1. Singleton, N., Maung, N. A., Cowie, J., et al. Mental Health of Carers. London: Office for National Statistics,2002.2. Oyebode JR.Carers as partners in mental health services for older people. Advances in Psychiatric Treatment.2005; 11: 297-3043. Magliano L., McDaid D., Kirkwood S. and Berzins K. Carers and families of people with mental health problems. In: Mental health policy and practice across Europe (eds). M. Knapp, D. McDaid, E. Mossialos, G. Thornicroft), pp. 374-396, McGraw-Hill: Berkshire.2007.4. Ostman M. and Hansson L. Stigma by association. British Journal of Psychiatry.2002; 181: 494-498.5. Lauber C., Eichenberger A. and Luginbuhl P. Determinants of burden in caregivers of patients with exacerbating schizophrenia. European Psychiatry.2003; 18: 285-289.6. Schulze, Beate. Caregiver Burden in Mental Illness: Review of Measurement, Findings and Interventions, 2004-2005. Current Opinion in Psychiatry.2005; 18(6).7. Andren, Signe,Elmstahl, Solve. The relationship between caregiver burden, caregivers' perceived health and their sense of coherence in caring for elders with dementia. Journal of Clinical Nursing,2008;vol./is. 17/6(790-799), 0962-1067;1365-2702.8. Hoenig J. and Hamilton M. The schizophrenic patient and his effect on the household. International Journal of Social Psychiatry.1966; 12: 165-1769. Ostman, M. and L. Hansson. Appraisal of caregiving, burden and psychological distress in relatives of psychiatric inpatients. European Psychiatry.2004; 19: 402-407.10. Magliano L., Fiorillo A., De Rosa C., Malangone C. and Maj M. Family burden in long-term diseases: a comparative study in schizophrenia vs. physical disorders. Social Science and Medicine.2005a; 61: 313-322.11. Holmes, T .H., and Rahe,R.H.The social readjustment rating scale.J.Psychosom.Res.1967; 11:213-218.12. Kanner,A. D.,Coyne, J.D.,Schaefer, C., and Lazarus,R. S.Comparison of two modes of stress measurement: Daily hassles and uplifts versus major life events.J.Behav.Med.1981;4:1-39.13. Pearlin,L.I.Role strains and personal stress. In Kaplan, H.B. (ed.), Psychosocial stress: Trends in Theory and Research, Academic Press, New York, pp.3-32.1983.14. Lazarus, R.S., & Folkman, S. Stress, Appraisal and Coping. New York: Springer.1984.15. Deimling,G.T;Bass,D.M;Townsend,A.L;and Noelker,L.S.Care Related stress: A comparison of spouse and adult child caregivers in shared and seperate households. Journal of Ageing and health.1989;1,67-82.16. Amirkhanyan, A.A., & Wolf, D.A. Caregiver stress and noncaregiver stress: Exploring the pathways of psychiatric morbidity. Gerontologist.2003; 43, 817-827.17. Danhauer, S.C.,McCann, J.J., Gilley,D.W., Beckett, L.A., Bienias, J. L., & Evans, D.A.Do behavioural disturbances in persons with Alzheimer's disease predict caregiver depression over time? Psychology and Aging.2004; 19, 198-202.18. Askey, Ryan,Holmshaw, Janet,Gamble, Catherine,Gray, Richard.What do carers of people with psychosis need from mental health services? Exploring the views of carers, service users and professionals. Journal of Family Therapy.2009;vol./is. 31/3(310-331), 0163-4445;1467-6427.19. Canadian Study of Health and Aging Working Group.Canadian Study of Health and Aging: Study methods and prevalence of dementia. Canadian Medical Association Journal.1994a; 150, 899-913.20. Yvonne Yueh-Feng Lu and Mary Guerriero Austrom. Distress Reponses and Self- Care Behaviours in Dementia Family Caregivers With High and Low Depressed Mood: J Am Psychiatr Nurses Assoc, 2005; 11(4), 231-240.21. Gallant, M.P., & Connel, C.M.Predictors of decreased self-care among spouse caregivers of older adults with dementing illnesses. Journal of Aging and Health.1997;9, 373-395.22. Gallagher,D.,Rose,J.,Rivera,P.,Lovett,S.,&Thompson,L.W.Prevalence of depression in family caregivers.The Gerontologist.1989;29,449-456.23. Dura,J.R;Stukenberg,K.W;and Kiecolt-Glaser,JK..Anxiety and depressive disorders in adult children caring for demented parents.Psychology and ageing.1991;6,467-473.24. Molyneux, C. J,McCarthy, G. M,McEniff, S,Cryan, M,Conroy, R. M. Prevalence and predictors of carer burden and depression in carers of patients referred to an old age psychiatric service. International Psychogeriatrics.2008; vol./is. 20/6(1193-1202), 1041-6102;1741-203X25. Cohen,D; Luchins,D; Eisdorfer,C;Paveza,G; Ashford,J.W;Gorelic,P; Hirsehman,R;Freels,S;Levy,P;Semla,T;&Shaw,H.Caring for relatives with Alzheimers Disease:The Mental Health Risks to Spouses,Adult children and other family