The British Journal of Medical Practitioners has adopted a “Continuous Publication” model from the beginning of year 2010 publishing articles online as soon as they are peer-reviewed and copy-edited. This provides faster publication of articles for the authors and a quicker access for readers.
The BJMP website will now be updated regularly with the latest articles and we will continue to collate published articles into archival "issues" (about 4 issues per year).
The Medical Training Initiative (MTI) is a training programme to assist doctors with proven capability in anaesthesia/Intensive Care/Pain Medicine from low and middle income countries to undertake further anaesthesia training in the UK, for a maximum of 24 months1.
Why MTI?
It offers an opportunity not only to fine-tune their clinical acumen, but also to assimilate non-clinical skills (medical education, leadership and management, quality improvement projects) 2. The exposure most of the MTIs receive overseas is heterogeneous - in terms of level of supervision/independence, access to modern equipment and medications, lines of management, level of expectations and communication or interaction with patients. Funding received by training hospitals overseas can be variable thereby impacting on the resources available to provide standardised training. Under the MTI scheme, anaesthetic trainees can also take the FRCA examination.
From home to UK
A general awareness of the scheme helps the department to provide the MTIs with an appropriate support system. Details of the MTI scheme are available on the Royal College of Anaesthetists (RCoA) website.
It takes about 3-6 months after verification of the educational qualification by Educational Commission for Foreign Medical Graduates (ECFMG) via Electronic Portfolio of International Credentials (EPIC). The planning involves resignation from the current job, applying for a Tier 5 Visa to be in time for the GMC identity check (3 month deadline) and collecting the Biometric Residence Permit to be able to start work in the UK.
Medical staffing has more paperwork, one of which is the Disclosure and Barring Service (DBS). Prior intimation to the MTIs on the need for police verification from their home country would be of great benefit to make the process smoother. Hospital accommodation should be offered and organised in advance.
Acquaintance with the system
The MTI trainees often join at a time that doesn’t coincide with the UK training programme. Hence, a one-to-one induction customised towards overseas doctors will be beneficial. In addition to a named Educational supervisor (a mandatory requirement stipulated by the RCoA), the MTIs will benefit from having a nominated mentor within the department. The trainees can also get familiarised to the new healthcare system via the RCoA approved training courses – ‘Simulation for MTIs’ and ‘New to NHS’.
Allocating MTIs to theatre lists with only a select number of consultants in the initial stages helps them to settle in a new healthcare environment before they commence on-call (out of hours) duties. The MTIs should be encouraged to attend resuscitation courses like Advanced Life Support (ALS) as most of them follow the Advanced Cardiac Life Support (ACLS). They should be encouraged to document their progress like any other UK trainee via the RCoA Lifelong Learning Platform (LLP).
Anaesthetic training in the UK is very structured. The three stages of training (core, intermediate and higher/advanced) are well defined. The curriculum is well laid out and assists trainees to not only develop clinical but also gain non-technical skills. A six-monthly ARCP (Annual Review of Competence Progression) like assessment with annual anonymised multi-source feedback helps to create professional development plans, monitor progress and put supportive plans in place (if needed ) for a struggling trainee. The curriculum provides an opportunity for all-round development to every overseas trainee.
Gaining experience in non-technical skills (leadership and management, medical education and QI/audit projects) can be lacking in some home countries as the curriculum back home could be heavily biased towards the development of clinical acumen only.
What to expect from an MTI?
The MTIs have at least 3-5 years (may be more) of anaesthetic experience. The NHS benefits from their skills and experience. Their experience helps the department to allocate them to provide out of hours work (on-call) sooner than a UK trainee after an appropriate period of induction. The journey of patient experience also improves with the presence of experienced staff on the shop floor.
Departments gain from increased service provision too. As an example, after obtaining the initial assessment of competency (IAC), the MTI anaesthetists can be allocated to do solo theatre lists with a named supervising consultant anaesthetist present within the theatre suite. The reliance on locum staff is reduced thereby reducing unnecessary cancellations of theatre lists for lack of permanent staff. It reduces the financial burden on the NHS as staffing the department with locums can add to increased costs.
Patient safety is of paramount importance in any healthcare setting. Since the MTIs have a two year working contract, they are familiar with the department policies and guidelines unlike a locum doctor who does the odd shift in a hospital.
Equally, new skills gained by the MTIs are ultrasound guided regional anaesthesia, using a fibre-optic scope and different airway gadgets, ICU training, experience in geriatric and bariatric anaesthesia, total intravenous anaesthesia (TIVA) / target controlled infusion (TCI) alongside access to new medications like remifentanil, sugammadex which may not be available in low to middle income countries. The NHS provides excellent opportunities in simulation training and teaching courses.
However, a system of protocols can be unnerving to the MTIs. One may find them taking a step back when it comes to ‘decision making’ as they are not sure if it would be approved or criticised. At times, some of the MTIs may come across as unyielding despite adequate teaching. It is essential to remember that the process of unlearning to re-learning takes time, and therefore, patience is the key. This is where the concept of teaching experienced medical practitioners with knowledge comes in handy.
Training learners with knowledge
Medical education comprises three inter-linked domains - knowledge, skills and attitude.3 Though trainees may differ in terms of their motivation for learning, it can manifest only after the basic needs are satisfied - the external barriers to motivation such as life events and transitions, opportunities, and barriers to learning or obtaining information are addressed and they feel respected in the educational environment. The MTIs are essentially adult learners with pre-existing knowledge, who bring a great deal of first-hand experience to any work-place. Learning should, therefore, be integrative, which forms the basis of constructivism theory of learning4. New knowledge and skills should be integrated into the existing bank of knowledge. They also have pre-set strong tastes and habits which can be a real asset or a hindrance to effective learning. The educational supervisor should be able to encourage or curb them accordingly5.
Being adults, MTIs enter training situations with a self-image as independent, mature beings as they have already passed the qualifying exams in their home country. They can direct their own learning, including decision making and plans for taking examinations. The supervisors should engage with the trainees in activities that create a sense of self-responsibility to facilitate better learning opportunities.
Many adult learners suffer from a fear of failure and living up to expectations6 and thus, educational supervisors should be cautious to avoid unnecessary criticism. Instead the focus should be to offer constructive positive feedback. Any educational plan for them should start with an awareness of their prior acquired knowledge, an assessment of their educational needs along with room for motivation and reflection. This helps the trainees retain the original “frame of reference” while continuing to constantly challenge and transform practice via reflection on-action and reflection in-action. The educational supervisors need to provide a supporting educational environment, a structured guide for reflection and constructive feedback to develop the trainees’ reflective practice7.
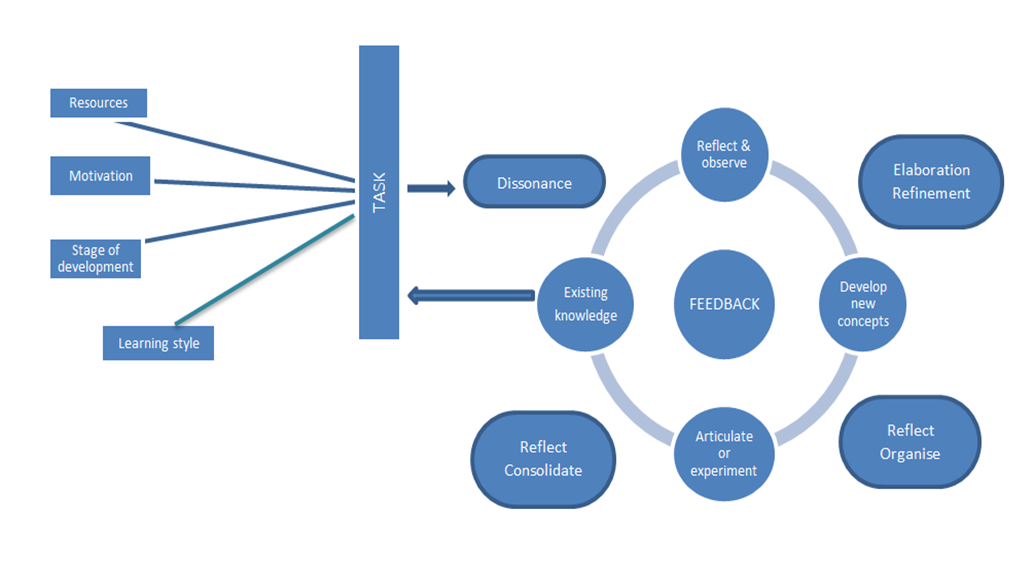
A simple multi-step approach involving active participation from both the trainee and the educational supervisor can be summarised into a model as below (Figure 1) 8. This model begins with the trainee’s prior knowledge.
Figure 1: Multi-step approach to training
The RCoA LLP, work-place based assessments and multi-source feedback along with the six-monthly meeting with educational supervisor are useful tools to deliver a holistic learning experience. It helps to refine the existing knowledge, reflect and provide constructive feedback. The supervisor can provide advance structures upon which the MTI can continue to build opportunities and gain confidence to rehearse and apply their new knowledge.
Summary
An organised induction programme, a period of familiarisation and good mentorship with patience helps to remove the barriers to learning for the MTI trainees. A dynamic trainee-supervisor relationship to accommodate the changing educational goals and an appropriate mix of strategies can help the MTI trainees attain medical competence, which is defined as “the habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values and reflection in daily practice for the benefit of the individual and the community being served3.”
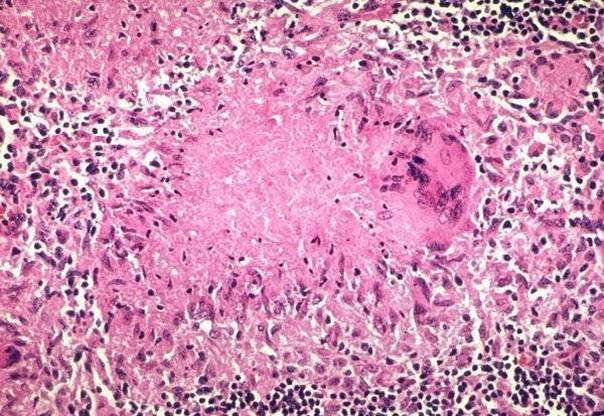
The spectrum of psychiatric illness in Systemic lupus erthyromatosus (SLE) include psychotic, depressive, subtle cognitive and personality disorders of histrionic type. The occurrence of psychiatric manifestations in SLE varies widely from 5 to 83%. It is postulated that there is a direct action of the disease on the central nervous system by autoantibodies namely anti phospholipid and anti-ribosome P auto antibodies or cytokines like interleukin 2, interleukin 6, alpha interferon 1. During the course of the disease side-effects of glucocorticosteroids and hydroxychloroquine or anxious reaction to chronic and potentially lethal illness is postulated to be another mechanism of psychiatric manifestation of SLE . SLE patients are prone to develop myriad of psychological distress in addition to neuropsychitric manifestations which require a social and psychological support. While some of these manifestations are treated by corticosteroids and psychotropic drugs1 medications with anticholinergic side-effects, like phenothiazines, tricyclic antidepressants and hydroxyzine which enhance the oral dryness should be avoided in SLE.
Clinical scenario:
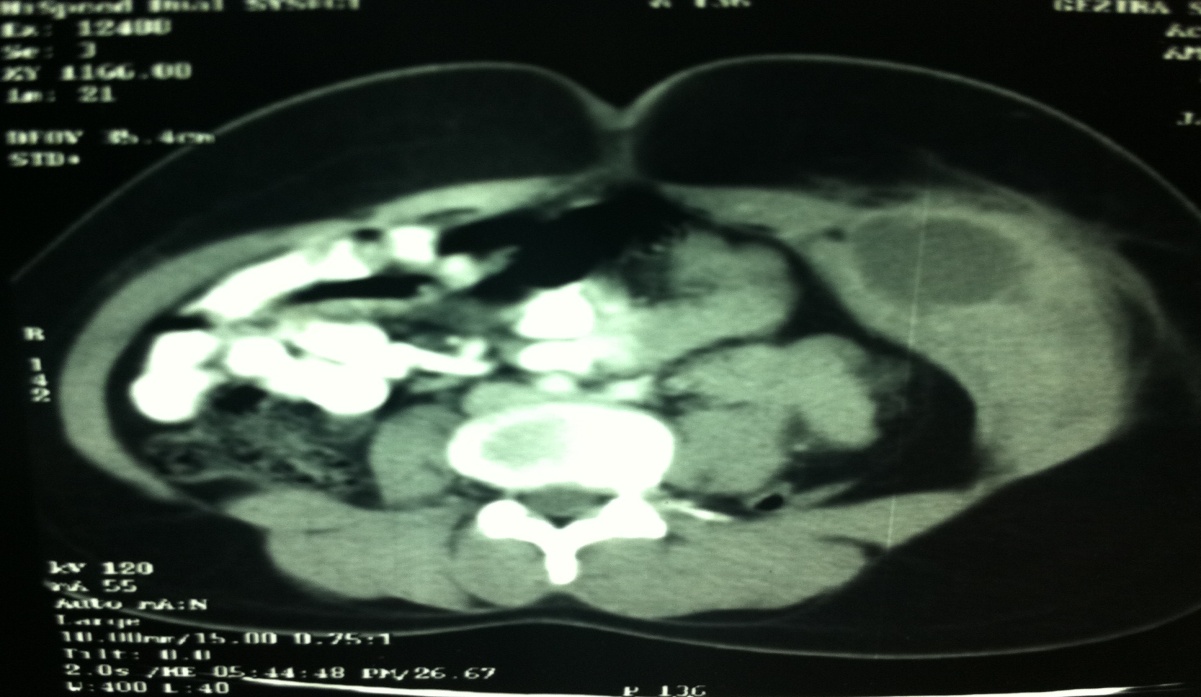
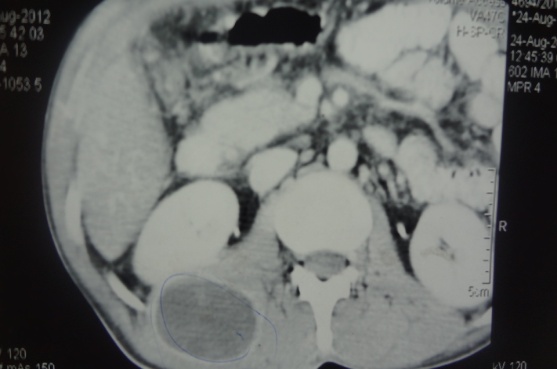
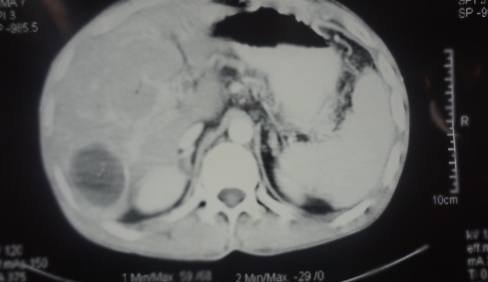
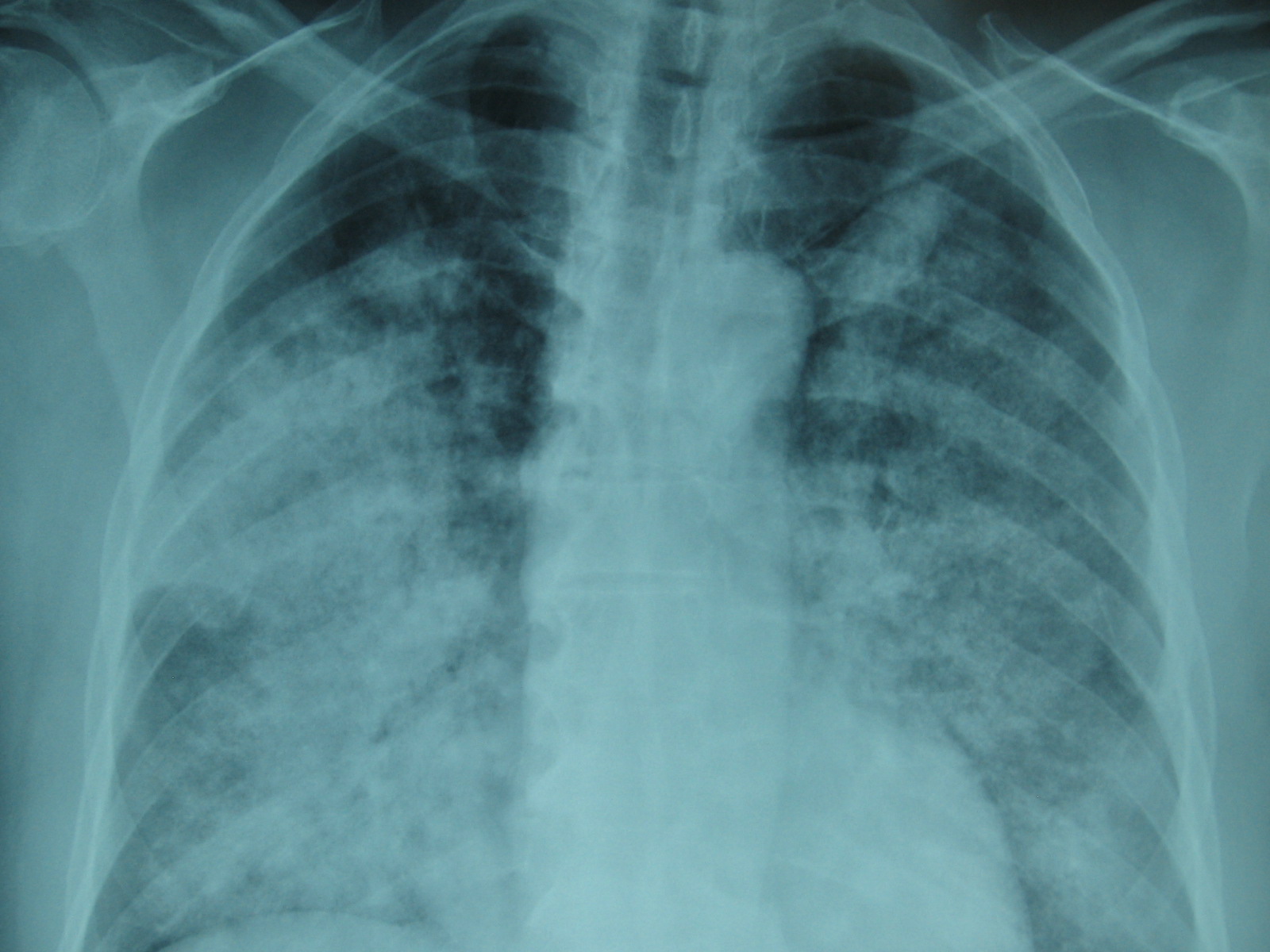
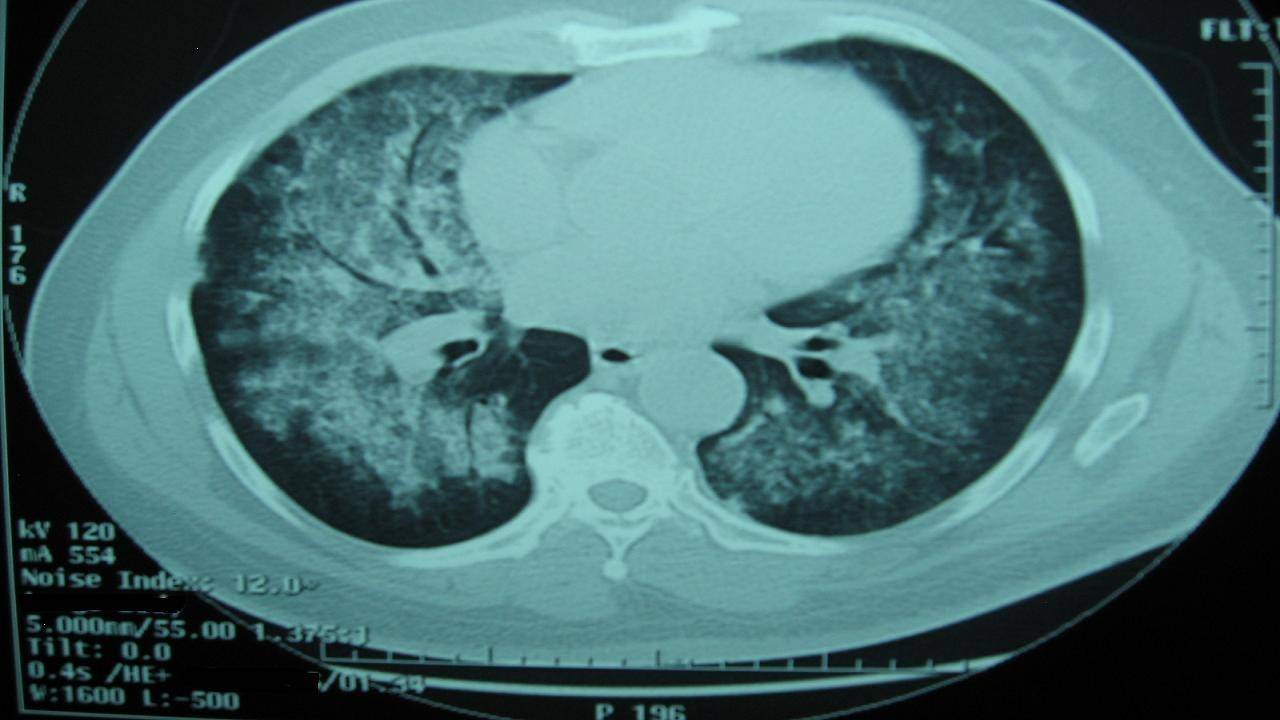
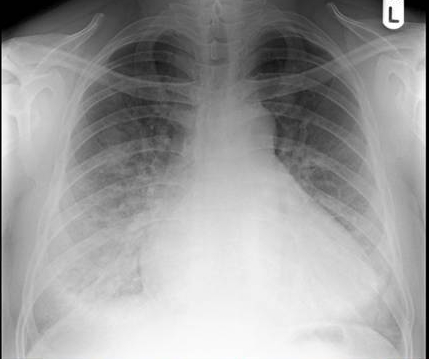
A 27-year-old male suddenly developed aggressive behaviour for the first time in his life ,while on his work place. The patient had no insight into his illness and was brought to the local psychiatric hospital by his colleagues where he was admitted as a case of acute mania. He was managed with electroconvulsive therapy (EST) in addition to antipsychotic medication as neuro imaging including CT scan and MRI brain were normal. A few days later , the patient was discharged on anti-psychiatric medicines. However, after six months while on antipsychotic medication, he developed a low grade fever .He was admitted to a local hospital where in addition to base line investigations a lymph node biopsy was done which revealed follicular hyperplasia, without any abnormal cell. Patient’s HBV, HCV, HIV were negative. The patient developed anorexia , significant weight loss and progressive difficulty in getting up from a sitting position .He also developed shortness of breath and presented to King Abdul Aziz specialist hospital in Taif, Saudi Arabia virtually in a bed bound state . He was admitted in the intensive care unit of the hospital .The examination revealed pallor, generalised lymph-adenopathy, palmer rash, alopecia and mouth ulcers. The patient had mild pericardial effusion and Mitral regurgitation (MR)++ on echocardiography. Further evaluation showed significant proteinuria. Serum ANA, dsDNA were positive .Lupus anticoagulant was negative. Keeping in view above symptoms and signs the patient was diagnosed as a case of SLE2 (Mouth ulcers, Pericardial effusion ,ANA positive , dsDNA positive ) The patient was managed with pulse dose of methylprednisolone 1g intravenously (IV) daily for 5days, followed by oral prednisone 60 mg once daily, which was tapered on follow up . Patient tolerated the treatment well and improved progressively . He became ambulatory and rejoined his job. The psychiatric medications were stopped.
However, on follow up the patient continued to have proteinuria 1.8 gm/24 hr. He was readmitted and the kidney biopsy revealed class IV lupus nephritis. He was given pulse cyclophosphamide 1gm/m2 intravenously and later started on tablet Mycophenolate 1.5gm once daily. The proteinuria improved and he is following our clinic for the last two years now .Patient’s follow up investigations are shown in table 1.
Table: 1 Patients’ hospital investigations and results
Test
Result Pre-treatment (On presentation )
Result Post-treatment (After 6 weeks )
Normal range
Haemoglobin
6.2
12.3
12. 2-15.3 gm/dl
White blood cell
3.2
6.7
6-16 × 109/l
Platelet
41,000
197
150-450 × 109/l
ESR
82mm first hour
56mm
Total bilirubin
1.2
1.0
.0.8 to 1mg/dl
Direct bilirubin
1.0
0.8
0.-0.6µmol/L
AST
335
30
5-30U/L
ALT
257
29
5-30U/L
ALP
182
100
50-100U/L
GTT
497
65
7-30 IU/l
Albumin
39
39
38-54 g/l
Total protein
5.2
4.5
INR
1.1
1.1
0.8-1.2
Urea
62
40
Creatinine
1.2
1.0
Na/K
131/3.8
142/3.6
Serum glucose
100
102
65-110mg/dl
ANA
Positive
Anti DsDNA
Positive
Lupus anticoagulant
Negative
24 hr urinary protein
2.3gm/L
500mg/L
<150mg/L
Discussion:
The correct diagnosis of central or even peripheral nervous system manifestations in patients with SLE can be challenging because of many SLE-related and non-SLE-related processes present in a patient. The index case proved to have acute mania as the first manifestation of SLE which remained under oblivion till he developed serositis another complication of SLE. While this patient came to clinical attention after one year a case of SLE masquerading schizophrenia for 14 years was reported by Funaunchi et al3. In another report, a 14-year-old boy with a two-year history of cognitive dysfunction and behavioural problems SLE was diagnosed after two years4 . It appears that the psychiatric symptoms may occur as the first manifestation of juvenile SLE. It will not be out of place to mention that the psychiatric manifestation can be at times dire which could even result in harm to others in a given society. The case of Folie a trios syndrome, characterized by the transfer of delusional ideas from one person to two other persons culminating in murder has been reported in a patient with SLE5 . In a significant retrospective data from China (a cohort of 518) neuropsychiatric manifestations in SLE were observed in 96(19%) of the above study cohort . The seizure disorder accounted for the most prevalent disorder of neuropsychiatric manifestations (NP) of SLE followed by cerebrovascular disease and acute confusional states. In the above study, 96 patients with psychiatric symptoms, acute psychosis was observed in 10(11%)patients. Authors in this study were of the opinion that this percentage could have been higher if subtle cognitive dysfunction were included as well. Authors of the same study further concluded that the antiphospholipid antibodies were significantly associated with NP manifestations, especially cerebrovascular disorders6.
The autoantibodies have been found to be biomarkers for future neuropsychiatric events in SLE. A prospective study throughout ten years conducted among 1047 SLE patients demonstrated that individuals who had evidence of lupus anticoagulant (LA) were at an increased future risk of intracranial thrombosis. Further, those with anti-ribosomal P antibodies were at an increased future risk of lupus psychosis7. The Lupus anticoagulant in the index case was negative, and anti-ribosomal P antibodies were not available . A study by Sanna et al8 have shown that an association exists between anti-NR2 antibodies and depressed mood in addition to decreased short-time memory and learning. Authors in this study concluded that antibodies to NMDA receptors thus might represent as one of the several mechanisms for cerebral dysfunction in patients with SLE.
The CT scan brain of the index case was normal. However, massive bilateral calcification of sub-cortical structures in a patient with SLE with the psychotic disorder has been reported9. The psychiatric diseases are related to vasculitis and non-inflammatory vasculopathy of the small cerebral blood vessels. Further, a study has shown that ninety per cent of the patients with psychosis, organic brain syndrome or generalised seizures had increased IgG antineuronal activity as compared with only 25 per cent of the patients who presented with hemiparesis or with chorea/hemiballismus. The authors in the above study concluded that the diffuse central nervous system manifestations of SLE are a direct result of the interaction of the antibody with neuronal cell membranes10.
The management neuropsychiatric manifestation in SLE should include treatment of the disease itself and specific psychotropic treatment. The index case had rapid improvement following Glucocorticosteroid therapy. Intravenous infusions of immunosuppressive agents, such as cyclophosphamide, have been found to be effective in such conditions 1 . Psychotropic drugs may be used, but it is prudent to mention that SLE-inducing drugs, like chlorpromazine, carbamazepine and lithium carbonate must be avoided. Following treatment with steroids, the index case improved and all his antipsychiatric medications were finally stopped and he resumed his job.
To conclude the index case highlights that even though SLE is more frequent among females of childbearing age but males are no way immune to SLE . While evaluating patients with multiple unexplained somatic complaints and psychiatric symptoms SLE ought to be ruled out. The existence of neuropsychiatric manifestations in SLE constitutes an indisputable clinical reality that every practitioner must be able to recognise and treat.
