Lung carcinoma the most common malignancy worldwide, presents as a metastatic disease in majority of the cases. The most frequent sites of distant metastases are liver, adrenal glands, bones, and brain. Skeletal muscle metastasis is an unusual presentation of lung adenocarcinoma.
Case report
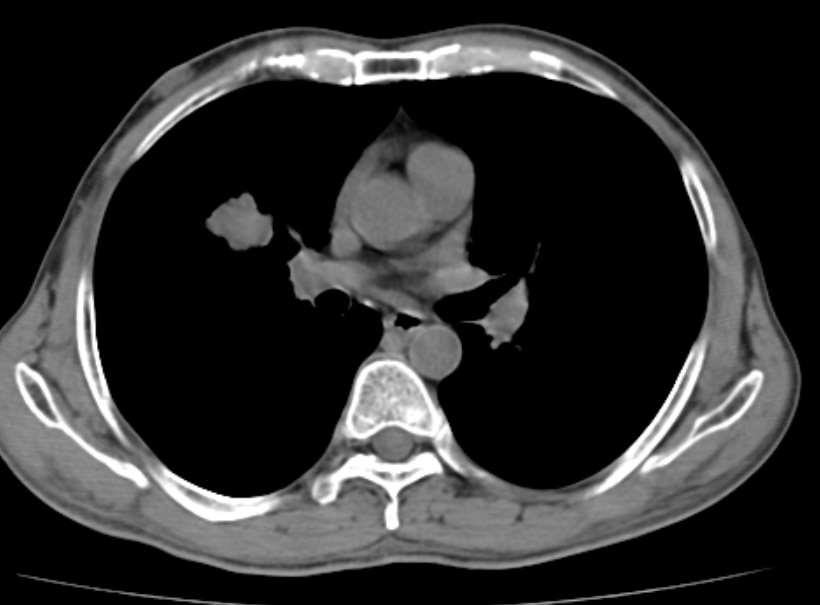
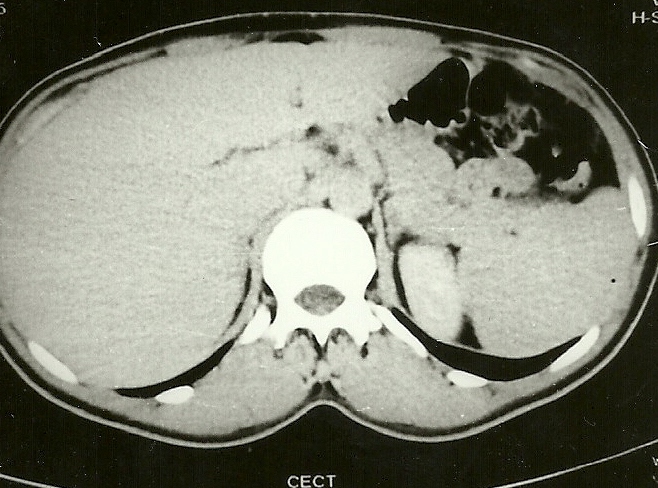
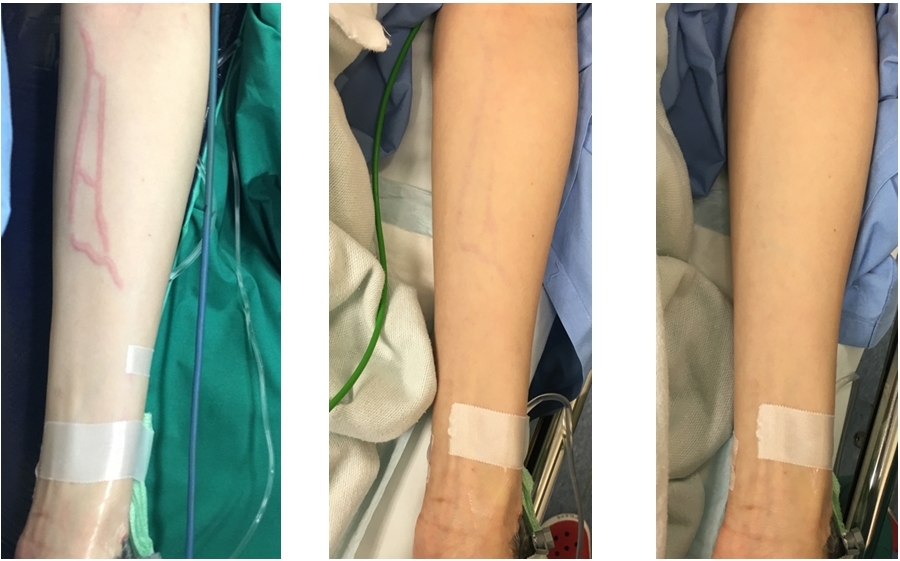
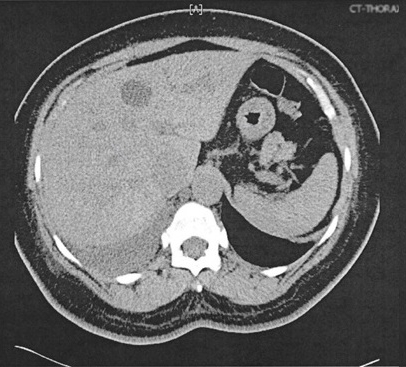
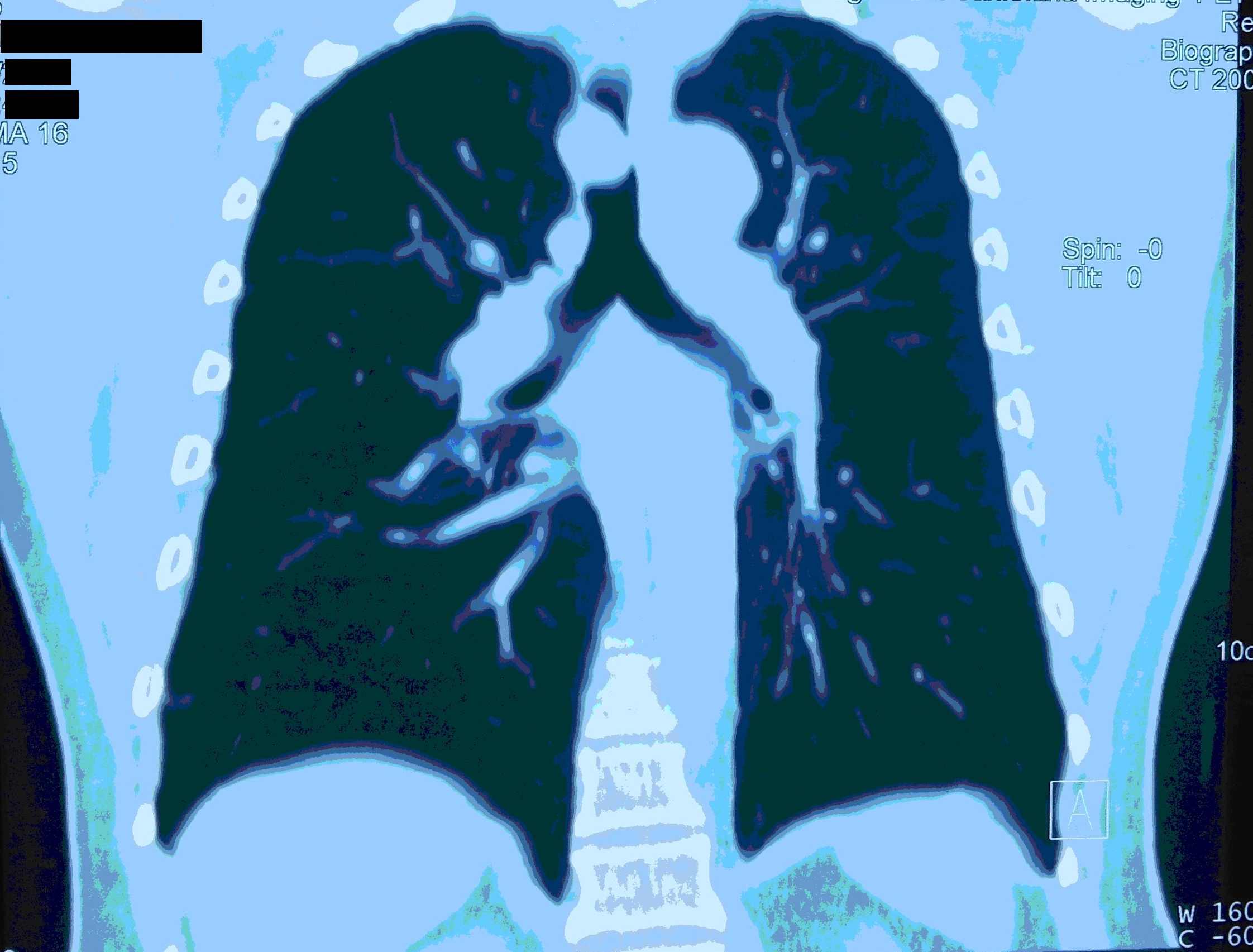
A fifty three year old male patient, labourer by occupation, beedi smoker for twenty five years, admitted to tertiary care hospital with pain and swelling over left arm, cough and expectoration for the past two months, accompanied with significant weight loss. There was no evidence of chest pain or haemoptysis. On local examination there was hard swelling over extensor compartment of left upper limb with mild tenderness, no loss of sensation and mild restriction of range of movements on flexion at elbow. Respiratory and other systemic examination was within normal results. Plain CT of thorax defined multilobulated lesion in right perihilar location in right middle lobe (Figure 1).
Figure 1: CT of Thorax: Well defined multi-lobulated lesion in right perihilar location in right middle lobe measuring 2.9 x 2.4 cm.
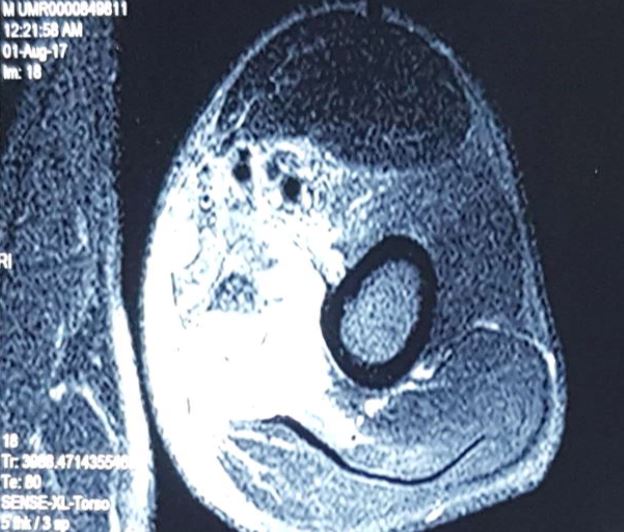
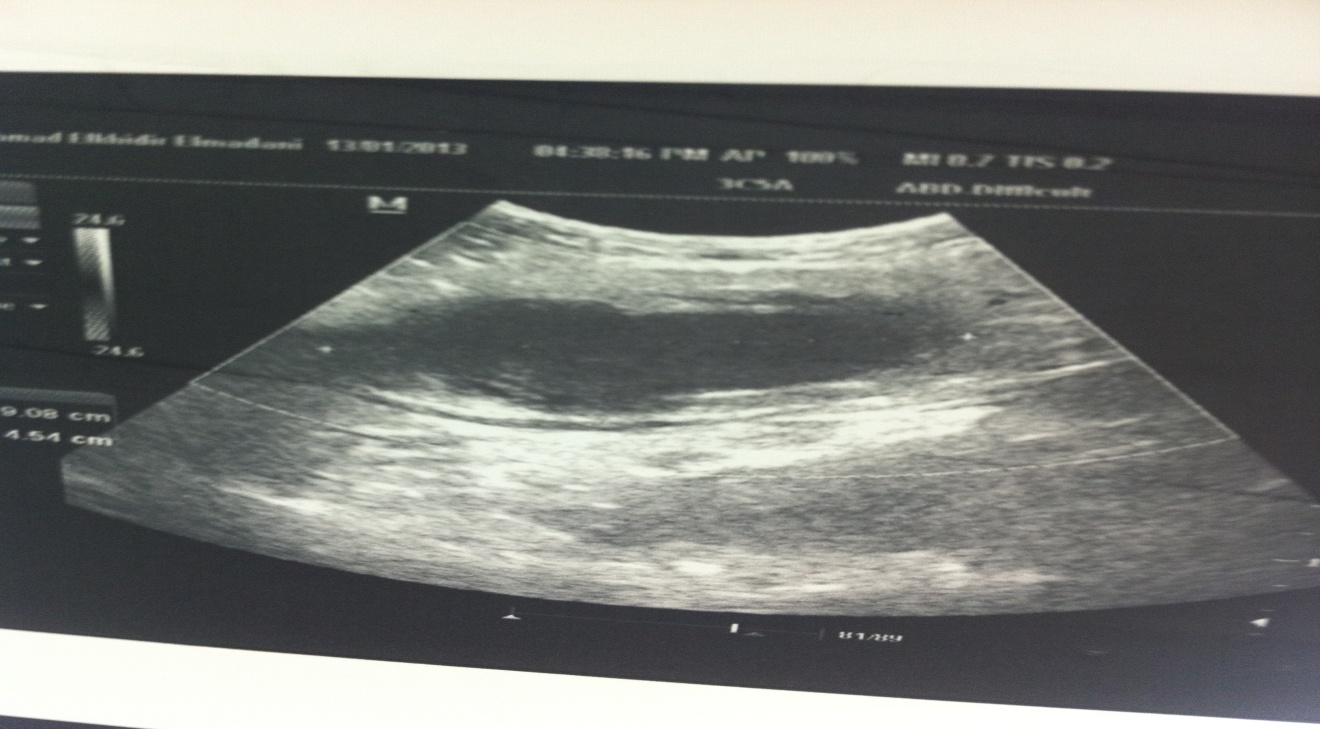
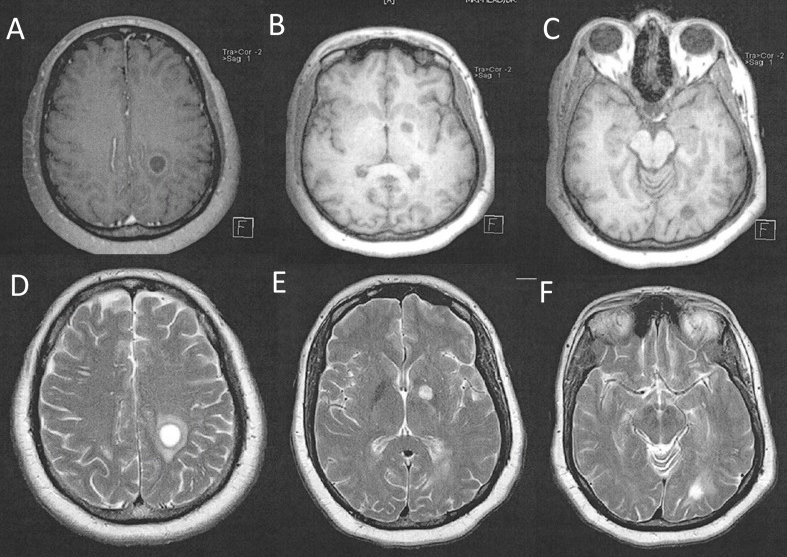
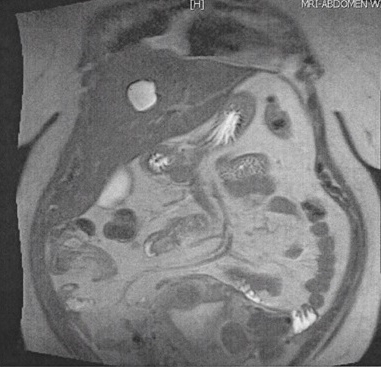
USG of left arm showed an irregular heterogenous soft tissue lesion noted within the triceps muscle with few areas of intra-lesional necrosis, MRI of left arm showed lobulated lesion in posteromedial aspect of mid and distal arm, involving triceps muscle, medial aspect of brachialis, encasing brachial artery, veins and median nerve (Figure 2).
Figure 2: MRI of Left arm: Well defined irregular lobulated enhancing T1 hypo intense, T2 and T2 flair hyperintense lesion in the posteromedial aspect of mid and distal arm.
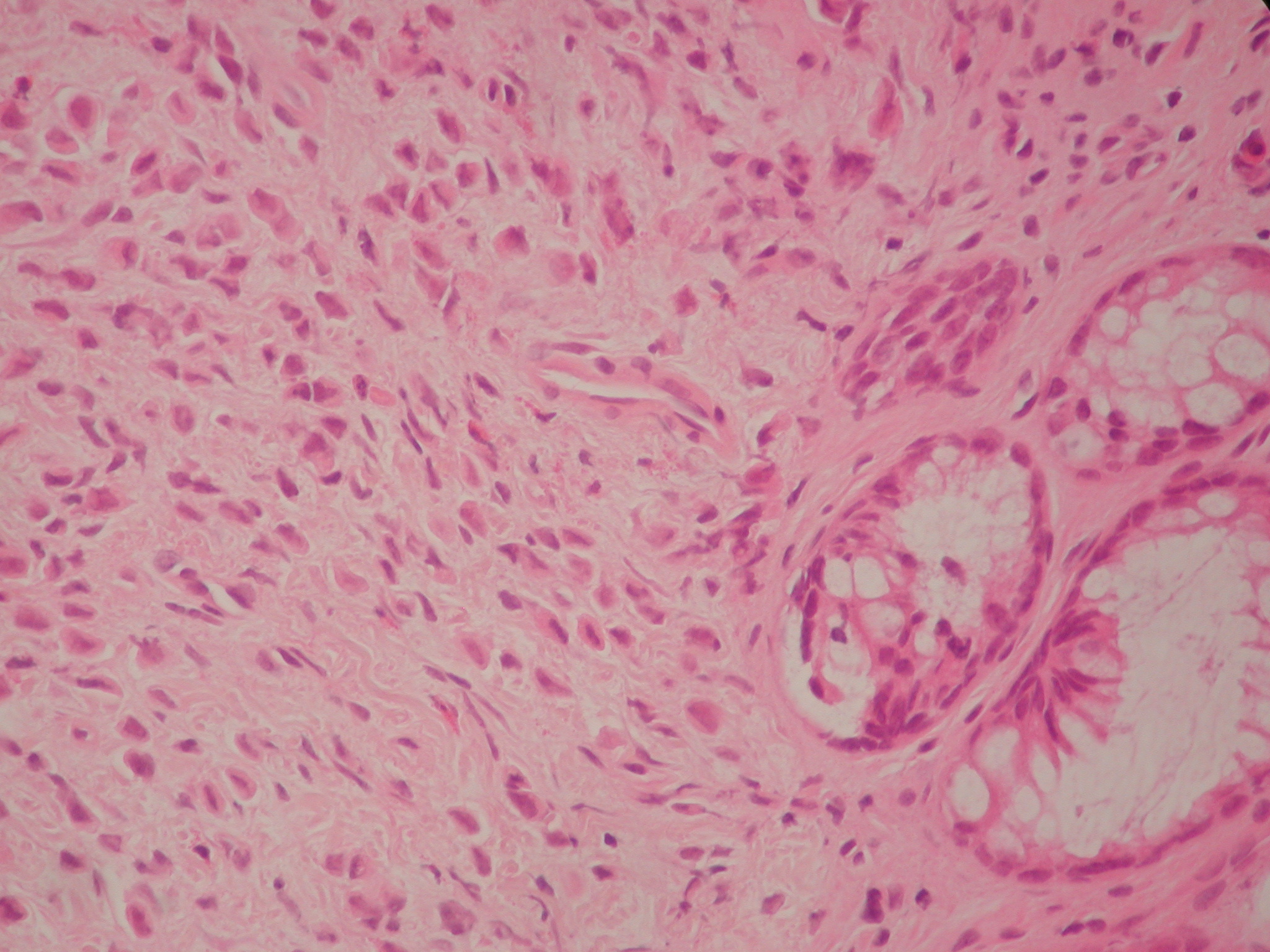
PET scan showed enhancing nodular soft tissue lesion noted in middle lobe of right lung, 2.9 x 2.4 centimetres. Biopsy revealed metastatic adenocarcinoma. For further studies Immunophenotyping was done which showed negative for EGFR and ALK. Patient was treated with palliative RT, Pem-Carbo f/b Pemtrexed maintenance and recently 3# of Gemcitabine. The patient died of metastasis to brain within eight weeks of diagnosis.
Discussion
Lung carcinoma is a leading cause of cancer-related mortality. The most common sites of distant metastasis in lung carcinoma are brain, bones, the liver, and the adrenal gland1. The most common tumours that cause skeletal muscle metastasis are tumours originating from thyroid, oesophagus, stomach, pancreas, colon, rectum, bladder, breast, ovary, and prostateand skeletal muscle metastasis of lung carcinoma was first reported by Fisher ER2. Willis RA reported four skeletal muscle metastases in their autopsy series composed of 500 lung carcinoma patients3. Skeletal muscle metastasis is a rare occurrence for any tumour with a reported incidence lees than one percent4-5. The most common sites of muscle metastasis are thigh muscles, iliopsoas, and paraspinous muscles6.
The mechanism of skeletal muscle metastasis is unclear. Despite its rich vascular blood supply and a large mass in the body, it is resistant to haematogenous metastases. Organs that are frequently metastasized, including liver, lung, and bone have rich capillary networks and blood supply. As a result of the muscle metabolism, substances such as lactic acid, free oxygen radicals, and low pH in the environment constitute an infertile medium for proliferating tumour cells. In addition, mechanical insults due to contractions, high tissue pressure, and widely alternating blood flow are also against the survival of tumour cells7.
There are several hypotheses proposed for skeletal muscle metastasis in lung carcinoma. The most widely accepted hypothesis is the haematogenous route. In this hypothesis, it is believed that tumour cells are formed through tumour embolism. Some authors suggested that skeletal muscle metastases might originate from abnormal lymph nodes found in the muscle. In a study by Bocchino M et al. 1754 lung carcinoma patients treated between 2007 and 2012 were analyzed and forty six (2.6%) had skeletal muscle metastasis8. Despite the variations between different studies in terms of the association between histological subtypes and skeletal muscle metastasis, forty patients in that study (87%) had non small cell lung carcinoma and six had (13%) small cell lung carcinoma. Among non small cell lung carcinoma patients, twenty four (60%) had adenocarcinoma. The most common initial manifestation of skeletal muscle metastasis is a pain. Pain can be accompanied by extremity swelling. The case presented herein also applied with pain and swelling. Diagnostic methods for skeletal muscle metastasis are not specific. Direct films usually show only soft tissue shadows. MRI usually reveals hypointense signal in T1 and hyperintense signal in T2. MRI is preferred to distinguish soft tissue metastasis from an abscess, sarcoma, and other conditions9, similarly; our patient had hypointense signal on T1 and the hyperintense signal on T2 series. The optimum treatment and prognosis of skeletal muscle metastasis from lung cancer is unclear. Depending on the clinical characteristics, treatment options include observation, surgery, chemotherapy and radiotherapy.
Conclusion
Lung carcinoma with skeletal muscle metastasis should be considered as a potential differential diagnosis in patients presenting with an intramuscular mass.
Acknowledgements
Authors acknowledge the immense co-operation received by the patient and the help received from the scholars whose articles are cited and included in references of this case report. The authors also acknowledge the authors/editors/publishers of all those articles, journals and books from where the literature for this case report has been reviewed and discussed.
Clozapine is an atypical antipsychotic, it is the treatment of choice for treatment resistant schizophrenia and more effective than conventional neuroleptic medications. Clozapine is associated with potentially life-threatening side effects, some of which appear early in treatment.
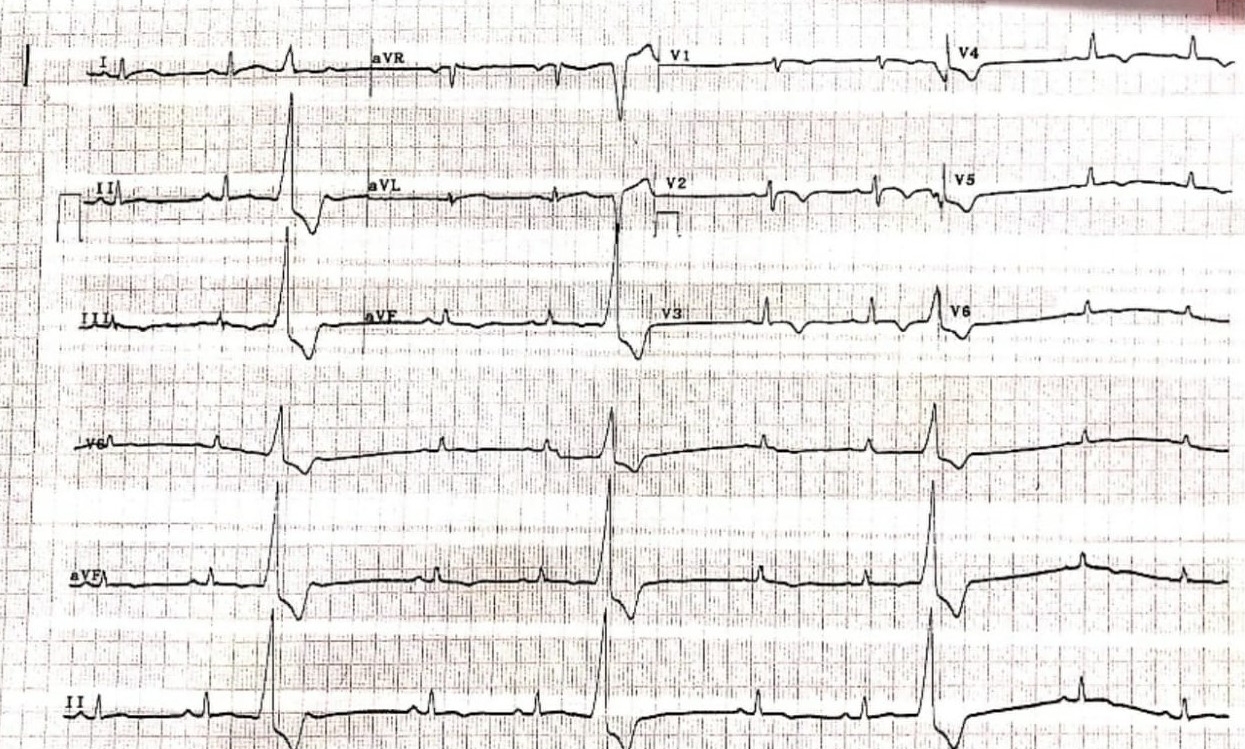
Myocarditis is an uncommon but serious early adverse event of Clozapine, the majority of reported cases occurring in the first 4-8 weeks.1 Clozapine induced myocarditis (CIM) can present with mild symptoms, but can progress rapidly to fulminant symptoms and thereafter heart failure and death.1 These symptoms and signs typically include dyspnoea, palpitations, chest pain, fatigue, flu-like symptoms, pyrexia and tachycardia.
Case Report
A 21-year-old Caucasian male with a two year diagnosis of schizophrenia and previously inadequate responses to Risperidone and Olanzapine was commenced on Clozapine. The patient had previously tolerated Risperidone and Olanzapine and did not experience adverse events, but there was inadequate therapeutic response to both; hence it was decided to commence Clozapine.
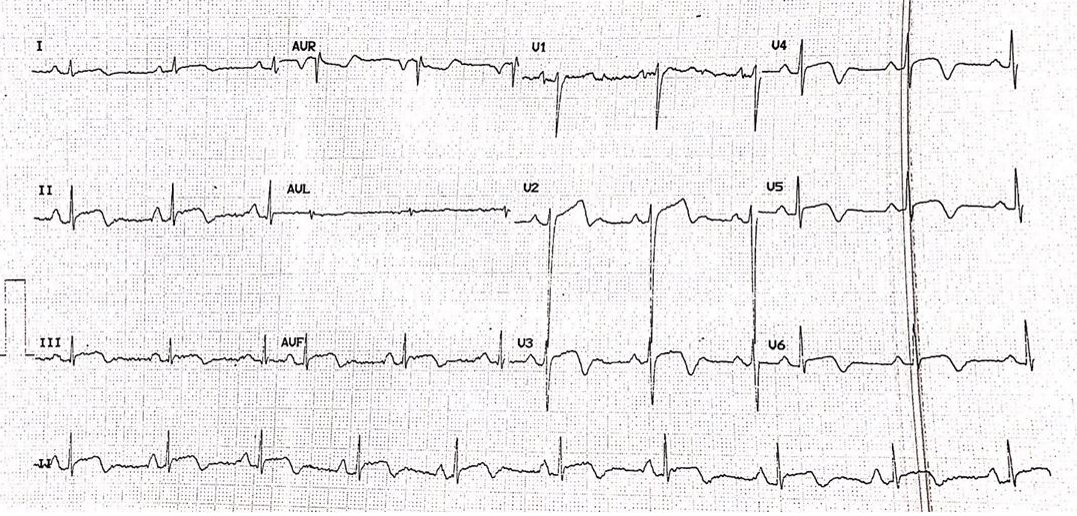
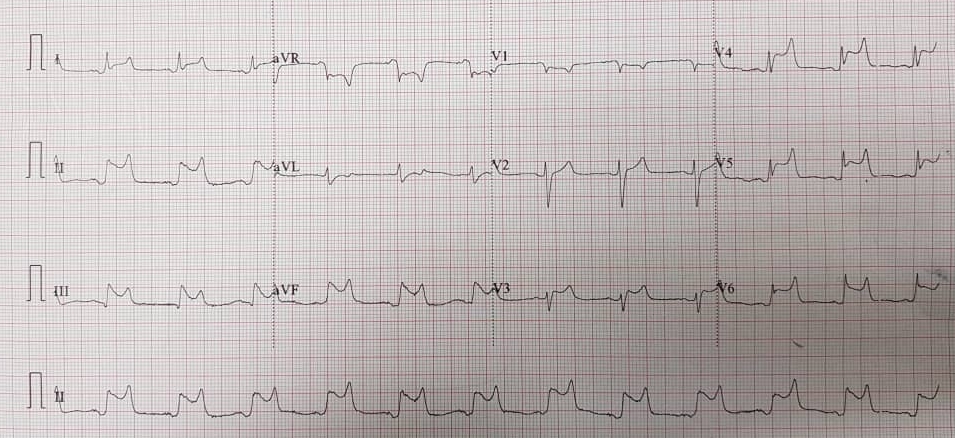
On admission, his physical examination, baseline blood investigations (these did not include cardiac markers such as troponin or C-reactive protein (CRP)) and electrocardiogram (ECG) were normal. His medical history was unremarkable and he did not have a family history of cardiac disease. He smoked 15 cigarettes per day.
A rapid Clozapine titration compared with the standard UK titration[2] was commenced with a target dose of 200 mg/day on day 14. He was not on any other psychotropic medication.
The patient remained asymptomatic in the first 3 days. On day 4, he developed tachycardia (114 BPM). A repeat physical examination and ECG was normal, eventually his heart rate settled to 94 BPM. The tachycardia was deemed to be a benign side effect of Clozapine, and the rate of titration was slowed down as a precaution.
On day 12, the patient reported dizziness when standing and a ‘cold air’ sensation in his chest. Nurses reported that blood pressure was normal with a heart rate of 145 BPM but when reviewed clinically his heart rate was 89 BPM. His titration was continued.
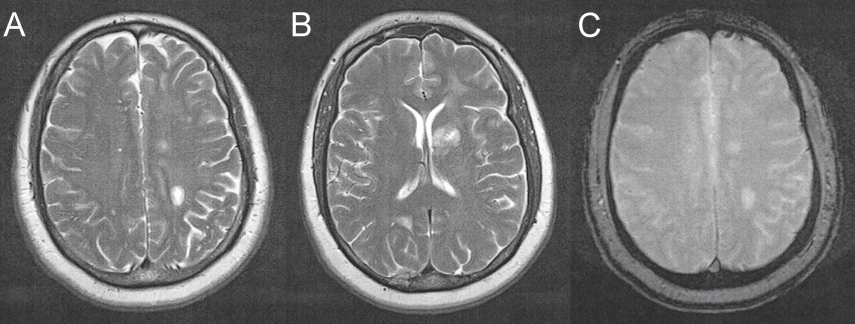
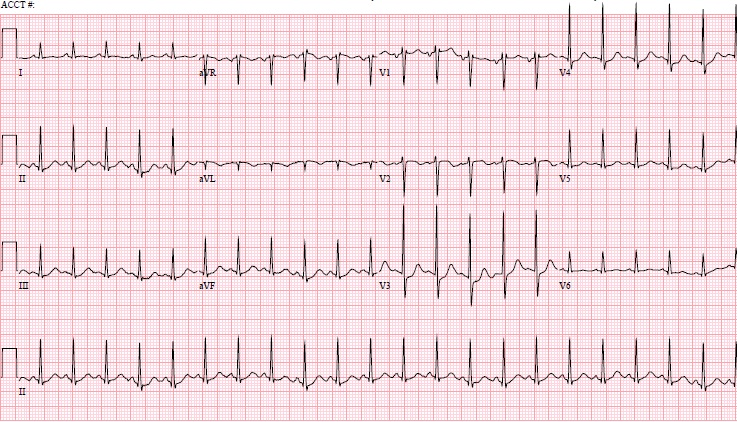
On day 14, the patient complained that his ‘internal organs were hurting’. His Clozapine dose was 125 mg/day at the time. He reported chest tightness with central pain, pain in his legs and abdomen, intermittent breathlessness and palpitations. The duration of his symptoms was 24-36 hours. Examination was normal except for a heart rate of 110 BPM. His ECG showed sinus rhythm with no ST segment or T wave changes. Blood tests showed markedly elevated troponin I—1211.5 ng/L (normal range: <34.3 ng/L), CRP—176 mg/L (normal range: 0-10 mg/L) and eosinophil count —1.28 109/L (normal range: 0.02-0.5 109/L).
The patient was afebrile throughout the titration period.
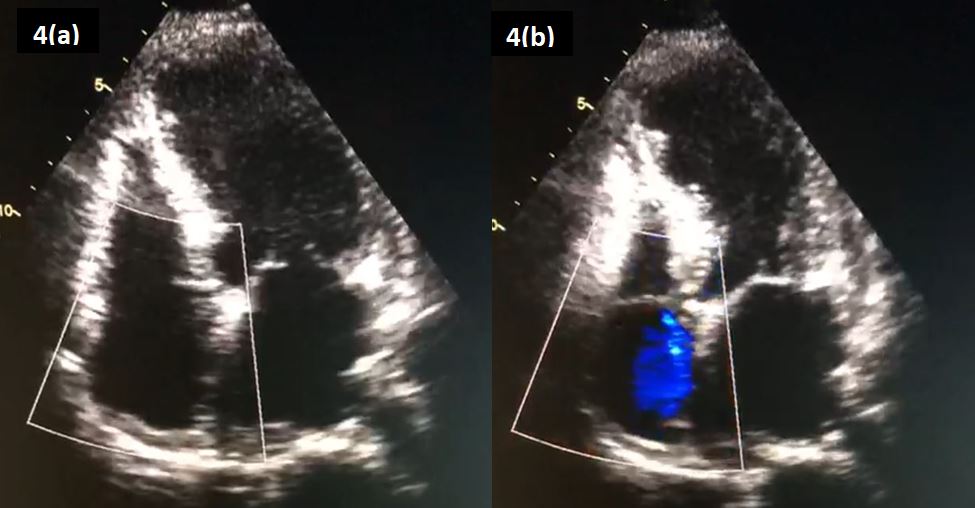
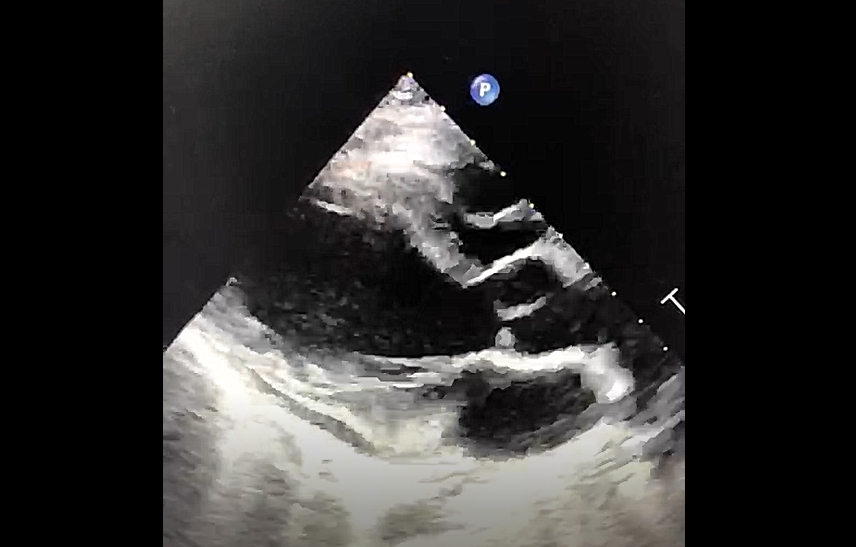
He was admitted to an acute hospital and a provisional diagnosis of Clozapine induced myocarditis was made. The echocardiogram did not reveal structural abnormalities or damage. An EBV (Epstein Barr Virus) serology was negative. Clozapine was withheld and the patient improved along with the blood markers, after 4-5 days he was discharged back to the psychiatric hospital.
Discussion
CIM is an often overlooked adverse event associated with Clozapine titration. Currently there is no mandatory requirement of laboratory monitoring for detecting myocarditis during Clozapine titration unlike the mandatory requirement for detecting neutropenia, despite roughly similar estimated incidence of the two adverse events at 3%.[3,4]
This case was unusual because of the very early appearance of symptoms, the patient’s age and atypical symptom presentation. Although CIM is an early adverse event, the onset within 2 weeks of initiation was unusual. Literature suggests that myocarditis typically presents within 4-8 weeks.[1] The patient was also younger than the reported median age of patients (30).[1] The symptoms appeared at a low dose of 125mg/day which literature suggests is unusual, although CIM at doses of 50mg/day has been reported.[5]
Tachycardia and fever are common early side-effects of Clozapine. Tachycardia usually settles after 4-6 weeks of treatment[6] and fever typically for 2-3 days.[7] Both symptoms can be suggestive of myocarditis, especially when they co-occur. CIM often presents in a non-fulminant form.[8] As this case demonstrates many patients may not report symptoms when CIM is mild.
Increasing age, concomitant administration of sodium valproate and increased rate of dose titration are significant risk factors for CIM.[9] In this case, the patient was young and sodium valproate was not co-administered. The titration was originally intended to be rapid but slowed down soon after commencement.
Given the clinical difficulties in detecting mild CIM, we suggest that all patients have baseline troponin, CRP, heart rate, blood pressure, temperature, resipatory rate and ECG. If medical history reveals history of heart disease, a baseline echocardiogram can be obtained. If there is history of congestive cardiac failure, then baseline brain natriuretic peptide (BNP) or N-Terminal pro-B-type natriuretic peptide (NTproBNP) should be measured.[10]
In clinically asymptomatic patients, if there is elevated baseline CRP (>100 mg/L), troponin, BNP or NTproBNP then Clozapine titration should not commence and further advice from cardiology should be sought.
Weekly CRP and troponin should be done in the first month of titration and levels repeated once after stable dose of Clozapine is reached. The dose increase should not be rapid.
Tachycardia developed should be checked with reference to the baseline heart rate measured before commencing Clozapine. A heart rate of greater than 120 BPM or increase of more than 20 BPM over the baseline pulse rate should lead to the review of physical health, blood monitoring, ECG, and Clozapine titration rate.
An increase in troponin above upper limits or an increase in CRP should trigger consideration of CIM. Literature suggests that troponin levels greater than 2x the upper normal limit are indicative of acute myocarditis.[9] CRP is raised on average 3 days before any increase in troponin levels is detected.[9] If the troponin levels are within the normal range and the CRP levels are raised but less than 100 mg/L, clozapine titration can continue, but the pace must be slowed. Troponin levels and CRP levels should be monitored daily and the patient should be closely monitored for clinical signs of developing cardiotoxicity.
We do not recommend routine eaosinophil monitoring as the marker in 90% of cases does not exceed normal limits at the onset of CIM and typically peaks 7 days after cessation of Clozapine.[11]
Conclusion
Clozapine induced myocarditis often presents with low level cardiotoxicity. Mild symptoms may be missed; however, progression to fulminant myocarditis can be rapid, with high mortality rates.[1] Myocarditis, including clinically asymptomatic myocarditis remains a risk with Clozapine every time the patient is titrated onto this medication[12]. Close clinical monitoring, high index of suspicion and monitoring of cardiac parameters will help early detection of adverse cardiac events.
Depression and osteoporosis are two extremely common comorbidities in geriatric patients. Each have their associated mental and physical impacts on the patient, and economically on the wider healthcare system. Staggeringly, up to 39% of frail patients suffer with depression.1 Selective serotonin reuptake inhibitors (SSRIs) have long since been used in the management of depression and anxiety states and are one of the fastest-growing classes of drugs prescribed. Their use is not without the potential for negative effects; their side effect profile includes nausea, anxiety, insomnia, sexual dysfunction and gastro-intestinal upset, with the impact on bone mineral density (BMD) being controversial.
Statistics from the International Osteoporosis Foundation (IOF) reveal that in 2015, 6.8% of men and 21.8% of women over the age of 50 had osteoporosis. The estimated lifetime risk of hip fractures for women over 50 is 17.2%, with fracture-related costs at 5.3 billion pounds in 2017.2 Osteoporosis is a progressive, systemic skeletal disorder characterised by loss of bone tissue and disruption of bone microarchitecture, that leads to increased bone fragility and consequently an increased risk of fracture. As well as increasing age and female sex, other well documented risk factors for reduced BMD include early menopause, alcohol use, corticosteroid use, smoking, sedentary lifestyle, low body weight, impaired eyesight, and recurrent falls. What is more, depression itself cannot be overlooked as a risk factor for osteoporosis.
The mechanism by which depression leads to lower BMD is by that of alternation of the hypothalamic-pituitary-axis system, resulting in hypercortisolism. Cortisol is a well-known factor in bone loss. Proinflammatory cytokines have been implicated in depressive disorders, and they may directly stimulate osteoclastic activity.3 What must also be considered is the impact that depression has on certain lifestyle choices such as the potential for increased alcohol and nicotine consumption, inadequate nutrition and low physical activity.
The presence of serotonin receptors, neurotransmitters, and transporters have been found within osteoclasts and osteoblasts.4 95% of serotonin is synthesised in the gut and cannot cross the heteroencephalic barrier. Gut derived serotonin reduces osteoblast proliferation, thereby leading to bone loss. Brain derived serotonin signals to the ventromedial hypothalamic neurones leading to decreased sympathetic output and therefore favours bone formation by action on the beta-2 adrenergic receptors on the osteoblasts. It appears that with shorter duration of use, decreased bone resorption predominates, and with longer term use, bone loss outweighs.4
The impact of SSRIs on bone health has long since been the subject of research, with a possible link with both increased risk of fractures, and reduced bone mineral density being identified. In response to emerging evidence, the MHRA issued advise to healthcare practitioners, stating that we “should be aware of epidemiological data showing a small increased risk of fractures associated with the use of TCAs and SSRIs, and should take this risk into account in discussions with patients and in prescribing decisions”, yet this has not yet filtered down to prescribing guidelines.5 The National Institute for Health and Care Excellence (NICE) guidelines state that on choosing the antidepressant to prescribe, healthcare practitioners must consider that there is currently no evidence to support using specific antidepressants for specific physical health problems.6
We therefore present a case of recurrent depressive disorder in a patient with a background of osteoporosis. We also include a review of the most up-to-date literature, with the aim of increasing awareness of the impact of SSRIs on bone health for fellow prescribers. We aim to highlight the difficulties we face as clinicians whilst there are no formal recommendations regarding the use of SSRIs in high risk populations.
Case Description
This 78-year-old was referred to our services in late 2019 with low mood and loss of motivation. She lives alone following the death of her husband 3 years ago and sadly has no family. She has a past medical history of depression, hypertension, acute pericarditis, subclinical hypothyroidism, hiatus hernia, cataracts, previous cholecystectomy, and osteoporosis.
She was diagnosed with osteoporosis in 2000. At that time, she had been seeing an osteopath due to back pain, who advised her to see her GP to investigate for arthritis or osteoporosis. She has a family history of osteoporosis on her mothers’ side. She was diagnosed by Dual-Energy X-ray Absorptiometry (DEXA) scan, with osteoporosis at the lumbar spine and pelvis, at which time she was started on calcium supplementation.
She was initially started on oral alendronic acid but developed reflux symptoms, so this was discontinued. Over the following years she was tried on various medications for bone protection but sadly developed side effects. Briefly, pamidronate infusion caused iritis, and nausea was reported whilst on sodium ranelate. Later she was to be commenced on sodium risedronate, however did not start this due to concerns she had following reading the information leaflet. Denosumab was discussed as the next suitable option, however she was undergoing dental work including tooth extraction and so this has been delayed due to the risk of avascular necrosis of the jaw.
DEXA scanning in March 2019 showed a T score of -0.8 at the neck of femur, -4.5 at the forearm, -1.3 at the total hip, and -4.2 at the spine. This had, unsurprisingly, worsened from her last DEXA in 2016 (-3.6 at the spine). Her risk of major osteoporotic fracture was last calculated at 21.6%, with the risk of hip fracture 11.5%. She has had no falls or fractures to date since her diagnosis.
Other than Adcal-D3 she is now no longer on bone protection. Her current medications also include levothyroxine, ramipril, bisoprolol, cetirizine, fluticasone nasal spray, and Hypromellose eye drops.
She had initially been started on citalopram by her GP which she had discontinued herself after a period of weeks as she felt it had no positive effect. In December 2019 she scored 92/100 on the Addenbrooke’s Cognitive Examination (ACE-III), with no significant deficits in any one category. As well as low mood and loss of motivation, she described frequent tearfulness, anhedonia, lack of energy, difficulty concentrating and poor sleep. There was no clear trigger for her current mental state, and her physical health was otherwise good. She had no suicidal ideation or thoughts of self-harm. There was some evidence of anxiety but no symptoms of psychosis. We could not identify any alcohol or substance use risks. Her mental state examination was unremarkable. She was given the diagnosis of moderate depressive episode, F32.1, and was started on sertraline. However, upon reading the patient information leaflet, she refused to start this medication due to it mentioning a link with bone disorders.
As a result of this discussion, we accessed the medicines.org patient information leaflet, where an increased risk of bone fractures is mentioned under the heading ‘symptoms that can occur when treatment is discontinued’. It also states that following clinical trials in adults, sertraline was found to cause ‘bone disorder’ in up to 1 in 1,000 people.7
Following in-depth discussions, our patient was very hesitant in agreeing to take any medication that may have an impact on her bone density. We were aware of the potential association between SSRIs and BMD but were unable to quantify this risk to our patient.
Discussion
Our case above represents a common situation; a patient that is worried about a side effect, concerning which there are no formal guidelines available to aid decision making. The link between depression, SSRIs and BMD is a complex one, with numerous confounders making analysis and application yet more difficult. We looked at the evidence surrounding SSRIs and their impact on bone health, in order to suitably advise our patient on the most appropriate treatment options.
Impact on BMD
We found several meta-analysis and systematic reviews concerning BMD. The majority showed no significant association between BMD and SSRI use.
Of note, a 2015 systematic review by Gebara et al, suggested that antidepressant use may well be associated with lower BMD. 4 of the included studies assessed the relationship with BMD, 3 of which highlighted an association with lower BMD. This association was reported with SSRIs but not TCAs. However, they concluded that there was insufficient evidence that SSRIs adversely affect bone health, and therefore a change in current recommendations for the use of antidepressants in older adults was not justified at the present time. They stated that the evidence did not satisfy the Bradford Hill criteria, it is inconsistent, and whilst there is biological plausibility, there are no experimental studies to support a causal relationship.8
Yet a 2012 literature review indicated effects on both BMD and fracture risk.9 Each and every study included, indicated a risk of reduced BMD, increased fracture risk, or both. Even when controlling for potential confounders this conclusion was drawn. Authors suggested on the basis of this evidence, that caution is advised when considering the use of SSRIs in those with osteoporosis or a history of osteoporotic fractures, despite there being no formal recommendations.
