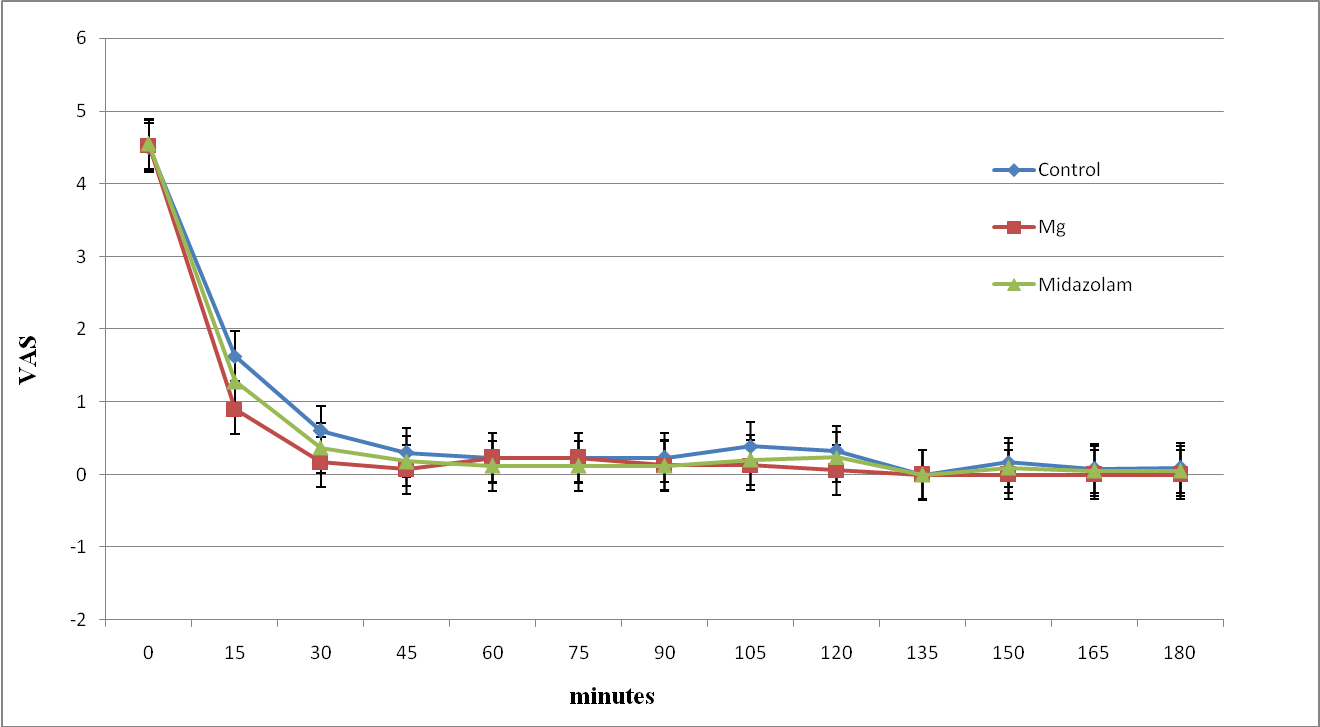

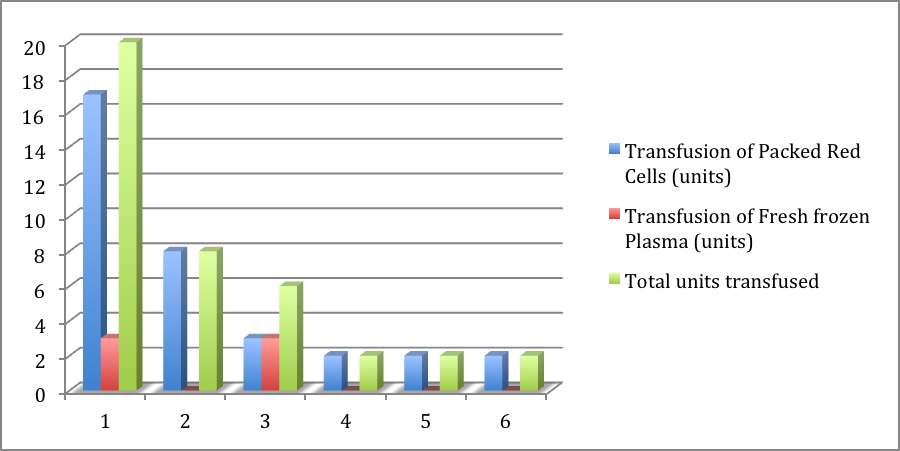
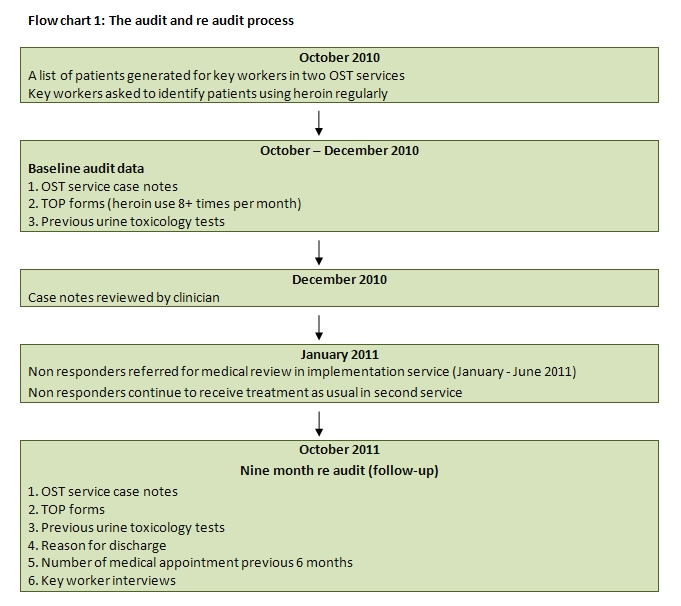
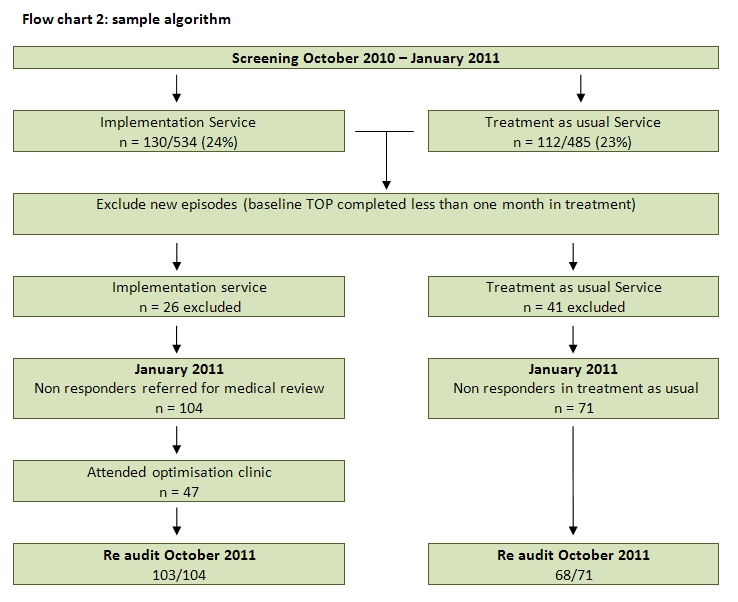
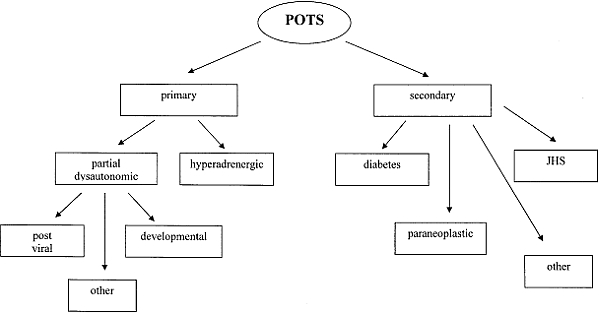
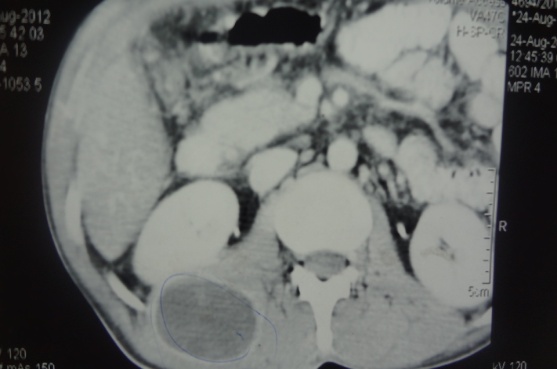
