World COVID-19 cases exceed 20 million as of today and the number of deaths surpass 733103. Behind these statistics is a great deal of pain and suffering. It is now increasingly getting recognized that COVID-19 is not just a respiratory disease at all. The face of COVID-19 is changing from a pulmonary disease to an inflammatory disease which particularly affects the blood vessels, the coronary vessels, the kidneys, the liver, brain and elsewhere. Its duration is also much longer with long term impact than initially speculated. Sufferers report a huge spectrum of problems beyond the three NHS-approved symptoms (persistent cough, fever and loss of taste or smell). These include fatigue, breathlessness, muscle aches, joint pain, 'brain fog,' memory loss, lack of concentration, and depression.
More morbidity is recognised in cases of infections among the aged populations and patients with suppressed immunity. The high incidence of complications among ethnic minority apparently points toward environmental factors of immunity rather than genetic factors. Underactive immune responses in cooler temperature and diminished synthesis of vit D and the genetic factors linked with these anomalies might explain only part of the higher incidence of COVID-19 among Black, Asian, and Minority Ethnic (BAME) communities.
Research on the first British patients to contract COVID-19 has shown that BAME people are more prone to critical impacts and care compared to white people. This research, conducted by the Intensive Care National Audit and Research Centre, observed that of nearly 2,000 COVID-19 patients, 35% were non-white, though people of BAME heritage only comprise 13% of the UK’s population.1 The study included data drawn from 286 critical care units across the UK and collected until 3 April 2020. According to another study from the UCL Institute for Global Health, Bangladeshi, Pakistani, Indian, Black African and Black Caribbean ethnic groups all had a substantially increased risk of death in comparison to white British and white Irish groups. Cook et al. pinpointed that of 119 NHS staff who died from COVID-19, 64 were from ethnic minority backgrounds.2 They also noted fewer deaths among critical care staff, highlighting PPE’s usefulness.
The UK BAME population’s mortality rate for the 2009 influenza A (H1N1) epidemic was nearly twice that of the white population.3 The Pakistani and Bangladeshi ethnic groups are now 1.8 times more likely to have a COVID-19-related morbidity than white males of a similar age, when other sociodemographic and health characteristics were compared.4Studies have also specified that Black men are 4.2 and Black women 4.3 times more likely to die from a COVID-19-related death than white people.5 Doherty et al. suggested that socioeconomic disadvantages and other circumstances only partially explicate this discrepancy, and that there are missing gaps that have not yet been expounded.6
There is some confusion regarding the cause of this higher incidence of morbidity and mortality among the BAME community, due to media propaganda failing to assess this relation’s intricacies. Higher morbidity and mortality have been observed among first-generation migrants to the UK, but not necessarily among the second generation, who were born and raised in the UK. Five months is a short period to develop any form of genetic immunity or susceptibility to a new viral infection. Each person’s genetic code differs only by 1% of 25,000 genes. The gene cluster largely responsible for our health is called the human leukocyte antigen (HLA), also known as the major histocompatibility complex (MHC). It also takes much longer for any sort of adaptation or mutation to occur. Suppressed general immunity due to various factors appears to be the main reason for the higher COVID-19 incidence among the BAME population. The following discussion examines the possible factors responsible for this anomaly.
a. Immunity and Temperature
Some data has suggested that immune cells are more active in higher temperatures, as supported by the fact that fevers are a bodily mechanism activated by the immune system to defend against pathogens. It has been established that if the body temperature is increased by 1°C, immunity instantly increases 5–6 times. Likewise, if the body temperature is reduced by 1°C, immunity decreases 5–6 times. This observation has some value in explaining the higher incidence of COVID-19 infection and mortality among BAME groups who were born and raised in warmer areas, then migrated to colder regions.
Temperature-dependent immune responses are linked to genetics. One probable explanation is that BAME individuals’ immune cells are genetically wired to function better in hot weather and are unable to optimally function in cold weather. Such a genetically determined immunological build-up means that their immune cells are slow to react to viral invaders. BAME individuals’ immune cells are well-adapted to warm weather but not so to cold weather, in comparison to white individuals who were born and raised in colder climates and adapted to lower temperatures. BAME individuals’ immune cells may even become underactive in cold weather. Though COVID-19 thrives equally well in hot and cold weather, the BAME population has immunity shortcomings in surviving colder months; this insight might prompt them to take special precautions in future cold seasons.
Low temperatures have been recognized as immunosuppressive. It has been observed that even coldblooded animals migrate to warmer places when they become ill. An increase in body temperature has long been a defence mechanism against infection and inflammation. The generation and differentiation of the lymphocytes CD8+ cytotoxic T-cells are enhanced by hyperthermia. Elevated body temperature changes T-cells’ membranes, which may help mediate micro-environmental temperature’s effects on cell function. Sub-thermoneutral laboratory housing temperature was shown to induce immunosuppression in mice experiments: when the mice were housed at a thermoneutral ambient temperature, striking reductions in tumour formation, growth rate and metastasis were observed.7
Mice experiments with antigens demonstrated that mice with antigen-induced raised temperatures showed a greater number of the CD8 T-cells capable of destroying infected cells.8,9 Parallels were observed in teleost fish.10 Higher temperatures also seem to interfere with microbe replication. This is particularly noticeable when a host has a high fever and their immune system temporarily enhances as their temperature rises. Hong Kong’s persistent cold weather was attributed to the rapid spread of SARS in 2003. BAME communities whose immune mechanisms are genetically evolved for survival in higher temperatures are compromised in Western countries’ lower temperatures. The cold weather puts additional stress on their immune cells, which give in to viral invaders.
This argument is further supported by the spread of the flu. During flu season, immune cells become less efficient and flu viruses, unaffected by low temperatures, are in an advantageous position to defeat these cells. Such a hypothesis explains the higher incidence of flu in the winter and challenges the misconception that the flu virus is killed by hot weather and thrives in cold weather. The 1918 Spanish flu that broke out in the United States in the winter seemed to ease off during the summer, but returned with a deadlier strain in the autumn, and a third wave followed the next year. The problem then seems to be in humans, as viruses are unaffected by seasonal temperature variations.
b. Diminished Vitamin D Synthesis
Other mitigating factors can explain the higher COVID-19 incidence among BAME people. Nearly all immune cells have vitamin D receptors that connect to vitamin D networks in the immune system. Vitamin D helps regulate both the innate and adaptive immune systems, and is critical for balancing immune function. Vitamin D has been demonstrated to reduce the production of pro-inflammatory cytokines associated with lung damage caused by acute viral respiratory infections, such as influenza and COVID-19.11 BAME communities are prone to vitamin D deficiency because higher melanin levels in their skin cause lower vitamin D absorption. Consequently, prolonged exposure to sunlight is required to accrue the equivalent vitamin D quantity produced in the white population. This is further exacerbated in colder countries like the UK, which see less sunlight, meaning BAME individuals spend more time indoors without much opportunity to absorb vitamin D. So, there may be a connection between lower vitamin D levels and more frequent COVID-19 cases in BAME communities, though there is no firm data defending this link.
Virtually all immune cells have vitamin D receptors, indicating vitamin D interacts with the immune system. Vitamin D is required to regulate both the innate and adaptive immune systems and its deficiency is associated with immune dysregulation. Many of the ways this vitamin affects the immune system are directly relevant to the body’s ability to defend against viruses. For example, vitamin D triggers the production of cathelicidin and other defensins, which are natural antivirals capable of preventing viruses from replicating and entering cells. Vitamin D also increases the number of CD8+ T-cells, which play a critical role in clearing acute viral infections in the lungs. Further, vitamin D suppresses pro-inflammatory cytokines and may also alleviate the cytokine storms occurring in the most severe COVID-19 cases. This vitamin plays an essential role as well in glucose homeostasis, insulin sensitivity and the regulation of adipokines, such as leptin and inflammatory cytokines.12
Evidence from randomized controlled trials suggested that regular vitamin D supplements may help protect against acute respiratory infections. Admittedly, the direct evidence of vitamin D’s role against COVID-19 is still scant. One study from the United States and another from Asia found a strong correlation between low vitamin D and severe COVID-19 infection. It is well-recognized that the elderly and people with pre-existing conditionsare more vulnerable to COVID-19. Notably, people with existing medical conditions are also often vitamin D–deficient. Studies assessing ICU patientshave reported these patients’ low vitamin D levels even before COVID-19. It appears logical to hypothesize a link between the high COVID-19 infection rates in UK and US BAME groups and their observed lower vitamin D levels. Moreover, it is not possible to gain a sufficient vitamin D supply through food alone, making exposure to sunlight indispensable.
c. Weakened Immunity
COVID-19’s spread in the UK is disproportionately high compared to its spread in the countries of origin of many BAME communities. BAME people should be mindful of their genetics in a new environment. These demographics also have higher rates of cardiovascular disease, type-2 diabetes and hypertension, conditions that have been linked to severe COVID-19 symptoms and complications. There may also be other genetic links that warrant further exploration.
Current evidence has illustrated that chronic stress can increase infection susceptibility by suppressing the T-helper 1 immune response in favour of the T-helper 2 immune response.40 Stress management, lifestyle changes and career management may reduce infection susceptibility in turn. When people are less mobile, food becomes a distraction and they can overindulge. Obesity is also an adaptation to cold weather, as fat protects against low temperatures. Black and South Asian populations in the UK have 3–5 times the prevalence of type-2 diabetes compared to the white population and are diagnosed 10–12 years sooner on average.13
Human immunity is generally fixed by age 5, as contributed to by bacterial flora, among other factors. Several trillion bacteria exist within our body, with the gut considered this bacterial colony’s front yard. We have 25,000 genes, but up to 3 million bacterial flora genes are the real immune cell trainers.14Bacterial worlds came into existence well before humans evolved. When people migrated to Western countries from tropical regions, their bacteria had to adjust to their host’s new lifestyle, with some even replaced. Others may not have survived at all; consequently, these individuals’ immunity may have weakened.
The high incidence of diabetes and coronary heart disease in the British Asian population has been well-recognized, along with many other risk factors and comorbidities, including obesity, chronic obstructive pulmonary disease, chronic kidney disease, hypertension, and age. These may partly account for this population’s increased COVID-19 mortality15,16, but warrant further exploration. Vitamin D level is also likely to drop with rising BMI and age.17Obesity is strongly associated with vitamin 19-22D deficiency.18 Admittedly, there are weaknesses in these data collections and interpretations, which are theoretical speculations yet to be confirmed, modified or falsified.
There are diverse genetically linked immune responses in a given population, and the spread and survival of complications in a pandemic like this are not well-defined. Research has suggested that people living in close communities, like certain regions of Lombardy, Italy, have a poor genetically linked immune response to COVID-19. Like our fingerprints, immunity genetics contribute to our physical identity, but our immunity is not permanently fixed by genetics. There thus remain many unknowns in immunity research.
It is now increasingly recognized that immune ageing and organismal ageing are intimately inter-related. Aging weakens the immune system and immunity decline further accelerates the aging process. Immune system protects the individuals against viruses and bacteria and it also helps identify and remove cancer cells and toxins. The potential for these elements to cause damage in the body increases as age advances. Critical cells in the immune system decrease in number and become less functional as people get older. COVID-19 affects seriously the aging people of the BAME community as in the case of general population, but they are more disadvantaged in terms of health care access.
d. Social Factors
Alongside these factors, many BAME individuals work in fields that carry a high risk of infection, such as healthcare, transport services and retail. In the UK, 40% of doctors, 20% of nurses and a large number of social care and unskilled migrant workers belong to BAME backgrounds. Another reason why these infections may become more prevalent among ethnic minorities is that BAME community members tend to spend more time indoors clustered together, often in cramped accommodations, which increases the likelihood of person-to-person transmission. A multigenerational family set-up is not helpful either to social distancing in a pandemic, so this lifestyle could contribute to higher infection rates. Some people living in this arrangement may also become stressed and obese due to unhealthy nourishment.
Migrant communities tend to visit and keep in contact with their country of origin, which involve international air travel and thus increased infection risk. Family studies demonstrate that BAME people living in the colder countries develop COVID-19 at a faster rate, but most of their family members living in the tropical climate in the countries of birth are spared from the infection. Such an observation point towards extrinsic factors like lifestyle and weather conditions rather than intrinsic genetic links-nurture than genetics. The second-generation immigrant population are less affected and the mixed-race individuals because of diversity of immune cells appear more resilient to the viral pandemic. There appears to exist an epidemiological trend of transmission concentrations within BAME communities living in colder countries, such a situation runs the risk of racial stigmatisation and discrimination and also risks to social cohesion.
BAME individuals should be cognizant of the additional risks and take preventive and precautionary measures. They should also adapt to balance their immunity. Enough sleep, healthy diet, moderate exercise, abstaining from excess alcohol and smoking and de-stressing are the cornerstones of enhancing immunity. Immunity is not absence of a specific disease or illness; rather, it is a balanced physiological and psychological state, the most sophisticated and elegant system of human physiology. Vaccines are pathogen-specific, and they do not bestow an overall balanced immunity.
Supporting Immunity
To defeat the tiger, one may need to become stronger than the tiger. To do this with COVID-19, we may need to foster our existing immune system, which can be done in many subtle ways. We all must grapple with the unprecedented threat posed by COVID-19, and frontline health workers must be mindful of their own immune systems when advising their patients to do the same. Unreasonable fear of COVID-19 only weakens the immune system, and fear attracts that which is feared. According to many COVID-19 survivors, remaining positive is a crucial factor in combatting this illness. Knowledge about the enemy and our potential resources lessens fears and helps us to plan strategies to defeat the adversary. With a quarter of the world’s population in the grip of COVID-19, it is a highly challenging period to learn to survive and strengthen our body and mind and enhance our immune system, even using the wisdom of unconventional medicines and faith traditions. We will have to battle with this invisible enemy until an effective vaccine is identified. Anything that fosters self-immunity should be encouraged in this time of a global medical emergency.
The two functions of immune system are defending the body’s health and maintaining health.The immune system is depicted as having two components: the innate and adaptive immune responses. The innate system is the more primitive and less specific. It is the body’s first line of defence against foreign substances that may lead to disease. The adaptive system, found only in vertebrates, is a much more specific, delayed response and requires sanction from the innate system to be instigated. Though considered separate, each interacts with the other in critical and complex manner. A basic understanding of both responses facilitates to clarify and further substantiate the significance of immune balance.
There are many myths surrounding immunity enhancement. Enrichment of the immune system is possible so that it becomes vigilant and active in the event of an invasion by pathogens and it may possibly prevent immunity anomalies. It is defending the defenders of the body. Immune system is our protective shield. Metaphorically, immune cells are the guardian angels of the body. Balancing of immunity can be achieved by focussing on ample sleep, healthy diet, moderate exercise, weight monitoring, restricting alcohol, free of smoking and destressing.In the nutshell, it warrants lifestyle changes- one size may not fit all and immune balancing has to be adjusted on an individual basis.
a. Restful Sleep
One healthy habit vital to preventing sickness is getting a full eight hours of sleep each night, which may help regulate immune function.19 Studies reveal that people who are deprived of quality sleep are more likely to get sick after being exposed to a virus. Respiratory infection has been linked to poor sleep.20 One study of over 22,000 people, for example, found that those who slept less than six hours per night or had a sleep disorder were more likely to suffer colds and other respiratory infections.21 Lack of sleep can affect immune system adversely.
During sleep, immune system releases cytokines, some of which even help promote sleep. Certain cytokines need to increase during an infection, or under stress. Sleep deprivation may decrease production of these protective cytokines. In addition, infection-fighting antibodies and cells are reduced during periods when person is deprived of ample sleep. Sleep and the circadian system are strong regulators of immunological processes.22 There is a bidirectional communication between CNS and immune system. This is mediated by shared signals though neurotransmitters, hormones and cytokines and direct innervations of the immune system by the autonomic nervous system. Differentiated immune cells with immediate effect or functions, like cytotoxic NK cells and terminally differentiated CTL, peak during the wake period. 23 These chemicals permit an efficient and fast combat of obtrusive antigens and reparation of tissue damage. The more slowly evolving adaptive immune response is initiated during nocturnal sleep and undifferentiated or less differentiated cells like naïve and central memory T cells peak during the night.
It is during sleep, the immune system heals, repairs, and prepares for the challenges of wakeful periods. During the deep stages of NREM sleep, the body repairs and recuperates, and this deep sleep also reinforces immunological memories of previous pathogens.23 The endocrine milieu during early sleep critically supports (a) the interaction between APC and T cells, as evidenced by an enhanced production of IL-12, (b) a shift of the Th1/Th2 cytokine balance towards Th1 cytokines and (c) an increase in Th cell proliferation and (d) probably also facilitates the migration of naïve T cells to lymph nodes.22 A feeling of lethargy when fighting an infection may be a signal from the body—which produces chemicals that act on the brain—to sleep, so that the body can recover. A single night of poor sleep can lead to a dramatic reduction in NK cells, the first line of defence against viruses and cancer cells, which negatively impacts other immune cells.
b. Nutrition
The size of the inoculum, the virulence of the exposure, the immune response of the host, and the health of the host are the four vulnerability factors of an infection. The former three ingredients are beyond the control of the host and the fourth one is within the control of the host and is very much based on the nutritional status. Food is generally viewed in terms of calories, but nutritionists have started appreciating the noncaloric micronutrients in the food, including those that are neither vitamins nor minerals, but phytochemicals (plant-chemicals) that strengthen and support normal immune function. The recent research discovery that food is not only a calorie supplier, but also adds to disease resistance and longevity benefits, has rekindled an interest in phytochemicals that support defensive and self-reparative functions. Modern diet consists of processed food mixed with additives, colouring agents, and preservatives; there is no room for unrefined vegetables in the dietary pie. Nutritional excellence can be achieved through green vegetations and friuts.
Antioxidants are vitamins, minerals and phytochemicals that support the clearance of free radicals and controlling its production in the body. Free radicals are molecules that contain an unpaired electron which causes them to be highly chemically reactive and these unstable molecules are destructive as they come in contact with structures and other molecules within the cells.24 Antioxidants are the natural enemy of free radicals which creates inflammation leading to dysfunctional immune system and to premature aging. Vitamin C, E, folate, selenium, and alpha and beta-carotene, as well as various other phytochemicals have antioxidant properties. They are available in plentiful amounts in vegetables and fruits and consumption of them enhances the immune functions. The Namboothiri caste of Kerala are famous for their strict vegetarian dietary habits and disease-free life, and longevity. The nutritional status of the host is critical in permitting or prophylaxis against viral and bacterial infections as well as the nutritional deficiencies in the host allow mutation of viruses into more lethal forms. 24 This is evident in the meat-eating food markets where the SARS-Cov-2 initially began to breed and mutate.
Pro-inflammatory foods can sabotage the immune system and should thus be checked in its quantity of consumption. Thirty minutes after they are consumed, carbohydrates may begin suppressing the immune system, and this effect may last for up to five hours. Foods with extreme diuretic properties also have detrimental effects on the immune system, which functions better when well hydrated. Drinking plenty of water facilitates efficient cell operation and allows the body to process food and eliminate waste. Following a diet rich in antioxidants is also essential to supporting the immune system, so eating fruits and vegetables is recommended. Fruits and vegetables are rich in antioxidants that combat free radicals—chemical by-products known to damage DNA and suppress the immune system.25 Choosing healthy fats—such as the omega-3 fatty acids found in oily fish, flaxseed and krill oil—over the saturated fats found in meat and dairy products is generally recommended by health authorities. These oils may help increase the body’s production of compounds involved in regulating immunity.26
Dietary supplements and medicines may be required for people who suffer from micronutrient deficiencies. Vitamin D is linked with a healthy immune system, and a large body of well-established data highlights its antiviral effects; it not only directly interferes with viral replication but also has immunomodulatory and anti-inflammatory effects.27-29 A research study in the U.S. suggests that having low levels of vitamin D doubles the risk of death due to heart attack compared to having higher levels.30 It is therefore recommended that all UK citizens take a vitamin D supplement between October and March to help maintain healthy levels during less sunny months. Such supplements are available in several forms, including capsules, sublingual sprays, and liquid drops, that are usually oil-based, as the vitamin is fat-soluble.
Nutritional excellence is in one’s own individual control. An over-boosted immune system, however, can lead to autoimmune reactions, so it is important to balance supplements and not over-boost. Moreover, vitamin D toxicity can cause hypercalcemia, which may lead to excess calcium deposits in the kidneys, lungs, or heart. A well-balanced diet is crucial in balancing immunity. An ideal immunity diet maintains caloric balance and consists of healthy fats, phytonutrients, fibre, quality carbs and diverse protein sources. Multiple micronutrients, including lutein, lycopene, folate, bioflavonoids, riboflavin, zinc, selenium, and many others have immune modulating functions.31 In general, the Mediterranean diet pattern has been praised as anti-inflammatory and good for fortifying immunity.32 The Mediterranean diet is associated with older age, as well as increased activity and reduced stress
c. Hygiene
Simply keeping the hands clean is one of the best ways to ward off illness, according to the Centres for Disease Control and Prevention (CDC). By washing the hands for 20 seconds using warm water and soap before preparing food or eating, as well as after coughing, sneezing, using the bathroom, or touching public surfaces can prevent the invasion of several pathogens. Hygiene hypothesis in medicine is quite often misinterpreted and misunderstood. It does not suggest that having more infections during childhood would be an overall benefit.
The hygiene hypothesis promulgates the view that early childhood exposure to particular microorganisms such as the gut flora and helminth parasites shields against allergic diseases by contributing to the maturation of the immune system. Lack of exposure is thought to lead to defects in the establishment of immune tolerance. The time period for exposure to microbes commences in utero and probably terminates at school age.
d. In Praise of Microbes and Nature
The preindustrial lifestyle that made available for the daily intake of trillions of friendly microbes is now replaced by a world of sanitisers and wet wipes. Alternative medicine takes into account the friendly bacterial flora inhabiting human body and we ought to be mindful of their role in balancing immunity. Even though humans are controlled by 25000 genes, the genes of the microbes cohabiting with ours are taken into account, it would be more than 3 million. In fact, these genes of the microbes are the immunity trainers and coaches of human immunological genes. Conventional medicine also takes into account the existence of intestinal microbes and their role in health and illness. Approximately, 95 percent of the total number of cells in the human body are constituted by these GI tract microflorae and play a prominent role in the health of our immune system. In fact, these guts bacterial flora is the meeting point of alternative medicine and modern medicine.33
The intestinal microflora serve several useful functions that may include the supplementation of the digestive process, produce vitamins, short-chain fatty acids, protect against the overgrowth of pathogenic bacteria and yeasts, strengthen immune abilities and generate beneficial nutrients that stop weight gain. 24 Pathogenic bacteria, on the other hand, produce toxic substances, become bacterial invaders, cause digestive disturbances, trigger immune system dysfunctions, and even stimulate weight gain.
Modern urban life is at a low level on microbial variety and has poor contact with helpful environmental microbes.34 Asthma and allergies are found to be much less among children brought up in farm and drunk farm milk.35 People living in urban areas are more susceptible to allergies and inflammatory diseases. Children exposed to outdoor microbes have more robust immunity. Obese people with 30% fewer intestinal microbes tend to gain more weight. 36
People should enjoy the smell of green grasses and appreciate the healing powers of mother nature. Ecopsychology, which is the study that explores the connection between the world of nature and the world of humans, is a new branch of psychology. Studies have revealed that spending some time outdoors, in the nature, can actually reduce stress, as well as improve our overall emotions and feelings of happiness and wellbeing, raise the levels of energy, and enhance immunity. It is healthier to do exercises outdoors than indoors. A lifestyle admirably adapted to mother nature alone can guarantee robust mental and physical health.
e. Antibiotic Overuse
Research findings suggest that antibiotic abuse can result in damage to the immune system, and memory problems caused by a lack of growth in new brain cells. Overusing antibiotics, which happens when antibiotics are overprescribed or prescribed inappropriately, has many negative outcomes. In the first place there is no relief of symptoms or rationale in prescribing antibiotics for a viral rather than bacterial infection. It results in disruption of the normal, healthy flora in the digestive system, which can take nearly two years to correct and lead to other infections. Antimicrobial resistance is another established complication of overprescribing antibiotics. Antibacterial adverse effects are attributed to 25% of all drug reactions in hospital patients.37
Even a single course of antibiotics has a detrimental effect on the gut flora and can result in harmful alterations in the composition and diversity of gut flora disrupting ecosystem. 38 Antibiotic exposure in children have long standing impact on the health and is linked with increased risk of immune system disorders. Antibiotic induced autoimmunity has been reported. Low levels of antibiotic administration lead to fatter mice by up to 40%.39
f. Physical Activity
To enjoy a good night sleep, one has to be pleasantly tired. Being active reduces stress and causes individuals to feel more energetic and alert, thereby helping the body prepare for better sleep. The main principle underlying exercise is keeping the body moving. Stress hormones are slowly released during exercise, which has a favourable effect on the immune system.40 Physical activity can also facilitate clearing of bacteria from the pulmonary system and can alter levels of white blood cells and antibodies. It is believed that during exercise, leucocytes and antibodies move faster in the circulatory system, allowing them to detect internal threats and diseases sooner; however, there is not yet proof that infections are prevented by these changes. Bacterial growth may also be blocked by the increased body temperature during and after exercise, which may help the body fight infection in a way similar to a fever.
Keeping muscles active releases high levels of interleukin 7 into the blood, which helps to stop the thymus from shrinking. This would help production of new T cells and balance our immunity. Maintaining a healthy basal metabolic rate is crucial. Walking is the simplest but highly effective exercise. Regular walks strengthen our immune system. It improves the mood and energizes the body. Walking in green spaces could give a big mood boost Walking has no set rules and can be carried out in the busiest cities and in the sprawling countryside. Too much of exercise can become a stressor for the body and turn out to be counterproductive.
g. Immunity and Obesity
Obesity is the result of a disruption of energy balance that leads to weight gain and metabolic disturbances that cause tissue stress and dysfunction. 41Metabolic syndrome is a cluster of metabolic disorders and is rampant in the 21st century. It results in conditions combining diabetes, hypertension, and obesity. Metabolic syndrome is also linked to several types of cancers and it has strong inflammatory underpinnings linked to dysregulated immunity.
Obesity and immunity are inversely related. It has been observed, for example, that the same amount of vaccine generates different immune responses from obese and lean people. Obesity has been identified as a modifiable risk factor of severe COVID-19, but weight loss also brings other health benefits. Having a healthy body weight is important in maintaining strong immunity because the presence of too many fat cells suppresses immunity. Obesity can depress the immune system by reducing the body’s ability to produce leucocytes, generate antibodies and locate infection sites. Persistently enlarged fat cells place a body in a constant state of inflammation, keeping the immune system permanently on the go. Maintaining the right amount of body fat is crucial to immunity and health.
h. Alcohol Impairs Immune Cells
Much remains unclear about the impact of alcohol consumption to immune system. Alcohol abuse result in diminished liver and pancreas functioning which can lead to immune system problems. Chronic alcohol abuse and pneumonia are linked. Alcohol has an immunosuppressant effect, and binge drinking is particularly detrimental. One study reports that after four shots of vodka within a 20-minute period, blood samples reveal initial ramping of the immune system followed by sluggish immune responses a few hours later. Acute and chronic alcohol use impedes cellular immune function, placing binge drinkers at greater risk for bacterial and viral infections. A multi-layered interaction between alcohol and immunity exists, and alcohol abuse has negative effects on both innate and adaptive immunity.42
Drinking alcohol immoderately can cause damage to the immune system in two ways. First, it reduces the availability of nutrients, thus depriving the body of resources that strengthen immunity. Second, it can hinder the ability of white blood cells to destroy microbes. It is well recognised that excessive alcohol consumption suppresses white blood cell replication, inhibits the action of killer white cells on cancer cells and hampers macrophages’ production of tumour necrosis factors. Immune system damage increases in proportion to the quantity of alcohol consumed. While wine promoters assert that one daily glass of red wine may be helpful to maintaining health, any amount of alcohol large enough to cause intoxication is also large enough to suppress immunity.
There is a perilous myth circulating among the inner quarters of the public that consuming high-strength alcohol can kill the COVID-19 virus and it has stemmed from fear and helplessness and is totally unfounded. Consuming any alcohol poses health risks, but consuming high-strength ethyl alcohol (ethanol), particularly if it has been adulterated with methanol, can result in severe health consequences, including death. Alcohol consumption is associated with a range of communicable and noncommunicable diseases and mental health disorders, which can make a person more vulnerable to COVID-19. In particular, alcohol compromises the body’s immune system as described above and increases the risk of harmful health effects. Though there is still limited data on the link between alcohol and COVID-19, past evidence shows alcohol consumption can worsen the outcomes from other respiratory illnesses by damaging the lungs and gut and impairing the cells responsible for immune function.
i. Avoiding Substance Use
Marijuana, cocaine, heroin, and other opiates are widely used illegal drugs. Drug abuse compromises immunity, so it is imperative to stay clear of illicit drugs during a pandemic. Numerous clinical reports indicate the association between infectious diseases and the use of illegal drugs. These drugs alter not only neurophysiological and pathophysiological responses but also immunity responses. Thus, it is vital to determine the mechanisms through which drugs compromise immune responses both independently and in concert with immunosuppressive viruses.43
Snorting cocaine harms mucous membranes in the nasopharynx and pulmonary areas. This increases the chance of upper respiratory infections.44Marijuana affects several kinds of cells in the body, which can ultimately harm the immune system. Smoking marijuana reduces the body’s ability to resist infections from viruses, bacteria, fungi, and protozoa. Because of the suppressed ability of the immune system, it may also reduce the ability of an immune system to be able to destroy cancer cells. Drugs of abuse include heroin, morphine, fentanyl, opium, and prescription painkillers. While all narcotics have some effect on the immune system, injecting drugs into the veins increases the risk of viral infections like HIV and hepatitis B or C (due to sharing needles) and bacterial or fungal infections. This is especially dangerous in people whose immune systems are already compromised. Crushing and snorting narcotic drugs can also increase the risk of upper respiratory infections due to damage to the mucous membranes in the nasopharyngeal regions. Morphine and related opioids have been found to directly impact white blood cells, which can reduce the ability of the immune system to react to diseases.45
j. Pulmonary Health
As with marijuana and crack cocaine, smoking cigarettes can lead to upper respiratory problems and a lowered immune system response to infections in the pulmonary system.46 Studies indicate that smoking increases the risk of more severe lung disease in cases of SARS-CoV-2 infection. It has been argued that exposure to cigarette smoke increased the number of infected and apoptotic cells in the airway and that SARS-CoV-2 prevented the usual repair response to airway injury.47 SARS-CoV-2, the causative agent of the COVID-19, infects cells by binding to the angiotensin-converting enzyme 2 (ACE2) receptor present on host cells. ACE2 is highly expressed in ciliated cells of the upper airways. Smoking is linked with both a negative progression and adverse outcomes of COVID-19.48
Smokers touch their lips frequently, which may accidentally pass the virus to their mouths, and they tend to have existing respiratory conditions consequent to their smoking habit. These factors make them more vulnerable to viral respiratory infections and more prone to COVID-19-related complications. Indeed, smoking has been linked to a plethora of respiratory diseases and poor disease prognosis.49 Smokers are more vulnerable to infectious diseases because smoking harms the immune system, adversely affecting how it responds to infections.50 During the previous MERS-CoV epidemic, for example, smokers were found to have high mortality rates.51 One retrospective analysis of 78 patients in China found that smoking was correlated with greater COVID-19 severity and poorer prognosis. Though analytical studies conflict,52 smoking continues to be linked with higher risk.53
k. Balancing Bodily Temperature
It has been recognised that an increase in body temperature by 1°C than normal would result in an instantaneous increase of immunity by 5 to 6 times. On the contrary, as soon as the body temperature drops, the activity of white blood cells will be retarded, resulting in a decrease in immunity. Low temperature is well recognised as immunosuppressive. It is an accepted fact that fever is the body’s defence mechanism that activates the immune system in response to inflammation. The immune system functions optimally at higher comfortable temperatures and becomes underactive in cold environments. This is why seasonal infectious diseases like influenza are more prevalent during lower temperatures. Warm temperature restricts viral replication through type I IFN-dependent and -independent mechanisms in vitro.54 In addition, both humidity and temperature affect the frequency of influenza virus transmission among guinea pigs.55 One way to warm the body is to be metabolically active while keeping a relatively high room temperature and/or wearing warm clothes. The significance of thermal balancing to maintain healthy immunity has been discussed in preceding paragraphs.
l. Destressing
Good relationships protect mental health and wellbeing. People who are more socially connected are happier, physically healthier and have longevity. One should put more time aside to connect with friends and family, learn to live in the present and switch out of work mode whenever possible. It is important to invest time on and value relationships and make them a priority, listen to others, and speak openly about feelings. People should be good listeners and concentrate on the needs of other people. Happiness is the reflection of what one does for others. People should make an effort to be surrounded by positive individuals and allow themselves to be listened and supported. The key to destressing and happiness is being honest and respecting others.