A 5-year longitudinal study involving 1988 women, 319 of which were using antidepressants, measured femoral neck BMD. A dose-response increase in bone mineral loss was evident.10 An older cohort study also showed that even after adjustment for potential confounders, mean total hip BMD decreased 0.47% per year in non-users, compared with 0.82% in SSRI users.11 A year later, and a community-based study revealed that after controlling for age, weight, height and smoking history, BMD among SSRI users was 5.6% lower at the femoral neck, 6.2% lower at the trochanter and 4.4% lower at the mid-forearm than nonusers.12
Fracture Risk
The evidence surrounding fracture risk is more unanimous. Of the systematic reviews and meta-analyses we found, all highlighted an increased risk of fracture in SSRI users.
Wu et al concluded that the significantly higher risks of fractures observed for patients who received SSRIs compared with patients with no exposure, remained statistically significant in studies that controlled for important risk factors and studies that scored highly in the quality assessment.13
Eom et al extrapolated their data, estimating that the increased risk of fractures translates to about one case of fracture for every 42 patients treated with SSRIs.14 The dose and duration of SSRIs also seems to contribute to fracture risk, with both an early increased risk (under 6 weeks), and a late risk associated with prolonged use.14,15
A notable literature review by Panday et al on medication-induced osteoporosis summarised that treatment decisions concerning SSRIs should be considered on an individual basis for patients with osteopenia, osteoporosis, or fracture risks greater than 3% and 20% for hip and major fractures respectively.16 Of particular note from this review, a 10-year cohort study revealed that 14.7% of SSRI users suffered at least one fragility fracture over the study period.17 Whilst those using SSRIs do tend to have more fracture risk factors than the general population; they are more likely to be women, have more comorbidities, use other antidepressants/ anxiolytics, and have a previous history of falls; the significant association remained even after these variables were controlled for. The risk of first fracture specifically was increased by more than 50%, and similar to other studies, a dose–response relationship was evident.17
Conclusion
The impact of SSRIs on bone health is clearly a topic of contention. Whilst the impact on BMD is unclear, the increased fracture risk is more unanimous. There are plausible biological mechanisms to explain these risks, yet there is also the fact that the risk of falls themselves are higher when taking SSRIs.
Yet why hasn’t this filtered down to making formal recommendations in prescribing guidelines? Questions remain as to whether we should be prescribing SSRIs in individual’s with osteoporosis at all. Regardless, the relatively high risk of fracture with SSRI use may have a significant clinical impact. These risks must be balanced against the benefits gained by the treatment for depression; both in terms of mental state and in osteoporosis risk factor modification. What would perhaps be more relevant would be to consider a patient’s falls risk independently to their bone health, when deciding whether to prescribe SSRIs. Consideration towards the use of concomitant medications, co-morbidities and other confounders is vital.
It is on this basis that we suggest discussing bone health with your patients (particularly those at high risk), prior to prescribing these medications, and being wary of prescribing SSRIs in those with osteoporosis or more importantly, those at high risk of falls.
Summary
Impact of SSRIs on bone health is complex with significant confounding factors
Whilst the impact on BMD is contentious, the increased fracture risk is more significant
Risk-benefit decision is needed
Consider the patients falls risk most importantly before prescribing an SSRI
The pituitary gland is a tiny gland located at the base of the brain and is connected to the hypothalamus. Dubbed as the body’s “master gland”, it produces important hormones that control many bodily functions such as those involved in the control of haemodynamics, glucose, fight or flight response, body growth and many more. Any of the pituitary hormones may be affected in pituitary disease, with acute adrenocorticotropic hormone (ACTH) deficiency being the most catastrophic and life-threatening.
Pituitary apoplexy occurs following acute haemorrhage or infarction of the pituitary gland, causing patients to be acutely unwell due to hormonal as well as local compressive effects. These effects cause the usual presentation of pituitary apoplexy such as severe headache, diplopia, visual loss and hypopituitarism.
We report a case of pituitary apoplexy that presented with a 2-week history of loss of peripheral vision and lethargy with stable vital signs.
CASE PRESENTATION
A 49 years of age gentleman complained of loss of peripheral vision in the left eye and lethargy for 2 weeks. The loss of vision was sudden, painless and non-progressive and had caused him considerable difficulties with driving where he would shift into the wrong lane and was honked at. He had no known medical or surgical history of note. Prior to presentation, he had no history of eye pain, eye redness or a history of trauma to the left eye. There were no headaches, neurological deficits or constitutional symptoms.
Clinically, he had bitemporal hemianopia with no other cranial nerve deficits. His Glasgow Coma Scale was 15/15, vital signs were stable and there was no postural change in blood pressure. Examination of other systems was unremarkable. Blood investigations revealed a decreased morning cortisol of 46 nmol/L and a normal thyroid stimulating hormone (TSH) with borderline low free thyroxine. Serum electrolytes, plasma glucose and all other anterior pituitary hormones were within reference range.
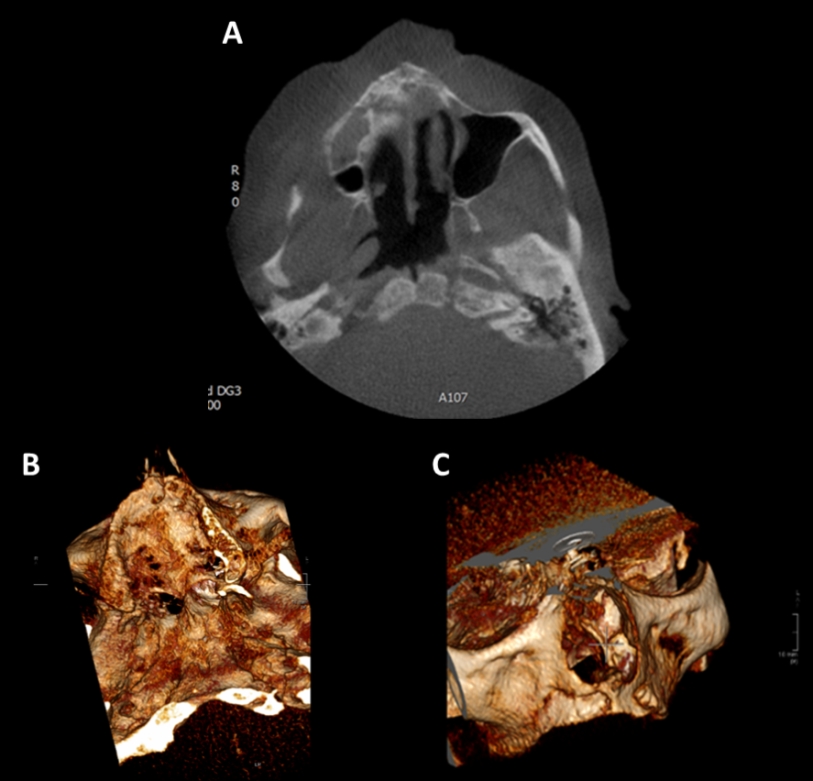
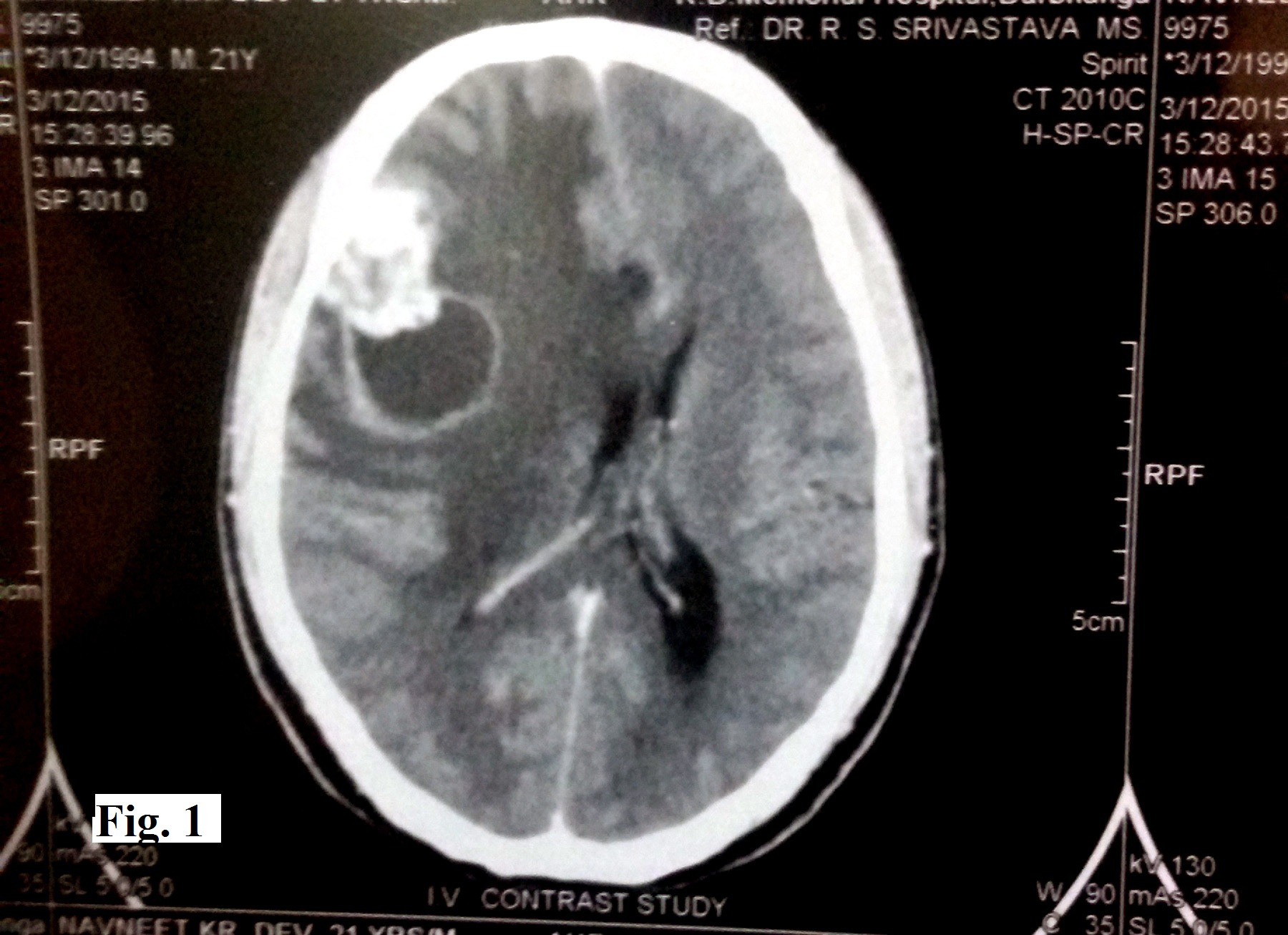
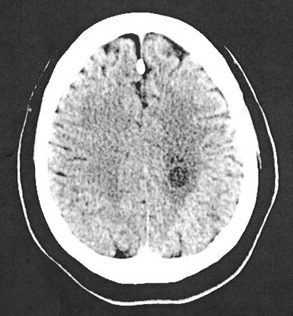
A computed tomography (CT) of the brain showed an enlarged pituitary sella with a large well-circumscribed and heterogeneously enhancing mass within. This mass measured 3.5cm x2.7cm x3.5cm (AP xW xCC) and had no calcifications within. It was also compressing onto the optic chiasm.
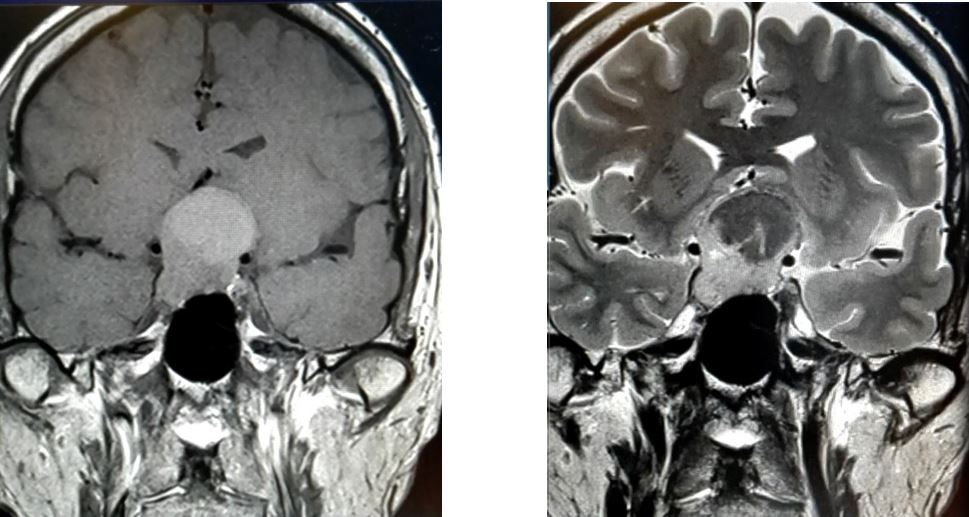
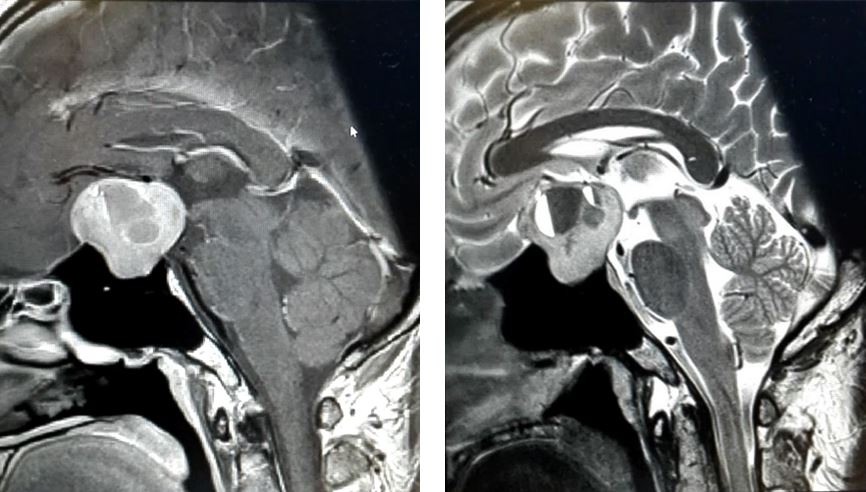
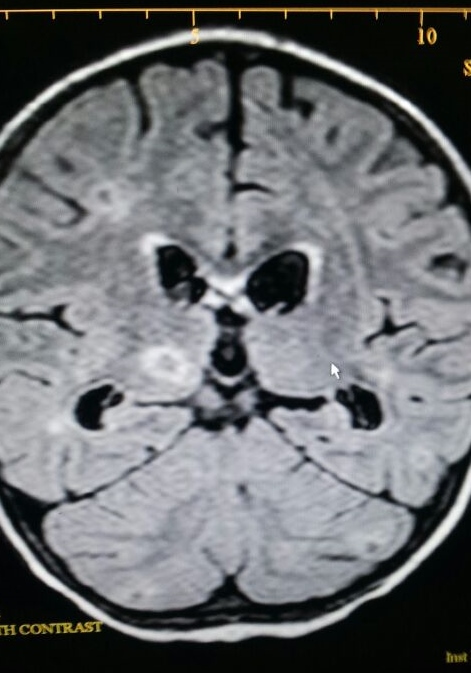
Two days later, a brain pituitary Magnetic Resonance Imaging (MRI) was done which reported a heterogeneous mass occupying the sella with suprasellar extension measuring 2.7 x2.8 x2.9cm (AP xW xCC) (Figures 1.1 & 1.2). This mass returned mixed solid-cystic intensity with significant enhancement post-contrast administration. There was evidence of layering within the cystic component of this mass. Inferiorly, the right border ended lower than the left (Figures 2.1 & 2.2).
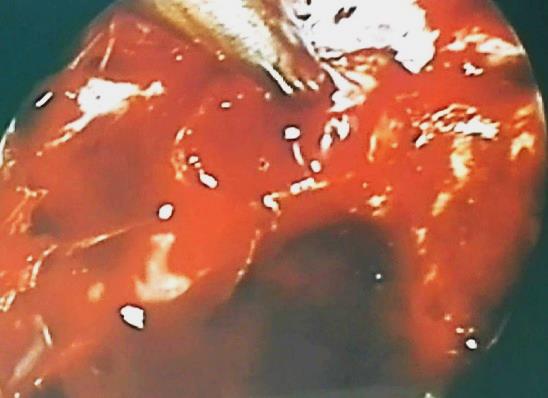
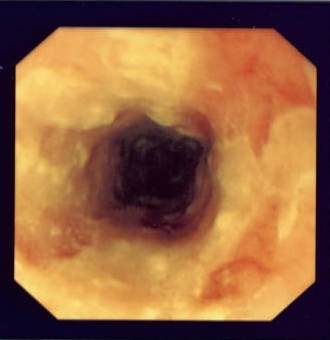
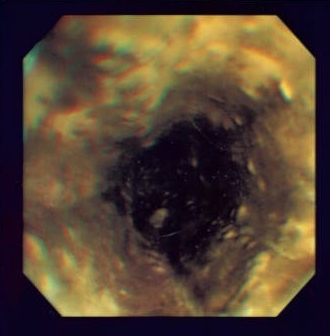
Following consultations with endocrinologists, neurosurgeons and radiologists, a clinical diagnosis of pituitary apoplexy with hypocortisolism and central hypothyroidism was reached. The patient was started on oral hydrocortisone 20mg in the morning and 10mg in the evening; and oral L-thyroxine 100mcg in the morning before he was referred to the neurosurgeon for trans-sphenoidal surgery. While awaiting surgery, no clinical deterioration was reported. An endoscopic trans-sphenoidal surgery successfully took place a week later which revealed an enlarged haemorrhagic pituitary gland (Figure 3.0). The patient was discharged well a week post-surgery.
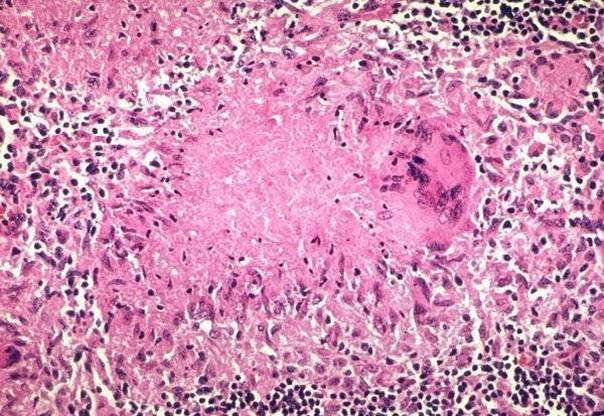
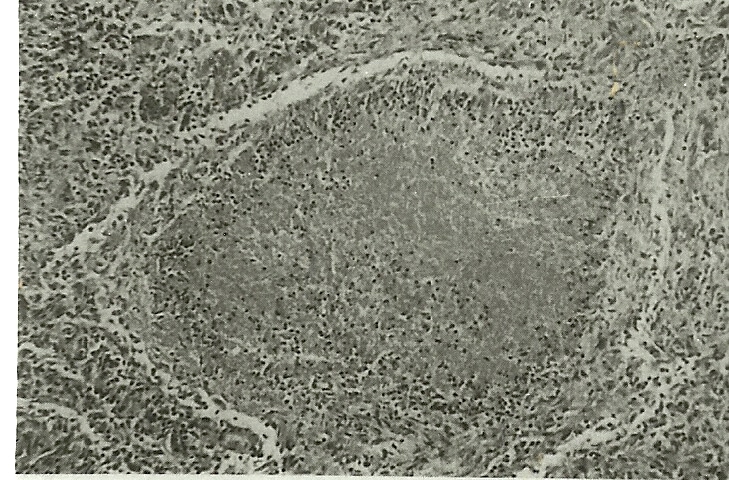
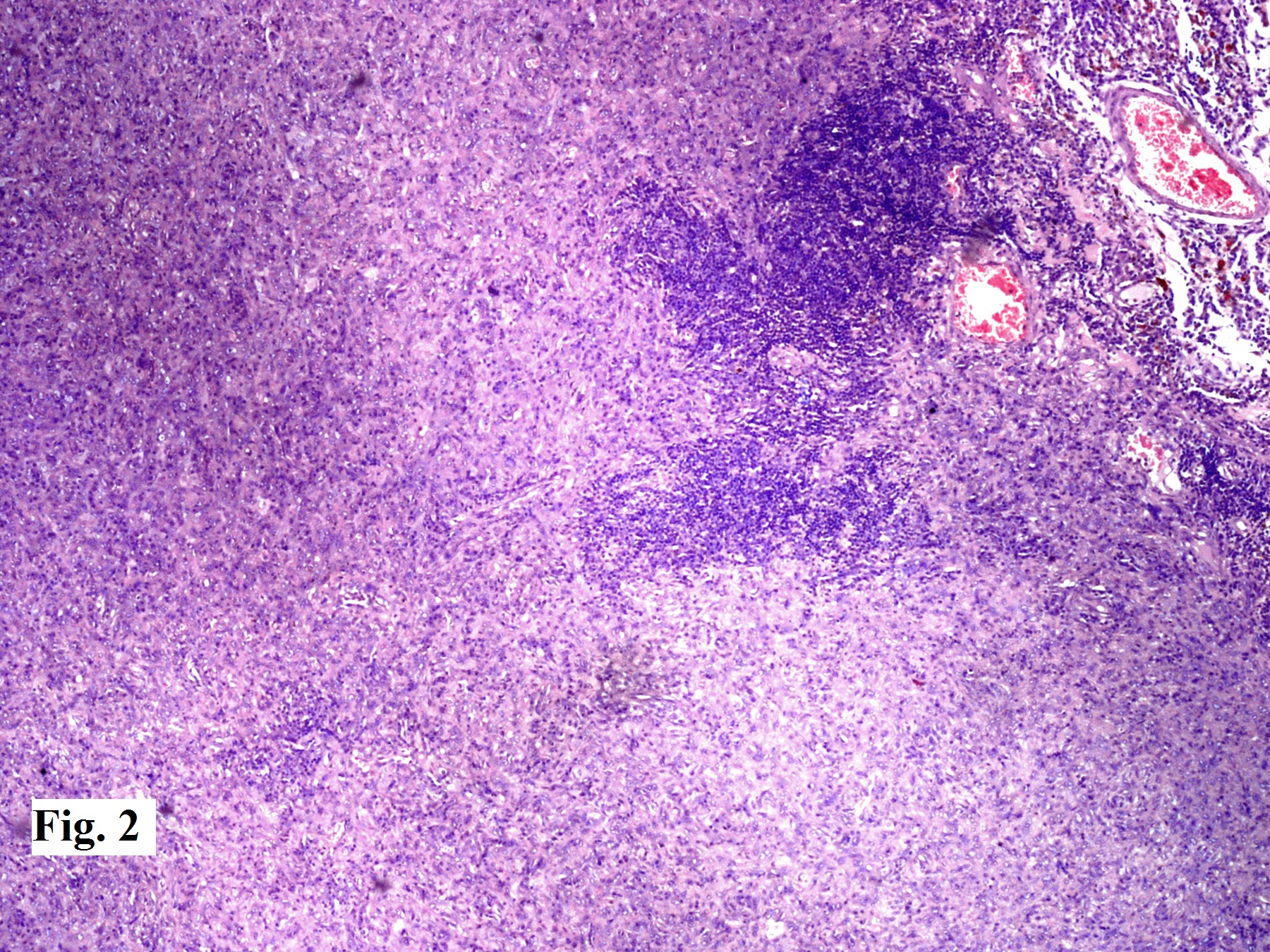
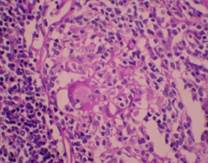
His histopathology report later confirmed pituitary adenoma where monomorphic tumour cells arranged in nests and trabeculae and some pseudorosettes were seen. The tumour cells exhibited mild pleomorphism with moderate amount of cytoplasm. The stroma was highly vascularised. No necrosis, calcification or mitosis was seen. Immunohistochemistry studies were positive for follicle-stimulating hormone (FSH) and luteinising hormone (LH) and negative for ACTH, growth hormone, prolactin and TSH.
Figure 1.1 and 1.2: MRI brain on coronal view illustrating well-defined and heterogenous suprasellar mass
Figure 2.1 and 2.2: MRI brain on sagittal view illustrating mixed solid-cystic intensity pituitary mass
Figure 3.0: Intraoperative finding showing haemorrhage of the pituitary gland
DISCUSSION
Pituitary apoplexy is a potentially fatal condition caused by haemorrhage or infarction or both. Most cases occur during the fifth decade of life, predominantly in males.1 In the majority of cases, it is associated with a pre-existing non-functioning macro-adenoma which accounts for 14-54% of pituitary adenomas and has a prevalence of 7-41.3/100,000 population. The standardised incidence rate is 0.65-2.34/100,00.2
The many clinical presentations of pituitary apoplexy result from local compression of adjacent structures or deficiency of pituitary hormones – the former being more common where affected individuals present with headaches, visual disturbances and other symptoms of raised intracranial pressure.3
Subclinical haemorrhages refer to asymptomatic individuals with evidence of pituitary haemorrhage on MRI. In a 2018 retrospective transversal analysis involving 64 patients, 34.38% had subclinical haemorrhage within a non-functional adenoma.4 In another retrospective overview by Turgut et al, 186 cases of apoplectic pituitary adenoma presenting with monocular or binocular blindness were published in the last century.5 In a case report by Sasaki et al, a 65-year-old gentleman was only diagnosed with pituitary apoplexy following weeks of blood investigations for hyponatraemia and repeat imaging. His only presenting complaints were anorexia, low energy and fever for two weeks.6 These studies show that while an early correct diagnosis of pituitary apoplexy is important, it is not necessarily urgent.
On the other end of the spectrum, pituitary apoplexy may also present as a life-threatening situation where patients are unconscious and hemodynamically unstable due to hypopituitarism. In its acutely deficient state, ACTH causes acute adrenal insufficiency hence resulting in hypotension, hypoglycaemia, hyponatraemia and hyperkalaemia. Sometimes, non-specific symptoms precede the symptoms of hypocortisolism. A drop in consciousness level may be due to the tumour’s mass effect transmitting pressure to the brainstem or causing hypothalamic compression.7 Espinosa et al reported a 48-year-old gentleman with pituitary apoplexy who presented with the worst headache of his life, requiring urgent neurosurgical intervention which proved to be life-saving.8
Complex as it already is, diagnosing pituitary apoplexy may be further complicated when non-specific symptoms can be explained by other causes such as post-general anaesthesia drowsiness, hyponatraemia in a patient on diuretics and headaches in post-partum women receiving spinal anaesthesia.9, 10
While most patients consequently suffer from pituitary insufficiency, the extent, type and duration of therapy differs between patients. Cases of spontaneous recoveries whether a surgical or conservative approach was adopted have also been reported.11, 12 However, robust control studies comparing the outcome of surgical with conservative management in patients with pituitary apoplexy have yet to emerge. Nonetheless, studies have proven that visual outcomes significantly improve with surgery.13, 14
Having discussed the varied presentations of pituitary apoplexy, it can be agreed upon that the life-threatening endocrinal condition should be considered in any patient with abrupt neuro-ophthalmic deficits despite the state of clinical stability. This is imperative as prompt medical and surgical management may not only be life-saving, but also significantly improve visual and cranial nerve outcomes.15
CONCLUSION
Pituitary apoplexy is an endocrinal emergency which requires immediate investigation and treatment. Despite its disastrous pathology, there have been cases where affected patients present with isolated visual disturbances or with no symptoms at all. It is therefore important to have early suspicion of pituitary apoplexy in stable patients with eye complaints as early detection and management are life-saving and significantly improve neuro-ophthalmic outcome.
In December 2019, the Wuhan province of China was struck by an outbreak of viral pneumonia due to the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) or COVID-19.1 On the 30th of January, WHO declared a state of global emergency due to the rapid spread of COVID 19 2 and since then it has developed into an epidemic, contributing to over 247,000 global deaths as of 4th May 2020. COVID-19 has commonly presented with respiratory symptoms, but some gastrointestinal symptoms have also been described.3, 4 Here we describe a rare case of COVID-19 presenting with acute psychosis with initially false negative RT-PCR nasopharyngeal swab upon hospital admission.
Case Review
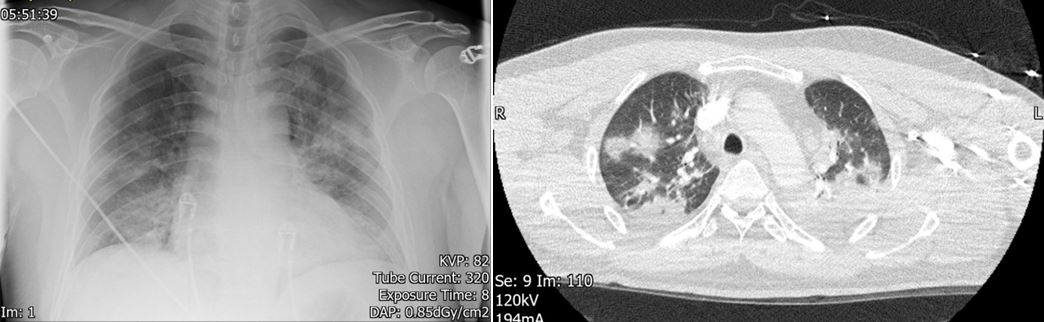
A 40 year old, previously fit and healthy male, with a six day history of dry cough, breathlessness and nasal congestion, presented to accident and emergency via ambulance. Prior to the respiratory tract symptoms, he had a progressively worsening fever, anosmia and intermittent diarrhoea for four days. His observations included a temperature of 39⁰C, oxygen saturations of 95% on room air and a respiratory rate of 30. His initial laboratory tests are shown in Table 1 and imaging in Figure 1.
Table 1: Table showing the relevant laboratory results of the patient upon admission
Investigations
Value
Reference Range
White cell count (x109/L)
12.0
3.7 - 11.1
Neutrophil count (x109/L)
10.3
1.7 - 7.5
Lymphocyte count (x109/L)
1.1
0.9 - 3.2
C-reactive protein (mg/L)
190
0 - 6
Cerebrospinal Fluid Protein (g/L)
2.4
0.15 - 0.45
Cerebrospinal Fluid Glucose (mmol/L)
3.7
2.5 - 4.5
Cerebrospinal Fluid White Cells (/µL)
0
0 - 5
Influenza A, B and RSV nasopharyngeal swab
Negative
COVID-19 nasopharyngeal swab
Negative
Pneumococcal urine antigen
Negative
Legionella urine antigen
Negative
Figure 1: (Left) An AP X-ray showing bilateral patchy consolidation. (Right) A cross-sectional CT thorax image showing multifocal, peripheral, bilateral, ground-glass opacities with bilateral consolidation.
Over the course of the next two days, he developed acute confusion. A CT scan of his head was done in the first instance to identify any intracranial cause of confusion, but the scan was unremarkable. His behaviour included severe anxiety, aggression, wandering and agitation. His wife confirmed that he had never behaved like this before and had no history of psychiatric illness. He felt as if he was living in a dream, exhibiting derealisation and depersonalization. Worryingly, he also experienced suicidal ideation which he hoped would bring him back to reality. One of the ways in which he tried to kill himself was by jumping out of the hospital window. Due to verbal and non-verbal de-escalations being ineffective, 5mg of Haloperidol was given, but failed to settle the patient. This was the maximum daily dose of haloperidol in accordance with the British Geriatric Society Guidelines for the management of COVID-19 related confusion5. Subsequently, the patient was successfully managed with intubation and ventilation for 24 hours, despite the absence of respiratory failure. After extubating, he recovered back to baseline over 2 days, during which a 2nd RT-PCR nasopharyngeal swab result returned positive for COVID-19. After recovery, he had insight into the events that took place prior to intubation. Retrospectively, he reported auditory hallucinations of hospital staff talking about him all day and night, and the delusions that the hospital staff were against him, and that he was in a dream which could only be escaped by committing suicide.
Discussion
There are two clinically relevant learning points to convey from this case relating to, firstly, the difficulties encountered in diagnosis and, secondly, the management of acute psychosis in COVID-19 with intubation. The diagnosis of COVID-19 was confounded by the first nasopharyngeal RT-PCR swab being negative. Since his symptoms were typical of COVID-19 and with strongly suggestive radiographic findings, it was deemed appropriate to send a repeat COVID-19 nasopharyngeal RT-PCR swab (which indeed came back positive). This patient thus had COVID-19 pneumonia and the official diagnosis was delayed due to a false negative nasopharyngeal RT-PCR swab upon hospital admission.
Various studies have identified a high false negative rate with the COVID-19 swab.6, 7 Ai et al., describes 287 patients (n=1014) who had radiographic findings suggestive of COVID-19 with negative nasopharyngeal swabs.8 It is important for clinicians to be aware of the poor sensitivity of the RT-PCR COVID-19 swab so that it can be interpreted appropriately when being used to make clinical decisions. Various studies have estimated the RT-PCR COVID-19 swab sensitivity to be approximately 70-75%.9 This is hypothesised to be even lower if clinical staff do not use the correct technique when taking the nasopharyngeal swab. Subsequently, there is a growing clinical need for more sensitive laboratory tests for COVID-19 such as antibody tests.10
Chest radiographs may be normal in early or mild disease, but can assist diagnosis. Of patients with COVID-19 requiring hospitalisation, only 69% had an abnormal chest radiograph at the initial time of admission. Findings are most extensive about 10-12 days after symptom onset. The most frequent findings are bi-basal, peripheral, consolidative and ground-glass airspace opacities. In contrast to parenchymal abnormalities, pleural effusion is rare.11, 12 Indeed, this patient’s chest radiograph shown in Figure 1 (left) was performed after 10 days of symptoms, showing features of COVID-19.
The primary findings on CT have been reported in multiple studies to include ground glass opacification, ‘crazy-paving’ texture, air space consolidation, broncho vascular thickening, adjacent pleural thickening and traction bronchiectasis. The ground glass, or consolidative, opacities are usually bi-basal, peripheral and ill-defined.13-18 Four stages on CT have been described, as shown in Table 2 below.19, 20 This patient’s CT Thorax shown above in Figure 1 (right), was performed after 12 days of symptoms and displays features in keeping with the ‘peak’ stage.
Table 2: Table showing the radiographic staging of COVID-19
Stage
Timescale
Radiographic Findings
Early/initial stage
0-4 days
Normal CT or GGO only
Progressive stage
5-8 days
Increased GGO and crazy paving appearance
Peak stage
9-13 days
Consolidation
Absorption stage
14 days<
With an improvement in the disease course, "fibrous stripes" appear and the abnormalities resolve at one month and beyond
It is important to mention that in a retrospective, COVID-19 case-controlled study of 104 patients, 54% of asymptomatic patients had CT radiographic features in keeping with COVID-19.21 CT scan changes are estimated to be as high as 97%-98% sensitive and can thus be useful when there is a strong suspicion of COVID-19 despite negative nasopharyngeal swabs.8, 9, 22 This can avoid clinicians having a false sense of security when managing potential COVID-19 patients who may otherwise be nursed in open bays, consequently exposing unprotected clinical staff and patients; a common problem that we unfortunately encounter in our clinical practise.
The second interesting learning point in this case is with regards to the clinical reasoning behind why this patient was intubated. Patients with severe COVID-19 symptoms such as hypoxaemia, respiratory distress, shock or an SpO2 of <90% are usually commenced on supplemental oxygen therapy of 5L/min, which should then be titrated to maintain an SpO2 of >94%. Continuous positive airway pressure or non-invasive ventilation can then be trialled, and if ineffective, the patient can be intubated for ventilation.23 This patient’s SpO2 prior to intubation was 94%. Interestingly in this case, the clinical reasoning behind intubation was not respiratory failure, but instead acute psychosis secondary to COVID-19 which had failed to respond to conservative de-escalation measures, as well as haloperidol.
The intubation of this patient aimed to reduce respiratory effort, cross-infection risk, as well as prevent further suicide attempts. As mentioned in the history above, this patient was non-compliant with isolation regulations as he was severely confused and wandering around clinical areas, thus posing a cross-infection risk to staff and other patients.24 Self-isolation precautions have been heavily implemented in the UK because COVID-19 is an extremely virulent infectious disease.25 The basic reproductive number of COVID-19 has been estimated to be 1.55-5.5,26,27 making it more infectious than the seasonal influenza, at 1.28.28 This highlights the importance of strictly following isolation protocols, and thus, the rationale behind intubation.
Conclusion
There are two primary learning points to be appreciated from this case report. Firstly, the false negative rate with RT-PCR COVID-19 nasopharyngeal swabs is high, and this identifies a crucial diagnostic role for CT Thorax in ‘swab-negative’, symptomatic patients with suspected COVID-19. Secondly, acute psychosis is an emerging indication for intubation to consider when managing patients with highly virulent respiratory infections, such as COVID -19. The mechanisms behind COVID-19 induced acute psychosis remained yet to be elucidated, but, in this case, COVID-19-induced encephalitis was amongst the differential diagnoses.
Nocardia sp. are aerobic, gram-positive microorganisms found mainly in soil and stagnant water. Nocardiosis commonly occur in immunocompromised patients, is often multi-systemic and easily mistaken for tuberculosis when involving the lungs 12. We report a complex case of disseminated nocardiosis in a patient already suffering from Myasthenia Gravis (MG) and azathioprine-induced myelosuppression, in which selection of antimicrobials and management planning became complex.
Case Report
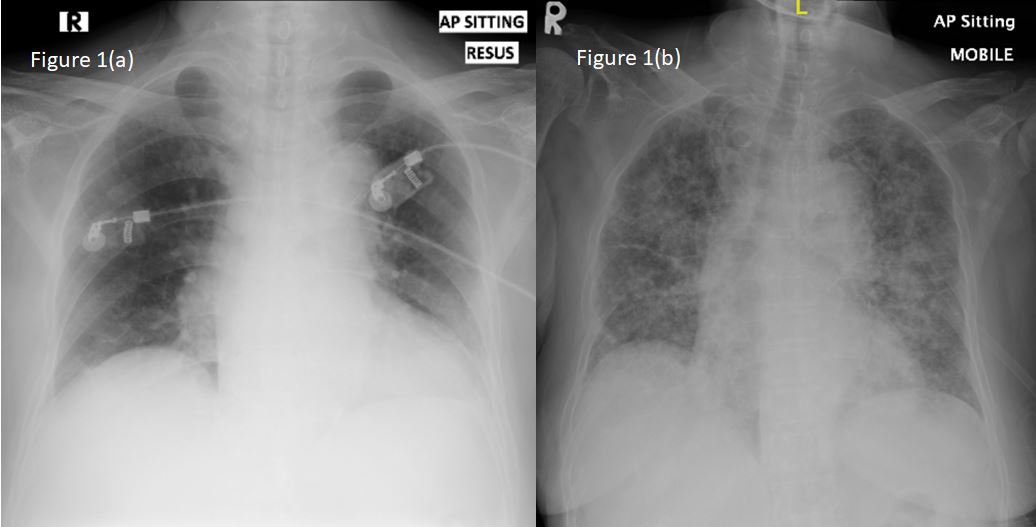
A 68-year old lady, known to have generalized MG for 12 years, presented to our centre following a week history of diarrhea and lethargy. She describes having loose stools, up to 8 times per day, chills and rigors, but denied per rectal bleeding or melaena. The patient was, on regular oral prednisolone (50mg a day). She had recently ceased her azathioprine 4 months prior due to severe anaemia, linked to myelosuppression following a bone marrow aspiration test revealing markedly reduced erythropoiesis, normal oesophageo-gastro-dudodenoscopy and colonosocopy, and having normal thiopurine methyltransferase levels prior to azathioprine initiation. The patient had several admissions in that 4 months due to her anaemia, requiring packed cell transfusions, and had recently sustained an interhemispheric subdural bleed two weeks prior following a mechanical fall. At the time, hemoglobin and platelet levels had returned within normal range. Clinical examination was unremarkable and her vitals on arrival included an oxygen saturation of 98% on room air with a normal chest radiography on arrival (Figure 1a). The patient was subsequently treated for infective gastroenteritis, and was started on metronidazole.
Figure 1: Chest radiography on (a) initial presentation and (b) 48-hours into admission, showing newly developed diffuse bilateral consolidation.
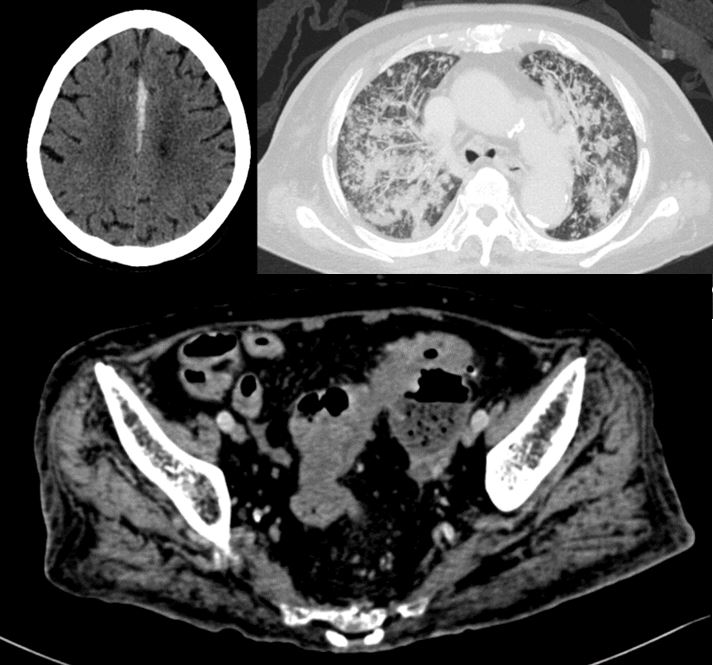
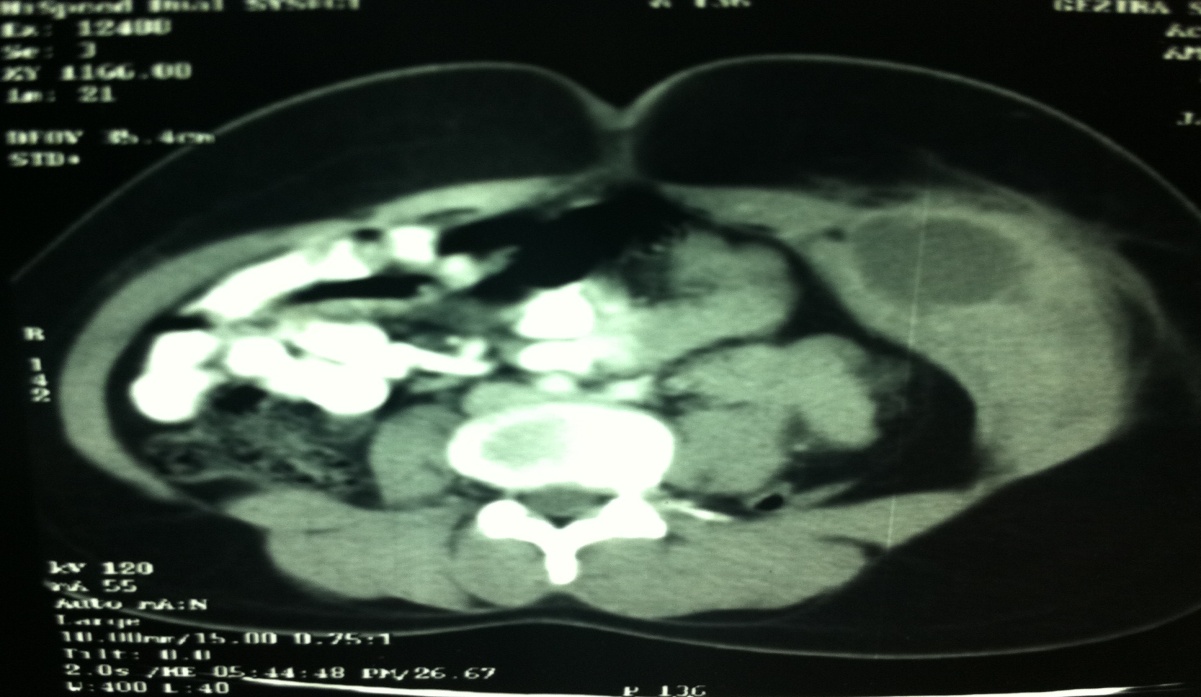
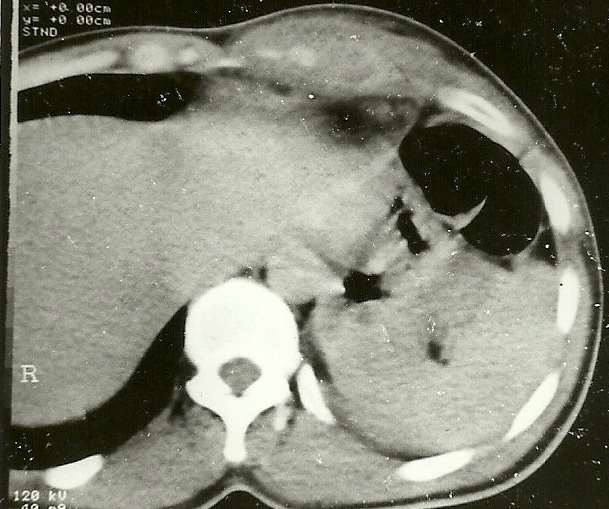
Unfortunately, 48 hours into her inpatient stay, the patient developed acute dyspnoea in which her oxygen saturation dropped to 77% under room air and examination revealed diffuse, coarse crepitations bilaterally. A repeat chest radiograph confirmed diffuse consolidation bilaterally (Figure 1b). She was subsequently treated for a hospital-acquired pneumonia, and had her antibiotics swapped to intravenous ceftriaxone. Unfortunately, the patient showed little improvement on the ward, which prompted further investigation. Her blood cultures revealed presence of nocardia farcinica which was resistant to ceftriaxone. In view of being immunosuppressed, a computed tomography (CT) imaging of the brain, thorax, abdomen and pelvis (Figure 2) was performed. Imaging showed extensive bilateral lung consolidation and reticulonodular opacities, predominantly in upper lobes. There was also evidence of sigmoid colon diverticulitis with a rim-enhancing collection adjacent to the posterior aspect of the proximal-to-mid sigmoid colon (2.9 x 2.6 x 2.6 cm).
Figure 2: Computed tomography (CT) imaging of (a) the brain, revealing inter-hemispheric hyperdensity consistent with a subdural haematoma, (b) the thorax, revealing extensive bilateral lung consolidation and reticulonodular opacities, predominantly in upper lobes, and (c) abdomen, showing sigmoid colon diverticulitis with a rim-enhancing collection adjacent to the posterior aspect of the proximal-to-mid sigmoid colon (2.9 x 2.6 x 2.6 cm).
Following consultation with our Infectious Disease team, the patient was treated for likely disseminated nocardiosis using intravenous trimethoprim/sulfamethoxazole as a recommended first line therapy. Unfortunately, following 72 hours of trimethoprim/sulfamethoxazole administration, the patient developed severe pancytopenia (haemoglobin 63 g/L, white cell count 2.0 x 109/L and platelets 33 x 109/L) requiring packed red cell and platelet transfusions, as well as immediate cessation of trimethoprim/sulfamethoxazole. Further decisions on antimicrobial proved difficult as it was noted that other effective alternatives against nocardiosis, including amikacin and fluoroquinolones may potentially exacerbate MG symptoms. Furthermore linezolid, another possible alternative, could potentially exacerbate her thrombocytopenia and worsen the pre-existing subdural haematoma. Thus, a decision was made to commence co-amoxiclav and meropenem concurrently despite neither being first-line therapy. The patient subsequently had an uneventful CT-guided drainage of the sigmoid abscess, with the assistance of our General Surgical colleagues, and was kept on prolonged intravenous antibiotic therapy for 3 months. Following improvement in clinical state, she was allowed discharge from hospital with ongoing oral co-amoxiclav and linezolid with regular bloods tests to monitor for myelosuppression as an outpatient, which has not occurred till this date. With support from clinical and radiological improvement, we aim for 12 months of therapy.
Discussion
Various cases of nocardia sp bacteraemia have been reported, in which immune system dysfunction was primarily due to chronic glucocorticoid therapy 134. A retrospective review of 40 patients from a Chinese tertiary hospital revealed that half of patient with nocardiosis were on corticosteroids prior to infection onset 5. An even larger case series reported up to 94% of pulmonary nocardial infection being linked to use of immunosuppressants 6.
