



ISSN 1757-8515
Jeune Syndrome
Ramya H S, Sushanth and Manjunath M N
Cite this article as: BJMP 2013;6(2):a617
|
|
Abstract Jeune syndrome or asphyxiating thoracic dystrophy is a rare autosomal recessive skeletal dysplasia characterised by a small chest and short ribs which restrict the growth and expansion of the lungs often causing life threatening complications. The inheritance is autosomal recessive. A locus has been identified on chromosome 15q13 , while recently, mutations were found in the IFT80 gene, encoding an intraflagellar protein. Other symptoms may include shortened bones in the arms and legs, unusually shaped pelvic bones, and extra fingers and/or toes (polydactyly). It is estimated to occur in 1 per 100,000 – 130,000 live births. Children that survive the breathing and lung challenges of infancy, can later develop life-threatening kidney problems. Heart defects and a narrowing of the airway (subglottic stenosis) are also possible. Other, very less common features of Jeune syndrome include liver disease, pancreatic cysts, dental abnormalities, and an eye disease called retinal dystrophy that can lead to the loss of vision. We report a preterm neonate with Jeune syndrome. Keywords: Jeune Syndrome,Thoracic deseaseAbbreviations: SGA - Small for Gestational Age, HMD - Hyaline Membrane Desease, CPAP - Contineous Positive Airway Ptressure, E/T - Endotracheal Tube, ATD - Asphyxiating Thoracic Dystrophy. |
Case Report
A 34 week preterm, small for gestational age, third born male neonate to a non consanguinous married couple with father having short extremities was admitted in our NICU prematurely with respiratory distress.
On examination the baby was tachypneic with grunt and lower chest indrawing. The baby was also found to have a narrow thorax, short fingers with postaxial polydactyly in both upper limbs and right lower limb, with syndactyly in right upper and lower limb (figures 1,2,3). The cardiovascular, respiratory, abdominal and neurological examination were unremarkable with no facial dysmorphism. The fundus examination was inconclusive.
The antenatal scan showed all long bones short in configuration. The liver function tests were normal except for mild elevation of alkaline phosphatase. The Ultrasound abdomen showed hepatomegaly and no evidence of any other mass lesions. The urine examination was negative for proteinuria and haematuria. The chest x ray showed short ribs, high position of clavicle and features of hyaline membrane disease (Figure 4).
The baby was put on continuous positive airway pressure and given surfactant through an endotracheal tube twice for two consecutive days, but as the condition deteriorated, with hypercarbia and hypoxia as evident on arterial blood gases, the baby was electively ventilated with minimal settings. The baby improved and hence was extubated. After a few hours of being extubation the baby gradually developed respiratory distress and started to deteriorate. Hence the baby was reintubated. The condition of baby was explained to attenders and as the attenders were not willing to continue the treatment, the baby was discharged from hospital against medical advice and later we were informed that the baby expired within few hours after discharge from the hospital.

