The concept of burnout has been used to describe emotional and psychological stress among healthcare workers in response to work-related stressors1. Maslach et al2 have defined burnout as a triad of characteristics: emotional exhaustion, depersonalisation (such as objectifying and treating patients indifferently) and lack of feelings of personal accomplishment. Since high time-pressure, high job- stress and excessive workload with poor support are among significant factors that contribute to burnout, physicians are at a greater risk of suffering from it as compared to the general population3.
Burnout affects approx. half of the doctors in the U.S. and in Western Europe working across multiple specialties including in family medicine and internal medicine4,5. Likewise, burnout is universally prevalent among healthcare workers from low and middle-income countries6.
Psychiatry presents specific range of stressors not encountered concurrently in other medical specialties, such as treating chronically ill patients, potentially difficult therapeutic relationships, threat of patient suicide/self-harm and stigma associated with this field of medicine7. Therefore, it is not surprising to discover that approx. 37% of psychiatric trainees working across 22 countries suffered from severe burnout8.
The COVID-19 pandemic resulted in a national lockdown in the U.K. with travel restrictions and unprecedented pressure on an already stretched healthcare system. Healthcare workers were, therefore, faced with extraordinary difficulties including increased working hours, heavy workload, staff shortages and lack of resources. A recent systematic review showed that a startling 40% of medical workers experienced acute stress disorder following COVID-19 pandemic, with burnout prevalent among 29% of them9.
During to the pandemic, there has been a huge increase in the pressure on mental health related admissions to hospitals10. A number of causative stressors may have instigated further strain on mental health workers, including bereavement, unemployment, and isolation, resulting in increased psychological morbidity11. Under such circumstances, ensuring the wellbeing of healthcare workers is of paramount importance to maintain a resilient healthcare system. However, limited research has been carried out so far on the effects of pandemics on psychiatrists and other frontline healthcare workers.
Following two surges of COVID-19 pandemic, we proposed to ascertain the frequency of burnout among doctors working in a large mental health trust in Southeast England, with a secondary aim of exploring possible contributory factors.
METHODOLOGY
We carried out a cross-sectional survey of all doctors working in a county-wide mental health Trust in England. Using the NHS Mail, a link to complete the online survey was sent to all doctors working at different experience levels and across a number of psychiatric specialties.
The survey was based on The Maslach Burnout Inventory12, which is considered to be a gold standard in assessing burnout among healthcare workforce. It consists of 22 questions, divided into domains that assess emotional exhaustion, depersonalisation and personal accomplishment based on a 7-point scale, ranging from “never” to “every day”. Scores for these domains range from 0 to 54, 0 to 30, and 0 to 48, respectively. High scores on the EE (≥ 30) and DP (≥ 12) subscales or a low score on the PA subscale (≤ 30) were considered highly suggestive of burnout symptoms.
The anonymised survey contained questions related to demographics, 22 questions as derived from the Maslach Burnout Inventory, and 14 other questions exploring specific work-related stressors regarding the COVID-19 pandemic. Responses to the questions were analysed and categorised into themes to allow further analysis and discussion.
RESULTS
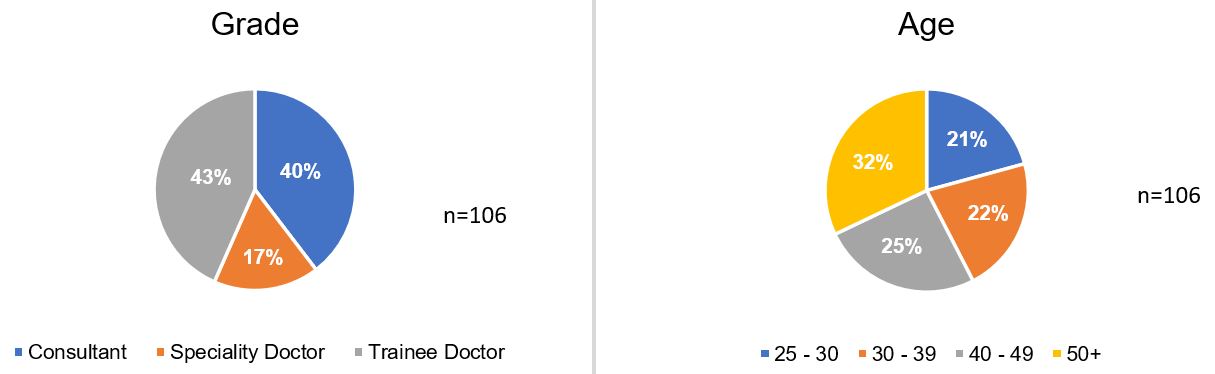
Our response rate was 42% as 106 out of 254 doctors filled the questionnaire. Not all participants answered all questions, and response numbers for each question are indicated where applicable in the respective tables. There was an even distribution between trainees and consultants, but less representation from speciality doctors, which was expected due to their fewer numbers. Where gender was equally split, we found that age was relatively evenly distributed in our sample.
Figure 1: Participant demographics
Regarding the Maslach Burnout Inventory questions, higher aggregates in emotional exhaustion and depersonalisation subscales indicate higher chance of burnout. When comparing these two subscales, the levels of emotional exhaustion were higher than that of depersonalisation. Conversely, in the personal accomplishment subscale, more common occurrences indicate a lower chance of burnout.
Table 1: Maslach Burnout Inventory Results
Question
Possible responses
n
Never
A few times/ year
Once/ month
A few times/ month
Once/ week
A few times/ week
Every day
I feel emotionally drained by my work
7.6% (8)
23.8% (25)
10.5% (11)
27.6% (29)
6.7% (7)
20% (21)
3.8% (4)
105
Working with people all day long requires a great deal of effort
11.3% (12)
23.6% (25)
11.3% (12)
26.4% (28)
5.7% (6)
16.0% (17)
5.7% (6)
106
I feel like my work is breaking me down
20.0% (21)
39.0% (41)
9.6% (10)
18.1% (19)
1.9% (2)
9.6% (10)
1.9% (2)
105
I feel frustrated by my work
16.2% (17)
33.3% (35)
10.5% (11)
21.9% (23)
5.7% (6)
10.5% (11)
1.9% (2)
105
I feel I work too hard at my job
12.4% (13)
21.0% (22)
8.6% (9)
25.7% (27)
5.7% (6)
17.1% (18)
9.5% (10)
105
It stresses me too much to work in direct contact with people
46.2% (49)
28.3% (30)
9.4% (10)
7.5% (8)
0.9% (1)
4.7% (5)
2.8% (3)
106
I feel like I’m at the end of my tether
42.9% (45)
33.3% (35)
4.8% (5)
6.7% (7)
2.9% (3)
7.6% (8)
1.9% (2)
105
I feel I deal with my team/colleagues impersonally, as if they are objects
70.8% (75)
19.8% (21)
4.6% (5)
2.8% (3)
0.9% (1)
0.0% (0)
0.9% (1)
106
I feel tired when I get up in the morning and have to face another day at work
15.1% (16)
36.8% (39)
13.2% (14)
11.3% (12)
1.9% (2)
17.0% (18)
4.6% (5)
106
I have the impression that my team/colleagues make me responsible for some of their problems
41.0% (43)
21.9% (23)
10.5% (11)
20% (21)
0.0% (0)
4.8% (5)
1.9% (2)
105
I am at the end of my patience at the end of my work day
31.7% (33)
36.5% (38)
5.8% (6)
11.5% (12)
3.8% (4)
9.6% (10)
0.9% (1)
104
I really don’t care about what happens to some of my team/colleagues
85.7% (90)
6.7% (7)
1.9% (2)
1.9% (2)
1.9% (2)
0.9% (1)
0.9% (1)
105
I have become more insensitive to people in the workplace
67.0% (71)
22.4% (24)
2.8% (3)
3.8% (4)
0.9% (1)
2.8% (3)
0.0% (0)
106
I’m afraid that this job is making me uncaring
62.3% (66)
25.5% (27)
2.8% (3)
1.9% (2)
3.8% (4)
1.9% (2)
1.9% (2)
106
I accomplish many worthwhile things in this job
2.9% (3)
8.6% (9)
6.7% (7)
15.2% (16)
6.7% (7)
25.7% (27)
34.3% (36)
105
I feel full of energy
4.7% (5)
6.6% (7)
8.5% (9)
20.8% (22)
8.5% (9)
33.0% (35)
17.9% (19)
106
I am easily able to understand what my team/colleagues feel
0.9% (1)
2.8% (3)
3.8% (4)
13.2% (14)
8.5% (9)
34.0% (36)
36.8% (39)
106
I look after my team/colleagues problems very effectively
0.9% (1)
1.9% (2)
5.8% (6)
12.5% (13)
7.7% (8)
44.2% (46)
26.9% (28)
104
In my work, I handle emotional problems very calmly
0.9% (1)
4.8% (5)
1.9% (2)
2.9% (3)
13.3% (14)
31.4% (33)
44.8% (47)
105
Through my work, I feel that I have a positive influence on people
0.9% (1)
4.8% (5)
4.8% (5)
8.6% (9)
9.5% (10)
38.1% (40)
33.3% (35)
105
I am easily able to create a relaxed atmosphere with my team/colleagues
0.9% (1)
3.8% (4)
2.8% (3)
9.4% (10)
11.3% (12)
34.0% (36)
37.7% (40)
106
I feel refreshed when I have been close to my team/colleagues
1.9% (2)
8.5% (9)
3.8% (4)
17.0% (18)
11.3% (12)
34.9% (37)
22.6% (24)
106
In other quantitative questions, all respondents reported that their screen time had increased during the pandemic. A majority reported it to be by more than 2 hours/week, and 71% registered an increase of more than 4 hours/week. Despite this, there appears to be no increase in their home-working that could account for this difference.
The results of the remaining questions reflected a poorer work experience. The strongest evidence was for a feeling that mask wearing had affected rapport with patients. Other more common experiences included poor outcomes for patients during the pandemic, with decreased staffing levels, increased workload, and delayed treatments.
Table 2: Other Question Responses – Quantitative only
Question
Possible responses
n
0-1 hours
1-2 hours
2-3 hours
4-6 hours
6 hours +
During the pandemic, my screen time (e.g. due to meetings and teaching) increased by
4.0% (4)
5.0% (5)
20.0% (20)
37.3% (37)
33.3% (33)
99
Question
Possible responses
n
Yes
No
Were you working from home more often during the pandemic?
48%(48)
52%(52)
100
Question
Possible responses
n
Strongly disagree
Disagree
Neither agree nor disagree
Agree
Strongly agree
I felt that the increase in screen time negatively affected my mood
10.0% (10)
23.0% (23)
35.0% (35)
24.0% (24)
8.0% (8)
100
I felt that the increase in screen time increased my level of exhaustion
14.3% (14)
16.3% (16)
19.4% (19)
39.8% (39)
10.2% (10)
98
I felt that the increase in screen time resulted in depersonalisation of my patients
11.0% (11)
25.0% (25)
33.0% (33)
25.0% (25)
6.0% (6)
100
I felt that the increased screen time hindered the working relationship between colleagues
10.0% (10)
25.0% (25)
20.0% (20)
33.0% (33)
12.0% (12)
100
I felt that the increase in screen time resulted in feelings of burnout
17.0% (17)
26.0% (26)
27.0% (27)
23.0% (23)
7.0% (7)
100
I felt dissatisfied with my online/telephone consultations
8.2% (8)
31.6% (31)
41.8% (41)
13.3% (13)
5.1% (5)
98
I felt that wearing masks affected my rapport with patients
8.1% (8)
17.1% (17)
9.1% (9)
49.5% (49)
16.2% (16)
99
I felt dissatisfied with the patient care provided to patients during the pandemic
7.1% (7)
36.4% (36)
33.3% (33)
21.2% (21)
2.0% (2)
99
I felt that patients did have poorer outcomes during the pandemic
5.1% (5)
27.2% (27)
28.3% (28)
35.4% (35)
4.0% (4)
99
I felt that working from home affected my work-life balance
10.4% (10)
24.0% (23)
42.7% (41)
17.7% (17)
5.2% (5)
96
I felt that working from home resulted in increased work related stressors
12.5% (12)
30.2% (29)
37.5% (36)
18.8% (18)
1% (1)
96
I felt that working from home resulted in more difficulties in my job e.g. communicating with my team or patient
11.5% (11)
29.2% (28)
35.4% (34)
21.9% (21)
2.0% (2)
96
DISCUSSION
Our study provides a snapshot of difficulties encountered by different grades of psychiatrists, while working in a large English county, during the COVID-19 pandemic. We found a burnout rate of 44.2%, which is higher than 36.7% observed by Jovanović et al8 among those working in other countries before the pandemic. Since a higher prevalence is also documented in other recent studies13, it is reasonable to assume that the higher rate of burnout is due to increased work-related stressors during the COVID-19 pandemic. These stressors could be linked to the newly introduced guidelines, which involved social distancing, high staff sickness and redeployment.
In the personal accomplishment subset of our study, highest number of doctors experienced burnout, possibly suggesting a link to the COVID-19 pandemic. Unfortunately, we do not have a pre-COVID pandemic survey for the sake of comparison, which could have confirmed causality with greater certainty.
71% of our cohort reported an increase of more than 4 hours of computer screen time a week, which was not due to increased amount of working from home. Various factors could explain this finding including the introduction of remote medical consultations, online multidisciplinary team meetings and teaching/training. Virtual consultations may provide an alternative to face-to-face assessments, but complications such as difficulty in discussing sensitive topics and demonstrating empathy could influence therapeutic relationship, medical errors, and screen fatigue resulting in increased levels of burnout14, 15.
A compromised professional identity and reduced job satisfaction are considered among significant predictors of job burnout16, 17. It is, therefore, reasonable to question whether the increased screen time and reduced patient contact could have impacted the professional identity of our cohort and their job satisfaction. This could also provide possible explanation for our cohort scoring highly for low personal accomplishment. However, one study that examined burnout in medical residents, who had used virtual telemedicine to replace outpatient clinics, found that the burnout actually decreased with increased use of virtual consultations18. Therefore, more consideration and research needs to be conducted on telemedicine practices in different medical subspecialties and their impact on medical professionals’ working lives.
Burnout is associated with an increase in clinical errors and may manifest in irritability, fatigue, and reduced cognitive functioning that ultimately result in a reduction in quality of patient care12,19. Medical errors on the other hand cost the National Health Service (NHS) £3.3 billion in litigation costs and additional bed days due to both systemic and individual factors20. Overall, 41% of our cohort were dissatisfied with remote consultations and the care provided to their patients during the pandemic. The reported difficulties with providing good patient care primarily consisted of poorer quality of and reduced patient interaction, patients being unable to engage with services and delayed treatments.
Wearing face masks could affect both verbal and non-verbal communication that in turn hinder the therapeutic relationship, as previous research has shown that patient engagement, understanding and treatment success are influenced by a clinician’s facial expressions21. Poorer patient outcomes found in our study could partly be due to the difficulties experienced during the pandemic as approx. 62% of our cohort felt that face masks affected their rapport with patients. Other factors that could have contributed to these poorer outcomes include redeployment of staff due to NHS pressures and reduced services. Further work is, however, needed to ascertain the associated casual pathway.
During the height of pandemic, carrying out frenetic clinical work with limited resources and little respite, coupled with the loss of loved ones and colleagues, could have undoubtedly impacted the mental health of medical workforce including psychiatrists. On the other hand, the pandemic may have also heightened the sense of vocation for some doctors. It is, therefore, difficult to assess the lasting effects of burnout until the pandemic is finally over and we resume normal therapeutic practices, in both clinical and personal settings.
There is considerable evidence for the benefit of simulation among foundation year doctors.1 Simulation training delivered during the 2 years has tended to focus on the management of the acutely unwell patient, procedures and practical aspects of delivering medical care, such as DNAR discussions, breaking bad news and capacity assessments.2-5 However, to date, there has been less focus on the benefits of developing more complex communication skills that may assist foundation year doctors in dealing with patients with mental health diagnoses or needs. These skills may include performing risk assessments, managing the agitated patient and forming initial management plans for patients in medical settings with mental health problems. This is important, as people with mental health needs have a higher burden of physical morbidity and are hence likely to be encountered in acute care settings.6
Since Health Education England’s Broadening the Foundation Programme report in 2014, there has been a surge in the number of foundation trainees working in psychiatry.7 The development of complex communication skills was an expected natural outcome of these rotations.8 However, this has not always happened – foundation trainees on a psychiatry rotation have stated that they are often recognised only for their medical skills, and that assessment and management was predominantly senior-led.9
Taking this into account, we set out to develop a simulation-based complex communication skills programme available for all F1s and F2s based in the North Central and East London Foundation School. Our focus was on the development of the transferable skills in communication and management that would be useful for dealing with patients with mental health diagnoses in a medical setting.
METHOD
Following a pilot study in 2018, funding was secured for 2019 from Health Education England to run half-day simulation sessions to foundation trainees in complex communication skills and the management of common mental health presentations to primary and secondary care settings.
Half-day sessions took place in hospitals in North and East London hospitals. A total of 121 foundation year doctors took part in the sessions; a breakdown of this can be seen in Table 1. All sessions took place between May 2019 and March 2020.
Table 1: Participants by Site and Year
Year
Region
Site
Cohort
Number of trainees
2019
North London
Whittington
FY1 & FY2
9
Royal Free
FY1 & FY2
11
Barnet
FY1 & FY2
8
East London
Homerton
FY2
16
Homerton
FY1
14
Royal London
FY1 & FY2
3
2020
North London
Whittington
FY1 & FY2
19
East London
Homerton
FY1 & FY2
33
Whipp’s Cross
FY1 & FY2
8
Facilitators
Each simulation group had one facilitator who offered feedback to participants. Facilitators were consultants, higher trainees and core trainees from the North and East London deaneries.
Session organisers
A session organiser was present at every session. They delivered the introductory briefing for participating doctors, provided a briefing for the actors, time-kept and held a feedback session at the end.
Venues
Four half-day sessions were run in North London, and five half-day sessions were run in East London. Three sessions were cancelled due to too few doctors registering to participate, and a further session was cancelled due to COVID-19.
Scenarios
Participants were presented with six scenarios in each session (Box 1), covering presentations in a range of settings: acute general hospitals, accident and emergency, general outpatient clinics and general practice. The sessions required skills in history taking and management when interviewing patients with complex communication needs.
Box 1 Scenarios
1. Attempting to de-escalate an elated patient with manic symptoms and explain the need for a physical medical examination
2. Conducting a risk assessment and liaising with the psychiatric team regarding a patient who has attempted suicide and taken a paracetamol overdose
3. Assessing a patient with drug-seeking behaviour requesting a benzodiazepine prescription
4. Conducting a capacity assessment in a depressed patient who is refusing carers following a recent myocardial infarction
5. Managing an agitated patient with antisocial personality disorder who is experiencing chest pain
6. Assessment of a patient with a likely eating disorder and formulating a preliminary management plan
Timing
Each session lasted 3 hours. Scenarios were 20 minutes each, with 10 minutes for participants to complete the set task, and 10 minutes for feedback from the facilitator, actor, and other participating doctors.
Data collection
Quantitative data
Foundation doctors were asked to complete pre- and post-session anonymous feedback forms, to ascertain their level of confidence in four domains (see Box 2): Participants were asked to rate their confidence level on a Likert scale from 1 (strongly disagree) to 5 (strongly agree) for each of these components.
Box 2 Quantitative data statements
“I feel confident in assessing patients with mental health diagnoses”
“I feel confident in making initial management plans for patients with mental health diagnoses”
“I feel confident in performing initial risk assessments in a medical setting”
“I feel confident in dealing with agitated patients in a medical setting”
Post-session feedback forms also included three questions, asking if anything could have been done differently about the day, if anything was done well, and a white space for any other comments.
Qualitative data
Qualitative data was recorded in the form of the written feedback documented post session and cross-checked by three members of the organising team.
Moderations to 2020 model
Minor changes to the format of the programme were made in August 2019, following presentation of interim findings to Health Education England. These were based on feedback generated from doctors and facilitators and are shown in Table 2. The logistics of the set-up on the day, scenarios, methods of feedback collection and analysis of data remained the same as in 2019.
Table 2: Moderations to 2020 Model
Feedback from 2019 Sessions
Updates made to 2020 Sessions
Title for the sessions ‘Psychiatry Communication Skills’ may have discouraged foundation trainees who were not interested in a career in psychiatry
Title changed to ‘Complex Communication Skills’
The sign-up process for foundation trainees required simplification
Foundation trainees were able to book onto the session via a centralised system, which also enabled their attendance to be tracked
Difficulties with room availability
Medical education managers contacted early in the academic year, with centralising to larger, well-equipped sites, improving room availability
Some trainees were less incentivised to attend with sessions held late in the academic year
Sessions held earlier in the academic year
Low trainee/facilitator numbers, limiting the ability to run scenarios simultaneously
Sessions centralised with the aim to run 2 sessions in North London & 2 sessions in East London
Clarity of brief needed on capacity assessment scenario
Slight amendments to scenario made with
input from old age psychiatry consultant,
including more details on occupational
therapy assessment in the doctors’ and
actors’ brief
RESULTS
Quantitative data
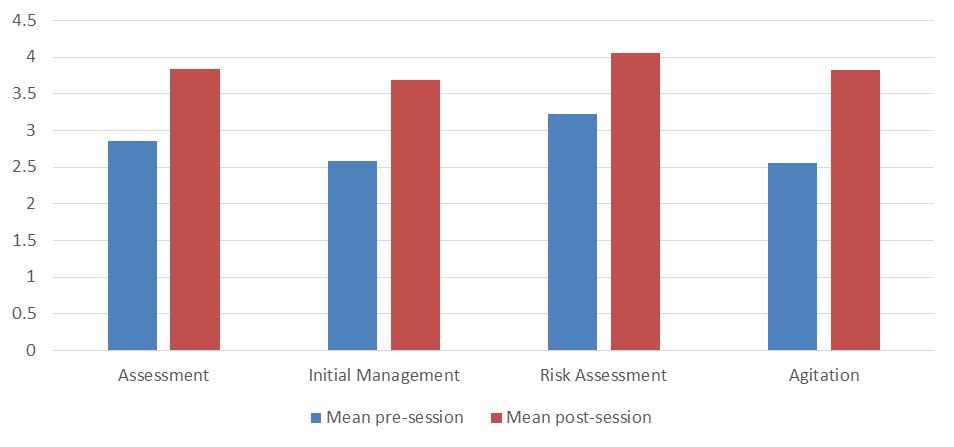
Results showed a consistent increase in confidence across all domains following participation in the simulation session. Increases ranged from 0.83 (“I feel confident in performing initial risk assessments in a medical setting”) to 1.27 points (“I feel confident in dealing with agitated patients in a medical setting”).
Figure 1: Trainee confidence pre- and post-session by domain
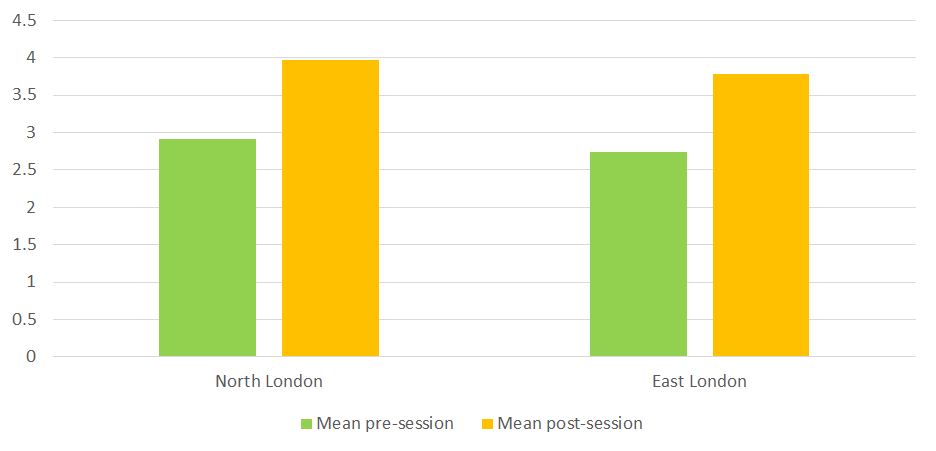
There were consistent increases in overall confidence ratings at every site, ranging from 1.03 to 1.25. Similar increases in overall confidence were observed in North London (1.04) and East London (1.06).
Figure 2: Trainee confidence pre- and post-session by region
There was a 94% (n=114) completion rate of pre-session feedback forms, and a 91% completion rate (n=110) of post-session feedback forms.
Qualitative data
No changes were made to the themes following cross-checking for validity.
Thematic analysis of the free text in the post-session questionnaires generated the following themes, as below.
Quality of the stations
Trainees consistently reported positive experiences regarding the quality of the scenarios (48), actors (43), feedback (30) and facilitators (20). In particular, there was a good breadth of scenarios, they were realisticand pitched at an appropriate level. Feedback was constructive and individualised.
“enjoyed how challenging and how true to life the scenarios were”
“right level of difficulty. Took me out of my comfort zone!”
“really good to have an agitated patient as it was a very challenging scenario”
“quite clever to have capacity assessment in somebody with capacity because it’s harder in some ways!”
Five trainees would have liked to have had more scenarios, and three suggested that it would have been useful for the facilitator to have demonstrated a ‘model’ example of a scenario at the end of the session.
Environment/logistics of the circuit
General comments included that the circuits were well organised, and that there was a comfortable atmosphere for giving and receiving feedback. Eight trainees commented that the group size was too big (all were attendees at the Homerton session in 2020, which was the largest session run with 33 trainees in attendance).
Preparation of candidates for the circuit
Ten trainees (seven in 2019; three in 2020) said they would have liked clearer briefings or objectives for the scenarios – two trainees specified that this was in relation to the capacity assessment station.
DISCUSSION
Our results suggest that simulation training involving actors with mental health diagnoses can help foundation year doctors build confidence in their approach to such patients in a medical setting.
The greatest increase occurred in participants’ confidence in dealing with an agitated patient. It is likely that participants felt the most anxious about this prior to and during the session. Thus, they were able to gain a more immediate sense of progress in this domain by being able to practice this in a ‘safe space’ and after being able to see a visible de-escalation of the patient during the station. Participants also valued receiving supportive feedback from the actor, facilitator and their peers.
Participants also demonstrated large increases in confidence with respect to formulating initial management plans. This was the domain trainees were second least confident in prior to the session. It is likely that some trainees would be anxious about whether they have enough clinical knowledge when formulating an initial management plan for mental health patients. The chance to practice this in a controlled setting, with pertinent feedback, appears to have bolstered confidence.
Results were consistent between sites, suggesting that the content of the course, the experience of being in the roleplay itself, and the chance to receive feedback from experienced clinicians were of the most importance to participants, and local variations in delivery did not impact on participants’ experience to a great extent. The wide participation among foundation trainees in North and East London (121 trainees across two regions of London, over nine simulation sessions) suggests that there is a demand for such sessions and there might be an unmet need across other deaneries.
Qualitative data analysis showed positive feedback relating to the quality of the actors, the facilitators and the scenarios themselves. This likely contributed to the trainees reporting that the simulation was realistic and pitched at the right level, hence they were able to find benefit from them.
Limitations
There was a large difference in the number of participants enrolled in each session (three in the smallest, 33 in the largest). This will have given rise to a difference in experience between these participants, with the smallest group being able to partake in all six scenarios, and the largest group only being able to partake in one. This may have meant that those undertaking all six scenarios may have been exhausted by their experience, whereas those undertaking one may have felt that they did not get enough opportunity to practise. Confidence scores between these two groups were relatively similar, but it is unclear whether there would have been a difference if they were of similar size.
Linking of pre- and post-session feedback questionnaires to the respective trainees would have also enabled testing for statistical significance. A paired t-test could have been used to assess the increase in confidence observed by our simulation sessions in each domain.
This study tracked changes in confidence among foundation year doctors following a simulation session, but it did not assess the impact on their actual practice. This would be important to ascertain, to see if the session has allowed foundation year doctors to build on their experience of assessing and managing mental health patients in a medical setting. As a result, a cohort of participants has been selected for future contact regarding this to determine the potential impact on their clinical work.
Clozapine is an atypical antipsychotic, it is the treatment of choice for treatment resistant schizophrenia and more effective than conventional neuroleptic medications. Clozapine is associated with potentially life-threatening side effects, some of which appear early in treatment.
Myocarditis is an uncommon but serious early adverse event of Clozapine, the majority of reported cases occurring in the first 4-8 weeks.1 Clozapine induced myocarditis (CIM) can present with mild symptoms, but can progress rapidly to fulminant symptoms and thereafter heart failure and death.1 These symptoms and signs typically include dyspnoea, palpitations, chest pain, fatigue, flu-like symptoms, pyrexia and tachycardia.
Case Report
A 21-year-old Caucasian male with a two year diagnosis of schizophrenia and previously inadequate responses to Risperidone and Olanzapine was commenced on Clozapine. The patient had previously tolerated Risperidone and Olanzapine and did not experience adverse events, but there was inadequate therapeutic response to both; hence it was decided to commence Clozapine.
On admission, his physical examination, baseline blood investigations (these did not include cardiac markers such as troponin or C-reactive protein (CRP)) and electrocardiogram (ECG) were normal. His medical history was unremarkable and he did not have a family history of cardiac disease. He smoked 15 cigarettes per day.
A rapid Clozapine titration compared with the standard UK titration[2] was commenced with a target dose of 200 mg/day on day 14. He was not on any other psychotropic medication.
The patient remained asymptomatic in the first 3 days. On day 4, he developed tachycardia (114 BPM). A repeat physical examination and ECG was normal, eventually his heart rate settled to 94 BPM. The tachycardia was deemed to be a benign side effect of Clozapine, and the rate of titration was slowed down as a precaution.
On day 12, the patient reported dizziness when standing and a ‘cold air’ sensation in his chest. Nurses reported that blood pressure was normal with a heart rate of 145 BPM but when reviewed clinically his heart rate was 89 BPM. His titration was continued.
On day 14, the patient complained that his ‘internal organs were hurting’. His Clozapine dose was 125 mg/day at the time. He reported chest tightness with central pain, pain in his legs and abdomen, intermittent breathlessness and palpitations. The duration of his symptoms was 24-36 hours. Examination was normal except for a heart rate of 110 BPM. His ECG showed sinus rhythm with no ST segment or T wave changes. Blood tests showed markedly elevated troponin I—1211.5 ng/L (normal range: <34.3 ng/L), CRP—176 mg/L (normal range: 0-10 mg/L) and eosinophil count —1.28 109/L (normal range: 0.02-0.5 109/L).
The patient was afebrile throughout the titration period.
He was admitted to an acute hospital and a provisional diagnosis of Clozapine induced myocarditis was made. The echocardiogram did not reveal structural abnormalities or damage. An EBV (Epstein Barr Virus) serology was negative. Clozapine was withheld and the patient improved along with the blood markers, after 4-5 days he was discharged back to the psychiatric hospital.
Discussion
CIM is an often overlooked adverse event associated with Clozapine titration. Currently there is no mandatory requirement of laboratory monitoring for detecting myocarditis during Clozapine titration unlike the mandatory requirement for detecting neutropenia, despite roughly similar estimated incidence of the two adverse events at 3%.[3,4]
This case was unusual because of the very early appearance of symptoms, the patient’s age and atypical symptom presentation. Although CIM is an early adverse event, the onset within 2 weeks of initiation was unusual. Literature suggests that myocarditis typically presents within 4-8 weeks.[1] The patient was also younger than the reported median age of patients (30).[1] The symptoms appeared at a low dose of 125mg/day which literature suggests is unusual, although CIM at doses of 50mg/day has been reported.[5]
Tachycardia and fever are common early side-effects of Clozapine. Tachycardia usually settles after 4-6 weeks of treatment[6] and fever typically for 2-3 days.[7] Both symptoms can be suggestive of myocarditis, especially when they co-occur. CIM often presents in a non-fulminant form.[8] As this case demonstrates many patients may not report symptoms when CIM is mild.
Increasing age, concomitant administration of sodium valproate and increased rate of dose titration are significant risk factors for CIM.[9] In this case, the patient was young and sodium valproate was not co-administered. The titration was originally intended to be rapid but slowed down soon after commencement.
Given the clinical difficulties in detecting mild CIM, we suggest that all patients have baseline troponin, CRP, heart rate, blood pressure, temperature, resipatory rate and ECG. If medical history reveals history of heart disease, a baseline echocardiogram can be obtained. If there is history of congestive cardiac failure, then baseline brain natriuretic peptide (BNP) or N-Terminal pro-B-type natriuretic peptide (NTproBNP) should be measured.[10]
In clinically asymptomatic patients, if there is elevated baseline CRP (>100 mg/L), troponin, BNP or NTproBNP then Clozapine titration should not commence and further advice from cardiology should be sought.
Weekly CRP and troponin should be done in the first month of titration and levels repeated once after stable dose of Clozapine is reached. The dose increase should not be rapid.
Tachycardia developed should be checked with reference to the baseline heart rate measured before commencing Clozapine. A heart rate of greater than 120 BPM or increase of more than 20 BPM over the baseline pulse rate should lead to the review of physical health, blood monitoring, ECG, and Clozapine titration rate.
An increase in troponin above upper limits or an increase in CRP should trigger consideration of CIM. Literature suggests that troponin levels greater than 2x the upper normal limit are indicative of acute myocarditis.[9] CRP is raised on average 3 days before any increase in troponin levels is detected.[9] If the troponin levels are within the normal range and the CRP levels are raised but less than 100 mg/L, clozapine titration can continue, but the pace must be slowed. Troponin levels and CRP levels should be monitored daily and the patient should be closely monitored for clinical signs of developing cardiotoxicity.
We do not recommend routine eaosinophil monitoring as the marker in 90% of cases does not exceed normal limits at the onset of CIM and typically peaks 7 days after cessation of Clozapine.[11]
Conclusion
Clozapine induced myocarditis often presents with low level cardiotoxicity. Mild symptoms may be missed; however, progression to fulminant myocarditis can be rapid, with high mortality rates.[1] Myocarditis, including clinically asymptomatic myocarditis remains a risk with Clozapine every time the patient is titrated onto this medication[12]. Close clinical monitoring, high index of suspicion and monitoring of cardiac parameters will help early detection of adverse cardiac events.
Depression and osteoporosis are two extremely common comorbidities in geriatric patients. Each have their associated mental and physical impacts on the patient, and economically on the wider healthcare system. Staggeringly, up to 39% of frail patients suffer with depression.1 Selective serotonin reuptake inhibitors (SSRIs) have long since been used in the management of depression and anxiety states and are one of the fastest-growing classes of drugs prescribed. Their use is not without the potential for negative effects; their side effect profile includes nausea, anxiety, insomnia, sexual dysfunction and gastro-intestinal upset, with the impact on bone mineral density (BMD) being controversial.
Statistics from the International Osteoporosis Foundation (IOF) reveal that in 2015, 6.8% of men and 21.8% of women over the age of 50 had osteoporosis. The estimated lifetime risk of hip fractures for women over 50 is 17.2%, with fracture-related costs at 5.3 billion pounds in 2017.2 Osteoporosis is a progressive, systemic skeletal disorder characterised by loss of bone tissue and disruption of bone microarchitecture, that leads to increased bone fragility and consequently an increased risk of fracture. As well as increasing age and female sex, other well documented risk factors for reduced BMD include early menopause, alcohol use, corticosteroid use, smoking, sedentary lifestyle, low body weight, impaired eyesight, and recurrent falls. What is more, depression itself cannot be overlooked as a risk factor for osteoporosis.
The mechanism by which depression leads to lower BMD is by that of alternation of the hypothalamic-pituitary-axis system, resulting in hypercortisolism. Cortisol is a well-known factor in bone loss. Proinflammatory cytokines have been implicated in depressive disorders, and they may directly stimulate osteoclastic activity.3 What must also be considered is the impact that depression has on certain lifestyle choices such as the potential for increased alcohol and nicotine consumption, inadequate nutrition and low physical activity.
The presence of serotonin receptors, neurotransmitters, and transporters have been found within osteoclasts and osteoblasts.4 95% of serotonin is synthesised in the gut and cannot cross the heteroencephalic barrier. Gut derived serotonin reduces osteoblast proliferation, thereby leading to bone loss. Brain derived serotonin signals to the ventromedial hypothalamic neurones leading to decreased sympathetic output and therefore favours bone formation by action on the beta-2 adrenergic receptors on the osteoblasts. It appears that with shorter duration of use, decreased bone resorption predominates, and with longer term use, bone loss outweighs.4
The impact of SSRIs on bone health has long since been the subject of research, with a possible link with both increased risk of fractures, and reduced bone mineral density being identified. In response to emerging evidence, the MHRA issued advise to healthcare practitioners, stating that we “should be aware of epidemiological data showing a small increased risk of fractures associated with the use of TCAs and SSRIs, and should take this risk into account in discussions with patients and in prescribing decisions”, yet this has not yet filtered down to prescribing guidelines.5 The National Institute for Health and Care Excellence (NICE) guidelines state that on choosing the antidepressant to prescribe, healthcare practitioners must consider that there is currently no evidence to support using specific antidepressants for specific physical health problems.6
We therefore present a case of recurrent depressive disorder in a patient with a background of osteoporosis. We also include a review of the most up-to-date literature, with the aim of increasing awareness of the impact of SSRIs on bone health for fellow prescribers. We aim to highlight the difficulties we face as clinicians whilst there are no formal recommendations regarding the use of SSRIs in high risk populations.
Case Description
This 78-year-old was referred to our services in late 2019 with low mood and loss of motivation. She lives alone following the death of her husband 3 years ago and sadly has no family. She has a past medical history of depression, hypertension, acute pericarditis, subclinical hypothyroidism, hiatus hernia, cataracts, previous cholecystectomy, and osteoporosis.
She was diagnosed with osteoporosis in 2000. At that time, she had been seeing an osteopath due to back pain, who advised her to see her GP to investigate for arthritis or osteoporosis. She has a family history of osteoporosis on her mothers’ side. She was diagnosed by Dual-Energy X-ray Absorptiometry (DEXA) scan, with osteoporosis at the lumbar spine and pelvis, at which time she was started on calcium supplementation.
She was initially started on oral alendronic acid but developed reflux symptoms, so this was discontinued. Over the following years she was tried on various medications for bone protection but sadly developed side effects. Briefly, pamidronate infusion caused iritis, and nausea was reported whilst on sodium ranelate. Later she was to be commenced on sodium risedronate, however did not start this due to concerns she had following reading the information leaflet. Denosumab was discussed as the next suitable option, however she was undergoing dental work including tooth extraction and so this has been delayed due to the risk of avascular necrosis of the jaw.
DEXA scanning in March 2019 showed a T score of -0.8 at the neck of femur, -4.5 at the forearm, -1.3 at the total hip, and -4.2 at the spine. This had, unsurprisingly, worsened from her last DEXA in 2016 (-3.6 at the spine). Her risk of major osteoporotic fracture was last calculated at 21.6%, with the risk of hip fracture 11.5%. She has had no falls or fractures to date since her diagnosis.
Other than Adcal-D3 she is now no longer on bone protection. Her current medications also include levothyroxine, ramipril, bisoprolol, cetirizine, fluticasone nasal spray, and Hypromellose eye drops.
She had initially been started on citalopram by her GP which she had discontinued herself after a period of weeks as she felt it had no positive effect. In December 2019 she scored 92/100 on the Addenbrooke’s Cognitive Examination (ACE-III), with no significant deficits in any one category. As well as low mood and loss of motivation, she described frequent tearfulness, anhedonia, lack of energy, difficulty concentrating and poor sleep. There was no clear trigger for her current mental state, and her physical health was otherwise good. She had no suicidal ideation or thoughts of self-harm. There was some evidence of anxiety but no symptoms of psychosis. We could not identify any alcohol or substance use risks. Her mental state examination was unremarkable. She was given the diagnosis of moderate depressive episode, F32.1, and was started on sertraline. However, upon reading the patient information leaflet, she refused to start this medication due to it mentioning a link with bone disorders.
As a result of this discussion, we accessed the medicines.org patient information leaflet, where an increased risk of bone fractures is mentioned under the heading ‘symptoms that can occur when treatment is discontinued’. It also states that following clinical trials in adults, sertraline was found to cause ‘bone disorder’ in up to 1 in 1,000 people.7
Following in-depth discussions, our patient was very hesitant in agreeing to take any medication that may have an impact on her bone density. We were aware of the potential association between SSRIs and BMD but were unable to quantify this risk to our patient.
Discussion
Our case above represents a common situation; a patient that is worried about a side effect, concerning which there are no formal guidelines available to aid decision making. The link between depression, SSRIs and BMD is a complex one, with numerous confounders making analysis and application yet more difficult. We looked at the evidence surrounding SSRIs and their impact on bone health, in order to suitably advise our patient on the most appropriate treatment options.
Impact on BMD
We found several meta-analysis and systematic reviews concerning BMD. The majority showed no significant association between BMD and SSRI use.
Of note, a 2015 systematic review by Gebara et al, suggested that antidepressant use may well be associated with lower BMD. 4 of the included studies assessed the relationship with BMD, 3 of which highlighted an association with lower BMD. This association was reported with SSRIs but not TCAs. However, they concluded that there was insufficient evidence that SSRIs adversely affect bone health, and therefore a change in current recommendations for the use of antidepressants in older adults was not justified at the present time. They stated that the evidence did not satisfy the Bradford Hill criteria, it is inconsistent, and whilst there is biological plausibility, there are no experimental studies to support a causal relationship.8
Yet a 2012 literature review indicated effects on both BMD and fracture risk.9 Each and every study included, indicated a risk of reduced BMD, increased fracture risk, or both. Even when controlling for potential confounders this conclusion was drawn. Authors suggested on the basis of this evidence, that caution is advised when considering the use of SSRIs in those with osteoporosis or a history of osteoporotic fractures, despite there being no formal recommendations.
A 5-year longitudinal study involving 1988 women, 319 of which were using antidepressants, measured femoral neck BMD. A dose-response increase in bone mineral loss was evident.10 An older cohort study also showed that even after adjustment for potential confounders, mean total hip BMD decreased 0.47% per year in non-users, compared with 0.82% in SSRI users.11 A year later, and a community-based study revealed that after controlling for age, weight, height and smoking history, BMD among SSRI users was 5.6% lower at the femoral neck, 6.2% lower at the trochanter and 4.4% lower at the mid-forearm than nonusers.12
Fracture Risk
The evidence surrounding fracture risk is more unanimous. Of the systematic reviews and meta-analyses we found, all highlighted an increased risk of fracture in SSRI users.
Wu et al concluded that the significantly higher risks of fractures observed for patients who received SSRIs compared with patients with no exposure, remained statistically significant in studies that controlled for important risk factors and studies that scored highly in the quality assessment.13
Eom et al extrapolated their data, estimating that the increased risk of fractures translates to about one case of fracture for every 42 patients treated with SSRIs.14 The dose and duration of SSRIs also seems to contribute to fracture risk, with both an early increased risk (under 6 weeks), and a late risk associated with prolonged use.14,15
A notable literature review by Panday et al on medication-induced osteoporosis summarised that treatment decisions concerning SSRIs should be considered on an individual basis for patients with osteopenia, osteoporosis, or fracture risks greater than 3% and 20% for hip and major fractures respectively.16 Of particular note from this review, a 10-year cohort study revealed that 14.7% of SSRI users suffered at least one fragility fracture over the study period.17 Whilst those using SSRIs do tend to have more fracture risk factors than the general population; they are more likely to be women, have more comorbidities, use other antidepressants/ anxiolytics, and have a previous history of falls; the significant association remained even after these variables were controlled for. The risk of first fracture specifically was increased by more than 50%, and similar to other studies, a dose–response relationship was evident.17
Conclusion
The impact of SSRIs on bone health is clearly a topic of contention. Whilst the impact on BMD is unclear, the increased fracture risk is more unanimous. There are plausible biological mechanisms to explain these risks, yet there is also the fact that the risk of falls themselves are higher when taking SSRIs.
Yet why hasn’t this filtered down to making formal recommendations in prescribing guidelines? Questions remain as to whether we should be prescribing SSRIs in individual’s with osteoporosis at all. Regardless, the relatively high risk of fracture with SSRI use may have a significant clinical impact. These risks must be balanced against the benefits gained by the treatment for depression; both in terms of mental state and in osteoporosis risk factor modification. What would perhaps be more relevant would be to consider a patient’s falls risk independently to their bone health, when deciding whether to prescribe SSRIs. Consideration towards the use of concomitant medications, co-morbidities and other confounders is vital.
It is on this basis that we suggest discussing bone health with your patients (particularly those at high risk), prior to prescribing these medications, and being wary of prescribing SSRIs in those with osteoporosis or more importantly, those at high risk of falls.
Summary
Impact of SSRIs on bone health is complex with significant confounding factors
Whilst the impact on BMD is contentious, the increased fracture risk is more significant
Risk-benefit decision is needed
Consider the patients falls risk most importantly before prescribing an SSRI
Insomnia is a disturbance of normal sleep patterns. It is characterised by sleep onset latency and/or sleep maintenance. Short term insomnia is defined as having symptoms for less than four weeks, whilst long term insomnia is symptoms lasting more than four weeks1. Hypnotics can provide relief from the symptoms of insomnia; they do not treat any underlying cause.
Several hypnotic agents are licensed for the treatment of insomnia, including the benzodiazepines and Non-benzodiazepine hypnotics (Z-drugs)2.
NICE guidance for Insomnia management states “After consideration of the use of non-pharmacological measures, hypnotic drug therapy is considered appropriate for the management of severe insomnia interfering with normal daily life; it is recommended that hypnotics should be prescribed for short periods of time only, in strict accordance with their licensed indications” 1.
NICE guidance also advises to use the lowest effective dose of the hypnotic agent for the shortest time frame possible. The exact duration will depend on the underlying cause, but treatment should not continue for longer than two weeks. We should also inform the patient that further prescriptions for hypnotics will not usually be given, ensure that the reasons for this are understood, and document this information in the patient’s notes.
Side effects are common with hypnotic usage including, most importantly, the development of tolerance and rebound insomnia. Other side effects can occur such as daytime sedation, poor motor coordination, cognitive impairment, hallucinations, anxiety, delusions and sleep disorders2.
Aims
To reduce the amount of hypnotic medication being prescribed to patients on an Acute Inpatient psychiatric ward in the Northwest of UK. The ward is in a semirural psychiatric hospital and is a Male ward containing 17 inpatient beds. The patients are 18 years old onwards with varying diagnosis including Generalised Anxiety Disorder, Bipolar Affective Disorder, Schizophrenia, Depression, and patients with mental and behavioural disorders due to psychoactive substance use.
The reason for doing this project was most importantly for improving patient safety by reducing unnecessary prescriptions and therefore administration of hypnotic medications, but also to reduce NHS expenditure and carbon footprint.
Inclusion criteria
Patients who have been an inpatient on the selected ward between the 09/12/2020-20/01/202 and 28/01/2020-10/03/2020.
Intervention
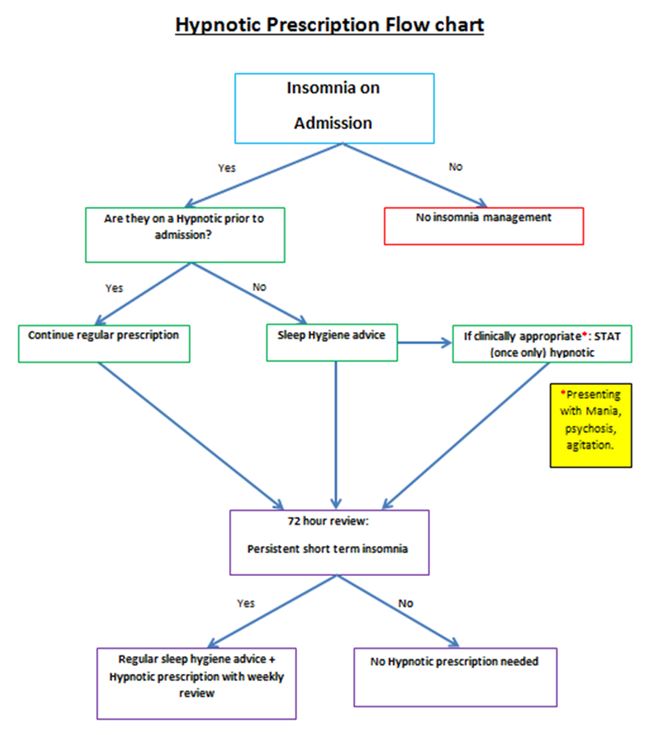
We developed a prescription aid flow chart (Appendix 1) for all newly admitted patients to the ward. This will guide doctors when making the decision if a hypnotic prescription is warranted.
All patients on the ward during this intervention period, who are currently on a hypnotic agent and are not newly admitted, will have their hypnotic prescription reviewed using the flow chart (Appendix 1) at their weekly consultant ward round.
We then decided on some interventions to fulfil our aims. The interventions were as follows:
1) Development of an educational presentation about Insomnia and sleep management.
2) Development of an Insomnia management Flow chart (Appendix 1) to be used at admission point.
3) Training sessions for ward staff.
4) Shared teaching programme with patients at their sleep management sessions.
5) Face to face and E-mail correspondence to inform medical trainees about this project.
6) Gather feedback from ward patients and staff before and after this project.
The Hypnotic prescription flow chart aid (Appendix 1), has been put on the ward office notice board, the clinic room and the On Call Doctors Room. It was also e-mailed out to the regular ward doctors, as well as all on-call doctors working during the intervention period.
As discussed above, we created an educational PowerPoint presentation entitled “Insomnia and hypnotic agents”. This included insomnia definitions and types, NICE guidance on insomnia, sleep hygiene advice, the medications used for insomnia, their mode of actions, side effects, cautions and cost of these medications. We also included our new hypnotic prescription flow chart aid (Appendix 1).
From the 21/01/2020-27/01/2020 we had two of these educational training sessions. This was to ensure that all staff working on this ward attended at least one of these sessions. Staff in attendance included the ward managers, nursing staff, health care assistants, the pharmacist, a junior doctor, and the ward consultant. This was very important as all these health care professionals are involved with the management of patients on the ward, and those suffering from insomnia. We felt that this session was vital as we wanted to ensure that all the staff knew the importance of this project and could raise their own concerns and issues that they have with regards to managing patients with insomnia. This proved to be very useful as we all brainstormed and voiced some realistic ward changes that could happen on an inpatient psychiatric ward. We also acknowledged that sleeping on the ward as an inpatient can often be disturbed, due to regular nursing checks and noise from the staff and other patients. We did however discuss some feasible interventions which included:
1) The time at which all the automatic ward lights are turned on in the morning could be delayed.
2) Caffeine –free coffee/tea available only after a particular time in the evening.
3) Discourage daytime napping.
4) Have regular sleep-hygiene sessions on the ward.
Between 28/01/2020 to the 10/03/2020 we started these interventions, and this is the time period for collection of our next six weeks of data. We had multiple patient group sessions on sleep hygiene during this time led by the occupational therapist. Other health professionals assisted with this, including the ward pharmacist and the junior doctor. During these sessions we asked for patients to give their feedback on the current management of insomnia on the ward. Some responses included:
· One patient with Severe Generalised Anxiety Disorder stated that he feels that the sleep hygiene advice is helpful, as he doesn’t like to “jump straight into taking tablets” and likes to “fix the root” of his sleeping problem.
· A second patient with a diagnosis of Mental and Behavioural Disorder due to use of cannabinoids, stated that he needs both sleeping medications and sleep hygiene advice, as sometimes he still cannot get to sleep on the ward by solely using relaxation methods.
· A third patient with Generalised Anxiety Disorder stated that he found the sleep hygiene sessions useful. He is now using relaxation methods and is trying to avoid daytime naps which are both helping with his sleep. However, he still on occasions struggles with sleep. He said it is important to have a tidy, clean and relaxing sleeping environment, which is sometimes difficult to implement on the ward.
Appendix 1
Results:
Data was collected prior to any intervention on the ward between the dates 09/12/2020 and 20/01/2020.
The table below (Table No.1) includes the type and number of sleeping tablets prescribed on the ward between the dates 09/12/2020 and 20/01/2020. The total number of patients treated from 9 December 2019 to 20 January 2020 were 28 and the total number of patients were prescribed hypnotic medication during this time were 14.
Table No.1 - Hypnotic medication prescribed:
Name
dose
Number of tablets
Zopiclone
7.5mg
191
Zopiclone
3.75mg
12
Zolpidem
10mg
4
Nitrazepam
5mg
7
Temazepam
10mg
10
The table below (Table No.2) includes the number of hypnotics prescribed and administered after the interventions mentioned above. The total number of patients treated from 28 January 2020 to 10 March 2020 were 25 and the total number of patients who had prescribed hypnotic medication were 11.
Table No. 2- Hypnotic medication prescribed:
Name
dose
Number of tablets
Zopiclone
7.5mg
96
Zopiclone
3.75mg
6
Zolpidem
10mg
0
Nitrazepam
5mg
0
Temazepam
10mg
0
With our ward interventions we have significantly reduced the amount of hypnotic tablets being administered. The total number of tablets administered during this 6 week period was 102. The total number of patients who were prescribed hypnotics was 11. Prior to our interventions the total number of tablets administered between 9th December 2019 and 20th January 2020 was 224 and 14 patients in total were treated. This demonstrates a 44.5% reduction in tablets which is significant.
Discussion
The total reduction in tablet administration was very significant with a 44.5% reduction post-intervention. This demonstrates the positive change in our clinical practice that has resulted from using the flow chart aid (Appendix 1) as well as patient and staff educational and feedback sessions. This will improve patient safety by reducing the risk of side effects. The risk of patients developing tolerance to hypnotic medications has been reduced, as well as reducing those being discharged on a regular prescription which will further improve long term expenditure of hypnotic medications for the NHS. With the changes that have occurred in our clinical practice, we have reduced the number of hypnotics being unnecessarily prescribed and administered.
Over prescribing/unnecessary prescribing is an issue within the NHS and is impacting negatively on the environment. The NHS constitution states that the NHS is ‘committed to providing the most effective, fair and sustainable use of finite resources’3. By reducing the number of inpatients being unnecessarily started on hypnotic medications, another positive from this project will be the reduction in the negative pharmaceutical impact on the environment. The number patients being discharged with hypnotic medications, who may no longer need them, due to their insomnia improving when they are discharged from the inpatient setting will also improve. Furthermore, if they are unnecessarily started on a hypnotic prescription as an inpatient, they may continue this prescription regularly and become tolerant, which will inevitably have an undesirable effect on the environment.
The feedback that we received from the educational insomnia teaching sessions also proved to be very useful. As stated above the staff sessions allowed us to brainstorm simple ward-based interventions, as well as discussing possible drawbacks which may result. This allowed us to modify the flow chart so that it worked for all staff effectively.
The feedback given from patients was also very encouraging. As health professionals we sometimes overlook how some patients want and need more involvement in making decisions on aspects of their care. Ensuring patients are informed about medications prior to prescribing, especially about side effects is something that is very important and allows patients to make informed decisions which is a more holistic approach to clinical practice. This is vitally important prior to prescribing any medications but especially medications with more severe side effects which some hypnotics have.
The patient educational sessions were a key part of this project. We gathered feedback and established that the patients involved found these sessions informative. Some, but not all, of the sleep hygiene advice was feasible to implement into their daily routine on the ward. The ward can be disruptive at night, due to other patients, or due to regular staff checks in patient rooms, as well as rooms not being familiar surroundings, were two of the difficulties raised from the patients. This is something that we appreciate can’t be changed, however with the interventions that can be feasibly made on the inpatient psychiatric ward, we continue to strive to implement and improve for patients. For these reasons both the staff and the patient educational sessions should be continued and proved a vital part of this project
Following on from this initial intervention, we feel that we can continue to make further changes and expand the changes we made on this ward, to other similar wards in our hospital and to other inpatient psychiatric wards in the Trust.
The Royal College of Psychiatrists and NICE Guidelines both stress the importance of carrying out physical examination on psychiatric in-patients due to their high level of physical health issues. Carrying out and carefully documenting these physical examinations at the time of admission allows physical health issues to be appropriately taken into account when creating management and medication plans and, in more severe cases, to allow diversion for medical treatment if that is required or the underlying cause of the presentation.
Monitoring physical health of patients in psychiatric settings is vital and is recommended by NICE in its guidelines; documentation of physical health assessment carried out at the right place is also imperative. According to Louth/Meath Mental Health Services Admission Policy, 2016, all psychiatric patients admitted should have their Physical Examination completed and recorded on Physical Examination Proforma.
Psychotropic medications can effect on physical health of psychiatric patients1. Patients with medical co-morbidities are more at risk from psychotropic medications compare to normal healthy population2. In addition, depression is considered as an independent risk factor for cardiac events in patients with coronary artery disease3. Adding that, depression may also possibly increase the risk of cardiovascular disease in population without medical co-morbidities. Hence, psychotropic medications are carefully chosen for treatment of individual patients to avoid any adverse events1. Depression is not the only risk factor for medical co-morbidities; other psychiatric problems also make patients vulnerable for physical health issues1. Moreover, prevalence of medical problems is relatively high in psychiatric patients compared to cohorts without mental health disorders4. The risk of medical co-morbidities do not always increase after prescribing psychotropic medications; the risk of cardiovascular disease also increases for patients suffering from anxiety and not necessarily using medications5.
Psychiatric patients receiving psychotropic medications should have their physical health monitored regularly as recommended by NICE6.
Methods
The audit cycle was completed in St Brigid’s Complex, Ardee. The audit cycle comprised initial audit (phase 1), implementing changes following recommendations and re-audit to compare results with initial audit. All patients in Unit 1, which is an acute admission ward, were included for the audit and re-audit. Patients admitted in another ward, which is a long stay ward, were excluded in the audit cycle. The rationale for not including patients admitted in long stay ward was that these cohorts of patients are already well established on psychotropic medications and their physical health is regularly monitored. Data collection was carried out from physical health proforma completed upon admission and filed in notes. No patient identifiable data was collected during the audit cycle.
During phase1, a review of the notes of all in-patients on a specific day in Unit 1, St Brigid’s Complex, Ardee was carried out. Data was collected from physical health proforma of each patient. This data was then entered in Xl-spread sheet for the analysis purpose. Results were analysed and feedback obtained from non-consultant hospital doctors. The findings were presented during local teaching to both the consultant and NCHD bodies and means of improving compliance were discussed openly. These discussions led to a redesign of the proforma to make it shorter and simpler to complete. This proforma was then attached to an assessment booklet, whereas physical health proforma was not part of an assessment booklet. A re-audit was carried out during a single day on all in-patients in Unit 1 several months after the first phase of the audit. In-patients who remained in Unit 1 since the initial phase of the audit were excluded from the re-audit.
Results
The results of initial audit demonstrated only 50% (10/20) compliance with physical health proforma. Furthermore, in phase 1 the proformas were only partially completed with elements of the physical exam documented on the proforma. In addition, other components were documented elsewhere in the admission notes and many elements omitted altogether. Only 15% (3/20) of the proformas contained a complete, documented physical examination.
One of the sections on proforma that lacked information significantly was information about patient’s current circumstances. On the other hand, demographic details were recorded for only 50% of patients. However, admitting doctor’s details were recorded on 35% (7/20) of proformas, the details of professional carrying out physical information was also not available on large number (19/20) of proformas.
Table 1:
Yes
No
Partial
Patient Demographics
10
10
0
Date & Time of Admission
6
11
3
Referral Agency
7
13
0
Admission Status
8
12
0
Drug Allergies
6
14
0
GP Details
7
13
0
NOK Details
3
17
0
Religion
1
19
0
Marital Status
2
18
0
No of Children
2
18
0
Occupation
2
18
0
Nationality
3
17
0
No of Previous Admissions
1
19
0
Medical Card No
0
20
0
V.H.I
0
20
0
Provisional Diagnosis
6
14
0
Admitting Doctor Name
7
13
0
Admitting Doctor Signature
7
13
0
General Examination
9
11
0
CVS
9
11
0
R.S
9
11
0
C.N.S
9
11
0
Alimentary System
6
14
0
G.U.S
3
17
0
L.M.P
1
19
0
Signature
1
19
0
Date
8
12
0
Data analysis of the re-audit shows that 80% (16/20) of the proformas were been completed. In overall, there was a huge improvement seen in the results of the re- audit and doctor’s details performing physical health was recorded on 75% of the proformas. Adding that, general examination section of the proforma demonstrated huge compliance of 80% along with Cardiovascular and Respiratory system.
Table 2:
Yes
% Yes
No
% No
Name
12
60%
8
40%
DOB
10
50%
10
50%
General Examination
16
80%
4
20%
CVS
15
75%
5
25%
R.S
15
75%
5
25%
C.N.S
14
70%
6
30%
Alimentary System
14
70%
6
30%
G.U.S
14
70%
6
30%
L.M.P
6
30%
14
70%
Signature
15
75%
5
25%
Date
15
75%
5
25%
Discussion
A total of 20 patients in each phase of the audit were included for data analysis. The number of patients included may seem small for a research study with a different design; however, quantitative number is not taken into account with this particular design used. On the other hand, number of patients admitted in any acute ward is similar.
During data collected, it was apparent that physical examination findings were recorded in the notes instead and proforma was not used for some of patients, which is evident through results. Even though physical examination may have been carried out, it was not possible to include in data analysis and results due to the study design.
The results of first phase demonstrated poor compliance with physical health proforma despite carrying out physical examinations and findings been recorded elsewhere in admission notes. It is an arguable fact that regardless of physical health proforma been filled, physical examination of patients are been carried out as per local and NICE guidelines. However, physical examinations documented elsewhere in the admission notes makes it difficult to locate; hence, a proforma is completed upon admission as a pre agreed standard procedure.
Once the results of initial audit were analysed, these results were presented in the local academic session to all the NCHDs and Consultant Psychiatrists. While all involved agreed the importance of carrying out physical examination on all patients upon admission; the design and complex nature of the initial proforma made very difficult for NCHDs to complete it. Adding that, some of the information, such as demographic details and personal information, was also repeated making it duplicate that had been recorded elsewhere in the notes. The physical health proforma was then redesigned and simplified to complete. Unnecessary and duplicate information was omitted in the new proforma and was attached with the initial psychiatric assessment booklet. The new physical health proforma was then implemented in the service after discussions with fellow NCHDs, Consultants and management.
Second phase of the audit cycle was conducted after number of months and redesigned physical health proforma been in circulation for some time. Data was again collected as per study design and methods and entered for analysis. These results demonstrated a huge improvement in compliance with physical health proforma after the change of practice. Although compliance with proforma has improved significantly, some gaps were noted to reach the desired outcome of 100% in practice. Case notes were studied to understand the reasons for not completing physical health proformas. Several themes emerged through case note reviews and one of the reasons was assumed that patient was transferred from medical ward of General Hospital after been medically cleared. Time and mode of admission also resulted in physical health proforma not been completed.
Conclusion
While all involved agreed that carrying out physical examination on all admissions was advisable; the length and complexity of the initial proforma contributed to poor completion rates by NCHDs. A combination of teaching to underline its importance and a redesign focused on usability and speed led to significantly increased completion of the proforma with attendant benefits for patient assessment and treatment.
Parkinson’s disease (PD) is the second most common neurodegenerative disease. It is associated with loss of dopamine leading to motor disorders 1. However, non-motor symptoms such as anxiety, stress, and depression as well as cognitive impairment are also abundant among patients 2. It has been hypothesized that non-motor symptoms can affect the quality of life in PD patients 3. The current therapeutic approach relies on dopamine substitution, which has no curative effect and does not improve non-motor symptoms. Studies have shown that meditation and other relaxation techniques can provide relief in non-motor symptoms. Mindfulness-based stress reduction (MBSR) is a technique used for improving stress-related symptoms in long-term conditions such as stroke, cancer, and PD 4-6. It involves focused attention, open monitoring, and self-awareness of body movements in a non-judgemental state in the present moment. Studies have shown that mindfulness improves brain plasticity in some areas of interest. The areas of plasticity are involved in emotional regulation and processing 7, 8. Thus, we hypothesized that mindfulness techniques could also have a positive effect on non-motor symptoms of PD patients which can enhance the quality of life after training sessions. This clinical trial aimed to investigate the impact of mindfulness training on the quality of life of PD patients.
Materials and Methods
Participants and Ethical issues
This randomized clinical trial was conducted at the neurology outpatient clinic of Imam Reza and Razi University-Hospital. Participants were 40 patients aged 67.95 ± 6.8 years (56-80) with a definite diagnosis of PD who were receiving dopaminergic drugs for at least one year. Twenty-seven of the patients were males, and 13 were females. They all were married, and 4 of them reported a family history of PD. Participants were randomly categorized into two experiment and control groups with 20 patients in each. For randomization, a list of random numbers was used based on the computer program and applied to the patients at the time of their neurologist visit at the clinic.
The inclusion criteria were: definite diagnosis of idiopathic PD based on UK Brain Bank criteria, mild and moderate forms of disease according to Hoehn and Yahr (HY) staging (1-3), stable and normal dosage of PD medications within last six months, normal cognitive function or mild cognitive impairment according to Mini-Mental State Examination (MMSE) score 17-30, enthusiasm and commitment to participate in mindfulness training sessions and to practice the required works at home.
The patients with the following criteria were excluded: focal neurologic deficit, abnormal brain imaging findings suggestive of brain lesions, other medical conditions that would affect the quality of life, use of antiepileptic drugs and symptoms of psychosis,
The protocol of the study was reviewed and confirmed by the local ethics committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1397.551). All patients received an informed written consent to participate in the study and to the use of their information. This trial was registered on the IRCT.ir website (IRCT20181007041258N1).
Mindfulness Training sessions
The interventions included 8-week mindfulness-based stress reduction (MBSR) sessions each for 2hours with a 15-minute break between the first and second hours. The sessions followed by a one-day retreat program between sixth and seventh sessions and took for 7 hours. The patients were asked to practice the requested homework at least for 30 minutes after each session. The protocol of the training sessions was conducted as per the steps described by Kabat-Zinn 9. The sessions were performed by a psychiatrist with over 5-year of experience in MBSR instructions. The instructions were based on the teaching of three techniques: body scanning, mindfulness meditation, and gentle yoga. The sessions focused on physical and mental awareness of body, how to diminish the physiological effect of pain and stress, how to perform less emotional reaction when facing distress, mental calmness in challenges through life, non-judgmental awareness, equity in stress management and joy of every moment.
Controls
The patients in the control group received eight 1-hour sessions during the same time as the experiment group. The sessions centered on basic information about PD based on brochures published by the American Parkinson Disease Association with topics: medications, symptoms of the disease, mood and sleep, and connecting with resources.
Assessments
All participant's general data, regarding age, gender, type of medication, and duration of disease were gathered according to patients' self-report and the information documented in patients' clinical records. Two neurologists assessed the HY stage, disease severity, and probable motor disturbance at baseline (within patient recruitment within one week before the initial session). The assessments of the quality of life were conducted at baseline (on the day of the first training session before the class), and after the experiment.
For the evaluation of the quality of life, the PDQ-39 questionnaire was used. PDQ-39 is a 39-item questionnaire based on the patient report of health status. It evaluates eight scales of daily activities including Mobility (MOB), Activities of daily living (ADL), Emotional well-being (EMO), Stigma (STI), Social support (SOC), Cognitions (COG), Communication (COM) and Bodily discomfort (BOD) and how these scales are being affected by PD. Participants are required to choose one of five orders of responses based on how often due to their disease, they have faced difficulties defined in each item. The final score of each item is calculated as a percentage score. The overall score is measured by calculating the mean percentage score of eight items as Parkinson`s disease summary Index(PDSI). The assessments were conducted in-person by the principal investigator (N.Gh) who was blinded about the group of study which patients were enrolled in.
Statistical Analysis
The scores of each item were described as mean ± SD. The between-group and within-group comparisons were made by the independent and sample T-test, respectively. The chi-square test was performed for the comparison of categorical variables. To investigate the change in the quality of life each PDQ-39 item scores and the PDSI scores were compared before and after the experiment in either control or experiment group by splitting the data into two study groups and comparing the mean scores of each item using independent T-test. All the analyses were performed using SPSS software version 19.0 (IBM Corp., Armonk, N.Y., USA). The boxplot figures were drawn using medCalc.ink software. Figures of the change in questionnaires' scores were provided by GraphPad.prism v.6.0.7 Ink software.
Results
All the 40 patients completed the training sessions in 8 weeks. The primary assessment was made after the last MBSR session and during their first neurologic visit at the clinic.
The general characteristics of the patients in each experiment and control group are shown in Table 1. The baseline characteristic data did not differ significantly between the two study groups.
As it is demonstrated in Table 2, at baseline, the PDQ-39 item scores did not differ significantly between two study groups, except for the SOC score, which was significantly higher in control subjects compared to the experiment group (35.80 ± 9.7 vs 29.11 ± 8.7, p = 0.02).
Quality of life assessment
The statistical analysis revealed a lower mean score in all PDQ-39 items in the experiment group compared to control subjects; however, the difference was insignificant for MOB, ADL, EMO, STI, COG, COM, and BOD and was only significant for SOC (34.13 ± 9.7 vs 26.19 ± 7.7 for control and experiment group, respectively. P = 0.007) (Table 2).
On the other hand, the within-group analysis yielded a significant improvement in the mean score of subjects in the experiment group. Their mean PDSI score was 31.88 ± 6.5 after one month compared to the baseline score of 33.93 ± 6.2 (p < 0.001). However, the mean scores of the participants in the control group did not significantly differ from the baseline.
A comparison of the delta values between the experimental and control groups showed MOB, ADL, and EMO to be significantly different.
The classification of the patients based on the stage of disease by HY revealed a significant improvement in PDSI score in patients in the experiment group at the severe stage (III). In contrast, the PDQ-39 item scores did not significantly differ (except for the ADL) after the training for mindfulness. The analysis also showed that patients in milder stages (I) have significant improvement after the experiment. However, the same improvement was noted in the control group (Table 3).
Table 1. Patients' demographic data in each study group
Table 2.PDQ-39 score items and PDSI before and after the mindfulness sessions in control and experiment group pf patients
Before Experiment
After Experiment
P ϯ value
95% CI €
The mean difference in score
Study Group
Mean Score
P* value
Mean Score
P* value
Delta
P* value
95% CI €
MOB
Control
47.87 ± 8.7
0.84
48.50 ± 8.4
0.62
0.26
-1.7 – 0.5
0.62 ± 2.4
0.02
0.24 – 3.28
Experiment
48.37 ± 6.8
47.23 ± 7.5
0.04
0.04 – 2.2
-1.14 ± 2.3
ADL
Control
34.72 ± 12.3
0.90
34.95 ± 13.8
0.47
0.75
-1.7 – 1.2
0.22 ± 3.2
0.004
1.11 – 5.60
Experiment
35.17 ± 10.8
32.04 ± 11.1
0.002
1.3 – 4.9
-3.13 ± 3.7
EMO
Control
37.41 ± 6.3
0.56
37.21 ± 7.0
0.43
0.83
-1.8 – 2.2
-0.23 ± 4.3
0.01
0.78 – 6.65
Experiment
38.92 ± 9.4
34.96 ± 10.4
0.001
1.7 – 6.1
-3.95 ± 4.7
STI
Control
25.94 ± 9.9
0.26
25.29 ± 10.2
0.26
0.47
-1.2 – 2.5
-0.65 ± 4.0
0.97
-2.24 – 2.18
Experiment
22.81 ± 7.3
22.18 ± 6.8
0.33
-0.6 – 1.9
-0.62 ± 2.7
SOC
Control
35.80 ± 9.7
0.02
34.13 ± 9.7
0.007
0.10
-0.3 – 3.7
-1.67 ± 4.3
0.40
-1.71 – 4.20
Experiment
29.11 ± 8.7
26.19 ± 7.7
0.01
0.6 – 5.2
-2.91 ± 4.8
COG
Control
28.43 ± 7.4
0.69
28.75 ± 7.9
0.15
0.71
-2.0 – 1.4
0.31 ± 3.7
0.09
-0.47 – 5.47
Experiment
27.60 ± 5.9
25.41 ± 6.3
0.08
-0.3 – 4.7
-2.18 ± 5.3
COM
Control
29.14 ± 9.9
0.47
29.97 ± 9.5
0.88
0.32
-2.5 – 0.9
0.83 ± 3.7
0.08
-0.36 – 5.35
Experiment
31.21 ± 8.0
29.54 ± 8.7
0.16
-0.7 – 4.0
-1.66 ± 5.1
BOD
Control
44.71 ± 11.2
0.08
43.05 ± 11.2
0.12
0.04
0.6 – 3.2
-1.66 ± 3.4
0.47
-3.11 – 1.46
Experiment
38.31 ± 11.9
37.47 ± 10.9
0.32
-0.9 – 2.5
-0.84 ± 3.7
PDSI
Control
35.50 ± 7.1
0.46
35.23 ± 7.5
0.14
0.29
-0.2 – 0.8
-0.27 ± 1.1
< 0.001
0.84 – 2.72
Experiment
33.93 ± 6.2
31.88 ± 6.5
<0.001
1.2 – 2.8
-2.05 ± 1.7
Note:Abbreviations:Confidence Interval (CI), Mobility (MOB), Activities of daily living (ADL), Emotional well-being (EMO), Stigma (STI), Social support (SOC), Cognitions (COG), Communication (COM), Bodily discomfort (BOD), Parkinson`s disease summary Index (PDSI). ϯ: P value of the differences before and after the experiment in each group; *: P value of the differences between mean score of experiment and control group; €: 95% CI of the differences between mean score of experiment and control group.
Table 3. The quality of life in patients with different stages of PD before and after the mindfulness sessions in each experiment and control group
Control group
Experiment group
Stage (HY)
PDQ-39
Before Experiment
After Experiment
P value
95%CI of difference
Before Experiment
After Experiment
P value
95%CI of difference
I
PDSI
25.93 ± 2.1
24.62 ± 2.0
0.03
0.31 – 2.30
26.60 ± 1.8
23.34 ± 0.9
0.009
1.55 – 4.95
MOB
37.50 ± 0.0
37.50 ± 2.5
1.00
-6.21 – 6.21
40.62 ± 1.2
38.12 ± 1.2
ADL
23.61 ± 2.4
18.01 ± 2.4
0.06
-0.42 – 11.62
23.93 ± 7.1
19.72 ± 6.2
0.09
-1.24 – 9.66
EMO
29.13 ± 4.1
29.13 ± 4.1
29.15 ± 7.6
22.87 ± 7.9
0.10
-2.27 – 14.84
STI
18.75 ± 10.8
14.58 ± 3.6
0.42
-13.76 – 22.09
17.18 ± 5.9
17.19 ± 5.9
0.39
-0.03 – 0.01
SOC
22.20 ± 4.8
22.16 ± 9.6
0.99
-20.70 – 20.77
22.80 ± 8.0
20.70 ± 8.4
0.39
-4.58 – 8.78
COG
20.83 ± 7.2
22.91 ± 9.5
0.42
-11.04 – 6.88
27.07 ± 4.1
20.31 ± 5.9
0.08
-1.51 – 15.04
COM
24.96 ± 8.3
24.96 ± 8.3
27.07 ± 4.1
22.87 ± 7.9
0.18
-3.51 – 11.91
BOD
30.50 ± 12.7
27.73 ± 9.6
0.42
-9.13 – 14.67
24.97 ± 6.8
24.97 ± 6.8
II
PDSI
32.02 ± 4.0
31.48 ± 3.8
0.21
-0.38 – 1.45
31.36 ± 3.2
30.03 ± 4.0
0.12
-0.48 – 3.14
MOB
43.12 ± 4.5
44.37 ± 4.1
0.31
-3.98 – 1.48
45.62 ± 4.9
44.65 ± 4.8
0.41
-1.71 – 3.66
ADL
27.59 ± 7.3
28.11 ± 6.9
0.35
-1.75 – 0.71
34.34 ± 6.9
31.22 ± 8.6
0.11
-0.91 – 7.16
EMO
36.93 ± 6.0
36.88 ± 7.5
0.98
-4.91 – 5.01
37.46 ± 6.3
32.77 ± 6.0
0.06
-0.03 – 9.40
STI
23.43 ± 9.8
22.61 ± 10.0
0.32
-1.01 – 2.65
21.87 ± 7.4
21.09 ± 7.4
0.35
-1.06 – 2.62
SOC
33.30 ± 7.6
30.18 ± 6.1
0.08
-0.47 – 6.70
27.05 ± 8.6
24.96 ± 7.7
0.17
-1.14 – 5.31
COG
25.78 ± 6.1
25.78 ± 7.0
1.00
-2.79 – 2.79
24.21 ± 5.3
25.25 ± 6.2
0.35
-3.49 – 1.41
COM
23.93 ± 8.2
24.97 ± 6.3
0.34
-3.49 – 1.41
27.06 ± 7.3
27.05 ± 8.6
0.99
-5.24 – 5.27
BOD
42.05 ± 8.9
38.92 ± 6.5
0.08
-0.48 – 6.73
33.30 ± 7.6
33.30 ± 6.2
1.000
-3.70 – 3.70
III
PDSI
41.79 ± 3.6
42.09 ± 3.6
0.43
-1.14 – 0.53
40.18 ± 3.1
37.99 ± 3.3
0.001
1.19 – 3.18
MOB
55.55 ± 5.6
55.83 ± 5.5
0.59
-1.43 – 0.87
55.00 ± 2.9
54.37 ± 4.1
0.35
-0.85 – 2.10
ADL
44.77 ± 10.0
46.67 ± 10.2
0.03
-3.63 – -0.16
41.64 ± 11.3
39.02 ± 10.1
0.04
0.02 – 5.20
EMO
40.60 ± 4.5
40.18 ± 5.5
0.74
-2.42 – 3.24
45.26 ± 8.7
43.20 ± 8.0
0.10
-0.55 – 4.67
STI
30.57 ± 8.5
31.23 ± 8.2
0.61
-3.59 – 2.26
26.56 ± 6.4
25.78 ± 5.2
0.59
-2.56 – 4.12
SOC
42.55 ± 6.5
41.62 ± 5.9
0.34
-1.21 – 3.08
34.32 ± 6.9
30.17 ± 6.1
0.10
-1.09 – 9.39
COG
33.33 ± 5.4
33.33 ± 6.2
0.99
-3.39 – 3.39
31.24 ± 5.7
28.12 ± 5.7
0.17
-1.70 – 7.94
COM
35.15 ± 9.0
36.07 ± 9.2
0.59
-4.75 – 2.91
37.42 ± 6.2
35.37 ± 5.8
0.17
-1.12 – 5.22
BOD
51.82 ± 6.9
51.82 ± 6.9
49.98 ± 4.4
47.88 ± 5.9
0.17
-1.15 – 5.35
Note:Abbreviations:Confidence Interval (CI), Mobility (MOB), Activities of daily living (ADL), Emotional well-being (EMO), Stigma (STI), Social support (SOC), Cognitions (COG), Communication (COM), Bodily discomfort (BOD), Parkinson`s disease summary Index (PDSI)
Discussion
Significant improvement in the quality of life between the patients who received mindfulness training and the control group was observed in this clinical trial of people with Parkinson’s disease within eight weeks of trial.
Overall PDSI decreased modestly in the experiment group by 2.05 points and decreased in the control group by 0.27 points after the experiment.
Among the PDQ items, MOB, ALD, and EMO significantly improved in the experiment group compared to the control group. These results show that mindfulness training has a significant impact on not only motor symptoms of the disease but also the non-motor emotional wellbeing of the patients. The most significant effect of mindfulness training was on patients’ daily activity, which was also obvious in the severe cases of the disease.
Up to now, a few trials have been conducted on the effect of mindfulness training on PD 10-13. The effect of mindfulness on different features of motor and non-motor symptoms has been measured. However, the outcome was discrepant regarding the time duration of the follow-up and improvement in the measured symptoms.
Similar to our findings, Geong son et al. found a significant difference in the quality of life and ADL of 33 experiment patients who received mindfulness training in comparison to 30 control subjects 13. Some other studies found mindfulness an effective modality for a few subscales of PDQ-3911, 12.
In a clinical trial by Cash et al. 39 patients were enrolled in 8-week mindfulness sessions and their EMO and COG improved after the experiment11. In a similar study conducted by Advocat et al., the effect of mindfulness training on the quality of life in 35 PD patients was compared with 37 control subjects within seven weeks and six months. In a two-step analysis, ADL was the only improved factor in experiment group 14.
In contrast, Dissanayaka et al. examined the effect of mindfulness on fourteen PD patients in the 8-week training program and compared the results with baseline at post-intervention assessment and 6-month follow up 15. Their results did not yield a significant improvement in any subscales of the quality of life in primary and secondary evaluation. Similarly, non-significant results were reported by Rodgers et al. and Pickut et al. 12.
Birtwell et al. also assessed the long-term efficacy (16 weeks) of mindfulness training on STI and EMO in thirteen individuals with PD. They found an insignificant change in these two subscales of PDQ-39 16.
In the present study, EMO and ADL were more subjective to the short-term effect of mindfulness training. The results of Rodger’s et al. study were consistent with our primary outcome. Their between-group analysis revealed a significant difference in depression subscale of DASS-21 after mindfulness intervention in PD patients 17. Cash et al. also found depression to improve after mindfulness interventions in PD patients 11.
In contrary to our findings, the difference between PD experiment and control subjects was not meaningful in Pickut et al.'s study 12. COG was unaffected to mindfulness training in our study. This finding was supported by the clinical trial of Cash et al. They found an insignificant change in PD patients' cognitive function in immediate pots-intervention assessment 11.
On the other hand, Dissanayaka et al. found post-interventional improvement in PD patients' cognition by obtaining PD Cognitive Rating Scale (PDCRS), extended for six months 15.
Similarly, Geong son et al. showed a significant difference between experiments who received mindfulness training with controls in the mean score of Korean Montreal Cognitive Assessment 13.
As described above, there are discrepant results regarding the role of mindfulness stress reduction sessions on quality of life in PD patients. Our results were consistent with some studies and contrary to others. The main factors that might have affected these differences are the size of the sample, including a control group in the study, subjective mood changes in the patients, the severity of the disease, and the likelihood of practicing the Learned lessons at home.
Mindfulness-based interventions aim to improve the current wellbeing of the individuals by self-awareness of present emotions and body movements. It might also help individuals to manage daily stress, have a better judgment of their own, and adjust to daily life. There is also evidence suggesting that mindfulness training leads to neuroplasticity in the brain areas which are involved in emotions 18.
Studies have also suggested that early therapeutic interventions are more practical in terms of diminishing the probable severity of the disease in the future 13, 18. In our study, patients in the early stages had improvement in their overall quality of life, which was also noted in controls of the same stage, too. However, a meaningful change in the quality of life of patients at the severe stage of PD was recorded after the training sessions. We suggest a long term follow up of the patients in each group and with different stages of the disease to find if the mindfulness training would help in diminishing the progress of the disease.
This study was a pilot study in which MBSR showed a great impact in improving the quality of life in PD patients. However, there were limitations in the study that must be considered. First, the sample size of the study was not large comparing to the prevalence of the disease, and it was constrained by other important factors such as disease severity and level of education. Patients needed to have a minimum level of education to be able to attend the sessions and apply them in their routine life. Second, the psychological nature of the intervention limited the blindness of the patients to the intervention.
We did not perform an intention to treat analysis or crossover randomization as all the randomly selected patients completed the trial, and none dropped out of the clinical trial.
Conclusion
In our study, mindfulness training improved the overall quality of life in PD patients. However, long-term follow up on a large-scale population is required to evaluate the impact of mindfulness-based stress reduction on each item.
The creative process is an enigma; there are conflicting opinions about creativity and creative people. Research studies on creativity have produced contradictory results. The long-standing belief that creativity results from a strange clairvoyant state is still occasionally associated with psychiatric disorders. 1 Although a decline in creativity with aging indicates that it is biologically based, a relationship between creativity and psychopathology is overstated in both print and media. Reductionism tends to misconstrue creativity as a product of psychopathology. Nonetheless, whilst psychopathology can facilitate creativity, it does not produce creativity. The inspirational characteristics of creativity remain shrouded in mystery.
Methodological issues that include both a definition and an evaluation of creativity impede the research into creativity. These challenges make the correlations between the studies problematic, and they deliver opposing outcomes. Although there is no confirmed relationship between psychopathology and creative accomplishment, the search for such a relationship hinders our understanding of human potential and the deeper levels of consciousness. Early detection of creative talents in children might enable providing them with special guidance, thereby averting potential psychiatric problems.
The superficial reductionism of 20th century biological psychiatry compressed all mental phenomena, including creativity, into compact neurobiological compartments, and the only way to achieve this was to medicalise it. Any assumed correlations between creativity and mental disorders will be clarified only when we gain a greater understanding of the creative process. In cases where creativity and mental illness indeed coexist, a psychiatric understanding of creativity may provide insights into patient functioning and assist in defining both normalcy and psychopathology.
Whilst human beings have existed on this planet for millions of years, the technological advancements of the last few centuries transpired without any perceptible changes in the development of the human brain. Historically, our ancestors were drawing two-dimensional pictures until just a few centuries ago. No one has hitherto been able to explain this sudden burst of creativity. An expanded model of brain-mind-consciousness that can appreciate the wonder of creativity is needed.
Defining Creativity
Researchers have long been interested in a potential connection between creativity and mental illness. The major challenge here is to define creativity and establish measurable indicators. Creativity has been described as the process of bringing something new into existence. It involves the capacity to take unrelated structures and combine them harmoniously in different ways for new purposes. The creative mind is alert to unexpected connections. An individual with a rich reservoir of knowledge is regarded as intelligent, whereas an individual who uses that knowledge in an original and constructive way is considered creative. 2 The creative process is not fully understood; some even feel that a precise definition is unattainable.3 Nonetheless, creativity can be described as the process of bringing something new into being where the outcome is larger than the input received by the creative mind. 4,5 Creative individuals are sensitive to gaps in human knowledge and these voids act as catalysts in their search for solutions. This is the highest form of human adaptation; whether to a greater or a lesser degree, it may exist in all people.
The creative process can be likened to a four-stage computer process.6 If information processing and storage is the primary process, the second stage is the incubation or pondering phase, during which ideas germinate at a subconscious level. The third phase involves illumination, or flashes of insight, and the fourth is the period of elaboration during which the new idea is developed and tested. These stages can be additionally likened to the biological rhythm of conception, gestation, birth and infancy. This pattern is not strict. As a rule, the process of illumination is gradual with countless small bursts of insight, such as with Charles Darwin’s elaborations on his theory of evolution.
Dream processes shed some light on creativity. As with poetry, dreams are replete with visual and highly idiosyncratic metaphors. Dreams are the art of the unconscious; whilst dreaming, we tap into a creative source. The dreaming psyche has seemingly unlimited creative potential. An anecdote about Kekule, the chemist, recounts that he conceived the benzene ring after a dream in which he saw a serpent biting its tail.
The Creative Personality
Creative people must be assessed on an individual basis. Not all persons of superior intelligence are creative, and not all creative people have superior intelligence. Although creative potential is dependent on intelligence, actual creative achievement is independent of intelligence (e.g. one does not have to be tall to be a successful basketball player). Highly intelligent people are prone to self-criticism, which has an inhibiting effect on the development of creativity. A combination of high intelligence and special aptitudes appears to promote creativity. Unconventionality, egocentrism, flexibility, tolerance for ambiguity and a preference for complexity are among the attributes of creative individuals. 7 Psychological testing has shown that creative individuals are frequently more emotionally troubled than are non-creative individuals; however, they also have more ego strength for dealing with problems. Their personal qualities include imagination, persistence, perseverance, dedication and stamina. Creative children tend to be egotistic and gullible. This egotism provides them with the confidence to believe that they are capable of unique achievements, whilst momentary gullibility enables them to break through scepticism and into creativity.
McClelland illuminated a controversial notion when he described the creative individual as one who is characterised by competition, either with an external standard of excellence or with his or her own internal aspirations. 8 Driving absorption, the ability to ignore failure and adversity and tremendous curiosity are noted as a predictive set of personality traits.9Although creative individuals are difficult to live with, whether their creativity flourishes or not frequently depends on the support that they receive from others. 10 Among the characteristics of creative people, Tarlaci (2014) included openness to experimentation and change, rebelliousness, individuality, sensitivity, playfulness, self-assertiveness, curiosity and simplicity. 11
Although there is a compulsion for order, symbolisation and communication are at the core of creativity. Intelligence, domain-specific knowledge/expertise, motivation and adaptive traits such as openness, broad interests and self-confidence are closely associated with creativity (Feist 1999). 12 Despite the fact that these characteristics of creative people are obviously independent of psychopathology, they point towards better mental health. Research on creativity in neuroscience has revealed that creativity is associated with ‘ordinary’ rather than psychopathological brain processes.13
Psychopathology
Since the time of Plato, philosophers have debated a conceivable connection between creativity and psychopathology. He proposed a logical paradox when he stated that a poet does not know what he is going to write, and yet he cannot produce a poem if he has no picture of what he describes. As a Greek philosopher, Plato was a reincarnationist. He obviously solved his own riddle by attributing hidden creative knowledge to remembrances of a previous life and to springing from ‘Divine madness’. Aristotle noted the predisposition of great artists and poets to melancholia, but he perceived creativity as a rational process. Shakespeare repeated the older perspective through one of his characters who states, ‘the lunatic, the lover, and the poet are of imagination, all compact’. During the 20th century, systematic investigations into this relationship were unable to either support or refute this association. Cesare Lombroso failed to clarify this confusion in his book, Genius and Mental Illness. Nonetheless, his influence led to speculation that genius is an ‘ancestral gift’ transmitted in families in the same manner as mental disorders.
