



ISSN 1757-8515
Pathological Fractures as the Presenting Symptom of Parathyroid Adenoma: A Report of Three Cases
Rajesh Rachha
Cite this article as: BJMP 2008:1(1) 26-29
|
|
Abstract Primary Hyperparathyroidism is usually diagnosed as an incidental finding of hypercalcemia in blood tests or due to symptoms secondary to the high calcium. Overt bone disease is an extremely rare presentation. Fractures in hyperparathyroidism are unusual and usually affect the vertebrae. Pathological fractures have been described in patients with parathyroid carcinoma. We report on three patients with benign parathyroid adenoma who primarily presented with pathological fractures of long bones. Excision of the parathyroid adenoma and immobilization of the fractures resulted in the return of the serum chemistry to normal, improvement of bone density and fracture union. |
INTRODUCTION
Patients who have untreated primary hyperparathyroidism with Ostitis Fibrosa Cystica have become a rarity. Primary hyperparathyroidism is usually diagnosed as a result of chance finding of raised serum calcium or complications associated with hypercalcemia such as polyuria, polydipsia, muscle weakness, gastrointestinal upsets and renal stone formation. Bone disease is rarely overt. Radiographic manifestations are seen in less than 2% of patients and include subperiosteal erosions, diffuse osteoporosis, cystic lesions (brown tumours), pathological fractures, ‘salt and pepper’ mottling of skull and loss of lamina dura in the mandible1.
The reported incidence of fractures in hyperparathyroidism is quite low, about 10% in two large series2 and apart from vertebral compression fractures, no characteristic fracture pattern have been described.
Extensive bony involvement with pathological fractures as a presenting feature due to parathyroid carcinoma has been documented3, but multiple pathological fractures, as a presenting feature of primary hyperparathyroidism due to parathyroid adenoma is extremely rare. Here we describe three patients seen at our institution in the period from 2001 to 2004 who presented with pathological fractures due to parathyroid adenoma.
CASE 1
A 50-year-old housewife was admitted with painful right thigh and inability to weight bear following a twisting injury of her right leg. She also complained of generalized weakness, lethargy and muscle pain over the past few months. Radiographs revealed segmental fracture of right femur (figure 1a) and gross osteopenia with a cortical index of 0.2 (normal: > 0.45). She also sustained a fracture of left femur following a very trivial injury while transferring her from trolley to bed.
Investigations (table–1) revealed hypercalcemia (12Mg/dl), hypophosphatemia (2.6Mg/dl) and elevated parathyroid hormone level (70 Pmmol/l). 25-hydroxyvitamin D value was in the lower limit of normal (22ng/ml). Renal parameters were normal.

Figure 1a. Gross osteopenia with segmental pathological fractures of right femur.
High-resolution ultrasound (HRUS) of neck revealed a hypoechoic mass measuring 4.1 x 1.7 cm in the posterior aspect of right thyroid lobe, suggestive of parathyroid adenoma. Bone scan showed patchy tracer uptake in almost entire skeleton with generalised osteoporosis and microfractures, suggestive of metabolic bone disease.

Figure1b. 12 Months post Parathyroid adenectomy showing improved bone density and Mallunion of fractures.
Patient underwent parathyroid adenectomy under the general surgeons. Histopathology confirmed the diagnosis of parathyroid adenoma. Following surgery patient developed hypocalcemic tetany and seizures, treated with intravenous calcium gluconate and followed by oral calcium supplements. Fractures were treated conservatively by splinting in groin to toe casts, as the bone quality was very poor. The biochemical tests came back to normal three months after surgery and radiographs revealed fracture healing and improvement in bone density. Casts were removed and mobilization commenced. Over next six months fractures healed but were mall-united (figure 1b). At eighteen months the patient was fully weight bearing with minimal functional disability.
CASE 2
A 32-year-old female patient presented with pain in the right thigh and inability to weight bear after a trivial fall at home. Radiographs revealed fracture middle one-third of right femur, osteopenia and with subperiosteal resorption (figure 2a)

Figure 2a. severe osteopenia with pathological fracture of right femur.
Biochemical tests and parathyroid hormone assay (see table-1) was suggestive of primary hyperparathyroidism. 25-hydroxyvitamin D was within normal limits (35ng/ml). High-resolution ultrasound of neck revealed hypoechoic lobulated lesion measuring 8.4x1.1x1.3 cm, on the inferior and posterolateral aspect of the left lobe of thyroid suggestive of parathyroid adenoma. Bones scan showed tracer uptake at the site of fracture and patchy sclerosis of femur, and increased uptake in left sacroiliac joint.
The patient underwent parathyroid adenectomy under the care of general surgeons. Histopathology confirmed the diagnosis of parathyroid adenoma. Patient received parentaral calcium supplements in the immediate post operative period and later by oral route. Femur fracture was initially treated in groin to toe cast and the calcium levels were controlled, after 2 months bone quality improved, despite callus formation there was mobility at the fracture site, and hence the fracture was managed with intramedullary nail and bone grafting (figure 2b).

