



ISSN 1757-8515
Photographic documentation of open fractures: A survey of current practice and proposed recommendations.
R Ahmad, SKM Annamalai, SMY Ahmed, SA Joseph and M Bould
Cite this article as: BJMP 2009:2(1) 32-34
|
Abstract
The primary objective of this survey was to check the availability and use of cameras in documentation of open fractures in emergency departments in England, Wales and Scotland. We also checked the use of mobile phone cameras in emergency departments without cameras. A telephone questionnaire posed questions to the first on-call orthopaedic doctor aboutthe availability of a functional camera in the emergency department. Altogether, 102 doctors replied in 115 hospitals that were surveyed. Only 63 emergency departments had a camera available for photography of open fractures, in which 53 orthopaedic doctors would always take photographs of an open fracture. In 7 emergency departments a mobile phone camera was used for documentation of open fractures, as a camera was not available.
Subsequently, recommendations for wound documentation using a mobile phone camera have been proposed as it is easily accessible and portable with good picture quality that can be transmitted to offsite senior colleagues for advice. This would prevent wound infection and also act as an adjunct to a narrative description of the wound.
Open fractures are quite common and account for a considerable number of admissions to the emergency department with a frequency of approximately 23 per 100000 patients per year1. Infections of open musculoskeletal injuries, especially open fractures, continue to pose a challenge to the Orthopaedic and Trauma surgeons. To reduce the risk of nosocomial infections these wounds need to be instantly photographed before the application of a sterile dressing which has to be left undisturbed until the surgical intervention in the theatre2.
The British Orthopaedic Association and British Association of Plastic surgeons recommend that a Polaroid photograph of every open fracture should be taken, this recommendation is not followed due to non availability of the equipment in some institutions1. This leads to unnecessary disturbance of the wound dressing, distress to the patient and nosocomial infection.
The objective of this study was to look at the availability and use of cameras in compound fractures in Hospitals across England, Wales and Scotland by using a telephone questionnaire.
Methods
We randomly selected 115 NHS hospitals with A&E departments from all the regions of the England, Wales and Scotland using the www.specialistinfo.com website and selected every third hospital on the list. The survey was conduction by the means of a telephone questionnaire (Table 1); the questions were answered by the first on call Orthopaedic doctor. 89% (102/115) first on-call doctors answered the questionnaire.
TABLE 1 Telephonic questionnaire
|
1. Do you have access to a camera in the A&E? 2. If yes, is the camera available 24/7? 3. Have you found a functional camera available every time you have wanted to use it? 4. Do you always take a picture of an open fracture? 5. Do you think that a picture is a useful tool in the assessment of a wound? 6. If a camera is not available in the A&E do you use your mobile phone camera? |
Y/N Y/N Y/N Y/N Y/N Y/N |
The questionnaire was meant to investigate if the doctor had access to a functional camera that was available round the clock in the Emergency department. It also questioned whether the doctor on call would always take a picture of an open fracture. They were also asked whether they thought that the picture was helpful in assessment of the wounds. Finally the respondents were asked whether they used a mobile phone camera in case of non availability of a camera in the emergency department.
Results
Of the 102 first on call Orthopaedic doctors questioned, 38% (39/102) stated that they were unable to photograph an open fracture due to non availability of a camera in the emergency department. A functional camera was not available in both trauma centers and small hospitals. Of the 61% (63/102) who had a camera available 22% (14/63) did not have 24 hour access to the camera. 33% (21/63) who have a Polaroid camera available have found occasions when they needed a camera but it was not functional. (Figure 2)