Medical Student Syndrome (MSS) is a unique type of hypochondriasis which specifically causes health anxiety related to the diseases medical students study during their medical training.1 However, this phenomenon does not translate into an increased number of consultations differentiating it from hypochondriasis.2 Nevertheless, the common denominator in both conditions is that the affected person persistently experiences the belief or fear of having severe disease, due to the misinterpretation of physical symptoms.3 The medical examination on multiple occasions does not identify medical conditions that fully account for the physical symptoms or the person’s concerns about the disease, making it a diagnosis of exclusion. Unfortunately, the fears frequently persist among medical students despite medical reassurance, affecting their concentration during their training.4
Earlier studies have shown a higher prevalence of MSS in various medical schools, but recent studies show a declining trend. While Howes et al5 demonstrated that 70% of medical students have groundless medical fears during their studies, Weck et al,6 on the contrary, recorded the prevalence of health anxiety only among 5-30 % of study participants. One of the reasons ascribed to this could be that earlier studies, showing a high prevalence of MSS, were uncontrolled. Also, age-matched peers were not used as controls in some studies, and no direct interviews had been conducted.7,8 Methodological issues in previous data have led to inaccurate interpretations and over-generalization of findings. For example, the high emotional disturbance in medical students resulted from comparisons made with the general population, rather than with other students of their age. 9-11
We were prompted to conduct this study because the magnitude of MSS is variable from region to region, and in this study we compared medical students with their peers, studying in different colleges of Taif University to avoid observational bias.
Methods
This study was carried out from September 2017 to June 2018 at the female campus of Taif University, Kingdom of Saudi Arabia (KSA) in medical (pre-clinical and clinical years) and non-medical colleges in accordance with research guidelines of the College of Medicine, Taif University, KSA.
Inclusion criteria
Age and gender-matched students were selected for inclusion in the study. These included:
1. Female medical students from the second to the sixth grades enrolled in the College of Medicine, Taif University, KSA.
2. Female non-medical students from first to fourth grades enrolled in colleges of Arts, Admin and Financial Sciences, Computer and Information Technology, Science and Islamic Law.
Exclusion criteria
Biology students were excluded due to the medical content of their courses. At the time of enrolment, permission for participant recruitment was obtained from the concerned faculty administrators.
The participants were approached in the common/study rooms or lecture halls. The students were informed of the voluntary nature of the participation and were randomly selected. They were not required to provide their names during completion of the questionnaire and were assured of confidentiality. The Hypochondria/Health Anxiety Questionnaire (HAQ), developed by the Obsessive Compulsive Centre of Los Angeles (http://ocdla.com/hypochondria-test), was used to collect the data. The questionnaire was translated into Arabic and underwent a revision in order to ensure compatibility with the original one. The questionnaire was not designed to provide a formal diagnosis but provided an indication as to whether or not the persons were exhibiting significant signs of the disease.
Results of this questionnaire were analyzed as under:
A) 1 to 3 test items checked: there is a low probability that the student has health anxiety, and it is unlikely that her concerns significantly impact his life.
B) 4 to 7 test items checked: there is a medium probability that she has health anxiety, and a moderately high amount of distress related to specific health-related thoughts. She spends more time than most people doing unnecessary behaviours related to these thoughts.
C) More than 7 test items checked: there is a high probability that she has health anxiety. She most likely has a significant amount of distress related to certain health-related obsessions, and likely spends a significant amount of time doing unnecessary compulsive and avoidant behaviours directly related to these obsessions.
Statistical methods
Data were statistically described regarding frequencies (number of cases) and valid percentages for categorical variables. The response of the two groups was analyzed by student t-test. P values less than 0.05 were considered to be statistically significant. All statistical calculations were done using computer program IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 21 for Microsoft Windows.
Results
400 students were included in the study. There were 200 medical students, and the other 200 students were from various non-medical colleges of Taif University (Colleges of Arts, Admin and Financial Sciences, Computer and Information Technology, Science and Islamic Law).
All participating students were females (100%), and the mean age of the medical students was 21 years (ranged from 19-22years). The mean age in the non-medical group was 20.5 years (ranged from 19-23 years).
All students in the non-medical colleges completed the HAQ while five students in the medical college (clinical years) did not complete it, so the data on 395 participants were finally analyzed.
According to the scaling criteria, this study showed that the overall prevalence of MSS among the total sample (medical and non-medical female students) was 16.2% (64 out 395 students). However, it was higher in the medical students (34 out of 195 students; 17.4%) than in the non-medical students (30 students out of 200; 15%) – see Table 1.
Non-medical students n=200
Medical students
p value
Pre-clinical (95)
Clinical (100)
Age
19-23
19-20
21-22
Medical student syndrome (MSS)
30 (15%)
20 (21.1%)
14 (14%)
0.22
One visit to doctor
33.3 % (10 /30)
20 % (4/20)
14.3 % (2/14)
0.0043
More than one visit to doctor
40 % (4/10)
25 % (1/4)
0 %
0.001
Table 1. The frequency of Medical Student Syndrome (MSS) among medical and non-medical students.
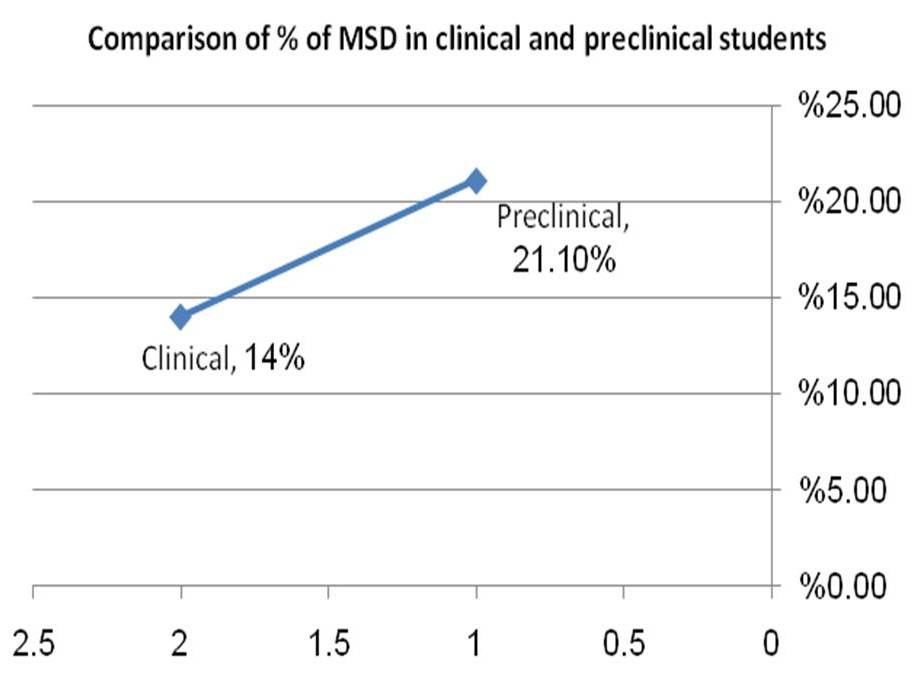
Figure 1. The difference of Medical Student Syndrome (MSS) between pre-clinical and clinical years (p=0.028).
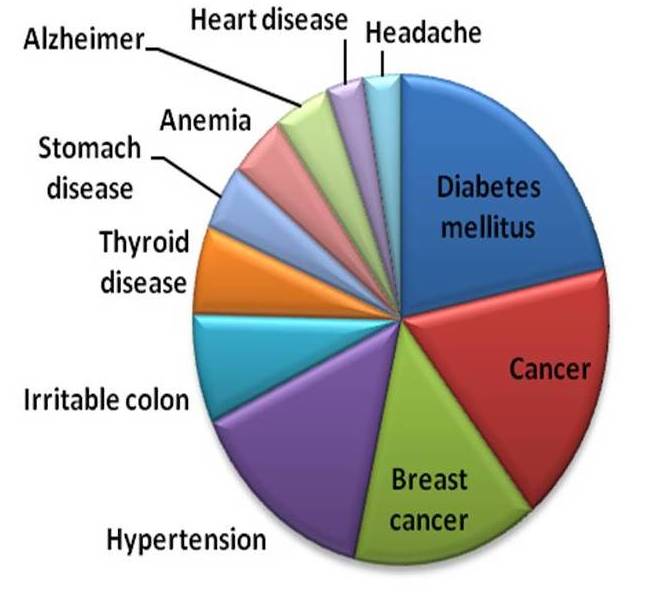
Figure 2. Fears related to diseases in the study cohort.
While comparing the response of the two groups by student t-test, there was no statistically significant difference between the responses obtained from medical and non-medical colleges (p=0.31). However, from the MSS diagnosed cases in the medical college, there was a significant difference between pre-clinical and clinical years – 21.1% vs 14% (p= 0.028) – see Figure 1.
Regarding the percentage of students who visited the doctors during the last year due to fears from disease, or medical condition, it was higher in the non-medical student's group than in the medical student's group with a significant difference observed (p=0.043).
The medical conditions that caused worry among medical and non-medical students were, diabetes mellitus followed by cancers especially breast cancer. The least worried diseases were headache and heart diseases – see Figure 2.
Regarding the percentage of students who consulted more than one doctor for the same medical concern, because of doubt about the previous doctor’s diagnosis and laboratory results, it was higher in the non-medical student's group compared to the medical student's group. The difference was significant (p=0.001).
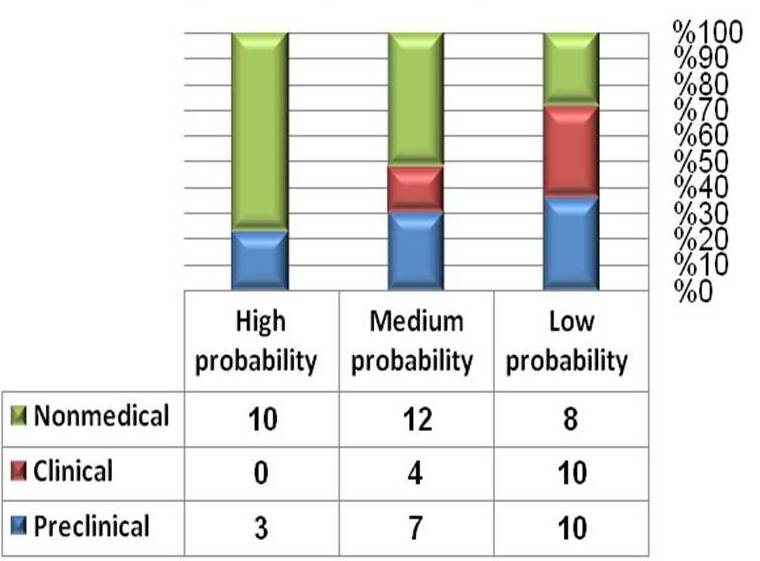
The students with MSS in the total sample (of 395 students) were categorized according to the degree of probability into low, medium and high as shown in Figure 3.
Figure 3. The probability of Medical Student Syndrome (MSS) among all groups compared to their non-medical peers.
Discussion
The unrealistic fears about illnesses recorded in this study among medical students were higher than their peers studying various non-medical courses at Taif University; however, the difference was not significant. The subgroup analysis revealed a correspondingly higher prevalence of health anxiety during pre-clinical years than clinical years as shown in Figure 1. Possibly during the pre-clinical years, students have an increased sense of body awareness and stress as demonstrated by Moss-Morris et al.7 The authors in the above study described this syndrome as a normal perceptual process and differentiated it from common hypochondriasis. Other researchers 8,12 as well affirmed this. Our results are in parallel with the finding of Azuri et al13 who recorded that first-year students visited a general practitioner (GP) or specialist more often than in other years. The authors in the above study suggested that the pre-clinical students` visits may be due to registering with a new doctor closer to university or due to necessary health checks before the beginning of their medical school. The dream content of pre-clinical medical students frequently involved a preoccupation with a personal illness of the heart, the eyes and the bowels in the above study.
Additionally, the fear of acquiring a future disease is a core feature of health anxiety, while fear of already having a disease is considered more central to the MSS.14 There is a number of instances where this syndrome manifests among students from time to time during their training. The students are even known to change their diagnosis depending upon their clinical rotation. For example, in a psychiatry rotation the student conceptualizes having schizophrenia and later shifts his or her diagnosis to Meniere's disease during an ear, nose and throat (ENT) rotation. The symptoms are thought to occur due to intensive exposure to knowledge affecting symptom perception and interpretation.15 The fact remains that the affected student is devoid of either. At times, the simple knowledge of the location of the appendix transforms the most harmless sensations in that region into symptoms of a serious threat.16 The students who study "frightening diseases" for the first time routinely experience intense delusions of having the disease, reflecting a temporary kind of hypochondriasis.17
In a study by Waterman et al18 it was observed that 80% of medical students conceptualize diagnoses ranging from tuberculosis to cancer while studying these diseases during training. This caused emotional distress and conflict in them. It was suggested that this phenomenon was present in approximately 70-80% of students in the study mentioned above. There may be multiple reasons for precipitation of this condition among medical students. The vastness of medical studies are undebatable, and medical schools cause students to experience a large amount of psychological pressure due to work required to grasp the subject matter, the stress of examinations, and the competitive environment.19
In this study, we compared medical students with the students of the same age and gender with the same cultural background in order to avoid any bias. Our results are in parallel with a more recent study, which compared three groups, medical students, non-medical students, and their peers who were not undergoing any academic course. The authors in the study mentioned above observed no significant differences between the groups on total scores in the questionnaires. However, when considering the individual components of the questionnaires, it was found that medical students were less aware of bodily changes and sensations than the other groups; nevertheless, they did not avoid seeking medical advice for any health-related fears.20
Regarding the percentage of students who visited doctors in the past 12 months due to fear of disease, it was observed in this study that the non-medical group had significantly higher visits to doctors compared to their peers studying in the medical college of the university. It is entirely possible that they had increased access to personal advice from peers, relatives, and various mentors. Of the various diseases, fear of diabetes mellitus was the highest, possibly due to a high prevalence of the disease in Saudi Arabia.21 Further, it is entirely possible that medical students subconsciously conceive these metabolic disorders as these are discussed in greater details during their courses.
MSS may lead to cyberchondria, a phenomenon of the public, seeking to diagnose themselves via the internet,11 which in turn may lead to hypochondriasis in any given student. Thus, it becomes imperative that students suffering from this disorder must be dealt with an empathetic approach and counselled properly after ruling out an organic cause of their illness. A step to circumvent it further would be that MSS must be thoroughly discussed among medical students during their training.
Limitation of the study
The drawback of this study is that that the questionnaire was translated from English into Arabic, and although it underwent a revision, there were no other formal tests such as linguistic and cultural validation to validate the translated version. Further, we believe that our focus was only on female students, and it is well known that females have better ability to cope up with anxiety and depression compared to males22,23 so the figures of MSS among male medical students needs to be studied as it may be different from what we reported in this female cohort.
Conclusion
In conclusion, the students who are suffering from MSS often overuse medical resources and outpatient’s services compared to others. Therefore, clinicians should be aware of these students, to avoid unnecessary procedures and treatments. However, it is vital that a proper evaluation is done before labelling a given student with MSS.
Stress-Induced Cardiomyopathy (SCM), also known as Takotsubo Cardiomyopathy or Apical Balooning Syndrome, is an acute, transient and non-ischaemic cause of left ventricular dysfunction often precipitated by periods of stress1. Diagnosis often follows evidence of left ventricular hypokinesia despite a normal coronary angiography. Prevalence is often underestimated, with an estimated 7% of suspected myocardial infarctions being in fact SCM2. We report a unique case of multi-nodal dysfunction following SCM.
Case Report
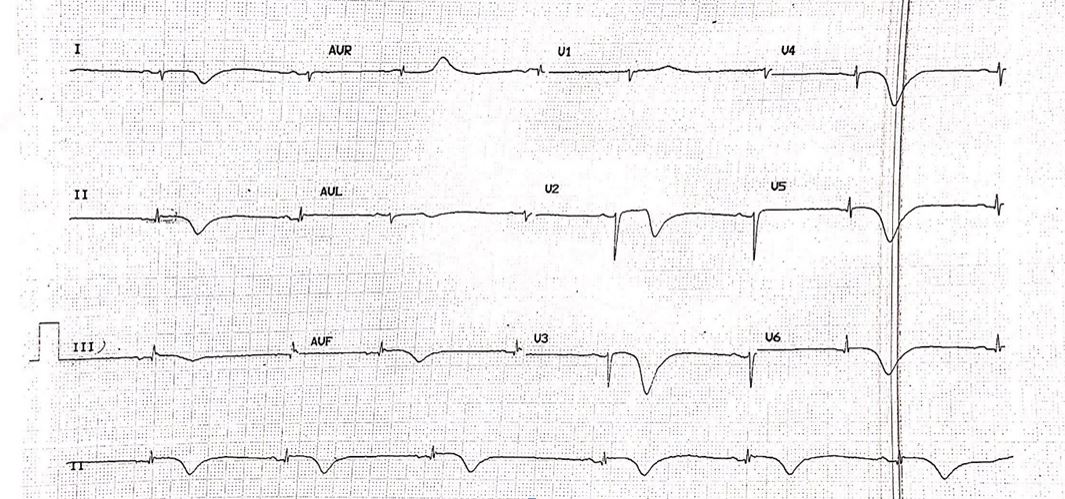
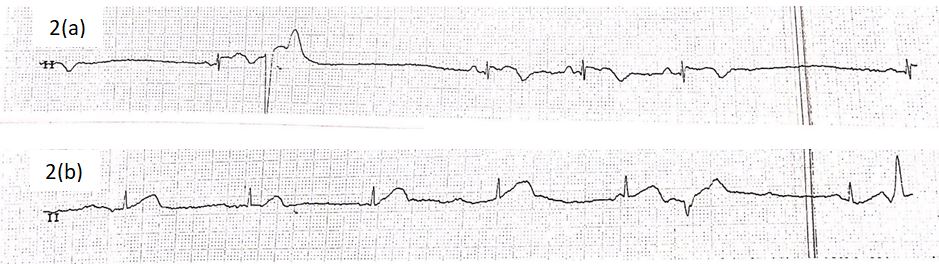
A 73-year old lady presented to our emergency department following a sudden onset of central, non-radiating chest heaviness 8 hours prior. She was a known chronic smoker of 20 pack years, and hypertension which had been left untreated for over 10 years. An initial electrocardiogram (ECG) revealed sinus bradycardia and T-wave inversions in the inferior, septal and lateral leads (Figure 1). Her Troponin-I levels was raised at 6532 pg/ml. She was treated as a Non-ST elevation myocardial infarction and was admitted to the coronary care unit for closer monitoring. She was kept on telemetry overnight, which disclosed several episodes of bradycardia. Rhythm strip revealed various transient conduction defects, including that of sinus node dysfunction (SND) and atrioventricular node (AVN) dissociation, although she remained asymptomatic throughout (Figure 2).
Figure 1: Electrocardiogram revealing sinus bradycardia, with T-wave inversion in the inferior, septal and lateral leads.
Figure 2: Telemetry rhythm strip revealing transient episodes of (a) sinus node dysfunction (SND) and (b) atrioventricular node (AVN) dissociation.
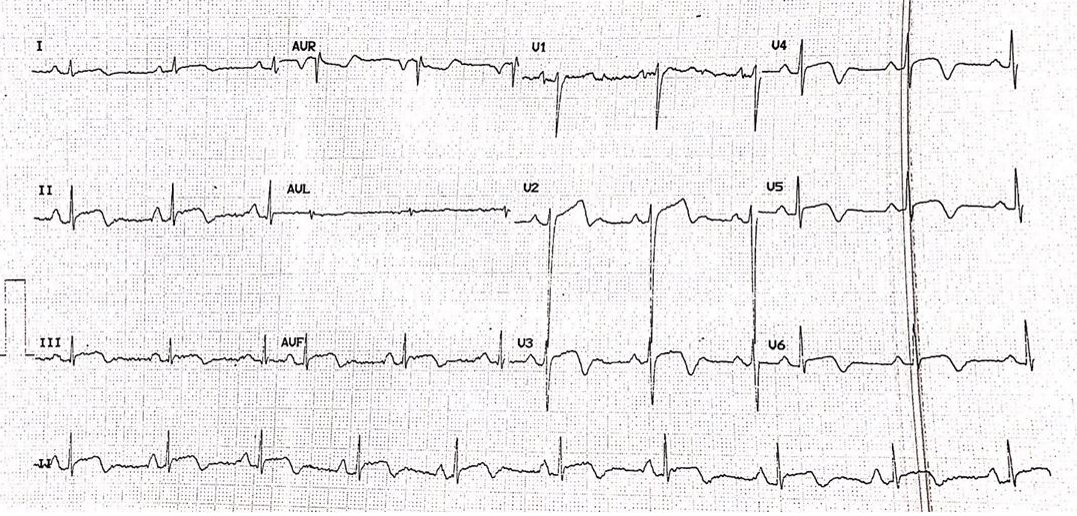
Figure 3: Electrocardiogram revealed ST-segment elevation with associated T-wave inversions in the inferior, septal and lateral leads.
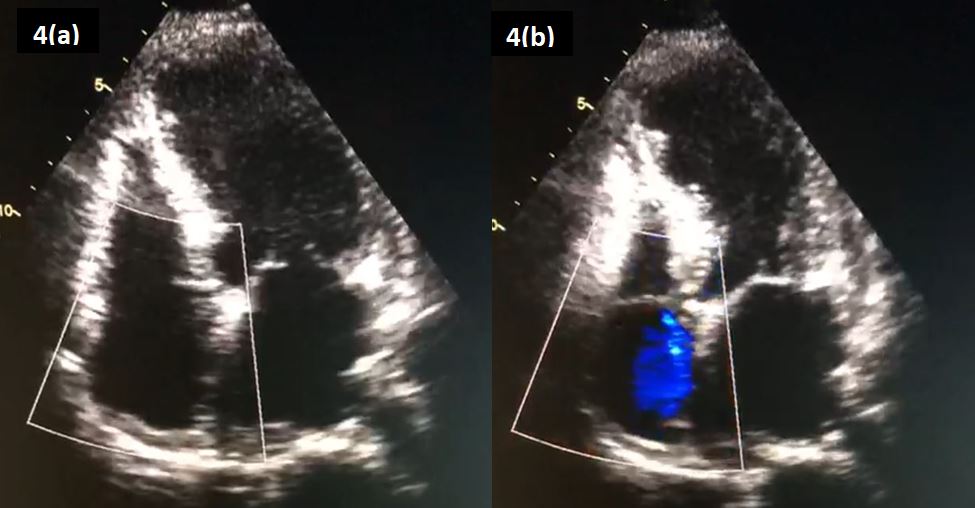
Figure 4: An ‘Apical 4-Chamber’ view on echocardiography, revealing an akinetic apex on (a) diastole and (b) systole.
Unfortunately, following an episode of chest pain the following morning, her troponin levels and an electrocardiogram were repeated, showing a rise of the former to 12 996 pg/ml. A repeat ECG revealed evidence of ST-segment elevation in previously affected leads (Figure 3). She was brought into the catheterization laboratory within 1 hour. Her coronary angiogram showed no evidence of coronary obstruction. An echocardiogram was performed, which revealed an akinetic apex (Figure 4).
Upon further history taking, it was revealed that she was recently made redundant from her job as a cleaner, several hours prior to her presentation to the emergency department. Prior to that, she denied any other emotional or physical stressors. She was diagnosed as having Stress-Induced Cardiomyopathy (SCM). Following an observational period of close to 48 hours, she was allowed home. A 48-hour Holter monitoring was performed approximately 3 weeks from her initial admission, which returned unremarkable. A repeat echocardiography was also performed, revealing normal wall motion abnormality which further support a transient SCM.
Discussion
Despite being transient, multiple complications can arise from the condition, including arrhythmias. Prevalence of arrhythmias varies greatly, depending on population and types of defect (15% suffering atrial fibrillation, 2-5% of tachyarrhythmias, 2-5% of bradyarrhythmias and 5% of AVN dissociation amongst others)3,4. This is largely due to evidence being based on retrospective case report and series, leading to severe underestimation of their true prevalence. We suspect cases of sinus node dysfunction are far more uncommon, with only a handful of case report of note, and one retrospective review of 816 patients quoting a rate of 1.3%5. There are no reports of concomitant sinus node and atrio-ventricular node dysfunction, to our knowledge.
Proposed mechanisms for SCM-induced nodal dysfunction include reduced coronary flow to conduction tissues due to left ventricular dyskinesia, cathecolamine-driven coronary and microvascular vasospasm leading to both reduced blood supply and direct cardio-toxicity effects, and continual ischaemia-driven fibrosis of nodal tissue6. However, there have been reports of SND-triggered SCM, likely secondary to adrenergic compensative activation following bradycardia events. In both scenarios, pre-existing, subclinical SND may lower the threshold of developing significant, symptomatic bradycardia7-10. This is important to note, as majority of patients affected by SCM are post-menopausal women whom are already at risk of age-related SND.
In our patient, the SCM may have likely induced both SND and AVN dissociation, as subsequent 48 hours Holter monitoring, 3 weeks from presentation, was unremarkable. Furthermore, the patient denies any previous syncopal or pre-syncopal symptoms. However, the possibility of subclinical SND could still have existed, as we had earlier discussed, and ideally an internal loop recorder for prolonged monitoring, catheter-based electrophysiology studies and a Cardiac Magnetic Resonance Imaging to detect nodal and conduction tissue fibrosis would assist in ruling out pre-existing nodal dysfunction. However, due to financial and pragmatic reasons (as patient was asymptomatic), the patient declined further investigations, opting for periodic clinic reviews instead.
Conclusion
Both nodal and conduction tissue blocks are a rare but significant complications that can occur following SCM. The occurrence of SND following SCM should lead clinicians to routinely investigate for pre-existing conduction tissue diseases, if not already performed and allows for earlier device implantation if deemed indicated.
Necrotising soft tissue infections (NSTI) are severe and rapidly progressive, requiring rapid recognitions and early, often surgically-based, management. Mono-microbial types of NSTI (i.e. Type 2 NSTI), which amounts for 20 to 30% of overall cases, are often linked to invasive Group A Streptococcus or Staphylococcus Aureus infections 1. Rarely, Group B Streptoccocus (GBS), also known as Streptococcus Agalactiae, are implicated 2. We report a unique case of NSTI of the lower limbs due to GBS, with acute pericardial dissemination leading to cardiac tamponade, leading to a diagnostic dilemma due to co-existing cardiogenic and septic shock.
Case Report
A 51-year old gentleman of Chinese ethnicity presented with right foot pain and swelling over 2 weeks, associated with chest pain and shortness of breath during that period. He had a 10-year history of poorly controlled diabetes mellitus with a Hba1c level of 8.8 %, hypertension and dyslipidaemia.
He was hypotensive on arrival, with a blood pressure of 91/60 mmHg and hypoxic, requiring high flow oxygen of 15L/min to maintain saturations at 100%. Otherwise other vitals were stable, pulse rate being 72 beats per minutes, respiratory rate 24 breaths per minute and a temperature of 37.4 degrees Celsius.
Clinical examination revealed a gangrenous lateral two toes extending into the lateral malleolus on the right foot, with evidence of pus discharge and associated warmth and crepitus up to hindfoot level on palpation. There was also evidence of dry gangrene in the fourth toe of the left foot, with presence of a small puncture at dorsum of foot with pus discharge. Similarly, crepitus was felt up to midfoot level on palpation of the left side. Bilateral dorsalis pedis and posterior tibialis pulses were palpable but feeble.
Table 1: Blood Investigations on Admission
Blood Test
Results
Blood Test
Results
White Cell Count
26.99 x109L
Alkaline Phosphatase
168 U/L
Neutrophil
90.30%
Alanine Aminotransferase
37 U/L
Lymphocyte
4.50%
Aspartate Aminotransferase
40 U/L
Platelets
210 x109L
Sodium
121 mmol/L
Hemoglobin
10.0 g/dL
Pottasium
7.6 mmol/L
Lactate Dehydrogenase
441 U/L
Urea
40.5 mmol/L
International Normalised Ratio
1.2
Creatinine
323 μmol/L
Activated Partial Thromboplastin Time
36.5 s
Creatinine Kinase
43 U/L
Prothrombin Time
14.6 s
Total Bilirubin
21 μmol/L
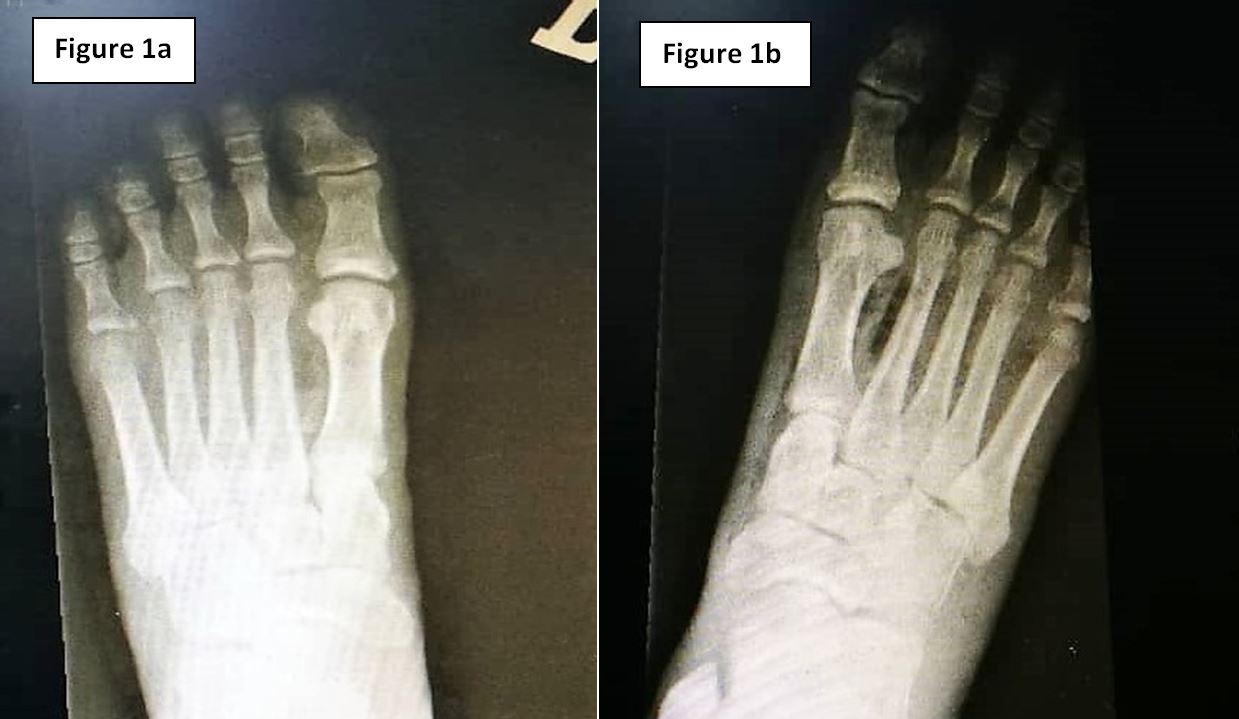
Figure 1a & 1b: Radiography of the (1a) left foot and (1b) right foot respectively, demonstrating gas within soft tissue bilaterally.
