Contact: Mrs. Kelly Westlake Tel: 011-44-29-2068-2131 Email: westlakekm@cf.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
June 15-17, 2009 United Kingdom / Cardiff
BASIC SKILLS IN HAND SURGERY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6336 Email: plastic@rcseng.ac.uk Website: www.rcseng.ac.uk
Plastic Surgery
June 15-17, 2009 United Kingdom / London
BRITISH FERTILITY SOCIETY PELVIC ULTRASOUND STUDY DAY
Contact: British Fertility Society Secretariat Tel: 011-44-454-642-217 Fax: 011-44-454-642-222 Email: bfs@bioscientifica.com Website: www.britishfertilitysociety.org.uk
Obstetrics/Gynecology / Radiology/Imaging
June 15-16, 2009 United Kingdom / London
REPRODUCTIVE AGEING IN OLDER MOTHERS
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Family Medicine / Obstetrics/Gynecology / Other Specialties
June 15, 2009 United Kingdom / London
BASIC TECHNIQUES IN ARTHROSCOPIC SURGERY BASK/RCS
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6337 Email: orthopaedic@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Orthopedics / Surgery
June 16, 2009 United Kingdom / London
SPECIALTY SKILLS IN EMERGENCY SURGERY & TRAUMA
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6328 Email: trauma@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Emergency Medicine / General Medicine
June 16-17, 2009 United Kingdom / Nottingham
CARE OF THE CRITICALLY ILL SURGICAL PATIENT
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6311 Email: ccrisp@rcseng.ac Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
June 17-19, 2009 United Kingdom / London
HOW TO PRACTICE EVIDENCE-BASED HEALTH CARE
Contact: Dr. Jane Ilsley, Western General Hospital Tel: 011-44-131-537-3355 Email: wtcrf.education@ed.ac.uk Website: www.rcpe.ac.uk
Other Specialties
June 18-19, 2009 United Kingdom / Edinburgh
BRITISH MATERNAL & FETAL MEDICINE SOCIETY 2009 ANNUAL CONFERENCE
Contact: Hampton Medical Conferences Tel: 011-44-20-8979-8300 Email: fetal@hamptonmedical.com Website: www.bmfms.org.uk
Obstetrics/Gynecology
June 18-19, 2009 United Kingdom / Liverpool
WRIST & HAND ARTHROPLASTY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6336 Email: plastic@rcseng.ac.uk Website: www.rcseng.ac.uk
Plastic Surgery
June 18, 2009 United Kingdom / London
HOW DOES RHEUMATOID ARTHRITIS NEED TO BE MANAGED?
Contact: Meetings & Events Office, Royal College of Physicians Tel: 011-44-20-7034-4900 Email: conferences@rcplondon.ac.uk Website: www.rcplondon.ac.uk/event
General Medicine / Orthopedics / Rheumatology
June 18, 2009 United Kingdom / London
3RD SYMPOSIUM ON ACETABULAR RECONSTRUCTION
Contact: Furlong Research Charitable Foundation Tel: 011-44-207-436-1919 Email: furlong@frcf.org.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Orthopedics / Surgery
June 19, 2009 United Kingdom / London
ROAD TRAFFIC FATALITIES, PASSENGERS, PEDESTRIANS, PATHOLOGISTS & POLICE
Contact: Conference Department, Royal College of Pathologists Tel: 011-44-20-7451-6715 Email: meetings@rcpath.org Website: www.rcpath.org
Pathology
June 19, 2009 United Kingdom / London
MANAGEMENT OF COMMON PROBLEMS IN OLDER PEOPLE
Contact: Joyce Achampong, Senior Regional Events Co-ordinator, Royal Society of Medicine Tel: 011-44-20-7290-2980 Fax: 011-44-20-7290-2989 Email: joyce.achampong@rsm.ac.uk Website: www.rsm.ac.uk/academ/condiary.php
Family Medicine / General Medicine / Internal Medicine
June 19, 2009 United Kingdom / York
UK THALASSAEMIA SOCIETY CONFERENCE
Contact: UK Thalassaemia Society Tel: 011-44-20-8882-0011 Fax: 011-44-20-8882-8618 Email: office@ukts.org Website: www.rsm.ac.uk/academ/condiary.php
Hematology
June 20, 2009 United Kingdom / Wilmslow
2009 ANNUAL MEETING OF BRITISH ASSOCIATION OF UROLOGICAL SURGEONS (BAUS)
Contact: BAUS Tel: 011-44-20-7869-6950 Fax: 011-44-20-7404-5048 Email: admin@baus.org.uk Website: baus.meeting.org.uk
Surgery / Urology
June 22-25, 2009 United Kingdom / Glasgow
GASTROENTEROLOGY FOR THE PCP BRITISH ISLES/NORWEGIAN FJORDS CRUISE
Contact: Continuing Education, Inc. Tel: 800-422-0711 (US) or 727-526-1571 Email: contactus@continuingeducation.net Website: www.continuingeducation.net
Family Medicine / Internal Medicine
June 22-July 04, 2009 United Kingdom / Harwich
BASIC PRACTICAL SKILLS IN OBSTETRICS & GYNAECOLOGY
Contact: Conference Office, Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/meetings
Obstetrics/Gynecology
June 22-24, 2009 United Kingdom / London
BYPASS, BALLOON PUMPS & CIRCULATORY SUPPORT
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: cardiothoracics@rcseng.ac.uk Website: www.rcseng.ac.uk
Surgery
June 22, 2009 United Kingdom / London
WORKSHOP IN PELVIC SURGERY
Contact: TMB Marketing and Communications, Conference Desk Tel: 011-44-1306-877-000 Fax: 011-44-1306-877-777 Email: info@wips-intl.com Website: www.wips-intl.com
Obstetrics/Gynecology
June 22-26, 2009 United Kingdom / London
SPECIALTY SKILLS IN VASCULAR SURGERY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: vascular@rcseng.ac.uk Website: www.rcseng.ac.uk
Surgery
June 22-23, 2009 United Kingdom / London
5TH INTERNATIONAL CONFERENCE ON CHILDREN'S BONE HEALTH
Contact: Clare Moloney, Oxford International Tel: 011-44-1865-511-550 Fax: 011-44-1865-511-570 Email: clare.moloney@oxfordint.co.uk Website: www.iccbh5.org
Endocrinology / Orthopedics / Pediatrics
June 23-26, 2009 United Kingdom / Cambridge
9TH ANNUAL INTERNATIONAL ASSOCIATION OF FORENSIC MENTAL HEALTH SERVICES (IAFMHS)
Contact: IAFMHS Tel: 604-924-5026 Fax: 604-924-5027 Email: tmoropito@iafmhs.org Website: www.iafmhs.org
Psychiatry
June 24-26, 2009 United Kingdom / Edinburgh
ADVANCED SKILLS IN VASCULAR SURGERY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: vascular@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
June 24-26, 2009 United Kingdom / London
INTERMEDIATE THORACIC SURGERY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: Cardiothoracics@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
June 24-25, 2009 United Kingdom / London
ASSOCIATION OF BREAST SURGERY AT BASO TRAINEES MEETING 2009
Contact: Krysia Cruickshank Tel: 011-44-141-211-6248 Email: krysia.cruickshank@northglasgow.scot.nhs.uk Website: www.baso.org
Oncology / Surgery
June 25-26, 2009 United Kingdom / Glasgow
RECENT ADVANCES IN MEDICINE
Contact: Sue Dent, University Hospital of North Tees Tel: 011-44-164-262-4791 Fax: 011-44-164-226-4918 Email: sue.dent@nth.nhs.uk Website: www.rcpe.ac.uk
Family Medicine / General Medicine / Internal Medicine
June 26, 2009 United Kingdom / Stockton-on-Tees
SYSTEMATIC TRAINING IN ACUTE ILLNESS RECOGNITION & TREATMENT FOR SURGERY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6311 Email: ccrisp@rcseng.ac.uk Website: www.rcseng.ac.uk
Surgery
June 27, 2009 United Kingdom / London
13TH CONFERENCE OF NATIONAL OSTEOPOROSIS SOCIETY
Contact: Sarah Phillips or Kelly Hall, Events Dep’t., National Osteoporosis Society Tel: 011-44-1761-473-106 or 011-44-1761-473-123 Fax: 011-44-1761-471-104 Email: s.phillips@nos.org.uk or k.hall@nos.org.uk Website: www.nos.org.uk
Other Specialties
June 29-July 01, 2009 United Kingdom / Manchester
2009 ANNUAL MEETING OF BRITISH SOCIETY FOR ALLERGY & CLINICAL IMMUNOLOGY (BSACI)
Contact: BSACI Tel: 011-44-207-340-9614 Email: info@bsaci.org Website: www.bsaci.org
Immunology/Allergy
June 29-July 01, 2009 United Kingdom / Nottingham
PATHOLOGICAL SOCIETY OF GREAT BRITAIN & IRELAND SUMMER MEETING 2009
Contact: Pathological Society of Great Britain & Ireland Tel: 011-44-20-7976-1260 Fax: 011-44-20-7930-2981 Email: admin@pathsoc.org Website: www.pathsoc.org
Pathology
June 30-July 03, 2009 United Kingdom / Cardiff
UPDATE IN MANAGEMENT OF DETRUSOR OVERACTIVITY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: urology@rcseng.ac.uk Website: www.rcseng.ac.uk
Surgery / Urology
June 30, 2009 United Kingdom / London
CARDIOTHORACICS FOR SURGICAL ASSISTANTS
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: Cardiothoracics@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
June 30, 2009 United Kingdom / London
RECONSTRUCTIVE TECHNIQUES IN UROLOGY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6340 Email: urology@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery / Urology
June 30, 2009 United Kingdom / London
CARE HOME MEDICINE
Contact: Meetings & Events Office, Royal College of Physicians of Edinburgh Tel: 011-44-20-7034-4900 Email: conferences@rcplondon.ac.uk Website: www.rcplondon.ac.uk/event
General Medicine / Geriatrics / Other Specialties / Pain Management
June 30, 2009 United Kingdom / London
SOUTH ASIA DAY: JOINT RCOG/AICC RCOG/SAFOG MEETING
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
July 03, 2009 United Kingdom / London
CANCER IN WOMEN BALTIC SEA CRUISE
Contact: Continuing Education, Inc. Tel: 800-422-0711 (US) or 727-526-1571 Email: available through web page Website: www.continuingeducation.net
Family Medicine / Internal Medicine / Obstetrics/Gynecology
July 04-16, 2009 United Kingdom / Harwich
6TH INTERNATIONAL ASSOCIATION FOR BIOLOGICALS SYMPOSIUM ON ADVANCES IN TRANSFUSION SAFETY
Contact: Department of Haematology, Cambridge Institute for Medical Research Tel: 011-44-122-354-8044 Email: jpa1000@cam.ac.uk Website: www.iabs.org
Hematology / Other Specialties
July 06-07, 2009 United Kingdom / Cambridge
4TH NATIONAL AUTISM TODAY
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Family Medicine / General Medicine / Neurology / Pediatrics / Psychiatry
July 06-07, 2009 United Kingdom / London
MRCOG PART 1 REVISION COURSE
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
July 06-10, 2009 United Kingdom / London
CURRENT CONCEPTS IN EXTERNAL FIXATION IN TRAUMA
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6337 Email: orthopaedics@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Orthopedics / Surgery
July 06, 2009 United Kingdom / London
WORKSHOP ON THE MOLECULAR PHARMACOLOGY & THERAPEUTICS OF BONE DISEASE
Contact: National Association for the Relief of Paget's Disease Tel: 011-44-161-799-4646 Fax: 011-44-161-799-6511 Email: director@paget.org.uk Website: www.paget.org.uk
Endocrinology / Other Specialties
July 06-09, 2009 United Kingdom / Oxford
89TH ANNUAL MEETING OF BRITISH ASSOCIATION OF DERMATOLOGISTS
Contact: Conference & Events Services, British Association of Dermatologists Tel: 011-44-20-7391-6358 Fax: 011-44-20-7388-0487 Email: conference@bad.org.uk Website: www.bad.org.uk
Dermatology
July 07-10, 2009 United Kingdom / Glasgow
13TH BRITISH ACADEMIC CONFERENCE IN OTOLARYNGOLOGY AND ENT EXPO
Contact: ENT UK Tel: 011-44-20-7404-8373 Fax: 011-44-20-7420-4200 Email: conferences@entuk.org Website: www.bacouk.org
Otolaryngology
July 08-10, 2009 United Kingdom / Liverpool
HANDS ON GYNAECOLOGICAL ENDOSCOPY SKILLS WORKSHOP
Contact: Therese Eleftheriou, Course Secretary Tel: 011-44-20-7795-0500 ext. 33863 Fax: 011-44-20-7431-1321 Email: courses@gynendo.com Website: www.gynendo.com/dates.htm
Obstetrics/Gynecology / Surgery
July 08-10, 2009 United Kingdom / London
INTERNATIONAL SYMPOSIUM ON PAGET’S DISEASE
Contact: National Association for the Relief of Paget's Disease Tel: 011-44-161-799-4646 Fax: 011-44-161-799-6511 Email: director@paget.org.uk Website: www.paget.org.uk
Endocrinology / Other Specialties
July 08-09, 2009 United Kingdom / Oxford
11TH NATIONAL CONFERENCE: THE DIABETES EPIDEMIC
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Endocrinology
July 13-14, 2009 United Kingdom / London
DEFINITIVE SURGICAL TRAUMA SKILLS FOR THE GENERAL SURGEON
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6336 Email: trauma@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
July 14-15, 2009 United Kingdom / London
3RD NATIONAL CRITICAL CARE SYMPOSIA
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Internal Medicine
July 15-17, 2009 United Kingdom / London
BRITAIN PACIFIC MEDICAL AND LEGAL CONFERENCE
Contact: Lorenzo Boccalbella Tel: 011-61-07-3254-3331 Fax: 011-61-07-3254-3332 Email: info@educationcpe.com Website: www.conferences21.com
Legal/Ethics
July 17-24, 2009 United Kingdom / Oxford
BRITAIN PACIFIC MEDICAL & LEGAL CONFERENCE
Contact: Continuing Professional Education Pty Ltd. Tel: 011-61-7-3254-3331 Fax: 011-61-7-3254-3332 Email: info@conferences21.com Website: www.conferences21.com
Legal/Ethics
July 17-24, 2009 United Kingdom / Stratford-upon-Avon
BASIC SCIENCE: CELL SIGNALLING AND THE GUT
Contact: United European Gastroenterology Federation Secretariat Tel: 011-43-1-997-1639 Fax: 011-43-1-997-1639 ext. 10 Email: office@uegf.org Website: www.uegf.org
Gastroenterology
July 19-21, 2009 United Kingdom / Cambridge
MRCOG PART 2 REVISION COURSE
Contact: Royal College of Obstetricians & Gynaecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
July 20-22, 2009 United Kingdom / London
FRCS (PLAST) AESTHETIC STUDY DAY
Contact: Royal College of Surgeons of England Tel: 011-44-20-7869-6336 Email: aesthetic@rcseng.ac.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Plastic Surgery
July 21, 2009 United Kingdom / London
2009 BRITISH ASSOCIATION FOR PSYCHOPHARMACOLOGY (BAP) SUMMER MEETING
Contact: Lynne Harmer, BAP Tel: 011-44-1223-358-421 Email: lynne@bap.org.uk Website: www.bap.org.uk
Clinical Pharmacology / Psychiatry
July 26-29, 2009 United Kingdom / Oxford
BASIC PRACTICAL SKILLS IN OBSTETRICS & GYNAECOLOGY
Contact: Royal College of Obstetricians & Gynecologists Tel: 011-44-20-7772-6245 Fax: 011-44-20-7772-6388 Email: conference@rcog.org.uk Website: www.rcog.org.uk/events
Obstetrics/Gynecology
July 27-29, 2009 United Kingdom / London
CORE SKILLS IN LAPAROSCOPIC SURGERY
Contact: Julie Bradley Tel: 011-44-121-424-1488 Email: julie.bradley@heartofengland.nhs.uk Website: www.rcseng.ac.uk/education/courses/course_list.html
Surgery
August 19-21, 2009 United Kingdom / Birmingham
11TH NATIONAL CONFERENCE: PARKINSONS DISEASE
Contact: Mark Allen Group Tel: 011-44-20-7501-6762 Fax: 011-44-20-7733-8174 Email: conferences@markallengroup.co.uk Website: www.mahealthcareevents.co.uk
Neurology
August 25, 2009 United Kingdom / London
Chest radiographs are one of the most common radiological procedures performed in medical practice. The chest radiograph should ideally include views of the heart, lungs, trachea, mediastinum, bones of the chest and upper part of the abdomen. Chest radiographs are normally taken in the posterior-anterior (PA) view with the patient in upright / standing position but for patients admitted in the intensive care unit (ICU) or other emergency situations, this is not possible and so they are taken in the supine (anterior-posterior views) or semi-erect position.
Chest radiographs are done not only for diagnostic reasons to look for abnormalities in the lungs, soft tissues and bones but also to check the position of various invasive lines and tubes. In this article, we aim to discuss and compare the normal and abnormal positions of central venous catheter (CVC) on chest radiographs.
Indications for Central Venous Catheter (Internal Jugular Vein Cannulation)
There are many indications for central venous cannulation 1. These include:
Central venous pressure (CVP) monitoring
Pulmonary artery catheterisation and monitoring
Transvenous cardiac pacing
Administration of drugs (vasoactive drugs, chemotherapy etc)
Aspiration of air emboli
Administration of fluids (in case of difficult peripheral venous access)
Confirming the position of the central venous catheter tip:
For accurate CVP measurement, the tip of the central venous catheter (CVC) should lie within the superior vein cava (SVC), above its junction with the right atrium and parallel to the vessel walls 1. After insertion of a CVC, the position of the catheter tip must be confirmed radiologically, as catheter tips located within the heart can cause cardiac perforation and tamponade 1. Hence, optimum positioning of the CVC tip is required to prevent complications.
If the CVC tip is situated high up (above the pericardial reflection), this can cause vessel wall erosion and if they are very low (in the right atrium), they can cause arrhythmias, placement in the coronary sinus and damage to the tricuspid valve 2.
The carina is a useful radiological landmark for CVC tip position. In this edition of pictorial essay, we aim to discuss the optimum position of both the right and left sided IJV cannula on chest radiographs.
Fig: 1 (CR-1819) shows the normal position of a right sided IJV catheter. The tip of the right sided IJV cannula should ideally lie just above the level of the carina 2. This is the junction of the left and right innominate veins with the superior vena cava (SVC).
Fig: 2 (CR-1829): The optimum position of the left sided IJV cannula is at or just below the level of the carina 2. This radiograph shows the comparison between the right and left sided IJV cannula in the same patient.
The right sided IJV cannula is too low (below the level of the carina) and is probably in the right atrium while the tip of the left sided IJV cannula is optimally placed.
Fig: 3 (CR-1832): In this radiograph, the right sided IJV cannula is too high in the neck. This will not give an accurate CVP measurement. Besides, there is also a risk that the CVC might get dislodged and lead to extravasation of administered fluids and drugs.
Seldinger technique for CVC insertions:
The CVC’s are usually inserted using the Seldinger technique. The IJV can be located by using anatomical landmarks or under direct vision with the help of an ultrasound machine. In the Seldinger technique, after puncture of the IJV, a thin J-shaped guide wire is introduced through the puncture needle. The needle is then slowly withdrawn leaving the J-shaped guide wire in place. A dilator is then introduced over the guide wire to dilate the skin and the subcutaneous tissue. Next, the dilator is removed and the CVC is introduced over the guide wire. Finally, it is important that the guide wire is removed and the CVC is secured.
Fig: 4 (CR-1831). This chest radiograph shows an unusual complication where the guide wire has been left accidentally in situ on the right side. (Note the presence of the J-shaped guide wire on the right side of the neck). This can result in serious complications if the guide wire migrates distally.
Conclusion:
In this article, we have highlighted the optimum placement of central venous catheters on chest radiographs. It is imperative that after every CVC insertion (via the IJV or subclavian vein), the position of the tip be confirmed radiologically and if any re-positioning is required, it must be done. The above discussion is true for even CVC’s inserted through the subclavian veins.
Self Assessment MCQ:
The tip of the right sided IJV cannula should be located a. below the level of the carina b. at the level of the clavicle c. just above the level of the carina d. in the right atrium
Answer: c
ACKNOWLEDGEMENTS We wish to thank the Department of Radiology in Bedford Hospital for helping us with the chest radiographs. COMPETING INTERESTS None Declared AUTHOR DETAILS DR. KRISHNAN MELARKODE, MD DNB FRCA, Specialist Registrar in Anaesthesia, Bedford Hospital NHS Trust, UK DR. M Y LATOO, MBBS FRCA, Consultant Anaesthetist, Bedford Hospital NHS Trust, UK CORRESPONDENCE: Dr. Krishnan Melarkode, Specialist Registrar in Anaesthesia, Bedford Hospital, Bedford, UK Email: drkrishnanmr@gmail.com
References
Mark JB, Slaughter TF and Gerald Reves J. Cardiovascular monitoring. In: Miller RD ed. Anesthesia. 5th edition. Churchill Livingstone; 1144-51.
Stonelake PA and Bodenham AR. The carina as a radiological landmark for central venous catheter tip position. British Journal of Anaesthesia 2006; 96: 335-340
The patient's
right to autonomy should always be respected and steps shall be taken
to make consent truly informed. There is, however, no absolute right
to consent on the basis of philosophical, ethical, legal and practical
considerations.
Introduction
Consent
to investigations and treatment is considered a cornerstone in the doctor-patient
relationship.1 The Oxford Dictionary (1998) defines consent
as “permission for something to happen or agreement to do something”.2
This definition does not entail understanding of the action agreed to
and for medical purposes the term ”informed consent” meaning “permission
granted in the knowledge of possible consequences” has been developed.2
General Medical Council (GMC) guidance requires the ability to comprehend
and weigh up information as well the ability to communicate for informed
consent.3
Most authors
describe consent as a principle relatively new to medicine.4-6
This is however incorrect as even Plato and Hippocrates used consent
in their medical practice.7
This review
addresses the issue whether the right to consent is an absolute right
by exploring the ethical and legal framework of consent or more specifically
informed consent. Whereas most of the ethical issues are universally
applicable, the legal aspects and guidance by the regulatory authorities
apply only to the United Kingdom (UK). Where law differs between Scotland
and the rest of the UK, I have focused on the laws for the latter.
Ethical
principles around consent
The four
main principles of medical ethics are justice, non-malificence, autonomy
and beneficence.8 Autonomy is the main ethical consideration
underlying informed consent. The patients’ right to determine what
investigations and treatment to undergo must be respected by all doctors.3
For consent to be informed patients rely on the information provided
by their doctor. Honesty and truthfulness are required to make the process
of consent valid.3 The ethical principle of justice needs
to be applied when deciding what treatments are offered to or withheld
from patients. This touches the process of informed consent and is further
explored when the right to demand certain treatments is discussed.
Philosophical
aspects
The debate
whether a right or a principle is absolute not only involves ethical
and legal aspects. It also touches on the philosophical argument of
absoluteness. Freedom as an example can’t exist as an absolute principle
because granting one individual absolute freedom will infringe the freedom
of a second individual considerably. Person A’s freedom to take any
good will influence the freedom of person B to have property. When applying
these principles to autonomy the same problem arises: Total autonomy
of one individual has a negative effect on autonomy of other individuals.
The modern democratic society has designed rules and laws to create
a fair way of living. On the one hand this restricts autonomy, while
on the other hand this same restricted autonomy guarantees the same
amount of it to all members of this society.
I argue
therefore that on a philosophical basis the principle of total autonomy
contradicts itself when applied to society. As autonomy is the main
ethical principle for informed consent an absolute right to consent
cannot exist.
Requirements
of informed consent
The basic
difference between consent and informed consent is the patients’ knowledge
behind the consent decision. Informed consent requires the patient to
understand the diagnosis and uncertainties about it as well as the different
treatment options (including doing nothing) and their advantages, disadvantages
and achievable outcomes.3 The amount of information required
to make consent informed may vary depending on complexity and risks
of treatment as well as the patient’s wishes.3 Furthermore
individual patients will have different intellectual capabilities and
understanding of their illness. It is therefore mandatory to tailor
information provided to the individual patient and the current situation.
An emergency like acute myocardial infarction for example will allow
less time to discuss diagnosis and treatment than an elective endoscopy.
To judge
whether a patient has really understood the information provided can
be difficult and often little of the information is retained (see practical
aspects chapter). This leaves physicians in doubt whether their patient’s
consent is truly informed. Consent based on partial information may
be invalid but this may go unnoticed by patient and treating physician.
The principal
of an absolute right to consent could be easily undermined by partial
information. It is highly dependant on the willingness to provide full
information and the patient’s capability to understand it and weigh
up the options.
Legal
framework
A medical
intervention without valid informed consent is a criminal offence and
the physician can be charged with battery. Examples of such situations
include treatment against the patient’s will, different treatment
than the one consented for and treatment after consenting deliberately
with wrong information.9
Guidance
for consent has been set up by the regulatory body (GMC). While no one
can consent for a competent adult UK laws are regulating consent for
minors, patients with acutely or permanent incapacity and patients suffering
form severe mental illness.
Minors
At the age
of 16 persons are to be considered as adults and can therefore be presumed
to have capacity. Children younger than 16 years may have capacity depending
on their understanding. When a competent child refuses treatment persons
with parental responsibility may authorise this or a court may overrule
the child’s decision.3 Incompetent children will be treated
with consent from a person with parental responsibility.
Acute
and permanent incapacity
The presumption
that every adult patient has capacity applies unless the opposite can
be clearly demonstrated.3, 10 Patients lacking capacity due
to an acute (i.e loss of consciousness after an accident or patients
on mechanical ventilation) or chronic illness (i.e dementia) cannot
make decisions about their treatments themselves. In those situations
it is the doctor’s duty to act in the “best interest of the patient”.
Views about the patient’s preferences may be sourced from a third
party (relatives for example). This third party can however not consent
or object to treatment.3 If a patient has clearly given an
advance directive while still competent, the treating physician is bound
to respect this (see advance directive).
To give
informed consent a patient needs to have mental capacity and the ability
to communicate.11 The physician needs to establish the patient’s
“ability to understand, retain, believe, evaluate, weigh and use information
that is relevant to a medical intervention or its withdrawal”.11
This test of capacity has been supported by several court rulings10,
12, 13 and is embedded in the Mental Capacity Act (2005).14
Making an
irrational choice does by no means constitute lack of capacity and a
competent patient’s irrational decision has to be accepted even if
this leads to an adverse outcome (including death).3
Mentally
ill patients
The Mental
Health Act (1983) regulates the treatment and hospital admission of
mentally ill patients not volunteering to undergo assessment and/or
treatment.15 These patients can only be admitted to hospital
if due to their mental illness they pose a threat to themselves or others.
Patients can be detained against their wishes to conduct an assessment
and if their condition is deemed treatable they can be detained to receive
such treatment. While this allows treatment for psychiatric conditions,
the treatment of physical conditions not related to mental illness cannot
be undertaken against the patient’s wishes. If needed, a court can
decide on treatment of non-psychiatric illnesses in those patients.
This aspect
of the law can leave physicians in difficult situations. If a depressed
patient takes an overdose of an anti-inflammatory drug he can be detained
in hospital using section 5.2 of the Mental Health Act. A resulting
medical complication like severe gastrointestinal bleeding is however
not covered by the mental health act. The patient therefore still remains
competent to refuse a life-saving endoscopy or blood transfusion.
Protecting
the public: infectious diseases, infection control and confidentiality
In order
to protect the public form contagious infectious diseases the Public
Health (Control of Disease) Act (1984) regulates notification of diseases
and mandatory treatment of conditions like tuberculosis (TB).16
The individual’s right to consent is severely restricted in two areas:
Firstly information about the patient’s diagnosis has to be given
to the relevant authorities. The patient should be informed about this
step. Section 11 regulates the disclosure of information. It is mandatory
for a medical practitioner to disclose personal details of the patient
and the diagnosis to the relevant authorities even if the patient does
not agree to this. The list of notify-able diseases ranges from food
poisoning and viral hepatitis to tuberculosis.
Secondly
patients suffering from communicable diseases can be forced to take
their medication by supervised administration or involuntary inpatient
treatment. Sections 37 and 38 of the Public Health (Control of Disease)
Act have recently been used to detain a man for inpatient treatment
of TB against his will at North Manchester General Hospital.17
The act was used to prevent the spread of TB to the wider public by
forcing treatment onto an individual, who was not compliant.
