



ISSN 1757-8515
A case of accidental carotid artery cannulation in a patient for Hemofilter: complication and management
Sanil Nair, Harshal Wagh, Kavita Mordani and Salim Bhuiyan
Cite this article as: BJMP 2009: 2(3) 57-58
|
|
Keywords: Carotid puncture, Haemofiltration, Surgical Repair |
Inadvertent carotid arterial puncture complication is reported to have an incidence of 2% - 8% 1, 2 and usually results in localised haematoma formation.
Case presentation
We present a case of a 72 year old man with acute on chronic renal failure referred for intensive care (ITU) management. History revealed dehydration and anuria for 3 days. His blood pressure was 80/40, sinus tachycardia around 130/min with cold clammy peripheries. Blood investigations revealed urea 23mmol, creatinine 800mmol, and potassium-7.7, with ECG changes of hyperkalemia. We attempted a right internal jugular (IJV) venous cannulation using landmark technique and inserted an Arrow-Howes central venous catheter with blue flexi tip, 8.5FR, 5 lumen, and 16cm length. The technique was difficult due to low blood pressure, and patient’s inability to lie flat. The ultrasound machine was unavailable at that moment.Soon after the catheter was introduced using seldinger technique, a swelling was noticed from the site of IJV cannulation .the blood sample analysis revealed arterial blood. The catheter was removed and pressure applied for 45 minutes. Thereafter, a left femoral vein catheter was inserted for central venous access and right femoral vascath –VYGON, DUALYSE Expert, 2 lumen catheter set, 12 fr, 20cm was inserted uneventfully.1 hour later the bleeding from the right carotid puncture site was examined and was found to have ceased. The patient was put on the continuous veno- venous haemofiltration (CVVHF), which clotted after 15minutes.Heparin was used as an anticoagulant for the filter. This was repeated thrice with same result. Three hours later, a haematoma was noticed in area of IJV puncture, which was gradually increasing in size. The haematoma spread to the neck and chest after which the patient complained of discomfort with breathing difficulty. In view of increasing airway compromise the patient was transferred to theatre for elective intubation and surgical intervention. Ultrasonongraphy by radiology consultant showed a large haematoma, but unable to see the damage in the vessel and a CT neck, thorax angiography was suggested.
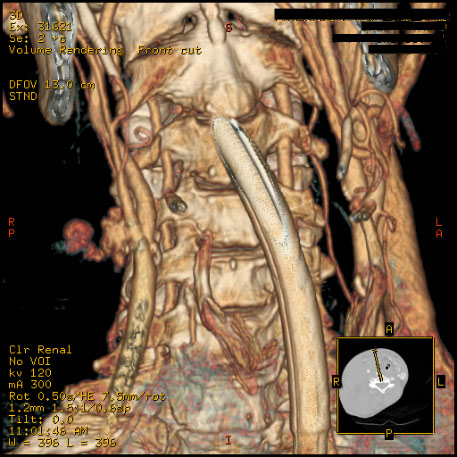
CT angiogram revealed a leak in the bifurcation of the carotid artery. Surgical access was difficult in view of the large persistent leak. Ultrasound probe was used to make the incision superficial to the leak. A small leak was identified in the artery, which was sutured uneventfully. He was then continued on CVVHF with no further complications Discussion Complications include arterial puncture, pneumothorax, neck or mediastinal haematoma and hemothorax3, 4. The haematoma may enlarge rapidly if the patient is coagulopathic, or if a large puncture wound is produced by the introduction of the sheath itself into the carotid artery. Airway obstruction 5, 6, pseudo aneurysm 7, 8, arterio-venous fistula formation 9 and retrograde aortic dissection 10 have all been reported as a consequence of carotid puncture. In the presence of occlusive (atheromatous) carotid disease, inadvertent puncture may carry the risk of precipitating a cerebrovascular accident 11. NICE guidelines 2002 recommended use of ultrasound for central venous cannulation12. The Royal College of Radiology (RCOR) recommends practical training in vascular ultrasound should involve at least two ultrasound lists per week over less than three months up to 6 months. Meta-analysis including 18 Randomised Controlled Trials by NICE concluded that ultrasonongraphic (USG) venous catheterisation was more effective than landmark technique for all outcomes 13 Royal College Of Anaesthetists feels guidance is fair and sensible but landmark technique is still acceptable alternative whether 2D available or not. Conclusion Complications following central venous cannulation are reduced if the procedure is USG guided and therefore must be used whenever possible. But landmark technique is still an acceptable alternative.