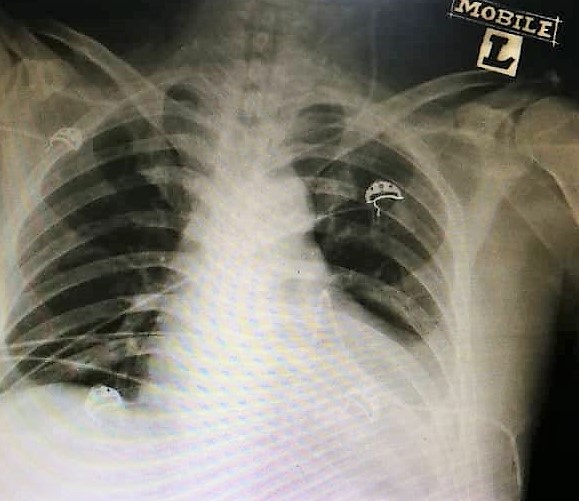
Figure 2: Chest radiography demonstrating cardiomegaly and globular-shaped heart, with loss of left-sided cardiophrenic and costophrenic angles.
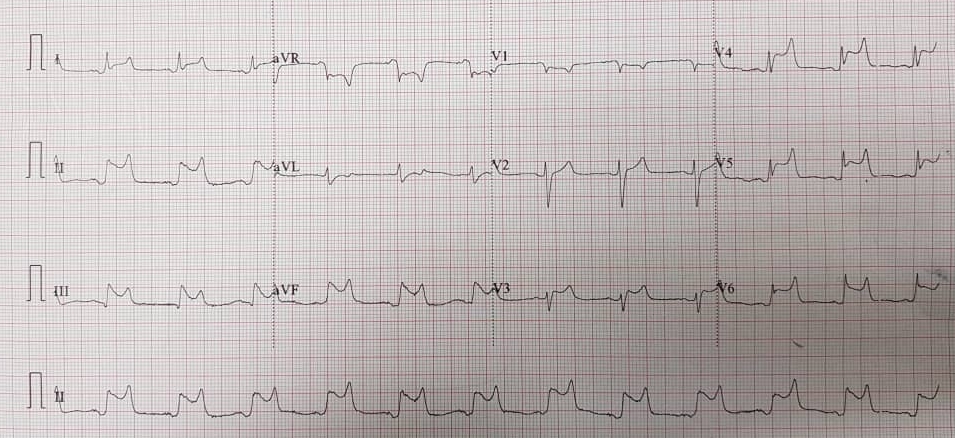
Figure 3: Electrocardiogram demonstrating widespread saddle-shaped ST-elevation, consistent with pericarditis.
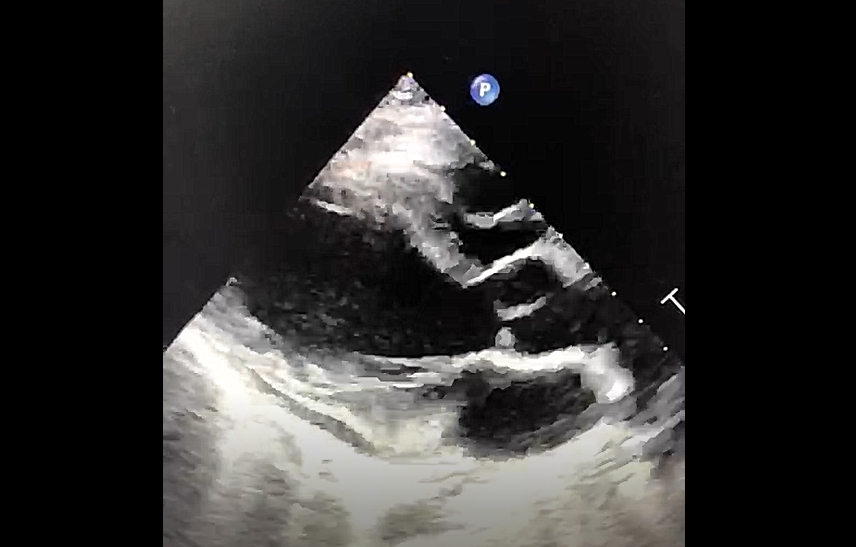
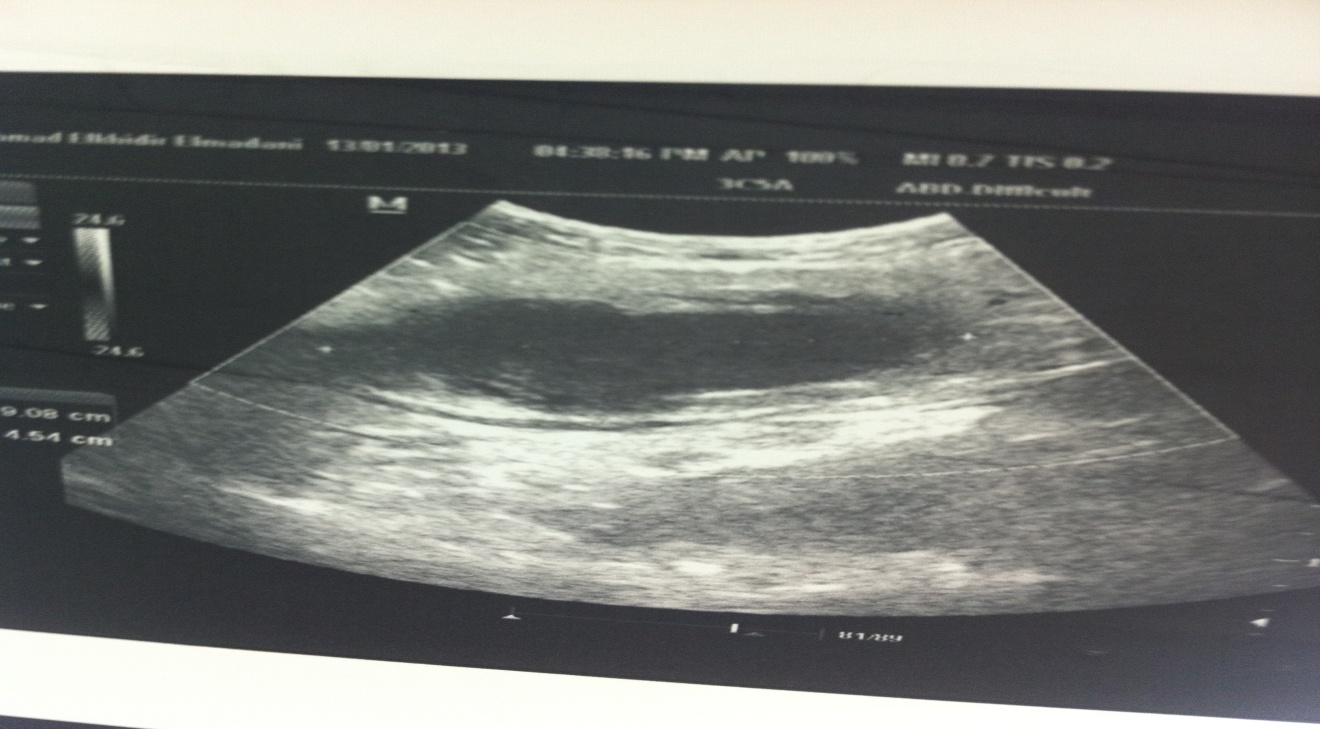
Figure 4: Parasternal Long Axis view of bedside echocardiography showing evidence of pericardial effusion and right atrial and ventricular collapse
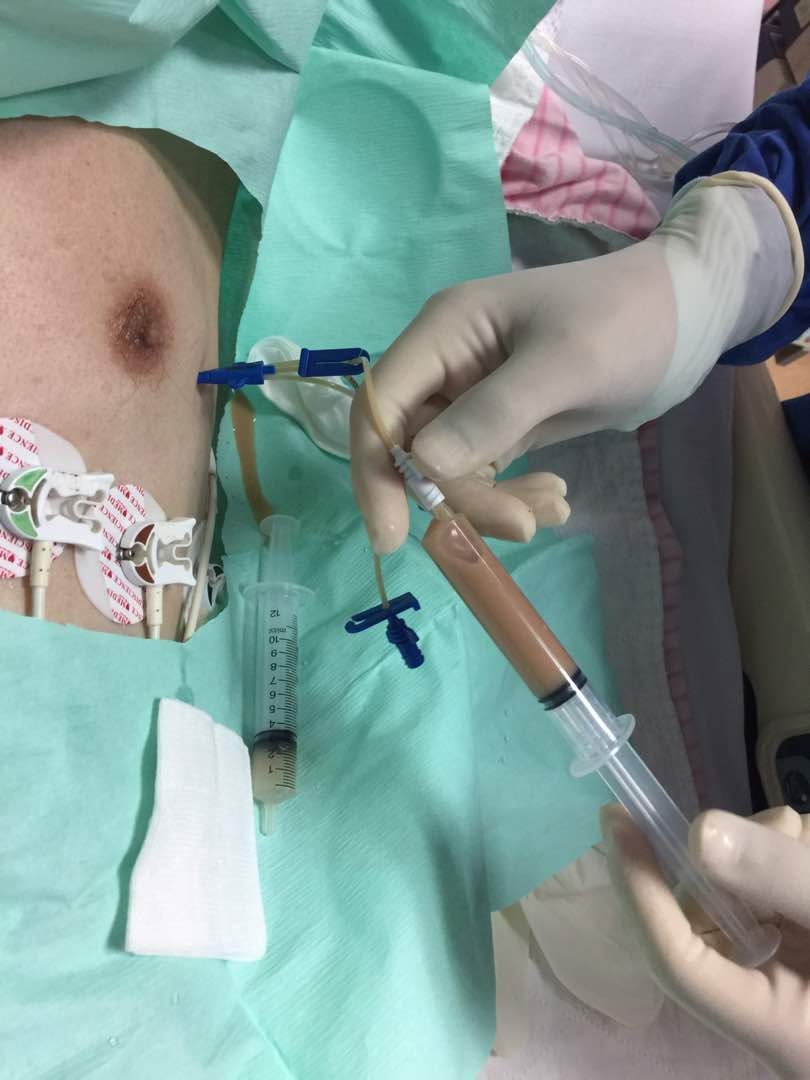
Figure 5: Purulent pericardial aspirate via pericardiocentesis
Initial blood investigations are highlighted in Table 1. HIV Antibody, Hepatitis B Surface Antigen and Hepatitis C Antibody serology were all negative. Lower limb radiography revealed evidence of gaseous shadows bilaterally (Figure 1). The clinical and radiological findings were consistent with necrotising soft tissue infection of bilateral feet, and the patient was advised for extensive wound debridement and possible amputation of the affected sites during an orthopaedic consult.
However, on closer review of the chest radiography, there was evidence of cardiomegaly with a globular-shaped heart (Figure 2). His electrocardiogram on arrival, revealed diffuse ST-segment elevations on majority of leads, ST-segment depression on lead aVR consistent with pericarditis (Figure 3).
A bedside echocardiogram was performed, revealing a massive pericardial effusion, measuring largest at 2 cm in depth, with evidence of both right atrial and ventricular collapse (Figure 4).
An urgent pericardiocentesis was performed, under echocardiographic guidance, which revealed turbid-looking aspirate (Figure 5). Urgent microscopic analysis revealed 45 Cells per mm3, majority of which were lymphocytes, and gram stain showed moderate amounts of pus cells with occasional gram positive cocci. Pericardial fluid was negative for acid-fast bacilli.
A repeat transthoracic echocardiogram was performed post-pericardial drain insertion, revealing minimal remnant pericardial fluid, with the pericardial drain in-situ, and no evidence of any mass or vegetation. Unfortunately, a transoesophageal echocardiography and Computed Tomography (CT) imaging of the mediastinum (to rule out mediastinitis and pneumonitis) was not performed, as management of the NSTI took precedence.
The patient was started on intravenous antibiotics, both tazobactom-pipericillin and clindamycin. There was a delay in performing limb saving wound debridement as the patient was reluctant for invasive management, but had later consented to the procedure which was performed only on day 3 of admission. Tissue cultures were taken peri-operatively. Unfortunately, the patient deteriorated post-operatively due to extensive blood loss and overwhelming septicaemia and succumbed to his illness 72 hours after. Subsequently, it was revealed that cultures from blood, pericardial aspirate and tissue aspirate were positive for GBS infection.
Discussion
GBS is a common microorganism, often colonising the gastrointestinal and reproductive tract 3. Rarely, GBS colonises the skin and can cause necrotising fasciitis, i.e. necrotising soft tissue infection (NSTI), with only 22 cases having been reported in the past ii. Majority of these patients are either immunocompromised or have other predisposing factors including recent thoracic intervention or trauma 4,5.
GBS-related infections of cardiac structures are rare, as a whole, with 2 to 3% of cases presenting as native valve endocarditis and far less as pericarditis, mycotic aneurysms and intraventricular abscesses 3. Parikh et al reviewed the types of microorganisms isolated from purulent pericarditis samples and revealed that only 5% were due to streptococcal organism, sansStreptococcus Pneumoniae, possibly less so due to GBS 6. Our literature search revealed only one case of GBS-related purulent pericarditis reported although the case was not linked in any way to a NSTI to our knowledge 7.
Our case was unique as, at the time of writing, there were no other reports of GBS-related lower limb NSTI in combination with mediastinal involvement. There have been only a handful of cases of necrotising fasciitis reported with mediastinal involvement, the majority of which were supra-diaphragmatic with only one reporting NSTI of the lower limb due to Aspergillus infection 89.
The similarity in culture results obtained from blood, tissue aspirate and the pericardial fluid in our patient suggest dissemination of GBS from the NSTI, possibly via a haematogenous route, although bacterial-related pericardial dissemination can also occur via direct spread from infected foci from neighbouring intra-thoracic structures or sub-diaphragmatic 4. The possibility of multi-routed spread should remind clinicians that, albeit rare, mediastinal involvement in NSTI is a possible complication of such disease.
Conclusion
This case highlights the rare possibility of cardiac involvement in cases of NSTI, and the possibility of cardiac tamponade causing cardiogenic shock masquerading alongside septic shock. It also highlights the importance of combining clinical findings with ancillary testing, including bedside echocardiography, when faced with challenging cases of sepsis to help look for possible foci of infection.
The Royal College of Psychiatrists (RCPsych) launched its five-year Recruitment Strategy in 2011 aiming to achieve a 50% improvement in recruitment to core psychiatry training and a 95% fill rate of posts by the end of the five-year campaign (1). The primary focus of this campaign was on recruiting UK medical graduates.
Two of the Strategy’s main aims were to highlight good practice in undergraduate teaching and to improve the teaching skills of psychiatrists to inspire and influence medical students during their psychiatry curriculum.
The Strategy stressed the importance of good clinical placements in psychiatry and recommended that medical students should ideally be placed only with ‘the best teachers and welcoming teams’ avoiding colleagues who are disillusioned with psychiatry or not happy with their jobs.
It is therefore essential that psychiatrists and other clinicians play an important role to improve the medical students placement in their workplace in order to give the students a positive expereince of this speciality and hopefully promote it as a future career option.
Background
Fourth-year medical students from the University of East Anglia (UEA) spend two months rotating through various mental health services as part of their clinical placement in the Mind Module (also known as Clinical Psychiatry or Module 11).
As part of this rotation, students are placed in Old Age Psychiatry for six days over a two-week period. They shadow clinicians in two community teams, two inpatient wards and the Electro-Convulsive Therapy (ECT) clinic. All of these teams are based at the Julian Hospital in Norwich.
The students are encouraged to talk to patients and carers and perform basic clinical tasks such as mental state examination and risk assessment. Table 1 summarises the learning outcomes for students during their placement.
Table 1- The learning outcomes for students during their Old Age Psychiatry placement
Gain clinical experience of diagnosis and management of mental health problems (including dementia) in older people.
Improve the communication skills with regard to interactions with older people with mental disorders and their carers.
Enhance the student’s understanding of the nature of the multi-disciplinary team (MDT) model in mental health for older people, particularly the social aspect of care and end of life care.
After each rotation, each student is asked to complete a feedback form regarding their placement. This feedback helps the module leads and clinicians to improve the students learning experience.
Before the implementation of our placement improvement project, the students did not feel that they were meeting their learning outcomes. Table 2 summarises the major areas that needed improvement.
Table 2- Areas needed to improve before the implementation of the new placement structure
Poor planning and organisation of the clinical placement.
Inadequate or no information sent before starting the placement.
Lack of a dedicated coordinator to design the placement timetable and allocate students to specific clinicians
Lack of multidisciplinary teaching and hence poor understanding of the various roles of professionals (e.g., memory assessors, community nurses, support workers, etc.).
Students felt that clinicians were too pressured to supervise students. Some students reported that they were sometimes sent off as the staff had been too busy or there insufficient volunteers from clinical staff to take a student.
Student dissatisfaction with clinical placements is not unique to psychiatry. Research has shown that educators and learners face significant challenges when teaching and learning take place in any clinical setting. See Table 3 for a summary.
Table 3- Challenges of teaching in clinical settings (modified from Spencer, 2003)
Limited clinician time allocated to teaching activities.
High number of students allocated to few clinicians.
Difficulty in seeing patients (e.g., patients refusing the presence of a student).
Clinical setting is not ‘teacher friendly’ (overcrowded, too small, noisy and/or lacking privacy to interview and examine patients).
Lack of rewards and recognition for the clinical educators.
One of the biggest challenges of teaching in clinical settings is how to provide a welcoming and supportive learning environment in a busy and time constrained practice. We found that one of the main reasons for clinicians to be reluctant to have students shadowing them is the challenge of providing a dual role of caring and teaching simultaneously.
The placement improvement project
The improved structure of the student's’ placement in Old Age psychiatry was based on the tenet that clinical placements should provide various clinical experiences that include interaction with patients and professionals from various grades in addition to face to face teaching in small groups (3). The authors took over full responsibility for coordinating the students’ placements and liaising with the various supervising clinical teams. This ensured clear leadership and consistency in organising the placement.
The improved placement structure started in October 2015 with the first cohort of medical students coming to their clinical placement after the summer break. Table 4 gives a summary of the changes implemented.
Table 4- Changes to improve the clinical placement in Old Age Psychiatry
Compiling a ‘welcome pack’ and sending it by email to the students before the clinical placement.
A “Meet and Greet” event on the first day of the clinical placement was introduced comprising of several clinicians who operate on a rota basis.
Involvement of all professionals in the MDT (including Staff and Associate Specialists, community and memory nurses, junior doctors and clinical psychologists in addition to consultant psychiatrists).
Introduction of a Balint-style psychotherapy group aiming to facilitate discussion in a safe and containing environment of the emotional impact of patients encountered.
Designing a weekly one-hour teaching session supervised by a senior clinician and facilitated by a trainee psychiatrist.
Each clinician received a formal letter of thanks from the Head of Norwich Medical School, the Module Lead and the Secondary Care Lead certifying their contribution to the education of medical students and thanking them for their work.
The information pack sent to the students before the placement contained information about the hospital environment (location, map, parking, travel arrangements, key codes and useful contact numbers) and a detailed timetable (and email address) of the clinician supervising the student each day during the placement. Also, it included useful information about the mental state examination and the Mental Health Act, information that had been requested previously by medical students.
Sending information before the placement has been shown to be beneficial in students’ electives (4) and this is especially important in psychiatry which can be experienced as less structured than other medical specialities and where students are required to travel to various hospitals and clinics bases. As a result, students felt that they were expected and had a clearer sense of where they should be and who would be supervising or teaching them. Later student feedback reported that these changes had contributed directly to an improved learning experience.
The timetable design ensured that every student would have the chance to experience working in several settings in Old Age Psychiatry, including community, inpatients, ECT and the Memory Clinic. It was also noted that a two-week placement in any psychiatric team could not easily give a student a sense of patient ‘recovery’. It was, therefore, decided that students see a patient who had been discharged from the ward, e.g. with the care coordinator.
The rota of the ‘Meet and Greet’ event on the first day of the placement ensured that the workload is spread among the clinicians and helped sustain the necessary levels of enthusiasm and energy. Previously, this task had repeatedly fallen to just a few clinicians.
The participation of all professionals in the clinical team in supervision and teaching helped the students to better understand the different roles of clinicians within the multidisciplinary team and enriched their learning experience. To achieve this, we attempted to allocate sessions with a clinical psychologist, care coordinators, memory assessment nurses and members of the intensive support team. It also had the bonus of ensuring that the workload of teaching was spread more equally among clinicians.
Attendance at ward rounds and community MDT meetings could be a valuable experience but only if the process is explained, and – in the ward round – the student is briefed on the clinical history and background of the patients. For these reasons, supervising clinicians were reminded to give this information to the students attending such meetings.
The weekly teaching sessions provided an opportunity for the students to present case histories of patients they had seen and to discuss their management. Clinicians could also give a formal didactic teaching on a specific topic, for example, mental state assessment or risk assessment in psychiatry.
The letters of thanks to the participating clinicians served as an added benefit (in addition to the satisfaction of teaching others) to sustain their motivation and reward them for their contribution to the teaching of medical students. The psychiatric trainees used the letter to demonstrate their skills in teaching in their portfolio.
Benefits of the new placement structure
Helping students to feel supported before, during and even after their placements was a high priority in this project. Research has shown that learners rank the need for support and guidance in workplace environments as high and it is an essential requirement for a successful learning experience (5). This extra support is particularly crucial in psychiatry which is perceived by many students to be difficult and challenging (6).
The support provided to the students in the improved structure was in the form of having the contact details of the rota coordinators, their supervising clinicians, the administration team (medical secretaries, site manager for parking permits) and some other useful numbers for various locations and clinics.
While improving the organisation of the placement, changes were aimed to reduce the commitment of teaching and supervision for clinicians and spread it more equally among the members of the team.
Students reported that they found home visits during the placement the most useful part of their placement and the most interesting. This is an invaluable experience with the student having a significant amount of time in a one to one interaction with a clinician (including during the travel from one location to another) and then observing the clinician ‘in action’ with patients at home. This experience highlights the role of ‘professional socialisation’ (7) that is considered by educators as a significant process in the development of a sense of a shared professional identity and responsibility in both the clinician and the learner.
Furthermore, using non-medical professionals to supervise and teach students has been valued by students (8). It enriched the clinical placement with the concept of (Inter-Professional Learning) which is an active learning from and with professionals from other disciplines allied to medicine. This style of education has been shown to improve students’ communication with professionals from different disciplines and to have a better understanding of the nature of the multidisciplinary teamwork and the roles of each member of the team (9).
While improving the organisation of the placement, changes were aimed to reduce the commitment of teaching and supervision for clinicians and spread it more equally among the members of the team.
Balint groups and improving student placements in psychiatry
Balint groups were pioneered by the Hungarian psychoanalyst Michael Balint who introduced this model in the late 1950s after running seminars for general practitioners in the UK with his wife, Enid. (10)
Balint recognised the intense emotions that affect the doctor and the patient and encouraged clinicians to talk about these feelings in groups, which later came to be known as Balint groups.
Research has shown that Balint groups for medical students can increase the students’ empathy towards patients with chronic mental illness and improve their ability to cope with complex clinical situations (11). It also helps them to engage in reflection about their professional growth and to develop their identity as future doctors (12). Most importantly, this psychotherapeutic approach it allows them to reach a deeper understanding of the emotional impact of their patients (13). It was felt that the students would benefit from this model to help with the various emotions evoked by dealing with patients they would encounter in Old Age Psychiatry, in particular, dementia.
The student feedback was very positive for the Balint group. One student commented. It is inevitable to have experiences with patients that leave you with a feeling, whether that be positive or negative. To be able to look back at those times, talk them through, be listened to and have others reflect things back that you may not necessarily have realised yourself, is invaluable’.
Patient and carer involvement in clinical education
Clinical education in the workplace has always depended on patients and carers in its design and delivery. Students value seeing patients and learning from their experiences. However, the evidence suggests that patients are not routinely involved in the design of the curriculum or clinical placements despite calls to actively engage them in teaching and training (14).
Students were given the opportunity to learn from patients and carers through regular and supervised contact with them. They also attended a workshop on dementia and viewed a DVD showing the experiences of a woman with dementia and depicting how the world might be seen from her perspective. Feedback from students was very positive for these opportunities.
Medical students placement and Electro-Convulsive Therapy (ECT)
Students are allocated to spend one day in ECT clinic during their two-week placement in Old Age Psychiatry. Research has shown that many medical students have negative attitudes and unjustified reservations about ECT and its therapeutic applications (15). However, these views can change with education about this therapy during clinical placements and encouragement of the students to talk to patients and read about its indications and effectiveness in people with severe mental illness (16). Seeing the procedure first hand would, therefore, help the student gain confidence to challenge the stigma attached to ECT and to explain this treatment to their future patients.
Feedback from the students following the implementation of the placement improvement project
The feedback from medical students and clinicians was very positive. The students enjoyed their placements and felt that they gained useful knowledge and skills. Above all, they felt welcomed in the clinical settings and settled very nicely into the teams.
Figures 1 and two summarise some comments from the medical students following the placement. This feedback was collected by Norwich Medical School as part of the regular monitoring of clinical placement for medical students.
Figures 1 and 2: Feedback from students after the implementation of the changes to the clinical placement:
‘Best part of placement. Doctors were all happy to have us and teach. It was well organised, I felt that we were welcomed and always expected. It was varied and generally useful to my learning needs’. Student ID 69. End of Module 11 feedback.
‘This was one of the best placements in psychiatry, each doctor was very helpful and especially keen on teaching. It was really good to not only see the patients on the ward but so helpful to go on home visits to see assessments in patients own home. Really enjoyed this placement’. Student ID 95.
Limitations
There were some challenges in the implementation of this improved model. First is not always easy to recruit non-medical members of the clinical teams to take students. There are some reasons for this including lack of confidence or experience in teaching, a belief that it is “not their role”, or concern about the increasing demands on their time. Others already had students in their discipline. This was addressed by briefing the professionals about what the students need to achieve at the end of the placement and encouraging them to be involved in the supervision. The introduction of nursing revalidation in April 2016 may help more nurses to get involved. (17)
Conclusions and recommendations
This paper describes a clinical placement improvement project for medical students in Old Age Psychiatry. The changes focused on the enhancement of organisation, supervision and teaching.
Our improvement project is ongoing, and there are areas needing further improvement, for example, more active involvement of patients and carers in the teaching and learning of medical students is necessary. It is planned to achieve this by inviting patients and carers to tell their personal stories to the students in a small group.
Organisers of students’ placement in secondary or primary care need a systematic approach to filling allocation slots to ensure that all students receive a similar and broad exposure to their speciality. It can be dispiriting and stressful to ask for volunteers constantly. They need to have good relationships with their clinical colleagues of all disciplines, and to be willing and assertive enough to go around and ask colleagues in person rather than sending email requests.
Psychiatric educators have a significant role to play in the improvement of clinical placements for students as this will hopefully contribute to improving recruitment to this medical speciality that is undergoing a recruitment crisis. Research has shown that there is a positive correlation between the length and quality of clinical placement and the likelihood of choosing psychiatry as a future career. (18)
Depression is a clinical syndrome. The International Classification of Diseases (ICD) diagnostic classification systems describe three core symptoms of depression; low mood, anhedonia and reduced energy levels1. Other symptoms include impaired concentration, loss of confidence, suicidal ideation, disturbances in sleep and changes in appetite. Symptoms must have been present for at least a period of two weeks for a diagnosis of depression to be made. Major depression refers to the presence of all three core symptoms and, in accordance with ICD criteria, at least the presence of a further five other symptoms1. See Table 1 for severity criteria of a depressive episode according to ICD criteria.