caregivers.Behaviour,Health,and Ageing.1990;1,171-182.26. Colerick,E.J;&George,L.K.Depression among Alzheimer's caregivers:Identifying risk factors.American Journal ..Journal of the American Geriatrics Society.1986;34,493-498.27. Magliano L., Marasco C., Fiorillo A., Malangone. C., Guarneri M. and Maj M. The impact of professional and social network support on the burden of families of patients with schizophrenia in Italy. Acta Psychiatrica Scandinavica.2002; 106: 291-298.28. Lefly H.P. (1997). Synthesizing the family caregiving studies: implications for service planning, social policy, and further research. Family Relations.1997; 46:443–450.29. Cohen C.A., Colantonio A. and Vernich L. Positive aspects of caregiving: rounding out the caregiver experience. International Journal of Geriatric Psychiatry.2002; 17: 184-188.30. Thomas P., Hazif-Thomas C., Delagnes V., Bonduelle P. and Clement J.P. La vulnérabilité de l’aidant principal des malades déments à domicile. L’étude Pixel. Psychologie et Neuropsychiatre Vieilissement.2005; 3: 207-220.31. Wittmund B., Wilms H.U., Mory C. and Angermeyer M.C. Depressive disorders in spouses of mentally ill patients. Social Psychiatry and Psychiatric Epidemiology.2002; 37: 177-182.32. Perlick D.A., Rosenheck R. R., Clarkin J.F., Raue P. and Sirey J. Impact of family burden and patient symptom status on clinical outcome in bipolar affective disorder. Journal of Nervous Mental Disorders.2001; 189: 31-37.33. Sartorius N. The economic and social burden of depression. Journal of Clinical Psychiatry.2001; 15: 8-11.34. Jungbauer J., Wittmund B., Dietrich S. and Angermeyer M.C. The disregarded caregivers: subjective burden in spouses of schizophrenia patients. Schizophrenia Bulletin.2004; 30: 665-675.35. van Wijngaarden B., Schene A.H. and Koeter M.W. Family caregiving in depression: impact on caregivers' daily life, distress, and help seeking. Journal of Affective Disorders.2004; 81: 211-222.36. Perlick D.A., Hohenstein J.M., Clarkin J.F., Kaczynski R. and Rosenheck R. A. Use of mental health and primary care services by caregivers of patients with bipolar disorder: a preliminary study. Bipolar Disorders.2005; 7: 126-135.37. Baldassano,C. “Reducing the Burden of Bipolar Disorder for Patient and Caregiver,” Medscape Psychiatry & Mental Health.2004; 9(2).38. Amir N., Freshman B.A. and Foa E. Family distress and involvement in relatives of obsessive-compulsive disorder patients. Journal of Anxiety Disorders.2002; 14: 209-217.39. Treasure J., Murphy T., Szmukler G., Todd G., Gavan K. and Joyce J. The experience of caregiving for severe mental illness: a comparison between anorexia nervosa and psychosis. Social Psychiatry and Psychiatric Epidemiology.2001; 36: 343-347.40. Perkins, S., S. Winn, J. Murray, R. Murphy and U. Schmidt. A qualitative study of the experience of caring for a person with bulimia nervosa. Part 1: The emotional impact of caring. International Journal of Eating Disorders.2004; 36(3): 256-268.41. Gruetzner, H.M. Alzheimer's: A Caregiver's Guide and Sourcebook. Wiley.2001.42. Mc Grath, E., Puryear Keita, G., Stricland, B.R., and Felipe Russo, N. Women and Depression: Risk Factors and Treatment Issues, American Psychological Association, Washington, DC.1992.43. Schulz, R., and Williamson, G.A Two-year longitudinal study of depression among Alzheimer's caregivers. Psychol. Aging.1991; 6:569-578.44. Gitlin, L.N., Corcoran, M., Winter, L., Boyce, A., & Marcus, S.Predicting participation and adherence to a home environmental intervention among family caregivers of persons with dementia .Family Relations.1999; 48, 363-372.45. Draper, B. Dealing With Dementia: A Guide to Alzheimer's Disease and Depression in Caregivers of Patients with Dementia.2004.46. Lawton,M.P., Rajgopal,D., Brody,E., & Kleban,M.H.The dynamics of caregiving for a demented elder among Black and White families.Journal of Gerontology:Social Sciences .1992;47, S156-S164.47. Baumgarten, M., Battista, R.N., Infante-Rivard,C.,Hanley, J.A., Becker, R.,& Gauthier, S.The Psychological and Physical health of family members caring for an elderly person with dementia. Journal of Clinical Epidemiology.1992; 45,61-70.48. Shaw WS,Patterson TL,Semple SJ,et al.Longitudinal analysis of multiple indicators of health decline among spousal caregivers.Ann Behav Med .1997;19:101-109.49. Schulz, R., O'Brien, A.T., Bookwala, J.,& Flessiner, K. Psychiatric and physical morbidity effects of dementia caregiving : Prevalence, correlates, and