Recent empirical research has shown that creative individuals have a higher tendency towards psychopathology than those in non-creative professions. This propensity is expressed in personality traits, behaviours and experiences similar to those identified in clinically ill patients (Jamison 1989). The evidence has not clarified whether the psychopathology linked to creativity relates more closely to features of schizophrenia or affective disorders. Countless novelists and dramatists have family histories of psychiatric disorders. Severe personality deviations have been observed among visual artists and writers and possibly among thinkers and scholars as well. Jamison noticed mood disorders among writers and artists. 14
Bipolar disorder may be more frequent among creative individuals than in the normal population. One study reported a higher incidence of depression and bipolar disorder among creative people, and especially among writers.15Another study noted a higher incidence of depression and alcoholism among writers and artists. Following recent epidemiological studies with large samples, Kyaga et al. (2013) argued in favour of an association between professional authors and psychiatric disorders. 16 They illuminated familial associations between the creative professions and schizophrenia, bipolar disorder, anorexia nervosa and possibly autism. 16They noted that this association was more evident in cases of self-employed artists and less so in scientific creativity, where the subjects had passed through several professional screening procedures.
In another epidemiological study, Parnas et al. (2019) found that the relatives of academics have a significantly increased risk of suffering from schizophrenia or bipolar disorder. 17 In another study, they suggested that ‘creativity and an increased risk for mental disorders seem to be linked by a shared vulnerability that is not manifested by clinical mental disorders in the academics.’ 18 The literature has made significant connections between bipolar disorder and creative accomplishment, with much of the thinking inspired by biographical accounts of poets and musicians who presented with signs of bipolar disorder. 19 Studies by Burkhardt et al. (2018) suggest that, in persons at-risk for bipolar disorder, their mood swings are strongly associated with creativity, but whilst there is evidence of increased creativity, there is no evidence of higher creative achievement. 20
Observations of the bipolar mood domain identify a high prevalence of changes in intuition, empathy, appreciation of danger and predictive capacity. However, these changes do not necessarily include supra-sensory changes in the primary senses of smell, taste, vision, touch or hearing. Parker et al. (2018) suggested that clinicians should be aware of non-psychotic, supra-sensory phenomena in patients with bipolar disorder and that the identification of such features could explain the increased creativity evident in those with a bipolar condition. 21
After examining the life of Charles Dickens, Longworth and Carlson (2018) maintained that there was very little historical evidence for the suggestion that he experienced bipolar disorder. 22 However, they did suggest that he displayed characteristic bipolar symptoms. They also maintained that his childhood was an outstanding example of personal resilience and that his own story was just as fascinating, if not even more intriguing, than any of those that he had created. Their investigations concluded that Dickens’ story confirmed the connection between writers, creativity and mood disorders. Retrospective psychiatric assessment of historical figures and the slotting of these celebrities into biological compartments may be risky. Biographical studies of creative people are criticised for having possible recall, interviewer, selection and cultural sampling bias. 23
The suicide rate is high among artists, and this has been linked to manic depression. Adverse financial circumstances and disappointments due to the rejection of their artistic productions are sufficient to explain this apparently high rate. In contrast, musicians have a low suicide rate, very likely reflecting the healing effect of music. In addition to alcohol, opium has been a historical favourite addictive drug of writers, of which Charles Dickens is an example; opium addiction was partially responsible for his death. 24 Ludwig’s study on 1000 outstanding individuals found an upsurge in alcohol abuse in artists, especially writers. 25 Post (1994) found a similar result among prose writers and playwrights. 26 Although Ernest Hemingway, the Nobel Prize winner for literature, may be a good example of this phenomenon, he committed suicide later in his life. Creative individuals may be notorious for their alcohol and drug misuse; however, it is not clear whether drug induced psychopathology promotes their creative expression. Whilst it is possible that the disinhibiting influence of mild psychopathology and the judicious use of alcohol or drugs could facilitate creativity, this phenomenon has potentially contributed to the confusion in which psychopathology is described as the ‘producer’ of creativity.
Absence of Psychopathology
Alongside these studies, other reports glorify the mental health of geniuses and eminent individuals. The Stanford 35-year follow-up study of over 1000 geniuses, the MacKinnon study of creativity in architects and Havelock Ellis’s psycho-biographical study of eminent men all emphasised the absence of psychopathology among these creative individuals. 27
In an investigation on the prevalence of psychopathology, in a sample of 291 famous men, Post (1994) noted that they all excelled by virtue of their abilities, originality, drive, perseverance, industry and meticulousness. 26Even though most of them had unusual personality characteristics and minor neurotic abnormalities, all of the subjects in this study were emotionally warm, with a gift for friendship and sociability. Post additionally noted that, among creative individuals, scientists show the fewest psychological abnormalities. Functional psychoses are less frequent than epidemiology would suggest. Depressive conditions, alcoholism and possible psychosexual problems are more prevalent than expected in some professional categories, particularly among writers. Hare (1987) noted that banning stimulant drugs in sports did not lower the achievements significantly, and that the same should be true of creativity. Poetic vision has been equated with psychedelic experiences. 28 Creative activity has been observed to be at its highest level in patients who are moderately ill, and at its lowest level in groups identified as severely ill. 29
Although there is no significant difference in the incidence of psychotic illness among males and females, there is less creativity among the latter. If the hypothetical connection between creativity and psychopathology were valid, the incidence of creativity should be proportional to gender. Historically, unfavourable social pressures and opposing cultural factors have represented major explanations for the lower incidence of creativity among women. This disparity points towards the fact that creativity has to be nurtured and is not automatically generated by psychopathology. Despite an equal incidence of mental illness in men and women, there have been few female geniuses in any culture; this challenge the probability of a clear connection between psychopathology and creativity. The same argument may be used against a pure biological view of creativity; both men and women have the same biological make up, yet fewer geniuses have been identified among female population.
Psychodynamic Perspectives
Psychoanalysts have postulated dynamic psychopathologies for the creative process. Analysts incline towards seeing artists as neurotics and their productions as sublimations of sexuality and regression in the service of the ego. 30 They consider the motives for creative activity as impulses that compensate for dissatisfaction and as defences against depression. Some perspectives differ from traditional psychoanalytical ideas, emphasise the crucial role of synthetic ego operations and draw distinctions between psychopathology and creativity. 31Analysts suggest that novel ideas exist in the subterranean regions of the mind. Whilst the conscious mind has no access to these hidden areas in the normal state, it is easier for a disturbed mind to tap information from the unconscious or preconscious. 32 Sims suggests that the psychotic and the creative states are subjectively indistinguishable and that delusions arrive in the minds of the mad in the same manner that ideas drop into the minds of the creative.33In contrast,Slater and Meyer report only minor psychiatric disorders among creative people. 34Although it would appear that psychopathology does not preclude creative activity, it may release it. In general, the creative person enjoys conflict free intimacy with the preconscious and is a model of psychological health. 35
Orderly Mind
The neurobiological model of schizophrenia suggests that a deficit in the systems involved in information-processing could contribute to its symptomatology. 36It has been hypothesised that such a deficit could favour the creative association between information units.37Psychopathology linked creativity has even been associated with abstract disciplines such as mathematics. If these views were accepted, creativity and schizophrenia would be separated only by a ’neurological difference’. Andreasen challenged the hypothesis of a connection between creativity and schizophrenia.38He argued that the bizarre nature of schizophrenic experiences is far from original, and that the cognitive impairment of such patients inhibits their creativity.
The creative intelligent person experiences an attention surplus, whereas a schizophrenic patient suffers from an attention deficit. As a case in point, a creative child may figure out in two seconds what the teacher is going to say, after which he may be looking around, waiting for the teacher to finish and appearing as if he is not paying attention. In contrast, because of a failure in the normal filtering of stimuli, schizophrenics tend to make unusual associations that result from over-inclusive thinking in which countless disconnected elements are included in their reasoning. 39 Although higher cognitive individuals also demonstrate ‘pseudo over-inclusive thinking’, this is due to their capacity to conceive and utilise two or more contradictory concepts simultaneously.40
Bleuler (1950) described intellectual ambivalence as both characteristic of schizophrenia and as superficially similar to the janusian process of oppositional thinking that involves conceiving of two or more opposites simultaneously. 41 The Kent-Rosanoff word association test has been used to assess this process. 42 In contrast to the creative thinker who is fully aware of logical contradictions, the schizophrenic patient is unconscious of the contradictory nature of his or her utterances. For example, when Albert Einstein derived his theory of relativity, derived from the fact that a man falling from the roof of a house was both in motion and at rest, he was fully aware of the contradictory nature of his thinking. 43 Another example is Frank Lloyd Wright’s revolutionary design of Falling water, in which nature and interior space coexist. The janusian process was initially identified in highly creative writers, visual artists and scientists. The fluency of association observed among creative individuals can be mistaken for over-inclusive thinking. 44Since their brains process increased sensory input effectively without cognitive overload, creative individuals derive an advantage from their higher levels of associative thinking.
Contrary to popular belief, in their cognitive and conceptual style, creative writers resemble those suffering from the manic phase of affective disorders, rather than schizophrenics. However, whereas the over-inclusiveness of maniacs is based on bizarre associations, that of writers is due to an imaginative recognition of original associations. Whilst writers are capable of controlled flights of fancy, manic imaginations are bizarre and based on personalised reason. The racing thoughts of a creative intellect are productive, whereas those of the manic are destructive. Albert Einstein claimed that he discarded a new idea every two minutes.
Creative thinking is polythetic and should not be confused with flight of ideas. Schuldberg (1990) investigated the overlap between schizotypal and hypomanic traits and suggested that affective symptoms may be more important than primary process thinking in determining creativity within the general population. 45 The fluctuation of thoughts experienced by higher cognitive ability individuals can be mistaken for mood swings. Fink et al. (2014) challenged the connection between creativity and psychopathology and proposed that the domains of artistic and scientific creativity should be analysed separately. 46
Although the creative potential of autistic people has been recognised, they differ from over perceptive children in many respects. One fundamental difference is that the creative potentials of the latter are polythetic, whereas such potentials of the of autistic individuals are generally monothetic. A key diagnostic criterion for autism—restricted and repetitive behaviours and interests—combined with a small number of research studies, suggest that generating original ideas or artefacts may be challenging for autistic individuals. 47Nonetheless, a minority within this population has exceptional artistic gifts, and a wider group embraces activities typically associated with creative expression, including visual art, music, poetry and theatre.
A three-level multilevel meta-analytic approach investigated the relationship between creativity and schizophrenia. The analyses of Acar et al. (2018), with 200 effect sizes gathered from 42 studies, detected a mean effect size of r =−0.324, 95%CI [−0.42, −0.23]. 48When the analyses focused on the moderators, they found that the relationship between schizophrenia and creativity was moderated by the type and content of the creativity measure, the severity of the schizophrenia and the patient status. The negative mean effect size was firmer with semantic-category or verbal-letter fluency tasks than the divergent thinking or associational measures. They submitted that when these findings are analysed along with previous meta-analyses on the association between creativity, psychoticism and schizotypy, creativity and psychopathology appear to have an inverted-U relationship. Whilst a mild expression of schizophrenia symptoms may support creativity, a full demonstration of the symptoms challenges it.
Schizophrenia and schizotypy have frequently been associated with above average creativity; nonetheless, empirical studies on the relationship between schizophrenia spectrum disorders and enhanced creativity have generated inconsistent results. 49 Even though some mental processes may appear to be similar in creative and psychotic thinking, the current literature challenges this conclusion. 50,51,52Psychopathology does not play a role in the genesis of higher order creativity; nonetheless, the psychological defence mechanism of overcompensation goes some distance towards explaining the high achievements of mentally or physically disabled individuals.53
The Myth of Drug Induced Creativity
The belief that brain alone is the source of creativity led to the idea that altering brain chemistry could make people more creative. The truth may be that the gentle psychopathology created in the brain might serve as a facilitator of creativity rather than a producer of creativity. The psychopathology generated by the psychedelic drugs might help to open Aldous Huxley’s ‘doors of perception.’ Huxley (1954) proposed “Doors of Perception” to illustrate the enlightenment induced by LSD etc.54 Interestingly, such a proposal is close to Zizzi and Pregnolato’s depiction of ‘very fast switches from the quantum logic of the unconscious to the classical logic of consciousness’ (Zizzi & Pregnolato,2012). 55Those who glorify such drug induced creativity are unaware that long term substance misuse can only kill creativity as the ‘switches’ become permanently damaged and lead to psychopathological states.
When one’s sense of self is suspended and space-time sense dissolves, psychedelic experiences occur, and such experiences should not be confused for true mystical experiences. Psychedelic experiences are pseudo-mystical experiences. True mystical perceptions and cognitions relate to what is essentially ineffable, pertaining to the nature of existence rather than being limited to familiar objects that are intrinsic to everyday experience. The hallucinating drug user or alcoholic is functioning at the level of impaired consciousness, while the mystic is operating at a higher level of consciousness. Mystics have full awareness of their altered state of consciousness and they are also in a position to switch back to their ordinary mode of perception, unlike a hallucinating patient. It may be true that psychedelic experience has created an interest in artistic activity and the raw materials obtained in such experience may be useful in eventual artistic creation, but the psychedelic experience as such is not a creative experience because motor functioning is impaired during psychedelic experience and information flow to the hands and fingers are affected. 56 The natural state of a relaxed, happy, and well-adjusted person is more creative rather than the perplexed psychedelic state. There may be ‘psychedelic artists,’ but not psychedelic scientists indicating the difference in the creative process of scientific generativity and artistic.
Drug induced creativity is a conundrum that need serious clarification as many young people are trapped in such faulty perceptions. Cannabis is the most widely used illegal substance globally. Schafer et al (2011) suggested that cannabis produces psychotomimetic symptoms, which in turn might lead to connecting seemingly unrelated concepts.57Such divergent thinking is considered primary to creative thinking. They argue that a drug induced altered state of mind may indeed lead to breaking free from ordinary thinking and associations, thereby, increasing the likelihood of generating novel ideas or associations. But the harmful effects of cannabis use have been extensively evaluated.58,59,60,61,62,63Cannabis abuse is quite unlikely to generate any sustainable creativity-‘the creative Big Bang’ would soon end up as a big crunch.
If creativity is a neurological phenomenon, creative people should have additional neural pathways, but psychedelic drugs have not been proven to create such new neural pathways. Speculations about specific brain regions promoting creativity is of great scientific interest. Creativity involve an architect and a set of engineers. According to Amit Goswami, quantum unconscious domain is the architect and the real source of creativity if brain does the engineering works. 64 Psychoactive substances do not act directly on the quantum consciousness but may help to open the gates to the hidden dimensions of consciousness. When quantum views of creativity are given due significance, the neurologically based psychedelic promotional views of creativity crumble. If not having creative abilities is deemed as a ‘brain deficit,’ use of illegal drugs to promote creativity can be compared to using medications to treat ADHD. But only if we use the ‘brain disease model’ of psychiatry, the argument of ‘brain deficit model’ will hold water. It may be even true that psychedelic drugs may have a quick and transient destressing effect and that could promote a creative mental state, but the production of any direct creativity through the use of such drugs is questionable.
Problematic Childhood
Some children of superior intelligence attempt to mask their creativity by being over-talkative and overactive. Such children run the risk of being misdiagnosed as ADHD. Creative children frequently have a unique sense of humour that their peer group cannot appreciate. Creative children are every so often resented by peers because of crazy or unusual ideas and their forcefulness and passion in presenting them or for pushing their ideas on others. Their divergent thinking is not helpful in school examinations, which require convergent thinking, and this could explain the poor academic achievement of several geniuses. The divergent thought processes of creative children must be differentiated from inattention and underachievement. For example, a highly intelligent child might fathom out what the teacher is going to say next and become inattentive. Although creativity is associated with divergent thinking, this alone does not correlate well with creative achievement.65 Creative children overflow with ideas and play with new ideas and concepts. They are not motivated or even concerned about high grades and need individualized attention lest they might fall on the wayside. There is nothing more frustrating than being a creative intelligent and become underachieved.
Creative children demonstrate certain unusual traits such as daydreaming, wanting to work alone, sharing bizarre thoughts and conflicting opinions. These qualities will not please the traditional teachers and bring them in conflict with them and their lack of conformity to the classroom structure can be even confused with attention deficit hyperactivity disorder. Highly critical parents kill creativity; unfortunately, countless creative individuals have chaotic childhoods leading to psychological problems in their adult lives. Mismatching due to variation in I.Q could lead to mismatching with parents and siblings. Mother and father may be of average intelligence, but the child can be above average intelligence, and could cause mismatching leading to behavioural problems.
There is a special group of children around the world who have high intelligence and intuition, healing abilities, and a strong spirituality and they are grouped as Indigo people in appropriate cultures. It can be stated that Indigo is people with high sensitivity level, unique creativity, high intuition ability, healer, and people with their own charisma for those around. 66According to the proponents of these new ideas, these children are often mislabelled as having behaviour disorders. Little is known from scientific research about the Indigo phenomenon. Indigenous populations are familiar with Indigo-like children. The purpose of studying these children when they are adults is to better understand these children when they are older and advance behaviour health sciences by increasing awareness of the Indigo phenomenon and learning about their lived experiences. There has been hardly any serious scientific study on the Indigo phenomenon.
A phenomenological study looked at the lived experiences of 10 adult Indigos. The study explored the lived experiences of 10 adult Indigos on the island of Oahu, Hawai'i (> or = 18+ years old-7 females, 3 males; mean age = 52.4 + SD). 67 Through in-depth semi-structured personal interviews, the experiences of these adults were analysed and interpreted to identify the common experiences faced during childhood, what worked for their assimilation into society, and recommendations for parents, educators, and health professionals on how to work with Indigos. Bioenergy field photographs of each participant were also taken. Statements related to the phenomenon were placed into themes, coded, and categorized as the investigators reached a consensus of common themes. Seven primary themes and nine secondary themes emerged from the findings.
The primary themes were: grandmother/mother had a similar gift; guided by a higher power to heal self and others; felt 'different' or misunderstood; did not openly share their unique abilities; having challenges with partner relationships; history of abuse/violence or frequently disciplined; and use of intuition at work and/or school. Secondary themes included: Using Hawaiian and cultural healing methods; everyone has a degree of intuition and the use of intuition to know when to see a doctor or not; various unique abilities from body and multiple careers; mental health institutions, and financial struggle. Self-reports on participants' life purpose, their unique abilities, and being misunderstood were also collected. It was concluded that Indigos felt mislabelled or misunderstood throughout their lives despite their belief that their life purpose was to help humankind.
Academic psychologists are sceptical about Indigo phenomenon and argue that the phenomenon is a cover up to normalise the odd behaviour of children who could otherwise be included under the category of attention deficit disorder, attention deficit hyperactivity disorder, autistic spectrum disorders and learning disabilities. Health experts are concerned that labelling a disruptive child an "indigo" may delay proper diagnosis and treatment that could help the child or investigate the parenting style that may be causing the behaviour.
Inspiration and Perspiration
Creativity is regarded as the product of inspiration or creative imagination combined with meticulous, disciplined effort. The Edisonian perception of invention as 1% inspiration and 99% perspiration is explained by the hypothesis of interactive creativity; it assumes that the inspirational aspect has a paranormal component. In his thesis on interactive creativity, Laszlo supported his hypothesis with observations on cultural creativity. 68These observations included the collective advance of entire populations through the typical creative activity of their members and by documented incidents in modern science in which different investigators developed scientific insights simultaneously, without any known contact. 68 Early cultures developed similar 7tools; calculus was discovered simultaneously by Newton and Leibni and biological evolution was described independently by Darwin and Wallace. Similarly, Graham Bell and Elisha Grey both applied to patent the telephone on the same day. The Rubic’s cube was conceived simultaneously and designed both by Rubic and a Japanese inventor. Nylon was discovered in both New York and London, hence, the name NyLon.
Jung’s research into the phenomenon of creative synchronicity helped him to formulate his concept of the collective unconscious. Psychological disturbances may represent the consequences of creative endeavour and Jung (1973) considered them the price to be paid for persistent exploration of the unknown.69 Polayni (1994) suggested that scientific discovery is informed by the imagination and integrated by intuition, and vice versa.70 This statement is close to the Edisonian perception of creativity: If imagination is a property of the brain, intuition occurs in the unconscious realm. Whilst Laszlo’s views are not definitive, they indeed supplement our existing knowledge about creativity. The inspirational aspect can be better explained by an expanded model of brain-mind-consciousness, and Xavier suggests a para-psychodynamic.71
Biological Perspectives
Particularly gifted individuals have determined the evolution of civilisation. Karlsson (1984) commented regarding creative individuals: ‘Without their genes, men might still live in caves’. 72Nonetheless, countless gifted individuals have a very ordinary family background, with no ancestral history of creativity. For example, Newton came from an undistinguished family. Genetics researchers look for the biological roots of creativity, with some believing that the mind is reducible to chemistry. Whilst intelligence may be a trait that can be cloned, creativity may not be attached, and it may prove even more complex than genetic manipulation. Kelly et al. (2007) suggested that creative inspiration is akin to mysticism. 35
Responses to both dopamine inhibiting drugs and to the psychoses triggered by the drugs that increase dopamine activity underlie the dopamine hypothesis of psychosis. However, dopamine over-activity in psychosis should not be confused with dopamine fluctuations in creative individuals. Dopamine diminishes with aging, which may explain the decreasing powers of creativity after the age of twenty.73
The relationship between age and outstanding achievement has captured the attention of researchers into creativity.Whilst Lehman maintained the perspective that creative achievement has a curvilinear single-peak function for age, other researchers have described two separate age-peaks.74Outstanding contributions among mathematicians after the age of fifty are exceptions. The age-related observations support a biological basis for creativity.
Future Directions
Study of creativity is an important area of research where consciousness studies and psychopathology meet each other. Cognitive scientists have pondered over the link between psychopathology and creativity for a long time without making any firm conclusions and appear to be barking at the wrong trees. The very process of creativity ought to be explored before any progress in this area of research could be achieved and the current reductionist model of mind stands as a hindrance. The following suggestions may be helpful for future researchers.
1. Establish the psychopathology of psychotic disorders
2. Creativity linked genetic studies are warranted, biological correlates of creativity need further elucidation.
3. Expand the current model of brain-mind-consciousness complex so as to explain the inspirational element of creativity.
4. More longitudinal, international and multicultural studies recommended.
5. Given the affinity of psychosis-proneness to the artistic creativity domain,
studies should be focussing artistic creativity and scientific creativity separately.
Clinical Implications
The study of creativity has clinical implications: A) Psychiatric understanding of creativity provides a better picture of patient functioning that could assist in clarifying the definitions of both normalcy and psychopathology. B) Early detection of creative talents in children might help to give special guidance for such children and thereby prevent potential psychiatric problems. C) When they coexist, differentiating creativity and mental illness is useful: The former might require nurturing and the latter warrant clinical intervention.
Discussion
Whilst it is true that investigators have observed a high incidence of psychiatric symptomatology of an affective nature among creative writers and artists, it is debatable whether this relationship is causal, an effect or a contributory factor. The increased psychopathological states observed in artistic creative individuals suggest that art and science reflect two different arenas of creativity. The mechanism of generation of novel ideas may be identical in art and scientific creativity, but they are evaluated differently by the two groups resulting in different types of products. Creativity and mental illness can coexist, and the creative impulse has a therapeutic effect on the psychiatric condition. Creativity can be therapeutic for those who are already suffering from mental illness; creative art therapies applied in clinical and psychiatric settings report positive health-related outcomes. 75 Even in rare cases of psychopathology induced creativity, the individual will require highly developed intellectual protective factors. It is the disciplined portion of the mind that enables outstanding creative achievements. Creativity of the highest order is a product of laborious intellectual effort. When they coexist, psychopathology is a mediator, not the producer of creativity, and the creativity may be cathartic.
There is no scientific consensus regarding the association between psychopathology and creative achievement. The literature does not substantiate the high reported incidence of mental illness among creative people. It is possible that predispositions to mental illness and creativity tend to co-occur because they reflect an underlying personality and cognitive style predisposed to both creativity and mood disorder. The high reported incidence of mental illness potentially signifies an ‘occupational hazard’ and creativity stands independent of psychopathology. The normal creative person can swing back to reality from a transient ‘creative psychical shift’ (e.g. such as a diver who searches for diamonds in the deep sea and then returns to the shore). The sensitivity and intensity that facilitate creative expression may additionally make highly creative people more susceptible to depression.
Early investigations of geniuses were retrospective. Formal meta-analyses were not considered justifiable. All forms of creativity were mixed in the studies, without distinguishing the different domains of creativity. Most of the studies were confined to English speaking people, whilst creativity is a global phenomenon. A multiplicity of literature does not mean that the ideas expressed are established scientific truth. This is true of creativity, which may be as mysterious as creation itself. The prevailing model of the mind may be inadequate for a full appreciation of the creative process. It would be easier for a ‘camel to pass through the eye of a needle’ than to explain creativity from a reductionist perspective. The inspirational component of creativity continues to be an enigma. It is my contention that creativity is essentially an inner, psychic phenomenon. We do not have even an approximate model of the brain-mind-consciousness complex, let alone know the true aetiology of schizophrenia and bipolar disorder. Therefore, it would be prudent to suspend our psychopathology allied perspectives of creativity until we develop a deeper understanding of consciousness.The association between creativity and psychopathology has soared to the level of cultural myth and this is evident in many films in which mentally ill persons are portrayed as extraordinarily creative. 76
Evidence suggests that Serotonin has an important role in bladder control through central and peripheral neurological pathways. The three main serotonin receptor sites involved in the micturition pathway are 5-HT1A, 5-HT4, and 5-HT7. 5-HT7 and 5-HT4 are excitatory to acetylcholine release and 5-HT1A is inhibitory. Increased serotonergic activity leads to parasympathetic inhibition, which results in urine retention. It is through this mechanism of action and their effect on pre-synaptic serotonin 1A and peripheral 5-HT3 receptors that SSRIs were observed to have anti-enuretic effect. However, the exclusive role of serotonin in this regard is not fully understood because along with serotonin, other neurotransmitters, particularly acetylcholine are also implicated in micturition physiology. Acetylcholine is released from nerves innervating the detrusor muscle and causes bladder contraction resulting in voiding. Contrarily, adrenergic pathways lead to constriction of the bladder sphincter and promote continence. There have been suggestions that at lower intrasynaptic 5-HT concentrations, there is prevalence of inhibitory control of micturition, whereas excitatory effect is more pronounced at higher concentrations of 5-HT. This may suggest a dose-dependent relationship between Sertraline and urinary side effects. 1
Case Reports:
Case 1
A 14 year old girl with a diagnosis of moderate depressive episode was prescribed Sertraline 150 mg once daily. On follow up with her community psychiatrist, mum reported that she had been having episodes of bedwetting on a regular basis for almost two weeks. There was no past history of enuresis, no medication changes, or changes to her diet or routine. She had been drinking fluids during the day and had limited fluid intake after 6 pm. On a visit to the Sheffield Children’s Hospital, she had been diagnosed with a urinary tract infection and was prescribed a five-day course of antibiotics. She denied symptoms of abdominal pain, dysuria or fever.
On discussion with the trust pharmacist, it was reported that urinary incontinence is a rare listed side effect of Sertraline with nocturia occurring in 1 in 100 to 1 in 1000.2 At further medication review appointments, the patient continued to report being incontinent on approximately every alternate night and had to use incontinence pads. It was agreed with the patient to reduce the dose of Sertraline to 100 mg once daily to test if her urinary incontinence was linked to Sertraline and review after 2 weeks in clinic. The reduction in Sertraline dose to 100mgs once daily did not alter the frequency of bedwetting that continued on most week nights and varied from being partial to full emptying of the bladder. As a result, she was then referred to the Paediatric Community Incontinence clinic for further investigation regarding the sudden onset of these night bedwetting episodes. Concurrently, Sertraline was gradually reduced and stopped. She was switched to Fluoxetine liquid for treatment of her depressive symptoms, which was titrated to a dose of 16 mg once daily. At the community continence clinic, urine dipstick was negative. Systemic examination including a neurological examination was unremarkable. Mum reported that since the change in medication from Sertraline to Fluoxetine, there was a remarkable improvement in her urinary symptoms.
Case 2
A 16 year old boy with a diagnosis of mixed anxiety and depressive disorder was initiated on Sertraline which was gradually titrated to a maximum dose of 200 mg once daily. He reported improvement in his symptoms of anxiety and depression. However, a few days into taking the higher dose, he experienced symptoms of hesitancy with micturition and failure to ejaculate. On reduction of Sertraline to 100 mg once daily, he reported complete resolution of urinary and sexual side effects, while still reporting a reactive and stable mood. Due to his significant progress, he was eventually discharged from CAMHS back to the care of his GP.
Case 3
A 12 year old girl with a diagnosis of Generalized Anxiety Disorder and Attachment Disorder reported three incidents of urinary incontinence whilst being on Sertraline 200 mg once daily. Sertraline was discontinued by the patient against medical advice. No follow up information was available to observe for resolution of symptoms after discontinuation of Sertraline.
Discussion:
Selective Serotonin Reuptake Inhibitors (SSRIs) are a very commonly used class of psychotropic medication in the CAMHS population to treat depression, anxiety, PTSD and OCD. 3 It is evident by the cases discussed above that SSRIs may have a key link in causing symptoms of urinary dysfunction, which may range from nocturnal enuresis to acute urinary retention. This could be explained by Serotonin’s pivotal role in micturition through central and peripheral pathways. There is not enough evidence on the links in a child and adolescent population as most of the studies are on an adult cohort.4
Conclusion:
In conclusion, it is important for clinicians to bear in mind the genitourinary side effects of SSRIs, which may be debilitating for patients in the CAMHS population. It is equally important for us as clinicians to educate young people and their parents about these potential side effects and how they can be managed. It has also been observed that higher doses of Sertraline have shown a possible link between onset of urinary side effects. In order to establish a significant causal and dose-related relationship on the onset and severity of genitourinary symptoms, studies with a larger sample size followed up over a longer period would be required.
Schizophrenia (SCZ) is a chronic relapsing and remitting disorder with a lifetime prevalence of 4 per 1000 persons.1Positive symptoms include delusions and hallucinations. Negative symptoms are characterised by deficits in normal behaviour, which are categorised into five domains: blunted affect, alogia, social withdrawal, anhedonia, and avolition. In clinical practice, when monotherapy fails multiple augmentation strategies – such as another antipsychotic, mood-stabilisers, benzodiazepines, lithium, electroconvulsive therapy, and repetitive trans-cranial magnetic stimulation – have been used to improve the clinical state of these patients, but evidence relating to the use of these interventions is lacking.2None of the regulatory bodies has openly endorsed polytherapy with antipsychotics.
The introduction of chlorpromazine in the 1950s revolutionised psychiatry, and the coming of slow-release, slow-acting forms (depot medication) contributed to the closure of asylums and paved the way to community psychiatry. Second-generation antipsychotics ameliorated the situation for a number of psychotic patients, but some remained resistant to all forms of psychopharmacology. In 1958, clozapine was formulated and marketed commercially in 1972. 3 The arrival of clozapine facilitated the rescue of some schizophrenia sufferers for a short time, but the drug disappeared from the scene because of initial untoward incidents. 4,5 The observation that clozapine has the potential to control the motor symptoms of tardive dyskinesia and to treat the psychotic symptoms of patients already diagnosed with tardive dyskinesia, led to its reintroduction, but with restrictions. 6,7,8 Clozapine is recommended for use only after a trial of two other antipsychotics. Combining depot antipsychotics with oral drugs of a different class has been the practice ever since the introduction of depot medications, and this practice has come to have general clinical acceptance.
Treatment resistance
Historically, it was observed that a specific group of chlorpromazine users remained symptomatic. They were considered to be refractory to phenothiazines. The availability of clozapine led to a better definition of treatment resistance. ‘Response to treatment’ means a reduction in the severity of symptoms, while ‘remission’ implies an absence of symptoms for a considerable period. ‘Recovery’ signifies absence of the disease for a long period.9‘Treatment resistant schizophrenia’ (TRS) is the term used for persistence of psychotic symptoms despite a certain number of adequate treatments. Since the introduction of first-generation antipsychotics, clinicians have been cognizant of TRS and operational definitions have been used such as those developed by Kane et al. 10 Sometimes, treatment has been based on algorithms such as the Texas Medication Algorithm Project (TMAP).
According to the most common definition of TRS, if patients present with persistent, moderate to severe, positive disorganization or negative symptoms together with poor social and work function over a prolonged period of time after at least 2 adequate trials of neuroleptic drugs, they may meet the criteria of having TRS. 11 A common agreement is that adequate drug treatment requires a duration of 4 to 10 weeks, a dosage equivalent to 1000 mg/d of chlorpromazine, and trials of 2 to 3 different classes of antipsychotic drugs. 12 The current treatment guidelines recommend 2 or more treatment trials of atypical antipsychotics at adequate dosages. Adequate response to treatment has been defined as at least a 20% reduction in symptoms as measured by rating scales. Typical antipsychotics can also be used for 4 to 6 weeks to screen for TRS.
Resistance to treatment and poor outcome are different from genuine TRS. Resistance to treatment may be defined as a state in which the patient has access to medication, but the effectiveness of the treatment is suboptimal. TRS may be conceptualised as a state in which medication has reached target receptors but does not seem to be effective. Chronicity has often been misconstrued with treatment-resistance. Schizophrenia is a chronic disorder that progresses to various levels of clinical deterioration without sustained remission or full recovery. Poor-outcome SCZ applies to 50% of patients, and TRS comprises a subset of such patients. In these, cognitive impairment, negative symptoms and mood symptoms are independent of positive symptoms, resulting in poor-outcome SCZ.
It is generally accepted that 30% of SCZ sufferers have TRS. Many people with SCZ do not achieve a satisfactory treatment response to their initial antipsychotic drug treatment. They may manifest a poor response to therapy because of intolerance to medication, poor adherence and inappropriate dosing, as well as true resistance of their illness to antipsychotic drug therapy. Assessing treatment resistance is a priority in the management of TRS. 13 TRS has to be closely evaluated before a comprehensive management plan is developed (Table 1). From a multidimensional point of view, TRS is dependent on manifold factors, such as longer duration, several episodes, gender, early onset, poor pre-morbid personality, family history, substance misuse, presence of soft neurological signs and a long untreated period.14 Genes are thought to be involved in the development of TRS; reliable genetic prediction of which patients will be TRS would have serious clinical implications. Structural neuroimaging techniques have revealed that TRS patients do not differ importantly than those responsive SCZ in terms of brain abnormalities.15
When clozapine fails or rejected
Clozapine may be the preferred drug for TRS – effectively the gold standard – but its side effects put off many patients to the extent that some of them refuse clozapine therapy. It is a unique atypical antipsychotic and there is robust evidence supporting its use in people with TRS. Though clozapine often represents the best hope for recovery, it is associated with severe and enduring adverse reactions that may delay its prescription and increase morbidity and mortality. The major side effects are a) agranulocytosis; b) metabolic side effects; c) myocarditis; d) seizures; e) severe constipation with gastrointestinal complications such as intestinal obstruction, bowel perforation, paralytics ileus and toxic megacolon; and f) sialorrhea. These side effects hinder the popular use of clozapine in TRS. It is a life-saving drug, but without extra care it may itself shorten the life span. Side effects are more common with higher doses. It has been estimated that between 10 and 60% of patients resistant or intolerant with other antipsychotic drugs respond to clozapine.
The side effects mentioned above are inevitably an impediment to its common use. When standard doses (300mg to 5oomg) do not produce the desired effects or patients develop unwanted effects, combining clozapine with other antipsychotics is a common practice for TRS. To mention a few antipsychotics, amisulpride and aripiprazole are atypical antipsychotics ordinarily used in combination with clozapine. The anti-salivatory effect of amisulpride and the alerting effect of aripiprazole are added advantages of such a combination, and these drugs are fairly weight neutral – in contrast to clozapine. Clozapine, representing a second generation of so-called atypical antipsychotic drugs, has shown positive effects in desperate cases of TRS. Furthermore, two epidemiological studies have shown that clozapine has the lowest mortality rate among antipsychotics.
Nevertheless, even supported by the literature as the best-known antipsychotic in terms of efficacy and rates of response, a sizeable number of patients remain resistant to clozapine therapy and continue as symptomatic and dysfunctional. It has been estimated that 40–70% of patients on clozapine may not respond satisfactorily to it.16 When patients do not respond to clozapine, they are categorised as super-refractory, but the very concept of super-refractory state is debatable. They do not differ from the refractory cases in terms of demographical factors but have high score of positive symptoms. It may be simply explainable that the aetiological mechanism of the illness of such patients may be different from the clozapine responders and that makes them unresponsive to clozapine. There are no operational definitions for super-refractory schizophrenia. According to the schizophrenia algorithm of the International Psychopharmacology Algorithm Project (www.jpap.org), persistence of psychotic symptoms after a trial with adequate doses of clozapine(300-900mg/day) for at least six months is designated as super-refractory cases. 17
Many predictors of clozapine response have been suggested without any firm ground. These include severe clinical symptoms, higher levels of functioning before the onset of schizophrenia, low levels of homovanillic acid and 5-hydroxyindoleacetic acid in cerebrospinal fluid, reduced metabolism in the prefrontal cortex, reduced volume of the caudate, and the improvement of P50 gating at the 500-ms prepulse interval. 18 However, none of these factors is consistent or specific as a predictor of clozapine response. More genetic and brain imaging studies are warranted with such patients. In these cases, augmenting strategies are necessary, and some have been in use: typical and atypical antipsychotics, mood stabilizers, antidepressants and electroconvulsive therapy. Some studies have favoured ECT, but no definitive conclusion has been drawn. So also, half of clozapine patients discontinue taking the medication on their own accord. In a retrospectively studied sample of patients who discontinued clozapine, the majority terminated the treatment as a result of their own decision or because of non-compliance with medical procedures such as blood sampling.19
There are currently no evidence-based pharmacotherapies for the TRS patients who do not respond to clozapine 20,21 or those who terminate clozapine therapy due to adversative reactions. 22 In the nutshell, clinicians should be prepared to try different alternative treatment options for TRS and super-refractory cases. Thus, combination therapy may become a choice as pre-clozapine therapy or post-clozapine therapy. Clozapine is not a drug that could normally be imposed on patients, but it has to be earned by the patient.
Combination therapy
The range of antipsychotic medications available is wide, with variable effectiveness, and there are also differing profiles for typical and atypical agents, adding to a confusing array of terminologies and dilemmas regarding what the best drug for service users is.23 Combination therapy involves the addition of a second antipsychotic to the therapy regimen. It is different from adjunctive therapy, in which a second agent is employed to reverse an emergent side effect or to obtain a complementary clinical effect. Augmentation involves the use of a non-antipsychotic along with the antipsychotic already in use. Combination therapy and augmentation therapy are sometimes used interchangeably. In general, ‘combination’ refers to the use of more than one type of disease-specific treatment to treat a particular illness.
A change from one antipsychotic to another in same class seldom produces any additional benefit, whereas switching to an antipsychotic with a different mechanism of action has proved to produce a more impressive response rate. Combination becomes desirable when the drug already in use produces some favourable effect, but that is not sufficient to control the symptoms. It is imperative to distinguish between partial response and no response when considering a change in medication. Past antipsychotic drug response, adverse effect profile differences, concomitant medical disorders and concurrent drug therapy are factors to be considered when choosing between switching and combination or augmentation approaches. A switch is indicated when there is no response to the drug and combination therapy; augmentation is recommended for partial response. Another antipsychotic combination may become necessary as an option for TRS patients who cannot be treated with clozapine for various reasons. It is common practice in such situations to add a second antipsychotic, in combination with the original one.
Clinical team do not have to be disheartened or disillusioned when clozapine therapy fails due to non-response or clozapine intolerance, and also when augmentation and combination therapies do not bring about the desired outcome. Switching back to atypical drugs once again may turn out to be effective in some cases and clozapine is not to be considered as the last resort. A multicentre open label 18-week trial evaluated a switch to olanzapine in 48 clozapine resistant or intolerant patients. 24 Switching to olanzapine 5-25 mg per day resulted in a mean drop in total scores on the Positive and Negative Syndrome Scale (PANNS) and Brief Psychiatric Rating Scale (BPRS) of 17.7 (14.2%) and 9.8 points (20.2%) respectively.
Cautions
Monotherapy is the most desirable form of treatment for SCZ. There is no good objective evidence to support dual antipsychotic therapy except in combination with clozapine. The evidence base supporting such combinations consists mostly of small open-label studies and case series.25 Combination therapy should be considered only when several attempts at monotherapy, including one atypical antipsychotic, fail. It is assumed that two different treatments together may have a different mechanism of action and therapeutic response from that of either drug alone. Studies have been conducted to determine whether treatment with antipsychotic combinations is effective for SCZ and whether such treatment is safe for the same illness. The results of trial studies are based on very low or low-quality results, and research that provides high-quality evidence is needed before firm conclusions may be drawn. The results so far show that there may be some clinical benefit in combination therapy in that more people receiving a combination of antipsychotics showed an improvement in symptoms. For other important outcomes – such as relapse, hospitalisation, adverse events and discontinuing treatment – no clear differences between the two treatment options were observed. Currently, most evidence regarding the use of antipsychotic combinations comes from short-term trials; the assessment of long-term efficacy and safety is limited. There is some very low-quality evidence that a combination of antipsychotics may improve the clinical response.
There are published case reports of serious side effects, such as a higher prevalence of extrapyramidal symptoms (EPS), metabolic side effects, paralytic ileus, grand mal seizures and prolonged QTc in association with a combination of antipsychotics.26Combining three antipsychotics may be extremely dangerous; studies have revealed that such a procedure substantially increases mortality.27A negative case control study exists.28 It should be usual practice to document the rationale for combined antipsychotic use in individual cases in clinical records, along with a clear account of benefits and disadvantages, including side effects.
Newer combinations and augmentation strategies are supported only by case reports and open trial data. Along with advantages, a number of potential concerns regarding antipsychotic combinations have been identified (Table 2) and specific clinical cautions have to be implemented in combination therapy (Table 3). Yet, fixed combinations of drugs are common in medicine and at one time were common in psychiatry. An example is small doses of an antipsychotic in combination with an antidepressant for treating major depression; this lost popularity because of side effects. Also, SNRI-NaSSA combination therapy (e.g. California Rocket Fuel) is prevalently used for treatment-resistant depression.
Olanzapine–amisulpride combination
In spite of the objections put forward against combination therapy, there are isolated case studies favouring the olanzapine–amisulpride combination. Zink et al. (2004) performed a retrospective study, aiming at the systematic evaluation of patients on combined olanzapine and amisulpride. The open study designed as a retrospective chart review of Zink et al. concludes that the olanzapine–amisulpride combination for TRS is encouraging, but requires further evaluation in prospective and randomised studies.29They point out that a reduction of the daily dose of both drugs helped to minimise the side effects of these drugs – such as weight gain and EPS – resulting in better compliance. They did not notice any additional side effects or undesirable drug interactions.
Within the heterogeneous group of atypical antipsychotics, the thienobenzodiazepine derivative olanzapine has a receptor profile that is quite similar to that of clozapine, indicated by having a greater affinity for serotonergic 5-HT2A receptors than for dopaminergic D2 receptors. The positive and negative symptoms of schizophrenic psychoses usually respond well to this drug. In contrast to clozapine, olanzapine does not induce major agranulocytosis but may, in a significant number of cases, lead to troublesome side effects including significant weight gain, type ii diabetes, sedation, anticholinergic effects and transient increases in liver enzymes. Assertive weight management from the start of treatment is recommended. Weight should be monitored and also waist circumference measurements made. In addition, blood lipids should be assessed routinely. A suggested schedule for these investigations would be at 3, 6, and 12-month intervals, and biannually thereafter.30The pharmacology of antipsychotics is not the only factor that determines their effect on weight. Olanzapine has also been shown to elevate prolactin significantly in some patients.31 As indicated earlier, Olanzapine can succeed in some cases even where clozapine fails.24
Amisulpride is an atypical antipsychotic of the benzamide class. It blocks D2 and D3 receptors (presynaptic in low doses, postsynaptic in higher). Unlike other atypical or typical antipsychotics, it has low affinity for serotonin, α-adrenergic, histaminergic, muscarinic and sigma receptors including D1, D4 and D5 receptors. It can lead to dose-related EPS that are significantly less than those of typical antipsychotics such as haloperidol and comparable to risperidone.32It is recognised that amisulpride is only sparingly metabolised by liver enzymes, and thus it is not known to participate in many drug interactions.33 Amisulpride may elevate prolactin, which may cause sexual dysfunction, osteoporosis, amenorrhoea, gynaecomastia or galactorrhoea. It is a weight-neutral compound and may ameliorate negative symptoms.34 Both olanzapine and amisulpiride are not associated with QTc prolongation.
One advantage of the combination of these drugs is that when olanzapine and amisulpride are combined, they may be given at a lower dose, which will spare the patients from the main unwanted side effects of the individual drugs: the over-sedation and weight gain of olanzapine; and the hyperprolactinemia of amisulpride, resulting in sexual side effects of a particularly undesirable extent. Our limited studies have found that this combination was well tolerated by TRS patients and its efficaciousness was similar to that of clozapine, but without any major side effects. Patients have been fully compliant. The combination of these drugs is managed by slowly introducing them one at a time and has been transformative in many cases. More studies of the olanzapine–amisulpride combination are needed in order to report on such outcomes as relapse, remission, social functioning, service utilisation, cost-effectiveness, satisfaction with care, and quality of life.
Table 1. Assessing Treatment Resistance
Re-evaluate current antipsychotic treatment Has an adequate trial been given? Suboptimal dose and non-adherence can lead to pseudo-resistance-poor adherence is unwaveringly associated with adverse effects, poor insight, and a poor therapeutic alliance. Consider exceeding BNF limits-recommended only in specialist centres Review the differential diagnosis eg schizo-affective disorder or bipolar affective disorder-Bipolar Disorder can present with first rank symptoms in the initial stages, it could take up to 10 years to establish a diagnosis of BD. Asses for psychotic symptoms Re-evaluate personal history and psychological pressures Investigate co-morbid psychiatric symptoms eg substance misuse or alcohol dependency, depression, obsessive compulsive disorder and panic attacks Investigate organic factors-temporal lobe epilepsy, endocrinopathies Check blood levels if facilities available Longer duration Multiple episodes Male gender Onset of illness at an earlier age Poor pre-morbid functioning Length of untreated psychosis Family history of schizophrenia Soft neurological signs-lateral and third ventricular enlargement and low catecholamine level in CSF Suicidal tendencies Aggression Asses adverse effects of psychiatric and other medications that may mimic worsening of positive and negative symptoms Complete physical and neurological examination and specialist consultation, as appropriate Rule out the desire to to be ill
Table 2. Advantages and disadvantages
Advantages: Discontinuation symptoms due to the withdrawal of the first antipsychotic could be avoided Patients unresponsive to the initial antipsychotic may achieve clinical response when the second agent is introduced Patient does not have to cope with another waiting period for the substituted drug to produce full results The benefits of the first drug are preserved in addition to the favourable effects of the added drug Switching involves tapering off the initial drug, wash out period and delay in the onset of the second drug Switching of antipsychotic drug requires additional supervision and care in the transitional period and could be delayed due to discontinuation symptoms; the addition of a second antipsychotic drug solves these problems Disadvantages: The possibility of unnecessarily high doses An increased acute and/or chronic side-effect burden Adverse pharmacodynamic and pharmacokinetic interactions Difficulties in determining cause and effect of multiple treatments Potential increased mortality, Higher costs Poorly documented risks and benefits of this practice Reduced compliance
Table 3 Physical cautions with combination
History of cardiac disorder (eg, MI, arrythmias, abnormal ECG) Hepatic impairment Renal impairment Obesity (high BMI) Heavy smoking High alcohol intake Substance misuse Hyperlipidaemia Above age 70 ECG, Haematological investigations. Side effect rating scales Physical effects Record justification for combination
Summary
Combination therapies are the second choice when monotherapy fails. Clozapine is the first choice in severe cases of TRS, but there are super-refractory cases of TRS where clozapine fails. At least in isolated cases, the combination of olanzapine and amisulpride (Ami-olan combination) is worth considering for TRS patients who are reluctant to go on to clozapine therapy or in instances when clozapine failed, or patents dropped out. Combination therapies are normally avoided, but clinicians’ helplessness and patients’ despair justifies such measures in hard-to-treat cases of TRS. Only time will tell whether this combination will become an important part of clinical practice in future or will be ruled out as just another dual antipsychotic therapy.
The aetiology of SCZ remains obscure. The symptoms of different psychotic disorders are not clearly demarcated and there are no physiological parameters on which to make a firm diagnosis. In such a situation, the treatment of TRS has to be tailored on an individual basis. Even though it is normally well calculated, it may be somewhat hit and miss. Finding the right combination of antipsychotics or augmenting agents when the clinician is stranded and torn between monotherapy and polypharmacy is a gargantuan task. Clinical judgement along with patient preference must take over when treatment algorithms fall short. Given the data on polytherapy with antipsychotics that is available, it is hard to make any firm recommendation regarding its efficacy and safety of its use. Clinicians should be reminded that they should try monotherapy in adequate dosages before considering combinations.
For the management of TRS, comprehensive treatment strategies that integrate pharmacological, psychological, and psychosocial approaches are highly relevant and for that to happen, TRS should be clearly recognised. NICE offers very little guidance on clozapine resistant cases of SCZ. Combination of antipsychotics is not a panacea or a permanent solution for TRS. More investigation of schizophrenic illness is the only way forward. In comparison with other medical conditions (eg,HIV), research into it is making little progress. As it stands now, deconstructing clozapine’s unique pharmacology may offer ‘light at the end of the tunnel’ for patients who are clozapine intolerant or non-responders.
A family carer or caregiver is someone who gives a substantial amount of unpaid care and support regularly to a relative, partner or friend. Currently, there are over 850,000 people living with dementia in the UK, of which two thirds are looked after in the community by primary carers, and the demands on individuals and families are set to increase1. Without the work of unpaid family carers, the formal care system would be likely to collapse.
Many people in the UK still do not feel comfortable talking about dementia, especially with their own families. A recent survey of more than 2,100 carers, of which 17% of respondents cared for a person with dementia, found that 75% of carers were not prepared for all aspects of caring. Nor were they prepared for the emotional impact, lifestyle or relationship changes of their caring role2. Failure to prepare and support carers in their role not only affects their own personal health and wellbeing, but can also lead to the early and potentially avoidable admission of people with dementia into formal care.
As dementia progresses, family members often provide care under high level of stress for longer periods of time. The effects of being a family caregiver, though sometimes positive, are generally negative on their psychological and physical health, life expectancy and quality of life 3. It is therefore important to educate carers of family members with dementia to improve their knowledge of, and attitude towards people with dementia. Poor knowledge about dementia has been found to result in the underutilisation of support and treatment services, and in poorer outcomes of people with dementia and their caregivers such as inadequate care of the disease, misinterpretation of behaviours and increased caregiver stress due to failure to seek appropriate support4.
Currently there is too much reliance on people with dementia and carers seeking out information for themselves. The result is that people do not receive the information they need because they do not know what to ask for. Despite the existence of information for carers, people report that their information needs are not met. Information is provided too late or not at all. A key problem is that people have to ask for information, rather than it being provided proactively.
It has been found that education and training programme covering the information5, or an individual training programme6, improve attitudes towards caring for people with dementia as well as general knowledge of dementia7. Psychosocial interventions have also been demonstrated to reduce caregiver burden and depression, and delay care home admission8. A systematic review9 of 44 randomised controlled trials has found statistically significant evidence that group-based supportive interventions impact positively on caregivers of people with dementia.
Coon et al (2003)10 found that psychoeducational skill training, in small groups, improved both the affective states and the type of coping strategies used by caregivers. On the other hand, an information-orientated programme failed to improve caregiver’s mood11, and a befriending scheme was not effective in improving carer’s wellbeing12. Similarly, a randomised controlled trial did not show preventive effects of family meetings on the mental health of family caregivers13. Livingstone et al (2013)6, on the other hand, have found encouraging results of a manual based coping strategy programme in their London study.
A suitable training programme is therefore required for building caregivers’ knowledge and skills. We have developed a Dementia First Aid (DFA) course for the family carers of people with early dementia. This is a problem solving, stress reducing, and crisis preventive training programme. The DFA course was inspired by the principles of Mental Health First Aid programme14, developed in Australia in 2001 and introduced to England in 2007 by the National Institute for Mental Health in England.
Dementia First Aid Course
Description of the course
Dementia First Aid course is delivered over 4 hour in a group setting. Each participant received a course manual prepared by the author AJ. The content covered an overview of dementia, impact of dementia on the individual, impact of caring on families, mindfulness-based stress reduction training, and a detailed discussion of Dementia First Aid Action Plan for crises associated with behavioural and psychological symptoms of dementia (BPSD).
In November-December 2013, a group of 8 health care professionals, working within the specialist mental health services for older people in Hertfordshire, were offered the 12-hour advanced Dementia First Aid course, followed by an additional 12-hour practice training of presenting the course to a group of family carers of people with recently diagnosed dementia.
Evolution of DFA course
The original 12-hour Dementia First Aid course was delivered over three half days. Although the course was well received by both carers and trainers, the dropout rate was high. This was mainly due to the carers struggling to make alternative arrangement to look after the person with dementia while they were away. The course was therefore changed to 8 hours and then reduced to 4 hours based on feedback received by the carers.
The main aim of this pilot evaluation was to investigate the potential benefits of a Dementia First Aid course in terms of the knowledge and attitude of family carers of people with newly diagnosed dementia.
Methods
The participants were the primary family caregivers of people with dementia residing in northwest Hertfordshire. The DFA course was organised once every two month from November 2015 till March 2017.
An invitation letter, along with details of the pilot assessment, was sent to all those carers of people whose dementia was diagnosed recently in memory clinic and all participants were given at least 4 weeks’ notice prior to the course.
Selection criteria included: being aged 18 or above, the primary carer of a person with newly diagnosed dementia (i.e. currently providing at least 20 hours of direct care per week) & residing in Hertfordshire.
The training was delivered by a pair of qualified DFA instructors, who were mental health professionals experienced in dementia care in the NHS. The training was conducted using a power point presentation, group work, and audio-visual clips based on a specially designed DFA manual.
Evaluation questionnaire
The participants were asked to complete a questionnaire on their own at the beginning of the programme. Oral consent from participants were obtained prior to filling out the questionnaire, the participants were made aware that participation in the pilot assessment was voluntary and would not pose any barrier for them to join the programme.
Participants were given Alzheimer’s disease Knowledge Scale15, a questionnaire comprising of 30 questions before and after the training. They were also asked to complete the Zarit Burden Scale a 12 item self-reported scale16 to measure carer burden.
After 6 months the participants were contacted to complete ADKS and Zarit Burden Scale. ADKS is therefore completed thrice and Zarit Burden Scale is completed twice during the study.
Statistical analysis
The data collected were analysed in two ways. First, ADKS data collected at pre-test were compared to post-test scores to examine change in participants’ knowledge. The participants’ knowledge at the end of 6 months was also compared to pre and post-test scores. Similarly Zarit Burden Scores at the time of initial assessment were compared to scores 6 month post training. To evaluate the effect of the training, answers to the structured questions given at pre- and post-test and scores at 6 months were compared using a correlated group t-test.
Results
The study sample comprised 65 people who had completed the DFA course. All completed ADKS pre- and post-training and completed Zarit Burden Scale, and a further 34 provided follow-up data approximately 6 months later.
Sample characteristics:
Mean (±SD) age = 66.9 (± 13.8) years (range 31-90). 23 attendees were male, 42 were female
ADK scores
Looking first at all 65 attendees:
ADK scores for whole sample
Pre-course
Post-course
Mean
16.7
21.2
SD
5.7
4.5
Min
0
10
Max
26
29
ADK scores improved significantly immediately after attending the course (p < 0.0001).
Score improvement was not predicted by gender (p > 0.3), and the correlation between score improvement and age was not significant (R = 0.023). We did not examine age and gender further.
Analysis of sample of 34 who provided long-term follow up data:
ADK scores for sub-sample
Pre-course
Post-course
6+ Month
Mean
17.2
22.0
21.0
SD
4.9
4.5
4.8
Min
1
11
7
Max
24
29
29
For the smaller sample, ADK scores improved significantly immediately after attending the course (p < 0.0001), and this was sustained at the longer-term follow up (p < 0.0001). Although the mean ADK score dropped by a point at 6+ months, this was still a significant improvement over the pre-course (baseline) score.
Comparing post-course ADK score with 6+ month follow-up ADK score, no significant difference was observed (t[33] = 1.48, p = 0.15), suggesting that knowledge was not lost to a significant degree.
Zarit Burden Scale Scores
The response rate Zarit Burden scores was not good as only 19 of the sample completed this at 6 month follow up. The score for this cohort increased by 3.58 points, which was borderline significant and is expected as dementia is a progressively declining condition.
Discussion
This is the first report on the level of dementia knowledge among family caregivers in the UK before and immediately after the implementation of a novel post-diagnostic dementia training programme, the Dementia First Aid Course and whether the knowledge sustains after 6 month.
The mean pre-course score on the ADKS in the sub-sample that completed test at 6 months was significantly lower at 17.2 than 22.7 reported by Smyth et al. (2013)7. It was expected that the level of dementia knowledge would improve after attending the course and the findings largely fulfilled this expectation. There was a significant difference between the pre and post training score with p value < 0.0001. Further there is evidence that the knowledge sustained after 6 months of the training.
The intervention studied in a recent British trial6 is an individual therapy programme, consisting of psychoeducation about dementia, carer’s stress, behaviour management, and relaxation techniques. The effectiveness of the programme on carer’s depression and abusive behaviour was significant. To provide individual training for a huge number of families may not be possible in the NHS. Therefore, a group based training approach employed in our study may well be more sustainable.
The carer’s burden of care as measured by Zarit burden scale at the time of training and 6 months later showed only a modest increase of 3.58 points. However, it was apparent that training could not affect the relentless progression of dementia, most of which were of the Alzheimer’s type.
Limitations
Being a pilot evaluation, the sample size of this study was small. This pilot assessment may be limited by the fact that participants were not randomly selected. Since the current evaluation was conducted in only one part of the County, the sample may not reflect a wider community. The knowledge gained during the course was sustained at the end of 6 months. However training did not reduce carer burden nor it was clear whether the new knowledge and skills will be effective in preventing crises. Brodaty et al (1989)17 reported reduced psychological morbidity of the carer following dementia carers’ programme but cautioned against delay in institutionalisation of patient at the expense of the morbidity of the carer.
Finally, the present pilot evaluation was uncontrolled and non-randomised, so we do not know to what extent any impact is due to the dementia first aid training, passage of time or experience of caring. A randomised controlled study with follow-up measurements on caregivers’ knowledge, sense of burden, psychological health and wellbeing, would be the ideal next step.
Key points
Most people with dementia live at home and are cared for by their spouses, children or other family members, but these carers are not usually offered adequate information and training about dementia and the impact of caring at the time of diagnosis.
This paper describes the effectiveness of a short (4-hour) version of a novel training programme, the ‘Dementia First Aid’ course, for family caregivers of people with early dementia.br> The Dementia First Aid course includes overview of dementia including Alzheimer’s disease, impact of dementia on the person and their family caregivers, principles and practice of ‘mindfulness’ to enhance coping ability, and first action plan for common behavioural and psychological symptoms of dementia.
‘Dementia First Aid’ course, appears to enhance caregivers’ knowledge of dementia.
Conclusions
The significance of these results can be placed in the wider context of proactive dementia training for family caregivers at the time of diagnosis. The results are important in demonstrating that having dementia training is associated with improved knowledge.
This study adds to the existing literature and has implications for both care and policy regarding community care of people with dementia, and emphasises the importance of dementia training as a routine component of post-diagnostic support.
Although knowledge alone does not necessarily translate into change in care, nor does high quality of care solely depend on broad education about dementia7, our results suggest that the dementia first aid course is effective in changing the knowledge and attitude of dementia caregivers. Hopefully, this will also enhance their ability and skills of caring, which may in turn reduce caregivers’ sense of burden and wellbeing. A randomised controlled study with follow-up measurements is required to support these claims.
Bipolar affective disorder (BPAD) is one of the commonest psychiatric disorders with a lifetime prevalence of about 3% in the general population and is the sixth leading cause of disability worldwide (1,2).This disorder is characterised by repeated episodes in which the patient’s mood and activity levels are significantly disturbed. This disturbance consists on some occasions of an elevation of mood and increased energy and activity (mania or hypomania), and on other occasions of a lowering of mood and decreased energy and activity (depression) (3). As the illness starts early in life, i.e., during teens or early adulthood, persons suffering from BPAD have symptoms of illness for the major part of their life (4, 5).
In India, since professional services, both in public and private sectors are not adequately developed due to shortage of trained human resources and infrastructure, the family support system plays a major role in caring for people with mental illnesses (6). The primary caregiver is identified as an adult relative (a spouse, parent or spouse equivalent) living with a patient, who is involved in the care of the patient on a day-to-day basis, takes the responsibility for bringing the patient to the treatment facility, stays with the patient during the inpatient stay, provides financial support and/or is contacted by the treatment staff in case of emergency (7). Intensive involvement in the care of the patient is often associated with significant caregiver burden.
Caregiver burden can be defined as the presence of problems, difficulties or adverse effects which affect the lives of caregivers of patients with various disorders or illnesses, e.g. members of the household or family (8). Family burden is broadly divided into objective and subjective burden. While the notion of the objective family burden relates to measurable problems (e.g. patients’ troublesome behaviours), the idea of subjective family burden is bound to caregivers’ emotions arising in response to the objective difficulties (9). Multiple studies across the world have shown that bipolar disorder is associated with significant caregiver burden (10-31). In view of the high caregiver burden, it is now suggested that the emphasis in psychiatric rehabilitation needs to shift from a patient-focused approach to a combined patient and caregiver-focused approach. Although there are studies from different parts of the country, there is a lack of data on caregiver burden from Kashmir, which is often faced with turmoil, which can influence caregiver burden. The present study is an effort in this direction to assess caregiver burden and its correlates among primary caregivers of patients with bipolar disorder.
Methodology
The present study was conducted on primary caregivers of patients with BPAD. Primary caregivers were defined as those caregivers who were closely involved in the care of the patient during the acute episodes and during the maintenance period in terms of bringing the patient to the hospital, supervising the medications and liaison with the treating team.
The study sample comprised of 100 caregivers of 100 patients diagnosed with BPAD as per the International Classification of Diseases classification of mental and behavioural disorders, 10th revision (ICD-10) (3), attending either the outpatient or inpatient services at the Department of Psychiatry, SKIMS, Bemina, Srinagar. The study was approved by the Ethics Committee of the institute and all the participants were recruited after obtaining written informed consent.
To be included in the study, the caregivers were required to be involved in the care of patients, aged 18 or above, living with the patient for at least 1 year and were a family member taking care of patients without any wages. Caregivers who were diagnosed with psychiatric illness and staying with the patient for less than 12 months were excluded.
The caregivers were assessed by following scales:
Family Burden Interview Schedule (FBIS) (32):This is a semi-structured interview schedule having 24 items, each of which is scored on a 3-point scale, i.e. 0 indicating no burden, 1 indicating a moderate level of burden and 2 suggesting severe burden. The items of the objective burden of the scale are divided into 6 domains, i.e. financial burden, disruption of routine family activities, disruption of family leisure, disruption of family interaction, physical health and mental health. Subjective burden is evaluated by a single item. This scale has been widely used in previous studies from India (26, 33-35).
DUKE-UNC Functional Social Support Questionnaire (FSSQ) (36):The Duke-UNC Functional Social Support Questionnaire (FSSQ) is an 8-item instrument to measure the strength of the person's social support network (36). Responses to each item were scored as 1 (‘much less than I would like’), 2 (‘less than I would like’), 3 (‘some, but would like more’), 4 (‘almost as much as I would like’) and 5 (‘as much as I would like’). The scores from all eight questions are summed (maximum 40) and then divided by 8 to get an average score. The higher score indicates better perceived social support. Cronbach’s alpha for this scale is 0.84.
Hindi General Health Questionnaire (GHQ-30) (37):The modified version of Goldberg's General Health Questionnaire (GHQ) (38) was used. This is a screening device for identifying minor psychiatric disorders in the general population and within the community or non-psychiatric clinical settings such as primary care or general medical outpatients. The self-administered questionnaire focuses on two major areas: the inability to carry out normal functions and the appearance of new and distressing phenomena. In each question of the 30-item GHQ, the caregivers were asked to choose among: Better than usual or same as usual = 0, less than usual or much less than usual = 1.The results were evaluated by the two-step assessment method (0-0-1-1-method). The minimum GHQ-30 total score was 0 and the maximum total score of GHQ-30 was 30. A cut-off of 6 was used to categorize those with and without psychiatric morbidity. Cronbach’s alpha value of the GHQ-30 was 0.93. The Kappa coefficient was 0.64 (p<0.001).
The recorded data was compiled and entered into a spreadsheet (Microsoft Excel) and then exported to data editor of SPSS Version 16.0 (SPSS Inc., Chicago, Illinois, USA). Continuous variables were summarised in the form of means and standard deviations and categorical variables were summarised as percentages. Student’s independent t-test and Chi-square tests were employed for comparing caregiver burden with different variables.
Results
Table 1: Description of socio-demographic variables of caregivers
Variables
Caregiver Frequency (n=100)(%)
Patients Frequency (n=100)(%)
Age (Years)
20-29
11(11%)
12(12%)
30-39
24(24%)
26(26%)
40-49
26(26%)
31(31%)
50-59
34(34%)
14(14%)
≥ 60
5(5%)
17(17%)
Mean± SD
43.4 ±11.25
34.3±12.86
Gender
Male
52(52%)
47(47%)
Female
48(48%)
53(53%)
Marital Status
Unmarried
7(7%)
37(37%)
Married
93(93%)
63(63%)
Educational Status
No formal education
48(48%)
36(36%)
Primary
5(5%)
6(6%)
Secondary
27(27%)
32(32%)
Graduate
20(20%)
26 (26%)
Occupation
Unemployed
3(3%)
10(10%)
Labourer
27(27%)
24(24%)
Student
3(3%)
16(16%)
House maker
44(44%)
34(34%)
Employed
23(23%)
16(16%)
Socio-economic Status
Low
60(60%)
60(60%)
Middle
40(40%)
40(40%)
High
0(0%)
0(0%)
Relationship of caregiver
Father
11(11%)
Mother
22(22%)
Spouse
55(55%)
Duration of care
1-5yrs
77(77%)
6-10yrs
16(16%)
>10yrs
7(7%)
Mean ± SD
4.8±4.16
Table 2: Clinical profile of patients.
Patient Variables
Frequency(n=100)(%)
Duration of illness
1-5 Yrs
77(77%)
6-10 Yrs
16(16%)
11-15 Yrs
5(5%)
16-20 Yrs
1(1%)
> 20 Yrs
1(1%)
Mean±SD
4.83±4.25
Number of hospitalisations
Never
47(47%)
Once
24(24%)
Twice
18(18%)
Thrice
6(6%)
Four Times
5(5%)
Mean±SD
0.98±1.16
Number of episodes of mania
1-2
55(55%)
3-4
39(39%)
5-6
6(6%)
Mean±SD
2.61±1.12
Number of episodes of depression
< 3
15(15%)
3-5
64(64%)
> 5
21(21%)
Mean±SD
4.05±1.87
Number of attempts of homicide
0
75(75%)
1
8(8%)
2
4(4%)
≥ 3
5(5%)
Mean±SD
0.37±0.93
Number of attempts of suicide
0
75(75%)
1
1(1%)
2
6(%)
≥ 3
2(2%)
Mean±SD
0.23±0.74
Compliance with medication
Yes
73(73%)
No
27(27%)
Table 3: Caregiver burden, social support and psychological morbidity among caregivers
Psychosocial parameters
Mean (SD)
Range
Caregiver burden (FBI scores)
Financial burden
7.01 (2.28)
3-12
Disruption of family routine activities
5.38(1.77)
3-9
Disruption of family leisure
4.12 (1.26)
2-8
Disruption of family interactions
4.04 (1.36)
3-9
Effect on physical health of others
2.28 (0.83)
1-4
Effect on mental health of others
1.51 (0.82)
0-4
Total family burden
24.31 (7.35)
13-44
Objective burden Score < 12 Score ≥12
3 97
Subjective Caregiver burden score
1.12(0.61)
0-2
DUKE UNC FSSQ
3.17 (0.84)
1.75-4.75
GHQ-30
13.14 (5.65)
2-25
GHQ score < 6 GHQ score ≥ 6
77 (77%) 23 (23%)
Table 4: Association of caregiver burden with socio-demographic variables of caregivers
Caregiver Variables
N
Mean
SD
P-value
Age (Years)
20-29 30-39 40-49 50-59 ≥ 60
11 24 26 34 5
20.63 22.67 25.08 26.93 29.25
4.860 7.409 6.211 5.839 6.675
<0.001*
Gender
Male Female
52 48
23.60 27.35
7.384 7.309
0.012*
Marital Status
Married Unmarried
93 7
26.97 21.29
7.409 6.211
0.041*
Educational Status
No formal education Primary Secondary Graduate
48 5 27 20
28.78 27.80 24.69 22.35
7.772 7.596 7.223 5.092
0.015*
Occupation
Unemployed Labourer Student House maker Employed
3 27 3 44 23
23.15 25.47 23.05 28.05 22.07
7.268 1.399 6.891 6.891 7.312
<0.001*
Socio-economic status
Low Middle High
60 40 0
26.88 23.38 0
7.958 5.687 0
0.018*
Type of family
Nuclear Joint
82 18
28.37 23.54
5.463 6.354
0.002*
Relationship to patient
Parent Spouse Offspring
33 55 12
24.47 28.04 21.57
7.972 7.038 6.024
0.008*
Duration of care
1-5 Years 6-10 Years > 10 Years
77 16 7
22.99 33.06 35.57
5.644 6.027 5.996
<0.001*
Table 5: Clinical Profile of patients with bipolar disorder
Disease Profile
No.
Mean
SD
P-value
Duration of illness
1-5 Yrs 6-10 Yrs ≥ 10Yrs
77 16 7
22.98 33.07 37.01
5.644 6.027 2.887
<0.001*
Number of Hospitalisations
Never Once Twice Thrice Four Times
47 24 18 6 5
22.21 25.83 26.54 28.50 31.00
7.896 7.438 6.527 4.506 6.042
0.045*
Number of episodes of mania
1-2 3-4 5-6
55 39 6
22.27 27.97 38.65
5.612 6.726 2.066
<0.001*
Number of episodes of depression
< 3 3-5 > 5
15 64 21
21.93 23.91 32.81
7.611 5.817 6.615
<0.001*
Compliance with medication (>75%)
Yes No
73 27
24.51 27.94
7.328 7.377
0.041*
Table 6: Clinical Profile of patients with bipolar disorder
The study included nearly equal number of male and female patients. About two-thirds of the patients were married (63%). About one-third of the patients had not received any formal education and another third had completed their secondary education and one-fourth had completed graduation (Table 1).
Description of socio-demographic variables of caregivers
The study included nearly equal numbers of male and female caregivers. The majority (55%) of the caregivers were spouses of the patient. The majority of the caregivers were married (93%). Nearly half of the caregivers had not received any formal education (48%), were homemakers (44%) and three-fifths of them were from low socioeconomic status (60%). The majority of caregivers (77%) had been caring for duration of one to five years (Table 1).
Clinical profile of patients.
In the present study, the majority of patients (77%) had duration of illness in the range of 1-5 years, nearly half of them were never hospitalised, the majority (55%) of patients had one to two manic episodes, most of them (64%) had three to five episodes of depression, and the majority (75%) of them never attempted suicide or homicide. The majority of patients (73%) were compliant with medication. (Table 2)
Caregiver burden, social support and psychological morbidity among caregivers
As is evident from Table 3, the highest burden was reported in the financial domain, followed by disruption in family routine activities, disruption of family leisure, disruption of family interactions, effect on physical health of others and least burden was reported in the form of effect on mental health of others. The mean DUKE UNC FSSQ score was 3.17 (SD=0.84) with range 1.75-4.75.
Mean GHQ-30 score was 13.14(SD=5.65) with a range of 2-25. Of the 100 caregivers, about one-fourth (N=23) had a GHQ-30 score of 6 or more, indicative of psychological morbidity.
Association of caregiver burden with demographic and clinical variables
As is evident from Table 4, higher caregiver burden was associated with higher age, female gender, lack of formal education, being a homemaker, lower socioeconomic status, a nuclear family set-up, being spouse of the patient and longer duration of being in the caregiver role.
Clinical Profile of patients with bipolar disorder
In terms of clinical variables, higher objective caregiver burden was associated with duration of illness more than 10 years, higher number of hospitalisations and higher number of manic and depressive episodes. Caregivers of patients consuming >75% of the prescribed medications reported lower caregiver burden (Table 5).
Advancing age of patient and caregiver, increasing duration of care, prolonged illness, greater number of hospitalisations and higher number of episodes of either polarity were significantly associated with higher caregiver burden. In terms of association of social support and caregiver burden, higher social support was associated with significantly lower caregiver burden, whereas higher caregiver burden was associated with higher psychological morbidity (Table 6).
Discussion
Families play an important role in care of patients with chronic mental illnesses. In the process of caring for such patients, relatives face a considerable burden.
Findings of the present study suggest that higher burden was seen among the caregivers who were relatively older, of female gender, uneducated or illiterate, homemakers and from nuclear families. Compared to parents and siblings, spouses reported significantly higher levels of caregiver burden. Furthermore, the caregivers involved in the care of the patient for longer durations reported significantly higher levels of caregiver burden.
In terms of clinical variables of patients, higher caregiver burden was associated with longer duration of illness, higher number of lifetime hospitalisations, higher number of manic and depressive episodes and poor medication compliance. Poor social support was associated with a higher level of caregiver burden. Higher caregiver burden was associated with higher psychological morbidity.
Many previous studies from India have evaluated caregiver burden among caregivers of patients with bipolar disorder (10-32). There is a lack of consensus with respect to caregiver variables and their association with caregiver burden (39). Some of the studies suggest that there is no significant difference in the caregiver burden as reported by caregivers of either gender (6), whereas others suggest that females report higher caregiver burden (13, 40). Our findings support the studies which have reported higher caregiver burden among female caregivers. This finding of ours could have been influenced by the relationship of caregivers with patients. In the present study, spouses of patients formed a large proportion of caregivers and they reported significantly higher burden, in contrast to parents and siblings. Cultural issues like restriction of females to household activities with lower opportunities to vent out their distress, inability to spend time on leisure activities, financial dependency and lack of independence could also be responsible for higher perceived burden. It was noticed that caregivers from nuclear families had higher caregiver burden as compared to those from joint families. The joint family system is considered to promote interdependence and possibly is associated with sharing of caregiver burden and this may explain why caregivers from joint families reported lower caregiver burden. Similar findings have been reported in earlier studies from India (41).
Findings of the association of higher caregiver burden with duration of illness are supported by existing literature (14). This finding suggests that possibly with passing time, frequent relapses of illness lead to caregiver burnout, which leads to higher caregiver burden. Previous studies have also noted an association of higher caregiver burden with higher numbers of hospitalisation (30). Findings of the present study too support this association. Higher caregiver burden with greater numbers of hospitalisations possibly indicate more severe episodes and hospitalisation associated with more expenditures and loss of earnings. This suggests that all efforts must be made to pick up relapses at the earliest and manage them effectively to minimise the chances of progression to severe episodes and resultant need for inpatient care. Previous studies have also reported association between higher caregiver burden and higher number of episodes, especially manic episodes (14) and more severe manic episodes (42). Manic episodes of the illness are very disruptive to daily life, work and family relationships. Due to this, these episodes place great demands on family members involved in caregiving. These demands can persist even during remission, where residual symptoms are often still present and lead to caregiver burden. Available data from India suggest that in contrast to patients from the West, patients from India have a higher number of manic episodes (43). Taken together, this finding has important implications as this suggests that efforts must be made to prevent frequent relapses in patients with bipolar disorder, especially in the Indian context to reduce the caregiver burden (44).
In the present study, higher burden was also associated with a higher number of depressive episodes and this finding is supported by existing literature (16).
Long-term management of bipolar disorder requires continuation of medications with good compliance. Poor medication compliance has been shown to be associated with many negative patient-related outcomes like higher risk of relapses, suicidality, poor quality of life, higher residual or sub-syndromal symptoms etc (45, 46). The present study adds to this body of literature and suggests that poor medication compliance in patients is also associated with higher caregiver burden and this finding is supported by the existing literature (11).
Among the demographic variables of caregivers, higher age of caregivers was associated with higher caregiver burden. This finding is also supported by existing literature (6). This association possibly suggests that with increasing age, the caregivers possibly experience more burnout, lose hope and also lose physical vigour to take care of the mentally ill relative.
Accordingly, it is important for the mental health professionals to support the ageing caregivers.
To conclude, the present study suggests that BPAD is associated with higher caregiver burden. Higher caregiver burden is associated with clinical variables of the patients and demographic variables of the caregivers. Among the patient-related variables, longer duration of illness, those with a higher number of lifetime episodes of either polarity and poor medication adherence are associated with higher caregiver burden. Hence, all measures must be taken to minimise relapse in patients with BPAD. Among the demographic variables of caregivers, higher caregiver burden is reported by caregivers who were relatively older, of female gender, uneducated or illiterate, homemakers and from nuclear families.
Our findings highlight the need for additional research on interventions to reduce burden among caregivers of patients with bipolar affective disorder. For better outcomes of disease, more attention needs to be given to the primary caregivers in terms of psycho-education and counselling.
There have been continuing initiatives to transform and improve the National Health Service (NHS) in recent years. Mental health services in England have similarly shown evolution with regards to service provision. There has been a shift away from the perceived “medicalisation” of treatment, with traditional long-stay institutions replaced with more targeted and personalised care in the community.1 Furthermore, community services themselves have seen much remodelling over the years including decommissioning and integration, as well as increased involvement in outreach and early intervention teams.2
Mental health services are sometimes perceived as relatively well funded from outside but, as with most healthcare sectors, compared to the population requiring this service, these resources are inadequate to support the growing demand. This has been the case for some time, but it has become more evident with a significant reduction in funding observed since 2010/11.1 In addition, constant governmental pressures to meet key performance targets, as well as unachievable expectations from the public, have further stretched an already resource-depleted mental health service.
The implementation of new National policies3 was supposed to be a shift from large psychiatric hospitals to smaller specialist community centres with a promised reduction in the demand placed on inpatient services. In England, a peak number of 150,000 inpatient psychiatric beds was reported in 1955; this has since rapidly declined to 22,300 in 2012. Between 2010/11 and 2013/14, a further rapid reduction of 7% of all beds available was seen.4
Despite the promise of changes in service delivery within mental health to mitigate the continued reduction in the number of inpatient beds, demand for inpatient beds has not in fact reduced nationally.1 The recommended level of occupancy, for example, is 85% but 119 wards surveyed5 were operating at 91%, with some at 138% level of occupancy. The occupancy levels of over 100% usually occurred when long-stay inpatients were discharged home on short-term leave and their beds got filled during their absence.4 Where numbers of inpatient beds fail to meet the demands, or waiting list for their first assessment or review grows, the inadequacy lends these facilities to issues with regard to providing high quality and safe patient care. Examples of this may include inappropriate use of the Mental Health Act for detention of patients as a means of securing an inpatient bed,5 incomplete assessments of people detained in places of safety due to time or space constraints,6 and an increase in violent incidents on overcrowded inpatient wards.7
What is a Crisis Resolution and Home Treatment Team (CRHTT)?
In the late 1980s and 1990s, community mental health teams provided acute crisis support. This posed a number of issues including that these teams usually operated during normal working hours of 9am-5pm (Monday to Friday) and were not always available to provide support to patients in a crisis, and did not have the desired impact of reducing the number of acute admissions.8 This gap in service provision inspired the experimentation with and subsequent development of intensive home treatment services, some of which showed evidence of reduced hospital admissions, and holistic-working often preferred by families who were happy to have their loved ones receive the required support in the home environment.9 Over the last two decades, with remodelling of services, increased investment, NHS funding rising from £49 billion in 2000 to £122 billion in 2016, and a migration of mental health professionals, CRHTTs were established and are now available in every mental health trust across the United Kingdom (UK).10
CRHTT is a team of mental health professionals including psychiatrists, community psychiatric nurses, social workers and support workers, who provide rapid and intensive support at home during a mental health crisis.11 They are a 24-hour service operating seven days a week, and acting as the “gatekeeper” for acute services accepting referrals from various sources including inpatient, community, liaison and from outside the Trust for providing support to patients experiencing crises. These teams risk-assess patients and determine whether they require inpatient or home treatment. In the latter case, CRHTTs provide intensive home treatment by offering up to 2-3 visits a day as well as 24/7 phone support. These teams are also involved in facilitating early discharges from hospitals; in cases where patients are past the initial acute crisis, but may need further input prior to discharge to community mental health teams for longer term support.8
Definition of diagnosis and second opinion.
A second opinion is defined as “advice from a second expert (such as a doctor/psychiatrist) to make sure advice from the first such expert is correct” whilst diagnosis is defined as “the art or act of identifying a disease from its signs and symptoms”.12 Due to increased pressure on inpatient facilities and remodelling of community services, there has been a huge increase in the number of referrals made to CRHTTs. Between 2011/12 and 2013/14, it has been noted that referrals to CRHTTs increased by 16%.13 Reduction in inpatient beds and high workloads within community services often result in the formulation of arbitrary diagnoses and treatment plans. With increased pressures on other mental health services, the role of CRHTTs has begun to evolve. In addition to the previously discussed functions, CRHTTs appear to be becoming second opinion services by default enabled by the psychiatrists working in these teams.
We organised a project to establish whether a typical CRHTT is fulfilling the criteria of being a diagnostic or second opinion service provider.
Method
We examined 100 consecutively accepted referrals to a CRHTT from 1st December 2016. The patients were divided into three groups: those being discharged/referred from hospital (HR), those referred from the community (CR), and those who were not open to secondary mental health services at the time of referral (NR). The age range and gender of the groups were noted. Thereafter, the NR group was excluded from analysis for the obvious reason that the CRHTT was not providing a second opinion in their case. The HR and CR groups were further reduced by excluding patients who were not seen by a CRHTT psychiatrist. The remaining patients in both groups were scrutinised regarding a change in medication; this was also recorded for the previous and next care occasions. The likelihood of medication change at the next treatment event was analysed to establish whether it was affected by the previous event. The numbers of patients with CRHTT diagnosis change were also recorded for both groups.
Results
Figure 1: Project Flowchart
Figure 2: Group Demographics
n
Patient Gender
Patient Age
Time with CRHTT
Male
Female
Average
Range
1-7 days
> 7 days
No prior referral open (NR)
43
20 (47%)
23 (53%)
36.0
19-60
5 (12%)
38 (88%)
Community referral (CR)
36
13 (36%)
23(64%)
37.8
19-66
7 (19%)
29 (81%)
Hospital referral (HR)
21
10 (48%)
11 (52%)
39.0
19-63
6 (29%)
15 (71%)
There was little difference in age between the three groups (average ages were: CR=37.8, HR=39.0, NR=36.0). There was a lower proportion of men in the CR group than were present in the HR and NR groups (36% as against 48% and 47%). Whether a psychiatrist saw a patient appeared to be related to both the referral source and the length of CRHTT stay. Most (n=16, 76%) patients in the hospital-referred group (HR) were not seen by a psychiatrist while most (n=24, 67%) of those referred from the community (CR) did receive such an outcome. No community-referred patient was seen by a psychiatrist if they were with the CRHTT for less than a week. These short-stay patients accounted for 7 out of the 12 community-referred patients who were not seen. This suggests that a psychiatric assessment should be scheduled more quickly after community referrals so as to offer patients a more comprehensive service.
Psychiatric assessment led to changed diagnoses for 28% (8/29) of patients. This figure was 40% (2/5) for the HR group and 25% (6/24) for the CR group.
Medications were changed for 69% (20/29) of patients seen by a psychiatrist. In the subgroups; 60% (3/5) of HR psychiatric assessments resulted in a change of medication while 71% (17/24) of CR psychiatric assessments led to medication changes.
The chi-square statistic was used to evaluate whether a recent medication change, during the inpatient stay or at the most recent outpatient appointment, made the CRHTT less likely to adjust medication. This indicated that there was no relationship between the two events. A similar analysis indicated that the likelihood of a medication change at the patient’s next community appointment was increased by seeing a CRHTT psychiatrist but unrelated to whether that assessment had resulted in a change of medication.
Discussion
We have demonstrated in this study that a typical CRHTT is providing a diagnostic and second opinion service. Changes in medication were more than twice as frequent as changes in diagnosis – this is perhaps unsurprising as diagnostic changes would be likely to require a different prescription.
Most community referrals were actively evaluated in terms of both diagnosis and treatment. This is a significant change to the original function of the CRHTT where a psychiatric assessment was not a standard aspect of care when very few of the original CRHTTs included a psychiatrist. This may also reflect the current pressures on community teams, which are frequently short-staffed, leading to more competition for the available clinic appointments. Consequently, patients may not have seen a psychiatrist for some time and their requirements may have changed. It is, however, also known1 that community patients who have not been reviewed recently or who have a long wait before their first assessment are more likely to present in crisis.
The diagnostic and second opinion function of the CRHTT is more prevalent when patients have been referred by the community team (67% reviewed, 47% medication changed) rather than on discharge from hospital (24% reviewed, 14% medication changed). This appears to largely reflect the fact that relatively few discharges were seen by the CRHTT psychiatrist because these patients had just received a full consultant-led discharge treatment plan. This may be another example of community service pressures leading to patient crises and thus engagement with alternative services – in this case inpatient care may be offering a second opinion service. The current separation of community and inpatient services will augment this effect as previously the patient would have been more likely to receive continuous care from the same consultant. This is an interesting view of current service configuration. The reduced continuity of care is often seen as a disadvantage but it does present an opportunity for a fresh evaluation of a patient’s diagnosis and medication by a different psychiatrist.
Longer lengths of stay with the CRHTT made psychiatric assessments more likely. It was particularly clear that discharge within a week made a psychiatric review unlikely. The proportion of community-referrals seen by a CRHTT psychiatrist could be increased to 83% if patients were to be seen within 24 hours. This figure is derived from the assumption that psychiatrists would then see the same proportion of both long and short stay patients. The residue would include those patients who refuse to engage with such an appointment.
It is interesting that chi-square statistical analysis suggests that the only influence on prescription change at the next appointment is whether the patient was seen by a CRHTT psychiatrist. It is not related to whether or not the CRHTT psychiatrist changed the medication. It is difficult to see why this should be the case unless the community psychiatrists consider the patients’ needs in more detail or are tempted to regain control after the referral to another psychiatrist.
In conclusion, the addition of psychiatric care to CRHTTs may be a valuable adjunct to the current pressures on community teams. The current trend to separate community, inpatient and CRHTT care is often cited as a disadvantage due to reduced continuity of care for patients. This project has drawn attention to the fact that it also offers opportunities for new teams to re-evaluate both diagnosis and treatment which offers patients the advantage of an internal second-opinion service. This advantage could be offered to more community-referred patients, albeit with more resources, by ensuring that they are assessed by the CRHTT psychiatrist within 24 hours.
Limitations
This is a small study conducted in a single CRHTT. It does, however, offer an indication of the evolving role of the CRHTT and its relationship to other services.
Psychiatric trainees in Iraq face many challenges that limit their immediate access to improved training opportunities. These include limited access to classroom teaching, regular clinical supervision meetings and fewer opportunities to attend international conferences and placements. These challenges are more acute in those specialities with the greatest shortage of consultants (for example, forensic and child and adolescent psychiatry).
Furthermore, the fragile security situation in the capital and larger cities and the post-conflict disruption to educational institutions consequent to these difficulties makes it difficult for those in the UK and elsewhere to visit the country and support educators and training on the ground.
Against this background and as a medical educational team in the UK (Oxford University Medical Education Fellows, OUMEF) with an interest in developing training opportunities for peers and colleagues in Iraq, we set up the Oxford Psychiatry in Iraq (OxPIQ) Project, beginning with a project development team that included Medicine Africa, an experienced online distance learning platform.
So what is the role of TEL in the delivery of online distance learning targeted at medical professionals in these circumstances?
Meeting the Challenge – the role of TEL
The concept of Technology-enhanced Learning (TEL), or Web-based learning (WBL), defined as the use of information and communication technologies in teaching and learning 1, is a relatively new phenomenon. Nevertheless, there is a considerable body of evidence supporting the use of TEL in various clinical and non-clinical settings.
Mccutcheon et al. 2 systematically reviewed thirteen studies and found that ten of these studies concluded that online learning is as effective as traditional or classroom teaching, despite the limitations of some of these studies.
In a large meta-analysis, Means and colleagues 3 concluded that students using online teaching performed modestly better compared to students learning similar material using face-to-face teaching. Combining face-to-face and online teaching resulted in larger benefit compared to the use of face to face methods only.
TEL can address the learning limitations in classroom settings due to expanding curriculum coverage and limits on contact time between students and lecturers/trainers alike. It can contribute to better use of such face-to-face classroom contact through the facilitation of the flipped classroom approach. 4 In this approach (also called inverted instruction and upside-down teaching), students acquire the basic information of the lesson outside the class (usually using online materials) and then develop their knowledge further in the class by sharing their learning, interacting with other classmates and teacher, and discussing various aspects of the study topic.These advantages have enabled TEL to revolutionise distance learning at many levels – enabling greater access to education by overcoming geographical and time-zone boundaries.
An allied concept within distance TEL is the concept of virtual teams 5 where health professionals come together to teach and learn from each other independent of location. Of itself, this offers some advantages. These include the possibility of addressing speciality-specific training gaps through the incorporation of the relevant expertise within the team - and to the creation of what is termed “connectivism”. This term refers to the use of internet technologies to enhance learning through online peer networks 6 and the development of communities of practice. 7 The latter allows for workplace-based learning with trainees learning from more experienced practitioners and moving towards the same through greater competency acquisition.