Table 1: Severity criteria of a depressive episode according to ICD-101
Criteria A – General:
Criteria B – Presence of ≥2 of the following:
Criteria C – ‘Other’ symptoms:
Symptoms for at least 2 weeks Symptoms not attributable to psychoactive substance use or organic mental disorder
Low mood Anhedonia Reduced energy levels/ increased fatigability
Loss of confidence and self-esteem Feelings of guilt Suicidal thoughts Impaired concentration/ability to think Changes in psychomotor activity Sleep disturbance Changes in appetite with weight changes
Criteria for severity of depressive episode:
Mild episode: 2 symptoms of criteria B
Moderate episode: ≥2 symptoms of criteria B + symptoms of criteria C until minimum of 6 symptoms in total
Major episode: all 3 symptoms of criteria B + symptoms of criteria C until a minimum of 8 symptoms in total
Depressive symptoms, which can be clinically significant, can be present in the absence of a major depressive episode. Depressive symptoms are those that do not fulfil diagnostic criteria for a diagnosis of depression to be made. Depressive symptoms can be collectively referred to as sub-threshold depression, sub-syndromal depression or minor depression2.
It has been proposed that there are two types of depression; early-onset and late-onset depression. Late-onset depression refers to a new diagnosis in individuals aged 65 years of age or older. Over half of all cases of depression in older adults are newly arising (i.e. the individual has never experienced depression before) and thus late-onset type depression. Late-onset type depression is associated more with structural brain changes, vascular risk factors and cognitive deficits. It has been suggested that late-onset depression could be prodromal to dementia3.
The Kings Fund has estimated that by 2032 the proportion of older adults aged 65-84 years old will have increased by 39% whereas the proportion over the age of 85 years will have increased by 106%4. This increase in population will consequently see the incidence and prevalence of depression rise. By 2020 it is estimated that depression will be the second leading cause of disability in the world regardless of age5. Recognising, and so diagnosing, depression in older adults will become more important because of a greater demand on existing healthcare services and provisions, due to physical health consequences, impact upon healthcare utilisation and greater economic healthcare costs.
Presentation of depression in older adults
The presentation of depression in older adults is markedly different to that in younger adults. The most significant and fundamental difference in presentation in older adults is that depression can be present with the absence of an affect component, i.e. subjective feelings of low mood or sadness are not experienced3,6-9. The absence of an affective component is referred to as ‘depression without sadness’8-9. It is common instead for older adults to report a lack of feeling or emotion when depressed8-9.
Anhedonia is also less prevalent in this population. However, reduced energy levels and fatigue are frequently reported8-9.
Compared to younger adults, psychological symptoms of depression occur more frequently and are more prevalent in older adults10. Such psychological symptoms include feelings of guilt, poor motivation, low interest levels, anxiety related symptoms and suicidal ideation. The presence of irritability and agitation are key features as well7. Hallucinations and delusions are also more common in older adults, particularly nihilistic delusions (i.e. a person believing their body is dead or a part of their body is not working properly or rotting).
Cognitive deficits are characteristic of depression in older adults7,11 and are described as ‘substantial and disabling’12. Such deficits mainly concern executive function13-14. Pseudodementia is a phenomenon seen in older adults15. The term refers to cognitive impairment secondary to a psychiatric condition, most commonly depression16. Pseudodementia has become synonymous with depression. Pseudodementia can be mistaken for an organic dementia and so older adults who are depressed can present primarily to mental health services with memory problems. Pseudodementia is classically associated with ‘don’t know’ answers, whereas older adults with a true dementia will often respond with incorrect answers17.
‘Depression-executive dysfunction syndrome’ is a more specific and descriptive term to describe the cognitive deficits found in older adults with depression14. It is associated with psychomotor retardation, which can be a core feature of depression in this population7,14,18. Psychomotor retardation describes a slowing of movement and mental activity19. Like pure cognitive deficits, psychomotor retardation contributes significantly to functional impairment19. Both executive dysfunction and psychomotor retardation have been found to be related to underlying structural changes in the frontal lobes14, 20-21. Psychomotor retardation is further related to white matter changes in the motor system, which leads to impaired motor planning21. There is conflicting evidence of whether the presence of psychomotor retardation is related to depression severity18-19.
Somatisation and hypochondriasis are associated with depression in older adults and increasing age in general22-23. Somatisation is often overlooked in older adults by healthcare professional who actively search to attribute such symptoms to a physical cause. Somatisation is more common in those who have physical comorbidities. Somatisation in older adults is associated with structural brain changes and cognitive deficits24.
Depression in older adults is associated with functional impairment cognitively, physically and socially7,12,25. Such functional impairment is linked to loss of independent function and increased rates of disability26. Withdrawal from normal social and leisure activities can be marked7,25. Social avoidance reduces interaction with others and is often a maintaining factor for depression25.
Self-neglect is a classical feature of depression7, with the presence of depressive symptoms in older adults being predictive of it27. Behavioural disturbances can be a common mode of presentation, especially for older adults living in institutionalised care 6-7. Behavioural disturbances include incontinence, food refusal, screaming, falling and violence towards others7.
Diagnostic difficulties
Depression in older adults has been a condition that has constantly been under-recognised. Several issues account for this. Firstly, phenomenological differences are present. Many have argued that phenomenological issues contribute heavily to diagnostic difficulties28; both the DSM and ICD classification systems do not have specific diagnostic criteria for depression in older adults. Potentially invalid diagnostic criteria for depression in older adults could result in fundamental difficulties in understanding, with consequent impact on both clinical practice and research.
Diagnostic difficulties are also encountered because depression in older adults can present with vague symptoms, which do not correspond to the classical triad of low mood, low energy levels and anhedonia, which can all be cardinal symptoms in a younger population. Reports of fatigue, poor sleep and reduced appetite can be attributed to a host of causes other than depression and therefore it is no surprise that a diagnosis of depression is overlooked and goes undetected by healthcare professionals29.
The absence of an affective component (i.e. low mood) can lead to healthcare professionals disregarding the potential for the presence of depression and consequently not exploring for other symptoms.
Furthermore, symptoms of depression, especially somatic ones, are often attributed to physical illnesses. Depressive somatic symptoms often lead to a diagnosis of depression being over looked; such symptoms ‘mask’ the clinical diagnosis of depression and hence the term ‘masked depression’30. Depressive somatic symptoms – e.g. low energy levels, insomnia, poor appetite and weight loss - are often attributed to physical illness and/or frailty by both the individual and healthcare professional7-8, 31.
Further complicating diagnostic difficulties and under-recognition is the fact that older adults are less likely to report any symptoms associated with mental health problems and ask for help in the first place7,10,32; explanations for this include older adults being less emotionally open, having a sense of being a burden or nuisance, and believing symptoms are a normal part of ageing or secondary to physical illness7,10,29,33.Older adults also have a reluctance to report mental health problems due to their perception of associated stigma; many older adults hold the view the mental health problems are shameful, represents personal failure and leads to a loss of autonomy7.
There is an overlap between symptoms of depression and symptoms of dementia. It is quite common for older adults with dementia to initially present with depressive symptoms. Depression has a high incidence in those with dementia, especially those with vascular dementia. Depression is particularly difficult to diagnose in dementia due to communication difficulties; diagnosis is often based on observed behaviours8,33.
Depression and comorbidity in older adults
In those with pre-existing physical health problems, depression is associated with deterioration, impaired recovery and overall worse outcomes34. For example, the relative risk of increased morbidity related to coronary heart disease is 3.3 in comparison to individuals without depression35. Mykletun et al. established that a diagnosis of depression in older adults increased mortality by 70%36. Several causative routes account for poor physical illness outcomes. Older adults with depression are less likely to report worsening health. Depressive symptomatology indirectly affects physical illness through reduced motivation (often secondary to feelings of helplessness and hopelessness) and engagement with management. Poor compliance with management advice, notably adherence to medications is observed37. Feelings of hopelessness, helplessness and negativity will contribute to the failure to seek medical attention in the first place or report worsening health when seen by a healthcare professional.
Depression affects biological pathways directly, which impairs physical recovery. Such biological effects include pro-inflammatory factors, metabolic factors, impact upon the hypothalamic-pituitary axis and autonomic nervous system changes38.
Older adults who are depressed are more likely to have existing physical health conditions and more likely to develop physical health conditions15. Depression is particularly associated with specific physical illnesses; cardiovascular disease and diabetes mellitus. A study by Win et al. found that cardiovascular mortality is higher in older adults with depression because of physical inactivity; the study established that physical inactivity was accountable for a 25% increased risk in cardiovascular disease39. The relationships between depression and cardiovascular disease and depression and diabetes have been described as “bidirectional”38.
Higher incidents of cardiovascular disease and diabetes mellitus are seen in people with depression regardless of age. A study by Brown et al. found that older adults with depression had a 1.46 relative risk increase for developing coronary heart disease compared to those without depression40. The hypothalamic-pituitary axis dysfunction found in depression leads to increased levels of cortisol, which in turn, increases visceral fat. Increased visceral fat is associated with increased insulin resistance, promoting diabetes mellitus, and increased cardiovascular pathology38.
Depression is a risk factor for the subsequent development of dementia; this is especially so if an older adult has no previous history of depression (i.e. depression is late-onset)13.
Healthcare utilisation and economic impacts
Older adults are less likely to report depressive symptoms to healthcare professionals explaining the under-utilisation of mental health services for depression32,41. Despite older adults under-utilising mental health services they over utilise other healthcare services26,41. For example, those presenting with non-specific medical complaints or somatisation have been found to have an increase use of healthcare services. Non-specific medical complaints and somatisation lead to an unnecessary use of resources, such as unnecessary consultations with healthcare professionals and investigations41. Increase in service utilisation means an increase in the associated economic cost of depression in older adults41-43.
Healthcare costs of older adults with a comorbid physical illness and depression are far greater than those without depression – findings in diabetes mellitus are a good example43. The majority of the increased healthcare costs are associated with the chronic physical disease and not the care and treatment of the depression44. Poor compliance with physical illness management is associated with missed appointments and a greater number of hospital admissions, which both have financial implications.
Aetiology and associations of depression in older adults
Late-onset type depression in older adults has been associated with the term ‘vascular depression’45-47. Studies have found a significant higher rate and severity of white matter hyperintensities on MRI imaging in older adults with depression compared to those without depression46,48,50. White matter hyperintensities represent damage to the nerve cells; such damage is a result of hypo-perfusion of the cells secondary to small blood vessel damage49. White hyperintensities are associated with vascular risk factors (e.g. age, hypertension, hypercholesterolaemia, obesity, diabetes mellitus, smoking) and are linked to cerebrovascular disease, such as stroke, vascular dementia. A relationship has been found between psychosocial stress and consequent development of vascular risk factors, which further supports the hypothesis of ‘vascular depression’46. Clinically, ‘depression-executive dysfunction syndrome’ and psychomotor retardation are associated with vascular changes48.
In older adults with depression, white matter hyperintensities are associated with structural changes to corticostriatal circuits and subsequent executive functional deficits. Loss of motivation or interest and cognitive impairment in depression are hallmark features of structural brain changes associated with the frontal lobes, which in turn are associated with a vascular pathology20. A study by Hickie et al. established that white matter hyperintensities in older adults with depression are associated with greater neurological impairment and poorer response to antidepressant treatment50. It is not fully understood why vascular depression responds less well to antidepressants; poor response has been linked directly to vascular factors but has also been associated with deficits in executive function46-47.
The relationship between cerebrovascular disease and depression is described as ‘bi-directional’45,51; depression has been found to cause cardiovascular disease and vice versa51. Baldwin et al. direct the reader to the presence of post-stroke depression and the occurrence of depression in vascular dementia45.
Younger and older adults share a number of fundamental risk factors for depression; such as female gender, personal history and family history7. Older adults have additional risk factors related to ageing, which are not just physiological in nature.
Age related changes:
Age related changes occurring in the endocrine, cardiovascular, neurological, inflammatory and immune systems have been directly linked to depression in older adults3.
The normal ageing process sees changes to sleep architecture and circadian rhythms with resultant changes to sleep patterns52. Thus sleep disturbances are common in older adults and positively correlated to advancing age52; over a quarter of adults over the age of 80 years report insomnia, and research has well-established that this is a risk factor for depression53-54. A meta-analysis by Cole et al. found sleep disturbances to be a significant risk factor for the development of depression in older adults53.
Sensory impairment:
Sensory impairments, whether secondary to the ageing or a disease process, are risk factors53,55. Research has found that hearing and vision impairments are linked to depression56. A sensory impairment can lead to social isolation and withdrawal, which, in turn, are further risk factors for depression.
Physical illness:
Physical illness, regardless of age, is a risk factor for depression. Older adults are more likely to have physical illnesses and so in turn are more at risk of depression. See Table 2. Physical illness is associated with sensory impairments, reduced mobility, impairment in activities of daily living and impaired social function, all of which can lead to depression. Physical illnesses associated with chronicity, pain and disability pose the greatest risk for the subsequent development of depression7,53,55. Physical illness affecting particular systems of the body, such as the cardiovascular, cerebrovascular and neurological, are more likely to cause depression3. Essentially, however, any serious or chronic illness can lead to the development of depression. It should be noted that a large proportion of older adults have physical illness but do not experience depression symptoms, therefore other factors must be at play5,57.
Treatments of physical illness are directly linked to aetiology in depression, for example, certain medications are known to cause depression; cardiovascular drugs (e.g. Propranolol, thiazide diuretics), anti-Parkinson drugs (e.g. levodopa), anti-inflammatories (e.g. NSAIDs), antibiotics (e.g. Penicillin, Nitrofurantoin), stimulants (e.g. caffeine, cocaine, amphetamines), antipsychotics (e.g. Haloperidol), anti-anxiolytics (e.g. benzodiazepines), hormones (e.g. corticosteroids), and anticonvulsants (e.g. Phenytoin, Carbamazepine)7,29. Polypharmacy is present in many older adults further increasing the risk of depression. Pharmacokinetic and pharmacodynamic age related changes also contribute to an increased risk of medication induced depression in older adults.
Table 2: Table of physical illnesses associated with depression3,7
Dementia is common in old age and those with dementia are at higher risk of developing depression compared to those who do not have it58. 20-30% of older adults with Alzheimer’s disease have depression59. Depression is a risk factor for the subsequent onset of dementia.
Psychosocial:
When compared to younger adults, older adults are at a greater risk of developing depression due to the increased likelihood of experiencing particular psychosocial stressors, in particular adverse life events. Stressors include lack of social support, social isolation, loneliness and financial hardship. Financial hardship and functional impairment often sees older adults downsizing in property. Deteriorating physical health often sees older adults no longer being able to manage living independently at home necessitating a move into institutional living. Bereavement, especially spousal, and the associated role change that follows this are risk factors for depression3.
Sub-threshold depression:
Sub-threshold depression is an established risk factor for major depression.
Prevalence and epidemiology
The prevalence of depression in older adults in England and Wales was found to be 8.7% in 2007; however, if those with dementia are included this figure rises to 9.7%60. A meta-analysis by Luppa et al. established a 7.2% point prevalence of major depression and a 17.1% point prevalence of depressive disorder in older adults61. The projected lifetime risk of an older adult developing major depression by the age of 75 years old is 23%62.
Sub-threshold depression is 2-3 times more prevalent than major depression in older adults26,63. These depressive symptoms are often clinically relevant26,29. 8-10% of older adults per year with sub-threshold depressive symptoms go onto develop a major depressive episode63.
Incidence and prevalence are greater in women; 10.4% of women over the age of 65 years have depression compared to 6.5% of men60. Older women are more likely to experience recurrent episodes of depression compared to older men62. The gender gap in incidence and prevalence becomes narrower with increasing age3. It should be acknowledged however that women are more likely to present to healthcare services and seek help in comparison to men64-65.
The prevalence of major depression in older adults varies by setting66. Highest rates are seen in long-term institutional care and inpatient hospital settings67. Table 3 summaries prevalence rates of major depression by setting.
Table 3: Prevalence rate of major depression by setting 7, 67
Setting
Prevalence rate (%)
Community
5 – 10
Primary care
10 – 30
Hospital inpatient
11 – 50
Long-term institutional care
10 – 43
Prognosis of depression in older adults
Depression in older adults is associated with a slower rate of recovery9, worse clinical outcomes compared to younger adults3 and is associated with higher relapse rates68. Worse prognosis in older adults correlates with advancing age, physical comorbidities and functional impairment70. The structural brain changes associated with depression in older adults are linked, as discussed, to poorer treatment response.
Morbidity and mortality associated with depression can be described as primary or secondary; primary morbidity and mortality arises directly from the depressive illness; whereas secondary morbidity and mortality arises from physical health problems, which are secondary to depression.
Outcomes from sub-threshold depression are on par with those of major depression; however sub-threshold depression which develops into major depression is associated with worse outcomes2.
Proportionally more people over the age of 65 years commit suicide compared to younger people71. Depression is the leading cause of suicide in older adults29,71; one study reports that 75% of older adults who killed themselves were depressed72.
The vast majority of older adults who commit suicide have had contact with a health professional within the preceding month9; this figure has been quoted as high as 70%3. This further supports and suggests the fact the depression is under-detected. Unlike younger adults, older adults are less likely to report suicidal ideation and can experience suicidal ideation without feeling low in mood3,7. Older adults have few suicide attempts, compared to younger adults, because their suicide methods are more lethal13.
Despite advances in the management of ectopic pregnancies an emphasis must be given on improving the understanding of the women and the healthcare professionals of the pathophysiology of haemorrhagic shock.
Educating the public and all health care professionals about the phrase “Think Ectopic” as a main differential in any women of childbearing age with atypical signs and symptoms of general ill health is paramount.
Précis
The significance of effective communication within multidisciplinary teams especially in emergency situations towards optimising patient care and saving lives cannot be understated.
Case Report
A 27-year-old woman who claimed to be unaware of her current pregnancy collapsed at her home. She was not known to have any co-morbidities. Paramedics were called and found her to be in cardiac arrest with pulseless electrical activity. Cardiopulmonary resuscitation (CPR) was immediately commenced. Spontaneous circulation returned after 13 minutes of CPR at home.
She was then transferred to the emergency department. On arrival to the emergency department her Glasgow Coma Scale (GCS) was 3. She had a pulse rate of 130 beats per minute; unrecordable blood pressure; haemoglobin of 55g/l; metabolic acidosis with a pH of 6.8; lactate > 15; and a potassium of 6.6 mmol/l. She was resuscitated and gradually regained consciousness with a GCS of 15.
In the midst of stabilising her condition and unaware of her pregnancy, a urine pregnancy test was obtained following siting of a urinary catheter. A positive pregnancy test prompted notification to the gynaecology team who performed ultrasonography imaging which revealed significant haemoperitoneum. An immediate decision was made to perform laparotomy in view of the most likely diagnosis of a ruptured ectopic pregnancy.
Laparotomy revealed a 3.5 litre of haemoperitoneum secondary to a ruptured right sided tubal ectopic pregnancy. A right salpingectomy was performed. The patient was subsequently transferred to the intensive care unit as her serology results were consistent with multi organ failure with a platelet count of 46 (109/L); creatinine of 194 mmol/L; estimated glomerular filtration rate (egfr) of 27 mls/min/ 1.73 m2; alanine transaminase (ALT) of 441 IU/L; and alkaline phosphatase (ALP) of 49 IU/L.
She made an uneventful recovery as demonstrated in figure 1 by the improving serological parameters and was discharged home after 6 days.
Figure 1: The cumulative serology- full blood count, liver function tests, urea and electrolytes, clotting profile.ankle
Investigations
Day 0
Day 0
Day 1
Day 1
Day 2
Day 3
Day 4
Day 5
Day 15
13:46
18:30
05:53
17:27
06:49
07:00
11:14
09:37
09:50
Hb g/L (115-150)
82
100
83
73
72
88
89
93
WCC 109/L (3.5-11.0)
19.8
23
18.1
13.2
11.8
11.2
9.5
9.1
Plts 109/L (140-400)
46
61
49
46
48
51
76
106
ALP IU/L (30-130)
49
42
44
51
57
73
74
100
ALT IU/L (0-40)
441
428
701
3197
2621
1807
1290
185
Bili mmol/L (0-21)
9
13
8
18
18
16
11
4
Na mmol/L (133-146)
139
142
143
141
143
142
140
141
139
K+ mmol/L (3.5-5.3)
6.8
4
4.3
4.2
3.9
3.9
3.7
4.6
Urea mmol/L (2.5-7.8)
9.6
12.4
14
14.2
11.5
7.9
7.4
8.3
Creat mmol/L (48-128)
194
174
230
279
319
269
163
137
88
egfr mls/min/ 1.73 m2
27
30
22
18
15
19
33
40
66
INR ratio
1.4
1.4
1.5
1.6
1.4
1.1
1
PT secs (9.7-12.3)
14.8
15.1
15.9
16.7
15.1
11.5
10.6
Fibrinogen g/L (1.9-3.1)
1.2
1.4
1.2
1.5
2.4
3.9
>4.5
Discussion
The confidential enquiry report into maternal deaths – UK has shown a decreasing trend in the case fatality rate in women with ectopic pregnancies. This has been suggested to reflect earlier detection and immediate treatment of ectopic pregnancies. However unforeseen tubal rupture with major haemorrhage continues to be a source of major morbidity and mortality. Ectopic pregnancies account for 3-4% of pregnancy related deaths. 4
The classical triad of symptoms encountered in ectopic pregnancy includes pain, vaginal bleeding and amenorrhoea. 1 Worryingly, as illustrated by our case, rarely these women may present in a state of collapse even before the diagnosis of pregnancy is made. 4
Pathophysiology of multi-organ failure following haemorrhagic shock
Our case clearly demonstrates the detrimental multi-systemic effects and subsequent threat to life created by haemorrhage from a ruptured ectopic pregnancy. Acute haemorrhage results in decreased cardiac output and pulse pressure that is detected by baroreceptors in the aortic arch and atrium. Neural reflexes subsequently cause an increased sympathetic outflow to the heart and other vital organs resulting in vasoconstriction, and redistribution of blood flow away from non-vital organs. Neuroendocrine responses activated by neural reflexes play a major role in homeostasis during haemorrhage. Elevated aldosterone and cortisol secondary to raised adrenocorticotrophic hormone secreted by the pituitary gland leads to increased water absorption in the kidneys. The reduced tissue perfusion to non-vital organs results in insufficient delivery of oxygen and nutrients required for cellular function. 2
The resultant hypoxia leads to anaerobic metabolism and hence lactate production and metabolic acidosis. Hyperlactaemia is defined when serum lactate is greater than 4 mmol/l. 3 A level of 15mmol/l as demonstrated by our case highlights the extent of shock the patient was in.
Endogenous heat production is restricted by anaerobic metabolism, which in turns exacerbates hypothermia that is likely to be predisposed by the administration of intravenous fluids and blood products. Hypothermia is one of the reversible causes of pulseless electrical activity and a core temperature of less than 35°C is itself an independent predictor of mortality after major haemorrhage.
Furthermore, our case revealed a severe acidosis with a pH of 6.8, which is reflective of widespread cellular anaerobic respiration secondary to hypoxia as a result of inadequate perfusion. Widespread literature has shown that a pH of less than 7.2 is associated with decreased contractility, low cardiac output, bradycardia, arrhythmias and decreased blood flow to the liver and kidneys. This can lead to multi-organ failure.6
Many patients with severe haemorrhage can establish coagulopathy very quickly as our case has demonstrated. At present there is nouniversally established definition of coagulopathy though many experts use prolonged prothrombin time as an indicator of coagulopathy. Our case presented with a prolonged prothrombin time of 14.8 seconds. The pathophysiology is complex and stems from immediate activation of multiple haemostatic pathways including fibrinolysis, platelet and endothelium dysfunction. Furthermore, acute phase response after resuscitation measures can create a prothrombotic state. Sometimes, disseminated intravascular coagulation can occur in those who are insufficiently resuscitated or not resuscitated in a timely manner. 7
Effective multi-disciplinary input
This case clearly highlights that the responsibility does not solely rely on the surgeon who is required to cease the bleeding but also on the multi-disciplinary specialists including paramedics, emergency clinicians, nursing staff, anaesthetists and haematologists. This is a vital component of resuscitation management during emergency situations.
Appropriate initial fluid management
The management with intravenous fluid resuscitation remains challenging as some evidence suggests that aggressive fluid resuscitation can be detrimental because it can lead to dislodging of clots and dilutional coagulopathy leading to increased risk of haemorrhage. 5
Clinicians supporting this hypothesis suggest to cautiously administer fluid resuscitation with the aim of maintaining a subnormal blood pressure (systolic of 70-90 mmHg), whilst allowing sufficient oxygen delivery. The very early use of crystalloids and blood products is paramount to help treat acute coagulopathy. 7
Immediate surgical treatment
Recourse to immediate surgical cessation of bleeding is a vital part of the resuscitation process, and must not be delayed. 7 The presence of free fluid in the abdomen and a positive pregnancy test immediately alerted an ectopic pregnancy as the most likely diagnosis. The majority of women of reproductive age are free of comorbidities with a greater ability to adapt to resuscitative measures and hence showing quicker recovery.
Conclusion
Despite advances in the management of ectopic pregnancies an emphasis must be given on improving the understanding of the women and the healthcare professionals of the pathophysiology of haemorrhagic shock. Educating the public and all health care professionals about the phrase “Think Ectopic” as a main differential in any women of childbearing age with atypical signs and symptoms of general ill health is paramount.
Furthermore, the significance of effective communication within multidisciplinary teams towards optimising patient care and saving lives cannot be understated.
Telephone triage has been used by many practices in primary care to manage workload and prioritise patients for same day appointments.1,2 Telephone triage may have benefits in terms of managing work load,3 but is also associated with certain risks,4 which has worried both clinicians and patients.5 The analysis of the use of telephone triage has so far focused on the ease of access, demand management, cost effectiveness, quality of consultations, safety and patient satisfaction. However, other effects in terms of patient outcome may exist. One of the main focuses in General Practice is to identify symptoms and signs of cancer for early diagnosis to improve outcome. Our study aims to assess whether telephone triage helps in prioritising early assessment and referral of patients who are subsequently diagnosed with cancer.
Methods
A retrospective analysis of all the patients at our practice who had a diagnosis of cancer made between April 2013 and December 2014 was carried out.
Patients have a choice of 2 different ways to book an appointment in our practice.
Telephone triage for same day appointment requests, where a triaging doctor decides about the urgency of a problem and books the appointment, arranges tests or gives advice after speaking to patients over the phone. This group is referred as “Group 1” in this study.
Patients book the next available appointment to see a GP through reception without any triage. This group is referred to as “Group 2” in this study.
The date of first contact with the GP practice for the symptoms which later lead to a diagnosis of cancer was noted for both groups. This was the telephone triage date for the first group and the date the appointment was booked by the patients for the second group. The date the patient was first seen in secondary care for further assessment and investigations was also noted. The duration between first contact with GP practice and GP appointment, and the duration between the first contact with practice and first hospital appointment were calculated. This information was gathered from practice computer records.
Patients who were diagnosed with cancer through screening were excluded. Slow growing tumours which do not merit a 2-week rule referral, such as basal cell cancer of skin were excluded. Patients whose appointments were initiated by the GP on reviewing the results of routine tests were not included. Patients diagnosed with cancer in hospital without going through primary care referral were also excluded from this study.
There are two research questions:
Is there a significant difference in the time required from the first contact with primary care to the GP Clinic appointment between Group 1 and Group 2 patients?
Is there a significant difference in the time required from the first contact with primary care to the date the patient was seen in the secondary care between Group 1 and Group 2 patients?
Descriptive statistics (such as the mean, standard deviation, median, minimum, and maximum) were used to present the time required from the first contact with primary care to the GP Clinic appointment; and the time required from the first contact with primary care to the date patient seen in the hospital, for Group 1 and Group 2 patients. Wilcoxon rank-sum test was used to answer each research question. A p-value less than 0.05 indicated significance at the 0.05 level.
All data analyses were conducted using SAS.
Results
A total number of 39 patients were included in the study. Among them, 13 (33%) used telephone triage to make their appointments and 26 (67%) booked their appointment by themselves.
Figure 1 shows the bar charts of the time required from the first contact to GP practice, to the GP clinic appointment for Group 1 and Group 2 patients. It took 0-3 days for 12 Group 1 patients and 8-11 days for 1 Group 1 patient. The time required from the first contact to GP practice to the GP Clinic appointment for Group 2 patients can be illustrated by the same manner.
Figure 1: Bar charts of the time (days) required from the first contact for surgery to the GP Clinic appointment for Group 1 and Group 2 patients. (Note that the midpoints 2, 6, 10, 14, 18, and 22 represented days within the range of 0-3, 4-7, 8-11, 12-15, 16-19, and 20-23, respectively.)
Table 1 shows the summary statistics for the time (days) required from the first contact with the practice, to the GP Clinic appointment for Group 1 and Group 2 patients. The average time required was 0.77 days for Group 1 patients and the average time required for Group 2 patients was 7.88 days. The results of Wilcoxon rank-sum test indicated that this was a statistically significant difference in time required from the first contact for surgery to the GP Clinic appointment between Group 1 patients (patients using Telephone triage to make their appointments) and Group 2 patients (patients booking their appointment by themselves) (p = 0.0020).
Number
Mean
SD
Median
Min
Max
Group 1
13
0.77
2.24
0
0
8
Group 2
26
7.88
7.53
6
0
23
Table 1:Summary statistics for the time (days) required from the first contact for surgery to the GP Clinic appointment for Group 1 and Group 2 patients. SD = standard deviation.
Figure 2 shows the bar charts of the time required from the first contact with the GP practice, to the date patients were seen in the secondary care for Group 1 and Group 2 patients. It took 0-5 days for 4 Group 1 patients, 10-19 days for 5 Group 1 patients, 20-29 days for 1 Group 1 patient, 30-39 days for 2 Group 1 patients, and 90-99 days for 1 Group 1 patient. The time required from the first primary care contact to the date patient seen in the secondary care for Group 2 patients can be illustrated by the same manner.