While above
regulations are clearly set out by law, a physician might encounter
situations in which no clear guidance is given. If a patient confesses
a crime or a planned crime to a doctor, it is left to him to decide
whether to pass on this information to the police. This decision requires
careful weighing up whether the right to consent on passing on information
is more important than the right of the public to be protected. GMC
guidance (Confidentiality: Protecting and Providing Information, 2004)
gives general advice on disclosure, but leaves the ultimate decision
with the medical practitioner.18
The legislative
has given clear laws stating when a right to consent does not apply
to a patient. Incompetent minors, adults lacking capacity and some mentally
ill patients do not have an absolute right to consent. Furthermore patients
suffering from some infectious diseases have limited right to consent
and can be detained and treated against their will. Using the principles
of capacity and justice towards other individuals the right to autonomy
has been cut in a few well-defined circumstances.
Advance
directives
When an
adult becomes incompetent he loses the right to decide on his medical
care. To allow patients to express their ideas and wishes before they
become incapacitated the Mental Capacity Act was introduced in 2005.19
Patients can give an advance directive or “living will” to outline
the treatments they wish or wish not to receive. A physician is required
to act within this advanced directive unless there is evidence that
the patient revoked the will when still competent. A “living will”
does not necessarily apply to all situations and it has to be checked
whether the patient’s current condition is covered by his will.
Practical
application of advance directives can be difficult: Unclear wording
like “no life-prolonging treatment” leaves room for interpretation
and the same intervention might have different outcomes depending on
underlying conditions. A healthy patient might set up an advance directive
to not receive mechanical ventilation without discussing the merits
of this intervention with a health care professional. This generally
prohibits any doctor from administering such treatment in any situation.
While this might be the patient’s wish should he suffer a devastating
stroke (very little chance of recovery), it could be argued that his
view would be different if the merits of ventilation after major emergency
surgery (reasonably good chance of full recovery) would have been explained
to him.
Furthermore
the act established the lasting power of attorney (LPA) concept. This
enables the patient to grant rights of consent and refusal to a LPA
while still competent. The LPA then takes over these powers when the
patient loses capacity.
Research
without consent
While consent
should always be sought for including patients in clinical research,
there are conditions that do not allow a delay: Unconscious patients,
patients in shock and studies with short therapeutic windows. While
including those patients without consent infringes their right to autonomy
society as a whole benefits from such research. The European Union (EU)
allows such studies to recruit patients without their consent under
strict regulation.20
The
right to refuse or demand treatment
British
law clearly gives competent patients the right to refuse any treatment
(the very few exceptions have been outlined in the chapter legal framework).
In contrast, however, no patient has a right to demand certain treatments.
GMC regulation (2008) states that if a patient wishes treatment that
in the doctor’s view is clinically not indicated there is no ethical
or legal obligation to provide such treatment.21
Burke, who
suffers from a chronic and progressing neurological illness, challenged
this guidance. He wishes to receive artificial nutrition and hydration
(ANH) when he loses his ability to swallow and he does not want doctors
to make decisions on his behalf. Arguing that the relevant GMC guidance
infringes his human rights he took the case to court achieving a favourable
ruling initially. Mr Justice Munby ruled in Burke22 that
the Human Rights Act (1998)23 entitles a person to demand
life-prolonging treatments such as ANH. He based his decision on article
2, 3 and 8 arguing that a competent person’s right to life and autonomy
constitute an entitlement to ANH.11
The Court
of Appeal overturned this ruling although the right-based analysis of
Munby’s decision was acknowledged. Two lines of argument were used
to justify the decision. Firstly the case of Bland24 (Airedale
NHS Trust 1993), an advance directive to withdraw treatment in a case
of persistent vegetative state must be respected, does not automatically
lead to a reverse decision in opposite cases.11
Secondly
an advanced directive demanding life-prolongueing treatment would not
be in consistence with the Mental Capacity Act, which requires the doctor
to take the incompetent patient’s best interest into consideration.11
Another
aspect of demanding treatment is the effect on the wider community.
Graber and Tansey argue that demanding certain (more expensive, equally
effective) treatments leads to injustice.25 While doctors
may feel pressured to please their patient’s wishes, financial and
organisational constraints in society (and a public health care system)
will mean that other patients might not get treatments they require.
Currently
there is no legal right in the UK to demand treatment. Furthermore such
demands infringe justice by prohibiting resources to be allocated by
need.
Practical
aspects of consent: understanding and retention of information provided
Informed
consent requires the ability to understand and weigh up information.
Several studies have addressed the issue of understanding and retention
of information provided. Even in a research setting where rigorous measures
for consent are applied severe defiencies have been identified: in a
randomized drug trial 44% of participants did not know that they were
assigned to treatment or placebo by chance.26 A capsule endoscopy
study recruited healthy volunteers, of whom 90% had university education
and 60% were medical students. Still vital information (drugs used,
potential risks) given during the consent was only completely recalled
by around 20%.27 These examples show that most patients or
research participants do not have a good understanding and/or recall
of the information provided by standard consent procedures. Despite
that treating doctors and researcher had treated or included patients
based on this “informed” consent.
Methods
like enhanced consent forms and multimedia interventions during informed
consent have shown mixed results, while only additional time spent in
one-on-one interviews significantly improved understanding and recall
of information.28
Discussion
Informed
consent is required for any investigation or treatment proposed to a
patient. Understanding of the nature of procedure, benefits and risks
are the cornerstones of informed consent. While autonomy is one of the
four main ethical principles, I argue that there is no absolute right
to autonomy or consent.
On a philosophical
basis an absolute right to autonomy and consent contradicts itself.
Several
restrictions in the right to consent are set by the legal framework
in the United Kingdom (or England). The main statuary instruments concerned
are: Mental Health Act, Mental Capacity Act and Public Health Act. UK
Law regulates the right to consent for minors, mentally ill patients,
patients with incapacity and patients with communicable diseases. Their
rights to consent are restricted and in special circumstances not granted.
Disclosure of information without consent is mandatory in infectious
diseases cases and legal in cases where the doctor believes that non-disclosure
will leave the public in danger. Furthermore patients can be recruited
to studies of emergency medical treatment without consent under strict
EU regulation. On a legal basis there is no absolute right to consent
therefore.
Patients
with anticipated incapacity can set advance directives to guide their
future treatment while still competent or a LPA can be given the right
to decide on treatment on the patient’s behalf. While this increases
the right of consent and improves patient autonomy to refuse treatment,
there is no right to demand treatment if this is considered medically
inappropriate (futile for example) by the treating medical practitioner.
Looking
at the practical aspects of consent shows that the information provided
is often poorly understood and retained. Patients giving consent are
doing so without being truly informed. In other words they can’t give
informed consent due to their lack of understanding. As shown in the
chapter practical aspects this will often not be noticed by the treating
doctor or researcher. It is difficult to conceive an absolute right
to consent in practice, when the effort to supply information required
for informed consent fails so often.
In summary
the patient’s right to autonomy should always be respected and step
shall be taken to make consent truly informed. On the basis of philosophical,
ethical, legal and practical considerations, however, there is no absolute
right to consent.
COMPETING
INTERESTS
None Declared AUTHOR
DETAILS
CHRISTIAN
P SELINGER, MD, MRCP, Royal Albert Edward Infirmary, Wigan, United Kingdom CORRESPONDENCE:
DR CHRISTIAN SELINGER, Royal Albert Edward Infirmary, Wigan Lane, Wigan,
WN1 2NN, United Kingdom Email:
Christian.selinger@web.de
References
1. Habiba MA (2000) Examining consent
within the patient-doctor-relationship. Journal of Medical Ethics 26:183-87 2. The Oxford
Dictionary of new English, Oxford. Oxford University Press, 1998 3. GMC (1998)
Seeking patients’ consent: The ethical considerations, General Medical
Council, London 4. King J
(1986) Informed consent: A review of empirical evidence. Institute of
Medical Ethics Bulletin supp 3: 1-17 5. Kour NW,
Rauff A (1992) Informed consent – historical perspective and
a clinician’s view. Singapore Medical Journal 33:44-46 6. Nelson-Marten
P, Rich RA (1999) A historical perspective of informed consent in clinical
practice and research. Oncology Nursing 15:81-8 7. Dalla-Vorgia
P, Lascaratos J, Skiadas P et al. (2001) Is consent in medicine a concept
only of modern times? Journal of Medical Ethics 27:59-61 8. Gillon
R. Medical ethics: Four principles plus attention to scope. BMJ 1994;
309:184-8<br>
9. MRHA guidance (2007): http://www.mhra.gov.uk;
as accessed on 01/06/2008 10. Re C
(adult refusal of treatment) [1994] 1WLR 290 11. Samata
A, Samata B (2006) Advance directives, best interests and clinical judgement:
shifting sands at the end of life. Clinical Medicine 6:274-78 12. Re MB
(an adult: medical treatment) [1997] 2 FLR 426 13. Re B
(consent to treatment: capacity) [2002] EWCH 429 14. Mental
Capacity Act 2005. The Stationary Office, 2005 15. Mental
Health Act 1983. The Stationary Office, 1983 16. Public
Health (Control of Disease) Act (1984). The Stationary Office, 1984 17. Crook
A (2007) TB patient under guard. Manchester Evening News 9/10/2007 18. GMC (2004)
Confidentiality: Protecting and Providing Information, General Medical
Council, London 19. Mental
Capacity Act 2005. The Stationary Office, 2005 20. Lecouturier
J, Rodgers H, Ford GA, et al. (2008) Clinical research without consent
in adults in the emergency setting: a review of patient and public views.
BMC Medical Ethics 9:9 21. GMC (2008)
Withholding and withdrawing life-prolonging treatments: Good practice
in decision making, General Medical Council, London 22. Re (Burke)
v General Medical Council (defendant) and Disability Rights Comission
(interested party) and the Official Solicitor (intervenor) [2004] EWHC
1879 23. Human
Rights Act (1998). The Stationary Office, 1998 24. Airedale
NHS Trust v Bland [1993] A.C. 789 25. Graber
MA, Tansey JF (2005) Autonomy, consent, and limiting healthcare costs.
Journal of Medical Ethics 31:424-426 26. Howard
JM, DeMets D (1981) How informed is informed consent: the BHAT experience.
Controlled Clinical Trials 2: 287-303 27. Fortun
P, West J, Chalkley L, Shonde A, Hawkey C (2008) Recall of informed
consent information by healthy volunteers in clinical trials. QJM an
international journal of Medicine in press, available online at:
http://qjmed.oxfordjournals.org/cgi/content/abstract/hc 28. Flory
J, Emanuel E (2004) Interventions to improve research participants’
understanding in informed consent for research. Journal of the American
Medical Association 292: 1593-1601
The incidence of caesarean section is rising1 and there is evidence that women who have a caesarean section may be at increased risk of complications in a subsequent pregnancy2. Compared with vaginal delivery in the first pregnancy, caesarean section has been found to be associated with significantly increased rates of: uterine rupture in labour;3 placenta previa and placental abruption;4 placenta previa leading to peri-partum hysterectomy;5 stillbirth;6 and perinatal death7. Sometimes some unusual complication develops with which, we are not familiar. Here an uncommon complication following caesarean section in a post caesarean pregnancy has been reported.
Case report
A 25 years old lady P 1+4 presented at the emergency department of NRS Medical College & Hospital, Kolkata as an unbooked sixth gravida with the complaint of leaking per vagina for last 4 hours and the period of amenorrhoea was 38weeks. Her past obstetric history revealed that she had caesarean section 4 years earlier (indication of caesarean section was not known to the patient) and 4 successive M.T.Ps, the last being done 1 year back. The baby was alive. The couple wanted ligation operation.
On examination, she was mildly anaemic. Pulse was 88/min and BP was 126/80 mm Hg. She was free of any medical or surgical complications like morbid obesity, COPD and umbilical hernia. Per abdominal finding revealed a term size uterus with cephalic presentation and average liquor. FHS was 144/min and regular. Her previous caesarean section scar was low transverse and there was no scar tenderness.
Per speculum examination showed dribbling of clear liquor. Vaginal examination revealed cervix was 1.5 cm dilated, tubular, station was high up (-3) and membranes were absent.
An emergency L.S.C.S. was performed under spinal anesthesia. The skin incision was Pfannenstiel with excision of the previous scar. On opening the abdomen, uterus was found to be adherent with anterior abdominal wall from which uterus was separated for delivery of the baby (a living male baby of 2.75 Kg) and bilateral tubectomy operation. Bladder was also pulled high up which was dissected and pushed down before opening the uterus. Parietal peritoneum was not closed and rectus sheath was repaired with no 1 chromic catgut. Duration of operation was one hour which was longer than usual operation time of 35 minutes.
First two post operative days were uneventful. On the 3rd day there was a small amount of serosanguinous discharge from the umbilicus. The caesarean section wound, which was located much below the umbilicus, was healthy. Methylene blue dye was introduced into the bladder to rule out any communication with umbilicus, through which no dye came out. On 4th post operative day a mass was seen protruding through the umbilicus and on gentle prodding it seemed to be omentum like structure (Fig-I) A provisional diagnosis of omental hernia through umbilicus was made.
Figure I showing omentum like structure protruding through umbilicus
Figure II showing omental tag held during herniorrhaphy operation
On the 5th post operative day, she underwent herniorrhaphy operation under general anesthesia. A tag of omentum was seen to herniate through anterior rectus sheath and skin (Fig-II). The protruding tag of omentum (sent for histopathological examination and confirmed) was excised and a double breasting of rectus sheath was done, keeping a drain which was removed after 48 hours. Her subsequent recovery was uneventful. She came for check up after 6 weeks, when no abnormality was detected.
Discussion
A review of literature has failed to demonstrate the type of complication mentioned above . Intra operative complication like dense intra abdominal adhesion resulting in injury to the bladder and the bowel is not uncommon8. Probably this case report presents an unusual complication for the first time. Probable explanation is that during too much dissection of anterior rectus sheath (to get access to the fallopian tubes) which was firmly adherent with uterus, there was inadvertent injury to the anterior rectus sheath and skin through which omentum had protruded.
COMPETING INTERESTS None Declared AUTHOR DETAILS CHANDANA DAS, MBBS, MD , Associate Professor ,Gynaecology & Obstetrics , NRS Medical College. SNEHAMAY CHAUDHURI, MBBS, MD, DNB , Assistant Professor, Gynaecology & Obstetrics, NRS Medical College. CORRESPONDENCE: DR SNEHAMAY CHAUDHURI, Sopan Kutir , Flat No 1G, 53 B Dr S C Banerjee Road , Kolkata -700010, West Bengal, India Email: snehamay_chaudhuri_dr@yahoo.com
References
Arjun G Caesarean section: evaluation, guidelines and recommendations Indian Journal of Medical Ethics available at www.ijme.in/163co117.html accessed on 29/09/2008
Taylor MK, Simpson JM, Roberts CL,Olive EC, Handerson- Smart D J Risk of complications in a second pregnancy following caesarean section in the first pregnancy: a population-based study MJA 2005; 183 (10): 515-519
Gregory KD, Korst LM, Cane P, et al. Vaginal birth after cesarean and uterine rupture rates in California. Obstet Gynecol 1999; 94: 985-989.
Lydon-Rochelle M, Holt VL, Easterling TR, Martin D. First-birth cesarean and placental abruption or previa at second birth. Obstet Gynecol 2001; 97: 765-769.
Crane JM, Van den Hof MC, Dodds L, et al. Maternal complications with placenta previa. Am J Perinatol 2000; 17: 101-105.
Smith GCS, Pell JP, Dobbie R. Caesarean section and risk of unexplained stillbirth in subsequent pregnancy. Lancet 2003; 362: 1779-1784.
Smith GCS, Pell JP, Cameron AD, Dobbie R. Risk of perinatal death associated with labour after previous cesarean delivery in uncomplicated term pregnancies. JAMA 2002; 287: 2684-2690
Sobande A, Eskander M. Multiple Repeat Caesarean Sections: Complications and Outcomes. J Obstet Gynaecol Can 2006;28(3):193–197
An 82 year old lady, who had suffered multiple strokes in the past and was currently on long term percutaneous endoscopic gastrostomy( PEG) feeding, was admitted as an emergency from a nursing home with a two week history of productive cough and fever. She had been on PEG feeding since her first stroke six years previously. The first PEG tube (placed in 2001) subsequently fell out of position, and a second tube (15 French Frecka PEG tube) was inserted in 2003.
On admission, she was pyrexial, dehydrated, and hypoxic on room air. Chest examination revealed bilateral crackles and neurological examination revealed expressive dysphasia, and spastic weakness in both lower limbs. Abdominal examination revealed an inflamed PEG site with purulent discharge. Blood tests revealed raised inflammatory markers with neutrophilia (WBC 20 x 109 /L with a neutrophil count of 12 x 109/L) and a raised C-reactive protein at 193 mg/L.
She was managed with intravenous fluids and antimicrobial therapy (tazocin and metronidazole) for possible aspiration pneumonia. Vancomycin was subsequently commenced as methicillin resistant staphylococcus aureus (MRSA) was isolated from the PEG site. As she remained stable, PEG feeding was recommenced.
A week following her admission she became unwell with an episode of vomiting and choking following PEG feeding. This was associated with difficulty in infusing feeds and medications through the PEG tube. Multiple flushes through the tube were unsuccessful. The tube was found to be persistently blocked and lacked free mobility within the tract.
Urgent upper gastro intestinal endoscopy revealed a buried bumper as the cause of blockage of the PEG tube. This necessitated insertion of a new PEG tube (9 French Frecka) for enteral feeding. The old PEG tube was removed surgically under local anaesthesia in due course. As the removal of the buried bumper was found to be very difficult endoscopically, and surgical intervention was deemed to be inadvisable in view of co morbidities, the bumper was left in situ. Feeding was recommenced through a new tube. In view of persistent discharge through the PEG site, abdominal ultrasound examination was performed, revealing a possible gastro-cutaneous fistula. No local collection was seen around the PEG wound.
As the patient remained clinically stable, she was discharged home with necessary instructions to her carers for regular flushing of the PEG tube with water, before and after each feed, to prevent further blockages.
Fig 1: Buried bumper (stomach-lower body)
Fig 2: New peg and buried bumper
Discussion
PEG is primarily used for long term (longer than 6 weeks) enteral alimentation for patients with impaired swallowing (e.g. from stroke, degenerative neurological disease, head injury, and oropharyngeal malignancy). However numerous complications have been reported since its introduction in 1980.
Buried bumper syndrome (BBS) is an uncommon but well documented complication of PEG insertion, first described in 1988 1. It is usually a late complication occurring up to 3 years post PEG insertion and reported to occur in 0.3-2.4 % of patients2.
The internal bumper of the PEG tube should normally sit snugly against the anterior gastric wall, and this is confirmed endoscopically at the time of initial placement. BBS develops when there is migration of the internal bumper/flange through or into the anterior abdominal wall. This probably occurs as a result of excessive tension between the internal and external bumpers, from over-tightening of the external flange, leading to gastric wall erosion. During migration it becomes lodged along the gastrostomy tube tract between the gastric and abdominal walls. Once epithelialisation occurs the bumper gets covered with gastric mucosa3.
The diagnosis of BBS should be suspected if localised abdominal pain, peri-tubal leakage or inability to infuse feed occurs. Initial measures to deal with a blocked tube include flushing with warmed water, and occasionally passage of a flexible wire through the lumen, in order to unblock any obstruction. Tube obstruction is usually related to the administration of protein-enriched formulae or medications, especially if the tube size is 9 French. Fungal colonisation may also lead to tube blockage, requiring specific solutions for flushing the tube4. Tube exchange should only be considered if the gastrocutaneous tract is mature (6 weeks or longer after placement of the tube).
Endoscopy is confirmatory in cases of BBS. The internal bumper is not seen, and the site of the PEG is indicated by an elevated area of submucosa with a central depression. Failure to recognise BBS can result in gastric perforation and gastrointestinal haemorrhage or intra abdominal sepsis, peritonitis and even death5.
Ideally, the buried bumper should be removed even if the patient is asymptomatic, to avoid potential complications from continued tube migration until it is completely impacted in the abdominal wall. The literature describes various methods of dealing with this complication. Endoscopic ultrasound of the gastric wall with a catheter US probe can facilitate the localisation of the bumper and also provides information regarding feasibility of surgical or endoscopic removal of PEG tube6.
Regular and optimal PEG care has been vital in identifying and prevention of this complication. During daily cleaning of the external PEG site, the PEG should be pushed in approximately 1 cm and rotated prior to repositioning of the external bumper. The length of the tube outside the abdominal wall should be examined at regular intervals so that migration can be recognised5.
This report reinforces the fact that physicians should be aware of this recognised risk of PEG feeding and prompt referral for endoscopy is necessary to avoid serious consequences including gastro-intestinal bleeding, peritonitis and death. Similarly specific instructions should be given to carers for prevention of BBS.
COMPETING INTERESTS None Declared AUTHOR DETAILS VIJAY JOSHI, Trust registrar in integrated medicine, Chase Farm Hospital, Enfield, UK ASHIS BANERJEE, Consultant in emergency medicine, Chase Farm Hospital, Enfield, UK CORRESPONDENCE: MR ASHIS BANERJEE, Consultant/honorary senior lecturer in emergency medicine, Chase Farm Hospital, The Ridgeway, Enfield EN2 8JL United Kingdom E-mail: libra19542003@yahoo.co.uk
References
Shallman RW, Norfleet RG, Hardache JM. Percutaneous endoscopic gastrostomy feeding tube migration and impaction in the abdominal wall. Gastrointest Endosc 1988; 34: 367–68.
Venu RP, Brown RD. Pastika BJ Erickson LW. The buried bumper syndrome: a simple management approach in two patients. Gastrointest Endosc 2002; 56: 582–84.
Anagnostopoulos GK, Kostopoulos P, Arvanitidis DM. Buried Bumper Syndrome with a fatal outcome, presenting early as gastrointestinal bleeding after percutaneous endoscopic gastrostomy placement. J Postgrad Med 2003; 49:325–27
Iber, FL, Lusak, A, Patel, M Importance of fungus colonization in failure of silicone rubber percutaneous gastrostomy tubes (PEGs) Dig Dis Sci, 1996, 41: 226-231
Braden B, Brandstaetter M, Caspary WF, Seifert H. Buried bumper syndrome: treatment guided by catheter probe US. Gastrointest Endosc 2003;57:747-51
Ma MM, Semalacher EA, Fedorak RN, Llor EA, Duerksen DR et al The buried gastrostomy bumper syndrome: prevention and endoscopic approaches to removal. Gastrointest Endosc 1995 ; 41:505-8
The acquired immunodeficiency syndrome (AIDS) was first recognized among homosexual men in the United States in 19811,2. While initially limited, infection with the human immunodeficiency virus (HIV) has immensely increased over the past two decades to become the biggest epidemic of the twentieth century. However, we have witnessed dramatic improvement in prevention of disease progression and long-term survival in the era of Highly Active Anti Retroviral Therapy (HAART).
Apart from biological factors associated with the virus and host which play a role in the transmission and progression of HIV infection, several demographic and social variables have been studied and described in different studies worldwide. Understanding the variety of non-biological factors and behavioral patterns which can affect care and prognosis of HIV patients gives us the opportunity to design non-pharmacological interventions and where possible, to facilitate better care for our HIV positive population.
BACKGROUND:
J.E. Wood clinic of Pennsylvania Hospital in Philadelphia is a teaching outpatient care facility where Internal Medicine residents of Pennsylvania Hospital acquire their ambulatory care experience under supervision of teaching attendings. We have once a week clinic sessions dedicated to the care and follow-up of HIV/AIDS patients under close supervision of Infectious Disease specialists. Our patients have diverse socio-economic, educational and stages of HIV infection.
OBJECTIVE:
We aimed at finding out basic understanding of HIV infection, degree of awareness regarding the ongoing treatment and reasons behind irregular follow-up visits of our HIV patients who attend J.E. Wood outpatient clinic of Pennsylvania Hospital, Philadelphia for treatment of HIV/AIDS.
PARTICIPANTS AND METHODS:
In order to collect relevant information from our patients, a two paged, anonymous, study questionnaire was given to all patients who attended the clinic during January 2007 to December 2007. The questionnaire looked into three different areas of patient related factors which can influence the disease outcome: demographic and social information (Age, Sex, level of education), patients’ knowledge about their HIV disease (source of the infection, duration of HAART, individual recent CD4 count, names of current medications, duration of therapy, medication side-effects) and their behavior (sexual precautions, reasons for medication and follow-up non-compliance). Out of the 75 patients who were given the questionnaire, 7 questionnaires were rejected from the study because of the information received was incomplete, illegible or not related to the questions. 68 completed questionnaires were evaluated and comparative data was tallied using Microsoft excel sheet. We also reviewed relevant literature in pubmed to understand our findings in the light of previous studies related to demographic, socio-economic and psychological aspects of HIV treatment.
RESULTS:
We analyzed the information which was obtained from 68 patients by means of the questionnaire. Our patients consisted of 35 male, 33 female (Table 1). We had a wide range of patients regarding distribution of their age as shown in Table 2 below. Significant numbers of our patients (36%) were diagnosed with HIV for >10 years ago and more than 60% had the diagnosis at least for 5 years (Table 3)
Table 1: Socio-demographic characteristics of patients (n=68)
Variables
Percentage
Gender
Male
51.5%
Female
48.5%
Education
<High school
34%
High school graduate
50%
>High school
16%
Table 2: Age distribution of patients (n=68)
Age group
Percentage
Upto 30 years
19%
31 to 40 years
22%
41 to 50 years
37%
51 to 60 years
18%
61 years and above
4%
Table 3: Duration of diagnosis (in years)
Duration of
diagnosis (years)
Percentage of
total patients (n=68)
Unknown
3%
< 5
36%
>5 to 10
25%
>10
36%
Half of our patients (n= 68) completed high school education or equivalent. About 34% quit education before attaining high school diploma. Roughly, 10% of our patients went to college for further education and 6% acquired some vocational training after high school.
We tried to establish the level of our patients’ participation in their treatment by gathering information through the questionnaire whether they could recall the names of their HIV medicines and the last CD4 count. We found that 74% of our patients, who are on HIV medicines, could recall the names of their medicines but only about 45% of our patients remembered their last CD4 count. Our patients who had completed high school education or equivalent were 2.5 times more likely to remember the names of their HIV medications(95 % confidence interval CI=1.42 to 4.98) and 1.75 times more likely to remember their last CD4 count(95 % confidence interval CI=1.12 to 4.38).
We asked our patients whether they knew that HIV medications need to be taken life long and we also enquired about their knowledge about their safe sexual practices. Only 48% patients of our study group knew that HIV medicines are for life. About 50% of all our patients mentioned that they ensure use of condom during sexual activity and another 40% claimed they practice sexual abstinence. Women patients in our practice were 2.0 times more likely to practice use protective measures during sexual activity (95 % confidence interval CI=1.22 to 4.67).
In our study, only 32 patients (47%) attempted to answer the question where we asked about reason behind not turning up for their follow up appointments as scheduled. Eight patients could not specify a cause, 7 mentioned transport related problems and 2 had insurance issues. Five patients thought their appointments were too often whereas 3 just forget to keep the appointment. Although we did not specifically ask questions on psychological state of our patients, 7 out of the 32 patients mentioned significant psychological problems in their daily life as the reason for non-adherence to medication or follow-up appointments. The responses included responses like “still dealing with the diagnosis mentally”, “feel lack of energy in life”, “life seems to have too many problems”, “been drinking heavy lately” etc.
DISCUSSION:
Interestingly, our small patient cohort roughly reflects the sex ratio of HIV patients globally in 2007 as published by World Health Organization (WHO). In our study the ratio was Male : Female = 51.5% : 48.5% and in the WHO worldwide survey it was 50% : 50%; At the end of 2007, estimated total global HIV positive adults = 33 million (30million – 36 million) 3.
Rates of progression of HIV disease appear to be similar by sex and race category if adjusted for the quality of care 4, 5. Multiple studies on chronic disease management showed that patients’ level of education and health literacy has direct influence on the treatment compliance. Moreover, limited health literacy is thought to be a strong contributing factor to racial disparities in health care. A study was published in 2007 which examined the mediating effect of limited health literacy on the relationship between race and HIV-medication adherence. For the study, a total of 204 patients infected with HIV were recruited and structured in-person interviews were conducted to obtain information. In an adjusted analysis that excluded literacy, African Americans were 2.40 times more likely to be non-adherent to their HIV-medication regimen than whites (95% confidence interval [CI]=1.14-5.08). When literacy was included in the final model, the effect estimates of race diminished from 25% to insignificant level. Therefore, health care providers need to consider the potential utility of responding to literacy and communication barriers in health care as part of interventions to reduce racial disparities 6. In our study, we found that patients who had completed high school education or equivalent were more conscientious regarding their HIV care as demonstrated by the fact that they were more likely to remember their last CD4 count and current HIV medications.
Multiple studies have demonstrated that increasing age at the time of HIV infection is associated with more rapid progression to AIDS in the absence of antiretroviral therapy. In one series, for example, the median time from seroconversion to AIDS without therapy was 15 years for patients aged 16 to 24 years at seroconversion, compared to 6 years for those 35 years or older at seroconversion 7. In our study, it is notable that 36% of patients were diagnosed with HIV >10 years ago and more than 60% had the diagnosis at least for 5 years. The reason behind the high survival rate is clearly attributable to HAART. Fifty-four patients out of the 68 are currently on HAART and 25 of them are on it for more than last 5 years.
