Schwannoma (neurilemmoma) is a peripheral nerve sheath tumour and commonly occurs on the head, neck and trunk. Giant schwannoma is rarely located in the retroperitoneum and the pelvis but rarer in the mesorectum. The majority of symptoms caused by the tumour are due to its mass effect. Surgical resection is enough to treat the tumour. Schwannoma is usually a benign tumour. Its malignant transformation is usually very rare. We report a 36 year old male patient with a giant mesorectal schwannoma who presented with vague symptoms.
Case Report
A 36 year old male patient presented with a lower abdominal mass since 2 months, urgency of defecation since 6 months and erectile dysfunction for more than 3 years. There was no history of urinary disturbances. General physical examination did not reveal any abnormality. Abdominal examination showed a non tender, firm, fixed mass with well defined borders over the suprapubic region which was extending into the pelvis. No organomegaly was detected. On rectal examination a hard, immobile mass was felt 5 cm away from the anal verge and lying anterior to the rectum.
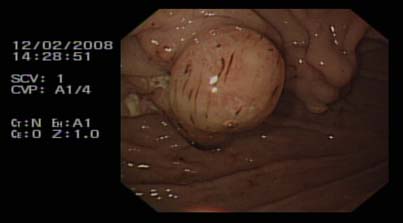
His urine analysis, routine hematological investigations and renal function test were within normal limits. Total bilirubin was raised to 24.9 µmol/l (3.42-20.52 µmol/l), direct bilirubin was also elevated 8.2 µmol/l (0-6.8 µmol/l) while all other results were within normal range. The patient was positively screened for Hepatitis B and Syphilis. CT scan (figure 1) of abdomen revealed a large soft tissue mass measuring 10x11 cm in the pelvis. It was a well defined mass without any infiltration to the following structures: sigmoid, rectum, prostate gland, the bladder and the sacral bone.
Figure 1 shows a large soft tissue mass measuring 10x11 cm which compresses the rectum.
FNAC of the mass which was taken 3 cm from the anal verge showed isolated fibrotic tumor.
The patient was advised for HIFU therapy (high intensity focused ultrasound) in view of eventual surgery. In HIFU therapy, the ultrasound beams are focused on the diseased tissue and due to the significant energy deposition at the focus, temperature within the tissue rises to 65° to 85°C, destroying the diseased tissue by coagulation necrosis and hence facilitating the dissection of the mass during surgery. After HIFU therapy, the patient no longer complained of urgency of defecation. But there was no significant change in the size of the mass after a rectal examination.
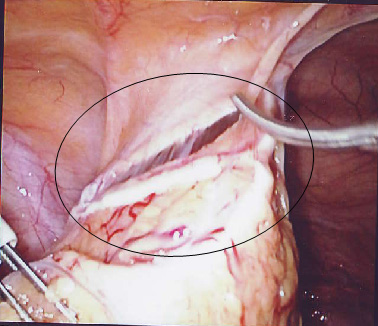
Hence, explorative laparotomy was carried out. The abdomen was opened through the lower midline incision. A huge mesorectal mass of 15x11x8 cm (figure 2), was identified on the right side of the rectum and behind the prostate gland extending upwards, without any posterior infiltration into the sacral bone. Complete excision of the mass was achieved by blunt dissection and the mass was sent for histopathological examination. The operation was uneventful.
Figure 2 shows the complete excision of a well encapsulated mass of 15x11x8 cm. The external surface of the mass was gray-white and smooth.
Figure 3: Histology showing typical pallisading arrangement of spindle cells (Antoni-A/Verocay Body) and less cellular myxoid areas (Antoni-B)
Discussion
Schwannoma (Neurilemmoma) is a benign neoplasm arising from the myelinated nerve sheaths. Malignant schwannoma despite their name, never arise from malignant degeneration of schwannomas. Instead they occur from transformation of a plexiform neurofibromatosis. This fact provides the basis for their association with neurofibromatosis1.
Schwannomas are frequently present in patients aged 20 to 50 years with a male predominance. They comprise 5% of all benign soft tissue tumors and have a predilection for the head and neck2, 3, 4 and flexor surfaces of the upper and lower extremities5. Pelvic schwannoma is rare and accounts for less than 1% of all benign schwannomas6. The rarity of this tumor and the lack of clinical manifestations make a pre-surgical diagnosis very difficult.
These tumors slowly increase in size before becoming symptomatic. Clinical signs or symptoms manifest themselves only by the compression or infiltration of adjacent organs. Therefore, detection is often accidental.
Schwannoma typically appears as a solitary, well encapsulated, firm and smooth-surfaced round mass. In large tumors (>8-10 cm), a degenerative pattern (cystic areas, calcifications, interstitial fibrosis, and hyalinization) is commonly found that identifies the “ancient” variant7. Histologically, typical schwannomas are composed of inter mixed Antoni A components (cellular and arranged in short bundles or interlacing fascicles) and Antoni B areas (less cellular and organized with more myxoid components).Schwannomas show uniform and intense staining for S 100 protein8.
Malignant transformation is very rare and controversial9. Malignant schwannomas are large in size and highly aggressive tumours. They are painful, and may cause many different symptoms depending on the location and size. They infiltrate into the adjacent structures and metastasize to distant sites. Histologically, the nuclear palisading may be a striking feature. There will be perineural and intraneural spread of tumour, lesional proliferation, or herniation into the lumina of the vessels10.
A combination of clinical, pathological and immuno-histochemial studies help to make the diagnosis.
However preoperative diagnosis of schwannomas is not easy owing to the difficulty in finding imaging features (with Ultrasonography, CT, or MRI) that enable the discrimination of schwannomas from other soft tissue tumors (fibrosarcoma or liposarcoma) and benign forms from malignant ones11. Schwannomas can frequently be misdiagnosed as psoas abscesses, pancreatic cysts, neoplasms, adnexal masses, adrenal, kidney or hepatic tumors, as reported in the literature12, 13, 14. Yet, radiological imaging is helpful in therapeutic planning, as it gives information about the tumor’s size, location, and possible invasion of other structures. Fine-needle aspiration biopsy may theoretically be useful if Schwann cells are found in the sample, but the tissue specimen collected for diagnosis is often inadequate and may be misleading because of cellular pleomorphism in degenerated areas which might be interpreted as consistent with malignancy15.
Hughes MJ et al11, in their largest radiological series of abdominal or pelvic schwannomas, showed that a smooth well defined border, ovoid or spherical shape and location in the pre sacral region or lower retro peritoneum at the pelvic brim, are frequent findings in primary abdominal or pelvic schwannomas ; 11 of 13 cases showed all these features. Evidence of degeneration was common, with 8 schwannomas showing cystic change and 3 showing areas of calcification. The cystic schwannomas tended to be larger, with a mean diameter of 10.5cm.
It is difficult to make an accurate pre operative diagnosis. The treatment depends solely on surgery. Malignant schwannomas are insensitive to chemotherapy and radiation, resulting in poor prognosis16.
Conclusion
Schwannoma is a benign encapsulating neoplasm with an overall low incidence, occurring mostly in the head, neck and trunk regions. Giant schwannoma is rarely located in the retroperitoneum, the pelvis and rarer in the mesorectum.
Schwannomas pose a difficult diagnostic challenge. Radiological findings are often non-specific. Ultrasonography can differentiate between solid and cystic tumours. CT can be helpful in determining the size, location, local involvement and distant spread. MRI provides similarly useful information as CT, but yields better visualization of the tumour. FNAC is not often helpful because the tissue architectural information required is not obtainable from cytological specimen. The only gold standard diagnostic investigation is histology of either biopsy or excised specimen.
Surgical excision has remained the mainstay of treatment. Although benign, large and incompletely excised lesions are capable of recurrence, malignant change is exceedingly rare.
Inadvertent carotid arterial puncture complication is reported to have an incidence of 2% - 8% 1, 2 and usually results in localised haematoma formation.
Case presentation
We present a case of a 72 year old man with acute on chronic renal failure referred for intensive care (ITU) management. History revealed dehydration and anuria for 3 days. His blood pressure was 80/40, sinus tachycardia around 130/min with cold clammy peripheries. Blood investigations revealed urea 23mmol, creatinine 800mmol, and potassium-7.7, with ECG changes of hyperkalemia. We attempted a right internal jugular (IJV) venous cannulation using landmark technique and inserted an Arrow-Howes central venous catheter with blue flexi tip, 8.5FR, 5 lumen, and 16cm length. The technique was difficult due to low blood pressure, and patient’s inability to lie flat. The ultrasound machine was unavailable at that moment.Soon after the catheter was introduced using seldinger technique, a swelling was noticed from the site of IJV cannulation .the blood sample analysis revealed arterial blood. The catheter was removed and pressure applied for 45 minutes. Thereafter, a left femoral vein catheter was inserted for central venous access and right femoral vascath –VYGON, DUALYSE Expert, 2 lumen catheter set, 12 fr, 20cm was inserted uneventfully.1 hour later the bleeding from the right carotid puncture site was examined and was found to have ceased. The patient was put on the continuous veno- venous haemofiltration (CVVHF), which clotted after 15minutes.Heparin was used as an anticoagulant for the filter. This was repeated thrice with same result. Three hours later, a haematoma was noticed in area of IJV puncture, which was gradually increasing in size. The haematoma spread to the neck and chest after which the patient complained of discomfort with breathing difficulty. In view of increasing airway compromise the patient was transferred to theatre for elective intubation and surgical intervention. Ultrasonongraphy by radiology consultant showed a large haematoma, but unable to see the damage in the vessel and a CT neck, thorax angiography was suggested. CT angiogram revealed a leak in the bifurcation of the carotid artery. Surgical access was difficult in view of the large persistent leak. Ultrasound probe was used to make the incision superficial to the leak. A small leak was identified in the artery, which was sutured uneventfully. He was then continued on CVVHF with no further complications Discussion Complications include arterial puncture, pneumothorax, neck or mediastinal haematoma and hemothorax3, 4. The haematoma may enlarge rapidly if the patient is coagulopathic, or if a large puncture wound is produced by the introduction of the sheath itself into the carotid artery. Airway obstruction 5, 6, pseudo aneurysm 7, 8, arterio-venous fistula formation 9 and retrograde aortic dissection 10 have all been reported as a consequence of carotid puncture. In the presence of occlusive (atheromatous) carotid disease, inadvertent puncture may carry the risk of precipitating a cerebrovascular accident 11. NICE guidelines 2002 recommended use of ultrasound for central venous cannulation12. The Royal College of Radiology (RCOR) recommends practical training in vascular ultrasound should involve at least two ultrasound lists per week over less than three months up to 6 months. Meta-analysis including 18 Randomised Controlled Trials by NICE concluded that ultrasonongraphic (USG) venous catheterisation was more effective than landmark technique for all outcomes 13 Royal College Of Anaesthetists feels guidance is fair and sensible but landmark technique is still acceptable alternative whether 2D available or not. Conclusion Complications following central venous cannulation are reduced if the procedure is USG guided and therefore must be used whenever possible. But landmark technique is still an acceptable alternative.