Management of nocardiosis can be challenging. Often, imipenem, trimethoprim/sulfamethoxazole, amikacin or a combination of these antibiotics are recommended, with treatment duration being guided by clinical and radiological improvement often extending up to a year 7. Bactericidal agents including carbapenems and amikacin are often recommended alongside trimethoprim/sulfamethoxazole in cases of disseminated nocardiosis to ensure greater success in treatment 7, 8. The use of amikacin however should be cautioned in cases of MG, and reports have described management using linezolid as an alternative 1, 9.
In our patient, the risk of worsening pancytopenia as illustrated following trimethoprim/sulfamethoxazole administration led to hesitance in using linezolid. Furthermore, the consequences of thrombocytopenia would have been devastating for the patient due to having residual subdural hematoma. Thus, the choice of antibiotics was limited to that of second-line agents including co-amoxiclav and meropenem on top of surgical drainage of existing abscesses, which has also been shown to be beneficial 15. However, it should be noted that the risk of pancytopenia remains to be multifactorial in our patient, ranging from pre-exisitng myelosuppression to ongoing sepsis and initiation of culprit medications
Mortality of nocardiosis infections ranges depending on organ involved, rates being under 40% in cases of pulmonary spread, and up to 100% when disseminated to the central nervous system (CNS) 6. Unfortunately, nocardia farcinica, the subtype reported in our case, has been shown to be more resistant to antimicrobials and carries a greater risk of dissemination to the CNS, a point being greatly considered as our centre continues to manage the patient 10.
Conclusion
Nocardiosis, although not uncommon in immunocompromised individuals, poses a unique challenge in the MG population due to limitations in suitable antibiotics. Our case highlights the importance of a multi-disciplinary approach, involving various specialties including the infectious disease, neurology, general surgical and microbiology to ensure successful management of such complex cases.
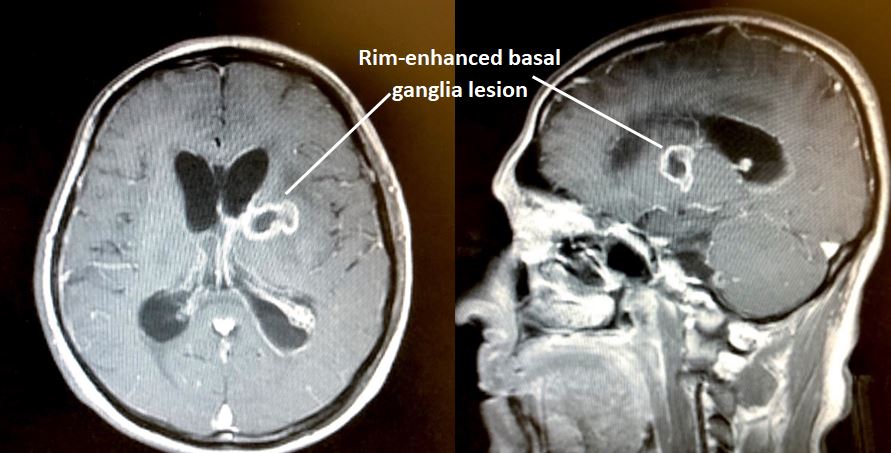
Tuberculosis (TB) involving the central nervous system (CNS) account for 2 to 5% of all TB cases1. Commonly it manifests in three ways – meningo-encephalitis, tuberculomas or abscesses2. Treatment should be guided by histological evidence, which unfortunately can be difficult to obtained in those with CNS dissemination. We present a rare case of solitary basal ganglia tuberculous abscess, which provided a diagnostic dilemma and led to complex management planning.
Case Report
A 53-year old man, with no known medical illness, presented with a 5-day history of fever, vomiting and altered mental behaviour. His vital signs were stable, on arrival aside from being pyrexial at 38°C. There was, however, neck stiffness noted on clinical examination as well as evidence of increased tone on the right upper and lower limbs, with an upgoing right-sided plantar response. Power was preserved in all limbs.
An initial contrast-enhanced computed tomography (CT) imaging of the brain revealed a hypodense lesion measuring 1.6 cm x 2.1 cm x 1.8 cm in the left basal ganglia region, with rim enhancement, complicated by cerebral oedema causing mass effect and mild hydrocephalus (Figure 1). A lumbar puncture was performed, and cerebrospinal fluid (CSF) analysis suggested the possibility of bacterial infiltration (Table 1). Initial, Ziehl-Neelsen (ZN) staining, mycobacterium tuberculosis (MTB) cultures and Gene Xpert nucleic acid amplification test (NAAT) from CSF were negative and a HIV antibody serology was negative as well. A transthoracic echocardiogram and CT imaging of the thorax and neck were both performed, failing to identify a possible source of spread. Furthermore, there was no evidence of focal lung infection or collection, and no evidence of lymphadenopathy of note.
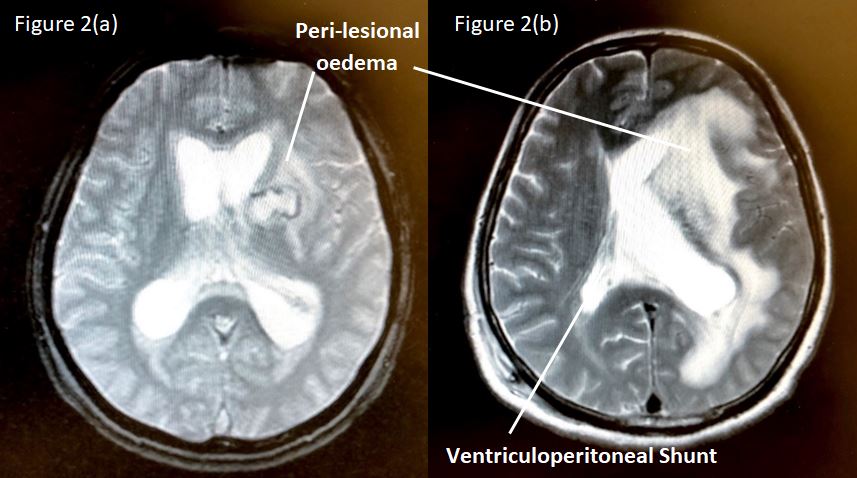
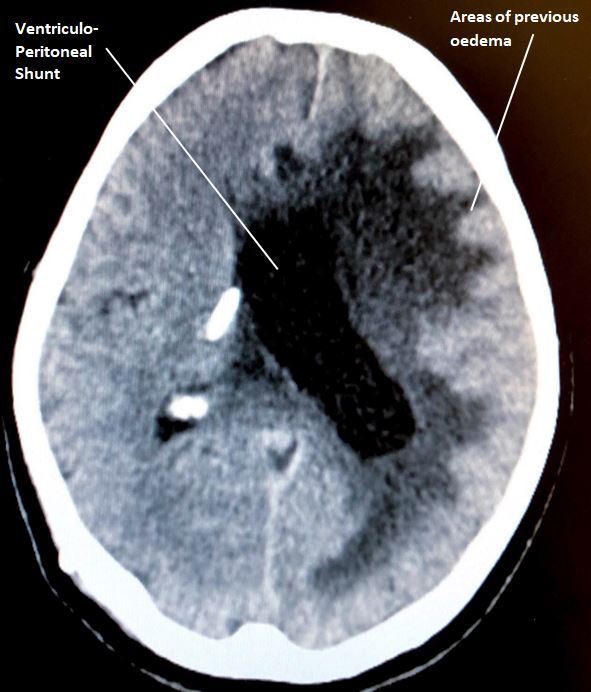
The patient was initially treated for 2 weeks with intravenous antibiotics, using intravenous Ceftriaxone 2g BD and Metronidazole 500mg TDS. Intravenous Dexamethasone was also commenced in view of the cerebral oedema. Unfortunately, the patient showed no clinical improvement, prompting repeat CT and Magnetic Resonance Imaging (MRI) which revealed an unchanged left basal ganglia enhancing lesion, with worsening obstructive hydrocephalus, perilesional oedema causing midline shift. The lesion was in contact with the lateral wall of the left lateral ventricle, with evidence of acute ventriculitis and involvement of the basal cisterns (Figure 2). A right-sided ventriculo-peritoneal shunt was inserted in view of the worsening hydrocephalus and persistent symptoms of headache and vomiting. Subsequently, stereotactic drainage and biopsy of the lesion was discussed but could not be performed in view of its deep location. A decision was thus made to initiate anti-tuberculosis therapy (ATT) empirically and to cease antibiotics. Subsequently, the patient’s clinical state improved with ongoing ATT and active inpatient rehabilitation, alongside improvement in the lesion, via radiological evidence (Figure 3).
Table 1: Cerebrospinal Fluid (CSF) test and other investigations performed during admission.
Test for Cerebrospinal Fluid (CSF)
Results
Other Test
Results
Micro-Total Protein
3.8 g/dL
Lumbar Puncture Opening Pressure
19 cm H20
Glucose
1.65 mmol/L
Lumbar Puncture Closing Pressure
16 cm H20
Culture & Sensitivity
Negative
Random Capillary Glucose
7.3 mmol/l
India Ink
Negative
Ziehl-Neelsen Stain
Negative
HIV Antibody
Negative
MTB Culture
Negative
Echocardiogram
No vegetation or mass
MTB NAAT (GeneXpert)
Negative
Cell Count & Cytology
No atypical cells. Mixed of pleomorphs and lymphocytes seen
Figure 1: CT imaging of the brain on (a) axial and (b) saggital view, illustrating a well-circumscribed, rim-enhanced lesion in the left basal ganglia region, suspicious of an abscess
Figure 2: T2-sequence of MRI brain on axial view (a) pre- and (b) post-procedure involving ventriculo-peritoneal shunting, illustrating a well-circumscribed hyperdense basal ganglia lesion, with peri-lesional oedema, as well as evidence of hydrocephalus.
Figure 3: Non-contrasted CT brain on axial view, illustrating less apparent left basal ganglia lesion, with hypodensities in areas of previous oedema, as well as an in-situ ventriculo-peritoneal shunt.
Discussion
Basal ganglia abscesses are very rare, incidence varying between 0.9 to 4% of total brain abscesses3. These are often disseminated lesions from sources such as congenital heart disease infections, intrathoracic and abdominal sepsis, dental caries, otitis media or sinusitis3-4. Solitary tuberculosis lesions, which includes tuberculous abscesses (TBA), in the basal ganglia are additionally more uncommon, even in endemic countries, as they normally have a predilection for the cerebellum and brainstem5. TBA has been seen in both the immunocompromised, or otherwise, where clinical presentation differs only slightly6-9.
Similar to other brain abscesses, stereotactic aspiration remains the gold standard diagnostic tool but there is a risk of rupture into ventricles or the subarachnoid space (leading to ependymitis or meningitis), worsening neurological deficits and more importantly the possible need for repeated procedures in as many as 70% of patients9.
Although experts advocate the combination of both surgical and chemotherapeutic therapy in managing TBA, the former was limited by the location of the lesion, whereas the latter was due to lack of histological evidence. Furthermore, the lack of risk factors, negative yield from cultures, NAAT and ZN stain, and inability to biopsy made the decision-making complex in our patient. Fortunately, there are evidence to support presumptive ATT for diagnostic and therapeutic purposes, which was adopted in our case5. This, however, requires cerebrospinal fluid examination, lung CT imaging and brain MRI that can provide circumferential evidence for diagnosis and to monitor treatment progress, all of which were performed in our gentleman5. In fact, CT imaging of the thorax is considered mandatory in cases suspicious of asymptomatic and subclinical extra-neurological tuberculosis, although yield remains poor (detecting abnormalities in only 38 to 56%)10.
Conclusion
Although CNS involvement in extra-pulmonary tuberculosis is not uncommon, TBA in the basal ganglia region remains a unique entity which poses a challenge in terms of diagnosis, as histological evidence is often difficult to obtain. As adopted in the case highlight, empirical therapy using ATT remains a valid option, especially in areas limited by resources and appropriate skills to perform intracranial biopsies, which is a common occurrence in endemic areas globally.
Evidence suggests that Serotonin has an important role in bladder control through central and peripheral neurological pathways. The three main serotonin receptor sites involved in the micturition pathway are 5-HT1A, 5-HT4, and 5-HT7. 5-HT7 and 5-HT4 are excitatory to acetylcholine release and 5-HT1A is inhibitory. Increased serotonergic activity leads to parasympathetic inhibition, which results in urine retention. It is through this mechanism of action and their effect on pre-synaptic serotonin 1A and peripheral 5-HT3 receptors that SSRIs were observed to have anti-enuretic effect. However, the exclusive role of serotonin in this regard is not fully understood because along with serotonin, other neurotransmitters, particularly acetylcholine are also implicated in micturition physiology. Acetylcholine is released from nerves innervating the detrusor muscle and causes bladder contraction resulting in voiding. Contrarily, adrenergic pathways lead to constriction of the bladder sphincter and promote continence. There have been suggestions that at lower intrasynaptic 5-HT concentrations, there is prevalence of inhibitory control of micturition, whereas excitatory effect is more pronounced at higher concentrations of 5-HT. This may suggest a dose-dependent relationship between Sertraline and urinary side effects. 1
Case Reports:
Case 1
A 14 year old girl with a diagnosis of moderate depressive episode was prescribed Sertraline 150 mg once daily. On follow up with her community psychiatrist, mum reported that she had been having episodes of bedwetting on a regular basis for almost two weeks. There was no past history of enuresis, no medication changes, or changes to her diet or routine. She had been drinking fluids during the day and had limited fluid intake after 6 pm. On a visit to the Sheffield Children’s Hospital, she had been diagnosed with a urinary tract infection and was prescribed a five-day course of antibiotics. She denied symptoms of abdominal pain, dysuria or fever.
On discussion with the trust pharmacist, it was reported that urinary incontinence is a rare listed side effect of Sertraline with nocturia occurring in 1 in 100 to 1 in 1000.2 At further medication review appointments, the patient continued to report being incontinent on approximately every alternate night and had to use incontinence pads. It was agreed with the patient to reduce the dose of Sertraline to 100 mg once daily to test if her urinary incontinence was linked to Sertraline and review after 2 weeks in clinic. The reduction in Sertraline dose to 100mgs once daily did not alter the frequency of bedwetting that continued on most week nights and varied from being partial to full emptying of the bladder. As a result, she was then referred to the Paediatric Community Incontinence clinic for further investigation regarding the sudden onset of these night bedwetting episodes. Concurrently, Sertraline was gradually reduced and stopped. She was switched to Fluoxetine liquid for treatment of her depressive symptoms, which was titrated to a dose of 16 mg once daily. At the community continence clinic, urine dipstick was negative. Systemic examination including a neurological examination was unremarkable. Mum reported that since the change in medication from Sertraline to Fluoxetine, there was a remarkable improvement in her urinary symptoms.
Case 2
A 16 year old boy with a diagnosis of mixed anxiety and depressive disorder was initiated on Sertraline which was gradually titrated to a maximum dose of 200 mg once daily. He reported improvement in his symptoms of anxiety and depression. However, a few days into taking the higher dose, he experienced symptoms of hesitancy with micturition and failure to ejaculate. On reduction of Sertraline to 100 mg once daily, he reported complete resolution of urinary and sexual side effects, while still reporting a reactive and stable mood. Due to his significant progress, he was eventually discharged from CAMHS back to the care of his GP.
Case 3
A 12 year old girl with a diagnosis of Generalized Anxiety Disorder and Attachment Disorder reported three incidents of urinary incontinence whilst being on Sertraline 200 mg once daily. Sertraline was discontinued by the patient against medical advice. No follow up information was available to observe for resolution of symptoms after discontinuation of Sertraline.
Discussion:
Selective Serotonin Reuptake Inhibitors (SSRIs) are a very commonly used class of psychotropic medication in the CAMHS population to treat depression, anxiety, PTSD and OCD. 3 It is evident by the cases discussed above that SSRIs may have a key link in causing symptoms of urinary dysfunction, which may range from nocturnal enuresis to acute urinary retention. This could be explained by Serotonin’s pivotal role in micturition through central and peripheral pathways. There is not enough evidence on the links in a child and adolescent population as most of the studies are on an adult cohort.4
Conclusion:
In conclusion, it is important for clinicians to bear in mind the genitourinary side effects of SSRIs, which may be debilitating for patients in the CAMHS population. It is equally important for us as clinicians to educate young people and their parents about these potential side effects and how they can be managed. It has also been observed that higher doses of Sertraline have shown a possible link between onset of urinary side effects. In order to establish a significant causal and dose-related relationship on the onset and severity of genitourinary symptoms, studies with a larger sample size followed up over a longer period would be required.
Calcinosis cutis involves deposition of calcium salts in skin and subcutaneous tissue. It is commonly associated with autoimmune connective tissue diseases and can be a source of pain and disability1. It can occur in damaged or devitalized tissues in the presence of abnormal or even normal calcium/phosphorus metabolism. These calcifications can lead to contractures, muscle atrophy, skin ulceration and infections2. There are four types of calcinosis cutis: idiopathic, dystrophic, metastatic, and iatrogenic. Determining the type of calcinosis is very important for accurate management3.Calcinosis cutis is a condition seen in the middle to elderly aged population and has rarely been described in neonates in the medical literature. We discuss a neonate in the succeeding text who presented to our Emergency department with a leg swelling.
Case Report
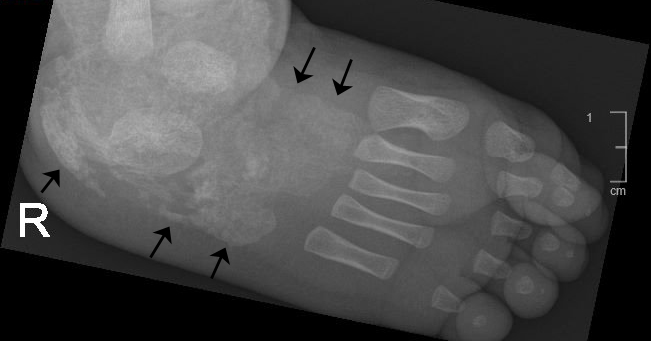
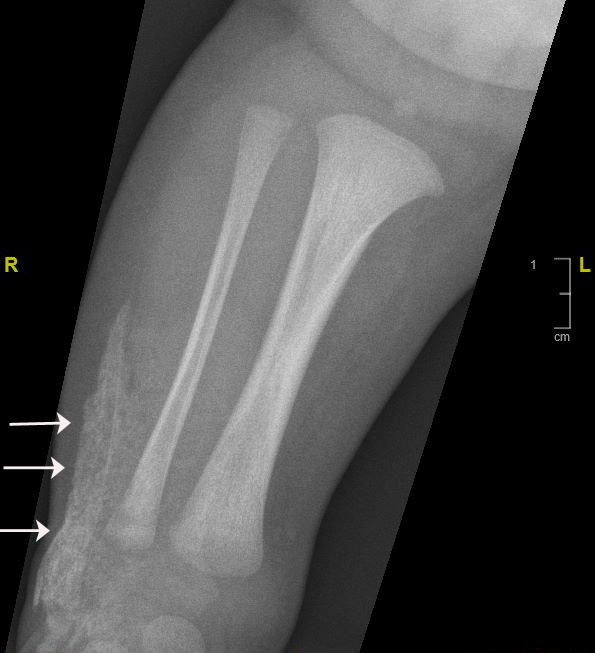
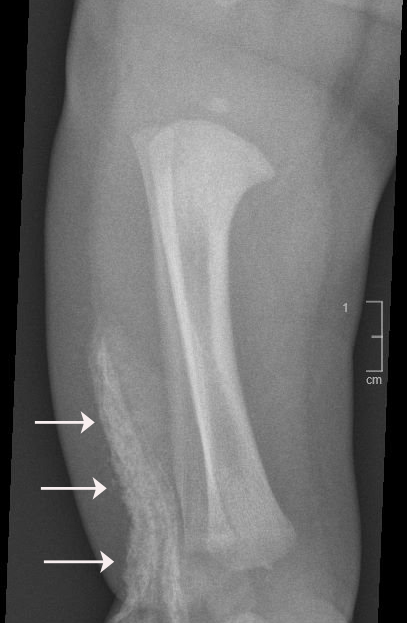
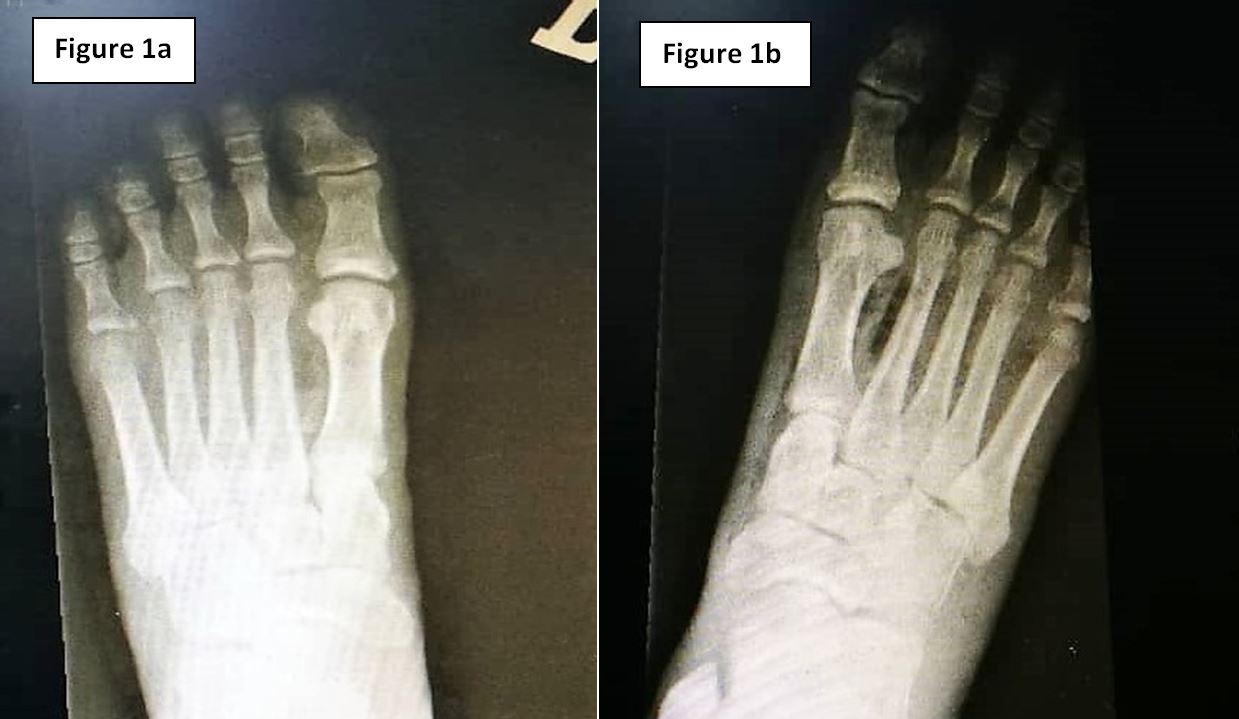
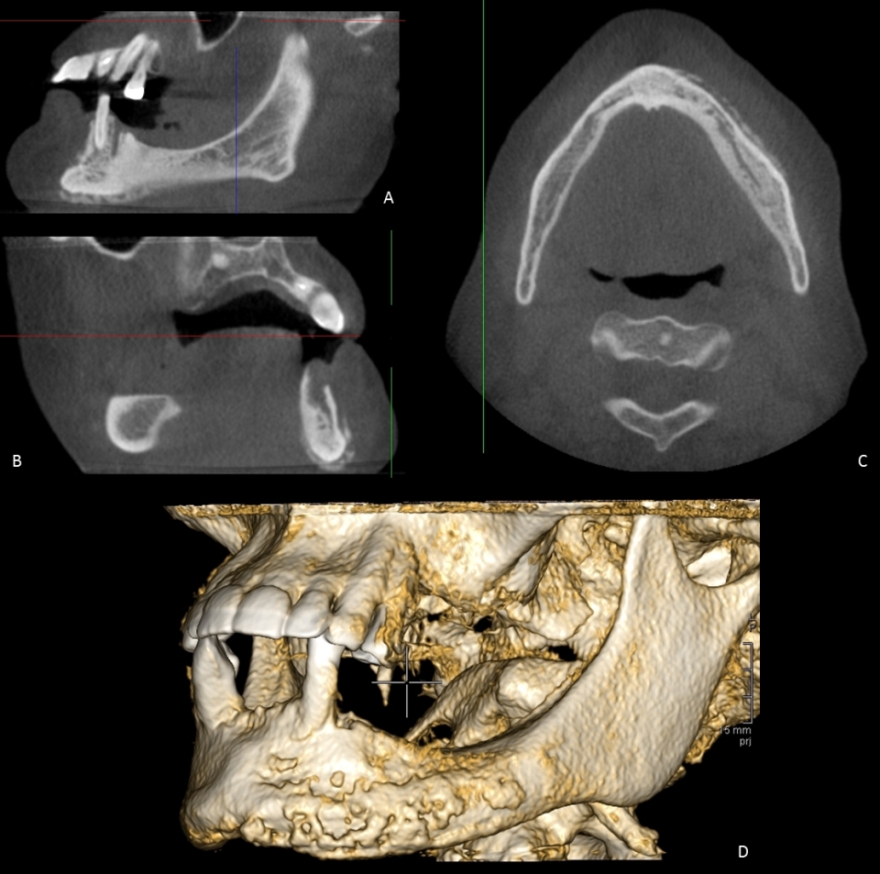
A 20 days old full term neonate was brought to our Emergency department with right leg swelling for the past ten days. He was feeding well and was afebrile. On examination there was swelling of right lower leg including the right foot with minimal redness of overlying skin. We did x-rays of the right foot and right leg, which showed a sheath of cutaneous calcification in right foot (Image A and Image B) and anterior-lateral of right leg (Image C and Image D).
Image A
Image B
Image C
Image D
There was no evidence of any bony destruction. White cell count and other inflammatory markers were normal. Upon reviewing the previous records we found that soon after the birth the neonate was admitted with pneumonia and during the hospital admission there was extravasation of calcium gluconate infusion at the dorsum of the right foot which explains the whitish sheath seen in the imaging. Musculoskeletal ultrasound did not reveal any signs of fluid collection or periosteal swelling. The patient was treated conservatively and regular follow up was insignificant and showed complete regression of the swelling three months later.
Discussion
Calcinosis cutis is an uncommon disorder caused by an abnormal deposit of calcium phosphate in the skin in various parts of the body. It is often noted in the subcutaneous tissues of connective tissues diseases primarily systemic lupus erythematosus, scleroderma and juvenile dermatomyositis4,7. Four main types of calcinosis cutis have been recognized according to etiology: associated with localized or widespread tissue changes or damage (dystrophic calcification), that associated with an abnormal calcium and phosphorus metabolism (metastatic calcification), not associated with any tissue damage or demonstrable metabolic disorder (idiopathic calcification), and Iatrogenic2-3,6-7.
It is recommended that patients be evaluated for abnormalities of calcium and phosphorus metabolism and that they be assessed for associated systemic conditions, such as collagen vascular diseases, renal insufficiency, and vitamin D poisoning. Determining the exact type of calcinosis cutis is very important for selecting accurate management3. Many agents have been used for treatment of calcinosis but none has been accepted as a standard therapy. Case studies have shown that aggressive treatment of the underling inflammatory condition with intravenous immunoglobulin, anti TNF agents, thalidomide and haematopoietic stem cell transplantation has also led to improvement of the calcinosis1,3. Moreover, agents such as warfarin, bisphosphonates and diltiazem have been aimed at treating the process of calcinosis with varying success3.Some experts have advocated surgical excision in severe resistant cases4.Calcinosis cutis has been rarely reported in neonates. It almost exclusively occurs due to iatrogenic causes8. Calcium gluconate has been widely used in the treatment of neonatal hypocalcemia which is a common problem confronted in this age group. When extravasation of calcium gluconate occurs; swelling, erythema, signs of soft tissue necrosis or infection may be seen. Rarely local calcification appears, called calcinosis cutis9-10.
Plain radiography is gold standard for diagnosis but are initially negative because calcium solutions used therapeutically are radiolucent. X-ray findings usually appear within 1-3 weeks9.This is consistent with our case. The pathogenesis of calcinosis cutis caused by extravasation of IV calcium is degeneration and soft tissue necrosis11. If extravasation of calcium gluconate is suspected; the IV line must be removed immediately. Cold packs should be applied for 15 minutes four times a day to treat edema at extravasation sites and limb elevation for 48 hours is suggested12. Supportive care remains the main element of the treatment and only in case of skin necrosis and secondary infection, debridement and antibiotics should be used8.
Calcinosis cutis in neonate can be easily misdiagnosed ascellulitis, arthritis, pyogenic abscess, osteomyelitis and thrombophelibitis8.In the present case also initially we were suspecting an infectious etiology. Initial x-rays can be misleadingly normal as it take about ten days to precipitate. The clinical and radiological findings usually disappear over a span of 2-6 months which is compatible with our case too13.
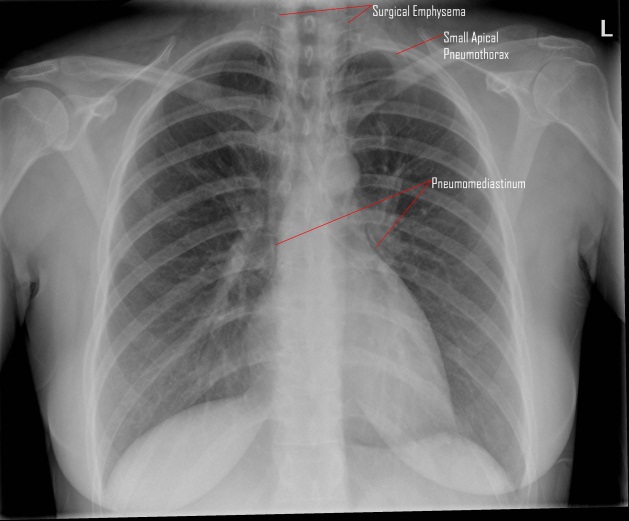
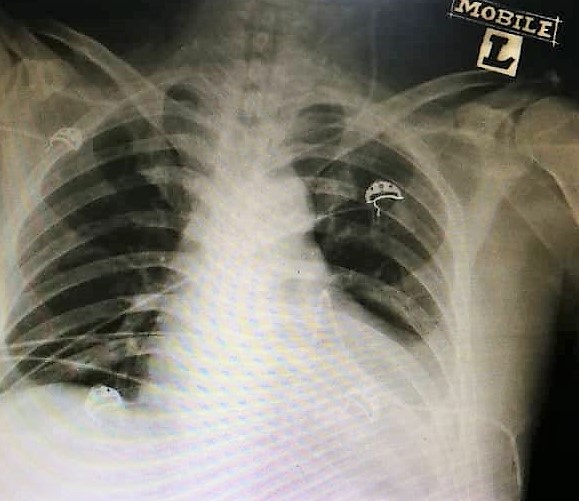
A 33 year-old ASA1, primigravida, presented to our delivery suite with spontaneous onset of labour at 38 weeks of gestation. Epidural analgesia was commenced to alleviate her labour pains. Subsequently, she underwent an assisted vaginal delivery of a live male baby (weighing 4660 gms) using Keiland’s outlet forceps after 90 min second stage of labour. 10 hours postpartum, she complained of dyspnoea & severe central substernal chest pain. She was noted to have an unusual swelling of face and neck with oxygen saturations of 90 % on room air. Ascultation of chest revealed normal bronchovesicular breath sounds, normal heart sounds with absence of added sounds. Arterial blood gases showed an O2 tension of 11 kpa, CO2 tension of 5 kpa and pH of 7.34. The diagnosis of subcutaneous emphysema, pneumomediastinum and small left apical pneumothorax (Hamman’s syndrome) was confirmed on chest X-ray (CXR 1). We ruled out differential diagnosis of pulmonary embolism, Tension pneumothorax, angina pectoris, pericarditis, dissection of aortic aneurysm, mediastinitis, cardiac tamponade, chest infection & oesophageal tear. She was managed conservatively by close monitoring for complications, administration of supplemental oxygen and use of simple analgesics. She demonstrated a complete uneventful recovery over the next 24 hours with normalising of chest signs (CXR 2).
CXR 1: shows pneumomediastinum, extensive surgical emphysema & a left apical pneumothorax.
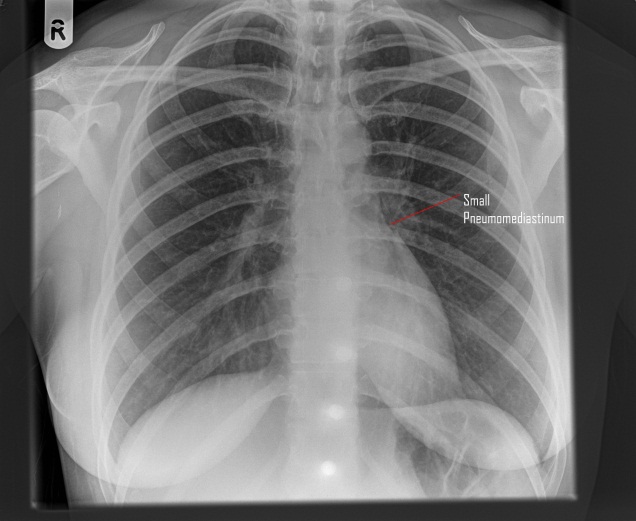
CXR 2: shows small pneumomediastinum, the surgical emphysema & pneumothorax resolved.
Discussion:
Hamman’s syndrome is named after Louis Hamman (1847-1946), the physician who first described it in 1945. The first reference to this condition was in 1618, when Louise Bourgeois, midwife to the Queen of France, wrote, “I saw that she tried to stop crying out and I implored her not to stop for the fear that her neck might swell”3.
Hamman’s syndrome usually occurs in the 2ndstage of labour & is associated with prolonged and protracted labour and larger than usual babies 4. However, the clinical presentation is often delayed to the postpartum phase as was clearly seen in our case. The condition seems to be provoked by any valsalva manoeuver such as vigorous coughing/vomiting/sneezing, forced physical activity & enormous efforts during spontaneous vaginal delivery. Its occurrence is usually related to the expulsive phase of labour when ‘pushing down’ actively raised the intraalveolar pressure. This may subsequently increase the intrathoracic pressure up to 50 mm of Hg or higher1. Rupture of marginal alveoli with air entering along the perivascular sheath into the mediastinum is the most likely mechanism, in our case. It is probable that, the air tracts through the fascial planes into subcutaneous and retroperitoneal tissues. Other reported mechanisms of Hamman’s syndrome include oesophageal rupture during childbirth, or pneumomediastinum related to asthmatic bronchospasm5 or chest infection, or dissection of pneumoperitoneum, secondary to epidural catheter placement or caesarean section1.
Palpable crepitus on face & neck is suggestive of subcutaneous emphysema & appearance of this emphysema in labour is the hallmark of pneumomediastinum. Other features of pneumomediastinum include substernal chest pain, dyspnoea, voice change, cough, sore throat and tachycardia1. Hamman’s sign, a fine auscultatory crepitation synchronous with the heartbeat, heard along the left sternal border; is sometimes observed in this condition2.
Chest X-ray and CT thorax are the diagnostic tests. Majority of the patients with Hamman’s syndrome have pneumomediastinum & subcutaneous emphysema without any pneumothorax and this requires supportive management with strict monitoring. Our patient demonstrated a small pneumothorax, which was managed conservatively. A surgical intervention in the form of subcutaneous air drainage may occasionally be indicated in severe cases.
Overall most cases have a benign, self-limiting course when the aggravating factors are no longer present. Published data indicates that subsequent pregnancies pose no additional risk of recurrence5.
Conclusion:
Since Hamman’s syndrome is a potentially dangerous complication of normal childbirth. We propose that every obstetric anaesthetist and obstetrician should be aware of this syndrome.
Fractures in surgically fused scoliotic spines are very uncommon and only a few cases have been reported in the literature. It is not possible to predict the outcome of traumatic injuries in fused spines. There is no reported prevalence or prognostic data in the published literature and all we have are a few case reports from different parts of the world.
In this case report we describe an unusual case of a spinal fracture in a 60-year-old patient, who had surgical fusion of her scoliotic spine 50 years ago.
Case Report
A 60-year-old lady presented to A&E after a trivial fall on an icy path approximately 10 days before presentation. She had pain in her back since the fall, gradually getting worse despite escalating doses of opiate analgesics. Past medical history revealed that she had congenital lympho-haemangioma causing deformity in her back and left foot. At the age of 6 months she underwent an extensive surgical excision of the tumour along with amputation of her left foot. Subsequently she developed scoliosis at the age of 6 years, which was treated conservatively in a Milwaukee brace between the ages of 7 and 10. At the age of 10 she underwent an extensive thoraco-lumbar postero-lateral inter-transverse fusion using iliac crest bone graft without instrumentation to treat her progressive scoliotic curve. She was supported in a Milwaukee brace for further 6 months. Following this she had no problems in her back although she had a considerable residual deformity.
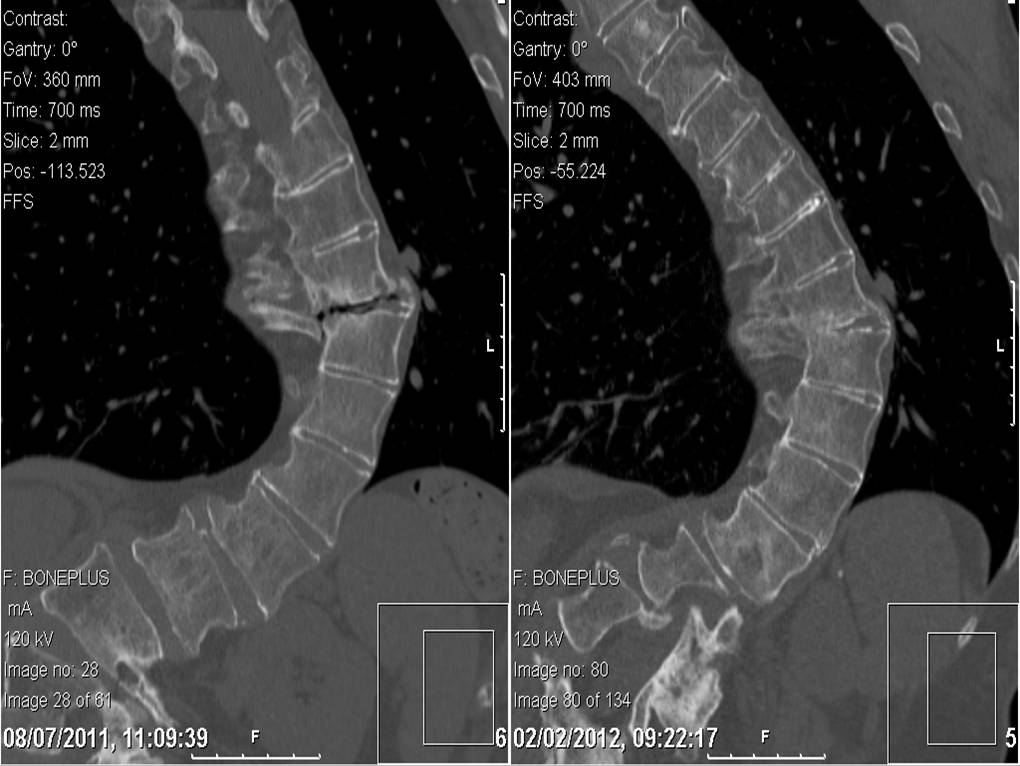
After this recent fall she developed pain in her right-sided thoracic hump. A full neurological examination revealed normal motor & sensory function in both lower limbs. Plain radiographs showed a thoracic scoliosis convex to the left and a broad fusion mass extending approximately from T4 to L1. There was no fracture seen. She was discharged from the A&E department with further analgesia. 3 days later she returned to A&E with increasing pain and respiratory depression due to excessive opiate usage. Investigations also revealed a very high level of serum lithium from her regular lithium medication combined with dehydration and deranged renal function. She was admitted in the high dependency unit for supportive care while the symptoms of pain and discomfort were progressively worsening. Another radiograph of her spine was again inconclusive of any bony injury. A CT scan was performed at this juncture. The CT scan (Fig. 1) showed a fracture line at the junction of T9-T10 extending through the fusion mass, with minimal displacement. She was neurologically stable on clinical examination.
The feasibility of surgical fixation of this fracture was discussed with a specialist scoliosis surgeon and a decision was made to pursue conservative treatment, considering her ongoing medical condition. Surgical fixation was deemed to be technically challenging and very risky. She was not found to be suitable for bracing either. She was advised bed rest with symptomatic management of pain, which was followed by protected and supervised mobilisation.
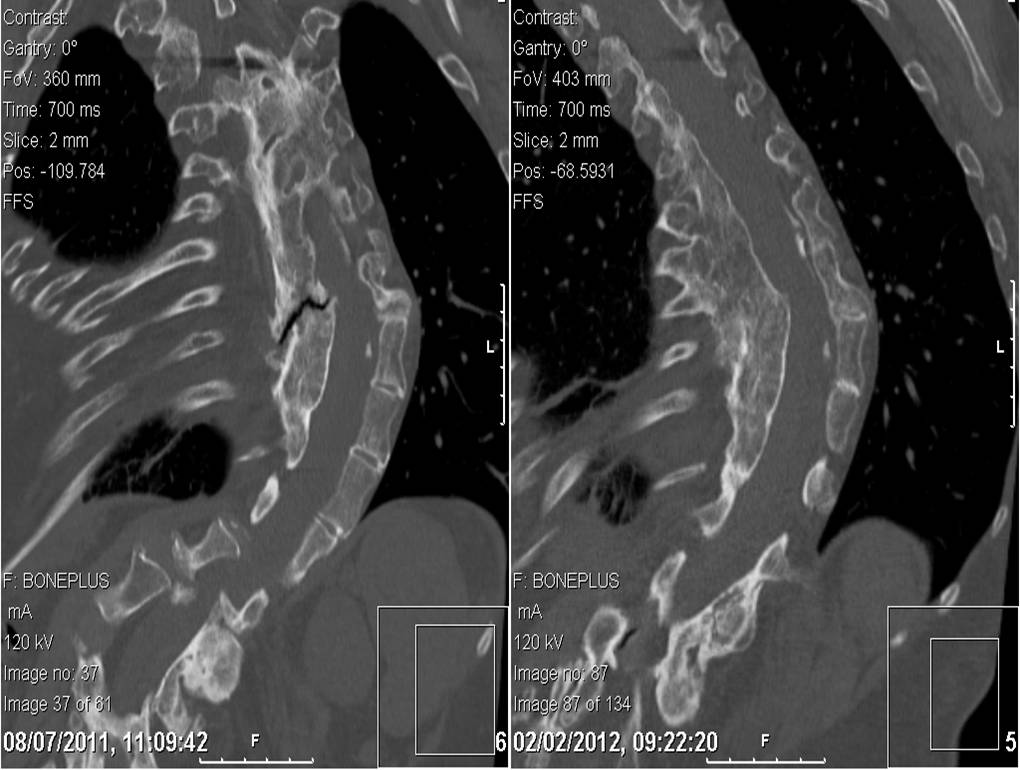
Further CT scans were performed after 6 weeks and after 12 weeks. These showed the fracture had remained stable but minimal signs of healing were observed with persistent gas shadows in the disc space. Throughout this she remained free of any neurological deficiency and her pain was under control. She was allowed mobilisation within the limits of comfort and under supervision. Serial CT scans were performed at the 7th month, which showed a stable spine and some callus formation at the fracture site. The latest follow up scans performed at the 12th month showed bony union had taken place (Fig 2 & 3). She was followed up in the outpatient clinic. She has resumed her normal activities and is now not requiring regular analgesia.
Figure 1- Coronal and Saggital CT Images of the Fracture from January 2011
Figure 2- Coronal Images compared between July 2011 and February 2012 showing healing
Figure 3- Saggital Images compared between July 2011 and February 2012 showing healing
Discussion
Fracture through a fused scoliotic spine is an uncommon entity. Healing of that fracture by conservative measure is fairly uncommon. Most authors point out that “the ankylosed spine breaks like a long bone, transversely, as a result of a bending force” (Bergmann)1. This fracture configuration results in higher rates of non-union and delayed union. In this light we have presented here a unique case report where a fractured fusion mass has healed without surgical intervention.
There are very few reported incidences of fracture through a spinal fusion mass after scoliosis surgery in the published literature in English. Two patients reported by Moskowitz et al2 had injuries as a result of traffic accidents. The exact mechanisms of the injuries were not described and their management was not discussed. One fractured through the fusion mass 20 years after surgery, the other 14 months after surgery.
King and Bradford3 described a fracture-dislocation of T11-T12 in a patient treated with Harrington rods. They decided to operate because of rod angulation and severe trunk de-compensation.
Tuffley and McPhee4 described a patient treated with posterior spinal fusion without instrumentation. The patient sustained a transverse fracture through the fusion mass without displacement after a fall. Posterior fixation with Harrington instrumentation was carried out.
Bagó et al5 described a 30 year old woman who had undergone anterior and posterior fusion with Cotrel-Dubousset instrumentation for progressive idiopathic scoliosis. Two years after surgery, she was in a car accident. A radiographic study and computer tomographic scanning depicted a fracture of T11 and bending of the rods. Observation was instituted and symptoms resolved.
Chung6 reported a post polio patient whose spine was fused from T7 to L4 as a teenager by spinal instrumentation, which was removed after achieving fusion. She fell down stairs fracturing the body of L2 without any neurological deficit. She was treated conservatively for 3 months after which non-union was observed. The fusion mass was fixed with an AO/ASIF broad dynamic compression plate rather than the convention spinal systems such as pedicle screws, Harrington or Luque system because of the absence of normal anatomical landmarks.
All the described case reports were from high-energy trauma unlike our case where the injury was very inconspicuous. We stress upon the fact that these injuries are very rare and can be very difficult to diagnose from plain radiographs. Our patient was fortunate not to have damaged her spinal cord, which is probably because of the low energy trauma she sustained. Our conservative management has worked well in alleviating her symptoms and achieving bony union.
The spectrum of psychiatric illness in Systemic lupus erthyromatosus (SLE) include psychotic, depressive, subtle cognitive and personality disorders of histrionic type. The occurrence of psychiatric manifestations in SLE varies widely from 5 to 83%. It is postulated that there is a direct action of the disease on the central nervous system by autoantibodies namely anti phospholipid and anti-ribosome P auto antibodies or cytokines like interleukin 2, interleukin 6, alpha interferon 1. During the course of the disease side-effects of glucocorticosteroids and hydroxychloroquine or anxious reaction to chronic and potentially lethal illness is postulated to be another mechanism of psychiatric manifestation of SLE . SLE patients are prone to develop myriad of psychological distress in addition to neuropsychitric manifestations which require a social and psychological support. While some of these manifestations are treated by corticosteroids and psychotropic drugs1 medications with anticholinergic side-effects, like phenothiazines, tricyclic antidepressants and hydroxyzine which enhance the oral dryness should be avoided in SLE.
Clinical scenario:
A 27-year-old male suddenly developed aggressive behaviour for the first time in his life ,while on his work place. The patient had no insight into his illness and was brought to the local psychiatric hospital by his colleagues where he was admitted as a case of acute mania. He was managed with electroconvulsive therapy (EST) in addition to antipsychotic medication as neuro imaging including CT scan and MRI brain were normal. A few days later , the patient was discharged on anti-psychiatric medicines. However, after six months while on antipsychotic medication, he developed a low grade fever .He was admitted to a local hospital where in addition to base line investigations a lymph node biopsy was done which revealed follicular hyperplasia, without any abnormal cell. Patient’s HBV, HCV, HIV were negative. The patient developed anorexia , significant weight loss and progressive difficulty in getting up from a sitting position .He also developed shortness of breath and presented to King Abdul Aziz specialist hospital in Taif, Saudi Arabia virtually in a bed bound state . He was admitted in the intensive care unit of the hospital .The examination revealed pallor, generalised lymph-adenopathy, palmer rash, alopecia and mouth ulcers. The patient had mild pericardial effusion and Mitral regurgitation (MR)++ on echocardiography. Further evaluation showed significant proteinuria. Serum ANA, dsDNA were positive .Lupus anticoagulant was negative. Keeping in view above symptoms and signs the patient was diagnosed as a case of SLE2 (Mouth ulcers, Pericardial effusion ,ANA positive , dsDNA positive ) The patient was managed with pulse dose of methylprednisolone 1g intravenously (IV) daily for 5days, followed by oral prednisone 60 mg once daily, which was tapered on follow up . Patient tolerated the treatment well and improved progressively . He became ambulatory and rejoined his job. The psychiatric medications were stopped.