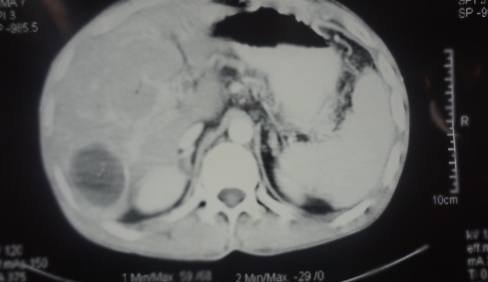
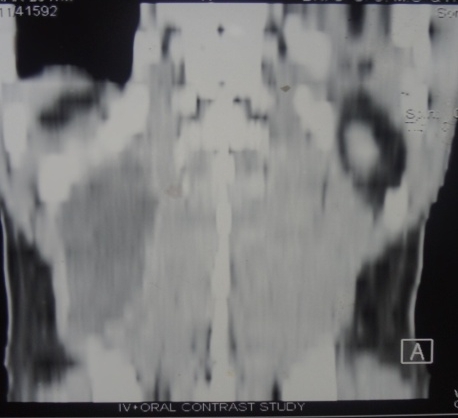


BJMP December 2013 Volume 6 Number 4
BJMP December 2013 Volume 6 Number 4
Editorial
Research Articles
Review Articles
Case Reports/Series