Patients' knowledge of their HIV condition and its treatment has been recognized as a factor that influences adherence to antiretroviral therapy. Patients’ knowledge & perception of the disease and participation in the treatment can be improved through targeted educational programs and support groups. One study done in Nigeria found that individuals living with HIV/AIDS who belonged to a support group and had availed themselves of relevant literature were more knowledgeable and positive about their illness than those who did not belong to support groups. The study concluded that HIV/AIDS support group membership is an important component of psycho-social care in HIV/AIDS patients 8. Another study done in France showed that an educational intervention improves adherence to antiretroviral regimens and health status and suggests that it should be initiated early in therapy 9. Communicating with patients about adherence issues is important issue, although this may not have an immediate impact on patients' behaviors. Health care professionals should play a pro-active role in this regard. The use of multi-disciplinary adherence teams to ensure that each HIV-positive patient receives the optimal amount of information and support for adherence is a practical approach. Health literacy should be provided in the context of different ethnicity, culturally sensitivity and individual needs associated with HIV, like any other chronic diseases. Epidemiological researches have shown that injection drug abusers and younger patients tend to have worse compliance, as well as subjects with depression and lack of self-perceived social support 10. Therefore, special care should be taken by health care providers to ensure treatment compliance and health literacy in these patients. In our J.E. Wood clinic, we have dedicated psychologist and social worker to for care of our HIV patients.
Psychological impact associated with treatment of any chronic illness is often neglected in clinical practice but indeed carries a huge significance in terms of long-term treatment compliance and outcome. We identified 7 of our patients who clearly expressed psychological issues related to their HIV infection and it was evident enough that those psychological problems were adversely affecting their treatment compliance. Formal and regular counseling sessions should be arranged for HIV/AIDS patients to promptly identify and manage any psychological or psychiatric disturbance that HIV patients might suffer from. We know that presence of a preexisting psychiatric disorder can increase the risk of HIV acquisition and can also complicate HIV treatment. Moreover, HIV infection can produce a number of psychiatric conditions and exacerbate many others; there is an intense co-morbidity and linkage between HIV and various types of psychiatric conditions. Personality disorders are more prevalent among HIV-infected (19 to 36 percent) and HIV at-risk (15 to 20 percent) individuals 11, 12 than the general population (10 percent). Antisocial personality disorder (ASPD) is the most common personality disorder among HIV infected individuals, and has been shown to significantly increase risk of HIV infection 13. Successful treatment can be achieved with even the most difficult patients by applying a comprehensive diagnostic formulation that includes psychiatric disease syndromes such as major depression, personality vulnerabilities, behavioral disorders such as addiction, and problems of life experiences such as trauma. With regards to anti-retroviral treatment of HIV positive or AIDS patients, nearly perfect compliance seems to be indispensable to obtain the maximum benefit from HAART. There is a clear relation between high adherence levels and virologic success. We reviewed relevant published literatures to understand the adverse effects and possible interventions of psychological problems in HIV patients. A prospective, randomized, two-arm controlled study was published in 2000 which included 116 patients starting their first-or second-line HAART who were randomized to receive psychoeducative intervention to implement adherence (experimental group [EG]) or a usual medical follow-up (control group [CG]). The study showed that specific and maintained psychoeducative interventions based on excellence on clinical practice are useful to keep high levels of adherence and therefore, high levels of viral suppression 14.
CONCLUSION:
Human Immunodeficiency Virus infection is one of the most serious disease entities in our modern time. We have witnessed dramatic improvement of long-term survival rate of HIV positive patients due to use of HAART in clinical practice. By identifying the demographic, socio-economic, behavioral and psychological variables which significantly influence patients’ adherence to treatment and understanding of the disease process, we can further improve treatment compliance and the long term prognosis of our HIV patients. These factors may not have very significant role individually, but collectively can dictate the course of success of HAART treatment in patients. Increasing awareness of these factors by practitioners caring for HIV-infected persons, recognizing and potentially treating some of them, should indirectly improve the effectiveness of antiretroviral therapy.
COMPETING INTERESTS None Declared AUTHOR DETAILS SUBHASISH BOSE, M.B.B.S., M.R.C.P, PGY1 in Internal Medicine, Pennsylvania Hospital, Philadelphia, USA. AJAY VARANASI, M.B.B.S.; PGY3 in Internal Medicine, Pennsylvania Hospital, Philadelphia, USA. GYI MO, M.B.B.S., M.P.H.; Director of J.E. Wood clinic, Pennsylvania Hospital, Philadelphia, USA. CORRESPONDENCE: DR SUBHASISH BOSE, Apartment 601, 269 South Ninth Street, Philadelphia, PA-19107, USA. Email: kumub@yahoo.com
Kaposi's sarcoma and Pneumocystis pneumonia among homosexual men--New York City and California. MMWR Morb Mortal Wkly Rep 1981; 30:305.
Status of the global HIV epidemic. http://data.unaids.org/pub/GlobalReport/2008/jc1510_2008_global_report_pp29_62_en.pdf. Accessed January 31, 2009.
Collaborative Group on AIDS Incubation and HIV Survival including the CASCADE EU Concerted Action. Time from HIV-1 seroconversion to AIDS and death before widespread use of highly-active antiretroviral therapy: a collaborative re-analysis. Lancet. 2000 Apr 1; 355(9210):1131-7.
Altisent, C, Montoro, JB, Ruiz, I, Lorenzo, JI. Long-term survivors and progression of human immunodeficiency virus infection. N Engl J Med 1996; 334:1065.
Osborn CY, Paasche-Orlow MK, Davis TC, Wolf MS. Health literacy: an overlooked factor in understanding HIV health disparities. Am J Prev Med. 2007 Nov; 33(5):374-8.
Mariotto, AB, Mariotti, S, Pezzotti, P, et al. Estimation of the acquired immunodeficiency syndrome incubation period in intravenous drug users. Am J Epidemiol 1992; 135():428.
Olley BO. The role of support group and duration of infection in HIV/AIDS patients' knowledge and attitudes to their illness. Afr J Med Med Sci. 2007 Mar; 36(1):11-6.
Goujard C, Bernard N, Sohier N, Peyramond D, Lançon F, Chwalow J, Arnould B, Delfraissy JF. Impact of a patient education program on adherence to HIV medication: a randomized clinical trial. J Acquir Immune Defic Syndr. 2003 Oct 1; 34(2):191-4.
Gordillo V, del Amo J, Soriano V, González-Lahoz J. Sociodemographic and psychological variables influencing adherence to antiretroviral therapy. AIDS. 1999 Sep 10; 13(13):1763-9.
Sher, KJ, Trull, TJ. Substance use disorder and personality disorder. Curr Psychiatry Rep 2002; 4:25.
Jacobsberg, L, Frances, A, Perry, S. Axis II diagnoses among volunteers for HIV testing and counseling. Am J Psychiatry. 1995; 152:1222.
Perkins, DO, Davidson, EJ, Leserman, J, et al. Personality disorder in patients infected with HIV: a controlled study with implications for clinical care. Am J Psychiatry. 1993; 150:309.
Tuldrà A, Fumaz CR, Ferrer MJ, Bayés R, Arnó A, Balagué M, Bonjoch A, Jou A, Negredo E, Paredes R, Ruiz L, Romeu J, Sirera G, Tural C, Burger D, Clotet B. Prospective randomized two-Arm controlled study to determine the efficacy of a specific intervention to improve long-term adherence to highly active antiretroviral therapy. J Acquired Immune Deficiency Syndrome. 2000; 25(3):221-8.
The significance of disturbed subjective sleep quality in the general population is important because of high prevalence rates (of up to 30%)1 and the association with decreased quality of life.2 Poor sleep affects cognitive and physical functioning, and insomnia is associated with a greater risk of falls and accidents,3 higher rates of absenteeism4 and increased health care utilization.4
Insomnia is commonly encountered in primary and secondary care settings, and can be symptomatic of many medical, neurological, substance abuse or primary sleep disorders.
Epidemiological and clinic-based studies consistently demonstrate high rates of psychiatric comorbidity.5,6 Sleep disturbance is an important clinical construct in psychiatry. It represents formal diagnostic criterion in mental illnesses such as affective and anxiety disorders.7,8
Insomnia is broadly defined as the subjective experience of poor or unrefreshing sleep, with some objective evidence of reduced time asleep or delayed sleep-onset. The subjective nature of such complaints remains key, because sleeping is a private event, and there is often no informant history. Furthermore, it is the perceptual aspects of sleep that influence patients’ help-seeking behaviour, such as consultation requests, demands for night sedation, and medication and substance use. It is noteworthy that despite the wide-ranging implications and subjectively distressing nature of this phenomenon, it remains arguably one of the least satisfying symptoms to treat. Seeking a better understanding of the extent and nature of patients’ sleep perception can help optimise appropriate therapeutic strategies.
This is the first study assessing the subjective sleep quality of a sample of psychiatric disordered in-patients in a UK psychiatric hospital setting, using the Pittsburgh Sleep Quality Index (PSQI).9 This study is framed in the context of increasing the awareness of the significance of patients’ complaints of insomnia and addressing the wider psychosocial issues that this raises.
Method
Design: This was a cross-sectional survey of the self-reported quality of sleep in a population of psychiatric in-patients on the acute adult wards of a London psychiatric hospital.
Participants and Procedure:Participants consisted of psychiatric in-patients (ages 18-65) on all five of the acute adult open psychiatric wards of the Highgate Mental Health Centre, London, currently admitted for the assessment or treatment of mental illness. Financial compensation was not provided for any subject.
Subjects were approached on the ward by a member of nursing staff and asked if they were interested in participating in a study about sleep. The researcher was then introduced to explain further details with the aid of the participant information sheet. After a minimum of 24 hours, patients were approached again by the researcher and asked if they were willing to participate. Recruitment of subjects took place if the patient was agreeable to take part and did not meet any of the exclusion criteria (listed below). A scheduled time and date was made with participants in order to obtain written informed consent and to administer the questionnaire. Questionnaire data was collected from each subject by the researcher in a private interview room located on the patient’s psychiatric ward. Demographic and clinical data required from the patient’s medical notes was recorded on the day of sampling. Exclusion criteria were: the presence of severely disturbed behaviour, or having received rapid tranquilisation for such behaviour on the day of sampling; a significant impairment in physical condition (e.g. infection, trauma); a history of a sleep disorder (e.g. obstructive sleep apnoea); the presence of organic illness including dementia; and lack of capacity to give informed consent.
Quality of Sleep:Subjects' quality of sleep was assessed by the administration of the Pittsburgh Sleep Quality Index (PSQI).9 This is one of the most widely used questionnaires employing standardised measures to assess subjective sleep quality in clinical and research settings. It assesses sleep quality and disturbances over a 1-month time interval. 19 individual items are used to generate 7 component scores (with a range of possible subscale scores from 0 to 3): 1) overall subjective sleep quality; 2) sleep latency; 3) sleep duration; 4) habitual sleep efficiency; 5) sleep disturbances 6) use of hypnotic or sedative medication; 7) daytime dysfunction. Higher scores indicate greater sleep disturbances. The sum of the component scores yields a global score (ranging from 0 to 21), which was used as the primary outcome measure in this study. A global PSQI score cut off score of 5 discriminates between good and bad sleepers and the PSQI gives acceptable measures of internal homogeneity, consistency (test-retest reliability) and validity.9,10
Other Variables:Demographic and clinical data recorded concurrently from participant's medical notes included: sex (male/female); age (years); ethnicity (Asian/Black/Mixed//Other); body mass index (BMI) (calculated as the ratio between weight [kilograms] and squared height [metres]); primary psychiatric diagnosis (based on ICD-10 criteria); duration of psychiatric illness (years); past medical history; number of currently prescribed medications; length of admission to date (days); current admission status (informal/detained under Section 2 of the Mental Health Act (MHA) (1983) (this is for a maximum period of 28 days for further assessment)/detained under Section 3 MHA (1983) (this is for a maximum period of 6 months for psychiatric treatment). A further category (detained under another type of section) was dropped as this did not apply to any of the subjects.
Ethics Committee Approval:Ethical and research governance authorisations were granted from Camden and Islington Community Local Research Ethics Committee, and from the North Central London Research Consortium, respectively.
Statistical Analysis:The aim was to compare clinical, demographic and PSQI data between the poor sleepers and good sleepers. The prevalence (%) of poor sleep was determined by the proportion of subjects with global PSQI score of 5 or more. Statistical analyses were predominantly performed using the software package Stata, version 9.2.
Results
Sample Characteristics
77 patients were initially identified as potentially eligible subjects. Of these, 31 (40%) were excluded due to: the presence of disturbed behaviour (n=1); inability to give informed consent (n=9); unwillingness to participate (n=19); absence from ward (either on leave or absent without leave) (n=2).
This left a total of 46 patients who were enrolled in to the study. Subject characteristics are given in Table 1. Table 1: Demographic and clinical characteristics of study subjects
Sex, n (%)
Male
24 (52)
Female
22 (48)
Ethnicity, n (%)
Asian
1 (2)
Black
9 (20)
Mixed
1 (2)
Other
1 (2)
White
34 (74)
Current Admission Status, n (%)
Detained under Section 3 MHA
22 (48)
Detained under Section 2 MHA
5 (11)
Informal
19 (41)
Age, years: mean (s.d.)
38 (11.1)
Range
18-62
Body Mass Index, kg/m²: mean (s.d.)
25.99 (4.96)
Range
17.9-41.5
Duration of mental illness, years: mean (s.d.)
10.51 (7.93)
Range
0.17-30
Length of admission, days: mean (s.d.)
42.43 (63.21)
Range
2-366
Prescribed regular medications, mean (s.d.)
1.83 (1.05)
Range
0-5
Medical comorbidities, mean (s.d.)
0.59 (0.98)
Range
0-3
s.d.: standard deviation
As defined by ICD-10 criteria, the most common subdivisions of patients’ psychiatric diagnoses in descending order were: paranoid schizophrenia, F20.0, (n=16); emotionally unstable personality disorder, F60.3, (n=6); depressive disorder, F32, (n=6); bipolar affective disorder, F31 (n=5). Other subdivisions of subjects’ diagnoses included: organic mood disorder, F06.3 (n=1); organic personality disorder, F07, (n=1); residual and late onset psychotic disorder due to alcohol use, F10.7, (n=1); persistent delusional disorder, F22, (n=1); acute and transient psychotic disorder, F23, (n=1); unspecified non-organic psychosis, F29, (n=1); post traumatic stress disorder, F43.1, (n=1). One patient was undergoing psychiatric evaluation and therefore had no formal diagnosis.
Medications prescribed regularly were: antipsychotics (for 40% of the total sample of patients), mood stabilizers (16%), antidepressants (14%) and benzodiazepines (7%). In terms of regular night time sedation, two patients out of a total of 46 were prescribed zopiclone and diazepam respectively. Zopiclone was prescribed on an “as required” basis for 15 patients (33% of the total sample).
Overall sleep quality evaluated by the PSQI revealed a mean score of 9.74 (standard deviation= 5.11). Poor sleep quality (defined as a global PSQI score of 5 or more) was present in 36 out of the total of 46 subjects (78% of the sample).
Comparison between good and poor sleepers
Comparison of numerical measurements between the two sleep groups is presented in Table 2. For the normally distributed variables the figures reported for each group are the mean (standard deviation) and the p-value from the t-test. For the non-normally distributed variables the figures reported are the median (inter-quartile range) and the p-value from the Mann-Whitney test.
Table 2: Comparison of demographic and clinical data between good and poor sleepers.
(*) Median (Inter-quartile range) reported. Analysis performed using Mann-Whitney test
The results indicate that there was no strong evidence of a statistically significant difference between good and poor sleepers for any of the variables examined. However, there was a possible difference for duration of admission, although this result was only of borderline statistical significance (p=0.06). The results indicate a median duration of admission of 44 days for good sleepers and 15 days for poor sleepers.
The difference between sleep groups for the categorical variables was examined using Fisher’s exact test. Results, presented in Table 3, show the number (and percentage) of subjects falling into each category, with the p-value indicating the significance of the results.
Table 3: Comparison of categorical data between good and poor sleepers
Variable
Group
Good sleepers
(total PSQI <5)
N (%)
Poor sleepers
(total PSQI ≥5)
N (%)
P-value
Sex
Female
3 (30%)
19 (53%)
0.29
Male
7 (70%)
17 (47%)
Admission status
Section 3
9 (90%)
18 (50%)
0.01
Section 2
0 (0%)
5 (14%)
Informal
1 (10%)
13 (36%)
Physical
comorbidities
None
7 (70%)
24 (67%)
1.00
1+
3 (30%)
12 (33%)
There was a significant difference between sleep groups with regard to their admission status. Almost all (90%) of the good sleepers were detained under Section 3 MHA (1983), whilst this applied to only half of those in the poor sleepers group. Being detained under Section 2 MHA and informal admission were more commonly found amongst those categorised as poor sleepers.
There was no significant difference between groups in terms of sex or the presence of physical comorbidities.
The final set of analyses compared the differences between groups for the PSQI measures, and the results are summarised in Table 4. The figures reported are the mean (standard deviation) score for each group. For the individual components the Mann-Whitney test was used to compare between groups, and the p-values from this analysis are reported. For the PSQI total score, the unequal variance t-test was used to compare between groups.
Table 4: Comparison of PSQI measures between the good and poor sleepers
Good sleepers
(total PSQI <5)
Mean (SD)
Poor sleepers
(total PSQI ≥5)
Mean (SD)
P-value
PSQI C1 score (quality) (*)
0.2 (0.84)
1.6 (0.9)
<0.001
PSQI C2 score (latency) (*)
0.9 (1.0)
1.8 (1.0)
0.02
PSQI C3 score (duration) (*)
0.1 (0.3)
1.7 (1.3)
0.002
PSQI C4 score (efficiency) (*)
0.1 (0.3)
1.7 (1.3)
0.001
PSQI C5 score (disturbances) (*)
0.7 (0.5)
1.4 (0.6)
0.003
PSQI C6 score (sedatives) (*)
0.4 (1.0)
1.5 (1.4)
0.04
PSQI C7 score (daytime dysfunction) (*)
0.7 (0.9)
2.1 (0.8)
0.004
PSQI total
3.1 (1.3)
11.6 (4.1)
<0.001
(*) Analysis performed using Mann-Whitney test
There was a statistically significant difference between good and poor sleepers for all PSQI components and for the PSQI total. The PSQI component values and PSQI total scores for poor sleepers were significantly higher than for good sleepers.
A profile of the mean PSQI individual component scores between the two groups (good sleepers versus poor sleepers) is displayed in Figure 1.
Figure 1: Mean component PSQI scores of good and bad sleepers Profiles of the PSQI represent group differences of individual component scores. Mann-Whitney test, *p<0.05).
Subjective Patient Comments
The PSQI also comprises an open ended question, providing subjects with the opportunity to cite “other” (subjective) reasons for difficult sleep. The most common response was anxiety (n=8). Other examples included: medication alterations (n=3); environmental noise (n=2); “thinking excessively” (n=1); “a desire to be creative” (n=1); hard mattress (n=1); “food eaten” (n=1); “sedentary lifestyle” (n=1); alcohol (n=1); hunger (n=1); asthma (n=1); symptoms of the menopause (n=1); and “voices”(n=1).
Discussion
Main Results
This is the first study to examine the subjective quality of sleep among a population of psychiatric in-patients in the UK. The prevalence of poor sleep, as defined by a cut off PSQI score of 5 or more, was present in 78% of the patients sampled. Patients detained under Section 3 MHA (1983) were more likely to report sleeping well when compared to informal patients or those detained under section 2 MHA (1983). There was some evidence of good subjective sleep quality being related to a longer duration of admission, but this requires further investigation.
There were no significant differences between good and poor sleepers for any of the other demographic and clinical variables studied, including age, body mass index, duration of psychiatric illness, number of prescribed medications, sex, and physical comorbidities.
Individual PSQI component scores and global scores were significantly lower for good sleepers compared to poor sleepers. This would be expected given that higher scores indicate more severe sleep complaints, and this supports the consistency of the PSQI as a research instrument.
Factors Affecting Sleep
In-patients’ disturbed sleep may be caused by a variety of exogenous factors such as unfamiliar surroundings, environmental noise, bright lighting and staff interactions or monitoring. Physical and psychological factors, such as the side-effects of medication and substance use, may also have a detrimental effect on sleep quality. In the added presence of a psychiatric disorder, each of these factors may act synergistically on the relationship between mental illness and sleep. Despite substantial research supporting the robust associations between insomnia and comorbid conditions, specific mechanisms linking sleep, medical and psychiatric factors have not been well established.
Sleep complaints may represent early symptoms and risk factors for new episodes of mental illness rather than simply representing phenomena secondary to experience of mental illness. For example, longitudinal studies have found insomnia to be a substantial risk factor for the development of a depressive disorder5,11,12 and the risk for developing new anxiety disorders and alcohol abuse is also greater for insomniacs.6
Stepanski & Rybarczyk13 present research arguing against the more traditional conceptualisation of insomnia as simply a consequence of another disorder. They propose the need for a revised model to understand insomnia that is comorbid with medical and/or psychiatric illness. Abnormalities of the hypothalamic-pituitary-adrenal (HPA) axis may represent the underlying pathophysiological process in many chronic insomnia patients.14 This may signify a common risk factor for insomnia and depression, thus predisposing the individual to a vulnerability to both conditions.15
In this study, detained patients (under Section 3 MHA (1983)) were significantly more likely to be classified as good sleepers. A suggestion for this finding could be that these patients may be less resisting of remaining and sleeping on the ward due to the involuntary nature of their admission. Alternatively these patients may represent the group with the most severe mental illnesses and with the least insight, and therefore less able to accurately recall their (poor) sleeping habits over the previous month.
There was also a potential association between longer admission status and better sleep quality. Explanations for this observation might include: patients’ acceptance over time of their admission and the consequent conditioning to, and familiarisation with, the ward environment; achievement of stability in mental state over time; or the adaptation of the perception of sleep quality to the sleep disturbances that accompany mental illness.
Limitations
This study is based on cross-sectional data and the relationship between the course of mental illness and sleep perception cannot be determined. In order to verify the direction of causality, it is necessary to demonstrate longitudinally that improvement in symptom severity is accompanied by an increase in subjective sleep quality.
This study was not designed to look at the prevalence of poor sleep across the different classes of psychiatric illnesses and dual diagnoses were not considered. It did not measure psychopathology or self-reported psychological distress. Possible confounding factors were not taken in to account, such as concurrent use of caffeine, alcohol, nicotine, illicit substances, hypnotics or other medications known to affect sleep.
The PSQI measures sleep quality averaged over the previous month. In cases where patients had only very recently been admitted to hospital, measurements would have been unlikely to accurately reflect the perspective of an in-patient’s experience. The mean length of admission for this population however was longer than one month (42 days).
These results were drawn from a small sample, with a fairly high proportion of excluded patients (40%). This may explain why this study did not identify factors previously found to more frequently affect sleep adversely such as female gender, the elderly and those with chronic medical conditions.16 In addition the population sample has little ethnic diversity which limits the generalisability of the results.
Implications
This study found that the prevalence of poor sleep quality was more common than previously reported in the general population17 and more comparable to the higher rates reported in similar patient populations. Two previous studies investigating subjective sleep quality using the PSQI, found prevalence rates of poor sleepers to be 45.5%18, and 91.22%19 among a population of schizophrenia patients and psychiatric in-patients respectively.
Complaints of poor sleep are important for diagnostic purposes and also raise the need to address the adequacy of therapeutic strategies, given the consequent adverse impact on patients’ mental state, physical health, daytime function and quality of life.
Improving Sleep
Hypnotics such as benzodiazepines and benzodiazepine receptor agonists can be efficacious for the treatment of insomnia.20,21 However the clinical benefits must be weighed against well known adverse effects, such as daytime sedation, agitation, memory impairment, confusion and ataxia. This, together with the recommendation that hypnotics should only be used for short periods of time because of the risk of drug tolerance and dependence,22 highlights the need for suitable non-pharmacological alternatives.
Recent reviews support the notion of the effectiveness of Cognitive Behavioural Therapy for insomnia in the treatment of people with psychiatric or medical conditions.13,23 Modified, lower cost education initiatives to promote good sleep could be employed by utilising the skills of the mental health professionals caring for patients on the ward, supplemented by the provision of clear written material.
Environmental variables to consider include adherence to regular ward routines including bedtime and awakening times, attention to ward layout and design (including the provision individual bedrooms), lighting, ambient noise, temperature, and the provision of comfortable mattresses and appropriate bed linen. Medication scheduling times, regular medication reviews, and avoidance of non-prescribed substances such as caffeine, alcohol and illicit substances are also important. Physical health problems, pain and psychological distress should be optimally managed. Moderate intensity exercise programs have also been found to bring about significant improvements in self-rated sleep quality.24 Finally, increased staff awareness and sensitivity to the sleep problems on the ward, supplemented with objective recording of such disturbances, would be informative in gaining a further understanding of patients’ insomnia experiences.
Future Directions for Research
The PSQI is simple and inexpensive to perform. Results could be followed longitudinally in order to examine the course of sleep problems throughout an episode of acute mental illness, or to examine the effects of specific therapeutic interventions for sleep disorders. Sleep diaries have been shown to provide reliable estimates of subjective sleep parameters25 and could be used as an adjunct to the PSQI. Ideally, concomitant objective measures such as polysomnography or wrist actigraphy (which detects physical motion), as well as cognitive and behavioural measures could be used to provide additional data.
This study represents the first attempt to examine the degree of self-reported poor sleep quality in a UK-based population of psychiatric in-patients and results suggest unsatisfactory sleep is a common finding. Large prospective longitudinal studies of sleep quality with control for confounding factors are needed to confirm the high prevalence rates in psychiatric in-patients. Studies comparing psychiatric patients with healthy controls, and also with insomniacs without psychiatric comorbidity, would further clarify the role of psychopathology in sleep disturbance.
ACKNOWLEDGEMENTS With thanks to Mr Paul Bassett, Statistical Consultant COMPETING INTERESTS None Declared AUTHOR DETAILS LUCINDA DONALDSON, BSc, MB BS, MRCPsych, Specialty Registrar, Barnet, Enfield and Haringey Mental Health Trust, United Kingdom PRAVEEN KUMAR CHINTAPANTI, MB BS, DPM, MRCPsych, Consultant Psychiatrist, Camden and Islington NHS Foundation Trust, United Kingdom CORRESPONDENCE: LUCINDA DONALDSON, Specialty Registrar, South West Complex Mental Health Team, 7th Floor Premier House, 112 Station Road, Edgware, Middlesex HA8 7BJ, United Kingdom Email: lucindadonaldson@yahoo.co.uk
References
1. Ancoli-Israel S, Roth T. Characteristics of insomnia in the United States: results of the 1991 National Sleep Foundation Survey. I. Sleep 1999;22 Suppl 2:S347-53.
2. Leger D, Scheuermaier K, Philip P, et al. SF-36: Evaluation of quality of life in severe and mild insomniacs compared with good sleepers. Psychosom Med 2001;63:49-55.
3. Roth T. Prevalence, associated risks, and treatment patterns of insomnia. J Clin Psychiatry 2005;66 suppl 9:10-13.
4. Leger D, Guilleminault C, Bader G, et al. Medical and socio-professional impact of insomnia. Sleep 2002;25(6):625-629.
5. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA 1989;262:1479-84.
6. McCall WV. A psychiatric perspective on insomnia. J Clin Psychiatry 2001;62 Suppl 10:27-32.
7. World Health Organisation. The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research. Geneva: World Health Organisation, 1993.
8. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th edn) (DSM-IV). Washington, DC: American Psychiatric Association, 1994.
9. Buysse DJ, Reynolds CF 3rd, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193-213.
10. Doi Y, Minowa M, Uchiyama M, et al. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res 2000;97:165-172.
11. Breslau N, Roth T, Rosenthal L, et al. Sleep disturbance and psychiatric disorders: a longitudinal epidemiological study of young adults. Biol Psychiatry 1996;39:411-418.
12. Chang PP, Ford DE, Mead LA, et al. Insomnia in young men and subsequent depression. The Johns Hopkins Precursors Study. Am J Epidemiol 1997;146:105-114.
13. Stepanski EJ, Rybarczyk B. Emerging research on the treatment and etiology of secondary of cormorbid insomnia. Sleep Med Rev 2006;10:7-18.
14. Richardson GS, Roth T. Future directions in the management of insomnia. J Clin Psychiatry 2001;62 suppl 10:39-45.
15. Roth T, Roehrs T. Insomnia: Epidemiology, Characteristics, and Consequences. Clin Cornerstone 2003;5(3):5-15.
16. Morin CM, Hauri PJ, Espie CA, et al. Nonpharmacologic treatment of chronic insomnia: an American Academy of Sleep Medicine review. Sleep 1999;22:1134-56.