Fig 1 : showing long narrow thorax and short upper extremities

Fig 2 : showing postaxial polydactyly with syndactyly in upper extremity

Fig 3 : showing polydactyly with syndactyly in lower extremity
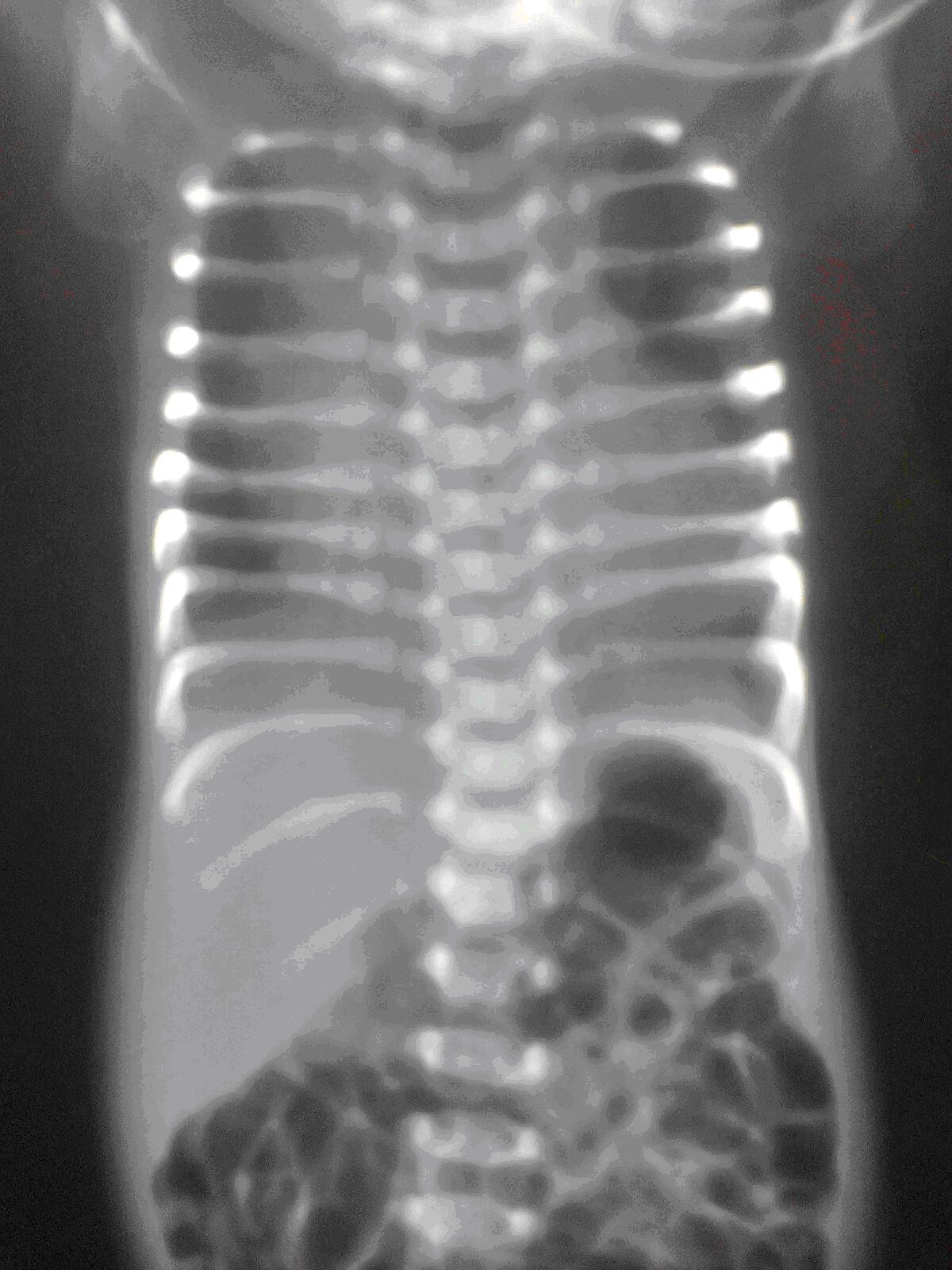
Fig 4 : chest xray showing long narrow thorax and short and horizontally oriented ribs with irregular costochondral junctions and bulbous and irregular anterior ends
Discussion
Jeune syndrome or asphyxiating thoracic dystrophy is a rare autosomal recessive skeletal dysplasia characterised by a small chest and short ribs which restrict the growth and expansion of the lungs1. The inheritance is autosomal recessive and a locus has been identified on chromosome 15q13 2. Other symptoms may include shortened bones in the arms and legs, unusually shaped pelvic bones, and extra fingers and/or toes (polydactyly)3 . It is estimated to occur in 1 per 1,00,000 -1,30,000 (again is this 130,000?) live births4.. The diagnosis is based on clinical and radiological findings. Our patient fulfills the diagnostic criteria for Jeune syndrome. The most consistent and characteristic findings were the abnormalities of the thoraxand limbs. Jeune syndrome was first described in 1955 by Jeune in two siblings with severely narrow thorax5. It is known to be genetically heterogeneous.
