



ISSN 1757-8515
An Unusual Manifestation of Adenocarcinoma of Lung - Skeletal Muscle Metastasis
Sharan Badiger & Siddarthkumar Chawath
Cite this article as: BJMP 2020;13(2):a016
|
|
Abstract Introduction: Lung carcinoma is the most common malignancy in adults and the leading cause of death globally. It is responsible for 25% of all malignancy-related death worldwide. Among various types of lung carcinoma, adenocarcinoma is the most common (50%) of all the variants. Lung adenocarcinoma metastasising to skeletal muscle is rare in clinical practice. Case report: A fifty three year-old male patient presented with complaints of swelling over left arm of size 5x4 centimetres which was irregular in shape, soft to hard in consistency and gradually increasing in size. He was symptomatically treated but there was no improvement in clinical condition. In due course of time, patient presented with cough with expectoration. On general physical examination, pulse rate was eighty beats per minute, blood pressure 120/80 mmHg, respiratory rate eighteen cycles per minute. On systemic examination, respiratory system revealed bilateral normal vesicular breath sounds, cardiovascular, abdominal and neurological systems were clinically within normal limits. Panel of investigations were done as a part of work up, inclusive of ultrasonography (USG) and magnetic resonance imaging (MRI) of left arm, computerized tomography (CT) of chest, fine needle aspiration cytology and positron emission tomography (PET) scan which concluded adenocarcinoma of right lung with left triceps muscle metastasis. Conclusion: Though the metastasis of adenocarcinoma lung is common, metastasis to the skeletal muscle is not so well-known. A clinical suspicion about such pathology can help a clinician to arrive at right diagnosis on time. This case report emphasizes that even a trivial swelling in triceps muscle could be hiding the grave adenocarcinoma in the lung. Keywords: Adenocarcinoma, Metastasis, Skeletal Muscle.Abbreviations: Computerized Tomography (CT), Magnetic Resonance Imaging (MRI), Positron Emission Tomography (PET), Ultrasonography (USG). |
Introduction
Lung carcinoma the most common malignancy worldwide, presents as a metastatic disease in majority of the cases. The most frequent sites of distant metastases are liver, adrenal glands, bones, and brain. Skeletal muscle metastasis is an unusual presentation of lung adenocarcinoma.
Case report
A fifty three year old male patient, labourer by occupation, beedi smoker for twenty five years, admitted to tertiary care hospital with pain and swelling over left arm, cough and expectoration for the past two months, accompanied with significant weight loss. There was no evidence of chest pain or haemoptysis. On local examination there was hard swelling over extensor compartment of left upper limb with mild tenderness, no loss of sensation and mild restriction of range of movements on flexion at elbow. Respiratory and other systemic examination was within normal results. Plain CT of thorax defined multilobulated lesion in right perihilar location in right middle lobe (Figure 1).
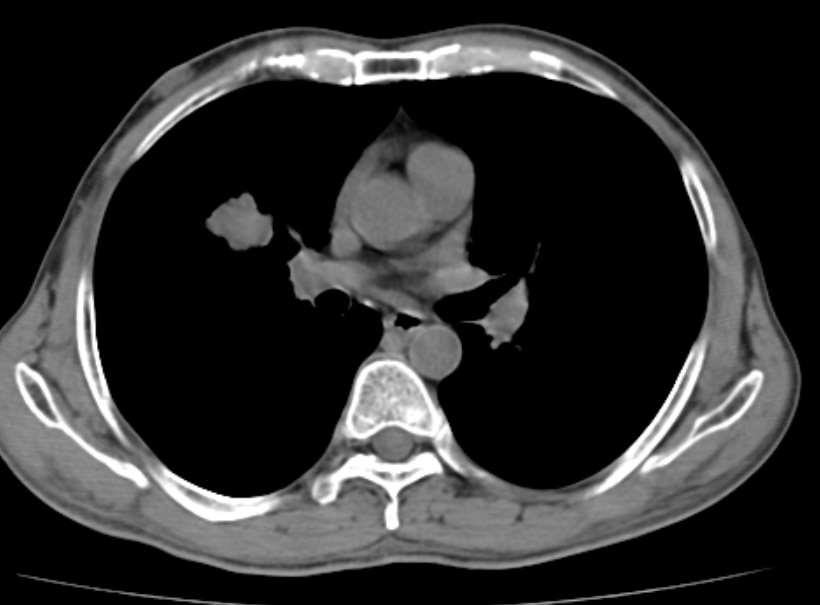
Figure 1: CT of Thorax: Well defined multi-lobulated lesion in right perihilar location in right middle lobe measuring 2.9 x 2.4 cm.