Figure 2b. Fracture union with intramedullary nail insitu.
It took ten months for the fracture to unite.
CASE 3
A 20-year-old female patient presented with diffuse pain in the left elbow of two months duration following a trivial injury to her elbow. Plain radiograph of the elbow showed a well-defined lytic lesion with sub cortical erosions and with break in the cortex suggestive of Brown tumour with pathological fracture (figure 3a).
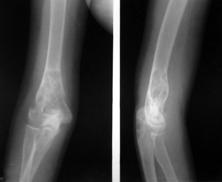
Figure 3a. Brown tumour lower end of humerus with pathological fracture
Biochemical analysis revealed hypercalcemia and hypophosphatemia and parathyroid hormone assay was suggestive of primary hyperparathyroidism (table-1). 25-hydroxyvitamin D levels were within normal limit (40ng/ml). High-resolution ultrasound neck showed 2.6 X 1.1 X 1.6 cm hypo echoic mass lesion inferior to lower pole of thyroid suggestive of left parathyroid adenoma.
Bone scan showed patchy increased tracer concentration in entire skeleton with increased tracer concentration in the distal end of humerus.
She underwent parathyroid adenectomy and histopathological examination confirmed the diagnosis of parathyroid adenoma. The fracture was managed in a cast.

Figure 3b. One year post parathyroid adenectomy shows healed fracture with increased bone density and sclerosis.
Patient was followed up with regular check on her calcium levels and serial radiographs of elbow. By 12 months the fracture was completely healed and brown tumour resolved with increased bone density and sclerosis (figure 3b).
|
Ca++
Mg/dl
|
Phosphorus
Mg/dl
|
Alk. Phos.
IU/L
|
Intact PTH
Pmmol/l
|
25-hydroxy Vit D
ng/ml
|
|
|
Normal |
8 -10 |
3 - 4.5 |
34-135 |
1.1 – 6.5 |
20 - 56 |
|
Case 1 |
12 |
2.6 |
3000 |
70 |
22 |
|
Case 2 |
11.5 |
2.0 |
745 |
56 |
35 |
|
Case 3 |
10.5 |
2.5 |
1184 |
48 |
40 |
|
TABLE –1 Serum biochemical parameters in the patients at presentation |
|||||
DISCUSSION:
Primary hyperparathyroidism is a well-recognised entity identified almost more than a century ago by Von Recklinghausen. He and his co-workers coined the term Osteitis fibrosa cystica1.
This condition is more common in females. Peak age incidence is between 30 to 50 years and incidence increases with age, though patient aged as young as 14 years was documented. In U.S.A annual incidence is around 0.2% in patients > 60 years1. All the patients in our series are females with florid changes observed in-patient aged 52 years other 2 patients are aged 20 years and 32 years.
Disease results from excessive secretion of parathyroid hormone either due to solitary (50-85%) or multiple (10%) adenomas, hyperplasia (10-40%), or rarely due to a carcinoma of a single parathyroid gland. Extensive bony involvement with pathological fractures as a presenting feature due to parathyroid carcinoma has been documented3. In our series of 3 patients all of them were diagnosed to have solitary parathyroid adenoma. Our first patient aged 52 years had coexisting vitamin D deficiency, which explains severe osteomalacia and multiple fractures. Coexistence of vitamin D deficiency in patients with Primary Hyperparathyroidism may put the patient at a significant higher risk of loosing bone mineral density and development of osteoporosis.
Two distinct types of bone lesions are described in primary hyperparathyroidism4. The slowly progressive type- leads to cortical thinning and osteoporosis & the rapidly progressive type. Pathological fractures may occur through a cyst or in a weakened long bone. A principal test at present is the ‘Immunoassay’ for PTH 1-84 as it distinguishes the hypercalcaemia of malignancy from that of hyperparathyroidism5.
Once the diagnosis of primary hyperparathyroidism has been made by biochemical analysis, the site or sites of adenomatous or hyperplastic parathyroid tissue must be identified6. Some authors advocated ‘Exploratory neck operation’ as most adenomas are localized in the neck7. CT scan and Thallium subtraction scans are useful for detecting parathyroid pathology in normal as well as ectopic locations.