Figure 2: the bar charts of the time required from the first contact for surgery to the date patient seen in the hospital for Group 1 and Group 2 patients. (Note that the midpoints 5, 15, 25, 35, 45, 55, 65, 75, 85 and 95 represented days within the range of 0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89 and 90-99, respectively).
Table 2 shows the summary statistics for the time (days) required from first contact with GP practice to the date patients were seen in the hospital for Group 1 and Group 2 patients. The average time required for Group 1 patients was 19.54 days and the average time required for Group 2 patients was 35.69 days. The results of Wilcoxon rank-sum test indicated that this was a statistically significant difference in time required from the first contact to the primary care to the date patient seen in the hospital between Group 1 patients (patients using Telephone triage to make their appointments) and Group 2 patients (patients booking their appointment by themselves) (p = 0.0474).
Number
Mean
SD
Median
Min
Max
Group 1
13
19.54
23.41
10.00
3
90
Group 2
26
35.69
26.28
32.50
1
88
Table 2: Summary statistics for the time (days) required from the first contact for surgery to the date patient seen in the hospital for Group 1 and Group 2 patients. SD = standard deviation.
Type of Cancer
Number of Patients
Lung
5
Breast
5
Colorectal
4
Malignant melanoma of Skin
3
Squamous Cell carcinoma of Skin
3
Oesophagous
2
Stomach
2
Urinary Bladder
2
Larynx
2
Pancreas
1
Endomtrium
1
Cervix
1
Kidney
1
Prostate
1
Testis
1
Tonsil
1
Lymphoma
1
Appendix
1
Myelodysplastic
1
Olfactory Neuroblastoma
1
Table 3: Number of patients with types of cancer.
Discussion
More than 90% of contacts with healthcare in the UK occur in primary care.6 The estimated numbers of consultation for a typical practice in England rose from 21,100 in 1995 to 34,200 in 2008 as per analysis conducted by Hippisley-Cox J et al.7 With increasing demands being placed upon General Practice, there is a need to explore innovative ways of working which enable the prioritisation of patients with concerning symptoms. Telephone triage has been considered to reduce the demand for face-to-face consultation with GPs,3 which can potentially free up time for effective use. NHS England report ‘Transforming Urgent and Emergency Care Service in England’ suggests GPs should offer more telephone consultations to reduce pressure on accident and emergency.8 However, a cluster-randomised controlled trial (The Esteem Trial) across 42 practices showed that telephone triage increased the number of primary care contacts in the following 28 days, after patients’ request for same day GP consultation.1
With increasing demands for consultations, it is important to have a system to identify and prioritise patients for early assessment; who may have a suspected cancer diagnosis. Our study demonstrates that telephone triage reduces the time from first primary care contact to face to face assessment in primary and secondary care for patients with suspected cancer. Patient numbers are small and the sample is from one practice, yet the difference seen is statistically significant.
Cancer stage at diagnosis is one of the major reasons for difference in cancer survival in different countries.9,10 The delay in cancer diagnosis can be due to multiple factors. Telephone triage can provide an opportunity to patients to discuss symptoms early with a GP, and this can reduce delays in the cancer diagnosis pathway. It has been shown that certain alarm symptoms are associated with the likelihood of cancer diagnosis 11 and these can be used to prioritise the patients in triage process. It may also reduce anxiety amongst patients waiting for an appointment, who are concerned about their symptoms.
Telephone triage should not only be seen as a way of managing demands and appointments but also as a system to improve patient outcome. Further research is clearly needed on a larger scale to determine if the results are reproducible in other settings as patients’ knowledge and understanding about cancer warning symptoms and healthcare seeking behaviour may vary among different population sets.
A 70-year-old man presented in the winter with a four-week history of redness of the left anterolateral leg. He first noticed a slight “tenderness” in the area when showering; the discomfort lasted only a few days. Over the next week, he noticed redness developing. It is now painless and not pruritic, warm, or peeling. He has not applied any topical lotions or creams. He has not had an exposure to new soaps or detergents. He feels well, without fever or weight loss. He has a diagnosis of hypertension and lumbar radiculopathy with an L5 discectomy and resultant leg numbness. He is retired and does not smoke or drink alcohol; his hobby is woodworking in his garage.
Physical examination reveals normal vital signs. On his left anterolateral leg, he has an 8 cm, irregular patch of reticulated erythema with both hyperpigmentation and scaling. The lesion is non-palpable. He has decreased sensation in an L5 distribution on that leg, which was unchanged from prior examinations. These skin findings are shown in Figure 1.
Figure 1
Question: Based on history and physical examination, which of the following is the most likely diagnosis?
Livedo reticularis
Erythema ab igne
Livedo racemosa
First-degree burn
Discussion
The answer is erythema ab igne (EAI; literally “redness from fire,”) which results from chronic exposure to moderate-intensity heat. EAI presents as a reticulated erythematous patch over the area of exposed skin. Possible secondary changes include epidermal atrophy and scaling.1,2 With repeated exposure, brown hyperpigmentation may develop.1 Most patients are asymptomatic, although some note a mild burning sensation. A history of repeated exposure to heat is key to the diagnosis. While cases were historically noted on skin exposed to fire, such as the arms of bakers and coal shovellers, EAI can result from our many, modern heat-sources, such as laptop computers, car seat heaters, heating pads, and, in this case, the portable space heater under the patient’s woodworking bench.2-4 With removal of the heat source, hyperpigmentation typically regresses but may take years.1,3 The diagnosis is clinical. A biopsy is not required to make the diagnosis, but is indicated if malignant transformation is suspected. EAI can increase risk of squamous cell carcinoma, Merkel cell carcinoma, and cutaneous marginal zone lymphoma.1,5 Treatment is typically not necessary; topical steroids or retinoids and laser have had variable success.1,3,4 If pre-malignant changes are detected, topical 5-flourouracil is recommended.1,4
See Table 1 for a summary of the key characteristics and distinguishing features of each diagnosis in this selected differential.
Table 1. Selected Differential Diagnosis of Reticulated Skin Lesions in Adults
Condition
Characteristics
Livedo reticularis
Violaceous mottled or reticulated patches; painless; typically temperature sensitive; may be physiologic or secondary to systemic disease; no hyperpigmentation.
Erythema ab igne
Erythematous reticulated patch, with possible secondary changes including epidermal atrophy and scaling; chronic exposure may lead to hyperpigmentation; painless or associated with a mild burning sensation; history of heat exposure.
Livedo racemosa
Violaceous reticulated patch with larger branching pattern than livedo reticularis, often with asymmetric or “broken” net appearance; typically involves the trunk and proximal limbs; generally secondary to chronic disease; frequently painful; no hyperpigmentation.
First-degree burn
Erythematous, dry, painful lesion which includes the entire area of skin that contacted the high-intensity heat source; not reticulated; no hyperpigmentation.
Livedo reticularis is typically more violaceous in appearance, with net-like, mottled discolouration of the skin due to deoxygenation and dilation of the venous plexus. Primary, physiologic livedo reticularis is often brought on by cold and alleviated by warming. It usually involves a larger area, such as the bilateral thighs, rather than a confined area of skin.1,2
Livedo racemosa is a persistent variant of livedo reticularis with a characteristic, large, broken, branching pattern, often on the trunk and proximal limbs. It is generally secondary to a systemic disease, such as antiphospholipid antibody syndrome or Sneddon syndrome.6
First-degree burns are erythematous, dry, and painful. Instead of a reticulated pattern, as shown here, the erythema of first degree burns covers the entire area of skin that contacted the high-intensity heat source.
Warfarin is a widely used anticoagulant, primarily for the prevention of thrombosis and thromboembolism. Warfarin is used as a prophylactic agent in conditions such as atrial fibrillation and coronary artery thrombosis.1
Although effective and safe, treatment with Warfarin is associated with risks. Because of its narrow therapeutic index, patients require regular blood monitoring for the international normalised ratio (INR) to determine the safe yet effective dose of Warfarin.
Warfarin has interaction with several medications which affect the availability of Warfarin. One class of drugs which is very commonly prescribed is the selective serotonin reuptake inhibitors (SSRIs) antidepressants.
Due to their supposedly favourable side-effect profile, e.g. less cardiotoxicity, and safety in overdose, SSRIs have become the first-line antidepressant 2, preferred over tricyclic antidepressants (TCA). However, SSRIs, have other serious side-effects including increased tendency to bleed, particularly gastrointestinal bleeding. SSRIs may increase the risk of bleeding due to the secondary effect of serotonin release which is essential for platelet aggregation. 3 This effect is especially significant when combined with anticoagulants. 1
Several of the SSRIs are inhibitors of the cytochrome P 450 enzyme system, which is responsible for the metabolism of some medications, including Warfarin. Both SSRIs and anticoagulants are frequently prescribed in the elderly population.
Fluvoxamine is a SSRI which is licensed for use in the treatment of depressive disorder, obsessive-compulsive disorder (OCD) 1, and is also used in the treatment of social phobia. While an interaction between Fluvoxamine and Warfarin is to be expected because of Fluvoxamine’s inhibitory action on a number of cytochrome P 450 enzymes, there have not been many case reports of the interaction between Fluvoxamine and Warfarin.
A Medline search revealed only two case reports of an interaction between Warfarin and Fluvoxamine. 4,5
We report a case of an elderly man who developed elevated INR when he was started on Fluvoxamine for the treatment of depression, while on Warfarin.
Case Report
A 75-year old male was admitted to the acute psychiatric unit with complaints of anxiety, depressed mood and suicidal ideation. In the previous months, he had developed a pre-occupation that his bowels were not functioning properly and that he would not be able to open his bowels. He was using excessive laxatives secondary to this preoccupation. He also described other depressive symptoms: anhedonia, insomnia with early morning wakening, poor concentration, and low motivation.
The patient was diagnosed with depression two years previously, requiring Electroconvulsive therapy (ECT). He was discharged on Mirtazapine 45mg and Venlafaxine-XL 150mg. Following a deterioration in mental state, the Venlafaxine-XL dose was increased to 225mg three months before this admission, without much improvement. Risperidone and Olanzapine were trialled as an adjunct without beneficial effect and were discontinued. Compliance with medication was reportedly good.
The patient had multiple physical health complaints: previous myocardial infarctions, hypertension and paroxysmal atrial fibrillation. He was prescribed tamsulosin, bisoprolol, perindopril, atorvastatin, and warfarin.
The patient’s preoccupation about bowel movements was, for the most part, deemed to have obsessive quality: he accepted that these worries were repetitive and came to his mind against his wishes. He said that he would rather not have these worries but was unable to distract himself.
The marked subjective anxiety, according to the patient, was entirely linked to the preoccupation. However, when the patient became agitated, it was difficult to persuade him to appreciate the anomalous nature of his thoughts. At such times he insisted that there was something definitely wrong with his bowels and nothing could help him.
Prior to admission, the patient was treated at different times with different antipsychotic medications, which made little impact on the symptoms. Following his admission he was referred to the psychology services, which concluded that he was too unwell to meaningfully participate in psychological therapies. The patient, too, was not keen on this option. He also declined ECT and was deemed to have the capacity to make the decision.
Venlafaxine-XL was switched, in light of the patient’s cardiac risk history, to an SSRI known to have an effect on obsessional symptoms. Accordingly, a dose of Mirtazapine was decreased to 30mg, and Venlafaxine-XL was tapered off over ten days.
Fluvoxamine was started at 50mg/day, and the dose was titrated to 150 mg/day over the next week. The dose was further increased to 200 mg/day.
INR was previously stable on warfarin dose of 5mg per day: blood results were between 2.32-2.68. Following fluvoxamine-initiation, INR started increasing: 2.98 after six days. INR increased further, to 3.82, with increase in Fluvoxamine’s dose
Warfarin-dose, as a result, was decreased, initially from 5mg to 4mg; however, INR remained above range (3.75). With further reduction in Warfarin’s dose, to 3mg/day, INR reduced but was still above range (3.51). INR eventually stabilised when warfarin-dose was reduced to 2mg/day. The dose adjustment took place over ten days.
Discussion
Management of depression in elderly population requires careful consideration of the choice of psychotropic medication, as elderly patients are more likely than younger patients to be on multiple medications for associated physical health problems, which increase the potential for drug interactions. Half-lives of drugs are also extended in the elderly.
The patient was prescribed Warfarin for the management of atrial fibrillation. Warfarin is a racemic mixture of S-warfarin and R-warfarin, of which S-warfarin is more potent than R-warfarin. 6
Warfarin has the potential to cause pharmacokinetic drug interactions (drugs affecting hepatic cytochrome P 450 enzyme system, which metabolises warfarin), which are thought to be more clinically relevant than pharmacodynamic interactions (highly protein bound drugs displacing Warfarin from its binding site) for warfarin. 6
Warfarin is metabolised by a number of P450 isoenzymes such as 2C9/2C19, 1A2, and 3A4. 6 Of these 2C9 is thought to be crucial, as it metabolises the more potent S-isomer. Isoenzyme 1A2 is the major route for the metabolism of the R-isomer, while 3A4 and 2C19 are considered to be minor routes.
The psychotropic medications that are thought to have the potential for significant pharmacokinetic interaction with warfarin include Fluoxetine, Fluvoxamine, Quetiapine, and Valproic Acid. 7 Venlafaxine is also considered a high-risk drug in patients taking warfarin. One study found that fluvoxamine and venlafaxine were associated with a more than double risk of having an INR value of 6 or more. 3
Fluvoxamine by dint of its inhibitory actions on 2C9/2C19, 3A4, and 1A2 8 inhibits all the isoenzymes that metabolise Warfarin and can be said to have the maximum potential for pharmacokinetic interaction with Warfarin.
National Collaborating Centre for Mental Health guidelines on depression in adults with chronic physical health problems advise avoiding SSRI in patients taking warfarin or heparin and instead offering an alternative antidepressant such as mirtazapine. 9 Therefore, caution is needed when prescribing these medications to patients who fail to respond to other safer options.
At the time of his admission, the patient was on a combination on Mirtazapine and Venlafaxine XL, both at high doses, for several months. Neither of the antidepressants has significant action on the P450 isoenzyme system, although both are substrates of some enzymes, such as 2D6, 1A2 and 3A4. 8 The patient’s INR was within normal limits when he was on these two medications (despite the aforementioned potential effect of venlafaxine on INR values).
During the period of admission, a decision was taken to change the antidepressant regime, for clinical reasons. The two antidepressants considered were Fluvoxamine and Sertraline.
It was felt that despite its higher potential to cause pharmacokinetic interaction with Warfarin, Fluvoxamine is chosen ahead of Sertraline (which inhibits 3A4 and 2D6). The more potent action of Fluvoxamine on the sigma1 receptors, which account for its significant anxiolytic properties and therapeutic action in the delusional depression 10 was felt to have the potential of benefit given the patient’s clinical symptoms.
It was also felt that Fluvoxamine would also be of more benefit than Sertraline with insomnia which was patient’s frequent complaint given its side-effect of somnolence. 11
Fluvoxamine was started at a low dose (50 mg/day) after Venlafaxine XL was completely withdrawn. The dose was titrated rapidly over the next one week, to 150 mg/day. The INR showed an upward trend within five days of commencing Fluvoxamine, and it exceeded three by the time the dose of Fluvoxamine was increased to 150 mg/day. This necessitated a reduction in Warfarin’s dose from 5 mg to 2 mg/day. The INR stabilised to between 2 and 3 when warfarin dose was more than halved.
Fluvoxamine has a half-life of 9-28 hours, and steady-state levels reach roughly after ten days. 8
The half-life is increased by almost 50% in the elderly. 3 The trajectory of increase in the INR was consistent with the pharmacokinetic of Fluvoxamine: it is a potent inhibitor of CYP4501A2, with a relatively little affinity for the other isoenzymes. The increase in INR was not dramatic, which is different from previous reports. 4 Throughout the period of Fluvoxamine –titration and Warfarin dose adjustment, there was no clinically untoward incident.
In conclusion, this case shows the need for close monitoring when warfarin is combined with another drug which significantly enhances warfarin’s anticoagulant effect. At the same time, it can be done safely, even in patients such as the elderly, who can be at a higher risk of adverse effects of interaction, when appropriate steps to monitor the patient are in place. The case also demonstrates the necessity of using clinical judgment while applying the guidance in individual patients.
The skeletal type of muscles are rarely affected by tuberculosis (TB) because they are not a preferred site for the survival and multiplication of Mycobacterium tuberculosis.1 Even in patients with widespread involvement of the disease, TB rarely involves muscles. Petter et al recorded only one case of primary skeletal muscles TB in over 8,000 cases of all types of TB, with an incidence of 0.015%.2 Few cases of tubercular myositis have been described in literature until now, mostly in adults. This, together with the decline in TB in general, makes it unlikely that one would immediately consider TB as the cause of a rectus sheath abscess.
There are only limited cases reports of isolated tubercular involvement of the anterior abdominal wall even though TB is rampant in developing countries, and with the rapid spread of acquired immune deficiency syndrome (AIDS) it has made inroads into the developed nations as well.3 We are presenting a case of primary tuberculous abdominal wall abscess, with no evidence of pulmonary, skeletal or gastrointestinal TB in an immunocompetent patient. This case report should serve as a reminder that TB, in all of its various manifestations, remains very much among us.
Case report
A 20-year-old female presented to the outpatient department of surgery, with a complaint of a progressive swelling in the left lower abdomen for the last three months. There was no history of preceding trauma, fever, cough, malaise or pain. There was no history of contact with any case of TB. On examination, there was a swelling in the left iliac fossa, measuring 8x8cm in size, non-tender with smooth and ill-defined margins, and normal overlying skin. The swelling was firm in consistency and moved with respiration. Examination of the cardiovascular and respiratory systems were within normal limits.
Laboratory investigation revealed: haemoglobin 11.5 g/dl; total leukocyte count 8510/cumm with a differential count of 54% neutrophils, 42% lymphocytes and 4% eosinophils; erythrocyte sedimentation ratio 70 mm; and enzyme-linked immunosorbent assay (ELISA) for human immunodeficiency virus (HIV) negative. The chest radiograph was unremarkable. Other biochemical blood investigations, including liver and kidney function tests, were within normal limits. Ultrasonography of the abdomen revealed a 6.5x8.5cm left iliac fossa cystic mass with a liquefied necrotic centre in the anterior abdominal wall (Fig. 1). Computerized Tomography (CT) scan of the abdomen showed an abscess in the left antero-lateral portion of the abdominal wall limited to the muscle layer (Fig. 2). Ultrasound-guided fine-needle aspiration and cytological examination revealed caseating granuloma with central necrosis, lymphocytes, and giant cells, consistent with TB (Fig. 3). The patient was diagnosed to have tuberculous abscess of the anterior abdominal wall and antituberculous treatment was started following internal medicine consultation. She improved rapidly over the next few days. After four weeks of antituberculous treatment, she responded well to the treatment and the abscess regressed considerably. The patient did not require any surgical intervention.
Figure 1. Ultrasonography of the abdomen revealed a left iliac fossa cystic mass.
Figure 2. Focal cystic collection seen in the anterior abdominal wall of the left iliac fossa with mild peripheral enhancement (white arrow)
Figure 3. Photomicrograph revealed caseating granuloma with central necrosis, lymphocytes, and giant cells, consistent with tuberculosis.
Discussion
TB of the anterior abdominal wall is a rare entity and only isolated cases are reported in the literature. Possible explanation for the rarity of muscle involvement in TB includes high lactic acid content, lack of reticulo-endothelial tissue in muscle, lack of lymphatic tissue, the abundant blood supply, and the highly-differentiated state of muscle tissue.4 Although none of them seems to be an adequate explanation, all theories (except the first one) have been criticized.2
Two forms of skeletal muscle involvement are recognized.5 In the first type the tuberculous process spreads into the muscle through direct extension from a neighbouring structure e.g. bone, joint, tendon, or lymph node. In the second type the spread is haematogenous. Our patient is of interest because she seems to have a primary tubercular anterior abdominal muscular lesion with no evidence of immunoincompetence.
A tuberculous focus in the muscle usually manifests as progressive swelling and pain. The infection is usually restricted to one muscle.6 There may be a frank tuberculous abscess (as seen in our case) or a nodular sclerosis followed by calcification. Ultrasonography usually shows a cystic mass of mixed echogenicity with irregular walls and a liquefied, necrotic centre. Computed scan of the abdomen usually shows a well-defined abscess in the abdominal wall.7, 8 Ultrasonography or CT-guided aspiration followed by cytological examination usually reveals tuberculous granulomas with areas of caseous necrosis.
Management of this entity is mainly in the form of antituberculous drugs. Surgical intervention in the form of sonography, CT-guided aspiration or open drainage is usually reserved to patients where medical treatment has failed.3 Our patient responded well to medical treatment.
Although localized swelling in the rectus abdominis muscle is commonly due to necrotizing fasciitis, rectus sheath haematoma or tumours (benign / desmoid / malignant), a rare possibility of TB should also be considered. The prognosis is good in tuberculous myositis with appropriate chemotherapy.
Conclusion
This case alerts clinicians and radiologists of the possibility of TB when considering the differential diagnosis of any lesion even in any unlikely anatomical area, especially in those regions where TB is endemic.
For decades the genus Acinetobacter has undergone several taxonomical modifications. Large number of non-fastidious, aerobic, Gram-negative bacteria (GNB) are included in this genus. In the last few years these organisms are genetically modifying into highly resistant forms resulting in untreatable nosocomial infections1 and health care associated infections.2 Acinetobacter is also a major cause of invasive type infections in children resulting in untreatable urinary tract infections (UTIs), skin infections and septicemia.3 One identified cause of the resistance mechanism in carbapenem resistant Acinetobacter spp. is the production of the MBL enzyme.4 It has been revealed through various published studies that Acinetobacter displays a specific type of mechanism of resistance against different antimicrobials. Some of them, for example β-lactam, are inhibited by enzymatic degradation, while quinolones are rendered ineffective due to a genetic mutation preventing the binding of an antibiotic to a distinct binding site. The same is true with aminoglycosides in which the resistant strains are noticed to acquire a gene involved in enzymatic modification.1
Although polymixin resistance in Acinetobacter spp. was reported the specific cause of resistance was unknown until 2008. In 2013, one study detected the presence of hetero-and adaptive resistance due to mutation in specific gene for the first time.1,21 Hence the aim of this current study was to evaluate the trend of sensitivity/resistance pattern of Acinetobacter spp. against broad spectrum antibiotics.
Method and Materials
The objective of the study was to evaluate the sensitivity of Acinetobacter spp. to 08 broad spectrum antibiotics. The Kirby Bauer Disc Diffusion method was used following the standard procedures as laid down by CLSI 2013.6 A total of 52 isolates were collected from Feb 2014-March 2014 from patients admitted to tertiary care hospitals in Karachi. The isolates were identified by routine lab procedures.
Antimicrobial agents and medium: Standard (Oxoid) discs of Amikacin (30 µg), Cefoperazone (75 µg), Ceftriaxone (30 µg), Ciprofloxacin (5 µg), Colistin (10µg), Fosfomycin (50 µg), imipenem (10 µg), Polymixin B (300units), Mueller Hinton Agar (Oxoid UK) and Mueller Hinton broth (Oxoid UK) were used.
0.5 McFarlan Standard: The inoculum was grown at 370C for 2-6 hrs. Turbidity Standard of 0.5 McFarland was achieved by incubating broth culture.
Inoculation of test plates:The plates were inoculated with the culture of Acinetobacter spp. by the help of sterile cotton swabs. The excess fluid was removed after the cotton swab was dipped into inoculum suspension. When the inoculum were dried the antibiotic discs were placed with sterile forceps onto the agar surface.15
Incubation of test plates: The isolates after application of antibiotic discs plates were incubated for 24 hours and results were interpreted according to CLSI standards 5,6. Interpretative standards for used antibiotics and Zone diameter of inhibition are shown in Table 25.
Control strain: Escherichia coli ATCC 25922was used as a control strain to maintain accuracy and precision of procedures.
Results
It is reported that out of all the samples 61.5% were obtained from male patients. Infections caused by Acinetobacter spp. had a high prevalence among both the genders among the age group 51-75 yrs. The most frequent site of isolate collection was tracheal aspirate (55.76%) among both genders and the second highest percentage of isolate was obtained from sputum (19.23%) as shown in Table 1. The Colistin and Polymixin B were found equally effective against Acinetobacter spp. by inhibiting 98% of isolates each and 19.23% isolates showed sensitivity against Amikacin. The isolate showed the highest degree of resistance against Imipenem (98%), followed by Cefoperazone (94.23%) and Ceftrioxone (92.3). Surprisingly 32.69% of isolates exhibited intermediate sensitivity (IS) against Fosfomycin as indicated in Table 3 and Figure 1.
Table 1: Age and gender specific distribution of Acinetobacter spp. among patients
Age
Male n=32(61.5%)
Female n=20(38.46%)
00-25
10
06
26-50
05
02
51-75
12
11
76-100
05
01
Table 2: Zone diameter interpretive standards for Acinetobacter spp. CLSI standards table of antibiotics for Acinetobacter spp.
Antibiotic
Disc Content
Zone of Inhibition (mm)
Resistance
Intermediate
Sensitive
Amikacin
30µg
≤14
15-16
≥17
Cefoperazone
75 µg
≤15
16-20
≥21
Ceftriaxone
30 µg
≤13
14-20
≥21
Ciprofloxacin
5 µg
≤15
16-20
≥21
Colistin٭
10µg
≤11
≥17
Fosfomycin٭
50 µg
≤12
13-15
≥16
Imipenem
10 µg
≤13
14-15
≥16
Polymixin B٭
300units
≤13
≥19
*Since the interpretive standards for Colistin, Fosfomycin and Polymixin B against Acinetobacter spp. is not established in CLSI 2013 mannual zone diameter interpretative standards for Enterobacter spp. and E. coli were used.20
Figure 1: Susceptibility pattern of Acinetobacter spp. against broad spectrum antibiotics
Table 3: Total % efficacy of different antibiotics among Acinetobacter spp. isolated (N= 52)
S.No.
Antibiotics
Disc Code
Resistance (%)
Intermediate (%)
Sensitivity (%)
1.
Amikacin
30µg
42(80.76)
00
10(19.23)
2.
Cefoperazone
75µg
49(94.23)
00
03(5.76)
3.
Ceftriaxone
30µg
48(92.3)
00
04(7.69)
4.
Ciprofloxacin
05µg
47(90.38)
01(1.9)
04(7.69)
5.
Colistin
10µg
01(1.9)
00
51(98)
6.
Fosfomycin
50µg
34(65.38)
17(32.69)
01(1.9)
7.
Imipenem
10µg
51(98)
00
01(1.9)
8.
Polymixin B
300 units
01(1.9)
00
51(98)
Discussion
Our present study shows that the Acinetobacter spp. were highly resistant to Cefoperazone (94.23%). This finding is further substantiated by research that observed Cefoperazone to be only effective when used in combination.7,8
We also observed that only 19% isolates were sensitive to Amikacin, which contradicts the findings of Liu et al 2013 3 who observed 100% efficacy. However, they also discovered that 82% were inhibited by Imipenem while Fluoroquinolone was also found to be effective against 70% of all isolated organisms and Cefoperazone as least effective.
Organisms isolated from sputum showed a high degree of resistance to most of antibiotics, Zheng W and Yuan S also observed such results9.Nwadike et al 201410 found a high prevalence of resistant Acinetobacter spp. isolates against Ciprofloxacin (100%) and Amikacin (50%).10
Polymixin inhibited 98% of isolates, which is similar to figures found by Haeili et al 20131 who observed 95.5% susceptibility to Polymixin B. The second most effective antibiotic was Colistin - Trottier et al 200712 also observed 100% susceptibility of A. baumanni to Colistin. Similarly, Vakilietal 201413 found a low rate (i.e, 11.6%) of Colistin resistance.
Colistin has emerged as a viable choice for treatment of multidrug resistant Acinetobacter strains. In several studies,13,14 where 98% of isolates were resistant to Imipenem these results support the work of Khajuria et al 201416 who also reported reduced efficacy. Our findings are in contradiction to the study by of Tripathi et al 201417 who reported that Imipenem was a highly effective drug in comparison to other broad spectrum antibiotics.Fosfomycin surprisingly exhibited unusual results in our study; 32% of Acinetobacter spp. were IS while 65% were resistant. However, previous studies showed that Fosfomycin were proved to be good option to treat infections caused by Acinetobacter spp.18 Zhang et al 201319 reported that Fosfomycin used alone was highly ineffective in treatment of Penicillin Drug Resistant-Acinetobacter baumannii (PDR-Ab).Another study revealed that Acinetobacter spp. has developed adaptive resistance against Polymixin.21
Acinetobacter spp. are emerging as a resistant bacteria and a common cause of nosocomial and hospital acquired infections. There is a serious need to take necessary measures by hospital administration in maintaining environmental and personnel cleanliness according to current Good Manufacturing Practices. Pharmacists should educate patients about the drawbacks of self-medication and not completing medication courses, which is resulting in development of resistant bacterial pathogens.