USG of left arm showed an irregular heterogenous soft tissue lesion noted within the triceps muscle with few areas of intra-lesional necrosis, MRI of left arm showed lobulated lesion in posteromedial aspect of mid and distal arm, involving triceps muscle, medial aspect of brachialis, encasing brachial artery, veins and median nerve (Figure 2).
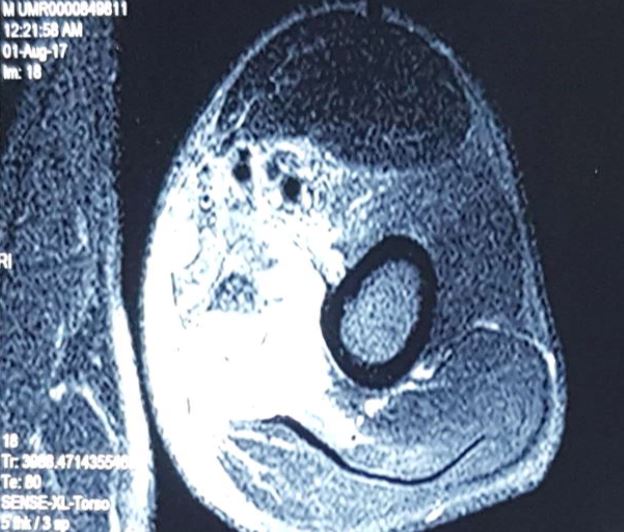
Figure 2: MRI of Left arm: Well defined irregular lobulated enhancing T1 hypo intense, T2 and T2 flair hyperintense lesion in the posteromedial aspect of mid and distal arm.
PET scan showed enhancing nodular soft tissue lesion noted in middle lobe of right lung, 2.9 x 2.4 centimetres. Biopsy revealed metastatic adenocarcinoma. For further studies Immunophenotyping was done which showed negative for EGFR and ALK. Patient was treated with palliative RT, Pem-Carbo f/b Pemtrexed maintenance and recently 3# of Gemcitabine. The patient died of metastasis to brain within eight weeks of diagnosis.
Discussion
Lung carcinoma is a leading cause of cancer-related mortality. The most common sites of distant metastasis in lung carcinoma are brain, bones, the liver, and the adrenal gland1. The most common tumours that cause skeletal muscle metastasis are tumours originating from thyroid, oesophagus, stomach, pancreas, colon, rectum, bladder, breast, ovary, and prostateand skeletal muscle metastasis of lung carcinoma was first reported by Fisher ER2. Willis RA reported four skeletal muscle metastases in their autopsy series composed of 500 lung carcinoma patients3. Skeletal muscle metastasis is a rare occurrence for any tumour with a reported incidence lees than one percent4-5. The most common sites of muscle metastasis are thigh muscles, iliopsoas, and paraspinous muscles6.
The mechanism of skeletal muscle metastasis is unclear. Despite its rich vascular blood supply and a large mass in the body, it is resistant to haematogenous metastases. Organs that are frequently metastasized, including liver, lung, and bone have rich capillary networks and blood supply. As a result of the muscle metabolism, substances such as lactic acid, free oxygen radicals, and low pH in the environment constitute an infertile medium for proliferating tumour cells. In addition, mechanical insults due to contractions, high tissue pressure, and widely alternating blood flow are also against the survival of tumour cells7.