In a similar vein, creating networks of professionals may help to establish more longer-lasting relationships of mutual benefit between the UK and Iraqi professionals (e.g. through collaboration on training programmes, conferences, etc.). Also, cross-cultural online learning has been shown to be very useful in improving language skills and cultural awareness of learners and educators. 8 With language translation technology, any language difficulties can also be overcome, especially if the educator can observe the learners’ responses to the translated text and offered the opportunity to give further explanations and clarifications when necessary. 9 Finally, as well as sharing knowledge and experience within groups, TEL enables opportunities for mentoring and coaching individuals. 10
For our purposes, these findings and opinions support the use of online learning as a suitable distance learning “add-on” to existing training opportunities in Iraq.
TEL and Learning Theories
Learning theorists suggest that experiential and constructive learning theories are most appropriate to learning in the clinical context. Both are possible with TEL (as well as being facilitative of behaviourist and cognitivist approaches).
For example, the virtual classroom environment can enhance the learning experience of the participants by improving their analytical skills by thinking through case formulation and management plans. 11 Participants in online learning could be assessed and receive the feedback immediately. Ideas can be shared, and there is no passive acquisition or transfer of knowledge as is the case with traditional lectures. These aspects have implications for the design of the educational sessions and are discussed below in the learning methods section.
Challenges of Online Distance Learning
There are many challenges associated with online distance learning. Firstly, there is the potential lack of the required technologies (internet access, laptops or desktop computers), the expenses of subscribing to these online learning templates, the need to have technical support, and similar technical and logistic issues. 12 These technical problems may impair access to and functioning of the virtual team. The choice of an experienced online platform must, therefore, be considered carefully.
Secondly, there may be ethical issues about the protection of patients’ confidentiality in these sessions, especially when there are different laws of privacy that are applied in the UK and Iraq. This will require knowledge of the relevant professional requirements by the tutor team for example.
Furthermore, the student-teacher relationship has traditionally been underpinned by direct face-to-face contact and being present at the same time and place. 11 Therefore, learners and educators might be less satisfied with online learning. For these reasons, the concept of blended learning (careful integration of online learning with face to face learning experience) has been developed to overcome the limitations of a standalone online or face to face learning and has been found effective and applicable in various settings. 13
Thirdly, any distance online learning programme must understand and support existing “local” training provision and arrangements, in the classroom and the workplace. This requires liaison and cooperation with the training providers and institutions on the ground.
For clinical training to be relevant, it needs to reflect the learning needs of trainees in the workplace – in keeping with adult learning principles and cognitive apprenticeship models of learning. 14 The latter includes the importance of clinical decision-making underscored by the higher levels of Bloom’s (1956) cognitive domain. 15 To this end, then appropriate learning and assessment methods are needed to enable effecting learning.
In other words, while necessary, TEL may be insufficient in enhancing learning outcomes if allied learning methods are not chosen appropriately. Also, in our view, TEL is not a substitute for bedside teaching.
Table 1 summarises this appraisal of online distance learning (using the online platform provided by MedicineAfrica).
Table 1 Strengths and limitation of using MedicineAfrica (web-based virtual classroom environment)
Strengths
Limitations
Better use of the participants time and resources
Limited or lack of internet access
Overcome geographical barriers between two countries
Technical and logistic issues
Improve critical thinking and communication skills
Subscription expenses Appropriate choice of learning methods
Form long-standing professional networks
Ethical and legal issues (e.g., confidentiality)
Interactivity
Lack of direct face to face contact
OxPIQ & Project Development Team
OxPIQ is a partnership between Medicine Africa and psychiatrist members of the Oxford University Medical Education Fellows, with experience of working in Iraq. The Oxford University Medical Education Fellows (http://OUMEF.org) is a group of trainees from across medical and surgical specialities with interest in medical education and training.
Medicine Africa (http://medicineafrica.com) is an innovative clinically targeted online platform developed in collaboration with King’s College London’s Centre for Global Health, within the King’s Somaliland Partnership. Built at low bandwidth, it enables collaboration between medical professionals in the UK and those in remote or fragile states to enhance education in various clinical specialities using online sessions (live courses and mentoring sessions). Please see Appendix 3 for a screenshot of one of the active sessions of OxPIQ.
The next step was to invite representation and support from the Iraqi Board of Psychiatry and the Medical Education Unit in Baghdad. These developments led to the formal launch of OxPIQ Partnership in March 2016. Later on, the many UK and Iraqi doctors joined the Partnership as tutors and learners.
The Virtual Learning Team: Trainees, Specialty Consultants & Tutors
Iraqi psychiatry trainees were then recruited, and their more pressing learning needs to be appraised based on their views and those of the Iraqi Board of Psychiatry supervisors. Learning needs to emerge included the management of older patients with dementia and functional disorders, assessment and management of children and adolescents (with autism and ADHD for example), forensic patients and those with drug and alcohol addiction. The team thus formed was composed of up to ten psychiatry trainees from Iraq and five senior psychiatrists/tutors each, from Iraq and the UK respectively. A schedule of fortnightly seminars was agreed and published on the learning platform. Case-based discussions were used as the main educational activity during these seminars.
Learning Methods and Processes
As noted earlier, the importance of experiential and constructivist learning methods are key to clinical education. Our literature appraisal revealed that they are essential elements of successful TEL in this context too. 16, 17 To these must be added learner engagement. 18
Virtual or online (anonymised) case-based discussions (CBDs) are valid and reliable learning tools. 16 They are interactive and centred around the students and their learning needs while a facilitator guides the process of learning. Learners are engaged through discussion of actual clinical cases, so preparing learners for real-life experience. 19 Also, expert facilitation and peer feedback to trainees promotes clinical knowledge and skills’ development. 20, 21
Effective small group teaching is characterised by four main strengths: flexibility, interaction, reflexivity and engagement. 22 Flexibility is when the teacher responds to the needs and learning of the students dynamically and helps them to explore wider pedagogic spaces. A higher degree of interactivity is usually seen in small group teaching compared to a larger group. Teachers are better able to continually engage in self-reflection and listen sensitively to students in a small group and observe the dynamics between the members of the group, leading therefore to better reflexivity. Engagement refers to encouraging the students to develop their academic identity and engage in lively debate about the various aspects of the topic discussed.
We aimed to replicate these characteristics. For example, a small group discussion allowed better interaction with each participant (interactivity); the presence of chat windows enables the facilitator to self-reflect on the process, monitor engagement and respond reflexively using questions and answers to stimulate interest and respond flexibly to individual trainee knowledge gaps. Tutors are encouraged to identify trainees’ learning needs and facilitate interactivity, and timely feedback as these are highly valued by the participants and help to keep them motivated and engaged. 18
For further reading in this area, we recommend Brindly and colleagues’ 23 ten strategies to increase students’ motivation towards and engagement with online learning (see table 2).
Table 2- Strategies to increase engagement in online teaching (modified from Brindly and colleagues, 2009) 23
1. Transparency of expectations: Making the learning objectives very clear and relevant to the participants learning needs. The teachers must be open to the learners’ suggestions and must be willing to discuss the process and purpose of the educational activities.
2. Clear instructions: The educational activity, its timing, duration, and the technical aspects are described in detail to the participants. They should not be left to ‘try out things’ and must be guided explicitly.
3. Appropriateness of task for group work: For the online activity to succeed, individual versus group tasks should be differentiated. In our example, this may be done by asking the participants to do a particular task before the session (e.g., read about severe and enduring mental illness), and then to work together on producing a formulation for the case discussed. This will increase their motivation to be involved in various tasks.
4. Meaning-making/relevance: The case-based discussions (and any online activity) should have relevance for the participants and aim to enrich their experience in their clinical work.
5. The motivation for participation embedded in course design: It is essential that participants in the online activity understand that the success of the group and the course depend on the individual effort of each participant.
6. The readiness of learners for group work: This aspect describes the development of a sense of community through a professional relationship which leads to better collaborative work.
7. The timing of group formation: Before the participants join in the educational activity, it is preferable to have some discussions before the tutorial on their learning needs to allow a time for rapport to develop to enable better group activities.
8. Respect for the autonomy of learners: Joining and leaving the educational activity (and the whole online course) should be voluntary. No penalties should be attached to leaving the course. Learners should have the freedom to choose what aspects of the online course is relevant to them.
9. Monitoring and feedback: The tutor should monitor the progress of the participants, and timely feedback is given respectfully to enhance the engagement and motivation of the participants. Please see Appendix 1 (lesson plan) for more details on feedback and evaluation.
10. Sufficient time for the task: Participants should be given time to be actively involved in the session. This is particularly important in a distant learning session when issues related to sound quality or speed of internet connection may prevent some participants from engagement.
The focus of the Lesson Plan Design
To these ends, the focus on the lesson design was on using problem-based learning methods (e.g. CBDs) within a small group setting (between 4-12 members) and a format that promoted learner engagement. A sample lesson plan is provided in Appendix 1.
In practical terms, tutorials were held fortnightly in term-time. All participants received an email notification to inform them of the session topic, and the tutor uploaded the slides from the session to the website beforehand. Participants logged-in to the site (http://medicineafrica.com) and interact with the tutor by voice (requiring only simple microphone equipment) and by writing in a chat window.
Evaluation and feedback gathering
The evaluation of the effectiveness of these sessions was reliant originally on trainees’ immediate reaction (table 3, level 1 evaluation, Kirkpatrick 24) using formal feedback tools provided online by MedicineAfrica. This feedback was shared with tutors and the Project Team. Please see Appendix 2 for the template used in collecting feedback after each session.
Subsequently, members of the project team approached trainee representatives, tutors and Iraqi Psychiatry Board leads separately for further feedback and appraisal of learning needs. Furthermore, some months after a tutorial we have asked trainees for evidence of learning across the higher levels of Kirkpatrick’s evaluation model.
Regular feedback from the Iraqi and UK participants has been positive. The sessions have been associated with improved clinical knowledge and skills of the Iraqi Psychiatry Trainees. Requests for certificates of tutorial participation have been agreed upon and provided by the project team addition, so supporting learners’ (and tutors) portfolio development.
Table 3 Kirkpatrick’s (1996) Levels of Training Assessment
Level
How to assess
Level 1: Reaction (the participants feeling about the training
Feedback during and after the tutorial using the feedback questionnaire
Level 2: Learning (improving the participants’ knowledge)
Post-tutorial questionnaire and interviews
Level 3: Behaviour-also called Transfer (improving the participant's performance)
Direct or indirect observation and assessment of the skills and competencies of the trainees
Level 4: Results (cost-effectiveness, engagement, sustainability, adherence to evidence-based practices)
regular meetings between the participants, tutors, and stakeholders.
Further cooperation
A surprising (and very welcome) outcome of the project was, through the facilitation and support of the Iraqi Board of Psychiatry, the introduction of educational workshops in Baghdad. These workshops were held in Medical City, Baghdad, in May 2017 and April 2018 and were facilitated by tutors (YH & H Al-T) from the OxPIQ Partnership. They covered targeted topics such as old age psychiatry, addiction, organic and forensic psychiatry. Trainees and senior psychiatrists from Iraq attended; their feedback showed how they valued the interactive nature of the teaching and use of CBDs as learning methods, resulting in high levels of engagement.
Conclusions
This paper describes the process of designing, delivering, and the early evaluation of an online distance TEL programme for mental health professionals based in the UK and Iraq.
TEL has had an important role in overcoming the geographical barriers and other challenges to developing training opportunities in Iraq and other developing countries. We are of the view that it could be used more often to connect professionals working in similar circumstances and with other disadvantaged groups, including refugee and asylum seekers. It is a flexible way of providing training to professionals working with those groups in relatively remote and resource-deprived environments.
Greenhalgh 25 suggests that three factors are needed for the success of online educational activity: ease of access, perceived usefulness of the activity to the learning requirements of the students, and the interactivity of the session. In our experience, these are important. Also, we believe that additional consideration should be given to (i) working with an experienced online platform provider; (ii) working with local educational institutions, trainers and learners to identify unmet learning needs and support existing learning opportunities/programmes; and (iii) adopting an iterative approach to feedback and evaluation.
Appendix 1: Example of a Lesson Plan
Session title
Case-based discussion on management of severe and enduring mental illness.
Duration of session
60 minutes
Tutor
A UK-based Psychiatrist
Learner group
Psychiatry Board Trainees and Senior Psychiatrists in Iraq and UK
Step 1– Learning outcomes
a) Describe the various stages in the management of the cases discussed during the session.
b) Enhance the participants learning using case-based discussion with peers and seniors in the UK and Iraq.
c) Improve the presentation and discussion skills of the participants and their communication skills.
d) Explore ethical, cultural, and social issues related to the management of mental disorders and improve cultural competency and awareness.
Step 2 – Learning Plan
Introduction to the online tutorial -10 minutes
a) Highlight the learning objectives of the tutorial
b) Stimulate the thinking of the participants by asking about their current knowledge of the subject, whether they managed similar cases in their clinical work, and what are their learning needs.
c) Outline the tutorial structure and further engage the participants by informing them about other details (e.g., if they can ask the question during or after the case presentation)
2. The tutorial in a case with severe and enduring mental disorder – 30 minutes
a) Participants are encouraged to interact with the tutor who should be invited to keep the tutorial interactive.
b) The case presented will provide an overview of the patient’s journey from the initial presentation, followed by the investigation, then treatment plans. Discussions of the differential diagnosis are important.
c) The tutor will assess the knowledge of the participants by asking questions on the various aspects of the case presentation (e.g., what is your differential diagnosis for a patient presenting with auditory and visual hallucination? What investigations would you request?).
3. Recap and Q&A time- 20 minutes
a) Tutor to give a summary of the main learning points from the tutorial and linking these to the learning outcomes presented at the beginning.
b) Participants are given enough time to ask questions and to participate actively in the session.
Step 3 – Assessment
Before Lesson
Before the tutorial, the tutor should know the current educational curriculum of the participants and their learning outcomes in that subject. UK and Iraqi Psychiatry curriculum are different, and therefore knowing what is relevant is important.
Stating the learning outcomes at the beginning of the tutorial will also help in the baseline assessment of the knowledge and skills of the participants.
Pre-session questionnaires could be used as well (for example, asking questions on the prognosis of various mental disorders and comparing the participant’s knowledge before and after the session).
After the lesson
· Ongoing assessment during the tutorial using questions on various aspects related to the case presented.
· Questions in the recap section at the end of the tutorial.
· Post tutorial feedback forms will allow the participants to give their views about their learning needs and if they feel the tutorial was relevant to their learning outcomes.
It is important to provide personalised feedback to the participants about their performance on these assessment tools as this will help them to identify gaps in their knowledge and improve their learning. 26
Step 4 – Resources required
MedicineAfrica is free to join and designed to work well even with low bandwidth. Hence it won’t be affected by slow internet connections which are likely to be the case in developing countries.
Trainees and Tutors will need a computer (desktop or laptop) with an internet connection. No other resources are needed. Recommended readings could be disseminated by email to the trainees after the session.
Step 5 – Evaluation
Student evaluation
Gathering feedback is an essential step to influence the learning outcomes favourable and continue to improve the structure and content of the tutorials (After the tutorial, the participants will be asked to fill an electronic feedback form (please see Appendix 2).
The form contains various questions with rating (from 1-5, ranging from strongly disagree to strongly agree) on various aspects of the tutorial. These include structure, organisation, the range of aids used and meeting of the learning outcomes.
Also, direct feedback from the trainees, tutors, facilitators, and the stakeholders responsible for running the online learning platform is gathered to assess the effectiveness of these tutorials.
Teacher evaluation
Professionals invest a significant amount of time and efforts in these lessons, and it is imperative to assess how the tutorials could be improved to meet the needs of the trainees and keep them and the tutors motivated and interested. Tutors in these tutorials meet regularly using Skype to reflect on their teaching sessions and discuss ways of improving the delivery and quality of the tutorials.
Mutual learning is another aspect that needs to be assessed (is the tutor also benefitting from these lessons, for example, by improving their cultural competencies or their teaching skills).
Appendix 2: Feedback form to be completed by the participants after the session
Session title
Case-based discussion on management of severe and enduring mental illness.
Speaker
Date
Content
The session was relevant to my training needs
Strongly disagree 1 2 3 4 5 Strongly agree
Organisation
Sufficient time was allowed for the session
Strongly disagree 1 2 3 4 5 Strongly agree
Presentation
The session was well presented
Strongly disagree 1 2 3 4 5 Strongly agree
The session was delivered at the right pace
Strongly disagree 1 2 3 4 5 Strongly agree
The session was interactive and encouraged discussion/questions
Strongly disagree 1 2 3 4 5 Strongly agree
Structure
The session was well organised and structured
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were clear
Strongly disagree 1 2 3 4 5 Strongly agree
The aims and objectives of the session were met
Strongly disagree 1 2 3 4 5 Strongly agree
Overall evaluation
Overall, I would rate this session as
Extremely poor 1 2 3 4 5 Extremely good
Appendix 3: MedicineAfrica screenshot during an active session
The recent increase in the number of patients presenting with a borderline personality disorder (BPD) in general adult psychiatry and primary care is creating pressure within the National Health Service (NHS)1.Currently, BPD is perceived to be like an ‘epidemic’ entity, particularly in areas with a high incidence of socioeconomic deprivation. Similarly, there is a parallel increase in the human and medical resources needed to manage this disorder efficiently. In fact, the authors have found that BPD tends to be comorbid with factitious disorders and depression (Tripolar syndrome) with a tendency to overuse hospital and medical facilities, inclusive of Accident and Emergency (A&E) departments, family doctors and General Practitioner (GP) surgeries2.
Consequently, patients with BPD require a constant and unlimited allocation of medical and psychiatric resources, together with targeted care plans. In fact, they might be prone to frequent self-referrals to A&E, seek hospital admissions and augment all their psychotropic medications in order to deal with their on-going crises not solvable in their homes. Also, the skills needed by healthcare personnel to reduce chronic self-harming and suicidal ideation in this vulnerable population are complex and need to be updated on an on-going basis also due to the tendency of these patients to raise allegations towards their healthcarers3. Nonetheless, the provision of treatment is often hindered by various healthcare system limitations, such as the lack of beds on medical and psychiatric units, forced reduction in the length of stay in a hospital and insufficient human resources. This scenario has mostly affected female patients with BPD who seek admission to psychiatric hospitals often for respite from chronic suicidal ideation4.Moments of amplified suicidal ideas become evident when internal voices, perceived as auditory hallucinations commanding to self-harm or to commit suicide, become more intense5.
As observed by the authors of the current editorial, increased suicidal ideation in persons with BPD also occurs during minor crises in life, when experiencing intensified flashbacks about past abuses, during minor losses, after significant conflicts with others and after the separation from influential people in their social network. Besides, admissions in psychiatric wards, very commonly, occur when there is an intensification of internal voices commanding BPD patients to take overdoses of the prescribed medication or to jump in front of a train, a car or off a pier to commit suicide. Police is often involved to stop these dramatic plans. At the same time, healthcare professionals are discouraged by the complex management of patients with BPD, which, in combination with their tendency to challenge or make unwarranted allegations against their health carers, results in feelings of sadness, rejection and alarm in the latter. Kanin reported that the reason to produce a false allegation is to create a defence or to get compassion6. Nonetheless, it is also likely that some healthcare professionals might have some preconceived ideas about people with Borderline Personality Disorder, which might reduce the depth of health carers’ empathy towards these patients and lead to burnout after prolonged treatment of BPD in hospital or community. Attempts to treat and to reduce suicidal ideation and self-harm in this group of patients are often thwarted as they challenge medical decisions and endeavour to sabotage the proposed care plans. The strain on the doctor-patient relationship is determined by the underlying ‘Mistrust/Abuse’ scheme of patients with BPD who expect from others, and are thus sensitive to, signals of relational wound, treachery and abuse7.
Consequently, a chronic feeling of inadequacy in patients with BPD translates itself in enduring dissatisfaction with any therapy and healthcare professionals. Hence, in the authors’ experience, any attempt to establish a long-term therapeutic relationship with BPD patients might have limited outcomes. Frustration in healthcare professionals aiming to create an enduring therapeutic alliance with patients with BPD happens as these patients tend to interpersonal biases and to ascribe undesirable experiences to people (hence to healthcare professionals) as opposed to circumstances8. Therefore, social interactions with primary carers result in dissatisfaction of people with BPD about any medical or psychiatric plan is set up for them. Consequently, community teams, general practitioners and hospital staff feel hopeless due to recurrent readmissions of people with BPD and the lack of definitive treatment for such pathology. Stress caused by difficulties encountered in ensuring that BPD patients comply with the therapy regularly places doctors and nurses at crisis point.
Once in the hospital, discharging patients with BPD can be difficult as they are frequently reluctant to return to the community, leading to recurrent readmissions within a short period. In fact, the period before discharge from a psychiatric hospital is complicated by mounting anxiety and distress in patients with BPD. The authors observed a regular escalation of self-harming behaviours and increased suicidal ideation in these patients just before discharge, possibly indicating their underlying anxiety in going back to the home environment. Many BPD patients suggest that they would rather stay in the hospital instead of returning to the community that is considered by them as unsafe or unstructured. Furthermore, as these patients have an intense vulnerability to social rejection, they rarely feel adequate during social interactions thus developing an enduring sense of solitude9. Therefore, any hospital discharge or a visit to the GP will be interpreted by them as disappointing and will lead patients with BPD to confirm their sense of rejection. As a reaction, the authors observed that BPD patients demand endless and unconditional attention from their primary carers. Attempts by patients with BPD to self-harm or commit suicide intensify over weekends or public holidays as their sense of solitude increases during these periods, especially when there is also a shortage of healthcare professionals available for immediate support.
The authors of the current editorial propose possible strategies of intervention both on the psychopharmacological and managerial side. The challenge is that patients with BPD often use overdoses of oral medication in a suicide attempt10. Hence, the authors recommend the use of long-lasting depot antipsychotic injections (e.g., Zuclopenthixol Decanoate) to stabilise their mood and reduce impulsivity, the risk of overdoses, pseudo-psychotic symptoms and command hallucinations leading to deliberate self-harm. The use of oral lithium to treat mood swings poses an ethical dilemma for doctors as it could be lethal when used as an overdose. Healthcare management is another way of intervention. One point of difficulty is the tendency of patients with BPD to split their teams and to create niches of protectors and opposers within staff with possible conflicts within the team that is treating them. In this case, inter-professional coordination, integrated care and constant information sharing are required11. Furthermore, several healthcare services treating patients with BPD are trying to find an integrated approach for their hospital and community treatment. The authors speculate that the increased number of admissions of patients with BPD is reducing the total capabilities of physical and mental wards to treat patients with other pathologies. Besides, the dramatic presentation of patients with BPD who tend to overuse the healthcare services poses ethical dilemmas in their management. This scenario has created discrepancies in health care policies about treatments and hospital (re)admissions of patients with BPD reaching an epidemic magnitude in many healthcare trusts. Hence, a new culture is required for the management and treatment of patients with BPD in the community.
Culture is defined as the character of an institution that affects employee gratification and organisational accomplishments12.What is needed is a frank and constructive dialogue between healthcare managers, leaders and medical staff in the hospital and in the community. Furthermore, clear and regional guidelines should exist to improve the efficacy of care which is offered to BPD patients at home and to reduce the constant risks which patients pose to themselves, their sense of solitude and their tendency to seek hospital admission in order to solve chronic existential difficulties. A model of integrated care comes from Max Weber who differentiated between ‘formal rationality’, the endorsement by healthcare managers of the most efficient ways of achieving organisational goals (e.g., ensuring more hospital beds by quick discharges of ‘bed blockers’), and ‘substantive rationality’, the expectation by healthcare professionals that values and morals should instead be based on tradition, compassion and dedication13;pertinent to the care of BPD patients in our case. The collaboration of all those involved parties is also important to reduce the risk of ‘silo management’ where confined and regional policies do not embrace a wider perspective for the management of specific problems while responding only within the confines of the own guidelines and procedures14.In these cases, integrated care in communities can halt self-harming and suicidal attempts of patients with BPD. The organigram sees inter-professional actions, targeted psychopharmacological policies and psychiatric crisis teams in A&E that can reduce the need to hospitalise patients with BPD at any ensuing crisis.
Several studies found that refugees develop post-traumatic stress disorder (PTSD) after having endured war trauma1, or certain circumstances related to migration like moving to a new country, being unemployed and poor housing2. PTSD is described as distress and disability due to a traumatic event that occurred in the past3. In 2013, the American Psychiatric Association revised the PTSD diagnostic criteria in the fifth edition of its Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and PTSD was included in a new category, Trauma- and Stressor-Related Disorders4. All of the conditions included in this category required exposure to a traumatic or stressful event as a diagnostic criterion4. The person with PTSD often avoids trauma-related thoughts and emotions, and discussion of the traumatic event4. PTSD patients are invariably anxious about re-experiencing the same trauma. The trauma is usually re-lived by the person through disturbing, repeated recollections, flashbacks, and nightmares4. Symptoms of PTSD generally begin within the first 3 months after the provocative traumatic event, but may not begin until several years later4. A large number of children (10-40%), 16 or younger, who have experienced a traumatic event in their life, tend to develop PTSD later on5. Moreover, many families with children growing in war zones and then moving to safer places, experience trauma, stress and reduced functioning6. These families have different resilience rates in their survival mechanisms, coping strategies and adaptation levels7.
The latest war in Syria has led to the migration of large parts of the Syrian population to neighboring countries such as Lebanon, Jordan and Turkey8.The United Nations High Commissioner for Refugees (UNHCR) estimates that approximately 1.5 million refugees are located in Lebanon9. These refugees have been exposed to several types of traumatic events that may increase the incidence of mental health problems10.
We hypothesize that the proportion of positive PTSD screens would be high among Syrian refugees with the presence of some specific related risk factors. Thus, the objective of our study was to examine PTSD symptoms and to determine the associated risk factors in a sample of Syrian refugees living in North Lebanon.
METHODS
1. Study design and population
This was a cross-sectional study that aimed to assess the proportion of Syrian refugees in North Lebanon who were at high risk of developing PTSD, and to examine the association of PTSD high risk with other factors. The survey was carried out during February and March 2016. A convenient sample of Syrian refugees of both gender, aged between 14 and 45 years, living in North Lebanon, was selected out of a population of 262,15111.
The estimated minimum sample size, calculated using Raosoft sample size calculator, with a margin of error of 5% and a confidence interval of 95%, was 384 refugees. A total number of 450 Syrian refugees, residing in individual tented settlements (ITSs), collective shelters (CS) or Primary Health Care Centers (PHCs) located in North Lebanon, was selected according to inclusion and exclusion set criteria.
The inclusion criteria were: Syrian refugees, aged (14-45 years), physically and mentally independent. Hence, all subjects that were younger than 14 or older than 45, speechless, deaf, physically and mentally dependent, or have undergone recent moderate or severe surgery (less than one week earlier), were excluded from the study.
2. Ethical considerations
The study protocol received approval from the Notre Dame University (NDU) Institutional Review Board (IRB). The approval comprised details about the procedure of the study and the rights of the participants. Informed consent was obtained from each participant. The questionnaires were answered anonymously, ensuring confidentiality of collected data.
3. The Interview questionnaire
The interview questionnaire was divided into six sections consisting of a total of 46 questions. The questions were dichotomous, close-ended and open-ended. A cover page described the purpose of the study, ensuring the anonymity and confidentiality, and soliciting the consent of participants. The questionnaire collected data on the demographic and socio-economic characteristics of the participants. Information about health status and stressful life events (SLE) were also obtained. The PC-PTSD (Primary Care Post-Traumatic Stress Disorder) tool was used to screen PTSD.
For the purposes of the study, subjects were classified as having/not having positive PC-PTSD. The results were used to calculate the proportion of Syrian refugees who are at high risk of developing PTSD.
PC-PTSD questionnaire: The PC-PTSD was initially developed in a Veteran Affairs primary care setting and is currently used to screen for PTSD, based on the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-4) diagnostic criteria12. The screen consisted of 4 questions related to a traumatic life event: In the past month you (1) Have had nightmares about it or thought about it when you did not want to?; (2) Tried hard not to think about it or went out of your way to avoid situations that reminded you of it?; (3) Were constantly on guard, watchful, or easily startled?; (4) Felt numb or detached from others, activities, or your surroundings? The answers to these questions were dichotomous (Yes/No) and the total screen was considered "positive" when a patient answered "yes" to three out of four questions. PC-PTSD showed a high sensitivity (86%) and moderate specificity (57%) when using a cutoff score of 213.
In order to validate the Arabic version of the PC-PTSD questionnaire, it was translated into Arabic and translated back into English. The original version of the Arabic questionnaire was pilot-tested on 10 Syrian refugees to ensure the validity of the answers, and to guarantee its reliability.
Anthropometric measurements: The main anthropometric measurements were weight and height. Participants were dressed in light clothes and barefooted, and standing height was measured to the nearest 0.1 cm using a stadiometer. Body weight was measured to the nearest 100g using an electronic scale. Body Mass Index (BMI) is a measure of weight adjusted to height (kg/m2), calculated by dividing weight (in kilograms) by the square of height (in metres). For the purposes of the study, BMI was recoded into four categories: underweight, normal, overweight and obese.
4. Data entry and statistical analysis
The Statistical Package for Social Science (SPSS) for Windows (version 22) was used for data entry and analysis.
First, bivariate analyses of categorical variables were performed using the Fisher exact tests, Chi-squared tests and Student’s t-test. The dependent variable was the high risk of PTSD, using the PC-PTSD tool. Thus, the PC-PTSD score was considered the dependent variable: a dichotomous variable of PC-PTSD (-) and PC-PTSD (+), and all variables that might be a risk factor or might lead to PTSD were set as the independent variables. Two main independent variables were: age and gender. Other variables included: marital status, place of residence, number of people and families living in the same household (crowding index), income, education status, profession, work status, lifestyle habits, medical or psychological problems, medication taken and SLE. Frequencies and percentages were calculated for qualitative variables, and mean and standard deviations for quantitative variables (BMI, crowding index). A p-value of 0.05 or less was considered to be statistically significant.
RESULTS
Table 1: Socio-demographic characteristics of the 450 Syrian refugees
Variables
Frequency (n) or Mean
Percentage (%) or Standard Deviation
Gender
· Male
69
15.3
· Female
381
84.7
Age (years)
27.9
8.1
Crowding index (co-residents/room)
4
2.4
Crowding index
· ≤ 2.5
135
30
· 2.51-3.5
108
24
· > 3.5
207
46
Current place of residence
· Tented settlements
62
13.8
· Collective shelters
92
20.4
· Building
296
65.8
Educational level
· Don’t know how to read and write
33
7.3
· Know how to read and write/Elementary
216
48
· Complementary/Secondary/Technical
178
39.6
· College degree
23
5.1
Marital status
· Single
54
12
· Married
378
84
· Divorced
5
1.1
· Widowed
13
2.9
Current employment status
· No
379
84.2
· Full-time job
40
8.9
· Part-time job
31
6.9
Presence of income
· No
379
84.2
· Yes
71
15.8
Perceived income (n=71)
· Satisfactory
25
35.2
· Non-Satisfactory
46
64.8
Table 2: Health characteristics and migration factors of the 450 Syrian refugees
Variables
Frequency (n)
Percentage (%)
BMI category (kg/m2)
· <18.5
11
2.4
· 18.5-24.9
176
39.1
· ≥ 25
263
58.5
Tobacco consumption
· Yes
97
21.6
· No
353
78.4
Presence of medical conditions
· No
337
74.9
· Yes
113
25.1
Migration status
· Before 2011
15
3.3
· 2011-2013
339
75.3
· After 2013
96
21.4
Seeking professional help for psychological disorders
· No
439
97.6
· Yes
11
2.4
Number of stressful life events
· None
22
4.9
· [1-2]
181
40.2
· [3-4]
235
52.2
· [5-6]
12
2.7
PC-PTSD
· Negative
237
52.7
· Positive
213
47.3
Table 3: Socio-demographic characteristics associated with positive screen for PTSD among the 450 Syrian refugees (bivariate analyses)
Variables
Positive PC-PTSD n(%) or mean±SD
Negative PC-PTSD n(%) or mean±SD
p-value
Gender
0.011*
· Male
23 (33.3)
46 (66.7)
· Female
190 (49.9)
191 (50.1)
Age (years)
28.9 ± 7.6
26.9 ± 8.5
0.009*
Crowding index (co-residents/room)
4.2 ± 2.7
3.8 ± 2.2
0.069
Crowding index
0.294
· ≤ 2.5
58 (43.0)
77 (57.0)
· 2.51-3.5
49 (45.4)
59 (54.6)
· > 3.5
106 (51.2)
101 (48.8)
Current place of residence
0.137
· Tented settlements
27 (43.5)
35 (56.5)
· Collective shelters
52 (56.5)
40 (43.5)
· Building
134 (45.3)
162 (54.7)
Educational level
0.479
· Don’t know how to read and write
16 (48.5)
17 (51.5)
· Know how to read and write/Elementary
95 (44.0)
121 (56.0)
· Complementary/Secondary/Technical
· University level
92 (51.7)
86 (48.3)
10 (43.5)
13 (56.5)
Marital status
0.000*
· Single
9 (16.7)
45 (83.3)
· Married
191 (50.5)
187 (49.5)
· Divorced
4 (80.0)
1 (20.0)
· Widowed
9 (69.2)
4 (30.8)
Current employment status
0.205
· No
184 (48.5)
195 (51.5)
· Full-time job
14 (35.0)
26 (65.0)
· Part-time job
15 (48.4)
16 (51.6)
Presence of income
0.233
· No
184 (48.5)
195 (51.5)
· Yes
29 (40.8)
42 (59.2)
Perceived income (n=71)
0.264
· Satisfactory
8 (32.0)
17 (68.0)
· Non-Satisfactory
21 (45.7)
25 (54.3)
*Significant with p-value < 0.05
Table 4: Health characteristics and migration factors associated with positive screen for PTSD among the 450 Syrian refugees (bivariate analyses)
Variables
Positive PC-PTSD n (%)
Negative PC-PTSD n (%)
p-value
BMI category (kg/m2)
0.183
· <18.5
7 (63.6)
4 (36.4)
· 18.5-24.9
75 (42.6)
101 (57.4)
· ≥ 25
131 (49.8)
132 (50.2)
Tobacco consumption
0.369
· Yes
42 (43.3)
55 (56.7)
· No
171 (48.4)
182 (51.6)
Presence of medical conditions
0.000*
· No
143 (42.4)
194 (57.6)
· Yes
70 (61.9)
43 (38.1)
Migration status
0.094
· Before 2011
5 (33.3)
10 (66.7)
· 2011-2013
154 (45.4)
185 (54.6)
· After 2013
54 (56.2)
42 (43.8)
Seeking professional help for psychological disorders
0.003*
· No
· Yes
203 (46.2)
236 (53.8)
10 (90.9)
1 (9.1)
Number of stressful life events
0.000*
· None
0 (0.0)
22 (100.0)
· [1-2]
66 (36.5)
115 (63.5)
· [3-4]
138 (58.7)
97 (41.3)
· [5-6]
9 (75.0)
3 (25.0)
* Significant with p-value < 0.05
All the socio-demographic, health and migration characteristics of our sample of Syrian refugees were described in Tables 1 and 2. Out of the 450 participants, 47.3% had positive PC-PTSD. In order to study the association between the socio-demographic characteristics among the Syrian refugeesand PTSD screening, abivariate association was explored as shown in Table 3. The results indicate a significant difference between gender groups, as almost half of the women (49.9%) had a positive screen for PTSD compared to 33.3% of the men (p=0.011). Mean age was significantly higher in refugees with positive PC-PTSD (28.9 ± 7.6 years) versus those with negative PC-PTSD (26.9 ± 8.5 years) (p=0.009). PTSD screening was shown to be significantly associated with marital status. In fact, positive PC-PTSD was mostly perceived in divorced participants (80%) compared to 69.2% of widowed, 50.5% of married, and 16.7% of single subjects (p=0.000). Yet, crowding index, current place of residence, educational level, employment status, and income were not significantly associated with positive PC-PTSD (p>0.05).
The association of health characteristics and migration factors among the Syrian refugees with PTSD screening was displayed in Table 4. A significant association was observed between the presence of medical condition and positive screen for PTSD, as 61.9% of subjects suffering from a medical condition had a positive PC-PTSD, compared to 42.4% of participants without medical conditions (p=0.000). However, BMI and tobacco consumption were not significantly associated with PTSD screening (p>0.05). PTSD screening was significantly associated with the presence of psychological disorders. Thus, 90.9% of refugees who sought professional help for psychological disorders had positive PC-PTSD, versus 46.2% of those who did not (p=0.003). Positive PC-PTSD was significantly associated with the increase in the number of SLE. In fact, none of the participants without any stressful event had a positive PC-PTSD, compared to 36.5% of participants with 1-2 SLE, 58.7% of participants with 3-4 SLE and 75% of participants with 5-6 SLE (p=0.000). On the other hand, no significant association was observed between PC-PTSD and migration status (p>0.05).
DISCUSSION AND CONCLUSION
PTSD represents the most frequently occurring mental disorder occurring among refugees14. PTSD prevalence rates ranging between 15% and 80% have been reported in refugees. A study of Cambodian refugees living in the Thailand-Cambodia border camp indicated that 15% had PTSD15. A cohort study aimed to show the prevalence of PTSD among Iranian, Afghani and Somalian refugees that have moved to the Netherlands at a 7-year interval [(T1=2003) - (T2=2010)]. Results displayed a high prevalence at both T1 (16.3%) and T2 (15.2%). The reason for this high unchanged prevalence may be due to the late onset of the PTSD symptoms, and the low use of mental health care centers16. De Jong and colleagues reported that 50% of the refugees in Rwandan and Burundese camps had serious mental health problems, mainly PTSD17. While Teodorescu and colleagues aimed to illustrate the prevalence of PTSD among refugees in Norway; results showed that 80% of the refugees had PTSD18. In our study, the high proportion of positive screen for PTSD among Syrian refugees was estimated at 47.3%. In 2006, a mental health assessment demonstrated that Lebanese citizens exposed to war were more likely to develop psychiatric problems such as PTSD19. Subsequently, a cross-sectional study was done in South Lebanon on 681 citizens in 2007 (1-year after the 2006 war in Lebanon). The aim of the study was to examine the prevalence of PTSD 12 months after 2006 war cessation. Results showed that the prevalence of PTSD was 17.8%19. A recent cross sectional study, aimed to show the prevalence of PTSD and explore its relationship with various variables. The study included 352 Syrian refugees settled in camps in Turkey. An experienced psychiatrist evaluated the participants, and results demonstrated that 33.5% of study participants had PTSD, mainly female refugees, people who experienced 2 or more SLE, or those who had a family history of psychiatric disorder20.
PTSD has been associated with a wide range of traumatic events: emotional or physical abuse21, sexual abuse22, parental break-up23, death of a loved one24, domestic violence25, kidnapping26, military services27, war trauma28, natural disasters29 and medical conditions including cancer30, heart attack31, stroke32, intensive-care unit hospitalization33, and miscarriage34.
Our findings should be interpreted taking into account several limitations. The first limitation is the use of screening tools, instead of the more accurate diagnosis of the clinician, in order to detect PTSD. Given that a standardized screening tool for PTSD was used, our rates are likely an overestimate of the true prevalence rates. Secondly, this study was conducted with a limited sample of Syrian refugees and therefore should not be generalized to all refugees of other eras or from other countries. The third limitation is represented by the lack of information on the presence of other Axis I psychiatric comorbidities such as anxiety or mood disorder that could facilitate the development of PTSD or influence its manifestations35-36.
Refugees are an important group to examine, given the high prevalence of mental health disorders. Although refugees are evaluated for health problems, currently there are no standardized screening and clinical practice guidelines for assessing PTSD in all refugees. Therefore, we may be missing opportunities to detect and treat these harmful and potentially fatal conditions. Our findings suggest the need to consider a standardized screening tool for PTSD in this population. In addition, a far greater percentage of patients may have “PTSD symptoms,” that are abnormal but do not meet full criteria of the DSM5 for PTSD diagnosis, but still cause functional impairment and may later develop into a diagnosable PTSD. Given the overall high prevalence, one possible model for evaluation would be a stepped screening approach: Positive screens for PTSD could trigger a standardized clinical diagnosis for PTSD with more comprehensive assessment and early intervention. Considering the high cost of treating individuals with PTSD, screening and intervention strategies should be addressed. Greater awareness among providers and increased targeted assessment and treatment efforts may increase early detection of a wide range of PTSD, preventing more serious future health problems and functional impairment among refugees.
The Royal College of Psychiatrists (RCPsych) launched its five-year Recruitment Strategy in 2011 aiming to achieve a 50% improvement in recruitment to core psychiatry training and a 95% fill rate of posts by the end of the five-year campaign (1). The primary focus of this campaign was on recruiting UK medical graduates.
Two of the Strategy’s main aims were to highlight good practice in undergraduate teaching and to improve the teaching skills of psychiatrists to inspire and influence medical students during their psychiatry curriculum.
The Strategy stressed the importance of good clinical placements in psychiatry and recommended that medical students should ideally be placed only with ‘the best teachers and welcoming teams’ avoiding colleagues who are disillusioned with psychiatry or not happy with their jobs.
It is therefore essential that psychiatrists and other clinicians play an important role to improve the medical students placement in their workplace in order to give the students a positive expereince of this speciality and hopefully promote it as a future career option.
Background
Fourth-year medical students from the University of East Anglia (UEA) spend two months rotating through various mental health services as part of their clinical placement in the Mind Module (also known as Clinical Psychiatry or Module 11).
As part of this rotation, students are placed in Old Age Psychiatry for six days over a two-week period. They shadow clinicians in two community teams, two inpatient wards and the Electro-Convulsive Therapy (ECT) clinic. All of these teams are based at the Julian Hospital in Norwich.
The students are encouraged to talk to patients and carers and perform basic clinical tasks such as mental state examination and risk assessment. Table 1 summarises the learning outcomes for students during their placement.
Table 1- The learning outcomes for students during their Old Age Psychiatry placement
Gain clinical experience of diagnosis and management of mental health problems (including dementia) in older people.
Improve the communication skills with regard to interactions with older people with mental disorders and their carers.
Enhance the student’s understanding of the nature of the multi-disciplinary team (MDT) model in mental health for older people, particularly the social aspect of care and end of life care.
After each rotation, each student is asked to complete a feedback form regarding their placement. This feedback helps the module leads and clinicians to improve the students learning experience.
Before the implementation of our placement improvement project, the students did not feel that they were meeting their learning outcomes. Table 2 summarises the major areas that needed improvement.
Table 2- Areas needed to improve before the implementation of the new placement structure
Poor planning and organisation of the clinical placement.
Inadequate or no information sent before starting the placement.
Lack of a dedicated coordinator to design the placement timetable and allocate students to specific clinicians
Lack of multidisciplinary teaching and hence poor understanding of the various roles of professionals (e.g., memory assessors, community nurses, support workers, etc.).
Students felt that clinicians were too pressured to supervise students. Some students reported that they were sometimes sent off as the staff had been too busy or there insufficient volunteers from clinical staff to take a student.
Student dissatisfaction with clinical placements is not unique to psychiatry. Research has shown that educators and learners face significant challenges when teaching and learning take place in any clinical setting. See Table 3 for a summary.
Table 3- Challenges of teaching in clinical settings (modified from Spencer, 2003)
Limited clinician time allocated to teaching activities.
High number of students allocated to few clinicians.
Difficulty in seeing patients (e.g., patients refusing the presence of a student).
Clinical setting is not ‘teacher friendly’ (overcrowded, too small, noisy and/or lacking privacy to interview and examine patients).
Lack of rewards and recognition for the clinical educators.
One of the biggest challenges of teaching in clinical settings is how to provide a welcoming and supportive learning environment in a busy and time constrained practice. We found that one of the main reasons for clinicians to be reluctant to have students shadowing them is the challenge of providing a dual role of caring and teaching simultaneously.
The placement improvement project
The improved structure of the student's’ placement in Old Age psychiatry was based on the tenet that clinical placements should provide various clinical experiences that include interaction with patients and professionals from various grades in addition to face to face teaching in small groups (3). The authors took over full responsibility for coordinating the students’ placements and liaising with the various supervising clinical teams. This ensured clear leadership and consistency in organising the placement.
The improved placement structure started in October 2015 with the first cohort of medical students coming to their clinical placement after the summer break. Table 4 gives a summary of the changes implemented.
Table 4- Changes to improve the clinical placement in Old Age Psychiatry
Compiling a ‘welcome pack’ and sending it by email to the students before the clinical placement.
A “Meet and Greet” event on the first day of the clinical placement was introduced comprising of several clinicians who operate on a rota basis.
Involvement of all professionals in the MDT (including Staff and Associate Specialists, community and memory nurses, junior doctors and clinical psychologists in addition to consultant psychiatrists).
Introduction of a Balint-style psychotherapy group aiming to facilitate discussion in a safe and containing environment of the emotional impact of patients encountered.
Designing a weekly one-hour teaching session supervised by a senior clinician and facilitated by a trainee psychiatrist.
Each clinician received a formal letter of thanks from the Head of Norwich Medical School, the Module Lead and the Secondary Care Lead certifying their contribution to the education of medical students and thanking them for their work.
The information pack sent to the students before the placement contained information about the hospital environment (location, map, parking, travel arrangements, key codes and useful contact numbers) and a detailed timetable (and email address) of the clinician supervising the student each day during the placement. Also, it included useful information about the mental state examination and the Mental Health Act, information that had been requested previously by medical students.
Sending information before the placement has been shown to be beneficial in students’ electives (4) and this is especially important in psychiatry which can be experienced as less structured than other medical specialities and where students are required to travel to various hospitals and clinics bases. As a result, students felt that they were expected and had a clearer sense of where they should be and who would be supervising or teaching them. Later student feedback reported that these changes had contributed directly to an improved learning experience.
The timetable design ensured that every student would have the chance to experience working in several settings in Old Age Psychiatry, including community, inpatients, ECT and the Memory Clinic. It was also noted that a two-week placement in any psychiatric team could not easily give a student a sense of patient ‘recovery’. It was, therefore, decided that students see a patient who had been discharged from the ward, e.g. with the care coordinator.
The rota of the ‘Meet and Greet’ event on the first day of the placement ensured that the workload is spread among the clinicians and helped sustain the necessary levels of enthusiasm and energy. Previously, this task had repeatedly fallen to just a few clinicians.
The participation of all professionals in the clinical team in supervision and teaching helped the students to better understand the different roles of clinicians within the multidisciplinary team and enriched their learning experience. To achieve this, we attempted to allocate sessions with a clinical psychologist, care coordinators, memory assessment nurses and members of the intensive support team. It also had the bonus of ensuring that the workload of teaching was spread more equally among clinicians.
Attendance at ward rounds and community MDT meetings could be a valuable experience but only if the process is explained, and – in the ward round – the student is briefed on the clinical history and background of the patients. For these reasons, supervising clinicians were reminded to give this information to the students attending such meetings.
The weekly teaching sessions provided an opportunity for the students to present case histories of patients they had seen and to discuss their management. Clinicians could also give a formal didactic teaching on a specific topic, for example, mental state assessment or risk assessment in psychiatry.
The letters of thanks to the participating clinicians served as an added benefit (in addition to the satisfaction of teaching others) to sustain their motivation and reward them for their contribution to the teaching of medical students. The psychiatric trainees used the letter to demonstrate their skills in teaching in their portfolio.
Benefits of the new placement structure
Helping students to feel supported before, during and even after their placements was a high priority in this project. Research has shown that learners rank the need for support and guidance in workplace environments as high and it is an essential requirement for a successful learning experience (5). This extra support is particularly crucial in psychiatry which is perceived by many students to be difficult and challenging (6).
The support provided to the students in the improved structure was in the form of having the contact details of the rota coordinators, their supervising clinicians, the administration team (medical secretaries, site manager for parking permits) and some other useful numbers for various locations and clinics.
While improving the organisation of the placement, changes were aimed to reduce the commitment of teaching and supervision for clinicians and spread it more equally among the members of the team.
Students reported that they found home visits during the placement the most useful part of their placement and the most interesting. This is an invaluable experience with the student having a significant amount of time in a one to one interaction with a clinician (including during the travel from one location to another) and then observing the clinician ‘in action’ with patients at home. This experience highlights the role of ‘professional socialisation’ (7) that is considered by educators as a significant process in the development of a sense of a shared professional identity and responsibility in both the clinician and the learner.
Furthermore, using non-medical professionals to supervise and teach students has been valued by students (8). It enriched the clinical placement with the concept of (Inter-Professional Learning) which is an active learning from and with professionals from other disciplines allied to medicine. This style of education has been shown to improve students’ communication with professionals from different disciplines and to have a better understanding of the nature of the multidisciplinary teamwork and the roles of each member of the team (9).
While improving the organisation of the placement, changes were aimed to reduce the commitment of teaching and supervision for clinicians and spread it more equally among the members of the team.
Balint groups and improving student placements in psychiatry
Balint groups were pioneered by the Hungarian psychoanalyst Michael Balint who introduced this model in the late 1950s after running seminars for general practitioners in the UK with his wife, Enid. (10)
Balint recognised the intense emotions that affect the doctor and the patient and encouraged clinicians to talk about these feelings in groups, which later came to be known as Balint groups.
Research has shown that Balint groups for medical students can increase the students’ empathy towards patients with chronic mental illness and improve their ability to cope with complex clinical situations (11). It also helps them to engage in reflection about their professional growth and to develop their identity as future doctors (12). Most importantly, this psychotherapeutic approach it allows them to reach a deeper understanding of the emotional impact of their patients (13). It was felt that the students would benefit from this model to help with the various emotions evoked by dealing with patients they would encounter in Old Age Psychiatry, in particular, dementia.
The student feedback was very positive for the Balint group. One student commented. It is inevitable to have experiences with patients that leave you with a feeling, whether that be positive or negative. To be able to look back at those times, talk them through, be listened to and have others reflect things back that you may not necessarily have realised yourself, is invaluable’.
Patient and carer involvement in clinical education
Clinical education in the workplace has always depended on patients and carers in its design and delivery. Students value seeing patients and learning from their experiences. However, the evidence suggests that patients are not routinely involved in the design of the curriculum or clinical placements despite calls to actively engage them in teaching and training (14).
Students were given the opportunity to learn from patients and carers through regular and supervised contact with them. They also attended a workshop on dementia and viewed a DVD showing the experiences of a woman with dementia and depicting how the world might be seen from her perspective. Feedback from students was very positive for these opportunities.
Medical students placement and Electro-Convulsive Therapy (ECT)
Students are allocated to spend one day in ECT clinic during their two-week placement in Old Age Psychiatry. Research has shown that many medical students have negative attitudes and unjustified reservations about ECT and its therapeutic applications (15). However, these views can change with education about this therapy during clinical placements and encouragement of the students to talk to patients and read about its indications and effectiveness in people with severe mental illness (16). Seeing the procedure first hand would, therefore, help the student gain confidence to challenge the stigma attached to ECT and to explain this treatment to their future patients.
Feedback from the students following the implementation of the placement improvement project
The feedback from medical students and clinicians was very positive. The students enjoyed their placements and felt that they gained useful knowledge and skills. Above all, they felt welcomed in the clinical settings and settled very nicely into the teams.
Figures 1 and two summarise some comments from the medical students following the placement. This feedback was collected by Norwich Medical School as part of the regular monitoring of clinical placement for medical students.
Figures 1 and 2: Feedback from students after the implementation of the changes to the clinical placement:
‘Best part of placement. Doctors were all happy to have us and teach. It was well organised, I felt that we were welcomed and always expected. It was varied and generally useful to my learning needs’. Student ID 69. End of Module 11 feedback.
‘This was one of the best placements in psychiatry, each doctor was very helpful and especially keen on teaching. It was really good to not only see the patients on the ward but so helpful to go on home visits to see assessments in patients own home. Really enjoyed this placement’. Student ID 95.
Limitations
There were some challenges in the implementation of this improved model. First is not always easy to recruit non-medical members of the clinical teams to take students. There are some reasons for this including lack of confidence or experience in teaching, a belief that it is “not their role”, or concern about the increasing demands on their time. Others already had students in their discipline. This was addressed by briefing the professionals about what the students need to achieve at the end of the placement and encouraging them to be involved in the supervision. The introduction of nursing revalidation in April 2016 may help more nurses to get involved. (17)
Conclusions and recommendations
This paper describes a clinical placement improvement project for medical students in Old Age Psychiatry. The changes focused on the enhancement of organisation, supervision and teaching.
Our improvement project is ongoing, and there are areas needing further improvement, for example, more active involvement of patients and carers in the teaching and learning of medical students is necessary. It is planned to achieve this by inviting patients and carers to tell their personal stories to the students in a small group.
Organisers of students’ placement in secondary or primary care need a systematic approach to filling allocation slots to ensure that all students receive a similar and broad exposure to their speciality. It can be dispiriting and stressful to ask for volunteers constantly. They need to have good relationships with their clinical colleagues of all disciplines, and to be willing and assertive enough to go around and ask colleagues in person rather than sending email requests.
Psychiatric educators have a significant role to play in the improvement of clinical placements for students as this will hopefully contribute to improving recruitment to this medical speciality that is undergoing a recruitment crisis. Research has shown that there is a positive correlation between the length and quality of clinical placement and the likelihood of choosing psychiatry as a future career. (18)
Depression is a clinical syndrome. The International Classification of Diseases (ICD) diagnostic classification systems describe three core symptoms of depression; low mood, anhedonia and reduced energy levels1. Other symptoms include impaired concentration, loss of confidence, suicidal ideation, disturbances in sleep and changes in appetite. Symptoms must have been present for at least a period of two weeks for a diagnosis of depression to be made. Major depression refers to the presence of all three core symptoms and, in accordance with ICD criteria, at least the presence of a further five other symptoms1. See Table 1 for severity criteria of a depressive episode according to ICD criteria.
Table 1: Severity criteria of a depressive episode according to ICD-101
Criteria A – General:
Criteria B – Presence of ≥2 of the following:
Criteria C – ‘Other’ symptoms:
Symptoms for at least 2 weeks Symptoms not attributable to psychoactive substance use or organic mental disorder
Low mood Anhedonia Reduced energy levels/ increased fatigability
Loss of confidence and self-esteem Feelings of guilt Suicidal thoughts Impaired concentration/ability to think Changes in psychomotor activity Sleep disturbance Changes in appetite with weight changes
Criteria for severity of depressive episode:
Mild episode: 2 symptoms of criteria B
Moderate episode: ≥2 symptoms of criteria B + symptoms of criteria C until minimum of 6 symptoms in total
Major episode: all 3 symptoms of criteria B + symptoms of criteria C until a minimum of 8 symptoms in total
Depressive symptoms, which can be clinically significant, can be present in the absence of a major depressive episode. Depressive symptoms are those that do not fulfil diagnostic criteria for a diagnosis of depression to be made. Depressive symptoms can be collectively referred to as sub-threshold depression, sub-syndromal depression or minor depression2.
It has been proposed that there are two types of depression; early-onset and late-onset depression. Late-onset depression refers to a new diagnosis in individuals aged 65 years of age or older. Over half of all cases of depression in older adults are newly arising (i.e. the individual has never experienced depression before) and thus late-onset type depression. Late-onset type depression is associated more with structural brain changes, vascular risk factors and cognitive deficits. It has been suggested that late-onset depression could be prodromal to dementia3.
The Kings Fund has estimated that by 2032 the proportion of older adults aged 65-84 years old will have increased by 39% whereas the proportion over the age of 85 years will have increased by 106%4. This increase in population will consequently see the incidence and prevalence of depression rise. By 2020 it is estimated that depression will be the second leading cause of disability in the world regardless of age5. Recognising, and so diagnosing, depression in older adults will become more important because of a greater demand on existing healthcare services and provisions, due to physical health consequences, impact upon healthcare utilisation and greater economic healthcare costs.
Presentation of depression in older adults
The presentation of depression in older adults is markedly different to that in younger adults. The most significant and fundamental difference in presentation in older adults is that depression can be present with the absence of an affect component, i.e. subjective feelings of low mood or sadness are not experienced3,6-9. The absence of an affective component is referred to as ‘depression without sadness’8-9. It is common instead for older adults to report a lack of feeling or emotion when depressed8-9.
Anhedonia is also less prevalent in this population. However, reduced energy levels and fatigue are frequently reported8-9.
Compared to younger adults, psychological symptoms of depression occur more frequently and are more prevalent in older adults10. Such psychological symptoms include feelings of guilt, poor motivation, low interest levels, anxiety related symptoms and suicidal ideation. The presence of irritability and agitation are key features as well7. Hallucinations and delusions are also more common in older adults, particularly nihilistic delusions (i.e. a person believing their body is dead or a part of their body is not working properly or rotting).
Cognitive deficits are characteristic of depression in older adults7,11 and are described as ‘substantial and disabling’12. Such deficits mainly concern executive function13-14. Pseudodementia is a phenomenon seen in older adults15. The term refers to cognitive impairment secondary to a psychiatric condition, most commonly depression16. Pseudodementia has become synonymous with depression. Pseudodementia can be mistaken for an organic dementia and so older adults who are depressed can present primarily to mental health services with memory problems. Pseudodementia is classically associated with ‘don’t know’ answers, whereas older adults with a true dementia will often respond with incorrect answers17.
‘Depression-executive dysfunction syndrome’ is a more specific and descriptive term to describe the cognitive deficits found in older adults with depression14. It is associated with psychomotor retardation, which can be a core feature of depression in this population7,14,18. Psychomotor retardation describes a slowing of movement and mental activity19. Like pure cognitive deficits, psychomotor retardation contributes significantly to functional impairment19. Both executive dysfunction and psychomotor retardation have been found to be related to underlying structural changes in the frontal lobes14, 20-21. Psychomotor retardation is further related to white matter changes in the motor system, which leads to impaired motor planning21. There is conflicting evidence of whether the presence of psychomotor retardation is related to depression severity18-19.
Somatisation and hypochondriasis are associated with depression in older adults and increasing age in general22-23. Somatisation is often overlooked in older adults by healthcare professional who actively search to attribute such symptoms to a physical cause. Somatisation is more common in those who have physical comorbidities. Somatisation in older adults is associated with structural brain changes and cognitive deficits24.
Depression in older adults is associated with functional impairment cognitively, physically and socially7,12,25. Such functional impairment is linked to loss of independent function and increased rates of disability26. Withdrawal from normal social and leisure activities can be marked7,25. Social avoidance reduces interaction with others and is often a maintaining factor for depression25.
Self-neglect is a classical feature of depression7, with the presence of depressive symptoms in older adults being predictive of it27. Behavioural disturbances can be a common mode of presentation, especially for older adults living in institutionalised care 6-7. Behavioural disturbances include incontinence, food refusal, screaming, falling and violence towards others7.
Diagnostic difficulties
Depression in older adults has been a condition that has constantly been under-recognised. Several issues account for this. Firstly, phenomenological differences are present. Many have argued that phenomenological issues contribute heavily to diagnostic difficulties28; both the DSM and ICD classification systems do not have specific diagnostic criteria for depression in older adults. Potentially invalid diagnostic criteria for depression in older adults could result in fundamental difficulties in understanding, with consequent impact on both clinical practice and research.
Diagnostic difficulties are also encountered because depression in older adults can present with vague symptoms, which do not correspond to the classical triad of low mood, low energy levels and anhedonia, which can all be cardinal symptoms in a younger population. Reports of fatigue, poor sleep and reduced appetite can be attributed to a host of causes other than depression and therefore it is no surprise that a diagnosis of depression is overlooked and goes undetected by healthcare professionals29.
The absence of an affective component (i.e. low mood) can lead to healthcare professionals disregarding the potential for the presence of depression and consequently not exploring for other symptoms.
Furthermore, symptoms of depression, especially somatic ones, are often attributed to physical illnesses. Depressive somatic symptoms often lead to a diagnosis of depression being over looked; such symptoms ‘mask’ the clinical diagnosis of depression and hence the term ‘masked depression’30. Depressive somatic symptoms – e.g. low energy levels, insomnia, poor appetite and weight loss - are often attributed to physical illness and/or frailty by both the individual and healthcare professional7-8, 31.
Further complicating diagnostic difficulties and under-recognition is the fact that older adults are less likely to report any symptoms associated with mental health problems and ask for help in the first place7,10,32; explanations for this include older adults being less emotionally open, having a sense of being a burden or nuisance, and believing symptoms are a normal part of ageing or secondary to physical illness7,10,29,33.Older adults also have a reluctance to report mental health problems due to their perception of associated stigma; many older adults hold the view the mental health problems are shameful, represents personal failure and leads to a loss of autonomy7.
There is an overlap between symptoms of depression and symptoms of dementia. It is quite common for older adults with dementia to initially present with depressive symptoms. Depression has a high incidence in those with dementia, especially those with vascular dementia. Depression is particularly difficult to diagnose in dementia due to communication difficulties; diagnosis is often based on observed behaviours8,33.
Depression and comorbidity in older adults
In those with pre-existing physical health problems, depression is associated with deterioration, impaired recovery and overall worse outcomes34. For example, the relative risk of increased morbidity related to coronary heart disease is 3.3 in comparison to individuals without depression35. Mykletun et al. established that a diagnosis of depression in older adults increased mortality by 70%36. Several causative routes account for poor physical illness outcomes. Older adults with depression are less likely to report worsening health. Depressive symptomatology indirectly affects physical illness through reduced motivation (often secondary to feelings of helplessness and hopelessness) and engagement with management. Poor compliance with management advice, notably adherence to medications is observed37. Feelings of hopelessness, helplessness and negativity will contribute to the failure to seek medical attention in the first place or report worsening health when seen by a healthcare professional.
Depression affects biological pathways directly, which impairs physical recovery. Such biological effects include pro-inflammatory factors, metabolic factors, impact upon the hypothalamic-pituitary axis and autonomic nervous system changes38.
Older adults who are depressed are more likely to have existing physical health conditions and more likely to develop physical health conditions15. Depression is particularly associated with specific physical illnesses; cardiovascular disease and diabetes mellitus. A study by Win et al. found that cardiovascular mortality is higher in older adults with depression because of physical inactivity; the study established that physical inactivity was accountable for a 25% increased risk in cardiovascular disease39. The relationships between depression and cardiovascular disease and depression and diabetes have been described as “bidirectional”38.
Higher incidents of cardiovascular disease and diabetes mellitus are seen in people with depression regardless of age. A study by Brown et al. found that older adults with depression had a 1.46 relative risk increase for developing coronary heart disease compared to those without depression40. The hypothalamic-pituitary axis dysfunction found in depression leads to increased levels of cortisol, which in turn, increases visceral fat. Increased visceral fat is associated with increased insulin resistance, promoting diabetes mellitus, and increased cardiovascular pathology38.
Depression is a risk factor for the subsequent development of dementia; this is especially so if an older adult has no previous history of depression (i.e. depression is late-onset)13.
Healthcare utilisation and economic impacts
Older adults are less likely to report depressive symptoms to healthcare professionals explaining the under-utilisation of mental health services for depression32,41. Despite older adults under-utilising mental health services they over utilise other healthcare services26,41. For example, those presenting with non-specific medical complaints or somatisation have been found to have an increase use of healthcare services. Non-specific medical complaints and somatisation lead to an unnecessary use of resources, such as unnecessary consultations with healthcare professionals and investigations41. Increase in service utilisation means an increase in the associated economic cost of depression in older adults41-43.
Healthcare costs of older adults with a comorbid physical illness and depression are far greater than those without depression – findings in diabetes mellitus are a good example43. The majority of the increased healthcare costs are associated with the chronic physical disease and not the care and treatment of the depression44. Poor compliance with physical illness management is associated with missed appointments and a greater number of hospital admissions, which both have financial implications.
Aetiology and associations of depression in older adults
Late-onset type depression in older adults has been associated with the term ‘vascular depression’45-47. Studies have found a significant higher rate and severity of white matter hyperintensities on MRI imaging in older adults with depression compared to those without depression46,48,50. White matter hyperintensities represent damage to the nerve cells; such damage is a result of hypo-perfusion of the cells secondary to small blood vessel damage49. White hyperintensities are associated with vascular risk factors (e.g. age, hypertension, hypercholesterolaemia, obesity, diabetes mellitus, smoking) and are linked to cerebrovascular disease, such as stroke, vascular dementia. A relationship has been found between psychosocial stress and consequent development of vascular risk factors, which further supports the hypothesis of ‘vascular depression’46. Clinically, ‘depression-executive dysfunction syndrome’ and psychomotor retardation are associated with vascular changes48.
In older adults with depression, white matter hyperintensities are associated with structural changes to corticostriatal circuits and subsequent executive functional deficits. Loss of motivation or interest and cognitive impairment in depression are hallmark features of structural brain changes associated with the frontal lobes, which in turn are associated with a vascular pathology20. A study by Hickie et al. established that white matter hyperintensities in older adults with depression are associated with greater neurological impairment and poorer response to antidepressant treatment50. It is not fully understood why vascular depression responds less well to antidepressants; poor response has been linked directly to vascular factors but has also been associated with deficits in executive function46-47.
The relationship between cerebrovascular disease and depression is described as ‘bi-directional’45,51; depression has been found to cause cardiovascular disease and vice versa51. Baldwin et al. direct the reader to the presence of post-stroke depression and the occurrence of depression in vascular dementia45.
Younger and older adults share a number of fundamental risk factors for depression; such as female gender, personal history and family history7. Older adults have additional risk factors related to ageing, which are not just physiological in nature.
Age related changes:
Age related changes occurring in the endocrine, cardiovascular, neurological, inflammatory and immune systems have been directly linked to depression in older adults3.
The normal ageing process sees changes to sleep architecture and circadian rhythms with resultant changes to sleep patterns52. Thus sleep disturbances are common in older adults and positively correlated to advancing age52; over a quarter of adults over the age of 80 years report insomnia, and research has well-established that this is a risk factor for depression53-54. A meta-analysis by Cole et al. found sleep disturbances to be a significant risk factor for the development of depression in older adults53.
Sensory impairment:
Sensory impairments, whether secondary to the ageing or a disease process, are risk factors53,55. Research has found that hearing and vision impairments are linked to depression56. A sensory impairment can lead to social isolation and withdrawal, which, in turn, are further risk factors for depression.
Physical illness:
Physical illness, regardless of age, is a risk factor for depression. Older adults are more likely to have physical illnesses and so in turn are more at risk of depression. See Table 2. Physical illness is associated with sensory impairments, reduced mobility, impairment in activities of daily living and impaired social function, all of which can lead to depression. Physical illnesses associated with chronicity, pain and disability pose the greatest risk for the subsequent development of depression7,53,55. Physical illness affecting particular systems of the body, such as the cardiovascular, cerebrovascular and neurological, are more likely to cause depression3. Essentially, however, any serious or chronic illness can lead to the development of depression. It should be noted that a large proportion of older adults have physical illness but do not experience depression symptoms, therefore other factors must be at play5,57.
Treatments of physical illness are directly linked to aetiology in depression, for example, certain medications are known to cause depression; cardiovascular drugs (e.g. Propranolol, thiazide diuretics), anti-Parkinson drugs (e.g. levodopa), anti-inflammatories (e.g. NSAIDs), antibiotics (e.g. Penicillin, Nitrofurantoin), stimulants (e.g. caffeine, cocaine, amphetamines), antipsychotics (e.g. Haloperidol), anti-anxiolytics (e.g. benzodiazepines), hormones (e.g. corticosteroids), and anticonvulsants (e.g. Phenytoin, Carbamazepine)7,29. Polypharmacy is present in many older adults further increasing the risk of depression. Pharmacokinetic and pharmacodynamic age related changes also contribute to an increased risk of medication induced depression in older adults.
Table 2: Table of physical illnesses associated with depression3,7
Dementia is common in old age and those with dementia are at higher risk of developing depression compared to those who do not have it58. 20-30% of older adults with Alzheimer’s disease have depression59. Depression is a risk factor for the subsequent onset of dementia.
Psychosocial:
When compared to younger adults, older adults are at a greater risk of developing depression due to the increased likelihood of experiencing particular psychosocial stressors, in particular adverse life events. Stressors include lack of social support, social isolation, loneliness and financial hardship. Financial hardship and functional impairment often sees older adults downsizing in property. Deteriorating physical health often sees older adults no longer being able to manage living independently at home necessitating a move into institutional living. Bereavement, especially spousal, and the associated role change that follows this are risk factors for depression3.
Sub-threshold depression:
Sub-threshold depression is an established risk factor for major depression.
Prevalence and epidemiology
The prevalence of depression in older adults in England and Wales was found to be 8.7% in 2007; however, if those with dementia are included this figure rises to 9.7%60. A meta-analysis by Luppa et al. established a 7.2% point prevalence of major depression and a 17.1% point prevalence of depressive disorder in older adults61. The projected lifetime risk of an older adult developing major depression by the age of 75 years old is 23%62.
Sub-threshold depression is 2-3 times more prevalent than major depression in older adults26,63. These depressive symptoms are often clinically relevant26,29. 8-10% of older adults per year with sub-threshold depressive symptoms go onto develop a major depressive episode63.
Incidence and prevalence are greater in women; 10.4% of women over the age of 65 years have depression compared to 6.5% of men60. Older women are more likely to experience recurrent episodes of depression compared to older men62. The gender gap in incidence and prevalence becomes narrower with increasing age3. It should be acknowledged however that women are more likely to present to healthcare services and seek help in comparison to men64-65.
The prevalence of major depression in older adults varies by setting66. Highest rates are seen in long-term institutional care and inpatient hospital settings67. Table 3 summaries prevalence rates of major depression by setting.
Table 3: Prevalence rate of major depression by setting 7, 67
Setting
Prevalence rate (%)
Community
5 – 10
Primary care
10 – 30
Hospital inpatient
11 – 50
Long-term institutional care
10 – 43
Prognosis of depression in older adults
Depression in older adults is associated with a slower rate of recovery9, worse clinical outcomes compared to younger adults3 and is associated with higher relapse rates68. Worse prognosis in older adults correlates with advancing age, physical comorbidities and functional impairment70. The structural brain changes associated with depression in older adults are linked, as discussed, to poorer treatment response.
Morbidity and mortality associated with depression can be described as primary or secondary; primary morbidity and mortality arises directly from the depressive illness; whereas secondary morbidity and mortality arises from physical health problems, which are secondary to depression.
Outcomes from sub-threshold depression are on par with those of major depression; however sub-threshold depression which develops into major depression is associated with worse outcomes2.
Proportionally more people over the age of 65 years commit suicide compared to younger people71. Depression is the leading cause of suicide in older adults29,71; one study reports that 75% of older adults who killed themselves were depressed72.
The vast majority of older adults who commit suicide have had contact with a health professional within the preceding month9; this figure has been quoted as high as 70%3. This further supports and suggests the fact the depression is under-detected. Unlike younger adults, older adults are less likely to report suicidal ideation and can experience suicidal ideation without feeling low in mood3,7. Older adults have few suicide attempts, compared to younger adults, because their suicide methods are more lethal13.
Warfarin is a widely used anticoagulant, primarily for the prevention of thrombosis and thromboembolism. Warfarin is used as a prophylactic agent in conditions such as atrial fibrillation and coronary artery thrombosis.1
Although effective and safe, treatment with Warfarin is associated with risks. Because of its narrow therapeutic index, patients require regular blood monitoring for the international normalised ratio (INR) to determine the safe yet effective dose of Warfarin.
Warfarin has interaction with several medications which affect the availability of Warfarin. One class of drugs which is very commonly prescribed is the selective serotonin reuptake inhibitors (SSRIs) antidepressants.
Due to their supposedly favourable side-effect profile, e.g. less cardiotoxicity, and safety in overdose, SSRIs have become the first-line antidepressant 2, preferred over tricyclic antidepressants (TCA). However, SSRIs, have other serious side-effects including increased tendency to bleed, particularly gastrointestinal bleeding. SSRIs may increase the risk of bleeding due to the secondary effect of serotonin release which is essential for platelet aggregation. 3 This effect is especially significant when combined with anticoagulants. 1
Several of the SSRIs are inhibitors of the cytochrome P 450 enzyme system, which is responsible for the metabolism of some medications, including Warfarin. Both SSRIs and anticoagulants are frequently prescribed in the elderly population.
Fluvoxamine is a SSRI which is licensed for use in the treatment of depressive disorder, obsessive-compulsive disorder (OCD) 1, and is also used in the treatment of social phobia. While an interaction between Fluvoxamine and Warfarin is to be expected because of Fluvoxamine’s inhibitory action on a number of cytochrome P 450 enzymes, there have not been many case reports of the interaction between Fluvoxamine and Warfarin.
A Medline search revealed only two case reports of an interaction between Warfarin and Fluvoxamine. 4,5
We report a case of an elderly man who developed elevated INR when he was started on Fluvoxamine for the treatment of depression, while on Warfarin.
Case Report
A 75-year old male was admitted to the acute psychiatric unit with complaints of anxiety, depressed mood and suicidal ideation. In the previous months, he had developed a pre-occupation that his bowels were not functioning properly and that he would not be able to open his bowels. He was using excessive laxatives secondary to this preoccupation. He also described other depressive symptoms: anhedonia, insomnia with early morning wakening, poor concentration, and low motivation.
The patient was diagnosed with depression two years previously, requiring Electroconvulsive therapy (ECT). He was discharged on Mirtazapine 45mg and Venlafaxine-XL 150mg. Following a deterioration in mental state, the Venlafaxine-XL dose was increased to 225mg three months before this admission, without much improvement. Risperidone and Olanzapine were trialled as an adjunct without beneficial effect and were discontinued. Compliance with medication was reportedly good.
The patient had multiple physical health complaints: previous myocardial infarctions, hypertension and paroxysmal atrial fibrillation. He was prescribed tamsulosin, bisoprolol, perindopril, atorvastatin, and warfarin.
The patient’s preoccupation about bowel movements was, for the most part, deemed to have obsessive quality: he accepted that these worries were repetitive and came to his mind against his wishes. He said that he would rather not have these worries but was unable to distract himself.
The marked subjective anxiety, according to the patient, was entirely linked to the preoccupation. However, when the patient became agitated, it was difficult to persuade him to appreciate the anomalous nature of his thoughts. At such times he insisted that there was something definitely wrong with his bowels and nothing could help him.
Prior to admission, the patient was treated at different times with different antipsychotic medications, which made little impact on the symptoms. Following his admission he was referred to the psychology services, which concluded that he was too unwell to meaningfully participate in psychological therapies. The patient, too, was not keen on this option. He also declined ECT and was deemed to have the capacity to make the decision.
Venlafaxine-XL was switched, in light of the patient’s cardiac risk history, to an SSRI known to have an effect on obsessional symptoms. Accordingly, a dose of Mirtazapine was decreased to 30mg, and Venlafaxine-XL was tapered off over ten days.
Fluvoxamine was started at 50mg/day, and the dose was titrated to 150 mg/day over the next week. The dose was further increased to 200 mg/day.
INR was previously stable on warfarin dose of 5mg per day: blood results were between 2.32-2.68. Following fluvoxamine-initiation, INR started increasing: 2.98 after six days. INR increased further, to 3.82, with increase in Fluvoxamine’s dose
Warfarin-dose, as a result, was decreased, initially from 5mg to 4mg; however, INR remained above range (3.75). With further reduction in Warfarin’s dose, to 3mg/day, INR reduced but was still above range (3.51). INR eventually stabilised when warfarin-dose was reduced to 2mg/day. The dose adjustment took place over ten days.
Discussion
Management of depression in elderly population requires careful consideration of the choice of psychotropic medication, as elderly patients are more likely than younger patients to be on multiple medications for associated physical health problems, which increase the potential for drug interactions. Half-lives of drugs are also extended in the elderly.
The patient was prescribed Warfarin for the management of atrial fibrillation. Warfarin is a racemic mixture of S-warfarin and R-warfarin, of which S-warfarin is more potent than R-warfarin. 6
Warfarin has the potential to cause pharmacokinetic drug interactions (drugs affecting hepatic cytochrome P 450 enzyme system, which metabolises warfarin), which are thought to be more clinically relevant than pharmacodynamic interactions (highly protein bound drugs displacing Warfarin from its binding site) for warfarin. 6
Warfarin is metabolised by a number of P450 isoenzymes such as 2C9/2C19, 1A2, and 3A4. 6 Of these 2C9 is thought to be crucial, as it metabolises the more potent S-isomer. Isoenzyme 1A2 is the major route for the metabolism of the R-isomer, while 3A4 and 2C19 are considered to be minor routes.
The psychotropic medications that are thought to have the potential for significant pharmacokinetic interaction with warfarin include Fluoxetine, Fluvoxamine, Quetiapine, and Valproic Acid. 7 Venlafaxine is also considered a high-risk drug in patients taking warfarin. One study found that fluvoxamine and venlafaxine were associated with a more than double risk of having an INR value of 6 or more. 3
Fluvoxamine by dint of its inhibitory actions on 2C9/2C19, 3A4, and 1A2 8 inhibits all the isoenzymes that metabolise Warfarin and can be said to have the maximum potential for pharmacokinetic interaction with Warfarin.
National Collaborating Centre for Mental Health guidelines on depression in adults with chronic physical health problems advise avoiding SSRI in patients taking warfarin or heparin and instead offering an alternative antidepressant such as mirtazapine. 9 Therefore, caution is needed when prescribing these medications to patients who fail to respond to other safer options.
At the time of his admission, the patient was on a combination on Mirtazapine and Venlafaxine XL, both at high doses, for several months. Neither of the antidepressants has significant action on the P450 isoenzyme system, although both are substrates of some enzymes, such as 2D6, 1A2 and 3A4. 8 The patient’s INR was within normal limits when he was on these two medications (despite the aforementioned potential effect of venlafaxine on INR values).
During the period of admission, a decision was taken to change the antidepressant regime, for clinical reasons. The two antidepressants considered were Fluvoxamine and Sertraline.
It was felt that despite its higher potential to cause pharmacokinetic interaction with Warfarin, Fluvoxamine is chosen ahead of Sertraline (which inhibits 3A4 and 2D6). The more potent action of Fluvoxamine on the sigma1 receptors, which account for its significant anxiolytic properties and therapeutic action in the delusional depression 10 was felt to have the potential of benefit given the patient’s clinical symptoms.
It was also felt that Fluvoxamine would also be of more benefit than Sertraline with insomnia which was patient’s frequent complaint given its side-effect of somnolence. 11
Fluvoxamine was started at a low dose (50 mg/day) after Venlafaxine XL was completely withdrawn. The dose was titrated rapidly over the next one week, to 150 mg/day. The INR showed an upward trend within five days of commencing Fluvoxamine, and it exceeded three by the time the dose of Fluvoxamine was increased to 150 mg/day. This necessitated a reduction in Warfarin’s dose from 5 mg to 2 mg/day. The INR stabilised to between 2 and 3 when warfarin dose was more than halved.
Fluvoxamine has a half-life of 9-28 hours, and steady-state levels reach roughly after ten days. 8
The half-life is increased by almost 50% in the elderly. 3 The trajectory of increase in the INR was consistent with the pharmacokinetic of Fluvoxamine: it is a potent inhibitor of CYP4501A2, with a relatively little affinity for the other isoenzymes. The increase in INR was not dramatic, which is different from previous reports. 4 Throughout the period of Fluvoxamine –titration and Warfarin dose adjustment, there was no clinically untoward incident.
In conclusion, this case shows the need for close monitoring when warfarin is combined with another drug which significantly enhances warfarin’s anticoagulant effect. At the same time, it can be done safely, even in patients such as the elderly, who can be at a higher risk of adverse effects of interaction, when appropriate steps to monitor the patient are in place. The case also demonstrates the necessity of using clinical judgment while applying the guidance in individual patients.
In the UK, all newly graduated doctors spend their first two years of work rotating between different specialities, usually spending four months in each placement, before applying for speciality training. This period is called the Foundation Programme.
In January 2016, the Royal College of Psychiatrists published its first ever strategy on Broadening the Foundation Programme to address the need to improve the psychiatric training experience for foundation doctors. The strategy’s aim is to “ensure the delivery of a high-quality training experience in all psychiatry foundation placements”.1
Over the last few years, the number of Foundation training posts in psychiatry in England and Wales has significantly increased. Health Education England aims that all Foundation doctors should rotate through a community or an integrated placement (psychiatry is considered as a community placement) from August 2017.2
As such, the College highlights the need to provide a supervised and well-structured psychiatric training experience for Foundation doctors. This aims not only to improve recruitment into psychiatry but also to ensure doctors have a good working knowledge and understanding of psychiatry and psychiatric services, no matter what career they pursue.
Mentoring provides an additional support and therefore can be helpful to improve the placement of Foundation doctors in psychiatry.
We implemented an ambitious mentoring scheme in Norfolk and Suffolk NHS Foundation Trust (the seventh largest mental health trust in the UK). The paper describes its essential component together with a brief review of the literature on mentoring in clinical settings, focusing on Foundation placements.
Why is mentoring is needed for Foundation doctors in psychiatry?
The literature on mentoring for medical professionals draws attention to the idea that it is beneficial to all doctors at all stages of their career to experience mentoring in some form or another. However, mentoring is of particular importance to doctors moving to a new job or organisation 3, thus making it highly relevant to Foundation trainees.
For newcomers, most of the mentoring support will focus on helping them settle into their new role, becoming familiar with, and developing an understanding of the expectations of their employers.4
Evidence shows that the quality of care in any organisation can be improved when clinical leaders support time for activities such as reflection, coaching and mentoring 5.
Most Foundation doctors will lack experience in psychiatry and will need a substantial amount of guidance from their supervisors and their teams.6 Research has shown that the transition from student to doctor is a difficult one and can be associated with significant levels of emotional stress.7
Foundation doctors find psychiatric assessments physically and emotionally challenging. They feel they lack the specialist knowledge and skills to deal with complex patients, especially concerning self-harm, personality and eating disorders. Dealing with such complex diagnostic categories requires knowledge, skill, understanding as well as physical and emotional robustness. Due to the relative lack of focus on such topics in most undergraduate medical training, a comprehensive support in psychiatric placements is essential.
Psychiatry is very different from other specialities in the way services are configured and delivered: junior doctors may face isolation as psychiatric units are typically spread across a wide geographical area and often lack a centralised meeting place for junior doctors (e.g. a doctors’ mess). In addition, they may find themselves the lone practitioner when on call, which can be daunting for many.
Clinical and Educational supervision is provided to Foundation doctors in similar ways to other rotations. However, the consultants delivering this essential support often focus only on clinical issues related to knowledge and skills. Furthermore, it is easy to see that the best guides to new trainees regarding the idiosyncrasies of the speciality and its services are likely to be trainees who have spent some time in those services and are more able to detect the specific stresses new doctors may experience and may find difficult to articulate.
Furthermore, mentoring fosters a productive peer-to-peer relationship. The learning needs of the Foundation doctor can be considered alongside their personal and professional interests and lifestyle. Questions can be posed in a non-judgmental forum, without fear of being ridiculed or condemned. The fundamentals of on-call systems, clinical cases and management options can all be considered at a level appropriate to their junior grade. Tips for examination success and information about essential courses and core texts can be shared. Job choices and research opportunities can be discussed. Day to day difficulties and mismatches between expectation and reality can be identified and possibly overcome. Where this is not possible next steps can be identified, and clinical and educational supervisors can be drawn in for higher level support. The benefits of the scheme are broad.
Finally, although mentoring is different from role-modelling (teaching by example and learning by imitation), it has been shown toserve some of the same aims of role-modelling, including enhancing problem-solving abilities of the mentee, improving professional attitudes, showing responsibility and integrity, and supporting career development. 8
What is mentoring?
Mentoring can mean different things to different people. There are various definitions which can create confusion between mentoring and other formal structures of support such as supervision, coaching, consultation, befriending or friend systems and even counselling. However, mentoring is none of the above but at the same time a combination of them.
The Standing Committee on Postgraduate Medical and Dental Education (UK) defined mentoring as ‘The process whereby an experienced, highly regarded, empathetic individual (the mentor) guides another individual (the mentee) in the development and re-examination of their ideas, learning, and personal and professional development”.9
The term “mentoring” takes us back to Greek mythology: Mentor was a person: he was the friend of Odysseus who was asked to look after Odysseus’ son Telemachus when Odysseus was fighting in the Trojan Wars. The name Mentor was later used to describe a trusted person, a supporter, or a counsellor.10
Mentoring as a professional developmental tool became popular in the private sector organisations in the USA during the 1970s and was introduced to the area of health during the 1990s 11. Since then, it has been widely used in various organisations.
Aims of mentoring
Mentoring has the advantage of being a flexible supporting tool, unlike other structured processes (e.g., clinical supervision or coaching) where the goals are set clearly from the start of the relationship between the supervisor and supervisee. The aims of mentorship are summarised in Table 1.
Table 1- Aims of mentorship
Help the mentees take the lead in managing their career and its development.
Provide support to discuss personal issues in a confidential and secure environment
Improve both the individual and the team performance
Types of mentoring
Buddeberg-Fischer and Herta 11 discussed various types of mentoring based on the numbers of mentors and mentees and their professional status or grade:
One to one mentoring (between a mentor and a mentee).
Group mentoring (one mentor and a small group of mentees)
Multiple-mentor experience model (more than one mentor assigned to a group of mentees).
Peer-mentoring (the mentor and mentee are equal in experience and grade): This mentoring is used mainly for personal development and improving interpersonal relationships. Mentor and mentee roles can be reversed. Also, called ‘co-mentoring’.
Distance or e-mentoring is becoming more popular, and it has the advantages of being “fast, focused, and typically centred on developmental needs”. 12
Structured vs. flexible mentoring
Evidence suggests that providing mentorship through a rigid and structured process can be counterproductive. 13 Mentors and mentees usually work in different locations, making it difficult for both to have a set of pre-planned meetings and topics for discussions.
Another advantage of the flexibility of mentoring is that it does not follow a “tick box” exercise but encourages informal discussions and exploration of whatever comes to mind during meetings. Doubtless, having some structure to the overall mentoring process is important as it ensures that the mentoring session doesn’t become an informal befriending or friend support system. Table 2 sets out the main benefits of mentoring.
Benefits to the organisations
Benefits to the mentee
Benefits to the mentor
Improve job satisfaction leading to improved performance, recruitment, and retention of employees
Enable early recognition and resolution of issues that face employees
Provide a valuable source of feedback that the organisations can use to improve working conditions
Ensure that the mentee has clear aims and objectives (development outcomes) at the start of their mentorship. These goals may include improving knowledge, performance and preparation for exams and interviews
Empowers the mentee to explore and pursue their career aims
Incorporates the mentee into a wider professional network and prevents isolation
Supports the mentee to use reflective practice and improve their self-awareness
Reducing stress and burnout
Formal recognition of informal practice within the profession
Structured program with support and supervision to the mentor
Development of knowledge and skills in management and supervision
Satisfaction of helping others and passing on their knowledge
Table 2-Benefits of mentoring. Developed from Mentoring – Chartered Institute of Personnel and Development (CIPD) Factsheet. Revised February 2009 14. Available from: https://www.shef.ac.uk/polopoly_fs/1.110468!/file/cipd_mentoring_factsheet.pdf
Are there any Disadvantages of mentoring?
There is extensive literature on the benefits of mentoring, but is there any harm associated with it?
As with any intervention, it does carry some potentially adverse effects. Mentoring can be perceived to “infantilise” junior employees rather than empowering them 10. This perception is probably more common among employees who see themselves as senior or very competent and think of themselves as able to adapt to change very quickly.
Mentoring might hinder creativity in new employees and inhibit them from thinking “outside the box” as it might re-enforce the message that ‘this is how we do things here’. 10
Clashes of personalities or other interpersonal factors could lead to a troubled mentor-mentee relationship and cause distress to both parties. Hence, plans must be put in place in any formal mentoring scheme to ensure an amicable ending to this relationship. Multiple mentor allocation mentioned earlier could also prevent such interpersonal problems and help to tackle them early on.
Furthermore, some mentees may feel uncomfortable with the influence or authority of the mentor, and this may hinder the progress of the mentoring relationship. 13 This is particularly relevant when the mentor is also involved in the formal assessment of the performance of the mentee (e.g. being the line manager or supervisor) or when a mentee who lacks self-confidence is paired with an overconfident mentor.
Good mentors avoid common pitfalls in the mentoring process, such as a patronising attitude, breaches of confidentiality and offering direct advice to the mentees. Instead, they encourage the mentee to reflect and come up with their answers. 15
Finally, mentoring can be perceived as an additional demand on doctors during their training, and some may feel that they are forced to provide it or receive it during placement. However, it must be remembered that mentoring should always be voluntary and flexible to meet the individual’s needs and not an additional ‘box to tick’ or a portfolio enrichment exercise.
The Mentoring Scheme for Foundation Doctors in Psychiatry Norfolk:
The scheme started in December 2015 and initially ran as a pilot in Norfolk with the support of all stakeholders. The mentoring scheme coordinator (YH) contacted twelve Foundation doctors by email, welcoming them to the Trust and inviting them to participate. The welcome email contained information about mentoring, including the benefits it may offer.
The voluntary nature of this scheme was highlighted so that the doctors didn’t feel they were being pressured to be enrolled.
Of the 12 doctors invited, five took up this opportunity. Uptake has remained constant over the consequent cohorts of Foundation doctors for many reasons. Those deciding not to enrol in this scheme explained that they felt happy with the support provided by their clinical supervisors. However, some doctors asked for a mentor halfway through their placement when they felt that they needed additional support. In these instances, a mentor was allocated to them as soon as possible.