We describe a case of a 32 year old primigravida with type III Klippel-Feil Syndrome for an elective Caesarean section. A preanaesthetic assessment at 32nd week of pregnancy revealed a history of mild asthma for which the patient was on regular salbutamol inhaler. She had no history of cardiovascular or respiratory insufficiency. There was no significant family history. Anaesthetic history included a repair of encephalomyelocele immediately after birth and a squint correction surgery at the age of 6 years under general anaesthesia which was uneventful.
Examination revealed a woman of small stature, 137 cm in height and weighing 52 kg. Airway examination revealed Mallampati III with a normal mouth opening, a reduced thyromental distance (3 cm) and inability to flex or extend the neck (Figure 1). She had thoraco-lumbar kyphoscoliosis and examination of the respiratory and cardiovascular system was unremarkable. Electrocardiogram was within normal limits as were haemoglobin, urea and electrolyte estimation. Radiography revealed fusion of atlanto-axial joint (flexion and extension views, Figure 2 ) and also fusion of lumbar vertebrae with associated scoliosis (Figure 3Cobb’s angle 25 degree) and Cobb’s angle 25 degree Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.
The incidence of caesarean section is rising1 and there is evidence that women who have a caesarean section may be at increased risk of complications in a subsequent pregnancy2. Compared with vaginal delivery in the first pregnancy, caesarean section has been found to be associated with significantly increased rates of: uterine rupture in labour;3 placenta previa and placental abruption;4 placenta previa leading to peri-partum hysterectomy;5 stillbirth;6 and perinatal death7. Sometimes some unusual complication develops with which, we are not familiar. Here an uncommon complication following caesarean section in a post caesarean pregnancy has been reported.
Case report
A 25 years old lady P 1+4 presented at the emergency department of NRS Medical College & Hospital, Kolkata as an unbooked sixth gravida with the complaint of leaking per vagina for last 4 hours and the period of amenorrhoea was 38weeks. Her past obstetric history revealed that she had caesarean section 4 years earlier (indication of caesarean section was not known to the patient) and 4 successive M.T.Ps, the last being done 1 year back. The baby was alive. The couple wanted ligation operation.
On examination, she was mildly anaemic. Pulse was 88/min and BP was 126/80 mm Hg. She was free of any medical or surgical complications like morbid obesity, COPD and umbilical hernia. Per abdominal finding revealed a term size uterus with cephalic presentation and average liquor. FHS was 144/min and regular. Her previous caesarean section scar was low transverse and there was no scar tenderness.
Per speculum examination showed dribbling of clear liquor. Vaginal examination revealed cervix was 1.5 cm dilated, tubular, station was high up (-3) and membranes were absent.
An emergency L.S.C.S. was performed under spinal anesthesia. The skin incision was Pfannenstiel with excision of the previous scar. On opening the abdomen, uterus was found to be adherent with anterior abdominal wall from which uterus was separated for delivery of the baby (a living male baby of 2.75 Kg) and bilateral tubectomy operation. Bladder was also pulled high up which was dissected and pushed down before opening the uterus. Parietal peritoneum was not closed and rectus sheath was repaired with no 1 chromic catgut. Duration of operation was one hour which was longer than usual operation time of 35 minutes.
First two post operative days were uneventful. On the 3rd day there was a small amount of serosanguinous discharge from the umbilicus. The caesarean section wound, which was located much below the umbilicus, was healthy. Methylene blue dye was introduced into the bladder to rule out any communication with umbilicus, through which no dye came out. On 4th post operative day a mass was seen protruding through the umbilicus and on gentle prodding it seemed to be omentum like structure (Fig-I) A provisional diagnosis of omental hernia through umbilicus was made.
Figure I showing omentum like structure protruding through umbilicus
Figure II showing omental tag held during herniorrhaphy operation
On the 5th post operative day, she underwent herniorrhaphy operation under general anesthesia. A tag of omentum was seen to herniate through anterior rectus sheath and skin (Fig-II). The protruding tag of omentum (sent for histopathological examination and confirmed) was excised and a double breasting of rectus sheath was done, keeping a drain which was removed after 48 hours. Her subsequent recovery was uneventful. She came for check up after 6 weeks, when no abnormality was detected.
Discussion
A review of literature has failed to demonstrate the type of complication mentioned above . Intra operative complication like dense intra abdominal adhesion resulting in injury to the bladder and the bowel is not uncommon8. Probably this case report presents an unusual complication for the first time. Probable explanation is that during too much dissection of anterior rectus sheath (to get access to the fallopian tubes) which was firmly adherent with uterus, there was inadvertent injury to the anterior rectus sheath and skin through which omentum had protruded.
COMPETING INTERESTS None Declared AUTHOR DETAILS CHANDANA DAS, MBBS, MD , Associate Professor ,Gynaecology & Obstetrics , NRS Medical College. SNEHAMAY CHAUDHURI, MBBS, MD, DNB , Assistant Professor, Gynaecology & Obstetrics, NRS Medical College. CORRESPONDENCE: DR SNEHAMAY CHAUDHURI, Sopan Kutir , Flat No 1G, 53 B Dr S C Banerjee Road , Kolkata -700010, West Bengal, India Email: snehamay_chaudhuri_dr@yahoo.com
References
Arjun G Caesarean section: evaluation, guidelines and recommendations Indian Journal of Medical Ethics available at www.ijme.in/163co117.html accessed on 29/09/2008
Taylor MK, Simpson JM, Roberts CL,Olive EC, Handerson- Smart D J Risk of complications in a second pregnancy following caesarean section in the first pregnancy: a population-based study MJA 2005; 183 (10): 515-519
Gregory KD, Korst LM, Cane P, et al. Vaginal birth after cesarean and uterine rupture rates in California. Obstet Gynecol 1999; 94: 985-989.
Lydon-Rochelle M, Holt VL, Easterling TR, Martin D. First-birth cesarean and placental abruption or previa at second birth. Obstet Gynecol 2001; 97: 765-769.
Crane JM, Van den Hof MC, Dodds L, et al. Maternal complications with placenta previa. Am J Perinatol 2000; 17: 101-105.
Smith GCS, Pell JP, Dobbie R. Caesarean section and risk of unexplained stillbirth in subsequent pregnancy. Lancet 2003; 362: 1779-1784.
Smith GCS, Pell JP, Cameron AD, Dobbie R. Risk of perinatal death associated with labour after previous cesarean delivery in uncomplicated term pregnancies. JAMA 2002; 287: 2684-2690
Sobande A, Eskander M. Multiple Repeat Caesarean Sections: Complications and Outcomes. J Obstet Gynaecol Can 2006;28(3):193–197
An 82 year old lady, who had suffered multiple strokes in the past and was currently on long term percutaneous endoscopic gastrostomy( PEG) feeding, was admitted as an emergency from a nursing home with a two week history of productive cough and fever. She had been on PEG feeding since her first stroke six years previously. The first PEG tube (placed in 2001) subsequently fell out of position, and a second tube (15 French Frecka PEG tube) was inserted in 2003.
On admission, she was pyrexial, dehydrated, and hypoxic on room air. Chest examination revealed bilateral crackles and neurological examination revealed expressive dysphasia, and spastic weakness in both lower limbs. Abdominal examination revealed an inflamed PEG site with purulent discharge. Blood tests revealed raised inflammatory markers with neutrophilia (WBC 20 x 109 /L with a neutrophil count of 12 x 109/L) and a raised C-reactive protein at 193 mg/L.
She was managed with intravenous fluids and antimicrobial therapy (tazocin and metronidazole) for possible aspiration pneumonia. Vancomycin was subsequently commenced as methicillin resistant staphylococcus aureus (MRSA) was isolated from the PEG site. As she remained stable, PEG feeding was recommenced.
A week following her admission she became unwell with an episode of vomiting and choking following PEG feeding. This was associated with difficulty in infusing feeds and medications through the PEG tube. Multiple flushes through the tube were unsuccessful. The tube was found to be persistently blocked and lacked free mobility within the tract.
Urgent upper gastro intestinal endoscopy revealed a buried bumper as the cause of blockage of the PEG tube. This necessitated insertion of a new PEG tube (9 French Frecka) for enteral feeding. The old PEG tube was removed surgically under local anaesthesia in due course. As the removal of the buried bumper was found to be very difficult endoscopically, and surgical intervention was deemed to be inadvisable in view of co morbidities, the bumper was left in situ. Feeding was recommenced through a new tube. In view of persistent discharge through the PEG site, abdominal ultrasound examination was performed, revealing a possible gastro-cutaneous fistula. No local collection was seen around the PEG wound.