There are several hypotheses proposed for skeletal muscle metastasis in lung carcinoma. The most widely accepted hypothesis is the haematogenous route. In this hypothesis, it is believed that tumour cells are formed through tumour embolism. Some authors suggested that skeletal muscle metastases might originate from abnormal lymph nodes found in the muscle. In a study by Bocchino M et al. 1754 lung carcinoma patients treated between 2007 and 2012 were analyzed and forty six (2.6%) had skeletal muscle metastasis8. Despite the variations between different studies in terms of the association between histological subtypes and skeletal muscle metastasis, forty patients in that study (87%) had non small cell lung carcinoma and six had (13%) small cell lung carcinoma. Among non small cell lung carcinoma patients, twenty four (60%) had adenocarcinoma. The most common initial manifestation of skeletal muscle metastasis is a pain. Pain can be accompanied by extremity swelling. The case presented herein also applied with pain and swelling. Diagnostic methods for skeletal muscle metastasis are not specific. Direct films usually show only soft tissue shadows. MRI usually reveals hypointense signal in T1 and hyperintense signal in T2. MRI is preferred to distinguish soft tissue metastasis from an abscess, sarcoma, and other conditions9, similarly; our patient had hypointense signal on T1 and the hyperintense signal on T2 series. The optimum treatment and prognosis of skeletal muscle metastasis from lung cancer is unclear. Depending on the clinical characteristics, treatment options include observation, surgery, chemotherapy and radiotherapy.
Conclusion
Lung carcinoma with skeletal muscle metastasis should be considered as a potential differential diagnosis in patients presenting with an intramuscular mass.
Acknowledgements
Authors acknowledge the immense co-operation received by the patient and the help received from the scholars whose articles are cited and included in references of this case report. The authors also acknowledge the authors/editors/publishers of all those articles, journals and books from where the literature for this case report has been reviewed and discussed.
|
Competing Interests None declared Author Details SHARAN BADIGER, MD, Professor and Head, Department of Medicine, Sri B M Patil Medical College, (Deemed to be University), Vijayapur, Karnataka, India. SIDDARTHKUMAR CHAWATH, Junior Resident, Department of Medicine, Sri B M Patil Medical College, (Deemed to be University), Vijayapur, Karnataka, India. CORRESPONDENCE: SHARAN BADIGER, Professor and Head, Department of Medicine, Sri B M Patil Medical College, (Deemed to be University), Vijayapur, Karnataka, India Email: sharanrb@rediffmail.com |
References
- Quraishi MA, Costanzi JJ and Hokanson J. The natural history of lung cancer with pericardial metastases. Cancer 1983; 51: 740-742.
- Fısher ER, Gıngrıch RM, Gruhn J, Laıng P. Ossifying metastatic carcinoma; report of a case with comments relative to histogenesis of ectopic ossification. Cancer 1959; 12:257-262.
- Wİllis RA. The Spread of Tumors in the Human Body. London: Butterworth; 1973. p. 282.
- Di Giorgio A, Sammartino P, Cardini CL, Al Mansour M, Accarpio F, Sibio S, et al. Lung cancer and skeletal muscle metastases. Ann Thorac Surg 2004; 78:709-711.
- Heyer CM, Rduch GJ, Zgoura P, Stachetzki U, Voigt E, Nicolas V. Metastasis to skeletal muscle from esophageal adenocarcinoma. Scand J Gastroenterol 2005; 40:1000-1004.
- Marioni G, Blandamura S, Calgaro N, Ferraro SM, Stramare R, Staffieri A, et al. Distant muscular (gluteus maximus muscle) metastasis from laryngeal squamous cell carcinoma. Acta Otolaryngol 2005; 125:678-682.
- Perisano C, Spinelli MS, Graci C, Scaramuzzo L, Marzetti E, Barone C, et al. Soft tissue metastases in lung cancer: A review of the literature. Eur Rev Med Pharmacol Sci 2012; 16:1908-1914.
- Bocchino M, Valente T, Somma F, de Rosa I, Bifulco M, Rea G. Detection of skeletal muscle metastases on initial staging of lung cancer: A retrospective case series. Jpn J Radiol 2014; 32:164-171.
- Schmidt GP, Reiser MF, Baur-Melnyk A. Whole-body imaging of the musculoskeletal system: The value of MR imaging. Skeletal Radiol 2007; 36:1109–1119.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.