USG of neck can be helpful in picking abnormal parathyroid tissue but CT scan and MRI are more sensitive to assess ectopic sites8. In our series of 3 cases, High Resolution Ultrasound Scan (HRUS) of neck helped in localizing the parathyroid adenoma (90% of adenomas are in the neck). Excised parathyroid gland has to be subjected to histopathological examination to confirm and differentiate adenoma, hyperplasia and malignancy. Histopathological examination in all our 3 cases confirmed the diagnosis of parathyroid adenoma.
Our experience with fractures in primary hyperparathyroidism revealed that these take longer to heal and are prone to malunion unless splinted internally or externally. Average time taken for fracture union in our series was 12 months. Non-union of fractures is rare and healing proceeds uneventfully after excision of an adenoma.
Bone histology returns to normal within 5-6 weeks6. Brown tumours usually resolve with increase in bone density and sclerosis after parathyroid adenectomy.
The extensive skeletal involvement due to hyperparathyroidism has rarely been reported. The substantial improvement in bone density, in promotion of fracture healing and in preventing pathological fractures after successful parathyroid adenectomy has been demonstrated in our series of 3 cases.
CONCLUSION:
In conclusion, a high index of suspicion is necessary to diagnose this unusual presentation of primary hyperparathyroidism. A pathological fracture in young lady with marked osteopenia is highly suggestive. A combination of biochemical tests, including serum levels of calcium, phosphorus, alkaline phosphatase and parathormone assay will help in diagnosing primary hyperparathyroidism in 90% of the cases. All patients with Primary Hyperparathyroidism should have Vitamin D level assessment in order to exclude the coexistance of Vitamin D deficiency with Primary Hyperparathyroidism. High Resolution Ultrasound Scan of neck provides valuable preoperative information in selected cases especially in those undergoing minimally invasive parathyroid surgery. Surgical excision and calcium supplementation along with external or internal splinting of fractures allowed the fractures to heal.
CONFLICT OF INTERESTS:
None declared
ACKNOWLEDGEMENTS:
Department of Orthopaedics, Nizam’s Institute of Medical Sciences (NIMS), HYDERABAD, INDIA.
AUTHOR DETAILS:
RAJESH RACHHA, Diploma (Orthopaedics), MRCS. Senior Clinical Fellow, Bedford hospital NHS trust, United Kingdom
CORESSPONDENCE: Dr R Rachha, Bedford Hospital, Kempston Road, Bedford, MK42 9DJ.
Email: drrajeshracha@yahoo.com
REFERENCES:
-
Henry,J.Mankin.: An instruction course lecture- Metabolic bone disease. The American Academy of orthopaedic surgeons. Journal of Bone & Joint Surgery; 1994;Vol- 76A, No.5; 760-788.
-
Chalmers J, Irvine GB: Fractures of the femoral neck in elderly patients with hyperparathyroidism. Clin Orthop Related Res. 1988 Apr;(229): 125-130
-
R.G.Deshmukh., S.A.L.Alsagoff., S.Krishnan et al. Primary hyperparathyroidism presenting with pathological fracture. The Royal College of Surgeons of Edinburgh, December 1998; Vol-43, 424-427.
-
Lancourt JE, Hochberg F. Delayed fracture healing in primary hyperparathyroidism Clin OrthoP 1977; 124: 214-218
-
Nussbaum,S.R., & Polt,J.T., Jr.: Immunoassays for parathyroid hormone 1-84 in the diagnosis of hyperparathyroidism. J Bone and Min. Res., 6 (supplement 2); s43- s50, 1991.
-
George,D.C., Incaro,S.J., Devlin,J.T et al .: Histology of bone after parathyroid adenectomy – A case report. J Bone & Joint Surgery .1990;Vol 72A, No: 10 ; pp 1558- 1561.
-
Satava,R.M., Jr., Beahrs, O.H., and Scholz, D.A.: Success rate of cervical exploration for hyper parathyroidism. Arch.Surg., 1975;Vol-110. 625-628.
-
Winzelberg,G.G.: Parathyroid imaging. Ann.Intern. Med.,1987;Vol-107: 64-70.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.