17. Doi Y, Minowa M, Uchiyama M, et al. Subjective sleep quality and sleep problems in the general Japanese adult population. Psychiatry Clin Neurosci 2001; 55(3): 213-215.
18. Ritsner M, Kurs R, Ponizovosky A, et al. Perceived quality of life in schizophrenia: Relationships to sleep quality. Qual Life Res 2004;13:783-791.
19. Prieto-Rincón D, Echeto-Inciarte S, Faneite-Hernández P, et al. [Quality of sleep in hospitalized psychiatric patients]. Invest Clin 2006;47:5-16.
20. Nowell PM, Mazumdar S, Buysse DJ, et al. Benzopdidazepines and zolpidem for chronic insomnia: a meta-analysis of treatment efficacy. JAMA 1997;278:2170-7.
21. Holbrook AM, Crowther R, Lotter A, et al. Meta-analysis of benzopdiazepine use in the treatment of insomnia. CMAJ, 2000; 162: 225-233.
22. National Institute for Health and Clinical Excellence. Guidance on the use of zaleplon, zolpidem and zopiclone for the short-term management of insomnia. London: NICE, 2004. (Technology Appraisal 77.) Available from: URL: http://www.nice.org.uk/TA077guidance
23. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev 2005;25:559-92.
24. King AC, Oman RF, Brassington GS, Bliwise DL, Haskell WL. Moderate-Intensity Exercise and Self-rated Quality of Sleep in Older Adults. A Randomized Controlled Trial. JAMA 1997;277:32-37.
25. Coates TJ, Killen JD, George J, et al. Estimating sleep parameters: A multitrait-multimethod analysis. J Consult Clin Psychol 1982;50:345-52.
Hepatitis B is one of the world’s major health problems 1. By recent estimates, worldwide more than 2 billion people have been infected with hepatitis B virus (HBV) globally and more than 350 million have chronic (long term) liver infections2. The infection is supposed to be causally related to 1 to 2 million deaths per year worldwide 3. Hepatitis B is a blood borne infection that is transmitted 1) by an infected mother to the newborn, 2) by contact with infected blood through unsafe injection, transfusion, open wounds, and sharing toothbrush or razors, and 3) by unprotected sex. Approximately 90% of newborns infected with HBV develop chronic infection, whereas 30-50% of children under age 5 years, 10% of adolescents aged 15 years, and 2-5% of older individuals develop chronic infection 4,5.
In Pakistan, it is Hepatitis (B & C) not Human immuno deficiency virus (HIV) that is the most common serious viral infection. Number of hepatitis B carriers in Pakistan is estimated at around seven million4 that is about 5% of the world wide 350 million carriers of hepatitis B 5. Unlike HIV, there was no large-scale national awareness campaign to educate the public and healthcare professionals in Pakistan about these infections before 2006, but now a comprehensive national strategy that will lead to the elimination and control of hepatitis B is becoming a top public health priority in Pakistan after inclusion of HBV immunization in government’s expanded Program for Immunization (EPI). The World Health Organization (WHO) Assembly endorsed the recommendation of its Global Advisory Group that all countries should implement a hepatitis B immunization program6. The threat of HBV to the health of the nation is frequently under-recognized by epidemiologists, policy makers and the public because unlike the influenza virus, it is often not the acute infection that makes people sick, but the consequences of chronic HBV infection that occurs after 20-30 years. Fortunately, hepatitis B is a vaccine preventable disease, global eradication is therefore possible if everyone worldwide receives the HBV vaccine before they become infected. Despite advances in antiviral therapy, only a minority of patients with chronic hepatitis B will have a sustained response. Thus, primary prevention by vaccination to increase herd immunity remains the main thrust in the control of HBV infection.
The development of hepatitis B vaccine is considered to be one of the major achievements of modern medicine. Three different classes of hepatitis B vaccine are available based upon how they are derived (from plasma, yeast, or mammalian cells).The first generation HBV vaccine was prepared by concentrating and purifying plasma from Hepatitis B surface antigen (HbsAg) carriers to produce 22 nm sub viral particles, which contain HBsAg alone. Derivation from plasma has left lingering concerns regarding the potential to transmit blood-borne infections, although this vaccine has excellent efficacy and safety7. Yeast-derived recombinant HBV vaccines were first introduced in the mid 1980s. They are produced by cloning of the HBV-S gene in yeast cells. These vaccines contain non-glycosylated HBV small S protein as the envelope antigen which must be released from the yeast during the manufacturing process 8. These vaccines do not contain antigens of the pre-S regions. The third class of HBV vaccine is the mammalian cell-derived recombinant vaccine. Three vaccines of this class have been developed. In addition to the S antigen, one of these contain antigen from the pre-S2 region while the other two contain antigens from both the pre-S1 and pre-S2 regions 9
The efficacy of universal immunization has been shown in different countries, with striking reductions of the prevalence of HBV carriage in children, most importantly; the HBV vaccine can be considered the first successful anti-cancer vaccine, as 20 years of mass vaccination has clearly reduced the incidence of hepatocellular carcinoma in children, at least in Taiwan 10. Currently available hepatitis B vaccine in Pakistan’s market are genetically engineered DNA recombinant vaccines and the recommended series of three intramuscular doses of hepatitis B vaccines induces a protective antibody response (anti-HBs > =10 milli-international units {mIU/ml}) in > 90% of healthy adults and in >95% of infants, children and adolescents 7, 11.
A vaccine consists of many parts, only one of which is the antigen by which it is known. Other components of the presentation may include, for instance, an adjuvant, a preservative or other ingredient. There may be components not stated on the information sheet that are classified as proprietary and therefore the manufacturers are not obliged to declare them. Thus, the effect the vaccine has, on an individual may be influenced in various ways by each and all of these components. Preservatives are just one of a number of additives to vaccines that are carefully regulated and which come under special scrutiny from time to time 12. Several case reports raised concerns that hepatitis B (HB) immunization might be linked to new cases or reactivation of multiple sclerosis, could shift the immune system toward an auto-immune direction, or may cause central nervous system (CNS) demyelinating diseases etc 13, 14, 15, 16. The present study sought to compare the safety of four hepatitis B vaccine regimens available in Pakistan’s market, in apparently healthy young females, and to determine the sero-response (i.e. reactogenicity and immunogenicity) to these vaccine in the same group of volunteers.
MATERIALS AND METHODS: Study Duration: Jan 2003 to Jan 2006 Study Design: Prevention, Open Label, Dose Comparison, Parallel Assignment, Safety/Efficacy Study. Subject: A total of 243 apparently young healthy female students of two Universities of the city were included in this study. Informed Consent: Prior to immunization, all volunteers were requested to give written informed consent to participate in this study. The volunteers were also advised that they are free to withdraw from the study at any time without any obligation to disclose her reason (s) for so doing. Criteria For Inclusion In The Study: All volunteers after submitting their signed consents were subjected to selection criteria on the basis of health checkups by a medical doctor to record the various factors including: a) Age: 18 – 30 years, b) History of Jaundice, blood transfusion, exposure to syringe, surgical and dental, c) Weight: > 45 Kg, d) Body Temperature: 96 – 98°F, e) Hemoglobin: > 10 g/ dl, f) Blood Pressure: Systolic 100 – 180 mm of Hg, Diastolic: 60 – 100 mm of Hg, g) Pulse rate: > 65/min.
After qualifying for inclusion in this study, volunteers were asked to give 10 cc of blood sample for different hematological (CP i.e. complete blood picture and Hb% i.e. hemoglobin percentage by Sysmex blood analyzer & ESR i.e. erythrocyte sedimentation rate by Westergreen method ), and Biochemical analysis (Direct Bilirubin, Indirect Bilirubin, ALT, AST and, Alkaline phosphatase by MicroLab- Merck chemistry analyzer), this data was used to keep the record of health status of participants and its comparison with adverse effects if appeared. Screening for HBs antigen, anti HBs antibodies and HBc IgM antibodies by Immunochromatography (ICT, Australia and Abbott, USA) and confirmation by enzyme linked immunosorbent assay (IMX ELISA - Abbott, USA) was also done before first dose of immunization. Test Vaccines: Fourrecombinant yeast derived HB vaccine were used as test regimens i.e. Euvax-B (LG Chemicals Ltd., Korea), Heptis-B (Boryang, Korea), Amvax-B (Amson, Pakistan) and Engerix-B (GS & K, Belgium). To avoid complications related to multi dose vials, it was strictly followed that the vaccination dose for each subject should be company packed, individually in a sealed container and, formulated for intra muscular injection. The dosage vial should contain same amount i.e. 20 μgm/ ml of HBs Ag absorbed on to approximately 0.5 μgm / ml adjuvant (aluminum hydroxide) and 100 μgm / ml preservative (Thiomersal/ Thimerosol) in a final volume of 1.1 ml (1 dose/ vial). Storage temperature should maintain as 2ºC to 8ºC to ensure integrity. Participants were injected with the vaccine of their own choice. Information broachers of the four vaccines were distributed among participants to help them make a choice. Out of total 729 doses administered to 243 individuals during this study, 195 were of Engerix-B, 420 were Heptis-B, 75 were Amvax-B, and 39 doses were of Euvax-B. Categories for Determining Severity of an Adverse Effect:
Local Symptoms: Soreness, indurations, swelling and redness.
General Symptoms: Fever, headache and dizziness.
Mild: Adverse events easily tolerated
Moderate: Adverse event of sufficient discomfort to interfere with daily activity or requiring simple treatment (e.g. Paracetamol, Generic name: Paracip).
Severe: Adverse event incapacitating and preventing usual activity or which may be life threatening, requiring hospitalization or completed treatment.
The course of an adverse event was described as:
Spontaneous recovery without discontinuation of vaccination
Recovery after discontinuation of vaccination
Continuation of recovery after symptomatic treatment
Eight samples of Peripheral blood (2-3 ml) were taken from all vaccinees before administration of each dose, and at different intervals after completion of immunization as per schedule given below; the sera were collected and stored at - 20°C.
Table 1: Visits Were Scheduled As Follows:
Vaccination number & sample collection
1.
First sample Before 1st dose of Vaccine (Jan, 2003)
2.
Second sample Before 2nd dose of Vaccine (Feb, 2003)
3.
Third sample Before3rd dose of Vaccine (June, 2003)
4.
Fourth sample After 6 months of 3rd dose (Dec, 2003)
5.
Fifth sample After 15 months of 3rd dose (Sep, 2004)
6.
Sixth sample After 19 months of 3rd dose (Jan, 2005)
7.
Seventh sample After 22 months of 3rd dose (May, 2005)
8.
Eighth sample After 30 months of 3rd dose (Jan, 2006)
Antibody Estimation and Statistics:
Anti-HBs were detected by ELISA using IMX- Abbott and quantitated using appropriate dilution of a positive sample with a known concentration of anti-HBs expressed as IU/L, provided by the manufacturer. The assay determined IgG type of anti- HBs antibody and the protective level of antibody was considered >10 IU/L. P values of less than 0.05 were considered significant. On the whole Hepatitis B antibodies titer was determined in participants using five standards i.e. <10 IU/ml, Between 10 – 100IU/ml, Between 100 – 1000 IU/ml, >1000 IU/ml, and no response or no antibody titer for the period of 36 months starting Jan’2003 till Jan’ 2006.
RESULTS:
Percentage of Geometric mean titer (GMT) of antibodiesbelow 10 IU/ml was in between 0.0% to 0.22% in case of Engerix-B, 0.0% to 0.20% in case of Euvax B, 0.0% to 0.30% in case of Amvax-B and 0.0% to 0.25% in case of Heptis-B. Percentage of GMT of antibodies between 10 – 100 IU/ml was in between 0.0% to 10% in case of Engerix-B, 0.0% to 9% in case of Euvax B, 0.0% to 8.9% in case of Amvax-B and 0.0% to 9.3% in case of Heptis-B. Percentage of GMT of antibodies between 100 – 1000 IU/ml was in between 0.0% to 35% in case of Engerix-B, 0.0% to 30.1% in case of Euvax B, 0.0% to 39.3% in case of Amvax-B and 0.0% to 40% in case of Heptis-B. While, Percentage of GMT of antibodies above 1000 IU/ml was in between 0.0% to 23% in case of Engerix-B, 0.0% to 25% in case of Euvax B, 0.0% to 26% in case of Amvax-B and 0.0% to 23.7% in case of Heptis-B. When Percentage of GMT of negative response was calculated we found that on the whole Engerix-B showed no response after 6 months of 3rd dose in 0.9% recipients leading towards no response in 31.78% of recipients after 30 months of 3rd dose. Euvax-B showed no response after 6 months of 3rd dose in 7.9% recipients leading towards no response in 35.68% of recipients after 30 months of 3rd dose. Amvax-B showed no response after 6 months of 3rd dose in 11.6% recipients leading towards no response in 25.5% of recipients after 30 months of 3rd dose. While, Heptis-B showed no response after 6 months of 3rd dose in 9.88% recipients leading towards no response in 26.75% of recipients after 30 months of 3rd dose. Period after 6 months of 3rd dose and before 15th month of 3rd dose was the period when highest Percentage of GMT of anti- HBs was observed .
Local and generalized adverse effects observed during and after the immunization of volunteers were recorded separately for each vaccine (Table 2, 3, 4 & 5).
Table 2 Incidence of Local and/or Generalized Symptoms on Vaccination With Engerix-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
N
%
n
%
n
%
1
65
19
29
5
8
10
15
38
58
2
65
11
17
3
5
7
11
29
45
3
65
8
12
0
0
0
0
18
28
Total
195
38
19
8
4
17
9
85
44
Table 3 Incidence of Local and/or Generalized Symptoms on Vaccination With Euvax-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
13
4
31
2
15
3
23
8
62
2
13
2
15
1
0
2
15
6
46
3
13
2
15
0
0
0
0
0
0
Total
39
8
21
3
8
5
13
14
36
Table 4 Incidence of Local and/or Generalized Symptoms on Vaccination With Heptis-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
140
53
38
10
7
34
24
95
68
2
140
25
18
25
18
27
19
70
50
3
140
22
16
7
5
32
23
84
60
Total
420
100
24
42
10
93
22
249
59
Table 5 Incidence of Local and/or Generalized Symptoms on Vaccination With Amvax-B
Dose
Total
Local
Only
General
only
Local &
General
With
symptoms
n
n
%
n
%
n
%
n
%
1
25
13
52
8
32
3
56
23
92
2
25
2
8
6
24
4
16
9
36
3
25
14
56
3
12
25
100
12
48
Total
75
29
39
17
27
32
43
44
59
As Shown in Table 6 that one month after the first dose, 180/243 subjects (74.45%) had seroprotection with respect to anti-HBs. One month after the second dose, 189/243 subjects (77.92%) showed seroprotection, four months after second dose, at month 6, 224/243 subjects (92.43%) were seroprotective. After 15 months of 3rd dose 231/243 subjects (95.27%) showed maximum seroprotection level in the immunized women. Later on seroprotection level was determined after 19, 22 and 30 months of 3rd dose. 170/243 subjects (70.08%) subjects were seroprotected even after 30 months of 3rd dose without having any booster dose.
Table 6: Over All Seroprotection Levels and Geometric Mean Titers (GMT) of Anti- HBs Antibodies
Timing
N
S+
% of S+
GMT
Range of Anti HBs Titer
PRE
Before Vaccination (Jan, 03)
243
0
0
0
0
M1
Before 2nd dose (Feb, 03)
243
180
74.45
16
0-50
M2
Before 3rd dose (June, 03)
243
189
77.92
143
1-700
M3
After 6 months of 3rd dose(Dec, 03)
243
224
92.43
18500
45-50000
M4
After 15 months of 3rd dose(Sep, 04)
243
231
95.27
23000
40-50000
M5
After 19 months of 3rd dose(Jan, 05)
243
222
91.57
12100
39-33000
M6
After 22 months of 3rd dose(May, 05)
243
195
80.53
1875
5-17000
M7
After 30 months of 3rd dose(Jan, 06)
243
170
70.08
690
1-1500
Comparative results of serum protection analysis of 04 candidate vaccines determined after 15 months of third dose without giving any booster dose, were found effective in healthy young female volunteers, demonstrating induction of very good immunogenicity. No significant differences were observed in seroprotection level of test vaccines (Table7). Overall serum protection rate achieved in case of Engerix-B was 95.9%, in case of Euvax-B, it was 95.2%, in case of Heptis-B was 95.0% , and in case of Amvax-B it was 95.1%. Calculated P values for all four test vaccines were lesser than 0.05 indicating significance of the used vaccines.
Table 7: Comparative Serum Protection analysis of 04 different Hepatitis-B Vaccines(n= 243; mean age= 21.5+3.7 Years)
As yet no such immunogenicity trials have been conducted in Pakistan or risk factors indigenous to the region assessed for any of the vaccine being utilized at the population level for such long period. Our study, is one of the longest study, conducted between Jan’2003 and Jan’ 2006, which includes total 243 healthy women subjects of child bearing age group. In this study we have demonstrated that there is no significant difference in reactogenicity and serum protection level among all four candidate vaccines we tested here, excellent immunogenicity of vaccines in volunteers recommends their usage for immunization purpose among different communities without having any doubts related to reactogenicity and side effects.
Recombinant hepatitis B vaccines have long been used for protection in the serum of and three doses have been shown to produce Anti HBs in the serum of approximately 95% of people who have not encountered the virus. The antibody response declines with increasing age. Patientsolder than 30 years have an increased risk of no response toHBV vaccine, as compared with younger persons 17. Thus, immunizationduring childhood or adolescence offers the greatest potentialfor protection 17 and provides lifelong immunity. Ninety percent of healthy adults and 95 percent of infants, children, and adolescents have protective serum anti-HBs antibody concentrations after the vaccine series has been completed 18.
Two kinds of recombinant vaccine are used for active immunization against hepatitis B; one of them contains the PreS1 and PreS2 antigenic domains while the other kind contains S and PreS polypeptide. No important differences between the effectiveness of these two types of vaccine have been detected 19. In a series of studies it has been demonstrated that 90-99% of healthy neonates, children, adolescents and adults develop protective levels of anti-HBs antibody following a standard vaccination course with hepatitis B vaccine 20, 21, 22, 23, 24, 25.
Efficacy of vaccines in the field have been measured long after the vaccine have been introduced at large scale population levels and only selected countries have record keeping such as the Centers for Disease Control in USA and the National Health Services in UK. Most developing countries do not have infra structure to support these activities and therefore the efficacy and risk indigenous to the population remains unknown.
Procurement and delivery of high-quality vaccine has national and international public health and ‘public good’ implications far beyond the scope of most products. People immunized with vaccines of inadequate quality can become ill and die from the disease that the vaccine should have prevented. Even more lives are placed at risk if vaccination coverage declines as a result of reduced public confidence in immunization programs. If we look at the outcome of immunization programs in different countries then we will have a good idea that how mass vaccination helped in reduction of disease burden?26
Importance of dose size, number of doses and dose response is another important issue related to immunization programs. Published studies regarding the dose-response relationship in terms of immunogenicity and sero-protection are highly varied. Chiaramonte et al 27reported that the sero-protection reached a level of 99.6% within one month after primary immunisation with the recombinant hepatitis B vaccine. The findings of Assateerawatt et al28 and Just et al 29 also were the same. Baldy JLS et al carried out a comparative study with three recombinant hepatitis B vaccines, one Brazilian (Butang, Instituto Butantan) and two Korean vaccines (Euvax-B, LG Life Sciences Ltd. and Hepavax-Gene, Green cross Vaccine Corp.), administered intramuscularly to students aged 17to19 years in three doses (corresponding to half the amount of antigen routinely used for adult vaccination) at intervals of one month between the first and second dose, and of four months between the second and third dose. The GMT of anti-HBs induced by the Euvax-Band Engerix-B vaccines were higher than those obtained with the Butangvaccine (p < 0.05); this difference was not significant when comparing the other vaccines two-by-two. No spontaneous adverse effects attributable to the application of any dose of the three vaccines were reported 30.
Vaccine efficacy is defined as the reduction in the incidence of a disease among people who have received a vaccine compared to the incidence in unvaccinated people. The efficacy of a vaccine is measured in clinical trials by giving one group of people a vaccine and comparing the incidence of disease in that group to another group of people who do not receive the vaccine. In our study overall efficacy of the vaccines used was satisfactory, without producing sever adverse effects, also there is no report of incidence of disease till now, in those who were vaccinated during this study(Table 2, 3, 4, 5).
Maximum protection level in terms of immunogenicity was observed in Euvax-B, which showed GMAT of 35.68% in test population. Engerix-B showed GMAT of 31.78%, Heptis-B showed GMAT of 26.75% and, Amvax-B showed GMAT of 25.5% after 30 months of 3rd dose of immunization While highest serum protection level was achieved in case of Engerix -B i.e. 95.9%. On the whole, r-hepatitis B vaccines showed high immunogenicity and good safety profile in the test population.
The inclusion of Hepatitis B in the list of compulsory and Extended Program for Immunization (EPI) in Pakistan since 2005 will result in mass vaccination of pediatric population. However, a big chunk of the adult population, especially healthcare workers, also needs to be immunized against Hepatitis B infection. We believe that all of the above mentioned HB vaccines, which are easily available in Pakistan’s market can be used for these mass vaccination programs without having any doubts related to Reactogenecity and Immunogenicity.
CONCLUSION:
In conclusion, this prospective study reinforces that the four different recombinant hepatitis B vaccines licensed in Pakistan have a good tolerability and are highly immunogenic among young women. It is also recommended that government should ensure the serosurvey of HBsAg and vaccine coverage at country level in order to reduce the disease burden on country’s economy.
ACKNOWLEDGEMENTS We are thankful to the administration of Jinnah University for Women, Karachi-Pakistan, administration of University of Karachi, Karachi-Pakistan, and team of Volunteer students from Microbiology Department, JUW for their cooperation during vaccination camps and manufacturers of test vaccines for giving consents to include their vaccines in this study. COMPETING INTERESTS None Declared AUTHOR DETAILS SHAZIA TABASSUM HAKIM, Ph.D., Virology and Tissue Culture Lab, Jinnah University for Women and I.I.D.R.Lab., University of Karachi, Pakistan SAYYADA GHUFRANA NADEEM, Virology and Tissue Culture Lab, Jinnah University for Women and I.I.D.R.Lab., University of Karachi, Pakistan SHAHANA UROOJ KAZMI, I.I.D.R.Lab., University of Karachi, Pakistan CORRESPONDENCE: SHAZIA TABASSUM HAKIM, Associate Professor & Chairperson, Department of Microbiology, Jinnah University for Women, Nazimabad, Karachi-74600, Pakistan Email: Shaz2971@yahoo.com
References
1.Kane MA, and Clements J. Hepatitis B. D. T. Jamison, W. H. Mosley, A. R. Meashan, and J. Bobadilla , editors. Disease control priorities in developing countries. New York: Oxford University Press N.Y; 1993:321–330.
2.World Health Organization, Revised fact sheet, August 2008.
3.Park K. Textbook of prevention and social medicine, 15th edition, Jabalpur, India: Banarsidas Bhanot Publishers;1997:159
4.Wasim J, Nadim J, Yakoob K , Muhammad I, Tirmizi SFA, et al. Hepatitis B and C: prevalence and risk factors associated with seropositivity among children in Karachi, Pakistan. BMC Infectious Disease. 2006;6:101
5.Zaman AS. 2003. Daily Dawn Internet Edition. 23 January.
6.WHO, 45th World Health Assembly, expanded programme on immunization and vaccine quality—progress report by the Director General, A45/8. World Health Organization, Geneva, Switzerland. 1992.
7.Szmuness W, Stevens CE et al. Hepatitis B vaccine: demonstration of efficacy in a controlled clinical trial in a high-risk population in the United States. N Engl J Med. 1980; 9;303(15):833-41.
8.Stephenne J. Development and production aspects of a recombinant yeast-derived hepatitis B vaccine. Vaccine. 1990;8 Suppl:S69-73; discussion S79-80.
9.Young MD, Schneider DL et al. Adult hepatitis B vaccination using a novel triple antigen recombinant vaccine. Hepatology. 2001;34(2):372-6.
10.Kao JH, Chen DS. Global control of Hepatitis B infection. Lancet Infect Dis. 2002;2(7):395-403.
11. Zajac BA, West DJ, McAleer WJ, Scolnick E M. Overview of clinical studies with hepatitis B vaccine made by recombinant DNA. J. Inf. 1986; Suppl A0:39–45.
12.Clements CJ. Vaccine preservatives: what is the big deal?. Indian J Med Res. 2006;124:5–8.
13.Duclos P. Safety of immunisation and adverse events following vaccination against hepatitis B. Expert Opin Drug Saf. 2003;2:225-31.
14.Hall A, Kane M, Roure C, Meheus A. Multiple sclerosis and hepatitis B vaccine? Vaccine. 1999;17:2473-2475.
15.DeStefano F, Verstraeten T, Jackson LA et al. Vaccinations and risk of central nervous system demyelinating diseases in adults. Arch Neurol. 2003;60:504-509.
16.Ascherio A, Zhang SM, Hernán MA et al. Hepatitis B vaccination and the risk of multiple sclerosis. N Engl J Med. 2001;344:327-332.
17.Fisman DN, Agrawal D, Leder K. The effect of age on immunologic response to recombinant hepatitis B vaccine: a meta-analysis. Clin Infect Dis. 2002;35:1368-1375.
18.Mast E, Mahoney F, Kane M, Margolis H. Hepatitis B vaccine. Plotkin SA, Orenstein WA, editors. Vaccines. Philadelphia: Saunders. 2004:299-337.
19.Bertino JS Jr, Tirrell P, Greenberg RN et al. A comparative trial of standard or high-dose S subunit recombinant hepatitis B vaccine versus a vaccine containing S subunit, pre-S1, and pre-S2 particles for revaccination of healthy adult nonresponders. J Infect Dis. 1997;175:678-681.
20.Zannolli R, Morgese G. Hepatitis B vaccine: current issues. Ann Pharmacother. 1997;31(9):1059-1067.
21.West DJ, Calandra GB. Vaccine induced immunologic memory for hepatitis B surface antigen: implications for policy on booster vaccination. Vaccine. 1996;14(11):1019-1027.
22.Jafarzadeh A, Shokri F. The antibody response to HBs antigen is regulated by coordinated Th1 and Th2 cytokine production in healthy neonates. Clin Exp Immunol. 2003;131(3):451-456.
23.Shokri F, Jafarzadeh A. High seroprotection rate induced by low doses of a recombinant hepatitis B vaccine in healthy Iranian neonates. Vaccine. 2001;19(31):4544-4548.
24.Jafarzadeh A, Kardar GA, Khoshnoodi J, Shokri F. Downregulation of IL-12 production in healthy nonresponder neonates to recombinant hepatitis B vaccine. Iran Biomed J. 2004;8:41-45.
25.Jafarzadeh A, Shokrgozar MA, Khoshnoodi J, Shokri F. Unresponsiveness to recombinant hepatitis B vaccine in healthy Iranian neonates: association with HLA antigens. Irn J Med Sci. 2002;27:51-55.
26.Proceedings of Who’s third expert working group meeting on hepatitis B. Tokyo, Japan 6-7 March 2007.
27.Chiaramonte M, Majori S, Ngatchu T et al. Two different dosages of yeast derived recombinant hepatitis B vaccines: A comparison of immunogenicity. Vaccine. 1996;14:135-7.
28.Assateerawatt A, Tanphaichitr VS, Suvatte V, Yodthong S. Immunogenicity and efficacy of a recombinant DNA hepatitis B vaccine, Gen Hevac B Pasteur in high risk neonates, school children and healthy adults. Asian Pac J Allergy Immunol. 1993;11:85-91.
29.Just M, Berger R, Just V. Reactogenicity and immunogenicity of a recombinant hepatitis B vaccine compared with a plasma derived vaccine in young adults. Postgrad Med J. 1987;63 (Suppl 2):121-3.
30.Baldy JLS, Lima GZ, Morimoto HK et al. Immunogenicity of three recombinant hepatitis B vaccines administered to students in three doses containing half the antigen amount routinely used for adult vaccination. Rev Inst Med Trop S Paulo. 2004;46(2):103-7.
Laparoscopic fundoplication (LF) has been emerging as the procedure of choice for selected patients with symptomatic and problematic reflux disease since the first described case by Dallemagne in 1991 (1). This was followed by a rapid expansion into routine clinical practice shortly afterwards. With increased acceptance and availability of laparoscopy as a safe surgical modality there has been a huge increase in the number of patients undergoing LF. This has probably been due to increased willingness of patients and referring doctors to consider the less invasive procedure, rather than the older ‘open’ surgical treatment, with its more rapid recovery, smaller incisions and earlier return to work and to normal daily activities.