However, on follow up the patient continued to have proteinuria 1.8 gm/24 hr. He was readmitted and the kidney biopsy revealed class IV lupus nephritis. He was given pulse cyclophosphamide 1gm/m2 intravenously and later started on tablet Mycophenolate 1.5gm once daily. The proteinuria improved and he is following our clinic for the last two years now .Patient’s follow up investigations are shown in table 1.
Table: 1 Patients’ hospital investigations and results
Test
Result Pre-treatment (On presentation )
Result Post-treatment (After 6 weeks )
Normal range
Haemoglobin
6.2
12.3
12. 2-15.3 gm/dl
White blood cell
3.2
6.7
6-16 × 109/l
Platelet
41,000
197
150-450 × 109/l
ESR
82mm first hour
56mm
Total bilirubin
1.2
1.0
.0.8 to 1mg/dl
Direct bilirubin
1.0
0.8
0.-0.6µmol/L
AST
335
30
5-30U/L
ALT
257
29
5-30U/L
ALP
182
100
50-100U/L
GTT
497
65
7-30 IU/l
Albumin
39
39
38-54 g/l
Total protein
5.2
4.5
INR
1.1
1.1
0.8-1.2
Urea
62
40
Creatinine
1.2
1.0
Na/K
131/3.8
142/3.6
Serum glucose
100
102
65-110mg/dl
ANA
Positive
Anti DsDNA
Positive
Lupus anticoagulant
Negative
24 hr urinary protein
2.3gm/L
500mg/L
<150mg/L
Discussion:
The correct diagnosis of central or even peripheral nervous system manifestations in patients with SLE can be challenging because of many SLE-related and non-SLE-related processes present in a patient. The index case proved to have acute mania as the first manifestation of SLE which remained under oblivion till he developed serositis another complication of SLE. While this patient came to clinical attention after one year a case of SLE masquerading schizophrenia for 14 years was reported by Funaunchi et al3. In another report, a 14-year-old boy with a two-year history of cognitive dysfunction and behavioural problems SLE was diagnosed after two years4 . It appears that the psychiatric symptoms may occur as the first manifestation of juvenile SLE. It will not be out of place to mention that the psychiatric manifestation can be at times dire which could even result in harm to others in a given society. The case of Folie a trios syndrome, characterized by the transfer of delusional ideas from one person to two other persons culminating in murder has been reported in a patient with SLE5 . In a significant retrospective data from China (a cohort of 518) neuropsychiatric manifestations in SLE were observed in 96(19%) of the above study cohort . The seizure disorder accounted for the most prevalent disorder of neuropsychiatric manifestations (NP) of SLE followed by cerebrovascular disease and acute confusional states. In the above study, 96 patients with psychiatric symptoms, acute psychosis was observed in 10(11%)patients. Authors in this study were of the opinion that this percentage could have been higher if subtle cognitive dysfunction were included as well. Authors of the same study further concluded that the antiphospholipid antibodies were significantly associated with NP manifestations, especially cerebrovascular disorders6.
The autoantibodies have been found to be biomarkers for future neuropsychiatric events in SLE. A prospective study throughout ten years conducted among 1047 SLE patients demonstrated that individuals who had evidence of lupus anticoagulant (LA) were at an increased future risk of intracranial thrombosis. Further, those with anti-ribosomal P antibodies were at an increased future risk of lupus psychosis7. The Lupus anticoagulant in the index case was negative, and anti-ribosomal P antibodies were not available . A study by Sanna et al8 have shown that an association exists between anti-NR2 antibodies and depressed mood in addition to decreased short-time memory and learning. Authors in this study concluded that antibodies to NMDA receptors thus might represent as one of the several mechanisms for cerebral dysfunction in patients with SLE.
The CT scan brain of the index case was normal. However, massive bilateral calcification of sub-cortical structures in a patient with SLE with the psychotic disorder has been reported9. The psychiatric diseases are related to vasculitis and non-inflammatory vasculopathy of the small cerebral blood vessels. Further, a study has shown that ninety per cent of the patients with psychosis, organic brain syndrome or generalised seizures had increased IgG antineuronal activity as compared with only 25 per cent of the patients who presented with hemiparesis or with chorea/hemiballismus. The authors in the above study concluded that the diffuse central nervous system manifestations of SLE are a direct result of the interaction of the antibody with neuronal cell membranes10.
The management neuropsychiatric manifestation in SLE should include treatment of the disease itself and specific psychotropic treatment. The index case had rapid improvement following Glucocorticosteroid therapy. Intravenous infusions of immunosuppressive agents, such as cyclophosphamide, have been found to be effective in such conditions 1 . Psychotropic drugs may be used, but it is prudent to mention that SLE-inducing drugs, like chlorpromazine, carbamazepine and lithium carbonate must be avoided. Following treatment with steroids, the index case improved and all his antipsychiatric medications were finally stopped and he resumed his job.
To conclude the index case highlights that even though SLE is more frequent among females of childbearing age but males are no way immune to SLE . While evaluating patients with multiple unexplained somatic complaints and psychiatric symptoms SLE ought to be ruled out. The existence of neuropsychiatric manifestations in SLE constitutes an indisputable clinical reality that every practitioner must be able to recognise and treat.
Stress-Induced Cardiomyopathy (SCM), also known as Takotsubo Cardiomyopathy or Apical Balooning Syndrome, is an acute, transient and non-ischaemic cause of left ventricular dysfunction often precipitated by periods of stress1. Diagnosis often follows evidence of left ventricular hypokinesia despite a normal coronary angiography. Prevalence is often underestimated, with an estimated 7% of suspected myocardial infarctions being in fact SCM2. We report a unique case of multi-nodal dysfunction following SCM.
Case Report
A 73-year old lady presented to our emergency department following a sudden onset of central, non-radiating chest heaviness 8 hours prior. She was a known chronic smoker of 20 pack years, and hypertension which had been left untreated for over 10 years. An initial electrocardiogram (ECG) revealed sinus bradycardia and T-wave inversions in the inferior, septal and lateral leads (Figure 1). Her Troponin-I levels was raised at 6532 pg/ml. She was treated as a Non-ST elevation myocardial infarction and was admitted to the coronary care unit for closer monitoring. She was kept on telemetry overnight, which disclosed several episodes of bradycardia. Rhythm strip revealed various transient conduction defects, including that of sinus node dysfunction (SND) and atrioventricular node (AVN) dissociation, although she remained asymptomatic throughout (Figure 2).
Figure 1: Electrocardiogram revealing sinus bradycardia, with T-wave inversion in the inferior, septal and lateral leads.
Figure 2: Telemetry rhythm strip revealing transient episodes of (a) sinus node dysfunction (SND) and (b) atrioventricular node (AVN) dissociation.
Figure 3: Electrocardiogram revealed ST-segment elevation with associated T-wave inversions in the inferior, septal and lateral leads.
Figure 4: An ‘Apical 4-Chamber’ view on echocardiography, revealing an akinetic apex on (a) diastole and (b) systole.
Unfortunately, following an episode of chest pain the following morning, her troponin levels and an electrocardiogram were repeated, showing a rise of the former to 12 996 pg/ml. A repeat ECG revealed evidence of ST-segment elevation in previously affected leads (Figure 3). She was brought into the catheterization laboratory within 1 hour. Her coronary angiogram showed no evidence of coronary obstruction. An echocardiogram was performed, which revealed an akinetic apex (Figure 4).
Upon further history taking, it was revealed that she was recently made redundant from her job as a cleaner, several hours prior to her presentation to the emergency department. Prior to that, she denied any other emotional or physical stressors. She was diagnosed as having Stress-Induced Cardiomyopathy (SCM). Following an observational period of close to 48 hours, she was allowed home. A 48-hour Holter monitoring was performed approximately 3 weeks from her initial admission, which returned unremarkable. A repeat echocardiography was also performed, revealing normal wall motion abnormality which further support a transient SCM.
Discussion
Despite being transient, multiple complications can arise from the condition, including arrhythmias. Prevalence of arrhythmias varies greatly, depending on population and types of defect (15% suffering atrial fibrillation, 2-5% of tachyarrhythmias, 2-5% of bradyarrhythmias and 5% of AVN dissociation amongst others)3,4. This is largely due to evidence being based on retrospective case report and series, leading to severe underestimation of their true prevalence. We suspect cases of sinus node dysfunction are far more uncommon, with only a handful of case report of note, and one retrospective review of 816 patients quoting a rate of 1.3%5. There are no reports of concomitant sinus node and atrio-ventricular node dysfunction, to our knowledge.
Proposed mechanisms for SCM-induced nodal dysfunction include reduced coronary flow to conduction tissues due to left ventricular dyskinesia, cathecolamine-driven coronary and microvascular vasospasm leading to both reduced blood supply and direct cardio-toxicity effects, and continual ischaemia-driven fibrosis of nodal tissue6. However, there have been reports of SND-triggered SCM, likely secondary to adrenergic compensative activation following bradycardia events. In both scenarios, pre-existing, subclinical SND may lower the threshold of developing significant, symptomatic bradycardia7-10. This is important to note, as majority of patients affected by SCM are post-menopausal women whom are already at risk of age-related SND.
In our patient, the SCM may have likely induced both SND and AVN dissociation, as subsequent 48 hours Holter monitoring, 3 weeks from presentation, was unremarkable. Furthermore, the patient denies any previous syncopal or pre-syncopal symptoms. However, the possibility of subclinical SND could still have existed, as we had earlier discussed, and ideally an internal loop recorder for prolonged monitoring, catheter-based electrophysiology studies and a Cardiac Magnetic Resonance Imaging to detect nodal and conduction tissue fibrosis would assist in ruling out pre-existing nodal dysfunction. However, due to financial and pragmatic reasons (as patient was asymptomatic), the patient declined further investigations, opting for periodic clinic reviews instead.
Conclusion
Both nodal and conduction tissue blocks are a rare but significant complications that can occur following SCM. The occurrence of SND following SCM should lead clinicians to routinely investigate for pre-existing conduction tissue diseases, if not already performed and allows for earlier device implantation if deemed indicated.
Necrotising soft tissue infections (NSTI) are severe and rapidly progressive, requiring rapid recognitions and early, often surgically-based, management. Mono-microbial types of NSTI (i.e. Type 2 NSTI), which amounts for 20 to 30% of overall cases, are often linked to invasive Group A Streptococcus or Staphylococcus Aureus infections 1. Rarely, Group B Streptoccocus (GBS), also known as Streptococcus Agalactiae, are implicated 2. We report a unique case of NSTI of the lower limbs due to GBS, with acute pericardial dissemination leading to cardiac tamponade, leading to a diagnostic dilemma due to co-existing cardiogenic and septic shock.
Case Report
A 51-year old gentleman of Chinese ethnicity presented with right foot pain and swelling over 2 weeks, associated with chest pain and shortness of breath during that period. He had a 10-year history of poorly controlled diabetes mellitus with a Hba1c level of 8.8 %, hypertension and dyslipidaemia.
He was hypotensive on arrival, with a blood pressure of 91/60 mmHg and hypoxic, requiring high flow oxygen of 15L/min to maintain saturations at 100%. Otherwise other vitals were stable, pulse rate being 72 beats per minutes, respiratory rate 24 breaths per minute and a temperature of 37.4 degrees Celsius.
Clinical examination revealed a gangrenous lateral two toes extending into the lateral malleolus on the right foot, with evidence of pus discharge and associated warmth and crepitus up to hindfoot level on palpation. There was also evidence of dry gangrene in the fourth toe of the left foot, with presence of a small puncture at dorsum of foot with pus discharge. Similarly, crepitus was felt up to midfoot level on palpation of the left side. Bilateral dorsalis pedis and posterior tibialis pulses were palpable but feeble.
Table 1: Blood Investigations on Admission
Blood Test
Results
Blood Test
Results
White Cell Count
26.99 x109L
Alkaline Phosphatase
168 U/L
Neutrophil
90.30%
Alanine Aminotransferase
37 U/L
Lymphocyte
4.50%
Aspartate Aminotransferase
40 U/L
Platelets
210 x109L
Sodium
121 mmol/L
Hemoglobin
10.0 g/dL
Pottasium
7.6 mmol/L
Lactate Dehydrogenase
441 U/L
Urea
40.5 mmol/L
International Normalised Ratio
1.2
Creatinine
323 μmol/L
Activated Partial Thromboplastin Time
36.5 s
Creatinine Kinase
43 U/L
Prothrombin Time
14.6 s
Total Bilirubin
21 μmol/L
Figure 1a & 1b: Radiography of the (1a) left foot and (1b) right foot respectively, demonstrating gas within soft tissue bilaterally.
Figure 2: Chest radiography demonstrating cardiomegaly and globular-shaped heart, with loss of left-sided cardiophrenic and costophrenic angles.
Figure 3: Electrocardiogram demonstrating widespread saddle-shaped ST-elevation, consistent with pericarditis.
Figure 4: Parasternal Long Axis view of bedside echocardiography showing evidence of pericardial effusion and right atrial and ventricular collapse
Figure 5: Purulent pericardial aspirate via pericardiocentesis
Initial blood investigations are highlighted in Table 1. HIV Antibody, Hepatitis B Surface Antigen and Hepatitis C Antibody serology were all negative. Lower limb radiography revealed evidence of gaseous shadows bilaterally (Figure 1). The clinical and radiological findings were consistent with necrotising soft tissue infection of bilateral feet, and the patient was advised for extensive wound debridement and possible amputation of the affected sites during an orthopaedic consult.
However, on closer review of the chest radiography, there was evidence of cardiomegaly with a globular-shaped heart (Figure 2). His electrocardiogram on arrival, revealed diffuse ST-segment elevations on majority of leads, ST-segment depression on lead aVR consistent with pericarditis (Figure 3).
A bedside echocardiogram was performed, revealing a massive pericardial effusion, measuring largest at 2 cm in depth, with evidence of both right atrial and ventricular collapse (Figure 4).
An urgent pericardiocentesis was performed, under echocardiographic guidance, which revealed turbid-looking aspirate (Figure 5). Urgent microscopic analysis revealed 45 Cells per mm3, majority of which were lymphocytes, and gram stain showed moderate amounts of pus cells with occasional gram positive cocci. Pericardial fluid was negative for acid-fast bacilli.
A repeat transthoracic echocardiogram was performed post-pericardial drain insertion, revealing minimal remnant pericardial fluid, with the pericardial drain in-situ, and no evidence of any mass or vegetation. Unfortunately, a transoesophageal echocardiography and Computed Tomography (CT) imaging of the mediastinum (to rule out mediastinitis and pneumonitis) was not performed, as management of the NSTI took precedence.
The patient was started on intravenous antibiotics, both tazobactom-pipericillin and clindamycin. There was a delay in performing limb saving wound debridement as the patient was reluctant for invasive management, but had later consented to the procedure which was performed only on day 3 of admission. Tissue cultures were taken peri-operatively. Unfortunately, the patient deteriorated post-operatively due to extensive blood loss and overwhelming septicaemia and succumbed to his illness 72 hours after. Subsequently, it was revealed that cultures from blood, pericardial aspirate and tissue aspirate were positive for GBS infection.
Discussion
GBS is a common microorganism, often colonising the gastrointestinal and reproductive tract 3. Rarely, GBS colonises the skin and can cause necrotising fasciitis, i.e. necrotising soft tissue infection (NSTI), with only 22 cases having been reported in the past ii. Majority of these patients are either immunocompromised or have other predisposing factors including recent thoracic intervention or trauma 4,5.
GBS-related infections of cardiac structures are rare, as a whole, with 2 to 3% of cases presenting as native valve endocarditis and far less as pericarditis, mycotic aneurysms and intraventricular abscesses 3. Parikh et al reviewed the types of microorganisms isolated from purulent pericarditis samples and revealed that only 5% were due to streptococcal organism, sansStreptococcus Pneumoniae, possibly less so due to GBS 6. Our literature search revealed only one case of GBS-related purulent pericarditis reported although the case was not linked in any way to a NSTI to our knowledge 7.
Our case was unique as, at the time of writing, there were no other reports of GBS-related lower limb NSTI in combination with mediastinal involvement. There have been only a handful of cases of necrotising fasciitis reported with mediastinal involvement, the majority of which were supra-diaphragmatic with only one reporting NSTI of the lower limb due to Aspergillus infection 89.
The similarity in culture results obtained from blood, tissue aspirate and the pericardial fluid in our patient suggest dissemination of GBS from the NSTI, possibly via a haematogenous route, although bacterial-related pericardial dissemination can also occur via direct spread from infected foci from neighbouring intra-thoracic structures or sub-diaphragmatic 4. The possibility of multi-routed spread should remind clinicians that, albeit rare, mediastinal involvement in NSTI is a possible complication of such disease.
Conclusion
This case highlights the rare possibility of cardiac involvement in cases of NSTI, and the possibility of cardiac tamponade causing cardiogenic shock masquerading alongside septic shock. It also highlights the importance of combining clinical findings with ancillary testing, including bedside echocardiography, when faced with challenging cases of sepsis to help look for possible foci of infection.
Arrhythmogenic Right Ventricular Dysplasia (ARVD) was first described in a case series of 24 patients back in 1982 1, 2. Since then, our understanding of its pathophysiology has improved dramatically, with dedicated guidelines and literature being published to help with both diagnosis and management. Prompt diagnosis remains a struggle in majority of developing countries, including Malaysia, where resources and expertise are scarce, and obtaining both cardiac magnetic resonance imaging or endomyocardial biopsies remain a challenge. Furthermore, diagnosis is difficult in most cases as clinical presentation may vary and wide range of clinical mimics exist. We present a unique case of ARVD, diagnosed early through the knowledge of having a deceased sibling, whom had endomyocardial tissue characterization performed in the past confirming the presence of the disease in a first degree relative.
Case Report
A 21-year old gentleman presented to the emergency department following an episode of loss of consciousness, lasting approximately 30 minutes which recovered spontaneously. He denies having any similar episodes in the past. However, he had been suffering from reduced exercise tolerance, with a New York Heart Association (NYHA) Class II, over the past 1 year. He had no known medical illness at the time but smoked 6 cigarettes a day for the past 7 years.
His vital signs were stable on arrival, with a heart rate of 73 beats per minute, regular in rhythm, a blood pressure of 143/84 mmHg, respiratory rate of 19 breaths per minute, temperature of 37 degrees Celcius and oxygen saturation of 98% on room air. Cardio-respiratory examination revealed no murmurs, and normal heart and breath sounds. There were no carotid bruits audible. There was no evidence of any neurological deficits on neurological examination.
Figure 2 – Electrocardiogram revealing T-wave inversions in leads V2 to V4 with ventricular ectopic beats
Chest radiography revealed cardiomegaly (Figure 1). Electrocardiogram (ECG) revealed deep T-wave inversions in leads V2 to V4, with ventricular ectopic beats (Figure 2). Due to the suspicious-looking ECG, a serum Troponin-I test was performed, which was elevated at 480 pg/ml. The patient was treated for acute coronary syndrome complicated by cardiac syncope, and was later referred to the medical team for further inpatient management.
However, on further history, it was revealed that the patient had a sibling who had died from an unknown cause, 5 years prior. His younger brother, 14 years of age at the time, was brought in after collapsing whilst playing basketball in a school compound. Unfortunately, he was pronounced dead on arrival to the clinic. A post-mortem was performed due to the unexpected nature of the event. Fortunately, our patient was brought into the same hospital as his sibling, allowing us to trace previous autopsy reports and images, with consent.
Macroscopic examination of the right ventricular cavity revealed epicardial surfaces showing infiltration of excessive fat tissue with nodular fibrosis. The right ventricular cavity appeared dilated and cut sections showed diffuse transmural fibro-fatty replacement of the right ventricular free wall, extending into the endocardium and involving the right ventricular septum (Figure 3a).
Figure 3a – Macroscopic examination of right ventricular cavity, which was dilated and showing signs of transmural fibrofatty infiltration. Figure 3b – Histological evidence of focal lymphocytic infiltration, myocyte hypertrophy and degenerative cytoplasmic changes.
Histology revealed extensive fatty infiltration with interstitial fibrosis, primarily in the epicardium. There was associated myocyte loss with hypertrophy of cardiac muscle cells remaining (Figure 3b). Both macroscopic and microscopic findings were suggestive of ARVD.
After learning of the autopsy results, changes in clinical management took place, with priorities being shifted towards obtaining an echocardiogram, cardiac Magnetic Resonance Imaging (MRI) and Holter recording, as opposed to diagnostic angiography and coronary evaluation. Echocardiography revealed an ejection fraction of 25 to 30%, with evidence of left ventricular dyssynchrony, a tethered posterior mitral valve leaflet with mild eccentric regurgitation, consistent with dilated cardiomyopathy.
Cardiac MRI revealed both left and right ventricular dilatation, end diastolic dimensions being 5.8 cm and 4.4 cm and end-diastolic volume being 153 ml/m2 and 149 ml/m2 respectively, with evidence of bi-ventricular dyssynchrony. Left ventricular and right ventricular ejection fraction measured 31% and 8% respectively. There was also bilateral atrial dilatation. Gadolinium study revealed late enhancement in areas of the right ventricular wall (Figure 4).
Figure 4 – Four-chamber view of cardiac magnetic resonance imaging revealing evidence of right ventricular enhancement following gadolinium study.
A 24-hours Holter recording revealed up to significant ventricular ectopic burden, many of which were bigeminy and trigeminy in nature. In view of symptoms and the above investigative findings, the patient consented to insertion of an implantable cardiac defibrillator (ICD) 4 weeks later in our centre, and has since recovered well with regular monitoring.
Discussion
ARVD is rare, prevalence ranging between 1 in 2000 to 1 in 5000 (taking into consideration geographical variations) and accounts for 5% of deaths in young adults and 25% of deaths in athletes 3, 4. Typical histopathological feature of ARVD is the loss of right ventricular myocardium, replaced heavily by fibro-fatty tissue. Less commonly, left ventricle involvement have been reported 5, 6. Consequence from such pathological process leads to arrhythmias, heart failure and more importantly sudden cardiac death (SCD), with mortality rate ranging between 4 to 20% and peaking in the fourth decade, equally in both males and females 5.
Diagnosis is difficult in most cases as clinical presentation may vary and wide range of clinical mimic exist, including myocarditis, sarcoidosis, Brugada syndrome, idiopathic RV outflow tract VT and congenital heart diseases with right chambers overload amongst others 6. A Diagnostic Criteria was developed in 1994, with further modification in 2010 to assist in the diagnosis of ARVD and although the criterion has been shown to be specific, it lacks sensitivity 7. Nevertheless, it highlights several key areas, a mix of clinical, radiological, histological and electrophysiological features, that assist in diagnosis 4.
Despite not having any further evaluation or investigations performed at the time of presentation, in view of circumstances, our patient’s deceased sibling had supportive histological features. Therefore, our patient met the major criteria of having a first degree relative affected by the disease. More importantly, the suspicious family history had prompted further evaluation for the disease, allowing the medical team to prioritize investigations performed, specifically the Cardiac MRI and Holter evaluation. This led to early risk stratification and decision to implant an ICD for the patient, as he was deemed at high risk of SCD.
Conclusion
This case highlights the importance of good history taking, including a detailed family history of SCD or cardiac-related diseases, especially in young patients presenting with typical cardiac-related symptoms. Early identification and appreciation of risk will subsequently affect the outcomes of such patients affected by ARVD. Furthermore, important diagnosis like ARVD will have implications to relatives and future off-springs, further highlighting the need for detailed evaluation of patients similar to ours described in the above case report.
Epidural anaesthesia is one of the favored and effective treatment options for labour pain. It is usually safe and only a handful situations lead to absolute contraindications to this technique such as patient’s refusal, lack of expertise and equipment, severe coagulopathy and infection at the site of puncture (1). However, as with any other technique and procedure, epidural anaesthesia is not flawless. The side effects and complications include hypotension, pruritus, inadequate analgesia, post puncture headache, nerve damage, infection, and epidural haematoma (1,2). Headache is common in one third of the patients after lumbar puncture however, the frequency is less in epidural anaesthesia as the fluid is injected in and not removed in the latter (3). Accidental dural damage and subsequent headache following epidural anaesthesia is uncommon and is an important cause of morbidity which can limit patient severely. Further, in rarest of rare cases Pneumocephalus can develop after epidural anaesthesia which has rarely been reported. We report a patient who developed Pneumocephalus after receiving epidural anaesthesia for labour pain.
Case Report:
A 39 year old female presented to our Emergency Department with severe headache not responsive to analgesics. The headache started developing 10 to 12 hours after she was given an epidural which was attempted three times for labour pain which was four days prior at a nearby medical center . The severity of the headache did not change with lying or the upright position. She had no symptoms of vomiting, no fever and no confusion. Neurological examination and vital signs were unremarkable. The site of the spinal anaesthesia did not reveal any swelling or any signs of infection. An urgent head CT scan was performed which revealed Pneumocephalus denoted by numerous left fronto-parietal extra axial air locules (Figure 1 and Figure 2). MRI spine revealed mild subcutaneous oedema at the site of the needle insertion without any haemorrhage or collection. The patient was admitted and treated conservatively for six days and follow up serial head CT scans showed complete resorption of the Pneumocephalus and the patient’s symptoms resolved completely. The patient was discharged and the follow up was uneventful.
Figure 1: Pneumocephalus seen as locules of air (black color) in the left fronto-parietal region denoted by arrows (Axial section)
Figure 2: Multiple pockets of air seen in the Saggital section marked by arrows demonstrate the Pneumocephalus.
Discussion:
Pneumocephalus is the presence of air in the intracranial cavity. It can be acute ( less than72 hours ) or delayed (more than 72 hours). The most common site is the frontal region (4). Plain skull x-rays can detect Pneumocephalus of about 2 ml, whereas it requires only 0.5 ml of air to be detected by a CT scan (5). Pneumocephalus is most commonly a result of traumatic brain injury, surgical intervention of the brain or infection (5). Trauma accounts for up to 75% percent of the total cases. Chronic infections of ENT especially otitis media also amounts to a number of significant cases. Surgical procedures of brain, spine and ENT like sinus surgery, nasal polypectomy and nasal septum resection accounts for the causes. The incidence after supratentorial craniotomy has been reported to be 100% (6, 7). However, it is very unusual for pneumocephalus to develop post epidural anaeasthesia possibly due to ball valve mechanism in which the air enters the space through the CSF leakage which allows input but not output. Headache post lumbar puncture and epidural anaesthesia is relatively not uncommon but certain situations may demand a more thoughtful approach (3).
In our patient we suspect there was a puncture of the dura during epidural anaesthesia which led to air being trapped and siphoned upwards in an inverted soda bottle fashion. This is supported by the meta-analysis done by Choi et al. which states the incidence of accidental dural puncture in epidural insertion to be 1.5% and among those 52 % will have post puncture headaches (8). In another extensive study performed over ten years, the overall incidence of accidental dural puncture and postdural puncture headache were 0.32% and 0.38%, respectively (9). The authors further stressed that if more than one attempt was required to identify the epidural space, the accidental dural puncture rate increased to 0.91%. In our patient we witnessed the same wherein three attempts were made to identify the epidural space which increased the risk of dural injury and subsequent leaking. Pneumocephalus usually gets absorbed without any clinical manifestations. The conservative treatment involves placing the patient at rest, avoiding Valsalva manoeuver, administering analgesics. With these measures, reabsorption was observed in 85% of cases after 2–3 weeks (5). Use of oxygen mask, nasal catheter, hyperbaric oxygen sessions and good hydration have also been reported. If conservative measures fail to provide the desired results then specific treatment like a epidural blood patch or even surgical closure of the dural gap is indicated (3, 10).
Adult Still’s disease (AOSD) is an inflammatory disorder of unknown etiology characterized by quotidian (daily) fevers, arthritis, and an evanescent rash and multi-organ involvement [1].First described in children by George Still in 1896, subsequently in 1971 Bywaters described 14 patients with similar presentation [2]. The clinical course of adult Still’s disease (AOSD) can be divided into three main patterns: monophasic (or monocyclic), intermittent, and chronic. Patients with monophasic AOSD have a disease course that typically lasts only weeks to months, completely resolving within less than a year in most patients [3]. Systemic features, including fever, rash, serositis, and hepatosplenomegaly, predominate in this group. The patient we diagnosed as AOSD, with monophasic course, went into remission after proper treatment and is symptom free even after stopping the treatment.
CASE REPORT
46 year old Indian male, non-smoker, married, nondiabetic, normotensive admitted at department of internal medicine in our hospital with history of high grade fever, polyarthritis, and skin rash for the last 4 weeks. The fever was high grade, with maximum temperature reaching 39.2°C. The patient also complained of joint pains involving the knee, ankle, wrist and proximal interphalangeal joints. There was no history of oral ulcers, morning stiffness, ocular symptoms, or contact with infected persons. In the hospital, during the febrile period, he developed macular rash mainly on chest and back [Figure 1]. On examination, the patient was sick looking, febrile-39.2°C. Chest on auscultation was normal, cardiovascular examination was unremarkable. Examination of abdomen revealed mild spleenomegaly. Neurological examination was unremarkable. Investigations revealed hemoglobin 12.7g/dl, erythrocyte sedimentation rate (ESR) 120 mm in 1st hour. Total leukocyte count-12.7 x10 9/L. Liver function showed elevated liver enzymes with Aspartate transaminase-125U/L, Alaninie aminotransferase 60 U/L, low albumin 2.3gms/dl. He was worked on lines of pyrexia of unknown origin and his blood, urine and sputum culture showed no growth. Procalcitonin level was less than 0.5ng/ml. Sputum for AFB was negative for three samples; qunatiferon gold test for tuberculosis was negative. IgM CMV, EBV, HIV, hepatitis B and C were negative malarial parasite, Widal and Brucella serology was negative. CT-chest and abdomen were normal, except for mild spleenomegaly. Echocardiogram was normal. ANA, rheumatoid factor was negative. Lactate dehydrogenase (LDH) 978 U/L, His CRP showed a progressive increase from 82mg/L to 284 mg/L, which decreased after starting steroids. His ferritin levels were 40, 000 (normal range 21.8 -274.6 ng/ml), which were reconfirmed by second sample and he had normal transferrin saturation. On the basis of his history, clinical examination and review of his laboratory investigations, diagnosis of AOSD was made. We started him on prednisolone 60 mgs daily along with Diclofenac potassium 50 mg twice daily, to which he responded and become afebrile. He was discharged with a tapering dose of steroids 5mgs weekly. He is doing well and is completely symptom free.
Figure 1: Skin Rash on the back
DISCUSSION
First described in children by George Still in 1896, “Still’s disease” has become the eponymous term for systemic juvenile idiopathic arthritis [4]. In 1971, the term “adult Still’s disease” was used to describe a series of adult patients who had features similar to the children with systemic juvenile idiopathic arthritis and did not fulfill criteria for classic rheumatoid arthritis.
The etiology of adult Still’s disease (ASD) is unknown; both genetic factors and a variety of infectious triggers have been suggested as important, but there has been no proof of an infectious etiology, and the evidence supporting a role for genetic factors has been mixed. It is uncertain whether all patients with AOSD share the same etiopathogenic factors. Proposed pathogens have included numerous viruses; suspected bacterial pathogens include Yersinia enterocolitica and Mycoplasma pneumoniae [5]. As an example of studies of the immunogenetics of ASD, in a series of 62 French patients, human leukocyte antigen (HLA)-B17, -B18, -B35, and -DR2 were associated with AOSD. However, other studies have not confirmed these findings [6].
Adult Still’s disease is very uncommon. Prevalence of AOSD is estimated to be 1.5 cases per 100, 000-1, 000, 000 people, with an equal distribution between the sexes [6]. There is a bimodal age distribution, with one peak between the ages of 15 and 25 and the second between the ages of 36 and 46. The diagnosis of AOSD is possible only by recognizing the striking constellations of clinical and laboratory abnormalities. It is also to be to remember that AOSD is a diagnosis of exclusion. AOSD has been associated with markedly elevated serum ferritin concentrations in as much as 70 percent of patients. Serum ferritin values above 3000 ng/mL in a patient with compatible symptoms should lead to suspicion of AOSD in the absence of a bacterial or viral infection. Abnormally high serum ferritin values were reported in some case reports and it was suggested that high ferritin levels may be a diagnostic marker of Still's disease [7]. Our patient showed almost all features as laid down in Yamaguchi criteria[Table 1] for the diagnosis of AOSD [8] along with a markedly high ferritin levels.
Table 1 : Diagnostic criteria for AOSD (Yamaguchi)8
Major criteria
Minor criteria
Fever > 39ºC, > 1 week
Sore throat
Arthralgia/ arthritis > 2 weeks or splenomegaly
Lymphadenopathy
Typical rash
Abnormal LFT
WBC > 10, 000 with > 80% PMNs and RF
Negative ANA
Exclusions: Infections, malignancy, rheumatological diseases. Five criteria with at least two major criteria. ASOD: Adult onset still’s disease. WBC: White blood cell, ANA: Antinuclear antibody, RF: Rheumatoid factor, PMN: Polymorphonuclea
Non-steroidal anti-inflammatory drugs (NSAIDs), such as aspirin, ibuprofen or naproxen, help to reduce inflammation [9]. Patients with high-fever spikes, severe joint glucocorticoids, such as prednisone (0.5- 1mg/kg/day)Methotrexate has been used successfully in a small series of people to treat adult Still's disease [10]. Some patients are refractory to these conventional therapies. Tumor necrosis factoralpha (TNF) blockers include infliximab, adalimumab, etanercept, anti-interleukin-1, antiinterleukin-6 agents, and most recently anti CD20-expressing B-cell antibodies are also effective in some cases. Other experimental drugs, including cyclosporine and anakinra, have also been successful in small groups of people [9]. Interleukin 6 inhibitors like tocilzumab showed a good result in patients with AOSD resistant to other immunosuppressive agents such as methotrexate, TNF inhibitors and anakinara [11]. Even with treatment, it's difficult to predict the course of adult Still's disease. Some people might only experience a single episode, while for others adult Still's disease may develop occasional flair up or a chronic condition. About one-third of people with the disorder may fall into each of the above groups.
CONCLUSION
A diagnosis of AOSD should be kept in mind in case of pyrexia of unknown origin particularly in a patient who presents with high-grade intermittent fever, polyarthritis and skin rash of more than two weeks duration. However, the patient should be extensively evaluated to rule out other differentials of AOSD like acute or chronic infections, autoimmune disorders, vasculitis and malignant disorders. Serum ferritin values can be powerful adjuncts in making the diagnosis of AOSD [12], where they are usually higher than other inflammatory diseases. Indeed, extreme elevation of serum ferritin up to 75, 500ng/ mL has been reported in AOSD[12]. Several investigators agree that ferritin levels above l, 000 ng/mL are suggestive of AOSD while levels greater than 4, 000ng/mL are very specific for this diagnosis when accompanied by a compatible clinical picture.
This case highlights a rare and interesting medical condition bought about by liquorice ingestion. While there have been many previous reports of liquorice toxicity secondary to eating confectionary, I have only found one case report of liquorice toxicity secondary to liquorice tea ingestion and the patient there had only a mild case of hypokalaemia and did not require hospital admission unlike patient X.1
Case presentation
Patient X is a usually fit and well 49-year-old woman who was admitted following a collapse. Prior to this collapse she had experienced a 3-week history of gradual onset, slowly worsening dull headache and a feeling of tingling in her hands which increased over this timeframe. On the day of admission, she experienced nausea. Her past medical history included migraines, for which she self-medicated with paracetamol, ibuprofen and codeine as necessary. She was also using Cerazette. She was in full time work, was a lifelong non-smoker and used alcohol very rarely. She had no family history of note.
On examination, Patient X was a slim individual who was hypertensive with a blood pressure of 170/100 mmHg. Her other observations were normal. Her general and neurological examinations were unremarkable.
While initially the medical team felt that Conn’s syndrome was a likely cause of the abnormalities, this was reconsidered on a ward round where, following research on the internet into her abnormalities, patient X brought it to the attention of the team that she had been consuming between six and eight liquorice tea infusions per day for the past two months and had been consuming around three a day for a significant period time prior to this (roughly 18 months). The diagnosis was made based on her history.
Investigations
A venous gas demonstrated a metabolic alkalosis with a pH of 7.57.
Blood tests revealed hypokalaemia (K+ = 2.2 mmol/L) and hypophosphataemia (PO4 = 0.35mmol/L). No other abnormalities were detected.
More specialist assays were undertaken, and demonstrated that her plasma renin was 2.3 ng/mL/hour (normal range 0.2 – 3.3 ng/mL/hour). Her morning supine plasma aldosterone level was 29 pg/mL (normal range 30 – 160 pg/mL). Her morning plasma cortisol level was 612 nmol/L (normal range 138-635 nmol/L).
In addition, the patient also underwent a CT head and a CT renal angiogram, both of which were normal.
DIFFERENTIAL DIAGNOSIS
Apparent mineralocorticoid excess
Exogenous mineralocorticoid excess
Liddle’s syndrome
Congenital adrenal hyperplasia
Cushing syndrome
Liquorice
Treatment
Intravenous potassium and phosphate replacement, cessation of liquorice intake and amlodipine 5mg OD.
Outcome and follow-up
The patient was discharged with a blood pressure of 132/66 mmHg on amlodipine, a potassium level of 2.9, and a phosphate level of 1.16. She was given oral potassium supplementation to be taken 3 times per day. After two weeks, the amlodipine was stopped as she became mildly hypotensive. Her blood pressure was 120/60 following cessation of amlodipine. Three months later her plasma potassium level was 4.6 without supplementation. Mrs X required no follow up although she reports an ongoing feeling of tingling in her hands.
Discussion
Liquorice is an extract of the roots of the Glycyrrhiza glabra plant and has been used as both a confectionary flavouring agent and a herbal remedy. It is also commonly used as a laxative, and as a flavouring agent in chewing gums, sweets, and food products.
The active ingredient in liquorice is glycyrrhetinic acid which inhibits the enzyme 11-β-hydroxysteroid dehydrogenase. This enzyme converts cortisol into inactive cortisone within the distal tubule of the kidney and so in liquorice toxicity there is a build-up of cortisol in distal tubular cells.2 This results in increased mineralocorticoid like activity as there are structural similarities between cortisol and aldosterone, with increased Na+ and water retention in conjunction with increased H+ and K+ excretion.3 Here hyperaldosteronism occurs, but with a low or low-normal plasma aldosterone and renin level. Serum glycyrrhetinic acid levels can be measured with enzyme-linked immunosorbent assay (ELISA) and high-performance liquid chromatography (HPLC). Urinary glycrrhetinic acid levels can be measured with gas chromatography-mass spectrometry (GC-MS).4
Pseudoaldosteronism secondary to liquorice consumption is a relatively rare occurrence. Case reports demonstrate a range of clinical manifestations from an asymptomatic patient fortuitously diagnosed to those with more severe presentations such as rhabdomyolysis, hypertensive encephalopathy, asthenia, paralysis, heart failure, and cardiac arrhythmias such as polymorphic ventricular tachycardia and ventricular fibrillation secondary to hypokalaemia. For these reasons, it has been suggested that the public should be made aware of the potential dangers associated with liquorice consumption. 5-13
The combination of alkalosis hypokalaemia and hypertension suggests increased mineralocorticoid activity leading to increased renal tubular Na+ reabsorption along with increased k+ and H+ excretion. Both primary and secondary hyperaldosteronism cause these abnormalities, the former via an appropriate response (renin release) to decreased renal perfusion pressure or decreased sodium concentration in the ultra filtrate, the latter an inappropriate release of aldosterone from the adrenal cortex, often a result of an adrenal adenoma.
Other genetic syndromes, such as Bartter’s or Gitelman’s, cause hypokalaemia with alkalosis but without hypertension.14
Features of low potassium include generalised weakness and lethargy, ascending paralysis, and rhabdomyolysis.15-17 Decreased intake is rarely a cause of low potassium as the western diet usually contains significantly more potassium than is needed and because the renal tubular reabsorption mechanism can be extremely effective in limiting potassium excretion.17
The maximum recommended dose of liquorice is 100mg/day although cases of liquorice toxicity have been reported in association with doses as low as 80mg/day. Each liquorice tea bag contains approximately 500mg of glycyrrhetic acid, of which approximately 20mg is ingested per infusion.
This is a relatively rare occurrence and it has been suggested that certain groups are more susceptible to toxicity than others – for example those with 11-β-hydroxysteroid dehydrogenase deficiency.18 It is also thought that those with essential hypertension are also more at risk.19
LEARNING POINTS/TAKE HOME MESSAGES
Consumption of liquorice can cause pseudoaldosteronism.
The clinical picture is similar to that of primary aldosteronism, but is characterised by low levels of both aldosterone and renin.
While liquorice toxicity can be asymptomatic, clinical manifestations are wide ranging and include cardiac arrhythmias, rhabdomyolysis, weakness and paralysis.
Pseudohyperaldosteronism caused by liquorice consumption is reversible and generally resolves upon cessation of liquorice consumption. Prior to resolution, potassium supplements are usually necessary.
Despite advances in the management of ectopic pregnancies an emphasis must be given on improving the understanding of the women and the healthcare professionals of the pathophysiology of haemorrhagic shock.
Educating the public and all health care professionals about the phrase “Think Ectopic” as a main differential in any women of childbearing age with atypical signs and symptoms of general ill health is paramount.
Précis
The significance of effective communication within multidisciplinary teams especially in emergency situations towards optimising patient care and saving lives cannot be understated.
Case Report
A 27-year-old woman who claimed to be unaware of her current pregnancy collapsed at her home. She was not known to have any co-morbidities. Paramedics were called and found her to be in cardiac arrest with pulseless electrical activity. Cardiopulmonary resuscitation (CPR) was immediately commenced. Spontaneous circulation returned after 13 minutes of CPR at home.
She was then transferred to the emergency department. On arrival to the emergency department her Glasgow Coma Scale (GCS) was 3. She had a pulse rate of 130 beats per minute; unrecordable blood pressure; haemoglobin of 55g/l; metabolic acidosis with a pH of 6.8; lactate > 15; and a potassium of 6.6 mmol/l. She was resuscitated and gradually regained consciousness with a GCS of 15.
In the midst of stabilising her condition and unaware of her pregnancy, a urine pregnancy test was obtained following siting of a urinary catheter. A positive pregnancy test prompted notification to the gynaecology team who performed ultrasonography imaging which revealed significant haemoperitoneum. An immediate decision was made to perform laparotomy in view of the most likely diagnosis of a ruptured ectopic pregnancy.
Laparotomy revealed a 3.5 litre of haemoperitoneum secondary to a ruptured right sided tubal ectopic pregnancy. A right salpingectomy was performed. The patient was subsequently transferred to the intensive care unit as her serology results were consistent with multi organ failure with a platelet count of 46 (109/L); creatinine of 194 mmol/L; estimated glomerular filtration rate (egfr) of 27 mls/min/ 1.73 m2; alanine transaminase (ALT) of 441 IU/L; and alkaline phosphatase (ALP) of 49 IU/L.
She made an uneventful recovery as demonstrated in figure 1 by the improving serological parameters and was discharged home after 6 days.
Figure 1: The cumulative serology- full blood count, liver function tests, urea and electrolytes, clotting profile.ankle
Investigations
Day 0
Day 0
Day 1
Day 1
Day 2
Day 3
Day 4
Day 5
Day 15
13:46
18:30
05:53
17:27
06:49
07:00
11:14
09:37
09:50
Hb g/L (115-150)
82
100
83
73
72
88
89
93
WCC 109/L (3.5-11.0)
19.8
23
18.1
13.2
11.8
11.2
9.5
9.1
Plts 109/L (140-400)
46
61
49
46
48
51
76
106
ALP IU/L (30-130)
49
42
44
51
57
73
74
100
ALT IU/L (0-40)
441
428
701
3197
2621
1807
1290
185
Bili mmol/L (0-21)
9
13
8
18
18
16
11
4
Na mmol/L (133-146)
139
142
143
141
143
142
140
141
139
K+ mmol/L (3.5-5.3)
6.8
4
4.3
4.2
3.9
3.9
3.7
4.6
Urea mmol/L (2.5-7.8)
9.6
12.4
14
14.2
11.5
7.9
7.4
8.3
Creat mmol/L (48-128)
194
174
230
279
319
269
163
137
88
egfr mls/min/ 1.73 m2
27
30
22
18
15
19
33
40
66
INR ratio
1.4
1.4
1.5
1.6
1.4
1.1
1
PT secs (9.7-12.3)
14.8
15.1
15.9
16.7
15.1
11.5
10.6
Fibrinogen g/L (1.9-3.1)
1.2
1.4
1.2
1.5
2.4
3.9
>4.5
Discussion
The confidential enquiry report into maternal deaths – UK has shown a decreasing trend in the case fatality rate in women with ectopic pregnancies. This has been suggested to reflect earlier detection and immediate treatment of ectopic pregnancies. However unforeseen tubal rupture with major haemorrhage continues to be a source of major morbidity and mortality. Ectopic pregnancies account for 3-4% of pregnancy related deaths. 4
The classical triad of symptoms encountered in ectopic pregnancy includes pain, vaginal bleeding and amenorrhoea. 1 Worryingly, as illustrated by our case, rarely these women may present in a state of collapse even before the diagnosis of pregnancy is made. 4
Pathophysiology of multi-organ failure following haemorrhagic shock
Our case clearly demonstrates the detrimental multi-systemic effects and subsequent threat to life created by haemorrhage from a ruptured ectopic pregnancy. Acute haemorrhage results in decreased cardiac output and pulse pressure that is detected by baroreceptors in the aortic arch and atrium. Neural reflexes subsequently cause an increased sympathetic outflow to the heart and other vital organs resulting in vasoconstriction, and redistribution of blood flow away from non-vital organs. Neuroendocrine responses activated by neural reflexes play a major role in homeostasis during haemorrhage. Elevated aldosterone and cortisol secondary to raised adrenocorticotrophic hormone secreted by the pituitary gland leads to increased water absorption in the kidneys. The reduced tissue perfusion to non-vital organs results in insufficient delivery of oxygen and nutrients required for cellular function. 2
The resultant hypoxia leads to anaerobic metabolism and hence lactate production and metabolic acidosis. Hyperlactaemia is defined when serum lactate is greater than 4 mmol/l. 3 A level of 15mmol/l as demonstrated by our case highlights the extent of shock the patient was in.
Endogenous heat production is restricted by anaerobic metabolism, which in turns exacerbates hypothermia that is likely to be predisposed by the administration of intravenous fluids and blood products. Hypothermia is one of the reversible causes of pulseless electrical activity and a core temperature of less than 35°C is itself an independent predictor of mortality after major haemorrhage.
Furthermore, our case revealed a severe acidosis with a pH of 6.8, which is reflective of widespread cellular anaerobic respiration secondary to hypoxia as a result of inadequate perfusion. Widespread literature has shown that a pH of less than 7.2 is associated with decreased contractility, low cardiac output, bradycardia, arrhythmias and decreased blood flow to the liver and kidneys. This can lead to multi-organ failure.6
Many patients with severe haemorrhage can establish coagulopathy very quickly as our case has demonstrated. At present there is nouniversally established definition of coagulopathy though many experts use prolonged prothrombin time as an indicator of coagulopathy. Our case presented with a prolonged prothrombin time of 14.8 seconds. The pathophysiology is complex and stems from immediate activation of multiple haemostatic pathways including fibrinolysis, platelet and endothelium dysfunction. Furthermore, acute phase response after resuscitation measures can create a prothrombotic state. Sometimes, disseminated intravascular coagulation can occur in those who are insufficiently resuscitated or not resuscitated in a timely manner. 7
Effective multi-disciplinary input
This case clearly highlights that the responsibility does not solely rely on the surgeon who is required to cease the bleeding but also on the multi-disciplinary specialists including paramedics, emergency clinicians, nursing staff, anaesthetists and haematologists. This is a vital component of resuscitation management during emergency situations.
