It is widely acknowledged that medicine can be a high-stress profession. The reasons behind this observation have been the focus of research over recent years, because concerns over the welfare of doctors have grown due to its relevance to burnout of individuals and safeguard of healthcare systems. However, a recent survey of hospital doctors still showed that 80% experienced workplace stress, and the junior doctors surveyed suffered significantly higher burnout rates than their consultants.1 Separate research has specifically found that junior doctors have a poor work-life balance, a composite measure of individual factors affecting wellbeing.2 There seem to be differences in the wellbeing of doctors in different specialities studied – a study in 2016 showed higher levels of leisure time enjoyed by general practitioners compared to doctors working in other specialities.3 Another survey showed that psychiatrists experienced lower levels of burnout than surgeons did.4 Furthermore, different burnout rates have been observed between consultants and junior doctors working in Psychaitry.5
We sought to build on existing research by studying the work-life balance of junior doctors and how some factors might affect that. We also decided to explore what factors might contribute to the differences in wellbeing between medical specialties and professional grades.
Method
Junior doctors working across an English county in general practice, medical and surgical specialities (the “non-psychiatric setting”), and in psychiatric specialities (the “psychiatric setting”), were recruited into a cross-sectional study between September and December 2019. To enable appropriate comparison between groups, junior doctors must have worked between the level of Foundation Year 2 (FY2) and consultant in their relevant speciality. This was necessary because the on-call responsibility of Foundation Year 1 (FY1) doctors in this locality varies significantly from that of more senior doctors.
All doctors were required to complete the SWING (Survey Work-home Interaction-NijmeGen), questionnaire6; a validated instrument measuring four aspects of work-home interaction. This questionnaire is split into negative (questions 1-12) and positive (questions 13-22) subscales, where lower and higher scores are better respectively. For each question four responses ranging from never to always could be returned. Demographic information was also collected to assess participant group similarity and identify any effect of these variables. These included age, gender, and whether they have children under the age of 18. No identifying information was requested to allow for staff anonymity, and no incentive was offered for participating.
Ethical approval for the study was granted by the local Medical Education Departments. Data from completed questionnaires was recorded in an Excel spreadsheet, which was used for collation and analysis. Significance of the between-group differences was calculated using the Chi-Squared test, with the threshold for statistical significance set at p<0.05. In order to allow comparison between the answers given for each questionnaire item, 1, 2, and 3 points were respectively allocated to each “sometimes”, “often”, or “always” response. The sum of these points for each question gave the “overall question score”, with lower and higher scores reflecting better work-life-balance on negative and positive subscales respectively. Overall question scores were also calculated as percentages of the maximum possible score for each question or subscale (i.e. if every respondent had answered “always”).
Results
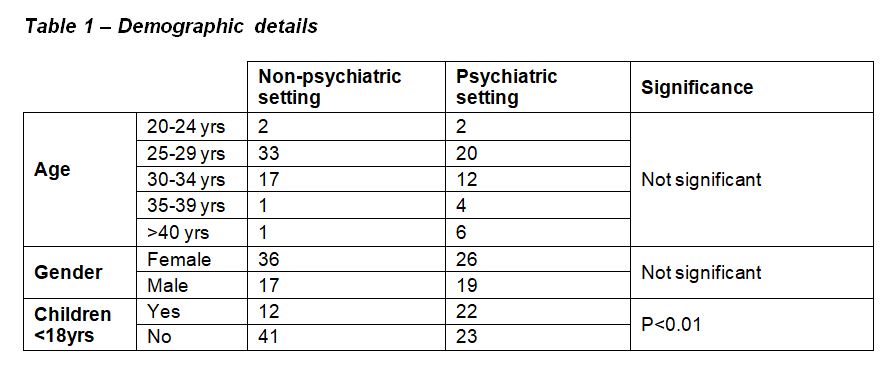
Questionnaires were returned by 99 junior doctors (54 working in the non-psychiatric setting, and 45 working in the psychiatric setting). Demographic details are shown in Table 1. Not all respondents returned demographic details. There were no significant differences in the ages and genders of respondents between the two settings, but there were significantly more doctors with children <18 years in the psychiatric setting.
Table 1
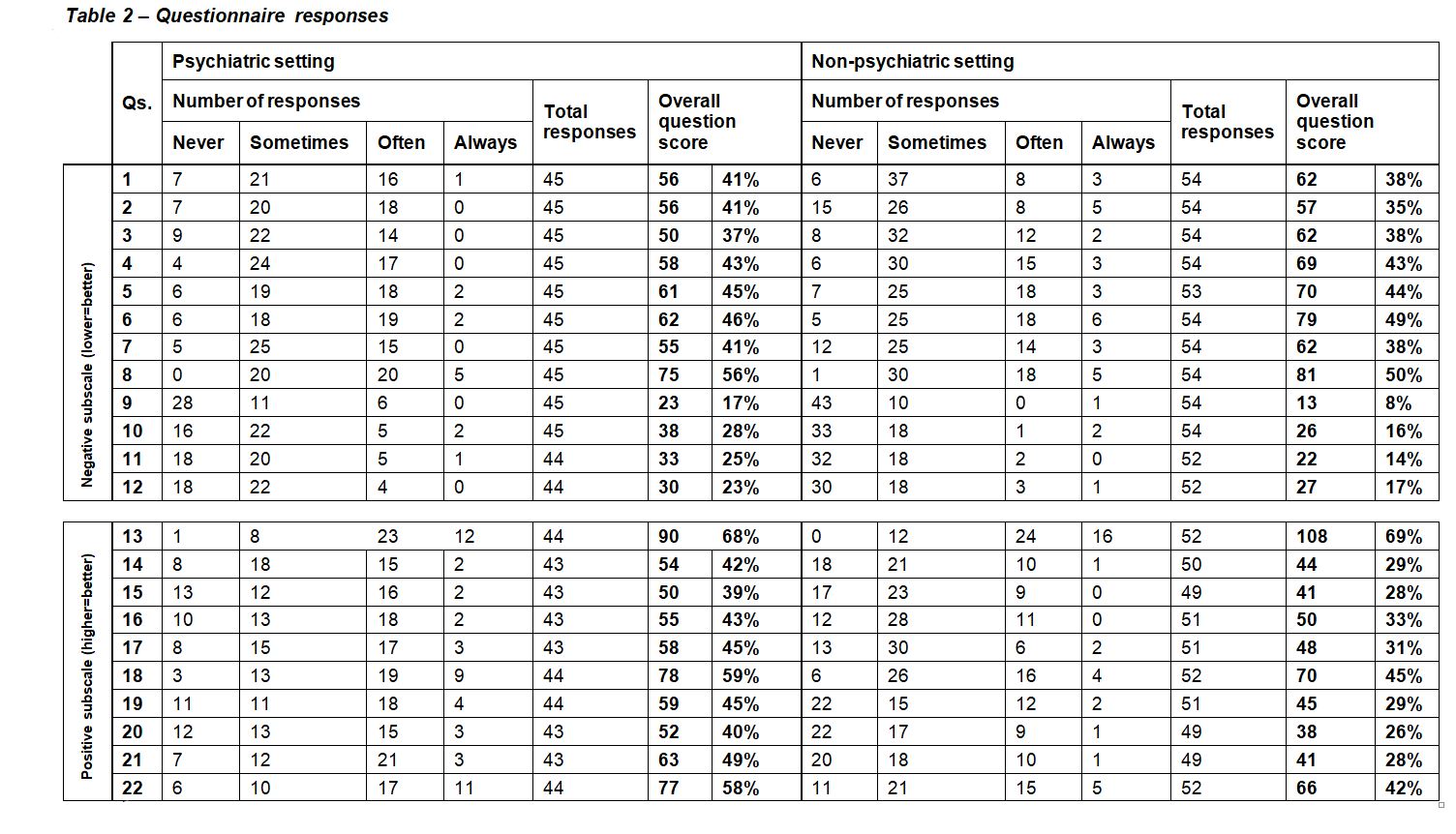
Table 2
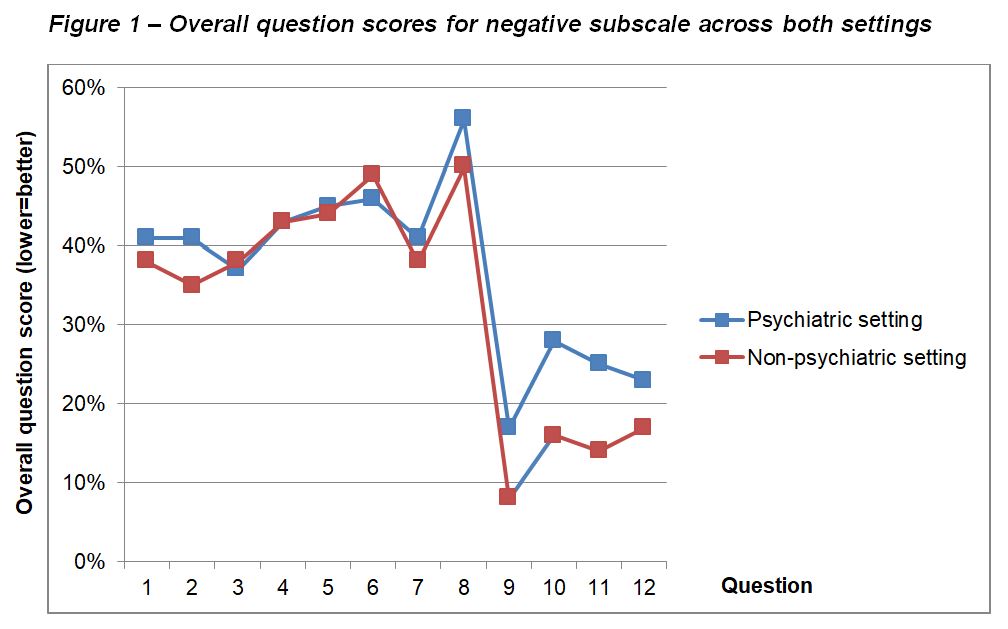
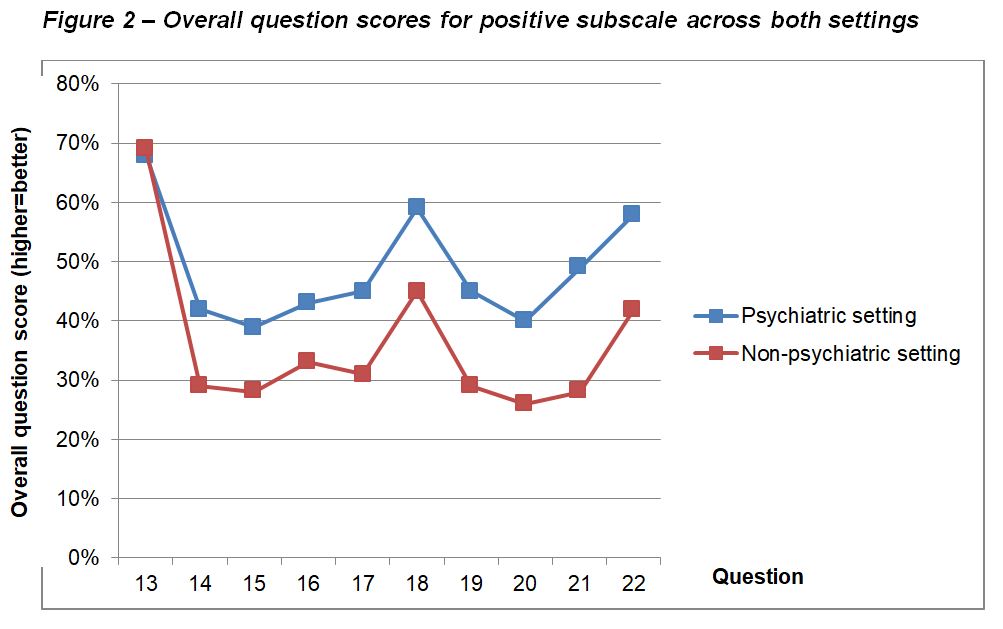
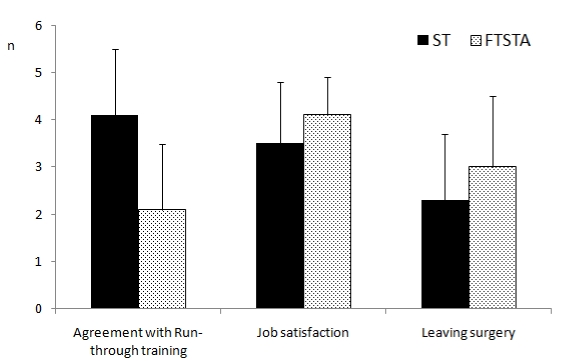
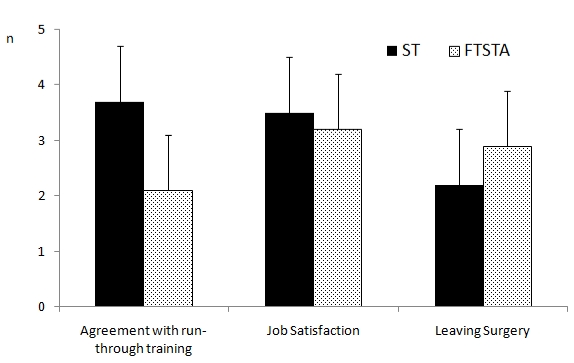
Questionnaire responses are shown in Table 2, along with calculated overall question scores and overall subscale scores for each subscale in both settings. Differences in overall question scores between settings are shown in Figure 1 and Figure 2.
Figure1
Figure 2
Overall question scores across the negative subscale were generally high, indicating a high incidence of negative work-home interaction among all respondents. Scores for questions 1-8, which ask about negative impact of work on home life, showed little/no difference between the two settings. Questions 9-12, which ask about negative impact of home life on work, recorded much lower scores in both settings, but there was separation between the settings, with scores in the psychiatric setting being higher than those in the non-psychiatric setting.
In the positive subscale, questions 13-17 ask about positive impact of work on home life, and questions 18-22 ask about positive impact of home life on work. Overall, there was a much more clear separation in scores between the two settings than that seen in the negative subscale. Aside from question 13, scores in the psychiatric setting being consistently higher than those in the non-psychiatric setting.
Main findings of this study can therefore be summarised as:
High negative impact of work on home life in both settings
Lower levels of negative impact of home life on work, but higher in the psychiatric setting
Higher positive impact of home life on work, and work on home life, in the psychiatric setting than in the non-psychiatric setting
Discussion
There has been a great interest in the wellbeing of junior doctors in recent years, resulting in a number of changes in working patterns, such as the move away from the old “firm” structure to medical training, and the introduction of the European Working Time Directive.7 However, the perceived wellbeing of junior doctors in the UK seems to still be poor, and has resulted in a so-called “Drexit” of junior doctors to other countries, such as Australia, providing a better quality of life or away from medicine altogether.7 One survey shockingly revealed that almost half of UK junior doctors have considered leaving the National Health Service, citing concerns over wellbeing.7 It is, therefore, unsurprising that in 2018, only 38% of FY2 doctors continued into speciality training.8
Various aspects of junior doctor wellbeing and contributory factors have been researched. For example, a large survey of Australian junior doctors published in 2020 showed that those working only a few more hours than the average were more than twice as likely to report common mental disorders.9 Many interacting themes have been qualitatively identified, such as those found in a recent Australian qualitative survey.10 These ranged from institutional issues such as discouragement to claim overtime, to cultural issues such as not wanting to ask for assistance, to personal issues such as time for personal care. Another study found multiple factors to be correlated with higher rates of burnout in hospital doctors, including male sex, younger age, and lower years of practice.1
It seems that wellbeing in junior doctors is a highly complex, multifactorial issue with many interacting contributory factors. In addition to considering the individual factors at work, it is also necessary to consider how these factors interact on a larger scale. One way which researchers have done this, and which we have replicated, is to consider the concept of “work-life balance”, which explores the interaction between work and home life, and vice-versa. Existing research in junior doctors has found work-life balance to be particularly poor in those with children and in women, who frequently cited that this had resulted in a change in career direction.2
Unsurprisingly, we have found high levels of work negatively impacting on home life in both psychiatric and non-psychiatric settings. Since work-life balance involves many interacting components, we speculated that it may differ between junior doctors working in different medical specialities. Indeed, we detected such differences, with the reported negative impact of home life on work being higher among those trainees in the psychiatric setting than those in the non-psychiatric setting. In a cross-sectional study like ours, it is not possible to comment on causality but we noted that there were significantly more trainees in the psychiatric setting who had children. This correlates with previous findings,2 and raises the possibility of a causative relationship between having children under 18 and negative impact on work. A study of stress in psychiatrists which gathered responses from 449 participants found that sickness of children and arranging childcare were among the top five stressors identified.11
Trainees in the psychiatric setting have consistently reported higher levels of positive impact of work on home life and vice-versa. One possible explanation is that the nature of psychiatry is inherently different to other areas of medicine, with a focus on promoting the quality of patient interaction, and training time dedicated to exploring this in detail. Supervision of patient contact is also conducted more thoroughly than in other specialities, which may lead to a greater sense of being supported in clinical decision making when trainees work in psychiatry.
Strengths and limitations
Regarding strengths of this study, we used an innovative method in seeking to compare trainees across two different settings. The questionnaire used was validated and holistic in examining bidirectional interaction between work and home life. Groups were well-matched in terms of the selection of trainees with broadly similar working rotas, and in their age and sex, which have been shown to be important variables which can affect work-life balance. We also used an innovative method in analysing the questionnaire responses which enabled us to compare directly between the two settings.
There are several limitations with this methodology which identify possible interesting and important areas for future research. For example, we did not investigate for differences in work-life balance between staff working in inpatient and community settings. Additionally, it was not possible to make conclusions about causality with this cross-sectional methodology, and the use of a longitudinal method with a more detailed exploration of demographic factors may provide interesting insights in the future. Due to local factors in the way psychiatric and general healthcare services are set up in our area, it was not practical to measure participant engagement with the study, and this would have presented a barrier making this study impossible. There were however 99 responses included in this study, with similar representation in both healthcare settings, which relative to the local population of doctors in the settings studied represents a good sample.
There will inherently be local differences in working patterns, and therefore the results of this study are not directly generalizable to a national or international population. The non-psychiatric setting is broad in its scope and includes trainees undertaking varied forms of medical and surgical training, and therefore there are likely to be more subtle variations which were missed in this approach.
Conclusion
This study adds to the literature on work-life balance in junior doctors, which is an important area of research in order to promote the wellbeing of the current and future medical workforce. It also explores how factors affecting wellbeing might interact on a higher level than when studied in isolation, and how these interactions may differ depending on the medical speciality in which the respective doctors work.
Because of the local variations in working patterns, we would suggest a replication of this research in other areas in the UK and abroad. We would also suggest that an interesting area for future research may be the exploration of differences in work-life balance between narrower groups of trainees, which may aid developmental policy generation in supporting doctors to maintain a healthy work-life balance across different specialities. The group we feel would benefit from further research in particular is the trainees with young children, as we found a possible negative association between this and impact of home life on work.
There is considerable evidence for the benefit of simulation among foundation year doctors.1 Simulation training delivered during the 2 years has tended to focus on the management of the acutely unwell patient, procedures and practical aspects of delivering medical care, such as DNAR discussions, breaking bad news and capacity assessments.2-5 However, to date, there has been less focus on the benefits of developing more complex communication skills that may assist foundation year doctors in dealing with patients with mental health diagnoses or needs. These skills may include performing risk assessments, managing the agitated patient and forming initial management plans for patients in medical settings with mental health problems. This is important, as people with mental health needs have a higher burden of physical morbidity and are hence likely to be encountered in acute care settings.6
Since Health Education England’s Broadening the Foundation Programme report in 2014, there has been a surge in the number of foundation trainees working in psychiatry.7 The development of complex communication skills was an expected natural outcome of these rotations.8 However, this has not always happened – foundation trainees on a psychiatry rotation have stated that they are often recognised only for their medical skills, and that assessment and management was predominantly senior-led.9
Taking this into account, we set out to develop a simulation-based complex communication skills programme available for all F1s and F2s based in the North Central and East London Foundation School. Our focus was on the development of the transferable skills in communication and management that would be useful for dealing with patients with mental health diagnoses in a medical setting.
METHOD
Following a pilot study in 2018, funding was secured for 2019 from Health Education England to run half-day simulation sessions to foundation trainees in complex communication skills and the management of common mental health presentations to primary and secondary care settings.
Half-day sessions took place in hospitals in North and East London hospitals. A total of 121 foundation year doctors took part in the sessions; a breakdown of this can be seen in Table 1. All sessions took place between May 2019 and March 2020.
Table 1: Participants by Site and Year
Year
Region
Site
Cohort
Number of trainees
2019
North London
Whittington
FY1 & FY2
9
Royal Free
FY1 & FY2
11
Barnet
FY1 & FY2
8
East London
Homerton
FY2
16
Homerton
FY1
14
Royal London
FY1 & FY2
3
2020
North London
Whittington
FY1 & FY2
19
East London
Homerton
FY1 & FY2
33
Whipp’s Cross
FY1 & FY2
8
Facilitators
Each simulation group had one facilitator who offered feedback to participants. Facilitators were consultants, higher trainees and core trainees from the North and East London deaneries.
Session organisers
A session organiser was present at every session. They delivered the introductory briefing for participating doctors, provided a briefing for the actors, time-kept and held a feedback session at the end.
Venues
Four half-day sessions were run in North London, and five half-day sessions were run in East London. Three sessions were cancelled due to too few doctors registering to participate, and a further session was cancelled due to COVID-19.
Scenarios
Participants were presented with six scenarios in each session (Box 1), covering presentations in a range of settings: acute general hospitals, accident and emergency, general outpatient clinics and general practice. The sessions required skills in history taking and management when interviewing patients with complex communication needs.
Box 1 Scenarios
1. Attempting to de-escalate an elated patient with manic symptoms and explain the need for a physical medical examination
2. Conducting a risk assessment and liaising with the psychiatric team regarding a patient who has attempted suicide and taken a paracetamol overdose
3. Assessing a patient with drug-seeking behaviour requesting a benzodiazepine prescription
4. Conducting a capacity assessment in a depressed patient who is refusing carers following a recent myocardial infarction
5. Managing an agitated patient with antisocial personality disorder who is experiencing chest pain
6. Assessment of a patient with a likely eating disorder and formulating a preliminary management plan
Timing
Each session lasted 3 hours. Scenarios were 20 minutes each, with 10 minutes for participants to complete the set task, and 10 minutes for feedback from the facilitator, actor, and other participating doctors.
Data collection
Quantitative data
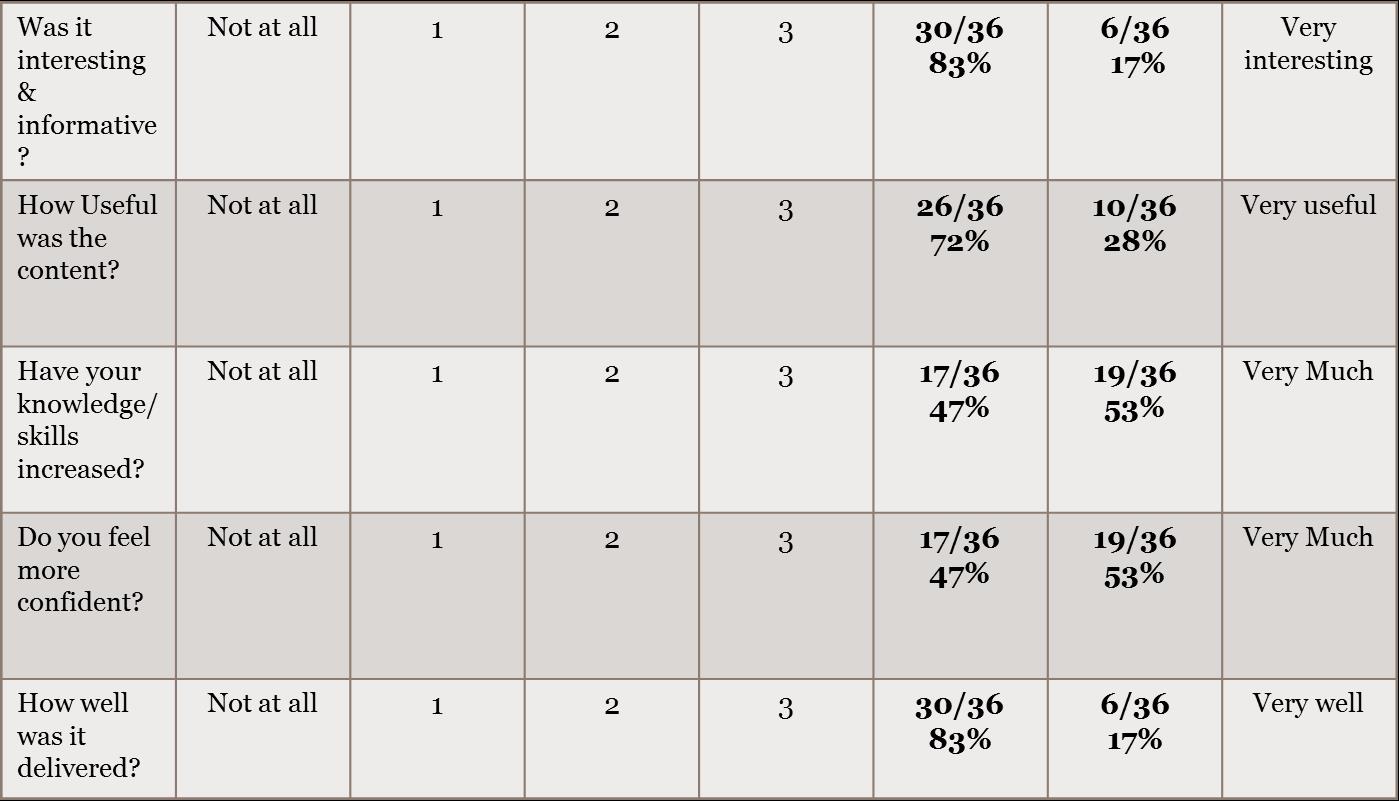
Foundation doctors were asked to complete pre- and post-session anonymous feedback forms, to ascertain their level of confidence in four domains (see Box 2): Participants were asked to rate their confidence level on a Likert scale from 1 (strongly disagree) to 5 (strongly agree) for each of these components.
Box 2 Quantitative data statements
“I feel confident in assessing patients with mental health diagnoses”
“I feel confident in making initial management plans for patients with mental health diagnoses”
“I feel confident in performing initial risk assessments in a medical setting”
“I feel confident in dealing with agitated patients in a medical setting”
Post-session feedback forms also included three questions, asking if anything could have been done differently about the day, if anything was done well, and a white space for any other comments.
Qualitative data
Qualitative data was recorded in the form of the written feedback documented post session and cross-checked by three members of the organising team.
Moderations to 2020 model
Minor changes to the format of the programme were made in August 2019, following presentation of interim findings to Health Education England. These were based on feedback generated from doctors and facilitators and are shown in Table 2. The logistics of the set-up on the day, scenarios, methods of feedback collection and analysis of data remained the same as in 2019.
Table 2: Moderations to 2020 Model
Feedback from 2019 Sessions
Updates made to 2020 Sessions
Title for the sessions ‘Psychiatry Communication Skills’ may have discouraged foundation trainees who were not interested in a career in psychiatry
Title changed to ‘Complex Communication Skills’
The sign-up process for foundation trainees required simplification
Foundation trainees were able to book onto the session via a centralised system, which also enabled their attendance to be tracked
Difficulties with room availability
Medical education managers contacted early in the academic year, with centralising to larger, well-equipped sites, improving room availability
Some trainees were less incentivised to attend with sessions held late in the academic year
Sessions held earlier in the academic year
Low trainee/facilitator numbers, limiting the ability to run scenarios simultaneously
Sessions centralised with the aim to run 2 sessions in North London & 2 sessions in East London
Clarity of brief needed on capacity assessment scenario
Slight amendments to scenario made with
input from old age psychiatry consultant,
including more details on occupational
therapy assessment in the doctors’ and
actors’ brief
RESULTS
Quantitative data
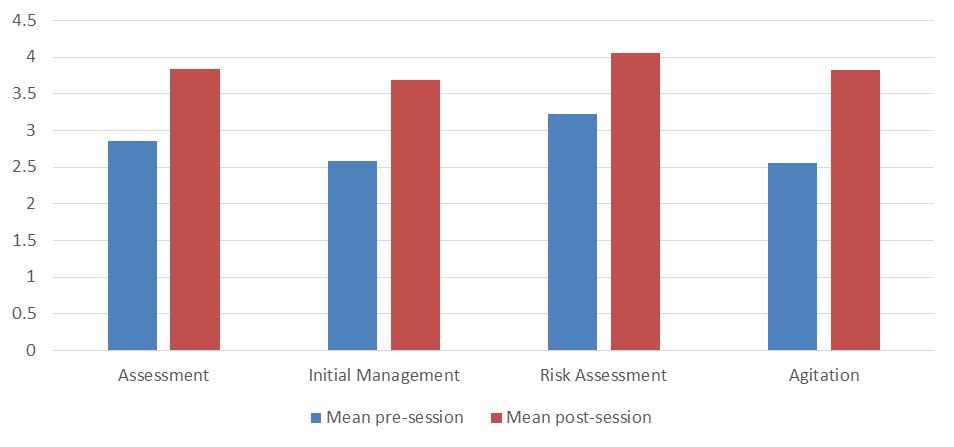
Results showed a consistent increase in confidence across all domains following participation in the simulation session. Increases ranged from 0.83 (“I feel confident in performing initial risk assessments in a medical setting”) to 1.27 points (“I feel confident in dealing with agitated patients in a medical setting”).
Figure 1: Trainee confidence pre- and post-session by domain
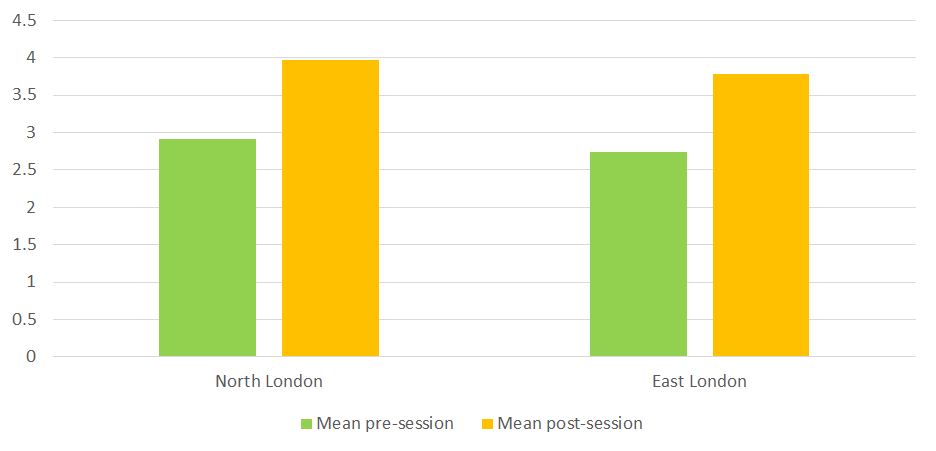
There were consistent increases in overall confidence ratings at every site, ranging from 1.03 to 1.25. Similar increases in overall confidence were observed in North London (1.04) and East London (1.06).
Figure 2: Trainee confidence pre- and post-session by region
There was a 94% (n=114) completion rate of pre-session feedback forms, and a 91% completion rate (n=110) of post-session feedback forms.
Qualitative data
No changes were made to the themes following cross-checking for validity.
Thematic analysis of the free text in the post-session questionnaires generated the following themes, as below.
Quality of the stations
Trainees consistently reported positive experiences regarding the quality of the scenarios (48), actors (43), feedback (30) and facilitators (20). In particular, there was a good breadth of scenarios, they were realisticand pitched at an appropriate level. Feedback was constructive and individualised.