Patient referral patterns have also changed over the last decade with the main indication for consideration of LF being patient choice, a general unwillingness to take long term medication as well as ineffective or intolerance of medications and relapse of symptoms (5-6). Several advantages of LF have been described by recent data including shorter hospital stay, less requirement for analgesia, and sooner return to work (7-9). These have to be offset against procedure specific complications including gastro-oesophageal perforation, pneumothorax, dysphagia, and bleeding (2-4). However, the other main downside to LF is the learning curve during which there are an increased number of complications. Previous reports have suggested the learning curve to be around 20 for an individual surgeon and 50 for an institution (10-12).
In a recent meeting of the Upper GI group at the Royal College of Surgeons there was discussion concerning the incidence and management of dysphagia following laparoscopic fundoplication (13 Bill Owen Day RCS (Eng) 2004). There is a paucity of data available in this regard with a general paucity of negative or unequivocal results in the literature equating to a selection bias towards only positive data and positive reporting of good results.
Therefore the aim of the present study was to look critically at the learning curve and, with respect to operative complications, with specific regard to the incidence and management of dysphagia in a personal series of patients who underwent a laparoscopic fundoplication in a District General Hospital in the United Kingdom.
Patients and Methods
From December 1997 to February 2004, 75 patients who underwent laparoscopic fundoplication under the care of a single consultant surgeon in a district general hospital were included in this study. It became routine practice for LF to be performed by one dedicated surgical team (JMT) who kept a complete prospective list of procedures. This series was complete and the hand written records of all the procedures were used to identify patients undergoing operations for LF with or without reduction and repair of Para-oesophageal hernia during the study period. These records were cross-checked with the theatre logbook, hospital computer system as well as with the surgeon’s own record. This ensured full inclusion in the analysis of patients.
The groups were not randomised and ‘all comers’ where included in the study. However, Group 1 consisted of the first 20 LF whereas Group 2 included LF (numbers 21-75). Informed consent was obtained in writing prior to surgery. At least a single dose of prophylactic antibiotics (of either a third generation cephalosporin or co-amoxiclav) was administered at induction; all patients received standard thromboprophylaxis (subcutaneous clexane, TEDS, intermittent pneumatic calf compression).
Patients underwent a laparoscopic fundoplication as briefly described below. The patient was placed in the lithotomy position with reversed Trendelberg tilt; a pneumoperitoneum was created and 4 ports inserted. The liver was elevated using a ‘Nathanson’ liver retractor placed through a 5 mm epigastric incision. Initially the right and left limbs of the right crus are dissected alongside the pancreaticogastric and phrenogastric ligaments. A window is created behind the distal oesophagus. A Penrose drain is passed through the gap. The short gastric vessels are divided using a harmonic scalpel (Ethicon, USA), if required. The crural limbs are approximated using 2, 2-0 ethibond sutures to leave a hiatus 1 cm wider than the oesophagus. A laparoscopic babcock is placed behind the oesophagus and the gastric fundus is brought left to right behind the oesophagus and bought round to meet with the remaining portion of the fundus anteriorly. Two (or rarely three) sutures of 2-0 ethibond were used for the fundoplication. The upper suture included a bite of the anterior hiatal margin to anchor the wrap. Of note, the important feature of the procedure is the creation of a ‘floppy’ tension free fundoplication. This is hugely aided by good mobilisation of the gastric fundus with its associated ligaments and if required, division of the short gastric vessels. Notably, one must carefully create a window behind the oesophagus and an overlap of no longer than 3 cms length and one must stay high up on the fundus in order to avoid the creation of a ‘2’ compartment stomach syndrome’.
Post-operatively all patients were treated in an identical manner. As soon as tolerated after the operations the patients were allowed the consumption of water; diet and analgesia were made available as soon after surgery as required by individual patients. Complications were noted as they occurred during the follow-up period. Both general and specific complications were documented for at least 6 months. Furthermore, patient demographics, details of operations, all complications and follow-up data were kept. Follow up for the purpose of this audit involved completion of a proforma at a minimum post operative period of one year and a maximum of eight years.
All patients where regularly reviewed daily on the ward whilst they were in-patients and in the outpatients at 4-6 week intervals or sooner should the need arise by the surgical team. Thereafter they were given a “see on request” appointment. Data on patient and procedure related morbidity and acceptability was also collected.
At the time of the study contact was made via the telephone and a questionnaire was completed. A telephone survey asking the patient four questions,
Where they happy with the operation
Would they reccomend the procedure to a friend
Had there symptoms resolved
If they had had post op dysphagia had it resolved
The data was reviewed and analysed in conjunction with our department of medical statistics. Analysis was performed using the Mann-U test. Multivariate analysis of the means was performed using the Kruskal-Wallis Test.
Results
Overall the 75 patients who underwent laparoscopic fundoplication consisted of 44 males (59%) and 31 females (41%). The mean age was 47.0 years (range 22-80 years). Group 1, which consisted of the first 20 LF cases included 11 male and 9 females. The mean age was 53.25 years (range 32-80). Group 2, which consisted of the LF cases numbering 21-75 included 33 male and 22 females. The mean age was 44.8 years (range 22-78). Both groups were well matched across the above parameters with no statistical differences (Table A). Only 4 patients were obese (5%), smoker (n=10, 14%), 7 patients suffering with Hypertension (10%) and one with diabetes mellitus (2%) and were equivalently represented in both groups (data not shown).
Presenting features are shown in Table B. Notably, the commonest presenting complaints included regurgitation of acid/ food in 79% (n=59), heartburn in 73% (n=55) and pain and discomfort 53% (n=35). Other complaints included dysphagia 21% (n=16), cough/wheeze 19% (n=14) and excess salivation 18% (n=13).
Table A: Patient Demographics
Group 1
Group 2
P value
Numbers
20
55
NS
Male: Female
9: 11
22: 33
NS
Age range (mean) yrs
32-80 (53)
22-78 (45)
NS
Operating time (median) mins
120-240 (190)
75-195 (144)
<0.05
Sliding/No sliding
11
44
NS
Type II/Type III hiatus hernia
9
11
NS
Table B: Presenting Features
No. of cases
Regurgitation (acid/food)
59 (79%)
Heartburn
55 (73%)
Dysphagia
16 (21%)
Cough/wheeze
14 (19%)
Excess Salivation
13 (17%)
Nausea
10 (14%)
Epigastric pain
6 (8%)
TOTAL
173 (100%)
Patients underwent pre-operative evaluation with Upper GI endoscopy 88% (n=66), pH manometry 47% (n=35) and barium swallow 32% (n=24). Previous to this procedure all patients (100%) were on or had been during some part of their illness on therapeutic doses of proton pump inhibitors.
There was a significant difference between the operating times in the two groups. Thus in Group 1 the average operating time was 190 minutes (range120-240 minutes) whereas in Group 2 the average operating time was 144 minutes (range 75-195 minutes, P <0.05).
Table C: Post Op Mild and Moderate Complications<
Cases (n=75)
Dysphagia
40
Regurgitation
7
Nausea
4
Diarrhoea
3
Heartburn
5
Excess Salivation
2
Portsite discomfort
6
Gas Bloat
4
Total
71
One of the major aims of the study was to record post-operative complications. Table C shows all mild and moderate complications which resolved completely with conservative management. Of note Table F shows that dysphagia occurred in up to 40 of our patients. Table F shows the distribution of dysphagia in both groups. In group A (n=20) the are 15 patients who complained with dysphagia (75%) of which 5 settled spontaneously and 10 required further investigation with OGD +/- dilation. in group B (n=55), 25 patients suffered with dysphagia all of which settled with conservative management. Our initial policy was to perform an OGD and dilate prophylactically; however, this was abandoned halfway through the study. It was found that the dysphagia settled in all patients with conservative management. Furthermore, other mild/moderate complications, of note included regurgitation of stomach contents (7/75) and port-site discomfort (6/75), all of which also resolved spontaneously
Table D: Major Complications Groups 1 & 2
Group 1
Group 2
P value
PE
1 (5%)
0
NS
Pneumonia
1 (5%)
1 (2%)
NS
Oesophageal Perforation
1 (5%)
1 (2%)
NS
Stomach perforation
0
1 (2%)
NS
Pneumothorax
0
1 (2%)
NS
Major desaturation
0
1 (2%)
NS
TOTAL
3 (15%)
5 (9%)
NS
Table E: Conversion to Open Surgery
Group 1(n=20)
Group 2(n=55)
P Value
Desaturation
0
1 (2%)
NS
Perforation viscus
1 (5%)
1 (2%)
NS
Pneumothorax
0
1 (2%)
NS
Technical (Obese/previous surgery)
2 (10%)
2 (4%)
NS
TOTAL
3 (15%)
5 (9%)
NS
Major complications are shown in Table D. Of note there are three conversions to ‘Open’ surgery in Group 1 and five in Group 2 (Table E). In detail, four cases (two in each group) were converted early because of poor or very difficult access. They included difficulty in reducing the stomach and omentum from the mediastinum into the abdomen, unable to reach the hiatus despite placing the ports as high as possible, dense adhesions between the liver and stomach and G-O junction thereby leaving no access to the hiatus and simply impossible access to the upper stomach. Further, oesophageal perforation which was caused by intra-operative insertion of a nasogastric bougie (Group 1), this was repaired laparoscopically with no sequelae. Other reasons for conversions included perforation of the greater curve of the stomach due to the fact that there was thickened fatty tissue around the greater curve of the stomach and spleen which produced a perforation while dissecting the stomach free. Also in Group 2 there was one pneumothorax and in another patient there was marked desaturation on creation of the pneumoperitoneum and in both cases it was deemed safer to open the patient.
Table F: Dysphagia Group
Group 1(n=20)
Group 2 (n=55)
P value
Dysphagia
15
25
NS
Resolved Spontaneously
5
25
<0.05
Investigated (swallow and OGD)
10
0
<0.05
Relaparotomy occurred in three patients; one developed severe pain and clinical shock at 24 hours and it was found on laparotomy to have a perforated oesophagus, the second patient we found disruption of the wrap (requiring re-operation and refashioning the wrap) and a final patient developed small bowel obstruction.
Finally a telephone survey at the conclusion of the study managed to contact 70/75 patients. It was found that overall 68/70 patients were satisfied with their procedure and would recommend the procedure to a relative or friend.
Discussion
Gastro-oesophageal reflux disease (GORD) is the commonest disorder of the Upper GI tract affecting approximately between 10-40% of most western populations and with rising incidence (11). In Australia it has shown to consume around 10% of the national expenditure on prescription drugs. Fortunately the majority of patients settle with simple measures including weight loss and reductions in smoking, caffeine and chocolate consumptions. Furthermore, better timing of meals as well as increasing the number of pillows and raising the head end of the bed can lead to improved symptoms. The advent of H2- receptor antagonist (H2RA) and later proton pump inhibitors (PPIs) has led to symptom control in the majority of patients. However, patients on maximum therapy who remain symptomatic or who develop complications (i.e. haemorrhage, oesophagitis, strictures) or those who refuse long term medication are deemed candidates for surgical intervention.
LF has emerged as the procedure of choice for GORD. The present study, which is a personal single surgeon series, shows that laparoscopic fundoplication is a safe and effective procedure with low rates of long-term complications. Importantly, post operatively these patients may develop dysphagia which settles with conservative measures in the vast majority of cases (13).
There is no doubt that for LF a ‘learning curve’ exists but there is debate about the actual numbers. Most studies suggest that it is around 20 for an individual and around 50 for a department (12), thus in the present study we compared our first 20 (classically thought to be within the learning curve) with the next 55 in order to assess major complications, conversions to open procedure. We found that in Group 1 there were 3 major complications (15%) whereas in the next 55 cases there were five (9%). Indeed only one major complication in Group 1 and two in Group 2 could be considered as technical, they were oesophageal and gastric perforations the rest being post operative pneumonia, PE and major desaturation. There were no deaths in either group. This was in keeping with previously published series (14-16).
Previously published data and our own observations revealed that there were significant post operative rates of dysphagia. In the present series dysphagia was the single commonest complication experienced by 53% of patients (n=40). Initially these were investigated with barium swallow and OGD and treated aggressively with early dilation (Group 1) however this strategy was abandoned after it was found that the vast majority of our patients resolved their dysphagia with conservative treatment. From thereon we adopted a very conservative approach reassuring the patient and keeping within close contact until the dysphagia resolved. We reserved dilatation for only highly resistant dysphagia or patients who where non-compliant with conservative treatment. We found that clear explanations pre-operatively, regular reassurance and assessment was generally all that was required. In Group 2 (21-75) none of the patients required dilation for dysphagia. It is almost universal that patients undergoing LF will have a degree of dysphagia. However what is now accepted and reflected from the experience from the present study is that dysphagia after LF should only cause concern if severe, presenting with severe pain, uncontrolled retching and vomiting requiring immediate surgical revision (17). Most commonly this is due to over-tightening of the hiatus or with poor mobilisation and a 360 degree wrap. This may be related to the learning curve, being more common in the earlier cases in a personal series. In our series 53% of patients (n=40) experienced dysphagia. This is comparable to previous reported data (2,16). Notably, Fontaumard et al reported a dysphagia rate of 78% (40/51). The reason for this post operative dysphagia has been thought to be related to the type of procedure. In our series all patients underwent a Nissen type of repair however evidence is now emerging that the incidence of dysphagia and gas related complications are reduced following anterior partial fundoplication (19,20). This is shown from the data of two recent randomised controlled studies. Baigrie et al (18) in a double-blind, randomized study compared laparoscopic Nissen total fundoplication and anterior partial fundoplication. There were no differences in mean heartburn scores between groups but dysphagia scores for both liquids and solids were lower after anterior fundoplication. Also Ludemann et al (19) compared total fundoplication for gastro-oesophageal reflux disease with an anterior 180 degrees partial fundoplication. Both achieved effective reflux control but the partial wrap was associated with fewer side-effects in the short term than total fundoplication. After 5 years, dysphagia, measured by a visual analogue score for solid food and a composite dysphagia score, was worse at 5 years after total fundoplication.
Our study confirms what has previously been shown with the learning curve for LF and its acceptability. It has also clearly highlighted that post operative dysphagia is common and affects a significant number of patients post operatively. However in our study we found that this was best managed conservatively and the almost all resolved spontaneously. There is no evidence to support early intervention unless the symptoms are very severe and occur very soon after surgery, when the patient should be taken back to theatre for another look. The specific causes of the dysphagia are not known but it is postulated that it is due to increased pressure as the upper part of the wrap augments the pressure of the lower oesophageal sphincter causing it to become over competent. Over time this mechanism relaxes leading to an improvement in dysphagia with simple conservative therapy. Furthermore, there was a hugely positive satisfaction score on a simple telephone survey suggesting symptom control from this procedure.
COMPETING INTERESTS None Declared AUTHOR DETAILS A A RIAZ, FRCS(I) FRCS(Eng) FRCS(Gen) PhD, Hunterian Professor RCS(Eng) and Senior Visiting Clinical Fellow, University of Hertfordshire, UK CORRESPONDENCE: A A RIAZ, Consultant Upper GI, Laparoscopic and General Surgeon, West Hertfordshire Hospitals NHS Trust, Waverley Road Hertfordshire, AL3 5PN, UK Email: mrariaz@hotmail.com
Watson DI, Johnson AG, Reed MWR, Stoddard CJ. Laparoscopic Fundoplication for gastroesophageal reflux. Ann R Coll Surg Engl 1994:76; 264-68.
Schauer PR, Meyers WC, Eubanks S et al. Mechanisms of avoidance of esophageal perforation during laparoscopic Nissens fundopliaction. Ann Surg 1996; 223:43-52.
Reid DB, Winning T, Bell G. Pneumothorax during laparoscopic dissection of the diaphragmatic hiatus. Br J Surg 1993;80:670
Perdikis G, Hinder RA. Lund J. Laparoscopic Nissens Fundoplication: where do we stand? Surg Laparosc Endosc 1997; 7; 17-21.
Laine S, Rantala A, Gullichsen R, Ovaska J. Laparoscopic vs. conventional Nissens Fundoplication. Surg Endosc 1997; 11:441-44.
Zacharoulis D, O'Boyle CJ, Sedman PC, Brough WA, Royston CM. Laparoscopic fundoplication: a 10-year learning curve. Surg Endosc. 2006; 20(11):1662-70.
Martin RC 2nd, Kehdy FJ, Allen JW. Formal training in advanced surgical technologies enhances the surgical residency. Am J Surg. 2005 Aug; 190(2):244-8.
Hwang H, Turner LJ, Blair NP. Examining the learning curve of laparoscopic fundoplications at an urban community hospital. Am J Surg. 2005 ;189(5):522-6;
7th Bill Owen Oesophago-Gastric Symposium 'Meet-the-Experts' The Royal College of Surgeons of England, London March 2005.
Watson DI, Baigrie RJ, and Jamieson GG. A learning curve for laparoscopic fundoplication. Definable, avoidable, or a waste of time? Ann Surg. 1996 August; 224(2): 198–203.
Champault GG, Barrat C, Rozon RC, Rizk N, Catheline JM. The effect of the learning curve on the outcome of laparoscopic treatment for gastroesophageal reflux. Surg Laparosc Endosc Percutan Tech. 1999 Dec; 9(6):375-81.
Cuschieri A, Hunter J, Wolfe B, Swanstrom LL, Hutson W. Multicenter prospective evaluation of laparoscopic antireflux surgery. Preliminary report. Surg Endosc. 1993; 7(6):505-10.
Jones NJ, Soper DB. Laparoscopic Nissens Fundoplication. Surg Rounds 1994:17;573-81
The Civil Rights Act 1964 remains of the greatest achievements in United States (US) history. It had implications internationally, making racial discrimination illegal, but its effectiveness in the employment domain remains contestable 2. The worldwide existence of workplace racism has attracted controversy and this is drawn out by psychiatry’s attempt to understand the nature of the problem 3. Discrimination at work, based on a person’s race, comes in different guises and can have negative consequences on both individuals and organisations 1. Despite legislation to protect individuals substantial progress needs to be made to eradicate the problem.
What is racism?
The concepts of “race”, “ethnicity” and “racism” are explained in figure 1.
Figure 1: Definition of race, ethnicity and racism 4, 5
Race
The group a person belongs to as a result of a mix of physical features, ancestry, and geographical origins, as identified by others or, increasingly, as self-identified. The importance of social factors in the creation and perpetuation of racial categories has led to a broadening of the concept to include social and political heritage, making its usage similar to ethnicity. Race and ethnicity are increasingly used synonymously.
Ethnicity
The group you belong to as a result of a mix of cultural factors that include language, diet, religion, ancestry, and race.
Racism
A belief that some races or ethnic groups are superior to others, used to devise and justify actions that create inequality between racial groups.
Racism is a social process associated with “overt and covert forceful establishment and maintenance of power by one social group over another” 3.
Racism can be seen as a misuse of power and, even today, power relations are signified by subtle cultural rules that perpetuate racial inequality 6.
What are the origins of racism?
That some races are superior to others has origins from the 19th century 5. The history of racism has stimulated considerable debate in understanding racism.
Racism may have origins in experiences derived from, what is known in analytical psychology as, the collective and personal unconscious. The personal unconscious arises from the lifetime experiences of the individual. This is distinct from the “collective unconscious” which psychiatrist Carl Jung described to represent a form of the unconscious common to mankind as a whole and originating in the inherited structure of the brain 7. This contains inherited primitive cultural and racial elements. Both the personal and collective unconscious, made from our individual and ancestral experiences respectively, may account for the manifestation of racism in society today.
In recent times the experience of overt racial bigotry and prejudice is seldom seen 8. Nevertheless discrimination against members of a social group may persist because it is so deeply entrenched within society, by the personal and collective unconscious, that it becomes the automatic response even when no conscious intent is present 9. “Everyday discrimination” is the discreet, pervasive discriminatory acts experienced by stigmatised groups on a daily basis 10, and highlights the modern perspective that racism is subtle.
The subtlety of racism
“Like a virus that has mutated, racism has evolved into a new form that is difficult to recognise and harder to combat” 8
As blatant forms of racism become extinguished, particularly in the current climate of political correctness, unconscious racial biases in subtle forms, known as ambivalent or modern racism 10, are appearing. This has been referred to as aversive racism occurring in people who possess strong egalitarian values, and who believe they are not prejudiced, but have negative racial feelings and beliefs that they are unaware of 8. These feelings and beliefs are rooted in the normal psychological processes of social categorisation, satisfaction of basic needs for power and control, and socio-cultural influences 8. The ambivalence involving positive and negative feelings creates a psychological tension that leads to an inconsistent pattern in their behaviour 8.
The cumulative effects of unpredictable and seemingly trivial behaviour such as avoidance of ethnic minorities, closed and unfriendly verbal and non verbal communication, and failure to provide assistance, is more damaging 10. Apparently harmless interactions, including racist assumptions and questioning about where somebody is from, also convey messages about marginality and not belonging 11. This subtle racism may contribute to the racism perceived by minority groups in higher status professions and organisations.
Does racism exist in healthcare organisations?
“American Medical Association apologizes for racism in medicine” (10th July 2008) 12.
This admission by the American Medical Association, of racial discriminatory practices against African-American physicians, reflects the recognition of racism in other western countries.
In the United Kingdom (UK) racism has been revealed in public institutions such as the metropolitan police 13 and widely reported in the nursing profession 14,15 within the National Health Service (NHS). Trevor Phillips, chairman of the Equality and Human Rights Commission, referred to the “snowy peaks of the NHS” 16 with a large number of ethnic minorities at the base. Less than 10% of senior managers and 1% of chief executives are from ethnic minority background 17. There is a “glass ceiling” 18 preventing promotion and black and minority ethnic (BME) managers feel they have to work twice as hard and have twice as many qualifications to succeed 19.
Since 2000, after a survey commissioned by Department of Health (DOH) reported that half of front-line NHS BME staff had been victims of racial harassment in the previous 12 months 20, reports of racism in healthcare have increased. In 2001 a Kings Fund report, “Racism in Medicine” 21, generated powerful debate after finding that bullying and discrimination were a daily fact of life for black and Asian doctors. Then in 2003 a British Medical Association (BMA) survey revealed that in ethnic minority doctors, who form nearly one third of the NHS workforce 22, more than 80 per cent believed that their ethnicity had a negative effect on their career advancement 23. In 2004 the Royal College of Psychiatrists accepted that racism existed in the NHS and in their own institution 24.
How does racism manifest itself in medicine?
“Discrimination can appear to be hidden when it is institutionalised, although it is not usually hidden from the person who is subjected to it” 3
Institutional racism is “the collective failure of an organisation to provide an appropriate and professional service to people because of their colour, culture and ethnic origin” 13. Health disparities among patients have been widely linked to racially biased discriminatory health practices 25, 26, 27 but how do structures, processes, and values within an organisation discriminate against those working in the medical profession?
There is considerable evidence to indicate that discriminatory practices against doctors evolved from medical school. For instance racial discrimination has operated at the time when students applied to study medicine 19, 28, through short-listing based on whether applications had Asian or English names 29, 30, and with downgrading of non-English names by computer 31. Discrimination has also been reported during medical school in the US and Canada 11. UK ethnic minority medical students also perform poorly in examinations compared to white students 32, 33 although the lack of evidence of explicit discrimination may suggest the involvement of more subtle communication styles and cultural differences 33.
If the problems at medical school are accountable by racial organisational processes it is not surprising that discriminatory practices persist after qualification (figure 2)
Figure 2: How BME doctors may experience racism 17, 19, 34, 35, 36
Bullying and harassment
More likely to experience bullying and harassment.
Recruitment and career advancement
More likely to be over-represented in junior grades. Reduced promotion and career advancement also seen in relation to academic careers. Underrepresented in senior leadership positions.
Disciplinary hearings
Over-represented at disciplinary hearings with nearly a third of complaints coming form other health professionals.
Disciplinary action and dismissals
Six times more likely to be disciplined e.g. in 2006 two thirds of the 54 doctors struck off in UK had trained outside UK.
Reward systems
Disadvantaged in the allocation of discretionary grants and NHS distinction awards.
What are the consequences of racism in healthcare?
“Racial discrimination damages both those discriminated against and those doing the discriminating” 37
The cost of workplace racism is that it acts as a chronic and acute stressor on the individual with a range of consequences (figure 3):
Figure 3: Consequences of racism on an individual 1, 10, 38, 39
Psychological
Poor well-being. Loss of confidence. Humiliation. Low morale. Gives a sense of thwarted aspirations.
Physiological
Increase blood pressure. Physical illness.
Behavioural
Bad work performance. Require time off work.
“Racial fatigue” characterises the potential emotional and psychological sequelae of feeling isolated in a work environment in which race regularly influences behaviour but is consistently ignored and nobody wants to discuss it (“racial silence”) 40. Racism may be underreported for the same reasons seen with workplace bullying: fear of making matters worse, belief that nothing will be done, concerns regarding confidentiality, fear of victimisation, and concern about being labelled as a troublemaker 41. In addition the individual may fear being regarded as having a “chip on one’s shoulder”.
Organisations may also suffer with disharmony at work, high sickness levels, and resignation 1. In medicine this results in the “double loss” of a speciality losing highly motivated people and gaining those where enthusiasm may be low 19. In addition victims of racial discrimination in healthcare may pursue legal action. In 2003 a surgeon won over £600,000 42 after being denied entry to the specialist registrar. Another surgeon successfully sued the BMA for more than £800,000 for racial discrimination after it failed to support his own claim against the DOH 43. In another case a UK trust paid £2.5m, including legal costs, for wrongful dismissal of a consultant obstetrician who was investigating discrimination 44.
What can be done if you are experiencing racism at work?
In the UK there is protection by legislation. It is unlawful to discriminate against anyone on racial grounds. The Race Relation Act 1976 defined three types of discrimination (direct, indirect, and victimisation) 1, 45,. Following this was the setting up of the Commission for Racial Equality (CRE) in the UK to tackle racism and promote racial equality 45. The Race Relations Act 1976 has now been superseded by the Race Relations (amendment) Act 2000 46 that requires public bodies to eliminate discrimination, promote equal opportunities, and ensure good race relations. However legal processes are stressful and there are some steps you can take before pursuing this route (figure 4).
Figure 4: Steps to take if you are a victim of racial discrimination 1
Talk to colleagues and friends who may have suffered a similar problem because it helps to share a problem and trying to cope on your own can be particularly stressful.
Keep a diary of events of who said what, when, circumstances and any witnesses – this will give a vital record of the nature of the racism.
Find out whether your employer has specific rules about racism at work or a grievance procedure you can use to raise a problem.
If you are in a union contact them to assist you with talking to management or approaching the perpetrator.
In the UK the Commission for Racial Equality is a national body that can help victims of racial discrimination.
Your local Citizens Advice Bureau or Law Centre may be able to help.
You may want to talk to a private law firm that specialises in discrimination issues.
Recommendations and Conclusion
“The law may be just but its implementation is another matter” 47
Despite legislation and procedures, to address racism at work, healthcare organisations are slow in introducing and supporting the policies for race equality 18. Suits come to legal action, not for a lack of policy, but because of not being enforced 48. Practice is not synonymous with policy 19. Reinforcement of policies depends on the degree to which upper management understands discrimination and harassment 48. Although implementation of policies could be successful in combating overt racism this is not so for the covert form.
The covert form of racism, as in institutional racism where organisational processes are “unwittingly” enacted 13, suggests that racism is inevitable. Even people with strong motivations to avoid it are subject to automatic cognitive activation of stereotypes, which can unconsciously influence behaviour, making diversity training courses and non-discrimination policies relatively ineffective 10. Attending to, and encouraging the reporting of, the “softer” aspects of racism may be the key to establishing a true “positively diverse climate” 10. New forms of racism require new approaches (Figure 5):
Figure 5: The STEEP model to approaching subtle racism in organisations 8
Structured Support
Visibly supported by senior management.
Training and Education
Educate people about subtle bias and training to recognise it.
Experience
Frequent and constructive interracial contact to decrease bias, enhance group cohesion, and increase productivity.
Personal Commitment
Individuals must be committed to recognise and combat subtle racism.
The most important part of the solution is education. Teaching on racism should be incorporated into the undergraduate and postgraduate curriculum 19. However of greater significance is recognising our own personal prejudices, at an early stage, so that prejudices we all harbour are challenged within ourselves.
“The hardest attitude to change is the one you don’t know you have” 8
KEY POINTS – RACISM:
Is associated with power and superiority
Has evolved from an overt to a covert form
Is commonplace in healthcare organizations
Is manifested at each stage of a doctors career
Has implications for individuals and organizations
Can be partly dealt with through policies and legislation
Requires a new approach to eradicate the problem
Useful UK online resources
http://www.oneworkplace.co.uk - “One Workplace Equal Rights” aims to tackle racism and promote equal opportunities in the workplace.
http://homepage.ntlworld.com/rajen/RacialEquality - Race Equality Ltd provides phone advice about racism in the medical establishment.
http://www.bidaonline.org.uk - The British International Doctors Association protects and promotes the interests of Ethnic Minority Doctors and Dentists working in the UK.
http://www.equalityhumanrights.com - A new commission working to eliminate discrimination, reduce inequality, protect human rights and build good relations.