As the patient remained clinically stable, she was discharged home with necessary instructions to her carers for regular flushing of the PEG tube with water, before and after each feed, to prevent further blockages.
Fig 1: Buried bumper (stomach-lower body)
Fig 2: New peg and buried bumper
Discussion
PEG is primarily used for long term (longer than 6 weeks) enteral alimentation for patients with impaired swallowing (e.g. from stroke, degenerative neurological disease, head injury, and oropharyngeal malignancy). However numerous complications have been reported since its introduction in 1980.
Buried bumper syndrome (BBS) is an uncommon but well documented complication of PEG insertion, first described in 1988 1. It is usually a late complication occurring up to 3 years post PEG insertion and reported to occur in 0.3-2.4 % of patients2.
The internal bumper of the PEG tube should normally sit snugly against the anterior gastric wall, and this is confirmed endoscopically at the time of initial placement. BBS develops when there is migration of the internal bumper/flange through or into the anterior abdominal wall. This probably occurs as a result of excessive tension between the internal and external bumpers, from over-tightening of the external flange, leading to gastric wall erosion. During migration it becomes lodged along the gastrostomy tube tract between the gastric and abdominal walls. Once epithelialisation occurs the bumper gets covered with gastric mucosa3.
The diagnosis of BBS should be suspected if localised abdominal pain, peri-tubal leakage or inability to infuse feed occurs. Initial measures to deal with a blocked tube include flushing with warmed water, and occasionally passage of a flexible wire through the lumen, in order to unblock any obstruction. Tube obstruction is usually related to the administration of protein-enriched formulae or medications, especially if the tube size is 9 French. Fungal colonisation may also lead to tube blockage, requiring specific solutions for flushing the tube4. Tube exchange should only be considered if the gastrocutaneous tract is mature (6 weeks or longer after placement of the tube).
Endoscopy is confirmatory in cases of BBS. The internal bumper is not seen, and the site of the PEG is indicated by an elevated area of submucosa with a central depression. Failure to recognise BBS can result in gastric perforation and gastrointestinal haemorrhage or intra abdominal sepsis, peritonitis and even death5.
Ideally, the buried bumper should be removed even if the patient is asymptomatic, to avoid potential complications from continued tube migration until it is completely impacted in the abdominal wall. The literature describes various methods of dealing with this complication. Endoscopic ultrasound of the gastric wall with a catheter US probe can facilitate the localisation of the bumper and also provides information regarding feasibility of surgical or endoscopic removal of PEG tube6.
Regular and optimal PEG care has been vital in identifying and prevention of this complication. During daily cleaning of the external PEG site, the PEG should be pushed in approximately 1 cm and rotated prior to repositioning of the external bumper. The length of the tube outside the abdominal wall should be examined at regular intervals so that migration can be recognised5.
This report reinforces the fact that physicians should be aware of this recognised risk of PEG feeding and prompt referral for endoscopy is necessary to avoid serious consequences including gastro-intestinal bleeding, peritonitis and death. Similarly specific instructions should be given to carers for prevention of BBS.
COMPETING INTERESTS None Declared AUTHOR DETAILS VIJAY JOSHI, Trust registrar in integrated medicine, Chase Farm Hospital, Enfield, UK ASHIS BANERJEE, Consultant in emergency medicine, Chase Farm Hospital, Enfield, UK CORRESPONDENCE: MR ASHIS BANERJEE, Consultant/honorary senior lecturer in emergency medicine, Chase Farm Hospital, The Ridgeway, Enfield EN2 8JL United Kingdom E-mail: libra19542003@yahoo.co.uk
References
Shallman RW, Norfleet RG, Hardache JM. Percutaneous endoscopic gastrostomy feeding tube migration and impaction in the abdominal wall. Gastrointest Endosc 1988; 34: 367–68.
Venu RP, Brown RD. Pastika BJ Erickson LW. The buried bumper syndrome: a simple management approach in two patients. Gastrointest Endosc 2002; 56: 582–84.
Anagnostopoulos GK, Kostopoulos P, Arvanitidis DM. Buried Bumper Syndrome with a fatal outcome, presenting early as gastrointestinal bleeding after percutaneous endoscopic gastrostomy placement. J Postgrad Med 2003; 49:325–27
Iber, FL, Lusak, A, Patel, M Importance of fungus colonization in failure of silicone rubber percutaneous gastrostomy tubes (PEGs) Dig Dis Sci, 1996, 41: 226-231
Braden B, Brandstaetter M, Caspary WF, Seifert H. Buried bumper syndrome: treatment guided by catheter probe US. Gastrointest Endosc 2003;57:747-51
Ma MM, Semalacher EA, Fedorak RN, Llor EA, Duerksen DR et al The buried gastrostomy bumper syndrome: prevention and endoscopic approaches to removal. Gastrointest Endosc 1995 ; 41:505-8
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) is a rare clinical syndrome, commonly seen in elderly patients who present with dorsal pitting edema of the hands and has a dramatic response to steroids, suggesting a benign nature. Sometimes it is associated with other rheumatologic conditions and potential underlying malignancy should be ruled out, especially when there is a poor response to steroids.
Elderly patients presenting with musculoskeletal symptoms such as painful, swollen or stiff jointsare challenging to physicians. The common conditions encountered are osteoarthritis, crystal arthropathies, spondyloarthropathies and rarely seropositive arthritis. RS3PE highlights a different inflammatory disease involving the tenosynovium of the tendons of the hands with a characteristic presentation. This case details such a presentation and aims to raise awareness amongst general physicians.
Case report:
An 83 year old man, with a history of chronic leg ulcers and poor mobility presented following a fall at home. On admission he also complained of a six to eight week history of bilateral hand swelling. This was of sudden onset, initially on the right hand and gradually progressed until the time of admission when it became prominent over the dorsum of both hands. Both hands were initially tender, but painfree at rest, and restricted in movement due to the swelling. Lately he had also noticed mild inactivity stiffness in his knees and shoulders, He had no previous musculoskeletal history, no skin rash or trauma to his hands.
Inspection of his hands revealed bilateral, symmetrical swelling, involving all the fingers and more pronounced on the dorsum. On palpation there was pitting oedema over the dorsum without signs of synovitis or joint deformity.(Figure 1 and 2).
On movement, finger flexion and opposition were limited, with reduced grip strength.
There was no girdle muscle weakness or pain. There was pitting oedema of both feet, with compression bandaging to the upper calf. This was chronic, and was likely to be secondary to peripheral vascular insufficiency.
Fig 1:Swollen hands
Fig 2: Dorsal pitting edema
Blood tests during this admission showed normocytic anaemia with low vitamin B12 levels but normal ferritin. Erythrocyte sedimentation rate (ESR) was raised at 100mm/hour and initial C-reactive protein (CRP) at 55 mg/l. Anti nuclear antibody (ANA) and rheumatoid factor were negative. X-rays of the hands revealed mild osteoarthrosis without any evidence of bony erosions. Computerised tomography (CT) of the chest and abdomen did not show any evidence of malignancy.
In view of the clinical presentation and seronegativity, a diagnosis of peritendinous rheumatoid arthritis was considered. He was commenced on low dose oral steroids following initial parenteral corticosteroid. Subsequent to the initiation of steroids, there was dramatic resolution of the swelling of the hands, within a week (Figure 3),
Fig 3: Response to steroids
Case discussion
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome was first described by McCarty et al in 1985 1 . It is also termed as peritendinous rheumatoid arthritis in Europe.
It predominantly affects elderly males and although not exceptionally rare, there is no clear documentation of the incidence of this condition (2).
The syndrome is a subset of symmetrical polyarthritis characterised by
Bilateral pitting oedema of both hands
Sudden onset of polyarthritis (A few cases report patients being able to state the time to the hour at which this occurred.1)
Age >50 years
Absence of rheumatoid factor (seronegativity).
Other features include symmetrical distal synovitis and tenosynovitis affecting the synovial sheaths of the flexor and extensor tendons of the hands and/or feet without evidence of joint erosions 2. It responds dramatically to corticosteroids with long term remission after withdrawal, suggesting a benign prognosis.
Although generally thought to be a characteristic benign syndrome with good outcomes, several studies have been published linking RS3PE to various rheumatic disorders such as spondyloathropathies, psoriasis (HLA associations), polymyalgia rheumatica, and temporal arteritis. 3 It may also be a paraneoplastic manifestation of haematological or solid malignancies 4 (eg. prostate, rectal, gastric and ovarian tumors) linked to the synthesis of interleukin, IL-6. Review of these cases suggested that RS3PE associated with neoplasia was associated with a poor response to steroid treatment. 4
Although MRI scanning offers the best imaging technique to diagnose the condition.,RS3PE is a clinical diagnosis. Scans typically demonstrate the tenosynovitis of the extensor tendons believed to cause the oedema which characterises the syndrome.3 MRIscans are valuable to exclude other bony pathologies like osteomyelitis.. An alternative imaging technique for identification of extensor tenosynovitis is ultrasonography. 5
Treatment generally involves steroids, but in some cases the patient may respond to NSAIDs or gold therapy
Learning points:
RS3PE should be considered as a diagnosis when a patient presents with bilateral symmetrical pitting oedema of the hands and or feet, and is found to be seronegative.
Patients are generally very responsive to corticosteroids.
A high index of suspicion is needed to search for underlying malignancy especially in the absence of associated rheumatic disorders and poor response to corticosteroid therapy.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
DR. VIJAY JOSHI MD, Registrar, Internal Medicine, Chase Farm Hospital, UK
DR ANNA GREEN MBBS, FY1 Doctor, Chase Farm Hospital, UK
DR. JANE GRIFFIN FRCP, Consultant Rheumatologist, Chase Farm Hospital, UK
CORRESPONDENCE: DR. VIJAY JOSHI, Chase Farm Hospital, Enfield, UK
Mehmet Sayarlioglu Remitting Seronegative Symmetrical Synovitis with Pitting Edema (RS3PE) Syndrome and Malignancy. Eur J Gen Med 2004; 1(2): 3-5.