Several complications of asphyxiating thoracic dystrophy have been described in the literature. The respiratory problems are the main concern. A large percentage of the children with asphyxiating thoracic dystrophy die as a result of these problems. Percentages up to 80% have been mentioned in literature6,7. In our case the baby experienced respiratory distress on day one of life needing ventilator support. The thoracic malformation tends to become less pronounced with age8. A possible explanation could be the improved mechanical properties of the chest wall with growth.
Clinically, Jeune syndrome is characterized by a small, narrow chest and variable limb shortness. Associated congenital abnormalities can be postaxial polydactyly of both hands and/or feet (20%). Typical radiographic findings include a narrow, bell-shaped thorax with short, horizontally oriented ribs and irregular costochondral junctions, elevated clavicles, short iliac bones with a typical trident appearance of the acetabula, relatively short and wide long bones of the extremities, and hypoplastic phalanges of both hands and feet with cone-shaped epiphyses9. The reported case has long narrow chest, short and horizontally oriented ribs with irregular costochondral junctions and bulbous and irregular anterior ends with post axial polydactyly in both upper extremities and right lower limb with left lower limb being normal.
Jeune syndrome is sometimes compatible with life, although respiratory failure and infections are often fatal during infancy. The severity of thoracic constriction widely varies. For those patients who survive infancy, the thorax tends to revert to normal with improving respiratory function. This suggests that the lungs have a normal growth potential and the respiratory problems are secondary to restricted rib cage deformity 10.
|
Acknowledgements Medical Records Department, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bangalore, India. Competing Interests None declared Author Details RAMYA H S, MD, Assistant Professor, NICU In-charge (2012), Department Of Paediatrics, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bangalore, India. SUSHANTH SHIVSWAMY, Consultant Neonatologist, Department Of Paediatrics, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bangalore, India. MANJUNATH M N, Department Of Paediatrics, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bangalore, India. CORRESPONDENCE: RAMYA H S, MD, Assistant Professor, Department Of Paediatrics, Kempegowda Institute of Medical Sciences Hospital and Research Centre, K R Road, V V Puram, Bangalore, India, 560004. Email: drhsramya@yahoo.com |
References
- Familial asphyxiating thoracic dysplasia: clinical variability and impact of improved neonatal intensive care.Kajantie E, Andersson S, Kaitila IJ Pediatr. 2001 Jul; 139(1):130-3.
- Morgan NV, Bacchelli C, Gissen P et al (2003) A locus for asphyxiating thoracic dystrophy, ATD maps to chromosome 15q13. J Med Genet 40:431–435. doi:10.1136/jmg.40.6.431.
- Hennekam RCM, Beemer FM, Gerards LJ, Cats B (1983) Thoracic pelvic phalangeal dystrophy (Jeune syndrome). Tijdschr Kindergeneeskd 51:95–10..
- Oberklaid F, Danks DM, Mayne V, Campbell P. Asphyxiating thoracic dysplasia: clinical, radiological, and pathological information on 10 patients. Arch Dis Child 1977; 52:758–765.
- Jeune M, Beraud C, Carron R. Dystrophie Thoracique asphyxiante de caractère familial. Arch Fr Pediatr 1955;12:886.
- Amirou M, Bourdat-Michel G, Pinel N et al (1998) Brief report: successful renal transplantation in Jeune syndrome type 2. Pediatr Nephrol 12:293–294.
- Morgan NV, Bacchelli C, Gissen P et al (2003) A locus for asphyxiating thoracic dystrophy, ATD maps to chromosome 15q13. J Med Genet 40:431–435.
- Hanissian AS, Riggs WW Jr, Thomas DA (1967) Infantile thoracic dystrophy—a variant of Ellis–Van Creveld syndrome. J Pediatr 71:855–864. doi:10.1016/S0022-3476(67)80011-80.1136/jmg.40.6.431.doi:10.1007/s004670050456.
- Hennekam RCM, Beemer FM, Gerards LJ, Cats B. Thoracic pelvic phalange dystrophy (Jeune syndrome). Tijdschr Kindergeneeskd 1983;51:95–100.
- de Vries J, Yntema JL, van Die CE, Crama N, Cornelissen EAM, Hamel BCJ. Jeune syndrome: description of 13 cases and a proposal for follow-up protocol. Eur J Pediatr 2010;169:77–88.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.