The term ‘designer drug’, coined in the 1980s, generally referred to various synthetic opioids based mostly on the fentanyl molecule (α-methylfentanyl) and MDMA (methylenedioxymethamphetamine) commonly known as ecstasy. Fentanyl is an extremely potent analgesic, some 100 times more potent than morphine. MDMA and fentanyl compounds were the most popular synthetic drugs initially. The terminology is confusing because although the description ‘designer drug’ seems to imply the creation of new drugs, many are not new. For example, cathinone derivatives have been reported since the late 1920s. MDMA was first synthesised in 1912, methcathinone in 1928, and mephedrone in 1929. Cathinone is chemically similar to ephedrine, cathine, methcathinone and other amphetamines.
Legal highs generally comprise cathinone stimulants and synthetic cannabinoids. Hallucinogenic agents such as salvia divinorum are also included, the latter sometimes described as herbal ecstasy. Synthetic amphetamines are not regarded as hallucinogenic, though hallucinations are experienced by some users.
Thus, the term ‘designer drugs‘ covers an array of substances which are used recreationally, are not controlled under the Misuse of Drugs Act (1971), are not licensed for ‘legal’ use, and are not regulated under the Medicines Act (1968). They are chemicals produced by tweaking or altering the molecular structure of previous well-known psychoactive agents. By stating they are ‘not for human consumption’, or are just ‘bath salts’, they can be sold legally. Hundreds of such substances are now available, reflecting the ease at which chemists can produce them.
Availability and Consumption
The World Drug Report (available on the Internet) produced annually by the UN Office on Drugs and Crime (UNODC), provides information on the worldwide manufacture and marketing of illegal drugs. The 2013 report highlights a striking rise in the availability of new substances. Part of the challenge lies in their variety - some are derived from plants, for instance, the mint plant Salvia divinorum, native to Mexico, with synthetic cathinones and cannabinoids also being major contributors in other countries.
Ease of synthesis, low cost, and resourceful marketing have contributed to the problem. Information provided via the internet, combined with minimal difficulty in the manufacture and transport from distant regions, together with lax legal enforcement, creates an ideal opportunity for legal highs to flourish. The low cost is particularly attractive though ironically legal highs probably cost more these days: for example, 1g of mephedrone costs about £16.00 more than when legislation was introduced in 2010. On the other hand MDAI (methylenedioxy-2-aminoindane), a legal stimulant and club drug which is snorted or bombed, costs about half the price of cocaine (£20 per gm). It is sometimes cheaper to buy legal highs over the internet than from a drug dealer. Part of the increase in use of legal highs may be a result of decreasing purity of other ‘buzz’ drugs such as cocaine and MDMA.As with other illegal drugs regulatory measures drive the drugs ‘underground’ and into the hands of drug dealers and the price then varies with the purity of the drug and its ease of manufacture and availability.
Some users will revert to taking an illegal drug when the legal alternative is prohibited. There is also a certain curiosity to experiment with new drugs. Even so, to keep things in perspective, consumption of more harmful familiar illegal drugs (for example, cocaine, amphetamines) has not abated, with over 315 million people worldwide thought to be using them. More worrying is that millions of individuals inject more harmful drugs such as opiates with resultant increased rates of HIV, hepatitis B and hepatitis C infection. Readers are also likely to be aware of the violence and deaths associated with drug manufacturing and supplying within countries such as Latin America.
Government Control
The Medicines Act 1968 (UK) governs the control of medicines for human and veterinary use. It defines three categories of medicines: a) prescription only medicines (POM), available solely from a pharmacist and requiring an appropriate practitioner to issue, b) pharmacy medicines (P), available only from a pharmacist, without the need for a prescription, and c) general sales list (GSL) meaning medicines bought without a prescription. The Medicines Act 1968was set up to protect patients from unscrupulous suppliers of medicines. Safeguarding the public from illegal medicines or any inaccurate and misleading labelling of medicines isparamount. However, manufacturers have managed to sell legal highs by passing them off as bath salts or research chemicals.
Phenylalkylamines analogues such as amphetamine are widely misused and because of their simple structure hundreds of amphetamine analogues have been introduced for decades. This is the reason why so many legal highs are available. Amphetamine (phenylisopropolamine), a familiar central nervous system (CNS) stimulant, has effects which last for several hours after oral intake. Methamphetamine is closely related to amphetamine and ephedrine (a mixed-acting sympathomimetic). Ephedrine and pseudoephedrine (often used for relief of nasal congestion) undergo reduction to methamphetamine, or oxidation to methcathinone. As with methamphetamines, methcathinones can be readily ‘cooked’ in the laboratory and hence the term ‘synthetic’.
Background biochemistry
Morphine, the most abundant opiate alkaloid found in the poppy plant, papaver somniferum, was first isolated in 1804. The actual term alkaloid is derived from "alkaloide" introduced in 1819 by the German chemist Carl Friedrich Wilhelm Meisner, from the Latin root ‘alkali’, and the Arabic word al-qalwī meaning "ashes of plants".
Alkaloids are a group of naturally occurring organic nitrogen-containing bases, a base being a substance with a pH above 7 which turns red litmus paper blue. They include related compounds with neutral and even weakly acidic properties and more than 3,000 different types have been identified. In addition to nitrogen, hydrogen and carbon, most alkaloids contain oxygen, sulfur, and to a lesser extent, chlorine, bromine, and phosphorus. Generally, an alkaloid contains at least one nitrogen atom in an amine-type structure, i.e. one derived from ammonia (NH3) replacing the hydrogen atoms with hydrocarbons, for example, CH3 or CH2. Alkaloids generally are weak bases and some act as acid or base (amphoteric).
Alkaloids are produced primarily by flowering plants and organisms such as bacteria, fungi, and animals. Several alkaloids may be extracted from one plant.They can be purified from crude extracts by acid-base extraction and tend to have a bitter taste. Those containing a ring system are known as indole alkaloids (for example, terpenoids and steroids). Some are named after the biological species from which they are derived (morphine from the poppy plant Papaver somniferum, cocaine from erythroxolon coca, and so on). Other common examples include psilocin, caffeine, nicotine, vincristine, reserpine, atropine, quinidine, ephedrine,strychnine and quinine. Atropine is the tropane alkaloid isolated from the deadlynightshade plant Atropa belladonna, and strychnine is derived from the seeds of the Strychnos nux-vomica tree. Caffeine, cocaine, codeine (methylmorphine) and nicotine are water-soluble alkaloids. Morphine and yohimbine are highly water-soluble. Other alkaloids dissolve poorly in water yet readily in organic solvents such as chloroform or ether. The biological precursors of most alkaloids are amino acids, such as phenylalanine, tyrosine, tryptophan, histidine, and aspartic acid, among others. 1
How are they used?
The synthetic cathinones (usually mephedrone and methylone, or M-Cats) are most commonly used intranasally (insufflated) or ingested. “Bombing” is a method of ingestion whereby mephedrone powder is wrapped in cigarette paper and swallowed. Because sniffing the drug may cause nasal burns users will often resort to ‘bombing’. “Keying” is the practice of dipping a key into powder and then insufflating, with approximately five to eight “keys” per gram. Rectal administration, gingival delivery, inhalation, intramuscular and intravenous injection have also been described. Multiple concomitant routes of administration are reported. Self-reported doses range from a few milligrams to over 1 g of powder. A typical dose of mephedrone would be 100-200mg every 1-2 hours.
Users cannot be certain of the actual contents or indeed of the purity of the drug, therefore actual dosage and exposure is highly variable. For example, when MDAI (methylenedioxy-2-aminoindane) known as Sparkle (a granular, brownish powder) is snorted or bombed, it has an effect similar to ecstasy causing mood enhancement and hallucinations. Onset of action is usually within one hour and the effects are then almost immediate, perhaps a minute or so. The high lasts about six hours with a peak of two hours. It may cause hyperthermia, paranoid ideation and panic attacks.2
Cathinone is a naturally-occurring beta-ketone amphetamine analogue found in the leaves of the khat plant. Other synthetic cathinones such as methcathinone and MDVP (methylenedioxypyrovalerone) produce similar effects. Beta-ketone refers to the possession of a ketone group in the beta position of the aminoalkyl chain attached to the main molecular methylenedioxyphenyl ring.
Synthetic cannabinoids share some functional similarities with Δ9-tetrahydrocannabinol (THC), the active principle of cannabis. Like THC, they can have sedative, depressant and hallucinogenic effects. They have been detected in herbal smoking mixtures such as ‘Spice’ as well as resins that mimic cannabis resin.
Khat (Catha edulis)
Some knowledge of this plant is necessary in order to explain the background to many of the synthetic designer drugs. Khat is an evergreen shrub the leaves of which are chewed for their stimulant properties. An understanding of its chemical composition helps to explain the use of its constituents in the formation of designer drugs. Khat contains more than 40 alkaloids as well as many other compounds. The khat pheylalkylamines consist of cathinone, cathine and norephedrine: these alkaloids are structurally related to amphetamine and noradrenaline. Although similar to methylamphetamine, methcathinone (variously known as Cat, Kat, Qat, Ghat, and Chat) possesses a chemical structure resembling cathinone; its side effects and addictive properties are more potent.
The plant is chewed into a ball and kept in the cheek for a while. When khat leaves dry, cathinone (benzoylethanamine) decomposes within 48 hours leaving behind the milder chemical, cathine (a phenethylamine compound). Therefore, to maintain the potency of the drug, harvesters transport khat by packaging the leaves and stems in plastic bags or wrapping them in banana leaves to preserve moisture. It is common to sprinkle the plant with water or use refrigeration during transportation. Khat is therefore best used within 12-48 hours when the leaves are still moist.
Catha edulis is a flowering plant (one that produces seeds) native to the Horn of Africa (Eritrea, Djibouti, Ethiopia and Somalia) and the Arabian Peninsula. In these countries chewing the leaves and stalks is a social custom dating back thousands of years. It may take 7-8 years for the shrub to reach its full height (6-12 feet or more). Globally it is estimated that some 10 million males (usually) use khat on a daily basis.
Cathaedulis leaves containa beta-ketone amphetamine analogue. Ketones contain a carbonyl group (C=O) bonded to two other carbon atoms. Phenylalkylamines (derived from phenethylamine) are often termed “bk-amphetamines” for the beta-ketone moiety.
The principal active components in khat are cathinone and cathine. By chewing khat these substances are secreted into saliva. The effects are similar to amphetamine though less potent. Psychological dependence does occur in some though generally khat is not addictive. It is freely available in many countries and its production, sale and consumption are legal, including the Horn of Africa. In the Arab Peninsula it is known as Arabian tea and in South Africa it is referred to as Bushman’s tea.
Although its stimulant effect was originally attributed to cathine, extracts from fresh leaves of khat were shown to contain cathinone, isolated in 1975 and its properties recognized in 1978. Cathinone is not very stable and breaks down to produce cathine and norephedrine which belong to the phenylpropanolamine family, a subset of the phenethylamines and the catecholamines adrenaline and noradrenaline.
When the leaves are chewed the active ingredients are absorbed through the oral and gastric mucous membranes. The action of cathine and cathinone on the reuptake of adrenaline and noradrenaline results in the wakefulness associated with amphetamine derivatives. The effects of cathinone peak after 30 minutes, with nearly 98% of the substance metabolized by the liver into noradrenaline. Cathine has a half-life of about three hours in humans. Typically, an individual consumes 100–200 g of khat leaves (one bundle) in a session, and its effects last for several hours.
Symptoms are rather similar to the ingestion of strong coffee or amphetamines, for example, overtalkativeness and hyperactivity. The effects of oral cathinone occur more rapidly than those of amphetamine, 15 minutes compared to 30 minutes respectively. Khat causes constipation, dilated pupils (mydriasis), tachycardia and increased blood pressure, reflecting the sympathomimetic effects of the drug. Withdrawal symptoms, as would be expected, include mild depression and irritability, lethargy, rebound anxiety causing nightmares, tremulousness and loss of appetite. Long-term use may cause hepatic dysfunction, a permanent greenish tinge darkening of the teeth, and diminished libido. Rarely, dilated cardiomyopathy and myocardial infarction result from chronic use. 3
Mephedrone
Mephedrone (‘meow meow’) is a synthetic stimulant chemically related to cathinone, the psychoactive substance present in the khat plant. It is usually sold as a white crystalline or off-white-yellow powder (as a hydrochloride salt) for about £10 per gram. Consumption is usually oral or intranasal and rarely, by injection. Sellers avoid attracting the attention of regulatory bodies by labelling the substance “not for human consumption,” which means that no advice on safer use and dosing is provided.4
In one study the most commonly seen drug class were piperazines, followed by the cathinones, with significant variation in the content in one quarter of these compounds. The authors stated that it was relatively easy to purchase a number of legal highs from different Internet suppliers, though there times when not all of the products were available leading to the problem of users buying different active drugs to those they are used to, raising the prospect of potential toxicity to unknown agents.5A cross-sectional survey of 947 of mephedrone users found it to be the sixth most frequently used drug in the previous month after tobacco, alcohol, cannabis, cocaine and MDMA. Users typically were young males; 15% reported using weekly or more frequently; nearly 50% used between 0.5 and 1g during a typical session; intranasal use was the most common route of use (70%). Almost 55% of those who used cocaine reported that the ‘high’ obtained with mephedrone was better: intranasal use was also more likely addictive than oral use. Mephedrone appears to be the most widely abused synthetic cathinone in Europe, in contrast to the USA where MDVP and methylone are the most frequently abused. 6 7
Classification of mephedrone has had a limited effect on controlling its availability and use. Before the introduction of the legislation users generally obtained it via the internet. Now it is bought from street dealers, on average at double the price. Mephedrone was defined as a Class B drug under the Misuse of Drugs Act (1971) in the UK in April 2010. 4
Mephedrone produces similar effects to ecstasy, amphetamines and cocaine. It is detected in 20% of ecstasy tablets. It simulates the release of and inhibits the reuptake of monoamine neurotransmitters. The onset of psychoactive effects after insufflation is usually 10–20 minutes with an expected duration of effect of 1–2 hours; after oral ingestion onset is about 15–45 minutes with duration of 2–4 hours, and intravenous users report symptoms peaking at 10–15 minutes with a 30-minute duration of the desired effect.
Mephedrone users report that it has a better quality high than cocaine. It is speculated that mephedrone’s popularity reflects dissatisfaction with the purity and consistency of available cocaine and ecstasy. Concerns are also raised when it is considered that mephedrone is readily available from street dealers and may be taken by young people who have little previous experience of drug use.
Blood or plasma mephedrone concentrations are expected to be in a range of 50–100 μg/l in persons using the drug recreationally, >100 μg/l in intoxicated patients and >500 μg/l in victims of acute overdose.
Mephedroneinduces a greater increase in dopamine than serotonin release whereas MDMA (‘ecstasy’) induces a huge increase in serotonin with an insignificant rise in dopamine. Amphetamine results in a surge in dopamine release with an insignificant increase in serotonin. Mephedrone, amphetamine, and MDMA have decay values of 25, 50 and 300 minutes respectively. Therefore, the rapid rise and fall of dopamine levels could explain the addictive properties of mephedrone in some users. The effects are often described as somewhere between ecstasy and cocaine. As with cocaine, the ‘high’ generally lasts around an hour before wearing off. Furthermore, prolonged high –dose use of the substances can produce long-lasting neurotransmitter deficits in humans. 8 9
According to Mixmag (the online drug-use clubbing survey magazine for the UK) published in March 2012, 42% of clubbers had tried mephedrone the drug, and 34% had taken it in the last month. Some 30% of mephedrone users had reported using more ecstasy since the ban came into effect, while 19% reported using more cocaine. Blood or plasma mephedrone concentrations are expected to be in a range of 50–100 μg/l in persons using the drug recreationally, >100 μg/l in intoxicated patients and >500 μg/l in victims of acute overdose.
In 2011, Mixmag and the Guardian newspaper which draws on previous Mixmag surveys collected 15,500 responses from around the world, mostly the United Kingdom. In 2010/11, reported levels of use of mephedrone in the last year and last month were three times higher among clubbers (30 % and 13 %) than non-clubbers (10 % and 3 %).
Mephedronepredictably, causes increased alertness, restlessness, euphoria, excitement, the urge to talk, openness, time rushes, hot flushes, increased libido and elation. Hyperhidrosis, headache, palpitations, a Raynaud–type syndrome, and nausea are other relatively common unpleasant effects. Dizziness, hallucinations, panic attacks, and psychosis may occur. Other physical symptoms include dry mouth, blurred vision, and epistaxis. Symptoms of intoxication include agitation, aggression, violence, seizures and hyperthermia. Fatigue and insomnia are common residual effects. Mephedrone is generally used by nasal insufflation or ingestion of powder, liquid, capsule or tablets. The majority of users source mephedrone from street level dealers.10 Mephedrone induces strong feelings of craving in most users. If the unstable ecstasy market situation persists, the potential of mephedrone to substitute for MDMA might be substantial. Mephedrone, sold as ecstasy, is therefore more likely to be a cause for concern in the future.
Bath salts
This is the street name for substances which contain synthetic cathinone stimulants, such as methylenedioxypyrovalerone (MDPV) and mephedrone.11Bath salts components act synergistically at the dopamine transporter site and enhanced dopamine transmission may increase the potential for abuse. MDPV is consumed with other illicit drugs of abuse. It is the primary ingredient in "bath salts." Being a synthetic, cathinone-derivative it produces a high similar to cocaine or methamphetamine. It can be administered orally, by nasal insufflation, smoking, intravenously/intramuscularly, or per rectum, and intoxication lasts many hours.
MDPV may cause cardiac problems and disturbance of perception. During the withdrawal period after MDPV use, bone and muscle pain, and visual disturbances may occur. In the metabolism of MDPV, the most important catalyst is the CYP2C19 isoenzyme; the CYP1A2 and the CYP2D6 isoenzymes also play a role. The formed catechols are conjugated with either glucuronic acid or sulphate.
These compounds are not true bath salts in the traditional sense of household products. Cathinone is an amphetamine-like stimulant found naturally in the khat plant, described in more detail below. MDPV is much more potent than cocaine and its effect is longer lasting.12
Because of the sympathomimetic activity side effects are predictable and include cardiac arrhythmias, hypertension, arrhythmias, and hyperthermia. Chest pain, myocardial infarction, sweating, rhabdomyolysis, seizures, stroke, cerebral oedema, cardiorespiratory collapse, and rarely, death, have been reported. Psychiatric manifestations include hypersomnia, panic attacks, agitation, paranoia, suicidal ideation, self-mutilation, and aggressive behaviour.
The mode of action is thought to be the result of disruption and interference with central monoamine systems. In other words, synthetic cathinones increase extracellular monoamines by blocking transporter reuptake and increasing presynaptic neurotransmitter release. The dopamine (DA) transporter (DAT) and serotonin (5-HT) transporter (SERT) tightly regulate the amount of neurotransmitters within the synaptic cleft. Monoamine release also may be driven by presynaptic input from cholinergic or glutaminergic systems.127
Psychoactive bath salts are sold as tablets, capsules, or powder and purchased in places such as tobacco and convenience stores, gas stations, head shops, and the Internet. Bath salts may mimic cocaine, lysergic acid diethylamide (LSD), methamphetamine, or MDMA. The most common bath salts are the cathinone derivatives MDPV, mephedrone and methylone. The drugs have the potential for addiction because they cause intense stimulation, euphoria, elevated mood, and a pleasurable "rush". 13 14
In the United Kingdom (UK) to avoid being controlled by the Medicines Act, legal highs are sometimes described as bath salts, fertilizer (plant food), or incense, even though they have never been used for these purposes. In other words, legal highs are not covered by current drugs laws yet are used by individuals in the same way as illegal drugs such as cocaine or cannabis. The easy availability of legal highs marketed as "bath salts", ‘incense’ and ‘plant foods’, with the added proviso that they are not to be consumed by humans allows the drugs to circumvent current legislation. When legislation is changed the molecular structure is easily altered to produce a new legal high.
Synthetic cannabinoids
Marketed as ‘incense’ and labeled “not for human consumption”, these drugs were increasingly popular with students and young adults being initially legal and easily available from stores, online, head shops (outlets selling drug paraphernalia/counterculture magazines) and petrol stations. The structure of synthetic cannabinoids does not resemble that of tetrahydrocannabinol (THC] contained in marijuana or hashish, yet the drugs affect individuals in the same manner and are much more potent. Synthetic cannabinoids are sold under countless names such as ‘Mr Nice Guy,’ ‘Spice’, ‘Sabbaba’ and ‘Lemon Grass’, to name a few. Spice is a designer drug derived from herbs sprayed with synthetic chemicals which mimic the effects of cannabis. The ingredients are thus similar to but not identical to THC. Synthetic cannabis can precipitate psychosis, especially in individuals with a previous history and a chronic psychotic disorder may persist in some vulnerable patients.
A great variety of synthetic cannabinoids, most often cannabicyclohexanol, are used in an attempt to avoid prosecution. Some are sold in 'herbal' smoking mixtures and the latter have been found on occasion not to contain any synthetic cannabinoids at all. Cannabicyclohexanol is a cannabinoid receptor agonist drug. It has been sold under various brands such as Black Mamba, Bombay Blue, Fake Weed, Genie, Bliss, Blaze, Yucatan Fire. Spice products sometimes sold as “incense,” more closely resemble potpourri. Although Spice is usually smoked, sometimes individuals mix it with cannabis or prepare a herbal infusion for drinking.
To create the herbal products, synthetic cannabimimetics are dissolved in an organic solvent (e.g. acetone) and the resulting solution is sprayed on plant material. The doped plant material is then dried and smoked in a similar fashion to actual cannabis. Spice products typically have a pleasurable smell and taste. They are often referred to as herbal or legal highs because of their legal status and ‘natural’ herbal make-up. They are distributed in the form of dried leaves or resin, and powder, and are sold without age restriction in metal-foil sachets, usually containing 3 g of vegetable matter, to which one or more of the synthetic cannabinoids have been added. Spice is typically smoked, using a pipe or by rolling in a cigarette paper, and can also be ingested as an infusion, or inhaled.1516
Drugs of the 2C family (phenethylamines containing methoxy groups attached to a benzene ring) have hallucinogenic and stimulant effects. The term ‘2C’' refers to the 2 carbon atoms between the benzene ring and the amino group in these compounds. The effects are a cross between MDMA and LSD. They are relatively new to the market and not widely available in the UK. An excited delirium presentation seems to be consistent in deaths attributed to 2C drugs and at least five deaths have been reported in the literature in patients intoxicated with 2C drugs. One agent known as 2C-1 or Smiles, which first appeared in 2003,has more potent effects than MDMA and LSD. Users report an intense energy with vivid visual and auditory hallucinations lasting hours to days.. Patients may exhibit symptoms consistent with serotonin toxicity. Doctors need to be vigilant as synthetic drugs do not show up on routine testing. Treatment of 2C intoxication is primarily supportive.17
Despite widespread Internet availability, many of these drugs remain unfamiliar to doctors and yet ‘bath salts’, have resulted in nationwide emergency department visits for severe agitation, sympathomimetic toxicity, and death. As with other illicit substances designer drugs may compromise cardiac function causing hypertension and tachycardia and users who inject run the well-known risks of contracting hepatitis C or HIV, thrombophlebitis and embolus formation.
Methoxetamine
Methoxetamine (also known as ‘mexxy’) is available on the Internet and marketed as ‘legal ketamine.’ It is an arylcyclohexylamine chemically related to ketamine and PCP (phencyclidine). Methoxetamine is longer acting and more potent than ketamine. The drug, a white powder, is usually taken sublingually, snorted, ‘bombed’, or injected intramuscularly. Doses are typically between 5mg-90mg orally. After snorting the drug it may take 30-90 minutes for its effects to become apparent. When injected the onset of action is usually within five to ten minutes. The overall duration of effect is within the range of 1–3 hours, sometimes longer. The drug induces feelings of detachment (dissociative state), paranoid symptoms, visual hallucinations, restlessness and increased energy in some. Other reported symptoms include confusion, catatonia, depression, tachycardia and hypertension. Methoxetamine is now a Class B drug under the Misuse of Drugs Act.18 19
Piperazine derivatives
The piperazine derivatives, a class of amphetamine-like compounds that includes BZP (benzylpiperazine) and TFMPP (trifluoromethylphenylpiperazine) are making a comeback as "legal ecstasy." Often perceived as safe by the public, adverse effects may range from minimal to life-threatening. Co-ingestion of BZP and TFMPP causes increased action of dopamine and serotonin, similar to MDMA. Severe symptoms include seizures, hyperthermia, hyponatremia, dystonic reactions, rhabdomyolysis, renal failure, metabolic acidosis, DIC, and respiratory failure. 20 Over the last few years piperazine derivatives are being sold as ecstasy pills, or under the names of “Frenzy”, “Bliss”, “Charge”, “Herbal ecstasy”, “A2”, “Legal X” and “Legal E”. Although piperazine designer drugs enjoy a market reputation of being safe, they may cause distorted perceptions after ingestion. There are several reports of toxic symptoms experienced by users after drug intake.The piperazinic compounds are derived from piperazine, a cyclic molecule containing two opposite nitrogen atoms and four carbon atoms distributed between the two and were originally used as anti-helminthic agents in the 1950s. Designer drugs of this class can be divided into the benzylpiperazines such as benzylpiperazine (BZP) and its methylenedioxy analogue methylenedioxybenzylpiperazine (MDBP), and phenylpiperazines such as chlorophenylpiperazine (CPP), trifluoromethylphenylpiperazine (TFMPP), and methoxyphenylpiperazine (MeOPP). A third group includes the thienylmethylpiperazines. Chlorophenylpiperazine is an active metabolite of drugs such as trazodone, and nefazodone used as antidepressants. A survey in the UK found that piperazines are among the most common active drugs in tablets purchased from internet supplier sites.Piperazine-derived compounds are therefore emerging designer drugs, whose abuse has increased remarkably worldwide.21
Naphyrone
Naphyrone(naphthylpyrovalerone) or NRG-1 (or Energy1) is a cathinone derivative available to buy on a number of websites and is gaining popularity. It is sold as an alternative to mephedrone. Belonging to the designer drugs class, it is similar in structure to pyrovalerone, a monoamine uptake inhibitor and as it is somewhat similar to other cathinone derivatives it has the potential to produce anxiety, paranoia, and cardiovascular side effects. Two products, both sold as NRG-2 from different internet suppliers, were found to contain the banned substituted cathinones - 4-methylethcathinone (4-MEC) and 4-methylmethcathinone (4-MMC), the latter being present in much smaller quantities. Although sold as research chemicals and labelled 'not for human consumption', they are essentially legal highs and are available online. 22 23
Table 2: Some commonly used psychoactive substances
Drug
Mode of Action
How used
MDMA (‘ecstasy’) ‘Molly’ is the pure crystalline powder form
Releases and inhibits reuptake of dopamine, serotonin and noradrenaline
Tablet or capsules
Sometimes one or more tablets taken at one time (‘bumping’)
Salvia divinorum
Partial dopamine receptor agonist; also works on kappa receptors
Smoked, inhaled, ingested, used sublingually
Mephedrone
Effects similar to MDMA, cocaine and amphetamines
Nasal insufflation, ingestion
MDVP (see text)
Related to cathinone. Effects similar to ‘ecstasy’
Nasal insufflation, inhalation, ingestion
Spice
Similar to THC
Smoked; sometimes prepared as a herbal infusion for drinking
Naphyrone
Effects similar to mephedrone
Usually snorted, sometimes swallowed in paper wraps (‘bombing’)
Discussion
New designer drugs have increased in popularity over the past several years because of their euphoric effects. Understanding the pharmacology and toxicology of these agents is essential in order to provide the best medical care for patients. They are all potentially dangerous. For example, an excited delirium presentation seems to be consistent amongst deaths attributed to 2C drugs.
From the above description it can be seen that synthetic drugs fall into three broad categories: synthetic cathinones (bath salts), synthetic cannabinoids (spice or incense), and amphetamine-like drugs (methamphetamine, ephedrine, MDMA). Cathinones being related to the amphetamine family will cause dilated pupils, hypertension, hyperventilation, paranoia, agitation, hyperthermia, tremors and seizures. Many countries have made certain cathinones illegal, for example, mephedrone, methylone and MDPV. Indeed, the robust stimulation of dopamine transmission by MDPV predicts serious potential for abuse and may provide a mechanism to explain the adverse effects observed in humans taking high doses of 'bath salts' preparations. Furthermore, pyrovalerone is much more potent than cocaine at inhibiting the uptake of dopamine and norepinephrine.
Methcathinone was previously used in Russia as an antidepressant, also known as “Cat” and “Jeff” when used recreationally. Nowadays the drugs are sold as bath salts, plant food, insecticides, chicken feed additives, or research chemicals with names such as like NRG (Energy) and meow, meow. Bath salts are water-soluble, usually inorganic, solid products designed to be added to water during bathing. Numerous nicknames are used to describe them including Ivory Wave, Purple Wave, Red Dove, Zoom, Bloom, Cloud Nine, Ocean Snow, Lunar Wave, Vanilla Sky, White Lightning, and Hurricane Charlie.