Oliveri I, Salvarani C,Cantini F. Remitting distal extremity swelling with pitting edema: a distinct syndrome or a clinical feature of different inflammatory rheumatic diseases.J.Rheumatol 1997;24:249-52
Sibilia J, Friess S, Schaeverbeke T et al. Remitting seronegative symmetrical synovitis with pitting edema (RS3PE): a form of paraneoplastic polyarthritis? J Rheumatol 1999;26:115-20
Agarwal et al . Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome: ultrasonography as a diagnostic tool. Clinical Rheumatology. Volume 25, Number 5/October 2005
Left ventricular free wall rupture is a serious complication of myocardial infarction (MI) with a mortality rate without intervention close to 100%. Its presentation is classically late following an MI but in some cases can present within 24 hours. There can be sudden overt clinical symptoms or it can present insidiously and therefore there must be a high index of suspicion. This report highlights the case of a gentleman with no prior history of ischaemic heart disease that presented with non-specific symptoms. A diagnosis of left ventricular (LV) free wall rupture near the atrial appendage, post MI was made and he was managed successfully.
Clinical Presentation
We present the case of a 75 year old gentleman who collapsed suddenly whilst riding his bicycle. According to an eye-witness he was unresponsive & confused for a few minutes after the episode. Paramedics attended and brought him to the Accident and Emergency department at a local hospital and he was subsequently transferred to the Admissions Unit. Initially he was confused with no recollection of the collapse however his confusion abated after a short period of time.
He was normally fit and well, his only past medical history of note being chronic neck pain requiring simple analgesia and mild asthma requiring when necessary salbutamol inhalers. He was however a life-long smoker with a minimal alcohol intake.
On arrival to the hospital, the patient was conscious, oriented, afebrile and not in any pain. His Glasgow Coma Scale (GCS) was 15/15, pulse was 92/min, regular but weak and the right radial and femoral pulses were absent. His systolic blood pressure was 55mmHg in the right arm and 105mmHg in the left arm. The only other positive finding on examination was muffled heart sounds. Bloods were taken and results are shown in Table 1 with normal ranges given for reference (results within normal limits are not shown).
Random Blood Glucose
16 mmol/l
<11.1 mmol/l
Troponin I (12 hour)
6.16 ng/ml
<0.04 ng/ml
WBC
14.0 x109/l
4-11 x109/l
CRP
179 mg/l
<10 mg/l
Hb
10.9 g/dl
13-18 g/dl (men)
Table 1. Blood results with normal ranges in italics.
In view of the high blood glucose and history of collapse, the patient was aggressively treated with insulin and intravenous fluids. However after receiving 2 litres of intravenous fluids, there was no haemodynamic response. An arterial blood gas on air was performed and the results are shown in Table 2 with normal ranges given for reference.
pH
7.40
(7.35-7.45))
pCO2
3.0 Kpa
(4.7-6.0 Kpa)
pO2
14.8 Kpa
(10.8-12.5 Kpa)
HCO3
13.6 mmol/l
(22-28 mmol/l)
Table 2. Arterial Blood Gas with normal ranges in italics.
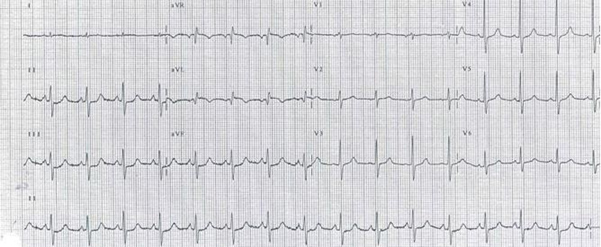
A Chest X-ray was performed and showed nothing unusual. However an ECG demonstrated ST depression in the inferior leads & T- wave inversion with a Q wave in aVL (see figure 1). Differential diagnosis at this stage was therefore aortic dissection, carotid dissection and left ventricular wall rupture (post myocardial infarction).
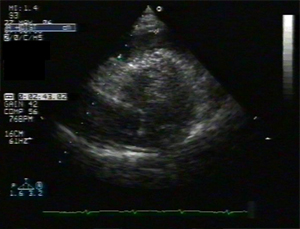
A subsequent CT scan showed no aortic dissection, but probable haemopericardium together with an occluded right common iliac artery (see figure 2). Trans-thoracic echocardiogram confirmed haemopericardium with no suggestion of tamponade (see figure 3) and in addition demonstrated some mild LV diastolic dysfunction. CT scan of the brain and the carotids showed no evidence of carotid dissection but did indicate significant stenosis of the right subclavian artery. The diagnosis of left ventricular free wall rupture was made at this juncture. It was noted that the variability in blood pressure between both arms and between upper limbs and lower limbs was exacerbated by coincidental stenosis in the right common iliac and right subclavian arteries which possibly delayed diagnosis.
Subsequent coronary angiogram showed a blocked intermediate coronary artery (a branch of the left main coronary artery), 2 stenosed areas in the left anterior descending coronary artery (LAD) and a 50% occlusion of the right coronary artery (RCA). Later a trans-oesophageal echocardiogram (TOE) demonstrated separation of the ventricular free wall between the LAD artery and the left atrial appendage, high up in the heart a very unusual position indeed. The diagnosis of Left Ventricular Free Wall Rupture following a Silent Myocardial Infarction was therefore confirmed. The patient was transferred to a nearby cardiac surgery centre and an emergency patch repair of the ventricular free wall rupture was performed.
Figure 1. ECG demonstrating ST depression in II, III and aVL & T-wave inversion with a Q wave in aVL.
The patient had a prolonged recovery, spending 2 weeks on the Cardiac ICU and then subsequently developed hospital acquired pneumonia and remained an inpatient on a general medical ward for a further 4 weeks where he made slow progress. He later spent 4 weeks in a rehabilitation centre before finally returning home.
Figure 2. Thoracic CT with obvious haemopericardium.
Figure 3. Transthoracic echo with evidence of pericardial fluid.
Discussion
First described by William Harvey in 1647, left ventricular (LV) free wall rupture is a dramatic complication of myocardial infarction where there is a rupture of infarcted LV free wall tissue. The rupture is commonly insidious with bleeding into the pericardial sac and subsequent cardiac tamponade. It is hard to assess as clinical and autopsy results vary considerably. It contributes to nearly 15% of deaths due to acute MI1, with the average age of those affected being 69 years. It is third only to cardiogenic shock and arrhythmias as the leading cause of death following a myocardial infarction.2 Hutchins et al reviewed 153 post mortem results with gross and histological evidence of acute myocardial infarction and reported that 30.7% of patients in this group who had died from sudden death had a cardiac rupture.3 It is more common in females and classically occurs 3 to 6 days post MI, however in some studies, up to 50% of cases have been reported less than 24 hours post MI.4There is a history of previous MI in 25% cases but often LV free wall rupture can be the first presentation of ischaemic heart disease.5 Around 50% of the cases of LV free wall rupture are due to anterior MIs with LAD involvement.6There is a new murmur in 25% cases and echocardiography may often demonstrate a pericardial effusion. The prior use of NSAIDS and corticosteroids and a presentation which may mimic major artery dissection often delays thrombolytic therapy.
Unfortunately the current mortality rate in the UK is around 90%. Of note the incidence of LV free wall rupture post MI has increased since the more widespread availability of coronary care units and it is thought that this is because more people are now surviving the first few days post MI.7
The pathophysiological process involves thinning of the myocardial wall with the intensity of necrosis occurring at the terminal end of the vessel (watershed area) where there is often poor collateral flow. The shearing effect of myocardial contraction against a stiffened necrotic area causes rupture. The most common rupture location is on the anterior or lateral wall of the left ventricle.8 A midventricular position along the apex to base axis is most common. It can present either with sudden death or can present sub acutely e.g. with nausea, hypertension or pericardial type chest discomfort or pain. The gentleman discussed in this report collapsed with no preceding symptoms and as mentioned the location of his rupture was in a very unusual place, high up near the atrial appendage.
Transoesophageal echo (TOE) is diagnostic for this condition and is the gold standard.9 However it is found to have only a 70% sensitivity rate for LV free wall rupture10 and therefore some centres advocate the use of cardiac MRI when available.11 Initial management is haemodynamic stabilization and this is often followed by blood transfusion, pericardiocentesis12, inotropic support and the use of an intra-aortic balloon pump but ultimately prompt surgical repair is required.
Various surgical techniques have been applied including suturing of the infarcted ventricle but modern surgical repair involves the application of a Teflon felt patch over the ruptured area with a synthetic biocompatible glue (e.g. cyanoacrylate) as an adhesive to keep the patch attached to the epicardium.13,14 Crucially it can be performed without the use of cardiopulmonary bypass in most of cases. The current overall operative mortality for surgical intervention is reported to be around 24-35%15.
Ultimately survival depends on early recognition of the condition, prompt investigations & diagnosis and urgent surgical treatment. Unfortunately at the present time the condition is usually diagnosed at post-mortem.
Conclusion
The patients presentation i.e. collapse with no proceeding symptoms coupled with the fact that he was suffering a silent MI with no prior indications of ischaemic heart disease e.g. angina, shortness of breath etc and the rapid subsequent development of left ventricular free wall rupture in such an high position made this quite an unusual case. Stenosis in the right common iliac and subclavian arteries did delay diagnosis slightly, as aortic and carotid dissection had yet to be ruled out but ultimately this patient survived probably because of early diagnosis despite these obstacles and subsequent prompt treatment.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
ANDREW PETER VANEZIS MBChB BSc, FY2 Doctor, Barts and The London NHS Trust, UK.