Severe anxiety suppresses the immune system and the coronavirus may thus literally feed on fear. Relaxing and focussing on the present, however, can improve mental health and counteract negative feelings. Various forms of meditation and progressive muscle relaxation techniques, for example, can help one unwind from the assault of daily stressors, and such post-work relaxation may enhance the immune system. Incorporating relaxing practices like meditation, yoga or deep breathing into a daily routine has been found to be helpful. Psychological health and immunity are causally related. The current pandemic is forcing us all to adjust to new and strange ways of life, which can adversely affect mental wellbeing.
While short-term exposure to stressors can accelerate immune defence, prolonged stress may wear down the immune system, increasing vulnerability to illness. 56 In this way, chronic stress can be a killer. Immuno-psychiatry is a fledgling sub-speciality which deals with the immunological components of psychosis and depression.57 The autoimmune aetiology of schizophrenia is gaining ground 58-60 and the neurotoxic effects of cytokine storm due to COVID-19 have recently caught high attention.
Extra-physiological Immunity?
The chemical effects of allopathic medicines are a scientific reality, but their therapeutic effects are also partially due to placebo effect. Placebos are aimed at the symptomatic relief of illnesses. Disease and illness have different connotations; disease is understood scientifically in terms of pathophysiology and illness is understood phenomenologically, as a lived experience. 61 It is increasingly being recognized that what we call the ‘placebo effect’ may involve changes in brain chemistry induced by quantum bioenergy fields. That implies the placebo effect may be a quantum reality that is created by the mobilisation of quantum bioenergy fields.62 The placebo effect is believed to be brought about when the subjective mind produces medicinal agents and accelerates the healing process. It is estimated that up to 40 per cent of the effects of medicinal drugs may be a placebo effect. The placebo effect often seems to be associated with measurable changes in brain chemistry and there have been observed quantifiable changes in neurotransmitters, hormones, and immune regulators. 63 Placebos also relate to the disposition to heal, no matter what treatment is offered, if those being treated believe the treatment is helpful. 64 Regarding the effects of drugs, expectations appear to have a significant influence. The very existence of placebos offers an indirect proof for the existence of extrasomatic energy system and we need to incorporate their effect in the immune balancing. A quantum conceptual model of placebo is essential to understand certain hidden channels of medical sciences. The placebo component of immunity is highly significant and needs further evaluation.
Immunity is not a single entity; it is a system, and for a system to function well, it requires balance and harmony. Not everything about the immune system is known to science, and according to integrated medicine, immunity may not be confined to physiology alone, but may have non-physiological aspects as well. Numerical age and physiological age are two different things. This is particularly so if extra-physiological energy system is brought into the equation of immunity. It is true that the existence of extra-physiological systems is not scientifically well established, but they are strong hypothetical possibilities.
Studies of quantum bioenergy fields should be an integral part of the science of human physiology and homeostasis should be redefined as the state of steady internal physical and chemical conditions maintained by different regulators, including extrasomatic energy fields.65 Humans are multidimensional or psycho-spiritual entities with several layers of energy bodies with increasing subtilty.66 Complementary medicines work on the assumption that humans are associated with a subtle energy system, in addition to their material body. Even though such extrasomatic energy systems are not recognised in the modern medical sciences, there are energy fields that cannot be explained by the classic Maxwell–Schrodinger equation.
The material body and energy bodies are in a complementary relationship: if the material body is the container, vital energy is the content.67 Beverly Rubik postulated that biological systems may be regarded as complex, non-linear, dynamic, self-organising systems of energy and field phenomena68,69 Many researchers have attempted to bring the existence of extrasomatic energy fields into the arena of mainstream sciences.70--73 If such quantum bioenergy fields really exist, they may play a major role in maintaining homeostasis in the human physiology, and it would be of great clinical interest to evaluate their role in immune system functionality, as long as they do not overrun the scientifically accepted views. To bring the concept of extra-physiological immunity into immunology, we may also have to accept the possibility of ‘nano immune cells’ and a ‘nano-level immune mechanism’.
Conclusion
The high incidence of complications among ethnic minority points toward the thermal conditioning and the role of immunogeneticsgenetics. Underactive immune responses in cooler temperature and diminished synthesis of vit D and the genetic factors linked with these anomalies might explain part of the higher incidence of COVID-19 among BAME. It is the physically and psychologically resilient people of a community who normally migrate to overseas countries. If migrants are to develop mental health problems, it would manifest within 6 months of migration, but physical health problems come about any time of their stay abroad as the weakening of immunity is a slow process. COVID-19 has a direct impact on co-existing disease processes worsening them because of the added immunity impairment. There are still missing gaps in the pervasive occurrence of this viral affliction among the BAME people. They should be mindful of the vulnerability factors and special precautionary measures should be adapted to prevent the infection.
COVID-19 appears to be a test of self-immunity. To combat COVID-19, efficient tests, novel treatments, and vaccines are the three means. An effective and safe vaccine would drastically change the pandemic situation for good. Vaccination and developing novel form of medication would take some time to become available. In such circumstances, one way of protecting from COVID-19 is by balancing one’s own immune mechanisms. It is a good thing that there is ample promotion of preventive measures of the contagion, there should be more awareness of improving personal immunity. More research works are warranted in immunology including extra-physiological immunity. Strengthening immunity is achievable for everybody if sufficient attention is paid. A safe and effective vaccine with long term immunological properties would drastically change the pandemic situation for good. Thus far, the research findings of the pandemic are inconsistent, and many dimensions of this pandemic warrant further clarification. COVID-19 will have a serious impact on virology and the neurotoxic effects of cytokine storm may be a stimulus for the growth of immuno-psychiatry.
Science is good enough to study the physical and visible, but it has obvious limitations when it comes to the unphysical and non-physical. Unphysical is undetectable only because they cannot be identified with the present-day instrumentation but can become detectable when our technology advances and their presence should not be stubbornly denied. The well-established placebo effects may point towards the existence of quantum bioenergy fields. Existence of extrasomatic energy system indirectly support the concept of extra-physiological immunity. Placebo effects are not psychological artefacts, but quantum manifestations. If extra-physiological immunity exists, it may be guarding and supervising the physiological immune system.
The way a doctor dresses is a fundamental part of establishing therapeutic alliance with patients.1,2 It has been shown that doctor’s dress can influence patient confidence, offer greater reassurance, higher levels of trust, better adherence to prescribed medication regimens, enhanced willingness to complete return visits, and discuss sensitive issues.3,4 The literature outcomes in this field are mixed; for example, some studies suggest a non-correlation with perceived courteousness or professionalism,5,6 but we believe there is enough evidence to suggest that the manner in which a doctor dresses forms an important part of non-verbal communication, which is important for their interaction with patients, carers and with other staff members.
Various studies have examined patient preferences towards doctors’ dress. Formal dress or a white coat have been cited as favoured due to their perceived association with empathy, competence and trust.2,4,7,8 This is in contrast to other studies which found semiformal dress as preferred.9
In psychiatry, studies of inpatients have indicated a preference for smart attire and white coats as part of their doctors' dress code.10,11 Mcguire et al also found that community patients preferred their psychiatrists to be dressed as “smart/formal”.12
In recent years, dress code policy for doctors in the UK has become more informal, and white coats have been abolished for a number of reasons.13 In this study, we sought to determine the attitudes of multiple stakeholders towards doctors’ dress in both general and psychiatric hospital settings.
Methods
We surveyed healthcare staff, patients, and carers in an emergency department at a district general hospital (“medical setting”), and in a psychiatric hospital (“psychiatric setting”) in the South East of England. The data was collected on a week day between 09.00 and 17.00 at both settings, using a questionnaire based on Rehman et al.14 There were no exclusion criteria.
The survey questionnaire sampled demographic details, and used nine questions and two sets of images (a male doctor & a female doctor) depicting three styles of dress; white coat, formal (tie & trousers for male; dark skirt and white shirt for female) and smart casual (“bare below the elbows”). The survey questionnaire was piloted amongst volunteer staff and assessed for their user-friendliness and ease of comprehension before use. It was amended in line with the feedback received.
Results
337 individuals responded to the questionnaire, giving a response rate of 94%. Our sample was predominantly white (72%), female (62%) and married (43%). Respondent age, ethnicity and employment status were broadly representative of the local population.
Overall (Table 1), we found that the majority of respondents felt that the way that doctors dress was important to them, and that the location of respondents significantly affected their preferences (p <0.001). Although in these overall results there was no majority preference for one dress code over another in either location, preferences within each varied significantly (medical: p<0.01 and psychiatric: p<0.001). This numerical preference appeared to be for formal dress in both settings, capturing 35% and 45% of respondent vote respectively.
Within the three stakeholder-specific breakdowns (Tables 2-4), differences in preference reached significance for medical staff (p<0.001), psychiatric staff (p<0.001), psychiatric patients (p<0.05), and psychiatric carers (p<0.01). Like the overall results, there was no majority preference in any of these groups, but formal dress captured the highest numerical vote in medical staff (41%), psychiatric staff (55%), and in psychiatric patients (41%). Psychiatric carers preferred formal and smart casual dress broadly equally, which captured 36% and 40% of the vote respectively. Carers were the only stakeholder whose preferences were significantly influenced by their location (p< 0.01).
Dress code statistically significantly influenced the attributes associated with the doctor wearing them (p< 0.0001), as shown in Table 5. Formal dress captured the greatest proportion of every attribute tested, and considering total responses, formally dressed doctors were almost twice as likely to be associated with these attributes as those dressed in smart causal or a white coat.
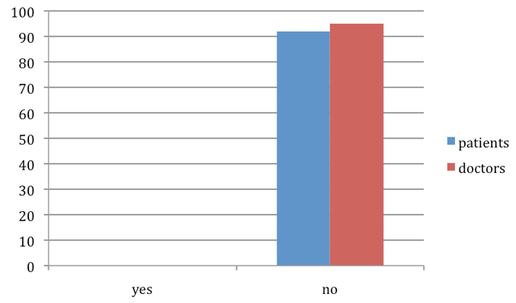
52% of respondents were not aware that a doctors’ dress code policy existed, and while 53% of respondents felt they should not be consulted when considering dress code, 41% believed they should. 59% of respondents believed doctors adhered to their sites’ dress code policies, while 27% did not think so.
Discussion
To our knowledge, this is the first study in the world to compare preferences in doctors’ dress code between a psychiatric hospital and a medical hospital. Also, no other study to our knowledge has simultaneously explored the attitudes of different key stakeholders in both medical and psychiatric settings regarding this important issue.
In this study, we have successfully captured the attitudes and perceptions of key stakeholders regarding doctors’ dress code. We found that overall, doctors’ dress code was felt to be important, and that in medical and psychiatric locations a formal dress code is preferred. Looking at staff, patients and carers specifically, we found a preference for formal dress among medical staff, psychiatric staff, and in psychiatric patients. Among psychiatric carers, formal dress was preferred equally to smart casual. There were no significant preferences among the other stakeholders surveyed.
This preference for formal dress is easily explained by the results shown in Table 5. Seeing a doctor in formal dress made it almost twice as likely that that doctor would be seen as possessing any of the eight positive attributes included. Clearly, in the eyes of the respondents to our survey, a formally dressed doctor was most likely to provide good care.
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
42
40
59
26
167
<0.01
-
Psychiatric
57
18
76
19
170
<0.001
-
Total
99
58
135
45
337
-
<0.001
Table 1. Dress code preferences among all stakeholders. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
22
10
27
7
66
<0.001
-
Psychiatric
22
4
35
3
64
<0.001
-
Total
44
14
62
10
130
-
NS
Table 2. Dress code preferences among staff. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
14
14
15
10
53
NS
-
Psychiatric
16
9
24
10
59
<0.05
-
Total
30
23
39
20
112
-
NS
Table 3. Dress code preferences among patients. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Location
Dress code preference
Total
Within-group p value
Between-group p value
Smart casual
White coat
Formal
No preference
Medical
6
16
17
9
48
NS
-
Psychiatric
19
5
17
6
47
<0.01
-
Total
25
21
34
15
95
-
<0.01
Table 4. Dress code preferences among carers. P values were calculated using Chi-squared test. NS = not significant (p=>0.05).
Dress code
Associated doctor attribute
Total
Trust
Advice
Conf.
Return
Knowl.
Caring
Resp.
Auth.
Smart casual
77
57
59
74
49
109
51
38
514
White coat
74
91
89
77
107
65
87
103
693
Formal
142
138
142
134
132
110
143
145
1086
Table 5. Doctor attributes associated with different dress codes.Respondents were shown images of each dress code asked “Which doctor would you…”: Trust the most (trust), Follow the advice of (advice), Have confidence in their diagnosis and treatment (conf.), Return to for follow-up care (return), Regard as knowledgeable & competent (knowl.), Regard as caring & compassionate (caring), Regard as responsible (resp.), Regard as authoritative & in control (auth.). P <0.0001.(calculated using Chi-squared test). Results were excluded for where more than one dress code was selected for an attribute, or where no choice was made.
Discussion (continued)
Interestingly, we also found that the location of healthcare influenced the preferences of carers to such an extent that it offset the non-significant results among staff and patients; such that this significance was carried through to the overall results. Exploring this in more detail, we see a marked preference for smart casual in the psychiatric setting over the medical setting (40% vs. 13%), for a white coat in the medical setting over the psychiatric setting (33% vs. 11%), and an almost equal preference for formal dress in both. This starkness in difference in preference between care locations indicates differences in the cultural perceptions of doctors by carers, but not by staff or patients. Perhaps an explanation for this difference is that historically, carers have been more involved and influential in the psychiatric setting, being an essential component to care, whereas in the medical setting they have tended to be more passive partners in care. A negative perception of mental health care portrayed to the public through film and media may have driven preferences away from white coat in the psychiatric setting, whereas in the medical setting perhaps a positive association with the white coat and physical health may have done the opposite.
Conclusion
We have identified a clear preference for a formal dress code for doctors from all stakeholders at medical and psychiatric care locations studied. However, we identified several interesting variations in preferences among individual stakeholders, and found that the location of care significantly impacted the preferences of carers. We believe these findings could be harnessed in the future development of dress code policies for doctors in order to enhance the doctor-patient relationship, and to improve the quality of doctors’ relationships with both carers and with other staff members. Additionally, there may be merit in involving these stakeholders during the policy development process.
In a contemporary medical practice caring for complex patients with utmost efficiency, primary care physicians and specialists are expected to work together to organize a seamless transfer from acute to chronic care. The job of the generalist is to sort out and integrate different recommendations from numerous specialists and apply those strategies in the care of the patient long after the index admission. During such interactions with specialists, primary care physicians often realize the impact of differing viewpoints on the overall patient care well beyond the anticipated time frame, whether acute or chronic. To that end, and to better inform such recommendations, this paper proposes the top 10 things primary care physicians wish every specialist knew when addressing problems on the busy hospital ward.
1. Organ-systems work together, not independently
As we see in examples such as the cardio-renal syndrome, hepato-renal syndrome, or hepato-pulmonary syndrome, as the patient gets sicker, the interaction of organ-systems begins to dominate. Indeed, predicting the outcome in comorbid conditions depends not only on understanding the culprit organ, but rather quantifying a complicated interaction of multiple organ-systems. For example, the ADHERE registry algorithm shows the most important predictor for in-hospital death in heart failure patients is not the cardiac function per se, but rather creatinine clearance and BUN[1]. In other words, the commonly used comments from a specialist asked to evaluate their system of expertise, ‘such and such organ is fine’, might soon become irrelevant and obsolete in the context of multiple complex systems.
Moreover, recent research revealed that genotype, endotype and phenotype are quite different in COPD and asthma[2]. Therefore, even though a disease may manifest in a single system, the pathophysiological process from which it arose may have been triggered in different organs.
2. Mortality is not the only outcome measure
Specialists seem to treat all-cause mortality as the most important outcome measure in most cases. Or, they choose strategies based on organ specific survival as an alternative, such as MACE (major adverse cardiac events) or creatinine-doubling time[3]. Life is far more than just being alive. Subsequently, the quality of life (QOL) measures, which capture patient-centred outcomes, provide insight into the effectiveness of interventions but also their meaningfulness to patients, and such measures are gauging previously uncaptured positive aspects of interventions[4]. The difficulty of defining well-being remains a challenge for researchers and arises from the differences brought about by cultural and societal elements which are context-bound and unique to each community.
3. ADL is one of the most critical prognostic indicators
New biological markers are numerous around here - new renal injury markers, such as NGAL or KIM, to name a few. But a quick, old-fashioned, bedside assessment can easily reveal impairments in Activities of Daily Living (ADL) at each patient visit; and ADLs by Functional Assessment Measures have been consistently shown as strong outcome predictors in acute and chronic illnesses, especially within elderly populations[5]. In fact, functional measures were deemed to be as important as other objective measures in some prognoses[6]; for instance, in the BODE score for COPD survival prediction, the ADL measure carries the same weight as the PFT (Pulmonary Function Test). In the management of elderly patients, hospitalization[7] and initiation of haemodialysis[8] significantly influence the worsening of ADLs. In the development of a 1-year mortality index after hospital admissions among elderly patients, ADL was of pivotal importance[9].
Functional impairment is also a strong indicator for readmission: there is a dose-response correlation of severity of impairment and the risk of readmissions[10]. Intensifying the in-hospital post-ICU physical and nutritional therapy has been shown to improve many aspects of recovery[11]. In patients with numerous chronic illnesses, the number of comorbidities strongly correlates with the decline of ADL[12]. Interventions to maintain pre-hospitalization ADL is important in facilitating recovery from hospitalization, and in one study in-hospital mobility programs helped patients to maintain pre-hospitalization ADL while the usual care group experienced significant decline[13].
4. Effectiveness, not efficacy, matters most in the real-world
“Doctor, I cannot afford the medicine prescribed to me when I was discharged!” This is oft-repeated in offices of generalist physicians. If a patient cannot afford medication and therefore does not take it, the treatment lacks efficacy. In the inpatient setting, efficacy of intervention determines the outcome since patients are most likely to receive the prescribed intervention. This is not the case in the outpatient setting, and the effectiveness of an intervention depends on many other elements, such as the accuracy of diagnosis, patient compliance to the proven intervention, prescription drug coverage, access to care, and finally, efficacy of the intervention[14].
5. Mental wellness is essential to physical wellness
Health is not limited to the physical body; it also involves mental wellness. In fact, mental and physical health are inseparable. Naturally, serious illnesses affect mood and cognition: therefore, it is important to acknowledge that mental health issues lie squarely within the spectrum of physical disease management. Generalists can help patients with multiple comorbidities manage depressive symptoms through brief psychological interventions; such symptoms related to cognition and mood are expected consequences of any serious illnesses.
Studies have shown that among elderly patients without dementia at baseline, noncritical hospitalization is associated with the development of cognitive dysfunction[15]. Among elderly patients, the prevalence of cognitive dysfunction is significantly higher in ADHF (acute decompensated heart failure) admissions[16] or survivors of severe sepsis[17]. Depression and depressed mood are prevalent in patients suffering serious illnesses[18]. New models are emerging to integrate psychotherapy in multiple comorbid patients and have been proven to be effective[19].
6. Pay heed to illness trajectory
“My grandma has never been the same after her hip surgery. Please fix her!”
Primary care physicians often note a decline in the general function and cognition of their patients after index admissions to the hospital. As noted earlier, acute hospital admissions have a strong independent effect on the severity of disability amongst elderly persons[20]. The multidimensional frailty score, which incorporates ADL and cognitive function, predicts one-year mortality based on a simple scoring system[21]. Poor functional status attributes to frailty and has led to poor surgical outcomes in the elderly[22]. The prevalence of functional impairment steadily increases from 28% in the 2 years prior to death to 56% in the last month of life[23]. Studies demonstrate that gait speed is an important predictor for survival amongst the elderly[24][25] as well as grip strength[26][27].
Furthermore, elderly patients sustain significant impairments long after the index hospitalization[28]. Amongst elderly patients discharged from the ICU, more than 50% die within a month[29]. At one-year follow-up, critical ADL capacity, such as taking medications or shopping, was impaired in more than 70% of ICU survivors who remained ventilated for longer than 48 hours[30]. Delirium sustains a long-lasting effect even after patients are discharged from the hospital, the longer the duration of delirium, the more sustained is the cognitive impairment[31].
7. Care for the care-givers
There is increasing evidence that caregivers sustain long lasting effects from patient illnesses. Depressive symptoms increase overall for surviving spouses regardless of hospice use[32]. The RECOVER study[33] demonstrated that caregivers suffered from high levels of depressive symptoms up to 1 year after a loved one’s ICU admission. In the era of chronic illnesses, it is essential to be mindful of the contributions made by caregivers in disease management. Tools are widely available for the clinician to assess caregiver burden[34]. This is important because family-support interventions have been shown to improve the quality of communication and decrease the patient’s length of stay in ICU[35].
8. ‘Exercise and diet’ trumps ‘medicine and surgery’
The COURAGE trial demonstrated that after 7 years, there is no difference between medical management and percutaneous intervention (PCI) in managing coronary disease[36]. As time progresses after the initial event, the benefits of surgical intervention become less apparent. Similarly, in the long run, intensive statin therapy has not proven to be of greater clinical significance compared to those receiving moderate levels of statin[37]. As the saying goes, in the long run, “we are what we eat.” Innumerable studies have shown that diet and physical habits have a lasting effect on the health of individuals[38]. Bariatric surgery has been demonstrating dramatic and long-lasting effects on diabetes control, while the DiRECT study demonstrated that intensive exercise and diet successfully achieved remission in nearly half of the intervention group, compared to only 4% of controls[39]. Despite the substantial increase in chronic illnesses that are closely tied to our lifestyle and eating habits, physicians of all specialties are poorly trained to provide nutritional counselling to patients[40].
9. Whose definition of health matters?
If health is defined, as defined by the WHO, is not simply the lack of illness, but “a state of complete physical, mental and social well-being,” it must incorporate many other elements dictated by societal, cultural, moral and philosophical norms and values. Furthermore, the definition of health and the path to attain it should come from the society and community it reflects, since neither healthcare personnel nor the healthcare industry own health. Therefore, the definition should emerge from community interventions and multidisciplinary groups filled with varied stakeholders, rather than from the ivory tower of healthcare researchers. Therefore, medical decision-making processes are rapidly moving away from the paternalistic approach to consensus-based, collegial decisions. Shared decision-making, informed consent, discussions of different treatment options and acquiring second opinions have become standard practice and reflect the empowerment of patients, and communities, to define their own healthcare. Ultimately, as long as patients are competent, they decide their treatment after consulting with physicians, who advocate for the patients’ goals in care and advise them accordingly.
10. Empower healthcare recipients
In the long-term management of chronic illness, participation of the patient is essential. And transparent communication is pivotal for better participation and shared decision-making[41]. In the new model of health, healthcare providers must play an active role in advocating for patients and promoting well-being while acknowledging that health is a dynamic concept[42]; these physicians do not simply “coordinate care.” This shift from the physician-centred to the patient-centred approach, in and of itself, will be empowering for patients.
CONCLUSION
Transition of care is one of the most important steps connecting hospital care to primary care. Those problems currently labelled as miscommunication might be more than just a lack of handoff tools or timely messaging; they rather stem from a difference in priorities and varied interpretations of patients’ problems by these two groups of providers. Many questions remain unanswered when facing the future of collaborative healthcare: what kind of doctors are most suited to address the complex interaction of illnesses involving multiple organs? Who can develop a new framework to capture this dynamic and complex interaction of systems, covering many organs in a single patient? Moreover, the next generation of healthcare providers will need to be trained to bear in mind this fundamental concept of patient management. As the twenty-first century progresses, discoveries within medical science will continue to advance the field further away from the current organ-based specialization to pathophysiology-based specialization. This article advances the discussion on the altering role of generalist physicians and the advice of their specialist colleagues, as together they face more and more changes within the practice of medicine.
Medical scientists who espouse a strict biological model of the mind tend to care less about the prolongation of life than do those who have faith in higher authority.1 The prevailing reductionist model of mind has recently been challenged effectively.2,3,4,5. That has led to a position in which there is some justification for claiming that there is scientific evidence to enable a suspension of disbelief in life after death. 6 Medical profession should respect the theology veiled in thanatology and should be careful not to become instrumental in creating a culture of death; alleviating suffering is not by eliminating the patient.
In the absence of spiritual conviction, human suffering lacks deep meaning and death is regarded as the ultimate tranquilliser. Prolonging life at any cost may be perceived as a worthless endeavour. To counter that, without suffering evolution would not take place and human consciousness would fail to expand. Without stress and struggle the spirit buds to which we may be likened would not mature and grow leaves and fruit, and our characters would not develop; we would lead the lives of lotus-eating sybarites. 7
Evidence for discarnate survival
According to those who are sceptical about after-death survival, there is only as much evidence to justify belief in life after death as there is for the historical existence of dinosaurs. Some scientific researchers however argue that there are compelling reasons to support those who are proponents of belief in life after death. Dr Vernon Neppe, a neuropsychiatrist turned parapsychologist, has declared that the combined body of evidence for discarnate survival is overwhelming – so great that it may be regarded as scientifically cogent.8 This emerging scientific view, coupled with the wisdom of the faith traditions, challenges the rationality of supporting assisted suicide. The following are examples of evidence for discarnate existence that are commonly cited:
clinical death experiences
pre-death visions
shared death experiences
collective apparitions
some forms of mediumistic incidents, particularly ones that involve cross-correspondence, drop-in communications and physical phenomena
children’s memories of previous lives
electronic voice phenomena
instrumental trans-communications
transplant cases
Scientifically studied Marian apparitions
The list is becoming longer as survival research progresses. Encouraged by the success of afterlife experiments with mediums,9 the multi-specialist professor Gary Schwartz of Arizona University claims to have invented a device to communicate with discarnate spirits; the holy grail of survival research that could possibly offer a fool proof scientific evidence of afterlife existence,10 but also takes account of all the potential negative consequences. He claims to have worked with black boxes in his laboratory, using a software programme that has generated proof that there is a spirit world by measuring light. 11It appears that he has developed a technique whereby faint light can be detected in a totally dark box. Measurements are taken at the beginning of an experimental session, and then a specific “hypothesized spirit collaborator” is asked to show a “spirit light” in the box and a second reading is taken. The finding is that instruction for specific spirits to enter a light sensing system was associated with reliable increase in the apparent measurement of photons. Such a curious result means that these communicating spirits are able to hear, respond and produce light in an otherwise dark enclosure. 12,13 The conclusion is that survival research opens up new vistas which seem much more important than cosmology or quantum electrodynamics.
Scientifically examined Marian apparitions are a recent addition to the evidences for discarnate existence. 14 Mainstream scientists seem never to have attempted to develop the conceptual tools and vocabulary needed to investigate the possibility of post-mortem existence. It may be that science will not accept the possibility of discarnate survival without a new theory of physical reality. In the early part of the twentieth century the prevailing view of scientists was that there was no possibility whatsoever of proving the existence of life after death. Over the years that have passed since then attitudes have evolved, and in the world, we are now in it is asserted by some researchers that there is scientific evidence for the existence of life after death. Some of the evidence relating to discarnate existence may not however satisfy the criteria of the physical sciences since the latter are based on speculative science and court room logic.
Paradigmatic shift
Demonstrating post-mortem existence as an irrefutable phenomenon is a route to establishing empirically that humans have a higher consciousness. Unfortunately, in survival research there are many phenomena that have multiple possible explanations, and these augments add to the complexity of this immensely significant area of scientific enquiry. All the types of evidence postulated as supporting discarnate survival are simultaneously a form of evidence of a non-biological component that operates in association with the brain. The existence of a non-biological component indirectly proves the possibility of survival after physical extinction. A huge paradigmatic shift towards non-reductionism is now taking place in the cognitive sciences – consciousness is no longer considered an epiphenomenon of brain activity, but asthe designer and prime mover of the material body. Nowadays, some mainstream scientists are themselves paradoxically trying to debunk mainstream science.
Suicide victims
Through suicide, a person is simply changing the location of their suffering. While wrapped in the physical planet by space and time, we are in an advantageous position for inducing personality changes swiftly, whereas in the timeless state of discarnate existence changes are sluggish and personality development is much slower. Contemporary data for survival research may be congruent with the wisdom of the faith tradition. 15 To use a simple analogy for this, carrying out assisted suicide is like destroying the shell of a pupa and forcefully freeing it in a premature state. Such a pupa will not be able to fly about like a butterfly. It is arguable that a person subjected to violent death – as in the case of suicide – may not be able to enjoy the beauty of God’s grand other-worldly dimensions until they have become spiritually compatible with them. They have to navigate through the physical plane like wingless birds. 10 To look at this way, if fruit that is unripe drops from a tree, it will be sour. Suicide breaks a solemn law because it deprives the conscious self of the natural growth that life in a physical body can best provide.7The Chinese saying “One day of earthly existence is not equivalent to a thousand days of ghostly existence” is a statement of the sanctity of terrestrial life.
Lord Alton has campaigned against the Assisted Suicide Bill of 2014 since its inception. Referring to his dying father’s account of how he had seen his own brother, a member of the Royal Air Force who had died in the Second World War, Lord Alton argued that a forced death, as opposed to a natural one, may deprive a person of their “healing moment.” 16 A graceful and natural death may be supposed to be accompanied by benign caretaker spirits with exuberant love who assist those who are dying by making them comfortable for the big transition.17,18 A person who terminates their own life prematurely may not be so fortunate as to get such benevolent assistance from the spiritual realm. Most hospice workers are very familiar with departing and death-bed visions such as that described by Lord Alton. Furthermore, it has been suggested that beings from the imperceptible spiritual sphere who assist in delivery from the terrestrial plane have a role in such matters as the timing of death, and it is arguable that their part in what happens should not be impeded by intervention.
It appears that human brain is designed to have some doubts about discarnate survival for some reason and a fool proof evidence of post-mortem existence may have its down side in that somebody who is fed up of life might use it to justify ending his earthly life voluntarily. 19An ultra-optimistic view of discarnate life is spiritually counterproductive and such an over optimism could be seen as a justification by the patient and carers in the decision making of assisted suicide. In a weak moment of extreme psychological or physical sufferings, such a belief can also become the final rationalization for ending one’s own life voluntarily. In my own clinical practice, I have come across suicidal patients telling me, “It will be always better on the other suicide.” A belief in discarnate existence based on parapsychological proof alone did not deter one such patient making a serious suicidal attempt
End-of-life concerns
The evening of life was considered as a great opportunity for spiritual, emotional and psychological growth and a celebration of one’s life journey. These are also times to harvest the wisdom of yesteryears and share them with the succeeding generation. Spiritually enlightened people consider this to be the time to conquer the fear of death. Fear of death is not the fear of the physical pain of death, but the fear of truthful self-judgement after death. Recent observations in thanatology favour a belief in post-mortem self-assessment and appraisal. For some, it would be voluntary or assisted, whereas for others it could turn out to be forced upon them. The final phase of life is the time to settle the errors committed against fellow beings that have not been remedied in life. Fortunately, modern medicine has prolonged this period, which grants an opportunity for most people to experience conscious ageing. Sadly, traditional attitudes towards the evening of life have changed in today’s youth-obsessed culture. For some, medical procedures have extended life and made dying a lingering process rather than a sudden event, and have contributed their own problems. For several reasons, terminally ill people who are in crisis may wish to die rather than being kept alive longer (Table 1).
From an evolutionary point of view, there can be only a survival instinct – no Freudian death instinct. Avoiding death rather than seeking it is a natural human urge and the fear of death may affect every individual action. The very concept of euthanasia is totally against the human make-up and is entirely artificial. Assisted dying and assisted suicide are the same thing when a member of the medical professional gives a lethal drug to a person so that they can take their own life. Euthanasia is different; it happens when, for example, someone injects a lethal substance into a patient. Involuntary euthanasia refers to a situation in which the patient has the capacity to give consent, but has not done so; and in non-involuntary euthanasia a person is unable to give consent, for example because of dementia or being in a coma. Mercy killing is claimed to be a compassionate act to end the life of a patient.
Table 1: End of Life Concerns
Losing autonomy
Less able to engage in activities making life enjoyable
Loss of dignity
Burden on family, friends/caregivers
Losing control of bodily functions
Inadequate pain control or concern about it
Financial implications of treatment
Moral and ethical issues
It has been observed that the risk of suicide is higher among people with a family history of suicide. Family culture and genetics may account for the increased incidence of suicide in such situations. Assisted suicide would create a trail in the culture of more families and more succeeding generations would perhaps be at increased risk of considering suicide as a serious option at a time of crisis. Kevil Yull (2013) comments that changes in the law of assisted suicide would have an additional impact on those left behind, because of their effect on the moral connections, assumptions and accepted responses to situations on which we base our relationships with fellow human beings and establish ourselves in the world. 20 He argues that the legalisation of assisted suicide would undermine freedom instead of promoting freedom of choice, and also that the proposed safeguards and regulations would breach the privacy of the death-bed.
Assisting someone to kill themselves is assisting them in murder. According to all the major faith traditions, life is a gift from God and ending it is like throwing a precious object back to the giver. All spiritual traditions teach and believe that bringing the human heart to a standstill is God's business (Table 2). There are patients who assert that even if all their limbs were amputated, they would still want to hold on to the treasured gift of life. It is very difficult to define what unbearable suffering is; extreme suffering is a subjective matter that it is not possible to separate from an individual’s outlook on life. A fundamental question is that of who would be the one to pronounce a verdict on when suffering is intolerable – the patient or medical personnel?
