



ISSN 1757-8515
The Hoffa Fracture: a case report
SKM Annamalai, JR Berstock and MN Shannon
Cite this article as: BJMP 2008:1(2) 36-37
|
ABSTRACT
We report a case of the rare coronal unicondylar fracture of the distal femur called Hoffa fracture. Hoffa fracture is a rare injury consisting of unicondylar tangential posterior fracture of the distal femur. These fractures are due to high energy trauma and sometime not easy to visualise on routine imaging, and therefore could represent a diagnostic challenge to the accident department and to the orthopaedics surgeon. Clinically however, our patient had obvious knee swelling, localised tenderness and was unable to weight bear. Plain radiograph and CT scan confirmed the fracture and was treated surgically with cancellous screws.
Case Presentation
A thirty-four year old male injured his left knee whilst turning on a motocross bike. He put his left leg on to the ground with his knee in 20 degrees of flexion to stabilise himself whilst turning a left hand corner at about 30 mph. He did not crash, but was unable to weight bear afterwards.
The initial AP and lateral radiographs showed a coronal fracture of lateral condyle of the distal femur.


[FIG 1: AP radiograph right knee / Lateral radiograph right knee].
This fracture could have been easily missed on the plain radiograph. Further imaging with the CT scan confirmed the fracture and its pattern.


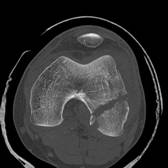
[FIG2: Axial CT of distal femur / Saggital CT of distal femur].
He had an open reduction and internal fixation via a lateral approach, vastus lateralis was reflected off the lateral intermuscular septum and the knee joint opened. Maintaining the knee flexed during the surgery relaxes the posterior capsule, gastrocnemius and protects the neurovascular structures. Soft tissue attachments of the fractured fragment constitute the sole source of blood supply and must be preserved. The joint was carefully inspected for associated injuries. After reduction the fragments were temporarily fixed with Kirschner wires. Partially threaded cancellous screws were used in the lag mode to secure compression across the fracture.

FIG3: Image Intensifier of ORIF with cancellous screw]
Discussion
This fracture pattern was initially described by Hoffa in 1904 1 hence the name for this fracture. The Hoffa fracture is an intra-articular fracture of the knee analogous to the capitellum fracture of the elbow 2. This injury is the result of violent force and generally occurs in young adults. There is usually a combination of forces: direct trauma, possibly with an element of abduction, the ground reaction is transmitted through the tibial plateau and the axial compression on a flexed knee concentrates the force in the posterior half of the femoral condyles1. In flexion the lateral condyle is the leading part of the knee to receive the impact1. Although the Hoffa fracture may be of either condyle4 the preponderance of lateral condylar fractures suggests an anatomic-biomechanical vulnerability due to the physiological valgus.
Few cases have been reported in literature with associated femoral shaft fracture 6, ligament entrapment with irreducible knee dislocation5, open and bicondylar fractures7. Our case is unique as it is a closed injury, uniconylar fracture with no associated ligamentous or meniscal disruptions. Open reduction has been shown to be mandatory for good long-term function 2, 3. High index of suspicion, further imaging with CT scan / 3D reconstruction, open reduction and internal fixation is necessary for good outcome following these types of fractures.
|
Competing Interests None Declared Author Details SURESH KM ANNAMALAI, MBBS, MRCS. Registrar in Orthopaedics, Weston General Hospital, United Kingdom JR BERSTOCK, MBBCh, Senior House Officer in Orthopaedics, Weston General Hospital, United Kingdom MN SHANNON, FRCS(South Africa, Ortho), Consultant Orthopaedic Surgeon, Weston General Hospital, United Kingdom CORRESPONDENCE: SURESH KM ANNAMALAI, Registrar in Orthopaedics, Department of Orthopaedics, Weston Area Healthcare Trust, Weston General Hospital, Grange Road South, Uphill, Weston Super Mare, BS23 4TQ Tel: 01937 636363 Email: sureshkumar.annamalai@gmail.com |
References
1. Hoffa A: Lehrbuch der Frakturen und Luxationen.4th ed.Stuttgart: Ferdinand Enke-Verlag 1904, 453.
2. Lewis SL, Pozo JL, Muirhead-Allwood WFG: Coronal fractures of the lateral femoral condyle. Journal of Bone and Joint Surgery (Br) 1989, 71:118–120.
3. Ostermann PAW, Neumann K, Ekkernkamp A, Muhr G. Long-term results of unicondylar fractures of the femur. Journal of Orthopaedics and Trauma 1994, 8(2):142–146.
4. Heuschen UA, Göhring U, Meeder PJ Bilateral Hoffa fracture--a rarity. Aktuelle Traumatol 1994 May; 24(3):83-6.
5. Shetty GM, Wang JH, Kim SK, Park JH, Park JW, Kim JG, Ahn JH Incarcerated Patellar tendon in Hoffa fracture: an unusual cause of irreducible knee dislocation Knee Surg Sports Traumatol Arthrosc. 2007 Oct 24
6. Miyamoto R, Fornari E, Tejwani NC. Hoffa fragment associated with a femora shaft fracture. A case report J Bone Joint Surg Am. 2006 Oct; 88(10):2270-4.
7. Calmet J, Mellado JM, García Forcada IL, Giné J. Open bicondylar Hoffa fracture associated with extensor mechanism injury. J Orthop Trauma. 2004 May-Jun; 18(5):323-5.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.