



ISSN 1757-8515
Open Mesh Repair Of Different Hernia. Is The Technique Free Of Complications?
Arshad M Malik, Asad Khan, K Altaf Hussain Talpur and Abdul Aziz Laghari
Cite this article as: BJMP 2009: 2(3) 38-41
|
|
Abstract OBJECTIVES: To study mesh related complications in various hernias and their management. |
INTRODUCTION:
Implantation of prosthetic mesh in repair of different hernias has gained a global acceptance and popularity. It is thought to be a potent safeguard against recurrence of hernias 1, 2.The use of prosthetic mesh in different types of hernias has brought a phenomenal change in the out look of hernia patients all over the world 3. Today, an ever increasing number of hernias are repaired by implanting prosthetic meshes either by conventional open method or by laparoscopic approach 4. Beside its well known advantages and global acceptance in every day hernia surgery, a number of complications are thought to be associated with the use of mesh in different types of hernias 5-15. We present our experience of mesh related complications in different open hernia repairs and their management in this study. MARERIALS AND METHODS It’s a descriptive observational study over 5 years during which a total number of 1008 patients with different types of hernias were repaired electively in a teaching hospital as well as in private hospitals by the same surgical team. Of these, 638 (63.29 %) hernias were repaired by implanting prolene mesh of different sizes depending on the size of the defect. A drain was left in place in selected cases .The patients were followed up to a period of three years after discharge from the hospital. The follow up visits were scheduled at 1 month, 6 months, and then yearly. Of the total patients , 432(67.71%) were followed up to three years while 159 (26%) patients were lost in the follow up from day of discharge from the hospital. Another 47 patients attended follow up up to 2 years only and then disappeared. Sixteen of these patients continued to complain about chronic pain and foreign body sensation up to two years and then they did not return while 4 of these patients developed recurrent hernia in one year time but they were lost in follow up. The data of every patient is recorded on a proforma and their follow up records are maintained. The variables studied included immediate, early and late post-operative complications in addition to the demographic details. The statistical analysis of the data is done on SPSS version 12. RESULTS The mean age of the patients is 41 years with a range of 73 years and a STD of 19.089. There is a male dominance (N=531, 83%) over females (N=107, 17 %). The commonest type of hernia in this series is inguinal hernia (n=518, 81%) followed by Para-umbilical hernia (n=83, 13 %). Distribution of different varieties of hernias among male and female study population is shown inTable-I. Table-1. Frequency of hernias and distribution among males and females
| Type of hernia | Total | ||||
| Inguinal | Para- umbilical | Incisional | Epigastric | ||
| Male | 518 | 4 | 3 | 6 | 531 |
| Female | 0 | 79 | 26 | 2 | 107 |
| Total | 518 | 83 | 29 | 8 | 638 |
Of the total number, 34 (5 %) hernias were recurrent hernias including 21 inguinal hernias, 11 Para-umbilical hernias and 2 Incisional hernias. The patients were operated after preliminary investigations and medical fitness. All the patients were operated by open conventional technique regardless of the type of hernia. Total duration of operation is shown in Figure -I with maximum patients (467, 73%) operated with in 60 minutes. 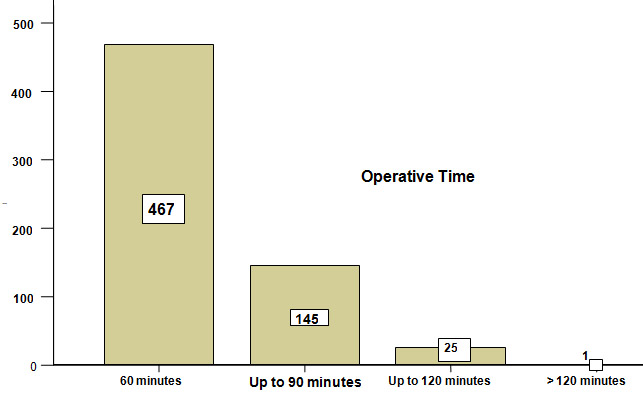 Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation
Figure-I. Total duration of operation: Various early complications during the same admission occurred in 9 % (n=55) of the patients. Their distribution according to the type of hernia is displayed inTable- II. Table-II Type of hernia * Complications during same hospitalization Cross tabulation
| Type of hernia | Complications during same hospitalization | Total | ||||||
| Wound infection | Reaction | Mechanical failure | Seroma | Pain | Mesh infection | Hematoma | ||
| Inguinal | 14 | 3 | 4 | 7 | 1 | 1 | 3 | 518 |
| paraumbilical | 5 | 1 | 2 | 3 | 0 | 3 | 3 | 83 |
| Incisional | 0 | 0 | 0 | 1 | 0 | 2 | 1 | 29 |
| Epigastric | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 8 |
| Total | 19 | 4 | 6 | 11 | 1 | 7 | 7 | 638 |