Laws are not precision-guided arrows and they may become perverted. In a world full of violence and crime, assisted suicide is unsafe and could be exploited. There would be many unintended consequences. For reasons of public safety alone, some people oppose assisted dying. Financial abuse by relatives of the elderly seems to be becoming more common; those with a vested interest could be tempted to put an inheritance before life.
The regulation of assisted dying has been modified in recent times in some countries, an example being the Netherlands in 2014. There it is now lawful to kill a patient without their consent, and euthanasia and assisted suicide may be offered to people with mental health problems (consensus with the family is required in all these situations). Inboth Belgium and the Netherlands the euthanasia of children is legal with family consent (in Belgium there is no age limit; in the Netherlands the child must be 12 or above and must give consent). In Belgium blind adults who were developing further problems were granted euthanasia at their own instigation a few years ago. There is public concern about collaboration between euthanasia teams and transplant surgeons in Belgium.
Table 2: Medical dilemmas
Assisted suicide promotes a human right to commit suicide and gives wrong messages to suicidal patients in psychiatry.
It undermines the Universal Declaration of Human rights and strikes at the foundations of all spiritual values.
It is hard to define unbearable sufferings.
Assisted suicide has many unintended consequences.
Death with dignity could deteriorate as death with indignity.
It might permit the unlawful killing of innocent people in certain circumstances.
It is founded on unethical principles-survival of the fittest.
In 2013, 1.7% of all deaths in Belgium were hastened without the explicit request of the patients. 21 Professor Cohen Almagor, the author of 2015 report on euthanasia in Belgium stated that the decision as to which is no longer worth-living is not in the hands of the patient but in the hands of the medical personal. 22 More than 500 people in the Netherlands are subjected to euthanasia without their consent.23 Data from Oregon where assisted suicide was legalised in 1977 shows that the top five reasons people choose assisted suicide are not because they are suffering from a terminal illness and 49% stated that feeling like a burden and a fear of loss of control are among the main reasons for choosing assisted suicide Oregon .24 In Washington state in 2013, 61% of people who were killed in assisted dying said that being a burden was a key factor for their choice of death. 25
Medical Dilemmas
Majority of British medical practitioners are against assisted suicide. 26 A 2013 survey showed that 77% hold the view that they would oppose a change in the current law to allow assisted dying, 18% favoured the RCGP moving to a neutral position, and only 5% favoured a change in the current law. They opined that a change in the law would make patients afraid of their doctor and would alter doctor –patient relationship, and would make vulnerable patients most at risk from assisted dying. According to Marris bill, some people should be given help to die meaning that some lives are worth less than others. Vulnerable people would feel pressurised to choose death and could be killed without their explicit consent. GPs feel that it is their privilege to protect the disadvantaged and vulnerable people of the society.
Assisted dying would lead to less focus on investment in palliative care. The RCGPs also cautioned in the survey that a change in the position of the law makers would become like abortion legislation, which started as something for extreme circumstances and is now effectively on demand. They are also anxious for the fact that legalisation of assisted dying would make it impossible to tell the real reason why patients decided to die, because illness can cause people to become depressed and frightened. As debate on assisted suicide has become hotter, in clinical practice suicidal patients have already started enquiring about the prospects of assisted death.
Thanatology
Medical sciences have not advanced enough in matters of death to offer details to make informed choice for those who want to die voluntarily and thanatology is only a fledgling science. Thanatology is the scientific study of death and investigates the mechanisms and forensic aspects of death, such as bodily changes that accompany death and the post-mortem period, as well as wider psychological, parapsychological and social aspects related to death. They are not particularly interested in the meaning of life and related philosophical issues, but this is an area where science and philosophy not be separate. In recent years, studies of parting visions by Elizabeth Kubler Ross and Raymond Moody’s NDE studies. 27,28,29,30,31,32 have given a spiritual dimension to thanatology. Theology and Thanatology are two major corpuses of human wisdom that cannot but overlap. Assisted dying would probably become also an issue of forensic sciences.
It is the job of the doctor to keep the patient alive whereas it is the job of the psychotherapist to have a sense of a bigger picture. 33 People wanting to hasten death should also have the choice of receiving pastoral and psychotherapeutic assistances to distract themselves from their preoccupations of death and allow nature take its own natural course. New generation psychotherapists will have to be well versed in all aspects of death related sciences. Thanatology has a rightful place in medical studies, but I content that medical professionals need not to be unduly concerned about the different forms of afterlife existences, the borderland between religion and thanatology. Medical professionals are expected to be above religion and politics. Thanatologists now fear that if assisted suicide is legalised, they might be pressurised to slip from the original goal of acquiring more knowledge of human dying to serve the dying into the pursuit of death.
Concluding Remarks
Assisted suicide or euthanasia is incongruous with the theological view that it is the weakest and the vulnerable who can teach us the values of life and the concepts of euthanasia or assisted suicide have an indirect message of discarding them. The right to die would soon deteriorate as duty to die to prepare room for fittest ones. Instead of looking for reasons to live, people will be looking for reasons to die. What is need is better understanding of death process and advancements in the palliative care of the terminally ill, rather than doing away with them. Until we know more about the death process, assisted dying debate should be kept on hold. More research in palliative care and allowing people to die naturally with dignity should be the concern of medical profession.
Evolution may be taking place in biological and spiritual streams and they are interconnected: biological sufferings maybe aiding spiritual evolution. 34. From a philosophical perspective, the rationale of terminal sufferings is to help the individual to disengage from the “pleasant illusions” of earthly life. The debate of assisted suicide raises the question whether human beings are mere electrical animals, quantum beings or fundamentally spiritual personalities-humans maybe all the three.The sanctity of human sufferings need to be brought into the equation of assisted suicide discussion. Assisted suicide would only add to the growing violence in the present world that could do with reintroduction of principles of non-violence.
USA may have better legal infrastructure to negate the unwanted and unintended errors of assisted suicide, but in many third world countries, where there is no such legal infrastructure, the procedure would easily get dishonoured. Oriental religions as well as Abrahamic faith traditions are opposed to ending life voluntarily. In general, all faith traditions believe that life that is nearing the biological end need not be preserved at all costs and that one does not have to go to extraordinary lengths to preserve a terminally ill person’s life. This means, for instance, that while a terminally ill person should not be denied basic care, he or she could refuse treatment that might prove to be futile or unduly burdensome for the dying person - passive voluntary euthanasia.
A scientific belief in after death existence is not without its pitfalls unless it is accompanied by the spiritual corollary of sanctity of earthly life. Science alone cannot highlight the sanctity of life; Divine standards are helpful in comprehending the sacredness of life. In fact, science has taken us to a cross road with Professor Schwartz’s new instrumental communication and it is time mark the boundaries of healthy survival research and the unhealthy ones.
Medical professional terminology is used to communicate with each other, allied professions and differentiates professionals from patients1. As a tradition, it has perhaps evolved into a language of its own with a vocabulary of terms used as expressions, designations or symbols such as ‘Patient’, ‘Ward Round’ and ‘Registrar’. This ‘language’ is not restricted to use by doctors or nurses - it is used among other professionals working in healthcare, e.g. medical coders and medico-legal assistants.
The National Health Service (NHS) in the U.K. has seen many changes in the last few decades. From within these changes, an interesting trend to change or alter the use of professional terminology, often without consultation with directly affected professionals or patients, has emerged. With new or changed roles, multidisciplinary teams have been observed to alter titles, even borrowing specific terms ascribed to doctors such as “consultant,” “practitioner” and “clinical lead”2,3. On the other hand, Modernising Medical Careers initiative4 has also led to changes in doctors’ titles reflecting their experience levels, which have been reported to be unclear to patients and fellow professionals5.
Medical professional terms can be traced back to Hippocratic writings and their development is a fascinating study for language scholars1. Psychiatric terminology is particularly interesting, as it has evolved through scientific convention while absorbing relevant legal, ethical and political trends along the way. Superficially, it may appear pedantic to quibble over terminology, but the power of language and its significance in clinical encounters is vital for high quality clinical care2,6. Since medical professional terminology is an established vehicle for meaningful communication, undue changes in its use can create inaccurate images and misunderstandings, leading to risks for professional identity. There is also evidence to suggest that such wholesale changes have been misleading7 and a source of inter-professional tension.
Understanding of a professional’s qualifications and experience is crucial for patient autonomy and for them to be able to give informed consent. We carried out a survey among foremost stakeholders of medical professional terminology, patients and doctors, within a psychiatric service to ascertain their attitudes to the changes they have experienced in recent years.
Method:
We gave out a self-report questionnaire to all adult psychiatric patients seen at a psychiatric service in the South East (U.K.) in a typical week and to all working psychiatrists/doctors. The questionnaire was developed after a review of the relevant literature and refined following feedback from a pilot project. The questionnaire contained demographic details and questions regarding attitudes towards medical professional terms for patient and professional identity, processes and working environments. The questions were mostly a “single best of four options” style, with one question involving a “yes” or “no” answer.
The datacollected was analysed by using SPSS statistical package8. Descriptive statistics were used to summarize the characteristics of the study population. The two sub-samples (patients & doctors) were compared with each other regarding different variables by using a t-test, which highlighted the absolute and relative differences among those.
Results:
196 subjects were approached to participate. 187 subjects (patients = 92, doctors = 95) participated, which represents a response rate of 95%.
Male to female ratio was roughly equal in the sample but there were more females in the medical group (56%) as compared to the patient (46%) group. Among responders, those over 40 years of age were more prevalent in the patient group (60% vs. 39%) compared to the medical group.
As shown in the Table 1, patients’ and doctors’ attitudes overwhelmingly leaned towards a patient being called a “patient” (as opposed to “client”, “service user” or “customer”); understanding “clinician” as a doctor (as compared to being a nurse, social worker or psychotherapist), and believing psychiatrist to be a “consultant” (preferred to nurse practitioner, psychologist or social worker).
Table1: Patients’ & doctors’ attitudes to medical professional terms = “patient”, “clinician” and “consultant”
What do you prefer to be called?
Doctors (%)
Patients (%)
Client
16 (17)
13 (14)
Patient
68 (72)
65 (71)
Service user
10 (11)
11 (12)
Customer
1 (1)
3 (3)
Don’t know
0
0
Total
95
92
Chi2 1.378, p = 0.710
Which of these is a clinician?
Doctors (%)
Patients (%)
Nurse
14 (15)
14 15)
Social worker
4 (4)
2 (2)
Doctor
56 (59)
70 (76)
Psychotherapist
7 (7)
6 (6)
Don’t know
14 (15)
0 (0)
Total
95
92
Chi2 16.3, p<0.05
Which of these is a consultant?
Doctors (%)
Patients (%)
Psychiatrist
71 (75)
68 (74)
Psychologist
3 (3)
6 (7)
Social worker
10 (11)
10 (11)
Nurse practitioner
3 (3)
8 (9)
Don’t know
8 (8)
0 (0)
Total
95
92
Chi2 11.3, p<0.05
Patients and doctors seemed to prefer (>70%) calling the person who provides the patient support in the community as “care-coordinator” or “key worker”.
It is worth noting that “key worker” is the main person looking after the patient admitted to hospital and “care-coordinator” has the same role when they are back in the community. Similarly, the majority of the patients deemed the terms “Acute ward” and “PICU” (psychiatric intensive care unit) appropriate for a psychiatric ward.
There was strong evidence to suggest that both patients and doctors were confused as to what a ‘medication review’ was; as approximately 35% of them thought it was a “nursing handover” and the rest were divided whether it was a “pharmacist meeting” or an “assessment”. See Table 2.
This is understandable because the patients are used to an “Out Patient Appointment/Review” where a psychiatrist reviews patients in a holistic manner, which includes prescribing and adjusting their medications. Similar confusion prevailed regarding what has replaced the term “ward round”, as both groups were universally divided among choices offered as “MDM” (multidisciplinary meeting), “Assessment”, “CPA” (Care Programme Approach) and “Review”.
Table 2: Patients’ & doctors’ attitudes to what a “ward round” and “medication review” means?
Which of these means a ward round?
Doctors (%)
Patients (%)
Assessment
26 (27)
34 (37)
MDM
18 (19)
15 (16)
Review
34 (36)
29 (32)
CPA
16 (17)
14 (15)
Don’t know
1 (1)
0 (0)
Total
95
92
Chi2 2.82, p = 0.588
Which of these is a medication review?
Doctors (%)
Patients (%)
OPD
19 (20)
11 (12)
Assessment
25 (26)
34 (37)
Pharmacist meeting
34 (36)
31 (34)
Nursing handover
14 (15)
12 (13)
Don’t know
3 (3)
4 (4)
Total
95
92
Chi2 3.89, p = 0.421
Both patients and doctors were clear (84% vs. 69%) that they expected to see a doctor when they attended a “clinic”. However, both groups were approximately equally divided between their preferences for what a psychiatry trainee should be called; “SHO” (37%) or “Psychiatric trainee” (36-40%). There was also a higher preference (approx. 50% vs. 30%) for the doctor a grade below consultant to be called a “Senior Registrar”.
Patients and doctors were equivocal in their response that they have never been consulted about medical professional terminology.
Fig. 1 Has anyone consulted you about these terms?
Discussion:
In a survey of attitudes to the use of medical professional terms among patients and doctors in a psychiatric service, we have found a significant preference for the older and established medical terms as compared to the newer terms such as MDM, CT trainee, Specialty Trainee, etc.
While replicating findings of other studies3,7, we also found that no single term was chosen by 100% of participants in either group, showing confusion surrounding most psychiatric terms. This lack of consensus and confusion can be explained by the fact that no participant had ever been consulted about the changes or new nomenclature.
Limitations to this study should be taken into account before generalising the results. The patients’ group is older than the doctors’ group, which could skew the results due to age related bias in favour of familiarity and against change9. In a questionnaire about preference and understanding, participants may intuitively prefer the easiest to understand terms and ignore the subtle difference between other styles. Possibility of bias may have been introduced by some of those giving out questionnaires being doctors
Our sample was drawn only from a psychiatric service, which may restrict the implications of our findings to mental health.
Furthermore, involvement of other professionals and carers working in the psychiatric service would have been useful to expand the scope of this study.
Inconsistency regarding doctors’ titles, unleashed by the Modernising Medical Careers (2008) initiative, has resulted in patients considering trainees as medical students5, not recognising ‘Foundation Year 1 Trainees’ as qualified doctors and being unable to rank doctors below consultant level3. Our findings have highlighted the uncertainty regarding qualifications and seniority of doctors – this can erode patients’ confidence in their doctors’ abilities, compromise therapeutic relationship10, especially in psychiatry, and result in poor treatment compliance. Medical students may also find themselves mistaken for doctors, and feel daunted by future job progression where training structures and status are unclear.
Title changes introduced by local management or Department of Health (DoH), without consultation with stakeholders, have the potential to create inter-professional tensions and devalue the myriad skills offered by healthcare workers other than doctors. This could also be damaging to their morale and the confidence instilled in patients. It is interesting to note, however, that titles that do not give the impression of status and experience, such as “trainee”, tend not to be adopted by non-doctor members of the multidisciplinary team3. On the other hand, in a profession steeped in tradition, there will be doctors who see other professionals’ adoption of their respect-garnering and previously uncontested titles as a threat to the status of the medical profession6. Previous studies have shown that terminology has a significant effect on the confidence and self-view of doctors5 and at a time where a multitude of issues has led to an efflux of U.K. junior doctors to other countries, and a vote for industrial action, re-examining a seemingly benign issue involving titles and terminology could have a positive impact.
Patients’ attitudes to development of surgical skills by surgical nurses show that they would like to be informed if the person doing a procedure is not a doctor7.
The roles of a number of professionals involved in an individual’s healthcare can be confusing and the possibility of mistaken identity could be considered misleading6, unethical, and even fraudulent. Introducing confusion by appropriating titles associated with doctors could be damaging to patients’ trust, and is inappropriate in a health service increasingly driven towards patient choice. The challenge lies in how to keep the terminology consistent and used in the best-understood contexts.
Commissioners and managers may instead evaluate the implications of changing professional terms by making sure that all stakeholders are consulted beforehand. Perhaps the pressing source of inconsistency in staff job titles could also be rectified by a broader scale study to find national, multidisciplinary and patient preferences, and taking simple measures such as standardising staff name badges.
Our study has highlighted once again how the landscape of nomenclature in psychiatry/medicine is pitted with inconsistency. While language naturally evolves with time and it may be understandable to see increasing application of business models & terminology in the NHS9, medical professional terms have been determined contextually over the years with significant implications for patient management and safety. Therefore, it is important to question how changes in terminology affect patients, whether it occurs by gradual culture change or due to new initiatives. It would benefit patient care if medical and psychiatric professional language could be standardised and protected from changes, which can lead to colleagues and patients being misled. DoH, Commissioners and Trust/Hospital management must recognise that changing terminology can have a significant impact and that serious discussion of such changes is important for reasons far beyond pedantry. For inter-professional communication a formalised consensus on titles would be beneficial for transparency, trust, patient safety and reducing staff stress levels.
The closure of asylums in the last century has resulted in an increased number of compulsory hospital admissions for psychiatric patients. Psycho-geriatric patients are highly vulnerable in this respect. Although the traditional buildings instituted for the care of the mentally afflicted have gone, misconceptions about provision and anecdotes about incarceration continue to haunt the community. Recent legislative changes have further extended the occurrence of involuntary hospital admission.1 Compulsory community care is under constant review. Concurrently the validity of the concept of mental illness, psychiatric classification and diagnostic dilemmas all continue to be debated. Confinement has regained respectability in the discourses of present-day British mental health system because of violent offences committed by psychiatric patients and the public media portraying them as a reflection of failure of community care.
Table 1, Advantages of Mental Health Acts
1. Mental health acts secure the safety of vulnerable people 2. Helps to regain control on their lives 3. Compulsory treatment helps to prevent further deterioration of mental health 4. Aimed to provide effective care and treatments 5. Ensure better after care 6. Protects the safety of other people 7. Prevents suicides 8. Provides opportunities for assessments and diagnosis 9. Can be therapeutic by unburdening personal responsibilities to an institution.
Numerical quantitative studies imply that generally involuntarily admitted patients show clinical improvement and retrospectively view their compulsory admission rather positively.2 It is an unquestionable fact that Mental Health Acts prevent suicides and homicides (table 1). Mental Health Acts have some unsatisfactory outcomes particularly on a subset of patients including senior citizens admitted formally. It is important to identify such patients and take additional precautions in their management as they run the risk of leaving hospital feeling inferior and inadequate. Patients’ specific characteristics, thought processes and past treatment experiences, colour their attitude towards coerced treatment and determine the gains and shortcomings of compulsory care.
Disadvantages
The Mental Health Acts are open to social abuse and elderly patients can be more defenceless in this respect. Specifically they may be: invoked to control behaviour; misused for material gain and implicated in subtle expressions of revenge. They are sometimes invoked to hasten divorce proceedings and to secure the custody of children by a specific parent. They are also used to control the behaviour of children by their parents. Mental Health Acts designed to control psychiatric patients are being enacted and enforced in some underdeveloped countries that lack an efficient tribunal system to monitor their effects.
A patient who has been detained is at risk of repeat detention and someone who has been inappropriately assessed becomes increasingly vulnerable to control on psychiatric grounds. The experience of being detained involuntarily has a reductive effect on behaviour after discharge – it may induce anxiety or post-psychiatric depression. The awareness of being deemed to require compulsory detention generates such negative attitudes as self-denigration, fear and unhealthy repression of anger. It may also impede self-direction and the normal sense of internal control and may encourage the view that in a world perceived as being divided into camps of mutually exclusive ‘normal’ and ‘abnormal’ people, the patient is in the latter category. Compulsory detention may lead to suicide because the patient loses their sense of integration within their own society. Furthermore, the fear and anxiety associated with involuntary admission delays the recovery process. There are other frequently occurring barriers to recovery for those affected such as, loss of capabilities, whether real or imagined, ineffectual medication due to poor elicitation of symptoms because of patient’s lack of cooperation and negative drug side effects.
Depressed patients have a higher suicide risk than the population at large and one of the reasons for detention is suicidality. Some of the subjective symptoms of depression can be ameliorated by denying them, while compulsory detention may reinforce depressive symptoms. Detention gives carers a false sense of security and this may lead them to relax their vigilance towards the patient. The Mental Health Acts increase the stigma associated with psychiatric illness and with the exuberant expression of emotions. Patients who are under section or are frightened of being placed under section may deliberately mask their symptoms in an attempt to have the section lifted or to avoid sectioning.
Trans-cultural studies
Trans-cultural studies show that members of migrated cultures, particularly the elderly, are more at risk of inappropriate sectioning than the rest of the population because of the lack of knowledge on part of professionals about the patient’s culture. For instance, the debate of over diagnosis of schizophrenia among Afro-Caribbean patients is still unsettled. A study conducted in South London has concluded that Black Africans and Black Afro-Caribbean patients with psychosis in that area are more likely than White patients to be detained under the Mental Health Act 1983.3 GreatBritain has become a multicultural society and a significant percentage of professionals working in psychiatric units have been trained overseas, in a wide range of countries. This creates further risk of inappropriate diagnosis. There needs to be more emphasis on the significance of trans-cultural psychiatry in the United Kingdom. In particular, psychiatrists should be aware that psychiatry is a medicine of language and culture as well as of the mind.
Medical Dilemmas
Countries in which Mental Health Acts are widely enforced have not achieved any reduction in suicide rates through their implementation. Sectioning is perceived by many patients affected as a psychological guillotine – a form of psychiatric terrorism. The medical profession is invested by the Acts with undue power over society. This is of particular concern because training in psychiatry does not include the study of free will and allied philosophical issues and also because there is no clear definition or description of mind and consciousness. In psychiatry there is a lack of clinical indicators and psycho-physiological parameters so the criteria for diagnosis are imprecise, with a concomitant risk of the Acts being erroneously implemented. It has been postulated that once a person has been classified as having deviant behaviour, that categorisation has a potent effect on the subsequent actions of the person concerned and those interacting with them.
Is it not justifiable to argue that even if a few mentally ill patients are underdiagnosed and not subjected to psychiatric admission, someone whom we would regard as normal should not be detained in a psychiatric hospital against their will? Such a view is analogous to the judicial view regarding capital punishment where even if ninety-nine murderers escape capital punishment because there is no death penalty, one innocent person should not be sentenced to death. Mental Health Acts may be a necessary evil but they present a dilemma for mental health professionals: the morality of helping patients and protecting the society from the consequences of their illness against the immorality of restricting their freedom. Clinicians become torn between the ideals of curing mental illness and defending the sanity of patients.
Patients’ Perception
A small survey conducted by the author revealed that no sectioned patient in the group studied sent a thank-you card after discharge to the ward in which they were confined. However, many voluntary patients expressed appreciation in that way. This is an indicator of the attitude of sectioned patients towards the Mental Health Acts. One reason must be that a record of being sectioned limits their freedom to travel and also affects their employment opportunities adversely. A patient has commented that it is easier for an ex-convict to gain employment than it is for a once-sectioned psychiatric patient.
There is anecdotal evidence illustrating the panic that may be generated with the word ‘section’ in psychiatric patients. A recovering elderly hypomanic patient explained that he misconstrued the word on hearing it when he was ill, taking it in relation to sectioning in Obstetrics and General Surgery. He remembered that as he resisted entering a taxi while being persuaded to agree to admission, the driver said that he was going to be sectioned if he refused hospital admission. The patient misunderstood this and interpreted it as he was going to be cut into pieces and tried to jump out of the vehicle.
Post-traumatic stress disorder
Any loss of intrinsic importance to an individual constitutes bereavement. Denial, anger and depression experienced in compulsory detention are comparable to bereavement.4 In the case of a detained patient, the loss of self-identity and of social functioning causes a grief reaction. It has been hypothesised that there are high levels of Post-traumatic Stress Disorder (PTSD) symptoms in detained patients.5 Very few repeat detainees become habituated to the implementation of the Mental Health Acts. The vast majority become increasingly frustrated and develop a pessimistic outlook towards their mental health. There is a high incidence of suicide among patients who have multiple detentions.
Post-hospitalisation Stress Disorder is much more common than generally recognised. Formal admission may lead to fear, anger, frustration, depression or loss of self-esteem, depending upon the individual’s psychological response.6 Involuntary admission may result in pervasive distress in any patient – this kind of hospital admission may be perceived as threatening and even as a catastrophe. Detained psychotic patients are less aware of their environment because of the preoccupation with their symptoms. Non-psychotic patients, when detained for instance because of a risk of suicide, are fully aware of their immediate environment and the chaos they have caused to themselves. They have a high risk of PTSD.
Preventive detention
Fear of liability may lead to compulsory hospitalisation solely to prevent violence on the part of patients who otherwise do not require in-patient care.6 Psychiatrists are not trained to police society and may lack sufficient knowledge and experience to participate in the social control responsibilities that are part of the remit of the criminal justice system - they are sometimes involved in that function. Psychiatry has to be safe and secure in the hands of individual psychiatrists and psychiatrists have to be protected when practising psychiatry. Mentally ill patients are sometimes mistakenly processed through the criminal justice system rather than the mental health system. When that happens, compulsory detention may be perceived as a form of criminalisation of mental illness. Unless there is scrupulous monitoring, mandatory treatment impinges on civil liberties. Preventive detention is legally ambiguous and clinically impractical.
Assessment
Amongst the government’s fundamental powers and responsibilities are, protecting people from injury by another and caring for less able people, whether physically or mentally incapacitated. These functions encompass the welfare and safety of both the individual concerned and the public.
A decision about compulsory detention is made on the basis of three considerations: loss of emotional control; psychotic disorder and impulsivity with serious thoughts, threats or plans to kill oneself or others. Any perceived risk must be imminent and provocative. The clinician is legally required to determine the least restrictive environment to which a patient may be safely assigned for continued care. To fulfil these requirements while implementing the Mental Health Acts, a psychiatrist needs the skills of a physician, lawyer, judge, detective, social worker and philosopher. The decision-making process is influenced by multiple factors such as: the clinician’s propensity to detain patients; the record of past untoward incidents involving the patient; attitude towards risk taking and availability of hospital beds and alternative safe treatment facilities. It is regrettable that in section 5(2) assessments, often it is a junior doctor, the least experienced person in the team, who is called upon to conduct the evaluation.4 A multitude of interviews with mental health staff, a social worker and solicitor will have to be endured by the patient - these are regarded as ordeals by most of them.
Non-detainable patients
Since the introduction of the Mental Capacity Act 2005, the number of assessments that are followed by a decision against compulsory detention is increasing. Patients who are assessed for formal admission but not found to be detainable may develop new risks subsequently as a result of the assessment procedure itself. Before assessment, mental health professionals may place themselves in covert locations around the patient’s house and neighbours may watch eagerly behind their curtains. Thereby the patient’s social image is damaged. After meticulous assessment, it may be a relief for the patient that they are not detained and that euphoria may continue for a short while but all too often damage has been done. The patient who is tormented by psycho-social stressors may find the assessment experience intensifies the injury. The decision about whether it is appropriate to assess someone is therefore an area in which more clarification and some management guidelines are much needed. In situations such as these, untoward incidents have been periodically reported. That may mean that the professionals involved and perhaps also family members who initiated the assessment, blame themselves and endure severe guilt feelings or blame each other. Furthermore, psychiatrists are not mind readers. It is possible that a patient will cleverly deny any suicidal intent during assessment, intending to fulfil a suicidal urge afterwards and that may falsely appear to be a reaction to the assessment. An interview for assessment may be the factor that takes them beyond their limit. Because of all these circumstances, the patient may need intensive home care and counselling after an assessment that does not lead to hospital care. In addition to treating mental illness, it is the duty of the psychiatrist to defend the sanity of patients. The difficulty of defining normalcy is notorious: it is easier to detect psychiatric symptoms than to describe normal behaviour.
Tribunals
Mental health tribunals are demanding and may be humiliating and intimidating. They are highly stressful for the patient and clinician and they involve the breach of patient confidentiality. Tribunals are often emotionally charged scenes for the patient and psychiatrist, they may result in traumatisation. The largely professional make-up of a tribunal is often perceived as intimidating by patients, who tend to be suspicious of collusion between professionals and above all of their reluctance to challenge the decision of a psychiatrist.7 Psychiatrists who are aware of legal profession’s ignorance on psychiatric issues dominate the tribunal scene by flamboyant linguistic expressions, while lawyers question the objectivity of psychiatry and the expertise of psychiatrists in legal matters. Tribunals are concerned with the legality of detention and not with the appropriateness of treatment. However, one study has shown that patients who appear before tribunals find it easy to accept they require compulsory admission. 8 Psycho-geriatric patients find it extremely distressing to attend tribunals. Hospital managers’ review hearings are often arranged and carried out promptly. Managerial hearings involve local people too which may make them less intimidating for detained patients.
Involuntary treatment
Although mental health staff usually have the best of intentions, when mandatory treatment is applied to patients it may prove traumatic and counter-therapeutic. The experience of undergoing forced treatment adds to the patient’s perception of stigma and discrimination. Involuntary psychiatric drug treatment is bound to be less effective than voluntary treatment. An outcome may be misdiagnosis, long-lasting and disabling side effects. Forced treatment potentially violates a person’s right to respect private life under Article 8 of the European Convention on Human Rights. Article 8 is violated only if patients can prove the treatment given is more harmful than the claimed therapeutic benefits, yet the clinician can administer the treatment if he thinks it is therapeutically necessary. Compulsory treatment makes patients feel infantilised, especially because forced psychiatric treatment often involves coercion, emotional intimidation, bullying and threats.
Community Treatment Order (CTO) is being constantly evaluated in terms of its merits and demerits. The results have been inconclusive and warrant more systematic studies. It was Section 41 of the Mental Health Act that inspired the introduction of CTO - the main purpose being to protect the community from the aggressive behaviour of some of the psychiatric patients as in the case of the successful Section 41. There are indications that CTO has fulfilled such a goal. It was also targeted to enhance compliance and concordance with the mental health services and to prevent suicides but studies indicate that those goals were not achieved.9,10 The Oxford Community Treatment Order Evaluation Trial (OCTET) substantiates a lack of any evident advantage in dropping relapse.
The “knee jerk” reaction from part of community service has apparently resulted in spontaneous readmissions of patients under CTO. It has also contributed to prolonged detention of patients awaiting community placement under CTO. This is because detained patients must stay on section 3 or 37 to allow the Mental Health Act to be converted to CTO upon discharge. Obviously, such a scenario curtails liberty. Patients always feel bitter about the “hanging feelings” of continued detention. Coercion runs the risk of weakening therapeutic alliance. It may be true that if fewer conditions are imposed, CTO could serve as a “memory knot” for patients with limited insight. Despite all the controversies surrounding the benefits of CTO, its use is increasing worldwide. 11
Assertive Human Rights
All human beings have individual rights and mental health professionals in particular must be mindful of those rights. Table 2 presents the list of assertive human rights, as modified from Gael Lindenfield (2001). 12
Table 2, Assertive Human Rights
1. The right to ask for what we want (realising that the other person has the right to say “No”). 2. The right to have an opinion, feelings and emotions and to express them appropriately. 3. The right to make statements which have no logical basis and which we do not have to justify (e.g. intuitive ideas and comments). 4. The right to make our own decisions and to cope with the consequences. 5. The right to choose whether or not to get involved in the problems of someone else. 6. The right to know about something and not to understand. 7. The right to be successful. 8. The right to make mistakes. 9. The right to change your mind. 10. The right to privacy. 11. The right to be alone and independent. 12. The right to change ourselves and be assertive people. 13. The right to be neutral. 14. The right to be empathetic and apathetic.
Discussion
Community care is more innovative than compulsory detention in hospital. For majority of patients, the best way forward is having high quality home treatment facilities as it is least restrictive and using compulsory detention should be the last resort. In some cases, forced psychiatric admission is indicative of failure in the supply of quality home treatment.One thing that sometimes leads to in-patient admission is lack of confidence in the service available. The perception of home treatment may be at fault here - it needs to be understood as more than merely staying outside hospital. Forensic patients and treatment resistant psychotic disorders lacking insight may be a different state of affairs. CTOs have serious impact on the autonomy and privacy interests of individuals and should not be applied to compensate for under-resourced community services.
Caring and supportive relationships between mental health staff and patients during involuntary in-patient care have considerable bearing on the outcome of compulsory detention. A recent study has revealed that among patients who have been detained involuntarily, perceptions of self are related to the relationships with mental health professionals during their inpatient stay. 13 Perceived coercion at admission predicts poor engagement with mental health staff in community follows up. When professionals demonstrate their genuineness and encourage patient participation in the treatment options, coercive treatment would be perceived as less of an infringement to the autonomy of patients and their sense of self-value. 14 If patients maintain both positive and negative views about detention, interventions should be designed to enhance positive experiences by focussing on respect and autonomy.Patients admit only compulsory detention gave them an opportunity to receive medication in a time of crisis and report it did not necessarily prevent thoughts relating to self-harm. It simply reduced the opportunities for impulsive acts.