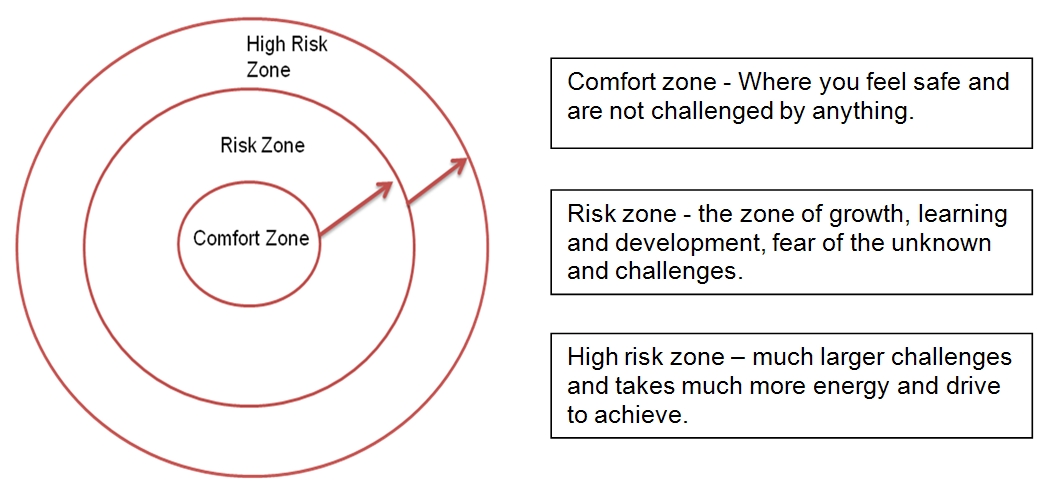
“enjoyed how challenging and how true to life the scenarios were”
“right level of difficulty. Took me out of my comfort zone!”
“really good to have an agitated patient as it was a very challenging scenario”
“quite clever to have capacity assessment in somebody with capacity because it’s harder in some ways!”
Five trainees would have liked to have had more scenarios, and three suggested that it would have been useful for the facilitator to have demonstrated a ‘model’ example of a scenario at the end of the session.
Environment/logistics of the circuit
General comments included that the circuits were well organised, and that there was a comfortable atmosphere for giving and receiving feedback. Eight trainees commented that the group size was too big (all were attendees at the Homerton session in 2020, which was the largest session run with 33 trainees in attendance).
Preparation of candidates for the circuit
Ten trainees (seven in 2019; three in 2020) said they would have liked clearer briefings or objectives for the scenarios – two trainees specified that this was in relation to the capacity assessment station.
DISCUSSION
Our results suggest that simulation training involving actors with mental health diagnoses can help foundation year doctors build confidence in their approach to such patients in a medical setting.
The greatest increase occurred in participants’ confidence in dealing with an agitated patient. It is likely that participants felt the most anxious about this prior to and during the session. Thus, they were able to gain a more immediate sense of progress in this domain by being able to practice this in a ‘safe space’ and after being able to see a visible de-escalation of the patient during the station. Participants also valued receiving supportive feedback from the actor, facilitator and their peers.
Participants also demonstrated large increases in confidence with respect to formulating initial management plans. This was the domain trainees were second least confident in prior to the session. It is likely that some trainees would be anxious about whether they have enough clinical knowledge when formulating an initial management plan for mental health patients. The chance to practice this in a controlled setting, with pertinent feedback, appears to have bolstered confidence.
Results were consistent between sites, suggesting that the content of the course, the experience of being in the roleplay itself, and the chance to receive feedback from experienced clinicians were of the most importance to participants, and local variations in delivery did not impact on participants’ experience to a great extent. The wide participation among foundation trainees in North and East London (121 trainees across two regions of London, over nine simulation sessions) suggests that there is a demand for such sessions and there might be an unmet need across other deaneries.
Qualitative data analysis showed positive feedback relating to the quality of the actors, the facilitators and the scenarios themselves. This likely contributed to the trainees reporting that the simulation was realistic and pitched at the right level, hence they were able to find benefit from them.
Limitations
There was a large difference in the number of participants enrolled in each session (three in the smallest, 33 in the largest). This will have given rise to a difference in experience between these participants, with the smallest group being able to partake in all six scenarios, and the largest group only being able to partake in one. This may have meant that those undertaking all six scenarios may have been exhausted by their experience, whereas those undertaking one may have felt that they did not get enough opportunity to practise. Confidence scores between these two groups were relatively similar, but it is unclear whether there would have been a difference if they were of similar size.
Linking of pre- and post-session feedback questionnaires to the respective trainees would have also enabled testing for statistical significance. A paired t-test could have been used to assess the increase in confidence observed by our simulation sessions in each domain.
This study tracked changes in confidence among foundation year doctors following a simulation session, but it did not assess the impact on their actual practice. This would be important to ascertain, to see if the session has allowed foundation year doctors to build on their experience of assessing and managing mental health patients in a medical setting. As a result, a cohort of participants has been selected for future contact regarding this to determine the potential impact on their clinical work.
The Medical Training Initiative (MTI) is a training programme to assist doctors with proven capability in anaesthesia/Intensive Care/Pain Medicine from low and middle income countries to undertake further anaesthesia training in the UK, for a maximum of 24 months1.
Why MTI?
It offers an opportunity not only to fine-tune their clinical acumen, but also to assimilate non-clinical skills (medical education, leadership and management, quality improvement projects) 2. The exposure most of the MTIs receive overseas is heterogeneous - in terms of level of supervision/independence, access to modern equipment and medications, lines of management, level of expectations and communication or interaction with patients. Funding received by training hospitals overseas can be variable thereby impacting on the resources available to provide standardised training. Under the MTI scheme, anaesthetic trainees can also take the FRCA examination.
From home to UK
A general awareness of the scheme helps the department to provide the MTIs with an appropriate support system. Details of the MTI scheme are available on the Royal College of Anaesthetists (RCoA) website.
It takes about 3-6 months after verification of the educational qualification by Educational Commission for Foreign Medical Graduates (ECFMG) via Electronic Portfolio of International Credentials (EPIC). The planning involves resignation from the current job, applying for a Tier 5 Visa to be in time for the GMC identity check (3 month deadline) and collecting the Biometric Residence Permit to be able to start work in the UK.
Medical staffing has more paperwork, one of which is the Disclosure and Barring Service (DBS). Prior intimation to the MTIs on the need for police verification from their home country would be of great benefit to make the process smoother. Hospital accommodation should be offered and organised in advance.
Acquaintance with the system
The MTI trainees often join at a time that doesn’t coincide with the UK training programme. Hence, a one-to-one induction customised towards overseas doctors will be beneficial. In addition to a named Educational supervisor (a mandatory requirement stipulated by the RCoA), the MTIs will benefit from having a nominated mentor within the department. The trainees can also get familiarised to the new healthcare system via the RCoA approved training courses – ‘Simulation for MTIs’ and ‘New to NHS’.
Allocating MTIs to theatre lists with only a select number of consultants in the initial stages helps them to settle in a new healthcare environment before they commence on-call (out of hours) duties. The MTIs should be encouraged to attend resuscitation courses like Advanced Life Support (ALS) as most of them follow the Advanced Cardiac Life Support (ACLS). They should be encouraged to document their progress like any other UK trainee via the RCoA Lifelong Learning Platform (LLP).
Anaesthetic training in the UK is very structured. The three stages of training (core, intermediate and higher/advanced) are well defined. The curriculum is well laid out and assists trainees to not only develop clinical but also gain non-technical skills. A six-monthly ARCP (Annual Review of Competence Progression) like assessment with annual anonymised multi-source feedback helps to create professional development plans, monitor progress and put supportive plans in place (if needed ) for a struggling trainee. The curriculum provides an opportunity for all-round development to every overseas trainee.
Gaining experience in non-technical skills (leadership and management, medical education and QI/audit projects) can be lacking in some home countries as the curriculum back home could be heavily biased towards the development of clinical acumen only.
What to expect from an MTI?
The MTIs have at least 3-5 years (may be more) of anaesthetic experience. The NHS benefits from their skills and experience. Their experience helps the department to allocate them to provide out of hours work (on-call) sooner than a UK trainee after an appropriate period of induction. The journey of patient experience also improves with the presence of experienced staff on the shop floor.
Departments gain from increased service provision too. As an example, after obtaining the initial assessment of competency (IAC), the MTI anaesthetists can be allocated to do solo theatre lists with a named supervising consultant anaesthetist present within the theatre suite. The reliance on locum staff is reduced thereby reducing unnecessary cancellations of theatre lists for lack of permanent staff. It reduces the financial burden on the NHS as staffing the department with locums can add to increased costs.
Patient safety is of paramount importance in any healthcare setting. Since the MTIs have a two year working contract, they are familiar with the department policies and guidelines unlike a locum doctor who does the odd shift in a hospital.
Equally, new skills gained by the MTIs are ultrasound guided regional anaesthesia, using a fibre-optic scope and different airway gadgets, ICU training, experience in geriatric and bariatric anaesthesia, total intravenous anaesthesia (TIVA) / target controlled infusion (TCI) alongside access to new medications like remifentanil, sugammadex which may not be available in low to middle income countries. The NHS provides excellent opportunities in simulation training and teaching courses.
However, a system of protocols can be unnerving to the MTIs. One may find them taking a step back when it comes to ‘decision making’ as they are not sure if it would be approved or criticised. At times, some of the MTIs may come across as unyielding despite adequate teaching. It is essential to remember that the process of unlearning to re-learning takes time, and therefore, patience is the key. This is where the concept of teaching experienced medical practitioners with knowledge comes in handy.
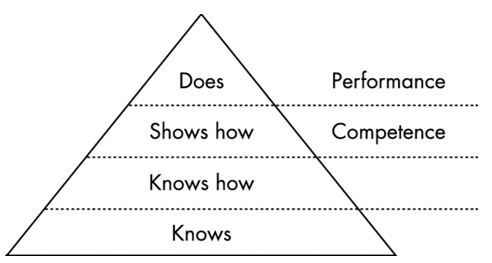
Training learners with knowledge
Medical education comprises three inter-linked domains - knowledge, skills and attitude.3 Though trainees may differ in terms of their motivation for learning, it can manifest only after the basic needs are satisfied - the external barriers to motivation such as life events and transitions, opportunities, and barriers to learning or obtaining information are addressed and they feel respected in the educational environment. The MTIs are essentially adult learners with pre-existing knowledge, who bring a great deal of first-hand experience to any work-place. Learning should, therefore, be integrative, which forms the basis of constructivism theory of learning4. New knowledge and skills should be integrated into the existing bank of knowledge. They also have pre-set strong tastes and habits which can be a real asset or a hindrance to effective learning. The educational supervisor should be able to encourage or curb them accordingly5.
Being adults, MTIs enter training situations with a self-image as independent, mature beings as they have already passed the qualifying exams in their home country. They can direct their own learning, including decision making and plans for taking examinations. The supervisors should engage with the trainees in activities that create a sense of self-responsibility to facilitate better learning opportunities.
Many adult learners suffer from a fear of failure and living up to expectations6 and thus, educational supervisors should be cautious to avoid unnecessary criticism. Instead the focus should be to offer constructive positive feedback. Any educational plan for them should start with an awareness of their prior acquired knowledge, an assessment of their educational needs along with room for motivation and reflection. This helps the trainees retain the original “frame of reference” while continuing to constantly challenge and transform practice via reflection on-action and reflection in-action. The educational supervisors need to provide a supporting educational environment, a structured guide for reflection and constructive feedback to develop the trainees’ reflective practice7.
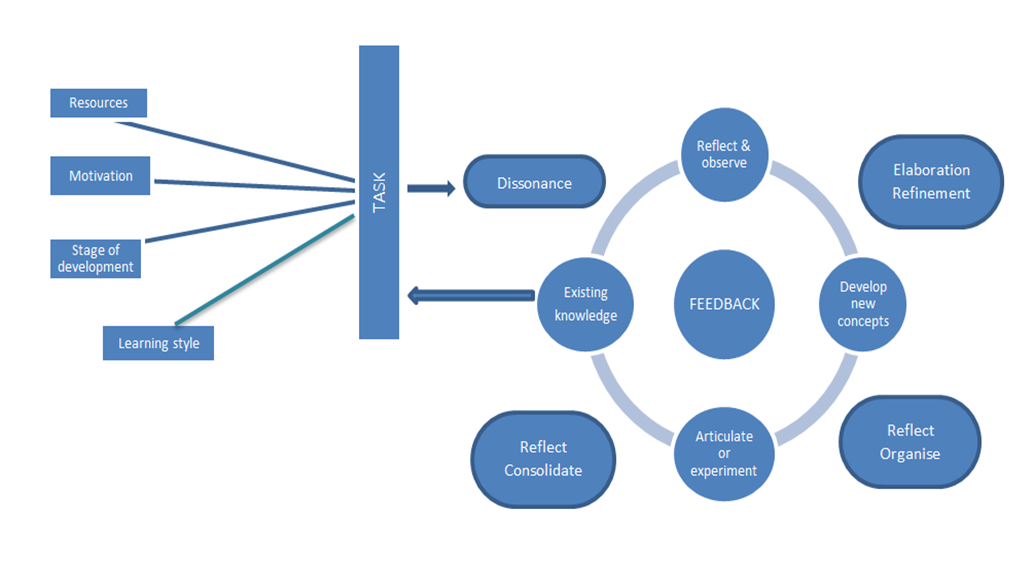
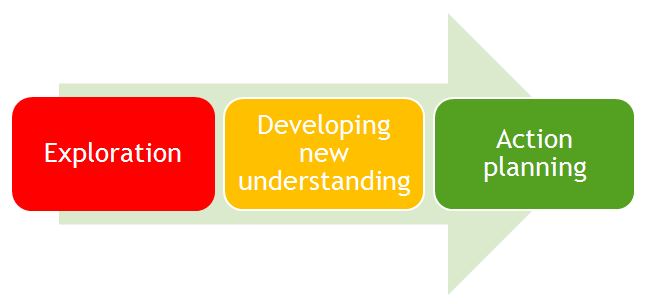
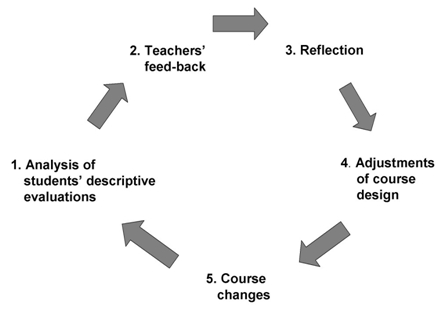
A simple multi-step approach involving active participation from both the trainee and the educational supervisor can be summarised into a model as below (Figure 1) 8. This model begins with the trainee’s prior knowledge.
Figure 1: Multi-step approach to training
The RCoA LLP, work-place based assessments and multi-source feedback along with the six-monthly meeting with educational supervisor are useful tools to deliver a holistic learning experience. It helps to refine the existing knowledge, reflect and provide constructive feedback. The supervisor can provide advance structures upon which the MTI can continue to build opportunities and gain confidence to rehearse and apply their new knowledge.
Summary
An organised induction programme, a period of familiarisation and good mentorship with patience helps to remove the barriers to learning for the MTI trainees. A dynamic trainee-supervisor relationship to accommodate the changing educational goals and an appropriate mix of strategies can help the MTI trainees attain medical competence, which is defined as “the habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values and reflection in daily practice for the benefit of the individual and the community being served3.”
Health Education England (HEE) runs the Medical Training Initiative (MTI) scheme on behalf of the Department of Health (the Government Sponsor) and is influenced by the Home Office Tier 5 Government Authorised Exchange Visa Scheme1. The Academy of Medical Royal Colleges is the national sponsor for visa purposes. Major stakeholders involved in this scheme are the GMC and GMC Approved Sponsors (e.g. Medical Royal Colleges), Postgraduate Deaneries/Local Educational Training Boards (LETBs), and National Health Services (NHS) Trusts, with support from the Department of Health.
The Royal College of Psychiatrists (RCPsych) Medical Training Initiative (MTI) Scheme enables qualified overseas psychiatrists to undertake training posts in the National Health Service (NHS) for a maximum of two years (2). The purpose of the scheme is to provide training opportunities for international psychiatrists in the UK to improve capacity as a professional and return home with broad knowledge and experience. Vacant core training (CT3) posts approved by Deaneries/LETBs are offered to eligible international doctors. Thus, the MTI psychiatry scheme can benefit overseas doctors, the NHS and the countries that trained them.
Although the MTI scheme was first established in 2009, the RCPsych only formally adopted the program in 2014. Some lessons were learned from the experience of the scheme in other specialities and provided an opportunity for the RCPsych to develop its own scheme. It developed a selection process for successful candidates and matches them with relevant placements in NHS trusts across the UK. This process takes into consideration the training needs of the overseas doctor and vacancies available in NHS trusts. The MTI Psychiatry Scheme is now in its sixth year and has gradually grown over the years as evidenced by an increase in annual allocation of the training post to 40 placements, a rise in the number of applicants from different regions of the world and an increase interest from employing NHS trusts. However, there are areas for further development in this scheme and there is a need to ensure that it consistently provides a good training experience to international doctors.
Various researches suggest that there are diverse difficulties faced by overseas doctors during their transition into a new country 3,4. Lack of information about NHS; clinical, educational and work-culture challenges; language and communication challenges; and discrimination challenges were issues experienced by international doctors while initially working in the UK hospital settings 5. The College has recognised these difficulties and wanted to understand how these are impacting on the international doctors and what can be done to help them.
Aims
The aim of this survey was to evaluate the trainee’s experience of the MTI psychiatry training scheme and explore difficulties during the training and what can be done to help. The purpose of this survey was to gather feedback on the current implementation of the MTI scheme.
Methods
An anonymous online survey consisting of 28 questions was sent to doctors using SurveyMonkey as part of the RCPsych Annual MTI survey. All doctors enrolled in MTI Scheme were identified through the RCPsych MTI mailing list. The survey was open in November 2018 for one month.
Results
Out of seventy-six, a total of thirty-one trainees completed the survey with a response rate of 40.78%. Most of them (n= 13) were from the age group 31-35 years. The findings of the survey are summarised in Table 1-3.
Table 1: Description of MTI doctors (n=31)
Gender
Male
17 (54.83%)
Female
13 (41.93%)
Prefer not to say
1 (3.22%)
Age (years)
<30
5 (16.12%)
31-35
13 (41.93%)
36-40
6 (19.35%)
41-45
5 (16.12%)
>45
2 (6.45%)
Year of MTI scheme
First
16 (51.61%)
Second
7 (22.58%)
Completed
8 (25.80%)
Country of Primary Medical Qualification
Egypt
3 (9.67%)
India
8 (25.80%)
Lebanon
2 (6.45%)
Nigeria
12 (38.70%)
Sri Lanka
3 (9.67%)
Trinidad & Tobago
1 (3.22%)
Skipped
1 (3.22%)
Previous psychiatric experience (Years)
3-5 years
17 (54.83%)
6-7 years
7 (22.58%)
8-10 years
5 (16.12%)
>10 years
2 (6.45%)
Worked in other countries besides the country of primary medical qualification prior to working in UK
Yes
2 (6.45%)
No
29 (93.54%)
Reason for choosing MTI Scheme
Recommendation from senior colleagues
15 (48.38%)
College reputation
16 (51.61%)
Training opportunities
24 (77.41%)
Research opportunities
6 (19.35%)
Job prospects
15 (48.38%)
Others
2 (6.45%)
Table 2: Induction, Supervision and Mentoring (n=31)
Initial induction at workplace prior to starting work
Yes
28 (90.32%)
No
3 (9.67%)
Allocation of educational supervisor
Yes
29 (93.54%)
No
2 (6.45%)
Frequency of educational supervision
Never
5 (16.12%)
1-2 times/year
14 (45.16%)
1-2 times/month
5 (16.12%)
Every week
5 (16.12%)
Other
2 (6.45%)
Able to attend course/study days
Yes
26 (83.87%)
Sometimes
4 (12.90%)
None
1 (3.22%)
Frequency of clinical supervision
Weekly
19 (61.29%)
Fortnightly
7 (22.58%)
Monthly
5 (16.12%)
Quality of clinical supervision
Excellent
7 (22.58%)
Good
16 (51.61%)
Fair
7 (22.58%)
Poor
1 (3.22%)
Access to out of hours support/advice
Always
18 (58.06%)
Sometimes
11 (35.48%)
Rarely
2 (6.45%)
Forced to cope with clinical problems
Weekly
2 (6.45%)
Monthly
3 (9.67%)
Rarely
17 (54.83%)
Never
9 (29.03%)
How often do you meet your MTI mentor?
I don’t have mentor
16 (51.61%)
1-2 times per year
5 (16.12%)
1-2 times per month
2 (6.45%)
Others
8 (25.80%)
Table 3: Work experience in MTI scheme (n=31)
Have you experienced any of the following?
Clinical training second to service
16 (51.61%)
Feeling unsafe
3 (9.67%)
Being punished for seeking help
4 (12.90%)
Being bullied
3 (9.67%)
Others
6 (19.35%)
Challenges encountered
Lack of relevant information about National Health Service (NHS)
14 (45.16%)
Lack of knowledge of regulatory framework
19 (61.29%)
Unfamiliarity with multidisciplinary teamwork approach
11 (35.48%)
Communication difficulties
8 (25.80%)
Cultural differences
15 (48.38%)
Varied level of training and support
11 (35.38%)
Others
7 (22.58%)
Reasons for choosing MTI Scheme
Training opportunities in the UK were considered by three quarters of the respondents for joining the MTI scheme. However, about half of the respondents reported job prospects, recommendation from senior colleagues and college reputation as pull factors.
Clinical and Educational Supervision
Three-fifths of trainees had weekly supervision with their designated clinical supervisor and three quarters (75%) of them rated the quality of supervision as either good or excellent. The majority (93.54%) of them had an educational supervisor and less than half met the supervisor 1-2 times per year. RCPsych has a mentoring scheme to support MTI doctors but half of the trainees (51%) did not have a mentor.
Out of hour support
Less than one-third of the trainees were never forced to cope with clinical problems beyond their competence. However, three-fifths of trainees reported that they always had access to out of hour support and advice.
Challenges encountered
Lack of knowledge of regulatory framework was reported by three-fifths of trainees while working in the UK settings. In addition to that, half of the trainees reported a lack of knowledge of NHS and cultural differences. One third had difficulty regarding multidisciplinary team settings and varied levels of support and training. About 51.61% felt that their clinical training was secondary to service and few reported feeling unsafe, being bullied and being punished.
Discussion
This is the first evaluation of the training experience of MTI psychiatric doctors. This study showed that most of the trainees had good work experience of psychiatry before coming to the UK. One of the undoubted strengths of the MTI psychiatry scheme is the recruitment of international psychiatrists with skills and experience of working in diverse cultural backgrounds and low resource settings. This is one of the potential benefits that the NHS can draw whilst delivering the health care smoothly. The majority of respondents in the present survey cited training opportunities as the main reason for choosing the MTI scheme. Child and Adolescent Psychiatry, Old Age Psychiatry, Addiction Psychiatry and Forensic Psychiatry were the subspecialties that received the highest interest in the MTI post in a 2017 survey 6. It is encouraging that most doctors were keen to gain further experience and training in subspecialties that were not readily available in their respective home countries.. A similar finding has been reported in the Royal College of Anaesthetists’ annual MTI survey where the majority chose subspecialties that were poorly developed in their respective countries, e.g. ICU and pain7.
Transition to the UK is not a smooth process for overseas doctors and must be supported during this transition phase (5). Lack of knowledge of the NHS, regulatory framework and cultural differences were the challenges faced by most MTI doctors in this study. The RCPsych International Medical Graduates (IMG) conference acknowledged that IMGs face more problems than British counterparts in succeeding in the system and recognised the importance of trainers, the role of employers in developing meaningful induction programmes and giving IMGs additional support and remediation if required8. This study showed that most of the trainees had attended local induction in the workplace before starting a job. Induction course content must be relevant and reflect issues concerning overseas doctors 9. It is particularly important to remember the specific needs of overseas doctors as they were trained in culturally diverse and low resource clinical settings. Several studies have shown that a structured induction program is a useful way to integrate doctors during the transition to the NHS10-12. Few trainees missed the local hospital induction as they arrived in the UK months later than expected and the trust could not arrange the training. With this hindsight, RCPsych organises the annual national MTI induction program to the new doctor in this scheme to complement and compensate for any shortcomings in the local hospital induction.
MTI posts should provide the trainee with an opportunity to train in a highly supported environment. Supervisors provide regular support and ongoing feedback during the training. Trainees value the support they receive through supervision, senior and peer support, and the opportunity to work in multidisciplinary team 13. It was reassuring to find that three-fifths of trainees had weekly clinical supervision as recommended by the Royal College of Psychiatrists.The quality of clinical supervision was rated as good by 51.61% of trainees and 22.58 % reported as excellent. Most of them had access to out-of-hour support/advice. Supervision is important for continued professional development as international doctors need more support than UK trained doctors 9. Unfortunately, few reported serious issues such as being bullied at the workplace and feeling unsafe. A survey of bullying of psychiatric trainees in the workplace reported that it was experienced equally by both IMGs and UK graduates, but IMGs were less likely to report the incident to the organisation14. It is important to educate IMGs about the mechanisms to escalate this concern for proper action. Besides that, it would also be prudent to include these pertinent issues during the annual MTI induction program to raise awareness among IMGs.
The MTI doctors had identified areas for additional support from the College, trusts, local deaneries, and senior colleagues in the 2017 annual survey6. The College took the following steps:
1. Annual MTI Induction Program: Full day induction program is held annually in the Royal College of Psychiatrists’ for new doctors in the scheme. The program is specifically tailored for doctors who are working in the UK for the first time. Highlights of the program include an introduction to the NHS, Good Medical Practice, Psychiatric training in the UK, ‘Person-Centred Care’, resources and support available for trainees and most importantly, communication skills workshop. It also provides an opportunity to meet with other MTI fellows and share experiences and set up informal support networks such as WhatsApp group. Twenty-three doctors attended the MTI induction program in 2019. Not all doctors recruited in the MTI scheme were able to attend the annual induction program because of the variable start date resulting from delay in visa processing. RCPsych could provide support to these IMGs by organizing the induction program two times a year.
2. MTI Mentoring Scheme: RCPsych runs a mentoring scheme and has been offering mentorship to MTI doctors for the past three years (15). Mentors are usually experienced RCPsych members who have volunteered in the mentoring scheme. RCPsych MTI team matches the mentor and mentee who will stay together for the duration of the placement. The current study shows that 50% do not have a mentor. We did not explore the reason for this, but we speculate that as doctors must actively express their interest in participating in this mentoring scheme and this might have shown less engagement.
3. Annual MTI Scheme Survey: Feedback is collected from MTI doctors each year as part of ongoing efforts to improve the RCPsych MTI scheme.
4. Sharing of experiences about the scheme between the trusts: Trust has varying levels of experience regarding the training scheme and the College has been facilitating the exchange of shared experience by the experienced trust to a new host trust.
This survey explored the experiences of doctors involved in the MTI scheme and it would be interesting to know findings from longer-term studies. Longer-term follow-up studies are needed to evaluate the positive impact of the scheme after the doctors return home on completion of the training. It is hoped that invaluable insight gained from the survey can be used to strengthen the scheme as well as provide learning points to other specialities with similar training scheme for international doctors.
Conclusions
This survey provides useful information regarding training experiences in the MTI psychiatry scheme. The first step in making the difference is getting feedback directly from those involved in the scheme. RCPsych MTI Scheme is an evolving program and measures were put in place to address the needs/concerns that emerged from the survey to enhance the training experience of the MTI doctors.
Temporomandibular joint disorder (TMD) refers to a broad spectrum of disease states characterised mainly by pain and tenderness in the temporomandibular joint (TMJ) and adjacent soft tissues, TMJ clicking and limitation in jaw movements. TMD symptoms vary in severity and if left untreated, may lead to debilitating pain and limited function with a significant impact on quality of life. The estimated prevalence of TMD is 2-6 % 1 although up to 25 % has also been reported. The aetiology of TMD is not fully understood and it is multifactorial including organic disease of the TMJ, trauma, malocclusion and stress. Treatment options include reassurance and education, physical and splint therapy, simple analgesia and other drugs, surgical intervention or combined treatment. Most cases of TMD can be managed non-surgically. Most patients with TMD have traditionally been initially managed by a GDP and are often referred to a specialist for further non-surgical or surgical therapies if symptoms are not controlled.
Andersen et al (1999) reported approximately 3 out of every 100 attendances to GMP services in Wales, UK were due to oral and dental problems 2. The number of people attending their GMP for dental problems has been increasing 3, 4. GMPs have expressed concerns about their ability to treat dental diseases 5 as these conditions are beyond the scope of their expertise.
Consulting GMPs for TMD has been observed dating back to over nearly six centuries 6. Similar to the rising trend of attending GMP for oral problems in general, there has been an increasing tendency for patients with TMD symptoms to approach their GMP as the first point of contact due to comparatively easier availability and financial feasibility. Prompt referral to a GDP or relevant speciality is likely to improve management and reduce the adverse impact on quality of life. This could potentially reduce the burden on overstretched NHS hospitals in UK. There is paucity of data on the management of TMD among GMPs in UK. To the best of our knowledge, there has been no prior survey of their knowledge of and attitude towards assessment and management of TMD. The objectives of this study are to assess the current experience of UK GMPs with the care of TMD patients in primary care.
Method:
Design
A Single-Centre Cross-sectional survey
Study population and survey development
GMPs listed within the Leicester City Clinical commissioning groups 7 with access to refer to the regional NHS Oral and Maxillofacial Services Providers. GMPs were formally invited to complete a specifically prepared postal questionnaire (See Appendix) consisting of their knowledge and management of TMD. In order to ensure the reliability and validity of the results of survey, the questionnaire was pretested on the GMPs in five different Urban GP surgeries other than Leicester city. To maximise response rates, a follow-up questionnaire and telephone calls were arranged after four weeks if no reply had been received. Confidentiality was maintained by number-coding the questionnaires. Selection bias was avoided by sending the questionnaire to all the GMPs in the Leicester city area.
The questionnaire Survey was conducted in February 2018 and comprised of 16 questions on TMD and two demographic questions .The questionnaire assessed knowledge of TMD including clinical features, diagnostic criteria, prevalence and aetiology. Participants were asked about awareness of current guidelines and treatment options, and their management practice, whether they would refer to a GDP, or oral and maxillofacial surgeon or TMD specialist. They were asked whether they update or have updated their knowledge about TMD. They were also invited to propose which means of TMD knowledge provision they would prefer to receive demographic data included information on the gender and clinical experience. There were no open-ended questions and participants were asked to select the most correct statement from more than one option in some of the questions. Participant GMPs were informed in the invitation letter that participation was voluntary, all responses were anonymous and that the study would be published in a peer-reviewed journal. Participation in the survey implied consent.
Data analysis
Data was analysed descriptively using IBM SPSS Statistics for Windows version 21 (IBM Corp, Armonk, USA). We aimed to determine whether there is any relationship between GMPs knowledge of diagnostic features of TMD and their length of experience in practice. We stratified GMPs into two groups according to the seniority [certificate of completion of specialist training (CCST) obtained within 5 years or earlier]. Chi square test was used to compare the proportion between two groups and a p value < 0.05 was considered to be statistically significant.
Results:
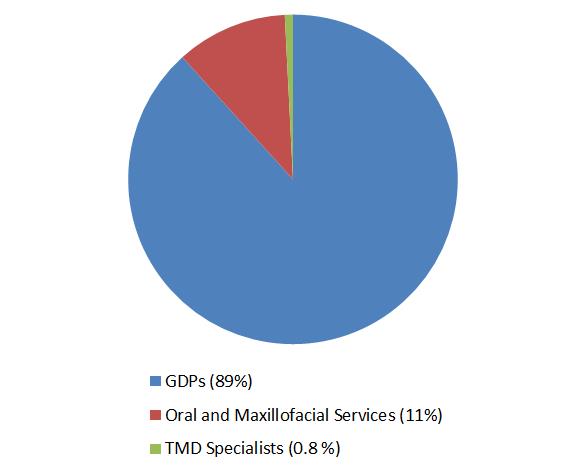
Out of 259 GMPs who were contacted and invited to participate, a total of 126 practitioners returned the questionnaire by post {response rate (48.6%)}. Of the respondents, 2 did not correctly fill the survey questionnaire; the remaining 124 responses were analysed. There was a slight male preponderance (55%). Only 12% GMPs rated themselves above average (score >4) in terms of being familiar in general with TMD. Five percent of responders were aware of published guidelines of TMD management. None of them were familiar of Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD). Seventy-four percent of participants, including both GMPs with experience less than 5 years and more described the clinical features consistent with the diagnosis of TMD. 4% selected the correct option when asked about the possible causative factors. None of them knew about the actual prevalence of TMD symptoms in the community and majority of GMPs underestimated the proportion of population with TMD. Fourteen percent were correct in identifying the age group affected by TMD. While majority of them (56%) chose ‘ No’ and 12 % of them selected ‘Don’t know’ , thirty-two percent, participants believed that subjects with TMD symptoms require initial radiographic assessment before any treatment is commenced. 95% of respondents believed that they have seen on average 2 to 4 TMD patients per month. Eighty nine percent of respondents referred patients to GDPs whereas remaining 11 % of GMPs contacted Oral and maxillofacial surgery service providers for TMD management (see Figure). Only one of the participants was familiar of specialist-clinical services for TMD who, in addition to sending these patients to GDPs, also referred TMD patients directly to specialists. Majority of them (66%) were not comfortable in seeing and provide initial management of TMD and 34% of GMPs, in addition to referring TMD patients to other services, also provided initial treatment to these patients. All those who offered this initial non-surgical treatment to manage TMD, selected combined modalities i.e. patient education, pharmacological and physical therapy. In every 25 participants (6%) has updated their knowledge through internet resources in order to increase their awareness and knowledge about the TMD management in community. Almost all (97%) of the GMPs would welcome relevant continued education programmes and receiving leaflets / published literature. The summary of GMPs responses from survey is given in Table 1. Group analysis of participants (See Table 2) did not show any statistical association between the experience of GMPs and their knowledge of TMD clinical features (Chi-square statistics 3.78, p = 0.5).