Wound infection has an alarmingly high incidence in our series (n=19, 3 %). Most of these infections are superficial and effectively controlled by intensive antibiotic therapy so that the failure of repair is saved and mesh rejection prevented effectively. Four of recurrences occurred during 2 years follow up but patient discontinued follow up afterwards. Remaining 07 recurrences occurred between 24 to 36 weeks. The complications observed during the follow up period of up to three years in different hernias are shown in Table-III. Table-III Type of hernia * Late Complications after discharge Cross tabulation
| Complications after discharge | Total | ||||
| Type of hernia | Pain | Recurrence of hernia | Thickening of spermatic cord | Testicular atrophy | |
| Inguinal | 10 | 4 | 7 | 2 | 518 |
| paraumbilical | 2 | 7 | 2 | 0 | 83 |
| Incisional | 2 | 0 | 0 | 0 | 29 |
| Epigastric | 1 | 0 | 0 | 0 | 8 |
| Total | 15 | 11 | 9 | 2 | 638 |
A remarkably low incidence of wound infection in para-umbilical and incisional hernia is attributable to the placement of suction drain which prevents hematoma formation and secondary infection. Seven (2%) recurrences occurred in para-umbilical hernias where suction drain did not work. Mesh infection with massive reaction , although, treated conservatively in 5 patients with vigorous antibiotic therapy led to the formation of a weaker scar which later on gave way and recurrence of hernia occurred. Follow up was not 100% and about 26% patients were lost in the follow up. Majority of the patients (n=457, 90 %) were discharged within 4 days while patients who were complicated had a longer stay up to 15 days (P <0.001). Late complications were mostly chronic pain and foreign body sensations with 2 cases of unilateral testicular atrophy. DISCUSSION A number of non-infectious and infectious complications are attributed to the use of mesh in the repair of most of the hernias5, 13, 16. The type of mesh as well as their composition seems to affect complications following their use and specific materials are related to specific complications. We present 638 patients of different types of hernias repaired by implanting polypropylene mesh of varying sizes depending upon the size of defect. Prolene meshes are monofilaments, non-absorbable, inert, sterile and porous synthetic materials commonly used for this purpose. The use of mesh in hernia repair has brought a phenomenal change in the overall outcome of hernia repair especially in terms of recurrence of hernia 17. We experienced wound infection as the commonest complication in our series (n=19, 3%) and this was more so in the inguinal hernias. Most of the wound infections are superficial and very easy to control on conservative measures. On the contrary deep seated mesh infections are always dreaded complications and if not treated vigorously can lead to total failure and rejection of prosthetic mesh. A number of similar studies have reported an increased infection rate in mesh hernia repair testifying our results 18-28. Grant AM 29, however claims no difference in the incidence of infection between mesh and non-mesh repair of groin hernias. A severe local reaction occurred in 4 (0.62%) patients which resolved in few days without any consequences. Seroma and hematoma occurred in 11(2 %) and 7(1.09%) patients respectively. Only 3 seromas and one hematoma needed evacuation. We report a recurrence of 11(2 %) hernias of which 4 are inguinal and 7 are para-umbilical hernias. All of the recurrent para-umbilical hernias had severe reaction and wound infection in the post-operative period which was effectively controlled by vigorous antibiotic therapy and local wound care. There is probably a weaker scar after resolution of the infective process which resulted in recurrence. A significantly low recurrence rate in inguinal hernias in our study (0.77%) is consistent with the results of other similar reports 30-32. Chronic pain and a foreign body sensation poses a real problem and though it occurred in only two cases but a similar study by Bay-Nielsen M 33 claims 22.9% study population having chronic pain and more so in the adult males. CONCLUSION Although mesh repair is an efficient method of hernia repair, a number of complications may be associated and can lead to failure. An aggressive antibiotic therapy and wound care may control even massive infections.