Appropriate initial fluid management
The management with intravenous fluid resuscitation remains challenging as some evidence suggests that aggressive fluid resuscitation can be detrimental because it can lead to dislodging of clots and dilutional coagulopathy leading to increased risk of haemorrhage. 5
Clinicians supporting this hypothesis suggest to cautiously administer fluid resuscitation with the aim of maintaining a subnormal blood pressure (systolic of 70-90 mmHg), whilst allowing sufficient oxygen delivery. The very early use of crystalloids and blood products is paramount to help treat acute coagulopathy. 7
Immediate surgical treatment
Recourse to immediate surgical cessation of bleeding is a vital part of the resuscitation process, and must not be delayed. 7 The presence of free fluid in the abdomen and a positive pregnancy test immediately alerted an ectopic pregnancy as the most likely diagnosis. The majority of women of reproductive age are free of comorbidities with a greater ability to adapt to resuscitative measures and hence showing quicker recovery.
Conclusion
Despite advances in the management of ectopic pregnancies an emphasis must be given on improving the understanding of the women and the healthcare professionals of the pathophysiology of haemorrhagic shock. Educating the public and all health care professionals about the phrase “Think Ectopic” as a main differential in any women of childbearing age with atypical signs and symptoms of general ill health is paramount.
Furthermore, the significance of effective communication within multidisciplinary teams towards optimising patient care and saving lives cannot be understated.
A 23 y/o male was brought to our Emergency Department after having a seizure. He was alert and his vital signs were stable. He is known to have epilepsy and is on regular anti-epileptic medication for three years. He is being followed up at a neighborhood medical center at his native village . On physical examination numerous brown papules were seen over his nose and both cheeks in a butterfly pattern which correspond to facial angiofibromas (Figure 1). Ash Leaf Hypomelanotic macules were seen over his extremities (Figure 2). Few hyperpigmented café au lait macules were observed over his trunk (Figure 3). A big fibroma was also seen over his scalp (Figure 4). Areas of thick leathery texture of orange peel known as Shagreen patches were observed on back (Figure 5).
Figure 1: Facial angiofibromas
Figure 2: Ash Leaf spot
Figure 3: Cafe au lait macule
Figure 4: Scalp fibroma
Figure 5: Shagreen patch
A Brain CT scan revealed multiple subependymal giant cell astrocytomas. Laboratory investigations were normal.
This patient was clinically diagnosed as Tuberous Sclerosis Complex having a myriad of skin lesions.1
Tuberous sclerosis complex is an autosomal-dominant, neurocutaneous, multisystem disorder characterized by cellular hyperplasia and tissue dysplasia.2 Seizures are commonly encountered in Emergency Room however, conspicuous lesions as described above must alert the physician to guide the patient for a multidisciplinary approach.3
Isolated splenic tuberculosis is extremely rare, particularly in the immunocompetent persons. Splenic tuberculosis, however, can be part of military tuberculosis in immunocompromised patients. Tuberculosis spleen invariably presents in the form of an abscess. The risk factors for splenic abscess described in the literature are sickle cell disease, hemoglobinopathies, splenic trauma endocarditis or tuberculosis elsewhere in an immunocompetent patient. Although rare cases of splenic tuberculosis in immunocompetent patients have been described in the past. With re-emergence of tuberculosis due to AIDS and use of immunosuppressive medications around the globe, it is very important to bear this rare clinical condition while evaluating pyrexia of unknown origin in a given case.
Case 1
A 54-year-old male vet nary doctor by profession presented with the history of off and on fever of 8 weeks duration. The fever was low grade, intermittent and was associated with weight loss of 4 kilograms. There was no evening rise of temp and no sweating. The patient denied any history of a cough, urinary symptoms or diarrhoea. There was no history of travel or contact with sick people. He had been type II diabetic for last 12 years controlled on oral hypoglycemic agents and had no history of acute or chronic complications. There was no history of tuberculosis in the past or in close contacts . He was non-alcoholic and denied any high-risk behaviour. The clinical examination revealed an average built person who was conscious oriented and had stable vitals. There was no jaundice or lymphadenopathy. Abdominal examination revealed moderate splenomegaly. The liver was not palpable and there was no ascites. Respiratory and cardiovascular systems were normal. During the hospitalisation temp. recorded ranged from 380 C to 390C with no night sweats during his hospital stay. Patient’s evaluation showed haemoglobin levels of 10.5g/dl Leukocyte and platelet counts were normal. ESR was 88mm for the first hour. The tests on kidney and liver functions were normal. An ultrasound abdomen showed the presence of two heterogenic space occupying lesions measuring 3×4cms suggestive of splenic abscesses. An echocardiogram was done to rule out any features of subacute bacterial endocarditis. All the valves of his heart were normal and no feature of endocarditis was noted. The patient had normal ejection fraction and the pericardial cavity was normal too. Blood cultures and urine cultures were found to be sterile. A 24-hour collection of urine showed no evidence of albuminuria and funduscopic examination ruled out retinopathy. Keeping in view splenic abscesses CT guided fine needle aspiration was done and acid-fast bacillus were demonstrated by Zeal-Neilson s stain and the patient was put on antitubercular treatment. The culture of the aspirate a few weeks later turned out to be positive for Mycobacterium tuberculosis. His HIV serology was negative .The patient continued standard four-drug regimen for two months followed by two drug regimen for another seven months. Patients fever settled after two weeks of treatment and followed our clinic till completion of his treatment.
CASE 2
A 24-year-old female student presented with the history of off and on fever of 5 weeks duration. The fever was low grade intermittent and not associated with sweating She also complained of loss of appetite and weight loss of 3 kilogrammes over a period of 2months She denied any history of a cough, urinary symptoms. The patient had no history of contact with sick persons or travel. She had no co morbid illness. On examination she was conscious oriented and had mild pallor, no lymphadenopathy or jaundice was noted. Her respiratory and cardiovascular system was normal. Abdominal examination showed splenomegaly 5cms below the costal margin. Her laboratory data showed haemoglobin levels of 9.8gm/dl WBC count of 4200 and platelets were 1.5×103. ESR was 90mm in the first hour. Blood culture, widal tests and Brucella serology were negative. Tests on liver and kidney functions were normal. An ultrasound abdomen showed the presence of three small space occupying lesions in the spleen.Each was measuring 2×2 cms. Portal vein diameter and spleno-portal axis were normal. CT scan abdomen confirmed splenic abscesses and no abdominal lymphadenopathy was noted. CT guided fine needle aspiration was done which turned out to be positive for AFB and cultures a few weeks later confirmed Mycobacterium tuberculosis. Her transthoracic echocardiography showed normal values and didn’t show any features of vegetations. Her HIV serology was negative. The patient was started on conventional four drugs antitubercular regimen for two months followed by two drug regimen for another seven months. Her fever settled and she had marked improvement in her appetite and her weight increased.
DISCUSSION:
Splenic abscesses presenting as fever of unknown origin is well known. Most of the cases of TB spleen present as fever, vague ache in left hypochondrium or weight loss. Although the frequency of splenic tuberculosis is more common in immunosuppressed patients but splenic abscess due to tuberculosis has been described in immune competent patients as well1. Due to the advent of AIDS epidemic prevalence of tuberculosis has increased globally and more cases are now getting reported. Another scenario leading to increased frequency of this previously rare entity is the widespread use of immunosuppressed therapies for chronic disorders like Rheumatoid arthritis, Crohn's disease Psoriasis etc. The index cases were neither HIV positive nor where on any immunosuppressant medication but developed splenic lesions, reflecting some other hitherto unknown predisposing factor for such lesions. The splenic abscess does occur in the setting of infective endocarditis as infective emboli get lodged in the spleen. Splenic abscess following endocarditis in an 80 year old male presenting with abdominal pain during the course of treatment was reported by Pereira et al2 and in another series3 of 3 patients with bacterial endocarditis, splenic abscess was diagnosed based on CT abdomen with evidence of endocarditis on Echocardiography. In the same series two of the patients underwent splenectomy before valve repair while as splenectomy was performed after the valve repair in the other patient .The echocardiogram in index cases, however, were normal without any evidence of endocarditis. After the diagnosis and initiation of ATT, the index cases became afebrile and splenectomy was thus averted . While one of the cases had well controlled diabetes mellitus but the other patient was euglycemic and had no other known risk factor for splenic tuberculosis as is described in the literature. What lead to splenic tuberculosis in the second case remained unidentified? .There is a well known linkage between diabetes mellitus and TB and as per WHO a bidirectional screening has been recommended. Sri Lankan data4 on 112 patients with TB found that 8 patients with TB already were already known cases of diabetes mellitus and in their study further screening unravelled TB in another 17 patients. It is thought that metabolic adaptation is critical during the pathogenesis of mycobacterium tuberculosis5,6..
In time management of tubercular abscess is very crucial as without treatment patients can have complicated clinical course.Splenic abscess can rarely rupture or lead to fistulous communication with adjacent organs. A gastrosplenic fistula has been reported by Lee et al7 in a 61-year-old male presenting with abdominal discomfort and cough. The authors demonstrated a fistulous tract between the spleen and the stomach on endoscopic examination. The fistulous track healed in their case after completion of anti-tubercular treatment. It is quite possible that delay in diagnosis may be a factor that leads to such complications. The index cases, however, had favourable outcome without any complications and successfully completed anti-tubercular treatment.
The other side of the coin is that complications are even known during the antitubercular treatment as a result of reaction to antitubercular treatment. Spontaneous rupture during treatment leading to splenectomy was reported by et Yea et al8 .Splenic tubercular abscess are known to be associated with miliary tuberculosis or with haematological diseases where leucopenia and thrombocytopenia are profound9.The index cases had normal platelet count and leucocytic count highlighting that there was neither bone marrow suppression nor hypersplenism. The patients with ITP on treatment are also prone to develop Tuberculosis of spleen and conversely, patients with TB spleen can per se develop thrombocytopenia.
The management of splenic abscess used to be splenectomy in the past but with the advent of FNAC splenectomy is avoided . Here a word of caution is that various other lesions in spleen can mimick splenic TB hence it is very important to confirm the disease especially in endemic areas where TB is prevalent. Kunnathuparambil et al10 described melioidosis in a 47 year old male who was treated as case of splenic tuberculosis based on splenic lesions on imaging and fever. The diagnosis of splenic tuberculosis in past was mainly reached after histological examination of surgical specimens but now fine needle aspiration has become the procedure of choice. Spleen being highly vascular organ bleeding is the most feared complication of any intervention but fine needle aspiration has been found to be technically safe and in a retrospective data no significant complication was observed11 .With the advent of non-invasive biomarkers diagnosis of tuberculosis has advanced further and a step further is Quantiferon Gold test which has come up another non-invasive modality in the diagnosis of TB. In various studies12, the sensitivity of this test to the tune of 75% has been demonstrated.
While treating an HIV patient the clinician requires high alert in patients presenting with pain abdomen as the splenic abscess is one of the differentials and it is recommended that initial ultrasound must be carried out to diagnose this condition13. In modern era ,Splenectomy may be offered only to resistant cases otherwise ATT is considered to be the therapy of choice.
To conclude tuberculosis of spleen must be kept in mind while evaluating fever of unknown origin in any patient on immunosuppressant treatment or having HIV and even in immunocompetent patients as well. The Fine needle aspiration is a safe diagnostic modality and treatment with antitubercular medication is rarely unsuccessful.
Warfarin is a widely used anticoagulant, primarily for the prevention of thrombosis and thromboembolism. Warfarin is used as a prophylactic agent in conditions such as atrial fibrillation and coronary artery thrombosis.1
Although effective and safe, treatment with Warfarin is associated with risks. Because of its narrow therapeutic index, patients require regular blood monitoring for the international normalised ratio (INR) to determine the safe yet effective dose of Warfarin.
Warfarin has interaction with several medications which affect the availability of Warfarin. One class of drugs which is very commonly prescribed is the selective serotonin reuptake inhibitors (SSRIs) antidepressants.
Due to their supposedly favourable side-effect profile, e.g. less cardiotoxicity, and safety in overdose, SSRIs have become the first-line antidepressant 2, preferred over tricyclic antidepressants (TCA). However, SSRIs, have other serious side-effects including increased tendency to bleed, particularly gastrointestinal bleeding. SSRIs may increase the risk of bleeding due to the secondary effect of serotonin release which is essential for platelet aggregation. 3 This effect is especially significant when combined with anticoagulants. 1
Several of the SSRIs are inhibitors of the cytochrome P 450 enzyme system, which is responsible for the metabolism of some medications, including Warfarin. Both SSRIs and anticoagulants are frequently prescribed in the elderly population.
Fluvoxamine is a SSRI which is licensed for use in the treatment of depressive disorder, obsessive-compulsive disorder (OCD) 1, and is also used in the treatment of social phobia. While an interaction between Fluvoxamine and Warfarin is to be expected because of Fluvoxamine’s inhibitory action on a number of cytochrome P 450 enzymes, there have not been many case reports of the interaction between Fluvoxamine and Warfarin.
A Medline search revealed only two case reports of an interaction between Warfarin and Fluvoxamine. 4,5
We report a case of an elderly man who developed elevated INR when he was started on Fluvoxamine for the treatment of depression, while on Warfarin.
Case Report
A 75-year old male was admitted to the acute psychiatric unit with complaints of anxiety, depressed mood and suicidal ideation. In the previous months, he had developed a pre-occupation that his bowels were not functioning properly and that he would not be able to open his bowels. He was using excessive laxatives secondary to this preoccupation. He also described other depressive symptoms: anhedonia, insomnia with early morning wakening, poor concentration, and low motivation.
The patient was diagnosed with depression two years previously, requiring Electroconvulsive therapy (ECT). He was discharged on Mirtazapine 45mg and Venlafaxine-XL 150mg. Following a deterioration in mental state, the Venlafaxine-XL dose was increased to 225mg three months before this admission, without much improvement. Risperidone and Olanzapine were trialled as an adjunct without beneficial effect and were discontinued. Compliance with medication was reportedly good.
The patient had multiple physical health complaints: previous myocardial infarctions, hypertension and paroxysmal atrial fibrillation. He was prescribed tamsulosin, bisoprolol, perindopril, atorvastatin, and warfarin.
The patient’s preoccupation about bowel movements was, for the most part, deemed to have obsessive quality: he accepted that these worries were repetitive and came to his mind against his wishes. He said that he would rather not have these worries but was unable to distract himself.
The marked subjective anxiety, according to the patient, was entirely linked to the preoccupation. However, when the patient became agitated, it was difficult to persuade him to appreciate the anomalous nature of his thoughts. At such times he insisted that there was something definitely wrong with his bowels and nothing could help him.
Prior to admission, the patient was treated at different times with different antipsychotic medications, which made little impact on the symptoms. Following his admission he was referred to the psychology services, which concluded that he was too unwell to meaningfully participate in psychological therapies. The patient, too, was not keen on this option. He also declined ECT and was deemed to have the capacity to make the decision.
Venlafaxine-XL was switched, in light of the patient’s cardiac risk history, to an SSRI known to have an effect on obsessional symptoms. Accordingly, a dose of Mirtazapine was decreased to 30mg, and Venlafaxine-XL was tapered off over ten days.
Fluvoxamine was started at 50mg/day, and the dose was titrated to 150 mg/day over the next week. The dose was further increased to 200 mg/day.
INR was previously stable on warfarin dose of 5mg per day: blood results were between 2.32-2.68. Following fluvoxamine-initiation, INR started increasing: 2.98 after six days. INR increased further, to 3.82, with increase in Fluvoxamine’s dose
Warfarin-dose, as a result, was decreased, initially from 5mg to 4mg; however, INR remained above range (3.75). With further reduction in Warfarin’s dose, to 3mg/day, INR reduced but was still above range (3.51). INR eventually stabilised when warfarin-dose was reduced to 2mg/day. The dose adjustment took place over ten days.
Discussion
Management of depression in elderly population requires careful consideration of the choice of psychotropic medication, as elderly patients are more likely than younger patients to be on multiple medications for associated physical health problems, which increase the potential for drug interactions. Half-lives of drugs are also extended in the elderly.
The patient was prescribed Warfarin for the management of atrial fibrillation. Warfarin is a racemic mixture of S-warfarin and R-warfarin, of which S-warfarin is more potent than R-warfarin. 6
Warfarin has the potential to cause pharmacokinetic drug interactions (drugs affecting hepatic cytochrome P 450 enzyme system, which metabolises warfarin), which are thought to be more clinically relevant than pharmacodynamic interactions (highly protein bound drugs displacing Warfarin from its binding site) for warfarin. 6
Warfarin is metabolised by a number of P450 isoenzymes such as 2C9/2C19, 1A2, and 3A4. 6 Of these 2C9 is thought to be crucial, as it metabolises the more potent S-isomer. Isoenzyme 1A2 is the major route for the metabolism of the R-isomer, while 3A4 and 2C19 are considered to be minor routes.
The psychotropic medications that are thought to have the potential for significant pharmacokinetic interaction with warfarin include Fluoxetine, Fluvoxamine, Quetiapine, and Valproic Acid. 7 Venlafaxine is also considered a high-risk drug in patients taking warfarin. One study found that fluvoxamine and venlafaxine were associated with a more than double risk of having an INR value of 6 or more. 3
Fluvoxamine by dint of its inhibitory actions on 2C9/2C19, 3A4, and 1A2 8 inhibits all the isoenzymes that metabolise Warfarin and can be said to have the maximum potential for pharmacokinetic interaction with Warfarin.
National Collaborating Centre for Mental Health guidelines on depression in adults with chronic physical health problems advise avoiding SSRI in patients taking warfarin or heparin and instead offering an alternative antidepressant such as mirtazapine. 9 Therefore, caution is needed when prescribing these medications to patients who fail to respond to other safer options.
At the time of his admission, the patient was on a combination on Mirtazapine and Venlafaxine XL, both at high doses, for several months. Neither of the antidepressants has significant action on the P450 isoenzyme system, although both are substrates of some enzymes, such as 2D6, 1A2 and 3A4. 8 The patient’s INR was within normal limits when he was on these two medications (despite the aforementioned potential effect of venlafaxine on INR values).
During the period of admission, a decision was taken to change the antidepressant regime, for clinical reasons. The two antidepressants considered were Fluvoxamine and Sertraline.
It was felt that despite its higher potential to cause pharmacokinetic interaction with Warfarin, Fluvoxamine is chosen ahead of Sertraline (which inhibits 3A4 and 2D6). The more potent action of Fluvoxamine on the sigma1 receptors, which account for its significant anxiolytic properties and therapeutic action in the delusional depression 10 was felt to have the potential of benefit given the patient’s clinical symptoms.
It was also felt that Fluvoxamine would also be of more benefit than Sertraline with insomnia which was patient’s frequent complaint given its side-effect of somnolence. 11
Fluvoxamine was started at a low dose (50 mg/day) after Venlafaxine XL was completely withdrawn. The dose was titrated rapidly over the next one week, to 150 mg/day. The INR showed an upward trend within five days of commencing Fluvoxamine, and it exceeded three by the time the dose of Fluvoxamine was increased to 150 mg/day. This necessitated a reduction in Warfarin’s dose from 5 mg to 2 mg/day. The INR stabilised to between 2 and 3 when warfarin dose was more than halved.
Fluvoxamine has a half-life of 9-28 hours, and steady-state levels reach roughly after ten days. 8
The half-life is increased by almost 50% in the elderly. 3 The trajectory of increase in the INR was consistent with the pharmacokinetic of Fluvoxamine: it is a potent inhibitor of CYP4501A2, with a relatively little affinity for the other isoenzymes. The increase in INR was not dramatic, which is different from previous reports. 4 Throughout the period of Fluvoxamine –titration and Warfarin dose adjustment, there was no clinically untoward incident.
In conclusion, this case shows the need for close monitoring when warfarin is combined with another drug which significantly enhances warfarin’s anticoagulant effect. At the same time, it can be done safely, even in patients such as the elderly, who can be at a higher risk of adverse effects of interaction, when appropriate steps to monitor the patient are in place. The case also demonstrates the necessity of using clinical judgment while applying the guidance in individual patients.
Sjögren’s syndrome (SS) is an autoimmune exocrinopathy characterised by a lymphoplasmacytic infiltration of the exocrine glands. Both xerophthalmia and xerostomia are the most common manifestations of the disease. However serious organ damage such as, pulmonary and neurological involvement, can occur. The prevalence of neurological manifestations of SS varies between 0% and 70% (average 20%), which is largely dominated by peripheral neuropathies¹. The cranial nerve involvement, especially when it is isolated, represents a rare facet of the peripheral neuropathy.
Observation
We report the case of a 62-year-old patient with no medical history, referred to the internal medicine department with a 6 years history of dry mouth and xerophthalmia. No other complaints were reported.
The mouth examination showed a fissured, smooth and left deviated tongue without evidence of atrophy or fasciculation (figure 1). The rest of the oropharyngeal examination was unremarkable with no angina or cervical lymphadenopathy. Neurological examination confirmed a deficit of the right XII cranial nerve and excluded other cranial nerve involvements, sensibility or motility deficit. A specialised ophthalmologic examination was performed and showed a bilateral superficial punctuate keratitis.
The search for antinuclear antibodies by indirect immunofluorescence was positive at the titre of 1/1280 (speckled) corresponding to Anti-SSA and Anti-SSB antibodies. Cryoglobulinemia search was negative.
The rest of the laboratory investigations (blood cell count, liver and renal function tests, thyroid balance and inflammation markers) were normal.
A labial salivary gland biopsy was performed and its histological examination showed a lymphoid cell cluster of more than 50 cells/ 4 mm² corresponding to a focus score 1.
Brain MRI was normal - no damage in the brain stem was seen. Electromyography was normal.
The diagnosis of SS was made according to the presence of five out of six criteria according to the European American study group. The diagnosis of primary SS was retained due to the lack of clinical or biological argues for an associated autoimmune disease. A symptomatic treatment of Sicca syndrome was prescribed but no specific therapy has been initiated for the hypoglossal nerve attempt because of its asymptomatic nature.
Discussion
In the case of our patient, the tongue deviation was discovered at physical examination and was totally asymptomatic. In other cases, the twelfth nerve palsy could be responsible for swallowing difficulties, and in advanced stages for a lingual or hemi lingual amyotrophy. The spectrum of its aetiologies is numerous. In a large case series of 100 patients, malignant tumors (about half of cases), neurological causes (16 %) and post-traumatic palsy (12% of cases) were the three most popular aetiologies². Other conditions could be associated with twelfth nerve palsy, such as, infections², vascular injury³ and non-invasive oxygen therapy⁴. Paroxysmal idiopathic hypoglossal nerve palsy has also been described⁵. Our patient had Sicca syndrome which was related to SS according to 5 criteria of the European American study group: it was a subjective sensation of dry mouth and dry eyes associated to a bilateral punctuated keratitis, a focus score > 1 at the histological examination of the salivary gland biopsy and positive anti-SSA and anti-SSB⁶.
SS is an autoimmune disease that often presents as dry eyes and dry mouth due to lacrimal and salivary gland involvement. It can be primitive or associated to other autoimmune diseases such as, Hashimoto’s Thyroiditis, Rheumatoid Arthritis or Systemic Lupus Erythematosus. Wide varieties of neurological complications are characteristic features of SS which occurs most frequently in the primary form. Peripheral neuropathy is the most frequent neurological manifestation. Its most common presentation is a symmetrical sensorimotor or pure sensory neuropathy of hands and feet. Sensitive neuropathy, small fiber neuropathy, multiple mononeuropathy and polyradiculoneuropathy have also been described¹. Cranial nerve involvement is rare. In a review of the literature, Colaci M found 267 patients suffering from SS with different types of cranial neuritis during their clinical history. The discovery of cranial neuritis was contemporary to SS diagnosis in 40% of the patients, as in the case of our patient.
Optic neuritis and trigeminal nerve injury were the most frequent attempts and represent respectively 46.4% and 38% of all cranial nerve palsies. All cranial nerves palsies have been described except the eleventh⁷. Involvement of the twelfth cranial nerve is very rare and only two cases have been described⁸′ ⁹. In these two cases, it was associated with an involvement of other cranial nerves (table 1). To the best of our knowledge, this is the first report of an isolated and permanent involvement of the twelfth cranial nerve in a patient with primary SS. Many mechanisms were proposed to explain the cranial nerve involvement in SS. Clinicopathological observations of Mori K⁸ suggest that an isolated trigeminal nerve attempt could be explained by an immune-mediated neuron death in the sensory gasser ganglion. Whereas, other cranial nerve involvements which are frequently associated together could be explained by a multiple mononeuropathy resulting from a vasculitis⁸.
Further clinical observations will be necessary to determine the exact mechanisms of such neurological involvement.
Table 1: Review of the literature regarding SS patients with hypoglossal nerve injury
Number of patients
Age
Nerves
involved
Treatment
Evolution
Mori/2005 [8]
1
No data
V, VII, IX, X, XII
No data
Paroxysmal
Ashraf/2009 [9]
1
47
V–IX–XII
No data
Paroxysmal
Our patient
1
62
XII
None
Permanent
Figure 1: Smooth and left deviated tongue
Conclusion
In front of cranial nerves neuritis, we should actively search for sicca syndrome, sometimes not spontaneously reported by patients. Examination of the mouth can be instructive and should not be omitted in the diagnosis and monitoring of Sjögren’s syndrome.
Metastatic bone disease is a relatively common event in the advanced stages of many malignancies.1 Bone-modifying agents decrease the incidence of skeletal-related events (SREs) such as spinal cord compression and bone fracture, as well as the need for skeletal radiotherapy or surgery.2
Bone modifying agents such as intravenous bisphosphonates (IV BPs) (e.g. pamidronate and zoledronic acid) and denosumab are approved for prevention of SREs. IV BPs are primarily used and effective in the treatment and management of cancer related conditions such as multiple myeloma (MM), and breast cancer with skeletal metastases, because they reduce bone pain, hypercalcemia, and the risk of pathologic fractures.3
Denosumab, a receptor activator of nuclear factor kappa-B ligand (RANKL) inhibitor, represents a breakthrough in the treatment of osteoporosis, MM, and bone metastases. The Food and Drug Administration (FDA) approved it in 2010 for the prevention of SREs in patients with bone metastases and in 2011 for the prevention of endocrine-therapy induced bone loss in patients taking aromatase inhibitors for breast cancer and in patients with non-metastatic prostate cancer.
Three international, randomised, double-blind, double-dummy phase III studies have evaluated denosumab versus zoledronic acid for the treatment of SREs in breast and prostate cancers, and in combined solid tumours and MM. Denosumab’s superior efficacy over zoledronic acid was demonstrated in the studies of patients with advanced breast or prostate cancer, as well as in a pre-specified integrated analysis of all patients enrolled across the three studies.4
In the 2014 position paper of the American Association of Oral and Maxillofacial Surgeons (AAOMS), the nomenclature “bisphosphonate-related osteonecrosis of the jaw” changed to “medication related osteonecrosis of the jaw” (MRONJ). MRONJ is defined as cases in which all of the following 3 characteristics are present5:
current or previous treatment with antiresorptive or antiangiogenic agents
exposed bone or bone that can be probed through an intraoral or extra-oral fistula in the maxillofacial region that has persisted for longer than 8 weeks
no history of radiation therapy to the jaws or obvious metastatic disease to the jaws
Other terminologies used previously include “denosumab related osteonecrosis of the jaw” (DRONJ), and “antiresorptive agent-induced ONJ” (ARONJ).
The aetiopathogenesis of MRONJ related to denosumab therapy remains enigmatic, and hypotheses have focused on reduced bony turnover, infection, toxicity of the soft tissue, and antiangiogenesis. The epidemiology also remains unclear, and reported incidence varies widely.6 Overall, it is estimated that bone necrosis can develop in about 0.7-1.9% of patients with malignancy who are given high-potency IV BPs (such as zoledronic acid), and in 0.01–0.1% of those with osteoporosis who take low-potency oral BPs (such as alendronate). Data relevant to denosumab given subcutaneously in patients with metastatic cancer and osteoporosis seem to replicate those when IV high-potency BPs are administered.7 The risk of osteonecrosis of the jaw (ONJ) is higher in patients exposed to concomitant antiagiogenic medication. The individuals’ risk of ONJ is further determined by factors such as the potency of agent, cumulative dosage or duration of antiresorptive treatment, route of administration, comorbidities and local factors such as periodontal disease.8,9 Oral hygiene plays a significant role with evidence supporting a strong correlation between bacteria associated with periodontal disease and MRONJ.10
MRONJ typically manifests as painful and often infected areas of necrotic bone, which subsequently may lead to severe chronic pain and facial disfigurement. This adversely affects the ability to eat, speak and lowers the quality of life. Adverse events related to RANKL inhibitors are usually considered to be infrequent and low in occurrence. Unfortunately from our recent clinical experience at Sheffield Teaching Hospitals' Trust, there have been several new cases presented in a very short period of time. In this paper we present a case series of MRONJ related to denosumab therapy since adverse events of denosumab in the mandible or maxilla have received relatively little attention.
The aim of this article is to highlight the elevated risk of MRONJ in patients receiving denosumab treatment and educate all health care providers involved in the management of such patients. Furthermore, the mechanisms of denosumab, comparison with bisphosphonates and the reported management strategies are reviewed.
Mechanism of Denosumab
Denosumab is an antiresorptive agent that exists as a human IgG2 monoclonal antibody and inhibits the binding of the receptor activator of nuclear factor kappa-B ligand (RANKL) to RANK (Receptor Activator of Nuclear Factor kappa-B). The binding normally signals the proliferation of osteoclasts, as RANK is expressed on the surface of osteoclasts and their precursors, whereas its ligand, RANKL, is a membrane bound protein expressed by bone marrow stromal cells, osteoblasts and T-lymphocytes. The activation of RANK is integral to the function of osteoclasts. Osteoprotegerin binds to membrane bound RANKL on osteoblast which in turns decreases the osteoclastic activity and in theory negatively effects bone turnover. Denosumab acts similarly to osteoprotegerin but has a higher affinity for RANKL.11-13
Denosumab follows nonlinear, dose-dependent pharmacokinetics. The bioavailability of one subcutaneous denosumab injection is 61% and serum concentrations are detected within 1 hour. Maximum serum concentrations occur in 5-21 days and cessation of osteoclast activity occurs within six hours of the subcutaneous injection. The normal function is restored approximately six to nine months later, whilst bone turnover returns to normal shortly after this.14 Based upon monoclonal antibody pharmacokinetics, denosumab is most likely cleared by the reticuloendothelial system with minimal renal filtration and excretion thus avoiding nephrotoxicity. Its elimination half-life is 32 days, and it does not incorporate into bone.15
It is currently marketed as Prolia® and Xgeva®, approved by FDA. Prolia® is administered subcutaneously every six months and has shown to reduce the incidence of new vertebral, non-vertebral, and hip fractures in osteoporotic patients.16,17 Xgeva® is also effective in reducing SRE related to metastatic bone disease from solid tumours when administered intravenously on a monthly basis.17,18
RANKL Inhibitors and BPs Pharmacokinetics
There are fundamental differences between denosumab and BPs with regard to their mode of action. Denosumab is an antibody and acts extracellularly whereas BPs act intracellularly. As such, BPs must be present in the circulation and available for reuptake into bone for prolonged periods to function.19 There is not any evidence of drug recycling with RANKL inhibitors, and therefore it is suggested that their adverse effects can be reversible with discontinuation, in fact leading to a transient rebound phenomenon, which can be restored, with subsequent treatment.14,20 On the other hand, recycling of BPs in the circulation system has been proposed as a reason for the long duration of action even after cessation which can be up to 12 years.
The US FDA-approved manufacturer’s package insert for both zolendronate and pamidronate states that “there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ in patients who require dental procedures during therapy and that clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/ risk assessment”. The package insert for denosumab does not address the issue of treatment continuation in patients who develop MRONJ to date.
Denosumab is a circulating protein capable of distributing throughout extravascular space. It is expected to reach all sites within bone including intracortical sites unlike with BPs. BPs have strong affinity for hydroxyapatite and bone mineral which limits their even distribution throughout the skeleton, particularly to sites deep within the bone.19,21 This can explain the more profound inhibition of bone remodelling with denosumab than that seen with BPs.
Case Series
Case 1
A 55 year-old lady referred to a dedicated Oral Surgery nerve injury clinic for an opinion and management of her left sided inferior alveolar nerve (IAN) paraesthesia. The patient presented with a history of numbness in the left sided inferior alveolar nerve distribution following removal of the left mandibular second premolar (LL5) in July 2014. She was asymptomatic until she had the LL5 removed and since had suffered with constant pain and numbness. A year later, she had removal of the left mandibular first molar (LL6) and gave a history of recurrent infections and excruciating pain in her mandible over the past two months. On presentation she had an obvious submental swelling and left sided IAN anaesthesia.
Medically she was diagnosed with breast cancer in 2011, for which she underwent wide local excision followed by chemotherapy. She then was placed on unknown clinical trial that we identified at the time to be denosumab trial, following liaison with the Oncology team. She is currently receiving intravenous denosumab every three months.
Clinical examination revealed a grossly mobile anterior mandible with widespread bony necrosis and associated osteomyelitis. Sensory testing revealed complete anaesthesia in the left sided IAN distribution secondary to MRONJ.
An OPG (Orthopantogram) and CBCT (Cone-Beam Computerised Tomography) revealed an extensive patchy area of ill-defined bone loss in the anterior mandible extending posteriorly to the premolar/molar areas bilaterally (Fig 1).
Figure 1 A) OPG showing non-healing sockets in the left mandible with extensive bony destruction together with periosteal reaction extending to the right mandible as shown by the arrows.
Rather interestingly, the bony destruction was evident bilaterally with the patient only having had extraction of teeth in the left mandible (Fig 1). This could be the case of spontaneous ONJ in the right mandible or an extensive ONJ arising from simple extractions on the left side.
Figure 2 3D reconstruction of the CBCT image demonstrating extensive bony destruction involving the lower border of anterior mandible in keeping with a spreading chronic bony infection and clinical presentation of submental swelling as showing by arrows.
Case 2
A 66-year-old female referred by her general medical practitioner (GMP) with a 3-month history of delayed healing following a tooth extraction in the left posterior mandible. She had moderate to severe discomfort and reported multiple previous infections and purulent discharge from the area, which treated with multiple courses of antibiotics. In addition, she reported discomfort from the root treated right mandibular first and second premolar teeth (LR4 and LR5).
Medically she was diagnosed with breast cancer over 10 years ago for which she underwent resection followed by chemotherapy. Three years ago, she diagnosed with metastatic deposits and therefore has been receiving intravenous denosumab every six weeks since then. Other medications include steroids, chemotherapy agents, antihypertensives and analgesics. She did not receive any radiotherapy or BPs treatment in the past.
Clinical presentation revealed a heavily restored dentition with chronic generalised periodontal disease. There was evidence of widespread bone loss clinically and radiographically. The slow healing socket in the left mandible was visible but did not have any exposed bone (Fig 3). The lower right first and second premolar teeth (LR4 and LR5) were clinically and radiographically sound.
Figure 3. Non-healing socket in the left posterior mandible with no evidence of exposed bone or suppuration as showing by white arrow. Gingiva recession (black arrows) is evident in the LL6 and LL5 teeth in keeping with chronic periodontal disease.
Figure 4 Coronal sections of CBCT A and B showing multiple lytic areas within the inferior cortex of the mandible and incomplete healing of the extraction sockets.
On follow-up appointments, the patient suffered multiple repeated infections in the right and left posterior mandible and due to deteriorating periodontal disease, the LR4, LR5, LR6 were extracted by her own general dental practitioner (GDP) due to severe mobility. All three extraction sockets failed to heal (Fig 5) leading to an extensive area of exposed bone in the right mandible, extending from the lower right first premolar (LR4) to lower left first molar (LL6) region. Conservative management was embarked which included antibiotics, chlorhexidine mouthwash and routine oral hygiene appointments. Selective sharp bone trimming and three sequestrectomies were undertaken. At the same time, liaison with the patient’s oncologist resulted in cessation of the denosumab therapy and complete resolution of her oral symptoms.
Figure 5 Clinical picture of exposed necrotic bone (white arrows) following simple extractions of periodontally involved teeth.
Case 3
A 76-year-old lady referred to the Oral Surgery department by her GDP with a 3-month history of a non-healing lower left first premolar (LL4) socket. The patient was treated with two courses of antibiotics prior to referral which provided only temporary relief to her symptoms.
Medically she was diagnosed with breast cancer 10 years ago and recently commenced intravenous denosumab for metastatic disease. She also receives hormone therapy and palliative radiotherapy to the spine.
On clinical examination, there was a partially healed LL4 socket with a rather granulomatous appearance. There was no clinical evidence of suppuration or bony exposure. Radiographs confirmed the absence of bony infill in the socket. Local debridement and biopsy of the granulomatous tissue was performed to exclude any metastatic disease. Biopsy report confirmed the presence of inflammation tissue.
Figure 6 CBCT scan; A and B sagittal views, C axial view and D 3D reconstruction. Extensive periosteal reaction extending from the midline of the mandible to the left molar region is evident in keeping with chronic osteomyelitis secondary to MRONJ.
Liaison with the microbiologist suggested a long-term antibiotic course to arrest osteomyelitis. Further liaison with the oncology team, resulted in denosumab being stopped for 4 months. On subsequent review appointments, patient’s symptoms improved however, there is now an area of exposed bone in the LL4 region as shown in Fig 7.
Figure 7 Clinical photo illustrating exposed bone (white arrow) in the LL4 region without evidence of local infection.
Case 4
A 65-year-old lady referred to the Oral Surgery department by her GDP with a history of a sore upper mouth and jaw underneath the dentures which is unable to wear.
Medically she was diagnosed with disseminated breast malignancy including bone metastases 3 years ago and for that, she is on exemestane and IV Denosumab monthly.
Clinical examination revealed multiple draining sinuses in the anterior maxilla. There was a partially healed LL4 socket with a rather granulomatous appearance and tenderness on palpation. There was neither discharge from the area nor any exposed bone. Radiographs confirmed the absence of bony infill in the LL4 socket. Local debridement and biopsy of the granulomatous tissue was performed to exclude any potential malignancy and it was confirmed as inflammation tissue.
Figure 8 CBCT scan; A axial view, B and C 3D reconstruction. A 25mm fragment of right anterior maxilla is beginning to sequestrate. This extends from the anterior margin of the right maxillary sinus approximately to the position of the upper left lateral incisor, crossing the midline. The sequestrated fragment involves the lateral margin of the nasal cavity. There is bilateral moderate mucosal thickening in the maxillary sinuses. Extensive periosteal reaction extending from the midline of the mandible to the left molar region is evident in keeping with chronic osteomyelitis secondary to MRONJ.
Table 1 Summary of cases
Cases
Indications
Duration (months)
Clinical Findings
Case 1
Metastatic deposits from primary breast malignancy
48
Anaesthesia in the distribution of the left inferior alveolar nerve Osteomyelitis Excruciating pain
Case 2
Metastatic deposits from primary breast malignancy
36
Chronic generalised adult periodontal disease Non-healing extraction sockets Exposed bone persisted for longer than 8 weeks Severe pain
Case 3
Metastatic deposits from primary breast malignancy and myeloma
24
Non-healing extraction socket with granulomatous tissue Severe pain
Case 4
Disseminated breast malignancy including bone metastases
30
Multiple draining sinuses in anterior maxilla Non-healing extraction socket with granulomatous tissue Severe pain
Discussion
ONJ associated with antiresorptive therapy deserves distinction from other causes and diseases/medications associated with the development of osteonecrosis of the jaw. AAOMS recently published stage specific treatment recommendation for MORNJ.22 The various stages and suggested stage-specific treatment strategies are not evidence-based, and in particular, stage 0 disease is not universally accepted. AAOMS recommendations echoed those stated in previous years for BRONJ, namely supporting conservative therapy, with aggressive surgery offered only to symptomatic patients. In contrast, the MRONJ guideline report from the German Dental and the German Oral and Maxillofacial Associations refrains from recommending therapy at least for certain stages of the disease. This might be attributed to the pitfalls of current MRONJ criteria. Furthermore, due to poor guidelines specifically related to RANKL inhibitors, no agreement exists on a universally acceptable therapy strategy of such cases.
Management strategies are largely based on expert opinion rather than experimental data. It includes prevention, conservative and surgical modalities. Prevention of the condition is the gold standard. It is highly recommended all patients have a comprehensive dental examination and preventive dentistry (pre-emptive extraction of unsalvageable teeth and optimised periodontal health) before commencing antiresorptive therapy.23,24 Oral hygiene should be kept meticulous during the course of therapy as periodontal disease and associated bacteria claim to be implicated in this condition and also observed in these cases.
The success rate of conservative treatment regimens range from less than 20% 25,26 to above 50%27,28 although some cases become chronic and develop complications.29
Microbial cultures from areas of exposed bone are not always helpful since normal oral microbes are isolated. However, when there is extensive soft tissue involvement, microbial cultures may help to define comorbid oral infections, which may guide the selection of an appropriate antibiotic regimen.30
Regardless of the stage of disease, areas of necrotic bone that are a source of chronic soft tissue irritation and loose bony sequestra should be removed or recontoured so that soft tissue healing can be optimised. This is in line with our clinical experience. The extraction of symptomatic teeth within exposed, necrotic bone should be considered as it appears unlikely that extraction will worsen the established necrotic process. Otherwise, surgical resection of necrotic bone should generally be reserved for refractory or advanced cases.31 Resection may occasionally result in even larger areas of exposed and painful infected bone.32
A recently published MISSION study7 reported that the AAOMS system misclassified/ underestimated the severity of the disease at a rate of about 1 in 3, in particular in patients suffering from MRONJ stage 1 and 2. The authors conclude that these findings may explain why the treatment of stage 3 ONJ, namely surgery with success rate over 85%33,34, has been deemed to be more predictable and therefore yields more favourable outcomes than the treatment of stages 1 and 2.35
Denosumab is characterised by reversibility of its effect after treatment discontinuation, in contrast with bisphosphonates. This is in line with our findings since cessation of denosumab in two cases helped to improve their symptoms significantly.
MRONJ has been reported to occur after a mean administration period of 39.3 months and 35 infusions in oncology patients.23 It is interesting that all published cases of denosumab-related ONJ occurred early after commencement of therapy, independent of the number of previous administrations.36,37 In our experience, all patients developed MRONJ within the first 3 months of teeth extractions; well ahead of the reported period and number of administrations of denosumab.
Furthermore, all four cases have had extensive lytic lesions developed following removal of a single tooth. The common radiographic findings in all cases include:
non-healing extraction socket
areas of focal and diffuse sclerosis
thickened lamina dura
early sequestrum formation
reactive periosteal bone
osteolysis of cortical and spongious bone
These findings, although common in MRONJ cases, have had extensive bony involvement and rapid progression of ONJ, demonstrating a far more aggressive nature of the disease compared to that seen with BPs.
In our experience, not all patients are adequately informed of the risks and adverse events of denosumab therapy. This highlights the importance of educating patients and inter-professional communication regarding the prevention and best management of MRONJ cases. In one of the cases, the lack of patient education concerning denosumab side effects and the failure of inter-professional communication had a detrimental effect on the patient’s overall management and subsequently patient’s oral health.
Table 2 Important Points
All patients prior to start of any antiresorptive medication should have a dental check-up and receive dental or surgical treatment beforehand to avoid the possibility of complications associated with antiresorptive medications
Strongly recommend regular dental check-ups to prevent
Patients should be advised to contact their Doctor/Dentist/Oral surgeon immediately if notice following symptoms:
Feeling of numbness, heaviness or other unusual sensation in the jaw
Pain in the jaw / toothache
Delayed healing to the gums, especially after dental work
Bad taste / infection
Swelling of the jaw
Loose teeth
Exposed bone
Pus like discharge from the affected area
Conclusion
We present our experience with denosumab-related ONJ from Sheffield Teaching Hospital’s NHS Trust. This case series should contribute to the existing sparse clinical literature on this topic. The pathogenesis, treatment and outcome of ONJ are complex and multifactorial. Patients treated with denosumab may be more prone to developing ONJ even without a precipitating dental event. ONJ may have a more aggressive profile and develop significantly earlier in patients receiving denosumab. Prevention of ONJ still remains the most important goal, and this is most directly accomplished by avoiding invasive dental procedures and establishing inter-professional communication.
The skeletal type of muscles are rarely affected by tuberculosis (TB) because they are not a preferred site for the survival and multiplication of Mycobacterium tuberculosis.1 Even in patients with widespread involvement of the disease, TB rarely involves muscles. Petter et al recorded only one case of primary skeletal muscles TB in over 8,000 cases of all types of TB, with an incidence of 0.015%.2 Few cases of tubercular myositis have been described in literature until now, mostly in adults. This, together with the decline in TB in general, makes it unlikely that one would immediately consider TB as the cause of a rectus sheath abscess.
There are only limited cases reports of isolated tubercular involvement of the anterior abdominal wall even though TB is rampant in developing countries, and with the rapid spread of acquired immune deficiency syndrome (AIDS) it has made inroads into the developed nations as well.3 We are presenting a case of primary tuberculous abdominal wall abscess, with no evidence of pulmonary, skeletal or gastrointestinal TB in an immunocompetent patient. This case report should serve as a reminder that TB, in all of its various manifestations, remains very much among us.
Case report
A 20-year-old female presented to the outpatient department of surgery, with a complaint of a progressive swelling in the left lower abdomen for the last three months. There was no history of preceding trauma, fever, cough, malaise or pain. There was no history of contact with any case of TB. On examination, there was a swelling in the left iliac fossa, measuring 8x8cm in size, non-tender with smooth and ill-defined margins, and normal overlying skin. The swelling was firm in consistency and moved with respiration. Examination of the cardiovascular and respiratory systems were within normal limits.
Laboratory investigation revealed: haemoglobin 11.5 g/dl; total leukocyte count 8510/cumm with a differential count of 54% neutrophils, 42% lymphocytes and 4% eosinophils; erythrocyte sedimentation ratio 70 mm; and enzyme-linked immunosorbent assay (ELISA) for human immunodeficiency virus (HIV) negative. The chest radiograph was unremarkable. Other biochemical blood investigations, including liver and kidney function tests, were within normal limits. Ultrasonography of the abdomen revealed a 6.5x8.5cm left iliac fossa cystic mass with a liquefied necrotic centre in the anterior abdominal wall (Fig. 1). Computerized Tomography (CT) scan of the abdomen showed an abscess in the left antero-lateral portion of the abdominal wall limited to the muscle layer (Fig. 2). Ultrasound-guided fine-needle aspiration and cytological examination revealed caseating granuloma with central necrosis, lymphocytes, and giant cells, consistent with TB (Fig. 3). The patient was diagnosed to have tuberculous abscess of the anterior abdominal wall and antituberculous treatment was started following internal medicine consultation. She improved rapidly over the next few days. After four weeks of antituberculous treatment, she responded well to the treatment and the abscess regressed considerably. The patient did not require any surgical intervention.
Figure 1. Ultrasonography of the abdomen revealed a left iliac fossa cystic mass.
Figure 2. Focal cystic collection seen in the anterior abdominal wall of the left iliac fossa with mild peripheral enhancement (white arrow)
Figure 3. Photomicrograph revealed caseating granuloma with central necrosis, lymphocytes, and giant cells, consistent with tuberculosis.
Discussion
TB of the anterior abdominal wall is a rare entity and only isolated cases are reported in the literature. Possible explanation for the rarity of muscle involvement in TB includes high lactic acid content, lack of reticulo-endothelial tissue in muscle, lack of lymphatic tissue, the abundant blood supply, and the highly-differentiated state of muscle tissue.4 Although none of them seems to be an adequate explanation, all theories (except the first one) have been criticized.2
Two forms of skeletal muscle involvement are recognized.5 In the first type the tuberculous process spreads into the muscle through direct extension from a neighbouring structure e.g. bone, joint, tendon, or lymph node. In the second type the spread is haematogenous. Our patient is of interest because she seems to have a primary tubercular anterior abdominal muscular lesion with no evidence of immunoincompetence.
A tuberculous focus in the muscle usually manifests as progressive swelling and pain. The infection is usually restricted to one muscle.6 There may be a frank tuberculous abscess (as seen in our case) or a nodular sclerosis followed by calcification. Ultrasonography usually shows a cystic mass of mixed echogenicity with irregular walls and a liquefied, necrotic centre. Computed scan of the abdomen usually shows a well-defined abscess in the abdominal wall.7, 8 Ultrasonography or CT-guided aspiration followed by cytological examination usually reveals tuberculous granulomas with areas of caseous necrosis.