‘Rooming-in’ is worth debating as an alternative to compulsory detention. This is the voluntary participation of so-called confidants, who may be chosen family members or trusted friends. They provide a 24-hour vigil for the patient in a safe hospital environment. An Australian study has suggested this system is highly valued by nursing staff, patients and their families.15 It is an initiative that needs further testing and evaluation. The resolution of angry feelings towards the mental health professionals has a significant bearing on their future compliance. The post-detention period tests the attention given to patients by mental health professionals. Here the staff members have to take the initial steps required to repair damaged relationships which may have developed in particular with angry patients. Detained patients should be offered counselling in post-discharge follow-ups and should be given satisfactory explanation of the circumstances for formal admission. Detained patients should be given the support to enable them to: rewrite their life story; reconstruct a sense of self; achieve healing of the assault of their illness and the treatment procedures inflicted on their personality. Specific interventions should be designed and evaluated in order to deal with any unresolved PTSD symptoms relating to formal psychiatric admission.
Angiogenesis is an integral process in biological programmes of embryonic development, tissue damage and regeneration, tumour growth and progression and pathogenesis of inflammatory and autoimmune diseases. MS (multiple sclerosis) is a demyelinating disease of the CNS (central nervous system). Angiogenesis has been a consistent feature of demyelinating plaques of MS1-3. Many inducers of angiogenesis are expressed in these plaques. They are also closely associated with the animal model of MS viz. EAE (experimental autoimmune encephalomyelitis)4 (Table 1). This has led to the suggestion that inhibition of angiogenesis by suppressing these effectors or inhibiting the elements of angiogenic signalling pathways might provide a viable way to target therapy to manage MS.
[Note: Inhibitory effects of thalidomides were described by Sherbet4; D’Amato et al.6; Kenyon et al.7; Lu et al.8]
Multiple sclerosis is an autoimmune inflammatory condition and so immunomodulators have been used in treatment. It is recognised that aberrant activation of the immune system and the associated network of its regulation are important events in the pathogenesis of the disease. This is the rationale for using immunomodulatory agents in disease control. Among immunomodulators of note are Fingolimod which prevents infiltration of auto-destructive lymphocytes into the CSF, Teriflunomide which reduces lymphocyte infiltration of the CNS, axonal loss and inflammatory demyelination, and dimethyl fumarate, which modulates the immune system by many mechanisms. Furthermore, much attention has been devoted to the immunomodulatory properties of MSCs (mesenchymal stem cells) 4,5. Thalidomides are also capable of modulating the function of key element of the immune system related to the pathogenesis of MS, but this brief article is intended to emphasise the potential of thalidomide and its analogues as potent inhibitors of angiogenesis and the latent possibility of their use as a therapeutic agent in the control of MS.
Thalidomide was introduced over four decades ago to treat respiratory infections and to combat morning sickness in pregnant women. It was withdrawn when it was found to be highly teratogenic. The teratogenic effects are a result of the binding of thalidomide to cereblon, a protein found in both embryonic and adult tissues. Cereblon is required for normal morphogenesis. It is inactivated by binding to thalidomide and this leads to teratogenesis9. Thalidomide possesses immunomodulatory, anti-inflammatory, anti-angiogenesis and cell proliferation inhibitory properties and this has suggested its use in the treatment of cancer5. Analogues of thalidomide, viz. lenalidomide and pomalidomide, have been synthesised and these possess reduced toxicity and greater efficacy10, 11. Recently, many studies have elucidated the signalling pathways which thalidomides inhibit and thereby suppress cell proliferation, promote apoptosis and inhibit angiogenesis. These have led to the suggestion of combining the modulators of these signalling pathways to synergise with thalidomides to deliver the suppressor effects with enhanced efficacy and at lower concentrations thus reducing the side effects5 (Figure 1).
Most of the work on the efficacy of thalidomide and the analogues has been carried out in preclinical models. Quite understandably, in the clinical setting very little effort is seen to check whether thalidomide or the analogues provide any beneficial effects in MS or neuro-inflammation. Clinically orientated investigations so far relate mainly to multiple myeloma and some other forms of haematological malignancies but not solid tumours5. Any perceived beneficial effects are probably outweighed by the side effects. We need to expend more effort and design and develop new analogues with reduced toxicity. In this context one should emphasise that pre-clinical exploration of the potential synergy between the thalidomides and the acknowledged modulators of the signalling pathways would be worthwhile. This might enable the delivery of benefits more effectively and at lower dosages. It is needless to say that safety of drug administration is of paramount importance.
It seems that psychiatry is gradually losing its allure for future doctors. All around, one can detect an air of pessimism from colleagues about the creeping 'socialisation' of this important field of medicine. There is no longer the breadth of interest in the subject and each sub-branch, for want of a better expression, has its followers and adherents. Proponents of one particular facet of treatment are zealous in the pursuit of their own interests. Psychotherapy is pitched against the neurobiological, rehabilitation and social psychiatry against the pharmacologists, all trying to mark out their own piece of territory, with some yearning for a place in the history books, or at the very least, an acronym. Some psychiatrists do not believe in diagnoses; others ridicule the concept of personality disorder, autistic spectrum disorder, or drug treatment; some believe psychiatric illness is the fault of governments, and there are probably a few who do not believe in psychiatry at all! 'Research' studies are cherry-picked by all sides to illustrate the ineffectiveness of 'alternative' treatments. The full picture or perspective of ill health is blurred and narrowed by a minority who believe they alone know what is right for patients, and psychiatry is 'intellectualised' by others to give it an air of authority and profundity it does not possess. Morale and training are suffering and, if this state of chaos and insanity continues, the discipline itself will implode and cease to be of interest to anyone, save the warring factions in the profession itself.
Once upon a time it was considered that a reasonably broad mixture of community and hospital services would provide benefit for patients with mental illness. Staff involved in their care, who have the rather cumbersome and oxymoronic description of being called 'mental' health professionals, would also widen their experience because of the continuity of care provided. It was hoped patients who clearly did not need to be in hospital (for example, waiting for appropriate accommodation) could be discharged. Clinical need would determine those who required further rehabilitation/treatment in hospital, and would not be swayed by pressures, often financial, to discharge. Now, with the setting up of Home Treatment and other teams the situation has ironically worsened, because there is an implicit opinion in this arrangement that hospital admission, even for the seriously ill or indeed violent patients, is the least desirable option and something to avoid at all cost, even when care in the community is not immediately available or adequate. Care provision for the elderly is a separate concern and is not under discussion here.
In the domain of general adult psychiatry those patients who are in need of care, be it medical or social, are languishing at home, desperate for help, being offered assessment after assessment by disparate teams. There are not enough care professionals to cope with the demand. Home Treatment Teams in particular, are under considerable sustained pressure and stress to ensure further reduction in beds. Rehabilitation beds are being closed. 'It is cheaper to keep patients in the community', we are told. Or, if that does not suit, the liberal stance might be, 'What does hospital admission achieve'? That's fine if the problem is not on your doorstep. Psychiatrists who oversee inpatient care are also pressurised to discharge patients as soon as possible, so the very old notion of 'incarceration' (that worn-out cliché from the antipsychiatry lobby) seems facile, to say the least. On the contrary, doctors now have the added worry of prematurely discharging partially treated ('we need the beds') as well as more vulnerable patients who cannot cope. Most patients who take up psychiatric hospital beds do not want to be in hospital in the first place as they often, rightly or wrongly, do not see themselves as ill. Many hospital beds are now occupied by 'Section patients', and conversely, many very ill patients are left to go it alone because they refuse hospital admission and do not want community team involvement, yet are not 'sectionable'. The inference seems to be, 'If not sectionable or under CPA (Care Programme Approach) it is not our concern.'
Where there are sufficient provisions for outpatient care, some of the damage may be mitigated. Overworked staff including community psychiatric nurses (CPNs), support time recovery workers (STRs) and occupational therapists (OTs) often have the thankless task and enormous responsibility of seeing patients at home, some of whom are threatening and potentially dangerous, others erratic with their outpatient clinics attendance not always through deliberate evasion but often the result of the very condition causing the problem, for example, lack of insight. Other patients do not engage either through hostility or loss of motivation induced by the underlying problem, say, drug and alcohol misuse. Chronic patients are not ill enough to be on CPA and diagnostic 'conundrums' are left to others to sort out. With the introduction of the New Ways of Working,1 the traditional outpatient clinics are being abolished and replaced with community clinics ('short-term' outpatients really). Ideally a community clinic should be run by CPNs as they usually understand the medical, psychiatric, psychological, and social needs of patients. In the authors' opinion the clinics should be Consultant-led because despite the tendency to classify everyone as 'clinicians' many staff feel uncomfortable with this role as it implies or infers a degree of clinical responsibility for which they are not qualified. Psychiatric nurses (especially those with a general nursing background) are ideally placed to carry out this function by virtue of their wide experience; also they are aware when to seek medical help when needed. Often they are more informed about patients than the primary physician or indeed the psychiatrist because of more frequent contact, either via liaison with the hospital wards or through home visits in their role as CPNs. Nurses and other staff (for example, social workers) are involved in patients' discharge from hospital (usually determined at pre-discharge meetings) and are therefore an essential link in the continuity of patient care before patients are eventually seen in the 'community clinics'. Requests for domiciliary visits from general practitioners (GPs) to physicians themselves have become a thing of the past, with the exception of those psychiatrists working with Home Treatment Teams and Assertive Outreach Teams. Nowadays it is not uncommon for patients to be waiting months on end (more assessments) before being deemed 'appropriate' to see a Consultant Psychiatrist.
Certainly there are patients who do not need to continue seeing a Consultant Psychiatrist for years on end and should be discharged back to the GP to reduce unnecessary costs and to avoid a dependency culture, in the same way a patient with mild arthritis does not need to see a rheumatologist or a patient with anaemia does not always need the expertise of a haematologist, to use simple analogies. However, sometimes GPs are unwilling to reciprocate or feel out of depth with 'psychiatry' that this is not always possible. The chronicity of many psychiatric disorders perhaps harnesses the belief that new treatments may emerge which only a psychiatrist, with his/her specialized knowledge, can implement and deal with. This type of scenario is seen with many other illnesses in all fields of medicine (chronic psoriasis, rheumatoid arthritis, multiple sclerosis) yet no one is suggesting that GPs solely should be left to manage these conditions. It seems the clinical risk to patient care is not thought through and this no doubt will lead to serious repercussions later. In our estimation, physical and mental illnesses are so often intertwined that their management should be equally shared by physicians and psychiatrists.2
Swings and Roundabouts
Such is the pressure by management (under the thumb of civil servants) and 'those in the know', reverentially referred to as ‘Commissioners’, that health professionals in psychiatry have to defend their clinical judgment and carry out numerous risk assessments (defensive medicine) of patients who are to be discharged from the outpatient clinic back to the GP in any event. Patients may be fortunate enough to receive a few last appointments with the Community Clinic (when they are up and running: some are at the time of writing) before they are shown the door and sent back to the GP, all to save money. Packages of care will not disguise the fact that vulnerable patients are being left to fend for themselves, just as they were in the past when the large institutions closed down without any forward planning as to how and where patients would survive. Yet ‘management training’ and ‘mandatory courses’ continue inexorably, often provided by 'expert' outside speakers, costing Trusts considerable amounts of hours lost, let alone the expense, instead of employing more nursing staff to cope with the ever-increasing workload. We are led to believe that reducing 'outpatient numbers' will lead to less pressurised work on staff, which really does not fit. All that will be happening to the extent that 'outpatients' will now be filling to the brim with CPA patients (read 'psychoses') instead of a good case-mix of patients required for general experience and training. It seems to be forgotten that there are patients who feel very unwell and are unable to cope, yet are not suffering from major psychiatric disorders.
The next scenario will be the revolving door ‘GP - Access/Assessment Team - possible Consultant Psychiatrist advice and at most two follow-up appointments (if one is really ill) - Community Clinic - discharge to GP system’, to replace the premature hospital discharge-readmission system which failed miserably in the past. When the patient relapses (or rather, when the illness remains static) the GP refers back into the system and the whole process begins again. In this way the Trusts receive money by reaching their targets (discharging patients) and are paid a second time when GPs 'purchase' more care. Those patients with 'minor problems' (not in their GP's estimation) will whittle away and remain unhappy. 'They can always see a counsellor' is the unspoken passive riposte. Furthermore, there will be less clinical variety for doctors and students, as their work will amount to prescribing 'powerful drugs' (we are told by the antipsychiatrists), monitoring serum lithium (and other drug) levels or checking blood results and clozapine dosages, because the Talking Therapies will be curing all and sundry. If only. We are reverting to the bad old days of pseudomedicine and pseudoscience.
Academicians and those who sit on government advisory bodies with grandiose names would have us believe there are far more effective ways to support people at home, or if they have no home, a crisis house will do. Meaningless, empty statements such as 'randomised controlled trials' (given the complexity of the issues under study) often with some reference to National Institute for Health and Clinical Excellence (NICE) guidelines, are used to support questionable findings. Despite all the 'new ways of working' national stress levels are at their highest because of rising unemployment, unexpected redundancies, increasing debt through credit card borrowing, and suicide rates are going up. New ways of Working is not working and any 'ad hoc survey' (note we did not say 'research') will reveal the depth of disillusionment all professionals in the discipline of psychiatry are experiencing, and not just the hallowed psychiatrists. Rudderless multidisciplinary teams are not the answer: teams require management. The term 'leadership' is becoming redundant (one only has to look at successive governments) and is often merely a spur for making money out of meaningless and time-wasting leadership courses which seem to be sprouting everywhere. Among the many qualities 'leadership' embraces are a sense of humour, assertiveness, fairness, creativity, openness, integrity and dedication, all to be found in one individual; presumably! Hierarchical structures may work, contrary to the sweeping statements of some,3 because people who are experienced in medical, academic and management matters (with perhaps a sense of humour) tend to command respect from team members. It is not enough to be an expert in cognitive behavioural therapy (CBT).
No place like home
How does one establish trust and rapport with patients when there will be less opportunity to do so because their care and progress are determined by market forces? Instead of decreasing outpatient volume or confining this aspect of care to CPA patients only, outpatient departments should cater for the mounting levels of stress in the community (poverty, debts, redundancies, threatened job losses) through increased staffing levels and training/supervision of more social workers, CPNs and occupational health workers. Where possible such staff should attend as many clinics as possible (not just CPAs) to offer a more holistic approach to patient care. If anything, policy makers, clinicians, managers, carers and user groups need to collaborate and clamour for a more integrative mental health service, not fracture the already fragile set-up. Community clinics are seen as a stepping stone to discharging from the mental health services (those who set them up don't like this analogy), which in theory is a good idea. The problem lies in the precipitous nature of transfer from outpatient to community clinics. Some very ill patients with chronic conditions are ironically not a burden to the system, in that they do not need to be seen frequently nor do they not require repeated admissions to hospital, yet if left to their own devices and discharged back to Primary Care would soon find life unmanageable as they rely on the expertise of health professionals to remain reasonably stable. Many patients have physical problems, some partly the result of the very treatments given to alleviate their underlying condition (obesity, hypertension, ECG disturbances, Type 2 diabetes and so forth), and need careful monitoring and supervision which is best provided by CPNs and other staff, in the same way a Health Visitor, Practice Nurse, or Diabetes Nurse Specialist might offer his/her expertise to a GP practice.
There will always be patients who need to be seen in the outpatient department with the emotional security and staff support this provides. We are aware that some 20% of patients miss their mental health appointments but then people miss appointments for other interviews and not always because they are unwell.4 Some people miss appointments because they feel better. This is surely not a reason for abandoning the outpatient system, which serves the remainder of the patient population quite well. We have experienced an unprecedented expression of worry and disappointment by patients who have been told they are not ill enough to be followed up at the outpatient department. Now mental health professionals are also frustrated, because they perceive their remit is to refer back to the GP as swiftly as possible, without having thoroughly assessed a patient over a period of time. First on the target list will be those patients who have not been seen by a psychiatrist for several months (‘We don't see them very often, therefore what is the point?') yet many chronically unwell patients may not want to attend outpatients, or have sufficient insight to realize they need to attend, for reasons outlined above. Will Outreach Teams in every Trust be abandoned to save money? Was it not their role in the first place to help those reluctant to receive treatment? What messages are we giving to patients other than being 'just a number, a hospital statistic’'? Those who have had the ‘luxury’ of a hospital admission usually comprise the very psychotic, and the personality disordered, and of the latter some consider they should not be in hospital anyway. The gains that have been made over the past decade in early intervention and engagement with patients by Assertive Outreach Teams will be lost. Yet, there is a continuing demand from patients and their carers to be seen by doctors.5
Here is how the 'new' system works. New Ways of Working, set up some years ago 1 and imposed on us, was meant to be an innovative approach to consultants' contracts by encouraging multidisciplinary teamwork ('When did consultants ever not consult their fellow professionals'?), reviewing the continued necessity for outpatient clinics, advocating more scheduled time for carers (colleagues we have spoken to cannot ever recall not seeing relatives or carers!) and more prominent roles for all team members, encouraging further education and training. Unfortunately we have gone to the other extreme and are being bombarded by all sorts of courses to the extent that much time is lost not seeing patients. Team members may and should undertake postgraduate studies. For doctors, continued professional development is mandatory. We are the only profession that requires revalidation every five years. Nothing can substitute for the medical training doctors undergo and it is a shame that the expertise of psychiatrists is diluted and devalued by their current roles as medication gatekeepers. It is a curious state of affairs or perhaps conveniently forgotten that when Trusts or 'Health Care Reformers' talk nowadays about working in teams and 'shared responsibility', the Consultant-led team concept is dismissed. Where there are Consultants who do not feel up to the role of leading a team, or are uncomfortable making assertive decisions and would rather take a back-seat thus avoiding the responsibility of being in charge of a team, then a Specialist Registrar nearing the end of training could fill this position. Multidisciplinary means 'several' not 'equal' disciplines of learning, ideally each discipline contributing a part to the whole. The medical member of the team is nowadays confronted with the added indignity of having his/her patients described in management-speak as customers, consumers, clients, service users, in fact any title that does not describe the ill person as a patient. It also reflects a creeping normalisation of 'political correctness' thrust upon us by the social engineers and should be resisted. We want patients to be treated with respect not as 'service users’, waiting for the next bus or train. Trusts are now seen to promote a business approach to health care, thereby gaining the approval of their masters, the civil servants and politicians.6 Lots of tick boxes and targets, with subtle threats of redundancies or talks about 'natural wastage'. Meanwhile, the College sits idly by.
Another concern is the training of future psychiatrists which is slip-shod and bureaucratic (lots of forms and assessments). There is hardly any room to accommodate medical students. Junior doctors who practice psychiatry are not receiving the continuity of supervision which existed years ago. The 'junior doctor' is less visible because of European working time directives, on-call commitments with days off in lieu, study leave, annual leave, and the inevitable sick leave. Passing the Member of the Royal College of Psychiatrists (MRCPsych) exams nowadays does not necessarily equate with clinical experience anymore. Even the nomenclature is confusing - not just to doctors and management (‘CT1’, ‘ST1’ and so forth) but also to staff, and reduces the profession to an anomalous set of categories no outsider understands, not to mention the loss of identity it creates in the individual doctor. What was wrong with Senior House Officer (SHO), Registrar, Senior Registrar, and Consultant? Unfortunately, we believe it is now too late to revert this shambles born out of the chaotic modernisation of medical careers. 7
The future is bleak and many doctors (and indeed nurses) are becoming disenchanted by psychiatry, feeling let down by a Royal College which seems to accommodate every new social trend rather than concentrating on improving the status of a once fascinating field of medicine. Lots of wake-up calls, but no-one is getting out of bed.8 Strange having a 'trade union' that ignores its members! Could someone inform the College that nowadays most General Adult Psychiatrists are almost reduced to measuring lithium levels, advising on clozapine doses, and attending meetings. No wonder the numbers of potential psychiatrists are falling. How would this dilution of responsibility work in a surgical unit? Would the team members decide how an operation is to be carried out because one of them is trained in resuscitation? Contrary to reports3 consultants are not happy with the present set-up, though it is unlikely our Royal College hierarchy will do anything about it. Many psychiatrists nowadays have an extensive academic knowledge of medicine, psychology, sociology, and neuropsychiatry, and no longer want to be minor players in the game, or undermined by a system that encourages power without responsibility.
Fragmentation breeds disinterest
What is the answer? The previous system, though not perfect, worked well. This had its shortcomings too (oversized catchments areas, Consultants in charge of many wards, and so forth)7 but the continuity of care was there. Patients discharged from hospital were seen by the same team. GPs could refer directly to Consultants (as is the case in other medical specialties) and patients were then seen in the outpatient clinic. However, often the patient would attend such clinics for years because GPs were reluctant to resume care. Nowadays the training and education of GPs is exemplary and most are more than capable and indeed willing, to continue to provide support for their patients provided there is a back-up plan. The academic training of psychiatrists has never been better but their clinical skills are suspect. Therefore there needs to be an overhaul in the examination system as well. Actors are not patients. Simulated psychiatry is not the same as simulated surgery. Simulation is a technique not a technology, we are told. It is not a substitute for doctors examining real patients in real contexts. The same applies to nurses. All nurses (CPNs) could easily be trained to do ECGs, act as phlebotomists, and arrange routine tests. Many already do. Give back to nurses the skills they enjoy in other fields of medicine. For psychiatrists there are numerous courses one can attend to broaden their medical knowledge. Most GPs take an interest in a holistic approach to their patients (social, psychological, physical). As matters stand GPs now refer to a borough 'Access and Allocation Team' with no one held accountable, and even though requested by the GP, a Consultant Psychiatrist's opinion is not always provided. Responsibility is the province of senior doctors and management and should not be diluted by putting pressure on the Team as a whole whose individual experience varies considerably. Doctors (and nursing staff) should have mandatory training in psychological therapies (cognitive and behaviour therapies specifically). A fixed number of sessions in addition to their usual duties could be part of the job plan for those doctors interested in the psychotherapies per se, or put another way, a holistic approach to patient care, which is what most doctors do in any event. Patients would then have the benefit of medical and psychological input simultaneously (let's call it a cognitive-medical model). Waiting lists would be dramatically reduced at a stroke and Trusts would no longer have the responsibility of finding and employing unqualified (in medicine or psychology) 'talking therapists'. People who are generally physically well and who do not have serious psychosocial problems or psychiatric illnesses could receive treatment elsewhere through their GP, counsellors or other psychotherapists (those with no medical or psychology degrees) of their own volition. There is no need to clog up the system with 'customers'. We are not a supermarket!
Complaints will inevitably follow when patient dissatisfaction begins to emerge, which is only a matter of time. More serious incidents will be a consequence of too many bed closures and staff shortages. Dilution of responsibility means that no one person seems to be accountable when things go wrong and patients are left stranded (read the Francis Report 9). Already GPs are frustrated by the lack of informal contact with psychiatrists who are once again seen to be retreating to their ivory towers, having been overwhelmed by lots of courses, lots of training, lots of meetings, lots of empty rhetoric. Too much emphasis nowadays is placed on the sociological/psychological aspects of patients' illness and so serious conditions are missed. GPs should be able to refer directly to their colleagues where there are immediate concerns and not have to wait for triage meetings which delay this process. After all, GPs know their patients best. Community clinics could take the bulk of moderate conditions (which are causing undue stress) and see patients for as long as necessary (not a determined number of appointments) before deciding the GP can resume responsibility. 'Packages of Care' and other outdated expressions should be confined to the dustbin. Patients are not fooled by promises of cardboard boxes with little pink ribbons. Continuity of patient care requires a flexible approach which encompasses easy access to information and a direct pathway to services and medical care when needed.
Knowledge in the making
Psychiatrists should concentrate on more difficult and complicated cases (as was the case in the past) as well as routine moderate conditions, enabling them to use their broad skills more efficiently and effectively. Some psychiatrists see too few patients and this should be changed. Perhaps there is a case for psychiatrists rotating through some specialties say, every five years, for example, between Rehabilitation and General Adult Psychiatry. There are many patients who are not on mood stabilisers or clozapine who require intensive input and combined medical expertise and rotating between posts would offer valuable experience. A more varied approach is thus needed but do we really need all those subspecialties? What ever happened to the general psychiatrist with a special interest? In our view at least one year of neurology training should be mandatory for psychiatrists during their training. No formal examinations, just certificates to prove the courses have been completed; otherwise the system grinds to a halt. Under this system a doctor could still theoretically become a consultant after nine years postgraduate training (three years in foundation training and neurology), and six years Psychiatry (to include neurology, psychology and sociology) which is not unreasonable. Equal emphasis on neuromedical, sociological and psychological factors causing health problems would foster a healthier and friendlier relationship between disciplines which deal with mental illness and primary care providers. As it stands, with the fragmented role of general adult psychiatric services and the emphasis on e-learning and internet training for junior doctors (no hands-on clinical experience) we are facing yet another era of overemphasis on social psychiatry (or rather reverting to ancient belief systems) with its 'neutral' politically correct denigrating sound bites (customers, clients, service users). All will be well if we can just sort out the social problems! The simplistic notion that problems will disappear if we do not smoke, drink, take illicit drugs, keep our weight down, and have a home to go to, is the stuff of social engineering by the 'experts in living,' and alas by doctors who have lost touch with medicine.
Doctors need reminding that psychiatry is that branch of medicine that is concerned with the study, treatment, and prevention of mental illness using medical and psychological therapies as well as paying special attention to social hardship and isolation where present. It is not philosophy or social science. It is to medicine what metaphysics is to philosophy. Psychiatrists need to broaden their horizons and take their heads out of the therapy books to witness the advances in neuroscientific techniques and genetic advancements that have already transformed the nature of medicine. To develop their psychological skills they need to take on board that patients want more than drugs to alleviate distress. Therefore practical techniques such as CBT or DBT (dialectical behaviour therapy) will further heighten their expertise as physicians. Many doctors are already familiar with applying CBT and other therapies. However, doctors should also be aware of the limitations of psychotherapies in general, recognizing and acknowledging that such therapies do not always work either and indeed in some instances may be harmful. Psychiatrists should be part of separate Wellbeing Clinics (perhaps one session per week) to becoming better acquainted and proficient again with physical examinations, investigations, routine procedures (ECGs for example) and interpretation of results (not just screen, but to intervene). This overseeing of the physical health of patients is not always possible in a busy outpatient clinic. Many potentially serious conditions would be revealed and information to the GP or tertiary services made known immediately. Psychiatrists are not 'stuck in a medical model' no more than a physician believes all myocardial infarcts are caused by psychosocial factors or life style. But to ignore the medical advances in molecular biology and neuroscientific diagnostic techniques portrays a profound ignorance of biological psychiatry and is insulting to those scientists who work tirelessly, often without much recognition, to further our understanding of 'brain disorders'. It is all very well to talk about art, philosophy, social sciences and literature as having a great bearing on our interest in psychiatry and congratulate ourselves as 'lateral thinkers' but an understanding of the philosophy of say, Bertrand Russell or indeed the school of Zen Buddhism, will not eliminate mental disorder. Romantic as it might sound in retrospect, Vincent Van Gogh did not enjoy cutting his ear off, nor did Robert Schumann feel ecstatic when jumping into the Rhine before being carted off to the asylum.
If we do not embrace a holistic view of mental ill-health we risk not only throwing the baby out with the bath water but the bath itself, thereby causing further dissatisfaction and low morale among doctors with an inevitable negative impact on patient care. Psychiatrists are not bemoaning their loss of hegemony - a favourite word and another myth propagated by the antipsychiatry lobby; rather, it is only too obvious to them (as qualified medical doctors) that patients will suffer in the long term by not being referred appropriately to those who have the expertise to recognize and distinguish between human difficulties and illness. There is also a need to re-examine the impact of psychological therapies and not succumb to the popular and naive notion that they are all evidence-based in scientific terms. In the meantime the 'worried well' can indulge themselves with all the peripheral talking therapies and current fads they desire. Likewise, performance management, outcome measures and payment by results have become relentless tick-box exercises creating unnecessary stress among health care professionals (threats of job losses) who 'must meet targets at all costs', all for a slice of the Commissioners' cake. What a way to run a health service! Patients become meaningless statistics in the meantime. No! The wake-up call should be aimed at those who are intent on destroying the good will and values of the very same people they purport to support, through their social engineering and outdated attitudes.
The Care Programme Approach (CPA) was introduced in England in 1993 to co-ordinate the care of patients with mental health disorders.1 Its aim was to ensure that there was a full assessment of the patient’s needs, that a care co-ordinator would see that the care was delivered, regular checks would be carried out to review progress, there would be collaboration between health and social services, and that patients (or the term used to ‘demedicalise’ them in psychosocial Newspeak 2 namely, ‘service users’) and carers (they also use the service) would have a greater say in the written management plan. Targets were set.
What has happened since? Prior to this I recall that most psychiatrists carried out full assessment needs, regular checks reviewed progress (outpatients), social services were involved when necessary, and patients and their families were nearly always involved in the discussion of after-care, when appropriate. Despite the condescending manner in which patients and carers were treated by the hierarchy, i.e. they would not understand the difference between social services management and other after-care, it was always quite clear to doctors that patients had no difficulty with the concepts of medical intervention (investigations, diagnosis, treatment), psychological therapies, and social help (housing, work, family, finances).
Rather than simplifying the process we now have two tiers of CPA, namely, standard and enhanced. Where the patient has ‘complex needs’ or is a ‘complicated case’ then you are in the enhanced bracket. For the rest – back to the General Practitioner (GP)! Not enough resources apparently. Not ill enough more likely. Remember – you have to have a severe and enduring mental health disorder – nothing else counts. Nowadays the GP is expected to be a specialist in mental health and run a risk assessment on every ‘psychiatric’ patient. The GP is frowned upon by the ‘experts in living’ should he/she for example, dare refer a mild or moderately (yes - those descriptions again!) ill patient to the Mental Health Services. Because there is no bottomless pit of money, the scenario was changed in 2008 so that those receiving only standard CPA were no longer entitled to it. However, not to appear callous and indifferent to the plight of those suffering from ‘less severe’ mental health problems, the usual lip service was paid to patients, assuring them that they should be respected and supported, and that their carers be also recognised as having ‘needs’. All the buzz words were put in place again – integrated care pathways, working together, reviews about the reviews, good practice, better training, and so forth. Now there is the Supervised Community Treatment Order, (whether you like it or not) and those subject to the new ‘order’ will be entitled to the ‘new’ CPA. Wonderful in theory.
So what happens to a patient who is not on CPA? We are informed that such patients should still be open to secondary mental health services, should continue to receive clinical support, that reviews should take place regularly, and a social assessment should be available under the new guidance to local authorities FACS (Fair Access to Care Services), readily available on the Internet. The truth of the matter is that only those patients on enhanced CPA will receive immediate support, the rest will have to jump through the usual hurdles to prove they have a severe, enduring mental illness (enduring is not enough) in order to gain access to NHS ‘support’ facilities. Some patients are seen as more deserving than others, for example, those admitted to hospital under the Mental Health Act (voluntary admission may count against you), current or potential risk (theoretically, any patient with a mental health disorder, which seems to defeat the purpose of the exercise) or the presence of a dual diagnosis (depression with alcoholism, or is it the other way round?). Anyway, if in doubt, the patient is entitled to a formal reassessment CPA and may be admitted to the ‘new’ CPA list. If all fails, the patient (remember, one with severe, enduring mental health symptoms) may make a complaint to the local authority or even hire a lawyer.
What is the true state of affairs? To begin with, many patients have enduring mental health problems which are not severe, are not life-threatening, and despite the hardship and drudgery endured, manage to trundle through work, relationships, and family life. Years of talking therapies or psychotropic medication, indeed both, may have only taken the edge off their symptoms. Often symptoms resurge and require alterations or adjustments in medication; sometimes a different psychological approach needs to be considered. Such patients are best left to the fountain of all wisdom, the GP, so it seems. Rather akin to telling the GP to treat for example, a ‘minor’ cardiac problem (say, palpitations) because the ‘specialist unit’ only deals with severe arrhythmias, severe pain, severe disability, ‘severe everything’. It is unfair to expect GPs to make informed decisions concerning psychotropic medication (no more than they should about adjusting chemotherapy drugs) and most would be familiar only with specific therapies such as Cognitive Behavioural Therapy (CBT) or Anger Management, where appropriate. The type of patients described here comprise the majority of those seen in outpatients, yet there is now a growing trend to discharge such patients back to the GP, because he/she is not ‘care co-ordinated’ on enhanced CPA. The burden is on the GP. It does not seem to have registered with politicians or management (doctors included) that chronic schizophrenia is not the same as chronic gastro-oesophageal reflux.
The trend now is for the setting up of Community Clinics (the patient does not necessarily get to see a doctor) where ‘all the other psychiatric problems’ are dealt with. The traditional psychiatric outpatient department is to be abolished, unless of course, GPs do something about this torrid state of affairs now. It could only happen in Psychiatry which seems to me a specialty doomed to oblivion. Family doctors are becoming increasingly irritated by a system or discipline (Psychiatry especially) which seems to ignore their concerns and is more preoccupied with targets (nothing has changed) and outcomes (back to the GP). Even referrals from GPs, who want a medical opinion, are filtered in order to weed out those not worthy to enter the hallowed walls of the Mental Health Institution. Those patients who ‘know the system’ or who are vociferous and make complaints (‘I know my rights’) get to be seen by the Great and Good. Lesser mortals, usually those with serious mental illnesses, do not make any undue demands and are therefore often forgotten or fall by the wayside. A patient with bipolar disorder on lithium is discharged back to a GP who is unsure whether or not the medication needs ‘fine tuning’ at times, should be discontinued, or reinstated were compliance is a problem in one heading for a relapse. As a corollary of that, I am sure most hospital doctors would not know what the acronym ABVD means in the chemotherapy treatment of Hodgkin’s disease. Adjusting psychotropic medication is not quite the same as adjusting an antihypertension regime. Unfortunately, if the patient needs to be referred back into the system the whole Kafkaesque scenario begins again.