causes. Gerontologist.1995; 35, 771-791.50. Connel, C.M., Janevic, M.R., & Gallant, M.P.The costs of caring: Impact of dementia on family caregivers. Journal of Geriatric Psychiatry and Neurology.2001; 14, 179-187.51. Calderon, V., & Tennstedt, S. Results of a qualitative study. Journal of Gerontological Social Work.1998;30, 159-178.52. Farran, C.J., Miller, B.H., Kaufman, J.E., & Davis, L. Race, finding meaning, and caregiver distress.Journal of Aging and Health.1997; 9, 316-333.53. Harwood DG, Barker WW, Cantillon, et al.Depression symptomatology in the first-degree family caregivers of Alzheimer disease patients: A cross-ethnic comparison. Alzheimer Disease & Associated Disorders.1998; 4: 340-346.54. Gallant, M.P., & Connel, C.M.Predictors of decreased self-care among spouse caregivers of older adults with dementing illnesses. Journal of Aging and Health.1997;9, 373-395.55. Clyburn L, Stones M, Hadjistavropoulos T, et al.Predict depression in caregiver burden and in Alzheimer's disease.J Gerontol B Psychol Sci Soc Sci.2000; 55:S2-S13.56. Williamson, G.M.,& Schulz, R. Coping with specific stressors in Alzheimer's Disease caregiving. The Geronotologist.1993;33, 747-755.57. Russo,J.,Vitaliano,P.P.,Brewer,D.D.,Katon,W.,&Becker,J.Psychiatric disorders in spouse caregivers of care recipients with Alzheimer's disease and matched controls:A diathesis-stress model of psychopathology,Journal of abnormal psychology.1995;104,197-204.58. McDonell M.G ., Short R.A ., Berry C.M ., Dyck D.G. Burden in Schizophrenia Caregivers: Impact of Family Psychoeducation and Awareness of Patient Suicidality. Family Process.2003; Vol. 42, No. 1.59. Tooth, Leigh,Russell, Anne,Lucke, Jayne,Byrne, Gerard,Lee, Christina,Wilson, Andrew,Dobson, Annette. Impact of cognitive and physical impairment on carer burden and quality of life. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care & Rehabilitation.2008;vol./is. 17/2(267-273), 0962-9343;1573-264960. Quayhagen. M.P.,& Quahagen. M.Alzheimer's stress: Coping wih the caregiving role. The Geronotologist.1998; 28, 391-396.61. Lazarus,R. S., and Folkman,S.Stress,Appraisal,and Coping,Springer Publishing Company,New York.1984.62. Fingerman, K.L., Gallagher-Thompson, D., Lovett, S., & Rose, J. Internal resourcefulness, task demands, coping, and dysphoric affect among caregivers of the frail elderly. International Journal of Aging &Human Development.1996; 42, 229-248.63. Woods RT, Wills W, Higginson IJ, Hobbins J, Whitby M.Support in the community for people with dementia and their carers: a comparative outcome study of specialist mental health service interventions. International Journal of Geriatric Psychiatry .2003;18:(4):298-307.64. Ballard, C.G., Saad,K., Patel, A., Gahir,M., Solis, M., et al. The prevalence and Phenomenology of psychotic symptoms in dementia sufferers. International Journal of Geriatric Psychiatry.1995a; 10, 477-485.65. Coppel, D.B., Burton, C., Becker, J. and Fiore, J. Relationships of cognitions associated with coping reactions to depression in spousal caregivers of Alzheimer's disease patients. Cog. Ther. Res.1985; 9, 253-266.66. Saad, K.,Hartman, J.,Ballard, C., Kurian, M.,Graham, C.and Wilcock, G.Coping in the Carers of dementia sufferes. Age Ageing.1995; 24 , 495-498.67. Horowitz, A. and Shindelman, L.W. Reciprocity and affection: Past influences on current caregiving. J. Gerontol. Soc. Work.1983; 5, 5-20.68. Lawton, M.P. Interventions in Dementia Care: Toward Improving Quality of Caregiving.200069. Levin, J.S.,Chatters,L.M., and Taylor, R.J. Religious effects on health status and life satisfaction among Black Americans. J.Gerontol. Soc. Sci.1995;50B: S154-S163.70. Picot, S.J, Debanne, SM., Namazi, K.H., and Wykle, M.L. Religiosity and perceived rewards of Black and Anglo caregivers. Gerontologist.1997; 37: 89-101.71. Dilworth-Anderson, P., Williams, I.C.,& Gibson, B.E.Issues of race , ethnicity, and culture in caregiving research :A 20-year review (1980-2000).The Gerontologist.2002; 42, 237-272.72. Coon, D.W., Rubbert, MP., Solano,N., Mausbach,B., Kraemer, H., Arguelles, T., et al.Well-being, appraisel, and coping in Latina and Caucasian female dementia caregivers:Finding from the REACH study. Aging and Mental Health.2004, 8(4), 330-345.73. Walls,CT.,&Zarit SH. Informal Support From Black Churches and the Well-Being of Elderly Blacks.The Gerontologist.1991; .31(4):490 495.74. Haley, W, E., Levine, E, G., Brown, S, L., Bartolucci, A, A. Stress appraisal, coping and social support as