REHAN QUADERY MBBS, ST3 Medicine, Bedford Hospital NHS Trust, UK
MOHAMMAD WASIL PhD, Assistant Director of Research & Development, Bedford Hospital NHS Trust, UK
MOHAMMED AZHER FCCP FRCP, Consultant Chest Physician, Bedford Hospital NHS Trust, UK
CORRESPONDENCE: REHAN QUADERY, Bedford Hospital NHS Trust, UK
Pohjola-Sintonen S, Muller JE, Stone PH, Willich SN, Antman EM, Davis VG, Parker CB, Braunwald E. Ventricular septal and free wall rupture complicating acute myocardial infarction: experience in the Multicenter Investigation of Limitation of Infarct Size. Am Heart J. 1989;117:809818
Hutchins, Kenneth D, Skurnick, Joan, Lavenhar, Marvin, Natarajan, Geetha A. Cardiac Rupture in Acute Myocardial Infarction: A Reassessment. American Journal of Forensic Medicine & Pathology. 23(1):78-82, March 2002.
Becker AE, Anderson RH. Cardiac pathology. An integrated text and colour atlas. London: Gower Medical Publishing; 1983.
Shirani J, Berezowski K, Roberts WC. Out-of-hospital sudden death from left ventricular free wall rupture during acute myocardial infarction as the first and only manifestation of atherosclerotic coronary artery disease. Am J Cardiol 1994 Jan; 73(1): 88-92
Slater J, Brown RJ, Antonelli TA, et al. Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction:A report from the SHOCK trial registry. J Am Coll Cardiology. 2000;36:1117-1122
Reddy SG, Roberts WC. Frequency of rupture of the left ventricular free wall or ventricular septum among necropsy cases of fatal acute myocardial infarction since introduction of coronary care units. Am J Cardiol 1989;63:90611
David, TE. Surgery for post infarction rupture of the free wall of the ventricle. In: David TE. , editor. Mechanical Complications of Myocardial Infarction. Austin, R.G. Landes Company; 1993. p. 142.
Cheitlin, MD et al. ACC/AHA/ASE 2003 Guideline update for the clinical application of echocardiography. J Am Coll Cardiol. 2003;42:95470
Lopez-Sendon J, Gonzalez A, Lopez de Sa E, Coma-Canella I, Roldan I, Dominguez F, et al. Diagnosis of subacute ventricular wall rupture after acute myocardial infarction: sensitivity and specificity of clinical, hemodynamic and echocardiographic criteria. J Am Coll Cardiol 1992;19: 114553.
Rajiv Agarwal, Pedro Diaz-Ortiz, Ravinder Reddy, Veronica Lenge, R. David Fish, David A. Ott, John Connelly, and Scott D. Flamm. Asymptomatic Incomplete Left Ventricular Apical Rupture Diagnosed by Cardiac Magnetic Resonance Imaging. Tex Heart Inst J. 2006; 33(1): 9395
Rolf Svedjeholma, Erik Hkansonb, Mrten Lindstrmc and Per Hjort. Case report - Cardiac general. Post-infarct left ventricular free wall rupture and ventricular septal defect managed by pericardial aspiration during transport to referral hospital. Interactive Cardiovascular and Thoracic Surgery. 2003; 2:193-195
Padro JM, Mesa JM, Silvestre J, Larrea JL, Caralps JM, Cerron F, Aris A. Subacute cardiac rupture: repair with a sutureless technique. Ann Thorac Surg. 1993;55:2023
Alejandro Aris. Surgical repair of left ventricular free wall rupture. Multimedia Manual of Cardiothoracics. 2004. doi:10.1510/mmcts.2004.
Malek G, Massas MD, Alexander SG. Surgical Repair of Mechanical Complications of Myocardial Infarction. World J Surg. 2004;28:847-856
The Mirena intrauterine system (IUS) has been licensed as a contraceptive in the UK since May 1995. Recent National Statistics suggest the Mirena IUS is used by only 1% of women aged 1649 years who are currently using contraception.1 The Mirena IUS now also has a licence for the management of idiopathic menorrhagia2 and may therefore be used by women who do not require contraception. Uterine perforation is a serious, albeit rare, potential complication of intrauterine device or system use. Women may be informed that uterine perforation occurs in fewer than 1 in 1000 of either copper intrauterine device (IUD) or IUS insertions.3,4 Rate of perforation reported with the Mirena IUS in a large observational cohort study was 0.9 per 1000 insertions.5 In this case report, an intraperitoneal Mirena IUS was detected nearly 4 years after its insertion and perforation of the uterus was diagnosed, despite vaginal hysterectomy and admissions to hospital. This case report demonstrates clearly that whenever there is suspicion from ultrasound scan report of an empty uterus that the IUS has fallen out, and in the persistence of symptoms, we should consider performing an abdominal X-Ray which is an easy, cheap method, to identify the IUS outside the uterus.
Case report
A 33-year-old woman, para 2, with a long standing history of menorrhagia, dysmenorrhoea and tiredness was referred by her GP to the hospital (2002). At the time she was treated for anaemia and felt tiredness. Also she was suffering from dysmenorrhoea; her periods had been regular although in the previous few months she was bleeding PV continuously. Her periods had become heavy after sterilisation (1996). She was anaemic. Cervical cytology had always been normal. In the past she had undergone a laparoscopy for pelvic pain for suspected endometriosis (1997), an appendicectomy (1997) and she was diagnosed with duodenal ulcer (1996). For management of her menorrhagia, she opted for Microwave Endometrial Ablation which was done in August 2002. After that she had an ultrasound scan for erratic bleeding which showed irregular endometrium. The patient was booked for hysteroscopy under general anaesthesia. The procedure was attempted in September 2003 and was abandoned due to difficulties passing the hysteroscope through the endocervical canal. The hysteroscopy was repeated in January 2004 and few intrauterine adhesions were reported. A Mirena IUS was inserted under the same general anaesthetic.
A month later she was admitted to the hospital with right upper quadrant pain and a problematic bleeding pattern. Ultrasound at this stage showed a normal size uterus but the Mirena IUS was not obviously in situ. It was assumed the Mirena IUS had fallen out and the patient was booked for vaginal hysterectomy, which was performed in September 2005.
In January 2007 was admitted to the hospital with right upper quadrant pain again and all investigations including chest X-ray, abdominal ultrasound scan and blood tests were normal. She had an upper GI endoscopy which showed a gastric ulcer (Cardia).
Fig.1 Abdominal X-Ray with the Mirena IUS (arrowed).
She was admitted again 1 year later with pelvic pain. An abdominal X-ray showed the lost IUS (fig. 1) and the CT scan showed the IUS to lie anteriorly under the rectus muscles and adjacent to the dome of the bladder. In April 2008 the IUS was retrieved laparoscopically. The omentum was adherent to anterior abdominal wall and the Mirena IUS was found in the omentum, (Fig.2). This was felt to be unlikely to be the cause of the pain. The IUS was removed easily from the abdominal cavity laparoscopically. The right tube and ovary were adherent to right pelvic side and they were freed up. The procedure was uneventful and the patient was discharged the same day and symptom free since.
Discussion
Uterine perforation is a serious, albeit rare, potential complication of Intrauterine contraceptive use. For informed consent, women should be informed that uterine perforation occurs in fewer than 1 in 1000 intrauterine LNG-IUS insertions4 Fig. 2 Mirena IUS (circled) within the omentum.
The rate of perforation reported with the LNG-IUS in a large observational cohort study was 0.9 per 1000 insertions.5 Current guidelines recommend that advice regarding the management of problems arising with the LNG-IUS use4 is similar to that for IUD use3. The problems are suspected perforation, lost threads, abnormal bleeding, pregnancy, presence of actinomyces-like organisms, pelvic infection, and postmenopausal removal.
The Royal College of Obstetricians & Gynaecologists recommends6 that women who present with persistent menorrhagia, despite LNG-IUS use, should be advised to return for further assessment of the uterine cavity (biopsy or ultrasound scan) to exclude pathology.
If menorrhagia persists despite medical treatments, women should be re-examined.6 An assessment of the uterine cavity should be performed using ultrasound scan. An endometrial biopsy should be considered in all women with persistent menorrhagia. When indicated, a hysteroscopy allows the assessment of the uterine cavity and biopsy under local anaesthesia.6 The WHO Selected Practice Recommendations for Contraceptive Use (WHOSPR) 7does not specifically refer to the Mirena IUS. Follow-up 36 weeks following IUD insertion is recommended and the Clinical Effectiveness Unit (CEU) advises similar follow-up for women using the Mirena-IUS.
In this case report, the detection of the Mirena IUS inside the peritoneal cavity was noted nearly 4 years after the insertion and the perforation of the uterus. The patient had several admissions to the hospital under the care of gynaecologists or gastroentero-logists always complaining for upper or lower abdominal pain. She even had a vaginal hysterectomy. Had she undergone an abdominal hysterectomy, the Mirena IUS may have been noted at that time.
This case report clearly demonstrates that following an ultrasound report showing an empty uterus in a symptomatic patient, an abdominal X-ray should be performed to identify whether or not the IUS is inside the peritoneal cavity. Also, we need to be aware of the peritoneal adhesion potential of Mirena IUS it is expected to be low. In another case report8, an intraperitoneal Mirena IUS resulted in plasma levonorgestrel levels 10 times higher (4.7 nmol/l) than the plasma level of levonorgestrel observed with Mirena IUS placed in utero. This high plasma LNG level suppresses ovulation. Therefore, aside from the adhesion potential, a misplaced Mirena IUS should be removed when pregnancy is desired9, 10.
The authors conclude that judicious use of the abdominal X-ray can lead to the early detection of a migrated IUS and expedite early removal.