Figure: GMPs Referral for TMD patients GMPs: General Medical practitioners, TMD: Temporomandibular joint disorders, GDPs: General Dental Practitioners
Table 1: Summary of the main responses from the GMPs survey about TMD knowledge
Familiarity of TMD rated as above average
12%
Awareness about TMD guidelines
5%
Familiarity with RDC Criteria of TMD
0%
Correctly identified the etiological factors of TMD
4%
Correctly identified TMD clinical features
74%
Correctly identified the TMD prevalence in General population
0%
Correctly identified the age group suffered most with TMD
14%
Selected ‘No’ about the need of radiograph before TMD management is initiated
56%
Not comfortable in seeing and provide initial management of TMD
66%
Selected combination of pharmacological and physiotherapy to treat TMD
34%
Have referred TMD patients to GDPs
89%
Have referred TMD patients to Oral and maxillofacial surgery
11%
Have updated the TMD knowledge through any resource
6%
Keen to receive further information about TMD
97%
GMPs: General Medical practitioners, TMD: Temporomandibular joint disorders
Table 2: Distribution of participant GMPs according to their seniority and familiarity with TMD clinical features
Experience as GMP
Correctly identified TMD features (n)
Incorrectly identified TMD features (n)
Greater than 5 years
50
11
Less than 5 years
42
21
Chi-square statistics 3.7894 p = 0.5 GMPs: General Medical Practitioners, TMD: Temporomandibular joint disorders
Discussion:
Main Findings
Our study is the first which has explored in-depth the experience of GMP with TMD management. Findings from the survey indicate that uncertainty exists among GMPs regarding their level of knowledge. Most GMPs had no awareness of TMD management guidelines. The RDC/TMD 8 is a valuable tool to assess signs and symptoms and to classify patients with TMDs. Participants were not aware of these guidelines. The response from GMPs indicated that the prevalence of TMD within the general population is not accurately recognised at all along. The majority of respondents do not appreciate that TMD patients require radiographic evaluation before treatment planning. None but one of the GMPs was aware of clinicians with a subspecialty in TMD. All patients with such condition were referred either to dentists or maxillofacial surgeons. This reflects an awareness of an appropriate chain of referral 9. There was a generalised consensus in considering the general medical practice environment as an unsuitable place to manage dental problems 5, including TMD. A positive finding of our study was that a significant proportion of GMPs in Leicester city are interested in learning about TMD. This indicates there is a need for designing formal training courses for GMPs. If appropriately trained, these practitioners will potentially have an enhanced capability of not only managing TMD at an initial level but also providing knowledge and guidance to other practices and community services
Comparison with existing literature
The knowledge, attitude and practices of GDPs regarding TMD management are widely reported 10-12 but there is hardly any study relating to General Medical Practice. Results of a questionnaire survey based on screening of TMD in 38 London teaching General Medical Practices were similar to our findings 13. .Thirty-six of 38 GMPs, who replied in that survey, routinely assess the TMJ as part of the physical examination for symptoms of TMD whereas TMJ assessment was not included in primary health care screening. Similarly to Cope et al 2015 5 another qualitative study in the North-west of England GMPs experiences of chronic orofacial pain, including TMD, revealed primary health care providers consider themselves unable to meet the diagnostic and management challenges of TMD 14 .GMPs in the face to face interviews explained that despite these limitations, they do offer TMD patients pharmacological and other complimentary approaches, particularly acupuncture. Similar experiences of GMPs are also reflected in our current findings.
Strength and limitations
The main strength of this survey is that, to the best of the authors' knowledge, it was the first study which determined Knowledge and experience of GMPs towards Management of TMD. In simple language but a comprehensive and pilot tested questionnaire was designed to assess GMPs knowledge of TMD which they were expected to have gained from available literature.
There were mainly two limitations in our survey. Firstly, the sample size was small as the study was confined only to the participant GMPs practising in Leicester City, hence it may not be representative of all GMPs across the country. Despite this weakness the results may serve as a scoping study to justify further research such as qualitative surveys. Secondly, there was a relatively low but acceptable response rate (48.6%). Although this raises concerns about the research validity, but studies have demonstrated that there is no direct correlation between response rate and validity 15. Also, Surveys with comparatively low response are only marginally less accurate than those with much higher reported response rates 16.
Implications for research and practice
In addition to other main areas of practice, the Royal College of General Practitioners (RCGP) curriculum also highlights the importance of Specialist GMP trainees attaining competency in learning about common oral and maxillofacial conditions 17. Considering the frequent attendance of patients with oral and facial diseases in primary care and the limited undergraduate Medical training, valuable suggestions have been made for GMPs to promote attendance at specialist oral medicine and oral surgery clinics to enhance exposure to common maxillofacial diseases. Despite these recommendations, surprisingly little no active interest has yet been shown by GMPs trainees. There is a need to integrate GMP training with some exposure to the specialty of Oral and Maxillofacial surgery to improve expertise in the management of TMD and other oral diseases, especially in view of the increasing trend for patients to initially present to their GMP for advice about TMD and other chronic orofacial pain conditions. .
Evidence based literature regarding dealing with TMD at a non-specialist level have been published in the medical literature 18-20. This provides clinicians including GMPs with sufficient knowledge to diagnose and refer TMD to the relevant clinician. The British association of Oral and Maxillofacial Surgeons (BAOMS) TMD commissioning guide 2014 8 suggests GMPs to refer TMD patients to a GDP in the first instance to start initial treatment. Early diagnosis, counselling and management of TMD tend to improve prognosis and reduces the severity of impact on the quality of life 21, 22. It is crucial that GMPs are have sufficient knowledge to make an early referral to an appropriate clinician in order to commence conservative measures including education and advice, use of a bite guard, medications and self-directed physical therapy. The limited access to dental care within the UK, despite a National Health Service (NHS), is a well-recognised challenge. There are multiple barriers to accessing dental care 23 including delays or failure in getting appointments which results in the patient turning to General Medical Practice for advice 4. GMPs have also expressed concerns regarding accessibility to and the collegiate relationship with GDPs in the management of chronic facial pain including TMD 14. Whether the aforementioned limitations are system related or simply patient factors, they are certainly hindrances to timely assessment and intervention. We suggest that suitably trained GMPs should be able to commence the initial conservative management of TMD patients whilst simultaneously referring patients to a GDP or appropriate specialist so as to optimize the management and possibly reduce subsequent referrals in the long term. There is an immense potential for primary care to be integral part of initial management of TMD. A large scale nationwide study could potentially help future planning for care within the community.
Conclusion:
Respondent GMPs in East midlands England, demonstrated limited knowledge and confidence related to the diagnosis and management of TMD. Appropriate post-graduate training and educational opportunities for ongoing continuing professional development related activities would improve the knowledge and awareness of TMD management, potentially leading to more effective care within the community.
Psychiatric trainees in Iraq face many challenges that limit their immediate access to improved training opportunities. These include limited access to classroom teaching, regular clinical supervision meetings and fewer opportunities to attend international conferences and placements. These challenges are more acute in those specialities with the greatest shortage of consultants (for example, forensic and child and adolescent psychiatry).
Furthermore, the fragile security situation in the capital and larger cities and the post-conflict disruption to educational institutions consequent to these difficulties makes it difficult for those in the UK and elsewhere to visit the country and support educators and training on the ground.
Against this background and as a medical educational team in the UK (Oxford University Medical Education Fellows, OUMEF) with an interest in developing training opportunities for peers and colleagues in Iraq, we set up the Oxford Psychiatry in Iraq (OxPIQ) Project, beginning with a project development team that included Medicine Africa, an experienced online distance learning platform.
So what is the role of TEL in the delivery of online distance learning targeted at medical professionals in these circumstances?
Meeting the Challenge – the role of TEL
The concept of Technology-enhanced Learning (TEL), or Web-based learning (WBL), defined as the use of information and communication technologies in teaching and learning 1, is a relatively new phenomenon. Nevertheless, there is a considerable body of evidence supporting the use of TEL in various clinical and non-clinical settings.
Mccutcheon et al. 2 systematically reviewed thirteen studies and found that ten of these studies concluded that online learning is as effective as traditional or classroom teaching, despite the limitations of some of these studies.
In a large meta-analysis, Means and colleagues 3 concluded that students using online teaching performed modestly better compared to students learning similar material using face-to-face teaching. Combining face-to-face and online teaching resulted in larger benefit compared to the use of face to face methods only.
TEL can address the learning limitations in classroom settings due to expanding curriculum coverage and limits on contact time between students and lecturers/trainers alike. It can contribute to better use of such face-to-face classroom contact through the facilitation of the flipped classroom approach. 4 In this approach (also called inverted instruction and upside-down teaching), students acquire the basic information of the lesson outside the class (usually using online materials) and then develop their knowledge further in the class by sharing their learning, interacting with other classmates and teacher, and discussing various aspects of the study topic.These advantages have enabled TEL to revolutionise distance learning at many levels – enabling greater access to education by overcoming geographical and time-zone boundaries.
An allied concept within distance TEL is the concept of virtual teams 5 where health professionals come together to teach and learn from each other independent of location. Of itself, this offers some advantages. These include the possibility of addressing speciality-specific training gaps through the incorporation of the relevant expertise within the team - and to the creation of what is termed “connectivism”. This term refers to the use of internet technologies to enhance learning through online peer networks 6 and the development of communities of practice. 7 The latter allows for workplace-based learning with trainees learning from more experienced practitioners and moving towards the same through greater competency acquisition.
In a similar vein, creating networks of professionals may help to establish more longer-lasting relationships of mutual benefit between the UK and Iraqi professionals (e.g. through collaboration on training programmes, conferences, etc.). Also, cross-cultural online learning has been shown to be very useful in improving language skills and cultural awareness of learners and educators. 8 With language translation technology, any language difficulties can also be overcome, especially if the educator can observe the learners’ responses to the translated text and offered the opportunity to give further explanations and clarifications when necessary. 9 Finally, as well as sharing knowledge and experience within groups, TEL enables opportunities for mentoring and coaching individuals. 10
For our purposes, these findings and opinions support the use of online learning as a suitable distance learning “add-on” to existing training opportunities in Iraq.
TEL and Learning Theories
Learning theorists suggest that experiential and constructive learning theories are most appropriate to learning in the clinical context. Both are possible with TEL (as well as being facilitative of behaviourist and cognitivist approaches).
For example, the virtual classroom environment can enhance the learning experience of the participants by improving their analytical skills by thinking through case formulation and management plans. 11 Participants in online learning could be assessed and receive the feedback immediately. Ideas can be shared, and there is no passive acquisition or transfer of knowledge as is the case with traditional lectures. These aspects have implications for the design of the educational sessions and are discussed below in the learning methods section.
Challenges of Online Distance Learning
There are many challenges associated with online distance learning. Firstly, there is the potential lack of the required technologies (internet access, laptops or desktop computers), the expenses of subscribing to these online learning templates, the need to have technical support, and similar technical and logistic issues. 12 These technical problems may impair access to and functioning of the virtual team. The choice of an experienced online platform must, therefore, be considered carefully.
Secondly, there may be ethical issues about the protection of patients’ confidentiality in these sessions, especially when there are different laws of privacy that are applied in the UK and Iraq. This will require knowledge of the relevant professional requirements by the tutor team for example.
Furthermore, the student-teacher relationship has traditionally been underpinned by direct face-to-face contact and being present at the same time and place. 11 Therefore, learners and educators might be less satisfied with online learning. For these reasons, the concept of blended learning (careful integration of online learning with face to face learning experience) has been developed to overcome the limitations of a standalone online or face to face learning and has been found effective and applicable in various settings. 13
Thirdly, any distance online learning programme must understand and support existing “local” training provision and arrangements, in the classroom and the workplace. This requires liaison and cooperation with the training providers and institutions on the ground.
For clinical training to be relevant, it needs to reflect the learning needs of trainees in the workplace – in keeping with adult learning principles and cognitive apprenticeship models of learning. 14 The latter includes the importance of clinical decision-making underscored by the higher levels of Bloom’s (1956) cognitive domain. 15 To this end, then appropriate learning and assessment methods are needed to enable effecting learning.
In other words, while necessary, TEL may be insufficient in enhancing learning outcomes if allied learning methods are not chosen appropriately. Also, in our view, TEL is not a substitute for bedside teaching.
Table 1 summarises this appraisal of online distance learning (using the online platform provided by MedicineAfrica).
Table 1 Strengths and limitation of using MedicineAfrica (web-based virtual classroom environment)
Strengths
Limitations
Better use of the participants time and resources
Limited or lack of internet access
Overcome geographical barriers between two countries
Technical and logistic issues
Improve critical thinking and communication skills
Subscription expenses Appropriate choice of learning methods
Form long-standing professional networks
Ethical and legal issues (e.g., confidentiality)
Interactivity
Lack of direct face to face contact
OxPIQ & Project Development Team
OxPIQ is a partnership between Medicine Africa and psychiatrist members of the Oxford University Medical Education Fellows, with experience of working in Iraq. The Oxford University Medical Education Fellows (http://OUMEF.org) is a group of trainees from across medical and surgical specialities with interest in medical education and training.
Medicine Africa (http://medicineafrica.com) is an innovative clinically targeted online platform developed in collaboration with King’s College London’s Centre for Global Health, within the King’s Somaliland Partnership. Built at low bandwidth, it enables collaboration between medical professionals in the UK and those in remote or fragile states to enhance education in various clinical specialities using online sessions (live courses and mentoring sessions). Please see Appendix 3 for a screenshot of one of the active sessions of OxPIQ.
The next step was to invite representation and support from the Iraqi Board of Psychiatry and the Medical Education Unit in Baghdad. These developments led to the formal launch of OxPIQ Partnership in March 2016. Later on, the many UK and Iraqi doctors joined the Partnership as tutors and learners.
The Virtual Learning Team: Trainees, Specialty Consultants & Tutors
Iraqi psychiatry trainees were then recruited, and their more pressing learning needs to be appraised based on their views and those of the Iraqi Board of Psychiatry supervisors. Learning needs to emerge included the management of older patients with dementia and functional disorders, assessment and management of children and adolescents (with autism and ADHD for example), forensic patients and those with drug and alcohol addiction. The team thus formed was composed of up to ten psychiatry trainees from Iraq and five senior psychiatrists/tutors each, from Iraq and the UK respectively. A schedule of fortnightly seminars was agreed and published on the learning platform. Case-based discussions were used as the main educational activity during these seminars.
Learning Methods and Processes
As noted earlier, the importance of experiential and constructivist learning methods are key to clinical education. Our literature appraisal revealed that they are essential elements of successful TEL in this context too. 16, 17 To these must be added learner engagement. 18
Virtual or online (anonymised) case-based discussions (CBDs) are valid and reliable learning tools. 16 They are interactive and centred around the students and their learning needs while a facilitator guides the process of learning. Learners are engaged through discussion of actual clinical cases, so preparing learners for real-life experience. 19 Also, expert facilitation and peer feedback to trainees promotes clinical knowledge and skills’ development. 20, 21
Effective small group teaching is characterised by four main strengths: flexibility, interaction, reflexivity and engagement. 22 Flexibility is when the teacher responds to the needs and learning of the students dynamically and helps them to explore wider pedagogic spaces. A higher degree of interactivity is usually seen in small group teaching compared to a larger group. Teachers are better able to continually engage in self-reflection and listen sensitively to students in a small group and observe the dynamics between the members of the group, leading therefore to better reflexivity. Engagement refers to encouraging the students to develop their academic identity and engage in lively debate about the various aspects of the topic discussed.
We aimed to replicate these characteristics. For example, a small group discussion allowed better interaction with each participant (interactivity); the presence of chat windows enables the facilitator to self-reflect on the process, monitor engagement and respond reflexively using questions and answers to stimulate interest and respond flexibly to individual trainee knowledge gaps. Tutors are encouraged to identify trainees’ learning needs and facilitate interactivity, and timely feedback as these are highly valued by the participants and help to keep them motivated and engaged. 18
For further reading in this area, we recommend Brindly and colleagues’ 23 ten strategies to increase students’ motivation towards and engagement with online learning (see table 2).
Table 2- Strategies to increase engagement in online teaching (modified from Brindly and colleagues, 2009) 23
1. Transparency of expectations: Making the learning objectives very clear and relevant to the participants learning needs. The teachers must be open to the learners’ suggestions and must be willing to discuss the process and purpose of the educational activities.
2. Clear instructions: The educational activity, its timing, duration, and the technical aspects are described in detail to the participants. They should not be left to ‘try out things’ and must be guided explicitly.
3. Appropriateness of task for group work: For the online activity to succeed, individual versus group tasks should be differentiated. In our example, this may be done by asking the participants to do a particular task before the session (e.g., read about severe and enduring mental illness), and then to work together on producing a formulation for the case discussed. This will increase their motivation to be involved in various tasks.
4. Meaning-making/relevance: The case-based discussions (and any online activity) should have relevance for the participants and aim to enrich their experience in their clinical work.
5. The motivation for participation embedded in course design: It is essential that participants in the online activity understand that the success of the group and the course depend on the individual effort of each participant.
6. The readiness of learners for group work: This aspect describes the development of a sense of community through a professional relationship which leads to better collaborative work.
7. The timing of group formation: Before the participants join in the educational activity, it is preferable to have some discussions before the tutorial on their learning needs to allow a time for rapport to develop to enable better group activities.
8. Respect for the autonomy of learners: Joining and leaving the educational activity (and the whole online course) should be voluntary. No penalties should be attached to leaving the course. Learners should have the freedom to choose what aspects of the online course is relevant to them.
9. Monitoring and feedback: The tutor should monitor the progress of the participants, and timely feedback is given respectfully to enhance the engagement and motivation of the participants. Please see Appendix 1 (lesson plan) for more details on feedback and evaluation.
10. Sufficient time for the task: Participants should be given time to be actively involved in the session. This is particularly important in a distant learning session when issues related to sound quality or speed of internet connection may prevent some participants from engagement.
The focus of the Lesson Plan Design
To these ends, the focus on the lesson design was on using problem-based learning methods (e.g. CBDs) within a small group setting (between 4-12 members) and a format that promoted learner engagement. A sample lesson plan is provided in Appendix 1.
In practical terms, tutorials were held fortnightly in term-time. All participants received an email notification to inform them of the session topic, and the tutor uploaded the slides from the session to the website beforehand. Participants logged-in to the site (http://medicineafrica.com) and interact with the tutor by voice (requiring only simple microphone equipment) and by writing in a chat window.
Evaluation and feedback gathering
The evaluation of the effectiveness of these sessions was reliant originally on trainees’ immediate reaction (table 3, level 1 evaluation, Kirkpatrick 24) using formal feedback tools provided online by MedicineAfrica. This feedback was shared with tutors and the Project Team. Please see Appendix 2 for the template used in collecting feedback after each session.
Subsequently, members of the project team approached trainee representatives, tutors and Iraqi Psychiatry Board leads separately for further feedback and appraisal of learning needs. Furthermore, some months after a tutorial we have asked trainees for evidence of learning across the higher levels of Kirkpatrick’s evaluation model.
Regular feedback from the Iraqi and UK participants has been positive. The sessions have been associated with improved clinical knowledge and skills of the Iraqi Psychiatry Trainees. Requests for certificates of tutorial participation have been agreed upon and provided by the project team addition, so supporting learners’ (and tutors) portfolio development.
Table 3 Kirkpatrick’s (1996) Levels of Training Assessment
Level
How to assess
Level 1: Reaction (the participants feeling about the training
Feedback during and after the tutorial using the feedback questionnaire
Level 2: Learning (improving the participants’ knowledge)
Post-tutorial questionnaire and interviews
Level 3: Behaviour-also called Transfer (improving the participant's performance)
Direct or indirect observation and assessment of the skills and competencies of the trainees
Level 4: Results (cost-effectiveness, engagement, sustainability, adherence to evidence-based practices)
regular meetings between the participants, tutors, and stakeholders.
Further cooperation
A surprising (and very welcome) outcome of the project was, through the facilitation and support of the Iraqi Board of Psychiatry, the introduction of educational workshops in Baghdad. These workshops were held in Medical City, Baghdad, in May 2017 and April 2018 and were facilitated by tutors (YH & H Al-T) from the OxPIQ Partnership. They covered targeted topics such as old age psychiatry, addiction, organic and forensic psychiatry. Trainees and senior psychiatrists from Iraq attended; their feedback showed how they valued the interactive nature of the teaching and use of CBDs as learning methods, resulting in high levels of engagement.
Conclusions
This paper describes the process of designing, delivering, and the early evaluation of an online distance TEL programme for mental health professionals based in the UK and Iraq.
TEL has had an important role in overcoming the geographical barriers and other challenges to developing training opportunities in Iraq and other developing countries. We are of the view that it could be used more often to connect professionals working in similar circumstances and with other disadvantaged groups, including refugee and asylum seekers. It is a flexible way of providing training to professionals working with those groups in relatively remote and resource-deprived environments.
Greenhalgh 25 suggests that three factors are needed for the success of online educational activity: ease of access, perceived usefulness of the activity to the learning requirements of the students, and the interactivity of the session. In our experience, these are important. Also, we believe that additional consideration should be given to (i) working with an experienced online platform provider; (ii) working with local educational institutions, trainers and learners to identify unmet learning needs and support existing learning opportunities/programmes; and (iii) adopting an iterative approach to feedback and evaluation.
Appendix 1: Example of a Lesson Plan
Session title
Case-based discussion on management of severe and enduring mental illness.
Duration of session
60 minutes
Tutor
A UK-based Psychiatrist
Learner group
Psychiatry Board Trainees and Senior Psychiatrists in Iraq and UK
Step 1– Learning outcomes
a) Describe the various stages in the management of the cases discussed during the session.
b) Enhance the participants learning using case-based discussion with peers and seniors in the UK and Iraq.
c) Improve the presentation and discussion skills of the participants and their communication skills.
d) Explore ethical, cultural, and social issues related to the management of mental disorders and improve cultural competency and awareness.
Step 2 – Learning Plan
Introduction to the online tutorial -10 minutes
a) Highlight the learning objectives of the tutorial
b) Stimulate the thinking of the participants by asking about their current knowledge of the subject, whether they managed similar cases in their clinical work, and what are their learning needs.
c) Outline the tutorial structure and further engage the participants by informing them about other details (e.g., if they can ask the question during or after the case presentation)
2. The tutorial in a case with severe and enduring mental disorder – 30 minutes
a) Participants are encouraged to interact with the tutor who should be invited to keep the tutorial interactive.
b) The case presented will provide an overview of the patient’s journey from the initial presentation, followed by the investigation, then treatment plans. Discussions of the differential diagnosis are important.
c) The tutor will assess the knowledge of the participants by asking questions on the various aspects of the case presentation (e.g., what is your differential diagnosis for a patient presenting with auditory and visual hallucination? What investigations would you request?).
3. Recap and Q&A time- 20 minutes
a) Tutor to give a summary of the main learning points from the tutorial and linking these to the learning outcomes presented at the beginning.
b) Participants are given enough time to ask questions and to participate actively in the session.
Step 3 – Assessment
Before Lesson
Before the tutorial, the tutor should know the current educational curriculum of the participants and their learning outcomes in that subject. UK and Iraqi Psychiatry curriculum are different, and therefore knowing what is relevant is important.
Stating the learning outcomes at the beginning of the tutorial will also help in the baseline assessment of the knowledge and skills of the participants.
Pre-session questionnaires could be used as well (for example, asking questions on the prognosis of various mental disorders and comparing the participant’s knowledge before and after the session).
After the lesson
· Ongoing assessment during the tutorial using questions on various aspects related to the case presented.
· Questions in the recap section at the end of the tutorial.
· Post tutorial feedback forms will allow the participants to give their views about their learning needs and if they feel the tutorial was relevant to their learning outcomes.
It is important to provide personalised feedback to the participants about their performance on these assessment tools as this will help them to identify gaps in their knowledge and improve their learning. 26
Step 4 – Resources required
MedicineAfrica is free to join and designed to work well even with low bandwidth. Hence it won’t be affected by slow internet connections which are likely to be the case in developing countries.
Trainees and Tutors will need a computer (desktop or laptop) with an internet connection. No other resources are needed. Recommended readings could be disseminated by email to the trainees after the session.
Step 5 – Evaluation
Student evaluation
Gathering feedback is an essential step to influence the learning outcomes favourable and continue to improve the structure and content of the tutorials (After the tutorial, the participants will be asked to fill an electronic feedback form (please see Appendix 2).
The form contains various questions with rating (from 1-5, ranging from strongly disagree to strongly agree) on various aspects of the tutorial. These include structure, organisation, the range of aids used and meeting of the learning outcomes.
Also, direct feedback from the trainees, tutors, facilitators, and the stakeholders responsible for running the online learning platform is gathered to assess the effectiveness of these tutorials.
Teacher evaluation
Professionals invest a significant amount of time and efforts in these lessons, and it is imperative to assess how the tutorials could be improved to meet the needs of the trainees and keep them and the tutors motivated and interested. Tutors in these tutorials meet regularly using Skype to reflect on their teaching sessions and discuss ways of improving the delivery and quality of the tutorials.
Mutual learning is another aspect that needs to be assessed (is the tutor also benefitting from these lessons, for example, by improving their cultural competencies or their teaching skills).
Appendix 2: Feedback form to be completed by the participants after the session
Session title
Case-based discussion on management of severe and enduring mental illness.
Speaker
Date
Content
The session was relevant to my training needs
Strongly disagree 1 2 3 4 5 Strongly agree
Organisation
Sufficient time was allowed for the session
Strongly disagree 1 2 3 4 5 Strongly agree
Presentation
The session was well presented
Strongly disagree 1 2 3 4 5 Strongly agree
The session was delivered at the right pace
Strongly disagree 1 2 3 4 5 Strongly agree
The session was interactive and encouraged discussion/questions
Strongly disagree 1 2 3 4 5 Strongly agree
Structure
The session was well organised and structured
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were clear
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were met
Strongly disagree 1 2 3 4 5 Strongly agree
Overall evaluation
Overall, I would rate this session as
Extremely poor 1 2 3 4 5 Extremely good
Appendix 3: MedicineAfrica screenshot during an active session
Within the United Kingdom, all doctors are expected to teach.1 It is assessed throughout their professional career, during annual appraisals for doctors in training and during consultant revalidation. But how are those just embarking on their medical career expected to develop the necessary teaching skills? As three educators at various stages in our clinical careers, we developed and delivered a small course with the aim of addressing this issue.
The General Medical Council within the United Kingdom, suggest that a basic comprehension of teaching should be gained during the undergraduate and postgraduate training of doctors.2 Dandavino et al. further suggest that early development of these teaching skills may have additional benefits for the clinician; such as improving communication and assisting undergraduates to develop their own ability to learn.3 Our local training region, Yorkshire and the Humber Deanery (HEYH), have a mandatory post-graduate training day in teaching skills which focuses on generic and clinical teaching skills. This is delivered towards the end of the first foundation year. It is delivered by doctors who have various roles in medical education. Whilst useful in its content, for many it comes late. Doctors have often already been involved in providing teaching to medical students on placement at this time.
AMC recalls from her first postgraduate (foundation) year. One peer was thrilled to have ‘shaken-off’ a final year medical student who was supposed to accompany them on a shift as a learning experience; stating that they were now able to ‘do some work’. She couldn’t understand the desperation to escape one-to-one teaching. On reflection, it was probable that her colleague found it overwhelming to incorporate the additional responsibility of teaching alongside an already stressful clinical workload. Many share these feelings, with new doctors finding time pressures along with competing clinical demands a challenge to implementing clinical teaching.4
We thought that giving our graduates simple tools to understand and overcome these challenges may empower them as teachers. It may also improve their confidence in other areas, such as in their own learning and presentation skills.5-6 This paper proposes a solution; after creating a short course to be delivered immediately following graduation, to empower new doctors as teachers by providing some basic training in clinical teaching. These doctors are then able to use this training as soon as they begin their foundation training, which is ultimately the beginning of their teaching career.
Methods
Two versions of a half-day course, titled ‘Teach the Medic’ were developed in HEYH which ran in successive years. The original course was designed by a surgical trainee (AMC) and a general practitioner running the undergraduate education curriculum (MS). Initial topics were chosen based on experiences of the authors and colleagues. The optional course (see figure 1), was offered to the cohort of Leeds medical students who were in the transition period between finishing their final examinations and commencing their first post as a doctor.
Figure 1: A representation of the initial course structure. Stations were developed as interactive lectures and delivered to participants by doctors of various training levels.
The initial course received encouraging verbal and written feedback from the participants, which was collected on the day of the course. Further feedback was collected a few months into foundation training, allowing enough time to pass for delegates to use this knowledge. This feedback, whilst encouraging, included that delegates were keen for additional workshop style sessions. Subsequently, a modified half-day course ran the following year, with the recruitment of additional postgraduate teachers (including LES). A further 17 newly qualified doctors from various medical schools completed the course, prior to commencing their HEYH foundation post. This modified course (see figure 2) included scenario based sessions around potentially difficult situations for the clinical teacher, and also explored alternative styles of teaching that could be adopted successfully in the workplace.
Figure 2: A representation of the modified course structure. Building on feedback from the initial course, the three co-authors incorporated new small group scenario based discussions, alongside the interactive lectures.
Results
Initial feedback received from evaluation of the day was positive for both courses. For the second course, initial feedback found that all participants found every session very good (71%) or good (29%) overall. 12/17 (71%) thought that the course should be made compulsory to medical students. We also sent a follow-up survey, distributed six months after the course which generated 14 responses. All respondents felt that the course should be run again. All participants either strongly agreed (n=2, 14%) or agreed (n=12, 86%) that they felt more confident in teaching compared with their peers. Regarding individual sessions, 10 participants (71%) had directly incorporated learning from the ‘Teaching Theory’ session, 12 (86%) from the ‘Teaching for your Learning and Portfolio’ session, 11 (79%) from the ‘Teaching your Peers’ session, and 10 (71%) from the ‘Scenarios’ workshop. All participants stated they would still recommend this course to colleagues. They also reported directly incorporating their learning from the sessions into their teaching practice. The responses gathered from the second course implied that participants felt more confident in teaching when compared to their peers.
Discussion
We feel the course content in ‘Teach the Medic’ complements other courses available later in one’s career, such as the Royal College of Surgeons’ ‘Train the Trainer’ course. We propose this course could be run by a junior doctor who has a strong interest in clinical teaching with involvement of a senior colleague with extensive medical education experience. We felt the course was especially beneficial as participants had continued to find it useful long after its delivery.
To expand this project to include a whole year group as a compulsory course is ambitious. It would require development and the use of more resources, but initial feedback suggested participants will find it extremely useful. Bing-You et al.6 agree, having found that undergraduate students would be willing to undertake formal instruction in clinical teaching prior to graduation.
As our short course gains momentum within HEYH, this prospect becomes more achievable. When considering a wider delivered course, one must remember that attendance to ‘Teach the Medic’ was optional; suggesting that those who attended had already identified an interest in teaching. This has the potential to bias our data to some degree. However, we still believe that making the session compulsory would allow skill development and empowerment for those who may not consider themselves aspiring medical educators, but who are still in positions to deliver teaching.
Conclusion
Our evolving teaching skills course suggests that close work with both local medical schools and deaneries is important to allow this course to be incorporated into the training of newly qualified doctors. This may be included as a compulsory part of the final year medical school curriculum, an option for a SSC, or as an integrated part of the new starter induction programme delivered by individual hospitals.
The Royal College of Psychiatrists (RCPsych) launched its five-year Recruitment Strategy in 2011 aiming to achieve a 50% improvement in recruitment to core psychiatry training and a 95% fill rate of posts by the end of the five-year campaign (1). The primary focus of this campaign was on recruiting UK medical graduates.