Mentors were core and higher trainees already involved in supporting more junior psychiatric trainees through informal mentoring. Their experience meant there was no need for formal training. However, reading material was circulated to them to highlight the roles and responsibilities of mentors and what to do if any problem arose during mentoring. Monthly mentors’ meetings were very helpful to discuss issues arising in mentoring and offer peer to peer support.
Also, there were regular meetings and discussions between the mentoring coordinator, the Director of Medical Education, and Medical Director of the Trust to resolve any issues facing the Foundation doctors and provide feedback to improve the Psychiatric placement.
During the first meeting, the mentors and mentees agreed on the aims of mentoring drawing up a list of objectives that the Foundation doctor would like to achieve by the end of the placement. Following this initial meeting, there should have been once monthly face to face meetings throughout the placement. The mentor and mentee agreed on the most convenient means of communication (e.g. using text messages, emails, etc.) outside scheduled meetings.
All mentors kept a record of the mentoring meetings, with the mentoring coordinator informed about these meetings. Issues discussed were confidential and not shared with the coordinator or supervisors unless the mentee gave specific consent.
At the end of the mentoring scheme, the coordinator collected feedback from mentees and mentors using a structured questionnaire that was designed by the coordinator using SurveyMonkey® website. The feedback highlighted the positive aspects of mentoring as well as areas for improvement.
End of mentoring survey
Mentors reported that acting as a mentor without being involved in clinical supervision allowed them to offer objective advice and support in a way that would have been harder if they were directly involved in the workplace. One Foundation doctor experienced bullying from another member of the team who was a locum doctor. The mentor supported the Foundation doctor, and the issue was addressed and resolved promptly. There was a significant risk that they would have been left isolated and unsupported during this time if the mentor scheme had not been in place.
The topics discussed were varied, and this suggested that mentoring was not limited to a aspect of the job (see Table 3)
Table 3- Topics discussed in mentoring meetings
General guidance about the job
Assistance on completing competencies on e-portfolio
Advice regarding personal health, bullying, career choices
Leadership and research opportunities.
Mentees reported that they found mentoring useful and supportive of learning and development. This was especially important in a speciality that they had little experience of as an undergraduate. With a mentor in Psychiatry, the Foundation doctors reported that they could identify areas of development, including leadership and teaching opportunities for Foundation doctors.
Overall, mentoring was shown to be a useful tool to improving Foundation doctors’ experience in Psychiatry by offering extra support during placement in a challenging medical speciality.
Table 4 summarises the areas of development suggested by the mentors and mentees.
Table 4- Recommendations from the feedback of mentors and mentees
Early allocation of mentors at the start of the placement is vital.
The need to provide e-learning and classroom training on mentoring to develop the skills of mentors
Maintain the independence of the mentor from the clinical team of the mentee
Enhance the flexibility of the scheme to meet the demands of the training and the time constraints of the mentees and mentors
Limitations
Feedback from mentors and mentees showed an overall satisfaction with the scheme, but it was not possible to measure such satisfaction quantitatively, this was expected from an approach which is willfully kept outside the realm of performance management.
According to the literature on mentoring, most mentoring schemes lack a clear structure, as well as a clear evaluation process of its short and long terms, benefits 11.In our scheme, we addressed this by continually monitoring the mentoring process and collecting feedback from mentees and mentors. Another limitation involves training the mentor himself and finding the time in a highly pressurised and heavy workload environment.
There are many questions that the literature on mentoring is yet to answer. For example, what are the long-term benefits of mentoring? Would our Foundation doctors who received mentoring be more successful professionally and personally compared to their peers who decided not to participate? These questions remain unanswered as our pilot was not set up to address this general shortcoming of current knowledge and understanding.
Conclusions and recommendations
Mentoring provides a focused opportunity to target the wider needs of the trainee. Not only could this encourage Foundation doctors to pursue a career in Psychiatry, but it also provides the space for them to learn how to incorporate psychiatric skills into whatever speciality they choose to pursue.
As a new doctor in a novel environment, being expected, welcomed, and gently guided into the job is invaluable. With the hindsight of our training experiences (good and bad), junior doctors are ideally placed to support more junior colleagues at all levels.
There is a need to develop links with other mentoring schemes to exchange experiences and learn lessons from others. Research has shown the importance of supporting mentors in their roles through regular meetings where mentors learn from each other. 13
In our experience, the mentoring scheme worked both alongside and separately to clinical and educational supervision and the opportunity for reflective practice offered in Balint groups. Mentoring added another level of support for the Foundation doctors, which was deemed beneficial by those participating.
We recommend more research is required to determine whether mentoring will increase recruitment to psychiatry. Organisations responsible for the training of doctors should support formal mentoring schemes and supervisors should ensure that mentors and mentees have protected time in their timetable due to the benefits of the mentoring experience to the doctors and the employing organisations.
Finally, funding should be available to support training of mentors in their workplace and aim to develop their skills in helping their mentees. Many private organisations offer mentoring training packages (including classroom and online training) for competitive prices. These courses provide useful resources to mentors and may help to increase the motivation of mentors to continue their participations in mentoring.
Appendix:
How does mentoring work? A simple three stage model:
Figure 1- The three stage model of mentoring. Developed from Alred et al (1998). Alred, G., Gravey, B. and Smith, R, 1998, Mentoring pocketbook. Alresford: Management Pocketbooks.
One of the unique characteristics of mentoring is that it is a partnership between two individuals (mentor and mentee) where both contribute to its growth and sustainability. It is based on trust, eagerness to learn and mutual respect. 16
Alred et al (1998) 4 described a model of mentorship with three stages: exploration, developing new understanding and then action planning (Figure 1). Both the mentors and mentee have certain roles and responsibilities in each stage and it is only through their collaborative work that the benefits of mentoring can be obtained.
The stage of exploration is characterised by the building of a relationship between the mentor and the mentee. Trust, confidence and rapport start to develop and hopefully grow throughout the mentoring process. Methods such as active listening, asking open questions, and negotiating an agenda are essential to facilitate this growth.
The second stage is where new understanding develops, is characterised by showing support to the mentee, demonstrating skills in giving constructive feedback and challenging negative and unhelpful cognitions.
Key methods employed in this stage include recognition of the strengths and weaknesses of the mentee, giving them information, sharing experience and establishing priorities for the mentee to work on.
In the third and last stage of the mentoring, action planning, the mentee takes the lead in negotiating and agreeing on the action plan, examining their options and developing more independent thinking and decision-making abilities.
A good mentor should help the mentee to gain confidence and knowledge over time. In order to achieve this, the mentor helps the mentee to develop new ways of thinking and improve their problem-solving abilities.
Monitoring the progress and evaluating the outcomes of the mentoring process is essential to ensure that the mentoring relationship is going in the right direction.
Acknowledgement
We would like to thank Dr Stephen Jones (Consultant CAMHS and former Training Programme Director), Dr Trevor Broughton (Consultant Forensic Psychiatrist, Director of Medical Education), Dr Bohdan Solomka (Medical Director) from Norfolk and Suffolk NHS Foundation Trust for their unlimited support for the mentoring scheme.
We also would like to thank Dr Calum Ross (Foundation Training Programme Director-FY1) and Mr Am Rai (Foundation Training Programme Director -FY2), Norfolk and Norwich University Hospital for their support in implementing this scheme. Dr Srinaveen Abkari (Specialist Registrar, Norfolk, and Suffolk NHS Foundation Trust) is one of our mentors who also contributed useful ideas to the development of this paper.
Finally, we would like to thanks all our mentors who provided the support for the Foundation, without their efforts, this scheme would not have succeeded.
Endocrine disorders are frequently accompanied by psychological disturbances. Conversely, psychiatric disorders, to significant extent demonstrate consistent pattern of endocrine dysfunctions. [1] Endocrinopathies manifests as myriad of psychiatric symptoms, as hormones affect a variety of organ systems function. The presence of psychiatric symptoms in patients with primary endocrine disorders provides a new insight for exploring link between hormones and affective function.[2] Disturbance of hypothalamic-pituitary-thyroidal axis is of considerable interest in psychiatry and is known to be associated with a number of psychiatric abnormalities.[3]Thus, the main focus of psychoneuroendocrinology is on identifying changes in basal levels of pituitary and end-organ hormones in patients with psychiatric disorders. Psychiatric symptoms may be the first manifestations of endocrine disease, but often are not recognized as such. Patient may experience a worsening of the psychiatric condition and an emergence of physical symptoms with the progression of the disorder.[4] Psychiatric manifestations of endocrine dysfunction include mood disturbances, anxiety, cognitive dysfunction, dementia, delirium, and psychosis. While dealing with treatment-resistant psychiatric disorder, endocrinopathies should also be considered as a possible cause in management. Psychotropics medicine may worsen the psychiatric symptoms and improves only once the underlying endocrine disturbance is corrected. [5]The lifetime prevalence of depression and anxiety is 11.8% to 36.8% and 5.0% to 41.2% respectively in the group with previously known thyroid disorder. [6,7].The occurrence of major depression in DM is mostly estimated around 12% (ranging from 8-18%). 15-35 % of individuals with DM report milder types depression. [8]. Depressive symptom is seen in almost half of patients with Cushing's syndrome and these experience moderate to severe symptoms. Some patients with Cushing's syndrome also experience psychotic symptoms [9]. Patients suffering from Addison's disease may be misdiagnosed with major depressive disorder, personality disorder, dementia, or somatoform disorders [4, 10]. Women with hyperandrogenic syndromes are at an increased risk for mood disorders, and the rate of depression among women with PCOS has been reported to be as high as 50 percent. Central 5-HT, system dysregulation that causes depression might simultaneously affect peripheral insulin sensitivity, or vice versa, possibly via behavioral or neuroendocrinological pathways, or both. [10]
Hollinrake 2007 showed prevalence of depression has shown it to be four times that of women without PCOS. Hollinrake screened patients with PCOS for depression and found total prevalence of depressive disorders which included women diagnosed with depression before the study, was 35% in the PCOS group[11]. No specific psychiatric symptoms have been consistently associated with acromegaly or gigantism or with elevated GH levels. Adjustment disorder may occur from changes in physical appearance and from living with a chronic illness [11]. Sheehan’s syndrome (SS) refers to the occurrence of varying degree of hypopituitarism after parturition (1). It is a rare cause of hypopituitarism in developed countries owing to advances in obstetric care and its frequency is decreasing worldwide. Reports of psychoses in patients with Sheehan’s syndrome are rare. [13] Psychiatric disturbances are commonly observed during the course of endocrine disorders .The underlying cause can be hyper- or hyposecretion of hormones, secondary to the pathogenic mechanisms. medical or surgical treatment of endocrine diseases, or due to genetic aberrations[14]. Psychiatric disorders frequently mimic the symptoms of endocrinological disorders. In view of sizable number of patients seeking treatment from our department present with comorbid endocrinolgical disorders, we planned the present study to investigate psychiatric morbidity preferably anxiety and depression pattern among endocrinolgical disorders patients. With this background, we studied the depression and anxiety in different endocrinogical disorders.
Methods
The present study was conducted in the SMHS Hospital of Government medical college Srinagar and the study sample was drawn from patients attending the endocrinogical OPD in the Department of Medicine at Government Medical College Hospital Srinagar (SMHS).The study was conducted over a period of one and half year, from April 2011 to September 2012 in patients attending the Department of Medicine Government Medical College Hospital Srinagar enrolling 152 cases of Endocrinological disorders. All patients were first examined by Consultant endocrinologist. The patients were then selected using simple random sampling choosing every alternate patient. General information including age, sex, residence, economic status, past history of thyroid disorders, family history of psychiatric disorders was included. An endocrinology specialist first examined the patients, while a psychiatrist administers Hospital Anxiety and Depression scale (HADS). Hospital Anxiety and Depression scale (HADS) was used for purpose of screening anxiety and depressive disorders in patients suffering from different endocrinogical disorders. Hospital Anxiety and Depression scale (HADS) is used for purpose of screening anxiety and depressive disorders in patient suffering from chronic somatic disease. HADS contain 14 items and consist of two subscales: anxiety and depression with seven question each. Each question is rated on four point scale (0 to 3) giving maximum total score of 21 each for anxiety and depression. Score of 11 or more is considered a case of psychological morbidity, while as score of 8-10 represents borderline and 0-7 as normal. The forward backward procedure was applied to translate HADS from English to Urdu by a medical person and professional translator. [15]
The participating physicians subjected select patient of chronic Endocrinological disorders to HADS Questionnaire and recorded scores both for anxiety and for depression.
The patients were subjected to inclusion and exclusion criteria as given below:
Inclusion criteria
1. All endocrinological disorders.
2. Both sexes will be included.
3. Age > 15 yrs.
4. Those who will give consent.
Exclusion criteria
1. Those who don’t consent.
2. If diagnoses is not clear.
3. Age less than 15 years.
4. Presence of pregnancy or a history of pregnancy in the last six months.
5. Those who are on steroids or drugs known to interfere with thyroid function
General description, demographic data and psychiatric history was be recorded using the semi structured interview which was pretested
Statistical methods: Statistical analyses were performed using the SPSS, version 16.0 for Windows. A secure computerized database was established and maintained throughout the study. Patient names were replaced with unique identifying numbers. Descriptive statics were used to generate a profiles of each illness group based on presence of depression only, anxiety only and those with both anxiety and depression. To determine whether there were any significant differences between each illness group in the prevalence of depression and anxiety disorders , an unadjusted 3×2×2 test chi square was conducted. Data were analyzed by the Pearson chi-squared test and t test. P<0.05 was considered as the significance level in the evaluations.
Consent: Informed consent was obtained from each patient; those who were considered incapable of consenting were allowed to participate with consent of their closest family member or custodian. All patients were informed about the nature of the research within the hospital and willingly gave their consent to participate. Information sheets and preliminary interviews made it clear that the choice to consent or otherwise would have no bearing on the treatment offered. The project ensured the anonymity of the subjects by replacing patient names with unique identifying numbers before the statistical procedures began.
Results
A total of 152 patients from the endocrinological departments of Govt. Medical College, Srinagar hospitals were taken up for study. They were evaluated in detail with regard to socio-demographic profile regard to presence of psychiatric co-morbidity by HADS and the results have been presented below in the tabulated form .Only patients who consented for complete interview and respond to all HADS questions were considered in final analyses.
Out of total 152 subjects 71 were males (46.72%)), and 81 were females (53.28%) (Table 1). Most of cases belong to 35-45 year age group (26.3%) followed by age group 25- 35 years (24.3%) and 67.7% were married and 18.4% were unmarried. More than half (51.97 %) of the study subjects were from nuclear families and 82 (53.9%) were illiterate and majority 84(55.4 %) belonging to middle class family. The socio-demographic profile of the studied patients is shown in Table-2 .
Out of 152 patients with endocrine disorders, 56(37%) patients elicited HADS score of 10 or less indicating absent or doubtful association anxiety or depression. 96 (63.15%) patients were found positive to HADS Questionnaire with anxiety/depression score of 11 or more. The mean HADS score for anxiety alone, depression alone and anxiety/depression patients were 13.42, 15.7 and 25.62 respectively. On the basis of HADS screening, 96(63.157%) patients had varying degree of psychiatric co morbidity. 27 (28.12%) had anxiety alone, 30(43.47%) had depression alone where 39(40.62%) as patients had anxiety and depression both.(Table 3) The breakdown of total number of different Endocrinological disorders is given in table. Maximum psychiatric comorbidity is found in thyroid patients (69.35%) followed by diabetic patients (68.05). (Table 4).
Table 1: Age and sex distribution
Sex
Total
Male
Female
Age group
< 25
14
20%
7
9%
21
14%
25 – 35
20
28%
17
21%
37
24%
35 – 45
17
24%
23
28%
40
26%
45 – 55
11
16%
19
24%
30
20%
55 & above
9
13%
15
19%
24
16%
Total
71
100%
81
100%
152
100%
Mean ± SD
51.4± 13.7
56.4± 13.1
54.1± 13.6
Table 2: Demographic Characteristics of the Studied Patients
Characteristic
N
%
Dwelling
Rural
98
64.47
Urban
54
35.52
Marital status
Unmarried
28
18.4
Married
103
67.7
Widowed
21
13.8
Occupation
Household
61
40.1
Unskilled
29
19
Semiskilled
39
25.6
Skilled
23
15.1
Professional
8
5.26
Family type
Nuclear
79
51.97
Joint
28
18.4
Extended
45
29.6
Literacy status
Illiterate
82
53.9
Primary
22
14.4
Secondary
16
10.5
Matric
13
8.55
Graduate
11
7.23
Postgraduate/Professional
8
5.26
Family Income(Rs)
< 5000
45
29.6
5000 to 10000
85
55.92
≥ 10000
22
14.4
Socioeconomic status ( Kuppuswamy Scale )
Lower
32
21
Upper lower
11
7.23
Middle
84
55.2
Upper middle
19
12.5
Upper
6
3.94
Table 3: Result of HADS Scoring
Variable
Total (n=96)
Anxiety alone
Depression Alone
Anxiety depression both
p value
Male
37(38.54%)
8(29.6%)
18(60 %)
11(28.2%)
-
Female
59(61.4%)
19( 70.3%)
12( 40%)
28(71.7 %)
-
Age (Years)
54.1± 13.6
51.4± 13.7
56.4± 13.1
54.1± 13.1
< 0.005
Mean HADS Score
-
13.42±3.4
15.73±3.3
25.62±4.3
< 0.005
Table 4: Types of endocrinological disorders
Endocrinological disorders
Number of patients(N=152)
Psychiatric comorbidity
percentage
Thyroid disorders
62 (40.7%)
43
69.35
Diabetes mellitus
47(30.92%)
32
68.05
PCOD
28(18.4%)
16
57.1
Cushings syndrome
5(3.289%)
2
40
Acromegally
2(1.31%)
0
0
Addisions disease
1(0.65%)
0
0
Sheehan’s syndrome
3(1.97%)
2
66.6
Miscellaneous
4(2.63%)
1
25
Table-5 Psychiatric Co-morbidity across Socio-demography of the Patients
Present
Absent
p value
n
%
N
%
Dwelling
Rural
59
60.02
39
39.7
<0.005 (Sig)
Urban
37
68.5
17
31.4
Marital status
Unmarried
8
28.5
20
71.4
>0.005 (NS)
Married
72
69.9
31
30
Widowed
16
76.1
5
23.8
Occupation
Household
57
93.4
4
6.55
>0.005 (NS)
Unskilled
14
48.2
15
51.7
Semiskilled
9
39.1
30
76.9
Skilled
14
60.8
9
39.1
Professional
2
25
6
75
Family type
Nuclear
45
56.9
34
43.0
>0.005 (NS)
Joint
22
78.5
6
21.4
Extended
29
64.4
23
51.1
Literacy status
Illiterate
70
85.2
12
14.6
>0.005 (NS)
Literate
26
36.1
46
63.8
Family Income(Rs)
< 5000
17
37.7
28
62.2
>0.005 (NS)
5000 to 10000
65
76.4
20
23.5
≥ 10000
14
63.6
8
36.3
Socioeconomic status
Lower
18
50
18
50
>0.005 (NS)
Upper lower
7
63.6
4
36.3
Middle
59
70.2
25
29.7
Upper middle
10
52.6
9
47.3
Upper
2
33.3
4
66.6
Discussion
This study is the first to offer data on psychiatric morbidity among endocrine patients in the Kashmiri population. 63.15% (96) patients were found positive to HADS questionnaire with anxiety/depression score of 11 or more in our study. The results of this study suggest patient suffering from endocrinological disorders are likely to have a co-morbid psychiatric disorder. [5, 16].Depressive disorders and anxiety disorders are the commonest psychiatric disorders in endocrinogical patients. [3].Numerous studies have shown a high correlation between depression and endocrinological disorders and this study supports these findings, with 43.47 %( 30) of the participants having depressive symptoms on the HADS. [3, 16] 40.62% (39) respondents had both depressive symptoms and an anxiety disorder. 28.12% (27) participants were diagnosed with an anxiety disorder, which is slightly higher than the lifetime prevalence of anxiety disorder in men [16]. Our findings of a high proportion of respondents with endocrinological disorders (45.7%) Female were more in number than their male counterparts 59(61.4%) vs. 37(38.54%) and the majority of men presenting with endocrinological disorders were between the ages of 35 and 45 years has also been reported in a previous studies. [4, 8].The findings of our study suggest that psychiatric disorders are highly prevalent in endocrinological disorders and is largely unrecognized in the primary care setting. Endocrine disorders of different kinds, irrespective of treatment have been associated with Psychological distress. Psychological wellbeing of endocrine disorders may provide new insights in clinical endocrinology. Further psychological disorders comorbid with endocrinological disorders adds to their disability as well as cost to the individual and the society.[17] Most of the clinicians do not suspect this important association of endocrinological disorders in the beginning resulting in delayed diagnosis. Thus, the high prevalence of anxiety and depression in endocrinological disorders in our study supports a case for screening for these disorders in endocrinological clinics. Furthermore, recognition and treatment of these comorbidities could improve patient outcomes. Future studies should focus on replicating or refuting these findings in larger samples as well as in testing interventions aimed at targeting psychological morbidities in this patient group. Under-recognition of psychiatric morbidity is not an uncommon phenomenon, and has been found in similar local studies of psychiatric morbidity in other medical illnesses[8].Thus, more attention should be paid to recognizing psychiatric morbidities in this group of patients.. The reasons for increase in the frequency of psychiatric disorders are multi-factorial. Being chronic illness leads to psychological stress .The major limitation of our study was relatively small sample size. Another limitation of our study is its crossectional design, which does not allow us to determine direction of causality in the relationship between endocrinological disorders and depression/anxiety. More community based studies are required to assess the magnitude of the problem and to lay down principles to help such patients.In order to clarify the temporal relationship prospective studies with a bigger sample size are essential in the future. As far as we are aware, this is a first of its kind study in kashmir. Endocrinological disorders accounts for a huge proportion of referrals to psychiatric clinics and misery is added upon an already devastating metabolic disease. To add the cost associated with psychiatric morbidity accounts individual and to the society are substantial. Thus, the high prevalence of anxiety and depression in endocrinological disorders in our study supports a case for screening for these disorders in Endocrinological clinics. Furthermore, recognition and treatment of these comorbidities could improve patient outcomes.
Global recruitment in psychiatry has been falling for several decades because medical students and graduates have been finding it consistently unattractive 1,2. An analysis of the career choices of newly qualified doctors in the United Kingdom (U.K.) found the same trend from 1974 to 2009; psychiatry was the first career choice for only 3-5% of medical graduates annually3. In the U.K., lack of recruitment into psychiatry had reached a crisis point by 2003 when 15% of all unfilled consultants posts in England were in psychiatry and the Royal College of Psychiatrists was finding recruitment into specialist psychiatry posts increasingly difficult4,5. In 2012, only 78% of the Core Training year one (CT1) posts in psychiatry were filled; a serious shortfall which was overcome by overseas recruitment up until changes in immigration rules.
The factors that seem to dissuade medical students from taking up psychiatry as a future career may include: stigma, bad prognosis of psychiatric disorders, poor scientific base of psychiatry, ‘bad-mouthing’ from medical colleagues, lack of respect among peers & public, threats of violence from patients and lack of resources1-5. However, there is evidence to suggest that many students’ attitudes towards career choice changed in a positive direction after working in psychiatry due to the perceived ‘job satisfaction’, ‘life-style’, ‘training available’ and ‘multidisciplinary approach’3.
Psychiatry has previously been ranked higher in career choice at the end of students’ clinical year6. To ensure a stable psychiatric workforce for the future, there is an obvious need to motivate current and future cohorts of young doctors to take up psychiatry as a career. Das & Chandrasena (1988) found that attitudes changed positively towards mental health following clinical placement in this specialty7. It is also known that medical students’ attitudes to psychiatry and career intentions can be improved by their experiences of teaching8. Students were found to develop more positive attitudes when encouraged by senior psychiatrists, had direct involvement in patient care, or saw patients respond well to treatment. Improvement in attitudes during the placement was also related to an increased intention to pursue psychiatry as a career.
Previous research into attitude to psychiatry as a specialty and career choice seems to have produced conflicting results and most of it was carried out among medical students. Since career choices in the U.K. are actually made in the first clinical year following graduation, we carried out a survey among a recent cohort of foundation year one (FY1) doctors in the South East England before and after their first clinical year.
Method
Our study sample consisted of all FY1 doctors (n=101) in one region of South East England. They participated in the study at the beginning and then at the end of their first clinical year. We used a 20–item questionnaire devised by Das & Chandrasena(1988) to ascertain their perceptions and attitudes towards psychiatry before they commenced their first clinical placement. The questionnaire was sent to them via their Medical Education Managers (MEMS). It was handed out to the FY1 doctors as part of their induction pack for completion along with a study information sheet.
At the end of their first year of working, the participants were asked to complete an amended version of the questionnaire. This included two additional questions which ascertained whether the doctor had an opportunity to work in a psychiatric post, or had any experience of psychiatry in practice (such as taster days or cases in A&E). These amended questionnaires were sent to the foundation doctors electronically via their MEMS for completion.
The data was collected and entered into a spreadsheet to prepare descriptive statistics. Comparisons for before and after exposure to psychiatry, and between the psychiatry and non-psychiatry groups were made using the chi-square test. As the data was binary, a latent class model was developed using LatentGOLD software9 to explore the associations between different items in the questionnaire. Responses from the questionnaires were coded as: responses which agree with a positive attitude to psychiatry or disagree with a negative attitude were coded as +1; those not sure were coded as 0; and responses which agree with a negative attitude to psychiatry or disagree with a positive attitude were coded as -1.
Results
A 100% (n=101) response rate was obtained for the first set of questionnaires completed at the beginning of the year. However, there was a significant drop in the number of questionnaires completed at the end of the year - a 53.5% response rate (n=54) generally but 61.1% (22 out of 36) for those FY1 doctors who had the opportunity or access to a post in psychiatry within their clinical year.
Initial cohort at beginning of the clinical year vs. those with no exposure to psychiatry at the end
Table 1 shows the group means for each questionnaire item, for the whole cohort at the beginning of the year compared to those with no exposure to psychiatry by the end of the year.
Table 1: All FY1 doctors before training placements started (initial cohort) versus FY1 doctors without a psychiatric post after FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.591
0.095
-0.169
0.359
0.476
I may consider pursuing a career in psychiatry in the future
-0.539
-0.136
0.403
0.046
0.760
0.028
Psychiatry is attractive because it is intellectually comprehensive
-0.500
0.273
0.773
0.436
1.000
0.000
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
-0.500
-0.069
-0.442
0.305
0.717
Physicians do not have time to deal with patients emotional problems
-0.294
0.273
0.567
0.142
0.991
0.009
Psychiatrists understand and communicate better than other physicians
-0.127
0.364
0.491
0.090
0.892
0.017
Psychiatrists don't overanalyse human behaviour
0.147
0.364
0.217
-0.200
0.633
0.306
Expressing an interest in psychiatry is not seen as odd
0.157
-0.136
-0.293
-0.727
0.141
0.184
Hospitalised patients are not given too much medication
0.167
0.591
0.424
0.116
0.732
0.007
Psychiatrists don't make less money on average than other physicians
0.255
0.045
0.209
-0.537
0.118
0.208
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.727
0.365
0.033
0.696
0.032
Psychiatric curriculum and training are not too easy
0.520
0.682
0.162
-0.112
0.436
0.243
Psychiatrists are not fuzzy thinkers
0.578
0.818
0.240
-0.082
0.561
0.142
Psychiatrists should have the legal power to treat patients against their will
0.608
0.955
0.347
0.051
0.642
0.022
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.864
0.246
-0.066
0.558
0.121
Psychiatry is scientific and precise
0.627
0.818
0.191
-0.098
0.480
0.194
There is a place for ECT in modern medicine
0.755
0.727
-0.028
-0.239
0.184
0.797
Psychiatric consultations are often helpful
0.853
0.864
0.011
-0.210
0.231
0.924
Entering psychiatry is not a waste of a medical education
0.873
1.000
0.127
-0.048
0.303
0.153
Psychiatrists don't often abuse their legal powers
0.892
1.000
0.108
-0.049
0.264
0.175
Those FY1 trainees who had not worked in psychiatry during the year were significantly more positive (p = < 0.05) for psychiatry’s future, psychiatrist being better at patient communication and not over-medicating their patients. However, they remained significantly less convinced as compared to the whole cohort about psychiatry’s intellectual attraction or taking it up as a future career.
Initial cohort at beginning of the year vs. those with exposure to psychiatry at the end
Table 2 shows the group means for each questionnaire item, for the whole
cohort at the beginning of the year compared to those with exposure to psychiatry at the end of the year.
Table 2: All FY1 doctors before training placements started versus FY1 doctors with a psychiatric post during FY1 training
Before
After
Difference
L
U
p-value
Within medicine, psychiatry has a high status
-0.686
-0.745
-0.058
-0.242
0.125
0.531
I may consider pursuing a career in psychiatry in the future
-0.539
-0.617
-0.078
-0.332
0.177
0.547
Psychiatry is attractive because it is intellectually comprehensive
-0.500
-0.468
0.032
-0.214
0.278
0.798
Most non-psychiatric medical staff are not critical of psychiatry
-0.431
0.106
0.538
0.248
0.827
0.000
Physicians do not have time to deal with patients emotional problems
-0.294
-0.383
-0.089
-0.401
0.224
0.575
Psychiatrists understand and communicate better than other physicians
-0.127
-0.085
0.042
-0.260
0.345
0.783
Psychiatrists don't overanalyse human behaviour
0.147
0.340
0.193
-0.123
0.510
0.229
Expressing an interest in psychiatry is not seen as odd
0.157
0.106
-0.050
-0.378
0.277
0.761
Hospitalised patients are not given too much medication
0.167
0.362
0.195
-0.044
0.434
0.109
Psychiatrists don't make less money on average than other physicians
0.255
0.404
0.149
-0.092
0.391
0.224
Psychiatry is a rapidly expanding frontier of medicine
0.363
0.064
-0.299
-0.569
-0.029
0.030
Psychiatric curriculum and training are not too easy
0.520
0.596
0.076
-0.128
0.281
0.464
Psychiatrists are not fuzzy thinkers
0.578
0.596
0.017
-0.233
0.268
0.892
Psychiatrists should have the legal power to treat patients against their will
0.608
0.532
-0.076
-0.323
0.171
0.545
A placement in psychiatry can change one's negative views of psychiatry
0.618
0.574
-0.043
-0.290
0.203
0.730
Psychiatry is scientific and precise
0.627
0.702
0.075
-0.155
0.304
0.521
There is a place for ECT in modern medicine
0.755
0.511
-0.244
-0.427
-0.061
0.009
Psychiatric consultations are often helpful
0.853
0.745
-0.108
-0.289
0.073
0.239
Entering psychiatry is not a waste of a medical education
0.873
0.808
-0.064
-0.218
0.090
0.412
Psychiatrists don't often abuse their legal powers
0.892
0.766
-0.126
-0.279
0.027
0.105
After a psychiatry placement, significant positive differences (p=<0.05) were observed in their responses to medical staff’s view of psychiatry, future of psychiatry and place of Electro Convulsive Therapy (ECT) in modern medicine. While there was a positive trend in most responses in favour of psychiatry, trainees remained negative about psychiatry’s status, its scientific base, curriculum & training and taking up psychiatry as a future career.
Those exposed to psychiatry vs. those not exposed to psychiatry
Table 3 compares responses between FY1 doctors exposed to psychiatry during the clinical year and those who were not.
Table 3: FY1 doctors who had a psychiatric post versus those who did not have one
Sorted by the size of the difference between the two groups.
t-test
ranksum
Psychiatry
No Psychiatry
Difference
L
U
p-value
p-value
Most non-psychiatric medical staff are not critical of psychiatry
0.106
-0.500
-0.606
-1.000
-0.144
0.011
0.011
Psychiatrists don't make less money on average than other physicians
0.404
0.045
-0.359
-0.694
-0.024
0.036
0.034
Expressing an interest in psychiatry is not seen as odd
0.106
-0.136
-0.243
-0.735
0.249
0.329
0.322
Psychiatrists don't overanalyse human behaviour
0.340
0.364
0.023
-0.421
0.467
0.917
0.907
Psychiatric curriculum and training are not too easy
0.596
0.682
0.086
-0.210
0.382
0.564
0.497
Psychiatry is scientific and precise
0.702
0.818
0.116
-0.187
0.419
0.447
0.777
Psychiatric consultations are often helpful
0.745
0.864
0.119
-0.173
0.411
0.419
0.388
Within medicine, psychiatry has a high status
-0.745
-0.591
0.154
-0.130
0.437
0.283
0.391
Entering psychiatry is not a waste of a medical education
0.808
1.000
0.191
-0.020
0.403
0.075
0.058
There is a place for ECT in modern medicine
0.511
0.727
0.217
-0.117
0.551
0.200
0.192
Psychiatrists are not fuzzy thinkers
0.596
0.818
0.222
-0.114
0.559
0.192
0.190
Hospitalised patients are not given too much medication
0.362
0.591
0.223
-0.139
0.597
0.218
0.192
Psychiatrists don't often abuse their legal powers
0.766
1.000
0.234
-0.005
0.473
0.055
0.040
A placement in psychiatry can change one's negative views of psychiatry
0.574
0.864
0.289
-0.045
0.623
0.088
0.064
Psychiatrists should have the legal power to treat patients against their will
0.532
0.955
0.423
0.097
0.748
0.012
0.011
Psychiatrists understand and communicate better than other physicians
-0.085
0.364
0.449
0.000
0.897
0.050
0.050
I may consider pursuing a career in psychiatry in the future
-0.617
-0.136
0.481
0.084
0.878
0.028
0.017
Physicians do not have time to deal with patients emotional problems
-0.383
0.273
0.656
0.195
1.000
0.006
0.007
Psychiatry is a rapidly expanding frontier of medicine
0.064
0.727
0.663
0.269
1.000
0.001
0.002
Psychiatry is attractive because it is intellectually comprehensive
-0.468
0.273
0.741
0.352
1.000
0.000
0.001
Those exposed to psychiatry agreed more often that non-psychiatric medical staffs were critical of psychiatry compared to the group not exposed to psychiatry. They also had comparatively negative responses for psychiatrists not abusing legal powers and to have the legal power to treat someone against their will. Trainees exposed to psychiatry also felt significantly (p=<0.05) positive towards psychiatry being intellectually comprehensive and adopting it as a career. However, they were less enthusiastic about psychiatrists treating patients against their will and psychiatry being the expanding frontier of medicine.
Discussion
In this study, we have ascertained attitudes of a regional cohort of FY1 doctors towards psychiatry as a specialty and as a career choice. Our findings are similar to previous research carried out among medical students, which found that there were generally negative attitudes towards psychiatry as a specialty and career choice but fairly positive attitudes towards the role of psychiatry in medicine and in society in general1-5,10. Like others, we also found that personal experience of psychiatry placement can improve trainees’ view of psychiatry as a specialty and as a future career 3,11.
It was interesting to find out that after a year in clinical practice but without any experience of psychiatry, trainees’ attitudes towards psychiatry as a specialty had been positive. It is difficult to know the exact reason but we can speculate that this respect for the specialty may have developed when they experienced limitations of the other specialties in medicine and/or perhaps due to the positive professional encounters with psychiatrists at the Accident & Emergency (A&E) or with psychiatric liaison teams during ward consultations. As opposed to previous research11, it was heartening to note that the group with no exposure to psychiatry agreed that non-psychiatric medical staff were not critical of psychiatry; a possible sign of reduced stigma for psychiatry within the medical profession.
Despite exposure to psychiatry, FY1 doctors’ attitudes to psychiatry’s status, scientific base, curriculum & training and career choice remained somewhat negative. Similar results were found by Lyons et al11 when they assessed students’ attitudes towards psychiatry after a clerkship in the specialty. There was a significant decrease in negative & stigmatising views towards mental illness after the clerkship, but no significant improvement in students' interest in psychiatry was detected1. Goldacre et al (2013) also acknowledged mixed outcomes of early experience of working in psychiatry as it might discourage some doctors. While highlighting positive effect of the doctors’ experience of the speciality, they also cited it as a negative factor that influenced some doctors who had previously considered psychiatry as a career3.
Our study has limitations because of having a small sample and being carried out in one small region of the country. It is also worth mentioning that the group exposed to psychiatry may not have had a psychiatry placement as it also included those who had had taster days or experience in A&E. The brevity of these latter exposures cannot give someone a real sense of the specialty. The nature of this and the overall experience needs to be differentiated and the exposure quantified in the future studies. Our study findings also need to be replicated with future cohorts and in other regions for confirmation because FY training programme in the U.K. is relatively recent and placements in psychiatry have evolved4 over the last few years through closer collaboration between different stakeholders in the Foundation Training Programmes.
Medical professional terminology is used to communicate with each other, allied professions and differentiates professionals from patients1. As a tradition, it has perhaps evolved into a language of its own with a vocabulary of terms used as expressions, designations or symbols such as ‘Patient’, ‘Ward Round’ and ‘Registrar’. This ‘language’ is not restricted to use by doctors or nurses - it is used among other professionals working in healthcare, e.g. medical coders and medico-legal assistants.
The National Health Service (NHS) in the U.K. has seen many changes in the last few decades. From within these changes, an interesting trend to change or alter the use of professional terminology, often without consultation with directly affected professionals or patients, has emerged. With new or changed roles, multidisciplinary teams have been observed to alter titles, even borrowing specific terms ascribed to doctors such as “consultant,” “practitioner” and “clinical lead”2,3. On the other hand, Modernising Medical Careers initiative4 has also led to changes in doctors’ titles reflecting their experience levels, which have been reported to be unclear to patients and fellow professionals5.
Medical professional terms can be traced back to Hippocratic writings and their development is a fascinating study for language scholars1. Psychiatric terminology is particularly interesting, as it has evolved through scientific convention while absorbing relevant legal, ethical and political trends along the way. Superficially, it may appear pedantic to quibble over terminology, but the power of language and its significance in clinical encounters is vital for high quality clinical care2,6. Since medical professional terminology is an established vehicle for meaningful communication, undue changes in its use can create inaccurate images and misunderstandings, leading to risks for professional identity. There is also evidence to suggest that such wholesale changes have been misleading7 and a source of inter-professional tension.
Understanding of a professional’s qualifications and experience is crucial for patient autonomy and for them to be able to give informed consent. We carried out a survey among foremost stakeholders of medical professional terminology, patients and doctors, within a psychiatric service to ascertain their attitudes to the changes they have experienced in recent years.
Method:
We gave out a self-report questionnaire to all adult psychiatric patients seen at a psychiatric service in the South East (U.K.) in a typical week and to all working psychiatrists/doctors. The questionnaire was developed after a review of the relevant literature and refined following feedback from a pilot project. The questionnaire contained demographic details and questions regarding attitudes towards medical professional terms for patient and professional identity, processes and working environments. The questions were mostly a “single best of four options” style, with one question involving a “yes” or “no” answer.
The datacollected was analysed by using SPSS statistical package8. Descriptive statistics were used to summarize the characteristics of the study population. The two sub-samples (patients & doctors) were compared with each other regarding different variables by using a t-test, which highlighted the absolute and relative differences among those.
Results:
196 subjects were approached to participate. 187 subjects (patients = 92, doctors = 95) participated, which represents a response rate of 95%.
Male to female ratio was roughly equal in the sample but there were more females in the medical group (56%) as compared to the patient (46%) group. Among responders, those over 40 years of age were more prevalent in the patient group (60% vs. 39%) compared to the medical group.
As shown in the Table 1, patients’ and doctors’ attitudes overwhelmingly leaned towards a patient being called a “patient” (as opposed to “client”, “service user” or “customer”); understanding “clinician” as a doctor (as compared to being a nurse, social worker or psychotherapist), and believing psychiatrist to be a “consultant” (preferred to nurse practitioner, psychologist or social worker).
Table1: Patients’ & doctors’ attitudes to medical professional terms = “patient”, “clinician” and “consultant”
What do you prefer to be called?
Doctors (%)
Patients (%)
Client
16 (17)
13 (14)
Patient
68 (72)
65 (71)
Service user
10 (11)
11 (12)
Customer
1 (1)
3 (3)
Don’t know
0
0
Total
95
92
Chi2 1.378, p = 0.710
Which of these is a clinician?
Doctors (%)
Patients (%)
Nurse
14 (15)
14 15)
Social worker
4 (4)
2 (2)
Doctor
56 (59)
70 (76)
Psychotherapist
7 (7)
6 (6)
Don’t know
14 (15)
0 (0)
Total
95
92
Chi2 16.3, p<0.05
Which of these is a consultant?
Doctors (%)
Patients (%)
Psychiatrist
71 (75)
68 (74)
Psychologist
3 (3)
6 (7)
Social worker
10 (11)
10 (11)
Nurse practitioner
3 (3)
8 (9)
Don’t know
8 (8)
0 (0)
Total
95
92
Chi2 11.3, p<0.05
Patients and doctors seemed to prefer (>70%) calling the person who provides the patient support in the community as “care-coordinator” or “key worker”.
It is worth noting that “key worker” is the main person looking after the patient admitted to hospital and “care-coordinator” has the same role when they are back in the community. Similarly, the majority of the patients deemed the terms “Acute ward” and “PICU” (psychiatric intensive care unit) appropriate for a psychiatric ward.
There was strong evidence to suggest that both patients and doctors were confused as to what a ‘medication review’ was; as approximately 35% of them thought it was a “nursing handover” and the rest were divided whether it was a “pharmacist meeting” or an “assessment”. See Table 2.
This is understandable because the patients are used to an “Out Patient Appointment/Review” where a psychiatrist reviews patients in a holistic manner, which includes prescribing and adjusting their medications. Similar confusion prevailed regarding what has replaced the term “ward round”, as both groups were universally divided among choices offered as “MDM” (multidisciplinary meeting), “Assessment”, “CPA” (Care Programme Approach) and “Review”.
Table 2: Patients’ & doctors’ attitudes to what a “ward round” and “medication review” means?
Which of these means a ward round?
Doctors (%)
Patients (%)
Assessment
26 (27)
34 (37)
MDM
18 (19)
15 (16)
Review
34 (36)
29 (32)
CPA
16 (17)
14 (15)
Don’t know
1 (1)
0 (0)
Total
95
92
Chi2 2.82, p = 0.588
Which of these is a medication review?
Doctors (%)
Patients (%)
OPD
19 (20)
11 (12)
Assessment
25 (26)
34 (37)
Pharmacist meeting
34 (36)
31 (34)
Nursing handover
14 (15)
12 (13)
Don’t know
3 (3)
4 (4)
Total
95
92
Chi2 3.89, p = 0.421
Both patients and doctors were clear (84% vs. 69%) that they expected to see a doctor when they attended a “clinic”. However, both groups were approximately equally divided between their preferences for what a psychiatry trainee should be called; “SHO” (37%) or “Psychiatric trainee” (36-40%). There was also a higher preference (approx. 50% vs. 30%) for the doctor a grade below consultant to be called a “Senior Registrar”.
Patients and doctors were equivocal in their response that they have never been consulted about medical professional terminology.
Fig. 1 Has anyone consulted you about these terms?
Discussion:
In a survey of attitudes to the use of medical professional terms among patients and doctors in a psychiatric service, we have found a significant preference for the older and established medical terms as compared to the newer terms such as MDM, CT trainee, Specialty Trainee, etc.
While replicating findings of other studies3,7, we also found that no single term was chosen by 100% of participants in either group, showing confusion surrounding most psychiatric terms. This lack of consensus and confusion can be explained by the fact that no participant had ever been consulted about the changes or new nomenclature.
Limitations to this study should be taken into account before generalising the results. The patients’ group is older than the doctors’ group, which could skew the results due to age related bias in favour of familiarity and against change9. In a questionnaire about preference and understanding, participants may intuitively prefer the easiest to understand terms and ignore the subtle difference between other styles. Possibility of bias may have been introduced by some of those giving out questionnaires being doctors
Our sample was drawn only from a psychiatric service, which may restrict the implications of our findings to mental health.
Furthermore, involvement of other professionals and carers working in the psychiatric service would have been useful to expand the scope of this study.
Inconsistency regarding doctors’ titles, unleashed by the Modernising Medical Careers (2008) initiative, has resulted in patients considering trainees as medical students5, not recognising ‘Foundation Year 1 Trainees’ as qualified doctors and being unable to rank doctors below consultant level3. Our findings have highlighted the uncertainty regarding qualifications and seniority of doctors – this can erode patients’ confidence in their doctors’ abilities, compromise therapeutic relationship10, especially in psychiatry, and result in poor treatment compliance. Medical students may also find themselves mistaken for doctors, and feel daunted by future job progression where training structures and status are unclear.
Title changes introduced by local management or Department of Health (DoH), without consultation with stakeholders, have the potential to create inter-professional tensions and devalue the myriad skills offered by healthcare workers other than doctors. This could also be damaging to their morale and the confidence instilled in patients. It is interesting to note, however, that titles that do not give the impression of status and experience, such as “trainee”, tend not to be adopted by non-doctor members of the multidisciplinary team3. On the other hand, in a profession steeped in tradition, there will be doctors who see other professionals’ adoption of their respect-garnering and previously uncontested titles as a threat to the status of the medical profession6. Previous studies have shown that terminology has a significant effect on the confidence and self-view of doctors5 and at a time where a multitude of issues has led to an efflux of U.K. junior doctors to other countries, and a vote for industrial action, re-examining a seemingly benign issue involving titles and terminology could have a positive impact.
Patients’ attitudes to development of surgical skills by surgical nurses show that they would like to be informed if the person doing a procedure is not a doctor7.
The roles of a number of professionals involved in an individual’s healthcare can be confusing and the possibility of mistaken identity could be considered misleading6, unethical, and even fraudulent. Introducing confusion by appropriating titles associated with doctors could be damaging to patients’ trust, and is inappropriate in a health service increasingly driven towards patient choice. The challenge lies in how to keep the terminology consistent and used in the best-understood contexts.
Commissioners and managers may instead evaluate the implications of changing professional terms by making sure that all stakeholders are consulted beforehand. Perhaps the pressing source of inconsistency in staff job titles could also be rectified by a broader scale study to find national, multidisciplinary and patient preferences, and taking simple measures such as standardising staff name badges.
Our study has highlighted once again how the landscape of nomenclature in psychiatry/medicine is pitted with inconsistency. While language naturally evolves with time and it may be understandable to see increasing application of business models & terminology in the NHS9, medical professional terms have been determined contextually over the years with significant implications for patient management and safety. Therefore, it is important to question how changes in terminology affect patients, whether it occurs by gradual culture change or due to new initiatives. It would benefit patient care if medical and psychiatric professional language could be standardised and protected from changes, which can lead to colleagues and patients being misled. DoH, Commissioners and Trust/Hospital management must recognise that changing terminology can have a significant impact and that serious discussion of such changes is important for reasons far beyond pedantry. For inter-professional communication a formalised consensus on titles would be beneficial for transparency, trust, patient safety and reducing staff stress levels.
The CASC (Clinical Assessment of Skills and Competencies) has been running since 2008 and is the final membership examination for the Royal College of Psychiatrists (MRCPsych).1 It is a clinical examination and follows an OSCE format (Objective Structured Clinical Examination), where candidates move through 16 short stations.2,3 We have been running a mock CASC in the West of Scotland for the last few years and have received consistently good feedback from candidates. This article describes our experience of organising the mock exam.
Step 1: Practicalities
The organising committee
Our mock CASC is arranged by the organising committee for the local core psychiatry education programme (MRCPsych course). This committee is comprised of a consultant chair, higher trainee chair and one or two trainee representatives from each higher subspecialty and each core training level. The higher trainee chair takes the lead with organising the mock, with the support of other committee members. This works well, as the trainees have recent experience of sitting or preparing for the exam and are enthusiastic about medical education.
Support from our postgraduate operations manager is invaluable. She works closely with the committee to book the venue and actors, and order equipment such as screens and a bell. She also has a key role in advertising the mock exam to trainees, booking places and being a point of contact for candidates. She assists with set up on the day of the exam and prints station instructions, marking schemes and labels for candidates.
Venue
Our mock exam is held in the same venue as our core trainee educational programme. We have 2 rooms to use for stations and a waiting area for candidates. Screens are borrowed from Glasgow University Medical School to create separate stations.
Timing
The mock exam takes place around 2 weeks before the CASC. This enables candidates to have prepared for the exam and leaves some time to work on any issues identified by the mock. Planning usually starts 4-5 months in advance of this, with increasing intensity and time commitment as the exam approaches.
Step 2: Mock Exam Format
CASC format and blueprint
The CASC itself includes morning and afternoon circuits, which all candidates will move through. There are 16 stations in total, with 90 seconds between each to read the task instructions. The morning session comprises 4 pairs of ‘linked’ stations, lasting 10 minutes each. In these paired stations, the second station is connected to the first in some way, such as taking a history in the first part then discussing with a family member in the second. Each station is marked independently. The afternoon consists of 8 single stations, lasting 7 minutes each. A passing list is posted online after a few weeks, with specific feedback made available to unsuccessful candidates.2
Mock CASC format
Our mock CASC is run in one afternoon session from 1.30-5pm. We have been able to include 16 stations by running the 2 circuits simultaneously. To make this possible, each station is 7 minutes in duration, with 90 seconds between stations. 4 candidates start after a delay, as it is not possible to start on part 2 of a linked station. Trainees are allocated candidate numbers and starting stations for both circuits to coordinate this effectively (figure 1). 16 candidates can take part in the mock exam.
Figure 1. Candidate numbers
Candidate Name
Number
1st loop starting station
2nd loop starting station
1
1a
5
2
2a
6
3
3a
7
4
4a
8
5
1a (8.5 min delay)
9
6
2a (8.5 min delay)
10
7
3a (8.5 min delay)
11
8
4a (8.5 min delay)
12
9
5
1a
10
6
2a
11
7
3a
12
8
4a
13
9
1a (8.5 min delay)
14
10
2a (8.5 min delay)
15
11
3a (8.5 min delay)
16
12
4a (8.5 min delay)
At least 3 other higher trainee helpers are recruited to assist the coordinator on the day of the exam. The same marking scheme is used for each station, covering domains common to all stations, such as building rapport and range and depth of questioning. There is also space for specific feedback, which examiners are encouraged to provide, though they do not interact with candidates directly during the exam. Forms are completed contemporaneously and distributed to candidates immediately after the mock exam.
Step 3: Writing the Stations
The content of the CASC follows a blueprint, which is available through the RCPsych website. A variety of skills are tested during the 16 stations of the exam, including history-taking, mental state examination, risk assessment, cognitive examination, physical examination, case discussion and difficult communication.3 We refer to the blueprint when selecting which stations to include in the mock. Each year, recent CASC candidates are asked to suggest stations and we combine these with previous stations to construct the mock exam. New stations are written by the trainee who suggested them, including candidate instructions and actor’s notes. The higher trainee organiser formats these to maintain consistency across the mock exam.
Role-play actors
For our most recent mock CASC, we employed paid actors for every station. These actors are part of a local agency which has experience in working as simulated patients for Glasgow University exams and communication skills sessions. In previous years, we have recruited a combination of core/higher trainees and actors. We have found pros and cons to each approach. The use of paid actors was more realistic for trainees but writing scripts proved more challenging as instructions required greater detailed in relation to specific psychiatric information, such as how a person with mania may present.
Step 4: Recruiting Examiners
There are a number of local consultant psychiatrists who are actively involved in teaching. They are supportive of the mock CASC and enthusiastic about examining stations. After the stations have been devised, consultants are invited to examine based on their areas of expertise. Higher trainees with particular interest in education are then asked to examine any remaining stations. Candidate instructions and actor’s notes are circulated to examiners in advance (figure 2). A simple guide to the mock exam is also sent to any new examiners. As we use the same marking scheme for each station, it is down to the experience of the examiner to consider whether the candidate has addressed the specific tasks appropriately.
Figure 2. Station template
Station
Title
Actor
Examiner
Written?
Sent?
1a
1b
2a
2b
3a
3b
4a
4b
5
6
7
8
9
10
11
12
Step 5: The Day of the Mock Exam
The higher trainee coordinators arrive at least 1.5 hours prior to the start time to set up the venue. Examiners, actors and candidates are asked to arrive 15-30 minutes before the scheduled start time. Each group is briefed on the exam format and given the opportunity to ask questions. Actors and examiners are shown to their stations and allowed time to discuss them. Candidates are provided with numbered labels to wear, for examiners to record on their marking sheets. The 4 candidates who will be starting later are asked to wait, while the others are shown to the examination rooms. They are shown which station they will be starting at, then queue in order at the door.
The mock exam coordinator stands where they can be heard by both rooms. There are 1 or 2 helpers in each room to guide the candidates around the circuit. The bell is rung to signify the start of the exam, the end of the 90 second preparation time (the start of each station), 1 minute warning and the end of each station. The candidates who were allocated to start later are brought into the circuit and shown to their station as the ‘end of station’ bell is rung, as this also signifies the start of the 90 second preparation time for the next station.
Marking schemes are collected and sorted during the break. Candidates are not kept separate from examiners, actors or each other. They are advised that they will get the most out of the afternoon if they don’t discuss the stations but this is ultimately their choice.
Examiners and actors return to their stations following the short break and candidates swap between circuits. Following the second round, there is another short break. Actors are excused at this point and most examiners remain for a feedback session. Marking schemes are collected, sorted and distributed to candidates. One room is re-set for group feedback. Examiners are thanked for their time and each is asked in turn for general feedback, hints and tips on their station (figure 3).
Figure 3. Mock CASC timing
11.30pm
Coordinators arrive & set up venue
12.30-12.45pm
Candidates, actors & examiners on site
1pm
Exam starts
2.15pm approx
Break
2.45pm
Exam re-starts - candidates switch circuits
4pm approx
Exam ends
4.30pm
Feedback forms distributed/ group feedback session
5pm
End
Overcoming Potential Problems
Examiners
Our examiners are all either higher trainee or consultant psychiatrists. It is therefore possible that unforeseen circumstances mean that they may have to cancel at very short notice, attend late or not at all, or be called away during the mock exam. Each of these has happened over the past few years but has been easily managed by the extra higher trainee helpers stepping in to examine a station.
Actors
All of our actors have attended as planned. If a paid actor has to cancel at short notice, the agency will find a replacement. If a trainee actor did not attend, one of the higher trainee helpers could step in. Another potential problem which we have encountered is actors not performing as intended. This can be minimised by preparing clear instructions for actors, with examiners providing some direction if needed.
Quality control of stations
It is difficult to know how a station will work until it is used in the mock exam. To minimise the risk of problems, stations are checked and formatted before the exam. They are circulated to actors and examiners in advance to allow time for them to raise any concerns and clarify any uncertainties. Despite following these processes, there are some stations which appear unclear or do not run smoothly on the day of the mock exam. It is helpful to receive feedback from examiners, so that stations can be amended or avoided in future.
Timing
Our mock exam follows a very tight schedule. If the mock exam itself overruns, then fewer examiners may be able to remain to provide feedback. The higher trainee coordinator should keep time carefully during the day of the mock exam, particularly during break times, which are very brief. Support from other higher trainee helpers is essential for this, in working together to collect and organise marking sheets and guiding examiners, actors and candidates to stations. Late arriving examiners remain a potential problem due to their other commitments. We provide a sandwich lunch to our examiners prior to the exam, which helps with prompt attendance.
Venue
The venue we use is quite cramped and can become noisy. We have access to only 14 screens to divide the 16 stations so they are close together and those at the ends of the room are not fully enclosed. The screens are thin so only muffle the noise from neighbouring stations. These issues of space and noise are difficult to overcome. Trainees are warned in advance and aim to focus on their own station as much as possible.
Recruiting actors, examiners and candidates
To date, we have not experienced any problems in recruiting actors, examiners or trainee helpers. We have been able to fill all candidate places and often have a waiting list. If necessary, the mock exam could be run with fewer stations and still provide helpful practice for trainees. If resources were tight, trainees could be role-play actors for some or all of the stations.
Conclusion
We run a local mock exam annually due to continued demand from trainees. It takes significant time and effort to arrange but is good experience for the organiser and local trainees and consultants remain enthusiastic. The mock CASC in the West of Scotland puts a strong emphasis on providing feedback for trainees to work on. The provision of completed marking sheets on the day of the exam and the group feedback session help with this ethos. Our experience has shown that a mock CASC can be delivered locally, at a low cost, while still providing trainees with a realistic exam experience.
Schizophrenia sufferers feel like abstract entities with non-animated bodies, often experiencing auditory verbal hallucinations (AVH) due to morbid “objectification” of inner dialogue.1 From the patient’s perspective, AVHs are a subjective–objective phenomenon. AVH is a non-consensual, dynamic and psychologically charged experience and the voices often echo significant emotions. Derogatory voices are common representations of unconscious self-hatred that cannot stand up to the external world’s logic. Thus, patients need help to incorporate it. Auditory hallucinations may be arising because of an interaction between biological predisposition, perceptual and cognitive factors. According to an integrated model of auditory hallucination (AHs) suggested by Waters et al,2 AHs arise from an interaction between abnormal neural activation patterns that generate salient auditory signals and top-down mechanisms that include signal detection errors, executive and inhibition deficits, a tapestry of expectations and memories. Recently, neuro-quantologists have proposed that AVHs may be an objectification of parallel thinking/quantum thinking.3 Parallel thinking is a source for thought insertion. There may be different variables of AVHs. Experiencing AVH has serious impact on the quality of life of the affected individual, and is a significant factor in prevalence of suicides among schizophrenic patients.4
Incidence
One in four schizophrenia sufferers experiences persistent AVH .5 AVHs are experienced by approximately 53% of schizophrenia sufferers 6 and are present in 28% of major affective disorders (Goodwin& Jamison, . 7 Evidence indicates that each patient responds differently to the voices, according to his/her evaluation of them (Table 1), which influences the degree of interventions. Specific dimensions of AVHs can give hints to the future likelihood of treatment resistance. Although the percentages differ in various studies, it is assumed that about 30% of patients have command hallucinations and they are seen as the ultimate betrayal of the mind. 8 Often, the content of such messages is negative; thus, commanding AVHs are more distressing than commenting ones. Schizophrenia predisposes them to a greater risk of suicides and homicides. Command hallucinations are more prevalent among forensic patients and contribute to their forensic status.
Table1. Patients’ Response to AVH
1.Anxiety and panic feelings 2.Fear 3.Feelings of humiliation 4.Entrapment 5.Self harm thoughts 6.Harm to others 7. Avoidant or withdrawn 8.Shouting and swearing 9.Ritualistic behaviour 10. Substance or alcohol abuse 11. Resistance. 12. Amusements 13. Engagement and courting the voices 14. Appeasement
The multi-factorial polygenic model of schizophrenic disorders has received great support and signifies that genetic factors play a bigger role than environmental factors in familial transmission of these disorders. Relevant studies provide little support for the mechanism of single major locus inheritance. A mechanism involving two, three, or four loci cannot be ruled out even though there is no compelling support for such models.9 It has also been proposed that a single gene may be even responsible for hallucinatory experiences 10 implying that those who have not inherited such a gene may not experience auditory hallucinations, but still could experience other characteristic symptoms of schizophrenia. One may also hypothesise that an individual who has inherited such a “hallucinatory gene” but not all the schizophrenia genes could hear non-clinical voices without having other schizophrenic symptoms. It is also arguable that those who carry such a specific gene are more vulnerable to experience hallucinations when they abuse psychoactive substances and could get misdiagnosed as having schizophrenia, but hallucinations may cease to occur once they abstain from illicit drug abuse.
Measurements for Assessment
AVH is a subjective experience and is hard to measure objectively. Several rating scales are now available for an efficient evaluation of different aspects of voice activities. Some are general and a number of them are specifically designed. Using rating scales facilitates better engagement with patients and helps in reinforcing the message that patients and the distress they experience are carefully considered.
Beliefs About Voice Questions (BAVQ) is an assessment scale useful in measuring the key beliefs about the voices.11 It is typically used in conjunction with the Cognitive Assessment Schedule (CAS).12 Voice Compliance Scale (VCS) is an observer rated scale aimed exclusively at measuring the frequency of command hallucinations and the level of obedience or confrontation with each recognized command.13 Voice Power Differential Scale (VPD) is another measure that can be applied to rate the perceived relative power differential between the voice and voice experience. 14 On the other hand, Omniscience Scale (OS) is intended to quantify the voice hearer’s beliefs about their voices’ knowledge regarding the bio data. 15 Another measure presently in use is Risk of Acting on Commands Scale (RACS), designed to assess the level of risk of acting on commands and the amount of associated distress. 16
The Bonn Scale (BSABS) is used for the assessment of basic symptoms, 17while the Schizophrenia Proneness Instrument (SPI-A) 18and the Examination of Anomalous Self Experience (EASE) 19 are useful aids in identifying minimal changes in subjective experience and for longitudinal monitoring (Table 2). In the extensively used Positive and Negative Syndrome Scale (PANSS), the hallucination item is one of seven in the positive subscale, which also includes delusions, conceptual disorganization, excitement, grandiosity, suspiciousness, and hostility. Given such a great number of scales in use, there is an obvious risk that differential anti-hallucinatory efficacy among antipsychotic drugs may be obscured by means of sum scores for the whole sample in clinical trials.
Table 2. Measurement scales
Beliefs About Voice Questions (BAVQ) Cognitive Assessment Schedule (CAS ). Voice co Voice Power Differential Scale (VPD) Voice Compliance scale (VCS) Voice Power Differential Scale (VPD) Omniscience Scale (OS) Risk of Acting on Commands Scale (RACS) Bonn Scale (BSABS) Schizophrenia Proneness Instrument (SPI-A) Examination of Anomalous Self Experience (EASE) Positive and Negative Syndrome Scale(PANSS)
Treatments
Although many forms of treatments aiming to eliminate AVH or improve quality of life are available, use of medication seems to be the most prevalent. Besides drug treatment, non-invasive physical treatments, such as TMS and different forms of psychological interventions, have recently evolved. Drug therapies are aimed at symptom eradication, whereas psychological therapies tend to foster healing, recovery and personal growth. Rather than being specifically anti-hallucinatory, typically, neuroleptics offer a generalised calming effect and patients are given some “breathing space” to work through their voices. Usage of non-pharmacological tools is needed in the long-term management of refractory cases. Presently, intervention strategies for AVH are based on different models of hallucinations, but regrettably no clear models have been established.
Pharmacotherapy
The current understanding of AVH and the neural mechanisms involved is limited, and knowledge on how CNS drugs, such as antipsychotics, influence the subjective experience and neurophysiology of hallucinations is inadequate. Consequently, using pharmacotherapy in the management of AVH remains very challenging. 20 Despite multiple trials of different combination and adjunctive therapies to an antipsychotic regime, AVH can remain drug resistant. It is also important to note that all antipsychotics are potentially anti-hallucinatory, even though these effects are usually modest. Moreover, given that, even when medications are effective, concordance can be an issue, antipsychotics should be used prudently and weighed up against effectiveness and side effects (Table 3). There are no clear guidelines for the drug treatment of AVH and comparisons of the efficacy of antipsychotics for AVHs are few. Clinical drug trials very rarely focus on single symptom scores, such as hallucinations, and tend to report group mean changes of overall psychopathology, or at best the positive subscale scores.
Evidences show that AVHs persist in spite of treatment in 32% of chronic patients 21 and 56% of acutely ill patients.22 Trifluperazine was popular as an anti-hallucinatory drug before the advent of atypical antipsychotic drugs. Clozapine is currently favoured for intractable AVHs and is beneficial in 30–60% of unresponsive patients.
Antipsychotic co-treatment is an option for clozapine augmentation. Olanzapine and risperidone may be alternative drugs in first episode psychosis. However, it is being debated whether clozapine should be used in such cases.
Table 3. Drug Treatment
Choice of antipsychotics Cautions and contraindications Titration of dose Switching antipsychotics Assessment of side effects, EPS, TD, Haematological effects etc. Measuring the beneficial effects Assess worsening of symptoms Compliance
Clozapine
Use of clozapine is suggested only after two other antipsychotics have been tried. It works better with continued usage and clinicians have to be patient in its upward titration. At six months, improvement in Global Assessment of Functioning score is significantly higher for clozapine in comparison to other antipsychotic drugs.23 However, when prescribing clozapine, cautions and contraindications must be noted (Table 4).
While higher doses of clozapine may not have more anti-hallucinatory effect, they still carry the risk of inducing the potential side-effects of this highly efficacious drug (Table 5). The most dreaded haematological side-effects are usually manifested within six months. For that reason, during clozapine therapy, patient has to be closely monitored, bearing in mind its limitations in achieving the anti-hallucinatory effects. If higher doses do not have the desired effect, clozapine dose should be titrated downwards to a point of its maximum anti-hallucinatory effect in a particular patient. Such an endeavour can prevent the emergence of serious side-effects, resulting in a complete failure of the therapy. The dose can also be adjusted to a safer level in cases where the psychological interventions are found to be successful. Clozapine can be effective even in lower doses, such as 200 mg/day. Only in the presence of command hallucinations, higher doses should be prescribed to patients whose other positive symptoms are well under control.
Prophylaxis with an antiepileptic drugs, such as lamotrigine or sodium valproate, or similar should be commenced before titrating the dose above 600 mg daily. Close monitoring and active treatment of metabolic dysregulation should be initiated concurrent with clozapine therapy. In clozapine therapy, weighing up safety and superior antipsychotic efficacy and educating the patients on “clozapine lifestyle” is immensely important, as it helps in treating refractory cases of AVH. Thirty percent of patients treated with clozapine may remain unresponsive and clinicians have to lower their expectations to the level of achievement without being cynical. Isolated cases of clozapine-induced joint visual and auditory hallucinations have been reported. 24 In spite of Clozaril treatment having the highest anti-hallucinatory effect, a good percentage of AVH sufferers remain symptomatic and are classed as super-refractory.8 According to Gonzales (2006), 25 50% of patients receiving antipsychotics achieve full remission, while 25% hear voices occasionally and 25% are unresponsive.
Table 4. Cautions & Contraindications of Clozapine
1.Patients with myeloproliferative disorders, a history of toxic or idiosyncratic agranulocytosis or severe granulocytopenia (with the exception of granulocytopenia / agranulocytosis from previous chemotherapy) 2.Bone marrow disorders 3-Patients with active liver disease, progressive liver disease and hepatic failure. 4-Severe CNS depression or comatose state, severe renal and cardiac disease, uncontrolled epilepsy, circulatory collapse, 5. Alcoholic/toxic psychosis and previous hypersensitivity to clozapine. 6.Pregnancy and breast feeding
Table 5. Benefits and risks of Clozapine
Benefits 1. Lower risk of suicide 2. Superior anti-delusional and anti-hallucinatory effects in refractory cases 3. Lower risk of tardive dyskinesia and suppression of TD. 4. Improvement in cognition 5.Higher quality of life and better adherence 6.Decreased relapse 7. Sexual functions unaffected Risks 1.Agranulocytosis 2.Metabolic syndrome 3.Myocardites 4.Chronic constipation and bowel complications 5.Incresed risk of seizure 6.Hypersalivation 7.Abrupt withdrawal cause marked discontinuation symptoms.
Benzodiazepines are often abused by voice hearers aiming to reduce their anxiety. Such patients might benefit by the addition of antidepressant, as this could enhance their mental resources to cope with the voices, even though they have no anti-hallucinatory effects per se. Mood stabilisers are sometimes used to augment the efficacy of antipsychotics without any clinical validation. Despite multiple trials of different adjuvant therapies to an antipsychotic regimen, there have been few promising results. Still, in practice, clinicians may get frustrated, as they struggle to provide symptomatic relief to the voice hearers at any cost. Recently allopurinol, an anti-gout agent has been used as an adjunctive therapy and based on three randomized controlled trials, the result has been encouraging. 26
Psychological Interventions
Persistent AVHs alone may not warrant pointless alteration of medication, as non-pharmacological interventions may achieve some control. When clinicians are not cognizant of non-pharmacological therapies, AVH patients that do not respond to antipsychotics alone may be mislabelled as having refractory AVH. In fact, they are only unresponsive to drug treatment, and could potentially respond to an integrated approach. Similarly, patients with treatment-refractory AVH are often over-diagnosed as suffering from hard to treat schizophrenia, even when other positive symptoms have been ameliorated.
There exists a false dichotomy between physical and psychological treatment approaches to AVH. In practice, both treatment modalities have to be modified in a personalised form. After all, psychiatry was originally known as psychological medicine. Presently, even though different forms of non-pharmacological interventions are available for drug-resistant AVH, some have questionable effects. 27,28,29 (Table 6).
Table 6. Psychological Interventions
1.Cognitive behavioural therapy (C.B.T.) 2. Acceptance and commitment therapy (ACT) 3. Competitive memory training (COMET) 4.Compassionate Mind Training therapy (CMT) 5.Hallucinations focussed integrative therapy (HIT) 6.Midfulness-based therapy 7.Normalizing techniques 8. Enhanced supportive psychotherapy 9. Attention training technique. 10. Distraction techniques 11. Self help approaches
CBT therapists predicate that AVHs are a manifestation of the morbid objectification of inner dialogue (thinking in words),and accordingly verbalised thoughts are the raw material for AVHs.Verbal thinking differs from external speech in many respects and has several distinct features. CBT therapists believe that cognitive dysfunctions underlie AVH and they target them with cognitive remediation strategies. Those experiencing voices commonly think that they are caused by a powerful external agency, and are controlling and potentially harmful. Psychological factors, such as meta-cognitive biases, beliefs, and attributions concerning the origins and intent of voices, also play critical modulatory role in shaping the experience of AVH. Teaching patients to recognize the source of the voices alone has yielded beneficial effects.
Specific techniques have been designed to modify the frequency of AVHs and restore a sense of control over them. Earlier methods involved behavioural approaches based upon addressing hypothesized antecedents and reinforcers of voices and explored a variety of specific interventions such as relaxation training, graded exposure to voice triggers, manipulation of environmental possibilities and even aversion therapy. 30 These behavioural techniques were eventually expanded on by the application of cognitive methods. The primary aim of psychological therapy is to change the belief that voices are omnipotent and uncontrollable and to suppress the associated attributes of false identity, wrong intentions, and urges to harm oneself and others. They encourage patients to challenge irrational interpretations and modify maladaptive behaviour, diverting attention from voices with distraction techniques (Table 7).
Reality testing and behavioural experiments are one form of CBT intervention, based on the view that behavioural changes can prompt cognitive changes. Attention switching can also be used to challenge the belief that hallucinations are uncontrollable. Command AVHs are more prevalent among the forensic population and are more distressing than the commenting ones. The risk of the sufferer acting on them is high when voices are perceived as omnipotent and uncontrollable. CBT has been proven beneficial in tackling command hallucinations. Lack of insight and formal thought disorder may not necessarily disqualify CBT for AVH; nonetheless, negative symptoms may pose a barrier to this form of psychological intervention. The current model of CBT for psychosis has been criticized, suggesting that it is simply an extension of general CBT concepts without taking into account the specificities of psychosis. 31 Patients with higher intelligence, who have the ability to grasp abstract concepts, might gain greater benefits from CBT. 32
Table 7. Goals of CBT
1. Change false beliefs about AVH . 2. Challenge irrational interpretations. 3. Modify maladaptive behaviour – e.g. fear of the voices or hiding from them. 4. Divert attention, using distraction techniques. 5. Build and maintain treatment strategies 6.Develop cognitive behavioural strategies 7.Develop newer understanding of hallucinatory experience 8. Address negative self-evaluation.
Combining psycho-education and supportive psychotherapy has been found to enhance the functioning and self-esteem of voice hearers, providing a therapeutic structure. In the increasingly popular self-help voice-hearing groups, the ethos of recovery is understanding, accepting and integrating the sufferer’s turmoil. Acceptance and non-judgemental support of people with similar experiences has helped many patients cope with the condition. In response, the number of books on AVH, aiming to educate the sufferers and carers, has grown considerably.
Newer Psychological Interventions
Attention Training Technique (ATT) focuses on negating psychological distress through cognitive and meta-cognitive modification. 33,34 Patients focus on up to five neutral sounds, such as a dripping tap, before switching their attention between different sounds. They then practise listening to all the sounds simultaneously. After a few weeks, they focus on neutral sounds and then on the AVH. Once this process is mastered, they switch attention between voices and other sounds, before being asked to divide their attention among them. This exercise continues for several weeks, whereby the aim is to replace the self-regulatory process with new processing configurations.
Acceptance and commitment therapy (ACT) is aimed at achieving psychological flexibility. It incorporates mindfulness and acceptance, considering AVH as a private experience and asserting that patients experience distress only when they try to deafen the voices. . By reducing struggle with voices and engagement with them, key responses such as arousal, attention and activation of brain areas are hypothesised to be reduced. 35 The ideas behind ACT are consistent with the emphasis on the recovery movement of finding a way to live a valued life despite the ongoing problems. To this effect, unique and effective coping strategies are offered, whereby patients are given the insights that parts of the self are behind the voices. Thus, accepting them means sending a loving message of compassion, acceptance and respect to oneself Two randomised control studies have yielded promising results. 36,37ACT follows a set manualised structure, rather than relying upon the complex and lengthy process of belief modification: therapy can be much briefer and potentially practiced by a wider range of clinicians and cost effective. 38
There are verbal and non-verbal routes to emotions. As CBT uses the former in voice therapy, it is less effective when patients are negatively involved with the voices. On the other hand, Competitive Memory Training (COMET) uses the non-verbal route. Generally COMET sessions involve four stages.39 A. identification of aspects of negative self-esteem reinforced by the voice; B. retrieval and re-living of memories associated with positive self-esteem; C. positive self-esteem is brought to compete with the content of the voices to weaken associations between voice content and negative self-valuation; and D. learning to disengage from the voices and to accept the voices as psychic phenomenon.
The significant past comes back to the conscious mind in AVH, as life experiences charged with emotion make a compelling impression on the brain. The observation that voices are knowledgeable about patients suggests that auditory hallucinations are linked to memory. In other words, negative experiences from memories evoke emotions, which should be deactivated. Distancing and decentring techniques could help patients to interpret voices as false mental events. As a result, incompatible memories could become tools to modify the power of voices—they are deactivated by new learning. Thus, when voices torment hearers, telling them that they are failures, a competing memory of such success as passing a significant examination is introduced. Posture, facial expression, imagination, self-verbalisation and music are all procedures included in the COMET protocol.40
Compassionate mind training (CMT) is used to encourage better resilience to unpleasant commenting voices.CMT involves practicing exercises which promote self-compassion and compassion towards others. It is targeted to activate brain systems involved in social and self-soothing that amend threat systems active when experiencing unfriendly voices. 41
Mindfulness is paying attention in a particular way – on purpose, in the present moment and non-judgementally. Clinical literature cautions against use of meditation in psychosis, but the effectiveness of mindfulness-based approaches for people with psychosis has been demonstrated in controlled clinical settings. 42and in the community. 43 Abba et al. 44 argue that effectiveness of mindfulness is a three-stage process: a. Becoming knowledgeable and developing more awareness of psychotic experiences and observing the thoughts and emotions that follow them. B. Permitting psychosis to come and go without reacting in order to cultivate understanding that distress is produced by the meanings one attaches to thoughts and sensations. C. Becoming autonomous by accepting psychosis and the self by acknowledging that the sensations only form part of the experience, and are not a definition of the self.
Neuroimaging studies are beginning to explain the neural mechanisms of how mindfulness might be working clinically. Structural changes have been observed in the anterior cingulate cortex, which is an area of the brain associated with emotional regulation. 45 . There is evidence to suggest that mindfulness practice is correlated to reduced brain activity in the default mode network. 46
Limited improvements with mono-therapy have prompted the development of multi-modular approaches. Hallucination-focused Integrative Therapy (HIT) is geared towards integrating CBT with neuroleptics, coping strategies, psycho-education, motivational intervention, rehabilitation and family treatment.47 Extant studies indicate that integrated treatment is more effective than TAU (treatment as usual).
The continuum model of psychosis and ordinary mental events has incited the development of normalisation of the voice hearing experience.48 Most psychiatric symptoms occur in normal people—just as breathlessness and palpitations occur while exercising—but are potential clinical symptoms. It is the frequency and duration that determine the borderline. According to the cognitive model, an internal mental event receives external attribution. Through normalisation, the external attribution can be reversed.
Although drug treatment may be the most practical way of managing AVH, refractory cases pose formidable challenges and it must be emphasized that psychological treatments are not counterproductive if applied skilfully. Clinicians who espouse the view that psychosis is a medical condition dismiss the usefulness of psychological interventions. The counter argument would be that a patient with a medical condition, such as stroke, benefits from physiotherapy, occupational therapy and psychological approaches.49
Repetitive Trans-cranial Magnetic Stimulation
There are several ongoing trials in which the aim is to treat refractory AVH (Table 4). Repetitive transcranial magnetic stimulation (rTMS) is thought to alter neural activity over language cortical areas. Several studies on rTMS have shown improvement in the frequency and severity of AVHs, albeit without offering any strong conclusive evidence for its efficacy .50 Moderate rates of AVH attenuation following rTMS have been noted in three meta analyses. Given that remarkable improvements in isolated cases have also been claimed, this suggests that rTMS may be appropriate mode of therapy for some patients.
Available data suggest that .rTMS selectively alters neurobiological factors that determine the frequency of AVH. However, a recent meta-analysis indicated that the effect of rTMS may be short-lived (less than one month).51 Studies seem to indicate that rTMS may be effective in reducing the frequency of AVHs, with little effect on their other topographical aspects.50,52 Sham stimulation has also led to improvements in a number of AVH parameters. Compared to bilateral stimulation, rTMS of left tempero-parietal region appears more effective in reducing the AVH frequency . 53 To reduce the distress associated with AVH and help patients to cope with hallucinatory predilection, rTMS could be combined with CBT. The side-effect profile is much cleaner for this biological approach when compared to medications. Still, like any other anti-hallucinatory treatments, neuro-stimulation technique does not guarantee long-term elimination of AVH. Electroconvulsive therapy (ECT) is considered a last resort for treatment resistant psychosis. Although several studies showed clinical improvement, a specific reduction in hallucinations severity has never been demonstrated.
Avatar Therapy
Computer-assisted voice therapy is a budding form of computerised psychological treatment that is currently undergoing trials.28 In this novel therapy, persecutory voices are directly depowered with the aid of a computerised dummy of the alleged persecutor through voice dialogue. Analytically-oriented therapists can even converse with “voices” and such committed clinicians will find computerised voice therapy as another helpful tool. It is hard to ascertain whether the benefits of the avatar therapy were due to the specific technique involved or simply the increased attention and care, and Leff’s team acknowledged the limitations of their work.54
Sound Therapy
Another important development in voice therapy is the use of tinnitus control instrument (TCI)—a form of sound therapy—in treating refractory AVH. Similar to AVH, subjective tinnitus is defined as the false perception of sound in the absence of acoustic stimuli. Even though their definitions are similar, the origin and underlying causes of these two conditions differ. Tinnitus is characterised by a simple sound—a monotone—and is non-verbal. In tinnitus, the brain is believed to interpret an internally generated electromagnetic signal as an acoustic sound or sounds.
Kaneko, Oda, and Goto29 reported successful intervention in two cases of refractory AVH with sound therapy, using tinnitus control instrument (TCI) alongside antipsychotic medications. They posited that, in sound therapy, the auditory system is directly helping the limbic nervous system and the neuro-mechanism for AVH is sensitive to sound therapy .55 They concluded that low-level auditory stimulation might be hindering the progression of voices and brain might be getting a breathing space to initiate self-healing process.
Future Directions
Hallucinogenic drugs, anti-hallucination medications and neuroimaging studies may lead to a better understanding of AVH. Animal models of hallucinations and pharmacogenetics might help to find more efficacious anti-hallucinatory drugs. AVHs themselves may have a genetic origin.10 Thus, not all patients that develop schizophrenia would experience AVHs. Such a finding might help shed more light on the genetics-linked mechanism and remedial measures of hallucinations in schizophrenia. Because the biological substrates facilitating drug effects on hallucinations remain largely unidentified, future studies with translational designs should address this important issue to find a more targeted drug treatment of psychosis.56
If a derivative of clozapine without the haematological side-effects is formulated in the future, it might be an important milestone in the treatment of refractory AVHs and schizophrenia because clozapine has the most potent anti-hallucinatory effect. Such a novel drug could become the first line of treatment for schizophrenia, as it would address many of schizophrenic symptoms at their onset. This is crucial, as symptoms and habits become stronger and more resistant the more frequently they occur. Fatty acid amide derivatives of clozapine, such as DHA-clozapine, are found to have better pharmacological properties and enhanced safety. However, such claims are awaiting substantiation in clinical trials.57 Thus, more attention needs to be directed into this potentially rewarding research arena. It is, however, very likely that, even after a better pharmacological cure is found for AVHs, a few symptoms might linger on for long periods. With this view, efficient non-pharmacological remedies have to be designed to deal with such residual symptoms.
Discussion
Medications help reduce the psychic pain, and protect the dignity of patients, as well as prevent suicides and homicides. From the patient’s perspective, the calming and relaxing effects of pharmacological therapies are a priority for relief from the distress due to AVH. Among the antipsychotics, clozapine has the maximum anti-hallucinatory effect and it is a shame that it cannot be used as a first line treatment choice. Treatment of AVH should be individualistic and clinicians should be prepared to apply several clinical and non-clinical approaches in concert to address them.
More research into the aetiology and mechanism of AVH is warranted in order to find effective treatment strategies. There is no shortage of theories about the mechanism of AVH, but there is no consensus among the investigators. It is unlikely that AVH is a pure neuro-chemical experience or a biological glitch, and this is where the currently available drug treatments fail. The distinction between primary and secondary symptoms was lost with the triumph of biological psychiatry in the last century. Thus, some authors presently claim that AVHs may even be a secondary symptom or a neuroquantological manifestation of an underlying biological disorder. We should not minimise the importance of eliminating symptoms when such symptoms are incapacitating, as in the case of hallucinatory experiences.
The present recovery model that emphasises and supports the patient’s potential for recovery involving hope, supportive relationship, empowerment, social inclusion, coping skills and meaning cannot be achieved without the help of psychological interventions. In this respect, CBT is a useful tool in the rehabilitation of psychotic patients with residual AVH. Jauhar et al.58 argued that the effectiveness of CBT in schizophrenia is influenced by failure to consider sources of bias. Consequently, the benefits are more apparent than real, prompting the question of whether CBT has been oversold.49 The verdict of Maudsley debate on the issue has been that CBT has not been oversold, but rather has a great impact on symptom reduction and enhancing concordance and insight. Perhaps the most informative trial so far accomplished has been the work on cognitive therapy for command hallucinations, which has proven the benefit of specific model development, and which productively, combined measurement of process and a targeted outcome.59
There is ample evidence suggesting that a combination of family and psychological interventions, alongside pharmacotherapy, can be the most effective way of dealing with refractory AVH.60 The inner dialogue hypothesis of AVH held by CBT therapists has its opponents.61 Patients respond to the voices they experience by utilising inner speech. Some observations with corresponding features weaken the inner-dialogue hypothesis. David and Lucas have demonstrated in a single case study that short-term maintenance of phonological representation (inner dialogue) may co-exist with AVHs – they are not synonymous experiences. The cost-effectiveness of psychological interventions is poorly studied, despite being highly relevant for policy decisions in healthcare.
Computerised voice therapy works better with technically minded, highly intelligent patients. In contrast, individuals of low to average intelligence may require a primarily behavioural approach, with limited efforts to understand concepts, such as automatic thinking and schema. Unlike sound therapy through music playing instruments (iPad, iPod, iPhone, etc.), TCI causes no disruption to daily functioning and can be used continuously. Computerised voice therapy and sound therapy warrant standardised case trials. When it comes to treating AVHs, optimizing compliance, reducing the burden of symptoms, and improving control, quality of life and social functioning should be the therapeutic goals.62 Neuroquantological views of AVHs63 explain the limitations of pharmacotherapy and the usefulness of psychological interventions.
During my placement in Psychiatry at the Brooker Centre, Runcorn, UK, I have come into contact with a wide array of psychiatric disorders, none more so than borderline personality disorder (BPD). It is undoubtedly one of the most prevalent problems in the area which the Brooker Centre serves. I can recall an example of a patient with BPD who had been quite unwell for a prolonged period of time and had struggled with affective instability. This patient had been quite successfully treated with Lithium therapy, has exhibited stability and is happy on the current treatment. There is a pattern of pharmacological treatment in BPD patients despite the fact that guidelines suggest otherwise…
Personality disorders are defined as ‘an enduring pattern of inner experience and behaviour that deviates markedly from the expectations of the individual’s culture, is pervasive and inflexible, has an onset in adulthood, is stable over time, and leads to distress or impairment’ . Personality disorders are representative of long-term functioning and are not considered in terms of episodes of illness 1.
The Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), groups the various personality disorders into three clusters based on their descriptive similarities.
Cluster A includes the Paranoid, Schizoid, and Schizotypal personality disorders which are categorised as ‘odd/eccentric’;
Cluster B includes the Antisocial, Borderline, Histrionic, and Narcissistic personality disorders which are categorised as ‘dramatic/emotional/erratic’;
Cluster Cincludes the Avoidant, Dependent, and Obsessive-compulsive personality disorders which are categorised as ‘anxious/fearful’ 2.
The International Classification of Diseases, 10th edition (ICD-10), specifies the condition of emotionally unstable personality disorder which has two subtypes: The impulsive type and the borderline type. The borderline type in essence overlaps with the DSM-5 definition 3.
It has proven difficult to provide robust clinical recommendations with regards to the treatment of personality disorder. This is, in part, due to the fact that study populations are diverse but also compounded by the use of different assessment criteria. Furthermore, it is important to consider that personality disorders often present with a great deal of psychiatric comorbidity. Of the personality disorders, particular attention has been paid to borderline personality disorder (BPD) as the symptom clusters which it involves have been shown to improve considerably with treatment 4.
Figure 1: Diagnostic Criteria for Borderline Personality Disorder according to DSM-5 2:
A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following: 1. Frantic efforts to avoid real or imagined abandonment. (Note: Do not include suicidal or self-mutilating behaviour covered in Criterion 5.) 2. A pattern of unstable and intense interpersonal relationships characterised by alternating between extremes of idealization and devaluation. 3. Identity disturbance: markedly and persistently unstable self-image or sense of self. 4. Impulsivity in at least two areas that are potentially self-damaging (e.g. spending, sex, substance abuse, reckless driving, binge eating). (Note: Do not include suicidal or self-mutilating behaviour covered in Criterion 5.) 5. Recurrent suicidal behaviour, gestures, or threats, or self-mutilating behaviour. 6. Affective instability due to a marked reactivity of mood (e.g. intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days). 7. Chronic feelings of emptiness. 8. Inappropriate, intense anger or difficulty controlling anger (e.g. frequent displays of temper, constant anger, recurrent physical fights). 9. Transient, stress-related paranoid ideation or severe dissociative symptoms.
Borderline personality disorder is characterised by a pervasive instability in mood, interpersonal relationships, self-image and behaviour. The condition was first recognised in the United States by Adolf Stern in 1938. He described that these are a group of patients who neither fit into psychotic or psychoneurotic group, which gave rise to the term ‘borderline’. BPD is often diagnostically comorbid with depression and anxiety, eating disorders (notably bulimia), post-traumatic stress disorder, substance misuse and bipolar affective disorder. Furthermore, psychotic disorders have also been found to overlap. Due to this extent of comorbidity it is rare to see a patient who has a pure BPD 5.
The pharmacological treatments of BPD are tailored according to the symptom clusters that present. These include impulsivity, affective instability, transient stress-related psychotic symptoms and suicidal & self-injurious behaviours 5,6.
Recommended Psychological and Pharmacological treatment, 2009 National Institute for Health and Clinical Excellence (NICE) guidelines on Borderline Personality Disorder5, 7:
Psychological
NICE guidelines state that when offering psychology for BPD or for the individual symptoms of the disorder, brief psychological interventions (i.e. less than a 3 month period) should not be used. It states that the frequency of psychotherapy sessions should be adapted to the patient’s needs and ‘context of living’ and suggests that twice-weekly session may be considered. The guidelines also specify that for women with BPD for whom recurrent self-harm is a priority, a comprehensive dialectical behaviour therapy programme should be considered. NICE recommends that when psychological treatment is provided in BPD, the effects should be monitored using a broad range of outcomes. These should include personal functioning, drug and alcohol use, self-harm, depression and the symptoms of BPD.
Pharmacological
The NICE guidance states that drug treatment should not be used specifically for BPD or for the individual symptoms or behaviour associated with the disorder (e.g. repeated self-harm, marked emotional instability, risk taking behaviour and transient psychotic symptoms). It goes on to suggest that antipsychotics should not be used for the medium- and long term treatment of BPD. However, with regards to the management of comorbidities, it specifies that drug treatment may be considered and that in each case, the NICE guidelines for each comorbid condition must be referred to. Antidepressants, mood stabilisers and antipsychotics are commonly used in clinical practice. The guidelines mention that short-term use of sedative medication may be considered in a crisis. ‘Short-term’ denotes treatment lasting no longer than one week.
With regards to drug treatment during a period of crisis, NICE recommends that there should be a consensus among prescribers and other involved professionals about the proposed drug treatment and also that a primary prescriber should be identified. There should be an appreciation of the likely risks of prescribing, including alcohol and illicit drug use. NICE emphasises that the psychological role of prescribing (both from the patient’s and prescriber’s perspective) should be taken into account, and the impact that such prescribing decisions may have on the therapeutic relationship and overall care plan. NICE recommends that a single drug be used and that polypharmacy is to be avoided as much as possible.
In a crisis NICE recommends prescribing ‘a drug that has a low side-effect profile, low addictive properties, minimum potential for misuse and relative safety in overdose.’ The minimum effective dose is favourable, prescribing fewer tablets more frequently if there is a significant risk of overdose and also agreeing with patient on the symptoms that are being targeted. NICE suggests that following a crisis, a plan should be made to stop drug treatment that was started during a crisis. If this is not possible, a regular review of the effectiveness, side effects, misuse and dependency of the drug is advised. BPD patients can often have concomitant insomnia and for this, NICE details basic advice regarding sleep hygiene and forwards on to the guidance on the use of zaleplon, zolpidem and zopiclone for the short-term pharmacological management of insomnia.