A thorough literature search of the Medline, Embase and Cochrane databases did not reveal case reports similar to this and also did not report any formal guidance as to the use of the Mirena IUS device following endometrial microwave ablation, but we did find an article regarding insertion of Mirena IUS, after endometrial resection.11
Endometrial resection is a surgical method to manage menorrhagia. Intrauterine scarring may occur following treatment, but it is not known if the risk of uterine perforation is increased.
The Clinical Effectiveness Unit (CEU) responded12 recently that the British National Formulary (BNF)13 suggested that intrauterine devices (IUDs) should be used with caution in severely scarred uteri.
The United Kingdom Medical Eligibility Criteria for Contraceptive Use (UKMEC)14 recommends that if women have a distorted uterine cavity (any congenital or acquired uterine abnormality distorting the uterine cavity in a manner that is incompatible with IUD insertion), then the IUD or the levonorgestrel-releasing intrauterine system (LNG-IUS) should not be used (UKMEC 4).
A narrative review paper on treatment after hysteroscopic surgery suggests that an acceptable post-operative method of contraception after endometrial ablation is the LNG-IUS, as it protects the endometrium and there is a high amenorrhoea rate.15 However, following successful endometrial ablation the uterine cavity is usually severely narrowed making insertion of IUS (or IUD) impossible and it would not normally be considered as an appropriate method in these circumstances. Significant bleeding would suggest failure of the procedure, and if IUS or IUD was to be considered it should only be done with hysteroscopic assistance by an experienced gynaecologist.
COMPETING INTERESTS
None Declared
AUTHOR DETAILS
SHAMBHU S MBChB Senior House Officer, Department of Obstetrics and Gynaecology, Hull Royal Infirmary, UK
PAPPAS M MBChB Specialist Registrar, Department of Obstetrics and Gynaecology, Hull Royal Infirmary, UK
CORRESPONDENCE: DR SHAMBHU S, Senior House Officer in Obstetrics and Gynaecology, Hull Royal Infirmary, Hull, UK
Email: siddesh@doctors.org.uk
References
Dawe F, Meltzer H. Contraception and Sexual Health, 2002. London, UK: Office for National Statistics, 2003; 149 http://www.statistics.gov.uk.
Faculty of Family Planning and Reproductive Health Care (FFPRHC). FFPRHC Guidance (January 2004). The copper intrauterine device as long-term contraception. J Fam Plann Reprod Health Care 2004; 30(1): 2942.
Faculty of Family Planning and Reproductive Health Care (FFPRHC). FFPRHC Guidance (January 2004). The levonorgestrel-releasing intrauterine system (LNG-IUS) in contraception and reproductive health. Journal of Family Planning and Reproductive Health Care 2004; 30(2): 99109
Zhou L, Harrison-Woolrych M, Coulter DM. Use of the New Zealand Intensive Medicines Monitoring Programme to study the levonorgestrel-releasing intrauterine device (Mirena). Pharmacoepidemiol Drug Saf 2003; 12: 371377
Royal College of Obstetricians and Gynaecologists (RCOG). The Management of Menorrhagia in Secondary Care. National Evidence- Based Clinical Guidelines. London, UK: RCOG, 1999.
World Health Organization (WHO). Selected Practice Recommendations for Contraceptive Use. Geneva, Switzerland: WHO, 2002.
Management of a perforated levonorgestrel - medicated intrauterine device: pharmacokinetic study: Case report Ronit Haimov-Kochman et al, Human Reproduction Vol.18, No.6 pp. 12311233, 2003.
Adoni, A. and Ben Chetrit, A. (1991) The management of intrauterine devices following uterine perforation. Contraception, 43, 7781.
Andersson, K., Ryde-Blomqvist, E., Lindell, K., Odlind, V. and Milsom, I. (1998) Perforations with intrauterine devices. Report from a Swedish survey. Contraception, 57, 251255.
MEMBERS ENQUIRY RESPONSE Enquiry Reference: 2268, Sent: 2nd April 2008 . Faculty of Family Planning and Reproductive Health Care. Clinical Effectiveness Unit
British National Formulary. BNF 54. 2007.
Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit. UK Medical Eligibility Criteria for Contraceptive Use. http://www.ffprhc.org.uk/admin/uploads/UKMEC200506.pdf. 2006.
Romer, T., Schmidt, T., and Foth, D. Pre- and postoperative hormonal treatment in patients with hysteroscopic surgery. Contributions to Gynecology and Obstetrics 20, 1-12. 2000.
We report a case of the rare coronal unicondylar fracture of the distal femur called Hoffa fracture. Hoffa fracture is a rare injury consisting of unicondylar tangential posterior fracture of the distal femur. These fractures are due to high energy trauma and sometime not easy to visualise on routine imaging, and therefore could represent a diagnostic challenge to the accident department and to the orthopaedics surgeon. Clinically however, our patient had obvious knee swelling, localised tenderness and was unable to weight bear. Plain radiograph and CT scan confirmed the fracture and was treated surgically with cancellous screws.
Case Presentation
A thirty-four year old male injured his left knee whilst turning on a motocross bike. He put his left leg on to the ground with his knee in 20 degrees of flexion to stabilise himself whilst turning a left hand corner at about 30 mph. He did not crash, but was unable to weight bear afterwards.
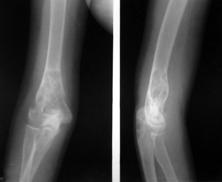
The initial AP and lateral radiographs showed a coronal fracture of lateral condyle of the distal femur.
[FIG 1: AP radiograph right knee / Lateral radiograph right knee].
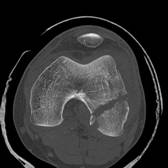
This fracture could have been easily missed on the plain radiograph. Further imaging with the CT scan confirmed the fracture and its pattern.
[FIG2: Axial CT of distal femur / Saggital CT of distal femur].
He had an open reduction and internal fixation via a lateral approach, vastus lateralis was reflected off the lateral intermuscular septum and the knee joint opened. Maintaining the knee flexed during the surgery relaxes the posterior capsule, gastrocnemius and protects the neurovascular structures. Soft tissue attachments of the fractured fragment constitute the sole source of blood supply and must be preserved. The joint was carefully inspected for associated injuries. After reduction the fragments were temporarily fixed with Kirschner wires. Partially threaded cancellous screws were used in the lag mode to secure compression across the fracture.
FIG3: Image Intensifier of ORIF with cancellous screw]
Discussion
This fracture pattern was initially described by Hoffa in 1904 1 hence the name for this fracture. The Hoffa fracture is an intra-articular fracture of the knee analogous to the capitellum fracture of the elbow 2. This injury is the result of violent force and generally occurs in young adults. There is usually a combination of forces: direct trauma, possibly with an element of abduction, the ground reaction is transmitted through the tibial plateau and the axial compression on a flexed knee concentrates the force in the posterior half of the femoral condyles1. In flexion the lateral condyle is the leading part of the knee to receive the impact1. Although the Hoffa fracture may be of either condyle4 the preponderance of lateral condylar fractures suggests an anatomic-biomechanical vulnerability due to the physiological valgus.
Few cases have been reported in literature with associated femoral shaft fracture 6, ligament entrapment with irreducible knee dislocation5, open and bicondylar fractures7. Our case is unique as it is a closed injury, uniconylar fracture with no associated ligamentous or meniscal disruptions. Open reduction has been shown to be mandatory for good long-term function 2, 3. High index of suspicion, further imaging with CT scan / 3D reconstruction, open reduction and internal fixation is necessary for good outcome following these types of fractures.
Patients who have untreated primary hyperparathyroidism with Ostitis Fibrosa Cystica have become a rarity. Primary hyperparathyroidism is usually diagnosed as a result of chance finding of raised serum calcium or complications associated with hypercalcemia such as polyuria, polydipsia, muscle weakness, gastrointestinal upsets and renal stone formation. Bone disease is rarely overt. Radiographic manifestations are seen in less than 2% of patients and include subperiosteal erosions, diffuse osteoporosis, cystic lesions (brown tumours), pathological fractures, ‘salt and pepper’ mottling of skull and loss of lamina dura in the mandible1.
The reported incidence of fractures in hyperparathyroidism is quite low, about 10% in two large series2 and apart from vertebral compression fractures, no characteristic fracture pattern have been described.
Extensive bony involvement with pathological fractures as a presenting feature due to parathyroid carcinoma has been documented3, but multiple pathological fractures, as a presenting feature of primary hyperparathyroidism due to parathyroid adenoma is extremely rare. Here we describe three patients seen at our institution in the period from 2001 to 2004 who presented with pathological fractures due to parathyroid adenoma.
CASE 1
A 50-year-old housewife was admitted with painful right thigh and inability to weight bear following a twisting injury of her right leg. She also complained of generalized weakness, lethargy and muscle pain over the past few months. Radiographs revealed segmental fracture of right femur (figure 1a) and gross osteopenia with a cortical index of 0.2 (normal: > 0.45). She also sustained a fracture of left femur following a very trivial injury while transferring her from trolley to bed.
Investigations (table–1) revealed hypercalcemia (12Mg/dl), hypophosphatemia (2.6Mg/dl) and elevated parathyroid hormone level (70 Pmmol/l). 25-hydroxyvitamin D value was in the lower limit of normal (22ng/ml). Renal parameters were normal.
Figure 1a. Gross osteopenia with segmental pathological fractures of right femur.
High-resolution ultrasound (HRUS) of neck revealed a hypoechoic mass measuring 4.1 x 1.7 cm in the posterior aspect of right thyroid lobe, suggestive of parathyroid adenoma. Bone scan showed patchy tracer uptake in almost entire skeleton with generalised osteoporosis and microfractures, suggestive of metabolic bone disease.
Figure1b. 12 Months post Parathyroid adenectomy showing improved bone density and Mallunion of fractures.