Two of the Strategy’s main aims were to highlight good practice in undergraduate teaching and to improve the teaching skills of psychiatrists to inspire and influence medical students during their psychiatry curriculum.
The Strategy stressed the importance of good clinical placements in psychiatry and recommended that medical students should ideally be placed only with ‘the best teachers and welcoming teams’ avoiding colleagues who are disillusioned with psychiatry or not happy with their jobs.
It is therefore essential that psychiatrists and other clinicians play an important role to improve the medical students placement in their workplace in order to give the students a positive expereince of this speciality and hopefully promote it as a future career option.
Background
Fourth-year medical students from the University of East Anglia (UEA) spend two months rotating through various mental health services as part of their clinical placement in the Mind Module (also known as Clinical Psychiatry or Module 11).
As part of this rotation, students are placed in Old Age Psychiatry for six days over a two-week period. They shadow clinicians in two community teams, two inpatient wards and the Electro-Convulsive Therapy (ECT) clinic. All of these teams are based at the Julian Hospital in Norwich.
The students are encouraged to talk to patients and carers and perform basic clinical tasks such as mental state examination and risk assessment. Table 1 summarises the learning outcomes for students during their placement.
Table 1- The learning outcomes for students during their Old Age Psychiatry placement
Gain clinical experience of diagnosis and management of mental health problems (including dementia) in older people.
Improve the communication skills with regard to interactions with older people with mental disorders and their carers.
Enhance the student’s understanding of the nature of the multi-disciplinary team (MDT) model in mental health for older people, particularly the social aspect of care and end of life care.
After each rotation, each student is asked to complete a feedback form regarding their placement. This feedback helps the module leads and clinicians to improve the students learning experience.
Before the implementation of our placement improvement project, the students did not feel that they were meeting their learning outcomes. Table 2 summarises the major areas that needed improvement.
Table 2- Areas needed to improve before the implementation of the new placement structure
Poor planning and organisation of the clinical placement.
Inadequate or no information sent before starting the placement.
Lack of a dedicated coordinator to design the placement timetable and allocate students to specific clinicians
Lack of multidisciplinary teaching and hence poor understanding of the various roles of professionals (e.g., memory assessors, community nurses, support workers, etc.).
Students felt that clinicians were too pressured to supervise students. Some students reported that they were sometimes sent off as the staff had been too busy or there insufficient volunteers from clinical staff to take a student.
Student dissatisfaction with clinical placements is not unique to psychiatry. Research has shown that educators and learners face significant challenges when teaching and learning take place in any clinical setting. See Table 3 for a summary.
Table 3- Challenges of teaching in clinical settings (modified from Spencer, 2003)
Limited clinician time allocated to teaching activities.
High number of students allocated to few clinicians.
Difficulty in seeing patients (e.g., patients refusing the presence of a student).
Clinical setting is not ‘teacher friendly’ (overcrowded, too small, noisy and/or lacking privacy to interview and examine patients).
Lack of rewards and recognition for the clinical educators.
One of the biggest challenges of teaching in clinical settings is how to provide a welcoming and supportive learning environment in a busy and time constrained practice. We found that one of the main reasons for clinicians to be reluctant to have students shadowing them is the challenge of providing a dual role of caring and teaching simultaneously.
The placement improvement project
The improved structure of the student's’ placement in Old Age psychiatry was based on the tenet that clinical placements should provide various clinical experiences that include interaction with patients and professionals from various grades in addition to face to face teaching in small groups (3). The authors took over full responsibility for coordinating the students’ placements and liaising with the various supervising clinical teams. This ensured clear leadership and consistency in organising the placement.
The improved placement structure started in October 2015 with the first cohort of medical students coming to their clinical placement after the summer break. Table 4 gives a summary of the changes implemented.
Table 4- Changes to improve the clinical placement in Old Age Psychiatry
Compiling a ‘welcome pack’ and sending it by email to the students before the clinical placement.
A “Meet and Greet” event on the first day of the clinical placement was introduced comprising of several clinicians who operate on a rota basis.
Involvement of all professionals in the MDT (including Staff and Associate Specialists, community and memory nurses, junior doctors and clinical psychologists in addition to consultant psychiatrists).
Introduction of a Balint-style psychotherapy group aiming to facilitate discussion in a safe and containing environment of the emotional impact of patients encountered.
Designing a weekly one-hour teaching session supervised by a senior clinician and facilitated by a trainee psychiatrist.
Each clinician received a formal letter of thanks from the Head of Norwich Medical School, the Module Lead and the Secondary Care Lead certifying their contribution to the education of medical students and thanking them for their work.
The information pack sent to the students before the placement contained information about the hospital environment (location, map, parking, travel arrangements, key codes and useful contact numbers) and a detailed timetable (and email address) of the clinician supervising the student each day during the placement. Also, it included useful information about the mental state examination and the Mental Health Act, information that had been requested previously by medical students.
Sending information before the placement has been shown to be beneficial in students’ electives (4) and this is especially important in psychiatry which can be experienced as less structured than other medical specialities and where students are required to travel to various hospitals and clinics bases. As a result, students felt that they were expected and had a clearer sense of where they should be and who would be supervising or teaching them. Later student feedback reported that these changes had contributed directly to an improved learning experience.
The timetable design ensured that every student would have the chance to experience working in several settings in Old Age Psychiatry, including community, inpatients, ECT and the Memory Clinic. It was also noted that a two-week placement in any psychiatric team could not easily give a student a sense of patient ‘recovery’. It was, therefore, decided that students see a patient who had been discharged from the ward, e.g. with the care coordinator.
The rota of the ‘Meet and Greet’ event on the first day of the placement ensured that the workload is spread among the clinicians and helped sustain the necessary levels of enthusiasm and energy. Previously, this task had repeatedly fallen to just a few clinicians.
The participation of all professionals in the clinical team in supervision and teaching helped the students to better understand the different roles of clinicians within the multidisciplinary team and enriched their learning experience. To achieve this, we attempted to allocate sessions with a clinical psychologist, care coordinators, memory assessment nurses and members of the intensive support team. It also had the bonus of ensuring that the workload of teaching was spread more equally among clinicians.
Attendance at ward rounds and community MDT meetings could be a valuable experience but only if the process is explained, and – in the ward round – the student is briefed on the clinical history and background of the patients. For these reasons, supervising clinicians were reminded to give this information to the students attending such meetings.
The weekly teaching sessions provided an opportunity for the students to present case histories of patients they had seen and to discuss their management. Clinicians could also give a formal didactic teaching on a specific topic, for example, mental state assessment or risk assessment in psychiatry.
The letters of thanks to the participating clinicians served as an added benefit (in addition to the satisfaction of teaching others) to sustain their motivation and reward them for their contribution to the teaching of medical students. The psychiatric trainees used the letter to demonstrate their skills in teaching in their portfolio.
Benefits of the new placement structure
Helping students to feel supported before, during and even after their placements was a high priority in this project. Research has shown that learners rank the need for support and guidance in workplace environments as high and it is an essential requirement for a successful learning experience (5). This extra support is particularly crucial in psychiatry which is perceived by many students to be difficult and challenging (6).
The support provided to the students in the improved structure was in the form of having the contact details of the rota coordinators, their supervising clinicians, the administration team (medical secretaries, site manager for parking permits) and some other useful numbers for various locations and clinics.
While improving the organisation of the placement, changes were aimed to reduce the commitment of teaching and supervision for clinicians and spread it more equally among the members of the team.
Students reported that they found home visits during the placement the most useful part of their placement and the most interesting. This is an invaluable experience with the student having a significant amount of time in a one to one interaction with a clinician (including during the travel from one location to another) and then observing the clinician ‘in action’ with patients at home. This experience highlights the role of ‘professional socialisation’ (7) that is considered by educators as a significant process in the development of a sense of a shared professional identity and responsibility in both the clinician and the learner.
Furthermore, using non-medical professionals to supervise and teach students has been valued by students (8). It enriched the clinical placement with the concept of (Inter-Professional Learning) which is an active learning from and with professionals from other disciplines allied to medicine. This style of education has been shown to improve students’ communication with professionals from different disciplines and to have a better understanding of the nature of the multidisciplinary teamwork and the roles of each member of the team (9).
While improving the organisation of the placement, changes were aimed to reduce the commitment of teaching and supervision for clinicians and spread it more equally among the members of the team.
Balint groups and improving student placements in psychiatry
Balint groups were pioneered by the Hungarian psychoanalyst Michael Balint who introduced this model in the late 1950s after running seminars for general practitioners in the UK with his wife, Enid. (10)
Balint recognised the intense emotions that affect the doctor and the patient and encouraged clinicians to talk about these feelings in groups, which later came to be known as Balint groups.
Research has shown that Balint groups for medical students can increase the students’ empathy towards patients with chronic mental illness and improve their ability to cope with complex clinical situations (11). It also helps them to engage in reflection about their professional growth and to develop their identity as future doctors (12). Most importantly, this psychotherapeutic approach it allows them to reach a deeper understanding of the emotional impact of their patients (13). It was felt that the students would benefit from this model to help with the various emotions evoked by dealing with patients they would encounter in Old Age Psychiatry, in particular, dementia.
The student feedback was very positive for the Balint group. One student commented. It is inevitable to have experiences with patients that leave you with a feeling, whether that be positive or negative. To be able to look back at those times, talk them through, be listened to and have others reflect things back that you may not necessarily have realised yourself, is invaluable’.
Patient and carer involvement in clinical education
Clinical education in the workplace has always depended on patients and carers in its design and delivery. Students value seeing patients and learning from their experiences. However, the evidence suggests that patients are not routinely involved in the design of the curriculum or clinical placements despite calls to actively engage them in teaching and training (14).
Students were given the opportunity to learn from patients and carers through regular and supervised contact with them. They also attended a workshop on dementia and viewed a DVD showing the experiences of a woman with dementia and depicting how the world might be seen from her perspective. Feedback from students was very positive for these opportunities.
Medical students placement and Electro-Convulsive Therapy (ECT)
Students are allocated to spend one day in ECT clinic during their two-week placement in Old Age Psychiatry. Research has shown that many medical students have negative attitudes and unjustified reservations about ECT and its therapeutic applications (15). However, these views can change with education about this therapy during clinical placements and encouragement of the students to talk to patients and read about its indications and effectiveness in people with severe mental illness (16). Seeing the procedure first hand would, therefore, help the student gain confidence to challenge the stigma attached to ECT and to explain this treatment to their future patients.
Feedback from the students following the implementation of the placement improvement project
The feedback from medical students and clinicians was very positive. The students enjoyed their placements and felt that they gained useful knowledge and skills. Above all, they felt welcomed in the clinical settings and settled very nicely into the teams.
Figures 1 and two summarise some comments from the medical students following the placement. This feedback was collected by Norwich Medical School as part of the regular monitoring of clinical placement for medical students.
Figures 1 and 2: Feedback from students after the implementation of the changes to the clinical placement:
‘Best part of placement. Doctors were all happy to have us and teach. It was well organised, I felt that we were welcomed and always expected. It was varied and generally useful to my learning needs’. Student ID 69. End of Module 11 feedback.
‘This was one of the best placements in psychiatry, each doctor was very helpful and especially keen on teaching. It was really good to not only see the patients on the ward but so helpful to go on home visits to see assessments in patients own home. Really enjoyed this placement’. Student ID 95.
Limitations
There were some challenges in the implementation of this improved model. First is not always easy to recruit non-medical members of the clinical teams to take students. There are some reasons for this including lack of confidence or experience in teaching, a belief that it is “not their role”, or concern about the increasing demands on their time. Others already had students in their discipline. This was addressed by briefing the professionals about what the students need to achieve at the end of the placement and encouraging them to be involved in the supervision. The introduction of nursing revalidation in April 2016 may help more nurses to get involved. (17)
Conclusions and recommendations
This paper describes a clinical placement improvement project for medical students in Old Age Psychiatry. The changes focused on the enhancement of organisation, supervision and teaching.
Our improvement project is ongoing, and there are areas needing further improvement, for example, more active involvement of patients and carers in the teaching and learning of medical students is necessary. It is planned to achieve this by inviting patients and carers to tell their personal stories to the students in a small group.
Organisers of students’ placement in secondary or primary care need a systematic approach to filling allocation slots to ensure that all students receive a similar and broad exposure to their speciality. It can be dispiriting and stressful to ask for volunteers constantly. They need to have good relationships with their clinical colleagues of all disciplines, and to be willing and assertive enough to go around and ask colleagues in person rather than sending email requests.
Psychiatric educators have a significant role to play in the improvement of clinical placements for students as this will hopefully contribute to improving recruitment to this medical speciality that is undergoing a recruitment crisis. Research has shown that there is a positive correlation between the length and quality of clinical placement and the likelihood of choosing psychiatry as a future career. (18)
In the UK, all newly graduated doctors spend their first two years of work rotating between different specialities, usually spending four months in each placement, before applying for speciality training. This period is called the Foundation Programme.
In January 2016, the Royal College of Psychiatrists published its first ever strategy on Broadening the Foundation Programme to address the need to improve the psychiatric training experience for foundation doctors. The strategy’s aim is to “ensure the delivery of a high-quality training experience in all psychiatry foundation placements”.1
Over the last few years, the number of Foundation training posts in psychiatry in England and Wales has significantly increased. Health Education England aims that all Foundation doctors should rotate through a community or an integrated placement (psychiatry is considered as a community placement) from August 2017.2
As such, the College highlights the need to provide a supervised and well-structured psychiatric training experience for Foundation doctors. This aims not only to improve recruitment into psychiatry but also to ensure doctors have a good working knowledge and understanding of psychiatry and psychiatric services, no matter what career they pursue.
Mentoring provides an additional support and therefore can be helpful to improve the placement of Foundation doctors in psychiatry.
We implemented an ambitious mentoring scheme in Norfolk and Suffolk NHS Foundation Trust (the seventh largest mental health trust in the UK). The paper describes its essential component together with a brief review of the literature on mentoring in clinical settings, focusing on Foundation placements.
Why is mentoring is needed for Foundation doctors in psychiatry?
The literature on mentoring for medical professionals draws attention to the idea that it is beneficial to all doctors at all stages of their career to experience mentoring in some form or another. However, mentoring is of particular importance to doctors moving to a new job or organisation 3, thus making it highly relevant to Foundation trainees.
For newcomers, most of the mentoring support will focus on helping them settle into their new role, becoming familiar with, and developing an understanding of the expectations of their employers.4
Evidence shows that the quality of care in any organisation can be improved when clinical leaders support time for activities such as reflection, coaching and mentoring 5.
Most Foundation doctors will lack experience in psychiatry and will need a substantial amount of guidance from their supervisors and their teams.6 Research has shown that the transition from student to doctor is a difficult one and can be associated with significant levels of emotional stress.7
Foundation doctors find psychiatric assessments physically and emotionally challenging. They feel they lack the specialist knowledge and skills to deal with complex patients, especially concerning self-harm, personality and eating disorders. Dealing with such complex diagnostic categories requires knowledge, skill, understanding as well as physical and emotional robustness. Due to the relative lack of focus on such topics in most undergraduate medical training, a comprehensive support in psychiatric placements is essential.
Psychiatry is very different from other specialities in the way services are configured and delivered: junior doctors may face isolation as psychiatric units are typically spread across a wide geographical area and often lack a centralised meeting place for junior doctors (e.g. a doctors’ mess). In addition, they may find themselves the lone practitioner when on call, which can be daunting for many.
Clinical and Educational supervision is provided to Foundation doctors in similar ways to other rotations. However, the consultants delivering this essential support often focus only on clinical issues related to knowledge and skills. Furthermore, it is easy to see that the best guides to new trainees regarding the idiosyncrasies of the speciality and its services are likely to be trainees who have spent some time in those services and are more able to detect the specific stresses new doctors may experience and may find difficult to articulate.
Furthermore, mentoring fosters a productive peer-to-peer relationship. The learning needs of the Foundation doctor can be considered alongside their personal and professional interests and lifestyle. Questions can be posed in a non-judgmental forum, without fear of being ridiculed or condemned. The fundamentals of on-call systems, clinical cases and management options can all be considered at a level appropriate to their junior grade. Tips for examination success and information about essential courses and core texts can be shared. Job choices and research opportunities can be discussed. Day to day difficulties and mismatches between expectation and reality can be identified and possibly overcome. Where this is not possible next steps can be identified, and clinical and educational supervisors can be drawn in for higher level support. The benefits of the scheme are broad.
Finally, although mentoring is different from role-modelling (teaching by example and learning by imitation), it has been shown toserve some of the same aims of role-modelling, including enhancing problem-solving abilities of the mentee, improving professional attitudes, showing responsibility and integrity, and supporting career development. 8
What is mentoring?
Mentoring can mean different things to different people. There are various definitions which can create confusion between mentoring and other formal structures of support such as supervision, coaching, consultation, befriending or friend systems and even counselling. However, mentoring is none of the above but at the same time a combination of them.
The Standing Committee on Postgraduate Medical and Dental Education (UK) defined mentoring as ‘The process whereby an experienced, highly regarded, empathetic individual (the mentor) guides another individual (the mentee) in the development and re-examination of their ideas, learning, and personal and professional development”.9
The term “mentoring” takes us back to Greek mythology: Mentor was a person: he was the friend of Odysseus who was asked to look after Odysseus’ son Telemachus when Odysseus was fighting in the Trojan Wars. The name Mentor was later used to describe a trusted person, a supporter, or a counsellor.10
Mentoring as a professional developmental tool became popular in the private sector organisations in the USA during the 1970s and was introduced to the area of health during the 1990s 11. Since then, it has been widely used in various organisations.
Aims of mentoring
Mentoring has the advantage of being a flexible supporting tool, unlike other structured processes (e.g., clinical supervision or coaching) where the goals are set clearly from the start of the relationship between the supervisor and supervisee. The aims of mentorship are summarised in Table 1.
Table 1- Aims of mentorship
Help the mentees take the lead in managing their career and its development.
Provide support to discuss personal issues in a confidential and secure environment
Improve both the individual and the team performance
Types of mentoring
Buddeberg-Fischer and Herta 11 discussed various types of mentoring based on the numbers of mentors and mentees and their professional status or grade:
One to one mentoring (between a mentor and a mentee).
Group mentoring (one mentor and a small group of mentees)
Multiple-mentor experience model (more than one mentor assigned to a group of mentees).
Peer-mentoring (the mentor and mentee are equal in experience and grade): This mentoring is used mainly for personal development and improving interpersonal relationships. Mentor and mentee roles can be reversed. Also, called ‘co-mentoring’.
Distance or e-mentoring is becoming more popular, and it has the advantages of being “fast, focused, and typically centred on developmental needs”. 12
Structured vs. flexible mentoring
Evidence suggests that providing mentorship through a rigid and structured process can be counterproductive. 13 Mentors and mentees usually work in different locations, making it difficult for both to have a set of pre-planned meetings and topics for discussions.
Another advantage of the flexibility of mentoring is that it does not follow a “tick box” exercise but encourages informal discussions and exploration of whatever comes to mind during meetings. Doubtless, having some structure to the overall mentoring process is important as it ensures that the mentoring session doesn’t become an informal befriending or friend support system. Table 2 sets out the main benefits of mentoring.
Benefits to the organisations
Benefits to the mentee
Benefits to the mentor
Improve job satisfaction leading to improved performance, recruitment, and retention of employees
Enable early recognition and resolution of issues that face employees
Provide a valuable source of feedback that the organisations can use to improve working conditions
Ensure that the mentee has clear aims and objectives (development outcomes) at the start of their mentorship. These goals may include improving knowledge, performance and preparation for exams and interviews
Empowers the mentee to explore and pursue their career aims
Incorporates the mentee into a wider professional network and prevents isolation
Supports the mentee to use reflective practice and improve their self-awareness
Reducing stress and burnout
Formal recognition of informal practice within the profession
Structured program with support and supervision to the mentor
Development of knowledge and skills in management and supervision
Satisfaction of helping others and passing on their knowledge
Table 2-Benefits of mentoring. Developed from Mentoring – Chartered Institute of Personnel and Development (CIPD) Factsheet. Revised February 2009 14. Available from: https://www.shef.ac.uk/polopoly_fs/1.110468!/file/cipd_mentoring_factsheet.pdf
Are there any Disadvantages of mentoring?
There is extensive literature on the benefits of mentoring, but is there any harm associated with it?
As with any intervention, it does carry some potentially adverse effects. Mentoring can be perceived to “infantilise” junior employees rather than empowering them 10. This perception is probably more common among employees who see themselves as senior or very competent and think of themselves as able to adapt to change very quickly.
Mentoring might hinder creativity in new employees and inhibit them from thinking “outside the box” as it might re-enforce the message that ‘this is how we do things here’. 10
Clashes of personalities or other interpersonal factors could lead to a troubled mentor-mentee relationship and cause distress to both parties. Hence, plans must be put in place in any formal mentoring scheme to ensure an amicable ending to this relationship. Multiple mentor allocation mentioned earlier could also prevent such interpersonal problems and help to tackle them early on.
Furthermore, some mentees may feel uncomfortable with the influence or authority of the mentor, and this may hinder the progress of the mentoring relationship. 13 This is particularly relevant when the mentor is also involved in the formal assessment of the performance of the mentee (e.g. being the line manager or supervisor) or when a mentee who lacks self-confidence is paired with an overconfident mentor.
Good mentors avoid common pitfalls in the mentoring process, such as a patronising attitude, breaches of confidentiality and offering direct advice to the mentees. Instead, they encourage the mentee to reflect and come up with their answers. 15
Finally, mentoring can be perceived as an additional demand on doctors during their training, and some may feel that they are forced to provide it or receive it during placement. However, it must be remembered that mentoring should always be voluntary and flexible to meet the individual’s needs and not an additional ‘box to tick’ or a portfolio enrichment exercise.
The Mentoring Scheme for Foundation Doctors in Psychiatry Norfolk:
The scheme started in December 2015 and initially ran as a pilot in Norfolk with the support of all stakeholders. The mentoring scheme coordinator (YH) contacted twelve Foundation doctors by email, welcoming them to the Trust and inviting them to participate. The welcome email contained information about mentoring, including the benefits it may offer.
The voluntary nature of this scheme was highlighted so that the doctors didn’t feel they were being pressured to be enrolled.
Of the 12 doctors invited, five took up this opportunity. Uptake has remained constant over the consequent cohorts of Foundation doctors for many reasons. Those deciding not to enrol in this scheme explained that they felt happy with the support provided by their clinical supervisors. However, some doctors asked for a mentor halfway through their placement when they felt that they needed additional support. In these instances, a mentor was allocated to them as soon as possible.
Mentors were core and higher trainees already involved in supporting more junior psychiatric trainees through informal mentoring. Their experience meant there was no need for formal training. However, reading material was circulated to them to highlight the roles and responsibilities of mentors and what to do if any problem arose during mentoring. Monthly mentors’ meetings were very helpful to discuss issues arising in mentoring and offer peer to peer support.
Also, there were regular meetings and discussions between the mentoring coordinator, the Director of Medical Education, and Medical Director of the Trust to resolve any issues facing the Foundation doctors and provide feedback to improve the Psychiatric placement.
During the first meeting, the mentors and mentees agreed on the aims of mentoring drawing up a list of objectives that the Foundation doctor would like to achieve by the end of the placement. Following this initial meeting, there should have been once monthly face to face meetings throughout the placement. The mentor and mentee agreed on the most convenient means of communication (e.g. using text messages, emails, etc.) outside scheduled meetings.
All mentors kept a record of the mentoring meetings, with the mentoring coordinator informed about these meetings. Issues discussed were confidential and not shared with the coordinator or supervisors unless the mentee gave specific consent.
At the end of the mentoring scheme, the coordinator collected feedback from mentees and mentors using a structured questionnaire that was designed by the coordinator using SurveyMonkey® website. The feedback highlighted the positive aspects of mentoring as well as areas for improvement.
End of mentoring survey
Mentors reported that acting as a mentor without being involved in clinical supervision allowed them to offer objective advice and support in a way that would have been harder if they were directly involved in the workplace. One Foundation doctor experienced bullying from another member of the team who was a locum doctor. The mentor supported the Foundation doctor, and the issue was addressed and resolved promptly. There was a significant risk that they would have been left isolated and unsupported during this time if the mentor scheme had not been in place.
The topics discussed were varied, and this suggested that mentoring was not limited to a aspect of the job (see Table 3)
Table 3- Topics discussed in mentoring meetings
General guidance about the job
Assistance on completing competencies on e-portfolio
Advice regarding personal health, bullying, career choices
Leadership and research opportunities.
Mentees reported that they found mentoring useful and supportive of learning and development. This was especially important in a speciality that they had little experience of as an undergraduate. With a mentor in Psychiatry, the Foundation doctors reported that they could identify areas of development, including leadership and teaching opportunities for Foundation doctors.
Overall, mentoring was shown to be a useful tool to improving Foundation doctors’ experience in Psychiatry by offering extra support during placement in a challenging medical speciality.
Table 4 summarises the areas of development suggested by the mentors and mentees.
Table 4- Recommendations from the feedback of mentors and mentees
Early allocation of mentors at the start of the placement is vital.
The need to provide e-learning and classroom training on mentoring to develop the skills of mentors
Maintain the independence of the mentor from the clinical team of the mentee
Enhance the flexibility of the scheme to meet the demands of the training and the time constraints of the mentees and mentors
Limitations
Feedback from mentors and mentees showed an overall satisfaction with the scheme, but it was not possible to measure such satisfaction quantitatively, this was expected from an approach which is willfully kept outside the realm of performance management.
According to the literature on mentoring, most mentoring schemes lack a clear structure, as well as a clear evaluation process of its short and long terms, benefits 11.In our scheme, we addressed this by continually monitoring the mentoring process and collecting feedback from mentees and mentors. Another limitation involves training the mentor himself and finding the time in a highly pressurised and heavy workload environment.
There are many questions that the literature on mentoring is yet to answer. For example, what are the long-term benefits of mentoring? Would our Foundation doctors who received mentoring be more successful professionally and personally compared to their peers who decided not to participate? These questions remain unanswered as our pilot was not set up to address this general shortcoming of current knowledge and understanding.
Conclusions and recommendations
Mentoring provides a focused opportunity to target the wider needs of the trainee. Not only could this encourage Foundation doctors to pursue a career in Psychiatry, but it also provides the space for them to learn how to incorporate psychiatric skills into whatever speciality they choose to pursue.
As a new doctor in a novel environment, being expected, welcomed, and gently guided into the job is invaluable. With the hindsight of our training experiences (good and bad), junior doctors are ideally placed to support more junior colleagues at all levels.
There is a need to develop links with other mentoring schemes to exchange experiences and learn lessons from others. Research has shown the importance of supporting mentors in their roles through regular meetings where mentors learn from each other. 13
In our experience, the mentoring scheme worked both alongside and separately to clinical and educational supervision and the opportunity for reflective practice offered in Balint groups. Mentoring added another level of support for the Foundation doctors, which was deemed beneficial by those participating.
We recommend more research is required to determine whether mentoring will increase recruitment to psychiatry. Organisations responsible for the training of doctors should support formal mentoring schemes and supervisors should ensure that mentors and mentees have protected time in their timetable due to the benefits of the mentoring experience to the doctors and the employing organisations.
Finally, funding should be available to support training of mentors in their workplace and aim to develop their skills in helping their mentees. Many private organisations offer mentoring training packages (including classroom and online training) for competitive prices. These courses provide useful resources to mentors and may help to increase the motivation of mentors to continue their participations in mentoring.
Appendix:
How does mentoring work? A simple three stage model:
Figure 1- The three stage model of mentoring. Developed from Alred et al (1998). Alred, G., Gravey, B. and Smith, R, 1998, Mentoring pocketbook. Alresford: Management Pocketbooks.
One of the unique characteristics of mentoring is that it is a partnership between two individuals (mentor and mentee) where both contribute to its growth and sustainability. It is based on trust, eagerness to learn and mutual respect. 16
Alred et al (1998) 4 described a model of mentorship with three stages: exploration, developing new understanding and then action planning (Figure 1). Both the mentors and mentee have certain roles and responsibilities in each stage and it is only through their collaborative work that the benefits of mentoring can be obtained.
The stage of exploration is characterised by the building of a relationship between the mentor and the mentee. Trust, confidence and rapport start to develop and hopefully grow throughout the mentoring process. Methods such as active listening, asking open questions, and negotiating an agenda are essential to facilitate this growth.
The second stage is where new understanding develops, is characterised by showing support to the mentee, demonstrating skills in giving constructive feedback and challenging negative and unhelpful cognitions.
Key methods employed in this stage include recognition of the strengths and weaknesses of the mentee, giving them information, sharing experience and establishing priorities for the mentee to work on.
In the third and last stage of the mentoring, action planning, the mentee takes the lead in negotiating and agreeing on the action plan, examining their options and developing more independent thinking and decision-making abilities.
A good mentor should help the mentee to gain confidence and knowledge over time. In order to achieve this, the mentor helps the mentee to develop new ways of thinking and improve their problem-solving abilities.
Monitoring the progress and evaluating the outcomes of the mentoring process is essential to ensure that the mentoring relationship is going in the right direction.
Acknowledgement
We would like to thank Dr Stephen Jones (Consultant CAMHS and former Training Programme Director), Dr Trevor Broughton (Consultant Forensic Psychiatrist, Director of Medical Education), Dr Bohdan Solomka (Medical Director) from Norfolk and Suffolk NHS Foundation Trust for their unlimited support for the mentoring scheme.
We also would like to thank Dr Calum Ross (Foundation Training Programme Director-FY1) and Mr Am Rai (Foundation Training Programme Director -FY2), Norfolk and Norwich University Hospital for their support in implementing this scheme. Dr Srinaveen Abkari (Specialist Registrar, Norfolk, and Suffolk NHS Foundation Trust) is one of our mentors who also contributed useful ideas to the development of this paper.
Finally, we would like to thanks all our mentors who provided the support for the Foundation, without their efforts, this scheme would not have succeeded.
Postgraduate medical training should equip trainees with the skills, knowledge and attributes for independent practice1. They need to be equipped with the skills to become lifelong learners and continually develop their abilities throughout their careers by learning from colleagues, mentors, patients and disease. The challenge for clinical teaching is how to provide an optimal learning environment in which trainees can achieve their competencies for practice within a defined training rotation; both the limitations in the number of hours within a working week and the balance between learning and service commitments all can negatively impact on the educational experience of trainees2. Moreover, trainees need to balance their own development of skills, knowledge and attributes for independent practice against the requirement to provide high quality and safe healthcare3. The appropriate level of supervision must be provided to trainees performing any patient interaction and this is gauged by the trainer-trainee relationship, regular assessment and feedback. The clinical workload of a trainee needs to be finely balanced between overstretching them with tasks outside their competencies and being left with all the routine and menial tasks4. Thus whilst trainees should work within their competencies, they must be given the opportunities to expand their repertoire of skills, which may result in errors (and potentially patient harm) – supervision should limit these errors, which should be reflected on to provide a learning opportunity within a ‘no-blame’ culture5. As a trainee gains competence of their necessary skills, the amount of supervision required can be stepped down, until distant supervision (i.e. advice via a telephone) may be all that is required.
An understanding of how each learning environment within the hospital setting can be maximized may enhance the learning opportunities conferred upon trainees. Both technical skills and the professional attributes of being a clinician can be learnt in clinical and non-clinical environments. These learning environments will be explored in the subsections below.
Bedside Teaching and Ward Rounds
Bedside teaching is a stalwart of medical education, allowing clinical history and examination to be performed under guidance, in an appropriate setting and with relevant clues (observation charts, oxygen, etc.) present. This patient-trainee interaction provides an opportunity to develop professionalism and communication, and can also be the source of training of diagnostic techniques ranging from venesection and cannulation to more invasive techniques (e.g., pleural aspiration, drainage of ascitic fluid)1.
Presentation of patients during ward rounds allows a professional conversation between trainees and trainers to occur, which justifies their role in management and provides an insight into understanding and thought processes6. The multidisciplinary nature of rounds creates a community of practice7, allowing social learning to occur, and an opportunity to voice differing perspectives on patient care3. In order to maximize these learning opportunities, learning objectives can be discussed prior to commencement and reflection undertaken once they it has been completed6. Teaching rounds should be carried out when the ward is quiet, at a suitable pace, with regular questioning and opportunities for trainees to ‘lead’ the process8. Factors that hinder this educational process include time pressures, patients not being available, and the availability of trainees8.