predictors of adptational outcome among dementia caregivers.Psychology and Aging.1987; 2, 323- 330.75. Kramer, B.J.Gain in the caregiving experience: Where are we ?What next? Gerontologist.1997; 37, 218-232.76. Pinquart, M., & Sorensen, S. Associations of stressors and uplifts of caregiving with caregiver burden and depressive mood: A meta-analysis. Journal of Gerontology: Psychological Sciences & Social Sciences.2003;58B, 112-128.77. Haley, W.E., Gitlin, L.N., Wisniewski, S. R., Mahoney, D.F., Coon, D.W.,Winter, L., et al. Well-being, appraisal, and coping in African- American and Cuacasian dementia caregivers: Findings from the REACH study. Aging & Mental Health.2004; 8(4), 316-329.78. Cox, C.Comparing the experience of Black and White Caregivers of dementia patients. Social Work.1995;3, 343-349.79. Alten, G.J. Racial variations in caregiver stress and burden among informal caregivers of impaired elderly persons.University of Florida, Gainesville.1993.80. Burton-Smith, Rosanne,McVilly, Keith R,Yazbeck, Marie,Parmenter, Trevor R,Tsutsui, Takako.Quality of life of Australian family carers: Implications for research, policy, and practice. Journal of Policy and Practice in Intellectual Disabilities.2009; vol./is. 6/3(189-198), 1741-112281. Rivera De J.L.G. Factores de estrés y enfermedad médica. Actas Luso-Españolas de Psiquiatría y Neurología.1991; 19: 290-297.82. Bourgeois,MS.,Burgio,LD.,Schulz,R.,Beach,S, and Palmer,B. Modifying repetitive verbalizations of community-dwelling patients with AD. The Gerontologist.1997; Vol 37, Issue 1 30-39.83. Stevens, A.B. & Burgio, L.D. Issues in training home-based caregivers of individuals with Alzheimer’s disease. Alzheimer’s Care Quarterly.2000; 1(1):55-68.84. Cheston, R. Psychotherapeutic work with people with dementia: a review of the literature. British Journal of Medical Psychology.1998; 71, 211-231.85. Marriott,A., Donaldson,C.,Tarrier,N and Burns,A. Effectiveness of cognitive-behavioural family intervention in reducing the burden of care in carers of patients with Alzheimer's disease,British Journal of Psychiatry.200086. Rigaux, Natalie. Informal care: Burden or significant experience? Psychologie & NeuroPsychiatrie du Vieillissement.2009; vol./is. 7/1(57-63), 1760-1703.87. Yarnoz, Adelaida Zabalegui,Diez, Montserrat Navarro,Torres, Esther Cabrera et al.Efficacy of interventions aimed at the main carers of dependent individuals aged more than 65 years old. A systematic review. Revista Espanola de Geriatria y Gerontologia.2008; vol./is. 43/3(157-166), 0211-139X.88. Sleath,B.,Thorpe,J.,Lawrence,MPH.,Landerman,R.,Doyle,M.and Clipp,E. African-American and white caregivers of older adults with Dementia:Differences in Depressive Syptomatology and Psychotropic Drug Use.2005; By the American Geriatrics Society.89. Helen C.Kales, MD, Frederic C. Blow, PhD, Deborah E.Welsh, MS, and Alan M.Mellow,MD, PhD. Herbal products and other Supplements: Use by Elderly Veterans With Depression and Dementia and Their Caregivers: J Geriatr Psychiatry Neurol 2004;17:25-31.90. Burdz, M.P., Eaton, W.O. and Bond, J.B.Effect of respite care on dementia and nondementia patients in caregiver', Psychology and Aging.1988; 3, 1:38-42.91. Harvey, K,Catty, J,Langman, A,Winfield, H,Clement, S,Burns, E,White, S,Burns, T. A review of instruments developed to measure outcomes for carers of people with mental health problems. Acta Psychiatrica Scandinavica.2008;vol./is. 117/3(164-176), 0001-690X;1600-0447.





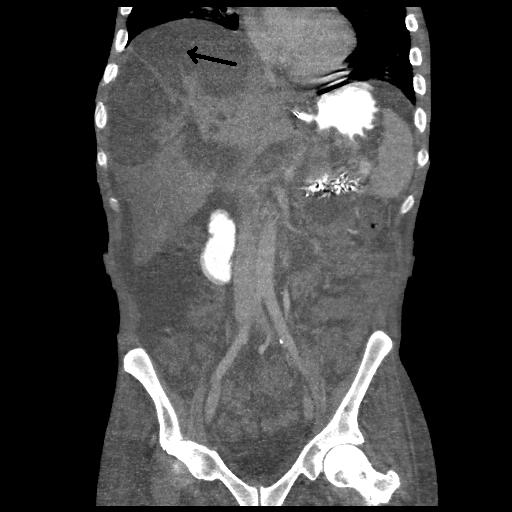
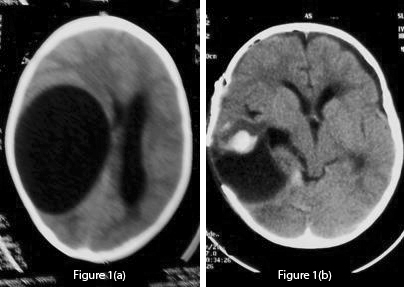 Fig 1 (a): Pre-operative unenhanced CT scan which shows a large CSF density cystic lesion on the right side causing mass effect and midline shift to the left. There is no peri-lesional oedema. Fig 1 (b): Post-operative CT scan of the lesion shows a large void which can lead to dangerous collapse. Mild haematoma is also seen.
Fig 1 (a): Pre-operative unenhanced CT scan which shows a large CSF density cystic lesion on the right side causing mass effect and midline shift to the left. There is no peri-lesional oedema. Fig 1 (b): Post-operative CT scan of the lesion shows a large void which can lead to dangerous collapse. Mild haematoma is also seen. 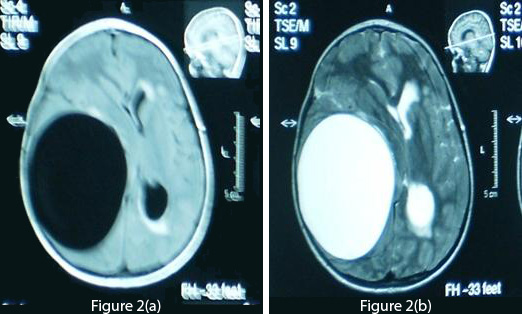 Fig 2 (a): T1-weighted axial MRI of the brain demonstrates a cyst density similar to CSF. Fig 2 (b): T2-weighted MRI shows no ring enhancement or oedema. The periventricular hyperintensity of the left side is probably due to obstructive hydrocephalus.