A medical colleague once bemoaned to me that psychiatrists are totally out of touch with Medicine. Alas, it seems they are also now out of touch with their medical colleagues.
Interest in cross-species transplantation has recently been rekindled1. This is due to many developments including the shortage of donor organs, advances in transplant medicine, investment in biotechnology research, and the non-availability of more ethically suitable alternatives to human organs. Increasing success rates in allotransplantations (organs from different member of the same species) has increased the demand on donor organs1, 2. Other types of transplantation include autotransplants (a person’s own organs or tissues are used for transplantation) and isotransplants (organs from one person are transplanted into another genetically identical person, like an identical twin). These options are limited in terms of body parts used and numbers.
Good facts inform good ethics. It is therefore obligatory to look into the current research knowledge about xenotransplants (organs from one species to another, for example animal to human) in more detail. The advocates of xenotransplantation argue that it could provide organs “relatively quickly” and hence save more lives. If animal organs were easily available for transplantation most eligible recipients would receive the transplantation much earlier on in their illness. It is argued that this may decrease distress and suffering. Whilst xenotransplantation may theoretically increase the survival time, it is unclear, however, whether the negative impact on recipients’ quality of life due to long-term immunosuppressant therapy and the risk of zoonotic infections would in fact worsen the overall long-term outcome3. Recent research suggests that xenotransplantation may be associated with the transmission of pig microorganisms including viruses, bacteria, fungi, and parasites. Because of the recipient’s likely immunosuppressed state, infection and pathologic consequences may be more pronounced. Transmission of most microorganisms with the exception of the porcine endogenous retroviruses may be prevented by screening the donor pig and qualified pathogen-free breeding. However, porcine endogenous retroviruses represent a special risk as they are present in the genome of all pigs and infect human cells in vitro. Until now, no porcine endogenous retrovirus transmission was observed in experimental and clinical xenotransplantations as well as in numerous infection experiments4. Nevertheless, strategies need to be developed to prevent their transmission to humans. It is equally possible that many eligible recipients may be denied having a trial of xenotransplantation by doctors who believe that there is an unfavourable risk-benefit ratio. The limited long-term data on outcomes of xenotransplants thus renders ethical analysis difficult.
There is some evidence to suggest that the recipients of animal organ donation may develop a different self image with possible consequences for their identity5,6. This happens with human organs at times, but may be a more significant problem with animal organs, as the recipient knows that they have been given a non-human organ. Loss of identity jeopardises the core principle of autonomy, which underpins all medical treatment.
The risk of zoonosis to the recipient and to the wider society cannot be accurately estimated7. Hence there is a requirement for vigilant post-operative monitoring5 with a possibility of engaging article5 and 8 of the European Convention of Human Rights (for England and Wales: Human Rights Act 1998)†. Article 12 may also be engaged as the recipients may be restricted from having physical relationships, carrying out their routine day to day activities and socialisation. This is because the prevention of possible risk to the wider public from zoonosis may require the recipient to be put under restrictions with regard to their engagement with others. This may include restrictions to go out, which can result into de facto temporary detentions at home. Hence consenting to xeno-transplantation would be “binding and contractual” over a long period of time. The subject may not have the right to withdraw. This is entering into a de facto contract with potential restrictions or even deprivation of human rights. This would restrict the ability to give informed consent even for a well informed patient, as it is difficult to be fully appreciative of future restrictions of one’s liberty.
Autonomous decision making and thus informed consent may also be put at risk by other factors surrounding xenotransplantation. The decision to embark on xenotransplantation may be primarily driven by an instinctual wish to survive due to a lack of other viable alternatives. Patients in these circumstances may have little or no consideration to medium and long-term effects on themselves and society. However, it is the consideration of such long-term consequences that make a truly autonomous decision, and differentiate it from a decision that is purely based on immediate instinct. Whilst the wish to survive is legitimate it is difficult to make decisions free of the pressure to survive when there is a lack of alternatives.
It also brings up an even more important question: Can any person everconsent to a future restriction or deprivation of their liberty or other human rights? Even if there were an option to define acceptable future restrictions it would be likely that patients could still challenge the legality of any such agreements. They could quite reasonably argue that they have agreed to the restrictions under duress because of a lack of viable alternatives to their xeno-transplants.
Xenotransplantation touches questions of utilitarianism (greatest good for the greatest numbers) and public protection2. Utilitarianism takes into account the reasonable interests of society in good outcomes, fairness in the distribution of resources, and the prevention of harm to others. The Nuffield council on bio-ethics embraces a utilitarian approach. However, there are limits to the utilitarian argument for xenotransplants. Even if they were widely available, the treatment would be immensely expensive. Production of a pathogen free donor organ would involve rearing animals in strictly controlled environments, subjecting them to rigorous standards of examination and surveillance. The additional costs of developing a sustainable work force to provide transplantation and post-transplant surveillance of the patient and the community would be high. The insurance providers may not cover expenses of a xenotransplant. Public health care providers may decline to provide this treatment as it may not be recommended by expert groups as cost effective. Xenotransplantation may commence in the developing world where the regulations are lax and the poor can be more easily exploited8. Patients who would potentially benefit from xenotransplantation may not be able to afford it due to its cost with serious implications for fairness.
Xenotransplantation also raises other ethical questions in relation to the wider community. We have seen that consent of an individual to a xenotransplant has significant bearing on the protection of society7. Should the members of a community therefore be consulted if there were any xeno-transplantation experiments in their region? The risk is primarily due to the risk of zoonotic infections, the need for surveillance, and possible quarantine of contacts7,9. In addition, if health authorities were to fund expensive experimental interventions like xenotransplantation, other routine treatments of greater potential benefits to society may be jeopardised. Society may also have views about particular animals being used as donor animals10. For example religions like Islam and Judaism may feel that pigs are ‘ritually unclean’. They may therefore not approve of certain animals to be used for donation, and more worryingly may fail to socially accept recipients with such ‘unclean’ transplants11.
From a deontological perspective (this judges the morality of an action based on the action's adherence to a ruleor principle) some authors assert that animals have rights similar to those considered appropriate for humans12,13. The protection of animals has legal status in many countries. Consequentialists may view the suffering and death of an animal as acceptable for the betterment of a human patient, as they would judge the morality of an action primarily by its end result. They would argue that potential benefits and improvement in human welfare arising from xenotransplantation may justify the loss of animal life. However, this will never satisfy the animal rights lobby; especially as whilst minimising the risk of acquired infections, the animals have to forgo greater suffering in the form of isolation, monitoring and investigations. Furthermore, genetic modification can have both immediate and long-term negative effects on animals.
In summary, xenotransplantation has significant ethical consequences. On an individual level, there are the questions of pressure to consent that may negate autonomy and the validity of that consent as well as the difficulties that arise when patients are asked to consent to future restrictions of their human rights. On a societal level there are questions of cost and benefit analysis as well as risks from zoonotic infections. In addition, questions of animal rights need to be addressed before any programs are likely to go ahead.
†Appendix of articles of the Human Rights Act.
Article 8 of the Human Rights Act 1998 (The right to respect for private and family life, home and correspondence)
Article 5 (The right to liberty).
Article 12 (The right to marry and found a family)
“The more we care for the happiness of others, the greater our own sense of well being becomes.” The Medicine of Altruism: Dalai Lama
Introduction
The fundamental mission of any medical school is to select those individuals who possess the qualities and personality traits best suited to becoming a good doctor. The first part of this article takes a critical look at how United Kingdom (UK) medical schools select doctors, which can vary considerably, and asks whether it can be improved. The qualities needed to be a good doctor are discussed and asks whether work experience illustrates at least some of these personal qualities and should therefore be an essential prerequisite for applying to medical school. Such experience helps the student to make an informed career choice and exploring it at interview can reflect student motivation to study medicine. My experience in Ghana gave me the opportunity to find out at first hand if I had what it takes to become a doctor. The trip was totally inspirational. It made me realise that medicine is much more than being master of all sciences. In Ghana I saw many of the qualities one needs to be a doctor, how this contrasts with the current selection criteria in the UK, and made me wonder whether the UK system offers our society the best practice available.
Critique of UK medical school selection
Applying to medical school has become increasingly competitive. Selection into medical schools is not an exact science but one assumes that best available evidence is being used. The present system almost certainly turns away students who would make good doctors and accepts some who are mediocre or poor or even drop out of medicine altogether. The selection criteria for entry into medicine have to be accurate. However, no system is fool proof and the number of drop-outs in UK training stands at 6.8 – 12%.1,2,3 I believe that better selection criteria would reduce the drop-out rate and save personal distress among those who made an unwise choice. This makes economic sense. There is widespread agreement that we should select medical students on wider criteria than scores of academic success,4, 5 though in practice many medical schools have valued academic scores at the expense of other considerations.6, 7 A Levels alone should not be sufficient to gain a place at medical school. True communication calls for some shared life experiences and empathy with others. I believe that students who are totally absorbed in their studies to the exclusion of almost everything else are less likely to make good doctors. In one study, a ten-year follow-up after entry into medical school showed no correlation between academic score at entry and drop-out rate, but significant correlation between low interview scores and later drop-out.8 Reasons for drop-out were a variety of personal reasons including lack of motivation for study or for medicine. In a medical school that carefully evaluates applicants, empathy and motivation to be doctors were found to be particularly important in predicting both clinical and academic success.9
Another major study, looking at the dropping out from medical schools in the UK over a ten year period (1990-2000), 10 showed that drop-out rates increased during this period and concluded that the probability of dropping out of medical school is 20% lower for students with a parent who is a doctor. The authors comment that this may be the result of greater commitment or better preparation and insight before starting the course. Ethnic background of students was recorded only between 1998-2000. The study found that Indian females were around 1.9% less likely to drop out compared with white females, whereas Indian males were no different from white males. Other ethnic groups were less likely to drop-out by around 0.8%. A concerning fact in this paper was the degree to which drop-out rates varied between different medical schools. No study to date has been done to find the reasons for these differences. Surely potential applicants need to be aware of these results. The differences could be accounted for by variable selection processes among the medical schools.11 Some medical schools shortlist for interview only on predicted academic performance or the number of A* GCSEs or decide by the UK Clinical Aptitude Test (UKCAT) / BioMedical Admissions Test (BMAT) scores. Some use information presented in the candidate’s personal statement and referee’s report while others ignore this because of concern over bias. In some cases candidates fill in a supplementary questionnaire. Interviews vary in terms of length, panel composition, structure, content, and scoring methods. Some schools do not interview.
The commonest reasons cited in many papers for dropping out of medical school were because it is not for them, they found it boring, they did not like patients, the work environment was not what they want to spend their time on, or they did not like responsibility.12 Essentially they had realised too late that Medicine was not for them. They had failed to find out what they were letting themselves in for before applying and the medical school had failed to pick this up. There is a strong argument for pooling resources so that applicants get one good assessment instead of four poor ones.
A levels, used for medical selection, do not indicate any personality attributes of the candidate and are affected by socio-economic bias. The UKCAT was introduced to level the playing fields. This test doesn’t examine acquired knowledge and candidates can’t be coached to pass, so in theory it should provide a fairer assessment of aptitude than A level grades. It was also thought that the various components of the UKCAT, namely verbal reasoning, quantitative reasoning, abstract reasoning, and decision making, could help to pick the students who have the personality attributes to make good doctors. Unfortunately, a recent paper suggests that the UKCAT does not provide any more assessment of aptitude than A levels.13 However, an inherent favourable bias towards students from well-off backgrounds or from grammar and independent schools was also found. Moreover the test does not compensate for talented candidates whose education has been affected by attending a poor school. Another paper looked at the predictive validity of the UKCAT.14 This showed that UKCAT scores did not predict Year 1 performance at two medical schools. Although early prediction is not the primary aim of the UKCAT, there is some cause for concern that the test failed to show even the small-to-moderate predictive power demonstrated by similar admission tools.
There is no doubt that potential doctors must have enough intellectual capacity to do the job but they must also possess other important traits (Table 1):
Table 1: Personality traits potential doctors ought to possess
Concern for people
Committed to self-learning
Sense of responsibility
Emotionally stable
Professionalism
Good judgement and perception
Good communication skills
Good listener
Highly motivated
An enquiring mind
Honesty
Well organised
Integrity
Patience
Ability to handle pressure
Mental strength
Confident
Resilience
Determination
Respect for other people
Perseverance
Respect for confidentiality
Decisiveness
Tolerance
Conscientious
Hard working
Team player
An open mind
Leadership qualities
A rational approach to problems
Humility
Critical reasoning
Flexible and adaptable to change
Separate important points from detail
Logical thinking
Recognise limits of professional competence
What patients rate highly among the qualities of a good doctor are high levels of empathy and interpersonal skills.15 Personality traits such as conscientiousness have been positively associated with pre-clinical performance.16
The criteria being used more and more by admission tutors include the candidate’s insight into medicine including as evidenced from work experience.17Surprisingly, very little has been written on work experience and the value placed on it varies considerably between medical schools. Many would regard this experience as a prerequisite for entry into medical school. It enables a student to experience at first hand what he/she is letting him/herself in for. Some find the experience fascinating and challenging while others may find it is not for them. Work experience should not be seen as a hurdle to climb, but part of the decision-making process in determining whether medicine really is for you. I fear that another contributing factor to the increase in drop-out rates from medical schools is the increasing difficulty in obtaining work experience. Gone are the days when students could join theatre staff and watch an exciting operation or shadow doctors in Accident and Emergency (A&E). Useful work experience is so important and it is becoming harder and harder to get, but is still possible. Therefore considerable desire, commitment and motivation by the student are required to obtain it. The work does not need to be medically related, but work experience in any care setting is essential. These placements can be used to illustrate at least some of the personal qualities that are sought after in a good doctor including: appreciation of the communication skills required of a doctor; a thorough awareness of the realities of medicine and the National Health Service (NHS); an understanding of teamwork; an ability to balance commitments; and observation of the caring and compassionate nature of the doctors. Furthermore, as demonstrated in general practice,18 personal experiences can have a highly positive influence on an individual’s attitude to a particular speciality. Encouraging school students to experience general practice would therefore not only increase their awareness of the life to which they are about to commit, but could aid recruitment to general practice as a speciality.
My Ghana Experience
I decided that, as part of my work experience, I would go to Ghana with a charity organisation (Motec UK Life). The reason was not to impress medical admissions tutors, but to discover if I had what it takes to become a doctor. I realised how comfortably we live in our small bubble, with little appreciation of what goes on in the rest of the world. Ghana is a third world country, which not only has great poverty and malnutrition but also has many deadly diseases such as Acquired Immunodeficiency Syndrome (AIDS)/Human Immunodeficiency Virus (HIV), malaria, hepatitis, typhoid and sickle cell disease. My trip was demanding as I was stripped of my luxuries and removed from my comfort zone, but it helped me to understand the real values in life through helping the most needy and vulnerable people. I felt the suffering and the pain they went through, day in and day out, but knew that making even the slightest difference to their lives motivated me and enabled me to persevere through my time there.
One of the hospitals we stayedwas Nkawkaw, which was in the middle of a shantytown with houses made of metal sheets. Yet, despite the presence of great poverty and disease, I did not find a single person who was not extremely kind and welcoming and always smiling. It made me think of the contrasting situation back home in the UK where people were relatively well off, and yet so unhappy. I spoke to as many people as possible, not realising that I was developing my people- and communication-skills. I played football with the children and made them smile. I was able to visit the AIDS/HIV clinic and gained a first-hand account of how this devastating disease was controlled and dealt with in a third-world country. The pain, grief and suffering were immense and difficult to comprehend unless one was actually there witnessing it. AIDS here hurts everyone, but children are always the most vulnerable. The children were born with HIV from their mothers, or infected through breast milk, or in the past infected by unsafe medical treatments. They were often orphaned and destitute, having to build their own homes, grow their own food, and care for younger brothers and sisters. That is the cruel reality.
Equally heartbreaking was seeing so many people in the HIV clinic who could
not afford the anti-retroviral drug that would improve the quality and duration of life. This feeling of helplessness motivated me even further to pursue a career in medicine in order to help people at their most vulnerable. On this trip I was greatly impressed by the dedication, commitment and professionalism shown by the doctors in difficult situations. I saw doctors working with little supervision and little equipment, and yet they seemed confident, well organised, and adapted themselves well to the conditions. Their enthusiasm and compassion never waned despite working long hours.
I saw many types of operation being performed including joint replacements, hernia repairs and caesarean sections. On one particular day, I observed the team performing many knee and hip joint replacements. The deformities of the joints were much more severe than seen in the UK. I enjoyed and appreciated the skills of the orthopaedic surgeons in carrying out these operations, which were being done under spinal anaesthesia, and so I was able to talk to the patients and comfort them. Throughout the day, after seeing many operations, I did not flinch or feel queasy at the sight, and this further encouraged me to believe that I could handle a career in medicine. On watching the caesarean sections, the excitement of bringing new life into the world was overwhelming. Seeing another baby being born with severe hydrocephalus marred this. No treatment facilities for this condition were available for hundreds of miles and the baby was too ill to be transferred such a large distance. I witnessed the doctors conveying the heartbreaking news to the family with compassion. It became clear to me that there are negative aspects to this career. There is a great deal of emotion and stress to cope with in such circumstances but I believe that, given training, I would be mentally stronger to take control of these situations.
I was always allowed to follow the doctors on their ward rounds, and was encouraged to ask questions and make comments, so that I often felt that I was being treated as a medical student, which was strange in some ways but also very gratifying. On this trip I was involved in teaching and in helping to set up a workshop, which lasted for a whole day for doctors from all over Ghana. This involved lectures as well as demonstrating the latest surgical and theatre equipment. I was impressed by the teamwork and organisation shown by the group. The communication skills of the group had to be of the highest quality in order to get the message across. I found that teaching about the devastating effects of HIV, in a local school in Ghana, was particularly challenging as some of the students before me were sufferers and so I found it difficult to look them in the eye, knowing that although they were being taught the safety precautions, many did not have much of a future. This reinforced my feeling of helplessness but, although this situation was heartbreaking, I remained enthusiastic for the children, to keep their morale high in order to prepare them for their inevitable future.
Conclusion
My trip was totally inspirational. It made me realise that medicine is much more than being a master of all sciences. In Ghana I observed in doctors the real passion and drive needed for medicine as well as many other essential qualities I believed doctors needed. This contrasts with the current selection criteria in the UK; sadly we are missing out on too many good doctors because of our obsession with grades rather than looking for real qualities that are going to make a difference to our patients.I discovered that seeing the immense suffering, and the close bond of doctors and patients in an entirely different social and economic context, helped me to evaluate and shape my own emotions and personal values. My motivation in wanting to become a doctor has increased tremendously since this trip. My trip to Ghana also inspired me to create a medical journal in my school as a fund-raising initiative. I brought together a group of fellow students to write articles about common teenage problems (teenage drinking, anorexia, obsessive compulsive disorder (OCD), stress, smoking, sexually transmitted diseases (STDs)) as well as articles on euthanasia and assisted suicide, stem cell research and the NHS. I wrote about my personal experiences in Ghana in addition to editing and publishing the school journal. All the funds raised from the school medical journal will be going to the HIV victims in Ghana.
A lifetime of happiness! No man alive could bear it: it would be hell on earth
George Bernard Shaw (1856-1950)
Guess what? Antidepressants do not work for mild or moderate depression! This amazing ‘revelation’ seems to surface periodically as a popular item in the media and platform for the experts in living, especially since talking therapies are now considered the panacea for all ills. Despite methodological flaws in the research (as with all studies)1 and noticeably, with less scrutiny of talking therapy research, this ‘fact’ is preferentially brought to our attention. That antidepressants have unpleasant side effects and are not always effective we have known all along. When one thinks about it, all drugs have adverse effects. Strange how antidepressants work - they seem to cause unpleasant adverse effects but not beneficial ones! No one doubts that neurotransmitters are involved in pain transmission or are responsible for muscle movement, yet biological pathways are dismissed when ‘emotional’ or ‘psychological factors’ are promoted as causing distress. By contrast, talking therapies cure the problem and are considered safe, it seems.
Am I alone in not being surprised? I have never understood how mild depression (whatever that is) becomes moderate, or how normal becomes mild, even with the International Classification of Diseases (ICD 10) and Diagnostic and Statistical Manual of Mental Disorders (DSM IV) to hand. And who has decided there be a minimum duration of two weeks for mild depression? Does it not count if one is suicidal for a week? The corollary of this is seen in another nugget of perceived wisdom masquerading as ‘research’ which informs us that 14 units and 21 units of alcohol per week are considered the upper limits of safe drinking for women and men, respectively. What if intake exceeds these magical figures? A rigid adherence to the dictum would castigate a woman or man as alcohol-dependent imbibing 15 and 22 units per week. This type of anecdotal research has no scientific meaning because one cannot equate units with a way of life, one’s metabolism, stature, weight, and so forth. In the laboratory I can detect mild anaemia from severe anaemia because haemoglobin can be measured, and when to treat is usually quite clear-cut. In mental health studies, as with the alcohol example quoted, the theory is also vague. The usual response from ‘researchers’ in this field is that rating scales are capable of detecting differences in mood, say, which then determines the ‘therapy’ one receives. This is a fallacy. For example, in medicine, small variations in haemoglobin do not make the slightest difference to how a patient feels, though such fluctuations are important.
How do you measure tiredness? One can feel tired and have a normal haemoglobin level. In the elderly, for example, abnormal blood indices are often present despite an outwardly well appearance. The anaemia still needs to be treated. Laboratory tests are therefore used to confirm the severity of an illness and are objective, regardless of outward appearances. Treatment is given and the haemoglobin (in this example) returns to normal, without the patient even being aware in many cases. The difference between the above example and a mental health ‘condition’ is that there is no realistic cut-off point between feeling well and being unwell. Therefore, when to intervene is arbitrary. Am I tired because I’m depressed, or is it the other way round? Do two or more weeks of mild happiness mean I am ill? ‘Is there such a thing as moderate happiness?’ ‘Should we be using mood stabilizing medication or talking therapies if we are mildly or moderately happy?’ Absurd. No one speaks of another individual as being mildly or moderately happy. So why should it make sense to talk of someone as mildly or moderately depressed? What next – mildly or moderately normal? Severe conditions require treatment; mild upsets can be managed by simple alterations in lifestyle, and one does not need a medical doctor or an expert in living to tell you so. There is little point in expecting a favourable drug treatment outcome for say, hypertension, if the patient continues to smoke or is grossly overweight. Take the metabolic syndrome of dyslipidaemia, central obesity, hypertension, and insulin resistance: treatment involves removing the causative factors, not prescribing drugs to reduce weight.
I am a kind of paranoiac in reverse. I suspect people of plotting to make me happy.
J.D. Salinger (1919-2010)
The norm for most people is to get on with matters in hand and tolerate life’s daily grind. Some good days, some bad. A lot depends on your financial status too. Nothing new there. It does not make sense to assume antidepressants will make the slightest difference to an individual’s ‘ups and downs,’ as there is no clinical syndrome to address. Living is not a genetic condition, though alterations in genes affect living. There is the risk of medicalising every difficulty one faces. Behaviour is often personality-driven and not a symptom of illness, and though personalities vary, one does not speak of a personality illness or personality condition. Even the term personality ‘disorder’ has come in for much criticism because of the difficulty in defining what is meant by personality.2 One individual may be overtly aggressive, another too passive, and to embrace all eventualities, there is the term passive-aggressive. No point in being perfectionist because nowadays you may fit the obsessive character description. On reflection though, I would rather the cardiologist, surgeon, airline pilot, concert musician and so forth, err on the side of perfectionism! It does not require much imagination to realize that the real test of a ‘condition’ is when an individual begins to feel he/she is not functioning at a healthy level because of a pervasive sense of inertia, lassitude, lack of motivation, persistent gloominess and despair, for reasons apparent or not. Most people feel despondent at times, say after bereavement, or losing one’s job, and likewise many individuals are more motivated, innovative, and ambitious than others. Some conditions, which seem to have a genetic basis, have stood the test of time, such as bipolar disorder, eating disorders, schizophrenia, borderline personality disorder and obsessive compulsive disorder; all other ‘disorders’ less so.
That antidepressants often fail to work is nothing new, even for severe depression because there are often too many factors at work. Patients who suffer from severe depression and suicidal ideation would be unlikely to be entering a clinical trial in any event. Furthermore, the theory of a chemical neurotransmitter imbalance is outmoded. It could be that an alteration in receptor sensitivity, either at the presynaptic or postsynaptic site, is the critical factor. Furthermore, it is conceivable that more neurotransmitters are involved than the handful we know of at present. What does the physician do then? Tell patients there is only a 70% chance of getting better with antidepressants and let them get on with it! Anyway, why should antidepressants be any different to other drugs used throughout the entire field of medicine? No drug has a 100% cure rate (save perhaps antibiotics or vaccines for specific infections). When one is well it is easy to be critical, cynical and dismissive. When a patient develops Hodgkin’s Lymphoma or any other serious nonsurgical illness and is told there is a 70% chance of survival with medication it is highly likely he/she would optimistically choose the latter. Why should severe depression be any different?
Rating scales cannot be robustly be relied on, at least in psychiatry, as most information is descriptive and there are few instances when a scale can be regarded as having proven validity.3 The Hamilton Rating Scale, a commonly used measure of depression, contains a large number of items relating to sleep and anxiety, and hence sedative antidepressants may seem to be appropriate. It could therefore be argued that the patient is benefiting from a good night’s sleep rather than any inherent antidepressant effect of the drug in question. Thus the side effect of the drug now has a therapeutic effect! This is akin to saying antihistamines work only through their sedative effect! Many scale items are poor contributors to the measurement of depression severity and others have poor interrater and retest reliability. Besides, mental and emotional diagnoses are so often ephemeral, and therefore defy ‘rateability’. Another example is the Beck Depression Inventory (BDI), often used as a screening tool: because it is a self-report questionnaire, it poses problems in that the person completing it may distort responses. The question therefore is: how does one prove that antidepressants are effective on the basis of flawed clinical trials even when the evidence in clinical practice is obvious?
Meta-analysis is often used as ‘proof’ that research shows or does not show evidence to support a particular theory. However, meta-analysis itself is not foolproof. The methodology is complex and fraught with difficulty.4 The sheer volume of material can impress the naïve and the search for negative outcomes, if it suits the preconceived, intended purpose, will be celebrated in the media as ‘scientists discover’ and so forth. A diligent search of the literature will uncover the sort of results one is looking for, because remember, there are lots of bad trials, no trials are identical, and there is heterogeneity among trial results.
It is clearly very difficult to devise a perfect rating scale, particularly in psychiatry where one is dealing in ‘mind matters’ and the pathoplasticity of mental disorders. Besides, leaving ‘research’ aside, the terminology in psychiatry as a whole is vague and interchanges between lay descriptions and ‘psychiatric’. Does ‘mad’ mean psychotic? What is madness anyway? Is neurotic the same as being a worrier or chronically anxious? Can one be neurotic about one thing and not another? Is a teenager worried about exams (assuming he/she is fully prepared of course) normal, anxious, neurotic or unduly concerned? In medicine, matters are clearer by and large: blood pressure is high, low or normal. We are not comparing like with like, is the usual retort.
To be stupid, selfish, and have good health are three requirements for happiness, though if stupidity is lacking, all is lost.
Gustave Flaubert (1821 - 1880)
Although it is easy to accept that antidepressants are ineffective for mild or moderate depression, one has to consider that in even in major depression the effects of spontaneous remission (75% in 12 weeks in some instances)5, 6 and natural fluctuations need to be taken into account. Even patients with chronic symptoms, who normally seek help when their symptoms are at their worst, sometimes improve anyway. Take a simple known fact: the prevalence of pain in patients with depression is high, around 65%, and the average prevalence of depression in pain clinics is nearly of a similar order. Pain symptoms in depression are not adequately treated by Selective Serotonin Reuptake Inhibitors (SSRIs) or indeed by amitriptyline (commonly used for pain relief) and hence depression is prolonged.7 On reflection it should not be too difficult to comprehend why drugs do not always work given that some three billion base pairs of deoxyribonucleic acid (DNA) make up the human genome. To add to the complexity, copy number variation refers to differences in the number of copies of a particular region in the genome, which is associated with susceptibility or resistance to disease.
Patients who are depressed and helped by medication are now being told by irresponsible ‘counsellors’ and sometimes by their own family doctors, that they are really only taking sugar pills, because of selective information taken from flawed antidepressant drug trials. By the same token should patients also give up their counselling sessions and take a sugar pill? It should not be forgotten that a true placebo control is impossible in psychotherapy unlike physical methods of treatment (though still difficult), whatever the flaws inherent in the latter. It seems odd that psychological data in ‘therapy studies’ carried out by non-clinicians and clinicians gets to be called ‘science’ whereas drug research carried out by scientists becomes ‘flawed science?’ Even so, countless dubious articles of ‘human interest’ manage to appear in prestigious medical journals under the apparent authorship of ‘leading figures in the field’ (being a pop celebrity physician or psychologist helps) where the psychobabble is fed to the reading classes who in turn regurgitate it to their naïve, well-intentioned adherents, and to the media. I don’t blame the latter: all the media want is a good story; ‘human interest’ items will sell newspapers regardless of their quality or accurateness. People who run the media have little understanding of science and wear their ignorance as a badge of honour.8 Therefore it comes as no surprise when it is discovered that antidepressants do not work for mild or moderate depression that the slogan becomes ‘antidepressants do not work at all,’ which is what the critical psychiatry faction wanted in the first place.
If you can’t explain it simply you don’t understand it well enough.
(Albert Einstein 1879-1955)
Ironically, as in neuropharmacology, it is through progress in molecular biology that advances in psychotherapy research will be made as molecular genetic findings unfold over the next few years; it is likely that biological vulnerability will become increasingly detectable; although single genes and polymorphisms will probably never account for a large proportion of variability, combinations of genes may increasingly identify specific types of environmental vulnerability.9, 10 No mental health condition is ‘all genetic or environmental.’ However, it is through neuropharmacological research that the mechanisms of action of various drugs used in neurology and psychiatry have been identified and helped to develop an understanding of biological substrates underlying the aetiology of psychiatric disorders. Genetic studies help us understand why some individuals are more prone to becoming ill given the same environmental stress factors.
The overriding clinical impression by doctors in clinical practice and in hospital settings is that patients tolerate minor side effects in the hope that benefits will accrue in the long term, as they do with the very unpleasant adverse effects from other drugs used in medicine (chemotherapy, for example). It is incumbent for doctors to stress that antidepressants do work for severe depression (though not in all cases) and mood stabilizers are helpful in bipolar disorder, and advise about untoward effects.11 Doctors should also emphasize that the therapeutic effect is not that of a placebo, much in the same way that methylphenidate helps many children with Attention Deficit Hyperactivity Disorder (ADHD) when it is properly diagnosed and not attributed to poor parenting skills. The beneficial effects of antidepressants when they do occur are noticed objectively, usually within four to eight weeks of taking the medication, sometimes sooner. Patients are not coerced into feeling better by the charismatic charm of the physician, who may be sceptical to begin with, in any event. Besides, ‘charisma’ wears a bit thin when one continues to feel miserable and unresponsive to treatment of whatever sort. Cognitive therapy is effective for those who are motivated and not too disabled with lethargic indifference to engage. Behavioural methods do work, because specific techniques are employed which allow accurate objective evidence (cessation of smoking, desensitisation for phobias, amelioration of obsessive rituals) to be gathered.
There is a vast grey area between what constitutes ‘normal’ and ‘mild or moderate’ depression. In most cases, even if one concedes that a patient is ‘mildly or moderately’ depressed there is usually no need to interfere, because everyday issues are usually the triggering factors. Most ‘psychiatric’ conditions are not psychiatric, and life’s ills and worries are best left to the General Practitioner (GP) to offer advice, perhaps a close friend, or even a next-door neighbour. Best to throw away all the psychobabble bibles and ‘treatment packages’ by the experts in living who earn a good income exploiting patients’ weaknesses. Instead, patients should be taught to rely more on their natural intuition and cultivate inner strengths and talents. When depression, mood swings, phobias, obsessive rituals, and inner turmoil (for example, derogatory hallucinations, tormenting thoughts) become overwhelming, that is the time to seek medical advice. Most people (unless delusional) know which category they fit into, and should be able to receive help or intervention to deal with mental anguish before it becomes too disabling.
Many patients get better with or without talking therapies or medication, through sheer determination. At least with pharmacotherapy the medication can be thrown out after a reasonable period of adequate dosage. Either the drug works or it does not. Psychotherapy theoretically, particularly psychoanalysis, has no end, and can prove very costly. The top-up sessions are not free either! Even the National Health Service (NHS) will only offer a certain number of sessions and then you are on your own. Of course, there is the homework and perhaps a few more top-up sessions, if you make enough fuss! By all means investigate the alleged fraudulent business practices of Big Pharma and eliminate the biased positive results of drug trials. Author bias should also be scrutinized to eliminate personal prejudice. There is no need for patients to be duped by the empty rhetoric perpetuated by the experts in living if we are simultaneously led to believe that life‘s ills will be resolved through the use of a sugar pill.