Although ‘legal highs’ are commonly referred to as bath salts they are not Epsom salts (magnesium sulphate) or other water softeners within the usual meaning. In many cases the chemical ingredients are changed without the consumer knowing, making risks unpredictable. Some legal highs contain active ingredients controlled under the Misuse of Drugs Act 1971 (UK). Therefore any individual found in possession of these products would be liable to prosecution and the associated penalties, even if unaware that he/she has purchased a controlled drug. However, claiming a product to be "not intended for human consumption" can potentially circumvent the entire legal process. Drug designers are already showing skilful exploitation of the law and remain far ahead of criminalization efforts. Furthermore, the irony of prohibition is that the supply and slump in the market for cocaine and ecstasy in 2009 led to individuals resorting to untried and untested substances that are now easily available online. 2425
Synthetic cathinones are mostly excreted via the urine and can be measured via gas or liquid chromatography-mass spectrometry in the blood, urine and stomach contents. They can also be analysed in hair. Unlike traditional cosmetic bath salts, which are packaged and sold for adding to bath water for soaking and cleaning, synthetic designer drugs sold as "bath salts" have no legitimate use for bathing and are intended for abuse. Baths salts contain one or more synthetic derivatives of the naturally-occurring stimulant cathinone. Low doses produce euphoria and increase alertness, but high doses or chronic use may cause serious adverse effects.26
Treatment
Treatment should be tailored to the specific drug of abuse. Medical and psychological needs require examining. Generally, treatment uses a combination of counselling and medication to reduce the need or desire (craving) for the drug and give the person the skills to refrain from future drug use. Other treatments might include cognitive behavioural therapy, detox, and relapse prevention techniques.
Supportive care is the mainstay of treatment for untoward serious side effects. Sedation with benzodiazepines is indicated for agitation, seizures, tachycardia, and hypertension. Extreme hypertension that persists despite benzodiazepines may be treated with vasodilators. Beta blockers should be avoided due to the potential to cause unopposed alpha-adrenergic stimulation, worsening the hypertension. Significant hyperthermia may require passive or active cooling. All moderately to severe symptomatic patients should have an electrocardiogram (ECG), be placed on a cardiac monitor, and receive serial temperature checks. Electrolytes, liver function tests, cardiac enzymes creatine, and toxicology should be carried out. Asymptomatic patients with no other suspected ingested drugs or psychiatric symptoms generally may be discharged.
Prevention
Banning legal highs is probably futile because it is impossible to keep up with newer drugs because they are synthesized as soon as the ‘illegal’ drug becomes banned. Some would argue that arresting users creates more harm for individuals, their families and society, as they are then caught up in the criminal system. Others may argue that ‘legal highs’ are not generally harmful and not as dangerous as opiates or their derivatives, or indeed alcohol. It might be more worthwhile making legal highs ‘uncool’, much in the same way that cigarette consumption is now frowned upon. However, it would require a great deal of public money to subsidise such an advertising venture.
Users of legal highs need to be made aware that such drugs purchased on-line may contain illegal substances and therefore may render them subject to prosecution if found in possession. 27
Pre-school family based programmes, and programmes involving the school and community, motivational interviewing for adolescents, and individual programmes, may be beneficial in reducing drug use and other harmful outcomes. Importantly, none of these approaches focus exclusively on particular substances or groups of substances, and although there have been relatively few investigations of intervention processes they most likely work by targeting a number of important precursors of drug use behaviour.28
Preventing designer drug abuse begins with understanding the warning signs of addiction which in many respects are similar to alcohol or more common street drugs.
Club drugs are now widely available and their harmful effects are increasingly becoming more evident. Their effects are unpredictable as they are often ‘contaminated’ with other harmful substances. It is unlikely that legislation will have a meaningful impact. Increasing public awareness about these drugs is paramount, and medical and nursing staff should consider intoxication in those patients who present with agitation and psychosis who have no previous history of mental health problems.
Pharmacists are in a pivotal position to observe changes in patterns of drug use and report worrying trends to health care practitioners. Counselling for young people especially and prevention programmes based in schools could prove useful in pointing out the dangers of these drugs to teenagers. Health care professional too should endeavour to keep up with recent information on these substances by attending hospital-based lectures or conferences as part of continuing professional education.
Urine drug testing will generally be unhelpful as many club drugs are undetectable on standard urine drug screens.29 Mental health staff should enquire about club drugs as part of routine drug and alcohol assessment and be aware that these patients may not fit the stereotype of a drug misuser.
Trigeminal Neuralgia (TN) is relatively rare in Multiple Sclerosis (MS) affecting approximately 2% of patients1. The severity of the pain is indistinguishable whether TN is an isolated impairment or is associated with MS. However, when associated with MS, TN is often bilateral, affecting younger patients and is more refractory to medical treatment 2.
Several pharmacological agents are reported to be effective in TN associated with MS. Topiramate3,4, gabapentin5 and lamotrigine6 were all reported to benefit patients with TN associated with MS in small uncontrolled trials. Several other drugs such as phenytoin, misoprostol and amitriptyline are routinely tried in patients with TN despite the lack of convincing evidence of their efficacy7.
In 2008, Both the American Academy of Neurology and the European Federation of Neurological Societies launched joint Task Force general guidelines for the management of TN. After systematic review of the literature the Task Force came to a series of evidence-based recommendations 8. Carbamazepine and oxcarbazepine had the strongest evidence of efficacy and were recommended as the first line treatment. An earlier Cochrane systematic review reached the same conclusion. 9.
Case report
A 62 year old female patient had been suffering from MS for about 20 years. The MS presented with trigeminal neuralgia from the outset and this was then followed by pyramidal lower limbs’ weakness and sphincteric dysfunction. The patient started to use a wheelchair 10 years ago but she became totally wheelchair dependent about 6 years later.
Trigeminal neuralgia remained active throughout the 20 years. Carbamazepine (300 mg daily) provided the patient with a satisfactory control of TN. Despite having occasional break through TN pain; the patient declined having higher doses of carbamazepine as excessive sedation was an unacceptable side effect.
Recently; the patient was admitted to hospital in two separate occasions complaining of increasing malaise and confusion. Plasma sodium levels were found to be low in both occasions (first presentation 118 mmol/l and second admission 114 mmol/l). Clinical evaluation confirmed Syndrome of Anti Diuretic Hormone Secretion (SIADH) as the cause of the hyponatremia and in the absence of any other explanation for the SIADH; carbamazepine was thought to be the main reason and was duly discontinued.
Unfortunately, TN attacks came back with vengeance. During the following 6 months, therapeutic trials using gabapentine, topiramate and amitriptyline failed to show any beneficial effect on either the severity or the frequency of the TN attacks. All three drugs were duly discontinued.
The patient was started on eslicrbazepine 400 mg on a single daily dose. This dose lead to almost complete eradication of the TN attacks. The control of TN and the plasma sodium levels remained stable a year following the initiation of the therapy.
Comments
Hyponatremia, defined as a sodium level < 135 mmol/l is a common side effect of carbamazepine and oxcarbazepine therapy. The incidence of hyponatremia secondary to carbamazepine therapy ranges between 4.8 and 40 % depending on the population studied10,11. In most cases, hyponatremia is asymptomatic and continuation of the carbamazepine use is possible whilst a close eye is kept on the plasma sodium level10. In rare occasions hyponatremia is symptomatic and discontinuation of carbamazepine is warranted. Administration of demeclocycline to normalise the sodium level was suggested by some authors12 However, the long term use of demeclocycline is associated with several complications and this approach is hardly a standard practice.
Clinicians often face a dilemma when carbamazepine is the only agent able to control a specific clinical problem. With many antiepileptics available, it is unusual to face such a problem in epileptic patients. Trigeminal neuralgia on the other hand can be extremely difficult to control and carbamazepine was found to have a unique ability to manage such unpleasant condition even before its antiepileptic effects were noticed on 196213.
Eslicarbazepine is promoted as an alternative to carbamazepine when side effects occurs on otherwise responsive patients to its favourable antiepileptic effects14. Hyponatremia is rare in eslacarbazepine users with only an incidence of less than 1% in the small populations studied15,16. Frequency of hyponatraemia increased with increasing eslicarbazepine dose. In patients with pre-existing renal disease leading to hyponatraemia, or in patients concomitantly treated with medicinal products which may themselves lead to hyponatraemia17.
Our patient showed the same favourable response to eslicarbazepine as she experienced with carbamazepine. However, hyponatremia did not occur with eslicarbazepine therapy. This enabled our patient to continue with pharmacological management and avoid surgical interventions.
With the exception of epilepsy, no reports are available commenting on the use of eslicarbazepine on the wide range of conditions that carbamazepine is traditionally used for such as mental health problems and neuropathic pain. When patients are well controlled on carbamazepine whatever the indication is, the occurrence of side effects such as hyponatremia is often managed by an automatic replacement with another agent. We feel that in such patients a therapeutic trial of eslicarbazepine might be appropriate especially if the control on carbamazepine was robust or if the benefits of carbamazepine therapy were clearly superior to other pharmacological agents potentially useful for the targeted clinical condition.
Driven by a global rise in opioid dependence, Opioid Substitution Treatment (OST), the prescribing of opioids (usually methadone or buprenorphine) as maintenance treatment, has expanded worldwide over the last two decades3. Participation in OST reduces the risk of death by overdose4, reduces the risk of HIV transmission5 and reduces participants’ involvement in property crime6. For these reasons, maintenance with methadone remains the major public health response to reduce the harms caused by heroin addiction.
In the United Kingdom (UK) in the late 1990s, government funding to expand access to OST was provided, with the explicit objective of reducing crime7. The expansion of treatment was supported with clinical guidelines2, and targets were set to try to ensure good outcomes. Given the research evidence on the importance of retention in producing better outcomes, service providers were set a target of retaining at least 75% of people in treatment for 3 months. A tool to monitor outcomes, the Treatment Outcomes Profile (TOP)8, was developed and service providers nationally were set a target of 80% of people in OST completing TOP at entry and after 6 months9. This 20-item self-report questionnaire records a set of core data for the previous 28 days, including the number of days on which heroin and cocaine have been used.
The amount of methadone prescribed in England and Scotland increased fourfold over the decade 1998 – 20083. However, in 2010, Britain’s newly-elected government signalled a change in the direction of drug policy1. The paradigm on which the new policy is based is “recovery”, a concept embracing self-help, mutual support, and optimism about the possibility of positive change. The policy is in part driven by the perception that treatment services have a defeatist attitude, expecting little positive change – hence the claim that there are too many patients “parked on methadone”. To counteract this perceived pessimism, the “recovery agenda” includes incentives to services to promote abstinence from all drugs including prescribed OST medication. This policy has been criticized as being inconsistent with the available evidence10, but has been defended on the grounds that many patients on methadone were doing poorly, and needed encouragement to make positive changes in their lives.
In 2010, we decided to investigate to what extent people were responding poorly to treatment, and whether this could be improved by implementation of evidence-based treatment.
Methods
This quality improvement project was undertaken in two OST clinics in Merseyside, managing in total over 1000 patients. The services had the same senior leadership and medical staff, but separate teams of nurses and key workers. Supervised administration was provided by local retail pharmacies.
In October 2010 key workers were provided with list of patients currently under their care and asked to identify patients they thought were using heroin regularly. A research assistant then checked case notes of identified patients, looking at self-reported heroin use as recorded in TOP monitoring forms, and at the results of previous urine toxicology tests. Those whose most recent TOP was performed at entry to treatment were excluded (since their self-reported heroin use covered a time when they were not in treatment). Among the remainder patients reporting use of heroin on at least 8 days in the 4 weeks preceding their last TOP interview were classified as “non-responding” patients. The case notes of all identified “non-responders” were reviewed using an audit tool covering age, sex, postcode, date of entry into treatment, duration of treatment, dose of medications, extent of supervised administration, dates and results of recent urine toxicology, and date and self-reported drug use from previous TOP questionnaires. This data was collected at baseline and again at re-audit (follow-up) 9 months later.
Postcodes were used to derive Index of Multiple Deprivation (IMD) scores11. The English index of multiple deprivation (IMD) is a measure of multiple deprivations, with domains including employment deprivation, health deprivation and disability, education skills and training deprivation, barriers to housing and services, living environment deprivation, and crime.
In one clinic, the “implementation clinic”, beginning January 2011, key workers were asked to refer all non-responders for a medical review. Patients were also screened for comorbidity, taking advantage of a separate project running concurrently which was designed to test the psychometric properties of a new questionnaire on mental health and well-being. All service users at the implementation clinic were invited to take part. The study had National Research Ethics approval and approval from the Merseycare NHS Trust R&D Office. Quality of life was assessed with the EQD12 which comprises 5 domains measuring health-related quality of life: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Depression was screened for with the Beck Depression Inventory13.
UK guidelines recommend for patients doing poorly “..ensuring medication is provided within evidence-based optimal levels, changing to another substitute medication, increasing key working or psychosocial interventions and increasing supervised consumption” 3. The recommended dosage for effective treatment is listed as in the range 60-120mg/day of methadone. At medical review, the plan was for the doctor to assess the non-responding patients, and propose raising methadone dose progressively until heroin use ceased, or a maximum dose of 120mg/day was reached; and requiring supervised consumption of methadone for patients persisting in heroin use.
Establishing the medical reviews in one of the two clinics was necessary for logistic reasons, but it also allowed an opportunity to assess the impact of the reviews, by comparing the outcomes of non-responders in the two clinics. If effective, it was proposed to extend this approach to the second ‘treatment as usual’ service. Referrals for medical review ceased in June 2011, and over the next three months staff feedback about the process was sought. In October 2011 a repeat audit of case notes including TOP results of all previously identified non-responders at both services was undertaken.
At follow-up data on the frequency of medical appointments in the preceding 6 months were also collected. In cases where people had left treatment, the TOP performed on exit from treatment was used. Those non-responders who had left treatment were identified and tabulated according to the reason for leaving treatment.
Flowchart 1: The audit and re-audit process
Ethics
The audit was approved by the local NHS Trust R&D Office. Funding was obtained to undertake the work by Mersey Care NHS Trust.
Analysis
Data was entered into SPSS version 18 (for windows). Summary statistics and standard hypothesis tests compared non responders in the intervention service to non responders in treatment as usual to ensure there were no statistically significant differences between the two groups at baseline. Chi-square and t-tests compared age, sex distribution, IMD scores, methadone dose and months in treatment this episode. Mann-Whitney U tests compared the number of TOP forms completed in each group during the previous 6 and 12 months. Regression analysis explored whether there was a relationship between attendance for supervised administration, self-reported quality of life and depression for non responders in the implementation group. Differences in baseline and at 9 month re audit methadone dose and heroin use were tabulated for each group. Mann-Whitney U-tests compared any differences between the two groups. Differences within each group were also compared using the Wilcoxon signed ranks test.
Results
The implementation service managed 534 patients, of whom 130 (24%) were initially identified as non-responders, reporting heroin use on 8 or more days in the previous month at their last TOP interview. At the TAU service there were 485 patients, of whom 112 (23%) were identified as non-responders. Of the 242 non-responders in total, 67 (28%) were new to treatment, and were excluded. This is illustrated in the flowchart 2.
Flowchart 2: Sample Algorithm
Approximately 50% of the non-responders in each group reported daily heroin use at baseline. The two groups of non-responders did not differ significantly in terms of age, sex distribution, nor on the Index of Multiple deprivation scores (mean of 62 reflecting very severe social exclusion across both groups). Non responders in the implementation service had been in treatment a median of 18 months compared to 17 months for those in treatment as usual. Urine testing was performed infrequently in both services, but a result was available from the six months prior to baseline for 133 of the remaining 175 subjects. The urine tests results were broadly consistent with the patients self-report. Aspects of treatment at the two services differed, as shown in Table 1. At baseline, doses did not differ significantly, but the treatment as usual group was significantly less likely to have their methadone administration supervised, and had less frequent TOP monitoring.
Table 1 Profile of non-responders and their treatment at baseline
Implementation
TAU
Total
N
104
71
175
Mean age in years (min, max)
42 (25,66)
43 (23,63)
42 (23,66)
Male (%)
65 (63%)
48 (68%)
113 (65%)
Mean IMD Score (SD)
62 (14.6)
62 (14.7)
62 (14.7)
Mean methadone dose in mg (SD)
60 (17.8)
60 (21.3)
60 (20.3)
Median Months in this Rx episode (IQR)
18 (20)
17 (10)
18 (14)
Any supervised doses
56 (54%)
22 (31%)*
78 (45%)
Last TOPS > 6/12 ago
15 (15%)
29 (42%)**
44 (25%)
*Pearson Chi square 9.995, df=2, p=0.007 **Mann-Whitney U =2654, p=0.002
Despite almost all non-responders being booked in for an appointment and given reminders at the implementation service, only 47 (45%) of the 104 identified attended at least one medical review. Keyworkers commented that the main reason for non-attendance was that clients were quite happy continuing heroin use and did not see stopping as something they wanted to do. When patients were told they would only receive their prescription renewal after attending, some patients chose to go without methadone and make contact a few days later, rather than attend an appointment. Among those who did attend, there was frequently resistance to increasing their methadone dose, and anger at the suggestion that medication administration should be supervised. Word of mouth spread through the service that doctors were proposing dose increases and more supervision. This increased resistance among patients, and appears to have generated some resistance among keyworkers, some of whom saw their role as advocates for the patients.
The attempt to implement change in one clinic appears to have had small effects in increasing average doses there, and having more patients seen by a doctor. Between baseline and 9 month re-audit (follow-up), mean methadone doses increased in the implementation group and fell in the TAU group, as shown in Table 2. There was a small and statistically significant increase in methadone dose in the implementation group compared to the TAU group. The difference in change in methadone dose between the two groups was statistically significant (Mann-Whitney U= 2745, p=0.002), but the mean dose increase (3mg) in the implementation group was small. In the 6 months prior to the collection of follow-up data, medical reviews in both services were infrequent; 36% of patients in the implementation group and 66% of patients in the TAU group had not seen a doctor in their OST service (Chi square =13.38, df=1, p=0.001).
In both groups, the reductions in heroin use over time were statistically significant (Wilcoxon signed ranks test p = <0.05), but the change in heroin use over time did not differ significantly between the two services (Mann-Whitney U 2832.5, p=0.7). The changes from baseline audit to 9 month re audit are shown in Table 2. Among the 47 patients who attended a medical review, the mean prescribed methadone dose rose from 58 to 66mg/day, but the number receiving supervised doses actually fell, from 23 at baseline to 20 at follow-up. Mean days of reported heroin use fell from 20 to 12 (6 patients reported abstinence) – changes almost identical to what was observed in the TAU group.
Table 2 Changes in dose and heroin use between baseline (T1) and follow-up/re audit (T2)
Implementation
TAU
Time 1
Time 2
Time 1
Time 2
N
104
103
71
68
Mean Self-report heroin days/28 (SD)
19.9 (8.6)
13.4 (10.8)
19.6 (8.3)
11.7 (10.8)
Reported daily heroin use
52 (50%)
33 (32%)
25 (42%)
17 (25%)
Heroin abstinence
-
14 (14%)
-
15 (22%)
Urine test positive morphine %
88%
76%
85%
70%
Mean daily methadone dose
59.5
62.9
60.1
57
Proportion self-report cocaine
67%
54%
53%
44%
Urine test cocaine positive
66%
57%
58%
45%
29 non responders (28%) from the implementation service, and 27 (38%) from the TAU service had left the service between baseline and 9 month re audit. Most discharges (31/56) were transfers to another service as part of a local policy to move more people into treatment in primary care. Eight patients from the Implementation service dropped out of treatment, and 4 patients from the TAU service did so. Differences in the pattern of leaving the two services did not approach significance.
Table 3 Reason for discharge
Reason
Implementation
TAU
Total
Transfer of Rx
13
17
30
Did not attend (DNA)
8 (28%)
4 (15%)
12
Elective Withdrawal
3
3
6
Deceased
2
0
2
Prison/drug diversion program
3
3
6
Total
29
27
56
44 non responders who attended a medical review at the implementaion service completed questionnaires on health, quality of life, and depression. Ninety-six percent were not in education, employment or training (NEET). On the Beck Depression Inventory, 50% of respondents reported depression in the moderate to severe range. Regression analysis indicated that having to attend for supervised doses was associated with less depression measured on the BDI (r=-.332, p=0.039), and with better quality of life in terms of EDQ scale of self-care (r=-.598, p<0.001) and being able to undertake usual activities (r=-.605, p<0.001).
Discussion
Many people persisting in heroin use were receiving care that was out of line with guidelines – doses below 60mg, often with no supervised doses, and seldom attending for medical reviews. However, the attempt to systematically implement guidelines was not effective. Most patients did not attend, and many of those who did attend resisted changes. Although patients who attended received slightly higher doses, changes in heroin use in the subset who actually attended for review were no different to the changes observed in the TAU group.
Higher methadone doses, and patients having control over their doses, have been shown in a meta-analysis to be independently predictive of better outcomes14. One possible explanation for the failure to implement guidelines is that it may have been perceived as challenging clients’ control over their treatment. If so, it was a challenge easily defeated. Patients clearly had substantial control over their treatment, choosing whether to attend appointments, whether to accept higher doses, and whether to accept supervised doses. However, this degree of control over their treatment did not appear to be beneficial. “Non-responders” reported depression, disability and a poor quality of life.
Guidelines need to move beyond systematic reviews of effectiveness, to include evidence about implementing evidence in a real world setting15. Our conclusion is that the failure to implement guidelines was that the approach adopted was not congruent with clinic culture, which emphasised “support” rather than “structure”. “Structure” refers to both cognitive and behavioural elements of treatment. The cognitive elements are defined and agreed objectives, a sense of the direction and purpose of treatment. In all areas of mental health, clinical interactions are most useful if focused on specific performance goals related to the patient’s circumstances16. In the OST services studied, there appeared to be a focus on process and on supporting patients, rather than achieving outcomes.
Structure also includes behavioural elements - expectations and rules regarding attendance, and daily attendance for supervised administration. Interviews with UK patients in OST have indicated that they understand and value the role of supervision, not only in minimizing diversion and misuse, but in providing an activity for many people without social roles17. Consistent with the benefits of supervision, in the current audit more supervision was associated with less depression and less-poor quality of life.
This audit had several limitations. It did not attempt to measure the proportion of patients responding poorly to long-term methadone treatment, and it is possible that the true proportion may be higher than the 17% identified by key workers. Documentation of treatment outcomes, using TOP reports and UDS results, was unsystematic, limiting the number of patients in whom complete data was available. “Non-responders” self-reported heroin use to keyworkers, who administered the TOP questionnaire, and there may have been under-reporting. However, while this study may not have identified all non-responding patients, this does not invalidate the observation that attempting to implement guidelines was not successful.
Most importantly, the observations from these clinics may not be generalisable to other treatment settings. However, certain key data are available suggesting the treatment and outcomes observed in this study were not atypical. A report on national TOP monitoring noted patchy availability of follow-up data, and confirmed a high rate of persisting heroin use in treatment, with 38% of participants reporting abstinence from heroin18. Despite this high rate of heroin use, a recent survey reported a mean dose of 56mg of methadone in a national survey19. In this regard, the clinics in this report thus seem representative.
Medical staff appeared to have a peripheral role in delivery of OST in these clinics. Most non-responders did not have a medical review in 6 months – despite persisting heroin use, and self-reported depression. In the 1980s in the US, methadone treatment underwent a process labelled “demedicalisation”, marginalisation of the role of medical practitioners, and a loss of the sense that methadone was a medical treatment with clearly defined objectives and guidelines20. This contributed to a situation in which much methadone treatment in the US was out of line with research evidence21. The current audit suggests that a similar process of demedicalisation and deviation from evidence-based treatment has been occurring in some NHS services in the UK.
If these observations are representative of at least some treatment culture in the UK, they lend support to the criticisms made of methadone treatment in the new UK drug strategy1. To the extent that the recovery agenda challenges clinic culture and shifts the focus of treatment onto outcomes, it is a positive development.
However, many well-intentioned policies have unintended consequences, and there are well-based fears that the new policy promoting abstinence from OST as an objective of recovery will lead to an increase in overdose deaths3. This is specifically because of the risk of overdose deaths after leaving treatment. The reason for the increased risk of overdose after leaving treatment is that newly abstinent addicts who have reduced opioid tolerance, and a dose of heroin they previously used during periods of addiction becomes a potentially fatal dose once they are abstinent. This risk attaches to all forms of drug free treatment, as well as to patients who have left methadone. The critical issue is that lapses to heroin use, and relapses to dependent heroin use, are very common among newly-abstinent addicts. It is the high probability of relapse to heroin use which is the basis of long-term maintenance treatment – better to keep people safe and functioning normally, albeit while still taking a medication, than the risk of relapse and re-addiction, or relapse and fatal overdose. In the UK, implementation of the recovery agenda has included incentives to abstinence, and this is not consistent with evidence about the risk of relapse. If the recovery agenda can accommodate the evidence that indefinite maintenance as a valid option for many, perhaps most heroin users, then the evidence of this study is that far from being in contradiction, the recovery agenda may facilitate the implementation of evidence-based practice.
Hydatid disease is due to Echinococcus species commonly granulosus sometimes multilocularis. The common locations of hydatid cyst are the liver (65% to 75%) and lungs (25%-30%) 1,2,3. Hydatid disease rarely develops in some locations such as the spleen, kidney, bones, heart, brain, peritoneum, myocardium and muscles (1-4%)1. In our review of literature, concomitant paraspinal and intrahepatic hydatid is reported rarely.
Case Report
A 25 year old male presented with backache on the right for 1 month and fullness in the right paraspinal region. No history of trauma, fever, burning micturition, pain in abdomen, weight loss or hematuria.
On clinical examination he had non ballotable lump in the right paraspinal region, measuring 15x5x5cm with ill defined margins intra muscular plane extending from the posterior subcostal margin to the iliac region with no overlying skin changes and no organomegaly.
Blood investigations including liver function tests and kidney function tests were normal. Ultrasound examination revealed hepatomegaly with thick walled cystic lesion in the right lobe of the liver and the in muscle plane in the right renal angle region.
CT abdomen (P+C) revealed a well defined hypodence non-enhancing cystic lesion measuring 45x40 cm seen in the right lobe of the liver with peripheral calcification with another lesion of similar morphology of size 14x5x3.6cm in the right paraspinal muscles with no intercommunication between them and no bone, spinal canal alteration or compression of the right kidney.
Figure 1: Right paraspinal hydatid
Figure 2: Intrahepatic hydatid
Figure 3: Coronal view of CT image
The diagnosis of paraspinal hydatid cyst was confirmed. As the patient was symptomatic for paraspinal hydatid cyst only and the size of the hepatic cyst was small, exploration of the right paraspinal region was done after 21 days of antiscolicidal treatment. There was a cyst measuring 15x5x5 cm beneath the oblique and lattisimus dorsi ,superficial to the psoas muscle without invasion into it .The cyst opened multiple daughter cysts along with pus evacuated. The cyst excised in totto without rupture & spillage. Negative suction drain was kept. Post operatively on day 3 the drain was removed, stitches removed on day 10 and discharged. Histopathology confirmed diagnosis.
Figure 4: Intraoperrative photograph
Figure 5: Photograph of multiple daughter cysts
Discussion
Hydatid disease is most prevalent in sheep and cattle-breeding areas, which is where the first step in the chain of transmission occurs. The causative agent is introduced to the dog (the primary host) through the faeces of livestock. The minute larval form of E. granulosus lives in the small intestine of the dog species. The eggs are passed in the faecesof an infected dog and can be transferred to mammal (man – intermediate host) that ingests them. After ingestion, the embryos are released from the eggs, traverse the intestinal mucosa and disseminate systemically via venous and lymphatic channels and develop into hydatid cysts in various body parts.
The cysts cannot easily grow in muscles due to their contractility and lactic acid content. The wall of a cyst in the muscle is formed by three layers: the inner germina, intermediate and outer granulomatous adventitial layer. The most common skeletal sites include hip, thigh, shoulder and humerus regions. Hydatid cysts are frequently asymptomatic1. The latent period of cyst development varies between 5 and 20 years4,5.
Serological tests are widely used to diagnose hydatid cysts. However, positive serological results do not confirm, nor negative results exclude the disease1,6. The imaging features of hydatid cysts are well described in the literature. Ultrasound scans are a sensitive, safe, non-invasive method. It is the procedure of choice for the diagnosis of cysts with a “honeycomb” pattern (type 3), as observed in our patient. Gharbi’s classification provides morphological description on ultrasound. Type 1-pure fluid collection, type 2-fluid collection with split wall (floating membrane), type 3-fluid collection with septa, type 4-heterogenous echographic pattern, type 5-reflecting thick walls.
As seen in our case the cyst fluid appears anechoic at USS, yields an attenuation value of 3-30HU at CT. Calcifications in the cyst wall as in our case are best detected on CT scans. CT has the advantage of detecting smaller cysts when located outside the liver and sometimes differentiating parasitic from non-parasitic cysts, for follow-up studies during chemotherapy. Other diagnostic means such as fine needle aspiration should be avoided because of dangerous anaphylactic reactions7.
Surgery is the optimal treatment for hydatid cyst. Open cyst evacuation is indicated for gharbi types 4 & 5, posterior cysts, central cysts, more than 3 cysts, large cysts, heavy calcification, infected cysts with above criteria, biliary communication, pulmonary communication and peritoneal rupture. Laparoscopic evacuation is indicated in Gharbi type 1 or 2, anterior cysts, peripheral cysts,1-3 cysts, small cysts, no or minimal calcification. Pericystectomy is complete resection of cyst wall without entering the cyst cavity.
Alternative therapy with non-toxic scolocidal agents or combination chemotherapy using imidazole derivatives, particularly albendazol, has been advocated in the management of patients with recurrence and high risk of contamination8.