|
Competing Interests None Declared Author Details <p>SANIL NAIR MBBS,DA Trust anaesthetist, Albans hospital West Herts NHS trust AL3 5PN<br /> HARSHAL WAGH MBBS,FRCA, Registrar Anaesthetics, St Albans Hospital West Herts NHS Trust, Waverley road AL3 5PN.<br /> KAVITA MORDANI MBBS,FRCA Consultant Anaesthetics St Albans Hospital West Herts NHS Trust Waverley Road AL3 5PN<br /> SALIM BHUIYAN MBBS FRCA Consultant Anaesthetics St Albans Hospital West Herts NHS Trust. Waverley road AL3 5PN</p> CORRESPONDENCE: SANIL NAIR MBBS,DA Trust anaesthetist, St Albans hospital West Herts NHS trust AL3 5PN Email: docsanil@gmail.com |
References
1. Davies MJ, Cronin KD, and Domaingue CM Pulmonary artery catheterization: an assessment of risks and benefits in 220 surgical patients. Anaesth Intensive Care 10:9, 1982.
2. Patel C; Laboy V; Venus B; Mathru M; Wier D Acute complications of pulmonary artery catheter insertion in critically ill patients. Crit Care Med, 14(3):195-7 1986 Mar
3. Abbound P, Kendall J.Ultrasound guidance for vascular access.Emerg Med Clin North Am 2004; 22:749-73
4..Randolf AG,Cook DJ,Gonzales CA, et al. Ultrasound guidance for placement of central venous catheters. A meta-analysis of the literature.Cric care Med. 1996; 24:2053-8
5. Knoblanche GE Respiratory obstruction due to haematoma following internal jugular vein cannulation. Anaesth Intensive Care 7: 286, 1979
6. Kua JS; Tan IK Airway obstruction following internal jugular vein cannulation. Anaesthesia, 52:776-80, 1997
7. Shield CF, Richardson JD, Buckley CJ, et al: Pseudoaneurysm of the brachiocephalic arteries: A complication of percutaneous internal jugular vein catheterization. Surgery 78:190-193, 1975
8. Aoki H. Mizobe T. Nozuchi S. et al: Vertebral artery pseudoaneurysm: A rare complication of internal jugular vein catheterization. Anesth Analg 75:296-298, 1992
9. Gobeil F. Couture P. Girard D, Plante R: Carotid Artery-lnternal Jugular Fistula: Another Complication following Pulmonary Artery Catheterization via the Internal Jugular Venous Route. Anaesthesiology 1994, 80:23-232.
10. Applebaum RM, Adelman MA, Kanschuger MS, Jacobowitz G, Kronzon I Transesophageal echocardiographic identification of a retrograde dissection of the ascending aorta caused by inadvertent cannulation of the common carotid artery. J Am Soc Echocardiogr 1997 Sep;10(7):749-51
11. Zaidi NA, Khan M, Naqvi HI, Kamal RS Cerebral infarct following central venous cannulation. Anaesthesia, 53:186-91, 1998 Feb
12. NICE guidelines on use of ultrasound devices for placing central venous catheters. Technology appraisal guidance no-49 September 2002.
13. Hind D Calvert N, McWilliams R, et al. Ultrasound locating devices for central venous cannulation: meta-analusisi.BMJ 2003, 32:361-7.

The above article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.