To be conscious that you are ignorant is a great step to knowledge.
Benjamin Disraeli (1804 - 1881)
Within the field of psychiatry (and psychology) there are those who do not believe in drug treatments, ADHD, eating disorders, to mention a few. Everything is environmentally induced or caused by bad parenting, we are told by some self-appointed ‘life experts‘. And there are those who thrive on being deliberately controversial in an effort to raise their media profile and income. What a pity. Cardiology does not compete with cardiothoracic surgery nor does gynaecology compete with obstetrics, for example. Debate - yes. Antagonism - no. It is time for psychiatry to re-examine and distance itself from the popular psychobabble of the agony aunts and uncles before it completely loses its sense of professionalism. Because there are so many overlapping clinical scenarios within psychiatry and neurology, the former needs to align itself with the latter specialty and by doing so will gain respectability. The ever-widening chasm between psychiatry and other medical disciplines has been gathering momentum over the years, leaving psychiatry more alienated than ever. Perhaps there is also a case for subsuming some psychiatry specialties back into general psychiatry, for example, a Consultant General Psychiatrist with a ‘special interest’ in the conditions a Child Psychiatrist might be expected to deal with, such as Tourette’s syndrome, ADHD, and psychoses. Fewer graduates are now interested in pursuing psychiatry because they do not want to study medicine for years only to end up being marginalized as an on-looker in some multidisciplinary setting, devoid of any responsibility or decision-making. It is not that Cinderella will not be going to the Ball; there will be no Ball to go to.
‘Everyone thinks of changing the world, but no one thinks of changing himself.’ Leo Tolstoy (1828-1910)
Readers surely must have noticed by now how ‘client’, ‘service user’, ‘customer’, and other business terms have gained momentum in health care settings over the years. Newspeak has insidiously worked its way into all health policy documents. For reasons that escape me, in mental health services particularly, there seems to be an unwritten diktat that hospital personnel use any terminology other than ‘patient’ for those attending for treatment. Anyone who sets foot inside a hospital is now deemed to be a service user even though the word patient (from the Latin, patiens, for ‘one who suffers’) has not changed its meaning for centuries. Yet curiously, management Newspeak is not questioned or discussed openly by medical or nursing staff, perhaps for fear of being labelled old-fashioned, trying to cling on to relics of a bygone era. Subtle, unspoken, ‘nannying’ of health professionals in general, and a casual, perfunctory dismissal of matters medical now seem to be the order of the day.
The term ‘patient’ is now viewed sceptically by some in the management hierarchy as depicting an individual dependent on the nurse or doctor, rather than a token of respect for that person’s privacy and dignity. Non-clinical therapists are not obliged to use the term patient. What follows from that however, is the abstruse rationale that it is probably best to describe everyone as a ‘client’, ‘customer’, or ‘service user’ so as not to appear judgemental or create confusion. This apparently avoids ‘inferiority’ labelling and ensures all are ‘treated’ the same. Using the term ‘patient’, implies a rejection by doctors of multi-disciplinary team working, we are led to believe. There is a perceived, albeit unfounded notion, that the medical profession want to dominate those with mental healthproblems in particular by insisting on a biological model of illness and, by inference, pharmacological ‘chemical cosh’ treatments. At the heart of all this mumbo-jumbo lies the social model of care with its aim of ‘demedicalising’ the management of mental illness. This, ironically, seems at odds with medical practice where the emphasis has always been on a holistic approach to patient care. Yet an insistence on a social model of mental illness is as patronising to the patients that hospital managers purport to be caring for, as is the imagined ‘disempowerment’ model they want to dismantle. Some in the health management hierarchy contend that the word ‘patient’ fits poorly with today’s views of‘users’ taking an ‘active part’ in their own health care.1 Or does it? One may decide to have the cholecystectomy or the coronary bypass, when the acute cholecystitis and chest pain respectively have settled down, and select the time and date of the procedure, but I doubt whether one has any real ‘choice’ in the matter when the condition becomes critical, or that one will play an active part in the procedure itself.
The concept of empowerment, which has been around for decades, also seems to be enjoying a renaissance, being one of the current buzzwords in ‘modern’ health care. Other buzz phrases, among many, include ‘freedom of choice’, ‘equity’, ‘right to participation’, ‘increased role of the consumer.’ Empowerment, theoretically, enables new customers to stand up for themselves, demand their therapeutic rights and choose their own treatment. Fine when you are well. However, should I develop a serious illness, particularly one in which I have no great expertise, and because I cannot conceivably amass the entire body of medical knowledge before I see the doctor or nurse about my condition, I would prefer the physician/nurse to outline the treatment plan. I do not want to be called a client, customer or punter, because such derisory terms are more apt to make me feel, ironically, ‘disempowered’.
Why the change?
‘If you want to make enemies, try to change something.’ Woodrow Wilson (1856-1924)
What is it about doctors using the word ‘patient’ that health managers and non-medical therapists find so irritating and difficult to accept? Perhaps the answer lies in the doctor-patient relationship, akin to the attorney-client privilege afforded to the legal profession, so loathed by the judicial system. We are being swept along on a current of neutral, incongruous words such as ‘client’ (the most popular at present), ‘service user’ (this applies across the board), ‘consumer’ (Consuming what? I know my rights!), ‘customer’ (Do I get a warranty with this service? May I return the goods if they are unsatisfactory?) Better still, ‘ambulatory health seekers’ (the walking wounded) and ‘punters’ (a day at the races). The general trend it seems is for doctors to name one attending an appointment as ‘patient,’ midwives opt for ‘people’, social workers tend to speak of the ‘service user’, psychologists and occupational therapists prefer ‘client’, and psychoanalysts sometimes use the rather cumbersome description ‘analysand’. What is usually forgotten is that the person waiting in the analyst’s reception is no different from the humble stomach-ache sufferer.2
To most people ‘service user’ infers someone who uses a train or bus, or brings their car to a garage or petrol station. The term ‘user’ often denotes one who exploits another; it is also synonymous with ‘junkie’ and a myriad of other derogatory terms for those dependent on illegal drugs; ‘client’ has ambiguous overtones, and ‘people’ refers generally to the population or race, not to individuals receiving treatment. For general purposes a ‘client’ could be defined as a person who seeks the services of a solicitor, architect, hairdresser or harlot. There is also talk of ‘health clients’. Someone who goes to the gym perhaps! A customer is a person who purchases goods or services from another; it does not specifically imply an individual patient buying treatment from a clinician. Try to imagine the scenario of being told in your outpatient setting that a client with obsessive compulsive disorder, or a service user who is psychotic, or a customer with schizophrenia, is waiting to be seen. Although it is defies belief, this is how non-medical therapists portray patients. Would a medical doctor describe a person with haemorrhagic pancreatitis as a customer? Picture a physician and psychiatrist talking about the same person as a patient and customer respectively. Patients make appointments with their general practitioners. In psychiatry the terms are an incongruous depiction of the actual clinic setting in that most patients are not consumers or customers in the market sense; indeed many have little wish to buy mental health services; some go to extraordinary lengths to avoid them.3 Those who are regarded as in greatest need vehemently avoid and reject mental health services and have to be coerced into becoming ‘customers’ through the process of the mental health act.
What do our medical and surgical colleagues make of all this? Despite Newspeak insidiously weaving its way through other specialties, it does not seem to have permeated medicine or surgery to the same extent. Is psychiatry therefore alienating itself even further from other fields in medicine by aligning itself with this fluent psychobabble? Do cardiologists refer to patients with myocardial infarctions as customers? Does a patient with a pulmonary embolism or sarcoidosis feel more empowered when described as a punter? Changing the name does not address the illness or the factors in its causation. Perhaps one could be forgiven for using terms other than ‘patient’ for someone who wants plastic surgery to enhance their facial appearance, or a ‘tummy tuck’ to rid themselves of fatty tissue induced by overindulgence, or in more deserving cases, successive pregnancies. Readers will have no difficulty adding to the list. Such people are not ill. However, when describing a person with multiple myeloma, acute pulmonary oedema, intravascular disseminated coagulopathy or diabetic ketotic coma, I’m not so sure ‘consumer’ or ‘ambulatory health client,’ fits the profile. After all, a customer usually wants to ‘buy something’ of his/her own choosing. Now this may apply to ‘gastric banding’ or silicone implants, but there is not much choice on offer when one is in a hypoglycaemic coma or bedridden with multiple sclerosis.
Despite the above, when people were actually asked how they would prefer to be described by a psychiatrist or by a general practitioner,67% and 75% preferred ‘patient’ respectively.4 Another survey revealed a slightly higher preference (77%) for ‘patient’.5 One might argue that such results depend on the setting where the surveys were carried out and by whom. However, logic dictates that if I am in the supermarket waiting to be served, I would assume I am a customer; while attending the general practitioner’s surgery for some ailment, I would imagine I am there as a patient. Such surveys are conveniently ignored by service providers. So what does it matter? It matters because the lack of direct contact between managers and patients puts the former at a great disadvantage and leads one to question their competence and credibility when accounting for patient preferences. Perhaps managers should ‘shadow’ physicians and surgeons to fully understand why the people they treat are called patients. Psychiatry is not a good example of normal medical practice since so many of its adherents possess the illusory fantasy of being ‘experts in living’, and not physicians whose aim is to diagnose and treat.
Be patient
‘The art of medicine consists in amusing the patient while nature cures the disease.’ Voltaire (1694-1778)
It is noticeable that ‘patient’ remains the preferred usage by the media, press, and cabinet ministers, and of course, by medical and surgical teams. The implicit meaning of the word ‘patient’ is that someone is being cared for, and the media at least seem to respect this. Ironically, in the field of mental health, clinicians will often write letters to other professionals referring to an ill person as a ‘patient’ in one paragraph, and a ‘client’ in the next! Doubt and equivocation reign. It is as if the stigma of mental illness will evaporate if we gradually stop talking about sufferers as patients, and ‘empower’ them by describing them as ‘customers.’ There is ambiguity in the terminology itself. The term service user is the most disliked term among those who consult mental health professionals.6 The terms are also used interchangeably, with ‘customers’ and ‘service users’ described in the same breath. What do we call a drug-user? - a service user drug-user or a drug-user service user, a customer who uses drugs, or a drug-using customer? How does one accurately describe an individual using alcohol and illegal drugs? Is an infant suffering from respiratory distress syndrome or a child moribund with bacterial meningitis an active participant in his/her health care? In theory, they are service users. What about young people among whom substance misuse is prevalent?7 Do we label and stigmatise them as drug clients or drug customers? Will the outpatient and inpatient departments be redesignated as out-service or in-service user clinics? Oxymoronic terms such as ‘health clients’ do not convey any meaning when applied to hospital patients. Doubtless, critics with their customary predictability will lamely and with gloating schadenfreude, accuse the medical profession of bemoaning their loss of hegemony in health care matters, but their arguments are specious, stem from a lingering resentment of the medical profession, and amount to little.
In other areas of health some argue that making choices about lifestyle, and seeking advice on matters such as fertility, liposuction, gastric banding, or cosmeticsurgery, do not require one to be called a patient, and rightly so. Such information is freely available at clinics and on the Internet, and therefore does not require the advice of a doctor per se, until the actual procedure is imminent. However, it would be inconceivable for a patient undergoing say, a laparoscopic bypass or sleeve mastectomy for obesity, not to heed the views of the surgeon performing the procedure itself, the success rate, and complications. Whether to have the operation is a different matter. Similarly, individuals who want to engage in psychological therapies such as cognitive or psychoanalytic, or who would rather indulge in an expensive course of ‘emotional healing’, can choose for themselves. Neither does one need to see a nurse practitioner or general practitioner for a mild upper respiratory tract infection. Such people are not suffering from any serious medical illness (an enduring feeling of being physically or mentally unwell) in the true sense of the word.
When all is said and done, most people are unschooled in etymology, and condemning words because of their remote origins is pointless. Words change in meaning over time. Often they take on a new meaning, all too obvious in teenage slang. The word ‘wicked’ used to mean sinful, now it refers to something ‘cool’ (another word that has changed its meaning). Besides, if ‘patient’ really is that offensive, it seems odd that it has retained unchallenged supremacy in the United States,the centre of consumerist medicine, where the patient is quite definitely a partner.8
Physicians do not want to return to the days of paternalistic and condescending medicine, where deferential, passive patients were at the mercy of the stereotypical omniscient, omnipotent doctor or nurse matron. Likewise, patients do not want to be treated like products in order to achieve targets for the government health police. Patients nowadays are generally more confident and better informed about their conditions, in other words, already empowered, than in days gone by, particularly with the advent of the Internet (alas, here misinformation also abounds) and this is welcome. Therefore, if you are relatively well you can choose a treatment to suit your lifestyle. Unfortunately, not many patients suffering from chronic illnesses, for example, schizophrenia in some cases, or a degenerative condition such as motor neurone disease, feel empowered. I might feel empowered when I can decide to have one therapy or another, say, cognitive as opposed to solution-focussed therapy. I somehow doubt whether I would feel equal in status to, or more empowered than, the surgeon who is performing a splenectomy on me for traumatic splenic rupture.
The thrust of all this is that nothing is thought through; everything consists of ‘sound bites’ and ‘catchphrases’, and the sound bites become increasingly absurd the more one scrutinises the terminology. The medical and nursing profession should only be tending to people who are ill or recovering from illness. Of course other staff are directly or indirectly involved in patient care and follow-up. Physiotherapy is a good example. Nonetheless the title patient remains the same. Therefore let us be clear about the definition: those who suffer from an illness are patients; those who are not ill can be called service users, or whatever term takes your fancy.
'The following article is another in a series of critical essays examining the current status of Psychiatry in the NHS'
In therapy
"Good advice is often a doubtful remedy but generally not dangerous since it has so little effect.’ Carl Jung (1875-1961)
The word ‘therapy’, as defined by the Oxford Dictionary as ‘to treat medically’, is derived from the Greek therapeuein, meaning to minister. Nowadays it can denote any treatment from massage therapy to music therapy. In mental health it has become synonymous with counselling or psychotherapy. Drug therapy, believe it or not, is included in the definition, though is frowned upon by many in the mental health industry, and is often the subject of derisory and ill-informed comments from both medical and non-medical practitioners. Many medical doctors who decide to embark on a career in psychotherapy generally forfeit all their knowledge of physiology, biochemistry, anatomy, pharmacology and many other subjects, in the pursuit of an ideal that somehow all life’s problems can be resolved through a particular brand of talking therapy. One wonders why they spend many years in medical school and in postgraduate teaching. Why devote all that time studying subjects, which have no relevance to common or garden psychotherapy? Would it not be more practical for those who specifically want to pursue such a career in psychotherapy to enrol in a psychotherapy training college, and then ‘specialise’ in whatever form of psychotherapy they aspire to? Such individuals, instead of wasting years training as medical doctors, could receive a diploma or certificate to practise psychotherapy. Likewise, you do not need to be a neurosurgeon to become a neuroscientist, or a physician to study virology. For some reason, however, scientists, including innovators in the fields of medicine and surgery, seem to be disparaged by both medical and non-medical psychotherapists, and seen as persons who can only conceptualise individuals as molecules, or objects to be examined with sophisticated machinery. Psychotherapy seems to induce a state of delusional intellectualism among some of its members, it would seem. Such intellectualism, if it be described as such, portrays an affected and misguided arrogance towards matters scientific. Yet curiously, published papers in mental health journals or in the press, when written by ‘experts’ are often interspersed with the words ‘science’ or ‘scientific’ even when they are little more than observations, studies, or comparisons between populations receiving a particular mode of this therapy or that therapy. We are not talking about advances in the treatment of neuroblastoma or other cancers here or a cure for dementia. It is one thing to describe Addison’s disease; it is another to discover the cause.
The panacea
‘Nice people are those who have nasty minds.’ Bertrand Russell (1872-1970)
The necessity for ‘therapy’ now seems to be deeply ingrained in our culture and the army of pop psychologists and psychiatrists, non-biological therapists, and agony aunts increases, it seems, by the day. In the media what is quoted as ‘research’ and passed off as science, is often no more than a street survey, or opinion poll on a current fad or passing headline grabber, rather like those ‘we asked a hundred people’ questions posed on popular family quiz shows. The therapy bandwagon rolls on and is quite lucrative if you are fortunate enough to capture the market with your own brand of snake oil cure to life’s woes. Admission is free to the Mind Industry and furthermore, there are no compulsory, nationally agreed standards for the conduct and competence of non-medical psychotherapists and counsellors. Even if removed from the membership of their professional body for inappropriate conduct say, therapists can continue to practise, there being no legal means to prevent them from doing so. Most members of the public are unaware of this lack of statutory regulation. It is not surprising then that many ‘therapists’ flagrantly sell their product and any attempt to question the authenticity of a particular ‘cure’ is met with vitriol and feigned disbelief. After all, one has to guard one’s source of income. The author Richard Dawkins was subject to such venom and hostility when he dared to question the reasons and need for religion in his book The God Delusion. Woe betide any practitioner who dares to criticise the favourable results of ‘carefully conducted positive outcome studies’ on, say, cognitive therapy, even when one’s own clinical experience attests to the opposite. Of course, some therapies work, some of the time, but not because of the outlandish claims made for them; rather, they work best when a ‘client’ harnesses the energy and motivation to get better and ‘chooses’ one brand of therapy over another, or feels at ease with a therapist who is empathic and understanding, much as one might confide in a best friend, rather than any inherent benefit from the ‘therapy’ itself. Certain therapies work because they have an intrinsic behavioural component to them, for example, dialectic therapy for ‘borderline personality’ disorder (as real a condition as ‘sociopathic’ disorder), or cognitive behaviour therapy for obsessive-compulsive disorder and phobic disorders. With other therapies one would almost have to admit feeling better given the enormous sums of money involved say, for a one-week course in a therapeutic healing centre. After all, it would be painful to admit an expensive holiday being a waste of time when a lot of hard-earned money has been spent.
The enemy within
‘Sorrow and silence are strong, and patient endurance is godlike.’ Henry W Longfellow (1807-1882)
Why does one who is vehemently opposed to psychiatry want to become a psychiatrist? Do as many medically qualified psychotherapists as non-medical therapists dismiss the role of biology in the causation of mental health disorders? Why do we speak of anti-psychiatrists and not anti-cardiologists? What about the claims for psychotherapy itself? Is it possible truthfully to scientifically evaluate whether or not it works? Criticism comes from within its own camp. To paraphrase one well-known psychologist, ‘Psychotherapy may be good for people, but I wish to question how far it changes them, and I strongly cast doubt on any assumption that it cures them’.1 The irony now is that the therapies themselves are being ‘dumbed down’, sometimes aimed at a younger audience to court popular appeal. Trite and stultifying sound bites such as ‘getting in touch with your feelings’, ‘it’s good to cry’, ‘promote your self-esteem’, ‘search for your inner child’, and many other inane phrases flourish. Failure to display distress or intense emotional turmoil outwardly (say, after a bereavement), is seen as weak, maladaptive, and abnormal, instead of being viewed as a strength, a mark of dignity, and an important way of coping. The corollary of course, is the spectacle of some psychiatrists, because of their medical training, endeavouring to explain every aspect of mental health psychopathology in terms of neurotransmitters and synapses. And then there is the scenario of non-medical ‘scientists’ critically evaluating and expounding on subjects completely outside their remit, for example, uttering pronouncements say, on the neuropharmacology of depression, or the reputed reduction in hippocampal volume caused by posttraumatic stress disorder, when they are not qualified to do so, having only a superficial knowledge of pharmacology and/or neuroimaging respectively. Instead of asking the engineer’s advice on the safety strength of a steel column supporting a bridge, why not ask the carpenter! The absurdity knows no bounds.
It seems that all life’s problems are self-inflicted or caused by ‘society’ or faulty upbringing. Back to the schizophrenogenic mother then. It is up to the client to seek the therapist’s help and advice by way of talking cures to set him/her on the road to recovery. To be fair to non-medical therapists and lay counsellors, some psychiatrists do not believe in the genetics of, or neurobiological contribution to, mental health. Some even believe mental illness to be a myth! Imagine an electrician who does not believe in electricity, or to compare like with like, an oncologist who does not believe in cancer. Many decades ago the psychiatrist Thomas Szasz described psychology as pseudoscience and psychiatry as pseudomedicine 2 .Since then others have reinforced Szasz's conclusions. Who can blame them? To illustrate by one example, many court cases (particularly in the forensic field) involve a psychiatrist/psychologist giving ‘expert’ testimony for the defence with the prosecution in turn calling for a psychiatrist/psychologist to offer a contradictory opinion on say, the defendant’s fitness to plead. The prosecution says the defendant is acting, the defence argues the defendant is suffering from a mental disorder. No surprises there as to why psychiatry has descended into farce.
Psychotherapy is all talk
‘There is no art to find the mind’s construction in the face.’ William Shakespeare (1564-1616)
One outspoken critic has had the courage, some might say the audacity, to assert that the psychology/psychiatry therapy hoax is still as widespread and dangerous as it was when the neurologist Sigmund Freud first invented what she describes as ‘the moneymaking scam of psychoanalysis.’ 3. Briefly, at the core of psychoanalysis lies the principle that the id, ego and superego (not originally Freud’s terms) are considered to be the forces underlying the roots of psychological turmoil. The id, or pleasure principle, is in conflict with the superego or conscience (the conscious part of the superego) and the resultant outcome is mediated by the ego. Any interference with this delicate balance results in symptoms. However, this simplistic theory has come in for much criticism over the years and many scholars now consider the claims of psychoanalysis as having little credibility. It is not philosophy and it is certainly not science. Research in this area is fraught with even more methodological problems than say, with cognitive therapy studies. There is no way of testing analysts’ reports or interpretations reliably, and their conclusions are speculative and subjective. One eminent psychotherapist pronounced ‘as far as psychoanalysis is concerned, the logistical problems of mounting a full-scale outcome study are probably insurmountable.’4 It is impossible to develop a truly valid research protocol in either cognitive or psychoanalytic treatments to account for all the subtle, different variables that make individuals so unique. How can one research the mind? There are no specific blood tests and brain investigations that diagnose mental illness in the same way one might diagnose neuroleptic malignant syndrome or Parkinson’s disease respectively, at least not yet. Measuring scales are a very crude way of conducting research into mental health, and are not always objective, particularly when researchers are keen to have a favourable result. This applies also to drug trials, I hasten to add.
Many people feel better simply by seeing and discussing their troubles with a friend, their physician, a member of the clergy, or their next-door neighbour for that matter. Such individuals are usually more than prepared to give considerable time to listening sympathetically and offering possible solutions to often intricate and personal problems. Nonetheless, talking about a negative experience or trauma does not necessarily alleviate the distress or pain felt by that event. One wonders then why a ‘client’ would be expected to get better simply by insisting changing his/her ‘negative set’, for instance, by doing homework exercises for the teacher/therapist. No doubt countless individuals move in and out of therapy and support groups; some may even benefit from self-help books. However, it is the earnest fatuity in such books that is so tragically funny, and that people take them so seriously is even more worrying.5 Some ‘clients’ find therapy a waste of time, but since they do not return for their follow-up sessions it is assumed they are well, or have moved on, or are simply unsuitable. On the other hand, there are countless individuals who find an inner resilience to withstand and improve themselves through their own volition, with a few prompts on the way, rather like finding one’s way through unfamiliar territory with the aid of a street map. Likewise, drug treatment is of very little value if one’s relationships are in disarray, or an individual is in great debt, for instance. The ‘worried well’ simply require practical help from appropriate advisors, not health care professionals and should they wish to spend money on counsellors and therapists, that is for them to decide.
Common sense and nonsense
‘He who exercises his reason and cultivates it seems to be both in the best state of mind and dear to the gods.’ Aristotle (384 -322 BC)
We have now reached a point where minor setbacks and irritations are seen as obstacles to be treated. By adopting this attitude we are succumbing to the might of the Therapies and Mind Industry, eliminating those experiences that define what it is to be human. Individuals freed from moral duty are now patients or victims. This abnegation, abdication and suffocation of individual responsibility for the sake of self-esteem is creating a society which needs only to be placated and made content.3 Anything that causes dismay or alarm is a trauma, and therefore needs therapy. Any crime or misdemeanour is not our fault. We have a psychological condition that absolves us from every sin or ailment. The opposite scenario is whether through scientific ignorance or a refusal to acknowledge that the human genome may play a part, perhaps both, some therapists accuse organic theorists of being ‘too ready’ to favour biological models, believing that dysfunctions in neuronal circuits have no part to play in ‘disorders of the psyche’. We are not all at the mercy of our neurotransmitters, they cry. Neither view is accurate. Psychoanalytic psychotherapy is no exception either. The nub of psychoanalysis is the therapist’s analysis of transference and resistance, which distinguishes this form of psychotherapy from all other types. With this brand of therapy absurd interpretations abound, leading one psychotherapist to openly admit that ‘jargon is often used to lend a spurious air of profundity to utterances which are nothing of the kind’.6 The author Frederick Crews writes: ‘I pause to wonder at the curious eagerness of some people to glorify Freud as the discoverer of vague general truths about human deviousness. It is hard to dispute any of these statements about “humans”, but it is also hard to see why they couldn't be credited as easily to Shakespeare, Dostoevsky, or Nietzsche - if not indeed to Jesus or Saint Paul - as to Freud’.7
One particular concept that is difficult to sustain is that repressed memories of traumatic events lead to psychiatric disorders. That such repressed memories in some instances encompass sexual preferences towards one or other parent, is even more perplexing to most people. The Oedipus and Electra complexes, expounded by Freud and Jung respectively, were founded on Greek mythology, hardly the basis for scientific study. Psychoanalysis set out to cure a disorder by uncovering repressed memories. However, traumatic memories by their very nature are actually difficult to ‘repress’. Of course individuals do forget. This is a normal part of the human condition. Memories are recollected or resurrected by association of ideas; multiple-choice format questionnaires work on the same principle. Familiar sights, smells and sounds, as famously depicted in Marcel Proust’s A La Recherché de Temps Perdu (‘and suddenly the memory revealed itself. The taste was that of the little piece of madeleine cake‘) often conjure up previously ‘forgotten’ memories, what used to be described as involuntary memory. Forgetting does not always equate with psychopathology; forgetfulness is common and becomes more common with age. In psychiatric treatment electroconvulsive therapy (ECT) is associated with a high prevalence of memory disturbances, often irreparable. With organic disorders, memory channels or traces are damaged, for example, through alcohol, or subcortical injury.8 However, even in Alzheimer’s disease, at least in the early stages, memories are often not totally erased, a fact utilised in reminiscence therapy. Memories in healthy people are not suppressed or repressed. Not wanting to talk about some painful issue is not necessarily ‘denial’, nor does it denote a fear of unleashing repressed/suppressed memories.
After the Trauma
‘We seldom confide in those who are better than ourselves.’ Albert Camus(1913-1960)
Mental health care workers often speak of posttraumatic stress disorder where memories of an especially overwhelming and upsetting event are ever-present and particularly distressing, leading to panic feelings, flashbacks, and recurrent nightmares. Such memories may be easily evoked, sometimes merely by watching a documentary, reading a news item, listening to a radio programme, and so forth. In other words, patients are all too quickly reminded of them - the memories are very vivid, not repressed. Often people simply do not want to be reminded. They are not in denial – they are simply avoiding the issue and should be allowed to do so. Whereas formerly such traumas were associated with catastrophic events such as the Holocaust or major natural disasters, nowadays the term posttraumatic has become over-inclusive. Some people have ‘trauma’ imposed on them in the form of invidious suggestions that they were subject to abuse of one form of another. On the contrary, there is no evidence that any of Freud’s patients who came to him without memories of abuse had ever suffered from sexual abuse. Furthermore, Freud ensured that his theory of repression could not be easily tested, and in practice the theory became ‘unfalsifiable’.9 Traumatic memories of abuse are very difficult to forget, and patients struggle to suppress them, in the author’s experience.
Undoubtedly, some memories are painful, and generally speaking, there are individuals who want to ‘forget the past’ in order to ‘move on’, which would strike most of us as being a reasonably healthy approach in certain circumstances. Many patients, for instance, would want to ‘move on’ to a healthier, more satisfying relationship, change job, alter their lifestyles, and so forth. When it comes to major catastrophic events, memories are not preconscious or unconscious: they are very often disturbingly real, and very difficult to live with; in many cases time is the only ‘healer’. Some traumatic memories never fade and in many cases no amount of talking will erase the painful memories. Witness the Holocaust survivors and those subject to horrendous atrocities throughout the Pol Pot regime, for example.
It is difficult to ascertain therefore whether so-called defence mechanisms such as repression or denial are truly separate entities operating in the human psyche, or merely part of a conscious natural survival instinct to ward off painful stimuli. How can such mechanisms be unconscious when it is commonplace to hear of people ironically talking about ‘being in denial’? Individuals who attempt to overcome their own addictions for example, are seen as suffering from a ‘perfectionist complex’, and reluctant to admit their failings. In other words, acknowledge you are unable to cope and are in denial about the true nature of your affliction and you will then be offered a place in the recovery programme.5 Therapists see denial as a mechanism deployed to avoid the pain of acknowledging a problem and taking action to seek help. It is not medical bodies but grass roots campaigners who are foremost in demanding that every ‘traumatic’ or ‘problematic’ condition be medicalised, creating more opportunities for counselling intervention.10 Hence the new breed of disorders to include shyness, inattentiveness, road rage, trolley rage, sex addiction, shopping addiction, internet addiction and so forth.
Beyond therapy
‘We are all born mad. Some remain so.’ Samuel Beckett (1906-1989)
Talking therapy is now the new religious cult and is what people have now turned to in order to find solace or answers (‘discover your real self’), and even cope with often inconsequential day-to-day events. The constant, pervasive emphasis on counselling diminishes the capacity of healthy people to confront commonplace problems they encounter in ordinary day life. Normal variants in behaviour are considered pathological and ‘psychologised’ or ‘medicalised’. Psychobabble prevails. We all need therapy or a pill. More and more ‘disorders’ are being invented. The endless proliferation and demand for ‘expertise’ in all areas of life is eroding the willingness of those who are best positioned to offer at least measured advice, accumulated from years of experience. There are no ‘experts in living’ and some individuals need to steer away from their excessive dependency and seeking self-approval of others who claim to be. Kierkegaard once wrote of people ‘taking refuge in a depersonalized realm of ideas and doctrines rather than confronting the fact that everyone is accountable to himself for his life, character and outlook’.11 In the words of John Stuart Mill, ‘Ask yourself whether you are happy, and you cease to be so.’
“The mind is its own place, and in itself can make a heaven of hell, a hell of heaven” John Milton
The word 'psychiatry' is derived from the Greek for "doctor of the soul" and was first coined in the early 19th century by the German physician and anatomist, Johann Reil (1759-1813), although the treatment of mental disturbances dates back hundreds of years prior to this. The specialty of Psychiatry is regarded as dealing with the prevention, assessment, diagnosis, treatment, and rehabilitation of ‘mind’ illnesses or mental disorders. Diseases of the brain itself, for example encephalitis, tumours, and so forth, fall within the realm of neurology, generally. There are, of course, many overlapping disorders which cause neurological symptoms (paresis, slurred speech, ataxia, to cite a few) and ‘mind’ symptoms (depression, anxiety, psychosis). Disorders which affect several organ systems, for example, the autoimmune diseases, often cause multiple, bewildering neurological and mental symptoms. The primary goal of the psychiatrist is relief of suffering associated with ‘psychiatric’ disorders which include inappropriate anxiety, clinical depression, and psychotic disorders. Attempts have also been made to categorize and ‘treat’ different types of personality disorder. The latter is a contentious issue (perhaps with the exception of antisocial and borderline types) sometimes based on value judgments rather than clear scientific evidence. Treatment for mental health problems nowadays is usually community-orientated for less severe conditions and often hospital-based for more intractable disorders. The vast majority of patients are treated on a voluntary basis, whether in hospital or the community.
Medical, biological, social or psychological?