Outpatient Clinics
Outpatients provides a mixture of new and follow-up patients that enables a trainee to learn management of patients in an ambulatory setting. Trainees may be in the same room as their supervisor (learning the basics of the consultation), or can practice semi-autonomously as their experience increases (with discussion with their supervisor as required); they must select an appropriate investigation and treatment plan, with a time frame for review, once the investigation or intervention has been performed3. Outpatient teaching is more highly valued by trainees and students compared to ward based tuition9. Factors that hinder this educational opportunity include room availability, time constraints, staffing levels and attitudes to teaching9.
Operating Theatre and Interventional Suites
Invasive procedures should be performed by adequately trained (or supervised) personal in the relevant area of the hospital (e.g. endoscopy, interventional radiology suites, theatre), with the necessary equipment and monitoring for the technique to be performed. Even before patients enter these environments, trainees have an opportunity to review the patient and their relevant investigations, discuss the procedure with the patient and obtain consent for the intervention1. Trainees can learn a wide spectrum of skills within these environments including both technical (both procedural related and anesthetic related) and non-technical skills, including Human Factors, anatomy, identification of instruments, aseptic technique, effective hand-washing and donning of surgical gowns10. Teaching invasive procedures represents a dichotomy for clinicians, not only do trainees need to gain exposure and experience in the relevant technique, but patients need to be prevented from undue harm. Prior to undertaking an intervention, trainees should be familiar with the relevant anatomy and physiology of the system they are about to operate upon, will have watched the procedure being performed and may have learnt the basics of the procedure in a simulated setting.
Trainees must to be able to self-reflect on their own skills and record of the number of procedures they have performed (which can act as a proxy for ability) to ensure that the correct level of supervision is provided alongside an intervention of suitable difficulty. Trainers need to be sure that their trainees have the necessary skills and knowledge to perform a technique, with experience often being gained in a stepwise reflecting both the difficulty of intervention and the gaining of skills, competence and confidence by the trainee11. This skills acquisition should be accompanied by regular discussion and feedback to maximise learning opportunities; when no supervision is available, trainees should consider video-recording the procedure as this allows reflection and review at a later date. A video diary can also be used as a portfolio of a trainee’s repertoire from beginner to expert during their training rotation. The challenge for trainees is to achieve competence in the relevant invasive technique within their training rotation; the number of interventions required to gain competence will vary between each trainee and technique11.
Handover
Handover allows the care of patients to be transferred from one group of individuals to another on a temporary or permanent basis. Handover confers an opportunity to present a clinical synopsis of patients with key information to ensure continuity of care and patient safety is maintained3. Most handovers are trainee led which provides an opportunity for peer learning to occur, checking comprehension and sharing interesting cases or tips for practice12. Handovers should be considered to be a high risk procedure, as communication errors can result in vital information being omitted; as such the process should be undertaken in suitable environment away from distractions, in a structured written and oral manner supported by an electronic format12. A further review at the patient’s bedside can be performed if required, which can highlight high risk patients.
Multidisciplinary Team Meetings
Multidisciplinary team (MDT) meetings are small formal meetings focused on all aspects of a patient’s care that involve a wide range of medical personal, nursing staff and allied health care professionals1. Meetings ensure that evidence-based guidelines are followed, and help to streamline management, removing unnecessary delays in treatment and improving cost effectiveness. MDTs represent a Community of Practice7 allowing social learning to occur as each individual can share their relevant expertise; MDTs enable best practice to be shared and help break down barriers between different specialties. Trainees can learn from the didactic teaching that occurs within the MDT (in relation to clinical details, investigation and management), but can also contribute to the meetings and practice their presentation skills.
Morbidity and Mortality Meetings
Morbidity and Mortality (M&M) meetings can help ascribe accountability and be used to highlight improvements in patient safety. They provide an opportunity for professional education, especially if the discussion can be held within a no-blame culture, and the meeting can voice discrepancies in how to manage patients, especially in ambiguous situations13. Trainees may be tasked with presenting a case and the potential learning aspects associated with patient care.
Grand Rounds/Formal Teaching
Grand rounds are traditional formal teaching opportunities that typically revolve around a case, whereby salient findings are presented prior to a discussion of management. These meetings allow opportunities for trainees to present cases and learn management, but their educational benefit may be decreasing as they are being replaced with lectures with limited clinical relevance14. However “audience apathy, deteriorating decorum and shrinking attendance” have diminished these learning opportunities14. Targeted teaching and the establishment of learning objectives for trainees can improve the educational content and the provision of feedback to the speakers can also enhance these meetings.
Journal Club
Journal clubs confer an opportunity for current scientific research and developments to be presented, critiqued and discussed by trainees. These clubs confer an opportunity to appraise the current literature and how that can be translated into evidence based patient care15. Journal clubs tend to be both voluntary and occur outside of working hours, resulting in highly motivated groups of participants whom are protected from interruptions.
eLearning and mLearning
Electronic learning (eLearning) and multimedia learning (mLearning) enable trainees to work informally, away from desks and computers, and at their own pace through a series of educational modules. Any intervention that engages trainees and promotes learning should be encouraged and these online learning platforms can be combined traditional learning resources should be promoted to ensure that all aspects of the curriculum are covered. mLearning in particular can be ‘dipped into’ allowing the learner optimal flexibility of how and when they want to use it. elearning can be referred to during point-of-care patient interactions when a trainee is unsure of how to proceed with patient management1. These increasingly important and under-utilized resources should be supported by educational institutions that support both undergraduate and post graduate trainees. By developing a virtual learning environment, individual tailored learning programs can be created that allow a trainee to develop and control their own online learning16.
Simulation
Simulation is becoming increasingly important for medical training. , anything can be simulated from learning clinical skills to human factors training, for both individuals and teams, focused on patient care and current medical practice in both the undergraduate and postgraduate setting. The availability of simulators coupled with competency based training and a decreased amount of training within the workplace has led to an increase use of this teaching format1. In addition, trainees need to understand how to use certain pieces of equipment prior to employing them on patients and this familiarity can only be gained in a simulated setting. Simulation can either occur within the workplace (allowing point-of-care simulation to see how teams react in a situation) or on formal taught courses; it can be low-technology and cheap (e.g., tying surgical knots on the back of a chair), but can also be high-fidelity and expensive (e.g., a virtual reality training simulator for laparoscopic operations), or use animal or cadaveric tissue. Simulation that increases trainee’s familiarity with certain techniques is likely to improve their clinical performance, decreasing potential patient harm and shorten the time taken for trainees to achieve competence1. A simulation should be completed with feedback from the supervisor to ensure that trainees gain the most from the session and clarify any facts or concerns about the simulation; a video recording of the session can also enable participants to reflect on their performance in a manner that is almost impossible in everyday clinical practice.
Global recruitment in psychiatry has been falling for several decades because medical students and graduates have been finding it consistently unattractive 1,2. An analysis of the career choices of newly qualified doctors in the United Kingdom (U.K.) found the same trend from 1974 to 2009; psychiatry was the first career choice for only 3-5% of medical graduates annually3. In the U.K., lack of recruitment into psychiatry had reached a crisis point by 2003 when 15% of all unfilled consultants posts in England were in psychiatry and the Royal College of Psychiatrists was finding recruitment into specialist psychiatry posts increasingly difficult4,5. In 2012, only 78% of the Core Training year one (CT1) posts in psychiatry were filled; a serious shortfall which was overcome by overseas recruitment up until changes in immigration rules.
The factors that seem to dissuade medical students from taking up psychiatry as a future career may include: stigma, bad prognosis of psychiatric disorders, poor scientific base of psychiatry, ‘bad-mouthing’ from medical colleagues, lack of respect among peers & public, threats of violence from patients and lack of resources1-5. However, there is evidence to suggest that many students’ attitudes towards career choice changed in a positive direction after working in psychiatry due to the perceived ‘job satisfaction’, ‘life-style’, ‘training available’ and ‘multidisciplinary approach’3.
Psychiatry has previously been ranked higher in career choice at the end of students’ clinical year6. To ensure a stable psychiatric workforce for the future, there is an obvious need to motivate current and future cohorts of young doctors to take up psychiatry as a career. Das & Chandrasena (1988) found that attitudes changed positively towards mental health following clinical placement in this specialty7. It is also known that medical students’ attitudes to psychiatry and career intentions can be improved by their experiences of teaching8. Students were found to develop more positive attitudes when encouraged by senior psychiatrists, had direct involvement in patient care, or saw patients respond well to treatment. Improvement in attitudes during the placement was also related to an increased intention to pursue psychiatry as a career.
Previous research into attitude to psychiatry as a specialty and career choice seems to have produced conflicting results and most of it was carried out among medical students. Since career choices in the U.K. are actually made in the first clinical year following graduation, we carried out a survey among a recent cohort of foundation year one (FY1) doctors in the South East England before and after their first clinical year.
Method
Our study sample consisted of all FY1 doctors (n=101) in one region of South East England. They participated in the study at the beginning and then at the end of their first clinical year. We used a 20–item questionnaire devised by Das & Chandrasena(1988) to ascertain their perceptions and attitudes towards psychiatry before they commenced their first clinical placement. The questionnaire was sent to them via their Medical Education Managers (MEMS). It was handed out to the FY1 doctors as part of their induction pack for completion along with a study information sheet.
At the end of their first year of working, the participants were asked to complete an amended version of the questionnaire. This included two additional questions which ascertained whether the doctor had an opportunity to work in a psychiatric post, or had any experience of psychiatry in practice (such as taster days or cases in A&E). These amended questionnaires were sent to the foundation doctors electronically via their MEMS for completion.
The data was collected and entered into a spreadsheet to prepare descriptive statistics. Comparisons for before and after exposure to psychiatry, and between the psychiatry and non-psychiatry groups were made using the chi-square test. As the data was binary, a latent class model was developed using LatentGOLD software9 to explore the associations between different items in the questionnaire. Responses from the questionnaires were coded as: responses which agree with a positive attitude to psychiatry or disagree with a negative attitude were coded as +1; those not sure were coded as 0; and responses which agree with a negative attitude to psychiatry or disagree with a positive attitude were coded as -1.
Results
A 100% (n=101) response rate was obtained for the first set of questionnaires completed at the beginning of the year. However, there was a significant drop in the number of questionnaires completed at the end of the year - a 53.5% response rate (n=54) generally but 61.1% (22 out of 36) for those FY1 doctors who had the opportunity or access to a post in psychiatry within their clinical year.
Initial cohort at beginning of the clinical year vs. those with no exposure to psychiatry at the end
Table 1 shows the group means for each questionnaire item, for the whole cohort at the beginning of the year compared to those with no exposure to psychiatry by the end of the year.
Table 1: All FY1 doctors before training placements started (initial cohort) versus FY1 doctors without a psychiatric post after FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.591
0.095
-0.169
0.359
0.476
I may consider pursuing a career in psychiatry in the future
-0.539
-0.136
0.403
0.046
0.760
0.028
Psychiatry is attractive because it is intellectually comprehensive
-0.500
0.273
0.773
0.436
1.000
0.000
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
-0.500
-0.069
-0.442
0.305
0.717
Physicians do not have time to deal with patients emotional problems
-0.294
0.273
0.567
0.142
0.991
0.009
Psychiatrists understand and communicate better than other physicians
-0.127
0.364
0.491
0.090
0.892
0.017
Psychiatrists don't overanalyse human behaviour
0.147
0.364
0.217
-0.200
0.633
0.306
Expressing an interest in psychiatry is not seen as odd
0.157
-0.136
-0.293
-0.727
0.141
0.184
Hospitalised patients are not given too much medication
0.167
0.591
0.424
0.116
0.732
0.007
Psychiatrists don't make less money on average than other physicians
0.255
0.045
0.209
-0.537
0.118
0.208
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.727
0.365
0.033
0.696
0.032
Psychiatric curriculum and training are not too easy
0.520
0.682
0.162
-0.112
0.436
0.243
Psychiatrists are not fuzzy thinkers
0.578
0.818
0.240
-0.082
0.561
0.142
Psychiatrists should have the legal power to treat patients against their will
0.608
0.955
0.347
0.051
0.642
0.022
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.864
0.246
-0.066
0.558
0.121
Psychiatry is scientific and precise
0.627
0.818
0.191
-0.098
0.480
0.194
There is a place for ECT in modern medicine
0.755
0.727
-0.028
-0.239
0.184
0.797
Psychiatric consultations are often helpful
0.853
0.864
0.011
-0.210
0.231
0.924
Entering psychiatry is not a waste of a medical education
0.873
1.000
0.127
-0.048
0.303
0.153
Psychiatrists don't often abuse their legal powers
0.892
1.000
0.108
-0.049
0.264
0.175
Those FY1 trainees who had not worked in psychiatry during the year were significantly more positive (p = < 0.05) for psychiatry’s future, psychiatrist being better at patient communication and not over-medicating their patients. However, they remained significantly less convinced as compared to the whole cohort about psychiatry’s intellectual attraction or taking it up as a future career.
Initial cohort at beginning of the year vs. those with exposure to psychiatry at the end
Table 2 shows the group means for each questionnaire item, for the whole
cohort at the beginning of the year compared to those with exposure to psychiatry at the end of the year.
Table 2: All FY1 doctors before training placements started versus FY1 doctors with a psychiatric post during FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.745
-0.058
-0.242
0.125
0.531
I may consider pursuing a career in psychiatry in the future
-0.539
-0.617
-0.078
-0.332
0.177
0.547
Psychiatry is attractive because it is intellectually comprehensive
-0.500
-0.468
0.032
-0.214
0.278
0.798
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
0.106
0.538
0.248
0.827
0.000
Physicians do not have time to deal with patients emotional problems
-0.294
-0.383
-0.089
-0.401
0.224
0.575
Psychiatrists understand and communicate better than other physicians
-0.127
-0.085
0.042
-0.260
0.345
0.783
Psychiatrists don't overanalyse human behaviour
0.147
0.340
0.193
-0.123
0.510
0.229
Expressing an interest in psychiatry is not seen as odd
0.157
0.106
-0.050
-0.378
0.277
0.761
Hospitalised patients are not given too much medication
0.167
0.362
0.195
-0.044
0.434
0.109
Psychiatrists don't make less money on average than other physicians
0.255
0.404
0.149
-0.092
0.391
0.224
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.064
-0.299
-0.569
-0.029
0.030
Psychiatric curriculum and training are not too easy
0.520
0.596
0.076
-0.128
0.281
0.464
Psychiatrists are not fuzzy thinkers
0.578
0.596
0.017
-0.233
0.268
0.892
Psychiatrists should have the legal power to treat patients against their will
0.608
0.532
-0.076
-0.323
0.171
0.545
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.574
-0.043
-0.290
0.203
0.730
Psychiatry is scientific and precise
0.627
0.702
0.075
-0.155
0.304
0.521
There is a place for ECT in modern medicine
0.755
0.511
-0.244
-0.427
-0.061
0.009
Psychiatric consultations are often helpful
0.853
0.745
-0.108
-0.289
0.073
0.239
Entering psychiatry is not a waste of a medical education
0.873
0.808
-0.064
-0.218
0.090
0.412
Psychiatrists don't often abuse their legal powers
0.892
0.766
-0.126
-0.279
0.027
0.105
After a psychiatry placement, significant positive differences (p=<0.05) were observed in their responses to medical staff’s view of psychiatry, future of psychiatry and place of Electro Convulsive Therapy (ECT) in modern medicine. While there was a positive trend in most responses in favour of psychiatry, trainees remained negative about psychiatry’s status, its scientific base, curriculum & training and taking up psychiatry as a future career.
Those exposed to psychiatry vs. those not exposed to psychiatry
Table 3 compares responses between FY1 doctors exposed to psychiatry during the clinical year and those who were not.
Table 3: FY1 doctors who had a psychiatric post versus those who did not have one
Sorted by the size of the difference between the two groups.
t-test
ranksum
Psychiatry
No Psychiatry
Difference
L
U
p-value
p-value
Most non-psychiatric medical staff are not critical of psychiatry
0.106
-0.500
-0.606
-1.000
-0.144
0.011
0.011
Psychiatrists don't make less money on average than other physicians
0.404
0.045
-0.359
-0.694
-0.024
0.036
0.034
Expressing an interest in psychiatry is not seen as odd
0.106
-0.136
-0.243
-0.735
0.249
0.329
0.322
Psychiatrists don't overanalyse human behaviour
0.340
0.364
0.023
-0.421
0.467
0.917
0.907
Psychiatric curriculum and training are not too easy
0.596
0.682
0.086
-0.210
0.382
0.564
0.497
Psychiatry is scientific and precise
0.702
0.818
0.116
-0.187
0.419
0.447
0.777
Psychiatric consultations are often helpful
0.745
0.864
0.119
-0.173
0.411
0.419
0.388
Within medicine, psychiatry has a high status
-0.745
-0.591
0.154
-0.130
0.437
0.283
0.391
Entering psychiatry is not a waste of a medical education
0.808
1.000
0.191
-0.020
0.403
0.075
0.058
There is a place for ECT in modern medicine
0.511
0.727
0.217
-0.117
0.551
0.200
0.192
Psychiatrists are not fuzzy thinkers
0.596
0.818
0.222
-0.114
0.559
0.192
0.190
Hospitalised patients are not given too much medication
0.362
0.591
0.223
-0.139
0.597
0.218
0.192
Psychiatrists don't often abuse their legal powers
0.766
1.000
0.234
-0.005
0.473
0.055
0.040
A placement in psychiatry can change one's negative views of psychiatry
0.574
0.864
0.289
-0.045
0.623
0.088
0.064
Psychiatrists should have the legal power to treat patients against their will
0.532
0.955
0.423
0.097
0.748
0.012
0.011
Psychiatrists understand and communicate better than other physicians
-0.085
0.364
0.449
0.000
0.897
0.050
0.050
I may consider pursuing a career in psychiatry in the future
-0.617
-0.136
0.481
0.084
0.878
0.028
0.017
Physicians do not have time to deal with patients emotional problems
-0.383
0.273
0.656
0.195
1.000
0.006
0.007
Psychiatry is a rapidly expanding frontier of medicine
0.064
0.727
0.663
0.269
1.000
0.001
0.002
Psychiatry is attractive because it is intellectually comprehensive
-0.468
0.273
0.741
0.352
1.000
0.000
0.001
Those exposed to psychiatry agreed more often that non-psychiatric medical staffs were critical of psychiatry compared to the group not exposed to psychiatry. They also had comparatively negative responses for psychiatrists not abusing legal powers and to have the legal power to treat someone against their will. Trainees exposed to psychiatry also felt significantly (p=<0.05) positive towards psychiatry being intellectually comprehensive and adopting it as a career. However, they were less enthusiastic about psychiatrists treating patients against their will and psychiatry being the expanding frontier of medicine.
Discussion
In this study, we have ascertained attitudes of a regional cohort of FY1 doctors towards psychiatry as a specialty and as a career choice. Our findings are similar to previous research carried out among medical students, which found that there were generally negative attitudes towards psychiatry as a specialty and career choice but fairly positive attitudes towards the role of psychiatry in medicine and in society in general1-5,10. Like others, we also found that personal experience of psychiatry placement can improve trainees’ view of psychiatry as a specialty and as a future career 3,11.
It was interesting to find out that after a year in clinical practice but without any experience of psychiatry, trainees’ attitudes towards psychiatry as a specialty had been positive. It is difficult to know the exact reason but we can speculate that this respect for the specialty may have developed when they experienced limitations of the other specialties in medicine and/or perhaps due to the positive professional encounters with psychiatrists at the Accident & Emergency (A&E) or with psychiatric liaison teams during ward consultations. As opposed to previous research11, it was heartening to note that the group with no exposure to psychiatry agreed that non-psychiatric medical staff were not critical of psychiatry; a possible sign of reduced stigma for psychiatry within the medical profession.
Despite exposure to psychiatry, FY1 doctors’ attitudes to psychiatry’s status, scientific base, curriculum & training and career choice remained somewhat negative. Similar results were found by Lyons et al11 when they assessed students’ attitudes towards psychiatry after a clerkship in the specialty. There was a significant decrease in negative & stigmatising views towards mental illness after the clerkship, but no significant improvement in students' interest in psychiatry was detected1. Goldacre et al (2013) also acknowledged mixed outcomes of early experience of working in psychiatry as it might discourage some doctors. While highlighting positive effect of the doctors’ experience of the speciality, they also cited it as a negative factor that influenced some doctors who had previously considered psychiatry as a career3.
Our study has limitations because of having a small sample and being carried out in one small region of the country. It is also worth mentioning that the group exposed to psychiatry may not have had a psychiatry placement as it also included those who had had taster days or experience in A&E. The brevity of these latter exposures cannot give someone a real sense of the specialty. The nature of this and the overall experience needs to be differentiated and the exposure quantified in the future studies. Our study findings also need to be replicated with future cohorts and in other regions for confirmation because FY training programme in the U.K. is relatively recent and placements in psychiatry have evolved4 over the last few years through closer collaboration between different stakeholders in the Foundation Training Programmes.
The CASC (Clinical Assessment of Skills and Competencies) has been running since 2008 and is the final membership examination for the Royal College of Psychiatrists (MRCPsych).1 It is a clinical examination and follows an OSCE format (Objective Structured Clinical Examination), where candidates move through 16 short stations.2,3 We have been running a mock CASC in the West of Scotland for the last few years and have received consistently good feedback from candidates. This article describes our experience of organising the mock exam.
Step 1: Practicalities
The organising committee
Our mock CASC is arranged by the organising committee for the local core psychiatry education programme (MRCPsych course). This committee is comprised of a consultant chair, higher trainee chair and one or two trainee representatives from each higher subspecialty and each core training level. The higher trainee chair takes the lead with organising the mock, with the support of other committee members. This works well, as the trainees have recent experience of sitting or preparing for the exam and are enthusiastic about medical education.
Support from our postgraduate operations manager is invaluable. She works closely with the committee to book the venue and actors, and order equipment such as screens and a bell. She also has a key role in advertising the mock exam to trainees, booking places and being a point of contact for candidates. She assists with set up on the day of the exam and prints station instructions, marking schemes and labels for candidates.
Venue
Our mock exam is held in the same venue as our core trainee educational programme. We have 2 rooms to use for stations and a waiting area for candidates. Screens are borrowed from Glasgow University Medical School to create separate stations.
Timing
The mock exam takes place around 2 weeks before the CASC. This enables candidates to have prepared for the exam and leaves some time to work on any issues identified by the mock. Planning usually starts 4-5 months in advance of this, with increasing intensity and time commitment as the exam approaches.
Step 2: Mock Exam Format
CASC format and blueprint
The CASC itself includes morning and afternoon circuits, which all candidates will move through. There are 16 stations in total, with 90 seconds between each to read the task instructions. The morning session comprises 4 pairs of ‘linked’ stations, lasting 10 minutes each. In these paired stations, the second station is connected to the first in some way, such as taking a history in the first part then discussing with a family member in the second. Each station is marked independently. The afternoon consists of 8 single stations, lasting 7 minutes each. A passing list is posted online after a few weeks, with specific feedback made available to unsuccessful candidates.2
Mock CASC format
Our mock CASC is run in one afternoon session from 1.30-5pm. We have been able to include 16 stations by running the 2 circuits simultaneously. To make this possible, each station is 7 minutes in duration, with 90 seconds between stations. 4 candidates start after a delay, as it is not possible to start on part 2 of a linked station. Trainees are allocated candidate numbers and starting stations for both circuits to coordinate this effectively (figure 1). 16 candidates can take part in the mock exam.
Figure 1. Candidate numbers
Candidate Name
Number
1st loop starting station
2nd loop starting station
1
1a
5
2
2a
6
3
3a
7
4
4a
8
5
1a (8.5 min delay)
9
6
2a (8.5 min delay)
10
7
3a (8.5 min delay)
11
8
4a (8.5 min delay)
12
9
5
1a
10
6
2a
11
7
3a
12
8
4a
13
9
1a (8.5 min delay)
14
10
2a (8.5 min delay)
15
11
3a (8.5 min delay)
16
12
4a (8.5 min delay)
At least 3 other higher trainee helpers are recruited to assist the coordinator on the day of the exam. The same marking scheme is used for each station, covering domains common to all stations, such as building rapport and range and depth of questioning. There is also space for specific feedback, which examiners are encouraged to provide, though they do not interact with candidates directly during the exam. Forms are completed contemporaneously and distributed to candidates immediately after the mock exam.
Step 3: Writing the Stations
The content of the CASC follows a blueprint, which is available through the RCPsych website. A variety of skills are tested during the 16 stations of the exam, including history-taking, mental state examination, risk assessment, cognitive examination, physical examination, case discussion and difficult communication.3 We refer to the blueprint when selecting which stations to include in the mock. Each year, recent CASC candidates are asked to suggest stations and we combine these with previous stations to construct the mock exam. New stations are written by the trainee who suggested them, including candidate instructions and actor’s notes. The higher trainee organiser formats these to maintain consistency across the mock exam.
Role-play actors
For our most recent mock CASC, we employed paid actors for every station. These actors are part of a local agency which has experience in working as simulated patients for Glasgow University exams and communication skills sessions. In previous years, we have recruited a combination of core/higher trainees and actors. We have found pros and cons to each approach. The use of paid actors was more realistic for trainees but writing scripts proved more challenging as instructions required greater detailed in relation to specific psychiatric information, such as how a person with mania may present.
Step 4: Recruiting Examiners
There are a number of local consultant psychiatrists who are actively involved in teaching. They are supportive of the mock CASC and enthusiastic about examining stations. After the stations have been devised, consultants are invited to examine based on their areas of expertise. Higher trainees with particular interest in education are then asked to examine any remaining stations. Candidate instructions and actor’s notes are circulated to examiners in advance (figure 2). A simple guide to the mock exam is also sent to any new examiners. As we use the same marking scheme for each station, it is down to the experience of the examiner to consider whether the candidate has addressed the specific tasks appropriately.
Figure 2. Station template
Station
Title
Actor
Examiner
Written?
Sent?
1a
1b
2a
2b
3a
3b
4a
4b
5
6
7
8
9
10
11
12
Step 5: The Day of the Mock Exam
The higher trainee coordinators arrive at least 1.5 hours prior to the start time to set up the venue. Examiners, actors and candidates are asked to arrive 15-30 minutes before the scheduled start time. Each group is briefed on the exam format and given the opportunity to ask questions. Actors and examiners are shown to their stations and allowed time to discuss them. Candidates are provided with numbered labels to wear, for examiners to record on their marking sheets. The 4 candidates who will be starting later are asked to wait, while the others are shown to the examination rooms. They are shown which station they will be starting at, then queue in order at the door.
The mock exam coordinator stands where they can be heard by both rooms. There are 1 or 2 helpers in each room to guide the candidates around the circuit. The bell is rung to signify the start of the exam, the end of the 90 second preparation time (the start of each station), 1 minute warning and the end of each station. The candidates who were allocated to start later are brought into the circuit and shown to their station as the ‘end of station’ bell is rung, as this also signifies the start of the 90 second preparation time for the next station.
Marking schemes are collected and sorted during the break. Candidates are not kept separate from examiners, actors or each other. They are advised that they will get the most out of the afternoon if they don’t discuss the stations but this is ultimately their choice.
Examiners and actors return to their stations following the short break and candidates swap between circuits. Following the second round, there is another short break. Actors are excused at this point and most examiners remain for a feedback session. Marking schemes are collected, sorted and distributed to candidates. One room is re-set for group feedback. Examiners are thanked for their time and each is asked in turn for general feedback, hints and tips on their station (figure 3).
Figure 3. Mock CASC timing
11.30pm
Coordinators arrive & set up venue
12.30-12.45pm
Candidates, actors & examiners on site
1pm
Exam starts
2.15pm approx
Break
2.45pm
Exam re-starts - candidates switch circuits
4pm approx
Exam ends
4.30pm
Feedback forms distributed/ group feedback session
5pm
End
Overcoming Potential Problems
Examiners
Our examiners are all either higher trainee or consultant psychiatrists. It is therefore possible that unforeseen circumstances mean that they may have to cancel at very short notice, attend late or not at all, or be called away during the mock exam. Each of these has happened over the past few years but has been easily managed by the extra higher trainee helpers stepping in to examine a station.
Actors
All of our actors have attended as planned. If a paid actor has to cancel at short notice, the agency will find a replacement. If a trainee actor did not attend, one of the higher trainee helpers could step in. Another potential problem which we have encountered is actors not performing as intended. This can be minimised by preparing clear instructions for actors, with examiners providing some direction if needed.
Quality control of stations
It is difficult to know how a station will work until it is used in the mock exam. To minimise the risk of problems, stations are checked and formatted before the exam. They are circulated to actors and examiners in advance to allow time for them to raise any concerns and clarify any uncertainties. Despite following these processes, there are some stations which appear unclear or do not run smoothly on the day of the mock exam. It is helpful to receive feedback from examiners, so that stations can be amended or avoided in future.
Timing
Our mock exam follows a very tight schedule. If the mock exam itself overruns, then fewer examiners may be able to remain to provide feedback. The higher trainee coordinator should keep time carefully during the day of the mock exam, particularly during break times, which are very brief. Support from other higher trainee helpers is essential for this, in working together to collect and organise marking sheets and guiding examiners, actors and candidates to stations. Late arriving examiners remain a potential problem due to their other commitments. We provide a sandwich lunch to our examiners prior to the exam, which helps with prompt attendance.
Venue
The venue we use is quite cramped and can become noisy. We have access to only 14 screens to divide the 16 stations so they are close together and those at the ends of the room are not fully enclosed. The screens are thin so only muffle the noise from neighbouring stations. These issues of space and noise are difficult to overcome. Trainees are warned in advance and aim to focus on their own station as much as possible.
Recruiting actors, examiners and candidates
To date, we have not experienced any problems in recruiting actors, examiners or trainee helpers. We have been able to fill all candidate places and often have a waiting list. If necessary, the mock exam could be run with fewer stations and still provide helpful practice for trainees. If resources were tight, trainees could be role-play actors for some or all of the stations.
Conclusion
We run a local mock exam annually due to continued demand from trainees. It takes significant time and effort to arrange but is good experience for the organiser and local trainees and consultants remain enthusiastic. The mock CASC in the West of Scotland puts a strong emphasis on providing feedback for trainees to work on. The provision of completed marking sheets on the day of the exam and the group feedback session help with this ethos. Our experience has shown that a mock CASC can be delivered locally, at a low cost, while still providing trainees with a realistic exam experience.
Supporting Professional Activities (SPA) time is a part of each consultant’s new contract. When the new consultant contract evolved in 2003, a suggested breakdown of the week was 7.5 sessions (1 session equates to 4 hours) for direct clinical care (DCC) and 2.5 sessions for SPAs.1 This was driven by the need for consultants to continue their own professional development (CPD) as well as having the time for input into the development of trainees and medical students.
Examples of CPD work for consultants could include audit for improvement of service or patient care, teaching of patients, medical students or trainees, research, publications, aspects of hospital management and involvement in simulation courses e.g. Advanced Life Support (ALS)/Advanced Paediatric Life Support (APLS).
The General Medical Council (GMC) requires that during annual appraisals, doctors should use supporting information to demonstrate they continue to follow “Good Medical Practice”. This mandates that doctors should ‘take part in educational activities that maintain and further develop’ their competence and performance.1 With regard to revalidation, the GMC states you will have to demonstrate that you regularly participate in these activities; at Annual Review of Competency Progression (ARCP) it is imperative that accurate records of these CPD activities are presented at the annual job plan review.2
It is clear, therefore, that the provision of allocated time during the working week to complete these aspects of work life are deemed necessary for consultants. The Royal College of Anaesthetists and Association of Anaesthetists of Great Britain and Ireland both support the original view that a consultant should “typically” have 2.5 SPAs in their contract (though this would have to be subject to individual workload). With the demands of service provision it is clear that consultant SPAs are under threat, with around 40% of new consultants offered jobs with fewer SPA sessions than are thought necessary to allow sufficient non-DCC work.3
Since trainees are subject to similar appraisal and development requirements, we wonder if trainees should be allocated SPA time? For progression through training years and to pass the ARCP, it is necessary to provide evidence of trainee development within clinical practice in a similar way to consultants. This can involve a great deal of extra time. Once (notoriously difficult) exams have been passed, each trainee must go through the application process and prove what skills they have assimilated during their training to date. In fact, the ST3 anaesthesia application criteria states that the following are some of the ‘desirable’ criteria that require evidence:
Relevant academic and research achievements
Involvement in an audit project, or quality improvement project
Interest and commitment to the specialty beyond the mandatory curriculum
Evidence of interest in, and experience of, teaching
Instructor status in an advanced life support course (ALS, APLS)
Involvement in management…and understanding of management
Effective multi-disciplinary team working and leadership
Effective leadership in and outside medicine
Achievement outside medicine
Altruistic behaviour, e.g. voluntary work
The list is extensive and clearly requires a lot of time and input outside of the normal working week. With the expectation that trainees should be prepared to move straight from CT2 to ST3 (assuming their exams are completed), these desirable criteria must be addressed alongside completing other mandatory aspects of training such as, for anaesthesia: an Initial Assessment of Competency (IAC), an Intensive Care Unit (ICU) module, an Initial Assessment of Obstetric Competency (IAOC) and 15 Units of Training. With all these challenges between a core anaesthetic trainee and potential specialist anaesthetic training, there seems little time to complete an adequate number of the desirable criteria; this is a compelling reason to facilitate some time into the trainee contract to help produce more well rounded trainees.