AIMS AND OBJECTIVES
This report will review the current guidelines specifically regarding the management of borderline personality disorder and explore the literature according to the research recommendations that are set by NICE. The report is to focus on the two aspects of the management of BPD – The psychological/psychosocial aspect and the pharmacological aspect.
CURRENT NICE GUIDELINES ON PSYCHOLOGICAL AND PHARMACOLOGICAL TREATMENT OF BPD 7:
Psychology
Mentalisation-based therapy and dialectical behavioural therapy are proposed in the setting of a ‘well structured, high quality community based service’ e.g. a day hospital setting or a community mental health team. NICE suggests that these techniques should be compared with ‘high-quality community care delivered by general mental health service without the psychological intervention for people with BPD’ in order to measure efficacy. For outpatients, cognitive analytic therapy, cognitive behavioural therapy, schema-focussed therapy and transference focussed therapy are suggested and are catered to those with less severe BPD (i.e. fewer comorbidities, higher level of social functioning, greater ability to depend on self-management methods). Randomised controlled trials reporting medium term outcomes (e.g. quality of life, psychosocial functioning, employment outcomes and BPD symptomatology) of a minimum of 18 months are recommended
Pharmacology
Mood stabilisers are proposed as it is detailed that emotional instability is a key feature in BPD. In particular, topiramate and lamotrigine are mentioned as they have been shown to produce encouraging results in small-scale studies. A randomised placebo-controlled trial with medium to long-term follow up is recommended.
ANALYSIS
Psychology: Dialectical Behaviour Therapy (DBT)
Dialectics can be defined as the art of investigating the relative truth of opinions, principles, and guidelines 8. Dialectical in DBT refers to a means of arriving at the truth by examination of the argument i.e. the ‘thesis’ and ‘antithesis’ and resolving the two into a rational synthesis. DBT was introduced in 1991 by Marsha Linehan (a psychology researcher) and colleagues tailored as a treatment for BPD. In this, patients are supported in understanding their own emotional experiences and are taught new skills for dealing with their stresses. A combination of individual and group sessions are used. More adaptive responses and effective problem-solving techniques are integrated to improve functioning and quality of life as well as improving morbidity and mortality 9, 10.
A study published in 2015 by M. Linehan et al detailed a randomized clinical trial that set out to compare
1) Standard DBT (DBT group skills training + DBT individual therapy) with
2) A treatment that evaluated DBT group skills training with manual case management (i.e. with the removal of DBT individual therapy) and
3) A treatment that removed DBT skills training by providing only DBT individual therapy with an activities group and prohibited individual therapists from teaching DBT skills.
All 3 versions of the treatment were found to be comparably effective at reducing suicide attempts, suicidal ideation, medical severity of intentional self-harm, use of crisis services owing to suicidality and improving reasons for living 11.
Psychology: Mentalization based therapy
Mentalization is ‘the process by which we make sense of each other and ourselves, implicitly and explicitly, in terms of subjective states and mental processes.’ It is a social construct suggesting that we are attentive to the mental states of those we are with, physically or psychologically 12. Mentalization based treatment is a psychosocial treatment for BPD in which therapists monitor attachment and mentalizing capacity, and use interventions that aim to reinstate or maintain the capacity of patients to mentalize 13.
A longitudinal study, published in 2008, involving an eight-year follow-up of patients treated for BPD evaluated the effect of mentalization-based treatment (MBT) with partial hospitalization compared with treatment as usual. Five years after discharge from MBT, the MBT group exhibited clinical and statistical superiority to treatment as usual measured on suicidality, diagnostic status, service use, medication use, global function and vocational status 14. A more recent review article, published in 2015, emphasises the consideration of disruptions in three closely related domains in individuals with BPD. These are ‘in attachment relationships, in different polarities of mentalizing, and in the quality of epistemic vigilance and trust’. It is suggested that this approach allows seemingly paradoxical features of BPD patients appear more coherent. It is supposed that this approach provides a clear focus for the therapist enabling them to monitor the therapeutic process in terms of imminent mentalizing impairments and epistemic mistrust due to activation of the attachment system.
The article goes on to assert that the effectiveness of MBT in BPD may be elucidated due to the fact that it ‘enables the therapist to maintain and foster a mentalizing stance, even–and perhaps particularly–under high arousal conditions that are so characteristic of work with these patients’ 15.
Psychology: Cognitive analytic therapy (CAT)
CAT is a brief focal therapy that is informed by cognitive therapy, psychodynamic psychotherapy and elements of cognitive psychology. It was originally developed by Anthony Ryle tailored towards the needs of the NHS 16. It is based on a collaborative therapeutic position which sets out to create narrative and diagrammatic reformulations with patients concerning their difficulties. The theory centres on descriptions of sequences of linked external, mental and behavioural events. At first, the emphasis was on how such procedural sequences prevented revision of dysfunctional ways of living. More recently, this has been extended to understanding the origins of reciprocal role procedures in early life and their repetition in current relationships and self-management 17.
One study detailed a randomised controlled trial which aimed to investigate the effectiveness of time-limited CAT for participants with personality disorder. The study found that participants receiving CAT exhibited reduced symptoms and showed considerable improvement compared with the control group who showed signs of deterioration during the treatment period. They concluded that CAT is superior to treatment as usual in improving outcomes associated with personality disorder 18.
Psychology: Cognitive behavioural therapy (CBT) and Schema-focussed therapy
CBT is a time-limited, problem focussed psychotherapy that has been applied to a wide range of psychiatric disorders. The development of this technique was born out of the observation that patients referred for psychotherapy often would hold ingrained, negatively skewed assumptions of themselves, their future and their environment. The therapy is based on the notion that disorder is caused not by life events, but by the view the patient adopts of events. The therapy focusses on current problems and helps to develop new skills to provide symptom relief and sustain recovery 9, 19.
Initially CBT was predominantly insight-orientated, using introspection to bring about change. Beck et al began to integrate a range of behavioural techniques to improve the impact on dysfunctional controlling belief systems (schemas). The goal of treatment is not to replace the dysfunctional schemas; it aims to modify beliefs and develop new ones allowing the patient to cope more effectively in challenging situations 20, 21.
A 2013 review article that set to explore schema-focussed therapy concluded that schema-therapy is based on a ‘cohesive theoretical model’ and that there seems to be sufficient evidence supporting its validity. Regarding effectiveness, it goes on to indicate that one should be encouraged by the results of studies, however it points out that due to the small number of ‘methodologically-good efficacy studies’ it is difficult to be certain. The article claims that when evaluated against other psychotherapeutic treatments, specifically DBT and MBT, schema-therapy requires more investigation 22. A pilot study (2013) set out to monitor the effects of group schema-based CBT on global symptomatic distress in young adults with personality disorders or features of personality disorder. Their findings provide preliminary evidence that schema-based CBT might be an effective treatment 23.
Furthermore, there is a multicentre randomized controlled trial being conducted with the aim of investigating schema-focussed therapy versus treatment as usual in BPD, which has a closing date of 1st February 2016 24.
Psychology: Transference focussed therapy (TFT)
The classic use of the term transference originates in psychoanalysis and comprises “the redirection of feelings and desires and especially of those unconsciously retained from childhood toward a new object” 25. Transference-focussed psychotherapy is an evidence-based manualised treatment using a psychodynamic approach with a focus on object relations theory 26. TFT aims to ‘facilitate the reactivation, under controlled circumstances, of the dissociated internalised object relations in the transference relationship to observe the nature of the patient’s split polarised internal representations, and then, through a multistep interpretive process, work to integrate them into a fuller, richer, and more nuanced identity 27.
Yeomans et al produced an article in 2013 consisting of vignettes to illustrate the techniques used in TFT with the view to evaluate its use in treating BPD. Their findings supported the validity of TFT in treating BPD patients who specifically had difficulty with relationships.
They distilled TFT down to three important components 28:
1) The treatment contracting/setting the frame
2) Managing one’s affective response
3) The interpretative process
Pharmacology
A Cochrane intervention review assessing the effects of drug treatments in BPD, included twenty-eight randomised control trials, published in the period 1979-2009 (20 of 28 trials dating from 2000 or later), involving a total of 1742 participants 29.
Figure 2: The pharmacological agents that were tested included the following:
The authors arrived at the conclusion that pharmacotherapy in BPD ‘is not based on good evidence from trials’. The review found that there is support for the use of Second-generation antipsychotics (in improving cognitive-perceptual symptoms and affective dysregulation); Mood stabilisers (in diminishing affective-dysregulation and impulsive-aggressive symptoms); and Omega-3 fatty acids.
However, these claims were made based on single study effects and therefore require replication. No drug was found to significantly affect the symptom clusters, specific to BPD, including avoidance of abandonment, chronic feelings of emptiness, identity disturbance, and dissociation.
One noteworthy finding was that Olanzapine was associated with an increase in self-harming behaviour. Furthermore, the review states that ‘special attention’ is needed in BPD when prescribing tricyclic antidepressants (due to toxic effects in overdose) and hypnotics & sedatives (due to there being potential for misuse or dependence). Another problem that was highlighted was that in comorbid eating disorders the use of Olanzapine can contribute to weight gain and Topiramate can produce weight loss.
The review goes on to elucidate that there is not any evidence from randomised controlled trials that any drug reduces the severity of BPD and that it consists of ‘distinct pathology facets’. They recommend that the pharmacotherapy of BPD should be targeted at ‘defined symptoms’ and that polypharmacy is not supported by the latest evidence and should be avoided as much as possible.
The authors end by reaffirming that the evidence is not robust and that the studies may not satisfactorily reflect certain characteristics of the clinical environment. They propose that further research is needed in order to produce reliable recommendations. They detail the complications that arise from the ‘polythetic nature’ of BPD i.e. each patient is likely to experience different aspects of the disorder. There lacks a consensus among researchers about a common battery of outcome variables and measures. They comment that there is a fragmentary view on drug effects and that it is unknown as to how the alteration of one symptom affects another.
Comorbidity
Comorbidity is a foremost concern in the interpretation of data concerning personality disorders 30. A majority of individuals diagnosed with one personality disorder often meet criteria for at least one other personality disorder 30. A large proportion of patients with personality disorder have one axis I 31 disorder comorbidly, mostly depression, anxiety and alcohol and substance use disorders 32. [Axis I is a reference to the multi-axial classification system used in the Diagnostic and Statistical Manual of Mental Disorders that was removed in the latest version, DSM-5 2
It is important to consider therefore that, an improvement in the symptom clusters in personality disorders might be an improvement in comorbid axis I disorder symptoms. It is reported that the rates of depression are very high in BPD 33 and that the response to antidepressants in depressed individuals with comorbid personality disorders appears lower than in those without comorbid personality disorder 32.
The most recent guidance on the treatment of BPD from the National Health and Medical Research Council of Australia (NHMRC), which reviewed the literature and integrated a series of meta-analyses, details that pharmacotherapy does appear to be effective in altering the nature and course of BPD and that evidence does not warrant the use of pharmacotherapy as a sole or first-line treatment for BPD 34.
DISCUSSION
All of the aforementioned psychotherapy techniques are shown to produce promising results when applied to the treatment of BPD, with some standing out, such as DBT and MBT, due to the presence of a relatively robust evidence base. With such a wide variety of different approaches that all show some propensity for successful treatment of BPD it is clear that these approaches must be taken more seriously in clinical practice. These treatments have been shown to considerably improve symptomatic outcomes however there is a shortcoming in that they have failed to significantly improve social functioning. Each of the therapies follow distinct theories, however, when each treatment modality is applied to BPD, similar effects are seen. This is intriguing and should be explored further.
An analysis of these therapies revealed some common features which are now suggested as core requirements for all effective psychotherapeutic treatments:
Figure 3: Five common characteristics of evidence-based treatments for BPD 35, 36.
1. Structured (manual directed) approaches to prototypic BPD problems 2. Patients are encouraged to assume control of themselves (i.e. sense of self-agency) 3. Therapists help connections of feelings to events and actions 4. Therapists are active, responsive, and validating 5. Therapists discuss cases with others, (including personal reactions)
An update to the aforementioned Cochrane review 29 was published in 2013. The update focussed on the psychotherapies that are available for the treatment of BPD and included a total of 1804 participants spread over 28 studies. The psychotherapies discussed were divided into ‘comprehensive’ if they substantially involved an individual psychotherapy element or as ‘non-comprehensive’ if they did not. The comprehensive therapies included dialectical behaviour therapy, mentalization-based therapy (delivered in either a partial hospitalisation or outpatient setting), transference-focussed therapy, cognitive behavioural therapy, dynamic deconstructive psychotherapy, interpersonal psychotherapy and interpersonal therapy for BPD. These were assessed against a control condition and also with some direct comparisons against each other. Non-comprehensive psychotherapies included DBT-group skills training, emotion regulation group therapy, schema-focussed group therapy, systems training for emotional predictability and problem solving for borderline personality disorder (STEPPS), STEPPS plus individual therapy, manual assisted cognitive treatment, and psychoeducation 37.
The authors concluded that both comprehensive and non-comprehensive therapies indicated beneficial effects for the core pathology of BPD and associated general psychopathology. The authors identified that dialectical behaviour therapy had been studied the most comprehensively followed by mentalization-based therapy, transference-focussed therapy, schema-focussed therapy and STEPPS. However, the authors do state that none of the treatments presented a very robust evidence base and that there are concerns over the quality of individual studies 37.
In terms of pharmacotherapy, the NICE and NHMRC guidelines agree with the 2006 Cochrane interventional review among others 38, 39 that there is some evidence that some second-generation antipsychotics (aripriprazole and olanzapine) and some mood stabilisers (topiramate, lamotrigine and valproate) could improve BPD symptoms in the short term. However, for some of these agents, it is necessary to balance risks against benefits as they have considerable long-term risks (e.g. with antipsychotics, extrapyramidal side effects such as tardive dyskinesia can persist even after withdrawal of the drug 40). Such risks are not a problem in psychological treatments and it is probable that this influences guidelines. In practice, off-label use of psychotropics is widespread, despite the fact that the NICE guidance negates their use. It is arguable that clinicians should preferentially use pharmacological treatments that have the strongest evidence base (i.e. antipsychotics and mood stabilisers) and refrain from using agents with the least evidence (i.e. antidepressants and benzodiazepines).
CONCLUSION
Specialist treatments, in particular DBT and MBT substantiate the use of psychotherapy in BPD and these findings support the validity of the NICE guidance. However, the array of such treatments must be amalgamated with the view to provide a comprehensive, multi-faceted treatment approach. Each treatment must be broken down in order to outline the components that are particularly useful in BPD with the view to understand the condition in greater depth and to provide more focussed therapies.
The 2013 Cochrane review 37 highlights that further psychotherapies are available and have been shown to successfully treat BPD core pathology, however, as it is clearly stated the evidence base lacks robustness and there is a need for further studies that can replicate results. The therapies that have been included in this Cochrane review that have not been covered in the guidelines (e.g. STEPPS) may prove to be superior to those put forward by NICE, and I recommend that these be explored thoroughly when the guidelines are due for update.
While the NICE guidance emphasises that the use of psychotropics is reasonable in the management of comorbidities, it worth noting that to understand BPD, it is necessary to explore both the underlying aberrant psychological processes and biological processes that manifest in the disorder. This will enable the use of more specific pharmacological therapies in targeting the symptoms of BPD in the future.
India ranks second in world not only in terms of its population but also in disaster proneness.1 Disasters, whether they are natural or man-made, result in a wide range of mental and physical health consequences.2 International public agenda has taken notice of protection and care of children in natural and man-made disasters. This, in large part, is due to observations that those affected and overlooked often include children and adolescents.3 There is continuous controversy about the impact of disasters on victims including children4, 5and some investigations deny that serious psychological effects occur.6, 7, 8However further researchhas found that the criterion used in these studies were extremely narrow and inadequate and hence more systematic, clinically relevant investigations are required.9 For children and adolescents, response to disaster and terrorism involve a complex interplay of pre-existing psychological vulnerabilities, stressors and nature of support in the aftermath. Previous research has shown that direct exposure to differenttypes of mass traumatic events is associated with an increasein post-traumatic stress symptoms, 10, 11, 12, 13 anxiety, and depression, 11, 14 which are frequently comorbid withpost-traumatic stress reactions among youth.15 To the best of our knowledge, studies on long term psychological effects of disasters on younger age groups from South Asian countries are only a handful even though the frequency and the extent of natural disasters in this part of the world are considerable. As trauma during childhood and adolescents can etch an indelible signature in the individual's development and may lead to future disorder,16 it underscores the need for such studies.
A snowstorm followed by an avalanche took over a small mountainous village “Waltengu Nard” in South Kashmir, India on 19th Feb. 2005, about a month after the devastating Indian Ocean Tsunami. Of the total population, 24.77% (n=164) had perished. 17 As reported, the total population of children and adolescents prior to disaster was 242, of whom 52 died (21.49%).17 The present study is a discreet one which aims to determine long term psychiatric morbidity among the surviving children and adolescents of this disaster affected region five years after the snowstorm disaster. This is based on the notion that psychiatric disturbances can be present in children and adolescents years after a disaster has occurred.18, 19, 20 The socio-demographic variables of the patients are also studied. The results may support the need to apply wide area epidemiological approaches to mental health assessment after any large scale disaster.
Material and Methods
The study was designed as a survey of children attending school. Children from ages 6 years to 17 years from the high school near Waltengu Nard were taken up for the study. Only those children who were present in the area during the disaster were included in the study. Those with presence of any psychiatric disorder prior to the time of disaster, mental retardation, organic brain disorder, serious physical disability prior to disease (e.g. blindness, polio, amputated limbs etc.) or severe medical condition (e.g. congenital or rheumatic heart disease, tuberculosis, malignancy etc.) were excluded from the study. Within the school, an alphabetically ordered list was prepared including all classes of school with children aged 6-17 years 11 months. Every 3rd student on this list was chosen and subjected to inclusion and exclusion criteria until a sample size of 100 children was complete. Informed consent was obtained both from the child and one of his/her caregivers or parents.
Selected children were subjected to the Mini International Neuropsychiatric interview for children and adolescents (MINI-KID) for evaluation of symptoms and diagnosis which is a DSM-IV based diagnostic interview with high reliability and validity. 21, 22 A semi structured proforma was prepared for socio-demographic profile. Kuppuswamy's Socioeconomic Status Scale, 2007 was used for determining socio-economic status. 23 Oslo-3 Social Support Scale (OSS-3) was used to calculate social support. 24
Interviews were conducted following formal training in instituting MINI-KID by trained psychiatrists of the Department of Psychiatry GMC Srinagar. The data was then subjected to appropriate statistical methods. A p-value less than 0.05 was taken as significant.
Results
Of the 100 children and adolescents studied (41.32% of the affected population of children and adolescents) 41 were noted to have at least one psychiatric diagnosis (patients). The socio-demographic profile of these patients is represented in Table 1. Age and sex distribution of diagnoses is presented in Table 2 and Table 3 respectively.
A total of 54 diagnoses were observed in these 41 patients (Figure 1), with comorbidities present in 12 patients (29.27%). 11 of these 12 patients were experiencing two psychiatric disorders present concurrently and 1 was enduring three concurrent psychiatric diagnoses. Post-Traumatic Stress Disorder (PTSD) was the commonest comorbidity seen in 6 patients. This comes to 42.86% of total PTSD cases. This was followed by Major Depressive Disorder (MDD), Generalized Anxiety Disorder (GAD), Suicidality, Social Phobia, Panic Disorder, Agoraphobia and Separation Anxiety Disorder (SAD) in 2 each. Attention Deficit/Hyperactivity Disorder (ADHD), Conduct Disorder (CD), Specific Phobia (dark), Substance Abuse and Dysthymia were comorbid in one patient each. Studies have consistently shown presence of psychiatric comorbidities post-disaster.48, 49 Of the total 54 diagnoses, the commonest were Anxiety disorders (except PTSD), PTSD and affective disorders (includes MDD, dysthymia and mania) comprising 37.04% (N=20), 25.93% (N=14) and 14.81% (N=8) of total diagnosis respectively.
Figure 1: Diagnostic profile of the patients
Discussion
When children and their families are involved in natural or man-made disasters they may be exposed to diverse stressors which may impact mental health of the survivors, including children.25 Studies have suggested that reliance on parental reports of children’s distress may not be valid as parents typically under-report symptoms compared with child and adolescent self-report in mental health surveys.26 Thus in our study the psychiatric interview of each child was done individually without getting leads from their parents. In the early "heroic" and "honeymoon" phases of disaster relief there is much energy, optimism, and altruism. As fatigue sets in over the time and frustrations and disillusionment accumulate, more stress symptoms may appear.27 Accordingly, the study was carried out five years after disaster to catch this delayed response to disaster in the form of psychiatric morbidity.
Consequences of the extensive amount of stress on our sample population due to the snowstorm resulted in a high prevalence of psychiatric disorders in our sample which was apparently not due to any other psychological stress during this period. Despite the fact that the study was done five years after the disaster, the research generated high psychiatric morbidity. Many young survivors reported restlessness and fear with the return of the season in which snowstorm occurred. All these kept the memories of the disaster and the losses fresh in their mind thus not allowing the wounds to heal. Some said that they couldn't keep their minds off the snowstorm during the weeks approaching the anniversary. This was much like the so called anniversary reactions.28 Even children and adolescents, who have rebuilt their homes or found new dwellings to rent, frequently feel a sense of loss at the anniversary. Though the area was provided with adequate relief in terms of better infrastructure, education, employment and financial help in years post disaster to make their life without psychological distress, but, perhaps four such anniversary reactions and the fact that they are still living in the same geographical area and climate conditions have not allowed them to settle down in a routine since the psychological distress. Of the total sample of 100 patients, 41 % (N=41) reported at least one diagnosis. This is almost similar to a study by Kar and Bastia after a natural disaster in Orissa (cyclone) who found 37.9 % of adolescents with any diagnosis.29 Similarly Margoob et al found that 34.39 % had a psychiatric disorder at the end of one year, after disaster.17 Other studies yielded results in the range of 12% to 70% in terms of total psychiatric morbidity.26, 30-33
PTSD was the commonest individual diagnosis in our study with 14% (N=14) of the total population. Studies have shown PTSD prevalence after disaster from as high as 72 %34 to as low as 8 %.35 However, these were done immediately or within a few months after the disaster and the longitudinal pattern was not studied. A study conducted by Margoob et al reported a prevalence of 18.51 % in a sample of survivors one year after the same snowstorm on which this present study is based.17 Similarly, Bockszczanin et al 2.5 years after a flood in Poland reported 18 % of children to be suffering from PTSD.36 Thus our results of 14 % patients suffering from PTSD are also similar to the trend as we are studying them after a period of five years following the disaster. Diagnosis of PTSD in our study was more common among the pre-adolescent age group, 22.58 % (N=7) and adolescents 33.33% (N=2). Similar findings were reported by Hoven et al who found a prevalence of 20.1 % in this age group.30 Also PTSD was more frequent in females in our study. It was observed in 16.98 % females (N=9) as compared to 10.64 % for males. Hoven et al also found high prevalence in girls (13.3 % vs. 7.4 %).30
Anxiety Disorders (excluding PTSD) formed the most common collective diagnostic category in our sample. Anxiety disorders were present in 20 % (N=20) of our sample population which formed about 37.04 % of total diagnosis. These included cases of GAD 5% (N=5), SAD 4% (N=4), Social Phobia 3% (N=3), Agoraphobia 3% (N=3), Panic Disorder 2% (N=2), OCD 2% (N=2) and Specific Phobia 1% (N=1). Similarly Norris et al found anxiety in various forms in 32% of their sample of disaster victims.25 Similar findings were also reported by Reijneveld et al.37 Hoven et al in an important study after 9/11 found prevalence of various anxiety disorders to the magnitude of 28.6%.30 Our study correlated very closely to the above mentioned study. GAD was the commonest anxiety disorder among the above group. A prevalence of 5% (N=5) was found in the study sample. This prevalence was almost half of the earlier studies in children and adolescents after a disaster by Kar and Bastia29 where it was 12% and by Hoven et al 30 where it came out to be 10.3 %. However these studies were conducted within a few months after the disaster and hence came out with a higher prevalence of GAD than ours. It was more common in girls in contrast to boys (7.55 % vs. 2.12%) similar to study by Hoven et al.30 SAD was also seen to predominate in anxiety disorders with 4 % (N=4) of the sample receiving the diagnosis. Some studies like one by Hoven et al found it to be prevalent in 12.3 % of their sample 6 months after 9/11.30 However other studies have found SAD to be comparatively less frequent post disaster in children and adolescents.34 Thus our findings are modest and lie somewhere between the above two studies. Also ours was a long term study hence SAD figures are a bit low. SAD in our study was more prevalent in girls than boys (5.66% vs. 2.12%). Moreover, it was exclusively seen in ages below 10 years. The above findings are in tune with the study by Hoven et al.30 Panic disorder showed a low prevalence in our study and was found in only 2 % (N=2) patients. In both of these patients it was found to be comorbid, with MDD in one and with Agoraphobia in another. Studies immediately post disaster found the prevalence to be around 10.8 % (Math et al)32 and 8.7% (Hoven et al).30 However in the survivors of the same area, in which our study is based, an earlier study one year after the disaster found 3.08 % prevalence of panic disorder which is very similar to our study.17 It was more prevalent in females and is well correlated to a study by Hoven et al.30 Agoraphobia was present in 3 % (N=3) patients. It was comorbid in two patients with panic disorder and with PTSD, and an individual diagnosis in one. Hoven et al have found high rates of Agoraphobia post disaster i.e., about 14.8%.30 But again this study was done only 6 months after 9/11 hence more morbidity. Female preponderance of the diagnosis was established (3.77 % vs. 2.12 %) as with earlier studies.30 Obsessive traits are known to increase subsequent to disaster in the surviving population.38 Similarly 2 % of cases satisfying the criteria for OCD were seen in our study. The commonest obsessions were recurrent intrusive and annoying themes related to the disaster and ruminations about whether it could have been prevented, followed by worries related to harm befalling themselves, family members, or fear of harming others due to losing control over aggressive impulses. Other obsessive themes were related to scenes of trauma and commonly blood. Obsessions regarding extreme fears of contamination were also present.
The affective disorders have been studied less often than PTSD after disaster. Depression is known to occur with increased frequency subsequent to disaster.25 MDD was present in 4 % (N=4) of the total sample population. Studies conducted immediately after disasters have found higher prevalence. Math et al,32 Kar & Bastia29 and Catani et al33 found the prevalence of 13.5 %, 17.6 % and 19.6 % in their studies respectively. A study at three months and at one year after disaster on the adults in the same population as our study found the prevalence of MDD as 29.6 % and 14.28 % respectively.17 This decreasing trend is substantiated by the findings of our study and is in line with it. MDD was more common in females (5.66 % vs. 2.12%) which is similar to the study of Hoven et al.30 Our findings of increased prevalence of MDD in middle adolescents (7.69 %) as compared to other age groups is also comparable to Hoven et al.30 Of the Dysthymia cases, 3 % (N=3) were observed in our studies. Increased prevalence of dysthymia has not been reported post disaster in earlier studies. Our findings could be a part of large affective diaspora with dysthymia resulting from diminished self-esteem and a sense of helplessness subsequent to disaster. In addition to the time period for depression these patients were given the diagnosis of dysthymia because the depressed mood in them was more apparent subjectively than objectively. Finally these patients could have been on a natural course of dysthymia which usually begins in childhood. Combined dysthymia and MDD accounted for 7 % (N=7) of patients which if taken as a collective depression category, the results are slightly more comparable with the above studies. One patient had Mania (past). This patient had a positive family history of Bipolar Affective Disorder. This could be an incidental finding even though psychological stress is known to precipitate mania.39 Also the prevalence is 1 % in our study which is even less than the prevalence in general population thus it could be an artifact.40Studies have consistently found increased prevalence of adjustment disorder after disaster.41 In our study prevalence of adjustment disorder was 3% (N=3, anxiety 2, depression 1). In a study by Math et al 3 months after tsunami it was 13.5%.32 A lower prevalence in our study was again due to the long term nature of study. The role of trauma, stress, and negative life events as risk factors for suicidal ideation and behavior has long been recognized.42 A longitudinal investigation looking at the trends in suicidality and mental illness in the aftermath of Hurricane Katrina found significant increases in suicidal ideation and plans in the year after the disaster as a result of unresolved hurricane related stresses.43 The suicidality in our population sample was found to be 2% (N=2) of sample. These results were in tune with that of Kessler et al, although it was immediately after hurricane Katrina and hence a higher prevalence of 6.4%.43
Many symptoms of PTSD overlap with the symptoms of ADHD and CD.44 In our study, each of the disorders were present in 2 % of the sample. In one patient, they were comorbid with each other (ADHD with CD). In a study by Hoven et al 6 months after 9/11, the prevalence of CD was found to be as high as 12.8 %.30 This could be because of immediate post disaster nature of the study. Also because of the symptom overlap more weight was given to the PTSD diagnosis.
Three patients had a diagnosis of Substance Abuse, Tic Disorder and PDD, 1 % each. Though substance abuse is known to increase subsequent to disaster in adolescents,30 no evidence was found for relation of tic disorder or PDD to the post-disaster psychiatric stress. The cause of a low prevalence of substance abuse in our sample was because of the fact that the area is inhabited by Muslim population and hence alcohol is not religiously sanctioned, and, harder substances are either not available or they can’t be afforded. The only substance which is available is marijuana or cannabis. However, most used it only recreationally and the criterion for abuse was not met. Even the sole patient of substance abuse was also taking cannabis. Also, it is a well known phenomenon that drug dependent subjects do not reveal the true information and deny any history of abuse at first contact with the investigating team.45 Tic disorder and PDD are regarded as biological disorders and their relation to trauma is only incidental.46, 47
Studies have consistently shown presence of psychiatric comorbidities post disaster.48, 49 The same was observed in our study where 29.27 % of total patients had comorbid psychiatric diagnosis. Similar results were found by Kar and Bastia who found comorbidities in 39% of adolescents.29 PTSD is the most common comorbid disorder observed during the period post disaster48, 49 and the same was observed in our study with PTSD comorbid in 14.63 % (N=6) of cases. However when all the anxiety disorders were combined except PTSD, they were found to exceed the comorbidity of PTSD and they were comorbid in 21.95 % (N=9) patients. There is expanding literature regarding comorbidity of anxiety and depression in children and adolescents.50, 51, 52Similar comorbidity of an anxiety disorder (including PTSD) and depressive disorder (including Dysthymia) were seen in 7.32 % (N=3) of patients in our study. These results show that psychiatric diagnoses are frequently comorbid after the disaster and there is a need to be vigilant about them for a holistic psychiatric assessment, treatment and rehabilitation of the survivors.
Sociodemographic Profile: In our sample the prevalence of psychiatric morbidity was at maximum in pre-adolescents (6-10 years age group) and it was 61.29 % of the sample of pre-adolescents.This is consistent with the research that has suggested that younger children possess fewer strategies for coping with both the immediate disaster impact and its aftermath, and thus may suffer more severe emotional and psychological problems.53 Second commonest group was of 11-13 years with 40 % morbidity in them which was consistent with an earlier study which also found significant morbidity in this age group.54 The age characteristics of the total population also closely matched the above findings. More females than males were found to exhibit psychiatric morbidity in our study (47.17 % vs. 34.04 %). Though these findings were in tune with those of Hoven et al,their findings were a little lower than ours (34.7 % vs. 21.8 %).30 Some studies have found that girls express more anxiety-depressive disorders30 and PTSD symptoms55, 56 and boys seen to exhibit more behavioral problems.57 Similarly in our study rates of anxiety disorders, depressive disorders and PTSD were higher in girls and conduct disorder was exclusively found in boys.
Our study suggested that children up to 5th standard were (51.02 %) more susceptible than those in higher classes. This was in accordance with an earlier study by Kar et al.54 These findings are also in accordance with the findings of a study by Hoven et al. which found maximum morbidity (34.1 %) in preschoolers.30 Thus it could be said that higher educational status was protective, in addition to increasing age. Psychiatric morbidity was highest in children who were from joint family systems (48.15%). This was followed by children from extended nuclear (37.5%) and nuclear (27.27%) families. This pattern is consistent with an earlier study by Margoob et al.58 This could be because of the fact that in the sample of joint families there was loss of more family members in the tragedy. There were no cases of upper and upper-middle socio-economic class and lower-middle class was significantly less in our sample. This was because of the demographics per se and was not a sampling error. Consequently, higher morbidity was seen in the upper-lower socio-economic class (49.09%) followed by the lower class (31.71%). All the above findings are in accordance with an earlier study by Margoob et al.58
Psychiatric morbidity was not found to be influenced by the source of family income. Same was observed by Kar and Bastia in their study.29 The majority of the patients had poor social support (52.17%, p=0.03). These findings are substantiated by earlier studies.59 Loss of a parent was strongly associated with lower social support and high psychiatric morbidity. This was also reported by earlier studies.31, 60 Our study reported higher psychiatric morbidity in first-born children (71.43%). This could be due to increased burden of family matters on an eldest child subsequent to a disaster especially when head of family or mother has perished in such a catastrophe. This was in accordance with earlier studies on birth order and psychiatric morbidity.61 However in our study only childs also documented significant morbidity which is in contrast to earlier studies.61 This could be due to the fact that an only child had significantly less social support due to fewer siblings and death in the family due to disaster considerably compounding the problem. Also, often the youngest born is more pampered and hence more likely to feel emotionally insecure when attention is shifted from him in the aftermath of a disaster.
There was an unavoidable limitation in the study; the disaster-affected population was not compared with a normal or control population. The difficulty we faced was finding a control population as the area has a racially, geographically and culturally distinct population of Gujjars and all of them were affected. So no appropriate control group could be found. However if we compare it with most of the studies done in populations from the north India, the prevalence in our study is largely greater than those found In those studies.62
Conclusion
This research portrays and scrutinizes the experience of children and adolescents in the aftermath of a snowstorm disaster and supports the idea that children are susceptible to morbid psychological experiences long after the traumatic event has occurred. With that said, we want to stress the decisive role of support agents for children. These agents include the adults and peers who help children and youth recuperate in the long term. Provision of an outreach psychosocial and clinical service long after the disaster when no one is around to help after the initial knee jerk response of relief agencies is also stressed.
The closure of asylums in the last century has resulted in an increased number of compulsory hospital admissions for psychiatric patients. Psycho-geriatric patients are highly vulnerable in this respect. Although the traditional buildings instituted for the care of the mentally afflicted have gone, misconceptions about provision and anecdotes about incarceration continue to haunt the community. Recent legislative changes have further extended the occurrence of involuntary hospital admission.1 Compulsory community care is under constant review. Concurrently the validity of the concept of mental illness, psychiatric classification and diagnostic dilemmas all continue to be debated. Confinement has regained respectability in the discourses of present-day British mental health system because of violent offences committed by psychiatric patients and the public media portraying them as a reflection of failure of community care.
Table 1, Advantages of Mental Health Acts
1. Mental health acts secure the safety of vulnerable people 2. Helps to regain control on their lives 3. Compulsory treatment helps to prevent further deterioration of mental health 4. Aimed to provide effective care and treatments 5. Ensure better after care 6. Protects the safety of other people 7. Prevents suicides 8. Provides opportunities for assessments and diagnosis 9. Can be therapeutic by unburdening personal responsibilities to an institution.
Numerical quantitative studies imply that generally involuntarily admitted patients show clinical improvement and retrospectively view their compulsory admission rather positively.2 It is an unquestionable fact that Mental Health Acts prevent suicides and homicides (table 1). Mental Health Acts have some unsatisfactory outcomes particularly on a subset of patients including senior citizens admitted formally. It is important to identify such patients and take additional precautions in their management as they run the risk of leaving hospital feeling inferior and inadequate. Patients’ specific characteristics, thought processes and past treatment experiences, colour their attitude towards coerced treatment and determine the gains and shortcomings of compulsory care.
Disadvantages
The Mental Health Acts are open to social abuse and elderly patients can be more defenceless in this respect. Specifically they may be: invoked to control behaviour; misused for material gain and implicated in subtle expressions of revenge. They are sometimes invoked to hasten divorce proceedings and to secure the custody of children by a specific parent. They are also used to control the behaviour of children by their parents. Mental Health Acts designed to control psychiatric patients are being enacted and enforced in some underdeveloped countries that lack an efficient tribunal system to monitor their effects.
A patient who has been detained is at risk of repeat detention and someone who has been inappropriately assessed becomes increasingly vulnerable to control on psychiatric grounds. The experience of being detained involuntarily has a reductive effect on behaviour after discharge – it may induce anxiety or post-psychiatric depression. The awareness of being deemed to require compulsory detention generates such negative attitudes as self-denigration, fear and unhealthy repression of anger. It may also impede self-direction and the normal sense of internal control and may encourage the view that in a world perceived as being divided into camps of mutually exclusive ‘normal’ and ‘abnormal’ people, the patient is in the latter category. Compulsory detention may lead to suicide because the patient loses their sense of integration within their own society. Furthermore, the fear and anxiety associated with involuntary admission delays the recovery process. There are other frequently occurring barriers to recovery for those affected such as, loss of capabilities, whether real or imagined, ineffectual medication due to poor elicitation of symptoms because of patient’s lack of cooperation and negative drug side effects.
Depressed patients have a higher suicide risk than the population at large and one of the reasons for detention is suicidality. Some of the subjective symptoms of depression can be ameliorated by denying them, while compulsory detention may reinforce depressive symptoms. Detention gives carers a false sense of security and this may lead them to relax their vigilance towards the patient. The Mental Health Acts increase the stigma associated with psychiatric illness and with the exuberant expression of emotions. Patients who are under section or are frightened of being placed under section may deliberately mask their symptoms in an attempt to have the section lifted or to avoid sectioning.
Trans-cultural studies
Trans-cultural studies show that members of migrated cultures, particularly the elderly, are more at risk of inappropriate sectioning than the rest of the population because of the lack of knowledge on part of professionals about the patient’s culture. For instance, the debate of over diagnosis of schizophrenia among Afro-Caribbean patients is still unsettled. A study conducted in South London has concluded that Black Africans and Black Afro-Caribbean patients with psychosis in that area are more likely than White patients to be detained under the Mental Health Act 1983.3 GreatBritain has become a multicultural society and a significant percentage of professionals working in psychiatric units have been trained overseas, in a wide range of countries. This creates further risk of inappropriate diagnosis. There needs to be more emphasis on the significance of trans-cultural psychiatry in the United Kingdom. In particular, psychiatrists should be aware that psychiatry is a medicine of language and culture as well as of the mind.
Medical Dilemmas
Countries in which Mental Health Acts are widely enforced have not achieved any reduction in suicide rates through their implementation. Sectioning is perceived by many patients affected as a psychological guillotine – a form of psychiatric terrorism. The medical profession is invested by the Acts with undue power over society. This is of particular concern because training in psychiatry does not include the study of free will and allied philosophical issues and also because there is no clear definition or description of mind and consciousness. In psychiatry there is a lack of clinical indicators and psycho-physiological parameters so the criteria for diagnosis are imprecise, with a concomitant risk of the Acts being erroneously implemented. It has been postulated that once a person has been classified as having deviant behaviour, that categorisation has a potent effect on the subsequent actions of the person concerned and those interacting with them.
Is it not justifiable to argue that even if a few mentally ill patients are underdiagnosed and not subjected to psychiatric admission, someone whom we would regard as normal should not be detained in a psychiatric hospital against their will? Such a view is analogous to the judicial view regarding capital punishment where even if ninety-nine murderers escape capital punishment because there is no death penalty, one innocent person should not be sentenced to death. Mental Health Acts may be a necessary evil but they present a dilemma for mental health professionals: the morality of helping patients and protecting the society from the consequences of their illness against the immorality of restricting their freedom. Clinicians become torn between the ideals of curing mental illness and defending the sanity of patients.
Patients’ Perception
A small survey conducted by the author revealed that no sectioned patient in the group studied sent a thank-you card after discharge to the ward in which they were confined. However, many voluntary patients expressed appreciation in that way. This is an indicator of the attitude of sectioned patients towards the Mental Health Acts. One reason must be that a record of being sectioned limits their freedom to travel and also affects their employment opportunities adversely. A patient has commented that it is easier for an ex-convict to gain employment than it is for a once-sectioned psychiatric patient.
There is anecdotal evidence illustrating the panic that may be generated with the word ‘section’ in psychiatric patients. A recovering elderly hypomanic patient explained that he misconstrued the word on hearing it when he was ill, taking it in relation to sectioning in Obstetrics and General Surgery. He remembered that as he resisted entering a taxi while being persuaded to agree to admission, the driver said that he was going to be sectioned if he refused hospital admission. The patient misunderstood this and interpreted it as he was going to be cut into pieces and tried to jump out of the vehicle.
Post-traumatic stress disorder
Any loss of intrinsic importance to an individual constitutes bereavement. Denial, anger and depression experienced in compulsory detention are comparable to bereavement.4 In the case of a detained patient, the loss of self-identity and of social functioning causes a grief reaction. It has been hypothesised that there are high levels of Post-traumatic Stress Disorder (PTSD) symptoms in detained patients.5 Very few repeat detainees become habituated to the implementation of the Mental Health Acts. The vast majority become increasingly frustrated and develop a pessimistic outlook towards their mental health. There is a high incidence of suicide among patients who have multiple detentions.
Post-hospitalisation Stress Disorder is much more common than generally recognised. Formal admission may lead to fear, anger, frustration, depression or loss of self-esteem, depending upon the individual’s psychological response.6 Involuntary admission may result in pervasive distress in any patient – this kind of hospital admission may be perceived as threatening and even as a catastrophe. Detained psychotic patients are less aware of their environment because of the preoccupation with their symptoms. Non-psychotic patients, when detained for instance because of a risk of suicide, are fully aware of their immediate environment and the chaos they have caused to themselves. They have a high risk of PTSD.
Preventive detention
Fear of liability may lead to compulsory hospitalisation solely to prevent violence on the part of patients who otherwise do not require in-patient care.6 Psychiatrists are not trained to police society and may lack sufficient knowledge and experience to participate in the social control responsibilities that are part of the remit of the criminal justice system - they are sometimes involved in that function. Psychiatry has to be safe and secure in the hands of individual psychiatrists and psychiatrists have to be protected when practising psychiatry. Mentally ill patients are sometimes mistakenly processed through the criminal justice system rather than the mental health system. When that happens, compulsory detention may be perceived as a form of criminalisation of mental illness. Unless there is scrupulous monitoring, mandatory treatment impinges on civil liberties. Preventive detention is legally ambiguous and clinically impractical.
Assessment
Amongst the government’s fundamental powers and responsibilities are, protecting people from injury by another and caring for less able people, whether physically or mentally incapacitated. These functions encompass the welfare and safety of both the individual concerned and the public.
A decision about compulsory detention is made on the basis of three considerations: loss of emotional control; psychotic disorder and impulsivity with serious thoughts, threats or plans to kill oneself or others. Any perceived risk must be imminent and provocative. The clinician is legally required to determine the least restrictive environment to which a patient may be safely assigned for continued care. To fulfil these requirements while implementing the Mental Health Acts, a psychiatrist needs the skills of a physician, lawyer, judge, detective, social worker and philosopher. The decision-making process is influenced by multiple factors such as: the clinician’s propensity to detain patients; the record of past untoward incidents involving the patient; attitude towards risk taking and availability of hospital beds and alternative safe treatment facilities. It is regrettable that in section 5(2) assessments, often it is a junior doctor, the least experienced person in the team, who is called upon to conduct the evaluation.4 A multitude of interviews with mental health staff, a social worker and solicitor will have to be endured by the patient - these are regarded as ordeals by most of them.
Non-detainable patients
Since the introduction of the Mental Capacity Act 2005, the number of assessments that are followed by a decision against compulsory detention is increasing. Patients who are assessed for formal admission but not found to be detainable may develop new risks subsequently as a result of the assessment procedure itself. Before assessment, mental health professionals may place themselves in covert locations around the patient’s house and neighbours may watch eagerly behind their curtains. Thereby the patient’s social image is damaged. After meticulous assessment, it may be a relief for the patient that they are not detained and that euphoria may continue for a short while but all too often damage has been done. The patient who is tormented by psycho-social stressors may find the assessment experience intensifies the injury. The decision about whether it is appropriate to assess someone is therefore an area in which more clarification and some management guidelines are much needed. In situations such as these, untoward incidents have been periodically reported. That may mean that the professionals involved and perhaps also family members who initiated the assessment, blame themselves and endure severe guilt feelings or blame each other. Furthermore, psychiatrists are not mind readers. It is possible that a patient will cleverly deny any suicidal intent during assessment, intending to fulfil a suicidal urge afterwards and that may falsely appear to be a reaction to the assessment. An interview for assessment may be the factor that takes them beyond their limit. Because of all these circumstances, the patient may need intensive home care and counselling after an assessment that does not lead to hospital care. In addition to treating mental illness, it is the duty of the psychiatrist to defend the sanity of patients. The difficulty of defining normalcy is notorious: it is easier to detect psychiatric symptoms than to describe normal behaviour.
Tribunals
Mental health tribunals are demanding and may be humiliating and intimidating. They are highly stressful for the patient and clinician and they involve the breach of patient confidentiality. Tribunals are often emotionally charged scenes for the patient and psychiatrist, they may result in traumatisation. The largely professional make-up of a tribunal is often perceived as intimidating by patients, who tend to be suspicious of collusion between professionals and above all of their reluctance to challenge the decision of a psychiatrist.7 Psychiatrists who are aware of legal profession’s ignorance on psychiatric issues dominate the tribunal scene by flamboyant linguistic expressions, while lawyers question the objectivity of psychiatry and the expertise of psychiatrists in legal matters. Tribunals are concerned with the legality of detention and not with the appropriateness of treatment. However, one study has shown that patients who appear before tribunals find it easy to accept they require compulsory admission. 8 Psycho-geriatric patients find it extremely distressing to attend tribunals. Hospital managers’ review hearings are often arranged and carried out promptly. Managerial hearings involve local people too which may make them less intimidating for detained patients.
Involuntary treatment
Although mental health staff usually have the best of intentions, when mandatory treatment is applied to patients it may prove traumatic and counter-therapeutic. The experience of undergoing forced treatment adds to the patient’s perception of stigma and discrimination. Involuntary psychiatric drug treatment is bound to be less effective than voluntary treatment. An outcome may be misdiagnosis, long-lasting and disabling side effects. Forced treatment potentially violates a person’s right to respect private life under Article 8 of the European Convention on Human Rights. Article 8 is violated only if patients can prove the treatment given is more harmful than the claimed therapeutic benefits, yet the clinician can administer the treatment if he thinks it is therapeutically necessary. Compulsory treatment makes patients feel infantilised, especially because forced psychiatric treatment often involves coercion, emotional intimidation, bullying and threats.
Community Treatment Order (CTO) is being constantly evaluated in terms of its merits and demerits. The results have been inconclusive and warrant more systematic studies. It was Section 41 of the Mental Health Act that inspired the introduction of CTO - the main purpose being to protect the community from the aggressive behaviour of some of the psychiatric patients as in the case of the successful Section 41. There are indications that CTO has fulfilled such a goal. It was also targeted to enhance compliance and concordance with the mental health services and to prevent suicides but studies indicate that those goals were not achieved.9,10 The Oxford Community Treatment Order Evaluation Trial (OCTET) substantiates a lack of any evident advantage in dropping relapse.
The “knee jerk” reaction from part of community service has apparently resulted in spontaneous readmissions of patients under CTO. It has also contributed to prolonged detention of patients awaiting community placement under CTO. This is because detained patients must stay on section 3 or 37 to allow the Mental Health Act to be converted to CTO upon discharge. Obviously, such a scenario curtails liberty. Patients always feel bitter about the “hanging feelings” of continued detention. Coercion runs the risk of weakening therapeutic alliance. It may be true that if fewer conditions are imposed, CTO could serve as a “memory knot” for patients with limited insight. Despite all the controversies surrounding the benefits of CTO, its use is increasing worldwide. 11
Assertive Human Rights
All human beings have individual rights and mental health professionals in particular must be mindful of those rights. Table 2 presents the list of assertive human rights, as modified from Gael Lindenfield (2001). 12
Table 2, Assertive Human Rights
1. The right to ask for what we want (realising that the other person has the right to say “No”). 2. The right to have an opinion, feelings and emotions and to express them appropriately. 3. The right to make statements which have no logical basis and which we do not have to justify (e.g. intuitive ideas and comments). 4. The right to make our own decisions and to cope with the consequences. 5. The right to choose whether or not to get involved in the problems of someone else. 6. The right to know about something and not to understand. 7. The right to be successful. 8. The right to make mistakes. 9. The right to change your mind. 10. The right to privacy. 11. The right to be alone and independent. 12. The right to change ourselves and be assertive people. 13. The right to be neutral. 14. The right to be empathetic and apathetic.
Discussion
Community care is more innovative than compulsory detention in hospital. For majority of patients, the best way forward is having high quality home treatment facilities as it is least restrictive and using compulsory detention should be the last resort. In some cases, forced psychiatric admission is indicative of failure in the supply of quality home treatment.One thing that sometimes leads to in-patient admission is lack of confidence in the service available. The perception of home treatment may be at fault here - it needs to be understood as more than merely staying outside hospital. Forensic patients and treatment resistant psychotic disorders lacking insight may be a different state of affairs. CTOs have serious impact on the autonomy and privacy interests of individuals and should not be applied to compensate for under-resourced community services.
Caring and supportive relationships between mental health staff and patients during involuntary in-patient care have considerable bearing on the outcome of compulsory detention. A recent study has revealed that among patients who have been detained involuntarily, perceptions of self are related to the relationships with mental health professionals during their inpatient stay. 13 Perceived coercion at admission predicts poor engagement with mental health staff in community follows up. When professionals demonstrate their genuineness and encourage patient participation in the treatment options, coercive treatment would be perceived as less of an infringement to the autonomy of patients and their sense of self-value. 14 If patients maintain both positive and negative views about detention, interventions should be designed to enhance positive experiences by focussing on respect and autonomy.Patients admit only compulsory detention gave them an opportunity to receive medication in a time of crisis and report it did not necessarily prevent thoughts relating to self-harm. It simply reduced the opportunities for impulsive acts.
‘Rooming-in’ is worth debating as an alternative to compulsory detention. This is the voluntary participation of so-called confidants, who may be chosen family members or trusted friends. They provide a 24-hour vigil for the patient in a safe hospital environment. An Australian study has suggested this system is highly valued by nursing staff, patients and their families.15 It is an initiative that needs further testing and evaluation. The resolution of angry feelings towards the mental health professionals has a significant bearing on their future compliance. The post-detention period tests the attention given to patients by mental health professionals. Here the staff members have to take the initial steps required to repair damaged relationships which may have developed in particular with angry patients. Detained patients should be offered counselling in post-discharge follow-ups and should be given satisfactory explanation of the circumstances for formal admission. Detained patients should be given the support to enable them to: rewrite their life story; reconstruct a sense of self; achieve healing of the assault of their illness and the treatment procedures inflicted on their personality. Specific interventions should be designed and evaluated in order to deal with any unresolved PTSD symptoms relating to formal psychiatric admission.
Drug abuse is a universal phenomenon and people have always sought mood or perception altering substances. Similarly the attitude of people towards addiction varies depending upon various factors and can come across as prohibition and condemnation to tolerance and treatment1. The United Nations Narcotics Bureau describes drug abuse as the worse epidemic in the global history 2.India like rest of the world has huge drug problem. Located between two prominent drug producing hubs in the world, i.e. Golden Triangle (Burma, Laos and Thailand) and Golden Crescent (Iran, Afghanistan and Pakistan), India acts as a natural transit zone and thus faces a major problem of drug trafficking. Similarly the geographic location of Jammu and Kashmir is such that the transit of drugs is easily possible across the state. In addition the prevailing turmoil is claimed to have worsened the drug abuse problem alongside an unusual increase in other psychiatric disorders in Kashmir 3.
There are not many studies about drug use from Kashmir and hardly any about the actual community prevalence. In addition, it is difficult to conduct a study in a community affected by drug abuse due to stigma associated with drug addiction. Furthermore people hesitate to volunteer information due to laws prohibiting sale and purchase of such substances and risk of being criminally charged. In view of this difficulty the present study was conducted on the treatment seeking patients at the Drug De-addiction Centers. The present study was aimed at highlighting the epidemiological profile and pattern of drug use in Kashmir Valley.
Material and Methods
This cross-sectional study was undertaken at two Drug De-addiction Treatment Centers (Government Psychiatric Disease Hospital and Police Hospital, Srinagar). Government Psychiatric Disease Hospital is the only psychiatric hospital in the Kashmir valley that also provides treatment for substance use disorder patients. The De-addiction center at the Police Hospital is run by Police Department in the capital city Srinagar. Both these centres have a huge catchment area comprising all districts of the valley, due to lack of such services outside the capital city, thus reflecting the community scenario to a greater extent.
The study was conducted for a period of one year from July 2010 to June 2011. Substance Use Disorder Patients were diagnosed as per the Diagnostic and Statistical Manual-IV (DSM IV 2004) criteria 4. Following informed consent, a total of 125 patients were included in the study. In case of minors (<18 years of age), the consent was obtained from the guardian. Information was collected regarding the age, sex, residence, religion, marital status, educational status, history of school dropout, occupation and type of family, reasons for starting the substance of abuse, type of the substance abused, and age of initiation. The socio-economic status of the patients was evaluated by using the modified Prasad’s scale for the year 2010, based on per capita income per month 5.
Results
A total of 125 Substance Use Disorder patients were studied and all were males. The majority of the patients (50.4%) were in the age group of 20-29 years and most (73.6%) were unmarried. Most of the patients were Muslims (96%). There was nearly an equal urban to rural ratio. Most of the patients had completed their educationup to high school level or higher. There was a high rate of school dropouts (41.7%) and among those, substance use being common reason (46%) for school dropout. 71.2% belonged to nuclear families. Most of the patients (53.6%) belonged to socio-economic class I as per Prasad’s scale [Table 1]. Majority of the patients started taking substances in the age group of 10-19 years [Table 2]. Besides nicotine (89.6%), the most common substances used were cannabis (48.8%), codeine (48%), propoxyphene (37.6%), alcohol (36.8%) and benzodiazepines (36%) [Table3].
Table 1: Socio-demographic profile
N
%
Age (years)
10 to 19
20
16.0
20 to 29
63
50.4
30 to 39
27
21.6
40 to 49
12
9.6
≥ 50
3
2.4
Gender
Male
125
100.0
Religion
Islam
120
96.0
Sikh
3
2.4
Hindu
2
1.6
Residence
Urban
56
44.8
Rural
69
55.2
Marital Status
Unmarried
92
73.6
Currently Married
27
21.6
Separated/Divorced
6
4.8
Education
Illiterate
5
4.0
</= high school
71
56.8
> high school
49
39.2
Occupation
Unemployed
21
16.8
Student
25
20.0
Government Job
16
12.8
Self employed
63
50.4
Type of family
Joint
36
28.8
Nuclear
89
71.2
Socio-economic status
Class I
67
53.6
Class II
36
28.8
Class III
18
14.4
Class IV
3
2.4
Class V
1
0.8
Table 2: Age at onset of initiation of Substance use by the patients seeking treatment for Substance Use disorder
Substance
< 10 years
10 to 19 years
> 19 years
N
%
N
%
n
%
Nicotine
11
9.8
86
76.8
15
13.4
Volatile Solvents
0
0
10
76.9
3
23.1
Cannabis
0
0
43
70.5
18
29.5
Codeine
0
0
33
55
27
45
Propoxyphene
0
0
24
51.1
23
48.9
Benzodiazepines
0
0
20
44.4
25
55.6
Alcohol
0
0
19
41.3
27
58.7
Table 3: Type of substance used by the patients seeking treatment for Substance Use disorder*
Table 4: Reason for starting the Substances among the patients seeking treatment for Substance Use disorder*
Reason
N
%
Peer Pressure
91
72.8
Relief from psychological stress**
49
39.2
Curiosity/Experimenting
27
21.6
Fun/Pleasure Seeking
13
10.4
Prescription medicine abuse***
12
9.6
Others****
6
4.8
*multiple responses ** (family tragedy like death or disease in the family; history of arrests, torture in jail or death and disability in the family due to the prevailing turmoil; conflicts within family; loss of job or job dissatisfaction. ***deliberate use of prescription medications for recreational purposes in order to achieve intoxicating or euphoric psychoactive effects, irrespective of prescription status ****Family history, routine work or boredom, availability.
Peer pressure was the most common (72.8%) reason for starting the use of substance [Table 4]. Majority of the patients started using substances in the age group of 10 to 19 years with 76.8% nicotine users, 76.9% volatile substances and 70.5% cannabis users among this group. The age of onset was higher (>19 years) in case of benzodiazepines and alcohol.
Discussion:
Kashmir Valley has a population of over 6 million with around 70% people living in rural areas.6
There is almost no data available on the community prevalence of drug use in the valley. Population is predominantly Muslim with strong taboo on use of alcohol and other drugs. Interestingly, none of the patients in our sample are female which could be due to stigma associated with drug use and hence reluctance to seek treatment. The police drug addiction centre is locally in the police lines with heavy security which requires frisking, which may also prevent people, especially women, from seeking help. This does not mean females do not use drugs as evident from clinical practice and previous studies 7. The sample is mostly comprised of a young age group of 20-29 years (50.4%) followed by 30-39 years (21.6%). Similar findings have been shown by the previous study conducted by Kadri et al.8 Another study on college going male students showed a prevalence of 37.5 %9, suggesting young age at initiation and high prevalence in students. The results also show high school dropout rate due to drug use which could be due to the associated problems with drug use and negative impact on the overall quality of life and future prospects.
There is a minor rural predominance in the sample. This is consistent with findings of Drug Abuse Monitoring System India and other studies 10-12, which reveal a nearly equal rural urban ratio with slight rural predominance. This could be due to the stigma associated with these centres and reluctance from local population to seek help due to fear of being identified and shamed.
73.6% of the patients were unmarried with 4.8% separated or divorced. Similar results have been shown by Hasin DS et al 13 and Martins SS et al14. The reason for predominant unmarried sample in our study could be due the higher number of younger age patients as compared to the current marriageable age.
The majority of the patients in our study were using cannabis, medicinal opioids (codeine and Propoxyphene), benzodiazepines and alcohol. One of the major reasons for high rate of opioids and benzodiazepines abuse in present study can be explained by over the counter sale of these drugs without the prescription from the doctor. This is a worrying trend as there is no proper drug control and it is easy to access any medication. Although there are only a few outlets selling alcohol in the whole of Kashmir, it is surprising how alcohol use is so common. It is speculated that current political turmoil may be responsible and people buy alcohol legally or illegally from army depots.
Most of the substance users had started taking drugs at the age of 10 to 19 years and more so in the case of nicotine, volatile substances and cannabis. Similar results have been found in the earlier studies. 15 Nicotine was typically the first substance of abuse. Tobacco is often considered as a gateway to other drugs 16.
The overall prevalence of volatile substance abuse in this study was 10.4% but significantly higher in the adolescent age group (53.8%). About three fourths of the patients had started using volatile solvents in the age group of 10-19 years. Inhalant use has been identified as most prevalent form of substance abuse among adolescents by different studies 17-18. The observation in present study could be explained by the easy accessibility, cheap price, faster onset of action, and a regular “high” with volatile substances like glues, paint thinners, nail polish removers, dry cleaning fluids, correction fluids, petrol, adhesives, varnishes, deodorants and hair sprays.
Peer pressure is the most common cause of initiation of drug use only to be followed by self-medication for psychological stress. Previous studies have shown similar results in relation to peer pressure and also the ongoing conflict situation to be responsible for increased drug use in the valley 19-20.
Conclusion:
There is a need for further studies to find the community prevalence of drug use. The service provision is very limited, restricted to the capital city and with none in the rural areas. There is a worrying trend of early age of initiation with adverse consequences including dropping out of school. The control of prescription drug use is another major issue which needs to be addressed. It is also worrying that female drug users are not able to seek help due to lack of appropriate facilities.
A clearer understanding of the aetio-pathogenesis of schizophrenia would ultimately lead to effective treatment strategies and provide the impetus for elucidation. The autoimmune hypothesis promulgates that it is the auto-antibodies that are responsible for schizophrenia and, according to the viral hypothesis, it may be the body’s abnormal response to a slow viral infection or the undefeated viral antigens causing the schizophrenia pathology. The autoimmune and viral hypotheses are interlinked, as autoimmune disorders can be triggered by microbial infection. Viral aetiology is less convincing than the autoimmune model, but from a treatment perspective, the former is more promising than the latter. To gain a detailed understanding of aetiological models of a subset of schizophrenia, herein the author has reported on a review of the literature relating to the immunity- and viral-based aetiological models of schizophrenia. Genetic vulnerability has been highlighted in the schizophrenia literature alongside environmental factors. The veracity and contestability of the immunity- and viral-based aetiological hypothesis of schizophrenia merits further investigation.
Schizophrenic Syndromes
A prerequisite for incorporating autoimmune and viral aetiology into a scientific discussion would be acceptance of the heterogeneous hypothesis of schizophrenias; they may be a cluster of entities with different aetiologies and the end-stage of different disease processes. 1 Autoimmune or viral aetiology may account for one subgroup.
Schizophrenia has diverse signs and symptoms, and a long history of controversy. Nosologists designate it as polythetic, whereas most other mental illnesses are monothetic, seemingly affecting only one brain system. 2 In the second half of the twentieth century, the psychosocial model gave way to evidence that it is a brain disorder. Schizophrenia has a long history of controversies and there has been much contention over the aetiology, psychopathology, nomenclature, and diagnostic criteria. Schizophrenia is currently seen as a neurodevelopmental encephalopathy, in which the cognitive deficits are produced due to the errors during the normal development of the brain 3 or a neuro-degenerative disorder and the cognitive deficits are derived from a degenerative process that goes on unalterably. Modern neuroimaging techniques and an intensification of studies of necropsy tissue have been responsible for this shift. Researchers seem to agree that a neurodevelopmental or degenerative assault precedes the symptoms by several decades.
The aetiology of the cognitive deficits is unidentified and several potential factors, genetic and epigenetic, are envisaged. Environmental factors—including infectious agents and disturbance in utero through malnutrition—account for a few cases. Autoimmunity and viral theories would fit in with the neuro-developmental and neurodegenerative hypotheses. Proponents of viral aetiology view viruses as acting alongside susceptible genes to initiate a trajectory that manifests as psychotic symptoms.
Lessons from Autoimmunity
Disorders of an autoimmune nature are known to occur with increasing frequency in patients with another autoimmune disease. This is somewhat like the coexistence of multiple psychosomatic disorders in a person; as per Halliday’s psychosomatic formula, association of other psychosomatic afflictions justifies the diagnosis of a new psychosomatic condition. 4 It is well recognised that the central nervous system (CNS) may be directly affected by autoimmune processes, as in the case of multiple sclerosis (MS) and autoimmune limbic encephalitis. A physical autoimmune disease, such as systemic lupus erythematosus (SLE) and antiphospholipid syndrome are also associated with psychiatric morbidity. Paediatric autoimmune neuropsychiatry disorder is a post-infection (group A Beta-haemolytic streptococcal infection) autoimmune disorder characterised by abrupt onset of obsessive compulsive disorder (OCD) and Tourette’s syndrome, brought about by molecular mimicry. 5 Nicholson et al observed that 20% of OCD patients were positive for anti-basal antibodies, considered to be part of a post-streptococcal autoimmune reaction. 6
Autoimmunity is a misdirected response occurring when the immune system attacks the body; it is the loss of tolerance to self-antigens. Immunological tolerance to one’s own tissue is probably normally acquired during foetal life, helping to prevent the occurrence of the autoimmune process (see Table1). Some clones of cells that can produce auto-antibodies (forbidden clones) are thought to be produced throughout life, and are suppressed by large amounts of self-antigens or antigen-specific T cells. Auto-antibodies are produced for a wide variety of antigens; some are organ-specific and others are non-organ-specific. Some microorganisms or drugs may trigger changes in individuals who are genetically vulnerable to autoimmunity.
Table 1- Mechanisms preventing and causing autoimmunity
Tolerance to self molecules a. Clonal deletion-removing any lymphocytes that might react to self molecules b. Clonal anergy-decreasing the responsiveness of lymphocytes that recognise self-molecules. c. Receptor editing-rearrangement of B-cell receptors. d. Reduction or inhibition of molecules or antigens that may cause self recognition. Failure of self tolerance a. Release of isolated auto antigens-tissue trauma or infection may cause breakdown of anatomic barriers and may expose the hidden antigens for recognition of T cells that were not deleted during development. b. Structural alterations in self peptides- Once structurally altered by a trigger such as infection , the self-peptides become more antigenic and are subsequently recognised by the undetected T-cells evoking immune response. c. Molecular mimicry-based on a structural similarity between a pathogen or metabolite and self structures, evoking an immune response against the foreign particles but also an autoimmune response against the self molecules they resemble. d. Polyclonal activation-Infectious agents activate our immune system, B cells and T cells are stimulated resulting in abnormal production of immunoglobulin specific for self molecules. e. Genetic predisposition
A human disease may be considered of autoimmune origin on the basis of knowledge from molecular biology and hybridoma technology, 7 along with the Witebsky postulations. It is established by the presence of auto-antibodies and T cells that react with host antigens. Approximately 25% of patients with an autoimmune disease (AD) tend to build up additional auto-antibodies. Strausburg et al (1996) explained several hypotheses for the virally-triggered autoimmune mechanism (see Table 2). 8 Allergy is the consequence of a strong response to a harmless substance, but ADs are caused when the destructive potential of the immune system is misdirected to oneself. ADs share common effect or mechanisms with hypersensitivity reactions and can be classified into three main types corresponding to the type ii, type iii, and type IV categories of hypersensitivity reactions (see Table 3)
Table 2 - Virally triggered autoimmune mechanisms
a. Molecular mimicry -a protein or polysaccharide on the virus may be structurally homologous to a host molecule and the immune system being unable to differentiate between the two, may then cross react with host cells and tissues expressing this molecule. b. The virus may cause release into the circulation of auto antigens that are normally hidden from the immune system. c. The virus might pick up host proteins from the cell membranes that become immunogenetic since they are present on the virus particle. d. The virus in the process of replication may structurally change the host proteins that in turn become recognized as foreign to the immune system.
Table 3 - Classification of Autoimmune disorders
Type i-no autoimmune diseases are caused by lgE, the source of type i hypersensitivity reactions. Type ii-caused by antibodies directed against components of cell surfaces or the extracellular matrix Type iii-caused by soluble immune complexes deposited in tissues Type iv- caused by effector T cells.
Shared Aetiology
ADs are characterised by shared threads in terms of their propensity to co-exist in a patient or direct relatives. Two major autoimmune clusters have been recognised via, thyrogastric—mostly organ-specific—diseases and lupus-associated—mainly multi systems—diseases. 9 Some ADs are distributed within either cluster and there are also overlaps within each cluster. These patterns of concurrence depend predominantly on genetic determinants.
Poly-autoimmunity is the term proposed for the association of multiple autoimmune disorders in a single patient and such co-occurrences indicate a common origin of the disease. 10 Adriana et al, by grouping diverse ADs in the same patient, demonstrated that they are true associations as part of autoimmune tautology rather than chance findings.
Co-Occurrence of ADs
Theories for autoimmune aspects of schizophrenia raise the concept of early infection by microorganisms with antigens so analogous to CNS tissue that resulting antibodies act against the brain.Some data suggest that an autoimmune process precedes schizophrenia, non-affective psychosis, and bipolar disorder, 11 but do not establish whether this is affected by viral attack, as viral footprints may be hard to detect, especially in the target organ, once the autoimmune process has begun. Psychosis is reported in 25% of SLE cases.
A Danish study revealed that schizophrenia is associated with a large range of ADs. 12 The researchers found that a history of any AD in the patient is allied with a 45% increase in the incidence of schizophrenia. Specifically, nine ADs have a higher prevalence rate among patients and 12 ADs have a higher prevalence rate among their parents than among comparison groups. In comparison with the control group, Thyrotoxicosis, Celiac disease, Acquired haemolytic anaemia, interstitial cystitis, and Sjogren’s syndrome had a higher prevalence rate among schizophrenia sufferers and their family members.
Three of the Ads—namely, celiac disease, thyrotoxicosis, and acquired haemolytic anaemia—have been previously associated with schizophrenia. Celiac disease involves an immune reaction to wheat gluten. This could be due to increased permeability of the intestine, raising the level of antigen exposure, resulting in increased risk of an autoimmune response to brain components or it may be that gluten proteins are broken down into psychoactive peptides. Eaton et al opined that the association of schizophrenia and ADs could be due to common genetic causes, perhaps related to the HLA or other genes, and some cases of schizophrenia may be consequential to the production of autoantibodies that disrupt the brain function.
Researchers for a Taiwan study identified a greater variety of ADs in schizophrenic patients than anticipated and recommended further research. 13 Chen et al. found that 15 ADs are significantly associated with the schizophrenia group. Their studies also confirmed an earlier observation of a negative relationship between schizophrenia and rheumatoid arthritis (RA). It has been observed in a small sample study that mothers of schizophrenia patients have a lower risk for RA.14
Rheumatoid Connection
The negative correlation between schizophrenia and RA is puzzling. 15 Such dissociation was interpreted as the effect of antipsychotic medication. Similarly, the metabolic changes associated with one disease may inhibit another.16 Genes predisposing a person to have one disorder may have a protective influence against another and, in that way, the negative rheumatoid connection with schizophrenia is consistent with an autoimmune model.
RA has a genetic predisposition partly mediated by major histocompatibility complex (MHC) alleles and triggered by infection. Similarly, schizophrenia has genetic and environmental associations and has been cautiously connected with MHC genes other than those perhaps involved in RA. In addition to gene products accountable for antigen presentation, the MHC gene complex holds a multitude of genes-controlling aspects of immune response. Hypothetically, depending on the set of genes an individual has inherited at the MHC complex, a viral assault will lead the immune system to an immune cascade toward the development of RA, or along a genetically-predetermined path with a network of cytokines and immune mediators and directed against CNS components, resulting in schizophrenia. 17
The negative rheumatoid connection may be attributable to two mutually-exclusive alleles of the same gene. Such associations may lead to novel treatment strategies; sickle cell anaemia patients are thought to be less affected by malaria. Of note, the combined research of Karolinska Institute in Sweden and John Hopkins’s University School of Medicine in the United States have recently discovered the genes and the specific deoxyribonucleic acid (DNA) sequences that regulate them plot together to the progress of RA; rheumatology may be inching close to an early detection method and effective treatments. Such a development could hopefully happen in the schizophrenia research.
Commonalities
Even though ADs superficially seem different, the vast majority of them share several similarities. Like ADs, schizophrenia, as such, is neither infectious nor congenital. Schizophrenia and ADs have well-established genetic propensities, and a combination of genes, rather than a single gene, is thought to be responsible for their manifestations. Both schizophrenia and ADs can be triggered by environmental toxins and they have a remitting and relapsing course. Worsening of symptoms is observed when patients are exposed to stress and both conditions have a peak increase in late adolescence or early adulthood. These similarities argue in favour of an autoimmune aetiological model of schizophrenia. 18
Apparently, there is an interesting epidemiological dissimilarity between ADs and schizophrenia. The incidence of ADs is on the increase in developed countries, whereas schizophrenia has a consistent incidence of 1% globally. According to the hygiene hypothesis of ADs, the widespread practice of hygiene, vaccination, and antibiotic therapy in rich countries have disabled children’s immune systems to deal with proper infections and are more geared to charge with one’s own tissues in highly-destructive ways. 19 The incidence between the sexes was thought to be almost similar in the case of schizophrenia, but a recent study shows that for every three males with schizophrenia, there are two females with the disease. 20 ADs are slightly higher among the female population.
Immune Modulation of Clozapine
Antipsychotics may have an immunosuppressant effect; plasma levels of IL-6, soluble IL-6R and transferrin-receptor (TfR) were significantly lower after antipsychotic drug treatment. Activation of cell-mediated immunity may occur in schizophrenia; neuroleptic agents may modulate this through suppression of IL-6 or IL-6R-related mechanisms. 21 The antipsychotic effect may involve a counter-effect on the brain-mediated immune system.
Clozapine, the gold standard for refractory schizophrenia, is a dibenzodiazepine and lowers D2 receptor occupancy and is also a 5-hydroxytryptamine antagonist. Studies indicate that among the atypical antipsychotics, clozapine seems to have an immunosuppressant effect along with neuro-modulatory effect. It has been suggested that clozapine may diminish antibody synthesis in hematopoietic cells and also argued that a possible immunosuppressive action may contribute to its superior antipsychotic efficacy. 22 The long-term immunosuppressive effects of antipsychotics may inhibit putative autoimmune responses against neurological sites and could, thus, act synergistically with the direct antagonistic action on brain receptors for the evident improvement of psychotic symptoms. 23 It is also conjectured that the increase of soluble IL-2 receptor levels in Clozapine-treated patients indicates an immunosuppressant mechanism. 24
Haloperidol may also be a neuro-immune-modulating drug. A study of in-vitro effects of clozapine and haloperidol on cytokine production by human whole blood suggested that both drugs, at concentrations within their therapeutic range, may exert immunosuppressive effects through an enhanced production of IL-1 receptor antagonists. 25
It is well recognised that unlike other antipsychotics, clozapine works better over time, as immune modulation may take longer than neuro modulation. In addition to the neuro modulation, antipsychotics may be working on the principles of immune modulation, as well. If a derivative of clozapine, without its haematological and metabolic side effects is discovered, such a drug would become the first line of choice among the antipsychotics, and that could be a significant event in schizophrenia research. The immunosuppressant effects of clozapine seem to have public health awareness that patients on clozapine are advised to have the winter flue jab. Elderly patients on antipsychotic medications are more prone to get pulmonary infections, indicating that such drugs have a delicate immunosuppressant property.
Autoimmune-Neuropsychiatric Disorder?
If schizophrenia is an AD, a higher rate of other ADs may be expected among schizophrenics. Most studies confirm that it is tied to irregularities affecting multiple levels of the immune axis.There are multiple interlinked causative factors in the aetiology of schizophrenia. There are suggestions that the neuro-behavioural changes follow an abnormal response to microbial invasion, but that does not necessarily lead to an autoimmune process. The literature deciphering the role of viruses in neurotransmitter abnormalities linking neurodevelopment assaults and the neuropsychological manifestations of schizophrenia is unhelpful. For those who adhere to the autoimmune model of schizophrenia, the simplest suggestion would be that the pathogenesis of the subset of schizophrenia studied may be caused by antibodies in the plasma and CSF that react with brain proteins, resulting in a neuro-autoimmune process.
Lessons from Viral Infections
The concept that certain psychiatric disorders are the neuro-behavioural sequel of the body’s immune response to viral infections was prevalent in the early part of the 20th century. That was an outcome of research conducted into rabies in the late 1880s, which revealed the affinity of viruses for the nervous system. Research into tertiary syphilis also provided evidence of an infectious aetiology for specific psychiatric disorders. Investigation of the encephalitis lethargica pandemic (1919 - 1928) contributed to recognition of viral causation on account of similarities apparent between the psychotic symptoms associated with encephalitis lethargica and the clinical presentation of schizophrenia. 26
Post-influenza depression, depression following mononucleosis, and hallucination associated with herpes encephalitis are well recognised. Menninger, who studied post-influenza psychosis, promulgated the first acceptable viral hypothesis for schizophrenia. 27 In the mid-twentieth century, psychodynamic studies began to encompass the origins of schizophrenia and viral aetiology lost its novelty. Dementias associated with Acquired Immune Deficiency Syndrome (AIDS) have reawakened interest in the correlation between virology and psychiatric disorders, and different authors have revisited these hypotheses in the last three decades. 28-36
The immune response to influenza and other viruses involves cell-mediated immunity and cytokine activity, which tend to turn tryptophan into kynurenic instead of serotonin. The outcome of this deviation is mood disturbance. It is the body’s immune response that blocks the conversion of tryptophan into serotonin, thereby resulting in post-influenza depression. It is arguable that there may be other psychiatric disorders consequential to a slow immune response of the body to viral infections. The possibility of viral oncogenesis was originally ridiculed, but now there is some evidence to support the view that viruses are responsible, at some stage, for approximately 20% of human malignant diseases. 31
In theory, a virus could induce schizophrenic symptoms or depression by stimulating antibodies that cross-react with brain tissue, without necessarily gaining entry into the brain. At different developmental stages, the immune response may become less efficient and viral agents may become potentiated, leading to neuropsychiatric conditions. The supposedly inflammation-mediated brain diseases occur at different stages—for instance, schizophrenia in late adolescence or early adulthood, and Alzheimer’s typically at an advanced age. It is well established that the human immunodeficiency virus (HIV) may lead to a form of AIDS dementia, and other common viruses that infiltrate the neurons may cause other types of dementia. HIV/AIDS and Borna Disease Virus (BDV) in animals help to bring the infection-based model of schizophrenia to the realm of scientific imagination
Viruses can influence the human genome. After becoming effective, viral sequences are integrated into the genome of brain cells. These sequences are not thought to be inheritable, but may cause mutations that interfere with brain functions and contribute to the development of psychiatric disorders. 37 It may be arguable that the combination of the body’s sustained immune response and the constant release of antigens of a hypothetical slow virus (schizovirus) may account for the neuro-behavioural alterations. In the following paragraphs, the author discusses how viral pathogens and other potential contributors could interact and lead to schizophrenic psychopathology.
Immune Responses
Neuro-developmental theories of schizophrenia fit the hypothesis that viral insult occurs early in sufferers, not proximally to a psychotic episode. The interaction between host and virus is affected by coordinated activity of the immune system and the brain. There is evidence that schizophrenia is accompanied by mutations in the immune system. Innate immunity is the first defence against microbes; infection results in invasion by live microorganisms and their toxic products, stimulating an inflammatory response. Neuronal functions are disrupted by pathogens and the brain’s inflammatory responses. Non-cytolytic viruses may affect neurones without causing cyto-architectural alteration, but disturbing neurotransmitter production and weakening hormones involved in neurodevelopment. 38 In schizophrenia, immune infiltration is absent, as are vital inclusion bodies and minimal gliosis. There is subtle disruption of neuronal function and brain development, but no significant loss of neuronal cells. Thus, the schizophrenia subset may have a viral aetiological origin, bringing about anomalous, specific immune responses, an autoimmune basis, or both. What triggers the autoimmune process is uncertain, but microbial triggers are a strong possibility.
Immune dysfunctions including lymphocytic abnormalities, protein abnormalities, auto-antibodies, and cytokines have been suggested in seriously-ill patients 39. One study showed significantly higher plasma levels of interleukin-6 (IL-6) in schizophrenics, and soluble IL-6R and soluble IL-2R were significantly high in mania. 40 A few early investigators claimed to have microscopically visualised virus-like particles in the cerebrospinal fluid (CSF) of patients or in chicken embryos inoculated with CSF. Studies of viral antibodies, viral antigens, viral genomes, the cytopathic effect of specimens on cell cultures, and animal transmission experiments are other avenues for exploring the viral infection hypothesis.
The subset of schizophrenics in question may have a highly-sensitive surveillance system, but a less-discerning immune mechanism than the general population. It could be the over-reaction of the immune system to the microbial adversary that may eventually lead to the schizophrenia pathogenesis. The fault may lie in the surveillance system, as well as in the body’s anomalous response to the microbial invasion. 17 In general, innate and acquired immune mechanisms interact and cooperate, but any derangement can lead to deviant immune responses that may result in neuropsychiatric abnormalities.
From an evolutionary perspective, innate immunity is less evolved and the mammalian brain is endowed with a complex immune response system, implying that the neurobehavioral aberrations of schizophrenia could be more linked with deviant and vigorous specific immune responses. 17 It is possible that the proposed subset of schizophrenia may have either an autoimmune basis or a viral aetiological origin, bringing about anomalous, specific immune responses, or both. It has been argued that a gene family involved in the specific immune system and autoimmunity is involved in schizophrenia. 41 The genome-wide association studies (GWAS) have been disappointing in schizophrenia, whereas the major histocompatability complex (MHC) region continues to be the best replicated.
Epidemiological Findings
Epidemiological studies offer useful supporting evidence for viral aetiology (see Table 4). Epidemiological studies characterised by certain broad patterns of incidence and distribution of schizophrenia offer evidence to suspend the scepticism of the viral causal hypothesis. In a study of adults at risk of exposure in utero to the 1957 influenza A2 epidemic in Helsinki, those at risk during the second trimester had significantly more hospitalisations for schizophrenia than those potentially exposed during the other trimesters or immediate years. 42 Researchers for nine subsequent epidemiological studies scrutinised the risk of schizophrenia after possible intrauterine exposure to influenza in Europe and the USA; these identified a small majority claiming to find an association.43 Falsifying the influenza link with the origin of schizophrenia does not altogether make the viral aetiology null and void. There could still be an unknown virus (schizo-virus) as the causative agent. The Hepatitis C virus came to medical attention only 15 years ago. At least these epidemiological studies illustrated that viruses can help set the stage for schizophrenia as a long-term sequel
Table 4 - Suggested Evidences for Viral aetiology
A. Direct evidences: 1.Neuropathology 2.Transmission to laboratory animal 3.Detection of viral genome 4. Sero-epidemiological studies-Detection of Antigen or antibody B. Indirect evidences: 1.Seasonality of schizophrenic births 2.Prevalence studies 3. Immune alterations 4.Antiviral effects of antipsychotic drugs 5.Possible immunosuppressant effect of antipsychotic drugs 6.Studies of identical twins 7. Migration and high risk 8. Gender differences-males are younger at disease onset and have a more severe course.
A worldwide average of 1% prevalence of “core schizophrenia” is generally accepted, 44 even though such a concept of universal distribution and gender equality has opposition. 45 However, there is evidence to assume that there may not be gross variations in this global prevalence. Cross-culturally stable rates, despite decreased fecundity in affected individuals, support an external biological aetiology. These point toward biologically-interlinked and multifactorial causation including an evolutionary genetic factor, as a single biological factor would be insufficient. The preservation of susceptibility genes for schizophrenia in the human gene pool is an evolutionary enigma; gene carriers or first-degree relatives may have some compensatory evolutionary advantage. 46 In a multifactorial aetiological model of schizophrenia, infectious theories are contestable. 17
Such a consistent prevalence, if true, could also be argued in favour of a biologically-inter-linked and multi-factorial causation of schizophrenia, as it is obvious that a single biological factor would be insufficient to maintain a delicate and consistent global prevalence of a disease. Many viruses are relatively constantly distributed, while genetic diseases present distinct geographical clustering due to inbreeding. One may hypothesise that where viral loading is high, genetic input may be less and vice versa. The consistent global incidence points toward universal microbes, a readily-available environmental factor, or, more specifically, a “schizovirus.” The interaction of vulnerable host genes with a virus could yield epidemiology like that of schizophrenia.
Birth patterns rank highly among epidemiological observations in schizophrenia. 47 Many more schizophrenics are born in winter and spring than in summer and fall. 48 Infectious aetiology is a plausible explanation, as many viruses show a surge in the same months and viral aetiology is a more convincing explanation of the consistency in question. While gene coding for particular proteins is inherited, environmental and developmental factors are undoubtedly implicated in modulating genes’ expression.
Exposure to prenatal infections and other obstetric complications are neuro-developmental assaults that increase vulnerability to schizophrenia. 49-52 In obstetrics, infection in the mother generates antibodies transmitted to the foetus, producing auto-antibodies that upset neural development and increase the schizophrenia risk. 53
Schizo-Virus or any Microbe?
It is not certain whether it is body’s abnormal response to any virus and other microbes or a specific unknown virus that results in “schizophrenic reactions.” It is even unclear that the unbeatable antigens of this hypothetical virus alone are capable of inducing the neuro-behavioural changes associated with schizophrenia. The hepatitis C virus came to medical attention only 15 years ago. The rotavirus was isolated in 1973 and the HIV virus was isolated in 1983. Non-detection of a pathogen does not exclude its role in the pathogenesis. If a specific virus is responsible for schizophrenia, it should have been with human society for a very long time, as the illness has been reported from the beginning of recorded human history. Some people may have a genetic vulnerability to the hypothetical schizovirus; inheritability would lie in contracting the specific virus. Poliomyelitis has a concordant rate of 36% among monozygotic twins; the rest are attributed to environmental factors. The majority of children exposed to the polio virus may not develop poliomyelitis and a genetic propensity may be required for the viral manifestation. It is even reported that 10% of the world population rarely catch influenza, in spite of its yearly mutation.
Cardiac disease due to endocarditis (caused by an autoimmune process affecting many parts of the body), a sequel to acute rheumatic fever, is an analogy to demonstrate how, theoretically, a microbial infection may lead to impaired neurodevelopment and psychiatric disorders in a different scenario. Endocarditis is triggered by a reaction to streptococcal bacteria, not a bacterial infection. It may begin a chronic process, leading to valvular cardiac disease. Generally, rheumatic heart diseases are diagnosed 10 - 20 years following rheumatic fever. Similarly, schizophrenia could be an autoimmune complication of a subtle microbial infection; finding and countering the antigenic triggers of ADs may lead to an effective cure.
HIV/AIDS
Patients with HIV are at risk for developing psychiatric symptoms and disorders similar to those seen in the general population, as well as those that are direct effects of HIV. HIV is a neurotropic and lymphotropic virus that causes immune suppression and allows the entry of opportunistic pathogens with an affinity for the CNS. There is some evidence that HIV may trigger a psychotic episode and contribute to first-onset schizophrenia. 54 Serious CNS complications occur late in the course of HIV infection, when the immunity function has diminished considerably. The viral load is closely associated with the degree of cognitive impairment. HIV-associated dementia (AIDS dementia complex) is defined as acquired cognitive abnormality in two or more domains and is associated with functional impairment and acquired motor or behavioural abnormality in the absence of other aetiology. It is estimated that 30% to 60% of patients experience some CNS complications during the course of their illness and 90% reveal neuropathological abnormalities at autopsy.
Pearce argued that HIV-related encephalitis could engender a scenario for a viral aetiology of schizophrenia. 17 HIV produces symptoms after being latent for several years. HIV was not identified as the aetiological agent of AIDS until the conditions for viral replication in lymphoid cell lines were identified. Prior to the evolution of PCR serology techniques, it was debatable whether the virus was in circulation at all. This indicates that the absence of a demonstrable virus does not mean the absence of a subtle virus-induced disease process. No virus, as such, is currently detectable in the schizophrenia disease process. Even in the absence of opportunistic infections, HIV infection of the brain causes severe neuro-behavioural syndromes, such as AIDS dementia, without infecting neurons, but by complex interaction with host molecules and non-neuronal cells. All these suggest that a rare or unknown infectious agent is involved; it would not be identified unless it was specifically tested for.
The finding that the neurophysiological and psychological stress of HIV infection can aggravate an underlying psychotic illness implies that viruses, without being a direct causative agent in psychotic episodes, can unmask pre-existing psychiatric vulnerabilities, acting on the brain physiology through unknown pathways. A curious aspect of HIV-related psychosis is that it responds to anti-psychotic treatment and to anti-retroviral drugs. Several anti-psychotic drugs have been shown to have antiviral properties, both in vitro 55 and in vivo. 56 The deduction is that a virus could initiate events resulting in psychosis, and anti-psychotic drugs can interrupt that sequence. All these features of HIV infections are consistent with the idea that a virus can cause neurobehavioral abnormalities after several years.
Borna Disease Virus
It has been recognised that Borna disease virus (BDV) could cause neuropsychiatric complications including neurological, behavioural, and mood alterations in animals. 57 A ribonucleic acid (RNA) virus from the family Bornaviridae, it is a neurotropic virus with an affinity to a variety of hosts, particularly hoofed animals, and can cause persistent infection of the CNS. Such an infection may be either latent or chronic and slow, but BDV presents with the latent type, characterised by a lack of viral particles. It may resemble the alleged pathogens in non-affective psychosis. The severity of clinical symptoms depends on the immune response of the host.BDV can directly influence the CNS through the binding of viral proteins with neurotransmitter receptors and indirectly through immune response and inflammatory reactions.
Depending on the host’s age and the integrity of the immune response, an infection may be asymptomatic or involve a broad spectrum of behavioural disorders. The severity of clinical symptoms depends on the immune response of the host.58, 59 Unusual features of BDV biology include nuclear localisation of replication and transcription, varied strategies for the regulation of gene expression, and interaction with signalling pathways, resulting in subtle neuropathology.60 BDV can directly influence the CNS through the binding of viral proteins with neurotransmitter receptors and indirectly through immune response and inflammatory reactions. The issue of human BVD infection has been recently questioned by American researchers who reported an absence of association of psychiatric illness with antibodies to BDV or with nucleic acids in serially-collected serum and white blood cell samples from 396 participants. 61 However, BDV in animals helps to bring the infection-based model of schizophrenia to the realm of the scientific imagination.