|
Author Details <p>ARSHA M MALIK Assistant Professor Surgery, Liaquat University Of Medical and Health Sciences Jamshoro, Pakistan.<br /> ASAD KHAN Post-graduate student (Surgery), Liaquat University Of Medical and Health Sciences, Jamshoro.<br /> K ALTAF HUSSAIN TALPUR Associate Professor Surgery, ,Liaquat University Of Medical and Health Sciences Jamshoro, Pakistan.<br /> ABDUL AZIZ LAGHARI Associate Professor Surgery,Liaquat University Of Medical and Health Sciences, Jamshoro Pakistan.</p> CORRESPONDENCE: ARSHAD M MALIK, Assistant Professor, Department of Surgery, Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan Email: arshadhamzapk@yahoo.com |
References
1. Sanjay P, Reid TD, Davies EL, Arumugam PJ, Woodward A.Retrospective comparison of mesh and suture repair for adult umbilical hernias. Hernia 2005; 9(3):248-51.
2. Cobb WS, Kerchief KW, Heniford BT. The argument for light weight polypropylene mesh in hernia repair.Surg innov,2005;12(1):63-9.3. DeBord JR. The historical development of prosthetics in hernia surgery. Surg Clin North Am 1998; 78:973-1006.4. Liem MSL, Van Der Graaf Y,Van Steensel CJ et al.Comparision of conventional anterior surgery and laparoscopic surgery for inguinal hernia repair.N Eng J Med 1997;336:1541-7.5. Bliziotis IA, Kasiakou SK, Kapaskelis AM, Falagas ME. Mesh-related infection after hernia repair: Case report of an emerging type of foreign – body related infection. Infection 2006;34(1):16. Chowbey PK, Bagchi N, Goel A, Sharma A, Khullar R, Sonni V, Baijal M.Mesh migration into the bladder after TEP repair: a rare case report. Surg Lapros Endosc Percutan Tech 2006; 16(5):377-8.7. Delikoukos S, Tzovaras G, Liakou P, Mantzos F, Hatzetheofilou C. Late-onset deep mesh infection after inguinal hernia repair. Hernia 2007; 11(1):15-17.8. Hoefkens MF, Vles WJ. A giant pseudocyst following repair of an incisional hernia by a propylene mesh. Ned Tijdschr Geneeskd 2008; 26; 152(4):216-20.9. Celdran A, Esteban j, Manas j, Grazino JJ. Wound infections due to Mycobacterium Fortuitum after polypropylene mesh inguinal hernia repair. J Hosp Infect 2007; 66(4):374-77.10. Singh-Ranger D, Taneja T, Sroden P, Peters J. A rare complication following laparoscopic TEP repair: Case report and discussion of literature. Hernia 2007; 11(5):453-56.11. Bendavid R. complications of groin hernia surgery.Surg Clin North Am 1998; 78:1089-103.12. Robinson TN, Clarke JH, Schoen J, Walsh MD. Major mesh related complications following hernia repair: events reported to the Food and Drug Administration. Surg endosc 2005; 19(12):1556-60.13. White TJ, Santos MC, Thompson JS. Factors affecting wound complications repair of ventral hernias. Am Surg 1998; 64(3):276-80.14. Sohail MR, Smilac JD. Hernia repair mesh –associatedMycobacterium goodie infection. J Clin Microbiol 2004; 42(6):2858-60.15. Delikoukos S, Fafoulakis F, Christodoulidis G, Theodorpoulos T, Hatzitheofilou C. Re-operation due to severe late-onset persisting groin pain following anterior inguinal hernia repair with mesh. Hernia 2008 ;{ Epub ahead of print}.16. Leber GE, Grab JL, Alexander AI, Reed WP. Long –term complications associated with prosthetic repair of