COMPETING INTERESTS None Declared AUTHOR DETAILS MINAL MISTRY, BSc, BM, MRCPsych, MSc, Hampshire Partnership NHS Trust, United Kingdom JAVED LATOO, MBBS, DPM, MRCPsych, North East London NHS Foundation Trust, United Kingdom CORRESPONDENCE: Dr MINAL MISTRY, Hampshire Partnership NHS Trust, Melbury Lodge, Winchester, United Kingdom Email: minalmistry@yahoo.co.uk
References
1. TUC. Racism at work - a crime in anyone’s language. Available from: http://www.tuc.org.uk/tuc/rights_racism.cfm
2. Stainback K, Robinson CL, and Tomaskovic-Devey D. Race and workplace integration: a politically mediated process? Am Behav Sci. 2005; 48(9): 1200-1228.
3. Moore LJ. Psychiatric contributions to understanding racism. Transcult Psychiatry. 2000; 37(2): 147-182.
4. Bhopal R. Racism in medicine. Br Med J. 2001; 322: 1503-1504.
5. Bhopal R. Spectre of racism in health and health care: lessons from history and the United States. Br Med J. 1998; 316: 1970-1973.
6. Baker LD. Racism in professional settings: forms of address as clues to power relations. J Appl Behav Sci. 1995; 31(2): 186-201.
7. Encyclopaedia Britannica. Collective unconscious. Available from: http://www.britannica.com/EBchecked/topic/125572/collective-unconscious
8. Dovidio J. The subtlety of racism. Train Dev J. 1993; 47(4): 50-57.
9. Craig-Henderson KM. The automaticity of stereotyping and discrimination. PsycCritiques. 2006; 51(40): abstract.
10. Deitch EA, Barsky A, Butz RM, Chan S, Brief AP and Bradley JC. Subtle yet significant: the existence and impact of everyday racial discrimination in the workplace. Hum Relat. 2003; 56(11): 1299-1324.
11. Beagan BL. ‘Is this worth getting into a big fuss over?’ Everyday racism in medical school. Med Educ. 2003; 37: 852-860.
12. Aluko Y. American Medical Association apologizes for racism in medicine. J Natl Med Assoc. 2008; 100(10): 1246-1247.
13. Macpherson W. The Stephen Lawrence inquiry report. London: Stationary office, 1999.
14. Beishon S, Virdee S and Hagell A. Nursing in a multi-ethnic NHS. London: Policy studies Institute, 1995.
15. Staines R. Is racism a problem in nursing? Nurs Times. 2006; 102(10): 12-13.
16. Duffin C and Parish C. Freedom from racism. Nurs Stand. 2005: 20(4): 22-23.
17. White C. Trusts are making slow progress in promoting race equality, says Healthcare Commission. Br Med J. 2009; 338: b1357.
18. Sheikh A. What’s to be done about racism in medicine? J R Soc Med. 2001; 94(10): 499-500.
19. Coombes R. Mountains to climb. Health Serv J. 2004; 114(5925): 39-46.
20. Chand K. Letter: NHS racism is swept under the carpet. GP. 2004: 33-34.
21. Coker N (ed). Racism in medicine: an agenda for change. London: Kings Fund, 2001.
22. Esmail A. The prejudices of good people. Br Med J. 1994; 328: 1448-1449.
23. Cooke L, Halford S and Leonard P. Racism in the medical profession: the experience of UK graduates, 2006. Available from: http://www.bma.org.uk/employmentandcontracts/equality_diversity/ethnicity/racism.jsp
24. Mamode N. Is the BMA a 21st century organisation? Br Med J. 2004; 329: 161-163.
25. Dennis GC. Racism in medicine: planning for the future. J Natl Med Assoc. 2001; 93(3) Suppl: 1S-5S.
26. Clark PA. Prejudice and the medical profession; a five year update. J Law Med Ethics. 2009: 118-133.
27. Johnstone M-J. Nurses must take a stand against racism in health care. Inter Council Nurses. 2006; 53: 159-160.
28. Mcmanus IC. Factors affecting likelihood of applicants being offered a place in medical schools in the United Kingdom in 1996 and 1997: retrospective study. Br Med J. 1998; 317: 1111-1117.
29. Esmail A and Everington S. Racial Discrimination against doctors from ethnic minorities. Br Med J. 1993; 306: 691-692.
30. Esmail A and Everington S. Letters: Asian doctors are still being discriminated against. Br Med J. 1997; 314: 1619.
31. Lowry S and Macpherson G. A blot on the profession. Br Med J. 1988; 296: 657-658.
32. McManus IC, Richards P, Winder BC and Sproston KA. Final examination performance of medical students from ethnic minorities. Med Educ. 1996; 30(3): 195-200.
33. Wass V, Roberts C, Hoogenboom R, Jones R and Van der Vleuten C. Effect of ethnicity on performance in a final objective structured clinical examination: qualitative and quantitative study. Br Med J. 2003; 326: 800-803.
34. Fox S and Stallworth LE. Racial/ethnic bullying: exploring links between bullying and racism in the US workplace. J Vocat Beh. 2005; 66(3): 438-456.
35. Carr PL, Palepu A, Szalacha L, Caswell C and Inui T. ‘Flying below the radar’: a qualitative study of minority experience and management of discrimination in academic medicine. Med Educ. 2007; 41: 601-609.
36. Pitcher G. NHS human resources staff accused of ignoring racism and bullying of Asian doctors. Available from: http://www.personneltoday.com/articles/2007/08/20/41980/nhs-human-resources-staff-accused-of-ignoring-racism-and-bullying-of-asian-doctors.html
37. Smith R. Deception in research, and racial discrimination in medicine. Br Med J. 1993; 306: 668-669.
38. Forman TA. The social psychological costs of racial segmentation in the workplace: a study of African Americans’ well-being. J Health Soc Beh. 2003; 44(3): 332-352.
39. McKenzie K. Racism and health. Br Med J. 2003 ;326: 65-66.
40. Nunez-Smith M, Curry LA, Bigby JA, Berg D, Krumholz HM and Bradley EH. Impact of race on the professional lives of physicians of African descent. Ann Intern Med. 2007; 146: 45-51.
41. Mistry M and Latoo J (2009). Bullying: a growing workplace menace. Available from: http://www.bjmp.org/content/bjmp-march-2009-volume-2-number-1
42. Newman M. Who’s representing doctors on racism? Hospital Doctor. 11th Oct 2005: p. 9
43. Saleem A. How racism blocked this doctor’s career. Hospital Doctor. 18th Mar 2004: p. 26-27.
44. Symon A. institutional racism and discrimination: are they endemic in the NHS? Br J Midwifery. 2006; 14(6): 366.
45. Dimond Bridgit. Race relations and the law. Br J Midwifery. 2002; 10(9): 580-583.
46. Race relations (amendment) act 2000: New laws for a successful multi-racial Britain. Available from: http://www.homeoffice.gov.uk/documents/cons-2001-race-relations/
47. Dhruev N. Institutional racism: not just skin-deep: how systems sustain racism. Nurs Times. 2002; 98(23): 26-27.
48. Root M P P. The consequences of racial and ethnic origins harassment in the workplace: conceptualisation and assessment. In Barrett K H and George W H (ed). Race, culture, psychology and law. 2005: p. 125.
Ventilator Associated Pneumonia (VAP) is defined as pneumonia occurring in a patient within 48 hours or more after intubation with an endotracheal tube or tracheostomy tube and which was not present before1, 2. Early onset VAP occurs within 48 hours and late onset VAP beyond 48 hours of tracheal intubation.
Incidence
Between 5-15% of hospital in-patients develop infection during admission to ICU3. Patients are 5-10 times more likely to acquire nosocomial infections than patients in the wards4and approximately 86% of hospital associated pneumonia is linked with mechanical ventilation5.
Approximately 10-28% of critical care patients develop VAP6. VAP is also the most common and fatal infection of ICU7,8 and in the United States it affects 9-27% of intubated patients and doubles the risk of mortality as compared with similar patients without VAP9-13.
VAP may account for up to 60% of all Healthcare-Associated Infections14. VAP increases length of ICU stay by 28%16 and each incidence of VAP is estimated to generate an increased cost of £6000- £2200015.
Diagnosis
Despite the high incidence, diagnosis remains challenging because many conditions common to ICU patients like ARDS, sepsis, cardiac failure and lung atelectasis have similar clinical signs. More than 50% of patients diagnosed with VAP do not have the disease whereas upto one-third are not diagnosed17, 18. Unfortunately there is no clearly accepted gold standard for diagnosis of VAP19.
Centres for disease control and prevention (CDC) national healthcare safety network definition for VAP
Radiology signs (2 or more serial chest x-rays with at least one of the following)
New or progressive and persistent infiltrate
Consolidation
Cavitation
Clinical signs
At least one of the following
Fever (temperature > 38 deg C with no other recognised cause)
Leucocytosis > 12000WCC/uL or leucopenia (<4000 WCC /uL)
For adults 70 years or older, altered mental status with no other recognisable cause
and at least 2 of the following
New onset of purulent sputum, or change in character of sputum, or increased respiratory secretions, or increased suctioning requirements
New-onset or worsening cough, or dyspnoea or tachypnoea
Rales or bronchial breath sounds
Worsening gas exchange (eg. O2 desaturations [PaO2/FiO2 ≤ 240], increased O2 requirements, or increased ventilation demand)
Microbiological criteria (optional)
At least one of the following:
Positive growth in blood culture not related to another source of infection
Positive growth in culture of pleural fluid
Positive quantitative culture from bronchoalveolar lavage (≥104 colony forming units/ml) or protected specimen brushing (≥103colony forming units/ml)
5% or more of cells with intracellular bacteria on direct microscopic examination of Gram-stained bronchoalveolar lavage fluid
Histopathological evidence of pneumonia
Histological landmark of VAP is multifocal disease favouring dependant lung segments, often at different stages of development and severity with cultures growing heterogenous microbial flora.20,21
Risk Factors
Mechanical ventilation with Endotracheal intubation including Tracheostomy
Prolonged mechanical ventilation
Advanced age
Pre-existing sinusitis and lung disease
Micro or macroaspiration of oropharyngeal or gastric contents
Malnuitrition and immunosuppression
Obesity
Chronic lung disease
Several factors affect the aetiology of VAP
Time of onset of hospitalisation
Stress induced flora change
Antibiotic induced flora change
Exposure to contamination with nosocomial pathogens
Patient interventions
Pathogenesis:
VAP that occurs within 48 hours after tracheal intubation is usually termed as early onset often resulting from aspiration, which complicates intubation process22. VAP occurring after this period is late onset. Early onset VAP is often due to antibiotic sensitive bacteria (eg oxacillin-sensitive Staphylococcus aureus, Hemophilious influenza and Streptococcus pneumoniae), whereas late onset VAP is frequently caused by antibiotic resistant pathogens (eg.oxacillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa, acinetobacter species and enterobacter species) 23,24,25
The pathogenesis of VAP usually requires that two important processes take place:
Bacterial colonisation of the aero-digestive tract
Aspiration of contaminated secretions into the lower airway26.
Therefore, the strategies to prevent VAP usually focus on reducing the burden of bacterial colonisation in the aero-digestive tract, decreasing the incidence of aspiration or both.
The presence of invasive medical devices is an important contributor to the pathogenesis and development of VAP27. Many patients have nasogastric tubes that predispose them to gastric reflux and increase the potential for aspiration. Endotracheal tubes facilitate bacterial colonisation of the tracheo-bronchial tree and lower airway aspiration of contaminated secretions through mucosal injury, pooling of contaminated secretions above the endotracheal tube cuff and elimination of the cough reflex26. The ventilator circuit and the respiratory-therapy equipment may also contribute to the pathogenesis of VAP if they become contaminated with bacteria, which usually originate in the patient’s secretions26, 28.
Prevention:
The National Institute of Clinical Excellence (NICE) in collaboration with National Patient Safety Agency (NPSA) is examining four technical patient safety solutions for the prevention of VAP and in the process of publishing guidelines. The latest technical patient safety solutions for VAP was published in August 2008 which says
1. Body position-mechanically ventilated and intubated patients should be positioned with their upper body elevated for as long as possible. This may be inappropriate in some patients. eg. spinal injuries. 2. Oral antiseptics e.g. 2% chlorhexidine should be included as part of oral hygiene regimen for all patients who are intubated and ventilated. There is insufficient evidence to recommend any particular antibiotic regimen. 3. Use of kinetic beds - a lack of robust evidence meant the Committee was unable to make recommendations for action on the use of kinetic beds. 4. Care bundles - although the evidence supported the use of elements of care bundles; there was insufficient evidence to recommend a care bundle of any specific design.
The Department of Health published the following ‘High impact intervention’ for ventilated patients in June 2007
Elevation of the head of bed to 35-40 degrees
Sedation holding
Deep Vein Thrombosis prophylaxis
Gastric ulcer prophylaxis
Appropriate humidification of inspired gas
Appropriate tubing management
Suctioning of respiratory secretions (including use of gloves and decontaminating hands before and after the procedure)
Routine oral hygiene as per local policy
In addition the following also may contribute to the prevention of VAP
Prolonged nasal intubation (more than 48hrs) should be avoided because of the association between nosocomial sinusitis and ventilator-associated pneumonia29.
Several investigations have suggested that secretions that pool above the inflated endotracheal tube cuffs may be a source of aspirated material and thus VAP. Endotracheal tubes with separate dorsal lumen above the cuff to suction pooled secretions from the subglottic space are now available. The pressure of the endotracheal tube cuff should be adequate to prevent the leakage of colonised subglottic secretions into the lower airway26,30.
Antibiotic Administration:
Previous administration of antibiotics is an important risk factor for VAP because of the presence of antibiotic-resistant bacteria31. In an attempt to reverse the trend towards increasing rates of antimicrobial resistance among hospital acquired infections, more effective strategies for using antibiotics have been advocated that restrict antibiotic use or offer guidelines for their use 32, 33. Eliminating or reducing the unnecessary use of antibiotics should be the primary goal in reducing antibiotic-resistant nosocomial infections32.
The routine use of prolonged courses of empirical therapy i.e. therapy not supported by results of clinical cultures should be avoided to minimise the subsequent development of antibiotic-resistant infections.
The use of aerosolised antibiotics for the prevention of VAP has been abandoned because of its lack of efficacy and subsequent emergence of antibiotic-resistant infections28.
Similarly the routine use of selective digestive tract decontamination has not gained acceptance in the UK and USA because of its lack of demonstrated effect on mortality, emergence of antibiotic resistant infections and additional toxicity. NICE is currently in consultation for selective decontamination of digestive tract guidelines. The technical patient safety solutions for VAP in adults were published in August 2008.
The Committee examined evidence, which suggested that selective decontamination of the digestive tract (SDD) using topical antibiotics may reduce the incidence of VAP and that SDD regimes that include systemic antibiotics may also reduce mortality. However, Specialist Advisers stated that UK intensive care specialists had particular concerns about the risk of infection with Clostridium difficile and the induction and/or selection of resistant, including multiresistant, microorganisms as a result of SDD. Therefore the Committee recommended further research into SDD in a UK setting.
Use of broad-spectrum antibiotics is also not recommended for the prevention of VAP because of increasing antibiotic resistance among subsequent hospital acquired infections. Targeted antibiotic therapy with appropriate dose of appropriate antibiotic is the sensible thing to do.
Vaccines:
Various vaccination programmes in adults and children have reduced the incidence of pneumonia caused by specific pathogens including H.influenzae type B, Streptococcus Pneumoniae and Influenza virus 34, 35.Vaccinations against these may prevent some hospital acquired infections. Pneumococcal and influenza vaccination must be considered before hospital discharge or included in the discharge planning for all patients at increased risk for subsequent respiratory infections including VAP.
Newer Developments:
There have been new advances in equipment and techniques to help prevention of VAP
Endotracheal and tracheostomy tubes with an extra subglottic port to clear pooled secretions above the endotracheal and tracheostomy tube cuff.
Continuous suctioning of the subglottic secretions.
Endotracheal tubes with specially designed cuffs that do not allow pooled secretions above the cuff to trickle down causing micro-aspiration and ultimately leading to VAP. eg. Endotracheal tubes with microthin polyurethane cuff.
Specially designed closed Tracheal Suctioning Systems (TSS) as compared to open tracheal suctioning systems. However a meta analysis of randomised controlled trial showed that closed suctioning system is not associated with a lower incidence of VAP or mortality as compared to open suctioning36
ACKNOWLEDGEMENTS We thank Dr. S. Parida (Consultant Microbiologist) for her valuable contribution in helping us write this manuscript. COMPETING INTERESTS None Declared AUTHOR DETAILS HARSHAL WAGH, Registrar in Anaesthesia, St Albans City Hospital, United Kingdom DEVARAJA ACHARYA, Consultant in Anaesthesia and Critical Care, St Albans City Hospital, United Kingdom CORRESPONDENCE: DR HARSHAL WAGH, Registrar, Dept of Anaesthesia, Level I, St Julians Ward, St Albans City Hospital, St Albans, UK, AL3 5PN Email: drhdw@hotmail.com
References
Prevention of ventilator-associated pneumonia: consultation NICE, Sept 2007
Eggimann P, Pittet D. Infection control in the ICU. Chest 2001; 120: 2059-93
Weber DJ, Raasch R, Rutala WA. Nosocomial infections in the ICU: the growing importance of antibiotic-resistant pathogens. Chest 1999; 115: 34S-41S
Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in medical intensive care units in the United States. National Nosocomial infections Surveillance System.Crtic Care Med.1999 May; 27950: 887-92
The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee 1995.
Legras A, Malvy D, Quinioux AI, et al. Nosocomial Infections: prospective survey of incidence in five French intensive care units. Intensive Care Med.1998; 24: 1040-1046.
Urli T, Perone G, Acquarolo A, Zappa S, Antonini B, Ciani A. Surveillance of infections acquired in intensive care: usefulness in clinical practise. J Hosp Infect. 2002; 52: 130-135
Heyland DK, Cook DJ, Griffith L, keenan SP, Brun-Buisson C; Canadian Critical Trials Group. The attributable morbidity and mortality of ventilator-associated pneumonia. Am J Respir Crit Care Med. 1999; 159:1249-1256
Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gilbert C. Nosocomial pneumonia and mortality among patients in intensive care units. JAMA 1996; 275:866-869.
Rello J, Quintana E, Ausina V, et al. Incidence, etiology and outcome of nosocomial pneumonia in mechanically ventilated patients. Chest, 1991; 100:439-444.
Jiménez P, Torres A, Rodriguez-roisin R, et.al. Incidence and etiology of pneumonia acquired during mechanical ventilation. Crit care Med.1998; 17:882-885.
Safdar N, Dezfulian C, Collard HR, Saint S. Clinical and economic consequences of ventilator-associated pneumonia; a systemic review.Crit Care Med.2005; 33:2184-2193
CDC. Guidelines for preventing Health -Care -Associated Pneumonia, 2003. Recommendation of the CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR 2004; 53(No.RR-3)
Nosocomial pneumonia: incidence, morbidity and mortality in the intubated-ventilated patient. Pittett 1994
Nosocomial viral ventilator-associated pneumonia in the intensive care unit: a prospective cohort study. Pfr Vincent 2005
Petersen IS, Aru A, SkØdt V, et al. Evaluation of pneumonia diagnosis in intensive care patients. Scand J infect Dis.1999; 31:299-303
Fagon JY, Chastre J, Hance AJ, Domart Y, Trouillet JL, Gilbert C. Evaluation of clinical judgement in the identification and treatment of nosocomial pneumonia in ventilated patients.Chest.1993; 103:547-553
American Thoracic Society; Infectious diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med.2005; 171:388-416.
Rouby JJ, Martin De Lassale E, Poete P, et al. Nosocomial bronchopneumonia in the critically ill: histologic and bacteriologic aspects. Am Rev Respir Dis.1992; 146:1059-1066.
Fabregas N, Torres A, El-Ebiary M, et al. Histopathologic and microbiologic aspects of ventilator-associated pneumonia. Anaesthesiology.1996; 84:760-761
Pingleton SK, Fagon JY, Leeper KV Jr. Patient selection for clinical investigation of ventilator-associated pneumonia: criteria for evaluating diagnostic techniques. Chest 1990; 97:170-81.
Niederman MS,Craven DE, Fein AM, Schultz DE. Pneumonia in the critically ill hospitalised patient. Chest 1990; 97:170-81.
Kollef MH, Silver P,Murphy DM, Trovillion E. The effect of late-onset ventilator-associated pneumonia in determining patient mortality. Chest 1995; 108:1655-62.
Rello J, ausina V, Ricart M, Castella J, Prats G. Impact of previous antimicrobial therapy on the therapy on the etiology and outcome of ventilator-associated pneumonia. Chest 1993; 104:1230-5.
Craven DE, Steger KA. Epidemiology of nosocomial pneumonia: new perspectives on an old disease. Chest 1995; 108: Suppl: 1S-16S.
Kollef M. Current concepts - the prevention of VAP. NEJM 340; 8:627-634.
Tablan OC, Anderson LJ, Arden NH, Breiman RF, Butler JC, Mcneil MM. Guideline for prevention of nosocomial pneumonia: The Hospital Infection Control Practices Advisory Committee, Centres For Disease Control And Prevention.Infect Control Hosp Epidemiol 1998; 19:304
Rouby JJ, Laurent P, Gosnach M et al. Risk factors and clinical relevance of nosocomial maxillary sinusitis in the critically ill. Am J Respir Crit Care Med 1994; 150: 776-83
Valles J, Artigas A, Rello J et al. Continuous aspiration of subglottic secretions in preventing ventilator associated pneumonia. Ann Intern Med 1995; 122:179-86.
Crouch Brewer S, Wuderink RG, Jones CB, Leeper KV Jr. Ventilator-associated pneumonia due to Pseudomonas aeruginosa. Chest 1996; 109:1019-29
Goldman DA, Weinstein RA, Wenzel RP, et al. Strategies to prevent and control the emergence and spread of antimicrobial-resistant microorganisms in hospitals: a challenge to hospital leadership. JAMA 1996; 275:234-40.
Evans RS, Pestotnik SL, Classen DC, et al. A computer-assisted management programme for antibiotics and other anti-infective agents. N Engl J Med 1998; 338:232-8.
Herceg A.The decline of Haemophilus influenza type b disease in Australia.Commun Dis Intell 1997; 21:173-6.
Gross PA, Hermogenes AW, Sacks HS, Lau J, Levandowski RA. The efficacy of influenza vaccine in elderly persons: a meta analysis and review of literature. Ann Intern Med 1995; 123:518-27.
I I Siempos, K Z Vardakas, M E Falagas. Br J Anaesth 2008; 100(3): 299-306.
Technical patient safety solutions for Ventilator-associated pneumonia in adults. NICE August 2008
Osteoporotic
fracture is common, expensive, and associated with increased morbidity
and mortality. The incidence of osteoporosis fracture annually is greater
than the risk of stroke, breast cancer, and heart attack combined. Bisphosphonates
(BPs) have recently been the subject of clinical controversies because
of the reported incidence of osteonecrosis of jaw (ONJ). Bisphosphonates
as a group of drugs were introduced for the management of various conditions
such as osteoporosis, Paget’s disease, multiple myeloma, and hypercalcemia
of malignancy. This group of drugs has improved the quality of life
in many patients with proven efficacy in limiting pain and skeletal-related
events. The efficacy of BPs as one method to prevent and treat osteoporosis
and avert future fractures, particularly vertebral fractures, is well
documented in large clinical trials. However, despite this evidence,
many patients at risk for osteoporosis are not screened or treated.
The controversy of osteonecrosis of the jaws and bisphosphonates is
a recent and growing problem.
Bisphosphonates:
Bisphosphonates
are fairly safe drugs to be used in the long term. There is a significant
amount of safety data for up to 10 years with alendronate or Fosamax
and up to 7 years with risedronate or Actonel. Every year, an estimated
30 million BP prescriptions are written in the U.S. alone.1
The bisphosphonates alendronate, risedronate, ibandronate, and zoledronic
acid are nitrogen containing compounds that increase bone mineral density
(BMD) by inhibiting osteoclast-mediated bone resorption.2
They have been shown to increase BMD approximately 2–8%, depending
upon the dose and site measured, and have demonstrated efficacy in primary
and secondary prevention of osteoporotic fractures.3–10
Nitrogen-containing
bisphosphonates are used widely for the management of metastatic cancer
in bone (intravenous zoledronic acid or Pamidronate), for the prevention
and treatment of osteoporosis (oral alendronate, risedronate, and ibandronate
and intravenous ibandronate), for the treatment of Paget’s disease
of bone (intravenous Pamidronate and oral alendronate and risedronate),
and for the short-term management of acute hypercalcemia (intravenous
zoledronic acid and Pamidronate).11 Bisphosphonates reduce
the survival and function of osteoclasts, the bone-resorbing cells.
The clinical pharmacology of intravenous (IV) BPs is characterized by
low intestinal absorption but highly selective localization and deposition
in bone. Oral BPs have a bioavailability of less than 5%.12
Once in the blood, BPs disappear very rapidly into the bone.13
After BPs are buried in the skeleton, they are released only when the
bone is destroyed in the course of turnover. In humans, the skeletal
half-lives of various BPs range from 3 months to as long as 10 years.
14
Osteoporosis:
Osteoporosis
is a devastating disease that may lead to significant morbidity and
mortality from resultant fractures. Approximately one in two women and
one in four men over age 50 will have an osteoporosis related fracture
in their remaining lifetime. 15 According to estimated
figures, osteoporosis was responsible for more than 2 million fractures
in US in 2005 15 (including approximately 297,000 hip fractures,
547,000 vertebral fractures, 397,000 wrist fractures , 135,000 pelvic
fractures , 675,000 fractures at other sites). The number of fractures
due to osteoporosis is expected to rise to more than 3 million by 2025.
15
Osteoporotic
fractures are associated with significant morbidity and mortality. Patients
who sustain a fracture are more likely to have lower health-related
quality of life, depression, pain, disability, physical deconditioning
due to inactivity, vertebral deformities with a resultant decrease in
pulmonary function and increase in gastrointestinal complications
(e.g., refractory reflux esophagitis), pressure ulcers, increased likelihood
of nursing home placement, and changes in self-image. 16-23
Hip fractures, which are the most serious complication of osteoporosis,
are associated with significant mortality. 24–27 Up to
38% of patients may die within one year after a hip fracture, and the
risk of death is approximately double that of patients who do not sustain
a hip fracture. 24, 25, 27
The economic
consequences of osteoporosis are enormous. In 1995 in USA, osteoporotic
fractures were responsible for approximately 432,000 hospital admissions,
2.5 million physician’s office visits, and 180,000 nursing home admissions.
15 Health care costs associated with osteoporotic fractures in
2005 were an estimated $19 billion. By 2025, experts predict that these
costs will rise to approximately $25.3 billion. 15 As the
population of the United States continues to age, these costs will likely
increase, with the number of hip fractures and associated costs possibly
tripling by 2040. 15
Oral
bisphosphonate associated osteonecrosis of the jaw:
Osteonecrosis
of the jaws (ONJ) is characterized by the death of bone as a natural
consequence of a wide variety of systemic and local factors compromising
the blood flow of the bone. Clinically it is diagnosed by an area of
exposed bone in the mandible, maxilla, or palate that typically heals
poorly or does not heal over a period of 6 to 8 weeks. The diagnosis
is primarily a clinical one, but imaging studies such as computed tomography
can be helpful. Approximately two thirds of cases involve the mandible
and the rest involve the maxilla. The lesion is painful in many, but
not all, patients, and infection is often present. In one unusual case,
osteonecrosis of the external auditory canal developed in a patient
with myeloma who had received intravenous zoledronic acid and amidronate.28
Predisposing factors for the development of osteonecrosis of the jaw
appear to be dental disease, dental surgery (e.g., tooth extraction),
oral trauma, periodontitis, and poor dental hygiene. The risk factors
for developing ONJ include trauma, female gender, advanced age, edentulous
regions, radiotherapy, chemotherapy, steroid therapy, blood dyscrasias/metastatic
disease, anemia, coagulopathy, surgical dental procedures, alcohol or
tobacco use, prior infection, and bisphosphonate therapy.29-32
Although there have been some reports in the literature about osteonecrosis
caused by steroids, this form is different from ONJ in the sense that
steroid-induced osteonecrosis does not cause bone exposure.