Grapefruit (Citrus paradise) is thought to have originated as a cross between the Jamaican sweet orange (Citrus sinensis) and the Indonesian pomelo (Citrus maxima) fruit. It was first bred in Barbados and brought to Florida in 1820s. Subsequently, different mutant and hybrid varieties were developed. Although the white and pink varieties were being popularly consumed, the ruby red variety has become very popular and commercially successful.
The taste is a mixture of the sweetness and tanginess of an orange and the sourness of a citrus fruit. It is a rich source of vitamins C and potassium. It is found to have antioxidant properties due to the presence of lycopene1and an ability to inhibit atherosclerosis due to the presence of pectin2,3. The seed extract is thought to have antimicrobial and antifungal properties.
With good publicity, marketing and coverage by health magazines, grapefruit juice has gained widespread use and in most Western Europe and America it is one of the common fruit juices consumed at breakfast. In the United Kingdom, in terms of fruit juice sales, it ranks second among citrus fruits and the fourth overall.4
Pharmacokinetic effects
The interaction of grapefruit juice with medication was first reported by Bailey et al in 1991 after their accidental discovery of up to four fold increase in the blood levels of filodipine when taken with grapefruit juice5. Further studies have identified similar interactions with more than 85 drugs6. The half life of the effects of grapefruit juice is estimated to be around 12 hours7, but these effects may last from 4 hours to 24 hours8. The effects are more pronounced with regular consumption of grapefruit juice prior to ingestion of the drug and there can be a cumulative increase in drug concentrations with continued grapefruit juice intake7,9.
As little as 200-250ml may be sufficient to induce its effects7,10. Some of the interactions involve medication that have narrow therapeutic window and can therefore cause potent adverse effects such as torsade de pointes, rhabdomyolysis, myelotoxicity, respiratory depression gastrointestinal bleeding, nephrotoxicity and sudden cardiac death.6 There is a lack of awareness among both doctors and patients about its effects and interaction with various medications.
Mechanism of action
These pharmacokinetic interactions with grapefruit juice are more observable in drugs with high first pass metabolism and in those with an innate low oral bioavailability. The oral bioavailability of affected drugs is increased but their half life usually remains unaltered11,12. Grapefruit juice is associated with the inhibition of Cytochrome P450 enzyme system, particularly the CYP3A4 enzyme7. The CYP3A4 enzyme is present both in the liver and intestinal mucosa. Once the drug is taken up by the mucosa, the susceptible drug may be metabolised by the CYP3A4 or pumped back into the intestine lumen by P-glycoprotein. The observed effects of grapefruit juice are thought to be mainly due to the inhibition of intestinal CYP3A4 activity, which leads to decreased first pass metabolism and hence increased bioavailability. This inhibitory action is fairly quick and may be due to the rapid degradation of the enzyme or any decrease in its production from the mRNA. The production of mRNA itself from DNA is not thought to be affected13. The susceptibility varies between individuals depending upon their genetic expression of CYP3A4, the effects being more prominent in those with high small intestinal CYP3A4 content7, 14.
The effect of grapefruit juice on the P-glycoprotein is unclear. The activation of P-glycoprotein pumps the drug back into the intestinal lumen which should reduce bioavailability and similarly the inhibition of P-glycoprotein increases the bioavailability. Some studies suggest that the inhibition of P-glycoprotein is the mechanism responsible for the increased bioavailability of certain drugs like cyclosporine15,16.
The active ingredients responsible for interactions of grapefruit juice with medication are not clearly identified. The compounds exerting this action are thought to be either the flavanoids such as naringin and naringinen17,18,19,20 or the furanocoumarins such as bergamottin and its derivatives21,22,23,24, but there is no clear consensus.
Drug interactions
Table 1 below lists some of the commonly used drugs whose bioavailability is affected by grapefruit juice. Although the best known interactions have been mentioned in the table, there are many other drugs like carvedilol, estrogens, itraconazole, losartan and methyl prednisolone whose bioavailibility is increased by grapefruit juice and the adverse effects are not yet clear.
Table 1: Potential risk of drug interactions with grapefruit juice6, 7,13,25,26,27
Risk of Interaction
Group
Drug
V High
High
Mod
Anaesthetic
Ketamine
+++
Anaesthetic
Alfentanil
++
Fentanyl
++
Antiarrhythmic
Dronedorone
+++
Amiodorone
++
Quinidine
+
Anti-Cancer
Dasatanib
++
Everolimus
++
Nilotinib
++
Pazopanib
++
Sunitinib
++
Vanetanib
++
Antidepressants
Buspirone
++
Sertraline
+
Clomipramine
+
Antiemetic
Domperidone
+++
Antiepileptics
Carbamazapine
++
Anti-HIV
Maraviroc
+++
Ripivirine
++
Anti-infective
Erythromycin
++
Quinine
++
Primaquine
++
Antiplatelet
Clopidogrel
++
Antipsychotics
Pimozide
++
Quetiapine
++
Ziprasidone
++
Benzodiazepines
Midazolam
+
Diazepam
+
Triazolam
+
Ca-channel bolckers
Felodipine
+
Nifedipine
+
Immunosuppressants
Cyclosporin
++
Tacrolimus
++
Sirolimus
++
Opiods
Oxycodone
++
Methadone
++
Statins
Simvastatin
+++
Atorvastatin
++
Urinary Tract
Solifenacin
+
Fesoterodine
+
Darifenacin
+
Tamsulosin
+
Implications on clinical practice
Clinicians should make themselves aware and educate their patients of these potential interactions, keeping in mind the individual variations in susceptibility. This may be particularly important for medications that have a very narrow therapeutic window, medication that have an innate low oral bioavailability and a high first pass metabolism mainly via CYP3A4.
A patient may develop exceptional beneficial effects or equally, significant adverse effects should he start consuming grapefruit juice mid- treatment. Conversely, a drop in efficacy of a drug is also possible, should a patient using grapefruit juice on a regular basis, stops it suddenly.
To achieve steady concentration of the medication and avoid such potential effects, it may be best to advise patients to avoid consuming grapefruit juice if there is a potential of interaction. The half life of the effect of grapefruit juice appears to be around 12 hours and therefore, it is advisable to discontinue grapefruit juice 72 hours prior to starting any drug with potential interactions. 8,9
Due to the prolonged effect of CYP3A4 inhibition which may last up to 24 hours, it is not possible to avoid these interactions by separating the times of drug and grapefruit juice consumption.8,9
There is more research needed to clarify the mechanism of action and to determine the active ingredients. The identification of the active ingredient can allow oral administration of drugs that undergo CYP3A4 mediated high first pass metabolism because of which currently, they can only be given systemically.
In light of the possible increase in bioavailability of specific drugs, although it might be possible for patients to use this to their advantage in reducing the dose of their medication under medical supervision, it is perhaps too early to recommend the use of grapefruit juice as an adjunctive or augmentation strategy.
Post- graduate medical education in the United Kingdom has seen numerous dramatic changes in the last decade, with the introduction of structured training programmes and changes in assessment of skills driven by Modernising Medical Careers.1 Overall these new developments emphasise a competency based curriculum and assessments. Alongside and contingent on these wider changes in medical education, psychiatric trainees have faced major transformations in their membership (MRCPsych) examinations.
The MRCPsych examination was first introduced in 1972, a year after the Royal College of Psychiatrists was founded. There have been various modifications in its structure since its inception but a radical change occurred in the last decade with the introduction of an OSCE in 2003 and the CASC, a modified OSCE in June 2008. The CASC is considered as a high- stakes examination as it is now the only clinical and final examination towards obtaining the membership of the College. The MRCPsych qualification is considered as an indicator of achieving professional competence in the clinical practice of psychiatry and has the main aim of setting a standard that determines whether trainees are suitable to progress to higher specialist training.2 In his commentary to Wallace et al3 , Professor Oyebode describes the aims, advantages and disadvantages of the various assessment methods used in the MRCPsych examination and conclude that the precise assessment of clinical competence is essential.4
Traditionally, assessment of clinical skills involved a long case examination since it was introduced in clinical graduating examination by Professor Sir George Paget at Cambridge, UK in 1842. This has been followed by most of the medical institutions worldwide and remained as the clinical component of the MRCPsych examination until 2003. There are some shortcomings with this assessment method and the outcome can be influenced by several factors such as varying difficulty of the cases, co-operation of the real patient and examiner- related factors. The reliability of assessment of clinical competency with a single long case is low and it is necessary for the candidate to interview at least ten long cases to attain the reliability required for a high stakes examination like MRCPsych.5 A fair, reliable and valid examination is necessary to overcome these difficulties. The OSCEs proved to be one of the answers to these difficulties.
One important aspect of assessing the validity and acceptability of assessment methods is asking the opinions of examiners and candidates about their experiences and views about the examination once it has been rolled out. As far as the authors are aware there has been one previous published survey of CASC candidates’ views on this method of examination and this was based at a revision course. Whelan et al6 showed that approximately 70% of the candidates did not agree with the statement “there is no longer a need to use real patients in post-graduate clinical psychiatry exams”. In addition, only 50% of the candidates preferred the CASC compared to previous long case and the other 50% remained undecided. This raises doubts about the acceptability of the CASC format and merits further exploration.
Method
We conducted a national on-line survey asking both candidates and examiners about their views on the CASC examination.
Questionnaire development
Two questionnaires (one each for examiners and candidates) based on previously available evidence on this exam format6,7,8 were developed following discussions among the authors.
The final version of the questionnaire for both groups had the same seven questions with a five point Likert scale. It included questions on whether the exam effectively assessed the competency needed for real life practice, whether there was over testing of communication skills, whether feedback was adequate, respondents’ views on validity and reliability of the method and finally whether the clinical examination should revert to the previous style of long case and viva.
Sampling procedure
The examiners and the candidates who have already appeared in the CASC examination were invited to complete the online survey. The links to the questionnaires were distributed via the Schools of Psychiatry in thirteen deaneries in the United Kingdom (including Wales, Northern Ireland and Scotland). We approached 400 candidates and 100 examiners from different deaneries making sure the wide geographical distribution. The sample size was chosen based on the data that around 500 candidates appear in CASC exam each time and there are approximately 431 examiners on CASC board (personal contact with the College).Participants were assured that their responses were confidential. The survey was open from mid-March to mid-April 2011. Reminders were sent half way through the survey period.
Results
A total of 110 candidates and 22 examiners completed the survey. The response rate was better for candidates (27.5%) compared to the examiners (22%). Albeit the low response rate, the responses showed good geographical spread. Responses were received from most of the deaneries (87%). The London, East and West Midlands deaneries showed higher response rate (14% each) while Scotland, Severn and North Western deaneries showed least response rate (2% each).
Among the 110 candidates, 52% were males and 48% were females and among the examiners, 73% were males and 27% were females. 55% of the examiners were involved in the previous Part 2 clinical exam while only 7% of the candidates had the experience of previous Part 2 clinical exam. The results are summarised in Tables 1 and 2.
Table 1. Candidates’ views ( n= 110 )
Survey questions
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
CASC examines the required competencies to progress to higher training
10%
38%
7%
26%
19%
CASC examines all skills and competencies compared to previous Part 2 clinical exam
4%
11%
46%
21%
18%
CASC scenarios reflects the real life situations faced in clinical practice
12%
36%
13%
22%
17%
CASC gives more emphasis on testing communication and interviewing skills than overall competencies
29%
31%
14%
19%
7%
CASC is more valid and reliable as a clinical exam
9%
19%
29%
20%
23%
Feedback system ‘areas of concern’ are helpful to the unsuccessful candidates
1%
11%
28%
26%
34%
CASC needs to be replaced by traditional style of exam – a long case and a viva
14%
22%
25%
24%
15%
Table 2. Examiners’ views ( n= 22 )
Survey questions
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
CASC examines the required competencies to progress to higher training
14%
45%
14%
18%
9%
CASC examines all skills and competencies compared to previous Part 2 clinical exam
4%
14%
23%
45%
14%
CASC scenarios reflects the real life situations faced in clinical practice
14%
63%
5%
9%
9%
CASC gives more emphasis on testing communication and interviewing skills than overall competencies
22%
26%
17%
22%
13%
CASC is more valid and reliable as a clinical exam
9%
37%
27%
9%
18%
Feedback system ‘areas of concern’ are helpful to the unsuccessful candidates
0%
36%
14%
27%
23%
CASC needs to be replaced by traditional style of exam – a long case and a viva
18%
14%
41%
9%
18%
Clinical competencies and skills
59% of the examiners and 48% of the candidates have accepted that CASC examines the required competencies to progress to higher training. Strikingly only 18% of the examiners and 15% of the candidates agreed that CASC allows the assessment of all the skills and competencies necessary for the higher trainees in comparison to the previous Part 2 clinical exam.
Content of the CASC
Majority of the examiners (77%) and nearly half of the candidates (48%) agreed that CASC scenarios reflect real life situations faced by clinicians in normal practice. However 60% of the candidates and 48% of the examiners felt that CASC excessively emphasizes communication and interview skills.
Feedback - “areas of concerns”
More than half of the candidates (60%) and half of the examiners (50%) felt that the feedback indicating “areas of concerns”, for the failed candidates was not helpful to improve their preparations before the next attempt.
Validity and reliability of the CASC as a clinical exam
Just over one fourth of the candidates (28%) and less than half of examiners (46%) considered CASC as a valid and reliable method of clinical examination. However, only 36% of the candidates and 32% of the examiners supported replacing CASC with a traditional clinical exam (a long case and a viva). Broadly comparable numbers (39% of the candidates and 27% of the examiners) disagreed with the statement that the CASC should be replaced by the previous examination style.
Discussion
To our knowledge this is the first study of candidate and examiner views since the introduction of the CASC. Its predecessor OSCEs has a good reliability and validity in assessing medical students8 and it has become a standard assessment method in undergraduate examinations. Whilst OSCEs have been held to be reliable and valid in a number of assessment scenarios,8 there have been doubts about their ability to assess advanced psychiatric skills,9 which was one of the main reasons to retain the long case in MRCPsych Part 2 clinical exam.2 Over the years, most of the Royal Colleges introduced OSCEs into their membership examinations and used simulated patients in some scenarios. However CASC is the first examination with only simulated patients in a combination of paired and unpaired stations. So far there has been no published literature evaluating this method systematically.
In a recent debate paper10 it has been argued that CASC may have significant problems related to its authenticity, validity and acceptability. The findings of our survey reflect similar doubts about the reliability and validity of the CASC exam amongst both the candidates and examiners. The content validity of CASC has been demonstrated by the College Blueprint11 and the face validity appears to be good. However, as far as we are aware, the concurrent and predictive validity testing data have not been published. Although the global marking system appears to have better concurrent validity than other checklists, it gives the examiners the similar flexibility as the long case in making judgements which may affect CASC transparency and fairness. This may indicate that this new and promising examination method requires further systematic evaluations and modifications before its user’s fully accept it.
According to the results of our study the content of the CASC exam satisfies its purpose of assessing the candidates’ competencies to progress to the higher professional training. However many of the respondents felt that it lacked the completeness of previous traditional clinical examination, which collate skills. Although there were some differences between the candidates and the examiners on how they perceived the CASC exam, most of the respondents agreed that CASC laid more emphasis on communication and interviewing skills rather than overall assessment of the candidate’s competency.
Harden et al,12 in their paper on OSCEs, criticised the compartmentalisation of knowledge and discouraging candidates from a broader thinking during the clinical examinations. They also suggested using a long case and/or workplace based assessments rather than relying on OSCEs only in assessing trainees. Benning & Broadhurst13 expressed similar concerns on the loss of long case in MRCPsych examination. Our findings support the arguments that CASC assesses competencies in a piecemeal fashion rather than being reflective of the demands on senior doctors in real practice which often involve deciding what is and is not important depending on context.
The OSLER14 (Objective Structured Long Examination Record) method might overcome the shortcomings and improve the objectivity and transparency of long case. In this method, two examiners assess the candidate and grade their skills individually in a ten item objective record. Later they decide together the appropriate grade for each item and agree an overall grade. The ten items include four on history, three on examination and another three covering investigations, management and clinical acumen. The OSLER method is also practical as no extra assessment time is required and it can be used for both norm referenced & criterion referenced exams. The case difficulty can be determined by the examiners and all candidates are assessed for identical items. Thus this method assesses the candidate’s overall clinical competency and eliminates the subjectivity associated with the long case.
Another alternative might be using a combination of assessment methods as suggested by Harden.12 An 8-10 stations OSCE can be combined with a long case assessment using OSLER method. The OSCE stations might include patient management scenarios along with interview and communication skills scenarios. The final score determining the result could also include marks from work place based assessments as they provide a clear indication of the candidate’s skills and competence in real life situation.
It is also evident from our findings that both candidates and examiners are largely unsatisfied with the extent and usefulness of feedback that is provided to unsuccessful candidates. The feedback system have been criticised for its inability to clarify the specific areas or skills which need to be improved by the unsuccessful candidates. The recent “MRCPsych Cumulative Results Report’’ 15 states that the pass rate of the candidates declines after the first attempt. Perhaps this could be improved if failed candidates receive more detailed feedback about their performance.
There are a number of limitations to this study. The response rate was low but it was broadly in the range of other online surveys16 and there was representation from most of the deaneries in the United Kingdom. There could be a number of reasons for low response rate. As far as we are aware few deaneries were not willing to distribute the questionnaire through their School of Psychiatry and we had to contact the individual trusts in the area to distribute the survey. The poor response rate from the examiners could be because of their low interests in participating and lack of time. Also older examiners and those with more experience of CASC may have had particular views which might have had an influence on the responses. But when this was examined further, there were no major differences between respondents who had the experience of previous Part 2 examinations from those who had not. In addition one of the survey questions consisted of two parts (views on validity and reliability) which could have been difficult to answer accurately.
The findings of this preliminary study raise some doubts on acceptability of the CASC by both candidates and examiners. There might be a possibility of subjective bias in the responders’ views, perhaps influenced by other ongoing and controversial changes in the NHS, including the role of GMC and the College in the post- graduate medical education. However on the other hand it might be a signal that it is worthwhile to reconsider the implications of the CASC on education and training and to evaluate systematically this assessment method further.
Diffuse Alveolar Haemorrhage (DAH) is a rare but serious and frequently life-threatening complication of a variety of conditions. DAH refers to a clinical syndrome resulting from injury to the alveolar capillaries, arterioles, and venules leading to red blood cell accumulation in the distal air spaces because of leakage of alveolar capillaries. Most cases of DAH are caused by capillaritis associated with systemic autoimmune diseases such as ANCA-associated vasculitis, anti-GBM disease, and systemic lupus erythematosus.1 Treatment is with immunosuppressants for patients with autoimmune causes and respiratory support if needed.
Diffuse alveolar haemorrhage syndrome is not a specific entity but is a syndrome that suggests a differential diagnosis and a specific sequence of testing.
Aetiology
Many disorders can cause alveolar haemorrhage; they include
Coagulation disorders caused by diseases or anticoagulant drugs
Isolated pauci-immune pulmonary capillaritis
Idiopathic pulmonary haemosiderosis
Bone marrow or solid organ transplantation.
Clinical Presentation
The clinical presentation of diffuse alveolar haemorrhage may reflect either alveolar bleeding alone or features of the underlying cause (e.g., haematuria in Wegener granulomatosis, arthritis in systemic lupus erythematosus). Hence, its recognition requires a high degree of suspicion. Some patients present with severe acute respiratory distress requiring mechanical ventilation. However, dyspnoea, cough, and fever are the common initial symptoms and are most often acute or subacute (i.e., present for less than a week). The fever is usually due to the underlying cause, such as lupus. Haemoptysis may be absent at the time of presentation in up to a third of patients because the total alveolar volume is large and can absorb large amounts of blood, without extending more proximally into the airways. Apparent haemoptysis, if present, must be differentiated from haematemesis or pseudohaemoptysis (alveolar flooding with fluid that resembles blood, as in Serratia marcescens pneumonia, in which the reddish hue of the infecting organism can create the impression of alveolar bleeding).
Chest X-ray and Chest CT scan typically shows bilateral infiltrates (figure 1 &2)
Figure 1
Figure 2
DAH & ANCA associated vasculitides
Wegener's Granulomatosis (WG) is an uncommon disease that affects about 1 in 20,000 to 1 in 30,000 people. WG is defined by the triad of granulomatous inflammation of the respiratory tract, vasculitis of small to medium-size vessels and necrotizing glomerulonephritis. The onset of WG may be indolent with few symptoms, or it may have a rapid and severe onset. About 90% of patients have symptoms of a cold or runny nose or sinusitis that fail to respond to the usual therapeutic measures and last considerably longer than the usual upper respiratory tract infection. Other symptoms include nasal membrane ulcerations and crusting, saddle-nose deformity, inflammation of the ear with hearing problems, inflammation of the eye with sight problems, cough (with or without the presence of blood), pleuritis, (inflammation of the lining of the lung), rash and/or skin sores, fever, lethargy weakness, loss of appetite, weight loss, arthritic joint pain, night sweats, and haematuria which may or may not be indicated by a change in urine colour.Thediagnosis of WG depends on the combination of clinical presentation, serological markers, and histopathological findings. ANCA is a sensitive and specific marker for ANCA-associated systemic vasculitis. In a study done by U. Schönermarck et al,9 624 ANCA- positive patients were included, (C-ANCA: 333, P-ANCA: 291). C-ANCA were highly sensitive (81%) and specific (99.5%) for WG, resulting in high positive predictive value (PPV) (94%). Many studies showed that combining proteinase 3 (PR3) and C-ANCA results(C-ANCA/PR3) increases specificity and Positive Predictive Value close to 100%, but reduces sensitivity close to 70%.10,11,13,14 In summary, the presence of C-ANCA & PR3 antibody is highly suggestive of WG. This led to reevaluation of the role of biopsy for diagnosis of WG in multiple studies.4, 14, 15
The site of biopsy is dependent upon the clinical status. A nasal or sinus biopsy may be the least invasive way to diagnose WG. Renal biopsy is helpful if there is evidence of renal insufficiency or glomerulonephritis. A lung biopsy should only be considered if potentially diagnostic tissue cannot be obtained from any other site.1 Hoffman et al performed a total of 82 open lung biopsies in patients with small vessel vasculitis of which 89% showed evidence of combined vasculitis and necrosis, granulomas and necrosis were found in 90%.16 59 transbronchial biopsies were performed in 48 patients and only four specimens had evidence of vasculitis and granulomas were identified in an additional three. Thus, the role of transbronchial biopsies in these patients is limited and open lung biopsies are more informative but carry a higher morbidity and mortality.
The incidence of DAH has beenreported as between 7-45% in Wegner’s Granulomatosis (WG), and 10-30% in Microscopic Polyangitis (MPA).3, 5, 6 The lungs are the most commonly affected organ in WG with evidence of involvement in over 90% of patients during the course of their disease; in 9% it is the only organ affected. 5,7 In MPA lung involvement is less common than inWG, and occurs in up to 50% of cases during the course of the disease.8 Pulmonary involvement ranges from subclinical changes on high resolution computed tomography to devastating haemoptysis. Approximately 5% of patients will have a fulminant presentation requiring assisted ventilation.
Treatment
Patients with DAH with or without glomerulonephritis, who are found to have ANCA positive can be generally assumed to have WG or MPA. The type of ANCA (PR3-ANCA or MPO-ANCA) found is irrelevant with respect to the initial management of this patients.1 The backbone of therapy is the early identification of disease followed by the rapid induction of disease control with immunosuppression. Early recognition is crucial, because the prompt institution of supportive measures and immunosuppressive therapy is required for survival. The intensity of the initial treatment depends on the severity of the disease. Based on the European Vasculitis Study Group (EUVAS), which categorized the patients in groups according to the severity of their disease, the presence of DAH put the patient in the severe disease group.17 The management of these patients is a combination of corticosteroid and cyclophospamide. S.L Hogan showed that cyclophosphamide reduces mortality and increase the likelihood of inducing remission in patients with ANCA-associated vasculitis. 18
DAH is animportant cause of morbidity and mortality in ANCA- associated vasculitis, the mortality rate may reach 66%, which is six times greater than vasculitis without alveolar hemorrhage.3,19,20,21 Based on the high mortality rate with DAH in ANCA-associated vasculitis, and reduction in mortality shown with cyclophosphamide, treatment with cyclophosphamide should be started as early as possible, based on the clinical presentation and the presence of ANCA, without waiting histological confirmation.
Conclusion
DAH leading to acute respiratory distress syndrome is a rare and life threatening condition in adults with ANCA positive vasculitis. Patients with DAH with or without glomerulonephritis, who are found to have ANCA positive can be generally assumed to have WG or MPA, and diagnostic lung biopsy may be deferred. Early institution of treatment with prednisone and cyclophosphamide can significantly reduce morbidity and mortality.
Key points
1.Patients with Wegner’s Granulomatosis often present with diffuse alveolar haemorrhage. These patients must be treated promptly as delay in treatment results in high morbidity and mortality.
2.Lung biopsy is very helpful if it shows granulomatous inflammation and vasculitis however it lacks sensitivity and specificity.
3.Detection of C-ANCA with Proteinase-3 can substitute for biopsy in the diagnosis of WG in patients who present with diffuse alveolar haemorrhage.
A 44 year old male presented to the emergency department complaining of shortness of breath. The symptoms had commenced suddenly four weeks ago. He had been breathless at rest, and subsequently developed a productive cough with white sputum. He denied chest pain. He was known to have the sickle cell trait but was otherwise in good health. He was a non-smoker.
Since the onset of symptoms, and prior to this admission, the patient presented to two different emergency departments. The working diagnosis was, and remained, community acquired pneumonia. On initial presentation empirical treatment for a community acquired pneumonia was commenced. Failure to improve resulted in additional cover for atypical organisms and the prescription of a short course of steroids on the subsequent admissions.
Initial observations revealed the patient was tachypnoeic and tachycardic, with a respiratory rate of 25 breaths per minute, heart rate of 114 beats per minute. He was apyrexial (temperature of 36.5°C ). Pulse oximetry showed an oxygen saturation of 94% on room air. His blood pressure was recorded as 183/99 millimetres of mercury.
On examination large volume peripheral pulses, raised jugular venous pressure (5 cm), bi-basal crepitations, and bilateral ankle oedema were elicited/identified. Auscultation of the heart revealed a loud diastolic murmur audible throughout the praecordium.
A 12 lead ECG showed normal sinus rhythm, normal axis and left ventricular hypertrophy. Arterial blood gas analysis on room air showed a pH of 7.46, pa02 9.6 kPa, pCO2 4.3 kPa, HCO3 23.8 mmol/L, BE + 0.8 and lactate of 0.7 mmol/L. Routine venous blood tests did not identify any elevated markers of infection or inflammation. A chest radiograph (Figure 1) showed cardiomegaly and pulmonary oedema.
Figure 1
The patient was administered oxygen and given a diuretic to improve his ventilation.
The working diagnosis was congestive cardiac failure in the presence of what was presumed to be a new murmur. Urgent echocardiography revealed an aortic root of 6.2cm diameter at sinus level, with an evident dissection flap. There was no obvious haematoma. Severe free flowing aortic regurgitation, a dilated hyperdynamic left ventricle and a 0.7 cm diameter pericardial effusion anteriorly were also noted. It was concluded that the patient had a sealed 7cm type A aortic dissection. This was confirmed by a CT scan (Figure 2).
Figure 2
Large bore venous access was obtained and an intravenous beta blocker (Labetalol) administered. Urgent transfer to a tertiary cardio-thoracic surgical centre was made. He underwent aortic root and valve replacement, along with coronary artery bypass grafting to the right coronary artery using a reversed long saphenous vein graft. Postoperatively, he was anticoagulated on Warfarin, and was also placed on beta blockade therapy (Bisoprolol), a diuretic (Frusemide), an ACE inhibitor (Ramipril), and a statin (Simvastatin).
Discussion
Aortic dissection is a medical emergency. If left unrecognised or untreated mortality can be as high as 80% in two weeks, or 90% within three months1,2. 96 % of patients with aortic dissection present primarily with chest pain. The remaining 10% present with symptoms secondary to impairment of blood supply to other organ systems3. Dissections involving the ascending aorta present with retrosternal chest pain, while interscapular pain suggests involvement of the descending aorta. Pleuritic pain may indicate haemorrhage in the pericardial sac, with the potential for acute cardiac tamponade.
Only 6% of aortic dissections present with acute congestive cardiac failure. Patients presenting with aortic dissection and congestive cardiac failure are more likely to present without chest pain and have a valvular abnormality. When chest pain is present, the pain is more often mild and less likely to be abrupt in onset. Patients are less likely to be hypertensive on presentation and more likely to present in shock. These patients are more likely to have Stanford type A dissection . Congestive cardiac failure does lead to a delay in surgical intervention4.
Congestive cardiac failure is usually due to aortic regurgitation from aortic valve disease, incomplete aortic leaflet closure, or aortic valve disruption. In the setting of unexplained cardiac failure aortic dissection should be considered, especially when an aortic regurgitant murmur has been detected clinically. Heart failure has been associated with supravalvular aortic stenosis in the presence of a painless type A dissection, in a patient presenting with persistent cough5. Rupture of aortic dissection into the right atrium, right ventricle, or main pulmonary artery may lead to a left to right shunt and congestive heart failure6.
Painless aortic dissection has been recorded in other contexts, particularly with chronic dissection and in patients with Marfan’s syndrome.The absence of chest pain should not exclude aortic dissection.