Incisional hernias. Arch Surg.1998; 133(4):378-82.17. Ove H, Kumar A. Complications of Incisional hernia repair: Delaminated mesh with incarcerated hernia.ANZJ Surg 2004; 74:705-6.18. Furtschegger A, Sandbichler P, Judmaier W, Gstir H, Steiner E, Egender G. Sonography in the post-operative evaluation of laparoscopic inguinal hernia repair.J Ultrasound Med 1995;14:679-84.19. Stoppa RE. The treatment of complicated groin and Incisional hernias .World J Surg 1989;13(5):54520. Lujendijk RW, Hop WC, van den Tol MP, de Lange DC, Braaksma MM, Ijzemans JN et al.A comparison of suture repair with mesh repair for Incisional hernia.N Engl J Med 2000;343(6):392-398.21. Cappelletti M, Attolini G, Cangioni G, Mascherini G, Taddeucci S, Gervino L. [The use of mesh in abdominal wall defects] Minerva Chir1999; 52(10):1169-76.22. Van’t Riet M, de Vos van steenwijk PJ, Bonger HJ, Steyerberg EW, Jeekel J.Mesh repair for post-operative wound dehiscence in the presence of infection: is absorbable mesh safer than non-absorbable mesh? Hernia 2007; 11(5):409-13.23. Falagas ME, Kasialkou SK.Mesh-related infections after hernia repair surgery. Clinic Microbio and infection 2004; 11(1):3-8.24. Yerdel ,Mehmet A,Akin, Emin B, Dolalan ,Surku,Turkcapar, Ahmet G,et al.Effect of single dose prophylactic Ampicillin and Sulbactam on wound infection after tension free inguinal repair with polypropylene mesh: The randomized double-blind ,prospective trials. Annals of surgery 2001; 233(1):26-33.25. Geoffrey E, Leber, Jane L, Garb, Alexender, William P, Reed.Long term complications associated with prosthetic repair of Incisional hernias. Arch surg 1998; 133:378-382.26. Farrow B, Awad S, Berger DH, Albo D, Lee L, Subramanian A, Bellows CF. More than 150 consecutive open umbilical hernia repairs in a major veteran administration medical centre.Am J Surg 2008;196(5):647-51.27. Cingi A; Manukyan MN; Gulluoglu BM; Barlas A; Yegen C; Yalin R; Yilmaz N; Aktan AO. Use of resterilized polypropylene mesh in inguinal hernia repair: a prospective, randomized study. J Am Coll Surg. 2005; 201(6):834-40.28. Terzi C; Kilic D; Unek T; Hosgorler F; Fuzun M; Ergor G. Single-dose oral ciprofloxacin compared with single-dose intravenous cefazolin for prophylaxis in inguinal hernia repair: a controlled randomized clinical study. J Hosp Infect. 2005; 60(4):340-7.29. Grant AM. Open mesh versus non-mesh repair of groin hernia: meta-analysis of randomized trials based on individual patient data [corrected]. Hernia. 2002; 6(3):130-6.30. Kurzer M, Belsham PA, Kark AE.The Lichtenstein repair. Surg Clin North Am 1998; 78:1025-46.31. Amid PK, Shulman AG, Lichtenstein IL, Simultaneous repair of bilateral inguinal hernias under local anesthesia. Ann Surg 1996; 223:249-52.32. Scott NW, Mc Cormacmok K, Graham P, Go PM, Ross SJ, Grant AM. Open mesh versus non-mesh for repair of femoral and inguinal hernia. Cochrane database syst Rev 2002 ;( 4):CD002197.33. BAY-NIELSEN M. (1) ; NILSSON E. (2) ; NORDIN P. (2) ; KEHLET H. Chronic pain after open mesh and sutured repair of indirect inguinal hernia in young males. Br j surg 2004. 91: 1372-1376.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.