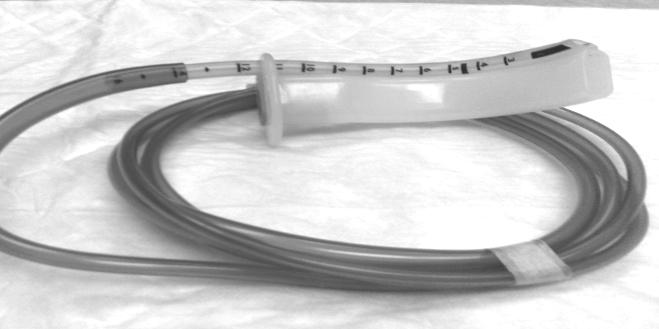
Fig 2 (a): T1-weighted axial MRI of the brain demonstrates a cyst density similar to CSF. Fig 2 (b): T2-weighted MRI shows no ring enhancement or oedema. The periventricular hyperintensity of the left side is probably due to obstructive hydrocephalus.  Fig 3: This shows the cyst removed in toto after operation. The cyst appears creamy and smooth. After summation of all the above data, the diagnosis of a hydatid cyst was made and a right frontotemporoparietal craniotomy was performed. A large cystic structure (14×14×12 cm) was delivered with utmost care to avoid rupture and spillage [fig 3]. A hydatid cyst was confirmed by pathology reports. A post-operative CT scan showed a large space without any residual matter [fig 1(b)]. Post-operatively, albendazole 15 mg/kg was started and continued for four weeks. The patient showed marked improvement in his neurological deficit and was discharged after one week with close follow-up. Discussion/Review Of Literature Life CycleHydatidosis is caused by Echinococcus granulosus, which occurs mainly in dogs. Humans who act as intermediate hosts get infected incidentally by ingesting eggs from the faeces of the infected animal. The eggs hatch inside the intestines and penetrate the walls, entering blood vessels and eventually reach the liver where they may form cysts or move on towards the lungs. Even after pulmonary filter, a few still make it to the systemic circulation and can lodge in almost any part of the body, including the brain, heart and bones.2,3,8,14,16,26 Brain hydatid cysts are relatively rare and only account for up to 2% of total cases.4,5,7 The actual percentage may be higher than what we have in literature, due to under-reporting. Brain hydatid cysts can be primary (single) or secondary (multiple).2,3,4,5,7 The latter are thought to arise from the multiple scolices released from the left side of the heart following cyst rupture in the heart2,3,5,27 or due to spontaneous, traumatic or surgical rupture of a solitary cranial cyst.3,5 Cysts mostly involve the territory of the middle cerebral artery4,7 but other regions like intraventricular, posterior fossa and the orbit have also been reported.15,17,18,28 The wall of the cyst consists of an inner endocyst (germinal layer) and outer ectocyst (laminated layer). The host reacts to the cyst forming a pericyst (fibrous capsule), which provides nutrients to the parasite. In the brain, due to minimal reaction, the pericyst is very thin. The endocyst produce scolices which bud into the cyst cavity and may sediment within the hydatid cavity, commonly known as hydatid sand.3,14,29,30 Presentation and DiagnosisMost hydatid cysts are acquired in childhood and are manifested during early adulthood.8,29 Cysts develop insidiously, usually being asymptomatic initially, and present with protean clinical and imaging features.3,5,6 In previous studies the most common presenting symptoms were headache and vomiting.4,5,7,14,15,28 Also in the literature, patients reported ataxia, diplopia, hemiparesis, abducens nerve palsy and even coma.5,7,15,28 Surprisingly, in the present study the patient did not have a headache and presented with parasthesia and numbness of the toes. Later he developed left sided weakness, convulsions and finally ataxia, which correlate with previous studies. Diagnosis of a hydatid cyst can sometimes be confused with other space occupying lesions of the brain, especially abscesses, neoplasms and arachnoid cysts.14,31 In this study the patient had bilateral frank papilloedema which is also mentioned in earlier reports.4,28 The Casoni and Weinberg tests, indirect haemagglutination, eosinophilia and ELISA are used in diagnosing hydatid cysts, but as brain tissue evokes minimal response many results tend to be false negatives.2,5,8,25 In our case also, serology for hydatid cyst was negative. CT scan and MRI are used frequently in diagnosing the cystic lesions.3,8,14,23,32,33 However, MRI is considered superior in demonstrating the cyst rim.5,8,11,21,32,34 On CT scan, a solitary cyst appears as well-defined, spherical, smooth, thin-walled and homogeneous, with an inner density similar to CSF, and non-enhancing walls.11,29,32The wall may appear iso-dense to hyper-dense on CT scan3,8, and rarely, may become calcified.11,29,32 There is usually no surrounding brain parenchymal oedema, which if exists along with ring enhancement, indicates inflammation and infection. 7,11,32,33,34,35 Ring enhancement and peri-lesional oedema differentiates brain abscesses and cystic neoplasms from uncomplicated hydatid cysts.3,8 These findings can in fact sometimes cause dilemma and misdiagnosis and lead to catastrophic events.14 The cyst shows low signal intensity on T1-weighted, and high signal intensity on T2-weighted MRI.2 MRI may also show peri-lesional oedema not seen on regular CT scan imaging.7 MRI may prove superior in determining exact cyst location, presence of super-added infections and cystic contents, and also in surgical planning and ruling out other diagnostic possibilities.14,33 We strongly recommend MRI for better evaluation of cystic brain lesions. Spontaneous cystic rupture can lead to different appearances depending on which layers have been obliterated, and