“ I think we ought always to entertain our opinions with some measure of doubt. I shouldn’t wish people to dogmatically believe any philosophy, not even mine.” Bertrand Russell
Psychiatry is sometimes criticized for adopting a ‘too’ medical or biological approach, despite the fact that many physical conditions masquerade initially with ‘mental’ symptoms. It would seem strange, if not irresponsible, were a psychiatrist, who is after all, a qualified medical doctor, not to enquire about a patient’s physical history. What is conveniently overlooked is that in everyday practice psychiatry uses a holistic approach to the patient, taking social and cultural backgrounds into account, as well as the general medical status. Treatment may thus involve medication, various forms of psychotherapy, or both, in addition to practical measures such as help with family problems, debts, housing, residential placements and so forth. In recent years, particularly in the UK, there has been a much greater emphasis on psychological treatments and social interventions. The ‘medical’ approach has taken a definitive back seat. Psychotropic drugs are frowned upon because of their side-effects, or perceived as a form of control used by psychiatrists towards their patients. Sweeping statements are made about their lack of efficacy and selective abstraction of the research is used to support such statements. Psychiatrists are denigrated for being in the grip of Big Pharma and are further demoralized by the being perceived as ‘drug pushers’. They are perceived by mostly non-medical ‘therapists’ as not being in touch with the psychological and sociological issues which are cited as underlying and perpetuating psychiatric disorders. Electroconvulsive therapy is considered barbaric; it is banned in some states in the USA. Complementary or ‘alternative’ therapies, regardless of whether or not they stand up to scientific scrutiny, are proliferating, and prescribed drugs are being replaced by ‘natural’ herbal products, despite the inherent dangers of the latter (1). Psychiatry is in decline and is becoming obsolete, a victim of its own psychobabble and increasingly mind-numbing research, understandable to the elite few. The profession is in danger of being ‘psychologised’ in order to appear acceptable and user-friendly, advocating therapies which in themselves do not stand up to scientific scrutiny. Outcome studies are quoted as favourable, when the very tenet of their foundations is very shaky, to say the least.
Perhaps there is not much reason for surprise when one considers not very long ago psychiatry advocated behaviour therapy for the treatment of homosexuality, orgone energy accumulators for neuroses, and insulin coma for schizophrenia. In hindsight such practices were totally unsound, unacceptable, and in the case of insulin coma therapy, dangerous; fortunately, they are now obsolete. Yet the history medicine is replete with such ‘cures’: mercury was once used to treat syphilis, and in surgery trepanation was widely used in ancient times for the treatment of seizures. In retrospect these procedures could be also be considered outrageous and barbaric, though with the development of scientific knowledge it is easy now to understand, reflect, and accept, that no other effective treatments were available at the time. Not so the case for psychiatry. Psychiatrists and other mental health professionals, who by and large genuinely have empathy and sympathy for their patients and want them to get better quickly, discharge them from hospital or outpatient clinics, and reunite them with their families whenever possible, are still unjustly accused of wanting to exert social control. There is no doubt that abuse of psychiatric practice does occur in some institutions and that political regimes throughout the world have used and still use powerful neurotropic drugs to subdue and control individuals who challenge the authority of the State. It is common knowledge that psychiatry was used by some totalitarian regimes as part of a system to enforce political control, for example in Nazi Germany, the Soviet Union, and the apartheid system in South Africa. Whether such abusive practices, which no doubt still exist, will ever be abolished will depend on the will of Governments and pressure from Human Rights campaigners such as Amnesty International.
What is madness?
“ Madness is rare in individuals - but in groups, parties, nations, and ages it is the rule” Friedrich Nietzche
It is not possible to delineate the boundary between sanity and insanity. Broad definitions of mental disorder have been attempted and an individual might be said to be ‘mentally disordered’, or as formerly described, ‘of unsound mind’, when there is a more than temporary impairment of cognitive functions such as memory, orientation and comprehension, an alteration of mood leading to a delusional appraisal of one’s situation, abnormal perceptions and disordered thinking. However, this concept is criticised for being overinclusive and precise definitions of mental illness remain elusive. It is probably easier to envisage mental health problems as being on a continuum from normal to abnormal for example, from a relative sense of well-being and contentment to a state of distress and unhappiness. Further exacerbations or stressors lead to a disintegration of oneself and that sense of oneness with the environment. Loss of reality ensues with further anxiety and perplexity, disordered and confused thinking or delusions, and perceptual disturbances (usually auditory hallucinations), in some cases. The same symptoms can be caused by drugs such as cocaine or amphetamines. It is known that these drugs alter the effects of dopamine, serotonin, noradrenaline, and perhaps other transmitters, leading to the assumption that anxiety, depression and psychoses are biologically driven, the often cited chemical imbalance approach. In the case of dopamine, implicating this neurotransmitter as a sole trigger factor in psychoses is simplistic and naïve. Likewise, depression and anxiety may have other biological causes such as hormone irregularities or fluctuating glucose levels. The dopamine hypothesis alone has largely been discredited in the aetiology of psychoses. Dopamine as an causative factor is only one small part of a much wider as yet unknown picture: for example, psychosis occurs in Parkinson’s disease where dopamine is actually deficient.
The ‘psychologised’ individual
‘Common sense is not so common’ Voltaire
One major criticism of psychiatry concerns the endless diagnostic categories or disorders which set out to describe and define the whole range of normal human expression, from the histrionic to the shy. No wonder then that psychiatry and allied specialties, for example, psychology and sociology, are accused of a sweeping disregard for the extraordinary complexity and richness of human behaviour. Whole subsets of psychiatric specialties have mushroomed over the last 30 or more years, to include substance misuse, forensic issues, autistic spectrum disorders and many others(2). Many disorders have variants, for example schizoaffective or schizomanic subtypes for schizophrenia, without any real scientific basis for such assertions. The eccentric individual becomes ‘schizotypal’; the individual who is detached from others and prefers his/her own company, is labelled ‘schizoid personality disorder’. Some would question whether many psychiatric descriptions are indeed ‘disorders’. There are very few ‘mental’ conditions which really could be regarded as disorders, save for example, severe clinical depression, bipolar disorder, obsessive compulsive states, and the psychoses, the latter often drug-induced. The diagnostic categories become bewildering and meaningless when subtypes are used, for example schizoaffective, bipolar I and bipolar II, depression with or without psychotic symptoms, and so forth; all have their supporters and detractors. Objectively, the symptoms are merely variations on a theme and cannot be accurately rated scientifically, unlike the gradings of say, Hodgkins or non-Hodgkins lymphoma. The distinction between normal and abnormal is blurred and varies among cultures. This is particularly pertinent when describing or defining personality disorder. For example, when does narcissistic behaviour become an illness? Why should it be seen as a disorder? Indeed, high self-esteem is encouraged in today’s’ climate and we are told to ‘love themselves more’. The usual response to the questioning of such behaviour is that it is ‘inappropriate’ or ‘out of proportion’ to the individual’s circumstances, or that ‘the patient is suffering’. Yet the entire media business, arts and entertainment, modelling and fashion industry is engaged in a narcissistic mind set, and the public love it! In other scenarios words are used interchangeably such that a psychopath, say, is perceived as a cold-blooded killer without conscience or feeling for his victim, or considered a creative genius, or indeed admired as a successful politician. The list of descriptions in the psychiatric disorders classification is wearisome and meaningless in many respects.
Much research in psychiatric journals nowadays is organic-based with ever intensive searches for newer receptors or transmitters, with increasing emphasis on the neurological basis for psychiatric conditions. In the past, emphasis was placed on the positive outcomes of drug trials, though this, fortunately, is now changing and reputable medical journals are now prepared to publish the results of negative findings. On the other hand, other researchers attempt to prove one type of psychotherapy is more effective than drug therapy, or that both together are better than either alone. Psychiatry has become polarized, with the ‘organic camp’ advocating a neurobiological basis and reductionist paradigm for psychiatric disorders, while the ‘psychotherapy model’ emphasizes the individual’s part in his/her illness with the development of strategies to defeat and overcome irrational beliefs and counterproductive emotions. There are problems with both approaches. A great deal of criticism is now being targeted against the psychology industry with its claims of treating serious illnesses through talking cures, and using labels to categorize almost every aspect of human behaviour (3). For example, how does one account for biological symptoms which are pervasive in severe depression without considering the role of neurotransmitters and regulatory hormones? How does one measure the complexity of suffering in any one individual and translate that into a rating scale for myriads of others whose problems have different origins? Are two people with severe depression really the same if they score identical marks on a depression scale? Whole books are written on the use of rating scales for research into psychological/psychiatric disorders. Yet there are over 250 different psychotherapy treatment approaches, which inevitably leads one to question the overall value of psychotherapy (4). In Epstein’s view, the whole field of psychotherapy is ‘pseudoscientific, an elaborate mysticism only differentiated from religion by a seemingly modern orientation and the cant of science (5). Research in psychotherapy is in any event notoriously difficult because of sample sizes, control groups, placebo effects and the nature of the therapeutic intervention itself (cognitive therapy, family therapy, psychoanalytic therapy). Besides, even when some patients show a moderate improvement, nonspecific factors are always operating in the period between therapy sessions and follow-up. Patients may have had a better social adjustment because of a new job, an increase in salary, or a change in a relationship and so forth, while others may have had a general decrease in life stresses, for example, through improved physical health (recovery from surgery, better control of diabetes). Some patients will deteriorate, despite ‘cognitive restructuring’, because of redundancy from a job, or ending of a relationship and so forth.
What next?
“Just trust yourself and you’ll learn the art of living” Goethe
Although many of the psychological treatments available nowadays were initially propounded by psychiatrists, psychotherapy and behavioural management are now more often carried out by psychologists, nurse practitioners and counsellors. Psychiatrists tend to deal with more severely affected individuals, ironically, those deemed to need psychotropic medication or where ‘counselling’ has failed. It could be argued that talking to a stranger for a fixed number of sessions (ranging from 10–12 one-hour slots) actually impedes the normal process of recovery and that a patient would benefit more from using his/her own social networks including family, friends, general practitioner and others, who are better placed to view the patient’s problems in context. Research claiming that depressed people are most likely to benefit from cognitive therapy, or that the majority of people suffering from panic attacks will recover with anxiety management, is deceptive and naively optimistic. Too many nonspecific factors are at play. The notion that a psychologist/counsellor/psychiatrist could turn a patient’s life around in 10 hours or so (10 sessions) is difficult to sustain when such problems have accumulated over that person’s lifetime, no matter how long or short-lived. The human mind is too complex and the human condition too intricate to be hoodwinked into such quick-fix solutions. Perhaps the best way forward is, ironically, to revert to an holistic approach with better education and training of both psychiatrists and psychologists. The former need further training in neurology (they already receive extensive training in psychology) and time spent in GP surgeries, the latter should be required to gain more experience of patients with severe types of psychiatric disorders (many hospital-affiliated psychologists already do), and general exposure to medicine via an acute emergency department or at a GP surgery (say, one year in total), preferably both, in order to broaden their horizons. The author appreciates the inherent, perhaps, unfortunately, insurmountable difficulties in setting up such a system involving the various disciplines. All ‘therapists’ should have a grounding in philosophy and sociology. It needs to be made clear that many patients simply feel better by talking to someone, though this ‘feeling better’ is not often sustained, and that knowing the cause of one’s problems does not equate with ‘cure’. Many patients have intractable conditions which are not amenable to ‘talking therapies’, and such individuals do not fit the category of the ‘worried well’, the usual ‘clients’ of counsellors and other therapists.
Healthcare organisations are a fertile breeding ground for interpersonal conflict and the development of dysfunctional relationships. The supervisory relationship between trainer and trainee is a particular area of concern for junior doctors. Aside from a problem trainee, such conflict can arise from a difficult supervisor, poor communication, personality clashes and power inequalities. This article will come from a trainee’s perspective in emphasising how these factors relate to the difficult supervisor. Recommendations are made for organisations and individuals on how the causes and consequences of this problem can be addressed .
The nature of working relationships
“Like a successful personal relationship, both sides must be able to acknowledge their goals, the obstacles they perceive in achieving their goals, and must be willing to compromise …” 1
Working relationships, like personal relationships, are embedded in a complex and diverse world with people of different personalities, backgrounds, motives and desires. Getting on with our fellow humans is a fundamental part of living and a challenge in our working lives. Garelick and Fagin (2004) have explored this area and have identified what facilitates a good working relationship (figure 1):
Figure 1: Factors that encourage good working relationships 2
Clarity about the organisation’s tasks and objectives
Clarity about the authority structure, with clear lines of accountability
The presence of a common goal or objectives
The opportunity to participate and contribute
The ability to trust and compromise
The possibility of setting aside inessential differences
Respect for alternative viewpoints
Protection of the weakest member of the team
Good leadership
A balance between individual aspirations and corporate needs
Sharing similar life experiences or cultural background
Dysfunctional Working Relationships
“Differences of perspectives … lead to interpersonal conflict that spirals into dysfunctional relationships” 3
Interpersonal conflict is a “dynamic process that occurs between interdependent parties as they experience negative emotional reactions to perceived disagreement and interference with the attainment of their goals” 4. Interpersonal work conflict can impact in terms of satisfaction, well-being, work disability, and mental health outcomes such as psychiatric morbidity, depression, fatigue and psychological distress 4. Factors that can play a role in conflict include perceived disagreements about tasks, ambiguities in role definition, or if the responsibilities are unclear 4.
One of the central issues inherent in workplace disputes is irrational behaviour on the part of one (or both) of the employees when the facts get confused with their highly charged feelings 5. In an attempt to avoid conflict the other individual may be uncomfortable about raising the issue, feel intimidated by someone with greater authority or power, or suspect a personal agenda, but does not want to sound argumentative. This can result in an emotionally charged situation with layer upon layer of faulty assumptions building up to a proverbial house of cards and the development of entrenched beliefs 3. Therefore what started as a misunderstanding can lead to a dysfunctional relationship3, which can result in multiple problems impacting on the organisation and the individuals involved. Specific consequences include complaints of bullying and racism against the trainer, labelling of the trainee as a doctor in difficulty, or the trainer developing a reputation as a “difficult supervisor”.
Causes of trainer-trainee conflict in medicine
In the field of medicine, particularly given the hierarchical structure of the profession, the potential for conflict is accentuated. Trainees tend to rotate around jobs, and educational supervisors, every 6-12 months. Trainees and trainers are expected to adapt to working with each other with differences in personality, styles of working, and expectations. It is therefore inevitable that difficulties will develop.The fundamental causes of the conflict between trainer and trainee in healthcare are:
1. The problem trainee
The problem junior doctor is a well-established area of concern 6. This type of doctor may be inflexible, clinically incompetent, arrogant, have poor time keeping or organisational skills, refuse to do what is asked, exhibit poor communication skills, lack enthusiasm, lack educational objectives, or have a difficult personality. Despite the “doctor in difficulty” being regarded as a “problem trainee” the dysfunctional relationship between trainer and trainee in medicine is usually a product of both parties.
2. The difficult supervisor
The most important factor in determining trainee satisfaction has been shown to be the quality of supervision provided by the consultant trainer 7. However the difficult supervisor, often a consultant, is an issue that is underreported. The problem consultant comes in various guises shown in figure 2:
Figure 2: The problem consultant 2
Authoritarian and bullying
Controlling
Indecisive and disorganised
Burnt-out
A consultant who is never there
A consultant biding time to retirement
The flirtatious consultant
Poor teacher and communicator
Generally a problem consultant would have, over the years, established a reputation as a difficult person to work with, usually confirmed by their peers and trainees. Unfortunately this aspect of their personality is ignored when they complain about a new trainee. Therefore the consultant is never identified as a difficult supervisor. Knowledge of what constitutes a bad supervisor should be accompanied by what is a good supervisor. In the field of psychology the notion of a good supervisor applies to any supervisory relationship (figure 3).
Figure 3: Good supervisor 8
Straddling the potentially conflicting roles of mentor and evaluator
Providing impartial and thorough evaluation within contexts that respect supervisee’s integrity
Having expertise
Being trustworthy
Modelling respect of differences in values, expectations and experiences
Tolerant of mistakes and facilitating trainees progress
Providing direct and clear feedback to trainees
Open to feedback about their own style of working
3. Communication problems
A supervisor should possess good communication skills in the form of: active listening, demonstrating understanding, using open questions, building areas of agreement and being open. As a good communicator the supervisor should refrain from stating unreasonable expectations, views, or opinions. They should avoid offering incentives / warning of consequences or revealing feelings. In the workplace, in times of pressure, dysfunctional communication is instrumental in trainer-trainee conflict.
These communication problems are prominent in the area of feedback 9. Feedback is a key role of the supervisor 10. Feedback should be honest, relevant, objective, specific, timely, and planned 9. It should be based on accurate information rather than hearsay and focused on behaviour and performance rather than personality and attitude. It should be constructive, conducted in private, descriptive rather than evaluative, and designed to avoid personalising and blaming 9. Feedback should not be given on things the trainee cannot change e.g. personality.
Should the trainee feel offended by feedback at any point then it may be that the supervisor has a hidden agenda or is a bully. A delay in feedback impedes efficient working so the giving and receiving of feedback should also be a balanced ongoing process in order to boost morale and motivation, leading to greater effectiveness and job satisfaction 9. If the supervisor has a good relationship with the trainee then constant feedback should be given about his/her performance: the final report should never be a surprise 11.
4. Personality clashes
Conflict may also reveal itself in personality differences between trainee and trainer. Personality characteristics of the latter that can significantly affect an otherwise healthy relationship include a trainer who is preoccupied with details, order, organisation and schedule. Such trainers may be seen as perfectionist, pedantic, rigid and stubborn, and often insist that others submit to their way of doing things, according to their own self-proclaimed high standards.
Personality clashes may arise from poor communication or underlying factors including racism, sexism, religion, or jealousy and envy interfering with the relationship on both sides 12. The crucial question to ask is whether the trainer-trainee conflict is a result of a difficult trainee, or whether it arises when a trainee does not fit the supervisor’s scheme of things.11
5. Power differential
The trainer/supervisor also has an evaluative function in relation to the trainee and therefore the potential for abuse and trainee vulnerability in respect of the supervisor, is clear 8. The dependence of trainees on trainers for references creates a “potential power imbalance and in some cases may lead to intentional or unintentional harm to the trainee” 13. This harm may be identified in the trainer’s assessment of the trainee when completing the end-of-post evaluation. The trainer taking a proactive approach in writing complaints and sending emails to sabotage a trainees’ career may also demonstrate abuse of power.
Equally an overpowering consultant may, consciously or unconsciously, take advantage of the situation by going on a fault-finding mission. This can become part of a self-fulfilling prophecy. If the trainee is perceived to be poorly performing the supervisor may feel under more pressure and become hostile towards the trainee, without addressing the main problem 12. The result is that the supervisor engages in “continuous criticism and academic humiliation” 12 which causes the trainee to feel more useless and helpless. This can lead to the trainee becoming a scapegoat in an already dysfunctional team12.
Another consequence of the power imbalance is that it causes a state of confusion for trainees who want things to change but will often tolerate the problem and endure it to avoid jeopardising their career prospects. The trainee may feel powerless and fearful about addressing the current problem and choose to be silent on the matter, rather than risk an unpleasant situation 12. Unfortunately such passive behaviour may result in the problem escalating and the trainer may, unconsciously and unwittingly, bully the trainee 8.
How to deal with trainer-trainee conflict?
“Conflicts are really a house of cards ... you can bring them down by getting to the bottom and getting to the facts” 3 .
Dealing with trainer-trainee conflict involves good emotional intelligence, self-awareness (being self aware and taking an honest look at oneself), self-regulation (ability to control emotions), empathy (ability to identify and understand the wants, needs and viewpoints of others), being well-motivated, and having good social skills 14. In other words, successful conflict resolution relies on first understanding ourselves, being aware of our personality, our prejudices, why we like some people and not others, and recognising that certain things will annoy us and not others 11.
From a trainee’s perspective conflict with the supervisor should be addressed at an early stage to prevent escalation of the problem 12. This should include self-appraisal, thinking about the root of the problem in a factual and non-personal way, and informal discussion with a discreet colleague to gain another perspective. Trainees should find out how their predecessor got on in the post. Finally, problems should be freely discussed with the supervisor. However, there may be supervisors with whom it is difficult to have a discussion; therefore the trainee must involve others to deal with the issues which escalate or remain unresolved. If the supervisor is considered the source of the problems there are steps to take to ensure the power of the supervisor is not misused against trainees (figure 4):
Figure 4: Steps to deal with a difficult supervisor 13
College / speciality tutors and clinical tutors / programme directors have an obligation to act as the trainee’s advocate
Where tutors and programme directors fail to act appropriately, a direct approach by the trainee to the local postgraduate dean or relevant college may be indicated
The local trainees’ committee, trade union, and its officers / representatives may also be helpful in acting as the trainee’s advocate in appropriate circumstances
Deanery contact monitoring and training programmes’ approval visits, involving the College and conducted on behalf of the Postgraduate Medical Education and Training Board, also afford opportunity to raise concerns about supervisors
If trainees consider their health affected by the stress of working with a difficult supervisor they should seek help from their occupational health department or postgraduate dean, who may offer confidential services and helpful advice for the assessment of mental health problems affecting doctors
Trainees may be reluctant to take the steps described in figure 4. The power differential between trainer and trainee, as well as acting as an antecedent to the conflict, is a perpetuating factor that ensures nothing is done about it. The difficult supervisor may be underreported for the same reasons seen with workplace bullying, namely, fear of making matters worse, belief that nothing will be done, concerns regarding confidentiality, fear of victimisation, and concerns about being labelled as a troublemaker 15. Ultimately it is the fear of the consequences that deters trainees from speaking out, though it is worth remembering that Franklin D Roosevelt stated in his first inaugural speech, “the only thing we have to fear is fear itself”.
What can healthcare organisations do about supervisory conflict?
Organisations must be proactive in identifying and dealing with problems between trainers and trainees, who in turn ought to be aware of their responsibilities. Organisations may be tempted to sweep problems under the carpet but there are recommendations on how they can address the causes of trainer-trainee conflict (figure 5):
Figure 5: Steps for organisations to tackle the causes of trainer-trainee conflict
Cause
Solution
Problem trainee
Training of supervisors in not only how to identify the problem junior, but how to constructively manage the problem at the outset. Adopting a positive, non-judgemental and non-confrontational approach, and having a problem-solving mindset are essential
Difficult supervisor
Training of supervisors regarding their roles as a educational and clinical supervisor
Training of supervisors in sensitive areas of diversity and equality, and self-reflection, with the support of college tutors and programme directors
360 degree feedback carried out frequently and acted upon promptly during the supervisor’s appraisal
Communication Problems
Communication skills training
Constructive feedback training
Personality Clashes
Training of supervisor and trainee in conflict resolution since there may be personality differences between the two, rather then an individual doctor in difficulty.
Power differential
Power imbalance of feedback can be countered if feedback from each trainee becomes part of appraisal and revalidation for consultants
Colleges should collect anonymous feedback about educational and clinical supervisors from trainees and review their future role as supervisor
Complaints of bullying and racism should be dealt with promptly and effectively by the organisation.
Paice (2002) describes an excellent mentor as someone who “will always inspire, teach by example, and excite admiration and emulation” 16. Mentoring can be beneficial in facilitating the development of the trainee but “faculty mentoring should be avoided’’ 17. In other words mentoring of doctors should not be carried out by the trainee’s educational supervisor or line manager, nor should they be involved in their assessment or appraisal, to avoid blurring the distinction between the roles 17. A good mentor should :
Motivate
Empower and encourage
Nurture self-confidence
Teach by example
Offer wise counsel
Raise the performance bar
However, the authors argue that these are the qualities that should be part of being a good supervisor 17.
Conclusion
“Differences in power and status, and dependence on references, places juniors in invidious positions when they experience problems in their relationships with trainers” 2
The relationship between trainer and trainee should reflect the same warmth and nurturing as in a parent-child relationship. There is a parallel with both types of relationship in that there is an imbalance of power that interacts with poor communication and personality conflicts. In medicine although the problem junior doctor is frequently highlighted it must be remembered that the trainer-trainee conflict may reflect a difficult supervisor. The supervisor needs to achieve a healthy relationship that is sensitive to the needs of the trainee, void of any of their preconceived beliefs and prejudices, and act as a role model in making a good doctor and achieving their full potential 16. Interpersonal conflict can nevertheless develop and escalate to the extent that the trainee may suffer in silence. Healthcare organisations can be more proactive in penetrating the causes of the dysfunctional working relationship. Trainees should be fearless in turning to existing support in face of a difficult supervisor.
KEY POINTS:
Professional working relationships are a major challenge in healthcare
Interpersonal conflicts can lead to a dysfunctional working relationship
Issues include problem trainees, poor communication, and personality clashes
Power inequalities and the difficult supervisor need to be addressed
Trainer-trainee conflict can be resolved with steps taken by the individual
Organisations must address the causes of dysfunctional working relationships
Trainees need to overcome their own fears when tackling conflict
The patient's
right to autonomy should always be respected and steps shall be taken
to make consent truly informed. There is, however, no absolute right
to consent on the basis of philosophical, ethical, legal and practical
considerations.
Introduction
Consent
to investigations and treatment is considered a cornerstone in the doctor-patient
relationship.1 The Oxford Dictionary (1998) defines consent
as “permission for something to happen or agreement to do something”.2
This definition does not entail understanding of the action agreed to
and for medical purposes the term ”informed consent” meaning “permission
granted in the knowledge of possible consequences” has been developed.2
General Medical Council (GMC) guidance requires the ability to comprehend
and weigh up information as well the ability to communicate for informed
consent.3
Most authors
describe consent as a principle relatively new to medicine.4-6
This is however incorrect as even Plato and Hippocrates used consent
in their medical practice.7
This review
addresses the issue whether the right to consent is an absolute right
by exploring the ethical and legal framework of consent or more specifically
informed consent. Whereas most of the ethical issues are universally
applicable, the legal aspects and guidance by the regulatory authorities
apply only to the United Kingdom (UK). Where law differs between Scotland
and the rest of the UK, I have focused on the laws for the latter.
Ethical
principles around consent
The four
main principles of medical ethics are justice, non-malificence, autonomy
and beneficence.8 Autonomy is the main ethical consideration
underlying informed consent. The patients’ right to determine what
investigations and treatment to undergo must be respected by all doctors.3
For consent to be informed patients rely on the information provided
by their doctor. Honesty and truthfulness are required to make the process
of consent valid.3 The ethical principle of justice needs
to be applied when deciding what treatments are offered to or withheld
from patients. This touches the process of informed consent and is further
explored when the right to demand certain treatments is discussed.
Philosophical
aspects
The debate
whether a right or a principle is absolute not only involves ethical
and legal aspects. It also touches on the philosophical argument of
absoluteness. Freedom as an example can’t exist as an absolute principle
because granting one individual absolute freedom will infringe the freedom
of a second individual considerably. Person A’s freedom to take any
good will influence the freedom of person B to have property. When applying
these principles to autonomy the same problem arises: Total autonomy
of one individual has a negative effect on autonomy of other individuals.
The modern democratic society has designed rules and laws to create
a fair way of living. On the one hand this restricts autonomy, while
on the other hand this same restricted autonomy guarantees the same
amount of it to all members of this society.
I argue
therefore that on a philosophical basis the principle of total autonomy
contradicts itself when applied to society. As autonomy is the main
ethical principle for informed consent an absolute right to consent
cannot exist.
Requirements
of informed consent
The basic
difference between consent and informed consent is the patients’ knowledge
behind the consent decision. Informed consent requires the patient to
understand the diagnosis and uncertainties about it as well as the different
treatment options (including doing nothing) and their advantages, disadvantages
and achievable outcomes.3 The amount of information required
to make consent informed may vary depending on complexity and risks
of treatment as well as the patient’s wishes.3 Furthermore
individual patients will have different intellectual capabilities and
understanding of their illness. It is therefore mandatory to tailor
information provided to the individual patient and the current situation.
An emergency like acute myocardial infarction for example will allow
less time to discuss diagnosis and treatment than an elective endoscopy.
To judge
whether a patient has really understood the information provided can
be difficult and often little of the information is retained (see practical
aspects chapter). This leaves physicians in doubt whether their patient’s
consent is truly informed. Consent based on partial information may
be invalid but this may go unnoticed by patient and treating physician.
The principal
of an absolute right to consent could be easily undermined by partial
information. It is highly dependant on the willingness to provide full
information and the patient’s capability to understand it and weigh
up the options.
Legal
framework
A medical
intervention without valid informed consent is a criminal offence and
the physician can be charged with battery. Examples of such situations
include treatment against the patient’s will, different treatment
than the one consented for and treatment after consenting deliberately
with wrong information.9
Guidance
for consent has been set up by the regulatory body (GMC). While no one
can consent for a competent adult UK laws are regulating consent for
minors, patients with acutely or permanent incapacity and patients suffering
form severe mental illness.
Minors
At the age
of 16 persons are to be considered as adults and can therefore be presumed
to have capacity. Children younger than 16 years may have capacity depending
on their understanding. When a competent child refuses treatment persons
with parental responsibility may authorise this or a court may overrule
the child’s decision.3 Incompetent children will be treated
with consent from a person with parental responsibility.
Acute
and permanent incapacity
The presumption
that every adult patient has capacity applies unless the opposite can
be clearly demonstrated.3, 10 Patients lacking capacity due
to an acute (i.e loss of consciousness after an accident or patients
on mechanical ventilation) or chronic illness (i.e dementia) cannot
make decisions about their treatments themselves. In those situations
it is the doctor’s duty to act in the “best interest of the patient”.
Views about the patient’s preferences may be sourced from a third
party (relatives for example). This third party can however not consent
or object to treatment.3 If a patient has clearly given an
advance directive while still competent, the treating physician is bound
to respect this (see advance directive).
To give
informed consent a patient needs to have mental capacity and the ability
to communicate.11 The physician needs to establish the patient’s
“ability to understand, retain, believe, evaluate, weigh and use information
that is relevant to a medical intervention or its withdrawal”.11
This test of capacity has been supported by several court rulings10,
12, 13 and is embedded in the Mental Capacity Act (2005).14
Making an
irrational choice does by no means constitute lack of capacity and a
competent patient’s irrational decision has to be accepted even if
this leads to an adverse outcome (including death).3
Mentally
ill patients
The Mental
Health Act (1983) regulates the treatment and hospital admission of
mentally ill patients not volunteering to undergo assessment and/or
treatment.15 These patients can only be admitted to hospital
if due to their mental illness they pose a threat to themselves or others.
Patients can be detained against their wishes to conduct an assessment
and if their condition is deemed treatable they can be detained to receive
such treatment. While this allows treatment for psychiatric conditions,
the treatment of physical conditions not related to mental illness cannot
be undertaken against the patient’s wishes. If needed, a court can
decide on treatment of non-psychiatric illnesses in those patients.
This aspect
of the law can leave physicians in difficult situations. If a depressed
patient takes an overdose of an anti-inflammatory drug he can be detained
in hospital using section 5.2 of the Mental Health Act. A resulting
medical complication like severe gastrointestinal bleeding is however
not covered by the mental health act. The patient therefore still remains
competent to refuse a life-saving endoscopy or blood transfusion.
Protecting
the public: infectious diseases, infection control and confidentiality
In order
to protect the public form contagious infectious diseases the Public
Health (Control of Disease) Act (1984) regulates notification of diseases
and mandatory treatment of conditions like tuberculosis (TB).16
The individual’s right to consent is severely restricted in two areas:
Firstly information about the patient’s diagnosis has to be given
to the relevant authorities. The patient should be informed about this
step. Section 11 regulates the disclosure of information. It is mandatory
for a medical practitioner to disclose personal details of the patient
and the diagnosis to the relevant authorities even if the patient does
not agree to this. The list of notify-able diseases ranges from food
poisoning and viral hepatitis to tuberculosis.
Secondly
patients suffering from communicable diseases can be forced to take
their medication by supervised administration or involuntary inpatient
treatment. Sections 37 and 38 of the Public Health (Control of Disease)
Act have recently been used to detain a man for inpatient treatment
of TB against his will at North Manchester General Hospital.17
The act was used to prevent the spread of TB to the wider public by
forcing treatment onto an individual, who was not compliant.
While above
regulations are clearly set out by law, a physician might encounter
situations in which no clear guidance is given. If a patient confesses
a crime or a planned crime to a doctor, it is left to him to decide
whether to pass on this information to the police. This decision requires
careful weighing up whether the right to consent on passing on information
is more important than the right of the public to be protected. GMC
guidance (Confidentiality: Protecting and Providing Information, 2004)
gives general advice on disclosure, but leaves the ultimate decision
with the medical practitioner.18
The legislative
has given clear laws stating when a right to consent does not apply
to a patient. Incompetent minors, adults lacking capacity and some mentally
ill patients do not have an absolute right to consent. Furthermore patients
suffering from some infectious diseases have limited right to consent
and can be detained and treated against their will. Using the principles
of capacity and justice towards other individuals the right to autonomy
has been cut in a few well-defined circumstances.
Advance
directives
When an
adult becomes incompetent he loses the right to decide on his medical
care. To allow patients to express their ideas and wishes before they
become incapacitated the Mental Capacity Act was introduced in 2005.19
Patients can give an advance directive or “living will” to outline
the treatments they wish or wish not to receive. A physician is required
to act within this advanced directive unless there is evidence that
the patient revoked the will when still competent. A “living will”
does not necessarily apply to all situations and it has to be checked
whether the patient’s current condition is covered by his will.
Practical
application of advance directives can be difficult: Unclear wording
like “no life-prolonging treatment” leaves room for interpretation
and the same intervention might have different outcomes depending on
underlying conditions. A healthy patient might set up an advance directive
to not receive mechanical ventilation without discussing the merits
of this intervention with a health care professional. This generally
prohibits any doctor from administering such treatment in any situation.
While this might be the patient’s wish should he suffer a devastating
stroke (very little chance of recovery), it could be argued that his
view would be different if the merits of ventilation after major emergency
surgery (reasonably good chance of full recovery) would have been explained
to him.
Furthermore
the act established the lasting power of attorney (LPA) concept. This
enables the patient to grant rights of consent and refusal to a LPA
while still competent. The LPA then takes over these powers when the
patient loses capacity.