Patient underwent parathyroid adenectomy under the general surgeons. Histopathology confirmed the diagnosis of parathyroid adenoma. Following surgery patient developed hypocalcemic tetany and seizures, treated with intravenous calcium gluconate and followed by oral calcium supplements. Fractures were treated conservatively by splinting in groin to toe casts, as the bone quality was very poor. The biochemical tests came back to normal three months after surgery and radiographs revealed fracture healing and improvement in bone density. Casts were removed and mobilization commenced. Over next six months fractures healed but were mall-united (figure 1b). At eighteen months the patient was fully weight bearing with minimal functional disability.
CASE 2
A 32-year-old female patient presented with pain in the right thigh and inability to weight bear after a trivial fall at home. Radiographs revealed fracture middle one-third of right femur, osteopenia and with subperiosteal resorption (figure 2a)
Figure 2a. severe osteopenia with pathological fracture of right femur.
Biochemical tests and parathyroid hormone assay (see table-1) was suggestive of primary hyperparathyroidism. 25-hydroxyvitamin D was within normal limits (35ng/ml). High-resolution ultrasound of neck revealed hypoechoic lobulated lesion measuring 8.4x1.1x1.3 cm, on the inferior and posterolateral aspect of the left lobe of thyroid suggestive of parathyroid adenoma. Bones scan showed tracer uptake at the site of fracture and patchy sclerosis of femur, and increased uptake in left sacroiliac joint.
The patient underwent parathyroid adenectomy under the care of general surgeons. Histopathology confirmed the diagnosis of parathyroid adenoma. Patient received parentaral calcium supplements in the immediate post operative period and later by oral route. Femur fracture was initially treated in groin to toe cast and the calcium levels were controlled, after 2 months bone quality improved, despite callus formation there was mobility at the fracture site, and hence the fracture was managed with intramedullary nail and bone grafting (figure 2b).
Figure 2b. Fracture union with intramedullary nail insitu.
It took ten months for the fracture to unite.
CASE 3
A 20-year-old female patient presented with diffuse pain in the left elbow of two months duration following a trivial injury to her elbow. Plain radiograph of the elbow showed a well-defined lytic lesion with sub cortical erosions and with break in the cortex suggestive of Brown tumour with pathological fracture (figure 3a).
Figure 3a. Brown tumour lower end of humerus with pathological fracture
Biochemical analysis revealed hypercalcemia and hypophosphatemia and parathyroid hormone assay was suggestive of primary hyperparathyroidism (table-1). 25-hydroxyvitamin D levels were within normal limit (40ng/ml). High-resolution ultrasound neck showed 2.6 X 1.1 X 1.6 cm hypo echoic mass lesion inferior to lower pole of thyroid suggestive of left parathyroid adenoma.
Bone scan showed patchy increased tracer concentration in entire skeleton with increased tracer concentration in the distal end of humerus.
She underwent parathyroid adenectomy and histopathological examination confirmed the diagnosis of parathyroid adenoma. The fracture was managed in a cast.
Figure 3b. One year post parathyroid adenectomy shows healed fracture with increased bone density and sclerosis.
Patient was followed up with regular check on her calcium levels and serial radiographs of elbow. By 12 months the fracture was completely healed and brown tumour resolved with increased bone density and sclerosis (figure 3b).
Ca++
Mg/dl
Phosphorus
Mg/dl
Alk. Phos.
IU/L
Intact PTH
Pmmol/l
25-hydroxy Vit D
ng/ml
Normal
8 -10
3 - 4.5
34-135
1.1 – 6.5
20 - 56
Case 1
12
2.6
3000
70
22
Case 2
11.5
2.0
745
56
35
Case 3
10.5
2.5
1184
48
40
TABLE –1 Serum biochemical parameters in the patients at presentation
DISCUSSION:
Primary hyperparathyroidism is a well-recognised entity identified almost more than a century ago by Von Recklinghausen. He and his co-workers coined the term Osteitis fibrosa cystica1.
This condition is more common in females. Peak age incidence is between 30 to 50 years and incidence increases with age, though patient aged as young as 14 years was documented. In U.S.A annual incidence is around 0.2% in patients > 60 years1. All the patients in our series are females with florid changes observed in-patient aged 52 years other 2 patients are aged 20 years and 32 years.
Disease results from excessive secretion of parathyroid hormone either due to solitary (50-85%) or multiple (10%) adenomas, hyperplasia (10-40%), or rarely due to a carcinoma of a single parathyroid gland. Extensive bony involvement with pathological fractures as a presenting feature due to parathyroid carcinoma has been documented3. In our series of 3 patients all of them were diagnosed to have solitary parathyroid adenoma. Our first patient aged 52 years had coexisting vitamin D deficiency, which explains severe osteomalacia and multiple fractures. Coexistence of vitamin D deficiency in patients with Primary Hyperparathyroidism may put the patient at a significant higher risk of loosing bone mineral density and development of osteoporosis.
Two distinct types of bone lesions are described in primary hyperparathyroidism4. The slowly progressive type- leads to cortical thinning and osteoporosis & the rapidly progressive type. Pathological fractures may occur through a cyst or in a weakened long bone. A principal test at present is the ‘Immunoassay’ for PTH 1-84 as it distinguishes the hypercalcaemia of malignancy from that of hyperparathyroidism5.
Once the diagnosis of primary hyperparathyroidism has been made by biochemical analysis, the site or sites of adenomatous or hyperplastic parathyroid tissue must be identified6. Some authors advocated ‘Exploratory neck operation’ as most adenomas are localized in the neck7. CT scan and Thallium subtraction scans are useful for detecting parathyroid pathology in normal as well as ectopic locations.
USG of neck can be helpful in picking abnormal parathyroid tissue but CT scan and MRI are more sensitive to assess ectopic sites8. In our series of 3 cases, High Resolution Ultrasound Scan (HRUS) of neck helped in localizing the parathyroid adenoma (90% of adenomas are in the neck). Excised parathyroid gland has to be subjected to histopathological examination to confirm and differentiate adenoma, hyperplasia and malignancy. Histopathological examination in all our 3 cases confirmed the diagnosis of parathyroid adenoma.
Our experience with fractures in primary hyperparathyroidism revealed that these take longer to heal and are prone to malunion unless splinted internally or externally. Average time taken for fracture union in our series was 12 months. Non-union of fractures is rare and healing proceeds uneventfully after excision of an adenoma.
Bone histology returns to normal within 5-6 weeks6. Brown tumours usually resolve with increase in bone density and sclerosis after parathyroid adenectomy.
The extensive skeletal involvement due to hyperparathyroidism has rarely been reported. The substantial improvement in bone density, in promotion of fracture healing and in preventing pathological fractures after successful parathyroid adenectomy has been demonstrated in our series of 3 cases.
CONCLUSION:
In conclusion, a high index of suspicion is necessary to diagnose this unusual presentation of primary hyperparathyroidism. A pathological fracture in young lady with marked osteopenia is highly suggestive. A combination of biochemical tests, including serum levels of calcium, phosphorus, alkaline phosphatase and parathormone assay will help in diagnosing primary hyperparathyroidism in 90% of the cases. All patients with Primary Hyperparathyroidism should have Vitamin D level assessment in order to exclude the coexistance of Vitamin D deficiency with Primary Hyperparathyroidism. High Resolution Ultrasound Scan of neck provides valuable preoperative information in selected cases especially in those undergoing minimally invasive parathyroid surgery. Surgical excision and calcium supplementation along with external or internal splinting of fractures allowed the fractures to heal.
CONFLICT OF INTERESTS:
None declared
ACKNOWLEDGEMENTS:
Department of Orthopaedics, Nizam’s Institute of Medical Sciences (NIMS), HYDERABAD, INDIA.
AUTHOR DETAILS:
RAJESH RACHHA, Diploma (Orthopaedics), MRCS. Senior Clinical Fellow, Bedford hospital NHS trust, United Kingdom
CORESSPONDENCE: Dr R Rachha, Bedford Hospital, Kempston Road, Bedford, MK42 9DJ.
Email: drrajeshracha@yahoo.com
REFERENCES:
Henry,J.Mankin.: An instruction course lecture- Metabolic bone disease. The American Academy of orthopaedic surgeons. Journal of Bone & Joint Surgery; 1994;Vol- 76A, No.5; 760-788.
Chalmers J, Irvine GB: Fractures of the femoral neck in elderly patients with hyperparathyroidism. Clin Orthop Related Res. 1988 Apr;(229): 125-130
R.G.Deshmukh., S.A.L.Alsagoff., S.Krishnan et al. Primary hyperparathyroidism presenting with pathological fracture. The Royal College of Surgeons of Edinburgh, December 1998; Vol-43, 424-427.
Lancourt JE, Hochberg F. Delayed fracture healing in primary hyperparathyroidism Clin OrthoP 1977; 124: 214-218
Nussbaum,S.R., & Polt,J.T., Jr.: Immunoassays for parathyroid hormone 1-84 in the diagnosis of hyperparathyroidism. J Bone and Min. Res., 6 (supplement 2); s43- s50, 1991.
George,D.C., Incaro,S.J., Devlin,J.T et al .: Histology of bone after parathyroid adenectomy – A case report. J Bone & Joint Surgery .1990;Vol 72A, No: 10 ; pp 1558- 1561.
Satava,R.M., Jr., Beahrs, O.H., and Scholz, D.A.: Success rate of cervical exploration for hyper parathyroidism. Arch.Surg., 1975;Vol-110. 625-628.