produce some specific signs.3 When only the endocyst ruptures, cyst contents are held by the outer pericyst giving a peculiar water lily sign, which is pathognomic.3,8 TreatmentThough still in infancy, medical therapy for small or inoperable brain hydatid cysts has been promising. Albendazole alone or in combination with other compounds, such as praziquantel, has been reported with favourable results as an adjunct and, in certain circumstances, as the primary mode of treatment.2,36,37,38 It is reported that albendazole results in the disappearance of up to 48% of cysts and a substantial reduction in size of the cysts in another 28%.2 The duration of the treatment is four weeks or more, and recently many authors have favoured a prolonged therapy. The change in levels of cyst markers such as alanine, succinate, acetate and lactate, measured before and during treatment on Proton Magnetic Resonance Spectroscopy (MRS), correlate well with shrinkage and resolution of cyst findings on conventional MRI and help in evaluating the efficacy of chemotherapy.39 Cysts may drain into ventricles or rupture completely, causing spillage of contents into the subarachnoid space, leading to fatal anaphylactic shock, meningitis or local recurrence.3,5,22,25 Surgery is the mainstay for treating intracranial hydatid cysts and the aim is to excise the cysts entirely without rupture, which can otherwise lead to catastrophic events as described earlier 2,3,14,25. The Dowling-Orlando technique remains the preferred method, in which the cyst can be delivered by lowering the head of the operating table and instilling warm saline between the cyst and the surrounding brain.40 Even minimal spillage can cause deleterious effects (1 ml of hydatid sand contains 400,000 scolices).14 The thin cyst wall, periventricular location and micro-adhesions to the parenchyma are the main problems encountered during the surgical procedure.1,22 The large cavity remaining after the cystic removal can lead to many serious complications, such as cortical collapse, hyperpyrexia, brain oedema and cardio-respiratory failure.5 Recurrence remains a major concern, which is managed by both antihelminthic chemotherapy and surgery. In a study conducted by Ciurea et al, 25% of the patients had recurrence, which highlights the need for long term follow up.23 In the present study, due to the huge size of the cyst and progressive neurological deficit, it was not wise to completely rely on medical therapy. Surgery was performed and post-operatively albendazole was started as an adjunct. We recommend that for treating brain hydatid cyst, the size of the cyst, multiplicity, location and neurological deficit must all be taken into consideration.
Fig 3: This shows the cyst removed in toto after operation. The cyst appears creamy and smooth. After summation of all the above data, the diagnosis of a hydatid cyst was made and a right frontotemporoparietal craniotomy was performed. A large cystic structure (14×14×12 cm) was delivered with utmost care to avoid rupture and spillage [fig 3]. A hydatid cyst was confirmed by pathology reports. A post-operative CT scan showed a large space without any residual matter [fig 1(b)]. Post-operatively, albendazole 15 mg/kg was started and continued for four weeks. The patient showed marked improvement in his neurological deficit and was discharged after one week with close follow-up. Discussion/Review Of Literature Life CycleHydatidosis is caused by Echinococcus granulosus, which occurs mainly in dogs. Humans who act as intermediate hosts get infected incidentally by ingesting eggs from the faeces of the infected animal. The eggs hatch inside the intestines and penetrate the walls, entering blood vessels and eventually reach the liver where they may form cysts or move on towards the lungs. Even after pulmonary filter, a few still make it to the systemic circulation and can lodge in almost any part of the body, including the brain, heart and bones.2,3,8,14,16,26 Brain hydatid cysts are relatively rare and only account for up to 2% of total cases.4,5,7 The actual percentage may be higher than what we have in literature, due to under-reporting. Brain hydatid cysts can be primary (single) or secondary (multiple).2,3,4,5,7 The latter are thought to arise from the multiple scolices released from the left side of the heart following cyst rupture in the heart2,3,5,27 or due to spontaneous, traumatic or surgical rupture of a solitary cranial cyst.3,5 Cysts mostly involve the territory of the middle cerebral artery4,7 but other regions like intraventricular, posterior fossa and the orbit have also been reported.15,17,18,28 The wall of the cyst consists of an inner endocyst (germinal layer) and outer ectocyst (laminated layer). The host reacts to the cyst forming a pericyst (fibrous capsule), which provides nutrients to the parasite. In the brain, due to minimal reaction, the pericyst is very thin. The endocyst produce scolices which bud into the cyst cavity and may sediment within the hydatid cavity, commonly known as hydatid sand.3,14,29,30 Presentation and DiagnosisMost hydatid cysts are acquired in childhood and are manifested during early adulthood.8,29 Cysts develop insidiously, usually being asymptomatic initially, and present with protean