Figure 1
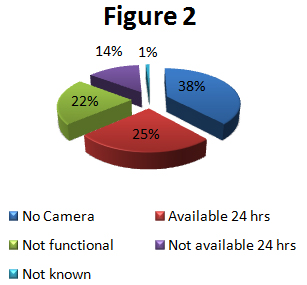
Figure 2 Availability of cameras in A&E.
84% (53/63) who had a camera available said that they always photographed an open fracture. (Figure 3) 28% (11/39) doctors who did not have a camera in the emergency department would use a mobile phone camera to photograph an open fracture (Fig 1). 4 doctors used it even though they had a Polaroid camera in the Accident and Emergency department (A&E) as they found a mobile phone camera easy to use and readily accessible.
All the doctors who responded to the questionnaire thought that a camera was a valuable tool in the documentation of an open fracture.
Discussion
The objective of this study was to look at the availability and use of cameras in compound fractures in hospitals across England, Wales and Scotland.
Figure 3 Percentage of doctors photographing open fractures in A&E.
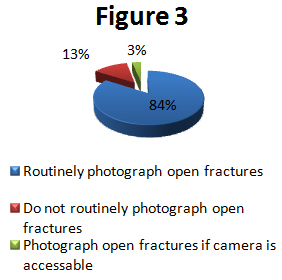
We found that 38% of hospitals did not have access to a camera at all, in a further 15% there wasnt 24 hour access and another 21% had a camera that was not functional when needed at some time in the Emergency department. Thus 74% of hospitals did not have a functional camera available in the emergency department at all times. Therefore the photographic documentation of an open fracture as recommended by the British Orthopaedic association and the British association of Plastic Surgeons working party could not be implemented2. 13% (8/63) respondents who had a camera in the Emergency department did not routinely photograph an open fracture. A similar study done in London and south-east UK hospitals found that 10% hospitals did not have a camera to photograph an open fracture and another 19% did not have it available 24 hours1.
The potential reasons for failure of photographic wound documentation could be difficulty to obtain funding for purchase of a camera, lack of secure storage space and unfamiliarity of the junior doctors with the guidelines of photographic wound documentation
Open wounds of the musculoskeletal system are usually contaminated at presentation with pathogenic organisms3. In the A&E the wound should be assessed and dressed until the formal debridement in the theatre. The ideal practice is to photograph the wound before application of the sterile dressing. These photographs are a vital tool as they act as an adjunct to a narrative description allowing the wound to be accurately described to colleagues. This avoids unnecessary disturbance of the sterile dressing over the wound which has a risk of nosocomial infection2.
The problem of non availability of Polaroid cameras in the emergency department can be overcome by using mobile phone cameras. We faced the same problem of non availability of a camera in our A & E department and we started using our camera phones for photographing open fractures. The authors found that images on mobile phone cameras allowed a useful presentation in the morning trauma meetings. The incidence of re- examining of the wound by the senior surgeons also dropped significantly. Mobile phones can be used in A & E as the maximum distance at which any phone causes interference is only two meters4.
We found the mobile phone camera a valuable alternative as it is easy to use and has excellent portability with an image quality that is sufficient for interpretation. In our study it is already being used by many doctors in different hospitals. With the advancement in technology the mobile phones have become more user friendly with the power to process medical images5. The advantage over a Polaroid picture is that these images can be transferred to another mobile phone or sent as an e-mail attachment for assessment by the offsite registrars and consultants for immediate advice. This is even more useful in hospitals with hospital at night where second on call doctors are usually nonresident. It has been shown that it takes only 3-4 minutes from image taking to remote reception6. The Integrated Service Digital Network (IDSN) used for image transfer in some hospitals is expensive and mobile camera phones are a suitable inexpensive substitute.
We recommend supplying a mobile phone camera to the on call doctor. Unlike Polaroid cameras they dont need a constant supply of batteries and expensive film and the risk of theft is negligible as they are smaller, lighter with excellent portability. The picture can be magnified and is easier to store than traditional cameras. Images must be stored in a manner that prevents tampering and preserves confidentiality. This could be done by deleting the images after they have been assessed, hard copies produced and kept in the case notes as done with pictures taken with a Polaroid camera or storing them by using specific software packages that do not allow image manipulation7 .
There have been two studies assessing the accuracy of the use of mobile phone cameras in diagnosing intracranial pathologies and interpretation of emergency Ear Nose and Throat (ENT) radiological investigations. 5, 8 They have also been used to take pictures of injured digits and then transmitted to camera phones of plastic surgeons for assessment 6. Tsai et al. in their study on teleconsultation by using the mobile camera phone showed that the camera phone is valuable for remote management of the extremity wound9 .Lam TK et al. showed that low cost and the ease of use make the mobile camera phones easily incorporated into clinical practice10.
Conclusion
A functional camera was not available at all the times for photographic documentation of open fractures in the majority of the hospitals. We also feel that mobile phone cameras may be used as a powerful graphic adjunct to a verbal clinical presentation to other health professionals located on or off site.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
MR R AHMAD, MBBS, MRCS, MR S K M ANNAMALAI, MBBS, MRCS, Registrars in T & O, Weston General Hospital, UK
MR SMY AHMED, Registrar T & O, Great Western Hospital, Swindon, UK
MR SA JOSEPH MBBS MRCS, Registrar T & , Wolverhampton General Hospital, UK
MR M BOULD FRCS, Consultant Orthopaedic Surgeon, Weston General Hospital, UK
CORRESPONDENCE: MR. SKM ANNAMALAI, Registrar, T & O, House 18, Staff Residence, Weston General Hospital, Weston Super Mare, BS23 4TQ
Email: suresh.annamalai@nhs.net
References
1. Solan MC, Calder JD, Gibbons CE, Ricketts DM. Photographic wound documentation after open fracture. Injury 2001; 32: 33-35.
2. The management of Open Tibial Fractures. British Orthopaedic Association and British association of Plastic Working Party, London, 1997.
3. Akinyoola AL, Ako-Nai AK, Dosumu O, Aboderin AO, Kassim OO. Microbial isolates in early swabs of open musculoskeletal injuries. Niger Postgrad Med J 2006; 13: 176-81.
4. Tri JL, Hayes DL, Smith TT, Severson RP. Cellular phone interference with external cardiopulmonary monitoring devices. Mayo Clin Proc 2001; 76: 11-5.
5. Eze N, Lo S, Bray D, Toma AG. The use of camera mobile phone to assess emergency ENT radiological investigations. Clin Otolaryngol 2005; 30: 230-3.
6. Hsieh CH, Tsai HH, Yin JW, Chen CY, Yang JC, Jeng SF. Teleconsultation with the mobile camera-phone in digital soft-tissue injury: a feasibility study. Plast Reconstr Surg 2004; 114:1776-82.
7. Bhangoo P, Maconochie IK, Batrick N, Henry E. Clinicians taking pictures a survey of current practice in emergency departments and proposed recommendations of best practice. Emerg Med J 2005; 22: 761-5.
8. Yamada M, Watarai H, Andou T, Sakai N. Emergency image transfer system through a mobile telephone in Japan: technical note. Neurosurgery 2003; 52: 986-8.
9. Tsai HH, Pong YP, Liang CC, Lin PY, Hsieh CH. Teleconsultation by using the mobile camera phone for remote management of the extremity wound: a pilot study. Ann Plast Surg 2004; 53:584-7.
10. Lam TK, Preketes A, Gates R.Mobile phone photo messaging assisted communication in the assessment of hand trauma. Lam TK, Preketes A, Gates R. ANZ J Surg 2004; 74:598-60

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.