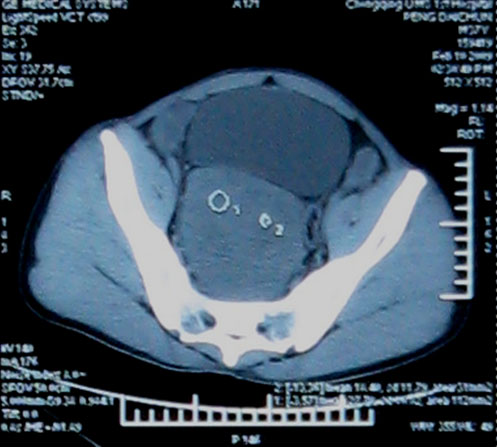
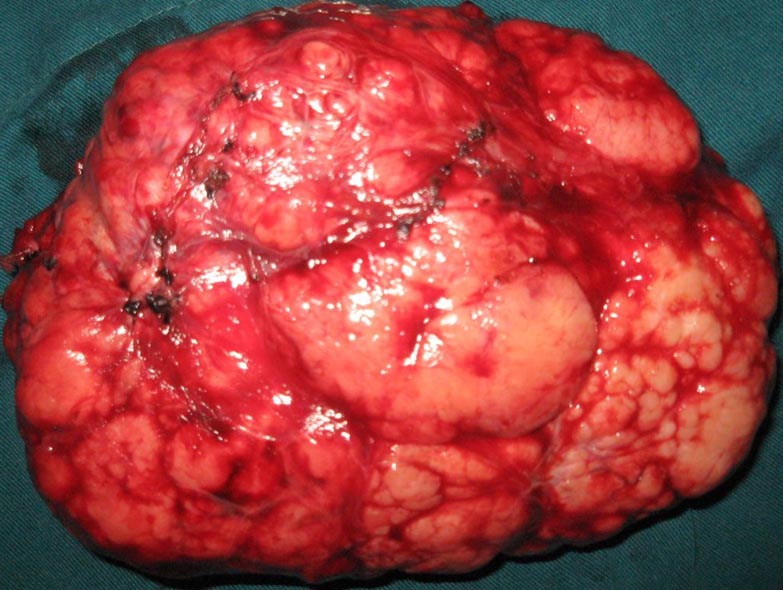
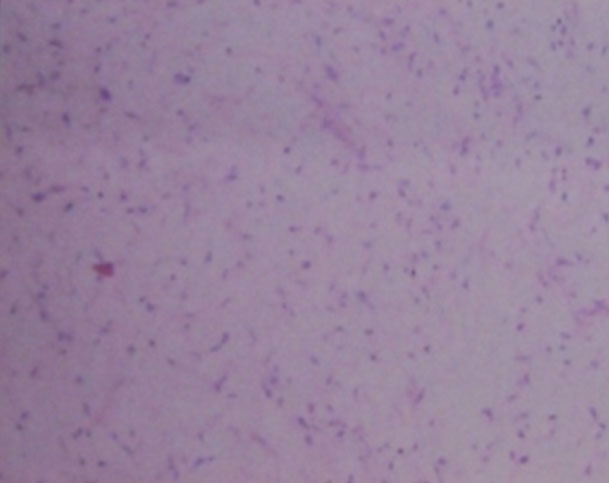
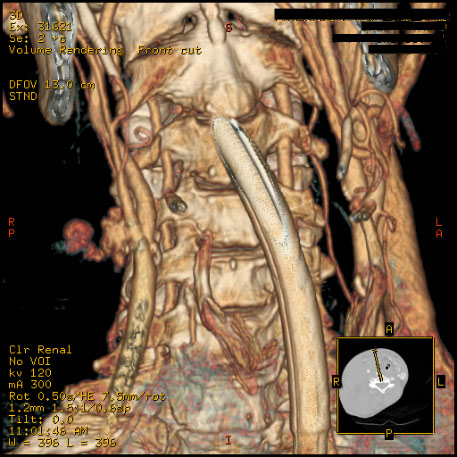
 Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements
Figure 1. A 32 year old parturient with Klippel-Feil syndrome with a short webbed neck and severely restricted neck movements 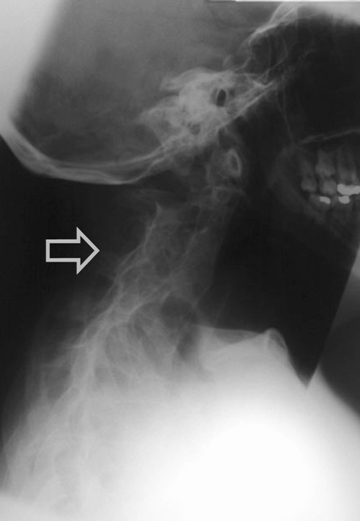 Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae
Figure 2. Radiograph of a Lateral view of cervical spine showing fusion of atlanto - occipital joint and cervical vertebrae 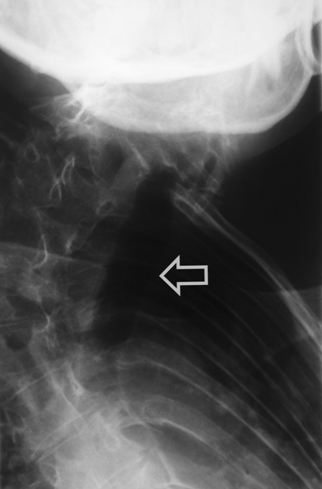 Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.
Figure 3. Antero - posterior view of dorsal spine showing deviation of trachea and marked kyphoscoliosis of thoracic spine She was scheduled to have an elective Caesarean section. The anaesthetic management options in this case included either a general anaesthetic with an anticipated difficult endotracheal intubation or a regional anaesthetic. After discussion with the patient, we planned a general anaesthetic technique with awake intubation using a fibreoptic bronchoscope (FOB) as we considered this safe. For FOB through oral route was preferred due to narrow anterior nares. Oral Ranitidine 150 mg was administered as a premedication the night before and on the morning of the planned section. After institution of standard monitoring and securing two peripheral intravenous cannulae (18G & 16 gauges), the upper airway was anaesthetised with nebulisation of 4% Lignocaine (5 ml) and 10% Lignocaine spray to the posterior pharynx. The FOB was passed through the Berman airway by using a ‘spray as you go” technique to anaesthetise the larynx and upper trachea using 4% Lignocaine and keeping well below the toxic dose (3 mg/kg). A 6.5 mm ID endotracheal tube was rail roaded over the FOB prior to its insertion and the airway was successfully secured. Once position of the endotracheal tube was confirmed, anaesthesia was then induced using intravenous Thiopentone 200 mg, Alfentanil 0.5 mg followed by Rocuronium 25 mg. Anaesthesia was maintained using oxygen with nitrous oxide (1:1 ratio) and Sevoflurane (1 MAC). Patient was ventilated with intermittent positive pressure ventilation to maintain normocapnia. The surgery lasted for 45 min and was uneventful. Using a nerve stimulator for assessing neuromuscular blockade she was reversed with Neostigmine 2.5 mg and Glycopyrrolate 0.5 mg towards the end of surgery. The patient was extubated in supine, head-low position when fully awake and in presence of protective airway reflexes. Discussion Klippel-Feil syndrome is an inherited autosomal dominant condition. In 1912, Klippel and Feil 1 first reported on a patient with a short neck, a low posterior hairline, and severe restriction of neck movements due to complete fusion of the cervical spine. These features now constitute the classic clinical triad which is the hallmark of Klippel-Feil syndrome. A great number of other anomalies associated with Klippel-Feil syndrome may pose a threat to the patient than the obvious deformity of neck. The spinal deformities may cause difficulties with both tracheal intubation and regional anaesthetic techniques. Anaesthetic management may therefore be challenging in these patients. In our case we opted for a general anaesthetic technique rather than a regional technique because of the following reasons: firstly, the patient was not keen to have regional anaesthesia, secondly, it would entail difficulty for regional anaesthesia keeping in view the spinal fusion and scoliosis and thirdly, the dose of a single bolus of spinal anaesthetic would be difficult to judge in this patient and epidural anaesthesia 2 might prove technically difficult and is associated with an increased risk of inadvertent dural puncture and poor spread within the epidural space. This patient’s abnormalities posed problems for all the commonly used anaesthetic techniques for Caesarean section. General anaesthesia could be complicated by difficult intubation. While greater use of regional anaesthesia may have reduced the number of deaths due to failed intubation in obstetric practice, several complications of epidural and spinal anaesthesia may still require intubation as part of their management. Some of these include total or high spinal anaesthesia, inadvertent intravascular injection, overdose of local anaesthetic, anaphylaxis and failure. For these reasons, the choice of regional anaesthesia for a patient with known difficult airway does not necessarily bypass the problem of unanticipated intubation. The most commonly associated anomaly in a series of 50 patients from Delaware, USA 3 was scoliosis (60% of cases), renal abnormalities (35%), Sprengel deformity (30%), deafness (30%), synkinesia (20%) and congenital heart disease (14%). The most common heart disease variant was ventricular septal defect. Less commonly associated were ptosis, lateral rectus palsy, facial nerve palsy and upper extremity anomalies. There are 3 variants of Klippel-Feil Syndrome. 4 Type I is an extensive abnormality where elements of several cervical and upper thoracic vertebrae are incorporated into a single block. In Type II variant, failure of complete segmentation occurs at one or two cervical interspaces. Type III variant includes Type I or II deformities with coexisting segmentation errors in the lower thoracic or lumbar spine. The incidence of Type II abnormalities was found to be 0.71% of Black and Caucasian skeletons that were between the ages of 17 and 102 years in a study from St Louis, Missouri, USA 5 and it is considered to be the most common form. C2-3 and C5-6 are the interspaces usually involved. It often remains unrecognised since the neck may appear normal and the patients are asymptomatic until later in life, when they present due to their increased susceptibility to cervical osteo-arthritis. Patients with Type I abnormalities are 50 times less common than Type II but are reported more frequently. This is probably because they exhibit the classic triad and thus have bizarre appearances. 6 These patients are frequently disabled by birth injuries, or have major anomalies in other organ systems. A planned elective section at term was considered as the best option for delivery of the baby by the obstetricians due to severe cephalo-pelvic disproportion and also due to anaesthetic issues regarding management. The case was managed successfully with a favourable outcome both for the mother and the baby.