clinical and imaging features.3,5,6 In previous studies the most common presenting symptoms were headache and vomiting.4,5,7,14,15,28 Also in the literature, patients reported ataxia, diplopia, hemiparesis, abducens nerve palsy and even coma.5,7,15,28 Surprisingly, in the present study the patient did not have a headache and presented with parasthesia and numbness of the toes. Later he developed left sided weakness, convulsions and finally ataxia, which correlate with previous studies. Diagnosis of a hydatid cyst can sometimes be confused with other space occupying lesions of the brain, especially abscesses, neoplasms and arachnoid cysts.14,31 In this study the patient had bilateral frank papilloedema which is also mentioned in earlier reports.4,28 The Casoni and Weinberg tests, indirect haemagglutination, eosinophilia and ELISA are used in diagnosing hydatid cysts, but as brain tissue evokes minimal response many results tend to be false negatives.2,5,8,25 In our case also, serology for hydatid cyst was negative. CT scan and MRI are used frequently in diagnosing the cystic lesions.3,8,14,23,32,33 However, MRI is considered superior in demonstrating the cyst rim.5,8,11,21,32,34 On CT scan, a solitary cyst appears as well-defined, spherical, smooth, thin-walled and homogeneous, with an inner density similar to CSF, and non-enhancing walls.11,29,32The wall may appear iso-dense to hyper-dense on CT scan3,8, and rarely, may become calcified.11,29,32 There is usually no surrounding brain parenchymal oedema, which if exists along with ring enhancement, indicates inflammation and infection. 7,11,32,33,34,35 Ring enhancement and peri-lesional oedema differentiates brain abscesses and cystic neoplasms from uncomplicated hydatid cysts.3,8 These findings can in fact sometimes cause dilemma and misdiagnosis and lead to catastrophic events.14 The cyst shows low signal intensity on T1-weighted, and high signal intensity on T2-weighted MRI.2 MRI may also show peri-lesional oedema not seen on regular CT scan imaging.7 MRI may prove superior in determining exact cyst location, presence of super-added infections and cystic contents, and also in surgical planning and ruling out other diagnostic possibilities.14,33 We strongly recommend MRI for better evaluation of cystic brain lesions. Spontaneous cystic rupture can lead to different appearances depending on which layers have been obliterated, and produce some specific signs.3 When only the endocyst ruptures, cyst contents are held by the outer pericyst giving a peculiar water lily sign, which is pathognomic.3,8 TreatmentThough still in infancy, medical therapy for small or inoperable brain hydatid cysts has been promising. Albendazole alone or in combination with other compounds, such as praziquantel, has been reported with favourable results as an adjunct and, in certain circumstances, as the primary mode of treatment.2,36,37,38 It is reported that albendazole results in the disappearance of up to 48% of cysts and a substantial reduction in size of the cysts in another 28%.2 The duration of the treatment is four weeks or more, and recently many authors have favoured a prolonged therapy. The change in levels of cyst markers such as alanine, succinate, acetate and lactate, measured before and during treatment on Proton Magnetic Resonance Spectroscopy (MRS), correlate well with shrinkage and resolution of cyst findings on conventional MRI and help in evaluating the efficacy of chemotherapy.39 Cysts may drain into ventricles or rupture completely, causing spillage of contents into the subarachnoid space, leading to fatal anaphylactic shock, meningitis or local recurrence.3,5,22,25 Surgery is the mainstay for treating intracranial hydatid cysts and the aim is to excise the cysts entirely without rupture, which can otherwise lead to catastrophic events as described earlier 2,3,14,25. The Dowling-Orlando technique remains the preferred method, in which the cyst can be delivered by lowering the head of the operating table and instilling warm saline between the cyst and the surrounding brain.40 Even minimal spillage can cause deleterious effects (1 ml of hydatid sand contains 400,000 scolices).14 The thin cyst wall, periventricular location and micro-adhesions to the parenchyma are the main problems encountered during the surgical procedure.1,22 The large cavity remaining after the cystic removal can lead to many serious complications, such as cortical collapse, hyperpyrexia, brain oedema and cardio-respiratory failure.5 Recurrence remains a major concern, which is managed by both antihelminthic chemotherapy and surgery. In a study conducted by Ciurea et al, 25% of the patients had recurrence, which highlights the need for long term follow up.23 In the present study, due to the huge size of the cyst and progressive neurological deficit, it was not wise to completely rely on medical therapy. Surgery was performed and post-operatively albendazole was started as an adjunct. We recommend that for treating brain hydatid cyst, the size of the cyst, multiplicity, location and neurological deficit must all be taken into consideration. 



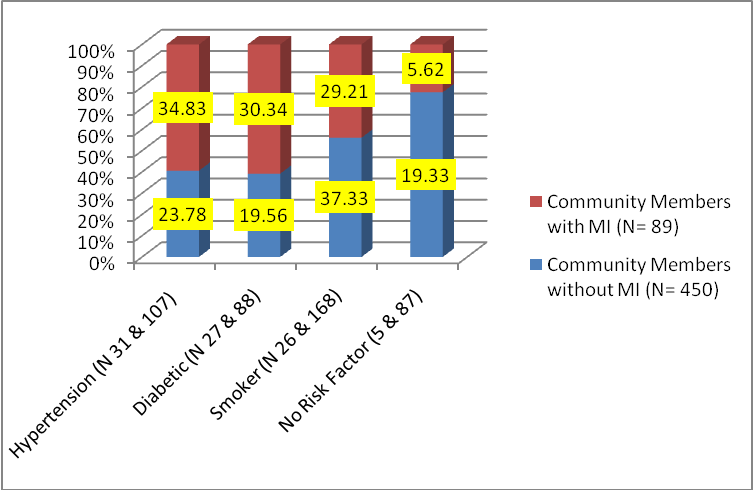
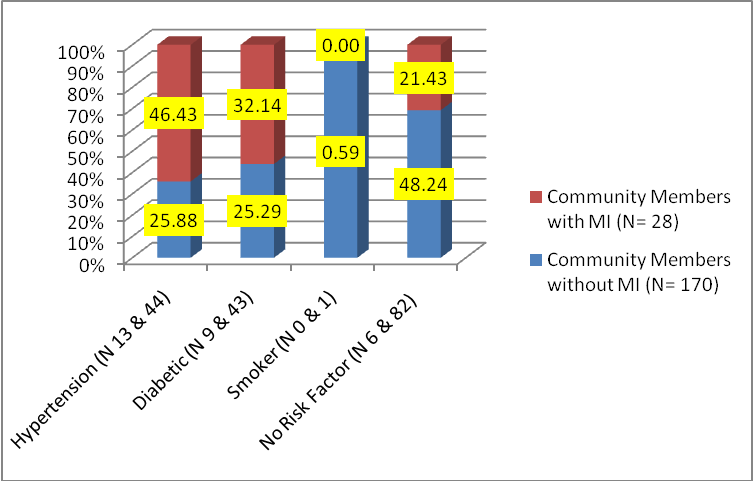 (Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI.