Management of this entity is mainly in the form of antituberculous drugs. Surgical intervention in the form of sonography, CT-guided aspiration or open drainage is usually reserved to patients where medical treatment has failed.3 Our patient responded well to medical treatment.
Although localized swelling in the rectus abdominis muscle is commonly due to necrotizing fasciitis, rectus sheath haematoma or tumours (benign / desmoid / malignant), a rare possibility of TB should also be considered. The prognosis is good in tuberculous myositis with appropriate chemotherapy.
Conclusion
This case alerts clinicians and radiologists of the possibility of TB when considering the differential diagnosis of any lesion even in any unlikely anatomical area, especially in those regions where TB is endemic.
Tuberculosis is an important and major infectious disease worldwide, especially in developing countries with an estimated global case fatality rate of 13% in 2007. The World Health Organization estimated that there were 13.7 million prevalent cases of TB infection worldwide, with each year bringing about 9.27 million new cases, 44% of which are new smear-positive cases1. Musculoskeletal tuberculosis is rare, chest wall tuberculosis is rarer and involvement of costochondral junction is among the rarest forms of tuberculosis. Tubercular costochondritis usually presents with insidious onset non-specific pain and swelling, resulting in delay in the diagnosis. Diagnosis is usually made by typical radiological findings and microbiological and histological evidence of tuberculosis. Treatment consists of antitubercular therapy with or without surgery.
Case report
30 year male, smoker, from low socio economic status presented with history of low grade fever, malaise and anorexia which began gradually two months back. For about one month he had pain in right side of chest just adjacent to lower part of sternum. The pain had started insidiously, gradually worsened with time, and was dull and aching in character. Pain was localized to the right lower parasternal area, occasionally radiating to the back. The pain was aggravated by physical activity and deep inspiration and was relieved to some extent by ordinary anti- inflammatory medications. There was significant history of pulmonary tuberculosis in the patient’s sister 1 year ago. There was no history of cough, haemoptysis, fever with chills or history of tuberculosis in the past.
On general physical examination, the patient was weak and febrile. On local examination, there was a bulge in the right lower parasternal area, corresponding to the right 9th costochondral junction. On palpation, there was severe tenderness in the same area. There was no peripheral lymphadenopathy and abdomen was soft and non-tender with no organomegaly. Chest examination was unremarkable. The rest of the examination was normal.
In terms of investigations, the chest radiograph, ECG, haemogram, kidney function tests and liver function tests were normal. ESR was high (34), Mantoux test was positive(15mm). Sputum for AFB was negative. Axial CT chest demonstrates expansion of the left 9th costal cartilage with soft tissue thickening on both the inner and outer aspect of the cartilage (Fig.1). FNAC (Fine Needle Aspiration Cytology) of the costochondral junction revealed Mycobacterium tuberculosis and on culture and histopathology of aspirated material revealed tubercular granuloma (Fig.2). A final diagnosis of tubercular costochondritis was made and the patient was treated with anti tubercular drugs for 9 months. Patient's symptoms improved after 2 weeks of treatment and swelling and tenderness subsided. Post treatment axial CT demonstrated complete resolution of soft tissue abnormality previously seen around the costal cartilage (Fig.3).
Figure 1: CT chest showing evidence of costochondritis.
Figure 2: Typical tubercular granuloma with central caseous necrosis on histopathology.
Figure 3: Post ATT CT showing complete resolution of costochondritis.
Discussion
Tuberculosis is very common infectious disease in developing countries like India, resulting in significant morbidity and mortality. Musculoskeletal tuberculosis is relatively uncommon and accounts for 1 to 2% of all the tuberculosis patients2,3 and accounts for about 10% of all extrapulmonary TB infections4. Tuberculosis of the chest wall constitutes 1 to 5% of all cases of musculoskeletal TB5,6. TB abscesses of the chest wall are usually seen at the margins of the sternum and along the rib shafts, and can also involve the costochondral junctions, costovertebral joints and the vertebrae7. In one study8, on the basis of the part of the rib involved, the roentgenographic findings for patients with rib tuberculosis was divided into four categories: Costovertebral (35%), Costochondral (13%),Shaft (61%), and Multiple cystic bone. TB of the thoracic wall is usually caused by reactivation of some latent foci of primary tuberculosis formed during hematogenous or lymphatic dissemination but direct extension from contiguous mediastinal lymph nodes can also occur9. In developing countries such as ours, tuberculosis is endemic and all the rare forms of the disease have been described, but in developed countries, resurgence of tuberculosis due to HIV may be responsible for atypical presentations .
Thoracic wall tuberculosis mostly presents insidiously with pain and swelling, but the diagnosis of chest wall TB is often delayed due to lack of specific symptoms and signs and gradual course10. Approximately less than 50% of chest wall TB patients may have active pulmonary TB11,12. Imaging techniques like X-Rays and CT scan play an important role in diagnosis and follow up of these patients. According to a study done by Vijay YB et al13, radiological signs may not be present initially at the time of presentation with symptoms, abscesses or sinuses may be present much before the imaging modalities detect them. Computed tomography (CT) scan is more valuable for localization and detection of bone destruction and soft tissue abnormalities. Atasoy et al demonstrated the role of Magnetic Resonance Imaging (MRI) for early detection of marrow and soft tissue involvement in sternal tuberculosis due to high contrast resolution of MRI14.Diagnosis is usually confirmed by finding acid fast bacilli (AFB) and positive AFB cultures of bone (positive in up to 75% of cases), and caseous necrosis and granuloma on histopathology11.
Complications of thoracic wall tuberculosis include secondary infection, fistula formation, spontaneous fractures of the sternum, compression or erosion of the large blood vessels, compression of the trachea and migration of tuberculosis abscess into the mediastinum, pleural cavity or subcutaneous tissues as discharging sinus. Chest wall TB needs to be differentiated from benign and malignant tumors [chondroma, osteochondroma, fibrous dysplasia, lipoid granuloma, chondrosarcoma, myeloma multiplex]11, metastatic carcinoma, lymphoma or other kinds of infection15,16.
The treatment of choice of chest wall TB is still not clear. Whether antitubercular therapy alone or surgical debridement (or excision based on lesion extension) combined with antitubercular therapy should be done needs further studies. But the general rule is if there are any complications, surgery is the treatment of choice followed by antitubercular therapy. We conclude that the diagnosis of thoracic wall tuberculosis is a challenge for physicians and is suspected by gradual onset clinical features and confirmed by microbiology, histopathology and radiography findings. Early diagnosis and treatment are important to prevent complications caused by bone and joint destruction.
Three and half year old male child presented to PICU, Narayana health BANGALORE, with a short history of fever of 8 days with headache and cough for 2 days. At admission the child was febrile, dull looking, haemodynamically stable with no meningeal signs or focal neurological deficit. He was admitted and evaluated for the cause of fever. Same day child developed generalized seizures along with fever, hence a possibility of meningitis or electrolyte imbalance (hyponatremia) kept as child had initial serum sodium of 128meq/l. The cause of hyponatremia was looked into and child managed with antiepileptic drugs and 3% normal saline infusion. The initial sepsis screen was in-conclusive and CSF analysis showed 3 lymphocytes with low glucose and elevated protein levels, hence partially treated meningitis was considered (as h/o admission to a hospital for 3 days prior to admission in our hospital). The antimeningitic dose of IV antibiotics were given. On day 3 of admission child developed meningeal signs with worsening sensorium, hence neuro imaging was done (MRI brain) which showed multiple well defined ring enhancing lesion at bilateral central and cerebrallar hemisphere, thalamus, pons with mild perilesional edema. This radiological picture suggested a possibility of nerucysticercosis, however the clinical picture did not match with the same, hence pediatric neurology opinion was taken and simultaneous workup for tuberculosis were started. Child was also started on IV steroid. A strong possibility of CNS toxoplasmosis was kept by neurologist based on radiological picture. The workup for TB was inconclusive (negative mantoux, normal ESR, negative gastric aspirate for AFB) however child was empirically started on category II ATT in view of deteriorating clinical state. Repeat CSF evaluation showed increasing cell counts and similar biochemical picture as before, the sample was also send for Gene-Xpert (DNA amplification study). On day 6 of admission child developed lethargy and drowsiness hence antiedema measures were initiated. Same day he developed tonic posturing with unequal pupil, hypertension and bradycardia indicating raised Intracranial pressure (ICP), for which he was intubated and ventilated and urgent repeat CT head was done which showed increase in ventricular size and hydrocephalus. Immediately EVD was put by neurosurgeons after which there was gradual improvement in child’s condition and he was extubated within 48 hours. The reports showed negative HIV and toxoplasma serology and positive CSF gene study for AFB confirming the diagnosis of CNS tuberculosis, hence ATT and antiedema measures were continued and the EVD was later converted into VP shunt. Child by 2nd week of illness became afebrile with improved sensorium and function.
Fig 1 & 2: MRI showing multiple ring enhancing lesions
Discussion
Tuberculosis remains a leading cause of morbidity and mortality in the developing world. CNS involvement is thought to occur in 2-5% of patients with tuberculosis and up to 15% of those with AIDS related tuberculosis 1,2. Although CNS involvement by tuberculosis is seen in all age groups, there is a predilection for younger patients, with 60-70% of cases occurring in patients younger than 20 years of age 2. Haematogeneous spread from the lungs or gastrointestinal tract is most common, leading to small subpial or subependymal infective foci. These are termed Rich foci and form a reservoir from which intracranial manifestations may arise 3,4. Tuberculomas often present with symptoms and signs of focal neurological deficit without evidence of systemic disease. The radiologic features are also nonspecific and differential diagnosis includes malignant lesions, sarcoidosis, pyogenic abscess, toxoplasmosis and cysticercosis.5,6
Regarding treatment, the Center for Disease Control and Prevention recommends 12 months of treatment for CNS TB when the MT strain is sensitive to all drugs.7 However numerous variables can affect the response of the disease to therapy and it has been suggested that treatment duration should be tailored to the radiological response.8 After 12 months of treatment more than two-thirds of the patients still have contrast enhancing lesions. Although it is not clear if this represents an active lesion or just inflammation, continuing treatment is probably prudent. Total resolution of the tuberculoma is observed when scans demonstrate no enhancing lesions or only an area of calcification.8
In the case described above child had tubercular mengitis, multiple tuberculous, hydrocephalus and raised ICP. Although clinical presentations were suggestive of same, however the radiological picture and initial CSF finding raised suspicion is diagnosis. As tuberculoma and NCC shows many common clinical features, there are few distinguishing features such as the cysticercosis is smaller, less perilesional edema, multiple numbers and less of midline shift as compared to tuberculoma. However in our patient the multiple tuberculi gave a suspicion of NCC. It was only gene expert which confirmed our diagnosis.
Hence clinical cases like Tuberculoma, the radiological findings of which can usually be distinguished from other common illness like Neurocysticercosis or Toxoplasmosis, sometimes pose challenge in terms of radiological diagnosis suggesting the need for detailed evaluation to reach the diagnosis and guide treatment.
Meningiomas are common intracranial neoplasms with a wide range of histopathological appearances. The WHO classification of tumours of the central nervous system recognises 15 subtypes of meningiomas, of which meningothelial, fibrous and transitional subtypes are most common. Lymphoplasmacyte-rich meningiomas (LPM) are rare WHO subtype that belong to Grade I meningiomas.1 The estimated incidence is less than 1% of all meningiomas.2 LPM usually occurs in young and middle age patients, with most common locations being cerebral convexities, skull base, parasagittal area within the superior sagittal sinus, cervical canal, optic nerve and tentorium.3 Histopathological examination shows extensive infiltrates of lymphocytes and plasma cells often obscuring the meningothelial component.
Case report
A 21-year-old man presented with a history of headache since 4 months. It was a dull pain not associated with vomiting, seizures or visual symptoms. The patient did not have any features suggestive of cranial nerve involvement. Physical examination was unremarkable except for the presence of papilloedema. Non-contrast CT scan showed a large isodense lesion with peri- lesional oedema and eccentric enhancing nodular component in the right fronto-parietal region (Figure 1). A radiological diagnosis of glioma with mass effect and shift to left was rendered. A right frontoparietal free bone flap craniotomy was performed. Operatively, a well encapsulated tumour probably arising from the dura mater was found. Gross total removal of the tumour was done and the excised tumour was sent for histopathological examination with a provisional clinical diagnosis of meningioma.
Histopathological examination revealed a tumour arranged as sheets and whorls of meningothelial cells without any mitoses or atypia. A dense infiltrate of lymphocytes and plasma cells was seen in large areas of the tumour (Figure 2).
On immunohistochemistry, tumour cells were positive for epithelial membrane antigen (EMA) (Figure 3) and vimentin. The lymphoplasmacytic infiltrate contained mixture of CD3 and CD20 positive lymphocytes. A diagnosis of lymphoplasmacyte- rich meningioma was given.
Figure 1. Non-contrast CT scan showing a large isodense cystic lesion with perilesional oedema and eccentric enhancing nodular component in the right frontoparietal region
Figure 2: Tumour arranged as sheets and whorls of meningothelial cells without any mitoses or atypia. A dense infiltrate of lymphocytes and plasma cells seen in large areas of the tumour (H & E x 100)
Meningiomas are common neoplasms accounting for 24-30% of all primary intracranial tumours. They arise from the arachnoidal cells, and are typically attached to the inner surface of the duramater.1 Most of the meningiomas are benign, corresponding to WHO grade I and associated with a favourable clinical outcome. LPM is a rare low grade histopathological subtype of meningioma, usually seen in younger patients, with the mean age of onset being 34 years.4,5 The patients with LPM have variable clinical manifestations according to the location of the tumour. The common presentations include headache, hemiparesis, seizure, vomiting, dizziness, visual disturbance, dyscalculia, dysgraphia and slurred speech.3 Although the natural history of LPM is often over one year, few cases might occur in short duration due to inflammatory cell infiltration and oedema.6 Systemic haematological abnormalities such as hyperglobulinemia and iron refractory anaemia have been documented in some patients with LPM, believed by some to be due to the plasma cell infiltrate.3,6,7
Radiologically, LPMs are usually globular, highly vascular, contrast- enhancing, and dural based tumours. The typical characters of LPM on MRI are isointense lesions on T1-weighted images and hyperintense lesions on T2-weighted images, with a strong homogenous enhancement after the administration of gadolinium; obvious peritumoural brain oedema and dural tail signs.3 Sometimes, cystic component and heterogeneous enhancement may also be encountered, making pre-operative diagnosis difficult, as in our case.8
On microscopic examination, this tumour is characterised by a conspicuous infiltrate of lymphocytes and plasma cells, sometimes completely obscuring the tumour cells. The massive infiltration of lymphocytes and plasma cells has been postulated to play a central role in the development of brain oedema associated with LPM. The origin of this tumour (neoplastic or inflammatory) is unclear, so it is considered closer to intracranial inflammatory masses rather than typical meningiomas.7
The differential diagnoses include collision tumour of meningioma and plasmacytoma, inflammatory pseudotumour, idiopathic hypertrophic pachymeningitis (IHP), and intracranial plasma cell granuloma.3,7 The use of staining for EMA and vimentin is useful in indicating the meningothelial origin of the tumour, and differentiates LPM from other intracranial lesions.9
The pathological findings of IHP usually include thickened fibrotic dura mater with marked infiltration of lymphocytes and plasma cells, occasionally accompanied with small islands of meningothelial proliferation mimicking those of LPM. Localised nodular lesion can sometimes rule out this diagnosis in that IHP usually shows diffused lamellar thickenings or plaque-like features.4
Chordoid meningiomas often contain regions that are histologically similar to chordoma, with cords or trabeculae of eosinophilic, vacuolated cells in a background of abundant mucoid matrix background.3 Detailed histological studies can aid the differential diagnosis. The plasma cell component is not neoplastic and thus plasmacytoma with reactive meningothelial hyperplasia or a collision tumour involving meningioma and plasmacytoma can both be excluded.10
The knowledge of this rare entity is important to avoid its underdiagnosis as an inflammatory pseudotumour or plasma cell granuloma and overdiagnosis as a plasmacytoma.
A 38 year old BMI 20.2 ASA 2 female underwent an elective robotic-assisted laparoscopic extirpation of endometriosis and dissection of endometriomas. Her medical history included hypertension, migraine, atopic dermatitis, sciatica, cervical spine spondylosis and dysplastic spondylolisthesis of L4/5. Of note, the patient had allergies to Aspirin (causing angioedema), Morphine and Tramadol (both causing generalized rash).
An 18gauge IV cannula was inserted into the cephalic vein at the left wrist, and connected to a bag of Hartmann’s solution. The patient was induced with Propofol 100mg, Rocuronium 30mg and a Remifentanyl infusion running at Ce 1ng/mL. Cefazolin 2g and Dexamethasone 4mg were also administered post-intubation. No rashes were noted on the patient’s skin, and her arms were subsequently enclosed with green towels by her sides for the duration of the surgery. During the procedure, the patient was sustained in a steep trendelenberg position, with her face and eyes checked periodically. No rashes were noted on any exposed skin. Peri-operatively, she was maintained with O2/air/Desfluorane, top-up doses of Rocuronium, and titration of the Remifentanyl infusion. At the end of the surgery, the patient was administered Ondansetron 4mg and Pethidine 50mg (in 2mL), and reversed with Neostigmine 2.5mg and Glycopyrrolate 0.4mg. The patient’s arms were subsequently exposed in preparation for transfer, and it was noted that she had developed severe erythema and inflammation in specific tributaries of the cannulated vein (Figure 1). The patient was extubated uneventfully five minutes later, and did not complain of any symptoms systemically or pertaining to the cord inflammation. She was monitored in recovery for three hours post-op, and the inflammation subsided significantly 90 minutes post-op (Figure 2) and completely 150 minutes post-op (Figure 3).
There have not been many reports of such a reaction in published materials, and we take this opportunity to provide further pictorial evidence of the possible sequelae of IV administration of a high concentration Pethidine solution. The variances in analgesia effectiveness and potential side effects between Morphine and Pethidine are negligible2. As such, and given that Pethidine is commonly used as a mode of analgesia on our wards and in the peri- and immediate post-operative periods when other classes of drugs are contraindicated, we hope to provide further pictorial support of such an extraordinary reaction for other interested clinicians. It is also interesting to note that in both cases the patient was female, around 40 years old, had a thin body structure, had an atopic tendency, and the concentration of injected solution was higher than 10mg/mL. Additionally, these are known factors believed to increase reaction severity3 4. We acknowledge that 3 other drugs were administered at the same approximate time as Pethidine, and as such any of the 4 medications could be culprit to the reaction, although this is unlikely as our patient had been given those medications in previous procedures with no issues or complications.
Figure 1: Post-op, Figure 2: 90 mins post-op, Figure 3: 150 mins post-op
A 61-year-old lady underwent a modified radical mastectomy and axillary clearance in 2008 for a carcinoma of the left breast. Histopathology examination revealed two tumours within the left breast; a 16mm Grade 2 lobular carcinoma with probable vascular invasion and a 9mm Grade 1 infiltrating ductal carcinoma with no vascular invasion. She had clear resection margins. 21 out of 34 removed lymph nodes were positive for metastatic deposits. The tumour was oestrogen receptor positive and HER2 negative. She was staged as T1 N3a Mx and the tumour had a Nottingham Prognostic Index of 5.32. Metastatic workup revealed no distant metastasis.
Postoperatively, she required aspiration of a seroma but her recovery was otherwise satisfactory. She received adjuvant chemotherapy in the form of three cycles of Fluorouracil, Epirubicin and Cyclophosphamide and 3 cycles of Docetaxel. In addition, she had postoperative radiotherapy to the chest wall and supraclavicular fossa (40 Gy in 15 Fractions over 3 weeks) and hormonal therapy with Letrozole 2.5mg once daily.
The patient opted to undergo a prophylactic right mastectomy in 2010. She was regular in follow up and appeared to be free of disease recurrence for 6 years.
Her past surgical history included abdominal hysterectomy and bilateral salpingo-ophorectomy for fibroid disease as well as varicose vein stripping. She is a non-smoker and doesn’t consume alcohol. She had a family history of colon and cervical cancer in her uncle and sister respectively.
The patient visited the surgical outpatient clinic complaining of abdominal cramps, altered bowel habits and fatigue of a few months duration. There was no associated rectal bleeding, haematemesis, melaena, weight loss or urinary symptoms. Physical examination was unremarkable but she was noted to have gradually worsening renal function. Her symptoms were at first attributed to side effects of intravenous antibiotic treatment, which she received during an admission for cellulitis. She had already undergone an upper GI endoscopy which showed oesophagitis and ulceration; biopsies were within normal limits. She received treatment with proton pump inhibitors but her symptoms persisted.
A non-contrast abdominal CT scan was done, on account of her poor renal function, which showed bilateral hydronephrosis and thickening of the postero-superior aspect of the bladder wall. Considering the limitations of the non-contrast study, there were no other abnormalities. A colonoscopy was also done to investigate her altered bowel habit and it revealed a benign-looking stricture in the sigmoid about 25cm from the anal verge which was easily bypassed by the scope.
Figure 1. Benign stricture on flexible sigmoidoscopy
Biopsies of the sigmoid stricture showed an infiltrate of small to medium sized tumour cells in the submucosa, which had an Indian file pattern. They were positive for AE1/AE3 (pancytokeratins) and negative for CD68. They were positive for CK7 and negative for CK20, strongly positive for oestrogen receptors and HER2 negative. Taken in conjunction with the patient’s past history of an invasive lobular carcinoma of the breast, the appearance was consistent with a metastatic lobular carcinoma.
Figure 2. Clusters and cords of cells with positive cytoplasm for the cytokeratin immunostain CK7. Although the classical ‘Indian filing’ of lobular carcinoma is not well seen, the image clearly demonstrates that the large bowel glands are negative (normally CK20+, CK7-) and that the infiltrate is beneath the glandular mucosa (i.e. not originating from dysplastic glands within the mucosa and raising the possibility of infiltration from outside the bowel wall). The magnification is x200. Lobular carcinoma is usually CK7 +, CK20 -, ER +.
Figure 3. The same cells with their nuclei staining positively with an immunostain to oestrogen receptors. There are a few short chains of ‘Indian filing’ with the cells appearing rather rectangular in shape with straight margins. You can make out slight ‘moulding’ of the nuclei as they press against one another. The magnification is x 400.
Figure 4. Haematoxylin and Eosin section at 400 magnification. This shows a diffuse infiltrate of single cells with eccentric nuclei.
The patient required a right nephrostomy and a cystoscopy with left double J ureteric stent insertion to address her hydronephrosis and deteriorating renal function before undergoing restaging of her disease.
DISCUSSION
In patients with history of breast cancer, isolated GI metastases are less common than benign disease processes or second primaries of the GI tract.1.2 In a retrospective review, 73 out of 12001 cases of breast cancer had gastrointestinal metastases, out of which 24 were to the colorectum3 and invasive lobular carcinoma was the commonest histological subtype. 3.4 However, sixteen percent of patients with breast cancer have GI metastases at postmortem examination1.
There might be a long interval of time between the diagnosis of breast cancer and development of gastrointestinal metastasis which together with their rare occurrence and nonspecific clinical and radiological manifestations adds to the diagnostic challenge. The median interval between the diagnosis and the development of GI metastasis was reported to be 6 years (range 0.25 to 12.5 years) by Schwarz et al 5with 25 years being the longest reported in the literature.6 Because of this long interval the history of a primary breast cancer can be missed. This also highlights the importance of long term follow up and maintaining an index of suspicion when these patients develop GI symptoms.
In our case, the interval between the diagnosis of breast cancer and colonic metastasis was 81 months. Her GI symptoms were initially attributed to side effects of antibiotic treatment for cellulitis and dyspepsia before investigating her with a colonoscopy. Even at colonoscopy the appearance was that of a smooth benign-looking stricture which did not seem to harbour any sinister pathology
Histological examination is probably the most reliable tool to make a diagnosis and it is prudent in such cases to compare the specimen with the original breast tumour. In this case, there were two primary tumours; an invasive ductal carcinoma as well as a lobular carcinoma but the metastatic disease favoured the lobular component, which is consistent with other published reports in the literature. The reasons why metastases favour lobular carcinoma are poorly understood. One explanation is the loss of E-cadherin expression, a molecule involved in cellular adhesion, in invasive lobular carcinoma7. A similar case in which the primary was a mixed ductal and lobular type with lobular subtype colonic metastasis was reported by Uygun et al.8 Immunohistochemistry can also help in establishing a diagnosis. Metastatic breast cancers tend to be positive for Oestrogen or Progesterone receptors as well as Gross Cystic Disease Fluid Protein-15.9, 10 It is, however, worth noting that primary colonic cancers can be oestrogen receptor positive in 30 to 70% of cases.11
Accurate histopathological diagnosis probably saved our patient an unnecessary surgical treatment for a primary colonic neoplasm as the main focus of her treatment should be systemic therapy for metastatic breast cancer.
CONCLUSION
GI tract metastases from breast cancer are a rare occurrence. The patients may present after a long interval from the original diagnosis and the clinical and radiological features are nonspecific with the diagnosis often established on histological examination. Moreover, the history of breast cancer may not be elicited in all cases and these patients may present to a gastroenterologist or colorectal surgeon rather than a breast surgeon or oncologist. Therefore, remaining vigilant to this possibility is advised in any patient with a history of breast cancer who presents with unexplained GI symptoms.
The NHS is supplied with approximately 300 000 NG tubes per year1. There are approximately 800-1000 incidents reported to the NPSA every year related to the insertion and use of NG tubes. Difficulties are often encountered with their insertion, especially in the setting of general anaesthesia. Whilst stridor and injury related to the use of NG tubes has been previously reported2,3, it has been related to prolonged siting. We describe a case acute stridor occurring in the recovery room due to direct trauma of the airway upon NG tube insertion.
Case report
A 61-year-old male presented with clinical symptoms of bowel obstruction. His medical history included atrial fibrillation (AF) treated with flecainide, and a 30-pack year smoking history. He was previously independent with a World Health Organisation performance status of 0. After CT confirmation of bowel obstruction, he was scheduled for an emergency laparotomy. A predicted P-Possum 30 day mortality was calculated at over 10%. He required no organ support pre-operatively, although his AF was poorly controlled. He had a low thoracic epidural sited awake, followed by induction of general anaesthesia with a rapid sequence induction. An arterial line, a central venous line, and an NG tube were inserted once anaesthetised. The NG tube was documented as difficult to site, and there were several attempts at a blind insertion via the oral and nasal route, before successfully inserting under direct vision using a laryngoscope.
The operative finding was that of an unresectable caecal tumour, and a defunctioning loop colostomy was formed. The total duration was 150 minutes. Following peripheral nerve stimulation and administration of 2mg/kg Sugammadex, he was woken, extubated and escorted to recovery.
Within minutes of being in the recovery area, he was acutely stridulous. Emergency assistance was called, and after assessment he was given nebulized adrenaline (1mg diluted in 4mls 0.9% saline), and 200mg of intravenous hydrocortisone. The nasogastric tube was removed, and his breathing was then supported with CPAP via a Mapleson C circuit and 100% oxygen. Direct examination of his airway, and indirect nasendoscopy with a Storz fibre-optic scope were performed. Significant bruising of his soft palate was seen, in addition to bruising and oedema of the soft tissues around the arytenoid cartilages with a small haematoma within the valleculae [Figure 1]. After approximately twenty minutes his stridor settled.
He was transferred to a level 2 high dependency unit later that day. He did not suffer from any further airway compromise, and his symptoms completely resolved.
Discussion
The insertion of an NG tube, whilst often deemed low risk, may result in life threatening consequences4. There even exists a “NG tube syndrome” 5, the pathophysiological mechanism of which is thought to be paresis of the posterior cricoarytenoid muscles secondary to ulceration and infection over the posterior lamina of the cricoid. There is no doubt that insertion of an NG tube in the anaesthetised patient can prove to be difficult, with a failure rate of up to 50% on first pass6, with repeated attempts at insertion being required. However, this case highlights the need for a controlled and ordered approach to managing the difficulties that can be encountered. Medical training incorporates NG insertion as a basic skill within the curriculum, but this affords new anaesthetic trainees little help with the anaesthetised and intubated patient.
There are several techniques described to insert NG tubes in anaesthetised, intubated patients7. There is evidence to suggest that modified techniques such as a reverse Sellick’s manoeuvre or neck flexion with lateral pressure are better than blind insertion in the neutral position. In the right hands, insertion under direct vision can overcome most difficulties, but is again not without risk.
We feel it is important to remember that NG insertion can cause patient harm, and potentially lead to life threatening consequences. Whatever the approach or technique that is chosen, having a logical and ordered approach is paramount. Using suitable alternative methods for insertion, or abandoning the procedure, as opposed to blindly continuing to repeat the same unsuccessful method must be key for success, as would be the case for approaching any clinical encounter.
Published with the written consent of the patient.
Multiple Sclerosis (MS) is an inflammatory, demyelinating disease of the central nervous system (CNS) that affects approximately 400,000 people in the United States and 2.5 million worldwide.1 There are rare variants of this disease that can profoundly delay diagnosis and treatment. Examples of such variants include: Tumefactive MS, Acute Disseminated Encephalomyelitis, Neuromyelitis Optica, Marburg’s MS and Balo Concentric Sclerosis.2 These variants have a uniquely aggressive presentation and do not exhibit classic MS features.2 Classic MS features include relapsing and remitting sensory and motor impairments, optic neuritis and pain. These aggressive variants are more likely to present with symptoms similar to neoplasm such as motor impairments and seizures. When dealing with these aggressive MS variants diagnostic options include Magnetic Resonance Imaging (MRI), Single Photon Emission Computed Tomography (SPECT) scan, MR spectroscopy and Cerebrospinal Fluid (CSF) analysis.3
Invasive tests such as brain biopsy are not warranted unless absolutely necessary. In MS, a biopsy must not be completed in order to confirm a diagnosis. However, to confirm a diagnosis of cancer a biopsy is required.
We present a rare case of Tumefactive MS that exhibited a clinical picture identical to brain metastasis. This was diagnosed with surveillance MRI and CSF analysis in the absence of a brain biopsy.
Case presentation
A 48-year-old African American female was brought in by emergency medical services after falling with a brief loss of consciousness. Associated symptoms included dull chest pain, diaphoresis and shortness of breath. While in the emergency department she also developed nausea, vomiting and dizziness. The patient reported no similar previous episodes and denied precipitating events. There was nothing else to note on review of systems. The past medical history included hypertension with no previous surgeries and family history included breast cancer of the mother diagnosed at age 47. The patient denied tobacco, alcohol and intravenous drug use. She noted an allergy to iodine.
On physical examination the patient was afebrile, normotensive and tachycardic with an oxygen saturation of 89% on room air. She was alert and oriented but pale and diaphoretic with mild left sided chest pain. Cardiac examination revealed a normal rhythm tachycardia and no murmurs were heard. Her neurological examination showed a normal mental status, normal cognition/comprehension and that Cranial Nerves II-XII were intact.
Laboratory findings included haemoglobin of 9.8 g/dL, 30.8% haematocrit and potassium of 3.3 mmol/L. Electrolytes were otherwise normal. Cardiac workup showed a normal ECG and slightly elevated cardiac enzymes of 0.319 ng/mL.
Given the patients tachycardia and desaturation, a stat Ventilation-perfusion (V/Q) scan was completed (patient had an iodine allergy). The V/Q scan revealed a perfusion defect suggesting pulmonary embolism (PE) as the cause of symptoms. Subsequently the patient was placed on appropriate anticoagulation.
Head CT (computed tomography) showed a left centrum semiovale round hypodense lesion measuring 1.4 cm, a left basal ganglia round hypodense lesion measuring 1.0 cm and a left occipital lobe round hypodense lesion measuring approximately 1.0 cm (Figure 1). No midline shift was seen. MRI showed multiple hypointense T1/hyperintense T2 nonenhancing lesions, mainly within the left cerebrum (Figure 2 A-F). The three largest lesions within the left posterior centrum semiovale (2A), left globus pallidus (2B) and left posterior corona radiata adjacent to the occipital horn (2C) measured 1.5 cm, 1.0 cm and 1.0 cm respectively. Perilesional vasogenic oedema was seen in all except the basal ganglia lesion. There were bilateral cerebral scattered foci of hyperintense FLAIR/T2 signals (D-F). The imaging suggested a differential diagnosis which included metastasis, infection or primary CNS malignancy.
Further work up in search for possible malignancy was completed. Skin map revealed no concerning nevi. Mammogram showed no tumor. CT of the abdomen and pelvis revealed a 2.6 cm indeterminate hypodense lesion in the left lobe of the liver (Figure 3A) along with an enlarged fibroid uterus (17x 7 x 14 cm). Liver biopsy was considered but a repeat MRI and ultrasound showed the lesion to be cystic, so this was deferred following surgical oncology recommendations (Figure 3B). For the hypertrophic uterus found on imaging, gynecology felt no further workup was necessary as they attributed the findings to a fibroid uterus.
Tumor markers CA 27-29, CA 19-9, CA 125 and AFP were all sent and came back negative. Initial lumbar puncture with CSF analysis was not completed secondary to possible complications that could be incurred while on necessary PE anticoagulation.
Due to a non-focal neurological examination, she was discharged on Levetiracetam 500 mg for seizure prophylaxis and Dexamethasone 4 mg for perilesional oedema. Over subsequent months the patient did well without headaches, vision changes or seizure like activity. On subsequent visits to the clinic, she had no evidence of focal neurological deficits except for mild bilateral symmetric hyperreflexia. Given that the metastatic work up remained negative, we considered obtaining a baseline Positron emission tomography (PET) scan to ensure we were not missing any possible metastasis.
She subsequently went back to work full-time and reported no symptoms. Repeat MRI of the head (Figure 4 A-C) showed predominantly T1 hypointense and T2 hyperintense (A-B) lesions with significant decrease in size from MRI done three months ago. These lesions demonstrated no enhancement to incomplete ring enhancement, with diminished vasogenic oedema (A). These findings suggested an inflammatory demyelinating process so a lumbar puncture was obtained after anticoagulation was held. CSF analysis was done using Isoelectric Focusing (IEF) and immunoblotting methodology. This revealed a normal myelin basic protein but with eight oligoclonal bands restricted to the CSF. These findings solidified the suspicion of Tumefactive MS.
Figure 1. Head CT without contrast: left centrum semiovale round hypodense lesions measures 1.4 cm with perilesional vasogenic edema
Figure 2. MRI of brain showing axial T1-weighted (A-C) hypodense lesions of the left centrum semiovale(A), left basal ganglia(B) and left occipital lobe(C). Axial T2-weighted (D-F) views show multiple hyperdense lesions corresponding to the same locations. Perilesional vasogenic edema is seen.
Figure 3A. Thorax CT without contrast. 2.6 cm left lobe liver lesion.
Figure 3B. MRI of abdomen showing coronal T2-weighted half-Fourier acquisition single-shot turbo spin-echo (HASTE) hyperdense lesion. A mildly enlarged liver measuring 18.7 cm in craniocaudal span. Simple 2.8 x2.4 cm cyct in the medial segment of left lobe.
Figure 4. MRI of brain (3 month after initial scans) showing axial T-2 weighted (A-B) hyperdense lesions of the left centrum semiovale(A) and left basal ganglia(B). There is irregular peripheral enhancement. Considerable decrease in size is seen from previous MRI (Figure 2). Left posterior centrum semiovale, left globus pallidus and left occipital lobe lesion measure 1.3 cm, <1 cm and <1 cm respectively. Vasogenic edema is diminished in comparison to previous study.
Discussion
Tumefactive MS lesions are defined as solitary demyelinating plaques greater than 2 cm.5 Lesions are difficult to distinguish between primary or metastatic given similarity of imaging features.5 Imaging features suggestive of Tumefactive MS include incomplete ring enhancement, absence of mass effect and absence of cortical involvement.6 7 Kim describes that CT hypoattenuation of magnetic resonance enhancing lesions was found to be highly specific for distinguishing Tumefactive MS lesions from CNS cancer pathology.6 It has been shown that SPECT using I-IMP is useful for diagnosing CNS malignancy.3 This is because there would be increased uptake in comparison to the MS lesions - implying increased metabolic activity.3 However this study has its limitations in diagnosis. In a few isolated cases I-IMP was found in greater quantities in MS tumor-like lesions.3
The imaging studies for this patient established a concern for metastasis, infection or primary malignancy. Extensive cancer workup was completed as previously discussed. Since all tumor markers were negative a baseline PET scan was considered however, was not done secondary to insurance denial. Due to the asymptomatic presentation of her disease, a primary differential diagnosis of brain metastasis and anticoagulation therapy for PE, a CSF analysis was not considered until much later. We were able to use surveillance MRI and CSF analysis to see some resolution of these lesions and confirm the diagnosis. Brain biopsy was never warranted but in unique symptomatic cases it may have been.6
The cornerstone of diagnosing MS is the demonstration of lesions in both time and space - termed the McDonald Criteria.8 The revised criteria allow a diagnosis of MS, “possible MS” or “not MS”.8 This is what made the diagnosis of our patient difficult, as no clinical symptoms or attacks were evident. It was demonstrated that over the course of three months the lesions seen on MRI evolved. From the size of 1.5 cm, 1.0 cm and 1.0 cm they became 1.3 cm, <1.0 cm and <1.0 cm respectively (Figure 2, Figure 4). This was likely the effects of steroids that the patient was on due to her vasogenic oedema. Here an evolution in time and space is demonstrated which excluded brain metastasis and infection. This brings into discussion the diagnostic value of surveillance MRI, which in our case was helpful and appropriate as the patient did not have clinical symptoms.
Conclusion
The diagnosis of Tumefactive MS can be extremely difficult and time consuming. As seen in our case, it can mimic other conditions. Our patient was able to be diagnosed with MRI surveillance and CSF analysis. The definitive diagnostic test for MS is a brain biopsy but this is not preferred due to the invasiveness of the procedure. With the advent of newer diagnostic tests such as SPECT, MR Spectroscopy, surveillance MRI and CSF analysis, diagnosis can be attained and treated presumptively.
Methamphetamine and related compounds are the most widely abused drugs in the world after cannabis 1. Methamphetamine is a synthetic stimulant which acts both on central and peripheral nervous system. It causes the release and blocks the reuptake of dopamine, norepinephrine, epinephrine and serotonin in neuronal synapse. Methamphetamine can be smoked, snorted, injected or ingested orally. Methamphetamine is more potent, and its effects last longer than cocaine 2, 3.
Methamphetamine intoxication causes various systemic complications like sympathetic over activity, agitation, seizure, stroke, rhabdomyolysis and cardiovascular collapse. Acute cardiac complications of methamphetamine like chest pain, hypertension, arrhythmias, aortic dissection, acute coronary syndrome, cardiomyopathy, and sudden cardiac death have been reported 4, 5. Chronic methamphetamine use is associated with coronary artery disease, chronic hypertension and cardiomyopathy 6.
Here we present a case of methamphetamine overdose, which presented with cardiomyopathy and severe systolic heart failure whose cardiac function was normalized after treatment.
Case presentation
A 38-year-old male presented with shortness of breath, chest tightness and sweating which started after he used intravenous crystal meth the day before presentation. He was an active poly substance abuser and used different drugs like marijuana, alprazolam, amphetamine, cocaine, percocet (oxycodone and acetaminophen) and clonazepam regularly. He was on methadone maintenance program as well. The patient did not have any cardiac problem in the past. He had a seizure disorder but he was not on medication. He had an episode of a seizure after methamphetamine use. His review of system was otherwise unremarkable.
On presentation he was tachycardic, his pulse was 128/min and his temperature was 98 degree Fahrenheit. He had bilateral diffuse crackles on lung bases. Troponin I was high 4.23 ng/ml (reference 0.01-0.05 ng/ml) and BNP was high 657 pg/ml (reference 0-100pg/ml). His electrolytes, renal function, liver function and creatinine kinase were normal. Urine toxicology was positive for opiate, methadone, amphetamine, benzodiazepine, cocaine and cannabinoid. Electrocardiogram showed sinus tachycardia at rate 130/min and QTc was prolonged at 488ms (Figure 1).
Figure 1 - Electrocardiogram: Sinus tachycardia at 130/min with prolonged QTc
Subsequently the patient became tachypnoeic and hypoxic, was intubated, put on a mechanical ventilator, and sedated with versed, fentanyl and propofol. Arterial blood showed respiratory acidosis and hypoxia. The patient was in cardiogenic shock and dopamine drip was started and intravenous Lasix was given. A subsequent chest X-ray showed newly developed pulmonary congestion. Echocardiogram showed left ventricular dilatation with diffuse hypokinesis and depressed systolic function. The left atrium was dilated. He had moderate diastolic dysfunction, mild mitral regurgitation and tricuspid regurgitation with a pulmonary artery pressure of 38mmHg. There was global left ventricular function was reduced and ejection fraction was 25-30%. His CT head was negative for an infarct or hemorrhage. He was managed in the cardiac care unit and responded very well to treatment. He became haemodynamically stable and dopamine was discontinued; aspirin, clopidogrel and carvedilol were started. The patient gradually improved and was extubated. Cardiac catheterization showed normal coronaries and normal left ventricular function. LVEDP was 18mmHg. His repeat echocardiogram one week later showed normal left ventricular systolic and diastolic function with an ejection fraction of 70%. The patient was discharged to drug rehab after eight days of treatment.
Discussion
This patient used intravenous crystal meth after which his problem started, so the most likely culprit was methamphetamine. Although he used multiple drugs including cocaine and amphetamine, which have acute and chronic effects on the heart, his cardiac function was normal before. Different mechanisms for cardiac injury due to methamphetamine have been proposed which include catecholamine excess, coronary vasospasm and ischaemia, increase in reactive oxygen species, mitochondrial injury, changes in myocardial metabolism, and direct toxic effects 3.Methamphetamine use is known to cause acute and chronic cardiomyopathy and the reversal of cardiac failure has been documented after discontinuing the drug. In one case report, a patient with chronic methamphetamine-associated cardiomyopathy did not demonstrate late gadolinium enhancement, consistent with an absence of significant fibrosis, and had left ventricular function recovered with 6 months of medical therapy and decreased drug abuse 7. Another case of a female 42 year old methamphetamine user who had transient left ventricular dysfunction and wall motion abnormalities and an index ventriculogram showed apical ballooning consistent with Takotsubo cardiomyopathy; her left ventricular function significantly improved after 3 days of medical treatment 8. In our patient, acute cardiomyopathy resolved quickly with intensive medical management. It is not clear how long it takes for cardiomyopathy to revert to normal after discontinuing the drug, or at what stage cardiac damage is irreversible. Many patients who use methamphetamine also ingest other drugs as well. It is unclear to what extent the use of multiple drugs play synergistic role in the cardiac complications that occur. Among patients who present with cardiomyopathy and cardiogenic shock, the usage of drugs like methamphetamine and co-ingestion of other drugs should be considered. Further study is needed to recommend treatment for methamphetamine and related drugs induced cardiomyopathy.
A 79 year old lady presented to the accident and emergency department with severe abdominal pain. On admission she was hypotensive and hypothermic. Blood tests demonstrated raised inflammatory markers and white count, but were otherwise unremarkable. A CT scan revealed no abnormalities. She was treated with intravenous fluids and empirical antibiotics.
She had multiple co-morbidities, including ischaemic heart disease, hypertension and chronic kidney disease.
Figure 1 – Upper Oesophagus
Figure 2 – Distal Oesophagus
Figure 3 - Gastro-eosophageal Junction
Figure 4 – Stomach (in retroflexion)
Figure 5 - Duodenum
Three days into her admission she had a single episode of hematemesis and a gastroscopy was arranged. Endoscopic features were as per figures 1- 5. Histology taken at the time showed necrotic tissue with evidence of candidiasis. Her treatment was optimised with a two-week course of fluconazole with the dose adjusted for her renal function and parenteral nutrition, with good clinical response. She was discharged after a two week hospital admission. A repeat gastroscopy 10 weeks later showed complete resolution of endoscopic features with no evidence of perforation or stricture formation.
DISCUSSION
The images seen at endoscopy demonstrate a region of oesophageal ulceration progressing to a diffuse, circumferential, black discoloration of the distal esophageal mucosa, with an abrupt transition to normal mucosa at the gastro-esophageal junction (Figs. 1-3). These endoscopic features, in the absence of a history of ingestion of caustic substances, are diagnostic of Acute Oesophageal Necrosis (AON), also known as ‘Black Oesophagus’. Whilst histology confirming necrosis is not necessary to make the diagnosis, it is confirmatory.
AON was first described in 1990 by Goldberg et al, since which over one hundred cases have been reported in the literature1. Population studies have suggested the incidence of this condition to be between 0.08% and 0.2%, although interestingly one post-mortem series of 1000 patients failed to reveal any cases2-4. There is a male preponderance, with an incidence four times greater than that for women and a peak incidence during the sixth decade of life5, 6.
The aetiology of this condition is not entirely clear; however case reports to date suggest that this is almost exclusively observed in those who are systemically unwell, usually in the context of multi-organ dysfunction5-7. It has been postulated that necrosis most commonly occurs as a consequence of hypo-perfusion caused by a low flow state in those with underlying vascular disease. This is likely to account for the predilection for the distal third of the esophagus, which is relatively less vascular5. Individual cases have occurred in association with bacterial, viral and fungal infections, whilst malnutrition, malignancy and immune-compromise appear to be important factors3, 5, 6.
The most common indication for the gastroscopy that makes the diagnosis of AON is hematemesis and melena, accounting for over 75% of cases6. It is therefore likely that AON is significantly under reported as endoscopy is often precluded in those who are clinically unstable. Further it is not clear whether hematemesis is a universal symptom of this condition; it is conceivable that AON may go undiagnosed in those in whom this is not a feature.
Whilst AON has no specific treatment, its presence is indicative of significant systemic compromise and predicts a poor prognosis. This diagnosis should alert physicians that close monitoring and aggressive treatment is required to optimise patient outcomes. There is no clear role for the use of anti-acid therapy, however this is commonly used in management due to patient symptoms, which usually includes hematemesis. Similarly, candidiasis may occur in conjunction with AON, whilst it is not thought to be causative, treatment is considered prudent given the poor prognosis associated with this condition.
For those that recover from their acute systemic insult the prognosis appears to be good. The long-term sequale of this condition includes oesophageal stenosis due to structuring. Evaluation with a repeat gastroscopy if therefore indicated if dysphagia develops.
CONCLUSION
The clinical course of AEN is variable, with an associated mortality of 32%5. The severity of the underlying clinical condition appears to be the most important factor in determining prognosis. There is no specific treatment for AON. The current body of experience suggests aggressive management of abnormal physiology optimises outcomes5, 6. Antibiotics, antifungals and nutritional support should be considered on an individual basis.
As syphilis is a notable clinical and pathological imitator, its diagnosis remains challenging. Physicians should be vigilant to suspect syphilis in cases of non-specific signs, such as lymphadenopathies, even in patients with no apparent risk for sexually transmitted infections or a history of primary syphilis.
Case Report
We report the case of a seventy-year old woman with a medical history of arterial hypertension. She had neither smoked cigarettes nor drunk alcohol and she had no significant medical family history. The patient presented with a history of swelling in the left axilla of one year duration. The swelling gradually increased in size and was painless. There was a history of occasional low-grade fever and weight loss, but no cough or night sweats.
On initial examination, the patient was thin with generalised lymphadenopathy: she had an axillary adenopathy that measured 4 cm in diameter in the right axilla and one measuring 3 cm in the left axilla. She also had two cervical lymph nodes that were less significant, and one enlarged right inguinal lymph node of about 3 cm in diameter. The existing lymph nodes were painless, mobile, mildly tender and smooth. Otherwise, breasts, limbs and other regions were essentially normal. No skin rash or suspect lesions were noticed. All her family members were well, with no contributory medical history, and none of them had similar symptoms.
A complete blood count revealed a white blood cell count of 5300/l (neutrophils 40%, eosinophils 19%, lymphocytes 30%, monocytes 10%), and a C-reactive protein of 14 mg/l. The remaining results of her full blood count, electrolytes, liver enzymes, lactate dehydrogenase and urine analysis were within normal limits. Calcium and phosphate levels were normal in both blood and urine analyses. Both human immunodeficiency virus screening and the serological tests for hepatitis B and C were negative. Mantoux test did not show any indurations. Smear and culture of the sputum were negative. Her chest x-ray and abdominal ultrasound were normal.