However, therein lies the challenge - anaesthetic training is such a busy programme. Trainees are involved with multiple areas within a hospital such as ICU, theatre work or Obstetric Delivery Suite that they must learn and practice a wide range of skills to demonstrate the proficiency expected of a consultant anaesthetist. With experience of clinical work already at a premium due to European Working Time Directive hours, creating a good teaching environment whilst providing service provision is a hard enough task. It might seem difficult, therefore, to justify taking away yet more clinical time for trainees.
The proposed “7 day National Health Service (NHS)” contract could also pose more difficulties. Current example rotas released by NHS Employers demonstrate an increased likelihood of shift-work for a typical ICU rota.4 This shows trainees will be working more weekends and nights than at present, which could reduce the time spent directly with consultants. This would make introducing more non-DCC work difficult to justify as it would likely occur during daylight hours – when training could occur.
How it could be introduced:
Assuming SPA sessions for trainees were implemented, there would also be practical aspects to address. For example, how many SPA sessions to allocate for each level of trainee and how to monitor that this time was spent effectively and efficiently.
Monitoring:
Trainees could propose which aspects to focus on during their SPA sessions, such as management, teaching, quality improvement projects or more time in their sub-specialty interest. The goals could then be set at the initial educational supervisor meeting, much like a Personal Development Plan (PDP), and monitored throughout the year. This would give focus to any SPA time and ensure it is effectively used. If a trainee abuses their time or is not using it appropriately then removal of SPA time could be enforced. This would give the trainees more ability to improve the skills so often considered additional to trainees.
Funding:
In times of NHS austerity, funding would also need addressing. Potentially neither Deanery nor Trust might be willing to pay a doctor for days spent working outside the hospital workload – such as in educational roles or as a college tutor.5 A trial in one single deanery could assess the efficacy of such a scheme.
A possible solution would be to remove a few days of study leave allowance, as many trainees do not use their whole entitlement, and re-assign these to SPA time, allowing a trainee more flexibility. Trainees could initially start with fewer SPA sessions when more junior, to allow more clinical time, increasing SPAs to one per week for intermediate or higher trainees who may well be approaching their Certificate of Completion of Training (CCT).
Conclusion:
There are some practical difficulties in establishing trainee SPA sessions and no doubt many feel all contracted time should be spent practicing anaesthesia. However, given the changing way trainees are recruited via a ‘tick-box’ national application system, together with the variety of non-clinical skills expected by consultancy such as an ability to teach, conduct audit work, engage in managerial roles etc., a small change in the training set-up could produce more rounded trainees, benefitting anaesthesia in general and training programmes in the future.
Communicating effectively with patients and families is a vital component of high quality care. Studies have shown that patients feel excellent communication in consultations is vital for instilling confidence in the medical practitioner.1,2 There is evidence that doctors are not meeting this fundamental need.3
Some consider it an ethical obligation of doctors to balance their training needs against providing optimal care for patients. It is well known that junior trainees have significant level of performance anxiety that translates through to their consultations.4
Simulation based training is now an integral part of postgraduate curriculum in training a variety of medical specialties in managing acute scenarios. As an education method it provides a controlled environment in which it is safe to learn from errors,5 and improves learner outcomes.6 Simulation has been shown to be a valid approximation of true clinical practice.7 It therefore allows trainees to reach higher levels of proficiency prior to embarking on real patient encounters.
Current Core Medical Trainees (i.e. junior doctors who have embarked on the first stage of physician training within England) in the London deanery are expected to be able to manage complex communication scenarios effectively prior to entering specialty training. This is demonstrated by requirements set out in the Core Medical Curriculum, as detailed in Box 1. Whilst significant emphasis is placed on communication skills training in basic scenarios at a medical student level, there is very little formal postgraduate communication skills training within this deanery and others.
Box 1: Excerpts from Core Medical Trainee curriculum
Counsel patients, family, carers and advocates tactfully and effectively when making decisions about resuscitation status, and withholding or withdrawing treatment
Able to explain complex treatments meaningfully in layman's terms and thereby to obtain appropriate consent even when there are problems of communication and capacity
Skillfully delivers bad news in any circumstance including adverse events
This deficit in training led us to conduct a survey exploring Core Trainees’ views regarding communication skills training in the London deanery. Findings from the survey are detailed in Box 2.
Box 2: Results from Core Trainee Survey
83% received less than 2 hours of post-graduate training in communication skills since the start of Core Medical Training
Only 50% felt somewhat competent in engaging in difficult communication scenarios
88% reported significant challenges when conducting these discussions. They have had difficult on-calls experiences relating to communication difficulties
100% displayed interest in attending further Simulation Training in advanced communication skills
Method
We devised a pilot project using simulation to develop trainees’ competencies in advanced communication skills. After application to our local training board, we secured funding to run a number of sessions for core medical trainees within the London area.
The objectives of our pilot project were to provide experience of realistic communication based scenarios in a structured and safe environment to core trainees; provide feedback on trainees’ communication styles and offer suggestions for improvement; improve confidence of trainees in difficult communication situations.
Each session was conducted in an afternoon session and candidates were divided into three groups of three trainees who would remain together for the entire session. We ran four sessions, with a total of 36 trainees. Each group was facilitated by a consultant or a higher trainee in either elderly or palliative care medicine, given our focus on resuscitation/end of life discussions and assessment of capacity. We employed three actors to rotate around each group performing a variety of roles including patients and relatives. With a total of six scenarios, each trainee had the opportunity to participate in at least two scenarios lasting approximately 15 minutes, with feedback thereafter for approximately 10 minutes.
The scenarios employed were based on personal experience of regularly occurring, challenging communication situations encountered in our own clinical practice. We created detailed scripts for the actors as well as corresponding clinical vignettes for the candidates.
The scenarios were:
End-of-life discussion with a challenging family regarding a patient with end-stage dementia.
Discussing resuscitation with a family opposed to do not attempt resuscitation (DNAR) regarding an acutely unwell patient with poor functional baseline.
Discussing resuscitation with a young patient with metastatic cancer undergoing palliative chemotherapy who has little understanding of the terminal nature of the disease.
Assessing mental capacity regarding discharge planning in a patient with mild to moderate dementia.
Assessing mental capacity regarding treatment in a patient with moderate learning difficulties.
Assessing mental capacity in a medically unwell patient with mental health issues who wishes to self discharge from the ward.
Box 3 outlines the session structure.
Box 3: Timetable for the session
12.30-12.45:
Actors briefing
12.45- 13.00:
Facilitators briefing
13.00-13.30:
Core trainee briefing
13.30-14.45:
Scenarios 1-3 in small groups
14.45-15.00:
Tea/Coffee break
15.00-16.15:
Scenarios 4-6 in small groups
16.15-16.45:
Feedback and closing
Results
Written feedback was obtained from all participants by distributing a post-course evaluation form, with a 100% response rate. A number of areas were assessed via a Likert scale of 1 – 5, with 1 being ‘not at all’ and 5 being ‘very much’. 100% of trainees felt the content was useful and their knowledge/skills had increased. 100% felt more confident after the session and all trainees and facilitators felt this would be beneficial for medical trainees. A full breakdown of results is detailed in Table 1.
Table 1: Results from post-course feedback
The post-course feedback form allowed for free text feedback from participants, with some individual examples given below:
“Realistic scenarios - good opportunity to experience them and get feedback in a safe environment, good practice of common communication problems”
“It builds confidence in dealing with these situations and provides basis for building up ”
“This work dealt with complicated cases and actors were not too easy which I liked. Good and unforgettable”
Discussion
With the European Working Timing Directive and resulting shorter working hours, gaining proficiency in a number of key skill areas is limited due to reduced patient encounters. A recurrent complaint among core medical trainees is the lack of observed clinical encounters that leads to individualised feedback.
Feedback from more experienced speciality practitioners was only one component of our attendees learning experience. They also benefited from personal practise in a non-threatening environment, observation of their colleagues communication styles and finally learning through reflection with their colleagues
This innovation has shown a clear benefit in amplifying the confidence and preparedness of our core medical trainees in approaching these higher level communication scenarios. Future directions include introducing quantitative assessments pre- and post- course to objectively demonstrate improved confidence and performance. Providing the course to trainees in other specialties as well as across the multidisciplinary team would also be beneficial given the universal requirement of healthcare professionals to communicate skilfully.
Claimants in medical negligence cases are increasingly making use of negligent failure to warn of risk in claims for compensation following medical mishaps when an inherent risk in a medical procedure has manifested itself resulting in injury. In order to succeed the claimant must establish firstly that the failure to warn was negligent and secondly that the negligence has caused a loss. This paper focuses on causation in failure to inform cases but briefly considers the shift in judicial attitudes to the requirement to give warnings in order to explain how the duty to inform and the available remedies have diverged.
Members of the medical profession commonly believe that to find a negligent failure to inform has caused a loss to the claimant a court must be satisfied that the patient would not have consented to the treatment had they been told of the risk. This was probably true until 2004 when the House of Lords came to a surprising decision which has since received a mixed reception.
The Changing nature of the requirement to give warnings
In the early days of medical litigation whether non-disclosure amounted to negligence was left to the standards of the medical profession. A medical professional was under a duty to at least equal the standards of a reasonably skilled and competent doctor; this would be assumed if s/he had acted in accordance with a body of professional opinion. This is referred to as the Bolam test.[i] There was disquiet amongst academic lawyers that doctors were being allowed to set their own standards and over time the courts have been wrestling back control.[ii],[iii] Following the Recent Supreme Court ruling in Montgomery[iv] there is now no doubt that patient autonomy is paramount and the need to inform will now be judged by reference to a reasonable person in the patient’s position.
In Montgomery the claimant, a diabetic, alleged she had been given negligent advice during her pregnancy. In particular she was not warned of risk of shoulder dystocia, the inability of the baby’s shoulders to pass through the pelvis, assessed at 9-10% for diabetic mothers and not informed of the possibility of delivery by elective caesarean section. The Consultant responsible for her care gave evidence (at paragraph 13) that she would not routinely advise diabetic mothers of this risk because if mentioned, “most women will actually say, ‘I’d rather have a caesarean section.’” The Supreme Court in finding (at paragraph 87) for the claimant held, “The doctor is therefore under a duty to take reasonable care to ensure that the patient is aware of any material risks involved in any recommended treatment, and of any reasonable alternative or variant treatments. The test of materiality is whether, in the circumstances of the particular case, a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it.” Although expressed as, “a duty to take reasonable care,” the medical professional is expected to, “ensure,” that the patient has the requisite knowledge. The test in failure to inform cases now focuses, not on the actions of the medical professional but, on the patient’s knowledge of the risks.
Chester v Afshar[v]
On 21st November 1994 Mr Afshar carried out a microdiscectomy at three disc levels on Miss Chester. There was no complication during the operation and the surgeon was satisfied that his objectives had been met. When Miss Chester regained consciousness she reported motor and sensory impairment below the level of L2. A laminectomy shortly after midnight the next day found no cause and the surgeon’s only explanation was cauda equine contusion during the retraction of the L3 root and cauda equine dura during the L2/L3 disc removal. During the legal proceedings Miss Chester brought against Mr Afshar it was found that the operation carried an unavoidable 1-2% risk of cauda equine syndrome (CES) and that the surgeon had not warned the patient about this risk. It was further found that, had the warning been given, Miss Chester would have sought a second (and possibly third) opinion meaning that the operation would not have taken place on 21st November.
The surgeon and the patient did not agree what was said about the risks of the operation before consent was obtained but the issue was decided in favour of the patient: the surgeon had failed to give a proper warning about the risk of CES. In order to succeed in her claim Miss Chester needed to establish that this failure had caused her loss but her lawyers did not argue that she would have refused consent if she had been informed. They took a different approach; the 1-2% risk of CES is not patient specific and is realised at random. If warned of the risk Miss Chester would have sought a second opinion meaning that the operation would have happened at a later date and possibly with a different surgeon. This subsequent operation would have carried the same 1-2% risk of CES. The High Court of Australia had previously accepted (in a different case) that the claimant can satisfy the burden by showing that, if informed, s/he would have chosen a different surgeon with a lower risk of adverse outcome but there was no evidence in this case that by choosing another surgeon Miss Chester could have reduced the risk.[vi]
At the time Mr Afshar failed to advise Miss Chester of the risks two paths should have been open to her. She could choose to have the operation with the defendant on 21st November which resulted in CES or to seek a second opinion and undergo the operation at a later date giving her a 98-99% (a better than balance of probabilities) chance of avoiding CES. Thus the failure to inform did not increase the 2% risk of CES but the court found, as a matter of fact, that it did cause the CES. Although the physical harm that Miss Chester had suffered (because of the inevitable risk) did not fall within the scope of the doctor’s duty to inform (to allow the patient to minimise risk) a majority of the House of Lords felt that the surgeon should be held liable because otherwise the patient would be left without a remedy for the violation of her right to make autonomous decisions about treatment.
There are two leaps in Chester the first is the notion that negligence causes a loss if it induces the claimant to follow a path with an associated risk that is realised when they could have followed another path with exactly the same risk. The second is that violating a patient’s right to make autonomous decisions should, as a matter of policy, make the surgeon liable for personal injury which happens after the patient is deprived of their right to make a decision about treatment. The next two paragraphs will consider these leaps in turn.
Equally risky paths: The first leap
In Wright[vii] the patient had developed a streptococcus pyogenes infection that had seeded into her proximal femur resulting in osteomyelitis. Her admission to hospital was delayed for two days by the defendant clinic’s negligent handling of her first presentation. On admission to hospital the patient had the additional misfortune to receive woefully inadequate treatment resulting in septic arthritis and permanently restricted mobility. The patient took the questionable decision to sue the clinic but not the hospital. One of the patient’s arguments against the clinic was that had she been admitted to hospital without the two day delay she would have been treated by different staff who would, almost certainly, not have been negligent. The claimant argued that, as in Chester, although the clinic’s negligence did not increase the random risk of receiving negligent hospital care it had, as a matter of fact, caused the negligent care. Lord Justice Elias rejected this suggestion precisely because the delay had not increased the risk that the hospital would provide the patient with inadequate treatment. However, the other members of the Court of Appeal found for the patient but for another reason; given two extra days the hospital would probably have realised their mistakes and been able to correct them before any permanent harm resulted.
Violated autonomy and personal injury: The second leap
There have been attempts to expand the scope of the majority reasoning in Chester. In Meiklejohn[viii] the patient was treated for suspected non-severe acquired apastic anaemia with Anti Lymphocyte Globulin and Prednisolone the latter causing an avascular necrosis. At an initial consultation a blood sample was taken from the patient for “research purposes” but possibly to exclude dyskeratosis congenital, the condition from which he was actually suffering. The patient argued he had not given informed written consent to the taking of a blood sample for research purposes and that had he been told about the uncertainty in the diagnosis he would have delayed treatment pending the result of the blood test or asked to have been treated with Oxymetholone instead. He further argued these violations of his autonomy required that he be given a remedy for the injury which had actually occurred through a reasonable misdiagnosis of his rare condition. Lady Justice Rafferty sitting in the Court of Appeal dismissed this argument stating at paragraph 34 that, “Reference to [Chester] does not advance the case for the Claimant since I cannot identify within it any decision of principle.”
Conclusion
Courts deciding failure to warn cases have shifted the emphasis from the reasonable practices of the medical profession to the autonomy of the patient; from the duty of the medical professional to the rights of the patient. Medical professionals are now required to give enough information to allow a reasonably prudent patient to make an informed decision about their own treatment. While this change has been taking place there has been no corresponding revision of the remedies available when a patient’s autonomy is infringed. If autonomous decision making is to be properly protected a remedy should be vested in every patient who has had their autonomy infringed whether or not that patient has suffered physical injury; autonomy infringements should be actionable per se (without proof of loss) and result in the award of a modest solatium (a small payment representing the loss of the right to make an informed decision about treatment.) Under the present arrangements the wrong that the patient complains of (infringement of autonomy) is not what they are seeking damages for (personal injury.)
In a small way, the court in Chester has sought to close this gap between the patient’s right and the remedy available by extending the existing law and widened the circumstances in which damages can be recovered by a patient following an infringement of autonomy. Medical professionals who fail to warn patients of small risks may be held liable if disclosing the risk might cause the patient to delay treatment while further deliberations take place. Paradoxically it could conceivably be argued that medical professionals who fail to disclose significant risks (greater than 50%) should escape liability because the loss was more likely than not to happen anyway!
Both Chester extensions to the law have been tested independently in Wright and Meiklejohn and rejected but this does not mean that it has been overruled. The two subsequent cases were heard by the Court of Appeal which cannot overrule the House of Lords (now the Supreme Court.) Both cases were distinguished meaning that the court was satisfied that they were not factually the same as Chester. Clearly Wright is not concerned with rights to autonomy and Meiklejohn is a failure to warn of uncertainties in diagnosis or failure to obtain written informed consent to research rather than risks inherent in treatment. If the facts of Chester were to come before the Courts again the decision would have to be the same; a surgeon could not necessarily escape liability by proving that, informed of the risk, the patient would have consented to the operation.
Summary points
Patients have a right to be informed of material risks inherent in medical treatment
An injured patient does not necessarily need to prove they would not have consented to the operation if the risks had been disclosed
A legal claim against a health care professional may be successful if the patient would have delayed the operation to a later date
This extension of the law has critics but the situation is unlikely to change in the near future
A 73 year old male retired civil servant with a background of spinal bulbar atrophy and hypertension presented to his General Practitioner (GP) for a routine health check. He was taking bendroflumethiazide, propranolol, atorvastatin and aspirin. His brother also has spinal bulbar atrophy.
The GP sent routine blood tests, which came back as follows: Haemoglobin 8.5 (13-17g/dL), Mean Cell Volume 84.9 (80-100fl), White Cell Count 3.4 (4-11 x10^9/L), Neutrophil Count 0.68 (2-8 x10^9/L), Platelets 19 (150-400 x10^9/L). A random blood sugar reading was 18 (3.9-7.8mmol/L). Renal function, bone profile and hepatic function tests were normal. The General Practitioner referred the patient urgently to the local Haematology unit for further assessment.
On further review the patient complained of tiredness but had had no infections or bleeding. There were no night sweats or recent foreign travel. Physical examination was unremarkable, with no lymphadenopathy or organomegaly.
A blood film showed marked anaemia with red cell anisopoikilocytosis, prominent tear drop cells and neutropenia with normal white cell morphology. There were no platelet clumps. A diagnostic investigation followed.
QUESTIONS
What are the differential diagnoses of pancytopenia and which causes are likely here given the findings on examination of the peripheral blood film?
Infections - Viral infections including cytomegalovirus, hepatitis A-E, Epstein-Barr virus, Parvovirus B19 and non A-E hepatitis viruses can cause aplastic anaemia1. The classical picture would be pancytopenia in a young patient who has recently had ‘slapped cheek syndrome’ from parvovirus B19 who has transient bone marrow aplasia. Tropical infections such as visceral leishmania may cause pancytopenia, splenomegaly and a polyclonal rise in immunoglobulins2. Overwhelming sepsis may also cause pancytopenia with a leucoerythroblastic blood film (myeloid precursors, nucleated red blood cells and tear drop red cells). HIV is also an important cause of cytopenias.
Medications - common medications may cause aplastic anaemia, such as chloramphenicol, azathioprine and sodium valproate. The history in this case did not have any recent medications introduced. The other very common cause of pancytopenia in modern practice would be in the context of chemotherapy.
Bone marrow disorders - tear drop cells are a key finding and clue in this case. They suggest an underlying bone marrow disorder and stress. In the context of a known active malignancy they are nearly indicative of bony metastases. Our patient did not have a known malignancy and there was nothing to suggest this on the history or physical examination, although in a man of this age metastatic prostate cancer should be considered. Other bone marrow disorders that would need to be considered are acute leukaemia (which was the diagnosis here), myelodysplasia and myelofibrosis. Splenomegaly would be especially significant in this case as it would be highly suggestive of myelofibrosis in combination with tear drop cells wit pancytopenia in an elderly patient3.
B12 and folate deficiency – this may cause pancytopenia, tear drop cells and leucoerythroblastic blood findings4&5. The mean corpuscular volume in this case however is normal which would somewhat argue against B12 and folate deficiency, as well as the fact that there were no hypersegmented neutrophils seen on the blood film. This cause is however very important given how it is easily reversible and treatable.
Haemophagocytosis – this is a bone marrow manifestation of severe inflammation and is a manifestation of systemic disease6. It has various causes including viruses (e.g. Epstein Barr virus), malignancy and autoimmune disease. It should be considered in patients with prolonged fever, splenomegaly and cytopenias. It is diagnosed by characteristic findings on bone marrow biopsy.
Paroxysmal nocturnal haemoglobinuria – this is a triad of pancytopenia, thrombosis and haemolysis caused by a clonal stem cell disorder with loss of membrane proteins (e.g. CD55 and CD59) that prevent complement activation7.
Genetic disease – Fanconi anaemia is a rare autosomal recessive disease with progressive pancytopenia, malignancy and developmental delay. It is caused be defects in DNA repair genes.
The key finding in this case was tear drop cells on the blood film. These are part of a leucoerythroblastic blood picture seen in bone marrow disease, malignant marrow infiltration, systemic illness and occasionally haematinic deficiency. See above for why this is unlikely to be haematinic deficiency. Although tear drop cells can occur in systemic illness such as severe infection, the history here was not in keeping with this. The diagnoses remaining therefore are malignant bone marrow infiltration or a primary bone marrow disorder (myelodysplasia, acute leukaemia or myelofibrosis). There were no features in the history pointing towards a metastatic malignancy and therefore primary bone marrow disorder is the most likely diagnosis. The diagnosis was later established as acute myeloid leukaemia on bone marrow examination.
What investigations would help to confirm or eliminate the possible diagnoses?
Blood tests including a clotting screen, liver function tests, inflammatory markers and renal function shall help to exclude other systemic disease such as disseminated intravascular coagulation, sepsis, liver disease and thrombotic thrombocytopenic purpura which may all give rise to cytopenias. Autoimmune screening may also suggest vasculitis which can cause cytopenias.
Microbiology studies including virology tests (e.g. human immunodeficiency virus, Epstein Barr virus and hepatitis viruses) may also be requested as appropriate given the clinical scenario and findings. Visceral leishmania should be tested for according to travel history and clinical likelihood. Leishmania may be identified through serology and light microscopy (for amastigotes) or polymerase chain reaction of the bone marrow aspirate. Tuberculosis could be cultured from the bone marrow is suspected.
Haematinics are a crucial test and the aim should be to try and withhold transfusion until these results are known in case they can easily be replaced thereby negating the need for blood products. Remember that if haematinics are not tested before transfusion then the blood products will confound the tests results.
Bone marrow biopsy, including aspirate and trephine are a crucial investigation for morphological examination and microbiological testing if indicated. This will distinguish the bone marrow disorders including acute leukaemia, myelofibrosis, bone marrow metastatic infiltration and myelodysplasia. Haemophagocytic syndrome may also be suggested by bone marrow examination findings.
Imaging if there is suspicion of an underlying malignancy (e.g. CT chest, abdomen and pelvis) and then further blood tests such as the prostate specific antigen. Ultrasound could also be used to check for splenomegaly where clinical examination has not been conclusive.
Medication review is vital as this may reveal the diagnosis (e.g. use of chloramphenicol)
Flow cytometry may be considered to investigate for an abnormal clone in the case of paroxysmal nocturnal haemoglobinuria and may be used on bone marrow samples to further evaluate the cells.
Unless a very clear cause for the pancytopenia is obvious (e.g. haematinic deficiency or malignant infiltration) then bone marrow examination is crucial for establishing a diagnosis. This will also prevent inappropriate treatments being initiated.
What immediate management steps and advice would be given to this patient?
General measures for pancytopenia include blood product support. Red cells and platelets can be given for symptomatic anaemia and bleeding. There is no need to transfuse platelets in the patient if there are no signs of bleeding. Alternatively he could also be treated with tranexamic acid as an alternative to avoiding risks associated with platelet transfusion. Infection should be treated urgently. Due to the neutropenia he should be advised to seek medical help if he develops a fever or sore throat. He should urgently be followed up in clinic with the results and given the contact details for the haematology department in the interim period in case he develops any problems.
The specific treatments for pancytopenia rests on the exact cause found after investigation. In this case the diagnosis was acute myeloid leukaemia arising from a background of myelodysplasia. The treatment for acute myeloid leukaemia in general, with curative intent, would consist of induction chemotherapy with DA (daunorubicin and cytosine arabinoside) followed by consolidation with further chemotherapy, the type of which (e.g. high dose cytosine arabinoside or FLAG-Ida) would depend on the risk assessment of the disease and possible consideration of an allograft bone marrow transplant after consolidation. Currently different approaches to consolidation chemotherapy, transplantation and small molecule inhibitors are being evaluated in clinical trial (e.g. AML 17 clinical trial).
The other options, in older more frail patients where high dose chemotherapy will be very toxic, are low dose palliative chemotherapy and support with transfusion.
PATIENT OUTCOME
He has been supported with blood products (platelets and packed red cells for bleeding and anaemia respectively). After discussion with him and his wife he has elected to have palliative chemotherapy with low dose cytosine arabinoside. He will be seen regularly in the haematology clinic and day unit for review. We do not suspect a link between the leukaemia and spinal bulbar atrophy.
Isaac Asimov famously said: ‘The only constant is change.’ (Cited in Hartung, 2004).
So why is it so difficult for most of us to understand, manage, or embrace change?
Coping with change can be challenging for many and, depending on the change and what the impact or outcome of the change means to the individual, will depend upon how well they embrace and accept it. Should a person be fearful of change then it is natural that they will attempt to resist it which in turn can cause high levels of stress and anxiety.
Understanding how we typically react to change also helps us to cope better and manage change. The Kubler-Ross (2009) Model of Change is perhaps one of the best known and most applied models within clinical environments (her original work being around the five stages of grief) which is now also applied to businesses and organisations when looking at changes in the work place such as loss or change of job.
The five stages she refers to are:
Denial
Anger
Bargaining
Depression
Acceptance
A common example used to explain this model is to understand how we would typically respond to an unexpected change such as a dead car battery.
The dead car battery
Just imagine it is a cold winter day and you are dashing to get to work already running late…
You jump into the car, place the key in the ignition and turn it on.
Nothing happens, the battery is dead.
Applying the Kubler Ross Model to this situation, this is how a person may typically react:
Denial - This cannot be happening! Try again. And again! Check the other things in the car are working such as the lights and radio. Try again but still nothing.
Anger - Arrrrgh you stupid car!!! I’m sick of this car!! Why is this happening today of all days!! Slamming a hand against the steering wheel.
Bargaining - (realising that it really isn’t going to start and that you're going to be late for work)..., Oh please car, if you will just start one more time I promise I'll buy you a brand new battery and keep you clean and tidy. Please just start this one time.
Depression - Oh no! What am I going to do? I'm going to be late for work. I give up. I don't really care any more. What's the use?
Acceptance - Right I need to do something. It is not going to start. I need to call the breakdown service and ring into work.
The above example is a simple example yet I’m sure most of us have experienced it or something similar quite often. If you apply this to a situation where the stakes are far higher such as a sudden loss or change of a job, bereavement, house, relationship etc which may impact upon so many things including stability of finances, family, health and other forms of security, then you may be able to see the harsh effect this could have on an individual during this time.
Often individuals add to their stress by expecting themselves to be able to cope with such events. It is important to understand it is not about strength or weakness but about human nature to react by demonstrating the signs of loss and grief. Organisations, managers and individuals need to be understanding and supportive when situations like this happen.
Another way of understanding and coping with change is to consider what goes on in the mind of the individual at the time of the change and what it ‘means’ to them. Some people see risk and uncertainty as exciting and embrace change (depending on the change), whereas others can be fearful of any change, even those perceived to be minor changes, as for them any change is seen as a risk and takes them out of their comfort zone.
The comfort zone
Your comfort zone is where you are fully able, competent and comfortable. The job that you can do with your eyes shut or routines of life where you know exactly what you are doing. You may feel slightly challenged now and then, but there’s nothing you cannot easily handle.
When invited to step outside their comfort zone – or if they’re pushed outside of it - many people react with resistance. This is because of the human fear of failure which, when you look into it more deeply, comes from a desire to be accepted, liked and even loved. When most people ‘fail’ they feel embarrassed, ashamed, silly or stupid because they feel they can’t or couldn’t do whatever it was they tried.
So it’s understandable if at work, or any area of life where there is change, people react with resistance. Change is the unknown, and if you don’t know whether you can do something – especially if you have a ‘Be Perfect’ driver – you could have fears over whether you can do it, can be a success or even cope. Everyday changes such as new computers or telephone systems, new staff, new jobs, new routines and procedures, new management, merging of departments, sections or whole companies or, on a personal level, exams, weddings, divorce, births, deaths, moving house and so on, are all high on the list of stressors due to change.
How big is your zone?
Are you resistant to change? If you are, you’re causing yourself stress. Imagine what size a child’s comfort zone would be compared to an adult’s. Children do not have inhibitions and fears; it’s only as we grow older that we learn to feel fear, that we learn what embarrassment is and how to feel silly or stupid – that is, we learn to have an ego. This restricts our ability to have the freedom to learn, grow and be open to change, as we are nervous about asking questions for fear of looking silly, or trying new things for fear of failure, and we avoid doing anything that may cause us to feel embarrassed.
By being more fluid and open to change, accepting any fear and dealing with it effectively, you would not only grow your confidence and self-esteem, but you will be free to develop your life with more happiness and less stress.
By looking at change differently (for example, recognising that change can also be a good thing; focusing on the possible positives from a situation rather than being quick to look at the negatives from a point of fear and therefore resistance) stress can be greatly reduced.
Choose to flow with change rather than resist; choose to step out of your comfort zone and grow the size of your comfort zone daily. Aim to have a comfort zone the size of a child’s where nothing can faze or worry you, and you will notice a huge difference to the amount of stress you have in your life.
‘The greatest discovery of my generation is that a human being can change their life by altering their attitude of mind.’ William James (cited in Maxwell, 2007).
Remember – the only failure is not trying again. If we fail at something at least we know what NOT to do next time!
Identifying your zones and being rational
Following are three simple exercises you can complete to help you to gain a rational perspective on understanding how you cope with change and also being solution focused when embracing change.
The zones of change help us to understand the different levels of comfort or ‘risk’ and where changes may sit in terms of their percieved meanings to the individual.
Zones of change
Exercise 1
Think back to a significant change in your life or work (something from the past).
What were your perceived risks at the time?
…………………………………………………………………………………
…………………………………………………………………………………
What did you lose?
…………………………………………………………………………………
…………………………………………………………………………………
What did you gain?
…………………………………………………………………………………
…………………………………………………………………………………
This exercise demonstrates that our ‘perceived risks’ at the time of a change were often far different than the reality of how the change occurred. It is also common for an individual to notice that their ‘gains’ can be larger than their ‘losses’ (time can play a factor in this too, often a change can seem a disaster at the time but over time a person can look back and be glad it happened in comparison to how their life is now.)
Exercise 2
Think of a change that you are currently undergoing.
What aspects of the change are in your ‘comfort zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What aspects are in your ‘risk zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What aspects are in your ‘high risk zone’?
…………………………………………………………………………………
…………………………………………………………………………………
What do you need to make the ‘high risk’ into ‘risk’ and the ‘risk’ into ‘comfort’?
…………………………………………………………………………………
…………………………………………………………………………………
This exercise is excellent for considering a current change and how it may affect a person.
Actually listing in categories the level of ‘risk,’ or even drawing the zones on a piece of paper and writing in each change in the place on the zone where the person believes it sits, will give a rational perspective.
Once all the ‘risks’ are highlighted then that is the time to minimize ‘risk’ and find solutions for the individual to cope or manage that change. This is good for action planning and allowing a person to take control to embrace a change rather than being reactive once the change has occurred.
Exercise 3
Think of a life or work change which is going to occur in the future.
Blockers
What I’d be sorry to lose.
…………………………………………………………………………………
…………………………………………………………………………………
My fears and concerns.
…………………………………………………………………………………
…………………………………………………………………………………
Drivers
Benefits of the change.