1,
33
ONJ in connection
with bisphosphonate use was first reported in 2003 34, or
5 to 10 years after these drugs were approved in the United States for
their current indications; it was rarely seen before then. Most of the
reported cases (95%) have been associated with zoledronic acid or Pamidronate
given intravenously to control metastatic bone disease. 35, 36,
11 Myeloma and breast cancer are by far the most common cancers
associated with intravenous bisphosphonate use and osteonecrosis of
the jaw.35
Osteonecrosis
of the jaw has developed far less often among patients who have received
oral bisphosphonates at the lower doses used for osteoporosis than among
patients who received the higher doses used for metastatic cancer. Among
several million patients who have received oral treatment for osteoporosis,
fewer than 50 cases of osteonecrosis of the jaw have been reported to
date.35 Moreover, with more than 60,000 patient- years of
exposure to nitrogen- containing bisphosphonates in clinical trials
of treatment for osteoporosis (involving follow-up for as long as 10
years in some patients), osteonecrosis of the jaw was not reported among
the adverse events. 11 The exact incidence of ONJ is unknown.
However, some reports have estimated it to be about 1 in 10,000 for
Intravenous use of BPs. 37 1 in 100,000 patient years
is a reasonable estimate of the incidence of osteonecrosis of the jaw
in patients receiving oral nitrogen-containing bisphosphonates for osteoporosis.
11 The risk of developing ONJ for patients taking alendronate,
the most commonly prescribed oral bisphosphonate, has been estimated
to occur in approximately 0.7 per 100,000 persons per years’ exposure
38; on the other hand, the incidence of ONJ for risedronate and
ibandronate cannot yet be quantified because too few cases have been
reported (12 cases for risedronate and one for ibandronate). 38
The Cartosos
medical claims database study also surveyed 260,000 subjects with osteoporosis,
and found an odds ratio for inflammatory necrosis of the jaw to be 0.65
in oral bisphosphonate users, and that for surgery for a necrotic process
to be 0.86. 39 Both these values are consistent with the
other data suggesting that oral bisphosphonate use does not increase
ONJ risk in osteoporosis patients. These findings are very similar to
those from a case-control study using a claims database, which found
that receiving at least
one oral bisphosphonate prescription was associated with an odds ratio for
jaw surgery of 0.91. 40 As per one consensus panel, there
have been 33 cases [reported] in the literature as of January 2007 --
out of the 33 million patients who have been treated worldwide with
an oral bisphosphonate -- which translates into approximately 200 million
prescriptions written. 41 In addition, there has been spontaneous
reporting in 1 of 100,000 patient-years for all of the approved bisphosphonates.
41 The fact that the majority of reported cases of osteonecrosis
of the jaw are associated with the use of high-dose intravenous bisphosphonates
for metastatic bone disease suggests that the dose, duration of treatment,
and route of administration, as well as coexisting conditions, concomitant
treatments (glucocorticoids or immunosuppressive agents), and dental
health, could all be related to the incidence of this complication.
11
Prevention
and management of bisphosphonate-associated osteonecrosis of the jaw:
Published
recommendations are based upon expert experience from a variety of sources.
35,36,1, 42-–45 As yet, there have been no randomized, controlled
trials that have evaluated strategies to prevent or manage ONJ in individuals
receiving long-term high-dose bisphosphonate therapy. Before initiating
BP therapy, all medical and dental practitioners are encouraged to follow
these guidelines:
All patients
should undergo a routine dental exam to rule out any dental source of
infection.
All medical practitioners
also should perform a baseline oral exam.
Invasive dental
or/and oral surgical procedures should be completed before initiating
therapy.
Practice preventive
dentistry, involving procedures such as oral prophylaxis, dental restorations,
and endodontic therapy, and check dentures for irritational foci.
Schedule routine
follow-up every 3 months to check for any signs of developing ONJ.
The risks associated
with oral surgical procedures such as dental implants, extractions,
and extensive periodontal surgeries must be discussed with the patient
and weighted against the benefits.
The following
recommendations are made by the American Association of Oral and Maxillofacial
Surgeons for management of patients on BP therapy and patients with
proven ONJ. 46
Management
of patients with proven ONJ based on staging of the condition:
Stage 1: Exposed/necrotic bone in patients who are asymptomatic and have no
evidence of infection
Stage 2: Exposed/necrotic bone in patients with pain and clinical evidence
of infection.
Stage 3: Exposed/necrotic bone in patients with pain, infection, and 1 or
more of the following: Pathologic fracture, extra oral fistula, or osteolysis
extending to the inferior border.
Treatment of patients with established ONJ:
Patients with stage 1 ONJ: Conservative management with oral rinse such as 0.12%
chlorhexidine.
Patients
with stage 2 ONJ: Manage with antibiotics and antimicrobial oral rinses.
Patients
with stage 3 ONJ: Surgical debridement/ resection in combination with
antibiotic therapy.
Extraction
of symptomatic teeth can be performed without any additional risks of
worsening the condition.
General
recommendations:
As with
all dental patients, routine dental examinations are recommended. A
comprehensive oral evaluation should be carried out of all patients
about to begin therapy with oral bisphosphonates (or as soon as possible
after beginning therapy). The dentist should inform the patient taking
oral bisphosphonates that there is a very low risk (estimated at 0.7
cases per 100,000 person-years’ exposure) of developing ONJ; there
are ways to minimize the risk, but not to eliminate the already low
risk; the consensus is that good oral hygiene along with regular dental
care is the best way to lower risk; there are no diagnostic techniques
to identify those at increased risk of developing ONJ.
Before undergoing
any invasive procedure that involves manipulation of the bone the patient
should understand that at this time, the risk of developing osteonecrosis
of the jaw is considered very small, and that the vast majority of patients
taking an oral bisphosphonate do not develop any oral complications.
(Dental management of patients receiving oral bisphosphonate therapy:
Expert panel recommendations)
Based on
the currently available information, National Osteoporosis Foundation
believes that in the vast majority of patient who are receiving them,
the benefits of oral bisphosphonate medications outweigh the potential
risk of ONJ. Patients for whom bisphosphonates are appropriate would
be at higher risk of fractures without treatment, and fractures are
the source of significant pain and disability that impact on function
and quality of life. If a patient receiving bisphosphonates has planned
dental surgery that involves the bone, a drug holiday beginning shortly
before the procedure and lasting until there is local healing could
be considered, although there is as yet no clinical evidence that this
will affect the incidence or severity of ONJ. (Osteonecrosis of the
Jaw (ONJ) June 14, 2006 / Reviewed and approved by the Science and Research
Committee of the NOF Board of Trustees March 3, 2007).
Conclusion:
There is
a need to clearly delineate the incidence of ONJ in osteoporosis patients
treated with oral bisphosphonates, and in appropriate control populations.
Based on current evidence, the risk of ONJ in osteoporosis patients
taking oral BPs appears to be comparable to that in the general population.
With the likely prevalence sitting at approximately 1 per 100,000 patient-years,
it is quite clear that this is no different from that in the general
population, since these problems can certainly occur in the absence
of bisphosphonate use. The documented benefits of using bisphosphonates
for established indications clearly outweigh whatever small risk of
osteonecrosis of the jaw might be incurred. 11, 47 Even if
the number of cases of ONJ in patients taking oral bisphosphonates are
still rare compared to the total exposure, primary care physicians treating
bone diseases with bisphosphonates need to be aware there is a small
risk their patients may develop this new complication, allowing for
prophylaxis, early diagnosis and prevention of potential consequences.
The benefits and risks of bisphosphonate therapy should be individually
discussed and, when necessary and possible, alternative therapy for
postmenopausal osteoporosis should be considered.
It is important
to understand that, based on the information currently available; the
risk for developing BON is much higher for cancer patients on intra
venous bisphosphonate therapy than the risk for patients on oral bisphosphonate
therapy. Therefore, there are different recommendations for dental management
of these patients.
In conclusion,
the risk of ONJ is extraordinarily low. The risk of being in a fatal
car accident is 10-15 times as high as the risk of ONJ from taking an
oral bisphosphonate. 41
Competeing Interests:
Serves as a speaker for Eisai Inc. and Pfizer Inc. for the 2008 ARICEPT LTC DELTA
2 (Dementia Education Leadership Training in Alzheimer's) Promotional
Education Program AUTHOR DETAILS
NASSEER A. MASOODI, MD,
FACP, CMD. Assistant Professor Clinical Sciences, Florida State University
College of Medicine, Tallahassee, FL-USA; Courtesy Assistant Professor
Geriatrics, University of Florida College of Medicine, Gainesville,
FL-USA; Medical Director Health Services, ACV Inc, Dowling Park, FL-USA
CORRESSPONDENCE: PO BOX: 4346, Dowling Park, FL-32064, USA.
Email: haadin@yahoo.com
References
Gutta R, Louis
P. Bisphosphonates and osteonecrosis of the jaws: Science and rationale.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:186-93
NIH Consensus
Conference. Optimal calcium intake. NIH Consensus Development Panel
on Optimal Calcium Intake. JAMA. 1994; 272:1942–8.
Cummings SR,
Black DM, Thompson DE et al. Effect of alendronate on risk of fracture
in women with low bone density but without vertebral fractures: results
from the Fracture Intervention Trial. JAMA. 1998; 280:2077–82.
Black DM, Cummings
SR, Karpf DB et al. Randomized trial of effect of alendronate on risk
of fracture in women with existing vertebral fractures. Lancet. 1996;
348:1535–41.
Harris ST, Watts
NB, Genant HK et al. Effects of risedronate treatment on vertebral and
nonvertebral fractures in women with postmenopausal osteoporosis: a
randomized controlled trial. JAMA. 1999; 282:1344–52.
Reginster J,
Minne HW, Sorensen OH et al. Randomized trial of the effects of risedronate
on vertebral fractures in women with established postmenopausal osteoporosis.
Osteoporos Int. 2000; 11:83–91.
McClung MR, Geusens
P, Miller PD et al. Effect of risedronate on the risk of hip fracture
in elderly women. N Engl J Med. 2001; 344:333–40.
Chesnut IC, Skag
A, Christiansen C et al. Effects of oral ibandronate administered daily
or intermittently on fracture risk in postmenopausal osteoporosis. J
Bone Miner Res. 2004; 19:1241–9.
Lyles KW, Colón-Emeric
CS, Magaziner JS et al. Zoledronic acid and clinical fractures and mortality
after hip fracture. N Engl J Med. 2007; 357:1799–809.
Black DM, Delmas
PD, Eastell R et al. Once-yearly zoledronic acid for treatment of postmenopausal
osteoporosis. N Engl J Med. 2007; 356:1809–22.
Bilezikian JP.
Osteonecrosis of the Jaw-Do Bisphosphonates pose a risk? N Engl J Med.
2006; 355:2278–81.
Conte P, Guarneri
V. Safety of intravenous and oral bisphosphonates and compliance with
dosing regimens. Oncologist 2004; 9(Suppl 4):28-37.
Bisaz S, Jung
A, Fleisch H. Uptake by bone of pyrophosphate, diphosphonates and their
technetium derivatives. Clin Sci Mol Med 1978; 54:265-72.
Kasting GB,
Francis MD. Retention of etidronate in human, dog, and rat. J Bone Miner
Res 1992; 7:513-22.
National Osteoporosis
Foundation. Physician’s guide to prevention and treatment of osteoporosis. www.nof.
org/physguide/index.htm (accessed Nov. 2008)
Lips P, Cooper
C, Agnusdei D et al. Quality of life in patients with vertebral fractures:
validation of the Quality of Life Questionnaire of the European Foundation
for Osteoporosis (QUALEFFO). Osteoporos Int. 1999; 10:150–60.
Gold DT, Shipp
KM, Lyles KW. Managing patients with complications of osteoporosis.
Endocrinol Metab Clin North Am. 1998; 27:485–96.
Hallberg I,
Rosenqvist AM, Kartous L et al. Health related quality of life after
osteoporotic fractures. Osteoporos Int. 2004; 15:834–41
Nevitt MC, Ettinger
B, Black DM et al. The association of radiographically detected vertebral
fractures with back pain and function: a prospective study. Ann Intern
Med. 1998; 128:793–800.
Fink HA, Ensrud
KE, Nelson DB et al. Disability after clinical fracture in postmenopausal
women with low bone density: the Fracture Intervention Trial (FIT).
Osteoporos Int. 2003; 14:69–76.
Ensrud KE, Thompson
DE, Cauley JA et al. Prevalent vertebral deformities predict mortality
and hospitalization in older women with low bone mass. J Am Geriatr
Soc. 2000; 48:241–9.
Margolis DJ,
Knauss J, Bilker W et al. Medical conditions as risk factors for pressure
ulcers in an outpatient setting. Age Ageing. 2003; 32:259–64.
Melton LJ 3rd.
Adverse outcomes of osteoporotic fractures in the general population.
J Bone Miner Res. 2003; 18:1139–41.
Empana JP, Dargent-Molina
P, Breart G. Effect of hip fracture on mortality in elderly women: the
EPIDOS prospective study. J Am Geriatr Soc. 2004; 52:685– 90.
Center JR, Nguyen
TV, Schneider D et al. Mortality after all major types of osteoporotic
fracture in men and women: an observational study. Lancet. 1999; 353:878–82.
Cauley JA, Thompson
DE, Ensrud KC et al. Risk of mortality following clinical fractures.
Osteoporos Int. 2000; 11:556–61.
Keene GS, Parker
MJ, Pryor GA. Mortality and morbidity after hip fractures. BMJ. 1993;
307:1248–50.
Hoff AO, Toth
B, Altundag K, et al. Osteonecrosis of the jaw in patients receiving
intravenous bisphosphonate therapy. J Bone Miner Res 2005; 20: Suppl
1:1218. Abstract
Bouquot JE,
McMahon RE. Neuropathic pain in maxillofacial osteonecrosis. J Oral
Maxillofac Surg 2000; 58:1003-20.
Assouline-Dayan
Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME. Pathogenesis and
natural history of osteonecrosis. Semin Arthritis Rheum 2002; 32:94-124.
Gruppo R, Glueck
CJ, McMahon RE, Bouquot J, Rabinovich BA, Becker A, et al. The pathophysiology
of alveolar osteonecrosis of the jaw: anticardiolipin antibodies, thrombophilia,
and hypofibrinolysis. J Lab Clan Med 1996;127:481-8.
Damato K, Gralow
J, Hoff A, Huryn J, Marx RE, Ruggiero S, et al. Available at: http://www.fda.gov/ohrms/dockets/ac/05/briefing/ 2005-4095B2_02_12-Novartis-Zometa-App-11.pdf.
(Accessed Oct, 2008).
Zigic TM, Marcous
C, Hungerford DS, Dansereau JV, Stevens MB. Corticosteroid therapy associated
with ischemic necrosis of bone in systemic lupus erythematosis. Am J
Med 1985;79:596.
Marx RE. Pamidronate
(Aredia) and zoledronate (Zometa) induced avascular necrosis of the
jaws: a growing epidemic. J Oral Maxillofac Surg 2003;61(9):1115–7.
Woo SB, Hellstein
JW, Kalmar JR. Bisphosphonates and osteonecrosis of the jaws. Ann Intern
Med 2006; 144:753-6. [Erratum, Ann Intern Med 2006; 145:235.]
Marx RE, Sawatari
Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis)
of the jaws: risk factors, recognition, prevention, and treatment. J
Oral Maxillofac Surg 2005; 63:1567-75.
Novartis Pharmaceuticals
Co. Updated safety: possible relationship of Aredia (Pamidronate disodium)
and/or Zometa (zoledronic acid) with osteonecrosis of the jaw [letter
to health care professionals]. Ottawa: Health Canada; Nov 2004. Available
at: www.hc-sc.gc.ca/ hpfb-dgpsa/tpd-dpt/aredia_zometa_hpc_e.html.
(Accessed Nov, 2008).
American Dental
Association Council on Scientific Affairs: Expert panel recommendations:
Dental management of patients receiving oral bisphosphonate therapy.
J Am Dental Assoc 2006, 137:1144-1150
Cartosos VM,
Zhu S, Zavras AI. Bisphosphonate use and the risk of adverse jaw outcomes.
JADA 2008; 139: 23-30.
Pazianas M,
Blumentals WA, Miller PD. Lack of association between oral bisphosphonates
and osteonecrosis using jaw surgery as a surrogate marker. Osteoporos
Int 2008;19: 773-779.
Postmenopausal
Osteoporosis: Putting the Risk for Osteonecrosis of the Jaw Into Perspective
Authors: Stuart L. Silverman, MD, FACR, FACP; Mone Zaidi, MD, PhD, FRCP;
E. Michael Lewiecki, MD, FACP; Regina Landesberg, DMD, PhD (Medscape
Online CME, accessed on April 23, 2007).
Migliorati CA,
Siegel MA, Elting LS. Bisphosphonate-associated osteonecrosis: a long-term
complication of bisphosphonate treatment. Lancet Oncol 2006;7(6):508–14
Expert panel
recommendations for the prevention, diagnosis, and treatment of osteonecrosis
of the jaws. LDA J 2005; 64(3):21–4.
Melo MD, Obeid
G. Osteonecrosis of the jaws in patients with a history of receiving
bisphosphonate therapy: strategies for prevention and early recognition.
J Am Dent Assoc 2005; 136(12):1675–81.
Hellstein JW,
Marek CL. Bisphosphonate induced osteochemonecrosis of the jaws: an
ounce of prevention may be worth a pound of cure. Spec Care Dentist
2006; 26(1):8–12.
AAOMS Position
Paper on Bisphosphonate-Related Osteonecrosisof the Jaws. Available
at: http://aaoms.org/docs/position_papers/osteonecrosis.pdf. (Accessed
October, 2008).
ASHP Therapeutic
Position Statement on the Prevention and Treatment of Osteoporosis in
Adults http://www.ashp.org/DocLibrary/BestPractices/TPS_Osteo.aspx (Accessed Nov 25, 2008)
Adjuvant
modes of breast cancer therapy following surgical intervention mainly
revolve round radiation therapy, chemotherapy, or hormone therapy designed
to eliminate residual cancer cells. The increase in the incidence of
breast cancer with age has sharply focused attention on the link between
incidence and progression. It follows from this that approaches to successful
treatment and patient management would converge on hormonal status as
a beneficial mode of targeted therapy. A number of growth factors, besides
the steroid hormones oestrogen and progesterone, are closely involved
in the growth and metastatic spread of breast cancer. Recent years have
seen intensive studies of the mechanisms of function of growth factors
and the pathways by which they stimulate the growth of cancer cells.
These studies have led the way to the targeting growth factor function
as a means of controlling breast cancer development and secondary spread.
The growth
factor receptors are transmembrane proteins. The binding of growth factors
to the external domain activates these receptors which have tyrosine
kinase activity. This activation therefore leads to the phosphorylation
of signalling proteins down stream in the signalling cascade. This in
turn leads to the expression of genes associated with cell proliferation
and often also to the inhibition of apoptotic loss of cells.
Growth
factors, growth factor receptors and tumour growth and progression
Growth factors
and their receptor play a major part in normal growth and differentiation
and also in tumour development and progression. Growth factors promote
proliferation and induce cancer invasion. Certain growth factors, e.g.
the insulin-like growth factor (IGF) might promote tumour growth by
inhibiting apoptotic loss of cells1. Mutations or over-expression
of growth factor receptors is associated with aggressive cancers and
poor prognosis for patients. Growth factor receptor genes are amplified
in a number of human cancers and this is reflected in the expression
of the respective receptor proteins in the cancers. Growth factor receptors
are transmembrane tyrosine kinase proteins and transduce the signals
imparted by the binding of the growth factors to their specific receptors;
this signal transmission ultimately results in the induction of cell
proliferation.
Among growth
factors of note in the context of this editorial are the epidermal growth
factor (EGF) and the Heregulins constituting a family of EGF related
growth factors. There are several isoforms of Heregulin generated by
alternative RNA splicing of the heregulin gene; these isoforms bind
to their receptors with different degree of affinity. The epidermal
growth factor receptor (EGFr) family (also often referred to as the
erb family) includes HER1 (human epidermal growth factor receptor 1
also called EGFr), HER2, HER3
and HER4. These receptor proteins significantly resemble one another
in aminoacid sequence2. Heregulin can bind HER3 and HER4
receptors but the ligand for HER2 has not been identified3
and so HER2 is often described as an orphan receptor. The receptor protein
consists of an external domain that binds growth factors, a transmembrane
domain and an intracellular domain which possesses tyrosine phosphorylation
sites4. Growth factors and their paralogues bind to these
receptors and induce receptor oligomerisation. This activates the cytoplasmic
kinase domains, which phosphorylate and activate target proteins that
induce the expression of genes responsive to the growth factors. The
binding and activation of the receptors is a highly specific process,
but often more than one receptor might be involved in the signalling
process. In this event heterodimerisation would occur between different
receptors; this seems to enhance the affinity of ligand binding5.
This process of engagement of co-receptors to enhance growth factor
signalling has been described as cross-talk between the receptors. HER2
is known to be involved in cross-talk with EGFr, HER3 as well as HER4.
So HER2 seems to occupy a pre-eminent position in the signalling cascade,
but recently it has been suggested that HER3 might also be a prominent
participant6.
The EGFr
family of receptors have been intensively investigated for their potential
relationship to cancer progression and prognosis and as a potential
route for treatment and patient management. Approximately 25% of breast
cancers show HER2 gene amplification and this correlates aggressive
behaviour and poor prognosis7-10. However, on the positive
side the presence of HER2 receptors has provided a new treatment modality
for many patients.
Monoclonal
antibodies (Herceptin) have been raised against the external domain
of HER2. Herceptin has provided a highly successful mode of treatment
for metastatic breast cancer showing high HER2 expression and HER2 gene
amplification11-13. Blocking receptor function with Herceptin
inhibits tumour growth and possibly also microvascular density associated
with tumours and vascular permeability. Furthermore, Herceptin treatment
appears to reduce VEGF (vascular endothelial growth factor) expression,
tumour associated microvascular density and cell proliferation in breast
cancers xenografted into mice14. Also in murine tumour models,
Herceptin reduces the number of circulating cancer cells even under
circumstances where the tumour is resistant to Herceptin treatment15,
which could be a manifestation of its effects on the vasculature independently
of its inhibition of HER2 signalling.
HER2
expression and tamoxifen resistance
Breast cancer
growth is influenced by the sex steroid hormones oestrogen and progesterone
and growth factors such as EGF and HER2 ligands. Patients with tumours
that are oestrogen receptor (ER) positive are treated with tamoxifen.
The latter binds ER and competitively blocks oestrogen signals. In the
context of the deployment of Herceptin to treat HER2+ patients, it has
emerged that tumours over-expressing HER2 are resistant to tamoxifen.
These patients could benefit from anti-oestrogen therapy combined with
blockade of HER2 signalling16. A randomized trial has indicated
that post-menopausal patients with advanced breast cancer can benefit
significantly from this combination therapy17.
Among other
factors that might confer tamoxifen resistance is AIB1, the steroid
receptor co-activator, which is often amplified in breast cancers. In
vitro studies with breast cancer cells and in vivo investigations of
murine tumours have suggested the involvement of AIB1 in tamoxifen resistance18
and in HER2 signalling19. In primary breast cancer also AIB1
has been linked with tamoxifen resistance20, 21. A second
factor deserving discussion in this context is the possibility that
EGFr and HER2 signalling systems might interact and contribute in this
way to resistance to hormonal therapy. As mentioned elsewhere in this
review, EGFr does recruit HER2 as a co-receptor in signal transduction.
This is of some significance for patients with ER-negative tumours.
For, we showed some years ago that a proportion of ER-ve tumours tended
to be EGFr+ve22-24. So this would suggest the possibility
that patients with ER-ve/EGFr+ tumours could conceivably benefit from
Herceptin treatment (see below).
Another
possible means by which tamoxifen resistance might arise has been suggested
by the finding that tamoxifen and Fulvestrant, also an anti-oestrogen,
appear to be able to induce breast cancer cell invasion in the absence
of E-cadherin25. Cadherins are transmembrane proteins, which
have considerable influence on cancer invasion because they alter intercellular
and cell-substratum adhesion. E-cadherin is regarded as a suppressor
of invasion and growth of carcinomas as the loss or mutation of E-cadherin
leads to the acquisition of invasiveness. Borley et al.25
showed that both tamoxifen and Fulvestrant induced invasion in E-cadherin
deficient MCF7 breast cancer cells, but this did not occur after oestrogen
depletion. These findings add a new dimension to tamoxifen resistance
as potentially being mediated by recurrence resulting from induced invasive
ability.
HER2
expression and adjuvant chemotherapy
It has been
recognised of late that combination of Herceptin with chemotherapy might
yield considerable benefits in terms of reduction of recurrence and
mortality. So HER2 expression has come into the reckoning when considering
the use of adjuvant chemotherapy. Combining Herceptin with either an
anthracycline plus cyclophosphamide or with Paclitaxel, as first-line
therapy for metastatic breast cancer over expressing the HER2 receptor,
has provided significant benefits in terms of objective response, duration
of response and survival as compared with chemotherapy alone. Furthermore,
the benefits were related to the degree of HER2 over-expression26.
A review of 35 clinical trials has indicated that patients with HER2+
cancers might benefit more from anthracycline-based and taxane-based
adjuvant chemotherapy than those with HER2-negative cancers27.
Indeed, anti-HER2 antibody combined with chemotherapy is superior to
HER2 anitibody and anti-oestrogen combination17. The benefits
of adjuvant chemotherapy with anthracyclines to patients with HER2 over-expressing
tumours seem to be beyond reasonable doubt. Gennari et al.28
have provided a combined analysis of eight studies. HER2+ patients on
anthracyclines had superior disease-free as well as overall survival
in comparison with patients on non-anthracycline regimen. No such benefits
emerged for HER2-ve patients, suggesting that one can exclude these
patients from anthracycline adjuvant therapy. Also being investigated
is potential synergy between antibodies against other growth factor
receptors and anti-HER2 antibodies.
Attempts
are also currently in progress to test the efficacy of conjugates of
anti-HER2 antibodies with cytotoxic drugs to achieve targeted delivery
of the cytotoxic agents. Laboratory studies are underway with Herceptin-platinum(II)
complexes29 and Herceptin-microtubule-depolymerising agents30.
Contraindications
of Herceptin regimen
The toxic
side-effects of the administration of monoclonal antibodies were recognised
some years ago. Cardiotoxicity, pulmonary toxicity and infusion-related
problems such as anaphylaxis occur, albeit infrequently with monoclonal
antibody therapies 31, 32. These toxicities have been described
with Herceptin treatment, more so in patients on anthracycline and cyclophosphamide
combined with Herceptin26. Cardiotoxicity could occur in
some patients when Herceptin is administered with anthracyclines33,
34. Herceptin itself can be cardiotoxic in patients receiving
concurrent or prior anthracyclines35, 36. Cardiotoxicity
is not due to structural abnormalities but Herceptin might cause myocardial
dysfunction. The toxicity of anthracyclines and Herceptin could be brought
about by different routes37. As Dinh et al.38
have emphasised, many questions relating to Herceptin treatment still
remain unanswered, e.g. optimising treatment, and combination with conventional
chemotherapeutic agents, among others. Even with these caveats Herceptin
may be regarded as a most efficacious agent in the treatment of HER2+
breast cancers.
EGFr
inhibitor Lapatinib (Tykerb) in breast cancer treatment
As stated
earlier, EGFr is over expressed in a proportion of breast cancers that
are ER-negative. EGFr expression also correlates with the expression
of metastasis promoting genes. Further, in the light of the function
of EGFr in conjunction with HER2, it would be of considerable clinical
benefit to test the effects of EGFr inhibitors in breast cancer treatment.
Lapatinib is a powerful dual inhibitor of EGFr and HER2 with marked
pharmacological potential.
Lapatinib
is a protein kinase inhibitor (a 4-anilinoquinazoline derivative), which
inhibits growth factor signalling by binding to the ATP-binding pocket
of both EGFr and HER2 receptor proteins and so prevents autophosphorylation
of the receptor and inhibits the signalling cascade leading to the suppression
of the growth of tumours, including advanced or metastatic breast cancers
resistant to Herceptin39. Objective responses have been achieved
in 28% of patients with untreated HER2-positive tumours40.
Clinical trials have provided promising results; Lapatinib is clinically
very effective especially in advanced or metastatic breast cancer and
patients with brain metastases. A phase III trial assessing the efficacy
of combination of Lapatinib with Capecitabine, which is converted to
5-Flurouracil and inhibits DNA synthesis, seems to suggest a significant
slowing down of disease progression by the combination as compared with
capecitabine alone41. The efficacy of combining Lapatinib
with other conventional chemotherapeutic agents is being evaluated.
First-line Paclitaxel-Lapatinib combination gave significant benefits
to HER-2-positive patients42.
Lapatinib
could be functioning synergistically with HER2 inhibitors, for its effect
on prominently EGFr over-expressing cancers, such as colorectal cancer
or squamous cell carcinoma of the head and neck, is said to be unexceptional
and moderate43. According to Press et al.44 the
benefits of Lapatinib appear to be restricted to patients with HER2
over-expressing cancers. Lapatinib has no cardiac toxicity but does
produce other toxic effects45. However, its toxicity whilst
administered in combination with other anticancer agents has not been
appraised.