A CT scan of the patient’s neck and chest showed a marked anterior mediastinal mass of about 50 mm diameter with multiple calcifications. Several small lymph nodes were also noticed in the cervical and axillary areas. An axillary lymph node biopsy was performed. Histopathological examination of the biopsy specimen revealed a granulomatous lesion with epithelioid and multinucleated giant cells (Fig.1) associated with calcifications and central areas of caseous necrosis (Fig.2), which were highly suggestive of tuberculosis.
Fig 1: Epithelioid granuloma with giant cell
Fig 2: Eosinophilic granuloma with acellular caseous necrosis
According to these clinical and pathological findings, the most common granulomatous diseases are mycobacterial diseases such as tuberculosis, hence why the diagnosis of tuberculous lymphadenitis was highly suspected, and the patient was given anti-TB drugs. However, other differential diagnoses were considered, including bacterial infections like syphilis or actinomycosis, protozoal infections such as toxoplasmosis, and miscellaneous diseases such as sarcoidosis, Crohn's disease and Wegener's granulomatosis. To distinguish disease processes and make a definitive diagnosis, further investigations, such as special stains, culture methods and serologic tests, were indicated.
Additional histological stains, including Ziehl-Nielsen, were performed and returned negative, excluding the diagnosis of tuberculosis. In the meantime, the serological tests showed a positive venereal disease research laboratory test (VDRL: 1/8) and Treponema Pallidum haemagglutination assay (TPHA: 1/350). As a result, the diagnosis of secondary syphilis was confirmed and tuberculosis treatment was ceased.
The patient received intramuscular injections of 2.4 million units of benzathine penicillin every three weeks. Additional clinical and laboratory examinations were performed for both the patient and her family. She did not present with any manifestations of cardiovascular or neurological syphilis. Her husband’s VDRL and TPHA tests were negative. After a nine-month follow-up, the patient had no clinical or laboratory evidence of syphilis.
Discussion
Syphilis is predominantly a sexually-transmitted disease with both local and systemic manifestations. The causative organism is the spirochete Treponema Pallidum (TP) which was first demonstrated on the 17th of May 1905 1.
Syphilis has many non-specific signs and symptoms that may be overlooked by the physician, because in some cases it may simply be indistinguishable from other more common diseases. In fact, syphilis can share clinical manifestations with other treponemal and non-treponemal diseases, and it may be asymptomatic in some stages. Unfortunately, undiagnosed and untreated syphilis may lead to life-threatening complications such as hepatitis, stroke and neurological damage 2. Therefore its clinical diagnosis must be supported by laboratory tests.
Several older methods can be used to confirm syphilis diagnosis such as direct identification of TP by dark-field microscopy or direct fluorescent antibody tests, but such tests are not practical in a routine clinical setting and these methods can only be performed on lesion exudate or tissue 3.
As a consequence, the diagnosis in most patients is based on serological tests. Guidelines from the United States of America (USA) and Europe recommend a combination of two tests: the first one is a non treponemal (cardiolipin, reaginic) test, essentially Venereal Disease Research Laboratory (VDRL) or rapid plasma reagin (RPR); and the second is a treponemal test, essentially TP haemagglutination assay (TPHA), TP particle agglutination, or the fluorescent treponemal antibody absorption (FTA-abs) test 3,4.
In our patient, the most significant clinical finding was lymphadenopathy. This case presented diagnostic difficulties because of its clinical and histopathological resemblance to other pathological conditions. In fact, the presence of generalised lymphadenopathy and the finding of granulomatous lesions with epithelioid cells in the biopsy were highly suggestive of tuberculosis. As a matter of fact, tuberculosis tops the list of aetiological causes of granulomatous infections5. Worldwide it is considered the leading cause of contagious disease leading to approximately 1.4 million deaths per year 6. Its prevalence is still extremely high in certain populations especially in low-and middle-income countries such as Tunisia where the disease is endemic.
Tuberculosis is caused by Mycobacterium tuberculosis (M. tuberculosis) and M. bovis, an acid and alcohol fast organism 7,8. Histopathology is characterized by the presence of epitheloid granuloma with Langerhans giant cells and central caseous necrosis 7.
Lymphadenitis is the most common extra-pulmonary manifestation of tuberculosis but its diagnosis is difficult, often requiring biopsy. In such granulomatous disease, and in cases of persisting doubts, it is necessary to identify the specific etiological agent by further investigations such as special stains, culture methods and molecular techniques like polymerase chain reaction (PCR) and serological tests, as in the case of syphilis.
In the case of tuberculosis infection, demonstration of the mycobacteria can be done with Ziehl-Neelsen staining or by immunofluorescence using auramine-rhodamine. Mycobacterial culture and detection of mycobacterial DNA using PCR are also used 7,9. Since the growth of mycobacterium in culture requires a long time, additional histological stain with Ziehl-Nielsen was performed, but returned negative in the case of our patient. As a consequence, the diagnosis of tuberculosis was excluded and syphilis was considered as a definitive diagnosis.
Conclusion
Granulomatous lesions can be seen in numerous diseases. A definitive diagnosis cannot be made on the basis of the history and physical examination alone, confirmatory testing should be performed in order to identify the specific etiologic agent correctly. Diagnosis of the disease in the initial stages would be beneficial not only to allow the patients to receive early treatment, but also to prevent the spread of the disease to others.
SSRIs (Selective Serotonin Uptake Inhibitors) are very commonly used in Depression and Anxiety. Though considered as safest antidepressants, they have some common side effects which include gastrointestinal side effects, headache and at times sexual dysfunction. Yawning is one of the rare side effects of SSRIs. SSRIs were found to be the commonest cause of not so common drug induced yawning in a meta-analysis1. Isolated cases of intractable yawning have been reported with citalopram2 fluoxetine, citalopram and sertraline3 in the literature .Excessive yawning can cause injury to Temporo-Mandibular Joint (TMJ) 4. Paroxetine has also been shown to cause intractable yawning5. Yawning possibly helps in thermoregulation and is an unconscious effort by the body to cool the brain 6, 7. It is known that yawning can be contagious. Reading, talking, seeing someone yawn or even thinking about yawning can induce yawning in the subjects8. Susceptibility to contagious yawning is different for different individuals depending upon their ability to process information about self9.
Case
A 60 year old postman presented with his first episode of depression. He attended the GP who started him on sertraline (an SSRI). He developed serious headaches and did not notice any therapeutic benefit. He was then referred to the psychiatric services for further management. He was assessed, Sertraline was stopped and Cipramil 20mg was introduced. He was reviewed after 2 months and the dose was increased to 40 mg to which he responded partially but relapsed within 4 months. There were no changes in his psycho- social circumstances. Cipramil was stopped and he was started on fluoxetine 20 mg. Once again the response was partial and was overshadowed by midnight insomnia and increased sleepiness in the daytime. Fluoxetine was increased to 40 mg and he was reviewed after 4 months when he reported clear and significant improvement in his depression but complained of “excessive yawning spells” causing him problems at his work place. The psychiatrist was surprised at the number of times he yawned at the Out Patient Clinic review. On further discussion it became clear that this side effect had become highly troublesome. He complained that his jaw was in severe pain. He was unable to do his delivery rounds and was having clear episodes of attention lapses leading to letters being put to wrong addresses. He was transferred to “sorting” the post at sorting counters and was taken off delivery rounds. Even here the intractable yawning continued and he was committing sorting errors. By now it was affecting his colleagues too and they also started yawning (it is known to be contagious).It was affecting his self-confidence and was extremely embarrassing in all social situations to an extent that he started avoiding social interactions. He was drowsy all the time. He was clearly suffering more due to excessive yawning than due to depression. He was unable to perform his employment duties and was signed off sick. At that point the dose of fluoxetine was reduced to 20 mg .After a couple of weeks his yawning reduced significantly but was still disruptive to his routines. He was advised to slowly taper off fluoxetine over next 4 weeks. Unfortunately his depression relapsed and his GP restarted him on Fluoxetine 20 mg. He was reviewed by the psychiatrist after a couple of weeks. Once again he reported return of intractable yawning.
Fluoxetine was stopped once again and he was started on Mirtazapine 15 mg. There was very little response. The dose was increased to 30 mg after around two weeks. This led to him to experience nausea and vomiting. Unfortunately Mirtazapine too had to be stopped. He was then tried on amitriptyline 50 mg which improved his sleep and symptoms of Depression. He was reviewed in the outpatient clinic after a couple of months .He did not develop any side effects and responded quite well. He then started his job starting from part time to full time within 6 weeks. After 6 months on the same dose of amitriptyline, did not have any symptoms of depression and was finally discharged from the mental health services.
Discussion
SSRI is the first line antidepressants used in the treatment of depression and Anxiety disorders. They are known to have least side effects and safest when it comes to overdosing. Intractable Yawning is quite an unusual and uncommon side effect. One has to be conscious of the fact that it may cause yawning that can be pathological and can cause severe disruption of patient’s life. It can contribute to poor compliance. It is quite easy to overlook and ignore this side effect as yawning usually seems to represent sleep problems which is also a significant feature of the associated depression itself.
Excessive yawning can cause Jaw/facial pain. It can even cause dislocation of temporo-mandibular-joint. It can cause severe problems with one’s work and self-esteem. The sufferer might be misunderstood for being inattentive, indolent and sluggish. It might affect relationships with spouse/friend/relatives and especially at place of work. It can be misunderstood by doctors and lead to unnecessary tests and investigations. One has to be aware when prescribing SSRIs in patients who are driving or are involved in handling heavy machinery, athletes, airline pilots, surgeons, life guards, air traffic controllers and many other professionals. Due to its contagious nature, it’s not only the patient who is affected but also others around him. Excessive yawning can adversely affect the level of arousal, the level of concentration and work efficiency leading to poor performances in tasks requiring undiverted attention.
Hence excessive or intractable yawning has to be kept in mind while prescribing the so called most safe anti-depressant class of medication, the SSRIs, in this case fluoxetine.
A 41-year-old woman with a 6-year history of mild psoriasis presented with a rash under her breasts. The differential diagnosis included flexural psoriasis, an allergy to the nickel in her under wired bra, and intertriginous dermatitis (moisture-associated skin damage). She was prescribed Trimovate cream (GlaxoSmith Kline) and developed a florid weeping eczema within 48 hours of application (Figure 1). The eczema settled with the withdrawal of Trimovate and application of Betnovate RD cream (GlaxoSmith Kline). The history was very suggestive of a contact dermatitis to Trimovate cream.
Figure 1 showing eczema
She was referred to the Dermatology department and was patch tested to the European standard, medicament and steroid batteries. She had a number of positives including cetearyl alcohol, sodium metabisulphite, and clobetasone butyrate. These are all components of Trimovate. She was given advice sheets on all her allergens and on avoiding them she has had no recurrence of eczema.
Discussion
Contact dermatitis is a type IV allergy and usually appears within 2 to 3 days after contact with an external allergen. This case is likely to be an example of concomitant sensitisation, where one sensitivity facilitates the acquisition of another sensitivity to a chemically unrelated ingredient within a product.Whilst there has been a previous case report of concomitant sensitivity to sodium metabisulphite and clobetasone butyrate in a patient using Trimovate cream,1 this is the first report of a patient reacting to three of the ingredients found in Trimovate - sodium metabisulphite, clobetasone butyrate, and cetearyl alcohol. Allergy to clobetasone butyrate is rare, with only 5 previously reported cases.1, 2, 3 Allergy to sodium metabisulphite is not uncommon, producing a positive reaction in approximately 4% of patients who are patch tested.4, 5 Allergy to cetearyl alcohol is also rare, with one study estimating the incidence of positive reactions to be 0.8% among 3062 patients that were patch tested.6
Detection of the allergen, or allergens, is important, as avoidance results in resolution of the eczema. Our patient highlights the fact that it is insufficient to simply advise a patient to avoid the topical medicament that has caused a reaction. Ideally, patients with a topical medicament allergy should be patch tested to identify which components the patient is allergic to, so that they can be avoided in all products. In this case, in addition to Trimovate, there are a number of other products that our patient will now avoid. This is of particular significance in view of her history of psoriasis, for which she has used moisturizers and topical steroid preparations in the past, and will likely need again in the future. Clobetasone butyrate is often used in facial and flexural psoriasis. Cetearyl alcohol is a particularly important allergen to identify, as it is found in many products including a number of commonly used moisturizers such as Diprobase (MSD), Cetraben (Genus) and Epaderm (Mölnlycke) cream, and most steroid creams although not steroid ointments. Our patient was therefore advised to use only steroid ointments and has had no recurrence of the contact dermatitis. To conclude, GPs should consider sending their patients with contact dermatitis for patch testing, as the identification of all allergens is valuable to management.
Blue discolouration of the skin can have a multitude of causes, including Mongolian spots, blue naevi, the naevi of Ito and Ota and metallic discolouration1 or the use of drugs such as minocycline. Here we report the case of a 61 year old gentleman who developed blue macular skin lesions that were not attributable to any obvious cause and may be the result of an unidentified occupational exposure.
A 61 year old Caucasian gentleman developed blue macular skin lesions over a 14 year period. The very first lesion appeared in the middle phalanx of the right middle finger (figure 1). It was light blue and pinpoint, eventually darkening and increasing in size to approximately 1mm x 1mm, at which point becoming permanent and non-evolving. The lesion had no notable associated features and the patient was in otherwise good health.
Figure 1: The first blue macular lesion on the middle phalanx of the right middle finger.
Figure 2: A blue macular lesion on the terminal phalanx of the left middle finger.
Figure 3: A lesion on the anterior abdomen from which a punch biopsy was taken.
Figure 4: Haematoxylin and Eosin stained slide at 10x magnification. Abdominal skin biopsy showing dermal interstitial and perivascular distribution of black coloured pigment deposits
At present, he has approximately thirteen blue macular lesions in total, all of which have developed in the same manner. They are distributed predominantly on his hands with one on his left forearm and one on the right abdominal flank. New spots still continue to arise on his hands (figure 2).
A punch biopsy of the abdominal lesion (figure 3) was carried out. The histological findings were those of skin with normal intact epidermis and the presence of black coloured pigment granular deposits, located largely within the papillary dermis and occasional smaller deposits in the superficial reticular dermis (figure 4). The deep reticular dermis and subcutaneous fat were normal. The pigment had a perivascular distribution and in dendritic histiocytic cells, with close association to fibroblasts. Histiocytic cells form part of the mononuclear phagocyte system and these cells are abducted mainly for phagocytosis removal or storing material2. Apart from the pigment, the remaining skin was normal. The use of light microscopy alone does not identify all substances on examination of a Haematoxylin and Eosin (H&E) stained section of tissue. Applying polarisation light microscopy enables the identification of numerous structures, for example crystals, pigments, bone and amyloid3. However, the black coloured material here was non polarisable (no refractile foreign material could be identified). These appearances as seen on light microscopy alone are most frequently seen where there is a history of tattoo artistry, but tattoo pigment is typically identified as showing reflective properties using polarisation4. Interestingly, the patient had no clinical history of deliberate tattooing and other causes were considered.
Discussion
The discovery of black coloured deposits in the dermis excludes the diagnoses of Mongolian spots or blue naevi and the naevi of Ito and Ota, all of which are disorders of dermal melanocytes. Another important differential is malignant melanoma, but it is not the diagnosis as the histopathological findings did not find any evidence of dysplasia or malignancy.
In a disorder known as anthracosis, similar findings of black coloured deposits can be seen in other organs such as within the lung and draining lymph nodes. It is often found in smokers and urban populations and reflects the deposition of carbon which is the most commonly identified exogenous mineral substance within tissue sections. The skin is not a site where such carbon pigment is typically seen and therefore, this is not a credible diagnosis in this case.
Agyria is a condition that occurs as a result of silver particle impregnation of skin leading to blue-grey skin discolouration. Silver exposure may be due to occupational or surgical exposure (by use of silver sutures) or medication with silver salts. On interview, the patient denied any occupational exposure to silver and the use of silver salts. Although the patient had had previous shoulder surgery, silver sutures are no longer used in modern day surgical practice and therefore this cannot be the cause of his skin discolouration.
Unfortunately, histological examination of paraffin embedded tissue sections can only confirm the presence and distribution of an exogenous substance and it is not possible to precisely differentiate the exact type of material which is present. The use of an electron probe micro analyser may have been useful in identifying the substance, however, such equipment is not currently available and was not used in this case.
Interestingly, in tattoo artistry, carbon black may be used to give blue tattoos their colour5 and this is also a component of tyres and industrial rubber products6. This provided us with a link to occupational exposure, given that this gentleman is a tyre worker and has been involved in both the manufacture and assembly of tyres for 34 years. Carbon can cause discoloration of the skin, depending on the extent of deposition.
It is notable that in his 34 years of working with tyres, this gentleman did not routinely use gloves or protective uniform until only 10 years ago. This was as workplace safety precautions were not as strongly enforced in previous times. He admitted to have been in direct contact with the materials involved in tyre building and also suffered accidental superficial cuts on his hands whilst working, which may be a route by which carbon may have been introduced into the dermis. This is supported by the observation that the majority of the blue macular lesions were on the hands. Adding credibility to this theory is the identification of a colleague of this gentleman’s (who did not wish to be identified), whose job also involved the manufacture and assembly of tyres, who also has a similar single blue macular lesion on his hand.
In addition to this we have identified a forum on the internet7 that reports other similar cases of blue pin-point macular lesions appearing on the skin of tyre factory workers – some of whom worked for the same tyre company that this gentleman did. This may suggest that there is an association between exposure to a chemical, possibly carbon black, involved in the manufacture of tyres, and the appearance of these blue macular lesions.
In this case report, the identity of the material deposited and the route by which it accumulated in the dermis is unclear, but may have been related to an occupational exposure – this was in keeping with the general consensus upon presentation of this case at the West Midlands Dermatology Conference at New Cross Hospital Wolverhampton. We welcome any new case reports or literature that may be able to shed further light on this subject.
The rate of primary and secondary syphilis reported in the United States is gradually increasing. Reported cases of syphilis decreased during the 1990s, were lowest in 2000, after which it gradually increased annually during 2001-20091. In a recent report published by CDC, primary and secondary syphilis rates have increased among men of all ages, races and ethnicities, largely among MSM, from 5.1 cases per 100,000 population in 2005 to 9.8 in 2013. Rates of 50%–70% HIV coinfection among MSM infected with primary and secondary syphilis have been reported2. Syphilis and the behaviours associated with acquiring it, increase the likelihood of acquiring and transmitting HIV. Although the incidence of HIV has remained stable, the incidence of syphilis has been increasing disproportionately possibly due to adaptive behaviour like serosorting among HIV concordant couples and oral sex that decrease transmission of HIV but not syphilis3.
Syphilis may manifest differently in patients with HIV. HIV positive patients present more often with secondary syphilis and the disease course is more aggressive4. Malignant syphilis also known as lues maligna or ulceronodular syphilis is a severe form of secondary syphilis and is more common among HIV infected persons5. Although HIV patients present with varied clinical symptoms, it is uncommon to present with florid secondary syphilitic skin lesions. Here we present a case report of a patient, who presented with diffuse ulceronodular skin lesions, whose serology and skin biopsy confirmed syphilis and was subsequently found to have HIV.
Case report
A 20-year-old African American man was admitted to Interfaith Medical Center with a generalised body rash for a month. He noticed a rash on his chest, which in few days spread centrifugally to his whole body, face and arms, including palms and soles. The rash was non-pruritic, painless, progressive in size and gradually oozed and crusted (Figure 1a). Besides significant unintentional weight loss of 26 pounds in the last two months, he did not report any other systemic complaints. He denied any travel or unwell contacts. He is a homosexual man and has had two male sexual partners in the last two years; one of them was treated for syphilis two years ago. He denied smoking, alcohol or drug use.
Figure 1a - Skin lesions reveal papulosquamous nodular and ulcerative changes in upper limbs
On admission, he was afebrile with normal vital signs. His physical examination revealed widespread papulonodular and ulcerated lesions on his whole body including the scalp and oral mucosa, and measured up to 2-3 cm. Skin lesions were prominent on his face, some with sero-purulent discharge and some covered with crusts and scabs, which would bleed on removal of crusts and scabs. No skin lesions were noted in genital area. Besides bilateral enlarged axillary lymph nodes, nosignificant lymphadenopathy was noted. Other systemic examinations were within normal limits.
His full blood count showed microcytic hypochromic anaemia with a mean corpuscular volume of 77.2 fL (normal reference range, 80-100 fL) and thrombocytosis with platelets of 546 per microliter (reference range, 130-400 per microliter). Renal and hepatic function tests were normal. He tested positive for HIV using serum enzyme linked immunosorbent assay (ELISA), rapid plasma reagin was 1:128 (reference range, nonreactive), fluorescent treponemal antibody absorption test was reactive (reference range, nonreactive) and neurosyphilis was ruled out with negative spinal fluid studies. Hepatitis B and Cserologieswere negative. Nucleic acid amplification test of the urine sample was negative for Neisseria gonorrhea and Chlamydia trachomatis. The patient was treated with doxycycline100 mg every 12 hours for secondary syphilis as he was allergic to penicillin.
The patient developed chills, fever, sweating, tachycardia and hypotension 18 hours after treatment with doxycycline. A Jarisch-Herxheimer reaction was suspected, which was managed with observation, intravenous hydration and a single dose of methylprednisone. Despite being on antibiotics, he had intermittent fever for two weeks, possibly related to the syphilis and its treatment. Further investigations included blood and urine culture, chest x-ray, CT scan of the head, chest, abdomen and pelvis and a gallium scan, which were unremarkable. Brucella IgM antibody, Q fever phase I and II antibodies, coccidioides antibody, histoplasma urine antigen, cryptococcal antigen and blood culture for acid fast bacilliwere all negative. His EBVserologies suggested past infection and CMV serologies for IgG and IgM were positive. Wound culture taken from the purulent skin lesions grew methicillin sensitive Staphylococcus aureus (MSSA)which was treated with antibiotics. His HIV-1 RNA was 1050118 (reference range, <20) and CD4 was 276 cells per microlitre (reference range, 317-1868 cells per microlitre), CD4 was 17.4% (reference range, 25.7-62.8%) and CD4:CD8 ratio was 0.32 (reference range, 0.20-3.50). Skin biopsy from the left forearm lesion showed lichenoid lymphohistiocytic infiltrate with plasma cells (Figure 1b). Immunochemical stain was positive for spirochetes, which confirmed secondary syphilitic skin lesions (Figure 1c). After three weeks of doxycycline therapy, significant clinical improvement in the skin lesions were noted. The skin lesions healed well with hyperpigmentation. Combination anti-retroviral therapy was initiated upon discharge and on follow-up a month later, the skin lesions had resolved and the RPR titre was 1:32; showing a four-fold reduction.
Figure 1b - A lymphocyhistiocytic infiltrate was present in the dermis and extended around blood vessels.
Figure 1c - Immunohistochemical stain showing delicate and spiral shaped spirochaetes, highly specific and sensitive of Treponema pallidum
Discussion
Skin lesions of secondary syphilis in patients with HIV may have varied appearance that mimic other diseases like cutaneous lymphomas, mycobacterial infections, bacillary angiomatosis, fungal infections or Kaposi’s sarcoma6. Detail workup was done in our patient and systemic fungal and bacterial infections were ruled out. He had secondary infection of the skin lesions due to MSSA and was treated with doxycycline. Skin biopsy confirmed secondary syphilitic skin lesions. Histology showed abundant plasma cells and lymphocytesandtreponomes were demonstrated in the special immuno-histochemical stains. Fisher’s diagnostic criteria for lues maligna include strongly positive RPR titre, a severe Jarisch-Herxheimer reaction, characteristic gross and microscopic morphology and rapid resolution of the lesions with antibiotics7. Our patient had all of these features. Because of variable presentation of skin lesions and increased rate of false negative serological tests due to prozone phenomenon in patients with HIV, alternative diagnostic techniques like biopsy of skin lesions and special stains should be performed8,9. The relative paucity of spirochetes in the biopsy of skin lesions makes the demonstration of microorganisms difficult. Yanagishawa et al were able to find 6 published cases of pathologically confirmed malignant syphilis with the demonstration of spirochetes10. Treatment of secondary syphilis in HIV infected patient is the same as that of HIV non infected patients. Benzathine penicillin is first line therapy and doxycycline is an alternative drug for penicillin allergic patients11. A severe Jarish-Herxheimer reaction occurred in our patient, which might not be observed in some cases with HIV and syphilis due to concurrent immunosuppression10. Experience from case reports have shown that malignant syphilitic skin lesions respond very well to antibiotics regardless of CD4 count12. With the increasing incidence of syphilis in HIV infected patients, it is important to recognise and diagnose malignant syphilis early and institute appropriate treatment as complete cure can be achieved.
Pellagra is a nutritional disorder due to an insufficiency in vitamin B3 also called vitamin PP (‘Pellagra preventing’). The disease was characterized by the following ‘3 D’s’: ‘Dermatitis’, ‘Dementia’ and ‘Diarrhoea’. When it is misdiagnosed, it can lead to the fourth ‘D’ which is ‘Death’.1 It was very common in past centuries, particularly in populations that had an exclusively maize diet. Nowadays, this diet problem is rare in developed countries, so the disease is less frequent. However, many recent studies suggest that the disease has not been eradicated and can be under-diagnosed. Alcohol, drugs and malabsorption seem to be the new aetiologies of the disease. So, it is important to recognize the ‘3 D’s’ triad in such situations to avoid fatalities.
Observation
A 61-year-old patient presented to the Internal Medicine Department with an 8-month history of deterioration in her general state. She had a medical history of Epilepsy treated by Phenobarbital since she was 16.
Review of systems revealed gastrointestinal symptomatology consisting of intermittent diarrhoea (6-7 watery stools a day without blood), dysphagia and diffuse abdominal pain. The patient also reported a skin photosensitive eruption affecting her hands and feet.
Physical examination showed a listless patient with a low Body Mass Index (17 kg/m²).
On dermatological examination, symmetric, well-defined, brown-coloured and scaly eruption was observed on the dorsa of her feet (Picture 1) and hands (Picture 2). The mucous examination showed a commissural Cheilitis and Glossitis.
Picture 1: Brown well-defined patches on feet.
Picture 2: Brown pigmentation and scales of hands.
Picture 3: Hands aspect after treatment.
The nervous system examination revealed a pyramidal and cerebellar syndrome. The response to neurocognitive tests was altered suggesting Dementia.
The rest of physical examination was normal. In particular, there were neither peripheral lymph nodes, nor spleen or liver enlargements, nor abdominal mass.
The laboratory tests (glucose, calcaemia, creatinine, liver function tests, urine analysis, haemoglobin, hematocrit, sedimentation rate, C-reactive protein and protein electrophoresis) were within normal limits.
Oesogastroduodenal endoscopy was normal. The cranial, thoracic and abdominal CT scans were normal.
The diagnosis of Pellagra was made on dermatological, abdominal and neurological signs. The patient was treated by Niacin (1000 mg/day) and multivitamin complex. Phenobarbital was discontinued and switched to Clobazam. The patient’s symptoms started to improve quickly. Ten days after the treatment began the skin lesions (Picture 3) and gastrointestinal signs completely disappeared.
Discussion
Pellagra was diagnosed clinically in our patient based on the skin aspects. The skin lesions have been described since 1771 by Frapolli whose name was given to the disease: Pellagra which means rough skin in Italian.1 The typical lesions consist of a brown pigmentation and scales with a photosensitive distribution and well-defined borders as seen in our patient. The face, the neck and the dorsa of the hands are the preferential locations.2 The skin lesions are not always found, and cases of Pellagra Sine Pellagra have been described.3 The extra-cutaneous manifestations are less specific, but their association with pellagrous skin lesions are sufficient to reach a diagnosis. The neurological involvement is classically a Dementia syndrome, but ‘Pellagrous Encephalopathy’ can also consist of delirium, insomnia, depression, cerebellar and extrapyramidal syndrome.4 The gastrointestinal signs are non-specific; they can be Glossitis, dysphagia, nausea, vomiting and abdominal pain. An intractable diarrhoea may occur in advanced stages of disease and can quickly lead to death.5
In 1929, Goldberger attributed such clinical manifestations to a Niacin (vitamin B3 or PP) deficiency. Niacin is a precursor for two important coenzymes namely ‘Nicotinamide Adenine Dinucleotide (NAD)’ and ‘NAD-Phosphate’ which are essential for many oxidative reactions. This probably explains why Pellagra affects tissues with a high rate of cell turnover such as the skin and digestive tract.4
Niacin can be directly absorbed by the gastrointestinal tract or synthesized from Tryptophan.
Primary Pellagra occurs when the diet is deficient in Niacin or Tryptophan as in poor populations with an exclusive maize diet (which contain Niacin but in an indigestible form).
Despite sufficient dietary Niacin, Secondary Pellagra may be caused by a problem in Niacin absorption or metabolism. Many causes of Secondary Pellagra were identified as alcohol, intestinal malabsorption, carcinoid tumours, Hartnup’s Syndrome, Anorexia Nervosa and drugs (Table 1).5 Our patient did not consume alcohol and had no biological signs of malabsorption, but she was taking Phenobarbital for about 45 years. In the English literature, we found only two cases of Phenobarbital-induced Pellagra, and with a fatality in one case.6, 7 The underlying mechanism of Pellagra caused by Phenobarbital, or other antiepileptic drugs, is an alteration in Niacinamide synthesis due to an enzymatic induction.5
Chemotherapy and immunosuppressive drugs 6-Mercaptopurine 5-Fluorouracil Chlorambucil Azathioprine Chloramphenicol
The treatment is first based on correction of predisposing factors. In our patient, it consisted of using another antiepileptic drug instead of Phenobarbital. Second-line treatment is a vitamin therapy based on Niacin. There is no consensus on the doses, form and duration of the treatment, but the minimal dose is 300 mg of Niacin/day. A multivitamin complex containing other B-vitamins is often necessary because of the frequency of other deficits in such patients.2 With treatment, the skin lesions and gastrointestinal symptoms generally disappear within a few hours or days, as in the case of our patient, and it is a good argument for a retrospective diagnosis of pellagra.1 Testing for Niacin levels or urinary metabolites is not frequently available and it’s not necessary for the diagnosis.
Conclusion
We described a typical case of Pellagra in which the ‘3 D’s’ were present. In such a case, we should begin the treatment before the results of the laboratory investigations are known. The improvement of all symptoms within a few days is sufficient to confirm the diagnosis. However, the ‘3 D’s’ triad is not always present, and the clinician should consider the diagnosis in face of unexplained abdominal or neurological signs in certain patient groups.
Dilated cardiomyopathy (DCM) is a cardiac muscle disease, characterized by dilatation and impaired contraction of the left ventricle or both ventricles, and leads to progressive heart failure and sudden or heart failure-related death [1]. The life expectancy is limited and varies according to the underlying etiology with a median survival time of about 5 years after diagnosis [2]. Although the pathogenesis of this disease has been extensively studied for decades, it remains ambiguous. Currently, myocarditis, immunological abnormalities, toxic myocardial damage, and persistent cardio-tropic viral infection are all assumed to be causes of DCM [3]. Dilated cardiomyopathy occurring in families, or the familial dilated cardiomyopathy (FDC) may occur in 25% to 35% of DCM cases, implicating a genetic contribution to the etiology [4-7]. More than 30 susceptibility genes have been shown to be associated with an increased risk of developing a DCM. Here we report three strange cases of FDC accompanied by hearing loss and rapid progressive course in brothers from Sichuan Province of China. The presentation of the family was really rare and it is anticipated that more susceptibility genes may be discovered.
Case report
The patient was a boy from Sichuan Province, and had lost his hearing when he was five years old. At the age of eight, the boy presented with cough and acute onset breathlessness. On examination, he had blood pressure (BP) of 90/60mmHg, heart rate (HR) 105/min, raised jugular venous pressure (JVP), crackles over the lung bases and a pansystolic murmur at the apex. A huge cardiomegaly was seen on chest X-ray (CXR), and the cardiothoracic ratio (CT ratio) was 0.721. ECG revealed primary atrioventricular block and left ventricular hypertrophy (LVH). Echocardiography (Echo) showed enlargement of both ventricles of the heart, a decreased left ventricular ejection fraction (LVEF), and severe mitral regurgitation (MR). The patient was treated in line with congestive cardiac failure (CCF). However, he died three months after the acute onset of breathlessness.
Surprisingly, the progression was nearly the same as two of his older brothers. Both of them also lost hearings at the age of five. Then presented with acute onset breathlessness and they were diagnosed with DCM aged seven to eight years. They also died three months later after the acute onset of breathlessness. Because of the terrible experience of his older brothers, the boys’ parents took him to hospital every year to be examined. ECG and Echo images were normal 6 months before the onset of breathlessness. Moreover, the boy had no symptoms 1 month before his presentation.
Discussion
The definition of FDC is clinically based on manifestation with at least two affected members from the same family [5]. The most common mode of inheritance is the autosomal dominant type, while X-linked, autosomal recessive and mitochondrial forms are less common [8, 9]. Although most people affected die in early adulthood, the age of onset, rate of progression, disease complications, as well as overall prognosis and outcome vary within families [5, 10]. Nevertheless, the age of onsets in this family were similar and with a rapid progressive course. All of the sons in the family suffered from DCM as well as hearing loss. The manifestation of the brothers haven’t been reported before. We traced back three generations of this family finding no other affected members. As all the patients were male, we speculated that the possible mode of inheritance in this family is X-linked. Regrettably, the parents had no daughters and we were not able to investigate the possible association between gender and FDC of this kind. Because of the rapid progressive course, we hypothesize that autoimmune abnormalities might be the pathogenic factors for this disease, but we do not have any solid evidence yet. Fortunately, we were able to get the blood samples from the patient and the relatives. Further studies are needed to explore new susceptibility genes as well as the molecular mechanisms that are involved in the disease.
Anaesthetic management of a patient with a tracheal tumour is challenging, as the airway is shared with the surgeon and patency must be maintained despite airway manipulation.
Several anaesthetic techniques have been used in patients requiring tracheal resection and reconstruction. Cardiopulmonary bypass standby after femoral artery and vein cannulation and then intravenous/inhalational induction while oxygenating the patient has been considered to be a reasonable approach. Intratracheal tumours are challenging to anaesthetists because of the difficulty in establishment of a patent airway before commencement of surgery. The principal anaesthetic consideration is ventilation and oxygenation in the face of an open airway.
CASE REPORT
A 56 year old male with no other co-morbidities presented to the Thoracic Oncology department with a history of progressive dyspnoea and orthopnoea.On examination he was found to have dyspnoea at rest and could not complete full sentences while talking. Change of position made no difference to his symptoms.
Routine blood investigations which included full blood count, renal and liver functions, coagulation profile, ECG and 2DEcho were within normal limits. PFT showed a typical intrathoracic obstructive picture.
His chest X-ray showed bilateral hyperinflated lungs suggesting airtrapping. CT of the chest showed an intratracheal growth about 4 cm above the carina almost completely obstructing the lumen. An awake flexible bronschoscopy confirmed the CT scan findings. A 2.7mm flexible bronschocope was passed with difficulty beyond the tumour to visualise the carina. Excision of the intratracheal tumour was planned with possible resection and anastomosis of the involved tracheal segment. A careful perioperative plan was discussed and decided in agreement with the thoracic surgeons, anaesthetist, cardiovascular surgeons and the rest of the team members.
Flexible and rigid bronchoscope, a Sanders venturi, an additional anaesthesia machine and various sizes of reinforced and normal endotracheal tubes and tracheostomy tubes were kept ready.
Preoperatively the patient had incentive spirometry and bronchodilator nebulisation and intravenous steroids. An awake epidural at T9-10 level and radial artery cannulation were done under local anaesthesia without any problems. Two 16 gauge peripheral IV lines were sited under local anaesthesia.
After adequate preoxygenation anaesthesia was induced with IV propofol along with oxygen and sevoflurane with BIS monitoring. As mask ventilation proved to be easy the patient was paralysed with suxamethonium. There was no difficulty in ventilation after muscle paralysis. An 8.5 number COETT portex tube was placed in the trachea with the cuff just beyond the cords to avoid possible trauma to the tumour. Since there was preoperative evidence of airtrapping, ventilator settings were set to an I:E ration of 1:3 with a tidal volume of 550ml, respiratory rate of 12-14 per minute and PEEP of 4. At these ventilator settings the airway pressures were reaching up to 22 cm of H20 and ETCO2 reaching a maximum of 40mmHg. Anaesthesia was maintained with oxygen: air with sevoflurane and atarcurium for muscle paralysis.
Flexible bronchoscopy was done to confirm the position of the endotracheal tube, which showed that the ETT was adequately above the tumour.
A laryngeal drop procedure was done in the supine position with neck extension to facilitate mobilisation of the trachea for resection anastomosis. After the laryngeal drop procedure a right thoracotomy was done in the left lateral position. At this point of the procedure, the patient was ventilated with low tidal volumes of 300 and respiratory rate of 16-20 to keep the ETCO2 at around 40.The right lung was surgically retracted and the trachea was exposed up to the carina. A repeat bronchoscopy was done through the ETT to help identify the upper and lower extent of the tumour. The trachea was then opened below the tumour, after which a 6.5 reinforced tube was introduced through the left bronchus to aid ventilation of the left lung. This ETT was withdrawn intermittently to help visualisation and aid surgical excision of the tumour and sleeve resection of the trachea. The left lung was ventilated till partial closure of the trachea. The left-sided tube was then removed. Ventilation resumed through the orotracheal tube with intermittent occlusion of the defect with gauze by the surgeon. The orotracheal tube was adjusted under vision before closure of the trachea to position it above the anastomotic site. The trachea was sutured and the thoracotomy incision closed without any adverse event. The neck was kept in a flexed position to avoid tension on the tracheal anastomotic area.
The patient was then extubated in the immediate postoperative period without any problems and the recovery was uneventful.
DISCUSSION
Anaesthetic management of a patient with a tracheal tumor is challenging, as the airway is shared with the surgeon, and patency must be maintained despite airway manipulation1, 2. Several anaesthetic techniques have been used in patients requiring tracheal resection and reconstruction 3–5.
Primary tracheal masses are very rare and mostly malignant, occurring in 0.2 in 1,00,000 persons per year 6 and among these squamous cell carcinomas form the main bulk. Cardiopulmonary bypass standby after femoral artery and vein cannulation and then intravenous/inhalational induction while oxygenating the patient with the oxygen inhalation has been considered to be a reasonable approach 7. Byrne JG et al (2004) advocated planned use of CPB to facilitate complete resection of thoracic malignancies after careful patient selection 8.
These patients are often mistaken to have asthma and require treatment with inhaled corticosteroids and beta agonists 9. They are generally treated for many years for asthma or COPD, unless a CT scan or endoscopic procedure is done for the symptoms 10. Intratracheal masses usually start getting symptomatic when 75% or more of the tracheal lumen is obstructed. Tracheal lesions present at lower level can have more complicated management of airway, anaesthesia and surgery for successful and safe removal of the mass. 10
Intratracheal tumours are challenging to anaesthetists because of the difficulty in establishment of a patent airway before commencement of surgery. The principal anaesthetic consideration is ventilation and oxygenation in the face of an open airway. Ventilation can be managed in many ways, including manual jet ventilation, high frequency jet ventilation, distal tracheal intubation, tracheostomy, spontaneous ventilation and CPB.11
Knowledge of various techniques available for management of such cases is vital. In order to have a successful and safe outcome it is extremely important to have good communication between the anaesthetic, surgical and intensive care team.
The challenge in managing such cases lies in establishing and maintaining a patent airway and also preventing seepage of blood and tumour particles distally into the tracheobronchial tree during the surgery.
There is a possibility of total airway obstruction during ventilation attempts using positive pressure because airway obstruction has a fixed and dynamic component. Dislodgement of the tumour, possibly from trauma following intubation causing total obstruction, should also be considered.
Thus an intratracheal tumour was successfully removed without any complications and by avoiding CPB. This case report also highlights the importance of proper planning and good communication between team members to ensure a successful and safe outcome.
A forty-eight year old man presented with unusual and distressing visual experiences with varying degrees of severity for over twenty years. Some of these included the following; red objects having a green shimmer around them like 3-D glasses, altered sense for distance estimation, people’s faces seeming to change shape when looked at, alteration of own reflection, anything patterned appearing to move all the time, words moving about while reading, things appearing to be multi-layered, bright lights throwing up shadows, vehicles appearing to stretch as they drive past, flying birds looking like animation and difficulty in focussing.
When present, his symptoms interfered markedly with his functioning. For example, he could not cross the road, could not read, and had to dim his lights. He struggled with knowing which visual perceptions were real and which were not. The patient felt his visual experiences were related to his past LSD use twenty-five years ago. He felt the drug had put him “in a coma” and he was “dreaming all of this”.
He specifically remembered a party with friends where he took a cocktail of illicit drugs, including LSD and marijuana, with alcohol. He said he would usually take drugs and alcohol in a binge pattern. The ‘trips’ would usually last twelve hours. He felt he experienced some memory loss of that particular night. When he woke up the next morning he was still experiencing the effects of LSD and said he has felt these effects ever since. He tried to explain that it was like drinking alcohol, waking up drunk and being drunk from that point on. After this incident he did not use illicit drugs again.
Prior to this particular night he said he may have used LSD about fifteen times, as Microdot tablets, usually one at a time, with cannabis. He said it was “like having a tripping switch in your brain”. When you took LSD, “the switch turned the tripping on and after a while it turned off”. He said his switch “was broken” and he therefore continued to re-experience the effects of the drug.
His other complaint was that of feeling he was “not real”; to the extent he even thought he should harm his family members so he could prove he was real.
He also complained of low mood, decreased concentration, anxiety and an inability to cope.
His first contact with mental health services was at the age twenty two years. He presented with symptoms of anxiety but it was not felt he had a mental illness. He was referred again a year later and was diagnosed to have Primary Depersonalization syndrome.
The patient himself reported that all his symptoms started after he had used LSD about fifteen times in six months. At the time he had described having undergone a complete personality change due to his experiences. He felt objects and experiences had a dream-like quality. His visual experiences caused so much distress he felt suicidal.
Over the next twenty-five years he has had various other diagnoses; LSD induced Depersonalisation Syndrome, Depersonalisation-Derealisation Syndrome, LSD induced Simple schizophrenia, depressive disorder and anxiety disorders. His visual disturbances had been interpreted as visual hallucinations. He had received treatment with antidepressants (Imipramine, Amitriptyline, and Venlafaxine); antipsychotics (Trifluperazine, Promazine); Benzodiazepines (Diazepam); Propranolol; and Fentazine. He was also prescribed Hydergine (which helped reduce symptoms briefly) at one point.
Investigations: EEG, MRI Brain, and Carotid ultrasound were normal.
He was admitted to a psychiatric hospital at the age of forty-eight years old where the admitting doctor described his symptoms as visual hallucinations and started him on Risperidone, which increased the intensity of his symptoms. He was also treated with Citalopram for his low mood. It was noted that his symptoms were different from common psychotic illnesses. Detailed history taking and assessment of his perceptual abnormalities over the following few weeks in hospital confirmed the diagnosis of hallucinogen persisting perception disorder (HPPD).
He was treated with Clonazepam 1 mg four times a day with good effect; as seen by the reduction of symptoms - see Table 1.
Table 1:
DSM IV/V Symptom Checklist
Prior to treatment with Clonazepam
3 months after initiation of Clonazepam treatment
Geometric hallucinations
Present
Absent
False perception of movement in peripheral fields
Present
Absent
Flashes of colour
Present
Absent
Intensified colours
Present
Absent
Trails of images of moving objects
Present
Absent
Positive after images
Present
Absent
Halos around objects
Present
Present but reduced in intensity and frequency
Macropsia
Present
Absent
Micropsia
Present
Absent
After discharge he had .a depressive episode and was treated with Escitalopram. This was later changed to Reboxetine.
Discussion:
This is the first case that we are aware of where symptoms of HPPD have persisted for over two decades after the cessation of the use of Lysergic acid diethylamide. There is a need for raising awareness about this condition to prevent misdiagnosis and delay in appropriate treatment.
This patient presented to psychiatric services over twenty-five years ago and at that time he felt his symptoms were related to his use of LSD. He was given a variety of different diagnoses before the correct diagnosis was established and treatment initiated with good outcome.
The patient had also experienced migraines and used alcohol excessively on occasions in the past. Although we are not aware of any connection between this disorder and these factors, future reports and studies may help provide further knowledge in these areas.
HPPD is a recognised condition described in DSM V and DSM IV with a diagnostic code 292.89. In DSM III it was referred to as post hallucinogen perception disorder (PHPD). It is described in ICD 10 under the code F16.983.
LSD has been known to alter perception and mood in the presence of an unaltered sensorium. HPPD was first described by Eisner and Cohen, who observed spontaneous recurrences of LSD like states in subjects, days to weeks following cessation of drug use1.
Other authors have described more or less the same clinical picture; for example, Rosenthal described patients suffering from post drug visual hallucinations lasting as long as five months from the time of drug use2
In a survey of sixty five users of LSD, Holsten found fifty users who described post LSD disturbances eighteen months to four years later3.
Flashbacks have been suggested to be a misnomer as patients described cases of continuous rather than paroxysmal visual disturbances from LSD 4
It is not clear what made our patient re-experience these visual disturbances however the literature suggests that emerging into a dark environment can precipitate or exacerbate post LSD visual symptoms. Among other precipitating factors are intentional inductions, marijuana use, medications like: neuroleptics (phenothiazine), amphetamines, cold remedies, anti-Parkinson’s agents and SSRI’s5.
The patient mentioned that he had ingested LSD approximately fifteen times before he developed this condition. The data suggests that peak incidence occurs with fifteen exposures and second smaller peaks at around forty to fifty exposures 6.
A number of hypotheses have been formulated in order to understand the underlying aetiology. HPPD is related to the recreation of symptoms experienced in intoxication. LSD has been shown to be excitotoxic to neurons. It is also known to be a partial agonist at post synaptic 5HT2 receptors and enhances glutaminergic transmission.
The patient had suffered from these rather distressing visual disturbances for more than two decades, which have had considerable impact on his daily living. He was given different diagnoses which included Induced depersonalisation, depersonalisation-derealisation syndrome, LSD induced simple schizophrenia, depressive disorder and anxiety disorders.
The patient had been treated with different psychotropic medications including antidepressants, antipsychotics, benzodiazepines, propranolol, fentazine and hydergine. Some had little effect like hydergine, whilst others worsened symptoms, in particular antipsychotic medications.
A case series of three HPPD patients treated with Risperidone reported an exacerbation of LSD-like panic and visual symptoms. Thus from these reports and our case report Risperidone could be contraindicated in patients with HPPD 7.
There have been some published case reports on treatment of HPPD, including the use of Reboxetine, which suggest it is beneficial in the treatment of the visual disturbances and depressive features associated with HPPD. This is possibly due to its alpha 2 adrenoceptor modulating effect on both Noradrenaline and Serotonin release8. Another case report suggested the use of a combination of Fluoxetine and Olanzapine in the treatment of HPPD9.
Benzodiazepines seem to be the most beneficial treatment so far and Clonazepam is the most effective due to its high potency compared to low potency Benzos and its long action at the GABA receptors10.
Conclusion:
Hallucinogen Persisting Perception Disorder is one of the outcomes associated with the ingestion of LSD. Symptoms can be present for years as demonstrated by different case reports, and for over two decades as reported in this report. The effect could be devastating to the person experiencing extremely distressing and disturbing perceptual phenomenon. It can last up to twenty five years after the cessation of the hallucinogenic drug. Early diagnosis and appropriate treatment can significantly help improve the quality of life of patients with this condition.
A 36 year old multiparous woman presented to the Labour Ward at 33 weeks’ gestation with lower abdominal pain. She had mild asthma and her obstetric history included 2 previous normal vaginal deliveries.
At 16 weeks’ gestation she was found during antenatal scanning to have a right ovarian cystic lesion measuring 59x34x50mm. This was monitored and a repeat scan at 25 weeks’ showed it had increased in size to 73x55x47mm.
At 32 weeks’ she was diagnosed with a DVT and was commenced on therapeutic enoxaparin (stopped two days before current presentation). (D-Dimer > 4000micrograms/L). An inferior vena cava filter was inserted. The patient declined any surgical intervention of the cystic lesion during pregnancy and an early elective Caesarean Section with surgical management of the cyst at 34 weeks’ gestation was planned. She had no symptoms or signs suggestive of a PE and was not formally investigated for one prior her current presentation.