…………………………………………………………………………………
…………………………………………………………………………………
What I’d be glad to leave behind.
…………………………………………………………………………………
…………………………………………………………………………………
Answering these questions assists a person to determine how much resistance they may feel/have towards a change. Listing potential blockers will identify fears and concerns of the change as well as the levels of risk and loss. Listing drivers will encourage the individual to consider the benefits of the change, the gains, and that change can also be a good thing.
Typically, whichever list is the longest or has the most meaning/impact will be the strongest for that person. If this is the blockers they will resist the change and cause themselves pressure and stress. Therefore addressing the zones of change and looking for ways to reduce risk would be a good strategy in action planning to manage the change well. Should the drivers be the strongest for the person then they are likely to embrace the change more readily although they may still need to address their thoughts and rationale for any blockers listed.
Change tips:
Embrace change, as if you don’t accept it someone will push you into it.
Take every opportunity to grow your comfort zone.
Have the attitude that there is no failure and only learning and development – when we ‘fail’ we know what NOT to do next time.
The worst rarely happens, so why waste energy focusing on it and enforcing irrational fears?
Change CAN be a good thing.
There is always a solution, it may take time for you to see it, but if you look, you will find it.
Sleep is a fundamental part of our lives and about one-third of it is spent sleeping. Sleep deprivation has been linked with such high profile public disasters, as Chernobyl, the Challenger shuttle disaster and the nuclear meltdown at Three Mile Island. According to the US Highway Traffic Safety Administration, approx. 100,000 motor vehicle accidents are the result of driver’s drowsiness and fatigue1. There is an association of sleep disorders with anxiety and depression which may be bidirectional. Patients with insomnia for 2 weeks or longer, without current depression are at increased risk of developing major depression. Both insomnia and hypersomnia are considered independent predictors of depression and anxiety2.
Key Milestones in the Development of American Sleep Medicine:
The history of treatment of sleep disorders dates back to at least the use of opium as a hypnotic reported in ancient Egyptian text. Sleep medicine, however did not emerge as a distinct discipline until the 1970’s. Drs. Kleitman and Dement were significant early contributors to this field in the United States. In 1957 they first described Non Rapid Eye Movement (NREM) sleep and Rapid Eye Movement (REM) sleep and proposed the 4 stages of NREM sleep. In 1972 Dr. Dement, a Professor of Psychiatry and Behavioural Sciences at Stanford University School of Medicine, contributed to the establishment of the first sleep disorder centre in Stanford. After Stanford, other centres in New York, Texas, Ohio and Pennsylvania started providing sleep evaluations for which patients stayed in the centre overnight. The Association of Sleep Disorders Centre (ASDC) was established in 1975 and Dr. Dement served as its first president for12 years. In 1999 ASDC was renamed American Academy of Sleep Medicine (AASM). The first textbook of sleep medicine “Principles and Practice of Sleep Medicine” was published in 80’s. The journal SLEEP started in 1978. In 1998 the AASM commissioned the fellowship training committee to develop guidelines for sleep medicine fellowship training. The first two programmes to be granted formal accreditation were Stanford University in California and the Centre for Sleep and Wake in Montefiore Medical Centre, New York. The American Medical Association recognized sleep medicine as a specialty in 1996. In 2004 the Accreditation Council on Graduate Medical Education (ACGME) took over the fellowship accreditation process and approved a one year training programme 1,3,4,5.
Sleep Medicine training in Europe:
Unlike United States, there are no formal sleep medicine training programmes or qualification in the United Kingdom or Europe. Sleep medicine is restricted to a small group of respiratory physicians with a special interest in sleep medicine. Psychiatry trainees are exposed to very little formal teaching in sleep medicine. However in the last 3 years the neuropsychiatry section of the Royal College of Psychiatrists of the United Kingdom has formed the “sleep working group” under the leadership of Dr. Hugh Selsick, this group is responsible for increasing awareness of sleep medicine among British psychiatrists, by emphasizing the importance of sleep medicine in psychiatric practice and encouraging psychiatrists to contribute to the field of sleep medicine. This group has developed a competency based curriculum that incorporates the training of sleep medicine into the psychiatry curriculum, to organize sleep medicine symposia at annual conferences of the Royal College and to develop professional training (CPD) modules for psychiatrists. British Sleep Society is another forum that brings together physicians from various backgrounds interested in sleep medicine. Royal Society of Medicine also has a sleep medicine section which organizes various conferences. There are two, week long courses on sleep medicine, the Edinburgh and Cambridge courses. Recently the University of Glasgow started a Master’s of Science (MSc) in behavioural sleep medicine program for healthcare providers working in Scotland, the rest of the United Kingdom and Europe 6, 7, 8, 9. There is a trans-European move to start a formal sleep medicine certification similar to what we have in the United States. European Sleep Research Society (ESRC), a professional body of sleep scientists in Europe responsible for promoting sleep research and sleep medicine is starting its “first ESRS certification examination” in sleep medicine; this examination is scheduled to take place on September 4th, 2012 at the 21st Congress of the European Sleep Research Society in Paris. Since there are no formal training programmes this will be for those without formal training 10.
Psychiatry and Sleep:
Asking about the patient’s sleep is an integral part of a psychiatric consultation. Almost all the medication that psychiatrists prescribe has an effect on sleep architecture. Some psychiatric medications are used to treat sleep disorders and others can cause sleep disorders like Restless Legs Syndrome and PMLD. Understanding sleep can help us understand the mechanism of psychiatric illness. Many psychiatric disorders have comorbid sleep disorders and several behavioural therapies have been used successfully for the treatment of sleep disorders. There is bidirectional association between sleep disorders and psychiatric disorders. With the growing population of military soldiers returning from Iraq and Afghanistan with post-traumatic stress disorder, sleep problems and depression, there is an increased need for psychiatrists who possess knowledge in both sleep disorders and comorbid psychiatric illness. Psychiatrists have a distinct advantage dealing with sleep disorders and can bring those skills to sleep medicine.
Are psychiatrists attracted towards sleep medicine? The answer is yes. In the recent years we have seen an increased interest among psychiatry trainees for a sleep fellowship in United States. In recognition of behavioural consequences of sleep problems and multidisciplinary approach in sleep disorders, fellowship programmes are increasingly taking applicants from various backgrounds and not just pulmonology and neurology. Many psychiatry trainees are choosing a sleep medicine elective earlier in residency. Currently there are more than 710 accredited sleep centres in the United States. Many major university medical centres have a one year fellowship programme accepting applications from physicians from various backgrounds including Psychiatry, Neurology, Internal Medicine, Pulmonology, Paediatrics, ENT and Anaesthesia 1. There are more than 24 AGME approved sleep medicine fellowship programmes in the United States 11. New fellowship programmes are being opened at the University of Kansas Medical Centre and the University of Texas Health Sciences Centre, San Antonio.
Conclusion:
Sleep medicine is a new and exciting field of medicine with potential to grow in future. It’s a multidisciplinary field. American sleep medicine has evolved greatly over the last 30 years and there appears to be much to learn from the American model. There is a need for the psychiatry training programs both in the United States and the Europe to encourage and prepare their trainees to consider training in sleep medicine. Psychiatry trainees in the United States interested in sleep medicine should speak with their programme directors early in their residency training to register their interest and residents should also contact the local sleep centre for more advice. Each year American Academy of Sleep Medicine (AASM) accepts 10 international physicians for its 4 week mini-fellowship programme. Three weeks of the fellowship are spent at an AASM-accredited U.S sleep centre with their last week of the fellowship spent at the annual SLEEP conference. A certificate of training is issued at the end of the mini fellowship 12.
Assessment and evaluation are the foundations of learning; the former is concerned with how students perform and the latter, how successful the teaching was in reaching its objectives. Case based discussions (CBDs) are structured, non-judgmental reviews of decision-making and clinical reasoning1. They are mapped directly to the surgical curriculum and “assess what doctors actually do in practice” 1. Patient involvement is thought to enhance the effectiveness of the assessment process, as it incorporates key adult learning principles: it is meaningful, relevant to work, allows active involvement and involves three domains of learning2:
Clinical (knowledge, decisions, skills)
Professionalism (ethics, teamwork)
Communication (with patients, families and staff)
The ability of work based assessments to test performance is not well established. The purpose of this critical review is to assess if CBDs are effective as an assessment tool.
Validity of Assessment
Validity concerns the accuracy of an assessment, what this means in practical terms, and how to avoid drawing unwarranted conclusions or decisions from the results. Validity can be explored in five ways: face, content, concurrent, construct and criterion-related/predicative.
CBDs have high face validity as they focus on the role doctors perform and are, in essence, an evolution of ‘bedside oral examinations’3. The key elements of this assessment are learnt in medical school; thus the purpose of a CBD is easy for both trainees and assessors to validate1. In terms of content validity, CBDs are unique in assessing a student’s decision-making and which, is key to how doctors perform in practice. However, as only six CBDs are required a year, they are unlikely to be representative of the whole curriculum. Thus CBDs may have a limited content validity overall, especially if students focus on one type of condition for all assessments.
Determining the concurrent validity of CBDs is difficult as they assess the pinnacle of Miller’s triangle – what a trainee ‘does’ in clinical practice (figure1)4. CBDs are unique in this aspect, but there may be some overlap with other work based assessments particularly in task specific skills and knowledge. Simulation may give some concurrent validity to the assessment of judgment. The professional aspect of assessment can be validated by a 360 degree appraisal, as this requests feedback about a doctor’s professionalism from other healthcare professionals1.
Figure 1: Miller’s triangle4
CBDs have high construct validity, as the assessment is consistent with practice and appropriate for the working environment. The clinical skills being assessed will improve with expertise and thus there should be ‘expert-novice’ differences on marking3. However the standard of assessment (i.e. the ‘pass mark’) increases with expertise – as students are always being assessed against a mark of competency for their level. A novice can therefore score the same ‘mark’ as an expert despite a difference in ability.
In terms of predictive validity performance-based assessments are simulations and examinees do not behave in the same way as they would in real life3. Thus, CBDs are an assessment of competence (‘shows how’) but not of true clinical performance and one perhaps could deduct that they don’t assess the attitude of the trainee which completes the cycle along with knowledge and skills (‘does’)4. CBDs permit inferences to be drawn concerning the skills of examinees that extend beyond the particular cases included in the assessment3. The quality of performance in one assessment can be a poor predictor of performance in another context. Both the limited number and lack of generalizability of these assessments have a negative influence on predictive validity3.
Reliability of Assessment
Reliability can be defined as “the degree to which test scores are free from errors of measurement”. Feldt and Brennan describe the ‘essence’ of reliability as the “quantification of the consistency and inconsistency in examinee performance” 5. Moss states that less standardized forms of assessment, such as CBDs, present serious problems for reliability6. These types of assessment permit both students and assessors substantial latitude in interpreting and responding to situations, and are heavily reliant on assessor’s ability. Reliability of CBDs is influenced by the quality of the rater’s training, the uniformity of assessment, and the degree of standardization in examinee.
Rating scales are also known to hugely affect reliability – understanding of how to use these scales must be achieved by all trainee assessors in order to achieve marking consistency. In CBD assessments, trainees should be rated against a level of completion at the end of the current stage of training (i.e. core or higher training) 1. While accurate ratings are critical to the success of any WBA, there may be latitude in the interpretation of these rating scales between different assessors. Assessors who have not received formal WBA training tend to score trainees more generously than trained assessors7-8. Improved assessor training in the use of CBDs and spreading assessments throughout the student’s placement (i.e. a CBD every two months) may improve the reliability and effectiveness of the tool1.
Practicality of Assessment
CBDs are a one-to-one assessment and are not efficient; they are labour intensive and only cover a limited amount of the curriculum per assessment. The time taken to complete CBDs has been thought to negatively impact on training opportunities7. Formalized assessment time could relieve the pressure of arranging ad hoc assessments and may improve the negative perceptions of students regarding CBDs.
The practical advantages of CBDs are that they allow assessments to occur within the workplace and they assess both judgment and professionalism – two subjects on the curriculum which are otherwise difficult to assess1. CBDs can be very successful in promoting autonomy and self-directed learning, which improves the efficiency of this teaching method9. Moreover, CBDs can be immensely successful in improving the abilities of trainees and can change clinical practice – a feature than is not repeated by other forms of assessment8.
One method for ensuring the equality of assessments across all trainees is by providing clear information about what CBDs are, the format they take and the relevance they have to the curriculum. The information and guidance provided for the assessment should be clear, accurate and accessible to all trainees, assessors, and external assessors. This minimizes the potential for inconsistency of marking practice and perceived lack of fairness7-10. However, the lack of standardization of this assessment mechanism combined with the variation in training and interpretation of the rating scales between assessors may result in inequality.
Formative Assessment
Formative assessments modify and enhance both learning and understanding by the provision of feedback11. The primary function of the rating scale of a CBD is to inform the trainee and trainer about what needs to be learnt1. Marks per see provide no learning improvement; students gain the most learning value from assessment that is provided without marks or grades12. CBDs have feedback is built into the process and therefore it can given immediately and orally. Verbal feedback has a significantly greater effect on future performance than grades or marks as the assessor can check comprehension and encourage the student to act upon the advice given1,11-12. It should be specific and related to need; detailed feedback should only occur to help the student work through misconceptions or other weaknesses in performance12. Veloski, et al, suggests that systemic feedback delivered from a credible source can change clinical performance8.
For trainees to be able to improve, they must have the capacity to monitor the quality of their own work during their learning by undertaking self-assessment12. Moreover, trainees must accept that their work can be improved and identify important aspects of their work that they wish to improve. Trainee’s learning can be improved by providing high quality feedback and the three main elements are crucial to this process are 12:
Helping students recognise their desired goal
Providing students with evidence about how well their work matches that goal
Explaining how to close the gap between current performance and desired goal
The challenge for an effective CBDis to have an open relationship between student and assessor where the trainee is able to give an honest account of their abilities and identify any areas of weakness. This relationship currently does not exists in most CBDs, as studies by Veloski, et al8and Norcini and Burch9 who revealed that only limited numbers of trainees anticipated changing their practice in response to feedback data. An unwillingness to engage in formal self-reflection by surgical trainees and reluctance to voice any weaknesses may impair their ability to develop and lead to resistance in the assessment process. Improved training of assessors and removing the scoring of the CBD form may allow more accurate and honest feedback to be given to improve the student’s future performance. An alternative method to improve performance is to ‘feed forward’ (as opposed to feedback) focusing on what students should concentrate on in future tasks10
Summative Assessment
Summative assessments are intended to identify how much the student has learnt. CBDs have a strong summative feel: a minimum number of assessments are required and a satisfactory standard must be reached to allow progression of a trainee to the next level of training1. Summative assessment affects students in a number of different ways; it guides their judgment of what is important to learn, affects their motivation and self-perceptions of competence, structures their approaches to and timing of personal study, consolidates learning, and affects the development of enduring learning strategies and skills12-13. Resnick and Resnick summarize this as “what is not assessed tends to disappear from the curriculum” 13. Accurate recording of CBDs is vital, as the assessment process is transient, and allows external validation and moderation.
Evaluation of any teaching is fundamental to ensure that the curriculum is reaching its objectives14. Student evaluation allows the curriculum to develop and can result in benefits to both students and patients. Kirkpatrick suggested four levels on which to focus evaluation14:
Level 1 – Learner’s reactions Level 2a – Modification of attitudes and perceptions Level 2b – Acquisition of knowledge and skills Level 3 – Change in behaviour Level 4a – Change in organizational practice Level 4b – Benefits to patients
At present there is little opportunity within the Intercollegiate Surgical Curriculum Project (ISCP) for students to provide feedback. Thus a typical ‘evaluation cycle’ for course development (figure 2) cannot take place15. Given the widespread nature of subjects covered by CBDs, the variations in marking standards by assessors, and concerns with validity and reliability, an overall evaluation of the curriculum may not be possible. However, regular evaluation of the learning process can improve the curriculum and may lead to better student engagement with the assessment process14. Ideally the evaluation process should be reliable, valid and inexpensive15. A number of evaluation methods exist, but all should allow for ongoing monitoring review and further enquiries to be undertaken.
Figure 2: Evaluation cycle used to improve a teaching course15
Conclusion
CBDs, like all assessments, do have limitations, but we feel that they play a vital role in development of trainees. Unfortunately, Pereira and Dean suggest that trainees view CBDs with suspicion7. As a result, students do not engage fully with the assessment and evaluation process and CBDs are not being used to their full potential. The main problems with CBDs relate to the lack of formal assessor training in the use of the WBA and the lack of evaluation of the assessment process Adequate training of assessors will improve feedback and standardize the assessment process nationally. Evaluation of CBDs should improve the validity of the learning tool, enhancing the training curriculum and encouraging engagement of trainees.
If used appropriately, CBDs are valid, reliable and provide excellent feedback which is effective and efficient in changing practice. However, a combination of assessment modalities should be utilized to ensure that surgical trainees are facilitated in their development across the whole spectrum of the curriculum.
Controlled teaching environment can be provided to undergraduate medical students for learning certain basic clinical skills through using manikins or models before they have to perform them on real patients. Many medical schools in the United Kingdom now have clinical skills laboratories which are equipped with a large host of such learning resources. Many medical schools promote their clinical laboratories and have dedicated lead consultants to teach, monitor and develop clinical skills. Furthermore, a wide variety of skills can be taught in these laboratories. For example, the University of Leeds Medical school offers teaching to second year undergraduate medical students in basic life support, vital signs, injections, blood glucose monitoring, cannulation and venepuncture while third year medical students are taught fundoscopy, rectal examination, urinary bladder catheterisation, doing an ECG and examination of the breast. Similarly, simulators have also been used in postgraduate medical teaching, for example, Colonoscopy simulators have been used to calculate efficiency ratio of learners. 1
However not all places in the world have clinical skills laboratories. Alternatively, some institutions teach the undergraduate medical students various basic skills in clinical supervised settings before they take up their first job as physicians. Some have assessed the level of training that their institutions have thus offered and tried to improve upon deficits. Mario Sicaja et al 2 from Zagreb University evaluated 252 students using a questionnaire asking the students to self assess their abilities on nine groups of skills and asked 129 faculty teachers to simultaneously assess the minimum necessary level of skills they expected from the graduating students. They concluded that the teachers expected higher level of clinical skills from students than that assessed by the students. Similarly, in postgraduate teaching, the students’ learning needs have been assessed by determining the difference in expectation of trainers and the trainees. 3
Effectiveness of basic clinical skills training programmes has been documented and it has been suggested that longitudinal skills training offers superior preparation for abilities during the clerkship 4. It has also been suggested that whereas students from medical schools using traditional curriculum may not differ in their knowledge based performance, (demonstrated by Multiple Clinical Questions i.e. MCQ scores) from students at medical schools with clinical skills training, the later perform better on clinical examination (measured by Objective Structured Clinical Examination i.e. OSCE). 5
However, in many other medical schools worldwide, which implement the traditional undergraduate medical curriculum, there are no clinical skills teaching sessions for undergraduate medical students. The students get to learn this first time when they are doing internship and are in direct contact with the patients. It was the same situation in Liaquat University of Medical and Health Sciences (LUMHS) in Hyderabad, Pakistan. This is a large medical school which is based in the second largest city of Sindh province of Pakistan. The first author was invited from United Kingdom to review and advise on the undergraduate medical curriculum at LUMHS. The professor of plastic surgery (second author) had started to run a voluntary clinical skills course in his department covering some general basic clinical skills and provided his data to the first author for analysis and review.
This study was devised to analyse the views of participating students regarding the course and determine their learning needs. Based on the learning needs, one could identify which resources are needed and what the University should aim to provide. Furthermore, there are no such published studies from Pakistan. This study was aimed at providing scientific information on the learning needs of undergraduate medical students from the developing world, which may be deemed to be different from the medical students in the western world.
Methods:
All medical students from fourth and final year at LUMHS were invited to attend four weeks of clinical skills course at the plastic surgery department voluntarily. The students had to attend the department after their normal working hours. There were dedicated junior doctors in the department who were given the responsibility to teach the attendees hands on clinical skills in a structured manner. The skills included history taking, organising blood tests, vene-puncture, giving intravenous and intra-muscular injections, intravenous cannulation, urinary bladder catheterisation, passing naso-gastric tube, dressing of surgical wounds, basic pre-operative assessment, basic post-operative assessment including haemo-dynamic stability, surgical theatre mannerism, principles of sterilization, identification of common surgical instruments and equipment and identification of types of drugs used in anaesthesia. The students were provided a questionnaire asking for feedback on the course which they had to fill at the end. The study was approved by the University Research and Ethics Committee. The data was computerised and statistically analysed using a statistical package. It involved all students who went through the course during consecutive sixteen months commencing from October 2008 and ending in January 2010.
Results:
90 students were recruited to the study. Students were from both sexes and both fourth year and final year. There were 32 male (35.6%) and 58 female (64.4%) students. Of the total 90 students, 62 (68.9%) were from 4th year while 28 (31.1%) students were from final year. They were all volunteers who were willing to attend the course after their normal working hours and were allocated seats on a first come first serve basis. No student was refused entry to the course and all participants were provided questionnaire on feedback at the time of completion of the course. The response rate was 100% although this may be because students were actively encouraged by the teaching staff to ensure that feedback questionnaires were filled in.
History taking and laboratory investigations were deemed least important by students, perhaps because these are taught to them during normal attachments in all wards for clinical teaching.
The Friedman mean rank was highest for catheterisation of urinary bladder (11.66) and passing of a naso-gastric tube (12.44). The students felt the greatest need to learn these two basic clinical skills perhaps because they are not taught elsewhere. This was followed by anaesthesia, sterilisation and passing an intravenous cannulation. The students ranked learning of the learning of the following skills in the middle: giving injections, taking blood, providing pre or post-operative care and being able to identify surgical instruments. Taking history and arranging laboratory investigations were both ranked the lowest at 6.22. The Friedman asymptotic significance was high (p<0.000). Despite being a good sample size, Monte Carlo significance at confidence interval of 99% was very high (p<000.0). Table below summarises the statistics
Ranks
Mean Rank
History taking
6.22
Lab investigations
6.22
Venesection
6.29
Giving injection
6.68
I/v cannulation
7.46
Catheterisation
11.66
Naso-gastric intubation
12.24
Dressing wound
6.29
Pre-operative assessment
6.71
Theatre environment
6.53
Post-operative assessment
6.62
Principles of sterilisation
7.73
Types of anaesthesia
7.81
Surgical instruments
6.54
Test Statistics a
N
90
Chi-Square
615.431
Df
13
Asymp. Sig.
0.000
Monte Carlo Sig.
0.000
99% Confidence Interval Lower Bound
0.000
99% Confidence Interval Upper Bound
0.000
a : Friedman Test
Discussion:
Our study has shown that undergraduate medical students from the developing world greatly value a basic clinical skills course, and are particularly keen on being taught naso-gastric intubation and urinary bladder catheterisation. They seem to get enough exposure in the wards on history taking and arranging laboratory tests, but identify learning needs in other clinical skills.
This study is limited to data collection from one large medical university, but the sample size has been large, observation has been over a period of one year, statistical significance has been very high and response rate has been extremely good. The teaching staff actively encouraged the students to fill the feedback questionnaires, and this could arguably lead to some response bias.
There are no such previous studies from Pakistan to compare our findings with. This study therefore can make a good baseline for local institutions to further develop and build upon. Roy Remmen’s group compared four medical schools on clinical skills of students, and demonstrated positive effect of both longitudinal skill training as well as utilisation of problem based approach in these skill courses. Our study did not provide any longitudinal data and problem based learning approach was not utilised either. Our data is a cross sectional study.
There seem to be three levels of engagement in learning basic clinical skills. One side of the spectrum has structured teaching in clinical skills laboratories with simulation, models and manikins, while the other has no teaching of clinical skills at all, until the physician starts to work with real patients. In the middle is the model of teaching clinical skills on the wards, before graduating as doctors. The former model with clinical skills laboratories requires the most resource. Which model of teaching is adopted by any individual medical university may be dependant upon the local resources, as well as the demands of the local regulatory bodies. During this study, we were able to realise the pattern of clinical skills teaching at some other medical universities in Pakistan, India and Bangladesh as random examples of southeast Asia. We learned that most institutions in this part of the world do not undertake any formal clinical skills teaching, and certainly there are hardly any clinical skills laboratories. This voluntary attempt by the professor of plastic surgery at LUMHS is therefore commendable.
This study has also identified the keenness of students to learn some specific skills through such courses prior to graduation. With a move to more globalisation of medical protocols and guidelines, a greater uniformity should also emerge in the ways in which doctors in the east or the west hemisphere of the world learn medical knowledge, attitudes and skills. There may thus be need for researchers in medical education to encourage and push for adoption of clinical skills teaching courses prior to medical graduation in the developing world.
Furthermore this study has yet again reiterated that student’s views should form a key part in the curriculum design when considering development of a clinical skills course, and resources should be geared to meet these learning needs of students.
There has been a concerted attempt by government to engage doctors in management and the importance of medical management in psychiatry has never been greater. This commenced with the Griffiths Report on management within the National Health Service1 (NHS) but had renewed emphasis 25 years later in Lord Darzi’s report.2 The NHS Next Stage Review Final Report ‘High Quality Care for All’ sets out a vision for an NHS with quality at its heart. It places a new emphasis on enabling NHS staff to lead and manage the organisations in which they work. It pledges to incorporate leadership and management training into postgraduate medical curriculum. The proposal that management training should be integral to the training of all doctors, including psychiatrists, is not new.3, 4
Although management as a component of training for doctors is generally accepted, new consultants are often poorly prepared to deal with the complex organisational issues involved in taking on managerial responsibility.5, 6 This is partly to do with prior training and partly because learning in this area needs to be based on experience. It is essential that they be adequately prepared to fulfil the responsibilities. Recent psychiatric literature has pointed to the need for psychiatrists to have skills to develop their management and leadership roles and has called for more than ‘on the job training.’7
Management training for trainees – why?
It is important to recognise that all doctors will have some management responsibilities and it is a requirement of all doctors to fulfil these duties effectively as part of appraisal and revalidation. Medical training has traditionally focused on the clinical skills necessary to be a safe and competent clinician. It is increasingly important that doctors are not only competent clinicians but also have the skills to enable them to function efficiently and effectively within a complex healthcare system.
The aim for the doctor in training is to develop management skills in readiness to take on the responsibilities of a consultant. The management role of consultants is becoming more widely accepted and continually increasing, e.g. this may involve responsibility for teams, people, and the resources they use.8 Furthermore, the changing role of consultant psychiatrists calls for consultants to have skills to fulfil management and leadership roles.9 However, while not always recognised, all doctors including trainees are required to achieve some managerial functions from an early stage in their careers. Acquisition and application of leadership and management skills will enable them to contribute to the effective delivery of healthcare for patients.
The fast pace of change within healthcare provision means that it is important that current trainees have the appropriate skills for effective delivery of healthcare.10 It is clearly no longer acceptable that development of management and leadership competencies is left as optional.
What are the competencies that we need to acquire?
Leadership and management are a key part of a doctor’s professional work and the development of appropriate competencies needs to be an integral part of a doctor’s training and development. The objectives of the skills of all psychiatrists in training has relied on a number of documents which include Good Medical Practice11 produced by the General Medical Council (GMC), Good Psychiatric Practice12 produced by the Royal College of Psychiatrists, and the Medical Leadership Competency Framework (MLCF).13 The Royal College of Psychiatrists recognise that psychiatrists will need to acquire a basic level of management skill, and this is reflected in the curriculum which outlines the knowledge and experience to be gained during specialty training.
The intended learning outcomes for trainees are to demonstrate the ability to work effectively with colleagues including team-working, developing appropriate leadership skills, and demonstrating the knowledge, skills and behaviours to manage time and problems effectively.14 Furthermore the MLCF describes the leadership competencies that doctors need to acquire (Box 1). The MLCF was introduced in response to the recognised need to enhance medical engagement in leadership and was jointly developed by the Academy of Medical Royal Colleges, GMC and the NHS Institute for Innovation and Improvement.15
Box 1: Leadership competencies to begained during speciality training
1. Demonstrating personal qualities
Developing self awareness
Managing yourself
Continuing personal development
Acting with integrity
2. Working with others
Developing networks
Building and maintaining relationships
Encouraging contribution
Working within teams
3. Managing services
Planning
Managing resources
Managing people
Managing performance
4. Improving services
Ensuring patient safety
Critically evaluating
Encouraging improvement and innovation
Facilitating transformation
5. Setting direction
Identifying the contexts for change
Applying knowledge and evidence
Making decisions
Evaluating impact
How to attain competencies in management and leadership - formal qualifications Versus ‘On the job training’
It is important to realise that the acquisition of management competencies is an ongoing experience which starts early in one's career. Any trainee embarking on management training should consider very carefully the alternatives, assess their needs, and determine their own aims and objectives. It is often necessary to choose and tailor an individual training package. We share our experiences of two routes that can lead the trainee to acquire the relevant skills. For the convenience of the reader we will discuss these under the headings of ‘formal qualifications’ and ‘on the job training.’
Formal qualifications (MSc in Health and Social Care Management)
There are many advanced courses on offer, leading to a management qualification, usually lasting several years. Some of these courses are MBA (Health Executive), MSc in Health and Social Care Management, MSc in Health and Public Leadership, Masters degree in Medical Leadership, and Masters in Medical Management.
We (OW and AS) are pursuing an MSc in Health and Social Care Management, through the Faculty of Health and Applied Social Sciences in Liverpool John Moores University, on a part-time basis using our dedicated special interest time (six sessions per month). This degree has been specifically designed to provide all health and social care professionals the opportunity to develop their knowledge and skills to facilitate their role as managers. The programme is structured in such a way as to facilitate the part-time student and enhance their learning experience.
The MSc is modular in structure. In the first year the student will undertake three core management modules. In the second year the student will undertake a research methods module, management module and an individual work-based project. The final year culminates in a dissertation involving a significant piece of research. The student can choose to register for CPDs and there is an option to exit after one year (60 credits) with a Postgraduate Certificate or after two years (120 credits) with a Diploma. University regulations allow students to gain credit for demonstration of relevant prior learning, whether certificated or not. The course format is shown in Box 2.
The ratio of coursework, in-house teaching and self-directed learning varies between modules. Each module usually requires half to one-day attendance of in-house teaching per week. The programme uses a variety of assessment procedures that include a written assignment of 2000–5000 words, video role-play, seminar presentations and work-based projects. Completion of the assignments represents the greatest challenges to time and requires commitment and motivation.
Box 2: Format of the MSc in Healthcare Managementat the Liverpool John Moores University
·Improving service delivery through human resource management (20 credits)
·The economics of World Class commissioning (20 credits)
·Advancing leadership for quality (20 credits)
·Research methods and data analysis (30 credits)
·Strategic management and entrepreneurship (20 credits)
·Individual study or work based learning (10 credits)
·Dissertation (60 credits)
Strengths and weaknesses of an MSc in Health and Social Care Management
Whilst on the course we were able to learn a variety of concepts that were completely new to us, but the main challenge was to put them into practice. As part of the course we had to work on management related projects in our workplaces, so that we could apply the learnt concepts in real time.
We believe that the MSc course has undoubtedly improved our understanding of team working and leadership whilst working on a work-based project. The projects were specific supervised experiences linked to key developmental objectives and enhanced our problem-solving and decision-making, the ability to analyse and reflect on situations, as well as the expected understanding of resource management and change management.
We have been able to analyse personal development needs to enhance personal effectiveness and leadership skills. It helped us to critically evaluate the impact of action learning for organisational development. We have gained an insight into the concepts of commissioning and the role of economic evaluation. We were able to critically appraise the impact of government policies on the commissioning process. Our skills and knowledge of human resource management within a framework of contemporary policy context has increased. We really do feel that it has improved our insight into change management.
We hope that completing a significant research project within an academic setting will further develop our research skills. So far it has been a valuable and stimulating experience that has provided us with both skills and knowledge in management. The teaching and learning approaches for all modules draw into the experiences of the workplace. All core module assessment tasks are linked to the workplace, which is particularly useful.
However the process of developing a dissertation proposal, finding a supervisor, gaining ethical approval and proceeding with the research is time consuming and at times frustrating. The financial cost is a significant consideration but can be partially funded through the study leave budget. Furthermore, there is funding available for some modules through the Strategic Health Authority. As we were using most of our special interest sessions to pursue the degree, we had to put an extra effort to develop additional clinical interests.
‘On the job training’- what does that mean?
On the job management training may entail clinical managerial experience (e.g. organising outpatient clinics, developing systems for prioritising clinical work, managing teams, and drawing up on-call rotas), specific skills (e.g. chairing meetings, organising training days, and representation on committees), specific management experience (e.g. participation in service development) and resource management (non-clinical aspects of management such as human resources and finance).