Avastin
in breast cancer treatment
A different
route to control of tumour growth and metastatic spread has been afforded
by inhibitors that target the microvasculature associated with tumours.
Tumours induce the formation of neovascularisation so that tumour cells
can access the vascular system and become disseminated to form distant
metastases. The neovasculature is induced by VEGF, which transduces
its effects by binding specifically to its receptors VEGFr (see46).
A strategy similar to that adopted with EGF family growth factors has
been used to target VEGFr, inhibit its function and inhibit the signalling
by VEGF. Avastin (Bevacizumab), a humanised monoclonal anti-VEGFr antibody,
is such an inhibitor. Avastin with Paclitaxel chemotherapy has been
found to enhance progression-free survival and improve response rate
in patients with advanced breast cancer47. However, on account
of possible side effects, there is some reluctance to the use of Avastin.
It has been approved in Europe for first line treatment of women with
metastatic breast cancer, but has not been approved for use by the National
Institute for Health and Clinical Excellence UK48.
ACKNOWLEDGEMENTS
The author
thanks Professor Leif Bergkvist of the Department of Surgery and Centre
for Clinical Research of Uppsala University Central Hospital at Västerås,
and Dr M.S. Lakshmi for reading the manuscript and making helpful suggestions,
and Professor Bayan Sharif and Professor Satnam Dlay for research and
literary facilities
COMPETING
INTERESTS
None Declared AUTHOR
DETAILS
GAJANAN
V SHERBET, The Institute for Molecular Medicine, Huntington Beach CA,
USA and School of Electrical, Electronic and Computer Engineering, University
of Newcastle upon Tyne UK
CORRESPONDENCE:
GAJANAN V SHERBET, School of Electrical, Electronic and Computer Engineering,
University of Newcastle upon Tyne, Merz Court, Newcastle upon Tyne,
NE1 7RU, U.K.
Email:
gajanan.sherbet@ncl.ac.uk
References
Werner H, Le
Roith D. The insulin-like growth factor-I receptor signaling pathways
are important for tumorigenesis and inhibition of apoptosis., Critical
Reviews Oncol 1997; 8: 71-92.
Schlessinger
J, Ullrich A. Growth factor signalling by receptor tyrosine kinases.
Neuron 1992; 9: 383-391
Tzahar E, Levkowitz
G, Karunagaran D, et al. ErbB-3 and ErbB-4 function as respective low
and high affinity receptors of all Neu differentiation factor Heregulin
isoforms. J Biol Chem 1994; 269: 25226-25233.
Ullrich A, Schlessinger
J. Signal transduction by receptors with tyrosine kinase activity. Cell
1990; 61: 203-212.
Karunagaran D,
Tzahar E, Beerli RR, et al. ErbB-2 is a common auxiliary subunit of
NDF and EGF receptors: Implications for breast cancer. EMBO J 1996;
15: 254-264.
Lee-Hoeflich
ST, Crocker L, Yao E, et al. A central role for HER3 in HER2-amplified
breast cancer: implications for targeted therapy. Cancer Res 2008; 68:
5878-5887.
Slamon DJ, Clark
G, Wong S et al. Human breast cancer: correlation of relapse and survival
with amplification of the HER-2/neu oncogene. Science 1987; 235: 177-181.
Slamon DJ, Godolphin
W, Jones L, et al. Studies of the HER-2/neu proto-oncogene in human
breast and ovarian cancer. Science 1989; 244: 707-711.
Venter D, Kumar
S, Tuzi N, et al. Over expression of the c-erbB-2 oncoprotein in human
breast carcinomas: immunohistochemical assessment correlates with gene
amplification. Lancet 1987; 2: 69-72.
Natali P, Nicotra
M, Brigotti A, et al. Expression of the p185 encoded by HER2 oncogene
in normal and transformed human tissues. Int J Cancer 1990; 45: 457-461.
Cobleigh MA,
Vogel CL, Tripathy D, et al. Multinational study of the efficacy and
safety of humanized anti-HER2 monoclonal antibody in women who have
HER2-overexpressing metastatic breast cancer that has progressed after
chemotherapy for metastatic disease. J Clin Oncol 1999; 17: 2639-2648.
Vogel CL, Cobleigh
MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single
agent in first-line treatment of HER2-overexpressing metastatic breast
cancer. J Clin Oncol 2002; 20: 719-726.
Shepard HM,
Jin P, Slamon DJ, et al. Herceptin Handbook Exp Pharmacol 2008;
181: 183-219.
Le XF, Mao WQ,
Lu CH, et al. Specific blockade of VEGF and HER2 pathways results in
greater growth inhibition of breast cancer xenografts that over express
HER2. Cell Cycle 2008; 7: 3747-3758.
Barok M, Balazs
M, Nagy P, et al. Trastuzumab decreases the number of circulating and
disseminated tumor cells despite trastuzumab resistance of the primary
tumor. Can Lett 2008; 260: 198-208.
Rastelli F,
Crispino S. Factors predictive of response to hormone therapy in breast
cancer. Tumori 2008; 94: 370-383.
Prat A, Baselga
J. The role of hormonal therapy in the management of hormonal-receptor-positive
breast cancer with co-expression of HER2. Nature Clin Pratice Oncol
2008; 5: 531-542.
Su QB, Hu SY,
Gao HD, et al. Role of AIB1 for Tamoxifen resistance in estrogen receptor-positive
breast cancer cells. Oncology 2008; 75: 159-168.
Fereshteh MP,
Tilli MT, Kim SE, et al. The nuclear receptor coactivator amplified
in breast cancer-1 is required for neu (ErbB2/HER2) activation, signaling,
and mammary tumorigenesis in mice. Cancer Res 2008; 68: 3697-3706.
Kirkegaard T,
McGlynn LM, Campbell FM, et al. Amplified in breast cancer 1 in human
epidermal growth factor receptor-positive tumors of tamoxifen-treated
breast cancer patients. Clin Cancer Res 2007; 13: 1405-1411.
Dihge L, Bendahl
PO, Grabau D, et al. Epidermal growth factor receptor (EGFR) and the
estrogen receptor modulator amplified in breast cancer (AIB1) for predicting
clinical outcome after adjuvant tamoxifen in breast cancer. Breast Cancer
Res Treat 2008; 109: 255-262.
Sainsbury JRC,
Farndon JR, Harris AL, Sherbet GV. Epidermal growth factor receptors
are present in human breast cancers. Br J Surg. 1984; 71: 902.
Sainsbury JRC,
Farndon JR, Harris AL, Sherbet GV. Epidermal growth factor receptors
on human breast cancers. Br J Surg 1985; 72: 186-188.
Sainsbury JRC,
Farndon JR, Sherbet GV, et al. Epidermal growth factor receptors and
oestrogen receptors in human breast cancer. Lancet 1985; l: 364-366.
Borley AC, Hiscox
S, Gee J, et al. Anti-oestrogens but not oestrogen deprivation promote
cellular invasion in intercellular adhesion-deficient breast cancer
cells. Breast Cancer Res 2008; 10: R103.
McKeage K, Perry
CM. Trastuzumab - A review of its use in the treatment of metastatic
breast cancer over expressing HER2. Drugs 2002; 62: 209-243.
Dhesy-Thind
B, Pritchard KI, Messersmith H, et al. HER2/neu in systemic therapy
for women with breast cancer: a systematic review. Breast Cancer Res
Treat 2008; 109: 209-229.
Gennari A, Sormani
MP, Pronzato P, et al. HER2 status and efficacy of adjuvant anthracyclines
in early breast cancer: a pooled analysis of randomized trials. J Natl
Cancer Inst. 2008; 100: 14-20.
Gao J, Liu YG,
Liu R, et al. Herceptin-platinum(II) binding complexes: Novel cancer-cell-specific
agents. Chem Med Chem 2008; 3: 954-962.
Phillips GDL,
Li GM, Dugger DL, et al. Targeting HER2-positive breast cancer with
Trastuzumab-DM1, an antibody-cytotoxic drug conjugate. Cancer Res 2008;
68: 9280-9290.
Cersosimo RJ.
Monoclonal antibodies in the treatment of cancer, part 1. Amer J Hlth-System
Pharm 2003; 60: 1531-1548.
Klastersky J.
Adverse effects of the humanized antibodies used as cancer therapeutics.
Current Opinion Oncol 2006; 18: 316-320.
Perez EA. Cardiac
toxicity of ErbB2-targeted therapies: What do we know? Clin Breast Cancer
2008; 8: S114-S120
McKeage K, Lyseng-Williamson
KA. Trastuzumab - A pharmacoeconomic review of its use in early breast
cancer. Pharmacogenomics 2008; 26: 699-719.
Ewer SM, Ewer
MS. Cardiotoxicity profile of trastuzumab. Drug Safety 2008; 31: 459-467.
Popat S, Smith
IE. Therapy insight: anthracyclines and trastuzumab - the optimal management
of cardiotoxic side effects. Nature Clin Pract Oncol 2008; 5: 324-335.
Bria E, Cuppone
F, Milella M, et al. Trastuzumab cardiotoxicity: biological hypotheses
and clinical open issues. Expert Opinion Biol Therapy 2008; 8: 1963-1971.
Dinh P, de Azambuja
E, Cardoso F, et al. Facts and controversies in the use of trastuzumab
in the adjuvant setting Nature Clin Pract Oncol 2008; 5: 645-654.
Nelson MH, Dolder
CR. Lapatinib: A novel dual tyrosine kinase inhibitor with activity
in solid tumors. Ann Pharmacotherapy 2006; 40: 261-269.
Johnston SRD,
Leary A. Lapatinib: A novel EGFR/HER2 tyrosine kinase inhibitor for
cancer. Drugs Today 2006; 42: 441-453.
Bilancia D,
Rosati G, Dinota A, et al. Lapatinib in breast cancer. Ann Oncol 2007;
18 Suppl 6: 26-30.
Di Leo A, Gomez
HL, Aziz Z, et al. Phase III, Double-blind, randomized study comparing
Lapatinib plus Paclitaxel with placebo plus Paclitaxel as first-line
treatment for metastatic breast cancer J Clin Oncol 2008; 26: 5544-5552.
Montemurro F,
Valabrega G, Aglietta M. Lapatinib: a dual inhibitor of EGFR and HER2
tyrosine kinase activity. Expert Opinon Biol Therapy 2007; 7: 257-268.5
Press MF, Finn
RS, Cameron D, et al. HER-2 Gene amplification, HER-2 and epidermal
growth factor receptor mRNA and protein expression, and Lapatinib Efficacy
in women with metastatic breast cancer. Clin Cancer Res 2008; 14: 7861-7870.
Sherbet GV,
Lakshmi MS. The genetics of cancer: Genes associated with cancer invasion,
metastasis and cell proliferation. 1997; Academic Press, London.
National Cancer
Institute and Eastern Cooperative Oncology Group ECOG, 2005
The National
Institute for Clinical Excellence in June 2008 guidelines.
Severe pulmonary
hypertension (PH) is a rare disorder characterized by multifactorial
etiology and shared pathophysiology. The belief that primary pulmonary
hypertension (PPH) is an idiopathic variety mostly affecting younger
women may still be held by some. However, PH has often been reported
in overweight and obese individuals and postmenopausal women.1
Earlier studies have also suggested that combination of obesity and
higher altitude favors the development of pulmonary arterial hypertension.
Hypercapnic acidemia and increased total blood volume have been implicated
in this group of patients. Pulmonary artery systolic pressures (PASP)
greater than 40 mmHg is found in 6% of otherwise normal individuals
age 50 years or older and in 5% of individuals with a BMI greater than
30kg/m2 . 2
Overall,
the widely held view has been that alveolar hypoxia is the main pathophysiologic
cause of vasoconstriction in obese patients living at sea level or higher
altitudes. In 1947, Motley et al demonstrated that breathing a gas mixture
containing 10% oxygen induced a rise in pulmonary artery pressure (PAP).3Papers
dating back more than three decades have documented increases in PAP
associated with hypoxemia related to sleep disordered breathing (SDB).
It is well known that apneic episodes during sleep are associated with
transient elevations in PAP, which return to baseline when breathing
resumes after relief of obstruction. Earlier studies suggested
that daytime hypoxemia attributable to abnormal lung function was the
main cause of pulmonary hypertension in patients with sleep apnea. Whether
transient hypoxemias and associated elevations in PAP with obstructive
events during sleep are adequate to produce daytime resting “fixed”
pulmonary vascular disease, or whether daytime hypoxemia is required
remains unclear. It is also less certain whether daytime pulmonary
arterial hypertension also occurs in OSA patients without underlying
pulmonary or cardiac disease. Additionally, studies have shown
that the severity of SDB as measured by apnea-hypopnea index (AHI) and
the PAP elevations often fail to correlate.
Sajkov et
al 4 were amongst the first to demonstrate that hypoxemia
in PH patients with obstructive sleep apnea syndrome (OSAS) could not
be explained by impairment of lung or cardiac function, BMI and smoking
history. However, most of the studies that have tackled this question
(including the one done by Sajkov) have used echocardiography based
pulmonary artery pressures and the few that have used the gold standard
Right heart catheterization (RHC) used a definition of mean pulmonary
artery pressure (mPAP) >20 mmHg. At present, pulmonary arterial hypertension
is defined as a mean PAP greater than 25mmHg at rest or 30 mmHg with
exercise, as measured by RHC. The largest such study found PAH in 17%
patients but it also included some patients with chronic obstructive
pulmonary disease (COPD).5
Smaller series of patients with OSA but no clinical history of COPD
have reported daytime PAH as measured by RHC in 20-42% patients.
6, 7
Thus, despite
acute nocturnal increases in PAP associated with obstructive apneas,
proof that OSA causes PH has been limited by other co-morbidities related
to obesity. The three biggest confounders making this issue difficult
to be explored are associated COPD in OSAS patients (overlap syndrome),
Obesity Hypoventilation Syndrome (OHS) and underlying concomitant left
ventricular dysfunction in patients with OSA. OHS as defined at present
is characterized by combination of obesity (BMI ≥30kg/m2)
and chronic daytime hypercapnia (PaCo2 >45 mmHg); and sleep disordered
breathing in the absence of other known causes of hypercapnia.8
PH has been shown to be more frequent and mean PAP higher in patients
with OHS or the overlap syndrome when compared to patients with pure
OSAS only. 9 Elevated mPAP associated with higher pulmonary
capillary wedge pressure (PCWP) from underlying elevated left
ventricular end-diastolic pressure and in some studies apnea associated
have been other potential confounders.10 Other difficulties
related to exploring this issue are technical concerns regarding non-invasive
measurement of pulmonary artery pressure in obese OSA patients and difficulties
in identifying suitable controls i.e, obese patients with PH and without
OSA. Studies are also needed to investigate the role of humoral vasoactive
factors like natriuretic peptides, nitric oxide or norepinephrine and
individual genetic predisposition to account for different remodeling
responses to hypoxia in the pulmonary circulation. In OSAS patients
no neutrally mediated effect of apneas on PAP has been demonstrated.
PH seen
in association with OSA is generally regarded as mild and can be attributed
to elevated pulmonary vascular resistance (PVR) because cardiac output
and PCWP are normal atleast at rest. Although the association between
left sided-heart disease and OSA is widely accepted, most studies of
OSA patients with PH do not differentiate between pre-capillary (PAH)
and post-capillary pulmonary hypertension (PVH). Additionally a good
proportion of the studies do not even report PCWP.6, 9 while
some explain higher PAP on the basis of PCWP alone.
Elevations in both PCWP and PVR have been reported to contribute to
PH in patients with OHS. A recent study of referred patients who met
the WHO criteria for PAH from Duke University reported PCWP> 15 mmHg
in 25% of the patients. These patients were predominantly obese (58%)
and all had normal LVEF%. 11
In ourretrospective analysis of 8254 patients who underwent
RHC for suspected PH, mean Right atrial pressure, mean PA diastolic
pressure, mean PCWP and mean cardiac output increased proportionately
with increase in BMI regardless of the underlying contributory disease
process. 12
The debate
about whether OSA alone can be a cause of sustained pulmonary arterial
hypertension continues, but based on the above literature, the latest
revision of the Clinical Classification of Pulmonary Hypertension identifies
SDB as a part of the category of respiratory disorders associated with
PH.13 The most direct evidence comes from observations that
treatment of OSA with continious positive airway pressure (CPAP)
may lower daytime PAP. OSA patients with PH seem to have increased pulmonary
vascular reactivity to hypoxia compared to patients without PH and CPAP
has been reported to decrease pulmonary vascular reactivity to hypoxia.14
In studies from Stanford as early as 1978, 50% reduction in PAP
was noted in six selected patients with OSA after tracheostomy. In a
recent randomized placebo-controlled cross-over trial of effective versus
sham CPAP in 23 patients with OSA, effective CPAP was associated with
decreases in echocardiographic measurements of PASP especially in patients
with PH or left ventricular diastolic dysfunction at baseline.
15 This trial was limited by baseline differences in obesity and
lung function between the two groups. Larger randomized studies are
needed to identify more definitively any sustained effects of CPAP therapy
on PH and right heart function and to better establish any role for
CPAP as one of the rapidly evolving therapeutic options for PH.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
ROOP KAW, MD, Assistant Professor of Medicine, USA
CORRESPONDENCE: DR ROOP KAW,
Cleveland Clinic Main Campus, A12, 9500 Euclid Avenue, Cleveland, USA. OH44197
Email: KAWR@ccf.org
References
Taraseviciute
A, Voelkel NF et al. Severe pulmonary hypertension in postmenopausal
obese women. Eur J Med Res.2006 May 5; 11(5): 198-202.
McQuillan BM,
Picard MH, Leavitt et al. Clinical correlates and reference intervals
for pulmonary artery systolic pressure among echocardiographically normal
subjects. Circulation 2001; 104: 2797-2802.
Motley HL, Cournand
A, Werko et al. The influence of short periods of induced acute anoxia
upon pulmonary artery pressures in man. Am J Physiol 1947; 150: 315-320.
Sajkov D, Crowie
RJ, Thronton TH et al. Pulmonary hypertension and hypoxemia in obstructive
sleep apnea syndrome. Am J Respir. Crit. Care Med. 1994; 149: 416- 422.
Chaouat A, Weitzenblum
E, Krieger J et al. Pulmonary Hemodynamics in the Obstructive Sleep
Apnea Syndrome: Results in 220 Consecutive patients. Chest 1996; 109;380-386.
Laks L, Lehrhaft
B, Grunstein R et al. Pulmonary hypertension in obstructive sleep apnea.
Eur Respir J 1995 (8): 537-541.
Sanner BM, Doberauer
C, Konermann M et al. Pulmonary hypertension in patients with obstructive
sleep apnea syndrome. Arch Int Med 1997; 157: 2483-2487.
Olson AL, Zwillich
C. The Obesity hypoventilation syndrome. Am J Med 2005(118): 948-56.
Kessler R, Chaouat
A, Schinkewitch P et al. The Obesity-Hypoventilation Syndrome revisited.
A prospective Study of 34 cases. Chest 2001; 120(2): 369-376.
Buda AJ,
Schroeder JS, Guilleminault C et al. Abnormalities of pulmonary
artery wedge pressures in sleep-induced apneas. Int J Cardiol 1981;
I: 67-74.
Fortin TA, Krichman
A, Hargett CW et al. Characteristics of pulmonary arterial hypertension
associated with elevated pulmonary capillary wedge pressure. Chest 2005
Abstracts, Monday October 31.
Kaw R, Thota
A, Minai O. Pulmonary hypertension in Obese patients: An analysis of
hemodynamic data. Chest 2008; 134: p 134003.
Simmonneau G,
Galie N, Rubin LJ et al. Clinical classification of pulmonary hypertension.
J Am Coll of Cardiol. 2004; 43;5S-12S
Sajkov D, Wang
T, Saunders NA et al. Continous positive airway pressure treatment improves
pulmonary hemodynamics in patients with obstructive sleep apnea. Am
J Resp Crit Care Med. 2002; 165: 152-158.
Arias MA, Garcia-Rio
F, Alonso Fernandez A et al. Pulmonary hypertension in obstructive sleep
apnoea: effects of continous positive airway pressure: a randomized,
controlled cross-over study. Eur Heart J 2006; 27: 1106-1113.




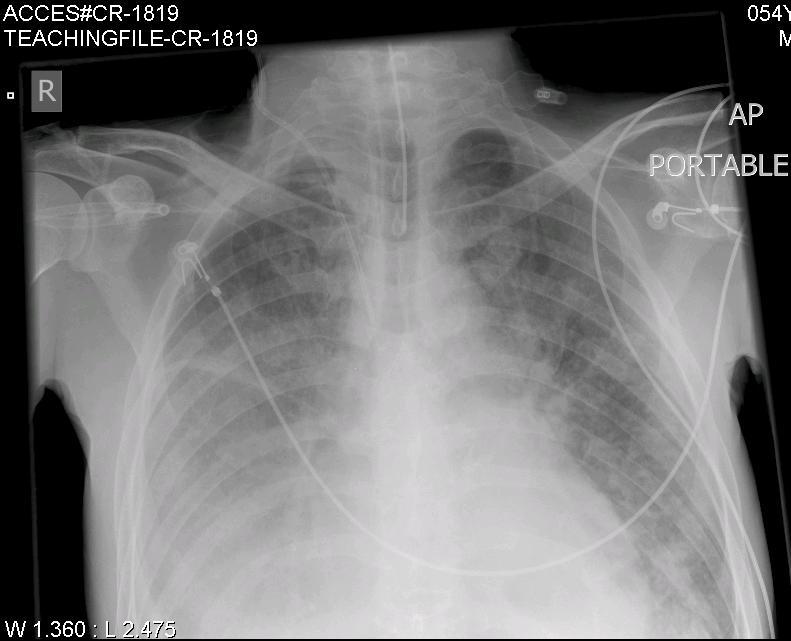
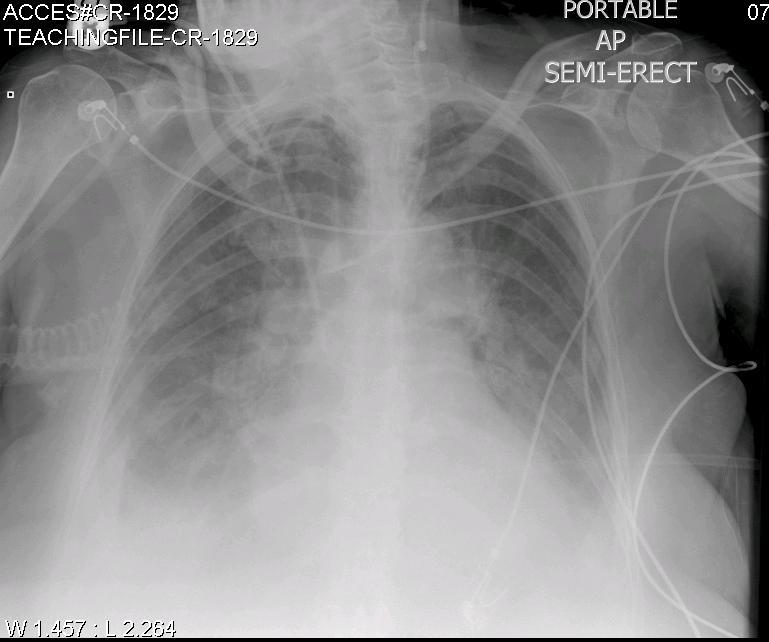
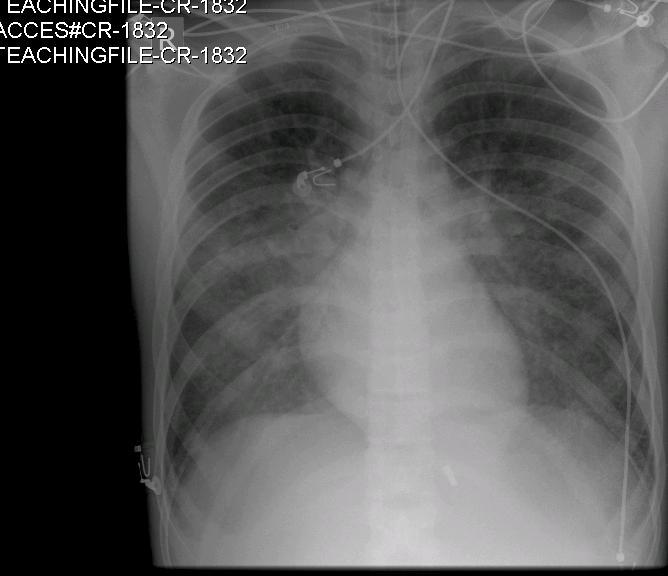
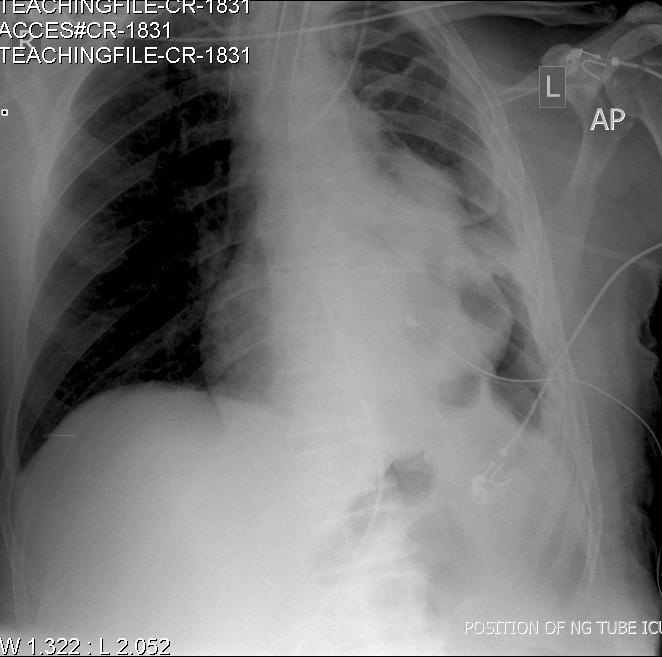


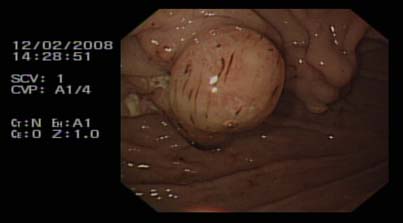
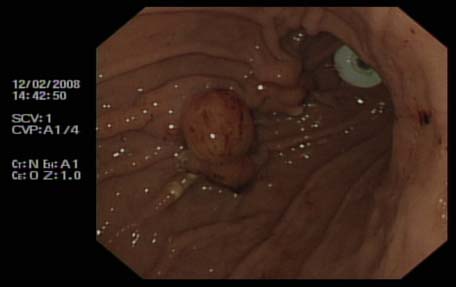
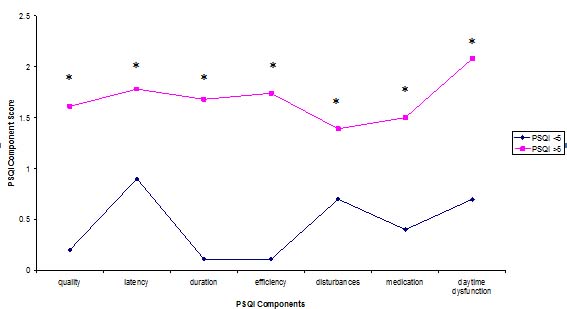
BJMP June 2009 Volume 2 Number 2
BJMP June 2009 Volume 2 Number 2
Full Issue Booklet (All Articles)
PDF
Full Booklet
Editorial
Obesity and Pulmonary Hypertension. What’s the Link?
Full Text
PDF
Review Articles
Breast cancer and therapeutic deployment of growth factor receptor
Full Text
PDF
Oral Bisphosphonates and the Risk for Osteonecrosis of the Jaw
Full Text
PDF
Ventilator Associated Pneumonia – an Overview
Full Text
PDF
Uncovering the face of racism in the workplace
Full Text
PDF
Original Articles
Laporoscopic Fundoplication: Not a simple wrap
Full Text
PDF
Comparative Evaluation of Four Hepatitis B vaccines Available in Pakistan: Reactogenecity and Immunogenecity
Full Text
PDF
Mental illness and comorbid insomnia: a cross- sectional study of a population of psychiatric in-patients
Full Text
PDF
Demographic, socio-economic and psychological determinants of HIV treatment: A community out-patient experience
Full Text
PDF
Case Reports
Blocked percutaneous endoscopic gastrostomy tube - an unusual cause
Full Text
PDF
Omental herniaton through umbilicus following lower segment caesarean section in a post caesarean pregnancy
Full Text
PDF
View Point
The right to consent: Is it absolute?
Full Text
PDF
Medicine in Pictures
Pictorial essay: central venous catheters on chest radiographs
Full Text
PDF
Miscellaneous
Upcoming Medical Meetings/Conferences
Full Text
PDF