On this presentation at 33 weeks’ gestation, her pain suddenly worsened with associated hypotension and evidence of foetal distress and so an emergency exploratory laparotomy was performed.
Admission haematology results: haemoglobin 10g/dL, platelets 158 x 109 /L, INR 1.0, APTT 28.4 seconds, APTT ratio 1, fibrinogen 3g/L.
She underwent a rapid sequence induction in the supine wedged position using thiopentone and suxamethonium. She was a Grade 1 intubation and anaesthesia was maintained with oxygen/nitrous oxide/sevoflurane and muscle relaxation was achieved with atracurium. A ruptured, torted right ovarian mass containing an estimated one litre of altered blood was noted. At Caesarean section a live male infant was delivered. A right oophrectomy was then performed. The infant was subsequently intubated and transferred to the Neonatal Intensive Care Unit.
Oxytocin 5IU followed by a 40IU infusion over 4 hours was administered following delivery of the baby. Effective haemostats was achieved, the uterus appeared well-contracted and the patient’s abdomen was closed. Surgical blood loss was estimated as 600mls (excluding blood within the ovarian mass).
Thirty minutes following completion of surgery the patient, fresh blood was noted vaginally. A HemoCue* reading was taken as 5.9g/dL. Four units of blood and two units of FFP were transfused whilst a second laparotomy was performed. Fresh blood was noted intra-abdominally and the uterus was markedly atonic. Ergometrine 500mcg and carboprost trimethamine 250mcg were administered intramuscularly, as well as, misoprostol 800mg vaginally. A hysterectomy was performed due to the rate of bleeding and the evident haemodynamic instability.
Coagulation studies: platelets 27 x 109/L, INR 1.4, APTT 101.8 seconds, APTT ratio 3.6 and fibrinogen 1g/L.
A further 4 units of blood, 4 units of FFP, 1 pool of platelets and 2 units of cryoprecipitate were transfused. Factor VII was also administered on advice from the Haematologist.
An internal jugular central venous catheter was inserted and a noradrenaline infusion started. Initial attempts to insert an arterial cannula were unsuccessful as peripheral pulses were difficult to palpate. Venous blood gas readings revealed hyperkalaemia (K+ 6.4mmol/L) which was treated with sodium bicarbonate, 10mls 10% calcium chloride and a continuous 50% dextrose and insulin infusion. Her abdomen was packed and percutaneous drains were inserted. Anaesthesia, close monitoring and resuscitation continued.
Ongoing output from drains prompted a third exploration after an hour. There was generalised oozing particularly around the bed of the resected ovary in the pouch of Douglas.
Coagulation profile: platelets 50 x 109/L, INR 1.4, APTT 89.6 seconds, APTT ratio 3.1 seconds, fibrinogen 1.4g/dL.
A further 10 units of blood, 3 pools of platelets, 5 units of FFP and 3 units of cryoprecipitate were transfused. Sequential coagulation profiles and thromboelastography were used to guide transfusion.
During this exploration, ECG revealed a broad complex tachycardia with no palpable pulse confirming cardiac arrest likely secondary to hypovolaemia and/or hyperkalaemia. Return of spontaneous circulation was achieved after 3 cycles of continuous cardiac massage, 4 direct current shocks and adrenaline 1mg.
A femoral artery cut-down was performed and arterial cannula was inserted by a general surgeon. IABP monitoring commenced.
A fourth exploration was carried out around two hours later for ongoing blood loss. Again only generalised oozing was noted particularly from the oophrectomy site. Her abdomen was re-packed.
Coagulation profile: haemoglobin 7.4g/dL, INR 1.2, APTT 48.9 seconds, APTT ratio 1.7, fibrinogen 1.9g/dL, platelets 94 x 109/L.
She was transferred to the ICU eight hours from the start of the primary operation. Estimated total blood loss was 13,200mls. Transfusions continued and her abdomen was closed two days later. She received haemofiltration therapy for acute kidney injury. She recovered to her premorbid level with no neurological deficit before being discharged with her baby a few weeks later. In total, she was transfused 64 units of blood, 35 units of FFP, 10 pools of platelets and 11 units of cryoprecipitate. Histology of the ovarian mass revealed high grade clear cell carcinoma for which she received chemotherapy but unfortunately she died two years later.
Discussion
The association between cancer and thromboembolism has been well established for many decades.1Ovarian cancer patients have one of the highest incidences of VTE amongst cancer patients, particularly clear cell carcinoma (CCC). One study found the incidence of thromboembolic complications to be significantly higher in CCC when compared with other epithelial types of ovarian cancer (27.3% vs 6.8%).2
The pathological mechanism behind the hypercoaguable state induced in ovarian cancer patients appears to be largely multi-faceted. A variety of procoagulant subtances may be involved. Of particular interest is tissue factor (TF), a potent procoagulant found in endothelial and blood cells, as well as, in tumour cells. TF may play an important role in this hypercoaguable state through activation of the coagulation cascade.3 TF is frequently over-expressed in ovarian cancer tissue and there is research suggesting it influences tumour progression.3,4
A hyperviscosity syndrome may also be seen in association with ovarian cancer which favours thrombosis and may accelerate tumour progression and metastasis.DVT is a recognised complicating factor of ovarian cancer which may adversely affect the course of the disease possibly as a component of this hyperviscosity syndrome5,6 Ovarian cancer patients are also vulnerable to developing cerebrovascular complications and carry a higher risk of developing ischaemic strokes which has a significant impact on morbidity and mortality.7
The hypercoagulable state seen in cancer patients can have a spectrum of manifestations that ranges from DIC to massive thromboembolism. DIC in these instances is usually chronic and subclinical.8
The degree of coagulopathy which was seen in this case could not be attributed solely to dilutional effects incurred through fluid resuscitation. Instead we propose the acute severe coagulopathy was a consequence of procoagulant factors inherent to neoplastic tissue, including TF, which were suddenly released into the circulation following rupture and surgery to the ovarian tumour. The overall result would be widespread activation of the clotting cascade and a consumptive coagulopathy.
This case aims to increase awareness of a refractory coagulopathy which may be seen following rupture and/or surgical resection of a malignant ovarian tumour. The presence of an ovarian cyst especially in conjunction with evidence of vascular thrombosis in pregnancy should raise suspicion for an ovarian malignancy and hence vigilance for this potential complication. Anticipation of such a severe coagulopathy and associated significant blood loss should pre-empt early establishment of invasive monitoring, ample intravenous access and ensuring quick access to blood and blood products. Bedside coagulation tests such as thromboelastography are useful guides to blood product transfusion.9 Prompt mobilisation of resources, multi-disciplinary input and effective team work were crucial factors which facilitated the management of this case.
Acute, severe DIC associated with ovarian intratumoural bleed which resolves following resection of the tumour has been reported previously.10 This is the first case to the best of our knowledge occurring following ovarian cancer torsion and rupture during pregnancy.
A 74 year old female presented to the A&E department after waking with a swollen tongue. She called for an ambulance and the paramedic crew initially treated her for an allergic reaction with 200mg hydrocortisone IV, 20mg chlorphenamine IV and four doses of 0.5mg adrenaline 1 in 1,000 IM. She did not improve and was transferred to the local A&E.
In A&E, she was initially stable with no stridor or difficulty in breathing but noticeably swollen tongue. Saturations were 98% on 5L nasal O2. Blood pressure was stable at 135/75 mmHg. GCS was 15/15, but the patient was agitated from not being able to speak or retract the tongue. No further history was taken other than an allergy to shellfish, with no recent exposure. An obese habitus was noted.
A&E doctors called the anaesthetic on-call team, and on their request called the on-call ICU consultant and the on-call ENT consultant. Further adrenaline 100mcg IV, hydrocortisone 200mg IV and chlorphenamine 10mg IV were given. An attempt to look inside the mouth with a tongue depressor and torch was made by the anaesthetics/ICU team and it was quickly realised that the swelling continued into the mouth and larynx and was rapidly progressing. Given the lack of suitable equipment and the severity of the case, a decision was made to transfer to emergency theatres.
Once in emergency theatres, the on-call ENT consultant was scrubbed and ready. 100% oxygen via facemask and routine monitoring was instituted. At the request of the ENT consultant, a micro-tracheostomy was attempted with local anaesthesia but failed to pass into the trachea given the patient’s habitus. The ENT surgeons attempted an awake tracheostomy, but this was difficult due to her being agitated and unable to lie still, and a calcified trachea.
The rapidly progressing swelling compromised oxygen delivery to the lungs and the saturations began to drop quickly. The patient became bradycardic and lost consciousness. At this point, it became easier to attempt the tracheostomy. The ALS protocol was followed and CPR started. An attempt was made for direct laryngoscopy – a grade 3b view was obtained and a size four microlaryngeal tube was passed successfully. 100% O2, two doses of 1mg adrenaline IV, and 3mg atropine IV were given and the heart rate improved. Pulses were present and the defibrillator showed sinus rhythm; CPR was stopped and tracheostomy was continued. Due to abundant peri-tracheal fat, a number of tracheostomy tubes were tried before a secure tracheostomy was placed. However the microlaryngeal tube maintained airway patency.
An arterial line and larger cannula was secured. Propofol infusion and fentanyl IV were given to maintain anaesthesia and the patient was transferred to ICU.
On ICU, there was further difficulty in ventilation, with high airway pressures and saturations falling to the low 90s despite 100% O2. It was thought the tracheostomy tube was abutting the carina or posterior tracheal walls. The ENT surgeons were called urgently and in the interim the patient was re-intubated with a size 7 ETT to maintain the airway. The ENT team changed the size 8 cuffed non-fenestrated tracheostomy tube for a size 7 Shiley with a proximal extension. Despite the change, ventilation remained difficult. An urgent chest X-ray was performed which showed a right-sided pneumothorax. A chest drain was inserted and a ‘hiss’ was noted on insertion, indicating a possible tension pneumothorax. Ventilation then improved.
Further history was taken from previous notes and discharge letters. It was noted that the patient had allergies to shellfish, penicillin, erythromycin, and diclofenac, but no history of exposure. She had a background of hypertension, angina, chronic kidney disease and previous breast cancer. She was taking Lisinopril, Diltiazem, Nicorandil, Tamoxifen, Sertraline and Omeprazole. Her tongue swelling improved markedly over the next two days with antibiotic treatment and regular dexamethasone. She was awakened once appropriate and haemodynamically stable. A nasendoscopy was performed by the ENT team on day six and nothing remarkable was noted, with swelling having regressed totally. She was decannulated on day eight and transferred to the ward. Lisinopril was stopped.
Discussion
This case demonstrated a severe, acute presentation of tongue swelling (glossitis) leading to upper airway obstruction. Although a number of conditions may cause glossitis: infection, trauma, anaemia, liver disease, malnutrition. Acute glossitis is a hallmark of angio-oedema. This is a rare, but life threatening condition that requires prompt recognition and treatment.
Angio-oedema may result from anaphylactic, hereditary, acquired or idiopathic processes. Some 12-24% of anaphylaxis cases present with angio-oedema.1, 2 Hereditary and acquired cases usually result from a deficiency of C1 esterase inhibitor deficiency, which causes an accumulation of bradykinin, leading to soft tissue oedema. Such an increase in bradykinin may be caused by angiotensin converting enzyme inhibitors, leading to angio-oedema.3 If no cause can be found, it is termed idiopathic.
Management of angio-oedema requires rapid airway assessment and management; resuscitation; and treatment of the underlying cause. Anaphylaxis should respond to standard management as outlined by the AAGBI.4 Angio-oedema from other causes requires cessation of the suspected causative agent3, and in an emergency, nebulized adrenaline to reduce airway swelling. Infusion of plasma derived or recombinant C1 Esterase Inhibitor may also rapidly improve symptoms.1
Although airway support is the cornerstone of anaesthetic management, an acute, rapidly progressing case such as this requires a multi-disciplinary approach.5 Anaesthetists will require help from operating department practitioners and nurses to manage the initial airway compromise. A compromised airway presents a significant hazard to any form of anaesthesia, especially if it results in cardio-respiratory depression, which will expedite hypoxemia and impair tissue oxygenation. An awake, spontaneously ventilating approach to secure the airway needs to be undertaken. ENT staff should be scrubbed and ready to perform an emergency surgical tracheostomy if complete airway obstruction occurs or airway access cannot be secured.
An awake fibre-optic intubation can be attempted but this requires an experienced anaesthetist, timely access to equipment, preparation and a co-operative patient. These are unlikely to be provided in the resuscitation room. Fibre-optic manipulation causing bleeding or further swelling can lead to complete airway obstruction.
An inhalational induction to maintain spontaneous ventilation and then followed by direct laryngoscopy or fibre-optic intubation is another option and reduces the required co-operation of the patient. But this may cause haemodynamic instability in an already compromised patient and can lead to complete airway collapse.
An elective awake tracheostomy under local anaesthetic is the most likely route to ensure airway access without haemodynamic compromise.6 This will require a co-operative patient, senior help from trained operating department staff, and the ENT surgeons scrubbed and ready to perform a surgical tracheostomy if a percutaneous approach fails.
The Intensive Care Unit should be aware of the patient and ICU teams will be required to help with airway access as well as manage haemodynamic instability, secure arterial and central venous access. The patient will need further airway support and treatment in the Intensive Care Unit.
An acute upper airway obstruction therefore requires an emergent, yet controlled, approach to secure airway access and maintain oxygenation. Staff should have clear roles, ideally decided beforehand and practiced, with experience in the use of the equipment available. Senior ENT help should be available readily and again be versed in securing an emergency awake tracheostomy should other means fail or are not suitable.
As with any critical incident a debriefing should be undertaken to highlight points in the management of such patients that were handled well and those that were not, so that existing management plans can be improved and skills honed to improve management of future incidents.
Polyarteritis nodosa (PAN) is a rare vasculitis in childhood. Since first described by Kussmaul and Maier in 1866 1, there have been approximately 140 pediatric case reports in the literature. Traditionally, children were classified as having one of three forms: infantile, cutaneous, and systemic. Infantile PAN is now recognized as a severe form of Kawasaki disease. Criteria for a diagnosis of systemic PAN in childhood have been proposed but not validated2.
Cutaneous PAN (cPAN) is recognized as a separate entity but there are no diagnostic criteria for cPAN2. cPAN is characterized by disease affecting the skin with no major organ system involvement. The cutaneous symptoms are similar to systemic PAN and mild fever, muscle, joint, and peripheral nervous system involvement may also occur. Fever, rash, and musculoskeletal symptoms are common in children and cPAN needs to be differentiated from other diagnostic entities. Definitive diagnosis is by histopathologic evidence of necrotizing inflammation of the medium and small-sized arteries. There is a paucity of knowledge of the spectrum of clinical presentation and management of children with cPAN. Here we describe a case of cPAN and summarize the clinical manifestations, laboratory data and treatment regimens of our patient.
Case report
This 10 year old female adolescent presented with pain in both the elbow joints followed by pain in the left knee joint and both the ankle joints in a course of 8 days and fever for the past 2 days .On admission her vitals were stable, both the elbow joints were tender and the knee and ankle joints were swollen and tender .She had multiple subcutaneous nodules over extensor aspect of both her forearms, both her tibial shins and few on her thighs. Systemic examination showed presence of a soft PSM of grade 2 intensity over left sternal edge. Blood investigations showed leucocytosis, elevated CRP, elevated ASLO titres and 2Decho revealed a mild tricuspid regurgitation. An initial diagnosis of acute rheumatic fever was made and child was started on penicillin and Aspirin. But child continued to have excruciating arthralgia and hence a rheumatologist opinion was taken. Child was advised a skin biopsy from the nodular lesions which showed small and medium vessel vasculitis suggestive of cutaneous polyarteritis nodosa. Hence she was stopped with aspirin therapy , given pulse therapy with methyl prednisolone and continued with penicillin therapy .Her arthralgia subsided within a day of pulse therapy and the subcutaneous nodules gradually disappeared .On discharge child was put on oral steroid therapy and penicillin prophylaxis and advised regular follow up.
Fig1 showing segmental fibrinoid necrosis with inflammatory infiltrates of small artery.
Fig2 showing leukocystoclastic vasculitis with fragmentation of neutrophils in and around blood vessels.
DISCUSSION:
cPAN is not common in the pediatric population with approximately 140 cases reported in the literature. Disease is limited to skin, joints, and muscles in the majority with a minority having nerve involvement. Constitutional symptoms are common. Most children have a chronic and relapsing benign course.
The precise etiology of cPAN remains to be unknown. However, an immune mediated mechanism has been postulated. Several infectious and noninfectious conditions have been associated both to initiation and relapse of the disease3,4,5. Among them, streptococcal infection has been commonly implicated6,7. Although some evidence of streptococcal infection as an initiating factor for cPAN is present, caution must be exercised when interpreting elevations in the serologic markers of streptococcal infection in the absence of an appropriate clinical presentation.
Cutaneous and systemic PAN share the same histopathologic features of necrotizing arteritis of small and medium sized vessels. Kussmaul and Meier described the first case of systemic PAN in 1866 1. Early reports 8,9 confirm that cPAN is a separate entity to systemic PAN. We have limited our definition of cPAN to disease affecting the skin, muscle, joints, and peripheral nervous system, with corresponding biopsy confirmation. Any evidence of visceral involvement, either clinically (central nervous system, pulmonary, cardiac, gastrointestinal, or renal), radiographically (abnormal angiography), or by histology (visceral biopsy) were classified as systemic PAN. Nakamura et al 10 proposed further restriction of the definition of cutaneous PAN in that any extracutaneous involvement such as peripheral neuropathy and myalgias must be limited to the same area as skin lesions. Systemic PAN and cPAN appear to be fairly distinct entities on a clinical continuum. There are only 5 reported cases of cPAN evolving into systemic PAN 11,12.
On review of treatment regimens reported in the literature, most children respond to corticosteroids. Penicillin should be considered in children with increased ASO titres 13,14. Recent case series report success with low-dose methotrexate, cyclophosphamide, intravenous immunoglobulin, and biologic therapies 15,16.
In summary, cPAN can be challenging to diagnose and manage. A diagnosis of cPAN should be considered in a child with fever, tender subcutaneous nodules, livido reticularis, and arthralgias/arthritis. Most children respond to corticosteroids and have a benign course, but some children may be corticosteroid dependent or corticosteroid resistant, necessitating other immunosuppressive agents including DMARDs and biologic therapy. Multicentre pediatric vasculitis disease registries are necessary to inform development and standardization of best clinical practice for childhood cPAN.
Our patient is a 40-year-old lady who presented to our department feeling unwell with fever and numbness in both hands. Past medical history showed recurrent urinary tract infections, rheumatoid arthritis, chronic eczema and epilepsy .She was taking Levetiracetam 500mg twice daily and Clobazam 5 mg twice daily for the epilepsy. She is also known to have learning difficulties. Mild hypocalcaemia was documented few years back in a previous admission in other hospitals, but the cause was unclear. On admission, she was hemodynamically stable with mild facial dysmorphism, and positive Trousseau's and Chvostek's signs.
Blood tests showed a low corrected calcium 1.5 mmol/L (NR 2.25-2.5 mmol/L), high C-reactive protein, Leukocytosis, and 3.0 mmol/L serum potassium level (NR 3.5-5.0 mmol/L). Other routine blood tests were normal. Further investigations showed low Serum parathyroid hormone levels, normal magnesium levels and normal TSH level. A CT scan of the brain was unremarkable. Electrocardiogram showed QT prolongation (with QTc of 520 ms). The diagnosis of hypoparathyroidism and urinary tract infection was established and the patient was treated with antibiotics to cover urinary tract infection and calcium supplements for hypocalcaemia. The patient symptoms improved significantly and was discharged on calcium supplements and Calcitriol (Rocaltrol 0.25 mcg) with a calcium level of 2.1 mmol/L. The presence of hypoparathyroidism in association with learning difficulties, eczema and epilepsy prompted chromosomal analysis for DiGeorge syndrome. The microdeletion of chromosome 22q11.2 was confirmed by FISH (fluorescent in situ hybridization) analysis. Cardiac echo examination demonstrated no abnormalities and abdominal ultrasound examination showed no renal abnormalities. The patient was offered Genetic counselling together with her family.
Discussion:
DiGeorge syndrome is a well-known genetic disorder with a prevalence of 1:4000 live births1. It was initially described by Angelo DiGeorge a physician and paediatric endocrinologist in 1968 2. DiGeorge is a developmental defect caused by a microdeletion of chromosome 22q11.2; it is also known as velocardiofacial syndrome or CATCH 22 syndrome to describe the classical features of this syndrome (C-Congenital heart disease, A-Abnormal facies, T-Thymus hypoplasia, C-Cleft Palate and H- Hypocalcaemia due to Hypoparathyroidism. Autoimmune disorders, skeletal defects, renal abnormalities, psychiatric and behavioural disorders are also associated with this syndrome.
DiGeorge is an autosomal dominant syndrome but the majority of patients have de novo mutations caused mainly by the microdeletion of chromosome 22q11.2 which leads to developmental disorders such as the failure of development of pharyngeal pouch system 3, 4. These developmental disorders are the main cause of the classic features and presentation of DiGeorge syndrome such as congenital heart diseases, hypoplasia of the parathyroid glands and thymus, congenital immune deficiency and renal abnormalities5 .
Congenital Conotruncal cardiac defects that involve truncoaortic sac can present in 70% patients with DiGeorge Syndrome. The most common cardiac anomalies are interrupted aortic arch, Tetralogy of Fallot, Atrial septal defect and ventricular septal defects 4, 5, 6 .
Hypocalcaemia is due to hypoparathyroidism and is present in about 60 % of patients 5, 7 . Hypocalcaemia is a strong predictor of DiGeorge syndrome if it is associated with other clinical features such as cardiac defect and immunodeficiency. Hypocalcaemia commonly presents as muscle cramps, numbness, tetany, focal or generalized seizures, prolong QT and hypotension.
Immunodeficiency is rare in adults and but it may present in up to 70-80% of the children with DiGeorge syndrome. Immunodeficiency occurs because of the low T cell count due to thymus hypoplasia. The function of T cells is however, usually preserved. Patients with immunodeficiency may have recurrent viral chest infection, systemic fungal infections frequent bacterial infections 8 .
The characteristic facies of DiGeorge include long face, narrow palpebral fissures, broad nasal bridge, micrognathia and asymmetrical crying face.
Psychiatric disorders have been reported with 22q11.2 deletion syndromes such as schizophrenia, bipolar disorder, anxiety and affective disorders.
Other conditions that may be associated with DiGeorge are atopic disorders (asthma and eczema) rheumatoid arthritis, autoimmune thyroiditis, renal abnormalities (such as multicystic kidneys andVesicoureteral reflux).
Conclusion:
Due to the variety of symptoms and the de novo mutations, DiGeorge Syndrome should be considered in adults presenting with hypocalcaemia due to hypoparathyroidism even in the absence of the classical features. The syndrome has significant health implications, and confirming the diagnosis is important for future family planning.
Although it is well appreciated that pancreatitis is frequently secondary to biliary tract disease and alcohol abuse, it can also be caused by drugs, trauma and viral infections, or even be associated with metabolic and connective tissue disorders.1 Knowledge of the true incidence of drug-induced acute pancreatitis is dependent on the clinician’s ability to exclude other possible causes, and by promptly reporting the occurrence. Based on individual case reports and case control studies of drug-induced acute pancreatitis, the estimated overall incidence ranges from between 0.1 and 2% of pancreatitis cases.2,3 In particular, drug-induced acute pancreatitis is of mild severity and usually resolves without significant complications.4
Attempts have been made to categorize the risk of drugs causing acute pancreatitis. A previous classification system described by Mallory and Kern Jr. categorized drugs associated with acute pancreatitis as definite, probable, or possible.5 Trivedi et al. proposed a newer classification system for commonly used medications associated with drug-induced pancreatitis. Class I drugs are those medications with at least 20 reported cases of acute pancreatitis and at least one case with a positive rechallenge. Drugs with fewer than 20 but more than 10 reported cases of acute pancreatitis, with or without a positive rechallenge, are designated into Class II. While those medications with 10 or less reported cases, or unpublished reports in pharmaceutical or FDA files, are grouped into Class III.6
Acute pancreatitis as a result of either doxorubicin or cyclophosphamide, or a combination of both, or fluorouracil or epirubicin is a rare occurrence and has seldom been reported in the literature. Even the drug package labels registered with the FDA do not indicate the possible occurrence of pancreatitis. In this case report, we present a rare occurrence of drug-induced acute pancreatitis after the completion of the first cycle of the chemotherapy protocol involving cyclophosphamide and doxorubicin in a patient with stage 3 breast cancer, with recurrences of acute pancreatitis after re-challenging with cyclophosphamide and a derivative of doxorubicin, given individually on two separate occasions.
CASE PRESENTATION
A 58 year-old female presented to the emergency room with a one day history of severe, diffuse, deep-seated abdominal pain that radiated to her back, associated with nausea and vomiting, and was unrelieved despite the intake of NSAIDs. There was no reported fever, chills, diarrhea, dysuria, or antecedent trauma. Her medical history is notable for well-controlled hypertension, hyperlipidemia and hypothyroidism for which she takes amlodipine, atorvastatin and levothyroxine. She was recently diagnosed with left-sided breast cancer, Stage III, two months prior to admission and underwent a left modified radical mastectomy. Three days prior to the hospital visit, she was given her first cycle of chemotherapy with Doxorubicin 60 mg/m2 and Cyclophosphamide 600 mg/m2 along with Pegfilgrastim 6 mg and Fosaprepitant 150 mg. She is a former cigarette smoker, drinks alcohol infrequently, and denies illicit drug use. Her family history is unremarkable.
Physical examination revealed stable vital signs without a fever (36.6◦C). She had non-icteric sclerae and a dry oral mucosa. Chest exam revealed a well-healed left mastectomy scar and an infusaport located on the right anterior chest wall. Her breath sounds were clear bilaterally. Her heart sounds were normal. Her abdominal exam was significant for mild tenderness to palpation in the epigastric area without palpable masses, organomegaly or ascites. There was no evident ecchymosis observed. The extremities were warm to touch with intact and symmetrical pulses, and without bipedal edema.
Initial work-up revealed an elevated leukocyte count of 42,000 with 80% neutrophils and 17% band forms. Basic metabolic panel was normal except for mild hyponatremia of 129 mEq/L. Serum amylase and lipase were markedly elevated at 2802 units/L and >2000 units/L, respectively. Liver function panel was normal (Alk phos 63 U/L [ref range 30-115 U/L], GGT 21 U/L [ref range 3-40 U/L], total bilirubin 0.90 mg/dL [ref range 0-1.5 mg/dL]). The coagulation profile was within normal range. Imaging of the abdomen with a CAT scan with intravenous and oral contrast showed haziness in the pancreatic fat plane suggestive of pancreatic inflammation, with no gallstones, focal abscesses, hepatic masses, or biliary ductal dilatation (Figure 1). Right upper quadrant ultrasound was essentially normal (Figure 2).
Figure 1. Coronal view of CT scan of abdomen and pelvis with IV and oral contrast showing haziness in the peripancreatic fat plane.
Figure 2. Sonogram of the right upper quadrant of the abdomen showing gallbladder devoid of gallstones and non-dilated common bile duct.
She was admitted to the medicine unit with the assessment of acute pancreatitis likely secondary to doxorubicin and cyclophosphamide. Intravenous fluid hydration with normal saline was initiated. She was kept NPO (nothing per os) and was started on empiric Imipenem and IV Esomeprazole. Her abdominal pain was controlled with intravenous morphine and her nausea with Ondansetron as needed. The serial basic chemistry panel was monitored and electrolyte deficits were replaced accordingly. Further work-up was performed to identify other possible etiologies of pancreatitis. The lipid panel was within normal limits (cholesterol 169 mg/dL [0-200 mg/dL], HDL 74 mg/dL, LDL 71 mg/dL and triglycerides 54 mg/dL [0-150 mg/dL]). The serum calcium levels remained within the normal range throughout her hospital stay. An abdominal sonogram demonstrated absence of gallstones or dilatation of the common bile duct, with a normal appearing liver parenchyma and pancreas. During her stay in the medicine unit, the patient’s abdominal pain improved and she was gradually started on an oral diet, which she tolerated well. Her serum electrolytes remained stable, while her serial CBC revealed progressively decreasing trends in leukocytes, hemoglobin, hematocrit, and platelet count, findings which were attributed to her prior chemotherapy. Repeat serum amylase and lipase both trended downward. The patient was discharged with follow up in the Oncology clinic. A month later, she was started on another chemotherapy regimen that consisted of weekly administration of Paclitaxel 80 mg/m2 which, over the next two months, the patient completed without any complications. Then, after explaining the risks of recurrent pancreatitis, the patient consented to have a trial of cyclophosphamide 500 mg/m2 along with fluorouracil 500 mg/m2. Five days after receiving the chemotherapy, the patient developed acute pancreatitis which was attributed to cyclophosphamide. She again made a full recovery at that time. Three weeks later, her chemotherapy regimen was again changed, to epirubicin 90 mg/m2 and fluorouracil. Four days after receiving this regimen, she again, for the third time, had a recurrence of acute pancreatitis. At this time, a repeat abdominal sonogram revealed a 4mm echogenic focus adherent to the anterior gallbladder wall with a comet tail sign, suggestive of cholesterol crystals lodged within Rokitansky-Aschoff sinuses of the gallbladder wall. There were no visible gallstones. A subsequent MRI of the abdomen with contrast revealed a small rounded hypointensity in the dependent portion of the gallbladder wall that was suggestive of a gallstone, however, there was no biliary obstruction, choledocholithiasis or an obstructing pancreatic mass. At this point, chemotherapy was stopped and anastrozole along with radiation therapy was initiated. The patient continues to be followed regularly and has had no recurrence of pancreatitis since her last episode.
DISCUSSION
The case presented described the development of acute pancreatitis in a patient with breast cancer three days after receiving the chemotherapy regimen consisting of cyclophosphamide and doxorubicin. After re-challenging the patient with cyclophosphamide, and again a few weeks later with a derivative of doxorubicin, epirubicin, acute pancreatitis recurred on each occasion. Despite the presence of cholelithiasis detected on the abdominal MRI, the temporal presentation of acute pancreatitis after chemotherapy exposure is highly suggestive of the role these chemotherapeutic agents played in triggering these three acute attacks. Acute pancreatitis was diagnosed based on the clinical suspicion and symptoms suggestive of the acute pancreatitis and was supported by the marked elevation in serum amylase and lipase, as well as, the radiologic evidence of pancreatic inflammation, both of which are markers of acute pancreatitis.
Chemotherapy-induced acute pancreatitis involving cyclophosphamide and doxorubicin either alone or in combination, is quite rare that even the drug labels registered with the FDA do not indicate acute pancreatitis as one of the possible complications. This scenario highlights the importance of drug surveillance and prompt reporting in order to maintain a credible drug safety database.
Though the drug latency, which is the interval between the initial exposure to the drug and the development of acute pancreatitis, differs variably, the present case is considered to have an intermediate latency (1-30 days). Other drugs may have short (< 24 hours) or long (>30 days) latency periods. Examples of drugs with short latency are acetaminophen, codeine, erythromycin and propofol. Intermediate latency drugs include L-asparaginase, pentamidine and stibugluconate. Drugs with long latency are estrogen, tamoxifen, valproate and dideoxyinosine.7
Based on the revised classification of Badalov et al, the combination of cyclophosphamide and doxorubicin is classified as Class IV drugs, which have the weakest association with acute pancreatitis due to limited information and the lack of adequate detailed case reports. Fluorouracil, which has been known to cause a gastrointestinal ulcer, is also categorized as a Class IV drug, while epirubicin, which is derived from doxorubicin, has not been classified, as it has not been reported before to cause acute pancreatitis. In implicating drugs in the etiology of acute pancreatitis, two conditions must be considered to weigh the strength of the association between the causality and the disease process, namely: a positive rechallenge test resulting in the recurrence of pancreatitis and a similar latency period between the drug exposure and development of the disease.7
The combination of drugs rather than a single agent was implicated for drug-induced pancreatitis in a previous case report that described the development of acute pancreatitis shortly after the second cycle of the chemotherapy regimen composed of cyclophosphamide, doxorubicin, and vincristine in a patient with mediastinal immunoblastic lymphoma. The pancreatitis episode resolved over 48 hours without complications.8
Another case was described in a patient with breast cancer developing acute pancreatitis four days after the third cycle of chemotherapy, which involved docetaxel and carboplatin.9
Toprak et al. reported the occurrence of acute pancreatitis in a patient with multiple myeloma after the initial treatment with the triple regimen chemotherapy protocol consisting of vincristine, doxorubicin, and dexamethasone. In this case report, symptoms suggestive of acute pancreatitis started to manifest on the first day of the treatment, with resolution following discontinuation of the drugs.10
Other antineoplastic agents for breast cancer associated with drug-induced pancreatitis are alemtuzumab, trastuzumab and tamoxifen. Extended use of these medications may cause chronic pancreatitis as a result of their causing repeated clinical or subclinical episodes of acute pancreatitis.6 Most cases of drug-induced pancreatitis follow a mild clinical course.7
In a retrospective study involving 1613 patients diagnosed with acute pancreatitis in a gastroenterology center, the incidence of drug-induced pancreatitis had been reported in 1.4% of patients treated for acute pancreatitis. It has been observed that a higher incidence of drug-induced acute pancreatitis occurs in elderly or pediatric patients, and in those patients with inflammatory bowel disease or AIDS.11
The pathophysiology behind drug-induced pancreatic injury remains unclear. Potential mechanisms underlying such pancreatic injury might be related to drug hepatotoxicity which can be secondary to intrinsic toxicity of the drugs affecting the tissue, or due to an idiosyncratic reaction. In the vast majority of the cases, an idiosyncratic reaction could be the main pathway for tissue injury through a hypersensitivity reaction or production of toxic intermediate metabolites. Idiosyncratic reactions have a longer latency period of months to years before the onset of pancreatitis while the onset of hypersensitivity reactions is earlier (i.e. 1-6 weeks).7
CONCLUSION
Due to a variable latent period between the initial drug exposure and the onset of clinical symptoms, drug-induced pancreatitis must remain as a differential diagnosis in patients receiving chemotherapy regimens and presenting with the constellation of symptoms typical of acute pancreatitis. Due to the unclear pathogenesis of chemotherapy-induced pancreatitis, post-marketing surveillance and adverse drug reporting are paramount in elucidating the effect these drugs have on the pancreas.
Sertraline is selective serotonin reuptake inhibitor (SSRI). It is a commonly prescribed antidepressant. The common side effects of SSRI’s are nausea, vomiting, diarrhoea, dyspepsia, anorexia and weight loss.
To our knowledge this is the only second reported case of sertraline-induced hyperpigmentation. It is interesting to note that in some cases sertraline has been used as replacement medication following antidepressant induced hyperpigmentation. So it is important that both clinicians and patients are aware of this potential rare side effect of sertraline.
Case Report:
In this case report we present a 27 years old Caucasian lady that developed hyper pigmentation, after starting sertraline.
The patient, a 27 years old lady was diagnosed with Bipolar Affective Disorder (ICD-10)2 years ago. She was prescribed sertraline 50mg for low mood. Her current medications also include semi sodium valproate 1000 mg orally daily, quetiapine modified release 400 mg orally daily, tramadol 50mg orally twice a day and co-codomol orally on an as required basis for back pain. She was not prescribed any depot medications. To our knowledge she was compliant with her medication.
She responded well but reported that she had developed hyperpigmentation after four weeks. This persisted after suffering a recurrence of low mood and being seen in clinic 5 months later.
There is no significant past medical or family history. She has been on various psychotropic medications in the past including fluoxetine, venlafaxine, olanzapine and procyclidine.
Physical examination revealed focal hyperpigmentation limited to the upper lip. It was dark brown in color with sharply defined outline and was not associated with itching, redness, rash or excoriation. It was gradually getting darker in color and she had to wear a lot of make up to conceal it. The patient was referred to a consultant dermatologist for an opinion but unfortunately she did not attend her appointment. This has been acknowledged as a limitation of our case report. Routine blood tests were within the normal range. She also reported some weight gain with sertraline.
She did not report any previous history of dermatological disorders or any endocrine conditions and Addison's disease was excluded. She did not begin any new medication or vaccines prior to onset of the hyperpigmentation and denied ever having chlorpromazine, tricyclics, tetracyclines, amiodarone, hormone replacement therapy, aspirin, chemotherapy or minocycline. However three years ago, she had taken anti malarial medication before going to the Dominican Republic. She also denied any intake of herbal medication, non-prescribed medication or illicit drugs.
She also denied excessive exposure to sunlight during the time of development of hyperpigmentation and she was not pregnant. There is no history of heavy metal exposure.
The probability of adverse drug reaction assessed by using Naranjo Scale indicated a probable association between the use of sertraline and hyperpigmentation. Subsequently her sertraline was stopped and replaced by duloxetine 30mg daily. Unfortunately the hyperpigmentation persisted after three off sertraline but is no longer worsening.
Discussion:
Bipolar Affective Disorder also known as bipolar disorder, manic-depressive disorder, or manic depression is characterised by two or more episodes in which patients mood and functionality is significantly disturbed, this disturbance on some occasions includes episodes of mania or hypomania with elevated mood and increased energy levels and on others episodes of depression with low mood, tiredness and diminished pleasure in activities. Recovery is usually complete between these episodes. 1
The pharmacological treatment of bipolar affective disorder depends on nature and degree of presenting episode and includes mood stabilisers like lithium, valproate, carbamazepine and lamotrigine, anti psychotics like olanzapine, quetiapine, aripiprazole and risperidone and antidepressants like sertraline, citalopram and venlafaxine.
Sertraline, citalopram, escitalopram, fluoxetine, fluvoxamine and paroxetine selectively inhibits reuptake of serotonin, hence named selective serotonin reuptake inhibitor (SSRI).
In our case the patient was on semi sodium valproate and modified release quetiapine and was later prescribed sertraline to help with low mood.
A literature review of English language using PubMed database was done on 15th June 2013. The terms searched were “sertraline”, “serotonin reuptake inhibitor”, “SSRI”, “anti depressants”, “hyperpigmentation”, “pigmentation”, and it found case reports of antidepressant associated hyperpigmentation with citalopram2, mirtazapine3 and imipramine.4, 5,6,7 It is interesting to note that in some of the case reports the antidepressants were replaced by sertraline after development of hyperpigmentation, but there was no record as to whether the lesion resolved.2, 3,4
Only one previous case of sertraline-induced hyperpigmentation was found8,which also unfortunately persisted after discontinuation of the antidepressant.
As hyperpigmentation has also been reported with other SSRIs, clinicians should be more aware that hyperpigmentation might be related to the class effect, rather than the individual drugs.
Though the exact biological mechanism for the development of hyperpigmentation is not clear and further research is needed, the secretion of melanocyte stimulating hormone (a-MSH) is closely associated with skin pigmentation, and serotonin and dopamine transmitters appear to be involved which may point to a possible mechanism for the hyperpigmentation.
Brain injury is a major cause of mortality and morbidity all over the world and in Europe there is an estimated incidence of 235 brain injury inpatients per 100,000 population 1. Over the years, the medical care of brain injuries has developed with a resultant fall in mortality. However, with this fall in death rates the proportions of people with complications, especially the neuro-behavioural effects of brain injury, has risen 2. Of the complications, psychiatric disorders have a significant impact on the patient’s quality of life and rehabilitation prognosis3 and so are an important consideration from both a care delivery and public health perspective. This paper therefore aims to analyse the prevalence of psychiatric disorders following brain injury and highlight the practical and personal implications of these through an illustrative case series.
Depression Following Brain Injury
Jorge et al in 20044 conducted a prospective case controlled study on a sample of 91 patients with traumatic brain injury (TBI). Patients with penetrating head injury, spinal cord injury and severe deficits of comprehension was excluded and 27 patients without brain injury but with other trauma was included as controls. The sample was analysed at 3, 6 and 12 months with Present State Examination (PSE), structured clinical interview for DSM1V, and analysed with Mann Whitney and chi squared tests. The results showed that 33% of the TBI group had major depression compared to 22 % in the control group. Neuropsychological testing also demonstrated that depressed patients had a greater degree of impaired cognitive function. An earlier study with a larger sample was conducted by Kreutzer in 20015, studying 722 TBI patients (average time post injury for evaluation 2.5 years). Data was collected via survey, using the Neurobehavioral Functioning Inventory to identify depression; the response was studied by trained neuropsychologists and compared with DSM-IV Criterion for depression. A significant proportion (42%) of survey respondents met the DSM-IV criterion for depression. Fatigue, low concentration and frustration were most commonly reported symptoms. A similar study done by Seel et al in 20036, where 666 TBI outpatients from 17 centres was reviewed using DSM-IV Criterion, showed rates of major depression to be 27%.
Mania Following Brain Injury
Jorge in 19937 reviewed 66 patients with brain injury at 3, 6 and 12 month intervals to evaluate the prevalence of mania. The inclusion criteria was age above 18 years and absence of delirium, no previous history of mood disorder and absence of grave injuries to other areas of the body. Using the Present State Examination to gather data, 9% of the sample had symptoms in correlation with the DSM III criteria for mania.
Van Reekum in 19968 recruited 18 TBI patients attached to a rehabilitation unit for a study to evaluate mental illness in this population. 44% of patients had severe TBI while 56% had mild/moderate TBI; the average duration since TBI was 4.9 years. 27% met the DSM II criteria for bipolar affective disorder and 61% met criteria for depressive illness. The rate of anxiety disorder was 38% but psychosis was not reported.
Psychosis & Other Mental Illness Following Brain Injury
Fann et al in 20049 conducted a large prospective cohort study involving 1939 randomly selected TBI patients 1 year pre injury and 3 years post injury to study rates of psychiatric illness including psychosis. The sample was divided into the moderate/severe TBI and mild TBI compared to matched controls. The presence of psychiatric illness was detected by utilisation of mental health services by subjects, usage of psychotropic medication and presence of a psychiatric diagnosis in the records. Psychotic disorders were seen in 49% of the moderate to severe TBI patient group and for the mild TBI group psychosis was seen in 34% of the sample. This is significantly greater than the rate seen in the control group. However the lack of definitive diagnostic criteria and confounding factors such as social circumstances and other physical health issues which may have strong associations with mental illness were not accounted for.
Another observational prospective study done by Rao et al in 200910 looked into prevalence rates of aggression in the 3 months following brain injury. Overt Aggression Scale was used by trained examiners in the assessment of aggression in a sample of 107 TBI patients. Comorbidities were analysed using General Medical Health Rating scale; psychosocial functioning was analysed by Social Functioning Exam and the Social Ties Checklist. Results showed the prevalence of aggression in the sample to be 28.4% and this subgroup was also associated with new-onset major depression. Only 63% of the already small sample completed the study and the drop out group was unaccounted for; this may negatively impact the results.
Keenan et al in 200811 studied prevalence of attention-deficit hyperactivity disorder(ADHD) in 2782 post TBI children and demonstrated chance of a diagnosis of ADHD two folds higher amongst children with a head injury before age 2. Jellinger in 200412 studied links between brain injury and dementia, and found that although cognitive deficit was associated with brain injury, there was no established link between development of dementia and brain injury. Oquendo et al in 200413 studied 325 depressed patients to analyse the link with mild TBI and suicidal behaviour; 44% of the sample had mild TBI and suicidal behaviour was more common in this subgroup. Suicide Intent Scale and the Lethality Rating Scale was used to measure suicidal behaviour. However, exclusion of moderate to severe TBI and inclusion of only inpatients in this study would affect any generalisability of the results.
Case series: Psychiatric Disorders Following Brain Injury
Case 1- Patient A: Epilepsy, interictal psychosis and organic personality disorder following head injury
Patient A is a 37 year old female under mental health services with a diagnosis of organic personality disorder and interictal psychosis. She suffered from epilepsy from the age of 9 but coped well at school and went on to work successfully as a hairdresser. However, in 1998 at the age of 22 she was admitted to ITU with status epilepticus as a result of encephalitis of unknown cause, and remained severely unwell for several months. She recovered but was left with residual tonic clonic and complex partial seizures.
Since this episode, marked changes in her personality were noted. She developed mood swings with recurrent episodes of low mood, and expressed paranoid beliefs about people in the street talking about her. These beliefs resulted in her being agitated and physically aggressive, resulting in harm to both herself and others. She has required numerous admissions to acute wards and rehabilitation units because of her paranoid and suspicious behaviour and aggressive outbursts that her family were not able to manage in the community. She required restraint under Section 3 of the Mental Health Act in 2010, believing that care staff were poisoning her. Psychotic symptoms are most marked around seizures, with her displaying self harming behaviour such as cutting off hair or painting face with nail polish. She frequently accuses staff and family of acting against her in these periods and her behaviour is very difficult to manage.
Her case has been challenging to manage successfully in the community by family and community teams, and she has needed several short and long term stays in acute wards and residential units. Her care has been coordinated jointly between neurological and psychiatric services. She currently lives with her parents and has carers to support her. Her epilepsy is yet to be successfully controlled; antipsychotics can lower the seizure threshold and so a delicate balance between these and her antiepileptic medication is warranted. There is an on-going concern that further mental health problems may develop in light of this.
Case 2- Patient B: Schizophrenia following head injury
Patient B is a 43 year old female with a diagnosis of schizophrenia, learning difficulties and epilepsy. She suffers from epilepsy in the form of absence and tonic-clonic seizures from the age of 7 months, when there is high suspicion that she sustained a head injury whilst in the care of extended family. Patient B has difficulties with numeracy and literacy, identified through psychological assessment, and an IQ of around 70. She has required three admissions under Section 2 of the MHA due to her paranoid delusions and poor self care. Patient B frequently reports feeling monitored by cameras, suspicions that her food has been poisoned and that her personal belongings are being tampered with. She has attempted to take her own life due to feeling unable to cope with these delusions, laying in the road to be run over by a bus.
She is currently managed well in the community on oral risperidone for her psychosis and sodium valproate for her epilepsy; she resides in supported accommodation and has required stints in long term residential and rehabilitation beds due to her mental health problems and learning difficulties.
Case 3- Patient C:Depression and Personality disorder after head injury
Patient C first came in to contact with psychiatric services in 2007 and was diagnosed with depression and organic personality disorder. At the age of 16 this gentleman was knocked off his bicycle and sustained a severe head injury, from which he was left in a coma for over three weeks, but recovered well enough to go home. In 1994 he started having blackouts, was investigated extensively by neurology, and diagnosed with non-epileptic attack disorder. As part of these investigations, Patient C underwent an MRI which demonstrated significant brain damage including traumatic damage to the frontal lobes. This was likely due to his accident at age 16. From his first assessment by psychiatric services, he eluded to thoughts and behaviours that were of serious concern to his team. He reported feeling emotionally detached from his family, gaining little pleasure from life, getting in to fights frequently and allegedly having stabbed someone in an altercation several years ago. He described to practitioners only getting excitement out of reading and watching programmes about serial killers, and occasionally became sexually aroused by this. He had made extensive written plans on how he would capture, torture and kill the couple he believed were responsible for his accident at 16. He also struggles with auditory command hallucinations telling him to harm himself and others. He frequently self harms, often using a Stanley knife to cut his arms and legs. Patient C has been jointly managed by adult psychiatry and neuropsychiatry on an outpatient basis. His risks of aggression and violence have been carefully managed through regular assessment and involvement of forensic services.
Conclusion:
The literature search indicates that the prevalence of psychiatric disorders in patients with brain injury is much higher compared to general population. The significance of the results are however greatly affected by response bias, the impact of patients’ cognitive impairment on their study participation, observer biases and the small study population sizes; however, we believe that these short-fallings should be seen as a trigger to stimulate more comprehensive and wide-scale research in to this field. The methodologies used by authors described in the literature review demonstrate the wide variance in the tools used to assess psychiatric illness in patients following TBI; we therefore argue that universal case definitions need to be agreed on and implemented to standardise studies and reduce bias. The economic impacts and impacts on quality of life have often been neglected by researchers and warrant formal assessment. From a service delivery perspective, rehabilitation programs need to identify patients with signs of psychiatric illness post TBI earlier and involve psychiatric service in the development of integrated care plans to improve the total outcome and quality of life of the patient. The impact on the patient’s family and carers also need to be explored further to provide an evidence base for more effective and holistic interventions.