Research
without consent
While consent
should always be sought for including patients in clinical research,
there are conditions that do not allow a delay: Unconscious patients,
patients in shock and studies with short therapeutic windows. While
including those patients without consent infringes their right to autonomy
society as a whole benefits from such research. The European Union (EU)
allows such studies to recruit patients without their consent under
strict regulation.20
The
right to refuse or demand treatment
British
law clearly gives competent patients the right to refuse any treatment
(the very few exceptions have been outlined in the chapter legal framework).
In contrast, however, no patient has a right to demand certain treatments.
GMC regulation (2008) states that if a patient wishes treatment that
in the doctor’s view is clinically not indicated there is no ethical
or legal obligation to provide such treatment.21
Burke, who
suffers from a chronic and progressing neurological illness, challenged
this guidance. He wishes to receive artificial nutrition and hydration
(ANH) when he loses his ability to swallow and he does not want doctors
to make decisions on his behalf. Arguing that the relevant GMC guidance
infringes his human rights he took the case to court achieving a favourable
ruling initially. Mr Justice Munby ruled in Burke22 that
the Human Rights Act (1998)23 entitles a person to demand
life-prolonging treatments such as ANH. He based his decision on article
2, 3 and 8 arguing that a competent person’s right to life and autonomy
constitute an entitlement to ANH.11
The Court
of Appeal overturned this ruling although the right-based analysis of
Munby’s decision was acknowledged. Two lines of argument were used
to justify the decision. Firstly the case of Bland24 (Airedale
NHS Trust 1993), an advance directive to withdraw treatment in a case
of persistent vegetative state must be respected, does not automatically
lead to a reverse decision in opposite cases.11
Secondly
an advanced directive demanding life-prolongueing treatment would not
be in consistence with the Mental Capacity Act, which requires the doctor
to take the incompetent patient’s best interest into consideration.11
Another
aspect of demanding treatment is the effect on the wider community.
Graber and Tansey argue that demanding certain (more expensive, equally
effective) treatments leads to injustice.25 While doctors
may feel pressured to please their patient’s wishes, financial and
organisational constraints in society (and a public health care system)
will mean that other patients might not get treatments they require.
Currently
there is no legal right in the UK to demand treatment. Furthermore such
demands infringe justice by prohibiting resources to be allocated by
need.
Practical
aspects of consent: understanding and retention of information provided
Informed
consent requires the ability to understand and weigh up information.
Several studies have addressed the issue of understanding and retention
of information provided. Even in a research setting where rigorous measures
for consent are applied severe defiencies have been identified: in a
randomized drug trial 44% of participants did not know that they were
assigned to treatment or placebo by chance.26 A capsule endoscopy
study recruited healthy volunteers, of whom 90% had university education
and 60% were medical students. Still vital information (drugs used,
potential risks) given during the consent was only completely recalled
by around 20%.27 These examples show that most patients or
research participants do not have a good understanding and/or recall
of the information provided by standard consent procedures. Despite
that treating doctors and researcher had treated or included patients
based on this “informed” consent.
Methods
like enhanced consent forms and multimedia interventions during informed
consent have shown mixed results, while only additional time spent in
one-on-one interviews significantly improved understanding and recall
of information.28
Discussion
Informed
consent is required for any investigation or treatment proposed to a
patient. Understanding of the nature of procedure, benefits and risks
are the cornerstones of informed consent. While autonomy is one of the
four main ethical principles, I argue that there is no absolute right
to autonomy or consent.
On a philosophical
basis an absolute right to autonomy and consent contradicts itself.
Several
restrictions in the right to consent are set by the legal framework
in the United Kingdom (or England). The main statuary instruments concerned
are: Mental Health Act, Mental Capacity Act and Public Health Act. UK
Law regulates the right to consent for minors, mentally ill patients,
patients with incapacity and patients with communicable diseases. Their
rights to consent are restricted and in special circumstances not granted.
Disclosure of information without consent is mandatory in infectious
diseases cases and legal in cases where the doctor believes that non-disclosure
will leave the public in danger. Furthermore patients can be recruited
to studies of emergency medical treatment without consent under strict
EU regulation. On a legal basis there is no absolute right to consent
therefore.
Patients
with anticipated incapacity can set advance directives to guide their
future treatment while still competent or a LPA can be given the right
to decide on treatment on the patient’s behalf. While this increases
the right of consent and improves patient autonomy to refuse treatment,
there is no right to demand treatment if this is considered medically
inappropriate (futile for example) by the treating medical practitioner.
Looking
at the practical aspects of consent shows that the information provided
is often poorly understood and retained. Patients giving consent are
doing so without being truly informed. In other words they can’t give
informed consent due to their lack of understanding. As shown in the
chapter practical aspects this will often not be noticed by the treating
doctor or researcher. It is difficult to conceive an absolute right
to consent in practice, when the effort to supply information required
for informed consent fails so often.
In summary
the patient’s right to autonomy should always be respected and step
shall be taken to make consent truly informed. On the basis of philosophical,
ethical, legal and practical considerations, however, there is no absolute
right to consent.
COMPETING
INTERESTS
None Declared AUTHOR
DETAILS
CHRISTIAN
P SELINGER, MD, MRCP, Royal Albert Edward Infirmary, Wigan, United Kingdom CORRESPONDENCE:
DR CHRISTIAN SELINGER, Royal Albert Edward Infirmary, Wigan Lane, Wigan,
WN1 2NN, United Kingdom Email:
Christian.selinger@web.de
References
1. Habiba MA (2000) Examining consent
within the patient-doctor-relationship. Journal of Medical Ethics 26:183-87 2. The Oxford
Dictionary of new English, Oxford. Oxford University Press, 1998 3. GMC (1998)
Seeking patients’ consent: The ethical considerations, General Medical
Council, London 4. King J
(1986) Informed consent: A review of empirical evidence. Institute of
Medical Ethics Bulletin supp 3: 1-17 5. Kour NW,
Rauff A (1992) Informed consent – historical perspective and
a clinician’s view. Singapore Medical Journal 33:44-46 6. Nelson-Marten
P, Rich RA (1999) A historical perspective of informed consent in clinical
practice and research. Oncology Nursing 15:81-8 7. Dalla-Vorgia
P, Lascaratos J, Skiadas P et al. (2001) Is consent in medicine a concept
only of modern times? Journal of Medical Ethics 27:59-61 8. Gillon
R. Medical ethics: Four principles plus attention to scope. BMJ 1994;
309:184-8<br>
9. MRHA guidance (2007): http://www.mhra.gov.uk;
as accessed on 01/06/2008 10. Re C
(adult refusal of treatment) [1994] 1WLR 290 11. Samata
A, Samata B (2006) Advance directives, best interests and clinical judgement:
shifting sands at the end of life. Clinical Medicine 6:274-78 12. Re MB
(an adult: medical treatment) [1997] 2 FLR 426 13. Re B
(consent to treatment: capacity) [2002] EWCH 429 14. Mental
Capacity Act 2005. The Stationary Office, 2005 15. Mental
Health Act 1983. The Stationary Office, 1983 16. Public
Health (Control of Disease) Act (1984). The Stationary Office, 1984 17. Crook
A (2007) TB patient under guard. Manchester Evening News 9/10/2007 18. GMC (2004)
Confidentiality: Protecting and Providing Information, General Medical
Council, London 19. Mental
Capacity Act 2005. The Stationary Office, 2005 20. Lecouturier
J, Rodgers H, Ford GA, et al. (2008) Clinical research without consent
in adults in the emergency setting: a review of patient and public views.
BMC Medical Ethics 9:9 21. GMC (2008)
Withholding and withdrawing life-prolonging treatments: Good practice
in decision making, General Medical Council, London 22. Re (Burke)
v General Medical Council (defendant) and Disability Rights Comission
(interested party) and the Official Solicitor (intervenor) [2004] EWHC
1879 23. Human
Rights Act (1998). The Stationary Office, 1998 24. Airedale
NHS Trust v Bland [1993] A.C. 789 25. Graber
MA, Tansey JF (2005) Autonomy, consent, and limiting healthcare costs.
Journal of Medical Ethics 31:424-426 26. Howard
JM, DeMets D (1981) How informed is informed consent: the BHAT experience.
Controlled Clinical Trials 2: 287-303 27. Fortun
P, West J, Chalkley L, Shonde A, Hawkey C (2008) Recall of informed
consent information by healthy volunteers in clinical trials. QJM an
international journal of Medicine in press, available online at:
http://qjmed.oxfordjournals.org/cgi/content/abstract/hc 28. Flory
J, Emanuel E (2004) Interventions to improve research participants’
understanding in informed consent for research. Journal of the American
Medical Association 292: 1593-1601
Indian medical education system has seen rapid growth in the last two decades. From a miniscule number, private medical colleges have grown to account for more than half of the 270 medical colleges in 2008 and consequently, India has the highest number of medical educators in the world. This unregulated unequal growth brings two issues to focus: the failing quality of medical education and implementing effective solutions to address an artificial faulty shortage due to doctor mal-distribution. The menace posed by the growing merchandisation of medical education has to be warded off and efforts should be made to ensure maintenance of standards and check the unplanned growth of substandard medical colleges and substandard education norms in universities or their constituent medical colleges. There is a strong case for a review of the entire system of medical education and examinations in the country. Some solutions like increasing retirement ages of MD faculty to 70 years, sharing of faculty, increasing MD seats, allowing clinical MDs to teach paraclinical and preclinical subjects or temporary merger of specialities have been proposed to address the faculty shortage instead of relying on inadequately qualified MSc non-medical faculty.
Keywords: Qualified Medical teacher, India, medical colleges, faculty shortage, Medical Council of India (MCI).Abbreviations DCI=Dental Council of India. MSc=Master of Science
Establishing a medical college is not similar to establishing a science or Arts College and apart from a huge capital requires a huge number of qualified, competent, MCI compliant manpower to produce quality doctors.1,4,7 Having established a Medical College, maintaining the standards of education to world acceptable levels with a vision to serve poor Indian masses has been a concern of the Indian planning committees. Also, the good name a college attains is due to the accomplishments of its faculty and alumni. In that regard, proper emphasis on the quality of medical education ,inspite of the recent rapid proliferation of private medical colleges, has rightly been the working domain of Medical Councils all over the country and has consumed energies of Medical Council of India over the last forty years. 1, 4, 7,10,12
The Medical Council of India (MCI), the regulatory and advisory body on medical education, approves medical curricula and permits medical school existence and allows for recognition of medical degrees issued by various universities. The accreditation process for medical schools focuses largely on the infrastructure and human resources required and little on the process and quality of education or outcomes.15 The implementation of the recommendations of MCI regarding recognition or de-recognition of a medical college is governed by the Ministry of Health and Family Welfare, whilst individual universities also have variable sets of regulations for their affiliated medical schools. As a result, there is no uniformity in the standard of medical education across the country. At the time of independence there were just 19 medical schools with an output of 1200 doctors.10 In 1965, there were 86 medical colleges in India with only a few private colleges7 The college total increased to 112 by 1980(at a rate of 30%), to 143 in next decade (rate of growth of 28%) and since 1990 over past 18 years the number has increased to 271, an increase of ~90% compared with the figure in 1990.7 Today, there are 271 medical colleges out of which about 31,000 medical graduates pass out every year and private sector medical colleges have grown to account for more than half of all medical education institutions in India 13
Evidently, medical education system seems to have had an unregulated growth over the last two decades. It has been pointed out that even the prestigious colleges window dress faculty lists or put up names of non-existing academic members in their staff list. 5 Most medical college permissions were gifts given out as largesse or patronage to political heavyweights from health ministry.1,14 Very few have had adequate space, laboratories or hospitals as per MCI norms. They were and remain ill- equipped and inadequately staffed.10 This unregulated rapid growth in enrolment of medical students and poorly implemented regulations relating to admissions, faculty strength and infrastructure in medical colleges adversely impacts quality of training in Indias medical institutions.
Many reputed physicians and surgeons, professors, directors and deans working in new private medical colleges fabricate and falsify records like even birth records and lie to the MCI and the courts in order to get their medical college of questionable standards approved or recognized. Illegal money is involved in the business of getting new private medical colleges approved or recognized by the MCI and the health ministry. The decay of medical colleges reflects the general trend in this country .4,5 Corruption and bribery have made permanent inroads into medical education since past few decades in health universities or entrance examinations. Even clerks in the universities leak question papers and manipulate marks. 1 Perhaps the worst kind of gross unethical practice in academic medicine happens around the time of inspection by the Medical Council of India (MCI) post 1998-2000, in new private medical colleges. In emergency-like frenzied two day shows, busloads of patients are mobilized to fill up empty wards, carloads of doctors are paraded before the inspectors, and even instruments are hired or shifted between colleges, during the period of MCI inspections.4
Privatization in general has been known to increase the gap between rich and poor, amounting to encouraging survival of the richest which cannot be a acceptable goal of any civil society.8 And, the policy of excessive privatization of medical care delivery system has undermined health services and further limited the access of the underprivileged.3,8
Privately, many managements agree that it is very difficult to get faculty and that it is even more difficult to retain them in the wake of continuous offers or lure from newly established medical colleges. Certain medical college locations in smaller cities or semi-urban areas do not have facilities, ambience, or charm of big cities hence attracting teachers or other qualified staff to such medical colleges has been difficult, and various inducements have been applied. Such colleges have been surviving council inspections by window dressing or luring faculty with money. In certain new colleges which are literally brick fresh, bereft of hostel or quarters or other amenities the teachers delay even more to move or settle down themselves. At times doubts are established whether an impossible set of conditions and heavy financial burden is imposed on Medical college managements, by the MCI just to make management fail MCI inspections, but at the same time, some stringent MCI regulations have helped faculty of Medical colleges by ensuring job availability.
Doubling of medical colleges over last 15 years has improved the number of medical practitioners in India, but will the mere increased numbers mean a higher quality health care delivery system is debatable. Most management fail to fulfill the excellent set of norms stipulated by Medical Council of India. It is worthwhile, in national interest to note that, we have been loosing medically qualified post graduates to Western countries since till recently Medical College teaching jobs were low paid and did not give that richness or respect attained by private practitioners. After the Karnataka Government & Pondicherry scales new implementation in 2007, with a heavy Non Practicing allowance teaching profession has gained respectability vis--vis elite in society like software engineers. Similar uniform pay scale implementation is need of the hour, all over the country to prevent medical teacher mass migrations.
Nearly 27000 teachers are required as per Ananthakrishnans calculations 7 to fill the faculty positions in 270 medical colleges purely for the purpose of teaching MBBS.He ignores the existence of ~300 Diplomate National Board hospitals across India and requirement of faculty for DNB courses. He also ignores MCI recognized institutions exist in other countries like China, Nepal, Malaysia, Netherlands and have been training MBBS doctors of Indian origin. All these institutions have been drawing medical teachers to satisfy MCI or DNB stipulations for accreditation. Hence we have to account loosing faculty to such Institutions. Also his manpower calculations are only for colleges purely teaching MBBS and ignore multiple course Colleges like KMC Mangalore, Manipal which harbor 90 MSc students per year per department and ignores existence of PhD students which evidently will require more teachers. He also ignores the net strain on the same faculty who are simultaneously teaching BPT, MPT, etc in allied institutions. A great academic strain on medical college teachers ,exists,which has never been accounted by MCI nor by Dr Ananthakrishnan.So, on the whole, it means that a great qualified medical teacher shortage exists in India. Either it is due to the excessive number of courses imposed on the same faculty or maybe it is inefficient use of existing qualified medical teachers for non teaching purposes.
Contrary to the opinion of Health ministry, eminent educationists Sood & Adkoli point out that the doctor: population ratio has already exceeded that required by the country and there is mal-distribution of their services. They feel that the menace posed by the growing merchandisation of medical education has to be warded off and efforts should be made to ensure maintenance of standards and check the unplanned growth of substandard medical colleges and substandard education norms in universities or their constituent medical colleges. This mal-distribution of medical manpower is the centered on biased political will and seat purchasing power in the community. With the correction of medical manpower maldisditribution medical standards will harmonize throughout India.11,12
Indeed, given the sharp increase in the number of medical colleges and the doubling of enrolment capacity after1980s it is difficult to imagine that enough trained full-time faculty exist to adequately staff the newly created colleges or DNB Hospitals and maintain reasonable teacher-student ratios.9 Dr Ananthakrishnan proposes to allow MSc from Non Medical Universities to teach Medicine. 7 It will be gross medical impropriety to allow such injustice to be allowed by Medical council of India which is supposed to uphold medical education standards across India. What glory does it give Indian medical education system to have a bunch of unqualified non medical doctor MSc teachers seeking to run coaching medical classes a la science tuition centers we fail to see. What is the necessity to increase number of medical college, or medical college seats, in inadequacy of appropriate medical teachers? Is it possible to permit inadequately trained staff to run these colleges, and will the output reflect quality abroad? Emphasis here is not on excellent university results, these MSc teachers, produce by mere mugging up of unconnected facts or figures or excellent power point teaching but what MBBS educated teachers can produce by moulding young doctor student minds by bringing in relevant clinical experience.
Some Solutions
Today, India has the highest number of medical colleges in the world and consequently the highest number of medical teachers. Yet, shortage of medical faculty and lack of medically oriented teaching by appropriately trained MD faculty have tarnished Indian medical glory. The unprecedented institutional growth has created a national quality challenge for medical education and has resulted in varying standards across medical graduates. There is a national need for well-trained faculty who will help improve programs to produce quality graduates. 5,14 Annual student intake is said to be a critical factor in assessing the requirement for teachers as per Ananthakrishnan,7 and should dictate the employment. A punitive MCI, DNB Board and vigilant state medical councils can act synergistically to decrease medical student intake in Medical Institutions where teachers are not ready to go or do not exist. MCI and DNB Board also need to do more for its medical teachers- give them more respect, recognition, arrange for their pensions, gratuity, relieving orders or get involved in pay scale recommendations as no entity exists till date to safeguard medical teacher interests. Measures are required to ensure private medical colleges proper regulation by the medical council. Further, Indian Health ministry has been known to interfere in the functioning of MCI, DCI and DNB Boards, override MCI, DCI and supreme courts decisions and this is undesirable.12,14,15
Increasing the retirement age of MD teachers up to 70 years will harness hard earned medical experience of senior professors to guide preparation of efficient faculty and will reemploy retired teachers . This will also lead to discipline enforcement, more projects, PhDs and papers of relevance. Else, MCI can think of sharing of medical faculty among medical colleges, or dental colleges, and ensure less burdened teaching schedules. Implementing integrated medical education system-will help, as has been experimented in -KMC Manipal, Sri Ramachandra Medical College. Present paramedical system is a confused network of PhDs who have not enriched Medical education system, a proof of which can be the absence of a single Nobel laureate or international repute medical scientist or of the glory of IISc departments, in 270 odd medical colleges across India, even Manipal, or AIIMS in spite of having the system for 50 years. Merging of homogenous specialities like merging of biochemistry with physiology or pathology, microbiology with pathology, or creation of a discipline of laboratory medicine merging pathology, microbiology and biochemistry has been suggested in yahoo groups like mdbiochemists. Merging of homogenous specialities decreases the requirement of professors in biochemistry and microbiology by providing MCI norm requirements of professors from pathology. Also merging of Anatomy with Surgery will be worthwhile and achieve similar objective of providing deficient staff from Surgery department, who happen to be plenty. It is said to bring about some integrated medical education also. This cure is supposed to provide a broad based intermingling for net objective of efficient medical teaching by qualified professors, peers in interrelated departments. We would further extend their argument in suggesting that the proposed speciality merger need not be complete and final but a temporary arrangement for next 20 years.
Acute shortage of medical teachers needs to be filled. Appropriate solution exists within medical education system itself and help can come from recruitment of medical brethren from clinical sciences to fulfill non clinical department norms, as has been happening successfully ,silently ,without MCI approval ,in Tamilnadu and Andhra pradesh government medical colleges. A whole lot of MD or MS or DNB doctors are ready to serve as Medical teachers, but colleges have never used their teachership as MCI does not permit this. Many such part-time consultants who are practicing in community could deliver excellent teaching assignments and help tide over the so called artificial medical teaching crisis.MCIs generosity to allow MDs of homogenous specialties to teach in Pre or Para clinical sciences for a honoraria, rewards system will effectively ,in a short time solve inadequate improper medical staffing problems forever. Number of seats available in various post-graduate medical courses is approximately 11,005 annually which is one third of MBBS graduates coming out every year. Nearly a third of these seats are diplomas and a diplomate cannot be considered for even a junior lecturer post like an MSc graduate, but will be considered for post of Tutor, the lowest cadre of medical teachership. Thus all DCP (Diploma in Clinical Pathology) and DFM (Diploma in Forensic Medicine) loose out Lecturership to their MD colleagues. Increasing the number of MD seats in Para clinical and preclinical sciences and replacing existing Diploma seats with corresponding MD seats is a just approach and should be the right approach for MCI to follow, since in contrast to before 1960s,in present days no postgraduate seat goes vacant-it means there are no shortage of MD aspirants as wrongly assumed by Dr Ananthakrishnan7 .MCI also has to think of giving Junior lecturership posts to MBBS graduates who have been serving as tutors for more than 3 years in any department .
Continuing medical education
Thus there is a strong case for a review of the entire system of medical education and examinations in India. The American style of giving credits for demonstrable good performance throughout the years can be introduced. It will, of course, be necessary to ensure objective evidence of such assessment and performance.1,8 The Indian Health ministry has realized that efficient medically qualified teachers are in the best position to mould young physician minds hence, Indian National Knowledge Commission (NKC-2008) proposes raising average standards and creating centers of medical excellence, revised medical accreditation; methods of attracting and retaining talented medical faculty members and devising measures to ignite, promote and sustain the research tradition in medical colleges and teaching hospitals.
Medical teacher incentivisation8, i.e increments, promotions, paid study leaves will also attract good teachers to stable institutions. In order to recruit good and gifted medical teachers, it is necessary to provide them with regular attractive salaries, amenities and retirement benefits which are realistic and at least on par with the earnings of those in practice.2 Emigration of high quality physicians who could potentially serve as medical teachers in local Medical colleges may lead to further declines in the quality of medical graduates produced. To address regional inequities for medical training and related availability of doctors, firstly, it may be useful to set up adequately staffed medical research and training institutions in economically backward areas. Secondly, the government could subsidize the medical education of individuals living in backward areas, perhaps by combining such a subsidy with a bond to serve in the backward areas for a limited number of years. Implementing this bond system will be in the control of the health ministry.
For existing medical teachers, high standards of teaching are to be maintained and improved upon with constant seminars and workshops. Teaching aids, computers, medical CDs, DVDs, medical e-books, Internet facilities and availability of the latest journals and literature on the subject should be provided in every medical college or diploma national board certified hospital.2At the post graduate level, it is the duty of the senior teacher to train the young doctor so that he learns to perform according to accepted international standards.2 As a long- term policy, no new medical colleges must be permitted in prosperous states, unless they demonstrate an MCI compliant infrastructure and facilities better than those in existing institutions. A revitalized Medical Council of India must be the only agency permitted to recognize such colleges and health ministry need not have any role.1 Since advent of the MCI it has been noted that Indian health ministry can not only ignore a negative rating by Medical Council of India, but also openly defy the Supreme Court.12
India needs also a MCI controlled and Supreme Court monitored screening system of students admitted to medical colleges under the discretionary management quota so that merit remains the paramount criterion. This requires common entrance examinations to assess student performance across colleges, publicly accessible information on admission standards practiced by colleges, including transparent nondiscriminatory ranking by performance, and enforcement of sanctions on colleges violating norms. A useful first step is the government policy of maintaining a accessible list of recognized colleges, but obviously much more needs to be done to implement ways to increase the supply of MD teaching personnel .Indian policy makers need to think proactively about developing a cadre of doctors focused more on medical education and research. Lastly, the Indian Medical Association, Association of Medical Biochemists of India, All India MD/MS Doctors Association, and other national medical and dental professional bodies must play a greater role to foster true medical and dental education and prevent governmental and political interference.1,12,14
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR P VALLYAMMA MD, Professor & Head of Biochemistry, Periyaram Medical College, Kerala, India
DR SRINIVAS R DESHPANDE MD, Associate Professor in Biochemistry, Melmarvathur Adiparashakti Institute of Medical Sciences, Tamilnadu, India.
DR GAYATHREE L, MD, Assistant Professor in Microbiology, Hassan Institute of Medical Sciences, Hassan, Karnataka, India
CORRESPONDENCE: Dr P Vallyamma MD, Professor & Head of Biochemistry, Periyaram Medical College, Periyaram, Kannur Dt, Kerala, India
Email: aimdda@yahoo.com
References
Madhok P.Medical tuitions .Issues in Medical Ethics 1997; 5: 23
Chinoy R. F: Medical ethics: relationships between doctors.Ind J Med Ethics
Qadeer I: The real crisis in medical education. Ind J Med Ethics
Chattopadhyay S: Black money in white coats: whither medical ethics? Ind J Med Ethics ;Jan-Mar 2008(1)
Bansal P, Supe A. Training of medical teachers in India: Need for change. Indian J Med Sci [serial online] 2007 [cited 2008 Oct 1]; 61:478-84. Available from: http://www.indianjmedsci.org/text.asp?2007/61/8/478/32930
Nair KR :Medical college teachers and some ethical issues in Kerala .Ind J Med Ethics
Ananthakrishnan N: Acute shortage of teachers in medical colleges: Existing problems and possible solutions.NMJI Jan/Feb 2007: Vol 20, No 1:1-8.
Aggarwal A. Strengthening the health care system in India: Is privatization the only answer? Editorial. Indian J Community Med: April 2008; Vol 33; Isuue 2; 69-70.
Dutta R. Rash of medical colleges spawns corruption and mediocrity. Express Healthcare Management, August 2002
Richards T. Impressions of Medicine in India; Medical education in India-in poor health. British Medical Journal Volume 290; 13 April 1985;1132-34.
Sood R & Adkoli BV. Medical Education in India Problems and Prospects. Journal of Indian Academy of Clinical Medicine Vol. 1, No. 3; October-December 2000; 210-12.
Mahapatra D .Ramadoss nod to medical college despite SC no-Times of India National edition;29 Sep 2008, 0054 hrs IST, TNN.
India to recognize foreign medical degrees :an article published in India Chronicle a monthly e-newsletter Issue No 002;March 2008 http://indianembassy.ru
Rajeev D & Mahapatra D Did Ramadoss flout dental council norms?-Times of India National edition;30 Sep 2008, 0449 hrs IST, TNN
Sood R. Medical education in India ;Medical Teacher, Volume 30, Issue 6 2008 , pages 585 - 591
“That element of tragedy which lies in the very fact of frequency, has not yet wrought itself into the coarse emotion of mankind; and perhaps our frames could hardly bear much of it. If we had a keen vision and feeling of all ordinary human life, it would be like hearing the grass grow and the squirrel’s heart beat, and we should die of that roar which lies on the other side of silence”. (George Elliot)
I wonder what would be the magnitude of the roar on the other side of silence when Depression, as WHO has it, becomes the second most common disabling condition worldwide by 20201. I don’t know about others but I myself would be relying on my chronic ailment of selective deafness to remain blissfully unaware of the enormity of emotional pain and ceaseless suffering, if these were to penetrate into the much narrowed range of my sensitivity. I am sure my wise colleagues won’t die of the roar either and would have plenty of effective safeguards to choose from. You might, however, argue that these measures may be gratuitous, as the emotional coldness, which is endemic in our circles, may suffice. You may have a point.
Okay let me cut out the rhetoric and tell you what it is basically about. Depression is a major health problem2 and 6% of the population meet the criteria for the disorder or Dysthymia at any one time3. In individuals between 15-44 years Depression accounts for 10% of all DALYS (disability-adjusted life-year), which is projected to rise to 15% by 2020, making Depression second only to Ischemic Heart Disease in terms of worldwide disease burden4. The irony is, while the time-bomb is ticking away and the race against time is underway, my learned colleagues seem to be engrossed in an endless duel over Antidepressants. “The term ‘antidepressants’ is a misnomer” and ‘they are not effective at all’5 sums up the stand ‘the Critical Psychiatry Network’ takes on this group of medications in particular while others dig their heels and maintain that ‘Antidepressants do work and there is lack of evidence for Cognitive Behavioural Therapy in mild Depression’6. The debate has raged on for decades now and this year it really came to a head when a major publication7 made a news headline writing off Antidepressants nearly completely and then only three months later we had fresh guidelines by another high impact association8 recommending their use.
It might sound alarmist but these days patients would be running a huge risk of getting bogged down by diametrically opposite views if they spend more than a few minutes on the internet only trying to find help. People with Depression may very likely find the College recommendations9on when and why to use Antidepressants as straightforward and easy to follow. But if they push a search engine to full throttle they will soon find themselves on a long and bumpy road that basically leads to nowhere. They may suddenly stumble on a view that ‘meta-analyses show selective serotonin reuptake inhibitors have no clinically meaningful advantage over placebo’10 after negotiating a number of trials suggesting otherwise. With a couple of further clicks on the keyboard they, like myself, will find themselves struggling to see any concordance between the argument that the effect of Antidepressants could be exaggerated by their sedative property10 and the conclusion that ‘Insomnia and REM sleep suppression were reported with all SSRIs’ 11. Surfing on they may even start to wonder whether the beneficial effects of a whole range of medications like Antihypertensives, Antiepileptics, Antibiotics, Hypoglycaemics etc. could be exaggerated, if they come across a view that ‘unblinding effects’ (for example those due to side effects) ‘may inflate the efficacy of antidepressants in trials using inert placebos’12. The doubt would be perfectly legitimate because the principle of testing medications against ‘active placebos’ appears to be so neatly applicable right across the board and naturally begs the question whether it is applied generally in actual practice. Unfortunately, after a while the answer to the question whether the Antidepressants are beneficial or not will start to appear ever so elusive and it won’t be long afterwards that a deep sense of disappointment will set in, making these desperate searchers to log off from the Net as well as hope.
Dividing the whole of Psychiatry into two warring parties is not what I have intended to do in the above lines. That would be too simplistic. My attempt is only about trying to get a couple of messages across to all of us who claim to have patients´ best interest at heart. I cannot think of any other way to convey the crux of my first message than to take a quote from ‘War is a Racket’13. The author says in the book, ‘For a great many years, as a soldier, I had a suspicion that war was a racket; not until I retired to civil life did I fully realize it’. So while we maintain a high quality of our research studies about treatments in Psychiatry by employing rigorous methods, observing scientific detachment and keeping every enquiry dispassionate, it is imperative that we remain on guard against the possibility of us turning into inadvertent racketeers for those who are only driven by their monstrous appetite for profiteering.
My second message is specifically for ‘the Critical Psychiatry Network’ and to those of similar persuasion. I have had an honour to work with one of your main proponents and I can safely claim that you are a group of exceptionally talented Psychiatrists. You are doing a great job of saving Psychiatry against a potential risk of it simply degrading into some kind of quackery. However, I am not entirely comfortable with the unidirectional nature of your works, which appear to be mainly focussing on disproving positive claims made about the efficacy of treatments. It is about time that an equal amount of your energy and time is devoted towards establishing what can effectively treat Depression and help rekindle hope.
CORRESPONDENCE: 90 Heathfield Park Drive, Essex RM6 4FJ
Email: jkhaja@yahoo.com
REFERENCES:
1. Murray, C. & Lopez, A. (1996) The Global Burden of Disease. Cambridge, MA: Harvard University Press.
2. Greenberg, P., Stiglin, L., Finkelstein, S., et al (1993) The economic burden of depression in 1990. Journal of Clinical Psychiatry, 54, 405–418.
3. Keller, M., Lavori, P., Mueller, T., Keller, M., Lavori, P., Mueller, T., et al (1992) Time to recovery, chronicity and levels of psychopathology in major depression: a 5 year prospective follow-up of 431 subjects. Archives of General Psychiatry, 49, 809–816.
4. Murray, C. & Lopez, A. (1996) The Global Burden of Disease. Cambridge, MA: Harvard University Press.
5. Joanna Moncrieff Canadian Journal of Psychiatry Feb. 2007;52,2; Pro Quest Medical Library pg 96.
6. SAGE Press Release in connection with BAP guidelines published in May 2008.
7. Irving Kirsch et al, Initial Severity and Antidepressant Benefits: A Meta-Analysis of Data Submitted to the Food and Drug Administration; PLoS Medicine, Feb. 2008, Vol. 5, Issue 2.
8. Anderson etal, Journal of Psychopharmacology May 2008 http://jop.sagepub.com/cgi/rapidpdf/0269881107088441v2
9. www.rcpsych.ac.uk
10. Joanna Moncrieff Canadian Journal of Psychiatry Feb. 2007;52,2; Pro Quest Medical Library pg 96.
11. Mayers A G, Baldwin D S, Antidepressants and their effect on sleep; Human Psychopharmacology: Clinical and Experimental 2005 Vol. 20(8), (Database of Abstracts of Reviews of Effects (DARE)).
12. Moncrieff J, Wessely S, Hardy R, Active placebo versus antidepressants for depression; January 2004 Systematic Review (Cochrane).
13. Major General Smedley D Butler (1898-1931), United States Marine Corps, author of War is a racket.