The clinical setting provides many opportunities to gain knowledge, skills, attitudes and behaviours that are identified in the management and leadership curriculum. The diversity of daily clinical practice will enable the acquisition of appropriate skills and trainees need to take advantage of all the formal and informal learning opportunities. These range from workplace-based ‘learning sets’16 and project based learning. It is the responsibility of the trainers to ensure adequate and appropriate educational opportunities are made available to the trainee. In turn the trainee should be enthusiastic and proactive in identifying their own gaps in knowledge, skills, attitudes and behaviour.
It is important to bear in mind that such training should be supplemented by selected formal courses. Some training schemes offer no organised management training, whilst some provide training as a short and often intense course.17 A variety of courses have been developed for trainees, both at regional and national level. Trusts, Deaneries, independent organisations, universities and the Royal Colleges run such courses. These courses are normally short, lasting a week or less. The components of ‘on the job training’ in Merseycare NHS Trust and generic management courses offered by Mersey Deanery are listed in Boxes 3 and 4 respectively.
Box 3: Components of ‘on the job training’ in Merseycare NHS Trust
Appropriate involvement of trainees in clinical teams
Appropriate involvement of trainees in service development
Shadowing arrangements in placements
Undertake a management project
Senior managers in the trust as mentors to trainees
Action learning sets for trainees
Trainees developing teaching and supervisory skills with junior colleagues
Management seminars
Representation on committees (e.g. school board, local negotiating committee, local education board etc)
Two-day and three-day residential management training for higher trainees
Generic management courses runby the deanery
Personal development and management courses hosted by the College
Box 4: Generic management courses offered by Mersey Deanery
Management and leadership
Mentoring, appraisal, interview skills
Effective team-working
Managing change
Time management
Preventing and managing stress
Negotiating skills
Managing meetings
Strengths and weaknesses of ‘on the job training’
‘On the job training’ may vary from one placement to another depending on the availability of resources and mentors. Achieving ‘on the job’ management experience depends on the enthusiasm of the senior trainee. It is more personalised and individually driven. Higher training posts do provide exposure to management issues, but do not necessarily provide in-depth management experience.
It is easier to gain experience in clinical management skills but it can be difficult to achieve specific management experience including resource management. Trainers with formal management roles do not routinely engage trainees in this aspect of their work, and similar experiences have been expressed in other training schemes.18 Even if there are opportunities available to get involved in service development and other operational issues, one may struggle to commit any time.
Furthermore the loss of protected training (reduction of special interest to only two sessions for specialist trainees) to service provision has impacted on training.19 The formal courses are confined to development of skills such as leadership, teamwork and management of conflict. Residential management courses are available, providing one week or less of intensive training. The amount of management theory and techniques that can be learned on such courses is limited. The limited theoretical training in management means that trainees are unlikely to be adequately prepared for the extensive management role.
Which one is for you?
Managing services and leading organisations is not for everyone. Nevertheless, the medical role has inherent elements of leading and managing patient care and therefore doctors are often involved in service improvement and development. Perhaps the key issue is whether qualifications alone are sufficient to equip a doctor to be an effective manager, or is experience simply enough? It is important to remember that management qualifications tend to involve real-time application of concepts (which may be the same as on the job training) but at the same time gives a solid knowledge base. Furthermore, limited experience (involvement in local management) is unlikely to be sufficient and therefore experience should ideally be supplemented by selected formal courses.
However, even with the most impressive portfolio of formal training, trainees will nevertheless have to demonstrate competence in leadership and management in their work. All trainees are adult learners who ought to take responsibility for their own education. Which route the trainee wants to take depends not only on what the trainee intends to do in his future role but also on where he trains and what resources are available. Training needs will differ depending on past experience, competence, and capabilities. It is important for the trainees to recognise that the training needs will differ depending on their interests and the type of consultant post to which they aspire.
Formal qualifications would suit those with a well-developed interest in management and a desire to make this a significant part of their ongoing career. If the trainee intends to take a lead management role it may be necessary and useful to complete a Master’s degree. It will provide the trainee with both skills and knowledge in management and a well-recognised and formal degree in management. Having established that, it is worthwhile appraising the variety of courses available, as they vary significantly. It is helpful to determine the course’s content, assess its relevance, and establish how much in-house teaching and self-directed learning is expected. For those who want to acquire management skills for better day-to-day functioning in their job, it is useful to analyse their personal development needs and complete relevant modules according to these needs. This could be attained through ‘on the job training’ if resources can be identified and secured. A final point to bear in mind is the Royal Colleges’ direct contribution to developing management and leadership in trainees. For example the Royal College of Psychiatrists promotes engagement of doctors in management and has a dedicated Special Interest Group for management.
The Department of Health’s Modernising Medical Careers (MMC) has been uniformly implemented into specialty training across the United Kingdom (UK). This began with the controversial and subsequently redundant Medical Training Application System (MTAS) selection process in Spring 2007, and ended with the first MMC specialty training posts commencing in August 2007. During the application process itself one preliminary study reported that 85% of candidates demonstrated decreased levels of enjoyment in their work, and 43% caring less about patient care.1 The emergency introduction of the ‘golden ticket’ Round 1b guaranteed interview - though arguably justified in the face of a flawed application system - was a cause of further discontent and division amongst junior trainees and the consultants responsible for appointing them.
For surgical training in particular, the advent of the MMC initiative combined with the European Working Time Directive (EWTD) represents an estimated 50% reduction in the amount of specialist training hours when compared to the previous system.2 This has raised concerns not only from current consultants, but also from the already increased number of surgical trainees having to share the same caseload. A previous survey of Ear, Nose, and Throat senior house officers reported 71% were willing to opt out of the EWTD to safeguard their training and patient care.3
In the Oxford Deanery the selection process of shortlisted surgical trainees in Rounds 1a and 1b consisted of six stations assessing curriculum vitae, portfolio, clinical examination, data interpretation, and pre- and post-operative management (totalling one hour). Candidates were offered generic or specialty themed Core Training (CT) posts at Speciality Training (ST) 1 or 2, or Fixed Term Speciality Training Appointments (FTSTA) 1 or 2, depending upon the candidate’s ranking at interview (plus application form for Round 1a) irrespective of speciality preference. Following acceptance, individual appointments were made based on candidates ranking job preferences. Round 2 appointments were made at a local level via traditional selection methods. The most recent information from the deanery states that those trainees who received an offer of run-through training in the region will be guaranteed an interview for an ST3 post in surgery, however individual specialty preference and job allocation will be determined by re-ranking based on continuous appraisal during the core surgical training years, further Higher Specialist Training interviews, and training numbers available.
The media coverage that surrounded MTAS clearly highlighted the dissatisfaction amongst trainees and consultants leading up to and during the application process,4, 5 but no study has yet assessed the views of surgical trainees following the start of their new MMC-based training posts. This survey aimed to obtain the views and outcomes of core surgical trainees in the Oxford Deanery.
Methods
At three and nine months following the commencement of speciality training posts, questionnaires were distributed to junior surgeons (CT 1-2) in the Oxford Deanery School of Surgery. Questions were structured to obtain information about level of experience and qualification(s), current and desired surgical speciality, job satisfaction, attitudes towards ‘run-through’ training and levels of support. In the Oxford Deanery there were 40 appointments at CT1 (18 ST1 and 22 FTSTA), and 29 at CT2 (17 ST2 and 12 FTSTA) in August 2007. Data were expressed as the mean ± standard deviation (SD). Statistical comparison was performed using Mann-Whitney’s U test, with the significance level at p<0.05.
Results
The questionnaire was completed by a total of 46 and 45 surgical trainees at three and nine months respectively. At the three-month time point this represented 67% of all trainees in the Oxford Deanery School of Surgery (male: female, 33:13) and included 11 at ST1, 16 at ST2, 11 at FTSTA1, and 8 at FTSTA2. Of these 52% (n=24) had obtained their post via Round 1a, 41% (n=19) via Round 1b, and 7% (n=3) via Round 2. At both CT1 (ST1 & FTSTA1) and CT2 (ST2 & FTSTA2), trainees were on average 3.7 ± 1.9 years post graduation (from time surveyed; CT1 range 1-11 years, CT2 range 3-8 years); 16% (n=7) of all trainees had previously studied Medicine at Oxford University, and 93% had studied medicine in the UK. (Figures 1a, b). Most popular desired specialties at three and nine months are displayed in figure 2. Of the 46 respondents, all had worked in the speciality of their career choice during the course of the year.
Figure 1a. Number of trainees selected in each MTAS round
Figure 1b. Surgical trainee graduating medical school distribution
At time of appointment, 52% of trainees had completed the Membership to the Royal College of Surgeons (MRCS) exams, and 35% (n=16) of all trainees had completed a higher degree. (Figure 3). Furthermore, 22% (n=10) felt that there should be a further exam in addition to the MRCS to rank candidates for appointment to higher specialist training (ST3 onwards), with half of this number having already obtained their MRCS.
Figure 2. Desired surgical specialty at three and nine months
Figure 3. Trainee postgraduate qualifications at time of appointment
Those who had been allocated to ‘run-through’ ST posts were more satisfied with the concept of run-through training than those in FTSTA posts (where scores were assigned on a scale from 1 - very unsatisfied, to 5 - very satisfied), with the mean score at three months for ST trainees 4.1 ± 1.4, and FTSTA trainees 2.0 ± 1.4 (p<0.01), and at nine months 3.7 ± 1.1 for ST trainees versus 2.1 ± 1.1 for FTSTA trainees (p<0.01). Job satisfaction levels between these two groups of trainees were similar: at three months, mean score 3.5 ± 1.3 in ST posts versus 4.1 ± 0.8 in FTSTA posts (p>0.05), and at nine months, mean score 3.5 ± 1.0 in ST posts versus 3.2 ± 1.3 in FTSTA posts (p>0.05). In addition, a similar comparison between ST and FTSTA trainees was found when determining if trainees had thought about leaving surgery. On a scale where a score of 1 – never thought of leaving surgery to 5 – very frequently thought of leaving surgery, the mean score at three months was 2.3 ± 1.4 for ST trainees versus 3.0 ± 1.6 for FTSTA trainees (p>0.05), and at nine months 2.2 ± 1.4 for ST trainees versus 2.9 ± 1.5 for FTSTA trainees (p>0.05). (Figures 4a, b).
Figure 4a. Trainee attitudes at three months
Figure 4b. Trainee attitudes at nine months
In fact, 43% (n=20) of all trainees surveyed reported having enquired about surgical training in another country, with 4% (n=2, both UK Medical School graduates) stating that if unsuccessful in securing a training post in their desired specialty for August 2008, they would move abroad to train.
At three months, 9% (n=4) of all trainees felt well-informed about what will happen in the future regarding their training, with 20% (n=9, ST to FTSTA ratio 2:7) responding that had they been better informed prior to August 2007, then they would not have accepted their current post, and 28% (n=13) felt well-supported by their senior colleagues with regard to their future training. However at nine months from appointment, 69% (n=29) of all trainees felt well informed, and nearly two thirds well supported by their seniors (n=27). (Figure 5). Ninety three percent (n=43) of applicants wished to remain in the region for their future training, with 61% (n=28) having initially selected Oxford as their first choice deanery.
Figure 5. How well informed and supported trainees felt at three and nine months
The majority of both ST2 (85%, n=11) and FTSTA2 (71%, n=5) trainees secured ST3 posts from August 2008, mainly within the Oxford Deanery, and all within their desired surgical specialty. All ST1 (n=16) trainees successfully moved into ST2 posts, and the majority of FTSTA1 (78%, n=7) trainees secured CT positions. (Table 1).
Grade (n)
August 2008 Post (n)
ST1 (16)
ST2 (16)
FTSTA1 (9)
CT1 (3) CT2 (4) FTSTA (2)
ST2 (13)
ST3 (11) Research Fellow (1) GP Trainee (1)
FTSTA2 (7)
ST3 (5) ST1 Radiology (1) CT2 (1)
Table 1. ST2 and FTSTA2 trainee outcomes from August 2008
Discussion
MMC has and will have profound implications on the way junior doctors will henceforth be trained in the National Health Service (NHS). Last year’s difficult introduction into specialist training, has for obvious reasons, directly affected the perceptions of trainees having to negotiate their careers through the ‘transition’ period.1, 6 This survey provides an interesting insight into the demographics, current viewpoints, and outcomes of the first cohort of MMC surgical trainees in the Oxford Deanery.
Just over half of all trainees in the survey were appointed after Round 1a (52%, n=24) of which two thirds (n=16) were to ST posts: a further 41% (n=19) were appointed after Round 1b, of which roughly half (n=9) were to ST posts. This highlights the large number of very good surgical trainees that may have been left unemployed had MTAS interim measures not been introduced to permit all candidates the opportunity of at least one interview, and that in the Oxford Deanery at least, candidates were given an equal chance of obtaining a ‘run-through’ post between the two rounds. Despite MMC person specifications at the time of application stating that MRCS was not an absolute requirement for entry at ST1-2, 52% (n=24) had completed their MRCS, with a further 20% (n=9) having completed at least Part I or more.
Overall job satisfaction levels were good amongst all trainees (mean score 3.7 ± 1.1), with 57% (n=26) still agreeing with the concept of ‘run-through’ training, and hence MMC. This view is maintained despite the problems associated with last years application process, and in the face of an uncertain future. However, nearly half (43%, n=20) of trainees had enquired about training abroad, with several committed to leaving the UK next year if unable to obtain their desired surgical specialty. With the average cost to train a UK medical graduate being at least £150,000,7 and the amount of dedication and effort needed to embark on a surgical career thereafter, care must be taken to improve morale amongst junior surgeons, and to provide adequate and timely information. Encouragingly, between the two time points surveyed, levels of senior support and how well informed surgical trainees felt with regards to their training, increased from 28% to 60% and from 9% to 69% respectively; this may be secondary to a combination of extensive effort from the Deanery and the Royal College of Surgery to address trainee concerns.
The realistic future of those in FTSTA posts is cause for concern. This is highlighted in the recently released Tooke Report, in which it is stated they are “in danger of becoming the next ‘lost tribe’, the very category of doctor MMC sought to avoid”, but at the same time that “core [training] should not repeat the errors of previous SHO arrangements and must be time limited”.6 Those in FTSTA posts face higher levels of future uncertainty than their ST colleagues, and this was reflected in reporting a higher likelihood of consideration of alternative careers outside of surgery. However, both groups of trainees demonstrated statistically similar scores when questioned about how frequently they had thought of leaving surgery (2.3 ± 1.4 for ST trainees versus 3.0 ± 1.6 for FTSTA trainees, p>0.05), and 71% of FTSTA2 trainees surveyed within the Oxford Deanery went on to secure ST3 level posts in their desired specialty.
The authors note the limitations inherent to surveys in general namely the validity and reliability of responses obtained to questions asked due to the self-report method of data collection, the questionnaire entirely constructing the information obtained, and that the data does not capture the decision process that produced the observed outcomes and is therefore descriptive rather than explanatory. More specifically, the authors note that candidates who were successful in obtaining an ST3 post may have been more likely to complete the questionnaire, leading to further potential bias.
Conclusion
MMC has crossed the threshold into higher specialist training, and the first cohorts of MMC surgeons are being trained. The majority of trainees we surveyed expressed good levels of job satisfaction, had successfully negotiated their first year of the new system, and encouragingly felt better informed and supported over the course of their first year. However, this study encompassed a proportion of surgical trainees in one Deanery in the UK, and further study on a larger scale at regular time intervals is certainly warranted. Consequent to the problems of MMC’s difficult introduction, positive steps included travelling tours by the Royal College of Surgeons (England), and in the Oxford Deanery at least, regional meetings to address concerns and expectations, and outline the realistic future for surgical trainees. Perhaps a key determinant of sustainability for MMC in surgery in 2008 and beyond will be the relative success of the Intercollegiate Surgical Curriculum Programme (ISCP), and this represents a significant area for further study.
The Royal College of Psychiatrists first introduced the CASC in June 2008. It is based on the OSCE style of examination but is a novel method of assessment as it tests complex psychiatric skills in a series of observed interactions.2 OSCE (Observed Structured Clinical Examination) is a format of examination where candidates rotate through a series of stations, each station being marked by a different examiner. Before the CASC was introduced, candidates appeared for OSCE in Part 1 and the ‘Long Case’ in Part 2 of the MRCPsych examinations. The purpose of introducing of the CASC was to merge the two assessments.3
The first CASC diet tested skills in 12 stations in one circuit. Subsequently, 16 stations have been used in two circuits - one comprising eight ‘single’ and the other containing four pairs of ‘linked’ scenarios. Feedback is provided to unsuccessful candidates in the form of ‘Areas of Concern’.4 The pass rate has dropped from almost 60% in the first edition to around 30% in the most recent examination (figure 1). Reasons for this are not known. The cost of organising the examination has increased and candidates will be paying £885 to sit the examination in 2010 in the United Kingdom (figure 2).
Figure 1
We are sharing our experience of the CASC examination and we hope that it will be useful reading for trainees intending to appear for the CASC and for supervisors who are assisting trainees in preparation. In preparing this submission, we have also made use of some anecdotal observations of colleagues. We have also drawn from our experience in organising local MRCPsych CASC training and small group teaching employing video recording of interviews.
Figure 2
CASC is an evaluation of two domains of a psychiatric interview: ‘Content’ (the knowledge for what you need to do) and ‘Process’ (how you do it). The written Papers (1, 2 and 3) test the knowledge of candidates. We therefore feel that the candidates possess the essentials of the ‘Content’ domain. Therefore, the more difficult aspect is demonstrating an appropriate interview style to the examiner in the form of the ‘Process’.
This article discusses the preparation required before the examination followed by useful tips on the day of the examination.
Before the examination day (table 1)
Table 1: Tips before the examination day
Factor
Technique
- The mindset
- Have a positive attitude
- Time required
- Start preparing early
- Analysing areas for improvement
- Use ‘Areas of Concern’
- Practice
- Group setting and individual sessions
- Feedback from colleagues using video
The mindset
In our view, preparation for the CASC needs to begin even before the application form is submitted. Having a positive mindset will go a long way in enhancing the chances of success.5 It is therefore a must to believe in ones ability and dispel any negative cognition. Understandably, previous failure in the CASC can affect ones confidence, but a rational way forward would be to consider the failure as a means of experiential learning, a very valuable tool. Experiential learning for a particular person occurs when changes in judgments, feelings, knowledge or skills result from living through an event or events.6
Time required
Starting to prepare early is crucial as it gives time to analyse and make the required changes to the style of the interview. For instance, a good interview requires candidates to use an appropriate mixture of open and closed questions. Candidates who have been following this technique in daily practice will find it easier to replicate this in examination conditions when there is pressure to perform in limited time. However, candidates who need to incorporate this into their style will need time to change their method of interview.
Analysing areas for improvement
Candidates need to identify specific areas where work is needed to improve their interview technique. The best way to accomplish this is by an early analysis of their interview technique by a senior colleague, preferably a consultant who has examined candidates in the real CASC examination. We think its best to provide feedback using the Royal College’s ‘Areas of Concern’ - individual parameters used to provide structured feedback in the CASC. This will help to accustom oneself with the expectation in the actual examination.
Requesting more than one ‘examiner’ to provide feedback is useful as it can provide insight into ‘recurring mistakes’ which may have become habit. In addition, different examiners might provide feedback on various aspects of the interview style. The Calgary-Cambridge guide7, 8 is a collection of morethan 70 evidence-based communication process skills and is a vital guide to learn the basics of good communication skills.
Practice
We believe that it is important to practice in a group setting. Group work increases productivity and satisfaction.9 The aim of group practice is to interact with different peers which will help candidates to become accustomed to varying communication styles. Group practice is more productive when the group is dynamic so that novelty prevails. Practising with the same colleagues over a period of weeks carries the risk of perceiving a false sense of security. We feel this is because candidates get used to the style of other candidates and, after a period of time, may not recognise areas for improvement.
Another risk of a static group is candidates may not readily volunteer areas for improvement - either because they may feel they are offending the person or, more importantly, because the same point may have been discussed multiple times before! Whenever possible, an experienced ‘examiner’ may be asked to facilitate and provide feedback along the lines of ‘Areas of Concern’. However candidates need to be conscious of the pitfalls of group work and negative aspects such as poor decisions and conflicting information.
In addition to group practice, candidates would benefit immensely from individual sessions where consultants and senior trainees could observe their interview technique. Candidates could interview patients or colleagues willing to role-play. We have observed that professionals from other disciplines like nurses and social workers are often willing to help in this regard. Compared to group practice, this needs more effort and commitment to organise. Consultants, with their wealth of experience, would be able to suggest positive changes and even subtle shifts in communication styles which may be enough to make a difference. We found that video recording the sessions, and providing feedback using the video clips, helps candidates to identify errors and observe any progress made.
The feedback of trainees who appeared in the CASC examination included that attending CASC revision courses had helped them to prepare for the examination. It is beyond the remit of this article to discuss in detail about individual courses. The majority of courses employ actors to perform role-play and this experience is helpful in preparing for the CASC. Courses are variable in style, duration and cost. Candidates attending courses early in their preparation seem to benefit more as they have sufficient time to apply what they have learnt.
During the examination (table 2)
Table 2: Tips during the examination
Factor
Technique
- Reading the task
- Fast and effective reading
- Focus on all sub-tasks
- Time management
- ‘Wrap up’ in the final minute
- The golden minute
- Establish initial rapport
- Leaving the station
- Avoid ruminating on previous station
- Expecting a surprise
- Fluent conversation with empathy
Reading the task
Inadequate reading and/or understanding of the task leads to poor performance. Candidates have one minute preparation time in single stations and two minutes in linked stations. We have heard from many candidates who appeared in the examination that some tasks can have a long history of the patient. This requires fast and effective reading by using methods such as identifying words without focusing on each letter, not sounding out all words, skimming some parts of the passage and avoiding sub-vocalisation. It goes without stating that this needs practice.
CASC differs from the previous Part 1 OSCE exam in that it can test a skill in more depth. For example it may ask to demonstrate a test for focal deficit in cognition that may not be detected by conducting a superficial mini mental state examination.
Candidates need to ensure they understand what is expected of them before beginning the interview. In some stations, there are two or three sub-tasks. We believe that all parts of a task have a bearing on the marking.
An additional copy of the ‘Instruction to Candidate’ will be available within the cubicles. We suggest that when in doubt, candidates should refer to the task so that they don’t go off track. Referring to the task in a station will not attract negative marking but it is best done before initiating the interview.
Time management
It is crucial to manage time within the stations. A warning bell rings when one minute is left for the station to conclude. This can be used as a reference point to ‘wrap up’ the session. If the station is not smoothly concluded before the end of the final bell candidates may come across as unprofessional. Candidates also run the risk of losing valuable time to read the task for the next station.
Single stations last for seven minutes and linked stations last for ten minutes. Candidates who have practiced using strict timing are able to sense when the warning bell will ring. They are also able to use the final minute to close the session appropriately.
Having stressed the importance of finishing the stations on time, it is also vital to understand that an early finish can lead to an uncomfortable silence in the station. This may give the examiner the impression that the candidate did not cover the task. We feel that there will always be something more the candidate could have explored!
The awkward silence in the above scenario can potentially make the candidate feel anxious and ruminate on the station which must be avoided.
The golden minute
First impressions go a long way in any evaluation and the CASC is no different in this regard.10 Candidates need to open the interview in a confident and professional manner to be able to make a lasting impact and establish a better rapport. Observing peers, seniors and consultants interacting with patients is a good learning experience for candidates in this regard.
Candidates who do well are able to demonstrate their ability to gain the trust of the actors in this crucial passage of the interaction. Basic aspects such as a warm and polite greeting, making good eye contact, and clear introduction and explanation of the session will go a long way in establishing initial rapport which can be strengthened as the interview proceeds.
The first minute in a station is important as it sets the tone of the entire interaction. A confident start would certainly aid candidates in calming their nerves. Actors are also put at ease when they observe a doctor who looks and behaves in a calm and composed manner.
Leaving the station behind
Stations are individually marked in the CASC. Performance in one station has no bearing on the marking process in the following stations. It is therefore important not to ruminate about previous stations as this could have a detrimental effect on the performance in subsequent stations. The variety of tasks and scenarios in the CASC means that candidates need to remain fresh and alert. Individual perceptions of not having performed well in a particular station could be misleading as the examiner may have thought otherwise. Candidates need to remember that they will still be able to pass the examination even if they do not pass all stations.
Expecting a sorprise
Being mentally prepared to expect a new station is good to keep in mind while preparing and also on the day of the examination. Even if candidates are faced with a ‘surprise station’, it is unlikely that the station is completely unfamiliar to them. It is most likely that they have encountered a similar scenario in real life. Maintaining a calm and composed demeanour, coupled with a fluent conversation focused on empathy and rapport, will be the supporting tools to deal with a station of this kind.
Conclusion
The CASC is a new examination in psychiatry. It tests a range of complex skills and requires determined preparation and practice. A combination of good communication skills, time management and confident performance are the key tools to achieve success. We hope that the simple techniques mentioned in this paper will be useful in preparing for this important examination. Despite the falling pass rate, success in this format depends on a combination of practice and performance and is certainly achievable.
Problem based learning (PBL) has been an important development in health professions education in the latter part of the twentieth century. Since its inception at McMaster University1 (Canada), it has gradually evolved into an educational methodology being employed by many medical schools across the globe2,3. PBL presents a paradigm shift in medical education, with a move away from ‘teacher centered’ to ‘student centered’ educational focus. The assumptive difference between a pedagogy learner and an androgogy learner (Table 1) was summarised by Knowles4, and the androgogy approach underpins PBL. This shift has redefined the role of a teacher in the PBL era, from being a teacher to a facilitator.
Table 1: Differences between Androgogy and Pedogogy learner (Knowles)
Characteristics
Pedagogy
Androgogy
Concept of the learner
Dependent personality
Self-directed
Readiness to learn
Uniform by age-level & curriculum
Develops from life tasks & problems
Orientation to learning
Subject-centered
Task- or problem-centered
Motivation
By external rewards and punishment
By internal incentives curiosity
It is well known that implementing PBL as an educational methodology required additional resources compared to a traditional lecture based curricula5. In addition, there was a need to recruit and train a large number of tutors to facilitate the PBL process6.Training PBL tutors is an important component of a successful curriculum change, and is a continuous process. Training workshops and role plays were employed to train conventional teachers, but challenges were faced in developing them into effective PBL tutors5.
The aim of this paper is to evaluate the literature for any evidence supporting the theory that a PBL background student may develop into an effective PBL tutor. The Medline, EMBASE and CINHAL databases were searched to look for any pre-existing literature or research supporting this theory.
Results:
To the best of my knowledge, there has been no reported evidence supporting this theory. With limited literature evidence, this paper aims to identify common grounds between a PBL student and a PBL tutor, and whether being a PBL student may contribute to the overall development as a PBL tutor. The discussion evolves around the following domains:
1. Teaching Styles:
The ideal teaching style of a PBL tutor is a facilitative-collaborative style, which augments and supplements the PBL process. The teaching style inventory developed by Leung et al7 hypothesised four domains of teaching styles: the assertive, suggestive, collaborative and facilitative styles. Though a PBL tutor assumes himself in possessing this style (facilitative), it does not necessarily match with the students perceptions, as reported by Kassab et al8.
Some of the characteristics of being a PBL student may foster the development of a collaborative teaching style. Being a student, you are expected to be a collaborative learner which is critical for achieving and improving group performance9. Initial years as a student in PBL may contribute to developing attributes required to develop a preferential teaching style.
2. Facilitating critical thinking:
PBL is grounded in cognitive psychology and is set out to stimulate curiosity and build durable understanding. One of the roles of the tutor is to foster critical thinking and enhance the group’s ability to analyse and synthesise the given information. This attribute stems from the tutors ability to facilitate, rather than teach. Irby10 opined that clinical teachers tended to teach as they themselves were taught using traditional approaches, which may affect the process of stimulating critical thinking among the students.
A tutor from a PBL background would have the ability to think critically, through a process of developing thoughtful and well-structured approach to guide their choices11. Tiwari et al12 showed in their study that PBL students showed significantly greater improvement in critical thinking compared to traditionalist courses. Hence, prior exposure to a certain learning style can create a cognitive psychology that can contribute to tutor development.
3. Group dynamics:
One of the prime roles of a PBL tutor is to facilitate the PBL process by keeping the group focused on tasks, and guiding them to achieve their goals. Tutors who are skilled in group dynamics are evaluated more highly than those who are not so skilled11,13 . Tutors need to develop sound appreciation of the group dynamics, failing which may lead to fostering uncertainty with in the group. Bowman et al13 commented about the lack of consideration on the emotional implications placed on prospective PBL tutors when tutoring small groups, especially the skills required to balance between short term anxieties and potential serious problems. This imbalance which usually serves as unconscious incompetence may affect group dynamics.
PBL students would have experience of group dynamics and the pressures of working within it. They would have developed a model of working with members with varying attributes. Blighet al14 showed in their study that students from a PBL curriculum rated themselves better in team working and motivation compared to conventional course peers. This highlights the fact that an apprenticeship model may be necessary in developing the right skills to be an effective tutor.
The characteristics of a student that may foster ideal attributes in a PBL tutor are briefly summarised in Table 2, and has evolved from the work of Samy Azer9,11 .
Table 2: Common ground
Ideal PBL student
Ideals of a PBL tutor
Knows his role within a group
Would help in identifying different roles students may play
Knows to ask empowering questions
Would help in guiding groups in achieving learning objectives
Monitors his own progress by self evaluation and motivation
Would help in monitoring individual progress and motivate group
Bonds with other members to achieve goals
Would help in building trust and encourage bonding of group members
Develops thoughtful and well structured approach to guide choices
Would help in facilitating critical thinking
Fosters collaboration with other group members to create a climate of trust
Would facilitate collaborative teaching style
4. Tutor training
Considerable resources are exhausted in teaching new tutors the art of facilitating a PBL group6, and the usual cohort is teachers from a conventional taught background. The shift from didactic expertise to facilitated learning is difficult for those tutors who feel more secure in their expert role. Finucane et al5 published their study which showed that only a minority of staff had volunteered to be PBL tutors, possibly reflecting the fact that absence of prior exposure to PBL style of learning may have contributed to this. In spite of tutor training workshops, they could only retain 73% at the end of two years.
Prior exposure as a student may help negate much of the stigma associated with PBL. They would have observed and learnt from their PBL tutors, and would have analysed their contribution to the PBL process. They could reflect on their experience and evolve into an ideal PBL tutor. This would help in minimising resource expenditure and contribute towards retention of staff.
5. Tutor comfort zones:
PBL contextualises learning to practical situations, with integration across disciplinary boundaries. Dornan et al15 reported on how some teachers felt PBL to be a frustrating drain on time as it did not fit their educational style, and was a distraction from clinical teaching, demonstrating the ‘conditioning effect’ of prior experiences. This further fuels the debate between content vs. process expertise, but prior knowledge of the process would benefit the students and the PBL process.
6. Role modeling:
Role models have long been regarded as important for inculcating the correct attitudes and behaviors in medical students. Being an ideal role model is considered as one of the prime requisites of a teacher. In a recent study, Mclean et al16 showed that PBL students tended to have a higher percentage of role models compared to students from a traditional programme (73% vs. 64%). In an ideal setting, a “content and process expert” would be the perfect role model for the PBL students, but this may not be realised in all settings.
Paice et al17 commented on the resistance to change within the medical profession, and highlighted the need for training to emphasise the values and attitudes required. This puts an added emphasis on the tutor to demonstrate tenacity and virtues to be an effective role model, avoiding ‘cognitive clouding’ from previous experiences.
As a PBL student, they would be exposed to variety of PBL tutors. They would have incorporated the good points of an effective PBL tutor, and would have reflected on the negative aspects. Reflective practice enables them to develop the right attributes. Though these attributes may be difficult to develop through training workshops, having a background of PBL education may help mould the tutor characteristics.
Conclusion:
As PBL continues to be employed across different specialties, there would be increased emphasis on the medical schools to match the resources needed to implement it. There is an argument for developing an apprenticeship model or recruiting tutors from PBL background, which would help in reducing the cost in training new tutors, along with nullifying the negative influences a new tutor may bring. The biggest limitation in the present setting is finding a cohort of PBL background tutors, but an apprenticeship model may benefit teachers from conventional background. A prospective research study exploring the attributes of tutors, successful and less successful, from traditional, PBL and hybrid curricula and those who have crossed the Rubicon from traditional to PBL can effectively answer this question.