Neurotransmitters
It is an overstatement to say that schizophrenia is a neurotransmitter disease, although it is well established that it incorporates a derangement of dopamine activity. Some viruses have been shown to alter dopamine metabolism. 62 The literature deciphering the role of viruses in bringing about neurotransmitter abnormalities linking neurodevelopment assaults and the neuropsychological manifestations of schizophrenia is unhelpful. 63 It has been reported that in rodents, BDV could crash neurotransmitter systems, including dopamine, neuropeptides, and glutamate. 64 How viruses alter neurotransmitters is a central issue. Communication between the immune system and the brain is crucial to defend against viral infection; this is mediated through neurotransmitters. Viruses are bound to tamper with the intrinsic communication system as part of their cellular offensive. Some viruses have been shown to alter dopamine metabolism. 65
Genetics
The undisputed genetic factor in schizophrenia may be posited to discount the viral hypothesis. However, genetic factors do not exclude environmental contributions. Monozygotic twins have a concordance rate of only 48%. Brief reactive psychosis due to acute sequels to viral infection, though regarded as unrelated to schizophrenia, may still be schizophrenic reactions and they do not progress to schizophrenia only because the sufferers are not genetically predisposed to schizophrenia. Genetic predilection may be attributable to genes that determine idiosyncratic differences in immune responsiveness to common viral pathogens.
Susceptibility and immune response to infectious agents are known to be subject of genetic control and may involve multiple interacting susceptibility genes. 66 The genetic component of schizophrenia may engross multiple interacting susceptibility genes. These together or singularly may moderate the virus, and the virus and gene product may act at different points. Many cases would have a genetic foundation and it may be extremely rare to develop schizophrenia independently of a genetic anomaly. A small subset of patients may have a purely genetic form. Research should also be directed at identifying risk genes and why they assert themselves and cause the disease. Any future research which sheds more light on some people are affected more readily than others would bring researchers closer to more effective treatments and early intervention (see Table 5).
Table 5 - Future Directions
1. Critical research studies should target in establishing the viral and autoimmune aetiology of a subset of schizophrenia as the illness may be due to both factors. Detection criteria/ tests are vital in isolating this subset from the rest of schizophrenia syndromes 2. Robust epidemiological studies to be conducted to find putative infectious agents and possible models of transmission. 3. Developing new methods for detection of viral agents, directed at the analysis of previously identified pathogens and identification of novel viruses. Vigorous studies with PCR and other sensitive methods for nucleic acid detection to be carried out for the detection of viral nucleic acids in the body fluids of schizophrenia sufferers. 4.To find a method to turn off autoimmune attacks from the body or selectively disable the immune response 5. Identify risk genes and to find the specific DNA molecules and their tagging patterns vital for the progress of the illness. 6. To develop drugs to target specific genes which would mean they would be far more effective and have fewer side effects. 7. Finding psycho-physiological parameters for early detection to minimise the damage. 8. In the event of future discovery of effective antiviral agents, the subset of schizophrenia in question could take advantage of the clinical benefits of such discoveries. 9. Viral aetiology, if proven true, could lead to finding a vaccine against the disease. 10. Selective immune-suppressants could be a future addition into the psychiatric armamentarium. 11. A derivative of cloazapine without its haematological and metabolic side effects would be highly promising.
Summary
There are multiple interlinked causative factors in schizophrenia and viral infection may be only a trigger. Viral infections may be the cause of vigorous immune responses or triggering an autoimmune process that lead to neuro-behavioural aberrations and a subset of schizophrenia would emerge as viro-immuno-neuropsychiatric disorder or autoimmuno-neuro-psychiatric disorder. If such a subset of schizophrenia contains an autoimmune component, either triggered by infectious agents or due to unidentified intrinsic factors, the disease process would be determined by genetic vulnerability. There is not sufficient evidence established to identify viruses as being implicated in the aetiology of schizophrenia, but researchers have reason to anticipate further laboratory studies, as newer, more sensitive laboratory technologies are evolving. A viral or autoimmune model of schizophrenia may illuminate its pathogenesis, but not necessarily the diversity of psychiatric symptomatology. In the last few decades, schizophrenia research has been focussed on neurotransmitter derangements and neuro-developmental anomalies. The cause of a tsunami is not in the sea water, but due to the tectonic shifts under the sea bed; the aetiology of schizophrenia may be similarly due to immune alterations.
Pellagra psychosis due to niacin deficiency was hidden under the schizophrenia umbrella. 67 There may be other psychotic disorders grouped under schizophrenia, and they may have a pure biological aetiology—chemical or infectious—but with genetic vulnerability. No one can be sure whether it is the toxic chemical of the pathogens or the immune response of the host, or both, that may lead to the psychopathology. Searching for this hypothetical virus is a challenging task, but if researchers found it, the benefits would be enormous. A viral aetiology of certain types of schizophrenia, if demonstrable, could affect radical changes in treatment and management. In fact, the hypothesis of viral aetiology is more promising than any other biological hypothesis, as it gives a message of potential drug cure. In this contest, it is interesting to note that the antigenic similarity between components of the streptococcus and cardiac tissue resulted in rheumatic heart diseases, but with the advent of penicillin, this disease has virtually disappeared. Only time will determine the validity and therapeutic prospects of the viral and autoimmune aetiology of schizophrenia.
Davison opined that as evidence accumulates about the autoimmune basis of at least a subset of psychiatric disorders, clinicians should keep abreast of immune-neuropsychiatric research. 68 Psychiatry must constantly expand to meet the growing needs with the emergence of novel ideas in other medical specialities and it is high time to introduce a new terminology—“Psycho-immunovirology”—to study the viral aetiological mechanisms involved in psychiatric disorders like schizophrenia. Neuro-virology and psycho-immuno-virology could develop as an interdisciplinary field which represents a melding of virology, psychiatry, the neurosciences and immunology.
SSRIs (Selective Serotonin Uptake Inhibitors) are very commonly used in Depression and Anxiety. Though considered as safest antidepressants, they have some common side effects which include gastrointestinal side effects, headache and at times sexual dysfunction. Yawning is one of the rare side effects of SSRIs. SSRIs were found to be the commonest cause of not so common drug induced yawning in a meta-analysis1. Isolated cases of intractable yawning have been reported with citalopram2 fluoxetine, citalopram and sertraline3 in the literature .Excessive yawning can cause injury to Temporo-Mandibular Joint (TMJ) 4. Paroxetine has also been shown to cause intractable yawning5. Yawning possibly helps in thermoregulation and is an unconscious effort by the body to cool the brain 6, 7. It is known that yawning can be contagious. Reading, talking, seeing someone yawn or even thinking about yawning can induce yawning in the subjects8. Susceptibility to contagious yawning is different for different individuals depending upon their ability to process information about self9.
Case
A 60 year old postman presented with his first episode of depression. He attended the GP who started him on sertraline (an SSRI). He developed serious headaches and did not notice any therapeutic benefit. He was then referred to the psychiatric services for further management. He was assessed, Sertraline was stopped and Cipramil 20mg was introduced. He was reviewed after 2 months and the dose was increased to 40 mg to which he responded partially but relapsed within 4 months. There were no changes in his psycho- social circumstances. Cipramil was stopped and he was started on fluoxetine 20 mg. Once again the response was partial and was overshadowed by midnight insomnia and increased sleepiness in the daytime. Fluoxetine was increased to 40 mg and he was reviewed after 4 months when he reported clear and significant improvement in his depression but complained of “excessive yawning spells” causing him problems at his work place. The psychiatrist was surprised at the number of times he yawned at the Out Patient Clinic review. On further discussion it became clear that this side effect had become highly troublesome. He complained that his jaw was in severe pain. He was unable to do his delivery rounds and was having clear episodes of attention lapses leading to letters being put to wrong addresses. He was transferred to “sorting” the post at sorting counters and was taken off delivery rounds. Even here the intractable yawning continued and he was committing sorting errors. By now it was affecting his colleagues too and they also started yawning (it is known to be contagious).It was affecting his self-confidence and was extremely embarrassing in all social situations to an extent that he started avoiding social interactions. He was drowsy all the time. He was clearly suffering more due to excessive yawning than due to depression. He was unable to perform his employment duties and was signed off sick. At that point the dose of fluoxetine was reduced to 20 mg .After a couple of weeks his yawning reduced significantly but was still disruptive to his routines. He was advised to slowly taper off fluoxetine over next 4 weeks. Unfortunately his depression relapsed and his GP restarted him on Fluoxetine 20 mg. He was reviewed by the psychiatrist after a couple of weeks. Once again he reported return of intractable yawning.
Fluoxetine was stopped once again and he was started on Mirtazapine 15 mg. There was very little response. The dose was increased to 30 mg after around two weeks. This led to him to experience nausea and vomiting. Unfortunately Mirtazapine too had to be stopped. He was then tried on amitriptyline 50 mg which improved his sleep and symptoms of Depression. He was reviewed in the outpatient clinic after a couple of months .He did not develop any side effects and responded quite well. He then started his job starting from part time to full time within 6 weeks. After 6 months on the same dose of amitriptyline, did not have any symptoms of depression and was finally discharged from the mental health services.
Discussion
SSRI is the first line antidepressants used in the treatment of depression and Anxiety disorders. They are known to have least side effects and safest when it comes to overdosing. Intractable Yawning is quite an unusual and uncommon side effect. One has to be conscious of the fact that it may cause yawning that can be pathological and can cause severe disruption of patient’s life. It can contribute to poor compliance. It is quite easy to overlook and ignore this side effect as yawning usually seems to represent sleep problems which is also a significant feature of the associated depression itself.
Excessive yawning can cause Jaw/facial pain. It can even cause dislocation of temporo-mandibular-joint. It can cause severe problems with one’s work and self-esteem. The sufferer might be misunderstood for being inattentive, indolent and sluggish. It might affect relationships with spouse/friend/relatives and especially at place of work. It can be misunderstood by doctors and lead to unnecessary tests and investigations. One has to be aware when prescribing SSRIs in patients who are driving or are involved in handling heavy machinery, athletes, airline pilots, surgeons, life guards, air traffic controllers and many other professionals. Due to its contagious nature, it’s not only the patient who is affected but also others around him. Excessive yawning can adversely affect the level of arousal, the level of concentration and work efficiency leading to poor performances in tasks requiring undiverted attention.
Hence excessive or intractable yawning has to be kept in mind while prescribing the so called most safe anti-depressant class of medication, the SSRIs, in this case fluoxetine.
An audit and re-audit on the monitoring of the physical health of patients on antipsychotic medication in the Early Intervention in Psychosis Service of the 5 Boroughs Partnership NHS Foundation Trust
Introduction
A growing number of studies suggest a causal relationship between antipsychotic treatment and metabolic disturbances. The most frequent problems linked to antipsychotic drugs have been abnormalities of glucose metabolism such as insulin resistance, hyperglycaemia or new onset diabetes mellitus and dyslipidemia, including increased levels of total cholesterol, LDL-cholesterol and triglycerides.1
Developing effective models of identifying and managing physical ill health among mental health service users has increasingly become a concern for psychiatric service providers. Individuals with Serious Mental Illness (SMI) defined as any Diagnostic and Statistical Manual (DSM) mental disorder leading to substantial functional impairment, have higher than expected risks of physical morbidity and mortality in comparison with members of the general population.2 People with mental health problems such as Schizophrenia or Bipolar Disorder have been shown to die on average 16 to 25 years sooner than the general population.3 One set of explanations for these vulnerabilities points to the lifestyles of people with serious mental illnesses, which are often associated with poor dietary habits, obesity, high rates of smoking, and the use of alcohol and street drugs.4 Illness related factors have also been cited. It has been suggested that individuals with serious mental illness are less likely to spontaneously report physical symptoms.5 Poor physical activity has also been shown to be a common occurrence in people with serious mental illness.6, 7
A greater inherent predisposition to develop metabolic abnormalities coupled with metabolic adverse effects of antipsychotic drug treatments may negatively influence physical health.8 Many of these problems can be avoided if close attention is paid to the physical health of patients on antipsychotic treatment. A longstanding debate persists concerning who is responsible for the physical care of patients with serious mental illness. Psychiatrists and physicians are advised to play an active role in ensuring that patients with mental illness are not disadvantaged.9
The Warrington and Halton Early Intervention in Psychosis Team is based in the 5 Boroughs Partnership (5BP) NHS Foundation Trust in the North West region of the United Kingdom, and in collaboration with Advancing Quality Alliance (AQuA), they embarked on a joint audit between November 2012 and May 2013 with the aim of reviewing the practice regarding the routine monitoring of physical health of service users on antipsychotic treatment. The study set out to reduce the cardio-metabolic effect of antipsychotic medication in service users. The study was also aimed at contributing to a reduction in the mortality rates in people with severe mental illness as well as testing out approaches to improve the physical health of people with serious mental illness who are receiving care from the Early Intervention in Psychosis Teams. The promotion of a more integrated approach to the physical health care of people with a SMI was also targeted.
Method
In November 2012, the Warrington and Halton Early Intervention in Psychosis service (EIP) conducted the initial audit, designed by AQuA as a baseline measure of the current standard of physical health screening amongst the Early Intervention patients in the two boroughs. The recommendations from the National Institute for Health and Care Excellence (NICE) and Maudsley prescribing guidelines were the frameworks for the AQuA design. The Research and Audit Governance Group in the 5 Boroughs Partnership NHS Foundation Trust approved the audit.
A retrospective review of the clinical records of all patients opens to the EIP, who were prescribed antipsychotics, was undertaken. Six physical health parameters were examined and these include; serum lipid profile and blood glucose levels. Others measures were body weight, height, Body Mass Index (BMI) and blood pressure. These parameters were entered into the survey monkey audit tool developed by AQuA.
Other items audited were the frequency of screening, the number of physical health parameters evaluated at each period of recording and the smoking status of the service users. Clinical records were checked for documented history of physical illness in all patients. The number of service users receiving physical health interventions as a result of the screening and the number of service users who were offered physical health interventions at the screening but either refused treatment or did not respond to the referral was also recorded. The results were presented at a Trust-wide forum and recommendations were made, and disseminated shortly afterwards. A re-audit was done in May 2013.
Results
Table 1, summarises the demographic details of patients at baseline and re-audit. 55 patients were involved in the baseline audit and 52 patients were involved in the re-audit. No significant differences were observed in both audits in terms of gender distribution and age. Majority of the patients involved in both audits were of white British ethnicity.
Table 1: Demographic details of patients at baseline audit and re-audit
Nov 2012
May 2013
Total number of patients
Male : female
35:20
22:30
Age
14-36
15-36
White British Ethnicity
52
48
Baseline audit: November 2012
Screening and monitoring
The table below indicates the number of service users receiving a screening for weight, height, BMI, glucose blood levels, lipid blood levels and blood pressure at the 4 week, 3 month, 12 month and 24 month assessments.
Table 2: Physical health screening of service users at baseline
4 weeks recorded screening
3 months recorded screening
12 months recorded screening
24 months recorded screening
1 type of screening
5 (9.1%)
12 (21.8%)
18 (32.7%)
18 (32.7%)
2 types of screening
14 (25.5%)
17 (30.9%)
5 (9.1%)
5 (9.1%)
3 types of screening
4 (7.3%)
4 (7.3%)
3 (5.5%)
6 (10.9%)
4 types of screening
5 (9.1%)
3 (5.5%)
5 (9.1%)
3 (5.5%)
5 types of screening
4 (7.3%)
0
1 (1.8%)
4 (7.3%)
6 types of screening
4 (7.3%)
3 (5.5%)
4 (7.3%)
2 (3.6)
There was no screening recorded for 19 (34.5%) patients at 4 weeks, 16 (29%) patients at 3 months, 19 (34.5%) patients at 12 months and 17 (30.9%) patients at 24 months.
Smoking status of service users
Based on the analysis of those referred to the smoking cessation service, it was concluded that around 35% of service users within the EIP Service smoke. The findings from this data also indicate high refusal rates to smoking cessation programmes (at over 80% of those service users who confirmed that they smoke).
Documented history of physical illness
The presence or absence of physical illness was documented in the records of 35 patients. Where physical health problems were identified, patients were offered a number of interventions. These include referral to the dietician/exercise programmes, smoking cessation and referral to primary care services for illnesses such as, hypertension, diabetes and hyperlipidemia.
Table 3, summarises the types of interventions available for patients when physical health issues were identified. A number of patients (N/A) required no interventions, as physical problems were not identified.
Number of service users receiving physical health interventions
Table 3: Physical health interventions
Yes
No
N/A
Referral to dietician/exercise programme
15 (28.8%)
26 (50%)
14 (25.5%)
Treatment for Diabetes
0
22 (45.8%)
33 (60%)
Treatment for
Hyperlipidemia
2 (4.2%)
23 (47.9%)
30 (54.5%)
Treatment for
Hypertension
0
22 (45.8%)
33 (60%)
Help with smoking
cessation
12 (24.5%)
19 (38.8%)
24 (43.6%)
Re-audit: May 2013
Screening and monitoring
The table below indicates the number of service users receiving a screening for weight, height, BMI, glucose blood levels, lipid blood levels and blood pressure at the 4 week, 3 month, 12 month and 24 month assessments. The table shows that 29 patients had their screening recorded at 4 weeks, 19 (66%) of which had 6 types of screening. At 24 months, out of the 16 patients who had their screening recorded, 15 (95%) had 6 types of screening. Patients with no screening parameters were omitted.
Table 4: Physical health screening of service users at re-audit
4 weeks recorded
screening
3 months recorded screening
12 months recorded screening
24 months recorded screening
1 type of screening
2 (7%)
0
0
0
2 types of screening
2 (7%)
2 (8%)
1 (4%)
1 (5%)
3 types of screening
1 (3%)
1 (4%)
3 (11%)
0
4 types of screening
3 (10%)
3 (12%)
1 (4%)
0
5 types of screening
2 (7%)
1 (4%)
1 (4%)
0
6 types of screening
19 (66%)
18 (72%)
21 (77%)
15 (95%)
Smoking status of service users
The overall data confirms that 25 patients, who were identified as smokers, were offered smoking cessation, 19 of which refused, thus giving an overall refusal rate of 76%
The table below compares the results of both audits with respect to “6 types of screening” done at 4 weeks, 3 months, 12 months and 24 months. The result shows an overall improvement over the audit period.
Comparing results of both audits with respect to “6 types of screening”
Table 5: Comparison of screening results
November 2012
May 2013
4 weeks
4 (7.4%)
19 (66%)
3 months
3 (5.5%)
18 (72%)
12 months
4 (7.4%)
21 (77%)
24 months
2 (3.7%)
15 (95%)
Discussion
The first audit revealed a suboptimal screening of the 6 targeted parameters at 4 weeks, 3 months, 12 months and 24 months in the service users audited when compared to the recommendations of the Maudsley guidelines (See Table 3). Some of the issues identified are summarised in the table below;
Table 6: Issues identified following the first audit
Sporadic health and wellbeing sessions
Ad-hoc physical health checks prior to commencing antipsychotics
Physical health screening was not perceived as priority
Physical screening were unsystematic and erratic
Poor referral links with local health promotion programmes
Poor attendance to physical health screening appointments
Poor recording of screening tests
Inadequate links with primary care services
Psychiatric clinics poorly equipped with instruments for basic health screening
No clarity about who takes responsibility for screening: Psychiatrists or GP?
Patients’ lack of interest and motivation in the screening process
SMI register not up-to-date
Recommendations made following the initial audit are outlined in the table below;
Table 7: Recommendations following the first audit
Need to finda comprehensive screening tool
Development of a documentation system
Building an alert system to remind when physical health checks are due
Improvement of links with primary care services
A more robust approach to ensure patient’s attendance at screening clinics
Improvement of links within secondary care agencies
Identification of further skills needed within the team e.g. venipuncture, ECG
A Plan, Do, Study, Act (PDSA) model was used which was useful in clarifying issues and actions needed.10 It helped us to identify issues and actions needed including:
1. Establishing physical health as a priority within the EIP
2. Involvement of primary care and health promotion
3. Establishing a database for physical health monitoring
4. Making physical health monitoring part of care planning
To tackle the identified issues a local project group was constituted. This group was made up of a consultant psychiatrist, business manager, nurse consultant, team manager, an occupational therapist (OT), a support worker (STR), a pharmacist, social services, public health leads, wellbeing nurses, a service user representative, and a locally based General Practitioner. The group had monthly meetings.
Patients in the Warrington and Halton Early Intervention in Psychosis Service were screened using the 5 Boroughs Partnership (5BP) Comprehensive Physical Health Assessment tool. This tool covered the 6 parameters targeted in the audit and other relevant health information such as, smoking, diet, exercise, sexual health, sleep, dental and optical health, ECGs, and other routine bloods checks. An in-house database in which results could be recorded was devised and implemented. A notification list which alerted on computer when a screening is due was developed; a GP DVD and information leaflet for the GP website and the Clinical Commissioning Group (CCG) Newsletter were produced. Wellbeing Nurse-led clinics were held in Halton and a STR-led physical health clinic was initiated in Warrington. Access into the path labs for both localities was established to help facilitate prompt access to blood results. Regular AQuA meetings took place in Salford, Manchester, and links were established with the Medical Director and the Clinical Commissioning Group, who were regularly, provided progress reports.
The re-audit in May 2013 showed an increase in the number of service users being screened and monitoring for the six identified parameters (see Table 8).A robust and comprehensive recording system has been developed, resulting in more service users receiving appropriate screening and physical health monitoring. Better links and working relationships have been established with primary care services and there is increased awareness of the need for physical health monitoring in professionals and service users. Regular and well-equipped physical health clinics with well-trained staff have been established across both localities. Other secondary care agencies within the Trust are now more aware of the requirements for physical health screenings.
Why should we be doing regular physical health monitoring? The benefits of monitoring the physical health of individuals with serious mental illness cannot be overemphasised; it allows early identification and subsequent management of cardiovascular and other risk factors in a timely manner.11 The Maudsley Guidelines recommend monitoring of blood lipids at baseline, at 3 months and yearly. Similar recommendations are made for the weight, which includes BMI and waist size when possible. Plasma glucose measurements are recommended at baseline, at 4 to 6 months and yearly. Blood pressure measurements are recommended at baseline and frequently during dose titration. Full blood count and electrolyte measurements are recommended at baseline and yearly.12 In the last few years, agencies worldwide have also developed clinical guidelines. In the United States, the American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologist and the North American Association for the Study of Obesity have released joint guidelines.13
Even though the side effects of antipsychotics are well established, many mental health services today have yet to adopt a practice of regular blood monitoring as recommended by international guidelines.14 The issue of responsibility for monitoring metabolic abnormalities remains a much debated topic today.9 The primary responsibility for managing the physical health of individuals with severe mental illness has been said to lie with primary care.7 Another side of the debate, however, exists, and two consensus conferences have called on mental health care providers to take responsibility for the physical health of their patients.8 It is widely recognized that mental health teams have a role to play in the monitoring of the physical health of their service users; however, many psychiatrists still consider psychiatric symptom control as their primary responsibility.14 15 Studies have also shown that Individuals with Serious Mental Illness do not readily access primary care.16 Despite the availability of Clinical Guidelines, screening for and monitoring of metabolic problems in patients with serious mental illness remains suboptimal.11
The usual practice in most centers for monitoring physical health parameters and guidelines used vary and are rarely regulated. Local resource availability is likely to play a significant role in guideline selection. Physical equipment, staffing levels and other resource issues may need to be taken into consideration prior to devising a local guideline. Development of a specialised phlebotomy service, for example, to the outpatient clinics will be a welcome addition, introduction of a key worker system as seen in the Warrington and Halton Early Intervention in Psychosis Team and consideration of the physical health needs of patients as part of the key worker’s duties, a simple one-page monitoring prompt attached to the patient’s medical file, educational intervention and oversight by the senior clinicians may all increase the adherence to routine blood testing guidelines. Regular liaison with General Practitioners regarding a joint approach to physical health monitoring would also help improve adherence to the guidelines.
Suicide and deliberate self-harm (DSH) have been recognised as major public health problems in India for some time, but there are significant obstructions to effective intervention including difficulties in following Western models to understand these behaviours.1, 2, 3
The World Health Organisation (WHO) recognises suicide as one of the three leading causes of death in young adults globally.4 The greatest burden of suicide is now in low- and middle-income countries like India where annual suicide rates are 10-11 per 100,000.5, 6, 7 India is second only to China in the absolute number of annual deaths by suicide.5 The number of individuals who die by suicide each year in India alone is more than the total number of suicides in the four top ranked European countries combined.3, 5, 8
DSH, defined as intentional self-poisoning or self-injury, is a closely related public health problem.9WHO estimates that for every suicide there are at least 10-20 DSH acts.10 If this estimated proportion, based on Western research, is also true in India then there are 1-2 million DSH acts in India each year.
Official data for 2005 suggest that 19.6% (n=22,327) of India's 113,914 officially recorded suicides were self-poisonings with pesticides7 (predominately organophosphates, which are freely available and widely used in agriculture). The official suicide rate for India, 10.3 per 100,000 in 2005,7 is thought to be an under-estimate.3, 11 Studies from several regions suggest that India's suicide rates may be as high as 40 per 100,000 and that 30% or more of these deaths are due to pesticide self-poisoning.11 The studies reporting the highest suicide rates within India are from Tamil Nadu (>60 per 100,000 – three times higher than the official figure for the state).12, 13, 14, 15 Whilst some of the discrepancies between official statistics and findings in local studies may be due to urban-rural differences in the incidence of suicide, data collated by the Indian police suggest that around 90% of suicides in India occur in non-urban areas.7, 11, 15 Extrapolating from these figures, it is conservatively estimated that there may be up to 420,000 suicides per annum in India (126,000 from pesticide self-poisoning).
India's centrally collated self-harm and suicide data are unreliable owing to a number of factors. Death registration processes are below Western standards. Only about 25% of deaths are registered and only about 10% are medically certified.16, 17 Attempted suicide is a crime in India.18 Survivors are interviewed by the police. Fear of legal and social consequences following an act of self-harm probably influence willingness to acknowledge DSH and preparedness to seek medical intervention.
India contributes almost 20% to the world's population, and suicides rates are increasing particularly amongst the young.11, 19 Obtaining reliable and nationally representative data on DSH rates in India should be a priority for health-funding agencies over the next decade. In order to reduce fatalities following self-harm, information and investment are needed to improve quality, affordability and accessibility of health care close to the affected communities.20
If, as seems likely, self-harm (especially pesticide poisoning) occurs predominantly in rural areas of India,11 Western models of data collection and intervention aimed at reducing pesticide poisoning (which is predominately accidental in developed economies) are likely to require significant modification to be reliable and effective. The WHO's global suicide prevention strategy is largely based on findings from research and models of suicide prevention developed in the West.21 Health care resources in rural areas of India are thinly spread, and are often rudimentary compared to those in the West. There is an urgent need for research in low- and middle-income communities – particularly in rural areas of India – to provide the evidence base to underpin public health strategies for preventing pesticide suicides in these countries.
The establishment of DSH registers is a first step towards the systematic collection of data in relation to self-harm, both for epidemiological purposes and to understand pesticide self-poisoning at an individual level. If DSH registers can be shown to generate reliable information in India, in due course it may be possible to identify the factors that put individuals at risk of behaving in this way, and create relevant evidence-based policies to develop interventions for reducing mortality and morbidity associated with DSH (particularly pesticide poisoning).
This paper explores the feasibility of setting up a DSH register in a resource-poor large State hospital in south India, where rates of suicide and DSH are high.
METHODS
Setting
This study was carried out at Mysore Medical College and Research Institution (MMCRI), a State-run hospital in Mysore, southern India. The hospital serves a catchment area of 1,500,000 population and 135 primary health centres. The hospital has most specialities, with 1050 beds and a 10-bedded intensive care unit. 800-1000 patients attend the hospital outpatient department daily. Daily attendance to the casualty department for the purpose of medico-legal registration (which includes self-harm) is between 110 and 130. All other presentations including emergencies are managed through respective speciality outpatient departments.
Figure 1. Care Pathway for deliberate self-harm (DSH) at Mysore Medical College and Research Institution (MMCRI)
Setting up of the register
The flow diagram (Fig. 1) illustrates the care pathway of those presenting with DSH to MMCRI highlighting that only a few receive psychosocial assessment. A working group of psychiatrists, psychologists, social workers, casualty medical officers, statisticians and hospital managers was formed to arrive at a consensus on the minimum dataset that could be gathered from DSH survivors for the purpose of setting up a register. Literature on establishing self-harm registers was reviewed along with international guidelines in relation to self-harm assessment in the general hospital.22, 23 Opinion was sought from senior psychiatrists and public health personnel from the private and public sector in Mysore and from the United Kingdom (UK). The team was visited, supported and advised by the Centre for Mental Health and Society, Bangor, UK.
The items listed in Table 1 were considered as ‘minimal yet essential’ for informing clinical practice, service development and patient engagement in future research. The study was not externally funded and, due to time and resource implications, it was agreed that outcomes of mental health assessments would not be recorded in the register. The method of DSH was coded according to the International Classification of Diseases 10th Revision (ICD-10) criteria24 and socio-economic indicators were derived from a modified Kuppuswamy’s scale25 that is validated for the south Indian urban population.
Table 1. Contents of the deliberate self-harm (DSH) register.
An electronic DSH register was set up in February 2013 and is currently held in the Department of Psychiatry, MMCRI, and Mysore. Two pre-registration House Officers (junior resident equivalent) visited the casualty department daily and identified those cases registered as self-harm from both the standard patient register and medico-legal case registers. If the individual was discharged from casualty (condition necessitated no further treatment, no intensive care bed available, or patient chose admission in private sector after first aid) the available information is captured from the registers and medical records. If they admitted to the general hospital they were traced and personally contacted. Information (as in Table 1) was collected from DSH survivors and from medical records. The data was verified by a Consultant Psychiatrist before being entered in the register. DSH survivors are asked to provide two contact details (postal address and phone number) for future tracing if they consent to further contact either in person or by phone. Table 2 is a list of the sources of data for the DSH register in Mysore and their limitations.
Table 2. Sources of data for deliberate self harm (DSH) register in Mysore and their limitations.
Feasibility
A DSH register should be representative, complete and accurate. The register should be acceptable to the entrants and only take a minimal time for data collection and registration. For the purpose of this study the following were identified as indicators of feasibility:
· Time between identifying that the patient should be included in the register and completion of data entry in the register. This was recorded for 80 randomly chosen inpatient DSH survivors.
· The proportion of patients presenting with alleged DSH who were correctly identified and, if admitted to the general hospital, traced for the purpose of inclusion to the register (representativeness).
· Proportion of those included in the register for whom a full data set could be captured (completeness).
· Proportion of the DSH survivors who were willing to be included in the register and provided contact details for future follow-up (acceptability).
· Over a period of a week, every month during study period February 2013 to July 2013, a Consultant Psychiatrist independently collected data from casualty registers and checked against the total number registered on the DSH register for the corresponding month (accuracy).
RESULTS
Between February 2013 and July 2013, a total of 19,563 patients attended the casualty department. Of these, 1072 attended in relation to self-harm. 1041 of them were hospitalised for further intervention. All of those who were hospitalised and survived (n=817) were traced and contacted. None objected to their details being entered on the register. However, only 253 of the 817 (30.9%) agreed to be contacted for future follow-up. Of the 817, only 109 (13%) had been formally referred to the psychiatry department for an assessment prior to contact with the research team. None of the 817 had any involvement with Social Services.
Out of the 1023 on the register, complete data was available and/or obtained for 740 (72.3%) individuals and data was incomplete for 283 (27.7%) patients. Either by reviewing the medical records or interviewing the patient, it was confirmed in all 1023 cases that there had been an act of self-harm necessitating medical intervention. The time between identifying that the patient should be included in the register and completion of data entry in the register varied between 30 minutes and 2 hours. When the data collected was cross-verified (n=315) by a Consultant Psychiatrist (author RR), entries of 310 individuals were accurate, with a minor discrepancy in less than 3 items for another 5 individuals.
Various terminologies were used to report a case of DSH in the case records (for example, suicide attempt, failed suicide, self-harm, poisoning, deliberate harm).
DISCUSSION
This is the first description of a method of successfully setting up and maintaining a DSH register in an Indian setting. It was a labour-intensive exercise due of lack of electronic patient data management, administrative support and the absence of an agreed care pathway for DSH in the hospital. Despite these obstructions, we have illustrated that it is feasible to set up a DSH register in a busy tertiary care hospital in India. Results of our study indicate that the register details are accurate and representative of those who seek help from the specialist centre. However, it cannot capture those patients whose DSH was managed successfully within primary health centres, those individuals who failed to seek help and those who died before admission.
Clinical Implications
The experience of establishing a DSH register has lead to changes in local clinical practice. DSH is associated with increased morbidity and increased utilisation of health services.26 DSH survivors who were contacted (n=817) by the psychiatry residents were offered psychosocial assessments. Under normal circumstances, 708 (87%) of this group would not have received any psychosocial assessment. The process of setting up the register has helped to identify DSH cases so that an intervention can be offered before discharge from the general hospital. The register has also played a major role in the identification of people who harmed themselves but were discharged without admission to a ward. This group can also be helped. We have now developed an education and service information leaflet which includes emergency contact details (similar to a crisis card in the UK), which is given to DSH patients on discharge. These are known to decrease the repetition of DSH in the developed world.27 Deaths from suicide are largely preventable if knowledge and understanding of this maladaptive behaviour is used to ensure timely intervention.8
By auditing DSH data in a systematic way, clinical decision-making will be based on pooled experience, not just on each clinician’s recall. Comprehensive registers of DSH provide clinicians with the opportunity to review cases of suicide where they have had clinical involvement, using techniques such as psychological autopsy, improving clinical skills and judgements. Overall there is a need for an attitude of vigilance about suicide risk, and of enthusiasm about pursuing initiatives for suicide prevention based on evidence. Better understanding of self-harm will assist in devising means of reaching out to those at risk of dying without having had contact with health care services.
Reporting of DSH in case records was inconsistent. There is a need for uniform recording, medical coding and reporting of DSH. In the DSH register, the method of self-harm is recorded using an international recognised coding system (e.g. ICD-10).
If we continue to offer psychiatric assessment to all cases of DSH, the much higher rate of ascertainment arising from the DSH register will place further strain on an already stretched psychiatric service. Further investment in services specifically targeting self-harm in India is urgently needed.
Service Implications
Use of the register
The register creates an opportunity for a standing DSH audit, allowing for identification of trends over time and comparisons with other services that establish DSH registers using similar methods. Systematic collection of demographic and clinical data will allow calculation of admission rates, repetition rates and other indices of importance in service development. Collaboration with non-governmental organisations in the region who work with those who self-harm will allow development and evaluation of specific culturally appropriate interventions.
Where the register should be held?
In the developed world DSH registers are normally held on electronic systems in the Accident and Emergency department or liaison psychiatric services. In India, it is a mandatory obligation to hold a medico-legal register (which includes DSH) in casualty. Maintaining an additional DSH register risks unnecessary duplication, but modification of a medico-legal register creates an ethical problem and risks under-reporting. There are few liaison psychiatry services in India. On balance, we suggest that our practice of holding the DSH register within the department of adult psychiatry is the optimal arrangement in the Indian setting.
Confidentiality
Confidentiality must be respected. In the UK, when establishing a DSH register, it is necessary to discuss issues of confidentiality and legality with the local Data Protection Officer, and to register under the Data Protection Act. Use of the data for research purposes requires approval from local Research Ethics Committees. In India, there is little regulation of this sort. In order to establish our register it was only necessary to obtain consultant approval and consent through the local medical committee. We suggest that good practice would demand that standards of confidentiality and oversight should, as far as possible, match Western standards.
Manpower and resources
Setting up this register in Mysore required input by a Consultant Psychiatrist, for 2 sessions per week for 6 months, to negotiate with casualty medical officers, consultant physicians and reception staff. The resident from the psychiatry department spent at least 2 hours a day collating and updating the register. The absence of a patient electronic data system and lack of administrative support has placed additional strain on residents and has prolonged the time to identify a case of DSH from the casualty records and trace them on the medical wards. We believe that once the register is established, these tasks could be managed by a trained Social Worker spending 1 session per day collecting the data and 1 session per week editing the register. The work load might vary in other hospitals, depending on the number of daily hospital attendances for DSH.
Integration with other data sources
Linking this register with post mortem records, local civil registration of deaths and police records is desirable but this needs co-ordinated effort from several civil bodies and public health organisations. In the absence of any legislation or national record linkage systems, there are few motivators to drive this change or the allocation of resources. However, a unique person identification number system is presently being rolled out across India. The development of cross-agency electronic databases will facilitate easier record linkage in the future, which creates the opportunity for collection of reliable and representative data at a regional level.
None of those who were contacted during the study period had any formal input from Social Services. Though the models and mode of delivery by Social Services in India is radically different to those in Europe, DSH survivors form a stigmatised vulnerable group who are frequently in need of social assessment and support.
Future investment and development
There are good humanitarian reasons to seek the de-criminalisation of acts of self-harm in India, and there is presently strong lobbying to bring this about. It is reasonable to suppose that this might lead to readier help-seeking and better reporting of self-harm and suspected suicide. However, there are other measures that would be necessary to reduce rates of DSH and completed suicide. Regulating the supply of organophosphate insecticides, so that they are only available in dilutions that make fatal overdose more difficult, would be one such measure. There is also a need to develop liaison psychiatric services, offering psychosocial assessments to a higher proportion of those who present with features indicative of probable self-harm. Other necessary developments include investment in patient electronic records and systematic strategies for destigmatisation of DSH.
The register has provided us with a cohort of individuals who are willing to be contacted for future studies. The register has continued beyond the study period. We presently have 3720 individuals on the register. The unit has established formal links with research centres in the UK. We intend to carry out longitudinal studies to examine the patterns of DSH, rates of repetition, compliance with follow-up and suicide rates. This will help to identify the culture-specific access, adherence and prognostic factors, and will influence the development and validation of brief psychosocial interventions in a social, economic and cultural context that is radically different to the West.
CONCLUSIONS
We have illustrated that it is feasible to set up a DSH register in a busy tertiary care hospital in India where rates of self-harm are high. Results of our study indicate that the register details are accurate and representative of those who seek help from the specialist centre.
Very few were referred for psychosocial assessment following an act of self-harm and none of them had any formal input from Social Services. Though the models and mode of delivery by Social Services in India is radically different to those in Europe, DSH survivors form a stigmatised vulnerable group who are frequently in need of social assessment and support.
A forty-eight year old man presented with unusual and distressing visual experiences with varying degrees of severity for over twenty years. Some of these included the following; red objects having a green shimmer around them like 3-D glasses, altered sense for distance estimation, people’s faces seeming to change shape when looked at, alteration of own reflection, anything patterned appearing to move all the time, words moving about while reading, things appearing to be multi-layered, bright lights throwing up shadows, vehicles appearing to stretch as they drive past, flying birds looking like animation and difficulty in focussing.
When present, his symptoms interfered markedly with his functioning. For example, he could not cross the road, could not read, and had to dim his lights. He struggled with knowing which visual perceptions were real and which were not. The patient felt his visual experiences were related to his past LSD use twenty-five years ago. He felt the drug had put him “in a coma” and he was “dreaming all of this”.
He specifically remembered a party with friends where he took a cocktail of illicit drugs, including LSD and marijuana, with alcohol. He said he would usually take drugs and alcohol in a binge pattern. The ‘trips’ would usually last twelve hours. He felt he experienced some memory loss of that particular night. When he woke up the next morning he was still experiencing the effects of LSD and said he has felt these effects ever since. He tried to explain that it was like drinking alcohol, waking up drunk and being drunk from that point on. After this incident he did not use illicit drugs again.
Prior to this particular night he said he may have used LSD about fifteen times, as Microdot tablets, usually one at a time, with cannabis. He said it was “like having a tripping switch in your brain”. When you took LSD, “the switch turned the tripping on and after a while it turned off”. He said his switch “was broken” and he therefore continued to re-experience the effects of the drug.
His other complaint was that of feeling he was “not real”; to the extent he even thought he should harm his family members so he could prove he was real.
He also complained of low mood, decreased concentration, anxiety and an inability to cope.
His first contact with mental health services was at the age twenty two years. He presented with symptoms of anxiety but it was not felt he had a mental illness. He was referred again a year later and was diagnosed to have Primary Depersonalization syndrome.
The patient himself reported that all his symptoms started after he had used LSD about fifteen times in six months. At the time he had described having undergone a complete personality change due to his experiences. He felt objects and experiences had a dream-like quality. His visual experiences caused so much distress he felt suicidal.
Over the next twenty-five years he has had various other diagnoses; LSD induced Depersonalisation Syndrome, Depersonalisation-Derealisation Syndrome, LSD induced Simple schizophrenia, depressive disorder and anxiety disorders. His visual disturbances had been interpreted as visual hallucinations. He had received treatment with antidepressants (Imipramine, Amitriptyline, and Venlafaxine); antipsychotics (Trifluperazine, Promazine); Benzodiazepines (Diazepam); Propranolol; and Fentazine. He was also prescribed Hydergine (which helped reduce symptoms briefly) at one point.
Investigations: EEG, MRI Brain, and Carotid ultrasound were normal.
He was admitted to a psychiatric hospital at the age of forty-eight years old where the admitting doctor described his symptoms as visual hallucinations and started him on Risperidone, which increased the intensity of his symptoms. He was also treated with Citalopram for his low mood. It was noted that his symptoms were different from common psychotic illnesses. Detailed history taking and assessment of his perceptual abnormalities over the following few weeks in hospital confirmed the diagnosis of hallucinogen persisting perception disorder (HPPD).
He was treated with Clonazepam 1 mg four times a day with good effect; as seen by the reduction of symptoms - see Table 1.
Table 1:
DSM IV/V Symptom Checklist
Prior to treatment with Clonazepam
3 months after initiation of Clonazepam treatment
Geometric hallucinations
Present
Absent
False perception of movement in peripheral fields
Present
Absent
Flashes of colour
Present
Absent
Intensified colours
Present
Absent
Trails of images of moving objects
Present
Absent
Positive after images
Present
Absent
Halos around objects
Present
Present but reduced in intensity and frequency
Macropsia
Present
Absent
Micropsia
Present
Absent
After discharge he had .a depressive episode and was treated with Escitalopram. This was later changed to Reboxetine.
Discussion:
This is the first case that we are aware of where symptoms of HPPD have persisted for over two decades after the cessation of the use of Lysergic acid diethylamide. There is a need for raising awareness about this condition to prevent misdiagnosis and delay in appropriate treatment.
This patient presented to psychiatric services over twenty-five years ago and at that time he felt his symptoms were related to his use of LSD. He was given a variety of different diagnoses before the correct diagnosis was established and treatment initiated with good outcome.
The patient had also experienced migraines and used alcohol excessively on occasions in the past. Although we are not aware of any connection between this disorder and these factors, future reports and studies may help provide further knowledge in these areas.
HPPD is a recognised condition described in DSM V and DSM IV with a diagnostic code 292.89. In DSM III it was referred to as post hallucinogen perception disorder (PHPD). It is described in ICD 10 under the code F16.983.
LSD has been known to alter perception and mood in the presence of an unaltered sensorium. HPPD was first described by Eisner and Cohen, who observed spontaneous recurrences of LSD like states in subjects, days to weeks following cessation of drug use1.
Other authors have described more or less the same clinical picture; for example, Rosenthal described patients suffering from post drug visual hallucinations lasting as long as five months from the time of drug use2
In a survey of sixty five users of LSD, Holsten found fifty users who described post LSD disturbances eighteen months to four years later3.
Flashbacks have been suggested to be a misnomer as patients described cases of continuous rather than paroxysmal visual disturbances from LSD 4
It is not clear what made our patient re-experience these visual disturbances however the literature suggests that emerging into a dark environment can precipitate or exacerbate post LSD visual symptoms. Among other precipitating factors are intentional inductions, marijuana use, medications like: neuroleptics (phenothiazine), amphetamines, cold remedies, anti-Parkinson’s agents and SSRI’s5.
The patient mentioned that he had ingested LSD approximately fifteen times before he developed this condition. The data suggests that peak incidence occurs with fifteen exposures and second smaller peaks at around forty to fifty exposures 6.
A number of hypotheses have been formulated in order to understand the underlying aetiology. HPPD is related to the recreation of symptoms experienced in intoxication. LSD has been shown to be excitotoxic to neurons. It is also known to be a partial agonist at post synaptic 5HT2 receptors and enhances glutaminergic transmission.
The patient had suffered from these rather distressing visual disturbances for more than two decades, which have had considerable impact on his daily living. He was given different diagnoses which included Induced depersonalisation, depersonalisation-derealisation syndrome, LSD induced simple schizophrenia, depressive disorder and anxiety disorders.
The patient had been treated with different psychotropic medications including antidepressants, antipsychotics, benzodiazepines, propranolol, fentazine and hydergine. Some had little effect like hydergine, whilst others worsened symptoms, in particular antipsychotic medications.
A case series of three HPPD patients treated with Risperidone reported an exacerbation of LSD-like panic and visual symptoms. Thus from these reports and our case report Risperidone could be contraindicated in patients with HPPD 7.
There have been some published case reports on treatment of HPPD, including the use of Reboxetine, which suggest it is beneficial in the treatment of the visual disturbances and depressive features associated with HPPD. This is possibly due to its alpha 2 adrenoceptor modulating effect on both Noradrenaline and Serotonin release8. Another case report suggested the use of a combination of Fluoxetine and Olanzapine in the treatment of HPPD9.
Benzodiazepines seem to be the most beneficial treatment so far and Clonazepam is the most effective due to its high potency compared to low potency Benzos and its long action at the GABA receptors10.
Conclusion:
Hallucinogen Persisting Perception Disorder is one of the outcomes associated with the ingestion of LSD. Symptoms can be present for years as demonstrated by different case reports, and for over two decades as reported in this report. The effect could be devastating to the person experiencing extremely distressing and disturbing perceptual phenomenon. It can last up to twenty five years after the cessation of the hallucinogenic drug. Early diagnosis and appropriate treatment can significantly help improve the quality of life of patients with this condition.
The term ‘designer drug’, coined in the 1980s, generally referred to various synthetic opioids based mostly on the fentanyl molecule (α-methylfentanyl) and MDMA (methylenedioxymethamphetamine) commonly known as ecstasy. Fentanyl is an extremely potent analgesic, some 100 times more potent than morphine. MDMA and fentanyl compounds were the most popular synthetic drugs initially. The terminology is confusing because although the description ‘designer drug’ seems to imply the creation of new drugs, many are not new. For example, cathinone derivatives have been reported since the late 1920s. MDMA was first synthesised in 1912, methcathinone in 1928, and mephedrone in 1929. Cathinone is chemically similar to ephedrine, cathine, methcathinone and other amphetamines.
Legal highs generally comprise cathinone stimulants and synthetic cannabinoids. Hallucinogenic agents such as salvia divinorum are also included, the latter sometimes described as herbal ecstasy. Synthetic amphetamines are not regarded as hallucinogenic, though hallucinations are experienced by some users.
Thus, the term ‘designer drugs‘ covers an array of substances which are used recreationally, are not controlled under the Misuse of Drugs Act (1971), are not licensed for ‘legal’ use, and are not regulated under the Medicines Act (1968). They are chemicals produced by tweaking or altering the molecular structure of previous well-known psychoactive agents. By stating they are ‘not for human consumption’, or are just ‘bath salts’, they can be sold legally. Hundreds of such substances are now available, reflecting the ease at which chemists can produce them.
Availability and Consumption
The World Drug Report (available on the Internet) produced annually by the UN Office on Drugs and Crime (UNODC), provides information on the worldwide manufacture and marketing of illegal drugs. The 2013 report highlights a striking rise in the availability of new substances. Part of the challenge lies in their variety - some are derived from plants, for instance, the mint plant Salvia divinorum, native to Mexico, with synthetic cathinones and cannabinoids also being major contributors in other countries.
Ease of synthesis, low cost, and resourceful marketing have contributed to the problem. Information provided via the internet, combined with minimal difficulty in the manufacture and transport from distant regions, together with lax legal enforcement, creates an ideal opportunity for legal highs to flourish. The low cost is particularly attractive though ironically legal highs probably cost more these days: for example, 1g of mephedrone costs about £16.00 more than when legislation was introduced in 2010. On the other hand MDAI (methylenedioxy-2-aminoindane), a legal stimulant and club drug which is snorted or bombed, costs about half the price of cocaine (£20 per gm). It is sometimes cheaper to buy legal highs over the internet than from a drug dealer. Part of the increase in use of legal highs may be a result of decreasing purity of other ‘buzz’ drugs such as cocaine and MDMA.As with other illegal drugs regulatory measures drive the drugs ‘underground’ and into the hands of drug dealers and the price then varies with the purity of the drug and its ease of manufacture and availability.
Some users will revert to taking an illegal drug when the legal alternative is prohibited. There is also a certain curiosity to experiment with new drugs. Even so, to keep things in perspective, consumption of more harmful familiar illegal drugs (for example, cocaine, amphetamines) has not abated, with over 315 million people worldwide thought to be using them. More worrying is that millions of individuals inject more harmful drugs such as opiates with resultant increased rates of HIV, hepatitis B and hepatitis C infection. Readers are also likely to be aware of the violence and deaths associated with drug manufacturing and supplying within countries such as Latin America.
Government Control
The Medicines Act 1968 (UK) governs the control of medicines for human and veterinary use. It defines three categories of medicines: a) prescription only medicines (POM), available solely from a pharmacist and requiring an appropriate practitioner to issue, b) pharmacy medicines (P), available only from a pharmacist, without the need for a prescription, and c) general sales list (GSL) meaning medicines bought without a prescription. The Medicines Act 1968was set up to protect patients from unscrupulous suppliers of medicines. Safeguarding the public from illegal medicines or any inaccurate and misleading labelling of medicines isparamount. However, manufacturers have managed to sell legal highs by passing them off as bath salts or research chemicals.
Phenylalkylamines analogues such as amphetamine are widely misused and because of their simple structure hundreds of amphetamine analogues have been introduced for decades. This is the reason why so many legal highs are available. Amphetamine (phenylisopropolamine), a familiar central nervous system (CNS) stimulant, has effects which last for several hours after oral intake. Methamphetamine is closely related to amphetamine and ephedrine (a mixed-acting sympathomimetic). Ephedrine and pseudoephedrine (often used for relief of nasal congestion) undergo reduction to methamphetamine, or oxidation to methcathinone. As with methamphetamines, methcathinones can be readily ‘cooked’ in the laboratory and hence the term ‘synthetic’.
Background biochemistry
Morphine, the most abundant opiate alkaloid found in the poppy plant, papaver somniferum, was first isolated in 1804. The actual term alkaloid is derived from "alkaloide" introduced in 1819 by the German chemist Carl Friedrich Wilhelm Meisner, from the Latin root ‘alkali’, and the Arabic word al-qalwī meaning "ashes of plants".
Alkaloids are a group of naturally occurring organic nitrogen-containing bases, a base being a substance with a pH above 7 which turns red litmus paper blue. They include related compounds with neutral and even weakly acidic properties and more than 3,000 different types have been identified. In addition to nitrogen, hydrogen and carbon, most alkaloids contain oxygen, sulfur, and to a lesser extent, chlorine, bromine, and phosphorus. Generally, an alkaloid contains at least one nitrogen atom in an amine-type structure, i.e. one derived from ammonia (NH3) replacing the hydrogen atoms with hydrocarbons, for example, CH3 or CH2. Alkaloids generally are weak bases and some act as acid or base (amphoteric).
Alkaloids are produced primarily by flowering plants and organisms such as bacteria, fungi, and animals. Several alkaloids may be extracted from one plant.They can be purified from crude extracts by acid-base extraction and tend to have a bitter taste. Those containing a ring system are known as indole alkaloids (for example, terpenoids and steroids). Some are named after the biological species from which they are derived (morphine from the poppy plant Papaver somniferum, cocaine from erythroxolon coca, and so on). Other common examples include psilocin, caffeine, nicotine, vincristine, reserpine, atropine, quinidine, ephedrine,strychnine and quinine. Atropine is the tropane alkaloid isolated from the deadlynightshade plant Atropa belladonna, and strychnine is derived from the seeds of the Strychnos nux-vomica tree. Caffeine, cocaine, codeine (methylmorphine) and nicotine are water-soluble alkaloids. Morphine and yohimbine are highly water-soluble. Other alkaloids dissolve poorly in water yet readily in organic solvents such as chloroform or ether. The biological precursors of most alkaloids are amino acids, such as phenylalanine, tyrosine, tryptophan, histidine, and aspartic acid, among others. 1
How are they used?
The synthetic cathinones (usually mephedrone and methylone, or M-Cats) are most commonly used intranasally (insufflated) or ingested. “Bombing” is a method of ingestion whereby mephedrone powder is wrapped in cigarette paper and swallowed. Because sniffing the drug may cause nasal burns users will often resort to ‘bombing’. “Keying” is the practice of dipping a key into powder and then insufflating, with approximately five to eight “keys” per gram. Rectal administration, gingival delivery, inhalation, intramuscular and intravenous injection have also been described. Multiple concomitant routes of administration are reported. Self-reported doses range from a few milligrams to over 1 g of powder. A typical dose of mephedrone would be 100-200mg every 1-2 hours.
Users cannot be certain of the actual contents or indeed of the purity of the drug, therefore actual dosage and exposure is highly variable. For example, when MDAI (methylenedioxy-2-aminoindane) known as Sparkle (a granular, brownish powder) is snorted or bombed, it has an effect similar to ecstasy causing mood enhancement and hallucinations. Onset of action is usually within one hour and the effects are then almost immediate, perhaps a minute or so. The high lasts about six hours with a peak of two hours. It may cause hyperthermia, paranoid ideation and panic attacks.2
Cathinone is a naturally-occurring beta-ketone amphetamine analogue found in the leaves of the khat plant. Other synthetic cathinones such as methcathinone and MDVP (methylenedioxypyrovalerone) produce similar effects. Beta-ketone refers to the possession of a ketone group in the beta position of the aminoalkyl chain attached to the main molecular methylenedioxyphenyl ring.
Synthetic cannabinoids share some functional similarities with Δ9-tetrahydrocannabinol (THC), the active principle of cannabis. Like THC, they can have sedative, depressant and hallucinogenic effects. They have been detected in herbal smoking mixtures such as ‘Spice’ as well as resins that mimic cannabis resin.
Khat (Catha edulis)
Some knowledge of this plant is necessary in order to explain the background to many of the synthetic designer drugs. Khat is an evergreen shrub the leaves of which are chewed for their stimulant properties. An understanding of its chemical composition helps to explain the use of its constituents in the formation of designer drugs. Khat contains more than 40 alkaloids as well as many other compounds. The khat pheylalkylamines consist of cathinone, cathine and norephedrine: these alkaloids are structurally related to amphetamine and noradrenaline. Although similar to methylamphetamine, methcathinone (variously known as Cat, Kat, Qat, Ghat, and Chat) possesses a chemical structure resembling cathinone; its side effects and addictive properties are more potent.
The plant is chewed into a ball and kept in the cheek for a while. When khat leaves dry, cathinone (benzoylethanamine) decomposes within 48 hours leaving behind the milder chemical, cathine (a phenethylamine compound). Therefore, to maintain the potency of the drug, harvesters transport khat by packaging the leaves and stems in plastic bags or wrapping them in banana leaves to preserve moisture. It is common to sprinkle the plant with water or use refrigeration during transportation. Khat is therefore best used within 12-48 hours when the leaves are still moist.
Catha edulis is a flowering plant (one that produces seeds) native to the Horn of Africa (Eritrea, Djibouti, Ethiopia and Somalia) and the Arabian Peninsula. In these countries chewing the leaves and stalks is a social custom dating back thousands of years. It may take 7-8 years for the shrub to reach its full height (6-12 feet or more). Globally it is estimated that some 10 million males (usually) use khat on a daily basis.
Cathaedulis leaves containa beta-ketone amphetamine analogue. Ketones contain a carbonyl group (C=O) bonded to two other carbon atoms. Phenylalkylamines (derived from phenethylamine) are often termed “bk-amphetamines” for the beta-ketone moiety.
The principal active components in khat are cathinone and cathine. By chewing khat these substances are secreted into saliva. The effects are similar to amphetamine though less potent. Psychological dependence does occur in some though generally khat is not addictive. It is freely available in many countries and its production, sale and consumption are legal, including the Horn of Africa. In the Arab Peninsula it is known as Arabian tea and in South Africa it is referred to as Bushman’s tea.
Although its stimulant effect was originally attributed to cathine, extracts from fresh leaves of khat were shown to contain cathinone, isolated in 1975 and its properties recognized in 1978. Cathinone is not very stable and breaks down to produce cathine and norephedrine which belong to the phenylpropanolamine family, a subset of the phenethylamines and the catecholamines adrenaline and noradrenaline.
When the leaves are chewed the active ingredients are absorbed through the oral and gastric mucous membranes. The action of cathine and cathinone on the reuptake of adrenaline and noradrenaline results in the wakefulness associated with amphetamine derivatives. The effects of cathinone peak after 30 minutes, with nearly 98% of the substance metabolized by the liver into noradrenaline. Cathine has a half-life of about three hours in humans. Typically, an individual consumes 100–200 g of khat leaves (one bundle) in a session, and its effects last for several hours.
Symptoms are rather similar to the ingestion of strong coffee or amphetamines, for example, overtalkativeness and hyperactivity. The effects of oral cathinone occur more rapidly than those of amphetamine, 15 minutes compared to 30 minutes respectively. Khat causes constipation, dilated pupils (mydriasis), tachycardia and increased blood pressure, reflecting the sympathomimetic effects of the drug. Withdrawal symptoms, as would be expected, include mild depression and irritability, lethargy, rebound anxiety causing nightmares, tremulousness and loss of appetite. Long-term use may cause hepatic dysfunction, a permanent greenish tinge darkening of the teeth, and diminished libido. Rarely, dilated cardiomyopathy and myocardial infarction result from chronic use. 3
Mephedrone
Mephedrone (‘meow meow’) is a synthetic stimulant chemically related to cathinone, the psychoactive substance present in the khat plant. It is usually sold as a white crystalline or off-white-yellow powder (as a hydrochloride salt) for about £10 per gram. Consumption is usually oral or intranasal and rarely, by injection. Sellers avoid attracting the attention of regulatory bodies by labelling the substance “not for human consumption,” which means that no advice on safer use and dosing is provided.4
In one study the most commonly seen drug class were piperazines, followed by the cathinones, with significant variation in the content in one quarter of these compounds. The authors stated that it was relatively easy to purchase a number of legal highs from different Internet suppliers, though there times when not all of the products were available leading to the problem of users buying different active drugs to those they are used to, raising the prospect of potential toxicity to unknown agents.5A cross-sectional survey of 947 of mephedrone users found it to be the sixth most frequently used drug in the previous month after tobacco, alcohol, cannabis, cocaine and MDMA. Users typically were young males; 15% reported using weekly or more frequently; nearly 50% used between 0.5 and 1g during a typical session; intranasal use was the most common route of use (70%). Almost 55% of those who used cocaine reported that the ‘high’ obtained with mephedrone was better: intranasal use was also more likely addictive than oral use. Mephedrone appears to be the most widely abused synthetic cathinone in Europe, in contrast to the USA where MDVP and methylone are the most frequently abused. 6 7
Classification of mephedrone has had a limited effect on controlling its availability and use. Before the introduction of the legislation users generally obtained it via the internet. Now it is bought from street dealers, on average at double the price. Mephedrone was defined as a Class B drug under the Misuse of Drugs Act (1971) in the UK in April 2010. 4
Mephedrone produces similar effects to ecstasy, amphetamines and cocaine. It is detected in 20% of ecstasy tablets. It simulates the release of and inhibits the reuptake of monoamine neurotransmitters. The onset of psychoactive effects after insufflation is usually 10–20 minutes with an expected duration of effect of 1–2 hours; after oral ingestion onset is about 15–45 minutes with duration of 2–4 hours, and intravenous users report symptoms peaking at 10–15 minutes with a 30-minute duration of the desired effect.
Mephedrone users report that it has a better quality high than cocaine. It is speculated that mephedrone’s popularity reflects dissatisfaction with the purity and consistency of available cocaine and ecstasy. Concerns are also raised when it is considered that mephedrone is readily available from street dealers and may be taken by young people who have little previous experience of drug use.
Blood or plasma mephedrone concentrations are expected to be in a range of 50–100 μg/l in persons using the drug recreationally, >100 μg/l in intoxicated patients and >500 μg/l in victims of acute overdose.
Mephedroneinduces a greater increase in dopamine than serotonin release whereas MDMA (‘ecstasy’) induces a huge increase in serotonin with an insignificant rise in dopamine. Amphetamine results in a surge in dopamine release with an insignificant increase in serotonin. Mephedrone, amphetamine, and MDMA have decay values of 25, 50 and 300 minutes respectively. Therefore, the rapid rise and fall of dopamine levels could explain the addictive properties of mephedrone in some users. The effects are often described as somewhere between ecstasy and cocaine. As with cocaine, the ‘high’ generally lasts around an hour before wearing off. Furthermore, prolonged high –dose use of the substances can produce long-lasting neurotransmitter deficits in humans. 8 9
According to Mixmag (the online drug-use clubbing survey magazine for the UK) published in March 2012, 42% of clubbers had tried mephedrone the drug, and 34% had taken it in the last month. Some 30% of mephedrone users had reported using more ecstasy since the ban came into effect, while 19% reported using more cocaine. Blood or plasma mephedrone concentrations are expected to be in a range of 50–100 μg/l in persons using the drug recreationally, >100 μg/l in intoxicated patients and >500 μg/l in victims of acute overdose.
In 2011, Mixmag and the Guardian newspaper which draws on previous Mixmag surveys collected 15,500 responses from around the world, mostly the United Kingdom. In 2010/11, reported levels of use of mephedrone in the last year and last month were three times higher among clubbers (30 % and 13 %) than non-clubbers (10 % and 3 %).
Mephedronepredictably, causes increased alertness, restlessness, euphoria, excitement, the urge to talk, openness, time rushes, hot flushes, increased libido and elation. Hyperhidrosis, headache, palpitations, a Raynaud–type syndrome, and nausea are other relatively common unpleasant effects. Dizziness, hallucinations, panic attacks, and psychosis may occur. Other physical symptoms include dry mouth, blurred vision, and epistaxis. Symptoms of intoxication include agitation, aggression, violence, seizures and hyperthermia. Fatigue and insomnia are common residual effects. Mephedrone is generally used by nasal insufflation or ingestion of powder, liquid, capsule or tablets. The majority of users source mephedrone from street level dealers.10 Mephedrone induces strong feelings of craving in most users. If the unstable ecstasy market situation persists, the potential of mephedrone to substitute for MDMA might be substantial. Mephedrone, sold as ecstasy, is therefore more likely to be a cause for concern in the future.
Bath salts
This is the street name for substances which contain synthetic cathinone stimulants, such as methylenedioxypyrovalerone (MDPV) and mephedrone.11Bath salts components act synergistically at the dopamine transporter site and enhanced dopamine transmission may increase the potential for abuse. MDPV is consumed with other illicit drugs of abuse. It is the primary ingredient in "bath salts." Being a synthetic, cathinone-derivative it produces a high similar to cocaine or methamphetamine. It can be administered orally, by nasal insufflation, smoking, intravenously/intramuscularly, or per rectum, and intoxication lasts many hours.
MDPV may cause cardiac problems and disturbance of perception. During the withdrawal period after MDPV use, bone and muscle pain, and visual disturbances may occur. In the metabolism of MDPV, the most important catalyst is the CYP2C19 isoenzyme; the CYP1A2 and the CYP2D6 isoenzymes also play a role. The formed catechols are conjugated with either glucuronic acid or sulphate.
These compounds are not true bath salts in the traditional sense of household products. Cathinone is an amphetamine-like stimulant found naturally in the khat plant, described in more detail below. MDPV is much more potent than cocaine and its effect is longer lasting.12
Because of the sympathomimetic activity side effects are predictable and include cardiac arrhythmias, hypertension, arrhythmias, and hyperthermia. Chest pain, myocardial infarction, sweating, rhabdomyolysis, seizures, stroke, cerebral oedema, cardiorespiratory collapse, and rarely, death, have been reported. Psychiatric manifestations include hypersomnia, panic attacks, agitation, paranoia, suicidal ideation, self-mutilation, and aggressive behaviour.
The mode of action is thought to be the result of disruption and interference with central monoamine systems. In other words, synthetic cathinones increase extracellular monoamines by blocking transporter reuptake and increasing presynaptic neurotransmitter release. The dopamine (DA) transporter (DAT) and serotonin (5-HT) transporter (SERT) tightly regulate the amount of neurotransmitters within the synaptic cleft. Monoamine release also may be driven by presynaptic input from cholinergic or glutaminergic systems.127
Psychoactive bath salts are sold as tablets, capsules, or powder and purchased in places such as tobacco and convenience stores, gas stations, head shops, and the Internet. Bath salts may mimic cocaine, lysergic acid diethylamide (LSD), methamphetamine, or MDMA. The most common bath salts are the cathinone derivatives MDPV, mephedrone and methylone. The drugs have the potential for addiction because they cause intense stimulation, euphoria, elevated mood, and a pleasurable "rush". 13 14
In the United Kingdom (UK) to avoid being controlled by the Medicines Act, legal highs are sometimes described as bath salts, fertilizer (plant food), or incense, even though they have never been used for these purposes. In other words, legal highs are not covered by current drugs laws yet are used by individuals in the same way as illegal drugs such as cocaine or cannabis. The easy availability of legal highs marketed as "bath salts", ‘incense’ and ‘plant foods’, with the added proviso that they are not to be consumed by humans allows the drugs to circumvent current legislation. When legislation is changed the molecular structure is easily altered to produce a new legal high.
Synthetic cannabinoids
Marketed as ‘incense’ and labeled “not for human consumption”, these drugs were increasingly popular with students and young adults being initially legal and easily available from stores, online, head shops (outlets selling drug paraphernalia/counterculture magazines) and petrol stations. The structure of synthetic cannabinoids does not resemble that of tetrahydrocannabinol (THC] contained in marijuana or hashish, yet the drugs affect individuals in the same manner and are much more potent. Synthetic cannabinoids are sold under countless names such as ‘Mr Nice Guy,’ ‘Spice’, ‘Sabbaba’ and ‘Lemon Grass’, to name a few. Spice is a designer drug derived from herbs sprayed with synthetic chemicals which mimic the effects of cannabis. The ingredients are thus similar to but not identical to THC. Synthetic cannabis can precipitate psychosis, especially in individuals with a previous history and a chronic psychotic disorder may persist in some vulnerable patients.
A great variety of synthetic cannabinoids, most often cannabicyclohexanol, are used in an attempt to avoid prosecution. Some are sold in 'herbal' smoking mixtures and the latter have been found on occasion not to contain any synthetic cannabinoids at all. Cannabicyclohexanol is a cannabinoid receptor agonist drug. It has been sold under various brands such as Black Mamba, Bombay Blue, Fake Weed, Genie, Bliss, Blaze, Yucatan Fire. Spice products sometimes sold as “incense,” more closely resemble potpourri. Although Spice is usually smoked, sometimes individuals mix it with cannabis or prepare a herbal infusion for drinking.
To create the herbal products, synthetic cannabimimetics are dissolved in an organic solvent (e.g. acetone) and the resulting solution is sprayed on plant material. The doped plant material is then dried and smoked in a similar fashion to actual cannabis. Spice products typically have a pleasurable smell and taste. They are often referred to as herbal or legal highs because of their legal status and ‘natural’ herbal make-up. They are distributed in the form of dried leaves or resin, and powder, and are sold without age restriction in metal-foil sachets, usually containing 3 g of vegetable matter, to which one or more of the synthetic cannabinoids have been added. Spice is typically smoked, using a pipe or by rolling in a cigarette paper, and can also be ingested as an infusion, or inhaled.1516
Drugs of the 2C family (phenethylamines containing methoxy groups attached to a benzene ring) have hallucinogenic and stimulant effects. The term ‘2C’' refers to the 2 carbon atoms between the benzene ring and the amino group in these compounds. The effects are a cross between MDMA and LSD. They are relatively new to the market and not widely available in the UK. An excited delirium presentation seems to be consistent in deaths attributed to 2C drugs and at least five deaths have been reported in the literature in patients intoxicated with 2C drugs. One agent known as 2C-1 or Smiles, which first appeared in 2003,has more potent effects than MDMA and LSD. Users report an intense energy with vivid visual and auditory hallucinations lasting hours to days.. Patients may exhibit symptoms consistent with serotonin toxicity. Doctors need to be vigilant as synthetic drugs do not show up on routine testing. Treatment of 2C intoxication is primarily supportive.17
Despite widespread Internet availability, many of these drugs remain unfamiliar to doctors and yet ‘bath salts’, have resulted in nationwide emergency department visits for severe agitation, sympathomimetic toxicity, and death. As with other illicit substances designer drugs may compromise cardiac function causing hypertension and tachycardia and users who inject run the well-known risks of contracting hepatitis C or HIV, thrombophlebitis and embolus formation.
Methoxetamine
Methoxetamine (also known as ‘mexxy’) is available on the Internet and marketed as ‘legal ketamine.’ It is an arylcyclohexylamine chemically related to ketamine and PCP (phencyclidine). Methoxetamine is longer acting and more potent than ketamine. The drug, a white powder, is usually taken sublingually, snorted, ‘bombed’, or injected intramuscularly. Doses are typically between 5mg-90mg orally. After snorting the drug it may take 30-90 minutes for its effects to become apparent. When injected the onset of action is usually within five to ten minutes. The overall duration of effect is within the range of 1–3 hours, sometimes longer. The drug induces feelings of detachment (dissociative state), paranoid symptoms, visual hallucinations, restlessness and increased energy in some. Other reported symptoms include confusion, catatonia, depression, tachycardia and hypertension. Methoxetamine is now a Class B drug under the Misuse of Drugs Act.18 19
Piperazine derivatives
The piperazine derivatives, a class of amphetamine-like compounds that includes BZP (benzylpiperazine) and TFMPP (trifluoromethylphenylpiperazine) are making a comeback as "legal ecstasy." Often perceived as safe by the public, adverse effects may range from minimal to life-threatening. Co-ingestion of BZP and TFMPP causes increased action of dopamine and serotonin, similar to MDMA. Severe symptoms include seizures, hyperthermia, hyponatremia, dystonic reactions, rhabdomyolysis, renal failure, metabolic acidosis, DIC, and respiratory failure. 20 Over the last few years piperazine derivatives are being sold as ecstasy pills, or under the names of “Frenzy”, “Bliss”, “Charge”, “Herbal ecstasy”, “A2”, “Legal X” and “Legal E”. Although piperazine designer drugs enjoy a market reputation of being safe, they may cause distorted perceptions after ingestion. There are several reports of toxic symptoms experienced by users after drug intake.The piperazinic compounds are derived from piperazine, a cyclic molecule containing two opposite nitrogen atoms and four carbon atoms distributed between the two and were originally used as anti-helminthic agents in the 1950s. Designer drugs of this class can be divided into the benzylpiperazines such as benzylpiperazine (BZP) and its methylenedioxy analogue methylenedioxybenzylpiperazine (MDBP), and phenylpiperazines such as chlorophenylpiperazine (CPP), trifluoromethylphenylpiperazine (TFMPP), and methoxyphenylpiperazine (MeOPP). A third group includes the thienylmethylpiperazines. Chlorophenylpiperazine is an active metabolite of drugs such as trazodone, and nefazodone used as antidepressants. A survey in the UK found that piperazines are among the most common active drugs in tablets purchased from internet supplier sites.Piperazine-derived compounds are therefore emerging designer drugs, whose abuse has increased remarkably worldwide.21
Naphyrone
Naphyrone(naphthylpyrovalerone) or NRG-1 (or Energy1) is a cathinone derivative available to buy on a number of websites and is gaining popularity. It is sold as an alternative to mephedrone. Belonging to the designer drugs class, it is similar in structure to pyrovalerone, a monoamine uptake inhibitor and as it is somewhat similar to other cathinone derivatives it has the potential to produce anxiety, paranoia, and cardiovascular side effects. Two products, both sold as NRG-2 from different internet suppliers, were found to contain the banned substituted cathinones - 4-methylethcathinone (4-MEC) and 4-methylmethcathinone (4-MMC), the latter being present in much smaller quantities. Although sold as research chemicals and labelled 'not for human consumption', they are essentially legal highs and are available online. 22 23
Table 2: Some commonly used psychoactive substances
Drug
Mode of Action
How used
MDMA (‘ecstasy’) ‘Molly’ is the pure crystalline powder form
Releases and inhibits reuptake of dopamine, serotonin and noradrenaline
Tablet or capsules
Sometimes one or more tablets taken at one time (‘bumping’)
Salvia divinorum
Partial dopamine receptor agonist; also works on kappa receptors
Smoked, inhaled, ingested, used sublingually
Mephedrone
Effects similar to MDMA, cocaine and amphetamines
Nasal insufflation, ingestion
MDVP (see text)
Related to cathinone. Effects similar to ‘ecstasy’
Nasal insufflation, inhalation, ingestion
Spice
Similar to THC
Smoked; sometimes prepared as a herbal infusion for drinking
Naphyrone
Effects similar to mephedrone
Usually snorted, sometimes swallowed in paper wraps (‘bombing’)
Discussion
New designer drugs have increased in popularity over the past several years because of their euphoric effects. Understanding the pharmacology and toxicology of these agents is essential in order to provide the best medical care for patients. They are all potentially dangerous. For example, an excited delirium presentation seems to be consistent amongst deaths attributed to 2C drugs.
From the above description it can be seen that synthetic drugs fall into three broad categories: synthetic cathinones (bath salts), synthetic cannabinoids (spice or incense), and amphetamine-like drugs (methamphetamine, ephedrine, MDMA). Cathinones being related to the amphetamine family will cause dilated pupils, hypertension, hyperventilation, paranoia, agitation, hyperthermia, tremors and seizures. Many countries have made certain cathinones illegal, for example, mephedrone, methylone and MDPV. Indeed, the robust stimulation of dopamine transmission by MDPV predicts serious potential for abuse and may provide a mechanism to explain the adverse effects observed in humans taking high doses of 'bath salts' preparations. Furthermore, pyrovalerone is much more potent than cocaine at inhibiting the uptake of dopamine and norepinephrine.
Methcathinone was previously used in Russia as an antidepressant, also known as “Cat” and “Jeff” when used recreationally. Nowadays the drugs are sold as bath salts, plant food, insecticides, chicken feed additives, or research chemicals with names such as like NRG (Energy) and meow, meow. Bath salts are water-soluble, usually inorganic, solid products designed to be added to water during bathing. Numerous nicknames are used to describe them including Ivory Wave, Purple Wave, Red Dove, Zoom, Bloom, Cloud Nine, Ocean Snow, Lunar Wave, Vanilla Sky, White Lightning, and Hurricane Charlie.
Although ‘legal highs’ are commonly referred to as bath salts they are not Epsom salts (magnesium sulphate) or other water softeners within the usual meaning. In many cases the chemical ingredients are changed without the consumer knowing, making risks unpredictable. Some legal highs contain active ingredients controlled under the Misuse of Drugs Act 1971 (UK). Therefore any individual found in possession of these products would be liable to prosecution and the associated penalties, even if unaware that he/she has purchased a controlled drug. However, claiming a product to be "not intended for human consumption" can potentially circumvent the entire legal process. Drug designers are already showing skilful exploitation of the law and remain far ahead of criminalization efforts. Furthermore, the irony of prohibition is that the supply and slump in the market for cocaine and ecstasy in 2009 led to individuals resorting to untried and untested substances that are now easily available online. 2425
Synthetic cathinones are mostly excreted via the urine and can be measured via gas or liquid chromatography-mass spectrometry in the blood, urine and stomach contents. They can also be analysed in hair. Unlike traditional cosmetic bath salts, which are packaged and sold for adding to bath water for soaking and cleaning, synthetic designer drugs sold as "bath salts" have no legitimate use for bathing and are intended for abuse. Baths salts contain one or more synthetic derivatives of the naturally-occurring stimulant cathinone. Low doses produce euphoria and increase alertness, but high doses or chronic use may cause serious adverse effects.26
Treatment
Treatment should be tailored to the specific drug of abuse. Medical and psychological needs require examining. Generally, treatment uses a combination of counselling and medication to reduce the need or desire (craving) for the drug and give the person the skills to refrain from future drug use. Other treatments might include cognitive behavioural therapy, detox, and relapse prevention techniques.
Supportive care is the mainstay of treatment for untoward serious side effects. Sedation with benzodiazepines is indicated for agitation, seizures, tachycardia, and hypertension. Extreme hypertension that persists despite benzodiazepines may be treated with vasodilators. Beta blockers should be avoided due to the potential to cause unopposed alpha-adrenergic stimulation, worsening the hypertension. Significant hyperthermia may require passive or active cooling. All moderately to severe symptomatic patients should have an electrocardiogram (ECG), be placed on a cardiac monitor, and receive serial temperature checks. Electrolytes, liver function tests, cardiac enzymes creatine, and toxicology should be carried out. Asymptomatic patients with no other suspected ingested drugs or psychiatric symptoms generally may be discharged.
Prevention
Banning legal highs is probably futile because it is impossible to keep up with newer drugs because they are synthesized as soon as the ‘illegal’ drug becomes banned. Some would argue that arresting users creates more harm for individuals, their families and society, as they are then caught up in the criminal system. Others may argue that ‘legal highs’ are not generally harmful and not as dangerous as opiates or their derivatives, or indeed alcohol. It might be more worthwhile making legal highs ‘uncool’, much in the same way that cigarette consumption is now frowned upon. However, it would require a great deal of public money to subsidise such an advertising venture.
Users of legal highs need to be made aware that such drugs purchased on-line may contain illegal substances and therefore may render them subject to prosecution if found in possession. 27
Pre-school family based programmes, and programmes involving the school and community, motivational interviewing for adolescents, and individual programmes, may be beneficial in reducing drug use and other harmful outcomes. Importantly, none of these approaches focus exclusively on particular substances or groups of substances, and although there have been relatively few investigations of intervention processes they most likely work by targeting a number of important precursors of drug use behaviour.28
Preventing designer drug abuse begins with understanding the warning signs of addiction which in many respects are similar to alcohol or more common street drugs.
Club drugs are now widely available and their harmful effects are increasingly becoming more evident. Their effects are unpredictable as they are often ‘contaminated’ with other harmful substances. It is unlikely that legislation will have a meaningful impact. Increasing public awareness about these drugs is paramount, and medical and nursing staff should consider intoxication in those patients who present with agitation and psychosis who have no previous history of mental health problems.
Pharmacists are in a pivotal position to observe changes in patterns of drug use and report worrying trends to health care practitioners. Counselling for young people especially and prevention programmes based in schools could prove useful in pointing out the dangers of these drugs to teenagers. Health care professional too should endeavour to keep up with recent information on these substances by attending hospital-based lectures or conferences as part of continuing professional education.
Urine drug testing will generally be unhelpful as many club drugs are undetectable on standard urine drug screens.29 Mental health staff should enquire about club drugs as part of routine drug and alcohol assessment and be aware that these patients may not fit the stereotype of a drug misuser.
The discharge summary is an integral part of continuing patient care. Apart from containing vital information regarding current admission, it also conveys key findings and plans to clinicians who will be taking over the care of the patient. This would mean communicating important information about patients to ensure appropriate and safe follow-up management. Studies involving discharge summaries have looked into role of communication from secondary to primary care and have highlighted the importance of accuracy and quality of information,1 errors2 and general practitioner (GP) preference.3 Systematic reviews have found low availability (12-34%) of discharge summary during first visit post-discharge as well as wide variations in content of discharge summaries thereby directly affecting patient management.4,5 The timing of discharge summary completion and reaching the follow-up physician is therefore of prime importance wherein this has been also found to influence and reduce the risk of rehospitalisation.6 The content necessary for a ‘good’ or ‘high-quality’ discharge summary has been studied via surveys. The inclusion of important data such as diagnosis, discharge drugs, complications, laboratory results and follow-up plans have been considered to be important clinical information by hospital physicians and GPs.7
Hospital discharge summaries can be hand-written, dictated or in electronic format. These formats have their benefits and downfalls. Hand-written summaries have been found to be well-accepted by primary care physicians although involve the factor of legibility.8 A randomised-controlled trial found no difference between electronic and dictated discharge summaries for primary care physician satisfaction.9 Although the use of electronic discharge summaries has significantly improved both the content and timing of discharge summaries reaching follow-up physician or healthcare staff,10 they have been found to contain higher number of errors in patient progress, additional diagnosis and free-text components.11
This audit examined the timing and content of discharge summaries at The Mount and whether they met local Trust standards. A follow-on audit was conducted to study the impact of recommendations that had been put forward at the end of Cycle 1 of the audit.
Aim and Objectives
Aim
Cycle 1: To study the content, accuracy and timing of discharge summaries at The Mount, Old Age Psychiatry hospital.
Cycle 2: To examine changes in clinical practice following recommendations from Cycle 1 of audit involving content and timing of discharge summaries from The Mount.
Objectives
Cycle 1: To ascertain whether Trust guidelines regarding content of discharge summaries are met and also whether the timeline guidance is being maintained.
Cycle 2: To examine adherence to the Trust guidelines as well as to study the changes brought about by recommendations at the end of Cycle 1.
Criteria/ Standards
Trust guidelines state:
Discharge summaries must be typed and sent in 5 working days post-discharge from hospital.
They must include the following information (Box 1):
Box 1 Trust guidelines for inclusion of information in discharge summaries
Patient ID
Date dictated
Patient Name
Date of Birth
Name of consultant
Admission address
Discharge address
Admission date
Discharge date
Reasons for admission
History of present illness
Past medical history
Past psychiatric history
Family history
Social history
Occupational history
Premorbid history
Mental health examination
Physical examination
Results of investigations
Progress & treatment during admission
Final diagnosis
Discharge medications
Follow-up arrangements
Name of key worker
Number of pages
Method
Audit Sample
Patients admitted and discharged from Ward 3 & 4 of The Mount, between 01.04.2011 to 31.10.2011. A total of 103 patient discharge summaries were therefore analysed in Cycle 1 of the study. For cycle 2, the audit sample comprised of patients admitted and discharged from Ward 3 & 4 of The Mount, between 01.04.2012 to 31.10.2012. A total of 97 patient discharge summaries were therefore analysed in this part of the study.
Data Collection
Data was collected using an anonymous data collection tool (Appendix 1) which was designed according to Trust guidelines. Administrative staff provided the clinical audit leads with list of patients discharged during the study dates. The electronic patient record system of the Trust (PARIS: Patient Record Information System) was used to study the discharge summary letters. Data collection was performed under the supervision of consultant responsible for the audit, between November 2011 and January 2012 for cycle 1 and for cycle 2 data collection was performed between October 2013 and November 2013. Patient confidentiality and anonymity was maintained.
Data Analysis
Qualitative data was gathered, coded and collated on to a Microsoft Excel spread sheet. The data collected was reviewed by the authors to ensure each aspect of data collection tool was filled. The data was analysed by the Clinical Audits Facilitator at the Trust Clinical Audit Support Team and placed into a report format for dissemination.
Results
The number of discharge summaries analysed in Cycle 1 and 2 of this study was 103 and 97 respectively.
Data were collected using the data collection tool (appendix 1). Dates of discharge, dictation and typing were recorded. Date of typing was used as a proxy of date sent to GP since there was no record of this. Seven days were permitted for discharges to be sent (equivalent to 5 working days). Discharge summaries were read and it was recorded if each stipulated heading from the Trust guidelines was present. No comment was made on quality of information; only consideration was whether information was present or absent.
Compliance with each point from the above categories is shown in the following series of tables and comparison is made between the studies in Cycles 1 and 2 (Table 1-4). The statistical significance of the differences found in the two audit cycles was evaluated using chi-square tests.
Table 1 Presence of information on discharge summary according to Trust guidelines
Criteria
Adherence % 2011 (n=103)
Adherence % 2013 (n=97)
Statistical significance
Patient code
100% (n=103)
97% (n=94)
p=0.721
Date dictated
72% (n=74)
98% (n=95)
p<0.001
Patient Name
100% (n=103)
100% (n=97)
No change
Date of birth
97% (n=100)
100% (n=97)
p=0.090
Name of consultant
98% (n=101)
99% (n=96)
p=0.596
Name of current GP
98% (n=101)
98% (n=95)
No change
Admission address
98% (n=101)
100% (n=97)
p=0.167
Discharge address
98% (n=101)
100% (n=97)
p=0.167
Admission date
97% (n=100)
100% (n=97)
p=0.090
Discharge date
97% (n=100)
99% (n=96)
p=0.342
Legal status
99% (n=102)
98% (n=95)
p=0.525
Reasons for admission
98% (n=101)
98% (n=95)
No change
History of present illness
100% (n=103)
99% (n=96)
p=0.301
Past medical history
89% (n=92)
95% (n=92)
p=0.150
Past psychiatric history
95% (n=98)
98% (n=95)
p=0.282
Family history
19% (n=20)
86% (n=83)
p<0.001
Social history
56% (n=58)
89% (n=86)
p<0.001
Occupational history
67% (n=69)
68% (n=66)
p=0.873
Premorbid history
37% (n=38)
52% (n=50)
p=0.036
Mental health examination
95% (n=98)
93% (n=90)
p=0.482
Physical examination
86% (n=89)
92% (n=89)
p=0.227
Results of investigations
84% (n=87)
78% (n=76)
p=0.265
Progress & treatment during admission
96% (n=99)
100% (n=97)
p=0.049
Final diagnosis
92% (n=95)
97% (n=94)
p=0.147
Discharge medications
98% (n=101)
97% (n=94)
p=0.602
Follow-up arrangements
86% (n=89)
79% (n=77)
p=0.007
Name of key worker
64% (n=66)
56% (n=54)
p=0.225
Number of pages
0% (n=0)
0% (n=0)
No change
Are there any spelling/typing errors in the list of medications?
90% (n=8)
98% (n=2)
p=0.064
Are there any spelling/typing errors in the diagnosis and medical terminology?
78% (n=21)
99% (n=1)
p<0.001
Table 1: The presence of information mentioned in the Trust guidelines is analysed. The percentage adherence in cycle 1 is compared with findings from cycle 2. Significant increase in inclusion of family history, social history, follow-up arrangements and date of dictation is observed. A healthy increase is also observed in inclusion of premorbid history and progression and treatment during admission. A significant reduction in spelling/typing errors is also seen. The decrease in inclusion of name of key worker, discharge medications, mental health examination and results of investigation amongst others is also noted. GP, general practitioner.
The comparison of findings from Cycle 1 and 2 establish a significant increase in adherence to family history (p<0.001), social history (p<0.001), premorbid history (p=0.036) as well as progress and treatment during hospital stay (p=0.049) components of the discharge summary. There was also a significant increase in inclusion of date of dictation of discharge summaries (p<0.001). Increase in adherence to most of the components of discharge summaries was observed. However, there was significant decrease in inclusion of follow-up arrangements (p=0.007) as well as a decrease in inclusion of name of key-worker assigned to patient (from 64% in cycle 1 to 56% in cycle 2; p=0.0225). A significant decrease in spelling/typing errors in diagnosis or medical jargon was observed (p<0.001).
Timing of Discharge Summaries
Table 2 Time taken between discharge of patient and dictation of letter
Days
Adherence % 2011 (n=74)
Adherence % 2013 (n=94)
Statistical significance
0-7
30% (n=22)
73% (n=69)
p<0.001
8-15
24% (n=18)
22% (n=21)
p=0.762
16-22
18% (n=13)
4% (n=4)
p=0.004
23+
29% (n=21)
0% (n=0)
p<0.001
Table 2: The time taken between discharge of patient and dictation of letter is analysed. A significant increase is observed in the dictation of letter as per Trust guidelines (within 5 working days).
Table 3 Time taken between dictation and typing of discharge letter
Days
Adherence % 2011(n=75)
Adherence % 2013 (n=94)
Statistical significance
0-5
84% (n=63)
73% (n=69)
p<0.001
6-11
7% (n=5)
24% (n=23)
p=0.192
12+
9% (n=7)
2% (n=2)
p<0.001
Table 3: The time taken between dictation of letter and typing of discharge letter is analysed. A significant decrease is observed in the time taken for typing of letter within 5 days of dictation of letter.
Table 4 Time take between discharge and typing of discharge letter
Days
Adherence % 2011 (n=100)
Adherence % 2013 (n=96)
Statistical significance
0-7
18% (n=18)
52% (n=50)
p<0.001
8-15
32% (n=32)
34% (n=33)
p=0.724
16+
60% (n=60)
14% (n=13)
p<0.001
Table 4: The time taken between discharge of patient and typing of discharge letter is analysed. A significant increase is observed in the early typing of discharge letter from the date of discharge of patient.
The number of discharge summaries being dictated and typed within 7 days of discharge was significantly increased (p<0.001) and a significant decrease in discharge letters being dictated more than 2 weeks (p=0.004) or 3 weeks (p<0.001) of patient being discharged was observed. The time taken between dictation of letter and it being typed up was also found to have dropped, with 73% being done within 7 days, significant decrease (p<0.001) being observed since the first cycle. Furthermore, a significant increase is observed in early (less than 7 days) typing of discharge letter since patient being discharged (p<0.001).
Discussion:
The discharge summary is a very important means to communicate medical (both physical and psychiatric) and nursing interventions to the GP or community mental health team. This in turn helps in making invaluable decisions to patient care in the community. Hence, it is worth spending time on doing a good discharge letter which includes relevant information. A timely discharge letter can also be very useful in this regard.
At the end of Cycle 1 of the audit, recommendations that were made included (Appendix 2):
Disseminating information amongst all junior doctors, consultants and administrative staff on each ward to include the above mentioned headings in accordance with Trust guidelines.
Information was also provided regarding finding out Name of Keyworker in PARIS system.
A specific note was also placed regarding to spell out medical terminologies that would assist in the typing of discharge summaries by administrative staff.
From the results, it is evident that the content of the discharge summary has largely been maintained. In other words, good practice was maintained and recommendations from previous audit were implemented in most spheres of discharge letters. However, despite the recommendation of finding out name of key-worker from PARIS system, there was a decrease (from 64% in first cycle to 56% in second cycle) in its inclusion (p=0.225). Thus, training in usage of information technology system is essential. Providing appropriate instruction and training to junior doctors has been found to be useful in improving the quality of discharge summaries.12 Therefore, it might be beneficial to include instructions or guidelines for appropriate discharge summaries at local Trust or departmental inductions. This will help junior doctors in ensuring completion of accurate and succinct discharge summaries that will aid in patient management.