(Fig.2) Distribution of Risk Factors in Females with and without MI (The total number of responses are more than number of respondents because of more than one risk factor being present in many respondents) Combination of risk factors Out of 48 males with MI, 22 (45.83%) had both diabetes and hypertension and half of them (22.92%) were also smokers. The next group among males having multiple risk factors were that of smokers 14 (29.17%), out of which half (14.58%) also had hypertension. Out of 22 females with MI, 13 (59.09%) had hypertension and 27.27 % out of them were also diabetic. The next group was that of diabetics 3 (13.64%). Hence looking at the combination of risk factors in both males and females with MI the most common risk factor in terms of prevalence was found to be hypertension followed by smoking in men and diabetes in women. As Hypertension and BMI in age group of 35 to 54 years were found to be significant and commonly present risk factors, the data was further explored. Systolic BP 140 and above: The percentage of persons with MI having a systolic BP of 140 and above in the age group 35 to 54 years was more than double in comparison to the percentage expected by number of persons present in this age group that is 66.67% as stated in Fig.3, against 30% as stated above in Table1. Hence in this age group there appears to be considerable opportunity of detecting and treating cases of hypertension in the general community before they reach to the advanced stage of coronary artery disease and MI. 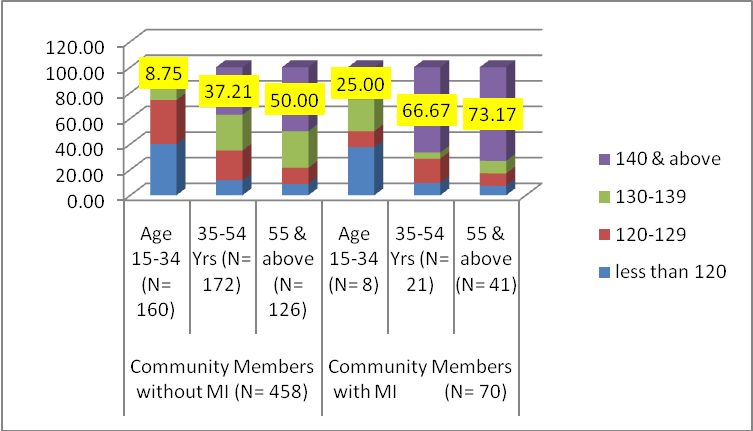 (Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years.
(Fig.3) Age wise distribution of blood pressure (both sexes) Body Mass Index: As presented below in Fig.4, the percentage of overweight and obese individuals were found to be 5 to 9 percent higher in those with MI than those without MI. The percentage of obese people increased by 2 times in both the groups that is with and without MI as age advanced to 35-54 years from 15-34 years. The percentage of overweight individuals was 1.48 times in those without MI and 1.77 times in those with MI in age group 35-54 years in comparison to the age group of 15-34 years. 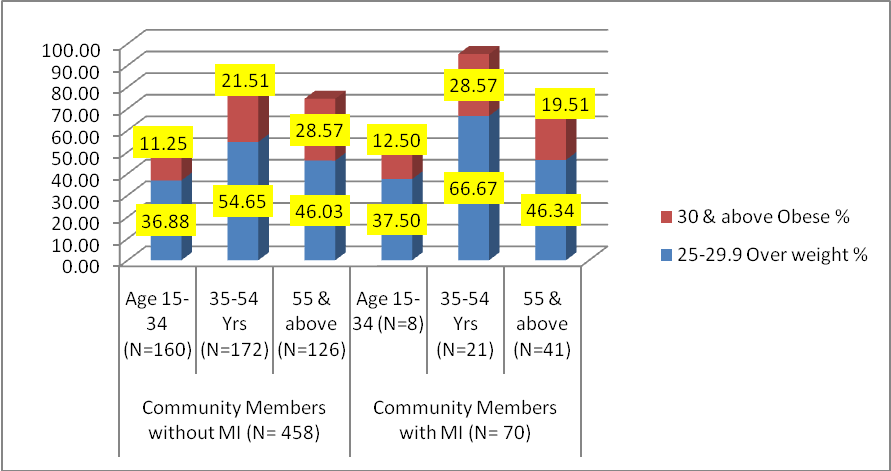













Browse the December 2010 PDF Booklet (Volume 3 Number 4)