There was a reduction in documentation of discharge medication, follow up arrangement, mental state examination and physical health investigation carried out as an in-patient. This certainly needs improving as these are the relevant areas to facilitate smooth transition of care in the community and follow-up arrangement. With regard to the timing of the discharge summary, this was found to have significantly improved from the previous audit cycle. For example, the timing between discharge and dictation (within 7 days) has increased from 30% to 73% and almost all discharge summaries are dictated no later than 3 weeks. The possible reasons for delays in dictation could be ongoing workload, availability of medical staff and of the medical notes, as these are sometimes requested by the Intermediate Community Service (ICS) team. There was a slight drop in the time between dictation and typing (from 84% to 73%), which could possibly due to availability of administrative staff, dictation tapes or medical notes and proof reading by medical staff. Significant increase was observed in inclusion of date of dictation of discharge summaries which will be a useful component for future audits. A significant decrease in spelling/typing errors in diagnosis or medical terminologies was observed. Furthermore, there was significant increase in inclusion of family history, social history, premorbid history as well as information on progress and treatment during hospital in the discharge summary. Therefore, timely audit and feedback can be very useful in improvement of discharge summaries and patient care.
Recommendations & Actions:
Raise awareness amongst senior house officers (SHO’s) and other doctors in the Trust regarding recording of pre-morbid history, occupational history, name of keyworker as this was only done in 52%, 62%, 56% cases respectively. This could be done by disseminating findings from this audit amongst SHO’s and other doctors of Trust through hand-outs to wards as well as through local teaching session.
Remove number of pages from the list of sub-headings needed in discharge summary as this is dependent on typing and not necessarily possible to estimate while dictating discharge summary. However, it is an important part of discharge summary. Therefore, send information with audit findings to medical secretaries informing the need to keep number of pages in the discharge summary.
Consider adding a section on documentation of risk assessment should be included in the discharge summary as well as ‘early relapse signature’ which would enable early intervention in the community to avoid inpatient admission. This could be included in the discharge summary. This would involve liaising with consultants and the responsible person for making/printing discharge summaries for Trust.
Sertraline is selective serotonin reuptake inhibitor (SSRI). It is a commonly prescribed antidepressant. The common side effects of SSRI’s are nausea, vomiting, diarrhoea, dyspepsia, anorexia and weight loss.
To our knowledge this is the only second reported case of sertraline-induced hyperpigmentation. It is interesting to note that in some cases sertraline has been used as replacement medication following antidepressant induced hyperpigmentation. So it is important that both clinicians and patients are aware of this potential rare side effect of sertraline.
Case Report:
In this case report we present a 27 years old Caucasian lady that developed hyper pigmentation, after starting sertraline.
The patient, a 27 years old lady was diagnosed with Bipolar Affective Disorder (ICD-10)2 years ago. She was prescribed sertraline 50mg for low mood. Her current medications also include semi sodium valproate 1000 mg orally daily, quetiapine modified release 400 mg orally daily, tramadol 50mg orally twice a day and co-codomol orally on an as required basis for back pain. She was not prescribed any depot medications. To our knowledge she was compliant with her medication.
She responded well but reported that she had developed hyperpigmentation after four weeks. This persisted after suffering a recurrence of low mood and being seen in clinic 5 months later.
There is no significant past medical or family history. She has been on various psychotropic medications in the past including fluoxetine, venlafaxine, olanzapine and procyclidine.
Physical examination revealed focal hyperpigmentation limited to the upper lip. It was dark brown in color with sharply defined outline and was not associated with itching, redness, rash or excoriation. It was gradually getting darker in color and she had to wear a lot of make up to conceal it. The patient was referred to a consultant dermatologist for an opinion but unfortunately she did not attend her appointment. This has been acknowledged as a limitation of our case report. Routine blood tests were within the normal range. She also reported some weight gain with sertraline.
She did not report any previous history of dermatological disorders or any endocrine conditions and Addison's disease was excluded. She did not begin any new medication or vaccines prior to onset of the hyperpigmentation and denied ever having chlorpromazine, tricyclics, tetracyclines, amiodarone, hormone replacement therapy, aspirin, chemotherapy or minocycline. However three years ago, she had taken anti malarial medication before going to the Dominican Republic. She also denied any intake of herbal medication, non-prescribed medication or illicit drugs.
She also denied excessive exposure to sunlight during the time of development of hyperpigmentation and she was not pregnant. There is no history of heavy metal exposure.
The probability of adverse drug reaction assessed by using Naranjo Scale indicated a probable association between the use of sertraline and hyperpigmentation. Subsequently her sertraline was stopped and replaced by duloxetine 30mg daily. Unfortunately the hyperpigmentation persisted after three off sertraline but is no longer worsening.
Discussion:
Bipolar Affective Disorder also known as bipolar disorder, manic-depressive disorder, or manic depression is characterised by two or more episodes in which patients mood and functionality is significantly disturbed, this disturbance on some occasions includes episodes of mania or hypomania with elevated mood and increased energy levels and on others episodes of depression with low mood, tiredness and diminished pleasure in activities. Recovery is usually complete between these episodes. 1
The pharmacological treatment of bipolar affective disorder depends on nature and degree of presenting episode and includes mood stabilisers like lithium, valproate, carbamazepine and lamotrigine, anti psychotics like olanzapine, quetiapine, aripiprazole and risperidone and antidepressants like sertraline, citalopram and venlafaxine.
Sertraline, citalopram, escitalopram, fluoxetine, fluvoxamine and paroxetine selectively inhibits reuptake of serotonin, hence named selective serotonin reuptake inhibitor (SSRI).
In our case the patient was on semi sodium valproate and modified release quetiapine and was later prescribed sertraline to help with low mood.
A literature review of English language using PubMed database was done on 15th June 2013. The terms searched were “sertraline”, “serotonin reuptake inhibitor”, “SSRI”, “anti depressants”, “hyperpigmentation”, “pigmentation”, and it found case reports of antidepressant associated hyperpigmentation with citalopram2, mirtazapine3 and imipramine.4, 5,6,7 It is interesting to note that in some of the case reports the antidepressants were replaced by sertraline after development of hyperpigmentation, but there was no record as to whether the lesion resolved.2, 3,4
Only one previous case of sertraline-induced hyperpigmentation was found8,which also unfortunately persisted after discontinuation of the antidepressant.
As hyperpigmentation has also been reported with other SSRIs, clinicians should be more aware that hyperpigmentation might be related to the class effect, rather than the individual drugs.
Though the exact biological mechanism for the development of hyperpigmentation is not clear and further research is needed, the secretion of melanocyte stimulating hormone (a-MSH) is closely associated with skin pigmentation, and serotonin and dopamine transmitters appear to be involved which may point to a possible mechanism for the hyperpigmentation.
Binge Eating Disorder (BED) was first defined by Stunkard in 19591; he identified peculiar food intake features characterized by a loss of control in a subgroup of obese patients. Various efforts have been made, ever since, to provide a non-sociological approach to individuals with such a behaviour disorder, which has long been considered a variant of Bulimia Nervosa.
Unlike patients affected by Bulimia Nervosa, patients with BED appear to be overweight and mainly obese. Thus, the treatment aims not only at reducing BED and its related psychopathology, but also at assessing the weight gain experienced by these patients to prevent a further worsening of physical health.
Walsh & Devlin2 evaluated the use of medication in the treatment of Bulimia Nervosa and BED, underlining the efficacy of antidepressant medication in the treatment of Bulimia Nervosa. The antidepressant efficacy led to consider its use in BED more accurately.
Williamson, Martin & Stewart3 stated that pharmacotherapy was not an effective treatment for Anorexia Nervosa. However, it did prove to be successful in Bulimia Nervosa and BED, although subjects affected with eating disorders apparently respond better to psychotherapy approaches.
Systematic investigations have been conducted on the aetiology of BED. Biological and genetic factors, neurotransmitters and hormones have been involved in the onset of binge eating and play an important role in the regulation of hunger and mood.4, 5 However, a definitive aetiological theory has not been developed and tested.3
BED is characterized by a relevant psychological component that in many cases is under-evaluated. Patients with BED have difficulty in interpreting the visceral sensations of hunger and satiety; they take large amounts of food even during regular meals and, moreover, their food contains more fat than protein.6, 7
In fact, Axis I and II disorders (DSM IV-TR) share common features with binge eating.8 Axis I psychiatric disorders (including depression, anxiety, body dysmorphic disorder, or chemical addiction) characterize many BED patients, and research has evidenced the presence of panic, loss of control, impulsivity, compulsive behavior, obsessive thoughts about food and social phobia.9 Axis II personality disorders (especially borderline personality disorder) are frequently related to patients suffering from eating disorder and comorbidity with Avoidant Personality Disorder and Obsessive-Compulsive Disorder was observed.10
BED is not associated with a restrained eating control, but probably with an increase of uncontrolled eating and emotional eating.11, 12
Pharmacological agents, compared to placebo, have been used in the treatment of BED. Appolinario, Bacaltuchuk, Sichieri et al13 evaluated the efficacy of Sibutramine to reduce the frequency of binge eating, while McElroy, Arnold, Shapira et al14 focused on Topiramate and evidenced a greater reduction in binge eating frequency but with side effects such as paraesthesia.
Other studies showed the efficacy of Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Noradrenaline Reuptake Inhibitors (SNRIs) in the treatment of obesity associated with BED15, 16, 17, 18 showing that SSRIs and Tricyclic Antidepressants (TCAs) reduced the frequency of BED compared to placebo.19 To determine which patients are most likely to benefit from medications, and how to sequence the various therapeutic interventions available better, are questions still open to debate.
Moreover, results in many cases appear to be divergent. Ciao, Latner and Durso20 underlined the influences of other factors that may influence treatment efficacy. They observed that many obese individuals who might benefit from weight loss treatment nevertheless do not plan or desire to seek treatment and perceive multiple barriers to treatments.
Pharmacotherapy may enhance weight loss,19 although other results suggest that pharmacotherapy may be associated with a reduction in binge frequency in obese patients with BED, but it does not lead necessarily to weight reduction.21 These medical treatments seem to be effective in reducing binge frequency over the short-term, and the subsequent discontinuation of the medication seems to be associated with a relapse of binge eating. Thus further studies of the role of pharmacotherapy in the treatment of BED need to be carried on.22
According to Williamson, Martin and Stewart3 the additive effects of psychotherapy, e.g. Cognitive Behavioural Therapy (CBT), and pharmacotherapy have to be investigated. At present it seems that adding pharmacotherapy to psychotherapy does not help to reduce binge frequency compared to psychotherapy alone.
The efficacy of CBT has been substantiated by scientific literature23, 24, 25, 26 and Vaidya27 stating that CBT helps patients reduce eating disorder habits by making them aware of the cause of their self-sabotage, while affecting weight indirectly.
Psychotherapy treatment over a one-year period deals with binge symptoms and aims at reducing the possibility of relapse by gathering different techniques for the maintenance of long-term results through the use of specific individual intervention protocols. The main target of the intervention is to facilitate the management of no-control food intake episodes and of impulsivity through the alteration of behaviour, and of cognitive and emotional factors related to eating disorders.
Thus, the main objective of this research was to verify the possible differences between those subjects with BED who underwent psychotherapy combined with pharmacotherapy and those who underwent psychotherapy only. In particular, it aimed at verifying possible differences between the various therapeutic strategies on eating behaviour (restrained eating, uncontrolled eating and emotional eating) and the behavioural and psychopathological features (psychopathic deviate, depression and hypomania).
The main hypothesis was to determine if patients who underwent CBT and pharmacotherapy with bio-equivalent doses of the SSRI Paroxetine or SNRI Venlafaxine obtained a considerable benefit from the pharmacotherapy on impulse regulation, on eating behavior and on personality features compared to those who underwent CBT alone.
The second hypothesis was to verify if Paroxetine and Venlafaxine treatments were equally effective on impulse regulation, eating behavior and on personality characteristics.
Methodology
Participants
A group of 30 subjects with BED were selected. All these subjects applied for support to the Inter-Service-Psychology Clinic for Eating Disorders and they were assisted by a Cognitive Behavioural Therapist. They were all of Italian nationality, aged 22 to 52, with a Body Mass Index (BMI) range of 26 to 35. All participants belonged to a middle class socio-cultural level. They were informed of the objectives of the research and signed a consent form. Those subjects who were diagnosed with binge eating less than two years ago, those aged over 65, or those who were suffering from other debilitating or chronic diseases were preliminarily excluded from this research.
Measures and procedure
Participants were recruited according to the nature of the assessments. More specifically, assessments had to address the effect of psychotherapy and pharmacotherapy in subjects with BED on their impulse regulation, their eating behavior (restrained eating, uncontrolled eating and emotional eating), and their personality features (Psychopathic Deviate, Depression and Hypomania). The 30 subjects selected were randomly assigned to three different treatments. Ten subjects had only CBT, ten subjects underwent psychotherapy with Paroxetine, and ten subjects underwent psychotherapy with Venlafaxine.
Each participant answered questionnaires during the assessment phase and in the post-training phase (after one year of psychotherapy). More specifically:
Binge Eating Scale (BES)28 is a 16-item questionnaire which assesses the presence of binge eating behaviour indicative of an eating disorder. The score ranges from 0 to 46 (non-binging <17; moderate binging = 18-26; severe binging = 27 and higher), which in this research had an adequate internal consistency (a = 0.84).
Eating Disorder Inventory-2(EDI-2)29 aims at quantifying some psychological and behavioural features. It consists of 64 questions grouped into 11 scales. For each item, the participants are asked to answer by using the following frequency adverbs: "always", "usually", "often", "sometimes", "rarely", and "never". The rating is measured with a score between 0 and 3: the maximum score of 3 corresponds to the intensity of the symptom ("always" or "never" depending on whether the direction of the item is positive or negative), score 2 corresponds to a degree intensity immediately below ("usually" or "rarely"), score 1 to an even lower level of intensity ("often" or "sometimes"), while a score of 0 is assigned to the three "asymptomatic" answers. So, those items with a positive direction are assigned the following scores: always = 3, usually = 2, often = 1, sometimes = 0, rarely = 0, never = 0; items with a negative direction are evaluated in the opposite way: never = 3, rarely = 2, occasionally = 1, and often, usually, always = 0. The sub-scale scores are calculated by simply adding all the scores of items of each specific sub-scale.
This research availed the Impulse Regulation Scale with an adequate internal consistency (a = 0.82). This scale shows the ability to regulate impulsive behaviour, especially binge behaviour.
Three Factor Eating Questionnaire (TFEQ)30 is a self-report questionnaire consisting of 51 items.The questionnaire refers to daily dietary practice and measures three different aspects of eating behaviour: (1) restrained eating (conscious restriction of food intake in order to control body weight or to promote weight loss – cut-off: ≤11; a = 0.79); (2) uncontrolled eating (tendency to eat more than usual due to a loss of control over intake accompanied by subjective feelings of hunger – cut-off: ≤8; a = 0.81): (3) emotional eating (inability to resist emotional cues – cut-off: ≤7; a = 0.83).
Minnesota Multiphasic Personality Inventory-2 (MMPI-2)31 consisting of 567 items with dichotomy answers (true/false) is most commonly used by mental health professionals to assess and diagnose mental illness. The MMPI is based on ten clinical scales that are used to indicate different psychotic conditions. In this research the scoring of the three following scales were taken into consideration: (1) Psychopathic Deviate Scale (Pd) (50 items) which measures social deviation, lack of acceptance of authority and amorality. This scale can be thought of as a measure of disobedience. High scorers tend to be more rebellious, while low scorers are more likely to accept authority. An adequate internal consistency was obtained in this research (a = 0.83); (2) Depression Scale (D) (57 items). The highest scores may indicate depression, while moderate scores tend to reveal a general dissatisfaction with one’s own life. A sound internal consistency was obtained through this research (a = 0.81); (3) Hypomania Scale (H), with 46 items, identifies such characteristics of hypomania as elevated mood, accelerated speech, locomotive activity, irritability, flight of ideas, and short periods of depression. In this research the internal consistency was a = 0.79.
Results
The Statistical Package for Social Science (SPSS 10.1) was implemented to verify the hypothesis. The limited number of subjects enabled analysis of data through non-parametric statistics. In order to verify statistical differences between simple comparisons on paired data the Mann-Whitney (U) test32 was applied. In order to verify statistical differences within phases (pre- Vspost-training), Wilcoxon Signed Ranks Tests33 were calculated separately on paired data.
Table 1 synthesizes the means and standard deviations of eating behaviour and of impulse regulation obtained by the three groups: CBT alone; psychotherapy with Paroxetine (CBT+P); and psychotherapy with Venlafaxine (CBT+V) in pre- and post-treatments.
Groups
Phases
Binge Eating Disorder
Impulse Regulation Scale
MIN
MAX
M
SD
MIN
MAX
M
SD
CBT (N=10)
Pre
28
35
31.43
2.41
74
94
85.93
6.84
Post
25
33
28.71
2.46
71
91
83.07
6.67
CBT+P (N=10)
Pre
26
35
30.90
3.54
77
94
86.80
5.29
Post
24
31
27.90
2.85
74
91
82.10
5.72
CBT+V (N=10)
Pre
27
35
30.80
2.78
83
94
87.80
3.91
Post
24
31
27.20
2.57
79
90
83.80
3.71
Table 1 – Minimum and maximum scores, Means and Standard Deviations of eating behaviour and of impulse regulation obtained by three differential groups.
By comparing the total scoring in BES during the pre-treatments phase, no statistical differences between groups were noticed. Subjects who only underwent CBT had the same result than those who had addition of Paroxetine (CBT+P) [U = 64; Z = 0.35; p = 0.75] and Venlafaxine (CBT+V) [U = 59; Z = 0.62; p = 0.55]. There were no initial statistical differences between the two groups that received pharmacotherapy [U = 50; Z = 0.1; p = 0.99].
In the post-treatment phases, the presence of binge eating behaviour appeared to be the same in all groups. Subjects belonging to the CBT group obtained the same results as those belonging to the CBT+P [U = 58; Z = 0.68; p = 0.5] and the CBT+V groups [U = 47; Z = 1.36; p = 0.19]. No statistical differences between medication use were noticed [U = 41; Z = 0.69; p = 0.53].
All groups in post-treatment phases seem to equally benefit from the treatment. Comparing scores obtained by participants in the pre- and post-treatments, statistically significant differences were found in subjects undergoing CBT [Z=3.38, p < 0.001] and those with the addition of Paroxetine [Z = 2.848; p < 0.004] and Venlafaxine [Z = 2.859, p < 0.004].
For this research, Impulse Regulation Scale scores were taken into consideration. In the pre-treatment phase relative to each group, all groups showed the same difficulties to regulate impulsive behaviour. The CBT group showed the same impulse regulation as those belonging to the CBT+P [U = 68; Z = 0.12; p = 0.93] and CBT+V group [U = 64; Z = 0.33; p = 0.75]. No initial statistical differences between pharmacotherapy groups were found [U = 45; Z = 0.39; p = 0.74].
In post-treatment, no statistical differences between groups were observed. The CBT group achieved the same results as the CBT+P [U = 60; Z = 0.56; p = 0.58] and CBT+V group [U = 64; Z = 0.32; p = 0.75]. No statistical differences between the use of Paroxetine and Venlafaxine were found either [U = 39; Z = 0.84; p = 0.44].
All groups seemed to benefit from the treatments. In fact, comparing the scores obtained by participants in the pre- and post-treatments, statistically significant differences were observed in subjects who underwent CBT [Z = 3.38, p < 0.001] as well as in subjects supported by Paroxetine [Z = 2.84; p < 0.005] and Venlafaxine [Z = 2.97, p < 0.003].
Table 2 synthesizes the means and standard deviations of different features of eating behavior (restrained eating,uncontrolled eating andemotional eating)showed by the three groups (CBT, CBT+P, and CBT+V) in pre- and post-treatment.
Groups
Scales
Pre-Treatment
Post-Treatment
MIN
MAX
M
SD
MIN
MAX
M
SD
CBT
restrained eating
5
9
6.64
1.28
5
8
5.86
.95
uncontrolled eating
13
16
14.71
1.07
11
15
12.93
1.21
emotional eating
8
13
9.93
1.21
7
11
8.57
1.22
CBT+P
restrained eating
5
9
6.50
1.43
5
7
6.00
.82
uncontrolled eating
13
16
14.10
1.11
10
13
11.60
1.07
emotional eating
8
13
10.70
1.64
8
11
9.80
1.03
CBT+V
restrained eating
5
8
6.10
1.11
4
7
5.50
.85
uncontrolled eating
12
16
13.90
1.37
10
13
11.40
1.17
emotional eating
9
13
10.60
1.43
7
11
9.10
1.19
Table 2 – Minimum and maximum scores, Means and Standard Deviations of different aspects of eating behavior (restrained eating, uncontrolled eating and emotional eating) obtained by three differential groups
In eating behaviour as well, all groups in pre-treatment phases appeared to be equivalent. The CBT group had the same mean result in restrained eating than those subjects who also underwent pharmacotherapy [CBT+P: U = 65; Z = 0.33; p = 0.74; and CBT+ V: U = 53; Z = 1.03; p = 0.55]. In the pre-training no statistical differences between groups with pharmacotherapy were noticed [U = 42; Z = 0.59; p = 0.58].
By analyzing the groups in pre-treatment phases no statistical differences in uncontrolled eating behaviour and emotional eating behaviour were found. In pre-treatment phase, the CBT subjects had the same statistical mean in uncontrolled eating [U = 48; Z = 1.33; p = 0.21] and in emotional eating [U = 48; Z = 1.32; p = 0.21] as those who took Paroxetine. No statistical differences were found when comparing CBT subjects with those that were taking Venlafaxine [uncontrolled eating: U = 48; Z = 1.33; p = 0.21; emotional eating: U = 48; Z = 1.32; p = 0.21]. In the pre-training phase there were no statistical differences between groups with pharmacotherapy [uncontrolled eating: U = 46; Z = 1.44; p = 0.17; emotional eating: U = 51; Z = 1.12; p = 0.28] were found.
All groups showed indistinctively less difficulty on restrained eating habits. In fact, by comparing post-training scores, the participants of CBT obtained the same results as those treated with Paroxetine [U = 61; Z = 0.56; p = 0.62] and Venlafaxine [U = 58; Z = 0.75; p = 0.51]. Therefore CBT alone appeared to be less effective on reducing uncontrolled eating than those with the addition of Paroxetine [U = 30; Z = 2.4; p < 0.02] and Venlafaxine [U = 26; Z = 2.6; p < 0.009]. Participants who underwent only CBT presented with less difficulties on emotional eating control than those with Paroxetine [U = 31; Z = 2.31; p < 0.02], but they achieved the same post-treatment score as those supported by Venlafaxine [U = 52; Z = 1.08; p = 0.31].
Comparing post-treatment outcomes, the effectiveness of Paroxetine and Venlafaxine appeared to be the same on restrained eating behaviour [U = 34; Z = 1.2; p = 0.25], on a better controlled eating behaviour [U = 45; Z = 0.39; p = 0.69] and on a higher emotional eating control behavior [U = 33; Z = 1.29; p = 0.2].
Comparing pre- and post-treatment results helped to observe a significant improvement in all groups. Participants who followed only CBT showed less difficulty to restrained eating behaviour [Z = 2.6; p < 0.009] in post-treatment. The same results were observed in those supported by Venlafaxine [Z = 2.12; p < 0.03], while no statistical differences were detected in a post-treatment phase in those groups supported by Paroxetine [Z = 1.89; p = 0.06].
Moreover it was possible to observe a considerable decrease in uncontrolled eating behaviour in all groups [CBT: Z = 3.49; p < 0.0001; CBT+P: Z = 2.84; p < 0.005; CBT+V: Z = 2.88; p < 0.004]. The same results were observed in the way emotional eating was handled. All groups benefited from treatments [CBT: Z = 3.27; p < 0.001; CBT+P: Z = 2.46; p < 0.01; CBT+V: Z = 2.87; p < 0.004].
Table 3 synthesizes means and standard deviations of Psychopathic Deviate (Pd), Depression (D) and Hypomania scales (H) obtained by the three groups (CBT, CBT+P, and CBT+V) in pre- and post-treatments.
Groups
Scale
Pre-Treatment
Post- Treatment
MIN
MAX
M
SD
MIN
MAX
M
SD
CBT
Psychopathic Deviate (Pd)
68
85
74.14
5.02
60
80
66
5.38
Depression (D)
63
81
72.50
5.58
61
78
69.86
5.39
Hypomania (H)
39
75
62
8.15
41
72
59.50
7.29
CBT+P
Psychopathic Deviate (Pd)
70
84
74.80
3.97
67
80
71.40
3.72
Depression (D)
66
76
70.80
3.91
64
74
67.80
3.58
Hypomania (H)
46
70
60.30
7.94
40
63
54.10
8.08
CBT+V
Psychopathic Deviate (Pd)
70
85
76.20
5.41
66
80
72.90
5.06
Depression (D)
65
80
70.80
4.76
61
75
66.60
4.69
Hypomania (H)
42
72
60.10
10.67
41
69
54
10.27
Table 3 – Minimum and maximum scores, Means and Standard Deviations of different aspects of Psychopathic Deviate obtained by three differential groups
As evidence of the homogeneity of the groups, the comparisons revealed no statistically significant differences in the pre-treatment phase. The CBT group subjects and those who received Paroxetine [Pd: U = 58; Z = 0.67; p = 0.51; D: U = 55; Z = 0.85; p = 0.39; H: U = 63; Z = 0.41; p = 0.71] showed similar scores. Likewise, the CBT group subjects and those treated with Venlafaxine [Pd: U = 53; Z = 0.99; p = 0.34; D: U = 58; Z = 0.71; p = 0.51; H: U = 65; Z = 0.26; p = 0.79] showed similar scores. The two groups treated subsequently with pharmacological support showed similar initial scores as well [Pd: U = 44; Z = 0.46; p = 0.68; D: U = 50; Z = 0.1; p = 0.99; H: U = 44; Z = 0.45; p = 0.68].
Comparing the results obtained in the post-treatment phase instead, those participants exposed to CBT alone showed a greater reduction of Pd compared to those who had taken Paroxetine [U = 23; Z = 2.76; p < 0.005] and Venlafaxine [U = 23; Z = 2.77; p < 0.005], whereas no differences were found comparing the scores obtained post-treatment in both groups of subjects with pharmacological treatments [U = 41; Z = 0.65; p = 0.53].
In post-treatment, the CBT group participants showed similar scores when compared to those taking Paroxetine [D: U = 54; Z = 0.91; p= 0.37; H: U = 41; Z = 1.67; p = 0.09] and Venlafaxine [D: U = 44; Z = 1.49; p = 0.14; H: U = 49; Z = 1.2; p = 0.23]. There have been no further significant differences in scores obtained post-treatment by the two pharmacotherapy groups [D: U = 39; Z= 0.84; p = 0.44; H: U = 0.47; Z = 0.23; p = 0.85].
All participants seem to have benefited from the proposed treatment. The CBT group had a significant reduction of Pd [Z = 3.3; p < 0.001], D [Z = 3.37; p < 0.001] and H [Z = 3.19; p < 0.001].
A similar result was found by comparing the pre- and post-treatment scores of the subjects supported by Paroxetine [Pd: Z = 2.7; p < 0.007; D: Z = 2.82; p < 0.005; H: Z = 2.82; p < 0.005].
Even in the group treated with Venlafaxine, a significant reduction of Pd [Z=2.87; p< 0.004], D [Z = 2.84; p < 0.004] and H [Z = 2.81; p < 0.005] was confirmed.
Discussion
The use of pharmacological therapy for overweight patients with BED has been less thoroughly studied. SSRIs (Citalopram, Sertraline, Fluoxetine, and Fluvoxamine) have mainly been used as the active compound in the pharmacological trials of patients with BED in order to improve mood symptoms and weight loss.34 Likewise, in many cases, promising results have been obtained with Venlafaxine in BED.35
Most of the research has focused on specific aspects of binge eating disorder, such as reduction in binge frequency and weight reduction. In general the results are associated with higher discontinuation rates.36
In this research, we did not only focus on the binge eating behaviour and impulse regulation in patients with BED. The main objective of this research was to analyze some aspects of eating behaviour (restrained eating, uncontrolled eating and emotional eating) and, more specifically, different psychotic conditions (psychopathic deviate, depression and hypomania).
The first hypothesis of this research was to verify differences between patients with binge eating disorder that followed CBT either with or without a pharmacotherapy support. The results confirmed that CBT and pharmacotherapy are equally effective in the treatment of BED and equally modified patients’ impulse regulation. Paroxetine and Venlafaxine medications did not enhance the control of binge eating or guarantee management of impulse regulation better than CBT alone.
This research also aimed at evaluating the efficacy of CBT with or without pharmacotherapy on some factors related to eating behaviour, such as the tendency to consciously monitor and reduce the caloric intake (restriction), the tendency to lose control on food intake (uncontrolled eating) and the conscious perception of the sensation of craving for food (emotional eating). The results suggest that CBT offers the same results regarding the reduction of caloric intake (restriction) as pharmacological treatment. It is less efficient in reducing the lack of control in food intake (uncontrolled eating), although it helps to reduce the sensation of craving for food (emotional eating) compared to pharmacotherapy.
In this research the effects of standardized treatments of CBT with or without the use of pharmacotherapy with bio-equivalent doses of Paroxetine and Venlafaxine were analyzed on psychopathic deviation, depression, and hypomania. The results confirmed that CBT showed a greater reduction of psychopathic deviation compared to those groups who underwent pharmacotherapy. Moreover, pharmacotherapy led to a higher reduction of depression and hypomania than CBT alone.
The second hypothesis was to verify if the SSRI Paroxetine and SNRI Venlafaxine were equally effective on impulse regulation, eating behaviour and personality features. The analysis showed that Paroxetine and Venlafaxine were equally effective on binge eating control and impulse regulation, but some differences in reducing dysfunctional eating behavior were found. Venlafaxine, compared to Paroxetine, seems to offer a greater improvement in emotional eating and restriction eating behavior. In fact CBT could be efficient to assess the tendency to reduce caloric intake (restriction) and to reduce the sensation of craving for food (emotional eating) more than Paroxetine alone. In order to reduce the tendency to lose control on food intake (uncontrolled eating) it could be helpful to administer Paroxetine or Venlafaxine.
Limitations
While the clinical groups were equivalent in all the parameters taken into consideration in the pre-treatment phase, the absence of a control group (no treatment) significantly reduced the possibility to accurately verify the conclusion. Due to ethical reasons we were not allowed to select a group of patients without any specific treatment. In order to correct this weakness in the research, it might be helpful to extend the sample and analyze the changes over a longer period of time.
It is relevant to analyze appropriately these aspects through controlled trials in order to test the efficacy and long-term outcome of psychotherapy, pharmacotherapy, and psychotherapy in combination with pharmacotherapy for treating BED.
Conclusion
In conclusion, patients with eating disorders usually suffer from other psychiatric disorders besides their eating disorder. Many results also confirm substantial comorbidity among obesity, BED, mood and anxiety disorders and metabolic syndrome in weight loss seeking populations.37
In such cases, it is important to understand the characteristics of the additional psychiatric disorders and the impact these ones have throughout the treatment.
As underlined by American Dietetic Association (ADA) Reports,38 understanding the complexities of eating disorders, such as influencing factors, comorbid illness, medical and psychological complications, is critical in the effectiveness of the treatment of eating disorders.
Eating disorders are complex medical illnesses since they have psychological, behavioural, and physiological components. Previous researchers underlined the importance to investigate gender differences in binge eating and associated behavioural correlates39 and, in order to prevent eating disorders, it is important to carry out individual treatment even on personality traits if the individual disorders have already occurred.40 Of course, a multidisciplinary approach involving a collaborative team of psychological, nutritional, and medical specialists as underlined in this research must be pursued in order to obtain important and at least short-term results.41
The results of this research confirm the need to analyze BED from an integrative perspective and to suggest treatments based on an interdisciplinary approach. The psychological (CBT) and pharmacological (Venlafaxine and Paroxetine) therapies were both efficient in different ways on the reduction of all the negative variables related to eating disorder. However any treatment could be inadequate in the absence of an accurate diagnosis that takes into consideration biological, genetic, psychological and nutritional components.
The assessment phase still plays an important role in determining which treatment is best for each patient. Accuracy in the medical examination when dealing with medical issues, as well as during the assessment examination and the psychological functioning evaluation is recommended.
Autism Spectrum Disorders (ASD) is the umbrella term increasingly used to describe the set of pervasive developmental disorders that included the diagnosis of Autism, Asperger’s Syndrome, and Pervasive Developmental Disorder Not Otherwise Specified under DSM IV. These are a group of disorders characterised by pervasive difficulties in a combination of the key areas of social communication interaction, and restrictive repetitive behaviours or activities 1, 2. The Diagnostic and Statistical Manual of Mental Disorders (the DSM-5), released by the American Psychiatric Association, officially eliminated many familiar autism spectrum diagnoses and now incorporated them into the single diagnosis of autism spectrum disorder. In DSM-IV, Asperger Syndrome was diagnostically differentiated from Autism by the lack of a significant language delay and intellectual functioning within the normal range.
The epidemiology of ASD is approximately estimated 30 in 10,000, although with increasing awareness of the disorder, this has led to greater rates of diagnosis, more recent estimates suggest the rate may be as high as 60 in 10,000 3. ASD may be as common as 1 in every 68 children according to the United States Centre for Disease Control 4.
Difficulties with an understanding of prevalence possibly related to early studies relying on clinically identified cases rather than community-based surveys, which may have resulted in cases not in treatment were being missed, and possibly only the most severe cases being recorded. Previous estimates may also have been incorrect due to previous narrower case definitions. As sampling methods have improved and better diagnostic instruments are used more cases have been identified and there has been a better delineation of ASD from other psychotic disorders. As more children with ASD are identified, there will be a likely rise in the number of families and children seeking treatment.
Comorbidities
There are very high levels of co-morbid psychiatric difficulties amongst this population with estimates ranging from 7-15%. Anxiety related concerns are among the most common presenting problems for school age children and adolescents with ASD 5. Several studies have examined the prevalence of anxiety within the ASD population. A review by white et al 6 of 11 such studies reported a prevalence to range from 11-84%. This large range in the prevalence may be accounted for by difference in methods used to measure anxiety, differences in definitions and in diagnostic subtypes.
Studies have also looked at prevalence rates of anxiety within the ASD population to other populations. Compared to groups of typically developing children, those with autism had a higher occurrence of anxiety 7, 8. Comparison with other groups considered to be at risk (children with conduct disorders and learning disabilities) children with ASD were more likely to be diagnosed with an anxiety disorder and/or have more intense anxiety symptoms 9,10.
A formal diagnosis of anxiety disorder in this group is hard for therapists due to overlap between comorbid anxiety and the core symptoms of ASD makes. Several anxiety disorders in DSM- IV and ICD 10 have autism as an exclusion criterion, implying that an anxious procession style is a feature of ASD.
The development of anxiety among children with ASD may relate to their cognitive impairment as they may lack the cognitive flexibility to generate strategies to adapt to varying circumstances and may experience distress over even trivial changes in the environment. The information processing style in children with ASD termed ‘weak central coherence’ is similar to non ASD anxious children whereby they selectively attend to threatening cues which results in the misinterpretation of ambiguous situations as threatening 11,12. As a consequence these cognitive deficits can result in a repertoire of social and communication difficulties resulting in children experiencing severe difficulties in social relationships which may in turn lead to the development of anxiety 13. If a child or adolescent has a co-occurring anxiety disorder, this could further negatively impact on the overall social impairment associated with ASD. This can impact on the child or adolescents ability to participate in activities at school, at home and within the community. Children with significant anxiety symptoms are at risk for serious educational difficulties, later unemployment, substance abuse and other psychiatric problems 14.
Some of the most frequently reported anxiety disorders and symptoms seen in children with Autistic Spectrum disorders are simple phobia, generalised anxiety disorder, separation anxiety disorder, obsessive-compulsive disorder and social phobia.
Treatment with Cognitive Behavioural Therapy
Pharmacological and psychosocial treatment have been the most common approaches to the treatment of anxiety in children with ASD but no single anxiety treatment has emerged to attain well established or probably efficacious empirically supported treatment status for children with an autistic spectrum disorder. Evidence for pharmacological intervention is limited. Also the effects of medication only appear to last as long as the medication is used, with relapse once regime is ceased.
The recommended treatment of choice by NICE guidelines for mood and anxiety disorders is cognitive behavioural therapy (CBT) and the primary psychosocial treatments have used CBT.
Despite the fact that CBT has been shown to be an effective empirically supported treatment for typical children, there continues to be differing views as to whether or not it can be used effectively with other populations. Some of the difficulties associated with treating children with ASD are due to suggestions from research that children with ASD have difficulty in identifying emotions and cognitions both in themselves and others. As CBT relies on the child’s ability to infer their own emotional states and thoughts in order to shift their cognitive style and in turn their anxious behaviour, standard CBT treatments need modification to address the difficulties associated with this.
Although there is recognition of the high comorbidity of anxiety with ASD, there have also been suggestions to the use of strict behavioural analysis 15 and an argument against using a cognitive component to treat this population. Lindsay 16 provides a different view, arguing children with ASD can benefit from the use of a cognitive component.
Various modifications have been proposed on the approach of CBT in this population. Some of the models have suggested adjustment of the developmental level to reflect the child’s ability, the use of coping model instead of curative model, the involvement of caretakers, and extending treatment both by the number of sessions and by overall session duration 17. Attwood 18 has recommended the use of role-plays and visuals, the involvement of special interests of the young person, the adjustment of material according to the developmental level and the incorporation of a social skills module due to the vast deficits associated with ASD. Anderson and Morris 19 recommend a more directive approach to treatment and the use of specifically in vivo practice to aid in the generalisation of skills. Each of these variations may contribute differently to the adaptation of CBT to meet the specific needs of the child being treated; however, the most appropriate pattern of practical and functional strategies is yet to be determined.
Chorpita and Daleiden 20 in their review of evidence based treatment for children and adolescents noted the most commonly used techniques to treat anxiety in typically developing children. These include exposure, relaxation, cognitive restructuring and modelling in that order. The most commonly used techniques to treat ASD include communication skills training, modelling, social skills training, goal setting and parent psycho-education.
CBT generally consists of six components which include assessment of the nature and degree of the disorder, affective education, cognitive restructuring, stress management, self-reflection and a schedule of activities to practice new cognitive skills. It is important to ensure that the young person has the same definition and interpretation of words, and affective education can help increase their vocabulary of emotional expression.
Attwood 21 has described several intervention components which can be added to CBT. Some of the suggestions include; a) Increasing the use of visual aids. b) Associating emotions with tangible objects. c) An emphasis on coping strategies that do not require the use of abstract language for instance the use of relaxation. d) Use of alternative communication modes. e) Embedding the use of preservative interests into CBT sessions. f) Increasing the focus on teaching social skills.
Attwood also developed the concept of an emotional toolbox and focused on working with the young person in identifying different tools to ‘fix’ problems that occur as a consequence of negative emotions including anger, anxiety and sadness. The ‘tools’ are further divided into those that constructively release or reduce energy and those that improve thinking. The therapist generally works together with the young person to draw a variety of tools and activities which encourage constructive emotions repair.
Cognitive restructuring aims to enable the young person to correct distorted conceptualisations and dysfunctional beliefs. It involves challenging the current thinking with logical evidence and ensuring rationalisation and cognitive control of their emotions. Young people with ASD can make false assumptions of their circumstances and intentions of others due to impaired or delayed theory of mind abilities. These young people also tend to make literal interpretations and are less able to seek alternative explanations or responses.
Summary of Case Reports, Case Series, and Randomised Control Trials
Method
Studies that used CBT with the aim of reducing anxiety symptoms in young people with an ASD diagnosis were looked at.
Search Procedures
A search was carried out in electronic bases: Psychinfo and Medline. The publication year was not restricted but the search was limited to English- language peer reviewed journals. Over the databases, the terms ‘Asperger’, ‘Autism’, or ‘developmental disability’, plus ‘anxiety’ or ‘CBT’ and the search was limited to children and adolescents.
Review of Case series and reports
There have been five case studies that used CBT in treatment of anxiety as well as one case report that used CBT in treatment of OCD in children with ASD.
The first case study by Reaven and Hepburn (2003)22 reported a 7 year old girl with Asperger syndrome who markedly responded to a 6 month modified CBT treatment which was primarily tailored for her OCD. Afterwards, Greig and MacKay (2005) 23, Sze and Wood (2007) 24 and (2008) 25, Reaven et al (2009) 26, and White et al (2009) 27 reported further successful outcomes of using modified CBT for treatment of Anxiety in children with ASD. See table 1 for a summary of published case reports and series of studies.
Table 1: A Summary of Published Case Reports and Series of studies using CBT for anxiety symptoms in young people with an ASD diagnosis
AUTHOR (year)
Sample
Anxiety Measure
Characteristics of intervention
Outcome
Reaven & Hepburn (2003)22
a 7 year old girl with Asperger syndrome
6 months modified CBT treatment based upon the work of March and Mulle
Obsessive-compulsive symptoms improved markedly
Greig and MacKay (2005) 23
12 year old male with ASD and unspecified anxiety disorder
TSCC, Teacher Report, SWQ
15 sessions
Anxiety score on TSCC reduced from 19 to 5. Teacher report suggested improvements at school.
Sze and Wood (2007) 24
11year old female SAD, OCD, GAD, HFA
ADIS
16 sessions 90 minutes each over 4 months family cognitive behavioural therapy (FCBT)
No longer met criteria for SAD, GAD or OCD on the ADIS by child or parent report
Sze and Wood (2008) 25
10 year old male with ASD,GAD, SAD
ADIS, CGI, MASC, CBCL, SSRS, VABS
Enhancing CBT
No longer met criteria for Social phobia or GAD, on the ADIS, improvement CGI , MASC
Reaven et al (2009) 26
7 male, 3 female mean age 11years, 12 weeks Active Treatment 10 parent-child dyads(n = 10) Wait List Control (n = 23)based on order of enrolment, not random assignment
SCARED
12 weekly sessions of 1.5 hours
Large group time, separate parent and child group meetings, and parent-child dyads
Parent report on SCARED showed significant decrease in severity of anxiety symptoms in treatment group
White et al (2009) 27
14 year old male with ASD, 14 yr old female with PDD-NOS,12 year old male with ASD, 12 year old female with ASD
ADIS
MCIT 12-13 individual therapy modules delivered over 11 weeks.
On the CASI-20 parent rated measure of anxiety, 3 out of 4 participants demonstrated significant improvement from baseline to endpoint.
There have been eight studies that have met criteria for a randomised controlled trial that identified CBT as a treatment for anxiety in children with ASD. See table 2 for published randomised controlled trials.
Table 2: Published randomised controlled trials of cbt
AUTHOR (year)
Age range/ Sample size
Anxiety Measure
Characteristics of intervention
Characteristics of Controlled
Outcome
Sofronoff, Atwood, Hinton (2005) 28
age 10-12
(n=71)
SCAS, SCAS-Parent,
child report measure
a 6 week CBT
child based (n=23) or combined child and parent (n=25) intervention
a waiting list group
Significant decreases Parent reports SWQ at follow-up and a significant increase in the child’s ability to generate positive strategies in an anxiety-provoking situation.
a 12 week group CBT based on ‘Cool Kids’ program(n=28)
Approx. 7 months waiting list (n=19)
71.4% of the treated children no longer met criteria for an anxiety disorder compared to 0% in the wait list condition (n=19)
Wood et al (2009) 30
ages 7-11 (n=40)
Anxiety symptom checklists at baseline and post treatment/ post waitlist
16 sessions of standard CBT augmented with multiple treatment components (n=17)
A 3 month wait list (n=23)
78.5% CGI improved compared to only 8.7% of the waitlist group, Remission of anxiety in CBT group, but child reported anxiety had no significant effect
Sung et al (2011) 31
age 9–16
(n=70)
SCAS-C,CGI-S
a 16-week CBT
program (n = 36)
a Social Recreational (SR) program on anxiety (n =34)
Children in both programs showed significantly lower levels of generalized
anxiety and total anxiety symptoms at 6-month follow-up on SCAS-C
Reaven et al (2012) 32
age 7-14
(n=50)
ADIS-P
modified CBT (n=24)
TAU (n=26)
50% in the CBT compared to 8.7% TAU group had a clinically meaningful positive treatment response, group CBT intervention specifically developed for children with ASD may be effective in decreasing anxiety
18 (75 %) of CBT arm, were treatment responders, versus only 3 of 21 (14%) in the TAU arm. CBT adapted for anxious youth with high-functioning ASD demonstrates large effects in reducing anxiety symptoms.
McNally et al (2013) 35
age 8-14
(n=22)
ADIS-P, SCAS-P, SCAS
a modified version of the Coping Cat program CBT package(n=12)
waiting-list
(n=10)
ADIS-P 58% of children with CBT had no anxiety / 36% after 2 month follow up. A modified version of the Coping Cat program may be a feasible and effective program for reducing clinically significant levels of anxiety in children with ASD.
Sofronoff, Atwood, and Hinton (2005) 28 evaluated the impact of a six week cognitive-behavioural intervention for anxiety in 71 school children aged between 10 to 12 with Asperger’s Syndrome. The authors also looked at the potential impact of parent involvement on outcome. The diagnosis of Asperger’s Syndrome was confirmed by semi-structured telephone interview and anxiety symptoms were based on parent report in the initial telephone interview. Children were randomly assigned to one of three groups: child based intervention, combined child and parent intervention or a waiting list group. The intervention focused on teaching the children strategies to manage feelings and expanding emotional knowledge and was delivered weekly in a group format. The focus was on teaching the children strategies to effectively manage feelings and expanding emotional knowledge. Parents served as co-therapists in the combined parent-child intervention as they were trained in all aspects of the intervention.
Using the Spence Child Anxiety Scale-Parent report, children in the combined parent-child intervention reported fewer symptoms of anxiety post–treatment and at a six week follow up than children in the child-only intervention. A child report measure (James and the Maths Test) was used to identify the number of strategies the child could identify for coping with anxiety. Compared to children on the waiting list, children who received either intervention were able to develop more coping strategies. Those in the combined intervention generated significantly more coping strategies at endpoint compared to those in the child only intervention.
Parental involvement is an important aspect of treatment of young people with ASD in ensuring better generalisation and therapy outcome. Authors of this study found that children whose parents were involved in treatment were significantly more improved at follow up than those whose parents were not involved. There are different models of parents involvement and include either only direct participation in each session or with a separate parent only component or both. It seems that regardless of which approach is used parent involvement increases the sustainability and success rate of CBT. Involvement of parents helps to improve their understanding of exposure and practice and helping the young person to learn how to master the skills on their own.
Limitations of this study include the reliance on the parent report of anxiety symptoms and both Asperger’s Syndrome and anxiety symptoms were not formally diagnosed. Parents who were involved in the delivery of treatment may have had a more vested interest in their children’s progress with higher expectations for improvement affecting outcome measure reports. However, no independent (blinded) ratings of anxiety were gathered.
Chalfant, Rapee, and Carroll (2006) 29 evaluated a 12 week group delivered cognitive –behavioural treatment for anxiety in 47 school children aged between 8 to 13 with ASD and no intellectual disability. The intervention was adapted from the ‘Cool Kids’ program (Lyneham et al, 2003), a 12 week group based activity for treatment of childhood anxiety. Cognitive strategies were simplified in the intervention, with a greater focus on visual aids, structured worksheets and homework and exposure and the programme was extended over a 6 month period of time.
The authors randomly assigned participants to either the CBT (n=28) or waiting list (n=19) before beginning of each treatment group. Those under waiting list condition were offered treatment after approximately 7 months, when the waiting list period ended. Multi-modal and Multi-person assessment of anxiety were used. At pre-treatment, over 75% of the sample met criteria for more than one anxiety disorder.
Structured diagnostic measures used in the study included the ADIS (Albano& Silverman, 1996), Spence Children’s Anxiety Scale (Spence, 1998), The Revised Children’s Manifest Anxiety Scale (Reynolds & Richmond, 1978), and Children’s Automatic Thoughts Scale (Schniering& Rapee, 2002). Parent report measures included the SDQ-Parent Report (Goodman, 1997), and SCAS-Parent Report (Spence, 1998).
At post treatment, 71.4% of the treated children (n=28) no longer met criteria for an anxiety disorder compared to 0% in the wait list condition (n=19). It was also found that children in the CBT condition were largely able to identify their automatic thoughts indicating some theory of mind ability and had a significant reduction in automatic thoughts, in comparison to the wait list condition.
Limitations of this study include the small sample size so the data may not be reflective of the wider population with high functioning autism and anxiety. Also the lack of confirmation of the diagnosis of ASD by the investigating clinicians reduced the validity of the participant’s diagnostic status. Participants were accepted based on previous evaluations completed within the community setting.
There was no time spent with the waiting list group to help ensure that the benefits of treatment could be attributed to the treatment alone and not to time spent with the therapist. Also the issue of the waiting list group being aware of the treatment programme and knowledge of future treatment may have attenuated the response of those on the waiting list. Clinicians who implemented the CBT groups and collected the relevant pre-and post-treatment data were not blind to the study’s aims.
Wood et al (2009) 30 used a standard CBT program augmented with multiple treatment components as a randomised controlled trial for 40 children aged between 7 to 11. It was designed to accommodate the social and adaptive skill deficit of children with ASD that could pose barriers to anxiety reduction. They also used a family based intervention program adapted for use with children with ASD. Enhancements included addressing of poor social skills, adaptive skill deficits, circumscribed interests and stereotypes, poor attention and motivation, common co-morbidities as well as school based problems. During modules, children were given social coaching by the therapist, parents and available school providers on appropriate ways to enter interactions and maintain conversation with peers.
Children were randomly assigned to 16 sessions of CBT (n=17) or a 3 month wait list (n=23). Independent evaluators blind to treatment condition, were involved in structured diagnostic interviews. Parents and children completed anxiety symptom checklists at baseline and post treatment/ post waitlist.
The Clinical Global Impressions Improvement Scale (CGI) criteria showed that 78.5% of the CBT group showed positive treatment response at post treatment as compared to only 8.7% of the waitlist group.
Children randomised to CBT had primary outcomes comparable to those of typically developing children receiving CBT for anxiety disorder, which were remission of all anxiety disorders for over half the children in immediate treatment at post treatment and follow up and a high rate of positive treatment response on the CGI. However child- reported anxiety did not yield a significant treatment effect.
Limitations of this study include the small sample size which precluded tests of moderation. The study was also undertaken by researchers who developed the intervention and would need independent replication to validate the intervention.
Also using measures not designed for children with ASD had major impact on the outcomes. The child report of Multidimensional Anxiety Scale for Children (MASC) scores did not yield a significant effect for treatment group largely due to a decrease in MASC scores from pre to post treatment for children in both groups. This may have been due to the MASC being not particularly effective in this population and children’s scores at baseline were relatively low on average. Parental scores showed less of a change from pre to post treatment in the waiting list group. The MASC does not specifically measure OCD and GAD symptoms and as there was a wide range of anxiety symptoms, the type of change that some children may have experienced may not have been properly assessed.
Sung et al (2011) 31 compared the effects of a 16-week cognitive-behavioural therapy program and a Social Recreational (SR) program for 70 children with ASD aged between 9 to16. 36 of them were randomised to CBT and 34 to Social Recreational program. Children in both programs showed significantly lower levels of generalized anxiety and total anxiety symptoms at 6-month follow-up on SCAS-C. They suggest factors such as regular sessions in a structured setting, consistent therapists, social exposure and the use of autism-friendly strategies are important components of an effective framework in the management of anxiety in children and adolescents with ASD.
Reaven et al (2012) 32 used a modified CBT intervention for anxiety in 50 children aged between 7 to 14 with high-functioning ASD and anxiety, who were randomized to group CBT (n=24) or treatment-as-usual (TAU) (n=26) for 12 weeks. Independent clinical evaluators blind to condition, completed structured ADIS-P pre- and post-intervention condition. They found a significant difference between CBT and TAU group.
47 children completed either the CBT or TAU condition. They also had 3 and 6 month follow-ups. Results indicated markedly better outcomes for the CBT group. Clinician Severity Ratings, diagnostic status, and clinician ratings of global improvement showed significant differences by group. In the intent-to-treat sample, the CBT group, 10 of 20 children (50%) had a clinically meaningful positive treatment response, compared to 2 of 23 children (8.7%) in the TAU group. Initial results from this randomized, designed treatment study suggest that a group CBT intervention specifically developed for children with ASD may be effective in decreasing anxiety.
Limitations of this study include small sample size, lack of an attention control group, use of outcome measures normed with typically developing children, and no use of teacher or child measures. TAU remained variable, and the study did not mention the situation of the children in TAU as were or weren’t receiving any treatment.
White et al (2012) 33 combined treatment approaches, and evaluated the feasibility and preliminary outcomes of the Multimodal Anxiety and Social Skills Intervention (MASSI) program in 30 adolescents aged between 12 to 17 with ASD and anxiety symptoms of moderate to greater severity who were randomised to CBT (n=15) or Wait list group (n=15). A 16 % improvement in ASD related social impairment (within-group effect size = 1.18) was observed on a parent-reported scale. Although anxiety symptoms declined by 26 %, the change was not statistically significant. These findings suggest MASSI as a feasible treatment program and further evaluation is warranted. High subject adherence and therapist fidelity demonstrate the treatment was acceptable to families.
Storch et al (2013) 34 examined the efficacy of the Behavioural Interventions for Anxiety in Children with Autism (BIACA), a modular cognitive behavioural therapy protocol, relative to treatment as usual (TAU) among 45 children with ASD aged between 7 to 11. Children with clinically significant anxiety (including OCD), and no intellectual disability, were randomised to receive 16 sessions of weekly CBT (n=22, 2 drop out) or TAU (n=21). After screening, assessments were conducted at baseline, post-treatment, and 3-month follow up for only CBT group which was not blind. The raters were blind to treatment condition. They did also use both child- and parent-report versions of ADIS. Children receiving CBT showed substantial improvement relative to TAU on primary anxiety outcomes. Of 24 children randomised to the CBT group, 18 (75 %) were treatment responders, versus only 3 of 21 children (14%) in the TAU group. Treatment gains were generally maintained at 3-month follow up for CBT responders. They concluded that relative to usual care, CBT adapted for anxious youth with high-functioning ASD demonstrates large effects in reducing anxiety symptoms.
The limitations of this study include that only about 75% of the TAU children were in fact getting treatment of any kind at all, as 25% of their TAU weren’t getting anything. Also TAU group was extremely variable, therefore the control group were getting a variety of treatments, or none, making comparisons with the children who received CBT difficult.
McNally et al (2013) 35 used a modified version of the Coping Cat Program in reducing anxiety in children with ASD. They randomly assigned 22 children with ASD aged between 8 to14, with clinically significant anxiety and no intellectual disability, to 16 sessions of the Coping Cat cognitive-behavioural therapy (CBT) program or a 16-week wait list group.
They used ADIS-parent at pre-treatment and post-treatment phases, and they also video-recorded therapy sessions to check for treatment fidelity. Children in the CBT condition evidenced significantly larger reductions in anxiety than those in the waitlist. Treatment gains were largely maintained at two-month follow-up. Results provide preliminary evidence that a modified version of the Coping Cat program may be a feasible and effective program for reducing clinically significant levels of anxiety in children with high-functioning ASD.
The limitations of this study include small sample size which recommended statistical and effect size to be interpreted with caution, and also the outcome measures were largely based on parent- ADIS reports by parents who were not blind to the treatment. Also, examining treatment response was limited to the primary author who delivered all of the treatment. Similarly, with waiting list as a comparison, there was a danger of getting placebo effects with the intervention arm, especially with parent-report measures, as most parents were very keen to get any help at all for their children.
Discussion and future perspective
It is clear from the 8 randomised controlled studies that young people on the autistic spectrum benefit from some form of CBT when modified as part of a therapeutic package. Unfortunately it is not clear what specific aspect of the therapy is making the difference. Cognitive Behavioural Therapy has many components to it as well as the actual cognitive, i.e. ‘thinking’ part and behavioural part. Which bit of the therapy is making a difference to the anxiety? Is it the cognitive reframing, the relaxation, the exposure, the parental involvement, or simply the therapeutic relationship with a therapist? As with CBT studies which are delivered as part of a package, positive results are often obtained when there is no control group or when compared to a waiting list.
Other limitation to research papers cited above include fairly small sample sizes, and outcome measures that are normed with a non ASD cohort.
Only 2 studies had non waiting list comparison 32, 34. These studies did show significant clinical improvement in anxiety levels. These studies have shown that CBT can be effective if modified for the ASD population. Many clinics often fail to pick up associated anxiety difficulties in the ASD cohort and if present, often are under the impression that CBT would not work in this population due to misunderstanding and ill informed prejudices about the ASD population. As there is such a high comorbidity with anxiety disorders, young people on the autistic spectrum should be offered effective interventions such as CBT. Research should focus on modifications of the CBT package to enable better engagement and better understanding of the CBT constructs.
Practice Points
Children with high-functioning Autism Spectrum Disorder (ASD) are at high risk for developing significant anxiety
Anxiety can adversely impact on functioning across school, home and community environments
Cognitive Behavioural Therapy (CBT) is frequently used with success for children with anxiety symptoms
Standard CBT treatments need modification to address the anxiety difficulties associated with ASD
Modified CBT interventions for anxiety in children with ASD have also yielded promising results
Brain injury is a major cause of mortality and morbidity all over the world and in Europe there is an estimated incidence of 235 brain injury inpatients per 100,000 population 1. Over the years, the medical care of brain injuries has developed with a resultant fall in mortality. However, with this fall in death rates the proportions of people with complications, especially the neuro-behavioural effects of brain injury, has risen 2. Of the complications, psychiatric disorders have a significant impact on the patient’s quality of life and rehabilitation prognosis3 and so are an important consideration from both a care delivery and public health perspective. This paper therefore aims to analyse the prevalence of psychiatric disorders following brain injury and highlight the practical and personal implications of these through an illustrative case series.
Depression Following Brain Injury
Jorge et al in 20044 conducted a prospective case controlled study on a sample of 91 patients with traumatic brain injury (TBI). Patients with penetrating head injury, spinal cord injury and severe deficits of comprehension was excluded and 27 patients without brain injury but with other trauma was included as controls. The sample was analysed at 3, 6 and 12 months with Present State Examination (PSE), structured clinical interview for DSM1V, and analysed with Mann Whitney and chi squared tests. The results showed that 33% of the TBI group had major depression compared to 22 % in the control group. Neuropsychological testing also demonstrated that depressed patients had a greater degree of impaired cognitive function. An earlier study with a larger sample was conducted by Kreutzer in 20015, studying 722 TBI patients (average time post injury for evaluation 2.5 years). Data was collected via survey, using the Neurobehavioral Functioning Inventory to identify depression; the response was studied by trained neuropsychologists and compared with DSM-IV Criterion for depression. A significant proportion (42%) of survey respondents met the DSM-IV criterion for depression. Fatigue, low concentration and frustration were most commonly reported symptoms. A similar study done by Seel et al in 20036, where 666 TBI outpatients from 17 centres was reviewed using DSM-IV Criterion, showed rates of major depression to be 27%.
Mania Following Brain Injury
Jorge in 19937 reviewed 66 patients with brain injury at 3, 6 and 12 month intervals to evaluate the prevalence of mania. The inclusion criteria was age above 18 years and absence of delirium, no previous history of mood disorder and absence of grave injuries to other areas of the body. Using the Present State Examination to gather data, 9% of the sample had symptoms in correlation with the DSM III criteria for mania.
Van Reekum in 19968 recruited 18 TBI patients attached to a rehabilitation unit for a study to evaluate mental illness in this population. 44% of patients had severe TBI while 56% had mild/moderate TBI; the average duration since TBI was 4.9 years. 27% met the DSM II criteria for bipolar affective disorder and 61% met criteria for depressive illness. The rate of anxiety disorder was 38% but psychosis was not reported.
Psychosis & Other Mental Illness Following Brain Injury
Fann et al in 20049 conducted a large prospective cohort study involving 1939 randomly selected TBI patients 1 year pre injury and 3 years post injury to study rates of psychiatric illness including psychosis. The sample was divided into the moderate/severe TBI and mild TBI compared to matched controls. The presence of psychiatric illness was detected by utilisation of mental health services by subjects, usage of psychotropic medication and presence of a psychiatric diagnosis in the records. Psychotic disorders were seen in 49% of the moderate to severe TBI patient group and for the mild TBI group psychosis was seen in 34% of the sample. This is significantly greater than the rate seen in the control group. However the lack of definitive diagnostic criteria and confounding factors such as social circumstances and other physical health issues which may have strong associations with mental illness were not accounted for.
Another observational prospective study done by Rao et al in 200910 looked into prevalence rates of aggression in the 3 months following brain injury. Overt Aggression Scale was used by trained examiners in the assessment of aggression in a sample of 107 TBI patients. Comorbidities were analysed using General Medical Health Rating scale; psychosocial functioning was analysed by Social Functioning Exam and the Social Ties Checklist. Results showed the prevalence of aggression in the sample to be 28.4% and this subgroup was also associated with new-onset major depression. Only 63% of the already small sample completed the study and the drop out group was unaccounted for; this may negatively impact the results.
Keenan et al in 200811 studied prevalence of attention-deficit hyperactivity disorder(ADHD) in 2782 post TBI children and demonstrated chance of a diagnosis of ADHD two folds higher amongst children with a head injury before age 2. Jellinger in 200412 studied links between brain injury and dementia, and found that although cognitive deficit was associated with brain injury, there was no established link between development of dementia and brain injury. Oquendo et al in 200413 studied 325 depressed patients to analyse the link with mild TBI and suicidal behaviour; 44% of the sample had mild TBI and suicidal behaviour was more common in this subgroup. Suicide Intent Scale and the Lethality Rating Scale was used to measure suicidal behaviour. However, exclusion of moderate to severe TBI and inclusion of only inpatients in this study would affect any generalisability of the results.
Case series: Psychiatric Disorders Following Brain Injury
Case 1- Patient A: Epilepsy, interictal psychosis and organic personality disorder following head injury
Patient A is a 37 year old female under mental health services with a diagnosis of organic personality disorder and interictal psychosis. She suffered from epilepsy from the age of 9 but coped well at school and went on to work successfully as a hairdresser. However, in 1998 at the age of 22 she was admitted to ITU with status epilepticus as a result of encephalitis of unknown cause, and remained severely unwell for several months. She recovered but was left with residual tonic clonic and complex partial seizures.
Since this episode, marked changes in her personality were noted. She developed mood swings with recurrent episodes of low mood, and expressed paranoid beliefs about people in the street talking about her. These beliefs resulted in her being agitated and physically aggressive, resulting in harm to both herself and others. She has required numerous admissions to acute wards and rehabilitation units because of her paranoid and suspicious behaviour and aggressive outbursts that her family were not able to manage in the community. She required restraint under Section 3 of the Mental Health Act in 2010, believing that care staff were poisoning her. Psychotic symptoms are most marked around seizures, with her displaying self harming behaviour such as cutting off hair or painting face with nail polish. She frequently accuses staff and family of acting against her in these periods and her behaviour is very difficult to manage.
Her case has been challenging to manage successfully in the community by family and community teams, and she has needed several short and long term stays in acute wards and residential units. Her care has been coordinated jointly between neurological and psychiatric services. She currently lives with her parents and has carers to support her. Her epilepsy is yet to be successfully controlled; antipsychotics can lower the seizure threshold and so a delicate balance between these and her antiepileptic medication is warranted. There is an on-going concern that further mental health problems may develop in light of this.
Case 2- Patient B: Schizophrenia following head injury
Patient B is a 43 year old female with a diagnosis of schizophrenia, learning difficulties and epilepsy. She suffers from epilepsy in the form of absence and tonic-clonic seizures from the age of 7 months, when there is high suspicion that she sustained a head injury whilst in the care of extended family. Patient B has difficulties with numeracy and literacy, identified through psychological assessment, and an IQ of around 70. She has required three admissions under Section 2 of the MHA due to her paranoid delusions and poor self care. Patient B frequently reports feeling monitored by cameras, suspicions that her food has been poisoned and that her personal belongings are being tampered with. She has attempted to take her own life due to feeling unable to cope with these delusions, laying in the road to be run over by a bus.
She is currently managed well in the community on oral risperidone for her psychosis and sodium valproate for her epilepsy; she resides in supported accommodation and has required stints in long term residential and rehabilitation beds due to her mental health problems and learning difficulties.
Case 3- Patient C:Depression and Personality disorder after head injury
Patient C first came in to contact with psychiatric services in 2007 and was diagnosed with depression and organic personality disorder. At the age of 16 this gentleman was knocked off his bicycle and sustained a severe head injury, from which he was left in a coma for over three weeks, but recovered well enough to go home. In 1994 he started having blackouts, was investigated extensively by neurology, and diagnosed with non-epileptic attack disorder. As part of these investigations, Patient C underwent an MRI which demonstrated significant brain damage including traumatic damage to the frontal lobes. This was likely due to his accident at age 16. From his first assessment by psychiatric services, he eluded to thoughts and behaviours that were of serious concern to his team. He reported feeling emotionally detached from his family, gaining little pleasure from life, getting in to fights frequently and allegedly having stabbed someone in an altercation several years ago. He described to practitioners only getting excitement out of reading and watching programmes about serial killers, and occasionally became sexually aroused by this. He had made extensive written plans on how he would capture, torture and kill the couple he believed were responsible for his accident at 16. He also struggles with auditory command hallucinations telling him to harm himself and others. He frequently self harms, often using a Stanley knife to cut his arms and legs. Patient C has been jointly managed by adult psychiatry and neuropsychiatry on an outpatient basis. His risks of aggression and violence have been carefully managed through regular assessment and involvement of forensic services.
Conclusion:
The literature search indicates that the prevalence of psychiatric disorders in patients with brain injury is much higher compared to general population. The significance of the results are however greatly affected by response bias, the impact of patients’ cognitive impairment on their study participation, observer biases and the small study population sizes; however, we believe that these short-fallings should be seen as a trigger to stimulate more comprehensive and wide-scale research in to this field. The methodologies used by authors described in the literature review demonstrate the wide variance in the tools used to assess psychiatric illness in patients following TBI; we therefore argue that universal case definitions need to be agreed on and implemented to standardise studies and reduce bias. The economic impacts and impacts on quality of life have often been neglected by researchers and warrant formal assessment. From a service delivery perspective, rehabilitation programs need to identify patients with signs of psychiatric illness post TBI earlier and involve psychiatric service in the development of integrated care plans to improve the total outcome and quality of life of the patient. The impact on the patient’s family and carers also need to be explored further to provide an evidence base for more effective and holistic interventions.
We report the case of 36 year old white Caucasian female who used to work as a driving instructor and living with her parents.
She has a diagnosis of congenital adrenal hyperplasia (21 hydroxylase deficiency) and is on long term corticosteroid replacement (prednisolone 4 mg once daily and fludrocortisone
100 mcg once daily) and she is under the care of an endocrinologist.
She was referred for psychiatric evaluation with “anxiety and depressive symptoms” and failure to respond to antidepressant treatment which was prescribed by her General Practitioner.
During the psychiatric assessment, she reported long history of recurrent episodes of elevated mood and depression dating back to her late teens with clear description of distinct periods of mood elevations lasting for few weeks and longer periods of persistent low mood. There was no history of psychotic symptoms and no family history of mental illness.
She was diagnosed with bipolar affective disorder and failed to achieve remission of symptoms on two different antipsychotic medications (quetiapine and olanzapine) and anticonvulsant medication (sodium valproate) before starting lithium carbonate.
The introduction of lithium and gradual titration resulted in significant improvement in her symptoms and mood stability. However, few months later, she reported relapse in her symptoms (mainly reporting features of bipolar depression) despite adequate lithium levels.
She agreed on the introduction of lamotrigine as an adjunctive medication to lithium. The initial dose of lamotrigine was 25 mg daily for two weeks in line with dose recommendation from manufacturer and drug guides.
On the same day of lamotrigine introduction, the patient started to experience visual hallucinations that she never had before (please see patient’s perspective for detailed description of her hallucinations).
With the dose of lamotrigine increased to 50 mg daily after the initial two weeks, she started to report worsening of these abnormal perceptions which developed into more complex visual and auditory hallucinations.
More importantly, there was no evidence of accompanying manic symptoms or severe depressive symptoms to explain these symptoms and also no alcohol or drug use.
Following a psychiatric review, the dose of lamotrigine was reduced to 25 mg which resulted in immediate reduction in the intensity of the abnormal perceptions. When the lamotrigine was eventually stopped after one week, there was complete cessation of abnormal perceptions.
Lamotrigine was never re-started again and she was maintained on a combination of lithium and quetiapine with good effect.
Investigation:
We used the Naranjo Adverse Drug Reaction Probability Scale (1) to determine the likelihood of whether an adverse drug reaction is related to this specific drug or may be related to other factors. This tool examine factors such as the temporal association of drug administration and event occurrence, alternative causes for the event, drug levels, dose – response relationships and previous patient experience with the medication.
The probability of the adverse drug reaction is concluded from the total score (Definite if the overall score is 9 or greater, Probable for a score of 5-8, Possible for 1-4 and Doubtful if the score is 0).
Questionnaire
1. Are there previous conclusive reports on this reaction? Yes (+1)
2. Did the adverse events appear after the suspected drug was given? Yes (+2)
3. Did the adverse reaction improve when the drug was discontinued or a specific antagonist was given?
Yes (+1)
4. Did the adverse reaction appear when the drug was re-administered? Do not know or not done (0)
5. Are there alternative causes that could have caused the reaction? No (+2)
6. Did the reaction reappear when a placebo was given? Do not know or not done (0)
7. Was the drug detected in any body fluid in toxic concentrations?
No (0)
8. Was the reaction more severe when the dose was increased or less severe when the dose was decreased?
Yes (+1)
9. Did the patient have a similar reaction to the same or similar drugs in any previous exposure?
No (0)
10. Was the adverse event confirmed by any objective evidence? Do not know or not done (0)
Scoring 7 (Probable Adverse drug reaction)
Discussion:
Lamotrigine is a phenyltriazine derivative used as an anticonvulsant drug with established mood stabilising properties. In the United Kingdom, it is recommended for use in bipolar affective disorder according to the guidelines from the National Institute of Health and Care Excellence (2) and the British Association for Psychopharmacology (3).
We performed a literature search to find similar case reports. We searched the following databases using the keywords (lamotrigine AND hallucinations): Complementary Medicine (AMED), British Nursing Index BNI), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta Medica Database (EMBASE), Health Business Elite (HMIC), Medline, PsycINFO and Health Management Information Consortium (HMIC).
The search returned 57 results. Only 8 articles discussed hallucinations and other psychiatric symptoms as side effects associated with lamotrigine and therefore were included in this review.
Psychotic symptoms have been reported with the use of lamotrigine (both as an anticonvulsant or mood stabiliser) but this reaction is mainly seen in patients with history of epilepsy. One study reported 4.8% incidence of psychiatric and behavioural side effects with lamotrigine in 546 patients with epilepsy. (4)
Another study on paediatric patients showed that reversible visual and auditory hallucinations were reported in one patient among 9 patients with epilepsy who received lamotrigine treatment (mean age 5 years). (5)
Villari et al published a literature review on psychiatric symptoms related to lamotrigine and included case reports documenting full acute psychotic episodes hallucinations and affective switching in patients with and without history of epilepsy.(6)
They found one case report on hallucination with lamotrigine in bipolar patient without epilepsy. In patients with epilepsy, they reported two cases reports and one case series (total number of patients 9) developing psychotic symptoms following lamotrigine and one randomised controlled trial in which four out of 216 patients stopped lamotrigine due to psychotic symptoms (including hallucinations and delusions).
The authors concluded that majority of the case reports concluded that these symptoms were lamotrigine-induced due to the temporal association with lamotrigine treatment and favourable outcome following drug withdrawal. It also appeared that more case reports were from patients with epilepsy, suggesting lower incidence in patients without this condition.
Chistyakova and Amos (7) reported a case of delirium associated with lamotrigine use. The dose of lamotrigine was increased from 200 to 400 mg over two weeks prior to her admission. The patient reported visual and auditory hallucination with confusion. She took an accidental overdose of her medication (200 mg of fluoxetine and 2800 mg of lamotrigine) due to her confusion and medications were stopped.
The authors concluded that delirium may result from lamotrigine toxicity or drug interaction with fluoxetine.
Uher and Jones in 2006 (8) reported a case of a 42-year-old woman with bipolar affective disorder with comorbid alcohol abuse and no history of neurological illness.
The patient tolerated an initial dose of lamotrigine 50 mg/day but following a dose increase to 100 mg/day, she reported vivid dream-like experiences and subsequently she reported visual hallucinations. These symptoms subsided over a few days when the dose was decreased to 50 mg/day.
The authors suggested a causal association through this dose dependent effect but also pointed out that the concurrent alcohol abuse may have been a contributing factor.
They also highlighted the paucity of case reports documenting this rare adverse reaction and identified two similar case reports in their references (which we were unable to get their full text) and a third paper reporting hallucination in 2 out of 108 patients with epilepsy on a combination of lamotrigine and sodium valproate (9)
Hallucination with lamotrigine when combined with valproic acid was also reported in a case report by Roberts et al (10) in 14 year old girl with epilepsy when it was added to valproic acid and it was suggested that this adverse effect may be due to an interaction between the two medications causing lamotrigine half-life to triple with valproic acid.
Learning points:
Lamotrigine is an anticonvulsant with an established role in management of bipolar affective disorder, particularly for the treatment and prevention of depressive episodes.
However, it appears to be associated with variable incidence of psychiatric symptoms which should be known to the prescriber and patient.
These adverse effects are mainly seen in patients with history of epilepsy but can occur in patients with mental health problem without epilepsy.
Different mechanisms for inducing these psychiatric symptoms have been suggested, including idiosyncratic reaction, lamotrigine toxicity as a result of concomitant use of another drug that affect lamotrigine metabolism (e.g., valproic acid) and delirium.
Examples of these psychiatric symptoms including affective switches in depressed patients with bipolar disorder, hallucinations in depressed patients, delirium and psychotic symptoms (mainly hallucinations and delusions) in patients with or without epilepsy.
Reversible and severe psychiatric disturbances associated with lamotrigine therapy are rarely reported in literature and more research is needed to identify population at risk.
Patient education about these rare but frightening side effects is essential to improve medication adherence and better outcome of the management of the mental disorder.
Patient perspective:
“The first hallucination I had was one hour roughly after taking lithium and lamotrigine. It was the Pope which appeared as bright light on my wall. He was wearing a white gown and he had gold jewellery. The picture was so clear and very detailed. I’m not religious and this image would not be something I would think of.
Every day on lamotrigine I had black spots moving quickly around the walls. They were in size of about an inch, 20-30 moving around at one time. Like spiders but without legs. I was really scared at first because I hate spiders. It was very unsettling and I changed my whole bed, away from my wall, and had trouble sleeping.
There was another night when I had similar to the black dots, where instead I had smaller black dots like bees moving into the corner of my room. They were all slightly moving as if they were getting their places. There were hundreds of them.
The scariest incident that happened was hearing voices downstairs. I was so sure that people had broken into the house; I went downstairs armed with razors. I was going to cut DNA from the burglars to give to the police as evidence. When I checked the house, there was no one there.
When I was taking lamotrigine with the lithium, it made me very unsettled, more anxious and mentally unstable. I was so tiered for not sleeping and my decisions irrational. It wasn’t a pleasant place to be for me personally.”
Electroconvulsive therapy (ECT) is an effective treatment for some individuals with severe neuropsychiatric illness. It is widely used to treat certain psychiatricdisorders, particularly major depression.1,2 ECT involves applying a brief electrical pulse to the scalp after the patients are administered muscle relaxants and general anaesthesia.3 This pulse excites the brain cells causing them to fire in unison and produce a seizure.
In 2003, the National Institute of Clinical Excellence (NICE) issued guidance on the use of ECT. Its use was recommended only to achieve rapid and short-term improvement of severe symptoms after an adequate trial of treatment options has proven ineffective and/or when the condition is considered to be potentially life-threatening in individuals with severe depressive illness, catatonia or a prolonged manic episode.4
The mechanism of action of ECT is not fully known. ECT affects multiple central nervous system components, including hormones, neuropeptides, neurotropic factors, and neurotransmitters. The induction of a bilateral generalized seizure is required for both the beneficial and adverse effects of ECT. Certain parameters like seizure duration, electric stimuli, seizure threshold, ECT practice factors and medication can influence its effectiveness. The degree to which electrical stimulation exceeds the seizure threshold, the positioning of electrodes on the head, pulse width, pulse frequency and seizure duration are all known to be important.5 This study aims to review the evidence base of these parameters in detail. The seizure duration and electric stimulus are the two critical parameters and are therefore the main focus of this review.
Literature Review
A review of literature regarding ECT was using search engines like MEDLINE, PsycInfo, and OVID using the key words “electroconvulsive therapy,” “seizure parameters,” “seizure duration,” “seizure threshold,” “stimulus dosing” and “effectiveness.”
Parameters Associated with Effectiveness of ECT
Seizure Duration Electrical Stimulus Seizure Threshold ECT Practice Factors Endocrine Factors Medication Other Parameters
Relationship between Seizure Duration and Effectiveness of ECT
Very little is documented on clinical studies that correlate ECT effectiveness and seizure duration. There is evidence that supports the direct relationship of seizure duration and the effectiveness of ECT. It was thought that measuring the seizure duration and the knowledge of measuring such parameters can help explain its therapeutic effect.6 There has been research which suggests that motor seizures of less than 15 seconds in duration do not exhibit tonic-clonic phases and are ineffective in treatment.7 Some of the studies in past years found a direct relationship between total seizure duration during a course of treatment and patient response to ECT.8
A retrospective study on ward patients found that a positive clinical outcome from depressive symptoms has a direct relationship with accumulative seizure time in the course of therapy.8 However, the study was neither randomized nor controlled. Stimulus intensity, diagnosis, and concurrent medication parameters were not properly considered. Another study that supports the correlation found that 88% of patients with cumulative seizure time of 300 seconds and over had a favourable response. The data was retrospectively and prospectively collected in a university hospital. It was mentioned that data gathering was very difficult specifically with regard to the variable number of patients’ ECT sessions; the confounding effect of medication and the treatment of different patients using unilateral or bilateral.9
However other studies challenge these statements. A prospective study of a sample of depressed patients undergoing ECT, the seizure duration did not correlate with Hamilton Depression Rating Scale (HAM-D) scores after treatment. However, it was found that significant nonverbal memory loss of patients was correlated with seizure duration.10 The seizure duration does not directly influence the frequency of ECT, longer seizures do not equate to fewer ECT treatments. Studies using HAM-D scores do not support the idea that seizure duration is a variable correlated to efficacy.11 Short seizures during ECT for few patients are the result of a medical condition or drug treatment interference. On the other hand, patients who have been subjected to ECT treatment encounter shortened seizures.12
There are studies which show that the length of the cerebral seizure activity or the tonic–clonic convulsion is not related to clinical effectiveness.6,13 However, the treating psychiatrist should question whether, or not, generalised cerebral seizure activity had occurred if, at the first treatment, the convulsion lasted less than 15 seconds or the EEG recording showed seizure activity lasting less than 25 seconds.14 Such brief seizure activity might be the result of a focal or partial seizure, and therefore be of questionable therapeutic efficacy. It has been noted that there are patients who recover with ECT and yet display only short tonic–clonic convulsions. This may be more likely in elderly patients.
Most recent evidence mentions that the quality of cerebral seizure activity and the quality of the desired activity cannot simply be related to its length in time alone. It is recommended that the convulsion be timed from the end of electrical stimulation to the end of generalised, that is, bilateral, clonic activity. EEG monitoring can also be done but one needs to have good experience using this technique and sometimes artefacts can cause misinterpretation of the results.15
Relationship between Electric Stimulus and Effectiveness of ECT
ECT is administered by a constant-current, brief-pulse ECT machine that is able to deliver a wide range of electrical dose, that is, 25–50 mC up to 750–800 mC. It is recommended that new machines deliver a range of dose from 25 to 1000 mC.15 One of the important parameters in predicting clinical response is the degree to which the electrical stimulus exceeds the seizure threshold.16 The maintenance of adequate seizure duration on patients is a complicated issue. Elderly patients are also more susceptible to cognitive side effects than younger patients.17 Patients regularly treated with ECT have records of shorten seizure duration over time, and clinicians need to increase stimulus to maintain duration, which in the long run can lead to complications.18
Electroencephalography (EEG) Findings
Voltage Suppression Studies. Postical voltage suppression refers to the decrease in resting EEG voltage after seizure activity as compared with baseline. Proper excitation of seizures invoke voltage-suppressing neural mechanisms intended to terminate and further seizure activity. This suppression is considered as a lower baseline on the EEG post ictus.19 According to studies, the degree of suppression correlates with seizure generalization, therapeutic adequacy, and bilateral stimulation.20
EEG Waveform Features. Greater ictal EEG amplitude, intensity, and symmetry obtained with bilateral ECT are not common with longer seizures, but they are related to antidepressant outcome.21 Studies found that the immediate post stimulus and mid ictal EEG amplitudes correlated with seizure therapeutic adequacy in depression. The symmetry of waveforms at the midpoint on the EEG tracing was also predictive.20 It was also proven that seizure duration had no impact as an EEG measure of treatment adequacy.21
Seizure Charge. The calculated product of EEG voltage, seizure uniformity throughout the brain, and seizure duration was hypothesized to be a measure of treatment intensity and efficacy.21 The variables included in total seizure charge are not physiologically independent of one another, which means longer seizure duration will not guarantee better results.
Low-dose bilateralelectroconvulsive therapy has a powerful antidepressant effectbut low-dose right unilateral therapy is ineffective.22 Evidence shows that the efficacy of rightunilateral electroconvulsive therapy depends on the electricaldose.23,24 There is some research showing that forboth unilateral and bilateral ECT, a higherelectrical dose leads to a more rapid clinical response.7,17,23
Seizure Threshold and Electroconvulsive Therapy
The knowledge of the seizure threshold is a guide to the selection of the electrical stimulus dose for ECT. In theory, the seizure threshold is the lowest dose of electrical charge for each particular patient that is required to induce seizure.25 In clinical applications the seizure threshold depends on individual patient’s characteristics, treatment history, and other stimulus factors.26
The therapeutic effectiveness of ECT is partly dependent on the degree that the stimulus intensity exceeds the seizure threshold.27,28 This statement is true on unilateral non-dominant electrode placement (UL) and on relative stimulus intensity. On bilateral (BL) ECT, the therapeutic response frequency is dependent on higher relative stimulus intensity,28 whereas barely suprathreshold UL ECT has significantly reduced antidepressant potency in contrast to moderately suprathreshold UL ECT (150% above threshold).6 The clinical use of this can be applied after determining the seizure threshold at the first treatment.22,29 The desired relative stimulus intensity to be maintained during treatments is confounded by variable increase in seizure thresholds during treatment.28 This rise in the seizure threshold lessens the degree to which a fixed stimulus dosage exceeds the seizure threshold which can result in possible diminished treatment therapeutic potency.
The seizure threshold can be higher in the elderly population and this may increase the difficulty of eliciting effective seizures.29,30,31 The choice of anaesthetic agent and other age related factors can also affect the seizure threshold. Propofol can reduce the seizure duration and has a possible effect on the seizure threshold.32 The seizure threshold may sometimes rise during the course of therapy. The dose would usually rise pari passu with a rise in the seizure threshold to maintain the dosing strategy. The seizure threshold can increase about 80% in bilateral ECT and 40% in unilateral ECT over a course of treatment.6 Some studies found increases of only 25–40% for bilateral ECT.33
ECT Practice Factors and Seizure Duration
As discussed earlier, the success of ECT treatment can be related to the degree to which the electrical stimulus exceeds seizure threshold and not the absolute dose that determines clinical outcome, especially in unilateral patients.6 Right unilateral (RUL) treatment at variable dosage can produce seizures of equal duration to bilateral treatment. With low levels electrical stimulation, RUL patients showed only 17% improvement inHAM-D scores compared to 70% in the BL group, despite the same mean seizure duration.22
Positioning electrodes over the non-dominant hemisphere causes lesssevere cognitive side effects than bilateral placement.11,24 In spite of extensive research however, the relative efficacy of right unilateraland bilateral electroconvulsive therapy is controversial.2,34,35 There are studies which have found superior efficacy with bilateral therapy,22,36,37 and then there are other studies which have reported equivalent efficacy.38,39 Because ofthis uncertainty, the American Psychiatric Association TaskForce on Electroconvulsive Therapy recommended thatelectrode placement be determined on a case-by-case basis.2
Multiple ECT stimuli (MECT) is given to patients to achieve longer cumulative seizure durations. The clinical improvement in depression correlates to patients’ total seizure time in MECT. But there is no proven study on the benefits of increased seizure time from the increased number of stimuli administered.40
Endocrine Measures
Oxytocin. According to studies, the measurement of oxytocin released from posteriorpituitary has a direct relationship with HAM-D measured improvement in depression.41 The concentration of oxytocin-associated neurophysin (AON) serum was calculated before and after the patient’s treatment of ECT. The increase in AON positively affects HAM-D. This neurophysin response was evident on ECT treatment but does not relate to EEG-measured seizure duration.
Prolactin. The surge of prolactin released during ECT treatment can be an indicator of clinical improvement. Seizure duration is associated with a rise in prolactin.42 However, the relationship between the magnitude of prolactin release and benefits of ECT is yet to be established.24
Cortisol. Although several variables have been studied as a possible predictor for the efficacy of ECT but results regarding hypercortisolism have been inconsistent. There has been a study to evaluate the relation between pre-treatment cortisol levels and the efficacy of ECT in a population of drug-free inpatients with severe major depression. This study suggests that higher levels of post-dexamethasone salivary cortisol at 9 AM are predictive of ECT efficacy.43
Elevated glucocorticoids may increase the vulnerability of the brain to the adverse effects of repeated seizures.This hypothesis was tested in a study and it was found that, ECT treatments delivered over 2 weeks resulted in a significant improvement in mood and a decline in most measures of cognitive performance. Elevated basal cortisol was associated with a greater decline in performance of executive function, visuospatial processing speed, and verbal memory. It was concluded that elevated cortisol predicts a greater degree of ECT-induced cognitive impairment. 44
Medication
Concurrent medication. Concurrent therapy can be considered under two headings: general medication and psychotropic medication. Both can affect seizure threshold. Anticonvulsants, hypnotics and membrane stabilisers tend to raise the seizure threshold, while preparations containing theophyllines can have the opposite effect. Concurrent psychotropic medication can have a significant effect upon ECT. Benzodiazepines are anticonvulsant and should be avoided if possible, but it is important to remember that there are risks associated with their sudden withdrawal. Some authorities have suggested short-term reversal with flumazenil if their presence is considered to be a limiting factor in the success of ECT, but experience is limited.45,46 Tricyclics tend to be proconvulsant, but there is little evidence of any detrimental effect on ECT. Selective serotonin reuptake inhibitors (SSRIs) tend to reduce seizure threshold and may be associated with prolonged seizures. Monoamine oxidase inhibitors increase seizure threshold and it is essential that the anaesthetist is aware that the patient is taking this class of medication or has done so within the previous 2 weeks. Lithium reduces seizure threshold and serum levels should be checked regularly and kept within a moderate range (0.4–1 mmol/l). Selective inhibitors of the reuptake of noradrenaline in common with SSRIs, can reduce seizure threshold and also cause hypertension. Neuroleptics tend to be proconvulsant at low dosage but increase seizure thresholds at higher dosage.
In a retrospective study of 455 patients involving 5482 treatments differences in tolerability and clinical effectiveness were found between combination therapy (ECT administered together with neuroleptic medication) and ECT monotherapy.47 Seizure duration which was assessed by EEG was significantly longer in patients treated with combination therapy using neuroleptics with lower antipsychotic potency; whereas seizure duration assessed by EEG-monitoring-electromyograph (EMG) was shorter in combination treatments done with atypical substances. In a parallel study, of ECT monotherapy or combination therapy with antidepressants using the same patient group, seizure duration was unaffected by most antidepressants but SSRIs lengthened seizure activity.48 In addition this study found that therapeutic effectiveness was significantly enhanced in the patients receiving tricyclic antidepressants, the tetracyclic antidepressant mirtazapine or SSRIs.
There may also be a role for antidepressants in the prevention of relapse following ECT. A small double-blind placebo controlled study of the tricyclic antidepressant imipramine involving 27 depressive inpatients who had failed on pharmacotherapy prior to ECT showed that imipramine, when compared to placebo, resulted in a significant decrease in the risk of relapse of patients receiving ECT.49 This study is in broad agreement with an earlier randomized, double-blind, placebo-controlled trial using another tricyclic antidepressant nortriptyline, or combination therapy of nortriptyline with lithium in the prevention of post-ECT relapse in patients with unipolar major depression.50 In 29 patients receiving placebo the relapse rate during the 24 week duration of the trial was 86%; whilst in 27 patients receiving nortriptyline 60% relapsed; and 39% of the 28 patients receiving nortriptyline and lithium combination therapy relapsed during the time of the study.
Other parameters
The effectiveness of the treatment is influenced by many other underlying factors, specifically the conditions and factors relating to individual patients. This would include age, sex, physical health status, co morbidities etc. Thus, one should always consider other factors that might affect the efficacy of ECT. Two recent small Japanese studies have suggested that some cardiovascular and EEG parameters may act as markers to predict the therapeutic response of ECT in depression. Postictal systolic heart rate and blood pressure were found to be significant predictors of the therapeutic efficacy of ECT in a study of 24 patients with depression;51 with higher systolic heart rate and blood pressure being associated with more effective ECT.
Discussion
ECT is widely used to treat certain psychiatricdisorders, particularly major depression. Although ECT has been extensively used there is little published information on the effect of seizure parameters and the effectiveness of ECT. There is evidence that supports the direct relationship of seizure duration and the effectiveness of ECT but the latest research suggests that the length in time of the cerebral seizure activity or the tonic–clonic convulsion is not related to clinical effectiveness.10,11 The effectiveness of ECT is related to the quality of cerebral seizure activity and cannot simply be related to its length in time alone. One of the important parameters in predicting clinical response is the degree to which electrical stimulus exceeds the seizure threshold.
Past research has shown that a generalized seizureof adequate duration is necessary and sufficient for antidepressanteffectsand that the intensity of the electrical stimuluscontributes to decreased cognitive function, the principal sideeffect, but not to effectiveness.7 Different types of anaesthetics, or concurrent medications can affect the seizure parameters and its efficacy.52,53 Research shows that a generalized seizureof adequate duration is necessary and sufficient for antidepressanteffects1,7 and that the seizures of less than 15 seconds duration are ineffective. There are other studies which mention that seizure duration does not influence the effectiveness of the ECT.10,11
The Future
Clinicians need to continue to research this difficult area within psychiatry to enhance the evidence base and fill such gaps in this evidence as highlighted by the ECT Handbook.54 On-going research is needed into what is a proven treatment of depressive illness and this should include more in depth research into the relationship of the above discussed parameters with its effectiveness.
“If ECT is ever legislated against or falls into disuse, it will not be because it is an ineffective or dangerous treatment, it will be because of a failure to supervise and monitor it correctly”55 and such supervision includes future quality research by concerned clinicians. Current NICE guidelines have limited the use of ECT to individuals with severe depressive illness, catatonia or a prolonged or severe manic episode who have been unresponsive to other treatment options.In addition, intervention of ECT should be considered to be short term and NICE does not recommend using it as maintenance therapy.56 As research into ECT develops, the consequences may be an even more targeted approach to the use of ECT as therapy.
We report a case of worsening psychiatric symptoms in a patient who was serendipitously diagnosed with Primary Hyperparathyroidism.
Behavioural change in form of aggression sometimes occurs as a component of psychiatric disorders such as psychosis, attention deficit hyperactivity disorder, autistic spectrum condition, conduct disorder and various mood disorders. It may also present as a psychiatric manifestation of an endocrine disorder such as Primary Hyperparathyroidism (PHPT)1,2.
PHPT is rare in children and adolescents with an incidence of 2-5 in 100000 3. It is characterized by hypercalcaemia and elevation of parathyroid hormone. Children with PHPT may present with non-specific complaints such as behavioural change and deteriorating school performance.
Patients who present with non-renal symptoms have a longer duration of symptoms prior to diagnosis of PHPT4,6. It seems probable that it takes much longer for diagnosis to be made in those with pre-existing mental disorder. When left undiagnosed and untreated, PHPT can be a serious disease with significant morbidity.
The finding of elevated serum calcium levels in young people is often fortuitous as they often present with non-specific symptoms3,4. A significant number of hyperparathyroidism cases with neuropsychiatric manifestation have been reported in patients without recorded pre-existing psychiatric diagnosis 3-6.
This case report highlights the need for clinicians to always consider endocrine disorder as a differential diagnosis when treating patients with psychiatric symptoms which are poorly responsive to standard treatment. It also demonstrates the relevance of an integrated approach in healthcare delivery including the importance of good communication between primary and tertiary care clinicians.
Case Report:
A 15yr old Caucasian male known to Child & Adolescent Mental Health Service (CAMHS) for management of his behavioural problems presented in crisis as a consequence of physical aggression, suicidal ideation and homicidal thoughts.
His first contact with CAMHS had been at the age of 10 when he was referred for management of his frequent aggressive outbursts. He had always been boisterous but had no previous history of significant emotional or behavioural difficulties. His developmental history was unremarkable and there were no features indicative of any neurodevelopmental disorder. There was no family history of mental illness.
His biological parents were involved in an acrimonious divorce at the time of his first referral to CAMHS so it was felt that this conflict may have contributed to his presentation.
He was referred a Child Psychotherapist for weekly sessions as the initial assessment suggested significant weakness in his attachment and identification which manifested in the instability and immaturity of mood and behaviour.
The family described minimal improvements in his capacity for self-control having had three years of psychotherapy. His behaviour remained challenging but manageable within the community until six months prior to him being re-referred by his General Practitioner (GP) for urgent psychiatric assessment.
Following parental divorce, his mum remarried but her new marriage was also turbulent and the couple had to separate. During this period of increased psychosocial stresses within his family, the patient’s behaviour escalated to a point that he was regarded as a significant risk to himself and others. It was thought that the separation between his mother and step-father might have triggered this deterioration.
The night before his urgent referral to CAMHS, he set a trap for his mother; he had put a rope around some curtains on the floor and was planning to throw another curtain over her. He also had a knife and hockey stick with him at the time. As his mother stepped into the room, he put the curtain over her head and attempted to hit her with the hockey stick. He was promptly restrained by his father, who had come to visit, before he could do much damage.
He presented as unpredictable and aggressive but would often deny recollection of any reported outbursts. He was very upset when incidents were talked about as he believed he had no control whatsoever over this behaviour – it was clear how upsetting his behaviour was to him.
He displayed uncontrollable rage on many occasions. It was usually directed at his mother and home furniture, and might last up to two hours. He appeared to seek immediate gratification and was clearly hypersensitive to his setting with a significant degree of paranoia and irritability.
He repeatedly stated that he had thoughts of wanting to kill his mother and himself especially when angry. He did not appear able to accept any responsibility for his actions, blaming his temper outbursts on his older sibling. We heard she was extremely frightened of him; he had on two occasions broken down her door.
When he came out of these rages he would become very tearful and profoundly apologetic. These difficulties had been noticed at school where his grades had been falling. He told teachers he felt suicidal and would sometimes go into the school toilet to cry especially when he thought about his inability to control himself.
Physical examination at this point was unremarkable. The Community Psychiatrist commenced him on Fluoxetine and referred him to an in-patient psychiatric unit for further psychiatric evaluation including a forensic assessment.
He was diagnosed with Asperger’s Syndrome and Attention Deficit Hyperactivity Disorder in the inpatient unit and was prescribed risperidone and methylphenidate. His GP was asked to arrange a baseline blood test, consisting of full blood count (FBC), liver function test (LFT), urea & electrolytes (U&E) and thyroid function test (TFT). There was no request for blood glucose level or serum calcium.
The GP asked for a serum calcium level estimate purely out of ‘habit’. The laboratory result showed a high level of calcium 3.89mmol/L (normal range 2.2-2.6). Based on this significantly elevated serum calcium level, a referral was sent to the Paediatric Endocrinologist.
At the Endocrinology Clinic, he described a twelve month history of generalised aches and pains in association with emotional lability. A history of fracture of his right wrist and left hallux occurring within 18 months prior to presentation was also obtained. The X-ray report showed presence of a radiolucent area in his right femur. An assay of his parathyroid hormone, Sestamibi scan and ultrasound scan of his neck were done.
The elevated parathyroid hormone level, increased serum calcium, history of fractures and X-ray features indicated the diagnosis of Primary Hyperparathyroidism. The endocrinologist was of the opinion that his PHPT has been present for a number of years. He was referred for parathyroidectomy.
His serum calcium level dropped to 2.47mmol/L two days post surgery. As calcium level normalised, his symptoms improved remarkably and his psychotropic medications were discontinued. Since then, he has successfully commenced college full time and has succeeded in obtaining good grades in his chosen courses.
Discussion:
Psychiatric symptoms cause significant impairment in children and adolescents. Having additional symptoms of hyperparathyroidism would exacerbate the psychiatric symptoms and increase the degree of impairment. This patient presented with neuropsychiatric symptoms and evidence of end organ damage which is similar to those in published reports3,4.
Research shows that diagnosis of primary hyperparathyroidism is often delayed in young people but we suspect that it may even be more delayed in those with a pre-existing psychiatric disorder as the symptoms may be more likely to be attributable to the psychiatric condition.
It is possible that the behavioural problems in this patient may have co-existed independently of each other, but the rapid resolution of the psychiatric symptoms suggests that they may have been exacerbated by hyperparathyroidism.
Our findings in this case are similar to those reported by Spivak and colleagues’ which showed that early diagnosis of hypercalcaemia can prevent unnecessary and potentially harmful treatment with psychotropic medications7.
Psychiatric diagnoses are usually formed from identification of collective symptoms some of which may occur in other medical conditions. Adopting a multidisciplinary team approach is most helpful in the management of complex psychiatric cases. This approach may encourage clinicians to take a holistic view in management of children.
It is important for clinicians to be familiar with common psychiatric symptoms and medical conditions that may mimic or cause them because the presence of non-specific symptoms in PHPT poses a significant emotional burden for affected children and their families. It is a potentially treatable condition which if not diagnosed early could lead to impaired psychosocial well-being and damage of vital organs. Parathyroidectomy has been shown to improve general health, quality of life and cognitive functioning in patients with PHPT8.
The outcome for this particular young person could have included further episodes of in-patient hospitalisation or involvement with the juvenile justice system as a consequence of further violent episodes. The achievement of adolescent milestones and his education could have been severely disrupted and may have resulted in labelling detrimental to his future.
In the current economic climate and because of the rarity of Primary Hyperparathyroidism, we do not advocate routine serum calcium estimation in all behavioural problems but clinicians should have lower threshold for screening for this condition especially in patients with worsening symptoms despite conventional treatment.
In conclusion, Primary Hyperparathyroidism should be considered in the differential diagnosis in young people with worsening neuropsychiatric symptoms which are unresponsive to standard psychiatric treatment.
Clozapine has shown to have superior efficacy compared to other antipsychotics and is the drug of choice for treatment-resistant schizophrenia. 1 However there is evidence that this treatment is actually under-prescribed. 2 Clozapine requires careful monitoring during the initial titration period. In the UK, this has originally been done in hospital settings to follow the manufacturer’s recommendations because of the risks of hypotension, excessive sedation and fits. Starting clozapine in a hospital setting ceased to be a mandatory regulatory requirement in the UK when the Summary of Product Characteristics was harmonised across Europe following an opinion and recommendation issued on the 12th of November 2002 by the Committee for Proprietary Medical Products of the European Medicines Agency. 3 Despite this happening several years ago, there is little information published about the practicality of successfully commencing clozapine in the community, with previous studies ranging from a single case report 4 to a few small case series of patients 5-8. Our study aimed to examine this practice in a larger sample to highlight the advantages and difficulties of initiating clozapine in the community.
Method
The Central Manchester day hospital was established in 1985, with a focus on acute psychiatric treatment as an alternative to in-patient care. From March 1997, the acute day hospital in Central Manchester was extended to 24 hours, seven days a week, adopting the name of the Home Option Service, focussing on flexible individualised care delivered at patient’s home or team base according to patient choice. 9 In 2007 as part of implementation of new teams across the city to comply with NHS policy guidance 10 the Home Option service developed further to become the crisis resolution and home treatment team (CRHT) for central Manchester, whilst CRHTs were set up de novo in North, and South Manchester, thereby, providing acute community psychiatric care to a metropolitan area of about 500,000 people.
This study describes a large case series of patients referred for clozapine titration in the community to these teams during a three year period. We collected data retrospectively from April 2007 to April 2010 of all the referrals to the three crisis teams, which have assumed the responsibility of providing the service of initiating clozapine in the community. The teams followed the Trust protocol for non-inpatient clozapine titration, which includes recommended monitoring parameters, dosing schedule and algorithms for the management of complications. This protocol is in essence similar to established guidelines. 4,5, 11
Statistical analysis was done using SPSS version 15 for Windows. Comparisons were made using the Student t-test, non parametric tests or the Chi-Square test according to the type of data.
Results
There were 6542 referrals to the crisis teams and 66 of those were related to clozapine initiation. Out of these, 36 were for a first time titration and 30 were referred for re-titration. The latter group were patients previously taking clozapine but who had discontinued it abruptly for a period longer than 48 hours. The reasons for stopping clozapine in those cases were lack of adherence (n=21), a supplying difficulty (n=5) and medical complications (n=4), such as neutropenia, collapse secondary to dehydration, or undergoing surgery. Two of the patients in the re-titration group restarted clozapine in hospital but were discharged early to continue the titration in the community under the care of the crisis team. Six patients in the titration group were initially referred to the crisis team for stabilisation of their mental state following a crisis; however, during the course of this intervention it was decided to start them on clozapine as they showed poor response to other antipsychotic trials.
Fig. 1 - Referrals, number of patients starting clozapine and drop-outs
The characteristics of the sample are presented in Table 1. The majority of patients were single white males, with a diagnosis of schizophrenia and a mean age of 38.8 years (standard deviation = 9.2). The flowchart in Figure 1 outlines the number of referrals, titrations, and reasons for stopping. Clozapine titration commenced in 54 cases (81.8% of referrals), the other 12 patients refused this treatment. Out of the patients who refused treatment, 8 were severely mentally unwell and were admitted to hospital compulsorily under the Mental Health Act. There were 46 (85.2%) patients who successfully completed the community titration. The attrition rate of 14.8% (8 cases) was due to 7 patients withdrawing their consent and one patient who was unable to tolerate the titration. This person was admitted to hospital with hypotension and vomiting. The other 7 patients withdrew their consent for the following reasons: lack of adherence (n=2), deterioration in mental state (n=1), refusal to continue with the physical monitoring (n=1), lack of motivation (n=1), and reluctance to continue due to side-effects (n=2). The mean final dose of clozapine was 309.1 mg (s.d. - 75.1 mg). The mean duration of titration was 34.6 days (s.d. - 20.3) and the mean length of admission to the crisis team was 45.9 days (s.d. - 39.5). The median waiting time for crisis team intervention after the referral was 2 days (range 140 days). The median waiting time to start clozapine was 7 days (range 217 days) from the point of referral.
Table 1. Sample characteristics
Total
Age in years, mean (s.d.)
38.8
(9.2)
Gender, n (%)
Male
45
(68.2)
Female
21
(31.8)
Ethnicity, n (%)
White
45
(68.2)
Black
14
(21.2)
Asian
3
(4.5)
Other
4
(6.1)
Marital Status, n (%)
Single
54
(81.8)
Married or cohabiting
5
(7.6)
Separated or divorced
6
(9.1)
Widowed
1
(1.5)
Diagnosis, n (%)
Schizophrenia
54
(81.8)
Schizoaffective disorder
8
(12.1)
Bipolar affective disorder
1
(1.5)
Other
3
(4.5)
Crisis Team, n (%)
North
21
(31.8)
Central
31
(47.0)
South
14
(21.2)
Days waiting to crisis team intervention
Mean (standard deviation)
9.5
(25.6)
Median (range)
2
(140)
Days waiting to start clozapine
Mean (standard deviation)
23.1
(40.9)
Median (range)
7
(217)
Days taken to complete the titration
Mean (standard deviation)
34.6
(20.3)
Median (range)
28
(101)
Days under the care of the crisis team
Mean (standard deviation)
45.9
(39.5)
Median (range)
34
(235)
Final dose in mg
Mean (standard deviation)
309.1
(75.1)
There were few significant differences between the group of patients starting clozapine for the first time (titration) and those restarting it following a treatment break (re-titration). There was a shorter wait for patients in the re-titration group to recommence clozapine from the time of referral to the service (median=6 days, range = 41 days), compared to those starting clozapine for the first time (median=13 days, range= 217 days). This difference was statistically significant (Mann Whitney U= 201.5, z=-2.529, p=0.01). Patients with first titration on clozapine reached a lower final dose (mean=288 mg, s.d.=50 mg), compared to those having re-titration (mean dose =340 mg, s.d.=94 mg). The mean difference of 52.7 mg (95% C.I. 8.7 to 96.8) between these two groups was significant (t test=-2.178, d.f 42, p=0.02). In terms of ethnicity, patients in the initial titration group were more likely to be Caucasian (n=30, 83%), whereas only half of the patients in the re-titration group were Caucasian (n=15, 50%). This difference was statistically significant (Chi-square with continuity correction = 6.915, df = 1, p=0.009).
There were also significant differences in the distribution of titrations and re-titrations across the three crisis teams. The Central Team dealt with more re-titrations (n=23) than the North (n=4) and the South (n=3) teams. Conversely, the Central Team had fewer patients referred for initial titration (n=8), compared to the North (n=17) and the South (n=11) teams. These differences were significant (Chi-square=19.493, df=2, p<0.0001). Another difference between the teams was the duration of clozapine titration, with the South team taking shorter time (mean=24.15 days, s.d.=7.151), compared to the North (mean=29.5 days, s.d=16.342) and the Central team (mean =43.67 days, s.d.= 23.797). This difference was statistically significant (Kruskal-Wallis chi-square=8.823, d.f.=2, p=0.0121).
No significant differences were found between teams and titration or re-titration groups in terms of patient’s diagnosis, gender, marital status, age, rate of accepted referrals, proportion of successfully finished titrations or waiting time to crisis team intervention.
With regards to adverse events, most patients experienced transient tachycardia (n=30, 55.5%). Other side-effects were excessive salivation (n= 15), hypotension (n= 13), sedation (n=10), hyperthermia (n=8), dizziness (n=6), constipation (n=6), hypertension (n=5), headaches (n=4), nausea (n=2), and heartburn (n=2). Less common adverse events (n=1) were syncope, seizures, transient neutropenia, atrial fibrillation, blurred vision, swelling of the arms , acute dystonic reaction, nocturnal incontinence, exacerbation of asthma, diabetes, erectile dysfunction and delayed ejaculation. Only the patient who developed syncope, which was associated with vomiting and severe hypotension, had to be advised to stop the treatment in the community and was admitted to hospital. For the rest of the patients, the other reported adverse events did not impede the successful completion of clozapine titration in the community.
In terms of longer term outcomes, a total of 50 patients (75.8% of the total sample) were still taking clozapine at the time the data was collected. This is after a median 337 days (range 824 days) from being referred to the crisis team. The majority of patients (n=14, 21.2%) who were not on clozapine had chosen to discontinue the treatment. One patient had died, but the cause of death was not related to clozapine treatment. One patient had developed neutropenia and needed to discontinue clozapine for this reason. Out of the 46 patients who successfully completed the titration, 40 (86.96%) were still continuing clozapine at the time we collected the data. This is after a median 365.5 days (range 824 days) after they commenced clozapine in the community.
Discussion
The results of this study confirm that clozapine can be safely and successfully started in the community. Comparing this to published evidence, we found only one case report 4 and a small study 5,6 previously conducted in the UK. O’Brien et al. 5,6 initially considered 26 patients in their study; however, only 14 patients started clozapine in the community as the rest were considered too unwell and were admitted to hospital. One patient refused daily access and therefore only 13 patients completed the titration. The side effects reported in this study were minor, including sedation in 5 cases, dizziness in 4 patients, hypotension in two and nausea and vomiting once. Compared to our results, O’Brien et al. described a larger proportion of patients needing to be admitted to hospital for clozapine titration.
We found two published studies 7,8 regarding clozapine community titration that were conducted in the United States. The first study included 47 patients who started clozapine in a partial hospitalisation program. Adverse reactions here were common. Patients were titrated much more quickly than in our report, (i.e. to 350 mg over 2 weeks), which might explain the higher incidence of side effects reported, including drowsiness (93.6%), hypersalivation (93.6%), constipation (89.4%), weight gain (72.3%) and tachycardia (57.4%). However no patient discontinued clozapine, and the potentially serious complications were much less frequent, including 3 cases (6%) of seizures and 2 of leukopenia. The other study 8 conducted in the US demonstrated some evidence of cost savings associated with decreased hospitalisation in 28 patients who started clozapine on an outpatient basis.
Johnson et al. 7 discuss in their report that the reluctance to start clozapine outside inpatient settings may be due partly to the potential adverse reactions, but also to clinicians’ fears of making mistakes, avoidance of additional duties, and anticipation of difficulties in patients with a history of non-adherence to treatment. The results of our study support a careful approach to starting clozapine at home in this latter group of patients, as they represented the bulk of cases not achieving the intended outcome of a successful community clozapine titration. However, our study confirms that other reasons to deny a patient the opportunity to start clozapine at home, such as potential adverse events, are hardly justified.
The general advantages of community psychiatric care as opposed to inpatient treatment have been described elsewhere 9. These include accessibility, flexibility and user satisfaction. Treating patients in their own homes avoids the stigma of hospital admission, prevents the breakdown of important social networks and avoids disruption to patients' benefits. A recent Cochrane review 12 found that crisis/home care reduces the number of people disengaging early, reduces family burden, and is a more satisfactory form of care for both patients and families. Some patients who might have been reluctant to start clozapine if they had to be admitted to hospital can therefore benefit from starting this treatment at home supported by crisis teams.
Although a detailed cost-benefit evaluation of this service was not undertaken, it is fair to assume that the costs associated with titrating clozapine at home would be significantly lower than those associated with in-patient care, as demonstrated in previous studies. 8,12
In summary, clozapine can be safely started in the community, but has to be carefully monitored. Patients’ adherence to the treatment and to the physical monitoring requirements is the key element to a successful outcome. Crisis teams are in an ideal position to support patients undergoing initiation of clozapine at home, although this specific role was not originally identified in policy guidance.10 The results of this multi-site study are encouraging and can be applicable to other crisis or community teams nationally.
Insomnia is chronic inability to obtain the amount of sleep needed for optimal functioning and well-being. Insomnia has received much attention in last few decades, since it has become a growing and complex problem in our society.1 Insomnia is defined as the chronic complaint of difficulty initiating or maintaining sleep, early awakening, and interrupting or non-restorative sleep. Furthermore, it must be accompanied by clinically significant impairment in day time function, for which there is no identifiable cause such as another sleep, psychiatric or medical disorder.1
General Criteria for Insomnia:2
A complaint of difficulty initiating sleep, difficulty maintaining sleep, or waking up too early or sleep that is non-restorative or poor in quality. In children, the sleep difficulty is often reported by the caretaker and may consist of observed bedtime resistance or inability to sleep inadequately.
The above sleep difficulty occurs despite adequate opportunity and circumstances for sleep.
At least one of the following forms of daytime impairment related to the night-time sleep difficulty is reported by the patient:
Fatigue or malaise
Attention, concentration or memory impairment
Social or vocational dysfunction or poor school performance
Mood disturbance or irritability
Daytime sleepiness
Motivation, energy or initiative reduction
Proneness for errors, or accidents at work or while driving
Tension, headaches or GI symptoms in response to sleep loss
Concerns or worries about sleep
Insomnia is prevalent condition in both the general population and in clinical practice, and it is associated with significant morbidity and mortality. It may present as the primary complaint or in association with physical or mental health problem.
Classification:
Insomnia can be classified into two main etiologic groups:
Primary Insomnia: When identifiable etiologies for insomnia have been ruled out, a diagnosis of primary insomnia can be made.
Secondary Insomnia: Related to other medical disorders, mental disorders or related to known organic factors.
Insomnia can be divided in to three types based on duration:
Less than one month called Acute or Transient insomnia.
One to six months called Sub-acute or Short-term insomnia.
More than six months called Chronic insomnia.
Following types of Insomnia recognized in The International Classification of Sleep Disorders (ICSD) second edition, Diagnostic and Coding manual:2
Adjustment Insomnia (Acute Insomnia)
Psycho-physiological Insomnia
Paradoxical Insomnia
Idiopathic Insomnia
Insomnia Due to Mental Disorder
Inadequate Sleep Hygiene
Behavioural Insomnia of Childhood
Insomnia Due to Drug or Substance
Insomnia Due to Medical Condition
Insomnia Not Due to Substance or Known Physiological Condition, Unspecified (Nonorganic Insomnia, NOS)
Physiological (Organic) Insomnia, Unspecified
Prevalence:
One third of adult population reports insomnia, 9 to 12% experience day time consequences and approximately 6% meet formal criteria for an insomnia diagnosis.3 Insomnia is more common among women, middle-aged and increases with age, shift workers and with medical or psychiatric disorders.
Consequences:
Persistent insomnia can produce an important burden for individual and society, as evidenced by reduced quality of life, impaired daytime functioning and increased absenteeism at work, and higher health-care cost. Persistent insomnia is also associated with increased risks of depression and chronic use of hypnotics.
Diagnosis of insomnia is based on subjective complaint of difficulties falling or staying asleep or non-restorative sleep that is associated with marked distress or significant daytime impairments. Several indicators such as intensity, frequency and duration, needs to be evaluated to assess severity of insomnia.
Evaluation:
Insomnia is an important public-health problem that requires accurate diagnosis and effective treatment (Standard).4 Insomnia is a symptom of an underlying disorder or condition. The insomnia may be a problem directly related to the sleep-wake regulatory system and/or it might be associated with a comorbid psychiatric, behavioural, medical, or neurological condition.4 Insomnia is primarily diagnosed by clinical evaluation through a careful, detailed medical, psychiatric, and thorough sleep history (which includes assessment of sleep patterns and waking processes) (Standard).4
Treatment options:
Pharmacotherapy is currently the most common treatment modality for insomnia,5 but long-term use of hypnotics in chronic insomnia can become complicated by drug tolerance, dependence or rebound insomnia. Since insomnia is a chronic condition, long-term and safe treatments are warranted. Non-pharmacological options provide longer lasting benefits.
If a cause of insomnia is identified, initial treatment should be directed at the specific factor. If insomnia persists, non-pharmacologic and/or pharmacologic interventions should be instituted. Hypnotic agents are the treatment of choice for the management of acute or transient insomnia. The expected goal is to normalize the sleep pattern within a few days to weeks. Behavioural interventions are important aspect of the treatment of chronic primary insomnia.
Classification of evidence (Table 1) is used to determine different level of recommendations (Table 2), which is available for behavioural therapies in management of insomnia.
Table 1: AASM (American Academy of Sleep Medicine) Classification of Evidence (Based on Sackett system,6 the criteria for grading evidence level of each study)
Randomized well-designed trials with low alpha and beta error (Grade I) Randomized trials with high alpha and beta error (Grade II) Non-randomized concurrently controlled studies (Grade III) Non-randomized historically controlled studies (Grade IV) Case series (Grade V)
(Alpha (Type I error) refers to the probability that the null hypothesis is rejected when in fact it is true (generally acceptable at 5% or less, or p<0.05). Beta (Type II error) refers to the probability that the null hypothesis is mistakenly accepted when in fact it is false (generally trials accept a beta error of 0.20). The estimation of Type II error is generally the result of a power analysis. The power analysis takes into account the variability and the effect size to determine if sample size is adequate to find a difference in means when it is present (Power generally acceptable at 80-90%).
Table 2: AASM Levels of Recommendations (The following are recommendations of the SPC (Standards of Practice Committee) approved by the Board of Directors of the AASM).7
Term
Definition
Standard
This is a generally accepted patient-care strategy, which reflects a high degree of clinical certainty. The term standard enerally implies the use of Level I evidence, which directly addresses the clinical issue, or overwhelming Level II evidence.
Guideline
This is a patient-care strategy, which reflects a moderate degree of clinical certainty. The term guideline implies the use of Level II evidence or a consensus of Level III evidence.
Option
This is patient-care strategy, which reflects uncertain clinical use. The term option implies either inconclusive or conflicting evidence or conflicting expert opinion.
Recommendations according to type of Insomnia:10, 11, 12
For both, chronic primary insomnia and secondary insomnia, the standard psychological and behavioural interventions are effective and recommended.
Recommendations for specific therapies:
1. Stimulus control therapy
Effective and recommended therapy in treatment of chronic insomnia (Standard)
Objective is to train the insomnia patient by a set of instructions designed to re-associate the bed and bedroom with sleep and to re-establish a consistent sleep-wake schedule:
Go to bed only when sleepy;
Get out of bed when unable to sleep;
Use the bed/bedroom for sleep only (no reading, watching TV etc.);
Arise at the same time every morning;
No napping.
2. Relaxation training
Effective and recommended therapy in treatment of chronic insomnia (Standard)
Aimed at reducing somatic tension (e.g. progressive muscle relaxation, autogenic training) or intrusive thoughts at bed time (e.g. imagery training, meditation) that interfere with sleep.
3. Cognitive Behavioural Therapy (CBT) with or without relaxation therapy
Effective and recommended therapy in treatment of chronic insomnia (Standard)
CBT includes various combinations of both cognitive as well as behavioural interventions. The cognitive component is aimed at changing patient's beliefs and attitudes about insomnia. The behavioural component may include therapies such as stimulus control therapy, sleep restriction or relaxation training. Sleep hygiene education is often also included.
4. Sleep Restriction
Effective and recommended therapy in chronic insomnia (Guideline)
It involves curtailing the amount of time in bed to actual amount of time spent asleep. For example, if a patient reports sleeping an average of 6 hours per night, out of 8 hours spend in bed, the initial recommended sleep window (from lights out to final arising time) would restrict to 6 hours. Periodic adjustments to this sleep window are made contingent upon sleep efficiency, until optimal sleep duration is reached. Therapy creating mild sleep deprivation, and then lengthening sleep time as sleep efficiency improves.
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
Combining stimulus control therapy, relaxation training, sleep hygiene education
Combining stimulus control therapy, sleep restriction therapy, sleep hygiene education
Combining sleep restriction therapy, stimulus control therapy
6. Paradoxical intention
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
It involves instructing the patient to remain passively awake and avoid any effort (i.e. intention) to fall asleep. The goal is to eliminate performance anxiety, as it may inhibit sleep onset. This parameter is limited to sleep initiation insomnia.
7. Biofeedback
Effective and recommended therapy in treatment of chronic insomnia (Guideline)
It provides visual or auditory feedback to patients to help them control some physiological parameters (e.g. muscle tension) in order to seek reduction in somatic arousal.
EEG Neurofeedback training: It is a self-regulation method that makes use of learning theory, more specifically, the paradigm of operant conditioning.8 While the EEG is measured; the patient receives instant feedback (visual and/or auditory) on the cortical activity of the brain. The goal of this treatment modality is to normalize the functioning of the brain by inhibiting and/or reinforcing specific frequency bands.
Recommendations relevant to specific patient groups:
Psychological and behavioural interventions are effective and recommended in treatment of insomnia in older adults (Standard) and among chronic hypnotic users (Standard)
Insufficient evidence is available for sleep hygiene education, imagery therapy, and cognitive therapy to be an option as a single therapy. (No recommendation level)
Sleep Hygiene Education: Please see table 3
Table 3: Sleep Hygiene Education:
1. Attempt to maintain a regular sleep-wake cycle 2. Obtain morning light exposure 3. Use the bedroom only for sleep and intimacy 4. Create a comfortable, quiet, dark and temperature-controlled bedroom environment 5. Develop a relaxing routine within an hour before bedtime 6. Exercise regularly, but not within a few hours of bed time 7. Avoid use of alcohol and other addicting substances 8. Avoid caffeine or nicotine, especially within a few hours of bedtime 9. Avoid empty stomach or heavy meals before bed time, a light snack may be of value 10. Avoid daytime napping, or if napping, be aware of the impact that napping has on nighttime sleep 11. Avoid disturbances at bedtime (e.g. disruptive noises, pets, family) 12. Avoid work, computers and emotional stress in the bedroom 13. Avoid keeping a clock close to the bed to prevent “clock watching” 14. Avoid excessive wakeful time in bed (>20 minutes)
Imagery therapy: It involves a visualization technique to focus on some pleasant or neutral images to block out unwanted thoughts before sleep.
Cognitive therapy: Psychological methods aimed at challenging and changing misconceptions about sleep and faulty beliefs and attitudes about insomnia and its perceived daytime consequences.
Limitations of non-pharmacological management:
Gains in sleep onset or total sleep time are not immediately attained.
Patient motivation and encouragement are required for success of management.
Non-pharmacological interventions are more expensive and time-consuming.
They require the availability of a skilled therapist.
Results:
Psychological and behavioural therapies produce reliable changes in several sleep parameters of individuals with either primary insomnia or insomnia associated with medical and psychiatric disorders.10 A Meta-analysis indicates that in patients with primary insomnia, behavioural interventions produce improvements in sleep parameters (sleep onset latency, time awake after sleep onset (WASO), number of awakenings and total sleep time) in about 70 to 80% of patients.9 Behavioural interventions are more expensive, time-consuming and require the availability of a skilled therapist, but the benefits are long lasting.13
Clinical Pearl:
Pharmacotherapy is currently the most common treatment modality for insomnia,5 but long-term use of hypnotics in chronic insomnia can become complicated by drug tolerance, dependence or rebound insomnia.
Psychological and behavioural therapies produce reliable changes in several sleep parameters of individuals with either primary insomnia or insomnia associated with medical and psychiatric disorders.
Behavioural interventions are important aspect of the treatment of chronic primary insomnia; they should be used in every patient of Insomnia.
Patients who present to physicians with altered mental health and behaviour may prematurely be diagnosed to have psychiatric illness. Psychiatric manifestations commonly accompany acute medical illnesses. As a rule of thumb, organic causes need to be ruled out before making a psychiatric diagnosis. A delay in arriving at a diagnosis could lead to prolonged psychiatric symptoms and unnecessary use of psychotropic medications. Prognosis and recovery will vary depending on the type of accompanying medical illness. Below, two cases are presented which varied significantly in terms of the sequelae.
Case 1
A female patient in her late 20’s was referred from primary care as she reported a sudden onset of “hearing voices”. The patient disclosed that she was bullied at work 6 months prior to this episode which resulted in change of job role and bullying has been dealt with. She described that the voices were talking about world politics and wanted her join MI5. She also believed that there were evil scientists who could read her mind through telepathy and felt that there were cameras and bugs planted in her house by a plumber. She became suspicious that her neighbours were spying on her. Her sleep was disturbed and she heard a ‘tick-tock ‘sound. This led to her checking pipes and walls to find the origin of the sounds. She believed that people were throwing things on to her bed and became very distressed - to the extent that the police were called on many occasions. She believed that people had been using telepathy on her and that aliens were invading the world. She was so distressed that she attempted to end her life by drinking bleach on one occasion and trying to cut her wrist on another.
There is no previous history of mental illness and no mental illness in the family.
Her medical history revealed that she had had mastoid surgery four years ago. Three weeks prior to the psychotic episode noted above, she had an ear infection with discharge from her ear. She presented to the general practitioner with psychotic symptoms at the same time. A CT scan of the brain was normal. A 2 week course of antibiotics in the form of Co-amoxiclav was given by the general practitioner. Her psychiatric manifestation resolved completely on follow up at two months without any psychotropics or Benzodiazepines, The patient was then kept under ‘wait and watch’ for six months in order to monitor any re-emergence of psychotic symptoms. She did not report any further episodes of ear infections during this period of follow up. Her diagnosis was Diseases of middle ear and mastoid (H65-H75).
Case 2
A 31 year old lady was referred to secondary mental health services from a Neurology team, presenting with psychotic symptoms following a viral encephalitis infection. A diagnosis of Herpes Simplex viral (HSV) encephalitis was confirmed by lumbar puncture and a CT scan by the Neurology team. She had made a gradual recovery from the encephalitis over a period of one month. She developed psychotic symptoms 2 weeks later, where she believed that doctors were trying to kill her and that she had been raped, with no evidence that this had occurred at any time. Her distress worsened which led to her informal admission to an inpatient mental health unit. A close assessment on the ward showed her to display an intermittent picture of worsening gait. A neuropsychiatry assessment confirmed that this lady had acquired brain injury following Herpes encephalitis. Single photon emission computed tomography (SPECT) showed extensive brain injury consistent with HSV. This lady presented with several acute episodes of psychosis where she complained of hearing voices and believed that people were trying to harm her. Her mood was labile and variably responsive to Olanzapine initially with a control of her psychotic symptoms as well as mood behaviour. She was diagnosed as suffering from Organic Delusional (Schizophrenia-like) Disorder (ICD 10 F06.2), with a picture of Paranoid Schizophrenia secondary to viral encephalitis. A maternal aunt was said to have suffered from Schizophrenia. Later on she had frequent relapses of psychosis and Quetiapine was initiated. As her symptoms did not respond to two different anti-psychotics, she was started on Clozapine which gave her reasonable stability. However, she still needs support while walking andhas been transferred to a suitable neuropsychiatric rehabilitation placement to maximise her independence and manage her ongoing needs.
Discussion
The two cases above display infective neurological diseases characterised by psychiatric presentations and greatly differing prognosis. The first case was an example of a chronic recurrent ear infection which was likely to have involved inner ear, mastoid or temporal lobe but has subsided without any long term sequelae. This was promptly treated with antibiotics at an early stage with complete recovery and there was no evidence of brain injury on imaging. The psychiatric manifestation was dramatically acute in this case and this could be partly attributable to stress at work. In particular there was neither previous history of mental illness nor a family history of psychiatric disorders.
In the second case, there was evidence of significant brain injury resulting in both physical and psychiatric sequelae following herpes encephalitis. Furthermore, this patient has a family history of schizophrenia which might have influenced the manifestation of the Mental Disorder.
There is significant evidence to suggest that childhood neurological viral infections increase the risk of psychotic illness 1. In both cases there was no suggestion of such illness in the childhood history. A recent study investigated whether HSV1 exposure was associated with structural brain abnormalities in individuals who, because of genetic or other factors, were deemed at high risk of developing psychosis. The results suggested that a history of HSV1 infection is associated with volumetric gray matter reductions in individuals at high risk for developing psychosis 2. In our second case, SPECT imaging confirmed grey matter loss and with the strong genetic risk would have led to the psychiatric illness.
The relationship between bacterial infections and psychotic illness in less well understood. Schizophrenic illnesses are often multifactorial in origin following a complex interplay between genetic and environmental factors such as infections. While there are various reports of Neurosyphilis, Mycoplasma Pneumoniae and Cryptococcal meningitis causing psychotic illness, specific bacteria could not be isolated in the first case presented 3-7. The improvement with antibiotics simply suggests that this could be a bacterial infection.
In summary, these cases clearly show the importance of identifying and treating medical illness presenting with psychiatric symptoms at the earliest to prevent long term complications.
Evidence has consistently shown that patients with mental illness have greater physical health morbidity and mortality compared to the general population.1 Many factors have been implicated and include a generally unhealthy lifestyle, side effects of medication, and inadequate physical healthcare.2, 3 Higher rates of suicide and accidents are other known risks. Psychiatric patients are more likely to smoke, have less inclination to exercise, and are prone to poor dietary habits and obesity, the latter through general inertia, the result of the adverse effects of neuroleptic medication, or increased alcohol use. Psychotropic medication is associated with impaired glucose tolerance and diabetes, metabolic syndrome, dyslipidemia, cardiovascular complications, extrapyramidal side effects and sexual dysfunction. A broad range of clinician and organisational factors prevent access to adequate physical healthcare that in turn compounds the above problems.
Scale of physical morbidity and mortality in mental illness
Patients suffering from depression are twice as likely to develop type 2 diabetes mellitus, and the prevalence of stroke and myocardial infarction is three- and five-fold respectively higher than people without depression.4 A mortality rate ratio (MRR) of 2 to 3 in patients with schizophrenia or bipolar disorder is a general finding.5 Schizophrenia is associated with higher rates of diabetes mellitus (side effects of medication partly to blame), osteoporosis (lifestyle risk factors play a role), obesity, and cardiovascular problems. 2, 6, 7, 8 It has been estimated that life expectancy is reduced by at least ten years. 9, 10 People with learning disabilities, particularly those with concurrent epilepsy, dementia and polypharmacy, are at greater risk of developing added complications.11 Eating disorders are associated with a high mortality because of physical disorders caused by anorexia/bulimia nervosa affecting other organ systems.12 Mental illness in general is associated with an increased risk of hepatitis, human immunodeficiency virus (HIV), tuberculosis, and poor dental health. 9, 10
Causes of raised physical health morbidity and mortality in psychiatric patients
Explanations for the higher morbidity and mortality in mental illness include cardiovascular and respiratory problems in addition to the increased suicide risk. Aetiological factors include adverse effects of medication (weight gain, diabetes, and dyslipidemia), lifestyle (smoking and the cost of smoking, poor diet and nutrition, lack of exercise, and obesity) and inability to access physical healthcare. Obesity, smoking and physical inactivity contribute to hypertension. Poor physical healthcare outcomes in mental illness are related to a combination of factors generally considered under the headings of patient/illness, psychiatrist/physician, and service provider/system issues.
De Hert and colleagues 9, 10 have outlined the factors that account for the raised physical health problems.For instance the patient/illness factors comprised difficulty in understanding health care advice combined with the motivation required to adopt new changes in lifestyle, poor compliance with treatment, cognitive deficits, reduced pain sensitivity (induced by antipsychotic medication), poor communication and deficient social skills (seen in many cases of schizophrenia, for example) which all accounted for the shortened life-span of patients with severe mental illness (SMI).
An additional patient/illness factor is that psychiatric symptoms may render patients less inclined to discuss physical problems. Some doctors are uncomfortable dealing with psychiatric patients because the latter may be cognitively compromised which may impair or impede a doctor’s clinical assessment. The stigma of mental illness, often the result of disparaging media coverage and negative stereotypes surrounding psychiatric patients, are other hurdles that prevent people from seeking treatment. Furthermore, psychiatric patients are less likely to see a primary care physician and therefore to receive other interventions such as screening for cancer.
Psychiatrist-related factors are characterised by an overemphasis on mental health to the exclusion of physical health, infrequent screening rates for metabolic abnormalities, omission of medical examination of patients because physical complaints frequently are part of the psychiatric presentation, poor communication with the patient and the primary care teams, a lack of awareness and perhaps adherence to treatment guidelines, insufficient medical knowledge, and erroneous, sometimes misguided beliefs about patients’ capability to change their lifestyle.9, 10 Even when risk factors are documented in the patient's clinical file, very little is done by way of further investigations or prevention.
Factors common to the psychiatrist and other physicians include a tendency to dismiss or interpret physical symptoms as psychosomatic, lack of good quality care, unequipped teams, insufficient assessment, and difficulties providing consistent monitoring and continuity of care. Other physician-related factors relate to problems coordinating psychiatric and medical care.9, 10
Service-provision factors included a lack of clarity and consensus as to where the responsibility of physical health lies.9, 10 Should general practitioners (GPs) supervise the majority of patients who do not suffer from severe, enduring mental illness? Should patients with acute alcohol withdrawal symptoms be managed at home by the GP, treated in a general hospital, or admitted to a psychiatric unit? The fragmentation of medical and mental health care systems, lack of integration of services (poor or absent liaison links) and insufficient funds to resource the mental health service, limit the ability of most psychiatrists to focus beyond their own speciality.
Service and system changes are prevalent in industrialised countries because reforms in mental health have led to reduced inpatient resources leading to shorter and infrequent hospital admissions with less time available to focus or investigate physical health problems. In the United Kingdom (UK) there is intense emphasis on community care and talking therapies, yet the management of physical health issues by community mental health teams may be poor because of inadequate training and learning.
Recommendations to improve physical health care in psychiatric patients
Health care professionals need to be more aware of these findings in order to improve medical screening and treatment of psychiatric patients. Currently there is no evidence this is happening, with increasing concerns regarding inequalities between those with and without mental illnesses.13
We propose the following recommendations to promote integration between mental and physical health care:
1.A greater effort to increase awareness of the problem among primary care and mental health care providers. The Royal College of Psychiatrists has launched a campaign called Fair Deal to highlight the importance of physical health of people with mental illness.1 Patients still feel stigmatised and therefore psychiatrists need to boost their efforts to reduce this discrimination. The excess mortality associated with this discrimination needs to be recognised as a human rights issue.13
2.Primary care providers need to change the culture of undertreating physical health in mental health patients. The National Institute for Health and Clinical Excellence (NICE) guidelines for schizophrenia and bipolar disorder highlight the importance of monitoring antipsychotics and mood stabilizers.14 The Royal College of Psychiatrists should lead by implementing the NICE guidelines for mental and behavioural conditions.
3.Education and training of doctors who pursue a career in psychiatry needs to be improved with mandatory trainee placements in acute medicine or neurology, regular personal development plan (PDP) courses, and training to update knowledge of recognising physical illness and the performance of basic medical tasks. The Royal College of Psychiatrists should develop a diploma in clinical psychiatry for GPs and clinicians with a specialist interest in psychiatry. The curriculum needs to be widened to include electrocardiogram (ECG) interpretation, basic endocrinology, and neurological investigations (magnetic resonance imaging and so forth). This would allow psychiatrists to develop better liaison with their fellow professionals and share responsibility with them, which undoubtedly would encourage good medical practice.
4.The Royal College Scoping Group’s report15 sets key standards for the physical healthcare of patients in a range of psychiatric services. It outlines the responsibilities of psychiatrists monitoring the physical health of patients, such as problems associated with adverse effects of medication. The report recommends that psychiatrists are trained and kept up to date in relevant physical health matters. These recommendationsneed to be followed.
5.Mental health professionals should encourage patients to monitor simple measures such as weight, dietary plans, and exercise programs, with the involvement of the voluntary sector (MIND, Mental Health Foundation) where possible. Patients and carers need to be educated about the health risks associated with unhealthy lifestyles: for example, smoking and alcohol misuse may interfere with the metabolism of neuroleptic medications. Smoking cessation clinics and alcohol treatment programmes may help. Advice from dieticians about patients' nutritional requirements to offset changes in metabolism caused by neuroleptics is important.
6.Because of the large-scale reduction of inpatient psychiatric beds and service redesign the majority of psychiatric care provision now exists in the community. Therefore community mental health teams and psychiatric outpatient clinics need to be appropriately designed and equipped to enable proper assessment of physical health monitoring. Annual health checks from the GP would benefit patients who require long-term monitoring in the community. Screening for deleterious effects of medication for example, hypothyroidism and renal dysfunction caused by lithium, at regular intervals would be appropriate.16 It should also be made clear to psychiatrists that they should resist working in clinical settings that compromise patient care and inhibit good medical practice.
7.Financial initiatives such as Commissioning for Quality and Innovation (CQUIN)17 may be used by commissioners to improve physical health monitoring.As part of this process, primary care commissioners could mutually agree with mental health providers to fulfil measured targets related to such monitoring.
8.In order to better understand the interplay between psychiatric conditions and medical complications contributing to the high physical morbidity and mortality, further studies are essential. To cite one example, we now know that psychotropic medications contribute to many physical problems (abnormal ECGs, weight gain, changes in plasma glucose) and lead to higher morbidity rates. The 'newer' generation of antidepressants and neuroleptics have not lived up to expectations and have as many untoward effects as the older drugs. Developments of newer drugs with different mechanisms of action are required, though this will take time.
9.The discrimination faced by people with mental illness and learning disabilities, with the accompanying excess mortality, represents a human rights issue13 that requires legislative changes. The Disability Right’s Commission18 has already recommended appropriate physical health care screening, for example, annual physical health checks. The government’s health inequality agenda should incorporate these conditions into its indicators of disadvantage and include mental illnesses and learning disability in the framework.
Conclusion
Traditionally the field of psychiatry involves a holistic approach in the management of patients. Unfortunately, over the decades psychiatry appears to have lost its way and therefore it is important to re-establish a more comprehensive system of treating mental illness that encompasses regular physical health monitoring. Physical morbidity and mortality in patients with mental illness is on the rise and is associated with a complex interplay of factors outlined above. The overall health care of psychiatric patients can be improved through the changes in education and training of clinicians, close liaison between primary and secondary care, implementation of recommendations by NICE and the Royal College of Psychiatrists, improved research through better funding, public health education of patients and carers, and legislative changes.
One in four people in general and one in five people in Canada suffer from a mental disorder and only half of these individuals will seek help for their mental health.1 Doctors have an increasingly demanding job with increasing expectations of excellence in clinical, academic and managerial roles. It seems surprising that with their rigorous training doctors have higher rates of suicide compared to the general population.2 Studies have revealed that two-thirds of Canada’s physicians consider their workload too heavy, and more than half say that personal and family life have suffered because of their career choice.3 One third of Canadian physicians disagreed with a statement that their work environment encourages them to be healthy .4
A systematic review of mental health studies of medical students in the US and Canada found consistently higher rates of psychological distress in medical students compared with both the general population and age-matched peers .5 Medical students were also less likely to seek help for psychological distress than their peers. 6
A survey of psychiatrists and physicians in the UK found that most would be reluctant to disclose personal mental illness to colleagues or professional institutions. Their choices regarding disclosure and treatment would be influenced by issues of confidentiality, stigma, and career implications rather than quality of care.7,8
To reduce stigma and ease physician access to mental healthcare it is important to understand and address the above issues. This will facilitate psychiatrists gaining optimized mental health as well as to improve recruitment and retention of these professionals.9 The objective of our study was to assess the understanding of Canadian psychiatrists to the incidence of mental illness amongst psychiatrists in comparison to the general population and also in comparison to their medical/surgical colleagues. The study also assessed the attitudes of psychiatrists towards preference for disclosure, and treatment should they develop a mental illness in addition to their own experience of mental illness.
Method
Ethics approval (Study code PSIY-336-11) from Queen’s University in Kingston, Ontario was granted. Funding was obtained from TH’s research initiation grant. A mailing list of all psychiatrists in the province of Ontario was provided by the College of Physicians and Surgeons of Ontario (CPSO) for specific use to this research project. The College of Physicians and Surgeons Ontario is a body similar to the General Medical Council (GMC) in the UK. Their role is to regulate the practice of medicine in the province of Ontario. Other provinces have their own respective College of Physicians and Surgeons. In the remainder of the text the term ‘psychiatrist’ refers to consultant psychiatrist.
The list obtained from the CPSO did not include approximately 10% of psychiatrists who opted out of having their postal details released for research purposes. In total 1231 psychiatrists were sent a survey package. This package included a covering letter, a 2-page questionnaire, and a stamped return addressed envelope. Consent was assumed based on taking part in the survey. The 10-item questionnaire was based on a review of the literature, previous research, and discussion with colleagues. It comprised broadly of three sections. The first collected information on the respondents’ perception of prevalence of mental illness in psychiatrists in comparison to the general population and then in comparison with other medical/surgical specialties. The second required psychiatrists to identify to whom they were most likely to disclose a mental illness and reasons for non-disclosure. The third asked psychiatrists their preference of treatment in both an outpatient and inpatient setting. The identifiable information requested was the amount of experience the respondent had as a psychiatrist and whether they had experienced mental illness in the past. A free-text box was included at the end for comments and complete anonymity was maintained. Psychiatrists were divided into 3 groups: Group 1 (less than 5 years of experience as a psychiatrist), Group 2 (5-10 years of experience) and Group 3 (greater than 10 years of experience).
Analysis
A series of two-sample chi-square tests (χ²) were conducted to examine associations between certain categorical variables. In cases where 20% of contingency cells were <5 or where any cell=0, Fisher’s Exact test was used. Phi (φ) or Cramer’s V (for associations >2x2) were used as measures of effect size, these provide an association coefficient between 0 and 1. All analyses were done using SPSS 19.
Results
Of the 1231 questionnaires sent to doctors 487 were returned, a response rate of 39.6%. The respondents were placed into three groups: those in attending for <5 years (55, 11.3%), 5-10 years (53, 10.9%) and >10 years (369, 75.8%). The frequency of responses to all questions, both overall and as a function of attending group are shown in Table 1.
Table 1. Responses to all questions and comparisons between attending groups. Discrepancies between the overall column and the sum of the attending group columns are due to missing cases in responses to the attending group question.
Attending Group
Overall
<5 years
5-10 years
>10 years
Incidence of psychiatric illness amongst doctors is higher than general population?
Yes
124 (25.5% )
15 (27.3%)
19 (35.8%)
89 (24.1%)
No
247 (50.7% )
30 (54.5%)
26 (49.1%)
184 (49.9%)
Don’t know
116 (23.8% )
10 (18.2%)
8 (15.1%)
96 (26.0%)
Incidence of psychiatric illness amongst medical/surgical professionals higher than that of psychiatrists?
Yes
37 (7.6% )
1 (1.8%)
8 (15.1%)
28 (7.6%)
No
285 (58.5% )
36 (65.5%)
29 (54.7%)
214 (58.0%)
Don’t know
165 (33.9% )
18 (32.7%)
16 (30.2%)
127 (34.4%)
Have you ever experienced a mental illness, which had affected your personal, social or occupational life?
Yes
151 (31.0%)
14 (25.5%)
18 (34.0%)
118 (32.0%)
No
336 (69.0%)
41 (74.5%)
35 (66.0%)
251 (68.0%)
If you were to develop a psychiatric illness affecting your personal, social or occupational life, to whom would you initially be most likely to disclose this?
Church/Clergy
3 (0.6% )
1 (2.0%)
0 (0.0%)
2 (0.6%)
GP/Family physician
153 (31.4%)
18 (35.3%)
16 (32.0%)
116 (32.3%)
Family/friends
204 (41.9% )
22 (43.1%)
27 (54.0%)
152 (42.3%)
Colleagues
54 (11.1% )
4 (7.8%)
1 (2.0%)
46 (12.8%)
Mental health profess.
32 (6.6%)
4 (7.8%)
5(10.0%)
22 (6.1%)
None
15 (3.1% )
1 (2.0%)
0 (0.0%)
14 (3.9%)
Other
9 (2.0% )
1 (2.0%)
1 (2.0%)
7 (1.9%)
What is the most important factor that would affect your decision not to disclose your mental illness?
Stigma
114 (23.4%)
12 (22.2%)
14 (26.4%)
86 (24.2%)
Career implications
168 (34.5%)
21 (38.9%)
22 (41.5%)
121 (34.1%)
Professional standing
80 (16.4%)
11 (20.4%)
6 (11.3%)
63 (17.7%)
Other
109 (22.4%)
10 (18.5%)
11 (20.8%)
85 (23.9%)
If you were to suffer from a mental illness affecting your personal, social or occupational life requiring out-patient treatment, what would be your first treatment preference?
Informal profess. advice
83 (17.0%)
6 (10.9%)
7 (13.5%)
70 (19.1%)
Formal profess. Advice
365 (74.9%)
42 (76.4%)
40 (76.9%)
275 (75.1%)
Self-medication
25 (5.1%)
7 (12.7%)
2 (3.8%)
15 (4.1%)
No treatment
9 (1.8%)
0 (0.0%)
3 (5.8%)
6 (1.6%)
If you were to develop a mental illness requiring in-patient treatment, where would be your first preference?
Local
109 (22.4%)
6 (10.9%)
5 (9.4%)
96 (26.5%)
Out of area
370 (76.0%)
49 (89.1%)
48 (90.6%)
266 (73.5%)
In choosing in-patient preference, which of the following influenced your decision most?
Quality of care
130 (26.7%)
7 (12.7%)
7 (13.2%)
112 (30.5%)
Convenience
44 (9.0%)
0 (0.0%)
5 (9.4%)
38 (10.4%)
Confidentiality
257 (52.8%)
39 (70.9%)
34 (64.2%)
180 (49.0%)
Stigma
32 (6.6%)
6 (10.9%)
4 (7.5%)
22 (6.0%)
Other
21 (4.3%)
3 (5.5%)
3 (5.7%)
15 (4.1%)
Perception of the incidence of mental illness
Just over half of respondents disagreed that the incidence of mental illness was higher in doctors than the general population (247, 50.7%). Just over a quarter (124, 25.5%) agreed and just under a quarter replied ‘don’t know’ (116, 23.8%). As can be seen in Table 1, the pattern of responding was similar across all attending groups on this question (χ²=5.92; df=4; p=.205; Cramer’s V=.08). Most disagreed that psychiatric illness was greater in medical/surgical professionals than in psychiatrists (285, 58.5%), a small minority agreed (37, 7.6%). Again the attending groups responded similarly on this question (χ²=7.06; df=4; p=.133; Cramer’s V=.09). Nearly a third of respondents (151, 31.0%) claimed to have experienced a mental illness, and once more the attending groups did not differ significantly in their responses to this (χ²=1.12; df=2; p=.57; Cramer’s V =.05).
Disclosure of mental illness
Respondents would be most likely to disclose their mental illness in the first instance to family and friends (204, 41.9%) although many would instead prefer to disclose to their family physician (153, 31.4%). Relatively few would disclose to a colleague (54, 11.1%) in the first instance or to a mental health professional (32, 6.6%), very few would choose no-one (15, 3.1%) and the clergy was the least endorsed option (3, 0.6%). When considering only the three most popular response options (family/friends, family physician, and colleague) the three attending groups responded similarly (χ²=6.63; df=4; p=.157; Cramer’s V=.09). When asked about the most important factor affecting the decision not to disclose, the most common response was career implications (168, 34.5%). However stigma (114, 23.4%) and professional standing (80, 16.4%) were also reasonably common responses.
Again, when including only the three most popular disclosure choices in the analysis, there emerged an association between choice of whom to disclose and factor affecting disclosure (χ²=12.52; df=6; p=.051; Cramer’s V=.13) (see Table 2). Those who would choose to disclose to their family physician or to family/friends were more likely to cite stigma as a factor influencing their choice than those who would choose to disclose to colleagues. Those who would disclose to colleagues would be more likely to cite professional standing as a factor influencing their choice compared to those who would disclose to their family physician or to their family/friends. There was no association between choice of whom to disclose and previous experience of mental illness (χ²=1.22; df=2; p=.545; Cramer’s V=.05).
Table 2. Preferences for disclosure and the factors influencing that preference.
Factors influencing disclosure
Stigma
Career implications
Professional standing
Other
Total
Preference for disclosure
Family Physician
33 (22.6%)
57 (39.0%)
29 (19.9%)
27 (18.5%)
146 (100.0%)
Family/friends
56 (28.1%)
71 (35.7%)
24 (12.1%)
48 (24.1%)
199 (100.0%)
Colleagues
7 (13.7%)
17 (33.3%)
14 (27.5%)
13 (25.5%)
51 (100.0%)
Treatment for mental illness
When considering out-patient treatment, the majority of respondents would opt for formal professional advice (365, 74.9%). A small proportion would choose informal professional advice (83, 17.0%) and very few would self-medicate (25, 5.1%) or have no treatment (9, 1.8%). With regard to in-patient treatment, the majority would opt for an out of area mental health facility (370, 76.0%). Only just over a quarter of respondents (130, 26.7%) claimed that quality of care would influence their choice of in-patient care, just over half would be most concerned about confidentiality (257, 52.8%) There was a strong association between in-patient preference and the factor influencing that preference (Fisher’s Exact=228.25; p<.001; Cramer’s V=.70). As shown in Table 3, those who would choose an out of area facility, were much more likely to cite confidentiality and stigma as factors influencing their choice, than those who would choose a local facility. Conversely, those choosing a local facility were more likely to cite quality of care and convenience as influencing factors.
Table 3. In-patient treatment choice and the factors influencing that choice.
Factors influencing in-patient choice
Quality of Care
Convenience
Confidentiality
Stigma
Total
In-patient treatment choice
Local MH Facility
57 (56.4%)
39 (38.6%)
4 (4.0%)
1 (1.0%)
101 (100.0%)
Out of area MH Facility
69 (19.4%)
4 (1.1%)
252 (70.8%)
31 (8.7%)
356 (100.0%)
There was an association between attending group and out-patient preference (Fisher’s Exact=12.00; p=.042; Cramer’s V=.13). As can be seen in Table 1, the >10 years group would be more likely to select informal advice than the <5 years group, but the >10 years group were less likely to self-medicate than the <5 years group. The >10 years group responded similarly to the 5-10 years group with regard to self-medication. There was also an association between attending group and in-patient preference (χ²=12.66; df=2; p=.002; Cramer’s V=.16). The >10 years group, although still largely in favor of out of area care, would be more likely than the other two groups to opt for local care. There was also a significant association between attending group and the factors influencing in-patient choice (Fisher’s Exact =25.335; p=.001; Cramer’s V=.16). As shown in Table 1, the >10 years group would be more influenced by quality of care and less influenced by confidentiality than the other two groups.
Finally, previous experience of mental illness was not associated with in-patient choice (χ²=0.542; df=1; p=.462; φ=-.04), but it was associated with out-patient choice (χ²=11.51; df=3; p=.009; Cramer’s V=.16). As Table 4 shows, although both groups are more likely to opt for formal over informal advice, this pattern is more pronounced in the group who have had mental illness, than in the group who have not previously had mental illness.
Table 4. Previous experience of mental illness and out-patient treatment preference.
Out-patient treatment preference
Informal prof. advice
Formal prof. advice
Self-medication
No treatment
Total
Previous experience of mental illness
No
69 (20.8%)
242 (72.9%)
17 (5.1%)
4 (1.2%)
332 (100.0%)
Yes
14 (9.3%)
123 (82.0%)
8 (5.3%)
5 (3.3%)
150 (100.0%)
Discussion
This is the first study to assess the attitudes of Canadian psychiatrists to becoming mentally ill themselves. As this study was carried out in one province of Canada and the results cannot be generalized across the country. There is a significantly large scope of research potential in this area especially among psychiatric residents and other healthcare professionals .10
Physician Impairment is any physical, mental or behavioral disorder that interferes with the ability to engage safely in professional activities.11 Impairment among medical practitioners and psychiatrists in particular is a significant problem characterized by chronicity, under reporting and in many cases, poor outcomes.12 However early detection, intervention and treatment programs that are more sensitive to the needs of impaired practitioners, that are more continuous, better structured, and rehabilitation and recovery focused may be more likely to produce a positive outcome. 13 It is extremely important to remember and advocate that although a physician may be mentally ill he/she is not necessarily impaired.
It is concerning that stigma continues to play a role in psychiatrists’ decision making process to obtain mental healthcare. This is consistent with the findings of a survey in the USA which showed that half of all psychiatrists with a depressive illness would self-medicate rather than risk having mental illness recorded in their medical notes.10 Both entertainment and news media provide a dramatic and distorted image of mental illness that emphasize dangerousness, criminality and unpredictability.14 With this increased stigma doctors subsequently are concerned whether to disclose a mental health problem to their Licensing Boards for fear of being discriminated.15 Studies of US medical licensing bodies have demonstrated a trend towards increasing stigmatizing approaches 16-19 and the concern is whether there is a similar trend in Canada.9 Most psychiatrists in Canada are not aware what to expect from provincial colleges once their mental illness is disclosed and as a result tend to expect the worst. More work is needed by psychiatrists to inform the Provincial Colleges on physician mental health. Only then can the Provincial Licensing Colleges do more to assure physicians that the recovery model of treatment applies to them as it does other psychiatric patients.
The gap however continues to lie between ‘I need help’ and active psychiatric management. Psychiatrists will be well aware of the profound impact that such illnesses can have on a person’s personal and professional competency. However to reflect it on oneself can at times be met with denial in the first instance. Dr. Mike Shooter (ex-President of the Royal College of Psychiatrists, UK) suffered from depression and he highlights the need to speak out and combat stigma. He points out the need to seek treatment early and how not doing so can adversely affect the doctor-patient relationship.20 For some however the fear of stigmatization by health professionals for health professionals can lead to very tragic consequences. Dr. Suzanne Killinger-Johnson was a family physician with a psychotherapy practice in Toronto. She suffered from postpartum depression and in November of 2000 she jumped in front of a subway train cradling her son. Her son died instantly and Dr. Killinger-Johnson died 9 days later.21
Over the past 15 years a greater understanding has developed on the incidence, stressors and complications of physician mental illness. 22 The CPA published its first position paper on the mentally ill physician as early as 1984 with the latest version in 1997 currently under review. 22 The Canadian Medical Association should be congratulated on the most comprehensive strategy document for mentally ill physicians. Physician Health Matters - A mental health strategy for physicians in Canada was published by the CMA in February 2010. In addition to outlining the mental health of medical students, residents and physicians it addresses the current gaps in services and strategic direction needed to achieve ‘optimal mental health for all physicians’. This sets out the necessary groundwork for institutions to implement based on current evidence. In Canada there was the inauguration of the position of ‘The Bell Mental Health and Anti-Stigma Research Chair’ with Queen’s University in February 2012. 23 This position was offered to Dr. Heather Stuart, Professor of Community Health and Epidemiology. Stigma is a social process characterized by exclusion, rejection, blame or devaluation resulting from an adverse social judgment about a person or group. 24 There is a cultural pressure amongst physicians not to be sick so that one can provide care resulting in physicians unfortunately trying to control their own illness and treatment. 25 This concept is exacerbated for mental health issues and the stigma is considerably attached to physicians acknowledging mental health issues or illness, as well as seeking help. 26
Over the past decade the physician health community has been working to destigmatise physician mental health and to provide support services in this regard. All Canadian provinces have Physician Health Programs (PHPs) to help physicians with mental health difficulties. Referrals can be from physicians, families, colleagues, and self. 9 Physicians with psychiatric or drug dependence problems are referred from outside the PHP though the PHP (depending on the province) may or will be involved in monitoring the physician.
One of the most important factors influencing where a doctor is treated is the issue of confidentiality. 8 At present in Canada many hospitals are either switching or have switched to electronic patient records. Patient data in an electronic environment will be accessed from multiple portals by different professionals. This potentially poses serious concerns for psychiatrists if they have significant concerns around confidentiality of their record. A mechanism by which patients can access a list of professionals who have accessed their information may alleviate some concern regarding confidentiality.
Conclusions
Education surrounding mental illness in physicians needs to begin in medical school. Medical students require more assurance that seeking help for psychological problems will not be penalized. Junior doctors are receptive to education on physician impairment and substance misuse and this should be a mandatory component of their training. 27 Education and training of medical students and psychiatric residents to assess doctors as patients would make this scenario less taboo than it is currently perceived.
CPSO in liaison with relevant partners must develop a clear and concise document outlining steps the CPSO will take in helping the mentally ill physician. This document must be clearly advertised on the CPSO website to ease access and would reduce the catastrophizing interpretation psychiatrists (and physicians) may make to the CPSO’s involvement with the mentally ill physician. By the CPSO taking a lead this will prove a stimulus for other provincial licensing colleges to follow suit.
The bridge from ‘I need help’ to ‘I am getting help’ is paved with multiple barriers. By addressing some of the concerns raised by psychiatrists will help the psychiatrist easily cross over.
It seems that psychiatry is gradually losing its allure for future doctors. All around, one can detect an air of pessimism from colleagues about the creeping 'socialisation' of this important field of medicine. There is no longer the breadth of interest in the subject and each sub-branch, for want of a better expression, has its followers and adherents. Proponents of one particular facet of treatment are zealous in the pursuit of their own interests. Psychotherapy is pitched against the neurobiological, rehabilitation and social psychiatry against the pharmacologists, all trying to mark out their own piece of territory, with some yearning for a place in the history books, or at the very least, an acronym. Some psychiatrists do not believe in diagnoses; others ridicule the concept of personality disorder, autistic spectrum disorder, or drug treatment; some believe psychiatric illness is the fault of governments, and there are probably a few who do not believe in psychiatry at all! 'Research' studies are cherry-picked by all sides to illustrate the ineffectiveness of 'alternative' treatments. The full picture or perspective of ill health is blurred and narrowed by a minority who believe they alone know what is right for patients, and psychiatry is 'intellectualised' by others to give it an air of authority and profundity it does not possess. Morale and training are suffering and, if this state of chaos and insanity continues, the discipline itself will implode and cease to be of interest to anyone, save the warring factions in the profession itself.
Once upon a time it was considered that a reasonably broad mixture of community and hospital services would provide benefit for patients with mental illness. Staff involved in their care, who have the rather cumbersome and oxymoronic description of being called 'mental' health professionals, would also widen their experience because of the continuity of care provided. It was hoped patients who clearly did not need to be in hospital (for example, waiting for appropriate accommodation) could be discharged. Clinical need would determine those who required further rehabilitation/treatment in hospital, and would not be swayed by pressures, often financial, to discharge. Now, with the setting up of Home Treatment and other teams the situation has ironically worsened, because there is an implicit opinion in this arrangement that hospital admission, even for the seriously ill or indeed violent patients, is the least desirable option and something to avoid at all cost, even when care in the community is not immediately available or adequate. Care provision for the elderly is a separate concern and is not under discussion here.
In the domain of general adult psychiatry those patients who are in need of care, be it medical or social, are languishing at home, desperate for help, being offered assessment after assessment by disparate teams. There are not enough care professionals to cope with the demand. Home Treatment Teams in particular, are under considerable sustained pressure and stress to ensure further reduction in beds. Rehabilitation beds are being closed. 'It is cheaper to keep patients in the community', we are told. Or, if that does not suit, the liberal stance might be, 'What does hospital admission achieve'? That's fine if the problem is not on your doorstep. Psychiatrists who oversee inpatient care are also pressurised to discharge patients as soon as possible, so the very old notion of 'incarceration' (that worn-out cliché from the antipsychiatry lobby) seems facile, to say the least. On the contrary, doctors now have the added worry of prematurely discharging partially treated ('we need the beds') as well as more vulnerable patients who cannot cope. Most patients who take up psychiatric hospital beds do not want to be in hospital in the first place as they often, rightly or wrongly, do not see themselves as ill. Many hospital beds are now occupied by 'Section patients', and conversely, many very ill patients are left to go it alone because they refuse hospital admission and do not want community team involvement, yet are not 'sectionable'. The inference seems to be, 'If not sectionable or under CPA (Care Programme Approach) it is not our concern.'
Where there are sufficient provisions for outpatient care, some of the damage may be mitigated. Overworked staff including community psychiatric nurses (CPNs), support time recovery workers (STRs) and occupational therapists (OTs) often have the thankless task and enormous responsibility of seeing patients at home, some of whom are threatening and potentially dangerous, others erratic with their outpatient clinics attendance not always through deliberate evasion but often the result of the very condition causing the problem, for example, lack of insight. Other patients do not engage either through hostility or loss of motivation induced by the underlying problem, say, drug and alcohol misuse. Chronic patients are not ill enough to be on CPA and diagnostic 'conundrums' are left to others to sort out. With the introduction of the New Ways of Working,1 the traditional outpatient clinics are being abolished and replaced with community clinics ('short-term' outpatients really). Ideally a community clinic should be run by CPNs as they usually understand the medical, psychiatric, psychological, and social needs of patients. In the authors' opinion the clinics should be Consultant-led because despite the tendency to classify everyone as 'clinicians' many staff feel uncomfortable with this role as it implies or infers a degree of clinical responsibility for which they are not qualified. Psychiatric nurses (especially those with a general nursing background) are ideally placed to carry out this function by virtue of their wide experience; also they are aware when to seek medical help when needed. Often they are more informed about patients than the primary physician or indeed the psychiatrist because of more frequent contact, either via liaison with the hospital wards or through home visits in their role as CPNs. Nurses and other staff (for example, social workers) are involved in patients' discharge from hospital (usually determined at pre-discharge meetings) and are therefore an essential link in the continuity of patient care before patients are eventually seen in the 'community clinics'. Requests for domiciliary visits from general practitioners (GPs) to physicians themselves have become a thing of the past, with the exception of those psychiatrists working with Home Treatment Teams and Assertive Outreach Teams. Nowadays it is not uncommon for patients to be waiting months on end (more assessments) before being deemed 'appropriate' to see a Consultant Psychiatrist.
Certainly there are patients who do not need to continue seeing a Consultant Psychiatrist for years on end and should be discharged back to the GP to reduce unnecessary costs and to avoid a dependency culture, in the same way a patient with mild arthritis does not need to see a rheumatologist or a patient with anaemia does not always need the expertise of a haematologist, to use simple analogies. However, sometimes GPs are unwilling to reciprocate or feel out of depth with 'psychiatry' that this is not always possible. The chronicity of many psychiatric disorders perhaps harnesses the belief that new treatments may emerge which only a psychiatrist, with his/her specialized knowledge, can implement and deal with. This type of scenario is seen with many other illnesses in all fields of medicine (chronic psoriasis, rheumatoid arthritis, multiple sclerosis) yet no one is suggesting that GPs solely should be left to manage these conditions. It seems the clinical risk to patient care is not thought through and this no doubt will lead to serious repercussions later. In our estimation, physical and mental illnesses are so often intertwined that their management should be equally shared by physicians and psychiatrists.2
Swings and Roundabouts
Such is the pressure by management (under the thumb of civil servants) and 'those in the know', reverentially referred to as ‘Commissioners’, that health professionals in psychiatry have to defend their clinical judgment and carry out numerous risk assessments (defensive medicine) of patients who are to be discharged from the outpatient clinic back to the GP in any event. Patients may be fortunate enough to receive a few last appointments with the Community Clinic (when they are up and running: some are at the time of writing) before they are shown the door and sent back to the GP, all to save money. Packages of care will not disguise the fact that vulnerable patients are being left to fend for themselves, just as they were in the past when the large institutions closed down without any forward planning as to how and where patients would survive. Yet ‘management training’ and ‘mandatory courses’ continue inexorably, often provided by 'expert' outside speakers, costing Trusts considerable amounts of hours lost, let alone the expense, instead of employing more nursing staff to cope with the ever-increasing workload. We are led to believe that reducing 'outpatient numbers' will lead to less pressurised work on staff, which really does not fit. All that will be happening to the extent that 'outpatients' will now be filling to the brim with CPA patients (read 'psychoses') instead of a good case-mix of patients required for general experience and training. It seems to be forgotten that there are patients who feel very unwell and are unable to cope, yet are not suffering from major psychiatric disorders.
The next scenario will be the revolving door ‘GP - Access/Assessment Team - possible Consultant Psychiatrist advice and at most two follow-up appointments (if one is really ill) - Community Clinic - discharge to GP system’, to replace the premature hospital discharge-readmission system which failed miserably in the past. When the patient relapses (or rather, when the illness remains static) the GP refers back into the system and the whole process begins again. In this way the Trusts receive money by reaching their targets (discharging patients) and are paid a second time when GPs 'purchase' more care. Those patients with 'minor problems' (not in their GP's estimation) will whittle away and remain unhappy. 'They can always see a counsellor' is the unspoken passive riposte. Furthermore, there will be less clinical variety for doctors and students, as their work will amount to prescribing 'powerful drugs' (we are told by the antipsychiatrists), monitoring serum lithium (and other drug) levels or checking blood results and clozapine dosages, because the Talking Therapies will be curing all and sundry. If only. We are reverting to the bad old days of pseudomedicine and pseudoscience.
Academicians and those who sit on government advisory bodies with grandiose names would have us believe there are far more effective ways to support people at home, or if they have no home, a crisis house will do. Meaningless, empty statements such as 'randomised controlled trials' (given the complexity of the issues under study) often with some reference to National Institute for Health and Clinical Excellence (NICE) guidelines, are used to support questionable findings. Despite all the 'new ways of working' national stress levels are at their highest because of rising unemployment, unexpected redundancies, increasing debt through credit card borrowing, and suicide rates are going up. New ways of Working is not working and any 'ad hoc survey' (note we did not say 'research') will reveal the depth of disillusionment all professionals in the discipline of psychiatry are experiencing, and not just the hallowed psychiatrists. Rudderless multidisciplinary teams are not the answer: teams require management. The term 'leadership' is becoming redundant (one only has to look at successive governments) and is often merely a spur for making money out of meaningless and time-wasting leadership courses which seem to be sprouting everywhere. Among the many qualities 'leadership' embraces are a sense of humour, assertiveness, fairness, creativity, openness, integrity and dedication, all to be found in one individual; presumably! Hierarchical structures may work, contrary to the sweeping statements of some,3 because people who are experienced in medical, academic and management matters (with perhaps a sense of humour) tend to command respect from team members. It is not enough to be an expert in cognitive behavioural therapy (CBT).
No place like home
How does one establish trust and rapport with patients when there will be less opportunity to do so because their care and progress are determined by market forces? Instead of decreasing outpatient volume or confining this aspect of care to CPA patients only, outpatient departments should cater for the mounting levels of stress in the community (poverty, debts, redundancies, threatened job losses) through increased staffing levels and training/supervision of more social workers, CPNs and occupational health workers. Where possible such staff should attend as many clinics as possible (not just CPAs) to offer a more holistic approach to patient care. If anything, policy makers, clinicians, managers, carers and user groups need to collaborate and clamour for a more integrative mental health service, not fracture the already fragile set-up. Community clinics are seen as a stepping stone to discharging from the mental health services (those who set them up don't like this analogy), which in theory is a good idea. The problem lies in the precipitous nature of transfer from outpatient to community clinics. Some very ill patients with chronic conditions are ironically not a burden to the system, in that they do not need to be seen frequently nor do they not require repeated admissions to hospital, yet if left to their own devices and discharged back to Primary Care would soon find life unmanageable as they rely on the expertise of health professionals to remain reasonably stable. Many patients have physical problems, some partly the result of the very treatments given to alleviate their underlying condition (obesity, hypertension, ECG disturbances, Type 2 diabetes and so forth), and need careful monitoring and supervision which is best provided by CPNs and other staff, in the same way a Health Visitor, Practice Nurse, or Diabetes Nurse Specialist might offer his/her expertise to a GP practice.
There will always be patients who need to be seen in the outpatient department with the emotional security and staff support this provides. We are aware that some 20% of patients miss their mental health appointments but then people miss appointments for other interviews and not always because they are unwell.4 Some people miss appointments because they feel better. This is surely not a reason for abandoning the outpatient system, which serves the remainder of the patient population quite well. We have experienced an unprecedented expression of worry and disappointment by patients who have been told they are not ill enough to be followed up at the outpatient department. Now mental health professionals are also frustrated, because they perceive their remit is to refer back to the GP as swiftly as possible, without having thoroughly assessed a patient over a period of time. First on the target list will be those patients who have not been seen by a psychiatrist for several months (‘We don't see them very often, therefore what is the point?') yet many chronically unwell patients may not want to attend outpatients, or have sufficient insight to realize they need to attend, for reasons outlined above. Will Outreach Teams in every Trust be abandoned to save money? Was it not their role in the first place to help those reluctant to receive treatment? What messages are we giving to patients other than being 'just a number, a hospital statistic’'? Those who have had the ‘luxury’ of a hospital admission usually comprise the very psychotic, and the personality disordered, and of the latter some consider they should not be in hospital anyway. The gains that have been made over the past decade in early intervention and engagement with patients by Assertive Outreach Teams will be lost. Yet, there is a continuing demand from patients and their carers to be seen by doctors.5
Here is how the 'new' system works. New Ways of Working, set up some years ago 1 and imposed on us, was meant to be an innovative approach to consultants' contracts by encouraging multidisciplinary teamwork ('When did consultants ever not consult their fellow professionals'?), reviewing the continued necessity for outpatient clinics, advocating more scheduled time for carers (colleagues we have spoken to cannot ever recall not seeing relatives or carers!) and more prominent roles for all team members, encouraging further education and training. Unfortunately we have gone to the other extreme and are being bombarded by all sorts of courses to the extent that much time is lost not seeing patients. Team members may and should undertake postgraduate studies. For doctors, continued professional development is mandatory. We are the only profession that requires revalidation every five years. Nothing can substitute for the medical training doctors undergo and it is a shame that the expertise of psychiatrists is diluted and devalued by their current roles as medication gatekeepers. It is a curious state of affairs or perhaps conveniently forgotten that when Trusts or 'Health Care Reformers' talk nowadays about working in teams and 'shared responsibility', the Consultant-led team concept is dismissed. Where there are Consultants who do not feel up to the role of leading a team, or are uncomfortable making assertive decisions and would rather take a back-seat thus avoiding the responsibility of being in charge of a team, then a Specialist Registrar nearing the end of training could fill this position. Multidisciplinary means 'several' not 'equal' disciplines of learning, ideally each discipline contributing a part to the whole. The medical member of the team is nowadays confronted with the added indignity of having his/her patients described in management-speak as customers, consumers, clients, service users, in fact any title that does not describe the ill person as a patient. It also reflects a creeping normalisation of 'political correctness' thrust upon us by the social engineers and should be resisted. We want patients to be treated with respect not as 'service users’, waiting for the next bus or train. Trusts are now seen to promote a business approach to health care, thereby gaining the approval of their masters, the civil servants and politicians.6 Lots of tick boxes and targets, with subtle threats of redundancies or talks about 'natural wastage'. Meanwhile, the College sits idly by.
Another concern is the training of future psychiatrists which is slip-shod and bureaucratic (lots of forms and assessments). There is hardly any room to accommodate medical students. Junior doctors who practice psychiatry are not receiving the continuity of supervision which existed years ago. The 'junior doctor' is less visible because of European working time directives, on-call commitments with days off in lieu, study leave, annual leave, and the inevitable sick leave. Passing the Member of the Royal College of Psychiatrists (MRCPsych) exams nowadays does not necessarily equate with clinical experience anymore. Even the nomenclature is confusing - not just to doctors and management (‘CT1’, ‘ST1’ and so forth) but also to staff, and reduces the profession to an anomalous set of categories no outsider understands, not to mention the loss of identity it creates in the individual doctor. What was wrong with Senior House Officer (SHO), Registrar, Senior Registrar, and Consultant? Unfortunately, we believe it is now too late to revert this shambles born out of the chaotic modernisation of medical careers. 7
The future is bleak and many doctors (and indeed nurses) are becoming disenchanted by psychiatry, feeling let down by a Royal College which seems to accommodate every new social trend rather than concentrating on improving the status of a once fascinating field of medicine. Lots of wake-up calls, but no-one is getting out of bed.8 Strange having a 'trade union' that ignores its members! Could someone inform the College that nowadays most General Adult Psychiatrists are almost reduced to measuring lithium levels, advising on clozapine doses, and attending meetings. No wonder the numbers of potential psychiatrists are falling. How would this dilution of responsibility work in a surgical unit? Would the team members decide how an operation is to be carried out because one of them is trained in resuscitation? Contrary to reports3 consultants are not happy with the present set-up, though it is unlikely our Royal College hierarchy will do anything about it. Many psychiatrists nowadays have an extensive academic knowledge of medicine, psychology, sociology, and neuropsychiatry, and no longer want to be minor players in the game, or undermined by a system that encourages power without responsibility.
Fragmentation breeds disinterest
What is the answer? The previous system, though not perfect, worked well. This had its shortcomings too (oversized catchments areas, Consultants in charge of many wards, and so forth)7 but the continuity of care was there. Patients discharged from hospital were seen by the same team. GPs could refer directly to Consultants (as is the case in other medical specialties) and patients were then seen in the outpatient clinic. However, often the patient would attend such clinics for years because GPs were reluctant to resume care. Nowadays the training and education of GPs is exemplary and most are more than capable and indeed willing, to continue to provide support for their patients provided there is a back-up plan. The academic training of psychiatrists has never been better but their clinical skills are suspect. Therefore there needs to be an overhaul in the examination system as well. Actors are not patients. Simulated psychiatry is not the same as simulated surgery. Simulation is a technique not a technology, we are told. It is not a substitute for doctors examining real patients in real contexts. The same applies to nurses. All nurses (CPNs) could easily be trained to do ECGs, act as phlebotomists, and arrange routine tests. Many already do. Give back to nurses the skills they enjoy in other fields of medicine. For psychiatrists there are numerous courses one can attend to broaden their medical knowledge. Most GPs take an interest in a holistic approach to their patients (social, psychological, physical). As matters stand GPs now refer to a borough 'Access and Allocation Team' with no one held accountable, and even though requested by the GP, a Consultant Psychiatrist's opinion is not always provided. Responsibility is the province of senior doctors and management and should not be diluted by putting pressure on the Team as a whole whose individual experience varies considerably. Doctors (and nursing staff) should have mandatory training in psychological therapies (cognitive and behaviour therapies specifically). A fixed number of sessions in addition to their usual duties could be part of the job plan for those doctors interested in the psychotherapies per se, or put another way, a holistic approach to patient care, which is what most doctors do in any event. Patients would then have the benefit of medical and psychological input simultaneously (let's call it a cognitive-medical model). Waiting lists would be dramatically reduced at a stroke and Trusts would no longer have the responsibility of finding and employing unqualified (in medicine or psychology) 'talking therapists'. People who are generally physically well and who do not have serious psychosocial problems or psychiatric illnesses could receive treatment elsewhere through their GP, counsellors or other psychotherapists (those with no medical or psychology degrees) of their own volition. There is no need to clog up the system with 'customers'. We are not a supermarket!
Complaints will inevitably follow when patient dissatisfaction begins to emerge, which is only a matter of time. More serious incidents will be a consequence of too many bed closures and staff shortages. Dilution of responsibility means that no one person seems to be accountable when things go wrong and patients are left stranded (read the Francis Report 9). Already GPs are frustrated by the lack of informal contact with psychiatrists who are once again seen to be retreating to their ivory towers, having been overwhelmed by lots of courses, lots of training, lots of meetings, lots of empty rhetoric. Too much emphasis nowadays is placed on the sociological/psychological aspects of patients' illness and so serious conditions are missed. GPs should be able to refer directly to their colleagues where there are immediate concerns and not have to wait for triage meetings which delay this process. After all, GPs know their patients best. Community clinics could take the bulk of moderate conditions (which are causing undue stress) and see patients for as long as necessary (not a determined number of appointments) before deciding the GP can resume responsibility. 'Packages of Care' and other outdated expressions should be confined to the dustbin. Patients are not fooled by promises of cardboard boxes with little pink ribbons. Continuity of patient care requires a flexible approach which encompasses easy access to information and a direct pathway to services and medical care when needed.
Knowledge in the making
Psychiatrists should concentrate on more difficult and complicated cases (as was the case in the past) as well as routine moderate conditions, enabling them to use their broad skills more efficiently and effectively. Some psychiatrists see too few patients and this should be changed. Perhaps there is a case for psychiatrists rotating through some specialties say, every five years, for example, between Rehabilitation and General Adult Psychiatry. There are many patients who are not on mood stabilisers or clozapine who require intensive input and combined medical expertise and rotating between posts would offer valuable experience. A more varied approach is thus needed but do we really need all those subspecialties? What ever happened to the general psychiatrist with a special interest? In our view at least one year of neurology training should be mandatory for psychiatrists during their training. No formal examinations, just certificates to prove the courses have been completed; otherwise the system grinds to a halt. Under this system a doctor could still theoretically become a consultant after nine years postgraduate training (three years in foundation training and neurology), and six years Psychiatry (to include neurology, psychology and sociology) which is not unreasonable. Equal emphasis on neuromedical, sociological and psychological factors causing health problems would foster a healthier and friendlier relationship between disciplines which deal with mental illness and primary care providers. As it stands, with the fragmented role of general adult psychiatric services and the emphasis on e-learning and internet training for junior doctors (no hands-on clinical experience) we are facing yet another era of overemphasis on social psychiatry (or rather reverting to ancient belief systems) with its 'neutral' politically correct denigrating sound bites (customers, clients, service users). All will be well if we can just sort out the social problems! The simplistic notion that problems will disappear if we do not smoke, drink, take illicit drugs, keep our weight down, and have a home to go to, is the stuff of social engineering by the 'experts in living,' and alas by doctors who have lost touch with medicine.
Doctors need reminding that psychiatry is that branch of medicine that is concerned with the study, treatment, and prevention of mental illness using medical and psychological therapies as well as paying special attention to social hardship and isolation where present. It is not philosophy or social science. It is to medicine what metaphysics is to philosophy. Psychiatrists need to broaden their horizons and take their heads out of the therapy books to witness the advances in neuroscientific techniques and genetic advancements that have already transformed the nature of medicine. To develop their psychological skills they need to take on board that patients want more than drugs to alleviate distress. Therefore practical techniques such as CBT or DBT (dialectical behaviour therapy) will further heighten their expertise as physicians. Many doctors are already familiar with applying CBT and other therapies. However, doctors should also be aware of the limitations of psychotherapies in general, recognizing and acknowledging that such therapies do not always work either and indeed in some instances may be harmful. Psychiatrists should be part of separate Wellbeing Clinics (perhaps one session per week) to becoming better acquainted and proficient again with physical examinations, investigations, routine procedures (ECGs for example) and interpretation of results (not just screen, but to intervene). This overseeing of the physical health of patients is not always possible in a busy outpatient clinic. Many potentially serious conditions would be revealed and information to the GP or tertiary services made known immediately. Psychiatrists are not 'stuck in a medical model' no more than a physician believes all myocardial infarcts are caused by psychosocial factors or life style. But to ignore the medical advances in molecular biology and neuroscientific diagnostic techniques portrays a profound ignorance of biological psychiatry and is insulting to those scientists who work tirelessly, often without much recognition, to further our understanding of 'brain disorders'. It is all very well to talk about art, philosophy, social sciences and literature as having a great bearing on our interest in psychiatry and congratulate ourselves as 'lateral thinkers' but an understanding of the philosophy of say, Bertrand Russell or indeed the school of Zen Buddhism, will not eliminate mental disorder. Romantic as it might sound in retrospect, Vincent Van Gogh did not enjoy cutting his ear off, nor did Robert Schumann feel ecstatic when jumping into the Rhine before being carted off to the asylum.
If we do not embrace a holistic view of mental ill-health we risk not only throwing the baby out with the bath water but the bath itself, thereby causing further dissatisfaction and low morale among doctors with an inevitable negative impact on patient care. Psychiatrists are not bemoaning their loss of hegemony - a favourite word and another myth propagated by the antipsychiatry lobby; rather, it is only too obvious to them (as qualified medical doctors) that patients will suffer in the long term by not being referred appropriately to those who have the expertise to recognize and distinguish between human difficulties and illness. There is also a need to re-examine the impact of psychological therapies and not succumb to the popular and naive notion that they are all evidence-based in scientific terms. In the meantime the 'worried well' can indulge themselves with all the peripheral talking therapies and current fads they desire. Likewise, performance management, outcome measures and payment by results have become relentless tick-box exercises creating unnecessary stress among health care professionals (threats of job losses) who 'must meet targets at all costs', all for a slice of the Commissioners' cake. What a way to run a health service! Patients become meaningless statistics in the meantime. No! The wake-up call should be aimed at those who are intent on destroying the good will and values of the very same people they purport to support, through their social engineering and outdated attitudes.